British Journal of Ophthalmology
164
British Journal of Ophthalmology October 2005 (Volume 89, Number 10). BJO at a glance BJO at a glance Creig Hoyt Br J Ophthalmol 2005; 89: 1231. Editorials Cataract surgery programmes in Africa T Y Wong Br J Ophthalmol 2005; 89: 1231-1232. Trachoma J D Chidambaram and T M Lietman Br J Ophthalmol 2005; 89: 1232-1233. Utility analysis tells all M Brown Br J Ophthalmol 2005; 89: 1233. Commentaries Reimbursement for internet based eye care S Kumar, I J Constable, and K Yogesan Br J Ophthalmol 2005; 89: 1234-1235. World view Increasing cataract surgery to meet Vision 2020 targets; experience from two rural programmes in east Africa S Lewallen, H Roberts, A Hall, R Onyange, M Temba, J Banzi, and P Courtright Br J Ophthalmol 2005; 89: 1237-1240. Utility values among glaucoma patients: an impact on the quality of life V Gupta, G Srinivasan, S S Mei, G Gazzard, R Sihota, and K S Kapoor Br J Ophthalmol 2005; 89: 1241-1244.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of British Journal of Ophthalmology

British Journal of Ophthalmology October 2005 (Volume 89, Number 10).
BJO at a glance
BJO at a glance Creig Hoyt Br J Ophthalmol 2005; 89: 1231.
Editorials
Cataract surgery programmes in AfricaT Y Wong Br J Ophthalmol 2005; 89: 1231-1232. Trachoma J D Chidambaram and T M Lietman Br J Ophthalmol 2005; 89: 1232-1233. Utility analysis tells all M Brown Br J Ophthalmol 2005; 89: 1233.
Commentaries
Reimbursement for internet based eye careS Kumar, I J Constable, and K Yogesan Br J Ophthalmol 2005; 89: 1234-1235.
World view
Increasing cataract surgery to meet Vision 2020 targets; experience from two rural programmes in east Africa S Lewallen, H Roberts, A Hall, R Onyange, M Temba, J Banzi, and P Courtright Br J Ophthalmol 2005; 89: 1237-1240. Utility values among glaucoma patients: an impact on the quality of life V Gupta, G Srinivasan, S S Mei, G Gazzard, R Sihota, and K S Kapoor Br J Ophthalmol 2005; 89: 1241-1244.

Direct costs of glaucoma and severity of the disease: a multinational long term study of resource utilisation in Europe C E Traverso, J G Walt, S P Kelly, A H Hommer, A M Bron, P Denis, J-P Nordmann, J-P Renard, A Bayer, F Grehn, N Pfeiffer, C Cedrone, S Gandolfi, N Orzalesi, C Nucci, L Rossetti, A Azuara-Blanco, A Bagnis, R Hitchings, J F Salmon, G Bricola, P M Buchholz, S V Kotak, L M Katz, L R Siegartel, and J J Doyle Br J Ophthalmol 2005; 89: 1245-1249. Traditional healers’ roles on eye care services in Nepal A K Poudyal, M Jimba, B K Poudyal, and S Wakai Br J Ophthalmol 2005; 89: 1250-1253.
Cover
An icy stare I R Schwab Br J Ophthalmol 2005; 89: 1236.
Clinical science - Scientific reports
Interferon as a treatment for uveitis associated with multiple sclerosis M D Becker, A Heiligenhaus, T Hudde, B Storch-Hagenlocher, B Wildemann, T Barisani-Asenbauer, C Thimm, N Stübiger, M Trieschmann, and C Fiehn Br J Ophthalmol 2005; 89: 1254-1257. Novel rhodopsin mutations and genotype-phenotype correlation in patients with autosomal dominant retinitis pigmentosa A Schuster, N Weisschuh, H Jägle, D Besch, A R Janecke, H Zierler, S Tippmann, E Zrenner, and B Wissinger Br J Ophthalmol 2005; 89: 1258-1264. PET/CT imaging: detection of choroidal melanoma S Reddy, M Kurli, L B Tena, and P T Finger Br J Ophthalmol 2005; 89: 1265-1269. Whole body PET/CT for initial staging of choroidal melanoma P T Finger, M Kurli, S Reddy, L B Tena, and A C Pavlick Br J Ophthalmol 2005; 89: 1270-1274. Infantile infection and diabetes insipidus in children with optic nerve hypoplasia S P Donahue, A Lavina, and J Najjar Br J Ophthalmol 2005; 89: 1275-1277. Social and visual function in nystagmus R F Pilling, J R Thompson, and I Gottlob Br J Ophthalmol 2005; 89: 1278-1281.

Clinical science - Extended reports
A randomised controlled trial of azithromycin following surgery for trachomatous trichiasis in the Gambia M J Burton, F Kinteh, O Jallow, A Sillah, M Bah, M Faye, E A N Aryee, U N Ikumapayi, N D E Alexander, R A Adegbola, H Faal, D C W Mabey, A Foster, G J Johnson, and R L Bailey Br J Ophthalmol 2005; 89: 1282-1288. Potential of the 1 CU accommodative intraocular lens G Sauder, R F Degenring, B Kamppeter, and P Hugger Br J Ophthalmol 2005; 89: 1289-1292. Effect of dorzolamide and timolol on ocular blood flow in patients with primary open angle glaucoma and ocular hypertension G Fuchsjäger-Mayrl, B Wally, G Rainer, W Buehl, T Aggermann, J Kolodjaschna, G Weigert, E Polska, H-G Eichler, C Vass, and L Schmetterer Br J Ophthalmol 2005; 89: 1293-1297. The relation between intraocular pressure peak in the water drinking test and visual field progression in glaucoma R Susanna, Jr, R M Vessani, L Sakata, L C Zacarias, and M Hatanaka Br J Ophthalmol 2005; 89: 1298-1301. Influence of change in body position on choroidal blood flow in normal subjects P Kaeser, S Orgül, C Zawinka, G Reinhard, and J Flammer Br J Ophthalmol 2005; 89: 1302-1305. 18 Years’ experience with high dose rate strontium-90 brachytherapy of small to medium sized posterior uveal melanoma R van Ginderdeuren, E van Limbergen, and W Spileers Br J Ophthalmol 2005; 89: 1306-1310. The achiasmia spectrum: congenitally reduced chiasmal decussation D A Sami, D Saunders, D A Thompson, I M Russell-Eggitt, K K Nischal, G Jeffery, M Dattani, R A Clement, A Liassis, and D S Taylor Br J Ophthalmol 2005; 89: 1311-1317. Randomised clinical trial of the effectiveness of base-in prism reading glasses versus placebo reading glasses for symptomatic convergence insufficiency in children M Scheiman, S Cotter, M Rouse, G L Mitchell, M Kulp, J Cooper, E Borsting and the Convergence Insufficiency Treatment Trial (CITT) Study Group Br J Ophthalmol 2005; 89: 1318-1323. Monocular and binocular reading performance in children with microstrabismic amblyopia E Stifter, G Burggasser, E Hirmann, A Thaler, and W Radner Br J Ophthalmol 2005; 89: 1324-1329.

Ocular motor dysfunction and ptosis in ocular myasthenia gravis: effects of treatment M J Kupersmith and G Ying Br J Ophthalmol 2005; 89: 1330-1334. Orbital exenteration: a 13 year Manchester experience I Rahman, A E Cook, and B Leatherbarrow Br J Ophthalmol 2005; 89: 1335-1340. Isolated visual symptoms at onset in sporadic Creutzfeldt-Jakob disease: the clinical phenotype of the "Heidenhain variant" S A Cooper, K L Murray, C A Heath, R G Will, and R S G Knight Br J Ophthalmol 2005; 89: 1341-1342.
Laboratory science - Scientific reports
Isolation, culture, and characterisation of human macular inner choroidal microvascular endothelial cells A C Browning, T Gray, and W M Amoaku Br J Ophthalmol 2005; 89: 1343-1347. An experimental study on the effect of encircling band procedure on silicone oil emulsification D J de Silva, K S Lim, and W E Schulenburg Br J Ophthalmol 2005; 89: 1348-1350.
Laboratory science - Extended reports
Contribution to comprehension of image formation in confocal microscopy of cornea with Rostock cornea module R Bochert, A Zhivov, R Kraak, J Stave, and R F Guthoff Br J Ophthalmol 2005; 89: 1351-1355. Hydroxyapatite promotes superior keratocyte adhesion and proliferation in comparison with current keratoprosthesis skirt materials J S Mehta, C E Futter, S R Sandeman, R G A F Faragher, K A Hing, K E Tanner, and B D S Allan Br J Ophthalmol 2005; 89: 1356-1362.
Perspective
Topical ciclosporin in the treatment of ocular surface disordersS Tatlipinar and E K Akpek Br J Ophthalmol 2005; 89: 1363-1367.

Letters
Bevacizumab suppresses choroidal neovascularisation caused by pathological myopia Q D Nguyen, S Shah, S Tatlipinar, D V Do, E V Anden, and P A Campochiaro Br J Ophthalmol 2005; 89: 1368-1370. Compliance: clear communication’s critical A J Buller, B Connell, and A F Spencer Br J Ophthalmol 2005; 89: 1370. Safety of phacoemulsification in a patient with an implanted deep brain neurostimulation device C F Parsloe and J M Twomey Br J Ophthalmol 2005; 89: 1370-1371. Vertical deviation exacerbated by convergence and accommodation S Thomas, S J Farooq, F A Proudlock, and I Gottlob Br J Ophthalmol 2005; 89: 1371-1372. Tetracycline induced green conjunctival pigment deposits V L Morrison, D O Kikkawa, and B G Herndier Br J Ophthalmol 2005; 89: 1372-1373. Corneal epithelial defects related to high postoperative astigmatism R Singh, T Umapathy, B B Kulkarni, and H S Dua Br J Ophthalmol 2005; 89: 1373-1374. Non-tuberculous mycobacteria related infectious crystalline keratopathy T Umapathy, R Singh, H S Dua, and F Donald Br J Ophthalmol 2005; 89: 1374-1375. Xanthogranulomatous disease in the lacrimal gland J A Sivak-Callcott, W K Lim, L L Seah, J Oestreicher, D Rossman, N Nijhawan, J Rootman, V White, H J Williams, W W L Chang, A DiBartolomeo, and D Howarth Br J Ophthalmol 2005; 89: 1375-1377. Management of phaeniciatic ophthalmomyiasis externa N Huynh, B Dolan, S Lee, J P Whitcher, and J Stanley Br J Ophthalmol 2005; 89: 1377-1378. Vitreous haemorrhage associated with Gingko biloba use in a patient with age related macular disease O P MacVie and B A Harney Br J Ophthalmol 2005; 89: 1378-1379. The legal requirement for driving in the United Kingdom is met following pupil dilatation J Siderov, D Mehta, and R Virk Br J Ophthalmol 2005; 89: 1379-1380.

Hydrated scleral buckle: a late complication of MAI explants N Bhagat, A Khanna, and P D Langer Br J Ophthalmol 2005; 89: 1380. Complex I respiratory defect in LHON plus dystonia with no mitochondrial DNA mutation K K Abu-Amero, T M Bosley, S Bohlega, and D McLean Br J Ophthalmol 2005; 89: 1380-1381. Retinal haemorrhages in a young patient with homocysteinuria R A Shah, M A Zarbin, and N Bhagat Br J Ophthalmol 2005; 89: 1381-1382. Internet based ophthalmology service: impact assessment S Kumar, M-L Tay-Kearney, I J Constable, and K Yogesan Br J Ophthalmol 2005; 89: 1382-1383. Temperature sensitive oculocutaneous albinism associated with missense changes in the tyrosinase gene T Wang, C T Waters, T Jakins, J R W Yates, D Trump, K Bradshaw, and A T Moore Br J Ophthalmol 2005; 89: 1383-1384. Choroidal neovascularisation associated with meningioma M S Lee and S Lessell Br J Ophthalmol 2005; 89: 1384-1385.
Mailbox
Intraoperative visual experiences of cataract patients can be both pleasant and unpleasant K-G Au Eong, C S H Tan, C L Ang, S S G Lee, R Venkatesh, R Muralikrishnan, G L Fanning, and C M Kumar Br J Ophthalmol 2005; 89: 1386. Cigarette pack warning: it can send you blind! S Chapman Br J Ophthalmol 2005; 89: 1386-1387.
Book reviews
Immunology of the lacrimal gland, tear film and ocular surfaceM Berry Br J Ophthalmol 2005; 89: 1387.

Glaucoma. 3rd ed. N Spencer Br J Ophthalmol 2005; 89: 1387.
From the library
From the Library Br J Ophthalmol 2005; 89: 1388.

Cataract surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Cataract surgery programmes in AfricaT Y Wong. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Towards evidence based public health
Readers of the BJO will be aware thatcataract is the leading cause ofblindness in Africa, affecting an
estimated half of the seven million blindpeople in that continent.1 This numberis likely to increase substantially, asapproximately 600 000 Africans becomeblind from cataract each year. Despitethe enormity of the problem, fewcataract operations are performed inAfrica. The cataract surgery rate (CSR),a measure of the volume of cataractsurgery performed in a population, isabout 500 per million per year in Africa.To tackle cataract blindness, the Vision2020 initiative, a programme involvingthe World Health Organization, theInternational Agency for Prevention ofBlindness, and various governmentaland non-governmental organisations,aims to increase the CSR in Africa toabout 2000 per million per year.2
Substantial progress has been madeon several fronts over the past few years.There has been a steady stream ofinformation on the epidemiology, dis-tribution, and impact of cataract indifferent parts of Africa.3 4 There is alsoincreasing evidence that well designedand well executed cataract surgeryprogrammes can provide effective highvolume and high quality cataract surgi-cal services in selected communities inAfrica.5
Despite encouraging signs, thereremain significant challenges and bar-riers. Thus, there may be importantlessons in the few ‘‘successful’’ cataractsurgery programmes that emerge fromAfrica. In this month’s issue of the BJO(p 1237), Lewallen and colleagues sharetheir experience of two such pro-grammes, both of which appeared tohave contributed towards a significantincrease in the number of cataractsurgeries performed in their commu-nities. Since the introduction of theseprogrammes, the authors estimate thatCSR have risen to 1583 per million inthe Kwale District in Kenya, and 1165per million in the Kilimanjaro Region inTanzania in 2004. These are remarkablefigures, all the more so given thatprevious estimates of the CSR wereapproximately 644 per million in
Kenya and 313 per million in Tanzaniain 2002.What were the key lessons learnt
from these ‘‘successful’’ cataract surgeryprogrammes? The authors describe sev-eral. These include a close link betweenthe community screening programmesand the hospital services that providethe cataract surgery services, a seamless‘‘patient friendly’’ referral chain, theutilisation of a community screeningexamination team that has appropriateophthalmic expertise to identify peoplemost likely to benefit from cataractsurgery, and selecting populations thatboth need the services and have theability to sustain such programmes.None of these concepts is very new, ofcourse. Indeed, many of the featuresdescribed in this article have beenproposed in other African communities,and apply elsewhere in other developingcountries (for example, India).6
Like changes in clinical practiceresulting from a heightened aware-ness of evidence based medicine,evidence based public health isnecessary in ensuring the majorparadigm changes needed in publichealth practice
A unique aspect of this study wasusing a quantitative outcome (in thiscase, the CSR) to qualify the success forthe programme, information that manyprevious descriptive studies havelacked.7 None the less, there are severallimitations in this study that may serveas areas for future research. For exam-ple, the authors argue in their articlethat one of the key lessons of thecataract surgery programme was to‘‘make specific changes at the hospitalessential to providing more service.’’ Alist of these changes is described in thearticle. However, the study lacked morequantitative analyses on the specificchanges described, which may make itdifficult to translate these features toother programmes. Future studiesshould more precisely quantify thespecific features or processes of a pro-gramme, and whether one feature orprocess is independent of and, more
important, relative to others. Secondly,although the article attributes the highCSR in the two communities to theintroduction of the cataract surgeryprogrammes, it would have been vastlymore instructive to have data on theactual change in CSR over time (that is,before and after the introduction of theprogramme).Some of this information will not be
readily available, given the resourcesand situation. Indeed, we recognise thatevaluating the effectiveness of cataractsurgery programmes is challengingenough, even in the most ideal circum-stances in developed Western countries.However, it is crucial for public healthophthalmology to move away frompurely descriptive, experience based casestudies towards evidence based publichealth.What is evidence based public health?
It is a variation of evidence basedmedicine, focusing instead on a publichealth intervention.8 Evidence basedpublic health seeks to answer severalquestions regarding the usefulness of anintervention.9 Firstly, has the researchperformed been sufficiently valid tosupport a decision on whether or notto implement an intervention (in thiscase, a particular cataract surgery pro-gramme)? Secondly, have all the impor-tant research outcomes been evaluated(CSR is one example, post-cataractsurgery visual outcome would beanother)? Thirdly, is the research applic-able to the potential recipients of theintervention (would such cataract sur-gery programme be transferable to otherAfrican communities and settings)?Although these questions are similar inmany respects to the evaluation ofevidence in medicine, there are somedifferences. Compared to a treatment inclinical medicine, public health inter-ventions tend to be multifaceted, morecomplex, and more dependent on spe-cific situations.10 Thus, it is more criticalto distinguish between the efficacy of anintervention, and the effectiveness of anintervention in terms of delivery andexecution.Evidence based public health is but
one factor in the process of translating aresearch observation into broad policydecisions regarding the implementationof a particular intervention. Likechanges in clinical practice resultingfrom a heightened awareness of evi-dence based medicine, evidence basedpublic health is necessary in ensuringthe major paradigm changes needed inpublic health practice. For public healthophthalmology, it will be the first steptowards the elimination of avoidableblindness from cataract in Africa andother developing countries.
EDITORIAL 1231
www.bjophthalmol.com

Br J Ophthalmol 2005;89:1231–1232.doi: 10.1136/bjo.2005.072645
Correspondence to: Tien Yin Wong, MD, PhD,Centre for Eye Research Australia, University ofMelbourne, 32 Gisborne Street, Victoria 3002,Australia; [email protected]
Competing interests: none declared
REFERENCES1 Lewallen S, Courtright P. Blindness in Africa:
present situation and future needs. Br JOphthalmol2001;85:897–903.
2 Foster A. Cataract and ‘‘Vision 2020—the right tosight’’ initiative. Br J Ophthalmol2001;85:635–7.
3 Congdon N, West SK, Buhrmann RR, et al.Prevalence of the different types of age-relatedcataract in an African population. InvestOphthalmol Vis Sci 2001;42:2478–82.
4 Rabiu MM. Cataract blindness and barriers touptake of cataract surgery in a rural community ofnorthern Nigeria. Br J Ophthalmol2001;85:776–80.
5 Limburg H, Foster A, Gilbert C, et al. Routinemonitoring of visual outcome of cataract surgery.Part 2: Results from eight study centres.Br J Ophthalmol 2005;89:50–2.
6 Natchiar G, Robin AL, Thulasiraj RD, et al.Attacking the backlog of India’s curable blind. The
Aravind Eye Hospital model. Arch Ophthalmol1994;112:987–93.
7 Rotchford AP, Rotchford KM, Mthethwa LP, et al.Reasons for poor cataract surgery uptake—aqualitative study in rural South Africa. Trop MedInt Health 2002;7:288–92.
8 Heller RF, Page J. A population perspective toevidence based medicine: ‘‘evidence forpopulation health’’. J Epidemiol CommunityHealth 2002;56:45–7.
9 Kohatsu ND, Robinson JG, Torner JC. Evidence-based public health: an evolving concept. J PrevMed 2004;27:417–21.
10 Rychetnik L, Frommer M, Hawe P, et al. Criteriafor evaluating evidence on public healthinterventions. J Epidemiol Community Health2002;56:119–27.
TRACHOMA. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
TrachomaJ D Chidambaram, T M Lietman. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
A tale of two diseases
Trachoma is in a sense two diseases:the infection most apparent inchildren and the blinding sequelae
found in adults. Ocular strains ofChlamydia trachomatis cause repeatedepisodes of conjunctivitis, with the peakprevalence of infection usually occurringin 3–5 year olds.1 Progressive scarring,entropion, and trichiasis lead to blind-ing corneal ulceration, typically some40 years or more later.2 This long lagtime between infection and blindnesshas always been somewhat of a puzzle.Several explanations have been offered.The normal, age related decrease intears, goblet cells, and lid elasticitymay make the elderly more prone tothe effects of scarring.3 Existing scarsmay contract slowly over time. Furtherepisodes of chlamydial infection maycause scarring to progress.4 5 If this lasthypothesis is the case, then the frequentrecurrence of trichiasis after surgicalrepair could in part be because ofrecurrent infection. This is a testablehypothesis. A single dose of oral azi-thromycin is effective in eliminatingchlamydial infection in an individual,6
and treatment given to a communitycan offer a sustained reduction ofinfection even a year later.7 With someeffort, infection can be prevented, atleast for the year or so after surgery.In this issue of the BJO (p 1282),
Burton et al report a trial in which theyrandomised patients receiving trichiasissurgery into two groups. One groupreceived topical tetracycline post-surgery as standard of care. The otherreceived topical tetracycline and, inaddition, they and their household
members received a dose of oral azi-thromycin at the time of surgery and6 months later. Recurrence of trichiasis12 months after surgery proved to be afairly common event, providing thestudy with some power to detect adifference. However, recurrence wasequally frequent in the two arms. Also,chlamydial infection was not a riskfactor for recurrence.
This trial makes us think abouttrachoma differently, even thoughazithromycia could not be shown toprevent recurrence of trichiasis aftersurgery
Although the authors could not impli-cate chlamydia in the failure of trichia-sis surgery, secondary analyses suggestthat other bacteria may have a role.Identification of a pathogenic species ofbacteria colonising the conjunctiva wasa twofold risk factor for recurrence ofsevere trichiasis. Bacterial colonisationmay just be a surrogate marker for moresevere scarring, which itself is a riskfactor for recurrence. However, it is alsopossible that bacterial infections them-selves cause progression of disease. Thiswould not be the first time that non-chlamydial bacteria have been impli-cated in trachoma,8 but it might be themost convincing evidence so far.Colonisation of the conjunctiva has alsobeen found in other cicatricial conjunc-tivitides, such as ocular cicatricial pem-phigoid (OCP). In fact, cornealulceration in OCP is often caused bythe same species of bacteria that hadcolonised the conjunctiva on previous
visits.9 In Western countries, prophylac-tic antibiotic drops are sometimes pro-vided to patients at such a high risk forcorneal ulcers. Burton et al’s resultssuggest that maybe we should considersuch prophylaxis in trachoma patientsafter trichiasis surgery.This was a well designed and well
organised trial. Strengths include a largenumber of patients, a large number ofsurgeons, good follow up, and excellentmicrobiology. However, it may not be thelast word on the importance of chlamydiain the progression of cicatricial trachoma.Azithromycin is already being distributedto everyone in endemic areas; some mayargue that extra doses in older, post-surgical patients are hardly necessarysince infection in adults is less common,1
of a shorter duration,10 and a lower load.11
On the other hand, estimates of thisprogression are higher in areas with moreinfection (Tanzania) than they are inareas with less infection (Gambia).12–14
Two other groups are examining thisquestion with somewhat similar designs(Emily West, Sheila West, WonduAlemayehu, and Deborah Dean, personalcommunications). One trial is beingperformed in an area of Ethiopia wheretrachoma is hyper-endemic and theopportunity for re-infection far greater.These studies may or may not producesimilar results.This trial makes us think about
trachoma differently, even though azi-thromycin could not be shown to pre-vent recurrence of trichiasis aftersurgery. Currently, programs treat tra-choma as two different diseases, redu-cing infection with antibiotics andeliminating trichiasis with surgery.Burton et al tested whether the linkbetween the two was stronger thanappreciated. Their bacteriological resultsmay even suggest an entirely new frontin trachoma control. The question ofhow cicatricial trachoma will progress inthe absence of recurrent chlamydialinfections is an important one. Even ifmass antibiotic distributions and othermeasures are successful in dramatically
1232 EDITORIAL
www.bjophthalmol.com

reducing infection in entire populations,there will still remain a generation ofindividuals with scarred conjunctivae.In some areas, we may no longer have tocontend with two trachomas, only thecicatricial form. It would have beencomforting had this trial found thattrichiasis would not recur in the absenceof chlamydia. Hopefully, furtherresearch will optimise the managementof cicatricial trachoma.
Br J Ophthalmol 2005;89:1232–1233.doi: 10.1136/bjo.2005.067322
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . . .
J D Chidambaram, T M Lietman, FI ProctorFoundation, University of California, SanFrancisco, CA, USAT M Lietman, Institute for Global Health, andDepartment of Ophthalmology, University ofCalifornia, San Francisco, CA, USA
Correspondence to: Dr Thomas M Lietman,WHO Collaborating Center, FI ProctorFoundation, Room 307, 95 Kirkham Street,University of California San Francisco, SanFrancisco, CA 94143-0944, USA;[email protected]
REFERENCES1 Bird M, Dawson CR, Schachter JS, et al. Does the
diagnosis of trachoma adequately identify ocularchlamydial infection in trachoma-endemic areas?J Infect Dis 2003;187:1669–73.
2 Mabey DC, Solomon AW, Foster A. Trachoma.Lancet 2003;362:223–9.
3 Bowman RJ, Jatta B, Cham B, et al. Naturalhistory of trachomatous scarring in the Gambia:results of a 12-year longitudinal follow-up.Ophthalmology 2001;108:2219–24.
4 Zhang H, Kandel RP, Sharma B, et al. Risk factorsfor recurrence of postoperative trichiasis:implications for trachoma blindness prevention.Arch Ophthalmol 2004;122:511–16.
5 West ES, Mkocha H, Munoz B, et al. Risk factorsfor postsurgical trichiasis recurrence in atrachoma-endemic area. Invest Ophthalmol VisSci 2005;46:447–53.
6 Bailey RL, Arullendran P, Whittle HC, et al.Randomised controlled trial of single-doseazithromycin in treatment of trachoma. Lancet1993;342:453–6.
7 Schachter J, West SK, Mabey D, et al.Azithromycin in control of trachoma. Lancet1999;354:630–5.
8 Jones BR. The prevention of blindness fromtrachoma. Trans Ophthalmol Soc UK1975;95:16–33.
9 Holsclaw DS. Ocular cicatricial pemphigoid. IntOphthalmol Clin 1998;38:89–106.
10 Bailey R, Duong T, Carpenter R, et al. Theduration of human ocular Chlamydia trachomatisinfection is age dependent. Epidemiol Infect1999;123:479–86.
11 Solomon AW, Holland MJ, Burton MJ, et al.Strategies for control of trachoma: observationalstudy with quantitative PCR. Lancet2003;362:198–204.
12 Munoz B, Bobo L, Mkocha H, et al. Incidence oftrichiasis in a cohort of women with and withoutscarring. Int J Epidemiol 1999;28:1167–71.
13 Bowman RJ, Faal H, Myatt M, et al. Longitudinalstudy of trachomatous trichiasis in the Gambia.Br J Ophthalmol 2002;86:339–43.
14 Lietman T. Trachoma control: the beginning of theend? Ophthalmology 2001;108:2163–4.
Utility analysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Utility analysis tells allM Brown. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
We must embrace it and foster its use
It is most gratifying to see the excellentarticle by Gupta et al in this issue ofBJO (p 1241), as advocates of pre-
ference based quality of life instrumentssuch as utility analysis (those that askpatients to make a choice about thedesirability of their quality of life)versus function based instruments(those that measure primarily function:physical, psychological, vocational, avo-cational, cognitive, social, and so forth).1
Why are we such fans of utilityanalysis? The answer lies in the defini-tion of what is the most desirablequality of life instrument.1 A goodinstrument should be:
(1) all encompassing with regard to thevariables that comprise quality of life
(2) sensitive to small changes in health
(3) reliable (reproducible)
(4) applicable across all medical spe-cialties
(5) able to be completed within areasonable time period
(6) able to be understood by patients,and
(7) able to demonstrate construct valid-ity (the ability to measure what it isintended to measure
(8) applicable for us in performinghealthcare economic analyses.
Utility analysis meets all of theseparameters and is a major pillar of valuebased medicine, the practice of medicinethat incorporates the best evidencebased data with patient preferences toassess the value conferred by our inter-ventions, whether medical, surgical,and/or pharmaceutical. Of special noteas well is the fact that these patientderived utility values that measure thequality of life associated with healthstates appear to be innate to humannature. How do we know? Becausedata2 3 suggest that, for the most part,utility values transcend sex, ethnicity,age, level of education, income, andeven nationality, There are, of course,exceptions, such as this analysis foundwith education, but overall humanattitudes towards illness are remarkablysimilar.Utility analysis incorporates improve-
ments in quality of life conferred byinterventions that can be integratedwith improvement in length of life toquantify the total value gained from theinterventions. This value (measuredusing the QALY, or quality adjusted life
year) is comparable across every inter-vention in health care. The most fre-quently utilised quality of lifeinstruments in ophthalmology, the VF-14 and the NEI-VFQ-25, are not espe-cially applicable across all specialtiesand have not been used in healthcareeconomic analyses.As policy makers and other stake-
holders in health care utilise quality oflife data to make allocation decisions, itseems natural that they would favour aninstrument than encompasses all inter-ventions in health care, rather than justophthalmology, which accounts for asmall fraction of the healthcare dollar.1
How should we, as ophthalmologists,approach the introduction of valuebased medicine? With open arms. Thegreat majority of ophthalmic interven-tions confer extraordinary value, and itis value that patients want. An addedbenefit is that the conferred value isgreat compared to the costs expended.Cataract surgery in the United Statescosts $600–$700/QALY. It is a bargain byany measure.
Br J Ophthalmol 2005;89:1233.doi: 10.1136/bjo.2005.074294
Correspondence to: Melissa Brown, Center forValue-Based Medicine, PO Box 335 Flourtown,PA 19031-1404, USA; [email protected]
REFERENCES1 Brown MM, Brown GC, Sharma S. Evidence-
based to value-based medicine. Chicago: AMAPress, 1995:1–324.
2 Brown MM, Brown GC, Sharma S, et al. Healthcare economic analyses and value-basedmedicine. Surv Ophthalmol 2003;48:204–23.
3 Brown MM, Brown GC, Sharma S, et al. Utilityvalues associated with blindness in an adultpopulation. Br J Ophthalmol 2001;85:327–31.
EDITORIAL 1233
www.bjophthalmol.com

Internet based eye care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Reimbursement for internet based eyecareS Kumar, I J Constable, K Yogesan. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
How long should we wait?
Medicare, Australia’s universalhealth insurance system, assuresaccess to public health services.
Although it is now 20 years sinceMedicare was introduced, marginalimprovements to Medicare are indi-cated.1 Fulfilling the specialist health-care needs of millions of ruralAustralians is crucial to the debate overMedicare’s future. Clinicians inAustralia are worried about inequity interms of access and outcome for theirpatients and are willing to be partners inhealthcare governance to improve thesituation.2 Yet, services like internetbased eye care, with a wide range ofusages, are candidates for regulation.3
The term internet based eye care refersto the delivery of eye care services,especially to remote and rural commu-nities, by means of modern telecommu-nications technology.4
Meanwhile, in the United States, theCongress has acknowledged internetbased healthcare as a viable, potentiallylife saving technology.5 Payers are sign-ing on to this trend, as major medicalcentres come to see the benefits.Beginning in October 2001, the HealthCare Financing Administration (HCFA)extended Medicare coverage to a widerange of internet based healthcare ser-vices and providers, allowing for medi-cal visits, consultations, mental healthservices, and pharmacological monitor-ing of patients living in rural areas.6
Payment to providers was at a ratesimilar to that paid without the use ofinternet based care. Furthermore,Medicare paid a facility fee of $20 perinternet based care session to theoriginating site in the remote region.Internet based care services are wellintegrated to regular healthcare systemsin Scandinavian countries.5
In Australia, integration of internetbased eye care to the healthcare systemmay become more feasible by reimbur-sing this service.2 7 Currently, with someexceptions, Australia does not haveprecise policies to reimburse for internetbased eye care services. For example,Medicare reimburses for some servicesthat do not require face to face contactbetween a patient and practitioner, such
as radiology or pathology interpretation.As a result, other internet based health-care specialty services have not found afirm financial foothold, and are primar-ily sustained through grants and shortterm funding.7
Initially, in the United States, thedebate centred on whether ‘‘Medicareshould pay for internet based careservices’’ and then shifted to ‘‘howMedicare should pay for internet basedcare services.’’8 Later, it became veryimportant to understand ‘‘why theprogram was not working and how tofix it.’’8 Learning from these US experi-ences can lead us to recognise whatneeds to be considered while formulat-ing future Medicare payment pro-grammes for internet based eye care inAustralia. There is a need to examineand debate what form of internet basedeye care reimbursement system isrequired in Australia. These discussionsare vital to work towards proposingMedicare payment guidelines for inter-net based eye care.
WHO ARE ELIGIBLE?In Australia, there are several remote,rural regions that have adequate pri-mary care resources but lack essentialspecialty services. For example, a ruralregion may have a nurse or generalpractitioner, but not cardiologists orophthalmologists. These rural commu-nities may greatly benefit by havingaccess to specialists via internet basedeye care,9 but providers servicing themcannot be reimbursed under the currentprovisions. Nevertheless, restriction ofcoverage only to rural societies mayseverely narrow the applicability ofinternet based eye care. Poor healthand inadequate public transportationcan pose hurdles to many urban/sub-urban residents as well. Hence, (propo-sal 1) internet based eye care guidelinesmust clearly define who are eligible forsuch services.
SERVICES AND TECHNOLOGYAs mentioned earlier, Medicare cur-rently reimburses some internet basedcare services that do not requiredirect patient-specialist contact such as
teleradiology. For other specialties, thecurrent definition of ‘‘consultation’’limits the reimbursement to thoseencounters where the patient must bepresent. A growing number of internetbased eye care programmes are usingstore and forward technology. Thesetechnologies engage asynchronoustransmission of medical information tobe reviewed later on by a physician at adistant site. The consultant reviews thecases without the patient being presentin real time. A familiar illustration of astore and forward consultation occurswhen a rural practitioner sends imagesof a retinal lesion to an ophthalmologistfor diagnostic and managementadvice.10 For many remote regionalcommunities in Australia, store andforward may be the only reasonableway to practise internet based eye care.In this scenario, Medicare coverage
for store and forward technologies inAlaska and Hawaii may represent asignificant outlook.11 In Alaska, begin-ning in December 2002, over a period of10 months, Medicaid has saved overUS$30 000 in travel costs alone by usingstore and forward internet based healthcare.12 Savings in lodging and per diemcosts accentuate these savings, alongwith significant time saving to patients.This may suggest that requirements fora patient to be ‘‘presented’’ by aphysician or practitioner at the originat-ing site in real time must be avoided bylegislation—unless medically necessary.The practitioner at the originating, dis-tant site must make the decision ofmedical necessity. Consequently, (pro-posal 2) consistent definitions need tobe developed regarding what constitutesa internet based eye care consultation.Even once these definitions are devel-
oped, the question will remain on whatbasis should the payment be set? Shouldthey be paid the same as for a face toface visit? Hence, (proposal 3) guide-lines must clearly define what servicesare to be covered. The services coveredmay include consultations, medicationmanagement, and any additional ser-vices.
ELIGIBLE PRACTITIONERInternet based eye care practitionersmay be divided into referring practi-tioners and consulting practitioners.Eligible referring practitioners mayinclude general practitioners and clin-ical nurses. But, in many instances, thereferring practitioner is not presentduring the consultation. The patient isoften ‘‘presented’’ by someone else likenursing assistants or healthcare techni-cians. Hence, (proposal 4) guidelinesmust clearly define the ‘‘presenter’’ aswell as consulting specialist requirement.
1234 COMMENTARY
www.bjophthalmol.com

To be reimbursed, presenters need to bean ‘‘eligible’’ referring practitioner.
PROCESS OF REIMBURSEMENTOne of the options is to split theteleconsultation fee equally among thereferring practitioner and consultingspecialist. However, this may prove tobe troublesome and both parties maynot accept the arrangement.13
Alternatively, the consulting specialistcould be paid the existing conventionalconsultation fee for the service provided.The originating site may receive afacility fee. Thus, (proposal 5) guidelinesmust clearly define internet based eyecare payment methodology.
ISSUES AND ACTIONSThis discussion of reimbursement forinternet based eye care may be only thebeginning. Even before the guidelinesare realised, it is apparent that someissues may be left unresolved. Studiesshould be conducted to monitor, evalu-ate, and refine the internet based eyecare reimbursement process.Additionally, it should be noted thatinternet based eye care licensure andindemnity laws might also need to beformulated. This issue, however,remains a misty region for healthcarestrategy that has implications for con-sulting specialist and ‘‘eligible practi-tioners’’ who practise across state orcountry lines.Healthcare reforms are often slow
because of varied factors. These mayinclude a lack of commitment to
change, resistance from vested stake-holders who fear losing some of theirexisting benefits, or failure by policy-makers to translate successful aspects ofthe reforms into something tangible tothe general public.14 Medicare, internetbased eye care service providers, andconcerned institutions should conveneto advance relationships leading to aworkable model regarding internetbased eye care service improvements.Several of these issues that call fordeliberation within the dominion ofinternet based eye care in Australiamay also be significant to other coun-tries.
ACKNOWLEDGEMENTSSupported by IPRS Scholarship fromUniversity of Western Australia and JackHoffman Scholarship from Lions Save SightFoundation.
Br J Ophthalmol 2005;89:1234–1235.doi: 10.1136/bjo.2005.077693
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . . .
S Kumar, I J Constable, K Yogesan, Centre ofExcellence in e-Medicine, Lions Eye Institute,The University of Western Australia, Australia
Correspondence to: Sajeesh Kumar, Lions EyeInstitute, Centre for Ophthalmology and VisualScience, University of Western Australia, 2Verdun Street, Nedlands, WA 6009, Australia;[email protected]
REFERENCES1 Duckett S. Medicare: where to now? Aust Health
Rev 1995;18:117–24.
2 Dwyer JM. The next Australian health careagreements: what clinicians want? Aust HealthReview 2002;25:17–23.
3 Kovac M. Rationing of hospital services in theAustralian health system. Croatian Med J1998;39:339–45.
4 Jakobsen KR. Space-age medicine, stone-agegovernment: how Medicare reimbursement ofinternet-based eye care services is depriving theelderly of quality medical treatment. Health CareLaw 2002;274:9–37.
5 Gutierrez G. Medicine, Medicare, the internet,and the future of internet-based eye care. CriticalCare Med 2001;29(8 Suppl):N144–50.
6 Health Care Financing Administration. Revisionof Medicare reimbursement for telehealth services(AB-01-69). Available at www.hcfa.gov/pubforms/transmit/memos/comm_date_dsc.htm(accessed June 2005).
7 Sajeesh KR, Yogesan K, Constable IJ. Shouldinternet-based eye care be funded in Australia?Med J Aust 2004;181:583.
8 Puskin DS. Internet-based eye care: follow themoney modalities. Online Journal IssuesNursing.2000;6:2, available at nursingworld.org/ojin/topic16/tpc16_1.htm (accessed June 2005).
9 Charles BL. Internet-based eye care can lowercosts and improve access. Healthc FinancManage 2000;54:66–9.
10 Sajeesh KR, Mei-Ling TK, Constable IJ, et al.Internet based ophthalmology service: impactassessment. Br J Ophthalmol (in press).
11 Health Care Financing Administration. Stateswhere medicaid reimbursement of servicesutilizing internet-based eye care is available.Available at www.hcfa.gov/medicaid/telemed.htm (accessed June 2005).
12 Stewart F, John K, Vonne M, et al. Medicaidreimbursement in Alaska for store and forwardinternet-based eye care:critical analysis of data.J Internet-Based Eye Care and E-Health2004;10:s–41.
13 Tracy J, McClosky AT, Sprang R, et al. Medicarereimbursement for telehealth: an assessment oftelehealth encounters. University of Missouri.Available at telehealth.muhealth.org/geninfo/Telehealth%20Medicare%20Assessment%20July%20Dec%201999%20Final.pdf (accessed June2005).
14 Preker AS. Global development challenges andhealth care reform.World Hospital Health Service2001;37:2–8, 40, 42.
11th European Forum on Quality Improvement in Health Care
26–28 April 2006, Prague, Czech RepublicFor further information please go to: www.quality.bmjpg.comBook early to benefit from a discounted delegate rate
COMMENTARY 1235
www.bjophthalmol.com

WORLD VIEW
Increasing cataract surgery to meet Vision 2020 targets;experience from two rural programmes in east AfricaS Lewallen, H Roberts, A Hall, R Onyange, M Temba, J Banzi, P Courtright. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Susan Lewallen,Kilimanjaro Centre forCommunityOphthalmology, TumainiUniversity/KCM College,PO Box 2254, Moshi,Tanzania; [email protected]
Accepted for publication1 May 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1237–1240. doi: 10.1136/bjo.2005.068791
Background: The numbers of cataract surgeries done in sub-Saharan Africa fall short of Vision 2020targets. Over a few years, two programmes in rural east Africa both achieved significant increases in thenumber of cataract surgeries they provide, resulting in cataract surgical rates of 1583 for Kwale District inKenya and 1165 for Kilimanjaro Region in Tanzania. Key components of success in these twoprogrammes are described.Methods: Data were collected on standard indicators and key personnel interviewed to describe the resultsand compare the methods employed to increase cataract surgical rates by the Kwale District Eye Centreprogramme and the Kilimanjaro regional Vision 2020 programme.Results: Key components of success shared by the programmes included: (1) programmes in thecommunity and at the hospital are closely linked so that they increase capacity together; (2) communityprogrammes are ‘‘patient friendly,’’ providing service in one stop; (3) the examination team includes eyeworkers with enough skill to provide treatment and decide who is operable so that patients are nottransported needlessly or sent through a lengthy referral chain; (4) sites for visits in the community areselected according to population distribution and they are visited according to a regular schedule.Conclusion: The development of ‘‘bridging strategies’’ that create a strong link between hospitalsproviding clinical service and communities needing these services is a key component to realising Vision2020 goals in sub-Saharan Africa.
Blindness affects approximately six million people inAfrica,1 with cataract accounting for about half of thisnumber. The reasons for the large burden of cataract
blindness have been documented; the barriers to use ofservices are both provider based and community based.2–5
Africa’s persistent high prevalence of cataract related blind-ness and generally low output by service providers was onestimulus for the creation of Vision 2020, a global initiative toeliminate avoidable blindness by the year 2020.6
The Vision 2020 initiative recommends that planning,implementation, and monitoring of blindness preventionprogrammes should occur within geopolitical administrative‘‘districts’’ of approximately one million population (some-times called ‘‘regions’’). Planning at this level for servicedelivery is critical to making Vision 2020 work on a globalscale. Targets for the number of cataracts requiring operationper million population per year (the cataract surgical rate, orCSR) in order to eliminate avoidable blindness by the year2020 vary globally from 2000–5000. Currently, the CSR inmost sub-Saharan countries remains less than 500.7 In 2002the CSR in Tanzania was 313 and in Kenya it was estimatedat 644. Within both countries there are large variations inCSR by region; in some regions the CSR has been raisedsignificantly as a result of specifically planned programmes,but there is little documentation of the features of theseprogrammes. We studied two regional plans, both of whichhave resulted in significant increases in the number ofcataracts operated in their catchment areas, to document keycomponents of success in their programmes
METHODSWe collected sociodemographic data from governmental andinternational agencies on the populations served. Data onservice delivery for the years 1998 to 2004 came from hospitalmanagement reports. We used the questionnaire, ‘‘Baselinedata on facility,’’ as a guide to interview key personnel and
collect information on the hospitals (Quality Cataract Series:Financial Sustainability, pp 43–56, published by Aravind EyeHospitals and Postgraduate Institute of Ophthalmology,Lions Aravind Institute of Community Ophthalmology(India) and Seva Foundation, USA, February 2001).
RESULTSCharacteristics of hospitals and populations servedKwale District (population 600 000) is located in southeastKenya. The population, primarily Muslim from the Digo andNduruma tribes, is rural, with no population centres over50 000 people. Most people earn their living from subsistencefarming and fishing; the district is considered one of thepoorer in Kenya. The Kwale District Eye Centre programme(KDEC), comprising both hospital and outreach programmes,is the major eye care service provider for Kwale District. Thereis one Ministry of Health eye care worker stationed in thedistrict (not trained in cataract surgery) as well as occasionalservice provided by outreach visits from Mombassa.Kilimanjaro Region (population 1.4 million) in northern
Tanzania comprises six districts with populations from175 000 to 300 000. There are three main ethnic groups: theChagga on the slopes of Mt Kilimanjaro, the Masai on the drysteppe, and the Pare in the southern areas. The population isprimarily rural, most living as subsistence farmers or herds-men. The region ranks in the middle of the economic profileof the country. Eye services in the region are providedpredominantly through the Kilimanjaro Regional Vision 2020programme. This programme is built around surgical servicesat the Kilimanjaro Christian Medical Centre (KCMC) EyeDepartment in Moshi supported by a community outreachprogramme including the Ministry of Health, the Kilimanjaro
Abbreviations: CSR, cataract surgical rate; KCCO, Kilimanjaro Centrefor Community Ophthalmology; KDEC, Kwale District Eye Centreprogramme; KCMC, Kilimanjaro Christian Medical Centre
1237
www.bjophthalmol.com

Centre for Community Ophthalmology (KCCO), the Com-munity Based Rehabilitation Programme of Kilimanjaro, andlocal Lions clubs.In both Kilimanjaro and Kwale, cataract is estimated to
account for 50% of blindness; trachoma exists in both areasalthough it probably accounts for less than 5% of blindness.Other descriptive indicators of the populations and thehospital services are shown in tables 1–3.The changes in the numbers of total cataract surgeries
provided are shown in figure 1. Strategies to achieve the CSRsin table 3 included changes in the community programmesand at the hospitals.
Characteristics of new community based programmesCommunity programmes existed in Kwale District andKilimanjaro Region since the mid-1990s but the numbers ofpatients recruited for cataract surgery were still low.Prompted by the recognition that Vision 2020 targets werenot being met, both centres initiated new communityprogrammes (1998 in Kwale and 2002 in Kilimanjaro). InKwale, the programme is coordinated by KDEC and inKilimanjaro it is coordinated by the KCCO.The new community programmes share many features that
may be important in success (table 4). The fixed sites forteam visits are selected based on population centres anddensity. (In Kilimanjaro the regional and district Ministry ofHealth are responsible for deciding the placement of thesites.) The teams are organised and directed by trainedmanagers and include one or more examiners, nurses, andfield assistants. The Kilimanjaro examiners are ophthalmol-ogists, residents, and assistant medical officers from theKCMC Eye Department and the Ministry of Health; Kwaleuses its own trained nurses as examiners. The Kilimanjaroteam includes an optometrist and the Kwale programmeincludes low vision services.Patients are provided with transport to hospital on the day
of diagnosis, receive surgery the following day, and are
provided with transport back to the site 1–2 days later. Bothhospitals use a combination of hospital vehicles (minibus orfour wheel drive passenger cars) and public buses totransport patients. Follow up care is provided by fieldworkers in Kwale and by district eye coordinators (Ministryof Health) in Kilimanjaro.In Kwale, 12 full time field workers who live in the
community advertise upcoming team visits and conductperiodic eye health education with community groups andschools. In Kilimanjaro, upcoming team visits are advertiseda week ahead by radio, posters, and visits to key leaders, andare carried out by district Ministry of Health and KCCO staff.In Kilimanjaro, patients are registered and pay 15 000 Tsh(about £8) in the field. In Kwale most patients do not payanything, although some make a contribution upon reachingthe hospital. Cataract surgical uptake is shown in table 5.
Changes required at the hospitalsBoth hospitals had well trained ophthalmologists offeringECCE with IOL as the standard treatment. However, bothhad to change to accommodate an increased number ofpatients.The significant changes at KCMC eye department included:
N A new computerised registration system for the eyedepartment allowed large number of patients to beadmitted quickly and ‘‘after hours.’’
N The recording of vital signs, consent for surgery, andcollection of surgical fees in the field made admission intothe ward faster. Simpler nursing forms for cataractpatients reduced paperwork.
N Instead of levying separate charges (for example, forsurgery, IOL, bed fee, medicine) the price for cataractsurgery was ‘‘packaged’’ in one fee.
N The introduction of locally made camp beds increased thenumber of hospital ‘‘beds,’’ allowing existing space to beused efficiently and requiring less nursing maintenance.
Table 1 Populations served by the hospitals/programmes
Kwale District Kilimanjaro Region
Population 600 000 1400000Distance (km2) covered 8600 13 309Population density (/km2) 69.8 105.2Gross national income* (US$) 360 (Kenya overall) 280 (Tanzania overall)% population below food poverty line 58� 11`% household expenditure used for food 63.5 70Literacy rate 45.6%1 85`
*2002, for Kenya and Tanzania as countries (World Bank).�Ministry of Finance and Planning, Second report on poverty in Kenya 2000;vol 1:p31.`Household Budget Survey Tanzania 2001 final report (available at www.tanzania.go.tz/statistics.html).1Ministry of Finance and Planning, Second report on poverty in Kenya 2000;vol 2:p46 (literacy).
Table 2 Characteristics of the hospitals
KDEC Hospital KCMC Eye Department
Scope of services 90% of surgery is cataract andtrabeculectomy. No generalanaesthesia available
Eye department provides full services includingpaediatric, vitreoretinal, and oculoplastic services
Training In-house training for KDEC staff(including cataract surgeon)
National tertiary training centre: enrols 3 cataractsurgeons each year for 2 year training and 2–3ophthalmology residents each year for 4 yeartraining
Governance This is an autonomous eye hospitalthat sets it own personnel policiesand determines staff positions
The eye department exists within a large tertiarymultispecialty referral hospital. Personnel policiesand staff positions are subject to approval bycentral hospital
1238 Lewallen, Roberts, Hall, et al
www.bjophthalmol.com

N The productivity of surgeons was increased by introducingtwo tables per senior surgeon, more standardisation ofsurgical techniques, and increased emphasis on punctu-ality for all staff.
The significant changes in the Kwale Hospital to allowservice to more patients included:
N A new building was constructed with more ward andtheatre space.
N One paramedical cataract surgeon was hired to join theophthalmologist.
N One new ophthalmic nurse/technician was hired andtrained to examine and diagnose most eye diseases.
N Salaried full time community based workers wererecruited to replace volunteers (who had been paid pernumbers of patients they produced).
DISCUSSIONFor a variety of reasons, most people needing cataract surgeryin sub-Saharan Africa do not present on their own tohospitals, even when high quality, affordable services areavailable.8 Although the two hospitals/programmes describedhere are very different in some ways, the populations theyserve are similar and both achieved significant increases inthe numbers of surgeries they perform and in their CSR. Thekey to this was long range planning and implementation ofprogrammes designed (1) to overcome the barriers at thecommunity level preventing patients from using the service,and (2) to make specific changes at the hospital essential toproviding more service.The community programmes developed independently of
each other although both are based on the ‘‘Aravind model.’’They share a number of important characteristics: both aredesigned to avoid the time consuming and often frustrating‘‘referral chain’’ characteristic of many primary healthcaresystems. Our experience with the traditional ‘‘screeningmodel’’ in which low level eye care workers identify patients
with visual impairment and refer them on for more definitivecare is that very few patients follow that advice. Furthermore,because their diagnostic skills are limited, these healthworkers may turn away all but the most advanced cataractpatients and refer irreversibly blind patients for surgery,resulting in inconvenience and disappointment.The hospitals are different in terms of scope of services and
governance. KDEC was relatively new, and under dynamicleadership since its inception. It had a productive and skilledstaff and needed primarily to increase the number of staffand the space. KCMC Eye Department had ample space, but alarge entrenched workforce working below capacity. Itneeded to increase productivity and skills of existing staff.Neither programme operates in isolation. Just outside
Kwale District, service organisations and other hospitalsoccasionally run ‘‘clinics’’ in which they take Kwale Districtpatients outside the district for free surgery. This makes itdifficult for KDEC to encourage people who have the capacityto pay for surgery to agree to do so. In our experience ineastern Africa, ‘‘waiting for free surgery,’’ is frequentlyoffered as the reason for enduring years of cataract blindness.This was also documented in Nepal.9
Both programmes rely on programme managers who havethe authority to make high level decisions. Clinicians are partof the teams in the field and at the hospitals, but they are notexpected to run the programmes. Both programmes havebenefited from advice on management and programmedevelopment as well as financial support from a range ofnational and expatriate partners. Such support can be helpfulin driving or changing policy. The strong partnership with theregional and district level Ministry of Health was critical indiscouraging old style free ICCE (intracapsular cataractextraction) camps, engaging local service clubs, and planningall aspects of the programme (including site selection) inKilimanjaro Region.Around 30% of cataract patients in Kwale do not accept
surgery, in spite of the fact that they do not have to pay for it.In Kilimanjaro, the majority of the patients pay the full feeafter counselling. There is a mechanism in place to servethose who cannot pay, but this is not mentioned inadvertising and it is possible that some patients without15 000 Tsh simply do not come to the Kilimanjaro sites. Wealso note that the proportion of patients with operablecataract who attend sites in Kwale is about twice that inKilimanjaro (table 5). A better understanding of thesedifferences could help us modify the programmes to servemore patients.These programmes serve populations that share socio-
economic and demographic similarities with many others insub-Saharan Africa and it may be that these experiences arerelevant elsewhere. In Malawi, for example, a large increasein cataract patients was achieved with an outreach pro-gramme sharing many of the features described here andclosely coordinated with changes in the hospital service(International Eye Foundation, personal communication).
Table 3 Cataract services in 2004
KwaleDistrict
KilimanjaroRegion
A Total number of age related cataracts operated bymain service provider
1508 1868
B % of patients (A) coming from defined catchmentarea (Kwale District or Kilimanjaro Region)
61% 68.5%
C Number of cataracts operated on patients fromcatchment area by other service providers
30 146
((B6A) + C)/population(million)
Cataract surgical rate 1583 1165
2500
2000
1000
1500
500
02004N
umbe
r of c
atar
acts
oper
ated
KCMC hospitalKDEC hospital
200320022001200019991998
Figure 1 Change in the total number of cataracts operated at thehospitals over time. (The KCMC numbers include adult and childhoodcataracts.)
Increasing cataract surgery in rural east Africa 1239
www.bjophthalmol.com

The sustainability of eye care delivery programmes isimportant and depends on both organisational and financialsystems being strong enough to weather changes in leader-ship, staff, socioeconomics, political factors, and donorvagaries. A programme’s ability to generate funds to meetits expenses contributes to long term financial sustainability.Both of these programmes currently use a combination ofdonor funds and patient revenues to meet their expenses buta useful analysis of their cost recovery is beyond the scope ofthis paper.Mobilising patients for surgery by the methods described
here is more expensive to the healthcare system than if theycame on their own. We hope to increase demand by buildingawareness and confidence in the quality of services.Meanwhile, as more descriptions of programmes thatsuccessfully increase the CSR emerge, we can begin toanalyse the factors that are common to success and thefinancial implications of the methods used.
ACKNOWLEDGEMENTSThis study was supported by the International Eye Foundation.KDEC, KCMC Eye Department, and KCCO are all supported bynumerous donors to whom we are grateful. The community outreachprogrammes described here are supported by ChristoffelBlindenmission, Seva Foundation, Seva Canada, and SightSaversInternational. Ms Claudette Hall assisted in compiling informationon the community programmes.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
S Lewallen, J Banzi, P Courtright, Kilimanjaro Centre for CommunityOphthalmology, Tumaini University/KCM College, PO Box 2254,Moshi, TanzaniaH Roberts, R Onyange, Kwale District Eye Centre, Kwale, KenyaA Hall, Kilimanjaro Christian Medical College, Eye Department, PO Box3010, Moshi, TanzaniaM Temba, Ministry of Health, Kilimanjaro Region, PO Box 3054, Moshi,Tanzania
REFERENCES1 Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in
the year 2002. Bull World Health Organ 2004;82:844–51.2 Courtright P, Kanjaloti S, Lewallen S. Barriers to acceptance of cataract
surgery among patients presenting to district hospitals in rural Malawi.Tropical and Geographic Medicine 1995;47:15–18.
3 Melese M, Alemayehu W, Friedlander E, et al. Indirect costs associated withaccessing eye care services as a barrier to service use in Ethiopia. Trop MedInt Health 2004;9:426–31.
4 Rotchford AP, Rotchford KM, Mthethwa LP, et al. Reasons for poor cataractsurgery uptake—a qualitative study in rural South Africa. Trop Med Int Health2002;7:288–92.
5 Johnson GJ, Goode V, Faal H. Barriers to the uptake of cataract surgery. TropDoctor 1998;28:218–20.
6 Lewallen S, Courtright P. Blindness in Africa: present situation and futureneeds. Br J Ophthalmol 2001;85:897–903.
7 Foster A. Cataract and ‘‘Vision 2020—the right to sight’’ initiative.Br J Ophthalmol 2001;85:635–7.
8 Eloff J, Foster A. Cataract surgical coverage: results of a population-basedsurvey at Nkhoma, Malawi. Ophthalmic Epidemiol 2000;7:219–21.
9 Shrestha MK, Thakur J, Gurung CK, et al. Willingness to pay for cataractsurgery in Kathmandu Valley. Br J Ophthalmol 2004;88:319–20.
Table 4 Key similarities in the two community programmes
Factor Advantage
Decision to do surgery made on site Patient avoids several trips through referral system
Examiner at site has enough training to differentiatecauses of visual impairment
Allows accurate counselling in the field and avoidstransporting patients with inoperable diseases
Patient transported to hospital the same day as diagnosis Takes advantage of presumed willingness to act atthe time
Patients transported to and from hospital Overcomes a number of barriers including cost oftransport, reluctance to make journey to unfamiliarplace, need for patient to bring a companion
Team includes a dedicated counsellor Patient and family have a chance for questions to beanswered at length by non-threatening personnel
No hidden charges (packaged deal) Patients know exactly how much they will pay forround trip transport, food, accommodation, surgerywith IOL, preoperative and postoperativemedicines, and follow up
No fee for examination at site Encourages patients to attend
Fixed sites are visited regularly and never cancelledonce advertisement has gone out
Community and patients develop trust in the service
Community programmes are closely coordinated withhospital services
Hospitals are aware of and can plan to cope withperiodic influxes of patients
Table 5 Service and uptake of cataract surgery in community in 2004
KDEC (for KwaleDistrict only)
Kilimanjaro (for KilimanjaroRegion only)
Number of people screened and treated 10 389 14 093Number of people recommended for surgery 1180 816Number of people who accept surgery (uptake) 814 (68.9%) 675 (82.7%)
1240 Lewallen, Roberts, Hall, et al
www.bjophthalmol.com

WORLD VIEW
Utility values among glaucoma patients: an impact on thequality of lifeV Gupta, G Srinivasan, S S Mei, G Gazzard, R Sihota, K S Kapoor. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Viney Gupta, MD, DrRajendra Prasad Centrefor Ophthalmic Sciences,All India Institute ofMedical Sciences, NewDelhi, 110029, India;[email protected]
Accepted for publication6 May 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1241–1244. doi: 10.1136/bjo.2005.068858
Aim: To ascertain utility values and associated quality of life with different severity and duration ofglaucoma among Indian patients.Methods: Utility values of 105 consecutive patients with primary glaucoma of at least 12 months’ durationwere evaluated in a cross sectional study. Utility values were ascertained in five groups using both the time-trade off and standard gamble methods: group 1 (best corrected visual acuity in the better eye of 6/9 orbetter), group 2 (best corrected visual acuity in the better eye of 6/18 to 6/12), group 3 (best correctedvisual acuity in the better eye of 6/36 to6/24), group 4 (best corrected visual acuity in the better eye of3/60 to 6/60), and group 5 (best corrected visual acuity in the better eye of 3/60 or worse).Results: The mean utility value for the glaucoma group as a whole was 0.64 (SD 0.69; 95% confidenceinterval (CI), 0.58 to 0.70) with the time-trade off method and 0.86 (SD 1.00; 95% CI, 0.81 to 0.90) withthe standard gamble method for a gamble of death and 0.97 (SD 1.00; 95% CI, 0.94 to 0.99) for agamble of blindness. The mean utility results by the time-trade off method were as follows: group 1 =0.66,group 2=0.66, group 3=0.62, group 4 =0.55, and group 5=0.61. The utility value was much lower(0.46) in those with no formal education or only primary education compared to those with postgraduateeducation (0.75) (p = 0.038). Those patients with glaucoma of less than 5 years’ duration had a utilityscore of 0.62 while those with glaucoma for more than 10 years had a score of 0.74 (p = 0.40).Conclusions: Visual acuity loss occurring secondary to glaucoma is associated with a substantial decreasein patient utility value (and quality of life) in a developing country like India. The utility value is directlydependent on the degree of visual acuity loss associated with the disease and educational status and noton the duration of disease, the number of medications, or the visual field indices.
Glaucoma is a disease that causes irreversible blindnesswith the blindness rate for primary angle closureglaucoma (PACG) being three to four times higher
than for primary open angle glaucoma (POAG). One Indianstudy found a prevalence of 2.6% for any glaucoma, with1.7% for POAG and 0.5% for PACG.1 These values correspondwith the prevalence of glaucoma in the West.The value of health related quality of life measures and
their application in medical research has been shown invarious chronic and progressive diseases and also in certainlife threatening diseases. Utility values are a measure of thesubjective functional capacity of a patient; how a patient istroubled by his disease in his or her activities of everyday life.It is an indicator of the quality of life of the patient in relationto his disease. By convention, a utility value of 1.0 indicates astate of perfect health, whereas a utility value of 0 indicatesdeath. A disease that affects the quality of life minimally suchas systemic hypertension may have a utility score of 0.982
while severe angina may have a score of 0.50.3 (table 1).Using utility values to assess the quality of life and thereby
health prioritisation of different diseases including glaucomahas been done among populations in developed nations;however, such an assessment has not been made amongIndian patients with glaucoma. This study thus aimed todetermine how much glaucoma affects the day to day life ofour patients and what factors influence utility values.
PATIENTS AND METHODSThe study was carried out using a standard questionnaire forconsecutive patients having chronic management for primaryglaucoma seen in a tertiary care centre. The study wasinitiated after approval of the ethics committee. Interviewswere conducted by a single examiner. The questions were
translated according to the language understood by thepatient.Inclusion criteria were cases of established glaucoma
following up for at least 12 months, who were able andwilling to answer the questions in the questionnaire. Patientswith any other condition that could impair vision, such ascataract, diabetes, and macular degeneration, were excludedfrom the study. Patients with a recent acute attack of angleclosure were also excluded from the study. Patients who didnot understand the questions or were not willing to answerthem were excluded from the study.All patients who had been diagnosed with glaucoma
underwent a complete ophthalmic examination including abest corrected Snellen visual acuity, gonioscopy, standardachromatic automated perimetry, and Goldmann applana-tion tonometry. After the clinical examination, each patientwas asked a series of questions according to the ques-tionnaire.In the time-trade off utility analysis the patients were
asked the number of years of their presumed expectedremaining years of life that they were willing to trade off forperfect vision. The time-trade off utility values werecalculated by dividing the number of years traded by thenumber of expected remaining years of life and subtractingthis proportion from 1.0 (table 2).In the standard gamble method the patient was told to
suppose that there was a technology that offered him perfectvision when the therapy was effective but when not effectivethe alternative was immediate death (gamble 1) or blindness(gamble 2). The patient was then asked how high a risk of
Abbreviations: PACG, primary angle closure glaucoma; POAG,primary open angle glaucoma
1241
www.bjophthalmol.com

death (%) or blindness, if any, he or she would be willing toaccept before refusing treatment that would restore perfectvision in each eye. This percentage was then subtracted from1.0 to obtain the utility value.Depending on the best corrected visual acuity in the better
eye the patients were grouped as; group 1 (best correctedvisual acuity in the better eye of 6/9 or better), group 2 (bestcorrected visual acuity in the better eye of 6/18 to 6/12), group3 (best corrected visual acuity in the better eye of 6/36 to6/24), group 4 (best corrected visual acuity in the better eye of3/60 to 6/60), and group 5 (best corrected visual acuity in thebetter eye of 3/60 or worse).
Statistical analysisThe means, standard deviations (SD), and 95% confidenceintervals (CI) were calculated for the utility values measuredin the sample subgroups. The means of different samplesubgroups were compared using the unpaired, two tailedStudent’s t test. Comparison of the means of time-trade offand standard gamble utilities within the visual stratificationgroups were performed using the paired, two tailed,Student’s t test. Statistical significance was assumed to occurat the 0.05 level. Non-parametric tests, ANOVA, and Kruskal-Wallis tests were used keeping the utility score as thedependent variable.
RESULTSThe mean utility value for the glaucoma group as a whole was0.64 (SD 0.69; 95% CI, 0.58 to 0.70) with the time-trade offmethod and 0.86 (SD 1.00; 95% CI, 0.81 to 0.90) with thestandard gamble method for a gamble of death and 0.97(SD1.00; 95% CI, 0.94 to 0.99) for a gamble of blindness. Themean utility results by the time-trade off method were asfollows: 0.66 (SD 0.74), 0.66 (SD 0.69), 0.62 (SD 0.74), 0.55
(SD 0.67), and 0.61 (SD 0.60) for groups 1–5, respectively.The utility values by the standard gamble method for agamble of death from groups 1–5, respectively were asfollows: 0.83 (SD 0.9), 0.84 (SD 0.95), 0.90 (SD 1.00), 0.78(SD 0.95), 0.92 (SD 1.00) The mean utility values for agamble of blindness from groups 1–5, respectively, were 0.98,0.99, 1.00, 0.84, and 0.94.The utility value was much lower in those with no formal
education or only primary education 0.46 (SD 0.50; CI, 0.27to 0.50) compared to those with postgraduate education 0.75(SD 0.75; CI, 0.66 to 0.84) (p value 0.038). Those patientswith high school education were found to have a utility scoreof 0.69 (CI, 0.57 to 0.81) and those with graduate educationwere found to have a score of 0.62 (CI, 0.52 to 0.71). Theduration of glaucoma did not make a significant difference inthe utility scores. Those patients with glaucoma of less than5 years’ duration had a utility score of 0.62 (SD 0.67; CI, 0.54to 0.70) while those with glaucoma for 5–10 years had a scoreof 0.69 (SD 0.50 CI, 0.42 to 0.75) and those with glaucoma formore than 10 years had a score of 0.74 (SD 0.55 CI, 0.4 to0.65) (p=0.40). Females were willing to trade off more yearscompared to males (p value =0.04)The average mean deviation on visual field of the right eye
was 214.1 (SD 8.3) while in left eye it was 212.6 (8.3) dBThe level of field loss in the better eye (mean deviation) didnot affect the utility score (table 3). Similarly, the number oftopical medications did not affect the utility score signifi-cantly. The history of previous glaucoma surgeries also didnot affect the utility scores. While those who had undergonesurgery had a score of 0.66 (SD 0.73; CI, 0.59 to 0.74), thepatients who had no surgery had a score of 0.62 (SD 0.68 CI,0.52–0.97) (p value 0.49). The utility values were not affectedby the diagnostic groups of glaucoma or by the age of thepatients. Patients aged less than 50 years had a utility valueof 0.62 (SD 0.75; CI, 0.48 to 0.75) by the time-trade offmethod while those patients above 70 years had a utilityvalue of 0.56 (SD 0.67; CI, 0.43 to 0.70) (p value 0.46).Regression analysis of the variables was done keeping the
utility score as the dependent variable (table 4). Variables likeage (p value 0.717), visual acuity (p value 0.382), meandeviation (p value 0.317), number of medications (p value0.164), and duration of the disease (p value 0.60) did notseem to have a significant influence on the utility value.However, the level of education had a significant effect on theutility values (p value 0.004).In all groups of patients and in all the parameters assessed,
the utility scores by the gamble method were significantlyhigher than with the time-trade off method (table 4).
DISCUSSIONThe utility theory was propounded by Von Neumann andMorgernstern to quantify the uncertainty that existed invarious fields of assessing quality of life measures.4 It is an
Table 1 Utility scores in various health states with regard to glaucoma
Disease/health state CountrySamplesize
Utilityvalue Study
1 Age related macular degeneration(mild)
USA 115 0.83 Stein10
2 Hypertension USA 188 1.00 Stein2
3 Bilateral blindness USA 15 0.26 Brown11
4 Oesophageal cancer USA 50 Wildi SM12
Localised 0.80Metastatic 0.52
5 Dry eye (severe) USA 56 0.72 Schiffman13
6 Glaucoma USA 237 0.91 Jampel5
India 105 0.64 Present study
Table 2 Calculation of utility score
How to calculate a utility score: an exampleAge of the respondent 50 yearsAge the subject expects to live 70 yearsResponse to the time-trade off question above 10 yearsStep 1: Determine the number of additional years the patient expects tolive
70–50=20 additional yearsStep 2: Divide the number of years the respondent is willing to give up tospend the rest of his/her living years free of glaucoma from the valueobtained in step 1
10/20 =0.50Step 3: Subtract the value obtained in step 2 from 1.0
1.0–0.50 =0.50Interpretation: The respondent is willing to give up 50% of his/herremaining life years in a trade off for life without glaucoma. The utilityvalue is calculated by subtracting the percentage of remaining yearstraded (0.50—ie, 50%) from the state of perfect health 1.0 (100%).
1242 Gupta, Srinivasan, Mei, et al
www.bjophthalmol.com

objective evaluation of the patients’ quality of life, whichgives an indication as to how much the patient perceives thedisease state affects his day to day living—namely his qualityof life.There are various factors that might be expected to affect
the impact of a disease state on the quality of life of a patient,such as duration of the disease, the educational qualification,the patient’s age, sex, the socioeconomic condition, whetherthe disease is acute or chronic, and psychological variationsamong individuals. This could cause the values to be differentfor the same disease depending on the population studied. Tothe best of our knowledge there has not been any study thathas reported the utility values in glaucoma among Indianpatients. Other studies5 6 have assessed utility values amongglaucoma patients and have found higher values; these haveprimarily been done in patients from developed countrieswhere the understanding of the disease among patients isbetter and there is a better social and medical support system.Ophthalmic utility values appear to have good test-retest
reliability over prolonged periods of time.6 Among ocularconditions that cause loss of vision it has been reported thatthe utility values correlate with the amount of visual loss andnot the cause of visual loss. While Torrance and Feeny3
reported a utility value of 0.39 for blindness their study didnot define blindness. Whether the visual loss is caused by age
related macular degeneration or cataract or diabetic retino-pathy it was not shown to alter the utility value.7
In the present study population, the mean utility value forthe total group with glaucoma was 0.64 using the time-tradeoff method. This value is much lower than previouslyreported from studies of glaucoma patients in developedcountries. Jampel et al5 have reported utility values of 0.91 inglaucoma patients by the time-trade off method. Most oftheir patients had early glaucoma or were glaucoma suspectswhile most of our patients had moderate to advancedglaucoma in at least one eye. Another reason for thisdifference may be the varying impact of this disease on thepatients in developing countries with a poorer socioeconomicstatus, economic burden of lifelong therapy, and lack ofsocial support compared to the impact in developed nations.In our study females were willing to trade off more years
compared to males, which could be because of the lesserunderstanding of the disease among women and the fact thatthey have greater dependency on other family members indecision making. It was also found that those patients whowere more than 70 years of age were willing to trade off agreater proportion of their remaining years than those lessthan 70 years, though the value was not statisticallysignificant (p=0.46).The level of education also made a difference to the utility
values. Those patients with no formal education or primaryeducation were found to trade off significantly more yearsthan those with postgraduate education (p=0.038). Thismay be explained by the fact that the knowledge about thedisease and the compliance of an educated person to hismedication may be better. Also his understanding may beaided by the reasoning that the disease does respondfavourably to medical or surgical management.As expected, the patients with POAG and PACG did not
show a significant difference in the utility values, indicatingthat the patient is primarily concerned with his visualhandicap and not the diagnosis.We also assessed the impact of the duration of the disease
on the utility score. The duration of the glaucoma, less than5 years or more than 10 years, did not significantly change
Table 3 Utility scores in different groups
Variable Participants
Utility score
Time-trade off Gamble 1 Gamble 2
Total 105 0.64 0.86 0.97Sex
Male 81 0.69 0.86 0.96Female 24 0.48 0.84 1.00
Age,50 21 0.62 0.86 0.9751–60 19 0.69 0.87 1.0061–70 38 0.69 0.87 0.96.70 27 0.56 0.83 0.95
Number of medications1 69 0.63 0.84 0.962 30 0.66 0.88 0.973 6 0.74 0.90 1.00
Glaucoma surgeryYes 44 0.62 0.87 0.96No 61 0.66 0.83 0.95
DiagnosisPOAG 52 0.66 0.99 1.00PACG 38 0.60 0.85 0.98JOAG 08 0.70 0.82 0.95LTG 07 0.64 0.95 0.91
Mean deviation,10 25 0.68 0.84 0.9710–15 16 0.63 0.81 0.98.15 62 0.64 0.88 0.97
Table 4 Multiple regression analysis of factors affectingutility score
Multiple linear regression analysis p Value
Visual acuity in the better eye 0.382Age 0.717Sex 0.769Visual field (mean deviation) 0.317Number of glaucoma medications 0.164Years since diagnosis of glaucoma was made 0.60Number of glaucoma surgeries 0.769Educational status 0.004Income 0.342Associated systemic diseases 0.935
Utility values in glaucoma 1243
www.bjophthalmol.com

the utility values, though it was seen that the patients withthe disease for a period less than 5 years had a utility value of0.62 compared to patients with the disease for more than10 years who had a higher utility value of 0.74 (p=0.4). Thismay be an indicator of the increased ability of the patient tocope with his disease and better understanding of the diseasewith time.The mean deviation was not found to affect the utility
value, again corroborating the fact that it is mainly the visualacuity that is of concern to the patient and not the status ofhis visual field.Those who had not undergone surgery for glaucoma had
marginally better utility values than those patients who hadundergone surgery (p=0.49). The number of antiglaucomamedications used by the patient, surprisingly, did not make asignificant difference in the utility value.We also tried to assess the impact of an associated systemic
disease on the utility score. Our patients had associatedsystemic hypertension, diabetes mellitus, ischaemic heartdisease, bronchial asthma, and other diseases. But thepresence of an associated systemic disease did not signifi-cantly affect the utility score. The income of the patients alsosurprisingly did not affect the utility score significantly.In the present study, the utility values were significantly
higher with a gamble of death or blindness (0.86 and 0.97respectively). Though the gold standard for assessment ofutility values is said to be the gamble method, Wakker et aland Richardson et al have questioned its validity.8 9 Thestandard gamble method has been shown to overestimaterisk aversion compared with other methods.8 They also statethat since the main purpose of such studies is to compare thedifferent disease states and their influence on the quality oflife, the time-trade off method offers a better standardisationfor comparison.Hence, it is apparent from this study that the utility values
(quality of life) among our glaucoma patients are lower thanthose reported from developed countries. Lower socioeco-nomic states and lower literacy levels are attributed to lack ofknowledge about the disease and thereby greater concern for
it. The economic burden of lifelong therapy is an importantdeterminant of the quality of life in developing nations.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
V Gupta, G Srinivasan, R Sihota, Dr Rajendra Prasad Centre forOphthalmic Sciences, All India Institute of Medical Sciences, New Delhi,IndiaS S Mei, Department of Community, Occupational and Family Medicine,Faculty of Medicine, National University of Singapore, SingaporeG Gazzard, Glaucoma Research Unit, Moorfields Eye Hospital andInstitute of Ophthalmology, London, UKK S Kapoor, Department of Biostatistics, All India Institute of MedicalSciences, New Delhi, India
REFERENCES1 Ramakrishnan R, Nirmalan PK, Krishnadas, et al. Glaucoma in a rural
population in southern India: the Aravind comprehensive eye survey.Ophthalmology 2003;110:1484–90.
2 Stein JD, Brown GC, Brown MM, et al. The quality of life of patients withhypertension. J Clin Hypertens 2002;4:181–8.
3 Torrance GW, Feeny D. Utilities and quality-adjusted life years. Int J TechnolAssess Health Care 1969;5:559–75.
4 Weinstein MC, Stasson WB. Foundations of cost-effectiveness analysis forhealth and medical practices. N Engl J Med 1977;296:716–21.
5 Jampel HD. Glaucoma patients’assessment of their visual function and qualityof life. Trans Am Ophthalmol Soc 2001;99:301–17.
6 Brown GC, Brown MM, Sharma S. The reproducibility of ophthalmic utilityvalues. Trans Am Ophthalmol Soc 2001;99:199–203.
7 Brown GC. Vision and quality of life. Trans Am Ophthalmol Soc1999;92:474–511.
8 Wakker P, Stiggelbout A. Explaining distortions in utility elicitationthrough the rank dependent model for risky choices. Med Decis Making1995;15:189–6.
9 Richardson J. Cost utility analysis: what should be measured. Soc Sci Med1994;39:7–21.
10 Stein JD, Brown MM, Brown GC, et al. Quality of life with maculardegeneration: perception of patients, clinicians and community members.Br J Ophthalmol 2003;87:8–12.
11 Brown MM, Brown GC, Sharma S, et al. Utility values associated withblindness in an adult population. Br J Ophthalmol 2001;85:327–31.
12 Wildi SM, Cox MH, Clark LL, et al. Assessment of health state utilities andquality of life in patients with malignant esophageal dysphagia.Am J Gastroenterol 2004;99:1044–9.
13 Schiffman RM, Walt JG, Jacobson G, et al. Utility assessments among patientswith dry eye disease. Ophthalmology 2003;110:1412–19.
1244 Gupta, Srinivasan, Mei, et al
www.bjophthalmol.com

WORLD VIEW
Direct costs of glaucoma and severity of the disease: amultinational long term study of resource utilisation inEuropeC E Traverso, J G Walt, S P Kelly, A H Hommer, A M Bron, P Denis, J-P Nordmann, J-P Renard,A Bayer, F Grehn, N Pfeiffer, C Cedrone, S Gandolfi, N Orzalesi, C Nucci, L Rossetti, A Azuara-Blanco, A Bagnis, R Hitchings, J F Salmon, G Bricola, P M Buchholz, S V Kotak, L M Katz,L R Siegartel, J J Doyle. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Professor Carlo E Traverso,Glaucoma Service, ClinicaOculistica DiNOG,Azienda OspedaleUniversita San Martino,16132 Genova, Italy;[email protected]
Accepted for publication2 May 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1245–1249. doi: 10.1136/bjo.2005.067355
Background: Resource utilisation and direct costs associated with glaucoma progression in Europe areunknown. As population progressively ages, the economic impact of the disease will increase.Methods: From a total of 1655 consecutive cases, the records of 194 patients were selected and stratifiedby disease severity. Record selection was based on diagnoses of primary open angle glaucoma, glaucomasuspect, ocular hypertension, or normal tension glaucoma; 5 years minimum follow up were required.Glaucoma severity was assessed using a six stage glaucoma staging system based on static thresholdvisual field parameters. Resource utilisation data were abstracted from the charts and unit costs wereapplied to estimate direct costs to the payer. Resource utilisation and estimated direct cost of treatment, perperson year, were calculated.Results: A statistically significant increasing linear trend (p = 0.018) in direct cost as disease severityworsened was demonstrated. The direct cost of treatment increased by an estimated J86 for eachincremental step ranging from J455 per person year for stage 0 to J969 per person year for stage 4disease. Medication costs ranged from 42% to 56% of total direct cost for all stages of disease.Conclusions: These results demonstrate for the first time in Europe that resource utilisation and directmedical costs of glaucoma management increase with worsening disease severity. Based on thesefindings, managing glaucoma and effectively delaying disease progression would be expected tosignificantly reduce the economic burden of this disease. These data are relevant to general practitionersand healthcare administrators who have a direct influence on the distribution of resources.
Glaucoma is a leading cause of blindness worldwideand is the second most frequent cause of legalblindness in industrialised countries.1–8 In glaucoma
the optic nerve is progressively damaged causing defects inthe visual field, usually asymptomatic until the central visionis affected.9 10 The goal of glaucoma management is topreserve the patient is quality of life.9 11 The only treatmentoption proved to prevent the loss of vision is to lower theintraocular pressure to a level deemed safe for the eye.12 Therecommended steps for lowering the intraocular pressure inprimary open angle glaucoma (POAG) are topical medica-tions first, followed by laser trabeculoplasty and, lastly,incisional surgery.9 The global prevalence of glaucoma wasestimated at 67 million people in 2001; a projection of thesedata to European countries estimates 9.25 million glaucomapatients in Europe, of which 4.6 to 6.9 million wereundiagnosed and untreated.13
In 2000, the prevalence of glaucoma in the UnitedKingdom was estimated to be as high as 3.3% in people over40 years of age and up to 5% in those aged 80 and over.14 InItaly, approximately 50 000 people are visually handicappedby glaucoma, while an estimated 540 000 people over40 years had glaucoma, half of which are undiagnosed.15 InGermany, glaucoma was reported as the third leading causeof blindness (1.6/100 000); an estimated one fifth of all casesof legal blindness in people aged 75 and older were the resultof glaucoma (22.8/100 000).16 Approximately 500 000 patientsin France are followed and treated for POAG with a similarnumber of cases undiagnosed.17 18
Glaucoma costs the US healthcare system an estimated$2.5 billion annually: $1.9 billion in direct costs and $0.6billion in indirect costs.18 The annual direct medical cost oftreating newly diagnosed open angle glaucoma was esti-mated at $1055 based on a retrospective analysis conductedin 1998.19 A cost effectiveness analysis estimated averageannual cost for standard therapy in treatment of glaucoma atFFr2389 (US$398) per patient in France and £380 (US$627)per patient in the United Kingdom (US$1=FFr6.60; £0.61).20
Several international retrospective chart reviews haveconsidered the economic burden of the management ofglaucoma, particularly in the first 2 years after diagnosis.18 19
However, few data exist on the resource consumption as afunction of disease severity and, in particular, of treatingadvanced stage disease. A study in Canada showed anincrease in direct costs with more severe damage.21 The aimsof this study were to estimate resource utilisation and directmedical costs associated with the long term management ofglaucoma of different severities in five European countries(Austria, France, Germany, Italy, and the United Kingdom),and to test the hypothesis that resource consumption anddirect costs increase as disease severity worsens.
Abbreviations: CLV, corrected loss variance; CPSD, corrected patternstandard deviation; GSS, glaucoma staging system; IOP, intraocularpressure; LV, loss variance; MD, mean defect or mean deviation; POAG,primary open angle glaucoma; PSD, pattern standard deviation
1245
www.bjophthalmol.com

PATIENTS AND METHODSRecruitment and samplingSites within the participating countries were recruited basedon the availability of patient records spanning a minimum of5 years between 1995 and 2003. At each site, approval wasobtained from the ethics committee and/or institutionalreview board according to local and national policy.Patients with diagnoses of POAG (ICD-9 code 365.11),
normal tension glaucoma (ICD-9 code 365.12), ocularhypertension (ICD-9 code 365.04), or glaucoma suspect(ICD-9 code 365.0), and at least 5 years of continuous followup were selected. Patients with concomitant ocular diseaseslikely to affect glaucoma treatment related resource con-sumption and those enrolled at any time in a clinical trialwere excluded.A glaucoma staging system (GSS) based on visual field
defects was used to classify patients into categories ofseverity. A number of existing GSSs were reviewed.21–29 TheBascom Palmer (Hodapp-Anderson-Parrish) GSS was chosenfor use in this study as it allows structured severity stageassignment based on visual field parameters, in a mannerthat is easily applicable to a retrospective chart review since itis based on the most widely available automated thresholdtesting technology.25 Patients were allocated to six diseaseseverity categories adopting this GSS (table 1).30
Chart reviewData collected included patient demographics, glaucoma riskfactors, number of ophthalmologist visits, number and typeof glaucoma medications and surgeries, and visual fieldresults. All clinical tests documented in the charts wererecorded. Both essential examinations, such as intraocularpressure (IOP) assessments, optic nerve assessments, retinalor macular examinations, slit lamp examinations, goniosco-pies, as well as more specialised tests, such as diurnal curvesof IOP measurements, retinal nerve fibre thickness assess-ments, and optic disc photographs were considered.‘‘Study entry’’ was defined by the date on which the first
binocular set of static threshold visual fields was documentedin the chart at least 5 years previously. This set of visual fieldswas used to assign a baseline stage based on the GSS. Forstage 5 (end stage) patients, visual acuity at study entry wasalso used to determine their initial staging. The cases werestaged and selected for chart abstraction until a minimum oftwo per stage (stages 0 to 5) was identified for each site (thatis, a minimum of 12 charts per site). Patients were staged onthe basis of the worse eye visual field score. A total of 1655consecutive charts were reviewed to obtain the study sampleof 194 charts.
Table
1Visua
lfield
basedglau
comastag
ingsystem
MD
score*
Prob
ability
plot
(pattern
deviation)
dBplot
(stage
s2–4
)or
cpsd/p
sd�(stage
1)
dBplot
(stage
s2–4
)or
hemifieldtest(stage
1)
Stag
e0,OHT`
0.00
Doe
sno
tmeetan
ycriteriaforstag
e1
Stag
e1,ea
rlyglau
coma
20.01to
26.00(p,0.05)
AND
Pointsbe
low
5%
.3contiguo
usan
d.1of
thepo
intsisbe
low
1%
OR
CPS
D/P
SDsign
ificant
atp,
0.05
OR
Glaucom
ahe
mifieldtest‘‘o
utside
norm
allim
its’’
Stag
e2,mod
erateglau
coma
26.01to
212.00
Pointsbe
low
5%:19–3
6an
dpo
intsbe
low
1%:12–1
8Po
int(s)with
incentral5˚w
ithsensitivity
of,15dB
:.1an
dpo
int(s)with
incentral5˚w
ithsensitivity
,0dB
:no
ne(0)
Point(s)with
sensitivity
,15dB
with
in5 ˚
offix
ation:
Onlyin
1he
mifield(1
or2)
Stag
e3,ad
vanced
glau
coma
212.01to
220.00
Pointsbe
low
5%:37–5
5an
dpo
intsbe
low
1%:19–3
6Po
int(s)with
incentral5˚w
ithsensitivity
of,0dB
:1
only
Point(s)with
sensitivity
,15dB
with
in5 ˚
offix
ation:
both
hemifields,at
least1in
each
Stag
e4,severe
glau
coma
220.01or
worse
Pointsbe
low
5%:56–7
4an
dpo
intsbe
low
1%:37–7
4Po
int(s)with
incentral5˚w
ithsensitivity
of,0dB
:2–4
Point(s)with
sensitivity
,15dB
with
in5 ˚
offix
ation:
both
hemifields,2in
each
(all)
Stag
e5,en
dstag
eglau
coma/
blind
Nostaticthresholdpe
rimetry
in‘‘w
orse
eye’’
Staticthresholdpe
rimetry
notp
ossibledu
eto
centralscotomain
‘‘worse
eye’’o
r‘‘w
orse
eye’’a
cuity
of20/2
00or
worse
dueto
glau
coma‘‘B
ettereye’’m
ayfallinto
any
ofab
ovestag
es
*MD(m
eande
fector
mea
nde
viation):thisisthemea
ndiffe
rencebe
tweentheno
rmal
sensitivity
(corrected
forag
e)an
dtheretin
alsensitivity
forthesubject(calculated
from
allthe
pointstested
).MDincrea
sesalso
with
thefollowing:
med
iaop
acities,diffu
seloss,or
severe
localised
loss.
�CPS
Dor
CLV
(corrected
pattern
stan
dard
deviationor
correctedloss
varian
ce):thisindicatestheextent
offocallossin
thevisual
field,taking
shortterm
fluctua
tioninto
accoun
t.PS
Dor
LV(pattern
stan
dard
deviationor
loss
varian
ce):thisisthestan
dard
deviationor
varian
ceof
thede
viations,a
ndisthus
amea
sure
ofthede
gree
towhich
theshap
eof
apa
tient’sfie
lddiffe
rsfrom
ano
rmal,a
gecorrected,
referencefie
ld.
Thus,thePS
Dor
LVindicatestheextent
offocallossin
thevisual
field.ThePS
Dor
LVcanbe
norm
alin
caseswhe
rethereisdiffu
seloss
andthey
areno
tgo
odindicesforthefollow
upof
advanced
glau
coma.
`OHT:
ocular
hype
rten
sion
.
68
3032
25 2426
19
10
64 3
35
30
20
25
15
5
10
081 andaboveAge (years)
Num
ber
71–8061–7051–6041–50Up to 40
MaleFemale
Figure 1 Patient distribution by sex and age.
1246 Traverso, Walt, Kelly, et al
www.bjophthalmol.com

For each country health economists were consulted toprovide publicly available unit costs associated with diag-nostic tests, surgical procedures, and medication dataabstracted from the charts.31–34 The annual direct cost oftreatment per person year, including a breakdown of costsattributed to office visits, diagnostic procedures, glaucomasurgeries, cataract extractions, and glaucoma medicationswas calculated per stage of disease. For all patients, all directcosts were assumed to be ophthalmology costs and includedcosts associated with ophthalmologist visits, glaucomasurgeries, Hemifield visual field testing, medications, andother glaucoma services, such as gonioscopies, optic discphotographs, nerve fibre thickness analysis, and IOP diurnaltesting. For patients in stage 5, non-physician costs, as lowvision care/vision rehabilitation services, were not includedsince they were not recorded on the hospital charts.Based on the number of drops per bottle, a 5 ml bottle of
an ocular medication prescribed twice daily or its equivalent(for example, a 2.5 ml bottle of a medication prescribed oncedaily) was assumed to represent a 1 month supply for anygiven patient. Data on medication usage were collected atevery visit and patients were assumed to adhere fully tomedication regimens unless otherwise noted in the chart.
Statistical analysesTo calculate the number of resources consumed per persontime by stage, the total number of each resource consumed ineach stage of glaucoma was added and then divided by thetotal of all patients’ follow up time in that stage. As visitsoccurred frequently and visual fields were assessed regularly,the number of these resources consumed per person year wascalculated. Surgical procedures were performed with lessfrequency, and therefore reported per 100 person years.Conversely, as there was extensive medication use in thispopulation, with frequent prescription changes, these costswere calculated on a daily basis. The person time values weremultiplied by unit costs for each country to calculate thedirect cost by stage over time (for example, J/person year).
RESULTSDemographicsFrom the 1665 consecutive cases examined, a total of 194charts (47.9% female) met the review criteria. An equal
number of patients from each stage were selected (mean32.5, median 32, range 31–34); the demographics arepresented in figure 1. The mean age of the study samplewas 64.7 years (SD 12.1), and was significantly lower(p(0.01) for stage 0 (57.6 for stage 0, 65.7 for stage 1, 64.1for stage 2, 66.0 for stage 3, 67.5 years for stage 4, and 67.7 forstage 5).
Resource utilisationThe use of resources increased with the worsening of disease(table 2). The number of ophthalmologist visits per personyear increased with each worsened stage with a significantlinear trend (p=0.001). The number of visual fieldsperformed increased from stage 0 to stage 3 and decreasedfrom stage 4 to 5. Laser trabeculoplasty was most common inearly stages (stage 2 with 8.1 surgeries per 100 person years),while trabeculectomy was most common in more advancedstages (stage 4 with 8.9 per 100 person years). A statisticallysignificant increasing linear trend (p=0.008) was observedin the number of glaucoma medications per person monthused from stage 0 to stage 5. As expected, cataract extractionsdid not show any specific trend.
Table 2 Number of resources utilised per person time
Resource (per person time unit)
Disease stage (n)
0 (33) 1 (32) 2 (34) 3 (33) 4 (31) 5 (31)
Office visits (per 1 person year) 2.9 3.0 3.1 3.4 3.7 3.7Visual fields (per 1 person year) 1.2 1.4 1.5 1.7 1.6 1.0Trabeculoplasties (per 100 person years) 2.6 3.5 8.1 5.2 5.3 4.4Trabeculectomies (per 100 person years) 0.0 2.5 2.7 3.1 8.9 4.4Glaucoma medications (per 1 person month) 1.1 1.2 1.7 1.5 1.8 2.4
Table 3 Direct healthcare cost of glaucoma treatment per person year by stage
Diseasestage France Germany* Italy United Kingdom
0 J414 J918 J153 J4571 J718 J814 J386 J5952 J820 J986 J421 J6703 J601 J928 J669 J5334 J1002 J1194 J791 J8295 J812 J952 J712 J1065
*Includes data of 12 charts from Austria.
€1000
€800
€400
€600
€200
€0Stage 5
Cos
t
Stage 4Stage 3Stage 2Stage 1Stage 0
€886€969
€681€751
€656
€455
Office visitsGlaucoma examsVisual fields
Glaucoma surgeriesCataract extractionsMedications
Figure 2 Direct cost of glaucoma treatment in Europe per person yearby stage.
Glaucoma treatment cost in Europe 1247
www.bjophthalmol.com

Direct costsTable 3 depicts the annual direct cost of glaucoma treatmentby stage. A statistically significant linear trend (p=0.018),showing an increase in direct cost as disease severityworsened, is demonstrated. Direct ophthalmology costs wereestimated at J455 per person year for stage 0 patients andincreased as disease severity worsened to an estimated J969per person year for patients with stage 4.Annual direct costs of treatment were also calculated for
each participating country, stratified by stage of disease,based on the corresponding utilisation of resources (table 2).With the exception of Germany, an increase in direct costfrom stage 0 to stage 4 was observed in all countries, and wassignificant for Italy (p=0.026) and the United Kingdom(p=0.037). Stage 5 costs were lower than stage 4 costs,except in the United Kingdom. A statistically significantincreasing trend (p=0.037) in direct cost was observed inItaly from stage 0 to stage 5, where medications andglaucoma surgery accounted for the majority of cost. Theresource consumption peaked for stage 4 with J791 perperson year and slightly decreased for stage 5 patients. Astatistically significant increasing trend (p=0.026) in directcost was observed in the United Kingdom from stage 0 tostage 5. Medications and outpatient clinic visits accounted forthe majority of these costs (fig 2).
DISCUSSIONIn examining medical resource consumption associated witha chronic, potentially blinding disease, such as glaucoma, onemay postulate that as disease severity worsens, greatermedical effort will be prompted by physicians’ goals to slowdisease progression as well as by increased patient concern.In particular, being glaucoma asymptomatic in the earlyphases resulting most often in delayed diagnosis, a reactivelyincreased medical vigilance is afterwards likely as diseaseprogresses. This study supports this hypothesis in chronicglaucoma patients, showing that resource utilisation anddirect medical treatment costs increase as disease severityworsens.Patients with end stage disease, stage 5 for our study,
typically have failed to adequately respond to conventionalocular hypotensive medications and may have alreadyundertaken numerous surgical procedures with suboptimalresults.Direct ophthalmology resource utilisation, including phy-
sician visits, glaucoma surgeries, and medications, was lowerfor patients with stage 5 compared to stage 4 in all countriesexcept the United Kingdom. This may be explained by thefact that ophthalmologists have less to offer to such severelyvisually impaired patients in terms of therapy to preservevision, compared with patients with less severe disease.Moreover, low vision care, vision rehabilitation services, andnon-physician resources where patients with end stagedisease may be referred to for further management werenot calculated as direct medical costs.When full compliance with medications is assumed,
medication costs represent a minimum of 42% of total directcost at any disease stage. Since topical ocular hypotensivemedications are as effective as early surgery in delaying therates of progression,35 the majority of physicians are likely tooffer medication therapy before advising surgery. In general,preventing patients progressing from stage 0 or 1 to stage 4 or5 will project a decrease between 30–50% of the costs.The overall results from this study appear to be within the
range of similar glaucoma resource utilisation studies,19–21 36 37
but there are methodological limitations. Glaucoma progressionmay be measured by ophthalmologists using visual fieldexamination, optic nerve head clinical assessment, or both.11
Visual field examination is the standard of care to evaluate
disease progression, and for clinicians it represents the driver foradjusting the management of the patient.9 36–40
Since the study retrospectively collected patient data fromthe previous 5–7 years, the number of years a patient mayhave been in his/her baseline stage before the study entrycould not be controlled. Patients with at least 5 years offollow up data may differ from patients who do not seekpersistent care for glaucoma for the same period, thuscreating a potential selection bias. Data on patients in endstage disease who may have been referred to low vision careand vision rehabilitation centres were not captured and thetotal medical and societal costs associated with end stagedisease were not fully estimated. Examining costs from asocietal perspective, as opposed to a payer perspective, mayhave an impact on treatment cost of end stage glaucoma; inparticular, as costs for low vision care and vision rehabilita-tion centres are likely to be borne by the patient or society,such resources are inherently excluded from medical costingmethods. The relatively small number of charts reviewed maylimit the generalisability of the results.Data on ocular hypotensive medication use were collected
at every ophthalmic visit and for cost calculations it wasassumed that patients fully adhered to medication regimens;this may overestimate real life resource utilisation and costsassociated with medication use. Medication costs aredistributed over periods of months to several years whilesurgical costs are incurred at a single point in time and arerepresented in the analysis as costs divided over the periodthat patients remain categorised within a given stage. Forexample, the relatively high unit cost of an incisional surgerywill be divided by the number of years of follow up and maytherefore be reported as a lower yearly cost. This costingapproach still represents the best approximation of actualsurgical costs given sample size and timelines. The possibilityof surgery to control the IOP for years in the majority ofpatients is well documented.41 42
Our study demonstrates a significant linear trend inresource consumption and total direct cost, both increasingwith worsening of disease severity. The direct cost oftreatment increased by an estimated J86 for each incre-mental increase in stage. The costs ranged from J455 perperson year for early stage (stage 0) to J969 per person yearfor late stage (stage 4) disease across Europe; similar trendswere observed across each analysed countries. Health policymodels have been constructed for other conditions, such asstroke, to allow for investigation of policy issues andoptions43; similar analyses in glaucoma are warranted.According to our results, glaucoma management strategiesaimed at slowing or stopping disease progression, if effective,would be expected to significantly reduce the healtheconomic burden of this chronic disease over many years.Ophthalmologists, general practitioners, and health admin-
istrators now have a European based set of data demonstratingthat managing glaucoma effectively, preventing progressionbeyond the early to moderate stages of the disease, will result ina decrease in direct costs. This should be used to offset theconstraints on resource delivery to manage patients with anunquestionable diagnosis of progressive glaucoma.
ACKNOWLEDGEMENTSThis study was supported by an unrestricted research grant fromAllergan, Inc, Irvine, CA, USA. The authors thank Karina Berensonfor designing electronic chart review forms, and Lisa Rosenblatt,Anthony Cuccia, and Gary Lebovics for structured chart abstractionsthroughout the study.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
C E Traverso, A Bagnis, G Bricola, Clinica Oculistica, DiNOG, AziendaOspedale Universita San Martino, Genoa, Italy
1248 Traverso, Walt, Kelly, et al
www.bjophthalmol.com

J G Walt, Allergan, Inc, Irvine, CA, USAS P Kelly, Bolton Hospitals NHS Trust, Bolton, UKA H Hommer, Hera Hospital, Vienna, AustriaA M Bron, Universite de Dijon, Dijon, FranceP Denis, Edouard Herriot Hopital, Lyon, FranceJ-P Nordmann, Hopital des Quinze-Vingts, Paris, FranceJ-P Renard, Hopital du Val de Grace, Paris, FranceA Bayer, Augenarzt, Weilheim, GermanyF Grehn, Department of Ophthalmology, University of Wurzburg,Wurzburg, GermanyN Pfeiffer, Johannes Gutenberg Universitat, Mainz, GermanyC Cedrone, C Nucci, Universita degli Studi di Roma, Tor Vergata, Rome,ItalyS Gandolfi, University Eye Clinic, Parma, ItalyN Orzalesi, L Rossetti, Ospedale San Paolo, Milan, ItalyA Azuara-Blanco, Grampian University Hospitals NHS Trust, Aberdeen,UKR Hitchings, Moorfields Eye Hospital, London, UKJ F Salmon, Oxford Eye Hospital, Oxford, UKP M Buchholz, Allergan, Inc, Ettlingen, GermanyS V Kotak, L M Katz, L R Siegartel, J J Doyle, The Analytica Group, Inc,New York, NY, USA
Competing interests: Allergan provided unrestricted research grants tothe departments where the following authors are based: A Azuara-Blanco, A Bayer, A M Bron, C Cedrone, P Denis, S Gandolfi, F Grehn, RHitchings, A H Hommer, S P Kelly, J-P Nordmann, C Nucci, N Orzalesi,N Pfeiffer, J-P Renard, L Rossetti, J F Salmon, and C E Traverso. J G Waltand P M Buchholz are employees of Allergan. S V Kotak, L M Katz, L RSiegartel, and J J Doyle’s organisation, the Analytica Group, receivedfunding from Allergan for their involvement in this study. J G Walt and PM Buchhols are employees of Allergan, Inc, and were involved in thestudy design, data interpretation, and writing of this manuscript.
REFERENCES1 Coulehan JL, Helzlsouer KJ, Rogers KD, et al. Racial differences in intraocular
tension and glaucoma surgery. Am J Epidemiol 1980;111:759–68.2 Dielemans I, Vingerling JR, Wolfs RC, et al. The prevalence of primary open-
angle glaucoma in a population-based study in the Netherlands. TheRotterdam Study. Ophthalmology 1994;101:1851–5.
3 Kahn HA, Milton RC. Revised Framingham eye study prevalence of glaucomaand diabetic retinopathy. Am J Epidemiol 1980;111:769–76.
4 Klein BE, Klein R, Sponsel WE, et al. Prevalence of glaucoma. The Beaver DamEye Study. Ophthalmology 1992;99:1499–504.
5 Leske MC, Connell AM, Schachat AP, et al. The Barbados Eye Study.Prevalence of open angle glaucoma. Arch Ophthalmol 1994;112:821–9.
6 Mason RP, Kosoko O, Wilson MR, et al. National survey of the prevalenceand risk factors of glaucoma in St Lucia, West Indies. Part I. Prevalencefindings. Ophthalmology 1989;96:1363–8.
7 Sommer A, Tielsch JM, Katz J, et al. Racial differences in the cause-specificprevalence of blindness in east Baltimore. N Engl J Med 1991;325:1412–17.
8 Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence ofprimary open-angle glaucoma. The Baltimore Eye Survey. J Am Med Assoc1991;266:369–74.
9 European Glaucoma Society. Terminology and guidelines for glaucoma, 2nded. Savona Italy: Dogma Srl, 2003 Ch 3, 3–38.
10 Quigley HA. Number of people with glaucoma worldwide. Br J Ophthalmol1996;80:389–93.
11 Coleman AL. Glaucoma. Lancet 1999;354:1803–10.12 Grant WM, Burke JF. Why do some people go blind from glaucoma?
Ophthalmology 1982;89:991–8.13 Michelson G, Groh MJ. Screening models for glaucoma. Curr Opin
Ophthalmol 2001;12:105–11.14 Gray SF, Spry PG, Brookes ST, et al. The Bristol shared care glaucoma study:
outcome at follow up at 2 years. Br J Ophthalmol 2000;84:456–63.15 Cerulli L, Cedrone C, Cesareo M, et al. L’epidemiologia del glaucoma. In:
Cerulli L, Miglior M, Ponte F, eds. L’epdimeiologia in Italia. Rome: Relazione
ufficiale al LXXVII Congresso della Societa Oftalmologica Italiana, Inc,1997:163–246.
16 Krumpaszky HG, Ludtke R, Mickler A, et al. Blindness incidence in Germany.A population-based study from Wurttemberg-Hohenzollern.Ophthalmologica 1999;213:176–82.
17 Sellem E. [Chronic glaucoma. Physiopathology, diagnosis, prognosis,principles of treatment]. Rev Prat 2000;50:1121–5.
18 Glick H, Brainsky A, McDonald RC, et al. The cost of glaucoma in the UnitedStates in 1988. Chibret Int J Ophthalmol 1994;10:6–12.
19 Kobelt-Nguyen G, Gerdtham UG, Alm A. Costs of treating primary open-angle glaucoma and ocular hypertension: a retrospective, observational two-year chart review of newly diagnosed patients in Sweden and the UnitedStates. J Glaucoma 1998;7:95–104.
20 Kobelt G, Jonsson L. Modeling cost of treatment with new topical treatmentsfor glaucoma. Results from France and the United Kingdom. Int J TechnolAssess Health Care 1999;15:207–19.
21 Iskedjian M, Walker J, Vicente C, et al. Cost of glaucoma in Canada: analysesbased on visual field and physician’s assessment. J Glaucoma2003;12:456–62.
22 Quigley HA. Identification of glaucoma-related visual field abnormality withthe screening protocol of frequency doubling technology. Am J Ophthalmol1998;125:819–29.
23 Advanced Glaucoma Intervention Study. 2. Visual field test scoring andreliability. Ophthalmology 1994;101:1445–55.
24 Anderson DR. Automated static perimetry. St Louis: Mosby, 1995.25 Hodapp E, Parrish RK, Anderson DR. Clinical decisions in glaucoma. St Louis:
Mosby, 1993.26 Katz J. Scoring systems for measuring progression of visual field loss in clinical
trials of glaucoma treatment. Ophthalmology 1999;106:391–5.27 Katz J, Sommer A, Gaasterland DE, et al. Comparison of analytic algorithms
for detecting glaucomatous visual field loss. Arch Ophthalmol1991;109:1684–9.
28 Mills RP, Drance SM. Esterman disability rating in severe glaucoma.Ophthalmology 1986;93:371–8.
29 Musch DC, Lichter PR, Guire KE, et al. The Collaborative Initial GlaucomaTreatment Study: study design, methods, and baseline characteristics ofenrolled patients. Ophthalmology 1999;106:653–62.
30 Mills RP, Budenz DL, Lee PP, et al. Categorizing the progression of glaucomafrom pre-diagnosis to end-stage disease by a novel six point staging system.Invest, Ophthalmol Vis Sci 2002;43:E-Abstract, 2160.
31 France costs. Base nationale PMSI—annee 2000, ATIH, Ministere de l’Emploiet de la Solidarite, 2000.
32 Germany costs. EBM (Statutory doctors fee scale) and GOA (Private doctorsfee scale) 2002.
33 Italy costs. CEIS—Health Economics and Health Care Management 2002.34 United Kingdom costs. NHS costing manual. London: Department of Health,
2003.35 Lichter PR, Musch DC, Gillespie BW, and the CIGTS Study Group, et al.
Interim clinical outcomes in the collaborative initial glaucoma treatment studycomparing initial treatment randomized to medication or surgery.Ophthalmology 2001;108:1943–53.
36 Gricar JA, Wilson PR, Cave DG. Glaucoma. Manag Care Interface1998;11:42–4.
37 Chen PP, Park RJ. Visual field progression in patients with initially unilateralvisual field loss from chronic open-angle glaucoma. Ophthalmology2000;107:1688–92.
38 Parrish RK 2nd, Gedde SJ, Scott IU, et al. Visual function and quality of lifeamong patients with glaucoma. Arch Ophthalmol 1997;115:1447–55.
39 Leske MC, Heijl A, Hussein M, Hyman L, Komaroff E, et al. Factors forglaucoma progression and the effect of treatment: the early manifestglaucoma trial. Arch Ophthalmol 2003;121:48–56.
40 The European Glaucoma Society. Terminology and guidelines for glaucoma.Savona, Italy: Dogma, I, 28–I.29, 2003.
41 Feiner L, Piltz-Seymour JR. Collaborative Initial Glaucoma Treatment Study: asummary of results to date. Curr Opin Ophthalmol 2003;14:106–11.
42 Membrey WL, Bunce C, Poinoosawmy DP, et al. Glaucoma surgery with orwithout adjunctive antiproliferatives in normal tension glaucoma: 2 Visual fieldprogression. Br J Ophthalmol 2001;85:696–701.
43 Matchar DB, Samsa GP, Matthews JR, et al. The Stroke Prevention PolicyModel: linking evidence and clinical decisions. Ann Intern Med 1997;127(Pt2):704–11.
Glaucoma treatment cost in Europe 1249
www.bjophthalmol.com

WORLD VIEW
Traditional healers’ roles on eye care services in NepalA K Poudyal, M Jimba, B K Poudyal, S Wakai. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Masamine Jimba, MD,PhD, MPH, Department ofInternational CommunityHealth, Graduate Schoolof Medicine, The Universityof Tokyo, 7-3-1 Hongo,Bunkyo-ku, Tokyo, 113-0033; [email protected]
Accepted for publication1 March 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1250–1253. doi: 10.1136/bjo.2004.065060
Aim: To evaluate the traditional healer (TH) training programme carried out by Nepal Netra Jyoti Sangh,a non-governmental organisation in Nepal, by measuring the changes in knowledge and practices oftrained THs in providing primary eye care services.Methods: 103 trained THs practising in six districts of Nepal were interviewed with a semistructuredquestionnaire. Their knowledge about various illnesses and eye care practices were compared before andafter the training.Results: A significant change in the number of THs with accurate perceived knowledge about trachoma(28.2% v 70.9%, p,0.0001) and cataract (54.4% v 94.2%, p,0.0001) was found after the training. Intotal, 98 (95%) THs stopped using traditional eye medicines after receiving the training (p,0.0001). Thereferral practices of THs improved significantly after the training (15% v 100%, p,0.0001). After thetraining, 95% of the THs used an eye care kit to treat patients with red eyes and simple ocular trauma.Conclusion: The findings show that a TH training programme on primary eye care services convincedtraditional healers to stop the use of traditional eye medicines and improve referral practices in Nepal.
The World Health Organization (WHO) estimates thatapproximately 45 million people in the world are blind.Ninety per cent of the blind live in developing countries,
and 80% of global blindness is avoidable.1 The 1981 NepalBlindness Survey showed that 0.84% of the Nepalesepopulation was bilaterally blind and 1.66% unilaterallyblind.2 No national blindness survey has been done sincethis time. The major causes of blindness in Nepal includecataracts, trachoma, corneal trauma, ulceration, glaucoma,and vitamin A deficiency.2–4
To improve eye care, Nepal has increased the number ofeye care professionals trained in western medicine. Nepal hasonly one ophthalmologist per 250 000 people, but hasapproximately 300 ophthalmic assistants and other eye careworkers such as optometrists and eye workers.5 Theseophthalmic assistants serve as the heads of primary eye carecentres (PECCs).5 PECCs are permanent eye care servicecentres in the districts. By the end of 2003, 32 PECCs and 11eye hospitals were providing eye care services in 40 of 75districts of Nepal (NNJS unpublished report, 2004).Health service utilisation in Nepal is very poor. The
National Planning Commission (HMG/N 1998) showed thatonly 12% of household used government health services andmore than 25% of households used non-government healthservices.6 Several studies have shown that traditional healers(THs) are the first people that the Nepalese contact whenseeking treatment for health problems, including eyeproblems.3 6–8
For the prevention of blindness, Nepal has launched aglobal initiative—Vision 2020: the right to sight—in whichhuman resource development is one of its three major goals.9
Research conducted in Zimbabwe and Malawi suggests that asustainable collaborative programme between traditional andwestern practitioners could help to reduce preventableblindness by advising against the use of harmful traditionalpractices.10–13
To improve such collaborations, some THs in Nepal havebeen trained in western medicine. The trained THs showedimproved knowledge of western medicine, and were morelikely to refer patients to modern health institutions.14–17
However, there is no documentation of the roles of trainedTHs in eye care services in Nepal.
In this study, we sought to evaluate the TH trainingprogramme carried out by a non-governmental organisation(NGO) by measuring the changes of their knowledge andpractices in providing primary eye care services.
MATERIALS AND METHODSBackgroundNepal Netra Jyoti Sangh (NNJS), an NGO, was established in1978 to improve eye care services in Nepal. NNJS started theTH training programme in 1994 for several reasons. Firstly,most of the patients who visited eye hospitals or eye carecentres had first consulted local THs. Secondly, more patientsvisited eye hospitals and eye care centres in the very latestages of their eye problems. Thirdly, communicationbetween THs and modern eye healthcare providers was poor.NNJS obtained this information from the hospital records
of the Nepal Eye Hospital in Kathmandu and a survey reportconducted by the NNJS at 15 PECCs of Nepal in 1993 (NNJSunpublished report, 1994).Considering these factors, NNJS started the TH training
programme for modern eye care services in Nepal (NNJS,unpublished report, 1994).NNJS selected THs who were highly respected and
renowned in their communities from those districts wherepermanent eye care service centres were available. Onaverage, NNJS trained 25 THs from each district. From1994 to 2003, NNJS trained 422 THs in 18 rural districts ofNepal.The training had three objectives. The first was to give basic
knowledge about eye related illnesses to the THs. The secondwas to encourage them to refer eye patients to PECCs and eyehospitals without delay. The third was to advise the THs notto use any traditional eye medicines.NNJS provided the THs with a 3 day long training on
primary eye care services. Then, once a year, NNJS provided1 day refresher training to all the previously trained THs.On the last day of both the initial and refresher training, an
eye care kit was distributed to all the participants free ofcharge. The kit contained a bottle of chloramphenicol eye
Abbreviations: NGO, non-governmental organisation; PECCs, primaryeye care centres; TH, traditional healer
Series editors: W V Good, S Ruit
1250
www.bjophthalmol.com

ointment (the bottle contained 100 small tubes of 1%chloramphenicol eye ointment), eye health education posters,recording and reporting forms, and referral slips.
Data collection and analysisOf 18 districts, we selected six districts; Kavrepalanchowk,Shindhupalchowk, Dhading, Chitwan, Palpa, and Gulmi forthis study. These districts were chosen as other districts hadsecurity risks caused by the current Maoist insurgency.Before the training, NNJS had interviewed all the THs to
collect baseline information. Based on the pretraining inter-view questionnaire and the training curriculum on primaryeye care services, we developed a semistructured interviewquestionnaire to evaluate the training programme. Thequestionnaire included questions about the causes of illness,knowledge of preventive measures, signs and symptoms ofeye illnesses, methods of treatment, and referral practices.We asked THs about various illnesses and categorised their
‘‘claimed knowledge’’ about any specific illness as the‘‘perceived knowledge.’’ Then, we examined their claimedknowledge by comparing their responses with the ‘‘standar-dised knowledge’’ taken from the TH training manualdeveloped by NNJS (NNJS, unpublished TH training manual,1994).The targets of this study were 162 trained THs of six
districts; of these 162, we interviewed 103. Fifty nine THscould not come to the interview because of the unstablepolitical situation.Before the interview, we informed each TH that we would
maintain their confidentiality and anonymity. We also toldthem that their participation was voluntary, and that if theywished to withdraw from the study, they could leave at anypoint without any obligation. We then obtained their consentfor their participation in the study. Nepal Health ResearchCouncil, Nepal approved this study and gave ethical permis-sion.Four experienced and trained research assistants inter-
viewed each TH for about 45 minutes. We completed theentire interview in April 2004.All the data were coded and entered into a Microsoft Visual
FoxPro 5.0 database. The data were then analysed with SPSS11.0 for Windows 2000. We used McNemar test and x2 test tocompare the knowledge and eye care practices of THs beforeand after the training.
RESULTSOf the 103 THs, two (2%) were female. The mean age of allthe respondents was 57.8 years (SD 11.4). Their meanduration of practising traditional healing was 32.4 years
(SD 14.3); 65% of them were literate. The median year oftraining after the initial training was 5 years (range 4–7 years). Agriculture was the major source of their income.However, 11% of them were earning their major income fromtraditional healing. Seventy six per cent of them mentionedthat they received payment in kind or cash when they treatedtheir patients.All the THs were living within 3 hours’ walking distance
from the nearest health posts or subhealth posts. Amongthem, 80% were living within 1 hour walking distance fromthe nearest health posts or subhealth posts. Forty per cent ofthem could reach the district PECCs within 1 day on foot orby vehicles from their communities. For 60% of them, it tookabout 2 days’ walk. Regardless of the TH’s number of annualrefresher training, we did not find any significant differencesin the knowledge about eye care among the trained THs.Table 1 summarises the THs’ perceived knowledge about
various illnesses before and after the training. The THs withyounger age groups (31–40, 41–50, and 51–60 years) showedchanges in the perceived knowledge in all the illnessescompared to the age group above 61 years. After the training,15 THs did not know about night blindness; among themnine (60%) were in the above 60 age group. Similarly, 17(57%) in the above 60 age group did not know abouttrachoma.Regarding treatment by the THs, 95% of the THs stated that
they treated patients who complained of red eye and simpleocular trauma with the chloramphenicol eye ointment tubesafter the training. As taught in the training, they treated eachpatient with three tubes of eye ointment. However, 79% ofthe THs stated that they had used up their medicines at thetime of our data collection. Of 103 THs, 95% wanted to havemore eye ointment tubes.We also saw striking changes in the THs’ referral practices.
Before the training, 15% of the THs stated that they referredtheir patients with general health problems to health posts/subhealth posts or hospitals when they could not diagnose ortreat them. After the training, all the THs referred patientswith general health problems to health posts/subhealth posts(p,0.0001). They referred eye patients directly to districtPECCs or eye hospitals. The THs reported that, on average, 60eye patients visited them last year. According to the reports ofthe THs, a TH referred 18 eye patients, on average, to thedistrict PECCs or hospitals last year. Three per cent of the THsreported that they used referral slips to refer the patients.Most of the trained traditional healers verbally referred eyepatients to the district PECCs or hospitals. Of the total, 73% ofthe THs said that they submitted the records of referredpatients to the training instructors at the refresher training.
Table 1 Traditional healers’ (THs) perceived knowledge about various illnesses
THs Before training After training p Value
Illness n = 103 (%) n = 103 (%)Communicable diseases
Know 60 (58.3) 85 (82.5) ,0.001Do not know 43 (41.7) 18 (17.5)
MalnutritionKnow 53 (51.5) 87 (84.5) ,0.0001Do not know 50 (48.5) 16 (15.5)
Night blindnessKnow 67 (65.0) 88 (85.4) ,0.001Do not know 36 (35.0) 15 (14.6)
CataractKnow 56 (54.4) 97 (94.2) ,0.0001Do not know 47 (45.6) 6 ( 5.8)
TrachomaKnow 29 (28.2) 73 (70.9) ,0.0001Do not know 74 (71.8) 30 (29.1)
We asked further questions to only those THs who claimed that they knew about various illnesses.
Traditional healers in Nepal 1251
www.bjophthalmol.com

Of six district PECCs, the ophthalmic assistants of threedistrict PECCs told us that they received referral patientsfrom THs, but the number of referral slips was small. Theyalso mentioned that some patients visited the PECCs on theTHs’ recommendation. An ophthalmic assistant in Chitwandistrict PECC said that a trained TH referred 45 patients withmature cataract in 1 year and all of them were operated.However, all six PECCs had no record keeping system for thereferred patients and THs. The last 5 years’ medical records inthe district PECCs and Nepal Eye Hospital showed that thenumber of patients with corneal ulcers was graduallydeclining compared to 5 years ago.For the use of traditional treatment methods, before the
training, 72% of the THs applied traditional eye medicines intheir patients’ eyes, whereas only 5% of them continued touse traditional eye medicines after the training (p,0.0001).Before the training, the THs used extracts of the roots, leavesof trees, seeds; herbs; powdered glass; breast milk andhuman urine; excreta from dog and birds as traditional eyemedicines.
DISCUSSIONSThis study showed that the TH training on primary eye careservices was successful in achieving three training objectives.Firstly, the training improved the THs’ knowledge aboutcommon illnesses and eye related problems. Secondly, mostTHs stopped using traditional eye medicines. Thirdly, theyreferred the eye patients to the district PECCs or eyehospitals.The study also revealed that the THs in the younger age
groups (31–40, 41–50, and 51–60 years) acquired morestandardised knowledge about eye care than the above60 year age group. This finding suggests that the futuretraining should target younger THs below 60 years old.We found a gap between perceived knowledge and
standardised knowledge in this study. As tables 2, 3, and 4showed, their perceived knowledge about various illnessesdid not match the standardised knowledge before thetraining.Table 2 shows that the THs’ knowledge on cataract and
trachoma increased after the training. In both cataract and
trachoma, all the incorrect knowledge was found among theabove 60 years age group.Table 3 shows that the training significantly improved the
THs’ knowledge about the preventive measures for malnutri-tion, night blindness, and trachoma. Among 22 THs who stillhad incorrect knowledge about preventive measures of nightblindness, nine (41%) were from the above 60 age group.Table 4 shows a significant difference between two groups
in their knowledge about the treatment of cataract andtrachoma.Two main reasons may explain the gap between the
perceived knowledge and standardised knowledge. Firstly,we assume they wanted to show us that they were knowl-edgeable healers and to maintain their reputation. In heranthropological study in Nepal, Pigg mentioned that THs donot want to lose their prestige by showing little knowledge.18
Secondly, they were afraid of losing chances of attending thetraining course by answering negative responses.Besides improving the standardised knowledge, the THs
also improved their practices after the training. Before thetraining, 60% of the THs were using traditionally used plantsalong with other substances for treating eye problems. Someof the traditional eye medicines are known to be contami-nated, and they may provide a vehicle for the spread ofpathogenic organisms.19 20 Therefore, NNJS advised the THsnot to use traditional eye medicines, and 95% of the THsstopped using them after the training.In this study, 79% of the THs mentioned that they had used
up chloramphenicol; and 90% of THs asked for more. To refillthe eye care kit, the THs had to wait up to 1 year till the nextrefresher training course. There was no system of supplyingeye medicines to the THs who used them up within a year. Ifsufficient eye ointments are provided to the THs free ofcharge, the THs will not suffer from the lack of medicines.Therefore, NNJS and the THs should develop an appropriatesystem to refill the eye care kit.As NNJS expected, most of the THs referred eye patients to
the district PECCs or hospitals when they could not treatthem. The THs knew that many health posts/subhealth postswere unable to provide eye care. Therefore, they directlyreferred eye patients to district PECCs and hospitals. Since2000, however, eye care has been integrated with the general
Table 2 Knowledge of traditional healers (THs) about signs and symptoms of cataractand trachoma
THs Before training After training p Value
Cataract N=56 (%) n = 97 (%)Correct 46 (82.1) 95 (97.9) ,0.001Incorrect 10 (7.9) 2 (2.1)
Trachoma N=29 (%) n = 73 (%)Correct 18 (62.1) 68 (93.2) ,0.0001Incorrect 11 (37.9) 5 ( 6.8)
Table 3 Traditional healers’ (THs) knowledge of preventive measures for various illnesses
THs Before training After training p Value
Malnutrition n = 53 (%) n = 87 (%)Correct 46 (86.8) 85 (97.7) ,0.001Incorrect 7 (13.2) 2 (2.3)
Night blindness n = 67 (%) n = 88 (%)Correct 7 (10.4) 66 (75.0) ,0.001Incorrect 60 (89.6) 22 (25.0)
Trachoma n =29 (%) n = 73 (%)Correct 18 (62.1) 68 (93.2) ,0.0001Incorrect 11 (37.9) 5 (6.8)
1252 Poudyal, Jimba, Poudyal, et al
www.bjophthalmol.com

healthcare system in Nepal. NNJS has thus started primaryeye care training to some of the health posts in charges oftheir target district. The THs have also started to be advised torefer their patients to the health posts. This practice is stillnew, but eye patients will be referred to the PECCs or eyehospitals through the health posts in future.Though NNJS started the TH training 10 years ago, a
systematic referral system has not yet been developed.Therefore, the referred patients were also not registeredaccording to the respective trained TH of each district.However, the last 5 years’ medical records in the districtPECCs and Nepal Eye Hospital showed that the number ofpatients with corneal ulcers was gradually declining. This mightbe because the THs stopped using traditional eye medicines.NNJS provided the training only to those THs who met the
selection criteria. Therefore, their average literacy rate washigher compared with the national average. Such selectionindeed may create a bias and the result may not be applicableto all THs in Nepal. However, this selection is practical andmeaningful as we can apply such selection methods in ruralNepal as long as THs remain as major health providers.In conclusion, the THs’ training programme on primary eye
care services was successful in convincing the THs to stopusing traditional eye medicines and improve referral practicesin Nepal. However, how to establish a sustainable medicinesupply system remains a challenge for future.
ACKNOWLEDGEMENTSWe acknowledge Dr Ram Prasad Pokhrel, the chairperson of NepalNetra Jyoti Sangh (NNJS) for allowing us to conduct this study ontheir traditional healer training programme on primary eye care. Wethank NNJS and staff members who helped us to conduct thefieldwork. We thank the district primary eye care centres’ staffmembers and the traditional healers for participating in this study.The views expressed in this paper are entirely those of the authors anddo not necessarily reflect the views of the organisations they serve.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
A K Poudyal, M Jimba, S Wakai, Department of InternationalCommunity Health, Graduate School of Medicine, The University ofTokyo, JapanA K Poudyal, Department of Community Medicine and Family Health,Institute of Medicine, Tribhuvan University, Kathmandu, Nepal
B K Poudyal, Nepal Netra Jyoti Sangh, Eye Health Education Unit,Kathmandu, Nepal
REFERENCES1 World Health Organization. Blindness: vision 2020. The global initiative for
the elimination of blindness, www.who.int/mediacentre/factsheets/fs213/en/ 2000 (accessed on 19 June 2004).
2 Brilliant G. The epidemiology of blindness in Nepal: report of the 1981 Nepalblindness survey. Chelsea, MI: Seva Foundation, 1988.
3 Upadhyaya MP, Karmacharya PCD, Koirala S, et al. Epidemiologiccharacteristics, predisposing factors and etiologic diagnosis of cornealulceration in Nepal. Am J Ophthalmol 1991;111:92–9.
4 Khatry SK, Lewis AE, Schein OD, et al. The epidemiology of ocular trauma inrural Nepal. Br J Ophthalmol 2004;88:456–60.
5 Nepal Netra Jyoti Sangh. Eye centres and eye hospitals: a profile of NepalNetra Jyoti Sangh. Kathmandu, Nepal: National Society for ComprehensiveEye Care, 2000.
6 HMG/N National Planning Commission. Service delivery survey: health andagriculture services. Nepal Multiple Indicator Surveillance Sixth Cycle 1998.
7 Jimba M, Poudyal AK, Wakai S. The need for linking healthcare-seekingbehaviour and health policy in rural Nepal. Southeast Asian J Trop Med PublicHealth 2003;34:2–3.
8 Mesko N, Osrin D, Tamang S, et al. Care for perinatal illness in rural Nepal: adescriptive study with cross-sectional and qualitative components. BMC IntHealth Hum Rights 2003;3:3.
9 World Health Organization. Vision 2020: the right to sight, www.v2020.org/right_to_sight/index.asp (accessed on 22 February 2005).
10 Lewallen S, Courtright P. Role for traditional healers in eye care. Lancet1995;345:456.
11 Courtright P, Lewallen S, Kanjaloti S. Changing patterns of corneal diseaseand associated vision loss at a rural African hospital following a trainingprogramme for traditional healers. Br J Ophthalmol 1996;80:694–7.
12 Chana HS, Schwab L, Foster A. With an eye to good practice: traditionalhealers in rural communities. World Health Forum 1994;15:144–6.
13 Courtright P. Eye care knowledge and practices among Malawian traditionalhealers and the development of collaborative blindness preventionprogrammes. Soc Sci Med 1995;41:1569–75.
14 Oswald IH. Are traditional healers the solution to the failures of primary healthcare in Rural Nepal? Soc Sci Med 1983;17:255–7.
15 Dhakal R, Graham-Jones S, Lockett G. Traditional healers and primary healthcare in Nepal. Kathmandu: Save the Children Fund-United Kingdom, 1986.
16 Gillam S. The traditional healer as village health worker. J Inst Med1989;11:67–76.
17 Poudyal AK, Jimba M, Murakami I, et al. A traditional healers’ training modelin rural Nepal: strengthening their roles in community health. Trop Med IntHealth 2003;8:956–60.
18 Pigg SL. Acronyms and effacement: traditional medical practitioners (TMP) ininternational health development. Soc Sci Med 1995;41:47–68.
19 Yorston D, Foster A. Traditional eye medicines and corneal ulceration inTanzania. J Trop Med Hyg 1994;97:211–14.
20 Whitcher JP, Srinivasan M, Upadhaya M. Corneal blindness: a globalperspective. Bull World Health Organ 2001;79:214–21.
Table 4 Traditional healers’ (THs) knowledge about where to refer patients with cataractand trachoma for treatment
THs Before training After training p Value
Cataract n = 56 (%) n = 97 (%)Correct 31 (55.4) 92 (94.8) ,0.0001Incorrect 25 (44.6) 5 (5.2)
Trachoma n =29 (%) n = 73 (%)Correct 19 (65.5) 71 (97.3) ,0.0001Incorrect 10 (34.5) 2 (2.7)
Traditional healers in Nepal 1253
www.bjophthalmol.com

SCIENTIFIC REPORT
Interferon as a treatment for uveitis associated with multiplesclerosisM D Becker, A Heiligenhaus, T Hudde, B Storch-Hagenlocher, B Wildemann, T Barisani-Asenbauer, C Thimm, N Stubiger, M Trieschmann, C Fiehn. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1254–1257. doi: 10.1136/bjo.2004.061119
Aim: In addition to optic neuritis (ON), multiple sclerosis(MS) may also involve the eye with a typically bilateralintermediate uveitis. The aim of this pilot study was toevaluate the efficacy of type I interferons (IFN) for thetreatment of MS associated uveitis.Methods: In this non-randomised, retrospective observa-tional case series 13 patients (eight female, five male) withproved MS and associated uveitis from five uveitis centreswho were treated with interferon b1a were included. Visualacuity (VA), cell count in the aqueous humour and vitreous,as well as the presence of cystoid macula oedema (CMO)were observed.Results: All except one patient had a bilateral form ofintermediate uveitis (total of 24 eyes). Seven patients haddocumented CMO before IFN treatment (n = 13 eyes).Median duration of treatment was 24.6 months (range7.9–78.7). VA improved in 17 eyes (comparing VA beforetherapy and at last follow up); while 10 eyes (36%) improved>3 Snellen lines. Aqueous cell count improved by 1.2 (SD1.1) grades in all eyes. Vitreous cell count improved by 1.7(1.4) in all eyes. Only two patients still had minimal CMO onlast follow up angiographically. CMO resolved after orduring IFN treatment in nine eyes.Conclusions: IFN has been shown to have beneficial effectsin patients with MS and/or ON. As shown in the models ofexperimental allergic encephalomyelitis (EAE) and uveitis,the neurological and ophthalmological manifestations seemto share similar pathogenic mechanisms. Treatment of MSassociated uveitis with IFN appears to have beneficial effectson VA, intraocular inflammation activity, and the presence ofCMO.
Optic neuritis is the most common ocular manifestationof multiple sclerosis (MS), occurring in an estimated30% of patients1; however, intraocular inflammation
also occurs. Originally described by Rucker2 the occurrence ofthis association varies widely, ranging from 0.4% to 26.9% inpatients with MS3–5 and from 0.8% to 14% in patients withuveitis.6–8 The most common type of uveitis is intermediateuveitis (according to Bloch-Michel and Nussenblatt9) withcharacteristic changes. Patients may also present withgranulomatous changes in the anterior segment.5 10–12 Inthese patients secondary changes like the formation ofcystoid macula oedema (CMO), or occlusive vasculitis withvasoproliferations often develop—changes that have aprofound effect on visual prognosis. If these secondarychanges occur, the disease is often difficult to manage,requires high doses of corticosteroids13 or laser treatment, andoften remains refractory to these standard therapies.Treatment with interferon b (IFN-b) is established for the
treatment of MS. Therefore, the aim of this pilot study was toevaluate the efficacy of IFN-b for MS associated uveitis in amulticentre, retrospective, uncontrolled study.
PATIENTS AND METHODSWe included 13 patients (eight females, five males) withproved MS and associated uveitis from five uveitis centres. Asthe data were analysed retrospectively (chart review) and thetreatment with IFN was started because of individualtreatment decisions for every patient, no informed consent,institutional, or ethics committee approval were required forthis study. Since this is a retrospective study, the five centresdid not coordinate the type of drug and treatment regimen,study design, inclusion/exclusion criteria, or follow upintervals for the individual patients in advance. Patientswere recruited independently based on the experience of theindividual centre after failure of systemic corticosteroids and/or systemic immunosuppressive treatment. In cooperationwith consulting neurologists the diagnosis of MS wasapproved in all patients after neurological examination andmagnetic resonance imaging (MRI) according to the guide-lines described by Poser et al.14
Median age of all patients at the time of data analysis(March 2004) was 48 years (range 34–58 years). All exceptone patient had bilateral uveitis (total of 25 eyes). In sevenpatients MS started a median of 8.2 years (range 2.8–24.2)before uveitis, in six patients uveitis was diagnosed a medianof 5.5 years (0.3–20.6) before MS. Seven of 13 patients hadhad ON in at least one eye during the previous course of theirdisease. In all patients ON happened before the onset ofuveitis. Aqueous humour and vitreous cell count were gradedas rare cells, 1+, 2+, 3+, and 4+ (according to BenEzra et al15).A change in this grading scale is given as +1 when cell countincreases by one step, and one when cell count improved(+/2 0.5 was used in the range of no cells, rare cells, 1+ cells).Change in VA is given as change of line in Snellen charts,respectively.
All patients received systemic corticosteroids for thetreatment of uveitis according to the experience and choiceof the individual centre or the urgency of uveitic complica-tions either with initial doses on a 1 mg/kg bodyweight basisor on a mega dose methylprednisolone scheme. Systemiccorticosteroids did not (or only in doses above 10 mg/day)improve disease activity sufficiently on a clinical basis(according to the documentation of the individual centres).Corticosteroid sparing agents were used before initiation ofIFN therapy in two patients (one patient methotrexate, oneazathioprine). However, this therapy was considered to bewithout success in those centres because of recurrences ofinflammation and further deterioration in VA. After a median
Abbreviations: CMO, cystoid macula oedema; EAE, experimentalallergic encephalomyelitis; IFN, interferon; MRI, magnetic resonanceimaging; MS, multiple sclerosis; ON, optic neuritis; VA, visual acuity
1254
www.bjophthalmol.com

of 2.3 years (range 0.3–27) after the onset of uveitis, patientswere put on IFN therapy. Median duration of treatment was24.6 months (range 7.9–78.7). The choice of drug was basedon the personal experience and preference of each individualcentre. According to the clinical response to IFN therapypatients who were treated with IFN-b1a either received 22 mgor 44 mg (Rebif, Serono Inc, n=10) three times per weeksubcutaneously or 30 mg once a week intramuscularly(Avonex, Biogen Inc, patients 8, 10, and 11).Primary outcome measures were defined as improvement
in VA and reduction of cell count in the aqueous humour andvitreous. Secondary outcome measures were the presence ofCMO. No statistical analysis was performed because of thesmall sample size.The characteristics of all patients including treatment
strategy and change of inflammatory activity and secondarycomplications during IFN treatment are summarised intable 1.
RESULTSDuring treatment with IFN, 17 eyes (71%) improved theirVA, five did not change (21%), and two eyes deteriorated(8%) because of development of cataract. Figures 1 and 2demonstrate the change of VA between initial and last visit.Aqueous cell count improved by 1.2 (1.1) grades in all eyes
(64% improved, no change in 21%). Vitreous cell countimproved by 1.7 (1.4) in all eyes (71% improved, 11% did notchange, and 4% deteriorated).At their last visit before IFN therapy was initiated seven
patients had CMO (13 eyes). At the last follow up during orafter therapy (median total observation time 18.7 months,range 7.9–74.8 months), in two patients CMO was stilldetectable angiographically but reduced before IFN therapyat their last follow up while CMO resolved after or during IFNtreatment in nine patients (82%).At the last visit nine patients were not on systemic
corticosteroids (69%). A reduction in the dose of prednisoneto 10 mg/day or less (or its equivalent for other corticoster-oids) while maintaining inactive uveitis during IFN therapywas considered a successful corticosteroid sparing in ourstudy. The corticosteroid sparing effect of IFN treatment hasbeen documented in almost all cases. At final follow upexamination only one of 13 patients had to use prednisone ata dose above 10 mg/day at her last follow up visit because of arecent flare up (patient 1, 50 mg/day).Three of 13 patients (23%) had side effects as documented
in table 1. However, in no patients did IFN therapy have to bediscontinued because of intolerable side effects.Details on the course of VA and intraocular inflammatory
activity as well as of the side effects and the surgical
Table
1Su
mmarises
allp
atientsof
ourstud
yan
dinclud
esde
mog
raph
ical
inform
ation,
descriptionan
dactivity
ofthedisease,
andcomplications
during
trea
tmen
twith
IFN
Patie
ntNo
Cen
tre*
Sex
Age
MSduratio
n(yea
rs)
Uveitis
duratio
n(yea
rs)
Bilateral
Granu
lomatous
chang
es?
Periphleb
itis/
vasculitis?
Optic
neuritis
Immun
osup
pression
beforeIFN
Duratio
nof
IFN
trea
tmen
t(m
onths)
Total
observatio
ntim
e(m
onths)
Sideeffects
from
interferon
1H
F35
6.1
13.9
yes
noyes
nono
19.7
7.9
none
2H
F48
9.2
1.7
nono
noyes
no25.6
25.9
minim
almyo
pathy
3H
M38
8.2
26.2
yes
noyes
nono
20.7
18.7
none
4H
F51
13.2
4.0
yes
yes
yes
nono
42.3
33.3
none
5H
F50
8.2
9.2
yes
yes
noyes
metho
trexate
17.7
11.2
none
6E
F58
5.3
4.0
yes
noyes
yes
azathiop
rine
24.6
7.9
depression
initially,trem
or,
restlessne
ss7
EF
43
25.2
3.8
yes
yes
yes
yes
no29.5
17.7
none
8W
M49
2.1
2.4
noyes
noyes
no78.7
74.8
none
9W
F41
6.2
3.0
yes
yes
yes
yes
no45.2
30.5
none
10
WM
54
9.6
30.2
yes
noyes
nono
24.6
21.9
none
11
WM
34
3.9
7.2
yes
noyes
nono
7.9
7.9
none
12
TM
39
3.8
2.8
yes
yes
yes
nono
28.7
22.7
none
13
MF
48
17.2
5.3
yes
yes
yes
yes
no18.1
17.8
dizz
iness
*H(Heide
lberg),E(Essen
),W
(Vienn
a),T(Tub
inge
n),M
(Mun
ster).
1.2
1.0
0.6
0.8
0.4
0.2
01.20.8 1.0
VA before IFN therapy
VA a
t las
t exa
min
atio
n
0.60.40 0.2
Figure 1 Comparison of the VA before treatment with IFN and at lastfollow up examination. Two eyes had reduced vision compared to initialexamination because of development of cataract.
IFN treatment for uveitis associated with MS 1255
www.bjophthalmol.com

procedures that were performed during the treatment periodwith IFN are summarised in table 2.
DISCUSSIONThis multicentre, retrospective, observational case series witha small number of patients suggests that treatment of MSassociated uveitis with IFN-b may improve intraocularinflammatory activity as well as the presence of CMO, andhence improve VA.IFN has been shown to have beneficial effects in patients
with MS16 17 and/or ON.18 Jacobs et al showed that initiatingtreatment with IFN-b1a at the time of a first demyelinatingevent, like optic neuritis, is beneficial for patients with brainlesions on MRI that indicate a high risk of clinically definitemultiple sclerosis.19
In the model of experimental allergic encephalomyelitis(EAE), a classic model for MS, animals also develop atemporary, mild, bilateral uveitis.20 21 This suggests sharedantigenic determinants between neurological and ophthal-mological manifestations with similar pathomechanisms.21
Treatment with IFN-b reduced ocular inflammation in thismodel.22
This beneficial effect may be useful, especially in patientswith partial resistance to systemic corticosteroids or immu-nosuppressive drugs. Side effects from IFN treatment did notappear in most of the patients, or were tolerable in mostpatients. The effects of IFN on posterior segment findingswere mostly related to a reduced vascular leakage and hencethe improvement of macular oedema. The pronounced anti-oedematous effect of type I IFNs in this small group of
patients should be further evaluated since chronic inflam-matory CMO is a known problem with conventionaltreatment.Whether glatiramer acetate (copolymer-1, Copaxone)
could be helpful in the treatment of uveitis would beinteresting to know. Its experimental effect has been shownin animal studies.23 Recently, a systematic Cochrane review ofall randomised controlled trials of glatiramer acetate foundlittle support for use of this drug in patients with MS.24 25 Tothe best of our knowledge there is no literature about theeffect of glatiramer acetate in uveitis.One of the limitations of our study is that the possibility of
spontaneous improvement is not recognised. Since MS can beof the relapsing/remitting type and since uveitis will some-times follow the pattern of the underlying MS, patients mighthave improved without regard to treatment. Owing toincomplete documentation in the different centres, the typeof MS was not specified and therefore cannot be correlatedwith the ocular response to treatment. Because of the lack ofa study protocol, all results are given as of ‘‘final visit’’—theactual pace of the clinical response cannot be deduced fromour data.These promising results are encouraging us to further
evaluate the effect of IFN on MS associated uveitis. We thinkespecially that patients with inflammatory CMO due tointermediate uveitis and with MS could benefit from IFNtherapy. An investigator initiated trial with controlled studiesis in preparation. This study could show if the preliminaryobservations herein can be confirmed and if the long termprognosis concerning VA and neurological MS may beimproved by this treatment, whose key concept is immuno-modulation rather than immunosuppression.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
M D Becker, C Fiehn, Interdisciplinary Uveitis Center, University ofHeidelberg, GermanyM D Becker, Department of Ophthalmology, University of Heidelberg,GermanyA Heiligenhaus, M Trieschmann, Department of Ophthalmology at StFranziskus Hospital, Munster, GermanyT Hudde, Department of Ophthalmology, University of Essen, GermanyB Storch-Hagenlocher, B Wildemann, Department of Neurology,University of Heidelberg, GermanyT Barisani-Asenbauer, Department of Ophthalmology, University ofVienna, AustriaC Thimm, N Stubiger, Department of Ophthalmology, University ofTubingen, GermanyC Fiehn, Department of Internal Medicine, University of Heidelberg,Germany and Centre of Rheumatic Diseases, Baden-Baden, Germany
40
35
30
20
25
15
10
0
5
≥3Lines gained or lost
% o
f eye
s
210–1–2≤–3
Figure 2 This graph shows the percentage of eyes that gained or lostSnellen lines. In two eyes VA deteriorated because of the development ofcataracts.
Table 2 Change in VA, cell count, and surgical procedures that were performed during the treatment period with IFN
NoCMOinitially
CMO atlast followup?
Proliferativechangesinitially
Proliferativechange at lastfollow up?
VAchangeRE
VAchangeLE
AC cellgradingchange RE
AC cellgradingchange LE
Vitreous cellgradingchange RE
Vitreous cellgradingchange LE
Surgical proceduresduring IFN treatment
1 no no no no 3 0 21 21 22 22 none2 yes no no no 6 0 23 0 24 0 none3 no no 22 0 21 21 21 0 none4 yes yes yes no 4 4 0 0 22 23 none5 no no 2 1 21 21 21 21 cataract extraction OD
6 yes yes no no2
10 0 20.5 20.5 argon laser coagulation,
vitrectomy + ILM-peeling7 no no no no 0 0 20.5 20.5 0 0 none8 no no no no 2 0 22 0 22 0 none9 yes no no no 0 3 22 24 1 21 none10 yes no no no 4 3 22 22 24 24 none11 yes no yes no 4 4 0 0 22 22 argon laser coagulation12 no no yes no 22 2 23 23 21 23 none13 yes no yes no 5 2 21 22 22 23 none
1256 Becker, Heiligenhaus, Hudde, et al
www.bjophthalmol.com

Correspondence to: Matthias D Becker, MD, PhD, FEBO,Interdisciplinary Uveitis Center, University of Heidelberg, ImNeuenheimer Feld 350, 69120 Heidelberg, Germany; [email protected]
Accepted for publication 1 May 2005
REFERENCES1 Optic Neuritis Study Group. The 5-year risk of MS after optic neuritis.
Experience of the optic neuritis treatment trial. Neurology 1997;49:1404–13.2 Rucker CW. Sheathing of the retinal veins in multiple sclerosis. Review of
pertinent literature. Mayo Clin Proc 1972;47:335–40.3 Breger BC, Leopold IH. The incidence of uveitis in multiple sclerosis.
Am J Ophthalmol 1966;62:540–5.4 Porter R. Uveitis in association with multiple sclerosis. Br J Ophthalmol
1972;56:478–81.5 Bamford CR, Ganley JP, Sibley WA, et al. Uveitis, perivenous sheathing and
multiple sclerosis. Neurology 1978;28:119–24.6 Malinowski SM, Pulido JS, Folk JC. Long-term visual outcome and
complications associated with pars planitis. Ophthalmology1993;100:818–24; discussion 825.
7 Rothova A, Buitenhuis HJ, Meenken C, et al. Uveitis and systemic disease.Br J Ophthalmol 1992;76:137–41.
8 James DG, Friedmann AI, Graham E. Uveitis. A series of 368 patients. TransOphthalmol Soc UK 1976;96:108–12.
9 Bloch-Michel E, Nussenblatt RB. International Uveitis Study Grouprecommendations for the evaluation of intraocular inflammatory disease.Am J Ophthalmol 1987;103:234–5.
10 Biousse V, Trichet C, Bloch-Michel E, et al. Multiple sclerosis associated withuveitis in two large clinic-based series. Neurology 1999;52:179–81.
11 Acar MA, Birch MK, Abbott R, et al. Chronic granulomatous anterior uveitisassociated with multiple sclerosis. Graefes Arch Clin Exp Ophthalmol1993;231:166–8.
12 Towler HM, Lightman S. Symptomatic intraocular inflammation in multiplesclerosis. Clin Experiment Ophthalmol 2000;28:97–102.
13 Wakefield D, Jennings A, McCluskey PJ. Intravenous pulsemethylprednisolone in the treatment of uveitis associated with multiplesclerosis. Clin Experiment Ophthalmol 2000;28:103–6.
14 Poser CM, Paty DW, Scheinberg L, et al. New diagnostic criteria for multiplesclerosis: guidelines for research protocols. Ann Neurol 1983;13:227–31.
15 BenEzra D, Ohno S, Secchi A, et al. Anterior segment intraocularinflammation guidelines. London: Martin Dunitz, 2000.
16 PRISMS-4. Long-term efficacy of interferon-beta-1a in relapsing MS.Neurology 2001;56:1628–36.
17 PRISMS. (Prevention of Relapses and Disability by Interferon beta-1aSubcutaneously in Multiple Sclerosis) Study Group. Randomised double-blindplacebo-controlled study of interferon beta-1a in relapsing/remitting multiplesclerosis. Lancet 1998;352:1498–504.
18 Group CS. Interferon beta-1a for optic neuritis patients at high risk for multiplesclerosis. Am J Ophthalmol 2001;132:463–71.
19 Jacobs LD, Beck RW, Simon JH, et al. Intramuscular interferon beta-1atherapy initiated during a first demyelinating event in multiple sclerosis.CHAMPS Study Group. N Engl J Med 2000;343:898–904.
20 Constantinescu CS, Lavi E. Anterior uveitis in murine relapsing experimentalautoimmune encephalomyelitis (EAE), a mouse model of multiple sclerosis(MS). Curr Eye Res 2000;20:71–6.
21 Adamus G, Amundson D, Vainiene M, et al. Myelin basic protein specific T-helper cells induce experimental anterior uveitis. J Neurosci Res1996;44:513–8.
22 Okada AA, Keino H, Fukai T, et al. Effect of type I interferon on experimentalautoimmune uveoretinitis in rats. Ocul Immunol Inflamm 1998;6:215–26.
23 Teitelbaum D, Meshorer A, Hirshfeld T, et al. Suppression of experimentalallergic encephalomyelitis by a synthetic polypeptide. Eur J Immunol1971;1:242–8.
24 Munari LM, Lovati R, Boiko A. Therapy with glatiramer acetate for multiplesclerosis (Cochrane Review). The Cochrane Library. 1 vol. Chichester: JohnWiley, 2004.
25 Munari LM, Filippini G. Lack of evidence for use of glatiramer acetate inmultiple sclerosis. Lancet Neurol 2004;3:641.
bmjupdates+
bmjupdates+ is a unique and free alerting service, designed to keep you up to date with themedical literature that is truly important to your practice.bmjupdates+ will alert you to important new research and will provide you with the best newevidence concerning important advances in health care, tailored to your medical interests andtime demands.
Where does the information come from?bmjupdates+ applies an expert critical appraisal filter to over 100 top medical journalsA panel of over 2000 physicians find the few ’must read’ studies for each area of clinicalinterest
Sign up to receive your tailored email alerts, searching access and more…
www.bmjupdates.com
IFN treatment for uveitis associated with MS 1257
www.bjophthalmol.com

SCIENTIFIC REPORT
Novel rhodopsin mutations and genotype-phenotypecorrelation in patients with autosomal dominant retinitispigmentosaA Schuster, N Weisschuh, H Jagle, D Besch, A R Janecke, H Zierler, S Tippmann, E Zrenner,B Wissinger. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1258–1264. doi: 10.1136/bjo.2004.063933
Aim: To identify novel or rare rhodopsin gene mutations inpatients with autosomal dominant retinitis pigmentosa anddescription of their clinical phenotype.Methods: The complete rhodopsin gene was screened formutations by DNA sequencing in index patients. Mutationspecific assays were used for segregation analysis andscreening for controls. Eight patients from five families andtheir relatives were diagnosed with autosomal dominantretinitis pigmentosa (adRP) by means of clinical evaluation.Results: Mutation screening identified five different rhodop-sin mutations including three novel mutations: Ser176Phe,Arg314fs16, and Val20Gly and two missense mutations,Pro215Leu and Thr289Pro, that were only reported once in amutation report. Electrophysiological and psychophysicaltestings provide evidence of an impaired rod system withadditionally affected cone system in subjects from eachgenotype group. Visual function tended to be less affected insubjects with the Arg314fs16 and Val20Gly mutations thanin the Ser176Phe phenotype. In contrast, Pro215Leu andThr289Pro mutations caused a remarkably severe pheno-type.Conclusion: The ophthalmic findings support a correlationbetween disease expression and structural alteration: (1)extracellular/intradiscal Val20Gly and cytoplasmicArg314fs16 mutation—mild adRP phenotype; (2)Ser176Phe mutation—‘‘mostly type 1’’ disease; (3) predictedalteration of transmembrane domains TM V and TM VIIinduced by Pro215Leu and Thr289Pro—severe phenotype.However, variation of phenotype expression in identicalgenotypes may still be a typical feature of RHO mutations.
Retinitis pigmentosa (RP) is a clinically and geneticallyheterogeneous group of inherited retinal degenerations.1
Patients with RP experience night blindness, visual fieldconstriction, and eventually loss of central vision, in mostcases caused by degeneration of the photoreceptor cells of theretina.1 2 There are autosomal dominant (adRP), autosomalrecessive (arRP), X linked (xlRP), and rare mitochondrial ordigenic forms.1 To date, 13 gene loci are known for adRP,3–13
21 for arRP, and five for xlRP (RetNet http://www.sph.uth.tmc.edu/RetNet/).The first photoreceptor specific gene found to be mutated
in adRP was rhodopsin (RHO).14 15 Rhodopsin is the lightabsorbing molecule that initiates the signal transductioncascade in rod photoreceptors. Mutations of the rhodopsingene account for approximately 25% of adRP.16 Numerousmutations in the RHO gene have been identified, most ofthem being point mutations.15 The analysis of mutant
rhodopsins suggest that some RP mutations impair proteinfolding, 11-cis retinal chromophore binding, G-proteincoupling/activation, and/or cellular trafficking of the rhodop-sin protein.17 18
In this study we report the results of the RHO genescreening in five independent adRP families.
PATIENTS AND METHODSRecruitment of patients, DNA isolation, and mutationanalysisEight patients were included into the study, all sufferingfrom adRP. The study was conducted in accordance with thetenets of the Declaration of Helsinki.
Mutation detection by direct sequencingPatient DNA was extracted using a standard salting outprocedure.19 For mutation detection by sequencing, PCR wasperformed using corresponding sense and antisense primersand 1 U Taq polymerase (Eppendorf, Hamburg, Germany).PCR products were separated on a DNA capillary sequencer(ABI 3100 Genetic Analyzer, Applied Biosystems, Foster City,CA, USA).
Mutation detection by DHPLCDenaturing high performance liquid chromatography(DHPLC) analysis was conducted with the WAVE nucleicacid fragment analysis system equipped with a L-7400 UVdetector (Transgenomic, Omaha, NE, USA). Samples withaberrant profiles were sequenced.
Mutation detection by RFLPA 588 bp PCR product encompassing Exon 1 was digestedwith 1 U RsaI restriction enzyme (NEB, Beverly, MA, USA).The Val20Gly missense change results in the loss of one ofthree genuine RsaI restriction sites. Restriction digest fornormal individuals results in two fragments of about 420 bpand 160 bp that can be visualised on a 4% agarose gel. Forindividuals heterozygous for the Val20Gly mutation, restric-tion digest results in an additional fragment of 178 bp.
Clinical studies of the RHO mutation phenotypePhenotype analysis comprised clinical examination,Goldmann perimetry, Panel D15 testing, dark adapted finalthresholds, Ganzfeld electroretinography (UTAS 2000 sys-tem; LKC Technologies, Gaithersburg, USA), according toISCEV standard20 and multifocal electroretinography usingthe VERIS system (EDI, San Francisco, CA, USA).21 22
Abbreviations: adRP, autosomal dominant retinitis pigmentosa; arRP,autosomal recessive retinitis pigmentosa; xlRP, X linked retinitispigmentosa; DHPLC, denaturing high performance liquidchromatography
1258
www.bjophthalmol.com

RESULTSMutation analysisThe index patient of each family was screened for mutationsin the RHO gene. Table 1 summarises the respective sequencealterations. Three of them were novel mutations (Val20Gly,Ser176Phe, Arg314fs16), and the other two mutations
(Pro215Leu, Thr289Pro) have only been reported once in abrief mutation report without clinical details.23
Clinical studiesFigure 1 (A to E) shows the pedigree of the patients/familiesinvestigated.
Table 1 RHO mutations
Nucleotidesequencealteration Consequence Location
Mutation carriers/families tested
Mutation carriers/controls
Previouslyreported
c.59T.G Val20Gly Exon 1 6/10 0/100 Noc.527C.T Ser176Phe Exon 2 1/1 0/100 Noc.644C.T Pro215Leu Exon 3 5/12 0/100 See ref 23c.865˚.C Thr289Pro Exon 4 1/1 0/100 See ref 23c.942insG Arg314fs16 Exon 5 1/1 Not performed No
B Family 2: R314fsx16
III
II1
I
2
1
3 4
2
5
1
6
Arg314fsx16
V1
IV1
III
Ser176Phe
II
I
A Family 1: S176F
2 3
2 3
1 2 3 4 5
1 2 3
1 2
4
4
5
5
4P215L/+
3+/+
2
Family 3: P215L
III
II
I
C
1+/+
1+/+
2 3 4 5 6 7 8
6P215L/+
9
7 +/+
10
8P215L/+
11P215L/+
9 +/+
10 113P215L/+
2+/+
4 5
12+/+
1
III1
II
I
D
2V20G/+
1
4 V20G/+
2
5 6+/+
3
1
7
4
8+/+
9
5
2
10
6
11+/+
12V20G/+
7V20G/+
13 V20G/+
8+/+
Family 4: V20G
3V20G/+
III
II
I
E Family 5: T289P
1Thr289Pro
1
2
2
1
3
3
2
Figure 1 (A to E) Pedigrees of adRPfamilies. Circles, females; squares,males; solid symbols, affectedmembers; open symbols, unaffectedmembers; slashed symbols, deceasedmembers; arrows, persons examinedophthalmologically; asterisks, DNAanalysis performed.
Rhodopsin mutations and autosomal dominant retinitis pigmentosa 1259
www.bjophthalmol.com

The clinical characteristics of affected patients are sum-marised in table 2. Original phenotype data is indicated infigures 2–4.
DISCUSSIONWe studied patients from five independent families showingtypical clinical features of autosomal dominant RP. Two ofthe novel mutations were missense mutations, and one was a1bp insertion (c.942insG) that results in a frameshift andsubsequent translation termination.We found considerable relation between the individual
mutation and disease expression. Cideciyan and colleaguesdistinguished two patterns of rod disease expression in avariety of rhodopsin mutations.24 Other widely acceptedclassification systems have been developed by Massof &Finkelstein,25 Lyness et al,26 and Fishman et al.27 According tothe latter systems the phenotypes of our study can besubdivided into distinct groups.
Patients with the novel mutations Arg314fs16 (family 2)and Val20Gly (family 4) express a remarkably mild ‘‘mostlytype 2’’ phenotype25 with late onset of symptoms and a morefavourable visual prognosis or ‘‘R’’-type26 and the Ser176Phephenotype (family 1) discloses an intermediate ‘‘mostly type1’’ or ‘‘D-’’ phenotype. In contrast, the Pro215Leu (family 3)and Thr289Pro (family 5) mutations result in a severe type 1-or D-phenotype with early onset of symptoms and rapid lossof visual field area, corresponding with a diffuse andprogressive loss of rod and cone function.Based on current models of rhodopsin (fig 5), two of the
novel mutations (Val20Gly and Ser176Phe) involve aminoacids on the intradiscal/extracellular side and one occurs atthe cytoplasmic side (Arg314fs16). Mutations Pro215Leu andThr289Pro involve transmembrane domains.Considering intradiscal/extracellular mutations, it has
been reasoned that missense mutations affecting residues2–428 or 15–1729 interfere with N-glycosylation or that the
Figure 2 Patient IV:4 (family 1;Ser176Phe). (A) Perimetry (targets V/4e, III/4e, I/4e, and I/2e). (B) MfERGresponses showing 61 single traces ofright eye (RE) (right lane) and left eye(LE) (left lane). (C) Ganzfeld-ERG. Leftcolumn: waveforms (top to bottom) areisolated rod b-wave of RE (1-R, 3-R, 5-R) and LE (2-L, 4-L, 6-L), scotopic mixedrod/cone response of RE (7-R) and LE(8-L). Right column: photopic 30 Hzflicker response of RE (1-R) and LE (2-L).Traces 3-R and 4-L show 30 Hzrepetition. ‘‘1’’: peaks of the 30 Hzflicker response. Left column:calibrations: 5 microV/div;5 ms/div(traces 1-R; 2-L) and 50 microV/div;5 ms/div for other traces. Rightcolumn: calibrations 20 microV/div;3 ms/div.
1260 Schuster, Weisschuh, Jagle, et al
www.bjophthalmol.com

replacement of cysteines 110 and 187 prevent the formationof the disulfide bridge.15
It could be speculated that the Ser176Phe mutation mayinduce a structural alteration of the cysteine 187 neighbour-hood.The Val20Gly missense mutation is close to previously
described mutations in the N-terminal region of thepolypeptide. The phenotype of patient III:13 carrying thisnovel mutation was extremely mild with moderately affectedrod and cone function even at age 34.The c.942insG mutation causes a frameshift mutation with
premature stop codon that results in an alteration andshortening of the cytoplasmatic domain, the first rhodopsinmutation to be described in a Bosnian family. The phenotypeof the single available patient is relatively mild with lateonset symptoms and relatively well preserved central conefunction. Cideciyan and colleagues described the phenotypeof other C-terminal truncated mutations (Gln312X andGln344X) and classified them as class B mutants.24
The Pro215Leu and Thr289Pro mutations involve aminoacid exchanges within transmembrane domains, and bothmutations eliminate or introduce proline residues. Recentpublications described mutations perturbing critical inter-helical interactions between TM III and TM V, namely theGlu122, His211 salt bridge, resulting in a severe type of adRPin vivo.30–33
The Thr289Pro phenotype (family 5, individual III:1) mayserve as another example of severe type adRP induced by amissense mutation in TMVII. Within TM VII, 11-cis-retinalcovalently binds to opsin at the epsilon amino group ofLys296.34 35 The phenotype presented in our study parallelsmany features of the unusually severe Lys296Glu pheno-type.36 37
Both intrafamilial and interfamilial phenotype differencesamong carriers of identical rhodopsin mutations have beendescribed.38 39 On the other hand, a disease course fairlyconstant in all affected persons within the same largepedigree has also been documented.40
Figure 3 Data of patient II:5 (family 2;Arg314fs16). (A) Perimetry (targets III/4e, I/4e, and I/2e). (B) See figure 2B.(C) Ganzfeld-ERG: waveforms areindicated as in figure 2. ‘‘3’’ indicatesa-wave, ‘‘4’’ indicates b-wave peak.Peaks of 30 Hz flicker signals areindicated by ‘‘1’’. Calibrations: seefigure 2.
Rhodopsin mutations and autosomal dominant retinitis pigmentosa 1261
www.bjophthalmol.com

Table
2RH
OMutations
andPh
enotyp
e
Family
number/
mutatio
nAgeof
onset/mod
eof
onset
(age)
VA:RE/
LEinitial
presentatio
n(age)
Refractiveerror:
RE/
LEVisua
lfie
ld:RE/
LE(age)
ERG
Fund
usDA/p
ane
lD15
1/S
er176Ph
e(G
erman
)IV:4
Night
blindn
ess;
field
constrictio
n(13)
60/1
00;
60/1
00(33)
21.75/2
1.75
Con
strictionto
15 ˚
(III/4e90)(33)
Scotop
ic:no
iselevel
Slight
optic
atroph
y,vessel
narrow
ing,
absent
macular
reflexes,
periph
eral
pigm
entmottling
,slight
periph
eral
hype
rpigmen
tatio
n
Sign
ificant
elevation/
desaturated:
norm
al
Loss
visual
acuity
(30)
Con
e30Hz-flicker:residu
alrespon
ses(33)
V:4
Night
blindn
ess,
glaresensitivity
(2)
80/1
00;
100/1
00(6)
+1.5/+
1.5
Nea
rno
rmal
(III/4e),
constrictio
nto
10–2
0 ˚(I/
4e90)(6)
notpe
rformed
Normal
optic
discs,
periph
eral
RPE
atroph
ywith
outbo
nespicules
Desaturated
:no
rmal
2/A
rg314fs16
(Bosnian
)II:5Night
blindn
ess,
glaresensitivity,fie
ldconstrictio
n(33)
100/1
00;
120/1
00(36)
Emmetropic
Con
strictionto
50–6
0 ˚with
large
scotom
as15–4
0 ˚(III/4e90)(36)
Scotop
ic:am
plitude
redu
ction
to10%
norm
alrang
eMild
optic
atroph
y,mod
erately
narrow
edvessels,
atyp
ical
macular
ILM
reflexes;
bone
-spiculesin
lower
sector,diffu
seRP
Eatroph
y
Sign
ificant
elevation/
desaturated:
norm
al
Photop
ic:am
plitude
redu
ction
to50%
norm
alrang
eMfERG
:preservedfoveal
cone
respon
ses
3/P
ro215Leu
(German
)II:3Night
blindn
ess(birth),
visual
acuity
loss,fie
ldconstrictio
n(33),glare
sensitivity
(45)
10/2
00;
10/2
00(48)
+1,25/+
1,25
Con
strictionto
5–7˚
(III/4e90)(48)
Noise
level(48)
Wax
yop
ticne
rveatroph
y,vessel
attenu
ation,
RPEatroph
y,an
dhype
rpigmen
tatio
n
Sign
ificant
elevation/
saturated:
disturba
nces
alla
xes
II:6Night
blindn
ess(birth)
Node
tails
Node
tails
Con
strictionto
5–1
0 ˚(III/4e90)(35)
Noise
level(35)
Node
tails
Node
tails
III:4
Night
blindn
ess
(birth),no
taw
areof
othe
rsymptom
s
120/1
00;
80/1
00(16)
+2.5/+
2.75
Con
strictionto
10–2
5 ˚(right
eye),7–1
5 ˚(lefteye)
(III/4e90)(16)
Rodrespon
ses:
noiselevel;
cone
30Hz:
residu
alrespon
ses(16)
Normal
optic
disc,slightly
narrow
edvessels,
cystoidmaculaoe
dema,
periph
eral
RPEatroph
ywith
hype
rpigmen
tatio
n
Sign
ificant
elevation/
desaturated:
slight
disturba
nces
alla
xes
4/V
al20Gly
(Austrian)
III:13Nosymptom
s100/1
00;
80/1
00(34)
0;+3
.5RE
:cataract
surgery
atag
e27
Not
performed
Scotop
ican
dph
otop
icam
plitude
redu
ctionwith
rest
functio
n;Electro-oculog
ram:
nolig
htpe
ak,pa
tholog
ical
Arden
ratio
Absen
tmacular
reflexes,
narrow
edvessels,
mid-periphe
ral
hype
rpigmen
tatio
n
Node
tails
5/T
hr289Pro
(Austrian)
III:1
Night
blindn
ess,
field
constrictio
n(3),
colorvision
(9),glare
sensitivity
(12),visual
acuity
(18),cataract
extractio
n(27)
10/2
50;
10/2
50(27)
Emmetropic
Con
strictionto
,5 ˚
(III/4e90)
Scotop
ic/p
hotopicno
iselevel
MfERG
noiselevel
Tempo
ralo
ptic
disc
pallor,
nomacular
reflexes,
mid-periphe
ral
hype
rpigmen
tatio
n
Sign
ificant
elevation
1262 Schuster, Weisschuh, Jagle, et al
www.bjophthalmol.com

In summary, the phenotype description of Ser176Phe givesat least consistent examples of mother (IV:4) and daughter(V:4) expressing an intermediate type of adRP with earlyonset of symptoms, but possibly long time preserved visualacuity. For the Arg314fsX16 and Val20Gly mutations, wecould describe an unusually mild phenotype. The alterationof transmembrane helices TM V or TM VII by the Pro215Leuand Thr289Pro missense mutation lead to severe adRP.However, more interfamilial and intrafamilial clinical datawill be necessary to draw conclusions on a constantgenotype-phenotype correlation in these mutations.
ACKNOWLEDGEMENTSWe are grateful to Dr Daxecker and Dr Lalehabbasi, Innsbruck/Austria for collaboration
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
A Schuster, H Jagle, D Besch, E Zrenner, University Eye Hospital,Department of Neuroophthalmology, Tuebingen, GermanyN Weisschuh, S Tippmann, B Wissinger, Molecular GeneticsLaboratory, Tuebingen, GermanyA R Janecke, Department of Medical Genetics, and Molecular andClinical Pharmacology, Innsbruck Medical University, Austria
Figure 4 (A) Fundus LE (patient II:3; family 3; Pro215Leu). Nasalperiphery (top) and posterior pole (bottom). (B) Fundus LE (patient III:4;family 3; Pro215Leu). Nasal periphery (top) and posterior pole (bottom).
Missense mutationArg314fsx16: Arg-Glu-Leu-His-Ala-His-His-His-Leu-Leu-Arg-Gln-Glu-Pro-Thr-Gly-STOP
ML
50
40 90
80
70
60
130
120
110
190
180200
2/3
1/2
170
160
230
220 260
5/4310
320
330
340
300
290
280
270210
150
4/3
240
250
140
30
10020
10
L
L
I
I
G
L
L
D
M
G
QW
PE
A
Ac-NH
LY Y Q P Y G F P S R V V G T A
M N G T E G P N F Y V P F
NS
S
TSLH G Y F V F G P T
GC S C Q L G E P
R YI
WGA
L
A
L
W
A
I
P
C
A
T
V
A
A
A
V
F
M
P
M
G
GI
DY Y T L K P E V
NN
ES
C
E
A
G
A
S
L
E
N
G
T
G
L
A
L
RYVVVC
Cytoplasm
TM I II III IV V VI VII
PK
NL
PT
RL
KKHQVT
M S N FR
FG
Q
QG
I
V
F
F
F
I
I
H
M
V
L
T
C
I
P
F
F
I
V
V
Y
F
M
T
V
Y
AA
A EK
QQ E S A T T Q K A
EKE
VTR
Diskmem-brane
ENH
L
E
W
V
I
F
LF
I
V
A
V
TY
I
N
A
F
G
T
Y
L
V
L
L
F
L
N
T
L
P
ML
Y
Y
F
F
V
V
F
F
S
AA
L
ST
P
K
I
V
I
S
F
I
I
M
I
Y
A
F
P
F
MN
KQ
F
NC M
LT
TI
C CG
KN
PL
GD
DE
ASATVSKTETSQVAGAHOOC-
R
Y
N
A
A
A
M
I
V
L
W
A
A
I
V
FFT
HQ G S N F
GP
Intradiscal/extracellular
V
M
F
C
Y
V
I
M
I
A
I
P
S
Y
Figure 5 Two dimensional model of rhodopsin (mutations boxed). The TM helices are labelled I-VII. Arg314fs16 mutation: Arg-Glu-Leu-His-Ala-His-His-His-Leu-Leu-Arg-Gln-Glu-Pro-Thr-Gly-STOP.
Rhodopsin mutations and autosomal dominant retinitis pigmentosa 1263
www.bjophthalmol.com

H Zierler, Institute of Medical Biology and Human Genetics, University ofGraz, Austria
Supported by the grants ZR 1/16-1 and ZR 1/16-2 of the DeutscheForschungsgemeinschaft (DFG)
Correspondence to: Dr A Schuster, University Eye Hospital, Departmentof Neuroophthalmology, Schleichstr 12–16, D-72076 Tuebingen,Germany; [email protected]
Accepted for publication 1 April 2005
REFERENCES1 Heckenlively JR, Daiger SP. In: Rimon DL, Conner JM, Pyeritz RE, eds.
Hereditary retinal and choroidal degenerations. New York: ChurchillLivingstone, 2001:2255–576.
2 Bird AC. Retinal photoreceptor dystrophies. Am J Ophthalmol1995;19:543–62.
3 Dryja TP, McGee TL, Reichel E, et al. A point mutation of the rhodopsin gene inone form of retinitis pigmentosa. Nature 1990;343:364–6.
4 Kajiwara K, Hahn LB, Mukai S, et al. Mutations in the human retinaldegeneration slow gene in autosomal dominant retinitis pigmentosa. Nature1991;354:480–3.
5 Farrar GJ, Kenna P, Jordan SA, et al. A three-base-pair deletion in theperipherin-RDS gene in one form of retinitis pigmentosa. Nature1991;354:478–80.
6 Bessant DA, Payne AM, Mitton KP, et al. A mutation in NRL is associated withautosomal dominant retinitis pigmentosa. Nat Genet 1999;21:355–6.
7 Sullivan LS, Heckenlively JR, Bowne SJ, et al. Mutations in a novel retina-specific gene cause autosomal dominant retinitis pigmentosa. Nat Genet1999;22:255–9.
8 Sohocki MM, Sullivan LS, Mintz-Hittner HA, et al. A range of clinicalphenotypes associated with mutations in CRX, a photoreceptor transcription-factor gene. Am J Hum Genet 1998;63:1307–15.
9 Wada Y, Abe T, Takeshita T, et al. Mutation of human retinal fascin gene(FSCN2) causes autosomal dominant retinitis pigmentosa. Invest OphthalmolVis Sci 2001;42:2395–400.
10 Bowne SJ, Sullivan LS, Blanton SH, et al. Mutations in the inosinemonophosphate dehydrogenase 1 gene (IMPDH1) cause the RP10 form ofautosomal dominant retinitis pigmentosa. Hum Mol Genet 2002;11:559–68.
11 Kennan A, Aherne A, Palfi A, et al. Identification of an IMPDH1 mutation inautosomal dominant retinitis pigmentosa (RP10) revealed followingcomparative microarray analysis of transcripts derived from retinas of wild-type and Rho(_/_) mice. Hum Mol Genet 2002;11:547–57.
12 Keen TJ, Hims MM, McKie AB, et al. Mutations in a protein target of the Pim-1kinase associated with the RP9 form of autosomal dominant retinitispigmentosa. Eur J Hum Genet 2002;10:245–9.
13 Rebello G, Ramesar R, Vorster A, et al. Apoptosis-inducing signal sequencemutation in carbonic anhydrase IV identified in patients with the RP17 form ofretinitis pigmentosa. Proc Natl Acad Sci USA 2004;101:6617–22.
14 Dryja TP, Li T. Molecular genetics of retinitis pigmentosa. Hum Mol Genet1995;4:1739–43.
15 Gal A, Apfelstedt-Sylla E, Janecke AR, et al. Rhodopsin mutations in inheritedretinal dystrophies and dysfunctions. Prog Retinal Eye Res 1997;16:51–79.
16 Chuang J-Z, Vega C, Jun W, et al. Structural and functional impairment ofendocytic pathways by retinitis pigmentosa mutant rhodopsin-arrestincomplexes. J Clin Invest 2004;114:131–40.
17 Franke RR, Sakmar TP, Graham RM, et al. Structure and function inrhodopsin. Studies of the interaction between the rhodopsin cytoplasmicdomain and transducin. J Biol Chem 1992;267:14767–74.
18 Sung CH, Schneider BG, Agarwal N, et al. Functional heterogeneity of mutantrhodopsins responsible for autosomal dominant retinitis pigmentosa. ProcNatl Acad Sci U S A 1991a;88:8840–4.
19 Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extractingDNA from human nucleated cells. Nucleic Acids Res 1988;16:1215.
20 Marmor MF, Zrenner E. Standard for clinical electroretinography (1999update). Doc Ophthalmol 1999;97:143–56.
21 Sutter EE, Tran E. The field topography of ERG components in man, I: thephotopic luminance response. Vis Res 1992;32:433–66.
22 Kretschmann U, Seeliger MW, Ruther K, et al. Multifocal electroretinographyin patients with Stargardt’s macular dystrophy. Br J Ophthalmol1998;82:267–75.
23 Martinez-Gimeno M, Trujillo MJ, Lorda I, et al. Three novel mutations (P215L,T289P, and 3811-2 A--.G) in the rhodopsin gene in autosomal dominantretinitis pigmentosa in Spanish families. Hum Mutat 2000;16:95–6.
24 Cideciyan AV, Hood DC, Huang Y, et al. Disease sequence from mutantrhodopsin allele to rod and cone photoreceptor degeneration in man. ProcNatl Acad Sci U S A 1998;95:7103–8.
25 Massof RW, Finkelstein D. Two forms of autosomal dominant primary retinitispigmentosa. Doc Ophthalmol 1981;51:289–346.
26 Lyness AL, Ernst W, Quinlan MP, et al. A clinical, psychophysical, andelectroretinographic survey of patients with autosomal dominant retinitispigmentosa. Br J Ophthalmol 1985;69:326–39.
27 Fishman GA, Alexander KR, Anderson RJ. Autosomal dominant retinitispigmentosa. A method of classification. Arch Ophthalmol 1985;103:366–74.
28 Bunge S, Wedemann H, David D, et al. Molecular analysis and geneticmapping of the rhodopsin gene in families with autosomal dominant retinitispigmentosa. Genomics 1993;17:230–3.
29 Sung CH, Davenport CM, Hennessey JC, et al. Rhodopsin mutations inautosomal dominant retinitis pigmentosa. Proc Natl Acad Sci U S A1991b;88:6481–5.
30 Patel AB, Crocker E, Eilers M, et al. Coupling of retinal isomerization to theactivation of rhodopsin. Proc Natl Acad Sci U S A 2004;101:10048–53.
31 Stojanovic A, Hwang I, Khorana HG, et al. Retinitis pigmentosa rhodopsinmutations L125R and A164V perturb critical interhelical interactions: newinsights through compensatory mutations and crystal structure analysis. J BiolChem 2003;278:39020–8.
32 Dryja TP, Hahn LB, Cowley GS, et al. Mutation spectrum of the rhodopsingene among patients with autosomal dominant retinitis pigmentosa. Proc NatlAcad Sci U S A 1991;88:9370–4.
33 Fuchs S, Kranich H, Denton MJ, et al. Three novel rhodopsin mutations(C110F, L131P, A164V) in patients with autosomal dominant retinitispigmentosa. Hum Mol Genet 1994;3:1203.
34 Bownds D. Site of attachment of retinal in rhodopsin. Nature1967;216:1178–81.
35 Wang JK, McDowell JH, Hargrave PA. Site of attachment of 11-cis-retinal inbovine rhodopsin. Biochemistry 1980;19:5111–17.
36 Keen TJ, Inglehearn CF, Lester DH, et al. Autosomal dominant retinitispigmentosa: four new mutations in rhodopsin, one of them in the retinalattachment site. Genomics 1991;11:199–205.
37 Owens SL, Fitzke FW, Inglehearn CF, et al. Ocular manifestations inautosomal dominant retinitis pigmentosa with a Lys-296-Glu rhodopsinmutation at the retinal binding site. Br J Ophthalmol 1994;78:353–8.
38 Berson EL, Rosner B, Sandberg MA, et al. Ocular findings in patients withautosomal dominant retinitis pigmentosa and a rhodopsin gene defect(Pro23His). Arch Ophthalmol 1991a;109:92–101.
39 Berson EL, Rosner B, Sandberg MA, et al. Ocular findings in patients withautosomal dominant retinitis pigmentosa with rhodopsin, proline-347-leucine.Am J Ophthalmol 1991b;111:614–23.
40 Rosas DJ, Roman AJ, Weissbrod P, et al. Autosomal dominant retinitispigmentosa in a large family: a clinical and molecular genetic study. InvestOphthalmol Vis Sci 1994;35:3134–44.
1264 Schuster, Weisschuh, Jagle, et al
www.bjophthalmol.com

SCIENTIFIC REPORT
PET/CT imaging: detection of choroidal melanomaS Reddy, M Kurli, L B Tena, P T Finger. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1265–1269. doi: 10.1136/bjo.2005.066399
Aim: To determine the size of untreated choroidal melano-mas resolved by whole body positron emission tomographyfused with computed tomography (PET/CT).Methods: 50 consecutive patients with untreated choroidalmelanomas underwent whole body PET/CT. A functionallyfused helical CT scan and 18-fluoro-2-deoxyglucose (FDG)PET scans were employed. The tumours were identified (bothquantitatively and qualitatively) and compared with clinicalmeasurements derived from ophthalmoscopic, angiographic,and ultrasonographic imaging. Standardised uptake values(SUV) of more than 2.5 were considered positive.Results: Among the 50 patients with choroidal melanoma,PET/CT scan SUVs of more than 2.5 were noted in 14 (28%)tumours. No AJCC T1 class tumours, 33.3% of T2melanomas, and 75% of T3 melanomas were physiologicallyidentifiable on PET/CT. With respect to COMS groupclassifications, no small choroidal tumours, 33% of medium,and 75% of large melanomas were physiologically identifi-able. The sole ring melanoma was identifiable on PET/CTimaging. The smallest tumour physiologically identifiable byPET/CT had basal dimensions of 365.9 and an apical heightof 2.9 mm.Conclusion: Though PET/CT was found to be capable ofphysiologically identifying certain medium (T2) and mostlarge sized (T3) choroidal melanomas, physiologicalimaging was not completely dependent upon tumour size.Functionally fused PET/CT localised the tumours within theeye and assessed their physiological activity.
Cancer cells require a great deal of sugar (glucose) formetabolism and growth. Positron emission tomogra-phy/computed tomography (PET/CT) scanning utilises
a radioactive form of glucose, called 18-fluoro-2-deoxyglu-cose (FDG) that accumulates within malignant cells becauseof their high rate of metabolism. The FDG injected patient isimaged on the whole body PET scanner in an effort to revealtumours that may have been overlooked or difficult tocharacterise (as benign or malignant) by conventionalcomputed tomography (CT), x ray, or magnetic resonanceimaging (MRI).The CT portion of a PET/CT provides detailed information
about the location, size, and shape of tumours but offers lessinformation that can be used to differentiate betweencancerous and normal structures (compared to PET). Thedual modality, PET/CT scanner fuses an image that puts formand function on the same diagnostic page.Choroidal melanomas are the most common primary
intraocular cancer in adults.1 The Collaborative OcularMelanoma Study (COMS) group and others have concludedthat indirect ophthalmoscopy, combined with ophthalmicultrasonography and fluorescein angiography, can yield adiagnostic accuracy rate greater than 99%.2 However, strictselection criteria (patient and tumour specific) for COMS
eligibility were based on size and. secondly, on appearance,shape, location, internal ultrasonic reflectivity, and angio-graphic evidence of tumour leakage.2 Though exhaustive, thediagnostic criteria employed by COMS did not includephysiological imaging.2
The importance of early detection of malignant melanomacannot be understated.3–7 Mathematical studies of tumourdoubling time and the COMS small tumour trial suggest thatmetastasis from choroidal melanomas can occur while asmall tumour is being observed as a ‘‘suspicious choroidalnaevus.’’4 5 Since COMS found that largest tumour dimensionis significantly correlated with the risk of metastasis, it isreasonable to assume that a physiological assessment oftumour metabolism could help differentiate between suspi-cious choroidal naevi and small choroidal melanomas beforegrowth.2 3
In the last few years PET/CT has emerged as a new imagingmodality for the detection and staging of cancer.8 Our studyevaluates the efficacy of FDG-PET/CT imaging for thedetection of primary choroidal melanomas, to assess theirphysiological activity and its relationship to tumour size.
METHODS AND MATERIALSPatientsSince August of 2003, 50 consecutive patients with choroidalmelanomas were evaluated by PET/CT before treatment(table 1). All patients had a clinical diagnosis confirmed byophthalmoscopy, fluorescein angiography, and ophthalmicultrasonography. Their initial metastatic investigationincluded liver function tests (c-glutamyl transpeptidase,aspartate aminotransferase, alanine aminotransferase, alka-line phosphatase, bilirubin), a chest x ray and whole bodyFDG-PET/CT imaging. Informed consent and health insur-ance portability and accountability act (HIPAA) forms wereobtained before treatment.
PET/CT protocolPET/CT imaging required that patients refrain from eating acarbohydrate based dinner the previous night and to fast4–6 hours before injection of 18-FDG. This diminishedphysiological glucose utilisation and reduced insulin serumlevels to baseline. The normal fasting glucose level wasoptimally less than 110 mg/dl, but the acceptable range was80 mg/dl to 160 mg/dl. The full body PET/CT scan began atthe top of the head and ended at the bottom of the feet. TheCT portion (General Electric Discovery ST, Piscataway, NJ,USA) with BGO (bismuth germanate) crystal consisted of amulti-detector helical CT scanner. The imaging parameterswere 80–140 kV, 40–80 mA, 0.8 s per CT rotation, and a tablespeed of 33.75 mm/rotation. The CT slice thickness was3.75 mm with an image interval of 3.27 mm. The CT
Abbreviations: AJCC, American Joint Cancer Committee; BGO,bismuth germanate; COMS, Collaborative Ocular Melanoma Study; CT,computed tomography; FDG, 18-fluoro-2-deoxyglucose; MRI, magneticresonance imaging; PET, positron emission tomography; SUV,standardised uptake values
1265
www.bjophthalmol.com

acquisition came before the PET emission acquisition, andthe acquisition time was dependent on the dose of FDG andranged from 19 seconds to 27 seconds. FDG was injectedwith a target dose of a 5 mCi (range 10 mCi to 20 mCi). Thedose was calculated by (weight in kilograms6 target dose inmCi)/70 kg. The FDG was injected via an intravenous line,followed by 10 ml of normal saline. Imaging began within45 minutes of injection and ended no later than 1.5 hoursafter injection.The resolution of the PET scan was 4 mm. The transmis-
sion time at each bed position was 2–3 minutes. Eight to ninebed positions were used. After each bed position, a 512 cm6512 cm CT matrix was converted to a 128 cm 6 128 cmmatrix that was fed into to the PET scan. The PET scanreconstructed the images on the fly and utilised the CT scanto correct for attenuation. Then, Xeleris (General Electricsoftware, Piscataway, NJ, USA), a computer software, wasused to fuse and display the PET and CT images to producethe final image. The images were graded positive when traceruptake of 2.5 SUV (standardised maximum uptake value) or
more was observed in comparison with the surroundingstructures. The SUVMAX was calculated for each site using theconventional formula using body weight normalisation:
RESULTSFifty patients (22 males and 28 females) with a mean age of64 years (range 39–95) and a clinical diagnosis of choroidalmelanoma underwent full body PET/CT scans (table 1). Ourstudy included 27 melanomas of the left eye and 23melanomas of the right. One of the melanomas was classifiedas a ring melanoma, and of the 49 remaining, the meanwidth, length, and height of the uveal melanomas were11.16 mm (range 5–19), 9.87 mm (range 3–19.1), and4.78 mm (range 1.6–14), respectively.
Table 1 Patients with uveal melanomas
PatientNo Age Sex Eye Location
Tumour size (mm)PET/CTdetectionWidth Length Height AJCC COMS
1 74 M RE 4I 5.9 3 2.9 T2 medium positive2 69 F LE 11P 13 11.5 3 T2 medium positive3 70 M LE 9EP 14.9 9.9 3.2 T2 medium positive4 69 M RE 12PE 13.5 11.5 4.5 T2 medium positive5 54 F RE 6P 15.8 15.1 6 T2 medium positive6 65 F RE 1E 14 13.8 7.3 T2 medium positive7 69 M LE 9EA 16 14 8.2 T2 medium positive8 83 F LE 12EA 14.9 14.1 8.6 T2 medium positive9 57 M LE 6EP 16 14 11.5 T3 large positive
10 88 F LE 2EA 16.2 15.3 11.9 T3 large positive11 60 F LE 230CB 15.5 14.5 12.2 T3 large positive12 65 M LE 730EA 16.9 19.1 12.3 T3 large positive13 67 F RE 9E 19 15.2 14 T3 large positive14 95 M LE ring melanoma T3 large positive15 53 F RE 430EP 8.8 8.2 1.6 T1 small no16 60 F RE CB 8.5 6.6 1.7 T1 small no17 66 M LE 1PE 6.4 5.4 1.7 T1 small no18 46 F RE 430E 7.9 7.4 1.8 T1 small no19 72 M RE 5PE 5.7 4.3 1.8 T1 small no20 55 F RE 2PE 9.5 9.1 2 T1 small no21 59 F RE 7PE 6.1 7.9 2 T1 small no22 67 F RE 2EP 8 6.8 2 T1 small no23 90 F LE 5PE 5 4 2.1 T1 small no24 59 F LE PE 7.9 7.6 2.1 T1 small no25 53 F RE 12EP 7.7 7 2.1 T1 small no26 70 F RE 9EP 9.6 6.4 2.1 T1 small no27 60 F LE 9PE 8 7.5 2.1 T1 small no28 65 M RE 9EP 8.7 8.9 2.2 T1 small no29 57 F LE 3PE 5 6 2.3 T1 small no30 54 F RE 11EP 7.7 6.8 2.4 T1 small no31 87 F RE 2EA 9 7.8 2.5 T1 small no32 56 F LE 3EP 8.5 6.2 2.5 T1 small no33 43 M LE 5CB 7 6.2 2.6 T2 medium no34 69 M LE 6EP 16 13.4 2.7 T2 medium no35 75 F LE 3EP 12 10.8 2.8 T2 medium no36 48 M RE 6EP 8 8 2.9 T2 medium no37 76 M LE 2EP 10 9.4 2.9 T2 medium no38 72 M RE 11PE 7.1 6.4 3 T2 medium no39 73 M RE 9EA 11 7 3 T2 medium no40 66 F RE 7EP 9.3 8.1 3.4 T2 medium no41 67 M LE 2EP 13.8 12.4 3.7 T2 medium no42 82 M RE 6EP 11.8 11 4.1 T2 medium no43 76 F LE 3EP 14.1 14 4.2 T2 medium no44 48 M LE 3E 13.8 11.2 4.3 T2 medium no45 51 M LE 430EP 11.8 8.3 4.8 T2 medium no46 48 M LE 6E 13.7 11.3 6.3 T2 medium no47 39 F LE 2EP 15.4 14.8 7.7 T2 medium no48 46 M LE 11PE 12.1 10.1 8.3 T2 medium no49 46 F RE 5CB 16 14 11.1 T3 large no50 48 F LE 11E 14.5 12.2 13.7 T3 large no
E, equator; P, posterior; A, anterior; I, iris; CB, ciliary body; AJCC, American Joint Cancer Committee; COMS, Collaborative Ocular Melanoma Study.
1266 Reddy, Kurli, Tena, et al
www.bjophthalmol.com

The analysis of PET/CT scans showed tumour uptake in 14(28%) patients. There were seven males, seven females, andtheir mean age was 70 years (range 54–95). The mean widthof the lesions identified by PET/CT, excluding the ringmelanoma, was 14.7 mm (range 5.9–19), the mean lengthwas 13.2 mm (range 3–19.1), and the mean height was8.1 mm (range 2.9–14). The PET/CT detected none of theAmerican Joint Committee on Cancer (AJCC) T1 stagedmelanomas (table 2). The PET/CT detected 33% of the AJCCT2 tumours and 75% of the AJCC T3 tumours. No smallchoroidal tumours (fig 1) as classified by COMS weredetected by PET/CT (table 2). Thirty three per cent of mediumsized melanomas (fig 2) and 75% of large tumour (fig 3) PET/CT scans showed tumour uptake (figs 4 and 5). The smallesttumour detected by PET/CT imaging was 365.9 mm in baseand 2.9 mm in height.
DISCUSSIONWith the introduction of positron emission tomography inthe 1960s, and its growing importance in clinical practicewithin the past decade, various studies addressed thequestion whether PET imaging can be used to diagnose and
stage malignant choroidal melanomas. A prospective studyby Spraul et al concluded that FDG-PET alone was not asensitive procedure for the diagnosis of choroidal melanomassince only two out of their four cases were visualised.9
Similarly, PET alone detected three of 12 uveal melanomasin one study and another reported only seven of 20.10 11
However, in the past few years, the PET/CT fusion scannersare helping bring molecular imaging to the forefront ofcancer diagnosis.12 A modern PET/CT scanner combines themetabolic/physiological findings of PET with the anatomiclocalisation/characterisation of CT.PET/CT increases the accuracy and confidence in judging
whether a tumour is malignant.13 This has been shown forcolorectal cancer as well as primary head and neckmalignancies.14 15 In addition, PET/CT has eliminated theneed for a full dose diagnostic CT to correlate inconclusivefindings demonstrated by PET alone.15 In addition, examina-tion times have been reduced by 30% (compared toconventional PET imaging) because PET attenuation correc-tion can now be based on the CT data. This eliminates theneed for separate transmission scanning.15 Compared withPET alone, PET/CT is also superior because it anatomically
Figure 1 Patient 20. PET/CT image ofa patient with an AJCC-T1 (COMSsmall) 9.169.562 mm choroidalmelanoma (arrow at tumour location).No FDG uptake was detected on PETand CT could not visualise the smalltumour in the right eye.
Table 2 PET/CT detection of uveal melanoma (AJCC/COMS classification)
Tumour size(AJCC/COMS)
Total numberof patients
Number of patientsdetected (AJCC)
Number of patientsdetected (COMS)
T1/small 18 0 (0%) 0 (0%)T2/medium 24 8 (33%) 8 (33%)T3/large 8 6 (75%) 6 (75%)
PET/CT in detection of choroidal melanoma 1267
www.bjophthalmol.com

Figure 2 Patient 6. An AJCC–T2(COMS medium) 13.861467.3 mmchoroidal melanoma was detected onPET/CT imaging in the right eye(arrow). There was increased FDGuptake and CT localised the uvealtumour.
Figure 3 Patient 9. PET/CT imagingdetected an AJCC–T3 (COMS large)14616611.5 mm choroidal melanoma(COMS/AJCC) in the left eye (arrow).
1268 Reddy, Kurli, Tena, et al
www.bjophthalmol.com

locates the melanoma and thereby increases the confidencethat it is the tumour that is being characterised by FDGuptake.In our study, neither AJCC-T1 uveal tumours nor small
COMS choroidal melanomas were identified by PET/CT.Therefore, it is unlikely that PET/CT can be used todifferentiate between small choroidal melanomas and suspi-cious choroidal naevi (at this time). Furthermore, 63% of T2tumours and 69% of small choroidal tumours (that wentundetected) were larger than the 4 mm resolution of ourscanner. This suggests that high metabolic activity wasintegral to making a tumour identifiable. PET/CT was mosteffective in detecting the physiological activity of AJCC-T3and large choroidal melanomas. Age, sex, or tumour locationdid not appear to affect SUV value.This study did not examine if the metabolic activity
revealed by PET/CT correlated with tumour metastasis. Thisstudy did not find PET/CT to be a more accurate method todiagnose intraocular choroidal melanoma (compared tostandard clinical evaluations). This study clearly demon-strated that current FDG-PET/CT technology can revealmetabolic activity of choroidal melanomas, that there appearsto be significant variability among melanomas of differentsizes, and that further research will define the role of PET/CTin ophthalmic oncology.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
S Reddy, M Kurli, L B Tena, P T Finger, The New York Eye CancerCenter, New York, NY, USAM Kurli, L B Tena, P T Finger, The New York Eye and Ear Infirmary, NewYork, NY, USAS Reddy, P T Finger, New York University School of Medicine, NewYork, NY, USAL B Tena, P T Finger, The Saint Vincent’s Comprehensive Cancer Center,New York, NY, USAL B Tena, New York Medical College, New York, NY, USA
This research was supported by The EyeCare Foundation, Inc, andResearch to Prevent Blindness, New York, NY, USA
Competing interests: none declared
Correspondence to: Paul T Finger, MD, FACS, The New York EyeCancer Center, 115 East 61st Street, New York City, NY 10021, USA;[email protected]
Accepted for publication 1 March 2005
REFERENCES1 Egan KM, Seddon JM, Glynn RJ, et al. Epidemiological aspects of uveal
melanoma. Surv Ophthalmol 1988;32:239–51.2 Collaborative Ocular Melanoma Study Group. Accuracy of diagnosis of
choroidal melanomas in the Collaborative Ocular Melanoma study. ArchOphthalmol 1990;108:1268–73.
3 Diener West M, Reynolds SM, Agugliaro DJ, et al. Screening for metastasisfrom choroidal melanoma: the Collaborative Ocular Melanoma Study GroupReport 23. J Clin Oncol 22:2438–44.
4 Elner VM, Flint A, Vine AK. Histopathology of documented growth in smallmelanocytic choroidal tumors. Arch Ophthalmol 2004;122:1876–8.
5 Eskelin S, Pyrhonen S, Summanen P, et al. Tumor doubling times in metastaticmalignant melanoma of the uvea. Tumor progression before and aftertreatment. Ophthalmology 2000;107:1443–9.
6 Eskelin S, Kivela T. Uveal melanoma: implications of tumor doubling time.Ophthalmology 2001;108:830–1.
7 Finger PT. Radiation therapy for choroidal melanoma. Surv Ophthalmol1997;42:215–232.
8 Townsend D, Carney J, Yap J, et al. PET/CT today and tomorrow. J Nucl Med2004;45(Supp 1):4S1–14S.
9 Spraul CW, Lang GE, Lang GK. Value of positron emission tomography in thediagnosis of malignant ocular tumors. Ophthalmologica 2001;215:163–8.
10 Lucignani G, Paganelli G, Modorati G, et al. MRI, antibody-guidedscintigraphy, and glucose metabolism in uveal melanoma. J Comp AssTomogr 1992;16:77–83.
11 Modorati G, Lucignani G, Landoni C. Glucose metabolism and pathologicalfindings in uveal melanoma: preliminary results. Nucl Med Comm1996;17:1052–6.
12 Beyer T, Townsend DW, Brun T, et al. A combined PET/CT scanner for clinicaloncology. J Nucl Med 2000;41:1369–79.
13 Cohade C, Osman M, Leal J, et al. Direct comparison of 18F-FDG PET andPET/CT in patients with colorectal carcinoma. J Nucl Med2003;44:1797–803.
14 Goerres G, Schulthess G, Steinert H. Why most PET of lung and head-andneck cancer will be PET/CT. J Nucl Med 2004;45(Suppl 1):66S–71S.
15 Von Schilthess GK. Cost consideration regarding an integrated CT-PETsystem. Eur Radiol 2000;10(suppl 3):S377–S380.
100
10
151494745434139373533312927252321191715139753 11
Patients
Tum
our s
ize
(siz
e in
mm
)AJCC T3/COMS large
AJCC T2/COMS medium
AJCC T1/COMS small
75%
33%
0%
25%
67%
100%
Tumours detected Tumours not detected
1
Figure 4 PET/CT detection of ocular melanoma.
10 000
1000
10
100
151494745434139373533312927252321191715139753 11
Patients
87.5%12.5%
12%
71.4% 28.5%
88%
Tumours detected
Tum
our v
olum
e (m
m c
ubed
)
Tumours not detected
1
Figure 5 PET/CT detection of ocular melanoma.
PET/CT in detection of choroidal melanoma 1269
www.bjophthalmol.com

SCIENTIFIC REPORT
Whole body PET/CT for initial staging of choroidalmelanomaP T Finger, M Kurli, S Reddy, L B Tena, A C Pavlick. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1270–1274. doi: 10.1136/bjo.2005.069823
Aim: To investigate the value of whole body positronemission tomography/computed tomography (PET/CT) inscreening for metastatic choroidal melanoma in patientsinitially diagnosed with choroidal melanoma.Methods: 52 patients with choroidal melanoma underwentwhole body PET/CT as part of their metastatic investigation.PET/CT scans were used as a screening tool at the time oftheir initial diagnosis. A physical examination, liver functiontests, and a baseline chest x ray were also obtained. PET/CTimages (utilising intravenous18-fluoro-2-deoxyglucose(FDG)) were studied for the presence of metastatic mela-noma. The standards for reference were further imagingand/or subsequent biopsies.Results: Two of 52 (3.8%) patients were found to havemetastatic melanoma before treatment. The most commonsites for metastases were the liver (100%), bone (50%), andlymph nodes (50%). Brain involvement was also present inone patient. One patient (50%) had involvement of multiplesites. Haematological liver enzyme assays were normal inboth patients. PET/CT showed false positive results in threepatients (5.7%) when further evaluated by histopathologyand/or additional imaging. In seven patients (13.4%) PET/CT imaging detected benign lesions in the bone, lung, lymphnodes, colon, and rectum.Conclusion: PET/CT imaging can be used as a screening toolfor the detection and localisation of metastatic choroidalmelanoma. Liver enzyme assays did not identify livermetastases, while PET/CT revealed both hepatic andextrahepatic metastatic melanoma. PET/CT imaging mayimprove upon the conventional methods of screening fordetection of metastatic disease in patients initially diagnosedwith choroidal melanoma.
Metastatic disease influences patient management;therefore, depending on the primary tumour, variousscreening procedures are recommended.1–6 Choroidal
melanoma metastases are most commonly found in the liver,therefore the COMS (Collaborative Ocular Melanoma Study)Group suggested baseline and periodic subsequent examina-tions (physical examination, liver function tests, and radio-graphic imaging of the chest).1–3 Abnormal elevated liverenzyme assays would prompt a subsequent MRI (magneticresonance imaging) or CT (computed tomography) abdom-inal scans and biopsy for histopathological evaluation.3
Others have recommended liver ultrasonography as a screen-ing test.4 However, recent reports have shown that liverultrasonography, chest radiographs, and liver function testshave high specificity but low sensitivity in the diagnosis ofmetastatic uveal melanoma.5 6 Clearly, baseline and regularscreening is warranted given the probability of micrometas-tases (at the time of diagnosis) and the current availability of
treatments (both standard and experimental) for metastaticdisease.7–11
Whole body PET/CT imaging is gaining worldwide accep-tance in the initial staging, screening, and management ofpatients with cancer.12–18 It combines the anatomic character-istics found on CT with the functional metabolic aspectsrevealed by PET. We have evaluated the role of whole body18-fluoro-2-deoxyglucose (FDG) PET/CT (positron emissiontomography/computed tomography) imaging in the initialstaging of patients diagnosed with choroidal melanoma.
MATERIALS AND METHODSSince August 2003, 52 untreated patients with choroidalmelanoma were referred for whole body PET/CT to screen formetastatic disease (table 1). Standard radiology relatedinformed consents were obtained from all patients beforePET/CT imaging as PET/CT has been approved for the stagingof malignant melanoma. A physical examination, liverfunction tests (c-glutamyl transpeptidase, aspartate amino-transferase, alanine aminotransferase, alkaline phosphatase,lactate dehydrogenase, bilirubin), and a chest x ray were alsoobtained.Patients underwent subsequent CT or MRI (with contrast)
and fine needle aspiration biopsy if abnormalities were notedon the PET/CT scan. The subsequent imaging studies wererequired to aid in performing a biopsy of the lesions detectedby PET/CT scans (for histopathological confirmation of thediagnosis).
PET/CT imagingPatients were instructed to refrain from eating a carbohy-drate based dinner the previous night and to fast 4–6 hoursbefore injection of 18-fluoro-2-deoxyglucose (FDG). Thesemeasures diminish physiological glucose utilisation andreduce insulin serum levels to baseline. The full body PET/CT scan began at the top of the head and ended at the bottomof the feet.The CT portion (General Electric Discovery ST, Piscataway,
NJ with BGO (bismuth germanate) crystal) consisted of amulti-detector helical CT scanner. The FDG was injected viaan intravenous line followed by 10 ml normal saline.The resolution of the PET scan was 4 mm. The PET scan
reconstructed the images and utilised the CT scan to correctfor attenuation. Then Xeleris workstation (General Electricsoftware, Piscataway, NJ, USA) was used to fuse and displaythe PET and CT images and to produce the final image (fig 1).
PET/CT image evaluationThe PET/CT images were studied for the presence of lymphnode and distant metastases and were based on qualitative
Abbreviations: AJCC, American Joint Cancer Committee Classification;BGO, bismuth germanate; COMS, Collaborative Ocular MelanomaStudy; CT, computed tomography; FDG, 18-fluoro-2-deoxyglucose;MRI, magnetic resonance imaging; PET, positron emission tomography;SUV, standardised uptake values
1270
www.bjophthalmol.com

and quantitative analysis. Data were evaluated for areas offocally increased glucose uptake and by maximally standar-dised uptake values (SUV). Glucose uptake above levels ofthe surrounding tissue qualitatively and an uptake valueabove 2.5 SUV quantitatively indicated malignancy. Distantmetastases were determined on an organ to organ basis.
RESULTSFifty two patients (24 males and 28 females) with a mean ageof 64 years (range 39–95) with a diagnosis of choroidalmelanoma (24 RE and 28 LE) were referred for a whole body
PET/CT scan (table 1). There were 13 anterior and 39posterior tumours. There were 16 T1 (30.8%), 28 T2(53.9%), and eight T3 (15.4%) tumours within the AJCC(American Joint Cancer Committee) classification. Using theCOMS (Collaborative Ocular Melanoma Study) Groupclassification, there were 16 small (30.8%), 28 medium(53.9%), and eight large (15.4%) tumours.Two patients (3.8%) were found on PET/CT imaging to
have distant metastatic disease (table 2). The mean age of thepatients was 80 years. One patient had a ring melanoma.Both tumours were classified as T3 (AJCC) and as large(COMS) tumours.
Table 1 Whole body PET/CT in initial staging of choroidal melanoma: results of PET/CT scans
PatientNo Age Sex Eye
Tumourlocation
Tumour size
LFT
Detection of tumour on PET/CT scan
AJCC COMS Liver Lung Breast OsseousLymphnode Subcutaneous Brain Rectum Colon Thyroid
Patients with metastatic disease1 65 M LE 730EA T3 large n + n n n n n n n n n2 95 M LE ring
melanomaT3 large n + n n + + n + n n n
Patients detected with other primary tumours3 65 F RE 1E T2 medium n n n + n n n n n n n4 48 M LE 3E T2 medium n n + n + + n n n n nPatients with false positive lesions on PET/CT5 54 F RE 11EP T1 small n n n n n + n n n n +6 69 M LE 6EP T2 medium n + n n n n n n n n n7 82 M RE 6EP T2 medium n n n n n + n n n n nPatients with negative PET/CT scans8 90 F LE 5PE T1 small n n n n n n n n n n n9 60 F RE 3CB T1 small n n n n n n n n n n n10 55 F RE 2PE T1 small n n n n n n n n n n n11 59 F LE 9PE T1 small n n n n n n n n n n n12 53 F RE 12EP T1 small n n n n n n n n n n n13 46 F RE 430E T1 small n n n n n n n n n n n14 53 F RE 430EP T1 small n n n n n n n n n n n15 65 M RE 9EP T1 small n n n n n n n n n n n16 57 F LE 3PE T1 small n n n n n n n n n n n17 67 F RE 2EP T1 small n n n n n n n n n n n18 72 M RE 5PE T1 small n n n n n n n n n n n19 70 F RE 9EP T1 small n n n n n n n n n n n20 66 M LE 1PE T1 small n n n n n n n n n n n21 60 F LE 9PE T1 small n n n n n n n n n n n22 59 F RE 7PE T1 small n n n n n n n n n n n23 43 M LE 5CB T2 medium n n n n n n n n n n n24 72 M RE 11PE T2 medium n n n n n n n n n n n25 69 M LE 9EA T2 medium n n n n n n n n n n n26* 87 F RE 2EA T2 medium n n n n n + n n n n n27 83 F LE 12EA T2 medium n n n n n n n n n n n28* 76 F LE 3EP T2 medium n n n n + n n n n n n29 46 M LE 11EA T2 medium n n n n n n n n n n n30 56 F LE 3EP T2 medium n n n n n n n n n n n31* 73 M RE 9EA T2 medium n n + n n n n n n n n32 48 M LE 6E T2 medium n n n n n n n n n n n33 66 F RE 7EP T2 medium n n n n n n n n n n n34 39 F LE 2EP T2 medium n n n n n n n n n n n35 69 F LE 11P T2 medium n n n n n n n n n n n36* 54 F RE 6P T2 medium n n n n + n n n n n n37 70 M LE 9EP T2 medium n n n n n n n n n n n38 48 M RE 6EP T2 medium n n n n n n n n n n n39 75 F LE 3EP T2 medium n n n n n n n n n n n40 76 M LE 2EP T2 medium n n n n n n n n n n n41* 67 M LE 2EP T2 medium n n n n n n n n + n n42 51 M LE 430EP T2 medium n n n n n n n n n n n43 69 M RE 12PE T2 medium n n n n n n n n n n n44 74 M RE 4I T2 medium n n n n n n n n n n n45 50 M LE 3E T2 medium n n n n n n n n n n n46 85 M RE 3EP T2 medium n n n n n n n n n n n47 60 F LE 230CB T3 large n n n n n n n n n n n48 48 F LE 11E T3 large n n n n n n n n n n n49* 57 M LE 6EP T3 large n n n n n n n n n n n50* 46 F RE 5CB T3 large n n n n n n n n n + n51 88 F LE 2EA T3 large n n n n n n n n n n n52* 67 F RE 9E T3 large n n + n n n n n n n n
E, equator; P, posterior; A, anterior; I, iris; CB, ciliary body; AJCC, American Joint Cancer Committee Classification; COMS, Collaborative Ocular MelanomaStudy; LFT, liver function tests; n, normal.*Benign lesions.
Whole body PET/CT for initial staging of choroidal melanoma 1271
www.bjophthalmol.com

Metastases were detected in the liver, bone, lymph nodes,and the brain (table 1). One patient (50%) was found to havemetastases in more than one site. Hepatic metastases weredetected in both patients ((100%) (figs 1 and 2)), bone in one((50%) (fig 3)), lymph nodes in one (50%), and braininvolvement in one (50%).Both patients with hepatic metastases had normal liver
enzyme assays and were found to have liver tumours on PET/CT. Liver biopsies confirmed the diagnosis and they werereferred to our medical oncologist (ACP) for further manage-ment.Two other patients were found to have small lung (n=1)
and breast tumours (n=1) on whole body PET/CT imaging.Histopathological evaluations revealed these tumours to besynchronous primaries and not metastatic melanoma. Theselesions were not detected on a previous chest x ray ormammogram.PET/CT imaging also detected inflammatory and other
benign lesions in seven (13.4%) of our patients. Benignlesions such as old fractures (n=2), benign pulmonarynodules (n=2), inflamed lymph nodes (n=1), lesions of thecolon (n=1) and rectum (n=1) were detected. PET/CTimaging was effective in differentiating these lesions frommalignancy by determining the glucose uptake in theselesions compared to the surrounding tissues and byquantitatively comparing them by standardised uptakevalues (SUV). PET/CT imaging also detected false positive
lesions in three patients (6%). But quantitative analysis(SUV) of these lesions, subsequent biopsies, and/or addi-tional radiographic imaging (CT/MRI) helped interpret thebenign nature of these lesions.
DISCUSSIONPET/CT imaging has been used in the diagnosis, staging, andrestaging of various cancers.12–18 The combination of meta-bolic and structural information provided by the PET and CTportions, respectively, has improved the accuracy of tumourstaging, detection of recurrences, and has an enormousimpact on patient management.12–18 Currently, clinical studiesmost commonly use FDG as the radioactive tracer in PET/CTimaging. Newer radiopharmaceuticals have been found to beuseful in the management of cancers (table 3). New tracersmay allow quantification of cellular processes (such ashypoxia and apoptosis) and enable identification of tumoursthat may respond to certain targeted therapies (for example,radiotherapy).15
PET/CT has been compared to PET imaging alone andwhole body MRI imaging in the staging of malignancies.14 15
Cohade and colleagues compared the use of PET/CT and PETin patients with colorectal carcinoma.14 There was poorvisualisation of normal organs and tissues on PET scansmaking lesion localisation suboptimal and there was asignificant increase in the certainty of lesion localisationand characterisation with PET/CT and was valuable in
Table 2 Metastatic disease detected at pretreatment evaluations
Author Year Tests usedMetastaticrate (%)
Wagoner19 1982 LFTs, liver spleen scan 2.47Pach20 1986 LFTs, CXR, liver scan or CT abdomen 2.2COMS6 2004 LFTs, CXR* ,1This study 2005 PET/CT 3.8
LFTs, liver function tests; CXR, chest x ray; CT, computed tomography; COMS, collaborative ocular melanomastudy.*Further imaging (CT/MRI) done if liver enzyme assays abnormal.
Figure 1 Patient 1. PET/CT fusedcoronal images demonstrate multipleareas of high SUV FDG uptake in theliver that correspond to low attenuationlesions seen on the transmission CTscan. These lesions were compatiblewith metastasis (arrow).
1272 Finger, Kurli, Reddy, et al
www.bjophthalmol.com

determining biopsy areas. The number of definite benign ormalignant lesions was increased by PET/CT as it enableddetermination between physiological variants and trueabnormalities.Whole body PET/CT imaging has also been compared with
whole body MRI for tumour staging.15 Both imagingprocedures showed a similar performance in detecting distant
metastases in 98 oncology patients, but superior performanceof PET/CT in overall TNM staging was established. This studysuggested the use of PET/CT as a first line modality for wholebody tumour staging.Even-Sapir and others found that PET/CT imaging was
both sensitive and specific for the detection of lytic andsclerotic malignant lesions.16 It accurately differentiatedmalignant and benign bone lesions. We found that PET/CTimaging was valuable in the detection of bone metastases inour patients. Benign bone lesions such as old fractures weredistinguishable on PET/CT imaging.Finger and colleagues reported the first use of PET/CT in a
patient with uveal melanoma and multiple hepatic andextrahepatic metastases.17 Also, Freudenberg and othersfound PET/CT imaging to be valuable in the detection ofpreviously undetected hepatic metastasis and staging ofadvanced uveal melanoma.18
Similar to the COMS Group findings that liver functiontests were highly specific but not sensitive for the detection ofhepatic metastases, we found that liver enzymes were notelevated our patients with hepatic metastases.7 The detectionof metastatic disease at the time of diagnosis influencesmanagement of the patient. This is particularly important inpatients with large choroidal melanomas in eyes that are notpainful, where enucleation can be avoided. Specification ofthe site of metastatic disease helps to develop betterstrategies for the evaluation and management of patients asPET/CT imaging can directly guide biopsies or other surgicalinterventions.Though the whole body PET/CT examination is (in itself)
expensive, discovering occult metastatic foci can be costeffective. The detection of extrahepatic tumours (as seen inour patients) may decrease the use of chemotherapyperfusions of the liver and surgical hepatic resections (bothmore expensive than PET/CT).We currently recommend whole body PET/CT as an
imaging tool for initial staging at the time of diagnosis. Itappears to be more sensitive than liver function tests and isespecially useful in the detection of extrahepatic tumours.Though a prospective randomised or comparative study
would be required to establish a statistical proof of therelative efficacy of whole body PET/CT imaging versus otherimaging modalities (for the detection of metastatic uvealmelanoma), this study suggests that PET/CT can be used forstaging of uveal melanoma.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
P T Finger, M Kurli, S Reddy, L B Tena, A C Pavlick, The New York EyeCancer Center, New York City, NY, USAP T Finger, L B Tena, The Saint Vincent’s Comprehensive Cancer Center,New York City, NY, USA
Figure 2 Patient 2. Abnormal PET/CT fused transaxial scansdemonstrate diffuse metastatic lesions involving the liver.
Table 3 Newer radiopharmaceuticals in PET/CTimaging
Newer radiopharmaceuticalsin PET/CT Cancer
18f-39-fluoro-39deoxy-L-thymidine (FLT) LungBreastRestaging of metastaticmelanoma
11C-choline Prostate11C-acetate ProstateIodine 124 Thyroid11C-metomidate Adrenal tumours11C-5-hydroxy-L-tryptophan(11C-5-HTP)
Neuroendocrine tumours
Whole body PET/CT for initial staging of choroidal melanoma 1273
www.bjophthalmol.com

P T Finger, M Kurli, L B Tena, The New York Eye and Ear Infirmary, NewYork City, NY, USAP T Finger, S Reddy, A C Pavlick, New York University School ofMedicine, New York City, NY, USAL B Tena, New York Medical College, New York City, NY, USA
Supported by The EyeCare Foundation, Inc, and Research to PreventBlindness, New York City, New York, NY, USA
Competing interests: none declared
Correspondence to: Paul T Finger, MD, The New York Eye CancerCenter, 115 East 61st Street, New York, NY 10021, USA; [email protected]
Accepted for publication 20 April 2005
REFERENCES1 Folberg R. Tumor progression in ocular melanoma. J Invest Dermatol
1993;100:326–31.2 Einhorn LH, Burgess MA, Gottlieb JA. Metastatic patterns of choroidal
melanoma. Cancer 1974;34:1001–4.3 Collaborative Ocular Melanoma Study Group. COMS manual of procedures.
Springfield, VA: National Technical Information Service, 1995. Accession NoPB95179693.
4 Eskelin S, Pyrhonen S, Summanen P, et al. Screening for metastatic malignantmelanoma of the uvea revisited. Cancer 1999;85:1151–9.
5 Hicks C, Foss AJE, Hungerford JL. Predictive power of screening tests formetastasis in uveal melanoma. Eye 1998;12:945–8.
6 Diener-West M, Reynolds SM, Agugliaro DJ, et al. Screening for metastasisfrom choroidal melanoma: The Collaborative Ocular Melanoma Study GroupReport 23. J Clin Oncol 2004;22:2438–44.
7 Albert DM, Ryan LM, Borden EC. Metastatic ocular and cutaneous melanoma:a comparison of patient characteristics and prognosis. Arch Ophthalmol1996;114:107–8.
8 Gragoudas ES, Egan KM, Seddon JM, et al. Survival of patients withmetastases from uveal melanoma. Ophthalmology 1991;98:383–90.
9 Collaborative Ocular Melanoma Study Group. Assessment of metastaticdisease at death in 435 patients with large choroidal melanoma in theCollaborative Ocular Melanoma Study (COMS). Arch Ophthalmol2001;119:670–6.
10 Leyvraz S, Spataro V, Bauer J, et al. Treatment of ocular melanomametastatic to the liver by hepatic arterial chemotherapy. J Clin Oncol1997;15:2589–95.
11 Nathan FE, Berd D, Sato T, et al. BOLD + interferon in the treatment ofmetastatic uveal melanoma: first report of active systemic therapy. J Exp ClinCancer Res 1997;16:201–8.
12 Schoder H, Larson SM, Yeung HWD. PET/CT in oncology: integration intoclinical management of lymphoma, melanoma and gastrointestinalmalignancies. J Nucl Med 2004;45:72S–81S.
13 Lardinois D, Weber W, Hany TF, et al. Staging of non-small cell cancer withintegrated positron emission tomography and computed tomography. J Med2003;348:2500–7.
14 Cohade C, Osman M, Leal J, et al. Direct comparison of 18F-FDG-PET andPET/CT in patients with colorectal carcinoma. J Nucl Med2003;44:1797–803.
15 Antoch G, Vogt FM, Freudenberg LS, et al.Whole body dual modality PET/CTand whole body MRI for tumor staging in oncology. JAMA2003;290:3199–206.
16 Even-Sapir E, Metser U, Flusser G, et al. Assessment of malignant skeletaldisease: initial experience with 18F-fluoride PET/CT and comparison between18F-fluoride PET and 18F-fluoride PET/CT. J Nucl Med 2004;45:272–8.
17 Finger PT, Kurli M, Wesley P, et al.Whole body PET/CT imaging for detectionof metastatic choroidal melanoma. Br J Ophthalmol 2004;88:1095–7.
18 Freudenberg LS, Schueler AO, Beyer T, et al. Whole body fluorine-18fluorodeoxyglucose positron emission tomography/computed tomography(FDG-PET/CT) in staging of advanced uveal melanoma. Surv Ophthalmol2004;49:537–40.
19 Wagoner MD, Albert DM. The incidence of metastases from untreated ciliarybody and choroidal melanoma. Arch Ophthalmol 1982;100:939–40.
20 Pach JM, Robertson DM. Metastasis from untreated uveal melanomas. ArchOphthalmol 1986;104:1624–5.
Figure 3 Patient 2. PET/CT fusedsagittal images demonstrate high SUVmetastatic melanoma in multiplevertebrae (arrows).
1274 Finger, Kurli, Reddy, et al
www.bjophthalmol.com

SCIENTIFIC REPORT
Infantile infection and diabetes insipidus in children withoptic nerve hypoplasiaS P Donahue, A Lavina, J Najjar. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1275–1277. doi: 10.1136/bjo.2005.069609
Background: Bilateral optic nerve hypoplasia (BONH) isoften associated with other central nervous system midlineabnormalities (septo-optic dysplasia). Hormonal dysfunction,caused by anterior (cortisol) and posterior (ADH) pituitaryinvolvement, can be sudden, severe, and life threatening.Methods: Case series. Three cases of septo-optic dysplasia(SOD) presenting as infantile infection with associateddiabetes insipidus are reported. The diagnosis of SOD wassuspected only after ophthalmological evaluation; furtherevaluation led to the diagnosis of panhypopituitarism.Conclusions: A high index of suspicion is required todiagnose SOD in children when the disorder presents withinfantile infection and hypernatraemia. Early warning signsof neonatal jaundice and hypoglycaemia should promptophthalmological evaluation.
Optic nerve hypoplasia (ONH) is a congenital abnorm-ality of the optic nerve characterised by a small opticdisc located within a normal scleral canal. It is often
associated with midline central nervous system anomaliessuch as absence of the septum pellucidum or agenesis of thecorpus callosum, and is then called septo-optic dysplasia (deMorsier’s syndrome). The associated hypothalamic andpituitary dysfunction can produce hypoglycaemia, hypothyr-oidism, growth retardation, diabetes insipidus, and a lack ofglucocorticoid response to stress, which can be life threaten-ing.1 We recently encountered three infants thought to benormal who presented with infantile infection severe enoughto warrant hospitalisation. All developed diabetes insipidus,and were later found to have bilateral ONH. Two had historyof neonatal jaundice and neonatal hypoglycaemia. We believethat undiagnosed pituitary and endocrine dysfunction con-tributed to the severity and morbidity of their infections. Thepresence of jaundice and hypoglycaemia in the neonatalperiod should prompt ophthalmological evaluation.
CASE 1An 11 week old white male was sent to a community hospitalby his grandmother after becoming ‘‘limp’’ and ‘‘floppy’’ andsleeping through his feeds. Gestational history was signifi-cant for recurrent maternal genital herpes, and alcohol,cocaine and marijuana abuse until the seventh month ofpregnancy. The child weighed 6 lb 7 oz (2.92 kg) at birth. Heexperienced hypoglycaemia and jaundice in the neonatalnursery, was treated and released, and appeared normal untilpresentation.Upon presentation, the child’s heart rate was 50 beats/min,
and he was lethargic and hypotonic. His serum sodium was154 mg/dl, and white blood cell (WBC) count was 17 000.Lumbar puncture revealed WBC=14, red blood cells (RBC)=295, protein=156 mg/dl, glucose=36 mg/dl, and a nor-mal gram stain. The child was given a presumptive diagnosis
of viral meningitis (based upon LP results and normalcerebrospinal fluid (CSF) cultures), but was started oncefotaxime (100 mg/kg/day) and aciclovir (30 mg/kg/day).The sodium remained high despite fluid replacement andhypo-osmolar urine output. The child was noted to haveunequal pupils, and a non-contrast head computed tomo-graph (CT) at that institution revealed a hypodense frontallobe irregularity of unclear aetiology.The child was then transferred to our institution, where
hydration was continued and 1-deamino-8-D-arginine vaso-pressin (DDAVP) was begun for central diabetes insipidus.Other laboratory abnormalities included anaemia (HCT 26%),hyperbilirubinaemia (3.7 mg/dl), and several transient epi-sodes of marginal hypoglycaemia (glucose in lower 60 sec-onds). TORCH titres were negative for acute infection.Thyroid hormone and serum cortisol levels were both low:TSH=14.7 mU/ml, FT4=0.5 mU/ml; serum cortisol=1 mg/dl.Brain magnetic resonance imaging (MRI) revealed anelongated and tubular fourth ventricle, absent septumpellucidum, small corpus callosum, small optic nerves andchiasm, interdigitation of the gyri in the frontal lobes, andatrophic basal ganglia. The normal posterior pituitary brightspot was absent.Our evaluation found nystagmus with no aversive response
to bright light. The right pupil was 4 mm and the left was3 mm, each with minimal reaction. Funduscopic examina-tion revealed small, pale optic nerves bilaterally. Followingcontrol of the endocrine problems, the child’s conditionstabilised, and he was sent home on DDAVP, hydrocortisone,and Synthroid.
CASE 2A 5 week old previously healthy girl had a 2 day history ofcough, congestion, and fever. Over 24 hours, she became lessactive and stopped eating. She was admitted to anotherhospital for a septic examination. Pregnancy was complicatedby gestational diabetes but birth was at 35 weeks gestationand she weighed 5 lb 7 oz (2.47 kg). There was no neonataljaundice or hypoglycaemia. The mother denied usingvalproate, nalidixic acid, or LSD.Admission laboratory tests showed a WBC count of 2500
with 9% segmented and 27% banded cells, and a serumsodium of 156 mg/dl with hypotonic urine. Initial lumbarpuncture revealed numerous Gram positive cocci with apositive group B streptococcal antigen. Cultures of blood andspinal fluid yielded group B streptococcus. The child wasplaced on ampicillin and gentamicin. The hospital course wascomplicated by fluctuating sodium levels, which respondedto DDAVP. Serum growth hormone and thyroid hormonewere low, but a cortisol stimulation test was normal.At age 8 months, the patient was evaluated and treated
elsewhere for large angle esotropia. Two years later, following
Abbreviations: ACTH, adrenocorticotrophic hormone; BONH, bilateraloptic nerve hypoplasia; SOD, septo-optic dysplasia
1275
www.bjophthalmol.com

two strabismus surgeries, the child was referred for ophthal-mological examination because of nystagmus and persistentesotropia. Visual acuity was uncentral, unsteady, andunmaintained in both eyes. She had nystagmus andapproximately 35 prism dioptres of esotropia. Both opticnerves were small and hypoplastic. The previous ophthalmol-ogy notes did not mention abnormal optic nerves, and did notindicate a examination for the nystagmus. Outpatient headMRI revealed encephalomalacia, schizencephaly in the righthemisphere, and an absent posterior pituitary bright spot. Adiagnosis of septo-optic dysplasia was made at this time. Shewas treated with replacement therapy for deficiencies ofgrowth hormone, thyroid hormone, and ADH.
CASE 3A 3K month old white male presented to an outside hospitalwith 3 days of cough, congestion, poor oral intake, increasedwork of breathing, and a fever of 102.4 F. He was born at39 weeks gestation to a nulliparous mother. The pregnancywas complicated by severe maternal dehydration secondaryto food poisoning and viral gastroenteritis at 6.5 months and7.5 months gestation respectively. The mother had beentreated with antibiotics before delivery for positive cultures ofgroup b streptococcus. Jaundice and hypoglycaemia occurredin the newborn nursery.Before transfer to our institution, he had been treated for
respiratory syncytial virus (RSV) bronchiolitis, and otitismedia, and had a serum sodium of 155 mg/dl.On admission at our institution, temperature was 100.7 F,
respirations 48/min, and pulse 177/min. Pus was visiblebehind the right tympanic membrane. Nystagmus, unequalpupils, and an exotropia were noted by the admitting service.Sodium reached 162 mg/dl despite intravenous fluid replace-ment.Our examination demonstrated right hemiparesis, right
amaurotic pupil, right gaze palsy, left relative afferentpupillary defect, left gaze paretic nystagmus, left ptosis, andan anisocoria consistent with left Horner’s syndrome. Dilatedfundus examination demonstrated bilateral optic nervehypoplasia. Given these findings and the persistent hyperna-traemia, we suspected septo-optic dysplasia with panhypo-pituitarism, and recommended urgent paediatricendocrinology consult and neuro-imaging.MRI showed hypoplastic optic nerves and optic tracts,
absent septum pellucidum, bilateral schizencephaly, bilateralcortical dysplasia, an attenuated small hypothalamic stalk,and anterior corpus callosum, and absent pituitary brightspot. The brainstem was remarkably normal. Paediatricendocrinology evaluation confirmed central diabetes insipi-dus, hypothyroidism, and low serum cortisol (6.6 mg/dl). Thepatient’s status eventually improved and he was discharged.
DISCUSSIONWe report three infants with previously undiagnosed bilateralONH who presented with infantile infection and hyperna-traemia. Two had neonatal jaundice and hypoglycaemia,which is often a harbinger of bilateral ONH and endocrineanomalies. One patient (case 2) had an intact septumpellucidum, but other abnormalities typically seen withBONH and SOD. In all three cases, the parents had noticedan ocular abnormality in early life. Neuro-imaging foundsignificant midline CNS abnormalities in all three, includingabsence of the normal posterior pituitary bright spot. In onecase, the pituitary images were read as normal until theywere reviewed by us. All three children had SOD diagnosedonly after our ophthalmological evaluation.The relation between bilateral ONH and mid-line CNS
abnormalities has been well documented.2–7 These midlinedefects are believed to be caused by an insult during
prosencephalic development (gestation week 13) whichaffects midline structures including the cerebral hemi-spheres, the hypothalamus, and the pituitary, and producespituitary and hypothalamic abnormalities.8–11 Ectopia orabsence of the posterior pituitary bright spot is a verysensitive MRI indicator of anterior pituitary dysfunction,5 12
and occurred in all three patients. This sign is also a markerfor diabetes insipidus in patients with BONH.In addition to diabetes insipidus, other associated endo-
crine abnormalities in BONH include adrenocorticotrophichormone (ACTH) deficiency,1 2 thyroid stimulating hormonedeficiency, and growth hormone deficiency.4 Cortisol insuffi-ciency often becomes manifest only during periods of stress.Brodsky et al recently reported five children with bilateralONH who experienced sudden death during stress, andpostulated this to be due to an abnormal cortisol response.1
We believe our patients began with mild childhood infectioussymptoms that progressed to meningitis because of insuffi-cient endocrine responses to the stress of the infection. Twoof our patients had abnormal cortisol response duringphysiological testing. Low cortisol levels lead to poorcounter-regulatory systems causing hypoglycaemia and/orlow blood pressure. This, in addition to diabetes insipiduswith resultant dehydration and hypernatraemia, can causesignificant morbidity. Therefore, it is important that evalua-tion of the hypothalamic-pituitary-adrenal axis be performedas part of the endocrine examination for patients diagnosedwith BONH, or those having unilateral ONH but neonataljaundice or hypoglycaemia.Our cases illustrate how the endocrinological abnormalities
seen with OHN can complicate a child’s normal response totypical childhood illnesses. SOD should be in the differentialdiagnosis of any infant with hypotonia, lethargy, or jaundice,who has unexplained hypoglycaemia or hypernatraemia,especially if ocular findings such as nystagmus or poor visualbehaviour are present. Prompt ophthalmological and endo-crine consultation and MRI imaging are mandatory forestablishing the extent of hypothalamic-pituitary axisabnormalities, and minimising morbidity.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
S P Donahue, A Lavina, Department of Ophthalmology and VisualSciences, Vanderbilt University School of Medicine, Nashville, TN, USAS P Donahue, Department of Neurology, Vanderbilt University School ofMedicine, Nashville, TN, USAJ Najjar, S P Donahue, Department of Pediatrics, Vanderbilt UniversitySchool of Medicine, Nashville, TN, USA
Support: In part by an unrestricted grant from Research to PreventBlindness (RPB), New York, NY to the Vanderbilt University Departmentof Ophthalmology. Dr Donahue was the recipient of a CareerDevelopment Award from Research to Prevent (RPB), New York, USA.
Correspondence to: Sean P Donahue, MD, PhD, Department ofOphthalmology and Visual Sciences, Vanderbilt University School ofMedicine, 8000 Medical Center East, Nashville, TN 37232-8808, USA;[email protected]
Accepted for publication 6 June 2005
REFERENCES1 Brodsky MC, Conte FA, Taylor D, et al. Sudden death in septo-optic dysplasia.
Report of 5 cases. Arch Ophthalmol 1997;115:66–70.2 Margalith D, Jan JE, McCormick AQ, et al. clinical spectrum of congenital
optic nerve hypoplasia: review of 51 patients. Develop Med Child Neurol1984;26:311–22.
3 Zeki SM, Hollman AS, Dutton GN. Neuroradiological features of patientswith optic nerve hypoplasia. J Pediart Ophthalmol Strabismus1992;29:107–12.
4 Siatkowski RM, Sanchez JC, Andrade R, et al. The clinical,neuroradiographic, and endocrinologic profile of patients with bilateral opticnerve hypoplasia. Ophthalmology 1997;104:493–6.
1276 Donahue, Lavina, Najjar
www.bjophthalmol.com

5 Brodsky MC, Glasier CM. Optic nerve hypoplasia: clinicalsignificance of associated central nervous system abnormalitieson magnetic resonance imaging. Arch Ophthalmol 1993;111:66–74.
6 Brodsky MC, Glasier CM, Pollock SC, et al. Optic nerve hypoplasia:identification by magnetic resonance imaging. Arch Ophthalmol1990;108:1562–7.
7 Brodsky MC. Optic nerve hypoplasia with posterior pituitary ectopia: malepredominance and non-association with breech delivery. Am J Ophthalmol1999;127:238–9.
8 Costin G, Murphree AL. Hypothalamic-pituitary function in children with opticnerve hypoplasia. AJDC 1985;139:249–54.
9 Margalith D, Tze WJ, Jan JE. Congenital optic nerve hypoplasia withhypothalamic-pituitary dysplasia: a review of 16 cases. AJDC1985;139:361–6.
10 Leaf AA, Ross RJM, Jones RB, et al. Response to growth hormone-releasinghormone as evidence of hypothalamic defect in optic nerve hypoplasia. ActaPediatr Scand 1989;78:436–9.
11 Sorkin JA, Davis PC, Meacham LR, et al. Optic nerve hypoplasia: absence ofposterior pituitary bright signal on magnetic resonance imaging correlateswith diabetes insipidus. Am J Ophthalmol 1996;122:717–23.
12 Phillips PH, Spear C, Brodsky MC. Magnetic resonance diagnosis ofcongenital hypopituitarism in children with optic nerve hypoplasia. J AAPOS2001;5:275–80.
Clinical Evidence—Call for contributors
Clinical Evidence is a regularly updated evidence-based journal available worldwide both asa paper version and on the internet. Clinical Evidence needs to recruit a number of newcontributors. Contributors are healthcare professionals or epidemiologists with experience inevidence-based medicine and the ability to write in a concise and structured way.
Areas for which we are currently seeking authors:
N Child health: nocturnal enuresis
N Eye disorders: bacterial conjunctivitis
N Male health: prostate cancer (metastatic)
N Women’s health: pre-menstrual syndrome; pyelonephritis in non-pregnant women
However, we are always looking for others, so do not let this list discourage you.
Being a contributor involves:
N Selecting from a validated, screened search (performed by in-house InformationSpecialists) epidemiologically sound studies for inclusion.
N Documenting your decisions about which studies to include on an inclusion and exclusionform, which we keep on file.
N Writing the text to a highly structured template (about 1500–3000 words), using evidencefrom the final studies chosen, within 8–10 weeks of receiving the literature search.
N Working with Clinical Evidence editors to ensure that the final text meets epidemiologicaland style standards.
N Updating the text every six months using any new, sound evidence that becomes available.The Clinical Evidence in-house team will conduct the searches for contributors; your task issimply to filter out high quality studies and incorporate them in the existing text.
N To expand the topic to include a new question about once every 12–18 months.
If you would like to become a contributor for Clinical Evidence or require more informationabout what this involves please send your contact details and a copy of your CV, clearlystating the clinical area you are interested in, to Klara Brunnhuber ([email protected]).
Call for peer reviewers
Clinical Evidence also needs to recruit a number of new peer reviewers specifically with aninterest in the clinical areas stated above, and also others related to general practice. Peerreviewers are healthcare professionals or epidemiologists with experience in evidence-basedmedicine. As a peer reviewer you would be asked for your views on the clinical relevance,validity, and accessibility of specific topics within the journal, and their usefulness to theintended audience (international generalists and healthcare professionals, possibly withlimited statistical knowledge). Topics are usually 1500–3000 words in length and we wouldask you to review between 2–5 topics per year. The peer review process takes placethroughout the year, and our turnaround time for each review is ideally 10–14 days.
If you are interested in becoming a peer reviewer for Clinical Evidence, pleasecomplete the peer review questionnaire at www.clinicalevidence.com or contact KlaraBrunnhuber ([email protected]).
ONH and diabetes insipidus 1277
www.bjophthalmol.com

SCIENTIFIC REPORT
Social and visual function in nystagmusR F Pilling, J R Thompson, I Gottlob. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1278–1281. doi: 10.1136/bjo.2005.070045
Aim: To investigate the influence of nystagmus on visual andsocial function and determine if parents are able to assessvisual and social function in children with nystagmus.Method: A postal questionnaire comprising 14 questionsrelated to visual function (VF-14) and questions pertaining tosocial function were sent to all 1013 members of theNystagmus Network—a UK based organisation for nystag-mus sufferers and their families. Visual and social functionscores were compared by regression analysis.Results: 180 adult, 233 parent, and 124 child question-naires were returned. Idiopathic nystagmus was the mostcommon cause. In adults the mean VF-14 score indicatedvery low visual function, in the same range as patientsassessed in low vision services. Children’s visual functionscored better than adults, between scores of patients with agerelated macular disease and corneal grafts. There was astrong correlation between perceived visual and socialfunction for adults (p,0.001) and parental assessment oftheir children (p,0.001), but not between child selfassessment of visual and social function. There was strongcorrelation between parental and child assessment of visualand social function (p,0.001, p,0.001)Conclusion: Questionnaires indicated that nystagmus isassociated with very low visual function. There is a strongcorrelation between visual and social impairment. Theauthors have shown for the first time in an ophthalmicdisease that parents are able to estimate the impact ofnystagmus on their child both in terms of visual and socialfunctioning, although they underestimate the impact ofnystagmus on emotional aspects of wellbeing.
Nystagmus often occurs in early childhood and can beidiopathic, associated with albinism, ocular, or neu-rological diseases. The prevalence of infantile nystag-
mus is one in 1000–6000.1 2 The impact of nystagmus onvisual function (VF; ability to perform activities of daily life)and social function (SF; self perception of wellbeing,interaction with and contribution to society) is unknown.Functional impairment in ocular disease can be explored
with questionnaires. The VF-14 is a valid, reliable tool formeasuring visual impairment. It was designed for patientswith cataract3 and has been used for other visual diseases.4–8
VF is variably affected depending on the eye disease.Experienced difficulties have found to be contrast and neartasks in cataract,3 sport in myopia,4 and fine details anddriving in macular degeneration.5
Disease specific tools3 9–13 have been developed. Thesequestionnaires contain items of little relevance for patientswith nystagmus who have, in addition to visual impairmentfrom unusual eye movements, abnormal head movementsand/or oscillopsia. Factors associated with quality of life invisual impairment include worry, independence, concernsabout the future, social relationships, and career.9 12 13
Because of altered cosmesis, teasing and self confidencewas found to be changed in myopia,4 while abnormal headposture and ocular deviation affected interpersonal commu-nication and employment in strabismus.12
Poor VF is associated with poor SF8 9 11–13; however, thepsychosocial implications of the effect of nystagmus has not,to our knowledge, been investigated. Our aim was to quantifyand compare VF and SF in nystagmus including a compar-ison of parental and child perception.
METHODSQuestionnaires were sent anonymously to all (1013) mem-bers of the Nystagmus Network UK (NN), a charity forpatients and families with nystagmus. Envelopes containedthree questionnaires—one for affected adults, one for parentsof affected children, and one for affected children. Uponrequest, additional questionnaires (for example, more thanone child affected) and questionnaires on disc and tape weresupplied. A reminder was placed in the NN newsletter after2 months. Questionnaires returned after 6 months wereincluded.The original VF-14 was used to assess VF3 (see appendix).
The question pertaining to driving was omitted for children.A SF questionnaire was derived from vision and socialfunction related questionnaires9 14 15 for adults and childrenwith nystagmus. Parents were asked to respond about theirchild and consider if their child could independentlycomplete an additional questionnaire. Returned parent andchild responses were directly compared using VF-14 and SFquestions appearing in the same form on both questionnaires(see appendix). There were variations between parental andchild questionnaires, to incorporate preschool child assess-ment (see appendix). Additional questions addressed sex,age, and nystagmus type.Following a pilot questionnaire sent to NN committee
members, the number of questions for children was reduced(questions 15–17 removed), wording was altered to aidcomprehension (question 11; ‘‘Do you feel lonely’’ to ‘‘Do youfeel isolated’’), and several social score questions werechanged to a positive turn (adult A, B, C, L: parent 15–17).SF questions were given scores between 1 and 4 (1=great
deal of difficulty, 2=moderate difficulty, 3= a little bit ofdifficulty, 4= no difficulty).3 Questions 1, 2, and 12 hadscores reversed to account for their positive turn. Scores weredivided by number of questions answered, then multiplied by25 to give total scores in the range 0-100: the higher thescore, the better the function. Results were compared usingregression analysis on SPSS.
RESULTSIn all, 398 (39%) of the 1013 envelopes were returned,containing 180 adult and 233 parent/child questionnaires; 22with more than one affected family member.
Abbreviations: NN, Nystagmus Network; SF, social function; VF, visualfunction
1278
www.bjophthalmol.com

Adult dataThe mean age of adult responders was 41 years (range 18–75,SD 15.6; 52% females and 48% males). The most commonnystagmus cause was idiopathic/no reason (table 1).Figure 1A shows the correlation between VF-14 and SF
scores for adults (R2=0.35, p,0.001). There was a trend forhigher VF-14 scores in idiopathic nystagmus than for otheraetiologies. Neither SF nor VF was associated with age or sex.
Parent and child dataOf the 233 datasets, 124 contained a non-affected parenttogether with an affected child response. The average age ofaffected children was 7.5 years (range 0–18, SD 4.3). Themale:female ratio was 60:40. The most common nystagmuscause was idiopathic/no reason (table 1). A trend was foundfor higher parental than child self assessment of VF andhigher VF-14 scores in both parental and child self assess-ment for idiopathic nystagmus than other aetiologies. Incontrast with adults, nystagmus associated with squint had ahigh VF. A weak positive association was found between VFand age (p,0.044). No association was found between sexand VF-14 score.
There was strong positive correlation between parentalassessment of child VF and SF (R2=0.39, p,0.001) (fig 1B).Figure 1C and D show correlations between SF scores(R2=0.72, p ,0.001) and VF-14 scores (R2=0.74,p,0.001) assessed by children and parents. A positiveassociation was found with age for SF scores for parentaland child assessment, but not for sex or type of nystagmus.
Table 1 Aetiologies, mean VF-14 score, and social score for adult, parental assessment of child and child self assessment
AetiologyAdult(n = 180)
Adult%
Child(n = 233)
Child(%)
VF-14 Social score
Adult Parent Child Adult Parent Child
Albinism 25 14 44 19 55 65 48 53 80 78Bad eyesight 9 5 5 2 44 53 50 47 87 64Neurological 19 10 12 5 46 51 33 46 67 78Pregnancy/birth 9 5 4 2 55 74 55 78 68Squint 4 2 5 2 58 81 83 67 76 83Not sure 41 23 21 9 56 77 67 53 83 83Idiopathic/no reason 61 34 95 41 65 73 77 59 82 83Missing data 12 7 48 21Mean 55 73 69 76 71 66SD 23 25 24 13 16 27Range 0–100 15–100 6–100 32–94 35–95 25–100
100
0
20
40
60
80
100VF14
A
Soci
al s
core
0 80604020
100
0
20
40
60
80
100VF14
B
Soci
al s
core
0 80604020
100
0
20
40
60
80
100Parent's social score
C
Chi
ld's
soc
ial s
core
0 80604020
100
0
20
40
60
80
100 Parent's VF14
D
Chi
ld's
VF1
4
0 80604020
Figure 1 (A) Adult VF-14 score versussocial function score. (B) Parentassessment of child VF-14 versus socialfunction score. (C) Parent versus childself assessment of social function score.(D) Parent versus child self assessmentof VF-14.
Table 2 Comparison of VF 14 scores from this studywith other chronic ocular diseases
Aetiology VF Ref
Low vision 54–62 8Adult nystagmus 55Age related macular degeneration 62 5Child nystagmus (self) 69Precorneal graft 72–76 6Child nystagmus (parent) 73Retinal disease 84 7Myopia 91 4
SF and VF in nystagmus 1279
www.bjophthalmol.com

Although parents’ and children’s assessment of social scorecorrelated highly, there was disagreement on two questions:11% of parents thought their child was bullied ‘‘a great deal’’because of nystagmus, whereas 26% children with nystagmusresponded this way; 3% of parents thought their childworried a great deal about eyesight but 32% childrenresponded likewise.VF-14 was higher in children than adults. Adults thought
they had a great deal of difficulty recognising people (11%);this was a problem for only a few children (2%) or theirparents (4%). Twenty seven per cent of adults reportedinability to participate in sports, in contrast with 3% ofchildren.
DISCUSSIONWe found a strong correlation between VF and SF for adultsand parental assessment of children with nystagmus andbetween parental and child self assessment of VF and SF.Children had lower SF scores than adults. Most children
scored low in areas concerned with appearance andconfidence, whereas few adults thought that career andeducation had been affected by nystagmus. This may reflectdifficulty in accepting those who are ‘‘different’’ by children.Children’s lifestyles affect their current wellbeing, develop-ment, and adult health.12 13 16 Studies on quality of life withstrabismus and amblyopia show interference with schooling,influence in job choice, and social activity.12 13 Research onchildhood strabismus concluded that psychological develop-ment and self esteem suffered because of other children’sattitudes.12
An association was found with age for parental assessmentof child VF and SF. Decreasing nystagmus amplitude withage17 might contribute to better VF and SF scores in olderchildren. However, measuring VF and SF is challenging inchildren because of difficulties in interpreting social interac-tion, varying parental experience, and rapid change in skills.18
The visual impairment caused by nystagmus is shown intable 2.4–8 For adults it is equivalent to patients requiring lowvision aids. In children it is above VF in patients with agerelated macular degeneration.A lower mean VF score was found for albinism than for
idiopathic nystagmus. Patients with idiopathic nystagmushave better visual acuity than in secondary nystagmus.1 Infuture studies it would be interesting to correlate visualacuity with VF and SF.It is possible nystagmus sufferers who are members of NN
are biased towards worse VF. A response rate of 39% mayreflect those with worse vision. However, VF ranged widely(0–100 adults: 6.25–100 children), enabling us to correlate awide range of VF with SF.In our study parents and children showed agreement
between SF and VF. To our knowledge no previous studiescompared parental assessment and child self assessment ofVF. Current research regarding chronic childhood disease19–21
shows parents overestimate the illness impact on physicalability, but underestimate emotional, cognitive, and socialimplications. This is confirmed here, where parents over-estimated difficulty with participating in sports and under-estimated the impact of appearance and the likelihood ofbeing bullied because of nystagmus. Children indicatingfewer problems with sports than adults could reflect on goodschool integration, the competitive nature of organised sportfor adults, or other neurological impairment in adults withacquired nystagmus.It is possible that children completing self assessment
questionnaires were influenced by parents. However, con-sistent differences in results (for example, bullying andappearance) support independent completion of question-naires.
The majority of ocular quality of life questionnairesconcentrate on tasks and symptoms rather than wellbeingand SF. It is important to develop quality of life instruments,which correlate visual acuity with functional ability andintegration in society, to judge the impact of visual disabilityand appropriately direct services.
CONCLUSIONPoor VF is associated with poor SF in nystagmus. This is thefirst study to show VF scores in nystagmus are low comparedwith other causes of chronic visual loss. We show for the firsttime in an ophthalmic disease that parents are able toestimate the impact of nystagmus on visual and socialfunctioning, and are well placed to assess their child’s needs.Children with nystagmus perceive social exclusion, whichshould be addressed by a multidisciplinary team.
ACKNOWLEDGEMENTSWe thank the members of the Nystagmus Network for help designingand piloting the questionnaires and members of the NystagmusNetwork who participated. This study was supported by theUlverscroft Foundation.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
R F Pilling, Department of Ophthalmology, University Hospitals Leicester,Infirmary Square, Leicester LE1 5WW, UKJ R Thompson, Department of Health Sciences, University of Leicester,22-28 Princess Road West, Leicester LE1 6TP, UKI Gottlob, Department of Ophthalmology, University of Leicester, RobertKilpatrick Clinical Sciences Building, Leicester Royal Infirmary, PO Box65, Leicester LE2 7LX, UK
Competing interests: none declared
Correspondence to: Professor Irene Gottlob, Department ofOphthalmology, Robert Kilpatrick Clinical Sciences Building, LeicesterRoyal Infirmary, PO Box 65, Leicester LE2 7LX, UK; [email protected]
Accepted for publication 25 May 2005
APPENDIX
VISUAL FUNCTION-14Do you have any difficulty, even with glasses…..1 Reading small print—eg, food label, phone book2 Reading a book or newspaper3 Reading a large print book or recognising numbers on TV4 Recognising people when they are close to you5 Seeing steps, stairs, or curbs6 Reading traffic signs, street signs, or shop signs7 Doing fine handwork—eg, sewing, knitting, crafts8 Filling in forms9 Playing games—eg, cards, dominoes, board games10 Taking part in sport11 Cooking12 Watching television13 Driving during the day—omitted from child questionnaire14 Driving at night—omitted from child questionnaire
ADULT SOCIAL SCORE (*SCORES REVERSED)Because of nystagmusA Do you enjoy making friends?*B Do you go out socially?*C Do you consider yourself independent?*E Were decisions about further education affected?F Were decisions about career choice affected?G Has career progression been affected?H Do you feel you have been prevented from working?I Do you worry about losing your job?J Do you dislike leaving home on your own?K Do you have problems getting along with people?
1280 Pilling, Thompson, Gottlob
www.bjophthalmol.com

L Do you have difficulty caring for family members?M Are you happy with life?*N Do you need help from other people?O Do you feel less inclined to meet new people?P Do you feel less inclined to meet family?Q Do you feel isolated from those around you?R Do you feel frustrated with life?S Have you been bullied or teased?T Do you worry about your eyesight?U Are you concerned about your appearance?
CHILD SOCIAL SCORE—SELF ASSESSMENT(Underlined questions used for direct comparison)1 Are you shy, withdrawn, or nervous?2 Do you spend time worrying about your vision?3 Do you feel frustrated?4 Have you been bullied or teased?5 Are you concerned about your appearance?6 Do you have difficulty making friends?7 Do you need help at school?8 Do you consider yourself disabled or handicapped?9 Do you feel less inclined to go out and meet friends?10 Do you feel less inclined to meet family?11 Do you feel lonely?
CHILD SOCIAL SCORE—PARENTAL ASSESSMENTBecause of nystagmus….1 Is he/she shy withdrawn or nervous?2 Does he/she spend time worrying about their vision?3 Is he/she frustrated?4 Has he/she been bullied or teased?5 Is he/she concerned about his/her appearance?6 Does he/she have difficulty making friends?7 Does he/she need help at school?8 Do you consider your child disabled or handicapped?9 Do you feel less inclined to meet new friends?10 Do you feel less inclined to meet family?11 Do you feel isolated from other parents?12 Do you feel downhearted?13 Do you worry about future children having nystagmus?14 Are you concerned about your child’s appearance?15 Is your child happy?*
16 Does your child get on well at school?*17 Does your child interact well with other children?*
REFERENCES1 Abadi RV, Bjerre A. Motor and sensory characteristics of infantile nystagmus.
Br J Ophthalmol 2002;86:1152–60.2 Hemmes GD. Hereditary nystagmus. Am J Ophthalmol 1924;10:149–50.3 Steinberg EP, Tielsen JM, Schien OD, et al. The VF14—an index of functional
impairment in patients with cataract. Arch Ophthalmol 1994;112:630–638.4 Ross K, Harper R, Tromans C, et al. Quality of life in myopia. Br J Ophthalmol
2000;84:1031–4.5 Riusala A, Sarna S, Immonen I. Visual function 14 in long duration age related
macular degeneration Am J Ophthalmol 2003;135:206–12.6 Boisjoly H, Grosset J, Fontaine N, et al. The VF14 index of functional visual
improvement in candidates for corneal graft. Am J Ophthalmol1999;128:38–44.
7 Linder M, Chang TS, Scott IU, et al. Validity of VF14 in patients with retinaldisease. Arch Ophthalmol 1999;117:1611–16.
8 Scott IU, Smeddy WE, Schiffman J, et al. Quality of life of low vision patientsand the impact of low vision services. Am J Ophthalmol 1999;128:54–6231.
9 Mangione CM, Berry S, Spritzer MS, et al. Identifying content area for the 51item NEI-VFQ. Arch Ophthalmol 1998;116:227–33.
10 Mangione CM, Phillips RS, Seddon JM, et al. Development of the Activities ofDaily Vision Scale’. Med Care 1992;30:1111–26.
11 Terwee CB, Gerding MN, Dekeer FW, et al. Development of a disease specificquality of life questionnaire for patients with Graves’ ophthalmopathy: theGO-QOL. Br J Ophthalmol 1998;82:773–9.
12 Sutterfield D, Keitner JL, Morrison TL. Psychosocial aspects of strabismusstudy. Arch Ophthalmol 1993;111:1100–5.
13 Packwood EA, Cruz O, Rychwalski PJ, et al. The psychosocial effects ofamblyopia study. J AAPOS 1999;3:15–17.
14 Jette AM, Davies AR, Cleary PD, et al. The functional status questionnaire:reliability and validity when used in primary care. J Gen Int Med1986;1:143–9.
15 Eiser C, Morse R. Can parents rate their child’s health-related quality of life?Results of a systematic review. Qual Life Res 2001;10:347–57.
16 Antwerp CA. The lifestyle questionnaire for school aged children: a tool forprimary care. J Paediatr Health Care 1995;9:251–5.
17 Reinecke RD, Guo S, Goldstein HP. Waveform evolution in infantilenystagmus: an electro-oculo-graphic study of 35 cases. Binoc Vis1988;3:191–202.
18 Felius J, Stager DR, Berry PM, et al. Development of an instrument to assessvision-related quality of life in young children. Am J Ophthalmol2004;138:362–72.
19 Erickson SR, Munzenberger PJ, Plante MJ, et al. Influence ofsociodemographics on the health-related quality of life of pediatric patientswith asthma and their caregivers. J Asthma 2002;39:107–17.
20 Ennett ST, DeVellis BM, Earp JA, et al. Disease experience and psychosocialadjustment in children with juvenile rheumatoid arthritis: children’s versusmothers’ reports. J Paediatr Psychol 1991;16:557–68.
21 Theunissen NC, Vogels TG, Koopman HM, et al. The proxy problem: childreport versus parent report in health-related quality of life research. Qual LifeRes 1998;7:387–97.
SF and VF in nystagmus 1281
www.bjophthalmol.com

EXTENDED REPORT
A randomised controlled trial of azithromycin followingsurgery for trachomatous trichiasis in the GambiaM J Burton, F Kinteh, O Jallow, A Sillah, M Bah, M Faye, E A N Aryee, U N Ikumapayi,N D E Alexander, R A Adegbola, H Faal, D C W Mabey, A Foster, G J Johnson, R L Bailey. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr Matthew Burton,International Centre forEye Health, London Schoolof Hygiene and TropicalMedicine, Keppel Street,London WC1E 7HT, UK;[email protected]
Accepted for publication29 January 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1282–1288. doi: 10.1136/bjo.2004.062489
Background/aim: Trachomatous trichiasis frequently returns following surgery. Several factors maypromote recurrence: preoperative disease severity, surgeon ability, surgical procedure, healing responses,and infection. This study investigates whether enhanced control of infection, both of Chlamydiatrachomatis and other bacteria, with azithromycin can improve surgical outcome in a trachoma controlprogramme.Methods: Individuals with trachomatous trichiasis were examined and operated. After surgery patientswere randomised to the azithromycin or control group. The azithromycin group and children in theirhousehold were given a dose of azithromycin. Antibiotic treatment was repeated at 6 months. All patientswere reassessed at 6 months and 12 months. Samples were collected for C trachomatis polymerase chainreaction and general microbiology at each examination.Results: 451 patients were enrolled. 426 (94%) were reassessed at 1 year, of whom 176 (41.3%) had oneor more lashes touching the eye and 84 (19.7%) had five or more lashes. There was no difference intrichiasis recurrence between the azithromycin and control group. Recurrent trichiasis was significantlyassociated with more severe preoperative trichiasis, bacterial infection, and severe conjunctivalinflammation at 12 months. Significant variability in outcome was found between surgeons. Visual acuityand symptoms significantly improved following surgery.Conclusion: In this setting, with a low prevalence of active trachoma, azithromycin did not improve theoutcome of trichiasis surgery conducted by a trachoma control programme. Audit of trichiasis surgeryshould be routine.
Trachoma is the leading infectious cause of blindnessworldwide. Recurrent infection with Chlamydia tracho-matis produces a chronic follicular conjunctivitis.
Conjunctival scarring develops, leading to entropion, trichia-sis, and blinding corneal opacification. Six million people areirreversibly blind from trachoma and a further 10 millionhave trachomatous trichiasis.1 To control trachoma the WorldHealth Organization promotes the SAFE strategy: Surgery fortrichiasis, Antibiotic distribution to reduce chlamydial infec-tion, Facial cleanliness, and Environmental improvements toreduce transmission.2
Trichiasis surgery probably reduces the risk of visual loss,although the evidence for this is limited.3 Various proceduresare used. The bilamellar tarsal rotation (BLTR) had the mostfavourable outcome in comparative trials and is recom-mended by the WHO.3–5 However, trichiasis returns in at least20% by 2 years.3 4 6 Longer term studies find trichiasisaccrues, reporting 3 year recurrence rates of more than60%.7–9 Recurrent trichiasis is poorly understood. Severalfactors may influence the outcome: preoperative diseaseseverity, surgical procedure, surgeon ability, wound healingresponses, and infection. C trachomatis infection has beenassociated with progression of conjunctival scarring totrichiasis and recurrent trichiasis after surgery.10 11 Non-chlamydial bacterial infection is associated with progressivecorneal opacification in eyes with unoperated trichiasis andrecurrent trichiasis following surgery.9 12 Therefore, interven-tions that reduce conjunctival infection after surgery mightimprove results.Azithromycin is effective against various bacteria including
C trachomatis.13 Mass azithromycin treatment controls ende-mic trachoma, with sustained reduction in infection a year
after distribution.14 Azithromycin is active against otherpathogens, including streptococci, staphylococci, andHaemophilus, which are commonly found in association withtrichiasis and it can produce a short term reduction inbacterial colonisation of the conjunctiva in children.9 15
This randomised controlled trial investigated whethertrichiasis surgery results could be improved by adjunctiveazithromycin treatment to an extent that would be ofprogrammatic significance in regions with low levels ofendemic active trachoma such as the Gambia.16
METHODSEthical permissionThe study was approved by the Gambian Government/Medical Research Council joint ethics committee. Informedconsent was required for participation.
Trichiasis patientsSubject with unoperated trichiasis were identified from theGambian National Eye Care Programme (NECP) database,community ophthalmic nurse records, and village screening.Individuals with recurrent trichiasis and pregnant women(self reported) were excluded. A series of 34 day surgerysessions were organised by the NECP at health posts betweenMay 2001 and April 2002.
Abbreviations: BLTR, bilamellar tarsal rotation; CON, communityophthalmic nurses; MMP, matrix metalloproteinases; NECP, NationalEye Care Programme; PCR, polymerase chain reaction; PLTR, posteriorlamellar tarsal rotation; RCT, randomised controlled trial; STGG,skimmed milk, tryptone, glycerol and glucose broth
1282
www.bjophthalmol.com

Preoperative assessmentAn ophthalmologist (MJB) conducted preoperative assess-ments. Height, weight, and logMAR visual acuity weremeasured.17 Clinical signs of trachoma were graded using2.56 loupes according to the WHO trachoma gradingsystem.18 The number of eyelashes touching the cornea andother parts of the globe in primary position were recorded.Lagophthalmos was measured. The conjunctiva was anaes-thetised with proxymetacaine 0.5% eye drops (Minims,Chauvin). A conjunctival swab sample was collected andplaced in sterile skimmed milk, tryptone, glycerol, andglucose broth (STGG) for bacteriology. A second swab wascollected for C trachomatis polymerase chain reaction (PCR)from the upper tarsal conjunctival surface. Both were kept onice before transfer to 270 C or 220 C freezers, respectively,later the same day.
SurgeryTrained community ophthalmic nurses (CON) from theNECP performed the surgery. Senior ophthalmic medicalassistants supervised to ensure the standard procedure wasperformed correctly. The surgical technique used in theGambia is the posterior lamellar tarsal rotation (PLTR).6 Thisis similar to the bilamellar tarsal rotation (BLTR), except skinand anterior lamella are not incised. Surgery was performedusing aseptic techniques under local anaesthesia (lignocaine1%). The district CON reviewed patients and removed suturesat 1week.
RandomisationRandomisation was to azithromycin or control group at theindividual patient level. Immediately following surgery anurse (OJ) not involved in clinical assessments or surgeryadministered the randomly allocated treatment. Treatmentallocations were concealed in opaque sequentially num-bered envelopes. Separate randomisation sequences weregenerated for each surgeon from random number tables andblocked in groups of four.19 Each patient was assigned theallocation in the next envelope in the sequence of theirsurgeon. This within surgeon blocked randomisation wasdone to reduce confounding from intersurgeon variability,by ensuring good balance between the two groups foreach surgeon. Examiners were ‘‘blinded’’ to treatmentallocation.
Antibiotic treatmentAll patients received unsupervised tetracycline eye ointmenttwice a day for 2 weeks, as per Gambian guidelines. Subjectsrandomised to azithromycin group also received a 1 g dose ofazithromycin. Children in the households of azithromycingroup subjects were given a dose of azithromycin (20 mg/kg),following informed consent from parents. This was done toreduce the risk of re-infection with C trachomatis from theimmediate environment of the patient. After the 6 monthassessment patients in the azithromycin group and thechildren were given a second dose of azithromycin by thetreatment nurse.
Follow up visitsPatients were reassessed (as above) 6 months (FK) and12 months (MJB) after surgery. At 12 months patients wereasked whether they considered the vision and pain in theoperated eye to be worse, the same or better, compared withhow it was before surgery. Recurrent trichiasis was managedaccording to national guidelines: epilation for a fewperipheral lashes; patients with multiple/central lashes werereferred for further surgery.
Laboratory testsConjunctival swab samples were tested for C trachomatis DNAusing a PCR based assay (Amplicor CT/NG Test, Roche) withpreviously described modifications.20 Bacteriology sampleswere plated out on blood agar (aerobic and anaerobic),McConkey’s agar, gentamicin blood agar, and bacitracinchocolate agar. Plates were incubated at 37 C for 48 hours.Gentamicin blood agar and bacitracin chocolate agar wereincubated in 5% carbon dioxide. Isolated organisms wereidentified using standard bacteriological techniques.Sensitivities were assessed using antimicrobial susceptibilitydiscs.
Sample sizeThis study was designed to evaluate whether azithromycin,used under the real life operational conditions of a trachomacontrol programme, is effective in reducing trichiasis recur-rence to an extent that would be of programmatic signifi-cance in regions with low levels of endemic trachoma.Previous studies indicate trichiasis recurs in at least 20% by1 year.3 6–8 We considered that for this intervention to beworth implementing the expected recurrence rate in theazithromycin group should be half that of the control group.Therefore, if the relative risk of failure in the azithromycingroup were taken to be 0.5 (10% failure at 1 year) then asample of 438 gives 80% power and 95% confidence to detecta difference. As well as being operationally important, thissize of effect was thought feasible, given the possible impactof azithromycin on both chlamydial and bacterial infection.
Data analysisThe primary outcome was recurrent trichiasis: one or morelashes touching any part of the globe in primary positionfollowing surgery. Secondary outcomes included visualacuity, conjunctival infection, and corneal opacification.18
For visual acuities of counting fingers or less, logMAR valueswere attributed: counting fingers 2.0, hand movements 2.5,and perception of light 3.0.Data were analysed in Stata 7. In bilateral cases only the
eye with more severe trichiasis was included in the studyanalysis. The Wilcoxon signed rank test was used to examinechange in degree of trichiasis before and after surgery. Pairedt tests were used to examine change in visual acuity.Multivariable logistic regression models were developed toinvestigate risk factors for recurrent trichiasis. All modelsincluded sex, age, and treatment allocation. Additional termswere added in a stepwise manner.
RESULTSA total of 451 people with trachomatous trichiasis wereenrolled; predominantly women (70.5%) with a mean age of57 years (table 1). Visually disabling corneal opacificationwas present in 30% of eyes (moderate/severe scarring over thepupil, CC2/CC3).18 Severity of trichiasis varied considerably(median: eight lashes, interquartile range: 5–16; total range:0 (epilating)–74). C trachomatis DNA was detected in 5% ofindividuals. Bacterial pathogens were cultured from 29.8% ofeyes.Following surgery 216 individuals were randomised to
receive azithromycin and 235 to the control group (fig 1).Baseline characteristics of the two groups were comparable(table 1). Follow up rates were 91% and 94% at 6 months and12 months, respectively; 98% of those alive at 12 months.Reasons for no follow up are given in figure 1.The prevalence of any trichiasis was 31.5% and 41.3% at
6 months and 12 months, respectively (table 2). The recur-rence rate was 37.9% at 12 months in fellow eyes that wereoperated on but not included in the study analysis. For allsubjects, the median number of lashes touching the globe at
RCT of azithromycin after trichiasis surgery 1283
www.bjophthalmol.com

12 months was 0 (interquartile range: 0–3; total range: 0–53). Trichiasis severity was significantly reduced (Wilcoxonsigned rank test: z=15.2, p,0.001). For subjects withrecurrent trichiasis the median was 10 lashes before surgery(interquartile range: 4–22; total range: 0 (epilating) – 74) andfour lashes at 12 months (interquartile range: 1–8; totalrange: 0 (epilating) – 53). This subgroup had a significantreduction in trichiasis severity (Wilcoxon signed rank test:z=7.1, p,0.001). Postoperatively, one patient developed alid infection, which settled with oral antibiotics and twoindividuals had defective lid closure (,2 mm lagophthal-mos).Univariate associations between various factors and
recurrent trichiasis at 12 months are presented in table 3.Multivariable logistic regression models were developed for
any trichiasis and 5+ lashes at 12 months (table 4).Azithromycin treatment did not affect the outcome.Recurrent trichiasis was associated with more severe pre-operative trichiasis, severe conjunctival inflammation, andbacterial infection at 12 months. C trachomatis infection wasnot associated with recurrent trichiasis in these models andtherefore dropped.Seventeen nurses performed surgery (mean: 26 cases, SD
22.9, range: 2–92). Trichiasis recurrence rates varied sig-nificantly between surgeons (median: 40%; interquartilerange: 22–49%; total range: 0–83%; Pearson x2: x2=63.1,df=16, p,0.001). Likelihood ratio testing between multi-variable logistic regression models for recurrent trichiasiswith and without surgeons was done. This indicatedintersurgeon variability remained significant after adjustingfor other factors, including preoperative disease severity(x2=55.9, p,0.001). The odds ratio for azithromycintreatment changed negligibly when models were adjustedfor surgeon (OR=0.99, 95% CI 0.63 to 1.59, p=0.989); thisis as expected, given the randomisation within surgeon.
Table 1 Patient characteristics and preoperative clinical parameters, subdivided by treatment allocation
All Azithromycin Control(n = 451) (n = 216) (n = 235)
Demographics:Sex, female 318 (70.5%) 152 (70.4%) 166 (70.6%)Age, mean (IQR) 57.3 (48–70) 57.3 (47–70) 57.2 (48–70)BMI (IQR) 20.4 (18.4–21.9) 20.3 (18.3–21.9) 20.6 (18.5–21.9)Ethnicity:
Mandinka 178 (39.4%) 88 (40.7%) 90 (38.3%)Wolof 154 (34.2%) 73 (33.8%) 81 (34.5%)Jola 58 (12.8%) 26 (12.0%) 32 (13.6%)Fula 33 (7.3%) 15 (6.9%) 18 (7.7%)Manjago 12 (2.7%) 6 (2.9%) 6 (2.5%)Sarahule 7 (1.6%) 4 (1.8%) 3 (1.3%)Other 9 (2.0%) 4 (1.9%) 5 (2.1%)
Corneal opacity:CC 0 235 (52.1%) 119 (55.1%) 116 (49.4%)CC 1 83 (18.4%) 34 (15.7%) 49 (20.1%)CC 2 62 (13.8%) 31 (14.4%) 31 (13.2%)CC 3 71 (15.7%) 32 (14.8%) 39 (16.8%)
Trichiasis (number of lashes):0 (epilate) 63 (14.0%) 24 (11.1%) 39 (16.6%)1–4 45 (10.0%) 26 (12.0%) 19 (8.1%)5–9 149 (33.0%) 70 (32.4%) 79 (33.6%)10–19 101 (22.4%) 50 (23.2%) 51 (21.7%)20 + 93 (20.6%) 46 (21.3%) 47 (20.0%)
Mean no of lashes (95% CI) 12.4 (11.2 to 13.5) 12.8 (11.1 to 14.5) 12.0 (10.4 to 13.7)Conjunctival inflammation:
P0 64 (14.2%) 33 (15.3%) 31 (13.2%)P1 118 (26.2%) 55 (25.5%) 63 (26.8%)P2 149 (33.0%) 64 (29.6%) 85 (36.2%)P3 120 (26.6%) 64 (29.6%) 56 (23.8%)
Infection:C trachomatis (PCR+) 22/443 (5.0%) 10/212 (4.7%) 12/231 (5.2%)Other bacteria 132/443 (29.8%) 60/210 (28.6%) 72/233 (30.9%)
IQR, interquartile range.
451 Trichiasis patients
Azithromycin216
6 month follow up:
199/216 (92%) seen17 not seen: 2 Died 4 Moved 11 Travelled
12 month follow up:
204/216 (94%) seen12 not seen: 8 Died 4 Moved
Control235
6 month follow up:
211/235 (90%) seen24 not seen: 4 Died 2 Moved 18 Travelled
12 month follow up:
222/235 (94%) seen13 not seen: 8 Died 3 Moved 2 Travelled
Figure 1 Flow diagram summarising the treatment and follow upcoverage at 6 months and 12 months after surgery.
1284 Burton, Kinteh, Jallow, et al
www.bjophthalmol.com

Table 2 Severity of recurrent trichiasis at 6 months and 12 months after surgery, subdivided by treatment allocation
All Azithromycin Control
6 Months n = 410 n =199 n =211Any trichiasis 129 (31.5%) 74 (37.2%) 55 (26.1%)Any touching the cornea 99 (24.1%) 54 (27.1%) 45 (21.3%)No of lashes touching eye:
0 281 (68.5%) 125 (62.8%) 156 (73.9%)1–4 70 (17.1%) 42 (21.1%) 28 (13.3%)5–9 25 (6.1%) 13 (6.5%) 12 (5.7%)10–19 15 (3.7%) 6 (3.0%) 9 (4.3%)20+ 19 (4.6%) 13 (6.5%) 6 (2.8%)
Mean no of lashes (95% CI) 4.1 (3.4 to 5.0) 3.9 (3.0 to 5.1) 4.4 (3.3 to 5.9)12 Months n = 426 n =204 n =222Any trichiasis 176 (41.3%) 84 (41.2%) 92 (41.4%)Any touching the cornea 139 (32.6%) 64 (31.4%) 75 (33.8%)No of lashes touching eye:
0 (No epilation) 250 (58.7%) 120 (58.8%) 130 (58.6%)0 (Epilate) 13 (3.1%) 7 (3.4%) 6 (2.7%)1–4 79 (18.4%) 34 (16.7%) 45 (20.3%)5–9 45 (10.6%) 26 (12.7%) 19 (8.5%)10–19 20 (4.7%) 6 (3.0%) 14 (6.3%)20+ 19 (4.5%) 11 (5.4%) 8 (3.6%)
Mean no of lashes (95% CI) 4.5 (3.7 to 5.3) 4.7 (3.6 to 6.0) 4.3 (3.4 to 5.4)
Table 3 Univariate associations between various factors and recurrent trichiasis (any trichiasis and 5+ lashes) at 12 monthsafter surgery
Any trichiasis 5+ Lashes
OR 95% CI p Value OR 95% CI p Value
Sex (female) 0.65 0.43 to 0.99 0.050 0.75 0.45 to 1.25 0.264Age 60+ years 1.63 1.10 to 2.41 0.015 1.73 1.05 to 2.84 0.031Azithromycin treatment 0.99 0.67 to 1.46 0.956 1.18 0.73 to 1.90 0.499Baseline trichiasis1–4 1 – – 1 – –5–9 1.06 0.49 to 2.26 0.889 1.10 0.29 to 4.20 0.88610–19 2.19 1.01 to 4.74 0.047 4.60 1.31 to 16.2 0.01720+ 3.93 1.78 to 8.65 0.001 10.28 2.95 to 35.8 ,0.00110+ lashes at baseline 2.03 1.37 to 3.00 ,0.001 4.51 2.67 to 7.60 ,0.001Severe inflammation (P3/TI)Baseline 1.92 1.24 to 2.97 0.003 2.42 1.46 to 3.99 0.00112 Months 7.38 3.78 to 14.4 ,0.001 6.53 3.62 to 11.8 ,0.001Bacterial Infection:Baseline 1.61 1.05 to 2.46 0.028 2.05 1.24 to 3.37 0.00512 Months 1.66 0.95 to 2.88 0.070 4.30 2.40 to 7.70 ,0.001C trachomatis infection:Baseline 2.73 1.07 to 7.00 0.036 1.37 0.48 to 3.88 0.55612 Months ‘ – ,0.001 4.12 0.57 to 29.8 0.159
Table 4 Multivariable logistic regression models for any trichiasis and 5+ lashes at 12 months after surgery
Variable
Any trichiasis 5+ Lashes
OR 95% CI p Value OR 95% CI p Value
Sex (female) 0.78 0.48 to 1.26 0.304 0.87 0.47 to 1.59 0.644Age (years):
,50 1.00 – – 1.00 – –50–59 0.94 0.48 to 1.83 0.872 0.73 0.30 to 1.78 0.48360–69 1.72 0.96 to 3.09 0.070 0.92 0.42 to 1.98 0.823.70 1.39 0.75 to 2.55 0.294 1.44 0.67 to 3.07 0.347
Azithromycin treatment 0.98 0.63 to 1.51 0.919 1.27 0.73 to 2.21 0.40710+ lashes at baseline 1.74 1.12 to 2.71 0.014 3.69 2.06 to 6.60 ,0.001Bacterial infection at baseline 1.33 0.81 to 2.17 0.261 1.11 1.22 to 4.94 0.722Bacterial infection at 12 months 0.84 0.44 to 1.61 0.604 2.45 1.22 to 4.94 0.012Severe inflammation at 12 months 6.41 3.17 to 12.9 ,0.001 5.90 3.02 to 11.5 ,0.001
RCT of azithromycin after trichiasis surgery 1285
www.bjophthalmol.com

C trachomatis was detected in 22, 16, and four samples atbaseline, 6 months, and 12 months, respectively. At6 months there was a significant reduction in chlamydialinfection in azithromycin compared to control group (OR0.14. p=0.010. 95% CI 0.03 to 0.63). At 12 months there wasone chlamydial infection in the azithromycin group and threein the control group.Bacterial pathogens were isolated from 29.8% before
surgery and 14.9% at 12 months (table 5). Twelve (9.1%)had mixed infections at baseline. Infection was morecommon as trichiasis severity increased. The principal riskfactor for bacterial infection was trichiasis. Azithromycintreatment was not associated with less infection at 6 monthsor 12 months. Various organisms were cultured (table 6).Seasonal variation in organisms was observed, with moreKlebsiella during the wet season (6 months).Corneal opacification at baseline was associated with
increasing age, severe trichiasis, severe inflammation, andbacterial infection (table 7). Corneal opacification progressedin 68 (16%), was unchanged in 303 (71%), and decreased in54 (13%) at 12 months. Progression of corneal opacificationwas associated with the presence of five or more lashes at12 months, when compared to individuals without cornealopacification (OR 2.76, 95% CI: 1.42 to 5.35, p=0.003). By1 year 27 individuals had developed new corneal opacifica-tion (CC2 or CC3), of whom 14 (52%) had no recurrent
trichiasis. Interobserver agreement for the diagnosis ofcorneal opacification (CC2/CC3) was good (kappa=0.76).Severe conjunctival inflammation (P3/TI) at 1 year was
independently associated with the presence of bacterialinfection and severe trichiasis at 12 months (table 8).Visual acuity improved in 57.6% and deteriorated in 28.4%
of eyes by 12 months. The 297 eyes with vision good enoughto be tested by logMAR had a mean improvement of 0.144logMAR units (paired two sided t test: p,0.0001, 95% CI0.108 to 0.180). When the additional 118 eyes with acuitybetween counting fingers and perception of light wereincluded the mean improvement was 0.121 logMAR units(paired two sided t test: p,0.0001, 95% CI 0.07 to 0.17).There was no significant difference in improvement betweenthose with or without recurrent trichiasis (unpaired twosided t test: mean difference 0.013, p=0.725, 95% CI: 20.060to 0.087). Before surgery 79% reported eye pain; 18% hadconstant pain. Epilation was common (38%.1 per week).Subjectively, 1 year after surgery 77% thought they could seebetter with the operated eye; 94.3% considered the operatedeye to be more comfortable, while 5.7% felt it was the same orworse.
DISCUSSIONBlinding trachoma is a progressive inflammatory cicatricialprocess, which is probably driven by recurrent infection with
Table 5 Conjunctival bacterial infection and relationship with trichiasis severity before surgery and at 12 months
Baseline 12 Months
Pathogen cultured 132/443 (29.8%) 61/410 (14.9%)No of lashes touching eye:
0 (No epilation) – – 30/242 (12.4%)0 (Epilate) 11/62 (17.7%) 2/22 (9.1%)1–4 10/45 (22.2%) 2/70 (2.9%)5–9 31/145 (21.4%) 10/39 (25.6%)10–19 25/101 (24.8%) 8/18 (44.4%)20+ 55/90 (61.1%) 9/19 (47.4%)
Association between infection and OR 95% CI p Value OR 95% CI p Value5+ lashes 2.02 1.19 to 3.43 0.009 4.15 2.33 to 7.42 ,0.00110+ lashes 2.77 1.82 to 4.22 ,0.001 6.03 2.96 to 12.3 ,0.001
Table 6 Pathological conjunctival bacterial isolates before and after surgery
Baseline 6 Months 12 Months
No % No % No %
Streptococcus pneumoniae 61 (42.4) 19 (20.7) 20 (26.0)S viridans 12 (8.3) 15 (8.7) 1 (1.3)Streptococcus group A 2 (1.4) 2 (2.2) 1 (1.3)Streptococcus group C 12 (8.3) 1 (1.1) 8 (10.4)Streptococcus group D 1 (0.7) 1 (1.1) –Streptococcus group G 3 (2.1) 1 (1.1) –Streptococcus spp 12 (8.3) 5 (5.4) 6 (7.8)Staphylococcus aureus 16 (11.1) 26 (28.3) 16 (20.8)Pseudomonas aeruginosa 3 (2.1) 1 (1.1) 1 (1.3)Moraxella 3 (2.1) 5 (5.4) 5 (12.0)Haemophilus influenzae 1 (0.7) 2 (2.2) 10 (12.0)Klebsiella 6 (4.2) 15 (16.3) 2 (2.6)Neisseria spp 3 (2.1) 1 (1.1) 1 (1.3)Coliform spp 5 (3.5) 3 (3.3) 3 (3.9)Proteus 1 (0.7) – –Escherichia coli 1 (0.7) – –Salmonella – 2 (2.2) –Serratia 1 (0.7) – 1 (1.3)Enterobacter sakazakii 1 (0.7) – –Fungus – – 2 (2.6)Total 144 92 77
1286 Burton, Kinteh, Jallow, et al
www.bjophthalmol.com

C trachomatis and bacterial pathogens. Trichiasis surgeryreduces the risk of blindness; however, trichiasis frequentlyreturns limiting the benefit.3 4 6–8 Recurrent trichiasis could bedue in part to progressive cicatricial disease driven byinfection.7 8 We investigated the impact of adjunctiveazithromycin on trichiasis surgery, within a trachoma controlprogramme. Preoperatively the azithromycin and controlgroups were comparable. There was no difference inrecurrence rates between the two groups. Therefore, in thissetting, which currently has a low prevalence of activetrachoma (6% in children 0–15 years), azithromycin did notimprove the 1 year surgical results of a control programme.16
C trachomatis was uncommon (5%) and not associated withrecurrent trichiasis. Azithromycin was associated withsignificantly less chlamydial infection at 6 months, comparedwith tetracycline alone. The overall downward trend in theprevalence of C trachomatis infection in the control group wasprobably the result of a combination of tetracycline treatmentand the downward secular trend previously observed in thisregion.16 In this low prevalence setting C trachomatis probablycontributes little to recurrent trichiasis. This study waspowered to detect a difference of practical programmaticsignificance (halving of recurrence rate), and does notexclude a more subtle effect of azithromycin. In higherprevalence regions the organism may contribute more torecurrence and azithromycin could improve outcomes.Bacterial infection was common preoperatively (29.8%).
Trichiasis was the principal risk factor for infection andisolation rates increased with severity. Trichiasis probablyfacilitates recurrent bacterial inoculation of the conjunctivaand impedes resolution of infection. Surgery probablyreduces susceptibility to bacteria, explaining the halving ofinfection at 12 months (14.9%). Azithromycin was notassociated with less bacterial infection 6 months aftertreatment; recurrent trichiasis (equally common in bothgroups) predisposes the conjunctiva to bacteria long after theantibiotic is active.13 We have reported a similar associationbetween bacterial infection and recurrent trichiasis 4 yearsafter surgery.9 Currently, it is unknown whether bacterialinfection is a cause or effect of recurrent trichiasis but thismerits further investigation.The recurrence rate (41%) was higher than some previously
reported series 3 6 but comparable with others.7–9 Comparisonsof alternative techniques found the BLTR to have the mostfavourable outcome.3 4 The Gambia, in common with several
trachoma endemic countries, uses the PLTR, which was notformally compared with the BLTR.6 It is possible that underoperational conditions they may have different intersurgeonreliability.There was significant intersurgeon variation in trichiasis
recurrence after adjusting for preoperative disease severity.Surgery followed national guidelines and was supervised bysenior staff. However, subtle variations in technique—forexample, in suture tension and dissection between anteriorand posterior lamellae, may influence outcome. This findingemphasises the importance of ongoing surgical audit, soappropriate training and support can be provided whereresults are less good. There is little published on intersurgeonvariability. One study reported variable recurrence ratesbetween three surgeons (28–73%), which were attributed tovariations in preoperative disease severity.4 Recurrence frompoor technique probably develops in the early postoperativeperiod. This was not assessed as the focus of this study wasthe long term impact of azithromycin. Within surgeonrandomisation of patients minimises potential confoundingfrom intersurgeon variability.Severe preoperative trichiasis was an independent risk
factor for recurrence. More severe trichiasis probably reflectsmore severe scarring, which makes surgery difficult and maybe associated with progressive postoperative cicatricial dis-ease. Others have reported similar associations.4 21 22 In manycountries, including the Gambia, epilation is practisedinitially and surgery is deferred until ‘‘major trichiasis’’ (5+lashes) develops. This study suggests that it may be better tooperate earlier in the natural history of the disease beforesevere trichiasis develops. It may also be appropriate todevelop graded referral systems in which severe trichiasiscases are operated on by senior surgeons.Severe inflammation was independently associated with
severe trichiasis and bacterial infection but not C trachomatis.Earlier studies found an association between conjunctivalinflammation and trichiasis.9 12 Several factors may promoteinflammation: infection, mechanical irritation from lashes,dry eye, or an immunological process. In many situationschronic, severe inflammation produces scarring. Severeinflammatory trachoma (TI) in children is associated withincreased expression of matrix metalloproteinases (MMP)and risk of subsequent scarring.23–25 Therefore, severeinflammation following surgery may produce additionalscarring and recurrent trichiasis. Pharmacological inhibition
Table 7 Multivariable logistic regression model for visually disabling cornealopacification (CC2 or CC3) before surgery
Variable OR 95% CI p Value
Age 60+ years 3.07 1.90 to 4.96 ,0.001Severe trichiasis (10+ lashes) 2.33 1.46 to 3.71 ,0.001Severe conjunctival inflammation (P3) 2.89 1.46 to 3.90 0.001Bacterial infection 2.12 1.32 to 3.45 0.002
Table 8 Multivariable logistic regression model for severe conjunctival inflammationbefore surgery and at 12 months
Variable
Baseline 12 Months
OR 95% CI p Value OR 95% CI p Value
Severe trichiasis (10+ lashes) 2.58 1.64 to 4.07 ,0.001 8.71 4.02 to 18.9 ,0.001Bacterial infection 2.02 1.27 to 3.22 0.003 2.47 1.12 to 5.11 0.015C trachomatis infection 1.86 0.73 to 4.71 0.190 1.68 0.13 to 21.8 0.691
RCT of azithromycin after trichiasis surgery 1287
www.bjophthalmol.com

of MMPs may offer a way to control the inflammatorycicatricial process before or after surgery.Surgery produced significant improvements in subjective
symptoms, visual acuity, burden of trichiasis and bacterialinfection. Improvement in visual acuity was similar to anearlier study.3 It was probably due to reduced oculardischarge and some restoration of the corneal surface.Corneal opacification progressed in 16% of individuals andwas significantly associated with recurrent trichiasis. Thedevelopment of new corneal opacification in the absence ofrecurrent trichiasis is an interesting observation, whichsuggests that other factors contribute to blinding trachoma.Mechanisms such as dry eye and conjunctival inflammationshould be investigated, as correcting trichiasis alone may beinsufficient to prevent blindness in some patients.In conclusion, this study does not support the use of
adjunctive azithromycin in trichiasis surgery in regions witha low prevalence of active trachoma such as the Gambia.Some useful insights into recurrent trichiasis have beengained. Recurrent trichiasis is a significant problem, whichwas associated with severe preoperative trichiasis, intersur-geon variability, conjunctival inflammation, and conjunctivalbacterial infection. There is a need for further research intothe causes of recurrent trichiasis and to evaluate interven-tions to improve the outcome of surgery.
ACKNOWLEDGEMENTSThe authors would like to thank the community ophthalmic nursesof the Gambian National Eye Care Programme who participated inthis study for all their hard work in identifying trichiasis patients andperforming the surgery. We would also like to thank the ProgrammeNational de Lutte Contre La Cecite de la Republique du Senegal andtheir ophthalmic nurses who participated in are of the surgery campsunder the auspices of the Health for Peace Initiative between theGambian and Senegalese governments. The authors thank Dr KatieBurton, Dr Heather Nunnerly, and Mrs Wendy Burton for preparingthe randomised treatment allocation sequences.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
M J Burton, N D E Alexander, D C W Mabey, A Foster, G J Johnson,R L Bailey, London School of Hygiene and Tropical Medicine, London,UKM J Burton, O Jallow, E A N Aryee, U N Ikumapayi, R A Adegbola,R L Bailey, Medical Research Council Laboratories, Fajara, GambiaF Kinteh, O Jallow, A Sillah, M Bah, H Faal, National Eye CareProgramme, GambiaM Faye, Programme National de Lutte Contre La Cecite de la Republiquedu SenegalG J Johnson, Division of Epidemiology and International Eye Health,Institute of Ophthalmology, London, UK
Funding: The funders of this study had no part in study design; in thecollection, analysis, and interpretation of data; in the writing of thereport; and in the decision to submit the paper for publication. This studywas principally funded by a grant from the International Trachoma
Initiative (01-030) with additional support from the Wellcome Trust andSight Savers International. The manufacturer, Pfizer Inc, donated theazithromycin used in the trial.
REFERENCES1 Thylefors B, Negrel AD, Pararajasegaram R, et al. Global data on blindness.
Bull World Health Organ 1995;73:115–21.2 World Health Organization. Global elimination of blinding trachoma.
Resolution WHA 51.11 adopted by the World Health Assembly 16 May1998.
3 Reacher MH, Munoz B, Alghassany A, et al. A controlled trial of surgery fortrachomatous trichiasis of the upper lid. Arch Ophthalmol 1992;110:667–74.
4 Reacher MH, Huber MJ, Canagaratnam R, et al. A trial of surgery for trichiasisof the upper lid from trachoma. Br J Ophthalmol 1990;74:109–13.
5 Reacher MH, Foster A, Huber MJ. Trichiasis surgery for trachoma. Thebilamellar tarsal rotation procedure. Geneva: World Health Organization,1993.
6 Bog H, Yorston D, Foster A. Results of community-based eyelid surgery fortrichiasis due to trachoma. Br J Ophthalmol 1993;77:81–3.
7 Bowman RJ, Jatta B, Faal H, et al. Long-term follow-up of lid surgery fortrichiasis in the Gambia: surgical success and patient perceptions. Eye2000;14:864–8.
8 Khandekar R, Mohammed AJ, Courtright P. Recurrence of trichiasis: a long-term follow-up study in the Sultanate of Oman. Ophthalmic Epidemiol2001;8:155–61.
9 Burton MJ, Bowman RJ, Faal H, et al. Long term outcome of trichiasis surgeryin the Gambia. Br J Ophthalmol 2005;89:575–80.
10 Munoz B, Bobo L, Mkocha H, et al. Incidence of trichiasis in a cohort ofwomen with and without scarring. Int J Epidemiol 1999;28:1167–71.
11 Zhang H, Kandel RP, Sharma B, et al. Risk factors for recurrence ofpostoperative trichiasis: implications for trachoma blindness prevention. ArchOphthalmol 2004;122:511–16.
12 Bowman RJ, Faal H, Myatt M, et al. Longitudinal study of trachomatoustrichiasis in the Gambia. Br J Ophthalmol 2002;86:339–43.
13 Burton MJ, Frick KD, Bailey RL, et al. Azithromycin for the treatment andcontrol of trachoma. Expert Opin Pharmacother 2002;3:113–20.
14 Schachter J, West SK, Mabey D, et al. Azithromycin in control of trachoma.Lancet 1999;354:630–5.
15 Chern KC, Shrestha SK, Cevallos V, et al. Alterations in the conjunctivalbacterial flora following a single dose of azithromycin in a trachoma endemicarea. Br J Ophthalmol 1999;83:1332–5.
16 Dolin PJ, Faal H, Johnson GJ, et al. Trachoma in the Gambia. Br J Ophthalmol1998;82:930–3.
17 Rosser DA, Laidlaw DA, Murdoch IE. The development of a ‘‘reducedlogMAR’’ visual acuity chart for use in routine clinical practice. Br J Ophthalmol2001;85:432–6.
18 Dawson CR, Jones BR, Tarizzo ML. Guide to trachoma control. Geneva:World Health Organization, 1981.
19 Smith PG, Morrow RH. Methods for field trials of interventions against tropicaldiseases: a ‘‘toolbox’’. Oxford: Oxford University Press, 1991.
20 Burton MJ, Holland MJ, Faal N, et al. Which members of a community needantibiotics to control trachoma? Conjunctival Chlamydia trachomatis infectionload in Gambian villages. Invest Ophthalmol Vis Sci 2003;44:4215–22.
21 Adamu Y, Alemayehu W. A randomized clinical trial of the success rates ofbilamellar tarsal rotation and tarsotomy for upper eyelid trachomatoustrichiasis. Ethiop Med J 2002;40:107–14.
22 Alemayehu W, Melese M, Bejiga A, et al. Surgery for trichiasis byophthalmologists versus integrated eye care workers: a randomized trial.Ophthalmology 2004;111:578–84.
23 Burton MJ, Bailey RL, Jeffries D, et al. Cytokine and fibrogenic geneexpression in the conjunctivas of subjects from a Gambian community wheretrachoma is endemic. Infect Immun 2004;72:7352–6.
24 Dawson CR, Marx R, Daghfous T, et al. In: Bowie WR, ed. Chlamydialinfections. Cambridge: Cambridge University Press, 1990:271–8.
25 West SK, Munoz B, Mkocha H, et al. Progression of active trachoma toscarring in a cohort of Tanzanian children. Ophthalmic Epidemiol2001;8:137–44.
1288 Burton, Kinteh, Jallow, et al
www.bjophthalmol.com

EXTENDED REPORT
Potential of the 1 CU accommodative intraocular lensG Sauder, R F Degenring, B Kamppeter, P Hugger. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr G Sauder, Universitats-Augenklinik, Theodor-Kutzer-Ufer 1-3, 68167Mannheim, Germany;[email protected]
Accepted for publication1 June 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1289–1292. doi: 10.1136/bjo.2005.068056
Aim: To assess the accommodative power of a new foldable monofocal intraocular lens.Method: A prospective randomised non-masked clinical interventional study. The study included 40patients attending the hospital for cataract surgery and who were randomly distributed into a study groupreceiving a new foldable monofocal intraocular lens with flexible haptics, and a control group receiving astandard foldable intraocular lens. Mean follow up period was 8.51 (SD 1.34) months (range 4–11 months) Standard cataract surgery consisted of clear cornea incision, capsulorrhexis, phacoemulsi-fication, and intraocular lens implantation, with topical anaesthesia. The main outcome measures werepreoperative and postoperative visual acuity for near and distance; range of accommodation; change inanterior chamber depth.Results: In the study group compared with the control group, range of accommodation was significantly(p = 0.01) higher (1.01 (SD 0.4) dioptres versus 0.50 (0.11) dioptres) and change in anterior chamberdepth was significantly more pronounced (0.82 (0.30) versus 0.40 (0.32), p = 0.01). Both groups did notvary significantly in best corrected vision (0.94 (0.12) versus 0.93 (0.18); p = 0.74).Conclusion: During a mean follow up period of 8 months after implantation, the new foldable monofocalintraocular lens with flexible haptics showed an accommodative power of about 1 dioptre, which wassignificantly higher than the accommodative power of a conventional monofocal flexible intraocular lens.The difference in the accommodative power between the two intraocular lenses was paralleled by adifference in the change of the anterior chamber depth.
Treatment of cataract as the most common surgicallytreatable reason for decreased vision in the elderlypopulation has almost been perfected by phacoemulsifi-
cation and implantation of intraocular lenses using localanaesthesia. All functions of the natural lens remaining inthe elderly patient can be restored such as transparency,refraction, compartmentalisation of the eye into a posteriorsegment and an anterior segment, and inner stabilisation ofthe eye. The only remaining function that has generally notyet been restored by surgery on its way to a ‘‘restitutio adintegrum’’ or functional rejuvenation of the eye, is accom-modation. It was, therefore, the aim of thsi study to evaluatethe accommodative power of a new foldable monofocalintraocular lens with flexible haptics, which may allow somedegree of accommodation.
PATIENTS AND METHODSThe prospective randomised, non-masked clinical interven-tional study included 80 eyes of 40 consecutive patients ineach group who presented with advanced cataract for routinecataract surgery. Exclusion criteria were age of less than40 years or higher than 80 years, diabetes mellitus, glau-coma, exudative age related macular degeneration, non-exudative age related macular degeneration with large softdrusen, history of ocular trauma, or previous ocular surgery.The total study population was randomised into a studygroup consisting of 40 patients undergoing standard cataractsurgery with implantation of the new foldable monofocalintraocular lens with flexible haptics (IOL 1 CU; HumanOptics AG, Erlangen, Germany) in both eyes, and a controlgroup consisting of 40 patients who underwent standardcataract surgery with implantation of a conventional foldablemonofocal intraocular lens (IOL AR 40e Sensar, Allergan,Irvine, CA, USA) in both eyes. For all patients included in thestudy, the density of cataract was estimated using a relativescale ranging from 0 for clear lens to 4 for mature cataract.Additonally, the duration of surgery, the width of the clear
cornea incision, and the diameter of the capsulorhexis weredetermined. Mean age was 73.29 (SD 5.89) years (range 62–82)in the study group, and 72.66 (4.78) years (range 59–80 years)in the control group. Mean axial length measured 22.87 (0.62)mm in the study group and 23.01 (0.47) mm in the controlgroup. Both groups did not vary significantly (p.0.40) in age,refractive error, axial length, anterior chamber depth, andanterior corneal curvature radius (table 1).Both intraocular lenses carrying the CE mark were certified
for intraocular implantation in the European Union.Informed consent was obtained from all patients beforeenrolment into the study. All patients were fully informedabout the new intraocular lens. Institutional ethics commit-tee approved that the methods applied in the study adheredto the tenets of the declaration of Helsinki for the use ofhuman subjects in biomedical research.The surgical procedure included a paracentesis performed
at the 10 o’clock position and the 1 o’clock position, a clearcornea incision in the horizontal meridian (nasal for righteyes, temporal for left eyes), injection of a viscoelasticsubstance into the anterior chamber, a continuous curvelined capsulorrhexis, phacoemulsification in the chop tech-nique, injection of a viscoelastic substance into the anteriorchamber and the capsular bag, endocapsular implantation ofthe intraocular lens, aspiration of the remaining viscoelasticsubstance, and injection of Ringer’s solution through theparacentesis into the anterior chamber to increase theintraocular pressure to normal values. The new intraocularlens was implanted either with the help of an implantationforceps or with a shooter. The conventional intraocular lensin the control group was inserted using a shooter. Allsurgeries were performed by the same surgeon (GS) withtopical anaesthesia using oxybuprocaine 0.4%.The study and control groups did not vary significantly in
intraoperative data such as duration of surgery, size of thecorneal incision, and diameter of the curvilinear capsulor-rhexis (table 2).
1289
www.bjophthalmol.com

All patients were examined preoperatively, and 1 monthand 6 months after surgery. The examination included slitlamp biomicroscopy of the anterior and posterior segment ofthe eye, gonioscopy, applanation tonometry. keratometry,optical interferometry (IOL Master, Zeiss-Humphrey, SanLeandro, CA, USA) , and visual acuity measurements. At thevisit 6 months after surgery, one patient in each group waslost to follow up.Accommodation was measured in five ways. Firstly, using
distance correction, visual acuity was determined for the nearat a distance of 30 cm using Nieden and Jaeger charts.Secondly, using distance correction and determining distantvisual acuity, minus lenses were added to the correction untilone Snellen line in visual acuity was lost. Thirdly, defocusingcurves were measured. With best corrected glasses fordistance, lenses ranging from +3.0 dioptres to 23.0 dioptreswere added in 0.5 dioptre steps. The best visual acuity witheach spherical addition was recorded. Fourthly, using opticalinterferometry (IOL Master, Zeiss-Humphrey, San Leandro,CA, USA), the change in anterior chamber depth wasmeasured during intended accommodation. Fifthly, usingoptical interferometry the anterior chamber depth wasmeasured in medical mydriasis using tropicamide 0.5% eyedrops (four times), and in medical miosis after installation ofpilocarpine 2% eye drops four times. Visual acuity wasmeasured using Snellen lines at a distance of 5 metres. UsingNieden and Jaeger charts held in a distance of 35 cm in frontof the patient and illuminated from above (about 70 cd/m2),near vision was assessed with best correction for the distancewithout added glasses, and with added glasses of 3 dioptres.For statistical analysis, the Mann-Whitney test was applied totest the significance of differences between the groups.
RESULTSAt the end of the follow up period, best corrected visualacuity in the distance measured in the study group 0.94(0.12) and 0.93 (0.18) in the control group with nosignificant (p=0.74) difference between the two groups(table 3). Correspondingly, best corrected visual acuity atnear did not vary significantly (p=0.34) between the twogroupsAccommodative power measured as visual acuity in the
near with glasses of the best correction for the distance,accommodative power measured as the power of minus
lenses added to the best correction for the distance until atleast one Snellen line was lost for the distance vision, andaccommodative power measured by the position of the apexof the accommodation curves, was significantly (p,0.01)higher in the study group than in the control group (table 3).Additionally, the change in the anterior chamber depthassociated with accommodation was significantly (p=0.01)more marked in the study group than in the control group(table 3). The difference between distance corrected nearvision and uncorrected near vision was statistically signifi-cant in both groups (p,0.05). Especially in the 1 CU groupthere was no dependency of the accommodative power andthe spherical power of the Intraocular lens.Anterior chamber haemorrhage originating from the
anterior chamber angle was the only complication observedintraoperatively (one patient in the study group). No othercomplication such as rupture of the posterior lens capsule,vitreous prolapse, postoperative decentration of the intrao-cular lens, shallowing of the anterior chamber, and opticallysignificant secondary cataract were detected in any group.
DISCUSSIONAccommodation is a delicate process leading to a change inthe focus of the eye by alternating the shape of the lens and,thus, the position of the anterior and posterior lens surface. Itis bound to the elasticity of the lens. The accommodativepower is strongly associated with age, being about 20 dioptresin a 10 year old subject, decreasing to 10 dioptres in a 20 yearold subject, and eventually decreasing to 4 dioptres or less inthe age beyond 40 years. Attempts to restore accommodationwith cataract surgery have been focused on several mechan-isms so far. For all eyes with intraocular lenses, pseudoac-commodation caused by the miosis in association with theconvergence reaction has been known for years.1 2 It usuallymeasures about 0.5 dioptres, a figure also found in thepresent study for patients in the control group (table 3).Methods specifically associated with cataract surgery torestore accommodation have been the implantation of bifocalor multifocal intraocular lenses, and in bilateral cataractsurgery, the implantation of monofocal intraocular lenseswith induced anisometropia to achieve so called monovi-sion.3–6 Independent of cataract surgery, anisometropia, andby that ‘‘monovision,’’ was induced by a laser assisted in situkeratomileusis.7 Additionally, experimental procedures have
Table 1 Preoperative data of the study group and the control group (mean (SD))
Study group (range) Control group (range) p Value
Number 40 40Age (years) 73.29 (5.89) (62–82) 72.66 (4.78) (59–80) 0.58Far vision
Best corrected 0.38 (0.17) (0.01–0.6) 0.33 (0.23) 0.62Near vision
Best corrected 0.35 (0.16) (0.01–0.6) 0.30 (1.45) (0.01–0.5) 0.54Axial length (mm) 22.87 (0.3) (21.62–23.55) 22.59 (0.28) (21.97–24.0) 0.71Intraocular pressure(mmHg)
16.7 (3.32) (10–24) 15.9 (4.31) (11–20) 0.43
Table 2 Intraoperative data of the study and the control groups (mean (SD))
MeasurementsDuration ofsurgery (minutes)
Density ofcataract (0–4)
Size of cornealincision (mm)
Rhexis diameter(mm) Complications
Study group 11.17 (2.85) (8–20) 2.27 (0.82) (1–4) 3.21 (0.31) (3–3.5) 4.91 (0.21) (4.5–5.3) AC bleeding n = 1Control group 9.57 (2.1) (7–15) 2.8 (0.56) (1–4) 3.3 (0.19) (3–3.5) 5.42 (0.18) (5.0–6.0) —p Value 0.18 (NS) 0.47 (NS) 0.51 (NS) 0.29 (NS) —
Mean (SD) and range. NS, statistically not significant.
1290 Sauder, Degenring, Kamppeter, et al
www.bjophthalmol.com

been performed, such as the substitution of the lens materialinside the lens capsular bag by an elastic substance.8 All ofthe clinical methods have had their limitations, such as a lackof binocularity in patients with ‘‘monovision,’’ and a possiblyreduced quality of the retinal image in patients with bifocalor multifocal intraocular lenses as a result of the multitude ofoptical foci of intraocular lenses.9
The intraocular lens used for patients in the study group inthis investigation has flexible haptics theoretically enablingthe intraocular lens to move its optical part forward and tochange its shape if the ciliary muscle contracts, releases thetension on the zonula fibres of the lens capsular bag, andindirectly relaxes the lens capsular bag. The results of thepresent study suggest that during the follow up period of6 months after surgery, a small accommodative effect inaddition to the pseudoaccommodative effect of 0.5 dioptres,may be measurable (table 3). The mean range of accom-modation measured in the control group of about 0.5 diop-tres is in agreement with preceding studies.10
The results of the present study are in agreement withprevious investigations by Kuechle and colleagues reportingan accommodative effect of about 1.57 dioptres for the newintraocular lens.11 The change in anterior chamber depthbetween medical miosis and medical mydriasis was smallerin the study performed by Kuchle and co-workers comparedto the measurements in this study.The present investigation has limitations. It has remained
unclear, so far, how to measure the range of accommodationin pseudophakic eyes. Using defocusing curves and measur-ing the difference between the near point and the far point asperformed by Kuechle et al and as carried out in the presentinvestigation may be one of the techniques to measure therange of accommodation.11 12 Using the device ‘‘IOL Master’’(Zeiss Company, Oberkochen, Germany) for laser interfero-matic measurement of the anterior chamber depth inpseudophakic eyes as performed in the present study maylead to inaccurate results, since the device has not beendesigned for that purpose. Interestingly, however, themeasured range of accommodation of about 1 dioptreparallels the mean change in anterior chamber depth of0.82 mm between medical mydriasis and medical miosis inthe study group. Additionally, the difference in the range ofaccommodation between the two groups of this study agreeswith the difference in the change of the anterior chamberdepth measurements between the two groups (table 3).Recently, laserinterferometric measurements reported an
anterior movement of the accommodative 1 CU intraocularlens that would result in a pseudophakic accommodation of0.5 dioptres if compared to a monofokal intraocular lens,13
with a great variability of movement during pilocarpineinduced ciliary contraction. These findings are comparable to
our clinical results concerning both the amount of accom-modative power and the great variability. Langenbucher et al14
compared different possibilities for measurement of accom-modation, indicating that the lowest fluctuation between the1 CU intraocular lens and a study group with a monofocalintraocular lens could be achieved by measuring andcomparing the subjective near point and by comparingdefocusing curves. This may lead to the assuption thatsubjective measurements are especially suitable for assessingthe effect of pseudophakic accommodation.The amount of the pseudophakic accommodative power of
the 1 CU certainly increases with the spherical power of thelens.15 Both study groups did not differ significantly in axiallength of the eye or in the spherical power of the implantedintraocular lens ranging from 18–24 dioptres.In conclusion, this pilot study may suggest that for a follow
up period of 6 months, the new monofocal foldableintraocular lens may offer the possibility of a small range ofaccommodation, in addition to the pseudoaccommodativeeffect monofocal intraocular lenses usually have.1 2
Considering that the study and the control groups did notdiffer significantly in best corrected visual acuity or in thenumber of complications, further studies on the accommo-dative properties of the new intraocular lens may bewarranted.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
G Sauder, R F Degenring, B Kamppeter, P Hugger, Department ofOphthalmology and Eye Hospital, Faculty of Clinical MedicineMannheim, University of Heidelberg, 68167 Mannheim, Germany
Competing interests: none declared
REFERENCES1 Altan-Yaycioglu R, Gozum N, Gucukoglu A. Pseudo-accommodation with
intraocular lenses implanted in the bag. J Refract Surg 2002;18:271–5.2 Thornton SP. Accommodation with monofocal IOLs. Ophthalmology
1992;99:1752.3 Leyland MD, Langan L, Goolfee F, et al. Prospective randomised double-
masked trial of bilateral multifocal, bifocal or monofocal intraocular lenses.Eye 2002;16:481–90.
4 Jacobi PC, Dietlein TS, Luke C, et al. Multifocal intraocular lens implantation inpresbyopic patients with unilateral cataract. Ophthalmology2002;109:680–6.
5 Walkow L, Klemen UM. Patient satisfaction after implantation of diffractivedesigned multifocal intraocular lenses in dependence on objective parameters.Graefes Arch Clin Exp Ophthalmol 2001;239:683–7.
6 Greenbaum S. Monovision pseudophakia. J Cataract Refract Surg2002;28:1439.
7 Jain S, Ou R, Azar DT. Monovision outcomes in presbyopic individuals afterrefractive surgery. Ophthalmology 2001;108:1430–3.
8 Nishi O, Nishi K. Accommodation amplitude after lens refilling with injectablesilicone by sealing the capsule with a plug in primates. Arch Ophthalmol1998;116:1358–61.
9 Steinert RF. Visual outcome with multifocal intraocular lenses. Curr OpinOphthalmol 2000;11:12–21.
Table 3 Postoperative results (mean (SD)) in the study and the control groups 6 months after surgery
Measurements
Best correctedvisual acuitydistance
Near vision withdistance correction*
Near visionuncorrected
Near visionbest corrected
Range ofaccommodation(dioptres)
Change of anteriorchamber (mm) frommydriasis to miosis (mm)
Study group (n = 38) 0.94 (0.12) 6.53 (0.91) (N) 8.07 (1.58) (N) 2.46 (0.9) (N) 1.01 (0.4) 0.82 (0.30)Range 0.7–1.25 5–9 (N) 5–10 (N) 1–4 (N) 0.5–1.7 0.41–1.14
8.53 (1.24) (J) 10.53 (2.45) (J)Range 6–12 (J) 6–14 (J)
Control group(n = 38)
0.93 (0.18) 9.61 (1.75) (N) 7.45 (1.63) (N) 2.01 (0.82) (N) 0.5 (0.11) 0.40 (0.32)
Range 0.8–1.0 7–14 (N) 6–10 (N) 1–4 (N) 0–0.75 0.29–0.6311.61 (1.75) (J) 9.73 (1.69) (J)
Range 8–14 (J) 6–14 (J)p Value 0.74 (NS) 0.03 0.29 (NS) 0.34 (NS) (N) 0.01 0.01
*J, Jaeger charts; N, Nieden charts.Mean (SD) and range. NS, statistically not significant.
Accommodative power of a new foldable intraocular lens 1291
www.bjophthalmol.com

10 Nakazawa M, Ohtsuki K. Apparent accommodation in pseudophakic eyesafter implantation of posterior chamber intraocular lenses: optical analysis.Invest Ophthalmol Vis Sci 1984;25:1458–60.
11 Kuchle M, Nguyen NX, Langenbucher A, et al. First six-month-results ofimplantation of a new accommodative posterior chamber intraocular lens (1CU). Spektrum Augenheilkd 2001;15:260–6.
12 Kuchle M, Nguyen NX, Langenbucher A, et al. Implantation of a newaccommodative posterior chamber intraocular lens. J Refract Surg2002;18:208–16.
13 Findl O, Kriechbaum K, Menapace R, et al. Laserinterferometric assessment ofpilocarpine-induced movement of an accommodating intraocular lens: arandomized trial. Ophthalmology 2004;111:1515–21.
14 Langenbucher A, Huber S, Nguyen NX, et al. Measurement ofaccommodation after implantation of an accommodating posterior chamberintraocular lens. J Cataract Refract Surg 2003;29:677–85.
15 Nawa Y, Ueda T, Nakatsuka M, et al. Accommodation obtained per 1.0 mmforward movement of a posterior chamber intraocular lens. J Cataract RefractSurg 2003;29:2069–72.
Video reports
To view the video reports in full visit our website www.bjophthalmol.com and click on the linkto the video reports.
N Suture of a Subluxated Posterior Chamber Lens within the Capsular Bag. LE Fernandez deCastro, KD Solomon
N Ocular Onchocerciasis: Anterior Chamber Microfilariae. WJ Flynn, HD Dillon
N Zero Phaco Microincision Cataract Surgey: The Hacc Technique. K Vaitheeswaran,S Gars, R Grover, M Nadar, S Sharma
N The presenting features of multiple sclerosis. VJM Barrett, J Walker, JS Elton
N Removal of INTACS: Stepped surgical complexity demonstrated with three cases.L Ilari, J C McAlister, D S Gartry
N The Nuclear Slide: A novel approach for unleashing the potential of the hydrodissectionwave. A Naseri
N Giant pleomorphic adenoma of the lacrimal gland: pre- and post-operative function.A Jain, V I Nehru, U N Saikia, C E E Reddy
N Limbal-sparing lamellar keratoplasty. S L Watson, S Rauz, J Dart
1292 Sauder, Degenring, Kamppeter, et al
www.bjophthalmol.com

EXTENDED REPORT
Effect of dorzolamide and timolol on ocular blood flow inpatients with primary open angle glaucoma and ocularhypertensionG Fuchsjager-Mayrl, B Wally, G Rainer, W Buehl, T Aggermann, J Kolodjaschna, G Weigert,E Polska, H-G Eichler, C Vass, L Schmetterer. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr L Schmetterer,Department of ClinicalPharmacology, WahringerGurtel 18-20, A-1090Vienna, Austria; [email protected]
Accepted for publication1 April 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1293–1297. doi: 10.1136/bjo.2005.067637
Background: There is evidence that perfusion abnormalities of the optic nerve head are involved in thepathogenesis of glaucoma. There is therefore considerable interest in the effects of topical antiglaucoma drugson ocular blood flow. A study was undertaken to compare the ocular haemodynamic effects of dorzolamideand timolol in patients with primary open angle glaucoma (POAG) or ocular hypertension (OHT).Methods: One hundred and forty patients with POAG or OHT were included in a controlled, randomised,double blind study in two parallel groups; 70 were randomised to receive timolol and 70 to receivedorzolamide for a period of 6 months. Subjects whose intraocular pressure (IOP) did not respond to eitherof the two drugs were switched to the alternative treatment after 2 weeks. Scanning laser Dopplerflowmetry was used to measure blood flow in the temporal neuroretinal rim and the cup of the optic nervehead. Pulsatile choroidal blood flow was assessed using laser interferometric measurement of funduspulsation amplitude.Results: Five patients did not respond to timolol and were changed to the dorzolamide group, and 18patients changed from dorzolamide treatment to timolol. The effects of both drugs on IOP and ocularperfusion pressure were comparable. Dorzolamide, but not timolol, increased blood flow in the temporalneuroretinal rim (8.5 (1.6)%, p,0.001 versus timolol) and the cup of the optic nerve head (13.5 (2.5)%,p,0.001 versus timolol), and fundus pulsation amplitude (8.9 (1.3)%, p,0.001 versus timolol).Conclusions: This study indicates augmented blood flow in the optic nerve head and choroid after6 months of treatment with dorzolamide, but not with timolol. It remains to be established whether thiseffect can help to reduce visual field loss in patients with glaucoma.
There is increasing evidence that ocular blood flowabnormalities are involved in the pathogenesis ofglaucoma,1 so there is considerable interest in the
potential ocular haemodynamic effects of currently availableantiglaucoma drugs. A large number of clinical studies havebeen performed to clarify this issue using different techni-ques for the assessment of ocular blood flow, yieldingpartially contradicting results.2 However, many publishedstudies suffer from the fact that only a small number ofpatients were included.We have compared the ocular haemodynamic effects of
dorzolamide and timolol in a larger number of patients withglaucoma or ocular hypertension (OHT). Dorzolamide waschosen on the basis of previous evidence that this drug mayincrease ocular blood flow,3–9 although not all studies showeda positive outcome.10–12 Timolol was chosen as a controlsubstance because the ocular hypotensive effect of this b-receptor antagonist is only slightly superior to that ofdorzolamide13 and comparable effects on ocular perfusionpressure (OPP) can be expected.Optic nerve head (ONH) blood flow was measured using
scanning laser Doppler flowmetry (SLDF)14 and pulsatilechoroidal blood flow was assessed by laser interferometricmeasurement of fundus pulsation amplitude (FPA).15
METHODSPatientsAfter approval from the ethics committee of the ViennaUniversity School of Medicine, 140 patients with primaryopen angle glaucoma (POAG) or OHT were included. For the
sample size calculation, which was based on the reproduci-bility data of the Heidelberg retina flowmeter (standarddeviation of 32% as calculated from monthly measurementsfor 6 months in POAG patients, unpublished data), arepeated measures ANOVA model was used with an a levelof 0.05 and a b level of 0.2. Differences of less than 10%between treatment groups were considered to be clinicallyirrelevant. Hence, the sample size calculation gave a totalnumber of 127 subjects. Originally, a drop out rate of 20%was anticipated and 160 patients were scheduled accordingly.Since it turned out that the drop out rate was smaller, only140 patients were included. The variability of topical funduspulsation measurement is smaller and was therefore notconsidered in our sample size calculation.The baseline characteristics of these patients have been
reported in detail previously.16 Inclusion criteria were eitherPOAG or OHT with an untreated intraocular pressure (IOP)of >21 mm Hg in at least one eye, which had to bedocumented on at least three different occasions. A washoutperiod of 2 weeks for previous antiglaucoma treatment wasscheduled for all patients. Any of the following excluded apatient from participation in the trial: exfoliation glaucoma,pigmentary glaucoma, history of acute angle closure, meandeviation (MD) of visual field testing (Humphrey 30-2program) .12, intraocular surgery or argon laser trabeculo-plasty within the last 6 months, ocular inflammation or
Abbreviations: FPA, fundus pulsation amplitude; HRF, Heidelbergretina flowmeter; IOP, intraocular pressure; OHT, ocular hypertension;ONH, optic nerve head; OPP, ocular perfusion pressure; POAG,primary open angle glaucoma; SLDF, scanning laser Doppler flowmetry
1293
www.bjophthalmol.com

infection within the last 3 months, bradycardia (heart rate,50 beats/min), second and third degree heart block, asthmabronchiale, chronic obstructive pulmonary disease, conges-tive heart failure, severe renal impairment (creatinineclearance ,1.8 l/h), history of hypersensitivity to one of thestudy drugs or drugs with similar chemical structure, historyof non-IOP responder to topical b-blockers or topical carbonicanhydrase inhibitors (CAIs), and pregnancy.The differentiation between POAG and OHT patients was
based on the criteria of the Ocular Hypertension TreatmentStudy.17 An abnormal visual field was accordingly defined asa glaucoma hemifield test outside normal limits and/or acorrected pattern standard deviation with p,0.05.
ProtocolThe study was performed in a randomised, double blind,parallel group design. Patients either received timolol twicedaily (Timoptic, MSD) or dorzolamide three times a day for6 weeks. To enable double blind conditions, patients in thetimolol group received a placebo bottle identical in appear-ance for lunch time instillation. The study schedule is shownin fig 1. During the 2 weeks before the start of the study,patients were assessed for eligibility and examined asoutlined above. If at least one eye was eligible for the study,a baseline visit was scheduled. If possible, both eyes weretreated with the study medication. If not, the contralateraleye was treated according to the clinical requirements. At thebaseline visit all outcome variables were assessed between08.00 and 12.00 hours.Patients were asked to return 2 weeks after the baseline
visit. During this visit they were divided into responders andnon-responders. Responders were defined as patients with anIOP (19 mm Hg or a decrease in IOP compared withbaseline of >25% in the index eye, and they continued thestudy as scheduled. Non-responders or patients who did nottolerate the study medication crossed over to the alternativetreatment and were scheduled for a further visit 2 weekslater. At the visit 2 weeks after changing the medicationthese patients were again divided into responders and non-responders. Non-responders to both medications wereeliminated from the study. Those patients who respondedto the second antiglaucoma drug continued the study asscheduled.Further visits were scheduled 3 months and 6 months
after the baseline visit. All haemodynamic outcome variablesand IOP were assessed during these visits. At the last visit avisual field test and an ophthalmic examination wereperformed again. A deviation of ¡3 days was accepted forthe 2 weeks visit and of ¡1 week for the other visits.The studies were performed at the Department of Clinical
Pharmacology and the Department of Ophthalmology,Allgemeines Krankenhaus, Vienna.
MeasurementsScanning laser Doppler f lowmetry (SLDF)SLDF was performed using the Heidelberg retina flowmeter(HRF; Heidelberg Engineering, Heidelberg, Germany). TheHRF is a confocal scanning laser ophthalmoscope employingthe principles of SLDF. The mean red blood cell velocity,blood volume, and blood flow can be calculated in relativeunits for any image point.18 In the present study one 10610pixel area (1006100 mm) in the cup of the optic disc (CupBF)and one 20620 pixel area (2006200 mm) at the temporalneuroretinal rim (RimBF) were chosen for calculation ofhaemodynamic parameters. The selection of the measure-ment areas was based on the method described by Nicolela etal.19 The neuroretinal rim was measured from images focusedon the superficial retina and the cup from images focused onthe lamina cribrosa. The measurements were performed inregions without major surface vessels.Reproducibility is a critical issue with SLDF.20 21 At least
two recordings were therefore taken and the mean of the twovalues from the best images obtained was calculated. Onlyflow readings with a coefficient of variation of less than 20%were included in the analysis.
Laser interferometric measurement of funduspulsationPulse synchronous pulsations of the eye fundus wereassessed by laser interferometry as described in detail bySchmetterer et al.15 The eye is illuminated by a laser beamwhich is reflected at both the front surface of the cornea andthe fundus. The two re-emitted waves produce interferencefringes from which the distance changes between the corneaand retina during a cardiac cycle can be calculated. Themaximum distance change is called the fundus pulsationamplitude (FPA) and estimates the choroidal pulsatile bloodflow.22 23 Again, two measurements were performed and themean was calculated. FPA values with a coefficient ofvariation of more than 20% were not included in the analysis.
Visual field testingVisual field testing was performed with the Humphrey Fieldanalyser (Full Threshold Program 30-2). All patients wereexperienced in visual field testing having performed at leastthree tests in total and one test during the 3 months beforethe beginning of the study. All measurements were super-vised by an experienced technician. Visual field eligibilitycriteria were less than 33% false positives, less than 33% falsenegatives, and less than 33% fixation losses.
Non-invasive measurement of systemichaemodynamicsSystolic and diastolic blood pressure (SBP, DBP) weremeasured on the upper arm by an automated oscillometricdevice; mean arterial pressure (MAP) was calculated as 1/3SBP + 2/3 DBP. Pulse rate was automatically recorded from afinger pulse oximetric device (HP-CMS patient monitor,Hewlett Packard, Palo Alto, CA, USA). Ocular perfusionpressure (OPP) was calculated as 2/3 * MAP 2 IOP.
Analysis of dataA two way repeated measures ANOVA model was used tocompare the effects of dorzolamide and timolol. Patients whoonly appeared at the baseline visit were not included in theanalysis. In all patients who did not complete the study butwho attended at least the 2 week visit, the last observationwas carried forward. The data from the last visit that actuallytook place were therefore used for all further missing entries.In patients who did not respond to the medication atrandomisation and switched over to the alternative treat-ment, the pretreatment values were taken as baseline. In
Positive inclusion criteria
2 weeks
6 months
RR
6 months
NR
Exclusion
Dorzolamide Timolol
6 months6 months
Figure 1 Study schedule (R = IOP responders; NR= IOP non-responders).
1294 Fuchsjager-Mayrl, Wally, Rainer, et al
www.bjophthalmol.com

these cases the values assessed at the 2 week visit were notincluded in the analysis. In addition, a multiple regressionanalysis model was performed using stepwise inclusion ofpredicting variables (for order of inclusion see table 3) tocharacterise potential determinants of dorzolamide andtimolol induced changes in blood flow parameters versusbaseline. Data are presented as mean (SD) values. The level ofsignificance was set at p=0.05.
RESULTSThe baseline characteristics of the study population havebeen presented in a previous report16 and are summarised intable 1.
Three patients appeared at the baseline visit only and werenot included in the analysis. Five patients did not respond totimolol and changed to the dorzolamide group after the first2 weeks of treatment. Eighteen patients did not show anadequate IOP response to dorzolamide or did not tolerate thetreatment and changed to the timolol group. The failure ratedue to inadequate IOP control or adverse reactions wassignificantly higher in the dorzolamide group than in thetimolol group (p,0.001). After switching to the alternativetreatment, all patients showed satisfactory IOP control andno subject had to be excluded at this stage of the study.After the 2 week and 3 month visits, seven and five
patients respectively were lost to follow up. The data on these12 subjects were carried forward. The study drugs had noinfluence on blood pressure or pulse rate (SBP: p=0.823between groups; DBP: p=0.644 between groups; pulse rate:p=0.511 between groups; table 2). Baseline IOP was similarin both treatment groups (timolol: 23.0 (3.1) mm Hg;dorzolamide: 22.8 (3.3) mm Hg). The reduction in IOP wassimilar in the two groups (p=0.32, fig 2). At the 6 monthvisit the reduction in IOP was 23.8 (1.4)% with timololtreatment and 19.9 (1.6)% with dorzolamide. Accordingly,the OPP tended to be increased in both groups to a similardegree (p=0.912 between groups; table 2). All ocularhaemodynamic variables increased during treatment withdorzolamide but did not change during timolol treatment(fig 2). This difference was significant for CupBF (p,0.001),RimBF (p,0.001), and FPA (p,0.001). After 6 months oftreatment CupBF increased by 13.5 (2.5)%, RimBF by 8.5(1.6)%, and FPA by 8.9 (1.3)% after treatment withdorzolamide; no effect was seen with timolol.The results of the multiple regression analysis are shown in
table 3. The increase in ocular haemodynamic parametersduring dorzolamide treatment was independent of thedecrease in IOP and independent of baseline IOP. In addition,the increase was comparable in POAG and OHT patients and
Table 1 Characteristics of the study population
POAG(n = 49)
OHT(n = 91)
Age (years) 63.0 (13.5) 61.2 (13.3)Sex (M/F) 19/30 48/43IOP (mm Hg) 22.6 (2.9) 23.2 (3.8)SBP (mm Hg) 141.0 (15.8) 142.8 (17.8)DBP (mm Hg) 75.7 (10.1) 74.8 (11.9)OPP (mm Hg) 39.0 (7.2) 40.6 (9.0)Pulse rate (/min) 78.1 (12.5) 78.0 (11.6)Mean deviation 21.58 (211.09–
+2.83)20.16 (25.35–+4.10)
Vertical C/D ratio 0.75 (0.11) 0.59 (0.12)Horizontal C/D ratio 0.77 (0.11) 0.62 (0.11)Optic disc area 1.58 (0.37) 1.46 (0.34)RimBF (au) 287 (51) 333 (111)CupBF (au) 192 (71) 212 (101)FPA (mm) 3.0 (0.8) 3.3 (0.9)
IOP, intraocular pressure; SBP, systolic pressure; DBP, diastolic pressure;OPP, ocular perfusion pressure; C/D ratio, cup to disc ratio; RimBF, rimblood flow; CupBF, cup blood flow; FPA, fundus pulsation amplitude.Data are presented as mean (SD) except for mean deviation which isshown as median (range).
0
–30
–25
–20
–15
–10
–5
Intra
ocul
ar p
ress
ure
(% c
hang
e)
12
9
6
3
0Rim
blo
od fl
ow (%
cha
nge)
2 weeks 3 months 6 months
16
14
12
10
8
6
4
2
0
–2
Cup
blo
od fl
ow (%
cha
nge)
12
9
6
3
0
A
C
B
D
Fund
us p
ulsa
tion
ampl
itude
(% c
hang
e)
2 weeks 3 months 6 months
Figure 2 Effects of dorzolamide (darker bars) and timolol (lighter bars) on (A) intraocular pressure, (B) cup blood flow, (C) rim blood flow, and (D)fundus pulsation amplitude. Data are presented as mean (SD). Asterisks indicate significant effects of dorzolamide compared with timolol.
Dorzolamide and ocular blood flow 1295
www.bjophthalmol.com

was not influenced by any other measured variable. After6 months of treatment with timolol or dorzolamide, visualfield parameters remained unchanged (data not shown).
DISCUSSIONThis study indicates that 6 months of treatment withdorzolamide, but not with timolol, is associated with anincrease in ocular blood flow. This was shown using twoindependent methods for the assessment of ocular haemo-dynamic parameters. Several arguments indicate that thisresult is caused by a direct vasodilator effect of dorzolamideand not secondary to a decrease in IOP. On the one hand,dorzolamide and timolol induced a comparable decrease inIOP and a comparable increase in OPP, whereas ocularhaemodynamic effects were only observed with dorzolamide.On the other hand, the results of our multiple regressionanalysis indicate that the increase in OPP is independent ofthe IOP lowering effects.The relevance of our results for the treatment of glaucoma
is critically dependent on whether reduced ONH blood flowcontributes to retinal ganglion cell loss in glaucoma. Manystudies have shown that blood flow in the ONH is reduced inpatients with glaucoma,19 24–27 but cross sectional studies donot provide a link between reduced perfusion and progres-sion of the disease. In recent years, however, there isincreasing evidence that reduced ocular blood flow is directlyassociated with visual field loss. In a longitudinal study inpatients with normal tension glaucoma, decreased blood flowvelocities in retrobulbar vessels were associated with pro-gression of visual field loss.28 This is in keeping with a morerecent retrospective study in which the rate of progression ofvisual field damage was related to reduced retrobulbar bloodflow velocities independently of the pre-existing visual fielddamage and the IOP.29 A significant correlation between ONHblood volume, as assessed by SLDF, and visual field loss in
POAG was recently reported in a longitudinal study with amean follow up of 33 months.30 In addition, numerousstudies indicate that glaucoma is not only related to reducedONH blood flow but also to abnormal ocular blood flowregulation; this is not easy to explain by a secondaryreduction in blood flow. Analysis of baseline blood flow inthe present study showed that there is an abnormalassociation between RimBF, CupBF and FPA and systemicblood pressure which is not seen in age matched healthycontrol subjects.16 While these trials do not establish directevidence for a beneficial treatment effect of enhancing ONHblood flow in patients with POAG, they provide a strongrationale for characterising antiglaucoma drugs with ocularhypotensive as well as ocular vasodilator properties.The exact mechanism underlying the vasodilator effects of
CAIs in ocular vessels is unclear. In rat retinal organ cultureCAIs decreased pH in the extracellular space and increasedpH in the intracellular space, related to an increase in retinalcapillary diameters and retinal pericyte relaxation.31
Intravenously administered dorzolamide induces acidosis ofarterial blood32 and of the extracellular space over the ONH.33
On the other hand, experiments in isolated precontractedbovine retinal arteries indicate that the vasodilator effects ofdorzolamide are independent of changes in pH becausedorzolamide induced dilatation is also seen when pH is keptconstant.34 Activation of nitric oxide does not appear to play amajor role in CAI induced vasodilation in the eye,35 andfurther studies are required to understand the mechanismsunderlying the vascular effects of CAIs.An interesting observation from the present study is that
all ocular haemodynamic parameters were virtuallyunchanged after treatment with timolol. Previous reportson the ocular haemodynamic effects of timolol are contra-dictory, which may be related to different treatment regi-mens, method related problems, and a lack of adequate study
Table 2 Effects of dorzolamide and timolol on blood pressure and pulse rate
Baseline 2 weeks 3 months 6 months
TimololSBP (mm Hg) 142.1 (16.5) 140.7 (19.2) 137.4 (20.7) 134.3 (24.1)DBP (mm Hg) 75.3 (9.5) 73.6 (9.9) 73.0 (10.3) 75.6 (11.7)OPP (mm Hg) 39.3 (7.4) 41.3 (7.6) 40.0 (6.3) 41.0 (8.3)Pulse rate (/min) 76.8 (12.0) 75.9 (12.0) 73.4 (11.8) 73.4 (11.7)
DorzolamideSBP (mm Hg) 142.3 (18.1) 140.7 (21.4) 136.8 (19.5) 138.1 (17.9)DBP (mm Hg) 75.0 (13.7) 75.6 (12.4) 72.8 (11.6) 71.4 (11.8)OPP (mm Hg) 39.0 (8.3) 41.8 (9.3) 40.6 (8.4) 39.4 (8.3)Pulse rate (/min) 79.9 (12.0) 82.1 (13.3) 81.2 (12.9) 79.2 (13.4)
SBP, systolic blood pressure; DBP, diastolic blood pressure; OPP, ocular perfusion pressure.Data are presented as mean (SD).
Table 3 Multiple regression analysis between dorzolamide induced changes in ocularhaemodynamic parameters and the other assessed parameters (p values are shown)
RimBF CupBF FPA
POAG/hypertension 0.52 0.60 0.59% change in OPP (after 6 months) 0.28 0.40 0.25% change in IOP (after 6 months) 0.20 0.60 0.23OPP 0.67 0.56 0.69Intraocular pressure 0.61 0.78 0.33Mean deviation 0.79 0.72 0.71Age 0.42 0.49 0.64SBP 0.66 0.56 0.73DBP 0.82 0.72 0.84Pulse rate 0.88 0.83 0.76
RimBF, rim blood flow; CupBF, cup blood flow; FPA, fundus pulsation amplitude; OPP, ocular perfusion pressure;IOP, intraocular pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure.
1296 Fuchsjager-Mayrl, Wally, Rainer, et al
www.bjophthalmol.com

design.36–41 Our results do, however, indicate that long termtopical administration of timolol is not associated withrelevant ocular haemodynamic effects.Both techniques used for the assessment of ocular
haemodynamics have limitations. With the HRF the sam-pling depth within ONH tissue is not known. In addition,reproducibility is a problem with this technique19 20 and ismore severe in patients with glaucoma than in healthycontrol subjects, leading to comparatively high sample sizes.With FPA measurement it is obvious that only the pulsatileportion of choroidal blood flow is measured. Accordingly, anyconclusion on the pharmacodynamic effects with thistechnique is critically dependent on the assumption thatthe ratio of pulsatile to non-pulsatile blood flow is constant.In the present study consistent results were observed withboth techniques, indicating that the observed effects are notinfluenced to a significant degree by the limitations of thetechniques.42
In conclusion, the data presented here indicate thatdorzolamide, but not timolol, increases ONH and choroidalblood flow in patients with POAG or OHT. It remains to beseen whether this effect is associated with a preservation ofvisual fields in patients with glaucoma.
ACKNOWLEDGEMENTSThe authors thank the following ophthalmologists for sending theirpatients to our unit for inclusion in the present study: Dr ElisabethArocker-Mettinger, Dr Helga Azem, Dr Alexandra Crammer, Dr PaulDrobec, Dr Marcela Hakl, Dr Christine Honigsmann, Dr Hans Kossler,Dr Eva Krammer, Dr Constanze Merenda, Dr Maria Reichel, DrGunther Reichelt, Dr Karin Schmetterer, Dr Herbert Schuster, DrNaresh Sheetal, Dr Elisabeth Sienko, Dr Eva Weingessl.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
G Fuchsjager-Mayrl, B Wally, T Aggermann, J Kolodjaschna,G Weigert, E Polska, H-G Eichler, L Schmetterer, Department of ClinicalPharmacology, Medical University of Vienna, AustriaG Fuchsjager-Mayrl, G Rainer, W Buehl, C Vass, Department ofOphthalmology, Medical University of Vienna, AustriaL Schmetterer, Institute of Medical Physics, Medical University of Vienna,Austria
Financial support from an unrestricted grant from Merck, Sharpe andDohme is acknowledged.
REFERENCES1 Flammer J, Orgul S, Costa VP, et al. The impact of ocular blood flow in
glaucoma. Prog Retin Eye Res 2002;21:359–93.2 Harris A, Jonescu-Cuypers CP. The impact of glaucoma medication on
parameters of ocular perfusion. Curr Opin Ophthalmol 2001;12:131–7.3 Harris A, Arend O, Arend S, et al. Effects of topical dorzolamide on retinal
and retrobulbar hemodynamics. Acta Ophthalmol Scand 1996;74:569–72.4 Martinez A, Gonzalez F, Capeans C, et al. Dorzolamide effect on ocular
blood flow. Invest Ophthalmol Vis Sci 1999;40:1270–5.5 Harris A, Arend O, Kagemann L, et al. Dorzolamide, visual function and
ocular hemodynamics in normal-tension glaucoma. J Ocul Pharmacol Ther1999;15:189–97.
6 Harris A, Arend O, Chung HS, et al. A comparative study of betaxolol anddorzolamide effect on ocular circulation in normal-tension glaucoma patients.Ophthalmology 2000;107:430–4.
7 Harris A, Jonescu-Cuypers CP, Kagemann L, et al. Effect of dorzolamidetimolol combination versus timolol 0.5% on ocular blood flow in patients withprimary open-angle glaucoma. Am J Ophthalmol 2001;132:490–5.
8 Avunduk AM, Sari A, Akyol N, et al. The one-month effects of topicalbetaxolol, dorzolamide and aprachlonidine on ocular blood flow velocities inpatients with newly diagnosed primary open-angle glaucoma.Ophthalmologica 2001;215:361–5.
9 Bernd AS, Pillunat LE, Bohm AG, et al. Okulare Hamodynamik undGesichtsfeld beim Glaukom unter Dorzolamid-Therapie. Ophthalmologe2001;98:451–5.
10 Grunwald JE, Mathur S, DuPont J. Effects of dorzolamide hydrochloride 2%on the retinal circulation. Acta Ophthalmol 1997;75:236–8.
11 Pillunat LE, Bohm AG, Koller AU, et al. Effect of topical dorzolamide on opticnerve head blood flow. Graefes Arch Clin Exp Ophthalmol1999;237:495–500.
12 Bergstrand IC, Heijl A, Harris A. Dorzolamide and ocular blood flow inpreviously untreated glaucoma patients: a controlled double-masked study.Acta Ophthalmol Scand 2002;80:176–82.
13 Balfour JA, Wilde MI. Dorzolamide. A review of its pharmacology andtherapeutic potential in the management of glaucoma and ocularhypertension. Drugs Aging 1997;10:384–403.
14 Michelson G, Schmauss B, Langhans MJ, et al. Principle, validity, andreliability of scanning laser Doppler flowmetry. J Glaucoma 1996;5:99–105.
15 Schmetterer L, Lexer F, Unfried C, et al. Topical measurement of funduspulsations. Opt Eng 1995;34:711–6.
16 Fuchsjager-Mayrl G, Wally B, Georgopoulos M, et al. Ocular blood flow andsystemic blood pressure in patients with primary open-angle glaucoma andocular hypertension. Invest Ophthalmol Vis Sci 2004;45:834–9.
17 Keltner JL, Johnson CA, Cello KF, et al. Classification of visual fieldabnormalities in the ocular hypertension treatment study. Arch Ophthalmol2003;121:643–50.
18 Bonner R, Nossal R. Principles of laser-Doppler flowmetry in laser-Dopplerblood flowmetry. In: Shepard AP, Oberg AP, eds. Developments incardiovascular medicine. Volume 107. Boston: Kluwer Academic Publishers,1990:17–45.
19 Nicolela MT, Hnik P, Drance SM. Scanning laser Doppler flowmetry study onretinal and optic disc blood flow in glaucomatous patients. Am J Ophthalmol1996;122:775–83.
20 Strenn K, Menapace R, Rainer G, et al. Reproducibility and sensitivity ofscanning laser Doppler flowmetry during graded changes in pO2.Br J Ophthalmol 1997;81:360–4.
21 Nicolela MT, Hnik P, Schulzer M, et al. Reproducibility of retinal and opticnerve head blood flow measurements with laser Doppler flowmetry.J Glaucoma 1997;6:157–64.
22 Schmetterer L, Dallinger S, Findl O, et al. A comparison between laserinterferometric measurement of fundus pulsation and pneumotonometricmeasurement of pulsatile ocular blood flow. 1. Baseline considerations. Eye2000;14:39–45.
23 Schmetterer L, Dallinger S, Findl O, et al. A comparison between laserinterferometric measurement of fundus pulsation and pneumotonometricmeasurement of pulsatile ocular blood flow. 2. Effects of changes in pCO2 andpO2 and of isoproterenol. Eye 2000;14:46–52.
24 Grunwald JE, Piltz J, Hariprasad SM, et al. Optic nerve and choroidalcirculation in glaucoma. Invest Ophthalmol Vis Sci 1998;39:2329–36.
25 Kerr J, Nelson P, O’Brien C. A comparison of ocular blood flow in untreatedprimary open-angle glaucoma and ocular hypertension. Am J Ophthalmol1998;126:42–51.
26 Michelson G, Langhans MJ, Groh MJ. Perfusion of the juxtapapillary retinaand the neuroretinal rim area in primary open angle glaucoma. J Glaucoma1996;5:91–8.
27 Findl O, Rainer G, Dallinger S, et al. Assessment of optic disc blood flow inpatients with open angle glaucoma. Am J Ophthalmol 2000;130:589–96.
28 Yamaaki Y, Drance SM. The relationship between progression of visual fielddefects and retrobulbar circulation in patients with glaucoma.Am JOphthalmol1997;124:287–95.
29 Saltimis M, Orgul S, Doubler B, et al. Rate of progression of glaucomacorrelates with retrobulbar circulation and intraocular pressure.Am J Ophthalmol 2003;135:664–9.
30 Zink JM, Grunwald JE, Piltz-Seymour J, et al. Association between lower opticnerve laser Doppler blood volume measurements and glaucomatous visualfield progression. Br J Ophthalmol 2003;87:487–91.
31 Reber F, Gersch U, Funk RW. Blockers of carbonic anhydrase can causeincrease of retinal capillary diameter, decrease of extracellular and increaseof intracellular pH in rat retinal organ culture. Graefes Arch Clin ExpOphthalmol 2003;241:140–8.
32 Stefansson E, Jensen PK, Eysteinsson T, et al. Optic nerve oxygen tension inpigs and the effect of carbonic anhydrase inhibitors. Invest Ophthalmol Vis Sci1999;40:2756–61.
33 Pedersen DB, Eysteinsson T, Kiilgaard JF, et al. The effect of intravenousadministration of carbonic anhydrase inhibitors and NH4Cl on pre-optic pH.Invest Ophthalmol Vis Sci. 2001;42: ARVO abstract, 4449.
34 Josefsson A, Sigurdsson SB, Bang K, et al. Dorzolamide inducesvasodilatation in isolated pre-contracted bovine retina arteries. Exp Eye Res2004;78:215–21.
35 Kiss B, Dallinger S, Findl O, et al. Acetazolamide-induced cerebral and ocularvasodilation in man is independent of nitric oxide. Am J Physiol1999;276:R1661–7.
36 Grunwald JE. Effect of topical timolol on the human retinal circulation. InvestOphthalmol Vis Sci 1986;27:1713–8.
37 Boles Carenini B, Brogliatti B, Boles Carenini A. Pulsatile ocular blood flowand antiglaucomatous drugs. New Trends Ophthalmol 1992;7:195–200.
38 Boles Carenini A, Sibour G, Boles Carenini B. Differences in long term effect oftimolol and betaxolol on the pulsatile ocular blood flow. Surv Ophthalmol1994;38(Suppl):S118–24.
39 Yoshida A, Feke GT, Ogasawara H, et al. Effect of timolol on human retinal,choroidal and optic nerve head circulation. Ophthalmic Res1991;23:162–70.
40 Harris A, Spaeth GL, Sergott RC, et al. Retrobulbar arterial hemodynamiceffects of betaxolol and timolol in normal-tension glaucoma. Am J Ophthalmol1995;20:168–75.
41 Schmetterer L, Strenn K, Findl O, et al. Effects of antiglaucoma drugs onocular hemodynamics in healthy volunteers. Clin Pharmacol Ther1997;61:583–95.
42 Polska E, Polak K, Luksch A, et al. Twelve hour reproducibility of choroidalblood flow parameters in healthy subjects. Br J Ophthalmol 2004;88:533–7.
Dorzolamide and ocular blood flow 1297
www.bjophthalmol.com

EXTENDED REPORT
The relation between intraocular pressure peak in the waterdrinking test and visual field progression in glaucomaR Susanna Jr, R M Vessani, L Sakata, L C Zacarias, M Hatanaka. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr R M Vessani, RuaItambe 422, apt 52, SaoPaulo, Sao Paulo, Brazil;[email protected]
Accepted for publication1 April 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1298–1301. doi: 10.1136/bjo.2005.070649
Aim: To compare the results of the water drinking test between glaucomatous eyes with and without visualfield progression.Methods: Retrospective analysis of 76 eyes of 76 open angle glaucoma patients followed for a meanperiod of 26.0 (SD 13.8) months. Patients were submitted to the water drinking test at the beginning of thefollow up period. Reliable achromatic automated perimetry tests performed during the studied period wereused to characterise visual field progression. All subjects were under clinical therapy and had anintraocular pressure (IOP) lower than 17 mm Hg monitored by isolated measurements during the followup period. The results of the water drinking test were compared between glaucomatous eyes with andwithout visual field progression.Results: Twenty eight eyes reached definite visual field progression. There were no significant differencesin the mean age, sex, race, basal IOP, number of antiglaucomatous drugs, initial mean deviation (MD),and corrected pattern standard deviation (CPSD) between eyes that showed visual field progression andthe ones who did not progress. A significant difference of 1.9 (SD 0.6) mm Hg (p = 0.001, analysis ofcovariance; 95% CI 0.8 to 3.0) was observed between glaucomatous eyes that showed visual fielddeterioration and glaucomatous eyes that did not progress. A significant difference of 16.8% (SD 4.6%) inthe mean percentage of IOP variation was also observed between the two groups (p,0.001, analysis ofcovariance; 95% CI 7.7 to 26.0).Conclusions:Mean IOP peak and percentage of IOP variation during water drinking test were significantlyhigher in patients with visual field progression compared with patients who did not progress.
Increased intraocular pressure (IOP) is the main risk factorfor the development of glaucoma and its progression.1
Lowering IOP is believed to be beneficial in slowing downglaucomatous changes of the optic nerves and visual field.2–4
However, reduction of IOP to a preselected level does notalways prevent deterioration.5–7 Factors independent of IOPmay be responsible, in part, for the sustained progression ofglaucoma8 but it has been suggested that in some cases theprogressive damage could be caused by peaks of IOP ordiurnal IOP variability not detected by tonometry duringoffice hours.9–12
A diurnal IOP curve gives a better estimate of anindividual’s IOP level and fluctuations than a singlemeasurement during the office visit, but demandshospital admission where IOP is measured over 24 hours.10
Some authors have demonstrated ‘‘home tonometry’’ asanother form to obtain 24 hour IOP data;11–13 however, thiskind of monitoring is demanding and may be susceptibleto bias.Many studies have been aimed at finding some way of
predicting the peak diurnal IOP. The water drinking test wasconsidered to have an inadequate diagnostic value in thepast14 15 but it has been proposed as a practical method topredict the IOP peak of the diurnal tension curve. Previousstudies observed a correlation between the IOP peak in thediurnal tension curve and in the water drinking test.16 17 Thistest may be used to access the efficacy of different forms ofIOP reduction (clinical or surgical).17 18
To study the risk associated with diurnal IOP variations inpatients with open angle glaucoma, we evaluated the waterdrinking test performance in open angle glaucoma eyesbefore a longitudinal follow up with periodic visual fieldexaminations.
METHODOLOGYOne hundred and eighty patients with diagnosis of openangle glaucoma who were submitted to the water drinkingtest between January 1998 and December 2003 had theircharts reviewed. Patients were selected based on inclusionand exclusion criteria. One eye of each patient was includedin this study. If both eyes of the same patient were eligible,one was randomly selected.All included eyes had a corrected visual acuity of 20/40 or
better during the entire period of the study, sphericalrefraction within plus or minus 5.00 dioptres, and cylindercorrection within plus or minus 3.00 dioptres. Eyes withclosed or narrow angles at gonioscopy exam were excluded.Patients submitted to any surgical procedure or laserintervention during the evaluation period and patients withretinal disease, non-glaucomatous optic neuropathy, or anyother disease that could interfere with visual field testingwere also excluded.Eyes with open angle glaucoma had to present an open
angle at gonioscopy and a glaucomatous optic disk associatedwith reproducible glaucomatous visual field defect based onAnderson’s criteria.19 Visual field defect was defined by thepresence of a cluster of three or more non-edge points thathave sensitivities with p,5% and one of the points has asensitivity with p,1% or corrected pattern standard deviation(CPSD) value with p,5% or glaucoma hemifield test (GHT)outside normal limits.All subjects were under clinical therapy and had IOP lower
than 17 mm Hg monitored by isolated measurements duringthe follow up period.
Abbreviations: CPSD, corrected pattern standard deviation; IOP,intraocular pressure.
1298
www.bjophthalmol.com

Patients were submitted to the water drinking test at thebeginning of the follow up period. The water drinking testwas performed after obtaining a baseline IOP measurement.Patients had to drink one litre of tap water in 5 minutes. IOPwas measured three times at 15 minutes intervals. Waterdrinking tests were performed between 4:00pm and 5:00pm.The maximum value of the three measurements wasconsidered as the maximum IOP during the water drinkingtest.IOP measurements were obtained with Goldmann appla-
nation tonometry. Achromatic perimetry was performed withthe Humphrey Visual Field Analyser (HumphreyInstruments, San Leandro, CA, USA) standard full threshold24-2). All patients had previous experience with visual fieldtests and only eyes with reliable exams (less than 20% offixation losses, and/or less than 33% of false positive and falsenegative rates) were included. The last reliable visual fieldexam performed before the evaluated period was consideredas the baseline exam. The method adopted to evaluate visualfield progression was based on Anderson’s progressioncriteria20 and was characterised by the rise of a new defector worsening of a previous defect. A new defect was definedby the presence of a new cluster of three or more non-edgepoints that have sensitivities with p,5% with one of thepoints having a sensitivity with p,1%. Worsening of apreviously defective region was characterised by the dete-rioration of three or more points in that region by 10 db.The end point for the eyes with visual field progression was
considered the day of confirmation of the visual fielddeterioration. For the patients without visual field progres-sion the last visual field exam performed during theevaluated period was considered the end point.The number of eyes that developed visual field progression
was determined. The performance of the water drinking testwas compared between the eyes that developed visual fielddeterioration and those that did not.Statistical analysis was performed with commercial soft-
ware (SPSS 10.0, SPSS Inc, Chicago, IL, USA). Analysis ofvariance and x2 test were used to compare, respectively,continuous and categorical demographic data betweengroups. The data included mean age, sex, ethnical group,basal IOP, number of antiglaucomatous drugs, initial meandeviation (MD) and correct pattern standard deviation(CPSD), period of follow up, and numbers of visual fieldsexams. Intraocular pressure peak and percentage of IOPfluctuation (intraocular pressure peak–baseline IOP/baselineIOP) during the water drinking test were evaluated in all eyesby analysis of covariance with initial IOP as a covariate.
RESULTSSeventy six eyes of 76 patients were included in this study.Demographic data are presented in table 1. The mean age ofall participants was 67.1 (SD 11.8) years. Thirty five (46.1%)patients were women. The majority of subjects were White(88.2%). The mean follow up period of all subjects was 26.0(SD 13.8) months (5–67 months).Twenty eight (36.8%) eyes reached definite visual field
progression based on the study criteria. No significantdifferences were found in the mean follow up time and thenumber of visual field exams performed between eyes withand without visual field deterioration (table 1). Similarly, nosignificant difference in the mean age, sex, race, basal IOP,initial MD, and CPSD was observed between groups (table 1).From a overall baseline of 12.7 mm Hg, a mean (standard
error of the mean) difference of 1.9 (SEM 0.6) mm Hg in themean IOP peak was observed between glaucomatous eyesthat showed visual field progression and the ones that didnot. This difference was significant (p=0.001, ANCOVA;95% CI 0.8 to 3.0) (see table 2).In the same way, a difference of 16.8% (SEM 4.6%) in the
mean percentage of IOP variation was observed betweenglaucomatous eyes which showed visual field deteriorationand the ones that did not progress. This difference was alsoconsidered significant (p,0.001, ANCOVA; 95% CI 7.7 to26.0).The mean (standard deviation) number of antiglaucoma-
tous drugs used in the eyes that demonstrated visual fieldprogression was 2.4 (SD 1.4) compared with 2.1 (SD 1.3) inthe non-progressive group (p=0.42). Prostaglandins werepart of the clinical treatment in 15 (53.6%) of the 28 eyes thatshowed visual field progression and in 32 (66.7%) of the 48eyes that remained stable (p=0.26). No significant differ-ence was observed in the number of eyes using beta blockers,carbonic anhydrase inhibitors, and alpha agonists betweenthe two groups (table 3). The number of eyes submitted to
Table 1 Demographic data of open angle glaucoma eyes with and without visual fielddeterioration
Eyes with visual fielddeterioration
Eyes without visual fielddeterioration p Value
Number of eyes 28 (36.8%) 48 (63.2%)Age (years) (mean (SD)) 66.8 (13.7) 67.4 (10.7) 0.83*Range (years) 40–88 39–86Sex (M/F) 11/17 30/18 0.06�Race
White 25 (89.3%) 42 (87.5%) 0.82�Asians 3 (10.7%) 6 (12.5%)
Period of follow up (months) (mean (SD)) 28.9 (16.7) 24.3 (11.6) 0.16*Number of visual field exams (mean (SD)) 4.3 (1.8) 4.7 (2.2) 0.37*Initial MD (db) (mean (SD)) 28.97 (5.63) 29.56 (7.20) 0.71*Initial CPSD (db) (mean (SD)) 7.73 (5.53) 6.67 (4.50) 0.37*Basal IOP (mmHg) (mean (SD)) 12.9 (2.7) 12.6 (2.0) 0.57*
*ANOVA.�x2 test.MD, mean deviation; CPSD, correct pattern standard deviation; IOP, intraocular pressure; db, decibels.
Table 2 Water drinking test results: IOP peaks andpercentage of IOP fluctuations
Water drinking testWith VFdeterioration
Without VFdeterioration
p Value at95% CI
IOP peak mm Hg (mean(SEM))
16.8 (0.4) 14.9 (0.3) ,0.01*
% IOP fluctuation mm Hg(mean (SEM))
34.0 (3.6) 17.2 (2.8) ,0.01*
*ANCOVA from an adjusted overall baseline IOP of 12.7 mm Hg.VF, visual field; IOP, intraocular pressure; CI, confidence interval.
The water drinking test and visual field progression 1299
www.bjophthalmol.com

glaucoma surgery (trabeculectomy) before the studied periodwas seven (25%) in the progressive group and 12 (25%) in thenon-progressive group (p=0.84).Among eyes that reached definite visual field progression,
25% (7/28) showed IOP .21 mm Hg during the waterdrinking test compared with 4.2% (2/48) observed in thegroup that remained stable (p=0.007). In this group, four of48 (8.3%) eyes had an IOP variation >6 mm Hg in the waterdrinking test compared with 35.7% (10/28) of eyes thatdemonstrated visual field progression (p=0.003).
DISCUSSIONThe water drinking test is a provocative test that was widelyused a few decades ago to help in the diagnosis of open angleglaucoma,15 16 but was found to be inadequate due to manyfalse positive and false negative results in 10 year prospectivestudies.15 However, after some years, the emphasis on thevalue of this test has changed. As a result of the correlationwith the diurnal tensional curve,16 the water drinking test hasbeen proposed as an alternative method to check IOP control.In this study we performed the water drinking test in
glaucomatous eyes with an IOP lower than 17 mm Hg underclinical and/or surgical therapy. Our findings revealed asignificant difference in the results of the water drinking testbetween eyes that showed glaucoma progression comparedwith eyes that remained stable.Previous studies had already suggested the importance of
the water drinking test to determine a risk factor for thedevelopment of glaucomatous visual field defect. In the1980s, based on a large prospective study (CollaborativeGlaucoma Study), Armaly and coworkers21 22 reported thepressure change after drinking water as one of five potentialrisk factors significantly related to the development ofglaucomatous visual field defects in patients with ocularhypertension.Another study performed by Yoshikawa et al23 in normal
tension glaucoma patients showed that the maximum IOPlevels after the water drinking test in patients withprogressive visual field loss was significantly greater thanthe levels observed for the non-progressive group. Unliketheir study, we also included open angle glaucoma patientswith an IOP higher than 21 mm Hg at the time of diagnosis.In agreement with their results, we observed a difference ofalmost 2 mm Hg in the IOP peak during the water drinkingtest between eyes that progressed and the ones that did not.In addition, more eyes with IOP peaks higher than21 mm Hg during the water drinking test were observed inthe progressive group.The importance of IOP peaks in the development of
glaucoma progression has been already reported by Zeimeret al11 and also by Martinez-Bello et al.24 In our study, we didnot observe a difference in the mean basal IOP obtainedduring isolated office visits between the two groups, but ourresults revealed that the percentage of IOP variation duringthe water drinking test in eyes with visual field progressionwas almost twice the value observed in the other group.
Despite the results obtained by our study and previousreports, the mechanisms involved in the water drinking testare not completely understood. After drinking water or anyhypotonic fluid, there is absorption of water into blood andbody tissues including the eye. This is associated with aconsequent rise in IOP. The ability of the eye to recover fromthis transient IOP rise depends on the outflow facility. Therapid inflow of aqueous humour and the low facility ofoutflow in the glaucomatous eye may lead, at least in part, tolarger IOP fluctuation.Recently, Brubaker25 proposed that the water drinking test
could be used as an indirect measurement of outflow facilityto compare the IOP responses of glaucoma eyes to differentdrugs. Drugs such as prostaglandins improve the outflowfacility and are expected to show less IOP variation secondaryto water challenge. Although eyes were under differenthypotensive medication regimen in this study, no significantdifference in the frequency of prostaglandins as part of theclinical treatment was observed between the two groups. Thepresence or not of any filtration surgery should also beconsidered when comparing water drinking test resultsbetween eyes. Earlier studies already showed a relativelysmall range of diurnal IOP variation in trabeculectomisedeyes.17 26 In our study no significant difference in the numberof eyes submitted to glaucoma surgery (trabeculectomy)before the studied period was found between the progressivegroup and the non-progressive group, reducing possible bias.This study may be vulnerable to some other biases related
to a retrospective analysis. Although no significant differencewas found in the number of visual fields performed betweeneyes that progressed and the ones that remained stable,visual field examination was not performed at the sameintervals in all patients. Despite this, no significant differencebetween groups was found in other baseline variables thatcould possibly influence the outcome parameters of the waterdrinking test.In this study we did not try identify which value of IOP
peak or IOP variation would suggest a higher risk ofprogression. Cutoffs may not be useful when evaluatingwater drinking test results to assess the risk of progression forall individuals. Each result of the water drinking test mayprovide important information when evaluating treatmentefficacy for a specific patient once the clinician hasestablished the target pressure.In summary, the water drinking test is a low cost and
feasible test and may reflect one of the important andcommon disturbances to steady state IOP during a commonactivity of daily living: drinking water.25 Our findings suggestthat the emphasis on the value of the water drinking testshould be changed. It may be useful as a complementaryexam to check IOP control in the clinical practice. The peakand percentage of IOP variation of this test should beconsidered when analysing risk factors for glaucoma pro-gression. Future randomised controlled longitudinal studiesmay give a better evaluation of this possibility.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
R SusannaJr, R M Vessani, L Sakata, L C Zacarias, M Hatanaka,Glaucoma Service, Ophthalmology Department, University of SaoPaulo, Brazil
REFERENCES1 Liu JH. Diurnal measurement of intraocular pressure. J Glaucoma
2001;10:S39–41.2 The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship
between control of intraocular pressure and visual field deterioration.TheAGIS Investigators. Am J Ophthalmol 2000;130:429–40.
3 The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Collaborative Normal-Tension Glaucoma Study Group.Am J Ophthalmol 1998;126:498–505.
Table 3 Percentage of eyes under each major kind oftopical antiglaucoma drugs
Topical antiglaucoma drugsWith VFdeterioration
Without VFdeterioration
p Value at95% CI
Beta blockers 75.0% 64.6% 0.35Carbonic anhydrase inhibitors 67.8% 45.8% 0.06Alpha agonists 28.6% 16.7% 0.2
x2 test.VF, visual field; CI, confidence interval.
1300 Susanna, Vessani, Sakata, et al
www.bjophthalmol.com

4 Leske MC, Heijl A, Hussein M, et al. Factors for glaucoma progression and theeffect of treatment: the early manifest glaucoma trial. Arch Ophthalmol2003;121:48–56.
5 Kass MA, Kolker AE, Becker B. Prognostic factors in glaucomatous visual fieldloss. Arch Ophthalmol 1976;94:1274–6.
6 Werner EB, Drance SM. Progression of glaucomatous field defects despitesuccessful filtration. Can J Ophthalmol 1977;12:275–80.
7 Chauhan BC, Drance SM. The relationship between intraocular pressure andvisual field progression in glaucoma. Graefes Arch Clin Exp Ophthalmol1992;230:521–6.
8 Brubaker RF. Delayed functional loss in glaucoma. LII Edward JacksonMemorial Lecture. Am J Ophthalmol, 1996;121:473–83.
9 Zeimer R. Circadian variations in intraocular pressure. In: Ritch R, Shields MB,Krupin T, eds. The glaucomas. St Louis: CV Mosby Co, 1996.
10 Hughes E, Spry P, Diamond J. 24-hour monitoring of intraocular pressure inglaucoma management: a retrospective review. J Glaucoma 2003;12:232–6.
11 Zeimer RC, Wilensky JT, Gieser DK, et al. Association between intraocularpressure peaks and progression of visual field loss. Ophthalmology1991;98:64–9.
12 Asrani S, Zeimer R, Wilensky J, et al. Large diurnal fluctuations in intraocularpressure are an independent risk factor in patients with glaucoma. J Glaucoma2000;9:134–42.
13 Zeimer RC, Wilensky JT, Gieser DK, et al. Application of a self-tonometer tohome tonometry. Arch Ophthalmol 1986;104:49–53.
14 Rasmussen KE, Jorgensen HA. Diagnostic value of the water drinking test inearly detection of simple glaucoma. Acta Ophthalmol (Copenh)1976;54:160–6.
15 Roth JA. Inadequate diagnostic value of the water-drinking test.Br J Ophthalmol 1974;58:55–61.
16 Miller D. The relationship between diurnal tension variation and the water-drinking test. Am J Ophthalmol 1964;58:243–6.
17 Medeiros FA, Pinheiro A, Moura FC, et al. Intraocular pressure fluctuations inmedical versus surgically treated glaucomatous patients. J Ocul PharmacolTher 2002;18:489–98.
18 Frankelson EN. The role of the water test in evaluation of glaucoma control.Can J Ophthalmol 1974;9:408–10.
19 Anderson DR. Automated Static Perimetry. St Louis: Mosby-Year Book, 1992.20 Anderson DR. Automated Static Perimetry, Second Edition. St Louis: Mosby-
Year Book, 1999.21 Armaly MF. Lessons to be learned from the Collaborative Glaucoma Study.
Surv Ophthalmol 1980;25:139–44.22 Armaly MF, Krueger DE, Maunder L, et al. Biostatistical analysis of the
collaborative glaucoma study. I. Summary report of the risk factors forglaucomatous visual-field defects. Arch Ophthalmol 1980;98:2163–71.
23 Yoshikawa K, Inoue T, Inoue Y. Normal tension glaucoma: the value ofpredictive tests. Acta Ophthalmol (Copenh) 1993;71:463–70.
24 Martinez-Bello C, Chauhan BC, Nicolela MT, et al. Intraocular pressure andprogression of glaucomatous visual field loss. Am J Ophthalmol2000;129:302–8.
25 Brubaker RF. Importance of outflow facility. IGR 2001;3:1.26 Saiz A, Alcuaz A, Maquet JA, et al. Pressure-curve variations after
trabeculectomy for chronic primary open-angle glaucoma. Ophthalmic Surg1990;21:799–801.
The water drinking test and visual field progression 1301
www.bjophthalmol.com

EXTENDED REPORT
Influence of change in body position on choroidal bloodflow in normal subjectsP Kaeser, S Orgul, C Zawinka, G Reinhard, J Flammer. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr S Orgul, University EyeClinic Basel, MittlereStrasse 91, P O Box, CH-4012 Basel, Switzerland;[email protected]
Accepted for publication1 April 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1302–1305. doi: 10.1136/bjo.2005.067884
Aim: To compare subfoveal choroidal blood flow (ChBF) in sitting and supine positions in normalvolunteers.Methods: ChBF was measured with laser Doppler flowmetry in 22 healthy volunteers of mean (SD) age 24(5) years. Six independent measurements of ChBF were obtained in one randomly selected eye of eachsubject while seated. The subjects then assumed a supine position for 30 minutes and a new series of sixmeasurements was obtained. The mean values of the two series were calculated. Systemic brachial arteryblood pressure and intraocular pressure were measured in the sitting and supine positions. Ocularperfusion pressure (OPP) was calculated based on formulae derived from ophthalmodynamometricstudies. The influence of changing OPP during change in body posture on the change in ChBF wasassessed by linear regression analysis.Results: ChBF decreased by 6.6% (p = 0.0017) in the supine position. The estimated ophthalmic bloodpressure in the supine position was adjusted to obtain a result of no change in OPP for no change in ChBF,yielding a mean decrease in the estimate of OPP of 6.7% (p = 0.0002). The necessary adjustment for theestimate of OPP in the supine position suggested a marked buffering of the change in perfusion pressureby the carotid system. The relative decrease in OPP correlated significantly with the relative decrease inChBF (R2 = 0.20; p =0.036) with a slope for the regression line of 1.04.Conclusions: The comparable degree of change in ChBF and OPP and the linear relationship between thetwo parameters suggest a passive response of the choroidal circulation to a change in posture. In contrast,the carotid system seems to control the gradient in perfusion pressure closely between the heart and itsbranches.
The functional integrity of the retina depends entirely onan adequate vascular perfusion level and an availabilityof vital metabolic nutrients and oxygen. In humans these
factors are promoted by a dual vascular system. The avascularregion of the retinal fovea, however, relies entirely on bloodflow in the subfoveal choroidal vasculature and, morespecifically, in the choriocapillaris. The understanding ofchoroidal blood flow (ChBF) regulation is therefore of utmostimportance when considering the pathophysiology of dis-eases such as age related macular degeneration, diabeticretinopathy, and others.Notwithstanding the concept of a passive vascular system,
investigations in rabbits have shown a non-linear relation-ship between ChBF and perfusion pressure.1 Even somestudies in humans have suggested that ChBF may be partlyindependent of perfusion pressure.2 3 On the other hand, arecent study suggested a passive response of the choroidalcirculation to perfusion pressure changes during changes inbody position.4 Because the alteration of body posture wasonly maintained for a few minutes in this latter study, it ispossible that some control mechanisms may not have hadtime to take effect. We therefore investigated the response ofthe subfoveal ChBF in healthy subjects in the sitting positionand 30 minutes after assuming a supine position.
METHODSCompact choroidal laser Doppler flowmeterChBF assessment was performed using laser Dopplerflowmetry.5 A confocal choroidal laser Doppler flowmeter(Choroidal Blood Flowmeter; IRO, Sion, Switzerland) wasused. The optical system for the delivery of the laser beamand the detection of the scattered light is based on a confocalarrangement and has been described in detail elsewhere.6
With this instrument, the scattered light is collected fromwithin the avascular zone of the fovea and ChBF in thesubfoveal region is computed.2 7–10
SubjectsTwenty two healthy non-smoking subjects (19 women) ofmean (SD) age 24.1 (4.7) years (range 18–40) were recruitedfrom volunteers in the University Eye Clinic, Basel. Based onprevious studies,4 11 this sample size was considered toprovide sufficient statistical power in the present study. Theprocedures were approved by the local ethical committee, thetenets of Declaration of Helsinki were followed, and eachsubject signed an informed consent form before anyexamination.Subjects were screened for ocular and systemic diseases. A
detailed medical and ophthalmic history was recorded, andall subjects completed an ophthalmologic examination. Onlyindividuals with no history of ocular or systemic disease, nohistory of chronic or current systemic or topical medication,and no history of drug or alcohol abuse were included in thestudy. Further inclusion criteria were a normal systolic bloodpressure (SBP, 100–140 mm Hg) and diastolic blood pressure(DBP, 60–90 mm Hg), best corrected visual acuity above 20/25 in both eyes, ametropia within 23 to +3 dioptres ofspherical equivalent and less than 1 dioptre astigmatism inboth eyes, a pupil diameter of at least 4 mm, an applanatory(Goldmann applanation tonometry) intraocular pressure
Abbreviations: ChBF, choroidal blood flow; DBP, diastolic bloodpressure; IOP, intraocular pressure; MBP, mean arterial blood pressure;OAP, ophthalmic arterial blood pressure; OPP, ocular perfusionpressure; SBP, systolic blood pressure
1302
www.bjophthalmol.com

(IOP) below 20 mm Hg in both eyes, and no pathologicalfindings on slit lamp examination and indirect fundoscopy.
Experimental procedureSubjects were studied at least 2 hours after a light meal andwere asked to refrain from alcohol and caffeine for 12 hoursbefore the trial days, as well as to avoid heavy exercising ormeals too rich in sugar and fat before the experimental day. Aresting period of at least 30 minutes was scheduled for eachsubject. Stable baseline conditions were established, whichwere ensured by repeated measurements of blood pressure(Profilomat, Roche, Basel, Switzerland). After stabilisation ofblood pressure, two measurements of SBP and DBP as well asheart rate (HR) were recorded and averaged. Immediatelyafterwards, IOP was determined with a handheld tonometer(Tonopen; Mentor, Norwell, MA, USA) after applying onedrop of 0.4% benoxinate hydrochloride and staining the tearfilm with a strip of fluorescein sodium. The subjects wereseated with the head stabilised in a slit lamp head rest. Carewas taken to standardise the subject’s head position whichwas held constant throughout the recordings by aligningmarks on the head rest with anatomical landmarks on thehead. The subjects were asked to fixate the red light spotwithin the ocular and to adjust the focus by turning theocular. The ocular-to-cornea distance was set between 1.5and 2 cm and held constant throughout the recordings. Inaddition, a constant very low level artificial room illumina-tion was used throughout all the experiments. The experi-mental eye was chosen randomly and measurements wereobtained without pupil dilatation. A stable direct currentduring a recording was used as a criterion of proper fixation.12
The same investigator performed all ChBF measurements(PK). A first series of six independent consecutive recordingsof 20–25 seconds each was obtained in a sitting position,with the subjects taking their head off the chin rest and theexaminer moving the laser Doppler flowmeter between themeasurements.13 Individual measurements were obtained atleast 1 minute apart. The subjects then assumed a supineposition for at least 30 minutes and, after stabilisation ofblood pressure, IOP, SBP, DBP, and HR were determined asoutlined above. The laser Doppler flowmeter mounted on aswivel arm was rotated by 90˚and the camera was aligned tothe subject’s eye, based on the landmarks identified in thesitting position. A second series of six independent measure-ments was obtained in the supine position and the meanChBF value was calculated for both series.
StatisticsThe SBP and DBP readings were used to calculate the meanarterial blood pressure (MBP) according to the formula: MBP= DBP + 0.42 (SBP – DBP).4 14 Mean ophthalmic arterialblood pressure (OAP) was calculated based on formulaederived from ophthalmodynamometric studies, with meanOAP in the sitting position calculated as OAP = 0.746MBPand OAP in the supine position calculated as OAP = 0.846MBP.4 14 15 The mean ocular perfusion pressure (OPP) was
calculated according to the formula: OPP = OAP 2 IOP. Thedifferences between sitting and supine positions werecalculated for OPP and ChBF by accounting for hetero-scedasticity.16 Departure from normal distribution of thevariables was assessed by means of the Shapiro-Wilk W testfor normality and measurements in the sitting position werecompared with those in the supine position using a paired ttest. The dependence of change in ChBF on change in OPPwas assessed by computing the significance of the slope ofthe line regressing the percentage difference in ChBF on thepercentage difference in OPP. A p value of (0.05 wasconsidered statistically significant.
RESULTSThe distribution of the data for ChBF in the sitting (p=0.28)and supine positions (p=0.46), MBP in the sitting (p=0.91)and supine positions (p=0.43), HR in the sitting (p=0.69)and supine positions (p=0.49), and OPP in the sitting(p=0.63) and supine positions (p=0.28) was normal.Changes in ChBF, MBP, HR, and OPP were also normallydistributed (p=0.86, p=0.09, p=0.13, and p=0.78, respec-tively). The variation (coefficient of variation) between thetwo series of ChBF measurements was comparable (10.28%and 9.58% in the sitting and supine positions, respectively:p=0.58, paired t test). The mean (SD) results for themeasured parameters IOP, SBP, DBP, MBP, HR, and ChBFare shown in table 1. MBP decreased by 7.8 (4.9)%, HR by 8.2(9.6)%, and ChBF by 6.6 (11.6)%. The mean (SD) estimatedOPP was 50.7 (5.9) mm Hg and 53.2 (4.8) mm Hg in the
Table 1 Mean (SD) parameters in the sitting and supine positions
Sitting position Supine position p value*
IOP (mm Hg) 13.0 (2.2) 14.0 (2.1) 0.0006SBP (mm Hg) 106.2 (12.6) 102.7 (7.2) 0.046DBP (mm Hg) 71.5 (8.6) 63.6 (6.9) 0.0001MBP (mm Hg) 86.1 (8.7) 80.0 (6.2) ,0.0001Heart rate (beats/min) 64.1 (8.1) 59.0 (10.1) 0.0006ChBF (arbitrary units) 9.5 (2.2) 8.9 (2.1) 0.0017
ChBF, choroidal blood flow; DBP, diastolic blood pressure; IOP, intraocular pressure; MBP, mean arterial bloodpressure; SBP, systolic blood pressure.*Paired t test.
20
15
10
5
0
–5
–10
–15
–20
–25
–306
Change in perfusion pressure (%)
Cha
nge
in c
horo
idal
blo
od fl
ow (%
)
–16 420–2–4–6–8–10–12–14
Figure 1 A curve fitted according to the distance-weighted leastsquares smoothing procedure and regressing the relative change inchoroidal blood flow on the relative change in ocular perfusion pressure(dotted line) suggested a nearly linear fit except for the lowest end of thecurve, suggesting an outlier. When the procedure was repeated afterexcluding the extreme points at the upper and lower end (solid line), thecurve showed a steady decrease in choroidal blood flow with decreasingocular perfusion pressure.
Influence of change in body position on choroidal blood flow 1303
www.bjophthalmol.com

sitting and supine positions respectively (p=0.0005), with amean (SD) increase of 5.4 (5.6)%.Because of a negative mean change in ChBF during an
estimated mean increase in OPP, it was hypothesised thatmean OAP in the supine position had been overestimated.Considering the measured parameters in table 1 and anadjusting factor for the estimate of the mean OAP in thesitting position of 0.74, a new adjusting factor for theestimate of the mean OAP in the supine position wascalculated in order to obtain no change in perfusion pressurefor no change in ChBF. Solving the equation yielded anadjusting factor of 0.767 instead of 0.84. With the newadjusting factor for the estimate of the mean OAP in thesupine position, the mean (SD) OPP was 50.7 (5.9) mm Hgand 47.3 (4.4) mm Hg (the latter parameter was stillnormally distributed: p=0.31) in the sitting and supinepositions respectively (p= 0.0002), with a mean (SD)decrease of 6.7 (5.0)%.Scrutinising distance-weighted least squares curves regres-
sing change in ChBF on change in OPP (fig 1), a steadydecrease in ChBF with decreasing OPP was observed. A linearfit was therefore computed to the entire data set and therelative change in OPP correlated positively with the relativechange in ChBF (R2=0.20, p=0.036; fig 2). Residualanalysis applying the 26 sigma limit did not unveil outliersin this regression analysis which showed a slope of 1.04.
DISCUSSIONThis study assessed the response of subfoveal ChBF to changein body posture. The experimental set up was designed toprovoke a change in OPP while limiting neurovegetativeinput during change in perfusion pressure. Enough time wasscheduled after the subjects had assumed the supine positionto allow the regulatory mechanisms to take effect. Thechange from a sitting position to a supine position resulted ina change in ChBF which depended linearly on the change inOPP, indicating a passive response of the choroidal circula-tion to changes in OPP. This finding suggests that thechoroidal vasculature has no intrinsic ability to regulateblood flow during changes in OPP. However, the experi-mental data suggest that the carotid system is able to bufferthe increase in perfusion pressure in the ophthalmic artery.A number of regulatory systems and factors such as
circulating hormones, as well as metabolic, myogenic andneurogenic factors, participate in the regulation of vasculartone.17 Autoregulation is said to occur when, within certainlimits, the effect of the decrease in perfusion pressure iscompensated by a decrease in vascular resistance and the
flow remains constant. A number of studies have shown thatthe human retina has some autoregulatory capacity inresponse to both an increase and a decrease in OPP. Incontrast to the choroid, the retina does not have neurovege-tative innervation so the elicited vascular response duringchange in perfusion pressure will be modulated by mechan-isms intrinsic to the vessels, whereas the choroidal vascu-lature may experience an important neuronal influence.Investigating blood flow autoregulation in the choroid maytherefore be challenging. While earlier studies had suggesteda linear pressure-flow relationship in the choroid ofprimates,18 19 more recent studies have implied some auto-regulatory capacity in the choroid of rabbits.1 Even inhumans, the response of the ChBF observed after changingthe OPP with a suction cup suggested some autoregulatorycapacity in the choroidal vasculature.2 A non-linear relation-ship between the genuine OPP and ChBF in a normalpopulation seemed to concur with such an interpretation.3
Finally, taking advantage of the increase in systemic bloodpressure resulting from neurovegetative stimulation duringisometric exercise, several studies have shown relativestability of the ChBF during increased OPP.8 10 However, itmust be remembered that the vascular response in thechoroid after exercise induced changes in OPP may be drivenby direct sympathetic input to the choroid and not representan autoregulatory response intrinsic to the choroidal vessels.Furthermore, a recent study—which also avoided directinterventions on the eye such as applying a suction cup orstimulation of the neurovegetative system—found a passiveresponse of the choroidal vasculature to changes in perfusionpressure.4 The inconsistency between the latter finding andan earlier result from the same group2 suggests that the use ofmeans such as a suction cup to increase IOP may elicitmechanisms responsible for a non-linear pressure-flowrelationship in the choroid.In the present study a relative increase in OPP was
observed when estimates of the blood pressure in theophthalmic artery were calculated with the same factors asin a previous study.4 Longo et al found that the increase incalculated OPP estimated using data based on ophthalmo-dynamometric measurements was much less than theincrease calculated with the hydrostatic model and, becausethe estimated change in perfusion pressure fitted themeasured change in ChBF, they hypothesised an activemechanism acting between the heart and the eye, bufferingthe increase in OPP. It is likely that this effect—possiblybased on myogenic mechanisms which usually need moretime to take effect20 21—may have been even more markedwhen the subjects were allowed to rest for 30 minutes in thesupine position. Obviously, the estimate of change in OPPwas erroneous and with a correcting factor of 0.767 instead of0.84 in the supine position, a zero change in OPPcorresponded to a zero change in ChBF. This suggests someexternal control mechanisms regulating the OPP in theophthalmic artery, similar to the control mechanisms in thecarotid system.22 Consequently, the change in the gradient inOPP between the heart and the cerebral circulation isbuffered in the supine position. As expected,14 a reductionin systemic blood pressure was observed after assuming thesupine position and OPP dropped. The decrease in OPP andChBF were of similar amplitude and amounted to 26.7% and26.6% respectively, confirming the findings of Longo et al.Furthermore, the regression line between the two variablesshowed a slope of 1.04 indicating an absence of a regulatoryresponse within the choroid.We confirmed the findings of Longo et al4 while allowing a
much longer time for the vasculature to adapt. Myogenicresponses of an autoregulated vessel may require severalminutes to induce stable vessel diameters following an acute
20
15
10
5
0
–5
–10
–15
–20
–25
–306
Change in perfusion pressure (%)
Cha
nge
in c
horo
idal
blo
od fl
ow (%
)
–16 420–2–4–6–8–10–12–14
Figure 2 Relative change in ocular perfusion pressure correlatedlinearly with the relative change in choroidal blood flow (R2 = 0.20,p = 0.036).
1304 Kaeser, Orgu l, Zawinka, et al
www.bjophthalmol.com

change in intravascular pressure,20 21 while metabolicmechanisms seem to occur within a few seconds.23 Becausethe supine position was assumed for at least 30 minutes,there is good reason to be confident that control mechanismshad enough time to take effect in the present experimentalset up and seem, in fact, to have influenced blood pressure inthe ophthalmic artery. However, as in the study by Longo etal, because ChBF was measured with a device which assessedonly the subfoveal choroid, the results presented hithertomay not apply to the remainder of the choroid.In conclusion, our results show that subfoveal ChBF
decreases proportionally with decreasing OPP, suggesting apassive response to changes in body posture. In contrast, thecarotid system seems to regulate the perfusion pressure in itsbranches.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
P Kaeser, S Orgul, C Zawinka, G Reinhard, J Flammer, University EyeClinic, Basel, Switzerland
REFERENCES1 Kiel JW, Shepherd AP. Autoregulation of choroidal blood flow in the rabbit.
Invest Ophthalmol Vis Sci 1992;33:2399–410.2 Riva CE, Titze P, Hero M, et al. Effect of acute decreases of perfusion pressure
on choroidal blood flow in humans. Invest Ophthalmol Vis Sci1997;38:1752–60.
3 Hasler PW, Orgul S, Gugleta K, et al. Vascular dysregulation in the choroid ofsubjects with acral vasospasm. Arch Ophthalmol 2002;120:302–7.
4 Longo A, Geiser MH, Riva CE. Posture changes and subfoveal choroidal bloodflow. Invest Ophthalmol Vis Sci 2004;45:546–51.
5 Riva CE, Cranstoun SD, Grunwald JE, et al. Choroidal blood flow in the fovealregion of the human ocular fundus. Invest Ophthalmol Vis Sci1994;35:4273–81.
6 Geiser MH, Diermann U, Riva CE. Compact laser Doppler choroidalflowmeter. J Biomed Opt 1999;4:459–64.
7 Riva CE, Cranstoun SD, Grunwald JE, et al. Choroidal blood flow in the fovealregion on the human ocular fundus. Invest Ophthalmol Vis Sci1994;35:4273–81.
8 Riva CE, Titze P, Hero M, et al. Choroidal blood flow during isometricexercises. Invest Ophthalmol Vis Sci 1997;38:2338–43.
9 Geiser MH, Riva CE, Dorner GT, et al. Response of choroidal blood flow in thefoveal region to hyperoxia and hyperoxia-hypercapnia. Curr Eye Res2000;21:669–76.
10 Kiss B, Dallinger S, Polak K, et al. Ocular hemodynamics during isometricexercise. Microvasc Res 2001;61:1–13.
11 Gherghel D, Orgul S, Dubler B, et al. Is vascular regulation in the centralretinal artery altered in persons with vasospasm? Arch Ophthalmol1999;117:1359–62.
12 Gugleta K, Orgul S, Flammer I, et al. Reliability of confocal choroidal laserDoppler flowmetry. Invest Ophthalmol Vis Sci 2002;43:723–8.
13 Preitner A, Orgul S, Prunte C, et al. Measurement procedures in confocalchoroidal laser Doppler flowmetry. Curr Eye Res 2004;28:233–40.
14 Sayegh FN, Weigelin E. Functional ophthalmodynamometry. Comparisonbetween brachial and ophthalmic blood pressure in sitting and supineposition. Angiology 1983;34:176–82.
15 Sayegh FN, Weigelin E. Functional ophthalmodynamometry. Comparisonbetween dynamometry findings of healthy subjects in sitting and supinepositions. Ophthalmologica 1983;187:196–201.
16 Pocock SJ, Assmann SE, Enos LE, et al. Subgroup analysis, covariateadjustment and baseline comparisons in clinical trial reporting: currentpractice and problems. Stat Med 2002;21:2917–30.
17 Orgul S, Meyer P, Cioffi GA. Physiology of blood flow regulation andmechanisms involved in optic nerve perfusion. J Glaucoma 1995;4:427–43.
18 Alm A, Bill A. Ocular and optic nerve blood flow at normal and increasedintraocular pressure in monkeys (Macaca irus): a study with radioactivelylabelled microspheres including flow determination in brain and some othertissues. Exp Eye Res 1973;15:15–29.
19 Alm A, Bill A. The oxygen supply to the retina. II: Effects of high intraocularpressure and of increased arterial carbon dioxide on uveal and retinal bloodflow in cats, a study with radioactively labelled microspheres, including flowdeterminations in brain and some other tissue. Acta Physiol Scand1972;84:306–19.
20 Halpern W, Osol G. Influence of transmural pressure of myogenicresponses of isolated cerebral arteries of the rat. Ann Biomed Eng1985;13:287–93.
21 Rajagopalan S, Dube S, Canty JM. Regulation of coronary diameter bymyogenic mechanisms in arterial microvessels greater than 100 microns indiameter. Am J Physiol 1995;268:H788–93.
22 Faraci FM, Heistad DD. Regulation of large cerebral arteries and cerebralmicrovascular pressure. Circ Res 1990;66:8–17.
23 Florence G, Seylaz J. Rapid autoregulation of cerebral blood flow:a laser-Doppler flowmetry study. J Cereb Blood Flow Metab1992;12:674–80.
Influence of change in body position on choroidal blood flow 1305
www.bjophthalmol.com

EXTENDED REPORT
18 Years’ experience with high dose rate strontium-90brachytherapy of small to medium sized posterior uvealmelanomaR van Ginderdeuren, E van Limbergen, W Spileers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Rita van Ginderdeuren,Department ofOphthalmology,Kapucijnenvoer 33, UZLeuven, B3000 Leuven,Belgium; [email protected]
Accepted for publication6 May 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1306–1310. doi: 10.1136/bjo.2005.068460
Aim: To analyse local tumour control, radiation related complications, visual acuity, enucleation rate, andsurvival after brachytherapy of small to medium sized choroidal melanoma (CM) with a high dose rate(HDR) strontium-90 (Sr-90) applicator.Methods: From 1983 until 2000, 98 eyes with CM were treated with Sr-90 brachytherapy. The mainoutcome measures were actuarial rates of the patients’ survival, ocular conservation rate, tumourregression, complication rates, and preservation of visual acuity. End point rates were estimated usingKaplan-Meier analysis.Results: The median follow up time was 6.7 years (0.5–18.8 years). Actuarial melanoma free patientsurvival rate was 85% (SE 4.8%) after 18 years. Actuarial rate of ocular conservation and completetumour regression was 90% (SE 3.8%) after 15 years. In 93% local tumour control was achieved, 88%showed a stable scar. Recurrence of the tumour on the border caused enucleation of six eyes (7%). In threecases (4%) retinal detachment was the end point. No cases of optic atrophy or of sight impairingretinopathy outside the treated area were found. Actuarial rate of preservation of visual acuity of 1/10was 65% at 5 years and 45% at 15 years of follow up (SE 5.9% and 8.8%).Conclusions: Sr-90 brachytherapy is as effective as iodine or ruthenium brachytherapy for small tomedium sized CM but causes fewer complications. The preservation of vision is better than with all otherdescribed radioisotopes. HDR Sr-90 brachytherapy can therefore safely be recommended for small tomedium sized CM.
Multiple techniques are used for the treatment of uvealmelanoma and different radioisotopes are used forbrachytherapy.1–6 We have used the high dose rate
(HDR) strontium-90 (Sr-90) applicator since 1983. The maindifference between Sr-90 and the other applicators is the veryhigh dose rate (10 200 cG/hour) of b irradiation: this reducesthe treatment to one session of 2–5 hours. Because Sr-90 hasa half life of 28.5 years, we have been able to use the sameapplicator for the past 21 years. Our preliminary results werereported in 1998.7 8 In this paper we review our results on alarger group of patients with a longer follow up time.
PATIENTS AND METHODSPatient characteristicsFrom 1983 to 2000, 98 eyes with CM were treated with HDRSr-90 brachytherapy. Eighty nine patients were treated withSr-90 as first treatment and are included in the study. Theother nine patients were treated first with another treatmentand are excluded. The patients comprised 49 women and 40men, with a median age of 64 years (range 29–85 years). Allpatients were followed for involution of the tumour andcomplications of the therapy until December 2003 or untildeath. Metastasis was proved by liver ultrasound andbiochemical tests. The exact date and cause of death wereknown for all patients.
Tumour characteristicsBefore treatment, the tumour had a median maximum basaldiameter of 9.5 mm (range 6–15.3 mm). The maximumheight of the tumour before treatment was measured byultrasound and ranged between 1.2 mm and 8.4 mm with amedian of 4.1 mm. Sixteen tumours (18%) belong to the
group of small tumours (thickness less than 3 mm anddiameter less than 10 mm) and 73 to medium size tumours.
Treatment protocolThe exact characteristics of the Sr-90 applicator, used in ourgroup, and the treatment protocols have already been fullydescribed.7 An epibulbar surface applicator (SIAQ 7321)produced by the Amersham Company was modified byremoving the shaft (figs 1, 2). It was loaded with 370 MBq(10 mCi) Sr-90 at the concave side and shielded with 0.1 mmplatinum. In 1983 the dose rate at the applicator’s surfacewas measured at 7.2 cGy/s. The dose delivered in thebeginning of the study was 75 Gy at the tumour apex (14patients), corresponding to a scleral dose between 299 Gyand 710 Gy. Because of recurrence of a small thin tumourand success of a tumour of 8 mm thickness, we believed thatit was more important to irradiate the base to a sufficientlarge dose. From June 1990 we treated 59 patients with ascleral dose of 600 Gy, administered in less than 2 hours.Because of the decay of Sr-90 the required time exceeded3 hours in 1999 and we decided to lower this scleral dose to450 Gy (12 patients). The size of the applicator was notsufficient for covering the whole tumour in four patients, anda shift of the applicator was performed in one treatment(total scleral dose 800 Gy). Sixty six patients were treatedwith one session. For insufficient regression or suspectedrecurrence at the tumour border, 18 patients were treated at alater point with a second session of Sr-90, and five patientswith a third session. For very small suspicious areas of thetumour xenon arc treatment was applied in nine patients and
Abbreviations: CM, choroidal melanoma; HDR, high dose rate; Sr-90,strontium-90
1306
www.bjophthalmol.com

in the latter part of the study diode laser in three patients,following the protocol of transpupillary thermotherapy (TTT).
AnalysesActuarial rates of patient melanoma free survival, tumourcontrol, ocular conservation, and preservation of visual acuityof 1/10 were estimated using Kaplan-Meier analysis(Statistica, Statsoft, Inc, USA).The study was approved by the ethics committee of
UZLeuven.
RESULTSSurvival rateThe median follow up time is 6.7 years (range 0.5–18.8 years). The number of patients followed for 3, 5, 8 and10 years is, respectively, 78, 57, 55, and 25. At 3, 5, and15 years post-treatment follow up, melanoma free patientsurvival was, respectively, 91%, 90%, and 85% (SE 2.9%,3.2%, and 4.8%). Eleven patients (12%) died of melanomarelated metastatic disease between 6 months and 9 years(fig 3). Six patients died in the follow up period as a result oftumour unrelated causes.
Tumour controlActuarial rate of tumour control after 3, 5, and 10 years was,respectively, 95%, 92%, and 90% (SE 2.0%, 3.0%, and 3.8%).Local tumour control was obtained in 83 eyes (93.3%), fromwhich 78 regressed to a scar: naked sclera or flat pigmentedchoroidal rest tissue, which could not be detected byultrasound (fig 4). The other five patients died as a resultof metastases during regression of the lesion but beforereaching a flat scar. Treatment failure (growth beyondcontrol at the tumour border) caused enucleation in sixpatients (7.3%). One eye presented with a second ciliary bodymelanoma after complete regression of macular treated
melanoma and was enucleated. No melanocytosis or connec-tion between the two locations was found histologically.8
There was no difference in regression between the differenttreatment protocols. Tumour control was obtained in 13/14patients with 75 Gy, 54/59 with 600 Gy, 11/12 with 450 Gy,and 4/4 with 26400 Gy.
Complication rateNo cases of sight impairing radiation retinopathy outside thetreated area were found. In 21% of cases mild radiationretinopathy was present with temporary small retinalexudates and haemorrhages; these regressed after years. Anexudative retinal detachment is seen around the treated area;this regressed spontaneously, except in four patients.Persistent complications comprised retinal detachment,3
macular fibrosis,1 diplopia.3 No painful eye, neovascularglaucoma, optic atrophy (distance tumour to optic disc was3 mm minimum) or scleral melting were observed. Non-tumour related surgery was performed in eight cases:vitrectomy4 for intravitreal bleeding or retinal detachment,argon laser photocoagulation for ischaemic retina because ofobliteration of retinal vessels passing over the tumour,2 anddiabetes.2 Actuarial rates of ocular conservation give acumulative survival of the eye of, respectively, 95%, 92%,and 90% after 3, 5, and 15 years (SR 2.3%, 3.0%, and 3.8%)(fig 5). No eyes were enucleated because of complications ofthe treatment.
Visual acuity resultsThe visual acuity before treatment, and at 3 years and 5 yearsof follow up is shown in table 1. Actuarial rate of visual acuityof at least 1/10 is 74%, 65%, and 45% at, respectively, 3, 5, and15 years follow up (SE 5.2%, 5.9%, and 8.8%), and isexpressed in figure 6. More than one third of patients hadat the end point a vision of more than 5/10; 58% of all our
7
6
4
5
3
2
0
1
54Depth (mm)
Radius 18 mm aftermodification
Shaft removed
15 mm
Dos
e ra
te (c
Gy/
s)
12 m
m16
mm
18.5
mm
320 1
7.2 c Gy/sBA Figure 1 (A) Modification of the
Amersham SIAQ 7321 Sr-90applicator. After removing the shaft, a16 mm diameter applicator wasobtained with a 12 mm radioactivezone. The perforated stainless steel ringto fix the applicator to the sclera has aninternal diameter of 16.5 mm. (B)Depth dose curve of the Sr-90applicator.
Figure 2 Picture of actual Sr-90 applicator with perforated stainlesssteel ring to fix the applicator to the sclera.
1.0
0.8
0.6
0.4
0.2
0.0250
Survival time (months)
Cum
ulat
ive
prop
ortio
n su
rviv
ing
0 20015010050
Figure 3 Kaplan-Meier melanoma free patients survival curve after Sr-90 treatment, expressed in months of follow up. (Survival function:#, complete (death by metastasis); +, censored.)
Strontium-90 brachytherapy for uveal melanoma 1307
www.bjophthalmol.com

patients retained vision 1/10 or more after a median follow uptime of 6.7 years. Only 13 of the 89 patients lost useful vision,including the enucleated eyes. From all patients with visionof 1/10 or more at the time of treatment, 69% retained 1/10vision after median follow up of 6.7 years.
DISCUSSIONIn this study small and medium sized CM were treated by anunconventional brachytherapy. This HDR Sr-90 treatmentcontrolled the tumour in 90% of cases, with preservation ofgood vision in 45% after 15 years. The long follow up timeindicates a persistent good result with survival times similarto other treatments.Sr-90 is a b emitter with high dose rate; because of the
decay the actual dose rate of our applicator is 4.5 cGy/s or10 200 cGy/hour. A high dose delivered at a high rate is radio-biologically very efficient in cell kill.2 We believe this explainsthe high rate of success with very fast shrinking of thetumour and high number of flat scars. After Sr-90 treatmentthe tumour shows swelling after 2 weeks. All the vessels inthe irradiated field are occluded in 2 weeks, proved byfluoroangiography performed after treatment.7 During thefirst 6 months after treatment the tumour shrinks veryquickly.The characteristics of Sr-90 show a very low penetration
depth (fig 1) and tumours thicker than 4 mm were never-theless successfully treated by treatment in two steps: afterthe initial treatment the tumour shrinks and after 6 monthsa second treatment is planned which reduces further theheight of the tumour.The major drawback of our Sr-90 applicator is its small
size. Because uveal melanoma can have lateral extensionsthat are undetectable with ophthalmoscopy or ultrasonogra-phy and our applicator has only a limited diameter whichrules out a safety margin of 2 mm, we re-marked tumourgrowth on the border after several months. In these cases wehad to re-treat borders with adjunctive methods such asxenon laser or diode laser; a second Sr-90 treatment wasperformed if the area was too large for laser.
The actuarial ocular survival rate was 90% after 18 years.Only seven eyes had to be removed after Sr-90 treatment,with six eyes because recurrence on the border.8 If we hadpossessed a larger applicator this complication could havebeen eliminated. Because of the low penetration depth of Sr-90 the complication rate is very low, no eyes were enucleatedbecause of pain or neovascular glaucoma.The final vision was mostly determined by the localisation
of the tumour, with poor central vision if the tumourinvolved the macular region. After 15 years, 45% of patientshad a minimum vision of 1/10. We did not see visualimpairment caused by radiation maculopathy or opticneuropathy, because of the limited penetration depth.
Strontium-90 compared with iodine-125Treatment with iodine-125 is popular, especially in NorthAmerica,9–12 and because of the COMS trial10 11 13 the resultsare known. The dose rate of this c emitter is between 50 cGy/hour and 100 cGy/hour, which is 100 times lower than Sr-90,and the application time varies between 30 and 300 hours.2
The safety procedures around the penetrating c rays with thelonger application time makes the procedure much morecomplex with more risks than Sr-90 treatment. The cost priceof iodine treatment is much higher than Sr-90, owing to thefrequent replacement of the iodine grains because of the veryshort half life of 60 days. The deeper penetration of the c raysallows treatment of larger and thicker tumours, but at thecost of causing more radiation damage to healthy surround-ing tissues and, hence, optic neuropathy, maculopathy, andvisual loss.14 In the medium sized arm of the COMS trial,12.5% of eyes were enucleated and 10% were enucleatedbecause of tumour recurrence during the first 5 years aftertreatment10; this is in the same range as our study.If we compare the results on the visual acuity with studies
of small and medium size tumours the rate of decline is muchhigher than in Sr-90 treated eyes. Nearly one half of thepatients treated with iodine-125 in the medium size tumourarm of the COMS lost substantial vision by only 3 years of
Figure 4 Picture of melanoma beforetreatment (left), after 6 months (centre),and after 5 years (right). The initialvision was 8/10; the lesion was 8 mmin diameter and 3 mm thick(ultrasound). Strontium treatment wasperformed for 2 hours 36 minutes. Themass regressed during the first6 months. After 5 years there was3/10 vision and no radiationretinopathy. No optic nerve atrophycould be detected.
1.0
0.8
0.6
0.4
0.2
0.0250
Survival time (months)
Cum
ulat
ive
prop
ortio
n su
rviv
ing
0 20015010050
Figure 5 Kaplan-Meier survival curve of the eye after Sr-90 treatment,expressed in months of follow up, showing the high proportion of non-enucleated eyes. (Survival function: #, complete (enucleated); +,censored.)
1.00.90.80.70.60.50.40.30.20.10.0
250Survival time (months)
Cum
ulat
ive
prop
ortio
n su
rviv
ing
0 20015010050
Figure 6 Kaplan-Meier estimates showing the proportion of patientsretaining visual acuity of 1/10; expressed in months of follow up. Allpatients are included, also patients with initial pretreatment visual acuityless than 1/10. (Survival function: #, complete (visus after treatment(1/10); +, censored.)
1308 van Ginderdeuren, van Limbergen, Spileers
www.bjophthalmol.com

follow up.10 Jones et al reported that only 33% of all patientsretained vision of 1/10 after 3 years.15 In the study of Wilsononly 29% of patients had a final vision of 1/10 of more after45 months.5 In the study of Shields and starting with onlythose patients with initial good vision (more than 1/10), 69%had poor vision (1/10 or less) at 10 years of follow up.9 Thevision decline continues also to progress with time: poorvision was seen in 1% of patients after 1 year, in 31% at5 years, and in 69% at 10 years.9 In all these studies on smallto medium sized tumours, the vision declines faster and witha much higher proportion of patients going legally blind thanin our group, because of the deeper penetration of c radiation.
Strontium-90 compared with ruthenium-106Ruthenium-106, a b emitter, is used for small and mediumsized tumours in Europe.4 16–20 All published studies incorpo-rated also small tumours with a range between 10% and 20%,which is similar to our study. The dose applied to the apex isbetween 60 Gy and 100 Gy. The dose rate of rutheniumvaries between 50 cGy/hour and 100 cGy/hour, which ishundred times less than Sr-90 (10 200 cGy/hour) and thiscorrelates with an application time of 1–7 days. Rutheniumhas a low dose rate, which means that during radiotherapyrepair of DNA destruction is possible; the high dose rate ofSr-90 excludes all repair during therapy. This lower dose ratemakes it less effective than Sr-90. The recurrence rate isbetween 6% and 36% after 5–15 years and the enucleationrate between 8% and 34% after 5–15 years.17–22
The vision decline is slower than with iodine-125 treat-ment, but is more pronounced than in strontium treated eyes.Loss of visual acuity to less than 1/10 is reported to bebetween 62% and 81% after 10–15 years; these studies do notdifferentiate between posterior and more anteriortumours.17 21 23 Rouberol et al reported in their study onposterior tumours (as were our tumours), that only 19% ofpatients had a vision more than 1/10 after 3 years.17 Only22.7% retained good vision at the end and 20% of patientswere enucleated.17 The complication rate of rutheniumtreated eyes is lower than in iodine treated eyes, but is stillmuch higher than in strontium treated eyes.17 20 Radio-insensitivity (persistence of cycling cells) is described inruthenium treated eyes, possibly related to the lower doserates.24–27 Histology of the enucleated eyes after Sr-90treatment showed tumour regrowth at insufficient treatedborders, but the irradiated regions were tumour free.8
Because Sr-90 delivers extremely high doses in a shorttime, all the blood vessels in the treated area are closed in lessthan 14 days.7 After a short swelling a shrinking process ofthe tumour sets in; the involution process is therefore muchfaster than in the other isotopes or proton treatment.6 13 17
Melanoma cells are not radiosensitive and a tumour necrosisrather than therapeutic dose of radiation is required todestroy this tumour.Survival rates of patients with Sr-90 treated eyes are
similar to other treatments, a logical consequence of totallydestroying the tumour.12 16 28–30
The cost of the strontium applicator (our applicator waspurchased in 1983 for J1250) should be far below all theother types because of the long half life; the treatmentprocedure should be safer because of the limited range of birradiation. Treatments should be completed more quicklybecause of the high dose rate. We regret that new applicatorsare not commercially available anymore, particularly plaqueshaving a greater diameter than the one we used. Strontiumplaques would enable brachytherapy of uveal melanomas beperformed in centres that do not receive enough patientswith this disease for other methods to be economically viable.
ACKNOWLEDGEMENTSWe thank Mrs M Bressinck for the help on the statistical program.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
R van Ginderdeuren, W Spileers, Department of Ophthalmology,Kapucijnenvoer 33, UZ Leuven, B3000 Leuven, BelgiumE van Limbergen, Department of Radiotherapy, Gasthuisberg UZLeuven, B3000 Leuven, Belgium
Competing interests: none declared
REFERENCES1 Damato BE. An approach to the management of patients with uveal
melanoma. Eye 1993;7:388–97.2 Potter R, Van Limbergen E. Uveal melanoma. In: The GEC ESTRO handbook
of brachytherapy. pp591–610.3 Robertson DM. Changing concepts in the management of choroidal
melanoma. Am J Ophthalmol 2003;136:161–70.4 Lommatzsch PK. Radiotherapie der intraokularen Tumoren,
insbesondere bei Aderhautmelanom. Klin Monatsbl Augenheilkd1979;174:948–58.
5 Wilson MW, Hungerford JL. Comparison of episcleral plaque and protonbeam radiation therapy for the treatment of choroidal melanoma.Ophthalmology 1999;106:1579–87.
6 Egger E, Schalenbourg A, Zografos L, et al. Maximizing local tumor controland survival after proton beam radiotherapy of uveal melanoma. Int J RadiatOncol Biol Phys 2001;51:138–47.
7 Missotten L, Dirven W, Van der Schueren A, et al. Results of treatment ofchoroidal malignant melanoma with high-dose-rate strontium-90brachytherapy. Graefes Arch Clin Exp Ophthalmol 1998;236:164–73.
8 Parys-Van Ginderdeuren R, Van den Oord JJ, Missotten L. Results of histo-pathologic examination of three enucleated eyes with a choroidalmelanoma afeter Strontium-90 irradiation. Bull Soc Belge Ophtalmol1997;265:47–54.
9 Shields CL, Shields JA, Cater J, et al. Plaque radiotherapy for uvealmelanoma. Long-term visual outcome in 1106 consecutive patients. ArchOphthalmol 2000;118:1219–28.
10 Jampol L, Moy C, Murray T, et al. The COMS randomised trial of iodine-125brachytherapy for choroidal melanoma. IV Local treatment failure andenucleation in the first 5 years after brachytherapy. COMS Report No 19.Ophthalmology 2002;109:2197–206.
11 Collaborative Ocular Melanoma Study Group. Collaborative ocularmelanoma study (COMS) randomised trial of I-125 brachytherapy formedium choroidal melanoma. Visual acuity after 3 years. COMS Report No16. Ophthalmology 2001;108:348–66.
12 Char D, Kroll S, Phillips T, et al. Late radiation failures after iodine 125brachytherapy of uveal melanoma compared with charged-particle (proton orhelium ion) therapy. Ophthalmology 2002;109:1850–4.
13 Sieving PA. Fifteen years of work. The COMS outcomes for medium-sizedchoroidal melanoma. Arch Ophthalmol 2001;119:1067–8.
14 Packer S, Stoller S, Lesser ML, et al. Long-term results of iodine 125 irradiationof uveal melanoma. Ophthalmology 1992;99:767–73.
Table 1 Visual acuity before treatment and after 3 years and 5 years
Number of eyes
Visual acuity
Beforetreatment After 3 years After 5 years
5/10–10/10 55 (62%) 32 (42%) 20 (38%)1/10–4/10 20 (22%) 17 (22%) 13 (25%)Less than 1/10 13 (15%) 20 (26%) 13 (25%)HM, LP, no LP 1 (1%) 7 (9%) 7 (13%)
HM, hand movements; LP, light perception.
Strontium-90 brachytherapy for uveal melanoma 1309
www.bjophthalmol.com

15 Jones R, Gore E, Mieler W, et al. Posttreatment visual acuity in patients treatedwith episcleral plaque therapy for choroidal melanomas: dose and dose rateeffects. Int J Radiation Oncology Biol Phys 2002;52:989–95.
16 Seregard S. Long-term survival after ruthenium plaque radiotherapy for uvealmelanoma. A meta-analysis of studies including 1066 patients. ActaOpthalmol Scand 1999;77:414–17.
17 Rouberol F, Roy P, Kodjikian L, et al. Survival, anatomic, and functional long-term results in choroidal and ciliary body melanoma after rutheniumbrachytherapy (15 years experience with beta-rays). Am J Ophthalmol2004;137:893–900.
18 Hungerford J. Current trends in the treatment of ocular melanoma byradiotherapy. Gregg Lecture 2001. Clin Experiment Ophthalmol2003;31:8–13.
19 Seregard S, Trmpe E, Lax I, et al. Results following episcleral ruthenium plaqueradiotherapy for posterior uveal melanoma. The Swedish experience. ActaOphthalmol Scand 1997;75:11–16.
20 Summanen P, Immonen I, Kivela T, et al. Radiation related complications afterruthenium plaque radiotherapy of uveal melanoma. Br J Ophthalmol1996;80:732–9.
21 Lommatzsch PK. Results after b irradiation (106Ru-106Rh) of choroidalmelanomas: 20 years’ experience. Br J Ophthalmol 1986;70:844–51.
22 Guthoff R, von Domarus D, Steinhorst U, et al. 10 Jahre Erfahrung mit derRuthenium-106/Rhodium106-Behandlung des malignen Melanoms derAderhaut – Bericht uber 264 bestrahlte Tumoren. Klin Monatsbl Augenheilkd1986;188:576–83.
23 Summanen P, Immonen I, Kiveal T, et al. Visual outcome of eyes withmalignant melanoma of the uvea after ruthenium plaque radiotherapy.Ophthalmic Surg Lasers 1995;26:449–60.
24 Pe’er J, Stafani FH, Seregard S, et al. Cell proliferation activity in posterioruveal melanoma after Ru-106 brachytherapy: an EORTC ocular oncologygroup study. Br J Ophthalmol 2001;85:1208–12.
25 Klaus H, Lommatzsch PK, Fuchs U. Histopathology studies in humanmalignant melanomas of the choroid after unsuccessful treatment with106Ru/106Rh ophthalmic applicators. Graefes Arch Clin Exp Ophthalmol1991;229:480–6.
26 Messmer E, Bornfeld N, Foerster M, et al. Histopathologic findings in eyestreated with a ruthenium plaque for uveal melanoma. Graefes Arch Clin ExpOphthalmol 1992;230:391–6.
27 Seregard S, Lundell G, Lax I, et al. Tumour cell proliferation after failedruthenium plaque radiotherapy in posterior uveal melanoma. ActaOphthalmol Scand 1997;75:148–54.
28 Kujala E, Makitie T, Kivela T. Very long term prognosis of patients withmalignant uveal melanoma. Invest Ophthalmol Vis Sci 2003;44:4651–9.
29 Collaborative Ocular Melanoma Study Group. The COMS randomised trialof Iodine 125 brachytherapy for choroidal melanoma, III: Initial mortalityfindings. COMS Report No 18. Arch Ophthalmol 2001;119:969–82.
30 Straatsma B, Diener-West M, Caldwell R, et al. Mortality after deferral oftreatment or No treatment for choroidal melanoma. Am J Ophthalmol2003;136:47–54.
1310 van Ginderdeuren, van Limbergen, Spileers
www.bjophthalmol.com

EXTENDED REPORT
The achiasmia spectrum: congenitally reduced chiasmaldecussationD A Sami, D Saunders, D A Thompson, I M Russell-Eggitt, K K Nischal, G Jeffery, M Dattani,R A Clement, A Liassis, D S Taylor. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr D S Taylor, VisualSciences Unit, Institute ofChild Health, 30 GuilfordStreet, London WC1N1EH, UK; [email protected]
Accepted for publication23 March 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1311–1317. doi: 10.1136/bjo.2005.068171
Aim: To describe the clinical spectrum of achiasmia, a congenital disorder of reduced relative decussationat the optic chiasm.Methods: A retrospective case note and patient review of nine children (four boys). Achiasmia was definedby the combination of a characteristic asymmetry of the monocular visual evoked potential (VEP) responseto flash and neuroimaging showing reduced chiasmal size.Results: Three of the children had an associated skull base encephalocele with agenesis of the corpuscallosum. In two patients achiasmia was associated with septo-optic dysplasia. Three patients had noneuroimaging abnormalities other than reduced chiasmal size and have no known pituitary dysfunction.One child had multiple physical deformities but the only brain imaging abnormality was reduced chiasmalsize.Conclusions: Some children with disorders of midline central nervous system development, includingsepto-optic dysplasia and skull base encephaloceles, have congenitally reduced chiasmal decussation.Reduced relative decussation may co-exist with overall chiasmal hypoplasia. Children with an apparentlyisolated chiasmal decussation deficit may have other subtle neurological findings, but our clinicalimpression is that most of these children function well.
The optic chiasm, shaped liked the letter X, is named afterthe Greek letter chi (x). Decussation of retinal fibres atthe chiasm appears to be the evolutionary ‘‘default
pathway’’ and the amount of ipsilateral projection correlateswith binocular specialisation.1 2 Clinically, most cases are dueto acquired abnormalities caused by compression, trauma, orinflammation. In some individuals, decussation of retinalganglion cell axons at the chiasm is selectively reducedduring development.3 4 Abnormal decussation could be theresult of disruption in molecular mechanisms that guidemidline axonal crossing. This is an area of active moleculargenetic research. Signalling pathways have been identifiedthat produce an achiasmic phenotype—for instance, retinalaxons do not decussate in Pax-2 deficient mice, entering theipsilateral optic tract instead.5 6 When Pax-2 is blocked, Sonichedgehog expression at the ventral midline is prolonged.7
Other molecular pathways implicated in midline attraction oravoidance of retinal ganglion cell axons include CD44 (asurface bound adhesion molecule),8 Zic2 (a zinc fingertranscription factor),2 and the Ephrins.9–11 An alternative tothe molecular genetic paradigm is a vascular disruptionsequence; during embryogenesis branches of the anteriorcerebral artery supply the chiasm, anterior hypothalamus,and septum pellucidum.12 In humans, chiasmal decussationof nerve fibres and development of the contralateral opticradiation has been reported despite unilateral optic nerveaplasia.13
Abnormalities of decussation can be revealed by hemi-spheric asymmetry of monocular visual evoked potentials(VEP).4 14 In humans, both reduced (in achiasmia)15 16 andexcess (in albinism)17 decussation correlate with nystagmus.However, a VEP asymmetry does not necessarily predictreadily visible nystagmus—as shown in albinism.14 18
Significant asymmetry of the monocular VEP response isnot always found in albinism with nystagmus.19 20
Complete absence of the chiasm (chiasmal aplasia) maynot be associated with other significant CNS abnormalities: a
girl with bilateral microphthalmos, bilateral aplasia of theoptic nerves, chiasm and tracts had no other apparentabnormalities and was developing normally up to the ageof 3.5 years.21 Also, aplasia of the chiasm was associated onlywith optic nerve hypoplasia and polymicrogyria.22
The term ‘‘non-decussating retinal fugal fibre syndrome’’(NDRFFS) has been used to describe isolated absence ofchiasmal crossing.23 There is an animal model—a strain ofBelgian sheep dogs with absent chiasmal decussation and thecombination of horizontal and seesaw nystagmus.24 Theclinical features of NDRFFS are combined horizontal andseesaw nystagmus, an achiasmic VEP pattern, absence ofendocrine abnormalities, normal visual fields, and normalfoveal reflexes.15 23 To our knowledge, the state of their opticdiscs on ophthalmoscopy has not been photographicallydetailed in the literature3 15 23 25–27 but is described asnormal.25–27 Head ‘‘shudder’’ or ‘‘tremor’’, torticollis, andalternating esotropia have been reported in at least three offour reported patients with the combined horizontal andseesaw nystagmus of NDRFFS.15 26 Nystagmus in patientswith a range of chiasmal disorders may be classically‘‘seesaw’’, but nystagmus is not necessarily present andmay be of many less specific types.There are other cases in which reduced chiasmal decussa-
tion does not fall within the strict criteria of NDRFFS. Aretrospective case note and patient review was undertaken todefine better the clinical spectrum of achiasmia.
METHODSPatient selectionFrom the records of the Great Ormond Street Hospital(GOSH) Ophthalmology Department, nine children (fourboys) aged 4–14 years were identified with a diagnosis of
Abbreviations: NDRFFS, non-decussating retinal fugal fibre syndrome;VEP, visual evoked potential
1311
www.bjophthalmol.com

achiasmia. All of these children had previously been clinicallyexamined and had undergone clinically appropriate neuro-imaging and VEP studies. One patient had died before thestart of this study, three were re-examined at routine followup visits to GOSH, one (who had been previously evaluated atGOSH) was reviewed locally by a paediatric ophthalmologist,and four were reviewed specially at GOSH. Inclusion criteriawere presence of nystagmus, VEP documentation of con-sistent positive contralateral crossed asymmetry to flash,16
and reduced chiasmal size on neuroimaging. Where appro-priate, VEPs and eye movement studies were repeated.Data on ocular motility, strabismus, refraction, and visual
acuity were recorded and the anterior segment and fundiwere examined in all cases. Whenever possible, eye move-ments, fundus photographs, and formal visual fields wererecorded. All previous hospital notes were reviewed.The study was approved by the Great Ormond Street
Hospital and the Institute of Child Health (University CollegeLondon) research ethics committee
ElectrophysiologyVEPs to flash16 were recorded from three occipital electro-des—one placed 2–3 cm above the inion and two placedmidway between the inion and mastoid process.Simultaneously, flash electroretinograms were recorded fromskin electrodes placed along the inferior eyelid margin.
Eye movement recordingQuantitative measurements of eye movements were madewith an infrared limbus tracking system (Skalar Medical,Delft, The Netherlands). Horizontal movements wererecorded from the right eye and vertical movements wererecorded from the left eye. A chin rest was used to stabilisethe head and the subject was asked to fixate on a red LEDlight subtending a quarter of a degree of visual angle. The eyemovement recordings were calibrated by asking the subjectsto fixate additional positions spaced ¡15 degrees aparthorizontally and ¡5 degrees apart vertically. Video record-ings of eye movements were also made to facilitateinterpretation of the quantitative eye movement recordings.
NeuroimagingAll previous brain neuroimaging results were reviewed toconfirm reduced chiasmal size and to review other associatedbrain deformities.
RESULTSThe case records and clinical examination results of the ninechildren are shown in table 1. The appearance of the opticnerves and relevant neuroimaging is shown in figs 1–9:fundus photographs were not available for cases 2 and 4 andonly one fundus was available for case 9. All patients had acharacteristic pattern of monocular VEP asymmetry to a flashof light (the VEPs for case 1 are shown in fig 1I and for case 6in fig 6G).16 Three of the children had a skull baseencepahalocele and agenesis of the corpus callosum (cases6, 7 and 8). In two patients achiasmia was associated withsepto-optic dysplasia, a combination of absent septumpellucidum, optic nerve hypoplasia, and hypopituitarism12
(cases 4 and 5). Three children had no neuroimagingabnormalities other than reduced chiasmal size and haveno known pituitary dysfunction (cases 1, 2 and 3); however,one had mild Asperger syndrome and one had subclinicalepileptiform seizure activity. One child had multiple defor-mities including microtia, hemifacial microsomia, oesopha-geal atresia, and hydronephrosis; the only brain imagingabnormality was reduced chiasmal size (case 9).Corrected acuities varied widely: one eye had 0.1 LogMAR,
the others between perception of light and 0.5, 10 eyes hadbetween 0.5 and 0.6. Eight patients had a best correctedbinocular acuity of at least 0.6 LogMAR (table 1). All childrenhad normal colour vision as tested with Ishihara colourplates. Stereo acuity as tested with Titmus fly and/or TNOstereo acuity tests was recorded as absent in all patients. Nospecific pattern of nystagmus was common to the studypatients. The sample includes pure horizontal, rotary, andcompound rotary or circumrotary and horizontal nystagmus(table 1). Further details can be seen on the video availableon the journal website (http://bjo.bmjjournals.com/supple-mental)Our patients seem mostly to fall into three subtypes: type A
(three patients) with isolated achiasmia on neuroimaging,
Table 1 Summary of study patients
Caseno Sex Type* Age (years) Refraction
Visual acuity(logMAR) Nystagmus Strabismus
1 M A 9 RE 21.50 + 0.50 690 1.0 Horizontal XT small angle�LE 0.00 + 1.00 690 0.6 R head turn V pattern
2 F A 4 RE 0.00 + 0.50 690 0.6 Horizontal XT small angleLE 0.00 + 1.50 690 0.5 Horizontal V pattern
3 F A 12 RE +1.50 sph 0.1 Minimal rotary nystagmus ET small angleLE +1.50 sph 0.6 Amplitude L..R
4 F B 4 RE +1.00 sph Very poor Rotary + horizontal Right XT angle 30LE +2.00 sph 0.6
5 F B 12 RE +3.0 sph Greater than 1.0 Highly variable Right ET angle 45LE +1.0 +4.0 690 0.6 Horizontal and vertical
(not seesaw)6 F C 10 RE 25.00 21.00 680 0.7 Seesaw variant: circumrotary
+ dysconjugate verticalNo detectable strabismus
LE 23.50 22.50 6120 0.57 M C 14 RE 20.50 +1.00 690 0.8 Horizontal No detectable strabismus
LE +1.00 +1.00 690 0.5 Left beating, rotarycomponent in 1˚
8 M C Deceased RE 24.50 + 2.00 6120 Greater than 1.0 Type unclear Vertical gaze palsyLE 21.50 + 1.00 6180 1.0
9 M Other 6 RE +0.50 +1.00 6120 0.6 Horizontal No detectable strabismusLE +0.50 +0.50 690 0.6 Head shake
XT = exotropia; ET = esotropia.*Type: A = no other midline abnormality on imaging except small chiasm; B = septo-optic dysplasia (optic nerve hypoplasia, hypopituitarism, deficient septumpellucidum); C = skull base encephalocele + agenesis of the corpus callosum + hypopituitarism.�Angle of strabismus in prism dioptres.
1312 Sami, Taylor, Saunders, et al
www.bjophthalmol.com

type B (two patients) with septo-optic dysplasia, and type C(three patients) with skull base encephalocele and agenesisof the corpus callosum (table 1). One patient (case 9) did notfit into any of these groups.
DISCUSSIONDefinition and classification of achiasmiaThere is probably some chiasmal hypoplasia whenever thereis optic nerve hypoplasia. In most of these cases, normalproportions of retinal ganglion cell axons have been directedipsilaterally and contralaterally but, overall, are fewer innumber. The optic chiasm in achiasmia is not just hypoplasticbut it has the essential absence or relative lack of crossingfibres; thus, optic nerve hypoplasia and achiasmia may co-exist (figs 5A and B, 6A and B, 7B). The term ‘‘achiasmia’’may strictly suggest an absence of the chiasm but, for clarity,it is used here to identify the essential abnormality ofcrossing fibres. Complete absence of the chiasmal structure,often associated with optic nerve aplasia, is thus notachiasmia; the term ‘‘chiasmal aplasia’’ is more appropri-ate.21 22
The definition of achiasmia is therefore not as strict asNDRFFS (defined above). The criteria for diagnosis arepositive contralateral asymmetry of the monocular VEPresponse to flash (figs 1I and 6G) and neuroimaging showingreduced chiasmal size (figs 1G, 2, 3A and B, 4, 5C, 6E, 8D,
and 9B). Although nystagmus was part of the inclusioncriteria for this study, it may not be a constant feature ofachiasmia—just as the excess decussation in albinism is notinevitably associated with clinical nystagmus.18
To our knowledge, four patients (all female) have beenreported with NDRFFS.15 23 26 A fifth female has beendescribed with isolated achiasmia but she only has horizontalnystagmus.25 The male:female ratio in our mixed group ofpatients with achiasmia is 4:5. One of three patients withisolated chiasmal deficit (our type A) is male (case 1).Another (case 9) who had an isolated small chiasm onneuroimaging but other associated facial and visceralproblems is also male.From our small sample and those in the literature, some
general patterns appear to emerge. While the numbers ofpatients with this rare finding are small, we feel that theremay be three main groups of patients with achiasmia:
N Type A: reduced decussation with optic nerves of normalappearance on clinical examination.25 26 A small chiasmmay be the only abnormality on the brain MRI scan. Thisgroup appears to overlap with NDRFFS. There may beseesaw23 or purely horizontal25 nystagmus, and the visualfields appear to be normal.23 In our patients, cases 1 and 3had normal formal visual fields, case 2 (who was 4 yearsold) had behaviourally normal fields. Abnormal head
Figure 1 Case 1 (type A). A 9 year old boy with a small chiasm as theonly neuroimaging abnormality. He also has mild Asperger syndrome.(A, right) and (B) There is a pigmented surround to the optic disc but thenerve substance is normal. (C, left) and (D) Normal Goldmann visualfields (stimulus i4E), the blind spot was difficult to define because ofnystagmus. (E) Normal calibre intracanilicular portion of the optic nerveson coronal T1 weighted MRI scan (white arrows). (F) Normal midlinestructures on a midline sagittal T1 weighted MRI scan except for verysmall chiasm (white arrow). Note normal corpus callosum (CC). (G)Severely reduced size of chiasm. Note the bright vessel signalsurrounding the very thin ‘‘gull wing’’ shaped chiasm. (H) Small chiasmat the level of the third ventricle. Note the bright signal from the terminalinternal carotid/proximal middle cerebral arteries (arrowheads)surrounding the very thin ‘‘gull wing’’ shaped chiasm (white arrow). (I)Visual evoked potential traces showing characteristic crossedcontralateral positivity of achiasmia. This abnormality was present in allcases.
The achiasmia spectrum 1313
www.bjophthalmol.com

posture, strabismus,26 and other subtle neurologicalabnormalities (mild autism in case 1 and subclinicalepileptiform temporal lobe activity in case 2) may bepresent.
N Type B: reduced decussation in combination with chiasmalhypoplasia and the midline defects of septo-optic dyspla-sia,16 28 a combination of absent septum pellucidum, opticnerve hypoplasia, and hypopituitarism (cases 4 and 5).12
N Type C: reduced decussation and chiasmal hypoplasia inassociation with clefting disorders and encephaloceles ofthe skull base (cases 6, 7, and 8). Agenesis of the corpuscallosum was present in all three of our patients with basal
encephaloceles. The association of corpus callosum agen-esis, morning glory disc, and optic nerve staphylomas withskull base encephaloceles has been previously reviewed.29
One patient in our series (case 9) did not fit into any of theabove categories. This child suffered from multiple facial(microtia, hemifacial microsomia), visceral (oesophagealatresia, hydronephrosis), and developmental problems inaddition to an isolated small chiasm; the MRI scan wasotherwise normal.
Visual fields in achiasmiaCongenitally reduced chiasmal decussation need not beassociated with visual field defects. The visual field may be
Figure 2 Case 2 (type A). A 4 year old girl with an isolated chiasmaldeficit as the only neuroimaging abnormality. She was noted to havesubclinical epileptiform activity. Optic nerve ophthalmoscopy wasnormal but photography was not possible. Behaviourally, the visualfields were normal and she has achieved all of her developmentalmilestones.
Figure 3 Case 3 (type A). A 12 year old girl with normal development and intelligence. (A) Serial coronal T1 weighted MRI scans showing an isolatedsmall chiasm (arrows) through the level of the pituitary gland (pg). (B) More posterior section through the anterior third ventricle. Note the subtle brightvessel signal surrounding the very thin ‘‘gull wing’’ shaped chiasm similar to case 1. (C, right) and (D) The optic discs were normal; there was a smallarea of myelination inferior on the disc in the right eye. (E) and (F) Automated perimetry (30-2) was normal.
Figure 4 Case 4 (type B). A 4 year old girl with septo-optic dysplasia.On examination the left optic nerve was smaller than the right. CoronalT1 weighted images through the chiasmatic recess reveal the chiasm tobe small and pulled down (arrow). The septum pellucidum is absent(arrowheads). Fundus photography was impossible due to lack of patientcooperation and nystagmus.
1314 Sami, Taylor, Saunders, et al
www.bjophthalmol.com

abnormal due to optic nerve hypoplasia (case 6, fig 2) butdoes not necessarily have a bitemporal hemianopia patternsuch as that seen with traumatic shearing of the chiasm.30–32
In cases 1 and 3 the appearance of the optic nerves andformal visual field testing were normal (figs 1C and D, 3E andF) The finding of normal visual fields in association with anisolated small chiasm on neuroimaging has been reportedpreviously.15 23 27 A full visual field is consistent with studiesof the lateral geniculate body (LGN) in the canine model ofisolated achiasmia: misdirected nasal fibres form ipsilateralmirror image maps in those LGN layers that normally wouldhave received nasal fibres from the contralateral eye.33 The
optic discs may appear normal in achiasmia.25–27 The size ofthe optic nerves, density of axons, and total number of axonsdo not differ between achiasmic mutant and normal dogs,but the area centralis of the achiasmic dogs is smaller and hasa lower peak ganglion cell density than that of normal dogs.34
Seesaw nystagmus and achiasmiaSeesaw nystagmus was described by Maddox in 1914.35 Thereis a conjugate torsional component and a dysconjugatevertical component. Both eyes rotate clockwise and thencounterclockwise. The intorting eye rises while the extortingeye falls. However, the definition of seesaw nystagmus has
Figure 5 Case 5 (type B). A 12 year old girl with septo-optic dysplasia. (A) Optic nerve hypoplasia, right eye. (B) Band hypoplasia, left eye. Formalvisual fields were not available but the appearances of the left optic disc suggest the likelihood of a left temporal hemianopia. (C) A coronal reformattedCT scan shows the optic nerves (arrows) but fails to reveal a chiasm suggesting that it is small (arrowhead).
Figure 6 Case 6 (type C). Optic nerve hypoplasia in a 10 year old girl. (A) Right optic disc showing mild hypoplasia and inferotemporal pallor. (B)Left optic disc showing possible mild hypoplasia and the suggestion of nasal pallor. (C) Left eye Goldmann visual field (stimulus IIVE) showingconstriction, especially superotemporally. (D) Right visual field showing superior constriction consistent with the optic disc findings of inferior pallor. (E)Midline T1 weighted sagittal MRI scan showing absence of the corpus callosum, a large empty sella (es), and a very thin chiasm (arrow) (see fig 1F for anormal corpus callosum). (F) Revised coronal T1 weighted MRI scan showing dragging of optic nerves (arrows) and chiasm into the repairedencephalocele. (G) VEP showing contralateral crossed asymmetry which, in combination with optic disc, visual fields, and MRI findings, demonstratesthe co-existence of overall chiasmal hypoplasia and relative decussation deficit. Although not shown for every case, this finding was present in all.
The achiasmia spectrum 1315
www.bjophthalmol.com

not remained strict over time. In 1946 Rucker36 describedseesaw nystagmus in a patient with vertical and torsionalmovements in the left eye (as described by Maddox), but onlyvertical movement in the right eye. Jensen described seesawnystagmus as a ‘‘rare disjunctive form of vertical nystagmusin which the eyes perform opposed vertical movements’’, butdid not specify a necessary torsional component.37
Disorders of the mesencephalon,38–40 chiasmal trauma,30 31
and chiasmal compressive lesions41 42 are associated withseesaw nystagmus. Achiasmia is a recent addition to thedifferential diagnosis of seesaw nystagmus.43
In initial reports the pattern of nystagmus in achiasmiawas limited to the combination of congenital horizontal andseesaw nystagmus.43 44 However, purely horizontal nystag-mus may be present in achiasmia, as illustrated by cases 1, 2and 9 in this study and in a previous case report.25 Combinedhorizontal and torsional nystagmus also appears to beconsistent with achiasmia as illustrated by cases 4 and 7.
Conclusions and general observationsCertainty of the diagnosis of achiasmia can only be achievedby a combination of MRI scanning and VEPs. A number ofour original sample of patients with VEP features ofcontralateral crossed positivity had to be excluded becausethe study was too noisy and/or was not reproducible onsubsequent testing. It is also not possible to determine ifthere is complete absence of decussation on the MRI scan;this would require extremely thin sections.Despite the wide spectrum of midline congenital CNS
malformations in our achiasmic patients, most function well;five of the nine patients attend mainstream schools and arenot behind their age matched peers. One (case 1) participatesin junior golf competitions; another (case 6) performs well inarts and crafts. Other reports corroborate our finding of ahigh level of functioning in these children.15 26 27
Full visual fields3 23 27 44 and ophthalmoscopically normaloptic discs25–27 are consistent with achiasmia, as shown by ourcases 1 and 3. There does not appear to be any single patternto the nystagmus: it may be rotary, seesaw, or purelyhorizontal. Subtle neurological problems may co-exist with‘‘isolated’’ forms, as reported elsewhere15 26 and in our cases 1and 2.Achiasmia appears to be rare, but a portion of children
diagnosed with ‘‘idiopathic congenital motor nystagmus’’may have reduced decussation as part of the underlyingabnormality—especially since VEPs and MRI scans are oftennot performed when the appearance of the nystagmus is‘‘classic’’.Relatively reduced decussation affects a subset of children
with developmental abnormalities that include midline facialdefects, basal encephaloceles, midbrain defects, pituitary and
Figure 7 Case 7 (type C). A 14 year old boy with a cleft lip and palate,an ethmoidal encephalocele, and agenesis of the corpus callosum.(A) Morning glory disc, right eye. (B) Band optic atrophy, left eye. Thepresence of band atrophy in one eye and an abnormal disc ofdevelopmental origin in the other suggest that the cause of the bandatrophy was most likely an early event, but it is possible that the bandatrophy may have been caused by a postnatal event. (C) Coronalreformatted CT scan on bone windows showing a nasal encephalocele.(D) Soft tissue windows reveal an attenuated optic chiasm (arrow).
Figure 8 Case 8 (type C). Deceased boy with frontonasal dysplasia, aspheno-ethmoidal encephalocele, and agenesis of the corpus callosum.(A) Right and (B) left fundi showing posterior pole staphyloma anddysplastic discs. (C) Coronal T1 weighted MRI scan through the frontalhorns of the lateral ventricles showing a spheno-ethmoidalencephalocele. (D) Midline sagittal image reveals an attenuated opticchiasm and agenesis of the corpus callosum (see fig 1F for normalcorpus callosum).
Figure 9 Case 9 (type unclassified). A 6 year old boy with an isolatedsmall optic chiasm on the MRI scan associated with multiple facial andvisceral anomalies. (A) Normal left optic disc. Photographs of the righteye had motion artefact. (B) Midline sagittal T1 weighted MRI scanshowing a small optic chiasm.
1316 Sami, Taylor, Saunders, et al
www.bjophthalmol.com

hypothalamic defects, alone or in combination. Wheneverthere is reason to suspect congenital chiasmal maldevelop-ment, VEPs, MRI scans, endocrine assessment, and visualfollow up until mature are recommended.
Video available on journal website athttp://bjojournals.com/supplemental
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
D A Sami, D Saunders, D A Thompson, I M Russell-Eggitt, K K Nischal,R A Clement, A Liassis, D S Taylor, Visual Sciences Unit, Institute of ChildHealth (University College, London), London and Department ofOphthalmology, Great Ormond Street Hospital for Children, London,UKG Jeffery, Institute of Ophthalmology, London, UKM Dattani, Department of Biochemistry, Institute of Child Health(University College, London), London and Department of Endocrinology,Great Ormond Street Hospital for Children, London, UK
Competing interests: none declared
REFERENCES1 Magnin M, Cooper HM, Mick G. Retinohypothalamic pathway: a breach in
the law of Newton-Muller-Gudden? Brain Res 1989;488:390–7.2 Herrera E, Brown L, Aruga J, et al. Zic2 patterns binocular vision by specifying
the uncrossed retinal projection. Cell 2003;114:545–57.3 Apkarian P, Bour L, Barth PG. A unique achiasmatic anomaly detected in non-
albinos with misrouted retinal-fugal projections. Eur J Neurosci1994;6:501–7.
4 McCarty JW, Demer JL, Hovis LA, et al. Ocular motility anomalies indevelopmental misdirection of the optic chiasm. Am J Ophthalmol1992;113:86–95.
5 Alvarez-Bolado G, Schwarz M, Gruss P. Pax-2 in the chiasm. Cell Tissue Res1997;290:197–200.
6 Torres M, Gomez-Pardo E, Gruss P. Pax2 contributes to inner ear patterningand optic nerve trajectory. Development 1996;122:3381–91.
7 Trousse F, Marti E, Gruss P, et al. Control of retinal ganglion cell axon growth:a new role for Sonic hedgehog. Development 2001;128:3927–36.
8 Lin L, Chan SO. Perturbation of CD44 function affects chiasmatic routing ofretinal axons in brain slice preparations of the mouse retinofugal pathway.Eur J Neurosci 2003;17:2299–312.
9 Guillery RW. Developmental neurobiology: preventing midline crossings. CurrBiol 2003;13:R871–2.
10 Williams SE, Mann F, Erskine L, et al. Ephrin-B2 and EphB1 mediate retinalaxon divergence at the optic chiasm. Neuron 2003;39:919–35.
11 Rasband K, Hardy M, Chien CB. Generating X: formation of the optic chiasm.Neuron 2003;39:885–8.
12 Lubinsky MS. Hypothesis: septo-optic dysplasia is a vascular disruptionsequence. Am J Med Genet 1997;69:235–6.
13 Margo CE, Hamed LM, Fang E, et al. Optic nerve aplasia. Arch Ophthalmol1992;110:1610–3.
14 Apkarian P, Shallo-Hoffmann J. VEP projections in congenital nystagmus. VEPasymmetry in albinism: a comparison study. Invest Ophthalmol Vis Sci1991;32:2653–61.
15 Apkarian P, Bour LJ, Barth PG, et al. Non-decussating retinal-fugal fibresyndrome. An inborn achiasmatic malformation associated with visuotopicmisrouting, visual evoked potential ipsilateral asymmetry and nystagmus.Brain 1995;118:1195–216.
16 Thompson DA, Kriss A, Chong K, et al. Visual-evoked potential evidence ofchiasmal hypoplasia. Ophthalmology 1999;106:2354–61.
17 Apkarian P, Reits D, Spekreijse H, et al. A decisive electrophysiological test forhuman albinism. Electroencephalogr Clin Neurophysiol 1983;55:513–31.
18 Sjodell L, Sjostrom A, Abrahamsson M. Transillumination of iris andsubnormal visual acuity–ocular albinism? Br J Ophthalmol 1996;80:617–23.
19 Soong F, Levin AV, Westall CA. Comparison of techniques for detectingvisually evoked potential asymmetry in albinism. J AAPOS 2000;4:302–10.
20 Bouzas EA, Caruso RC, Drews-Bankiewicz MA, et al. Evoked potentialanalysis of visual pathways in human albinism. Ophthalmology1994;101:309–14.
21 Scott IU, Warman R, Altman N. Bilateral aplasia of the optic nerves, chiasm,and tracts in an otherwise healthy infant. Am J Ophthalmol1997;124:409–10.
22 Waheed K, Jan W, Calver DM. Aplasia of the optic chiasm and tracts withunifocal polymicrogyria in an otherwise healthy infant. J Pediatr OphthalmolStrabismus 2002;39:187–9.
23 Apkarian P, Bour LJ. See-saw nystagmus and congenital nystagmus identifiedin the non-decussating retinal-fugal fiber syndrome. Strabismus2001;9:143–63.
24 Dell’Osso LF, Williams RW, Jacobs JB, et al. The congenital and see-sawnystagmus in the prototypical achiasma of canines: comparison to the humanachiasmatic prototype. Vis Res 1998;38:1629–41.
25 Jansonius NM, van der Vliet TM, Cornelissen FW, et al. A girl without achiasm: electrophysiologic and MRI evidence for the absence of crossing opticnerve fibers in a girl with a congenital nystagmus. J Neuroophthalmol2001;21:26–9.
26 Korff CM, Apkarian P, Bour LJ, et al. Isolated absence of optic chiasmrevealed by congenital nystagmus, MRI and VEPs. Neuropediatrics2003;34:219–23.
27 Victor JD, Apkarian P, Hirsch J, et al. Visual function and brain organizationin non-decussating retinal-fugal fibre syndrome. Cereb Cortex2000;10:2–22.
28 Miller SP, Shevell MI, Patenaude Y, et al. Septo-optic dysplasia plus: aspectrum of malformations of cortical development. Neurology2000;54:1701–3.
29 Hodgkins P, Lees M, Lawson J, et al. Optic disc anomalies and frontonasaldysplasia. Br J Ophthalmol 1998;82:290–3.
30 Arnott EJ, Miller SJ. See saw nystagmus. Trans Ophthalmol Soc UK1970;90:491–6.
31 Hassan A, Crompton JL, Sandhu A. Traumatic chiasmal syndrome: a series of19 patients. Clin Exp Ophthalmol 2002;30:273–80.
32 Heinz GW, Nunery WR, Grossman CB. Traumatic chiasmal syndromeassociated with midline basilar skull fractures. Am J Ophthalmol1994;117:90–6.
33 Williams RW, Hogan D, Garraghty PE. Target recognition and visual maps inthe thalamus of achiasmatic dogs. Nature 1994;367:637–9.
34 Hogan D, Williams RW. Analysis of the retinas and optic nerves ofachiasmatic Belgian sheepdogs. J Comp Neurol 2004;352:367–80.
35 Maddox EE. See-saw nystagmus with bitemporal hemianopia. Proc R SocMed 1914;7:12–3.
36 Rucker CW. Seesaw nystagmus associated with choroiditis and positiveneuralization test for toxoplasma. Arch Ophthalmol 1946;35:301–2.
37 Jensen OA. Seesaw nystagmus. Br J Ophthalmol 1959;43:225–9.38 Halmagyi GM, Hoyt WF. See-saw nystagmus due to unilateral
mesodiencephalic lesion. J Clin Neuroophthalmol 1991;11:79–84.39 Halmagyi GM, Aw ST, Dehaene I, et al. Jerk-waveform see-saw nystagmus
due to unilateral meso-diencephalic lesion. Brain 1994;117:789–803.40 Sparks DL. The brainstem control of saccadic eye movements. Nat Rev
Neurosci 2002;3:952–64.41 Arnott EJ. Vertical see-saw nystagmus. Trans Ophthalmol Soc UK
1964;84:251–7.42 Unsold R, Ostertag C. Nystagmus in suprasellar tumors: recent advances in
diagnosis and therapy. Strabismus 2002;10:173–7.43 Dell’Osso LF, Daroff RB. Two additional scenarios for see-saw nystagmus:
achiasma and hemichiasma. J Neuroophthalmol 1998;18:112–3.44 Apkarian P. Chiasmal crossing defects in disorders of binocular vision. Eye
1996;10:222–32.
The achiasmia spectrum 1317
www.bjophthalmol.com

EXTENDED REPORT
Randomised clinical trial of the effectiveness of base-inprism reading glasses versus placebo reading glasses forsymptomatic convergence insufficiency in childrenM Scheiman, S Cotter, M Rouse, G L Mitchell, M Kulp, J Cooper, E Borsting, and the ConvergenceInsufficiency Treatment Trial (CITT) Study Group*. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Professor M Scheiman, EyeInstitute, PennsylvaniaCollege of Optometry,1200 West Godfrey Ave,Philadelphia, PA 19141,USA; [email protected]
Accepted for publication1 March 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1318–1323. doi: 10.1136/bjo.2005.068197
Purpose: To compare base-in prism reading glasses with placebo reading glasses for the treatment ofsymptomatic convergence insufficiency (CI) in children aged 9 to ,18 years.Methods: In a randomised clinical trial, 72 children aged 9 to ,18 years with symptomatic CI wereassigned to either base-in prism glasses or placebo reading glasses. Symptom level, measured with aquantitative symptom questionnaire (CI Symptom Survey-V15), was the primary outcome measure. Nearpoint of convergence and positive fusional vergence at near were secondary outcomes.Results: The mean (SD) CI Symptom Survey score decreased (that is, less symptomatic) in both groups(base-in prism glasses from 31.6 (10.4) to 16.5 (9.2); placebo glasses from 28.4 (8.8) to 17.5 (12.3)).The change in the CI Symptom Survey scores (p = 0.33), near point of convergence (p = 0.91), and positivefusional vergence (p = 0.59) were not significantly different between the two groups after 6 weeks ofwearing glasses.Conclusions: Base-in prism reading glasses were found to be no more effective in alleviating symptoms,improving the near point of convergence, or improving positive fusional vergence at near than placeboreading glasses for the treatment of children aged 9 to ,18 years with symptomatic CI.
There is a lack of consensus regarding the most appro-priate treatment for convergence insufficiency (CI).Various treatments are commonly prescribed including
home based pencil push ups, vision therapy/orthoptics, andbase-in prism reading glasses.1–11 Base-in prism readingglasses are commonly recommended in ophthalmic text-books2 8 9 12 13 as part of ‘‘conventional’’ wisdom in ophthal-mic practice.14 This treatment is cost effective and easy toadminister. However, all of the published research on theeffectiveness of base-in prism for the treatment of CI hasfundamental design flaws including lack of a control group,no randomisation, and non-masked outcome examina-tions.14–16 Thus, in spite of the common use and rather broadacceptance of base-in prism for the treatment of CI, there islittle scientific evidence showing its effectiveness.This prospective randomised, double blind, placebo con-
trolled clinical trial was designed to evaluate the effectivenessof base-in prism for the treatment of children withsymptomatic CI. The purpose of the study was to determinewhether base-in prism reading glasses were more effectivethan placebo reading glasses in improving the symptoms andsigns associated with symptomatic CI in children aged 9 to,18 years.
METHODSThe study was conducted by the Convergence InsufficiencyTreatment Trial (CITT) Group at nine clinical sites (seeAppendix 1). The research followed the tenets of theDeclaration of Helsinki and the protocol and informedconsent forms were approved by each institutional reviewboard. The parent or guardian (referred to subsequently as
‘‘parent’’) of each study patient gave written informedconsent and the child gave written assent, as required.
Patient selectionChildren aged 9 to ,18 years with symptomatic CI wereeligible for the study. The eligibility criteria are listed intable 1. The 15-item version of the CI Symptom Survey (CISymptom Survey-V15) was administered to determine if thechild was symptomatic (fig 1).17 18 Each answer was scored 0–4, with 4 representing the highest frequency of symptomoccurrence (that is, always). The 15 items were then summedto obtain the CI Symptom Survey score (range 0–60).Other eligibility tests included best corrected visual acuity,
cover testing, near point of convergence, positive andnegative fusional vergence at near, near stereoacuity, mono-cular accommodative amplitude, monocular accommodativefacility (accommodative facility testing evaluates the speedand latency of the accommodative response by testing thepatient’s ability to alternately clear +2.00/22.00 lenses over a1 minute time span),19 and a cycloplegic refraction. Alltesting was performed using previously reported standardisedprotocols.20
If a patient had clinical emmetropia or was wearing glassesand no change in prescription was necessary, randomisationoccurred immediately. If a significant change in refractivecorrection was required, new glasses were prescribed.Refractive errors requiring correction were defined as>1.50 D of hyperopia, >0.50 D of myopia, >0.75 D ofastigmatism, or >0.75 D of anisometropia in sphericalequivalent, or >1.50 D of anisometropia in any meridianAfter wearing the new glasses for at least 2 weeks, eligibilitytesting was repeated to determine if the patient still met theeligibility criteria before he or she could be randomised.
Abbreviations: CI, convergence insufficiency; D, dioptre; D, prismdioptre
*A list of the investigators who participated in the study appears inAppendix 1.
1318
www.bjophthalmol.com

Treatment protocolsThe data coordinating centre randomly assigned eligiblepatients with equal probability to either base-in prismreading glasses or placebo reading glasses. Randomisationwas accomplished with the study’s website using a permutedblock design stratified by site.
Base-in prism reading glassesPatients in this group received glasses that corrected for thepatient’s refractive error, if necessary, and base-in prism. Theamount of prism was based on the minimum amountnecessary to meet Sheard’s criterion,21 with no less than1 D prescribed. Sheard21 suggested that, for a patient with asignificant phoria to be comfortable, the fusional reservemust be at least twice the amount of the phoria. To determinethe amount of prism necessary to achieve this relationship heproposed the following formula: prism to be prescribed = 2/3phoria – 1/3 compensating fusional vergence. The amount ofprism was rounded up to the nearest half prism dioptre andsplit equally between the two eyes if the magnitude exceeded1 D. The patient was asked to wear these glasses for allreading and near tasks requiring more than 5 minutes.
Placebo reading glassesPatients in this group received glasses that corrected theirrefractive error, or plano lenses were prescribed for those whodid not require a refractive correction. The patient was asked
to wear these glasses for all reading and near tasks requiringmore than 5 minutes.
MaskingNeither the patient nor the examiner performing testing atthe outcome examination was aware of the treatmentassignment. To prevent potential examiner unmasking byobservation of the glasses, the study coordinator placed Tac’N StikH reusable adhesive around the edges of the eyeglasses(fig 2). The edges of the lenses were therefore obscured,making it impossible for the examiner to see the edgethickness of the lenses.
Outcome examination proceduresThe primary outcome examination was conducted after amean (SD) of 6 (1) weeks of study glasses wear. At this visitan examiner who was masked to the patient’s treatmentgroup administered the CI Symptom Survey-V15, the covertest at distance and near, near point of convergence, andpositive fusional vergence at near. Testing was performedwith the assigned glasses.
Outcome measuresThe CI Symptom Survey-V15 score was the primary outcomemeasure. Secondary outcome measures were the near pointof convergence and positive fusional vergence at near.
Convergence Insufficiency Symptom Survey – V15
Clinician instructions: Read the following subject instructions and then each item exactlyas written. If subject responds with "yes" – please qualify with frequency choices.Do not give examples.
Subject instructions: Please answer the following questions about how your eyes feel whenreading or doing close work.
Response options: NeverInfrequently (not very often)SometimesFairly oftenAlways
Survey items: 1. Do your eyes feel tired when reading or doing close work?2. Do your eyes feel uncomfortable when reading or doing close work?3. Do you have headaches when reading or doing close work?4. Do you feel sleepy when reading or doing close work?5. Do you lose concentration when reading or doing close work?6. Do you have trouble remembering what you have read?7. Do you have double vision when reading or doing close work?8. Do you see the words move, jump, swim or appear to float on the page when reading or
doing close work?9. Do you feel like you read slowly?10. Do your eyes ever hurt when reading or doing close work?11. Do your eyes ever feel sore when reading or doing close work?12. Do you feel a "pulling" feeling around your eyes when reading or doing close work?13. Do you notice the words blurring or coming in and out of focus when reading or doing
close work?14. Do you lose your place while reading or doing close work?15. Do you have to re-read the same line of words when reading?
Figure 1 CI Symptom Survey (CI Symptom Survey-V15).
Base-in prism reading glasses versus placebo reading glasses for CI in children 1319
www.bjophthalmol.com

Adherence to the treatment protocolAdherence to treatment was assessed by asking the patient:‘‘What percentage of the time did you wear the glasses wegave you while you were reading or doing near work (0%,25%, 50%, 75%, or 100%)?’’ We also asked the child: ‘‘Howsure are you about this answer (very sure, pretty sure,somewhat sure, a little sure, not sure at all)?’’ Parents wereasked the same questions about their child’s wearing of thereading glasses.
Assessment of success of maskingTo assess the success of masking we asked the examiner toreport what treatment he/she thought the child had receivedor if he/she was unsure. This question was asked after testingwith the assigned reading glasses was completed. In addition,the children and parents were asked which treatment theythought they had received or if they did not know. The
children and parents were also asked to report how sure theywere about this answer (very sure, pretty sure, somewhatsure, a little sure, not at all sure).
Statistical methodsOne sample t tests were used to compare the mean change ineach outcome measure. Two sample t tests were used to makecomparisons between the two groups when the outcome ofinterest was interval scaled. x2 tests were used to comparegroups when the outcome of interest was a categoricalvariable, and a Wilcoxon rank sum test was used to comparegroups in the case of ordinal scaled outcome variables. ThePearson correlation coefficient was used to assess theassociation between amount of prism and CI symptom score.
RESULTSEnrollment and follow upSeventy two children were enrolled at nine clinical sites.Thirty one of the 36 patients (86%) assigned to receive base-in prism reading glasses and 34 of the 36 (94%) assigned toplacebo reading glasses completed their 6 week outcomeexamination (fig 3). There was no statistically significantdifference in the percentage loss to follow up between thetwo treatment groups (p=0.43, x2 test).
Baseline dataDemographic data for patients assigned to the two treatmentgroups are shown in table 2. The only statistically significantdifference at baseline between the groups was accommoda-tive amplitude (p=0.011), although this was not clinicallysignificant (table 3).
Prism prescribedIn the group receiving base-in prism, the mean (SD) prismprescription was 4.14 (2.4) D (range 1–10) and in the placebogroup the mean (SD) prism prescription that would havebeen prescribed was 3.78 (2.4) D (range 1–11). There was nostatistically significant difference in these values (p=0.48).
Adherence to treatmentIn the base-in prism group, 90% of patients reported wearingtheir glasses at least 75% of the prescribed time and 81% ofparents said their child wore his or her glasses at least 75% ofthe prescribed time. There was agreement between child andparent on percentage of time worn for 55% of the responses.In the placebo group, 79% of patients reported wearing theirglasses at least 75% of the prescribed time and 79% of parentssaid their child wore his or her glasses at least 75% of theprescribed time. Patient and parent agreed on the percentageof time the placebo glasses were worn 42% of time. Reported
72 patientsrandomised
36 assigned toplacebo
reading glasses
34 included inanalysis
2 lost tofollow up
36 assigned tobase-in prism
reading glasses
31 included inanalysis
5 lost tofollow up
Figure 3 Flow chart showing study completion for each group.
Table 1 Eligibility and exclusion criteria
Eligibility criteria:l Age 9 to ,18 years.l Best corrected visual acuity of 20/25 or better in both eyes at distance
and near.l Willingness to wear eyeglasses to correct refractive error, if
necessary.l Exophoria at near at least 4 D greater than at far.l Insufficient positive fusional convergence at near (fails Sheard’s
criterion).l Receded near point of convergence of >6 cm break.l Appreciation of at least 500 seconds of arc on the forms part of the
Randot Stereotest.l CI Symptom Survey-V15 score >16.l Informed consent and willingness to participate in the study and be
randomised.
Exclusion criterial CI previously treated with prism, pencil push ups, or office based
vision therapy/orthoptics (no more than 2 months of treatment withinthe past year).
l Amblyopia.l Constant strabismus.l History of strabismus surgery.l Anisometropia .1.50 D (spherical equivalent) difference between
eyes.l Previous refractive surgery.l Vertical heterophoria greater than 1 D.l Systemic diseases known to affect accommodation, vergence, and
ocular motility such as multiple sclerosis, Grave’s thyroid disease,myasthenia gravis, diabetes, and Parkinson’s disease.
l Any ocular or systemic medication known to affect accommodation orvergence.
l Monocular accommodative amplitude less than 4 D in either eye asmeasured by the push up method.
l Manifest or latent nystagmus.l Attention deficit hyperactivity disorder or learning disability diagnosis
by parental report that, in the investigator’s opinion, would interferewith treatment.
Figure 2 Tac ’N StikH reusable adhesive around the edges of theeyeglasses used to prevent unmasking.
1320 Scheiman, Cotter, Rouse, et al
www.bjophthalmol.com

wearing time was not statistically different between the twogroups using the patients’ (p=0.18) or parents’ responses(p=0.24).
Primary outcome measure: CI Symptom Survey scoreThere were statistically significant changes in the mean CISymptom Survey score in both the base-in prism group(p,0.001) and placebo group (p,0.001). The CI SymptomSurvey score decreased to less than 16 (previously found todifferentiate children with symptomatic CI from those withnormal binocular vision18) at the outcome examination in51.6% of the base-in prism group and 47.1% of the placebogroup. This difference is not statistically significant(p=0.71).Pearson correlation coefficients were calculated to assess
the relationship between amount of prism prescribed and theprimary outcome. In the base-in prism group, neither the CISymptom Survey score at the 6 week visit (R=0.263,p=0.15) nor the change in CI Symptom Survey score(R=20.078, p=0.68) were related to the amount of prismprescribed.
Secondary outcome measuresThere were no clinically significant changes in either nearpoint of convergence or positive fusional vergence at near.Few patients in either group achieved a normal near point ofconvergence or positive fusional vergence at near (table 3).
Placebo treatment: assessment of maskingExaminers performing the outcome examination correctlyidentified group assignment for 23 of the 64 patients (36%)who completed the outcome examination (information wasnot collected for one patient); 39% of these were in the base-in prism group and 33% were in the placebo group. Thepercentage correctly identified was significantly lower thanwould have been expected by chance (p=0.024).Sixteen of the 65 patients (25%) correctly identified their
group assignment which is significantly less than would beexpected by chance (p,0.001). Eleven of the 31 (35.5%)assigned to base-in prism and five of the 34 (14.7%) assignedto placebo reading glasses responded correctly (table 4). Fortyof the 65 patients (61.5%) responded ‘‘don’t know’’.Thirty two percent of the parents correctly identified their
child’s group assignment. This is significantly less thanexpected by chance (p=0.004). Twelve of the 31 parents(38.7%) whose child was assigned to base-in prism and nineof the 33 parents (27.3%) whose child was assigned toplacebo reading glasses correctly identified the assignedtreatment (table 4; data missing for one parent). Thirty fourof the 64 parents (53.1%) responded ‘‘don’t know’’.
DISCUSSIONIn this prospective, randomised, placebo controlled clinicaltrial, the prescription of base-in prism reading glasses (basedon Sheard’s criterion) was no more effective than placeboreading glasses for the treatment of symptomatic CI in
Table 2 Demographic data of study groups and clinical measures at randomisation
CharacteristicBase-in prism readingglasses (n = 36)
Placebo reading glasses(n = 36)
Mean (SD) age (years) 11.5 (2.3) 11.0 (2.0)Sex (%)
Boys 36.1 52.8Girls 63.9 47.2
Race (%)African American 36.1 36.0American Indian 2.8 2.0White 55.6 61.1Other 5.6 0.0
Mean (SD) accommodative amplitude (D) 8.5 (4.3) 10.8 (4.3)Mean (SD) accommodative facility (cycles/min) 6.6 (4.6) 6.7 (5.0)Mean (SD) exophoria (D)
Distance 2.36 (2.9) 1.61 (1.9)Near 11.19 (3.7) 10.44 (3.9)
Mean (SD) refractive error (spherical equiv) (D)OD 0.30 (0.84) 0.17 (1.09)OS 0.23 (0.84) 0.20 (1.04)
D, dioptre; D, prism dioptre; OD, oculus dexter; OS, oculus sinister.
Table 3 Comparison of treatment groups with respect to clinical measures at baselineand the 6 week outcome examination
CharacteristicBase-in prism reading glasses(n = 31)
Placebo reading glasses(n = 34)
CI symptom scoreBaseline 31.63 (10.41) 28.38 (8.79)Outcome 16.53 (9.25) 17.54 (12.26)Change 215.10 (11.91) 210.84 (13.41)
Near point of convergence break (cm)Baseline 17.95 (11.56) 15.87 (7.17)Outcome 13.81 (8.24) 14.54 (10.58)Change 24.14 (9.99) 21.33 (8.25)
Positive fusional vergence break (D)Baseline 10.55 (4.13) 10.05 (3.49)Outcome 12.56 (5.76) 12.71 (7.16)Change 1.97 (4.65) 2.66 (8.43)
Data shown as mean (SD) values.
Base-in prism reading glasses versus placebo reading glasses for CI in children 1321
www.bjophthalmol.com

children. Although neither treatment group showed clinicallysignificant changes in the near point of convergence orpositive fusional convergence at near, nearly half of thechildren assigned to each of the two treatment groupsreported a statistically significant decrease in symptoms(although neither group achieved a decrease in symptoms toa level considered clinically asymptomatic).Because the children assigned to placebo reading glasses
were just as likely to report a decease in symptoms as werethose assigned to the base-in prism reading glasses, thesedata suggest that the ‘‘placebo effect’’ was probablyresponsible for the reduction in symptoms in the base-inprism group. The placebo effect has been viewed as a changein a patient’s illness attributable to the symbolic aspect of atreatment and not to any specific pharmacological orphysiological property.22 In his review of 15 studies oftreatment for a variety of medical disorders ranging fromangina pectoris and headaches to the common cold, Beecher23
found the placebo response rate ranged from 15% to 58%with an average effectiveness of 35%. We are unaware of anystudies related to placebo effect and the use of spectacles inophthalmic care.Only one other study has investigated the effectiveness of
base-in prism glasses for the treatment of CI. In this study15
patients reported subjective improvement in asthenopicsymptoms and headaches after 2 weeks of wear. However,the authors did not have a placebo control group, so there isno way of knowing whether the reported improvement insymptoms was due to a placebo effect.One of the primary challenges of this study was to
maintain masking of the examiners, children, and parents.Our data suggest that the majority of examiners, patients,and parents were successfully masked to treatment assign-ment.We could identify no sources of bias or confounding factors
to explain our findings. The follow up visit rate was high inboth groups and missing data from patients who dropped outof the study did not influence the interpretation of theresults. Baseline findings were similar between the twotreatment groups, with the exception of accommodativeamplitude which was lower in the base-in prism group to astatistically but not clinically significant degree.Potential limitations of the study may be related to the
method used for determining the magnitude of prismprescribed and the length of follow up. There is no consensusabout the best method for prescribing prism for patients withCI. Our decision to use Sheard’s criterion was based on
previous research indicating its value as a discriminator ofsymptomatic from asymptomatic exophoric patients,24 25 andits perceived wide acceptance in the optometric community.We chose to re-evaluate our patients after 6 weeks of prismuse based on the assumption that, if symptomatic reliefoccurred, it would be likely to happen within 6 weeks.In conclusions, this first prospective multicentre, masked,
randomised clinical trial of the treatment of symptomatic CIin children aged 9 to ,18 years shows that base-in prismreading glasses prescribed on the basis of Sheard’s criterionare not an effective treatment. Our data suggest that theplacebo effect of prescribing glasses was most probablyresponsible for the decrease in symptoms achieved in thebase-in prism reading glasses group. Based on these findings,investigators may want to evaluate other spectacle lenstreatments such as low plus lenses and yoked prism, whichare anecdotally reported by some clinicians to be beneficialfor the treatment of various vision disorders in children. Itshould be noted that the results of our study can only beapplied to children aged 9 to ,18 years with symptomatic CI,and treatment effects may be different in other populationssuch as adults.26
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
M Scheiman, Eye Institute, Pennsylvania College of Optometry,Philadelphia, PA, USAS Cotter, M Rouse, E Borsting, Southern California College ofOptometry, Fullerton, CA, USAG L Mitchell, M Kulp, Optometry Coordinating Center, The Ohio StateUniversity, Columbus, OH, USAJ Cooper, College of Optometry, State University of New York, NewYork, NY, USA
This study was supported by grants from the Pennsylvania and OhioLions.
APPENDIX 1: CLINICAL SITESSites are listed in order of number of patients enrolled intothe study, with city, state, site name and number of patientsin parentheses. PI=principal investigator; I= investigator;C= coordinator; M=masked examiner.
N NOVA College of Optometry (13): R A Coulter (PI), A Bade(C), M Taub (M), M Bartuccio (M)
N Pennsylvania College of Optometry (11): M Scheiman(PI), T Yamada (M), K Pollack (C)
N Bascom Palmer (10): S Tamkins (PI), C Cannon, (M), JDel Pino (M), N Oveido, (I), E Olivares (C)
Table 4 Perception of treatment group assignment versus actual assigned treatmentgroup (week 6 visit)
Patients/parents believed assigned toReporting a specificgroup (%)
Pretty sure or very sureof answer (%)
Patient’s responsePatients assigned to base-in prism reading glasses
Base-in prism reading glasses 35.5 90.9Placebo reading glasses 3.2 100.0
Patients assigned to placebo reading glassesBase-in prism reading glasses 23.5 75.0Placebo reading glasses 14.7 100.0
Parent’s responseChild assigned to base-in prism reading glasses
Base-in prism reading glasses 38.7 91.7Placebo reading glasses 12.9 75.0
Child assigned to placebo reading glassesBase-in prism reading glasses 15.2 100.0Placebo reading glasses 27.3 88.9
1322 Scheiman, Cotter, Rouse, et al
www.bjophthalmol.com

N The Ohio State University College of Optometry (10): MKulp (PI), A Toole (M), M Earley (M), G Gabriel (M), KReuter (M), M Ackerman-Hemmer (M)
N University of Alabama, Birmingham (10): K Hopkins (PI),M Frazier (M), C Baldwin (C)
N Southern California College of Optometry (9): R Chu (PI),C Barnhardt (I), E Borsting (I), S Cotter (I), M Nguyen (I),M Rouse (I), S Shin (I), Y Flores (C)
N State University of New York, College of Optometry (5): JCooper (PI), E Samonte (C), A Steiner (I), H Friedman (I)
N Indiana University College of Optometry (3): D W Lyon(PI), D Plass (M), D Warren (M), M Varvel (C)
N University of Houston (1): J Wensveen (PI)
N The Ohio State University Optometry Coordinating Center:G L Mitchell (PI), L Barrett (data entry operator)
REFERENCES1 Duke-Elder S, Wybar K. Ocular motility and strabismus. In: Duke-Elder S, ed.
System of ophthalmology. Mosby: St Louis, 1973:547–51.2 von Noorden GK. Binocular vision and ocular motility: theory and
management of strabismus, 5th ed. St Louis: Mosby-Year Book, 1996.3 Abrams D. Duke-Elder’s practice of refraction, 10th ed. Edinburgh: Churchill
Livingstone, 1993.4 Cibis G, Tongue A, Stass-Isern M. Decision making in pediatric
ophthalmology. Philadelphia: Mosby-Year Book, 1993.5 Pratt-Johnson JA, Tillson G. Management of strabismus and amblyopia, 2nd
ed. New York: Thieme Medical Publishers, 2001.6 von Noorden G, Helveston E. Strabismus: a decision making approach. St
Louis: Mosby-Year Book, 1994.7 Griffin JR, Grisham JD. Binocular anomalies: diagnosis and vision therapy,
4th ed. Boston: Butterworth-Heinemann, 2002.8 Press LJ. Applied concepts in vision therapy. St Louis: Mosby-Year Book,
1997.9 Scheiman M, Wick B. Clinical management of binocular vision: heterophoric,
accommodative and eye movement disorders. Philadelphia: Lippincott,Williams and Wilkins, 2002.
10 Hugonnier R, Clayette-Hugonnier C. Strabismus, heterophoria and ocularmotor paralysis. St Louis: CV Mosby, 1969.
11 Gallaway M, Scheiman M, Malhotra K. Effectiveness of pencil push uptreatment for convergence insufficiency: a pilot study. Optom Vis Sci2002;79:265–7.
12 Saladin J. Horizontal prism prescription. In: Cotter S, ed. Clinical uses ofprism: a spectrum of applications. St Louis: Mosby, 1995:109–47.
13 Cotter S. Clinical uses of prism: a spectrum of applications. St Louis: Mosby,1995.
14 Worrell BEHM, Morgan MW. An evaluation of prism prescribed by Sheard’scriterion. Am J Optom Arch Am Acad Optom 1971;48:373–6.
15 Stavis M, Murray M, Jenkins P, et al. Objective improvement from base-inprisms for reading discomfort associated with mini-convergence insufficiencytype exophoria in school children. Binocul Vis Strabismus Q2002;17:135–42.
16 Haase H. Binocular testing and distance correction with the Berlin Polatest.J Am Optom Assoc 1962;34:115–25.
17 Borsting E, Rouse MW, De Land PN. Prospective comparison of convergenceinsufficiency and normal binocular children on CIRS symptom surveys.Convergence Insufficiency and Reading Study (CIRS) Group. Optom Vis Sci1999;76:221–8.
18 Borsting EJ, Rouse MW, Mitchell GL, et al. Validity and reliability of therevised convergence insufficiency symptom survey in children ages 9–18years. Optom Vis Sci 2003;80:832–8.
19 Zellers JA, Alpert TL, Rouse MW. A review of the literature and anormative study of accommodative facility. J Am Optom Assoc1984;55:31–7.
20 Scheiman M, Mitchell GL, Cotter S, et al. A randomized trial of theeffectiveness of treatments for convergence insufficiency in children. ArchOphthalmol 2005;123:14–24.
21 Sheard C. Zones of ocular comfort. Am J Optom 1930;7:9–25.22 Brody H. Placebo effect: an examination of Grunbaum’s definition. In:
White LTB, Schwartz GE, eds. Placebo: theory, research, and mechanisms.New York: Guilford Press, 1985.
23 Beecher HK. Powerful placebo. JAMA 1955;159:1602–6.24 Sheedy JE, Saladin JJ. Phoria, vergence and fixation disparity in oculomotor
problems. Am J Optom Physiol Opt 1977;54:474–8.25 Sheedy JE, Saladin JJ. Association of symptoms with measures of oculomotor
deficiencies. Am J Optom Physiol Opt 1978;55:670–6.26 Scheiman M, Mitchell GL, Cotter S, et al. A randomized trial of the
effectiveness of treatments of convergence insufficiency in young adults.Optom Vis Sci 2005;82:583–93.
Base-in prism reading glasses versus placebo reading glasses for CI in children 1323
www.bjophthalmol.com

EXTENDED REPORT
Monocular and binocular reading performance in childrenwith microstrabismic amblyopiaE Stifter, G Burggasser, E Hirmann, A Thaler, W Radner. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Wolfgang Radner, MD,Department ofOphthalmology, Universityof Vienna, WaehringerGuertel 18-20, A-1090Vienna, Austria;[email protected]
Accepted for publication2 May 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1324–1329. doi: 10.1136/bjo.2005.066688
Aim: To evaluate if functionally relevant deficits in reading performance exist in children with essentialmicrostrabismic amblyopia by comparing the monocular and binocular reading performance with thereading performance of normal sighted children with full visual acuity in both eyes.Methods: The reading performance of 40 children (mean age 11.6 (SD 1.4) years) was evaluatedmonocularly and binocularly in randomised order, using standardised reading charts for the simultaneousdetermination of reading acuity and speed. 20 of the tested children were under treatment for unilateralmicrostrabismic amblyopia (visual acuity in the amblyopic eyes: logMAR 0.19 (0.15); fellow eyes 20.1(0.07)); the others were normal sighted controls (visual acuity in the right eyes 20.04 (0.15); left eyes20.08 (0.07)).Results: In respect of the binocular maximum reading speed (MRS), significant differences were foundbetween the children with microstrabismic amblyopia and the normal controls (p = 0.03): whereas thecontrols achieved a binocular MRS of 200.4 (11) wpm (words per minute), the children with unilateralamblyopia achieved only a binocular MRS of 172.9 (43.9) wpm. No significant differences between thetwo groups were found in respect of the binocular logMAR visual acuity and reading acuity (p.0.05). Forthe monocular reading performance, significant impairment was found in the amblyopic eyes, whereas nosignificant differences were found between the sound fellow eyes of the amblyopic children and the controlgroup.Conclusion: In binocular MRS, significant differences could be found between children withmicrostrabismic amblyopia and normal controls. This result indicates the presence of a functionallyrelevant reading impairment, even though the binocular visual acuity and reading acuity were bothcomparable with the control group.
Reading is an important vision dependent ability ineveryday private and business life. For adults andchildren, reading impairments may reduce the indivi-
dual’s quality of life by negative effects on work and schooleducation.1 2 With an overall prevalence of 2% to 4%,amblyopia is the most frequent cause of visual impairmentin children and young adults in our population.3–5 Theincidence of amblyopia is high among children withstrabismus, and the child with obvious strabismus is likelyto come to medical attention earlier than the childwith microstrabismus or amblyopia in the absence ofstrabismus.6–9 This delayed beginning of amblyopia treatmentmay significantly influence the visual outcome.9–12 Inparticular, a typical monocular ‘‘reading amblyopia’’ wasdescribed in microstrabismus, causing functionally relevantimpairments in the amblyopic eyes.13 In a previous studyevaluating the reading performance of children with uni-lateral microstrabismic amblyopia, functional discrepanciesin monocular reading performance could be reliably eluci-dated between the amblyopic eyes and the normal sightedfellow eyes.14 In order to avoid functional deficits, it has beenrecommended to continue occlusion treatment until readingperformance has fully recovered.15
However, monocular reading tests do not imply thatchildren with unilateral amblyopia are poor readers underbinocular conditions. It has even been postulated thatchildren with microstrabismus causing a monocular readingamblyopia have no difficulty in binocular reading.16 17 Incontrast, others reported functionally relevant deficits.18
Therefore, the present study was designed to compare thebinocular reading performance of children with unilateralmicrostrabismic amblyopia with the measurements of the
monocular reading tests in the amblyopic and the normalfellow eye as well as with the binocular reading performanceof a control group of children with full visual acuity in botheyes.In order to obtain comparable and reliable measurements,
a standardised reading chart system with three equivalentreading charts for the simultaneous determination of readingacuity and speed was used in the present study.19 The highlycomparable sentence optotypes of the Radner reading charts(RR charts) have been designed, considering the interna-tional standards for vision tests,20–25 as well as the character-istics of amblyopic vision.19 26 The print sizes of the optotypeswere logarithmically scaled to provide constant geometricproportions controlling contour interaction. For adults, theRR charts represent a valuable clinical test for evaluatingfunctional differences in reading performance.27 All childrenperformed the reading test without any difficulties. Thereading tests were quick to administer and well accepted bythe children. Considering the syntactic complexity of the testsentences, the RR charts are a suitable and reliable readingtest for children starting from the third school grade19 andwere used in the present study to investigate the binocularreading performance of children with unilateral microstra-bismic amblyopia.
MATERIALS AND METHODSThis prospective clinical study evaluated the reading perfor-mance of 40 children (21 males and 19 females). The mean
Abbreviations: CPS, critical print size; logRAD, logarithm of thereading acuity determination; MRS, maximum reading speed; RR charts,Radner reading charts; wpm, words per minute
1324
www.bjophthalmol.com

age was 11.6 (SD 1.4) years, ranging from 10 years to12 years. In 20 of the tested children a unilateral amblyopiacaused by primary microstrabismus had been diagnosed; theother 20 children were normal controls without any oculardisease. The two study groups were comparable in age, sexdistribution, educational level, and the mean school marks(p.0.05). The study was performed in accordance with theDeclaration of Helsinki. Before all examinations, the parents’oral informed consent was obtained. The demographiccharacteristics of the study population are given in table 1.In the first group, 20 children with monocular amblyopia
caused by microstrabismus were included. Microstrabismusis defined by a small angle of squint (either convergent ordivergent) with less than 5 degrees.13 16 Children with a largeangle strabismus or a secondary microstrabismus (micro-strabismus that remains after operation for a large angle ofstrabismus) were not included in the study population. Also,patients with other ocular diseases or dyslexia were excludedfrom the study population.Cover-uncover tests and alternate cover tests were per-
formed for the clinical diagnosis of microstrabismus. Thesquint angle was evaluated with simultaneous prism alter-nate cover test (,5 prism dioptres). Accommodation wastested by dynamic retinoscopy. Convergence and motilitywere tested and monocular fixation was evaluated by directophthalmoscopy. As a sensory test, the Worth four dot testwas performed. Near stereoacuity was tested with the Titmusstereo test.All children included in the amblyopic group were under
continuing amblyopia treatment. Treatment was startedbefore the age of 4–5 years when microstrabismic amblyopiahas been first diagnosed. Treatment included correction ofany refractive error and occlusion therapy, resulting at leastin the expected age dependent physiological improvement ofvisual acuity.18 In all children, the improvement in visualacuity ranged from two to five acuity lines in the past 2 years.For the control group, children with no ocular disease and
full visual acuity (,logMAR 0.1) in both eyes undermonocular and binocular conditions were included aftercomplete eye examination. Any interocular difference invisual acuity or reading acuity of more than one line led toexclusion from the study population.All tests were performed with the patient’s optimal
correction. In the amblyopic group, refractive errors wereevaluated objectively by retinoscopy (cyclopentolate 1%)1 week before the reading tests and subjectively adjusted atthe beginning of the testing session. All tests were performedwith the child’s optimal correction for far and near vision.Accommodative deficits were compensated by an adequatenear addition to guarantee best corrected near performance.10
In all tested children, best corrected reading ability wastested using the RR charts19 at a reading distance of 25 cm.All tests were performed at a constant luminance of 80–90 cd/m2. The sentences were covered with a piece of paper,and the children were asked to uncover sentence aftersentence, reading each one aloud as quickly and accurately aspossible. The children were instructed to read each sentenceto the end without correcting any reading errors. Reading
time was measured with a stopwatch. Reading speed inwords per minute (wpm) was calculated based on thenumber of words in a sentence and the time needed to readthe sentence. The maximum reading speed (MRS) was thebest reading speed achieved in the test. Reading acuity wasset at the smallest print size the patient was able to readcompletely and expressed in terms of logRAD (= logarithmof the reading acuity determination/reading equivalent oflogMAR). LogRAD print size is defined by the height of alower case ‘‘x’’ and is calculated as follows: log10 [(anglesubtended by x height)/(5 arc min)]. Based on thepsychophysical function of reading speed, defining thatreading speed increases with print size up to the criticalprint size (CPS; the smallest print size the patients read withoptimal reading speed), and then plateau at the MRS,29 largerprint sizes were tested until this asymptotic level wasreached. Visual acuity was tested at a testing distance of4 metres, using ETDRS logMAR charts.22 Both eyes weretested monocularly and binocularly in randomised orderaccording to the orthogonal Latin square design, usingequivalent RR charts.27 28
Statistical methodsAll calculations were performed with SAS Release 8.2.Differences between the two groups in respect of the binocularreading performance were analysed by two sample t tests.Differences between the normal eyes and the amblyopic eyeswith respect to visual acuity, reading acuity, maximum readingspeed (MRS), and CPS were analysed for significance by pairedt test. For non-parametric data, the Mann-Whitney U test wasused. For all analyses, a two sided p value ,0.05 wasconsidered to indicate statistical significance.
RESULTSComparing the monocular and binocular readingperformance of children with unilateralmicrostrabismic amblyopiaIn the microstrabismic group, the reading performance of thesound fellow eyes was comparable to the binocular readingperformance. No significant differences were found for any ofthe tested reading parameters (p.0.05).Reading performance was significantly impaired in the
amblyopic eyes. In comparison with the sound fellow eyesand the binocular reading tests, significant differences werefound for the monocular reading acuity and the MRS(p,0.05; table 2). In the amblyopic eyes, the functionallyrelevant impairment was also found in respect of the readingspeed based on print size (fig 1) and the reading errors basedon print size (fig 2). Also for the visual acuity, a small, butsignificant residual deficit was found between the amblyopiceyes (logMAR 0.19 (0.15)) and the sound fellow eyes(logMAR 20.1 (0.07)).
Comparing the reading performance of the amblyopicgroup and the normal sighted control groupNo significant differences between the two groups werefound in respect of the binocular logMAR visual acuity andreading acuity (p.0.05; table 4).
Table 1 Demographic characteristics of the study population
Microstrabismicgroup (n = 20)
Control group(n = 20) p Value*
Age (years, mean (SD)) 11.5 (1.1) 11.7 (1.7) 0.6Females (%) 55 45 0.54Mean school marks (possible range:1 = best; 5 =worst)
1.6 (0.7) 1.7 (0.8) 0.66
*p,0.05 statistically significant.
Monocular and binocular reading performance in microstrabismic amblyopia 1325
www.bjophthalmol.com

In respect of the binocular MRS, significant differenceswere found between the children with unilateral microstra-bismic amblyopia and the normal sighted controls (p=0.03;fig 3): whereas the controls achieved a binocular MRS of200.4 (11) wpm, the children with unilateral amblyopiaachieved only a binocular MRS of 172.9 (43.9) wpm.There was also a small, but statistically significant
difference in the number of reading errors between the twogroups for the binocular tests (p,0.05; fig 2).Comparing the sound eyes of the amblyopic group with the
normal sighted controls in respect of the monocular visualacuity and reading parameters, no significant differenceswere found (visual acuity: p=0.4; reading acuity: p=0.2;MRS: p=0.11; CPS: p=0.77; logRAD/logMAR ratio:p=0.07).In the amblyopic group, nine of the tested children
achieved a relatively high MRS of more than 180 wpm.Additional analyses were performed, searching for significantdifferences in the main visual and demographic character-istics between the microstrabismic children with higher andlower MRS: No significant differences were found for thechildren’s age, visual acuity, accommodative impairment,
strabismic angle, and refractive error (p.0.05). In contrast,significant differences were found for fixation: for thechildren with high MRS, fixation was central or unstablecentral in all patients, none had an eccentric fixation in thedeviating eye. Analysing the mean duration of amblyopiatreatment, the children with high MRS were significantlylonger under treatment (mean duration 7.2 (0.7) years v 6.3(1) years; p=0.03). Also for the sensory Worth four dot testand the Titmus stereo test, the children with the high MRSshowed a significantly better performance.
DISCUSSIONIn this study, the average binocular maximum reading speedof children with microstrabismic amblyopia was significantlyreduced when compared to normal sighted, age matchedcontrols (p=0.03; table 5), indicating a functionally relevantreading impairment. Whereas the controls achieved abinocular MRS of 200.4 (11) wpm, the children withunilateral amblyopia achieved only a binocular MRS of172.9 (43.9) wpm. These differences in reading speed werefound to be above the level for a ‘‘real change’’ in visionevaluated for the RR charts.27 In contrast, no significantdifferences between the two groups were found in respect of
5
4
2
3
1
00.00.20.40.60.81.01.21.4
Print size (logRAD)
Read
ing
erro
rs (n
)
B Monocular, right eyesMonocular, left eyesBinocular
12
10
8
4
6
2
00.00.20.40.60.81.01.21.4
Print size (logRAD)
Read
ing
erro
rs (n
)
A Monocular, amblyopic eyesMonocular, normal eyesBinocular
Figure 2 Reading errors based on print size: (A) in children withunilateral microstrabismic amblyopia; (B) in normal sighted controls(n = 40).
Table 2 Monocular visual acuity and reading parameters in children with unilateralmicrostrabismic amblyopia (n = 20)
VariableAmblyopiceyes
Fellownormal eyes p Value*
Visual acuity (logMAR) 0.19 (0.15) 20.1 (0.07) ,0.001Reading acuity (logRAD) 0.52 (0.21) 0.07 (0.09) ,0.001Maximum reading speed (wpm) 139.4 (42.1) 172.4 (46.7) ,0.001CPS (logRAD)� 0.89 (0.25) 0.55 (0.18) ,0.001LogRAD/logMAR ratio (%)` 57.3 (18) 85.1 (9.2) ,0.001
*p,0.05 statistically significant.�A small CPS indicates that the patient is able to read smaller print sizes with optimal reading speed.`High logRAD/logMAR ratios indicate that the reading acuity reaches the level of distance visual acuity, whereaslower logRAD/logMAR ratios indicate a deficit in reading acuity.
250
200
100
150
50
00.00.20.40.60.81.01.21.4
Print size (logRAD)
Read
ing
spee
d (w
pm)
Monocular, right eyeB
Monocular, left eyeBinocular
250
200
100
150
50
00.00.20.40.60.81.01.21.4
Print size (logRAD)
Read
ing
spee
d (w
pm)
Monocular, amblyopic eyesA
Monocular, normal eyesBinocular
Figure 1 Reading speed (words per minute = wpm) based on printsize (logRAD) (A) in children with unilateral microstrabismic amblyopia;(B) in normal sighted controls (n = 40).
1326 Stifter, Burggasser, Hirmann, et al
www.bjophthalmol.com

the binocular logMAR visual acuity and reading acuity(p.0.05, table 5). Since reading speed is known to be closelyrelated to visual function,29–32 these findings indicate thepresence of a functionally relevant deficit that would beunderestimated by acuity measurements. Differences inreading practice between the groups cannot be consideredto significantly bias the above mentioned results, since nosignificant differences were found for the monocular visualacuity and reading parameters in the sound eyes of theamblyopic group when compared to the normal sightedcontrols (p.0.05; table 4).Reading speed measurements provide more information
about functional impairment than the visual acuity.33–36 Alsofor amblyopic children, it has been shown that high contrastvisual acuity is not always representing the full visualdeficit.37 Testing adults with unilateral anisometropicamblyopia, reading speed measurements evaluated relevantfunctional differences in monocular reading speed, whencompared with the normal fellow eyes.38 Also in children withunilateral microstrabismic amblyopia, functional discrepan-cies in reading performance could be reliably elucidatedbetween the amblyopic eyes and the normal sighted felloweyes.14 Even relatively mild forms of microstrabismic amblyo-pia with no persistent acuity deficit lead to an impairment ofmonocular reading ability.16 On the other hand, it has beenreported that these children had no difficulty in binocularreading, explained by the fact that patients with primarymicrostrabismus rarely alternate.16 The present study, how-ever, evaluated a significantly lower binocular MRS inchildren with monocular microstrabismic amblyopia whencompared with normal sighted controls, indicating thepresence of a functional reading impairment.The significance of particular changes in reading speed has
been evaluated recently for various eye diseases— age relatedmacular degeneration, cataract, and anisometropic amblyo-pia.27 29 30 33 38 As in the present study, statistically significantdifferences in reading speed were found, which have beenused for discriminating affected and sound eyes or differenteye diseases by reading tests.29 33
Patients with primary microstrabismus have a high degreeof binocularity, which may suggest that the ocular misalign-ment may have a sensory rather than an oculomotor origin,
as in large angle strabismus.39 However, as in large anglestrabismus, the anomalous retinal correspondence anddefective stereopsis of microstrabismus appear to beconsequences of abnormal visual experience caused by aninterocular deviation or by anisometropia.39 In addition,reading impairment may be significantly influenced by oneof the following deficits: abnormal contour interaction,40
which can be assessed using the difference between linearand single optotypes acuity; abnormal eye movements,41
which can be assessed using the difference between a highcontrast and repeat letter format acuity measure; andpositional uncertainty.42 Consequently, fixation is only oneof many aspects influencing the visual performance inamblyopic patients and may not be considered to sufficientlyexplain visual function in amblyopic vision. Nevertheless,binocular confusion, deficits in quality of binocular coordina-tion of saccades, or the presence of suppression scotomatacentred around the fixation point of the squinting eye mayexplain the significantly impaired binocular MRS of theamblyopic group.39 43 However, in the present study, thereading performance of children with microstrabismicamblyopia was compared with the reading performance ofnormal sighted controls, not with monofixators withoutamblyopia. In future research, it will be interesting to
Table 3 Monocular visual acuity and reading parameters of the control group (n = 20)
Variable Right eyes Left eyes p Value*
Visual acuity (logMAR) 20.04 (0.15) 20.08 (0.07) 0.4Reading acuity (logRAD) 0.03 (0.06) 0.03 (0.07) 0.2Maximum reading speed (wpm) 189.1 (15.6) 191.1 (18.8) 0.11CPS� (logRAD) 0.54 (0.14) 0.56 (0.15) 0.7LogRAD/logMAR ratio (%) 95.6 (16) 89.9 (6.4) 0.77
*p,0.05 statistically significant; �CPS = critical print size.
Table 4 Comparing monocular visual performance of the sound fellow eyes of theamblyopic group (n = 20) and the right eyes of the control group (n = 20)
VariableAmblyopic group,normal eyes
Control group,cight eyes p Value*
Visual acuity (logMAR) 20.1 (0.07) 20.04 (0.15) 0.4Reading acuity (logRAD) 0.07 (0.09) 0.03 (0.06) 0.2Maximum reading speed (wpm) 172.4 (46.7) 189.1 (15.6) 0.11CPS� (logRAD) 0.55 (0.18) 0.54 (0.14) 0.07LogRAD/logMAR ratio (%) 85.1 (9.2) 95.6 (16) 0.77
*p,0.05 statistically significant; �CPS, critical print size.Similar results were found for the controls’ left eyes.
250
200
100
150
50
0
Read
ing
spee
d (w
ords
per
min
ute)
Control groupAmblyopic group
Figure 3 A statistically significant difference in binocular maximumreading speed (words per minute) was found between the children withunilateral microstrabismic amblyopia and the normal sighted controlgroup (p =0.03).
Monocular and binocular reading performance in microstrabismic amblyopia 1327
www.bjophthalmol.com

investigate if monofixators without amblyopia show similarreading impairment, in order to discriminate between read-ing impairment caused by amblyopia or fixation disparity.In the amblyopic group, nine of the tested children
achieved relatively high MRS measurements of more than180 wpm. In comparison with the other children of theamblyopic group with a significantly lower MRS, significantdifferences were found in respect of fixation, sensory tests,and the duration of treatment, which was significantly longerin the better reading group.Besides the above mentioned visual factors influencing
reading performance, it is important to also consider thefundamental influence of comprehension. Reading andunderstanding a sentence is a complex process that requirescomprehension of the meaning of the individual words andalso the assignment of the structural relations between thesewords.44
In case of dyslexia, a type of learning disability that affectsreading ability, the child may have problems remembering,recognising, and or reversing written letters, numbers, andwords, might read backwards, and may have poor hand-writing. Neurological dysfunction is suspected as the cause ofthe reading disability in dyslexia, since the development ofintelligence, learning ability, and visual function may benormal. Consequently, dyslexic children might have animpaired reading acuity and speed in reading tests usingshort test sentences and were excluded from the presentstudy.In summary, this study determined that monocular read-
ing tests do not imply that children with unilateral amblyopiaare poor readers under binocular conditions. The binocularvisual acuity and reading acuity of the amblyopic group wereboth comparable with the control group. However, thebinocular MRS was significantly reduced in the amblyopicgroup, indicating functional reading impairment in compar-ison with normal sighted controls.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
E Stifter, G Burggasser, A Thaler, W Radner, Medical University ofVienna, Department of Ophthalmology, Vienna, AustriaE Hirmann, A Thaler, Orthoptic Academy, General Hospital, Vienna,Austria
Supported by the ‘‘Jubilaumsfonds der osterreichischen Nationalbank.’’
Competing interests: none declared
REFERENCES1 Monestam E, Wachtmeister L. The impact of cataract surgery on low vision
patients. A population based study. Acta Ophthalmol Scand1997;75:569–76.
2 Uusitalo RJ, Brans T, Pessi T, et al. Evaluating cataract surgery gains byassessing patients’ quality of life using the VF-7. J Cataract Refract Surg1999;25:989–94.
3 Duke-Elder S, Wybar K. Ocular motility and strabismus. St Louis: CV Mosby,1973:294.
4 Von Noorden GK. Burian-von Noorden’s binocular vision and ocular motility:theory and management of strabismus, 2nd ed. St Louis: CV Mosby,1980:436–47.
5 Vinding T, Gregersen E, Jensen A, et al. Prevalence of amblyopia in oldpeople without previous screening and treatment: an evaluation of the presentprophylactic procedures among children in Denmark. Acta Ophthalmol1991;69:796–8.
6 Shaw DE, Fielder AR, Minshull C, et al. Amblyopia: factors influencing age ofpresentation. Lancet 1988;2:207–9.
7 Friendly DS. Preschool visual acuity screening tests. Trans Am Ophthalmol Soc1978;76:383–480.
8 Campbell LR, Charney E. Factors associated with delay in diagnosis ofchildhood amblyopia. Pediatrics 1991;87:178–85.
9 Kutschke PJ, Scott WE, Keech RV. Anisometropic amblyopia. Ophthalmology1991;98:258–63.
10 Haase W. Amblyopien Teil II: Vorsorge und Therapie. Ophthalmologe2003;100:160–74.
11 Kivlin JD, Flynn JT. Therapy of anisometropic amblyopia. J PediatrOphthalmol Strabismus 1981;18:47–56.
12 Pollard ZF, Manley D. Long-term results in the treatment of unilateral highmyopia with amblyopia. Am J Ophthalmol 1974;78:397–9.
13 Lang J. Microtropia. Int Ophthalmol 1983;6:33–6.14 Stifter E, Burggasser G, Hirmann E, et al. Evaluation reading acuity and speed
in children with microstrabismic amblyopia using a standardized readingchart system. Graefes Arch Clin Exp Ophthalmol 2005 July 8; [Epub ahead ofprint].
15 Zurcher B, Lang J. Reading capacity in cases of ‘cured’ strabismic amblyopia.Trans Ophthalmol Soc UK 1980;100:501–3.
16 Lang J. Management of microtropia. Br J Ophthalmol 1974;58:281–92.17 Lang J. Microtropia. Arch Ophthalmol 1969;81:758–62.18 Haas W. Amblyopien Teil I Diagnostik. Ophthalomologe 2003;100:69–87.19 Radner W, Willinger U, Obermayer W, et al. A new German reading chart
for the simultaneous evaluation of reading acuity and speed [Article inGerman]. Klin Monatsbl Augenheilkd 1998;213:174–81.
20 NAS-NRC Committee on Vision. Recommended standard procedures for theclinical measurement and specification of visual acuity. Adv Ophthalmol1980;41:103–48.
21 CEN (European Committee of Norms). Europaische NormSehscharfenprufung EN ISO 8596. Berlin: Beuth-Verlag, 1996.
22 Ferris F, Kassoff A, Bresnick G, et al. New visual acuity charts for clinicalresearch. Am J Ophthalmol 1982;94:91–6.
23 Wesemann W. Sehscharfebestimmung mit Freiburger Visustest, Bailey-Lovie-Tafel und Landoltring-Tafel. Klin Monatsbl Augenheilkd 2002;219:660–7.
24 Bailey IL, Lovie JE. The design and use of a new near-vision chart. Am JOptom Physiol Opt 1980;57:378–87.
25 Bailey IL, Lovie JE. New design principles for visual acuity letter charts. Am JOptom Physiol Opt 1976;53:745–53.
26 Radner W, Obermayer W, Richter-Mueksch S, et al. The validity andreliability of short German sentences for measuring reading speed. GraefesArch Clin Exp Ophthalmol 2002;240:461–7.
27 Stifter E, Konig F, Lang T, et al. Reliability of a standardized reading chartsystem: variance component analysis, test-retest and inter-chart reliability.Graefes Arch Clin Exp Ophthalmol 2004;242:31–9.
28 John PWM. Statistical design and analysis of experiments. New York:Macmillan, 1971.
29 Elliott D, Patel B, Whitaker D. Development of a reading speed test forpotential-vision measurements. Invest Ophthalmol Vis Sci 2001;42:1945–9.
30 Stangler-Zuschrott E. Decreased reading speed and rapid fatigue as signs ofdisordered visual function [in German]. Klin Monatsbl Augenheilkd1990;196:150–7.
31 Legge GE, Rubin GS, Pelli DG, et al. Psychophysics of reading. II. Low vision.Vis Res 1985;25:253–66.
32 Ahn S, Legge G, Luebker A. Printed cards for measuring low-vision readingspeed. Vis Res 1995;35:1939–44.
33 Stifter E, Sacu S, Weghaupt H, et al. Reading performance in dependency ofthe type of cataract and its predictability on the visual outcome. J CataractRefract Surg 2004;30:1259–67.
34 Elliott DB, Hurst MA, Weatherill J. Comparing clinical tests of visual function incataract with the patient’s perceived visual disability. Eye 1990;4:712–17.
35 Martin BK, Kaplan Gilpin AM, Jabs DA, et al. Reliability, validity, andresponsivenes of general and disease-specific quality of life measures in aclinical trial for cytomegalovirus retinitis. J Clin Epidemiol 2001;54:376–86.
36 Riusala A, Sarna S, Immonen I. Visual Function Index (VF-14) in exudativeage-related macular degeneration of long duration. Am J Ophthalmol2003;135:206–12.
Table 5 Binocular visual acuity and reading parameters of the amblyopic and the controlgroup (n = 40)
Variable Amblyopic group Control group p Value*
Visual acuity (logMAR) 20.1 (0.06) 20.07 (0.08) 0.23Reading acuity (logRAD) 0.05 (0.09) 0.02 (0.1) 0.25Maximum reading speed (wpm) 172.9 (43.9) 200.4 (11) 0.03CPS� (logRAD) 0.48 (0.2) 0.5 (0.14) 0.11LogRAD/logMAR ratio (%) 86.9 (9.5) 92.8 (12.6) 0.72
*p,0.05 statistically significant; �CPS, critical print size.
1328 Stifter, Burggasser, Hirmann, et al
www.bjophthalmol.com

37 Simmers AJ, Gray LS, McGraw PV, et al. Functional visual loss in amblyopiaand the effect of occlusion therapy. Invest Ophthalmol Vis Sci1999;40:2859–71.
38 Osarovsky-Sasin E, Richter-Mueksch S, Pfleger T, et al. Reduced readingability of eyes with anisometropic amblyopia. Invest Ophthalmol Vis Sci2002;43:E-Abstract 4691.
39 Harwerth RS, Fredenburg PM. Binocular vision with primary microstrabismus.Invest Ophthalmol Vis Sci 2003;44:4293–306.
40 Giaschi ED, Regan D, Kraft SP, et al. Crowding and contrast in amblyopia.Optom Vis Sci 1993;70:192–7.
41 Simmers AJ, Gray LS, Winn B. The effect of abnormal fixational eye movementsupon visual acuity in congenital nystagmus. Curr Eye Res 1999;18:194–202.
42 Levi DM, Klein SA, Yap YL. Positional uncertainty in peripheral and amblyopicvision. Vis Res 1987;27:581–97.
43 Joosse MV, Simonsz HJ, Van Minderhout HM, et al. Quantitative perimetryunder binocular viewing conditions in microstrabismus. Vis Res1997;37:2801–12.
44 Martin-Loeches M, Casado P, Hinojosa JA, et al. Higher-order activity beyondthe word level: cortical dynamics of simple transitive sentence comprehension.Brain Lang 2005;95:332–48.
Monocular and binocular reading performance in microstrabismic amblyopia 1329
www.bjophthalmol.com

EXTENDED REPORT
Ocular motor dysfunction and ptosis in ocular myastheniagravis: effects of treatmentM J Kupersmith, G Ying. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Mark J Kupersmith, MD,Neuro-ophthalmology,Roosevelt Hospital, 100010th Avenue, New York,NY 10019, USA;[email protected]
Accepted for publication11 January 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1330–1334. doi: 10.1136/bjo.2004.063404
Aim: The optimal treatment of ocular myasthenia gravis (OMG) remains unknown. The authors evaluatedthe efficacy of prednisone and pyridostigmine in reducing diplopia, ocular motor dysfunction, and ptosisin patients with OMG.Methods: Review of records from a clinical database from one neuro-ophthalmology service of patientspresenting with OMG between 1990 and 2002, excluding those who developed generalised MG withinthe first month after diagnosis. Institutional review board approval was obtained for this study.Participants/interventions: Non-randomised, unmasked, therapy was given. 55 patients with diplopia inprimary or downward gaze and clinically demonstrable extraocular muscle dysfunction receivedprednisone. 34 patients who had contraindications to steroids or who refused treatment with prednisonereceived pyridostigmine only. Over 5 days the daily prednisone dose was increased to 50–60 mg andthen gradually reduced to 10 mg, followed by further reduction as tolerated. The pyridostigmine dose wasbegun at 180 mg daily and increased as tolerated. Main outcome measures: Follow up evaluations,performed at 1, 3–6, 12, and 24 months, detailed the frequency of ptosis and diplopia and the amount ofocular motor deviation in primary and downward gaze.Results: The prednisone and pyridostigmine groups were similar for age, sex, acetylcholine receptorantibody level, prism cover test results for primary and downward gaze, diplopia in primary anddownward gaze, and unilateral ptosis. Bilateral ptosis was present in 32.4% of the pyridostigmine groupand 10.9% of the prednisone group (p = 0.02). The prednisone group showed resolution in primary gazediplopia, downgaze diplopia, unilateral ptosis, and bilateral ptosis in 73.5%, 75.5%, 85.7%, and 98%,respectively at 1 month. The benefit persisted at 3–6, 12, and 24 months except for the bilateral ptosis.The pyridostigmine group showed resolution in primary gaze diplopia, downgaze diplopia, unilateralptosis, and bilateral ptosis in 6.9%, 17.2%, 50%, and 76.7% of patients after 1 month of treatment. Theprism cover results improved (p = 0.003) in the prednisone group only. In the prednisone group, fourpatients had no response to therapy. Among the 51 prednisone responsive patients, there were 33recurrences in 26 patients. 12 patients, all prednisone treated, had remissions. Except for three patientswho developed diabetes, no patient developed a clinically significant systemic corticosteroid complication.Conclusion: These results suggest that 50–60 mg daily prednisone followed by lower doses (10 mg or less)has the benefit of resolving ptosis and diplopia that lasts for at least 2 years in approximately 70% ofpatients.
Ocular myasthenia gravis (OMG) is an autoimmunedisorder that causes ptosis, diplopia, and extraoculareye muscle and orbicularis oculi weakness without
dysfunction of other muscles. Previous reports emphasisedOMG diagnosis1 2 and development of generalised myasthe-nia gravis (GMG).3–6 Few studies investigated therapy toimprove ocular motor function and restore single vision.3 7
Generally, pyridostigmine alleviates ptosis but may beineffective in resolving diplopia.3 In contrast, oral prednisone(up to 100 mg on alternate days) improved ocular motorfunction in seven of eight patients in one study8 andalleviated diplopia for 2 years in 66% of 32 OMG patientswith lower doses.9
Using lower doses of prednisone and a more uniformtreatment protocol than the previous study,9 we evaluated theeffect of prednisone and pyridostigmine in reducing diplopiaand ocular motor dysfunction in 89 OMG patients. Thedevelopment of GMG in this group has been describedrecently.10
METHODSThe charts of patients with OMG, evaluated by one neuro-ophthalmology Service (from 1990 through 2002) were
reviewed and the data extracted for a confidential OMGdatabase collected with consent from each patient. The agerange was 4–82 years at the first examination when OMGwas diagnosed (table 12). No patient had symptoms, such asswallowing, chewing, respiratory, or limb weakness orfatigue, or clinical examination findings of weakness in themuscles of the lower face or below the neck, suggestive ofGMG. We excluded any patient with signs of a restrictiveocular myopathy or who developed GMG within a month ofdiagnosis as a result of use of a different treatment regimen.Patients were not randomised for therapy. Patients with
diplopia in primary or downward gaze and extraocularmuscle dysfunction were offered prednisone therapy. Thirtyfour patients who refused or had contraindications tocorticosteroid therapy, or who had only mild ptosis at thefirst examination were treated with pyridostigmine (pyridos-tigmine group). Five of the 55 patients in the prednisonegroup received pyridostigmine (mean dose of 120 mg daily).Additionally, 10 patients initially treated with pyridostig-mine, who did not improve, were later treated with
Abbreviations: GMG, generalised myasthenia gravis; OMG, ocularmyasthenia gravis; PCT, prism cover test
1330
www.bjophthalmol.com

prednisone. The medication dose was recorded at each visit,without other controls for compliance. No patient receivedother immunosuppressive agents. One patient in the pre-dnisone group had a thymectomy for a thymoma, and wasone of the patients who failed prednisone.The prednisone dose, starting with 10 mg daily, was
escalated over 5 days to 50–60 mg daily, and after 4 daysthe dose was reduced by 10 mg per day each week until10 mg per day was achieved. The dose was further reduced by2.5 mg per day each week in response to controllingsymptoms and findings of diplopia in primary gaze, difficultyreading, or ptosis that interfered with vision. Most patients inthe prednisone group remained on a daily or alternate daydose of 2.5–10 mg. For analysis, alternate day prednisonewas recorded as a daily dose that was half the alternate daydose (for example, a patient taking 10 mg of prednisoneevery other day was considered to be taking 5 mg a day).Recurrences were treated with reinstitution of half of themaximal dose originally given. All prednisone treatedpatients were prescribed a histamine receptor 2 blockingagent and calcium 1000–1500 mg and vitamin D 400–800 IUdaily.The pyridostigmine group started therapy with 180 mg
daily in divided doses and received higher doses until theocular symptoms did not interfere with vision function orside effects developed despite medical co-interventions. Themean maximum daily dose was 272 mg (median 240 mg;range 180–720 mg) and 24 patients received at least 240 mgper day.In the prednisone group (including 10 patients switched
from the pyridostigmine group), a recurrence was defined asthe return of resolved diplopia in primary or downward gaze,as the dose of prednisone was reduced, and failed to resolvewith an increase of 10 mg daily. The time from reaching adaily dose of 10 mg of prednisone before a recurrence and thedaily dose of prednisone when the recurrence occurred wererecorded. A treatment failure was defined as persistentdiplopia in primary or downward gaze or ptosis that coveredeither pupil with the eyes in primary gaze despite higherprednisone doses or if 20 mg of daily prednisone was needed.A remission was defined as having no ptosis, no diplopia, andnormal ocular muscle ductions after stopping therapy for atleast 6 months.The baseline examination was performed when treatment
was prescribed. At each visit patients were questioned
whether diplopia was present in primary or downward gaze,particularly while reading or descending stairs over theprevious week. All examinations detailed the presence ofptosis and prism cover test (PCT) measurement (in dioptres)for distance primary and downward gaze. To account forvariability with worsening of the findings typically observedafter repeated testing in untreated patients, only initialmeasurements of ptosis and the cover test were recordedPatients were evaluated at each visit for GMG and inprednisone treated patients, for corticosteroid complications.
Analysis (using SAS 8.2)The descriptive analysis was performed for the baselinecharacteristics and longitudinal outcome measurements. Forsubsequent examinations, we evaluated whether the diplopiain primary or downward gaze or the ptosis in one or both eyespersisted, developed, or resolved, and if the PCT measure-ments were reduced. The PCT measurements at baseline werecompared with the measurements at each subsequentexamination. We devised a calculation, which considers thatin some patients the vertical and horizontal PCT measure-ments might worsen or improve independently of each other.We computed a vector determination composed of both thehorizontal and vertical measurements of the PCT measure-ment for each direction of gaze.The comparison of baseline characteristics between two
treatment groups was performed using x2 test for thecategorical measurements and Wilcoxon rank sum test forthe continuous measurements because of the skeweddistributions. For each treatment, the efficacy was evaluatedby the comparison of measurements from follow up withthose from baseline using the generalised equation estimateto adjust the correlation from the longitudinal repeatedmeasurements.11 The paired t test was used to evaluate thebaseline and 1 month vector calculations of the PCT results.The efficacy difference between two treatments was assessedusing the generalised equation estimate with the adjustmentof baseline characteristics. For the prednisone group, theeffect of baseline characteristics on the treatment failure,remission and recurrence was examined using the linearregression. For the prednisone group, the treatment failure,no response, remission, and recurrence data were consideredwith and without the data for the 10 patients switched toprednisone after failing pyridostigmine.
RESULTSThe baseline features (table 2) were comparable between thegroups except the pyridostigmine group had more frequentbilateral ptosis (p=0.02).Compared with the baseline evaluation, there was a
significant frequency of resolution of ptosis and diplopiaand improvement in the PCT measurements in the pre-dnisone group (table 3). The pyridostigmine group did notshow the same frequency of diplopia resolution or improve-ment of PCT measurements at 1 month and 3–6 months.Except for bilateral ptosis, the prednisone group hadsignificant benefit for all features that persisted at 3–6, 12,and 24 months. The prednisone group was significantlybetter than the pyridostigmine group at the 1 month and3–6 month evaluations (table 3). The prednisone group hadsignificantly better PCT measurements at 1 month and 3–6 months except for the vertical prism measurement inprimary gaze at 3–6 months (table 4). The patients in theprednisone group had significant reduction in the meanvector measurement comparing baseline and 1 month, forprimary gaze (15.9, SD 11.1 and 4.2, SD 8.1, p=0.001) andfor downward gaze (12.8, SD 8.6 and 3.3, SD 7.4, p=0.001).The pyridostigmine group did not show the same improve-ment in the vector measurements for baseline and 1 month
Table 1 Criteria for diagnosing ocular myastheniagravis
(1) Ptosis in one or both upper lids not due to local lid disease, preferablythat could fatigue or recover with rest.(2) Extraocular muscle weakness in one or both eyes not in a strict thirdnerve muscle innervation pattern. If solely lateral rectus weakness,clearcut fatiguability, recovery, or positive edrophonium test.(3) Weakness can be present in one or both orbicularis oculi but no otherweakness of the muscles of the head and neck.(4) No pupillary abnormality other than from previous local disease orsurgery.(5) (A) plus (B), or (C) or (D) or (E) has to be present:(A) Fatigue of the affected muscle with clear cut worsening of the ptosis
after upward gaze for 30 to 60 seconds or worsening of themonocular duction after 120 seconds of gaze in the direction ofaction.
(B) Recovery of the upper lid ptosis to almost normal after 30 seconds to10 minutes of eyelid closure. Recovery of the monocular duction after120–180 seconds of gaze in the direction of the antagonist muscle.
(C) A positive edrophonium test(D) Abnormal repetitive stimulation electromyography with a minimum
decrement of 10%.(E) Abnormal serum acetylcholine receptor binding level.
Ocular myasthenia gravis 1331
www.bjophthalmol.com

follow up primary gaze (17.9, SD 10.5 and 16.5, SD 10.4) ordownward gaze (14.7, SD 8.5 and 13.3, SD 7.8).In patients treated with prednisone, at 12 months, the
diplopia resolved in five of 10 patients with diplopia at3–6 months and at 24 months, in five of 14 patients withdiplopia at 12 months. Of the patients withdrawn fromprednisone, diplopia was absent in 10/17 at 12 months and in10/16 at 24 months.Of the 61 patients who responded to prednisone, there
were 43 recurrences in 31 patients occurring at a mean of5.2 months after the prednisone was reduced to 10 mg daily(table 5). There were eight failures in the prednisone group,four who never resolved their diplopia and four who had arecurrence as the dose was reduced below 20 mg daily; 12prednisone treated patients (18.5%) had remissions. Age, sex,abnormal acetylcholine receptor antibody level, ptosis, anddiplopia in primary or downward gaze at baseline were notcorrelated with treatment failure or the number of remissionsor recurrences.Two patients in the pyridostigmine group had the diplopia
resolve at 1 month. The diplopia recurred in one of the two by6 months. Because of the onset of diplopia in two additionalpatients at 1 month, the percentage of patients with diplopiawas the same as at baseline when accounting for missingdata. No patient in the pyridostigmine group had a remission.
The 12 month and 24 month results for the pyridostigminegroup are not reported owing to a large drop out rate.No patient developed a clinically apparent fracture, new
onset systemic hypertension, or an infection that requiredhospitalisation. Three of 65 patients treated with prednisonedeveloped new onset diabetes mellitus.
DISCUSSIONIn the present study, less than 10% of patients had ptosisonly, less than 30% had diplopia only, while the majority(64%) had both diplopia and ptosis, which differs from OMGin children where ptosis is frequent and diplopia isuncommon.12 Combined horizontal and vertical ocular mis-alignment was most frequent (43.5%) but horizontal (34.1%)or vertical (22.4%) deviations alone occurred.Our results confirm the findings of a previous study9 that
moderate dose (50–60 mg) daily prednisone, reduced over6 weeks, followed by 10 mg or less daily, resolves diplopia inprimary and downward gaze more frequently than withpyridostigmine alone. This treatment regimen also reducesthe amount of PCT measured ocular deviation in primary anddownward gaze. The immediate and long term benefit alsooccurred in patients who failed pyridostigmine alone.Prednisone decreased the frequency of ptosis in one or bothupper lids from 56.4% to 16.3% at 1 month and to 15.8% at
Table 2 Baseline characteristics of patients in prednisone and pyridostigmine treatmentgroups
CharacteristicsPrednisone group(n = 55)
Pyridostigminegroup (n = 34)
p Value*Abnormal acetylcholine receptor antibody(n = 26)Mean (SD)
(n = 15)Mean (SD)
Age (years) 48.4 (15.5) 52.6 (23.8) 0.16Acetylcholine receptor antibody (nmol/l) 2.7 (9.6) 2.8 (6.4) 0.35Primary gaze, horizontal PCT (dioptres) 12.2 (12.1) 13.3 (10.8) 0.54Primary gaze, vertical PCT (dioptres) 5.5 (6.3) 5.4 (6.4) 0.84Downward gaze, horizontal PCT (dioptres) 9.8 (10.4) 11.1 (9.5) 0.44Downward gaze, vertical PCT (dioptres) 6.3 (6.2) 5.5 (6.9) 0.50
n (%) n (%) p Value�Sex—male 30 (54.6%) 17 (50.0%) 0.83Abnormal acetylcholine receptor antibody 26 (47.2%) 17 (50%) 0.71Diplopia primary gaze 52 (94.6%) 29 (85.3%) 0.25Diplopia downward gaze 45 (81.8%) 27 (79.4%) 0.79Ptosis, unilateral 25 (45.5%) 17 (50.0%) 0.83Ptosis, bilateral 6 (10.9%) 11 (32.4%) 0.02
PCT, prism cover test.*From Wilcoxon rank sum test.�From exact x2 test.
Table 3 Comparison of treatment effect on outcome measurements for baseline groups for categorical outcome measurements
TreatmentMean daily dose(mg)
Follow upcompleted
Diplopia primarygaze Diplopia downgaze Ptosis, unilateral Ptosis, bilateral
Yes (%) No of patients (%) No of patients (%) No of patients (%) No of patients (%)
Times(months) Pred Pyrid Pred Pyrid Pred Pyrid Pred Pyrid Pred Pyrid Pred Pyrido
0 55 34 52 (94.6) 29 (85.3) 45 (81.8) 27 (79.4) 25 (45.5) 17 (50.0) 6 (10.9) 11 (32.4)1 13 272 49 30 13 (26.5) 27 (93.1) 12 (24.5) 24 (82.8) 7 (14.3) 15 (50.0) 1 (2.0) 7 (23.3)3–6 5 323 50 20 13 (26.0) 16 (76.2) 15 (30.0) 15 (71.4) 8 (16.0) 8 (40.0) 1 (2.0) 7 (35.0)12 2.5 308 41 5 12 (28.6) 7 (100)* 10 (23.8) 7 (100)* 8 (19.5) 4 (57)* 1 (2.4) 2 (28.5)*24 3.0 330 38 6 11 (29.0) 4 (67)* 11 (29.7) 4 (67)* 4 (10.5) 1 (16.7)* 2 (5.3) 2 (33.3)*p Value� ,0.0001 0.20 ,0.0001 0.55 0.002 0.62 0.07 0.22p Value` ,0.0001 0.0001 0.004 0.04
Pred, prednisone; Pyrid, pyridostigmine.*No or insufficient data available for analysis�For the comparison of outcome measure at follow up with that at baseline within the same treatment group`For the comparison of the outcome measure at follow up of 1 month and 3–6 months between the prednisone and pyridostigmine groups after adjustment forbaseline level, age, sex, and antibody level.
1332 Kupersmith, Ying
www.bjophthalmol.com

2 years. Our results contrast with those reported for child-hood OMG where only 29% of 24 patients treated withunspecified doses of prednisone, pyridostigmine, or both foran unspecified time improved ocular motility.12 In the currentstudy, the frequency of maintaining improved ocular motorand lid function might have been higher if the prednisonedose was reduced more slowly, as is recommended forcontrolling systemic muscle weakness.13 We reduced theprednisone dose quickly to avoid adverse effects. Somebenefit was probably gained by the combination of pyridos-tigmine and prednisone.Our failure rate of 12.3% contrasts with Evoli’s study where
6/18 (33%) failed to improve ocular motor function withprednisone 25–50 mg alternate day therapy.7 In fact, of oureight failures, only four (6.1%) failed to improve withmoderate doses. Although azathioprine appears to beeffective, it can take 6 months to improve the ocular motordysfunction and is less practical for patients needing a rapidresponse.14 Also, azathioprine (mean dose 145 mg) improved,but did not necessarily normalise, the OMG in 19 of 22patients.14 Azathioprine or other immunosuppressive agentscould be considered for patients who fail prednisone.Generally, thymectomy, in patients without a thymoma,has not been as the primary treatment of OMG, althoughreports suggest it is effective.1516 As new safer surgicalapproaches evolve, thymectomy may be investigated inOMG.17
The remission frequency was 18.5% for all patientstreated with prednisone and zero for patients treated with
pyridostigmine alone. The remission rate in the pyridostig-mine group could have been artificially low owing to poorfollow up. Remission rates of 11% in 108 patients4 and 30% in43 patients2 with OMG who did not generalise have beendescribed, without reference to treatment.A review of OMG treatment emphasised the complications
of rate of chronic corticosteroid use,18 but chronic low dosedaily or alternate day prednisone, particularly with co-interventions to prevent complications, may not result infrequent severe adverse effects.19 20 Our prednisone treatedpatients had no uncontrollable corticosteroid complications,possibly due to the effort to reduce the dose, not to use highmaintenance doses, to accept a degree of ocular symptoms,and not to continue prednisone in patients who failedtherapy, and the use of daily calcium and vitamin D. Therewere no clinically symptomatic hip or lumbar fractures.In our pyridostigmine group, only two of 34 patients with
diplopia had the diplopia resolve and one of these recurred.This contrasts with studies where pyridostigmine markedlyimproved ocular signs of OMG in 9/13 patients but thedefinition of ‘‘improved’’ was unspecified.7 In another report,50% of 14 patients treated with pyridostigmine, approxi-mately 150 mg per day, had ‘‘considerable improvement,’’but this term was also not defined.17 In the current study,after 1 month of pyridostigmine, 50% of patients had ptosisof an upper lid, similar to the baseline frequency, butapproximately one third of patients with bilateral ptosis hadresolution of the ptosis. The pyridostigmine treatment resultsmight have been better but side effects precluded using
Table 4 Comparison of treatment effect on outcome measurements for baseline groups for continuous outcome measurements(prism cover test)
Mean (SD)Follow upcompleted
Primary gaze,horizontal
Primary gaze,vertical
Downward gaze,horizontal
Downward gaze,vertical
No of dioptres (SD) No of dioptres (SD) No of dioptres (SD) No of dioptres (SD)
Times(months) Pred Pyrid Pred Pyrid Pred Pyrid Pred Pyrid Pred Pyrid
0 55 34 12.2 (12.1) 13.3 (10.8) 5.5 (6.2) 5.4 (6.4) 9.8 (10.4) 11.1 (9.5) 6.3 (6.2) 5.5 (6.9)1 49 30 4.1 (8.3) 13.0 (12.5) 0.8 (2.0) 5.0 (6.7) 2.1 (6.0) 10.9 (11.6) 1.1 (3.7) 4.6 (5.4)3–6 50 20 5.3 (9.4) 6.2 (5.9) 3.2 (6.8) 3.0 (5.6) 2.8 (6.6) 8.9 (9.5) 1.6 (3.3) 4.2 (6.7)12 41 5 5.2 (11.0) 22 (9.3)* 1.3 (3.9) 25* 3.2 (8.3) 17.7 (15)* 1.7 (4.6) 12*24 38 6 3.7 (8.1) * 1.1 (2.9) * 2.9 (7.9) * 0.6 (2.6) *p Value� 0.003 0.12 0.0008 0.25 0.008 0.73 0.006 0.71p Value` 0.007 0.11 0.01 0.02
Pred, prednisone; Pyrid, pyridostigmine.*No or insufficient data available for analysis�For the comparison of outcome measure at follow-up with that at baseline within the same treatment group`For the comparison of the outcome measure at follow up of 1 month and 3–6 months between the prednisone and pyridostigmine groups after adjustment forbaseline level, age, sex, and antibody level.
Table 5 Various outcome measurements in patients treated with prednisone initially orlate
Outcome
Patients initiallytreated withprednisone (n = 55) % of 55
Patients treatedwith prednisoneany time (n = 65) % of 65
Treatment failure 7 12.7 8 12.3Remission 11 20.0 12 18.5Unknown 1 1.8 1 1.5Never responded 4 7.3 4 6.2Number of recurrencesamong responder0 23 41.8 28 43.11 21 38.2 23 35.42 4 7.3 6 9.24 1 1.8 2 3.1
Two patients (3.6%) had incomplete or missing data. Age, sex, antibody level, ptosis at baseline were all notsignificantly associated with any above outcomes.
Ocular myasthenia gravis 1333
www.bjophthalmol.com

higher doses and we had limited follow up at 12 months and24 months, possibly because of treatment failure. Ourconclusions are biased towards prednisone treatment sinceour goal was to restore visual function as rapidly as possible.Prednisone and pyridostigmine for OMG are not truly
comparable therapies since prednisone alters the autoim-mune disease process and pyridostigmine does not. It appearsthat prednisone, given judiciously, is a reasonable therapy forrestoring visual function in OMG. Long term follow up withmeasures of patient visual function and safety documenta-tion of chronic low dose prednisone therapy are neededbefore final recommendations can be made.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
M J Kupersmith, Neuro-ophthalmology Service of Roosevelt Hospital,and New York Eye and Ear Infirmary, New York, NY, USAG-S Ying, University of Pennsylvania School of Medicine, Philadelphia,PA, USA
Supported by the Michael Fischer Foundation.
REFERENCES1 Osserman K. Ocular myasthenia gravis. Invest Ophthalmol Vis Sci
1967;6:277–86.2 Oosterhuis H. The ocular signs and symptoms of myasthenia gravis. Doc
Ophthalmol 1982;52:363–78.3 Schlezinger N, Fairfax W. Evaluation of ocular signs and symptoms in
myasthenia gravis. Arch Ophthalmol 1959;62:985–90.4 Bever C, Aquino A, Penn A, et al. Prognosis of ocular myasthenia. Ann Neurol
1983;14:516–19.
5 Oosterhuis H. The natural course of myasthenia gravis: a long term follow upstudy. J Neurol Neurosurg Psychiatry 1989;52:1121–7.
6 Grob D. Natural history of myasthenia gravis. In Engel AG, eds. Myastheniagravis and myasthenic disorders. Oxford: Oxford University Press,1999:135–6.
7 Evoli A, Tonali P, Bartoccioni E, et al. Ocular myasthenia: diagnostic andtherapeutic problems. Acta Neurol Scand 1988;77:31–5.
8 Fischer K, Schwartzman R. Oral corticosteroids in the treatment of ocularmyasthenia gravis. Ann NY Acad Sci 1976;274:652–8.
9 Kupersmith MJ, Moster M, Bhuiyan S, et al. Beneficial effects of corticosteroidson ocular myasthenia gravis. Arch Neurol 1996;53:802–4.
10 Kupersmith MJ, Latkany R, Homel P. Development of generalized disease at 2years in patients with ocular myasthenia gravis. Arch Neurol 2003;60:243–8.
11 Liang, KY, Zeger SL. Longitudinal data analysis using generalized linearmodels. Biometrika 1986;73:13–22.
12 Kim JH, Hwang JM, Hwang Y, et al. Childhood ocular myasthenia gravis.Ophthalmology 2003;110:1458–62.
13 Mann JD, Johns TR, Campa JF. Long-term administration of corticosteroids inmyasthenia gravis. Neurology 1991;26:729–40.
14 Sommer N, Sigg B, Melms A, et al. Ocular myasthenia gravis: response tolong term immunosuppressive treatment. J Neurol Neurosurg Psychiatry1997;62:156–62.
15 Schumm M, Wietholter H, Fateh-Moghadam A, et al. Thymectomy inmyasthenia with pure ocular symptoms. J Neurol Neurosurg Psychiatry1985;48:332–7.
16 Nakamura H, Taniguchi Y, Suzuki Y, et al. Delayed remission afterthymectomy for myasthenia gravis for the purely ocular type. J ThoracCardiovasc Surg 1996;112:371–6.
17 Shrager J, Deep M, Mick R, et al. Transcervical thymectomy for myastheniagravis achieves results comparable to thymectomy by sternotomy. Ann ThoracSurg 2002;74:320–6.
18 Kaminski H, Daroff R. Treatment of ocular myasthenia. Steroids only whencompelled. Arch Neurol 2000;57:752–3.
19 Caldwell J, Furst D. The efficacy and safety of low-dose corticosteroids forrheumatoid arthritis. Sem Arth Rheum 1991;21:1–11.
20 Spiera RF, Mitnick HJ, Kupersmith MJ, et al. A prospective double-blindrandomized placebo-controlled trial of methotrexate in the treatment of giantcell arteritis (GCA). Clin Experimental Rheumatol 2001;19:495–501.
1334 Kupersmith, Ying
www.bjophthalmol.com

EXTENDED REPORT
Orbital exenteration: a 13 year Manchester experienceI Rahman, A E Cook, B Leatherbarrow. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Imran Rahman,Manchester Royal EyeHospital, Lister Centre,Nelson Street, ManchesterM13 9WL, UK;[email protected]
Accepted for publication3 February 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1335–1340. doi: 10.1136/bjo.2004.062471
Background/aims: Orbital exenteration is a psychologically and anatomically disfiguring procedurereserved for the treatment of potentially life threatening malignancies or relentlessly progressive conditionsunresponsive to other treatments. In this study the authors aimed to review their experience withexenteration, including indications, outcomes, and reasons for the increased rate of exenterations over thepast 15 months.Method: This retrospective study reviewed operating department records via a computerised database toidentify all patients who had undergone exenteration of the orbit from 1 January 1991 to 1 April 2004inclusive, at the Manchester Royal Eye Hospital. Where case records were unavailable, attempts weremade to obtain patient data from general practitioners, local health authorities, and referring hospitals.Results: 69 orbits of 68 patients were identified. The mean age of the cohort was 68.2 years, with 33males and 35 females having undergone exenterations. In total, 31 patients had previously undergonetreatments undertaken by the referring specialty with a mean time from the primary procedure toexenteration of 115 months. 14 different tumours were encountered, of which basal cell carcinoma (28),melanoma (10), sebaceous cell carcinoma (nine), and squamous cell carcinoma (six) were the mostcommon. An increasing incidence was observed in cases of BCCs requiring exenteration. 30 patientsreceived orbital prosthesis within an 11 month period post-exenteration.Conclusion: Exenteration is a procedure performed with increasing frequency in this unit over the past15 months, the majority the result of BCCs. A large proportion of these exenterations had undergoneprevious treatments under a variety of non-ophthalmic specialties in other units. Exenterations aredisfiguring procedures that may, therefore, be reduced in incidence by aggressive removal at the time ofprimary removal. Once performed, the cosmetic rehabilitation is long, with multiple postoperative visits,independent of the method used to close the orbital defect.
Orbital exenteration, first described by George Bartischin 1583,1 is a radical procedure consisting of removalof the orbital contents, including orbital fat, con-
junctival sac, globe, and part or all of the eyelids. Thispsychologically and anatomically disfiguring procedure isreserved to treat potentially life threatening malignancies orrelentlessly progressive conditions unresponsive to othertreatments. Less often, orbital exenteration may aid inpalliation of severe deformity, pain, or less often as treatmentfor non-malignant disease.2
Cosmetic reconstruction is a major dilemma in exenteratedpatients, especially in the younger age group. Eyelid sparingtechniques,3 retention of conjunctiva,4 and preservation of theperiorbita5 are methods that have been introduced asmodifications of exenteration to aid in facial rehabilitation.In its currently practised form, orbital exenteration is
performed by only a few ophthalmic surgeons in the UnitedKingdom, mainly in large tertiary referral units. This reflectsthe rarity of such surgery and the reluctance to performorbital exenteration, especially as specialised reconstructivesurgery may also be needed to mask the disfigurement. Mohrand Esser6 reported their experience of 77 cases over a 20 yearperiod; Naquin7 described 48 cases over 25 years; Rathbun etal8 detailed 48 cases over a 30 year period; likewise, Levin andDutton presented their experience of 99 cases over 20 years.9
The largest series in the western literature is described byBartley et al10 of 102 patients from the Mayo Clinic over a20 year period.We report our experience and analyses of 69 cases of orbital
exenteration over a 13 year period from 1 January 1991 to1 April 2004.
METHODS AND SUBJECTSThis retrospective study reviewed operating departmentrecords via a computerised database to identify all patientswho had undergone exenteration of the orbit from 1 January1991 to 1 April 2004, inclusive, at the Manchester Royal EyeHospital. All surgical records were examined to determineindications for exenteration, referral methods, diagnosis andsurgical treatment elsewhere, location and extension ofpathological lesions, and histological diagnosis. In the caseof orbital and periorbital malignancies the histological reportswere examined to determine whether or not clear histologicalmargins had been obtained. Surgical technique, adjunctivepostoperative treatments (further surgery, radiotherapy,chemotherapy), intraoperative and postoperative complica-tions, recurrences, choice of aesthetic camouflage (occlusivepatch, opaque spectacle lens, orbitofacial prosthesis), andtime from exenteration to rehabilitation of the facialdisfigurement with a formal prosthesis were also noted.Recurrence of any malignant disease was also noted.Where surgical notes were unavailable, data were compiled
from correspondence letters from the department of ocularprosthetics, general practitioners, and the referring hospitalrecords.
RESULTSBetween 1 January 1991 to 1 April 2004, 69 orbits of 68patients were identified (one patient having bilateralexenterations for severe contracted sockets secondary to
Abbreviations: BCC, basal cell carcinoma; SCC, squamous cellcarcinoma
1335
www.bjophthalmol.com

Stevens-Johnsons syndrome) from the theatre database ashaving undergone orbital exenteration (fig 1). Case notes for57 patients were available for review. Histological data, lettersfrom general practitioners, and clinic letters were used tocollate the data for the remaining 12 patients. A total of 35females and 33 males made up the study group, with 35 rightorbits and 34 left orbits being affected. The mean age of thecohort was 68.2 years (median of 72, range 4–91 years), atthe time of exenteration.Preoperative visual acuity was unavailable in 18 patients;
21 of the remaining 51 patients (41%) had a Snellen visualacuity of 6/12 or better. In the eye not exenterated, Snellenvisual acuity of 6/12 or better was observed in 41 out of 53eyes (77%), in whom visual acuity measurements wereavailable preoperatively.Five orbits of four patients underwent exenteration for
non-malignant disease. One patient had a chronic dischar-ging socket, another a contracted socket, and the third (twoeyes) had severe Stevens-Johnson syndrome. The last patienthad severe chemical injury necessitating facial cosmeticrehabilitation. This report deals chiefly with those patientswith neoplastic indications for exenteration, and these fivepatients with non-neoplastic conditions are not consideredfurther, except where surgical technique and complicationsare concerned. An overview of indications for exenteration ispresented in table 1.Although the surgery was carried out by a senior
ophthalmic surgeon in all cases, referrals were made fromvarying specialties including dermatology, plastic surgery,neurosurgery, ENT, oncology, and from general practitioners.In total, nine patients had previous treatment in Manchesterand a further 31 patients had previously undergone treat-ments undertaken by the referring specialty. Sixteen had hada local tumour excision, one had undergone orbital radio-therapy, and a further 10 had had a combination of surgeryand orbital radiotherapy. Two patients proceeded to orbitalexenteration following failed attempts at Mohs’ micrographicsurgical excision of extensive periocular malignancies. Of thefinal two patients, one underwent enucleation and the othermultiple incisions with curettage. The mean time from the
primary procedure to exenteration was 115 months (range 1–600 months). Treatment modalities undertaken before exen-teration are outlined in table 2.Table 3 shows the histological diagnosis of the tumour.
Fourteen different tumours were encountered, of which basalcell carcinoma (BCC) (28), melanoma (10), sebaceous cellcarcinoma (nine) and squamous cell carcinoma (SCC) (six)were the most common. The remaining 10 tumour typesaccounted for the other 11 cases.Seventeen exenterations have been performed over a
15 month period since the beginning of 2003. Of these, 11(65%) had orbitally invasive BCC. In the previous 12 years atotal of 47 exenterations were performed, 17 (36%) of whichhad orbital invasion by BCCs. It, therefore, appears thatinvasive BCC as an indication for orbital exenteration hasincreased. It is also interesting that 39% in the group withexenterations over 12 years compared to an increased 69% inthe group in the most recent 15 months had at least oneprevious attempt at cure of the lesion. This may imply a trendtowards less destructive surgical techniques, resulting ininadequate surgical clearance of the tumour or inappropriatefollow up before exenteration is undertaken.The anatomical location of these lesions is outlined in
table 4. The eyelids were the most common sites of tumour,occurring in 38 of the 64 exenterated patients. Malignantdisease originating in the orbit and lacrimal gland accountedfor a further 18 cases, with the globe and conjunctivaaccounting for a further five cases.
14
12
8
10
6
4 3
1
43
8
45 5
45
6
3
12
5
0
2
Year
Num
ber o
f pat
ient
s
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
Up to 1
Apri
l 200
4
Figure 1 Distribution of exenteration patients over 13 year period.
Table 1 Indications for orbital exenteration
IndicationNumber of patients(n = 69)
Lid neoplasm 38Orbital neoplasm 18Non-neoplastic 5Conjunctival neoplasm 3Globe neoplasm 2Unknown 3
Table 2 Previous therapy
TherapyNumber of patients(n = 64)
None 24Local excision 16Local excision and radiotherapy 10Mohs’ abandoned 2Radiotherapy alone 1Unknown/not documented 8Other 3
Table 3 Histological diagnosis of patients undergoingexenteration
Histological diagnosisNumber ofpatients (n = 69)
Basal cell carcinomawith no previous treatment 9with previous surgery only 10with previous radiotherapy/surgery 8with previous radiotherapy 1
Sebacous cell carcinoma 9Squamous cell carcinoma 6Melanoma
Globe with extrascleral spread 8Lids 1Ethmoid sinuses 1
Adenocystic carcinoma (lacrimal gland) 2Adenocarcinoma 1Liposarcoma 1Merkel cell 1Lymphoma 1Apocrine carcinoma 1Rhabdomyosarcoma 1Secondary metastasis-gastrointestinal primary 1Malignant schwannoma 1Malignant medulloepithelioma 1Non-malignant disease 5
1336 Rahman, Cook, Leatherbarrow
www.bjophthalmol.com

In the overall total of 68 patients (69 orbits) undergoingorbital exenteration, including those for non-malignantdisease, 25 required a subtotal exenteration and a further35 a total orbital exenteration. In nine cases the procedurewas not clearly documented or the information was notretrievable. Surgery was performed under local anaesthesiawith intravenous sedation in seven cases and under generalanaesthesia in the remaining 62 cases. Patients were selectedfor local anaesthetic with sedation on the basis of co-existingmedical problems, in whom general anaesthesia was deemedunsafe following advice from a consultant anaesthetist.In three of the 64 cases requiring exenteration for
malignant disease, it was deemed necessary to remove partof the bony orbit to ensure tumour clearance at the time ofsurgery. Overall, 29 patients demonstrated tumour to bepresent in excision margins on histological examinationfollowing exenteration. Nineteen of these 29 underwentfurther postoperative adjunctive treatment; 16 underwentorbital radiotherapy, one patient required a combination ofradiotherapy and chemotherapy, one patient needed radio-therapy and further surgery, and one patient required furtherremoval of tissue to achieve histologically clear margins.The orbit was allowed to granulate in a total of 43 of the 64
patients. In a further 21 a split skin graft was applied.Postoperatively the most common complication was sino-orbital fistulas occurring in 15 patients. These occurred in 12patients in whom the orbit was allowed to granulate and inonly three patients in whom a split skin graft was placed.Fistula, therefore, developed more commonly with socketsleft to granulate (80%) than with the concomitant use of skingrafts (20%). Seven further patients had graft failure, four ofwhom required regrafting and three others were allowed togranulate. A cerebrospinal fluid leak was observed intra-operatively in one patient who had previously undergone acraniotomy, but this was managed at the time of theexenteration with a local pericranial flap with no furtheradverse sequelae. Another patient had chronic socketdischarge in the absence of a fistula. These complicationsand co-morbidity are detailed in table 5.
There were eight cases of local or regional recurrence oftumours, outlined in table 6. This group included two SCCs,one liposarcoma, one SCC, one BCC, one melanoma, oneadenocarcinoma from a gastrointestinal tumour, and oneadenocarcinoma occurring in a lacrimal gland pleomorphicadenoma. Of these eight cases, six patients had tumourpresent on histological examination. Two had clear resectionmargins. Seven of the eight patients underwent adjunctiveradiotherapy postoperatively.In total, 31 patients had facial prostheses fitted at an
average of 10 months (range 2–38 months) postoperatively(fig 2). Of these, four patients underwent successful 2 stageosseointegration before prosthesis fitting. There was nodifference in the mean time to prosthesis fitting whether ornot a split skin graft was applied (11 months for orbitsallowed to granulate compared to 10 months using a skingraft). However, 25 patients were satisfied with the cosmeticoutcome without a facial prosthesis and opted for a ‘‘pirate’’patch to cover the exenterated defect. A further eight patientshad not completed prosthesis fitting at the time of writing.Of the five orbits exenterated for non-malignant disease,
four were satisfied with the cosmetic outcome without facialprosthesis. One further orbit had prosthesis fitting 3 monthsafter exenteration with the application of a skin graft.A complete review of morbidity and mortality is beyond the
scope of this paper and will be presented in a follow up study.
DISCUSSIONOrbital exenteration is a disfiguring procedure requiringpreoperative and postoperative counselling by a multidisci-plinary team consisting of an ocularist, orbital surgeon,specialist wound care nurse, and a clinical psychologist.Preoperative counselling with an ocularist is pivotal indeciding on the timing and best surgical approach—forexample, whether osseointegration at the time of exentera-tion and before radiotherapy will save the patient later needfor hyperbaric oxygen. Tumour eradication, however, shouldtake precedence over cosmetic concerns. Often, removal ofpart of the bony orbit is necessary adding to the postoperativefacial rehabilitation management plan. Recently, we haveadapted the successful use of intravenous sedation with localanaesthetic (seven cases) as a means of exenterating theolder patient with systemic co-morbidity.Although non-malignant disease may occasionally be the
indication for orbital exenteration, the vast majority ofexenterations are undertaken to treat malignant disease.Bartley et al10 reported that 100 of their 102 exenterated casesresulted from malignant disease. This is similar to Levin et al(93 of 99 cases)9 and Mohr and Esser (74 of 77 cases).6 Wefound a similar ratio in our series of 64 of 69 cases requiringexenteration for malignant disease.Healing of the orbital defect is dependent on the method
used for reconstruction. Options include temporalis muscletransposition,11 midline forehead flaps,12 dermal graft,13
dermis fat graft,14 split skin graft,15 globe sparing exentera-tion,16 eyelid sparing techniques17 and spontaneous granula-tion.18 Allowing granulation of the defect may delay healingby up to 2–3 months. The need for regular dressing changesmust be weighed against the potential benefits of healing bysecondary intention—namely, an easier, quicker procedurethat allows recurrences to be detected early. This provides acomparable colour match to the surrounding skin whengranulation is complete.10 In our practice, postoperativedressing changes are undertaken by experienced nursepractitioners using a moist wound bed healing technique.The orbit is packed with Aquacel (Convatec Ltd, Deeside,UK), and dressings changed on a weekly basis until completehealing of the orbit.
Table 4 Location of lesion
Origin of lesionNumber of patients(n = 64)
LidsMedial canthus 17Upper lid 8Lower lid 8Lateral canthus 5
Orbital 16Lacrimal gland 2Globe 2Conjunctiva 3Other/unknown 3
Table 5 Complications and co-morbidity experienced inthe 64 patients undergoing exenteration for neoplasm
Complication/comorbidityNo of patients(n = 64)
None 35Sino-orbital fistula 15Failed skin graft requiring regrafting 4Failed skin graft allowed to granulate 3Chronic discharge 1Cerebrospinal fluid leak 1Complications not documented 5
Orbital extenteration 1337
www.bjophthalmol.com

Significant numbers of patients may develop sino-orbitalfistulas from perforated sinuses occurring intraoperatively. Inour series, 12 of the 43 (28%) orbits allowed to granulatedeveloped permanent fistula formation following granulationof the orbit. This is a lower rate when compared to other largestudies, 17/25 (68%) cases6 and 17/49 (35%) cases.10 Otherdisadvantages of secondary healing of an exenterated orbitinclude delayed healing, prolonged postoperative socket care,and delayed facial rehabilitation. The method employed toclose the orbital defect must take into account severalimportant issues: local and systemic tumour control andthe likely survival of the patient. For instance, in cases whererecurrence is unlikely and survival good, granulation may bebeneficial to allow local detection of tumour. Conversely, incases where exenteration is preformed for palliation of theneoplasm, a split skin graft will give rapid rehabilitation ofthe socket, and minimise hospital attendance. The use ofsuch a graft, however, lengthens the duration of surgery andcan have morbidity in older patients. Furthermore, in ourstudy, there was no significant difference in the time to facialrehabilitation with prosthesis for those orbits allowed togranulate (11 months) compared to those orbits in which asplit skin graft was applied (10 months).In our series, BCC was the most common neoplasm (44%),
followed by melanoma of the eyelids, sinuses, and globe withextrascleral spread, and then SCC. Combined, these threetumours accounted for 73% of cases requiring exenteration.Other large studies have reported varying rates of BCC.However, our rate of 44% is significantly higher. Rathbun etal8 reported 14 cases of BCC in their series of 48 (29%)exenterations, Bartley et al10 21 of 100 (21%) cases, Mohr andEsser6 six of 74 (8%) exenterations, and eight of 99 (8%)cases reported in the series by Levin and Dutton.9 Two casesof orbital exenteration in our BCC group had Gorlin-Goltzsyndrome,19 one of which underwent exenteration forpalliative reasons.It is interesting to note that 23/28 (82%) cases of those
orbits exenterated for orbital invasion of a BCC hadpreviously experienced failed treatments (surgery/radiother-apy) elsewhere. This was similar to the overall figuredocumented by Bartley et al of 80%.10 More recently, therehas been a significant increase in the number of exentera-tions being undertaken at our institution for orbital invasionby a BCC. Since 1 January 2003, 11/17 cases of orbitalinvasive BCC have undergone exenteration compared to 17/47 cases in the previous 12 years. Further, in the most recent15 months 69% of patients have had treatment of neoplasticlesions before exenteration. In comparison, in those withexenteration over a 12 year period, 39% received previousattempts at tumour removal before referral for exenteration.There has been a trend towards a greater number of patients
Table 6 Characteristics of patients with local or regional recurrence
Age/sex Diagnosis Clear margin Adjuvant treatment Previous treatment Cause of death Comment
70/M Sebaceous cell No Radiotherapy No Secondary metastases Had previousradiotherapy
27/F Liposarcoma No Radiotherapy No Secondary metastases Local bone involvement*80/M Metastases No None No Secondary metastases Gastrointestinal primary74/M Sebaceous cell No Radiotherapy Surgery Secondary metastases Delayed diagnosis.85/F BCC No Radio/surgery Radio/surgery Alive Cryotherapy for
recurrence72/M Melanoma with
extrascleral spreadYes Radiotherapy Radio/surgery Unknown status Neck metastasis at last
visit72/F SCC No Radio/surgery No Secondary metastases Local bone involvement*63/M Adenocarcinoma in
lacrimal glandpleomorphic adenoma
Yes Radiotherapy Radio/surgery Secondary metastases Local bone involvement*
*Noted at time of exenteration.
Figure 2 (A) Patient before facial prosthesis. (B) Patient with facialprosthesis. (Pictures reproduced with permission of patient and herparents.)
1338 Rahman, Cook, Leatherbarrow
www.bjophthalmol.com

being treated before exenteration over the past 15 months(69%) compared to the previous 12 years (39%).Since 2001, almost 50% of cases with orbitally invasive
BCCs have been treated and referred by allied specialties—that is, plastic surgery, dermatology, and oncology, and theremaining 50% or so by regional ophthalmologists. Precedingthis period, however, the majority (70%) had been treatedand referred by ophthalmologists. This may reflect the morediverse interest of eyelid tumour surgery among alliedspecialties, often using non-Mohs’ micrographic techniques,resulting in recurrence of tumours.A high rate of recurrence is observed in medial canthal
tumours and was confirmed in our series where 12 of 23cases of recurrence were from medial canthal lesions,necessitating exenteration.20 Only one case of BCC hadrecurrence after Mohs’ micrographic surgery. This may reflectthe medial canthal area as an area where BCCs are commonor a site where recurrence and invasion may be prominent.Many of these cases may have avoided exenteration if treatedearly; factors that are likely to have influenced their outcomeinclude inappropriate surgery, inappropriate observation and/or follow up, and neglect of the lesion by the patient until alate stage in the disease.Management of uveal tumours remains controversial, but
it is now generally agreed that primary exenteration does notincrease survival rates and may even hasten progress of thedisease process.21–26 In our series, there was a 100% survivalafter 1 year. The 3 year survival fell to 33%, although only sixpatients have been followed up for this length of time.Furthermore, three patients had an exenteration for pallia-tion of symptoms.Two schools of thought exist when deciding on exentera-
tion for these highly malignant uveal tumours with extra-scleral spread. Those opposing exenteration think that thehighly metastatic nature of these tumours necessarily involvemicro-metastases when extrascleral extension is identifiedand, thus, carry a poor prognosis with or without treatment.Those advocating exenteration believe that removing thetumour as early as possible may increase survival by limitingthe time for systemic spread to occur. Shammas and Blodi23
reported an overall 73% mortality of patients when extra-scleral extension of the tumour was observed, compared to22% when extrascleral extension was not observed. Kersten etal27 found a similar tumour related mortality of 81% inpatients undergoing extrascleral extension. Furthermore,there was no clinically significant difference in overallsurvival probabilities of patients undergoing early exentera-tion (21%) compared to enucleation (17%) alone on extendedfollow up, and a 100% incidence of metastasis related toorbital recurrences needing only palliation. Thus, thepreferred treatment for extrascleral extension of uvealmelanomas appears to be local resection of the tumour,including enucleation and tenonectomy.Sebaceous gland carcinoma of the eyelid is a slow growing
lesion, often mimicking benign conditions, such as achalazion.28 Of the eight cases in our series, only one hadhad previous surgery on the assumption that the lesion was achalazion. After several recurrences over a 24 month periodbefore referral, a biopsy confirmed sebaceous cell carcinoma.However, the remaining seven patients had biopsy confirma-tion without previous surgery elsewhere. All had confirmedpagetoid conjunctival spread. A mortality rate of 3–40% hasbeen reported.29–34 Early diagnosis can, however, preventmutilating exenteration and may be amenable to lessdestructive surgery. We found a mortality rate of 25% (twopatients) in this subgroup from metastatic disease and afurther one patient with metastatic disease, but havingpalliative treatment. All three of these patients did notachieve clear surgical margins at the time of exenteration.
CONCLUSIONExenteration is a procedure performed with increasingfrequency in our unit over the past 15 months, the majoritybecause of BCCs. The incidence of 44% of exenterations at ourunit being performed for orbitally invasive BCC is signifi-cantly higher than other large studies; 39% of these wereperformed in the past 15 months. A large number of patientswith these exenterations had undergone previous treatmentsunder a variety of non-ophthalmic specialties in other units,using non-Mohs’ micrographic techniques. Coupled withpossible inappropriate observation and/or follow up, orneglect of the lesion by the patient, eyelid tumours arepresenting at an advanced stage.Exenterations are disfiguring procedures that may, there-
fore, be reduced in incidence by primary removal of tumoursby those most skilled at tumour removal. Once performed,the cosmetic rehabilitation is long, with multiple post-operative visits, independent of the method used to closethe orbital defect. Our rate of fistula formation is significantlylower than other reports, which may reflect surgicaltechnique. Further, we have found the use of localanaesthetic with sedation to be very effect in specific patientswith medical co-morbidity without difficulties during exen-teration.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
I Rahman, A E Cook, B Leatherbarrow, Manchester Royal Eye Hospital,Lister Centre, Nelson Street, Manchester M13 9WL, UK
Competing interests: none declared
REFERENCES1 Bartisch G. Ophthalmodoulcia, Dresden, 1583;3:208.2 Rose GE, Wright JE. Exenteration for benign orbital disease. Br J Ophthalmol
1994;78:14–18.3 Sheilds JA, Sheilds CL, Suvarnamani C, et al. Orbital exenteration with eyelid
sparing: indications, technique and results. Ophthalmic Surg 1991;22:292–7.4 Frezotti R, Nuti A. Repair after orbital exenteration. Acta Neurochir
1982;60:119–24.5 Shore JW, Burks WR, Leone C, et al. Dermis fat graft for orbital exenteration
after subtotal exenteration. Am J Ophthalmol 1986;102:228–36.6 Mohr C, Esser J. Orbital exenteration: surgical and reconstructive strategies.
Graefes Arch Clin Exp Ophthalmol 1997;235:288–95.7 Naquin HA. Exenteration of the orbit. Arch Ophthalmol 1954;51:850–62.8 Rathbun JE, Beard C, Quickert MH. Evaluation of 48 cases of orbital
exenteration. Am J Ophthalmol 1971;72:191–9.9 Levin PS, Dutton JJ. A 20 year series of orbital exenteration. Am J Ophthalmol
1991;112:496–501.10 Bartley GB, Garrity JA, Waller RR, et al. Orbital exenteration at the Mayo
Clinic 1967–1986. Ophthalmology, 1989;96;468–74..11 Reese AB, Jones IS. Exenteration of the orbit and repair by transplantation of
the temporalis fascia. Am J Ophthalmol 1961;51:217–27.12 Dortzbach R, Hawes M. Midline forehead flap in reconstructive procedure of
the eyelids and exenterated socket. Ophthalmic Surg 1981;12:257–68.13 Mauriello JA Jr, Han KH, Wolfe R. Use of autogenous split-thickness dermal
graft for reconstruction of the lining of the exenterated orbit. Am J Ophthalmol1985;100:465–7.
14 Shore JW, Burks R, Leone CR Jr, et al. Dermis fat graft for orbitalreconstruction after subtotal exenteration. Am J Ophthalmol1986;102:228–36.
15 Harting F, Koorneef L, Peeters HJF, et al. Glued fixation of split-skin graft to thebony orbit following exenteration. Plast Reconstruc Surg 1985;76:633–5.
16 Catalano PJ, Laidlaw D, Sen C. Globe sparing orbital exenteration.Otolaryngol Head Neck Surg 2001;125:379–84.
17 Sheilds JA, Sheilds CL, Suvarnamani C, et al. Orbital exenteration with eyelidsparing: indications, technique and results. Ophthalmic Surg1991;122:292–7.
18 Putterman AM. Orbital exenteration with spontaneous granulation. ArchOphthalmology 1986;104:139–40.
19 Gorlin RJ, Goltz RW. Multiple nevoid basal-cell epithelioma, jaw cyst andbifid rib. A syndrome. N Engl J Med 1960;262:908–12.
20 Robins P, Rodriguez-Sains R, Rabinovitz H, et al.Moh’s surgery for periocularbasal carcinomas. J Dermatol Surg Oncol 1985;11:1203.
21 Pach JM, Robertson DM, Taney BS, et al. Prognostic factors in choroidal andciliary body melanomas with extrascleral extension. Am J Ophthalmol1986;101:325–31.
22 Rini FJ, Jackobiec FA, Hornblass A, et al. The treatment of advance choroidalmelanoma with massive orbital extension. Am J Ophthalmol 1987;104:634.
23 Shammas HF, Blodi FC. Orbital extension of choroidal melanomas. ArchOphthalmol 1977;95:2002–5.
Orbital extenteration 1339
www.bjophthalmol.com

24 Liarikos S, Rapidis AD, Roumeliotis A, et al. Secondary orbitalmelanomas: analysis of 15 cases. J Craniomaxillofac Surg2000;28:148–52.
25 Augsburger JJ, Schneider S, Narayana A, et al. Plaque radiotherapy forchoroidal and ciliochoroidal melanomas with limited nodular extrascleralextension. Can J Ophthalmol 2004;39:380–7.
26 Blanco G. Diagnosis and treatment of orbital invasion in uveal melanoma.Can J Ophthalmol 2004;39:388–96.
27 Kersten RC, Tse DT, Anderson RL, et al. The role of orbital exenteration inchoroidal melanoma with extrascleral extension. Ophthalmology1985;92:436–43.
28 McLean IW, Jackobiec FA, Zimmerman LE, et al. Tumours of the eye andocular adnexa. Washington: Maryland Armed Forces Institute of Pathology,1993;3:28–35.
29 Zurcher M, Hintschich CR, Garner A, et al. Sebaceous carcinoma of theeyelid: a clinicopathological study. Br J Ophthalmol 1998;82:1049–55.
30 Doxanas MT, Green WR. Sebaceous gland carcinoma: a review of 40 cases.Arch Ophthalmol 1984;102:245–9.
31 Boniuk M, Zimmerman LE. Sebaceous carcinoma of the eyelid, eyebrow,caruncle and orbit. Trans Am Acad Ophthalmol Otolarngol1968;72:619–41.
32 Ni C, Kuo PK. Mebomian gland carcinoma: a clinicopathologic study of 156cases with long-period follow-up of 100 cases. Jpn J Ophthalmol1979;23:388–401.
33 Rao NA, Hidayat AA, McLean JW, et al. Sebaceous carcinoma of the ocularadnexa. Hum Pathol 1982;13:113–22.
34 Muqit MMK, Roberts F, Lee WR, et al. Improved survival rates in sebaceouscarcinoma of the eyelid. Eye 2004;18:49–53.
1340 Rahman, Cook, Leatherbarrow
www.bjophthalmol.com

EXTENDED REPORT
Isolated visual symptoms at onset in sporadic Creutzfeldt-Jakob disease: the clinical phenotype of the ‘‘Heidenhainvariant’’S A Cooper, K L Murray, C A Heath, R G Will, R S G Knight. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr Sarah Cooper, TheNational Creutzfeldt-JakobDisease Surveillance Unit,Western General Hospital,Crewe Road, EdinburghEH4 2XU, UK; [email protected]
Accepted for publication15 July 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1341–1342. doi: 10.1136/bjo.2005.074856
Background: The Heidenhain variant of sporadic Creutzfeldt-Jakob disease (sCJD) is commonlyunderstood to represent cases with early, prominent visual complaints. The term is clarified to representthose who present with isolated visual symptoms. This group may pose diagnostic difficulties and oftenpresent to ophthalmologists where they may undergo needless invasive procedures.Method: A retrospective review of 594 pathologically proved sCJD cases referred to the UK National CJDSurveillance Unit over a 15 year period to identify Heidenhain cases.Results: 22 cases had isolated visual symptoms at onset with a mean illness duration of 4 months. Themean age at disease onset was 67 years. Most displayed myoclonus, pyramidal signs, and a delay in theonset of dementia for some weeks. 17 (77%) were referred initially to ophthalmology. Two underwentcataract extraction before diagnosis. All tested cases were homozygous for methionine at codon 129 ofthe prion protein gene.Conclusions: This rare, but clinically distinct, group of patients with sCJD may cause diagnostic difficulties.Because ocular intervention carries with it the risk of onward transmission awareness of this conditionamong ophthalmologists is important.
Sporadic Creutzfeldt-Jakob disease (sCJD) is a rare anduniformly fatal prion disease classically presenting as arapidly progressive dementia resulting in death usually
within 6 months.1 2
A subgroup of cases of sCJD present with isolated visualsymptoms. These can persist in the absence of cognitivedecline for some weeks.3 Historically, these are termed the‘‘Heidenhain variant’’ of sCJD after work by Heidenhain in1929.4 He described three cases of spongiform encephalo-pathy, two of which had prominent, early visual symptoms.The third presented with sensory complaints and athetosis.Meyer et al described, in 1954, the case of a 38 year old manwho ‘‘became forgetful, experienced difficulty in concentra-ting…suffered from headaches and his vision began to fail.’’A right homonymous hemianopia was detected and deathoccurred 6 months after the onset of symptoms.5
Subsequently, the term has been used rather imprecisely inall cases where visual symptoms occur along with otherwisecharacteristic early features. Visual symptoms are common insCJD and, in the early stages of the disease, have beendescribed in 20%.6 This study seeks to clarify Heidenhaincases as a clinically distinct group where visual symptomsoccur initially in isolation. These cases may cause diagnosticdifficulty and raise particular public health concerns. Theyare likely to present to ophthalmologists and may be subjectto needless ocular intervention, with risks of onwardtransmission.
MATERIALS AND METHODSA retrospective case file review was performed on allpathologically proved cases of sCJD referred to the UKNational CJD Surveillance Unit (NCJDSU) between January1990 and March 2005 inclusive. Case files comprised clinicaland epidemiological information collected by NCJDSU staffand copies of hospital and general practitioner records. Aclinical assessment and interview with patients’ relatives wasconducted by a surveillance neurologist whenever possible
and usually while the patient was alive.Electroencephalogram (EEG) recordings and magnetic reso-nance brain imaging (MRI) were reviewed at the NCJDSU.Cases were identified whose first symptom was visual and
who exhibited no other cognitive, behavioural, or physicalsymptoms for at least 2 weeks. The presence or absence ofcognitive decline was assessed by a review of case files,including a detailed discussion with relatives and a ques-tionnaire completed by the NCJDSU neurologist. Patientswere excluded if there were any memory difficulties,behavioural changes, episodes of confusion or disorientation,speech problems, or other neurological symptoms or signswithin 2 weeks of the first symptom. Cases were identifiedon a clinical basis without awareness of PRNP codon 129genotype data. Genetic analysis was performed withinformed consent of the patient or the next of kin.
RESULTSTwenty two patients out of 594 (3.7%) with pathologicallyproved sCJD had clearly documented purely visual symptomsfor at least the first 2 weeks of the illness. The nature of theseinitial symptoms is summarised in table 1.Fourteen (64%) cases were women. Mean age at onset was
67 years (median 66 years, range 50–88 years). Mean dura-tion of illness was 4 months (median 3 months, range 1–17 months). Seventeen patients (77%) lived for 3 months orless.
Clinical featuresThroughout the illness myoclonus was observed in 21 (95%),pyramidal signs in 19 (86%), cerebellar signs in 12 (55%),psychiatric symptoms in seven (32%), other involuntarymovements in six (27%), sensory symptoms in four (18%),
Abbreviations: EEG, electroencephalogram; MRI, magnetic resonanceimaging; NCJDSU, National CJD Surveillance Unit; sCJD, sporadicCreutzfeldt-Jakob disease
1341
www.bjophthalmol.com

and extrapyramidal signs in one (5%). None had documentedseizures. A rapidly progressive dementia was observed in allafter the initial period of cognitive preservation which lastedfrom 2–6 weeks.
Case 1A 73 year old man complained of difficulty reading, withblank spaces appearing in words. He also complained ofcolours appearing abnormally enhanced. He was assessed byan ophthalmologist when there was normal visual acuity butdense scotomata lying to the right of fixation bilaterally. Aprovisional diagnosis of an occipital infarct was made. Sixweeks after onset he developed myoclonus, followed byataxia and ultimately dementia. His vision deteriorated withoculomotor apraxia and cortical blindness. He died 3 monthsafter disease onset.
Case 2A 62 year old woman presented with deteriorating visualacuity. She felt that her vision was ‘‘fogging up’’ andcomplained of tunnel vision. She attended an optician butno abnormality was identified. A week later she complainedthat everything appeared green. An MRI brain scan wasordered following referral to the ophthalmology departmentbut no diagnosis made. Over the next month her gait becameunsteady and she was increasingly forgetful. By the time shedeveloped myoclonus she could only perceive light. She diedin an akinetic and mute state 4 months after onset.
Investigation resultsTwenty patients had at least one EEG. These were consideredtypical for sCJD1 after review at the NCJDSU in seven cases(35%). CSF 14-3-3 was analysed in five patients (positive inall). Cerebral MRI was available for review in only six cases,showing high signal in the basal ganglia in two (33%) andbeing normal in four. Sixteen cases (73%) had PRNP genecodon 129 genotype data. All of these were homozygous formethionine. In nine the glycotype was known and was type 1in all.1
Seventeen patients (77%) were initially referred to theophthalmology department. Two underwent cataract extrac-tion after the onset of symptoms and before a diagnosis ofsCJD. Thirteen (59%) were referred to the NCJDSU within2 months of onset. Three cases were referred after death, oneof these after a necropsy revealed sCJD.
DISCUSSIONAlthough visual symptoms in sCJD are not uncommon theyoften occur in the context of symptoms indicative of a morewidespread cortical involvement. These cases are distinctbecause of the isolated visual symptoms at onset and thestriking early preservation of cognitive function. Aside fromthe onset the cases are remarkably ‘‘typical’’ for sCJD. Themajority display an extremely rapid decline with associatedmyoclonus once dementia has supervened. Nearly 60% of
these patients were referred to the NCJDSU within 2 monthsof onset and only one case was referred as a result ofdiagnosis at necropsy (compared to 19% of total cases of sCJDreferred in this way7). Two cases underwent cataractextraction before the diagnosis of sCJD was considered.Previous work has highlighted the incidence of ocular surgeryin sCJD cases with visual symptoms8. Although there havenot been any reports of CJD transmission following cataractsurgery, it has been reported after corneal grafting. Abnormalprion protein has been isolated from ocular tissue.9 It isimportant that ophthalmologists are aware of the conditiondespite its rarity as onward transmission through ocularsurgical intervention remains a concern.All tested cases were homozygous for methionine at codon
129 of the PRNP gene. This genotype is associated with aclinically typical disease course10 rather than isolated visualsymptoms themselves. The methodology in this study differsfrom that previously employed as unselected, consecutivecases from surveillance in one country were obtained byapplying a careful definition of a ‘‘Heidenhain’’ case. We haveshown that 22 cases have been identified over 15 years out ofa population of approximately 58 million in the UnitedKingdom. The more defined inclusion criteria for visual onsetcases used here compared to those employed in the past6 mayhave identified a distinct subgroup of cases as reflected in thegenotype findings.Defining a group of cases with isolated visual symptoms at
onset may aid future recognition of similar cases. Byclarifying the definition of Heidenhain cases we haveidentified a group who generally exhibit short illnessduration, myoclonus, and a PRNP codon 129 MM genotype.As well as aiding diagnosis these findings may contribute tothe understanding of the how abnormal prion protein causesdisease within the central nervous system.
ACKNOWLEDGEMENTSWe would like to thank the referring clinicians and the patients andrelatives of patients with CJD for their assistance with thesurveillance work.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
S A Cooper, K L Murray, C A Heath, R G Will, R S G Knight, TheNational Creutzfeldt-Jakob Disease Surveillance Unit, Western GeneralHospital, Crewe Road, Edinburgh EH4 2XU, UK
Competing interests: none declared
REFERENCES1 Knight R, Collins S. Human prion diseases: cause, clinical and diagnostic
aspects. In: Rabenau HF, Cinatl J, Doerr HW, eds. Prions. a challenge forscience, medicine and public health systems. Basle: Karger, 2001;68–92).
2 Brown P, Cathala F, Sadowsky D, et al. Creutzfeldt-Jakob disease in France:II. Clinical characteristics of 124 consecutive verified cases during the decade1968–1977. Ann Neurol 1979;6:430–7.
3 Vargas ME, Kupersmith MJ, Savino PJ, et al. Homonymous field defect as thefirst manifestation of Creutzfeldt-Jakob disease. Am J Ophthalmol1995;119:497–504.
4 Heidenhain A. Klinische und anatomische Untersuchungen uber eineeigenartige organische Erkrankung des Zentralnervensystems im Praesenium.Zeitschrift fur die gesamte Neurologie und Psychiatrie 1928;118:49–114.
5 Meyer A, Leigh D, Bagg CE. A rare presenile dementia associated withcortical blindness (Heidenhain’s syndrome). J Neurol Neurosurg Psychiatry1954;17:129–33.
6 Kropp S, Schulz-Schaeffer WJ, Finkenstaedt M, et al. The Heidenhain variantof Creutzfeldt-Jakob disease. Arch Neurol 1999;56:55–61.
7 National UK Creutzfeldt-Jakob Disease Surveillance Unit, 2005. Unpublishedwork.
8 S-Juan P, Ward HJT, De Silva R, et al. Ophthalmic surgery and Creutzfeldt-Jakob disease. Br J Ophthalmol 2004;88:446–9.
9 Head MW, Northcott V, Rennison KA, et al. Prion protein accumulation ineyes of patients with sporadic and variant Creutzfeldt Jakob disease. InvestOphthalmol Vis Sci 2003;44:342–6.
10 Parchi P, Giese A, Capellari S, et al. Classification of sporadic Creutzfeldt-Jakob disease based on molecular and phenotypic analysis of 300 subjects.Ann Neurol 1999;46:224–33.
Table 1 Visual symptoms at onset (n = 22)
Visual symptomNumber of patients(n = 22)*
Decreased visual acuity 8Blurred vision 6Peripheral visual field defect 2Visual distortions 3Impaired colour vision 2Palinopsia 1Tunnel vision 1
*One patient experienced both impaired colour vision and visualdistortions at onset.
1342 Cooper, Murray, Heath, et al
www.bjophthalmol.com

SCIENTIFIC REPORT
Isolation, culture, and characterisation of human macularinner choroidal microvascular endothelial cellsA C Browning, T Gray, W M Amoaku. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1343–1347. doi: 10.1136/bjo.2004.063602
Aim: To develop a method for the reliable isolation of adulthuman macular inner choroidal endothelial cells (ICECs) andto subsequently characterise them for their expression of arange of endothelial cell associated surface markers.Method: Human ICECs were isolated after manual dissectionof maculas from fresh human posterior segments. Followingenzyme digestion to form a single cell suspension, the ICECswere isolated using anti-CD31 coated Dynabeads. Theisolated cells were grown in culture and examined for typicalendothelial cell morphology, surface expression of vWf, CD31, CD 105, VEGF receptors 1 and 2, and expression of E-selectin after stimulation with TNF-a. The cells were alsoexamined for their ability to form fenestrations and capillary-like tubes in Matrigel.Results: The method enabled the rapid isolation of viablecells that demonstrated typical endothelial cobblestonemorphology in culture. The cells stained positive for CD31,vWf, CD105, VEGF receptors 1 and 2, and E-selectin (afterstimulation with TNF-a). The cells stained negative for a
smooth muscle actin and fibroblast surface protein. The cellsalso developed fenestrations when cultured on fibronectincoated plates and formed capillary-like tubes structures whencultured on Matrigel.Conclusions: This technique isolates cells from the humanmacular inner choroid that display features consistent withvascular endothelial cells. These cells could subsequently beused to further the understanding of the pathophysiologicalmechanisms of diseases of the inner choroid, such aschoroidal neovascularisation.
The neovascular or ‘‘wet’’ form of age related maculardegeneration (ARMD) is characterised by the growth ofnew blood vessels from the inner choroid (including the
choriocapillaris).1–3 While the initiating event causing wetARMD is unknown, it is widely acknowledged that themicrovascular endothelial cell plays a pivotal part in thedisease process.It is widely accepted however, that endothelial cells derived
from different species, vascular organs and from withindifferent vascular beds within those organs display differentmorphological, biochemical and phenotypical heterogeneity.4–15
This suggests that the use of bovine, umbilical vein, orheterogeneous mixtures of human choroidal endothelialcells to study the pathophysiological mechanisms ofARMD16–19 may not be truly representative.To understand the angiogenic mechanisms important in
the development of ARMD, it would be advantageous tostudy the behaviour of endothelial cells derived from the sitewhere the disease occurs—that is, within the inner choroid ofthe human macula. In this study, we describe a method that
allows the reliable isolation and culture of human macularinner choroidal microvascular endothelial cells (ICECs).
MATERIALS AND METHODSIsolation of macular inner choroidal endothelial cellsHuman posterior segments free of any known ocular diseasewere obtained from UK Transplant. The research had theapproval of the local research ethics committee (Nottingham2 LREC). After the iris had been removed, an 8 mm biopsypunch was positioned over the macula and pressure wasapplied, sufficient to penetrate the full thickness of the sclera.The macular sample was removed and transferred to a petridish where the retina was discarded and retinal pigmentepithelium (RPE) removed by gentle brushing with a sterilespatula and irrigation with sterile phosphate buffered saline(PBS). The choroid was then gently teased from the attachedsclera and turned upside down. With the use of a dissectingmicroscope, the outer choroidal vessels along with adherentpigmented fibrous tissue were peeled off, leaving therelatively non-pigmented inner choroid and choriocapillaris/Bruch’s membrane complex. The tissue was cut into 1 mmpieces and washed three times in minimum essentialmedium (MEM) (Invitrogen Ltd, Paisley, UK) containing30 mM HEPES, 0.25 mg/ml amphotericin B, 100 mg/mlstreptomycin, 50 mg/ml kanamycin, and 30 mg/ml penicillin(isolation medium). The pieces were incubated in 0.1%collagenase I (Sigma-Aldrich) in MEM for 2 hours at 37 C,with frequent agitatation. The collagenase was neutralisedwith MEM containing 10% fetal calf serum (Invitrogen Ltd,Paisley, UK). and the mixture filtered through sterile 40 mmand 20 mm filters (Millipore Ltd, Watford, UK). The eluatewas centrifuged (75 g) and washed three times in isolationmedium, and resuspended in 1 ml of PBS/0.1%BSA. Theendothelial cells were then isolated as in the manufacturer’sinstructions (Dynal Ltd, Wirral, UK). The Dynabeads wereresuspended in endothelial growth medium (EGM2-MV withhydrocortisone omitted, Cambrex Biosciences, Wokingham,Berks, UK) and seeded onto fibronectin coated 35 mmculture dishes (Beckton Dickinson, Oxford, UK). The cellswere incubated at 37 C in a humidified atmosphere of 5%CO2 and the medium changed every 2 days. Cells werepassaged with 0.025% trypsin and 0.01% EDTA in sterile PBS.All reagents were from Sigma-Aldrich, Poole, Dorset, UKunless otherwise specified.
Endothelial cell characterisationAfter growing the cells (passage 1) on 1% gelatin coated glasscover slips (VWR Ltd, Poole, UK) and fixing them in ice cold
Abbreviations: a-SMA, a smooth muscle actin; ARMD, age relatedmacular degeneration; EGM, endothelial growth medium; FITC,fluorescein isothiocyanate; ICECs, inner choroidal endothelial cells;MEM, minimum essential medium; PBS, phosphate buffered saline; RPE,retinal pigment epithelium; TEM, transmission electron microscopy;VEGF, vascular endothelial growth factor
1343
www.bjophthalmol.com

methanol at 220 C for 20 minutes, a standard two stageimmunofluorescence technique was applied,20 using primaryantibodies detailed in table 1. (E-selectin expression wasexamined after exposure to TNF-a (100 pg/ml) (R and DSystems, Abingdon, UK) or PBS for 4 hours before fixation.)The secondary antibody used was rabbit anti-mouse F(ab’)2fragment, fluorescein isothiocyanate (FITC) conjugated (1:20dilution) (Dako, Ely, Cambridgeshire, UK) in all cases exceptvWf, for which swine anti-rabbit F(ab’)2 fragment FITCconjugate was used (1:20 dilution) (Dako). The slides weremounted in glycerol containing 2.5% 1–4 diazabicyclo[2, 2, 2]-octane (DABCO) (Sigma-Aldrich) and observedby confocal fluorescence microscopy (Leica TCS40D, Leica,Milton Keynes, UK). Frozen sections of fresh human placentawere used as a positive control for the vascular endothelialgrowth factor (VEGF) receptor antibodies, while HUVEC cellswere used as a positive control for all other antibodies exceptfor anti-a smooth muscle actin (anti-a-SMA) and anti-human fibroblast, for which human retinal pigment epithe-lial cells and human Tenon’s capsule fibroblasts were usedrespectively.
Transmission electron microscopy (TEM)Isolated cells were grown to confluence on 35 mm fibronec-tin coated culture dishes (Becton Dickinson, Oxford, UK) The
cells were fixed by immersion in 2.5% glutaraldehyde (in0.1 M cacodylate buffer, pH 7.4) for 16–24 hours andprocessed for TEM as previously described.21 22
In vitro tube formationA 1:1 mixture of chilled Matrigel (Beckton DickinsonBiosciences, Oxford, UK) and endothelial growth medium(EGM2-MV) was dispensed into pre-chilled wells of a 96 wellplate. The Matrigel was allowed to solidify at 37 C for30 minutes before isolated cells suspended in endothelialgrowth medium were seeded at a density of 4.86104 per well.The wells were observed hourly for the formation of tubes.For TEM, the endothelial growth medium was removed andreplaced by 2.5% glutaraldehyde (in 0.1 M cacodylate buffer,pH 7.4) for 16–24 hours at 37 C. The fixed Matrigel was thengently removed from the well and processed as describedpreviously.21 22
RESULTSHuman posterior segments of six donors were obtained. Theage of the donors (years) and the time from death toendothelial cell isolation (hours) were: 45 (52), 76 (42), 70(43), 37 (60), 83 (60), and 56 (60).Light microscopy after dissection showed the sample to
comprise Bruch’s membrane along with adherent chorioca-pillary and inner choroidal vessels (fig 1A and B).After isolation, the cells from all donors grew with a
cobblestone morphology typical of endothelial cells (fig 2).The isolated cells showed a positive expression for vWf(fig 3A), CD31 (fig 3B), CD105 (fig 3C), VEGF receptor 1(fig 3D), and receptor 2 (fig 3E), E-selectin before and afterstimulation with TNFa (100 pg/ml) (fig 3F and G). The cellswere negative for mouse anti-rat isotype control (fig 3H), a-SMA (fig 3I) and anti-fibroblast surface protein (fig 3J).Human RPE cells and Tenon’s capsule fibroblasts showedexpression of a-SMA (fig 3K) and fibroblast surface protein(fig 3L), respectively.
Table 1 Primary antibodies used in study
Epitope Class Dilution Source
CD31 murine IgG1 1:20 Dako, Cambridgeshire, UKCD105 murine IgM 1:20 Novo Castra Laboratories,
Peterborough, UKvWf rabbit immunoglobulin fraction 1:200 Dako, Cambridgeshire, UKReceptor 1 VEGF murine IgG1 1:100 Sigma-Aldrich, Poole, UKReceptor 2 VEGF murine IgG1 1:800 Sigma-Aldrich, Poole, UKa-SMA murine IgG1 1:50 Dako, Cambridgeshire, UKFibroblast surface protein murine IgG1 1:200 Dako, Cambridgeshire, UKE-selectin/CD62E murine IgG1 1:20 Serotec, Oxford, UKNegative murine IgG1 1:20 Dako, Cambridgeshire, UK
Figure 1 Histological section of human submacular choroid stainedwith toludine blue (A) before and (B) after removal of the outer choroidalvessels. (B) Shows the residual choriocapillaris and inner choroidalvessels attached to Bruch’s membrane.
Figure 2 Phase contrast photomicrograph of confluent primary cultureof ICECs demonstrating a typical cobblestone appearance (206originalmagnification).
1344 Browning, Gray, Amoaku
www.bjophthalmol.com

Fenestrations were found scattered throughout the cells onTEM (fig 4). Cells seeded onto Matrigel formed capillary-liketube structures within 3 hours (fig 5), and TEM showed thatthese structures possessed a lumen (fig 6) and each lumenwas surrounded by up to three cells joined by junctionalcomplexes.
DISCUSSIONIn view of the known heterogeneity of endothelial cells,4–15 itwould appear logical to study endothelial cells derived fromthe macular inner choroidal/choriocapillaris area of humanswhen studying the disease mechanisms of ARMD. Whilemethods have been described for the isolation of humanchoroidal endothelial cells that contain a mixture of bothinner and outer choroidal endothelial cells,23 24 to date it hasnot been possible to reliably isolate human macular innerchoroidal/choriocapillaris endothelial cells.
Figure 3 Immunofluorescent photomicrograph of human inner ICECs staining for (A) vWf, (B) CD31, (C) CD 105, (D) VEGF receptor 1, (E) VEGFreceptor 2, (F) E-selectin (unstimulated), (G) E-selectin (post-TNF-a stimulation), (H) ) mouse anti-rat isotype negative control, (I) a-SMA, (J) fibroblastsurface protein, (K) human RPE cells stained for a-SMA, (L) human Tenon’s capsule fibroblasts stained for fibroblast surface protein. (All 636originalmagnification.)
Figure 4 Transmission electron micrograph of human ICECs grown ona collagen IV coated Thermanox coverslip showing a typical fenestration(arrow) (bar = 200 nm).
Isolation of inner choroidal endothelial cells 1345
www.bjophthalmol.com

We describe a method to isolate human macular ICECscells that utilise observations made around 100 years ago. In1892, Nuel described a natural cleavage plane within thehuman choroid between the layers of Haller (inner choroid)and Sattler (outer choroid),25 while in 1912, Salzmann notedthat dissection of the choroid was easiest by teasing apart thelayers from the outside.26 With the aid of a dissectingmicroscope and a microdissection technique, we easily peeledthe large outer choroidal vessels from the underlying innerchoroid/choriocapillaris complex. The subsequent isolation ofendothelial cells was achieved using anti-CD31 coatedparamagnetic beads. This purification technique replacesthe laborious manual method of cell sweeping or the relianceon preferential EC proliferation by using endothelial cellspecific culture medium and produces isolates with a purityin excess of 99%.23 27–29
When grown in microvascular endothelial culture medium,the isolated cells formed typical cobblestone patternsconsistent with their endothelial cell lineage.The cells were found to stain strongly for CD31, a
ubiquitous endothelial cell marker important in cell-celladhesion, vWf, VEGF receptors 1 and 2, and CD105. Thelatter is a subunit of the TGF-b receptor found on proliferat-ing vascular endothelial cells and has been suggested as asuitable antigen for antibody directed attack (immunother-apy) on the proliferating endothelial cells within choroidalneovascularisation complexes.30 31 The cells also showedexpression of E-selectin (CD62E) after stimulation withTNF-a, a feature that is reported to be unique to endothelialcells.32 There appeared to be no contamination with RPE cellsor fibroblasts.In this study, the isolated cells also formed fenestrations
when grown on fibronectin and formed capillary-like tubeswhen cultured in Matrigel. The lumen of these tubes wassurrounded by two or more cells joined by junctionalcomplexes, suggesting that the cells had not simplyaggregated together randomly.In summary, we have developed a method to isolate and
culture human ICECs. During early passages, these cellspossess the morphological characteristics of vascularendothelial cells, form fenestrations and capillary tube-likestructures, and express a number of surface markersconsistent with their endothelial cell origin. These cells maybe useful in studying the pathophysiology and cellularmechanisms involved in choroidal neovascularisation.
ACKNOWLEDGEMENTSWe are grateful to the Kelman Foundation, USA, the British EyeResearch Foundation (formerly the Iris Fund), and QMC UniversityHospital Trust for grant funding this project. The authors thank SAnderson and I Ward, School of Biomedical Sciences, University of
Nottingham, for their assistance in conducting the confocal micro-scopy of the cells and I Zambrano, Eye Bank, Manchester RoyalInfirmary, for the provision of the donor eye tissue.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
A C Browning, W M Amoaku, Division of Ophthalmology and VisualSciences, Eye, Ear, Nose and Throat Centre, University Hospital,Queen’s Medical Centre, Nottingham NG7 2UH, UKT Gray, Division of Histopathology, University Hospital, Queen’sMedical Centre, Nottingham NG7 2UH, UK
Competing interests: none declared
Correspondence to: Winfried M Amoaku, Division of Ophthalmologyand Visual Sciences, Eye, Ear, Nose and Throat Centre, UniversityHospital, Queen’s Medical Centre, Nottingham NG7 2UH, UK; [email protected]
Accepted for publication 13 May 2005
REFERENCES1 Gass JDM. Biomicroscopic and histopathologic considerations regarding the
feasibility of surgical excision of subfoveal neovascular membranes.Am J Ophthalmol 1994;118:285–98.
2 Sarks JP, Sarks SH, Killingsworth MC. Morphology of early choroidalneovascularisation in age-related macular degeneration: correlation withactivity. Eye 1997;11:515–22.
3 Killingworth MC. Angiogenesis in early choroidal neovascularisationsecondary to age-related macular degeneration. Graefes Arch Clin ExpOphthalmol 1995;233:313–23.
4 Liu X, Ye X, Yanoff M, et al. Regulatory effects of soluble growth factors onchoriocapillaris endothelial growth and survival. Ophthalmic Res1998;30:302–13.
5 Aird WC. Endothelial cell heterogeneity. Crit Care Med 2003;31:S221–S230.6 Fajardo LF. The complexity of endothelial cells. A review. Am J Clin Pathol
1989;92:241–50.7 Thorin E, Shreeve SM. Heterogeneity of vascular endothelial cells in normal
and disease states. Pharmacol Ther 1998;78:155–66.8 Rhodin JAG. Ultrastructure of mammalian venous capillaries, venules and
small collecting veins. J Ultrastruct Res 1968;25:452–500.9 Graier WF, Holzmann S, Hoebel BG, et al. Mechanisms of L-NG
nitroarginine/indomethacin-restant relaxation in bovine and porcine coronaryarteries. Br J Pharmacol 1996;119:1177–86.
10 Imegwu OJ, Entersz I, Graham AM, et al. Heterotypic smooth muscle cell/endothelial cell interactions differ between species. J Surg Res 2001;98:85–8.
11 Ram JI, Hiebert LM. Dextran sulfate protects porcine but not bovinecultured endothelial cells from free radical injury. Can J Vet Med2003;67:81–7.
12 Lehmann I, Brylla E, Sittig D, et al. Microvascular endothelial cells differ intheir basal and tumor necrosis factor-alpha-regulated expression of adhesionmolecules and cytokines. J Vasc Res 2000;37:408–16.
13 Craig LE, Spelman JP, Strandberg JD, et al. Endothelial cells from diversetissues exhibit differences in growth and morphology. Microvasc Res1998;55:65–76.
14 Muller AM, Hermanns MI, Skrzynski C, et al. Expression of the endothelialmarkers PECAM-1, vWf, and CD34 in vivo and in vitro. Exp Mol Pathol2002;72:221–9.
15 Muller AM, Hermanns MI, Cronen C, et al. Comparative study of adhesionmolecule expression in cultured human macro- and microvascular endothelialcells. Exp Mol Pathol 2002;73:171–80.
Figure 5 Phase contrast photomicrograph of human ICECs 3 hoursafter seeding onto Matigel showing typical capillary-like tubes (206original magnification).
Figure 6 Transmission electron micrograph of a lumen of a capillary-like tube surrounded by ICECs. The cells are joined by tight junctions(higher magnification in inset) and project villi into the lumen(bar = 2 mm).
1346 Browning, Gray, Amoaku
www.bjophthalmol.com

16 Yang QR, Smets RME, Neetens A, et al. Human retinal pigment epithelialcells from different donors continuously produce a vascular endothelialcell-stimulating factor into serum free medium. J Cell Sci1993;104:211–18.
17 Sakamoto T, Ishibashi T, Kimura H, et al. Effect of Tecogalan sodium onangiogenesis in vitro by choroidal endothelial cells. Invest Ophthalmol Vis Sci1995;36:1076–83.
18 Zubilewicz A, Hecquet C, Jeanny JC, et al. Proliferation of CECs requires dualsignaling through both MAPK/ERK and PI 3-k/AKT pathways. InvestOphthalmol Vis Sci 2001;42:488–96.
19 Liu X, Ye X, Yanoff M, et al. Extracellular matrix of retinal pigment epitheliumregulates choriocapillaris endothelial survival in vitro. Exp Eye Res1997;65:117–26.
20 Folkman J, Haudenschild CC, Zetter BR. Long term culture of capillaryendothelial cells. Prog Natl Acad Sci 1979;76:5217–21.
21 Robinson G, Gray T. Electron microscopy 2: practical procedures. In:Bancroft JD, Stevens A, eds. In:Theory and practice of histologicaltechniques.4th ed. London: Churchill Livingstone, 1996:585–626.
22 Browning AC, Shah S, Dua HS, et al. Alcohol debridement of the cornealepithelium in PRK and LASEK: an electron microscopic study. InvestOphthalmol Vis Sci 2003;44:510–3.
23 Sakamoto T, Sakamoto H, Hinton DR, et al. In vitro studies of human choroidalendothelial cells. Curr Eye Res 1995;14:621–7.
24 Penfold PL, Wen L, Madigan MC, et al. Modulation of permeability andadhesion molecule expression by human choroidal endothelial cells. InvestOphthalmol Vis Sci 2002;43:3125–30.
25 Nuel IP. De la vascularisation de la choroide et de la nutrition de la retineprincipalement au niveau de la fovea centralis. Arch D’Ophtal1892;12:70–87.
26 Saltzmann M. The anatomy and histology of the human eyeball in the normalstate. Leipzig, Chicago: Franz Deuticke, 1912:52–63.
27 Silverman MD, Zamora DO, Pan Y, et al. Cell adhesion molecule expressionin cultured human iris endothelial cells. Invest Ophthalmol Vis Sci2001;42:2861–6.
28 Hull MA, Hewett PW, Brough JL, et al. Isolation and culture of human gastricendothelial cells. Gastroenterology 1996;111:1230–40.
29 WongHC, BoultonM,Marshall J,et al.Growthof retinal capillary endothelia usingpericyte conditioned medium. Invest Ophthalmol Vis Sci 1987;28:1767–75.
30 Duff SE, Li C, Garland JM, et al. CD105 is important for angiogenesis:evidence and potential applications. FASEB J 2003;17:984–992.
31 Yasukawa T, Kimura H, Tabata Y, et al. Active drug targeting withimmunoconjugates to choroidal neovascularisation. Curr Eye Res2000;21:952–61.
32 Bevilacqua MP, Pober JS, Mendrick DL, et al. Identification of an inducibleendothelial-leukocyte adhesion molecule. Proc Natl Acad Sci1987;84:9238–42.
Isolation of inner choroidal endothelial cells 1347
www.bjophthalmol.com

SCIENTIFIC REPORT
An experimental study on the effect of encircling bandprocedure on silicone oil emulsificationD J de Silva, K S Lim, W E Schulenburg. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1348–1350. doi: 10.1136/bjo.2004.063768
Aim: Silicone oil is a useful tamponading material used incomplex vitroretinal surgery. However, the use of silicone oilis associated with emulsification which can lead to visionthreatening complications. The authors developed an experi-mental model to study the effect of encircling band on siliconeoil emulsification.Methods: Two identical artificial eye chambers were con-structed with circumferential indentations placed at thesphere’s equator (mimicking an encircling band indentation),and filled with varying amounts of Silicone Oil 1000centistrokes (Adato, Bausch and Lomb, UK) and balancedsalt solution. The chambers were then placed on a horizontalrotating shaker, mimicking physiological saccadic eye move-ments, which spun the chambers at 100 Hz for 5 days at37 C. Emulsification was then quantified by dark fieldmicroscopy, digital photography, and manual counting bya masked observer.Results: The mean (standard deviation (SD)) values ofsilicone emulsification bubbles were as follows: in the 90%silicone oil filled chamber with no encircling band, 139.1 (SD313.4); in the 90% silicone oil filled chamber with encirclingband, 10.9 (SD 22.2) (p,0.0001); in the 75% silicone oilfilled chamber with no encircling band, 103.6 (SD 272.6); inthe 75% silicone oil filled chamber with encircling band, 18.5(SD 32), (p = 0.001).Conclusions: The emulsification of silicone oil results fromfriction between the silicone oil and aqueous liquids. Theresults from this study suggest silicone oil emulsification isreduced by (1) more complete silicone oil fill and (2)indentation from an encircling band. The authors hypothesisethat both these measures resulted in reduced emulsificationby reducing silicone oil/aqueous movement and resultingshearing forces.
The management of complicated retinal detachment isfrequently facilitated by the use of intravitreal materialsthat assist with retinal reapposition. Silicone oil is a
useful tamponading material used in complex vitroretinalsurgery. However, the use of silicone oil is associated withemulsification which can lead to vision threatening compli-cations such as silicone keratopathy and secondary glau-coma.1–3 We developed an experimental model using anartificial eye chamber and mechanical shaker to assesswhether the use of an encircling band or varying levels ofsilicone oil fill would effect silicone oil emulsification.
METHODSTwo identical artificial eye chambers were constructed usingclear perspex. Each sphere was constructed of two perspexhalves that were sealed together with four bolts (fig 1) Eachchamber had a spherical volume of 4 ml and a single access
port to allow easy filling of the chamber. One model had acircumferential band placed at the sphere’s equator thatmimicked an encircling band indentation height of 1.5 mm.One chamber with no encircling band was filled with 90%Silicone Oil 1000 centistrokes (Adato, Bausch and Lomb, UK)and 10% balanced salt solution, this is considered to be thecontrol. A second chamber with an encircling band was filledwith 90% silicone oil and 10% balanced salt solution. Theexperiment was repeated with the two chambers filled with75% silicone oil. Syringes were used to inject the liquids intothe eye chamber and care taken to avoid mixing of the liquidsor the introduction of air bubbles. The two liquids formedtwo immiscible phases when injected into the chambers, withthe silicone oil forming the upper phase. The two eyechambers with the encircling band positioned in the verticalmeridian were then placed on a horizontal rotating shaker.The shaker mimicked physiological saccadic eye movementsand spun the chambers at 100 Hz for 5 days at 37 C. Allexperiments were repeated five times. An emulsifying agentwas not used; however the eye chambers were immediatelyopened and the contents emptied, thereby not allowingsufficient time for the two mediums to separate. The order ofthe opening with and without an encircling band wasalternated. The extent of emulsification was then quantifiedby dark field microsopy, using a magnification factor of610.Ten random digital photographs (fig 2) were taken in thecentral field of view, quantification was done by manualcounting of emulsification bubbles by a masked observer, andthe mean number of emulsification bubbles for eachindividual eye chamber was calculated, using a previouslydescribed technique.4
RESULTSExamples of the dark field photographs from the silicone oilwith emulsification are shown in figure 2. Results are shownin table 1 and figure 3. The Mann Whitney non-parametrictest was used to analyse the results; 90% silicone oil filledchamber with no encircling band was the control.Emulsification was significantly reduced in the eye
chambers with an encircling band in both the 90% and 75%silicone oil filled models. The mean of emulsification bubbleswere also significantly lower in the 90% oil filled withencircling band compare to 75% oil filled with encirclingband (p=0.001).
DISCUSSIONSilicone oil emulsification is a key factor in the complicationsof silicone oil use as an intraocular tamponade. Previousstudies have investigated physiochemical properties of thesilicone oil and their role in emulsification. The purpose ofour experiment was to assess physical factors that mayreduce silicone oil emulsification in vitro. We comparedsilicone oil emulsification in two identical eye chambersassessing the use of an encircling band and a more completefill of silicone oil.
1348
www.bjophthalmol.com

Silicone keratopathy, cataract formation, and siliconeretinopathy have been attributed with silicone oil toxicityand their physiochemical properties.2 5 Silicone oil dropletsgenerated by emulsification may enter the anterior chamberthrough an intact zonular framework and droplets have beenfound in the trabecular meshwork, iris, ciliary body, retina,and optic nerve.6 7 Silicone oil droplets can enter the anteriorchamber angle and may lead to refractory glaucoma. Visionthreatening complications may result from silicone oilemulsification and may occur over a spectrum of thepostoperative period, removal of the oil may not reverse itstoxic effects.3 7 The mechanism of silicone oil induced toxicityremains unclear.5
Previous studies have found multiple factors effecting theemulsification of silicone oil: viscosity of silicone oil, surfacetension agents, and fraction of silicone oil.4 Emulsification isdefined as a dispersion of fine liquid particles in anotherliquid medium and results from shearing forces between thetwo mediums, causing droplets to be pinched off into theother medium due to surface tension. Droplets start at theinterface of the two liquids and give rise to an emulsion. Forthe emulsification to progress, kinetic energy is required andmay be counteracted by surface agent stabilisers.5 The processundergoes three stages—creaming, flocculation, and coales-cence—and is characterised by the accumulation of fine oildroplets on the surface of the intraocular fluids. The processof coalescence results in a variation of droplet size and isaided in vivo by the presence of emulsifiers.8–10 Low molecularweight components such as phospholipids, proteins, and ionsare likely to influence the emulsification process, howevertheir role in vivo is not known.4 Our results were consistentwith previous models of silicone oil emulsification: thebubbles were stable, demonstrated regular borders, and
showed a variation in size.4 Emulsification occurs at theinterface between the silicone oil and aqueous layers as aconsequence of shearing forces. In vivo, some aqueous fluidis likely to line the wall of the eye and emulsification mayoccur both at the wall and at the silicone oil/aqueousinterface.A number of studies have looked at the use of experimental
eye chambers and the use of silicone oil as a tamponadingagent.11–15 Perspex, a hydrophilic material, is a material whichmimics the surface properties of the retina. In addition, theuse of a protein solution to coat the surface of the artificial
Figure 1 (A) Two artificial eyechambers placed on a horizontalrotating shaker. (B) Two artificial eyechambers; the right chamber contains acircumferential plastic band placed atthe sphere’s equator which mimickedencircling band indentation.
Figure 2 Dark field photomicrographs (610) demonstrating effects ofencircling band procedure on silicone oil emulsification. (A) Silicone oilbubbles of the 90% silicone oil filled eye chamber without encirclingband. (B) Silicone oil bubbles of the 90% silicone oil filled chamber withencircling band.
500
400
300
200
100
0
Experiment number
90% SO unbanded
Silic
one
oil e
mul
sific
atio
nbu
bble
s/m
ean
num
ber
1 2 3 4 5
90% SO banded
A
500
400
300
200
100
0
Experiment number
75% SO unbanded
Silic
one
oil e
mul
sific
atio
nbu
bble
s/m
ean
num
ber
1 2 3 4 5
75% SO banded
B
Figure 3 Graphs showing silicone oil emulsification in the eyechambers with and without encircling band. (A) 90% silicone oil filled.(B) 75% silicone oil filled.
Table 1 Silicone emulsification in the eye chambers withand without encircling band
Silicone oil emulsification,mean (SD) p Value*
90% silicone oil filled withoutencircling band
139.1 (313.4)
90% silicone oil filled withencircling band
10.9 (22.2) ,0.0001
75% silicone oil filled withoutencircling band
103.6 (272.6) 0.001
75% silicone oil filled withencircling band
18.5 (32.0) 0.039
*Mann-Whitney non-parametric test.
Silicone oil emulsification 1349
www.bjophthalmol.com

eye chamber has been found to further represent the contactof silicone oil to the retina in vivo. In this experiment wechose not to coat the chamber with protein—a layer ofprotein may not impact on emulsification as the interface of athin film of aqueous solution may not deform sufficiently tocause emulsification into the film. In addition, shaking thechambers at 100 Hz may cause the protein layer to detachfrom the artificial chamber walls. We believe our model isvalid, and offers some insight into the effects of encirclingband procedure on silicone oil emulsification.The results from this study suggest two important factors
in the process of emulsification of silicone oil and how thisprocess may be reduced: (1) the more complete the siliconeoil fill in the eye chamber, the lower the level of silicone oilemulsification and (2) the indentation from the encirclingband exerted a stabilising effect on the silicone oil globuleduring eye movement resulting in reduced shearing forcesand silicone oil emulsification.The results of our experiment may be explained by the
physical properties of silicone oil and its interaction with theartificial eye chamber. The contact angle between the siliconeoil and the artificial eye chamber is small, and to induce an180˚ tamponade, an 80% fill is estimated.11 It follows thatwith an increased silicone oil fill, the total area of contactbetween silicone oil and the surrounding aqueous layer isincreased. With an increased silicone oil fill we propose thatthe increased size of the silicone oil bubble resulted inreduced movement of the silicone oil and aqueous layers.This resulted in an increased stability, a reduction of shearingforces, and silicone oil emulsification.Encircling scleral buckle procedure induces a geometric
alteration in the anatomy of the eye. This configurationalchange influences both axial length and induces indentationof the globe resembling an hourglass shape.12 13 The influenceof an encircling band in our artificial model eye resulted asignificant reduction of silicone oil emulsification. Wehypothesise that the encircling band leads to reducedemulsification by reducing silicone oil/aqueous movementand resulting shearing forces.Silicone oil emulsification can lead to vision threatening
complications and removal of the oil may not reverse thesechanges. Our in vitro experiments suggest an encircling bandprocedure and increased silicone oil fill may result in reducedsilicone oil emulsification.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
D J de Silva, K S Lim, W E Schulenburg, Western Eye Hospital,Marylebone Road, London, UKK S Lim, Ocular Repair and Regeneration Biology Unit and Departmentof Pathology, Institute of Ophthalmology, London, UK
Sponsor details: none.
Competing interests: none declared
Correspondence to: Mr W E Schulenburg, Consultant inOphthalmology, Western Eye Hospital, Marylebone Road, LondonNW1 5YE, UK; [email protected]
Accepted for publication 18 April 2005
REFERENCES1 Leaver PK, Grey RHB, Garner A. Complications following silicone injection.
Mod Probl Ophthalmol 1979;20:290–4.2 Gabel VP, Kampik A, Burkhardt J. Analysis of intraocularly applied silicone
oils of various origins. Graefes Arch Clin Exp Ophthalmol 1987;225:160–2.3 Laqua H, Lucke K, Foerster MH. Development and current status of silicone oil
surgery. Klin Monatsbl Augenheilkd 1988;192:277–83.4 Crisp A, de Juan E Jr, Tiedeman J. Effect of silicone oil viscosity on
emulsification. Arch Ophthalmol 1987;105:546–50.5 Heidenkummer HP, Kampik A, Thierfelder S. Emulsification of silicone oils
with specific physicochemical characteristics. Graefes Arch Clin ExpOphthalmol 1991;229:88–94.
6 Valone J Jr, McCarthy M. Emulsified anterior chamber silicone oil andglaucoma. Ophthalmology 1994;101:1908–12.
7 Kirchhof B, Tavakolian U, Paulmann H, et al. Histopathological findings ineyes after silicone oil injection. Graefes Arch Clin Exp Ophthalmol1986;224:34–7.
8 Nakamura K, Refojo MF, Crabtree DV. Factors contributing to theemulsification of intraocular silicone and fluorosilicone oils. Invest OphthalmolVis Sci 1990;31:647–56.
9 Becher P, ed. Encyclopedia of emulsion technology, Vol 2: Applications. NewYork: Marcel Dekker, 1985:1–69.
10 Sherman P. Emulsion science. London: Academic Press, 1968:59–65.11 Fawcett IM, Williams RL, Wong D. Contact angles of substances used for
internal tamponade in retinal detachment surgery. Graefes Arch Clin ExpOphthalmol 1994;232:438–44.
12 Wong D, Williams RL, German MJ. Exchange of perfluorodecalin for gas oroil: a model for avoiding slippage. Graefes Arch Clin Exp Ophthalmol1998;236:234–7.
13 Williams R, Wong D. The influence of explants on the physical efficiency oftamponade agents. Graefes Arch Clin Exp Ophthalmol 1999;237:870–4.
14 Herbert E, Stappler T, Wetterqvist C, et al. Tamponade properties of double-filling with perfluorohexyloctane and silicone oil in a model eye chamber.Graefes Arch Clin Exp Ophthalmol 2004;242:250–4.
15 Wetterqvist C, Wong D, Williams R, et al. Tamponade efficiency ofperfluorohexyloctane and silicone oil solutions in a model eye chamber.Br J Ophthalmol 2004;88:692–6.
1350 de Silva, Lim, Schulenburg
www.bjophthalmol.com

EXTENDED REPORT
Contribution to comprehension of image formation inconfocal microscopy of cornea with Rostock cornea moduleR Bochert, A Zhivov, R Kraak, J Stave, R F Guthoff. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr Ralf Bochert RobertKraak, Universitat Rostock,Universitatsaugenklinik,Doberaner Strasse 140, D-18055 Rostock, Germany;[email protected]
Accepted for publication1 February 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1351–1355. doi: 10.1136/bjo.2004.063743
Aim: To investigate the influence of refractive index of aqueous humour on imaging of cornealendothelium in confocal microscopy. To clarify the phenomenon of dark endothelial and bright epithelialcell membranes in confocal images of corneas.Methods: Use of a novel digital confocal laser scanning microscope, a combination of the Heidelbergretina tomograph (HRT II) and the Rostock cornea module. Exchange of aqueous humour solution fromdomestic pigs against glycerol/water solutions (refractive indices g=1.33721.47). Transelectronmicroscopy of endothelial and epithelial cell morphology.Results: Under the terms of variable refractive indices no differences were observed for general imaging ofendothelium. Bright cells were bordered by dark cell membranes in all experiments. Electron microscopy ofendothelium and epithelium revealed differences in intracellular and cell membrane structure of both celltypes.Conclusion: Source of specific confocal optical behaviour of endothelium does not come from interfaceconditions to aqueous humour, but may result from intracellular variations and ultrastructure of cellmembranes.
Confocal in vivo microscopy is becoming a usefuldiagnostic tool for corneal imaging.1–4 Normal cornealmorphology has been described intensively by in vivo
confocal microscopy.5 The only source of image contrast inconfocal microscopy arises from the interaction of theincident light beam with the specimen. This interaction iscomplex and may include absorption, fluorescence, refrac-tion, reflection, phase shift, scattering, or changes inpolarisation on cell structures and cell components.Contrast can be defined as the difference in signal strengthbetween various parts of an image or between details ofinterest and the background.6 A modern digital confocal laserscanning microscope, comprises the combination of Rostockcornea module with conventional Heidelberg retina tomo-graph (HRT II), makes in vivo imaging of the human corneapossible. Like other confocal microscopes, the Rostock corneamodule uses backscattered light, where the light signalproceeds from an interaction with the specimen towards thedetector.The main variables influencing confocal optical behaviour
of an object are refraction index, surface structure, and depthwithin tissue. The backscattered light signal strengthdepends of the degree of reflection which depends on thegradient of the refractive index (g) between two media.6 Thesmaller the difference in g between the two media, the loweris the reflectance (the ratio of illumination intensity toreflected intensity). The refractive indices are approximatelyg=1.37 for cytoplasm, g=1.45 for lipid cell membrane,7 and1.336 for aqueous humour.8 Furthermore, the reflectancedepends on the surface structure of the objects in the focalplane. Highest reflectance occurs on smooth surfaces, but ona rough surface the reflectance decreases as the tilt angle of astructure within the specimen increases. In living specimensthe image contrast degrades as the objective lens focusesdeeper into the tissue. Small structures, with an g differentfrom that of the surrounding medium and in the optical path,can cause pronounced degradation of image quality byscattering both the excited and the backscattered light. Incorneal confocal microscopy, differences are visible between
imaging of cells in the epithelium and the endothelium. Allcells of the five to six cellular layers of the epithelium arevisible with bright cell borders and dark homogeneouscytoplasm. In contrast, the one layer of endothelial cells atthe border of the anterior chamber is pictured with dark cellborders and bright cytoplasm.6
This study describes to what extent the refractive index, g,of aqueous humour and the overlying cell layers affects theimage formation of the corneal endothelium. A simplestacking experiment of two corneas is used to describepotential influence of focal depth within tissue on back-scattered light intensity. Electron microscopic investigationmagnifies morphological structures of different cell types forcomparison.
MATERIAL AND METHODSConfocal microscopyA novel digital confocal laser scanning microscope (LSM), acombination of the Heidelberg retina tomograph (HRT II)and the Rostock cornea module (Heidelberg EngineeringGmbH) was used.9 The LSM has a computer controlledhydraulic linear scanning device (Nikon hydraulic manip-ulator, Tokyo, Japan) and a water contact objective (Zeiss,636/NA 0.95 W). A diode laser emits a beam of 670 nmwavelength. One enucleated eye ball of a domestic pig wasfixed in front of the LSM objective. The eye was in closecontact with a Plexiglas disc, which covered the LSMobjective and allowed the objective to move in z-axis whilethe eye rested in close contact to the Plexiglas surface. A dropof carbomer gel (Visidic, Dr Mann Pharma, Berlin, Germany)served as the coupling medium. A feature of the LSM is theability to perform hydraulic z-scans, beginning from thecontact area of the Plexiglas disc/surface of the cornea to amaximum of 2000 mm depth. The actual focus depth withinthe cornea is displayed. The saving of images (3006300 mmcorneal area) of all layers from the superficial epithelium to
Abbreviations: FDTD, finite difference time domain; LSM, laserscanning microscope
1351
www.bjophthalmol.com

endothelium of the corneas is possible. A digital colour photocamera at one side can be use to assess and document thealignment of eye within laser beam.All image contrast arises from the interaction of the
incident light beam with the object. The focus depth of theLSM is 10 mm. This is the volume (voxel) which is imaged bythe confocal microscope to form an image pixel. Allinvestigations were performed in the central region of thecornea.Investigation objects were eyeballs from the domestic pig
(Sus scrofa f domestica). Domestic pigs were about 6 monthsold and slaughtered in the research institute for the biologyof farm animals (Dummerstorf, Germany).To clarify the extent of several variables on image
formation different study designs were used. Changes ofconditions at the interface endothelium/aqueous humourdescribe the influence of refractive index. The amount ofweakening on laser beam through tissue layers overlying thefocal plane describes an experiment of two corneas. Divergentfrom numerical measurement of intrinsic light scatteringintensity as a useful objective parameter, only the clear visiblescattering contrast of cytoplasm and cell membranes wasused for evaluation. Additionally, electron microscopicinvestigation magnifies morphological structures of differentcell types for comparison.
Experiment 1To test the influence of refractive index, g, on imaging of theendothelial cells a dilution series of glycerol (Merck,Germany) and distilled water was made (table 1). Therefractive index value of each solution was measured bymeans of an Abbe refractometer model G (C Zeiss Jena,Germany).Altogether, 18 eyes (three per set) were used. Eyeballs of
domestic pigs were prepared for investigation as followed.The cornea was punctured peripherally with a small needleand the aqueous humour was extracted with a syringe. Theanterior chamber was subsequent filled by injecting one ofthe glycerol/water solutions. This procedure took 2 minutesand endothelium was then imaged by the confocal micro-scope.
Experiment 2To test the amount of contrast degradation of the cell layersoverlying the endothelium, two eyeballs were used simulta-neously. A portion of the central cornea with a diameter ofabout 6 mm was cut from one eyeball (specimen 1). Thispiece of cornea was placed on top with the endothelium sideof the epithelium of specimen 2. A drop of carbomer gel(Visidic, Dr Mann Pharma, Berlin, Germany) served ascoupling medium. This double cornea was then imaged bythe confocal microscope.
Trans-electron microscopyCorneas of domestic pigs were prepared for trans-electronmicroscopic investigation. Specimens were fixed with 4%
glutaraldehyde in 0.2 M Sorrensen’s phosphate buffer(pH 7.4) for 2 hours and then post-fixed with 1% osmiumtetroxide for 1 hour. After dehydration in acetone, thecorneas were embedded in araldite. Sections were contrastedby immersion in saturated uranyl acetate solution in 50%methanol for 30 minutes and Reynolds lead citrate solutionfor 4 minutes. Ultrathin sections parallel to corneal surface ofthe epithelium and the endothelium were examined under aZeiss EM 902A electron microscope.
RESULTSExperiment 1The exchange of aqueous humour against different solutionsof glycerol/water revealed relatively clear imaging of theendothelium. Under refractive index values from 1.337 to1.47, no differences in endothelium morphology were seen.In all investigations the cells were revealed with dark cellborders and bright cytoplasms (fig 1). Additionally, darkspots in the cytoplasm at 20%, 60%, and 100% glycerol/watersolution were visible, denoting the nuclei of each cell.
Experiment 2Confocal image of the corneal endothelium of specimen 1showed normal appearance. Dark cell borders, brightcytoplasm, and dark cell nuclei were visible. The contrast ofepithelial cells of a second underlying cornea of specimen 2was noticeably reduced. Nevertheless, the normal picture wasrecognisable. Superficial and wing epithelial cells showedbright cell membranes, bright nuclei, and dark cytoplasm(fig 2).
Trans-electron microscopyElectron microscopic investigations showed the polygonalshape of the wing cells of the corneal epithelium (fig 3A). Thecell membranes of this layer show deep interdigitations(fig 3B). Numerous desmosomal junctions join these cells toeach other. The cytoplasm of the wing cells contained onlymoderate numbers of small thin mitochondria. Vesicles ofdifferent size were a prominent finding in the cytoplasm. Theoval nuclei contained dense packages of heterochromatin.The lateral cell membranes between adjacent endothelialcells appeared smooth and showed no complex interdigita-tions. Desmosomes were lacking (fig 4). With respect to theanterior-posterior axis of the cornea, the lateral cell mem-branes of the endothelium have an oblique and tortuouscourse. The endothelial cell cytoplasm is rich in organelles.The numerous mitochondria are elongated and their cristaeare oriented longitudinally. Both rough and smooth surfacedendoplasmic reticulum were present. The oval nuclei showeda homogeneous appearance without dense heterochromatin.
DISCUSSIONThe source of contrast in backscattered confocal microscopicimages of living species is based upon a variety of physicalprocesses and species specific morphological, anatomical, andbiochemical conditions. The incident light beam interacts inmultiple ways with structures of the object in and above thefocus plane of the objective.6 The specific source of contrast inbackscattering confocal microscopy of detailed cellularstructures, such as cell membranes, organelles, or cytoplasmwithin a tissue layer of a living object—for instance, thecornea, is not measurable directly.Scattering in tissue arises from local changes in the index
of refraction between cell components and other small tissuestructures, and the scale over which these changes occurvaries from tissue to tissue.10 The amount of scattered lightdepends on changes in local absorption and transmission.The light could be further affected by these differentprocesses again, while the backscattered beam passes
Table 1 Refractive index values of a dilutionseries of glycerol and distilled water
Percentage glycerol/distilled water gD (20)
5% 1.33720% 1.35540% 1.38160% 1.41180% 1.440100% 1.470
1352 Bochert, Zhivov, Kraak, et al
www.bjophthalmol.com

different tissue layers again on the way to the detector. Inaddition to light intensity loss by virtue of these processes,amplification could occur as a result of the forward scatteringof local structures. The calculated scatter intensity of smallorganelles is about 5000 times higher in the forward directionof the light beam than backwards.10
Confocal imaging of the cornea in vivo revealed obviousdifferences in contrast of similar cellular structures.5 Cellmembranes of the epithelium are illuminated more brightlythan equivalent endothelial membranes. Conditions of thecytoplasm are reversed. The refractive index differs forvarious cellular structures and averages—for extracellularfluid g=1.35–1.36, for cytoplasm g=1.36–1.375, for nucleig=1.38–1.41, for mitochondria and organelles g=1.38–1.41, for dried protein g=1.58, for cell membrane g=1.47,and for lipid g=1.48.11–16 Endothelial cells border theanterior chamber with a conspicuously lower refractive indexof aqueous humour of g=1.336,8 whereas epithelial cells lieembedded in layers of similar refractive conditions atg.1.35. Our study showed that variation of the refractiveindex from 1.337–1.47 of the anterior chamber produced nodifferences in image contrast of endothelial cell structures.The endothelium showed for all cases dark cell borders andbright cytoplasm. Hence, the location of the endothelial layerat the interface to aqueous humour was not the source ofvarying optical behaviour of epithelial and endothelial cellsbecause of higher refraction index differences.These differences are also not explainable by loss of
intensity, as the effect of overlying structures, if the lightgoes back from the endothelium, through about 500–600 mmbroad cellular structures to the detector. The imaging of asecond epithelial cell layer underlying the first corneal
endothelium revealed in fact lower image quality as a resultof experimental arrangement and procedure, but brightcontrasted cell membranes and bright nuclei were visibleduring our experiment.There are some morphological differences between
endothelial and epithelial cells found by our trans-electronmicroscopic investigations. The cell membranes of epitheliumcontained many desmosomes and showed deep interdigita-tions. In contrast, desmosomes were lacking in endothelium,and cell membranes were smooth. Cell membranes consist oflipids. The membrane interdigitations lead to an abidingappearance of media interfaces with refractive index for lipidof g=1.48 and for cytoplasm of g=1.48. Reflection occursat each interfacing media. For the protein rich desmosomes avalue of g.1.5 could be assumed, given that dried proteinhas a refractive index of g=1.58.15 Therefore, the highconcentration of desmosomes could be the source for cellmembrane brightness in epithelial images.Our ultrastructural investigations revealed large numbers
of mitochondria in endothelial cells, whereas the number oforganelles in epithelial cells was much lower. The effects ofvarious organelles and size of nucleus on the far fieldscattering patterns of cells were examined with a mathema-tical model, the finite difference time domain (FDTD)method.10 The scattering patterns were computed for cellscontaining different organelles to determine the effect ofeach cell component on the total amount of scatter.Scattering functions of two cells with diameters of 11 mmwere calculated. In the first case the cell contained only anucleus, membrane, and cytoplasm, in the second case smallorganelles have been added to the cell. The scattering from acell was highly peaked in the forward direction.10 Small
Figure 1 Confocal images ofendothelium of domestic pig eyes. Theanterior chamber was filled withglycerol/water solution of (A) 5%(gD=1.337), (B) 20% (gD=1.355), (C)60% (gD=1.411), and (D) 100%(gD=1.47). Magnification 6240.
Image formation in confocal microscopy 1353
www.bjophthalmol.com

organelles can have a large effect on the scattering pattern.The total amount of scattered light was 1.7 times greater forthe cell with small organelles than for the same cell withoutthe organelles.10 This predicts that the small organelles cancontribute significantly to the total scattering. Cells contain-ing large nuclei (diameter 6 mm) cause increasing amounts ofscattering relative to cells with smaller nuclei (diameter3 mm). In the absence of a nucleus, the amplitude of thescattering pattern decreased further.10
Our investigations were performed on pig eyes ex vivo. Incontrast, this confocal system is applicable to in vivodiagnosis of the human cornea. The experimental use ofhuman eyes is not practicable in vivo and has ethical practicaldifficulties ex vivo. Therefore, domestic pig eyes, withcomparable corneal morphology, are a good study object.However, tissues of ex vivo objects undergo several processessuch as cell hydration, and this may change their opticalbehaviour. The extent of this problem is hard to ascertain.Our confocal observations of pig eyes ex vivo in sequencesover a 24 hour period revealed corneal thickening on account
of stromal hydration, but the optical behaviour of cellsremained similar.By means of in vivo confocal microscopy, many corneal
diseases have been described, as changes in the physiologicalstructure of the tissue produce changes in the contrast ofobtained images.5 However, the ability to differentiatebetween normal and abnormal tissue depends on the abilityto interpret the source of reflected light within the sample.Our study contributes to the clinical application of theRostock cornea module and to confocal laser microscopy ingeneral. Observed variations of optical behaviour of cornealendothelium are a result of cell physiology, cell structure, andcell ingredients in the first place. Comparative studiesincluding confocal microscopy and conventional microscopichistology are necessary for further understanding the sourcesof image contrast.
Figure 2 Confocal images of two stacker domestic pig corneas. (A)Endothelium of specimen 1 lying above specimen 2. (B) Superficial cellsof specimen 2. (C) Wing cells of specimen 2. Magnification6240
Figure 3 Ultrathin sections of epithelial cells of domestic pig eyes.Magnification61500.
Figure 4 Ultrathin section of endothelial cells of domestic pig showingsmooth cell membrane, numberous mitochondria, and homogeneousnuclei. Magnification612 000.
1354 Bochert, Zhivov, Kraak, et al
www.bjophthalmol.com

ACKNOWLEDGEMENTSThe authors thank Professor Jonas of the Institute of Pathology at theUniversity of Rostock for use of the electron microscope, and we aregrateful to G Fulda for technical assistance. Many thanks to Angus, anative English speaker from Cambridge, for linguistic editing of themanuscript.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
R Bochert, A Zhivov, R Kraak, J Stave, R F Guthoff, Department ofOphthalmology, University of Rostock, Doberaner Strasse 140, 18055Rostock, Germany
REFERENCES1 Calvillo MP, McLaren JW, Hodge DO, et al. Corneal reinnervation after
LASIK: prospective 3-year longitudinal study. Invest Ophthalmol Vis Sci2004;45:3991–6.
2 Nakano E, Oliveira M, Portellinha W, et al. Confocal microscopy in earlydiagnosis of Acanthamoeba keratitis. J Refract Surg 2004;20(Suppl):737–40.
3 Patel S, McLaren J, Hodge D, et al. Normal human keratocyte density andcorneal thickness measurement by using confocal microscopy in vivo. InvestOphthalmol Vis Sci 2001;42:333–9.
4 Guell JL, Velasco F, Guerrero E, et al. Confocal microscopy of corneas with anintracorneal lens for hyperopia. J Refract Surg 2004;20:778–82.
5 Mastropasqua L, Nubile M. Confocal microscopy of the cornea. Thorofare,NJ: Slack, 2002.
6 Cheng PC, Kriete A. Image contrast in confocal light microscopy. In: Pawley JB,eds. Handbook of confocal microscopy. New York: Plenum Press,1995:281–310.
7 Smithpeter C, Dunn A, Drezek R, et al. Near real time confocal microscopy ofcultured amelanotic cells: sources of signal, contrast agents and limits ofcontrast. J Biomed Opt 1998;3:429–36.
8 Laing RA, Sandstrom MM, Leibowitz HM. Clinical specular microscopy. II.Qualitative evaluation of corneal endothelial photomicrographs. ArchOphthalmology 1979;97:1720–25.
9 Stave J, Zinser G, Grummer G, et al. Modified Heidelberg retinal tomographHRT. Initial results of in vivo presentation of corneal structures. Ophthalmologe2002;99:276–80.
10 Dunn A, Smithpeter C, Welch AJ, et al. Finite-difference time-domainsimulation of light scattering from single cells. J Biomed Opt1997;2:262–6.
11 Maier J, Walker S, Fantini S, et al. Possible correlation between blood glucoseconcentration and the reduced scattering coefficient of tissues in the nearinfrared. Opt Lett 1994;19:2062–4.
12 Liu H, Beauvoit B, Kimura M, et al. Dependence of tissue optical properties onsolute-induced changes in refractive index and osmolarity. J Biomed Opt1996;1:200–11.
13 Brunsting A, Mullaney P. Differential light scattering from sphericalmammalian cells. Biophys J 1974;14:439–53.
14 Beuthan J, Minet O, Helfman J, et al. The spatial variation of the refractiveindex in biological cells. Phys Med Biol 1996;41:369–82.
15 Barer R, Joseph S. Refractometry of living cells. Quart J Microscop Sci1954;95:399–423.
16 Maier J, Walker S, Fantini S, et al. Possible correlation between blood glucoseconcentration and the reduced scattering coefficient of tissues in the nearinfrared. Opt Lett 1954;19:2062–4.
Image formation in confocal microscopy 1355
www.bjophthalmol.com

EXTENDED REPORT
Hydroxyapatite promotes superior keratocyte adhesion andproliferation in comparison with current keratoprosthesisskirt materialsJ S Mehta, C E Futter, S R Sandeman, R G A F Faragher, K A Hing, K E Tanner, B D S Allan. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Mr J S Mehta, MoorfieldsEye Hospital, City Road,London EC1V 2PD, UK;[email protected]
Accepted for publication18 April 2005. . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1356–1362. doi: 10.1136/bjo.2004.064147
Aim: Published clinical series suggest the osteoodontokeratoprosthesis (OOKP) may have a lowerextrusion rate than current synthetic keratoprostheses. The OOKP is anchored in the eye wall byautologous tooth. The authors’ aim was to compare adhesion, proliferation, and morphology fortelomerase transformed keratocytes seeded on calcium hydroxyapatite (the principal mineral constituent oftooth) and materials used in the anchoring elements of commercially available synthetic keratoprostheses.Methods: Test materials were hydroxyapatite, polytetrafluoroethylene (PTFE), polyhydroxyethyl metha-crylate (HEMA), and glass (control). Cell adhesion and viability were quantified at 4 hours, 24 hours, and1 week using a calcein-AM/EthD-1 viability/cytotoxicity assay. Focal contact expression and cytoskeletalorganisation were studied at 24 hours by confocal microscopy with immunoflourescent labelling. Furtherstudies of cell morphology were performed using light and scanning electron microscopy.Results: Live cell counts were significantly greater on hydroxyapatite surfaces at each time point (p,0.04).Dead cell counts were significantly higher for PTFE at 7 days (p,0.002). ß1 integrin expression washighest on hydroxyapatite. Adhesion structures were well expressed in flat, spread out keratocytes on bothHA and glass. Keratocytes tended to be thinner and spindle shaped on PTFE. The relatively few keratocytesvisible on HEMA test surfaces were rounded and poorly adherent.Conclusions: Keratocyte adhesion, spreading, and viability on hydroxyapatite test surfaces is superior tothat seen on PTFE and HEMA. Improving the initial cell adhesion environment in the skirt element ofkeratoprostheses may enhance tissue integration and reduce device failure rates.
Corneal opacification is the second most common causeof world blindness affecting an estimated 10 millionpeople.1 Although endothelial failure is the most
common cause of corneal opacification in the developedworld, developing world populations—in which cornealblindness is far more prevalent—are typically blind as aresult of ocular surface disease leading to corneal neovascu-larisation and scarring.1 The prognosis for successful visualrehabilitation with conventional corneal grafting in thesepatients is often poor,2 and most of them have no access toallograft donor material. Exciting progress is currently beingmade in the development of tissue engineered alternatives tocadaveric corneal donor material.3 But, as with conventionalallograft material, collagen based constructs may fail tosustain a normal corneal epithelial phenotype or stromaltissue clarity in a hostile ocular surface environment.Techniques for promoting ocular surface regeneration4 5 thatcould be used in tandem with corneal tissue replacementcurrently require extensive laboratory back up and are notavailable, even in the developed world, outside specialistcentres. For the foreseeable future, the best hope of wideningaccess to treatment for corneal blindness probably lies in thedevelopment of an improved synthetic keratoprosthesis.6 7
Keratoprostheses incorporate a clear central optic and anannular porous surround, or skirt element, designed toprovide tissue integration.7 The osteoodontokeratoprosthesis(OOKP), consisting of an annular wafer of alveolar toothglued to a central polymethyl methacrylate optic has beenimplanted since the 1960s with continuing relative success.In particular, the device failure rate in association with poortissue integration for this keratoprosthesis would appear tobe significantly less than that for totally synthetic devices.8
Two totally synthetic keratoprostheses are currently available
commercially: the Legeais BioKpro III (FCI Ophthalmics,Paris, France) and the AlphaCor (Argus Biomedical, Perth,Australia). Published results from clinical series of patientsimplanted with the Legeais BioKpro I and II suggest that upto 40% of these devices fail within one year of implantation,9
with retraction of the surface tissues over the haptic elementof the device, retroprosthesis membrane formation, infection,or aqueous leakage necessitating device removal or revisionof implantation. Results have not yet been published for theLegeais BioKpro III, but this device incorporates the sameskirt material as earlier embodiments. Because inclusioncriteria vary between case series, direct comparison of resultsbetween devices is difficult. But problems with poor tissueintegration may be equally common with the AlphaCor Kpro.In a series of 40 implanted eyes followed for up to 36 months,the overall rate of surgical revision for complicationsassociated with poor tissue integration was 30%.10 Thesecases were a selected group comprised mainly of patientswith a normal ocular surface, and included 14 patients whohad not yet completed stage II of the implantation process inwhich the surface tissues are opened over the device optic.Most tissue integration problems are not clinically evidentuntil after this surgical stage.11 In contrast to these relativelypoor results for CE (Conformite Europeene) marked fullysynthetic Kpros, only five of 85 (5.8%) patients implantedwith the OOKP and followed for up to 16 years had clinicalproblems with tissue integration.8 Indications for implanta-tion in this series included severe ocular surface disease
Abbreviations: BSA, bovine serum albumin; Ethd-1, ethidiumhomodimer-1; HEMA, polyhydroxyethyl methacrylate; OOKP,osteoodontokeratoprosthesis; PBS, phosphate buffered saline; PTFE,polytetrafluoroethylene; PHEMA, poly(2-hydroxyethyl methacrylate).
1356
www.bjophthalmol.com

secondary to ocular cicatricial pemphigoid, Stevens-Johnsonsyndrome, and previous chemical injury. The skirt materialsused as a porous framework for tissue integration are porouspolytetrafluoroethylene (PTFE) in the Legeais BioKpro III,porous polyhydroxyethyl methacrylate (HEMA) in theAlphaCor device, and autologous tooth (biological calciumhydroxyapatite) in the OOKP.Stable tissue integration is vital for keratoprosthesis
survival. Fibroblast invasion and matrix deposition has beendemonstrated in vivo in preclinical studies of porous HEMA12
and PTFE13 explanted from rabbit corneal stroma. Butcomparative studies to determine whether the balancebetween matrix synthesis and degradation may be modifiedby the interfacial properties of different candidate kerato-prosthesis materials have not been performed in vivo.Sandeman et al14 have recently described a systematicapproach to the evaluation of novel keratoprosthesis materi-als based on polyurethane based interpenetrating co-poly-mers. Integral to the range of assays they describe are studiesof cell adhesion, viability, and morphology using a keratocytecell strain EK1.BR. As an initial step towards exploring thecellular basis for differential extrusion rates observedclinically between these leading contemporary keratopros-theses, we performed comparative studies of cell adhesion,survival, and morphology in standard culture conditionsusing telomerase transformed EK1.BR keratocytes seeded onplane surfaces of PTFE, HEMA, hydroxyapatite, and glass(control).Cellular interaction with the extracellular matrix is
mediated via integrins—that is, cell surface molecules whichlink the extracellular matrix to the actin cytoskeleton.15).Integrins are composed of an a and a b (18 a and 8 bsubunits) giving a diverse range of ab combinations withtheir own binding specificity and signalling properties; manyof the most widely expressed integrins contain the b1subunit. Clustering of integrins into supramolecular com-plexes (with cytoskeletal proteins and signalling molecules)is required to form focal contacts or adhesions. These serve asattachment sites to the underlying ECM and can also act assignalling centres regulating cell growth, survival, and geneexpression.16 Further comparative work was performed toanalyse the initial cellular interaction with the interfacialprotein layer coating candidate keratoprosthesis materialsincubated in serum enriched culture media by immunoflour-escent labelling to characterise the actin cytoskeleton, focalcontact, and b1 integrin expression.
MATERIALS AND METHODSCells and materialsTelomerase transformed keratocytes were used throughout.The EK1.BR embryonic keratocyte cell strain has previouslybeen characterised with respect to lifespan, fraction ofdividing cells, and maintenance of a keratocyte phenotypein culture.17
pBABE-hTERT is a puromycin resistant amphotropicretrovirus, based on a pBABE series vector backbone, thatexpresses the catalytic subunit of human telomerase(hTERT), and has been described previously.18 For retroviralinfections EK1.BR keratocytes were seeded at a density of8.46104 cells in 60 mm diameter standard tissue culturedishes. This seeding was performed about 24 hours beforeinfection so that the cultures were still substantiallysubconfluent at the time of infection.One hour before infection the cells were fed with fresh
medium containing 8 mg/ml of polybrene (Sigma, St Louis,MO, USA). Two ml of supernatant from psiCRIP producer celllines containing either pBABE-hTERT or control (pBABE-puro) retrovirus was then added to each 60 mm dish keepingthe polybrene concentration constant at 8 mg/ml. The cultures
were then incubated for 2 hours in a tissue culture incubatorat 37 C, after which time the retroviral supernatant wasdiluted with fresh medium. After 24 hours the supernatantwas replaced with fresh medium and cells were incubated fora further 48 hours. The cultures were then fed with selectivemedium (MEM containing the supplements given abovetogether with 1.5 mg/ml puromycin). The concentration ofpuromycin required to provide effective selection had beendetermined by cytotoxicity studies undertaken in advance. Ateach subsequent passage total cell numbers were estimatedand the population doublings estimated. EK1.BR wereconsidered immortal after 150 population doublings.Test materials were hydroxyapatite (Plasma Biotal,
Tideswell, UK) produced by isostatic pressing hydroxyapatitepowder at a nominal pressure of 50 MPa into discs andsintering the compacts at 1250 C, PTFE (GoodfellowCambridge Ltd, Huntingdon, UK); and HEMA (34% water)(Cantor & Nissel, Northampton, UK). Glass coverslips wereused as a positive control material. The individual discs ofmaterial were stored together at room temperature beforetesting. All test materials were sterilised with ultravioletirradiation for one hour before use in the experiments. Allmaterials were used as either solid flat discs (hydroxyapatiteand glass coverslips) or as flat non-porous sheet material(PTFE and HEMA).
Cell adhesion, proliferation, and viabili tyA viability/cytotoxicity assay using calcein-AM and ethidiumhomodimer-1 (EthD-1) (Molecular Probes, Eugene, OR,USA) was used to quantify viable cell growth for cells seededat a standard concentration on each of the test materials at4 hours, 24 hours, and 7 days. Calcein-AM is cleaved bycellular esterases present within viable cells to form afluorescent green product which is membrane impermeable.Ethidium homodimer-1 is a fluorescent red marker whichbinds to nucleic acids and only passes through thecompromised membrane of non-viable cells.10 mm diameter discs of each test material were placed in
the wells of a standard 12 well plate and sterilised byultraviolet irradiation. The discs were washed three timesthen incubated in serum free MEM culture medium for3 hours at 37 C in 5% carbon dioxide/air. Telomerasetransformed EK1.BR keratocytes (56103 in 2 ml MEMcontaining 10% FCS) were then seeded onto each of thediscs before further incubation at 37 C in 5% carbon dioxide/air. At 4 hours, 24 hours, and 1 week (n=3 per material foreach time point) culture medium was carefully removed fromthe wells and the cells were washed in phenol red-freemedium. The discs were then incubated for 5 minutes at 37 Cin 5% carbon dioxide/air in phenol red-free MEM containingcalcein-AM (2 mM) and EthD-1 (1 mM) before invertedplacement in a new 12 well plate containing 1 ml of phenolred-free MEM in each well. Cells adherent to the discsurfaces were then viewed by fluorescence microscopy.Sequential illumination at wavelengths of 500 nm and625 nm was used to highlight calcein-AM positive (live)and EthD-1 positive (dead) cells respectively. Live/dead cellcounts in five preselected fields per specimen were performedat a magnification of610.
Cell morphologyImmunofluorescent labelling was used to examine surfaceexpression of integrin (b1), and focal contact/adhesionformation. Organisation of the actin cytoskeleton was studiedusing FITC-phalloidin staining. These studies were essentiallyqualitative.For immunofluorescent studies, primary labelling was with
(1:100) mouse anti-b1 integrin IgG (courtesy of ProfessorFiona Watt, Cancer Research, UK) and (1:50) Hvin 1 mouse
Keratoprosthesis skirt integration 1357
www.bjophthalmol.com
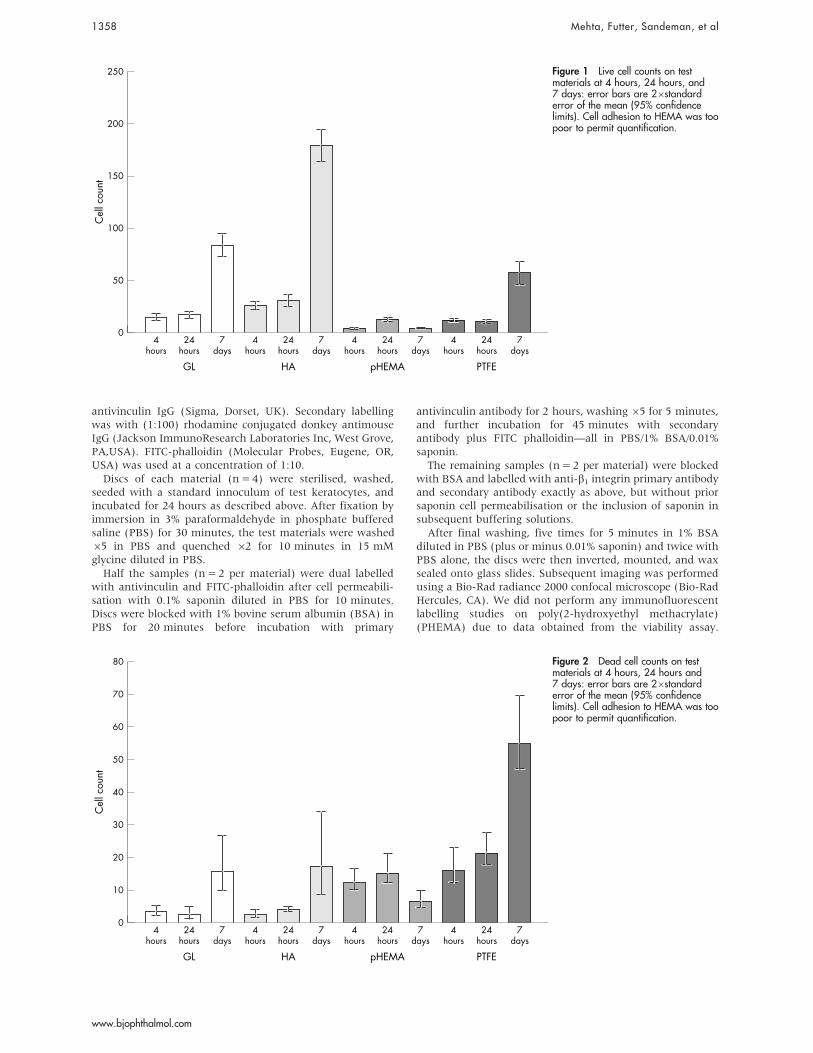
antivinculin IgG (Sigma, Dorset, UK). Secondary labellingwas with (1:100) rhodamine conjugated donkey antimouseIgG (Jackson ImmunoResearch Laboratories Inc, West Grove,PA,USA). FITC-phalloidin (Molecular Probes, Eugene, OR,USA) was used at a concentration of 1:10.Discs of each material (n=4) were sterilised, washed,
seeded with a standard innoculum of test keratocytes, andincubated for 24 hours as described above. After fixation byimmersion in 3% paraformaldehyde in phosphate bufferedsaline (PBS) for 30 minutes, the test materials were washed65 in PBS and quenched 62 for 10 minutes in 15 mMglycine diluted in PBS.Half the samples (n=2 per material) were dual labelled
with antivinculin and FITC-phalloidin after cell permeabili-sation with 0.1% saponin diluted in PBS for 10 minutes.Discs were blocked with 1% bovine serum albumin (BSA) inPBS for 20 minutes before incubation with primary
antivinculin antibody for 2 hours, washing65 for 5 minutes,and further incubation for 45 minutes with secondaryantibody plus FITC phalloidin—all in PBS/1% BSA/0.01%saponin.The remaining samples (n=2 per material) were blocked
with BSA and labelled with anti-b1 integrin primary antibodyand secondary antibody exactly as above, but without priorsaponin cell permeabilisation or the inclusion of saponin insubsequent buffering solutions.After final washing, five times for 5 minutes in 1% BSA
diluted in PBS (plus or minus 0.01% saponin) and twice withPBS alone, the discs were then inverted, mounted, and waxsealed onto glass slides. Subsequent imaging was performedusing a Bio-Rad radiance 2000 confocal microscope (Bio-RadHercules, CA). We did not perform any immunofluorescentlabelling studies on poly(2-hydroxyethyl methacrylate)(PHEMA) due to data obtained from the viability assay.
250
200
150
100
50
0
Cel
l cou
nt
4hours
24hours
7days
4hours
24hours
7days
4hours
24hours
7days
4hours
24hours
GL HA pHEMA PTFE
7days
Figure 1 Live cell counts on testmaterials at 4 hours, 24 hours, and7 days: error bars are 26standarderror of the mean (95% confidencelimits). Cell adhesion to HEMA was toopoor to permit quantification.
80
70
40
20
60
50
30
10
0
Cel
l cou
nt
4hours
24hours
7days
4hours
24hours
7days
4hours
24hours
7days
4hours
24hours
GL HA pHEMA PTFE
7days
Figure 2 Dead cell counts on testmaterials at 4 hours, 24 hours and7 days: error bars are 26standarderror of the mean (95% confidencelimits). Cell adhesion to HEMA was toopoor to permit quantification.
1358 Mehta, Futter, Sandeman, et al
www.bjophthalmol.com

The number of viable cells at 24 hours on this material wereto few to obtain any useful images with the confocal laser.
Electron microscopyCells inoculated and cultured on test materials for 24 hoursas described above were fixed in 2% paraformaldehyde/2%glutaraldehyde/0.1 M cacodylate for 30 minutes at roomtemperature. Specimens were then treated with 1%osmium/0.1 M cacodylate at 4 C for 1 hour before dehydra-tion in ethanol, washing in hexamethyl disilazane, anddrying by evaporation. After fixation, the discs were mountedon stubs using conductive silver paint and sputter coatedwith gold. Specimens were then examined in a JOEL 6100(JOEL, Peabody, MA, USA) scanning electron microscope.
StatisticsSPSS version 11.5 was used to for analysis of variance toexamine differences between live/dead cell counts acrossmaterials (SPSS Inc, Chicago, IL, USA). The Mann-WhitneyU test was used to examine differences in b1 integrinexpression across materials. Error bars on all graphs arepresented as 95% confidence limits (plus or minus 26stan-dard error of the mean).
RESULTSCell adhesion, proliferation, and viablityLive cell counts were significantly greater for hydroxyapatitespecimens at each time point than for the other test materials(p=0.02 (4 hours), p=0.04 (24 hours), p=0.003 (1 week)(fig 1). Cell counts increased between 24 hours and 7 days onglass, hydroxyapatite, and PTFE, indicating that cellsproliferated on all these materials. However, dead cell countswere significantly higher for PTFE than for other materials at7 days (p=0.002) (fig 2), indicating that this material,
although supporting initial adhesion, was significantly morecytotoxic than glass or hydroxyapatite.
Cell morphologyQualitative observation of immunofluorescent labelled cells(fig 3) suggested expression of ß1integrin onhydroxyapatite.glass.PTFE. Stress fibres (phalloidin stain-ing) were equally prominent on hydroxyapatite and glass butless prominent on PTFE (fig 3). Focal adhesions (vinculinimmunostaining) were more prominent on hydroxyapatitethan on glass or PTFE (fig 3). Representative images shownin figure 4 suggest that cell spreading was greater onhydroxyapatite and glass, with cells on PTFE adopting amore spindle shaped, elongated form.Light microscopic observation during the cell adhesion,
proliferation, and viability assays suggested more rapid cellspreading on hydroxyapatite than the other test materials(fig 4). After 4 hours cells were round on the HEMA, amixture of round and spreading on glass and PTFE, andmainly spreading on hydroxyapatite. At 24 hours cells onHEMA were still mainly round with few cells spreading out;but on glass, hydroxyapatite, and PTFE the cells were mainlyspread out. At 1 week there was a mass of cells on the glass,hydroxyapatite, and PTFE; however the scant cell deposits onHEMA were still round and poorly adherent. Scanningelectron microscopy, at 24 hours, was consistent with theseobservations (fig 5). On hydroxyapatite cells were spread sothinly that the surface texture of the test material was clearlyvisible through flattened lamellipodia. Lamellipodia of cellson glass were not as thin as those on hydroxyapatite, butwere, nevertheless, well spread and showed more filopodiathan cells cultured on hydroxyapatite. Cells cultured on PTFEwere much less well spread than those on HA or glass,
GL HA PTFE
β1 integrin
Phalloidin
Vinculin
Figure 3 b1 integrin, F-actin andvinculin distribution on test materials at24 hours. Montage of confocalmicrographs of representative cells onvarious test materials: b1 integrinexpression (immunofluorescentlabeling) on glass, hydroxyapatite, andPTFE; stress fibre expression (phalloidinstaining) on glass, hydroxyapatite,PTFE; and focal contact (vinculin)expression on glass, hydroxyapatite,and PTFE. Cell adhesion to HEMAsurfaces was too poor to obtainconfocal images.
Keratoprosthesis skirt integration 1359
www.bjophthalmol.com

produced numerous long extensions, and were frequentlyblebbing.
DISCUSSIONThese basic studies of cell adhesion, proliferation, andsurvival suggest that hydroxyapatite is superior, as an initialadhesion environment for keratocytes, to inert plastics usedas a porous tissue integration framework in contemporary CEmarked keratoprosthesies. Cell adhesion to pHEMA was poorand cell death was prominent on PTFE.We used telomerase transformed keratocytes in an effort to
standardise our experimentation through the use of a cell linewith a near normal phenotype. Transduction of cells toexpress the catalytic subunit of telomerase permits them toretain their telomeres and divide indefinitely without globalalterations of gene expression produced by earlier methods ofcellular immortalisation.19 The use of telomerase transformedcells is increasing in ophthalmic research20 21 and should helpto enhance both the reproducibility and biological validity ofexperimental results.
Cells were derived from the previously characterised EK1-BR1 human keratocyte strain.17 In the presence of serum, andspecifically TGF-b, keratocytes develop a myofibroblastphenotype.22 Clinically, keratoprosthesis skirts may be colo-nised by fibroblasts derived from sclera, or the overlyingmucous membrane flap. Although we have not performedcomparative studies, these cells have similar adhesionstructures, and it is unlikely that their behaviour woulddiffer significantly from keratocyte derived myofibroblasts.The study was restricted to plane surfaces. Cells may
behave differently in colonising a 3D porous keratoprosthesisskirt.7 Surface texture also exerts an important influence oncell behaviour,23 and this was uncontrolled. Despite theselimitations, the fit between our principal findings and therelatively good tissue integration observed clinically for theOOKP8 is striking.Our failure to observe cell adhesion on unmodified HEMA
surfaces is consistent with earlier published results.24 25
Peluso et al demonstrated human embryonic lung fibroblastsplated on HEMA fail to spread after 24 hours and remainspherical in shape, while those plated on modified HEMA
4 hours 24 hours 7 days
GL
HA
HEMA
PTFE
Figure 4 Light microscopy showing cell morphology on test materials. Montage of calcein-AM stained keratocytes illustrating cell morphology atdifferent time points (4 hours, 24 hours, 7 days) on glass (GL), hydroxyapatite (HA), HEMA, and PTFE.
1360 Mehta, Futter, Sandeman, et al
www.bjophthalmol.com

demonstrated good cell attachment and spreading.24
Sandeman et al also observed poor cellular attachment tounmodified HEMA at 24 hours using the EK1.BR cell linebut showed spreading of cells if the HEMA was modifiedwith 15% phenoxyethyl methacrylate (PEM) or of 20%2-(dimethylamino)ethyl methacrylate (DEM).25 Even at1 week, little evidence of cellular attachment to unmodifiedHEMA was observed. Although inferior to glass or hydro-xyapatite, cell adhesion to PTFE surfaces was relatively good,but characterised by high levels of cell death.Failure of cell adhesion to pHEMA and relatively high
levels of cell death observed for PTFE may adversely influencetissue integration for the AlphaCor and Legeais BioKpro 111respectively. Both keratoprostheses have a published trackrecord of development which includes histological studies ofexplants from intralamellar corneal implantation.26 27 Thesestudies, and others,7 demonstrate cellular ingrowth, collagenand matrix deposition, but do not demonstrate matrixstability. Future studies of gene expression focussing onmatrix synthesis and degradation may reveal important
differences among fibroblasts colonising different candidatekeratoprosthesis materials.Hydroxyapatite is similar to the principal mineral consti-
tuent of bone and tooth, and is thought to promoteintegration between hard and soft tissues by adsorbingextracellular adhesion molecules in a 3D configuration thatpreferentially exposes a high density of integrin bindingsites.28 We observed qualitatively greater b1 integrin expres-sion in cells adherent to hydroxyapatite versus other testmaterials. The strength of cell adhesion to a surface isdetermined not only by the numbers of surface integrinreceptors, but also by their organisation. Integrins areorganised into oligomeric complexes, termed focal adhe-sions/complexes, which link the extracellular matrix with theactin cytoskeleton. Increased numbers of focal adhesionsobserved in cells adherent to hydroxyapatite may account forthe increased adhesion to hydroxyapatite seen in live/deadcell counts and the close apposition of keratocytes to thehydroxyapatite shown by standard error of the mean.A range of bioactive ceramic materials has been developed
to encourage bonding with soft tissues through an interfaciallayer of hydroxyapatite. Existing applications include ossi-cular replacement, periodontal bone regeneration, and orbitalfloor repair.28 Porous hydroxyapatite coral implants arewidely used in ophthalmology as post enucleation ballimplants.29 A keratoprosthesis with a coral skirt elementhas also been described.30 However, a rigid hydroxyapatiteskirt could potentially lead to problems with device fracture,and stress concentrations at the skirt/sclera interface couldencourage tissue breakdown. Although bioactive ceramics areavailable as resorbable gels and metallic surface coatings,coating a flexible polymer is less easy. The ideal keratoprosth-esis would have a modulus of elasticity similar to the eyewall.7 Flexible polymer surfaces incorporating integrin adhe-sion ligands such as the RGD or YIGSR motif have recentlybeen developed.31 A logical future extension of our studywould encompass these materials.The selection of inert plastic materials such as PTFE and
HEMA as keratoprosthesis skirt materials has been based ontheir record of safe implantation rather than any specialmerit as an interfacial surface to promote normal tissuedifferentiation.7 27 We have demonstrated that hydroxy-apatite is a superior starting adhesion environment forkeratocytes. This may help to explain relatively low extrusionrates observed clinically for the OOKP,8 and suggests thatmaterial selection for the next generation of keratoprosthesesshould move away from inert plastics towards materialsdesigned to promote normal adhesion and differentiation incontacting cells.
ACKNOWLEDGEMENTSThe hTERT vector supplied under a material transfer agreement withGeron Corporation (Geron Corporation, Menlo Park, CA). Theauthors acknowledge funding from the Special Trustees ofMoorfields Eye Hospital and the Sir Jules Thorn Charitable Trust.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
J S Mehta, B D S Allan, Cornea & External Disease Service, MoorfieldsEye Hospital, London, UKJ S Mehta, C E Futter, B D S Allan, Division of Cell Biology, Institute ofOphthalmology, London, UKS R Sandeman, R G A F Faragher, University of Brighton, School ofPharmacy and Biomolecular Science, University of Brighton, Brighton,UKK A Hing, K E Tanner, IRC in Biomedical Materials, Queen MaryUniversity of London, London, UK
Competing interests: none declared
This paper was a presentation at the Association for Research in Visionand Ophthalmology, April 2004, Fort Lauderdale, FL, USA.
GL
HA
PTFE
Figure 5 Scanning electron microscopy showing cell morphology ontest materials. Montage of scanning electron micrographs showingkeratocyte morphology at 24 hours on glass, HA, and PTFE.Bar = 10 mm.
Keratoprosthesis skirt integration 1361
www.bjophthalmol.com

REFERENCES1 World Health Organisation. The World Health Report 1998: life in the 21st
century. Geneva: WHO, 1998:47.2 Williams KA, Roder D, Esterman A, et al. Factors predictive of corneal graft
survival: report from the Australian Corneal Graft Registry. Ophthalmology1992;99:403–14.
3 Li F, Carlsson D, Lohmann C, et al. Cellular and nerve regeneration within abiosynthetic extracellular matrix for corneal transplantation. Proc Nat AcadSci 2003;100:15346–51.
4 Pellegrini G, Traverso CE, Franzi AT, et al. Long-term restoration of damagedcorneal surfaces with autologous cultivated corneal epithelium. Lancet1997;349:990–3.
5 Grueterich M, Espana EM, Tseng SC. Ex vivo expansion of limbal stem cells:amniotic membrane serving as a stem cell niche. Surv Ophthalmol2003;48:631–46.
6 Allan BDS. Artificial corneas. BMJ 1999;318:821–2.7 Hicks CR, Fitton HF, Chirila TV, et al. Keratoprostheses: advancing toward a
true artificial cornea. Surv Ophthalmol 1997;42:175–89.8 Marchi V, Riici R, Pecorella I, et al. Osteo-odonto-keratoprosthesis.
Description of the surgical technique with results in 85 patients. Cornea 192,13:125–30.
9 Legeais J-M, Renard G. A second generation of artificial cornea (Biokpro II).Biomaterials 1998;19:1517–22.
10 Hicks CR, Crawford GJ, Lou X, et al. Corneal replacement using a synthetichydrogel cornea Alphacor device preliminary outcomes and complications.Eye 2003;17:385–92.
11 Dohlman CH, Doane MG. Some factors influencing outcome afterkeratoprosthesis surgery. Cornea 1994;13:214–18.
12 Chirila TV, Constable IJ, Crawford GJ, et al. Poly(2-hydroxy-ethylmethacrylate) sponges as implant materials: in vivo and in vitro evaluation ofcellular invasion. Biomaterials 1993;14:26–38.
13 Legeais JM, Rossi C, Renard G, et al. A new fluorocarbon forkeratoprosthesis. Cornea 1992;11:538–45.
14 Sandeman SR, Llloyd AW, Tighe BJ, et al. A model for the preliminaryscreening potential keratoprosthetic biomaterials. Biomaterials2003;24:4729–39.
15 Van der Flier A, Sonnenberg A. Functions and interactions of integrins. CellTissue Res 2001;305:285–98.
16 Giancotti FG, Ruoslahti E. Integrin signalling. Science 1999;285:1028–32.
17 Dropcova S, Denyer S, Lloyd A, et al. A standard strain of human ocularkeratocytes. Ophthalmic Res 1999;31:33–41.
18 Wyllie FS, Jones CJ, Skinner JW, et al. Telomerase prevents acceleratedcell ageing of Werner syndrome fibroblasts. Nat Genet 2000;24:16–17.
19 Jiang XR, Jimenez G, Chang E, et al. Telomerase expression in somatic cellsdoes not induce changes associated with a transformed phenotype. NatureGenet 1999;21:111–14.
20 Ranbhatla L, Chiu CP, Glickman RP, et al. In vitro differentiation capacity oftelomerase immortalised human RPE cells. Invest Ophth Vis Sci2002;43:1622–30.
21 Gipson IK, Spurr Michaud S, Argueso P, et al. Mucin gene expression inimmortalised human corneal-limbal and conjunctival epithelial cell lines. InvestOphth Vis Sci 2003;44:2496–506.
22 Jester J, Ho-Chang T. Modulation of cultured corneal keratocyte phenotype bygrowth factors/cytokines controls in vitro contractility of extracellular matrixcontraction. Exp Eye Res 2003;77:581–92.
23 Curtis AS, Wilkinson CD. Reactions of cells to topography. J Biomater SciPolym Ed 1998;9:1313–29.
24 Peluso G, Petillo O, Anderson JM, et al. The differential effects of poly(2-hydroxyethylmethacrylate) and poly(2-hydroxyethyl methacrylate) /poly(caprolactone) polymers on cell proliferation and collagen synthesis byhuman ling fibroblasts. J Biomed Mater Res 1997;34:327–36.
25 Sandeman SR, Faragher RGA, Allen MCA, et al. Novel materials to enhancekeratoprosthesis integration. Br J Ophthalmol 2000;84:640–4.
26 Chirila TV, Constable IJ, Crawford GJ, et al. Poly (2-hydroxyethylmethacrylate) sponges as implant materials: in vivo and in vitro evaluation ofcellular invasion. Biomaterials 1993;14:26–38.
27 Legeais JM, Rossi G, Renard G, et al. A new fluorocarbon forkeratoprosthesis. Cornea 1992;11:538–45.
28 Allan BDS. Closer to nature: new biomaterials and tissue engineering inophthalmology. Br J Ophthalmol 1999;83:1235–40.
29 Ashworth JL, Rhatigan M, Sampath R, et al. The hydroxyapatite orbitalimplant: a prospective study. Eye 1996;10:29–37.
30 Leon CR, Baraquer JL Jr, Barraquer JL Sr. Coralline hydroxyapatitekeratoprosthesis in rabbits. J Refract Surg 1997;13:74–8.
31 Dee KC, Anderson TT, Bizios R. Design and function of novel osteoblastadhesive peptides for chemical modification of biomaterials. J Biomed MaterRes 1998;40:371–2.
1362 Mehta, Futter, Sandeman, et al
www.bjophthalmol.com

PERSPECTIVE
Topical ciclosporin in the treatment of ocular surfacedisordersS Tatlipinar, E K Akpek. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Br J Ophthalmol 2005;89:1363–1367. doi: 10.1136/bjo.2005.070888
Mounting evidence suggests that inflammation is the keyfactor in the pathogenesis of various ocular surfacediseases, with a complex interplay of genetic,environmental, and psychosocial factors. Management ofthese conditions is often challenging. Topicalcorticosteroids, with their associated side effects, are themainstay of current treatments for patients with visionthreatening disease. Ciclosporin A is an immunomodulatorthat specifically inhibits T lymphocyte proliferation.Recently, a topical ciclosporin preparation was approvedby the US Food and Drug Administration and becameavailable for use in ophthalmology. Given the increasinguse of ciclosporin eye drops, the goal of this article is toprovide the reader with an overview of the well establisheduses of ciclosporin and to help refine the questions thatshould be addressed by future investigations.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Esen Karamursel Akpek,MD, Ocular Surface andDry Eye Clinic, The WilmerEye Institute, 600 NorthWolfe Street, MaumeneeBuilding 317, Baltimore,MD 21287–9238, USA;[email protected]
Accepted for publication15 June 2005. . . . . . . . . . . . . . . . . . . . . . .
The ocular surface encompasses the entireepithelial surface of the cornea, limbus, andconjunctiva. The primary purpose of this
functional unit is to maintain corneal clarity, acritical component of the eye’s optical system.Even a small change in corneal clarity, such as aless than adequate tear film, can lead to visualdisturbances.Ocular surface diseases are a large group of
disorders with a variety of aetiologies, symptoms,and clinical findings. These disorders range fromsimple meibomian gland dysfunction, with excel-lent prognosis, to Stevens-Johnson syndrome,which can cause permanent scarring of theconjunctiva, loss of corneal transparency and henceloss of vision, with considerable impairment inquality of life. Ironically, most patients with ocularsurface disease have a healthy posterior segmentwith otherwise favourable visual prognosis.Whatever the initial aetiological factor of
ocular surface disease, once the disease hasdeveloped, inflammation becomes the keymechanism of injury to the ocular surface.1 2
There is a diversity of initiating insults, such astear film insufficiency, chemical injury, orhypersensitivity mechanisms. When present,inflammation is augmented by mediatorsreleased from damaged cells and invadingleucocytes. Hence, eyes with ocular surfacedisease may be trapped in a vicious cycle ofinflammation and resultant injury.Currently, the anti-inflammatory treatment of
ocular surface disorders mainly relies on topical
or systemic corticosteroids, which carry the riskof serious side effects. A topical ciclosporin A(CsA) preparation has recently become commer-cially available. CsA is an established immuno-modulating drug that was originally used toprevent rejection after organ or tissue transplan-tation. Systemic CsA has also been employed as atreatment for a variety of autoimmune diseases,including those with ocular involvement.3–5
CsA is a neutral, hydrophobic, cyclic undeca-peptide metabolite of the fungus Tolypocladiuminflatum. Its major clinical effect is the perturba-tion of expression of interleukin-2 (IL-2) byhelper T cells, preventing the proliferation of Tcells.3 CsA was discovered in the early 1970s asan antifungal agent. Later, owing to its lack ofbone marrow toxicity,6 it assumed a leading rolein solid organ transplant surgery,7 with drama-tically improved patient prognosis. In ophthal-mology, topically applied CsA in various oil basedsolvents was first used to inhibit experimentalcorneal allograft reaction in the early 1980s8 9;this was followed by human studies.10 Later, thedrug proved useful for patients with variousinflammatory ocular surface disorders.11 12
The main problems with the eye drop prepara-tion of CsA were sterility, pH, particles, and itslipophilic properties. A licensed topical CsA (0.2%in ointment form, Optimmune, Schering-Plough)has been available in veterinary ophthalmology forthe treatment of canine keratoconjunctivitis sicca,but the introduction of a similar preparation forhuman pharmacy (0.05% eye drop form, Restasis,Allergan Inc) did not occur until April 2003. Thispreparation has now been approved by the Foodand Drug Administration for use in the treatmentof dry eye condition in humans. Given theincreasing use of this product in patients bypractising ophthalmologists for various indica-tions, the goal of this analysis was to evaluate thepeer reviewed published scientific literature, todefine well established uses of CsA eye drops, andto help refine the important questions to beaddressed by future investigations.
DRY EYE SYNDROMEDry eye syndrome is a common disorder of thetear film that results in epithelial damage andthe disruption of normal homeostasis at theocular surface. Clinical features of dry eyesyndrome include an unstable tear film, ocularsurface inflammation, and epitheliopathy, result-ing in symptoms ranging from discomfort toblindness.13
Abbreviations: CsA, ciclosporin A; IL-2, interleukin-2;PUK, peripheral ulcerative keratitis
1363
www.bjophthalmol.com

Dry eye syndrome is widespread with as many as 25% ofpatients visiting ophthalmologists reporting dry eye symp-toms.14 The current understanding of the pathogenesis of dryeye disease has proceeded from the mere recognition of a lackof, or altered quality of, tears to recognition of inflammationas the key pathogenetic mechanism, whether from a systemicautoimmune disease or a local autoimmune event.15
Inadequate tear production and low tear clearance, forwhatever reason, lead to chronic inflammation of the ocularsurface, mediated mainly by T lymphocytes.15 Moreover, theconjunctival T cell subpopulations do not differ significantlyin Sjogren’s syndrome and non-Sjogren’s syndrome patientswith dry eye.16 Androgens also represent an important trophicfactor for the ocular surface, and their deficiency predisposesto inflammation from both lacrimal and meibomian glanddysfunction.17 Immune based inflammation can thereforeinterconnect and negatively reinforce these different patho-genetic mechanisms, resulting in a vicious cycle andsubsequent ocular surface damage.The traditional approach to treating dry eye has been to
lubricate the ocular surface by replacing or conserving thepatient’s tears, without correcting the underlying diseaseprocess. Yet these treatments do not directly address theocular surface inflammation.Anti-inflammatory therapies are considered for patients
with moderate to severe dry eye syndrome who continue tohave symptoms or who have evidence of corneal disease onaqueous enhancement therapies. Several clinical studies haveshown topical corticosteroids to improve both signs andsymptoms of dry eye.18 19
In preliminary studies on small groups of patients,treatment with topical CsA improved the signs and symp-toms of dry eye syndrome.20–22 Evidence of the inflammatorynature of dry eye syndrome and the success of thepreliminary investigations led to large scale multicentre,randomised, placebo controlled, double masked, dose ran-ging clinical trials of the efficacy and safety of topical CsAtherapy in moderate to severe dry eye syndrome. A CsA oil inwater emulsion formulation significantly improved theocular signs and symptoms of moderate to severe dry eye inpatients with or without Sjogren’s syndrome, and was foundto be safe and well tolerated.23 In this phase 2 study, of thefour different CsA dosing regimens (0.05%, 0.1%, 0.2%, and0.4%), the 0.05% dose gave the most consistent improvementin symptoms. Following this study, the efficacy and safety oftopical 0.05% and 0.1% CsA were compared with vehicle inpatients with moderate to severe dry eye syndrome.24 As inthe phase 2 study, both formulations were reported to be safeand effective, and the 0.05% formulation produced signifi-cantly greater improvements in signs (that is, cornealstaining and Schirmer values) and symptoms (blurred vision,need for concomitant artificial tears, and the physician’sevaluation of global response to treatment). The 877 patients(293 in the 0.05% CsA group, 292 in the 0.1% group, and 292in the vehicle group) in the study were treated for 6 months.In addition, a subset of patients from the phase 3 studyunderwent conjunctival biopsy before and after treatmentwith topical CsA, in order to investigate the effect oftreatment on ocular surface histopathology. An increase ingoblet cell counts was reported in association with clinicalimprovement.25 Reduced numbers of activated lymphocytesin conjunctiva 26 and a decrease in IL-6 in conjunctivalepithelium27 were also observed.Evidence obtained from these studies supports the efficacy
of topical CsA treatment through its immunomodulatoryaction and a possible direct lacrimogenic effect as shown in acanine model in reversing inflammation of the ocular surfaceand lacrimal glands and in improving the signs andsymptoms of dry eye syndrome in patients with or without
Sjogren’s syndrome. However, the optimal dosing andrequired duration of treatment are not known.
VERNAL KERATOCONJUNCTIVITISVernal keratoconjunctivitis is a severe, chronic allergicdisorder, seen primarily in young males, often with a historyof atopy. The hallmark sign of vernal keratoconjunctivitis isgiant papillae on the upper tarsal conjunctiva, although insome patients limbal oedema may be predominant.The disease tends to be self limited and frequently
disappears after the teen age period, but a chronic, moresevere form of disease can be seen in adults. In certaincountries it is the most common form of conjunctivitis.28
The management of vernal keratoconjunctivitis is deter-mined by the severity of involvement. Mast cell stabilisers aregenerally considered effective, based on studies from Europeand North America.29–31 However, results from the MiddleEast and Africa have not consistently shown benefit.32–34
Vision threatening corneal complications include centralepithelial keratitis and shield-like ulcers. Topical steroidsusually alleviate the acute symptoms,32 but unsupervisedtreatment leads to glaucoma and cataract formation in asignificant proportion of patients.35 Particularly in thedeveloping countries, vernal keratoconjunctivitis is consid-ered a potentially blinding disease.36 37 The search for new,effective, safe treatments of this potentially blinding diseasecontinues. Recently, a 2 week trial of topical 0.01% mitomy-cin C, four times daily, proved safe and effective in thetreatment of patients with severe, blinding vernal kerato-conjunctivitis resistant to topical steroids.38
The immunopathogenetic mechanism is complex andinvolves an IgE mediated immediate hypersensitivityresponse as well as a Th2 type of immune reaction.39 40
Multiple studies on the efficacy of topical CsA for treatingvernal keratoconjunctivitis have consistently shown a bene-ficial effect of the drug.41–46 The improvement produced bytopical CsA usually took an average of 2 weeks using 1% or2% CsA in oil solvents, four times daily. The duration oftreatment depends on the activity of the inflammation. Nomajor adverse effect was reported, except for mild burningand stinging. A rebound phenomenon occurred soon afterdiscontinuation of the treatment, indicating the need for aslow taper.41
ATOPIC KERATOCONJUNCTIVITISAtopic keratoconjunctivitis is a bilateral, inflammatoryexternal ocular disease that manifests in the context ofatopic dermatitis. There appears to be an increasing incidenceof atopic dermatitis worldwide in recent years,47 possiblybecause of increased exposure to airborne allergens orirritants. About 25% to 40% of patients with atopic dermatitishave ocular involvement.48
Atopic keratoconjunctivitis is the most important of theallergic ocular surface disorders, because of its chronic courseand frequent corneal complications that can lead topermanent loss of vision.49–51 Unlike vernal keratoconjuncti-vitis, atopic keratoconjunctivitis can involve both upper andlower palpebral conjunctivae, with resultant scarring indis-tinguishable from other causes of cicatrising conjunctivitis.The pathogenesis of atopic keratoconjunctivitis is not fully
understood, but investigators have proposed a compleximmunomodulatory dysfunction at the ocular surface,including type I and type IV hypersensitivity reactions52 53
with a predominantly Th1 cytokine profile, perhaps becauseof the chronicity of the disorder.54
Currently available therapies are aimed, at best, at relievingsymptoms; there is no evidence for a significant effect on thedisease course. Corticosteroids are the mainstay of treatment,with dramatic improvement in acute symptoms. However,
1364 Tatlipinar, Akpek
www.bjophthalmol.com

the efficacy of steroids in preventing the crippling con-sequences of atopic keratoconjunctivitis is not known.Corneal complications are seen in up to 60% to 70% ofpatients.49 55 Despite a combination treatment with topicalmast cell stabilisers + oral antihistamines + intermittenttopical corticosteroid, about 30% of patients require cornealtransplantation for visual or tectonic purposes.49 Also,resistance to topical steroids may necessitate systemic CsAtherapy.56
In two prospective, randomised, double masked, placebocontrolled trials, topical CsA was found to be an effective andsafe treatment in both steroid dependent and steroidresistant cases of atopic keratoconjunctivitis.57 58 In the earlierstudy,57 21 patients used either topical 2% CsA or the vehiclealone four times daily for 3 months, in addition to their usualtherapy with topical corticosteroids and/or mast cell stabi-lisers. The great majority of the treated patients were able todiscontinue their topical steroid treatment. The later study58
included 20 patients with topical steroid resistant, severeatopic keratoconjunctivitis; they had moderately activedisease despite topical steroid therapy with or without mastcell stabilisers. Treatment (CsA or placebo) lasted for 28 dayswith a dosing schedule of six times daily during the first2 weeks and four times daily during the last 2 weeks.Significant improvement was observed in the CsA group,and none of these patients had a worsening of the disorder,in contrast with the placebo group.Another study involving both atopic keratoconjunctivitis
and vernal keratoconjunctivitis patients who had experiencedno improvement with conventional therapy documented thebeneficial effect of topical CsA as an additive treatment, witha reduced need for topical steroid use.59
Laboratory studies of the immunomodulatory effects oftopical CsA in atopic keratoconjunctivitis have showndecreased numbers of leucocytes and CD4+ and IL-2 receptorpositive T cells in conjunctival biopsy specimens of subjectswith atopic keratoconjunctivitis following therapy.60
Topical CsA seems to be an effective steroid sparing agentin patients with severe atopic keratoconjunctivitis. However,its efficacy as a first line agent during long term treatmentwarrants additional studies.
NON-INFECTIOUS KERATITISImmune mediated, sterile central or paracentral cornealulceration may develop in patients with connective tissuedisease, most commonly in rheumatoid arthritis or Sjogren’sdisease. These conditions need to be distinguished fromperipheral ulcerative keratitis (PUK), because PUK isessentially a vasculitis of limbal blood vessels and isconsidered to be associated with (re)activation of systemicillness.61 Central ulcerations or keratolysis, by contrast, arenot associated with a limbal vasculitis.62
Immunohistochemical studies demonstrated infiltration withmacrophages, T lymphocytes, and aberrant expression of HLAclass II antigens, suggesting a cellular immune reactiontargeted at the cornea.63 64
The treatment should be aimed at stopping melting andencouraging re-epithelialisation. In severe cases, with cornealmelting and perforation, tissue adhesives may be used.Controlling the underlying illness is essential. However,unlike PUK, the central/paracentral ulcerations may notrespond well to systemic immunosuppressive therapy.64 65
Several small, uncontrolled case series have reported thebeneficial effect of topical CsA in treating paracentral cornealulcers associated with connective tissue disease. In one study,topical 2% CsA, four times daily, was instituted in fivepatients with unilateral paracentral rheumatoid cornealulceration who had not responded to systemic immunosup-pression.64 Treatment resulted in an immediate arrest of
keratolysis and re-epithelialisation. In another study, sys-temic immunosuppressive therapy either could not beinitiated owing to a systemic contraindication or wasdiscontinued because of side effects in five patients withcollagen vascular diseases.65 The patients were treated withtopical 2% or 0.5% CsA, four to six times daily. All but one ofthe eyes responded favourably with an intense neovascular-isation within 48 hours of initiating treatment. In other smallseries sterile marginal corneal ulcers in the context ofrheumatoid arthritis responded to use of 2% CsA eye dropstwice daily with healing of the ulcers within several days.63 66
Observation of macrophages, T lymphocytes, and aberrantexpression of HLA class II antigens in the corneal andconjunctival tissues of patients with immune corneal ulcersassociated with collagen vascular disorders suggests a cellularimmune reaction. However, the current clinical evidencesupporting the role of topical CsA in the treatment is weak.
THYGESON’S SUPERFICIAL PUNCTATE KERATITISThygeson’s superficial punctate keratitis is a bilateral,idiopathic epithelial keratitis characterised by recurrentattacks of tearing, photophobia, blurred vision, and foreignbody sensation.67 The classic finding is multiple cornealepithelial lesions that appear during the exacerbations of thedisease.68 Although clinical features are similar to those ofviral infections, responsiveness to corticosteroids suggests animmune process, perhaps a post-infectious delayed hyper-sensitivity.69 However, no infectious aetiology has yet beenfound.70
Mild cases are often treated with lubricants and bandagelenses.71 72 More symptomatic cases are generally treated withweak topical steroids.68 Recurrences are common followingthe cessation of therapy. Some patients may require regularsteroid use for years.68
Reports have indicated that most patients with Thygeson’ssuperficial punctate keratitis respond to topical CsA.73–75 Inmore than two thirds of the patients, topical CsA suppressedthe epithelial and subepithelial opacities as long as the drugwas administered. Recurrences occurred during the taperingoff period. In one third of patients this therapy seemed to becurative. The results are encouraging and suggest that topicalCsA may be a safe alternative to corticosteroids for thetreatment of Thygeson’s superficial punctate keratitis, parti-cularly for patients who will require long term topical steroidtreatment.
LIGNEOUS CONJUNCTIVITISLigneous conjunctivitis is a rare form of chronic conjunctivitischaracterised by the development of firm, fibrin rich, woody-like pseudomembranous lesions mainly on the tarsalconjunctiva.76 Cornea may be involved secondarily, withscarring and vascularisation.The disorder is generally bilateral, and the onset is
frequently during childhood.77 The pseudomembranes arecharacterised by subepithelial deposition of amorphoushyaline material; a cellular component composed of lympho-cytes, plasma cells, neutrophils, eosinophils, and mast cells;and neovascularisation. The amorphous material has beenshown to contain fibrin(ogen), immunoglobulins, andalbumin, suggesting an increased permeability of bloodvessels.77 Histopathological findings from affected humansand (plasminogen deficient) mice indicate that woundhealing, mainly in injured mucosal tissues, is impairedbecause of markedly decreased (plasmin mediated) extra-cellular fibrinolysis.78 Rare immunohistochemical studieshave revealed a predominance of T cells,79 80 particularly withIL-2 receptor expression. The management of ligneousconjunctivitis is difficult, and no satisfactory treatmentexists.
Topical ciclosporin 1365
www.bjophthalmol.com

Several small, uncontrolled case series of CsA therapy haveindicated improvement in patients with ligneous conjuncti-vitis that is refractory to other modes of treatment.79 81
However, contradictory reports also exist.80
LICHEN PLANUSLichen planus is an inflammatory dermatosis of unknownaetiology that affects the skin and mucous membranes.Classic lesions appear as recurrent, violaceous, pruriticpapules distributed symmetrically on the flexor surfaces ofthe extremities and trunk. These lesions are often accom-panied by lesions of the oral, genital, and, rarely, ocularmucosa.82 Conjunctival lichen planus, albeit rare, can lead toirreversible damage to the ocular surface and loss of visionfrom corneal scarring.83 84
Although the pathogenesis is not fully understood, currentfindings suggest an autoimmune process mediated by T cellsinfiltrating the basement membrane and the basal layers ofepithelium.Most patients with skin involvement can be treated
successfully with topical corticosteroids. Chronic, aggressivelesions may need additional therapy ranging from psoralenplus ultraviolet A to retinoids or CsA.85 Low dose systemicCsA may be required for patients with severe diseaseunresponsive to systemic steroids.86
Reported treatments of conjunctival lichen planus includeCsA, mycophenolate mofetil, and azathioprine used systemi-cally.83 87 Because of its ability to accelerate apoptosis infibrotic tissues,88 topical CsA alone was used in a few patientshaving conjunctival involvement from lichen planus, andproved effective in controlling inflammation and scarring.84 89
In particular, patients with isolated lichen planus of theconjunctiva may be candidates for topical CsA treatment withor without topical corticosteroids.90
SUPERIOR LIMBIC KERATOCONJUNCTIVITISSuperior limbic keratoconjunctivitis is a chronic, local ocularsurface disease characterised by episodes of recurrent inflam-mation of the upper palpebral and superior bulbar conjuncti-vae, as well as of the superior limbus and cornea.91 The classicfinding of this condition is bilateral local hyperaemia of thesuperior bulbar conjunctiva. Patients often complain ofburning, foreign body sensation, and photophobia. The exactpathophysiology is unknown. A mechanical theory proposedsoft tissuemicrotrauma between tarsal and bulbar surfaces andbetween conjunctival stroma and sclera.92
Topical CsA was reported to be helpful as a primary oradjunctive therapy for superior limbic keratoconjunctivitis ina single study involving five patients.93 In patients withconcomitant dry eye and superior limbic keratoconjunctivitis,topical CsA may be used for both increasing tear productionand controlling inflammation.
LESS COMMON USES OF TOPICAL CICLOSPORIN AThere are also several, unconfirmed small case series or casereports on the use of topical CsA in the treatment of Mooren’sulcer,94 Cogan syndrome,95 chronic sarcoidosis of the conjunc-tiva,96 conjunctival manifestations of actinic prurigo,97 keratitisof Senter syndrome (keratitis-ichthyosis deafness),98 delayedonset bilateral diffuse lamellar keratitis after laser in situkeratomileusis,99 and microcrystalline keratopathy caused bystreptococcus.100 However, the evidence seems inadequate tojustify the use of topical CsA in these conditions.
CONCLUSIONSTopical CsA has been used in ophthalmology since the early1980s. Based on the available evidence, CsA eye drops seemto be safe. No serious side effects were reported with the0.05%, 0.5%, or 2% preparations, used for periods of up to
12 months. Current literature supports the efficacy of topicalCsA in the treatment of various ocular surface disorders,particularly the dry eye syndrome and severe allergickeratoconjunctivitis. Future studies should be directed tocomparing the efficacy of topical CsA with that of corticos-teroids and to its ability to change the natural course of someof these disorders during longer term follow up.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
S Tatlipinar, E K Akpek, The Wilmer Eye Institute, Johns Hopkins Schoolof Medicine, Baltimore, MD, USAS Tatlipinar, Department of Ophthalmology, Pamukkale UniversitySchool of Medicine, Denizli, Turkey
Competing interests: none declared
Dr Akpek received unrestricted research grant from Allergan Inc, Irvine,CA (see reference 58). She is supported in part by a William and MaryGreve Scholarship from Research to Prevent Blindness.
REFERENCES1 Baudouin C. The pathology of dry eye. Surv Ophthalmol 2001;45:211–20.2 Johnson ME, Murphy PJ. Changes in the tear film and ocular surface from dry
eye syndrome. Prog Retin Eye Res 2004;23:449–74.3 Nussenblatt RB, Palestine AG. Cyclosporin: immunology, pharmacology and
therapeutic uses. Surv Ophthalmol 1986;31:159–69.4 Belin MW, Bouchard CS, Phillips TM. Update on topical cyclosporin A:
background, immunology, and pharmacology. Cornea 1990;9:184–95.5 Williams DL. A comparative approach to topical cyclosporin therapy. Eye
1997;11:453–64.6 Borel JF, Feurer C, Gubler HU, et al. Biological effects of cyclosporin A: a new
antilymphocytic agent. Agents Actions 1976;6:468–75.7 Calne RY, White DJ, Thiru S, et al. Cyclosporin A in patients receiving renal
allografts from cadaver donors. Lancet 1978;2:1323–7.8 Coster DJ, Shepherd WF, Fook TC, et al. Prolonged survival of corneal
allografts in rabbits treated with cyclosporin A. Lancet, 1979;2, 688–9.9 Hunter PA, Wilhelmus KR, Rice NS, et al. Cyclosporin A applied topically to
the recipient eye inhibits corneal graft rejection. Clin Exp Immunol1981;45:173–7.
10 Hoffmann F, Wiederholt M. [Local treatment of corneal transplants in thehuman with cyclosporin A.] Klin Monatsbl Augenheilkd, 1985;187:92–6.
11 Holland EJ, Olsen TW, Ketcham JM, et al. Topical cyclosporin A in thetreatment of anterior segment inflammatory disease. Cornea 1993;12:413–9.
12 Gunduz K, Ozden O. Therapeutic use of topical cyclosporine. AnnOphthalmol 1993;25:182–6.
13 Lemp MA. Report of the National Eye Institute/Industry Workshop on ClinicalTrials in Dry Eyes. CLAO J 1995;21:221–32.
14 Doughty MJ, Fonn D, Richter D, et al. A patient questionnaire approach toestimating the prevalence of dry eye symptoms in patients presenting tooptometric practices across Canada. Optom Vis Sci 1997;74:624–31.
15 Stern ME, Gao J, Siemasko KF, et al. The role of the lacrimal functional unit inthe pathophysiology of dry eye. Exp Eye Res 2004;78:409–16.
16 Stern ME, Gao J, Schwalb TA, et al. Conjunctival T-cell subpopulations inSjogren’s and non-Sjogren’s patients with dry eye. Invest Ophthalmol Vis Sci2002;43:2609–14.
17 Sullivan DA, Wickham LA, Rocha EM, et al. Androgens and dry eye inSjogren’s syndrome. Ann N Y Acad Sci 1999;876:312–24.
18 Marsh P, Pflugfelder SC. Topical nonpreserved methylprednisolone therapyfor keratoconjunctivitis sicca in Sjogren syndrome. Ophthalmology1999;106:811–6.
19 Sainz De La Maza Serra M, Simon Castellvi C, Kabbani O. Nonpreservedtopical steroids and lacrimal punctal occlusion for severe keratoconjunctivitissicca. Arch Soc Esp Oftalmol 2000;75:751–6.
20 Laibovitz RA, Solch S, Andriano K, et al. Pilot trial of cyclosporin 1%ophthalmic ointment in the treatment of keratoconjunctivitis sicca. Cornea1993;12:315–23.
21 Power WJ, Mullaney P, Farrell M, et al. Effect of topical cyclosporin A onconjunctival T cells in patients with secondary Sjogren’s syndrome. Cornea1993;12:507–11.
22 Gunduz K, Ozdemir O. Topical cyclosporin treatment of keratoconjunctivitissicca in secondary Sjogren’s syndrome. Acta Ophthalmol (Copenh)1994;72:438–42.
23 Stevenson D, Tauber J, Reis BL. Efficacy and safety of cyclosporin Aophthalmic emulsion in the treatment of moderate-to-severe dry eye disease: adose-ranging, randomized trial. The Cyclosporin A Phase 2 Study Group.Ophthalmology 2000;107:967–74.
24 Sall K, Stevenson OD, Mundorf TK, et al. Two multicenter, randomized studiesof the efficacy and safety of cyclosporin ophthalmic emulsion in moderate tosevere dry eye disease. CsA Phase 3 Study Group. Ophthalmology2000;107:631–9.
25 Kunert KS, Tisdale AS, Gipson IK. Goblet cell numbers and epithelialproliferation in the conjunctiva of patients with dry eye syndrome treated withcyclosporin. Arch Ophthalmol 2002;120:330–7.
1366 Tatlipinar, Akpek
www.bjophthalmol.com

26 Kunert KS, Tisdale AS, Stern ME, et al. Analysis of topical cyclosporintreatment of patients with dry eye syndrome: effect on conjunctivallymphocytes. Arch Ophthalmol 2000;118:1489–96.
27 Turner K, Pflugfelder SC, Ji Z, et al. Interleukin-6 levels in the conjunctivalepithelium of patients with dry eye disease treated with cyclosporin ophthalmicemulsion. Cornea 2000;19:492–6.
28 Ukponmwan CU. Vernal keratoconjunctivitis in Nigerians: 109 consecutivecases. Trop Doct 2003;33:242–5.
29 El Hennawi M. A double blind placebo controlled group comparative study ofophthalmic sodium cromoglycate and nedocromil sodium in the treatment ofvernal keratoconjunctivitis. Br J Ophthalmol 1994;78:365–9.
30 Bonini S, Barney NP, Schiavone M, et al. Effectiveness of nedocromil sodium2% eyedrops on clinical symptoms and tear fluid cytology of patients withvernal conjunctivitis. Eye 1992;6:648–52.
31 Foster CS. Evaluation of cromolyn sodium in the treatment of vernalkeratoconjunctivitis. Ophthalmology 1988;95:194–201.
32 Resnikoff S, Cornand G, Filliard G, et al. Limbal vernal keratoconjunctivitis inthe tropics. Rev Int Trach Pathol Ocul Trop Subtrop Sante Publique1988;65:21–72.
33 Baryishak YR, Zavaro A, Monselise M, et al. Vernal keratoconjunctivitis in anIsraeli group of patients and its treatment with sodium cromoglycate.Br J Ophthalmol 1982;66:118–22.
34 Abiose A. Paediatric ophthalmic problems in Nigeria. J Trop Pediatr1985;31:30–5.
35 Tabbara KF. Ocular complications of vernal keratoconjunctivitis.Can J Ophthalmol 1999;34:88–92.
36 Tabbara KF, Ross-Degnan D. Blindness in Saudi Arabia. JAMA1986;255:3378–84.
37 Herse P, Gothwal VK. Survey of visual impairment in an Indian tertiary eyehospital. Indian J Ophthalmol 1997;45:189–93.
38 Akpek EK, Hasiripi H, Christen WG, et al. A randomized trial of low-dose,topical mitomycin-C in the treatment of severe vernal keratoconjunctivitis.Ophthalmology 2000;107:263–9.
39 Abu el-Asrar AM, Van den Oord JJ, Geboes K, et al. Immunopathologicalstudy of vernal keratoconjunctivitis. Graefes Arch Clin Exp Ophthalmol1989;227:374–9.
40 El-Asrar AM, Tabbara KF, Geboes K, et al. An immunohistochemical study oftopical cyclosporin in vernal keratoconjunctivitis. Am J Ophthalmol1996;121:156–61.
41 BenEzra D, Pe’er J, Brodsky M, et al. Cyclosporin eyedrops for the treatment ofsevere vernal keratoconjunctivitis. Am J Ophthalmol 1986;101:278–82.
42 Secchi AG, Tognon MS, Leonardi A. Topical use of cyclosporin in thetreatment of vernal keratoconjunctivitis. Am J Ophthalmol 1990;110:641–5.
43 Bleik JH, Tabbara KF. Topical cyclosporin in vernal keratoconjunctivitis.Ophthalmology 1991;98:1679–84.
44 Avunduk AM, Avunduk MC, Erdol H, et al. Cyclosporin effects on clinicalfindings and impression cytology specimens in severe vernalkeratoconjunctivitis. Ophthalmologica 2001;215:290–3.
45 Pucci N, Novembre E, Cianferoni A, et al. Efficacy and safety of cyclosporineyedrops in vernal keratoconjunctivitis. Ann Allergy Asthma Immunol2002;89:298–303.
46 Cetinkaya A, Akova YA, Dursun D, et al. Topical cyclosporin in themanagement of shield ulcers. Cornea 2004;23:194–200.
47 Hanifin JM. Epidemiologyofatopicdermatitis.MonogrAllergy1987;21:116–31.48 Garrity JA, Liesegang TJ. Ocular complications of atopic dermatitis.
Can J Ophthalmol 1984;19:19–24.49 Power WJ, Tugal-Tutkun I, Foster CS. Long-term follow-up of patients with
atopic keratoconjunctivitis. Ophthalmology 1998;105:637–42.50 Belfort R, Marbeck P, Hsu CC, et al. Epidemiological study of 134 subjects
with allergic conjunctivitis. Acta Ophthalmol Scand Suppl 2000;230:38–40.51 Tuft SJ, Kemeny DM, Dart JK, et al. Clinical features of atopic
keratoconjunctivitis. Ophthalmology 1991;98:150–8.52 Foster CS, Rice BA, Dutt JE. Immunopathology of atopic keratoconjunctivitis.
Ophthalmology 1991;98:1190–6.53 Metz DP, Hingorani M, Calder VL, et al. T-cell cytokines in chronic allergic eye
disease. J Allergy Clin Immunol 1997;100:817–24.54 Calder VL, Jolly G, Hingorani M, et al. Cytokine production and mRNA
expression by conjunctival T-cell lines in chronic allergic eye disease. Clin ExpAllergy 1999;29:1214–22.
55 Foster CS, Calonge M. Atopic keratoconjunctivitis. Ophthalmology1990;97:992–1000.
56 Hoang-Xuan T, Prisant O, Hannouche D, et al. Systemic cyclosporine A insevere atopic keratoconjunctivitis. Ophthalmology 1997;104:1300–5.
57 Hingorani M, Moodaley L, Calder VL, et al. A randomized, placebo-controlled trial of topical cyclosporin A in steroid-dependent atopickeratoconjunctivitis. Ophthalmology 1998;105:1715–20.
58 Akpek EK, Dart JK, Watson S, et al. A randomized trial of topical cyclosporin0.05% in topical steroid-resistant atopic keratoconjunctivitis. Ophthalmology2004;111:476–82.
59 Tomida I, Schlote T, Brauning J, et al. [Cyclosporin A 2% eyedrops in therapyof atopic and vernal keratoconjunctivitis.] Ophthalmologe 2002;99:761–7.
60 Hingorani M, Calder VL, Buckley RJ, et al. The immunomodulatory effect oftopical cyclosporin A in atopic keratoconjunctivitis. Invest Ophthalmol Vis Sci1999;40:392–9.
61 Foster CS, Forstot SL, Wilson LA. Mortality rate in rheumatoid arthritis patientsdeveloping necrotizing scleritis or peripheral ulcerative keratitis: effects ofsystemic immunosuppression. Ophthalmology 1984;91:1253–63.
62 Pfister RR, Murphy GE. Corneal ulceration and perforation associated withSjogren’s syndrome. Arch Ophthalmol 1980;98:89–94.
63 Zierhut M, Thiel HJ, Weidle EG, et al. Topical treatment of severe cornealulcers with cyclosporin A. Graefes Arch Clin Exp Ophthalmol1989;227:30–5.
64 Kervick GN, Pflugfelder SC, Haimovici R, et al. Paracentral rheumatoidcorneal ulceration: clinical features and cyclosporin therapy. Ophthalmology1992;99:80–8.
65 Gottsch JD, Akpek EK. Topical cyclosporin stimulates neovascularization inresolving sterile rheumatoid central corneal ulcers. Trans Am Ophthalmol Soc2000;98:81–7.
66 Liegner JT, Yee RW, Wild JH. Topical cyclosporin therapy for ulcerativekeratitis associated with rheumatoid arthritis. Am J Ophthalmol1990;109:610–2.
67 Thygeson P. Superficial punctate keratitis. JAMA 1950;144:1544–9.68 Nagra PK, Rapuano CJ, Cohen EJ, et al. Thygeson’s superficial punctate
keratitis: ten years’ experience. Ophthalmology 2004;111:34–7.69 Hardten DR, Doughman DJ, Holland EJ, et al. Persistent superficial punctate
keratitis after resolution of chlamydial follicular conjunctivitis. Cornea1992;11:360–3.
70 Reinhard T, Roggendorf M, Fengler I, et al. PCR for varicella zoster virusgenome negative in corneal epithelial cells of patients with Thygeson’ssuperficial punctate keratitis. Eye 2004;18:304–5.
71 Goldberg DB, Schanzlin DJ, Brown SI. Management of Thygeson’s superficialpunctate keratitis. Am J Ophthalmol 1980;89:22–4.
72 Forstot SL, Binder PS. Treatment of Thygeson’s superficial punctatekeratopathy with soft contact lenses. Am J Ophthalmol 1979;88:186–9.
73 Reinhard T, Sundmacher R. [Local cyclosporin A therapy in Thygeson superficialpunctate keratitis--a pilot study.] Klin Monatsbl Augenheilkd, 1996;209:224–7.
74 Reinhard T, Sundmacher R. Topical cyclosporin A in Thygeson’s superficialpunctate keratitis. Graefes Arch Clin Exp Ophthalmol 1999;237:109–12.
75 Del Castillo JM, Del Castillo JB, Garcia-Sanchez J. Effect of topical cyclosporinA on Thygeson’s superficial punctate keratitis. Doc Ophthalmol 1996–97;93:193–8.
76 Schuster V, Seregard S. Ligneous conjunctivitis. Surv Ophthalmol2003;48:369–88.
77 Hidayat AA, Riddle PJ. Ligneous conjunctivitis: a clinicopathologic study of 17cases. Ophthalmology 1987;94:949–59.
78 Watts P, Suresh P, Mezer E, et al. Effective treatment of ligneous conjunctivitiswith topical plasminogen. Am J Ophthalmol 2002;133:451–5.
79 Holland EJ, Chan CC, Kuwabara T, et al. Immunohistologic findings andresults of treatment with cyclosporin in ligneous conjunctivitis. Am JOphthalmol1989;107:160–6.
80 Rao SK, Biswas J, Rajagopal R, et al. Ligneous conjunctivitis: aclinicopathologic study of 3 cases. Int Ophthalmol 1998–99;22:201–6.
81 Rubin BI, Holland EJ, de Smet MD, et al. Response of reactivated ligneousconjunctivitis to topical cyclosporin. Am J Ophthalmol 1991;112:95–6.
82 Boyd AS, Neldner KH. Lichen planus. J Am Acad Dermatol1991;25:593–619.
83 Thorne JE, Jabs DA, Nikolskaia OV, et al. Lichen planus and cicatrizingconjunctivitis: characterization of five cases. Am J Ophthalmol2003;136:239–43.
84 Neumann R, Dutt CJ, Foster CS. Immunohistopathologic features and therapyof conjunctival lichen planus. Am J Ophthalmol 1993;115:494–500.
85 Oliver GF, Winkelmann RK. Treatment of lichen planus. Drugs1993;45:56–65.
86 Levell NJ, Munro CS, Marks JM. Severe lichen planus clears with very low-dose cyclosporin. Br J Dermatol 1992;127:66–7.
87 Crompton DO. Immuno-suppressive drug treatment of keratitis sicca, includingan example of lichen planus of the conjunctiva. Aust N Z J Surg1968;38:143–6.
88 Leonardi A, DeFranchis G, Fregona IA, et al. Effects of cyclosporin A onhuman conjunctival fibroblasts. Arch Ophthalmol 2001;119:1512–7.
89 Rhee MK, Mootha VV. Bilateral keratoconjunctivitis associated with lichenplanus. Cornea 2004;23:100–5.
90 Pakravan M, Klesert T, Akpek EK. Isolated conjunctival lichen planus. Cornea(in press).
91 Theodore FH. Further observations on superior limbic keratoconjunctivitis.Trans Am Acad Ophthalmol Otolaryngol 1967;71:341–51.
92 Cher I. Superior limbic keratoconjunctivitis: multifactorial mechanicalpathogenesis. Clin Experiment Ophthalmol 2000;28:181–4.
93 Perry HD, Doshi-Carnevale S, Donnenfeld ED, et al. Topical cyclosporin A0.5% as a possible new treatment for superior limbic keratoconjunctivitis.Ophthalmology 2003;110:1578–81.
94 Zhao JC, Jin XY. Immunological analysis and treatment of Mooren’s ulcer withcyclosporin A applied topically. Cornea 1993;12:481–8.
95 Shimura M, Yasuda K, Fuse N, et al. Effective treatment with topical cyclosporinA of a patient with Cogan syndrome. Ophthalmologica 2000;214:429–32.
96 Akpek EK, Ilhan-Sarac O, Green WR. Topical cyclosporin in the treatment ofchronic sarcoidosis of the conjunctiva. Arch Ophthalmol 2003;121:1333–5.
97 McCoombes JA, Hirst LW, Green WR. Use of topical cyclosporin forconjunctival manifestations of actinic prurigo. Am J Ophthalmol2000;130:830–1.
98 Derse M, Wannke E, Payer H, et al. [Successful topical cyclosporin A in thetherapy of progressive vascularising keratitis in keratitis-ichthyosis-deafness(KID) syndrome (Senter syndrome).] Klin Monatsbl Augenheilkd2002;219:383–6.
99 Chung MS, Pepose JS, El-Agha MS, et al. Confocal microscopic findings in acase of delayed-onset bilateral diffuse lamellar keratitis after laser in situkeratomileusis. J Cataract Refract Surg 2002;28:1467–70.
100 Touzeau O, Borderie V, Razavi S, et al. [Use of topical cyclosporin inmicrocrystalline keratopathy due to streptococcus.] J Fr Ophtalmol1999;22:662–5.
Topical ciclosporin 1367
www.bjophthalmol.com

Bevacizumab suppresseschoroidal neovascularisationcaused by pathological myopiaBevacizumab (Avastin, Genentech) is arecombinant humanised, full length, anti-VEGF monoclonal antibody that binds allisoforms of VEGF-A. It has been shown toprolong survival of patients with advancedcolon cancer when combined with 5-fluoro-uracil.1 In this report, we describe the effectof bevacizumab in two patients with chor-oidal neovascularisation (CNV) secondary topathological myopia, which was refractory toother treatment.
Case reportsPatient 1AM is a 36 year old white man who wasdiagnosed with subfoveal CNV caused bypathological myopia (right eye = 211.50 D,left eye = 211.50 D) in his left eye inSeptember 2002 for which he received threephotodynamic therapy (PDT) treatments. Hedeveloped subfoveal CNV in his right eye inJune 2003 and received one PDT treatmentcombined with an intravitreous injection of4 mg of triamcinolone acetonide. In May2004, he presented with recurrent subfovealCNV in his right eye and refused PDT. Off-label use of bevacizumab was discussed andafter informed consent, the patient decided toproceed.Just before treatment in July 2004, best
corrected visual acuity (VA) was 20/40 in theright eye and 20/25 in the left eye. There wasa ring of hyperpigmentation centred on thefovea with a surrounding ring of subretinalblood and substantial subretinal fluid in theright eye (fig 1A). An optical coherencetomography (OCT) scan through the centreof the fovea confirmed the presence of
extensive subretinal fluid (fig 1B, asterisks)with subretinal tissue in the centre of thefovea (arrowheads). An OCT map showedsevere thickening and subretinal fluidthroughout the centre of the macula (fovealthickness 510 mm, macular volume9.29 mm3). In the left eye, there werepigmentary changes and no subretinal bloodor fluid (foveal thickness, 201 mm). In theright eye, the early phase of a fluoresceinangiography (FA) scan showed a central areaof hyperfluorescence surrounded by blockedfluorescence from subretinal blood (fig 2A).Central fluorescence increased in the mid
phase (fig 2B) and in the late phase the areaof hyperfluorescence was larger with indis-tinct borders indicating leakage of dye intosurrounding tissue (fig 2C).The patient received an intravenous infu-
sion of 5 mg/kg of bevacizumab, which hetolerated well. He noted subjective improve-ment in vision in both eyes within 7 days and2 weeks after the infusion, VA was 20/20 inboth eyes and biomicroscopy showed lesssubretinal fluid (fig 1C), confirmed by OCT(fig 1D, asterisk). Compared to the pre-infusion OCT, the retinal thickness mapshowed substantial improvement with adecrease in foveal thickness (330 mm from510 mm) and macular volume (6.89 mm3
from 9.29 mm3). In the early phase of a FAin the right eye (fig 2D), the hyperfluorescentarea was reduced compared to a correspond-ing frame of the baseline FA (fig 2A). Theintensity of hyperfluorescence increasedbetween the early and mid phase (fig 2E)and there was evidence of dye leakage fromthe CNV during the late phase (fig 2F). Thepatient received second and third infusions of5 mg/kg of bevacizumab without any diffi-culty. Six weeks after the first infusion andjust before the fourth infusion, VA was 20/20in each eye and biomicroscopy showed noidentifiable subretinal fluid in the right eyeand resorption of almost all of the subretinalblood (fig 1E). OCT confirmed that there wasno subretinal fluid (fig 1F) and the retinalthickness map showed further improvementcompared to the map after the first infusion.Foveal thickness measured 244 mm andmacular volume was 5.80 mm3. Early phaseof the FA showed further reduction in thearea of hyperfluorescence (fig 2G) comparedto a corresponding frame of the FA done afterthe first infusion (fig 2D). There was only amild increase in brightness of the hyperfluor-escent area in the mid phase of the FA
Figure 1 Fundus appearance and optical coherence tomogram of patient 1 at baseline and afterstarting infusions of bevacizumab.
Figure 2 Fluorescein angiography of patient 1 at baseline and after starting infusions ofbevacizumab.
LETTERS
PostScript . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1368 Br J Ophthalmol 2005;89:1368–1387
www.bjophthalmol.com

(fig 2H) and sharp borders with no furtherincrease in brightness in the late phase(fig 2I). This indicates that there was littlecollection of dye within the CNV and noleakage into surrounding tissue—two favour-able signs. Nine months after the fourthinfusion, the patient was asymptomatic andvisual acuity was 20/20 in each eye. FAshowed no evidence of leakage in either eye.
Patient 2LL is a 52 year old white woman withpathological myopia (refractive error 217.75sphere and 218.75 + 0.756165). The left eyedeveloped subfoveal CNV in February 2002and the patient had six PDT treatments withthe last in January 2004. The right eyedeveloped juxtafoveal CNV and was treatedwith photocoagulation in April 2002.Recurrent CNV occurred beneath the foveaand was treated with PDT on two occasions,the most recent in January 2004.The patient presented in July of 2004
complaining of progressive loss of vision inboth eyes. Visual acuity was 20/100 in theright eye and 20/200 in the left eye. In theright eye, there was a laser scar between thedisc and the nasal border of the fovea. Therewere flecks of subretinal haemorrhage andmild subretinal fluid. In the left eye there washypopigmentation surrounded by a ring ofhyperpigmentation with subretinal fluid,blood, and thickening in the macula(fig 3A). OCT in the left eye showedprominent retinal thickening surrounding asmall central area of retinal atrophy (fig 3B,arrow). The retinal thickness map showedthe thickest region of the retina to be locatedon the inferotemporal side of the fovea.Foveal thickness was 311 mm and macularvolume was 7.30 mm3. In the right eye, OCTshowed retinal thinning in the region of thelaser scar inferonasal to the fovea (fig 3C,arrows), and thickening superotemporal tothe fovea with a pocket of subretinal fluid(asterisk). Foveal thickness was 296 mm andmacular volume was 5.91 mm3. There wassubfoveal CNV in both eyes, and it wasdecided to transit the left eye because there
was more retinal thickening in the left eye.The early phase of the FA showed a centralarea of hyperfluorescence and surroundingblocked fluorescence from subretinal blood(fig 4A). The hyperfluorescence becamemuch brighter during the mid phase of theFA (fig 4B) and leaked during the late phase(fig 4C). The patient refused additional PDTand after careful consideration of potentialrisks and benefits and signing a consentform, the patient was given four intravenousinfusions of 5 mg/kg of bevacizumab atintervals of 2 weeks, which she toleratedwell.Examination before the fourth infusion
showed a VA of 20/64 in the right eye and 20/
200 in the left eye. Biomicroscopy in the lefteye showed reduced subretinal blood com-pared to the baseline examination, butpersistent macular thickening (fig 3D) con-firmed by OCT, which showed a fovealthickness of 304 mm and a macular volumeof 7.37 mm3. In the right eye, there was mildresidual subretinal fluid and a few flecks ofsubretinal blood temporal to the laser scar.OCT in the right eye showed reduced retinalthickening and minimal subretinal fluid withfoveal thickness of 249 mm and a macularvolume of 5.78 mm3 (fig 3F). In the left eye,early phase of a FA (fig 4D) showed a similararea of hyperfluorescence as that seen in theearly phase of the baseline FA (fig 4A), butsubstantially less fluorescence during the mid(fig 4E) and late (fig 4F) phases than thecorresponding phases of the baseline FA,indicating less filling of the CNV with dye.There was still substantial leakage of dye intosurrounding tissue in the late phase (fig 4F).The patient returned 2 months after thefourth infusion noting subjective visualimprovement that had allowed her to resumemany activities that she had previouslystopped. VA was 20/64 in the right eye and20/200 in the left. Contact lens biomicroscopyin the left eye showed no identifiablesubretinal blood or fluid, and macular thick-ness appeared reduced (fig 3G). This wasconfirmed by OCT (fig 3H; foveal thickness253 mm, macular volume 6.40 mm3). In theright eye, there was no identifiable subretinalblood or fluid and OCT showed no changesfrom the scan at week 6. FA in the left eyeshowed reduced hyperfluorescence comparedto previous FAs at all phases, early (fig 4G),mid (fig 4H), and late (fig 4I), and noleakage.
CommentIn two patients, intravenous infusions ofbevacizumab resulted in reduced fluoresceinangiographic evidence of leakage from CNVand decreased retinal thickening and sub-retinal fluid. This anatomical evidence of
Figure 3 Fundus appearance and optical coherence tomogram of patient 2 at baseline and afterstarting infusions of bevacizumab.
Figure 4 Fluorescein angiography of patient 2 at baseline and after starting infusions ofbevacizumab.
PostScript 1369
www.bjophthalmol.com

improvement was accompanied by visualimprovement in two of the three eyes inwhich there was active subfoveal CNV atbaseline. The one eye that did not showobjective evidence of visual improvement hadprominent subretinal fibrosis and a centralarea of retinal atrophy at baseline. Althoughspontaneous improvement cannot be ruledout with certainty, the course of these twopatients suggests that antagonism of VEGFwith bevacizumab provided benefit. No ocu-lar or systemic side effects were observed.Recent studies have suggested that VEGF
may be an important stimulus for neovascu-lar age related macular degeneration(AMD).2 3 Despite differences in pathogenesisamong the disease processes, the effect ofbevacizumab in the two patients reportedhere suggests that VEGF may be an impor-tant stimulus for CNV in pathological myopiaas well as AMD. While uncontrolled observa-tions in two patients do not justify wide-spread use of bevacizumab in patients withCNV, additional studies are warranted. Acontrolled clinical trial is needed to determineif bevacizumab is safe and effective inpatients with subfoveal CNV caused bypathological myopia and, if so, to determinethe appropriate frequency of administration.
Q D Nguyen, S Shah, S Tatlipinar, D V Do,E V Anden, P A Campochiaro
Department of Ophthalmology, Johns HopkinsUniversity School of Medicine, 600 North Wolfe
Street, Baltimore, MD, USA
Correspondence to: Peter A Campochiaro, MD,Maumenee 719, Wilmer Eye Institute, Johns Hopkins
University School of Medicine, 600 North WolfeStreet, Baltimore, MD 21287-9277, USA; pcampo@
jhmi.edu
doi: 10.1136/bjo.2005.066431
References
1 Hurwitz H, Fehrenbacher L, Novotny W, et al.Bevacizumab plus irinotecan, fluorouracil, andleucovorin for metastatic colorectal cancer.N Engl J Med 2004;350:2335–42.
2 Gragoudas ES, Adamis AP, Cunningham ET Jr,et al. Pegaptanib for neovascular age-relatedmacular degeneration. N Engl J Med2004;351:2805–16.
3 Schwartz SD, Blumenkranz M, Rosenfeld PJ, et al.Safety of rhuFab V2, an anti-VEGF antibodyfragment, as a single intravitreal injection insubjects with neovascular age-related maculardegeneration. Invest Ophthalmol Vis Sci (suppl)2001;42:S522.
Compliance: clearcommunication’s criticalNon-compliance can be subdivided intovoluntary and involuntary types. Voluntarynon-compliance is patients deciding not touse their medication. Involuntary non-com-pliance refers to situations where medica-tions are used incorrectly, such as eye dropsmissing the conjunctival sac, using incorrectmedication, or following an incorrect regime.The impact of non-compliance is particularlyimportant for patients with chronic diseasessuch as glaucoma.1
We collected data from patients in ourclinic to try to ascertain the frequency andnature of any discrepancies between the dropregimes patients were using and what theirnotes said their current regimes should be.
MethodsOne hundred consecutive patients usingtopical medication to lower intraocular pres-sure attending a UK teaching hospital’sglaucoma service clinics were asked whichdrops they were using and how often theyput them in. Each patient was only enteredinto the study once. If any deviation from thedrop regime described in their notes wasidentified then further questioning was usedto identify the cause of that discrepancy.
ResultsIn total, 30 of the 100 patients were not usingthe antiglaucoma medication as described intheir notes. Eighteen cases were caused byophthalmologists either changing a regimewithout informing the general practitioner ornot giving clear instructions to the patient.Examples include transcription errors by theophthalmologist when dictating the letter tothe general practitioner (four cases), patientsstopping treatments because of side effectswithout contacting clinic (four cases),patients stopping their glaucoma drops aftercataract surgery (three cases), and ambiguitybetween Xalatan and Xalacom (one case).Patient error can be attributed to nine
cases. Examples include patient using dropsless frequently than prescribed (three cases),patient using drops in the wrong eye or oneeye only (two cases), patients changing thedose frequency of their own accord (onecase), and using drops too frequently (onecase).The other three cases were the result of
‘‘unreliable’’ nursing home staff (two cases),and failure to prescribe eye drops on admis-sion to a general medical ward.
CommentOphthalmologists communicating poorlywith patients or with general practitionerscaused nearly one in five patients to use thewrong regime. The responsibility for ensuringthat all communication between the ophthal-mologist and patients or general practitionersis intelligible and unambiguous lies with theophthalmologist.One frequent cause of non-compliance is
newly diagnosed patients thinking that theinitially prescribed bottle is the full course oftreatment, and ceasing treatment when thisbottle expires. This is a well recognisedphenomenon on the literature on persistencywith treatment for glaucoma.2
We were alarmed that 30% of the samplewere using an incorrect drop regime.Involuntary non-compliance merits furtherresearch and poses a considerable threat tothe control of patients’ disease. Furthermore,failure to identify compliance as the cause ofa patient’s apparent lack of response totreatment may result in prescription of moretoxic medication, and increasingly complexdrop regimes, which can lead to furthercompliance problems.3
A J Buller, B Connell, A F SpencerManchester Royal Eye Hospital, Manchester, UK
Correspondence to: A J Buller, Manchester Royal EyeHospital, Oxford Road, Manchester M13 9WH, UK;
doi: 10.1136/bjo.2005.066175
References
1 Schwartz GF. Persistency and tolerability ofocular hypotensive agents: population-basedevidence in the management of glaucoma.Am J Ophthalmol 2004;137(Suppl):S1–S2.
2 Reardon G, Schwartz GF, Mozaffari E. Patientpersistency with topical ocular hypotensivetherapy in a managed care population.Am J Ophthalmol 2004;137(Suppl):S3–S12.
3 MacKean JM, Elkington AR. Compliance withtreatment of patients with chronic open-angleglaucoma. Br J Ophthalmol 1983;67:46–9.
Safety of phacoemulsification ina patient with an implanted deepbrain neurostimulation deviceA 69 year old woman with nuclear scleroticcataracts was examined. She was awaitingneurosurgery for treatment of drug refractorytitubation (head tremor). Before cataract sur-gery, she underwent successful neurosurgery.The implanted Medtronic deep brain stimula-tion device rendered her asymptomatic oftremors. At the cataract preoperative clinicshe showed the device identification card thatstated ‘‘ultrasound diathermy … anywhere onyour body … can result in severe injury ordeath.’’1 Following confirmation fromMedtronic that it was safe to proceed, thepatient had an uneventful left phacoemulsifi-cation performed under general anaesthesiawith the neurostimulator turned ‘‘off.’’ Sevenmonths later she underwent a similar success-ful right phacoemulsification.
CommentDeep brain neurostimulation of the thalamus isthe treatment of choice for drug refractoryessential tremor.2 Indications for its use arewidening and include use in multiple sclerosis,advanced Parkinson’s disease, and movementdisorders such as dystonia.3 The deep brainneurostimulator has three implanted compo-nents. The electrodes are implanted into thesubthalamic nucleus or the globus pallidusinterna,1 2 4 then an insulated lead is placedsubcutaneously from the burr hole to a sealedneurostimulator device beneath the clavicle.The neurostimulator electrical stimulationpulses can be adjusted from external devices.4
There are two recorded fatalities in patientswith implanted deep brain neurostimulation
Accepted for publication 14 January 2005
Accepted for publication 9 January 2005Figure 1 Implanted deep brainneurostimulation device.
1370 PostScript
www.bjophthalmol.com

devices who had received short wave dia-thermy ‘‘as used by physiotherapists.’’5
Medtronic also report two similar patientswho were still comatose.1 Another reportdescribed permanent, severe central nervoussystem injury following stimulation of aspinal cord neurostimulator by a radiofre-quency antitheft device.6
Brain damage results from heating of theimplanted electrodes.7 Heat energy releaseddirectly to the body from an external source canbe conducted via the insulated lead of animplanted neurostimulation device, raising thetemperature at the electrode. Furthermore, ifan external source generates an electric currentin the insulated lead, this will result in a rise inthe temperature at the electrode. Ultrasounddiathermy transfers heat directly to the bodywhere short wave diathermy results in aninduced electrical current.8 One study calcu-lated a potential rise of 9.76 C at the deep brainneurostimulator electrode when short wavediathermy was used.7 For phacoemulsificationto be safe in patients with deep brain neuro-stimulators, it must not produce significantheat or generate an electric current.The phacoemulsification hand piece uses
the piezoelectric effect to drive the phacoe-mulsification needle tip in a linear jackham-mer-like movement, physically cutting thelens.9 Acoustic cavitation results from anexplosive collapse of vacuoles formed in fluidaround the swiftly moving phacoemulsifica-tion needle tip.9 A study showed a maximumtemperature rise of 3.5 C in the anteriorchamber during routine phacoemulsifica-tion.10 The risk of this generated heat spread-ing to the implanted electrodes must be low.The phacoemulsification tip does not gener-ate an oscillating magnetic field that mightinduce an electrical current. Theoretically,this should render ultrasound phacoemulsi-fication safe in the presence of implanteddeep brain neurostimulators.With expanding technology, there will
naturally be situations with the potential forinteractions between equipment from differ-ent specialties. Consent should include thepossibility of heat conduction to theimplanted neurostimulation device. The useof local anaesthesia may allow early detectionof discomfort or neurological sequelae. Thesurgeon should make use of all techniques toreduce the heat generated during phaco-emulsification. Medtronic advise turning theneurostimulator off and not placing anycables over the patient’s chest and neck (RCoffey, 3 February 2005, personal commu-nication). There are various neurostimula-tors, including cortical devices, that may haveincreased sensitivity to localised temperatureincreases. Heat formation at the phacoemul-sification needle tip has been analysed;however, further research on the extent ofheat dissipation is required.
C F Parsloe, J M TwomeyMusgrove Park Hospital, Taunton, Somerset
Correspondence to: Mr J M Twomey, Musgrove ParkHospital, Taunton TA1 5DA, Somerset, UK; john.
doi: 10.1136/bjo.2005.066209
References
1 Medtronic. Important safety information.www.medtronic.co.uk/UK/patients/neuro/safety_informationhtml, accessed 4 January, 2005.
2 Gross RE, Lozano AM. Advances inneurostimulation for movement disorders. NeurolRes 2000;22:247–58.
3 Joshua A, Bryant B, et al. The impact of thalamicstimulation on activities of daily living for essentialtremor. Surg Neurol 2003;59:479–85.
4 Medtronic. What is deep brain stimulation?www.medtronic.co.uk/UK/patients/neuro/brain_stimulation.html, accessed 4 January,2005.
5 Medicines and Healthcare Products RegulatoryAgency. Patients with active/powered implants:risk of serious injury from therapeutic diathermytreatment. www.medical-devices.gov.uk/mda/mdawebsitev2.nsf/webvwIndex/3FE48E06AB1F64F200256AB6003F1C6D?OPEN, accessed 4 January, 2005.
6 Eisenberg E, Waisbrod H. Spinal cord stimulatoractivation by an antitheft device. J Neurosurg1997;87:961–2.
7 Ruggera PS, Witters DM, et al. In vitro assessmentof tissue heating near metallic medical implants byexposure to pulsed radio frequency diathermy.Phys Med Biol 2003;48:2919–28.
8 Anderson DM, ed. Dorland’s illustrated medicaldictionary. Philadelphia: WB Saunders, 2000.
9 Dondrea CL, ed. Surgery for cataract. In: Basicand clinical science course. San Francisco:American Academy of Ophthalmology,2004:89–162.
10 Heisler JM, Barmbek AK, et al. In vivomeasurement of the temperature changes duringphacoemulsification. Ophthalmologe2002;99:448–56.
Vertical deviation exacerbatedby convergence andaccommodationWe report a patient with hypertropia causingdiplopia exacerbated by convergence andaccommodation.
Case reportA 36 year old man presented with 8 yearhistory of worsening intermittent doublevision. Visual acuities were 6/5 in each eye.For near there was manifest left hypertropiaand left hyperphoria at distance (fig 1A,table 1). Extraocular movements were fullwith no overactions. No significant differencein vertical deviation in different gaze posi-tions or cyclotropia was found, the deviationincreased on head tilt to the left (table 2).There was no dissociated vertical deviation.1
The angle of deviation varied between 2and 7 prism dioptres at distance and 24and 45 prism dioptres at near on repeatedexaminations. Stereovision was 55 secondsof arc when deviation was prism corrected.The AC/A ratio was normal using gradientmethod. The vertical fusion range was13 prism dioptres at distance (9 prismdioptres base-down and 4 prism dioptresbase-up).The vertical deviation increased on accom-
modation with concave lenses and the devia-tion decreased with 10 dioptre base-in prismsat near (table 1). Eye movement recordingsare shown in figure 1C. Pupil reactions andfundoscopy were unremarkable. Thyroidfunctions, thyroid peroxidase and acetylcho-line receptor antibodies were normal.Tensilon test was negative. Orbicularis oculimuscle single fibre electromyogram wasunremarkable. Neurological examinationand magnetic resonance imaging of the brainand orbits were normal.
CommentKlein-Scharff and Kommerell2 first reportedthree patients with hypotropia and two with
Accepted for publication 21 February 2005
Table 1 Angle of deviation on fixation at distance and near measured with thealternating prism cover test
At 6 metres 5 prism dioptres L/R*At 6 metres with –1D lens 8 prism dioptres L/RAt 6 metres with –2D lens 14 prism dioptres L/RAt 6 metres with –3D lens 25 prism dioptres L/RAt 33 cm 30 prism dioptres L/RAt 33 cm with +3D lens 30 prism dioptres L/RAt 33 cm with 10 prism dioptres base in 15 prism dioptres L/R
*Left over right
Table 2 Harms Wall measurements in nine directions of gaze (upper panel) andhead tilt to the right and left in primary position (lower panel) with left fixation
Left fixation (red filter over left eye)
Elevation+2 14 L/R +1 12 L/R +4 17 L/R0 0 0
+2 17 L/R +4 15 L/R +4 15 L/RLeft 2 Ex 0 2 int Right
+3 15 L/R +5 14 L/R +5 14 L/R2 Ex 0 0
Depression 0
Left fixation
R tilt L tilt+14 9 L/R 27 20 L/R0 0
For each direction of gaze the first number indicated the horizontal deviation (ie, +2 = 2 degreesesotropia), the second measurement indicates the vertical deviation (ie, 14 L/R = 14 degrees left overright) and the number under the horizontal and vertical measurements indicated the cyclodeviation (ie,0 = no cyclodeviation, 2 int = 2 degrees incyclotropia, 2 ex = 2 degrees excyclotropia).
PostScript 1371
www.bjophthalmol.com

hypertropia modulated by accommodationand/or convergence. In contrast with ourpatient, +3 dioptre lenses reduced the verticaldeviation at near in at least one case. Theyconcluded that the patient had verticalaccommodative vergence. Four of five of theircases had additional forms of strabismus.Graf and Weinand3 described a case of left
hyperphoria increasing on convergence. Useof convex lenses and concave lenses did notchange the vertical deviation. Similar to ourpatient, this child had an increase in verticaldeviation when the head was tilted to theside of the hyperphoria/tropia. Graf hasrecently attributed this to the unidirectionalfusional vertical vergence tonus that deve-lopes to compensate for the vertical devia-tion.4 Graf5 described three additional caseswith vertical accommodative vergence with
hypotropia. As in our patients concave lensesat distant fixation increased the verticaldeviation. Subsequently, a series of 19patients with differences in the verticaldeviation between near and distance werereviewed.6 Most cases were combined withstrabismus sursoadductorius and strabismusdeorsoadductorius. In 15 of the 19 patientsthe vertical deviation increased and in fourpatients it decreased at near fixation. Weagree that supranuclear or internuclear mis-innervation most likely explains the connec-tion between elevation and accommodationand convergence.2 3 A more peripheral inner-vational abnormality can be excludedbecause there is no elevation of the left eyewhen the patient is looking to the right (noaberrant innervation between the fibres tothe medial rectus and superior rectus).
In our patient it is unclear whether theabnormality was congenital and decompen-sation of hyperphoria increased symptoms, orwhether it was acquired. Increased verticalfusion range argues for a longstandingsquint. The history of most patients in theliterature1 2 was similar, with slow increase ofdiplopia and vertical deviation at near overseveral years. In several patients, combinedamblyopia or other strabismus forms—suchas dissociated vertical deviation—argue foran early onset of the eye motility problem.2 3
Interestingly, one patient5 seemed to havedeveloped the vertical deviation in combina-tion with convergence after trauma. It ispossible that the aberrant re-innervation canbe either congenital or acquired. It would beinteresting to investigate systematically theinfluence on near and distance fixation inpatients with vertical squint.
S Thomas, S J Farooq, F A Proudlock, I GottlobUniversity of Leicester, Robert Kilpatrick Clinical
Sciences Building, Leicester Royal Infirmary, PO Box65, Leicester LE2 7LX, UK
Correspondence to: Professor Irene Gottlob,Department of Ophthalmology, PO Box 65, RKCSB,
University of Leicester, Leicester LE2 7LX, UK;[email protected]
doi: 10.1136/bjo.2005.069351
References
1 Bielschowsky A. Disturbance of the vertical motormuscles of the eye. Arch Ophthalmol1938;20:175–200.
2 Klein-Scharff U, Kommerell G. Verticalaccommodative vergence. Klin MonatsblAugenheilkd 1991;199:344–5.
3 Graf M, Weinand K. Vertical deviation coupled toconvergence. Klin Monatsbl Augenheilkd2000;216:51–3.
4 Graf M, Krzizok T, Kaufmann H. Head-tilt test inunilateral and symmetric bilateral acquiredtrochlear nerve palsy. Klin Monatsbl Augenheilkd2005;222:142–9.
5 Graf M. Drei Falle von vertikaler accomodativerVergenz. Klin Monatsbl Augenheilkd1993;202:136–7.
6 Graf MH, Rost D, Becker R. Influence of viewingdistance on vertical strabismus. Graefes Arch ClinExp Ophthalmol 2004;242:571–5.
Tetracycline induced greenconjunctival pigment depositsThere have been no reports, to our knowl-edge, of a clinical presentation of ocularpigmentation secondary to the use of oraltetracycline only. Tetracycline hydrochlorideis not a well recognised cause of ocularpigmentary changes, but has been reportedto cause pigmentation of teeth and nails.1 Ofall the tetracyclines, minocycline (a secondgeneration drug) is most often associatedwith the adverse effect of pigmentation.1
There have been several case reports ofminocycline induced scleral pigmentation.2–6
Ocular pigmentary changes reportedly causedby tetracycline have been noted in associationwith use of minocycline.7 8 Both patients inthese case reports had had tetracycline/minocycline therapy for more than 10 yearsfor acne vulgaris and had their depositionlocalised within the tarsal conjunctiva.7 It isbelieved that most of the cysts are found atthe inferior border of the lower tarsusbecause of the frequency of pre-existinginvaginations of conjunctival epithelium in
5
–5
0
2 seconds
near near neardist dist dist distC
B
A
Verti
cal
right
(°)
5
–5
0
Verti
cal
left
(°)
5
–5
0
Hor
izon
tal
right
(°)
5
–5
0
Hor
izon
tal
left
(°)
Figure 1 Patient fixating at near with large left over right squint (A) and at distance with nomanifest vertical deviation (B). Eye movement recordings of patient during near and distancefixation demonstrating a slow upward drifting of the left eye, which occurred simultaneously withthe convergence movement (C).
Accepted for publication 13 March 2005
1372 PostScript
www.bjophthalmol.com

this location.7 The question was raised thatlong term tetracycline has an effect on thelipid layer of the tear film; noting that thepigmentary deposits were only seen in theconjunctival cysts over the tarsal conjunc-tiva.8 Recently, there has been a case report ofa patient with a 5 year history of minocyclineuse for rheumatoid arthritis who developedfocal palpebral conjunctival pigment depos-its. This patient did not have a reported use oftetracycline.2
Our patient was taking only tetracyclinewithout concomitant or previous minocyclineuse and had bulbar conjunctival lesions. Ourpatient had also been on tetracycline for2K years.
Case reportA 48 year old healthy white asymptomaticman presented for evaluation of ‘‘greencrystals’’ on the conjunctiva of both eyes(fig 1). The patient had noted the onset ofthis pigmentation over the previous severalmonths. The patient was treated for acnevulgaris with tetracycline 500 mg a day forthe past 2K years. He denied the use of anytopical ophthalmic drops. He took Lotensinfor the treatment of hypertension. Pastmedical history was otherwise unremarkable.On examination the patient was noted to
have several dark green granular deposits onthe temporal bulbar conjunctiva of both eyes.The granules appeared discrete, crystalline,and varied in size. Otherwise, the examina-tion was unremarkable. Pigmentation wasnot noted in any other region.
PathologyPathology confirmed the presence of tetra-cycline. The specimen was positive for a non-polarisable foreign material in a submucosaland intraepithelial distribution (fig 2). Thismaterial was calcified and had a faint
brown-yellow tinge. There was no appreci-able inflammatory reaction or giant cellreaction to the material. Pathology wasconsistent with that of previously describedreports of tetracycline.7
CommentTetracyclines of the first generation (tetra-cycline, oxytetracycline, and tetracyclinechloride) are the most commonly prescribedoral antibiotics for acne.9 Tetracycline hasalso been shown to result in improvement ofthe ocular manifestations of rosacea.10 11 Bothconditions are frequent; thus, the ophthal-mologist will encounter many patients beingtreated with tetracycline. Tetracycline fluor-escence has been detected in the conjunctivaof all patients who have taken tetracyclineorally.12 Fluorescence was not generalised butwas restricted to a thin film-like layer on thesurface and to small areas in the surface layerof cells.12
This is the first case report, to our knowl-edge, of clinically visible conjunctival bulbardeposits caused by the use of tetracyclinewithout a history of minocycline use.Pigmentary changes may initially be notedby the ophthalmologist, as in our case report.It is important to recognise signs of
tetracycline pigmentation as it is a commonlyused medication, and cessation of the med-ication may help avoid further pigmentarychanges.
V L Morrison, D O KikkawaUCSD Department of Ophthalmology, UCSD School
of Medicine, La Jolla, CA 92093-0946, USA
B G HerndierUCSD Department of Pathology, UCSD School of
Medicine, La Jolla, CA 92093-0946, USA
D O KikkawaDivision of Ophthalmic Plastic and Reconstructive
Surgery, UCSD Department of Ophthalmology, UCSDSchool of Medicine, La Jolla, CA 92093-0946, USA
Correspondence to: Don O Kikkawa, MD, UCSDDepartment of Ophthalmology, Shiley Eye Center,
9415 Campus Point Drive, La Jolla, CA 92093-0946,USA; [email protected]
doi: 10.1136/bjo.2005.069526
References
1 Eisen D, Hakim MD. Minocycline-inducedpigmentation; incidence, prevention andmanagement. Drug Safety 1998;18:431–40.
2 Bradfield YS, Robertson DM, Salomao DR, et al.Minocycline-induced ocular pigmentation. ArchOphthalmol 2003;121:144–5.
3 Morrow GL, Abbott RL. Minocycline-inducedscleral, dental, and dermal pigmentation.Am J Ophthalmol 1998;125:396–7.
4 Fraunfelder FT, Randall JA. Minocycline-inducedscleral pigmentation. Ophthalmology1997;104:936–8.
5 Sabroe RA, Archer CB, Harlow D, et al.Minocycline-induced discolouration of thesclerae. Br J Dermatol 1996;135:314–16.
6 Angeloni VL, Salasche SJ. Nail, skin, and scleralpigmentation. Cutis 1987;40:229–33.
7 Messmer E, Font RL, Sheldon G, et al. Pigmentedconjunctival cysts following tetracycline/minocycline therapy. histochemical and electronmicroscopic observations. Ophthalmology1983;90:1462–8.
8 Brothers DM, Hidayat AA. Conjunctivalpigmentation associated with tetracyclinemedication. Ophthalmology 1981;88:1212–15.
9 Zouboulis CC, Piquero-Martin J. Update andfuture of systemic acne treatment. Dermatology2003;206:37–53.
10 Del Rosso JQ. A status report on the medicalmanagement of rosacea: focus on topicaltherapies. Cutis 2002;70:271–5.
11 Brown SI, Shahinian L. Diagnosis and treatmentof ocular rosacea. Ophthalmology1978;85:779–86.
12 Dilly PN, Mackie IA. Distribution of tetracycline inthe conjunctiva of patients on long term systemicdoses. Br J Ophthalmol 1985;69:25–8.
Corneal epithelial defects relatedto high postoperativeastigmatismHigh and sometimes irregular astigmatism isnot an infrequent complication followinganterior segment surgery such as suturingof large wounds and corneal transplants.Abnormal corneal topography may affect tearfilm stability adversely. We present the caseof two patients who had persistent post-operative epithelial defects in the lower thirdof the cornea, in the presence of high cornealastigmatism despite aggressive lubrication.Upon addressing their high corneal astigma-tism their epithelial defects resolved.
Case 1An 84 year old man underwent a repeat, HLAmatched, penetrating keratoplasty followinga failed graft for pseudophakic bullouskeratopathy. He had had dry eye symptomswith his primary graft with signs of punctatekeratitis treated with non-preserved lubrica-tion. His repeat graft was uneventful. He wastreated with tacrolimus postoperatively tominimise risk of rejection.Postoperatively, he had persistent dry eye
symptoms for which he was prescribed non-preserved topical lubricants. Six monthspostoperatively sutures in the horizontalmeridian were removed to address ‘‘againstthe rule’’ astigmatism. He presented a monthlater with an epithelial defect in the lowerthird of his graft with an underlying super-ficial stromal melt (fig 1A). Corneal topogra-phy at this time revealed significant ‘‘withthe rule’’ corneal astigmatism of 13 dioptres(fig 1B). Tight sutures were cut and non-preserved lubrication, dexamethasone 0.1%and chloramphenicol 0.5%, was continued.Resolution of the epithelial defect followedrapidly with no further progression of stro-mal melting.
Case 2A 72 year old woman with progressivecataract underwent uncomplicated extracap-sular cataract surgery. She had been diag-nosed with keratoconjunctivitis sicca15 years previously, which at times requiredaggressive topical lubrication to control.Postoperatively, she developed a large centralcorneal defect in the lower third of thecornea. Despite aggressive lubrication theepithelial defect persisted for weeks. Shehad tight superior wound sutures causing11.0 dioptres of astigmatism. It was sus-pected that this could be impeding normalcorneal wetting. Upon their release andcontinued topical lubrication the epithelialdefect resolved.
CommentIt is possible that an irregular corneal surfaceinterferes with normal maintenance of theocular surface tear film. This abnormal teardistribution is likely to be exacerbated by an
Figure 2 Light microscopy of the pathologyspecimen of the conjunctival biopsy showing anon-polarisable foreign material in asubmucosal and intraepithelial distribution.
Accepted for publication 15 March 2005
Figure 1 Clinical photograph of theconjunctival pigmentary deposits.
PostScript 1373
www.bjophthalmol.com

underlying dry eye state. If tear deficiencyand degree of astigmatism are extreme,desiccation of the corneal epithelium ispossible, leading to non-healing defects andassociated sequelae.In cases where high or irregular astigma-
tism is associated with postoperative non-healing corneal defects, addressing thedegree of corneal astigmatism may helprestore physiological tear dynamics and reso-lution of the epithelial defect. Corneal suturesmay themselves impede epithelial migration,1
but if this were the only explanation all graftswould be exposed to the same risk.Conversely, not all patients with high astig-matism (non-surgical) have epithelialdefects. This would suggest that more thana single factor is at play in such situations. Toour knowledge high astigmatism as a con-tributory factor to development of persistentepithelial defects post operatively, has notbeen previously considered.
R Singh, T Umapathy, B B Kulkarni, H S DuaUniversity Hospital, Queens Medical Centre,University of Nottingham, Nottingham, UK
Correspondence to: Professor H S Dua, Division ofOphthalmology, University Hospital, Queens MedicalCentre, B Floor, Eye ENT Centre, Nottingham NG7
2UH, UK; [email protected]
doi: 10.1136/bjo.2005.069260
Reference
1 Lemp MA. The surface of the corneal graft: in vivocolour specular microscopic study in the human.Trans Am Ophthalmol Soc 1989;87:619–57.
Non-tuberculous mycobacteriarelated infectious crystallinekeratopathyNon-tuberculous mycobacteria (NTM) oratypical mycobacterial keratitis is an uncom-mon condition causing indolent cornealulceration. The infection mimics herpetic,mycotic, and Nocardia keratitis and diagnosisrequires a high index of suspicion. We reporttwo cases of NTM infection where thepresenting sign was that of crystalline kera-topathy. Both cases were diagnosed bymicrobial culture and successfully treated.
Case 1A 44 year old white female contact lenswearer presented with a 3 week history of
an inflamed eye with a 1.5 mm diameter areaof corneal stromal infiltration. Vision was 6/6in each eye. She was being treated withantivirals and later unsuccessfully with anti-bacterials and steroids. Three active stromalcrystalline infiltrates appeared in the mid-stroma 3 weeks later (fig 1). Culture from acorneal biopsy revealedMycobacterium chelonei.The keratitis responded to topical amikacin
and amphotericin B, which was started onthe suspicion of fungal keratitis, beforemicrobial culture results were available. Thekeratitis resolved over a 4 week period andvision settled at 6/9.
Case 2An 80 year old white woman with pseudo-phakic bullous keratopathy had a penetratingkeratoplasty and was given systemic tacroli-mus. Three months postoperatively she pre-sented with endothelial dusting and a 1 mmmid-stromal abscess with a crystallineappearance (fig 2). A corneal scrape revealedacid fast bacilli for which she was com-menced on topical ciprofloxacin and amika-cin 2.5% but was slow to respond. Cultureconfirmed Mycobaterium chelonei resistant toamikacin. Topical moxifloxacin was addedand oral clarithromycin commenced. Threemonths later, the ulcer healed with a cleargraft but the vision did not improve (count-ing fingers) on account of pre-existingmacular oedema.
CommentNon-tuberculous mycobacteria cause indo-lent corneal ulceration resembling herpesvirus, fungal, or Nocardia keratitis. The vari-able clinical presentations and poor suscept-ibility to conventional antibacterials usuallyresults in a delay in diagnosis.1–3 The twocommon types of NTM causing keratitis are
M chelonei and M fortutium. The clinicalfeatures of NTM include pseudodendriticepithelial defects, subepithelial white fluffyinfiltrates with crystalline satellite lesionsand ulcers with an overhanging necrotic edgeand a grey sloughed base.1 Keratic precipi-tates and endothelial deposits may appear.Early diagnosis is difficult and absence oforganisms in smears and cultures does notexclude the diagnosis of NTM. Repeat scrapesor a corneal biopsy should be considered inall indolent corneal ulcers.Amikacin has been the drug of choice in
Nocardia and atypical mycobacterial infec-tion.1 2 However, approximately 60% ofpatients will not respond to topical amikacin,as with our second case, and use of combina-tion therapy with ciprofloxacin, gatifloxacin,moxifloxacin, and clarithromycin is recom-mended.4–7 Penetrating keratoplasty is per-formed when stromal infiltration isextensive4 but immunosuppression may pre-dispose to recurrent infection. Both ourpatients were treated successfully. The firstpatient had a good visual outcome but thesecond had poor vision due to pre-existingpathology. Successful treatment requires dis-ease awareness, deferring the use of steroidswhen no organism has been isolated and useof effective antibiotics.
T Umapathy, R Singh, H S DuaDivision of Ophthalmology and Visual Sciences,
Queens Medical Centre, University Hospital,Nottingham, UK
F DonaldDepartment of Microbiology, Queens Medical Centre,
University Hospital, Nottingham, UK
Correspondence to: H S Dua, Division ofOphthalmology, B Floor, Eye ENT Centre, UniversityHospital, Queens Medical Centre, Nottingham NG7
2UH, UK; [email protected]
doi: 10.1136/bjo.2005.069856
References
1 Kinota S, Wong KW, Biswas J, et al. Changingpatterns of infectious keratitis: overview of clinicaland histopathologic features of keratitis due toacanthamoeba or atypical mycobacteria, and ofinfectious crystalline keratopathy.Indian J Ophthalmol 1993;41:3–14.
2 Hu FR, Huang WJ, Huang SF. Clinicopathologicstudy of satellite lesions in nontuberculousmycobacterial keratitis. Jpn J Ophthalmol1998;42:115–18.
3 Sridhar MS, Gopinathan U, Garg P, et al. Ocularnocardia infections with special emphasis on thecornea . Surv Ophthalmol 2001;45:361–78.
4 Matoba A. Mycobacterium chelonei keratitis of acorneal graft. Am J Ophthalmol1987;103:595–96.
Figure 1 (A) Diffuse slit lamp photograph of the corneal graft showing an epithelial defect andsuperficial stromal melting in the lower third. (B) Corneal topography showing steep with the ruleastigmatism.
Accepted for publication 23 March 2005
Figure 1 Case 1 showing three active stromalcrystalline infiltrates central to the edge of theulcer.
Figure 2 Case 2 showing a mid-stromalabscess with a crystalline appearance at 5o’clock region of the graft-host junction.
Accepted for publication 23 March 2005
1374 PostScript
www.bjophthalmol.com
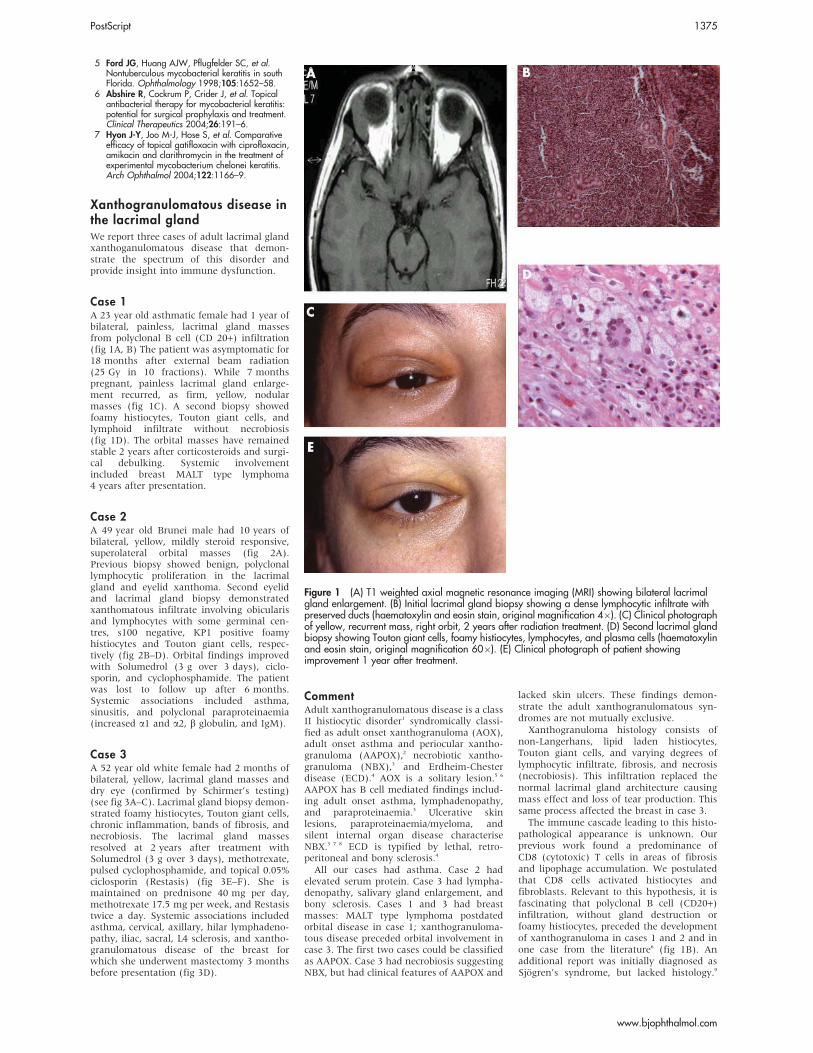
5 Ford JG, Huang AJW, Pflugfelder SC, et al.Nontuberculous mycobacterial keratitis in southFlorida. Ophthalmology 1998;105:1652–58.
6 Abshire R, Cockrum P, Crider J, et al. Topicalantibacterial therapy for mycobacterial keratitis:potential for surgical prophylaxis and treatment.Clinical Therapeutics 2004;26:191–6.
7 Hyon J-Y, Joo M-J, Hose S, et al. Comparativeefficacy of topical gatifloxacin with ciprofloxacin,amikacin and clarithromycin in the treatment ofexperimental mycobacterium chelonei keratitis.Arch Ophthalmol 2004;122:1166–9.
Xanthogranulomatous disease inthe lacrimal glandWe report three cases of adult lacrimal glandxanthoganulomatous disease that demon-strate the spectrum of this disorder andprovide insight into immune dysfunction.
Case 1A 23 year old asthmatic female had 1 year ofbilateral, painless, lacrimal gland massesfrom polyclonal B cell (CD 20+) infiltration(fig 1A, B) The patient was asymptomatic for18 months after external beam radiation(25 Gy in 10 fractions). While 7 monthspregnant, painless lacrimal gland enlarge-ment recurred, as firm, yellow, nodularmasses (fig 1C). A second biopsy showedfoamy histiocytes, Touton giant cells, andlymphoid infiltrate without necrobiosis(fig 1D). The orbital masses have remainedstable 2 years after corticosteroids and surgi-cal debulking. Systemic involvementincluded breast MALT type lymphoma4 years after presentation.
Case 2A 49 year old Brunei male had 10 years ofbilateral, yellow, mildly steroid responsive,superolateral orbital masses (fig 2A).Previous biopsy showed benign, polyclonallymphocytic proliferation in the lacrimalgland and eyelid xanthoma. Second eyelidand lacrimal gland biopsy demonstratedxanthomatous infiltrate involving obicularisand lymphocytes with some germinal cen-tres, s100 negative, KP1 positive foamyhistiocytes and Touton giant cells, respec-tively (fig 2B–D). Orbital findings improvedwith Solumedrol (3 g over 3 days), ciclo-sporin, and cyclophosphamide. The patientwas lost to follow up after 6 months.Systemic associations included asthma,sinusitis, and polyclonal paraproteinaemia(increased a1 and a2, b globulin, and IgM).
Case 3A 52 year old white female had 2 months ofbilateral, yellow, lacrimal gland masses anddry eye (confirmed by Schirmer’s testing)(see fig 3A–C). Lacrimal gland biopsy demon-strated foamy histiocytes, Touton giant cells,chronic inflammation, bands of fibrosis, andnecrobiosis. The lacrimal gland massesresolved at 2 years after treatment withSolumedrol (3 g over 3 days), methotrexate,pulsed cyclophosphamide, and topical 0.05%ciclosporin (Restasis) (fig 3E–F). She ismaintained on prednisone 40 mg per day,methotrexate 17.5 mg per week, and Restasistwice a day. Systemic associations includedasthma, cervical, axillary, hilar lymphadeno-pathy, iliac, sacral, L4 sclerosis, and xantho-granulomatous disease of the breast forwhich she underwent mastectomy 3 monthsbefore presentation (fig 3D).
CommentAdult xanthogranulomatous disease is a classII histiocytic disorder1 syndromically classi-fied as adult onset xanthogranuloma (AOX),adult onset asthma and periocular xantho-granuloma (AAPOX),2 necrobiotic xantho-granuloma (NBX),3 and Erdheim-Chesterdisease (ECD).4 AOX is a solitary lesion.5 6
AAPOX has B cell mediated findings includ-ing adult onset asthma, lymphadenopathy,and paraproteinaemia.3 Ulcerative skinlesions, paraproteinaemia/myeloma, andsilent internal organ disease characteriseNBX.3 7 8 ECD is typified by lethal, retro-peritoneal and bony sclerosis.4
All our cases had asthma. Case 2 hadelevated serum protein. Case 3 had lympha-denopathy, salivary gland enlargement, andbony sclerosis. Cases 1 and 3 had breastmasses: MALT type lymphoma postdatedorbital disease in case 1; xanthogranuloma-tous disease preceded orbital involvement incase 3. The first two cases could be classifiedas AAPOX. Case 3 had necrobiosis suggestingNBX, but had clinical features of AAPOX and
lacked skin ulcers. These findings demon-strate the adult xanthogranulomatous syn-dromes are not mutually exclusive.Xanthogranuloma histology consists of
non-Langerhans, lipid laden histiocytes,Touton giant cells, and varying degrees oflymphocytic infiltrate, fibrosis, and necrosis(necrobiosis). This infiltration replaced thenormal lacrimal gland architecture causingmass effect and loss of tear production. Thissame process affected the breast in case 3.The immune cascade leading to this histo-
pathological appearance is unknown. Ourprevious work found a predominance ofCD8 (cytotoxic) T cells in areas of fibrosisand lipophage accumulation. We postulatedthat CD8 cells activated histiocytes andfibroblasts. Relevant to this hypothesis, it isfascinating that polyclonal B cell (CD20+)infiltration, without gland destruction orfoamy histiocytes, preceded the developmentof xanthogranuloma in cases 1 and 2 and inone case from the literature6 (fig 1B). Anadditional report was initially diagnosed asSjogren’s syndrome, but lacked histology.9
Figure 1 (A) T1 weighted axial magnetic resonance imaging (MRI) showing bilateral lacrimalgland enlargement. (B) Initial lacrimal gland biopsy showing a dense lymphocytic infiltrate withpreserved ducts (haematoxylin and eosin stain, original magnification 46). (C) Clinical photographof yellow, recurrent mass, right orbit, 2 years after radiation treatment. (D) Second lacrimal glandbiopsy showing Touton giant cells, foamy histiocytes, lymphocytes, and plasma cells (haematoxylinand eosin stain, original magnification 606). (E) Clinical photograph of patient showingimprovement 1 year after treatment.
PostScript 1375
www.bjophthalmol.com

Moreover, case 1 developed a monoclonalproliferation of B cells in the breast 1 yearafter the orbital xanthogranuloma.Our cases are unusual because the orbital
xanthogranuloma were limited to the lacri-mal gland, which is devoid of fat. We foundfour similar reports (table 1). Perhapsimmune dysregulation leads to tissuedestruction, and the resultant cell membranefatty acids are scavenged by malfunctioninghistiocytes.The best treatment for xanthogranulo-
matous disease is unknown. Our patientshad some response to steroids, with cases 2and 3 responding to B cell (cyclophospha-mide and methotrexate) and T cell(ciclosporin) suppressors.These cases raise questions regarding the
pathogenesis of non-Langerhans histiocytosisand demonstrate that histopathological andclinical findings must be used for diagnosis in
the spectrum of disorders that is xanthogra-nulomatous disease.
J A Sivak-CallcottDepartment of Ophthalmology, West Virginia
University, Morgantown, WV, USA
W K Lim, L L SeahSingapore National Eye Centre, Singapore
J Oestreicher, D Rossman, N NijhawanDepartment of Ophthalmology, University of Toronto,
Toronto, Ontario, Canada
J RootmanDepartment of Ophthalmology and Visual Sciences,
University of British Colombia, Vancouver, BC,Canada
J Rootman, V WhiteDepartment of Pathology, University of British
Colombia, Vancouver, BC, Canada
H J Williams, W W L ChangDepartment of Pathology, West Virginia University,
Morgantown, WV, USA
A DiBartolomeo*Department of Rheumatology, West Virginia
University, Morgantown, WV, USA
D HowarthDepartment of Pathology, University of Toronto,
Toronto, Ontario, Canada
Correspondence to: Jennifer A Sivak-Callcott, MD,West Virginia University Eye Institute, PO Box 9193,Morgantown, WV 26506, USA; [email protected]
doi: 10.1136/bjo.2004.063578
References
1 Moschella SL. An update of the benignproliferative monocyte-macrophage and dendriticcell disorders. J Dermatol 1996;23:805–15.
2 Jakobiec F, Mills M, Hidayat A, et al. Periocularxanthogranulomas associated with severe adult-onset asthma. Trans Am Ophthalmol Soc1993;91:99–129.
3 Kossard S, Winkelmann RK. Necrobioticxanthogranuloma with paraproteinemia. J AmAcad Dermatol 1980;3:257–70.
4 Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D,et al. Erdheim-Chester disease: clinical andradiologic characteristics of 59 cases. Medicine1996;75:157–69.
5 Mencia-Gutierrez E, Gutierrez-Diaz E, Madero-Garcia S. Juvenile xanthogranuloma of the orbitin an adult.Ophthalmologica 2000;214:437–40.
6 Rouhianen H, Nerdrum K, Puustjarvi T, et al.Xanthogranuloma juvenile—a rare cause oforbital swelling in adulthood. Ophthalmologica1992;204:162–5.
7 Novak P, Robbins T, Winkelmann R. Necrobioticxanthogranuloma with myocardial lesions andnodular transformation of the liver. Hum Pathol1992;23:195–6.
8 Ugurlu S, Bartley GB, Gibson LE. Necrobioticxanthogranuoma: long term outcome of ocularinvolvement. Am J Ophthalmol 2000;129:651–7.
9 Karcioglu ZA, Sharara N, Boles TL, et al. Orbitalxanthogranuloma: clinical and morphologicfeatures in eight patients. Ophthalmic PlastReconstruct Surg 19:372–81.
10 Miszkiel KA, Sohaib SAA, Rose GE, et al.Radiological and clinicopathological features oforbital xanthogranuloma. Br J Ophthalmol2000;84:251–8.
Table 1 Xanthogranulomatous disease presenting in the lacrimal gland
Reference DurationPathologyfirst biopsy
Time to2ndbiopsy
Pathology2nd biopsy
Systemicfindings
Treatment/response Age Sex Diagnosis
Rouhianen6 1 month ‘‘chronicinflam’’
8 months Xantho NR Prednisone, variedcourse
45 F AOX
Miszkiel,10
case 91 year xantho Asthma, eosinophilia,
neutrophiliaSurgery 60 F AAPOX
Tucker11 2–3 months Xantho Paraproteinaemia,polyarticularmigratory arthritis.Later, conjunctivallesions
Prednisone 43 F NBX
Karcioglu9 Xantho Initially ‘‘diagnosedas Sjogren’s’’
23 F Notenoughinfo toclassify
Other cases report dry eye, or lacrimal gland involvement, but not specifically presentation in the lacrimal gland.
Figure 2 (A) Clinical photograph showing bilateral lacrimal gland enlargement and,xanthochromia of the upper eyelids. (B) Second lacrimal gland biopsy demonstrating infiltrationand destruction of the lacrimal gland by lymphorrhages with follicular centres (haematoxylin andeosin stain, original magnification 106). (C) Higher power view of follicular centres and occasionalTouton giant cell (arrows) (haematoxylin and eosin stain, original magnification 206). (D) Toutongiant cells with background of foamy histiocytes, lymphocytes, and plasma cells (haematoxylin andeosin stain, original magnification 606). Photograph reproduced with permission.
Accepted for publication 1 April 2005
None of the authors have any financial interestsregarding this paper.
*Published posthumously.
1376 PostScript
www.bjophthalmol.com

11 Tucker N, Discepola M, Blanco G, et al.Necrobiotic xanthogranuloma withoutdermatologic involvement. Can J Ophthalmol1997;32:396–9.
Management of phaeniciaticophthalmomyiasis externaOphthalmomyiasis, maggot or fly larvaeinfestation of the eye, is a rare condition thatcan have variable presentation depending on
the type of fly, the ocular structures involved,and the level of larval infiltration.
Case reportA 60 year old African-American male pre-sented with a chief complaint of a swollen,moderately painful red right eye since 4 amthat day. Ocular history was significant forforeign body lid trauma of unknown aetiol-ogy (presumably a rock or insect) 2 days
earlier while riding his motorcycle withoutprotective goggles.Ocular examination revealed 20/20 vision
in each eye with correction. Pupils, extra-ocular motilities, and confrontation fieldswere normal. Slit lamp evaluation revealedupper and lower lid oedema with milderythema in the right eye. A 1.5 mm roundulcerated lesion was noted on the right outercanthal region that appeared to pulsate as thepatient was examined in the slit lamp (fig 1).The left eye and other ocular structures in theright eye were unremarkable.Upon external digital pressure of the
ulcerated lesion, a foreign organism was seento retreat into the ocular tissue. Manualforceps were used to remove a 1.0 cm longwhite segmented maggot (fig 2). This speci-men was identified by an entomologist undera microscope, as being of the Calliphoridaefamily, Phaenicia lucilia, otherwise known as ascrewworm fly.The patient was given erythromycin oint-
ment for use twice a day over the lesion. After3 days, the patient returned with completeresolution of the lid oedema and erythema(fig 3).
CommentOphthalmomyiasis is generally caused bysheep botflies and flesh flies. The mostcommonly reported organism in the literatureis Oestrus ovis, a botfly highly prevalent insheep herding and farming communities.1 2
These flies typically lay their eggs on decayingorganic material, but are also attracted toopen mucopurulent human sores. Within24 hours, these eggs hatch, producing larvaewhich then feed on human tissue.2 3 This casewas somewhat unusual in that trauma wasthe mechanism by which the fly eggs were
Figure 3 (A, B) Clinical photographs showing bilateral lacrimal gland masses with yellowdiscoloration, parotid/submandibular salivary gland enlargement, and cervical lymphadenopathy.(C) Coronal computed tomography scan showing bilateral lacrimal gland enlargement. (D)Histopathology of mastectomy specimen showing foamy histiocytes, Touton giant cells (arrows),lymphocytes with follicular centres, and necrobiosis (haematoxylin and eosin stain, originalmagnification 106). (E) Clinical photograph 24 months after diagnosis, showing improvement. (F)Coronal computed tomography scan showing resolution of lacrimal gland masses. Photographreproduced with permission.
Figure 2 Manual forceps removal produces a1.0 cm long white segmented maggot.
Figure 1 A 1.5 mm ulcerated lesion thatappears to pulsate.
PostScript 1377
www.bjophthalmol.com

deposited. Clinical features of externalophthalmomyiasis can include conjunctivitis,conjunctival hemorrhage, corneal abrasion,and iritis. Internal ophthalmomyiasis canproduce vitreous haemorrhage, tractionalretinal detachment, endophthalmitis, andhypopigmented linear and arcuate subretinaltracks. Some of the cases of presumedinternal ophthalmomyiasis have been basedon hypopigmented subretinal tracks withoutdocumentation of an actual maggot.1
Treatment strategies depend upon the typeof ocular involvement and the level ofdamage. In cases of external ophthalmomyia-sis, manual forceps removal of the larvae isideal. Ophthalmic ointment can be used toblock the larvae’s respiratory pore, therebysuffocating the organism to facilitate manualremoval. Treatment strategies in cases ofinternal ophthalmomyiasis are case specific,ranging from iridectomy, vitrectomy, andretinotomy to laser photocoagulation. This isthe first reported case of ophthalmomyiasisexterna by a screwworm fly, CalliphoridaePhaenicia sp successfully treated with manualforceps removal.
AcknowledgementsThanks to Kipling Will and David Faulkner for theirassistance from the University of California,Berkeley, Entomology Department. Thanks to ABitanga for the photographs. Thanks also toThomas Lietman for his help with the manuscript.
N Huynh, B DolanSan Francisco VA Medical Center, CA, USA
S Lee, J P WhitcherProctor Foundation, CA, USA
J Stanley, J P Whitcher, S LeeUCSF Department of Ophthalmology, CA, USA
Correspondence to: Dr Scott Lee, UCSF Department ofOphthalmology, CA 94122, USA; [email protected]
doi: 10.1136/bjo.2005.071597
References
1 Heyde RR, Seiff SR, Mucia J. Ophthalmomyiasisexterna in California. West J Med1987;144:80–1.
2 Neva FA, Brown HW. Basic clinical parasitology,6th ed. Norwalk, CT: Appleton and Lange,1994:292–4.
3 Sigauke E, Beebe WE, Gander RM, et al. Casereport: ophthalmomyiasis externa in DallasCounty, Texas. Am J Trop Med 2003;68:46–7.
4 Buettner H. Ophthalmomyiasis interna. ArchOphthalmol 2002;120:1598–9.
Vitreous haemorrhage associatedwith Gingko biloba use in apatient with age related maculardiseaseGingko biloba extract is a widely used herbalextract that is readily available as an ‘‘overthe counter’’ product. It is most commonlyused for improving mental alertness andmemory. One of its components, gingkolideB is a potent inhibitor of platelet activatingfactor.1 Long term use has been associatedwith increased bleeding time and it canpotentate the anticoagulant effects of aspirinand warfarin.2
This is a case in which the regular use ofGinkgo biloba was associated with a vitreoushaemorrhage in a woman with a subretinalneovascular membrane, who had no otherrisk factors for haemorrhage.A 78 year old woman, who was otherwise
fit and well, first presented in July 2001to the ophthalmology department inCheltenham General Hospital with a historyof floaters in both eyes. Her visual acuitieswere 6/6 in the right eye and 6/12 correctingto 6/9 in the left eye. Fluorescein angiographyconfirmed exudative age related maculardisease (ARMD) on the left but no treatablediscrete neovascular membrane. She hadfurther loss of vision in the left eye and byOctober 2002 her left eye vision had deterio-rated to 3/60. She experienced a gradualdeterioration of vision in the right eye untilFebruary 2004, when she presented withrapid visual loss in the right eye to 6/24. Anuntreatable occult choroidal neovascularmembrane was demonstrated on fluoresceinangiography. In June 2004 she noted afurther sudden drop in central vision in theleft eye. On examination she had extensivepreretinal and subretinal haemorrhage.Within the next month she developed adense vitreous haemorrhage reducing hervisual acuity to hand movements. A B-scanultrasound confirmed the vitreous haemor-rhage and showed a flat retina with ahaemorrhagic elevation at the posterior poleconsistent with exudative age related macu-lar disease (fig 1). On further questioning sherevealed that she had been taking Gingkobiloba for the past 5 months. She was alsotaking vitamin C 1 g daily, zinc, lutein, Bcomplex, fish oil, Fossamax, and a steroidinhaler for asthma. She was advised to stopthe Gingko biloba and the vitreous haemor-rhage gradually resolved. There has been nofurther bleeding in the follow up period of8 months, but she has been left with exuber-ant macular fibrosis (fig 2).Another case of vitreous haemorrhage
associated with the use of Gingko biloba hasbeen reported in a patient with no other risk
factors for haemorrhage. A 59 year old manunderwent liver transplant for cirrhosiscaused by hepatitis B infection. This wascomplicated postoperatively by a large sub-phrenic haematoma. Three weeks later hedeveloped a right vitreous haemorrhage.3
There are several reports in the literaturelinking the use of Gingko biloba with sponta-neous haemorrhage. These include the reportof a subdural haematoma,4 hyphaema,5 sub-arachnoid haemorrhage,6 and intracerebralhaemorrhage.7
CommentA study evaluating the causes of 653 cases ofspontaneous vitreous haemorrhage foundARMD to be a small yet significant cause.8
A study by el Baba et al showed that in 19% ofreported cases of ARMD complicated bymassive intraocular haemorrhage, thepatients were taking warfarin or aspirin.9
Vitreous haemorrhage is found to have asignificantly higher incidence in patientstaking warfarin or aspirin when the bleedingoccurred.10
This case supplements a series of casereports implicating the use of Gingko bilobain spontaneous haemorrhage. There is adanger in the widely held belief that herbalremedies are benign. Patients often omit totell their doctors of these supplementalmedicines when being asked about their drughistory. Herbal remedies have been exemptfrom scientific scrutiny and product regula-tion and, as a result, we are largely unawareof their full adverse effects profile andpossible drug interactions. It should be maderegular practice to specifically ask patientsabout the use of any herbal remedies orunconventional medicines.
O P MacVie, B A HarneyGloucestershire Eye Unit, Cheltenham, UK
Correspondence to: Olivia P MacVie, GloucestershireEye Unit, Cheltenham General Hospital, Sandford
Road, Cheltenham GL53 7AN, UK;[email protected]
doi: 10.1136/bjo.2005.072454
References
1 Chung KF, Dent G, McKusker M, et al. Effect of aginkolide mixture (BN52063) in antagonising skinand platelet responses to PAF in man. Lancet1987;I:248–51.
2 Fugh-Berman A. Herb-drug interactions. Lancet2000;355:134–8.
3 Hauser D, Gayowski T, Singh N. Bleedingcomplications precipitated by unrecognizedGingko biloba use after liver transplantation.Transplant Int 2002;15:377–9.
Figure 2 B-scan showing vitreoushaemorrhage and haemorrhagic elevation atposterior pole.
Accepted 1 April 2005
Figure 3 Complete resolution of the lidoedema and erythema.
Figure 1 Colour fundus photograph of left eyeshowing extensive macular scar.
Accepted for publication 3 April 2005
1378 PostScript
www.bjophthalmol.com

4 Gilbert GJ. Gingko biloba. Neurology1997;48:1137.
5 Rosenblatt M, Mindel J. Spontaneous hyphaemaassociated with ingestion of Gingko bilobaextract. N Engl J Med 1997;336:1108.
6 Vale S. Subarachnoid haemorrhage associatedwith Gingko biloba. Lancet 1998;35:36.
7 Benjamin J, Muir T, Briggs K, et al. A case ofcerebral haemorrhage, can Gingko biloba beimplicated? Postgrad Med J 2001;77:112–13.
8 Butner RW, McPherson AR. Spontaneous vitreoushaemorrhage. Ann Ophthalmol1982;14:268–70.
9 El Baba F, Jarrett WH, Harbin TS, et al. Massivehaemorrhage complicating age-related maculardegeneration. Clinicopathologic correlation androle of anticoagulants. Ophthalmology1986;93:1581–92.
10 Tilanus MA, Vaandrager W, Cuypers MH, et al.Relationship between anticoagulant medicationand massive intraocular haemorrhage in age-related macular degeneration. Graefes Arch ClinExp Ophthalmol 2000;238:482–5.
The legal requirement for drivingin the United Kingdom is metfollowing pupil dilatationDilatation of the pupil (mydriasis) is a corecomponent of a comprehensive ophthalmicexamination and is becoming part of the eyeexamination routine for optometrists in theUnited Kingdom.1 As many patients drive toattend their examinations, concerns havebeen raised regarding the effects of pupillarydilatation on driving and whether or not thevisual standard for driving is met afterdilatation.2–4 Therefore, we investigated theeffect of mydriasis on the visual standard fordriving a private vehicle in the UnitedKingdom.
ReportTwenty adult subjects (mean age 24 years)with normal or corrected to normal visualacuity participated in the study. A selection ofsix different pairs of number plates (black onwhite and black on yellow), which con-formed to the current UK visual standardfor driving (that is, after 1 September 2001),5
was constructed for the study. Monocularand binocular distance logMAR visual acuity
and binocular number plate readings weremade before and after mydriasis (of at least6 mm diameter) with 0.5% tropicamide. Eachsubject performed the number plate testunder standard Driving Standards Agencyconditions (outside) at a fixed test distance of20 metres.6 A pass at the number plate testrequired all numbers and letters to be readcorrectly. Letter by letter scoring was used torecord visual acuity. Data were analysedusing paired t tests (one tailed) as appro-priate. Subjects were also asked for theirviews on the effects of mydriasis using aquestionnaire.3 The study followed the tenetsof the Declaration of Helsinki and approval ofthe protocol was obtained from the institu-tional human research ethics committee.All subjects met the legal requirement for
driving both before and after dilatation,irrespective of the number plate used. Visualacuity decreased (average of three lettersworse) following dilatation (p,0.05 for righteye, left eye and binocular visual acuityresults) (table 1).4 7
Following mydriasis, 13 subjects reportedan increase in glare, 15 felt more sensitive tolight, 14 reported blurry distance vision, fivereported blurry near vision, and one subjectreported no effect of the drops. Most subjectsreported a slight (nine) or moderate (10)effect of the drops; however, the majority(19) felt confident enough to safely drivehome after dilatation.
CommentDespite a loss in visual acuity after dilatation,all subjects passed the number plate test bothbefore and after dilatation and irrespective ofthe background colour of the number plate.Recently, Goel et al found a significantnumber of patients (four of 28) did not passthe number plate test after mydriasis.8
However, subjects in our study were relativelyyoung, wore the appropriate refraction andwere free from signs of ocular disease. Giventhe small effect of mydriasis on visualacuity,4 7 9 it is not surprising that, for oursubjects, mydriasis did not affect the UKvisual standard for driving. Notwithstandingthe relatively small loss in visual acuity, mostsubjects in our study reported a slight or
moderate effect of mydriasis on their vision.Nevertheless, all subjects but one felt con-fident enough to drive home.Wood et al have shown that mydriasis has a
measurable decrease on real life drivingperformance, specifically on the detectionand recognition of low contrast road obsta-cles and the ability to navigate around them.9
These findings, together with our results,suggest that satisfying the UK visual stan-dard for driving does not preclude a decreasein driving performance. Therefore, allpatients should be advised that althoughthe visual standard for driving may be metfollowing mydriasis, caution is advised whendriving after pupillary dilatation.
J Siderov, D Mehta, R VirkAnglia Vision Research, Department of Optometry
and Ophthalmic Dispensing, Anglia PolytechnicUniversity, Cambridge CB1 1PT, UK
Correspondence to: Dr John Siderov, Department ofOptometry and Ophthalmic Dispensing, Anglia
Polytechnic University, Cambridge CB1 1PT, UK;[email protected]
doi: 10.1136/bjo.2005.070722
References
1 Siderov J. Pupillary dilation in primary careoptometry. Part 1. Optician2004;228(5965):18–19.
2 Keightly S. Pupil dilation and driving. Eye2000;14:261–2.
3 Siderov J, Bartlett JR, Madigan CJ. Pupillarydilation: the patient’s perspective. Clin ExperimentOptom 1996;79:62–6.
4 Watts P, O’Duffy D, Riddell C, et al. Can I driveafter those drops, doctor? Eye 1998;12:963–6.
5 DVLA. At a glance guide to the current medicalstandards of fitness to drive. Swansea: DriversMedical Unit, Driver and Vehicle LicensingAuthority, 2003.
6 DSA. Technical Standards Branch, DrivingStandards Agency, UK, personal communication.2005.
7 Montgomery DMI, Macewan CJ. Pupil dilatationwith tropicamide: the effects on acuity,accommodation and refraction. Eye1989;3:845–8.
Table 1 Monocular (RE and LE) and binocular (BE) visual acuity results
Subject Age (years)
Pre-dilatation Post-dilatation
Confident to drive?RE LE BE RE LE BE
1 23 6/623 6/623 6/4.822 6/621 6/622 6/622 Yes2 23 6/6 6/6 6/6+2 6/6 6/7.5+2 6/6+1 Yes3 21 6/6 6/6 6/4.822 6/623 6/623 6/623 Yes4 23 6/6+2 6/6+1 6/6+3 6/7.5+2 6/7.521 6/621 Yes5 24 6/621 6/6+2 6/621 6/621 6/622 6/621 No6 36 6/7.521 6/622 6/621 6/7.521 6/7.522 6/7.5 Yes7 23 6/4.822 6/621 6/4.821 6/621 6/7.521 6/6+2 Yes8 27 6/4.8+3 6/4.821 6/3.823 6/6 6/4.821 6/4.8+1 Yes9 22 6/3.821 6/4.821 6/4.821 6/4.8 6/4.822 6/4.821 Yes10 21 6/6+1 6/6+2 6/6+3 6/621 6/6 6/6 Yes11 20 6/621 6/622 6/4.821 6/6+2 6/621 6/622 Yes12 23 6/4.821 6/622 6/4.821 6/6+2 6/621 6/6+3 Yes13 23 6/621 6/622 6/621 6/7.5+1 6/7.5+2 6/6 Yes14 20 6/4.823 6/622 6/4.822 6/4.822 6/4.822 6/4.822 Yes15 26 6/7.522 6/7.5+3 6/621 6/9.521 6/7.523 6/7.522 Yes16 22 6/4.822 6/7.5 6/4.8 6/4.8 6/621 6/4.822 Yes17 24 6/6+3 6/6+2 6/4.8+1 6/7.5 6/7.5+1 6/6 Yes18 22 6/4.823 6/4.821 6/4.8+1 6/622 6/621 6/6+1 Yes19 22 6/4.821 6/4.8+1 6/4.8+1 6/622 6/621 6/6 Yes20 23 6/6+2 6/6+3 6/4.821 6/7.522 6/7.523 6/7.5 Yes
Accepted for publication 8 April 2005
Competing interests: none declared
PostScript 1379
www.bjophthalmol.com

8 Goel S, Maharajan P, Chua C, et al. Drivingability after pupillary dilatation. Eye2003;17:735–8.
9 Wood JM, Garth D, Grounds G, et al. Pupildilatation does affect some aspects of daytimedriving performance. Br J Ophthalmol2003;87:1387–90.
Hydrated scleral buckle: a latecomplication of MAI explantsSeveral long term complications have beenreported with MAI scleral buckles,1–3 asynthetic hydrophilic scleral buckling ele-ment, first introduced in the 1970s.1 Wepresent a case of an extruding, hydratedMAI scleral buckle that presented as anorbital lesion. The magnetic resonance ima-ging (MRI) characteristics of the hydratedMAI buckle are also described.
Case reportAn 81 year old woman was referred to theorbital service for evaluation of a freelymobile non-painful subconjunctival lesionin the left eye present for at least a year.The extraocular movement was full but witha small left exotropia in primary gaze.Anterior segment examination revealed afirm, nodular subconjunctival lesion in thesuperomedial quadrant. The diagnosis ofextruding scleral buckle versus a large orbitalconjunctival inclusion cyst was entertained.She, however, denied a history of retinaldetachment repair.The patient underwent MRI of the orbits
with and without gadolinium infusion whichrevealed a 2.560.7 cm2 elongated, ellipticalmass in the medial intraconal space. Thehyperintensity of the mass on T2 weightedimages, indicative of high water content, ledto the mistaken radiological diagnosis of acystic, fluid filled lesion (fig 1).Introperatively, a swollen intact segmentalbuckle was encountered that disintegratedinto small and large pieces when graspedwith a forceps. Complete meticulous removalof these small fragments was performed(fig 2).
CommentMAI hydrogel explant is made of polymethylacrylate-co-2-hydroxyethyl acrylate crossedlinked with ethylene diacrylate with 15%water2 and was considered an ideal scleralbuckling material since it was as effective assolid silicone rubber buckle and sponge butwith lower incidence of erosion.4 However,long term complications are being morefrequently recognised with the MAI buckle.3
Complications include hydration of the
buckle with erosion and extrusion of theexplant.2 Owing to their hydrophilic nature,buckles tend to swell, become bulky, anddisplace from their intended position. Theseexplants change from an opaque, soft,spongy, whitish appearance to a translucent,gel-like, cream coloured material with hydra-tion.2 They become extremely friable andfragment easily with slight traction uponremoval.1–3 Scanning electron microscopy ofthese hydrated buckles has revealed distor-tion of their micropore architecture.1 2
The presentations of hydrated MAI bucklesare varied. They can become extremely looseand migrate anteriorly, or enlarge in situ andpresent as orbital masses. Since complica-tions do not occur until many years after theorbital surgery, the history of a retinaldetachment repair may not be elicited. Inaddition, these loose buckles usually do notindent the globe and may not be recognisedas being present on indirect ophthalmoscopy.Radiological imaging may be helpful. MRI
T1 weighted images of a hydrated bucklereveal a well defined, hypointense mass,while T2 weighted images reveal a hyper-intense mass as a result of high watercontent. (In contrast, a silicone element willbe black on MRI images.)Removal of hydrated MAI buckles can be
very difficult. Careful sub-Tenon dissectionshould be carried out since any pressure onthe buckle can lead to its fragmentation. Theprocedure is often complicated because of theextremely friable nature of these buckles.Cryoprobe has been used successfully in somecases for removal of the buckles.5 Le Rouic etal demonstrated that removal of MAI buckleswith a cryoprobe is a safe and effectivetechnique with lower fragmentation ratecompared to the use of forceps.5 The cryo-probe allows the water in the swollen explantmaterial to freeze, which helps to reducefragmentation.In conclusion, ophthalmologists should be
aware of the possible complications of theMAI hydrogel buckles. Knowledge of theMRI characteristics of hydrated MAI bucklesmay be helpful in identifying them in theevent they present as a space occupyingorbital mass.
N Bhagat, A Khanna, P D LangerInstitute of Ophthalmology and Visual Science, New
Jersey Medical School, Newark, NJ 07103, USA
Correspondence to: Paul D Langer, MD, Institute ofOphthalmology and Visual Science, New Jersey
Medical School, DOC, Suite 6168, 90 Bergen Street,Newark, NJ 07103, USA; [email protected]
doi: 10.1136/bjo.2005.072280
References
1 Oshitari K, Hida T, Okada AA, et al. Long-termcomplications of hydrogel buckles. Retina2003;23:257–61.
2 Marin JF, Tolentino FI, Refojo MF, et al. Long-termcomplications of the MAI hydrogel intrascleralbuckling implant. Arch Ophthalmol1992;110:86–8.
3 Hwang KI, Lim JI. Hydrogel exoplantfragmentation 10 years after scleral bucklingsurgery. Arch Ophthalmol 1997;115:1205–6.
4 Ho PC, Chan IM, Refojo MF, et al. The MAIhydophilic implant for scleral buckling: a review.Ophthalmic Surg 1984;15:511–15.
5 Le Rouic JF, Bejjani RA, Azan F, et al.Cryoextraction of episcleral Miragel buckleelements: a new technique to reducefragmentation. Ophthalmic Surg Lasers2002;33:237–9.
Complex I respiratory defect inLHON plus dystonia with nomitochondrial DNA mutationLeber hereditary optic neuropathy (LHON)sometimes occurs with dystonia1 in associa-tion with mitochondrial DNA (mtDNA)mutations in complex I.2 We describe apatient with LHON plus dystonia who had asevere complex I respiratory defect with nopathological mtDNA mutation, implying amitochondrial abnormality of nuclear origin.
Case reportThe proband was healthy until age 17 yearswhen she developed progressive right sidedweakness followed 5 years later by a lefthemiparesis with involuntary posturing ofthe left arm and leg. Intelligence was average,and she finished grade 6 at school. Herparents were unrelated, and she had fivehealthy siblings.Neuro-ophthalmological examination at
age 23 documented excellent afferent andefferent visual functioning with no Kaiser-Fleischer ring. Optic discs were hyperaemicand slightly elevated with peripapillary tel-angiectasias in both eyes (fig 1A and B). Shehad modest right sided weakness, diffusehyper-reflexia greater on the right, bilateralBabinski signs, and dystonic posturing on theright while walking.On return 21 months later, she reported
that the vision of both eyes had declined9 months previously. Visual acuity was 20/100 in both eyes with poor colour vision inboth eyes, a mild left afferent pupillarydefect, and bilateral optic atrophy with noresidual hyperaemia or peripapillary telan-giectasias (fig 1C). Gait was somewhat worse,and she was modestly dysarthric. Vision didnot improve during 18 months of follow up.Normal laboratory studies included hae-
mogram, liver and renal function, serumlactate, pyruvate, and 24 hour urine copperexcretion. Cerebral spinal fluid (CSF) lacticacid was slightly elevated (2.8 mm/l withnormal range 0.6–2.2 mm/l), and brain MRIrevealed abnormalities in both basal ganglia(fig 1D).After signing informed consent, the pro-
band, her mother and father, and foursiblings had blood drawn for DNA extraction,polymerase chain reaction amplification, andsequencing of the entire mitochondrial geno-mic coding region as previously described.3
Sequence results were compared to Mitomap(www.mitomap.org/mitomap/mitoseq.html),the human mitochondrial genome database(www.genpat.uu.se/mtDB), GenBank (www.ncbi.nlm.nih.gov/Genbank/index.html), and
Figure 2 Hydrated, friable buckle removed inmultiple small fragments.
Figure 1 T2 weighted MRI image reveals ahyperintense mass exhibiting a mass effect onthe left globe.
Accepted for publication 10 April 2005
Supported by an unrestricted grant from Research toPrevent Blindness.
Competing interests: none declared
1380 PostScript
www.bjophthalmol.com

a normal control group of 119 people with nomedical problems, who share similar ethni-city with the proband. Mitochondrial respira-tory function in complexes I, III, IV, and Vwas assessed in the proband and oneunaffected sibling using a previouslydescribed flow cytometric functional analysismethod.3 4
The proband, her siblings, and theirmother had one mtDNA sequence variantrecognised as a polymorphism in theJapanese population,5 which was not present
in the 119 normal controls of similar ethni-city. Thirteen previously reported homoplas-mic mtDNA polymorphisms were detected inthe proband, her family, and the controlgroup. The proband, but not her unaffectedbrother, had a severe respiratory defect incomplex I (fig 1E, F, and G).
CommentThis young woman’s initial examination wassignificant for normal vision with hyperaemic
optic discs, pseudopapilloedema, and peripa-pillary telangiectasias. She went on todevelop bilateral optic nerve injury typical ofLHON. She also had progressive basal gang-lion and upper motor neuron disease culmi-nating in bilateral spasticity, a broad basedand unsteady gait, dystonia, and dysarthria.Her clinical course, elevated CSF lactate,normal urinary copper excretion, and severecomplex I respiratory defect imply a mito-chondrial mechanism for optic nerve andbrain injury.Mitochondrial complex I dysfunction in
the absence of a pathological mtDNA muta-tion provides presumptive evidence of amitochondrial abnormality of nuclear origin.Complex I dysfunction has been identified inpatients with sporadic focal dystonia,6 and atleast one familial generalised dystonia syn-drome had a defined nuclear mutationaffecting a mitochondrial protein.7 Otherpatients with LHON plus dystonia have hadcomplex I mtDNA mutation(s), so thispatient broadens the genetic circumstancein which the phenotype may be expected.
K K Abu-AmeroGenetics Department, King Faisal Specialist Hospital
and Research Centre, Riyadh, Saudi Arabia
T M Bosley, S Bohlega, D McLeanNeuroscience Department, King Faisal Specialist
Hospital and Research Centre, Riyadh, Saudi Arabia
Correspondence to: Dr Khaled K Abu-Amero,Department of Genetics, King Faisal SpecialistHospital and Research Center (MBC No 03),PO Box 3354, Riyadh 11211, Saudi Arabia;
doi: 10.1136/bjo.2005.072819
References
1 Nikoskelainen EK, Marttila RJ, Huoponen K, et al.Leber’s ‘‘plus’’: neurological abnormalities inpatients with Leber’s hereditary optic neuropathy.J Neurol Neurosurg Psychiatry 1995;59:160–4.
2 Tarnopolsky MA, Baker SK, Myint T, et al. Clinicalvariability in maternally inherited leber hereditaryoptic neuropathy with the G14459A mutation.Am J Med Genet A 2004;124:372–6.
3 Abu-Amero KK, Bosley TM, Bohlega S, et al.Mitochondrial T9957C mutation in associationwith NAION and seizures but not MELAS.Ophthalmic Genet 2005;26:31–6.
4 Setterfield KWA, Donald J, Thorburn DR, et al.Flow cytometry in the study of mitochondrialrespiratory chain disorders. Mitochondrion2002;1:437–45.
5 Tanaka M, Cabrera VM, Gonzalez AM, et al.Mitochondrial genome variation in eastern Asiaand the peopling of Japan. Genome Res2004;14:1832–50.
6 Schapira AH, Warner T, Gash MT, et al. ComplexI function in familial and sporadic dystonia. AnnNeurol 1997;41:556–9.
7 Binder J, Hofmann S, Kreisel S, et al. Clinical andmolecular findings in a patient with a novelmutation in the deafness-dystonia peptide (DDP1)gene. Brain 2003;126(Pt 8):1814–20.
Retinal haemorrhages in a youngpatient with homocysteinuriaThe most common ocular complication inhomocysteinuria is lens subluxation.1 Wepresent a patient with homocysteinuria whodeveloped subhyaloid haemorrhages duringpars plana vitrectomy/lensectomy for a sub-luxated lens in the right eye. She had alsodeveloped preretinal and intraretinal hae-morrhages in her fellow eye 6 months earlier,
40E
A
B
C
D
30
20
10
0105
FL3 height
Cou
nts
104103102101
40F
30
20
10
0105
FL3 height
Cou
nts
104103102101
40G
30
20
10
0105
FL3 height
Cou
nts
104103102101
Figure 1 (A) Fundus photograph of left optic disc showing hyperaemia and peripapillarytelangiectasias. The right disc had a similar appearance. (B) Intravenous fluorescein angiogram ofleft optic disc confirming tortuous vessels with no leakage of fluorescein typical of thepseudopapilloedema of LHON. This photograph was taken at 5:45. The right disc had a similarappearance. (C) Fundus photograph of left optic disc taken 9 months after visual loss showingmodest diffuse pallor of the disc with resolution of disc elevation and peripapillary telangiectasias.The right disc had a similar appearance. (D) Brain magnetic resonance imaging (MRI, Flair TR9502 TE 138/EF) showing bilateral basal ganglion lesions affecting predominantly the putamen,left.right, with parenchymal loss and hyperintense signal implying gliosis without mass effect.Small T2 hyperintense signal abnormalities were also present in the diencephalon, the cerebralpeduncles, and the periaqueductal region. (E), (F), and (G) Overlain histograms showingfluorescence in uninhibited lymphoblasts (dark grey peaks) and in lymphoblasts inhibited withrotenone (light grey peaks) in the patient (E), unaffected sibling (F), and normal control (G). X axis isa logarithmic scale quantifying pulse of fluorescence detected by the flow cytometer; Y axis is alogarithmic scale of number of cells. Dark grey peaks represent fluorescence of cells incubated withdihydroethidium (DHE) only. Light grey peaks represent fluorescence of cells incubated with DHEand rotenone, which inhibits activity of mitochondrial complex I. Fluorescence increased almostthree-fold in control cells (G) and cells of the unaffected sibling (F) after incubation with rotenone(20 mM), while the patient’s cells showed no increase in fluorescence because of pre-existinginhibition, indicating a complex I respiratory defect. This experiment was repeated four times withsimilar results.
Accepted for publication 10 April 2005
PostScript 1381
www.bjophthalmol.com

after phacoemulsification of the subluxatedlens. No preoperative or intraoperative antic-oagulation was used for either eye surgeries.
Case reportA 12 year old girl with homocysteinuriapresented with decreased vision in the righteye as a result of an anteriorly luxated lenscausing pupillary block glaucoma with anintraocular pressure (IOP) of 50 mmHg. Theposterior segment was normal. She hadundergone phacoemulsification and anteriorvitrectomy for pupillary block glaucomacaused by subluxated lens in the fellow eye6 months earlier. Retinal examination post-operatively revealed preretinal and intraret-inal haemorrhages in the mid-periphery(fig 1), which cleared spontaneously overthe next 5 months.Since medical therapy was ineffective in
the right eye, she underwent pars planalensectomy and vitrectomy. As the corevitrectomy was initiated, small subhyaloidhaemorrhages were noted to develop in themid-periphery. The vitrectomy settings werechanged to a high cutting speed and lowaspiration but the haemorrhages continuedto form. Induction of the posterior vitreousdetachment was aborted when peripapillaryintraretinal haemorrhages were noted todevelop.On the first postoperative day, a 2 disc
diameter subhyaloid haemorrhage (not seenat the end of the surgery) was noted in themacula (fig 2). All haemorrhages resolvedspontaneously over the next 10 weeks.
CommentThe precise mechanism of action of homo-cysteine on the vascular tree is not wellunderstood. Elevated homocysteine levelscan cause endothelial disruption, structuraldamage by toxic effects on the intima andmedia, increased oxidation of low densitylipoproteins, and alterations of clotting fac-tors leading to a hypercoagulable state.2
Histopathological data derived primarilyfrom animal models demonstrate smoothmuscle cell hypertrophy and hyperplasiaof the arteries.3 Postmortem studies of
hyperhomocysteinaemic patients have shownintimal and medial thickening with disrup-tion of the internal elastic lamina of smalland large vessels.4 Histopathology of smallarteries reveal focal proliferation of connec-tive tissue with increased fibroblasts, col-lagen, and irregular elastic fibres.4 Thesechanges may contribute to the fragility ofsmall arteries and capillaries.Valsalva retinopathy sometimes occurs
with general anaesthesia. We do not believethis patient experienced this mainly becauseValsalva retinopathy is bilateral. The retinalhaemorrhages occurred only in the operatedeye and not the fellow eye each time thepatient underwent surgery.The haemorrhages noted postoperatively in
the left eye may have occurred because ofocular decompression retinopathy. An acutelowering of IOP can decrease the resistance ofthe retinal and choroidal circulation, tem-porarily overwhelming the capacitance of thecapillary bed and resulting in multipleendothelial leaks and intraretinal haemor-rhages.5 Hyperhomocysteinaemia can affectthe autoregulation of small arteries.2 3 Thismay have contributed to the development ofretinal haemorrhages in the left eye. Thesubhyaloid haemorrhages in the right eye,however, were unlikely to be related to oculardecompression retinopathy since no haemor-rhages were seen during pars plana lensect-omy, but these developed soon aftervitrectomy was initiated. Minimal tractiontransmitted to the internal limiting mem-brane and nerve fibre layer by the vitrectomymay have caused the extremely friable super-ficial capillaries to rupture. Indeed, defects inretinal vascular autoregulation due to homo-cysteinuria, may have contributed to thedevelopment of the observed haemorrhages.We hypothesise that individuals with
chronic hyperhomocysteinaemia are at anincreased risk for retinal haemorrhagesbecause of homocysteine mediated destruc-tive changes in small vessel walls and anautoregulatory defect that results in extremecapillary fragility.
R A Shah, M A Zarbin, N BhagatInstitute of Ophthalmology and Visual Science, New
Jersey Medical School, Newark, NJ 07103, USA
Correspondence to: Neelakshi Bhagat, MD, MPH,Institute of Ophthalmology and Visual Science, NewJersey Medical School, Doctor’s Office Center; No6168, 90 Bergen Street, Newark, NJ 07103, USA;
doi: 10.1136/bjo.2005.072330
References
1 Michalski A, Leonard JV, Taylor DS. The eye andinherited metabolic disease: a review. J Roy SocMed 1988;81:286–90.
2 Cook JW, Taylor LM, Orloff SL, et al.Homocysteine and arterial disease. Experimentalmechanisms. Vasc Pharmacol2002;38:293–300.
3 Van Guldener C, Stehouwer CD.Hyperhomocysteinemia, vascular pathology, andendothelial dysfunction. Sem ThrombosisHemostasis 2000;26:281–9.
4 McCully KS. Vascular pathology ofhomocysteinemia: implications for thepathogenesis of arteriosclerosis. Am J Pathol1969;56:111–28.
5 Nah G, Aung T, Yip C. Ocular decompressionretinopathy after resolution of acute primaryangle closure glaucoma. Clin ExperimentOphthalmol 2000;28:319–20.
Internet based ophthalmologyservice: impact assessmentIn 2003, the Department of Health, WesternAustralia, commenced a teleophthalmologyservice between Carnarvon Regional Hospital(CRH) and Lions Eye Institute (LEI) at City ofPerth (at 940 km), pioneering the use ofremote, interactive consultations in ophthal-mology. This assessment (a) reports theimpact of teleophthalmology service onpatient diagnosis, management, outcomes,and satisfaction; and (b) estimates the costsof teleophthalmology service.
Case reportAn internet based system (www.e-icare.com)developed and evaluated at LEI, was used tostore and transmit multimedia data to asecure, central database.1 Practitioners atCRH collected these data, which includedpatients’ demographic details, medical his-tory, and ocular images. A portable slit lampdeveloped at LEI,2 tonometer (Keeler Pulsair3000, Japan), and digital retinal camera(Canon CR4-45NM, Japan) were also used.A questionnaire and interview approachassessed the satisfaction of the patients andpractitioners. Estimation of costs analysedadditional activity data and associated costs.During the 12 month study period, there
were 118 teleophthalmology consultations(42% men, 58% women, mean age 42 years,range 4–73 years). Most patients (53%)became aware of the service through localmedia, while health professionals inCarnarvon referred 36% for teleophthalmol-ogy consultation. Of the 118 cases, 3% of thepatients used teleophthalmology for emer-gency consultation, 94% for testing forglaucoma and diabetic retinopathy; 3% ofthe cases were for expert second opinion andpostoperative follow up.Teleophthalmology proved to have impact
on all the patients, by improving the eye carefacility at CRH itself, instead of the need totravel 940 km to the city. Following telecon-sultation, only 3% of patients were referred toa city hospital. While 55% of patients had noabnormalities detected, 3% of patientsreceived treatment at CRH itself. Theophthalmologist recommended regular fol-low up for 36% of patients seen by tele-medicine.
Figure 2 Fundus photographs of the right eye1 day after pars plana vitrectomy and parsplana lensectomy for an anteriorly subluxatedlens. A 2 disc diameter subhyaloidhaemorrhage is seen in the macula along withone preretinal haemorrhage temporal to themacula. Photographs of other mid-peripheralretinal haemorrhages could not be taken owingto the patient’s non-cooperation.
Figure 1 Fundus photographs of the left eye3 days after undergoing phacoemulsificationand anterior vitrectomy for an anteriorlysubluxated lens. Multiple ovoid subhyaloidpreretinal and intraretinal haemorrhages arenoted in the mid-periphery of the retina.
Accepted for publication 12 April 2005
This work was supported by Research to PreventBlindness Inc, the Lions Eye Research Foundation ofNew Jersey, and the Eye Institute of New Jersey.
1382 PostScript
www.bjophthalmol.com

The teleophthalmology consultation costper patient, at current efficiency level, is$279.96 including fixed cost. A cost neutralanalysis estimated, at optimal efficiency of352 patients per annum, cost per patientwould decrease to $107.72. In the remotearea, without teleophthalmology, the cost tothe service provider for a face to faceconsultation with an ophthalmologist is ashigh as $665.44 per patient. The minimumnumber of patients needed to make a costeffective teleophthalmology consultation is126 per annum.The majority of patients (98%) expressed
satisfaction with the internet based consulta-tion and observed it as convenient. Lack ofphysical contact with ophthalmologist wasnot a major concern to many patients (74%).CRH practitioners spoke favourably of usingteleophthalmology, in that they were able toget advice from colleagues and discuss alter-native management strategies. Practitionersat LEI found the experience informative andchallenging.
CommentWhile acknowledging that face to face con-sultations with ophthalmologists are unique,its costs are enormous in remote healthcentres.3–5 The project is a technical andclinical success and one that led to directpotential benefits for patients in terms ofimproved outcomes, as well as considerableeducational experience for the participatingmedical practitioners. However, currentassessment brought to light the importanceof redefining utilisation criteria in order toachieve efficiency. For example, 126 patientsper annum are required for a cost effectiveteleophthalmology service while the currentefficiency rate is 118 per annum (2.2 patientsper week). Better coordination between thelocal healthcare workforce and CRH mayincrease the number of teleophthalmologyconsultations, which in turn will help toachieve breakeven or even establish netsavings. Overall, this assessment indicatesthat the success of teleophthalmology will bebased upon identifying the requirements ofthe service and using appropriate technology.
AcknowledgementsSupported by an IPRS Scholarship and UPA(IS)
Award from University of Western Australia. The
authors thank the Department of Health, Western
Australia, Mr Francisco Chaves (health economist),
and Ms Beth Hudson for her support and assistanceespecially in data collection. The authors also thank
the patients, clinical staff, and administrative
officers in CRH, Carnarvon and at LEI, City of
Perth for their assistance.
S Kumar, M-L Tay-Kearney, I J Constable,K Yogesan
Lions Eye Institute, University of Western Australia,Nedlands, WA 6009, Australia
Correspondence to: Sajeesh Kumar, Lions EyeInstitute, University of Western Australia, 2 VerdunStreet, Nedlands, WA 6009, Australia; sajeesh@
cyllene.uwa.edu.au
References
1 Yogesan K, Constable IJ, et al. Internationaltransmission of tele-ophthalmology images.J Telemed Telecare 2000;5:41–4.
2 Yogesan K, Cuypers M, et al. Tele-ophthalmologyscreening for retinal and anterior segmentdiseases. J Telemed Telecare 2000;5:96–8.
3 Keeffe JE, Weih LM, et al. Utilisation of eye careservices by urban and rural Australians.Br J Ophthalmol 2002;86:24–7.
4 Whitten PS, Mair FS, et al. Systematic review ofcost effectiveness studies of telemedicineinterventions. BMJ 2002;324:1434–7.
5 Sajeesh KR, Mei-Ling TK, Chaves F, et al. Remoteophthalmology services: cost comparison oftelemedicine and alternate scenarios. J TelemedTelecare (in press).
Temperature sensitiveoculocutaneous albinismassociated with missensechanges in the tyrosinase geneOculocutaneous albinism (OCA) describes agroup of autosomal recessive disorders char-acterised by reduced or absent pigmentationof the eye, skin, and hair as a result of acongenital reduction in melanin synthesis.Additional findings in the eye includedecreased visual acuity, nystagmus, iris trans-illumination, hypopigmentation of the uvealtract and retinal pigment epithelium, fovealhypoplasia, and abnormal decussation of theoptic nerve fibres at the optic chiasm leading toa lack of binocular vision.1 2 Type I OCA resultsfrom mutations in the tyrosinase gene andleads to either total absence of tyrosinaseactivity (OCA Ia) associated with absence ofpigmentation (‘‘tyrosinase negative’’), or amarked reduction in tyrosine activity (OCAIb) associated with reduced pigmentation
(‘‘tyrosinase positive’’ or ‘‘yellow albinism’’).We report a new case of the rare varianttemperature sensitive albinism and our identi-fication of missense mutations in the tyrosi-nase gene, not previously found in this form ofalbinism.
Case reportThe patient, a 31 year old woman, wasreferred to us for genetic advice. She hadoriginally presented at 6 weeks old withnystagmus and white hair; her parents bothhave dark hair and olive skin. The diagnosisof oculocutaneous albinism was made at9 months. As she grew older the hair of herhead darkened and, particularly in her teens,the hair on her lower legs and forearmsdarkened. As an adult she has light blondehair, darker eye lashes and eyebrows, whiteaxillary and pubic hair, but strongly pigmen-ted hair on forearms and lower legs (fig 1).When examined in the clinic she had reducedvisual acuity (6/36 bilaterally), marked iristranslucency, and an albinotic retina withfoveal hypolasia bilaterally. Visually evokedpotential revealed crossed asymmetry consis-tent with oculocutaneous albinism. We madea diagnosis of temperature sensitive albinismand searched for mutations in the tyrosinasegene. Blood was taken, with informed con-sent, from the patient and her parents andDNA extracted using standard techniques.Using polymerase chain reaction we ampli-fied each of her tyrosinase gene exons3 andsequenced the entire coding region andintron-exon boundaries. Our patient did nothave the R422Q mutation previously reportedin patients with this phenotype and also didnot have two other mutations known to betemperature sensitive.4 We did identify twomissense mutations: R217Q and A355P, inexons 1 and 3 respectively (fig 2). The exon 1mutation had been inherited from her
Competing interests: none declared
Ethical approval was obtained from the University ofWestern Australia Human Ethics Committee and the
Western Australia Aboriginal Health InformationEthics Committee.
doi: 10.1136/bjo.2005.072579
Accepted for publication 12 April 2005Figure 1 Clinical photographs of patient. Note the yellow blonde hair, dark eyebrows, andstrongly pigmented forearm hair. (Photograph reproduced with permission of the patient.)
PostScript 1383
www.bjophthalmol.com

mother and the exon 3 mutation from herfather. R217Q has been previously reported inOCA1,5 and A355P in OCA1b in a patientwith ‘‘little apparent pigmentation’’ but withno description of the distribution of thepigmentation.6 Neither has previously beenassociated with a temperature sensitive phe-notype.
CommentTemperature sensitive albinism is a rarevariant, first described in 19911 and subse-quently associated with a particular missensemutation in the tyrosinase gene.1 The muta-tion, R422Q, results in a temperature sensi-tive trafficking defect preventing thetranslocation of the mutant tyrosinase intomelanosomes.4 Thus, at 37 C mutant R422Qtyrosinase is retained in the endoplasmicreticulum and degraded by proteasomes andno pigment is produced. At lower tempera-tures (31 C) the enzyme can be successfullytranslocated into the melanosomes and canproduce pigment. This leads to a phenotypereminiscent of the Siamese cat with nopigment centrally but pigmentation developsin the peripheries (lower legs and forearms).Our patient is heterozygous for missense
mutations in the tyrosinase gene that haveboth previously been reported in OCA1 butneither with a temperature sensitive pheno-type. We are not aware of other patients withthis particular combination of mutations. Ithas been shown that co-expression of wildtype tyrosinase can correct the mutant con-formation in temperature sensitive allelessuch that exit from the endoplasmic reticu-lum and complex carbohydrate processing inthe Golgi is promoted even at the non-permissive temperature.7 It may be that oneof the mutant alleles identified in our patientmodulates the expression of the other,revealing its temperature sensitive naturewhereas coexpression with a different allelemay give no residual activity. Alternatively,this phenotype may be much commoner thanpreviously thought. To date there have beenno studies of function or response to tem-perature variation of these particular mutantforms of tyrosinase. In light of the phenotypewe describe here these studies would bevaluable. Furthermore, it is not unusual for
patients with albinism to report developmentof some pigmentation with age and it wouldbe interesting to review other patients withthese mutations. Unless patients with albin-ism are reviewed later in life this developingphenotype will not be noted.
T Wang, C T Waters, T Jakins, J R W Yates,D Trump
Department of Medical Genetics, Cambridge Institutefor Medical Research, University of Cambridge, UK
K BradshawDepartment of Ophthalmology, Addenbrooke’s
Hospital Trust, Cambridge, UK
A T MooreInstitute of Ophthalmology and Moorfields Eye
Hospital, London, UK
T Wang, D TrumpAcademic Unit of Medical Genetics, St Mary’s
Hospital and Centre for Molecular Medicine, Facultyof Medical and Human Sciences, University of
Manchester, UK
Correspondence to: Professor Dorothy Trump,Academic Unit of Medical Genetics, St Mary’s
Hospital, Hathersage Road, Manchester M13 0JH,UK; [email protected]
doi: 10.1136/bjo.2005.070243
References
1 King RA, Jackson IJ, Oetting WS. Humanalbinism and mouse models. In: Wright AF, Jay B,eds. Molecular genetics of inherited eyedisorders. New York: Harwood AcademicPublishers, 1994;89–122).
2 Abrams LS, Traboulsi E. Albinism. In: Traboulsi E,eds. Genetic diseases of the eye. New York:Oxford University Press, 1998;697–722).
3 Giebel LB, Strunk KM, Spritz RA. Organizationand nucleotide sequences of the human tyrosinasegene and a truncated tyrosinase-related segment.Genomics 1991;9:435–45.
4 Toyofuku K, Wada I, Spritz RA, et al. Themolecular basis of oculocutaneous albinism type 1(OCA1): sorting failure and degradation ofmutant tyrosinases results in a lack ofpigmentation. Biochem J 2001;355(Pt2):259–69.
5 Oetting WS, King RA. Molecular analysis of typeI-A (tyrosinase negative) oculocutaneous albinism.Hum Genet 1992;90:258–62.
6 Spritz RA, Oh J, Fukai K, et al. Novel mutations ofthe tyrosinase (TYR) gene in type I oculocutaneousalbinism (OCA1). Hum Mutat 1997;10:171–4.
7 Halaban R, Cheng E, Hebert DN. Coexpressionof wild-type tyrosinase enhances maturation oftemperature-sensitive tyrosinase mutants. J InvestDermatol 2002;119:481–8.
Choroidal neovascularisationassociated with meningiomaThis report documents the occurrence inthree patients of subretinal choroidal neovas-cular membranes (CNVM) ipsilateral tomeningiomas involving the optic nerve. Wepropose that the association might not becoincidental.
Case 1A 31 year old woman developed a centralscotoma in the left eye that led to thediagnosis of a left sphenoid wing menin-gioma involving the optic canal. The tumourwas resected and her vision returned tonormal. At age 56 a generalised seizure ledto recognition of a recurrence. When therecurrent tumour was resected it proved to bea malignant meningioma. She was thentreated with photon radiation from a 10 MVsource using a three field technique (rightlateral, left lateral, and superior). The totaldose was 45 Gy administered in 25 fractions.Thereafter, on regular follow up eye exam-inations she had normal visual function,pupils, and fundi. At the age of 64 she hada single episode in which for several secondsshe lost all vision in the left eye except for anasal island. There were no residua but herophthalmologist found a new fundusabnormality that prompted referral.Her medical history included migraine and
a cutaneous malignant melanoma. There wasno pertinent family history.The patient’s visual acuities were 20/15 in
each eye. Her colour vision (Ishihara) andpupils were normal. The Goldmann visualfield of her right eye was full but she had arelative inferior altitudinal defect to the I2ewhite stimulus in the left eye. There was3 mm of proptosis of the left eye with normalorbital resiliency. Fundus examination of theleft eye revealed a peripapillary superotem-poral retinal elevation associated with lipid(fig 1, top left). There were no maculardrusen. Echography showed 1.1 mm of ele-vated retina adjacent to the left disc withnormal acoustics. The rest of her neuro-ophthalmological examination was normal.There was hyperfluorescence in the area ofelevation with late leakage of dye on fluor-escein angiography consistent with a peripa-pillary CNVM (fig 1). At that time magneticresonance imaging (MRI) scans showed noevidence of recurrent meningioma.Five years later the vision declined to 20/30
in the left eye. There was neither opticatrophy nor optic disc swelling, but a leftafferent pupillary defect and dyschromatop-sia were observed. MRI showed that thesphenoid meningioma had recurred andinvolved the intracanalicular and posteriororbital segments of the left optic nerve. Therealso was enlargement of the posterior belliesof the left inferior and lateral rectus muscles.
Case 2An 89 year old woman had cataract surgeryon her left eye in December 2000 and herright eye in February 2001. She initially sawwell following surgery; however, in August
Figure 2 Mutations in tyrosinase gene.
Accepted for publication 18 April 2005
1384 PostScript
www.bjophthalmol.com

2001 she noted blurring of the vision in herleft eye and a peripapillary CNVM wasdiscovered. Despite two laser applicationsthe patient’s vision continued to worsen.Her medical history included rheumatic
heart disease, hypertension, and hypercho-lesterolaemia. In February 2001 she hadendocarditis complicated by a left hemiplegia.There was no family history of any pertinentdisorder.Her visual acuities were 20/20 in the right
eye and 7/200 in the left. She had dyschro-matopsia of the left eye with 2 mm ofproptosis and a relative afferent pupil defect.Goldmann perimetry revealed a full visualfield in the right eye and only a residual nasalisland in the left. The fundus of the right eyewas normal without drusen. Her left opticdisc was pale and there was nerve fibre layerswelling and haemorrhage adjacent to thenerve. MRI showed a 1.461.261.2 cm homo-geneously enhancing mass along the leftplanum sphenoidale extending into the leftoptic canal consistent with a meningioma.
Case 3A 47 year old woman noticed that she had apainless visual disturbance of her right eye‘‘like looking through a glass of water.’’ Thesymptom persisted, and 2 months later sheawoke with a blind right eye. An MRI scanwas interpreted as normal and her blindness
was ascribed to optic neuritis. She wastreated with a course of corticosteroidsduring which she recovered some vision buther vision failed again after the steroids werediscontinued and thereafter she was unableto see light.She had a history of asthma and obesity.
Her father had age related macular degenera-tion.At the age of 49 she noticed metamor-
phopsia in the left eye, and a large, elevated,extrafoveal CNVM was found. Echographyrevealed 1.3 mm of elevation, which wasacoustically normal. Vision was then 20/20.The right optic disc was atrophic and the leftwas normal. There were no macular drusen.She failed to respond to laser photocoagula-tion and proton beam radiation. Vision failedto 3/200 and the left disc became oedema-tous. MRI scanning showed bilateral opticnerve sheath enlargement and gadoliniumenhancement of the mid and posterior seg-ments of both optic nerves and extension ofthe lesion on the right side over the planumtowards the chiasm. The lesions were inter-preted as primary optic nerve sheath menin-giomas.
CommentChoroidal neovascularisation has been asso-ciated with macular degeneration, histoplas-mosis, pathological myopia, angioid streaks,
optic nerve drusen, optic nerve pits, pseudo-tumour cerebri, chronic inflammation, infec-tion, malignant melanoma, choroidalosteomas, choroidal naevi, photocoagulation,and choroidal rupture. A break in Bruch’smembrane seems to be a common feature inCNV, but the exact pathogenesis remains asubject of debate.1 2
While we cannot eliminate the possibilitythat the association of CNV with meningio-mas and CNV in our patients is merely bychance, several observations suggest other-wise. In each case the fundus of the felloweye was free of drusen, let alone moresubstantive evidence of macular degenera-tion. None of the patients had a disorderknown to predispose to CNV. There has beenone report of CNV after radiation but in thatcase the patient also had significant radiationretinopathy.3 Our irradiated patient (case 1)had no evidence of radiation retinopathy andthe radiation portals spared the eye. One ofour patients was only 49 years old when themembrane was recognised. In two of ourpatients the membrane was peripapillary.Schatz et al published the histopathological
findings in a patient with a primary opticnerve sheath meningioma in which there wasa CNV. However, their patient had chronicdisc oedema and venous collaterals and hadantecedent age related macular degenerationin both eyes.4 Shields et al described aninstance of CNV in a child with an opticnerve glioma. That patient’s disc was alsooedematous.5 Peripapillary CNV has beendescribed with chronic disc oedema of othercauses as well,6 but two of our patients neverhad disc swelling and the third developeddisc oedema only after the CNV was recog-nised.How might a meningioma cause an ipsi-
lateral CNV? The pathophysiological mechan-ism by which these two conditions occurtogether is unclear. It is possible that thetumour tissue could have invaded the eye.CNV has been associated with other tumoursinvolving the choroid.1 2 Ocular invasion wasnot evident on ultrasound (cases 1 and 3) orMRI scans but absence of proof is not proof ofabsence. In the case of Schatz et al there weresmall foci of the meningioma in the peripa-pillary sclera and retrolaminar optic nerve,which were not seen before enucleation.4
Dutton reviewed meningiomas involving theoptic nerve and primary optic nerve sheathmeningiomas. CNV was not mentioned as apresenting sign. None the less, he calculated3.7% of 477 reported cases described intra-ocular invasion by meningiomas.7 Otherauthors have reported histopathological casesof meningioma invading the optic nerve anddisc.8–10
We believe that the association of CNVwith ipsilateral meningiomas in our patientswas not one of chance. The presumedmechanism is invasion of the globe by thetumour sufficient to cause the CNV but belowthreshold for detection by MRI, ultrasound,or ophthalmoscopy.
M S LeeCole Eye Institute, The Cleveland Clinic Foundation,
Cleveland, OH 44195, USA
S LessellNeuro-ophthalmology Unit, Massachusetts Eye and
Ear Infirmary, Harvard Medical School, Boston,MA 02114, USA
Correspondence to: Michael S Lee, MD, Cole EyeInstitute/I-32, The Cleveland Clinic Foundation, 9500
Figure 1 Patient 1. Retinal elevation and lipid exudation superotemporal to the left optic disc (topleft). Venous laminar (top right), arteriovenous transit (bottom left), and late phases (bottom right) ofthe fluorescein angiogram demonstrates peripapillary hyperfluorescent area growing in size andfluorescence consistent choroidal neovascularisation.
PostScript 1385
www.bjophthalmol.com

Euclid Avenue, Cleveland, OH 44195, USA;[email protected]
References
1 Green WR, Wilson DJ. Choroidalneovascularization. Ophthalmology1986;93:1169–76.
2 Lopez FP, Green WR. Peripapillary subretinalneovascularization: a review. Retina1992;12:147–71.
3 Spaide RF, Borodoker N, Shah V. Atypicalchoroidal neovascularization in radiationretinopathy. Am J Ophthalmol2002;133:709–11.
4 Schatz H, Green WR, Talamo JH, et al.Clinicopathologic correlation of retinal tochoroidal venous collaterals of the optic nervehead. Ophthalmology 1991;98:1287–93.
5 Shields JA, Shields CL, De Potter P, et al.Choroidal neovascular membrane as a feature ofoptic nerve glioma. Retina 1997;17:349–50.
6 Jamison RR. Subretinal neovascularization andpapilledema associated with pseudotumorcerebri. Am J Ophthalmol 1978;85:78–81.
7 Dutton JJ. Optic nerve sheath meningiomas. SurvOphthalmol 1992;37:167–83.
8 Rodrigues MM, Savino PJ, Schatz NJ. Spheno-orbital meningioma with optociliary veins.Am J Ophthalmol 1976;81:666–70.
9 Coston TO. Primary tumor of the optic nerve: withreport of a case. Arch Ophthalmol1936;15:696–702.
10 Dunn SN, Walsh FB. Meningioma (duralendothelioma) of the optic nerve. ArchOphthalmol 1956;56:702–7.
Intraoperative visual experiencesof cataract patients can be bothpleasant and unpleasantWe read with interest Zia et al’s article, whichhighlights a professional artist’s and a poet’srespective renditions of their visual experi-ences during phacoemulsification and intra-ocular lens implantation under localanaesthesia.1 While it is unclear from thereport whether the artist’s elaborate drawingresembling a ‘‘colourful monkey’’ was asso-ciated with a pleasant or frightening visualexperience, it appears from the poem that thepoet’s visual experience was most probablypleasant and delightful.We have previously reported that the visual
experience during cataract surgery underlocal anaesthesia can be frightening in up to16.2% of patients.2–8 The anxiety that mayresult from the intraoperative visual experi-ence is clinically significant because it maycause patients to become uncooperative dur-ing the procedure and trigger a sympatheticstress response. This may result in hyperten-sion, tachycardia, ischaemic strain on theheart, hyperventilation, and acute panicattacks. These stress responses are particu-larly undesirable in cataract patients who areoften elderly, with systemic co-morbiditiessuch as hypertension and ischaemic heartdisease.2 9 The frightening experience may
also lower patients’ satisfaction with thesurgery.10 11
The poet’s experience reported by Zia et alreminds us that the intraoperative visualexperience during cataract surgery can bepleasant for some patients.1 In fact, ourexperience has shown that the majority ofpatients find their visual experiences pleasantand, in some cases, the visual experienceactually increases their satisfaction with thesurgery. In a recently reported randomisedcontrolled trial conducted in India involving304 patients who underwent phacoemulsifi-cation under either topical anaesthesia (TA)or retrobulbar anaesthesia (RA), the visualexperience was reported by 106 out of 154(68.8%) TA and 102 out of 150 (68%) RApatients to be pleasant and by 47 (30.5%) TAand 46 (30.7%) RA patients to be unplea-sant.12 In a separate unpublished studyconducted in Singapore, eight of 98 patients(8.2%) who had phacoemulsification underTA reported that their satisfaction with thesurgery increased because of their visualexperiences, whereas only two patients(2.0%) experienced a decrease in satisfaction.The remaining 88 patients (89.8%) reportedthat their visual experience did not affecttheir satisfaction with the surgery. Some ofthe patients who found their visual experi-ences pleasant commented on the ‘‘fantasticcolours’’ that they experienced. In anothersimilar study on patients who had cataractsurgery under RA, nine of 152 patients (5.9%)experienced an increase in satisfaction,whereas five patients (3.3%) thought thattheir satisfaction had decreased as a result ofthe visual experiences and the remaining 138patients (90.8%) experienced no change intheir satisfaction.An additional observation is from video-
taped interviews conducted by one of us(CMK) with several leading ophthalmicanaesthesia providers in the United Stateswho had cataract surgery under local anaes-thesia themselves. The video recordings weremade during the annual scientific meeting ofthe Ophthalmic Anaesthesia Society held inChicago in October 2004. The videos clearlyshowed they reported seeing pleasant andbeautiful images during their surgery.In summary, patients may experience
pleasant or unpleasant visual sensationsduring cataract surgery under local anaes-thesia. Further investigation is warranted tohelp ascertain how we can reduce thepossibility of the experience being unpleasantor frightening.
K-G Au EongThe Eye Institute at Alexandra Hospital, National
Healthcare Group, Singapore, The Eye Institute at TanTock Seng Hospital, National Healthcare Group,
Singapore, Department of Ophthalmology, NationalUniveristy of Singapore, Singapore, Singapore Eye
Research Institute, Singapore
C S H Tan, C L Ang, S S G LeeThe Eye Institute at Tan Tock Seng Hospital, National
Healthcare Group, Singapore
R VenkateshAravind Eye Hospitals, Pondicherry, India
R MuralikrishnanLions Aravind Institute of Community Ophthalmology,
Modurai, India
G L FanningHauser-Ross Eye Institute, Sycamore, IL, USA
C M KumarAcademic Department of Anaesthesia, The James
Cook University Hospital, UK
Correspondence to: Dr Kah-Guan Au Eong,Alexandra Hospital 378 Alexandra Road Singapore,Singapore 159964; kah_guan_au_eong@alexhosp.
com.sg
doi: 10.1136/bjo.2005.074823
References
1 Zia R, Schlichtenbrede FC, Greaves B, et al.‘‘Only rarely seen in dreams’’—visualexperiences during cataract surgery.Br J Ophthalmol 2005;89:247–8.
2 Au Eong KG. 6th Yahya Cohen lecture: visualexperience during cataract surgery. Ann AcadMed Singapore 2002;31:666–74.
3 Prasad N, Kumar CM, Patil BB, et al. Subjectivevisual experience during phacoemulsificationcataract surgery under sub-Tenon’s block. Eye2003;17:407–9.
4 Au Eong KG. The Royal College ofOphthalmologists cataract surgery guidelines:what can patients see with their operated eyeduring cataract surgery? Eye 2002;16:109–10.
5 Au Eong KG, Lim TH, Lee HM, et al. Subjectivevisual experience during phacoemulsification andintraocular lens implantation using retrobulbaranaesthesia. J Cataract Refract Surg2000;26:842–6.
6 Au Eong KG, Low CH, Heng WJ, et al. Subjectivevisual experience during phacoemulsification andintraocular lens implantation under topicalanaesthesia. Ophthalmology 2000;107:248–50.
7 Au Eong KG, Lee HM, Lim ATH, et al. Subjectivevisual experience during extracapsular cataractextraction and intraocular lens implantation underretrobulbar anaesthesia. Eye 1999;13:325–8.
8 Tranos PG, Wickremasinghe SS, Sinclair N, et al.Visual perception during phacoemulsificationsurgery under topical and regional anaesthesia.Acta Ophthalmol Scand 2003;81:118–22.
9 Tan CSH, Rengaraj V, Au Eong KG. Visualexperiences of cataract surgery. J CataractRefract Surg 2003;29:1453–4.
10 Leo SW, Au Eong KG. Comments on anaesthesiafor cataract surgery. J Cataract Refract Surg2003;29:633–5.
11 Leo SW, Au Eong KG, Rengaraj V, et al. TheMisericordia Health Centre cataract comfortstudy. Can J Ophthalmol 2003;38:23–4.
12 Rengaraj V, Radhakrishnan M, Au Eong KG, etal. Visual experience during phacoemulsificationunder topical versus retrobulbar anaesthesia:results of a prospective, randomised, controlled,trial. Am J Ophthalmol 2004;138:641–8.
Cigarette pack warning: it cansend you blind!The growing research implicating smoking inage related macular degeneration (AMD)prompted us to write an editorial in 19991
urging the Australian government to warnsmokers of this little appreciated risk.In 2000, the Australian National Quit
campaign ran an advertisement as part of aseries titled ‘‘Every cigarette is doing youdamage,’’ which explicitly addressed AMD. Awebsite describes the campaign here inAustralia (www.quitnow.info.au/script/eye.html) and the television ad may be down-loaded (www.quitnow.info.au/smokescreen/smokescreen.html).In 2006 the Australian government will
require new mandatory pictorial pack warn-ings, one of which will be about AMD. Thiswarning was one of the strongest testedamong smokers in the research conductedfor the government before the announce-ment. The full report and other relatedinformation can be found at tobacco.health.
Presented in part at the North American Neuro-ophthalmology Society annual meeting, Snowbird,
UT, USA, February 2003.
doi: 10.1136/bjo.2005.071696
Accepted for publication 1 May 2005
Supported by the Heed Foundation, Cleveland, OH,USA (MSL).
Competing interests: none declared
Accepted for publication 13 May 2005
MAILBOX
1386 PostScript
www.bjophthalmol.com

usyd .edu .au/ site / supersite / resources /docs/gallery_ packwarnings.htm.
Correspondence to: Professor S Chapman, School ofPublic Health, University of Sydney, Sydney 2006,
Australia; [email protected]
doi: 10.1136/bjo.2005.076562
Reference
1 Mitchell P, Chapman S, Smith W. ‘‘Smoking is amajor cause of blindness’’: a new cigarette packwarning? Med J Aust 1999;171:173–4.
Accepted for publication 9 June 2005
BOOK REVIEWS
The next chapter deals with antimetabolitesin filtration surgery; established antimetabo-lites are covered (5-fluorouracil and mitomycinC), new agents such as antibodies to TGF-b arealso mentioned. The final chapter is ondrainage implants, the Molteno, Baerveldt,and Ahmed implants are discussed. Finallythe actual surgical techniques and the compli-cations are well described.Overall, this is an excellent book, it is
concise, with only 163 pages of illustratedtext, easy to read, and extremely pertinent toclinical practice. A text I thoroughly recom-mend for any trainee ophthalmologist oroptometrist and anyone wanting a brief,contemporary revision text on the diagnosisand management of glaucoma. Although,fortunately or unfortunately, in the end itmay only whet your appetite for informationand leave you wanting more.
N SpencerBristo Eye Hospital, Lower Maudlin Street,
Bristol B S1 2LX UK;[email protected]
Immunology of the lacrimal gland,tear film and ocular surface
Eds Manfred Zierhut, Michael E Stern, David ASullivan. £75, pp 288. London: Taylor andFrancis, 2005, ISBN 184184568X
A short quotation (p 152) summarises thebook: ‘‘These systems are all part of themultiple and redundant and protectivemechanisms…[that] maintain a functioningcornea.’’ Reflecting this complexity, chaptersrange from the pathogenesis of herpetickeratitis to dry eyes, to mucosal immunityand the use of topical ciclosporin, to tear filmand contact lenses and, of course, inflamma-tion. The book includes more unusual chap-ters on ocular surface: these integrate the eyeinto the upper aerodigestive tract. Parallelsbetween lacrimal and salivary glands, whichare not often conducted, focus attention tothe inflammatory and immune processescommon to these mucosae and the diagnosticmarkers they might offer.Some chapters are dense and scholarly:
‘‘Sex, sex steroids and dry eye syndromes’’has no fewer than 232 references, andprovides a ‘‘must read’’ synthesis ofapproaches, results and hypotheses of theresearch undertaken to understand sexrelated differences in lacrimal and meibo-mian gland (dys)function. Other chaptershave a narrower focus: events leading toAcanthamoeba infections and candidates fortherapy are presented in an very clearlyorganised and chapter.Equally elegantly and authoritatively pre-
sented are hypotheses and results showingthat constant parasympathetic input is neces-sary for tear production and thus ocularsurface homeostasis.Though not stated by the editors, this book
contains contributions to a meeting with thesame title, which provided a wonderfulopportunity for discussions. It is rather a pitythat these are not part of the book. Putting upwith different styles is a small price to pay forthis highly informed and expertly abstractedstate of knowledge publication.
M BerryBristol Eye Hospital, Lower Maudlin Street,
Bristol, UK; [email protected]
Glaucoma. 3rd ed.
This excellent text has been in print since 1989and its longevity is testament to its highquality. This is the third edition, with a newco-author John Salmon. Since its previousedition over 8 years ago there have been manyadvances in both the genetics, and the diag-nosis, monitoring and treatment of glaucoma.This text successfully updates the previousedition, and provides a concise, systematic,detailed and well balanced representation ofmodern glaucoma diagnosis and management.This book is aimed at the trainee ophthal-
mologist and optometrist, although it is alsogood basic revision for the practising ophthal-mologist. This is a comprehensive text in thateach type of glaucoma is described in terms ofits main clinical features and management.There are many colour illustrations and photo-graphs, these help the reader to correctlyinterpret clinical signs and diagnostic tests. Italso covers current controversies and newtechniques such as non-penetrating glaucomasurgery. The landmark glaucoma studies andtheir significance are also mentioned. It isperhaps too brief in sections, particularly in thechapters looking at glaucoma diagnosis, peri-metry, and imaging; however, adequate andkey references are provided to allow furtherpursuit of these topics in more depth.The text begins by covering the basic
sciences including the physiology of aqueoussecretion. Then there is a comprehensivedefinition and classification of glaucoma.The different types of glaucoma are describedat length. Tonometry is covered well, includ-ing the range of tonometers, potential errorsin tonometry, and calibration. Gonioscopy isdiscussed including angle structure identifi-cation and the different systems of angleclassification.Retinal nerve fibre and optic nerve head
assessment is described briefly including thenew imaging techniques of scanning lasertomography (Heidelberg retinal tomogramII), ocular coherence tomography (OCT),and scanning laser polarimetry (GDx nervefibre analyser). The images or readoutsproduced by each machine are provided incolour along with a very brief description oftheir interpretation. The various modalities ofperimetry are described, their interpretationis given, and new techniques such as thefrequency doubling contrast test (FDT) andshortwave automated perimetry (SWAP) arediscussed and examples provided.Glaucomamedications are covered very well.
Long standing medication are discussed as wellas new treatment options, including combinedtopical preparations. Neuroprotective agentsare covered with the recent research regardingthese agents. There is a chapter on laser therapywhich covers argon, diode, and selective lasertrabeculoplasty, Nd-YAG laser iridotomy, anddiode laser cycloablation.Trabeculectomy surgery with early and late
complications are discussed comprehensively.There is an excellent and concise chapter onnon-penetrating filtration surgery, coveringthe two most popular techniques—deepsclerectomy and viscocanalostomy.
Eds J Salmon, J Kanski. £46, pp 169.Oxford: Butterworth-Heinemann, 2004, ISBN0750655283.
NOTICES
World Ophthalmology Congress2006 – BrazilThe World Ophthalmology Congress (whichis replacing the International Congress ofOphthalmology) is meeting in February 2006in Brazil.For further information on the congress
and committees, scientific program andcoordinators of different areas are availableat the congress website www.ophthalmolo-gy2006.com.br
Thoughts on Ophthalmology andDevelopmentThe Mathis Eye Foundation is a small,privately financed organisation, established17 years ago by a former international bankerwho began his medical studies at age 40,with the specific intention of working inthird world surgical ophthalmology. TheFoundation’s experiences and lessons learnedare presented in a 26 page bound summaryentitled Thoughts on Poor World OphthalmologyDevelopment, an often critical look at eyesurgery programs in Latin America, Africa,and Haiti. To obtain this report without cost,please contact [email protected].
Vision 2020The latest issue of Community Eye Health (No54) assesses the progress of Vision 2020 atthe district level. For further informationplease contact: Journal of Community EyeHealth, International Resource Centre,International Centre for Eye Health,Department of Infectious and TropicalDiseases, London School of Hygiene andTropical Medicine, Keppel Street, LondonWC1E 7HT, UK (tel: +44 (0)20 7612 7964;email: [email protected]; online edi-tion: www.jceh.co.uk). Annual subscription(4 issues) UK £28/US$45. Free to developingcountry applicants.
PostScript 1387
www.bjophthalmol.com

‘‘The Hakim was a doctor in the medievalsense; rather than learning the traditionalmedical sciences, he studied theology,literary history, logic, and grammar.Often he was a member of a pious societyof dervishes, at times a student of theKoran and a poet. Lev witnessed cures ofvarious local diseases—for example, onecalled pindinka, a horrible skin diseasethat would begin with one red spot andthen spread to engulf the face in flamingred masks of scabs. If it went untreated,the disease could spread to the conjunctivaand cause the loss of an eye. ‘I had aninsane fear of pindinka, but luckily wasspared its suffering,’ remarked Lev. (Reiss,Tom. The Orientalist. New York: RandomHouse, 2005:59)
The Ebola and Marburg viruses are naturaldeadly pathogens that could be manipu-lated for use as agents of bioterrorism. Noapproved vaccines or therapies againstthese pathogens currently exist. However,in the 5 July online edition of NatureMedicine, a vaccine that appears to offercomplete protection in non-human pri-mates infected with the viruses is reported.(www.nature.com\naturemedicine)
Meningiomas of the anterior skull baseaccount for 40% of all intracranial menin-giomas. About 25% are tumours of thetuberculum sellae. Women are affectedthree times more commonly than men. Ina report from Germany, encouragingresults are reported in a large series ofsurgically treated tuberculum sellaemeningiomas. Total macroscopic resectionwas achieved in 48 patients. Visual acuityimproved in 20 patients with only sevenexperiencing deterioration. The reportunfortunately does not document pre-operative and postoperative visual fieldsin each case. (J Neurol Nerosurg Psychiatry2005;76:977–83)
The use of statins to reduce cholesterollevels is now a well established therapyto prevent cardiovascular disease.Recommendations that supplementationof the diet with psyllium fibre might alsolower cholesterol are less well validated.However, in a study comparing dietarypsyllium supplementation in patients tak-ing statins, psyllium soluble fibre appearedto be safe and well tolerated. This dietarysupplement was as effective in lowering
cholesterol as 20mg of simvastatin alone.(Arch Intern Med 2005;165:1161–6)
The potential complications of hormonetherapy for the treatment of menopausalsymptoms has now been well documen-ted. Current recommendations suggestthat this therapy should be at the lowesteffective dose for the shortest durationpossible to assess the patient’s symptoms.However, in a study of more than 8000women, investigators documented thatmore than half of women with symptomsassociated with menopause will haverecurrence of these symptoms after dis-continuing hormonal therapy. The inves-tigators suggest that alternative strategiesto manage menopausal symptoms areclearly warranted. (JAMA 2005;294:183–93)
The overview of systemic antibiotics andthe problem of induction of antibioticresistance in certain bacterial strains iswell known. Now, in a study of the use ofchloramphenicol eye drops in the treat-ment of children with conjunctivitis,investigators have concluded that primarycare doctors should stop prescribing anti-biotic (chloramphenicol) eye drops forchildren with uncomplicated conjunctivi-tis. This is based on a study of more than300 children, in which the clinical curerates of children treated with placebodrops were similar to those who receivedinitial antibiotic therapy. The economicbenefit of adopting this policy is clear asthe authors point out that every year onemillion children present in the UnitedKingdom to general practitioners withconjunctivitis. (Lancet 2005 June 22;doi10.1016\SO140 6736)05)66709-8)
Controversy surrounds the question ofwhether neuromyelitis optica (Devic’ssyndrome) is a distinct entity separatefrom multiple sclerosis. Recent opinions,however, suggest that it is. The aetiology ofneuromyelitis optica is unknown,although connective tissue disorders,tuberculosis, and acute disseminated ence-phalomyelitis have been associated with it.Neurologists at the Royal InfirmaryLeicester have recently reported two casesof neuromyelitis optica apparently asso-ciated with gluten sensitivity. The authorssuggest that patients presenting withmyelitis with or without optic neuritis
should be investigated for possible glutensensitivity. (J Neurol Neurosurg Psychiatry2005;76:1028–30)
Immigration has always played an impor-tant part in population growth in theUnited States. A surge in immigration tothe United States has occurred since theImmigration and Nationality Act of 1965.One of the benefits of this increase inimmigration has been the availability ofstudents interested in science, medicine,and engineering. It appears that too fewAmericans born in the United States areinterested in the sciences. Today, only2.2% of native born citizens of the UnitedStates hold higher degrees such as PhDsand MDs, whereas 3.3% of citizens born inforeign countries hold similar degrees. (SciAm 2005;293:25)
The benefits of breast feeding have beenrepeatedly documented. Surprisingly,however, a study from Singapore suggeststhat breast feeding is associated with asignificant reduction in the developmentof myopia in children. In a study of morethan 500 children investigators demon-strated that there is a link between breastfeeding and a reduced incidence in myo-pia. (JAMA 2005;293:3001–2)
‘‘How about eyes? Would the first bilater-ian have had eyes? It isn’t enough to saythat all modern descendents of Concestor26 have eyes. It isn’t enough, because thevarious kinds of eyes are very diverse: somuch so that it has been estimated thatthe eye has evolved independently morethan 40 times in various parts of theanimal kingdom. How do we reconcile thiswith the statement that Concestor 26 hadeyes? To give intuition a steer let me sayfirst that what is claimed to have evolvedforty times independently is not light-sensitivity per se, but image-formingoptics. The vertebrate camera eye and thecrustacean compound eye evolved theiroptics (working on radically differentprinciples) independently of one anotherbut both these eyes are descended fromone organ in the common ancestor(Concestor 26) which was probably aneye of some kind.’’ (Dawkins, Richard. TheAncestor’s Tale. A Pilgrimage to the Dawn ofEvolution. New York: Houghton Mifflin,2004:388)
www.bjophthalmol.com
on 11 October 2005 bjo.bmjjournals.comDownloaded from