Can recent advances in stroke rehabilitation technologies be of benefit to children
75
Can recent advances in stroke rehabilita2on technologies be of benefit to children? Jane Burridge Prof of Restora2ve Neuroscience University of Southampton Bri2sh Paediatric Neurology Associa2on Friday January 31 st 2014
Transcript of Can recent advances in stroke rehabilitation technologies be of benefit to children

Can recent advances in stroke rehabilita2on technologies be of
benefit to children?
Jane Burridge
Prof of Restora2ve Neuroscience
University of Southampton
Bri2sh Paediatric Neurology Associa2on Friday January 31st 2014

Grown-‐ups like to play games but children like to play even more

What this talk is about
• Drivers for the use of technology in neurorehabilita2on • Differences between CP and stroke • Neuroplas2city -‐ a key factor in rehabilita2on • Current evidence for technologies in stroke and CP • Where to now?
– Evidence is cri2cal, but is the RCT appropriate? – Development of technologies

Clinical and Social drivers for the use of technologies in neurorehabilita2on
• Cost effec2veness: – More intensive therapy without increased therapist 2me
– Home-‐based therapy
• Technological advances • Advances in understanding of neuroplas2city

• Most neurorehabilita2on, including CP, prac2ced today is based on tradi2onal concepts developed over many years.
• But this is also an era for the development of new approaches.
The goal of physical therapy
• develop coordina2on • build strength • improve balance
• control spas2city and maintain flexibility
• op2mize physical func2on
• maximize independence

Conven2onal Therapy
• Neuro-‐development Treatment (Bobath)
• Exercise and Func2onal Strength Training • Mul2-‐modal approach to managing spas2city and preven2ng contractures

Evidence for conven2onal therapy in stroke
• Shi[ from compensa2on to recovery • No clear evidence that any par2cular therapy approach is superior to another1-‐5
• Evidence that outcomes are related to therapy intensity, but stronger evidence from cohort studies that RCTs
• The effect of conven2onal therapy on neuroplas2city following stroke is unknown
1Stern et al, 1970 2Logigian et al, 1983 3Dickstein et al, 1986 4Lord and Hall, 1986 5Wagenaar et al, 1990.
The great hope for sensory-‐motor rehabilita2on
• Advances in understanding of neuroplas2city • Technological advances in motor training devices, including robo2cs that may enhance recovery beyond current approaches
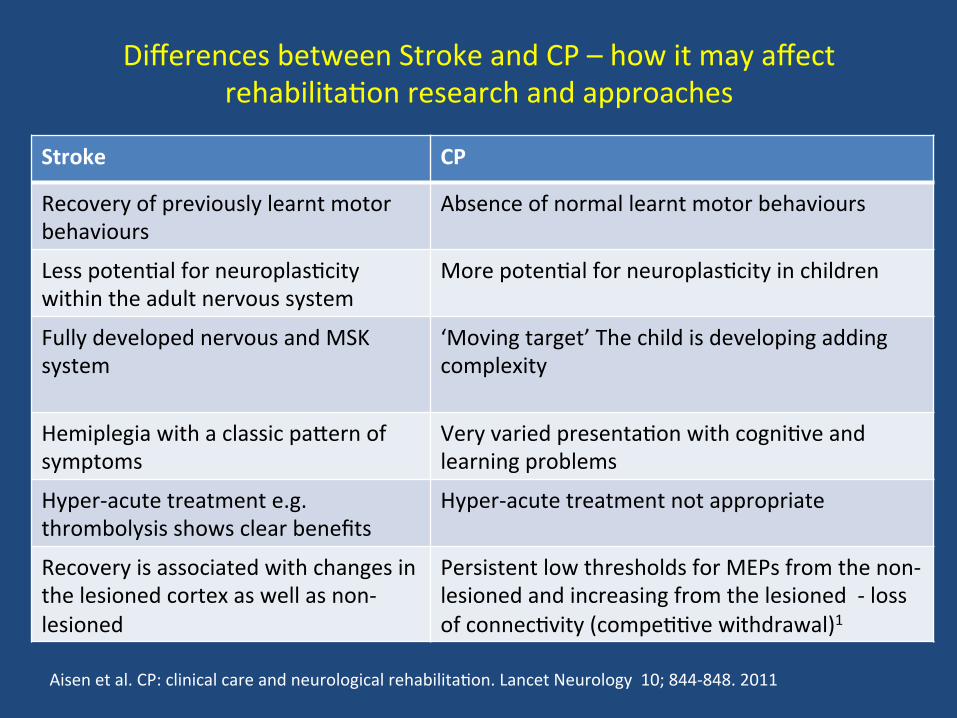
Differences between Stroke and CP – how it may affect rehabilita2on research and approaches
Stroke CP
Recovery of previously learnt motor behaviours
Absence of normal learnt motor behaviours
Less poten2al for neuroplas2city within the adult nervous system
More poten2al for neuroplas2city in children
Fully developed nervous and MSK system
‘Moving target’ The child is developing adding complexity
Hemiplegia with a classic pabern of symptoms
Very varied presenta2on with cogni2ve and learning problems
Hyper-‐acute treatment e.g. thrombolysis shows clear benefits
Hyper-‐acute treatment not appropriate
Recovery is associated with changes in the lesioned cortex as well as non-‐lesioned
Persistent low thresholds for MEPs from the non-‐lesioned and increasing from the lesioned -‐ loss of connec2vity (compe22ve withdrawal)1
Aisen et al. CP: clinical care and neurological rehabilita2on. Lancet Neurology 10; 844-‐848. 2011
Evidence for Neuroplas2city associated with recovery and prac2ce
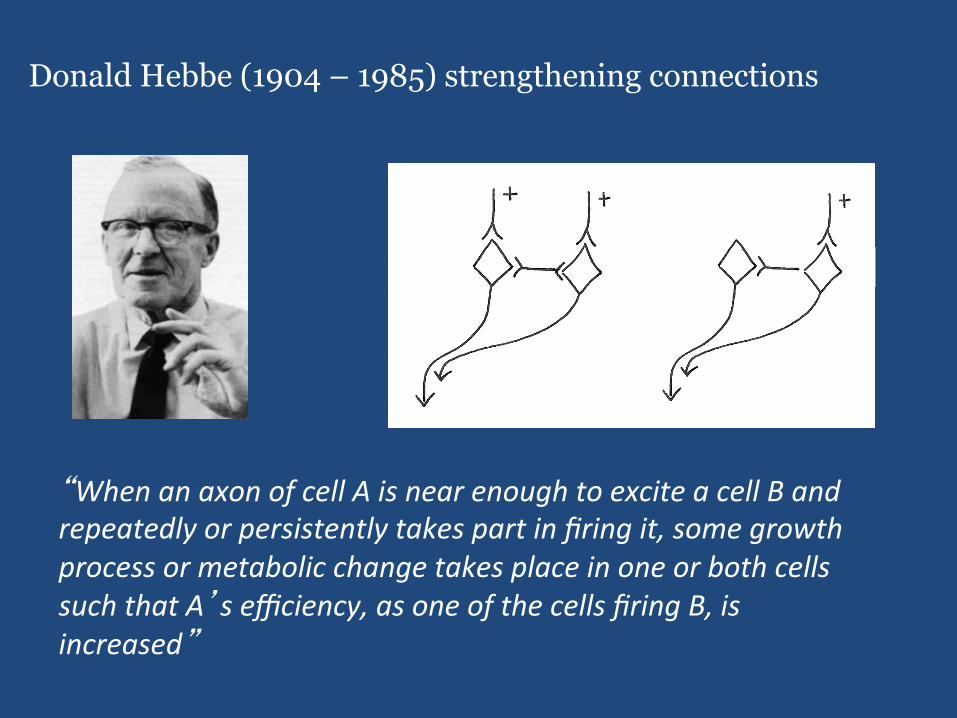
Donald Hebbe (1904 – 1985) strengthening connections
A B A B
“When an axon of cell A is near enough to excite a cell B and repeatedly or persistently takes part in firing it, some growth process or metabolic change takes place in one or both cells such that A’s efficiency, as one of the cells firing B, is increased”
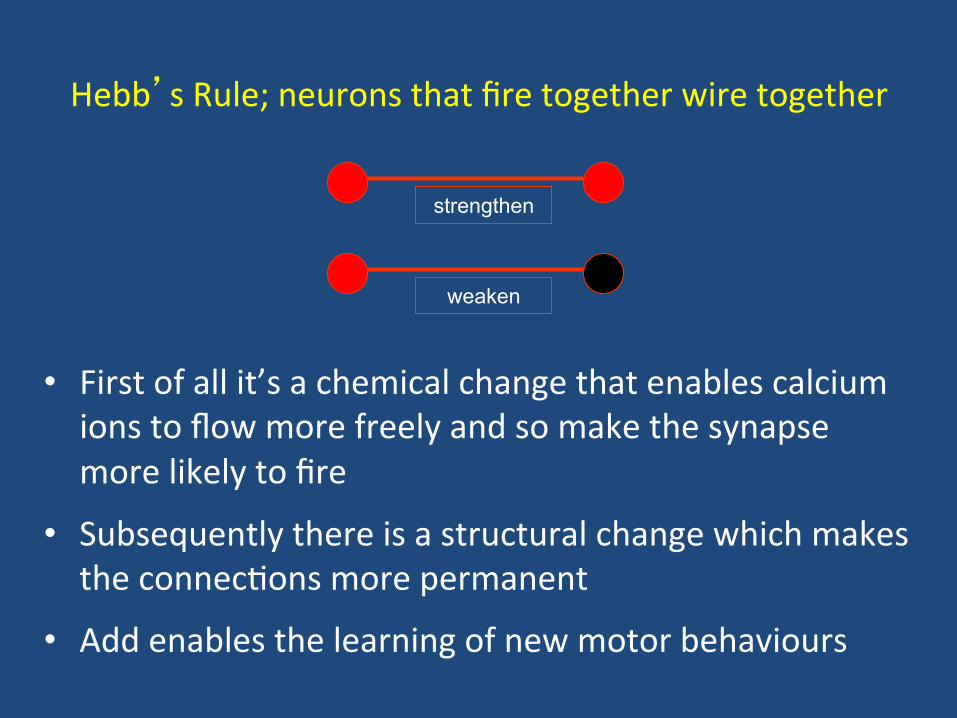
• First of all it’s a chemical change that enables calcium ions to flow more freely and so make the synapse more likely to fire
• Subsequently there is a structural change which makes the connec2ons more permanent
• Add enables the learning of new motor behaviours
Hebb’s Rule; neurons that fire together wire together
strengthen
weaken
14
Flexibility of the motor cortex: implica2ons for rehabilita2on
• Hebbian learning – fire together – wire together • Areas have the ability to adapt their func2on – rather than acquiring new func2ons
• Intensive training of one cor2cal area may be at the expense of other surrounding areas

15
Neuroplas2c changes in response to environment
• In the absence of sensory input and motor ac2va2on (learnt non-‐use) – Constraint Induced Therapy (CIT) – rat model (Taub)
• In response to repe22ve, successful and challenging prac2ce with posi2ve feedback
• Changes in excitability in response to: – Peripheral s2mula2on and paired associa2ve s2muli (PAS) – Repe22ve Transcranial Magne2c S2mula2on (rTMS) – Transcranial direct current s2mula2on (tDCS)
• Synaptogenesis – e.g. An2-‐Nogo A
Hummel & Cohen Lancet Neurology 2006

16
Representa2on of the hand in the motor cortex of the squirrel monkey

Evidence-‐Based Treatment
• How does this basic research translate into clinical prac2ce? • Well designed, rigorously conducted randomized controlled
clinical trials are a recent development in rehabilita2on • Rehabilita2on does not fit into the tradi2onal model -‐ so
useful for conduc2ng pharmacological trials
Problems with experimental studies of motor treatments following stroke (and maybe CP)
• We do not know which are the cri2cal variables to control – Time a[er stroke onset – Type and severity of neurological deficits
• Difficulty in providing true control treatment • Delivery of interven2ons
– Therapist – pa2ent interac2on – Dose / delivery – clinically appropriate vs. standardized
• Current research suggests that technology is not superior to intensive therapy
• We need a beber understanding of the mechanisms -‐ who benefits, when and why
Natural History
• The RCT is an inadequate tool to advance stroke (and maybe CP) rehabilita2on
• There are too many (and unknown) variables to control • If we could control them, then findings would not be generalizable • We have such an inadequate understanding of the mechanisms of
recovery that designing a RCT is based on guesswork • To answer our ques2ons at this stage Natural History studies may
be more useful • Recording medical treatment, therapy and psychosocial data with
retrospec2vely analysis • Cohort studies of intensity of stroke therapy show beber outcomes
that RCTs

Objec2ve measurement
• Lack of valid and reliable objec2ve measurement tools is cri2cal to: – Evalua2ng therapy – Understanding mechanisms of recovery
• Technology has the poten2al to provide this – e.g. – Neuroimaging and TMS
– Wearable sensors (e.g. iner2al sensors – ac2vity)
Technology in Stroke Rehabilita2on (mainly upper limb) and parallels in CP
Why use it?
• Poten2ally cost effec2ve • Promotes self management, mo2va2on and responsibility
• Allows intensive, poten2ally self-‐directed training • May lead to beber outcomes
• A means of extending the rehabilita2on period

What is the evidence that new approaches for enhancing motor recovery are superior to tradi2onal
approaches?

Examples of upper limb technologies
• Constraint Induced Movement Therapy (CIMT)
• Robot therapy • Interac2ve computer play and Virtual Reality e.g. the Wii and systems that use the Kinect mo2on sensing technology
• Peripheral (NMES) and cor2cal electrical (tDCS) and magne2c (TMS) s2mula2on
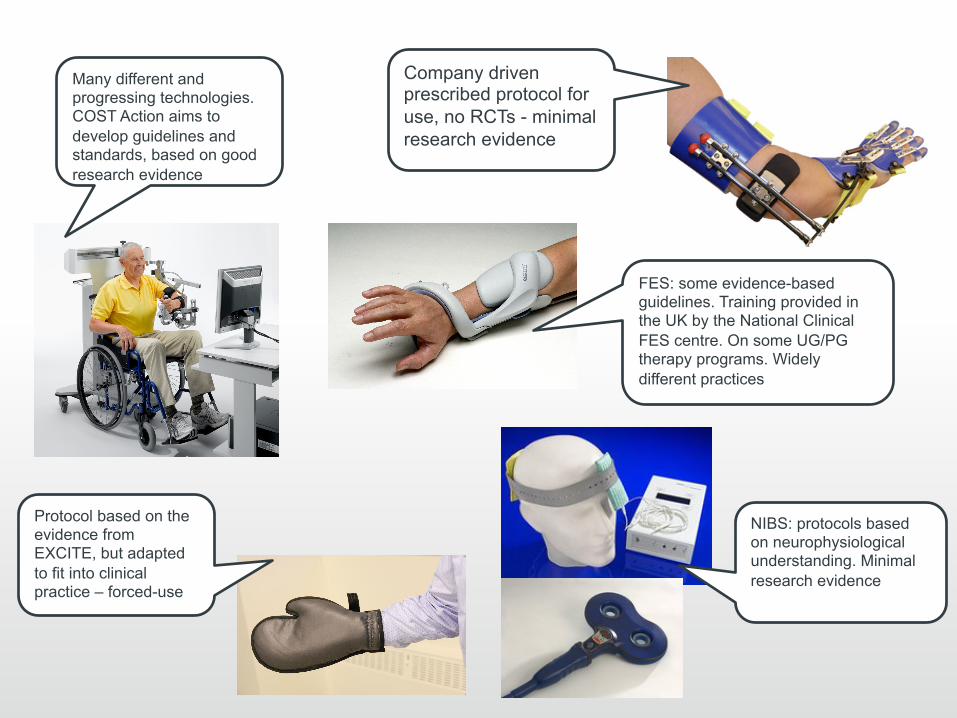
Company driven prescribed protocol for use, no RCTs - minimal research evidence
FES: some evidence-based guidelines. Training provided in the UK by the National Clinical FES centre. On some UG/PG therapy programs. Widely different practices
Many different and progressing technologies. COST Action aims to develop guidelines and standards, based on good research evidence
Protocol based on the evidence from EXCITE, but adapted to fit into clinical practice – forced-use
NIBS: protocols based on neurophysiological understanding. Minimal research evidence

Sarah Rosen, 5, struggled to play video games because of mobility issues caused by cerebral palsy. When her father bought a Kinect, she played until she fell asleep in a chair.

Constraint-‐Induced Movement Therapy
(CIMT)

CIMT is the most comprehensively studied new technique
• Based on animal models
• Extensive preliminary data
• First randomized mul2center trial of a training technique for stroke
• Good evidence that CIMT is associated with changes in cor2cal re-‐organiza2on in humans
• 1Cochrane Review 1Sirtori V, Corbeba D, Moja L, Gam R. Constraint-‐induced movement therapy for upper extremi2es in stroke pa2ents (Review) Cochrane 2009
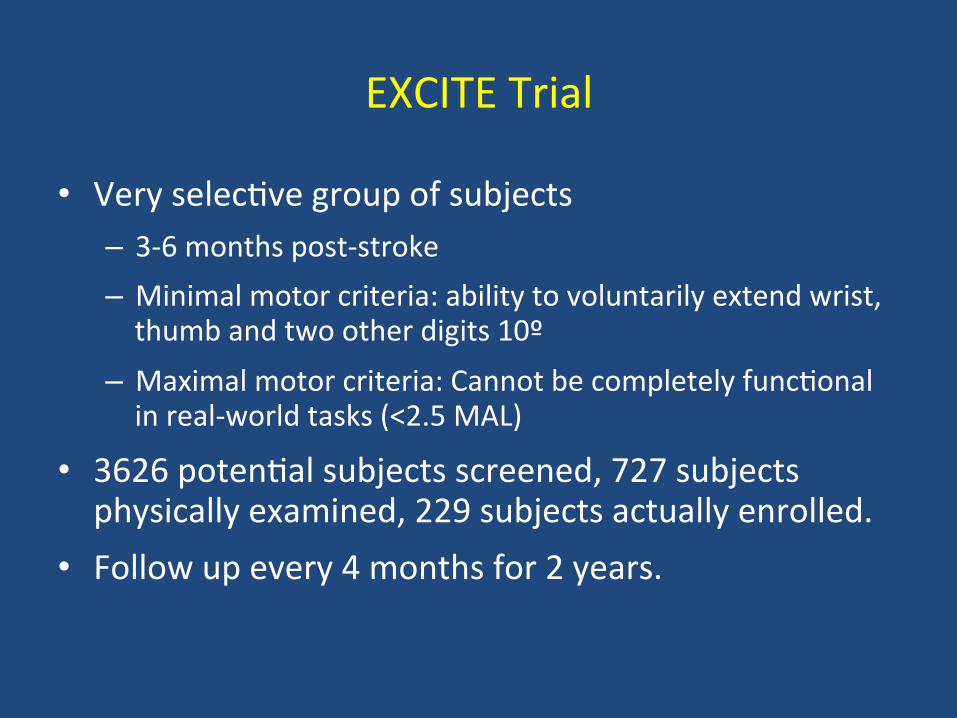
EXCITE Trial
• Very selec2ve group of subjects – 3-‐6 months post-‐stroke – Minimal motor criteria: ability to voluntarily extend wrist, thumb and two other digits 10º
– Maximal motor criteria: Cannot be completely func2onal in real-‐world tasks (<2.5 MAL)
• 3626 poten2al subjects screened, 727 subjects physically examined, 229 subjects actually enrolled.
• Follow up every 4 months for 2 years.
EXCITE Interven2on
• Wear “mib” 90% of waking hours during 2 weeks interven2on.
• Directed interven2on 6 hrs/day, 5 days/week • One-‐to-‐one repe22ve task prac2ce
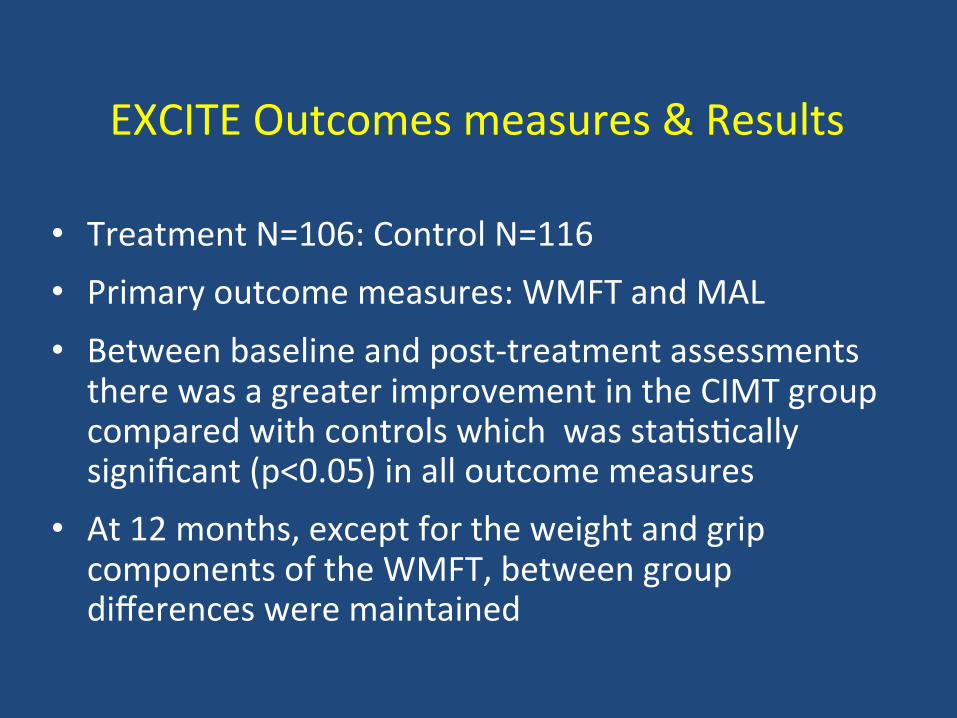
EXCITE Outcomes measures & Results
• Treatment N=106: Control N=116 • Primary outcome measures: WMFT and MAL • Between baseline and post-‐treatment assessments there was a greater improvement in the CIMT group compared with controls which was sta2s2cally significant (p<0.05) in all outcome measures
• At 12 months, except for the weight and grip components of the WMFT, between group differences were maintained

CIMT in children with CP
• Strong body of literature suppor2ng improved hand func2on1 (23 RCTs total N=814)
• Wide varia2on in:
– Type of constraint – Amount of wear and exercise
1Novak et al DMCD 55:885-‐910 2013
Guidelines for future research into CIMT in CP1
• Nine experts – reviewed the literature followed by a consensus mee2ng
• Iden2fied cri2cal issues for future research • Outcome:
– All models of CIMT demonstrated benefits (no large trials)
– Need for validated outcome measures
• Key ques2ons to be addressed – Predic2ve factors e.g. age – Is one model superior -‐ does dosage of training maber
– Effect of repeated use
1Eliasson et al DMCN 2014 56:125-‐137

Children and Robots
hbp://www.youtube.com/watch?v=sq6Qdz31d-‐o
• There have been no adequately powered RCTs to evaluate robot therapy in CP
• There have been no systema2c reviews
• Evidence is based on small studies and descrip2ve reviews

VA Robot Trial with stroke pa2ents1
• N=127 subjects >6 months post-‐ stroke randomized to:
-‐ Robot-‐assisted therapy (36 x 1 hour sessions)
-‐ Intensive conven2onal therapy (36 x 1 hour sessions)
-‐ Usual care (effec2vely no therapy)
• Outcome measures
-‐ Primary: Fugl-‐Meyer (FM)
-‐ Secondary: WMFT, SIS
1Lo et al, Robot assisted therapy for long-term upper limb impairment after stroke. NEJM 2010

VA Robot Trial1 Results • Subjects:
– Robot-‐assisted therapy (RT) (n=49) – Intensive comparison therapy (ICT) (n=50) – Usual care (UC) (n=28)
• At 12 weeks there was no significant difference in motor func2on between any groups
• Both intensive therapy and Robot assisted therapy were sta2s2cally significantly beber than usual care (at 36 weeks) (SIS)
• There was no difference between robot and intensive therapy
1Lo et al, Robot assisted therapy for long-term upper limb impairment after stroke. NEJM 2010
Summary of Evidence for UL Robot Therapy
• Evidence for improved motor control (impairment) and some evidence for improved func2on [Kwakkel 2008, EBRSR & Prange 2006]
• Merholz Cochrane review 2008 (11 studies n=328) – Safe, well accepted and improved func2on but lible evidence for improvement in ADL.
• People with moderate impairment may respond beber (stroke)
• Proximal training = proximal benefit

Evidence for robots in children1
• Upper limb robot and VR games (New jersey Ins2tute of Technology Robot Assisted VR rehabilita2on – NJIT-‐RAVR) for 9-‐12 hours over 3-‐weeks
• Nine children with CP
• Sta2s2cally significant improvement in kinema2c (path length, smoothness of movement and speed) measures taken in the robot
• Sta2s2cally significant improvement in the Melbourne Assessment (Pmes for: forward reach; sideways reach; hand-‐to-‐mouth and composite Pme)
• Suggests improvement in motor performance and control
1Fluet et al. Developmental Neurorehabilita2on October 2010; 13(5): 335-‐345

Interac2ve computer play as motor therapy
• Systema2c review -‐ 17 studies (6 upper limb, 5 lower, I fitness and 5 upper & lower limb)1
• Total: N=187 UL and N=114 lower limb • Two types:
– VR games e.g. Wii – VR + robot
• Level B evidence for LL and Level U for UL • Lack of evidence mainly due to small,
heterogenic samples, weak design • Promising trends especially in gross motor
func2on
1Fehlings et al Pediatric Neurology 20: 127-‐138 2013

Using technologies to improve motor control and co-‐ordina2on but with real rather than virtual objects

Technology supported Task Orientated Arm Training (T-‐TOAT)
A. A wireless iner2al sensors
B. Example of drinking
C. Picking up objects
D. Ea2ng with a fork
• Pa2ent mo2va2on and system U2lity
• Nine pa2ents 2x30 mins / day for 4 days /week for 8 weeks
• Iner2al sensors (Phillips II Node) incorpora2ng accelerometers, magnetometers, gyroscopes, radio transmiber and power supply worn on the sternum, upper and lower arm
• Ac2ve exercise board & so[ware toolkit – real objects and feedback via a PC – error between expected and actual angles etc.
• Outcome measures: ARAT, Fugl-‐Meyer, MAL (all improved sta2s2cally significantly @ 8 weeks and 6-‐months post interven2on). HR QoL improved @ 8 weeks
• T-‐TOAT Training: repe22ve, graduated prac2ce of the components of skills
• Followed by prac2ce of the skill • Skills included: ea2ng with a
knife and fork and drinking from a cup
Timmermans et al IEEE TNSRE Vol18 (3) 2010
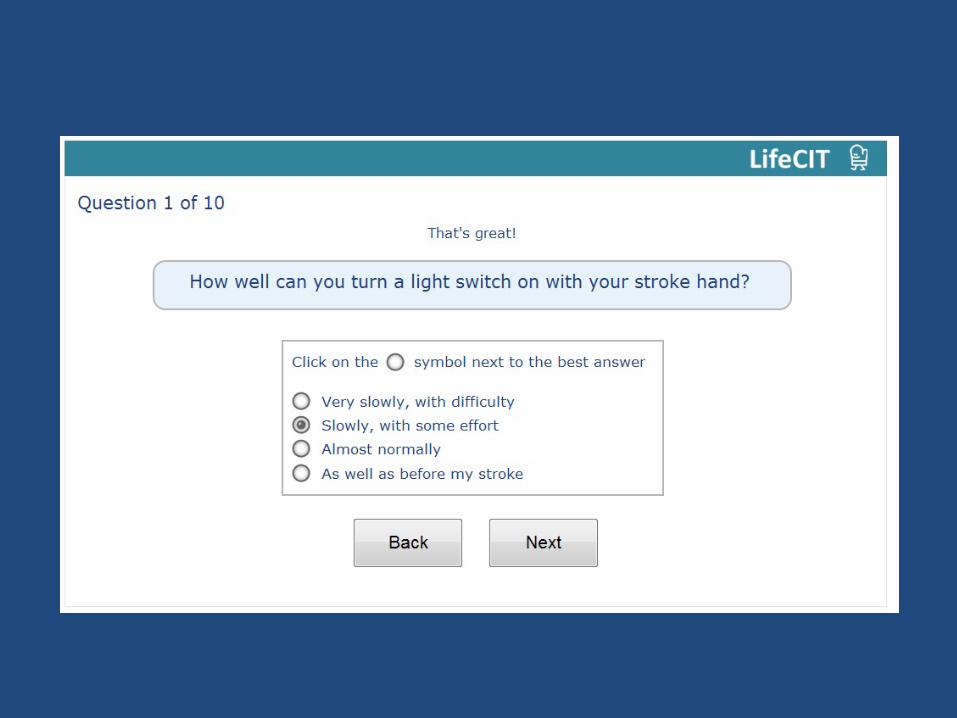
LifeCIT
A web-‐based support programme for people using Constraint Induced Movement Therapy (CIMT) at
home
Jane Burridge, Lucy Yardley, Ann-‐Marie Hughes, Sebas2en Pollet and Claire Meagher
This presenta2on presents independent research funded by the Na2onal Ins2tute for Health Research (NIHR)
under its Research for Pa2ent Benefit (RfPB) Programme (Grant Reference Number PB-‐PG-‐0909-‐20145). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
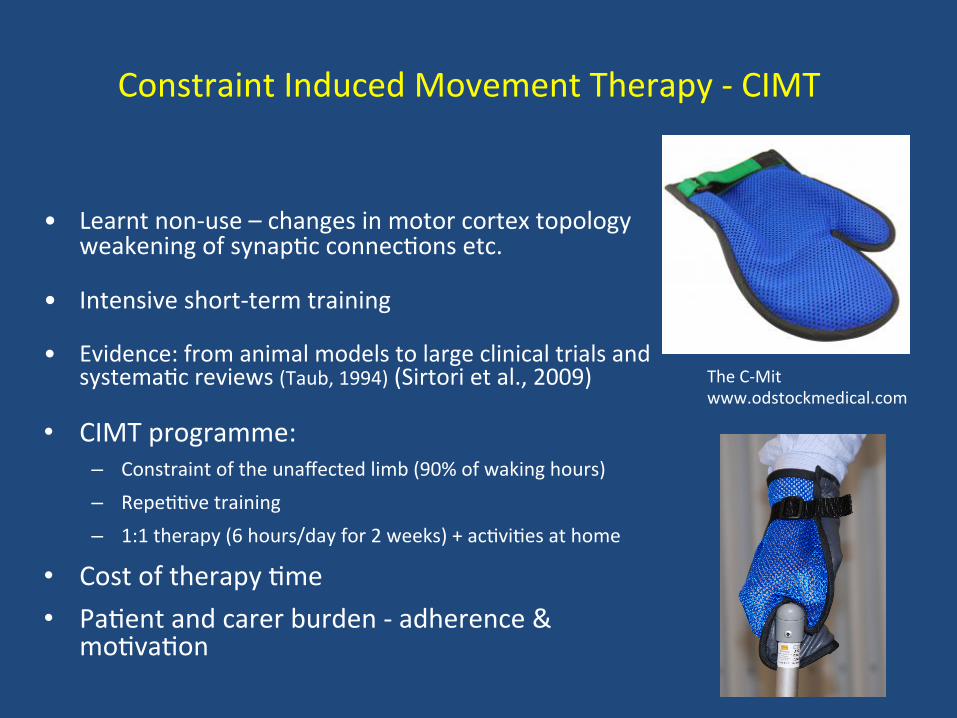
Constraint Induced Movement Therapy -‐ CIMT
• Learnt non-‐use – changes in motor cortex topology weakening of synap2c connec2ons etc.
• Intensive short-‐term training
• Evidence: from animal models to large clinical trials and systema2c reviews (Taub, 1994) (Sirtori et al., 2009)
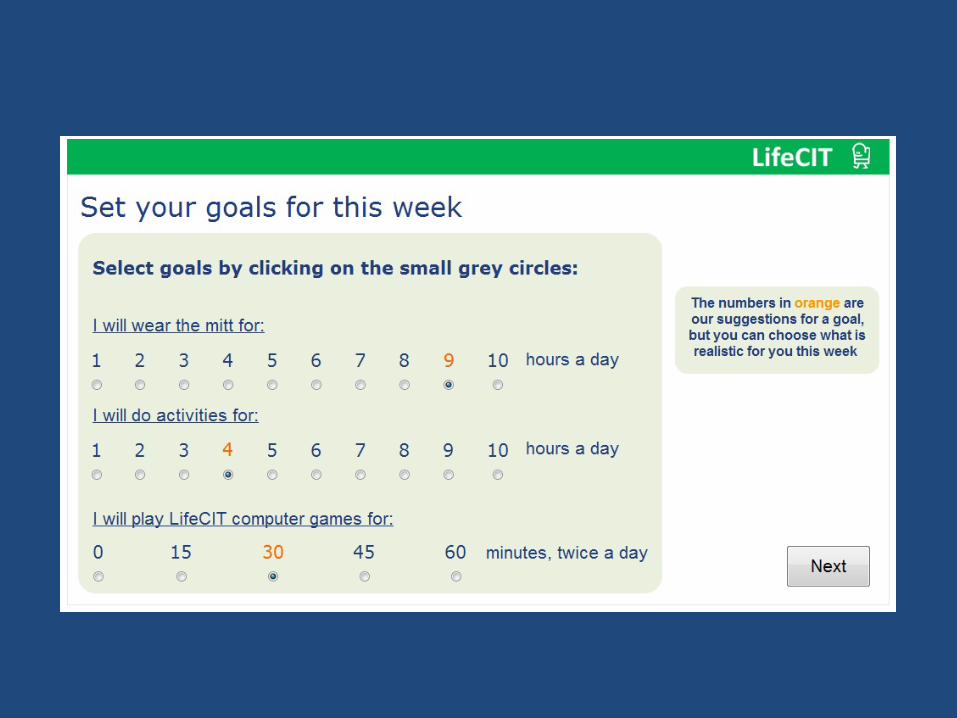
• CIMT programme: – Constraint of the unaffected limb (90% of waking hours) – Repe22ve training – 1:1 therapy (6 hours/day for 2 weeks) + ac2vi2es at home
• Cost of therapy 2me • Pa2ent and carer burden -‐ adherence &
mo2va2on
The C-‐Mit www.odstockmedical.com
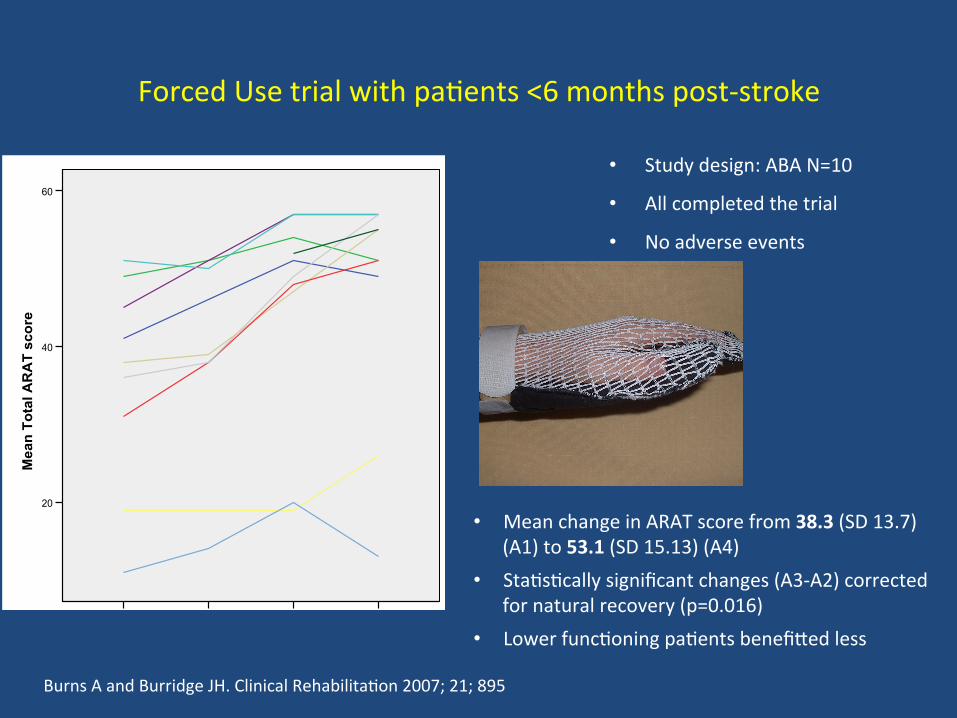
Forced Use trial with pa2ents <6 months post-‐stroke
• Study design: ABA N=10
• All completed the trial
• No adverse events
!
Burns A and Burridge JH. Clinical Rehabilita2on 2007; 21; 895
4321
Assessment
60
40
20
Mea
n To
tal A
RA
T sc
ore
29282726252423222120
Participant ID Stacked
• Mean change in ARAT score from 38.3 (SD 13.7) (A1) to 53.1 (SD 15.13) (A4)
• Sta2s2cally significant changes (A3-‐A2) corrected for natural recovery (p=0.016)
• Lower func2oning pa2ents benefibed less

• Phase 1: development (18 months) (2011-‐2012)
• Phase 2: mul2-‐centre pilot RCT (24 months)(2012-‐2013)
Phases of the study

Phase 1: Prototype 2. Developed via think-‐aloud studies with 12 sub-‐acute (<12 weeks) pa2ents in hospital and
home
Developments based on observed pa2ents’ behavior naviga2ng the website and simultaneous oral feedback
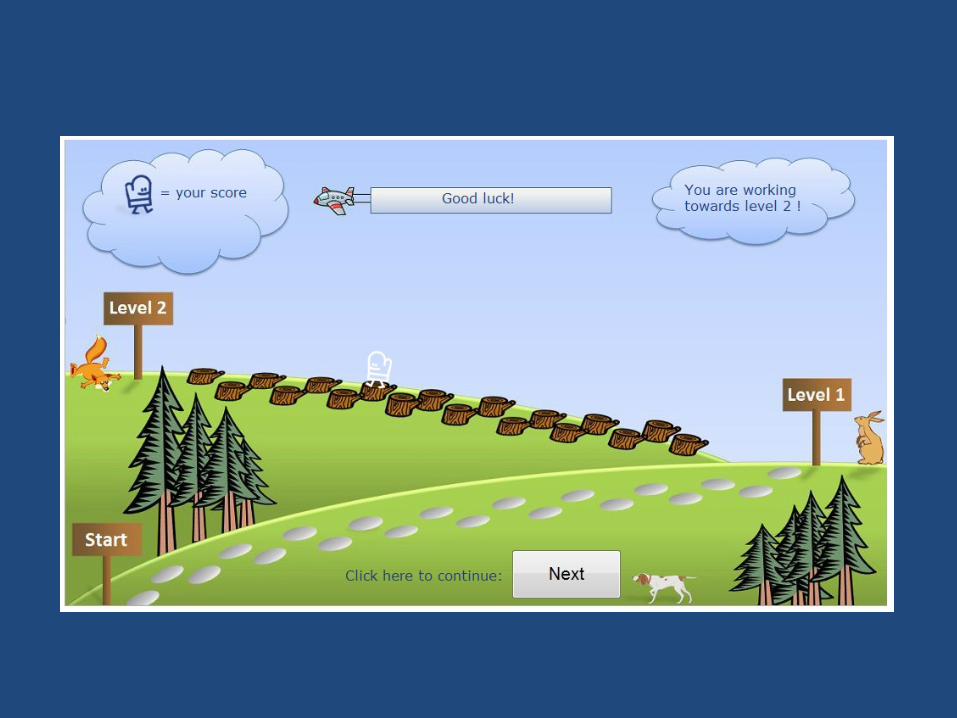
• Forced use therapy – 3 weeks • Interac2ve website • Mo2va2ng support and feedback
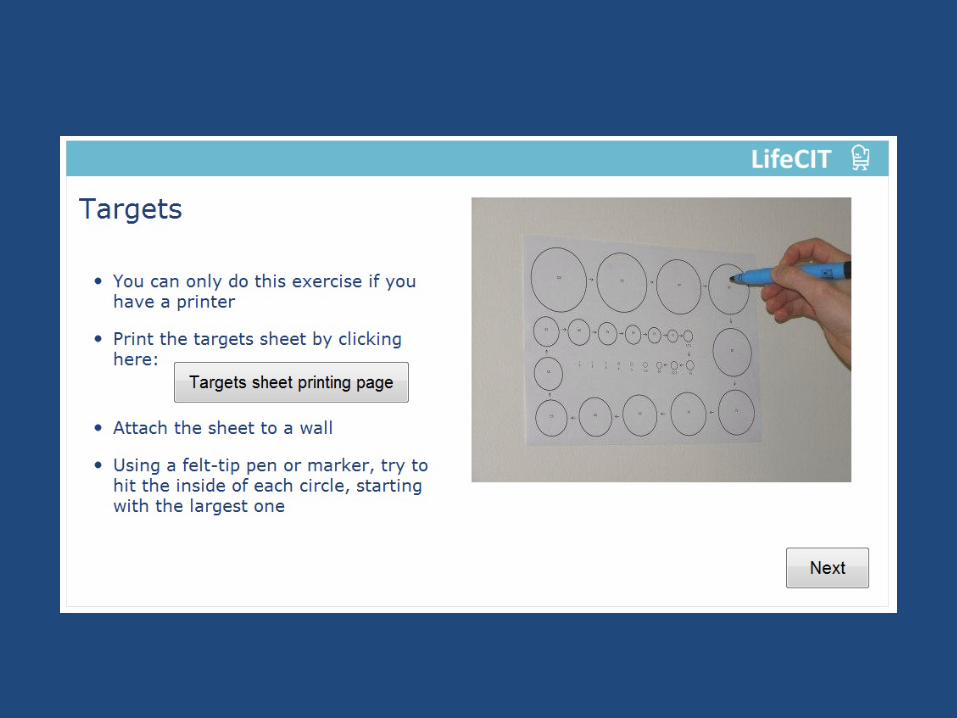
• Exercises and games
• Minimal cost: £50 for the constraint mib
The LifeCIT concept

Final Version of the Website







Developments based on observed pa2ents’ behavior naviga2ng the website and simultaneous oral feedback
• Website naviga2on:
– avoid mul2ple menu op2ons -‐ linear progression through the pages
– no scrolling – all informa2on on one page
• Clarity of instruc2ons:
– minimal text and avoiding ambiguity
– mo2va2onal language and illustra2ons e.g. ‘congratula2ons’ ‘use or lose it’
– Instruc2ons via video with a voice-‐over rather than text






CP literature has considered the importance of mo2va2on in therapy
• Acknowledged in both the stroke and CP communi2es that mo2va2on and engagement and cri2cal to outcomes
• And that technologies may enhance this
• Review of CP mo2va2on therapies combines results from studies of many different technologies
• Main finding: Mo2va2on is rarely measured – despite claims that the technologies improve mo2va2on
• Contribu2ng factors: loose defini2on and lack of consensus on the nature of mo2va2on
• Mo2va2on is mul2faceted construct -‐ need for effec2ve measures
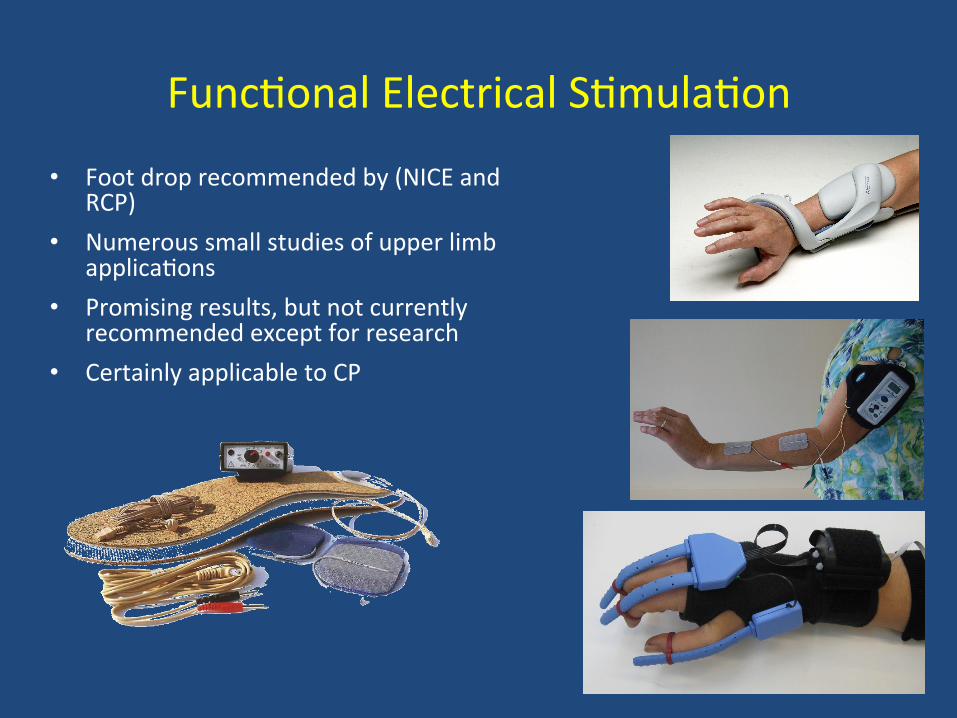
Func2onal Electrical S2mula2on
• Foot drop recommended by (NICE and RCP)
• Numerous small studies of upper limb applica2ons
• Promising results, but not currently recommended except for research
• Certainly applicable to CP

Direct Cor2cal S2mula2on

Cor2cal s2mula2on is based on the theory that increased excitability of cor2co-‐spinal projec2ons to pare2c muscles facilitates func2onal recovery

tDCS
• Current flows from anode to cathode through the brain
• May increase or decrease cor2cal excitability dependent on the direc2on and intensity of the current
• The effects of a single s2mula2on session persist for up to 1 hour
• Anodal tDCS has an excitatory effect on local cortex by depolarizing neurons
• Cathodal tDCS has an inhibitory effect due to hyperpolarisa2on

Meta-‐analysis of evidence for cor2cal s2mula2on (tDCS and TMS) in recovery of UL func2on 1
• Safe and promising tool demonstrated with mainly mild to moderate stroke pa2ents
• Methodological issues remain – rTMS vs. tDCS
– Dose – Time post-‐stroke
– Type and extent of lesion – Inhibi2on / excita2on
• There is currently lible evidence that tDCS or TMS is effec2ve in children, but the case for explora2on has been proposed2
73
1Nowak et al. NeurorehabilitaPon and Neural Repair 641-‐656 2009 2Adam Kirton Seminars in Pediatric Neurology 20:116-‐126 2013
Conclusions
• Many technology-‐based treatments seem to enhance motor recovery in stroke pa2ents
• Strong evidence for CIMT alone and in combina2on in stroke and some in CP
• Intensity of treatment, and probably task-‐oriented training, are the key variables – technologies may be useful in achieving this
• Mo2va2on and access to technologies • Technology is s2ll being developed and evaluated

Conclusions
• Currently there is lible evidence for either conven2onal or technology based neurorehabilita2on
• Providing high level evidence is very difficult in our field
• Objec2ve measurement is key to achieving this
• Incremental changes will not achieve our ambi2ons – a different approach to providing rehabilita2on and genera2ng evidence in needed
• Be BOLD!