
Cardiovascular magnetic resonance imaging of hypoplastic left heart syndrome in children
14
REVIEW Cardiovascular magnetic resonance imaging of hypoplastic left heart syndrome in children Jonathan R. Dillman & Adam L. Dorfman & Anil K. Attili & Prachi P. Agarwal & Aaron Bell & Gisela C. Mueller & Ramiro J. Hernandez Received: 30 July 2009 / Revised: 31 October 2009 / Accepted: 9 November 2009 / Published online: 27 January 2010 # Springer-Verlag 2010 Abstract Cardiovascular magnetic resonance imaging (CMR) plays an important complementary role to echocar- diography and conventional angiography in the evaluation of hypoplastic left heart syndrome. This imaging modality is particularly useful for assessing cardiovascular postsur- gical changes, extracardiac vascular anatomy, ventricular and valvular function, and a variety of complications. The purpose of this article is to provide a contemporary review of the role of CMR in the management of untreated and surgically palliated hypoplastic left heart syndrome in children. Keywords Cardiovascular MRI . Hypoplastic left heart syndrome . Congenital heart disease . Children Introduction Hypoplastic left heart syndrome (HLHS) is a form of complex congenital heart disease characterized by underdevelopment of the left ventricle and associated left ventricular outflow obstruction [1, 2]. Cardiovascular magnetic resonance imaging (CMR) is an important complementary imaging modality to echocardiography and conventional angiography in the noninvasive evaluation of children with untreated and surgically palliated HLHS, and, in some instances, may obviate the need for conventional angiography. Today, CMR may be used to assess cardiovascular postsurgical changes, extracardiac vascular anatomy, ventricular and valvular function, and a variety of complications. The purpose of this article is to review the role of CMR in the evaluation of untreated and surgically palliated HLHS in children. Overview of HLHS HLHS is the most common single ventricle congenital heart defect, occurring in approximately one in 5,000 live births [3–5]. This condition is a frequent cause of congenital heart disease-related death during the neonatal period and, without intervention, is invariably fatal during the first few weeks of life [1–3]. Morbidity and mortality is typically due to right ventricular failure, pulmonary venous obstruction, progressive cyanosis, and metabolic acidosis secondary to lack of systemic cardiac output following ductus arteriosus closure [3]. There is a spectrum of disease severity in HLHS, ranging from mild hypoplasia to complete absence of the left ventricle [1, 3, 4]. A rudimentary left ventricle is typically present (Figs. 1 and 2)[4]. A variety of additional lesions are typically present in addition to an underdeveloped left J. R. Dillman (*) : A. L. Dorfman : R. J. Hernandez Department of Radiology, Section of Pediatric Radiology, C.S. Mott Children’ s Hospital, University of Michigan Health System, 1500 East Medical Center Drive, Ann Arbor, MI 48109, USA e-mail: [email protected] A. L. Dorfman Department of Pediatrics, Division of Pediatric Cardiology, C.S. Mott Children’ s Hospital, University of Michigan Health System, Ann Arbor, MI, USA A. K. Attili : P. P. Agarwal : G. C. Mueller Department of Radiology, Division of Cardiothoracic Imaging, University of Michigan Health System, Ann Arbor, MI, USA A. Bell Division of Imaging Sciences, King’ s College London, Guy’ s & St. Thomas’ Hospital, London, UK Pediatr Radiol (2010) 40:261–274 DOI 10.1007/s00247-009-1473-5
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Cardiovascular magnetic resonance imaging of hypoplastic left heart syndrome in children
REVIEW
Cardiovascular magnetic resonance imaging of hypoplasticleft heart syndrome in children
Jonathan R. Dillman & Adam L. Dorfman &
Anil K. Attili & Prachi P. Agarwal & Aaron Bell &Gisela C. Mueller & Ramiro J. Hernandez
Received: 30 July 2009 /Revised: 31 October 2009 /Accepted: 9 November 2009 /Published online: 27 January 2010# Springer-Verlag 2010
Abstract Cardiovascular magnetic resonance imaging(CMR) plays an important complementary role to echocar-diography and conventional angiography in the evaluationof hypoplastic left heart syndrome. This imaging modalityis particularly useful for assessing cardiovascular postsur-gical changes, extracardiac vascular anatomy, ventricularand valvular function, and a variety of complications. Thepurpose of this article is to provide a contemporary reviewof the role of CMR in the management of untreated andsurgically palliated hypoplastic left heart syndrome inchildren.
Keywords Cardiovascular MRI . Hypoplastic left heartsyndrome . Congenital heart disease . Children
Introduction
Hypoplastic left heart syndrome (HLHS) is a form of complexcongenital heart disease characterized by underdevelopmentof the left ventricle and associated left ventricular outflowobstruction [1, 2]. Cardiovascular magnetic resonanceimaging (CMR) is an important complementary imagingmodality to echocardiography and conventional angiographyin the noninvasive evaluation of children with untreated andsurgically palliated HLHS, and, in some instances, mayobviate the need for conventional angiography. Today, CMRmay be used to assess cardiovascular postsurgical changes,extracardiac vascular anatomy, ventricular and valvularfunction, and a variety of complications. The purpose ofthis article is to review the role of CMR in the evaluation ofuntreated and surgically palliated HLHS in children.
Overview of HLHS
HLHS is the most common single ventricle congenital heartdefect, occurring in approximately one in 5,000 live births[3–5]. This condition is a frequent cause of congenital heartdisease-related death during the neonatal period and,without intervention, is invariably fatal during the firstfew weeks of life [1–3]. Morbidity and mortality istypically due to right ventricular failure, pulmonary venousobstruction, progressive cyanosis, and metabolic acidosissecondary to lack of systemic cardiac output followingductus arteriosus closure [3].
There is a spectrum of disease severity in HLHS, rangingfrom mild hypoplasia to complete absence of the leftventricle [1, 3, 4]. A rudimentary left ventricle is typicallypresent (Figs. 1 and 2) [4]. A variety of additional lesionsare typically present in addition to an underdeveloped left
J. R. Dillman (*) :A. L. Dorfman : R. J. HernandezDepartment of Radiology, Section of Pediatric Radiology,C.S. Mott Children’s Hospital,University of Michigan Health System,1500 East Medical Center Drive,Ann Arbor, MI 48109, USAe-mail: [email protected]
A. L. DorfmanDepartment of Pediatrics, Division of Pediatric Cardiology,C.S. Mott Children’s Hospital,University of Michigan Health System,Ann Arbor, MI, USA
A. K. Attili : P. P. Agarwal :G. C. MuellerDepartment of Radiology, Division of Cardiothoracic Imaging,University of Michigan Health System,Ann Arbor, MI, USA
A. BellDivision of Imaging Sciences, King’s College London,Guy’s & St. Thomas’ Hospital,London, UK
Pediatr Radiol (2010) 40:261–274DOI 10.1007/s00247-009-1473-5
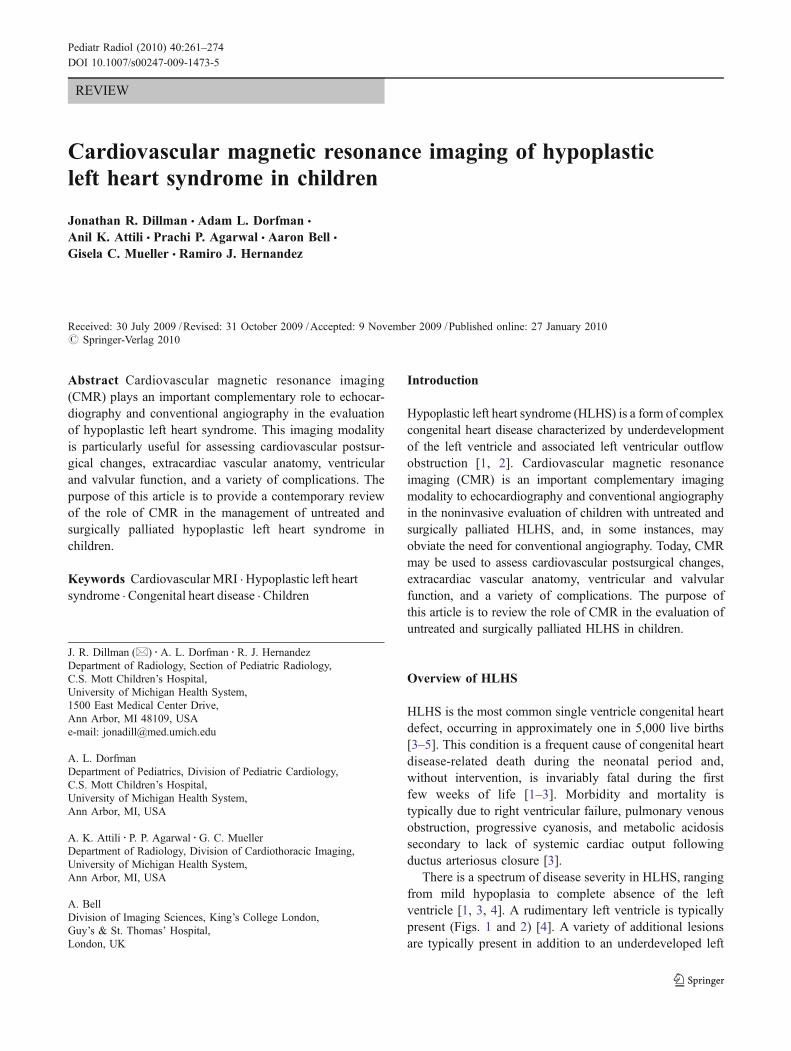
ventricle (Figs. 1 and 2). Both the mitral and aortic valvesare characteristically either underdeveloped or atretic [3],and the ascending thoracic aorta is usually severelyhypoplastic [3]. As outflow of blood from the left ventricleis obstructed, pulmonary venous return must be shuntedfrom the left atrium to the right atrium through either anatrial septal defect (ASD) or patent foramen ovale (PFO)[3]. Severe pulmonary venous congestion may result in thesetting of a restrictive interatrial septum, while a large atrialseptal defect may result in shunt pulmonary vascularity [3].The right ventricle must supply blood flow to the lungs viathe main pulmonary artery and to the descending aorta via a
patent ductus arteriosus (PDA) [3]. The PDA frequentlyalso provides retrograde blood flow to the aortic arch, greatvessels, ascending aorta, and coronary arteries [3]. Avariety of other cardiovascular anomalies may be associatedwith HLHS, including coarctation of the aorta, coronaryartery fistula, and endocardial fibroelastosis [3].
Role of CMR in untreated HLHS
CMR has a limited role in the evaluation of neonates withuntreated HLHS, as echocardiography is usually adequatefor complete evaluation. On occasion, CMR may be used toassist surgical planning, including the decision for univen-tricular versus biventricular repair. In a study of 20 neonateswith borderline left ventricle hypoplasia, Grosse-Wortmannet al. [6] compared CMR to echocardiography in the assess-ment of left ventricular volume. They concluded that echo-cardiography consistently underestimates left ventricularvolumes and may unfairly preclude some patients from abiventricular repair in whom CMR findings are reassuring[6]. The Simpson method for determining left ventricularvolume by echocardiography assumes a “bullet-shaped”cavity. The left ventricles of children with borderline andfrankly hypoplastic left ventricles are generally not “bullet-shaped.” This finding and associated leftward bowing ofthe interventricular septum lead to underestimation oftrue volume [6]. A left ventricular end-diastolic volume(LVEDV) of at least 20 ml/m2 is associated with improvedoutcome when undergoing biventricular repair [6].
In children with untreated HLHS, CMR can accuratelyassess left ventricular cavity volume in order to establish theexact degree of hypoplasia, right and left ventricle function,mitral and aortic valve patency and function, and ascendingaorta caliber (Figs. 2 and 3). Additionally, CMR can furthercharacterize ambiguous echocardiographic findings as wellas delineate extracardiac vascular anatomy. Extracardiacvascular structures that may be incompletely delineated byechocardiography and can be accurately depicted by CMR
Fig. 1 Illustration of prototypical HLHS. The left ventricular (LV)cavity is abnormally small and the ascending aorta (black arrow) ishypoplastic. There is abnormal communication between the atriaallowing for left-to-right shunting of blood. The ductus arteriosus ispatent (white arrow). LA left atrium; RA right atrium; RV rightventricle (Illustration by Anne Phillips, University of Michigan HealthSystem, Department of Radiology Media Services)
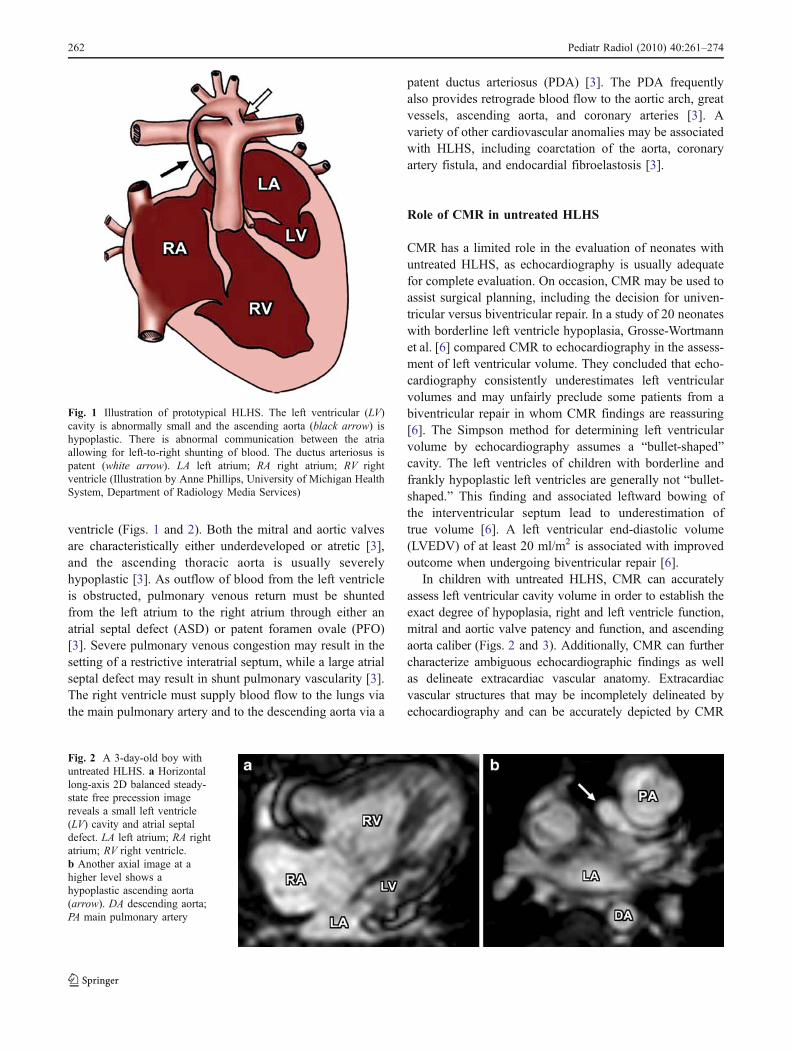
Fig. 2 A 3-day-old boy withuntreated HLHS. a Horizontallong-axis 2D balanced steady-state free precession imagereveals a small left ventricle(LV) cavity and atrial septaldefect. LA left atrium; RA rightatrium; RV right ventricle.b Another axial image at ahigher level shows ahypoplastic ascending aorta(arrow). DA descending aorta;PA main pulmonary artery
262 Pediatr Radiol (2010) 40:261–274
include the central pulmonary arteries, pulmonary veins,aortic arch and great vessels, ductus arteriosus, and descend-ing thoracic aorta.
Principles of HLHS surgical management
HLHS is most commonly managed using a three-step surgicalpalliative repair [3, 5]. The goal of surgical palliation is toconstruct separate, nonobstructed pulmonary and systemicvascular circulations, with systemic venous return flowingpassively into the lungs and the functional single ventricleproviding systemic blood flow [1]. At certain centers, cardiactransplantation may be the preferred treatment of choice[1, 3, 7]. Cardiac transplantation is advantageous in that it ismore physiologic than staged surgical palliation and it is asingle operation [1]. Disadvantages of cardiac transplantationinclude limited cardiac allograft availability, requirement ofimmunosuppressive therapy in order to prevent rejection,risk of post-transplant lymphoproliferative disorder (PTLD),and need for possible retransplantation with time due toallograft rejection, vasculopathy, and/or dysfunction [1]. Incertain circumstances, particularly in the setting of associatedanomalies and expected poor outcomes, a decision may bemade not to intervene surgically [1].
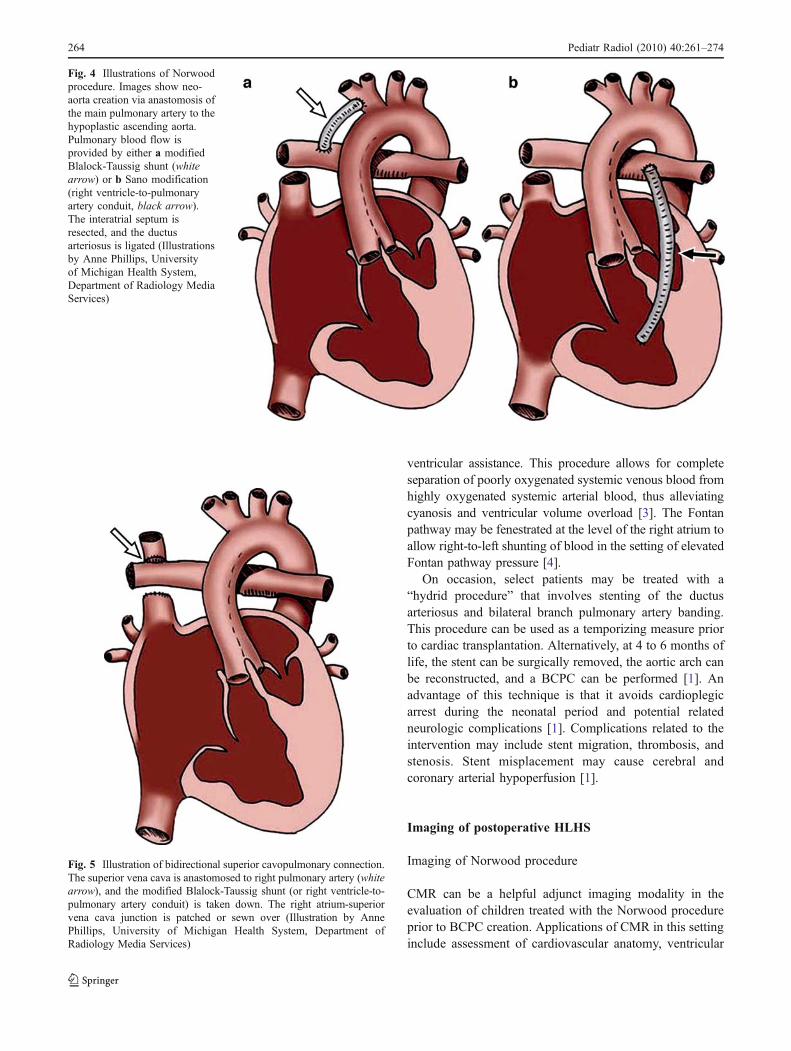
During the first few days of life prior to surgical inter-vention, prostaglandin E1 is intravenously administered tomaintain ductus arteriosus patency [1, 3]. The Norwoodoperation is the first stage employed in the surgicalpalliation of HLHS (Fig. 4) [1, 2, 8]. This complex surgicalprocedure is typically performed during the first few days oflife [4, 5]. With this procedure, the main pulmonary artery isligated and a portion is anastomosed to the hypoplasticascending aorta in order to create a neoaorta [3]. The neo-aorta is frequently augmented with a patch. As a result, thesingle functional (right) ventricle pumps blood through thenative pulmonary (or neoaortic) valve and neoaorta in order
to provide systemic blood flow. The interatrial septum isresected (atrial septectomy) to allow shunting of blood fromthe left atrium to the right atrium [1, 3]. Finally, the PDA isligated [3], and a controlled source of pulmonary blood flowis provided using either a modified Blalock-Taussig shunt(conduit placed between a subclavian/innominate artery andcentral pulmonary artery) [3, 4, 11] or Sano modification(right ventriculotomy with placement of a right ventricle-to-pulmonary artery valveless conduit) [4, 9–11].
The second surgical palliative stage is usually performedbetween the third and ninth months of life after pulmonaryarterial resistance has fallen and involves creation of abidirectional superior cavopulmonary connection (BCPC)(Fig. 5) [1, 3–5]. The purpose of this stage is to direct aportion of systemic venous return to the lungs, therebybypassing the single functional ventricle and helping torelieve ventricular volume overload [1, 3]. Two surgicaltechniques are commonly utilized: the hemi-Fontan proce-dure (HFP) and bidirectional Glenn shunt (BDG). Both ofthese procedures reroute a portion of systemic venousreturn via a superior vena cava (SVC)-to-pulmonary arteryanastomosis. With both techniques, inferior vena cava(IVC) blood flow is excluded from the surgically createdsuperior cavopulmonary pathway. Finally, the modifiedBlalock-Taussig shunt (or right ventricle-to-pulmonaryartery conduit) is ligated [3, 5].
The third and concluding surgical palliative stage is usuallyperformed between 18 and 48 months of life [1, 4, 5]. Thisstage, known as the Fontan operation, reroutes systemicvenous return from the IVC directly to the lungs via either anintracardiac lateral tunnel or extracardiac conduit, therebybypassing the single functional ventricle (the originallydescribed Fontan operation utilized a direct right atrium-to-pulmonary artery anastomosis and is only rarely used today)(Fig. 6) [4]. As a result, a total cavopulmonary connection(TCPC) is established with essentially all systemic venousblood flow passively returning to the lungs without direct
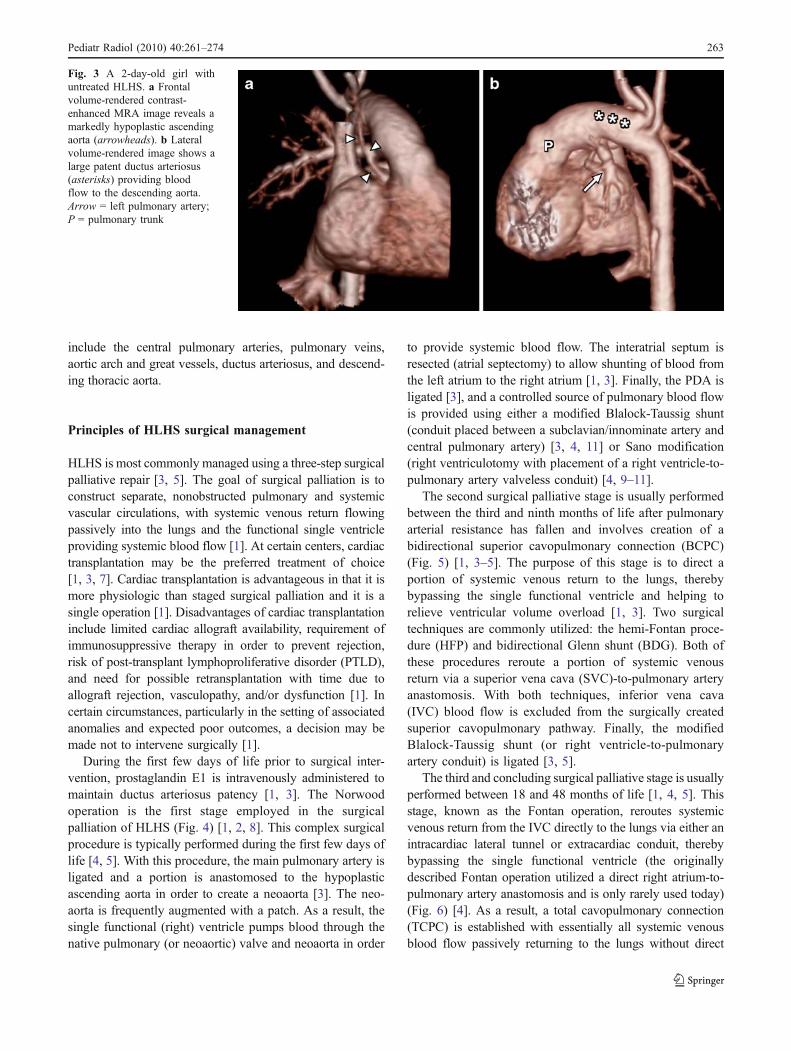
Fig. 3 A 2-day-old girl withuntreated HLHS. a Frontalvolume-rendered contrast-enhanced MRA image reveals amarkedly hypoplastic ascendingaorta (arrowheads). b Lateralvolume-rendered image shows alarge patent ductus arteriosus(asterisks) providing bloodflow to the descending aorta.Arrow = left pulmonary artery;P = pulmonary trunk
Pediatr Radiol (2010) 40:261–274 263
ventricular assistance. This procedure allows for completeseparation of poorly oxygenated systemic venous blood fromhighly oxygenated systemic arterial blood, thus alleviatingcyanosis and ventricular volume overload [3]. The Fontanpathway may be fenestrated at the level of the right atrium toallow right-to-left shunting of blood in the setting of elevatedFontan pathway pressure [4].
On occasion, select patients may be treated with a“hydrid procedure” that involves stenting of the ductusarteriosus and bilateral branch pulmonary artery banding.This procedure can be used as a temporizing measure priorto cardiac transplantation. Alternatively, at 4 to 6 months oflife, the stent can be surgically removed, the aortic arch canbe reconstructed, and a BCPC can be performed [1]. Anadvantage of this technique is that it avoids cardioplegicarrest during the neonatal period and potential relatedneurologic complications [1]. Complications related to theintervention may include stent migration, thrombosis, andstenosis. Stent misplacement may cause cerebral andcoronary arterial hypoperfusion [1].
Imaging of postoperative HLHS
Imaging of Norwood procedure
CMR can be a helpful adjunct imaging modality in theevaluation of children treated with the Norwood procedureprior to BCPC creation. Applications of CMR in this settinginclude assessment of cardiovascular anatomy, ventricular
Fig. 4 Illustrations of Norwoodprocedure. Images show neo-aorta creation via anastomosis ofthe main pulmonary artery to thehypoplastic ascending aorta.Pulmonary blood flow isprovided by either a modifiedBlalock-Taussig shunt (whitearrow) or b Sano modification(right ventricle-to-pulmonaryartery conduit, black arrow).The interatrial septum isresected, and the ductusarteriosus is ligated (Illustrationsby Anne Phillips, Universityof Michigan Health System,Department of Radiology MediaServices)
Fig. 5 Illustration of bidirectional superior cavopulmonary connection.The superior vena cava is anastomosed to right pulmonary artery (whitearrow), and the modified Blalock-Taussig shunt (or right ventricle-to-pulmonary artery conduit) is taken down. The right atrium-superiorvena cava junction is patched or sewn over (Illustration by AnnePhillips, University of Michigan Health System, Department ofRadiology Media Services)
264 Pediatr Radiol (2010) 40:261–274
and valvular (tricuspid and neoaortic) function, singlefunctional ventricular volume, and a variety of postsurgicalcomplications. Anatomic structures that can be accuratelydepicted include the SVC (right and/or left), IVC, centralpulmonary arteries, pulmonary veins, postsurgical commonatrium, single functional ventricle, neoaorta, aortic arch andgreat vessels, modified Blalock-Taussig shunt or rightventricle-to-pulmonary artery conduit, descending thoracicaorta, and any collateral vessels (Fig. 7). The ratio ofpulmonary-to-systemic blood flow (Qp/Qs) can also bedetermined using phase-contrast imaging. Complicationsfollowing Norwood procedure that can be detected by CMR
include branch pulmonary artery narrowing (Fig. 8), valvularregurgitation (Fig. 9), Blalock-Taussig or right ventricle-to-pulmonary artery shunt malfunction (pseudoaneurysm for-mation, stenosis, and occlusion), and aortic arch and greatvessel stenosis (Fig. 7). Our institutional CMR protocolused to evaluate children status post-Norwood procedure isdescribed in Table 1. Additional technical informationregarding the CMR imaging of HLHS can be found inAppendix.
MR allows for accurate appraisal of cardiac chamber size,shape, and function on a three-dimensional (3-D) basis,independent of mathematical assumptions that are required
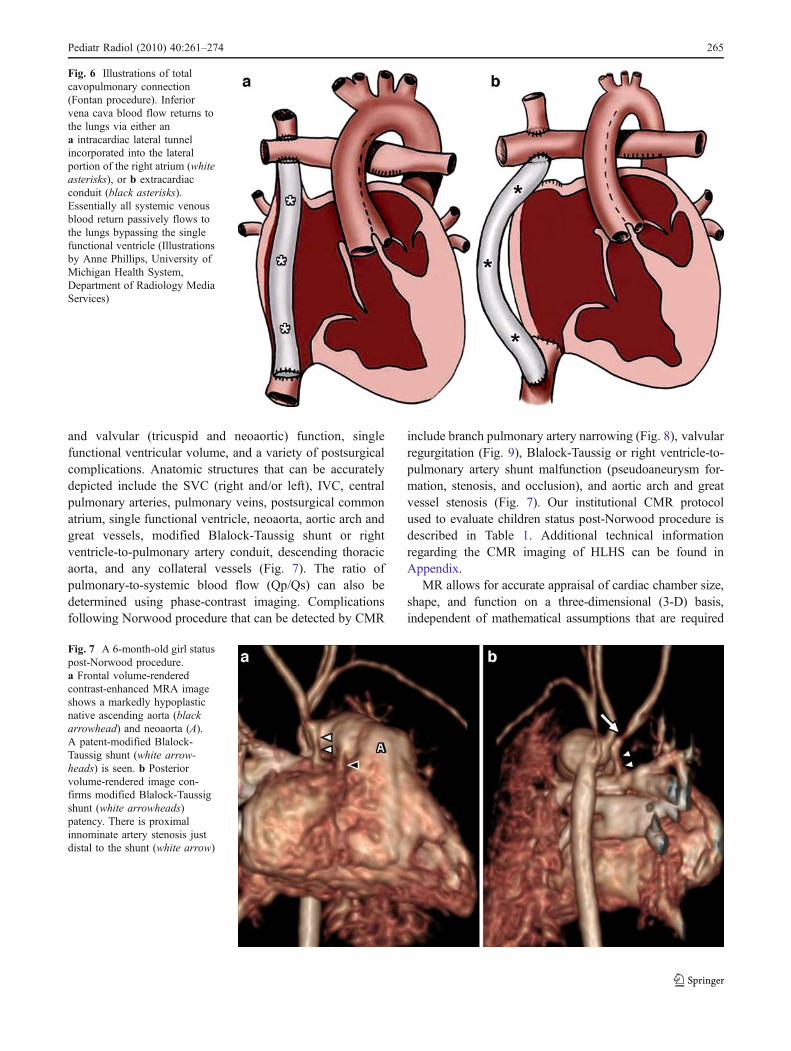
Fig. 6 Illustrations of totalcavopulmonary connection(Fontan procedure). Inferiorvena cava blood flow returns tothe lungs via either ana intracardiac lateral tunnelincorporated into the lateralportion of the right atrium (whiteasterisks), or b extracardiacconduit (black asterisks).Essentially all systemic venousblood return passively flows tothe lungs bypassing the singlefunctional ventricle (Illustrationsby Anne Phillips, University ofMichigan Health System,Department of Radiology MediaServices)
Fig. 7 A 6-month-old girl statuspost-Norwood procedure.a Frontal volume-renderedcontrast-enhanced MRA imageshows a markedly hypoplasticnative ascending aorta (blackarrowhead) and neoaorta (A).A patent-modified Blalock-Taussig shunt (white arrow-heads) is seen. b Posteriorvolume-rendered image con-firms modified Blalock-Taussigshunt (white arrowheads)patency. There is proximalinnominate artery stenosis justdistal to the shunt (white arrow)
Pediatr Radiol (2010) 40:261–274 265
for two-dimensional (2-D) echocardiography [6, 12]. Whilestudies by Altmann et al. [13] and Soriano et al. [14] showedagreement between CMR and 3-D echocardiography regard-ing estimation of single functional ventricular volumes, ejec-tion fraction, and ventricular mass, a lack of agreement wasnoted between 2-D echocardiography and both 3-D echo-cardiography and CMR [13].
Although invasive conventional angiography traditionallyhas been performed prior to BCPC creation, CMR is playingan increasingly important role in this setting. Brown et al.[15] performed a prospective randomized single-center trialcomparing CMR to conventional angiography prior to BCPCcreation. Following exclusion of patients with known pul-monary vein stenosis, pulmonary hypertension, severeventricular dysfunction, severe tricuspid valvular regurgita-tion, large aortopulmonary or venovenous collateral vessels,and aortic coarctation, 82 patients between the ages of2 months and 5 years were identified. In their study,conventional angiography was associated with longer pre-
operative hospital stay (p<0.001), increased cost (p<0.001),and increased frequency of minor adverse events (p<0.0001)[15]. Upon 3-month follow-up, there were no statisticaldifferences in clinical status, oxygen saturation, or frequencyof reintervention between the two groups [15]. The authorsconcluded that CMR is safe, effective, and a less costlyalternative to conventional angiography in select patientsprior to BCPC creation [15]. While conventional angiogra-phy has a few advantages over CMR, including thecapabilities to measure pulmonary vascular resistance andperform a variety of catheter-based therapies, Brown et al.[15] noted a general lack of evidence for the clinical benefitsof such interventions.
Another study by Muthurangu et al. [5] evaluated 37infants following Norwood procedure with CMR prior toBCPC creation. They study found that CMR has highsensitivity and specificity for both neoaortic and left pulmo-nary artery obstruction, findings typically delineated bypreoperative conventional angiography and often requiringintervention at surgery [5]. Based on their results, the authorsconcluded that CMR can be used to assess ventricular and
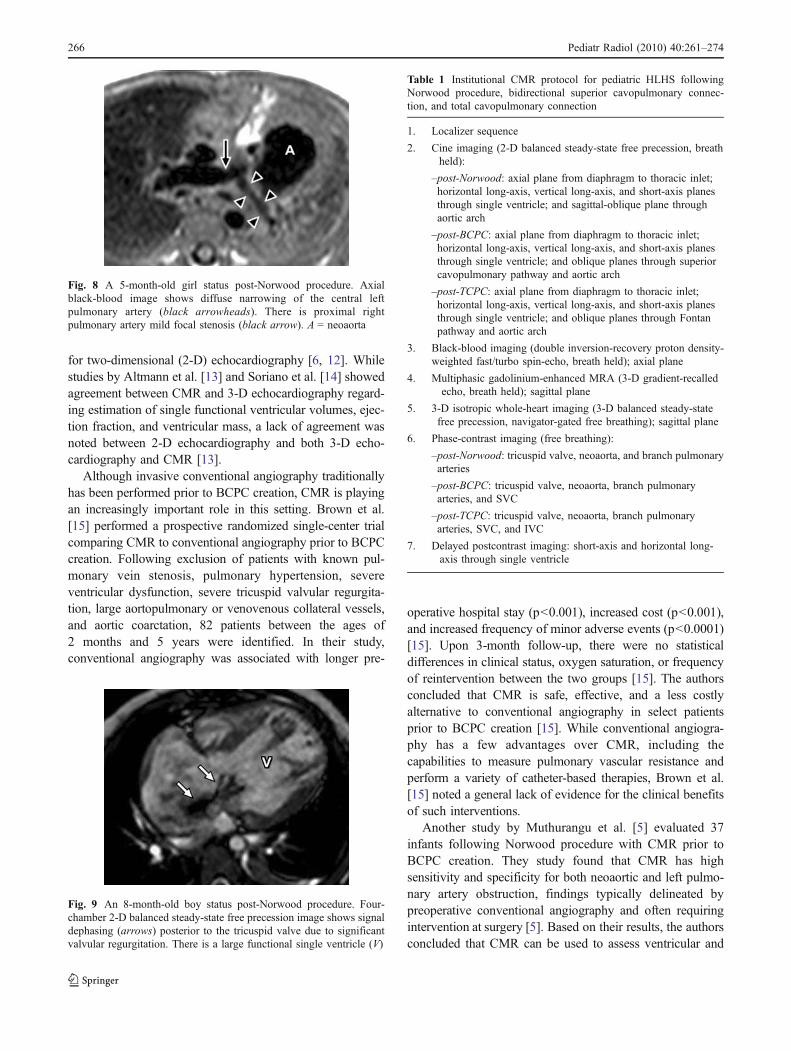
Fig. 9 An 8-month-old boy status post-Norwood procedure. Four-chamber 2-D balanced steady-state free precession image shows signaldephasing (arrows) posterior to the tricuspid valve due to significantvalvular regurgitation. There is a large functional single ventricle (V)
Fig. 8 A 5-month-old girl status post-Norwood procedure. Axialblack-blood image shows diffuse narrowing of the central leftpulmonary artery (black arrowheads). There is proximal rightpulmonary artery mild focal stenosis (black arrow). A = neoaorta
Table 1 Institutional CMR protocol for pediatric HLHS followingNorwood procedure, bidirectional superior cavopulmonary connec-tion, and total cavopulmonary connection
1. Localizer sequence
2. Cine imaging (2-D balanced steady-state free precession, breathheld):
–post-Norwood: axial plane from diaphragm to thoracic inlet;horizontal long-axis, vertical long-axis, and short-axis planesthrough single ventricle; and sagittal-oblique plane throughaortic arch
–post-BCPC: axial plane from diaphragm to thoracic inlet;horizontal long-axis, vertical long-axis, and short-axis planesthrough single ventricle; and oblique planes through superiorcavopulmonary pathway and aortic arch
–post-TCPC: axial plane from diaphragm to thoracic inlet;horizontal long-axis, vertical long-axis, and short-axis planesthrough single ventricle; and oblique planes through Fontanpathway and aortic arch
3. Black-blood imaging (double inversion-recovery proton density-weighted fast/turbo spin-echo, breath held); axial plane
4. Multiphasic gadolinium-enhanced MRA (3-D gradient-recalledecho, breath held); sagittal plane
5. 3-D isotropic whole-heart imaging (3-D balanced steady-statefree precession, navigator-gated free breathing); sagittal plane
6. Phase-contrast imaging (free breathing):
–post-Norwood: tricuspid valve, neoaorta, and branch pulmonaryarteries
–post-BCPC: tricuspid valve, neoaorta, branch pulmonaryarteries, and SVC
–post-TCPC: tricuspid valve, neoaorta, branch pulmonaryarteries, SVC, and IVC
7. Delayed postcontrast imaging: short-axis and horizontal long-axis through single ventricle
266 Pediatr Radiol (2010) 40:261–274
vascular anatomy following Norwood procedure and canreplace conventional angiography with good postoperativeoutcomes [5].
Imaging of bidirectional superior cavopulmonaryconnection
CMR has also shown value in the assessment of children whohave undergone BCPC creation prior to the Fontan operation.Similarly to CMR performed following Norwood operationprior to BCPC, the overall goal of imaging at this stage is toassess cardiovascular anatomy, ventricular and valvular(tricuspid and neoaortic) function, single functional ventric-ular volume, and any postsurgical complications. At thisstage, dedicated imaging of the SVC-to-pulmonary arteryanastomosis should also be performed. CMR protocol shouldbe tailored particularly to evaluate systemic venous return,pulmonary artery size and configuration, valvular compe-tency, ventricular function, and aortic anatomy, as these arefactors that can influence the decision to proceed with Fontanpalliation. Our institutional CMR protocol used to evaluatechildren status post-BCPC is described in Table 1.
BCPC pathway patency and flow can be thoroughlyevaluated using a variety of CMR techniques, includingblack-blood, 2-D and 3-D balanced steady-state freeprecession, phase-contrast, and gadolinium-enhanced mag-netic resonance angiography (MRA) imaging sequences.The SVC, pulmonary arteries, and cavopulmonary anasto-mosis are exquisitely depicted by MRI (Figs. 10 and 11).Complications following BCPC creation that may bedetected by CMR include branch pulmonary artery narrow-ing (Figs. 10 and 11), valvular regurgitation, aortic arch andgreat vessel stenosis (Fig. 10), BCPC pathway narrowing,
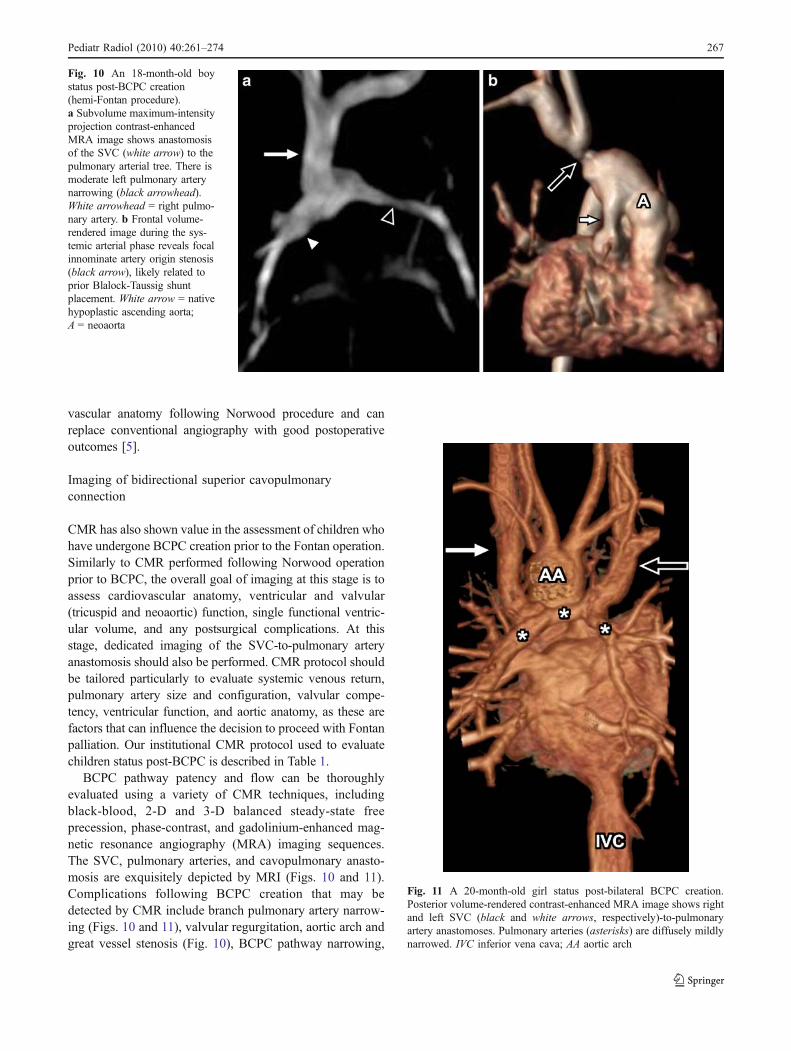
Fig. 10 An 18-month-old boystatus post-BCPC creation(hemi-Fontan procedure).a Subvolume maximum-intensityprojection contrast-enhancedMRA image shows anastomosisof the SVC (white arrow) to thepulmonary arterial tree. There ismoderate left pulmonary arterynarrowing (black arrowhead).White arrowhead = right pulmo-nary artery. b Frontal volume-rendered image during the sys-temic arterial phase reveals focalinnominate artery origin stenosis(black arrow), likely related toprior Blalock-Taussig shuntplacement. White arrow = nativehypoplastic ascending aorta;A = neoaorta
Fig. 11 A 20-month-old girl status post-bilateral BCPC creation.Posterior volume-rendered contrast-enhanced MRA image shows rightand left SVC (black and white arrows, respectively)-to-pulmonaryartery anastomoses. Pulmonary arteries (asterisks) are diffusely mildlynarrowed. IVC inferior vena cava; AA aortic arch
Pediatr Radiol (2010) 40:261–274 267
and systemic venous-to-systemic venous collateral vesselformation.
Knowledge of pulmonary artery size and anatomy prior tothe Fontan operation is thought to be particularly important as“one of the most powerful risk factors for death or takedownof the Fontan operation was the dimensions of the right andleft pulmonary arteries” based on a study of 334 patientsundergoing the Fontan operation [16]. In a study by Julsrudet al. [17], 53 patients were evaluated with CMR prior to amodified Fontan operation. In their study, MRI accuratelydepicted 97% of pulmonary arteries, 95% of pulmonaryveins, and 98% of systemic veins when compared toconventional angiography or surgery [17]. A study of 36patients at differing stages of HLHS surgical palliation(pre- and post-BCPC and post-Fontan) used CMR axialT1-weighted imaging to successfully detect five of fivenonconfluent branch pulmonary arteries and six of sixpulmonary artery stenoses [18]. In their study, 2-D echocar-diography with color Doppler failed to detect any instance ofnonconfluent branch pulmonary arteries and detected onlytwo of six pulmonary artery stenoses [18]. The authorsconsequently concluded that CMR is a useful, noninvasivetool that may be used to determine pulmonary artery size andconfluency, may prevent the need for cardiac catheterization,and may provide knowledge that directly affects surgicaldecision-making [18].
Imaging of total cavopulmonary connection
CMR serves a variety of purposes following the Fontanoperation. Perhaps most importantly, it can be used to thor-oughly evaluate the Fontan pathway (Figs. 12, 13 and 14). In
addition to establishing Fontan pathway patency and patternof blood flow, CMR can recognize an assortment of relatedcomplications, including pathway stenosis (Fig. 14), dilata-tion, and leak. CMR is also particularly useful in the detec-tion of intraluminal Fontan pathway and central pulmonaryartery thrombus (Fig. 15) [19]. Thrombus can be detectedusing a variety of MR imaging techniques, including black-
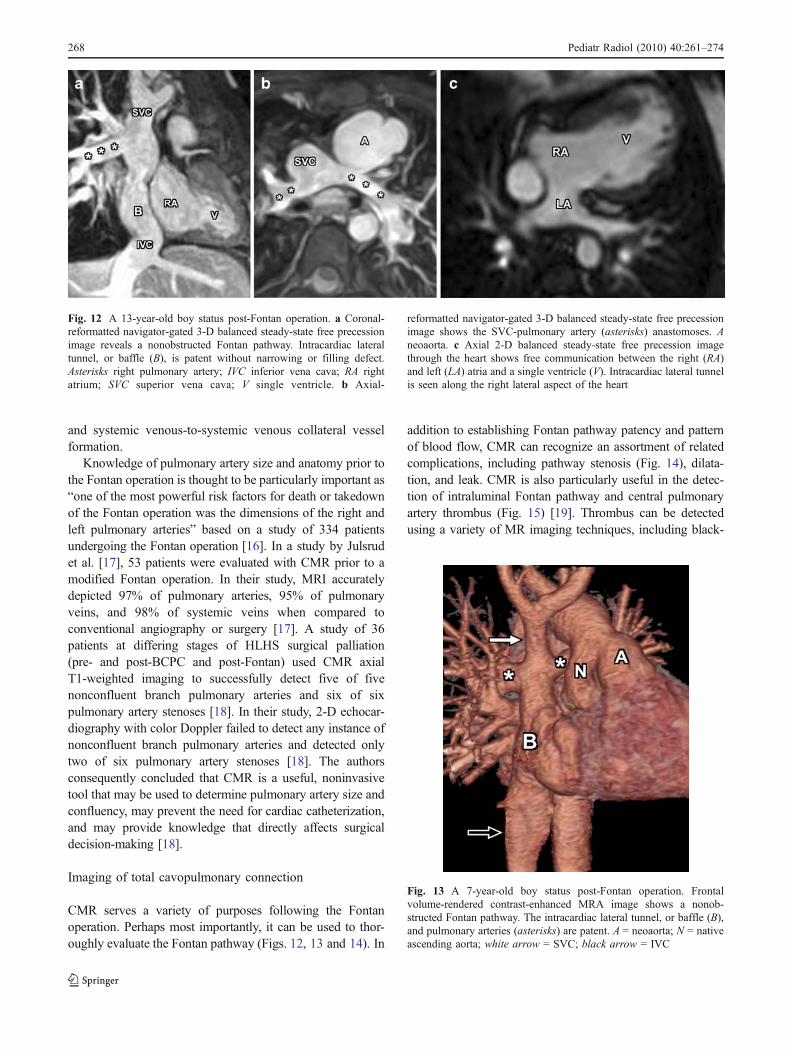
Fig. 13 A 7-year-old boy status post-Fontan operation. Frontalvolume-rendered contrast-enhanced MRA image shows a nonob-structed Fontan pathway. The intracardiac lateral tunnel, or baffle (B),and pulmonary arteries (asterisks) are patent. A = neoaorta; N = nativeascending aorta; white arrow = SVC; black arrow = IVC
Fig. 12 A 13-year-old boy status post-Fontan operation. a Coronal-reformatted navigator-gated 3-D balanced steady-state free precessionimage reveals a nonobstructed Fontan pathway. Intracardiac lateraltunnel, or baffle (B), is patent without narrowing or filling defect.Asterisks right pulmonary artery; IVC inferior vena cava; RA rightatrium; SVC superior vena cava; V single ventricle. b Axial-
reformatted navigator-gated 3-D balanced steady-state free precessionimage shows the SVC-pulmonary artery (asterisks) anastomoses. Aneoaorta. c Axial 2-D balanced steady-state free precession imagethrough the heart shows free communication between the right (RA)and left (LA) atria and a single ventricle (V). Intracardiac lateral tunnelis seen along the right lateral aspect of the heart
268 Pediatr Radiol (2010) 40:261–274
blood 2-D and 3-D balanced steady-state free precession,time-of-flight, and 3-D contrast-enhanced MRA pulsesequences.
Additional applications of CMR following TCPC includeappraisal of cardiovascular anatomy, ventricular and valvular(tricuspid and neoaortic) function, single functional ventric-ular volume, and a variety of non-Fontan pathway-relatedcomplications. Non-Fontan pathway-related complicationsfollowing TCPC creation that can be detected by CMRinclude branch pulmonary artery narrowing, neoaortic dila-tation (Fig. 16), aortic and great vessel stenosis (Fig. 17),valvular regurgitation (Fig. 18), and development ofsystemic venous-to-pulmonary venous collaterals (a causeof persistent hypoxemia and cyanosis) (Fig. 19) [4]. Ourinstitutional CMR protocol used to evaluate children statuspost-TCPC creation is described in Table 1.
One potential limitation of CMR in the evaluation ofsurgically palliated HLHS patients is the presence ofimplanted metal-related artefact. Artefact may arise fromstructures such as metallic sternal wires, vascular emboliza-tion coils, and vascular stents. In a study by Garg et al. [20],101 consecutive Fontan patients were evaluated for theeffects of metallic endovascular implants on the ability ofCMR to assess both cardiovascular anatomy and ventricularsize and function. Metallic endovascular implants werepresent in 54% of these CMR examinations. Seventy-sevenpercent of anatomic segments were adequately imaged inpatients with such implants compared to 100% of anatomicsegments in patients without such implants (p<0.001) [20].A statistically significant difference was also observed in theability to assess ventricular function between the two patientgroups (p<0.001) [20].
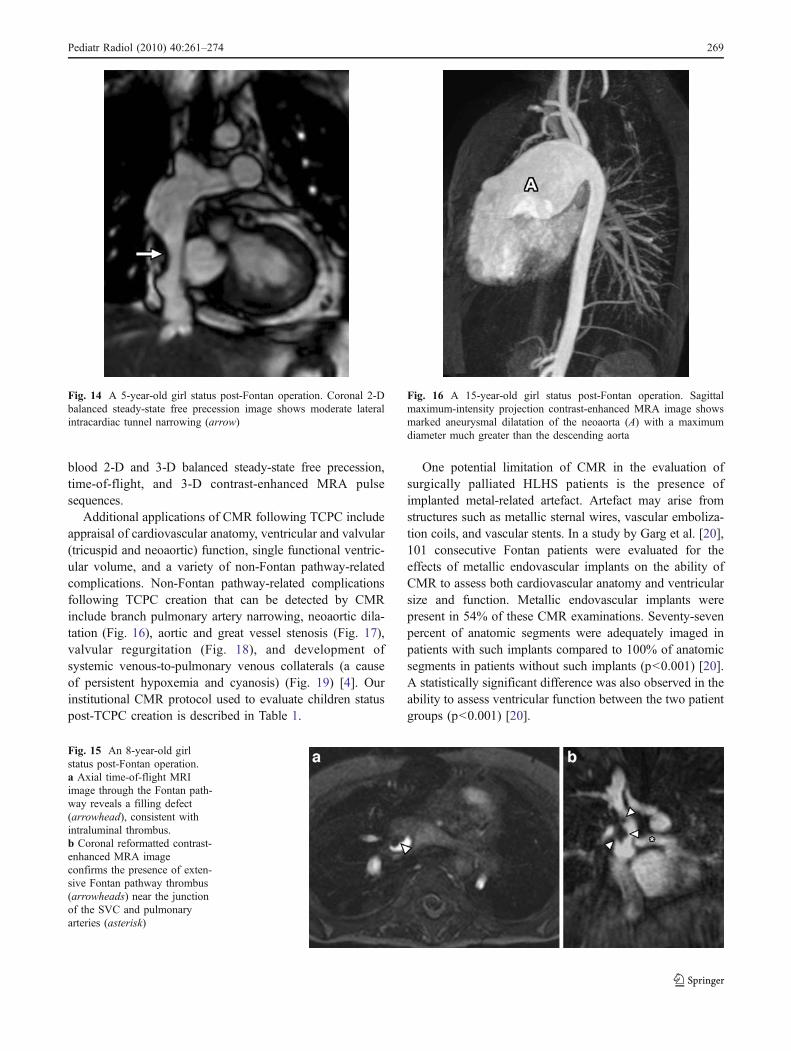
Fig. 14 A 5-year-old girl status post-Fontan operation. Coronal 2-Dbalanced steady-state free precession image shows moderate lateralintracardiac tunnel narrowing (arrow)
Fig. 15 An 8-year-old girlstatus post-Fontan operation.a Axial time-of-flight MRIimage through the Fontan path-way reveals a filling defect(arrowhead), consistent withintraluminal thrombus.b Coronal reformatted contrast-enhanced MRA imageconfirms the presence of exten-sive Fontan pathway thrombus(arrowheads) near the junctionof the SVC and pulmonaryarteries (asterisk)
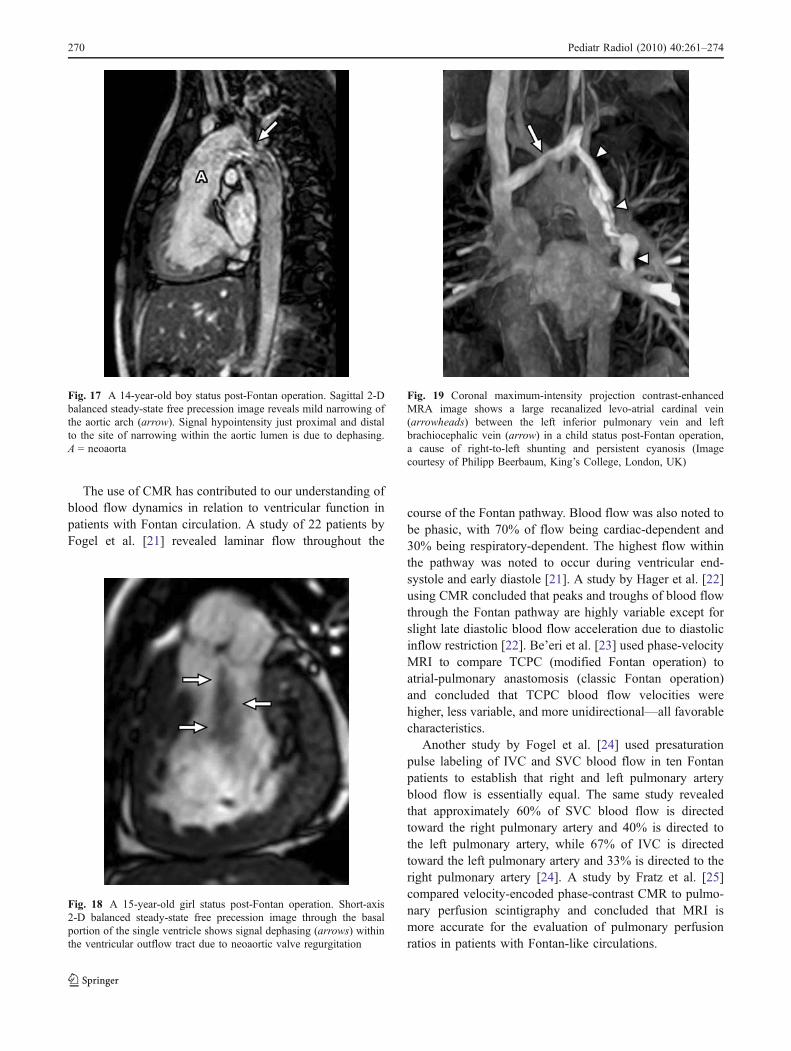
Fig. 16 A 15-year-old girl status post-Fontan operation. Sagittalmaximum-intensity projection contrast-enhanced MRA image showsmarked aneurysmal dilatation of the neoaorta (A) with a maximumdiameter much greater than the descending aorta
Pediatr Radiol (2010) 40:261–274 269
The use of CMR has contributed to our understanding ofblood flow dynamics in relation to ventricular function inpatients with Fontan circulation. A study of 22 patients byFogel et al. [21] revealed laminar flow throughout the
course of the Fontan pathway. Blood flow was also noted tobe phasic, with 70% of flow being cardiac-dependent and30% being respiratory-dependent. The highest flow withinthe pathway was noted to occur during ventricular end-systole and early diastole [21]. A study by Hager et al. [22]using CMR concluded that peaks and troughs of blood flowthrough the Fontan pathway are highly variable except forslight late diastolic blood flow acceleration due to diastolicinflow restriction [22]. Be’eri et al. [23] used phase-velocityMRI to compare TCPC (modified Fontan operation) toatrial-pulmonary anastomosis (classic Fontan operation)and concluded that TCPC blood flow velocities werehigher, less variable, and more unidirectional—all favorablecharacteristics.
Another study by Fogel et al. [24] used presaturationpulse labeling of IVC and SVC blood flow in ten Fontanpatients to establish that right and left pulmonary arteryblood flow is essentially equal. The same study revealedthat approximately 60% of SVC blood flow is directedtoward the right pulmonary artery and 40% is directed tothe left pulmonary artery, while 67% of IVC is directedtoward the left pulmonary artery and 33% is directed to theright pulmonary artery [24]. A study by Fratz et al. [25]compared velocity-encoded phase-contrast CMR to pulmo-nary perfusion scintigraphy and concluded that MRI ismore accurate for the evaluation of pulmonary perfusionratios in patients with Fontan-like circulations.
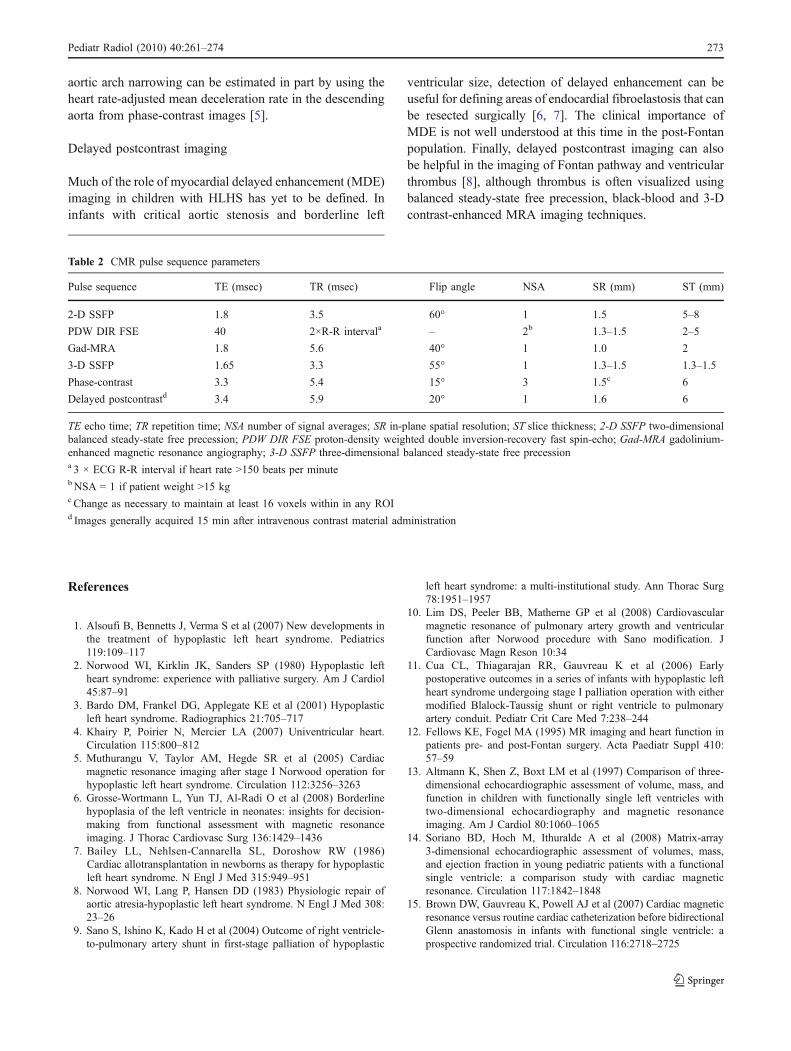
Fig. 19 Coronal maximum-intensity projection contrast-enhancedMRA image shows a large recanalized levo-atrial cardinal vein(arrowheads) between the left inferior pulmonary vein and leftbrachiocephalic vein (arrow) in a child status post-Fontan operation,a cause of right-to-left shunting and persistent cyanosis (Imagecourtesy of Philipp Beerbaum, King’s College, London, UK)
Fig. 18 A 15-year-old girl status post-Fontan operation. Short-axis2-D balanced steady-state free precession image through the basalportion of the single ventricle shows signal dephasing (arrows) withinthe ventricular outflow tract due to neoaortic valve regurgitation
Fig. 17 A 14-year-old boy status post-Fontan operation. Sagittal 2-Dbalanced steady-state free precession image reveals mild narrowing ofthe aortic arch (arrow). Signal hypointensity just proximal and distalto the site of narrowing within the aortic lumen is due to dephasing.A = neoaorta
270 Pediatr Radiol (2010) 40:261–274

CMR can also be used to assess ventricular mass,volume, and systolic function accurately following a Fontanoperation. A study of 23 individuals status post-Fontanpalliation with a mean age of 19.4 years revealed normalventricular mass and volume when compared to the leftventricles of healthy volunteers [26]. Median ejectionfraction following the Fontan operation was 49.3% com-pared to 64.8% in the healthy volunteers (p=0.00001),causing the authors to conclude that long-term survivorshave depressed systolic ventricular function [26].
Conclusion
CMR can be used to accurately evaluate cardiovascularanatomy and function in children with untreated andsurgically palliated HLHS. This imaging modality is comple-mentary to echocardiography, does not require ionizingradiation, and, in select patients, may obviate the need forinvasive conventional angiography. CMR is particularlyuseful for assessing single ventricle and valvular function,extracardiac vascular anatomy, and a variety of complications.Information acquired byCMR can directly influence decision-making in the HLHS surgical palliative process, including thedecisions to perform a univentricular versus biventricularrepair and whether or not to proceed to BCPC or TCPC.
Appendix
CMR imaging technique in HLHS: how we do it
Numerous MR imaging techniques and pulse sequences areavailable for the comprehensive assessment of cardiovas-cular morphology and function in congenital heart disease,including hypoplastic left heart syndrome (HLHS). Thecardiovascular MR (CMR) examination should begin witha review of available prior clinical and surgical medicalrecords and imaging data for each patient. The imagingexamination should be tailored to answer the specificquestions posed by the referring clinician in as an efficientmanner as possible in order to minimize scan time. Themajority of patients younger than 8 years of age referred forCMR will require either general anesthesia with endotra-cheal intubation due to pulse sequences that necessitatebreath-holding or intravenous deep sedation with pulsesequences modified for free-breathing. Dedicated cardiacphased-array multi-element surface coils with parallelimaging capabilities are typically used for older childrenand adults, while multi-element knee coils can be used ininfants and younger children with good results.
The CMR examination typically begins with the acqui-sition of non-gated two-dimensional (2-D) balanced steady-
state free precession (SSFP) localizer images in the coronal,axial and sagittal planes that cover the entire chest andupper abdomen. These localizer images provide a basicoverview of situs (cardiac and visceral) and cardiovascularanatomy as well as serve as the basis for establishing planesof imaging throughout the examination. Alternatively,many newer MRI scanners are now equipped with real-time interactive gradient echo sequences that can be usedwithout breath-holding to construct quickly all imagingplanes that will be needed for a given CMR examination.Using this technique, the specific imaging geometries canbe labeled and stored prior to performing higher qualitybreath-hold images, and they can be quickly accessed atany time during the examination.
Anatomic imaging
Two-dimensional SSFP imaging sequences are the main-stay of CMR anatomic imaging in children with HLHS.This pulse sequence provides bright blood cine images withexcellent myocardium-to-blood pool contrast and fastacquisition times. Our protocol typically begins with anaxial 2-D SSFP imaging series extending from thediaphragm through the thoracic inlet. These images providean initial overview of cardiovascular anatomy. Cine 2-DSSFP imaging series are acquired in the vertical long-axis,horizontal long-axis, and short-axis of the ventricle(s) inorder to further assess cardiac anatomy. Additional obliqueimaging series are then acquired through the aortic arch,superior cavopulmonary pathway, and Fontan pathwaybased upon the clinical needs of a given patient. Cine 2-DSSFP imaging series are ECG gated, typically contain 20 to30 cardiac cycle phases, and have a temporal resolution of20–50 msec. We do not generally use parallel processingimaging techniques for 2-D SSFP imaging sequences. Thebreath-hold time for a single slice (20–30 images) is usuallybetween 8 and 14 s. Breath holds are performed in end-expiration for better reproducibility of diaphragm position.
Additional anatomic imaging is performed using a double-inversion recovery fast (turbo) spin-echo (FSE or TSE) pulsesequence with proton-density weighting. These static black-blood images have better spatial resolution than balancedsteady-state free precession images and are less susceptible tometal-related artifact, which is particularly important in thispatient population. They provide useful anatomic imagingregarding blood vessel walls, small pulmonary arteries andveins, and the relationship of vascular structures to theairway. We do not typically use parallel processing tech-niques for black-blood imaging, and the breath-hold time fora single slice is usually between 10 and 15 s. As withbalanced steady-state free precession imaging sequences,breath holds are performed in end-expiration for betterreproducibility of diaphragm position.
Pediatr Radiol (2010) 40:261–274 271

Thoracic extracardiac vascular structures are depicted inexcellent detail using contrast-enhanced MR angiography(MRA). We specifically use a three-dimensional (3-D)gradient-recalled echo pulse sequence with radiofrequency(RF) spoiling following the intravenous injection of 0.1–0.2 mmol/kg of gadolinium-based contrast material (we useeither gadopentetate dimeglumine [Magnevist; BayerHealthCare, Wayne, NJ] or gadoteridol [ProHance; BraccoDiagnostics, Princeton, NJ]). A field-of-view covering theregion of interest is chosen, and images are acquired in thesagittal plane. The breath-hold time for a single 3-D volumeis typically between 20 and 25 s, and imaging is usuallyperformed during end-inspiration without ECG gating. Forchildren being imaged under general anesthesia, the breathhold can be performed in whatever phase of the respiratorycycle is safest for a given patient’s physiology. Theseimages have excellent spatial, contrast-to-noise, and signal-to-noise resolution for thoracic extracardiac vascular struc-tures. The 3-D isotropic data set can be reformatted in anyplane, and it allows for the creation of a variety of 3-Dreconstructions [(most commonly maximum intensity pro-jection [MIP] and volume-rendered images)].
Isotropic 3-D SSFP imaging is a newly developed pulsesequence that can be used to evaluate intracardiac andextracardiac anatomy as well as the coronary arteries incomplex congenital heart disease [1–3]. This imagingtechnique does not require the administration of intravenouscontrast material. A chemically selective fat saturationprepulse can be used to increase the contrast betweenblood, fat, and myocardium. A field of view covering theregion of interest is chosen, and images are acquired in thesagittal plane. ECG gating is used to acquire images whenthe heart is relatively motionless, usually during the periodof diastasis between early diastolic filling and atrial systole,or sometimes with higher heart rates at end-ventricularsystole. Imaging is performed during free breathing withrespiratory navigator gating. The 3-D isotropic data set canbe reformatted in any plane, and it allows for the creation ofa variety of 3-D reconstructions (most commonly MIP andvolume-rendered images).
Assessment of ventricular volume and function
Ventricular function can be assessed both subjectively andobjectively using cine 2-D SSFP imaging. Subjective orqualitative assessment of ventricular function can be per-formed using a combination of vertical long-axis, horizontallong-axis, and short-axis images. Wall motion and myocar-dial thickening can be assessed using these images.
The objective or quantitative assessment of ventricularfunction and volume is performed using a stack of short-axis cine images through the entire ventricle (30 imagingphases per cardiac cycle). We typically use a slice thickness
of 6–8 mm, with 12 slices usually sufficient to cover theventricle. Care must be taken to include the entire ventriclein the stack and not exclude portions of the ventricular apexor base. Using a dedicated computer program on a separateworkstation, the endocardial surface of the ventricularcavity is traced on all short-axis images during both end-diastole and end-systole. The ventricular cavity area of eachslice is then multiplied by slice thickness to acquire avolume (ml), and the volumes from each slice are thensummated to obtain end-diastolic and end-systolic ventric-ular cavity volumes (ml). These volumes are then used tocalculate ejection fraction [ end�diastolic volume�end�½ðsystolic volume�=end�diastolic volume � 100% Þ].
Phase contrast imaging
The assessment of blood flow direction and velocity usingvelocity-encoded phase contrast imaging is essential in thecomplete CMR appraisal of children with HLHS. This pulsesequence can be used to evaluate blood flow across thetricuspid and neoaortic valves, pulmonary arteries, Fontanpathway, and any area of abnormal aortic narrowing. Prior toassessing blood flow using this pulse sequence, the user mustselect an encoding velocity (VENC), a velocity just above theexpected blood flow maximum velocity in a given region ofinterest (ROI). If the blood flow velocity in an ROI is greaterthan the VENC, aliasing will occur [4].
Phase contrast imaging of the tricuspid and neoaorticvalves is generally performed to evaluate for regurgitation.When evaluating the tricuspid and neoaortic valves, ROIsare placed just beyond the valve plane in the right ventricleand proximal neoaorta, respectively. Phase contrast imagingof the neoaorta can also be used to determine stroke volumeand cardiac output in post-Fontan patients.
Phase contrast imaging of the pulmonary arteries can beused to assess differential blood flow to each lung. Addition-ally, an ROI can be placed distal to an area of branchpulmonary artery stenosis to estimate a pressure gradientacross the narrowing and determine clinical significance andneed for intervention. Blood flow measurements from ROIsplaced in the neoaorta and central pulmonary arteries can beused to determine the ratio of systemic to pulmonary bloodflow (Qp:Qs) in post-Fontan patients.
In children with Fontan circulation, blood flow throughthe total cavopulmonary pathway can be assessed by phasecontrast imaging by placing ROIs in the inferior vena cava(IVC) and superior vena cava (SVC). This assesses theproportion of venous return via the IVC and SVC, and is analternative method to measure systemic cardiac output. Ifthere is clinical concern for proximal aortic obstruction (forexample, aortic coarctation), an ROI should be placed in thedescending thoracic aorta near the level of the diaphragm.The hemodynamic significance of residual or recurrent
272 Pediatr Radiol (2010) 40:261–274
aortic arch narrowing can be estimated in part by using theheart rate-adjusted mean deceleration rate in the descendingaorta from phase-contrast images [5].
Delayed postcontrast imaging
Much of the role of myocardial delayed enhancement (MDE)imaging in children with HLHS has yet to be defined. Ininfants with critical aortic stenosis and borderline left
ventricular size, detection of delayed enhancement can beuseful for defining areas of endocardial fibroelastosis that canbe resected surgically [6, 7]. The clinical importance ofMDE is not well understood at this time in the post-Fontanpopulation. Finally, delayed postcontrast imaging can alsobe helpful in the imaging of Fontan pathway and ventricularthrombus [8], although thrombus is often visualized usingbalanced steady-state free precession, black-blood and 3-Dcontrast-enhanced MRA imaging techniques.
References
1. Alsoufi B, Bennetts J, Verma S et al (2007) New developments inthe treatment of hypoplastic left heart syndrome. Pediatrics119:109–117
2. Norwood WI, Kirklin JK, Sanders SP (1980) Hypoplastic leftheart syndrome: experience with palliative surgery. Am J Cardiol45:87–91
3. Bardo DM, Frankel DG, Applegate KE et al (2001) Hypoplasticleft heart syndrome. Radiographics 21:705–717
4. Khairy P, Poirier N, Mercier LA (2007) Univentricular heart.Circulation 115:800–812
5. Muthurangu V, Taylor AM, Hegde SR et al (2005) Cardiacmagnetic resonance imaging after stage I Norwood operation forhypoplastic left heart syndrome. Circulation 112:3256–3263
6. Grosse-Wortmann L, Yun TJ, Al-Radi O et al (2008) Borderlinehypoplasia of the left ventricle in neonates: insights for decision-making from functional assessment with magnetic resonanceimaging. J Thorac Cardiovasc Surg 136:1429–1436
7. Bailey LL, Nehlsen-Cannarella SL, Doroshow RW (1986)Cardiac allotransplantation in newborns as therapy for hypoplasticleft heart syndrome. N Engl J Med 315:949–951
8. Norwood WI, Lang P, Hansen DD (1983) Physiologic repair ofaortic atresia-hypoplastic left heart syndrome. N Engl J Med 308:23–26
9. Sano S, Ishino K, Kado H et al (2004) Outcome of right ventricle-to-pulmonary artery shunt in first-stage palliation of hypoplastic
left heart syndrome: a multi-institutional study. Ann Thorac Surg78:1951–1957
10. Lim DS, Peeler BB, Matherne GP et al (2008) Cardiovascularmagnetic resonance of pulmonary artery growth and ventricularfunction after Norwood procedure with Sano modification. JCardiovasc Magn Reson 10:34
11. Cua CL, Thiagarajan RR, Gauvreau K et al (2006) Earlypostoperative outcomes in a series of infants with hypoplastic leftheart syndrome undergoing stage I palliation operation with eithermodified Blalock-Taussig shunt or right ventricle to pulmonaryartery conduit. Pediatr Crit Care Med 7:238–244
12. Fellows KE, Fogel MA (1995) MR imaging and heart function inpatients pre- and post-Fontan surgery. Acta Paediatr Suppl 410:57–59
13. Altmann K, Shen Z, Boxt LM et al (1997) Comparison of three-dimensional echocardiographic assessment of volume, mass, andfunction in children with functionally single left ventricles withtwo-dimensional echocardiography and magnetic resonanceimaging. Am J Cardiol 80:1060–1065
14. Soriano BD, Hoch M, Ithuralde A et al (2008) Matrix-array3-dimensional echocardiographic assessment of volumes, mass,and ejection fraction in young pediatric patients with a functionalsingle ventricle: a comparison study with cardiac magneticresonance. Circulation 117:1842–1848
15. Brown DW, Gauvreau K, Powell AJ et al (2007) Cardiac magneticresonance versus routine cardiac catheterization before bidirectionalGlenn anastomosis in infants with functional single ventricle: aprospective randomized trial. Circulation 116:2718–2725
Table 2 CMR pulse sequence parameters
Pulse sequence TE (msec) TR (msec) Flip angle NSA SR (mm) ST (mm)
2-D SSFP 1.8 3.5 60° 1 1.5 5–8
PDW DIR FSE 40 2×R-R intervala – 2b 1.3–1.5 2–5
Gad-MRA 1.8 5.6 40° 1 1.0 2
3-D SSFP 1.65 3.3 55° 1 1.3–1.5 1.3–1.5
Phase-contrast 3.3 5.4 15° 3 1.5c 6
Delayed postcontrastd 3.4 5.9 20° 1 1.6 6
TE echo time; TR repetition time; NSA number of signal averages; SR in-plane spatial resolution; ST slice thickness; 2-D SSFP two-dimensionalbalanced steady-state free precession; PDW DIR FSE proton-density weighted double inversion-recovery fast spin-echo; Gad-MRA gadolinium-enhanced magnetic resonance angiography; 3-D SSFP three-dimensional balanced steady-state free precessiona 3 × ECG R-R interval if heart rate >150 beats per minuteb NSA = 1 if patient weight >15 kgc Change as necessary to maintain at least 16 voxels within in any ROId Images generally acquired 15 min after intravenous contrast material administration
Pediatr Radiol (2010) 40:261–274 273

16. Fontan F, Fernandez G, Costa F et al (1989) The size of thepulmonary arteries and the results of the Fontan operation. JThorac Cardiovasc Surg 98:711–724
17. Julsrud PR, Ehman RL, Hagler DJ et al (1989) Extracardiacvasculature in candidates for Fontan surgery. Radiology 173:503–506
18. Fogel MA, Donofrio MT, Ramaciotti C et al (1994) Magneticresonance and echocardiographic imaging of pulmonary arterysize throughout stages of Fontan reconstruction. Circulation90:2927–2936
19. Casolo G, Rega L, Gensini GF (2004) Detection of right atrial andpulmonary artery thrombosis after the Fontan procedure bymagnetic resonance imaging. Heart 90:825
20. Garg R, Powell AJ, Sena L et al (2005) Effects of metallicimplants on magnetic resonance imaging evaluation of Fontanpalliation. Am J Cardiol 95:688–691
21. Fogel MA, Weinberg PM, Hoydu A et al (1997) The nature offlow in the systemic venous pathway measured by magneticresonance blood tagging in patients having the Fontan operation. JThorac Cardiovasc Surgery 114:1032–1041
22. Hager A, Fratz S, Schwaiger M et al (2008) Pulmonary bloodflow patterns in patients with Fontan circulation. Ann Thorac Surg85:186–191
23. Be’eri E, Maier SE, Landzberg MJ et al (1998) In vivo evaluationof Fontan pathway flow dynamics by multidimensional phase-velocity magnetic resonance imaging. Circulation 98:2873–2882
24. Fogel MA, Weinberg PM, Rychik J et al (1999) Cavalcontribution to flow in the branch pulmonary arteries of Fontanpatients with a novel application of magnetic resonance presatu-ration pulse. Circulation 99:1215–1221
25. Fratz S, Hess J, Schwaiger M et al (2002) More accuratequantification of pulmonary blood flow by magnetic resonanceimaging than by lung scintigraphy in patients with fontancirculation. Circulation 106:1510–1513
26. Eicken A, Fratz S, Gutfried C et al (2003) Hearts late after Fontanoperation have normal mass, normal volume, and reduced systolic
function: a magnetic resonance imaging study. J Am Coll Cardiol42:1061–1065
References for Appendix
1. Sørensen TS, Körperich H, Greil GF et al (2004) Operator-independent isotropic three-dimensional magnetic resonance imagingfor morphology in congenital heart disease: a validation study.Circulation 110:163–169
2. François CJ, Tuite D, Deshpande V et al (2008) Unenhanced MRangiography of the thoracic aorta: initial clinical evaluation. AJR190:902–906
3. KrishnamMS, Tomasian A, Deshpande Vet al (2008) Noncontrast 3Dsteady-state free-precession magnetic resonance angiography of thewhole chest using nonselective radiofrequency excitation over a largefield of view: comparison with single-phase 3D contrast-enhancedmagnetic resonance angiography. Invest Radiol 43:411–420
4. Powell AJ, Geva T (2000) Blood flow measurement by magneticresonance imaging in congenital heart disease. Pediatr Cardiol 21:47–58
5. Nielsen JC, Powell AJ, Gauvreau K et al (2005) Magneticresonance imaging predictors of coarctation severity. Circulation111:622–628
6. Tworetzky W, del Nido PJ, Powell AJ et al (2005) Usefulness ofmagnetic resonance imaging of left ventricular endocardial fibro-elastosis in infants after intervention for aortic valve stenosis. Am JCardiol 96:1568–1570
7. Stranzinger E, Ensing GJ, Hernandez RJ (2008) MR findings ofendocardial fibroelastosis in children. Pediatr Radiol 38:292–296
8. Weinsaft JW, Kim HW, Shah DJ et al (2008) Detection of leftventricular thrombus by delayed-enhancement cardiovascular mag-netic resonance prevalence and markers in patients with systolicdysfunction. J Am Coll Cardiol 52:148–157
274 Pediatr Radiol (2010) 40:261–274




















