
CD4+CD25+ Regulatory T Cell Depletion Improves the Graft-Versus-Tumor Effect of Donor Lymphocytes...
10
DOI: 10.1126/scitranslmed.3001302 , 41ra52 (2010); 2 Sci Transl Med , et al. Sébastien Maury Hematopoietic Stem Cell Transplantation Graft-Versus-Tumor Effect of Donor Lymphocytes After Allogeneic Regulatory T Cell Depletion Improves the + CD25 + CD4 http://stm.sciencemag.org/content/2/41/41ra52.full.html figures, can be found at: and other services, including high-resolution A complete electronic version of this article http://stm.sciencemag.org/content/suppl/2010/07/20/2.41.41ra52.DC1.html "Supplementary Material" can be found at: Supporting Online Material http://stm.sciencemag.org/content/2/41/41ra52.full.html#ref-list-1 , 24 of which can be accessed free: cites 43 articles This article http://www.sciencemag.org/about/permissions.dtl in whole or in part can be found at: reproduce this article permission to of this article or about obtaining reprints Information about obtaining is a registered trademark of AAAS. Science Translational Medicine rights reserved. The title NW, Washington, DC 20005. Copyright 2010 by the American Association for the Advancement of Science; all last week in December, by the American Association for the Advancement of Science, 1200 New York Avenue (print ISSN 1946-6234; online ISSN 1946-6242) is published weekly, except the Science Translational Medicine on July 21, 2010 stm.sciencemag.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of CD4+CD25+ Regulatory T Cell Depletion Improves the Graft-Versus-Tumor Effect of Donor Lymphocytes...
DOI: 10.1126/scitranslmed.3001302, 41ra52 (2010);2 Sci Transl Med, et al.Sébastien Maury
Hematopoietic Stem Cell TransplantationGraft-Versus-Tumor Effect of Donor Lymphocytes After Allogeneic
Regulatory T Cell Depletion Improves the+CD25+CD4
http://stm.sciencemag.org/content/2/41/41ra52.full.htmlfigures, can be found at:
and other services, including high-resolutionA complete electronic version of this article
http://stm.sciencemag.org/content/suppl/2010/07/20/2.41.41ra52.DC1.html "Supplementary Material"
can be found at: Supporting Online Material
http://stm.sciencemag.org/content/2/41/41ra52.full.html#ref-list-1, 24 of which can be accessed free:cites 43 articlesThis article
http://www.sciencemag.org/about/permissions.dtl in whole or in part can be found at: reproduce this article
permission to of this article or about obtaining reprintsInformation about obtaining
is a registered trademark of AAAS. Science Translational Medicinerights reserved. The title NW, Washington, DC 20005. Copyright 2010 by the American Association for the Advancement of Science; alllast week in December, by the American Association for the Advancement of Science, 1200 New York Avenue
(print ISSN 1946-6234; online ISSN 1946-6242) is published weekly, except theScience Translational Medicine
on
July
21,
201
0st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
R E S EARCH ART I C L E
CANCER IMMUNOLOGY
CD4+CD25+ Regulatory T Cell Depletion Improves theGraft-Versus-Tumor Effect of Donor Lymphocytes AfterAllogeneic Hematopoietic Stem Cell TransplantationSébastien Maury,1,2* François M. Lemoine,3,4 Yosr Hicheri,1,2† Michelle Rosenzwajg,3,4†
Cécile Badoual,5,6 Mustapha Cheraï,3,4 Jean-Louis Beaumont,7 Nabih Azar,3 Nathalie Dhedin,8
Anne Sirvent,9 Agnès Buzyn,10 Marie-Thérèse Rubio,10 Stéphane Vigouroux,11
Olivier Montagne,2,12 Dominique Bories,1,2 Françoise Roudot-Thoraval,2,13 Jean-Paul Vernant,8
Catherine Cordonnier,1,2 David Klatzmann,3,4‡ José L. Cohen4,8*‡
(Published 21 July 2010; Volume 2 Issue 41 41ra52)
on
July
21,
201
0tm
.sci
ence
mag
.org
Donor T cells play a pivotal role in the graft-versus-tumor effect after allogeneic hematopoietic stem cell trans-plantation. Regulatory T cells (Tregs) may reduce alloreactivity, the major component of the graft-versus-tumoreffect. In the setting of donor lymphocyte infusion after hematopoietic stem cell transplantation, we postulatedthat Treg depletion could improve alloreactivity and likewise the graft-versus-tumor effect of donor T cells. Thesafety and efficacy of Treg-depleted donor lymphocyte infusion was studied in 17 adult patients with malignancyrelapse after hematopoietic stem cell transplantation. All but one had previously failed to respond to at least onestandard donor lymphocyte infusion, and none had experienced graft-versus-host disease. Two of the 17 patientsdeveloped graft-versus-host disease after their first Treg-depleted donor lymphocyte infusion and experienced along-term remissionof theirmalignancy. Four of the 15patientswhodidnot respondafter a first Treg-depleteddonorlymphocyte infusion received a second Treg-depleted donor lymphocyte infusion combined with lymphodepletingchemotherapy aimed to also eliminate recipient Tregs. All four developed acute-like graft-versus-host disease that wasassociated with a partial or complete and durable remission. In the whole cohort, graft-versus-host disease inductionthroughTregdepletionwasassociatedwith improvedsurvival. These results suggest that Treg-depleteddonor lymphocyteinfusion is a safe, feasible approach that induces graft-versus-host or graft-versus-tumor effects in alloreactivity-resistantpatients. In patients not responding to this approach, the combinationof chemotherapy-induced lymphodepletionof therecipient synergizeswith theeffect of Treg-depleteddonor lymphocyte infusion. These findingsoffer a rational therapeuticapproach for cancer cellular immunotherapy.
sm
Downl
oade
d fr
o
INTRODUCTIONAllogeneic hematopoietic stem cell transplantation (HSCT) is the treat-ment of choice for several types of severe hematological malignancy.Donor transplants contain HSCs that mediate engraftment and T cellsthat favor engraftment (1), promote peripheral T cell reconstitution (2),and, moreover, provide the graft-versus-tumor (GVT) therapeutic ef-fect of HSCT (3). The GVT effect is due to the alloreactivity of trans-
1Department of Hematology, Assistance Publique-Hôpitaux de Paris, Hôpital HenriMondor, Créteil F-94010, France. 2Université Paris-Est Créteil Val de Marne, CréteilF-94010, France. 3Department of Biotherapies, Assistance Publique-Hôpitaux de Paris,Hôpital Pitié-Salpêtrière, Paris F-75013, France. 4Centre National de la Recherche Sci-entifique UMR 7211, Université Pierre et Marie Curie Paris 06, Paris F-75013, France.5Department of Pathology, Assistance Publique-Hôpitaux de Paris, Hôpital EuropéenGeorges Pompidou, Paris F-75015, France. 6Ecole Nationale Vétérinaire d’Alfort, EA4054,Paris Descartes University, Paris F-75005, France. 7Department of Hemapheresis, Etablis-sement Français du Sang d’Ile de France, Créteil F-94010, France. 8Department ofHematology, Assistance Publique-Hôpitaux de Paris, Hôpital Pitié-Salpêtrière, Paris F-75013,France. 9Department of Hematology, Hôpital Archet, Nice F-06000, France. 10Departmentof Hematology, Hôpital Necker, Paris F-75015, France. 11Department of Hematology,Hôpital Haut-Leveque, Bordeaux F-33000, France. 12Center for Clinical Investigation inBiotherapy, Assistance Publique-Hôpitaux de Paris, Hôpital Henri Mondor, Créteil F-94010,France. 13Department of Public Health, Assistance Publique-Hôpitaux de Paris, HôpitalHenri Mondor, Créteil F-94010, France.*To whom correspondence should be addressed. E-mail: [email protected] (S.M.); [email protected] (J.L.C.)†These authors contributed equally to this work.‡These authors contributed equally to this work.
www.
planted T cells, which has been demonstrated by the increased risk ofmalignancy relapse after syngeneic twin graft or T cell–depleted allo-geneic HSCT (4). Alloreactivity results from the stimulation of donor Tcells by host dendritic cells presenting both human leukocyte antigens(HLAs) and minor histocompatibility antigens (mHAs) (5). The im-munotherapeutic effect of donor T cells is further illustrated by the suc-cessful application of donor lymphocyte infusion (DLI) in the treatmentof malignancy relapses after HSCT (3, 6). However, the beneficial effectsof donor T cells must be counterbalanced by their implication in thepathogenesis of graft-versus-host disease (GVHD), a major cause oftransplant-related morbidity and mortality after HSCT and DLI (7).
Although routinely used for relapse after HSCT, DLI is often notsuccessful in controlling malignancy (3). In DLI failure, as after HSCT(4), the absence of the GVT effect correlates with lack of GVHD. In-deed, despite disparities that may exist between donor and recipient inHLAs and/or mHAs, some grafted patients never display any clinicalmanifestation of donor T cell alloreactivity after HSCT and DLI. Thisillustrates that histo-incompatibility in HLAs and/or mHAs is not theonly determinant of alloreactivity. For instance, the subpopulation ofCD4+CD25+FoxP3+ immunoregulatory T cells (Tregs), in addition tocontrolling autoimmunity, has been shown to play a key role in thecontrol of alloreactive immune responses (8). They physiologicallyregulate tolerance to paternal alloantigens during gestation in mice(9, 10). Their capacity to modulate allogeneic immune responses has
ScienceTranslationalMedicine.org 21 July 2010 Vol 2 Issue 41 41ra52 1

R E S EARCH ART I C L E
also been demonstrated in experimental solid organs (11) and HSCtransplantation models (12). In the HSCT setting, we and others ob-served that the addition of donor-derived Treg to the transplant couldcontrol GVHD in mice while preserving the GVT effect (13–16). Con-versely, Treg depletion from the transplant led to significantly accel-erated GVHD in different murine models of allogeneic HSCT (13, 17).
Therefore, on the basis of these observations, we hypothesized thatHSCT recipients who did not respond to DLI treatment for a relap-sing hematological malignancy and who never experienced GVHDcould benefit from Treg-depleted DLI (d-DLI) with the potential toimprove alloreactivity and induce a GVT effect.
on
July
21,
201
0st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
RESULTS
d-DLI facilitates GVH or GVT effects inalloreactivity-resistant patientsSeventeen patients were included between December 2005 and De-cember 2008 in a phase I/II clinical trial (18). One patient was ex-cluded from the analysis owing to protocol violation in DLI celldosing. Our patients experienced relapse of their hematological malig-nancy at a mean interval of 18 months (range, 3 to 90 months) afterHSCT. This regimen involved bone marrow infusion preceded by amyeloablative conditioning regimen (n = 12) or peripheral blood stemcells after a nonmyeloablative regimen (n = 5) from a sibling (n = 13)or a matched unrelated (n = 4) donor (Table 1 and Fig. 1). Only onepatient received d-DLI as first-line DLI because of a persisting excessof blasts in marrow after salvage chemotherapy of acute myeloid leu-kemia (AML) relapse. All the other patients received an average of twostandard DLIs (std-DLI) (range, 1 to 4) before inclusion with a meanmaximal cell dose of 8 × 107 CD3+ cells/kg (range, 4 to 18). Of those,11 needed to receive chemotherapy for progressive disease betweentheir last std-DLI and d-DLI. Finally, all but three patients had detect-able disease at the time of d-DLI. Overall, the patients received d-DLIafter a mean interval of (i) 33 months after HSCT (range, 8 to 93months), (ii) 14 months after relapse (range, 3 to 36 months), and(iii) 9 months after their last std-DLI (range, 2 to 26 months).
Tregs were depleted from DLI with anti-CD25 magnetic micro-beads and a CliniMACS device. The extent of Treg depletion was con-firmed by multicolor flow cytometry analyzing CD3, CD4, CD25, andFoxP3 coexpression before and after cell manipulation (fig. S1). TheCD25 magnetic depletion led to a CD3+CD25+, as well as CD4+FoxP3+,cell depletion rate of 96 ± 7% and 98 ± 5% (mean ± SE), respectively.In accordance, FoxP3 messenger RNA (mRNA) expression was de-creased by 92 ± 5% (fig. S1). The effect of CD25 Treg depletion onother cell types was also analyzed. CD25 depletion led to significantlydecreased proportions of CD3+ and CD19+ cells among total cells (P =0.003 and P < 0.0001, respectively), whereas CD14+ monocytes wereenriched (P = 0.01; fig. S1). The CD25 procedure did not affect theproportion of CD3−CD56+ natural killer (NK) cells, which representeda mean of 8% of the injected cells. A mean d-DLI cell dose of 4.3 × 107
CD3+ cells/kg (range, 1 × 107 to 10 × 107 cells/kg) was infused withoutany acute infusion-related toxicity.
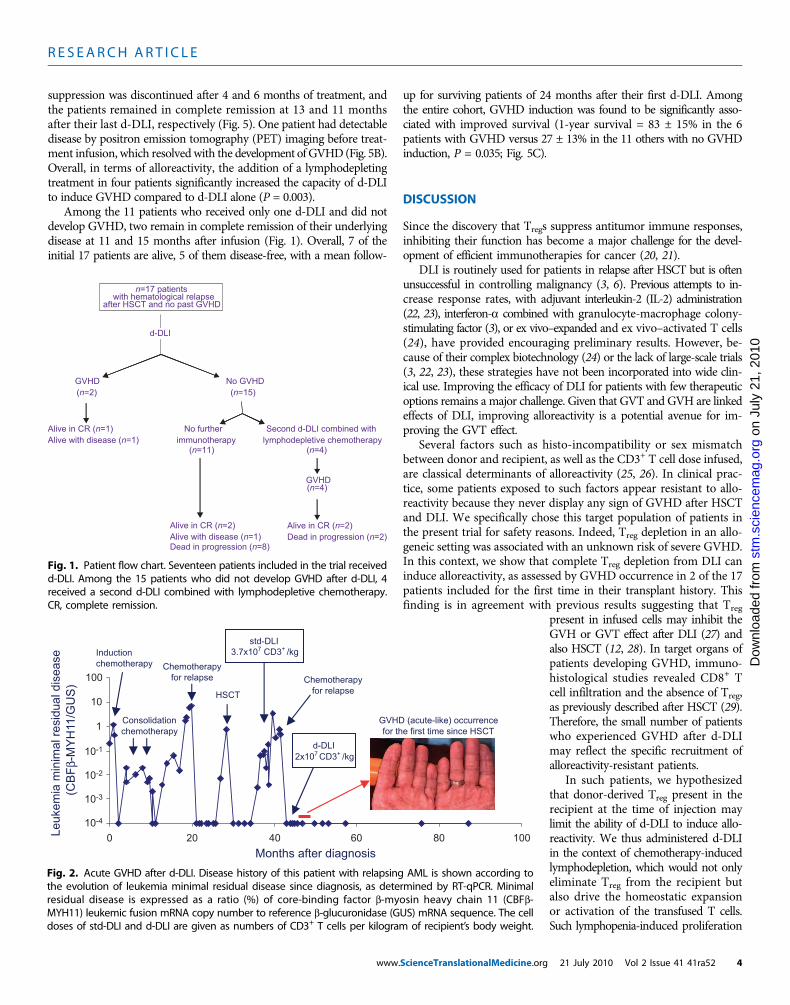
Of the 17 patients treated, 2 developed GVHD after d-DLI, whichwas the first GVHD occurrence in their transplant history. Patient 4manifested an acute-like grade 1 dermal disease, initially involvingpalms and soles (Fig. 2 and Table 1). GVHD occurred 20 days afterd-DLI and resolved after 10 days of topical steroid application. This
www.
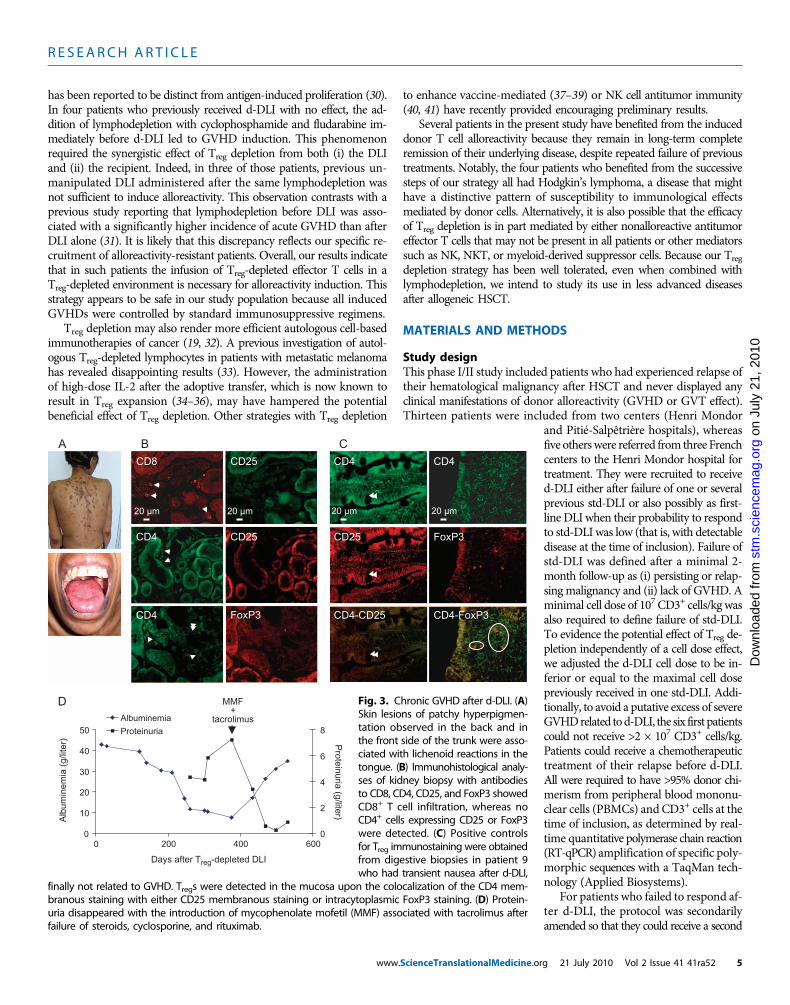
patient, who failed to respond to a previous std-DLI of a higher T lym-phocyte dosage, remains in complete molecular remission 43 monthsafter d-DLI (Fig. 2). Because this individual was already in remissionof his hematological malignancy at the time of d-DLI, it is difficult todirectly attribute this prolonged remission to d-DLI. Patient 12 devel-oped a chronic-like form of GVHD, with skin and oral involvement,266 days after d-DLI (Fig. 3A). Skin lesions appeared concomitantlywith kidney involvement, which was characterized by increased protein-uria associated with profound low albuminemia, leg swelling, ascites,and weight gain. Renal biopsy revealed histopathologic features of ex-tramembranous glomerulonephritis, evidenced by a CD8+ T cell infil-trate and no CD4+ cells expressing CD25 or FoxP3 (Fig. 3, B and C).The proteinuria persisted during treatment by various combinations ofimmunosuppressive drugs [steroids combined with cyclosporine andthen rituximab, a monoclonal antibody (mAb) to B cells] but finallyresolved with mycophenolate mofetil combined with tacrolimus. After4 months, this treatment could finally be discontinued without relapseof GVHD (Fig. 3D). This patient, who was in partial remission atd-DLI with an excess of blasts in marrow, is still alive with persistingtransfusion-dependent myelodysplasia at 37 months after d-DLI. Over-all, despite the low rate of alloreactivity induced by d-DLI in this cohort,the induction of GVHD in those two patients indicated that d-DLIhad the capacity to break alloreactivity resistance in some patients.
Improved alloreactivity of d-DLI afterlymphodepleting chemotherapyWe hypothesized that the low rate of alloreactivity induced by d-DLI(2 of 17 patients with GVHD induction) could be due to endogenousTreg of donor origin present in the recipient at the time of injection.Indeed, in the cohort, the mean (±SE) CD3+ T cell content inperipheral blood at the time of d-DLI was 994 ± 222 per microliter,with Treg constituting 4.3 ± 0.65% of CD4+ T cells. We hypothesizedthat Treg depletion in the recipient before d-DLI may favor the induc-tion of GVH and GVT effects in such alloreactivity-refractory patients.We therefore used a cyclophosphamide and fludarabine lymphode-pleting treatment adapted from Dudley et al. (19) in four patientswho previously received d-DLI and did not develop GVHD manifes-tations (Table 1). This regimen always led to profound lymphopeniaand to a significant decrease in Treg counts at the time of d-DLI (fig.S2). It was associated with a mean 3-day period of neutropenia withvalues below 500 polymorphonuclear leukocytes per microliter.
In one patient (patient 6) who had stable Hodgkin’s lymphoma at2 months after d-DLI, a second d-DLI was injected at a lower dose(1.25 × 107 versus 2.0 × 107 CD3+/kg for the previous d-DLI) aftercyclophosphamide-fludarabine chemotherapy. The patient developedan acute-like grade 3 dermal and hepatic GVHD 28 days after the in-fusion (Fig. 4). Dermal immunohistological analyses showed CD8+ Tcell infiltration in GVHD lesions, whereas no CD4+ cells expressingCD25 or FoxP3 were detected (Fig. 4). The patient was treated withmethylprednisolone (1 mg/kg per day) to quickly control for GVHD.The lymphoma remained stable for 6 months but progressed there-after, and the patient died 9 months after the second d-DLI.
Because of the strong and early GVHD that occurred in this pa-tient, we aimed to discriminate the effects of (i) the lymphodepletingchemotherapy and (ii) d-DLI on the induction of clinically detectable allo-reactivity. To this aim, the following three patients who were eligible for asecond infusion (patients 8, 13, and 15) received the cyclophosphamide-fludarabine lymphodepleting regimen followed by std-DLI instead of
ScienceTranslationalMedicine.org 21 July 2010 Vol 2 Issue 41 41ra52 2
R E S EARCH ART I C L E
d-DLI. With a mean follow-up of 5 months, none developed clinicalmanifestations of GVHD and one (patient 8) required chemotherapyfor progressive disease. Given this lack of GVHD induction after lym-phodepletion and std-DLI, the same three patients received a combi-nation of the same lymphodepletion followed by d-DLI. All threepatients developed an acute-like dermal GVHD associated with diges-
www.
tive (n = 2) or liver involvement (n = 1) at a mean interval of 26 daysafter the infusion. One patient with a grade 2 disease was not treatedto preserve a potential GVT effect. However, lymphoma progressed1 month later and the patient died of uncontrolled malignancy.Two patients had grade 3 GVHD that required treatment withmethylprednisolone (2 mg/kg per day) and cyclosporine. Immuno-
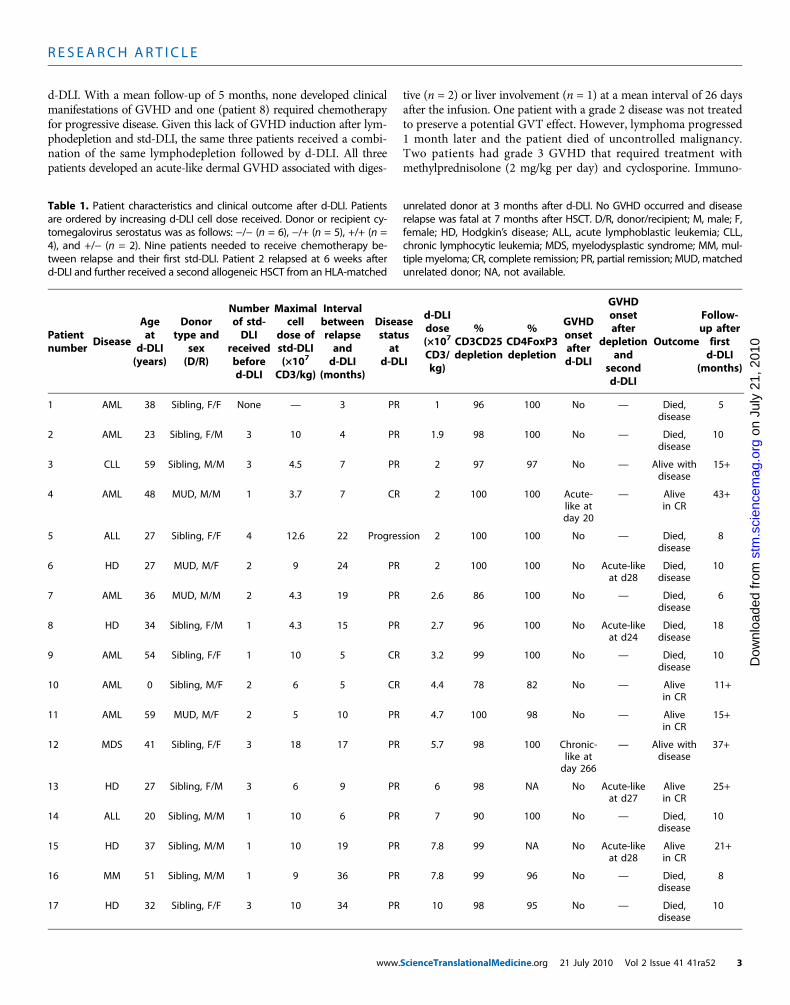
Table 1. Patient characteristics and clinical outcome after d-DLI. Patientsare ordered by increasing d-DLI cell dose received. Donor or recipient cy-tomegalovirus serostatus was as follows: −/− (n = 6), −/+ (n = 5), +/+ (n =4), and +/− (n = 2). Nine patients needed to receive chemotherapy be-tween relapse and their first std-DLI. Patient 2 relapsed at 6 weeks afterd-DLI and further received a second allogeneic HSCT from an HLA-matched
unrelated donor at 3 months after d-DLI. No GVHD occurred and diseaserelapse was fatal at 7 months after HSCT. D/R, donor/recipient; M, male; F,female; HD, Hodgkin’s disease; ALL, acute lymphoblastic leukemia; CLL,chronic lymphocytic leukemia; MDS, myelodysplastic syndrome; MM, mul-tiple myeloma; CR, complete remission; PR, partial remission; MUD, matchedunrelated donor; NA, not available.
10
Patientnumber
D
iseased20
Ageat-DLI
(years)
Donortype and
sex(D/R)
N
r
1,
umberof std-DLI
eceivedbefored-DLI
M
C
aximalcell
dose ofstd-DLI(×107
D3/kg)
Ib
(
ntervaletweenrelapseandd-DLImonths)
Diseasestatusat
d-DLI
dd(C
Scie
-DLIose×107
D3/kg)
Cd
nceTran
%D3CD25epletion
Cd
slationalMe
%D4FoxP3epletion
G
dicine.org
VHDonsetafterd-DLI
d
21 July 2
2
GVHDonsetafter
epletionand
secondd-DLI
010 Vol 2
Outcomeu
Issue 41 41
Follow-p afterfirstd-DLI
(months)
uly
1
AML 38 Sibling, F/F None — 3 PR 1 96 100 No —J
Died,disease
5
on
2
AML 23 S ibling, F/M 3 10 4 PR 1.9 98 100 No —rg
Died,disease
10
g.o
3
CLL 59 S ibling, M/M 3 4.5 7 PR 2 97 97 No — Aa
live withdisease
15+
cem
4
AML 48 MUD, M/M 1 3.7 7 CR 2 100 100cien
Acute-like atday 20
—
Alivein CR43+
.s
5 ALL 27 Sibling, F/F 4 12.6 22 P rogression 2 100 100 No —tm
Died,disease
8
sm
6
HD 27 MUD, M/F 2 9 24 PR 2 100 100 Noro
Acute-likeat d28
Died,disease
10
d f
7
AML 36 MUD, M/M 2 4.3 19 PR 2.6 86 100 No —de
Died,disease
6
loa
8
HD 34 S ibling, F/M 1 4.3 15 PR 2.7 96 100 Non
Acute-likeat d24
Died,disease
18
ow
9 AML 54 Sibling, F/F 1 10 5 CR 3.2 99 100 No —D
Died,disease
10
10
AML 0 S ibling, M/F 2 6 5 CR 4.4 78 82 No — Alivein CR11+
11
AML 59 MUD, M/F 2 5 10 PR 4.7 100 98 No — Alivein CR15+
12
MDS 41 Sibling, F/F 3 18 17 PR 5.7 98 100 C hronic-like atday 266— A
live withdisease37+
13
HD 27 S ibling, F/M 3 6 9 PR 6 98 NA No Acute-likeat d27Alivein CR
25+
14
ALL 20 S ibling, M/M 1 10 6 PR 7 90 100 No — Died,disease10
15
HD 37 S ibling, M/M 1 10 19 PR 7.8 99 NA No Acute-likeat d28Alivein CR
21+
16
MM 51 S ibling, M/M 1 9 36 PR 7.8 99 96 No — Died,disease8
17
HD 32 Sibling, F/F 3 10 34 PR 10 98 95 No — Died,disease10
ra52 3
R E S EARCH ART I C L E
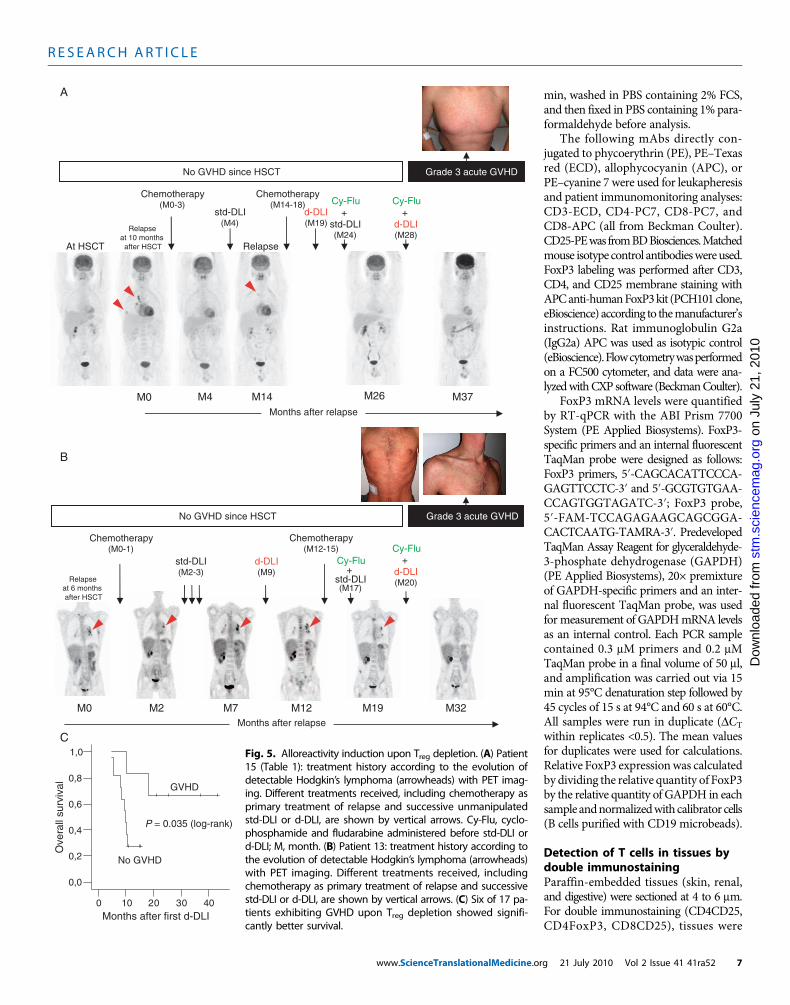
suppression was discontinued after 4 and 6 months of treatment, andthe patients remained in complete remission at 13 and 11 monthsafter their last d-DLI, respectively (Fig. 5). One patient had detectabledisease by positron emission tomography (PET) imaging before treat-ment infusion, which resolved with the development ofGVHD(Fig. 5B).Overall, in terms of alloreactivity, the addition of a lymphodepletingtreatment in four patients significantly increased the capacity of d-DLIto induce GVHD compared to d-DLI alone (P = 0.003).
Among the 11 patients who received only one d-DLI and did notdevelop GVHD, two remain in complete remission of their underlyingdisease at 11 and 15 months after infusion (Fig. 1). Overall, 7 of theinitial 17 patients are alive, 5 of them disease-free, with a mean follow-
www.
up for surviving patients of 24 months after their first d-DLI. Amongthe entire cohort, GVHD induction was found to be significantly asso-ciated with improved survival (1-year survival = 83 ± 15% in the 6patients with GVHD versus 27 ± 13% in the 11 others with no GVHDinduction, P = 0.035; Fig. 5C).
on
July
21,
201
0st
m.s
cien
cem
ag.o
rgde
d fr
om
DISCUSSION
Since the discovery that Tregs suppress antitumor immune responses,inhibiting their function has become a major challenge for the devel-opment of efficient immunotherapies for cancer (20, 21).
DLI is routinely used for patients in relapse after HSCT but is oftenunsuccessful in controlling malignancy (3, 6). Previous attempts to in-crease response rates, with adjuvant interleukin-2 (IL-2) administration(22, 23), interferon-a combined with granulocyte-macrophage colony-stimulating factor (3), or ex vivo–expanded and ex vivo–activated T cells(24), have provided encouraging preliminary results. However, be-cause of their complex biotechnology (24) or the lack of large-scale trials(3, 22, 23), these strategies have not been incorporated into wide clin-ical use. Improving the efficacy of DLI for patients with few therapeuticoptions remains a major challenge. Given that GVT and GVH are linkedeffects of DLI, improving alloreactivity is a potential avenue for im-proving the GVT effect.
Several factors such as histo-incompatibility or sex mismatchbetween donor and recipient, as well as the CD3+ T cell dose infused,are classical determinants of alloreactivity (25, 26). In clinical prac-tice, some patients exposed to such factors appear resistant to allo-reactivity because they never display any sign of GVHD after HSCTand DLI. We specifically chose this target population of patients inthe present trial for safety reasons. Indeed, Treg depletion in an allo-geneic setting was associated with an unknown risk of severe GVHD.In this context, we show that complete Treg depletion from DLI caninduce alloreactivity, as assessed by GVHD occurrence in 2 of the 17patients included for the first time in their transplant history. Thisfinding is in agreement with previous results suggesting that Treg
ScienceTranslationalMedicine.org
Dow
nloa
present in infused cells may inhibit theGVH or GVT effect after DLI (27) andalso HSCT (12, 28). In target organs ofpatients developing GVHD, immuno-histological studies revealed CD8+ Tcell infiltration and the absence of Treg,as previously described after HSCT (29).Therefore, the small number of patientswho experienced GVHD after d-DLImay reflect the specific recruitment ofalloreactivity-resistant patients.
In such patients, we hypothesizedthat donor-derived Treg present in therecipient at the time of injection maylimit the ability of d-DLI to induce allo-reactivity. We thus administered d-DLIin the context of chemotherapy-inducedlymphodepletion, which would not onlyeliminate Treg from the recipient butalso drive the homeostatic expansionor activation of the transfused T cells.Such lymphopenia-induced proliferation
n=17 patients
with hematological relapse
after HSCT and no past GVHD
No GVHD
(n=15)
GVHD
(n=2)
Second d-DLI combined with
lymphodepletive chemotherapy
(n=4)
GVHD
(n=4)
Alive in CR (n=2)
Alive with disease (n=1)
Dead in progression (n=8)
No further
immunotherapy
(n=11)
d-DLI
Alive in CR (n=2)
Dead in progression (n=2)
Alive in CR (n=1)
Alive with disease (n=1)
Fig. 1. Patient flow chart. Seventeen patients included in the trial receivedd-DLI. Among the 15 patients who did not develop GVHD after d-DLI, 4
received a second d-DLI combined with lymphodepletive chemotherapy.CR, complete remission.10-4
10-3
10-2
10-1
1
10
100
0 20 40 60 80 100
Months after diagnosis
Induction
chemotherapy
HSCT
std-DLI
3.7x107
2x107
CD3+
/kg
CD3+
/kg
Chemotherapy
for relapse
Chemotherapy
for relapse
GVHD (acute-like) occurrence
for the first time since HSCT
d-DLI
Consolidation
chemotherapy
(C
BF
β-M
YH
11/G
US
)
Leukem
ia m
inim
al resid
ual dis
ease
Fig. 2. Acute GVHD after d-DLI. Disease history of this patient with relapsing AML is shown according tothe evolution of leukemia minimal residual disease since diagnosis, as determined by RT-qPCR. Minimal
residual disease is expressed as a ratio (%) of core-binding factor b-myosin heavy chain 11 (CBFb-MYH11) leukemic fusion mRNA copy number to reference b-glucuronidase (GUS) mRNA sequence. The celldoses of std-DLI and d-DLI are given as numbers of CD3+ T cells per kilogram of recipient’s body weight.21 July 2010 Vol 2 Issue 41 41ra52 4
R E S EARCH ART I C L E
Jul
y 21
, 201
0
has been reported to be distinct from antigen-induced proliferation (30).In four patients who previously received d-DLI with no effect, the ad-dition of lymphodepletion with cyclophosphamide and fludarabine im-mediately before d-DLI led to GVHD induction. This phenomenonrequired the synergistic effect of Treg depletion from both (i) the DLIand (ii) the recipient. Indeed, in three of those patients, previous un-manipulated DLI administered after the same lymphodepletion wasnot sufficient to induce alloreactivity. This observation contrasts with aprevious study reporting that lymphodepletion before DLI was asso-ciated with a significantly higher incidence of acute GVHD than afterDLI alone (31). It is likely that this discrepancy reflects our specific re-cruitment of alloreactivity-resistant patients. Overall, our results indicatethat in such patients the infusion of Treg-depleted effector T cells in aTreg-depleted environment is necessary for alloreactivity induction. Thisstrategy appears to be safe in our study population because all inducedGVHDs were controlled by standard immunosuppressive regimens.
Treg depletion may also render more efficient autologous cell-basedimmunotherapies of cancer (19, 32). A previous investigation of autol-ogous Treg-depleted lymphocytes in patients with metastatic melanomahas revealed disappointing results (33). However, the administrationof high-dose IL-2 after the adoptive transfer, which is now known toresult in Treg expansion (34–36), may have hampered the potentialbeneficial effect of Treg depletion. Other strategies with Treg depletion
www.
to enhance vaccine-mediated (37–39) or NK cell antitumor immunity(40, 41) have recently provided encouraging preliminary results.
Several patients in the present study have benefited from the induceddonor T cell alloreactivity because they remain in long-term completeremission of their underlying disease, despite repeated failure of previoustreatments. Notably, the four patients who benefited from the successivesteps of our strategy all had Hodgkin’s lymphoma, a disease that mighthave a distinctive pattern of susceptibility to immunological effectsmediated by donor cells. Alternatively, it is also possible that the efficacyof Treg depletion is in part mediated by either nonalloreactive antitumoreffector T cells that may not be present in all patients or other mediatorssuch as NK, NKT, or myeloid-derived suppressor cells. Because our Tregdepletion strategy has been well tolerated, even when combined withlymphodepletion, we intend to study its use in less advanced diseasesafter allogeneic HSCT.
MATERIALS AND METHODS
Study designThis phase I/II study included patients who had experienced relapse oftheir hematological malignancy after HSCT and never displayed anyclinical manifestations of donor alloreactivity (GVHD or GVT effect).Thirteen patients were included from two centers (Henri Mondor
ScienceTranslationalMedicine.or
on
stm
.sci
ence
mag
.org
Dow
nloa
ded
from
and Pitié-Salpêtrière hospitals), whereasfive otherswere referred from three Frenchcenters to the Henri Mondor hospital fortreatment. They were recruited to received-DLI either after failure of one or severalprevious std-DLI or also possibly as first-line DLI when their probability to respondto std-DLI was low (that is, with detectabledisease at the time of inclusion). Failure ofstd-DLI was defined after a minimal 2-month follow-up as (i) persisting or relap-sing malignancy and (ii) lack of GVHD. Aminimal cell dose of 107 CD3+ cells/kg wasalso required to define failure of std-DLI.To evidence the potential effect of Treg de-pletion independently of a cell dose effect,we adjusted the d-DLI cell dose to be in-ferior or equal to the maximal cell dosepreviously received in one std-DLI. Addi-tionally, to avoid a putative excess of severeGVHDrelated tod-DLI, the six first patientscould not receive >2 × 107 CD3+ cells/kg.Patients could receive a chemotherapeutictreatment of their relapse before d-DLI.All were required to have >95% donor chi-merism from peripheral blood mononu-clear cells (PBMCs) and CD3+ cells at thetime of inclusion, as determined by real-time quantitative polymerase chain reaction(RT-qPCR)amplification of specific poly-morphic sequences with a TaqMan tech-nology (Applied Biosystems).
For patients who failed to respond af-ter d-DLI, the protocol was secondarilyamended so that they could receive a second
CBA
CD8
CD4
CD4
CD25
CD25
FoxP3
20 µm
CD4-FoxP3
CD4CD4
CD4-CD25
FoxP3CD25
D
20 µm 20 µm 20 µm
0
10
20
30
40
50
0 200 400 600
0
2
4
6
8
Albuminemia
Proteinuria
MMF
+
tacrolimus
Days after Treg
-depleted DLI
Pro
tein
uria
(g
/liter)
Alb
um
ine
mia
(g
/lite
r)
Fig. 3. Chronic GVHD after d-DLI. (A)Skin lesions of patchy hyperpigmen-tation observed in the back and inthe front side of the trunk were asso-ciated with lichenoid reactions in thetongue. (B) Immunohistological analy-ses of kidney biopsy with antibodiesto CD8, CD4, CD25, and FoxP3 showedCD8+ T cell infiltration, whereas noCD4+ cells expressing CD25 or FoxP3were detected. (C) Positive controlsfor Treg immunostaining were obtainedfrom digestive biopsies in patient 9who had transient nausea after d-DLI,
finally not related to GVHD. Tregs were detected in the mucosa upon the colocalization of the CD4 mem-branous staining with either CD25 membranous staining or intracytoplasmic FoxP3 staining. (D) Protein-uria disappeared with the introduction of mycophenolate mofetil (MMF) associated with tacrolimus afterfailure of steroids, cyclosporine, and rituximab.
g 21 July 2010 Vol 2 Issue 41 41ra52 5

R E S EARCH ART I C L E
on
July
21,
201
0st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
d-DLI combined with previous lymphodepleting chemotherapy (Fig.1).We used cyclophosphamide (1 g/m2 at day −5 before infusion) andfludarabine (30mg/m2 per day at days−5, −4, −3, and −2) given intra-venously with granulocyte colony-stimulating factor support [filgrastim(5 mg/kg per day) from day +2 until neutrophil recovery]. The CD3+ Tcell dose administered for this d-DLI was adjusted to be equal to that ofthe previous std-DLI.
www.
Written informed consent was obtained from all patients anddonors before enrollment and again before secondary infusions.The study was approved in October 2005 by the French Drug Eval-uation Agency (Agence Française de Sécurité Sanitaire des Produitsde Santé) and the institutional ethics committee of Hôpital Pitié-Salpêtrière (Paris, France). It was conducted in accordance with theDeclaration of Helsinki. Consensual published criteria were used todefine (i) acute and chronic GVHD (42, 43) and (ii) antitumoral re-sponses (44, 45).
Preparation of CD25-depleted leukapheresis productsLeukapheresis products (two to three blood masses, ≤12 liters) werefreshly collected from donors according to institutional guidelines. Upto 2 × 1010 PBMCs were collected in standard leukapheresis collectionbags on acid citrate dextrose anticoagulant. All donors were negativefor HIV, human T cell leukemia virus, hepatitis C virus, and hepatitisB virus. Leukapheresis products were first washed to remove contam-inating platelets: Briefly, PBMCs were transferred from the collectionbag into 500-ml transfer pack (TP) bags (MacoPharma) under sterileconditions and with tubing connector (Terumo Sterile Connection De-vice). The 500-ml TP bags were previously prepared with phosphate-buffered saline (PBS)–EDTA buffer supplemented with human serumalbumin (HSA) at a final concentration of 0.5% (w/v) (LFB), this buf-fer being named as CliniMACS buffer. PBMCs were diluted withCliniMACS buffer, and cells were centrifuged at 20°C at 3000g for3 min, without brake (KR4i centrifuge, Thermo Fisher Scientific). Then,the supernatant was removed with a plasma extractor. The PBMC pelletwas recovered in a second 500-ml TP bag and resuspended in 400 ml ofCliniMACS buffer. Cells were washed again, and the supernatant wasdiscarded and resuspended in CliniMACS buffer at 5 × 107 to 5 × 108
cells/ml. They were further labeled with CD25 microbeads (CliniMACSCD25 reagent, Miltenyi Biotec) at 20°C on a rotator at 25 rpm for 30min. Then, cells were transferred into a 600-ml TP bag (MacoPharma),washed once at 300g for 15min, and resuspended at a concentration of nomore than 1 × 108 cells/ml in CliniMACS buffer. The 600-ml TP bagwas connected to the CliniMACS device (Miltenyi Biotec), which wasused following the manufacturer’s standard operating procedure withthe depletion 1.2 program. After depletion, cells were harvested in a cellcollection bag in 180 ml of CliniMACS buffer, washed once, and finallyresuspended at 108 cells/ml in a 4% HSA buffer before infusion intopatients. At different steps of the procedure, aliquots were taken for var-ious quality controls.
Immunological analysesCell counts and viability (trypan blue dye exclusion assay) were per-formed from (i) initial leukapheresis samples, (ii) after removing con-taminating platelets, and (iii) after CD25+ T cell depletion. For flowcytometry analysis, 5 × 105 to 5 × 106 cells were incubated in 100 ml withthe appropriate mAbs at 4°C for 20 min, washed twice in PBS–2% fetalcalf serum (FCS), and immediately analyzed.
For patientmonitoring,CD3+,CD4+, and CD8+ T cells were countedfrom fresh blood samples with CYTO-STAT tetraCHROME kits ac-cording to the manufacturer’s instructions (Beckman Coulter). PBMCswere isolated from blood sample with Ficoll-Hypaque density gradientcentrifugation, washed twice in PBS containing 2% FCS, and numeratedbefore labeling. The flow cytometry analysis of lymphocyte subpopula-tions was performedwith a panel ofmAbs. Briefly, cells were incubatedin PBS containing 2% FCS with the appropriate antibodies at 4°C for 20
CD8
CD4
CD4
20 µm
20 µm
20 µm
20 µm
20 µm 20 µm
A
B
CD25
CD25
FoxP3
Fig. 4. Induction of GVHD upon d-DLI after chemotherapy. (A) Skinpapular lesions were observed on the face, members, and trunk. (B)
Dermal immunohistological analyses with antibodies to CD8, CD4, CD25,and FoxP3 evidenced a CD8+ T cell infiltrate under the epithelioma (redmembrane staining in the left upper panel). No colocalization with thegreen CD25+ membrane staining could be found (right upper panel). Alower number of CD4+ T cells were observed under the epithelioma(green membrane staining in left middle and lower panels) with no co-localization with the green membranous CD25 or intracytoplasmicFoxP3 staining. A diffuse nonspecific staining of collagen fibers can beobserved.ScienceTranslationalMedicine.org 21 July 2010 Vol 2 Issue 41 41ra52 6
R E S EARCH ART I C L E
www.ScienceTranslationalMedicine.or
on
July
21,
201
0st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
min, washed in PBS containing 2% FCS,and then fixed in PBS containing 1% para-formaldehyde before analysis.
The following mAbs directly con-jugated to phycoerythrin (PE), PE–Texasred (ECD), allophycocyanin (APC), orPE–cyanine 7 were used for leukapheresisand patient immunomonitoring analyses:CD3-ECD, CD4-PC7, CD8-PC7, andCD8-APC (all from Beckman Coulter).CD25-PEwas fromBDBiosciences.Matchedmouse isotype control antibodieswereused.FoxP3 labeling was performed after CD3,CD4, and CD25 membrane staining withAPCanti-humanFoxP3kit (PCH101clone,eBioscience) according to themanufacturer’sinstructions. Rat immunoglobulin G2a(IgG2a) APC was used as isotypic control(eBioscience).Flowcytometrywasperformedon a FC500 cytometer, and data were ana-lyzedwithCXP software (BeckmanCoulter).
FoxP3 mRNA levels were quantifiedby RT-qPCR with the ABI Prism 7700System (PE Applied Biosystems). FoxP3-specific primers and an internal fluorescentTaqMan probe were designed as follows:FoxP3 primers, 5′-CAGCACATTCCCA-GAGTTCCTC-3′ and 5′-GCGTGTGAA-CCAGTGGTAGATC-3′; FoxP3 probe,5′-FAM-TCCAGAGAAGCAGCGGA-CACTCAATG-TAMRA-3′. PredevelopedTaqMan Assay Reagent for glyceraldehyde-3-phosphate dehydrogenase (GAPDH)(PE Applied Biosystems), 20× premixtureof GAPDH-specific primers and an inter-nal fluorescent TaqMan probe, was usedfor measurement of GAPDHmRNA levelsas an internal control. Each PCR samplecontained 0.3 mM primers and 0.2 mMTaqMan probe in a final volume of 50 ml,and amplification was carried out via 15min at 95°C denaturation step followed by45 cycles of 15 s at 94°C and 60 s at 60°C.All samples were run in duplicate (DCT
within replicates <0.5). The mean valuesfor duplicates were used for calculations.Relative FoxP3 expressionwas calculatedby dividing the relative quantity of FoxP3by the relative quantity of GAPDH in eachsampleandnormalizedwith calibrator cells(B cells purified with CD19 microbeads).
Detection of T cells in tissues bydouble immunostainingParaffin-embedded tissues (skin, renal,and digestive) were sectioned at 4 to 6 mm.For double immunostaining (CD4CD25,CD4FoxP3, CD8CD25), tissues were
0 10 20 30 40Months after first d-DLI
0,0
0,2
0,4
0,6
0,8
1,0
Ove
rall
surv
ival GVHD
No GVHD
P = 0.035 (log-rank)
M26M0
Relapseat 10 monthsafter HSCT
M4
At HSCT
M14
Relapse
M37
d-DLI(M19)
Cy-Flu+
d-DLI(M28)
No GVHD since HSCT Grade 3 acute GVHD
Chemotherapy(M14-18) Cy-Flu
+std-DLI(M24)
Chemotherapy(M0-3)
std-DLI(M4)
Cy-Flu+
std-DLI(M17)
M0
Relapseat 6 monthsafter HSCT
No GVHD since HSCT Grade 3 acute GVHD
M32
Cy-Flu+
d-DLI(M20)
M2 M7 M12 M19
d-DLI(M9)
std-DLI(M2-3)
Chemotherapy(M0-1)
Chemotherapy(M12-15)
Months after relapse
A
B
C
Months after relapse
Fig. 5. Alloreactivity induction upon Treg depletion. (A) Patient15 (Table 1): treatment history according to the evolution ofdetectable Hodgkin’s lymphoma (arrowheads) with PET imag-ing. Different treatments received, including chemotherapy asprimary treatment of relapse and successive unmanipulatedstd-DLI or d-DLI, are shown by vertical arrows. Cy-Flu, cyclo-phosphamide and fludarabine administered before std-DLI ord-DLI; M, month. (B) Patient 13: treatment history according tothe evolution of detectable Hodgkin’s lymphoma (arrowheads)with PET imaging. Different treatments received, includingchemotherapy as primary treatment of relapse and successivestd-DLI or d-DLI, are shown by vertical arrows. (C) Six of 17 pa-tients exhibiting GVHD upon Treg depletion showed signifi-cantly better survival.
g 21 July 2010 Vol 2 Issue 41 41ra52 7

R E S EARCH ART I C L E
on
July
21,
201
0rg
stained with various primary and secondary antibodies, such as poly-clonal goat antibody to human CD4 (AF379NA, 100 mg/ml, IgG,1:10 dilution; R&D Systems), mouse antibody to human CD25 (NCL-CD25-305, IgG2b, 1:200 dilution; Novocastra), polyclonal rabbit anti-body to human CD8 (ab4055, 3 mg/ml, IgG, 1:100 dilution; Abcam),or mouse antibody to human FoxP3 (ab20034, IgG1, 450 mg/ml, 1:50dilution; Abcam), followed by fluorescein isothiocyanate–conjugateddonkey antibody to goat (705-095-147, IgG, 1 mg/ml, 1:100 dilution;Jackson ImmunoResearch), cyanine 3 donkey antibody to rabbit (711-165-152, IgG, 1 mg/ml, 1:500 dilution; Jackson ImmunoResearch), orbiotinylated donkey antibody to mouse (715-066-150, IgG, 1 mg/ml,1:100 dilution; Jackson ImmunoResearch), followed by cyanine 3–conjugated streptavidin (PA43001, 1 mg/ml, 1:300 dilution; AmershamBiosciences) or cyanine 2–conjugated streptavidin (PA42001, 1 mg/ml,1:800 dilution; Amersham Biosciences). For the CD8CD25 staining, apretreatment at PH9was needed. Fluorescent images ofmounted sectionswere analyzed with an epifluorescence microscope DMR (Leica Micro-systems). Positive controls for CD4CD25 and CD4FoxP3 Treg stainingwere obtained from digestive biopsies (Fig. 3C), as previously reportedin the same context of patients receiving HSCT (29).
StatisticsOverall survivals were calculated from the date of first d-DLI with theKaplan-Meier method and then compared by the log-rank test. Type1 error was fixed at the 5% level.
tm.s
cien
cem
ag.o
SUPPLEMENTARY MATERIAL
www.sciencetranslationalmedicine.org/cgi/content/full/2/41/41ra52/DC1Fig. S1. Complete Treg depletion from DLI products.Fig. S2. A cyclophosphamide and fludarabine regimen leads to profound lymphodepletion inrecipients’ peripheral blood before DLI.
sD
ownl
oade
d fr
om
REFERENCES AND NOTES
1. P. J. Martin, J. A. Hansen, C. D. Buckner, J. E. Sanders, H. J. Deeg, P. Stewart, F. R. Appelbaum,R. Clift, A. Fefer, R. P. Witherspoon, M. S. Kennedy, K. M. Sullivan, N. Flournoy, R. Storb, E. D.Thomas, Effects of in vitro depletion of T cells in HLA-identical allogeneic marrow grafts.Blood 66, 664–672 (1985).
2. C. L. Mackall, R. E. Gress, Pathways of T-cell regeneration in mice and humans: Implicationsfor bone marrow transplantation and immunotherapy. Immunol. Rev. 157, 61–72 (1997).
3. H. J. Kolb, Graft-versus-leukemia effects of transplantation and donor lymphocytes. Blood112, 4371–4383 (2008).
4. M. M. Horowitz, R. P. Gale, P. M. Sondel, J. M. Goldman, J. Kersey, H. J. Kolb, A. A. Rimm,O. Ringdén, C. Rozman, B. Speck, R. L. Truitt, F. E. Zwaan, M. M. Bortin, Graft-versus-leukemiareactions after bone marrow transplantation. Blood 75, 555–562 (1990).
5. W. D. Shlomchik, M. S. Couzens, C. B. Tang, J. McNiff, M. E. Robert, J. Liu, M. J. Shlomchik, S. G.Emerson, Prevention of graft versus host disease by inactivation of host antigen-presentingcells. Science 285, 412–415 (1999).
6. S. Mackinnon, Donor lymphocyte infusion after allogeneic stem cell transplantation, in ASCO 2008Educational Book (American Society of Clinical Oncology, Alexandria, VA, 2008), pp. 334–337.
7. J. L. Ferrara, J. E. Levine, P. Reddy, E. Holler, Graft-versus-host disease. Lancet 373, 1550–1561(2009).
8. K. J. Wood, S. Sakaguchi, Regulatory T cells in transplantation tolerance. Nat. Rev. Immunol.3, 199–210 (2003).
9. V. R. Aluvihare, M. Kallikourdis, A. G. Betz, Regulatory T cells mediate maternal tolerance tothe fetus. Nat. Immunol. 5, 266–271 (2004).
10. G. Darrasse-Jèze, D. Klatzmann, F. Charlotte, B. L. Salomon, J. L. Cohen, CD4+CD25+ regulatory/suppressor T cells prevent allogeneic fetus rejection in mice. Immunol. Lett. 102, 106–109 (2006).
11. O. Joffre, T. Santolaria, D. Calise, T. Al Saati, D. Hudrisier, P. Romagnoli, J. P. van Meerwijk,Prevention of acute and chronic allograft rejection with CD4+CD25+Foxp3+ regulatory T lym-phocytes. Nat. Med. 14, 88–92 (2008).
www.
12. J. L. Cohen, O. Boyer, The role of CD4+CD25hi regulatory T cells in the physiopathogeny ofgraft-versus-host disease. Curr. Opin. Immunol. 18, 580–585 (2006).
13. J. L. Cohen, A. Trenado, D. Vasey, D. Klatzmann, B. L. Salomon, CD4+CD25+ immunoregulatoryT cells: New therapeutics for graft-versus-host disease. J. Exp. Med. 196, 401–406 (2002).
14. A. Trenado, F. Charlotte, S. Fisson, M. Yagello, D. Klatzmann, B. L. Salomon, J. L. Cohen,Recipient-type specific CD4+CD25+ regulatory T cells favor immune reconstitution andcontrol graft-versus-host disease while maintaining graft-versus-leukemia. J. Clin. Invest.112, 1688–1696 (2003).
15. M. Edinger, P. Hoffmann, J. Ermann, K. Drago, C. G. Fathman, S. Strober, R. S. Negrin, CD4+CD25+
regulatory T cells preserve graft-versus-tumor activity while inhibiting graft-versus-host diseaseafter bone marrow transplantation. Nat. Med. 9, 1144–1150 (2003).
16. A. Trenado, M. Sudres, Q. Tang, S. Maury, F. Charlotte, S. Grégoire, M. Bonyhadi, D. Klatzmann,B. L. Salomon, J. L. Cohen, Ex vivo-expanded CD4+CD25+ immunoregulatory T cells preventgraft-versus-host-disease by inhibiting activation/differentiation of pathogenic T cells. J. Immunol.176, 1266–1273 (2006).
17. P. A. Taylor, C. J. Lees, B. R. Blazar, The infusion of ex vivo activated and expanded CD4+CD25+
immune regulatory cells inhibits graft-versus-host disease lethality. Blood 99, 3493–3499(2002).
18. ClinicalTrials.gov NCT00987987.19. M. E. Dudley, J. R. Wunderlich, P. F. Robbins, J. C. Yang, P. Hwu, D. J. Schwartzentruber, S. L.
Topalian, R. Sherry, N. P. Restifo, A. M. Hubicki, M. R. Robinson, M. Raffeld, P. Duray, C. A. Seipp,L. Rogers-Freezer, K. E. Morton, S. A. Mavroukakis, D. E. White, S. A. Rosenberg, Cancer regres-sion and autoimmunity in patients after clonal repopulation with antitumor lymphocytes.Science 298, 850–854 (2002).
20. M. P. Colombo, S. Piconese, Regulatory T-cell inhibition versus depletion: The right choicein cancer immunotherapy. Nat. Rev. Cancer 7, 880–887 (2007).
21. O. J. Finn, Cancer immunology. N. Engl. J. Med. 358, 2704–2715 (2008).22. E. Nadal, A. Fowler, E. Kanfer, J. Apperley, J. Goldman, F. Dazzi, Adjuvant interleukin-2 therapy
for patients refractory to donor lymphocyte infusions. Exp. Hematol. 32, 218–223 (2004).23. S. Slavin, E. Naparstek, A. Nagler, A. Ackerstein, S. Samuel, J. Kapelushnik, C. Brautbar, R. Or, Allo-
geneic cell therapy with donor peripheral blood cells and recombinant human interleukin-2 totreat leukemia relapse after allogeneic bone marrow transplantation. Blood 87, 2195–2204(1996).
24. D. L. Porter, B. L. Levine, N. Bunin, E. A. Stadtmauer, S. M. Luger, S. Goldstein, A. Loren, J. Phillips,S. Nasta, A. Perl, S. Schuster, D. Tsai, A. Sohal, E. Veloso, S. Emerson, C. H. June, A phase 1 trial ofdonor lymphocyte infusions expanded and activated ex vivo via CD3/CD28 costimulation. Blood107, 1325–1331 (2006).
25. C. Fozza, R. M. Szydlo, M. M. Abdel-Rehim, E. Nadal, J. M. Goldman, J. F. Apperley, F. Dazzi,Factors for graft-versus-host disease after donor lymphocyte infusions with an escalatingdose regimen: Lack of association with cell dose. Br. J. Haematol. 136, 833–836 (2007).
26. A. M. Raiola, M. T. Van Lint, M. Valbonesi, T. Lamparelli, F. Gualandi, D. Occhini, S. Bregante,C. di Grazia, A. Dominietto, M. Soracco, C. Romagnani, F. Vassallo, M. Casini, B. Bruno, F. Frassoni,A. Bacigalupo, Factors predicting response and graft-versus-host disease after donor lymphocyteinfusions: A study on 593 infusions. Bone Marrow Transplant. 31, 687–693 (2003).
27. Y. Hicheri, A. Bouchekioua, Y. Hamel, A. Henry, H. Rouard, C. Pautas, J. L. Beaumont, M. Kuentz,C. Cordonnier, J. L. Cohen, S. Maury, Donor regulatory T cells identified by FoxP3 expressionbut also by the membranous CD4+CD127low/neg phenotype influence graft-versus-tumor ef-fect after donor lymphocyte infusion. J. Immunother. 31, 806–811 (2008).
28. K. Rezvani, S. Mielke, M. Ahmadzadeh, Y. Kilical, B. N. Savani, J. Zeilah, K. Keyvanfar, A. Montero,N. Hensel, R. Kurlander, A. J. Barrett, High donor FOXP3-positive regulatory T-cell (Treg) contentis associated with a low risk of GVHD following HLA-matched allogeneic SCT. Blood 108,1291–1297 (2006).
29. K. Rieger, C. Loddenkemper, J. Maul, T. Fietz, D. Wolff, H. Terpe, B. Steiner, E. Berg, S. Miehlke,M. Bornhäuser, T. Schneider, M. Zeitz, H. Stein, E. Thiel, R. Duchmann, L. Uharek, MucosalFOXP3+ regulatory T cells are numerically deficient in acute and chronic GvHD. Blood 107,1717–1723 (2006).
30. S. Maury, B. Salomon, D. Klatzmann, J. L. Cohen, Division rate and phenotypic differencesdiscriminate alloreactive and nonalloreactive T cells transferred in lethally irradiated mice.Blood 98, 3156–3158 (2001).
31. J. S. Miller, D. J. Weisdorf, L. J. Burns, A. Slungaard, J. E. Wagner, M. R. Verneris, S. Cooley,R. Wangen, S. K. Fautsch, R. Nicklow, T. Defor, B. R. Blazar, Lymphodepletion followed by donorlymphocyte infusion (DLI) causes significantly more acute graft-versus-host disease than DLIalone. Blood 110, 2761–2763 (2007).
32. R. A. Morgan, M. E. Dudley, J. R. Wunderlich, M. S. Hughes, J. C. Yang, R. M. Sherry, R. E. Royal,S. L. Topalian, U. S. Kammula, N. P. Restifo, Z. Zheng, A. Nahvi, C. R. de Vries, L. J. Rogers-Freezer,S. A. Mavroukakis, S. A. Rosenberg, Cancer regression in patients after transfer of geneticallyengineered lymphocytes. Science 314, 126–129 (2006).
33. D. J. Powell Jr., C. R. de Vries, T. Allen, M. Ahmadzadeh, S. A. Rosenberg, Inability to mediateprolonged reduction of regulatory T cells after transfer of autologous CD25-depletedPBMC and interleukin-2 after lymphodepleting chemotherapy. J. Immunother. 30, 438–447(2007).
ScienceTranslationalMedicine.org 21 July 2010 Vol 2 Issue 41 41ra52 8

R E S EARCH ART I C L E
on
July
21,
201
0ci
ence
mag
.org
34. H. Zhang, K. S. Chua, M. Guimond, V. Kapoor, M. V. Brown, T. A. Fleisher, L. M. Long, D. Bernstein,B. J. Hill, D. C. Douek, J. A. Berzofsky, C. S. Carter, E. J. Read, L. J. Helman, C. L. Mackall, Lympho-penia and interleukin-2 therapy alter homeostasis of CD4+CD25+ regulatory T cells. Nat. Med. 11,1238–1243 (2005).
35. M. Ahmadzadeh, S. A. Rosenberg, IL-2 administration increases CD4+CD25hi Foxp3+ regulatoryT cells in cancer patients. Blood 107, 2409–2414 (2006).
36. E. Zorn, E. A. Nelson, M. Mohseni, F. Porcheray, H. Kim, D. Litsa, R. Bellucci, E. Raderschall,C. Canning, R. J. Soiffer, D. A. Frank, J. Ritz, IL-2 regulates FOXP3 expression in human CD4+CD25+
regulatory T cells through a STAT-dependent mechanism and induces the expansion of thesecells in vivo. Blood 108, 1571–1579 (2006).
37. M. A. Morse, A. C. Hobeika, T. Osada, D. Serra, D. Niedzwiecki, H. K. Lyerly, T. M. Clay, De-pletion of human regulatory T cells specifically enhances antigen-specific immune re-sponses to cancer vaccines. Blood 112, 610–618 (2008).
38. K. L. Knutson, Y. Dang, H. Lu, J. Lukas, B. Almand, E. Gad, E. Azeke, M. L. Disis, IL-2 immunotoxintherapy modulates tumor-associated regulatory T cells and leads to lasting immune-mediatedrejection of breast cancers in neu-transgenic mice. J. Immunol. 177, 84–91 (2006).
39. M. T. Litzinger, R. Fernando, T. J. Curiel, D. W. Grosenbach, J. Schlom, C. Palena, IL-2 im-munotoxin denileukin diftitox reduces regulatory T cells and enhances vaccine-mediatedT-cell immunity. Blood 110, 3192–3201 (2007).
40. A. Lundqvist, H. Yokoyama, A. Smith, M. Berg, R. Childs, Bortezomib treatment and regu-latory T-cell depletion enhance the antitumor effects of adoptively infused NK cells. Blood113, 6120–6127 (2009).
41. W. H. Hallett, E. Ames, M. Alvarez, I. Barao, P. A. Taylor, B. R. Blazar, W. J. Murphy, Combi-nation therapy using IL-2 and anti-CD25 results in augmented natural killer cell–mediatedantitumor responses. Biol. Blood Marrow Transplant. 14, 1088–1099 (2008).
42. D. Przepiorka, D. Weisdorf, P. Martin, H. G. Klingemann, P. Beatty, J. Hows, E. D. Thomas,1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 15, 825–828(1995).
43. H. Glucksberg, R. Storb, A. Fefer, C. D. Buckner, P. E. Neiman, R. A. Clift, K. G. Lerner, E. D.Thomas, Clinical manifestations of graft-versus-host disease in human recipients of marrowfrom HL-A-matched sibling donors. Transplantation 18, 295–304 (1974).
44. B. D. Cheson, J. M. Bennett, K. J. Kopecky, T. Büchner, C. L. Willman, E. H. Estey, C. A. Schiffer,H. Doehner, M. S. Tallman, T. A. Lister, F. Lo-Coco, R. Willemze, A. Biondi, W. Hiddemann, R. A.Larson, B. Löwenberg, M. A. Sanz, D. R. Head, R. Ohno, C. D. Bloomfield, Revised recommenda-tions of the International Working Group for Diagnosis, Standardization of Response Criteria,Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leu-kemia. J. Clin. Oncol. 21, 4642–4649 (2003).
www.
45. B. D. Cheson, B. Pfistner, M. E. Juweid, R. D. Gascoyne, L. Specht, S. J. Horning, B. Coiffier, R. I.Fisher, A. Hagenbeek, E. Zucca, S. T. Rosen, S. Stroobants, T. A. Lister, R. T. Hoppe, M. Dreyling,K. Tobinai, J. M. Vose, J. M. Connors, M. Federico, V. Diehl; International Harmonization Projecton Lymphoma, Revised response criteria for malignant lymphoma. J. Clin. Oncol. 25, 579–586(2007).
46. Acknowledgments: We thank E. Itti (Nuclear Medicine, Hôpital Henri Mondor) and B. Paulmier(Nuclear Medicine, Hôpital Européen Georges Pompidou) for providing PET imaging illustrations;N. Ortonne for help in collecting biopsy samples; L. Grégoire, C. Giverne, H. Trebeden-Negre,C. Bernard, P. Jouany, P. Maison, and V. Millul for study management; C. Pautas, M. Kuentz,I. Gaillard, T. ElGnaoui, K. Belhadj, and C. Haioun (Hematology) and M. Matignon and P. Grimbert(Nephrology) for clinical care (all in Assistance Publique-Hôpitaux de Paris); and G. Socié,O. Boyer, D. A. Landau, and C. Besson for their indispensable advice. The authors dedicate thispaper to J. P. Bessège who played a major role in the achievement of this study. Funding: Thisstudy was sponsored and monitored by the Regional Clinical Research Office (Paris, France)and supported by a grant from the Programme Hospitalier de Recherche Clinique (PHRC ID,AOR04047) and from Clinigene. These sponsors had no role in study design, data analysis,data interpretation, or writing of the report. Author contributions: S.M. and J.L.C. conceivedthe study and obtained funding. S.M., F.M.L., M.R., M.C., O.M., F.R.-T., J.-P.V., C.C., D.K., and J.L.C.participated in study design. J.-L.B. and N.A. were responsible for donor harvesting. F.M.L.,M.R., M.C., and D.K. were responsible for cellular manipulation and biological analyses. S.M.,Y.H., N.D., A.S., A.B., M.-T.R., S.V., J.-P.V., and C.C. participated in patient care. C.B. was respon-sible for immunohistological analyses. D.B. was responsible for chimerism analyses. S.M.,F.M.L., Y.H., M.R., C.B., C.C., D.K., and J.L.C. analyzed data. S.M. performed statistical analysesand wrote the initial version of the manuscript. F.M.L., Y.H., M.R., C.C., D.K., and J.L.C. contributed tothe final version of the manuscript, which was approved by all the authors. Competing interests:The authors declare that they have no competing interests.
Submitted 20 May 2010Accepted 2 July 2010Published 21 July 201010.1126/scitranslmed.3001302
Citation: S. Maury, F. M. Lemoine, Y. Hicheri, M. Rosenzwajg, C. Badoual, M. Cheraï, J.-L. Beaumont,N. Azar, N. Dhedin, A. Sirvent, A. Buzyn, M.-T. Rubio, S. Vigouroux, O. Montagne, D. Bories, F. Roudot-Thoraval, J.-P. Vernant, C. Cordonnier, D. Klatzmann, J. L. Cohen, CD4+CD25+ regulatory T cell depletionimproves the graft-versus-tumor effect of donor lymphocytes after allogeneic hematopoietic stem celltransplantation. Sci. Transl. Med. 2, 41ra52 (2010).
.s
ScienceTranslationalMedicine.org 21 July 2010 Vol 2 Issue 41 41ra52 9
stm
Dow
nloa
ded
from




















