Causes of delay in seeking treatment for heart attack symptoms
14
Pergamon 0277-9536(94)00278-9 Sot'. Sci. Med. Vol.40, No. 3, pp. 379-392, 1995 Copyright © 1995Elsevier Science Ltd Printed in Great Britain. All rights reserved 0277-9536/95$7.00 + 0.00 CAUSES OF DELAY IN SEEKING TREATMENT FOR HEART ATTACK SYMPTOMS KATHLEENDRACUP, ~ DEBRAK. MOSER, 2 MICKEYEISENBERG, 3 HENDRIKAMEISCHKE, 4 ANGELOA. ALONZO 5 and ALLAN BRASLOW 6 ~School of Nursing, University of California, Los Angeles, CA, U.S.A., 2School of Nursing, Ohio State University, Columbus, OH, U.S.A., 3School of Medicine, University of Washington, Emergency Medical Services, University of Washington Medical Center, Seattle, WA, U.S.A., 4School of Medicine, Depart- ment of Health Services, University of Washington, Seattle, WA, U.S.A., 5Department of Sociology, The Ohio State University, Columbus, OH, U.S.A. and 6Braslow and Associates, Alexandria, VA, U.S.A. A~traet--With the advent of thrombolytic therapy and other coronary reperfusion strategies, rapid identification and treatment of acute myocardial infarction greatly reduces mortality. Unfortunately, many patients delay seeking medical care and miss the benefits afforded by recent advances in treatment. Studies have shown that the median time from onset of symptoms to seeking care ranges from 2 to 61/2 hours, while optimal benefit is derived during the first hour from symptom onset. The phenomenon of delay by AMI patients and those around them needs to be understood prior to the design of education and counseling strategies to reduce delay. In this article the literature is reviewed and variables that increase patient delay are identified. A theoretical model based on the health belief model, a self regulation model of illness cognition, and interactionist role theory is proposed to explain the response of an individual to the signs and symptoms of acute myocardial infarction. Finally, recommendations are made for future research. Key words-~ielay, acute myocardial infarction Every year, approx. 1,250,000 persons in the United States experience a heart attack, 500,000 of whom die [l, 2]. About one-half (250,000) of these deaths occur suddenly, defined as within 1 hr of the onset of symptoms [1]. This early time period is critical be- cause patients are highly vulnerable to life-threaten- ing arrhythmias. In fact, approximately 50% of all heart attack deaths occur before patients reach the hospital [3, 4]. The high mortality associated with acute myocar- dial infarction (AMI) is dismaying in view of recent advances in medical therapy. Prior to the availability of thrombolytic agents, the management of AMI was mostly passive and reactive. Physicians and nurses watched and responded to complications as they occurred. There was no way to prevent myocardial damage. Clinical goals were limited to preventing or reducing serious complications. If a fatal arrhythmia did not occur, a delay in receiving therapy in the prethrombolytic era was generally not serious. This situation has now changed. If the patient receives care soon enough, thrombolytic therapy can alter the course of AMI and limit the extent of damage and subsequent morbidity. Since the mid-1980s, several large-scale studies have demonstrated that thrombolytic therapy can significantly reduce mortality from AMI [5-13]. The benefits of thrombolytic therapy are directly related to the interval between the onset of symptoms and the administration of the drug. The shorter the interval, the better the outcome. When administered within 3 hr of the onset of symptoms, mortality is reduced by 23%. Mortality can be reduced by approx. 50% if thrombolytic therapy is started within l hr of the onset of symptoms [6]. Similarly, the shorter the interval between symptom onset and treatment, the higher the resulting cardiac function [12, 14, 15]. Cardiac function is the best predictor of subsequent mortality and is also a good indicator of morbidity [16]. Thus, early treatment with thrombolytic agents can reduce mortality and morbidity [ 17]. Regrettably, delays in arriving at the hospital are a major reason that patients are pronounced as ineligible for throm- bolytic therapy [18]. DELAY TIMES Studies of the time from symptom onset to hospital arrival have reported considerable variation. The median total time in these studies ranges from just under 2 hr [19] to 6.5 hr [20]. Mean delay times are significantly longer than the median times in all reported trials, with many exceeding 6 hr [21-33] and one >21 hr [20]. The difference between mean and median times is a result of the skewing effect caused by individuals who wait many hours or even days before seeking medical care for their AMI. When the data are viewed in an alternative way, 26-44% of patients wait longer than 4 hr before seeking medical care for their cardiac symptoms [23-25]. It is clear 379
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Causes of delay in seeking treatment for heart attack symptoms
Pergamon 0277-9536(94)00278-9
Sot'. Sci. Med. Vol. 40, No. 3, pp. 379-392, 1995 Copyright © 1995 Elsevier Science Ltd
Printed in Great Britain. All rights reserved 0277-9536/95 $7.00 + 0.00
CAUSES OF DELAY IN SEEKING TREATMENT FOR HEART ATTACK SYMPTOMS
KATHLEEN DRACUP, ~ DEBRA K. MOSER, 2 MICKEY EISENBERG, 3 HENDRIKA MEISCHKE, 4 ANGELO A. ALONZO 5 and ALLAN BRASLOW 6
~School of Nursing, University of California, Los Angeles, CA, U.S.A., 2School of Nursing, Ohio State University, Columbus, OH, U.S.A., 3School of Medicine, University of Washington, Emergency Medical Services, University of Washington Medical Center, Seattle, WA, U.S.A., 4School of Medicine, Depart- ment of Health Services, University of Washington, Seattle, WA, U.S.A., 5Department of Sociology,
The Ohio State University, Columbus, OH, U.S.A. and 6Braslow and Associates, Alexandria, VA, U.S.A.
A~traet--With the advent of thrombolytic therapy and other coronary reperfusion strategies, rapid identification and treatment of acute myocardial infarction greatly reduces mortality. Unfortunately, many patients delay seeking medical care and miss the benefits afforded by recent advances in treatment. Studies have shown that the median time from onset of symptoms to seeking care ranges from 2 to 61/2 hours, while optimal benefit is derived during the first hour from symptom onset. The phenomenon of delay by AMI patients and those around them needs to be understood prior to the design of education and counseling strategies to reduce delay. In this article the literature is reviewed and variables that increase patient delay are identified. A theoretical model based on the health belief model, a self regulation model of illness cognition, and interactionist role theory is proposed to explain the response of an individual to the signs and symptoms of acute myocardial infarction. Finally, recommendations are made for future research.
Key words-~ielay, acute myocardial infarction
Every year, approx. 1,250,000 persons in the United States experience a heart attack, 500,000 of whom die [l, 2]. About one-half (250,000) of these deaths occur suddenly, defined as within 1 hr of the onset of symptoms [1]. This early time period is critical be- cause patients are highly vulnerable to life-threaten- ing arrhythmias. In fact, approximately 50% of all heart attack deaths occur before patients reach the hospital [3, 4].
The high mortality associated with acute myocar- dial infarction (AMI) is dismaying in view of recent advances in medical therapy. Prior to the availability of thrombolytic agents, the management of AMI was mostly passive and reactive. Physicians and nurses watched and responded to complications as they occurred. There was no way to prevent myocardial damage. Clinical goals were limited to preventing or reducing serious complications. If a fatal arrhythmia did not occur, a delay in receiving therapy in the prethrombolytic era was generally not serious. This situation has now changed. If the patient receives care soon enough, thrombolytic therapy can alter the course of AMI and limit the extent of damage and subsequent morbidity.
Since the mid-1980s, several large-scale studies have demonstrated that thrombolytic therapy can significantly reduce mortality from AMI [5-13]. The benefits of thrombolytic therapy are directly related to the interval between the onset of symptoms and the administration of the drug. The shorter the interval,
the better the outcome. When administered within 3 hr of the onset of symptoms, mortality is reduced by 23%. Mortality can be reduced by approx. 50% if thrombolytic therapy is started within l hr of the onset of symptoms [6]. Similarly, the shorter the interval between symptom onset and treatment, the higher the resulting cardiac function [12, 14, 15]. Cardiac function is the best predictor of subsequent mortality and is also a good indicator of morbidity [16]. Thus, early treatment with thrombolytic agents can reduce mortality and morbidity [ 17]. Regrettably, delays in arriving at the hospital are a major reason that patients are pronounced as ineligible for throm- bolytic therapy [18].
DELAY TIMES
Studies of the time from symptom onset to hospital arrival have reported considerable variation. The median total time in these studies ranges from just under 2 hr [19] to 6.5 hr [20]. Mean delay times are significantly longer than the median times in all reported trials, with many exceeding 6 hr [21-33] and one >21 hr [20]. The difference between mean and median times is a result of the skewing effect caused by individuals who wait many hours or even days before seeking medical care for their AMI. When the data are viewed in an alternative way, 26-44% of patients wait longer than 4 hr before seeking medical care for their cardiac symptoms [23-25]. It is clear
379
380 KATHLEEN DRACUP et al.
that patient delay is a substantial problem and that there has been little success over the past three decades in reducing delay time [21,25].
PHASES OF DELAY
Delay time is usually defined as the amount of time between the first awareness of symptoms and the arrival of the individual at the hospital. Given the importance of new therapies for AMI, it is now more important to speak of total delay time, which is the interval from the onset of symptoms to the initiation of definitive therapy, such as thrombolytic therapy. Investigators have divided total delay time into a variety of phases, using as few as three [26] and as many as 11 [27]. We use a simplified modification of Alonzo's [28] schema and speak of three phases of delay: patient/bystander recognition, prehospital and hospital. The word 'action' is added as a descriptor to the phases to emphasize the dynamic nature and importance of action by appropriate individuals, relative to each of the phases.
1. Patient/bystander recognition and action phase
The patient/bystander recognition and action phase encompasses the interval from symptom onset to accessing the emergency response system or to initiating travel to the hospital when transport occurs by some other method. This phase includes action taken by the patients and those around them in response to the symptoms and signs of an AMI. This phase begins when the patient becomes aware of 'something wrong,' or, in other words, begins to experience symptoms.
From interviewing hundreds of patients with symp- toms of an AMI, we have observed that approxi- mately one-third do not report an abrupt onset of symptoms and that they frequently have difficulty identifying the time of the onset of symptoms. These patients may report a prodrome of vague symptoms or symptoms that wax and wane over time, some- times disappearing completely (prodromal period). Although it may be more accurate to speak of initial and acute symptoms, a majority of patients can usually define the time of onset of acute symptoms (definition period). Acute symptoms are the constel- lation of symptoms that lead to the decision to seek medical care. Initial symptoms, when present, are the symptoms preceding the acute symptoms. Initial symptoms are milder than acute symptoms and do not in themselves cause an individual to seek medical care.
During the patient/bystander recognition and ac- tion phase, patients may engage in a variety of behaviors that can increase or decrease delay time. Patients may decide to seek medical care at once (i.e. call an ambulance or drive themselves to the hospi- tal); they may decide to wait and periodically evaluate or self-treat their symptoms; or they may decide to seek consultation from friends, relatives, or medical personnel (lay and medical consultation period). In
Alonzo's study of 1102 AMI patients, 93.2% of the patients told someone that they were ill [29]. The remainder decided to travel to the hospital without seeking advice from someone else.
2. Prehospital action phase
The prehospital action phase encompasses the in- terval from accessing the emergency response system to arriving at the hospital or, when the emergency response system (EMS) is bypassed, from initiating travel to the hospital to arriving at the hospital. The travel period, or the time spent traveling to the hospital, is a fundamental component of this phase. For transport by EMS, this phase is defined as the interval from calling the emergency telephone num- ber to the arrival of the ambulance at the hospital. Its components are public access (e.g. via the telephone 'call for help'), EMS professional response, and transportation. The prehospital action phase in- cludes, therefore, action taken by communications systems personnel, emergency medical dispatchers, and prehospital providers. For transport in a private vehicle, this phase is defined as the interval from leaving the site of symptom recognition and action (generally the home or workplace) to arriving at the hospital.
3. Hospital action phase
The hospital action phase encompasses the interval from the patient's arrival at the hospital to receiving definitive care, such as thrombolytic or other phar- macologic therapy. It includes, notably, action taken by health professionals in the emergency department.
Delays can occur in any one of these three phases. However, the prehospital action phase in most com- munities only adds an average delay time of 7-22min. [21,23,27,30], and the hospital action phase has recently been reported as lasting approx. 60--90 min [31-33]. Given that the average total delay time is >4 .5hr (with a median of 2.0-6.4hr), it is apparent that the prehospital and the hospital phases together represent but a small fraction of total delay time. Therefore this paper focuses on the patient/bystander recognition and action phase.
It is important to understand the factors that contribute to patient indecision and to develop and test interventions directed toward reducing the amount of time patients take to make the decision to seek care. To promote this understanding and assist the development of these interventions, this paper describes a theoretical framework for understanding why patients delay seeking care, considers the vari- ables affecting delay time, and provides recommen- dations for future research and community education.
WHY PATIENTS DELAY: A THEORETIC FRAMEWORK
Several investigators have identified care-seeking behavior during AMI and nonhospitalized sudden
Causes of delay in seeking treatment for heart attack symptoms 381
cardiac death [3,4, 19-25, 27, 29-30, 34-48]. With few exceptions [29, 40, 42, 43], researchers have used a medical model orientation and have focused on the demographic and clinical characteristics of the patient as predictors of delay [49]. Although it is possible to characterize patients as being at high or low risk for delaying seeking medical treatment by virtue of their sociodemographic or clinical profile (i.e. such as is---conveyed with the medical model orientation), this knowledge does not then suggest what the essential components of appropriate inter- vention programs should be.
Researchers working in the area of patient compli- ance (adherence) have used three models: the health belief model, a self regulation model of illness cogni- tion and behavior, and the interactionist role theory or symbolic interactionism. These models have the advantage of including many personality and so- cioenvironmental variables not considered in the medical model. Their strengths and limitations have been extensively analyzed [50--54] and are only briefly reviewed here. These models appear to hold promise for helping health professionals understand how and why AMI patients seek help when they do.
Health belief model
The health belief model [51] which is based on motivational theory, has been the most frequently used framework for identifying variables for study and for interpreting findings related to compliance [52]. According to this model, a heart attack victim who experiences symptoms of ischemia is likely to make the decision to seek medical attention based on two variables:
(1) the amount of threat perceived by the victim related to the symptoms; and
(2) the attractiveness or value of the action in question.
The degree of perceived threat is determined by the patient's feeling of vulnerability to cardiac disease and to illness in general, the perceived extent of bodily harm, the extent of possible disruption of social roles, the presence of symptoms, and previous experiences with symptoms. The value of the action is based on the probability that in the patient's view the decision to go to the hospital will reduce the threat and will not be too costly in terms of time, money or emotional energy. These two variables are modulated by demographic and structural (treatment-related) factors, patient attitudes and physician-patient interaction.
The health belief model is attractive to many investigators because it poses the decision in a cost/benefit framework that is easy to understand and easy to explain. Nonetheless, it has several limi- tations. First, like the medical model, the focus is on the patient and his or her belief system. The literature about delay emphasizes the important role that other people can play in a patient's decision to seek medical
care, but this importance is not reflected in the health belief model. Second, the health belief model is most accurate in describing preventive behaviors (e.g. seat- belt use) and less accurate in predicting care-seeking behaviors [52]. Third, prospective studies have gener- ally documented weak relationships within the model structure [53], suggesting that a significant portion of the variance in delay behavior is not explained by the model alone.
Self regulation model of coping with health threats
Levanthal and colleagues [54-56] argued persua- sively from both a theoretic perspective and from empirical data that patients use implicit theories of illness (illness schemata) to understand the threats to their health and to make decisions regarding health behavior. They proposed that patients' beliefs about their health are structured in a hierarchical fashion and that these structures are based on previous illness experiences and information presented in the social environment [54].
In the self regulation model [56] the individual who is faced with a health crisis experiences three stages:
(1) mental representation of the health threat; (2) coping or action plan, and (3) appraisal.
The first stage is triggered by a stimulus (such as chest pain or shortness of breath). It is affected by the patient's subjective experience, a sense of vulner- ability to illness and general knowledge about disease and illness. The second stage involves coping mech- anisms and behaviors designed to meet the health threat. Some will be primarily automatic, e.g. stop- ping activity when chest pain begins, and others will be consciously considered, e.g. calling a physician's office for advice or taking an antacid medication. Finally, the individual appraises or evaluates the coping plans in light of both perceived barriers and perceived success in reducing the health threat. The mental representation of the health threat may be altered as a result of the appraisal.
In his early work, Leventhal emphasized the need to look at people's everyday beliefs and procedures for coping with health threats rather than their personalities [54]. According to Leventhal and Diefenbach [55], people's past experience with illness is organized in a complex memory structure that is then used to cluster and organize illness knowledge. The construction and updating of these illness representations guide choices of behavior and ap- praisal.
The unique contribution of this model is its ex- planatory power in the face of a symptom or constel- lation of symptoms of unknown cause. For example, when a person experiences intermittent chest pain he may hypothesize an explanation (e.g. muscle pain from overexertion) and initiate behavior appropriate to the hypothesis. Failure to eradicate the symptom by resting or ingestion of muscle relaxants will cause

382 KATHLEEN DRACUP et al.
him to reappraise. This scenario of symptom attribu- tion in the context of a hierarchical order is described by many patients who experience the symptoms of AMI [28, 29, 40]. Leventhal's model incorporates the cost/benefit analysis inherent in the Health Belief Model, while providing insight into the cognitive processes which accompany an AMI.
Symbolic interactionism
The third model, symbolic interactionism, is de- rived from sociology and is based on role theory. According to interactionists, a role is a patterned sequence of learned behaviors performed by a person in an interactive situation. Roles are tentative, constantly being redefined on the basis of inter- actions with other people who serve in reciprocal roles (e.g. wife-husband, patient-doctor, employer- employee). Interactions are fluid, providing cues to individuals that assist them in modifying their own roles and altering their behavior. The interactionist position stresses the ongoing process by which roles are taken, assumed and modulated. According to Alonzo [57], "the interactionist perspective places considerable emphasis on the emergent and interac- tional nature of symptoms and signs, the interpretive, evaluative, and constructive nature of the individual's response, and the relationship which the social psychological individual maintains between his (or her) body and his (or her) social and physical en- vironments."
In this perspective, the biomedical changes of heart disease are a given, and the analysis is focused on the processes of how the individual defines and evaluates the symptoms of the disease and the relationship he or she maintains between his or her body and his or her social and physical environments. This view is particularly helpful because it focuses on 'labeling' as an essential process of an interaction [57, 58]. In the setting of an evolving AMI, the ability of the patient to label the symptoms and signs of a heart attack correctly together with the ability of any other indi- viduals in the victim's environment to reinforce the veracity of that label is key to reducing delay in seeking medical treatment.
The enactment of a given role involves four essen- tial components: the identification of self, behaviors that are appropriate to this identification, related acts by others in counterroles that serve as cues to guide specific performance, and an evaluation by the indi- vidual and others in counterroles as to how well the role is being enacted [59]. Therefore, the variables surrounding the phenomenon of delay are centered on the following four concepts:
1. The act of decision, which involves labeling the deviant health pattern, and the behaviors that evolve from that decision (e.g. seeking help from family members, friends, or coworkers; calling 9-1-1; driv- ing to an emergency facility). The act of decision is influenced in part by the severity of the deviation and
the experience the patient has had with previous symptoms.
2. The individual's self-concept, particularly as it is affected in the transition from a well role to a sick role. This self-concept is partially revealed through sociodemographic characteristics and personality traits.
3. The counterroles played by the patient's spouse, other family members, friends, and health pro- fessionals. The context in which the patient experi- ences cardiac symptoms (e.g. setting and times of day) affects which individuals will enact counterroles. For example, in one study of 1102 patients, 93% experienced their symptoms in the presence of another person. Eighty percent were at home or at a friend's house, 8% were at work, and 12% were in a public setting. Seventy-eight percent of the witnesses were family members [28].
4. The periodic evaluation of the role enacted by the patient and by those in counterroles. In the instance of chest pain or other cardiac symptoms, the individual evaluates the severity of the symptoms (e.g. pain) and how it is affected by self-treatment or coping strategies.
VARIABLES AFFECTING DELAY TIME
The decision to seek medical help for the symptoms of an AMI is made within the complex framework of multiple interrelated variables. These variables affect delay time in seeking medical care and can be catego- rized within an interactionist framework. Act-of- decision variables include coping mechanisms/denial, clinical status and medical history. Self-concept vari- ables include the sociodemographic factors of age, gender, race, socioeconomic status and education, as well as personality type. Counterrole variables are contextual and include witnessing, consulting a phys- ician, time of day, day of week, activity and place. Periodic evaluation variables are related to self- treatment. This section summarizes what the litera- ture reveals about these variables and their relationship to delay time. Variables related to in- creased delay are listed in Table 1.
Table 1. Effect of various factors on an individual's decision to seek medical care in response to heart attack symptoms
Characteristk's of Patients Likely to Delay ---older age (> 55 years) --female -- low socioeconomic status --history of angina or diabetes --family member as witness --self treatment --failure to perceive or recognize symptoms as cardiac in origin
----consultation with a physician -- low somatic or emotional awareness
Characteristics That Do Not ,4fJect Delay Time --years of education - -Type A/B personality --history of coronary artery disease or myocardial infarction--
severity of chest pain
Causes of delay in seeking treatment for heart attack symptoms 383
Act of decision
Coping Mechanisms--denial and related mechan- isms. Psychological adaptation to the stress of a sudden change in health status can be achieved through a number of mental mechanisms. These mechanisms vary in scope and intensity from distrac- tion of attention or suppression of unpleasant thought through contradiction and repression to gross denial of reality and even delusion-illusion formation. Each of these mechanisms may affect both the level of awareness of reality and the action taken by the patient in response to that awareness. Compli- cating the assessment of these effects is the fact that the patient's awareness of cardiac symptoms and the emotions that flow from that awareness are very much influenced by the person to whom the patient makes the acknowledgment.
All patients probably experience some degree of denial when they are experiencing a heart attack. The significance of denial in relation to a decision and its role in the interpersonal interaction that occurs during lay evaluation (the period of self-evaluation that occurs between the onset of symptoms and the seeking of medical advice) have not been assessed thoroughly. Given the long delay time that is usually reported during self-evaluation, it is tempting to identify denial as an important psychological re- sponse that significantly increases delay time.
Two methodological problems make it difficult to understand the role of denial in delay time. The first is that all data related to the patient's decision process must, of necessity, be collected retrospectively. For many variables, such as demographic or clinical characteristics, retrospective collection does not pre- sent any problem. However, denial is a transitory coping mechanism that is difficult to evaluate after the fact. Investigators can ask patients how serious they thought their symptoms were or if they labeled their symptoms as cardiac in origin, but in the end it is impossible to assess the degree to which the patient used denial to ward off anxiety.
The second methodological problem concerning denial is the lack of an appropriate psychometric instrument. Hackett and associates [60] used a denial rating scale in their study of response to the symp- toms of infarction; there is still no evidence related to the reliability and validity of the rating scale. Gentry and Haney [61] used a measure of denial defined as the difference between current self-reported health status (i.e. during a hospital stay for AMI) and reported health status in the week before infarction. A potential confounding factor in this approach exists if the patient had been in poor health before the infarction or had a long prodromal phase. Other investigators [23,41, 60] who have assessed denial have concluded that it does not contribute signifi- cantly to delay. This finding may relate more to the difficulty inherent in measuring denial than to the relationship of denial and delay.
Suppression is related to denial. The few investi- gators who have attempted to measure suppression as a way of coping with AMI symptoms have found that patients who report using it do not delay longer than patients who do not use it [41]. In contrast, patients who use distraction as a coping mechanism in the face of AMI symptoms experience significant delays in seeking treatment [42].
Symptom appraisal. Although a patient's subjective appraisal of the significance of AMI symptoms is an important factor in determining response to those symptoms, few researchers have investigated this phenomenon. Patients who believe their symptoms are cardiac in origin are more likely to seek medical attention quickly than those patients who ascribe their symptoms to another cause such as indigestion [34, 38, 43]. In one study, the factor most strongly as- sociated with early arrival at the hospital in response to AMI symptoms was the belief that the symptoms were those of a heart attack [38]. However, the perception of severity of chest pain does not appear to discriminate those who do not delay from those who do [4, 19, 41]. Moreover, the presence or absence of chest pain as an initial presenting symptom does not differentiate delayers from nondelayers [41,43].
Clinical status. Patients who were hemodynami- cally unstable [19, 37] and/or had large transmural infarctions [4] have been found to have significantly decreased delay times. Patients with slowly progress- ing symptoms experienced significant delays, whereas patients with rapidly developing symptoms quickly seek appropriate medical attention [29, 41].
Medical history. Many of the individuals who delay seeking medical treatment are at known risk for coronary heart disease (CHD) and are being treated for one or more conditions related to that risk (e.g. angina, diabetes) or already suffer from CHD or have had an AMI. Medical professionals often assume that these patients will not delay seeking medical care because of their familiarity with the medical system and the symptoms and signs of AMI. However, researchers have consistently documented that past medical history has no effect on delay time [19, 23, 30, 34, 36, 37, 41, 43, 45] or that delay times actually increase in these patients [36, 37, 46, 48].
A striking finding across several studies is that a history of prior AMI does not decrease delay times [4, 19, 21, 30, 34, 37,43]. Similarly, a history of CHD, coronary artery bypass surgery, angina, or congestive heart failure does not reduce delay time [21-24, 30, 36, 41,43, 45]. In some studies, angina ac- tually lengthens delay time [21,36, 46]. The chronic high-risk condition of diabetes mellitus also is related to increased delay times in most studies [23, 27, 46].
Self-concept
Sociodemographic factors
Age. The evidence regarding the effect of age on delay time is conflicting, but suggests that older age

384 KATHLEEN DRACUP et al.
is associated with an increase in delay time. Although some researchers report that age does not affect delay time [21, 23, 29, 34--36, 40, 43, 45] others have found a direct relationship between age and delay with older patients delaying more than younger patients [19, 30, 37, 41, 46]. These conflicting findings are likely the result of methodological issues [37]. Many studies reporting no difference in delay time based upon age have been small and thus lack the statistical power to detect differences. For example, an early study of factors contributing to delay in responding to symptoms of AMI was conducted among 100 randomly selected coronary care unit patients admit- ted with a diagnosis of suspected or proved AMI [34]. Age of the patient was not related significantly to delay, although there was a trend for older individ- uals to delay longer indicating that inadequate power contributed to the negative finding. In a Canadian study of 201 consecutive patients admitted for sus- pected AMI (only 42 of whom were interviewed and included in data analysis of the relationship between sociodemographics and delay times), age was not related to degree of delay [23]. A British investigator [39] also failed to find an association between age and time of delay in 50 hospitalized AMI patients. Similar findings were reported in the U.S. in studies of 160 [36] and 43 hospitalized AMI patients [40]. Moss and Goldstein [35] interviewed 160 patients admitted to coronary care units for an AMI and found no association, although there was a trend for younger patients to have shorter delay times than older patients.
In contrast, in the Multicenter Investigation of Limitation of Infarct Size (MILLS), a clinical study of 778 patients with AMI, Turi and associates [37] found that older age significantly contributed to increased delay time. This finding has been replicated in other studies with large sample sizes [19]. Data from a large Seattle AMI registry (n = 3258) show that older patients delay longer from chest pain onset until hospital admission [48] Although the median time delay of about 2 hr was similar for all age groups, the average delay increased substantially with increasing age: 4.1 hr in patients <55 years old, 5.2 hr in those 55-64 years old, 5.1 hr in those 65-74 years old, and 6.1 hr in patients >~ 75 years old (24% of whom, came to the hospital >/6 hr after symptom onset). Karlson and associates [62] found that the median delay time for those under age 50 was 0.9-1.7 hr compared to 3.5-4 hr for those over the age of 70. Adding to the evidence that older age contributes to increased delay are reports from two recent studies using multivariate analyses that identified older age as an independent risk factor for increased delay [41, 46].
Gender. Many investigators have not included gen- der in their study of factors contributing to delay. For those who have, conflicting findings have been re- ported on the role of gender in influencing delay. Some [19, 21, 23, 35-36, 39-40, 43] have reported no relationship between gender and time of delay, while
others [22, 29-30, 37, 41,46, 63] have concluded that women delay longer than men. Comparison of delay times in some investigations in which there were no statistically significant differences reveals large differences that were clinically significant [34, 38, 62] suggesting that inadequate sample size was a factor in failure to find statistical significance. For example, Karlson and associates [62] reported no statistical difference in delay time between men and women, but median delay was one hour longer in women than men. Similarly, in one of the earliest reports of pre-hospital delay, Hackett and Cassem [34] studied 64 men and 24 women admitted to a coronary care unit for suspected or established AMI and found no statistical difference in delay time. However, women delayed a median of 1 hr longer than men.
All researchers who have documented a difference in delay times between men and women have noted that women delayed longer. For example, Turi [37] reported that women delayed significantly longer than men in seeking medical care for symptoms of AMI. Although median time to treatment for women was only 0.2 hr longer than for men (3.2 hr vs 3.0 hr), at least 31% of the women in their study delayed longer than 5 hr. In another study, women delayed a mean of 3.3 hr longer than men in seeking treatment for cardiac symptoms [30]. Alonzo [29] reported increased delay times for women (a median of 47 min longer from symptom onset to medical evaluation) due primarily to a longer self-evaluation phase, while Schmidt and Borsch [41] reported that half of the women in their study delayed longer than 6 hr in coming to the hospital. Cunningham and associates [63] studied 7734 patients admitted to emergency rooms with chest pain and found that women who were subsequently diagnosed as having an AMI delayed one hour longer than men diagnosed with an AMI.
Race. The vast majority of CHD research studies, including those investigating factors contributing to delay in seeking care, have been conducted with white middle- and upper-class males. This fact limits our ability to generalize findings to other sociocultural groups. The few studies that have been conducted among members of other sociocultural groups indi- cate that their delays in care seeking may be consider- ably worse than those of white males and females [20, 38,47]. Cooper and associates [20] studied 111 blacks admitted with a documented AMI to a Chicago hospital serving poor and working-class minorities. Median elapsed time from onset of symp- toms to arrival at the hospital was 6 hr, with a mean of 21 hr for women and 24 for men. Compared with the results of studies among white populations, the median time in this study was twice as long, and the mean time was three times as long. Similarly, in a study of 74 chest pain patients in a population consisting mainly of African-Americans and the un- derprivileged, Ghali and associates [47] documented significant prehospital delay (mean time from onset

Causes of delay in seeking treatment for heart attack symptoms 385
of chest pain to decision to seek medical care of 11.3 ___ 18 hr). In a study of prehospital delay among inner-city patients with symptoms of an AMI, Clark and associates [38] reported longer median and mean delay times for blacks (median 3 hr, mean 13.1 +27 .5hr ) and Hispanics (median 4hr, mean 12.4+ 19.3hr) than for whites (median 2hr), mean 3.3 ___ 2.9 hr). In Alonzo's [29] series of 1102 subjects, blacks delayed longer than whites, with the increased delay times being attributed to the search for a physician by relatively young black men who had little or no prior contact with the medical care system. Turi and associates [37] compared mean time to emergency room arrival from symptom onset for whites (n ---611) and nonwhites (n = 167) and found it to be identical. The racial breakdown of the nonwhite group in this study was not reported; however, its probable heterogeneity limits the gener- alizability of the findings.
Socioeconomic status. Many investigators who have explored the effect of socioeconomic status on prehospital delay have concluded that it has no effect [23, 34, 36, 39-40,43]. However, there is scant re- search among truly economically disadvantaged populations, and comparisons between the poor and middle class have begun to reveal the deleterious effects of low socioeconomic status on delay [20, 22, 41, 47]. Cooper's [20] and Ghali 's [47] studies of delay among African-Americans were conducted in hospitals serving populations they classified as poor and underprivileged. Their findings raise ques- tions about the effects of delay on the interaction between ethnicity and economic status and suggest that delay may be more a result of socioeconomic disadvantage than an independent ethnic or cultural effect. A recent study by Ell and colleagues [22] supports this view. The time from symptom onset to the decision to seek care was 2.5 times longer for African-American patients who sought care at a public hospital compared to those who sought care at a private hospital. In their study, African-American patients who were poor, uninsured or without a regular physician had significantly longer delay times than African-American patients with the opposite characteristics.
Education. The effect of education on care-seeking behavior in general has received significant research interest as researchers discovered that higher edu- cational levels do not necessarily result in increased compliance or appropriate utilization of services [49]. Consistent with these findings, educational level has been shown to neither increase nor decrease delay time [22, 23, 30, 35-37, 41]. In one small series of 43 patients [40], delay time was decreased for those patients with less education.
Knowledge about AML Interestingly, knowledge of the symptoms of AMI does not ensure that a patient will recognize or acknowledge his or her own AMI symptoms as such [38] and does not reduce delay in seeking medical care [24]. There are no
differences in delay time between patients who know about thrombolytic therapy, the advantages of early treatment, risk factors for AMI [41], or who believe that heart disease is controllable [38]. The failure of large community based education campaigns in the United States to reduce prehospital delay in response to AMI symptoms [25] is further indication that knowledge alone of AMI symptoms and the import- ance of a timely response is not enough to reduce delay.
Personality factors--type A/type B. Investigators have examined the effect of personality traits, particu- larly the coronary-prone personality constellation (type A/type B), on the decision to seek medical care for cardiac symptoms. Matthews and colleagues [40], identified patients with type A personality to be slow to label their symptoms as cardiac. However, once these patients determined the nature of the deviation, they were quick to seek medical care. Patients with type B personality were quick to label their symptoms correctly but delayed seeking appropriate medical treatment. These findings, however, were contra- dicted by those of Wielgosz and associates [23], who found coronary-prone personality had no effect on delay time. Of note are the facts that the sample sizes of the two studies were identical and that the re- searchers used the same interview method, thus mak- ing the contradictory findings more perplexing. Other investigators have concluded that type A/type B behavior has no effect on delay time [42, 43].
Other psychological factors. Patients with the psychological characteristics of somatic and emotional awareness have significantly shorter pre- hospital delay than patients who are less capable of identifying inner experiences of emotion and body sensations [43]. Neither locus of control nor de- pression assessed after hospital admission distin- guished between delayers and nondelayers in one series of 161 AMI patients [41]. However, patients who initially responded to their symptoms with de- pression or fatigue, or who were pessimistic about the state of their health at the time of symptoms experi- enced long delays in deciding that their symptoms were significant [40].
Counterroles
It is too simplistic to rely on sociodemographic factors alone to explain delays in seeking medical care for an AMI. Consequently, researchers have exam- ined other factors in an effort to identify variables that are amenable to intervention. Among these factors, the context in which the AMI symptoms occur affects the counterroles that other people play in influencing the patient's decision to seek treatment. These contextual factors include who witnesses the symptoms (i.e. the person's relationship to the patient), whether a physician is consulted, the time and day of symptom onset, patient activity at the time of symptom onset, and the place symptoms initially occurred.

386 KATHLEEN DRACUP et al.
Witnessing an AMI. To gain information related to counterroles, a few investigators have examined the social context in which an AMI occurs. Among their findings was the observation that most patients arrive at the decision to seek medical care for cardiac symptoms with the assistance of a family member [34] but that patients who come to the decision themselves have shorter delay times [30, 34]. Another finding was that the spouse or other family member was usually the first to be informed of a patient's AMI symptoms, which turned out to be a choice that resulted in considerable delays [29, 34]. The median delay was 12 hr when patients told family members first of their symptoms, compared with 2 hr when friends were told first. The shortest delays were found when an unrelated person (friend, coworker, or stranger) as- sisted the patient in making the decision to seek medical care [29].
In explaining these intriguing findings, the re- searchers postulated that family members may have been motivated to share the denial of the patient or may have been less willing than a coworker or stranger to confront the patient's delay. A coworker or stranger may be less willing to bear the responsibil- ity of a wrong decision and less tempted to share the patient's wishful thinking.
Consulting a physician. For many patients, consult- ing or attempting to consult their physician is a logical first step in making the decision to go to the hospital for cardiac symptoms. Unfortunately, this decision results in significantly increased delay times [21,24,29, 36,64]. Increases in delay times occur for a variety of reasons, including physicians not perceiving the symptoms as cardiac in nature, recommendations from physicians to try self-medi- cation, inability of patients to contact physicians immediately, and inappropriate counseling by office staff.
Time and day. The onset of cardiac symptoms during the daytime hours has been reported to in- crease delay time [29, 30, 35]. A British investigator, however, found that delay time was significantly increased if AMI symptoms began at night and attributed this finding to a cultural unwillingness to bother a physician at night [39]. Time of day was not found to be a factor in delay in a Canadian study [23] and in recent U.S. studies [41,45].
When AMI symptoms occurred during the week- end, researchers have identified both an increase in delay time [30] and a decrease in delay time [23]. As with the effect of time of day on delay, inconsistent findings for the day of the week may be the result of cross-cultural comparisons in which traditional pat- terns of accessing the medical system and the medical systems themselves are different.
Activity. Only a few investigators have explored how a person's activity at the time of symptom onset affects delay. One who did [29] noted that subjects engaged in strenuous activity at the time of symptom onset had a decrease in delay time.
Place. It is difficult to draw conclusions concerning the effect of place because of conflicting study results. The setting in which the AMI occurred has been variably found to have no effect on prehospital delay [41], to increase delay if symptoms occurred at home [37], to increase delay if symptoms occurred some- where other than at home and the person then went home [37] and to decrease delay if symptoms oc- curred at home [29]. Because AMI symptoms occur in a social context and not simply an environmental one, the inconsistent findings reported may be the result of a failure to consider who a person is with in addition to where the person is when symptoms OCCUr.
Periodic evaluation
Self-treatment. As might be expected, the decision to try self-treatment, whether with over-the-counter or prescription medications or by reduction in activi- ties, results in significantly increased delay times [4, 29, 36, 37, 42].
Conclusions about variables affecting delay time
Methodological differences and study limitations make comparison across studies difficult and prob- ably account for the conflicting results found in some studies. One problem is that in retrospective studies investigators are forced to rely on the memory of the patient or family members. A person's memory of an emotional and stressful time is subject to inaccurate interpretation. In some studies, patients were inter- viewed alone. In others, a patient, a family member or both were interviewed, and it was obvious that interpretation and memory of a subjective event differ, depending on who was interviewed. Another problem is that many studies included only proven AMI patients, but others included both suspected and documented AMI patients. Across the studies prehospital delay was variably defined, making comparison difficult. Additionally, regional and inter- national differences in medical systems and differ- ences in accessing the systems for AMI symptoms make comparison problematic.
Nonetheless, it is possible to draw some con- clusions from these studies about the effects of se- lected variables on patient and bystander delay time. Delay times are shorter in hemodynamically unstable patients, in patients with large infarcts, and in patients who recognize their symptoms as being cardiac in origin rather than attributing them to some other organ system. Patients at risk for a myocardial infarction (those with diabetes or angina) often ex- perience considerable delays before arriving at an emergency department for treatment. A history of heart disease, myocardial infarction and congestive heart failure does not presume to decrease delay time. An increase in delay time appears to be more com- mon in females and in older age people. It is also more common in extremely economically disadvan- taged populations. African-Americans and Hispanics
Causes of delay in seeking treatment for heart attack symptoms
have substantially increased delay times, but this may be due to the interaction between socioeconomic status and ethnicity. Educational level does not affect delay time, nor does knowledge of AMI symptoms or the importance of a timely response to symptoms. Coronary-prone behavior differentially affects delay time. Other personality characteristics have been studied by only a few investigators, but preliminary findings suggest that certain traits predict increased delay (e.g. somatic and emotional awareness, per- ceived vulnerability to reinfarction). Seeking the as- sistance of a spouse in making a decision to go to the hospital for AMI symptoms is associated with in- creased prehospital delay time, as is the decision to consult a physician when confronted with cardiac symptoms. However, if the individual consults an unrelated individual, delay time is significantly de- creased. Patients experiencing an onset of symptoms during the daylight hours generally have increased delays. However, the effects of the time of day as well as the day of the week and the place symptoms occur are dependent on other factors, particularly on whom the patient was with when symptoms occurred and whom they told about their symptoms. Finally, the decision to try self-treatment for cardiac symptoms results in a significant increase in patient and by- stander delay.
DEVELOPING AN INTEGRATED MODEL
It is important to recognize that the effect of variables on delay time may change as the context from which they arise changes. Failure to view vari- ables as contextual may also account for the conflict- ing findings of past research. Therefore, having examined the variables separately to present the simplest picture of the abundance of research findings in this area, it is necessary to consider how these variables might be interrelated in a larger context. One way of investigating the relationships among
387
these variables is to rely on the three theoretical frameworks discussed earlier for a possible expla- nation of the overall process. This section of the paper investigates the larger context of the phenom- enon of prehospitalization delay time by combining the theoretical principles suggested by the health belief model, the self regulation model and symbolic interactionism,
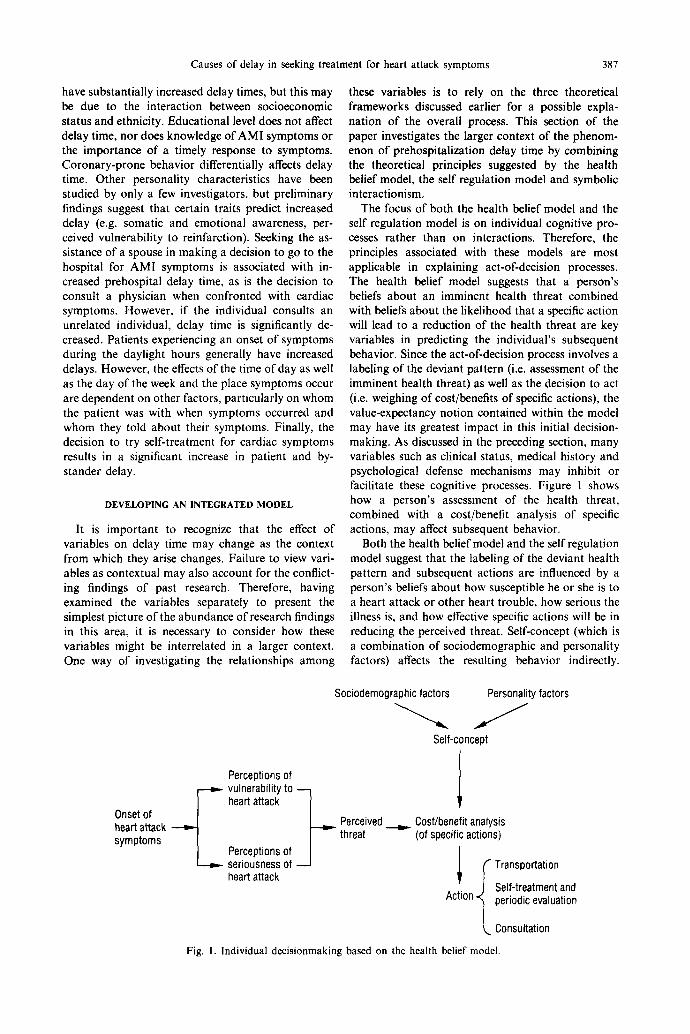
The focus of both the health belief model and the self regulation model is on individual cognitive pro- cesses rather than on interactions. Therefore, the principles associated with these models are most applicable in explaining act-of-decision processes. The health belief model suggests that a person's beliefs about an imminent health threat combined with beliefs about the likelihood that a specific action will lead to a reduction of the health threat are key variables in predicting the individual's subsequent behavior. Since the act-of-decision process involves a labeling of the deviant pattern (i.e. assessment of the imminent health threat) as well as the decision to act (i.e. weighing of cost/benefits of specific actions), the value-expectancy notion contained within the model may have its greatest impact in this initial decision- making. As discussed in the preceding section, many variables such as clinical status, medical history and psychological defense mechanisms may inhibit or facilitate these cognitive processes. Figure 1 shows how a person's assessment of the health threat, combined with a cost/benefit analysis of specific actions, may affect subsequent behavior.
Both the health belief model and the self regulation model suggest that the labeling of the deviant health pattern and subsequent actions are influenced by a person's beliefs about how susceptible he or she is to a heart attack or other heart trouble, how serious the illness is, and how effective specific actions will be in reducing the perceived threat. Self-concept (which is a combination of sociodemographic and personality factors) affects the resulting behavior indirectly.
Sociodemographic factors Personality factors
Self-concept
Perceptions of ~ vulnerability to ~
heart attack Onset of heart attack symptoms
Perceptions of seriousness of heart attack
Perceived threat
Cost/benefit analysis (of specific actions)
l I Transportation Self-treatment and
Action periodic evaluation
Consultation
Fig. I. Individual decisionmaking based on the health belief model.
388 KATHLEEN DRACUP et al.
Although the behavior that evolves from these cogni- tive processes may vary, it seems plausible that a person who has an AMI can take one of three kinds of actions: go to the hospital directly (either by calling 9-1-1 or by driving), decide to wait and periodically evaluate the situation (or engage in some sort of self-treatment), or decide to involve somebody else (calling a physician, telling a spouse or coworker). This last action in particular results in subsequent decisionmaking processes that are based in part on interaction rather than on individual action. This stage of the decisionmaking process is characterized by the importance of the counterroles played by a spouse, other family members, physicians or other persons in the individual's social environment. Thus, at this stage, the theoretical focus shifts from the individual to the interaction as the unit of analysis.
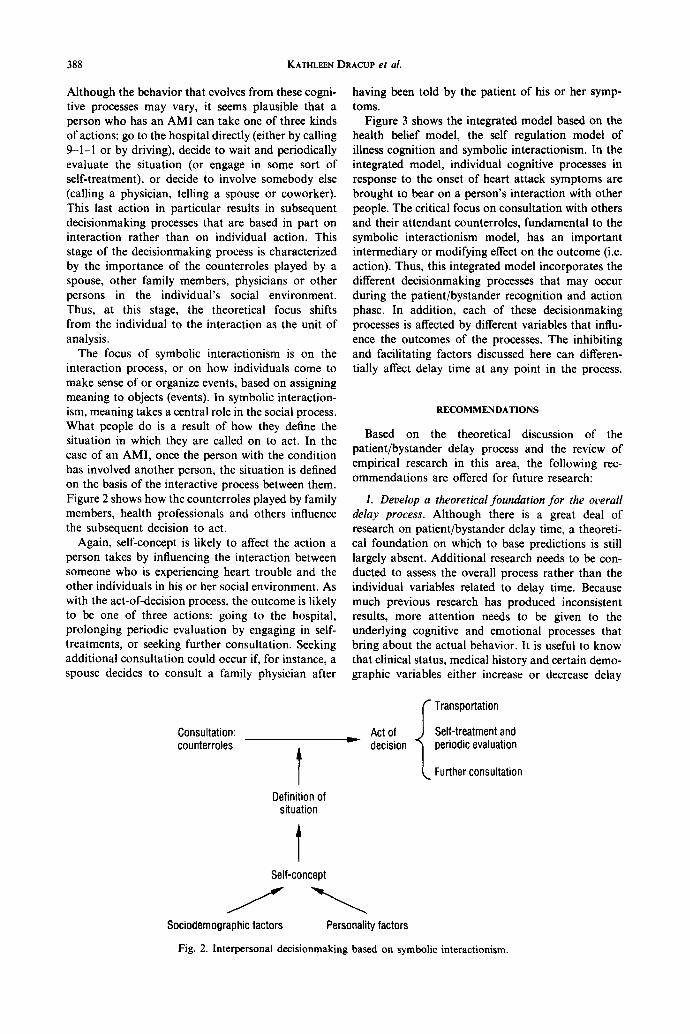
The focus of symbolic interactionism is on the interaction process, or on how individuals come to make sense of or organize events, based on assigning meaning to objects (events). In symbolic interaction- ism, meaning takes a central role in the social process. What people do is a result of how they define the situation in which they are called on to act. In the case of an AMI, once the person with the condition has involved another person, the situation is defined on the basis of the interactive process between them. Figure 2 shows how the counterroles played by family members, health professionals and others influence the subsequent decision to act.
Again, self-concept is likely to affect the action a person takes by influencing the interaction between someone who is experiencing heart trouble and the other individuals in his or her social environment. As with the act-of-decision process, the outcome is likely to be one of three actions: going to the hospital, prolonging periodic evaluation by engaging in self- treatments, or seeking further consultation. Seeking additional consultation could occur if, for instance, a spouse decides to consult a family physician after
having been told by the patient of his or her symp- toms.
Figure 3 shows the integrated model based on the health belief model, the self regulation model of illness cognition and symbolic interactionism. In the integrated model, individual cognitive processes in response to the onset of heart attack symptoms are brought to bear on a person's interaction with other people. The critical focus on consultation with others and their attendant counterroles, fundamental to the symbolic interactionism model, has an important intermediary or modifying effect on the outcome (i.e. action). Thus, this integrated model incorporates the different decisionmaking processes that may occur during the patient/bystander recognition and action phase. In addition, each of these decisionmaking processes is affected by different variables that influ- ence the outcomes of the processes. The inhibiting and facilitating factors discussed here can differen- tially affect delay time at any point in the process.
RECOMMENDATIONS
Based on the theoretical discussion of the patient/bystander delay process and the review of empirical research in this area, the following rec- ommendations are offered for future research:
I. Develop a theoretical foundation for the overall delay process. Although there is a great deal of research on patient/bystander delay time, a theoreti- cal foundation on which to base predictions is still largely absent. Additional research needs to be con- ducted to assess the overall process rather than the individual variables related to delay time. Because much previous research has produced inconsistent results, more attention needs to be given to the underlying cognitive and emotional processes that bring about the actual behavior. It is useful to know that clinical status, medical history and certain demo- graphic variables either increase or decrease delay
Consultation: counterroles
Definition of situation
Self-concept
h v
S
I Transportation
Act of Self-treatment and decision periodic evaluation
Further consultation
Sociodemographic factors Personality factors Fig. 2. Interpersonal decisionmaking based on symbolic interactionism.

Causes of delay in seeking treatment for heart attack symptoms
Sociodemographic factors Personality factors
Self-concept
389
Onset of heart attack symptoms
Perceived Cos t /bene f i t Consultation: threat analysis counterroles
(of specific actions)
f Transportation
Self-treatment and Action " ~ periodic evaluation
L Further consultation
Fig. 3. An integrated model of decisionmaking in acute myocardial infarction.
time, but exploring why these variables affect delay time is even more useful. For instance, does male gender decrease delay time because men:
(1) feel more vulnerable to having heart trouble than women;
(2) are more sensitive to somatic changes and consequently more quickly aware of a devi- ant health pattern; or
(3) have a generally higher perceived threat to illness and are therefore quicker to act?
In other words, what cognitive processes mediate the relationship between these more 'static' variables and delay time?
2. Explore the decisionmaking processes involved in seeking care. Theoretical models need to be developed especially to clarify the social and psychological pro- cesses that contribute to delay. What cognitive pro- cesses and problem-solving strategies differentiate individuals who take a long time to seek care from those who respond immediately and therefore are able to take advantage of lifesaving and myocardium- preserving medical interventions? Studies conducted to date contain consistent references to the defensive mechanism of denial but little empirical support as to its actual occurrence. Although the term 'denial' is used, we do not know if we are dealing with the actual process of denial, reasonable problem-solving behavior or a social hesitancy to seek emergency medical care. Studies need to be done to explore the decision making processes involved in care seeking to delineate possible points of intervention in the processes of symp- tom and sign recognition, evaluation and management.
3. Study anomalous findings. To understand the anomalous findings, we also need to study emergency medical care seeking. That is, why does a person's history of a myocardial infarction not have a more
pronounced effect on the duration of care seeking? Much more research needs to be done in the area of theory building. Additional research is also needed on the ethnic, sexual, cultural and socioeconomic differ- ences in symptom manifestation and treatment-seek- ing behavior for patients who are experiencing an AMI.
4. Study behavior of bystanders and witnesses. Ad- ditional research is needed to understand the behav- ior of bystanders and witnesses related to delays in seeking care. We need to specify a role for family, friends and bystanders as to their behavior in assist- ing potential cardiac patients in obtaining definitive medical care. We need to understand the behavior of bystanders and witnesses and the factors that influ- ence it. Why does consulting with a coworker or stranger result in less delay time than consulting with a family member? What psychosocial processes occur between the heart attack victim and the bystander? What should a community education program ad- dress in the way of bystander behavior?
5. Study the effect o f emotion and cognition on delay. All researchers have found that delay decreases dramatically when patients are able to label their symptoms as cardiac in origin. What are the cognitive processes that occur when an individual weighs the possibility that certain prodromal symptoms may be an impending heart attack? Do specific personality traits enhance rapid assessment and decision making? What role do appraisal, coping, attitudes and beliefs about health, and knowledge about the symptoms of heart attack play in the decision to seek medical care?
6. Test education and counseling strategies. Edu- cation and counseling strategies to reduce delay in individuals at high risk for acute myocardial infarc- tion need to be developed and tested in prospective,
390 KATHLEEN DRACUP et al.
randomized trials. In developing these interventions, attention should be given to the cognitive processes involved in problem solving and the coping behaviors surrounding sign and symptom recognition and differentiation among significant medical and social groups,
7. Use new research strategies. Previous re- searchers have relied on quantitative measures and have focused on sociodemographic and clinical characteristics that might predict increased delay. All data were collected retrospectively. In the future, researchers need to use both quantitative and quali- tative techniques to identify the dynamic processes that surround the decision to seek care. For example, the role and nature of denial probably can only be understood using qualitative methodology.
In research on pain, mult icomponent (e.g. cogni- tive, behavioral, emotional and social) assessment instruments are used to resolve how personality and environmental factors contribute to decision-making behavior. Similar mult icomponent research instru- ments need to be developed and tested in patients with cardiac symptoms [65].
Multivariate approaches to data analysis are re- quired to help unravel the complex interactions of sociodemographic, clinical, personality and cultural characteristics on decision making. Prospective clini- cal trials conducted to test educational and counsel- ing strategies in patients at high risk for future myocardial infarction would not only provide infor- mation about the effectiveness of various interven- tions, but would also provide prospective data on a control group. The latter could be used to confirm previous research findings collected retro- spectively.
Acknowledgements--The authors would like to acknowl- edge the contributions of James Atkins, John Bradley, Mary McDonald Hand and Michael Horan in their review of early versions of this paper. The paper was developed as part of the National Heart Attack Alert Program of the National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland.
REFERENCES
1. National Heart, Lung, and Blood Institute. Morbidity and Mortality: Chartbook on Cardiovascular, Lung, and Blood Diseases. Bethesda (MD): U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, Bethesda, MD, 1992.
2. U.S. Bureau of the Census. Statistical Abstract o f the United States: 1991, l l l th edn. U.S. Bureau of the Census, Washington, DC, 1991.
3. Herlitz J., Blohm M., Hartford M., Hjalmarsson A., Holmberg S. and Karlson B. W. Delay time in suspected acute myocardial infarction and the importance of its modification. Clin. Cardiol. 12, 370, 1989.
4. Hofgren K., Bondestam E., Johansson F. G., Jern S., Herlitz J. and Holmberg S. Initial pain course and delay to hospital admission in relation to myocardial infarct size. Heart Lung 17, 274, 1988.
5. European Cooperative Study Group for Streptokinase Treatment in Acute Myocardial Infarction. Streptoki-
nase in acute myocardial infarction. N. Engl. J. Med. 301, 797, 1979
6. Gruppo Italiano per 1o Studio della Streptochinasi nell' Infarto Miocardico (GISSI). Effectiveness of intra- venous thrombolytic treatment in acute myocardial infarction. Lancet 1 (8478), 397, 1986.
7. Gruppo Italiano per 1o Studio della Streptochinasi nell' Infarto Miocardico (GISSI). Long-term effects of intra- venous thrombolysis in acute myocardial infarction: final report of the GISSI study. Lancet 2, (8564), 871, 1987.
8. Second International Study of Infarct Survival (ISIS-2) Collaborative Group. Randomized trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancet 2, 349, 1988.
9. Kennedy J. W., Ritchie J. L., Davis K. B., Stadius M. L., Maynard C. and Fritz J. K. The Western Washington randomized trial of intracoronary strep- tokinase in acute myocardial infarction: a 12-month follow-up report. N, Engl. J. Med. 312, 1073, 1985.
10. Marder V. L. and Sherry S. Thrombolytic therapy: current status (second of two parts). N. Engl. J. Med. 318, 1585, 1988.
11. Simoons M. L., Serruys P. W., van den Brand M., B~ir F., de Zwaan C., Res J., Verheugt F. W. A., Krauss X. H., Remme W. J. Vermeer F. et al. Improved survival after early thrombolysis in acute myocardial infarction. Lancet 2, (8455), 578, 1985.
12. White H. D., Norris R. M., Brown M. A., Takayama M., Maslowski A., Bass N. M., Ormiston J. A. and Whitlock T. Effect of intravenous streptokinase on left ventricular function and early survival after acute myocardial infarction. N. Engl. J. Med. 317, 850, 1987.
13. Yusuf S., Collins R., Peto R., Furberg C., Stampfer M. J., Goldhaber S. Z. and Hennekens C. H. Intra- venous and intracoronary fibrinolytic therapy in acute myocardial infarction: overview of results on mortality, reinfarction and side-effects from 33 randomized con- trolled trials. Eur. Heart J. 6, 556, 1985.
14. Koren G., Weiss A. T., Hasin Y., Appelbaum D., Welber S., Rozenman Y., Lotan C., Mosseri M., Sapoznikov D., Luria M. H. et al. Prevention of myocardial damage in acute myocardial ischemia by early treatment with intravenous streptokinase. N. Engl. J. Med. 313, 1384, 1985.
15. Simoons M. L., Serruys P. W., van den Brand M., Res J., Verheugt F. W. A., Krauss H., Remme W. J., B~ir F., de Zwaan C., van der Laarse A. et al. Early thrombolysis in acute myocardial infarction: limitation of infarct size and improved survival. J. Am. Coll. Cardiol. 7, 717, 1986.
16. Eisenberg M. S., Hallstrom A. and Bergner L. Long- term survival after out-of-hospital cardiac arrest. N. Engl. J. Med. 306, 1340, 1982.
17. Second International Study of Infarct Survival (ISIS-2) Steering Committee. Intravenous streptokinase given within 0-4 hours of onset of myocardial infarction reduced mortality in ISIS-2. Lancet 1, (8531), 502, 1987.
18. Grines C. L. and DeMaria A. N. Optimal utilization of thrombolytic therapy for acute myocardial infarction: concepts and controversies. J. Am. Coll. Cardiol. 16, 223, 1990.
19. Maynard C., Althouse R., Olsufka M., Ritchie J. L., Davis K. B. and Kennedy J. W. Early versus late hospital arrival for acute myocardial infarction in the Western Washington thrombolytic therapy trials. Am. J. Cardiol. 63, 1296, 1989.
20. Cooper R. S., Simmons B., Castaner A., Prasad R., Franklin C. and Ferlinz J. Survival rates and prehospi- tal delay during myocardial infarction among black persons. Am. J. Cardiol. 57, 208, 1986.
Causes of delay in seeking treatment
21. Schroeder J. S., Lamb I. H. and Hu M. The prehospital course of patients with chest pain: analysis of the prodromal, symptomatic, decision-making, transpor- tation and emergency room periods. Am. J. Med. 64, 742, 1978.
22. Ell K., Haywood L. J., Sobel E., deGuzman M., Blumfield D. and Jia-Ping N. Acute chest pain in African Americans: factors in the delay in seeking emergency care. Am. J. Pub. Hlth 84, 965, 1994.
23. Wielgosz A. T. J., Nolan R. P., Earp J. A., Biro E. and Wielgosz M. B. Reasons for patients' delay in response to symptoms of acute myocardial infarction. Can. Med. Assoc. J. 139, 853, 1988.
24. Leitch J. W., Birbara T., Freedman B., Wilcox I. and Harris P. J. Factors influencing the time from onset of chest pain to arrival at hospital. Med. J. Aust. 150, 6, 1989.
25. Ho M. T., Eisenberg S., Litwin P. E., Schaeffer S. M. and Damon S. K. Delay between onset of chest pain and seeking medical care: the effect of public education. Ann. Emerg. Med. 18, 727, 1989.
26. Safer M. A., Tharps Q., Jackson T. C. and Leventhal H. Determinants of three stages of delay in seeking care at a medical clinic. Med. Care 17, 11, 1979.
27. Gillum R. F., Feinleib M., Margolis J. R., Fabsitz R. R. and Brasch R. C. Delay in the prehospital phase of acute myocardial infarction: lack of influence on inci- dence of sudden death. Arch. Intern. Med. 136, 649, 1976.
28. Alonzo A. A. Acute illness behavior: a conceptual exploration and specification. Soc. Sci. Med. 14A, 515, 1980.
29. Alonzo A. A. The impact of the family and lay others on care-seeking during life-threatening episodes of sus- pected coronary artery disease. Soc. Sci. Med. 22, 129% 1986.
30. Moss A. J., Wynar B. and Goldstein S. Delay in hospitalization during the acute coronary period. Am. J. Cardiol. 24, 659, 1969.
31. Kereiakes D. J., Weaver W. D., Anderson J. J., Feld- man T., Gibler B., Aufderheide T., Williams D. O., Martin L. H., Anderson L. C., Martin J. S. et al. Time delays in the diagnosis and treatment of acute myocar- dial infarction: a tale of eight cities. Report from the Pre-hospital Study Group and the Cincinnati Heart Project. Am. Heart J. 120, 773, 1990.
32. Moses H. W., Bartolozzi J. J. Jr, Koester D. L., Colliver J. A., Taylor G. J., Mikell F. L., Dove J. T., Katholi R. E., Woodruff R. C., Miller B. D. et al. Reducing delay in the emergency room in administration of thrombolytic therapy for myocardial infarction as- sociated with ST elevation. Am. J. Cardiol. 68, 251, 1991.
33. Sharkey S. W., Brunette D. D., Ruiz E., Hession W. T., Wysham D. G., Goldenberg I. F. and Hodges M. An analysis of time delays preceding thrombolysis for acute myocardial infarction. J A M A 262, 3171, 1989.
34. Hackett T. P. and Cassem N. H. Factors contributing to delay in responding to the signs and symptoms of acute myocardial infarction. Am. J. Cardiol. 24, 651, 1969.
35. Moss A. J. and Goldstein S. The pre-hospital phase of acute myocardial infarction. Circulation 41, 737, 1970.
36. Simon A. B., Feinleib M. and Thompson H. K. Jr. Components of delay in the pre-hospital phase of acute myocardial infarction. Am. J. Cardiol. 30, 476, 1972.
37. Turi Z. G., Stone P. H., Muller J. E., Parker C., Rude R. E., Raabe D. E., Jaffe A. S., Hartwell T. D., Robertson T. L., Braunwald E. (and the AMILIS Study Group). Implications for acute intervention related to
for heart attack symptoms 391
time of hospital arrival in acute myocardial infarction. Am. J. Cardiol. . ~ 203, 1986.
38. Clark L. T., Bellam S. V., Shah A. H. and Feldman J. G. Analysis of prehospital delay among inner-city patients with symptoms of myocardial infarction: impli- cations for therapeutic intervention. J. Natl. Med. As- soc. 84, 931, 1992.
39. Gilchrist I. C. Patient delay before treatment of myocar- dial infarction. Br. Med. J. 1, 535, 1973.
40. Matthews K. A., Siegel J. M., Kuller L. H., Thompson M. and Varat M. Determinants of decisions to seek medical treatment by patients with acute myocardial infarction symptoms. J. Pers. Soc. Psychol. 44, 1144, 1983.
41. Schmidt S. B. and Borsch M. A. The prehospital phase of acute myocardial infarction in the era of thromboly- sis. Am. J. Cardiol. 65, 1411, 1990.
42. Nolan R. P. and Wielgosz A. T. Assessing adaptive and maladaptive coping in the early phase of acute myocar- dial infarction. J. Behav. 14, 111, 1991.
43. Kenyon L. W., Ketterer M. W., Gheorghiade M. and Goldstein S. Psychological factors related to prehospital delay during acute myocardial infarction. Circulation 84, 1969, 1991.
44. Ridker P. M., Manson J. E., Goldhaber S. Z, Hen- nekens C. H. and Buring J. E. Comparison of delay times to hospital presentation for physicians and non- physicians with acute myocardial infarction. Am. J. Cardiol. 70, 10, 1992.
45. Goldberg R. J., Gurwitz J., Yarzebski J., Landon J., Gore J. M., Alpert J. S., Dalen P. M. and Dalen J. E. Patient delay and receipt of thrombolytic therapy among patients with acute myocardial infarction from a community-wide perspective. Am. J. Cardiol. 70, 421, 1992.
46. Meischke H., Eisenberg M. S., and Larsen M. P. Prehospital delay interval for patients who use emer- gency medical services: the effect of heart-related medi- cal conditions and demographic variables. Ann. Emerg. Med. 22, 1597, 1993.
47. Ghali J. K., Cooper R. S., Kowalty I. and Liao Y. Delay between onset of chest pain and arrival to the coronary care unit among minority and dis- advantaged patients. J. National. Med. Assoc. 85, 180, 1993.
48. Weaver W. D., Litwin P. E., Martin J. S., Kudenchuk P. J., Maynard C., Eisenberg M. S., Ho M, T., Cobb I. A., Kennedy J. W. and Wirkus S. (the MITI Group). Effect of age on use of thrombolytic therapy and mortality in acute myocardial infarction. J. Am. Coll. Cardiol. 18, 657, 1991.
49. Sacket D. L. and Haynes R. B. Compliance with Thera- peutic Regimens. Johns Hopkins University Press, Balti- more, 1976.
50. Dracup K. A. and Meleis A. I. Compliance: an interac- tionist approach. Nurs. Res. 31, 31, 1982.
51. Becker M. H., Drachman R. H. and Kirscht J. P. Motivations as predictors of health behavior. Hlth Serv. Rep. 87, 852, 1972.
52. Kasl S. V. Social-psychological characteristics associ- ated with behaviors which reduce cardiovascular risk. In: Applying Behavioral Science to Cardiovascular Risk: Proceedings o f a Conference (Edited by Enelow A. J. and Henderson J. B.) 17-19 June, 1974; Seattle, WA, pp. 173-190. American Heart Association, Dallas (TX), 1975.
53. Haynes R. B. A critical review of the determinants of patient compliance with therapeutic regimens. In: Com- pliance with Therapeutic Regimens (Edited by Sackett D. L. and Haynes R. B.), pp. 2(~39. The Johns Hopkins University Press, Baltimore, MD, 1976.
54. Skelton J. A. and Croyle R. T. Mental Representation in Health and Illness. Springer-Verlag, Berlin, 1991.
SSM 40/3--H
392 KATHLEEN DRACUP et al.
55. Leventhal H. and Diefenbach M. The active side of illness cognition. In Mental Representation in Health and Illness (Edited by Skelton J. A. and Croyle R. T.), pp. 247-272. Springer-Verlag, Berlin, 1991.
56. Leventhal H., Nerenz D. and Steele D. Illness represen- tation and coping with health threats. In A Handbook of Psychology and Health (Edited by Baum A. and Singer J.), pp. 219-252. Lawrence Erlbaum Associates, Hillsdale, N J, 1984.
57. Alonzo A. A. An illness behavior paradigm: a concep- tual exploration of a situational-adaptation perspective. Soc. Sci. Med. 19(5), 499, 1984.
58. Lorber. J. Deviance as performance: the case of illness. Soc. Probl. 14, 302, 1967.
59. Lindesmith A. R. and Strauss L. Social Psychology. Holt, Rinehart and Winston, New York, 1968.
60. Hackett T., Cassem N. H. and Wishnie H. A. The coronary-care unit: an appraisal of its psychologic hazards. N. Engl. J. Med. 279, 1365, 1968.
61. Gentry W. D. and Haney T. Emotional and behavioral reaction to acute myocardial infarction. Heart Lung 4(5), 738, 1975.
62. Karlson B. W., Herlitz J., Sjolin M. et al. Clinical factors associated with delay time in suspected acute myocardial infarction. Am. Heart. J. 120, 1213, 1990.
63. Cunningham M. A., Lee T. H., Cook E. F. et al. The effect of gender on the probability of myocardial infarction among emergency department patients with acute chest pain: a report from the Multicenter Chest Pain Study Group. J. Gen. Intern. Med. 4, 392, 1989.
64. Gray D., Keating N. A., Murdock J., Skene A. M. and Hampton J. R. Impact of hospital thrombolysis policy on out-of-hospital response to suspected myocardial infarction. Lancet 341, 654, 1993.
65. Wielgosz A. T. and Nolan R. P. Understanding delay in response to symptoms of acute myocardial infarction: a compelling agenda. Circulation 84, 2193, 1991.