
Odontogenic cutaneous sinus tract associated with ... - Springer
Upload
independentCategory
view
0download
0
Calcifying Cystic Odontogenic Tumour: immuno-histochemical expression of matrix metalloproteinases,their inhibitors (TIMPs and RECK) and inducer (EMMPRIN)
F�abio C. Prosd�ocimi1, Camila O. Rodini2, Mari C. Sogayar3, Suzana C. O. M. Sousa1, Fl�avia C. A. Xavier4,Kati�ucia B. S. Paiva1,5
1Department of Oral Pathology, Dental School, University of S~ao Paulo, S~ao Paulo, Brazil; 2Laboratory of Histology, Department ofBiological Sciences, Bauru Dental School, University of S~ao Paulo Bauru, S~ao Paulo, Brazil; 3Cell and Molecular Therapy Center(NUCEL), Department of Biochemistry, Chemistry Institute, University of S~ao Paulo, S~ao Paulo, Brazil; 4Department of Propedeutics andIntegrated Clinic, Dental School, Federal University of Bahia, Salvador, Brazil; 5Extracellular Matrix Biology and Cellular InteractionGroup, Laboratory of Molecular Mechanisms of Cytoprotection, Department of Biochemistry, Chemistry Institute, University of S~ao Paulo,S~ao Paulo, Brazil
BACKGROUND: Calcifying cyst odontogenic tumour
(CCOT) is a rare benign cystic neoplasm of odontogenic
origin. MMPs are responsible for extracellular matrix
remodelling and, together their inhibitors and inducer,
determinate the level of its turnover in pathological
processes, leading to an auspicious microenvironment for
tumour development. Thus, our goal was to evaluate
matrix metalloproteinases (MMPs-2, -7, -9 and -14), their
inhibitors (TIMPs-2, -3, -4 and RECK) and its inductor
(EMMPRIN) expression in CCOT.
MATERIALS AND METHODS: We used 18 cases of
CCOT submitted to immunolocalization of the target
proteins and analysed in both neoplastic odontogenic
epithelial and stromal compartments.
RESULTS: All molecules evaluated were expressed in
both compartments in CCOT. In epithelial layer, immu-
nostaining for MMPs, TIMPs, RECK and EMMPRIN was
found in basal, suprabasal spindle and stellate cells
surrounding ghost cells and ghost cells themselves,
except for MMP-9 and TIMP-2 which were only expressed
by ghost cells. In stromal compartment, extracellular
matrix, mesenchymal (MC) and endothelial cells (EC)
were positive for MMP-2, -7, TIMP-3 and -4, while MMP-9,
TIMP-2 and RECK were positive only in MC and MMP-14
only in EC. Statistical significance difference was found
between both compartments for MMP-9 (P < 0.001),
RECK (P = 0.004) and EMMPRIN (P < 0.001), being more
expressed in epithelium than in stroma. Positive corre-
lation between both stromal EMMPRIN and RECK
expression was found (R = 0.661, P = 0.003).
CONCLUSIONS: We concluded that these proteins/
enzymes are differentially expressed in both epithelium
and stroma of CCOT, suggesting an imbalance between
MMPs and their inducer/inhibitors may contribute on the
tumour behaviour.
J Oral Pathol Med (2014)
Keywords: Calcifying Cystic Odontogenic Tumour; EMMPRIN;
matrix metalloproteinases; RECK; tissue inhibitors of MMPs
Introduction
After the first description of the currently named calcifyingcystic odontogenic tumour (CCOT) as a benign odontogeniccyst in 1962 by Gorlin and colleagues (1), the question onthe cystic or neoplastic nature of this lesion raised severalmode of classifications. Then, considering the differenthistomorphological and clinicopathological features of thisset of tumours, the World Health Organization (WHO) in2005 renamed these lesions as tumours exhibiting threevariants (2): (I) calcifying cystic odontogenic tumour(CCOT) defined as a benign cystic neoplasm characterizedby an ameloblastoma-like epithelium with ghost cells thatmay calcify; (II) dentinogenic ghost cell tumour (DGCT)defined as a locally invasive neoplasm characterized byameloblastoma-like islands of epithelial cells in a matureconnective tissue stroma; and (III) ghost cell odontogeniccarcinoma (GCOC) defined as an uncommon malignantneoplasm that exhibits prominent mitotic activity, nuclearatypia and cellular pleomorphism, groups of ghost epithelialcells, necrosis, sometimes scarce mineralized or osteoden-tine-like (‘dentinoid’) material and infiltrative growth
Correspondence: Kati�ucia B. S. Paiva, Department of Oral Pathology,Dental School, University of S~ao Paulo, Avenida Lineu Prestes, 748 bloco9 superior, sala 959/974/976, Cidade Universit�aria, S~ao Paulo, SP 05508-000, Brazil. Tel/Fax: +551130913820, E-mail: [email protected] for publication December 21, 2013
doi: 10.1111/jop.12154
J Oral Pathol Med
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
wileyonlinelibrary.com/journal/jop
pattern (3). Thus, CCOT was classified as an epithelialodontogenic tumour with a contribution from odontogenicectomesenchyme, showing histological evidence of aninductive change (4).
Matrix metalloproteinases (MMPs) are the most impor-tant enzyme family responsible collectively for cleavage anddegradation of all components of the extracellular matrix(ECM) and then generating bioactive molecules. Severalpericellular and extracellular proteins are degraded orprocessed by MMPs (5). Nowadays, the proteolytic targetspectrum of MMPs was amplified, including other mole-cules on cell membrane and pericellular proteins non-relatedto ECM (other proteinases, intracellular substrates, latentgrowth factors, proteinase inhibitors, chemostatic mole-cules, growth factor binding proteins, cell membranereceptor, cell–cell and ECM–cell adhesion molecules),leading to the regulation of cell behaviour in severalpathways, mainly signal transduction (6–10).
Mammalian MMPs (24 members) are classified insoluble and cell membrane anchor-MMP (MT-MMP) inrelation to enzyme-substrate in vitro specificity and molec-ular structure, as well as discovery chronology. MMPs aredivided in collagenases (MMP-1, -8 and -13), gelatinases(MMP-2 and -9), stromelysins (MMP-3 and -10), matrily-sins (MMP-7 and -26), MT-MMPs (MMP-14, -15, -16,1-7, -24 and -25) and heterogeneous group (MMP-12, -19,-20, -21, -23, 27 and -28). Mostly, soluble MMPs aresecreted as pro-enzymes, and activation is requested intoECM (11), whereas MT-MMPs are activated in intracellu-lar space and expressed on cell membrane as active form(12).
MMPs are regulated at transcriptional and post-transcrip-tional levels by their inhibitors and inductors, as well asinteraction with specific ECM components (13). Geneexpression is controlled by several stimulant and suppressorfactors that influence many signalling pathways, such asintegrins, ECM proteins, hormones, growth factors, oncog-enes, cytokines, epigenetic regulation, cell stress, morpho-logical changes and extracellular matrix metalloproteinaseinducer (EMMPRIN/CD147) (14, 15). Regarding enzymaticinhibition, pro-MMP and its active form can be inhibited inthe ECM by their inhibitors anchored on the cell membraneas reversion-inducing cysteine-rich protein with Kazalmotifs (RECK) (16) and secreted into the ECM as tissueinhibitor of MMPs (TIMPs) (17). Most MMPs play centralrole in physiological conditions (stem cell differentiation,proliferation, cell mobility, tissue remodelling, wound
healing, angiogenesis and apoptosis), and an imbalancebetween MMPs, their inhibitors and inducer is implicated indifferent pathological processes (cancer, degenerative dis-eases) through several mechanisms, mainly related to tissuedestruction, fibrosis and changes in the microenvironment(ECM composition).MMP overexpression has already been correlated with
tumoural aggressiveness, stage and prognosis in a largerange of malignant tumours (18–20); however, little isknown about ECM changes and cell–ECM interactions inodontogenic tumours. Thus, our aim was to evaluate theimmunoexpression of some MMPs (-2, -7, -9 and -14),TIMPs (-2, -3 and -4), RECK and EMMPRIN in epithelialand stromal compartments of CCOT.
Material and methodsPatient tissue samplesThe research was approved by the Ethics Committee of theDental School, University of S~ao Paulo. Eighteen cases ofcalcifying cystic odontogenic tumour (CCOT), intra-osseous and without other associated odontogenic tumourswere obtained from the files of the Pathology Laboratory,Department of Stomatology (from 2000 to 2012). Histo-pathological diagnosis was confirmed by an oral pathologist
Table 1 Primary antibodies applied for immunohistochemistry
Antibody Clonality Specificity Source Cataloge Dilution
MMP-2 Rabbit polyclonal Pro- and active forms Abcam ab37150 1:250MMP-7 Rabbit polyclonal Pro-form Novus Biologicals NB600-1153 1:500MMP-9 Rabbit monoclonal Pro-form Abcam ab76003 1:200MMP-14 Rabbit monoclonal Active form Novus Biologicals NB110-57216 1:500TIMP-2 Mouse monoclonal C-terminal region Calbiochem IM56 1:500TIMP-3 Rabbit polyclonal C-terminal region Abcam ab39185 1:200TIMP-4 Rabbit polyclonal C-terminal region Abcam ab58425 1:200RECK Rabbit monoclonal Total protein Cell signalling 3433 1:50EMMPRIN Rabbit polyclonal C-terminal region Abcam ab70062 1:500
Table 2 Main clinical data of Calcifying Cystic Odontogenic Tumourcases in the studied sample
Patient Gender Age (years) Site
1 Male 39 Maxilla2 Male 40 Maxilla3 Male 36 Maxilla4 Female 21 Maxilla5 Female 27 Mandible6 Male 28 Uninformed7 Female 26 Anterior maxilla8 Male 19 Anterior maxilla9 Female 14 Right maxilla10 Female 20 Anterior maxilla11 Female 20 Anterior maxilla12 Male 26 Right angle mandible13 Female 28 Uninformed14 Female 21 Maxilla15 Male 47 Mandible16 Male 39 Mandible17 Male 15 Right maxilla18 Male 25 Anterior maxilla
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
2
(S.O.M.S.) through the slides review stained with haemat-oxylin and eosin, according to the WHO classification ofhead and neck tumours (3). The main clinical data asgender, age and tumour site were also collected.
ImmunohistochemistryFormalin-fixed paraffin-embedded (FFPE) CCOT tissuesections (4 lm thickness) were mounted on silane-coatedslides. After deparaffinization and rehydration in ethanol-graded series, the endogenous peroxidase was blocked by
3% H2O2 solution for 45 min, and the free charges wereneutralized by 1% borax solution for 15 min. Heat-inducedepitope retrieval (HIER) was performed with phosphate-citrate buffer – 93–96°C, pH 6.0 for 20 min (P4809; Sigma-Aldrich, St. Louis, MO, USA – except for MMP-2, forwhich no epitope retrieval was recommended by themanufacturer), and non-specific binding was blocked byProtein Block Serum-Free (X0909; DAKO, Carpinteria,CA, USA) for 10 min. The sections were incubated withprimary antibodies (Table 1) in a humid chamber at 4°C
A B
C D
E F
G H
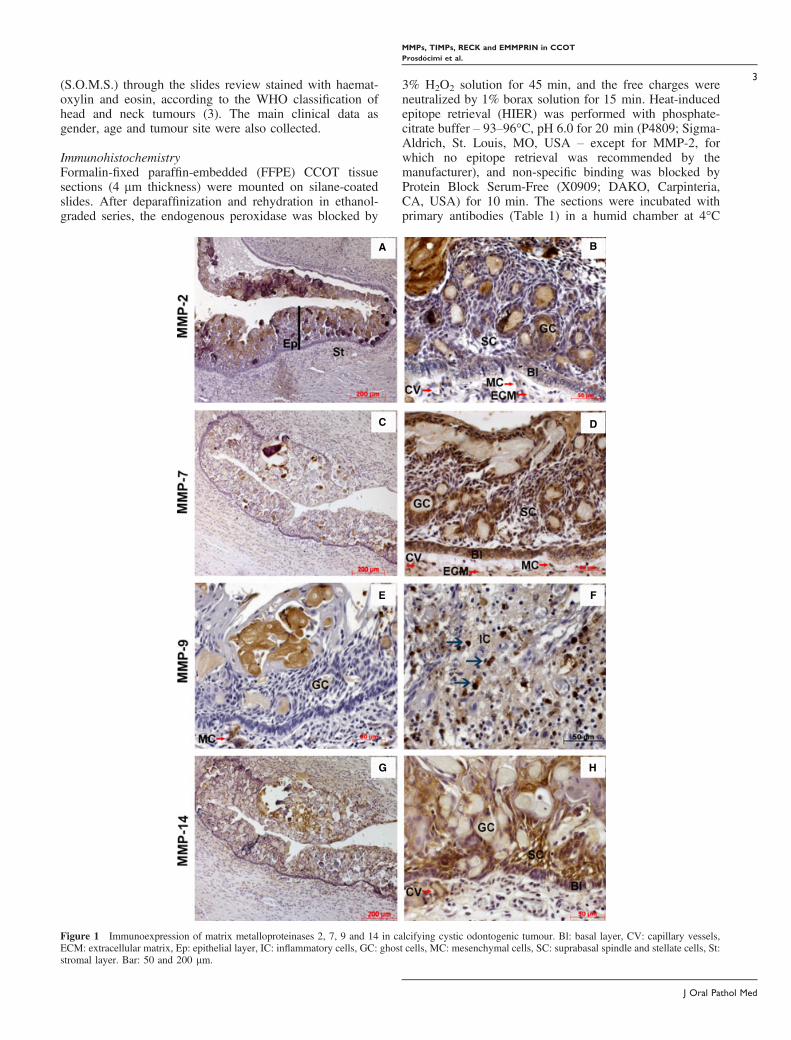
Figure 1 Immunoexpression of matrix metalloproteinases 2, 7, 9 and 14 in calcifying cystic odontogenic tumour. Bl: basal layer, CV: capillary vessels,ECM: extracellular matrix, Ep: epithelial layer, IC: inflammatory cells, GC: ghost cells, MC: mesenchymal cells, SC: suprabasal spindle and stellate cells, St:stromal layer. Bar: 50 and 200 lm.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
3
overnight, and detection was performed using EnVisionTM +Dual Link System-HRP (K4061; DAKO) or LSAB +System-HRP (K0690; DAKO). The immunostaining wasrevealed by Liquid DAB+Substrate-Chromogen System(K3468; DAKO), and the sections were counterstained withMayer′s haematoxylin. All rinses were performed using0.1% Triton X-100/PBS. Antibody diluent with backgroundreducing components (S3022; DAKO) was used for bothprimary antibody dilution and negative control (primaryantibody was replaced by this solution). Human oral
squamous cell carcinoma biopsy was used as positivecontrol for all antibodies.
Interpretation of immunohistochemical stainingThe immunohistochemical analysis was performed by twotrained examiners (F.C.A.X. and C.O.R.) at different times.Semi-quantitative analysis of immunostained cells in bothneoplastic odontogenic epithelium and adjacent stroma wasperformed according to immunostaining intensity: no stain-ing (�), weak (+), moderate (++) and intense (+++). The
A B
C D
E F
G H
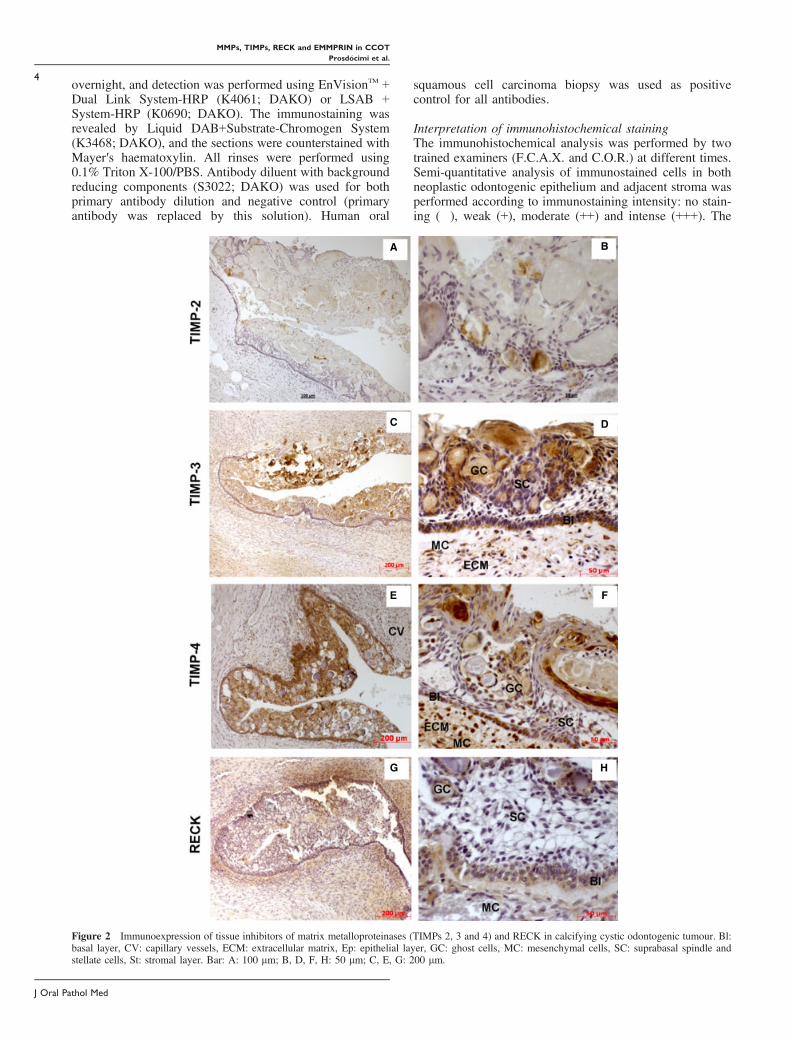
Figure 2 Immunoexpression of tissue inhibitors of matrix metalloproteinases (TIMPs 2, 3 and 4) and RECK in calcifying cystic odontogenic tumour. Bl:basal layer, CV: capillary vessels, ECM: extracellular matrix, Ep: epithelial layer, GC: ghost cells, MC: mesenchymal cells, SC: suprabasal spindle andstellate cells, St: stromal layer. Bar: A: 100 lm; B, D, F, H: 50 lm; C, E, G: 200 lm.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
4
percentage of immunopositive cells restricted to the neo-plastic odontogenic epithelium was estimated in 2009microscopic magnification and scored as 1 (≤ 10% ofstained epithelial cells), 2 (> 10 ≤ 50%), 3 (> 50 ≤ 75%)and 4 (> 75%). Immunostaining distribution was describedwithin epithelium (basal layer, suprabasal fusiform, stellateand ghost cells) and within stroma (mesenchymal andendothelial cells and extracellular matrix) and regardingcellular compartment as cell membrane, cytoplasmic and/ornuclear for all molecules.
Statistical analysisStatistical analysis was accomplished using the statisticalpackage Statistical Package for Social Sciences (SPSS),version 20.0 (IBM Corp., Armonk, NY, USA). Comparisonof absence (negative cases – no detected staining) orpresence (all positive cases independently of immunostain-ing intensity) found for each protein assessed between tissuecompartments (neoplastic odontogenic epithelium or adja-cent stroma) was performed using Fisher’s exact test, whilethe correlation between proteins expression within tissuecompartments was performed using Spearman’s rank cor-relation coefficient test. For both tests, P-value < 0.05 wasconsidered to indicate statistical significance.
Results
Clinical data demonstrated that the gender distribution ofCCOT was almost equal between males and females (10:8),and the individuals were usually young to middle-aged(age mean 27.7, SD = 9.36). The maxilla, predominantlythe anterior region, was in fact the most affected site(Table 2).
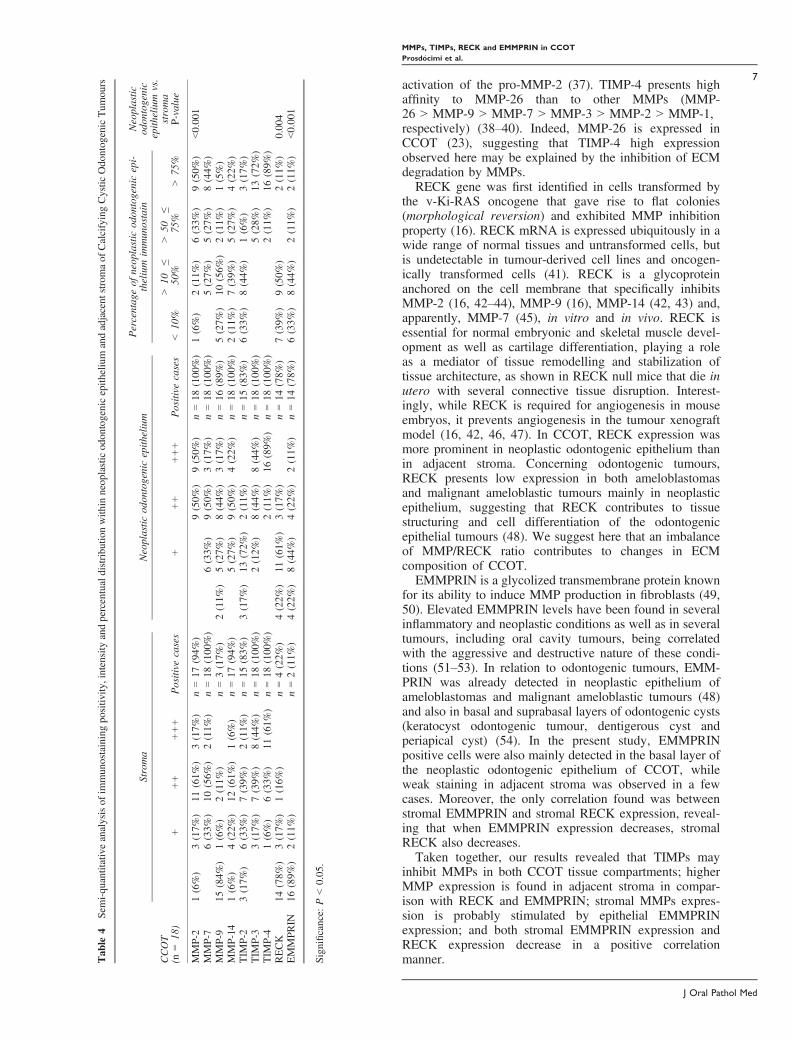
Immunohistochemical evaluation showed that allenzymes/proteins were expressed in variable amounts inboth neoplastic odontogenic epithelium and adjacent stromain all cases of CCOT. Regarding epithelial immunostaining,wide positivity for MMP-2 (n = 18/18) (Fig. 1A, B), MMP-7 (n = 18/18) (Fig. 1C, D), MMP-14 (n = 18/18) (Fig. 1G,H), TIMP-3 (n = 18/18) (Fig. 2C, D), TIMP-4 (n = 18/18)(Fig. 2E, F), RECK (n = 14/18) (Fig. 2G, H) and EMM-PRIN (n = 14/18) (Fig. 3A, B) was found in basal, spindlesuprabasal and stellate epithelial cells surrounding ghostcells as well as ghost cells themselves. MMP-9 (n = 16/18)
(Fig. 1C, D) and TIMP-2 (n = 15/18) (Fig. 2A, B) wereonly seen in ghost cells (Table 3). Cytoplasmic immuno-staining alone was found for MMP-2, MMP-7 and TIMP-3,while simultaneous cytoplasmic and cell membrane immu-nostaining were found for MMP-14, RECK and EMM-PRIN. Only TIMP-4 showed both cytoplasmic and nuclearimmunostaining patterns (Table 4). Concerning the per-centage of neoplastic epithelial immunopositive cells inCCOT, MMP-2, MMP-7, MMP-14 and TIMP-3 presentedscore 3, while TIMP-4 showed score 4. On the other hand,scarce immunostaining corresponding to score 2 wasobserved for MMP-9, TIMP-2, RECK and EMMPRIN inmost cases (Table 4). Regarding immunostaining intensity,cells were intense or moderately stained for MMP-2(n = 18/18), MMP-7 (n = 12/18), MMP-9 (n = 11/18),MMP-14 (n = 13/18), TIMP-3 (n = 16/18) and TIMP-4(n = 18/18), whereas weak staining was observed forTIMP-2 (n = 13/18), RECK (n = 11/18) and EMMPRIN(n = 8/18) in most cases (Table 4).When adjacent stroma was analysed, both mesenchymal
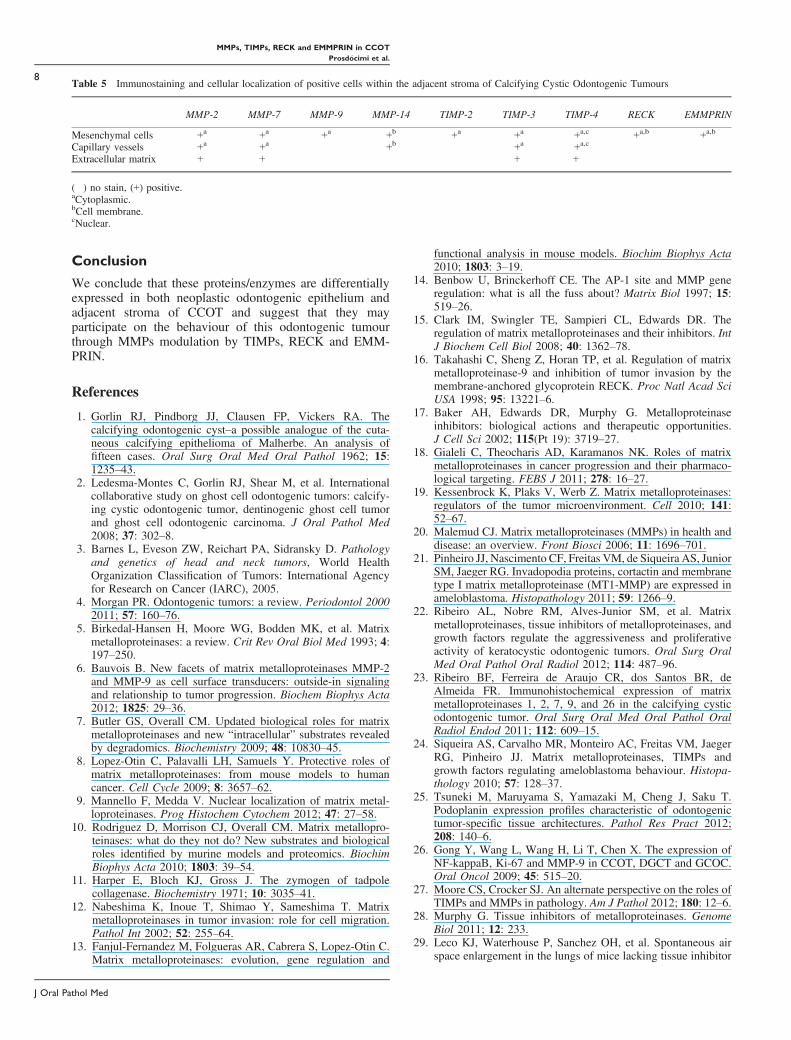
and endothelial cells, as well as the ECM, were alsoimmunopositive for MMP-2, MMP-7, TIMP-3, TIMP-4.MMP-9, TIMP-2, while positivity for RECK was only seenwithin mesenchymal cells, and MMP-14 was restricted toendothelial cells (Table 5). Cytoplasmic immunostainingalone was detected for MMP-2, MMP-7, MMP-9 andTIMP-2, and cell membrane immunostaining alone wasseen for MMP-14. Simultaneous cytoplasmic and nuclearimmunostaining were found for TIMP-4, and both cyto-plasmic and cell membrane immunostaining were found forRECK and EMMPRIN. Regarding immunostaining inten-sity, intense or moderate staining was observed for MMP-2,MMP-7, MMP-14, TIMP-2, TIMP-3 and TIMP-4, whereasweak staining for MMP-9 was observed in most cases. ForRECK and EMMPRIN, only a few cases presented weakpositivity (n = 3 and n = 2, respectively) (Tables 3 and 5).Comparing the immunostaining positivity for each pro-
tein between tissue compartments (neoplastic odontogenicepithelium and adjacent stroma), a statistically significantpositivity for MMP-9 (P < 0.001), RECK (P = 0.004) andEMMPRIN (P < 0.001) was found within the neoplasticodontogenic epithelium (Table 4). Furthermore, strongpositive correlation between stromal EMMPRIN andstromal RECK expression was found (P = 0.003 and
A B
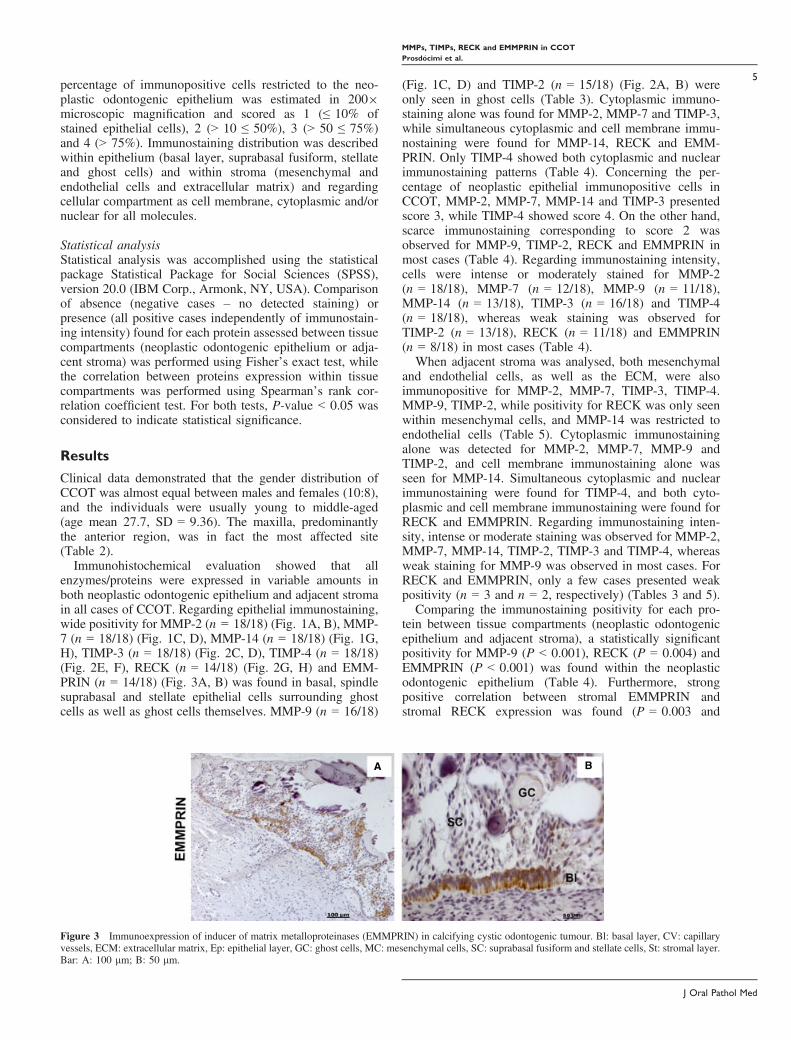
Figure 3 Immunoexpression of inducer of matrix metalloproteinases (EMMPRIN) in calcifying cystic odontogenic tumour. Bl: basal layer, CV: capillaryvessels, ECM: extracellular matrix, Ep: epithelial layer, GC: ghost cells, MC: mesenchymal cells, SC: suprabasal fusiform and stellate cells, St: stromal layer.Bar: A: 100 lm; B: 50 lm.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
5

r = 0.661), showing that when EMMPRIN expressiondecreases, stromal RECK expression also decreases.
Discussion
We presented in this study the distribution of MMPs, TIMPs,RECK and EMMPRIN in both neoplastic odontogenicepithelium and adjacent stroma of CCOT. To our knowledge,this is the first report of TIMP-3, TIMP-4, RECK andEMMPRIN in this tumour and, because CCOT is a rareodontogenic lesion, the results obtained from the 18 samplesused here represent robust information on the expression anddistribution of these markers within the tumour.
Traditionally, MMP biological functions have beenassociated with degradation and turnover of most ECMcomponents. This functional simplistic conception has beenused through the years to explain MMP involvement inembryonic development, homeostasis and disease. Forinstance, this has lead to the employment of MMP inhibitorsin clinical trials for cancer treatment without success, raisingthe question of whether they can be really therapeutictargets. Recent studies using degradomics and proteomicsapproaches in MMP knockout mice models have changedMMP function dogma revealing dubious functions intissues, both protective and destructive depending on thebiological process involved (6–10).
All MMPs evaluated in the present study were detectedboth in neoplastic odontogenic epithelium and adjacentstroma of CCOT in variable amounts, confirming previousfindings (21–24). Although MMPs expression level in bothneoplastic odontogenic epithelium and adjacent stroma ofCCOT is known to be lower than in ameloblastoma (21, 25)and keratocystic odontogenic tumour (22, 25), our resultsrevealed a higher expression ratio of MMP-9 in neoplasticepithelium compared to stroma in CCOT, mainly in ghostcells as already reported by others (25, 26).
TIMPs have comparable abilities to inhibit the activeforms of the MMPs and have shown to form tightcomplexes with active MMPs in a 1:1 stoichiometry.TIMPs inhibit all MMPs, but TIMP-1 is a poor inhibitorof MMP-14, MMP-17, MMP-19 and MMP-24. In additionto inhibiting MMP activity, TIMP-2 unique feature is toselectively interact with MMP-14 to facilitate the cellsurface activation of pro-MMP-2 (tertiary complex TIMP-2/MMP-14/pro-MMP-2). TIMPs show tissue-specific, con-stitutive or inducible expression, which is regulated at thetranscriptional level by various cytokines and growth
factors. The roles of TIMPs in both normal physiologyand in pathological processes have been investigated, andthese have indicated that there is some functional redun-dancy. Elevated MMP/TIMP expression ratios have beenassociated with many diseases, while elevated MMP/TIMPprotein level ratios are often viewed and interpreted withrespect to the net increase in proteolytic activity of MMPsand disease pathology (27, 28).All TIMPs evaluated here were detected in both
neoplastic odontogenic epithelium and adjacent stromaalso in variable amounts, confirming previous findings ofothers (22, 24), with the exception of TIMP-3 and TIMP-4,which are described for the first time in this study. AmongTIMPs, TIMP-3 is a glycoprotein that has complex sugarchains and is unique on interacting strongly with the ECMcomponents (sulphated glycosaminoglycans) (28). Timp-3gene deletion causes lung emphysema-like alveolar damage(29) and faster apoptosis of mammary epithelial cells afterweaning (30). TIMP-3 has conflicting activities accordingto cell type; in some cells, it appears to promote thedevelopment of a transformed phenotype, promotingapoptosis in several tumour cell lines and in smoothmuscle cells, but this appears to involve the modulation ofMMPs activities. This suggests that TIMP-3 is a majorregulator of MMP activities in vivo. Furthermore, TIMP-3plays a key role in innate immunity by regulating theprocessing of tumour necrosis factor-a (TNF-a) byADAM17 (31) is implicated in vascular inhibitionby blockage of VEGF binding to its receptor (32), byinteraction to angiotensin II type 2 (33), as well as TIMP-3knockout mice have been showed neovascularization (34).Although TIMP-3 was strongly detected in both neoplasticodontogenic epithelium and adjacent stroma of CCOT,nothing is known in the literature about its expression inodontogenic tumours. Recent study demonstrated thatTGF-b/Smad signalling in CCOT and adenomatoid odon-togenic tumour is higher than in ameloblastoma, suggestinglow and high neoplastic dynamics in these tumours,respectively (35). In our study, we could speculate thatTIMP-3 might be expressed by TGF-b induction and act onthe inhibition of MMP-2, MMP-7, MMP-9 and MMP-14 toprevent excess ECM degradation and avoid tumourexpansion and progression.Human TIMP-4 is a non-glycosylated protein more
closely related to TIMP-2 and -3 than to TIMP-1, binds topro-MMP-2, and it is also a strong inhibitor of MMP-2 andMMP-14 (36); however, it is unable to promote the
Table 3 Immunostaining and cellular localization of positive cells in neoplastic odontogenic epithelium of Calcifying Cystic Odontogenic Tumours
MMP-2 MMP-7 MMP-9 MMP-14 TIMP-2 TIMP-3 TIMP-4 RECK EMMPRIN
Basal layer +a +a � +a,b � +a +a,c +a,b +a,b
Suprabasalfusiform andstellate cells
+a +a � +a,b � +a +a,c +a,b +a,b
Ghost cells + + + + + + + + +
(�) no stain, (+) positive.aCytoplasmic.bCell membrane.cNuclear.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
6
activation of the pro-MMP-2 (37). TIMP-4 presents highaffinity to MMP-26 than to other MMPs (MMP-26 > MMP-9 > MMP-7 > MMP-3 > MMP-2 > MMP-1,respectively) (38–40). Indeed, MMP-26 is expressed inCCOT (23), suggesting that TIMP-4 high expressionobserved here may be explained by the inhibition of ECMdegradation by MMPs.RECK gene was first identified in cells transformed by
the v-Ki-RAS oncogene that gave rise to flat colonies(morphological reversion) and exhibited MMP inhibitionproperty (16). RECK mRNA is expressed ubiquitously in awide range of normal tissues and untransformed cells, butis undetectable in tumour-derived cell lines and oncogen-ically transformed cells (41). RECK is a glycoproteinanchored on the cell membrane that specifically inhibitsMMP-2 (16, 42–44), MMP-9 (16), MMP-14 (42, 43) and,apparently, MMP-7 (45), in vitro and in vivo. RECK isessential for normal embryonic and skeletal muscle devel-opment as well as cartilage differentiation, playing a roleas a mediator of tissue remodelling and stabilization oftissue architecture, as shown in RECK null mice that die inutero with several connective tissue disruption. Interest-ingly, while RECK is required for angiogenesis in mouseembryos, it prevents angiogenesis in the tumour xenograftmodel (16, 42, 46, 47). In CCOT, RECK expression wasmore prominent in neoplastic odontogenic epithelium thanin adjacent stroma. Concerning odontogenic tumours,RECK presents low expression in both ameloblastomasand malignant ameloblastic tumours mainly in neoplasticepithelium, suggesting that RECK contributes to tissuestructuring and cell differentiation of the odontogenicepithelial tumours (48). We suggest here that an imbalanceof MMP/RECK ratio contributes to changes in ECMcomposition of CCOT.EMMPRIN is a glycolized transmembrane protein known
for its ability to induce MMP production in fibroblasts (49,50). Elevated EMMPRIN levels have been found in severalinflammatory and neoplastic conditions as well as in severaltumours, including oral cavity tumours, being correlatedwith the aggressive and destructive nature of these condi-tions (51–53). In relation to odontogenic tumours, EMM-PRIN was already detected in neoplastic epithelium ofameloblastomas and malignant ameloblastic tumours (48)and also in basal and suprabasal layers of odontogenic cysts(keratocyst odontogenic tumour, dentigerous cyst andperiapical cyst) (54). In the present study, EMMPRINpositive cells were also mainly detected in the basal layer ofthe neoplastic odontogenic epithelium of CCOT, whileweak staining in adjacent stroma was observed in a fewcases. Moreover, the only correlation found was betweenstromal EMMPRIN and stromal RECK expression, reveal-ing that when EMMPRIN expression decreases, stromalRECK also decreases.Taken together, our results revealed that TIMPs may
inhibit MMPs in both CCOT tissue compartments; higherMMP expression is found in adjacent stroma in compar-ison with RECK and EMMPRIN; stromal MMPs expres-sion is probably stimulated by epithelial EMMPRINexpression; and both stromal EMMPRIN expression andRECK expression decrease in a positive correlationmanner.T
able
4Semi-quantitativeanalysisof
immunostainingpositiv
ity,intensity
andpercentualdistributio
nwith
inneoplasticodontogenicepith
elium
andadjacent
stromaof
CalcifyingCystic
OdontogenicTum
ours
CCOT
(n=
18)
Stroma
Neoplastic
odon
togenicepith
elium
Percentageof
neoplastic
odontogenicepi-
thelium
immunostain
Neoplastic
odon
togenic
epith
elium
vs.
stroma
P-value
�+
++
+++
Positive
cases
�+
++
+++
Positive
cases
<10
%>
10�≤
50%
>50�≤
75%
>75
%
MMP-2
1(6%)
3(17%
)11
(61%
)3(17%
)n=17
(94%
)�
�9(50%
)9(50%
)n=18
(100
%)
1(6%)
2(11%
)6(33%
)9(50%
)<0.00
1MMP-7
�6(33%
)10
(56%
)2(11%
)n=18
(100
%)
�6(33%
)9(50%
)3(17%
)n=18
(100
%)
�5(27%
)5(27%
)8(44%
)MMP-9
15(84%
)1(6%)
2(11%
)�
n=3(17%
)2(11%
)5(27%
)8(44%
)3(17%
)n=16
(89%
)5(27%
)10
(56%
)2(11%
)1(5%)
MMP-14
1(6%)
4(22%
)12
(61%
)1(6%)
n=17
(94%
)�
5(27%
)9(50%
)4(22%
)n=18
(100
%)
2(11%
)7(39%
)5(27%
)4(22%
)TIM
P-2
3(17%
)6(33%
)7(39%
)2(11%
)n=15
(83%
)3(17%
)13
(72%
)2(11%
)�
n=15
(83%
)6(33%
)8(44%
)1(6%)
3(17%
)TIM
P-3
�3(17%
)7(39%
)8(44%
)n=18
(100
%)
�2(12%
)8(44%
)8(44%
)n=18
(100
%)
��
5(28%
)13
(72%
)TIM
P-4
�1(6%)
6(33%
)11
(61%
)n=18
(100
%)
��
2(11%
)16
(89%
)n=18
(100
%)
��
2(11%
)16
(89%
)RECK
14(78%
)3(17%
)1(16%
)�
n=4(22%
)4(22%
)11
(61%
)3(17%
)�
n=14
(78%
)7(39%
)9(50%
)�
2(11%
)0.00
4EMMPR
IN16
(89%
)2(11%
)�
�n=2(11%
)4(22%
)8(44%
)4(22%
)2(11%
)n=14
(78%
)6(33%
)8(44%
)2(11%
)2(11%
)<0.00
1
Significance:
P<0.05
.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
7
Conclusion
We conclude that these proteins/enzymes are differentiallyexpressed in both neoplastic odontogenic epithelium andadjacent stroma of CCOT and suggest that they mayparticipate on the behaviour of this odontogenic tumourthrough MMPs modulation by TIMPs, RECK and EMM-PRIN.
References
1. Gorlin RJ, Pindborg JJ, Clausen FP, Vickers RA. Thecalcifying odontogenic cyst–a possible analogue of the cuta-neous calcifying epithelioma of Malherbe. An analysis offifteen cases. Oral Surg Oral Med Oral Pathol 1962; 15:1235–43.
2. Ledesma-Montes C, Gorlin RJ, Shear M, et al. Internationalcollaborative study on ghost cell odontogenic tumors: calcify-ing cystic odontogenic tumor, dentinogenic ghost cell tumorand ghost cell odontogenic carcinoma. J Oral Pathol Med2008; 37: 302–8.
3. Barnes L, Eveson ZW, Reichart PA, Sidransky D. Pathologyand genetics of head and neck tumors, World HealthOrganization Classification of Tumors: International Agencyfor Research on Cancer (IARC), 2005.
4. Morgan PR. Odontogenic tumors: a review. Periodontol 20002011; 57: 160–76.
5. Birkedal-Hansen H, Moore WG, Bodden MK, et al. Matrixmetalloproteinases: a review. Crit Rev Oral Biol Med 1993; 4:197–250.
6. Bauvois B. New facets of matrix metalloproteinases MMP-2and MMP-9 as cell surface transducers: outside-in signalingand relationship to tumor progression. Biochem Biophys Acta2012; 1825: 29–36.
7. Butler GS, Overall CM. Updated biological roles for matrixmetalloproteinases and new “intracellular” substrates revealedby degradomics. Biochemistry 2009; 48: 10830–45.
8. Lopez-Otin C, Palavalli LH, Samuels Y. Protective roles ofmatrix metalloproteinases: from mouse models to humancancer. Cell Cycle 2009; 8: 3657–62.
9. Mannello F, Medda V. Nuclear localization of matrix metal-loproteinases. Prog Histochem Cytochem 2012; 47: 27–58.
10. Rodriguez D, Morrison CJ, Overall CM. Matrix metallopro-teinases: what do they not do? New substrates and biologicalroles identified by murine models and proteomics. BiochimBiophys Acta 2010; 1803: 39–54.
11. Harper E, Bloch KJ, Gross J. The zymogen of tadpolecollagenase. Biochemistry 1971; 10: 3035–41.
12. Nabeshima K, Inoue T, Shimao Y, Sameshima T. Matrixmetalloproteinases in tumor invasion: role for cell migration.Pathol Int 2002; 52: 255–64.
13. Fanjul-Fernandez M, Folgueras AR, Cabrera S, Lopez-Otin C.Matrix metalloproteinases: evolution, gene regulation and
functional analysis in mouse models. Biochim Biophys Acta2010; 1803: 3–19.
14. Benbow U, Brinckerhoff CE. The AP-1 site and MMP generegulation: what is all the fuss about? Matrix Biol 1997; 15:519–26.
15. Clark IM, Swingler TE, Sampieri CL, Edwards DR. Theregulation of matrix metalloproteinases and their inhibitors. IntJ Biochem Cell Biol 2008; 40: 1362–78.
16. Takahashi C, Sheng Z, Horan TP, et al. Regulation of matrixmetalloproteinase-9 and inhibition of tumor invasion by themembrane-anchored glycoprotein RECK. Proc Natl Acad SciUSA 1998; 95: 13221–6.
17. Baker AH, Edwards DR, Murphy G. Metalloproteinaseinhibitors: biological actions and therapeutic opportunities.J Cell Sci 2002; 115(Pt 19): 3719–27.
18. Gialeli C, Theocharis AD, Karamanos NK. Roles of matrixmetalloproteinases in cancer progression and their pharmaco-logical targeting. FEBS J 2011; 278: 16–27.
19. Kessenbrock K, Plaks V, Werb Z. Matrix metalloproteinases:regulators of the tumor microenvironment. Cell 2010; 141:52–67.
20. Malemud CJ. Matrix metalloproteinases (MMPs) in health anddisease: an overview. Front Biosci 2006; 11: 1696–701.
21. Pinheiro JJ, Nascimento CF, Freitas VM, de Siqueira AS, JuniorSM, Jaeger RG. Invadopodia proteins, cortactin and membranetype I matrix metalloproteinase (MT1-MMP) are expressed inameloblastoma. Histopathology 2011; 59: 1266–9.
22. Ribeiro AL, Nobre RM, Alves-Junior SM, et al. Matrixmetalloproteinases, tissue inhibitors of metalloproteinases, andgrowth factors regulate the aggressiveness and proliferativeactivity of keratocystic odontogenic tumors. Oral Surg OralMed Oral Pathol Oral Radiol 2012; 114: 487–96.
23. Ribeiro BF, Ferreira de Araujo CR, dos Santos BR, deAlmeida FR. Immunohistochemical expression of matrixmetalloproteinases 1, 2, 7, 9, and 26 in the calcifying cysticodontogenic tumor. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2011; 112: 609–15.
24. Siqueira AS, Carvalho MR, Monteiro AC, Freitas VM, JaegerRG, Pinheiro JJ. Matrix metalloproteinases, TIMPs andgrowth factors regulating ameloblastoma behaviour. Histopa-thology 2010; 57: 128–37.
25. Tsuneki M, Maruyama S, Yamazaki M, Cheng J, Saku T.Podoplanin expression profiles characteristic of odontogenictumor-specific tissue architectures. Pathol Res Pract 2012;208: 140–6.
26. Gong Y, Wang L, Wang H, Li T, Chen X. The expression ofNF-kappaB, Ki-67 and MMP-9 in CCOT, DGCT and GCOC.Oral Oncol 2009; 45: 515–20.
27. Moore CS, Crocker SJ. An alternate perspective on the roles ofTIMPs and MMPs in pathology. Am J Pathol 2012; 180: 12–6.
28. Murphy G. Tissue inhibitors of metalloproteinases. GenomeBiol 2011; 12: 233.
29. Leco KJ, Waterhouse P, Sanchez OH, et al. Spontaneous airspace enlargement in the lungs of mice lacking tissue inhibitor
Table 5 Immunostaining and cellular localization of positive cells within the adjacent stroma of Calcifying Cystic Odontogenic Tumours
MMP-2 MMP-7 MMP-9 MMP-14 TIMP-2 TIMP-3 TIMP-4 RECK EMMPRIN
Mesenchymal cells +a +a +a +b +a +a +a,c +a,b +a,b
Capillary vessels +a +a � +b � +a +a,c � �Extracellular matrix + + � � � + + � �
(�) no stain, (+) positive.aCytoplasmic.bCell membrane.cNuclear.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
8
of metalloproteinases-3 (TIMP-3). J Clin Invest 2001; 108:817–29.
30. Fata JE, Leco KJ, Voura EB, et al. Accelerated apoptosis inthe Timp-3-deficient mammary gland. J Clin Invest 2001; 108:831–41.
31. Smookler DS, Mohammed FF, Kassiri Z, Duncan GS, MakTW, Khokha R. Tissue inhibitor of metalloproteinase 3regulates TNF-dependent systemic inflammation. J Immunol2006; 176: 721–5.
32. Qi JH, Ebrahem Q, Ali M, et al. Tissue inhibitor ofmetalloproteinases-3 peptides inhibit angiogenesis and choroi-dal neovascularization in mice. PLoS ONE 2013; 8: e55667.
33. Kang KH, Park SY, Rho SB, Lee JH. Tissue inhibitor ofmetalloproteinases-3 interacts with angiotensin II type 2receptor and additively inhibits angiogenesis. CardiovascRes 2008; 79: 150–60.
34. Ebrahem Q, Qi JH, Sugimoto M, et al. Increased neovascu-larization in mice lacking tissue inhibitor of metalloproteinas-es-3. Invest Ophthalmol Vis Sci 2011; 52: 6117–23.
35. Karathanasi V, Tosios KI, Nikitakis NG, et al. TGF-beta1,Smad-2/-3, Smad-1/-5/-8, and Smad-4 signaling factors areexpressed in ameloblastomas, adenomatoid odontogenictumors, and calcifying cystic odontogenic tumors: an immu-nohistochemical study. J Oral Pathol Med 2013; 42: 415–23.
36. Melendez-Zajgla J, Del PL, Ceballos G, Maldonado V. Tissueinhibitor of metalloproteinases-4. The road less traveled. MolCancer 2008; 7: 85.
37. Bigg HF, Morrison CJ, Butler GS, et al. Tissue inhibitor ofmetalloproteinases-4 inhibits but does not support the activa-tion of gelatinase A via efficient inhibition of membrane type1-matrix metalloproteinase. Cancer Res 2001; 61: 3610–8.
38. Liu YE, Wang M, Greene J, et al. Preparation and character-ization of recombinant tissue inhibitor of metalloproteinase 4(TIMP-4). J Biol Chem 1997; 272: 20479–83.
39. Troeberg L, Tanaka M, Wait R, Shi YE, Brew K, Nagase H.E. coli expression of TIMP-4 and comparative kinetic studieswith TIMP-1 and TIMP-2: insights into the interactions ofTIMPs and matrix metalloproteinase 2 (gelatinase A). Bio-chemistry 2002; 41: 15025–35.
40. Zhang J, Cao YJ, Zhao YG, Sang QX, Duan EK. Expressionof matrix metalloproteinase-26 and tissue inhibitor of metal-loproteinase-4 in human normal cytotrophoblast cells and achoriocarcinoma cell line, JEG-3. Mol Hum Reprod 2002; 8:659–66.
41. Noda M, Takahashi C. Recklessness as a hallmark ofaggressive cancer. Cancer Sci 2007; 98: 1659–65.
42. Oh J, Takahashi R, Kondo S, et al. The membrane-anchoredMMP inhibitor RECK is a key regulator of extracellular matrixintegrity and angiogenesis. Cell 2001; 107: 789–800.
43. Sasahara RM, Brochado SM, Takahashi C, et al. Transcrip-tional control of the RECK metastasis/angiogenesis suppressorgene. Cancer Detect Prev 2002; 26: 435–43.
44. Takagi S, Simizu S, Osada H. RECK negatively regulatesmatrix metalloproteinase-9 transcription. Cancer Res 2009; 69:1502–8.
45. Omura A, Matsuzaki T, Mio K, et al. RECK forms cowbell-shaped dimers and inhibits matrix metalloproteinase-catalyzedcleavage of fibronectin. J Biol Chem 2009; 284: 3461–9.
46. Echizenya M, Kondo S, Takahashi R, et al. The membrane-anchored MMP-regulator RECK is a target of myogenicregulatory factors. Oncogene 2005; 24: 5850–7.
47. Welm B, Mott J, Werb Z. Developmental biology: vasculo-genesis is a wreck without RECK. Curr Biol 2002; 12: R209–11.
48. Kumamoto H, Ooya K. Immunohistochemical detection ofMT1-MMP, RECK, and EMMPRIN in ameloblastic tumors.J Oral Pathol Med 2006; 35: 345–51.
49. Biswas C, Zhang Y, DeCastro R, et al. The human tumor cell-derived collagenase stimulatory factor (renamed EMMPRIN)is a member of the immunoglobulin superfamily. Cancer Res1995; 55: 434–9.
50. Guo H, Zucker S, Gordon MK, Toole BP, Biswas C.Stimulation of matrix metalloproteinase production by recom-binant extracellular matrix metalloproteinase inducer fromtransfected Chinese hamster ovary cells. J Biol Chem 1997;272: 24–7.
51. Kanekura T, Chen X. CD147/basigin promotes progression ofmalignant melanoma and other cancers. J Dermatol Sci 2010;57: 149–54.
52. Richard V, Pillai MR. The stem cell code in oral epithelialtumorigenesis: ‘the cancer stem cell shift hypothesis’. BiochimBiophys Acta 2010; 1806: 146–62.
53. Weidle UH, Scheuer W, Eggle D, Klostermann S, StockingerH. Cancer-related issues of CD147. Cancer Genomics Prote-omics 2010; 7: 157–69.
54. Ali MA. Expression of extracellular matrix metalloproteinaseinducer in odontogenic cysts. Oral Surg Oral Med Oral PatholOral Radiol Endod 2008; 106: 258–63.
Acknowledgements
The authors express special thanks to Elisa dos Santos and Juvani Lago
(Department of Oral Pathology, Dental School, University of S~ao Paulo) for the
histotechnical processing of the tissue samples.
J Oral Pathol Med
MMPs, TIMPs, RECK and EMMPRIN in CCOT
Prosd�ocimi et al.
9
Copyright © 2022 FDOKUMEN




















