Caprospinol: moving from a neuroactive steroid to a neurotropic drug
12
Review 10.1517/13543780902762827 © 2009 Informa UK Ltd ISSN 1354-3784 265 All rights reserved: reproduction in whole or in part not permitted Caprospinol: moving from a neuroactive steroid to a neurotropic drug Laurent Lecanu † , Laurent Tillement, Georges Rammouz, Jean Paul Tillement, Janet Greeson & Vassilios Papadopoulos McGill University Health Centre, The Research Institute of the McGill University Health Centre, Montreal, Quebec, Canada In search of new drugs for Alzheimer’s disease, we departed from the classic concepts and investigated the ability of normal and Alzheimer’s disease brain to convert cholesterol to steroids, otherwise known as neurosteroids. We identified 22 R-hydroxycholesterol to be present in much lower levels in the hippocampus and frontal cortex of Alzheimer’s disease than in tissue from age-matched controls. 22 R-hydroxycholesterol was shown to protect against β-amyloid (A β 42 )-induced neurotoxicity and block the formation of A β oligomers. In search of a 22 R-hydroxycholesterol stable analog, we identified the naturally occurring heterospirostenol, (22 R,25 R)-20 α-spirost-5-en-3 β-yl hexanoate (caprospinol). The mechanism of action underlying the neuro- protective properties of caprospinol involves, first, the ability of the compound to bind A β 42 and, second, its interaction with components of the mitochon- dria respiratory chain. Samaritan Pharmaceuticals is developing caprospinol as a disease-modifying drug for the treatment of Alzheimer’s disease. Samaritan Pharmaceuticals filed for an Investigational New Drug application with the FDA in 2006. The pharmacokinetic and pharmacodynamic parts of the application were found satisfactory, and the FDA has requested that additional information is submitted in support of caprospinol’s safety prior to initiating the Phase I clinical study. Keywords: Alzheimer’s disease, amyloid peptide binding, amyloid plaques, caprospinol, disease-modifying drug, drug development, memory disorders, neurosteroids Expert Opin. Investig. Drugs (2009) 18(3):265-276 1. Introduction For a long time, the scientific community has primarily focused on improving cholinergic network dysfunction for the treatment of Alzheimer’s disease. This led to the creation of the therapeutic class of acetylcholinesterase inhibitors (AchEI), with tacrine as the class leader. The clinical benefits of tacrine were modest and hampered by its significant liver toxicity. The new generation of AchEI represented by galantamine, rivastigmine, and donepezil did not improve the delay in symptom onset compared with tacrine. The evaluation of the true benefit of these AchEI for the treatment of mild, moderate, and severe Alzheimer’s disease cases, as well as in mild cognitive impairment (MCI), has been the subject of extensive studies and consequently much discussion. A number of clinical studies claim that these three AchEI have a beneficial effect in mild to moderate Alzheimer’s disease [1-4], with these three drugs having a comparable efficacy [1]. Two studies showed that donepezil and rivastigmine efficacy is maintained over a 2- to 3-year period [5,6]. However, a 2006 Cochrane review of donepezil efficacy in Alzheimer’s disease treatment concluded that, although this AchEI is clinically effective, the treatment effects are small and not 1. Introduction 2. Caprospinol development 3. Conclusion 4. Expert opinion
Transcript of Caprospinol: moving from a neuroactive steroid to a neurotropic drug

Review
10.1517/13543780902762827 © 2009 Informa UK Ltd ISSN 1354-3784 265All rights reserved: reproduction in whole or in part not permitted
Caprospinol: moving from a neuroactive steroid to a neurotropic drug Laurent Lecanu † , Laurent Tillement , Georges Rammouz , Jean Paul Tillement , Janet Greeson & Vassilios Papadopoulos McGill University Health Centre, The Research Institute of the McGill University Health Centre, Montreal, Quebec, Canada
In search of new drugs for Alzheimer’s disease, we departed from the classic concepts and investigated the ability of normal and Alzheimer’s disease brain to convert cholesterol to steroids, otherwise known as neurosteroids. We identified 22 R -hydroxycholesterol to be present in much lower levels in the hippocampus and frontal cortex of Alzheimer’s disease than in tissue from age-matched controls. 22 R -hydroxycholesterol was shown to protect against β -amyloid (A β 42 )-induced neurotoxicity and block the formation of A β oligomers. In search of a 22 R -hydroxycholesterol stable analog, we identified the naturally occurring heterospirostenol, (22 R ,25 R )-20 α -spirost-5-en-3 β -yl hexanoate (caprospinol). The mechanism of action underlying the neuro-protective properties of caprospinol involves, first, the ability of the compound to bind A β 42 and, second, its interaction with components of the mitochon-dria respiratory chain. Samaritan Pharmaceuticals is developing caprospinol as a disease-modifying drug for the treatment of Alzheimer’s disease. Samaritan Pharmaceuticals filed for an Investigational New Drug application with the FDA in 2006. The pharmacokinetic and pharmacodynamic parts of the application were found satisfactory, and the FDA has requested that additional information is submitted in support of caprospinol’s safety prior to initiating the Phase I clinical study.
Keywords: Alzheimer’s disease , amyloid peptide binding , amyloid plaques , caprospinol , disease-modifying drug , drug development , memory disorders , neurosteroids
Expert Opin. Investig. Drugs (2009) 18 (3):265-276
1. Introduction
For a long time, the scientific community has primarily focused on improving cholinergic network dysfunction for the treatment of Alzheimer’s disease. This led to the creation of the therapeutic class of acetylcholinesterase inhibitors (AchEI), with tacrine as the class leader. The clinical benefits of tacrine were modest and hampered by its significant liver toxicity. The new generation of AchEI represented by galantamine, rivastigmine, and donepezil did not improve the delay in symptom onset compared with tacrine. The evaluation of the true benefit of these AchEI for the treatment of mild, moderate, and severe Alzheimer’s disease cases, as well as in mild cognitive impairment (MCI), has been the subject of extensive studies and consequently much discussion.
A number of clinical studies claim that these three AchEI have a beneficial effect in mild to moderate Alzheimer’s disease [1-4] , with these three drugs having a comparable efficacy [1] . Two studies showed that donepezil and rivastigmine efficacy is maintained over a 2- to 3-year period [5,6] . However, a 2006 Cochrane review of donepezil efficacy in Alzheimer’s disease treatment concluded that, although this AchEI is clinically effective, the treatment effects are small and not
1. Introduction
2. Caprospinol development
3. Conclusion
4. Expert opinion

Caprospinol: moving from a neuroactive steroid to a neurotropic drug
266 Expert Opin. Investig. Drugs (2009) 18(3)
always apparent in practice [7] . In addition, the long-term cost-effectiveness of donepezil is unknown [8,9] , and the scientific relevance of the use of AchEI to treat Alzheimer’s disease has been questioned [10,11] . Nevertheless, except for AchEI, no major advances have been made in drug development for Alzheimer’s disease. Even the beneficial effects of the low-affinity N -methyl- D -aspartate (NMDA) receptor antagonist are still unclear. Recent Cochrane reviews confirm a small beneficial effect of the NMDA receptor antagonist, memantine, at 6 months in moderate to severe Alzheimer’s disease [12,13] . On the other hand, they rule out any beneficial effect of this agent in mild to moderate Alzheimer’s disease [13] . Memantine was also shown to induce subtle psychotic symptoms in an Alzheimer’s disease patients [14] , raising concerns about this treatment.
Thus, despite substantial effort and some success [15] , there is currently no real reason to be overly optimistic about the drug development status in Alzheimer’s disease. Indeed, the widely reported failure of the vaccine, AN1792, in Phase I studies for safety reasons and more recently, of the amyloid peptide ligand/plaque formation inhibitor, tramiprosate, and the γ -secretase modulator, tarenflurbil, in Phase III studies due to lack of clinical efficacy represent major setbacks in Alzheimer’s disease drug research and develop-ment (R&D). A cross-search on PubMed and ClinicalTrials.gov databases shows that these failures are not isolated cases, with multiple failures occurring in Phase II/III studies.
In addition, some of the ongoing successful trials should be considered with caution. The first example is the Phase II trial conducted on dimebon, a broad-spectrum activity molecule developed as an anti-histaminic in the former Soviet Union in the early 1970s [16] . This Phase II study (ClinicalTrials.gov number NCT00377715) demonstrated clinical improve-ment in dimebon-treated versus placebo-treated Alzheimer’s disease patients [17] . However, the FDA has not yet validated these results, nor has it validated previous preclinical results generated in Russia or in the former Soviet Union. The second example is the now-complete Phase II trial for the γ -secretase inhibitor, LY540139, performed on 45 patients with mild to moderate Alzheimer’s disease. The primary outcome measures were safety and tolerability, while the secondary outcome measures were amyloid peptide levels in the blood and cerebro-spinal fluid (CSF), changes in thinking and memory, changes in daily living activities, and pharmacokinetics (ClinicalTrials.gov number NCT00244322). Surprisingly, when the results of this Phase II trial were published [18] , no data related to cognitive improvement were reported, whereas the data related to the secondary outcomes were extensively discussed. Since cognitive performance is still the primary outcome for Alzheimer’s disease, the lack of such information for LY450139 raises concerns about the true clinical efficacy of this drug in Alzheimer’s disease. Considering these observations, finding a treatment – and, eventually, a cure – is critical.
Difficulty in finding an Alzheimer’s disease treatment arises from lack of knowledge of the origin of this disease.
Although the etiology of the familial form of Alzheimer’s disease is known, that of the sporadic form, which represents 95% of the cases, remains unidentified [19] . Consequently, most animal models currently used in the proof-of-concept stage of preclinical studies in Alzheimer’s disease R&D were developed based on knowledge acquired from studying the familial form of the disease. This represents a second obstacle in finding effective treatments, as these models have limited usefulness for studying the sporadic form of the disease and as an investigational tool in drug development. A third obstacle lies in the multiplicity of the deleterious pathways that are activated during the progression of the disease, probably at distinct time points. These multiple pathways explain the limited efficacy of the classical single-target drugs. Future treatments for Alzheimer’s disease will necessarily include drugs aimed at different targets. Alternatively, in accord with the current trend, they will evolve toward the development of compounds [20] that target several mechanisms leading to different pathological endpoints.
Here, we will review the drug candidate, caprospinol, an analog of the neurosteroid 22 R -hydroxycholesterol, and its potential as a disease-modifying drug for the treatment of Alzheimer’s disease.
2. Caprospinol development
2.1 Caprospinol mechanism of action: pharmacology 2.1.1 Caprospinol discovery 22 R -hydroxycholesterol ( Figure 1 ) is a steroid intermediate formed during the conversion of cholesterol to pregnenolone, a reaction catalyzed by cytochrome P450 C27 side chain cleavage (P450scc, CYP11A1) [21] . We have previously shown that in Alzheimer’s disease, 22 R -hydroxycholesterol is present at lower levels in the hippocampus and frontal cortex of the brain than in these brain regions of age-matched controls, and that this substance protects against cell death induced by amyloid β -peptide (A β ) in both rat sympathetic nerve pheochromocytoma (PC12) cells and differentiated human NT2N neurons [22] . The effect of 22 R -hydroxycholesterol is stereospecific, as its enantiomer 22 S -hydroxycholesterol fails to protect the neurons from A β -induced cell death. Moreover, the protective effect of this steroid is specific for A β -induced cell death, as it does not protect against glutamate-induced neurotoxicity.
In search of the mechanism underlying 22 R -hydroxy-cholesterol action, we found that 22 R -hydroxycholesterol binds to A β and that the resulting 22 R -hydroxycholesterol-A β complex is not toxic to rodent and human neurons [22] . Although the theoretical use of 22 R -hydroxycholesterol to treat Alzheimer’s disease is highly attractive, the fact that 22 R -hydroxycholesterol is an intermediate of pregnenolone synthesis indicates that it will be rapidly metabolized to a final steroid product by the major steroid-synthesizing endocrine systems (i.e., adrenals and gonads) and produce

Lecanu, Tillement, Rammouz, Tillement, Greeson & Papadopoulos
Expert Opin. Investig. Drugs (2009) 18(3) 267
steroid-related side effects. This makes development of 22 R -hydroxycholesterol as a drug unlikely.
To circumvent this pitfall, we used the 22 R -hydroxycholesterol chemical structure as a probe to screen naturally occurring compound databases. This ultimately led to the identification of caprospinol [23] ( Figure 1 ). Caprospinol [diosgenin 3-caproate; (22 R ,25 R )-20 α -spirost-5-en-3 β -yl hexanoate] is a heterospirostenol that occurs naturally in Gynura japonica , a plant from the Asteraceae family.
2.1.2 Caprospinol and A b 1 – 42 The first in vitro experiments conducted in rat pheochromo-cytoma PC12 cells revealed that caprospinol protects against neurotoxicity induced by the soluble amyloid species, A β 1 – 42 [23] . This effect is dose-dependent and is observed against increasing concentrations of A β 1 – 42 . The neuro-protective effect of caprospinol is more potent than that observed for 22 R -hydroxycholesterol in PC12 and human neuronal NT2 cells [22] . The neuroprotective properties of 22 R -hydroxycholestol are attributed to the ability of this neurosteroid to bind and inactivate A β 1 – 42 [22] . The kinetics of amyloid peptide aggregation and plaque formation are
still unresolved, but recent studies suggest that A β 1 – 42 first aggregates into what has been defined as critical oligomers [24] , probably corresponding to the previously identified amyloid-derived diffusible ligands (ADDLs) [25] . ADDLs are non-fibrillar oligomers with an approximate size range of 13 – 108 kDa [26] ; they are highly neurotoxic [26-28] . These critical oligomers assemble into protofibrils and then into fibrils. The conformational transition of amyloid peptide into β -sheets may occur during fibril formation in vivo .
Different strategies have been used to develop compounds that might prevent fibril formation and ultimately, plaque formation [29] . The resulting compounds differ in their chemical structure, as well as the amyloid species to which they bind. Binding studies show that caprospinol partially displaces 3 H-22 R -hydroxycholesterol from its binding site on amyloid peptide [23] , demonstrating for the first time that caprospinol might share part of the 22 R -hydroxycholesterol mechanism of action. Further molecular modeling studies confirmed the presence of a binding site for caprospinol on A β 1 – 42 [30] ( Figure 2 ). However, the binding site appeared to be different from that for 22 R -hyroxycholesterol. Indeed, 22 R -hydroxycholesterol was initially reported to bind A β 1 – 42
HO
OH
O
O
O
O
22R-hydroxycholesterol
CaprospinolDiosgenin 3-caproate(22R,25R)-20α-spirost-5-en-3β-yl hexanoate
Figure 1 . Chemical formulas of caprospinol and 22 R -hydroxycholesterol.

Caprospinol: moving from a neuroactive steroid to a neurotropic drug
268 Expert Opin. Investig. Drugs (2009) 18(3)
between residues 19 – 36 [22] , whereas the caprospinol binding site is located in a pocket formed between residues 23 – 42 [29] .
This limited, 13-amino acid overlap between the binding sites might explain why caprospinol only partially displaces 22 R -hydroxycholesterol from its binding site, and this slight difference in binding might be responsible of differences in the mechanisms of action. Indeed, as previously reported, 22 R -hydroxycholesterol binding to the monomeric A β 1 – 42 does not affect oligomerization of the peptide [22] , and the neuroprotective effect of 22 R -hydroxycholesterol is probably due to a conformational change in the monomeric and oligomeric form of the amyloid species. On the other hand, caprospinol inhibits the formation of highly neurotoxic ADDLs in a dose-dependent manner [23] . Moreover, capros-pinol decreases the amount of monomers available for ADDL formation, further suggesting that this compound binds to both oligomeric and monomeric amyloid species.
We recently investigated the in vivo effect of caprospinol on a pharmacological, non-transgenic, Alzheimer’s disease rat model [31] . A 4-week treatment of caprospinol (10 mg/kg once a day, intraperitoneal injection) almost completely eliminated the amyloid deposits present in the hippo-campus. To better reproduce the situations encountered clinically, we started treatment at a time when the animals displayed a severe Alzheimer’s disease phenotype, which has been previously described by our group [23] . Caprospinol was not only able to clear existing amyloid plaques present in the hippocampus, but also able to prevent the formation of new ones. Caprospinol was also able to remove and prevent intraneuronal A β 1 – 42 deposition aggregation.
These findings are extremely interesting given that intra-neuronal A β 1 – 42 accumulation is an early event in Alzheimer’s disease and Down’s syndrome, and occurs prior to A β 1 – 42 aggregation and plaque formation [32-35] . However, the fate of the caprospinol-bound amyloid remains to be determined. Whether the caprospinol A β 1-42 complex is eliminated through the blood–brain barrier into the arterial blood or
Figure 2 . Computational fl exible docking of caprospinol on A b 1 – 42 . The binding site corresponds to the amino acids 23 – 42.
via the cerebrospinal fluid into the venous blood is unknown. Likewise, whether caprospinol favors the amyloid degradation within the brain tissue remains to be established. However, we can hypothesize that since caprospinol prevents A β 1-42 polymerization into higher species, most of the amyloid is kept into the monomeric form, and is therefore available for all or some of the clearing pathways that normally process A β 1-42 in the brain.
Others have studied naturally occurring compounds such as the polyphenolic compound, catechin gallate. The hypothesis that tea consumption may reduce the risk of age-related neurodegenerative pathologies justified an interest in the polyphenolic compounds present in black and green teas. Interestingly, epigallocatechin gallate is the most active flavan-3-ol in protecting cultured neuronal cells against A β 1 – 42 and A β 25 – 35 neurotoxicity, and it prevents the formation of ADDLs [36] . Another phenolic compound, curcumin, reduces plaque formation and amyloid burden in the brains of Tg2576 mice treated intravenously with this compound until they reach 22 months of age [37] . Even more interesting, two clinical trials showed that the well-characterized Ginkgo biloba extract, EGb761, is efficacious in the treatment of mild to moderate Alzheimer’s disease [38,39] . It also rescues cultured neuronal cells from β -amyloid-induced death by preventing A β 1 – 42 aggregation and ADDL formation [40] . However, in a recent Phase IV clinical trial conducted to assess the effect of EGb761 in reducing the incidence of Alzheimer’s disease in elderly patients with normal cognition and mild cognitive impairment (NCT00010803), no preventive effect of the Ginkgo biloba extract was shown [41] .
Two more clinical trials to assess the effect of EGb761 on different parameters on patients with mild to moderate Alzheimer’s disease are in progress. A Phase II study investi-gated the effect of EGb761 on the ratio of the isoform of the protein precursor of β -amyloid in the platelets (NCT00500500). The results from this study have not yet been released. In another Phase II study (NCT00814346), which is still recruiting patients, the effect of EGb761 on the brain glucose metabolism and cognitive performances is under investigation. In addition, a large Phase III study is currently being conducted (NCT00010803) in order to determine a potential preventive effect of EGb761 on the incidence of Alzheimer’s disease in the elderly.
Epigallocatechin gallate, curcumin, EGb761, and caprospinol have attracted interest in the use of natural compounds present in food as potential treatments for Alzheimer’s disease, since they are expected to produce much less toxicity than newly designed compounds and they (or their starting materials) are readily available in commercially compatible amounts.
Meanwhile, the caprospinol mechanism of action raises another question. Tramiprosate and caprospinol belong to the same therapeutic class with regard to their main activity. They are both ligands for A β 1 – 42 , acting to inhibit its

Lecanu, Tillement, Rammouz, Tillement, Greeson & Papadopoulos
Expert Opin. Investig. Drugs (2009) 18(3) 269
oligomerization and aggregation into amyloid deposits [42] . However, the failure of tramiprosate necessarily poses the question of whether this is a therapeutic class failure or a compound-specific failure. Despite sharing a similar mecha-nism of action, tramiprosate and caprospinol are extremely different. First, caprospinol binds to the C-terminal portion of A β 1 – 42 . In contrast, the carboxy-terminal residue is not required for binding of tramiprosate, which binds to amino acids 1 – 28 of the A β 1 – 42 peptide [42] . Second, tramiprosate is a very small hydrophilic analog of the amino acid, taurine, and has zwitterionic properties. Caprospinol is a much larger steroidal compound that is not ionized at any physiological pH and is highly lipophilic. Finally, unlike caprospinol, tramiprosate is not of natural origin, a feature that could significantly affect how this compound behaves in a biological matrix.
2.1.3 Caprospinol and mitochondria In vitro , the neuroprotective effects of caprospinol are accompanied by the preservation of intracellular ATP [23] . The effect of A β on mitochondrial function has been extensively investigated during the past 10 years, and the data generated by these studies indicate that various effects of the peptide could lead to mitochondrial dysfunction. In neuronal mitochondria, A β 1 – 42 and the A β 25 – 35 fragment inhibit respiration and activities of key enzymes such as succinate dehydrogenase, α -ketoglutarate dehydrogenase, pyruvate dehydrogenase, and cytochrome oxidase [43,44] . Inhibition of the respiratory chain complexes has also been reported in neuronal mitochondria exposed to A β 25 – 35 [45-47] , and this peptide fragment promotes opening of the mitochondrial transition pore [48-50] .
Several natural compounds currently being investigated at various clinical trial stages displayed specific protective activity towards mitochondrial function during the preclinical, discovery phase. Epigallocatechin gallate [51] , EGb761 [52,53] , resveratrol [54,55] , and curcumin [56] demonstrated ‘mito-protective’ properties and ATP preservation in various mitochondrial preparations. We confirmed the protective effect of caprospinol on isolated brain mitochondria, showing that caprospinol restores respiratory function of these mito-chondria in the presence of monomeric A β 1 – 42 [57] . We also found that, in human neuroblastoma cells exposed to A β 1 – 42 , amyloid peptide co-localizes with complex II of the respiratory chain, indicating that A β 1 – 42 is capable of crossing both the outer cell membrane and the mito-chondrial membrane. When caprospinol and A β 1 – 42 are both present in the incubation medium, amyloid peptide labeling is abolished, and this ‘scavenging’ effect of caprospinol is accompanied by a partial restoration of mitochondrial respiratory function [57] .
This finding is of particular interest in view of recent results showing that amyloid deposits are present in the mitochondria of cortical pyramidal neurons in the post-mortem Alzheimer’s disease brain [58] . However, these results raise
the unanticipated question of whether these ‘mitoprotective’ properties are dependent on the A β 1 – 42 -binding ability of caprospinol or are due to a distinct mechanism of action. Indeed, since mitochondria are a direct site of A β 1 – 42 accumulation in Alzheimer’s disease neurons [59] , determining whether caprospinol has multiple mechanisms of action is critical. In this regard, caprospinol was able to abolish uncoupling triggered by carbonyl cyanide 3-chlorophenyl-hydrazone (an agent that mimics A β 1 – 42 -induced uncoupling) in isolated brain mitochondria, an effect that translated into neuroprotection in neuronal culture models [57] . Capros-pinol was also shown to specifically target complex IV of the respiratory chain, resulting in a neuroprotective effect against A β 1 – 42 [57] .
Interestingly, epigallocatechin gallate, curcumin, and EGb761 also preserve mitochondria function independently of their ability to bind to A β 1 – 42 . This finding warrants attention since tramiprosate does not exert neuroprotective properties by acting on mitochondria, despite the fact that it is an analog of taurine, which does preserve mitochondrial function in the face of various insults [60,61] . The various neuroprotective mechanisms uncovered by our in vitro studies were validated in a pharmacological rat model of Alzheimer’s disease. The effect of caprospinol on amyloid plaque formation mentioned earlier was associated with a dramatic protective effect on neuronal cells in the hippocampus and cortex [31] . Caprospinol stopped the progression of neurodegeneration in various brain structures, with the most dramatic effect being observed in the CA1 of the hippocampus and in the temporal cortex. Caprospinol also had a neuroprotective effect in the CA3 of the hippocampus, although this was less prominent.
2.1.4 Caprospinol and cognition The histological and biochemical effects of potential Alzheimer’s disease treatments would be meaningless were they not also associated with an improvement in memory and cognitive function. The primary goal of such treatments is to restore brain function to levels seen before the onset of the disease, as determined by phenotypic changes. The rat model that we have used in our studies exhibits poor cognitive performances in the Morris watermaze task compared to unaltered littermates [62] . Caprospinol treatment, when initiated at the time of observable disease, dramatically improves rat cognitive performances [31] . Treated animals perform as well as control rats, showing that caprospinol not only stops deterioration of the cognitive processes, but also restores cognition to a level comparable to that seen in healthy age-matched littermates. Caprospinol does not affect rat locomotor ability, excluding the possibility that changes in mobility interfered with the experimental observations.
2.1.5 Absence of steroid-related pharmacology Unlike its analog 22 R -hydroxycholesterol, caprospinol is not metabolized to steroid products when applied to steroidogenic

Caprospinol: moving from a neuroactive steroid to a neurotropic drug
270 Expert Opin. Investig. Drugs (2009) 18(3)
cells such as testicular Leydig cells. Therefore, caprospinol is unlikely to induce steroid synthesis in the human body. In addition, binding studies of human recombinant steroid receptors using high-throughput screening technology showed that caprospinol does not bind to any of the classical steroid receptors (i.e., glucocorticoid, progesterone, estrogen α , estrogen β , androgen, and vitamin D). Taken together, these results suggest that caprospinol treatment is incapable of producing steroid-like side effects.
2.2 Chemistry Conducting large studies such as long-term toxicity or Phase III trials will require large amounts of caprospinol. Moreover, should caprospinol show promise in clinical trials, a simple and reliable method would be required to produce large quantities of FDA-grade compound. Caprospinol chemical synthesis is extremely straightforward, comprising a single esterification reaction between diosgenin and caproic acid ( Figure 3 ). Caprospinol chemistry has two major advantages for pharmaceutical development. First, a one-step synthesis is rapid and financially attractive. Second, the starting material is available in very large quantities. These features make caprospinol an ideal candidate for chemical development.
2.3 Caprospinol pharmacokinetics and metabolism Caprospinol pharmacokinetics have been investigated in rats and dogs ( Table 1 ). After intravenous dosing in rats, caprospinol undergoes extremely low clearance (2% of liver blood flow) and exhibits a low volume of distribution (7% of total body water). After intraperitoneal dosing in rats, caprospinol undergoes slow absorption as seen by a median T max value of 3 h and has a bioavailability of 42%. The mean half-life, as calculated from the terminal declining phase, is much higher after intraperitoneal dosing than after intravenous dosing, suggesting that intraperitoneal adminis-tration is associated with a marked flip-flop phenomenon (i.e., an absorption rate slower than the elimination rate). This phenomenon has been reported for other steroids such as methylprednisolone [63] and epitiostanol [64] . After oral
dosing in rats, plasma concentrations of caprospinol are negligible compared to plasma concentrations following intravenous and intraperitoneal dosing. Caprospinol concen-trations are quantifiable up to 2 h after oral dosing of rats, with oral bioavailability being estimated to be < 1%.
Following intravenous administration in dogs, caprospinol undergoes very low plasma clearance, at about 3% of normal liver blood flow. It also exhibits a very low volume of distribution, which is about 15% of total body water. As in rats, caprospinol is poorly absorbed after oral adminis-tration. Caprospinol concentrations are negligible following oral administration as compared to concentrations following intravenous administration. The concentrations are quantifiable for up to 12 h after oral dosing, and oral bioavailability is estimated to be approximately 2%.
Caprospinol is not metabolized by liver microsomes from rats, dogs, or humans ruling metabolic interactions with other drugs. In rats, daily intraperitoneal injections of caprospinol (5 mg/kg/day) over 2 weeks resulted in an accumulation of the compound in the brain tissue. Liquid chromatography and tandem mass spectrometry analysis revealed that rat brains contained 17 – 24% of the total amount administered, unequivocally demonstrating that caprospinol crosses the blood–brain barrier [65] . Thus, caprospinol could be summarized to be a highly lipophilic compound with low oral bioavailability that crosses the blood–brain barrier in considerable quantities when injected intraperitoneally. Caprospinol is a lead compound for which we are currently developing derivatives with various side-chains in position 3. The main purpose of these modifications is to reduce the lipophilicity of the compound in order to improve its oral bioavailability without modification of the bioactivity. In addition, this compound undergoes low liver metabolism, exhibits flip-flop characteristics, and is probably tightly bound to plasma proteins of an unknown nature.
The low oral bioavailability of caprospinol does not preclude the future development of this drug, for several reasons. First, oral bioavailability studies were performed with a ‘basic’ oral formulation that was not meant to specifically enhance caprospinol absorption in the digestive tract. The
O
O
O
O
O
O
O
Figure 3 . One-step chemical synthesis of caprospinol. Caprospinol is generated through an overnight esterifi cation reaction between diosgenin and caproyl chloride.

Lecanu, Tillement, Rammouz, Tillement, Greeson & Papadopoulos
Expert Opin. Investig. Drugs (2009) 18(3) 271
technologies currently available for formulation development are likely to resolve this issue. Second, although the ability of caprospinol to cross the blood–brain barrier has not yet been fully characterized, in vivo data show that caprospinol does so in a therapeutically relevant amount. Third, the flip-flop properties and lack of liver metabolism of this drug indicate that metabolism will not limit its distribution, a feature that is desirable for a drug most likely to be prescribed to the elderly.
2.4 Toxicologic profi le The toxicologic profile of caprospinol is extremely favorable. Reverse mutation assays have revealed that this compound has no mutagenic activity in histidine-requiring auxotroph strains of Salmonella typhimurium ( S. typhimurium TA98, TA100, TA1535, and TA1537) or the tryptophan-requiring auxotroph strain of Escherichia coli ( E. coli WP2 uvrA). Caprospinol does not induce any chromosome aberrations in Chinese hamster ovarian (CHO-KI) cells. In addition, it does not induce in vivo genotoxicity, as assessed by micro-nucleus assays. Acute toxicity was not reached in general toxicology studies, precluding estimation of the no-observed-adverse-effect level. In an acute toxicity study in mice, no toxicity was detected in any organ, even at the highest dose tested (30 mg/kg, intravenous or oral route). The low aqueous solubility of caprospinol prevented us from testing higher concentrations in mice. To circumvent this problem, we are currently testing caprospinol toxicity in larger animals.
3. Conclusion
Alzheimer’s disease is a multifactorial – and up to now, irreversible – neurodegenerative disease with an etiology and pathological pathways that remain largely unknown. The main consequence of this lack of knowledge is a drug development process with a high failure rate, as illustrated by the results of the latest clinical trials. Despite challenges in Alzheimer’s disease drug development,
tremendous efforts are under way to generate disease-modifying therapeutics that not only alleviate Alzheimer’s disease symptomatology, but also efficiently stop and someday reverse the progression of this disease. We have attempted to provide an accurate overview of one such drug currently in development, caprospinol.
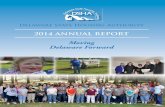
Caprospinol is a naturally occurring steroid with a favorable profile for drug development. It binds to A β 1 – 42 , preventing the formation of neurotoxic ADDLs and amyloid plaques as well as decreasing amyloid accumulation in the mitochondria. Caprospinol also possesses pharmacological properties that directly target the mitochondrial respiratory chain. Thus, both effects contribute to preservation of mitochondria function. Importantly, caprospinol significantly decreases neurodegeneration in a rat model of Alzheimer’s disease and maintains cognitive function ( Figure 4 ).
Caprospinol possesses several features that favor its pharmaceutical development: i) it crosses the blood–brain barrier, ii) it is not metabolized by the liver, iii) it is devoid of steroid activity, implying that it will not produce steroid-related side effects; and iv) it has a very safe toxicologic profile. In conclusion, we believe that the overall profile of caprospinol warrants its future development as one of the next disease-modifying drugs for the treatment of Alzheimer’s disease.
4. Expert opinion
Although promising therapeutic concepts are currently being developed [29] , the achievements of Alzheimer’s disease drug development remain limited. Since the release of tacrine in the early 1990s, no long-term successful therapeutic, preventive, or disease-stabilizing entities have been developed. Tacrine was discovered to be a germicidal and antimalarial acridine derivative, with its synthesis being reported in 1945 [66] . The use of tacrine in the clinic can be traced back to the late 1940s, when it was used as an antidote to treat anticholinergic drug overdose. The drug was further investigated in the 1960s as an anesthetic adjuvant [67,68] .
Table 1 . Caprospinol pharmacokinetics in rats and dogs (mean values).
Rat Dog
Intravenous Intraperitoneal Oral Intravenous Oral
Cl (mL/min/kg) 1.4 n.m. n.m. 0.92 n.m.
V D (L/kg) 0.05 n.m. n.m. 0.09 n.m.
C max (µg/ml) 88.9 7.72 0.03 24.78 0.38
AUC 0 – last (µ g.h/ml) 77.4 32.6 0.04 41.8 5.79
T max (h) n/a 3 1.3 n/a 2
t 1/2 (h) 0.67 4.6 1.7
AUC 0 – last : Total amount of caprospinol measured over time in the plasma; CI: Plasma clearance; C max : Plasma peak concentration; n/a: Not applicable; n/m: Not measured; t ½ : Half-life; T max : Plasma peak concentration time; V D : Distribution volume.

Caprospinol: moving from a neuroactive steroid to a neurotropic drug
272 Expert Opin. Investig. Drugs (2009) 18(3)
OO
O
OOO
O
O
A.
B.
C.
E.
F.
D.
OO
O
O
2
1
Figure 4 . Anti-amyloid and neuroprotective effects of caprospinol. Accumulation of amyloid peptide in the brain tissue ( A ) leads to its aggregation into neurotoxic ADDLs ( B ) and formation of amyloid plaques ( C ). A β 1 – 42 uncouples mitochondrial respiration and targets the complex IV. Increasing intracellular concentrations of amyloid peptide alters mitochondria respiratory chain function ( E ). Both ADDLs and mitochondria dysfunction lead to neurodegeneration ( D and F ). Caprospinol binds to the amyloid peptide, inhibiting its oligomerization into neurotoxic ADDLs ( 1 ) and subsequent aggregation in amyloid plaques. Caprospinol binding to A β 1 – 42 prevents the peptide from entering the mitochondria and therefore prevents it from disrupting mitochondrial function ( 2 ). In addition, caprospinol protects complex IV and prevents uncoupling independently of its ability to bind to amyloid peptide. These mitoprotective properties and the ability to block ADDL formation both contribute to the neuroprotective properties of caprospinol. ADDL: Amyloid-derived diffusible ligands.

Lecanu, Tillement, Rammouz, Tillement, Greeson & Papadopoulos
Expert Opin. Investig. Drugs (2009) 18(3) 273
One of the first tacrine clinical trials, which was performed on a very small cohort of Alzheimer’s disease patients, was published much later [69] , and was followed by three reports showing that tacrine lacks clinical benefit when given at doses of < 120 mg/day [70-72] . A dose of 125 mg/day is required to reach clinical efficacy, but also produces major liver toxicity.
These historical facts show that tacrine was never purposely developed to treat Alzheimer’s disease but was opportunistically used under circumstances in which treatments were unavailable and knowledge of the mecha-nisms underlying the onset and progression of Alzheimer’s disease was lacking. From this perspective, the release of the new generation of AchEI was not a break-through, since these inhibitors are nothing more than tacrine-like molecules with clinical efficacy that still remains questionable [7-9,11] .
Released in 2004, the non-competitive NMDA receptor antagonist memantine has thus far been shown to have an excellent safety profile [73] and clinical efficacy [74,75] . However, like tacrine, memantine was never purposely developed as a treatment for Alzheimer’s disease. In 1974, an amantadine derivative termed D145 (now known as memantine) was developed as a potent dopaminergic agonist [76] . A clinical trial was then conducted to investigate the effect of memantine on the plasma growth hormone levels in acromegalic subjects [77] . A second clinical trial provided evidence of a beneficial effect of this dopaminergic drug in patients with Parkinson’s disease [78] . Thus, the therapeutic arsenal available for Alzheimer’s disease today relies on two concepts developed in the 1940s and 1970s.
The recent history of Alzheimer’s disease drug development is essentially benchmarked by three regrettable failures, namely the AN1792 vaccine [79,80] , the amyloid peptide ligand/plaque formation inhibitor, tramiprosate, and the γ -secretase modulator, tarenflurbil. In our opinion, these failures illustrate lack of compliance with some of the fundamental principles ruling drug development. The first principle is the validity of the animal model. The meningo-encephalitis cases observed during the AN1792 clinical trial resulted from a type of immune reaction that was not observed in the rodent brain due to immune system differences. This questions the validity of the transgenic animal model used to study Alzheimer’s disease. Also, the role of transgenic mouse models in the failure of tramiprosate and tarenflurbil should not be overlooked, since both compounds produced beneficial effects in preclinical studies using Alzheimer’s disease transgenic mice. Transgenic mice used in Alzheimer’s disease research have been developed since the early 1990s [81,82] . These mouse models carry one or several mutated human genes ( APP , PS1 , and PS2 ) that account for familial Alzheimer’s disease, representing a maximum of 5% of cases. They also carry mutations in the gene encoding tau protein, though these mutations do not exist in Alzheimer’s disease.
Thus, these transgenic mice may not be relevant for exploration of the sporadic form of the disease. Indeed, these mouse models address the consequences of a geneti-cally driven alteration in APP metabolism, but they do not address the origin of the alteration that occurs in sporadic Alzheimer’s disease, nor the mechanisms (which have yet to be identified) underlying the progression of the sporadic form of the disease that represents 95% of cases [83] . This situation could have been anticipated, as there is no reason to expect that an animal model intended to mimic a form of Alzheimer’s disease affecting a small group could faithfully mimic all forms of this poorly understood disease. The relevance of an animal model depends on the extent to which the disease to be modeled has been characterized. On average, 15 years are required to develop a drug, yet in the 18 years of existence of these transgenic mouse models, they have made a limited contribution to Alzheimer’s disease drug development. Nevertheless, these mouse models have allowed us to better understand the pathophysiology of a number of brain proteins that ultimately may or may not be part of a successful therapy for Alzheimer’s disease.
Another basic principle of drug development that seems to have been ignored is the concept of target validation. This principle can be best illustrated with the γ -secretase inhibitors. The first report mentioning possible use of γ -secretase inhibitors in the treatment of Alzheimer’s disease was published in 1995 [84] , and the rational design of specific inhibitors was first reported in 1998 [85] . Surpris-ingly, the first studies reporting the relationship between γ -secretase/presenilins, A β 1 – 42 production, the Notch pathway, and Alzheimer’s disease were published much later [86-89] , clearly indicating that inhibitors were developed before the γ -secretase drugability assessment was complete. A warning that γ -secretase inhibitors may produce Notch pathway-related side-effects was published the same year [90] , and the results of the first and (to our knowledge) the only clinical trial with a γ -secretase inhibitor raised concerns [18] .
Similarly, the risk of inducing an autoimmune disease with a vaccine targeting a native protein has never really been debated, leaving open the question of what will happen to the physiological functions of A β 1 – 42 following vaccination. Since the only criteria that can be used to measure the success of drug R&D are the number of novel therapeutics released to market, the drug R&D record in the case of Alzheimer’s disease is poor at best. We believe that the drug development approaches being used for Alzheimer’s disease need to be reconsidered and the basic biology of the disease re-evaluated. In addition, new tools should be developed, along with new animal models that are based on fundamental knowledge and better represent the complexity of the disease. Future success in treating Alzheimer’s disease is not possible if the therapies continue to be based on strategies that have failed for almost 40 years.

Caprospinol: moving from a neuroactive steroid to a neurotropic drug
274 Expert Opin. Investig. Drugs (2009) 18(3)
Declaration of interest
A patent on the use of the described compound, caprospinol, for the treatment of Alzheimer’s disease was recently filed at the US Patent Office. Drs Lecanu, Greeson and Papadopoulos are named inventors in the patent. In addition, Dr Lecanu serves as a consultant and has stock options of Samaritan
Pharmaceuticals, as well as being a member of the Board of Directors and Scientific Advisory Board of Samaritan Pharmaceuticals. Dr Jean-Paul Tillement is member of the Scientific Advisory Board of Samaritan Pharmaceuticals. Dr Greeson is the CEO of Samaritan Pharmaceuticals. Dr Papadopoulos serves as a consultant and has stock options of Samaritan Pharmaceuticals.
Bibliography Papers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers.
1. Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst Rev 2006 ; 25 ;(1): CD005593
2. Johannsen P, Salmon E, Hampel H, et al. Assessing therapeutic effi cacy in a progressive disease: a study of donepezil in Alzheimer’s disease. CNS Drugs 2006 ; 20 : 311 -25
3. Orgogozo JM, Small GW, Hammond G, et al. Effects of galantamine in patients with mild Alzheimer’s disease. Curr Med Res Opin 2004 ; 20 : 1815 -20
4. Small GW, Kaufer D, Mendiondo MS, et al. Cognitive performance in Alzheimer’s disease patients receiving rivastigmine for up to 5 years. Int J Clin Pract 2005 ; 59 : 473 -7
5. Bullock R, Touchon J, Bergman H, et al. Rivastigmine and donepezil treatment in moderate to moderately-severe Alzheimer’s disease over a 2-year period. Curr Med Res Opin 2005 ; 21 : 1317 -27
6. Winblad B, Wimo A, Engedal K, et al. 3-year study of donepezil therapy in Alzheimer’s disease: effects of early and continuous therapy. Dement Geriatr Cogn Disord 2006 ; 21 : 353 -63
7. Birks J, Harvey RJ. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database Syst Rev 2006 ; 25 ;(1): CD001190
8. Courtney C, Farrell D, Gray R, et al. Long-term donepezil treatment in 565 patients with Alzheimer’s disease (AD2000): randomised double-blind trial. Lancet 2004 ; 363 : 2105 -15
9. Schneider LS. AD2000: donepezil in Alzheimer’s disease. Lancet 2004 ; 363 : 2100 -1
10. Kaduszkiewicz H, Zimmermann T, Beck-Bornholdt HP, et al. Cholinesterase inhibitors for patients with Alzheimer’s
disease: systematic review of randomised clinical trials. BMJ 2005 ; 331 : 321 -7
11. Kaduszkiewicz H, van den Bussche H, Zimmermann T. The evidence is not convincing. Int Psychogeriatr 2008 ; 6 : 1 -20
12. Areosa SA, Sherriff F, McShane R. Memantine for dementia. Cochrane Database Syst Rev 2005 ; 18 ;(2): CD003154
13. McShane R, Areosa SA, Minakaran N. Memantine for dementia. Cochrane Database Syst Rev 2006 ; 19 ;(2): CD003154
14. Huey ED, Dustin IH, Overman GP, et al. Development of subtle psychotic symptoms with memantine: a case report. J Clin Psychiatry 2005 ; 66 : 658 -9
15. Aisen PS. Tarenfl urbil: a shot on goal. Lancet Neurol 2008 ; 7 : 468 -9
16. Romanovskaia MG. Effect of cyproheptadine and dimebon on bacterial infection in animals receiving chlorazicin or aminazin. Farmakol Toksikol 1971 ; 34 : 698 -701
17. Doody RS, Gavrilova SI, Sano M, et al. Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer’s disease: a randomised, double-blind, placebo-controlled study. Lancet 2008 ; 372 : 207 -15
18. Siemers ER, Quinn JF, Kaye J, et al. Effects of a gamma-secretase inhibitor in a randomized study of patients with Alzheimer disease. Neurology 2006 ; 66 : 602 -4
19. Rocchi A, Pellegrini S, Siciliano G, et al. Causative and susceptibility genes for Alzheimer’s disease: a review. Brain Res Bull 2003 ; 61 : 1 -24
20. Youdim MB, Buccafusco JJ. Multi-functional drugs for various CNS targets in the treatment of neurodegenerative disorders. Trends Pharmacol Sci 2005 ; 26 : 27 -35
21. Hall PF. Role of cytochrome P-450 in the biosynthesis of steroid hormones. Vitam Horm 1985 ; 42 : 315 -68
22. Yao ZX, Brown RC, Teper G, et al. 22R-Hydroxycholesterol protects neuronal cells from beta-amyloid-induced cytotoxicity by binding to beta-amyloid peptide. J Neurochem 2002 ; 83 : 1110 -19
23. Lecanu L, Yao W, Teper GL, et al. Identifi cation of naturally occurring spirostenols preventing beta-amyloid-induced neurotoxicity. Steroids 2004 ; 69 : 1- 6
24. Modler AJ, Gast K, Lutsch G, et al. Assembly of amyloid protofi brils via critical oligomers–a novel pathway of amyloid formation. J Mol Biol 2003 ; 325 : 135 -48
25. Catalano SM, Dodson EC, Henze DA, et al. The role of amyloid-beta derived diffusible ligands (ADDLs) in Alzheimer’s disease. Curr Top Med Chem 2006 ; 6 : 597 -608
26. Klein WL. Abeta toxicity in Alzheimer’s disease: globular oligomers (ADDLs) as new vaccine and drug targets. Neurochem Int 2002 ; 41 : 345 -52
27. Dahlgren KN, Manelli AM, Stine WB Jr, et al. Oligomeric and fi brillar species of amyloid-beta peptides differentially affect neuronal viability. J Biol Chem 2002 ; 277 : 32046 -53
28. Lambert MP, Barlow AK, Chromy BA, et al. Diffusible, nonfi brillar ligands derived from Abeta1-42 are potent central nervous system neurotoxins. Proc Natl Acad Sci USA 1998 ; 95 : 6448 -53
29. Lecanu L, Papadopoulos V. Cutting-edge patents in Alzheimer’s disease drug discovery: anticipation of potential future treatments. Recent Patents CNS Drug Discov 2007 ; 2 : 113 -23
30. Teper GL, Lecanu L, Greeson J, et al. Methodology for multi-site ligand-protein docking identifi cation developed for the optimization of spirostenol inhibition of beta-amyloid-induced neurotoxicity. Chem Biodivers 2005 ; 2 : 1571 -9
31. Lecanu L, Sidahmed EL, Greeson J, Papadopoulos V. Caprospinol improves brain histopathology and recovers

Lecanu, Tillement, Rammouz, Tillement, Greeson & Papadopoulos
Expert Opin. Investig. Drugs (2009) 18(3) 275
memory function in a rat model of Alzheimer’s disease. Proceedings of the 8th International Conference AD/PD;14 – 18 March, 2007, Salzburg, Austria
32. Gouras GK, Tsai J, Naslund J, et al. Intraneuronal Abeta42 accumulation in human brain. Am J Pathol 2000 ; 156 : 15 -20
33. Gyure KA, Durham R, Stewart WF, et al. Intraneuronal a-beta-amyloid precedes development of amyloid plaques in Down syndrome. Arch Pathol Lab Med 2001 ; 125 : 489 -92
34. McGeer PL, Akiyama H, Kawamata T, et al. Immunohistochemical localization of beta-amyloid precursor protein sequences in Alzheimer and normal brain tissue by light and electron microscopy. J Neurosci Res 1992 ; 31 : 428 -42
35. Takahashi RH, Milner TA, Li F, et al. Intraneuronal Alzheimer abeta42 accumulates in multivesicular bodies and is associated with synaptic pathology. Am J Pathol 2002 ; 161 : 1869 -79
36. Bastianetto S, Yao ZX, Papadopoulos V, et al. Neuroprotective effects of green and black teas and their catechin gallate esters against beta-amyloid-induced toxicity. Eur J Neurosci 2006 ; 23 : 55 -64
37. Yang F, Lim GP, Begum AN, et al. Curcumin inhibits formation of amyloid beta oligomers and fi brils, binds plaques, and reduces amyloid in vivo. J Biol Chem 2005 ; 280 : 5892 -901
38. Kanowski S, Herrmann WM, Stephan K, et al. Proof of effi cacy of the ginkgo biloba special extract EGb 761 in outpatients suffering from mild to moderate primary degenerative dementia of the Alzheimer type or multi-infarct dementia. Pharmacopsychiatry 1996 ; 29 : 47 -56
39. Maurer K, Ihl R, Dierks T, et al. Clinical effi cacy of Ginkgo biloba special extract EGb 761 in dementia of the Alzheimer type. J Psychiatr Res 1997 ; 31 : 645 -55
40. Yao Z, Drieu K, Papadopoulos V. The Ginkgo biloba extract EGb 761 rescues the PC12 neuronal cells from beta-amyloid-induced cell death by inhibiting the formation of beta-amyloid-derived diffusible neurotoxic ligands. Brain Res 2001 ; 889 : 181 -90
41. DeKosky ST, Williamson JD, Fitzpatrick AL, et al. Ginkgo biloba for prevention of dementia: a randomized controlled trial. JAMA 2008 ; 300 : 2253 -62
42. Gervais F, Paquette J, Morissette C, et al. Targeting soluble abeta peptide with
tramiprosate for the treatment of brain amyloidosis. Neurobiol Aging 2007 ; 28 : 537 -47
43. Kaneko I, Yamada N, Sakuraba Y, et al. Suppression of mitochondrial succinate dehydrogenase, a primary target of beta-amyloid, and its derivative racemized at Ser residue. J Neurochem 1995 ; 65 : 2585 -93
44. Casley CS, Canevari L, Land JM, et al. Beta-amyloid inhibits integrated mitochondrial respiration and key enzyme activities. J Neurochem 2002 ; 80 : 91 -100
45. Casley CS, Land JM, Sharpe MA, et al. Beta-amyloid fragment 25-35 causes mitochondrial dysfunction in primary cortical neurons. Neurobiol Dis 2002 ; 10 : 258 -67
46. Pereira C, Santos MS, Oliveira C. Involvement of oxidative stress on the impairment of energy metabolism induced by A beta peptides on PC12 cells: protection by antioxidants. Neurobiol Dis 1999 ; 6 : 209 -19
47. Canevari L, Clark JB, Bates TE. Beta-amyloid fragment 25-35 selectively decreases complex IV activity in isolated mitochondria. FEBS Lett 1999 ; 457 : 131 -4
48. Bachurin SO, Shevtsova EP, Kireeva EG, et al. Mitochondria as a target for neurotoxins and neuroprotective agents. Ann NY Acad Sci 2003 ; 993 : 334 -44
49. Moreira PI, Santos MS, Moreno A, et al. Amyloid beta-peptide promotes permeability transition pore in brain mitochondria. Biosci Rep 2001 ; 21 : 789 -800
50. Moreira PI, Santos MS, Moreno A, et al. Effect of amyloid beta-peptide on permeability transition pore: a comparative study. J Neurosci Res 2002 ; 69 : 257 -67
51. Chen L, Yang X, Jiao H, et al. Tea catechins protect against lead-induced ROS formation, mitochondrial dysfunction, and calcium dysregulation in PC12 cells. Chem Res Toxicol 2003 ; 16 : 1155 -61
52. Eckert A, Keil U, Scherping I, et al. Stabilization of mitochondrial membrane potential and improvement of neuronal energy metabolism by Ginkgo biloba extract EGb 761. Ann NY Acad Sci 2005 ; 1056 : 474 -85
53. Eckert A, Keil U, Kressmann S, et al. Effects of EGb 761 Ginkgo biloba extract on mitochondrial function and oxidative stress. Pharmacopsychiatry 2003 ; 36 (Suppl 1): S15 -23
54. Morin C, Zini R, Albengres E, et al. Evidence for resveratrol-induced preservation of brain mitochondria functions after hypoxia-reoxygenation. Drugs Exp Clin Res 2003 ; 29 : 227 -33
55. Zini R, Morin C, Bertelli A, et al. Effects of resveratrol on the rat brain respiratory chain. Drugs Exp Clin Res 1999 ; 25 : 87 -97
56. Mancuso C, Bates TE, Butterfi eld DA, et al. Natural antioxidants in Alzheimer’s disease. Expert Opin Investig Drugs 2007 ; 16 : 1921 -31
57. Tillement L, Lecanu L, Yao W, et al. The spirostenol (22R, 25R)-20alpha-spirost-5-en-3beta-yl hexanoate blocks mitochondrial uptake of Abeta in neuronal cells and prevents Abeta-induced impairment of mitochondrial function. Steroids 2006 ; 71 : 725 -35
58. Fernandez-Vizarra P, Fernandez AP, Castro-Blanco S, et al. Intra- and extracellular Abeta and PHF in clinically evaluated cases of Alzheimer’s disease. Histol Histopathol 2004 ; 19 : 823 -44
59. Manczak M, Anekonda TS, Henson E, et al. Mitochondria are a direct site of A beta accumulation in Alzheimer’s disease neurons: implications for free radical generation and oxidative damage in disease progression. Hum Mol Genet 2006 ; 15 : 1437 -49
60. Palmi M, Davey G, Tipton KF, et al. Taurine, taurine analogues, and mitochondrial function and dysfuntion. Adv Exp Med Biol 2006 ; 583 : 469 -79
61. El IA. Taurine increases mitochondrial buffering of calcium: role in neuroprotection. Amino Acids 2008 ; 34 : 321 -8
62. Lecanu L, Greeson J, Papadopoulos V. Beta-amyloid and oxidative stress jointly induce neuronal death, amyloid deposits, gliosis, and memory impairment in the rat brain. Pharmacology 2006 ; 76 : 19 -33
63. Hazra A, Pyszczynski N, DuBois DC, et al. Pharmacokinetics of methylprednisolone after intravenous and intramuscular administration in rats. Biopharm Drug Dispos 2007 ; 28 : 263 -73
64. Ichihashi T, Kinoshita H, Shimamura K, et al. Absorption and disposition of epithiosteroids in rats (1): route of administration and plasma levels of epitiostanol. Xenobiotica 1991 ; 21 : 865 -72
65. Rammouz G, Papadopoulos V, Lecanu L. The neuroprotective steroid caprospinol crosses the blood brain barrier; analysis by

Caprospinol: moving from a neuroactive steroid to a neurotropic drug
276 Expert Opin. Investig. Drugs (2009) 18(3)
liquid chromatography and tandem mass spectrometry. Proceedings of the International Congress on Hormonal Steroids and Hormones & Cancer; 27 – 30 September, 2008, Quebec City, Canada
66. Albert A, Gledhill W. Improved synthese of aminoacridiens. Part IV. Substituted 5-aminoacridines. J Soc Chem Indus 1945 ; 64 : 169 -72
67. Speirs I. The use of tacrine and suxamethonium in anaesthesia for caesarean section. Br J Anaesth 1966 ; 38 : 394 -400
68. Benveniste D, Hemmingsen L, Juul P. Tacrine inhibition of serum cholinesterase and prolonged succinylcholine action. Acta Anaesthesiol Scand 1967 ; 11 : 297 -309
69. Summers WK, Viesselman JO, Marsh GM, et al. Use of THA in treatment of Alzheimer-like dementia: pilot study in twelve patients. Biol Psychiatry 1981 ; 16 : 145 -53
70. Chatellier G, Lacomblez L. Tacrine (tetrahydroaminoacridine; THA) and lecithin in senile dementia of the Alzheimer type: a multicentre trial. Groupe Francais d’Etude de la Tetrahydroaminoacridine. BMJ 1990 ; 300 : 495 -9
71. Fitten LJ, Perryman KM, Gross PL, et al. Treatment of Alzheimer’s disease with short- and long-term oral THA and lecithin: a double-blind study. Am J Psychiatry 1990 ; 147 : 239 -42
72. Gauthier S, Bouchard R, Lamontagne A, et al. Tetrahydroaminoacridine-lecithin combination treatment in patients with intermediate-stage Alzheimer’s disease. Results of a Canadian double-blind, crossover, multicenter study. N Engl J Med 1990 ; 322 : 1272 -6
73. Farlow MR, Graham SM, Alva G. Memantine for the treatment of Alzheimer’s disease: tolerability and safety data from clinical trials. Drug Saf 2008 ; 31 : 577 -85
74. Emre M, Mecocci P, Stender K. Pooled analyses on cognitive effects of memantine in patients with moderate to severe Alzheimer’s disease. J Alzheimers Dis 2008 ; 14 : 193 -9
75. Atri A, Shaughnessy LW, Locascio JJ, et al. Long-term course and effectiveness of combination therapy in Alzheimer disease. Alzheimer Dis Assoc Disord 2008
76. Maj J, Sowinska H, Baran L, et al. Pharmacological effects of 1,3-dimethyl-5-aminoadamantane, a new adamantane derivative. Eur J Pharmacol 1974 ; 26 : 9 -14
77. Camanni F, Massara F, Fassio V, et al. Effect of fi ve dopaminergic drugs on plasma growth hormone levels in acromegalic subjects. Neuroendocrinology 1975 ; 19 : 227 -40
78. Fischer PA, Jacobi P, Schneider E, et al. Effects of intravenous administration of memantine in parkinsonian patients (author’s transl). Arzneimittelforschung 1977 ; 27 : 1487 -9
79. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005 ; 64 : 1553 -62
80. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoencephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003 ; 61 : 46 -54
81. Quon D, Wang Y, Catalano R, et al. Formation of beta-amyloid protein deposits in brains of transgenic mice. Nature 1991 ; 352 : 239 -41
82. Wirak DO, Bayney R, Ramabhadran TV, et al. Deposits of amyloid beta protein in the central nervous system of transgenic mice. Science 1991 ; 253 : 323 -5
83. Duyckaerts C, Potier MC, Delatour B. Alzheimer disease models and human neuropathology: similarities and differences. Acta Neuropathol 2008 ; 115 : 5 -38
84. Schenk DB, Rydel RE, May P, et al. Therapeutic approaches related to amyloid-beta peptide and Alzheimer’s disease. J Med Chem 1995 ; 38 : 4141 -54
85. Wolfe MS, Citron M, Diehl TS, et al. A substrate-based difl uoro ketone selectively inhibits Alzheimer’s gamma-secretase activity. J Med Chem 1998 ; 41 : 6 -9
86. Lukinova NI, Roussakova VV, Fortini ME. Genetic characterization of cytological region 77A-D harboring the presenilin gene of Drosophila melanogaster. Genetics 1999 ; 153 : 1789 -97
87. Struhl G, Greenwald I. Presenilin is required for activity and nuclear access of Notch in Drosophila. Nature 1999 ; 398 : 522 -5
88. De SB, Annaert W, Cupers P, et al. A presenilin-1-dependent gamma-secretase-like protease mediates release of Notch intracellular domain. Nature 1999 ; 398 : 518 -22
89. Wolfe MS, De Los AJ, Miller DD, et al. Are presenilins intramembrane-cleaving proteases? Implications for the molecular mechanism of Alzheimer’s disease. Biochemistry 1999 ; 38 : 11223 -30
90. Hardy J, Israel A. Alzheimer’s disease. In search of gamma-secretase. Nature 1999 ; 398 : 466 -7
Affi liation Laurent Lecanu † 1 , Laurent Tillement 1 , Georges Rammouz 1 , Jean Paul Tillement 2 , Janet Greeson 3 & Vassilios Papadopoulos 1 † Author for correspondence 1 McGill University Health Centre, The Research Institute of the McGill University Health Centre, 6100 Royalmount Avenue, Montreal, Quebec, H4P 2R2, Canada Tel: +1 514 283 6239; Fax: +1 514 283 6282; E-mail: [email protected] 2 Académie Nationale de Médecine, 16 Rue Bonaparte, Paris, 75272, France 3 Samaritan Pharmaceuticals, 101 Convention Center Drive, Las Vegas, 89109, USA