Color Atlas & Synopsis of Clinical Ophthalmology - Wills Eye ...
384
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Color Atlas & Synopsis of Clinical Ophthalmology - Wills Eye ...



COLOR ATLAS & SYNOPSIS OFCLINICAL OPHTHALMOLOGY
W i l l s Ey e In s t i t u t e
Corne aSECOND EDITION
LWBK9 6 1 -FM_ i-1 .indd i 7 / 2 2 / 1 1 7 :2 7 PM

EDITORChristopher J. Rapuano, MD
Director and Attending Surgeon, Cornea ServiceCo-Director, Refractive Surgery Department
Wills Eye InstituteProfessor of Ophthalmology
Jefferson Medical College of Thomas Jefferson UniversityPhiladelphia, Pennsylvania
SERIES EDITORChristopher J. Rapuano, MD
Director and Attending Surgeon, Cornea ServiceCo-Director, Refractive Surgery Department
Wills Eye InstituteProfessor of Ophthalmology
Jefferson Medical College of Thomas Jefferson UniversityPhiladelphia, Pennsylvania
LWBK9 6 1 -FM_ i-1 .indd ii 7 / 2 2 / 1 1 7 :2 7 PM

COLOR ATLAS & SYNOPSIS OFCLINICAL OPHTHALMOLOGY
W i l l s Ey e In s t i t u t e
Corne aSECOND EDITION
LWBK9 6 1 -FM_ i-1 .indd iii 7 / 2 2 / 1 1 7 :2 7 PM

Senior Executive Editor: Jona han W. Pine, Jr.Senior Product Managers: Emilie Moyer and Grace Capu oSenior Manufacturing Coordinator: Benjamin Rivera Marketing Manager: Lisa LawrenceCreative Director: Doug SmockProduction Services: Ap ara, Inc.
© 2012 by LIPPINCOT WILLIAMS & WILKINS, a Wolters Kluwer business
First edition, © 2003 e McGraw-Hill Companies, Inc.
wo Commerce Square2001 Market StreetPhiladelphia, PA 19103 USALWW.com
All righ s reserved. T is book is pro ec ed by copyrigh . No par o his book may be reproduced in any orm by any means, including pho ocopying, or u ilized by any in orma ion s orage and re rieval sys em wi hou writ en permission rom he copyrigh owner, excep or brie quo a ions embodied in cri ical ar icles and reviews. Ma erials appearing in his book prepared by individuals as par o heir of cial du ies as U.S. governmen employees are no covered by he above-men ioned copyrigh .
Prin ed in China
Library of Congress Cataloging-in-Publication DataRapuano, Chris opher J. Cornea / Chris opher J. Rapuano. – 2nd ed. p. ; cm. – (Color a las & synopsis o clinical oph halmology–Wills Eye Ins i u e) Includes bibliographical re erences and index. ISBN 978-1-60913-338-2 (alk. paper) 1. Cornea–Diseases–A lases. 2. Cornea–Diseases–Handbooks, manuals, e c. I. i le. II. Series: Color a las and synopsis o clinical oph halmology series. [DNLM: 1. Corneal Diseases–A lases. WW 17] RE336.R37 2011 617.7'19–dc23 2011025133
Care has been aken o con rm he accuracy o he in orma ion presen ed and o describe generally accep ed prac ices. However, he au hors, edi ors, and publisher are no responsible or errors or omissions or or any con sequences rom applica ion o he in orma ion in his book and make no warran y, expressed or implied, wi h respec o he currency, comple eness, or accuracy o he con en s o he publica ion. Applica ion o he in orma ion in a par icular si ua ion remains he pro essional responsibili y o he prac i ioner. T e au hors, edi ors, and publisher have exer ed every e or o ensure ha drug selec ion and dosage se or h in his ex are in accordance wi h curren recommenda ions and prac ice a he ime o publica ion. However, in view o ongo-ing research, changes in governmen regula ions, and he cons an ow o in orma ion rela ing o drug herapy and drug reac ions, he reader is urged o check he package inser or each drug or any change in indica ions and dosage and or added warnings and precau ions. T is is par icularly impor an when he recommended agen is a new or in requen ly employed drug. Some drugs and medical devices presen ed in he publica ion have Food and Drug Adminis ra ion (FDA) clearance or limi ed use in res ric ed research set ings. I is he responsibili y o he heal h care provider o ascer ain he FDA s a us o each drug or device planned or use in heir clinical prac ice.
o purchase addi ional copies o his book, call our cus omer service depar men a (800) 638-3030 or ax orders o (301) 223-2320. In erna ional cus omers should call (301) 223-2300.
Visi Lippincot Williams & Wilkins on he In erne : a LWW.com. Lippincot Williams & Wilkins cus omer service represen a ives are available rom 8:30 am o 6 pm, ES .
10 9 8 7 6 5 4 3 2 1
LWBK961-FM_i-1.indd iv 28/07/11 10:54 AM

To my wonderful wife, Sara, an essential partner at home and at work; we continue to make a perfect team;our children—Michael, Patrick, Daniel, and Megan—for always reminding me what is important in life;
my parents, Cathie and Al, for all their love and support over the years; andmy three brothers, sisters-in-law, brothers-in-law, and their children, who demonstrate how essential family
really is in our lives.
LWBK9 6 1 -FM_ i-1 .indd v 7 / 2 2 / 1 1 7 :2 7 PM

Abou he SeriesThe beau y o he a las/ synopsis concep is
he power ul combina ion o illus ra ive pho ographs and a summary approach o he ex . Oph halmology is a very visual discipline ha lends i sel nicely o clinical pho ographs. While he seven oph halmic subspecial ies in his series—Cornea, Re ina, Glaucoma, Oculoplas ics, Neurooph halmology, Uvei is, and Pedia rics—employ varying levels o visual recogni ion, a rela ively s andard orma or he ex is used or all volumes.
T e goal o he series is o provide an up- o-da e clinical overview o he major areas o oph halmology or s uden s, residen s, and prac i ioners in all he heal hcare pro essions. T e abundance o large, excellen -quali y pho- ographs and concise, ou line- orm ex will help achieve ha objec ive.
Chris opher J. Rapuano, MDSeries Editor
vi
LWBK9 6 1 -FM_ i-1 .indd vi 7 / 2 2 / 1 1 7 :2 7 PM

vii
he main objec ive o basic oph halmic educa ion is o rain he user o discover
he ull his ory o he pa ien ’s illness, rec-ognize he abnormal physical signs, make a diagnosis, and sugges appropria e me hods o rea men . T e aim o higher raining is o ampli y hese capabili ies in bread h and dep h hrough prac ical experience and subspecial y raining. During case presen a ions and even clinical examina ions, i is no uncommon o encoun er residen s making he wrong diag-nosis and arriving a he wrong rea men plan. T ere are wo principal reasons or his error. Firs , hey may ail o de ec all he abnormal signs, and, second, hey are unable o in egra e and in erpre he ac s ha are collec ed. T e f rs s ep in he managemen o any condi ion is making a correc diagnosis. One mus be able o de ec all he abnormal signs and know wha one is observing.
T e goal o his book is o use color pho o-graphs o he impor an corneal, an erior seg-men , and ex ernal diseases wi h ou line- orm ex o succinc ly illus ra e and describe hese condi ions. T is a las is in ended no only or oph halmic residen s and cornea ellows bu also or prac icing physicians. Each sec ion covers he clinical ea ures o he impor an cornea and ex ernal eye diseases, diagnos ic
es s, di eren ial diagnoses, and rea men . In addi ion o providing prac ical in orma ion on he approach and managemen o each con-di ion, his book aids recogni ion o clinical signs by including a selec ion o classic pho- ographs. In he f eld o cornea s udy, he old saying, “A pic ure is wor h a housand words,” is inadequa e because no even a housand words can subs i u e or a good pic ure o he condi ion. I is hoped ha he ex ensive use o color pho ographs hroughou his a ordable a las will have a grea impac on he memory and acili a e learning.
o emphasize he impor ance o sign recogni- ion and he powers o observa ion, he ollow-ing quo a ions may serve as use ul reminders or all o us:
Credi mus be given o observa ion ra her han heories, and o heories only in so ar as hey are conf rmed by he observed ac s.
Aris o le
T e more I see, he more I see here is o see.
John Sebas ian
Chris opher J. Rapuano, MDEditor
Pre aceT
LWBK9 6 1 -FM_ i-1 .indd vii 7 / 2 2 / 1 1 7 :2 7 PM

I would like o acknowledge he many people who helped make his book a reali y. Mos
o he clinical pho ographs came rom my pa ien s. I am gra e ul o hem or allowing me o subjec hem o ash pho ography. Several colleagues generously supplied addi ional pho os, including Kris in Hammersmi h, MD, Elisabe h Cohen, MD, Pe er Laibson, MD, Irving Raber, MD, Wee-Jin Heng, MD, and also Rolande Michaud, MD, via Pa ricia Laughrea, MD, rom Quebec, Canada.
I also hank Jack Scully and Roger Barone o he Audio-Visual Depar men a Wills Eye
or all heir help and exper ise wi h he pho- ographic needs or his book and or all he volumes in his series.
I wish o hank Jona han Pine, Emilie Moyer, Grace Capu o, and he eam a LippincotWilliams & Wilkins or giving me he oppor- uni y o be par o his series and or keeping he process moving orward.
Finally, I hank all o our ellows and residen s, pas and presen , or all hey do o encourage me o con inue eaching and learning in our wonder ul subspecial y o cornea and an erior segmen disease.
Acknowledgmen s
viii
LWBK9 6 1 -FM_ i-1 .indd viii 7 / 2 2 / 1 1 7 :2 7 PM

ix
Con en sAbou he Series vi
Pre ace vii
Acknowledgmen s viii
Ch apt er 1 Conjunctival In ections and Inf ammations 2Blephari is and Meibomi is 2Chalazion (In ernal Hordeolum, S ye) 4Bac erial Conjunc ivi is (Nongonococcal) 6Gonococcal Bac erial Conjunc ivi is 8Viral Conjunc ivi is ( ypically Adenovirus) 10Chlamydial Conjunc ivi is (Adul Inclusion Conjunc ivi is) 14 rachoma 16Molluscum Con agiosum 18Ligneous Conjunc ivi is 20Pediculosis 21Parinaud’s Oculoglandular Syndrome 22Oph halmia Neona orum 24Allergic Conjunc ivi is 26A opic Kera oconjunc ivi is 28Vernal Kera oconjunc ivi is 30Superior Limbic Kera oconjunc ivi is 33Floppy Eyelid Syndrome 35 oxic and Fac i ious Kera oconjunc ivi is
(Kera i is Medicamen osa) 37Ocular Rosacea 40
Ch apt er 2 Conjunctival Degenerations and Mass Lesions 42Pinguecula and P erygium 42O her Conjunc ival Degenera ions 46
Amyloidosis 46Calcium Concre ions 46
Melanocy ic Conjunc ival Lesions 48Conjunc ival Epi helial Melanosis (Racial Melanosis) 48Oculodermal Melanosis (Nevus o O a) 48Nevus 48Primary Acquired Melanosis 48Secondary Acquired Melanosis 49Malignan Melanoma 49
LWBK9 6 1 -FM_ i-1 .indd ix 7 / 2 2 / 1 1 7 :2 7 PM

x CONTENTS
Benign Amelanocy ic Conjunc ival Lesions 52Granulomas 52Epibulbar Dermoid 52Lipodermoid 52Heredi ary Benign In raepi helial Dyskera osis 52
Po en ially Malignan Amelanocy ic Conjunc ival Lesions 58Squamous Papilloma 58Conjunc ival In raepi helial Neoplasia 58Squamous Cell Carcinoma 58O her Carcinomas 58Reac ive Lymphoid Hyperplasia and
Non-Hodgkin’s Lymphoma 59Cys ic Lesions 64
Primary Conjunc ival Cys 64Ia rogenic Cys s 64
Vascular Lesions 67 elangiec asias 67Hema ologic Disorders 67Hemorrhagic Lymphangiec asia 67Capillary Hemangioma 67Lymphangioma 67Kaposi’s Sarcoma 67S urge-Weber Syndrome (Encephalo rigeminal
Angioma osis) 67Caro id–Cavernous Sinus and Dural-Sinus Fis ulas 67
Ch apt er 3 Anterior Segment Developmental Anomalies 70Anomalies o Corneal Size and Shape 70
Microcornea 70Megalocornea 72Nanoph halmos 74Microph halmos 74Buph halmos 76Congeni al An erior S aphyloma/ Kera ec asia 78Sclerocornea 79Cornea Plana 81
An erior Segmen Dysgeneses 82Pos erior Embryo oxon 82Axen eld’s Anomaly 82Rieger’s Anomaly 82Rieger’s Syndrome 82Pe ers’ Anomaly 82Localized Pos erior Kera oconus 82Aniridia 86Iris Coloboma 88
LWBK9 6 1 -FM_ i-1 .indd x 7 / 2 2 / 1 1 7 :2 7 PM

CONTENTS xi
Ch apt er 4 Ectatic Conditions of the Cornea 90Kera oconus 90Pellucid Marginal Degenera ion 98Kera oglobus 100
Ch apt er 5 Corneal Dystrophies 102An erior Corneal Dys rophies 102
Epi helial Basemen Membrane Dys rophy (An erior Basemen Membrane Dys rophy, Map-Do -Fingerprin Dys rophy, Cogan’s Microcys ic Dys rophy) 102
Meesmann’s Corneal Dys rophy ( Juvenile Heredi ary Epi helial Dys rophy) 108Reis-Bücklers Dys rophy 110Gela inous Drop–Like Corneal Dys rophy 114
S romal Corneal Dys rophies 116Granular Dys rophy 116Lat ice Dys rophy 120Macular Dys rophy 123Avellino Corneal Dys rophy (Granular-Lat ice) 126Schnyder’s Corneal Dys rophy 128
Pos erior Corneal Dys rophies 131Endo helial Dys rophy and Fuchs’ Dys rophy 131Pos erior Polymorphous Corneal Dys rophy 136Congeni al Heredi ary Endo helial Dys rophy 140
Ch apt er 6 Corneal Degenerations and Deposits 142Involu ional Changes 142
Corneal Arcus 142Whi e Limbal Girdle of Vog 142Crocodile Shagreen 142Cornea Farina a 143Polymorphic Amyloid Degenera ion 143
Corneal Deposi s—Nonpigmen ed 148Band Kera opa hy 148Salzmann’s Nodular Degenera ion 151
O her Corneal Degenera ions 153Spheroidal Degenera ion 153Lipid Kera opa hy 153Coa s’ Whi e Ring 153
Corneal Deposi s—Pigmen ed 156Cornea Ver icilla a (Vor ex Kera opa hy) 156Crys alline Kera opa hy 158Corneal Iron Deposi s 160Kayser-Fleischer Ring 163Terrien’s Marginal Degenera ion 164Iridocorneal-Endo helial Syndrome 166
LWBK961-FM_i-1.indd xi 23/07/11 1:08 PM
xii CONTENTS
Ch apt er 7 Corneal In ections, Inf ammations, and Sur ace Disorders 168Bac erial Kera i is 168Fungal Kera i is 174Acanthamoeba Kera i is 178Herpes Simplex Kera i is 182
Primary Ocular Herpes 182Recurren Ocular Herpes Simplex 184HSV: Epi helial Kera i is (Dendri ic Ulcer) 184HSV: Nonnecro izing S romal Kera i is (Disci orm Kera i is) 188HSV: Necro izing S romal Kera i is 192HSV: Neuro rophic Kera i is (Me aherpe ic Kera i is) 194
Herpes Zos er Kera i is 196In ers i ial Kera i is (Syphili ic, Nonsyphili ic) 202Subepi helial Inf l ra es 206Superf cial Punc a e Kera opa hy (Punc a e Epi helial Erosions) 208T ygeson’s Superf cial Punc a e Kera opa hy 210Kera oconjunc ivi is Sicca (Dry Eye Syndrome) 212Filamen ary Kera opa hy 216Exposure Kera opa hy 218Neuro rophic Kera opa hy 220Recurren Corneal Erosion 222Bullous Kera opa hy 225Acquired Immunodef ciency Syndrome 228Con ac Lens Complica ions 230
oxic/ Allergic Conjunc ivi is 230Gian Papillary Conjunc ivi is 230Con ac Lens Kera opa hy (Con ac Lens–Associa ed
Superior Limbic Kera oconjunc ivi is) 230Con ac Lens Overwear Syndrome 230 igh Lens Syndrome 231Corneal Warpage 231Corneal Neovasculariza ion 231S erile Kera i is 231Microbial Kera i is 232
Ch apt er 8 Systemic and Immunologic Conditions A ecting the Cornea 236Wilson’s Disease (Hepa olen icular Degenera ion) 236Vi amin A Def ciency 238Cys inosis 240Mucopolysaccharidoses and Lipidoses 242Collagen Vascular Diseases 244Ocular Cica ricial Pemphigoid 249S evens-Johnson Syndrome (Ery hema Mul i orme Major) 252Mooren’s Ulcer 255
LWBK9 6 1 -FM_ i-1 .indd xii 7 / 2 2 / 1 1 7 :2 7 PM
CONTENTS xiii
Phlyc enulosis 257S aphylococcal Hypersensi ivi y 259Corneal Gra Rejec ion 261
Ch apt er 9 Anterior Sclera and Iris 266Episcleri is 266An erior Scleri is 269Iris Cys s 274
Iris Pigmen Epi helial Cys 274Iris S romal Cys 274
Iris umors 276Iris Nevus 276Malignan Melanoma 276Me as a ic umor 276Vascular umor 276
Ch apt er 10 Surgery and Complications 278Ca arac Ex rac ion and In raocular Lens Implan a ion 278Full-T ickness Corneal ransplan a ion (Pene ra ing Kera oplas y) 282Endo helial Kera oplas y 290An erior Lamellar Kera oplas y 295Corneal Biopsy 298Superf cial Kera ec omy 299Excimer Laser Pho o herapeu ic Kera ec omy 300Conjunc ival Flap 303Limbal S em Cell ransplan a ion 306Amnio ic Membrane ransplan a ion 308Corneal Per ora ion 311Re rac ive Surgery 313
Ch apt er 11 Trauma 324Chemical Burns 324T ermal and Elec rical Burns 330
T ermal Burns 330Elec rical Burns 330
Ul raviole Kera opa hy (Arc Welder’s Flash) 332Corneal Abrasion 334Corneal and Conjunc ival Foreign Bodies 336Subconjunc ival Hemorrhage 340Corneoscleral Lacera ion and Wound Dehiscence 342 rauma ic Hyphema 350Epi helial Downgrow h 353Desceme ’s De achmen 356
Index 359
LWBK9 6 1 -FM_ i-1 .indd xiii 7 / 2 2 / 1 1 7 :2 7 PM

LWBK9 6 1 -FM_ i-1 .indd xiv 7 / 2 2 / 1 1 7 :2 7 PM

COLOR ATLAS & SYNOPSIS OFCLINICAL OPHTHALMOLOGY
W i l l s Ey e In s t i t u t e
Corne aSECOND EDITION
LWBK9 6 1 -FM_ i-1 .indd 1 7 / 2 2 / 1 1 7 :2 7 PM


C H A P T E R
2
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
lashes (s aphylococcal), sleeves along eyelashes (seborrheic), and pou ing o meibomian gland orif ces, which can be expressed o produce a hickened lipid secre ion, some imes o oo hpas e-like consis ency ( Fig. 1-1 )
Fro hy and oamy ear f lm, conjunc ival injec ion, in erior superf cial punc a e kera opa hy, phlyc enulosis, corneal inf l ra es
Treatment Warm compresses 5 o 10 minu es b.i.d.,
eyelid margin scrubs wi h mild commercially available cleansers (e.g., Ocuso Lid Scrub, Advanced Vision Research S erilid)
ear supplemen s while awake, opical azi hromycin drops or ery hromycin, baci racin, or e racycline oin men a bed ime
Oral e racycline 250 mg b.i.d. o q.i.d. or doxycycline 100 mg q.d. o b.i.d. in severe or recurren cases. T ese medica ions can o en be apered o a much lower dose or long- erm use (e.g., doxycycline 20 mg
Conjunc ival In ec ions and In amma ions
BLEPHARITIS AND MEIBOMITIS
Chronic blephari is and meibomi is are very common, bila eral in amma ions o
he eyelid margins ha may cause nonspecif c ocular irri a ion, which is o en worse in he morning. On he o her hand, some pa ien s have severe blephari is bu no symp oms.
Etiology S aphylococcal in ec ion, acne rosacea,
seborrheic derma i is
Symptoms Burning, i ching, discom or , oreign-body
sensa ion, earing, crus ing, mild discharge, uc ua ion in vision
Signs Associa ed a opic and seborrheic derma i-
is, and ocular rosacea Hyperemia, elangiec asias, crus ing, scal-
ing, orma ion o collaret es around bases o
LWBK961-C01_p02-41.indd 2 22/07/11 8:48 AM

Blepharitis and Meibomitis 3
b.i.d. or 50 mg q.d.). Oral ery hromycin (approxima ely 200 mg/ day) can be used or children.
Judicious shor - erm use o opical cor i-cos eroids or phlyc enulosis or inf l ra es
FIGURE 1-1. A. Blepharitis. S ignif can crus ing a he base o he eyelashes is seen. A ew collaret es are presen . B. Meibomitis. Severe pou ing o he meibomian glands o he in erior eyelid can be seen. T e eyelid margin is hickened and in amed, wi h some conjunc ival injec ion visible.
A
B
Prognosis Good or signif can improvemen in
symp oms over weeks, bu pa ien s need o unders and ha he condi ion is con rolled ra her han cured.
LWBK961-C01_p02-41.indd 3 22/07/11 8:48 AM

4 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
CHALAZION ( INTERNAL HORDEOLUM, ST YE)
A chalazion is a ender eyelid mass, o en wi h surrounding ery hema and swell-
ing. I may be small or large, and can cause sig-nif can eyelid in amma ion when severe.
Etiology Blockage o meibomian gland orif ces and
s agna ion o sebaceous secre ions Associa ed wi h blephari is/ meibomi is
and acne rosacea
Symptoms Eyelid swelling, pain, and redness O en a his ory o previous chalazia Rarely, large, cen ral chalazia can cause
corneal at ening, especially a er re rac ive surgery, or induced as igma ism.
Signs Subcu aneous round, f rm, swelling in he
arsal pla e ( Fig. 1-2 ) May have an associa ed pyogenic granu-
loma on eversion o eyelid Some imes may be associa ed wi h signif -
can eyelid in amma ion (presep al celluli is)
Dif erential Diagnosis Ex ernal hordeolum: an acu e s aphylo-
coccal in ec ion o a lash ollicle and i s asso-cia ed gland o Zeis or Moll
Pyogenic granuloma: a vascularized mass pro ruding rom he conjunc iva
Sebaceous carcinoma: suspec in recurren chalazia, eyelid margin excoria ion, or loss o lashes, especially i unila eral
Diagnosis Eyelid biopsy i suspicious or sebaceous
carcinoma
Treatment Warm compresses, eyelid massage,
and hygiene (see Blephari is/ Meibomi is above)
opical azi hromycin drops or ery hromy-cin, baci racin, or e racycline oin men or blephari is/ meibomi is
Oral e racycline 250 mg b.i.d. o q.i.d. or doxycycline 100 mg q.d. o b.i.d. in in amed, severe, or recurren cases, o preven recur-ren chalazia
Cor icos eroid injec ion can be considered o reduce scarring in recalci ran cases.
Incision and curet age i no improvemen wi h medical rea men .
Prognosis Very good wi h medical rea men
I medical rea men is unsuccess ul, surgi-cal rea men is qui e e ec ive.
LWBK961-C01_p02-41.indd 4 22/07/11 8:48 AM

Chalazion (Internal Hordeolum, Stye) 5
FIGURE 1-2. Chalazion. A. A large, in amed chalazion o he upper eyelid. Severe blephari is and crus ing o he eyelid margin, predisposing ac ors or developmen o chalazia, are also presen . B. Lower-eyelid eversion reveals a large indura ed mass consis en wi h a chalazion.
A
B
LWBK961-C01_p02-41.indd 5 22/07/11 8:48 AM

6 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
BACTERIAL CONJUNCTIVITIS (NONGONOCOCCAL)
Bac erial conjunc ivi is is a rela ively uncom-mon, usually bila eral condi ion, charac er-
ized by a mucopurulen or purulen discharge.
Etiology Staphylococcus aureus, Staphylococcus
epidermidis Streptococcus pneumoniae Haemophilus inf uenzae (especially in
children), o hers
Symptoms Redness, discharge, oreign-body sensa-
ion, burning, i chiness, pho ophobia
Signs Purulen or mucopurulen discharge
( Fig. 1-3 ) Conjunc ival hyperemia, maximal in he
ornices Pseudomembranes may be presen in
severe in ec ions. Corneal punc a e epi heliopa hy
Preauricular lymphadenopa hy is usually absen .
Diagnostic Evaluation Conjunc ival swab or Gram s ain, cul-
ures, and sensi ivi ies i severe or recurren
Treatment Spon aneous resolu ion in days o 1 o
2 weeks is usual. Ar if cial ears o wash away discharge Empiric broad-spec rum opical an ibi-
o ic drops (e.g., polymyxin B/ rime hoprim, uoroquinolones, gen amicin, obramycin, neomycin/ gramicidin/ baci racin) q.i.d. or 1 week or azi hromycin b.i.d. or 2 days hen q.d. or 5 days
An ibio ic oin men s (e.g., cipro oxacin, obramycin, gen amicin, e racycline, baci- racin, polymyxin B/ baci racin) can be used q.i.d. or 1 week in pa ien s in whom he drops wash ou very quickly, such as crying children.
Prognosis Very good Severe in ec ions can cause permanen
conjunc ival scarring.
LWBK961-C01_p02-41.indd 6 22/07/11 8:48 AM

Bacterial Conjunctivitis (Nongonococcal) 7
FIGURE 1-3. Bacterial conjunctivitis. A. Di use conjunc ival injec ion and a purulen discharge are presen in his eye wi h bac erial conjunc ivi is. B. A severe purulen discharge wi h crus ing can be seen in his pa ien who has bac erial conjunc ivi is. T ere is also modera e conjunc ival injec ion.
A
B
LWBK961-C01_p02-41.indd 7 22/07/11 8:48 AM

8 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
GONOCOCCAL BACTERIAL CONJUNCTIVITIS
Gonococcal conjunc ivi is is a rare, occa-sionally bila eral condi ion, charac erized
by acu e onse o a severe purulen discharge.
Etiology Primarily Neisseria gonorrhoeae Occasionally Neisseria meningitidis I is ypically sexually ransmit ed.
Symptoms Redness, severe purulen discharge, oreign-
body sensa ion, burning, pho ophobia Hyperacu e onse (wi hin 12 o 24 hours)
Signs Severe purulen discharge; pseudomem-
branes may be presen Marked conjunc ival in amma ion and
chemosis ( Fig. 1-4 A) Eyelid swelling Preauricular lymphadenopa hy o en presen Corneal punc a e epi heliopa hy, epi helial
de ec , inf l ra e, ulcer, or per ora ion ( Fig. 1-4 B)
Diagnostic Evaluation Conjunc ival scraping or immedia e
Gram s ain, cul ures, and sensi ivi ies. T e
diagnosis is conf rmed i he Gram s ain demons ra es gram-nega ive in racellular diplococci.
Treatment Sys emic ce riaxone 1 g IM in a single
dose i here is no corneal involvemen . I he pa ien is allergic o cephalosporins, uoro-quinolones are he drugs o choice.
I here is corneal involvemen or corneal involvemen canno be excluded because o a limi ed sli -lamp examina ion, he pa ien should be rea ed wi h ce riaxone 1 g IV q12h o q24h or 3 days.
opical uoroquinolone (e.g., cipro- oxacin) drops q2h, or q1h i he cornea is involved.
Ocular irriga ion wi h saline q.i.d. o q2h o elimina e he discharge.
Evalua e and rea or possible coin ec ion wi h Chlamydia (e.g., azi hromycin 1 g PO once).
Evalua e sexual par ners or sexually ransmit ed in ec ions.
Prognosis Very good i diagnosed and rea ed appro-
pria ely be ore corneal involvemen occurs. I he cornea is involved, he prognosis is guarded.
LWBK961-C01_p02-41.indd 8 22/07/11 8:48 AM

Gonococcal Bacterial Conjunctivitis 9
FIGURE 1-4. Gonococcal conjunctivitis. A. Severe in amma ion and chemosis are presen hroughou he conjunc iva in his righ eye. Some purulen discharge is presen on he eyelid and conjunc iva nasally. T e cornea is no involved. B. A large corneal ulcer wi h signif can issue loss is ound in he superior cornea; i is cri ical o examine he en ire cornea in eyes wi h gonococcal conjunc ivi is o de ermine whe her here is corneal involvemen .
A
B
LWBK961-C01_p02-41.indd 9 22/07/11 8:48 AM
10 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
VIRAL CONJUNCTIVITIS (T YPICALLY ADENOVIRUS)
Viral conjunc ivi is is a common, highly con agious, usually bila eral condi ion,
charac erized by he rapid onse o redness, i chiness, and earing, f rs in one eye and hen he o her.
Etiology Adenovirus sero ypes 8, 19, 37: epidemic
kera oconjunc ivi is Adenovirus sero ypes 3, 7: pharyngocon-
junc ival ever, usually in children O hers: herpes simplex virus, en erovi-
ruses, Newcas le disease virus, Eps ein-Barr virus
Symptoms earing, i ching, burning, redness, oreign-
body sensa ion, pho ophobia His ory o con ac wi h someone wi h a
red eye, recen upper respira ory rac in ec- ion, or recen eye examina ion
Signs Eyelid edema Wa ery discharge Generalized conjunc ival hyperemia, sub-
conjunc ival hemorrhages Conjunc ival ollicles, which are requen ly
mos apparen in he in erior ornices ( Fig. 1-5 A)
Membranes or pseudomembranes in severe cases
Conjunc ival membranes consis o coagula ed exuda e adheren o in amed
conjunc ival epi helium. Clinically, a rue membrane causes bleeding on at emp ed removal and a pseudomembrane does no , bu his rule is no universal. T e causes o rue membranes and pseudomembranes are similar.
Cen ral punc a e epi helial kera i is, and occasionally an epi helial de ec ( Fig. 1-5 B).
Mul iple small corneal inf l ra es wi h overlying punc a e s aining may also be seen in he acu e phase o severe in ec ions ( Fig. 1-5 C).
Preauricular lymphadenopa hy is o en presen .
Subepi helial inf l ra es (SEIs) can occur weeks a er he onse o he acu e in ec ion and may persis or mon hs o years ( Fig. 1-5 D)
Treatment Ar if cial ears and cool compresses our o
eigh imes a day An ihis amines (e.g., an azoline, naphazo-
line) q.i.d. or i ching Removal o membranes or
pseudomembranes Cor icos eroid drops in severe cases wi h
membranes or pseudomembranes or ero-sions. A long, slow aper o mild cor icos e-roid drops can be used in eyes wi h SEIs ha a ec visual unc ion.
S ric observa ion o hygienic measures is needed o avoid spreading he in ec ion.
Prognosis Very good. I clinically signif can subepi-
helial inf l ra es develop, he rea men course can be prolonged. Severe in ec ions wi h membranes or pseudomembranes can cause permanen conjunc ival scarring ( Fig. 1-5 E).
LWBK961-C01_p02-41.indd 10 22/07/11 8:48 AM

Viral Conjunctivitis (Typically Adenovirus) 11
FIGURE 1-5. Viral conjunctivitis. A. Di use conjunc ival injec ion wi h a severe ollicular reac ion, grea es in eriorly, is presen in his eye wi h viral conjunc ivi is. B. A cen ral punc a e epi helial kera i is as seen in his eye is o en ound early in he course o viral conjunc ivi is, mos commonly caused by adenovirus.
(continued)
A
B
LWBK961-C01_p02-41.indd 11 22/07/11 8:48 AM

12 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
C
D
FIGURE 1-5. (Continued) Viral conjunctivitis. C. In he acu e phase, small superf cial corneal inf l ra es wi h overlying punc a e s aining can develop. No e he irregular ligh re ex. D. Mul iple subepi helial inf l ra es (SEIs) o he cornea can be seen 2 mon hs a er resolu ion o adenoviral kera oconjunc ivi is. T ese SEIs end o resolve on heir own. I hey are severe, hey can a ec visual acui y and cause glare symp oms. SEIs generally respond o low-dose opical cor icos eroid drops; however, i hey are s ar ed, hese drops need o be apered very slowly, over mon hs.
(continued)
LWBK961-C01_p02-41.indd 12 22/07/11 8:48 AM

Viral Conjunctivitis (Typically Adenovirus) 13
E
FIGURE 1-5. (Continued) Viral conjunctivitis. E. In erior conjunc ival scarring is seen in his eye several mon hs a er adenoviral conjunc ivi is.
LWBK961-C01_p02-41.indd 13 22/07/11 8:48 AM

14 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
CHLAMYDIAL CONJUNCTIVITIS ( ADULT INCLUSION CONJUNCTIVITIS)
Adul chlamydial conjunc ivi is is a rela- ively common, usually unila eral condi-
ion ha is ypically ransmit ed sexually and generally a ec s young adul s.
Etiology Chlamydia trachomatis sero ypes D
hrough K ypically sexually ransmit ed
Symptoms earing, i ching, burning, redness, oreign-
body sensa ion, pho ophobia, discharge o longer han 3 o 4 weeks in dura ion
May be associa ed wi h ure hri is, vagini- is, or cervici is
Signs S ringy, whi e mucopurulen discharge Large ollicles in he in erior ornices
( Fig. 1-6 ) Superior arsal ollicles, occasionally ol-
licles a he limbus Superior limbal or peripheral nummular
corneal inf l ra es and pannus
Mild preauricular lymphadenopa hy may be presen .
Diagnosis His ory o sexual exposure; pa ien
may have concomi an geni ourinary symp oms
Direc immuno uorescen an ibody es o conjunc ival smears
Giemsa s ain cy ology or basophilic cy o-plasmic inclusion bodies o Halbers aed er-Prowazek; more common in newborns han adul s
McCoy chlamydial cell cul ure
Treatment Azi hromycin 1 g PO once, doxycycline
100 mg PO b.i.d., or e racycline, ery hromy-cin or clari hromycin 250 mg q.i.d. or 2 o 6 weeks
opical azi hromycin drops b.i.d. or 2 days, hen q.i.d. or 1 o 6 weeks, or e racy-cline or ery hromycin oin men q.i.d. or 4 o 6 weeks
Re erral or rea men o sexual par ners and o her sexually ransmit ed in ec ions should be done.
Prognosis Very good
LWBK961-C01_p02-41.indd 14 22/07/11 8:48 AM

Chlamydial Conjunctivitis (Adult Inclusion Conjunctivitis) 15
FIGURE 1-6. Chlamydial conjunctivitis. A severe in erior conjunc ival ollicular reac ion can be seen in his eye wi h chronic chlamydial conjunc ivi is. T ere were similar conjunc ival ollicles superiorly. T ere is also di use bulbar conjunc ival injec ion.
LWBK961-C01_p02-41.indd 15 22/07/11 8:48 AM

16 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
TRACHOMA
Trachoma is a bila eral conjunc ivi is ha is common in underdeveloped coun ries
where hygiene is poor. I is endemic in A rica and cer ain par s o Asia and is one o he mos common causes o preven able blindness, a ec -ing millions o people around he world.
Etiology Chlamydia trachomatis sero ypes A, B, Ba,
and C
Signs World Heal h Organiza ion Classif ca ion
rachoma ous ollicular in amma ion ( F): more han f ve ollicles grea er han 0.5 mm on he upper arsus
rachoma ous in ense in amma ion ( I): hickening obscuring more han 50% o arsal vessels
rachoma ous scarring ( S): cica riza- ion wi h whi e lines or bands in arsal con-junc iva (Arl ’s line) ( Fig. 1-7 )
rachoma ous richiasis ( ): richia-sis o a leas one eyelash
Corneal opaci y (CO): corneal opac-i y involving a leas par o he pupillary margin
Cica riza ion o limbal ollicles resul s in depressions known as Herber ’s pi s.
Diagnostic Evaluation Diagnos ic inves iga ion is similar o ha
or adul inclusion conjunc ivi is.
Treatment SAFE s ra egy: s urgery or richiasis,
a n ibio ics (repea ed every 6 o 12 mon hs in endemic areas), acial and e nvironmen al hygiene
An ibio ic rea men similar o ha or adul inclusion conjunc ivi is
Prognosis Very good unless signif can corneal scar-
ring has developed. Rein ec ion is common i hygienic condi ions do no improve.
LWBK961-C01_p02-41.indd 16 22/07/11 8:48 AM

Trachoma 17
FIGURE 1-7. Trachoma. Whi e scarring o he superior arsal conjunc iva is presen . T e whi e line is called an Arl ’s line.
LWBK961-C01_p02-41.indd 17 22/07/11 8:48 AM

18 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
MOLLUSCUM CONTAGIOSUM
Molluscum con agiosum is an uncom-mon cause o chronic ollicular con-
junc ivi is, which is usually unila eral and may be missed i he eyelid margin is no examined closely.
Etiology Viral par icles rom molluscum con agio-
sum lesions o he eyelid may cause a oxic response o he conjunc iva.
Symptoms earing, i ching, burning, redness, oreign-
body sensa ion. May be chronic.
Signs Single or mul iple, dome-shaped, umbili-
ca ed, molluscum con agiosum eyelid lesions
associa ed wi h ollicular conjunc ivi is. May be chronic ( Fig. 1-8 ).
Wa ery or mucoid discharge Corneal micropannus i long-s anding In immunocompromised pa ien s, here
may be ex ensive eyelid lesions wi h minimal conjunc ival in amma ion.
Treatment Removal o eyelid lesion by incision and
curet age, shaving, excision, cau eriza ion, or cryo herapy.
I severe, consider a workup or an immune def ciency disorder such as HIV in ec ion.
Prognosis Very good, bu i can ake many weeks or
he ollicular conjunc ivi is o resolve a er he lesion is rea ed.
LWBK961-C01_p02-41.indd 18 22/07/11 8:48 AM

Molluscum Contagiosum 19
A
B
FIGURE 1-8. Molluscum contagiosum. A. A severe in erior palpebral conjunc ival ollicular reac ion o several mon hs’ dura ion is apparen . Generally, he bulbar conjunc iva is much less injec ed han he palpebral conjunc iva. B. In he same pa ien , an umbilica ed creamy-colored nodule is seen a he upper eyelid margin. I hey are no searched or care ully, molluscum con agiosum lesions can easily be overlooked. Small incision and curet age in o he cen er o he lesion, causing bleeding, is o en cura ive.
LWBK961-C01_p02-41.indd 19 22/07/11 8:48 AM

20 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
LIGNEOUS CONJUNCTIVITIS
Ligneous disease is a very rare cause o chronic unila eral or bila eral conjunc i-
vi is wi h charac eris ic “woody,” hick mem-brane orma ion.
Etiology Due o a plasminogen def ciency, o en
au osomal recessive, may be sporadic Symptoms
earing, i ching, burning, redness, oreign-body sensa ion
May have an eyelid mass Generally chronic
Signs Chronic conjunc ivi is wi h woodlike,
hick membrane orma ion on he upper
arsus and occasionally he lower arsus ( Fig. 1-9 )
May have similar involvemen o he mou h, nasopharynx, rachea, and geni ouri-nary mucous membranes.
Treatment Removal o pseudomembranes
opical cyclosporine, heparin, hyaluroni-dase, or cor icos eroids
opical or sys emic lys-plasminogen replacemen herapy may be benef cial.
Prognosis Poor wi h previous rea men s
opical or sys emic lys-plasminogen replacemen herapy is a promising rea men or his rare condi ion.
FIGURE 1-9. Ligneous conjunctivitis. Prominen whi e, “woody” membranes at ached o he superior palpebral conjunc ivas o bo h eyes are presen in his baby wi h ligneous conjunc ivi is. (Cour esy o Rolande Michaud, MD.)
LWBK961-C01_p02-41.indd 20 22/07/11 8:48 AM

Pediculosis 21
PEDICULOSIS
Pediculosis is a sexually ransmit ed in ec ion ha is caused by con ac wi h pubic lice.
Etiology Eyelid in ec ion wi h pubic lice
Symptoms earing, i ching, burning, redness, oreign-
body sensa ion. May be unila eral or bila eral May be chronic
Signs Lice, ni s (eggs), and blood- inged debris
on eyelids and lashes ( Fig. 1-10 ) Mild o severe chronic ollicular
conjunc ivi is
Treatment Remove all lice and ni s under sli -lamp
illumina ion. opical an ibio ic oin men (e.g., e racy-
cline, baci racin, or ery hromycin) on eyelids .i.d. or 1 o 2 weeks o smo her he lice and ni s.
Oral ivermec in, wo doses (exac dose depends on body weigh ), 1 week apar , has been shown o be e ec ive.
Use an ilice shampoo and lo ion o rea nonocular areas. Wash and machine dry all clo hes and linens.
rea sexual par ners.
Prognosis Good i all he lice and ni s are removed.
Rein ec ion can occur i sexual par ners and clo hes and linens are no rea ed appropria ely.
FIGURE 1-10. Pediculosis. Several lice can be seen at ached o he base o he eyelashes in his le eye wi h pediculosis. T e mos obvious one is loca ed emporally. Numerous ubular ni s are presen on he eyelash sha s. Some blood- inged debris can be seen a he base o he lashes.
LWBK961-C01_p02-41.indd 21 22/07/11 8:48 AM
22 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
PARINAUD’S OCULOGLANDULAR SYNDROME
Parinaud’s oculoglandular syndrome is an uncommon, usually unila eral condi ion
wi h diverse causes, charac erized by conjunc- ival granulomas and ex remely swollen preau-ricular and submandibular lymph nodes.
Etiology Ca -scra ch ever is he mos common cause. Mononucleosis ularemia uberculosis Rare causes: sporo richosis, syphilis, coc-
cidioidomycosis, chancroid, lymphogranu-loma venereum
Symptoms Redness, oreign-body sensa ion,
discharge Fever, malaise, skin rash
Signs Unila eral conjunc ival granulomas and
large ollicles ( Fig. 1-11 ) Severe ipsila eral preauricular or subman-
dibular lymphadenopa hy
Diagnostic Evaluation Appropria e blood es s, conjunc ival
s ains, cul ures, and conjunc ival biopsy Comple e blood coun , serology, and ches
radiograph as needed
Treatment opical an ibio ic oin men (e.g., e racy-
cline, ery hromycin, cipro oxacin, baci ra-cin, polymyxin B/ baci racin) q.i.d. or 4 weeks
Sys emic rea men varies according o cause.
Prognosis Generally good, al hough i depends on
he specif c e iology.
LWBK961-C01_p02-41.indd 22 22/07/11 8:48 AM

Parinaud’s Oculoglandular Syndrome 23
FIGURE 1-11. Parinaud’s oculoglandular syndrome. Severe di use conjunc ival in amma ion along wi h a supero emporal conjunc ival granuloma is presen in his child wi h ca -scra ch disease. No e he skin abrasions near he nose, which were presumably caused by a ca scra ch. (Cour esy o Pe er Laibson, MD.)
LWBK961-C01_p02-41.indd 23 22/07/11 8:48 AM

24 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
OPHTHALMIA NEONATORUM
Neona al conjunc ivi is (oph halmia neo-na orum) is unila eral or bila eral con-
junc ival in amma ion occurring during he f rs mon h o li e.
Etiology Chemical: Usually causes rela ively mild
di use injec ion wi hou discharge, which las s no longer han 24 hours. ypically due o prophylac ic silver ni ra e drops.
Neisseria gonorrhoeae: Causes copious purulen discharge, which may be associa ed wi h membrane orma ion. Presen s wi hin f rs ew days o li e.
Herpes simplex ype 2: Associa ed wi h eyelid margin vesicles. Presen s wi hin 1 week o bir h.
Chlamydia trachomatis: Causes a purulen papillary conjunc ivi is because he in an can-no produce ollicles. May have pseudomem-branes. Presen s during he second week o li e.
Simple bac erial (e.g., Staphylococcus, Streptococcus, gram-nega ive species): Presen s wi hin f rs ew days a er bir h.
Signs Eyelid edema, conjunc ival injec ion, che-
mosis, purulen discharge ( Fig. 1-12 ) Kera i is is uncommon bu may occur i
rea men or gonococcal conjunc ivi is is delayed.
Dif erential Diagnosis Nasolacrimal duc obs ruc ion: earing,
nonpurulen discharge, and no in ec ion
Diagnostic Evaluation Conjunc ival scrapings or Gram s ain,
Giemsa s ain, bac erial cul ure, immuno uo-rescen es s, and viral cul ure
Never assume ha only one pa hogen is responsible.
Treatment Evalua e bo h paren s or geni al in ec ion
and rea accordingly. Empiric: opical e racycline, cipro oxa-
cin, baci racin, polymyxin B/ baci racin or ery hromycin oin men q.i.d. and ery hromy-cin 25 mg/ kg PO b.i.d. or 2 weeks
Chemical: Ar if cial ears drops or gels, or no rea men
Neisseria gonorrhoeae: opical saline irriga- ion our o eigh imes a day. opical penicil-lin or a uoroquinolone (e.g., cipro oxacin) q1h. Sys emic single-dose ce riaxone 125 mg IM. Ery hromycin 12.5 mg/ kg PO q.i.d. or 2 weeks
Herpes simplex ype 2: opical ganciclovir (e.g., Zirgan) gel drops or vidarabine (e.g., Vira-A) oin men f ve imes a day and aper over 1 o 2 weeks. Consider IV acyclovir.
Chlamydia trachomatis: opical azi hromy-cin drops b.i.d. or 2 days, hen q.d. or e ra-cycline or ery hromycin oin men q.i.d. plus ery hromycin 12.5 mg/ kg PO q.i.d. or 2 weeks
Simple bac erial: Cipro oxacin, baci ra-cin, polymyxin B/ baci racin, gen amicin, or obramycin oin men q.i.d. or 2 weeks
Prognosis Generally good i diagnosed and rea ed
appropria ely be ore any corneal or sys emic involvemen occurs
LWBK961-C01_p02-41.indd 24 22/07/11 8:48 AM

Ophthalmia Neonatorum 25
FIGURE 1-12. Ophthalmia neonatorum. T is in an had a severe di use conjunc ivi is rom a Chlamydia in ec ion. (Cour esy o Irving Raber, MD.)
LWBK961-C01_p02-41.indd 25 22/07/11 8:48 AM

26 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
ALLERGIC CONJUNCTIVITIS
Allergic conjunc ivi is (e.g., hay ever conjunc ivi is) is a very common ype I
hypersensi ivi y reac ion ha causes conjunc- ival injec ion and i ching and generally occurs during he hay ever season.
Etiology Pollen, grass, spores, hair, pe s, wool, dus ,
mi es, e c.
Symptoms I ching, mucous discharge, earing, red-
ness, his ory o allergy. Symp oms are ypi-cally seasonal and vary wi h exposure.
Signs Eyelid edema Wa ery or mucoid discharge Conjunc ival hyperemia wi h a mild papil-
lary response ( Fig. 1-13 A) Chemosis ( Fig. 1-13 B) T e cornea is generally no involved.
Dif erential Diagnosis Perennial varian can occur a any ime o
or hroughou he year.
Treatment Avoid exposure o o ending allergen,
including requen change o clo hes, shower-ing, and washing o clo hes and bed linens.
Cool compresses, ar if cial ears opical an ihis amines (e.g., emedas ine,
levocabas ine, naphazoline, an azoline) q.i.d. opical mas cell s abilizers (e.g., cromo-
lyn, lodoxamide, pemirolas ) q.i.d. opical an ihis amine/ mas cell s abilizers
(e.g., azelas ine, epinas ine, ke o i en, nedo-cromil, olopa adine, bepo as ine, alca adine) q.d. o b.i.d.
Oral an ihis amine (e.g., diphenhydramine 25 mg PO .i.d., ce irizine 5 o 10 mg PO q.d., exo enadine 30 o 60 mg PO b.i.d., lora adine 5 o 10 mg PO q.d.), especially i rhini is is presen
Mild opical cor icos eroid i severe (e.g., lo eprednol 0.2%, uorome holone 0.1%) q.i.d. or shor dura ion
Skin es ing and desensi iza ion herapy can be help ul in some cases.
Prognosis Good, bu mild chronic symp oms o en
persis .
LWBK961-C01_p02-41.indd 26 22/07/11 8:48 AM

Allergic Conjunctivitis 27
A
B
FIGURE 1-13. Allergic conjunctivitis. A. Modera e conjunc ival injec ion and in erior papillary reac ion is presen in his eye wi h chronic allergic conjunc ivi is. B. Conjunc ival chemosis can be seen emporally, resul ing rom an acu e allergic reac ion o ca ur ouching he eye.
LWBK961-C01_p02-41.indd 27 22/07/11 8:48 AM

28 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
ATOPIC KERATOCONJUNCTIVITIS
A opic kera oconjunc ivi is is an uncom-mon, bila eral perennial condi ion ha
may also involve he eyelids and occurs pri-marily in pa ien s wi h a opic derma i is.
Etiology Chronic ype I hypersensi ivi y allergic
reac ion similar o vernal kera oconjunc ivi is, bu causing more prominen eyelid and peri-orbi al skin involvemen
Symptoms I ching, earing, redness, discharge His ory o a opy
Signs Eyelid crus ing, eczema, and s aphylococ-
cal blephari is ( Fig. 1-14 A) Mucoid discharge Small papillae on he palpebral conjunc-
iva wi h edema giving a velve y appearance Conjunc ival scarring and symblepharon
orma ion in advanced cases Corneal punc a e epi helial erosions,
peripheral vasculariza ion and scarring ( Fig. 1-14 B)
May have associa ed kera oconus, ca arac , and re inal de achmen
Dif erential Diagnosis Di ers rom vernal kera oconjunc ivi is
in ha a opic kera oconjunc ivi is presen s
in adul li e, papillae are small, here is an absence o limbi is and ran as’ do s, and i may cause neovasculariza ion and cica riza ion.
Treatment Cool compresses, ar if cial ears opical mas cell s abilizers (e.g., cromo-
lyn, lodoxamide, pemirolas ) q.i.d. or an ihis- amine/ mas cell s abilizers (e.g., azelas ine, epinas ine, ke o i en, nedocromil, olopa a-dine, bepo as ine, alca adine) q.d. o b.i.d.
opical cor icos eroid i severe (e.g., uo-rome holone oin men b.i.d. on eyelids and/or lo eprednol 0.2% o 0.5%, uorome ho-lone 0.1%, or prednisolone 0.125% o 1.0% drops q.i.d.) as shor - erm rea men
Pimecrolimus 1% cream (e.g., Elidel) or acrolimus 0.03% oin men (e.g., Pro opic) b.i.d. can be applied o a ec ed skin in pa ien s older han 2 years or several weeks. T ese medica ions have been associa ed wi h skin cancer and lymphoma.
An oral an ihis amine may be help ul (e.g., diphenhydramine 25 mg PO .i.d., ce irizine 5 o 10 mg PO q.d., exo enadine 30 o 60 mg PO b.i.d., lora adine 5 o 10 mg PO q.d.).
Cyclosporine drops (e.g., cyclosporine 0.05% o 2% b.i.d. o q.i.d.) can have a cor i-cos eroid-sparing e ec in severe cases.
Prognosis Fair o good, depending on he severi y o
he condi ion. In raocular pressure mus be moni ored regularly when cor icos eroids are used, even i only on he eyelids.
LWBK961-C01_p02-41.indd 28 22/07/11 8:48 AM

Atopic Keratoconjunctivitis 29
A
B
FIGURE 1-14. Atopic keratoconjunctivitis. A. Eyelid ery hema, hickening, and scaling are apparen in his pa ien wi h a opic disease. T e skin has a lea hery ex ure, and here is loss o lashes. Conjunc ival injec ion and an old in erior corneal scar can be apprecia ed. B. Severe superior and in erior corneal scarring has developed in his eye wi h chronic a opic kera oconjunc ivi is.
LWBK961-C01_p02-41.indd 29 22/07/11 8:48 AM

30 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
VERNAL KERATOCONJUNCTIVITIS
Vernal kera oconjunc ivi is (spring ca arrh) is a seasonal, recurren , bila eral, ype I
hypersensi ivi y reac ion ha usually presen s in childhood and resolves gradually a er puber y.
Etiology and Epidemiology ype I hypersensi ivi y allergic reac ion
similar o a opic kera oconjunc ivi is, bu wi h a seasonal exacerba ion and less eyelid and skin involvemen .
Males are a ec ed more commonly han emales.
Symptoms I ching, earing, oreign-body sensa ion,
burning, discharge
Signs S ringy, mucopurulen discharge Milky-whi e pseudomembranes Superior arsal papillae o medium o gian
size, p osis ( Fig. 1-15 A) Occasionally, limbal papillae (limbi is)
ha may be associa ed wi h small whi e spo s con aining eosinophils ( ran as’ do s) ( Fig. 1-15 B and C)
Superior corneal punc a e epi helial ero-sions, corneal ulcera ion (“shield” ulcer) ( Fig. 1-15 D)
Mild subepi helial corneal scarring
Dif erential Diagnosis Gian papillary conjunc ivi is (GPC) is
much less severe, and is charac erized by small- o medium-sized superior arsal papil-lae. I can be unila eral or bila eral, depend-ing on he cause. Also, GPC is caused by an allergic reac ion o pro ein buildup on con ac lenses, par icularly so lenses; ocular pros he ics; or pro ruding su ures ollowing ocular surgery.
Treatment I mild, rea as or a opic conjunc ivi is. An ihis amine/ mas cell s abilizers are
e ec ive, especially i ini ia ed be ore he allergy season. T ey also have a cor icos e-roid-sparing unc ion.
I severe or in he presence o shield ulcer, use a shor course o opical cor icos eroids wi h an ibio ic drops or oin men s our o six imes a day. Prolonged use o cor icos eroids is discour-aged, and moni oring o in raocular pres-sure and lens clari y should be per ormed regularly.
Shield ulcers may require surgical removal o he adheren plaque.
Prognosis Fair o good, depending on he severi y o
he condi ion.
LWBK961-C01_p02-41.indd 30 22/07/11 8:48 AM

Vernal Keratoconjunctivitis 31
FIGURE 1-15. Vernal conjunctivitis. A. Large, con uen papillae o he superior arsal conjunc iva are presen . T ese are a - opped and are ermed “cobbles one” papillae. B. Papillae can be more prominen a he limbus han he arsal conjunc iva in cer ain pa ien s, mos commonly o A rican heri age. In hese pa ien s he condi ion is called limbal vernal conjunc ivi is and he whi e spo s are ermed ran as’ do s. In his pa ien , limbal ollicles and ran as’ do s can be seen superiorly, especially a he 10 o’clock and 1 o 3 o’clock limbus.
(continued)
A
B
LWBK961-C01_p02-41.indd 31 22/07/11 8:48 AM

32 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
C
D
FIGURE 1-15. (Continued) Vernal conjunctivitis. C. Mul iple small whi e ran as’ do s are visible a he in erior limbus D. An ovoid epi helial de ec loca ed in he superior one- hird o he cornea (a “shield” ulcer) is apparen in his eye. T ere is also modera e surrounding punc a e kera opa hy. No e he poor corneal ligh re ex.
LWBK961-C01_p02-41.indd 32 22/07/11 8:48 AM

Superior Limbic Keratoconjunctivitis 33
SUPERIOR LIMBIC KERATOCONJUNCTIVITIS
Superior limbic kera oconjunc ivi is (SLK) is an uncommon, usually bila eral, chronic,
relapsing, in amma ory reac ion ha is re-quen ly associa ed wi h hyroid dys unc ion. I usually a ec s middle-aged emales.
Etiology Unknown, bu mos likely rela ed o
mechanical rauma involving he superior pal-pebral and lax bulbar conjunc iva
Symptoms Foreign-body sensa ion, burning, occa-
sionally redness
Signs Hyperemia, hickening, redundance, and
laxi y o superior bulbar conjunc iva ( Fig. 1-16 A)
Lack o lus er and posi ive s aining o superior bulbar conjunc iva wi h uorescein, lissamine green, and rose bengal dyes
Fine, velve y, superior arsal papillae
Superior corneal f lamen s, punc a e ero-sions, and occasionally pannus
Treatment Preserva ive- ree ar if cial ear drops q2h.
Consider emporary or permanen punc al occlusion.
Cyclosporine 0.05% o 2% b.i.d. o q.i.d. may be help ul.
Ace ylcys eine (e.g., Mucomys ) 10% drops q.i.d. or rea men o corneal f lamen s
opical an ihis amine/ mas cell s abilizers (e.g., azelas ine, epinas ine, ke o i en, nedo-cromil, olopa adine, bepo as ine, alca adine) q.d. o b.i.d. may be help ul.
Applica ion o silver ni ra e 0.5% solution o superior bulbar and palpebral conjunc iva or 15 o 30 seconds
Local cau ery or surgical resec ion o supe-rior bulbar conjunc iva ( Fig. 1-16 B)
Prognosis Good or improvemen in symp oms, air
or comple e resolu ion o symp oms. May be recalci ran o rea men
LWBK961-C01_p02-41.indd 33 22/07/11 8:48 AM

34 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
A
B
FIGURE 1-16. Superior limbic keratoconjunctivitis (SLK). A. In SLK, here is localized conjunc ival injec ion o he superior bulbar conjunc iva. T ere is pannus and hickened conjunc iva a he superior limbus. B. Medical rea men ailed. Localized conjunc ival cau ery a er injec ion o local anes hesia was per ormed. T is rea men is o en success ul in signif can ly improving he pa ien ’s symp oms.
LWBK961-C01_p02-41.indd 34 22/07/11 8:48 AM

Floppy Eyelid Syndrome 35
FLOPPY EYELID SYNDROME
Floppy eyelid syndrome, an uncommon condi ion, is due o a spon aneous eversion
o he upper eyelid during sleep, hereby expos-ing he upper arsal conjunc iva and cornea o rauma rom pillows or bed linens. I mos o en a ec s obese men who have a his ory o sleep apnea. I is associa ed wi h kera oconus.
Etiology An ex remely lax, oppy upper eyelid
ever s, causing corneal exposure.
Symptoms Chronic redness, oreign-body sensa ion,
discharge. O en worse in he morning Symp oms are mos commonly on he side
on which he pa ien sleeps.
Signs Easy eversion o upper eyelid. arsus eels
so and rubbery ( Fig. 1-17 A) Chronic papillary conjunc ivi is o he
upper arsus, superf cial punc a e kera opa hy ( Fig. 1-17 B)
Treatment Pro ec he eye by aping i closed or plac-
ing an eye shield during sleep. Ar if cial ears or an ibio ic oin men or
lubrica ion, especially a bed ime A horizon al eyelid- igh ening proce-
dure may be necessary o e ec long- erm improvemen .
Prognosis Good o very good wi h a horizon al
eyelid- igh ening procedure.
LWBK961-C01_p02-41.indd 35 22/07/11 8:48 AM

36 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
FIGURE 1-17. Floppy eyelid syndrome. A. Li ing he upper eyelid easily demons ra es he severe laxi y o he eyelid in his pa ien wi h oppy eyelid syndrome. B. T e upper eyelid is ex remely lax and easily ever ed by pulling he eyelid margin superiorly. T ere is a f ne, di use papillary reac ion o he upper palpebral conjunc iva.
A
B
LWBK961-C01_p02-41.indd 36 22/07/11 8:48 AM

Toxic and Factitious Keratoconjunctivitis (Keratitis Medicamentosa) 37
TOXIC AND FACTITIOUS KERATOCONJUNCTIVITIS (KERATITIS MEDICAMENTOSA)
Chronic oxic conjunc ivi is may be unila -eral or bila eral, depending on he cause.
Fac i ious conjunc ivi is is caused by sel -ins illa ion o ma erial o cause a red eye.
Etiology Aminoglycoside an ibio ics, especially or-
if ed medica ions An iviral agen s Glaucoma agen s, par icularly epinephrine,
brimonidine, pilocarpine, carbonic anhydrase inhibi ors
opical nons eroidal an i-in amma ory agen s
opical anes he ics Any preserved eyedrops Sel - rauma, o en or secondary gain, such
as missing work or school
Dif erential Diagnosis Mucus f shing syndrome: a rare, unila eral
or bila eral condi ion resul ing rom repea ed sel - rauma iza ion o he conjunc iva while rying o remove mucus rom he conjunc iva—o en a vicious cycle, as he rauma causes addi ional mucus produc ion. Pa ien s o en do no admi o his ac ivi y unless pressed.
Symptoms Chronic redness, i ching, oreign-body
sensa ion, mild discharge
Signs Ini ially a papillary conjunc ival reac ion,
la er ollowed by orma ion o ollicles,
predominan ly involving he in erior ornices ( Fig. 1-18 A)
In erior corneal punc a e epi heliopa hy In erior conjunc ival erosions.
Conjunc ival necrosis can occur in severe cases.
Severe corneal involvemen may cause a s erile s romal ring inf l ra e, which is some imes mis aken or in ec ious kera i is, especially wi h anes he ic abuse ( Fig. 1-18 B).
Rarely, s erile corneal, conjunc ival, or scleral mel ing can occur ( Fig. 1-18 C).
Diagnostic Evaluation De ailed his ory aking is mos impor an .
Treatment Discon inue o ending medica ion or
sel -abuse. Frequen preserva ive- ree ar if cial ear
drops our o eigh imes a day Mild an ibio ic oin men (e.g., ery hromy-
cin) i here is signif can epi heliopa hy Consider pressure pa ching (marking he
pa ch o make sure i is no removed) or 1 o 2 days o preven he pa ien rom placing any hing in he eye.
Hospi aliza ion may some imes be required or pa ien s who are unresponsive o rea men o ensure ha hey do no con inue o use he o ending medica ion or abuse he eye, especially or anes he ic abuse. A comple e emporary arsorrhaphy is rarely required o break he o ending cycle.
Prognosis Very good i he o ending medica ion or
sel -abuse can be s opped be ore signif can corneal damage has occurred.
LWBK961-C01_p02-41.indd 37 22/07/11 8:48 AM

38 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
FIGURE 1-18. Toxic/ allergic conjunctivitis. A. A chronic ollicular conjunc ivi is secondary o an allergic reac ion o opical apraclonidine (Iopidine) . I resolved over weeks once he medica ion was discon inued. Topical anesthetic abuse. B. T is pa ien was rea ed or a ungal ulcer loca ed rom he 9 o 11 o’clock posi ions. I was resolving slowly un il he s ole proparacaine rom he physician’s o ce and developed a large ring inf l ra e and hypopyon consis en wi h opical anes he ic abuse.
(continued)
A
B
LWBK961-C01_p02-41.indd 38 22/07/11 8:48 AM

Toxic and Factitious Keratoconjunctivitis (Keratitis Medicamentosa) 39
C
FIGURE 1-18. (Continued) Toxic/ factitious keratoconjunctivitis. C. T is eye has a localized conjunc ival abrasion and injec ion. T ere is some associa ed subconjunc ival hemorrhage. A er ob aining a sys emic workup (which was nega ive) , and rying several medical regimens wi hou success, i was learned ha he pa ien was poking hersel in he eye wi h a needle o ge ou o work. She was re erred or a psychological evalua ion.
LWBK961-C01_p02-41.indd 39 22/07/11 8:48 AM

40 1 CONJUNCTIVAL INFECTIONS AND INFLAMMATIONS
OCULAR ROSACEA
Acne rosacea is a common skin disease o unknown e iology wi h requen ocular
involvemen , ypically occurring in middle-aged adul s. I is o en associa ed wi h dry-eye syndrome.
Etiology Rosacea is an idiopa hic derma ologic con-
di ion a ec ing he pilosebaceous uni s o he acial and eyelid skin.
Symptoms Chronic, bila eral ocular irri a ion, red-
ness, burning, earing, crus ing
Signs Skin: chronic hyperemia, elangiec asias,
papules, pus ules o nose, orehead, and cheeks. Rhinophyma in advanced s ages, especially in men ( Fig. 1-19 A)
Eye: blephari is, meibomi is, eyelid-margin elangiec asias, recurren chalazia, conjunc ival or episcleral injec ion ( Fig. 1-19 B)
Superf cial punc a e kera opa hy, periph-eral corneal vasculariza ion, s erile marginal inf l ra es, phlyc enules, peripheral corneal
scarring, pannus, hinning, and occasionally corneal mel ing and per ora ion ( Fig. 1-19 C)
Treatment Warm compresses 5 o 10 minu es b.i.d.
and eyelid hygiene or blephari is/ meibomi is Minimally preserved or preserva ive- ree
ar if cial ears or dry eyes Judicious opical cor icos eroid or s erile
kera i is. When in doub , rea an inf l ra e as in ec ious kera i is.
opical azi hromycin drops a bed ime (q.h.s.), or e racycline, baci racin, or ery hro-mycin oin men b.i.d. or q.h.s.
Oral e racycline or ery hromycin 250 mg b.i.d. o q.i.d. or doxycycline 100 mg q.d. o b.i.d. or 1 week, hen hal dose or 4 o 6 weeks. Can aper down o a minimum dosage (e.g., doxycy-cline 20 mg b.i.d. or 50 mg q.d.) or long- erm rea men ?
Consider a derma ology consul i here is signif can skin involvemen .
Prognosis Good or improvemen in symp oms, poor
or o al resolu ion o symp oms. Pa ien s mus realize ha rosacea is a chronic condi- ion ha can be e ec ively rea ed in mos cases bu no “cured.”
LWBK961-C01_p02-41.indd 40 22/07/11 8:49 AM

Ocular Rosacea 41
FIGURE 1-19. Ocular rosacea. A. T ere are signif can papules and pus ules o he cheeks, nose, and eyebrow areas. Rhinophyma is apparen . No e he peripheral corneal scarring in ero emporally on he le rom previous corneal inf l ra e and mel ing. B. T ere are severe elangiec asias o he eyelid margin, which is no iceably hickened. No pa en meibomian gland orif ces are visible. C. elangiec asias and hickening o he eyelid margin, along wi h crus ing o he eyelashes, are seen in his pa ien wi h severe ocular rosacea. Di use conjunc ival injec ion and a dense corneal scar rom previous rosacea-rela ed ulcera ion a he 7 o’clock posi ion are presen .
A
B
C
LWBK961-C01_p02-41.indd 41 22/07/11 8:49 AM

C H A P T E R
42
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
Signs Pinguecula: yellow-whi e, of en riangular,
sligh ly eleva ed conjunc ival lesion adjacen o he nasal or emporal side o he limbus ( Fig. 2-1 A). T ey may become mildly o modera ely in amed ( Fig. 2-1 B).
P erygium: riangular, wing-shaped bro-vascular shee o issue ex ending on o he cor-nea a he 3 and 9 o’clock posi ions ( Fig. 2-1 C). An iron line (S ocker’s line) in he corneal epi helium may be presen cen ral o he apex o he p erygium.
An area o hinning due o desicca ion (delle) may be presen in he cornea adjacen o an eleva ed lesion.
Large or recurren p erygia can cause sym-blepharon orma ion and even res ric ocular mo ili y ( Fig. 2-1 D).
Dif erential Diagnosis Pseudop erygium: An adhesion o conjunc-
iva on o he corneal sur ace af er corneal injury ( Fig. 2-1 E). Unlike a rue p erygium, he adhe-sion is only a he apex and no hroughou he underlying sur ace. I is ypically unila eral and of en no a he 3 and 9 o’clock posi ions.
Conjunc ival Degenera ions and Mass Lesions
PINGUECULA AND PTERYGIUM
Pingueculae and p erygia are ex remely common conjunc ival/ corneal degen-
era ions ha ypically a ec pa ien s living in equa orial regions where here is high expo-sure o sunligh .
Etiology Ul raviole exposure Chronic dryness and ho , dus y
environmen T ese ac ors lead o elas o ic degenera-
ion o he subs an ia propria o he conjunc iva, resul ing in subepi helial proli era ion o brovascular issue, ini ially on he conjunc iva and hen on he cornea.
Symptoms Irri a ion, redness nasally or emporally,
earing, occasionally decreased vision Occasionally, con ac lens in olerance Rarely, pain i in amed
LWBK961-C02_p42-69.indd 42 22/07/11 8:50 AM

Pinguecula and Pterygium 43
Fuchs’ marginal kera i is: Associa ed wi h mild o severe peripheral corneal hinning ( Fig. 2-1 F).
Conjunc ival papilloma, nevus, in raepi- helial neoplasia, or squamous cell carcinoma: I no ypical or a p erygium or pinguecula, consider a conjunc ival biopsy.
Diagnostic Evaluation Sli -lamp examina ion o look or unusual
ea ures suspicious o o her diagnoses. Pingueculae and p erygia have classic appearances.
Excisional biopsy in cases suspicious or malignancy
Treatment Avoid excessive sunligh exposure and wear
good-quali y ul raviole -blocking sunglasses. Ar i cial ears o preven dry eyes opical an ihis amines (e.g., emedas ine,
levocabas ine, naphazoline, an azoline), nons eroidal an i-in amma ory agen s (e.g., ke orolac, brom enac, nepa enac), or, rarely,
cor icos eroids (e.g., lo eprednol 0.2%, uo-rome holone 0.1%) q.d. o q.i.d. o reduce redness or in amma ion.
Surgical excision is indica ed i here is excessive irri a ion, di cul y wi h con ac lens wear, or cosme ic reasons, or when here is progression oward he visual axis. T e recurrence ra e is much lower when excision is combined wi h a conjunc ival au ograf . I inadequa e conjunc ival issue is available, an amnio ic membrane graf can be used o cover he bare sclera.
In raopera ive applica ion o mi omycin C and pos opera ive use o be a radia ion may decrease he recurrence ra e, bu bo h are associa ed wi h an increased risk o corneo-scleral necrosis and are usually no necessary when a conjunc ival au ograf is per ormed.
Prognosis Good o very good, depending on severi y P erygia can recur in abou 10% o 15% o
pa ien s, occasionally worse han he original p erygium.
LWBK961-C02_p42-69.indd 43 22/07/11 8:50 AM

44 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
A
B
C
FIGURE 2-1. Pinguecula. A. A riangular, creamy-whi e eleva ed conjunc ival mass is seen a he nasal limbus rom he 3 o he 4:30 clock posi ion. B. T is pinguecula, also loca ed be ween he 3 o 4:30 posi ions, is sligh ly inf amed, as demons ra ed by mild surrounding conjunc ival injec ion. Pterygium. C. A nasal wing-shaped brovascular grow h is apparen in his pa ien ’s righ eye wi h a classic nasal p erygium. T is p erygium is reaching in o he visual axis.
(continued)
LWBK961-C02_p42-69.indd 44 22/07/11 8:50 AM

Pinguecula and Pterygium 45
D
E
F
FIGURE 2-1. (Continued) Pterygium. D. T is large recurren nasal p erygium has resul ed in signi can symblepharon orma ion and res ric ion o ocular mo ili y. Pseudopterygium. E. T is large nasal pseudop erygium developed as par o he healing process a er an episode o peripheral ulcera ive kera i is. Some residual peripheral scarring is seen in ero emporally. Fuchs’ marginal keratitis. F. T is eye has a his ory o unila eral chronic nasal peripheral corneal inf amma ion, hinning, and neovasculariza ion due o Fuchs’ marginal kera i is. Six years prior, i had developed a small Seidel-posi ive leak, which resolved wi h medical rea men . T e eye has remained quie on low-dose opical s eroids. No e he severe corneal hinning in eronasally.
LWBK961-C02_p42-69.indd 45 22/07/11 8:50 AM

46 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
OTHER CONJUNCTIVAL DEGENERATIONS
AMYLOIDOSIS Amyloidosis is a degenera ive condi ion in
which he noncollagenous pro ein amyloid is deposi ed in he conjunc iva ( Fig. 2-2 A and B).
I may be primary or secondary. I may be localized o he conjunc iva
or be rela ed o a sys emic disorder such as amyloidosis, plasma cell dyscrasias, or, rarely, lymphoma.
Primary localized amyloidosis is he mos common orm. Primary sys emic amyloidosis involves amyloid deposi ion hroughou he eye and eyelids and can a ec he hear and kidneys.
Rule ou sys emic amyloid condi ions.
CALCIUM CONC ETIONS Calcium concre ions are yellow-whi e
calcium deposi s ha are embedded in he upper and/ or lower palpebral conjunc iva.
Generally hey are loca ed below he sur- ace o he conjunc iva and do no cause any symp oms. Occasionally, he concre ions erode hrough he sur ace o he conjunc- iva, s ain wi h uorescein dye, and cause oreign-body symp oms ( Fig. 2-2 C).
I hey are mild, he symp oms can be rea ed wi h opical lubrica ion; i hey are severe, he concre ions can be removed, bu hey of en recur.
FIGURE 2-2. Conjunctival amyloidosis. A. An eleva ed yellow-colored conjunc ival mass is no ed in his elderly pa ien . I was mobile over he sclera, and i did no have he classic appearance o a p erygium or he papilloma ous pat ern o a squamous cell umor. Conjunc ival biopsy revealed amyloidosis. T ere is o en associa ed subconjunc ival hemorrhage, as seen in his case.
(continued)
A
LWBK961-C02_p42-69.indd 46 22/07/11 8:50 AM

Other Conjunctival Degenerations 47
B
C
FIGURE 2-2. (Continued) Conjunctival amyloidosis. B. A creamy whi e, rubbery conjunc ival lesion covered he superior and nasal bulbar conjunc iva o his le eye. Conjunc ival biopsy revealed amyloidosis. Conjunctival calcium concretions. C. Mul iple whi e calcium concre ions have eroded hrough he conjunc ival epi helial sur ace o he upper eyelid, resul ing in f uorescein s aining, seen upon eyelid eversion. T ese exposed concre ions cause a chronic oreign-body sensa ion and require removal.
LWBK961-C02_p42-69.indd 47 22/07/11 8:50 AM

48 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
MELANOCYTIC CONJUNCTIVAL LESIONS
CONJUNCTIVAL EPITHELIAL MELANOSIS (R CIAL MELANOSIS)
Common in pigmen ed races, usually bila eral, bu may have asymme ric ocular involvemen
Becomes more pronounced during puber y. Fla , pa chy, brownish pigmen a ion sca -
ered over he conjunc iva, bu requen ly involves he perilimbal regions ( Fig. 2-3 A).
Mobile over he sclera. May be per ora ed by an erior ciliary ar eries or nerves.
No malignan po en ial.
OCULODE MAL MELANOSIS (NEVUS OF OTA)
A congeni al condi ion charac erized by blue-gray hyperpigmen a ion o skin and mucous membranes in he dis ribu ion o he f h cranial nerve
Almos always unila eral. T ree varian s are seen: dermal, ocular,
and oculodermal melanoses. Involves he dermis o he skin and epi-
sclera o he eye, hus he lesion does no move over he sclera.
May a ec ipsila eral uveal issues, orbi , and cen ral nervous sys em.
Malignan rans orma ion, uveal mela-noma, and glaucoma can develop, and pa ien s should be ollowed up regularly.
NEVUS Develops during puber y or early
adul hood. Mos are subepi helial or compound nevi.
Appears as a well-demarca ed, a or sligh ly eleva ed lesion, usually in he in er-palpebral areas. I is usually soli ary, and has a predilec ion or he limbus, plica, caruncle, and eyelid margin. Cys ic spaces wi hin he nevus are common and are he key o diagno-sis. T e degree o pigmen a ion may vary and may increase a puber y ( Fig. 2-3 B).
Enlargemen can occur bu may be a sign o malignan rans orma ion. Nevi involving he cornea, arsal, or orniceal conjunc ivae are ex remely rare and should be excised or his opa hologic evalua ion.
Periodic pho ographic documen a ion o he lesion may be help ul or ollow-up.
P IMA Y ACQUI ED MELANOSIS T is is an uncommon, unila eral, premalig-
nan condi ion ha is usually seen in middle-aged o elderly whi e pa ien s.
Uni ocal or mul i ocal a pa ches wi h indis inc margins ha may involve any par o he conjunc iva. Cys ic spaces are absen ( Fig. 2-3 C).
Follow-up wi h clinical documen a ion (e.g., sli -lamp pho ography) should be per- ormed every 6 mon hs. Malignan change should be suspec ed i he pa ches become nodular.
Local wide excision wi h cryo herapy is of en per ormed or suspicious lesions. Pos opera ive opical chemo herapy (e.g., wi h mi omycin C) may be bene cial. Incomple e excision and/ or recurrence is common, requiring more aggressive rea -men (e.g., local radia ion herapy or opical chemo herapy). opical mi omycin C has also been used success ully o rea primary acquired melanosis wi hou wide excision.
LWBK961-C02_p42-69.indd 48 22/07/11 8:50 AM

Melanocytic Conjunctival Lesions 49
SECONDA Y ACQUI ED MELANOSIS
Causes include: Adrenochrome deposi s: discre e
clumps o melanin on arsal and orniceal conjunc iva associa ed wi h long- erm use o opical epinephrine—becoming rare
Alkap onuria: in erpalpebral, bluish-gray or black pigmen a ion o he con-junc iva, episclera, sclera, and endons o horizon al rec us muscles due o accumula- ion o homogen isic acid
Mascara deposi s Age-rela ed Addison disease Hemochroma osis Argyrosis: As a resul o long- erm use
o drops con aining silver, becoming rare Dark oreign bodies
MALIGNANT MELANOMA Malignan melanoma is an uncommon,
malignan umor ha may be pigmen ed or nonpigmen ed. I may arise de novo, rom preexis ing primary acquired melanosis, or rom a nevus.
Eleva ed nodule ha can a ec any par o he conjunc iva, bu has a predilec ion or he limbus and may ex end on o he cornea. Feeder vessels may be seen ( Fig. 2-3 D and E). Advanced melanomas may invade he eyelids and orbi .
rea men is local excision wi h cryo- herapy. Local radia ion herapy may also be bene cial. Exen era ion may be neces-sary or orbi al involvemen . Use pallia ion wi h chemo herapy i me as asis is presen ( lymph nodes, cen ral nervous sys em, liver, e c.).
FIGURE 2-3. Conjunctival epithelial (racial) melanosis. A. An area o poorly demarca ed conjunc ival epi helial melanin pigmen is seen in his A rican American pa ien . T ese lesions have minimal o no malignan po en ial.
(continued)
A
LWBK961-C02_p42-69.indd 49 22/07/11 8:50 AM

50 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
B
C
FIGURE 2-3. (Continued) Conjunctival nevus. B. A pigmen ed pa ch can be seen in he superior conjunc iva o his A rican American woman. I is well demarca ed, has no changed in size, and has numerous microcys s, all poin ing o he diagnosis o a nevus. Primary acquired melanosis. C. An area o f a conjunc ival pigmen a ion is seen a he limbus rom he 3 o 5 o’clock posi ions. T ere is a mild increase in vasculariza ion. T is lesion is suspicious or malignan rans orma ion.
(continued)
LWBK961-C02_p42-69.indd 50 22/07/11 8:50 AM

Melanocytic Conjunctival Lesions 51
D
E
FIGURE 2-3. (Continued) Malignant melanoma o the conjunctiva. D. Biopsy o his large, solid conjunc ival mass revealed malignan melanoma. I is rela ively amelano ic, bu pigmen ed areas can be seen a he 3 and 9 o’clock aspec s o he lesion. T ere is also signi can surrounding vasculariza ion, indica ing an aggressive process. E. A small recurren conjunc ival malignan melanoma is seen a he limbus a he 5 o’clock posi ion a er surgical excision. I was reexcised and rea ed wi h a radioac ive plaque.
LWBK961-C02_p42-69.indd 51 22/07/11 8:50 AM

52 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
BENIGN AMELANOCYTIC CONJUNCTIVAL LESIONS
GR NULOMAS Chalazion: Single nodule on he arsal
conjunc iva (see Fig. 1-2A and B) Pyogenic granuloma: vascularized
nodule(s) o he bulbar or palpebral conjunc- iva. T ey mos commonly occur af er con-junc ival injury such as surgery or a chalazion ( Fig. 2-4 A). T ey may be rela ed o a oreign body, such as a punc al plug ( Fig. 2-4 B).
Sarcoidosis: mul iple yellow-colored nodules involving he arsal or orniceal conjunc iva ( Fig. 2-4 C). When hese are presen , biopsy can con rm he diagnosis o sarcoidosis.
Rhinosporidiosis: very rare ungal in ec- ion ha may cause conjunc ival granulomas
Vasculi ides (e.g., polyar eri is nodosa, Churg-S rauss syndrome): very riable lesions
EPIBULBA DE MOID Epibulbar dermoid is an uncommon, con-
geni al lesion ha may occur in isola ion or in associa ion wi h o her ocular or sys emic anomalies. I may be unila eral or bila eral.
Solid, smoo h, round whi e mass ypically loca ed a he in ero emporal limbus, bu may be elsewhere, even he cen ral cornea. Lesions may encroach on o he cornea, causing as ig-ma ism. May have hair ollicles ( Fig. 2-4 D, E, and H)
Surgical resec ion may resul in corneo-scleral hinning and may have o be com-bined wi h a corneal lamellar pa ch graf or, rarely, a pene ra ing graf ( Fig. 2-4 F and G). Ul rasound biomicroscopy may be
help ul in de ermining he dep h o he lesion preopera ively.
Ocular associa ions: Eyelid coloboma, ocular coloboma
Sys emic associa ions: Goldenhar syndrome, mos common, of en bila eral dermoids; reacher Collins syndrome; Franceschet i syndrome
LIPODE MOID A lipodermoid is an uncommon and of en
bila eral condi ion, ypically ound in adul s. Large, yellow, sof , movable, subconjunc-
ival lesions consis ing o adipose and dermal issues mos commonly loca ed supero em-porally. Hair ollicles may be seen on he sur- ace. T e lesions can ex end in o he superior ornices, where i is impossible o visualize heir pos erior limi s. Comple e surgical exci-sion is unnecessary and should be avoided o preven damage o he rec us muscle, lacrimal gland, and he leva or muscle.
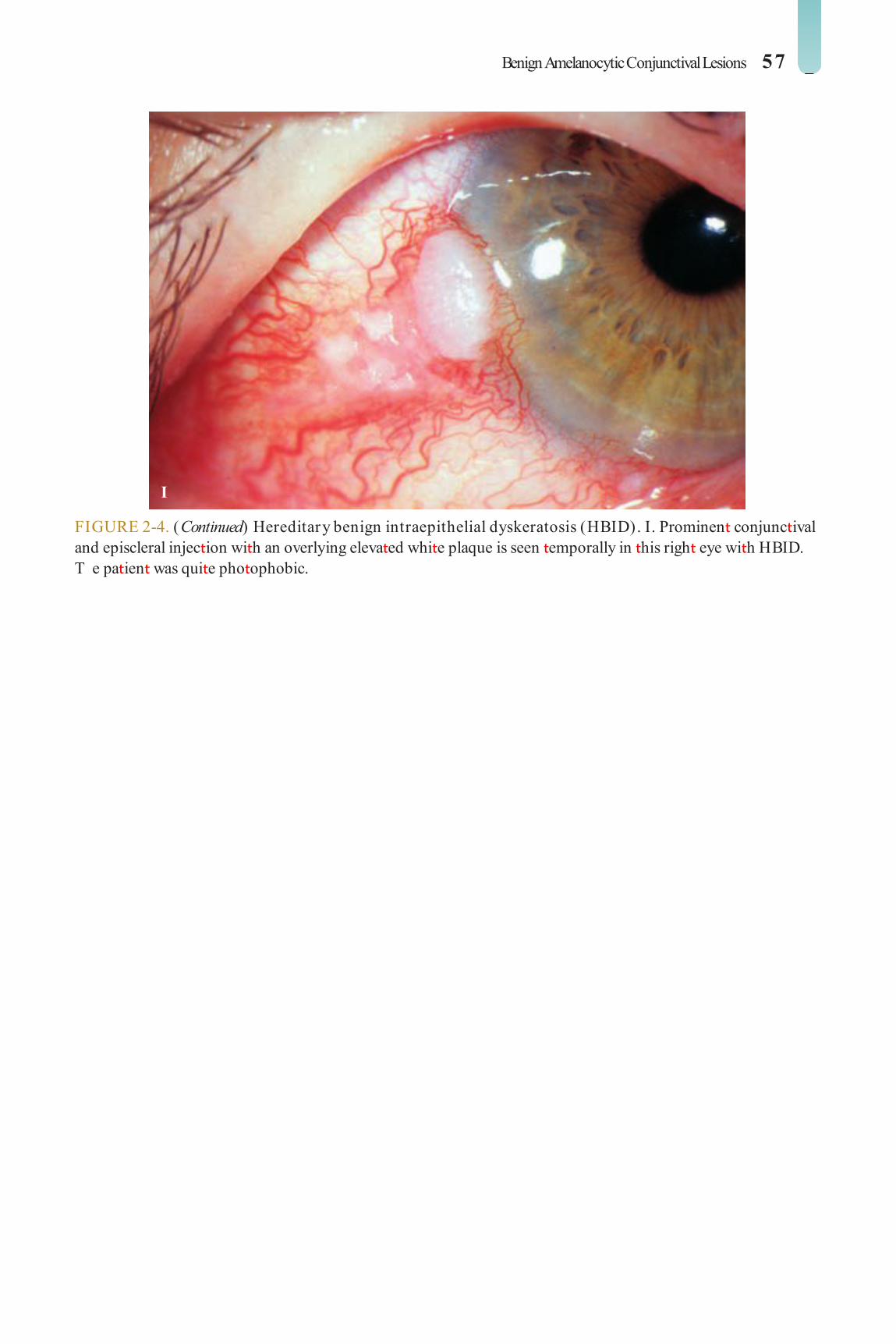
HE EDITA Y BENIGN INTR EPITHELIAL DYS ER TOSIS
Heredi ary benign in raepi helial dyskera o-sis (HBID) is a rare disorder charac erized by marked conjunc ival and episcleral vessel injec- ion wi h overlying whi e plaques o acan ho ic and dyskera o ic epi helial cells ( Fig. 2-4 I).
I is loca ed primarily in he nasal and em-poral in erpalpebral zones.
I is mos commonly ound in members o he Haliwa Indian ribes o Nor h Carolina.
No good rea men exis s curren ly, al hough occasionally a conjunc ival biopsy may be required o rule ou a conjunc ival umor.
LWBK961-C02_p42-69.indd 52 22/07/11 8:50 AM

Benign Amelanocytic Conjunctival Lesions 53
A
B
FIGURE 2-4. Pyogenic granuloma. A. T is large collec ion o granula ion issue occurred as an inf amma ory response a er an in erior eyelid chalazion resolved. B. A small pyogenic granuloma developed in his punc um, rela ed o a silicone punc al plug. I resolved once he plug was removed.
(continued)
LWBK961-C02_p42-69.indd 53 22/07/11 8:50 AM

54 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
C
D
FIGURE 2-4. (Continued) Sarcoid granulomas. C. Mul iple yellowish nodules are seen in he upper bulbar conjunc iva in his pa ien wi h sarcoidosis. In pa ien s wi h suspec ed sarcoidosis and a conjunc ival nodule, he diagnosis o sarcoidosis can o en be con rmed wi h a simple conjunc ival biopsy. Epibulbar dermoid. D. An in eronasal dermoid can be seen in his 7-year-old girl. Al hough her uncorrec ed vision was 20/ 20, she and her paren s were unhappy wi h i s cosme ic appearance.
(continued)
LWBK961-C02_p42-69.indd 54 22/07/11 8:50 AM

Benign Amelanocytic Conjunctival Lesions 55
FIGURE 2-4. (Continued) Epibulbar dermoid. E. T is 6-year-old boy was essen ially asymp oma ic rom his in ero emporal dermoid. T ere are several modera ely large cilia pro ruding rom he cen er. F. T is 12-year-old girl was becoming very unhappy wi h he cosme ic appearance o his dermoid, which was subsequen ly removed.
(continued)
E
F
LWBK961-C02_p42-69.indd 55 22/07/11 8:50 AM

56 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
G
H
FIGURE 2-4. (Continued) Epibulbar dermoid. G. A 2 years a er excision o he dermoid wi h a lamellar corneal gra , he pa ien seen in F had an excellen cosme ic resul . H. T is in ero emporal dermoid encroaches on he cornea wi h secondary corneal scarring.
(continued)
LWBK961-C02_p42-69.indd 56 22/07/11 8:50 AM
Benign Amelanocytic Conjunctival Lesions 57
I
FIGURE 2-4. (Continued) Hereditary benign intraepithelial dyskeratosis (HBID). I. Prominen conjunc ival and episcleral injec ion wi h an overlying eleva ed whi e plaque is seen emporally in his righ eye wi h HBID. T e pa ien was qui e pho ophobic.
LWBK961-C02_p42-69.indd 57 22/07/11 8:50 AM

58 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
POTENTIALLY MALIGNANT AMELANOCYTIC CONJUNCTIVAL LESIONS
SQUAMOUS PAPILLOMA Peduncula ed squamous papilloma is an
uncommon, benign umor caused by he human papillomavirus. I ypically occurs in children and young adul s.
Papillomas have ngerlike projec ions and are loca ed in he palpebral conjunc iva, ornix, or caruncle ( Fig. 2-5 A). T ey may be mul i ocal or bila eral.
T ey of en resolve on heir own. T ey can be excised when hey are large
or chronic, bu hey may recur, occasionally worse han he original lesion. Applica ion o cryo herapy a he base o he lesion af er excision may decrease he risk o recurrence. Oral cime idine has been repor ed o be e ec ive.
A nonviral, sessile orm ha occurs in he elderly and involves he perilimbal conjunc- iva should be considered precancerous or cancerous and should be comple ely excised wi h wide margins and supplemen al cryo- herapy and sen or his opa hologic evalua- ion. Al erna ive rea men includes opical or subconjunc ival in er eron alpha 2b, generally af er biopsy con rma ion.
CONJUNCTIVAL INTR EPITHELIAL NEOPLASIA
Conjunc ival in raepi helial neoplasia is a unila eral, premalignan condi ion ha is seen in older, air-skinned individuals. T is condi ion was ormerly re erred o as Bowen’s disease, in raepi helial epi helioma, and con-junc ival dyskera osis.
T e lesions are usually loca ed a he limbus and may involve adjacen cornea ( Fig. 2-5 B–D). T e hree clinical ypes are
(1) a eshy gela inous lesion wi h variable kera iniza ion, (2) a whi e plaque (leukopla-kic ype), and (3) papillary.
rea men is mos commonly com-ple e surgical excision wi h supplemen al cryo herapy.
Success ul rea men has also been achieved wi h opical and subconjunc ival in er eron alpha 2b.
SQUAMOUS CELL CA CINOMA Invasive squamous cell carcinoma is a rare,
slow-growing, locally invasive umor ha occurs mos requen ly a he limbus. I mos likely progresses rom conjunc ival in raepi helial neoplasia ha breaks hrough he conjunc ival basemen membrane.
Papillary or gela inous umor. Frequen ly associa ed wi h eeder blood vessels ( Fig. 2-5 E)
rea men is mos commonly comple e surgical excision wi h supplemen al cryo her-apy. A lamellar sclerec omy may be required o excise he lesion comple ely.
Success ul rea men has also been achieved wi h opical and subconjunc ival in er eron alpha 2b.
May be aggressive in immunocompro-mised pa ien s.
OTHE CA CINOMAS Mucoepidermoid carcinoma and spindle
cell carcinoma are similar o squamous cell carcinoma bu are more aggressive, and hey may arise anywhere on he conjunc iva.
Sebaceous carcinoma is an uncommon and aggressive umor ha ypically involves he upper eyelid o elderly pa ien s, bu may rarely arise de novo rom he arsal conjunc- iva as a papilloma ous or plaquelike lesion ( Fig. 2-5 F). May masquerade as chronic unila eral conjunc ivi is or recurren chalazia.
LWBK961-C02_p42-69.indd 58 22/07/11 8:50 AM

Potentially Malignant Amelanocytic Conjunctival Lesions 59
May require mul iple biopsies. May have pag-e oid spread wi h skip areas.
EACTIVE LYMPHOID HYPE PLASIA AND NON-HODG IN LYMPHOMA
T e appearance o he wo condi ions is similar.
Smoo h, eshy, subconjunc ival mass ha may involve a large area ( Fig. 2-5 G–I). T e lesions may be single or mul iple, and hey
involve bo h eyes in abou 20% o cases. Small a ec ed areas are called “salmon pa ches,” and hey occur mos commonly in he bulbar or orniceal conjunc iva.
Incisional or excisional biopsy should be per ormed and sen or immunohis ochemi-cal s udies (which may require non xed issue).
A sys emic evalua ion should be per ormed by an in ernis or oncologis .
FIGURE 2-5. Conjunctival papilloma. A. T is squamous papilloma in a pedia ric pa ien is likely o viral origin. I had numerous papillary vascular ronds at ached o a s alk (peduncula ed) .
(continued)
A
LWBK961-C02_p42-69.indd 59 22/07/11 8:50 AM

60 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
B
C
FIGURE 2-5. (Continued) Conjunctival intraepithelial neoplasia. B. No e he large, well-demarca ed, sessile papilloma ous lesion adjacen o he limbus rom he 6 o he 8 o’clock posi ion. Excisional biopsy revealed conjunc ival in raepi helial neoplasia. C. T is f eshy, sessile, mildly eleva ed mass lesion has a kera inized, leukoplakic componen . Excisional biopsy revealed conjunc ival in raepi helial neoplasia.
(continued)
LWBK961-C02_p42-69.indd 60 22/07/11 8:50 AM
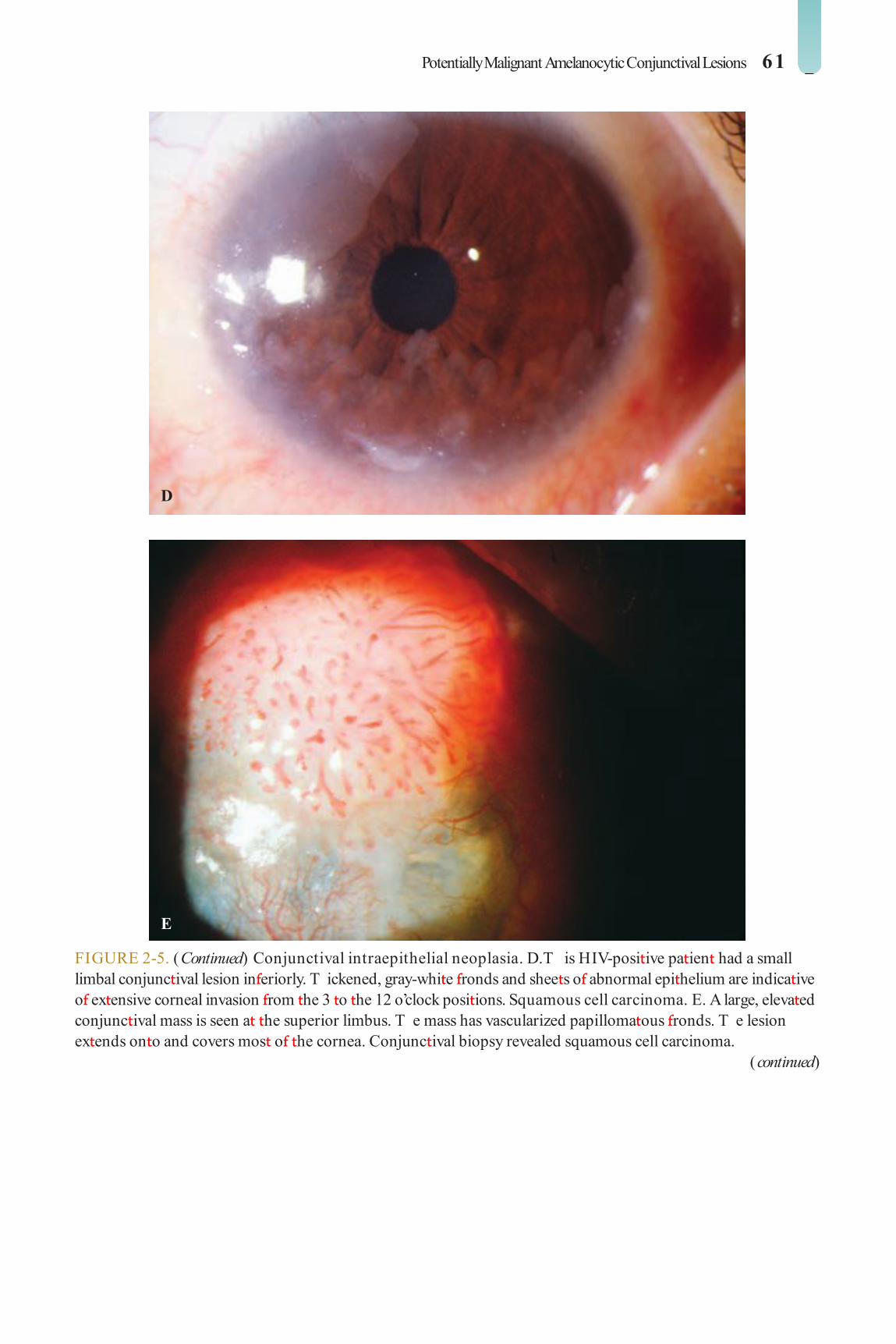
Potentially Malignant Amelanocytic Conjunctival Lesions 61
D
E
FIGURE 2-5. (Continued) Conjunctival intraepithelial neoplasia. D. T is HIV-posi ive pa ien had a small limbal conjunc ival lesion in eriorly. T ickened, gray-whi e ronds and shee s o abnormal epi helium are indica ive o ex ensive corneal invasion rom he 3 o he 12 o’clock posi ions. Squamous cell carcinoma. E. A large, eleva ed conjunc ival mass is seen a he superior limbus. T e mass has vascularized papilloma ous ronds. T e lesion ex ends on o and covers mos o he cornea. Conjunc ival biopsy revealed squamous cell carcinoma.
(continued)
LWBK961-C02_p42-69.indd 61 22/07/11 8:50 AM

62 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
F
G
FIGURE 2-5. (Continued) Sebaceous carcinoma. F. T e righ upper eyelid is ever ed in his elderly pa ien wi h a chronic unila eral blepharoconjunc ivi is demons ra ing a di use hickened papilloma ous conjunc ival sur ace. Eyelid biopsy revealed sebaceous carcinoma. Conjunctival lymphoma. G. Mul iple eleva ed pinkish nodules are presen in he lower palpebral conjunc iva o his le eye. Similar nodules were seen in he righ eye. Biopsy revealed conjunc ival lymphoma.
(continued)
LWBK961-C02_p42-69.indd 62 22/07/11 8:51 AM

Potentially Malignant Amelanocytic Conjunctival Lesions 63
H
I
FIGURE 2-5. (Continued) Conjunctival lymphoma. H. T is f eshy, salmon-colored mass adjacen o he caruncle was a conjunc ival lymphoma. I was rea ed wi h surgical excision and local radia ion herapy, as workup did no reveal evidence o sys emic involvemen . I. A large f eshy, well-delinea ed, sligh ly nodular conjunc ival mass can be seen occupying he en ire in erior ornix o his le eye; biopsy was posi ive or lymphoma.
LWBK961-C02_p42-69.indd 63 22/07/11 8:51 AM

64 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
CYSTIC LESIONS
P IMA Y CONJUNCTIVAL CYST A common, ranslucen cys con aining
clear uid on he bulbar conjunc iva. May be at ached o he conjunc iva or reely mobile under he conjunc iva ( Fig. 2-6 A–C). May cause a oreign-body sensa ion.
Di eren ial diagnosis includes conjunc- ival lymphangiocele, which is of en more or uous.
rea men is usually unnecessary. I i is symp oma ic, he cys should be comple ely excised by shelling i ou rom under he
conjunc iva. Punc uring he cys wi h a nee-dle or incomple e excision ypically resul s in recurrence.
IAT OGENIC CYSTS T ese cys s may ake he ollowing orms:
Secondary implan a ion cys s ollowing surgery or rauma.
Drainage bleb ollowing l ra ion sur-gery or blebs ha may be a and di use or localized af er ca arac surgery ( Fig. 2-6 D).
enon’s cys associa ed wi h a l ra ion bleb, charac erized by an eleva ed cys like cavi y wi h engorged sur ace vessels.
LWBK961-C02_p42-69.indd 64 22/07/11 8:51 AM

Cystic Lesions 65
FIGURE 2-6. Conjunctival cyst. A. A large, mobile conjunc ival cys is seen near he limbus. I was big enough o cause chronic irri a ive symp oms. T ese can o en be removed in o o by care ully incising he conjunc iva and gen ly shelling ou he cys . B. A large mobile nasal conjunc ival cys covers he caruncle nasally in his righ eye.
(continued)
A
B
LWBK961-C02_p42-69.indd 65 22/07/11 8:51 AM

66 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
C
D
FIGURE 2-6. (Continued) Conjunctival cyst. C. T e same cys as in B can be seen o be pro ruding rom he palpebral ssure when he eye is closed. T is caused drying and kera iniza ion o he sur ace o he cys . T e en ire cys and i s kera inized sur ace were excised and did no recur. D. T is nonmobile conjunc ival cys was probably rela ed o superior limbal surgery. A nylon su ure can be seen a he base o he cys .
LWBK961-C02_p42-69.indd 66 22/07/11 8:51 AM

Vascular Lesions 67
VASCULAR LESIONS
TELANGIECTASIAS T e ollowing me abolic disorders may
rarely be associa ed wi h dila ed and or uous blood vessels o he bulbar conjunc iva:
Diabe es melli us Fabry disease: Frequen ly associa ed
wi h small aneurysm orma ion O her me abolic disorders (e.g., ucosi-
dosis, GM 1 gangliosidosis) Mul iple endocrine neoplasia IIb: asso-
cia ed wi h prominen paralimbal nerve bundles
HEMATOLOGIC DISO DE S T e ollowing hema ologic disorders may
be associa ed wi h sludging o he blood: Dyspro einemias (e.g., mul iple
myeloma) Sickle-cell anemia: isola ed, corkscrew-
or comma-shaped vessels Polycy hemia vera
HEMO HAGIC LYMPHANGIECTASIA
Hemorrhagic lymphangiec asia is a rare condi ion ha may occur af er mild in am-ma ion or rauma. I may also be associa ed wi h vascular mal orma ions o he eyelid and paro id gland.
Dila ed and or uous bulbar lympha ic vessels may become lled wi h blood i hey communica e wi h conjunc ival veins.
CAPILLA Y HEMANGIOMA Capillary hemangioma is an uncommon
umor ha may be associa ed wi h hemangio-mas o he eyelids and orbi .
Brigh red lesion ha blanches wi h pres-sure. I may bleed spon aneously or ollowing minor rauma.
LYMPHANGIOMA Lymphangioma is a rare umor ha may
be associa ed wi h similar lesions o he orbi , ace, sinuses, and oropharynx.
Brigh red lesion which is similar o, bu may be larger han, a hemangioma
K POSI’S SA COMA Kaposi’s sarcoma, occurring mos com-
monly on he skin, including he eyelids and occasionally on he conjunc iva, may be seen in AIDS pa ien s.
A reddish vascular conjunc ival lesion ha may be di use or nodular (see Fig. 7-20B). A di use umor may resemble a subconjunc ival hemorrhage upon cursory examina ion.
No speci c rea men is required. I severe, and sys emic AIDS rea men and chemo- herapy have been maximized, local excision, cryo herapy, or radia ion can be used or ocu-lar Kaposi’s sarcoma.
STU GE-WEBE SYND OME (ENCEPHALOT IGEMINAL ANGIOMATOSIS)
Localized elangiec asias, probably associ-a ed wi h episcleral hemangiomas ( Fig. 2-7 A)
Associa ed wi h glaucoma, iris hyperchro-mia, and di use choroidal hemangioma.
CA OTID–CAVE NOUS SINUS AND DUR L-SINUS FISTULAS
T ere are wo ypes o ar eriovenous s u-las ha a ec he eye. T ey produce reversal o ow hrough he superior oph halmic vein ha can be seen on color Doppler s udies and dila ion o he superior oph halmic vein ha can be seen on compu ed omography or magne ic resonance imaging.
A caro id–cavernous sinus s ula is a high- ow communica ion be ween he in er-nal caro id ar ery and he cavernous sinus.
LWBK961-C02_p42-69.indd 67 22/07/11 8:51 AM

68 2 CONJUNCTIVAL DEGENERATIONS AND MASS LESIONS
I mos commonly occurs af er rauma or surgery bu can arise spon aneously. I can produce severe conjunc ival vessel engorge-men and chemosis, eyelid swelling, pulsa ing exoph halmos, eleva ed in raocular pressure, and an orbi al brui .
A dural-sinus s ula is a low- ow com-munica ion be ween he meningeal branches o he caro id ar ery and he cavernous sinus. T ey occur spon aneously, mos commonly in middle-aged and elderly women. T e clinical ndings are much milder han in caro id–cavernous sinus s ulas, al hough he
in raocular pressure can be qui e eleva ed. T e chronic red eye is of en mis aken or chronic conjunc ivi is ( Fig. 2-7 B and C).
Bo h orms can cause ar erializa ion o he conjunc ival blood vessels resul ing in he charac eris ic corkscrew pat ern.
rea men is wi h closure o he s ula hrough an endoar erial balloon emboliza ion or surgery, al hough dural-sinus s ulas may close spon aneously or af er angiography. Signi can ly eleva ed in raocular pressure needs o be addressed.
A
FIGURE 2-7. Sturge Weber syndrome. A. Prominen episcleral vessels are seen superiorly in his pa ien wi h S urge-Weber syndrome. Eleva ed episcleral venous pressure can cause glaucoma.
(continued)
LWBK961-C02_p42-69.indd 68 22/07/11 8:51 AM

Vascular Lesions 69
B
C
FIGURE 2-7. (Continued) Cavernous sinus f stula. B. T is pa ien had a low f ow dural-sinus s ula. No e he engorged corkscrew episcleral vessels. T e in raocular pressure was modera ely eleva ed. C. Mul iple prominen dila ed corkscrew episcleral vessels are seen in his eye wi h a low f ow dural-sinus s ula. (Cour esy o Wee-Jin Heng, MD.)
LWBK961-C02_p42-69.indd 69 22/07/11 8:51 AM

C H A P T E R
70
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
Shallow an erior chamber, angle-closure or open-angle glaucoma, corneal f at ening, and hyperopia
May have associa ed nanoph halmos ( Table 3-1 )
O her ocular dimensions are normal.
Treatment Manage re rac ive error and search or
o her ocular and sys emic anomalies.
Prognosis Varies depending on associa ed ocular and
sys emic abnormali ies
An erior Segmen Developmen al Anomalies
ANOMALIES OF CORNEAL SIZE AND SHAPE
MIC OCO NEA
Microcornea is an uncommon con-geni al unila eral or bila eral condi-
ion. Inheri ance is au osomal dominan or recessive.
Signs In an horizon al corneal diame er less
han 10 mm; adul horizon al corneal diam-e er less han 11 mm ( Fig. 3-1 )
TABLE 3-1. Associa ion o Microcornea
Ocular Systemic Syndromes• Anterior segment
dysgeneses • Congenital cataract • Congenital glaucoma • Corneal leukoma • Cornea plana • Hyperopia • Microphakia • Uveal coloboma
• Cornelia de Lange’s • Ehlers-Danlos • Nance-Horan • Trisomy 13, 18, 21 • Turner’s • Waardenburg’s • Weill-Marchesani
LWBK961-C03_p70-89.indd 70 22/07/11 8:54 AM

Anomalies of Corneal Size and Shape 71
FIGURE 3-1. Microcornea. T is cornea measured 8.5 o 9.0 mm in diame er. O herwise he eye was essen ially normal.
LWBK961-C03_p70-89.indd 71 22/07/11 8:54 AM

72 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
MEGALOCO NEA
Megalocornea is an uncommon congeni- al, bila eral condi ion ha is usually
inheri ed in an X-linked recessive manner and is here ore ound mos ly in males.
Signs Clear cornea wi h a horizon al diame er
o grea er han 12 mm in he neona e and 13 mm in adul s ( Fig. 3-2 )
Very deep an erior chamber Normal in raocular pressure Corneal s eepening, high myopia, and
as igma ism, bu good visual acui y
Lens subluxa ion may occur as a resul o zonular s re ching.
May develop glaucoma secondary o angle abnormali ies
Treatment Manage re rac ive error and search or
o her ocular and sys emic anomalies, espe-cially glaucoma and lens abnormali ies.
Prognosis Generally good, bu depends on associ-
a ed ocular and sys emic abnormali ies ( Table 3-2 )
TABLE 3-2. Associa ions o Megalocornea
Ocular Systemic Syndromes • Astigmatism • Axenfeld-Rieger
anomaly • Cataract • Congenital glaucoma • Ectopia lentis • Myopia
• Albinism • Alport’s • Apert’s • Craniosynostosis • Down’s • Ehlers-Danlos • Marfan’s • Osteogenesis
imperfecta • Progressive facial
hemiatrophy
LWBK961-C03_p70-89.indd 72 22/07/11 8:54 AM

Anomalies of Corneal Size and Shape 73
FIGURE 3-2. Megalocornea. T is cornea measured 14 mm in diame er. T e cornea is clear excep or some calcif c degenera ion nasally and emporally.
LWBK961-C03_p70-89.indd 73 22/07/11 8:54 AM

74 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
TABLE 3-3. ypes o Microph halmos
Noncolobomatous ColobomatousIsolated Isolated • Sporadic • Inherited (dominant,
recessive, X-linked recessive)
• Sporadic • Inherited (dominant)
With anterior persistent hyperplastic primary vitreous
With systemic syndromes: • Patau’s (trisomy 13) • Edward’s (trisomy 18) • Cat-eye (partial
trisomy 22) Intrauterine infections (rubella, toxoplasmosis, cytomegalovirus, varicella)
• CHARGE • Meckel • Lenz microphthalmia
CHARGE syndrome is c oloboma, h eart anomaly, choanal a tresia, r etardation, and g enital or e ar anomalies.
NANOPHTHALMOS
Nanoph halmos is an uncommon, con-geni al, bila eral condi ion in which he
globe has reduced volume bu is o herwise grossly normal.
Signs Very high hyperopia (e.g., + 12D o + 15D) Adul corneal diame er is reduced, bu he
lens has a normal volume. Shor axial leng h (e.g., 16–18 mm) Shallow an erior chamber T ick sclera Fundus may show a crowded disc, vascular
or uosi y, and macular hypoplasia
Associated Problems Angle-closure glaucoma Uveal e usion Re inal de achmen Poorly olera ed in raocular surgery
MIC OPHTHALMOS
Microph halmos is an uncommon uni-la eral or bila eral condi ion in which
he axial leng h o he eye is reduced and he eye is mal ormed ( Fig. 3-3 ) . T e e ec s on vision depend on i s severi y and he pres-ence o associa ed anomalies. T ere are wo ypes o microph halmos: noncoloboma ous and coloboma ous ( Table 3-3 ) .
LWBK961-C03_p70-89.indd 74 22/07/11 8:54 AM

Anomalies of Corneal Size and Shape 75
FIGURE 3-3. Microphthalmos. T is microph halmic eye has a small cornea, abnormal iris, and overall small size. (Cour esy o Pe er Laibson, MD.)
LWBK961-C03_p70-89.indd 75 22/07/11 8:54 AM

76 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
BUPHTHALMOS
Buph halmos is an uncommon, usually bila eral condi ion in which he globe is
enlarged as a resul o s re ching o he cornea and sclera because o increased in raocular pres-sure be ore bir h or during he rs 3 years o li e.
Signs Large cornea wi h variable scarring; may
develop corneal edema la er in li e Horizon al or curvilinear rup ures in
Desceme ’s membrane (Haab’s s riae) ( Fig. 3-4 )
Very deep an erior chamber Angle anomalies Myopia Op ic disc cupping
Associations o In antile Glaucoma Ocular
Aniridia An erior segmen dysgeneses Congeni al ec ropion uveae
Sys emic Down’s syndrome Lowe’s syndrome Mucopolysaccharidoses Neuro broma osis ype 1 Nevus o O a Pa au’s syndrome ( risomy 13) Pierre Robin’s syndrome Rieger’s syndrome S urge-Weber syndrome
Treatment Managemen o glaucoma by a glaucoma
specialis
Prognosis Guarded, depending on amoun o
op ic nerve damage prior o diagnosis, e cacy o rea men , and associa ed ocular and sys emic disorders. Haab’s s riae o he cornea do no preven good vision.
LWBK961-C03_p70-89.indd 76 22/07/11 8:54 AM

Anomalies of Corneal Size and Shape 77
FIGURE 3-4. Haab’s striae. A. T ese breaks in Desceme ’s membrane occurred secondary o congeni al glaucoma. No e he mul iple parallel swirling lines, which are rolled-up edges o Desceme ’s membrane. B. Mul iple parallel swirling lines are eviden in his eye wi h congeni al glaucoma.
A
B
LWBK961-C03_p70-89.indd 77 22/07/11 8:54 AM

78 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
CONGENITAL ANTE IO STAPHYLOMA/ KER TECTASIA
Congeni al an erior s aphyloma and kera- ec asia are ex remely rare, congeni al,
usually unila eral condi ions resul ing in severe corneal pro rusion and occasionally per ora- ion ( Fig. 3-5 ).
Etiology I is probably due o in rau erine kera i is.
Signs Severe corneal opaci ca ion and pro rusion
o corneal issue beyond he plane o he eyelids.
Endo helium, Desceme ’s, and pos erior corneal issue are absen .
I may be lined by uveal issue pos eriorly.
Treatment A pene ra ing kera oplas y or an e-
rior segmen ransplan can be at emp ed in bila eral cases, bu he success ra e is ex remely poor. Mos eyes will undergo an enuclea ion.
Prognosis Poor
FIGURE 3-5. Keratectasia. Gross specimen a er enuclea ion o an eye wi h a large corneal s aphyloma a er suspec ed in rau erine in ec ion. No e he massive pro rusion an erior o he corneal limbus. (Cour esy o Pe er Laibson, MD.)
LWBK961-C03_p70-89.indd 78 22/07/11 8:55 AM

Anomalies of Corneal Size and Shape 79
SCLE OCO NEA
Sclerocornea is a rare, congeni al, usually bila eral bu o en asymme ric, nonpro-
gressive, noninf amma ory condi ion. I can be par ial or comple e.
Etiology Unknown Mos cases are sporadic.
Signs Opaci ca ion and vasculariza ion o he
peripheral or en ire cornea. I only he periph-eral cornea is involved, he resul ing “scleral-iza ion” makes he cornea appear smaller han normal ( Fig. 3-6 ).
O en associa ed wi h cornea plana May have associa ed glaucoma
Ocular Associations An erior segmen dysgeneses Blue sclera Congeni al ca arac Cornea plana Glaucoma Iris abnormali ies (e.g., aniridia, coloboma) Microph halmos
Treatment I unila eral, may op o ollow he eye. I
bila eral, consider a pene ra ing kera oplas y or kera opros hesis.
Prognosis Pene ra ing kera oplas y has a rela-
ively poor prognosis in sclerocornea. Kera opros hesis surgery in in an s is a recen developmen and has a guarded prognosis.
A
FIGURE 3-6. Peripheral sclerocornea. A. T e en ire corneal periphery, bu especially he superior and in erior cornea, are scleralized.
(continued)
LWBK961-C03_p70-89.indd 79 22/07/11 8:55 AM

80 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
B
C
FIGURE 3-6. (Continued) Peripheral sclerocornea. B. T e superior, nasal, and in erior peripheral cornea are vascularized in his eye wi h ex ensive peripheral sclerocornea. Total sclerocornea. C. T e en ire cornea is scleralized. T ere is a sligh ly less opaque area cen rally, which urned ou o be he cen ral cornea during pene ra ing kera oplas y.
LWBK961-C03_p70-89.indd 80 22/07/11 8:55 AM

Anomalies of Corneal Size and Shape 81
CO NEA PLANA
Cornea plana is a rare, congeni al, bila eral condi ion. Many physicians consider i a
mild orm o sclerocornea.
Etiology Unknown
Symptoms None or poor vision
Signs Hyperopia Severely f a corneal curva ure, where he
sclera and cornea have he same curva ure ( Fig. 3-7 )
Shallow an erior chamber Glaucoma
Ocular Associations Aniridia An erior segmen dysgeneses Microcornea Microph halmos Sclerocornea
Treatment Correc re rac ive error. Con ac lenses can be di cul o
due o f a ness o he cornea and he lack o di erence be ween he corneal and scleral curva ure. A scleral lens may be bene cial.
Prognosis Good
FIGURE 3-7. Peripheral sclerocornea/ cornea plana. A sli -beam view o he eye seen in Figure 3 6 A demons ra es he lack o change in corneal curva ure be ween he sclera and he cornea. T e cornea had a a corneal curva ure and he eye was hyperopic.
LWBK961-C03_p70-89.indd 81 22/07/11 8:55 AM

82 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
ANTERIOR SEGMENT DYSGENESES
POSTE IO EMB YOTOXON Pos erior embryo oxon is a creamy-whi e,
hickened, an eriorly displaced Schwalbe’s line seen in he corneal periphery ( Fig. 3-8 A).
I is ypically a bila eral condi ion ha occurs o some ex en in approxima ely 15% o normals. I is presen in all pa ien s wi h Axen eld’s and Rieger’s anomaly.
AXENFELD’S ANOMALY Axen eld’s anomaly is a rare, bila eral,
au osomal dominan or sporadic anomaly. I is charac erized by s rands o iris ha span across he angle and at ach o a pos erior embryo oxon ( Fig. 3-8 B).
Glaucoma develops in 50% o cases, and he disorder is hen known as Axen eld’s syndrome.
IEGE ’S ANOMALY Rieger’s anomaly is a rare, bila eral, au o-
somal dominan or sporadic anomaly. I is charac erized by pos erior embryo oxon wi h adheren iris s rands and iris s romal hypopla-sia ( Fig. 3-8 C). T ere may be pseudopolyco-ria, corec opia, and ec ropion uveae.
O hose a ec ed, 50% o pa ien s develop glaucoma.
IEGE ’S SYND OME Au osomal dominan rai . Usually bila -
eral bu asymme ric. Consis s o Rieger’s anomaly plus den al
(hypodon ia, microdon ia) or acial (maxil-lary hypoplasia, elecan hus, hyper elorism) mal orma ions.
O hose a ec ed, 50% o pa ien s develop glaucoma.
PETE S’ ANOMALY Sporadic inheri ance, al hough au osomal
recessive and dominan pat erns have been repor ed.
Bila eral in 80% o cases bu o en asymme ric.
Cen ral corneal opaci y, pos erior Desceme ’s membrane or s romal de ec , o en iridocorneal adhesions, possible lens–cornea adhesion and shallow an erior cham-ber ( Fig. 3-8 D and E).
May be associa ed wi h lens displacemen and ca arac
O hose a ec ed, 50% o pa ien s develop glaucoma.
May have associa ed sys emic abnormali- ies (e.g., skele al, den al)
LOCALIZED POSTE IO KER TOCONUS
Very rare, sporadic, usually unila eral developmen al anomaly presen ing a bir h
Nonprogressive pro rusion o cen ral area o he pos erior corneal sur ace ( Fig. 3-8 F)
May have a mild corneal scar Myopic as igma ism can occur.
Diagnosis o Anterior Segment Dysgeneses Family his ory or similar condi ion and
sys emic his ory or associa ed anomalies Examine under anes hesia i unable o do an
adequa e evalua ion in he o ce, including a sli -lamp examina ion, measuremen o corneal diame er, in raocular pressure, gonioscopy, oph- halmoscopy, and re inoscopy. Ul rasound bio-microscopy and op ical coherence omography can be help ul in imaging he an erior segmen , A-scan ul rasonography is help ul o measure he axial leng h o moni or or glaucoma, and B-scan ul rasonography can be used o image he pos erior segmen when necessary.
Treatment o Anterior Segment Dysgeneses Visual rehabili a ion: correc re rac ive
errors, rea amblyopia, con rol glaucoma wi h medica ions or surgery, ca arac ex rac ion and corneal ransplan a ion as necessary. May need combined e or s o specialis s in cornea, glau-coma, re ina, and pedia ric oph halmology
LWBK961-C03_p70-89.indd 82 22/07/11 8:55 AM

Anterior Segment Dysgeneses 83
FIGURE 3-8. Posterior embryotoxon. A. A prominen Schwalbe’s line can be seen rom he 7 o he 9 o’clock posi ions. (Cour esy o Irving Raber, MD.) Axenfeld’s anomaly. B. A prominen Schwalbe’s ring wi h iris adhesions can be seen in eriorly in his eye wi h Axen eld’s anomaly. (Cour esy o Elisabe h Cohen, MD.)
(continued)
A
B
Re er o a pedia rician or managemen o sys emic abnormali ies.
Chromosomal analysis and gene ic counseling
Prognosis or Anterior Segment Dysgeneses Excellen or pos erior embryo oxon
and localized pos erior kera oconus; air
o good or Axen eld’s and Rieger’s anoma-lies; guarded or Pe ers’ anomaly. he prognosis depends grea ly on he severi y o he glaucoma. Eyes wi h Pe ers’ anomaly can do well wi h corneal ransplan a ion; he success ra e is worse when he lens is involved.
LWBK961-C03_p70-89.indd 83 22/07/11 8:55 AM
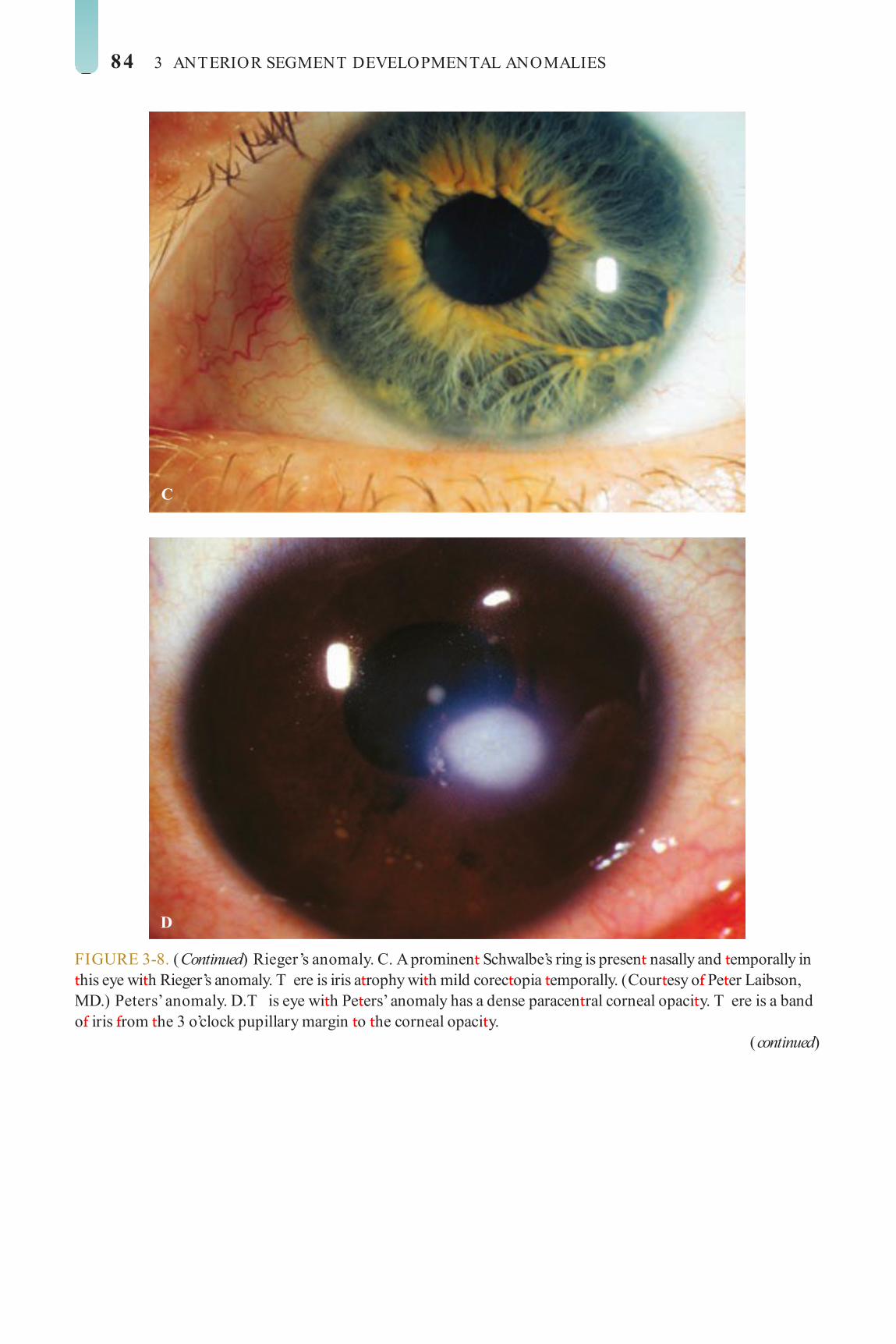
84 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
C
D
FIGURE 3-8. (Continued) Rieger’s anomaly. C. A prominen Schwalbe’s ring is presen nasally and emporally in his eye wi h Rieger’s anomaly. T ere is iris a rophy wi h mild corec opia emporally. (Cour esy o Pe er Laibson, MD.) Peters’ anomaly. D. T is eye wi h Pe ers’ anomaly has a dense paracen ral corneal opaci y. T ere is a band o iris rom he 3 o’clock pupillary margin o he corneal opaci y.
(continued)
LWBK961-C03_p70-89.indd 84 22/07/11 8:55 AM

Anterior Segment Dysgeneses 85
E
F
FIGURE 3-8. (Continued) Peters’ anomaly. E. T is dense cen ral corneal opaci y was associa ed wi h iris adhesions rom he pupillary margin o he pos erior aspec o he corneal opaci y in his 4-year-old girl born in China. Her o her eye had a similar condi ion requiring corneal ransplan s in bo h eyes. Posterior keratoconus. F. An inden a ion o he pos erior cornea can be seen cen rally, which is charac eris ic o pos erior kera oconus. T ere is a mild associa ed corneal opaci y. T ere is minimal an erior corneal change, bu here may be as igma ism.
LWBK961-C03_p70-89.indd 85 22/07/11 8:55 AM
86 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
ANI IDIA
Aniridia is a rare, bila eral condi ion ha is associa ed wi h glaucoma in 75% o
cases. wo- hirds o pa ien s have an au o-somal dominan orm ha is no associa ed wi h Wilms’ umor. Approxima ely one- hird o cases are sporadic; 25% o sporadic cases will develop Wilms’ umor.
Signs Par ial or essen ially comple e absence o
he iris Synechial angle-closure glaucoma occurs
in 75% o cases as a resul o pulling orward o rudimen ary iris issue.
Associa ed ocular and sys emic disorders
Classif cation AN-1: isola ed; au osomal dominan :
Vision is poor due o oveal hypoplasia. AN-2: isola ed; au osomal dominan :
Vision is normal. AN-3 (Gillespie’s syndrome): au osomal
recessive. Men al handicap, cerebellar a axia AN-4 (Miller’s syndrome): dele ion o
he shor arm o chromosome 11, sporadic. Wilms’ umor, geni ourinary anomalies, men- al re arda ion
AN-5: variable inheri ance. Iris hypoplasia wi h o her ocular mal orma ions (e.g., Pe ers’ anomaly, microcornea, congeni al aphakia, ec opia len is)
AN-6: variable inheri ance. Iris hypo-plasia wi h o her sys emic syndromes (e.g., Biemond’s syndrome, absence o pa ella)
Ocular Associations Glaucoma Corneal lesions: pannus, opaci y
( Fig. 3-9 A–C), kera olen icular adhesions, microcornea, sclerocornea
Lens and iris changes: congeni al aphakia, an erior polar, pos erior subcapsular ca arac , subluxa ion, ec opia len is, persis en pupil-lary membranes
Fundus lesions: oveal hypoplasia, disc hypoplasia, colobomas
Nys agmus
Diagnosis Family his ory or similar condi ion and
sys emic his ory or associa ed anomalies. Examine under anes hesia i unable o
do an adequa e evalua ion in he o ce, including a sli -lamp examina ion, measure-men o corneal diame er and in raocular pressure, gonioscopy, oph halmoscopy, and re inoscopy.
Treatment Visual rehabili a ion: Correc re rac ive
errors, rea amblyopia, and con rol glau-coma wi h medica ions or surgery. Ca arac ex rac ion and corneal ransplan / limbal s em cell ransplan / kera opros hesis as necessary
Chromosomal analysis and gene ic counseling
Renal evalua ion by pedia rician or pedia ric oncologis o moni or or Wilms’ umor
Prognosis Fair, depending on severi y o glaucoma
and corneal abnormali ies. T e limbal s em cell abnormali y o en leads o corneal haze and scarring. Corneal ransplan s o en ail because o limbal s em cell de ciency. Limbal s em cell ransplan a ion wi h chronic sys emic immunosuppression has a reasonably good prognosis. Kera opros hesis surgery also has a reasonably good prognosis.
LWBK961-C03_p70-89.indd 86 22/07/11 8:55 AM

Anterior Segment Dysgeneses 87
FIGURE 3-9. Aniridia. A. T is eye wi h aniridia demons ra es corneal pannus and severe corneal scarring. Al hough here is a hazy view, no iris was seen upon sli -lamp examina ion. B. S ignif can peripheral pannus and di use pa chy an erior s romal corneal haze is presen in his eye wi h aniridia. C. Re roillumina ion o he eye in B reveals a well-posi ioned pos erior chamber in raocular lens implan and perhaps a very small amoun o peripheral iris.
A
B
C
LWBK961-C03_p70-89.indd 87 22/07/11 8:55 AM

88 3 ANTERIOR SEGMENT DEVELOPMENTAL ANOMALIES
IRIS COLOBOMA
Iris coloboma is an uncommon, unilateral or bilateral condition caused by de ective clo-
sure o the embryonic f ssure, usually in ero-nasally. Isolated iris colobomas are either sporadic or dominantly inherited.
Signs A total coloboma is a segmental absence o iris
rom pupil to root, giving rise to a “keyhole” pupil. A partial coloboma does not involve the
iris root ( Fig. 3-10 ).
Ocular Associations Colobomas o the ciliary body, lens, retina,
choroid, and optic nerve Microphthalmos
Systemic Associations Cat-eye syndrome (partial trisomy 22) CHARGE syndrome ( c oloboma, h eart
anomaly, choanal a tresia, r etardation, and g enital or e ar anomalies)
Edward’s syndrome (trisomy 18)
Patau’s syndrome (trisomy 13) Rubinstein-Taybi syndrome
Diagnosis Family history or similar condition and
systemic history or associated anomalies. Examine under anesthesia i unable to do an
adequate evaluation in the o ce, including a slit-lamp examination, measurement o corneal diameter and intraocular pressure, gonioscopy, ophthalmoscopy, and retinoscopy. Ultrasound biomicroscopy and optical coherence tomogra-phy can be help ul in imaging the anterior seg-ment, and B-scan ultrasonography can be used to image the posterior segment when necessary.
Treatment Manage re ractive error and search or other
anterior and posterior segment anomalies. Chromosomal analysis and genetic counseling
Prognosis Depends on severity o the coloboma and
on the extent o other ocular and systemic abnormalities
FIGURE 3-10. Iris coloboma. A. An in erior iris coloboma is present in this newborn with numerous systemic abnormalities. T ere are f ne iris strands in eriorly. T e other eye, which had severe sclerocornea, is seen in Figure 3 6 C.
(continued)
A
LWBK961-C03_p70-89.indd 88 28/07/11 7:58 AM

Anterior Segment Dysgeneses 89
B
C
FIGURE 3-10. (Continued) Iris c oloboma. B . A large in erior iris coloboma has been covered wi h an iris- in ed so con ac lens. C. T e con ac lens in he eye in B has been moved superiorly wi h a cot on- ipped applica or o reveal he large in erior iris coloboma. T ere is also a cor ical ca arac .
LWBK961-C03_p70-89.indd 89 22/07/11 8:55 AM

C H A P T E R
90
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
Signs Early
Progressive myopia and as igma ism Scissors ref ex on re inoscopy Irregular mires on kera ome ry In erior s eepening on compu erized
corneal opography ( Fig. 4-1 A) and omography. Eyes wi h “low sagging cones” can demons ra e a mild crab-claw opo-graphic pat ern ( Fig. 4-1 B), which is simi-lar o he pat ern seen in pellucid marginal degenera ion.
Cen ral or paracen ral s romal hinning o he cornea wi h pro rusion a he apex o he hinning ( Fig. 4-1 C)
Fleischer’s ring: epi helial iron deposi s a he base o he cone ( Fig. 4-1 D)
Prominen corneal nerves ( Fig. 4-1 E) La e
Vog ’s s riae: ne ver ical deep s romal ension lines ha disappear emporarily
Ec a ic Condi ions o he Cornea
KERATOCONUS
Kera oconus is a airly common condi ion charac erized by corneal hinning, pro-
rusion, and irregulari y. I is usually bila eral, al hough he severi y o involvemen is o en asymme ric.
Etiology Sporadic or au osomal dominan wi h
incomple e pene rance
Symptoms Gradually decreasing vision, ypically
beginning in adolescence and progressing in o adul li e
Pa ien s o en rela e a his ory o no being able o at ain good vision despi e mul iple changes o glasses or so con ac lenses.
May have a his ory o eye rubbing Can develop acu ely decreased vision and
pain due o hydrops wi h advanced disease
LWBK961-C04_p90-101.indd 90 22/07/11 8:59 AM

Keratoconus 91
wi h digi al pressure applied o he limbus ( Fig. 4-1 F)
Abnormal “oil drople ” red ref ex Rizut i’s sign: conical ligh ref ec ion on
he nasal limbus when ligh is shone rom he emporal side
Variable corneal scarring, depending on severi y ( Fig. 4-1 G–I). May develop an eleva ed apical nodule ( Fig. 4-1 J)
Munson’s sign: bulging o he lower eye-lid in downgaze
Acu e hydrops: severe corneal edema resul ing rom a ear in Desceme ’s mem-brane ( Fig. 4-1 K–M)
Associations Ocular: vernal disease, blue sclera, re ini is
pigmen osa, Leber’s congeni al amaurosis, f oppy eyelid syndrome
Sys emic: Down’s syndrome, Ehlers-Danlos syndrome, Aper ’s syndrome, ocular allergies, os eogenesis imper ec a
Dif erential Diagnosis Pellucid marginal degenera ion: in erior
peripheral corneal hinning wi h pro rusion o he cornea above he area o maximal hinning
Treatment Mild cases: glasses and so con ac lenses
Modera e cases: rigid gas-permeable con ac lens (RGPCL), hybrid lens, or scleral lens
Severe and con ac lens–in oleran cases:
Lamellar kera ec omy wi h a blade or excimer laser or an erior nodules
Placemen o in racorneal ring segmen s
Deep an erior lamellar kera oplas y Pene ra ing kera oplas y Epikera oplas y and hermokera oplas y
are rarely per ormed. Re rac ive surgery in pa ien s wi h kera-
oconus is unpredic able and generally no recommended.
Corneal collagen crosslinking: Generally per ormed by placing ribof avin drops on he cornea and hen rea ing he cornea wi h ul raviole ligh , i is being used o “s reng hen” he cornea o preven worsen-ing o kera oconus in pa ien s wi h docu-men ed progression. While no curren ly FDA-approved, shor - erm resul s are promising.
Prognosis Mos pa ien s do well wi h RGP or hybrid
CLs. T e success ra e wi h corneal ransplan- a ion in kera oconus is high.
LWBK961-C04_p90-101.indd 91 22/07/11 8:59 AM

92 4 ECTATIC CONDITIONS OF THE CORNEA
FIGURE 4-1. Keratoconus corneal topography. A. Signif can irregular in erior corneal s eepening is apparen using compu erized corneal opographic analysis in his eye wi h modera e kera oconus. As seen on he color scale on he le , he red colors indica e corneal s eepening and blue colors indica e corneal at ening. T e f gure on he righ shows he Placido’s rings; his image is impor an o veri y he quali y and cen ra ion o he s udy. B. T e irregular in erior s eepening seen on compu erized corneal opographic analysis o his eye wi h kera oconus reveals a sligh crab-claw pat ern, which is reminiscen o pellucid marginal degenera ion. Eyes wi h “low sagging cones” can demons ra e his opographic pat ern. Keratoconus. C. Sli -beam view o his eye wi h signif can kera oconus demons ra es in erocen ral corneal hinning and s eepening. No e he hinnes and mos pro ruded areas o cornea coincide.
(continued)
A
B
C
LWBK961-C04_p90-101.indd 92 22/07/11 8:59 AM

Keratoconus 93
D
FIGURE 4-1. (Continued) Keratoconus. D. A prominen Fleischer’s ring, iron pigmen deposi ion a he base o he cone, is presen in his eye wi h kera oconus. E. Prominen corneal nerves can be seen in his eye wi h kera oconus. T ese nerves can be dis inguished rom corneal “ghos ” blood vessels because “ghos ” vessels have a lumen, making hem appear as wo parallel lines.
(continued)
E
LWBK961-C04_p90-101.indd 93 22/07/11 8:59 AM

94 4 ECTATIC CONDITIONS OF THE CORNEA
F
FIGURE 4-1. (Continued) Keratoconus. F. Fain , ver ical pos erior s romal s ress lines, Vog ’s s riae, are visible a he apex o he cone. Gen le pressure on he limbus can cause hese lines o change direc ion or disappear. G. Signif can cen ral s romal scarring is presen in his eye wi h advanced kera oconus.
(continued)
G
LWBK961-C04_p90-101.indd 94 22/07/11 8:59 AM

Keratoconus 95
H
FIGURE 4-1. (Continued) Keratoconus. H. Modera e in erocen ral corneal scarring can be seen in his eye a er resolu ion o corneal hydrops. An iron line is visible a he superior edge o he scarring. I. Sli -beam image o he same eye demons ra es signif can hinning in he area o scarring.
(continued)
I
LWBK961-C04_p90-101.indd 95 22/07/11 8:59 AM

96 4 ECTATIC CONDITIONS OF THE CORNEA
J
FIGURE 4-1. (Continued) Keratoconus. J. A hyper rophic nodule is presen a he apex o he cone. T ese nodules can occur de novo or rela ed o rigid con ac lens wear. Such a nodule can a ec vision and/ or in er ere wi h com or able con ac lens wear. T ese nodules can be removed wi h a superf cial kera ec omy wi h a blade or excimer laser pho o herapeu ic kera ec omy (P K). K. Acu e corneal hydrops occurs when he cornea s re ches o such a degree ha a ear develops in Desceme ’s membrane, allowing sudden in ow o aqueous uid in o he corneal s roma. T e corneal s roma can swell o grea er han f ve imes i s normal hickness. Acu e hydrops is associa ed wi h a sudden decrease in vision and increase in pain.
(continued)
K
LWBK961-C04_p90-101.indd 96 22/07/11 8:59 AM

Keratoconus 97
L
FIGURE 4-1. (Continued) Keratoconus. L. Sli -beam view o he same cornea. No e he severe corneal hickening. A prominen cle is apparen cen rally, where corneal lamellae are separa ed by a large degree o aqueous uid. M. Severe corneal whi ening rom acu e corneal hydrops is presen . T e ellow eye has scarring rom previous corneal hydrops (see Fig. 4-1 H and I ) .
M
LWBK961-C04_p90-101.indd 97 22/07/11 8:59 AM

98 4 ECTATIC CONDITIONS OF THE CORNEA
PELLUCID MARGINAL DEGENERATION
Pellucid marginal degenera ion is an uncommon, bila eral condi ion wi h in e-
rior corneal hinning, pro rusion, and irregu-lari y. I usually presen s in early adul hood.
Etiology Sporadic
Symptoms Gradually decreasing vision beginning
in young adul hood. Can develop acu e decreased vision and pain due o hydrops wi h advanced disease
Signs High irregular agains - he-rule as igma-
ism (f a a 90 degrees, s eep a 180 degrees) Recognizable “crab-claw” pat ern o irregu-
lar as igma ism on compu erized corneal opography and omography ( Fig. 4-2 A), al hough a similar pat ern can be ound in eyes wi h kera oconus wi h “low sagging cones.”
In erior, crescen -shaped band o periph-eral corneal hinning, 1 o 2 mm in wid h, ex ending rom he 4 o’clock o he 8 o’clock posi ion, which is separa ed rom he limbus by normal cornea ( Fig. 4-2 B).
T e area o pro rusion is loca ed above he band o hinning ( Fig. 4-2 C and D).
Fleischer’s ring and Vog ’s s riae are absen . Corneal hydrops occurs on rare occasions.
Dif erential Diagnosis Kera oconus: in erocen ral corneal hin-
ning wi h pro rusion o cornea in he area o grea es hinning. A Fleischer’s ring and Vog ’s s riae may be presen .
Treatment Mild and modera e cases: RGPCL, hybrid
lens, or scleral lens. Severe and con ac lens–in oleran cases
Large in erior pene ra ing kera oplas y Deep an erior lamellar kera oplas y In erior crescen ic wedge resec ion Crescen ic pene ra ing kera oplas y
(some imes ollowed by a cen ral pene ra ing kera oplas y) and placemen o in racorneal ring segmen s are occasionally per ormed.
Re rac ive surgery in pa ien s wi h pel-lucid marginal degenera ion is unpredic -able and generally no recommended.
Prognosis Mos pa ien s do well wi h RGPCLs,
al hough hey are harder o han in kera o-conus pa ien s. T e success ra e wi h corneal ransplan a ion in pellucid marginal degener-a ion is good, bu no as good as kera oconus, due o more peripheral disease.
A FIGURE 4-2. Pellucid marginal degeneration corneal topography. A. Signif can irregular nasal and emporal corneal s eepening is apparen in his compu erized corneal opographic analysis o his eye wi h modera e pellucid marginal degenera ion. Classically, he s eepening is seen o curve around in eriorly in his condi ion. As seen on he color scale on he le , he red colors indica e corneal s eepening and blue colors indica e corneal at ening. T e f gure on he righ shows he Placido’s rings; his image is impor an o veri y he quali y and cen ra ion o he s udy. No e he severe dis or ion o he Placido’s rings in his eye, wi h pellucid marginal degenera ion.
(continued)
LWBK961-C04_p90-101.indd 98 22/07/11 8:59 AM

Pellucid Marginal Degeneration 99
B
D
C
FIGURE 4-2. (Continued) Pellucid marginal degeneration. B. Side view demons ra es corneal pro rusion in eriorly wi h signif can s eepening near he limbus. C. T is sli -beam pho o reveals in erior corneal hinning approxima ely 2 mm rom he limbus, below he area o maximal pro rusion. D. Sli -beam view o his eye wi h severe pellucid marginal degenera ion also reveals corneal hinning approxima ely 2 mm rom he in erior limbus. T ere is signif can corneal s eepening in eriorly. No e ha he mos pro ruded por ion o he cornea is above he hinnes area.
LWBK961-C04_p90-101.indd 99 22/07/11 8:59 AM

100 4 ECTATIC CONDITIONS OF THE CORNEA
KERATOGLOBUS
Kera oglobus is an ex remely rare, bila -eral condi ion o severe uni orm periph-
eral corneal hinning. I usually presen s a or shor ly a er bir h.
Etiology Unknown
Symptoms Poor vision, occasionally pain due o
hydrops
Signs o al corneal hinning wi h maximal hin-
ning in he midperiphery, resul ing in pro ru-sion o he en ire cornea ( Fig. 4-3 )
T e cornea can be very hin. Normal corneal diame er; very deep an e-
rior chamber Acu e hydrops may occur in advanced
cases.
Pa ien may develop a corneal per ora ion rom minimal rauma because o he severe corneal hinning.
Systemic Associations A syndrome comprising blue sclera,
hyperex ensible join s, den al and hearing abnormali ies
Hyper hyroidism Rubins ein- aybi syndrome
Treatment Mild and modera e cases: Spec acles,
which improve vision and provide some pro- ec ion agains rauma
Severe cases: Some pa ien s do well wi h a scleral lens.
Surgical rea men is problema ic. A large ec onic lamellar gra ollowed many mon hs la er by a smaller pene ra ing gra is an op ion.
Prognosis Fair. Surgical rea men has a low success
ra e.
LWBK961-C04_p90-101.indd 100 22/07/11 8:59 AM

Keratoglobus 101
FIGURE 4-3. Keratoglobus. A. A hin, bulging cornea is eviden in his eye wi h kera oglobus. B. A sli -beam view demons ra es ha he hinnes por ion o he cornea is in he periphery in his eye wi h kera oglobus.
A
B
LWBK961-C04_p90-101.indd 101 22/07/11 8:59 AM

C H A P T E R
102
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
be a–induced [ GFBI] gene o chromosome 5q31)
Symptoms Mos commonly asymp oma ic Recurren erosion syndrome: may have
unila eral or bila eral recurren episodes o pain in he middle o he nigh or upon opening he eyes af er sleep. Can occur af er rauma wi h a sharp objec such as a nger-nail, ree branch, or paper edge
May no e painless dis or ion o vision when he cen ral cornea is involved
Signs Sli -lamp examina ion shows maplike
lines, do s (microcys s), and/ or ngerprin -like epi helial lesions, which may occur singly or in various combina ions ( Fig. 5-1 ). T ese ndings are bes seen wi h re roillumina ion and wi h a broad sli beam rom he side. “Nega ive s aining” rom sligh ly eleva ed areas o epi helium may be seen wi h uores-cein dye.
Corneal Dys rophies
ANTERIOR CORNEAL DYSTROPHIES
EPI HELIAL BASEMEN MEMBR NE DYS OPHY (AN E IO BASEMEN MEMBR NE DYS OPHY, MAP-DO -FINGE P IN DYS OPHY, COGAN’S MIC OCYS IC DYS OPHY)
Epi helial basemen membrane (EBM) dys rophy is a common epi helial dys ro-
phy ha can cause pain ul recurren corneal erosions and/ or decreased vision.
Etiology and Pathology EBM dys rophy is due o an abnormali y
o produc ion o epi helial basemen mem-brane ha ex ends in o he epi helium, lead-ing o mul iple basemen membranes in he corneal epi helium. rapped epi helial cells can orm “Cogan’s microcys s.”
ypically degenera ive, occasionally au o-somal dominan ( rans orming grow h ac or
LWBK961-C05_p102-141.indd 102 22/07/11 9:01 AM

Anterior Corneal Dystrophies 103
Eyes wi h recurren erosions may have minimal clinical ndings, localized areas o loose epi helium, or a rank epi helial de ec .
Dif erential Diagnosis O her an erior corneal dys rophies, such
as Meesmann’s dys rophy and Reis-Bücklers dys rophy
Treatment I vision is decreased due o cen ral
involvemen , he irregular epi helium can be debrided.
Pain ul erosions can be rea ed wi h lubrica- ion, hyper onic drops and oin men (sodium chloride 5%), pressure pa ching, opical cor icos eroids and oral doxycycline, epi he-lial debridemen , bandage sof con ac lens, an erior s romal micropunc ure, diamond burr polishing o Bowman’s membrane, or excimer laser pho o herapeu ic kera ec omy (P K).
Prognosis Very good wi h appropria e rea men ,
al hough some pa ien s have recalci ran recurren erosions
FIGURE 5-1. Epi helial basemen membrane dys rophy. A. Reduplica ed epi helial basemen membrane causing maplike changes are readily visible cen rally.
(continued)
A
LWBK961-C05_p102-141.indd 103 22/07/11 9:01 AM

104 5 CORNEAL DYSTROPHIES
B
C
FIGURE 5-1. (Continued) Epi helial basemen membrane dys rophy. B. Large maplike opaci ies are presen hroughou he cen ral cornea, causing complain s o monocular “diplopia,” bet er described as “shadow vision.” C. Maplike changes in his eye are almos conf uen cen rally, resul ing in signi can visual dis or ion.
(continued)
LWBK961-C05_p102-141.indd 104 22/07/11 9:01 AM
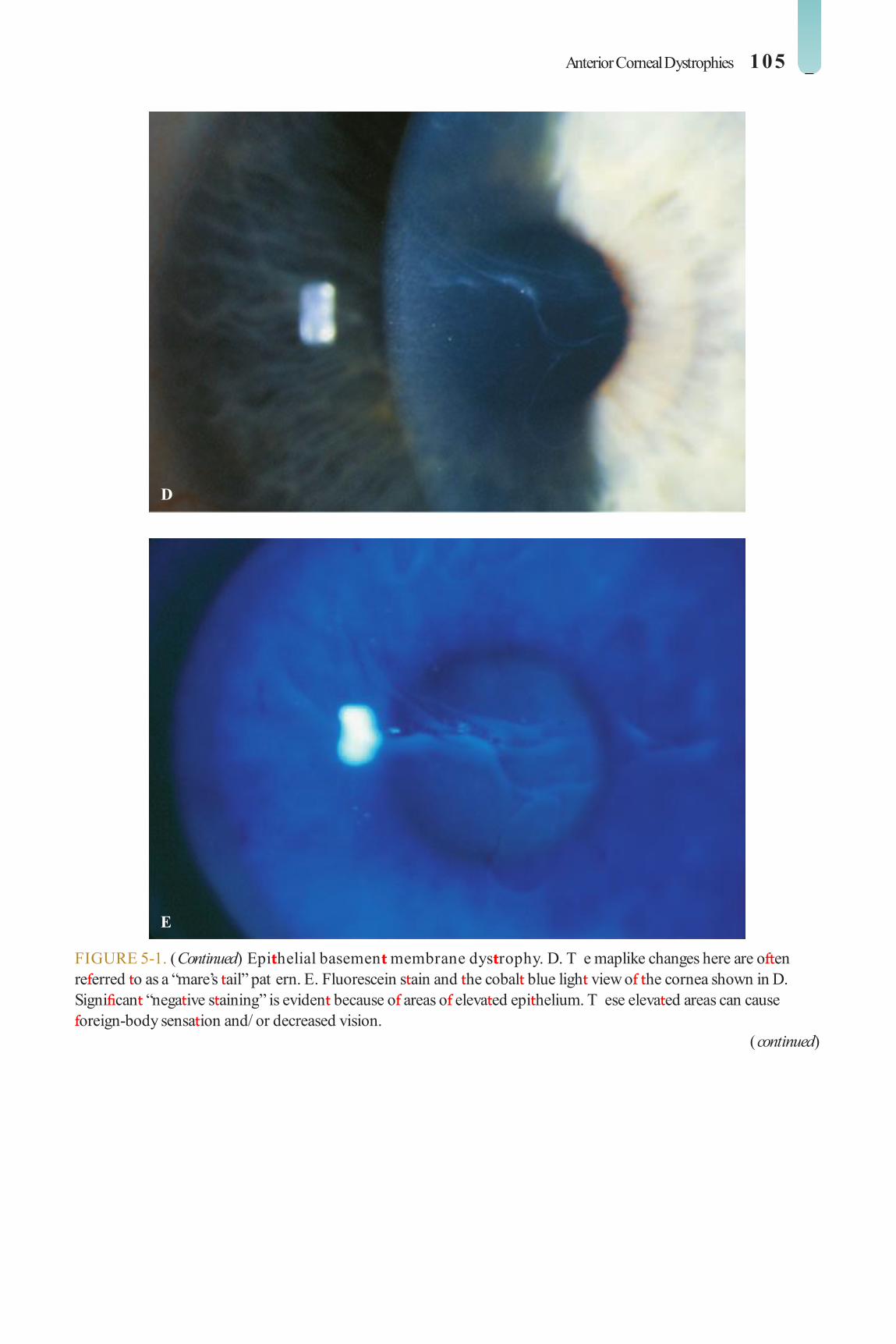
Anterior Corneal Dystrophies 105
D
E
FIGURE 5-1. (Continued) Epi helial basemen membrane dys rophy. D. T e maplike changes here are o en re erred o as a “mare’s ail” pat ern. E. Fluorescein s ain and he cobal blue ligh view o he cornea shown in D. Signi can “nega ive s aining” is eviden because o areas o eleva ed epi helium. T ese eleva ed areas can cause oreign-body sensa ion and/ or decreased vision.
(continued)
LWBK961-C05_p102-141.indd 105 22/07/11 9:01 AM

106 5 CORNEAL DYSTROPHIES
F
G
FIGURE 5-1. (Continued) Epi helial basemen membrane dys rophy. F. Do changes o EBM dys rophy. T ese creamy whi e Cogan microcys s are iny pocke s o sur ace epi helial cells rapped benea h an abnormal epi helial basemen membrane. G. A large area o epi helial microcys s is seen superiorly.
(continued)
LWBK961-C05_p102-141.indd 106 22/07/11 9:01 AM
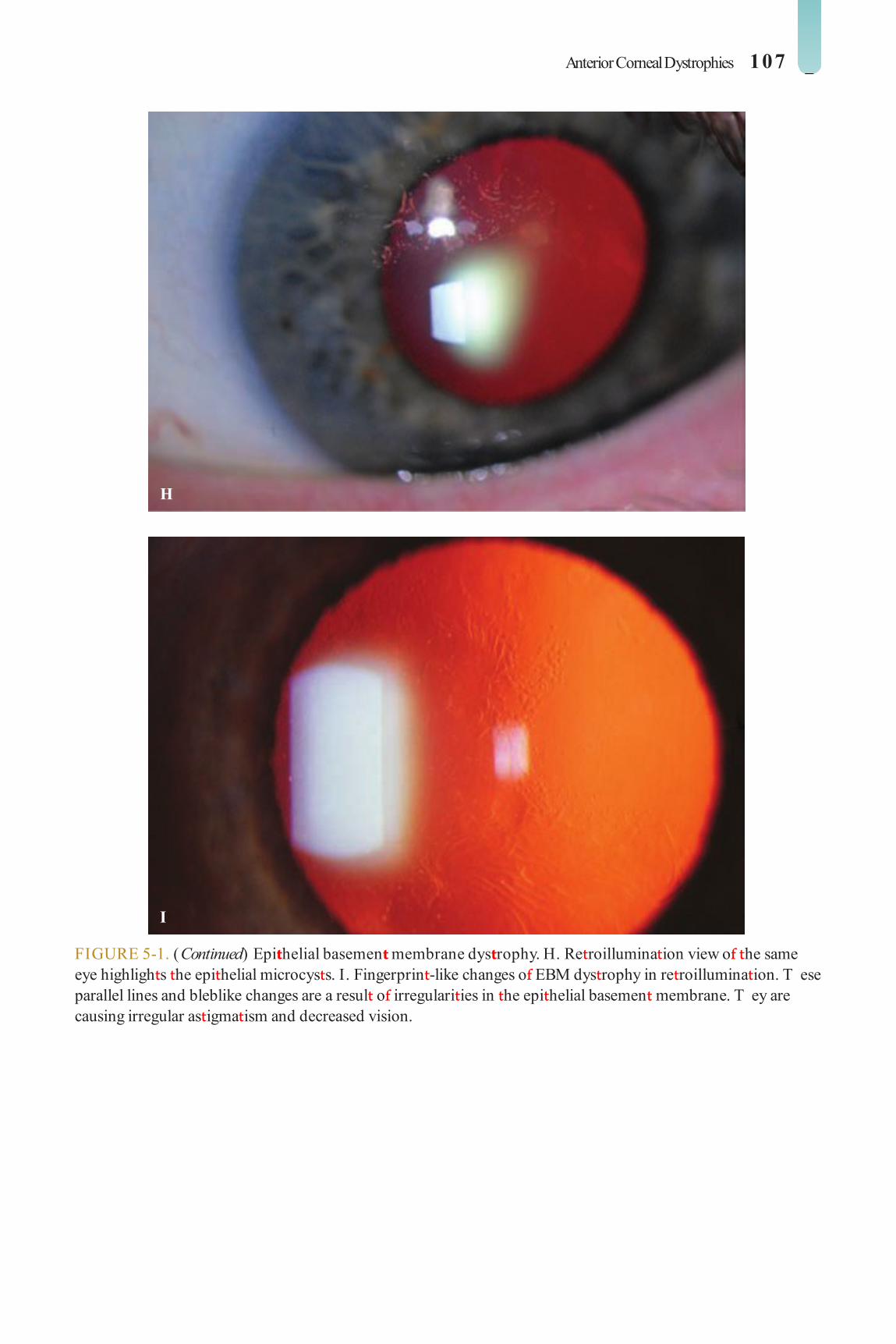
Anterior Corneal Dystrophies 107
H
I
FIGURE 5-1. (Continued) Epi helial basemen membrane dys rophy. H. Re roillumina ion view o he same eye highligh s he epi helial microcys s. I. Fingerprin -like changes o EBM dys rophy in re roillumina ion. T ese parallel lines and bleblike changes are a resul o irregulari ies in he epi helial basemen membrane. T ey are causing irregular as igma ism and decreased vision.
LWBK961-C05_p102-141.indd 107 22/07/11 9:01 AM

108 5 CORNEAL DYSTROPHIES
MEESMANN’S CO NEAL DYS OPHY (JUVENILE HE EDI A Y EPI HELIAL DYS OPHY)
Meesmann’s dys rophy is a rare bila eral epi helial disorder ha can cause ocu-
lar irri a ion and pho ophobia.
Etiology and Pathology Meesmann’s dys rophy is an au osomal
dominan (kera in K3 and K12 genes o chro-mosomes 12q13 and 17q12, respec ively) condi ion in which hundreds o iny vesicles con aining periodic acid-Schi (PAS)–posi ive “peculiar subs ance” are ound in he epi helium.
Symptoms Pa ien s are usually asymp oma ic bu may
no e irri a ion, glare, and pho ophobia. Mild
pain may develop in adul hood as a resul o recurring corneal erosions.
Signs Re roillumina ion demons ra es myriad
iny, ranslucen , epi helial cys s ha ex end o he limbus and are mos numerous in he in erpalpebral region. T e lesions appear gray or clear under direc illumina ion ( Fig. 5-2 ).
Treatment Mos pa ien s require no rea men .
Consider lubrica ion and sunglasses or mild symp oms. Rarely, a bandage sof con ac lens can be used or a super cial kera ec omy can be per ormed or severe symp oms, bu he dys rophy will recur.
Prognosis Good, al hough rare pa ien s will have
chronic symp oms
LWBK961-C05_p102-141.indd 108 22/07/11 9:01 AM

Anterior Corneal Dystrophies 109
FIGURE 5-2. Meesmann’s dys rophy. A. Mul iple iny, ranslucen , epi helial cys s are apparen in re roillumina ion. T ey end o be more prominen in he in erpalpebral zone. B. On direc illumina ion, he microcys s are gray in color bu are di cul o see. On illumina ion o he iris, a he 3 o’clock edge o he pupil, myriad microcys s are visible.
A
B
LWBK961-C05_p102-141.indd 109 22/07/11 9:01 AM

110 5 CORNEAL DYSTROPHIES
EIS-BÜCKLE S DYS OPHY
Reis-Bücklers dys rophy is an uncom-mon, bila eral, symme ric dys rophy o
Bowman’s membrane ha causes pain and decreased vision early in li e.
Etiology Reis-Bücklers dys rophy is an au osomal
dominan ( GFBI gene o chromosome 5q31) disorder ha causes damage and scar-ring o Bowman’s membrane and he an erior s roma.
Symptoms Severe recurren corneal erosions rom a
young age, even soon af er bir h Progression o he condi ion leads o
reduced vision ha occurs in he second o hird decades o li e, al hough in severe cases i can occur in he rs decade.
Signs Honeycomb appearance due o re icular,
ring-shaped, subepi helial opaci ies ha are mos dense cen rally bu may involve he
en ire cornea. Wi h ime, hey can progress deeper in o he s roma ( Fig. 5-3 A–D).
Dif erential Diagnosis O her an erior or s romal dys rophies
(e.g., epi helial basemen membrane dys ro-phy, granular dys rophy, macular dys rophy)
Treatment Mild cases: lubrica ion More severe cases: bandage sof con ac
lenses, super cial kera ec omy, excimer laser P K, mid-s romal or deep an erior lamellar kera oplas y, or pene ra ing kera oplas y may be necessary.
Prognosis Excimer laser P K can be qui e success ul
in improving vision and decreasing pain ul episodes in many cases. Kera oplas y may be required in advanced cases. Recurrence in he donor graf is common af er corneal ransplan- a ion and also af er P K ( Fig. 5-3 E and F). P K can of en be repea ed or per ormed or recurrence af er kera oplas y.
LWBK961-C05_p102-141.indd 110 22/07/11 9:01 AM

Anterior Corneal Dystrophies 111
FIGURE 5-3. Reis Bücklers dys rophy. A. A sligh re icular pat ern can be seen mainly in he cen ral cornea in his eye wi h rela ively mild Reis-Bücklers dys rophy. B. T is eye has modera e changes o Reis-Bücklers dys rophy. I primarily involves he cen ral cornea, bu he opaci y approaches he limbus in eriorly.
(continued)
A
B
LWBK961-C05_p102-141.indd 111 22/07/11 9:01 AM

112 5 CORNEAL DYSTROPHIES
C
D
FIGURE 5-3. (Continued) Reis Bücklers dys rophy. C. T is eye wi h advanced Reis-Bücklers dys rophy has di use, re icular, limbus- o-limbus subepi helial and an erior s romal opaci y. T ere are ew i any clear spaces. D. T is eye also has advanced Reis-Bücklers dys rophy. For una ely, he vision improved signi can ly a er excimer laser P K.
(continued)
LWBK961-C05_p102-141.indd 112 22/07/11 9:01 AM

Anterior Corneal Dystrophies 113
E
F
FIGURE 5-3. (Continued) Reis Bücklers dys rophy. E. Recurren Reis-Bücklers a ew years a er a pene ra ing kera oplas y. Un or una ely, Reis-Bücklers recurs rela ively rapidly a er corneal ransplan a ion. F. T is eye also has recurren Reis-Bücklers dys rophy several years a er pene ra ing kera oplas y. No e he honeycomb opaci y cen rally and involvemen o he en ire corneal periphery.
LWBK961-C05_p102-141.indd 113 22/07/11 9:01 AM

114 5 CORNEAL DYSTROPHIES
GELA INOUS D OP–LIKE CO NEAL DYS OPHY
Gela inous drop–like corneal dys rophy is a rare condi ion ha causes signi can
symp oms early in li e.
Etiology and Pathology Gela inous drop–like corneal dys rophy
is an au osomal recessive condi ion ( umor-associa ed calcium signal ransducer 2 gene o chromosome 1p32)
His opa hology: subepi helial and s romal amyloid deposi s
Symptoms Severe decreased vision, pain, redness,
pho ophobia, and earing beginning in he rs wo decades o li e.
Signs T ere are a varie y o presen a ions,
including rela ively a subepi helial opaci- ies similar o band kera opa hy, small or large groups o eleva ed nodules (“mulberry”
pat ern) ( Fig. 5-4 A), and larger nodular lesions (“kumqua ” pat ern).
Super cial and deep neovasculariza ion may develop.
Super cial and deep s romal opaci ca ion may also develop.
Dif erential Diagnosis O her an erior or s romal dys rophies
(e.g., macular dys rophy, Reis-Bücklers dys- rophy, granular dys rophy)
Treatment Mild cases: lubrica ion More severe cases: bandage sof con ac
lenses, super cial kera ec omy, excimer laser P K, mid-s romal or deep an erior lamellar kera oplas y, or pene ra ing kera oplas y may be necessary.
Prognosis Poor, because he condi ion ypically
recurs wi hin a ew years ( Fig. 5-4 B). Rarely, a kera opros hesis may be required i here is good op ic nerve and macular unc ion.
LWBK961-C05_p102-141.indd 114 22/07/11 9:01 AM

Anterior Corneal Dystrophies 115
FIGURE 5-4. Gela inous drop–like dys rophy. A. C onf uen severe cen ral “mulberry-like” eleva ed lesions are seen in his man wi h gela inous drop–like dys rophy. Ob aining good pho ographs was di cul due o in ense pho ophobia. B. Approxima ely 2 years a er pene ra ing kera oplas y, here was signi can symp oma ic recurrence o he nodules. T is pa ien is he sis er o he pa ien seen in A .
A
B
LWBK961-C05_p102-141.indd 115 22/07/11 9:01 AM

116 5 CORNEAL DYSTROPHIES
STROMAL CORNEAL DYSTROPHIES
GR NULA DYS OPHY
Granular dys rophy is an uncommon dis-order ha can cause decreased vision
and recurren pain ul erosions in young adul s.
Etiology and Pathology Granular dys rophy is an au osomal domi-
nan ( GFBI gene o chromosome 5q31) disorder ha becomes mani es during he rs or second decade o li e.
His opa hology: Hyaline deposi s s ain brigh red wi h Masson richrome.
Symptoms Pain ul recurren erosions are uncommon,
bu hey may occur be ore vision is signi -can ly a ec ed.
Decreased vision occurs in young adul -hood and middle age, when he corneal opaci ies become con uen .
Signs Small, discre e, whi e granules (“crushed
breadcrumbs”) wi hin he cen ral an erior s roma, separa ed by clear in ervening spaces. Wi h ime, he lesions ex end deeper wi hin
he s roma and become larger and more numerous. Wi h more ime, super cial lesions become con uen over he pupillary axis, severely a ec ing vision. T e periphery is spared ( Fig. 5-5 ).
Dif erential Diagnosis O her an erior or s romal dys rophies (e.g.,
Reis-Bücklers dys rophy, macular dys rophy)
Treatment Mild cases: lubrica ion More severe cases: bandage sof con ac
lenses, super cial kera ec omy, excimer laser P K, mid-s romal or deep an erior lamellar kera oplas y, or pene ra ing kera oplas y may be necessary.
Prognosis Excimer laser P K can be qui e success ul
in improving vision and decreasing pain ul episodes in many cases. Lamellar or pene ra -ing kera oplas y may be required in advanced cases. Recurrence in he donor graf is com-mon af er corneal ransplan a ion and also af er P K, al hough i akes longer han af er surgery or Reis-Bücklers dys rophy. P K can of en be repea ed or per ormed or recurrence af er kera oplas y.
LWBK961-C05_p102-141.indd 116 22/07/11 9:01 AM

Stromal Corneal Dystrophies 117
FIGURE 5-5. Granular dys rophy. A. T is eye wi h mild granular dys rophy has minimal opaci y and s ill re ains excellen vision. T ere are numerous discre e whi e, “crushed breadcrumb” opaci ies cen rally wi h clear in ervening spaces. B. T e same eye seen in re roillumina ion o he re ina; he granules are highligh ed.
(continued)
A
B
LWBK961-C05_p102-141.indd 117 22/07/11 9:01 AM

118 5 CORNEAL DYSTROPHIES
C
D
FIGURE 5-5. (Continued) Granular dys rophy. C. T is eye wi h granular dys rophy has rela ively conf uen opaci ies al hough he granules are small and no very dense. D. T is sli -beam view demons ra es some o he granular opaci ies o be ra her super cial.
(continued)
LWBK961-C05_p102-141.indd 118 22/07/11 9:01 AM

Stromal Corneal Dystrophies 119
E
F
FIGURE 5-5. (Continued) Granular dys rophy. E. T is eye has a combina ion o he f a “crushed breadcrumb” opaci ies and he more hree-dimensional dense whi e s ella e opaci ies. T e in ervening spaces are s ill rela ively clear. F. T e larger, denser, deeper granules are hidden by almos conf uen , very an erior s romal opaci ies. T e Vision is poor. For una ely, he conf uen an erior opaci ies are o en rea able wi h excimer laser P K.
LWBK961-C05_p102-141.indd 119 22/07/11 9:01 AM

120 5 CORNEAL DYSTROPHIES
LAT ICE DYS OPHY
Lat ice dys rophy is an uncommon disor-der ha ypically causes recurren pain ul
erosions in young adul s and decreased vision la er in li e.
Etiology and Pathology Lat ice dys rophy can be subdivided in o
several ypes: ype I: au osomal dominan inheri-
ance ( GFBI gene o chromosome 5q31). Fine, branching, re rac ile lines wi hin he an erior or mid-s roma, sparing he corneal periphery. T is is by ar he mos common orm.
ype II (Mere oja’s syndrome): associa ed wi h sys emic amyloidosis and has au osomal dominan inheri ance (gelsolin gene o chro-mosome 9q34). Lat ice lines are hicker bu less numerous han in ype I; he lines begin peripherally and progress cen rally. Visual acui y is usually good, wi h minimal recurren erosions.
ypes III and IV: au osomal dominan inheri ance ( GFBI gene o chromosome 5q31). Lat ice lines are coarser or hinner han in ype I and go rom limbus o lim-bus. T ere may no be recurren erosions.
His opa hology: amyloid deposi s, which s ain pinkish red wi h Congo red dye, me achroma ic wi h crys al viole s ain, and demons ra e apple-green bire ringence when viewed wi h polarized ligh .
Symptoms Pain ul recurren corneal erosions are
common and can occur in childhood or early
adul hood. Vision ypically declines af er early adul hood.
Signs Cen ral, branching, re rac ile lines (seen
well wi h re roillumina ion), subepi helial whi e do s, and di use an erior s romal haze can be seen early in he disease. La er, signi -can subepi helial brosis and scarring can occur ( Fig. 5-6 ).
Dif erential Diagnosis Polymorphic amyloid degenera ion (PAD):
a condi ion o older pa ien s, wi h no pain ul erosions, no decreased vision, and no am-ily his ory o cornea problems. Few or many re rac ile amyloid do s or lines are seen in he s roma, ypically cen rally (see Fig. 6-1 E–H in Chap er 6).
Treatment Mild cases: lubrica ion More severe cases: bandage sof con ac
lenses, super cial kera ec omy, excimer laser P K, mid-s romal or deep an erior lamellar kera oplas y, or pene ra ing kera oplas y may be necessary.
Prognosis Excimer laser P K can be success ul in
improving vision and decreasing pain ul episodes in some cases. Lamellar or pene ra -ing kera oplas y may be required in o hers. Recurrence in he donor graf is common af er corneal ransplan and also af er P K, al hough i akes longer han af er surgery or Reis-Bücklers dys rophy. P K can of en be repea ed or per ormed or recurrence af er kera oplas y.
LWBK961-C05_p102-141.indd 120 22/07/11 9:01 AM

Stromal Corneal Dystrophies 121
A
B
FIGURE 5-6. Lat ice dys rophy. A. T is eye has mild ype I lat ice dys rophy. No e he ne, branching lines ha appear gray-whi e on direc illumina ion and re rac ile on re roillumina ion o he iris. B. T is eye wi h ype I lat ice dys rophy has modera ely advanced disease. T ere are mul iple, rela ively hick lat ice lines cen rally and in he m idperiphery.
(continued)
LWBK961-C05_p102-141.indd 121 22/07/11 9:01 AM

122 5 CORNEAL DYSTROPHIES
C
D
FIGURE 5-6. (Continued) Lat ice dys rophy. C. T is eye wi h ype I lat ice dys rophy has cen ral an erior s romal haze due o numerous previous episodes o recurren erosions. T ere is subepi helial brosis cen rally. O en, his scarring leads o diminished recurren erosions bu grea ly impedes vision. Re rac ile lat ice lines are s ill visible. D. Re roillumina ion o he re ina highligh s he re rac ile amyloid deposi s in lat ice dys rophy.
LWBK961-C05_p102-141.indd 122 22/07/11 9:01 AM

Stromal Corneal Dystrophies 123
MACULA DYS OPHY
Macular dys rophy is a rela ively rare dis-order ha ypically causes glare and
decreased vision in young adul li e.
Etiology and Pathology Macular dys rophy is an au osomal reces-
sive (carbohydra e sul o rans erase 6 gene o chromosome 16q22) disorder. I can be subdivided in o wo ypes hrough blood es ing:
ype I: presen s in childhood and is more common; lacks kera an sul a e in he cornea
ype II: presen s in he second decade, and kera an sul a e is presen in he cornea
His opa hology: acid mucopolysaccha-ride (glycosaminoglycan) deposi s, which s ain wi h colloidal iron and Alcian blue s ains
Symptoms Glare and decreased vision in young adul s May have pain ul recurren erosion
symp oms
Signs Cen ral, gray-whi e, ill-de ned bu rela-
ively ocal opaci ies wi h di use cloudiness o he in ervening s roma (Fig. 5-7A–C).
T e cornea is usually hinner han normal. T e lesions ex end rom limbus o limbus
and even ually involve he en ire s romal hickness.
T e cen ral lesions are super cial, while he peripheral lesions are deep ( Fig. 5-7D ). May have associa ed cornea gut a a.
Dif erential Diagnosis O her an erior or s romal dys rophies
(e.g., Reis-Bücklers dys rophy, granular dys rophy)
Treatment Vision is usually a ec ed by he hird
decade and requires a corneal ransplan . Excimer laser P K may be help ul o remove super cial cen ral opaci ies.
Prognosis Good wi h corneal ransplan a ion.
Recurrence af er kera oplas y is uncommon and occurs la e.
LWBK961-C05_p102-141.indd 123 22/07/11 9:01 AM

124 5 CORNEAL DYSTROPHIES
FIGURE 5-7. Macular dys rophy. A. Small paracen ral ovoid creamy-whi e opaci ies are seen in his eye wi h rela ively mild macular dys rophy. No e ha he en ire cornea is sligh ly hazy. B. T is eye wi h macular dys rophy has cen ral opaci ies o various shapes and sizes. Al hough hey are ain , hese opaci ies are also presen in he corneal periphery. T e en ire cen ral cornea is involved, wi h a conf uen s romal opaci y, so here are no clear zones be ween he dense macules.
(continued)
A
B
LWBK961-C05_p102-141.indd 124 22/07/11 9:01 AM
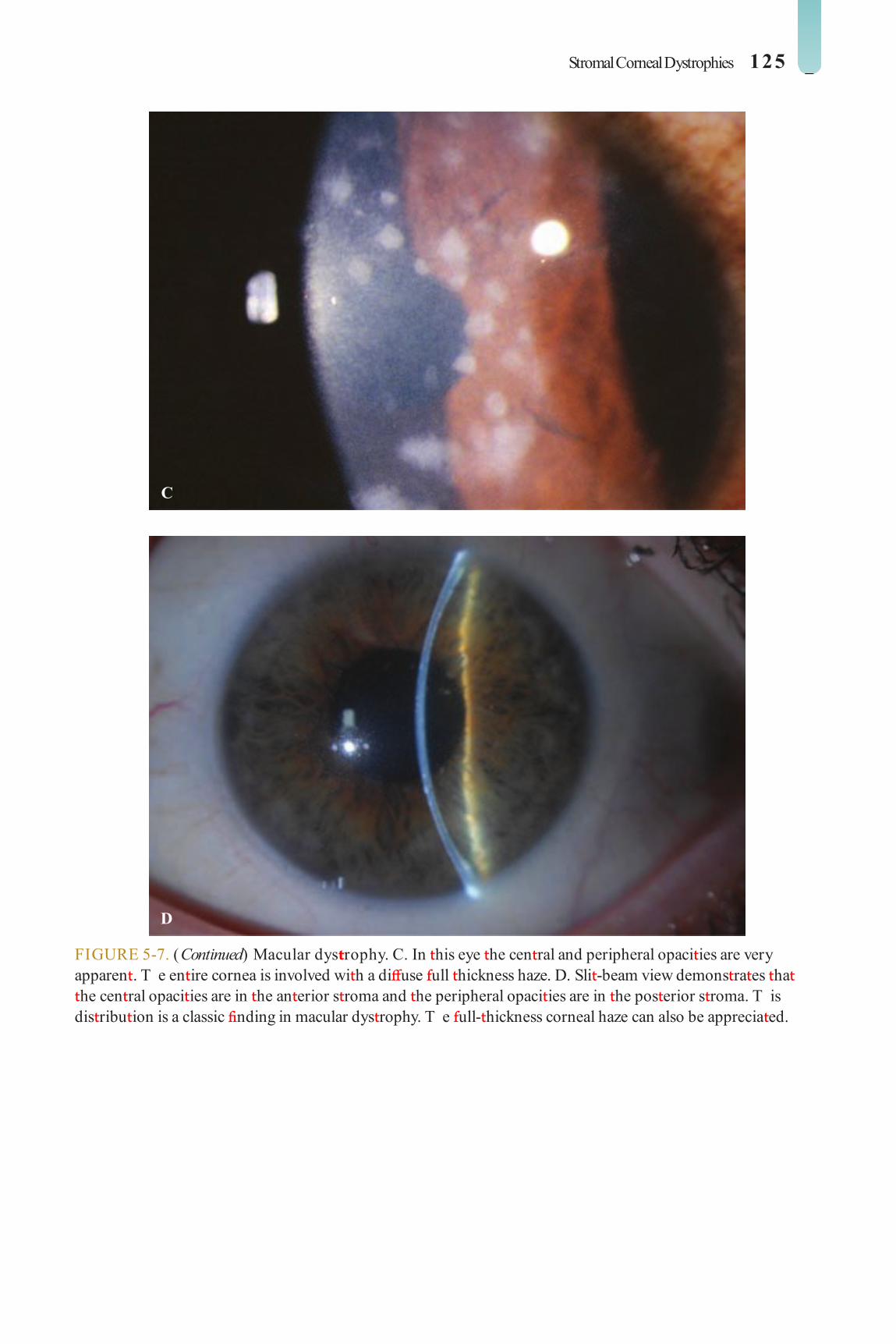
Stromal Corneal Dystrophies 125
C
D
FIGURE 5-7. (Continued) Macular dys rophy. C. In his eye he cen ral and peripheral opaci ies are very apparen . T e en ire cornea is involved wi h a di use ull hickness haze. D. Sli -beam view demons ra es ha he cen ral opaci ies are in he an erior s roma and he peripheral opaci ies are in he pos erior s roma. T is dis ribu ion is a classic nding in macular dys rophy. T e ull- hickness corneal haze can also be apprecia ed.
LWBK961-C05_p102-141.indd 125 22/07/11 9:01 AM

126 5 CORNEAL DYSTROPHIES
AVELLINO CO NEAL DYS OPHY (GR NULA -LAT ICE)
Avellino dys rophy is a varian o granular dys rophy wi h signi can amyloid depo-
si ion similar o lat ice dys rophy. I causes symp- oms similar o hose o granular dys rophy.
Etiology and Pathology Avellino dys rophy is an au osomal domi-
nan ( GFBI gene o chromosome 5q31) disorder ha becomes mani es during he rs ew decades o li e.
His opa hology: consis s o bo h hyaline and amyloid deposi s
Symptoms Pain ul recurren erosions are more com-
mon han in granular dys rophy. Decreased vision occurs in middle age,
when he cen ral corneal opaci ies become con uen .
Signs An erior s romal “crushed breadcrumb”
opaci ies sugges ive o granular dys rophy, associa ed wi h deeper s romal re rac ile lines
similar o hose ound in lat ice dys rophy ( Fig. 5-8 )
Dif erential Diagnosis O her an erior or s romal dys rophies
(e.g., Reis-Bücklers dys rophy, granular dys- rophy, lat ice dys rophy)
Treatment Mild cases: lubrica ion More severe cases: bandage sof con ac
lenses, super cial kera ec omy, excimer laser P K, mid-s romal or deep an erior lamellar kera oplas y, or pene ra ing kera oplas y may be necessary.
Prognosis Excimer laser P K can be qui e success ul
in improving vision and decreasing pain ul episodes in many cases.
Lamellar or pene ra ing kera oplas y may be required in advanced cases.
Recurrence in he donor graf is common af er corneal ransplan and also af er P K, al hough i akes longer han af er surgery or Reis-Bücklers dys rophy. P K can of en be repea ed or per ormed or recurrence af er kera oplas y.
LWBK961-C05_p102-141.indd 126 22/07/11 9:01 AM

Stromal Corneal Dystrophies 127
FIGURE 5-8. Avellino dys rophy. A. T is righ eye demons ra es charac eris ics o bo h granular and lat ice dys rophy. T ere are several “crushed breadcrumb” opaci ies along wi h he re rac ile lines o lat ice dys rophy. B. T e pa ien ’s le eye has similar ea ures.
A
B
LWBK961-C05_p102-141.indd 127 22/07/11 9:01 AM

128 5 CORNEAL DYSTROPHIES
SCHNYDE ’S CO NEAL DYS OPHY
Schnyder’s corneal dys rophy is a condi ion associa ed wi h choles erol deposi ion in
he cornea. T ere are ew ocular symp oms un il la e in li e, al hough he deposi s may be seen early.
Etiology T is is an uncommon, au osomal domi-
nan (UBIAD1 gene o chromosome 1p36) condi ion associa ed wi h hypercholes erol-emia and hyper riglyceridemia.
I can be associa ed wi h sys emic hyper-lipidemia or hypercholes erolemia. I may also be associa ed wi h genu valgum and xan helasma.
Symptoms Glare symp oms in adul hood. In advanced
cases, pa ien s can develop decreased vision.
Signs Fine ring o yellowish-whi e crys alline
choles erol deposi s mainly involving he
cen ral an erior s roma in hal o pa ien s ( Fig. 5-9 A–C)
Of en associa ed wi h a prominen arcus lipoides
A ull- hickness cen ral s romal haze devel-ops in la er s ages ( Fig. 5-9 D).
Dif erential Diagnosis O her causes o corneal crys als (e.g.,
in ec ious crys alline kera opa hy, cys ino-sis, gou , mul iple myeloma, monoclonal gammopa hies)
Treatment Check as ing choles erol and riglyceride
levels. Excimer laser P K or corneal ransplan a-
ion is occasionally needed la e in li e in eyes wi h severe corneal opaci y.
Prognosis Vision is usually good, and corneal rans-
plan is ypically no necessary. P K can be used o remove he super cial crys als in pa ien s wi h severe glare. Recurrence af er P K or kera oplas y is rare.
LWBK961-C05_p102-141.indd 128 22/07/11 9:01 AM

Stromal Corneal Dystrophies 129
FIGURE 5-9. Schnyder’s corneal dys rophy. A. T is young adul wi h Schnyder’s corneal dys rophy has he cen ral super cial crys als, bu minimal cen ral s romal haze and arcus lipoides. B. T e hree classic charac eris ics o Schnyder’s corneal dys rophy are eviden in his eye. T e cen ral, super cial crys alline opaci ies, ull- hickness s romal haze, and dense peripheral arcus lipoides are all apparen . T e cen ral crys als can have a denser annular pat ern as in his eye.
(continued)
A
B
LWBK961-C05_p102-141.indd 129 22/07/11 9:01 AM

130 5 CORNEAL DYSTROPHIES
C
D
FIGURE 5-9. (Continued) Schnyder’s corneal dys rophy. C. In his high-magni ca ion view, he super cial crys als and underlying s romal haze are visible. T e edge o he arcus lipoides can also be seen. D. T is pa ien , wi h a amily his ory o Schnyder’s corneal dys rophy, had he noncrys alline orm. T e cen ral ull- hickness opaci y and arcus lipoides are presen . Approxima ely 50% o eyes wi h Schnyder’s corneal dys rophy do no have crys als.
LWBK961-C05_p102-141.indd 130 22/07/11 9:01 AM

Posterior Corneal Dystrophies 131
POSTERIOR CORNEAL DYSTROPHIES
ENDO HELIAL DYS OPHY AND FUCHS’ DYS OPHY
Endo helial dys rophy and Fuchs’ dys ro-phy represen a con inuum o disease
involving abnormali ies in Desceme ’s mem-brane ha a ec he endo helial cells. Be ore s romal edema occurs, he condi ion is ermed endo helial dys rophy; af er s romal edema develops, i is ermed Fuchs’ dys rophy.
Etiology, Epidemiology, and Pathology Endo helial dys rophy is a common condi-
ion ha may proceed o Fuchs’ dys rophy over a period o years.
Fuchs’ dys rophy ypically occurs af er he f h or six h decade, more commonly in women.
Inheri ance is ypically au osomal domi-nan bu can be recessive. Associa ed wi h gene ic varia ion in he ranscrip ion ac or 4 gene on chromosome 18q21.
His opa hology: iny, cen ral excrescences o a hickened Desceme ’s membrane known as cornea gut a a; pigmen on he endo helium
Specular microscopy: variable endo helial size (polymege hism) and shape (pleomor-phism), numerous dark areas, reduced num-ber o endo helial cells
Symptoms Generally asymp oma ic in endo helial
dys rophy. Mildly decreased visual acui y and poor-quali y vision can be seen in eyes wi h modera e endo helial dys rophy, which wors-ens in early s ages o Fuchs’ dys rophy.
Modera e visual loss develops la er, as pos erior s romal edema increases. When epi helial edema develops, here is of en a signi can decrease in vision. Pa ien s gener-
ally have worse vision upon awakening in he morning, which improves over several hours.
As epi helial edema worsens, bullae, which can rup ure, can cause severe pain.
Signs iny, cen ral excrescences o Desceme ’s
membrane known as cornea gut a a are seen. T e con uence o lesions gives rise o a “bea en-me al” appearance ( Fig. 5-10 A and B).
A variable amoun o pigmen on he endo helium and a gray, hickened appear-ance o Desceme ’s membrane ( Fig. 5-10 C)
S romal edema develops, giving rise o a hickened cornea (Fuchs’ dys rophy) ( Fig. 5-10 D and E).
Epi helial edema and bullae (bullous kera- opa hy) orm, which may rup ure, causing irri a ion and pain ( Fig. 5-10 F). Years o bul-lae orma ion can cause scarring and brosis, wi h ewer pain ul symp oms bu poorer vision ( Fig. 5-10 G).
Increased incidence o hyperopia, narrow angles, and glaucoma.
Dif erential Diagnosis Aphakic and pseudophakic bullous kera-
opa hy: af er ca arac surgery Pos erior polymorphous corneal dys ro-
phy: linear, bandlike, vesicular, or grouped con gura ions wi h irregular edges a he level o Desceme ’s membrane
Treatment rea men in early s ages includes hyper-
onic saline, lubrica ion, and lowering in ra-ocular pressure. When mild epi helial edema is presen , blowing warm air rom a hair dryer held a arm’s leng h over he eyes or 5 o 10 minu es each morning can improve some pa ien s’ vision earlier in he day.
LWBK961-C05_p102-141.indd 131 22/07/11 9:01 AM

132 5 CORNEAL DYSTROPHIES
When vision is signi can ly impaired, endo- helial or pene ra ing kera oplas y is indica ed.
Prognosis Endo helial dys rophy uncommonly pro-
gresses o Fuchs’ dys rophy. Ca arac surgery
may precipi a e developmen o persis en corneal edema in eyes wi h endo helial dys- rophy. Mild o modera e Fuchs’ dys rophy can of en be managed success ully wi hou surgery, bu i a corneal ransplan is required, he success ra e is very good.
FIGURE 5-10. Fuchs’ dys rophy. A. A hickened Desceme ’s membrane wi h a corruga ed or “orange peel” pat ern o he endo helial cell layer is apparen in his eye wi h mild Fuchs’ dys rophy. B. Using re roillumina ion o he re ina, he “bea en-me al” pat ern o cornea gut a a can easily be apprecia ed.
(continued)
A
B
LWBK961-C05_p102-141.indd 132 22/07/11 9:01 AM

Posterior Corneal Dystrophies 133
C
D
FIGURE 5-10. (Continued) Fuchs’ dys rophy. C. T is eye wi h mild Fuchs’ dys rophy has mild s romal edema wi h some Desceme ’s olds. T ere are some secondary epi helial basemen membrane changes a he 5 o’clock edge o he pupil. Brown pigmen on he endo helium can be seen cen rally. D. In his eye wi h modera e Fuchs’ dys rophy, s romal edema has caused cen ral corneal clouding and decreased vision.
(continued)
LWBK961-C05_p102-141.indd 133 22/07/11 9:01 AM

134 5 CORNEAL DYSTROPHIES
E
F
FIGURE 5-10. (Continued) Fuchs’ dys rophy. E. Sli -beam view o he same eye demons ra es cen ral corneal hickening. T e irregular ligh ref ex is due o mild microcys ic edema. F. Sli -beam view o his eye wi h more advanced Fuchs’ dys rophy no only reveals cen ral s romal edema, bu also a large epi helial bulla in erocen rally.
(continued)
LWBK961-C05_p102-141.indd 134 22/07/11 9:01 AM
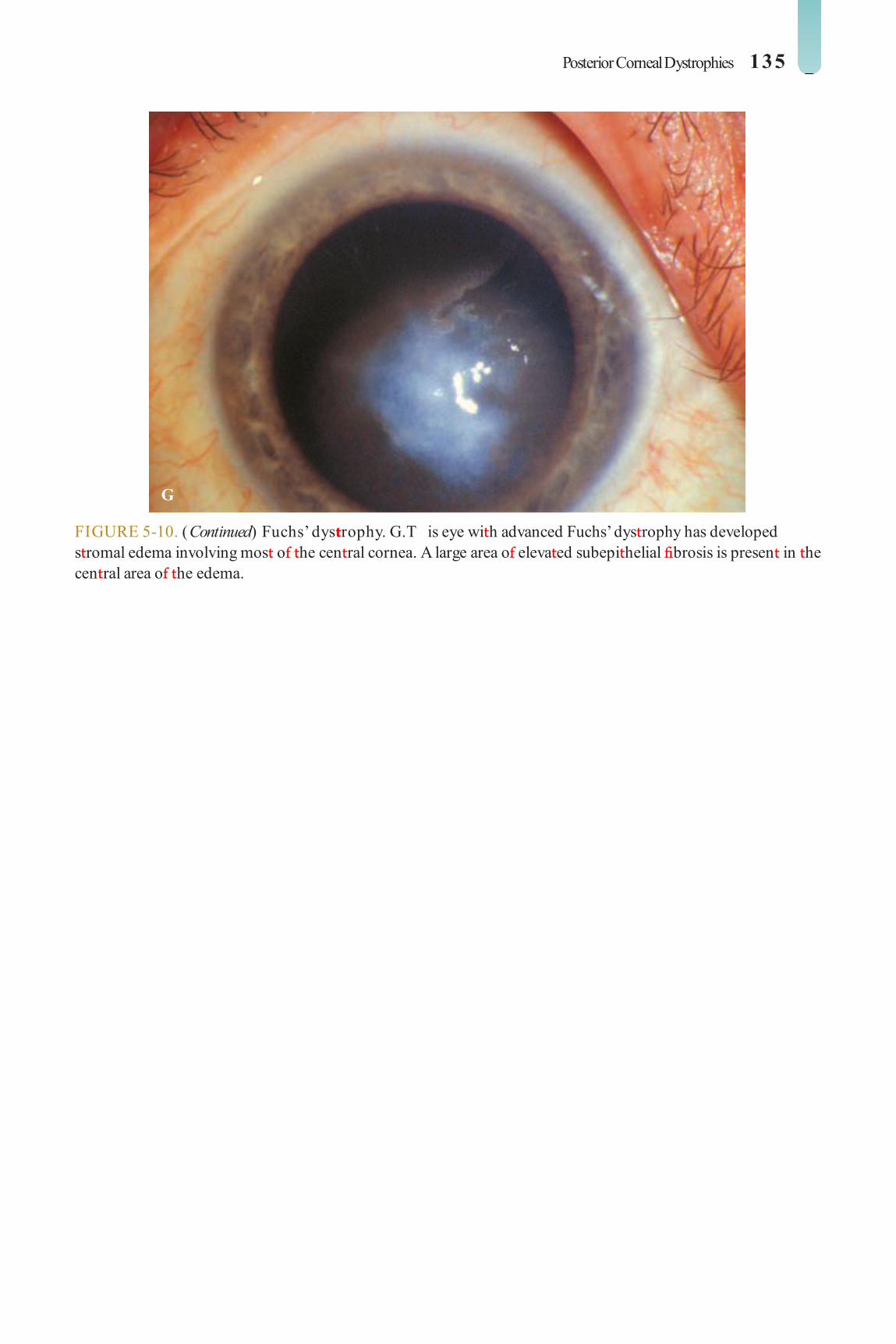
Posterior Corneal Dystrophies 135
G
FIGURE 5-10. (Continued) Fuchs’ dys rophy. G. T is eye wi h advanced Fuchs’ dys rophy has developed s romal edema involving mos o he cen ral cornea. A large area o eleva ed subepi helial brosis is presen in he cen ral area o he edema.
LWBK961-C05_p102-141.indd 135 22/07/11 9:01 AM

136 5 CORNEAL DYSTROPHIES
POS E IO POLYMO PHOUS CO NEAL DYS OPHY
Pos erior polymorphous corneal dys ro-phy is an uncommon condi ion charac-
erized by various abnormali ies o Desceme ’s membrane and he endo helium.
Etiology and Pathology T is is an uncommon, au osomal domi-
nan , markedly variable condi ion a ec ing Desceme ’s membrane and endo helium. T e signs and symp oms can be very variable even wi hin members o he same amily.
His opa hology: Endo helial cells look like epi helial cells in ha hey have microvilli and s ain posi ive or kera in.
Symptoms Onse o symp oms may occur a bir h,
bu many pa ien s are asymp oma ic. T e main symp om is decreased vision
due o corneal edema. Pain can occur i cor-neal bullae develop.
Signs Linear, bandlike, vesicular, or grouped
con gura ions wi h irregular, of en scalloped edges a he level o Desceme ’s membrane. T e lesions are requen ly asymme ric. T ere
may be corneal edema in advanced cases ( Fig. 5-11 ).
O hose a ec ed, 15% have glaucoma. May be associa ed wi h iridocorneal adhe-sions and corec opia
May be associa ed wi h Alpor ’s syndrome (heredi ary nephri is and sensorineural hear-ing loss)
Dif erential Diagnosis Iridocorneal endo helial syndrome: unila -
eral and nonheredi ary
Treatment Mos pa ien s require no rea men .
Pa ien s need o be moni ored or glaucoma. I corneal edema develops, i can be
rea ed similarly o Fuchs’ dys rophy. When vision is signi can ly impaired, endo helial or pene ra ing kera oplas y is indica ed.
Prognosis Very good or re aining good vision.
When signi can iris changes are presen , he chances o glaucoma increase. Pos erior polymorphous corneal dys rophy rarely requires corneal ransplan a ion, bu i a cor-neal ransplan is required, he success ra e is good.
LWBK961-C05_p102-141.indd 136 22/07/11 9:01 AM

Posterior Corneal Dystrophies 137
A
B
FIGURE 5-11. Pos erior polymorphous corneal dys rophy. A. A large cen ral horizon al scalloped band is visible in his eye wi h pos erior polymorphous corneal dys rophy. B. Mul iple small gray areas are eviden on he endo helial sur ace in his eye wi h pos erior polymorphous corneal dys rophy.
(continued)
LWBK961-C05_p102-141.indd 137 22/07/11 9:01 AM

138 5 CORNEAL DYSTROPHIES
C
D
FIGURE 5-11. (Continued) Pos erior polymorphous corneal dys rophy. C. On direc illumina ion, a scalloped band in he endo helium is visible jus superior o he visual axis. D. On re roillumina ion o he re ina, he scalloped band is more apparen .
(continued)
LWBK961-C05_p102-141.indd 138 22/07/11 9:01 AM

Posterior Corneal Dystrophies 139
E
F
FIGURE 5-11. (Continued) Pos erior polymorphous corneal dys rophy. E. Mul iple gray-whi e opaci ies o various shapes and sizes can be seen on direc illumina ion. F. Sli -beam view o he same eye demons ra es ha he opaci ies are a he level o Desceme ’s and endo helium.
LWBK961-C05_p102-141.indd 139 22/07/11 9:01 AM

140 5 CORNEAL DYSTROPHIES
CONGENI AL HE EDI A Y ENDO HELIAL DYS OPHY
Congeni al heredi ary endo helial dys ro-phy (CHED) is an ex remely rare con-
di ion involving corneal edema a bir h or shor ly hereaf er.
Etiology and Pathology Au osomal recessive and au osomal domi-
nan orms have been described. His opa hology: abnormal or absen endo-
helial cells
Symptoms Au osomal dominan orm: presen s in
he rs 1 o 2 years o li e, is progressive, wi h no nys agmus, bu pain and pho ophobia are common
Au osomal recessive orm: presen s a bir h, is nonprogressive, nys agmus is presen , and here is no pain
Signs Bila eral, limbus- o-limbus corneal s romal
edema wi h a blue-gray ground-glass appear-ance ( Fig. 5-12 )
Corneal hickness can be wo o hree imes normal
No increase in corneal diame er or ele-va ed in raocular pressure
Dif erential Diagnosis Congeni al glaucoma: enlarged corneal
diame er, eleva ed in raocular pressure Bir h rauma: unila eral, parallel oblique
breaks in Desceme ’s membrane
Treatment Depends on degree o corneal edema.
Endo helial or pene ra ing kera oplas y may be indica ed i corneal edema is severe.
Prognosis Fair, because o he di cul y o per orm-
ing corneal ransplan a ion in children.
LWBK961-C05_p102-141.indd 140 22/07/11 9:01 AM

Posterior Corneal Dystrophies 141
FIGURE 5-12. Congeni al heredi ary endo helial dys rophy. D i use limbus- o-limbus corneal edema wi h a blue-gray ground-glass appearance is presen in his eye wi h congeni al heredi ary endo helial dys rophy.
LWBK961-C05_p102-141.indd 141 22/07/11 9:01 AM

C H A P T E R
142
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
WHITE LIMBAL GI DLE OF VOGT Whi e limbal girdle o Vog is a very com-
mon, bila eral, innocuous, age-rela ed condi- ion charac erized by chalky-whi e, crescen ic deposi s (elas o ic degenera ion) along he nasal and emporal perilimbal cornea. I may or may no be separa ed rom he limbus by a clear zone ( Fig. 6-1 B).
Pa ien s are asymp oma ic, and ocular rea men is no necessary.
C OCODILE SHAG EEN Crocodile shagreen is charac erized by
grayish-whi e, polygonal s romal opaci ies separa ed by rela ively clear spaces. T e lesions usually involve he an erior s roma (an erior crocodile shagreen), bu hey may also be ound more pos eriorly (pos erior crocodile shagreen) ( Fig. 6-1 C).
Pa ien s are asymp oma ic, and ocular rea men is no necessary.
Corneal Degenera ions and Deposi s
INVOLUTIONAL CHANGES
CO NEAL A CUS Corneal arcus is a very common, bila eral
condi ion ha may be ei her age-rela ed (arcus senilis) or associa ed wi h hyperlipid-emia in younger individuals (arcus lipoides).
Lipid deposi s begin in eriorly, hen superi-orly, and la er ex end circum eren ially o orm a whi e perilimbal band abou 1 mm in diame- er wi h a sharp ou line peripherally and a more dif use boundary cen rally. A clear zone o cor-nea separa es i rom he limbus ( Fig. 6-1 A).
May be accompanied by mild, nonprogres-sive hinning o he clear zone o he cornea ( urrow degenera ion)
Check or hyperlipidemia in pa ien s under age 40 years. I unila eral, check or caro id disease on he uninvolved side.
Pa ien s are asymp oma ic, and ocular rea men is no necessary.
LWBK961-C06_p142-167.indd 142 22/07/11 9:02 AM

Involutional Changes 143
CO NEA FA INATA Cornea arina a is a rela ively common
condi ion charac erized by bila eral, innocu-ous, minu e, “ our-dus ” lipo uscin-like deposi s in he deep s roma near Desceme ’s membrane. I is mos prominen cen rally.
T ese opaci ies are bes seen wi h re roil-lumina ion of he iris ( Fig. 6-1 D).
Pa ien s are asymp oma ic, and ocular rea men is no necessary.
POLYMO PHIC AMYLOID DEGENER TION
Polymorphic amyloid degenera ion is a airly common, bila eral, innocuous,
degenera ive condi ion usually seen a er he age o 50 years.
I is charac erized by varying sizes o re rac ile, punc a e, comma-shaped, and lamen ous amyloid deposi s hroughou he s roma, bu is generally mos prominen cen rally and pos eriorly. T ese deposi s are bes seen wi h re roillumina ion of he re ina ( Fig. 6-1 E–H).
I is no associa ed wi h any sys emic disorder.
Dif eren ial diagnosis: cornea arina a and lat ice dys rophy
Pa ien s are asymp oma ic, and ocular rea men is no necessary.
LWBK961-C06_p142-167.indd 143 22/07/11 9:02 AM

144 6 CORNEAL DEGENERATIONS AND DEPOSITS
B
A
FIGURE 6-1. Corneal arcus. A. A circular yellow-whi e lipid deposi ion is presen adjacen o he limbus or 360 degrees. No e he clear zone be ween he arcus and he limbus. Limbal girdle o Vogt. B. A crescen ic, rela ively dense whi e opaci y is seen a he limbus a he 9 o’clock posi ion. T ere is a small clear zone be ween he limbal girdle and he limbus.
(continued)
LWBK961-C06_p142-167.indd 144 22/07/11 9:02 AM

Involutional Changes 145
FIGURE 6-1. (Continued) Crocodile shagreen. C. Gray-whi e polygonal s romal opaci ies are eviden in his cornea. T ey may be loca ed in he an erior or he pos erior s roma. Cornea arinata. D. iny, “f our-dus ” deposi s are seen a he pupillary margin. T ese pinpoin opaci ies are loca ed in he deep s roma. T ey do no a ec vision.
(continued)
C
D
LWBK961-C06_p142-167.indd 145 22/07/11 9:02 AM

146 6 CORNEAL DEGENERATIONS AND DEPOSITS
F
FIGURE 6-1. (Continued) Polymorphic amyloid degeneration. E. Amyloid deposi s in various shapes, including do s, commas, and lines, are seen in he corneal s roma. T is condi ion is a degenera ion, no a dys rophy. I is similar o lat ice dys rophy in ha hey bo h involve amyloid deposi ion; however, lat ice dys rophy is an inheri ed condi ion ha is ypically associa ed wi h recurren erosions and decreased vision in young adul hood. F. T is eye wi h polymorphic amyloid degenera ion has dense cen ral amyloid deposi s readily seen in re roillumina ion o he re ina.
(continued)
E
LWBK961-C06_p142-167.indd 146 22/07/11 9:02 AM

Involutional Changes 147
G
H
FIGURE 6-1. (Continued) Polymorphic amyloid degeneration. G. Mul iple small gray-whi e polymorphic amyloid degenera ion opaci ies are presen , primarily in he mid-periphery, in his elderly woman H. T e polymorphic amyloid degenera ion opaci ies in he same eye are highligh ed in re roillumina ion.
LWBK961-C06_p142-167.indd 147 22/07/11 9:02 AM

148 6 CORNEAL DEGENERATIONS AND DEPOSITS
CORNEAL DEPOSITS—NONPIGMENTED
BAND ER TOPATHY
Band kera opa hy is a common condi ion charac erized by calcium deposi s in he
subepi helial space, Bowman’s layer, and an e-rior s roma.
Etiology Ocular
Chronic ocular in amma ion (e.g., iridocycli is, juvenile rheuma oid ar hri is, corneal edema, in ers i ial kera i is, ph hi-sis bulbi)
Silicone oil in he eye, especially he an erior chamber
Me abolic Hypercalcemia or hyperphospha emia Gou Chronic renal ailure
Heredi ary: amilial O her
Chronic exposure o oxic vapors (e.g., mercury)
Idiopa hic (age-rela ed)
Symptoms O en asymp oma ic. I cen ral, vision may
be af ec ed. Ocular irri a ion can develop i hick calcium plaques ake of and cause an epi helial de ec .
Signs Peripheral, in erpalpebral plaque o cal-
cium deposi usually separa ed rom he limbus by a hin line o clear cornea ( Fig. 6-2 A–C)
T e plaque ypically begins a he nasal and emporal cornea and ex ends cen rally.
I o en con ains small holes and cle s, giving i a “Swiss cheese” appearance.
Advanced lesions may become plaquelike, nodular, and eleva ed ( Fig. 6-2 D).
Treatment Mild cases may be observed or rea ed
wi h lubrican s (e.g., ar i cial ear drops or oin men s).
Severe cases (wi h visual, pain ul, or cosme ic indica ions) can be rea ed wi h chela ion using disodium e hylenediamine e raace ic acid 3% or super cial kera ec omy using he excimer laser (pho o herapeu ic kera ec omy, or P K) or a blade.
Prognosis Excellen or he ocular calcium deposi s.
T e band kera opa hy can recur, especially i he underlying condi ion persis s.
Calcium chela ion can be repea ed i necessary.
Epi helial healing problems may occur. Vision is o en limi ed, as a resul o residual corneal scarring or o her ocular pa hology.
LWBK961-C06_p142-167.indd 148 22/07/11 9:02 AM

Corneal Deposits—Nonpigmented 149
FIGURE 6-2. Band keratopathy. A. A hin layer o calcium deposi ion can be seen adjacen o he limbus nasally and emporally. No e he hin line o clear cornea be ween he band kera opa hy and he limbus. B. T is eye had cen ral calcium deposi ion obscuring he view o he iris and pupil.
(continued)
A
B
LWBK961-C06_p142-167.indd 149 22/07/11 9:02 AM

150 6 CORNEAL DEGENERATIONS AND DEPOSITS
C
D
FIGURE 6-2. (Continued) Band keratopathy. C. T is eye has he classic limbus- o-limbus horizon al “band” o band kera opa hy. D. T is eye wi h chronic corneal edema rom herpes zos er kera opa hy has a dense cen ral plaque o calcium deposi ion. Some o he plaque spon aneously f aked o cen rally.
LWBK961-C06_p142-167.indd 150 22/07/11 9:02 AM

Corneal Deposits—Nonpigmented 151
SALZMANN’S NODULA DEGENER TION
Salzmann’s nodular degenera ion is a airly common, unila eral or bila eral condi ion
charac erized by smoo h gray-whi e eleva ed lesions o he cornea.
Etiology I is o en ound in eyes wi h a his ory o
chronic kera opa hy, such as in ers i ial kera i- is, vernal kera oconjunc ivi is, kera oconjunc- ivi is sicca, phlyc enulosis, and rachoma, bu requen ly appears in o herwise normal eyes.
Symptoms O en asymp oma ic. May af ec vision
i i involves he paracen ral or cen ral cor-nea; may cause a oreign-body sensa ion i i becomes very eleva ed
Signs Single or mul iple, discre e, whi e or gray-
whi e or occasionally bluish, smoo h, eleva ed
nodules anywhere on he sur ace o he cor-nea ( Fig. 6-3 )
Long-s anding nodules may have iron pig-men deposi ion in he epi helium a he base o he nodule.
Dif erential Diagnosis Spheroidal degenera ion: small, globular,
yellow-brown granules are ound in he super- cial corneal s roma.
Treatment Mild cases are observed or rea ed wi h lubri-
ca ion. I he nodules are causing symp oms, hey may be rea ed wi h super cial kera ec omy wi h a blade or excimer laser P K. opical mi omycin C a he ime o surgical excision may decrease he ra e o recurrence. Rarely, i severe, i may require a lamellar kera oplas y.
Prognosis Very good o excellen . Can recur a er
surgical excision
A
FIGURE 6-3. Salzmann’s nodular degeneration. A. A gray-whi e eleva ed lesion is seen in he peripheral cornea rom he 9 o 11 o’clock posi ions. T ese lesions may be single or mul iple and peripheral or cen ral. I hey are causing symp oms, hey can usually be rea ed wi h a super cial kera ec omy or excimer laser P K.
(continued)
LWBK961-C06_p142-167.indd 151 22/07/11 9:02 AM

152 6 CORNEAL DEGENERATIONS AND DEPOSITS
B
C
FIGURE 6-3. (Continued) Salzmann’s nodular degeneration. B. T is eye has approxima ely six Salzmann’s nodules superiorly. Flat er Salzmann’s opaci ies can be seen in be ween he more dis inc eleva ed nodules. C. Severe paracen ral and peripheral Salzmann’s nodular degenera ion is obvious rom approxima ely 9 o 6 o’clock.
LWBK961-C06_p142-167.indd 152 22/07/11 9:02 AM

Other Corneal Degenerations 153
OTHER CORNEAL DEGENERATIONS
SPHE OIDAL DEGENER TION Also known as Labrador’s kera opa hy,
ac inic kera opa hy, clima ic drople kera- opa hy, corneal elas osis, and Biet i’s nodular dys rophy
Spheroidal degenera ion is a rare, unila -eral or bila eral condi ion ha ypically af ec s people who work ou doors.
In erpalpebral, small, globular, yellow-brown granules are ound in he super cial corneal s roma ( Fig. 6-4 A).
T e lesions o en begin peripherally and progress cen rally. Advanced lesions can become nodular and eleva ed.
Vision becomes af ec ed when lesions are cen ral. Pa ien s can develop a oreign-body sensa ion rom eleva ed nodules.
When vision becomes impaired, rea men is wi h super cial kera ec omy wi h a blade, excimer laser P K, or lamellar or pene ra ing kera oplas y. Lesions may recur.
LIPID ER TOPATHY T is is a rela ively common unila eral con-
di ion mos requen ly associa ed wi h previ-ous herpes simplex or herpes zos er kera i is.
Unila eral, ocal, whi e or yellowish deposi s wi h ea hery edges ( Fig. 6-4 B). Secondary lesions are associa ed wi h corneal neovasculariza ion, whereas primary lesions (rare) are avascular. May appear crys alline ( Fig. 6-4 C). Rarely, he lipid may involve he en ire cornea.
Vision can be af ec ed by cen ral lipid deposi ion.
rea men is wi h opical cor icos eroids o decrease in amma ion and vasculariza- ion. I he blood vessels diminish, he lipid may improve. Laser abla ion o vessels can be at emp ed, bu hey ypically reopen. opical or subconjunc ival vascular endo- helial grow h ac or (VEGF) inhibi ors may decrease he blood vessels. Advanced cases causing poor vision may bene rom a cor-neal ransplan .
COATS’ WHITE ING Small, oval, whi e ring, 1 mm or less
in diame er, usually loca ed in he in erior cornea a he level o Bowman’s layer wi h an in ac overlying epi helium ( Fig. 6-4 D)
Represen s old me allic oreign-body injury.
Pa ien s are asymp oma ic, and ocular rea men is no necessary.
LWBK961-C06_p142-167.indd 153 22/07/11 9:02 AM
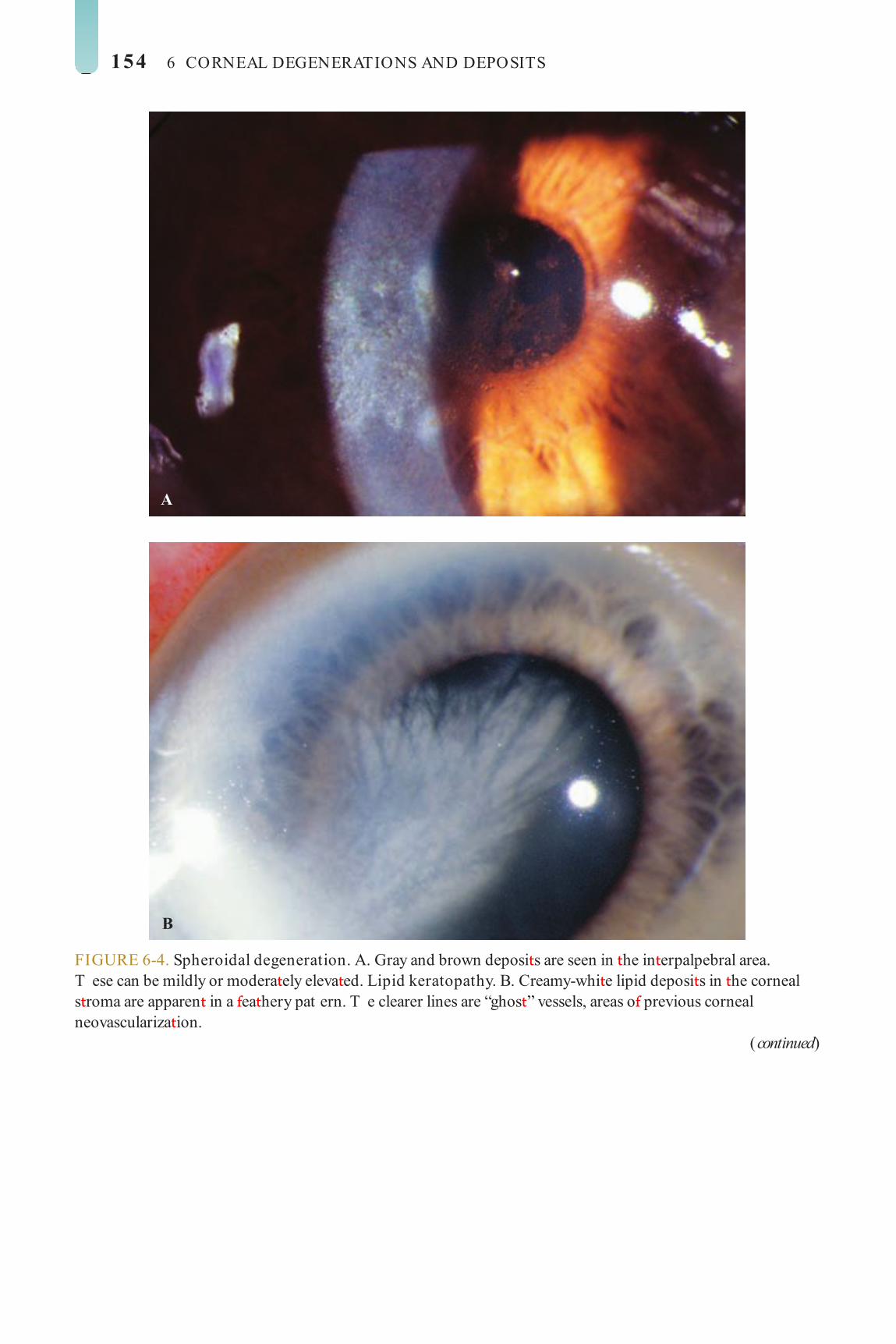
154 6 CORNEAL DEGENERATIONS AND DEPOSITS
A
B
FIGURE 6-4. Spheroidal degeneration. A. Gray and brown deposi s are seen in he in erpalpebral area. T ese can be mildly or modera ely eleva ed. Lipid keratopathy. B. Creamy-whi e lipid deposi s in he corneal s roma are apparen in a ea hery pat ern. T e clearer lines are “ghos ” vessels, areas o previous corneal neovasculariza ion.
(continued)
LWBK961-C06_p142-167.indd 154 22/07/11 9:02 AM

Other Corneal Degenerations 155
C
D
FIGURE 6-4. (Continued) Lipid keratopathy. C. Whi e s romal lipid deposi s in a crys alline pat ern are no ed cen ral o an area o corneal neovasculariza ion. Coats’ white ring. D. T is small, brigh whi e oval ring is he resul o an old me allic oreign-body injury.
LWBK961-C06_p142-167.indd 155 22/07/11 9:02 AM

156 6 CORNEAL DEGENERATIONS AND DEPOSITS
CORNEAL DEPOSITS—PIGMENTED
CO NEA VE TICILLATA (VO TEX ER TOPATHY)
Cornea ver icilla a is a condi ion ha occurs in pa ien s wi h Fabry’s disease,
bu i is ound much more commonly caused by a varie y o drugs.
Etiology Fabry’s disease: an X-linked recessive sphin-
golipidosis charac erized by cornea ver icilla a, small conjunc ival aneurysms, lens opaci ies, papilledema, op ic a rophy, and macular and re inal edema. Cornea ver icilla a is seen in males wi h Fabry’s disease and he emale car-riers. See also Mucopolysaccharidoses and Lipidoses in Chap er 8.
Drugs ha can cause cornea ver icilla a: Amiodarone (mos common)
( Fig. 6-5 )
Chloroquine Hydroxychloroquine Chlorpromazine Indome hacin A ovaquone
Signs Bila eral, symme rical, golden-brownish
epi helial deposi s arranged in a curvilinear ashion rom a poin below he pupil and swirling ou ward bu sparing he limbus
Treatment T is corneal disorder is asymp oma ic, and
no rea men is required.
Prognosis Excellen . T e drug-rela ed deposi s
end o resolve upon discon inua ion o he medica ion.
LWBK961-C06_p142-167.indd 156 22/07/11 9:02 AM

Corneal Deposits—Pigmented 157
FIGURE 6-5. Cornea verticillata. Super cial brown deposi s appearing o emana e rom a poin in he in erior cornea are apparen in his pa ien aking amiodarone. T ese deposi s do no a ec vision. T ey even ually disappear upon discon inua ion o he drug.
LWBK961-C06_p142-167.indd 157 22/07/11 9:02 AM
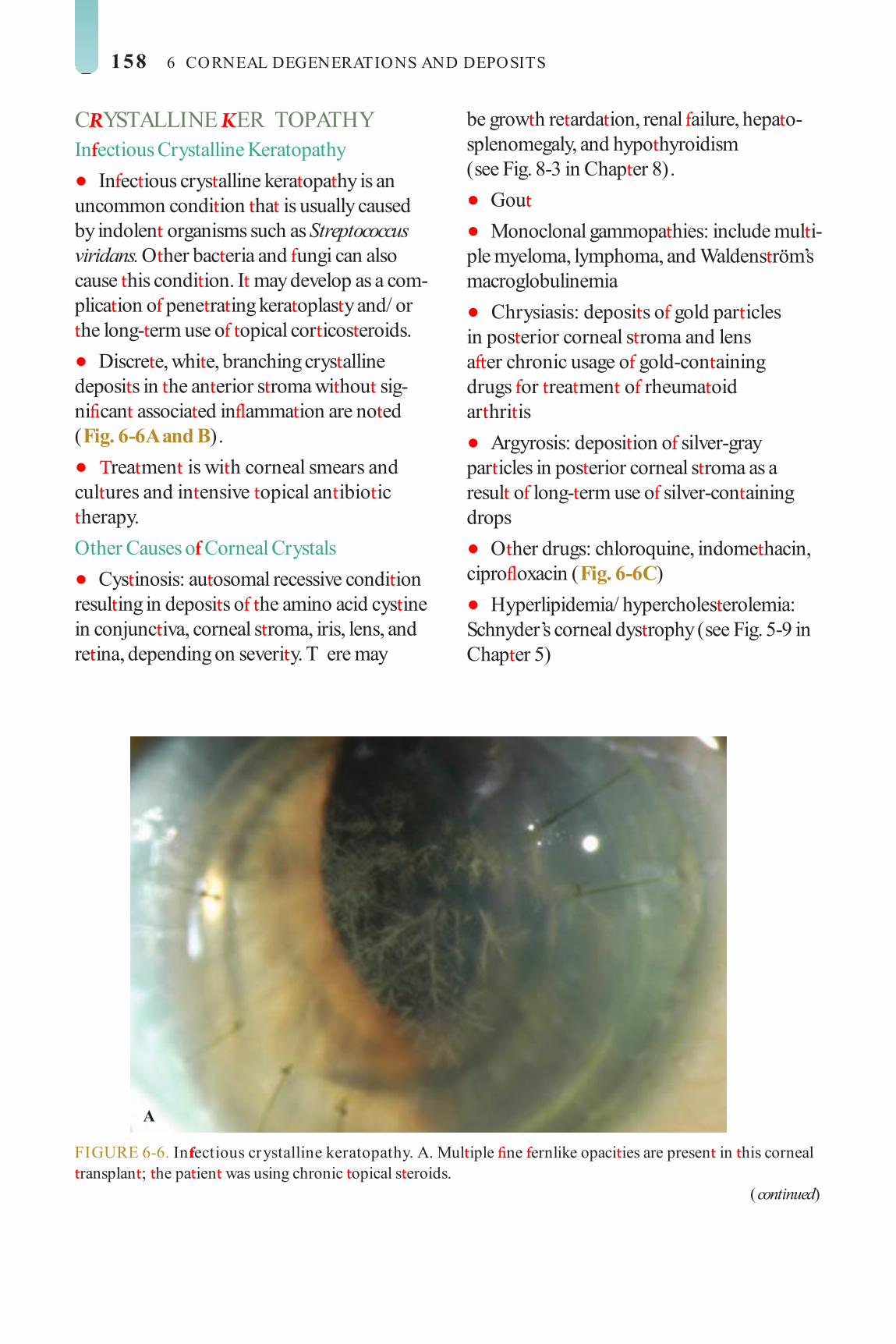
158 6 CORNEAL DEGENERATIONS AND DEPOSITS
C YSTALLINE ER TOPATHY In ectious Crystalline Keratopathy
In ec ious crys alline kera opa hy is an uncommon condi ion ha is usually caused by indolen organisms such as Streptococcus viridans. O her bac eria and ungi can also cause his condi ion. I may develop as a com-plica ion o pene ra ing kera oplas y and/ or he long- erm use o opical cor icos eroids.
Discre e, whi e, branching crys alline deposi s in he an erior s roma wi hou sig-ni can associa ed in amma ion are no ed ( Fig. 6-6 A and B).
rea men is wi h corneal smears and cul ures and in ensive opical an ibio ic herapy. Other Causes o Corneal Crystals
Cys inosis: au osomal recessive condi ion resul ing in deposi s o he amino acid cys ine in conjunc iva, corneal s roma, iris, lens, and re ina, depending on severi y. T ere may
be grow h re arda ion, renal ailure, hepa o-splenomegaly, and hypo hyroidism (see Fig. 8-3 in Chap er 8).
Gou Monoclonal gammopa hies: include mul i-
ple myeloma, lymphoma, and Waldens röm’s macroglobulinemia
Chrysiasis: deposi s o gold par icles in pos erior corneal s roma and lens a er chronic usage o gold-con aining drugs or rea men o rheuma oid ar hri is
Argyrosis: deposi ion o silver-gray par icles in pos erior corneal s roma as a resul o long- erm use o silver-con aining drops
O her drugs: chloroquine, indome hacin, cipro oxacin ( Fig. 6-6 C)
Hyperlipidemia/ hypercholes erolemia: Schnyder’s corneal dys rophy (see Fig. 5-9 in Chap er 5)
FIGURE 6-6. In ectious crystalline keratopathy. A. Mul iple ne ernlike opaci ies are presen in his corneal ransplan ; he pa ien was using chronic opical s eroids.
(continued)
A
LWBK961-C06_p142-167.indd 158 22/07/11 9:02 AM
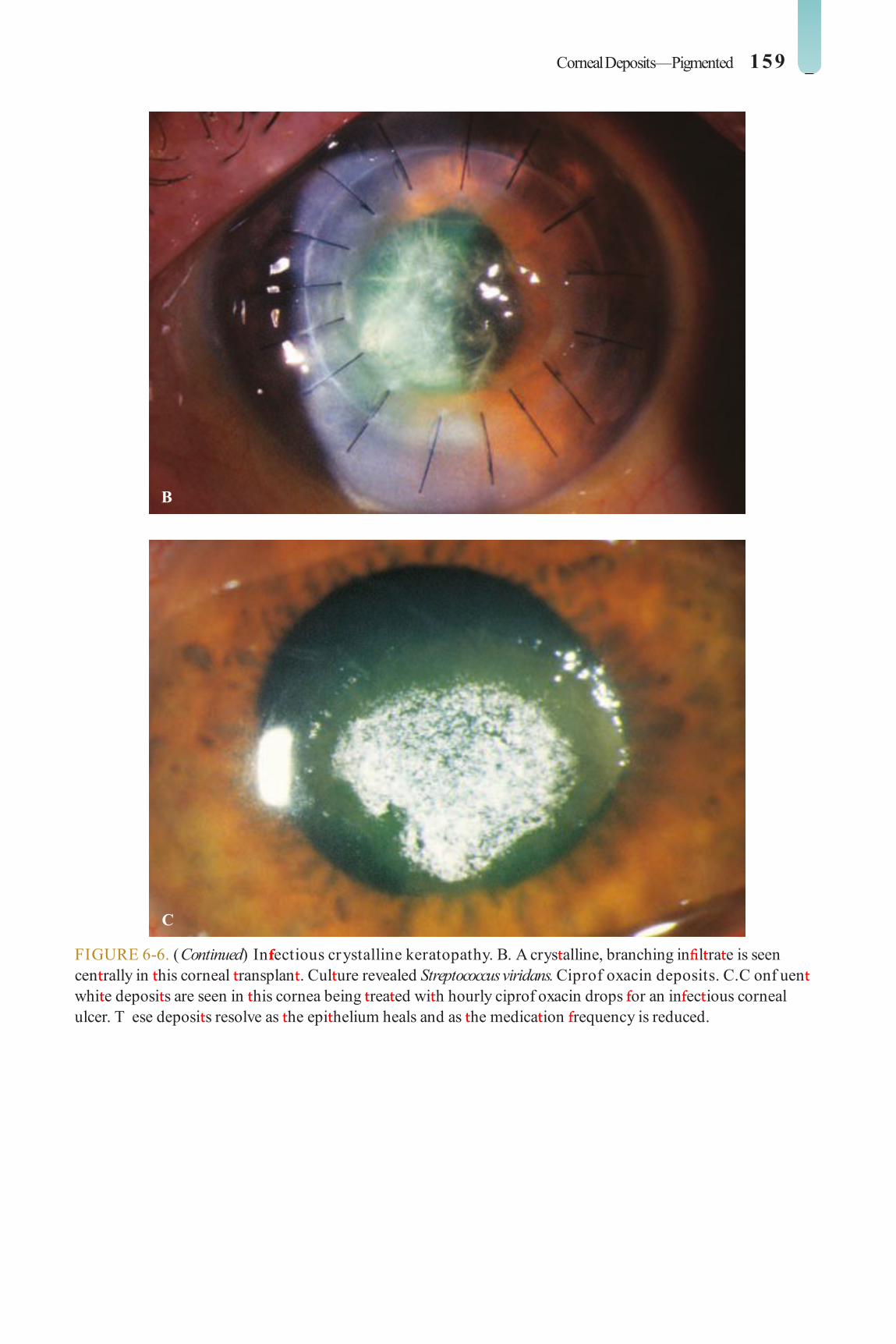
Corneal Deposits—Pigmented 159
B
C
FIGURE 6-6. (Continued) In ectious crystalline keratopathy. B. A crys alline, branching in l ra e is seen cen rally in his corneal ransplan . Cul ure revealed Streptococcus viridans. Ciprof oxacin deposits. C. C onf uen whi e deposi s are seen in his cornea being rea ed wi h hourly ciprof oxacin drops or an in ec ious corneal ulcer. T ese deposi s resolve as he epi helium heals and as he medica ion requency is reduced.
LWBK961-C06_p142-167.indd 159 22/07/11 9:02 AM

160 6 CORNEAL DEGENERATIONS AND DEPOSITS
CO NEAL I ON DEPOSITS
Epithelial Rus ring: consis s o residual rus ollow-
ing he removal o a me allic oreign body Hudson S ahli’s line: occurs a he junc-
ion o he upper wo- hirds and he lower one- hird o an o herwise normal cornea
Ferry’s line: occurs in ron o a l ering bleb ( Fig. 6-7 A)
S ocker’s line: occurs in ron o a p eryg-ium ( Fig. 6-7 A)
Fleischer’s ring: occurs a he base o he cone in kera oconus (see Fig. 4-1D in Chap er 4)
O her iron lines may be ound adjacen o corneal eleva ions in Salzmann’s degenera ion, ( Fig. 6-7 B), corneal gra s, and a er re rac- ive surgery such as radial kera o omy ( Fig. 6-7 C), pho ore rac ive kera ec omy (PRK), and laser-assis ed in si u kera omileu-sis (LASIK).
Stromal Siderosis: as a resul o an in raocular iron
oreign body Corneal blood s aining: due o hyphema,
especially an “eigh -ball” hyphema. Clears slowly rom he periphery ( Fig. 6-7 D and E)
FIGURE 6-7. Iron lines adjacent to a trabeculectomy bleb and pterygium. A. T is eye demons ra es iron lines jus cen ral o he superior rabeculec omy bleb (Ferry’s line) and nasal p erygium (S ocker’s line) .
(continued)
A
LWBK961-C06_p142-167.indd 160 22/07/11 9:02 AM

Corneal Deposits—Pigmented 161
B
C
FIGURE 6-7. (Continued) Iron line at the base o an elevated lesion. B. An iron line can be seen a he base o his long-s anding eleva ed Salzmann’s nodule. Iron line a er re ractive surgery. C. A s ella e iron line is presen cen rally in his eye wi h corneal f at ening several years a er radial kera o omy or myopia.
(continued)
LWBK961-C06_p142-167.indd 161 22/07/11 9:03 AM

162 6 CORNEAL DEGENERATIONS AND DEPOSITS
D
E
FIGURE 6-7. (Continued) Corneal blood staining. D. T ere is signi can brown corneal s romal deposi ion in his eye. T e pa ien had previously undergone an ex racapsular ca arac ex rac ion and subsequen rauma resul ing in dehiscence o he ca arac wound and a o al hyphema. T e wound was repaired, bu signi can blood s aining developed. No e ha here is some clearing o he blood s aining rom he periphery. E. C orneal blood s aining can be seen resolving rom he corneal periphery in his eye 6 mon hs a er severe ocular rauma.
LWBK961-C06_p142-167.indd 162 22/07/11 9:03 AM

Corneal Deposits—Pigmented 163
K YSE -FLEISCHE ING Bila eral, greenish brown, peripheral band
1 o 3 mm in wid h a he level o Desceme ’s membrane, which occurs primarily in Wilson’s disease
T e band rs appears in he ver ical meridian, hen ex ends o involve he en ire corneal circum erence. Early cases may require gonioscopy o visualize he deposi s ( Fig. 6-8 ; see also Fig. 8-1 in Chap er 8).
May have associa ed subcapsular len icular deposi s resul ing in a “sun ower” ca arac in Wilson’s disease.
Etiology Wilson’s disease (hepa olen icular degen-
era ion): mos common cause o a Kayser-Fleischer ring. A rare au osomal recessive condi ion caused by a de ciency o he enzyme ceruloplasmin. Charac erized by liver cirrhosis and mo or disorders. rea men wi h copper chela ing agen s such as D-penicillamine or e ra hiomolybda e may improve he condi ion and be ollowed by resolu ion o corneal deposi s.
Primary biliary cirrhosis Chronic ac ive hepa i is Mul iple myeloma
FIGURE 6-8. Kayser Fleischer ring . Sli -beam view o he in erior cornea o a pa ien wi h Wilson’s disease. No e he brown pigmen a he level o Desceme ’s membrane peripherally. In early cases, he pigmen may be seen bes using gonioscopy. See also Figure 8 -1.
LWBK961-C06_p142-167.indd 163 22/07/11 9:03 AM

164 6 CORNEAL DEGENERATIONS AND DEPOSITS
TE IEN’S MA GINAL DEGENER TION
Terrien’s marginal degenera ion is an uncom-mon, o en bila eral, painless, slowly pro-
gressive peripheral corneal hinning condi ion.
Etiology Unknown. Af ec s males more commonly
han emales, generally in he second o our h decades
Symptoms Pa ien s are asymp oma ic wi h mild dis-
ease. More advanced disease causes decreased vision rom severe agains - he-rule as igma- ism, which is commonly irregular.
Signs Nonin amed, peripheral hinning associ-
a ed wi h a vascularized pannus and lipid
deposi s cen ral o he hinned edge. T e hinning usually begins superiorly and ex ends circum eren ially, al hough i can begin in eriorly. Epi helium remains in ac ( Fig. 6-9 ).
Per ora ion is rare and is usually associa ed wi h blun rauma.
Treatment Mild cases can be rea ed wi h glasses
or so con ac lenses. Modera e cases can achieve good vision wi h rigid gas-permeable, hybrid, or scleral con ac lenses. Advanced cases may require a crescen ic inlay lamellar kera oplas y or ec onic purposes.
Prognosis Good or mild and modera e disease, air
or severe disease
FIGURE 6-9. Terrien’s marginal degeneration. A. Superior peripheral corneal hinning wi h overlying pannus is seen. A dense arc o lipid deposi ion is seen a he cen ral edge o he hinning.
(continued)
A
LWBK961-C06_p142-167.indd 164 22/07/11 9:03 AM

Corneal Deposits—Pigmented 165
B
C
FIGURE 6-9. (Continued) Terrien’s marginal degeneration. B. Sli -beam view reveals corneal hinning, pannus, and lipid deposi ion superiorly. C. In his eye, which has signi can errien’s marginal degenera ion, sli -beam view demons ra es superior corneal hinning and neovasculariza ion wi h lipid a he leading edge.
LWBK961-C06_p142-167.indd 165 22/07/11 9:03 AM

166 6 CORNEAL DEGENERATIONS AND DEPOSITS
I IDOCO NEAL-ENDOTHELIAL SYND OME
Iridocorneal-endo helial (ICE) syndrome is a rare, unila eral, noninheri ed condi ion
af ec ing he cornea, iris, and an erior chamber angle and is associa ed wi h glaucoma.
Etiology More common in young o middle-aged
emales ICE syndrome consis s o hree overlap-
ping ypes: Essen ial iris a rophy—iris hinning, iris
holes, corec opia, pseudopolycoria Chandler syndrome—mild iris hinning
and corec opia, marked corneal edema Cogan-Reese (iris nevus) syndrome—
mul iple small pigmen ed iris nodules His opa hology: Epi helioid me aplasia o
corneal endo helium, which can grow across he an erior chamber angle
Symptoms Asymp oma ic in early s ages. Cosme ic
symp oms can resul rom iris changes. Decreased vision occurs rom corneal edema and occasionally glaucoma.
Signs Common ea ures include an abnormal
corneal endo helium wi h a ain ly hazy, bea en-me al appearance and broad periph-eral an erior synechiae ex ending beyond Schwalbe’s line ( Fig. 6-10 ).
Glaucoma resul s rom synechial angle closure and is mos severe in Chandler’s syndrome.
Dif erential Diagnosis Axen eld-Rieger syndrome: prominen
an eriorly displaced Schwalbe’s line, peripheral iris s rands, possible sys emic abnormali ies
Pos erior polymorphous corneal dys ro-phy: au osomal dominan and bila eral, more corneal and ewer iris changes
Treatment rea men includes medical or surgi-
cal herapy o lower in raocular pressure and corneal ransplan a ion or corneal decompensa ion.
Prognosis Good o very good i he glaucoma can be
con rolled. T e glaucoma can be di cul o con rol wi hou surgery and increases he risk o gra ailure.
A
FIGURE 6-10. Iridocorneal endothelial syndrome. A. T is eye has mild essen ial iris a rophy. No e he ec ropion uveae and corec opia.
(continued)
LWBK961-C06_p142-167.indd 166 22/07/11 9:03 AM

Corneal Deposits—Pigmented 167
B
C
D
FIGURE 6-10. (Continued) Iridocorneal endothelial syndrome. B. T is eye has essen ial iris a rophy wi hperipheral an erior synechiae in eriorly and a large s re ch hole superiorly. C. T ere is an updrawn pupil due o progressive peripheral an erior synechiae orma ion superiorly and di use iris hinning in his eye wi hessen ial iris a rophy. Mild corneal edema is presen . D. Severe corec opia wi h he pupil drawn oward he 3 o’clock limbus can be seen in his eye wi h essen ial iris a rophy. T ere are several large s re ch holes. T is pa ien underwen a corneal gra or severe corneal edema.
LWBK961-C06_p142-167.indd 167 22/07/11 9:03 AM

C H A P E R
168
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA E E EEEEEE E EE E RRRRRRRRRRRRRRRRC H A P E R
Moraxella A ypical mycobac eria, o hers
Symptoms Pain, irri a ion, redness, pho ophobia,
discharge, decreased vision, con ac lens in olerance
Signs Vary according o he severi y o he in ec-
ion and, o a lesser ex en , he causa ive organism
Whi e s romal inf l ra e associa ed wi h conjunc ival injec ion and ypically wi h an overlying epi helial de ec . T ere may be s ro-mal loss (ulcer) ( Fig. 7-1 A and B).
T ere may be surrounding s romal edema, Desceme ’s olds, secondary reac ive iri is, and hypopyon ( Fig. 7-1 C–H).
S aphylococcal kera i is is charac erized by a well-def ned, whi e-gray or creamy s romal inf l ra e ha may enlarge o orm a dense s romal abscess.
S rep ococcal kera i is may be suppura ive or have a crys alline appearance. Severe an erior uvei is and hypopyon orma ion are common.
Corneal In ec ions, In amma ions, and Sur ace Disorders
BACTERIAL KERATITIS
Bac erial kera i is is a serious, po en ially sigh - hrea ening corneal in ec ion ha
ypically develops in pa ien s wi h a compro-mised corneal sur ace.
Predisposing Factors Con ac lens wear, especially ex ended-
wear so lenses Corneal rauma, oreign bodies Ocular sur ace disease (e.g., exposure/
neuro rophic kera opa hy, chronic bullous kera opa hy, dry eye syndrome, richiasis, dis ichiasis, en ropion)
opical immunosuppressive herapy (e.g., cor icos eroids)
Immunocompromised pa ien Pos opera ive: corneal wound or su ure-
rela ed (e.g., corneal gra )
Etiology Staphylococcus Streptococcus Pseudomonas
LWBK961-C07_p168-235.indd 168 22/07/11 10:15 AM

Bacterial Keratitis 169
Pseudomonal kera i is ypically presen s as a rapidly progressive, suppura ive inf l ra e associa ed wi h hypopyon and a mucopuru-len discharge. Corneal per ora ion may occur ( Fig. 7-1 G).
Dif erential Diagnosis S erile ulcers: vernal shield ulcer, neuro-
rophic or exposure kera i is, au oimmune kera i is, con ac lens–induced s erile kera- i is, medicamen osa kera i is. Usually less pain ul, minimal or no iri is or corneal edema, and cul ure is nega ive.
S aphylococcal hypersensi ivi y kera i is: Inf l ra es may be bila eral; mul iple; periph-eral; o en loca ed a he 2, 4, 8, or 10 o’clock posi ion; associa ed wi h blephari is; epi he-lial de ec is absen or is smaller han he inf l- ra e; and here is minimal an erior chamber ac ivi y.
O her microbial (nonbac erial) kera i is: Bac erial cul ures are nega ive. Fungal and special cul ures and s ains are necessary or diagnosis.
Diagnosis Corneal scraping or Gram’s s ain, Giemsa
s ain, calco uor whi e s ain, cul ures, and sen-si ivi y es ing. Rou ine media include blood, chocola e, Sabouraud’s agars, and hioglyco-la e bro hs.
For deep lesions or when repea ed cul ures are nega ive in recalci ran cases, a corneal biopsy may be necessary.
Treatment Empirical ou pa ien rea men wi h
broad-spec rum, opical, non or if ed an ibi-o ic drops may be su cien or small (2 mm or less) peripheral ulcers wi h minimal symp- oms and minimal an erior chamber ac ivi y. opical uoroquinolone (e.g., moxi oxacin, ga i oxacin, besi oxacin, levo oxacin, cipro- oxacin, o oxacin) drops q30–60min around
he clock ini ially, a er a loading dose o 1 drop q5min or 15 minu es.
For larger ulcers or when he ulcers involve he visual axis, or are associa ed wi h signif can discharge, an erior chamber ac ivi y, and hypo-pyon, rea men may require in ensive or if ed an ibio ic drops. Some pa ien s may need hos-pi aliza ion. For if ed ce azolin (50 mg/ mL) or vancomycin (25 mg/ mL) and or if ed gen a-micin or obramycin (15 mg/ mL). Frequency o ins illa ion: 1 drop q5min or 30 minu es, hen q30–60min, o each drop. Wai 5 minu es be ween adminis ra ions o each medica ion.
Subconjunc ival an ibio ics are necessary only i or if ed eye drops canno be s ar ed soon.
Oral an ibio ics (e.g., moxi oxacin 400 mg q.d., cipro oxacin 500 mg b.i.d., or levo oxacin 500 mg q.d.) are help ul i he ulcer involves he sclera or has ex ended in o he eye. Sys emic an ibio ics are also required or Neisseria and Haemophilus in ec ion (e.g., ce riaxone 1 g IV or IM q12–24h).
Cycloplegics are o en used o reduce cili-ary spasm and o preven pos erior synechiae (e.g., scopolamine 0.25% or a ropine 1% .i.d.).
Modi y regimen according o clinical response and cul ure and sensi ivi y resul s.
opical cor icos eroids can be used or severe in amma ion only a er he organ-ism is iden if ed and he in ec ion is under con rol.
Urgen corneal ransplan a ion may be necessary in severe cases ha are progressing despi e aggressive rea men or or ulcers ha have per ora ed.
Prognosis Close ollow-up is required. Prognosis is
very good or small ulcers, good or modera e ulcers, poor or severe ulcers. Bet er prognosis or ulcers ou side he visual axis han ulcers in he visual axis.
LWBK961-C07_p168-235.indd 169 22/07/11 10:15 AM

170 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
A
FIGURE 7-1. Bacterial keratitis. A. T is small in erior corneal inf l ra e in an overnigh so con ac lens wearer has some underlying corneal edema. Because i may be an early in ec ious kera i is, i should be rea ed wi h requen opical an ibio ics and ollowed closely. B. T is modera ely large, dense, paracen ral, con ac lens–rela ed corneal inf l ra e has an overlying epi helial de ec and surrounding edema.
(continued)
B
LWBK961-C07_p168-235.indd 170 22/07/11 10:15 AM

Bacterial Keratitis 171
C
D
FIGURE 7-1. (Continued) Bacterial keratitis. C. T is small o medium-sized paracen ral inf l ra e is modera ely dense. T e area o ac ive inf l ra ion is eleva ed as a resul o he in amma ory response. No e also he surrounding edema and he dis inc circular immune ring, bes seen cen rally. D. T is dense cen ral corneal ulcer has a large overlying epi helial de ec and modera e underlying corneal edema. T ere is a small hypopyon in eriorly, jus blun ing he in erior angle.
(continued)
LWBK961-C07_p168-235.indd 171 22/07/11 10:15 AM
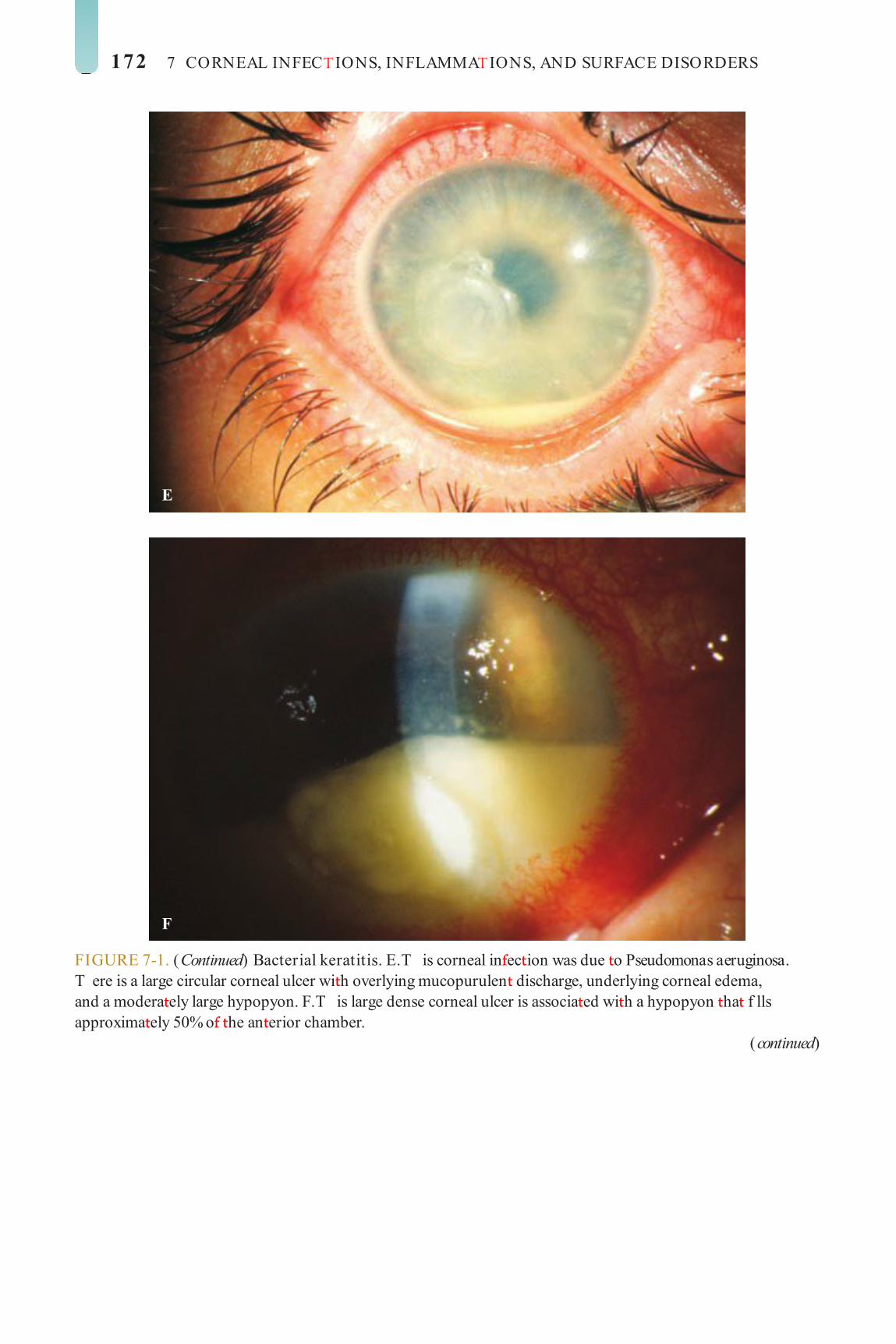
172 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
E
F
FIGURE 7-1. (Continued) Bacterial keratitis. E. T is corneal in ec ion was due o Pseudomonas aeruginosa. T ere is a large circular corneal ulcer wi h overlying mucopurulen discharge, underlying corneal edema, and a modera ely large hypopyon. F. T is large dense corneal ulcer is associa ed wi h a hypopyon ha f lls approxima ely 50% o he an erior chamber.
(continued)
LWBK961-C07_p168-235.indd 172 22/07/11 10:15 AM

Bacterial Keratitis 173
G
H
FIGURE 7-1. (Continued) Bacterial keratitis. G. T is in ec ed corneal ulcer caused a per ora ion. Iris is plugging he wound. T e an erior chamber is shallow bu ormed. H. A o al corneal ulcera ion and epi helial de ec is presen in his eye. Sli -beam view demons ra es signif can cen ral hinning. T ere is no view o he an erior chamber.
LWBK961-C07_p168-235.indd 173 22/07/11 10:15 AM

174 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
FUNGAL KERATITIS
Fungal kera i is is a very serious, po en- ially sigh - hrea ening corneal in ec ion
ha mos commonly develops in pa ien s a er rauma or in hose wi h a compromised cor-neal sur ace.
Etiology Nonf lamen ous (e.g., Candida ): Candida
kera i is is a rare, unila eral, insidious ungal in ec ion ha usually occurs in eyes wi h preexis ing chronic corneal disease (e.g., dry eyes, herpes kera i is, exposure kera opa hy, pos kera oplas y, chronic use o cor icos e-roid drops) or in severely debili a ed pa ien s. Fea ures include a gray-whi e s romal inf l- ra e similar o a bac erial ulcer. May have an an erior chamber reac ion and hypopyon ( Fig. 7-2 A and B).
Filamen ous (e.g., Aspergillus, Fusarium ): Filamen ous kera i is is a rare, unila eral, insidious or aggressive ungal in ec ion ha requen ly a ec s normal eyes ollowing ocu-lar rauma associa ed wi h vege a ive mat er and in wearers o so con ac lens. Fea ures include a grayish-whi e inf l ra e wi h indis- inc ea hery borders, ypically surrounded by f ngerlike sa elli e inf l ra es in adjacen s roma. T e inf l ra es may ex end beyond he epi helial de ec . May have an associa ed ring inf l ra e, an erior chamber reac ion, and hypopyon ( Fig. 7-2 C–F).
Symptoms Pain, pho ophobia, earing, decreased
vision; may have a his ory o rauma, con ac lens use or cor icos eroid eye drop usage
Dif erential Diagnosis Fungal kera i is should be considered
in he di eren ial diagnosis o bac erial or herpe ic kera i is ha does no respond o conven ional rea men or ha has an unusual his ory or suspicious appearance.
Diagnostic Evaluation His ory o rauma (which is o en
minor) involving vege a ive mat er is highly sugges ive.
Lack o response o conven ional an ibac- erial herapy
Corneal scrapings or Gram, Giemsa, cal-co uor whi e, or Gomori me henamine silver s ain, and cul ure (may ake up o a week or ungus o grow)
Corneal biopsy may be required i smears and cul ures are nega ive.
Treatment opical na amycin 5% (especially or
f lamen ous ungi) and/ or ampho ericin B 0.15% (especially or Candida ) q1h around he clock and aper over 4 o 6 weeks. Pa ien s may require hospi aliza ion ini ially. opical voriconazole 1% may also be e ec ive.
Oral voriconazole 200 mg b.i.d. or i racon-azole or uconazole 200 o 400 mg loading dose ollowed by 100 o 200 mg q.d. may be help ul in addi ion o he in ensive opical medica ions.
Cycloplegics (e.g., scopolamine 0.25% or a ropine 1% .i.d.)
Cor icos eroids are con raindica ed. Epi helial debridemen may acili a e
opical herapy by enhancing pene ra ion o an i ungals.
Modi y regimen according o clinical response and cul ure resul s.
T erapeu ic corneal ransplan a ion may be necessary or unresponsive cases or per o-ra ed ulcers. Lamellar kera oplas y is rela ively con raindica ed because here is a high risk o recurrence o in ec ion.
Prognosis Fair or mild o modera e in ec ions; poor
or severe in ec ions
LWBK961-C07_p168-235.indd 174 22/07/11 10:15 AM

Fungal Keratitis 175
A
FIGURE 7-2. Fungal keratitis. A. T is mul ilobula ed dense inf l ra e was caused by a Candida i n ec ion. T ere is an overlying epi helial de ec . Peripheral corneal neovasculariza ion sugges s ha i is a long-s anding ulcer. B. T is Candida corneal ulcer is slowly improving. T e denser inf l ra e a he in erior pupillary margin is surrounded by mul iple sa elli e lesions.
(continued)
B
LWBK961-C07_p168-235.indd 175 22/07/11 10:15 AM

176 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
C
D
FIGURE 7-2. (Continued) Fungal keratitis. C. T is dense whi e inf l ra e wi h ea hery borders was a resul o a Fusarium in ec ion. A ring inf l ra e is beginning in eriorly. D. T is large cen ral pa chy corneal inf l ra e and hypopyon enlarged rapidly over several days, leading o an urgen corneal ransplan . His opa hology demons ra ed numerous f lamen ous ungi.
(continued)
LWBK961-C07_p168-235.indd 176 22/07/11 10:16 AM

Fungal Keratitis 177
E
F
FIGURE 7-2. (Continued) Fungal keratitis. E. Several mon hs a er removal o a corneal oreign body, a pa chy cen ral corneal inf l ra e is seen. T ere is also old in erior scarring and neovasculariza ion. Ini ial cul ures were nega ive. F. wo mon hs la er, he eye seen in E has worsened and has a much more dense cen ral inf l ra e. Cul ures a his poin grew Alternaria, which even ually responded o opical and oral voriconazole.
LWBK961-C07_p168-235.indd 177 22/07/11 10:16 AM

178 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
ACANTHAMOEBA KERATITIS
Acanthamoeba kera i is is a rare parasi ic in ec ion o he cornea associa ed wi h
he use o so con ac lenses and inadequa e con ac lens hygiene (e.g., using ap wa er or home-made saline solu ion, swimming or ho ub use while wearing con ac lenses), and occasionally, rauma. I should be considered in nonhealing, cul ure-nega ive kera i is.
Etiology Acanthamoeba species
Symptoms Severe pain ou o propor ion o severi y
o kera i is, redness, earing, decreased vision, pho ophobia, minimal discharge. Symp oms ypically develop over a period o weeks, bu onse can be more rapid.
His ory o so con ac lens use and occa-sionally rauma
Signs Epi helial or subepi helial inf l ra es
appearing as pseudodendri es early on ( Fig. 7-3 A and B)
Pa chy an erior s romal inf l ra es may be presen early on.
Radial kera oneuri is ( Fig. 7-3 C) A nonsuppura ive s romal ring inf l ra e,
o en wi h variable epi helial breakdown, can develop over weeks. T e degree o in amma- ion is dispropor iona ely mild rela ive o he amoun o pain ( Fig. 7-3 D–F).
In advanced cases, corneal hinning or per ora ion, scleri is, or hypopyon may develop.
Dif erential Diagnosis Herpes simplex kera i is Fungal kera i is Bac erial kera i is
Diagnosis Pain dispropor iona e o severi y o
in amma ion Lack o response o an ibac erial and an i-
viral herapy Ring inf l ra e and radial kera oneuri is are
highly sugges ive. Corneal scrapings or Gram, Giemsa, or
calco uor whi e s ain or amoebic cys s Cul ure on non-nu rien agar wi h
Escherichia coli overlay or special media (e.g., bu ered charcoal yeas ex rac agar).
Corneal biopsy may be necessary i smears and cul ures are nega ive.
Treatment Polyhexame hylene biguanide (PHMB)
0.02% drops q1h. Chlorhexidine 0.02% can be used as an al erna ive o PHMB.
Propamidine ise hiona e 1% (e.g., Brolene) drops q1h.
Oral voriconazole 200 mg b.i.d. or i racon-azole 200 o 400 mg q.d. may be used in addi- ion o he opical medica ions.
O her drops (e.g., clo rimazole 1%) may be added, depending on he severi y or rea -men response o he in ec ion.
Cycloplegics (e.g., scopolamine 0.25% or a ropine 1% .i.d.)
Low-dose opical cor icos eroids may be help ul in reducing in amma ion once he in ec ion appears o be under con rol.
Oral nons eroidal an i-in amma ory agen s or narco ics or pain relie
LWBK961-C07_p168-235.indd 178 22/07/11 10:16 AM

Acanthamoeba Keratitis 179
FIGURE 7-3. Acanthamoeba keratitis. A. A curvilinear, sligh ly eleva ed, “pseudodendri ic” epi helial irregulari y can be seen in his eye wi h con ac lens–rela ed Acanthamoeba kera i is. B. T is early Acanthamoeba in ec ion has several subepi helial inf l ra es in a linear pat ern reminiscen o a dendri e, hence he erm pseudodendri e. T ere was no rank epi helial de ec , bu here was epi helial irregulari y.
(continued)
Modi y regimen according o clinical response.
Corneal ransplan a ion may be required i medical herapy ails, bu here is risk o recurrence.
Prognosis Fair o good i diagnosed and rea ed
appropria ely wi hin he f rs mon h or so o developmen o symp oms; poor i signif can corneal involvemen is presen
A
B
LWBK961-C07_p168-235.indd 179 22/07/11 10:16 AM

180 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
C
D
FIGURE 7-3. (Continued) Acanthamoeba k eratitis. C. Classic radial kera oneuri is is very apparen peripherally in his eye wi h con ac lens–rela ed Acanthamoeba kera i is. D. A er several weeks, a ring inf l ra e can develop, as can be seen especially superiorly. T ere is a small epi helial de ec in erocen rally.
(continued)
LWBK961-C07_p168-235.indd 180 22/07/11 10:16 AM

E
F
FIGURE 7-3. (Continued) Acanthamoeba keratitis. E. A large ring inf l ra e is presen in his eye. Despi e very aggressive medical rea men , his eye required a corneal ransplan . F. A er several mon hs o an iacan hamoeba rea men , his dense inf l ra e is f nally scarring. T e ac ive in ec ion even ually resolved, bu he eye was le wi h a signif can corneal scar.
Acanthamoeba Keratitis 181
LWBK961-C07_p168-235.indd 181 22/07/11 10:16 AM

182 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
HERPES SIMPLEX KERATITIS
Herpes simplex virus (HSV) in ec ion is an ex remely common condi ion ha
a ec s a major propor ion o he popula ion, al hough mos in ec ions are subclinical. T e eyes may be a ec ed in primary ocular herpes or in recurren disease.
Etiology HSV ype 1: causes in ec ion above he
wais , especially o he ace, lips, and eyes. ransmit ed by close con ac . Much more common in he eye han ype 2
HSV ype 2: causes in ec ion below he wais , par icularly o he geni alia. ransmit ed sexually, bu neona es can be in ec ed during vaginal delivery. Uncommon in he eye
P IMA Y OCULA HE PES Unila eral or bila eral acial and/ or eye
in ec ion
Etiology and Epidemiology Primary con ac wi h HSV Usually occurs in children or adolescen s
Symptoms Fever, ulike symp oms Facial vesicular rash. Ocular redness, pain,
decreased vision, and earing
Signs T ere may be vesicular blepharocon-
junc ivi is or periorbi al derma i is. T e vesicles usually progress o orm crus s ( Fig. 7-4 ). T ere may be associa ed acu e ollicular conjunc ivi is wi h preauricular lymphadenopa hy.
T e cornea may be involved in he orm o coarse macropunc a e epi helial kera i is or mul iple small branching epi helial dendri es wi hou s romal involvemen .
Treatment Blepharoconjunc ivi is: ganciclovir (e.g.,
Zirgan) gel, ri uridine (e.g., Virop ic) drops, vidarabine (e.g., Vira-A) oin men , or acyclo-vir (e.g., Zovirax oph halmic) oin men f ve imes a day
Corneal involvemen : ganciclovir (e.g. Zirgan) gel f ve imes a day or ri uridine drops (e.g., Virop ic) nine imes a day
Consider acyclovir 200 o 400 mg PO f ve imes a day, valacyclovir 500 mg .i.d., or am-ciclovir 250 mg .i.d. or 7 o 14 days.
Consider opical an ibio ic or acyclovir oin men o help heal skin lesions away rom he eyelid margin.
Prognosis Good. T is is usually a benign and sel -
limi ed condi ion, bu he virus subsequen ly es ablishes a la en in ec ion in he rigeminal ganglion and may reac iva e, especially during periods o physical or emo ional s ress, caus-ing recurren disease.
LWBK961-C07_p168-235.indd 182 22/07/11 10:16 AM

Herpes Simplex Keratitis 183
A
FIGURE 7-4. Herpes simplex dermatitis. A. T is pa ien had recurren herpes simplex derma i is. No e he numerous ulcera ed skin lesions around he righ eye and cheek. T e righ eye appears uninvolved, bu i should receive prophylac ic an iviral rea men because o skin lesions on he eyelid margin. B. Mul iple ulcera ed skin lesions o herpes simplex can be seen in he upper eyelid. Con uen skin ulcera ions are presen in he lower eyelid wi h a mucoid discharge.
B
LWBK961-C07_p168-235.indd 183 22/07/11 10:16 AM

184 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
ECU ENT OCULA HE PES SIMPLEX
Recurren ocular herpes may ake he orms o in ec ious epi helial kera i is,
non-necro izing s romal kera i is (disci orm kera i is), necro izing s romal kera i is, neuro- rophic kera i is, and kera ouvei is.
Etiology and Epidemiology Recurren HSV is due o a reac iva ion o
la en in ec ion in he rigeminal ganglion, especially during periods o physical or emo- ional s ress.
I occurs in children and adul s. I is usually unila eral, bu i can be bila -
eral, especially in immunocompromised pa ien s and hose wi h a opy.
HSV: EPITHELIAL KER TITIS (DEND ITIC ULCE )
Epi helial kera i is is a common, usually unila eral condi ion due o he presence
o live virus wi hin corneal epi helial cells.
Symptoms Unila eral redness, earing, irri a ion,
decreased vision, pho ophobia, his ory o previous episodes
Signs Single or mul iple branching, ulcera ing
epi helial lesions wi h raised edges and ermi-nal bulb orma ion ( Fig. 7-5 A–C)
Enlargemen o ulcers can lead o he orma ion o an amebic-shaped “geographic” ulcer ( Fig. 7-5 D and E).
T e ulcer bed s ains wi h uorescein. T e buil -up, swollen, opalescen margins o he lesion con aining virus-laden cells s ain wi h rose bengal.
An erior s romal haze called “ghos den-dri es” may develop below he epi helial lesions ( Fig. 7-5 F).
Corneal sensa ion is o en diminished.
Dif erential Diagnosis Herpes zos er kera i is: associa ed wi h a
his ory o herpes zos er oph halmicus wi h ypical skin vesicles ound along derma omal dis ribu ion o he ace. May have eleva ed epi helial lesions wi h apered ends, which lack erminal bulbs. T e en ire “mucous plaque dendri e” s ains wi h rose bengal and mildly wi h uorescein. Prior o develop-men o he ypical zos er rash, early zos er dendri es can look very similar o HSV dendri es.
Acanthamoeba pseudodendri es Healing epi helial de ec s oxic epi heliopa hy
Treatment Ganciclovir (e.g., Zirgan) gel f ve imes a
day, ri uridine (e.g., Virop ic) drops q2h dur-ing he day, vidarabine (e.g., Vira-A) oin men f ve imes a day or acyclovir (e.g., Zovirax oph halmic) oin men f ve imes a day
I he pa ien is already on cor icos eroids, he s eroids should be apered rapidly.
Epi helial debridemen can help reduce viral load.
I here is no response o rea men a er 1 week, hen poor compliance, resis ance o an iviral herapy, an iviral oxici y, or neuro- rophic disease should be considered.
A shor course o sys emic acyclovir is unnecessary, because i does no preven sub-sequen developmen o s romal kera i is or uvei is, bu i can be used in place o requen opical an ivirals.
Consider long- erm oral an iviral prophy-laxis (e.g., acyclovir 400 mg b.i.d.) i a pa ien has had mul iple episodes o herpe ic eye disease.
Prognosis Good, bu recurrences are common
LWBK961-C07_p168-235.indd 184 22/07/11 10:16 AM

Herpes Simplex Keratitis 185
A
B
FIGURE 7-5. Herpes simplex keratitis. A. Fluorescein s aining wi h a cobal blue ligh o an ac ive herpes simplex epi helial dendri e. No e he “ ree branching” pat ern o he dendri e. T e cen ral bed s ains well wi h uorescein, while he eleva ed edges do no . T e ends o he dendri e have classic erminal “end bulbs.” B. R ose bengal dye on his ac ive dendri e s ains he heaped-up edges ha con ain virus-laden cells.
(continued)
LWBK961-C07_p168-235.indd 185 22/07/11 10:16 AM

186 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
C
D
FIGURE 7-5. (Continued) Herpes simplex keratitis. C. A recurren epi helial dendri e is seen in his eye, which is 15 years s a us pos a corneal ransplan or herpes simplex kera i is scarring. D. T e cen ral area o a very large “geographic” lesion s ains readily wi h uorescein. T e edge o he epi helial de ec has herpes simplex dendri ic branching and erminal end bulbs.
(continued)
LWBK961-C07_p168-235.indd 186 22/07/11 10:16 AM

Herpes Simplex Keratitis 187
E
F
FIGURE 7-5. (Continued) Herpes simplex keratitis. E. Broad sli -beam view o he same eye highligh s he classic herpes simplex dendri ic ea ures. F. T is resolving epi helial dendri e barely s ains wi h uorescein. T ere is residual underlying corneal haze in he pat ern o he previous dendri e, o en ermed a “ghos dendri e.”
LWBK961-C07_p168-235.indd 187 22/07/11 10:16 AM

188 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
HSV: NONNEC OTIZING ST OMAL KER TITIS (DISCIFO M KER TITIS)
Disci orm kera i is is a primarily in am-ma ory condi ion caused by a hyper-
sensi ivi y reac ion o he herpes simplex viral an igen in he cornea.
Symptoms Unila eral redness, earing, irri a ion,
blurred vision, pho ophobia, his ory o previ-ous episodes
Signs Cen ral disc o s romal and epi helial
edema ( Fig. 7-6 A and B) Small kera ic precipi a es localized o he
underlying endo helium Folds in Desceme ’s membrane Surrounding s romal immune ring
(Wessley ring) may be presen . T e limbal issue may be hickened and
in amed (limbi is) ( Fig. 7-6 C). An erior uvei is ( Fig. 7-6 D and E) In raocular pressure may be eleva ed. Corneal sensa ion is ypically reduced.
Dif erential Diagnosis Herpes zos er disci orm kera i is Fuchs’ endo helial dys rophy
Acu e corneal hydrops o kera oconus Con ac lens overwear
Treatment I in amma ion is mild and vision is good,
he condi ion can be observed. In more severe cases, opical cor icos e-
roids (e.g., prednisolone 1%, dexame hasone 0.1%, or lo eprednol 0.5% drops q.i.d.) can be s ar ed, main ained or several days o weeks, hen gradually apered over weeks or mon hs. O en, a very low dose o opi-cal cor icos eroid (once or wice a week) may be required o preven recurren in amma ion.
While on cor icos eroids more han once a day, concomi an oral an iviral herapy (e.g., acyclovir 400 mg b.i.d.) is o en used as prophylaxis.
I an epi helial lesion is presen , i should be rea ed be ore s ar ing cor icos eroids.
Recommend long- erm oral an iviral prophylaxis (e.g., acyclovir 400 mg b.i.d.) i a pa ien has had mul iple episodes o s romal kera i is.
Prognosis Good. S romal scarring may occur and
reduce vision ( Fig. 7-6 F). O en recurs
LWBK961-C07_p168-235.indd 188 22/07/11 10:16 AM

Herpes Simplex Keratitis 189
FIGURE 7-6. Herpes simplex disci orm keratitis. A. T is eye has modera e cen ral corneal edema in a circular pat ern, hence he erm “disci orm.” T e sli -beam view demons ra es cen ral corneal hickening. T is disci orm kera i is represen s an in amma ory reac ion o previous herpes simplex in ec ion. I may resolve spon aneously, bu i o en responds ex remely well o opical cor icos eroids wi h an iviral coverage. B. T is eye has severe cen ral corneal edema wi h underlying kera ic precipi a es.
(continued)
A
B
LWBK961-C07_p168-235.indd 189 22/07/11 10:16 AM

190 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
C
D
FIGURE 7-6. (Continued) Herpes simplex limbitis. C. T is eye, wi h a previous his ory o herpes simplex kera i is, has severe limbal in amma ion. No e he hickened, eleva ed limbal conjunc iva. T is limbi is responded o opical cor icos eroids and an iviral coverage. Herpes simplex iritis. D. Hundreds o granuloma ous kera ic precipi a es are presen in his eye wi h a his ory o previous herpes simplex kera i is. No e he ain cen ral corneal scarring o old herpes kera i is. O en he in raocular pressure is eleva ed in eyes wi h herpe ic iri is. Herpes simplex iri is responds o opical cor icos eroids wi h an iviral coverage. I o en benef s rom rea men wi h oral an iviral agen s in addi ion.
(continued)
LWBK961-C07_p168-235.indd 190 22/07/11 10:16 AM

Herpes Simplex Keratitis 191
E
F
FIGURE 7-6. (Continued) Herpes simplex keratitis. E. Re roillumina ion o he re ina reveals signif can iris s romal a rophy and iris ransillumina ion de ec s a er mul iple episodes o herpes simplex kera i is and iri is. F. A large, dense corneal scar wi h neovasculariza ion remains a er repea ed episodes o herpes simplex kera i is.
LWBK961-C07_p168-235.indd 191 22/07/11 10:16 AM

192 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
HSV: NEC OTIZING ST OMAL KER TITIS
Necro izing s romal kera i is is unusual. I is mos likely caused by viral inf l ra ion
and in amma ion o he corneal s roma.
Symptoms Unila eral redness, earing, irri a ion,
blurred vision, pho ophobia, pain, his ory o previous episodes
Signs Necro ic, cheesy, s romal inf l ra ion,
usually associa ed wi h an epi helial de ec ( Fig. 7-7 A)
T e appearance o he inf l ra e can be con used wi h secondary bac erial or ungal kera i is.
Corneal hinning, s romal neovasculariza- ion, scarring, or per ora ion may develop ( Fig. 7-7 B).
T ere may be associa ed kera ic precipi- a es, an erior uvei is, or hypopyon.
In raocular pressure can be eleva ed even in he presence o minimal an erior chamber reac ion.
Dif erential Diagnosis Primary or secondary bac erial or ungal
kera i is: T ere is generally an overlying epi helial de ec . T ese condi ions should be considered when here is lack o response o an iviral rea men , and when here are increased or new signs o in ec ion and in amma ion.
Treatment T e f rs priori y is o rule ou a bac erial
or ungal in ec ion and o rea any associa ed epi helial de ec .
Once he epi helium has healed, opical cor icos eroids can be judiciously added o reduce s romal and an erior chamber in amma ion (e.g., prednisolone 1% or dexa-me hasone 0.1% drops q.i.d.), combined wi h opical or oral an iviral prophylaxis.
Cor icos eroid drops should be apered gradually (s reng h and requency) over weeks or mon hs, depending on he level o in amma ion and he herapeu ic response.
Cycloplegics (e.g., scopolamine 0.25% or cyclopen ola e 1% .i.d.).
rea any eleva ed in raocular pressure. Avoid mio ics and pros aglandin analogs.
Sys emic an iviral medica ions (e.g., acy-clovir 400 mg f ve imes a day or weeks o mon hs) are ypically indica ed, especially when here is an erior uvei is.
Corneal ransplan during acu e s ages o he in ec ion is discouraged because o he high ailure ra es
Recommend long- erm oral an iviral prophylaxis (e.g., acyclovir 400 mg b.i.d.) i a pa ien has had pas episodes o s romal kera i is.
Prognosis Fair. ypically, signif can s romal scarring
remains, and i i is in he visual axis, i can severely a ec vision.
LWBK961-C07_p168-235.indd 192 22/07/11 10:16 AM
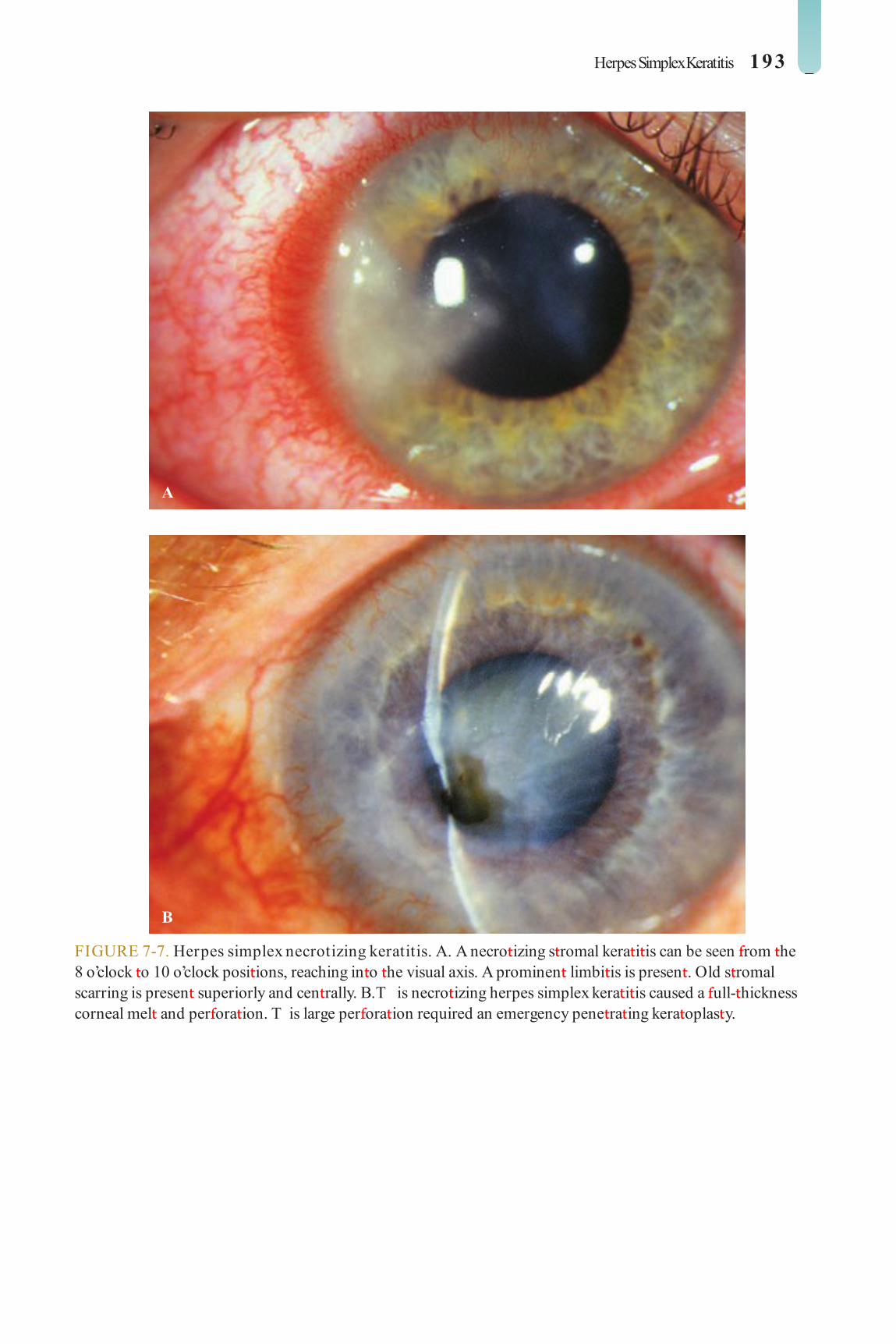
Herpes Simplex Keratitis 193
FIGURE 7-7. Herpes simplex necrotizing keratitis. A. A necro izing s romal kera i is can be seen rom he 8 o’clock o 10 o’clock posi ions, reaching in o he visual axis. A prominen limbi is is presen . Old s romal scarring is presen superiorly and cen rally. B. T is necro izing herpes simplex kera i is caused a ull- hickness corneal mel and per ora ion. T is large per ora ion required an emergency pene ra ing kera oplas y.
A
B
LWBK961-C07_p168-235.indd 193 22/07/11 10:16 AM

194 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
HSV: NEU OT OPHIC KER TITIS (METAHE PETIC KER TITIS)
Neuro rophic kera i is is no due o ac ive viral in ec ion bu is a healing problem
caused by a combina ion o decreased sensa ion, drug oxici y, and a damaged basemen mem-brane rom epi helial in ec ion due o herpes.
Symptoms Unila eral redness, earing, irri a ion,
blurred vision, pho ophobia, his ory o previ-ous episodes
Signs Persis en epi helial de ec wi h heaped-up
borders. T e edges do no s ain well wi h rose bengal. T e base s ains readily wi h uores-cein ( Fig. 7-8 ).
T ere may be mild o modera e corneal haze or scarring.
Epi helial dendri es and erminal bulbs are absen .
May progress o corneal mel ing and per ora ion, especially i also using opical cor icos eroids
Decreased corneal sensa ion Reac ive iri is may be presen .
Dif erential Diagnosis Geographic herpes simplex ulcer: Edges
have branching dendri ic ex ensions and s ain well wi h rose bengal.
Treatment Discon inue oxic opical medica ions. O her measures o heal he epi helium are
similar o hose or neuro rophic kera opa hy (see sec ion on Neuro rophic Kera opa hy in his chap er).
Prognosis Good or small lesions, air or large
lesions. O en corneal haze/ scar remains a er he epi helial de ec resolves.
LWBK961-C07_p168-235.indd 194 22/07/11 10:16 AM

Herpes Simplex Keratitis 195
FIGURE 7-8. Herpes simplex neurotrophic keratitis. A neuro rophic corneal ulcer is presen is his eye wi h recen herpes simplex kera i is. T e ac ive herpes in ec ion was rea ed wi h opical an iviral agen s and he ac ive dendri e resolved. However, he epi helial de ec remained, causing s romal hinning. No e he heaped-up edges o epi helium.
LWBK961-C07_p168-235.indd 195 22/07/11 10:16 AM

196 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
HERPES ZOSTER KERATITIS
Herpes zos er virus (HZV) in ec ion is caused by a reac iva ion o he chicken-
pox virus in he dorsal roo ganglion ha has migra ed down along he sensory nerves o a ec he skin o ha par icular derma ome. When he oph halmic division (V1) o he rigeminal nerve is involved, he condi ion is called herpes zos er oph halmicus.
Etiology and Epidemiology Varicella zos er virus Unlike chickenpox, i is rare in children and
ypically a ec s older pa ien s, bu i can also a ec young adul s, especially hose who are immunocompromised (e.g., hose wi h HIV, cancer).
Symptoms Fever, malaise, and headache, which
may precede he rash by a ew days. May be di cul o diagnose during he prodromal s age.
Derma omal skin rash, ingling, burning, i ching sensa ion, pain
Eye redness, irri a ion, earing, decreased vision, pho ophobia
Signs Unila eral vesicular skin rash ha does no
cross he midline ( Fig. 7-9 A). T e rash sub-sequen ly orms blis ers and crus s ha heal wi h scarring. Hu chinson’s sign, vesicles on he ip o he nose, indica es presence o naso-ciliary nerve involvemen and may predic a higher risk o ocular disease.
Periocular derma i is, conjunc ivi is, episcleri is, scleri is
Corneal involvemen includes superf cial punc a e kera i is, microdendri ic kera i- is, nummular kera i is, disci orm kera i is ( Fig. 7-9 B), and neuro rophic kera i is.
Neuro rophic ulcers and persis en epi helial de ec s can lead o secondary in ec ion, hin-ning, and, even ually, corneal per ora ion ( Fig. 7-9 C).
Zos er pseudodendri es are eleva ed, “s uck-on” mucous-plaque lesions ha s ain wi h rose bengal bu do no s ain well wi h uorescein and do no have erminal end bulbs ( Fig. 7-9 D and E).
Iri is, glaucoma, re ini is, op ic neuri is, cranial nerve palsy, and cranial ar eri is may be seen.
Pos herpe ic neuralgia (neuropa hic pain syndrome las ing longer han 3 mon hs a er he ini ial rash) may also develop.
Dif erential Diagnosis Herpes simplex kera i is: Pa ien s are
generally younger, have a his ory o recurren episodes, skin involvemen has no derma o-mal dis ribu ion, dendri es have erminal end bulbs, and he cen ral par s are depressed and s ain well wi h uorescein.
Treatment Skin involvemen
Oral acyclovir 800 mg f ve imes a day or amciclovir 500 mg .i.d. or valacyclovir 1000 mg .i.d. or 7 o 10 days o be s ar ed as soon as possible
H2 an agonis (e.g., cime idine 400 mg b.i.d. PO) may reduce i ching and pain.
An iviral (e.g., acyclovir) and/ or an ibac erial (e.g., e racycline, baci racin, or ery hromycin) oin men q.i.d. o he skin
Conjunc ivi is and episcleri is T ese are sel -limi ed, and rea men is
or symp oma ic relie . Cool compresses, ar if cial ears, or
an ibio ic oin men (e.g., ery hromycin, baci racin, or e racycline) b.i.d. or .i.d.
LWBK961-C07_p168-235.indd 196 22/07/11 10:16 AM
Herpes Zoster Keratitis 197
Scleri is: Consider oral nons eroidal an i-in amma ory agen s (e.g., urbipro en 100 mg .i.d.) or cor icos eroids (e.g., prednisolone 1 mg/ kg/ d q.d. or 2 weeks, hen aper) in severe cases.
Disci orm kera i is: opical cor icos eroids in more severe cases (e.g., prednisolone 1%, dexame hasone 0.1%, or lo eprednol 0.5% our o eigh imes a day). aper slowly. A very low dose may be required chronically o preven recurrences.
Pseudodendri es Generally sel -limi ed and rea ed wi h
lubrica ion wi h ar if cial ear drops or oin men
May respond o opical an iviral agen s (e.g., vidarabine oin men or gan-ciclovir gel), especially i he pa ien is immunocompromised
Neuro rophic kera i is: See sec ion on Neuro rophic Kera opa hy in his chap er.
Re ini is, choroidi is, op ic neuri is: in ra-venous acyclovir and oral cor icos eroids
Pos herpe ic neuralgia: opical capsaicin or doxepin creams, sys emic neuropa hic pain medica ions (e.g., gabapen in or pregabalin), and/ or sys emic an idepressan medica ion may be help ul. In severe cases, re erral o a neurologis or pain specialis is indica ed.
All pa ien s Con rol iri is wi h opical
cor icos eroids. Con rol glaucoma. Beware o
cor icos eroid-induced pressure rise as a possible cause.
Prognosis Good o poor, depending on he sever-
i y o he corneal involvemen ( Fig. 7-9 F). Chronic recurren bou s o ocular in amma- ion are common. Pos herpe ic neuralgia can be devas a ing in some pa ien s.
LWBK961-C07_p168-235.indd 197 22/07/11 10:16 AM

198 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
A
FIGURE 7-9. Herpes zoster dermatitis. A. A herpes zos er derma i is (shingles) in ec ion in he V 2
dis ribu ion. No e he ulcera ed skin vesicles. (continued)
LWBK961-C07_p168-235.indd 198 22/07/11 10:16 AM

Herpes Zoster Keratitis 199
B
C
FIGURE 7-9. (Continued) Herpes zoster keratitis. B. Herpes zos er virus can cause a similar disci orm kera i is o herpes simplex virus. In his eye, cen ral corneal edema and mul iple small kera ic precipi a es are seen using he sli -bean view. Herpes zoster keratitis. C. S ignif can limbal in amma ion and an ac ive corneal mel are presen in his eye wi h a his ory o herpes zos er kera i is. I responded well o a conjunc ival ap procedure.
(continued)
LWBK961-C07_p168-235.indd 199 22/07/11 10:16 AM

200 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
FIGURE 7-9. (Continued) Herpes zoster keratitis. D. Mul iple eleva ed, plaquelike pseudodendri es are presen in his eye several weeks a er a herpes zos er derma i is around his eye. E. Fluorescein s ain wi h a cobal blue ligh highligh s he pseudodendri es seen in D. No e ha hey lack he classic “ ree branch” pat ern, eleva ed edges, and erminal end bulbs o herpes simplex dendri es.
(continued)
D
E
LWBK961-C07_p168-235.indd 200 22/07/11 10:16 AM
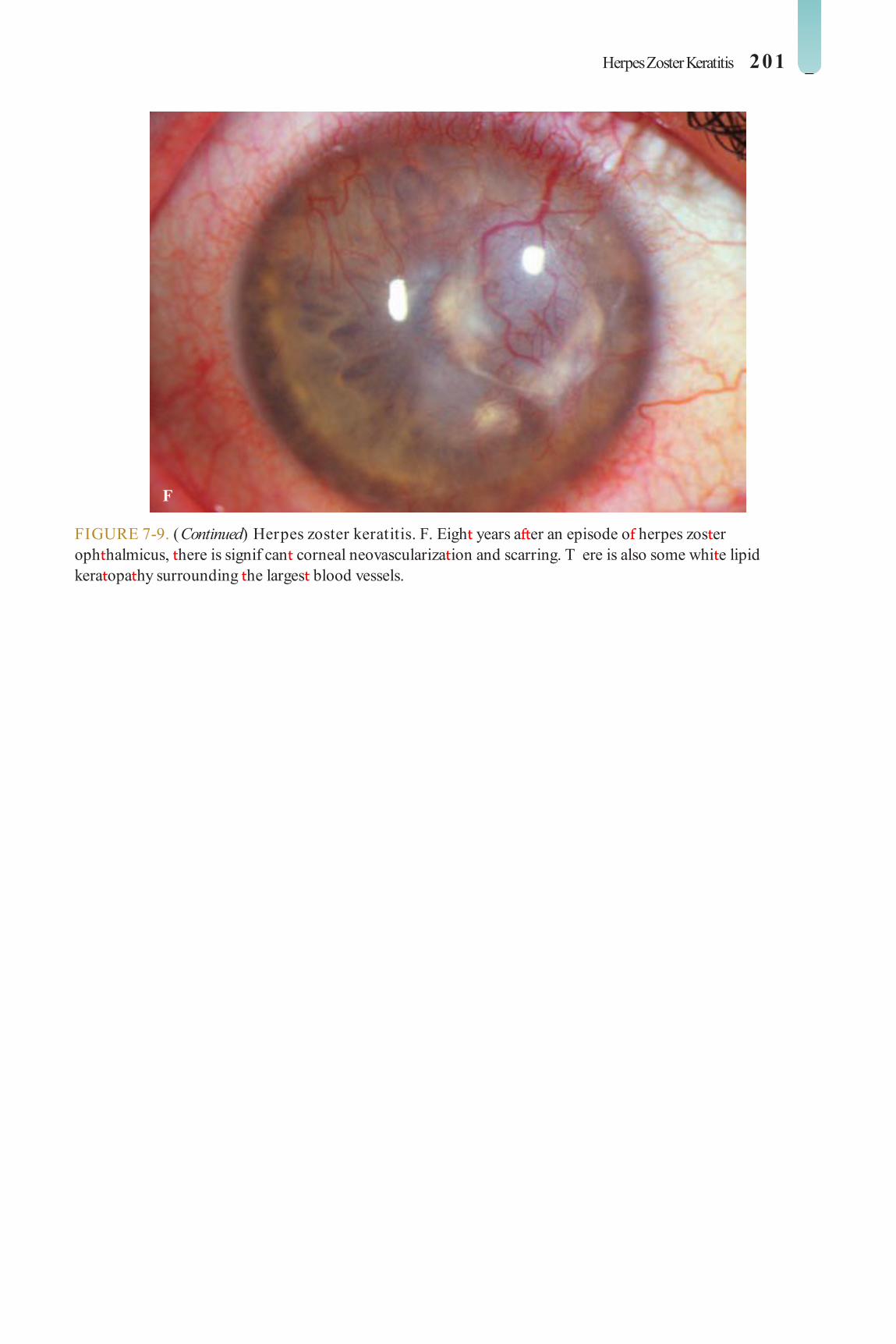
Herpes Zoster Keratitis 201
FIGURE 7-9. (Continued) Herpes zoster keratitis. F. Eigh years a er an episode o herpes zos er oph halmicus, here is signif can corneal neovasculariza ion and scarring. T ere is also some whi e lipid kera opa hy surrounding he larges blood vessels.
F
LWBK961-C07_p168-235.indd 201 22/07/11 10:16 AM
202 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
INTERSTITIAL KERATITIS (SYPHILITIC, NONSYPHILITIC)
In ers i ial kera i is is an uncommon, bila eral in amma ion o he corneal s roma wi h-
ou primary involvemen o he epi helium or endo helium. I has a wide varie y o causes.
Etiology Congeni al or acquired syphilis
( Treponema pallidum ) Lyme disease ( Borrelia burgdorferi ) uberculosis (Mycobacterium tuberculosis) Herpes simplex, herpes zos er, Eps ein-
Barr, mumps virus Leprosy (Mycobacterium leprae) Cogan’s syndrome: inni us, ver igo,
and dea ness. Associa ed wi h polyar eri is nodosa, Wegener granuloma osis, and rheu-ma oid ar hri is. Cogan’s syndrome is a rare condi ion.
Symptoms Bila eral pain, redness, earing, blurred vision
Nonspeci c Corneal Features Di use mids romal edema, neovascular-
iza ion, and nonsuppura ive inf l ra ion Mild iri is, kera ic precipi a es Inac ive signs include deep s romal scar-
ring associa ed wi h nonper used (ghos ) vessels ( Fig. 7-10 A–D)
Speci c Ocular Features Syphilis
Congeni al syphilis is associa ed wi h acu e in ers i ial kera i is in he f rs wo decades o li e.
Acquired syphilis has ewer corneal f ndings and more pos erior segmen involvemen .
uberculosis: in ers i ial kera i is, phlyc- enulosis, granuloma ous iridocycli is, re inal vasculi is, choroidi is
Lyme disease: enlarging skin rash (ery hema chronicum migrans), conjunc ivi is, episcleri is, in ers i ial kera i is ( Fig. 7-10 E), granuloma- ous iridocycli is, in ermedia e uvei is, cranial nerve, re inal, and orbi al abnormali ies
Leprosy: conjunc ivi is, episcleri is, scle-ri is, in ers i ial kera i is, hickened corneal nerves, corneal hypes hesia, granuloma ous iridocycli is, iris pearls, nodular leproma, iris a rophy, anisocoria, eyelid and lacrimal abnormali ies, ca arac , acial nerve palsy
Diagnosis Syphilis
Fluorescen reponemal an ibody absorp ion (F A-Abs) or microhemagglu- ina ion- Treponema pallidum (MHA- P) es (specif c es s or reponemal an ibod-ies). Usually remains posi ive or li e
Venereal Disease Research Labora ory (VDRL) or rapid plasma reagin (RPR) es (nonspecif c es s are posi ive during acu e in ec ion). Use ul or screening and or moni oring ac ivi y o disease
uberculosis: examina ion o spu um or acid- as bacilli, ches radiograph, purif ed pro ein deriva ive (PPD) skin es . New in er- eron release assay (e.g., Quan iFERON- B Gold) may also be help ul.
Lyme disease: his ory o exposure o deer, mouse, or ick bi e, direc immuno uorescen an ibody es
Leprosy: skin scrapings or Ziehl-Neelsen s ain
Cogan’s syndrome: Consul an o orhinolaryngologis .
Treatment Kera ouvei is: opical cor icos eroids
(prednisolone 1% or dexame hasone
LWBK961-C07_p168-235.indd 202 22/07/11 10:16 AM

Interstitial Keratitis (Syphilitic, Nonsyphilitic) 203
0.1% q2–4h) and cycloplegics (scopolamine 0.25% or cyclopen ola e 1% .i.d.)
Syphilis, uberculosis, Lyme disease, lep-rosy: Re er o an in ernis , pulmonologis , or in ec ious disease specialis or appropria e rea men .
Cogan’s syndrome: Re er o an o orhi-nolaryngologis or sys emic cor icos eroid
rea men o preven permanen hearing loss.
Prognosis Generally good wi h appropria e rea -
men . Signif can permanen corneal scarring can resul and may require corneal ransplan- a ion when nonin amed.
FIGURE 7-10. Interstitial keratitis. A. T is pa ien wi h a his ory o congeni al syphilis has old corneal s romal scarring. T e clearer lines are old blood vessels. T e scarring may be mid-s romal or pos erior s romal, and here is o en modera e corneal hinning.
(continued)
A
LWBK961-C07_p168-235.indd 203 22/07/11 10:16 AM

204 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
C
FIGURE 7-10. (Continued) Interstitial keratitis. B. Numerous corneal s romal “ghos ” vessels are seen. T e pa ien had a his ory o congeni al syphilis. C. T is le eye has signif can pa chy and ea herlike cen ral scarring rom in ers i ial kera i is. T ere are also many ghos vessels nasally.
(continued)
B
LWBK961-C07_p168-235.indd 204 22/07/11 10:16 AM

Interstitial Keratitis (Syphilitic, Nonsyphilitic) 205
D
E
FIGURE 7-10. (Continued) Interstitial keratitis. D. Sli -beam pho o o he same eye nicely demons ra es ha he scarring in in ers i ial kera i is is primarily pos erior. E. Nummular corneal inf l ra es are presen in his eye o a pa ien wi h Lyme disease. T e pa ien was rea ed sys emically or Lyme disease, and he inf l ra es responded o opical cor icos eroids.
LWBK961-C07_p168-235.indd 205 22/07/11 10:16 AM

206 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
SUBEPITHELIAL INFILTRATES
Subepi helial inf l ra es are a common uni-la eral or bila eral kera opa hy ha is ypi-
cally caused by viruses.
Etiology Adenovirus or Eps ein-Barr virus in ec ion Blephari is, ocular rosacea Con ac lens–induced reac ion, may be
exacerba ed by preserva ives in lens care solu ions
T ygeson’s superf cial punc a e kera opa hy S aphylococcal or chlamydial in ec ions Lyme disease Epi helial corneal gra rejec ion in donor
cornea (Krachmer’s spo s)
Symptoms Pho ophobia, oreign-body sensa ion, red-
ness, earing, mild blurring o vision, may be asymp oma ic
Signs Few or mul iple, unila eral or bila eral,
granular, small, oval or circular, subepi helial
opaci ies, which may s ain wi h rose bengal bu s ain poorly wi h uorescein ( Fig. 7-11 )
Dif erential Diagnosis Superf cial punc a e kera opa hy: mul iple
punc a e epi helial de ec s ha s ain well wi h uorescein bu no wi h rose bengal
Treatment rea underlying condi ion. Discon inue
con ac lens wear. Preserva ive- ree ar if cial ear drops or
gels q2–6h and lubrica ing oin men q.h.s. or b.i.d.
Mild opical cor icos eroid (e.g., lo epred-nol 0.2% or uorome holone drops 0.1% q.i.d.) i vision is a ec ed or symp oms are severe. May require a slow aper o preven recurrence
Prognosis Good, especially i underlying condi ion
can be iden if ed. When cor icos eroids are used, hey o en mus be apered very slowly o preven recurrence. Long-s anding sub-epi helial inf l ra es can resul in permanen scars.
FIGURE 7-11. Subepithelial inf ltrates a er viral conjunctivitis. A. T is eye has numerous ac ive cen ral subepi helial inf l ra es a er adenoviral kera oconjunc ivi is. T ese responded well o opical s eroids.
(continued)
A
LWBK961-C07_p168-235.indd 206 22/07/11 10:16 AM

Subepithelial Inf ltrates 207
B
C
FIGURE 7-11. (Continued) Subepithelial inf ltrates a er viral conjunctivitis. B. Over 100 ac ive subepi helial inf l ra es recurred a er opical s eroids were apered rapidly. T ey improved grea ly on a slower s eroid aper. Some eyes need o be on low-dose opical s eroids or mon hs o years o preven recurrence. C. M ul iple subepi helial inf l ra es can be seen cen rally in his eye many mon hs a er adenoviral kera oconjunc ivi is causing glare, halos, and decreased vision. Some o hese inf l ra es appear sligh ly ac ive, while o hers appear more s carred.
LWBK961-C07_p168-235.indd 207 22/07/11 10:16 AM

208 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
SUPERFICIAL PUNCTATE KERATOPATHY (PUNCTATE EPITHELIAL EROSIONS)
Superf cial punc a e kera opa hy is a com-mon nonspecif c f nding seen in a wide
varie y o corneal disorders.
Etiology Primarily superior
Sub arsal oreign body or concre ions Vernal kera oconjunc ivi is Superior limbic kera oconjunc ivi is rachoma Poorly f t ing con ac lens Floppy eyelid syndrome richiasis or dis ichiasis
Primarily in erpalpebral Kera oconjunc ivi is sicca Neuro rophic kera opa hy Exposure o ul raviole ligh Con ac lens–rela ed (chemical
oxici y, igh lens syndrome, overwear syndrome)
Primarily in erior Rosacea, blephari is Exposure kera opa hy, including noc-
urnal lagoph halmos Lower eyelid margin lesions oxici y rom drops or chemical injury En ropion or ec ropion richiasis or dis ichiasis
rauma, chemical injury Sel -in ic ed, eye rubbing
Symptoms Foreign-body sensa ion, earing, and
decreased o vision i cen ral cornea is a ec ed
Signs Mul iple, iny, pinpoin epi helial de ec s
ha s ain well wi h uorescein. T ey may be con uen i severe ( Fig. 7-12 ).
Dif erential Diagnosis Subepi helial inf l ra es: ew or mul iple,
unila eral or bila eral, granular, small epi helial or subepi helial opaci ies ha may s ain wi h rose bengal bu s ain poorly wi h uorescein
Treatment rea underlying disorder. Discon inue con ac lens wear and oxic
medica ions. Preserva ive- ree ar if cial ear drops or
gels q1–6h and lubrica ing oin men q.h.s. or b.i.d., depending on severi y. Consider punc- al occlusion wi h plugs or cau ery.
opical an ibio ic oin men (e.g., ery h-romycin, baci racin, polymyxin B/ baci racin, or e racycline) wo o our imes a day may be added.
Avoid opical medica ions con aining preserva ives.
Prognosis Generally good, bu depends on he
underlying condi ion.
LWBK961-C07_p168-235.indd 208 22/07/11 10:16 AM

Superfcial Punctate Keratopathy (Punctate Epithelial Erosions) 209
A
B
FIGURE 7-12. Superf cial punctate keratopathy. A. Fluorescein dye and cobal blue ligh reveal signif can in erior corneal punc a e s aining. B. Fluorescein dye and cobal blue ligh demons ra e severe cen ral punc a e s aining. T e s aining is almos con uen in eriorly.
LWBK961-C07_p168-235.indd 209 22/07/11 10:16 AM

210 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
THYGESON’S SUPERFICIAL PUNCTATE KERATOPATHY
Thygeson’s superf cial punc a e kera opa- hy is an uncommon, usually bila eral,
idiopa hic condi ion ha has a chronic course wi h exacerba ions and remissions. I may resolve spon aneously a er many years.
Etiology Unknown. Some physicians believe i is o
viral origin.
Symptoms Pho ophobia, oreign-body sensa ion,
earing, mildly decreased vision, may be asymp oma ic
Signs A ew o hundreds o course, punc a e or
s ella e, round o oval grayish-whi e clus ers o epi helial lesions ha occur hroughou he cornea, are sligh ly eleva ed, and s ain mini-mally wi h uorescein ( Fig. 7-13 )
T e conjunc iva is no injec ed, and he an erior chamber is quie .
Treatment Ar if cial ear drops q2–6h and lubrica ing
oin men q.h.s. or b.i.d., depending on severi y Mild opical cor icos eroid (e.g., lo epre-
dnol 0.2% o 0.5% or uorome holone drops 0.1% q.i.d.) i vision is a ec ed or symp oms are severe. Cor icos eroid drops can usu-ally be apered, bu recurrence is common. Pa ien s may need long- erm low-dose cor i-cos eroids o remain asymp oma ic.
T erapeu ic so con ac lenses may pro-vide symp oma ic relie i cor icos eroid herapy ails or is con raindica ed.
opical cyclosporine drops have been repor ed o help in cer ain pa ien s and may allow he dosage o opical cor icos eroid o be reduced.
Prognosis Good or signif can ly improved symp oms,
bu he condi ion is o en chronic and recurren .
LWBK961-C07_p168-235.indd 210 22/07/11 10:16 AM

T ygeson’s Superfcial Punctate Keratopathy 211
A
B
FIGURE 7-13. T ygeson’s superf cial punctate keratopathy. A. Mul iple small epi helial lesions are presen in he cen ral cornea. T ey may s ain minimally wi h uorescein dye. B. T e same eye seen wi h re roillumina ion o he re ina. No e he coarse, sligh ly s ella e na ure o he epi helial lesions.
LWBK961-C07_p168-235.indd 211 22/07/11 10:16 AM
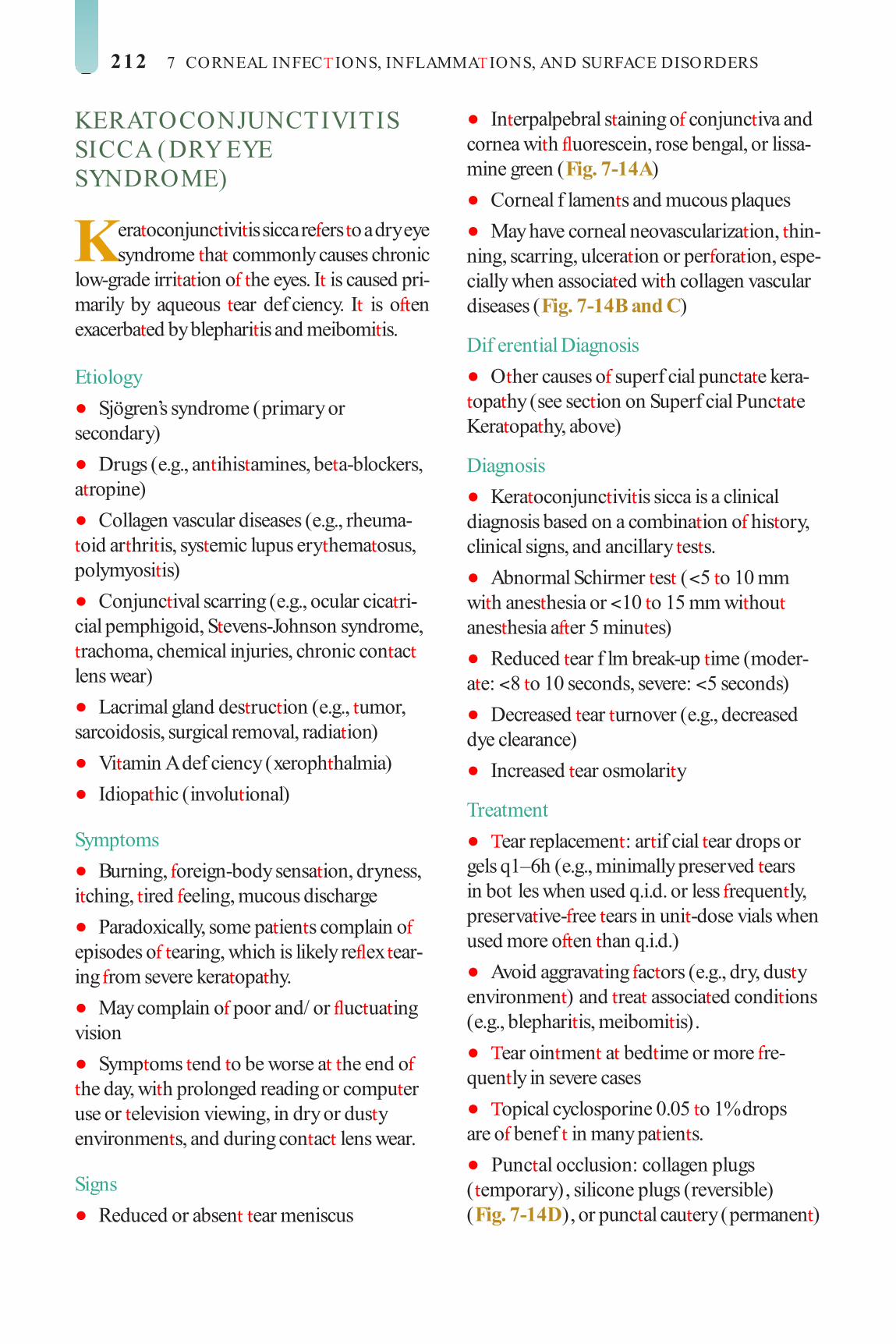
212 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
KERATOCONJUNCTIVITIS SICCA (DRY EYE SYNDROME)
Kera oconjunc ivi is sicca re ers o a dry eye syndrome ha commonly causes chronic
low-grade irri a ion o he eyes. I is caused pri-marily by aqueous ear def ciency. I is o en exacerba ed by blephari is and meibomi is.
Etiology Sjögren’s syndrome (primary or
secondary) Drugs (e.g., an ihis amines, be a-blockers,
a ropine) Collagen vascular diseases (e.g., rheuma-
oid ar hri is, sys emic lupus ery hema osus, polymyosi is)
Conjunc ival scarring (e.g., ocular cica ri-cial pemphigoid, S evens-Johnson syndrome, rachoma, chemical injuries, chronic con ac lens wear)
Lacrimal gland des ruc ion (e.g., umor, sarcoidosis, surgical removal, radia ion)
Vi amin A def ciency (xeroph halmia) Idiopa hic (involu ional)
Symptoms Burning, oreign-body sensa ion, dryness,
i ching, ired eeling, mucous discharge Paradoxically, some pa ien s complain o
episodes o earing, which is likely re ex ear-ing rom severe kera opa hy.
May complain o poor and/ or uc ua ing vision
Symp oms end o be worse a he end o he day, wi h prolonged reading or compu er use or elevision viewing, in dry or dus y environmen s, and during con ac lens wear.
Signs Reduced or absen ear meniscus
In erpalpebral s aining o conjunc iva and cornea wi h uorescein, rose bengal, or lissa-mine green ( Fig. 7-14 A)
Corneal f lamen s and mucous plaques May have corneal neovasculariza ion, hin-
ning, scarring, ulcera ion or per ora ion, espe-cially when associa ed wi h collagen vascular diseases ( Fig. 7-14 B and C)
Dif erential Diagnosis O her causes o superf cial punc a e kera-
opa hy (see sec ion on Superf cial Punc a e Kera opa hy, above)
Diagnosis Kera oconjunc ivi is sicca is a clinical
diagnosis based on a combina ion o his ory, clinical signs, and ancillary es s.
Abnormal Schirmer es ( < 5 o 10 mm wi h anes hesia or < 10 o 15 mm wi hou anes hesia a er 5 minu es)
Reduced ear f lm break-up ime (moder-a e: < 8 o 10 seconds, severe: < 5 seconds)
Decreased ear urnover (e.g., decreased dye clearance)
Increased ear osmolari y
Treatment ear replacemen : ar if cial ear drops or
gels q1–6h (e.g., minimally preserved ears in bot les when used q.i.d. or less requen ly, preserva ive- ree ears in uni -dose vials when used more o en han q.i.d.)
Avoid aggrava ing ac ors (e.g., dry, dus y environmen ) and rea associa ed condi ions (e.g., blephari is, meibomi is).
ear oin men a bed ime or more re-quen ly in severe cases
opical cyclosporine 0.05 o 1% drops are o benef in many pa ien s.
Punc al occlusion: collagen plugs ( emporary), silicone plugs (reversible) ( Fig. 7-14 D), or punc al cau ery (permanen )
LWBK961-C07_p168-235.indd 212 22/07/11 10:16 AM

Keratoconjunctivitis Sicca (Dry Eye Syndrome) 213
Cus om-f , wrap-around glasses (e.g., 7eye, Panop x)
Eye pa ch, mois chamber, or small la eral arsorrhaphy can aid in ear preserva ion.
Filamen s can be removed mechanically wi h orceps. Ace ylcys eine 10% drops (e.g., Mucomys ) q.i.d. can help in f lamen ary kera opa hy.
Hydroxypropyl cellulose inser (e.g., Lacriser ) may be help ul.
Au ologous serum drops or a scleral lens in severe cases.
Work up and rea underlying sys emic disorders, especially collagen vascular condi- ions, i severe.
Prognosis Good or improvemen in symp oms, bu
i depends on he underlying e iology. Mos causes are chronic and require prolonged herapy.
LWBK961-C07_p168-235.indd 213 22/07/11 10:17 AM

214 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
FIGURE 7-14. Keratoconjunctivitis sicca. A. Severe superf cial punc a e epi heliopa hy is presen cen rally and in eriorly in his pa ien wi h severe dry eye syndrome. In eriorly he kera opa hy is con uen . B. A deep s erile corneal mel is presen in his eye wi h severe dry eye syndrome. T e sli -beam view reveals approxima ely 90% issue loss.
(continued)
A
B
LWBK961-C07_p168-235.indd 214 22/07/11 10:17 AM
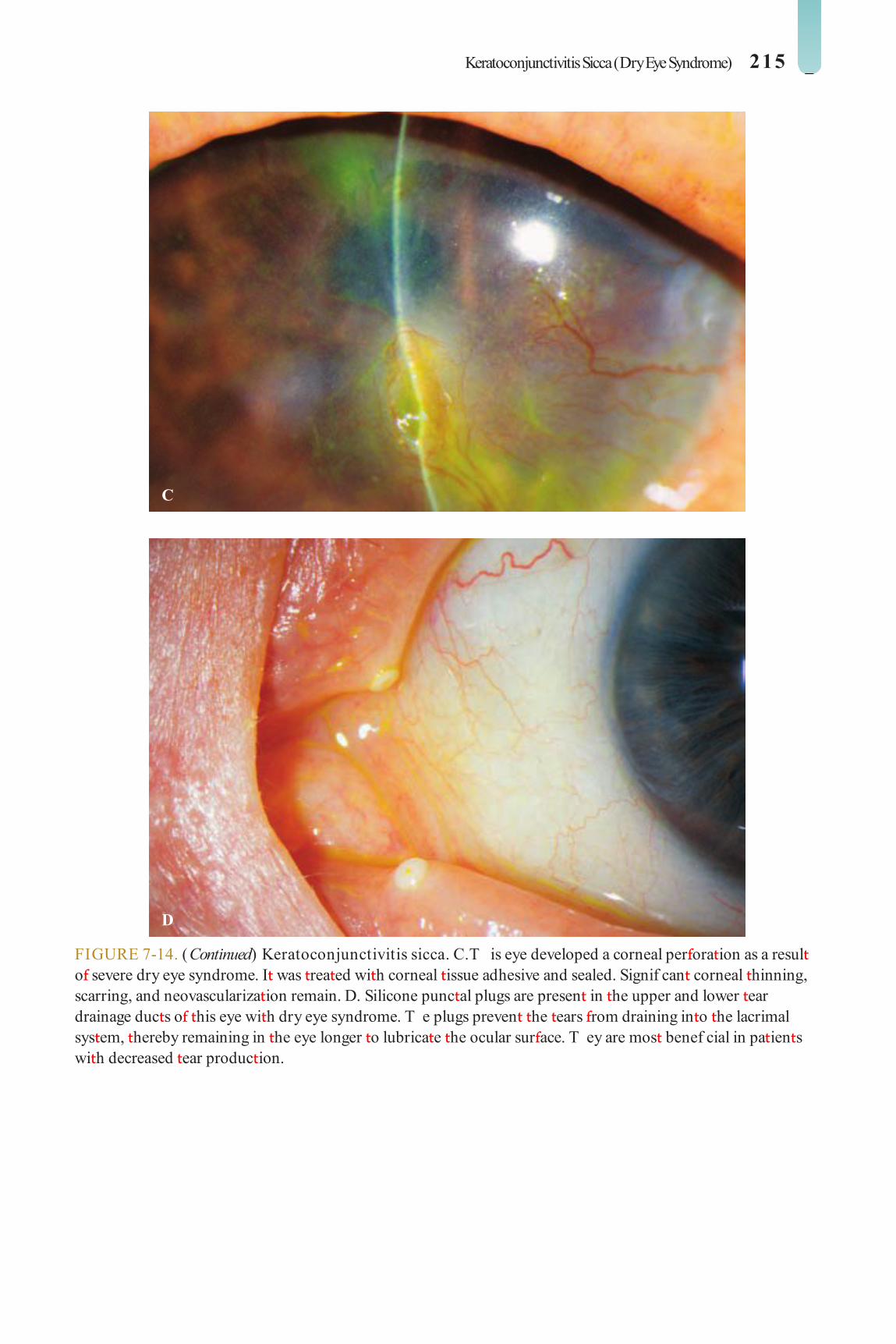
Keratoconjunctivitis Sicca (Dry Eye Syndrome) 215
C
D
FIGURE 7-14. (Continued) Keratoconjunctivitis sicca. C. T is eye developed a corneal per ora ion as a resul o severe dry eye syndrome. I was rea ed wi h corneal issue adhesive and sealed. Signif can corneal hinning, scarring, and neovasculariza ion remain. D. Silicone punc al plugs are presen in he upper and lower ear drainage duc s o his eye wi h dry eye syndrome. T e plugs preven he ears rom draining in o he lacrimal sys em, hereby remaining in he eye longer o lubrica e he ocular sur ace. T ey are mos benef cial in pa ien s wi h decreased ear produc ion.
LWBK961-C07_p168-235.indd 215 22/07/11 10:17 AM

216 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
FILAMENTARY KERATOPATHY
Filamen ary kera opa hy is a rela ively com-mon, unila eral or bila eral condi ion aris-
ing rom aberran healing o he epi helium. I can be caused by a varie y o disorders.
Etiology Kera oconjunc ivi is sicca Prolonged eye pa ching or p osis Superior limbic kera oconjunc ivi is Recurren corneal erosions Neuro rophic/ exposure kera opa hy Diminished corneal sensa ion Essen ial blepharospasm Pos opera ive, near wound Midbrain s rokes
Symptoms Foreign-body sensa ion, pain, redness,
decreased vision
Signs Mucus hreads con aining desquama ed
epi helial cells ha s ain wi h uorescein
at ached a one end o he corneal epi he-lium, conjunc ival injec ion, punc a e epi helial erosions, abnormal ear f lm ( Fig. 7-15 )
Treatment Work up and rea underlying disorder. Lubrica ion wi h preserva ive- ree ar i-
f cial ear drops q1–6h and oin men q.h.s. Punc al occlusion wi h plugs or cau ery i dry
Debridemen o f lamen s a heir base using a pair o jeweler’s orceps or a cot on- ipped applica or under opical anes hesia
Ace ylcys eine 10% drops (e.g., Mucomys ) q.i.d.
Bandage so con ac lens wi h opical an i-bio ic drops .i.d. or a ew weeks i symp oms are severe or i medica ions have ailed, i no associa ed wi h signif can dry eye.
Prognosis Good or improvemen in symp oms, bu
prognosis depends on he underlying e iol-ogy. Mos causes are chronic and require pro-longed herapy.
LWBK961-C07_p168-235.indd 216 22/07/11 10:17 AM

Filamentary Keratopathy 217
A
B
FIGURE 7-15. Filamentary keratopathy. A. Several f lamen s (epi helial mucoid s rands) ha s ain wi h uorescein dye are presen superiorly in his pa ien wi h dry eye syndrome. B. Mul iple s aining f lamen s are seen using he cobal blue ligh in his eye wi h a poor ocular sur ace and a his ory o old severe in ers i ial kera i is.
LWBK961-C07_p168-235.indd 217 22/07/11 10:17 AM

218 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
EXPOSURE KERATOPATHY
Exposure kera opa hy is caused by drying o he ocular sur ace as a resul o abnormal
eyelid blinking or incomple e eyelid closure.
Etiology Facial nerve palsy Eyelid malposi ions (e.g., ec ropion or
scarring a er p osis surgery or rauma) Noc urnal lagoph halmos Prop osis (e.g., dys hyroid eye disease) Eyelid coloboma A er blepharoplas y or eyelid excision or
umors
Symptoms Irri a ion, burning, oreign-body sensa-
ion, earing, epiphora, decreased vision, o en worse upon awakening
May have a his ory o sleeping wi h eyes open
Signs Incomple e blinking or closure o eyelids
( Fig. 7-16 A) Eyelid de ormi y or malposi ion may be
no ed ( Fig. 7-16 B).
Corneal desicca ion wi h loss o normal lus er, punc a e epi helial erosions, or epi he-lial de ec a ec ing mainly he in erior in er-palpebral region
In more severe cases, pannus, s erile ulcer-a ion, secondary in ec ion, or, rarely, per ora- ion can develop.
Treatment Correc underlying eyelid disorder. Lubrica e wi h ar if cial ears/ gels (more
viscous prepara ions are pre erred) q1–4h during he day and ear oin men or an ibio ic oin men a nigh .
Al erna ively, ar if cial ear or an ibio ic oin men q.i.d. can be used.
Eyelid aping, pa ching, or mois ure cham-ber a bed ime wi h oin men s
arsorrhaphy or gold weigh implan in he upper eyelid can be considered or more permanen rea men .
Prognosis Fair o good, depending on he under-
lying e iology. Worse i associa ed wi h decreased corneal sensa ion or a poor Bell’s phenomenon
LWBK961-C07_p168-235.indd 218 22/07/11 10:17 AM

Exposure Keratopathy 219
FIGURE 7-16. Exposure keratopathy. A. A band o in erior punc a e uorescein s aining is apparen in his eye o a pa ien wi h exposure rom noc urnal lagoph halmos. B. T is pa ien has an in erior eyelid abnormali y leading o poor eyelid coverage and exposure kera opa hy. Corneal hinning and scarring rom previous corneal ulcera ion can be no ed in erocen rally.
A
B
LWBK961-C07_p168-235.indd 219 22/07/11 10:17 AM

220 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
NEUROTROPHIC KERATOPATHY
Neuro rophic kera opa hy occurs in eyes wi h diminished corneal sensa ion. I is
usually acquired bu can rarely be congeni al.
Etiology Previous herpes zos er or simplex
in ec ion A er ocular surgery (e.g., corneal rans-
plan a ion, corneal re rac ive surgery such as laser-assis ed in-si u kera omileusis [LASIK] or sur ace abla ion)
Radia ion kera opa hy Eye drops (e.g., anes he ic, imolol, non-
s eroidal an i-in amma ory agen s) Chronic con ac lens wear Surgery on he rigeminal nerve or ic
douloureux S roke Long-s anding diabe es, especially a er
eye surgery Leprosy Familial dysau onomia (Riley-Day
syndrome)
Symptoms Redness, earing, burning, oreign-body
sensa ion, decreased vision
Signs In erpalpebral punc a e epi helial erosions Epi helial de ec s wi h heaped-up edges
ha are slow o heal and s ain wi h uorescein ( Fig. 7-17 A)
Secondary in ec ion may occur. In severe cases, s erile ulcera ion, kera i is,
iri is, and hypopyon can be seen ( Fig. 7-17 B). Corneal per ora ion may occur in
advanced cases.
Treatment T e mains ay o rea men is lubrica ion
wi h preserva ive- ree ar if cial ears/ gels (more viscous prepara ions are pre erred) q1–4h during he day and ear oin men or an ibio ic oin men (e.g., ery hromycin, baci- racin) a nigh .
Al erna ively, ar if cial ear oin men or an ibio ic oin men (e.g., ery hromycin, baci- racin) q2–6h can be subs i u ed.
In cases wi h ulcera ion, pa ching, arsor-rhaphy, bo ulinum oxin injec ion o induce p osis, amnio ic membrane gra , or conjunc- ival ap can be employed.
Prognosis Fair, depending on underlying e iology.
T e goal is o preven secondary complica- ions, because he nerves may no regenera e a grea deal.
LWBK961-C07_p168-235.indd 220 22/07/11 10:17 AM
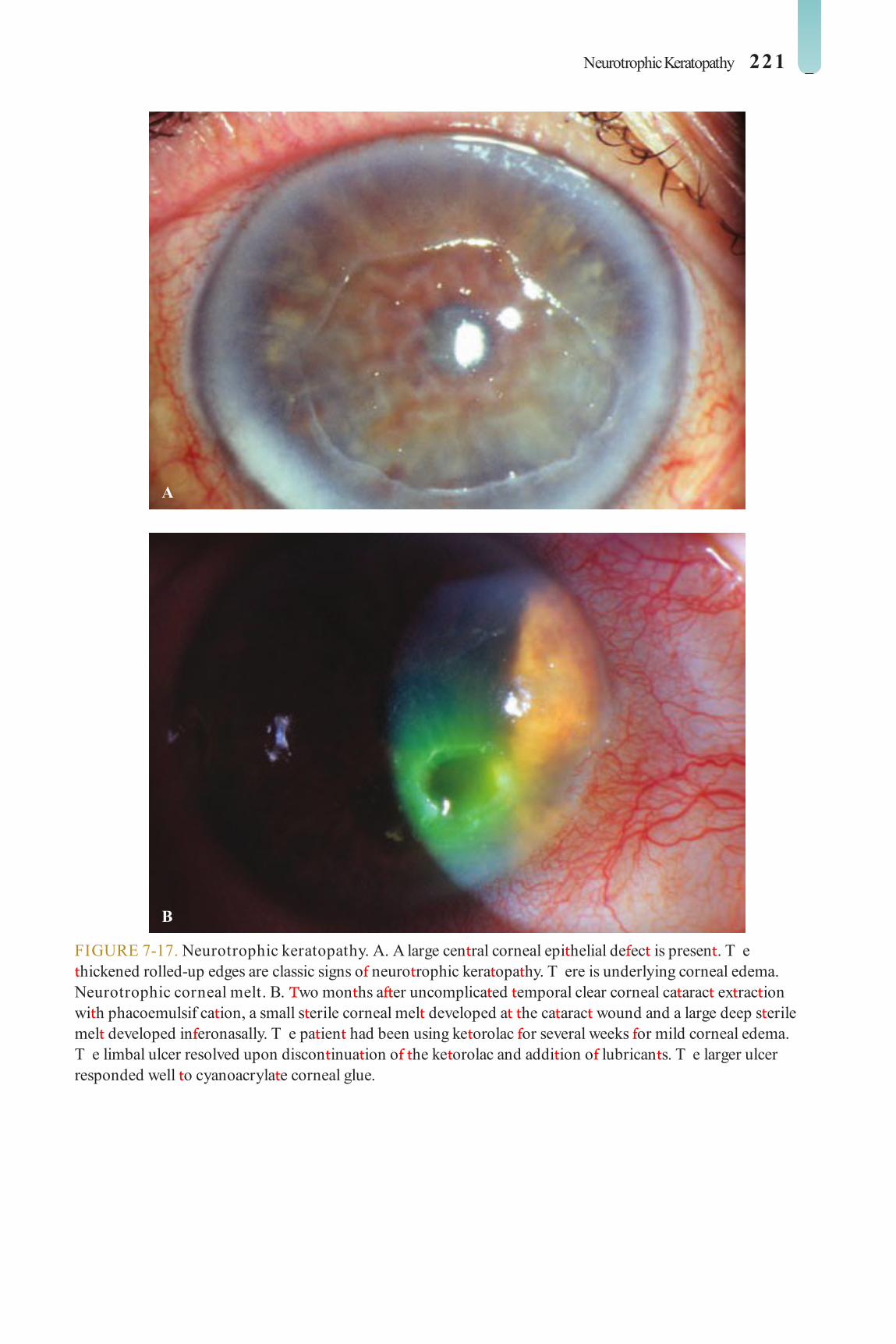
Neurotrophic Keratopathy 221
FIGURE 7-17. Neurotrophic keratopathy. A. A large cen ral corneal epi helial de ec is presen . T e hickened rolled-up edges are classic signs o neuro rophic kera opa hy. T ere is underlying corneal edema. Neurotrophic corneal melt. B. wo mon hs a er uncomplica ed emporal clear corneal ca arac ex rac ion wi h phacoemulsif ca ion, a small s erile corneal mel developed a he ca arac wound and a large deep s erile mel developed in eronasally. T e pa ien had been using ke orolac or several weeks or mild corneal edema. T e limbal ulcer resolved upon discon inua ion o he ke orolac and addi ion o lubrican s. T e larger ulcer responded well o cyanoacryla e corneal glue.
A
B
LWBK961-C07_p168-235.indd 221 22/07/11 10:17 AM

222 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
RECURRENT CORNEAL EROSION
Recurren corneal erosion ypically occurs in eyes ha have previously sus ained an
acu e, sharp abrasion (e.g., rom a f ngernail, ree branch, or paper-edge injury) o he cor-nea and in eyes wi h corneal dys rophies.
Etiology and Pathophysiology Previous rauma ic corneal abrasion Corneal dys rophy (e.g., epi helial base-
men membrane [EBM], Meesmann’s, Reis-Bücklers, lat ice, granular dys rophies); may have a amily his ory
Diabe es melli us Dis urbance o Bowman’s layer, resul ing
in de ec ive hemidesmosomal at achmen o he epi helium o he basemen membrane. T e loosely at ached epi helium is easily eroded, and his perpe ua es he dis urbance and is responsible or he recurren na ure o he disorder.
Symptoms Recurren at acks o acu e, sharp pain,
ypically during sleep or upon awakening earing, pho ophobia, mild o severe blur-
ring o vision His ory o superf cial corneal injury in
recen or dis an pas
Signs Minimal o severe localized epi helial
irregulari ies wi h nega ive uorescein s ain-ing ( Fig. 7-18 A and B)
Frank epi helial de ec may some imes be seen during acu e s ages.
Do s, microcys s, and f ngerprin pat erns o EBM dys rophy may bes be seen wi h
re roillumina ion. O her corneal dys rophies can be seen on sli -lamp examina ion, so bo h eyes should be examined.
Treatment Ar if cial ear drops q2–6h and lubrica -
ing oin men q.h.s. or lubrica ing oin men q2–6h.
opical an ibio ic oin men (e.g., ery hro-mycin or baci racin) hree o our imes a day un il he epi helial de ec has healed.
Cycloplegics (scopolamine 0.25% or cyclopen ola e 1% .i.d.) i iri is is presen .
Consider a pressure pa ch or 24 hours during acu e s ages.
Once healing is comple e: ar if cial ear drops q.i.d. and oin men q.h.s. or sodium chloride 5% drops q.i.d. and oin men q.h.s. or a leas 3 o 6 mon hs
I epi helium is grossly loose, recurrence is requen , or when medical herapy ails, he ollowing measures can be considered:
Epi helial debridemen An erior s romal micropunc ure or
small areas o erosions ou side he visual axis ( Fig. 7-18 C and D)
Diamond burr polishing o Bowman’s membrane or larger areas o erosions
Excimer laser pho o herapeu ic kera ec- omy (P K) or larger areas o erosions
Ex ended wear o a bandage so con ac lens or 3 o 6 mon hs (wi h appropria e replacemen )
Prognosis Very good o excellen wi h proper
managemen . Recurrences can occur even wi h surgical rea men , bu surgery can be repea ed.
LWBK961-C07_p168-235.indd 222 22/07/11 10:17 AM

Recurrent Corneal Erosion 223
FIGURE 7-18. Recurrent erosion syndrome. A. An area o loose, gray, hickened epi helium is seen in his eye wi h a healing recurren erosion. In eyes wi h mild erosions, he sli -lamp examina ion may be essen ially normal several hours a er an erosion. One mus look care ully or epi helial irregulari ies. B. A er uorescein s ain using a cobal blue ligh , a large area o loose epi helium is qui e apparen . Areas o nega ive s aining indica e eleva ed, hickened epi helium. Cen rally, mild uorescein s aining is presen where he epi helial de ec has almos comple ely healed.
(continued)
A
B
LWBK961-C07_p168-235.indd 223 22/07/11 10:17 AM

224 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
C
D
FIGURE 7-18. (Continued) Recurrent erosion syndrome. C. T is pho ograph was aken immedia ely a er an erior s romal micropunc ure was per ormed. Under sli -lamp illumina ion, approxima ely 150 small punc ures in o he an erior 20% o he cornea were per ormed wi h a 25-gauge needle in he area o recurren erosion. Numerous iny air bubbles under he epi helium are presen . D. T ree mon hs a er an erior s romal micropunc ure or recurren erosion syndrome, mul iple iny linear scars can be seen. Ideally, his procedure is per ormed ou side he visual axis, as occasionally hese scars can a ec vision.
LWBK961-C07_p168-235.indd 224 22/07/11 10:17 AM

Bullous Keratopathy 225
BULLOUS KERATOPATHY
Bullous kera opa hy is a airly common con-di ion resul ing rom endo helial decom-
pensa ion, which is charac erized by corneal edema.
Etiology Pos opera ive endo helial damage (e.g.,
aphakic or pseudophakic bullous kera opa- hy) ( Fig. 7-19 A–C)
Endo helial dys rophy (e.g., Fuchs’, pos e-rior polymorphous, congeni al heredi ary)
Corneal gra ailure Blun or pene ra ing an erior segmen
rauma (e.g., orceps delivery, ocular rauma) Iridocorneal endo helial syndrome (e.g.,
Chandler’s syndrome) Acu e angle-closure glaucoma Brown-McLean syndrome: peripheral
corneal edema o en associa ed wi h aphakia ( Fig. 7-19 D)
Symptoms Decreased vision, redness, earing, oreign-
body sensa ion, pain, pho ophobia
Signs Corneal s romal and epi helial edema,
superf cial vesicles or bullae, epi helial de ec s rom rup ured bullae, Desceme ’s olds, cor-nea gut a a
In long-s anding cases, may have neovas-culariza ion, subepi helial or s romal scarring
Diagnosis Pachyme ry shows an increase in corneal
hickness. Specular microscopy demons ra es
decreased endo helial cell densi y.
Treatment opical sodium chloride 5% drops q.i.d.
and oin men q.h.s. o reduce epi helial edema.
opical an ibio ic oin men q.i.d. or rup- ured bullae. Pa ching or bandage so con ac lenses can also be considered.
Cycloplegics (scopolamine 0.25% or cyclopen ola e 1% .i.d.) i iri is is presen .
Blow warm air over he cornea or 10 min-u es in he morning o reduce corneal edema.
Endo helial or pene ra ing corneal rans-plan or visual rehabili a ion i medical rea men ails. Old-s yle (closed-loop and iris-f xa ed) in raocular lenses should be removed.
For symp oma ic relie in a pain ul eye wi h poor vision po en ial, consider an erior s romal micropunc ure, P K, amnio ic mem-brane ransplan , or conjunc ival ap.
Con rol glaucoma and any associa ed iri is.
Prognosis Mild cases may re ain reasonable
vision and good com or or years, bu he endo helial cell loss is usually progressive. Success ra e is generally good wi h corneal ransplan a ion.
LWBK961-C07_p168-235.indd 225 22/07/11 10:17 AM

226 7 CORNEAL INFECTIONS, INFLAMMATIONS, AND SURFACE DISORDERS
A
B
FIGURE 7-19. Bullous keratopathy. A. Mild o modera e cen ral corneal edema causing decreased vision occurred af er uncomplica ed ca arac surgery. T e eye had pre-exis ing endo helial disease rom mild Fuchs’ dys rophy. A Desceme ’s s ripping endo helial kera oplas y was success ully per ormed. B. T is eye has signi can corneal edema, grea er in eriorly han superiorly. T ere is a closed-loop, Leiske an erior chamber in raocular lens implan . Closed-loop an erior chamber in raocular lens implan s were s rongly associa ed wi h causing bullous kera opa hy, of en requiring corneal ransplan a ion o achieve bet er vision. During corneal ransplan a ion, hese lenses are removed.
(continued)
LWBK961-C07_p168-235.indd 226 28/07/11 7:58 AM

Bullous Keratopathy 227
C
D
FIGURE 7-19. (Continued) Bullous keratopathy. C. T is eye developed poor vision a er complica ed ca arac surgery. Signif can corneal edema and a malposi ioned an erior chamber in raocular lens implan can be seen. T is eye underwen success ul corneal ransplan a ion and in raocular lens exchange. Brown McLean syndrome. D. Pronounced peripheral corneal edema is presen in his aphakic eye. T e chronic corneal edema has caused subepi helial f brosis. Vision remains ra her good because he cen ral cornea is rela ively clear.
LWBK961-C07_p168-235.indd 227 22/07/11 10:17 AM

228 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
ACQUIRED IMMUNODEFICIENCY SYNDROME
Acquired immunodef ciency syndrome (AIDS) is a condi ion charac erized
by he presence o oppor unis ic in ec ions, Kaposi’s sarcoma, and/ or lymphoma in an immunocompromised pa ien in ec ed wi h he human immunodef ciency virus.
Etiology Human immunodef ciency virus (HIV)
Symptoms May be asymp oma ic; o her symp oms
depend on he specif c problem.
Signs Nonspecif c ollicular conjunc ivi is,
punc a e epi helial kera i is, conjunc ival microangiopa hy, episcleri is, iri is may occur ( Fig. 7-20 A).
Herpes zos er oph halmicus Molluscum con agiosum: may have ex en-
sive lesions wi h minimal conjunc ivi is Kaposi’s sarcoma o eyelid or conjunc iva:
reddish-purple subepidermal or subepi helial nodule. T e subconjunc ival lesion may be mis aken or a subconjunc ival hemorrhage ( Fig. 7-20 B).
Microsporidial kera i is: chronic superf -cial punc a e kera i is ha does no respond
o conven ional rea men ( Fig. 7-20 C). Diagnosed by corneal scraping or Giemsa s ain. rea men is wi h opical umagillin and oral albendazole. Improves as immune s a us improves
Fungal, herpes simplex, or cy omegalovi-rus kera i is may also be seen.
Re inal microangiopa hy, cy omegalovirus (CMV) or Candida re ini is, Pneumocystis carinii or cryp ococcal choroidi is, oxo-plasma re inochoroidi is, ocular large-cell lymphoma
Syphilis Cranial nerve palsies, op ic neuropa hy
Diagnosis Enzyme-linked immunosorben assay
(ELISA) or serum HIV an ibody Wes ern blo es o conf rm diagnosis
Treatment Sys emic rea men by an in ernis or
in ec ious disease specialis Oppor unis ic in ec ions are rea ed
accordingly wi h an imicrobial medica ions. Kaposi’s sarcoma: local irradia ion,
excision, cryo herapy, and/ or sys emic chemo herapy
Prognosis Good o poor, depending on he severi y
o he HIV disease
LWBK961-C07_p168-235.indd 228 22/07/11 10:17 AM

Acquired Immunodefciency Syndrome 229
FIGURE 7-20. Acquired immune def ciency syndrome. A. Severe persis en conjunc ivi is has caused a chronic kera i is and dry eye s a e. T ere is signif can corneal neovasculariza ion, especially in eriorly. T e cen ral cornea is kera inized rom chronic sur ace disease. B. T is subconjunc ival vascular mass is a Kaposi’s sarcoma. I may be mis akenly hough o be a subconjunc ival hemorrhage, bu i does no resolve over a ew weeks. C. Mul iple cen ral and mid-peripheral small s ella e subepi helial opaci ies wi h mild overlying punc a e s aining are seen in his eye wi h cul ure-proven Microsporidia. (Pho o cour esy o Wee-Jin Heng, MD.)
A
B
C
LWBK961-C07_p168-235.indd 229 22/07/11 10:17 AM

230 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
CONTACT LENS COMPLICATIONS
TOXIC/ ALLE GIC CONJUNCTIVITIS Etiology
A hypersensi ivi y or oxic reac ion usually caused by preserva ives (e.g., himerosal or chlorhexidine) in he con ac lens solu ion
Symptoms Burning, i ching, redness soon a er lens
inser ion
Signs Conjunc ival injec ion, ollicular conjunc-
ivi is, superf cial punc a e kera opa hy
Treatment Lubrica ion wi h preserva ive- ree ar if cial
ears. Avoid solu ions con aining preserva- ives. Swi ch o a hydrogen peroxide sys em. Consider daily-wear disposable lenses.
GIANT PAPILLA Y CONJUNCTIVITIS Etiology
A hypersensi ivi y reac ion o pro ein buildup in con ac lenses, especially wi h so lenses and poor lens hygiene
Symptoms I ching, mucous discharge, burning,
reduced lens olerance
Signs Modera e- o gian -sized papillae on he
upper arsal conjunc iva; deposi s may be seen on con ac lens ( Fig. 7-21 A and B). Con ac lens may be high-riding.
Treatment Op imize lens hygiene and lens f -
ing. Increase requency o enzyme
depro einiza ion. Reduce dura ion o lens wear. Consider swi ching o daily disposable or rigid gas-permeable lenses. opical lubrica- ion and mas -cell s abilizer (e.g., pemirolas , lodoxamide, or cromolyn).
CONTACT LENS KER TOPATHY (CONTACT LENS–ASSOCIATED SUPE IO LIMBIC KER TOCONJUNCTIVITIS) Etiology
Usually rela ed o con ac lens preserva ive hypersensi ivi y or oxici y or overwear
Symptoms Burning, i ching, redness, reduced lens ol-
erance, occasionally decreased vision
Signs Superior conjunc ival injec ion, superf cial
punc a e kera i is, subepi helial inf l ra es, and haze. May have a superior corneal epi heli-opa hy ( Fig. 7-21 C and D)
Treatment Avoid solu ions con aining preserva ives.
Lubrica e wi h preserva ive- ree ar if cial ears. Swi ch o a hydrogen peroxide sys em. Consider swi ching o daily disposable or rigid gas-permeable lenses.
CONTACT LENS OVE WEA SYND OME Etiology
Chronic, long periods or ex ended wear o so lenses
Symptoms Redness, oreign-body sensa ion, earing,
burning, blurred vision
Signs Di use conjunc ival injec ion, epi helial
edema, punc a e epi helial erosions, mild
LWBK961-C07_p168-235.indd 230 22/07/11 10:17 AM

Contact Lens Complications 231
iri is. Superf cial or deep corneal neovascular-iza ion may be seen in chronic cases.
Treatment Lubrica e wi h ar if cial ears. Discon inue
ex ended wear and swi ch o daily wear. Reduce daily wearing ime. Ref wi h more oxygen-permeable, looser lenses.
TIGHT LENS SYND OME Etiology
Acu e, igh f t ing o a so lens or, rarely, a rigid lens. Overnigh wear o a daily lens. Acu e hypoxia
Symptoms Irri a ion, redness, pain, blurred vision a
ew hours a er lens inser ion. Pa ien s o en have di cul y removing lenses.
Signs Absence o lens movemen on blinking,
imprin o lens on conjunc iva a er so lens removal (or cornea a er rigid lens removal) ( Fig. 7-21 E), corneal epi helial and an erior s romal edema, punc a e kera opa hy, iri is, and s erile hypopyon
Treatment Discon inue con ac lens wear. Lubrica e
wi h ar if cial ears. Consider cycloplegic drops. Ref wi h a daily-wear, at er, looser lens.
CO NEAL WA PAGE Etiology
ypically a resul o prolonged wear o impermeable (polyme hylme hacryla e) hard lenses, bu can be seen wi h rigid gas-permeable lenses and even so lenses
Symptoms Spec acle blur (poor vision wi h glasses
a er removal o he con ac lens)
Signs Modera e o severe irregular as igma ism
on kera ome ry and compu erized corneal opography
Treatment Discon inue lens wear and allow corneal
curva ure o re urn o normal, which may ake weeks o mon hs. Once normalized, ref wi h a rigid gas-permeable lens or so lens and moni or or s abili y.
CO NEAL NEOVASCULA IZATION Etiology
Ex ended wear o so lenses or chronic overwear o igh , low-oxygen-permeable lenses
Symptoms May be asymp oma ic
Signs Peripheral, superf cial, and occasionally
s romal neovasculariza ion, usually a ec -ing he superior limbus, bu may occur 360 degrees. May be accompanied by lipid inf l ra es
Treatment Discon inue con ac lens wear. Consider
opical cor icos eroids in severe cases. Ref wi h daily-wear disposable lenses or rigid gas-permeable lenses.
STE ILE KER TITIS Etiology
May be rela ed o allergic conjunc ivi is, superior limbic kera oconjunc ivi is, over-wear or igh -lens syndrome, reac ion o lens-care preserva ives
LWBK961-C07_p168-235.indd 231 22/07/11 10:17 AM

232 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
Symptoms May be asymp oma ic or have mild
irri a ion
Signs Single or mul iple, small, peripheral, epi-
helial or subepi helial opaci ies ( Fig. 7-21 F). Occasionally, a s erile an erior s romal inf l- ra e or haze may be seen. I is impor an o dis inguish i rom an early microbial kera i is.
Treatment Discon inue lens wear. Broad-spec rum
an ibio ic drops wi h excellen pseudomo-nas coverage (e.g., a uoroquinolone) q.i.d. Judicious use o opical cor icos eroid q.i.d. once in ec ion has been ruled ou . Follow up pa ien in 1 o 2 days.
MIC OBIAL KER TITIS Etiology
Bac erial, ungal, Acanthamoeba corneal in ec ion
Symptoms Pain, irri a ion, redness, earing, discharge,
pho ophobia, blurred vision. May have a his- ory o ex ended wear or opical cor icos e-roid usage or con ac lens–rela ed problem.
Signs Conjunc ival injec ion, corneal inf l ra e,
corneal ulcer, iri is, hypopyon
Treatment See Bac erial Kera i is a he beginning o
his chap er.
FIGURE 7-21. Contact lens complication. A. Severe gian papillary conjunc ivi is is presen upon eversion o he upper eyelid in his pa ien who never enzymed his so con ac lenses and replaced hem once a year.
(continued)
A
LWBK961-C07_p168-235.indd 232 22/07/11 10:17 AM

Contact Lens Complications 233
B
C
FIGURE 7-21. (Continued) Contact lens complication. B. T is so con ac lens is covered wi h hick, eleva ed pro ein deposi globules. T e lens needs o be cleaned, enzymed, and disin ec ed. T e pa ien needs o be ins ruc ed in proper lens care, including more requen enzyming and/ or more requen replacemen . C. T is long- ime so con ac lens wearer no ed decreased vision. A large ongue o irregular epi helium emana ing rom he superior limbus is apparen . Chronic irri a ion rom con ac lens wear can cause damage o he limbal s em cells resul ing in abnormal epi helial cell produc ion and irregular as igma ism.
(continued)
LWBK961-C07_p168-235.indd 233 22/07/11 10:17 AM
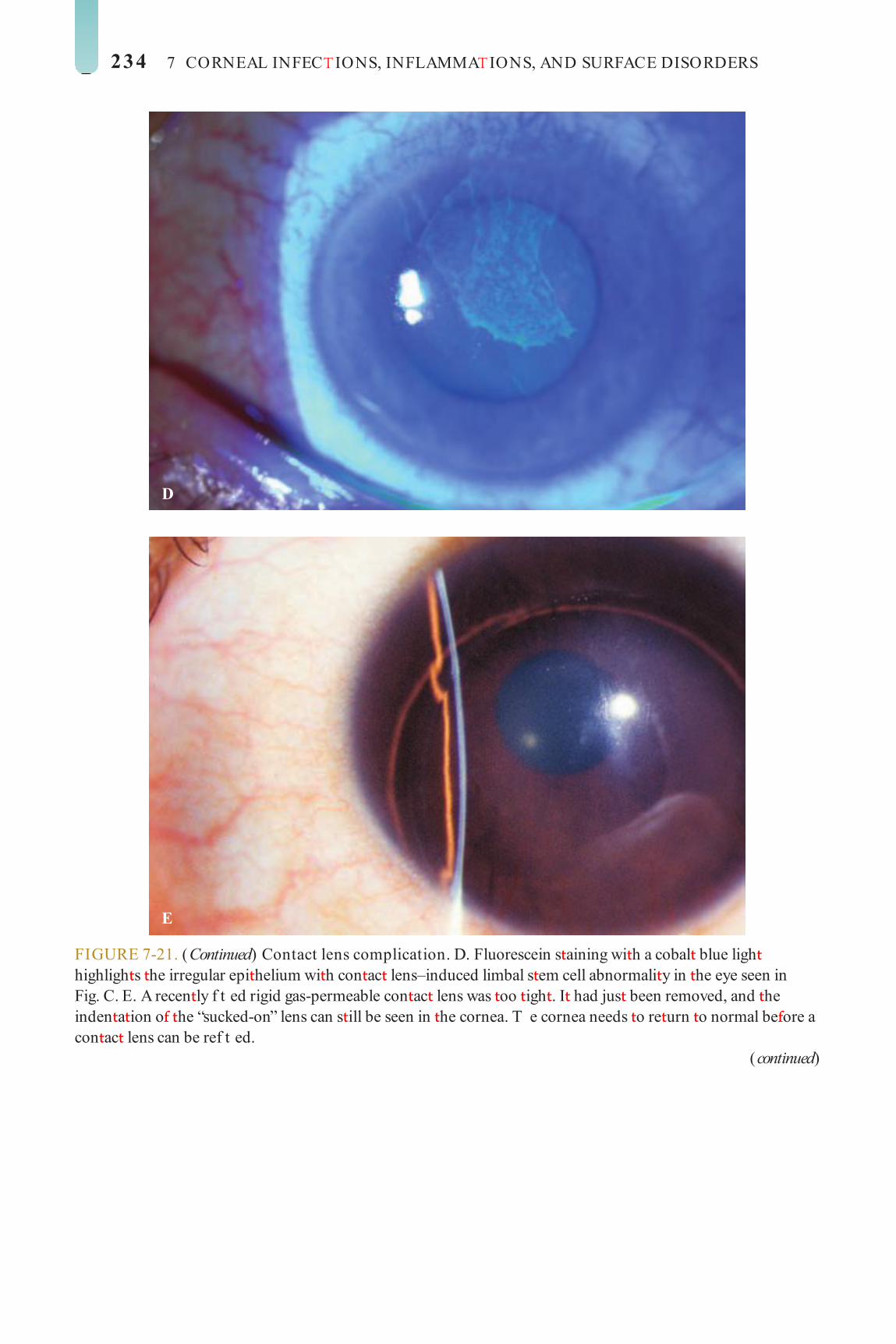
234 7 CORNEAL INFEC IONS, INFLAMMA IONS, AND SURFACE DISORDERS
D
E
FIGURE 7-21. (Continued) Contact lens complication. D. Fluorescein s aining wi h a cobal blue ligh highligh s he irregular epi helium wi h con ac lens–induced limbal s em cell abnormali y in he eye seen in Fig. C. E. A recen ly f t ed rigid gas-permeable con ac lens was oo igh . I had jus been removed, and he inden a ion o he “sucked-on” lens can s ill be seen in he cornea. T e cornea needs o re urn o normal be ore a con ac lens can be ref t ed.
(continued)
LWBK961-C07_p168-235.indd 234 22/07/11 10:17 AM

Contact Lens Complications 235
F
FIGURE 7-21. (Continued) Contact lens complication. F. Mul iple peripheral corneal inf l ra es are seen in his so con ac lens wearer’s eye. I was hough o be due o a oxic reac ion o preserva ives in he con ac lens cleaning solu ion.
LWBK961-C07_p168-235.indd 235 22/07/11 10:17 AM

C H A P T E R
236
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
Ca arac is ound in less han 10% o cases. A disc-shaped, cen ral, polychroma ic opaci y wi h peripheral radia ions can be seen (sunf ower ca arac ).
Dif erential Diagnosis O her causes o a Kayser-Fleischer ring:
primary biliary cirrhosis, chronic ac ive hepa i is, mul iple myeloma
Chalcosis: corneal copper deposi ion rom an in raocular copper oreign body
Diagnostic Evaluation Sli -lamp or gonioscopic examina ion Serum copper and ceruloplasmin levels,
urine copper level
Treatment rea men by an in ernis and/ or neurolo-
gis wi h copper chela ing agen s such as D-penicillamine or e ra hiomolybda e
Prognosis Good wi h early recogni ion and rea -
men . T e Kayser-Fleischer ring may resolve wi h rea men .
Sys emic and Immunologic Condi ions A ec ing he Cornea
WILSON’S DISEASE (HEPATOLENTICULAR DEGENERATION)
Wilson’s disease is a rare condi ion ha resul s in abnormal copper deposi ion
hroughou he body.
Etiology and Epidemiology Au osomal recessive condi ion caused by a
de ciency o he enzyme ceruloplasmin Onse under age 40 years
Symptoms Usually no ocular symp oms May experience cirrhosis, renal disease,
or neurologic dys unc ion ( ypically mo or disorders)
Signs Kayser-Fleischer ring: green-brown band
o copper deposi ion in he peripheral zone o Desceme ’s membrane ( Fig. 8-1 ; see also Fig. 6-8). T is ring usually begins in he ver i-cal meridians and may be seen earlies wi h gonioscopy. A Kayser-Fleischer ring may be he presen ing sign o he disease.
LWBK961-C08_p236-265.indd 236 22/07/11 10:18 AM

Wilson’s Disease (Hepatolenticular Degeneration) 237
FIGURE 8-1. Wilson’s disease. A prominen Kayser-Fleischer ring can be seen. Brown copper pigmen deposi ion is very apparen in he corneal periphery in his 18-year-old woman wi h Wilson’s disease. T e deposi s are a he level o Desceme ’s membrane and deep s roma. In mild cases, he copper pigmen is seen earlies using gonioscopy. See also Chap er 6, Figure 6-8.
LWBK961-C08_p236-265.indd 237 22/07/11 10:18 AM

238 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
VITAMIN A DEFICIENCY
Vi amin A de ciency is a rare, po en ially blinding disorder ha usually a ec s he
malnourished and is common in areas where polished rice is he main source o ood.
Etiology Die ary de ciency o vi amin A, ypically
rom chronic malnu ri ion Celiac diseases, biliary obs ruc ion, cys ic
brosis, pancrea ic or in es inal (e.g., gas ric band or s apling) surgery, which impairs absorp ion o vi amin A
Symptoms Nigh blindness is he earlies symp om;
dry eye, oreign-body sensa ion, gradual loss o vision in severe cases
Signs Xerosis (severe drying) o cornea and
conjunc iva Kera iniza ion o conjunc iva (Bi o ’s spo :
super cial, riangular, silvery-gray, oamy, kera inized pa ch on he in erpalpebral bulbar conjunc iva)
S erile corneal ulcers and mel s (kera oma-lacia), which may lead o scarring or per ora- ion ( Fig. 8-2 )
Dif erential Diagnosis Kera oconjunc ivi is sicca
Diagnostic Evaluation Serum vi amin A level Consider impression cy ology o he con-
junc iva (demons ra es decreased goble cell densi y) and elec rore inogram.
Treatment Sys emic vi amin A orally or in ramuscu-
larly and repea ed 1 mon h la er Frequen preserva ive- ree ar i cial ear
drops or oin men o lubrica e ocular sur ace rea o he malnu ri ion Corneal ransplan a ion or scars or per ora-
ion. Consider a kera opros hesis or bila eral severe scarring wi h good macular unc ion.
Prognosis Very good i diagnosed and rea ed be ore
signi can corneal ulcera ion has occurred. Fair o poor i signi can corneal damage is presen .
LWBK961-C08_p236-265.indd 238 22/07/11 10:18 AM

Vitamin A Defciency 239
FIGURE 8-2. Vitamin A def ciency. T is malnourished pa ien had severe xerosis o he cornea and conjunc iva. T ere was a deep s erile corneal mel near he limbus rom he 6 o he 7 o’clock posi ion. T e xerosis and mel resolved over a week wi h sys emic vi amin A herapy.
LWBK961-C08_p236-265.indd 239 22/07/11 10:18 AM

240 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
CYSTINOSIS
Cys inosis is a rare disorder ha resul s in accumula ion o cys ine in he body.
Etiology and Epidemiology Au osomal recessive disorder Resul s in deposi s o he amino acid cys-
ine in he conjunc iva, corneal s roma, iris, lens, and re ina, depending on severi y
T ree main orms In an ile: associa ed wi h dwar sm and
progressive kidney dys unc ion. Poor prog-nosis wi hou a renal ransplan
Adolescen (in ermedia e): Kidneys may be involved, bu re inas are normal.
Adul : minimal o no kidney disease, cys ine deposi s limi ed o an erior segmen
Symptoms Irri a ion, oreign-body sensa ion, pain,
occasionally decreased vision
Signs Myriad iny, glis ening crys als in he cor-
neal s roma, conjunc iva, iris, lens, and re ina, depending on he severi y o he disease ( Fig. 8-3 )
May have super cial punc a e kera opa hy, lamen s, and recurren erosions
Grow h re arda ion, renal ailure, hepa o-splenomegaly, and hypo hyroidism
Dif erential Diagnosis See Crys alline Kera opa hy in Chap er 6.
Treatment Lubrica ion or ocular sur ace disease Cys eamine eye drops have been repor ed
o be use ul. Rarely, a corneal ransplan is required.
Prognosis Poor or he in an ile orm; good or he
in ermedia e and adul orms.
LWBK961-C08_p236-265.indd 240 22/07/11 10:18 AM

Cystinosis 241
FIGURE 8-3. Cystinosis. A. C onf uen ull- hickness iny re rac ile corneal deposi s are seen. T ese opaci ies are cys ine crys als. Generally, he deposi s do no a ec vision; however, i hey are severe, hey can cause signi can visual symp oms. B. Sli -beam view o he eye wi h cys inosis seen in A. No e he ull- hickness dis ribu ion o he crys als.
A
B
LWBK961-C08_p236-265.indd 241 22/07/11 10:18 AM
242 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
All have progressive corneal clouding except Hunter’s and Sanf lippo’s syndromes ( Fig. 8-4 ).
Lipidoses: All may have macular cherry-red spots and optic atrophy. Bilateral, sym-metric, brownish corneal epithelial deposits arranged in a vortex ashion rom a point below the pupil and swirling outward but sparing the limbus (cornea verticillata) are seen in males with Fabry’s disease and emale carriers. Conjunctival aneurysms, lens opacities, papill-edema, optic atrophy, and macular and retinal edema are also seen in Fabry’s disease.
Treatment Severe corneal opacity may require a
corneal transplant. No ocular treatment is required or cornea verticillata.
Follow-up with a pediatrician or pediatric endocrinologist and a geneticist
Prognosis Poor to good, depending on the specif c
metabolic disorder
MUCOPOLYSACCHARIDOSES AND LIPIDOSES
The mucopolysaccharidoses and lipidoses comprise a group o inherited systemic
metabolic disorders that result in abnormal accumulation o material in the body.
Etiology and Epidemiology Mucopolysaccharidoses: lysosomal storage
diseases, including Hurler’s, Scheie’s, Hunter’s, Sanf lippo’s, Morquio’s, Maroteaux-Lamy, and Sly’s syndromes. All are autosomal recessive except Hunter’s syndrome, which is X-linked recessive.
Lipidoses: Numerous disorders o lipid metabolism, including Fabry’s disease. All lip-idoses are autosomal recessive except Fabry’s disease, which is X-linked recessive.
Signs Mucopolysaccharidoses: All may have
optic nerve, retinal, and CNS abnormalities.
LWBK961-C08_p236-265.indd 242 28/07/11 7:58 AM

Mucopolysaccharidoses and Lipidoses 243
FIGURE 8-4. Maroteaux Lamy syndrome. Di use ull- hickness corneal haze can be seen in his child wi h Maro eaux-Lamy syndrome.
LWBK961-C08_p236-265.indd 243 22/07/11 10:18 AM

244 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
COLLAGEN VASCULAR DISEASES
Collagen vascular diseases can cause a wide varie y o ocular abnormali ies, he mos
impor an o which are peripheral ulcera ive kera i is and scleri is.
Etiology Rheuma oid ar hri is (mos common) Wegener’s granuloma osis (o en causes a
necro izing scleri is) Polyar eri is nodosa Relapsing polychondri is Sys emic lupus ery hema osus (SLE) O hers
Symptoms Range rom none o signi can pain, red-
ness, discharge, and decreased vision
Signs Corneal ndings include kera oconjunc-
ivi is sicca, s romal kera i is, corneal s romal in l ra es or ulcera ion, which is ypically peripheral bu may be cen ral. T e peripheral corneal ulcera ion may occur wi h or wi hou symp oma ic inf amma ion. T e ulcera ion can be similar o Mooren’s ulcer in ha i can ex end circum eren ially and cen rally. However, unlike Mooren’s ulcer, he sclera is commonly involved. Corneal per ora ion may occur ( Fig. 8-5 A–C).
O her ndings include episcleri is, scleri is (necro izing wi h or wi hou inf amma ion) and sclerokera i is ( Fig. 8-5 D and E). Healed episodes o scleri is can lead o scleral hin-ning and uveal show ( Fig. 8-5 F).
T e corneal changes in SLE are o en unremarkable.
Dif erential Diagnosis Mooren’s ulcer: no underlying sys emic
disease In ec ious in l ra e or ulcer: pain, iri is,
more purulen discharge, cul ures posi ive
Treatment Ar i cial ear drops, gels, and oin men ,
cyclosporine 0.05% drops and punc al occlu-sion are used or kera oconjunc ivi is sicca. opical cor icos eroids are help ul in s romal kera i is bu should generally be avoided in corneal and scleral ulcers. opical cyclospo-rine 0.5% o 2% q.i.d. may also be bene cial.
Oral nons eroidal an i-inf amma ory agen s and/ or cor icos eroids are used or peripheral ulcera ive kera i is and scleri is. opical rea men is aimed a reepi helializa- ion and preven ion o secondary in ec ion (e.g., ar i cial ear and an ibio ic oin men q.i.d., punc al occlusion, la eral arsorrhaphy).
S ronger immunosuppressive agen s (e.g., me ho rexa e, aza hioprine, cyclosporine, or cyclophosphamide) or biologics (e.g., inf iximab, adalimumab, or ri uximab) may be required, especially or scleri is or severe corneal s romal inf amma ion.
Resec ion o inf amed conjunc iva adja-cen o a peripheral corneal ulcer may be help ul on rare occasions. Cyanoacryla e is-sue glue can be used or small per ora ions ( Fig. 8-5 G and H). Larger per ora ions will require corneal pa ch gra s.
Prognosis Fair o good, depending on he severi y and
response o he underlying sys emic disease
LWBK961-C08_p236-265.indd 244 22/07/11 10:18 AM

Collagen Vascular Diseases 245
A
B
FIGURE 8-5. Rheumatoid arthritis. A. Sli -beam view o a pa ien wi h rheuma oid ar hri is demons ra es a peripheral corneal mel wi h severe ulcera ion. T ere is approxima ely 90% issue loss. T ere is modera e corneal neovasculariza ion peripherally and superiorly. No e he area o clear cornea superiorly; i is an addi ional large area o corneal mel ing. B. T is pa ien wi h rheuma oid ar hri is has hree separa e peripheral corneal in l ra es rom he 9 o he 11 o’clock posi ions. T ere is an addi ional, larger peripheral in l ra e wi h corneal mel ing rom he 12 o he 2 o’clock posi ions. T e in l ra es are mos likely s erile, inf amma ory in l ra es.
(continued)
LWBK961-C08_p236-265.indd 245 22/07/11 10:18 AM

246 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
C
D
FIGURE 8-5. (Continued) Rheumatoid arthritis. C. T is eye has a large s erile corneal mel leading o per ora ion in he midperiphery a he 4:30 posi ion. T e radia ing s romal olds and peaked pupil sugges a per ora ion. Peripheral corneal neovasculariza ion and scarring rom he 3 o he 4 o’clock posi ions indica e 0 previous corneal inf amma ion in ha area. Wegener’s granulomatosis. D. T is pa ien wi h a necro izing scleri is and peripheral corneal mel had no known medical problems. Emergency sys emic work-up revealed Wegener’s granuloma osis. She was rea ed aggressively wi h sys emic cor icos eroids and cyclophosphamide, and her scleri is resolved. Appropria e diagnosis and rea men o Wegener’s granuloma osis can be li e-saving.
(continued)
LWBK961-C08_p236-265.indd 246 22/07/11 10:18 AM
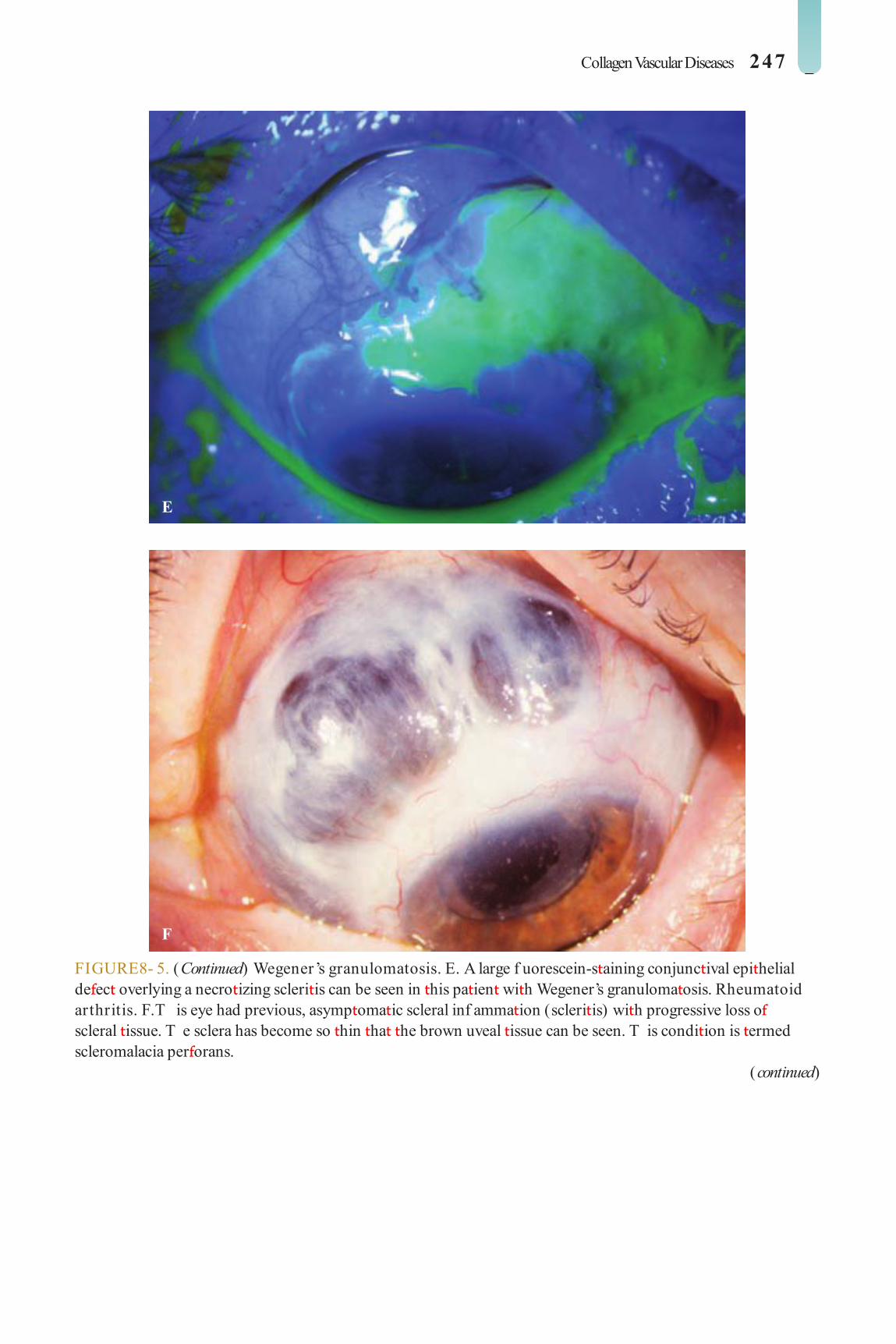
Collagen Vascular Diseases 247
E
F
FIGURE 8- 5. (Continued) Wegener’s granulomatosis. E. A large f uorescein-s aining conjunc ival epi helial de ec overlying a necro izing scleri is can be seen in his pa ien wi h Wegener’s granuloma osis. Rheumatoid arthritis. F. T is eye had previous, asymp oma ic scleral inf amma ion (scleri is) wi h progressive loss o scleral issue. T e sclera has become so hin ha he brown uveal issue can be seen. T is condi ion is ermed scleromalacia per orans.
(continued)
LWBK961-C08_p236-265.indd 247 22/07/11 10:18 AM

248 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
G
H
FIGURE 8-5. (Continued) Rheumatoid arthritis. G. A large crescen ic area o peripheral ulcera ive kera i is can be seen in his pa ien wi h rheuma oid ar hri is. T e an erior chamber was f a , and a small per ora ion was ound in he ulcera ion a he 10 o’clock posi ion. H. Due o he per ora ion and f a an erior chamber, he eye was rea ed wi h cyanoacryla e issue glue. T e an erior chamber re- ormed nicely over he nex hour.
LWBK961-C08_p236-265.indd 248 22/07/11 10:19 AM
Ocular Cicatricial Pemphigoid 249
OCULAR CICATRICIAL PEMPHIGOID
Cica ricial pemphigoid is an uncommon, chronic cica rizing mucocu aneous dis-
order. Many pa ien s also have lesions o he oral mucosa. Skin lesions are less common. Bila eral conjunc ival involvemen occurs in he majori y o cases, and in some i may be he only mani es a ion o he disease.
Etiology and Epidemiology Idiopa hic ype II hypersensi ivi y reac-
ion caused by an i–basemen membrane an ibodies
Primarily emale pa ien s over 60 years o age
Has been associa ed wi h numerous opical drugs (e.g., pilocarpine, imolol, idoxuridine)
Symptoms Chronic remit ing and relapsing course,
ocular redness, irri a ion, oreign-body sensa- ion, decreased vision, generally progressive
Oral ulcera ions
Signs Bila eral, o en asymme ric, conjunc ival
inf amma ion, ne subepi helial brosis o conjunc iva wi h shrinkage and obli era ion o he in erior ornix, o en wi h progressive symblepharon orma ion ( Fig. 8-6 A and B)
richiasis and dis ichiasis may lead o corneal pannus, scarring, hinning, ulcera ion, and occasionally per ora ion.
Punc a e epi helial erosions, poor ear lm, dry eye, blepharoconjunc ivi is
Corneal pannus or kera iniza ion and usion be ween he upper and lower eyelids a he ou er can hus ( Fig. 8-6 C)
Corneal ulcera ion and vasculariza ion, which may be complica ed by in ec ion,
persis en epi helial de ec s, exposure, and per ora ion
Mucous membrane vesicles and ulcer-a ions (oral cavi y, nose, anus)
Dif erential Diagnosis S evens-Johnson syndrome: acu e onse ,
precipi a ed by drug or in ec ion, gener-ally does no run a remit ing and relapsing course
Chemical injury: acu e onse , diagnosis is obvious rom his ory
Diagnostic Evaluation Pull down he lower eyelids while ask-
ing pa ien o look up, o observe or in e-rior orniceal oreshor ening and in erior symblepharon.
Look or lesions in he oral cavi y and skin. Conjunc ival biopsy o look or subepi he-
lial bullae and subepi helial brosis, and or immunof uorescen iden i ca ion o an igen–an ibody complexes in he conjunc- ival basemen membranes
Treatment Ar i cial ear drops or oin men s (e.g.,
drops q2–6h or oin men b.i.d. o q.i.d.). Punc al occlusion or severe cases, wi h ei her punc al plugs or punc al cau ery
rea any associa ed blephari is wi h eyelid hygiene, opical an ibio ic oin men , and oral e racycline, doxycycline, or ery hromycin. rea richiasis wi h epila ion, elec rolysis, and cryo herapy as needed.
opical cor icos eroids (e.g., prednisolone 1%, dexame hasone 0.1%, or lo eprednol 0.5% q.i.d.) or ac ive conjunc ival inf amma- ion. opical cyclosporine 0.05% o 2%, 2 o 4 imes per day, may also be help ul.
Oral dapsone can be used alone or as a complemen o o her sys emic rea men .
LWBK961-C08_p236-265.indd 249 22/07/11 10:19 AM
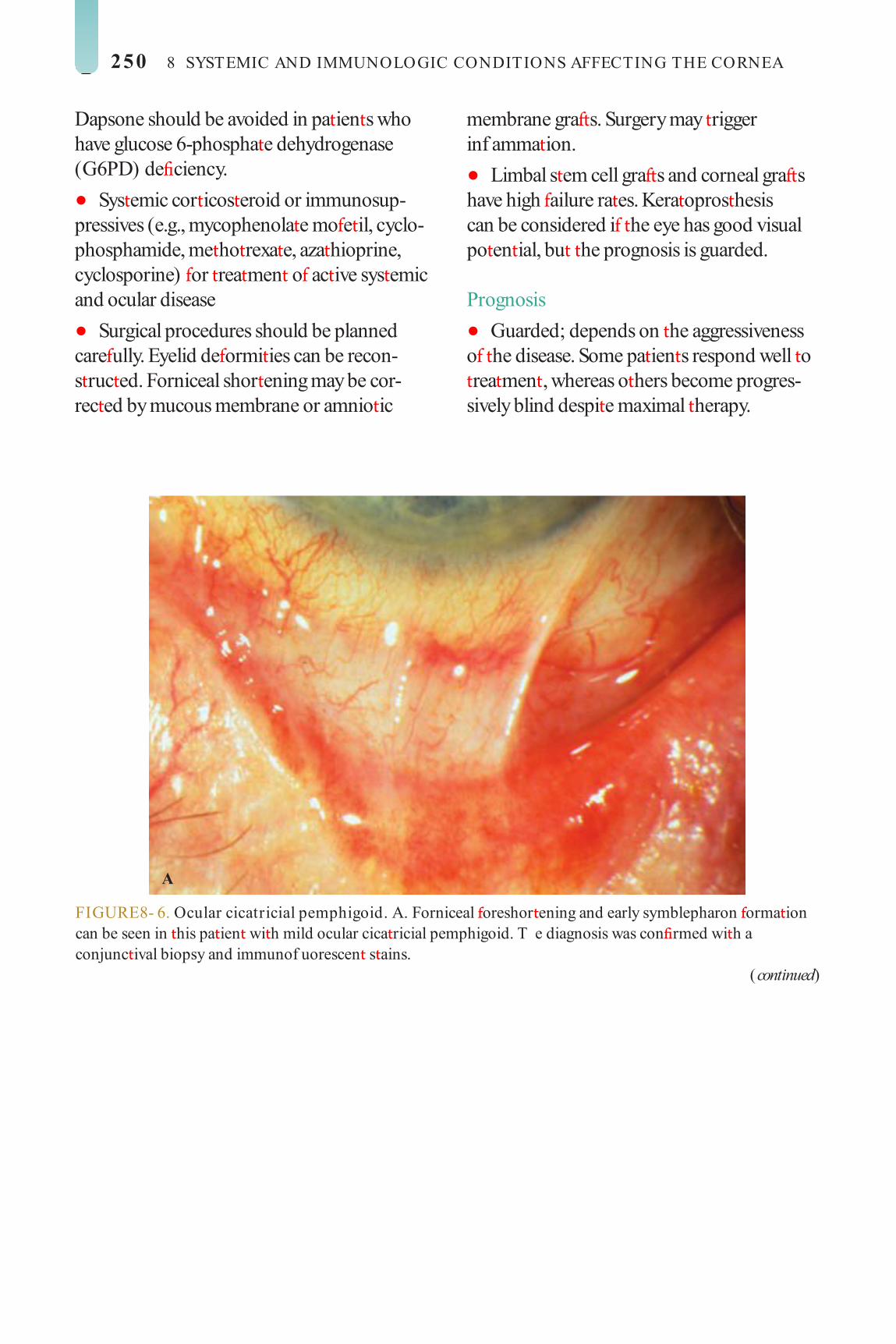
250 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
Dapsone should be avoided in pa ien s who have glucose 6-phospha e dehydrogenase (G6PD) de ciency.
Sys emic cor icos eroid or immunosup-pressives (e.g., mycophenola e mo e il, cyclo-phosphamide, me ho rexa e, aza hioprine, cyclosporine) or rea men o ac ive sys emic and ocular disease
Surgical procedures should be planned care ully. Eyelid de ormi ies can be recon-s ruc ed. Forniceal shor ening may be cor-rec ed by mucous membrane or amnio ic
membrane gra s. Surgery may rigger inf amma ion.
Limbal s em cell gra s and corneal gra s have high ailure ra es. Kera opros hesis can be considered i he eye has good visual po en ial, bu he prognosis is guarded.
Prognosis Guarded; depends on he aggressiveness
o he disease. Some pa ien s respond well o rea men , whereas o hers become progres-sively blind despi e maximal herapy.
A
FIGURE 8- 6. Ocular cicatricial pemphigoid. A. Forniceal oreshor ening and early symblepharon orma ion can be seen in his pa ien wi h mild ocular cica ricial pemphigoid. T e diagnosis was con rmed wi h a conjunc ival biopsy and immunof uorescen s ains.
(continued)
LWBK961-C08_p236-265.indd 250 22/07/11 10:19 AM

Ocular Cicatricial Pemphigoid 251
B
C
FIGURE 8- 6. (Continued) Ocular cicatricial pemphigoid. B. Obli era ion o he in erior ornix wi h severe, progressive scarring o he eyelid o he cornea is presen in his pa ien wi h advanced ocular cica ricial pemphigoid. C. o al corneal scarring and kera iniza ion occurred in his eye despi e aggressive sys emic rea men or ocular cica ricial pemphigoid. When bo h eyes are similarly involved, a permanen kera opros hesis may be an op ion al hough he prognosis is guarded.
LWBK961-C08_p236-265.indd 251 22/07/11 10:19 AM

252 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
STEVENS-JOHNSON SYNDROME (ERYTHEMA MULTIFORME MAJOR)
S evens-Johnson syndrome is an acu e, ypically sel -limi ed, inf amma ory vesic-
ulobullous disease o he skin and mucous membranes ha is mos requen ly riggered by drugs or in ec ions.
Etiology and Epidemiology Caused by a ype III hypersensi ivi y reac-
ion in he dermis and conjunc ival s roma and is po en ially a al (mor ali y ra e, 5% o 10%) because o mul isys em involvemen
May a ec all age groups bu is more com-mon in young adul s, and is more common in emales.
oxic epidermal necrolysis is a severe orm ha is occasionally seen in young children, rarely in adul s; mor ali y ra e approaches 40%.
Causes Drugs: sul onamides, penicillins, barbi u-
ra es, salicyla es, an iconvulsan s, o hers In ec ions: herpes, mycoplasma, Coxsackie
virus, echovirus, s rep ococcus, o hers
Symptoms Acu e onse o skin rash, ocular redness,
discharge, oreign-body sensa ion, decreased vision
May have a prodrome o headache, ever, malaise, ar hralgias
Signs Bila eral di use conjunc ivi is ha may be
associa ed wi h pseudomembranes Oral mucous membrane bullous erosions,
hemorrhagic crus ing o lips Skin lesions: di use ery hema, classic
“ arge ” lesions, macular epidermal lesions, sloughing o skin ( Fig. 8-7 A)
Long- erm sequelae include conjunc ival brosis, symblepharon, dis ichiasis, richiasis, punc al occlusion, dry eye, en ropion, corneal neovasculariza ion, kera iniza ion o conjunc- iva and cornea, persis en epi helial de ec , mel ing, and per ora ion ( Fig. 8-7 B–D)
Dif erential Diagnosis Ocular cica ricial pemphigoid: See above. S aphylococcal scalded skin syndrome: In
young children, mucous membranes are no involved. Caused by an ex olia ive oxin pro-duced by some species o Staphylococcus aureus
Treatment Consider hospi aliza ion; pa ien may
require rea men in a burn uni . rea underlying in ec ion or discon inue
he o ending medica ion. opical cor icos eroids (e.g., prednisolone
1% or dexame hasone 0.1%) drops q2–6h or 3 o 7 days. I is necessary o moni or or epi- helial de ec , corneal hinning, and microbial kera i is.
opical an ibio ic oin men (e.g., ery hro-mycin, baci racin, polymyxin B/ baci racin, or e racycline) q2–6h
Ar i cial ear drops or oin men s q2–6h Consider breaking symblepharon daily
wi h a cot on- ipped applica or or glass rod under opical anes hesia.
Sys emic cor icos eroids are con roversial. T e long- erm managemen o ocular
complica ions is similar o ha or ocular cica ricial pemphigoid.
Prognosis Good or mild cases, which may resolve
wi h minimal sequelae. Modera e o severe cases can resul in signi can corneal and con-junc ival damage wi h permanen ly decreased vision. Corneal ransplan s and kera opros- heses have a poor success ra e.
LWBK961-C08_p236-265.indd 252 22/07/11 10:19 AM

Stevens-Johnson Syndrome (Erythema Multi orme Major) 253
FIGURE 8- 7. Stevens Johnson syndrome. A. T is pa ien has severe scaling o he skin and a mucopurulen conjunc ivi is as a resul o S evens-Johnson syndrome rom pheny oin (Dilan in) . B. S igni can corneal and conjunc ival scarring is eviden 1 mon h a er his 2-year-old boy developed S evens-Johnson syndrome as a resul o aking amoxicillin.
(continued)
A
B
LWBK961-C08_p236-265.indd 253 22/07/11 10:19 AM

254 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
C
D
FIGURE 8-7. (Continued) Stevens Johnson syndrome. C. S igni can super cial corneal scarring and neovasculariza ion can be seen in his eye a er an episode o S evens-Johnson syndrome. D. End-s age corneal scarring and comple e kera iniza ion o he ocular sur ace is presen in his eye a er a severe case o S evens-Johnson syndrome. When bo h eyes are similarly involved, a permanen kera opros hesis may be an op ion, bu he prognosis is poor.
LWBK961-C08_p236-265.indd 254 22/07/11 10:19 AM

Mooren’s Ulcer 255
MOOREN’S ULCER
Mooren’s ulcer is a rare, unila eral or bila -eral, pain ul, inf amma ory, chronic
progressive ulcera ive disease o he peripheral cornea. wo orms have been described. T e rs is a airly benign unila eral condi ion in he elderly, and he second is a bila eral a ic- ion wi h relen less progression ha is seen in younger males.
Etiology Idiopa hic, by de ni ion, bu presumably
immunologically based A rare orm rela ed o hepa i is C in ec ion
has been iden i ed.
Symptoms Redness, pain, pho ophobia, decreased
vision, discharge
Signs Peripheral ulcera ive kera i is wi h an
epi helial de ec . ypically begins nasally or emporally ( Fig. 8-8 A)
T e ulcer ex ends circum eren ially and cen rally, wi h a leading undermined edge. T e en ire corneal circum erence and he sclera may be involved in severe cases ( Fig. 8-8 B).
Per ora ion is uncommon bu may occur in he progressive orm.
Healing akes place rom he periphery, resul ing in a hinned, vascularized cornea.
Dif erential Diagnosis Peripheral ulcera ive kera i is associa ed
wi h collagen vascular diseases: peripheral, unila eral or bila eral s romal in l ra es wi h hinning
S aphylococcal hypersensi ivi y kera i is: mul iple, usually bila eral s romal in l ra es
wi h in ac epi helium in early s ages, and requen ly associa ed wi h blephari is and meibomi is
errien’s marginal degenera ion: bila eral, painless, eye is no inf amed, epi helium is in ac , hinning usually begins superiorly
Diagnosis Diagnosis is made clinically, a er excluding
o her causes o peripheral ulcera ive kera i is.
Treatment An ibio ic oin men (e.g., polymyxin B/
baci racin, ciprof oxacin) q2–6h Cycloplegics (e.g., scopolamine 0.25% or
a ropine 1% .i.d.) Sys emic cor icos eroids (e.g., predniso-
lone 1 o 2 mg/ kg PO q.d.) opical cor icos eroids (e.g., prednisolone
1% or dexame hasone 0.1%) q2–6h. T ese should be used wi h cau ion i signi can cor-neal hinning is presen .
opical cyclosporine 0.05% o 2% q2–6h may have cor icos eroid-sparing ac ion.
opical (e.g., ace ylcys eine 10% drops q.i.d.) and sys emic (e.g., doxycycline 100 mg b.i.d.) collagenase inhibi ors may be help ul.
S ronger immunosuppressive agen s (e.g., me ho rexa e, aza hioprine, cyclosporine, or cyclophosphamide) or biologics (e.g., inf iximab, adalimumab, or ri uximab) may be required or pa ien s wi h more severe disease.
Conjunc ival recession or resec ion wi h or wi hou cryo herapy may reduce he s im-uli or peripheral corneal inf amma ion.
La eral arsorrhaphy, amnio ic membrane gra , or conjunc ival f ap or may be help ul in nonhealing epi helial de ec and ulcera ion.
Small per ora ions can be rea ed wi h cya-noacryla e issue adhesive.
LWBK961-C08_p236-265.indd 255 22/07/11 10:19 AM

256 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
Larger per ora ions or impending per o-ra ions may require lamellar or pene ra ing kera oplas y.
When hepa i is C rela ed, consider rea -men wi h in er eron- α .
Prognosis Fair o good in he unila eral orm, poor in
he bila eral orm
A
B
FIGURE 8-8. Mooren’s ulcer. A. Peripheral corneal ulcera ion rom 6 o’clock o 10 o’clock, and also a 12 o’clock, can be seen. Corneal scarring and neovasculariza ion are presen or almos 360 degrees as a resul o previous bou s o inf amma ion. T is pa ien had bila eral Mooren’s ulcers. B. T is Mooren’s ulcer has ex ended circum eren ially or abou 270 degrees. T e peripheral cornea has healed wi h scarring and neovasculariza ion, bu an epi helial de ec can be seen a he leading aspec o he ulcera ion, wi h an undermined ledge.
LWBK961-C08_p236-265.indd 256 22/07/11 10:19 AM

Phlyctenulosis 257
PHLYCTENULOSIS
Phlyc enulosis is an uncommon, usually unila eral condi ion ha a ec s he con-
junc iva and/ or cornea as a resul o hypersen-si ivi y ype IV reac ion o microbial an igens.
Etiology S aphylococcal in ec ion: associa ed wi h
blephari is. Mos common uberculosis Less common: Chlamydia, Candida,
coccidioidomycosis
Symptoms Redness, oreign-body sensa ion, pain,
earing, pho ophobia More severe when he cornea is involved,
and may a ec vision May have a his ory o mul iple chalazia
Signs Small, round, eleva ed pinkish-whi e nodule,
which may involve he conjunc iva, limbus, or cornea. Usually based a he limbus ( Fig. 8-9 )
T e phlyc en may or may no have an epi helial de ec .
Dif erential Diagnosis Inf amed pinguecula Rosacea kera i is
Limbal herpes kera i is Microbial kera i is
Diagnosis Exclude underlying in ec ion, especially
uberculosis.
Treatment rea underlying in ec ion and/ or blepha-
ri is i presen . An ibio ic oin men s (e.g., ery hromycin,
baci racin, polymyxin B/ baci racin, or e ra-cycline) b.i.d.
opical cor icos eroids (e.g., prednisolone 1%, lo eprednol 0.5%, or dexame hasone 0.1%) q4–6h
Cycloplegics (e.g., cyclopen ola e 1% or scopolamine 0.25% .i.d.)
Oral e racycline 250 mg PO q.i.d. or doxycycline 100 mg PO b.i.d. in severe cases associa ed wi h blephari is. Children can be rea ed wi h ery hromycin, approxima ely 200 mg PO q.d.
Super cial kera ec omy may occasionally be per ormed or corneal scars a er resolu- ion o he condi ion.
Prognosis Very good. T ere may be residual corneal
scarring and decreased vision.
LWBK961-C08_p236-265.indd 257 22/07/11 10:19 AM

258 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
A
B
FIGURE 8-9. Phlyctenulosis. A. A small paracen ral in l ra e wi h a leash o corneal neovasculariza ion can be seen in his eye wi h signi can blephari is. I is ypically due o eyelid disease such as blephari is and s aphylococcal hypersensi ivi y, bu may be due o more serious in ec ions such as uberculosis. B. T is eleva ed nodule wi h a neovascular leash rom he limbus is classic or a corneal phlyc enule.
LWBK961-C08_p236-265.indd 258 22/07/11 10:19 AM

Staphylococcal Hypersensitivity 259
STAPHYLOCOCCAL HYPERSENSITIVIT Y
S aphylococcal hypersensi ivi y is a very common, ransien , o en bila eral condi-
ion ha is associa ed wi h chronic s aphylo-coccal blephari is.
Etiology Hypersensi ivi y reac ion o s aphylococ-
cal exo oxins or an igens
Symptoms Irri a ion, mild pain, redness, mild earing,
minimal o no discharge, his ory o previous episodes
Signs Begins as single or mul iple, unila eral or
bila eral, nons aining, peripheral corneal in l- ra es ( Fig. 8-10 )
T ese subepi helial/ an erior s romal in l- ra es are separa ed rom he limbus by clear cornea.
In l ra es are usually ound a he 2, 4, 8, and 10 o’clock posi ions o he peripheral cornea, where he eyelid margin crosses he limbus.
Secondary epi helial breakdown is common.
Resolves over a ew days, leaving behind mild hinning, super cial vasculariza ion, and peripheral scarring
Dif erential Diagnosis See Mooren’s Ulcer above. In addi ion, consider in ec ious kera i is i
symp oms are severe, in l ra e is loca ed more cen rally, an epi helial de ec is presen prior o or simul aneous wi h he onse o in l ra e, and i here is signi can an erior chamber reac ion.
Treatment rea underlying blephari is. opical an ibio ic oin men (e.g., ery hro-
mycin, baci racin, polymyxin B/ baci racin, or e racycline) b.i.d. or gel (e.g., azi hromycin) q.d. o b.i.d.
opical cor icos eroids (e.g., prednisolone 0.125% o 1%, lo eprednol 0.2% o 0.5%, or f uorome holone 0.1%) q.i.d. and hen apered, once in ec ion has been ruled ou
Prognosis Very good. Chronic rea men o blephari-
is is ypically required o preven recurrences.
LWBK961-C08_p236-265.indd 259 22/07/11 10:19 AM

260 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
A
B
FIGURE 8-10. Staphylococcal hypersensitivity. A. Mul iple creamy-whi e corneal in l ra es can be seen in he periphery rom he 1 o he 3 o’clock posi ions. T ere is a clear zone be ween he in l ra es and he limbus. S aphylococcal hypersensi ivi y in l ra es are mos commonly loca ed a he 2, 4, 8, and 10 o’clock posi ions, where he eyelid margin crosses he limbus. B. Numerous small o medium-sized, dense whi e corneal in l ra es are eviden superiorly in his eye wi h signi can eyelid disease.
LWBK961-C08_p236-265.indd 260 22/07/11 10:19 AM

Corneal Gra Rejection 261
CORNEAL GRAFT REJECTION
Corneal allogra rejec ion is one o he leading causes o la e gra ailure a er
corneal ransplan a ion.
Etiology ype IV hypersensi ivi y o major his o-
compa ibili y complex an igens presen in donor cornea
Symptoms Blurred vision, mild discom or , red-
ness, pho ophobia, irri a ion, bu may be asymp oma ic
La er, may have markedly decreased vision, irri a ion, pain, earing
Signs Circumcorneal conjunc ival injec ion,
an erior chamber reac ion Subepi helial in l ra es (Krachmer’s
spo s) ( Fig. 8-11 A), epi helial rejec ion line ( Fig. 8-11 B and C), kera ic precipi a es ( Fig. 8-11 D and E), endo helial rejec ion line (Khodadous ’s line) presen in he donor cornea ( Fig. 8-11 F and G)
Epi helial or s romal edema, super cial or s romal neovasculariza ion in o he donor cornea ( Fig. 8-11 H)
Dif erential Diagnosis Primary gra ailure: gra edema presen
rom he rs pos opera ive day. Absence o whi e-cell in l ra ion. T is is usually a resul o poor quali y o he donor cornea or in raopera ive damage o he donor cornea.
Reac iva ion o herpes kera i is: epi helial dendri e or geographic ulcer, s romal in l- ra es, and kera ic precipi a es are presen in bo h recipien and donor cornea. May worsen wi h opical cor icos eroid herapy alone
Uvei is: may be con used wi h early gra rejec ion. When in doub , rea as rejec ion.
Epi helial downgrow h: appears as advanc-ing line wi h smoo h or scalloped edges on bo h recipien and donor corneal endo he-lium, wi h minimal o no corneal edema early on. May grow on o he sur ace o he iris, causing f at ening o he normal iris cryp s. Progresses despi e in ense cor icos eroid herapy
Treatment Urgen herapy wi h opical cor icos e-
roids (e.g., prednisolone 1% or dexame ha-sone 0.1% q1h or dif upredna e 0.05% q2h) or a week during waking hours and aper o q.i.d. by 3 o 4 weeks. Cor icos eroid oin -men q.h.s. may be used in addi ion.
opical cyclosporine 0.05% o 2% q2–6h can be added.
Sys emic cor icos eroids (e.g., predniso-lone 1 mg/ kg/ d PO q.d.) or 2 weeks and hen apered over 1 week may be considered i here is a lack o response o opical herapy or or recurren rejec ion. Al erna ively, pa ien can be rea ed wi h a single-dose me hylprednisolone 500-mg IV in usion given over a ew hours. Rarely, in racameral riamcinolone ace onide 4% may be used.
opical cycloplegics (e.g., cyclopen ola e 1% or scopolamine 0.25% b.i.d.) i signi can iri is is presen
LWBK961-C08_p236-265.indd 261 22/07/11 10:19 AM

262 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
Consider opical an ibio ic prophylaxis (e.g., ery hromycin, baci racin, polymyxin B/baci racin, or e racycline oin men b.i.d. o q.h.s.).
Prognosis Very good i diagnosed and rea ed wi hin
a ew days, poor i rea men is delayed more han 1 o 2 weeks
A
B
FIGURE 8-11. Corneal gra rejection. A. Mul iple subepi helial in l ra es are presen in his pene ra ing kera oplas y. Originally hough o represen pos viral in l ra es, hey are really evidence o mild gra rejec ion. Al hough hey ypically do no cause signi can damage o he gra or decrease vision, hey are o en harbingers o more severe orms or rejec ion, such as endo helial rejec ion, which can signi can ly harm he ransplan . B. An irregular, raised, epi helial line is no ed curving around he periphery o he gra rom he 8:30 o 4:30 posi ions. T is represen s an epi helial rejec ion line, he bat le line be ween he donor and hos epi helium. T is ype o rejec ion is also ypically no gra or vision hrea ening, bu indica es an ac ive immune response wi h an increased risk o more severe rejec ion.
(continued)
LWBK961-C08_p236-265.indd 262 22/07/11 10:19 AM

Corneal Gra Rejection 263
C
D
FIGURE 8-11. (Continued) Corneal gra rejection. C. A raised curvilinear epi helial rejec ion line, which s ains ain ly, can be seen near he periphery o he corneal gra winding around rom he 10 o 6 o’clock posi ions. D. Numerous pigmen ed kera ic precipi a es are visible on he endo helial sur ace o his corneal gra . Sligh corneal haze indica ing mild corneal edema is also seen. New kera ic precipi a es represen endo helial rejec ion. T e corneal edema indica es some endo helial compromise. Endo helial rejec ion needs o be rea ed aggressively o preserve as much heal hy endo helium as possible.
(continued)
LWBK961-C08_p236-265.indd 263 22/07/11 10:19 AM

264 8 SYSTEMIC AND IMMUNOLOGIC CONDITIONS AFFECTING THE CORNEA
E
F
FIGURE 8-11. (Continued) Corneal gra rejection. E. S romal edema and kera ic precipi a es are ound involving he in erior wo- hirds o his pene ra ing kera oplas y. F. An early line o kera ic precipi a es can be seen ex ending rom he 6 o’clock o approxima ely 9 o’clock posi ions, which is an endo helial rejec ion line (Khodadous ’s line) . No e he corneal edema peripheral o his endo helial rejec ion line. Endo helial rejec ion lines require aggressive an irejec ion rea men .
(continued)
LWBK961-C08_p236-265.indd 264 22/07/11 10:19 AM

Corneal Gra Rejection 265
G
H
FIGURE 8- 11. (Continued) Corneal gra rejection. G. An endo helial rejec ion line can be seen ex ending rom he 2 o he 7 o’clock posi ions. Such lines end o move rom he corneal periphery oward he cen er o he cornea and can cross he en ire cornea. H. Severe di use corneal edema wi h mul iple kera ic precipi a es (some in a linear pat ern a he in erior edge o he pupil) indica e advanced endo helial rejec ion. T ere is o en associa ed conjunc ival injec ion and iri is. rea men is wi h in ensive opical and occasionally sys emic or in racameral cor icos eroids o spare as many endo helial cells as possible.
LWBK961-C08_p236-265.indd 265 22/07/11 10:19 AM

C H A P T E R
266
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA TTTTT ET ET EEEEEETT ETT EET ET RRRRRRRRRRRRRRRRC H A P T E R
T e inf amed episcleral vessels have a straight, radial con guration.
opical phenylephrine 2.5% will cause blanching and enhance visualization o the normal deep vascular plexus over the sclera.
Nodular episcleritis Somewhat tender, usually solitary, local-
ized injected nodule that can be moved slightly over the sclera
A localized area o corneal thinning sec-ondary to desiccation (delle) may develop adjacent to an episcleral nodule.
Dif erential Diagnosis Conjunctivitis: usually associated with
papillary or ollicular response in the tarsal conjunctiva. May have a mucoid or purulent discharge
Scleritis: Pain is deeper and more severe, sclera has a purple or bluish hue under natural light, injected scleral vessels have criss-cross-ing con guration, vessels are immobile over the globe, patients tend to be older.
Inf amed pinguecula: located in the com-pletely mobile conjunctiva
Anterior Sclera and Iris
EPISCLERITIS
Episcleritis is a benign, transient, recur-rent, sel -limited, and usually nonspeci c
condition that a ects young adults. It rarely progresses to scleritis and should not be con-sidered a milder orm o scleritis. T ere are two orms, simple and nodular.
Etiology Idiopathic Collagen vascular diseases Rosacea Gout Herpes zoster, herpes simplex, syphilis
Symptoms Acute onset o redness, mild irritation,
tearing, rarely, pain
Signs Simple episcleritis
Sectorial or di use hyperemia, primar-ily involving the middle episcleral plexus, with some secondary involvement o the overlying conjunctival vessels ( Fig. 9-1 )
LWBK961-C09_p266-277.indd 266 26/07/11 4:50 PM

Episcleritis 267
Diagnostic Evaluation Examina ion is made wi h he sli lamp
and under na ural or room ligh . At emp o move he episcleral vessels over
he sclera using a cot on- ipped s ick under opical anes hesia.
Apply phenylephrine 2.5% and observe or blanching o episcleral vessels a er 15 minu es.
Sys emic work-up i his ory is sugges ive o collagen vascular disease or gou .
Treatment Ar i cial ears and cool compresses q.i.d. Consider a shor course o a opical
NSAID (e.g., diclo enac q.i.d., ke orolac
q.i.d., brom enac q.d. or b.i.d., or nepa enac .i.d.).
Oral NSAID (e.g., ibupro en 400 o 600 mg .i.d. o q.i.d., indome hacin 12.5 o 25 mg q.d. o .i.d. or f urbipro en 100 mg b.i.d. o .i.d.) or modera e o severe cases.
Consider a shor course o opical cor- icos eroids (e.g., f uorome holone 0.1% o 0.25%, lo eprednol 0.2% o 0.5%) q.i.d. in recalci ran cases. Rarely, oral cor icos eroids are required.
Prognosis Good o very good. Episcleri is is o en a
recurren condi ion.
A
FIGURE 9-1. Episcleritis. A. Localized injec ion o he episcleral vessels is eviden in his pa ien wi h sec orial episcleri is.
(continued)
LWBK961-C09_p266-277.indd 267 22/07/11 10:20 AM

268 9 ANTERIOR SCLERA AND IRIS
B
FIGURE 9-1. (Continued) Episcleritis. B. Dif use injec ion o he episcleral vessels is presen in his eye. Episcleri is can be di cul o dif eren ia e rom scleri is in some pa ien s. Episcleral vessels end o blanch wi h opical phenylephrine 2.5%, whereas scleral vessels do no .
LWBK961-C09_p266-277.indd 268 22/07/11 10:20 AM

Anterior Scleritis 269
ANTERIOR SCLERITIS
Scleri is is a severe, po en ially sigh - hrea -ening ocular disorder ha has a o ally
di eren prognosis han episcleri is. I may be mild and benign or severe and des ruc ive. Females are a ec ed more o en han males, and he condi ion is requen ly bila eral. Mos scleri is a ec s he an erior sclera. An erior scleri is can be divided in o he clinical orms described below.
Classi cation Nonnecro izing scleri is
Di use: di use hyperemia and dis or- ion o he pat ern o he deep vascular plexus, associa ed wi h variable episcleral and conjunc ival injec ion ( Fig. 9-2 A). T is is he mos benign orm and is associa ed wi h he leas severe sys emic condi ions.
Nodular: ender, usually soli ary, deep, localized injec ed nodule ha canno be moved over he sclera ( Fig. 9-2 B)
Necro izing scleri is Wi h inf amma ion
T is is he mos des ruc ive orm o scleri is. I is associa ed wi h ocular or sys emic complica ions in 60% o pa ien s, and 40% may have loss o vision. One- hird o pa ien s may die wi hin a ew years as a resul o severe au oimmune disease i hey are inad-equa ely rea ed.
Gradual appearance o pain ul, local-ized, avascular pa ch overlying an area o scleral necrosis ( Fig. 9-2 C)
Inf amma ion may be localized o he surrounding sclera or may become di use.
T e underlying uvea becomes pro-gressively visible hrough he hinned and necro ic sclera.
Wi hou inf amma ion (scleromalacia per orans)
ypically seen in pa ien s wi h long-s anding rheuma oid ar hri is
Asymp oma ic developmen o enlarg-ing gray-blue pa ches o scleral hinning
Exposure o underlying uvea hrough areas o hin, devi alized sclera wi h large bridging vessels
An erior scleral s aphylomas can occur.
Etiology Hal o pa ien s wi h scleri is have an asso-
cia ed sys emic disease. Idiopa hic Ia rogenic
Surgery (e.g., ca arac surgery, rabecu-lec omy, scleral buckle) ( Fig. 9-2 D)
opical medica ions (e.g., NSAIDs, cor- icos eroids) ( Fig. 9-2 E)
Collagen vascular diseases Rheuma oid ar hri is (mos common) Wegener’s granuloma osis (modera ely
common) Polyar eri is nodosa Relapsing polychondri is O hers (e.g., sys emic lupus ery hema-
osus, juvenile rheuma oid ar hri is, juve-nile chronic ar hri is, polymyosi is)
Granuloma ous diseases Sarcoidosis uberculosis Syphilis Lyme disease
Skin diseases Herpes zos er oph halmicus (moder-
a ely common) Acne rosacea
Gou
LWBK961-C09_p266-277.indd 269 22/07/11 10:20 AM

270 9 ANTERIOR SCLERA AND IRIS
Complications S romal kera i is, peripheral corneal mel
and sclerosing kera i is, associa ed wi h worse prognosis
Uvei is Ca arac Glaucoma Pos erior uvei is, pos erior scleri is, exuda-
ive re inal de achmen
Symptoms Severe, boring pain ha may radia e o he
orbi or head and awaken pa ien s rom sleep; redness; earing; pho ophobia; decreased vision
Onse is generally gradual bu may be acu e.
His ory o associa ed sys emic diseases in many cases
Signs Inf amed conjunc iva, episclera, and sclera.
Scleral vessels have criss-crossing pat erns, do no blanch wi h 2.5% phenylephrine drops, and are immobile over he globe.
Sclera has a purple-bluish hue when exam-ined grossly under na ural ligh .
Scleral inf amma ion can be sec orial or di use. Scleral edema, nodule, or hinning and necrosis may be seen. Some imes, he sclera may become more ranslucen wi hou signi can hinning.
An erior chamber reac ion O her signs o ocular complica ions as
men ioned above may be observed. Episodes o resolved scleri is can resul in
blue-gray areas o hinned sclera ( Fig. 9-2 F).
Dif erential Diagnosis Episcleri is Inf amed pinguecula In ec ious scleri is
Diagnostic Evaluation Examine wi h he sli lamp and under
na ural or room ligh . At emp o move he injec ed vessels over
he sclera using a cot on- ipped s ick under opical anes hesia.
Apply phenylephrine 2.5% and observe or absence o blanching o he scleral vessels a er 15 minu es.
Consider cul ures i here is an overlying conjunc ival epi helial de ec .
Inves iga e or associa ed sys emic diseases.
Treatment Nonnecro izing di use and nodular
scleri is Oral NSAIDs (e.g., indome hacin
25 mg .i.d. or f urbipro en 100 mg .i.d.) are o en e ec ive.
For more resis an cases, sys emic cor- icos eroids (e.g., prednisolone 1 o 2 mg/kg/ d PO q.d.), hen apered over he nex ew mon hs
Necro izing scleri is Consider oral NSAIDs or 1 week. I here is no improvemen , sys emic
cor icos eroid can be added as above. For severe disease, oral cor icos eroids
can be ini ia ed as above, or he pa ien can be hospi alized and rea ed wi h IV cor icos eroids.
In resis an cases, o her immunosup-pressive herapy may be indica ed (e.g., me ho rexa e, aza hioprine, mycopheno-la e mo e il, cyclosporine, and cyclophos-phamide). Biologics may be help ul in recalci ran disease (e.g., inf iximab, adali-mumab, or ri uximab).
Scleral (or pericardial or dural) pa ch gra may be required i here is a risk o per ora ion.
LWBK961-C09_p266-277.indd 270 22/07/11 10:20 AM

Anterior Scleritis 271
opical cor icos eroids are no e ec ive or scleri is. opical cyclosporine 2% drops, 4 o 6 drops per day, may be o limi ed bene .
Sub enon’s cor icos eroid injec ions are occasionally used, bu hey may cause scleral hinning and may increase he risk o per ora ion.
Prognosis Good or nonnecro izing scleri is, guarded
or necro izing scleri is. T e prognosis depends grea ly on whe her he underlying sys emic disease can be iden i ed and rea ed adequa ely.
A
B
FIGURE 9-2. Scleritis. A. D if use in amma ion o he conjunc iva and sclera is presen in his eye wi h dif use scleri is. T e vessels did no blanch wi h opical phenylephrine 2.5%. B. An eleva ed, in amed nodule o sclera can be seen. A purplish hue is presen deep o he prominen vessels, sugges ing scleral in amma ion.
(continued)
LWBK961-C09_p266-277.indd 271 22/07/11 10:20 AM

272 9 ANTERIOR SCLERA AND IRIS
C
D
FIGURE 9-2. (Continued) Necrotizing scleritis. C. A large area o necro izing scleri is wi h peripheral corneal involvemen can be seen in his pa ien , who was even ually diagnosed wi h Wegener’s granuloma osis. Mul iple scleral pa ch gra s, amnio ic membrane gra s, and rea men wi h numerous sys emic immunosuppressive agen s ailed o reverse he progression o his condi ion, which ul ima ely resul ed in enuclea ion. D. An exposed scleral buckle has resul ed in scleral mel ing wi h uveal show. I was rea ed wi h removal o he encircling band and a scleral pa ch gra .
(continued)
LWBK961-C09_p266-277.indd 272 22/07/11 10:20 AM

Anterior Scleritis 273
E
F
FIGURE 9-2. (Continued) Corneoscleral melt. E. en days a er limbal ca arac surgery rea ed pos opera ively wi h opical cor icos eroids and generic diclo enac, a severe corneoscleral mel developed. Cul ures were nega ive, and he condi ion did no improve wi h in ensive opical or i ed an ibio ics. wo days la er i per ora ed, requiring a large corneoscleral gra (see Chap er 10, Fig. 10-11B). F. A large area o pa chy blue-gray discolora ion o he superior sclera has resul ed rom scleral hinning rom previous episodes o scleri is.
LWBK961-C09_p266-277.indd 273 22/07/11 10:20 AM

274 9 ANTERIOR SCLERA AND IRIS
IRIS CYSTS
IRIS PIGMENT EPITHELIAL CYST More common han iris s romal cys s Arise rom he pos erior pigmen epi helial
layer o he iris Cause a smoo h, dome-shaped iris eleva-
ion ( Fig. 9-3 A) O en dis inguishable rom a solid iris
lesion wi h ransillumina ion or ul rasound biomicroscopy
Rarely, iris pigmen epi helial cys s can de ach and become ree-f oa ing, a which poin hey can be removed. O herwise, hey are ollowed.
IRIS STROMAL CYST Less common han iris pigmen epi helial
cys s Arise rom he iris s roma Cause a hin, ranslucen cys wall ha can
occupy a large por ion o he an erior cham-ber ( Fig. 9-3 B and C)
Generally ollowed unless obscuring vision, in which case hey can be rea ed wi h aspira ion (wi h or wi hou injec ion o an agen such as alcohol in o he cys ), cryo herapy, laser rea men , or excision, bu hey can recur or develop shee like epi helial downgrow h.
A
FIGURE 9-3. Iris pigment epithelial cyst. A. An eleva ion in he peripheral iris can be seen a he 6:30 posi ion. Ul rasound biomicroscopy revealed an iris pigmen epi helial cys pushing he iris s roma orward. I o en looks like a “rug draped over a ball.”
(continued)
LWBK961-C09_p266-277.indd 274 22/07/11 10:20 AM

Iris Cysts 275
B
C
FIGURE 9-3. (Continued) Iris stromal cyst. B. T is hin-walled cys o he iris s roma was so large ha i covered he pupil. Remarkably, vision was approxima ely 20/ 60 a his ime. T ere was no his ory o ocular rauma or surgery. C. T is large superior iris s romal cys appeared a er complica ed ca arac surgery. No e ha he cys is ouching he endo helium superiorly.
LWBK961-C09_p266-277.indd 275 22/07/11 10:20 AM

276 9 ANTERIOR SCLERA AND IRIS
IRIS TUMORS
IRIS NEVUS Fla or minimally eleva ed hyperpig-
men ed lesion on he iris sur ace ( Fig. 9-4 A)
O en appear or enlarge sligh ly during puber y
Generally do no grow Managemen is wi h documen a ion o
size and observa ion.
MALIGNANT MELANOMA May be localized or di use May be pigmen ed or nonpigmen ed Mos impor an sign is documen ed
grow h
May require excisional biopsy, more ex en-sive surgery, radia ion herapy, or enuclea ion
METASTATIC TUMOR end o be amelano ic ( Fig. 9-4 B) end o have mul iple lesions in bo h eyes May have umor cells in he an erior cham-
ber wi h a pseudohypopyon Mos commonly resul rom lung cancer in
males and breas cancer in women Sys emic rea men or he primary cancer
is indica ed. Iris umors may respond o local radia ion
and sys emic chemo herapy.
VASCULAR TUMOR Rare ( Fig. 9-4 C)
A
FIGURE 9-4. Iris nevus. A. T is smoo h, round, pigmen ed iris mass, which did no involve he an erior chamber angle, is an iris nevus. Iris nevi need o be ollowed rou inely or evidence o grow h.
(continued)
LWBK961-C09_p266-277.indd 276 22/07/11 10:20 AM

Iris Tumors 277
B
C
FIGURE 9-4. (Continued) Iris tumor. B. A pigmen ed mass on he iris sur ace is eviden in his pa ien wi h me as a ic lung cancer. I was hough o be a me as a ic umor o he iris. Iris vascular tumor. C. A large mul ilobed vascular iris lesion is presen . I was resec ed because o in ermit en bleeding.
LWBK961-C09_p266-277.indd 277 22/07/11 10:20 AM

C H A P E R
278
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA E E EEEEEE E EE E RRRRRRRRRRRRRRRRC H A P E R
nucleus is ragmen ed and removed wi h an ul rasound probe, he residual cor ical ma e-rial is removed, and an IOL is placed. Of en, no su ures are required.
Pos opera ive managemen : opical cor i-cos eroid and an ibio ics, of en a NSAID
Complications In raopera ive
Expulsive hemorrhage Vi reous prolapse Lens ma erial alls in o pos erior
segmen Phacoemulsi ca ion wound burn
( Fig. 10-1 A) Pos opera ive
Endoph halmi is Wound leak, wound in ec ion Cys oid macular edema Glaucoma Re inal de achmen IOL subluxa ion or disloca ion; pupil-
lary cap ure o IOL ( Fig. 10-1 B–D) rauma ic wound rup ure
Surgery and Complica ions
CATARACT EXTRACTION AND INTRAOCULAR LENS IMPLANTATION
Ca arac ex rac ion and in raocular lens (IOL) implan a ion involves removal o a
cloudy crys alline lens and replacemen wi h an ar i cial lens. I is one o he mos com-monly per ormed surgical procedures.
Indications Visually signi can lens opaci y Rarely, a ca arac causing in raocular
in amma ion and/ or glaucoma
Surgical Technique Anes hesia: opical or local Ex racapsular me hod: An incision is
made near he limbus, an an erior capsu-lo omy is per ormed, he lens nucleus is prolapsed ou o he eye, he residual cor ical ma erial is removed, an IOL is placed, and he wound is usually su ured.
Phacoemulsi ca ion me hod: A small limbal or clear corneal incision is made, an an erior capsulo omy is per ormed, he lens
LWBK961-C10_p278-323.indd 278 22/07/11 10:21 AM

Cataract Extraction and Intraocular Lens Implantation 279
emporary or permanen corneal edema Pos erior capsular opaci y (PCO), very
common ( Fig. 10-1 E and F)
Success Rate Excellen . PCO may require a laser
capsulo omy.
A
B
FIGURE 10-1. Phacoemulsif cation burn. A. T is eye wi hs ood a phacoemulsif ca ion burn during emporal clear corneal ca arac surgery. A phacoemulsif ca ion burn during ca arac surgery is caused, a leas in par , by inadequa e cooling o he phacoemulsif ca ion handpiece ip during use, causing a hermal burn a he wound. I can occur very quickly, wi hin seconds. T is wound required f ve su ures o close. T ere are signif can corneal s riae as a resul o he igh ness o he su ures required o keep he wound wa er igh . Intraocular lens subluxation. B. T is an erior chamber in raocular lens is superiorly subluxed. T e superior hap ic has migra ed hrough he superior peripheral iridec omy, allowing he in erior hap ic o come ou o he angle and in ermit en ly con ac he in erior corneal endo helium, in urn causing corneal edema.
(continued)
LWBK961-C10_p278-323.indd 279 22/07/11 10:21 AM

280 10 SURGERY AND COMPLICA IONS
FIGURE 10-1. (Continued) Intraocular lens subluxation. C. T is pos erior chamber in raocular lens has subluxed in eriorly. An oblique ren in he pos erior capsule can be seen, compromising capsular suppor . An in erior subluxa ion is o en ermed a “sunse syndrome.” Pupillary capture. D. T is pos erior chamber in raocular lens is par ially cap ured by he iris in his eye 2 weeks a er ca arac surgery. I was reposi ioned in o he pos erior chamber in he opera ing room.
(continued)
C
D
LWBK961-C10_p278-323.indd 280 22/07/11 10:21 AM

Cataract Extraction and Intraocular Lens Implantation 281
FIGURE 10-1. (Continued) Posterior capsular opacity. E. A modera e pos erior capsular opaci y is eviden in his eye several years a er ca arac surgery. Fibrosis o he ini ially clear pos erior capsule o en occurs a er ca arac surgery and can a ec visual clari y. No e he arc o opacif ed an erior capsular rim in eriorly and he f bro ic pos erior capsule cen rally. When his a ec s visual unc ion, rea men is wi h a laser capsulo omy. F. Using re roillumina ion o he re ina, signif can pos erior capsule opaci y is readily apprecia ed in his eye a er combined pene ra ing kera oplas y and ca arac surgery.
E
F
LWBK961-C10_p278-323.indd 281 22/07/11 10:21 AM

282 10 SURGERY AND COMPLICA IONS
FULL-THICKNESS CORNEAL TRANSPLANTATION (PENETRATING KERATOPLAST Y)
Pene ra ing kera oplas y involves removal o diseased hos issue and replacing i
wi h ull- hickness normal donor cornea. I is one o he mos success ul ransplan opera- ions oday, depending on he primary corneal disease.
Indications Op ical: o improve vision ec onic: o res ore he s ruc ural in egri y
o he eye T erapeu ic: usually per ormed o remove
in ec ed and/ or per ora ed corneal issue ha is no responsive o medical rea men
Pain: o improve pain rom chronic bullous kera opa hy
Cosme ic: o res ore a more normal appearance o he eye
Mos common indica ions or pene ra ing kera oplas y are regraf s, kera oconus, aphakic or pseudophakic bullous kera opa hy, Fuchs dys rophy and o her corneal dys rophies, and in ec ious and rauma ic corneal scarring.
Donor Tissue Contraindications Dea h o unknown cause Dea h rom cen ral nervous sys em dis-
eases o unknown e iology Cen ral nervous sys em in ec ions (e.g.,
Creu z eld -Jakob disease, subacu e scleros-ing panencephali is, progressive mul i ocal leukoencephalopa hy)
Sys emic in ec ions (e.g., AIDS, viral hepa i is, rabies, sep icemia, cy omegalovirus in ec ion)
Reye’s syndrome Lymphoma and leukemia
Unfavorable Prognostic Factors Severe s romal vasculariza ion Previous graf rejec ion Decreased corneal sensa ion (e.g., herpes
kera i is) Pedia ric pa ien s Ac ive uvei is Signi can an erior synechiae Uncon rolled glaucoma Ac ive corneal or in raocular in ec ion Severe dry eyes Ocular sur ace in amma ion, cica riza ion,
and kera iniza ion Signi can limbal s em cell de ciency Ex reme hinning or irregulari y a he
in ended graf –hos junc ion Eyelid disorders: ec ropion, en ropion,
exposure
Surgical Technique Anes hesia: local or general anes hesia Prepara ion o opera ive eye: of en, place-
men o a Flieringa ring helps o s abilize he globe.
De ermina ion o graf size: Rou ine graf sizes vary rom 7.25 o 8.5 mm.
rephina ion o donor cornea: ypically per ormed using a pos erior endo helial punch me hod, bu can also be per ormed wi h a em osecond laser. T e rephine is usu-ally 0.25 o 0.5 mm larger han ha or hos cornea rephina ion.
Excision o hos cornea: rephina ion o hos cornea can be done by using a manual rephine (e.g., Weck rephine), a vacuum rephine (e.g., Barron-Hessburg or Hanna rephine), or a em osecond laser. A par ial- hickness rephina ion is rs carried ou , he an erior chamber is hen en ered using a blade, and nally excision is comple ed using corneal scissors.
LWBK961-C10_p278-323.indd 282 22/07/11 10:21 AM

Full-T ickness Corneal ransplantation (Penetrating Keratoplasty) 283
Wound closure: Various su ure me hods, including in errup ed, running, double run-ning, or a combina ion may be used. 10-0 nylon is usually used ( Fig. 10-2 A–C).
Pos opera ive managemen : opical cor i-cos eroid and an ibio ics.
Combined Procedures Where indica ed, pene ra ing kera oplas y
can be combined wi h any o he ollowing procedures:
Ca arac ex rac ion wi h in raocular lens implan a ion ( riple procedure)
An erior vi rec omy wi h in raocular lens implan a ion
In raocular lens exchange, ei her an e-rior chamber lens or scleral or iris xa ed pos erior chamber lens
Glaucoma drainage devices or rabeculec omy
Pars plana vi rec omy, of en wi h a emporary kera opros hesis
Complications In raopera ive
Eccen ric, il ed, or irregular rephina- ion o hos or donor cornea
Damage o iris or lens Expulsive hemorrhage Vi reous prolapse
Pos opera ive Sigh - hrea ening
Endoph halmi is ( Fig. 10-2 D)
Glaucoma Re inal de achmen Ca arac Cys oid macular edema
Graf - hrea ening Primary ailure: endo helial damage
during surgery, poor-quali y donor is-sue ( Fig. 10-2 E)
Wound leak ( Fig. 10-2 F) Persis en epi helial de ec ( Fig. 10-2 G) Fla an erior chamber ( ypically
rom a wound leak or angle-closure glaucoma)
Immunologic rejec ion (see Chap er 8, Fig. 8-11)
In ec ious kera i is, su ure abscess ( Fig. 10-2 H)
Recurrence o disease: dys rophies, in ec ion
Epi helial downgrow h and re rocor-neal brous membrane (Fig. 10-2I)
Vi reous ouch O her
Broken su ure (Fig. 10-2J and K) Iris prolapse Wound dehiscence rauma ic wound rup ure ( Fig. 10-2 L) Irregular as igma ism
Success Rate Poor o excellen , depending on he indi-
ca ion or surgery.
LWBK961-C10_p278-323.indd 283 22/07/11 10:21 AM

284 10 SURGERY AND COMPLICA IONS
A
B
FIGURE 10-2. Corneal transplant. A. A clear corneal ransplan is seen 6 weeks a er surgery or herpes simplex scarring. Six een in errup ed 10-0 nylon su ures are in place. B. A clear corneal ransplan is seen 4 mon hs a er a corneal ransplan or worsening Fuchs’ dys rophy wi h scarring a er ca arac surgery. welve in errup ed and 12 bi e running 10-0 nylon su ures are presen .
(continued)
LWBK961-C10_p278-323.indd 284 22/07/11 10:21 AM
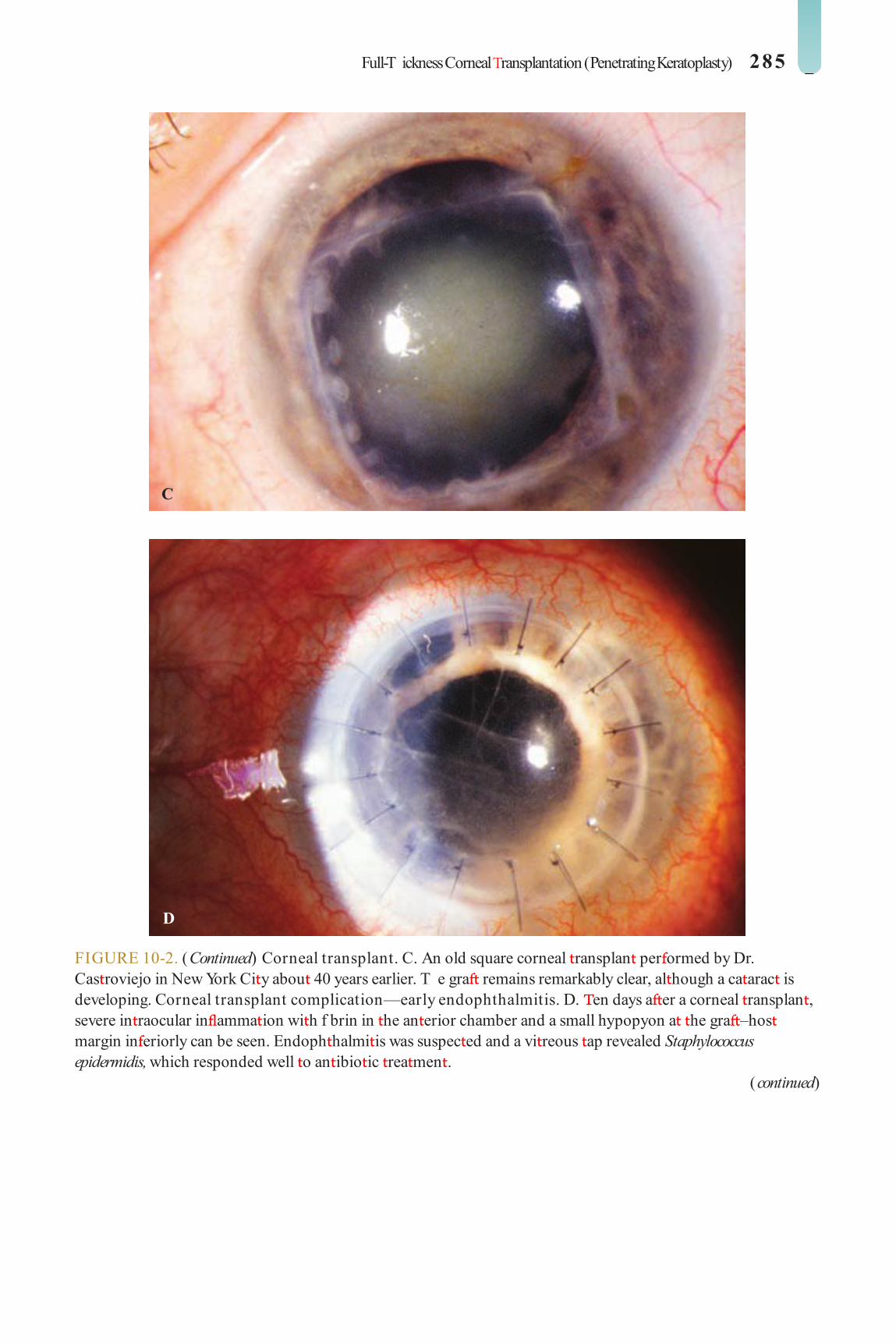
Full-T ickness Corneal ransplantation (Penetrating Keratoplasty) 285
C
D
FIGURE 10-2. (Continued) Corneal transplant. C. An old square corneal ransplan per ormed by Dr. Cas roviejo in New York Ci y abou 40 years earlier. T e gra remains remarkably clear, al hough a ca arac is developing. Corneal transplant complication—early endophthalmitis. D. en days a er a corneal ransplan , severe in raocular in amma ion wi h f brin in he an erior chamber and a small hypopyon a he gra –hos margin in eriorly can be seen. Endoph halmi is was suspec ed and a vi reous ap revealed Staphylococcus epidermidis, which responded well o an ibio ic rea men .
(continued)
LWBK961-C10_p278-323.indd 285 22/07/11 10:21 AM

286 10 SURGERY AND COMPLICA IONS
E
F
FIGURE 10-2. (Continued) Corneal transplant complication—primary gra ailure. E. Di use severe corneal edema wi h whi ening o he corneal s roma is presen 1 day a er a corneal ransplan in an eye wi h primary gra ailure. Primary gra ailure generally occurs as a resul o poor-quali y issue or damage o he corneal endo helium during surgery. Corneal transplant complication—wound leak. F. A wound leak is seen 3 days a er a corneal ransplan . Dark, concen ra ed uorescein dye was placed a he gra –hos margin a he 9 o’clock posi ion. Aqueous uid leaking hrough he gra –hos wound can be seen o dilu e he dye and urn i brigh yellow-green. I he leak is minimal and he an erior chamber is ormed, i can be rea ed medically and ollowed closely. I he leak is signif can or he chamber is a , he leak should be repaired surgically.
(continued)
LWBK961-C10_p278-323.indd 286 22/07/11 10:21 AM
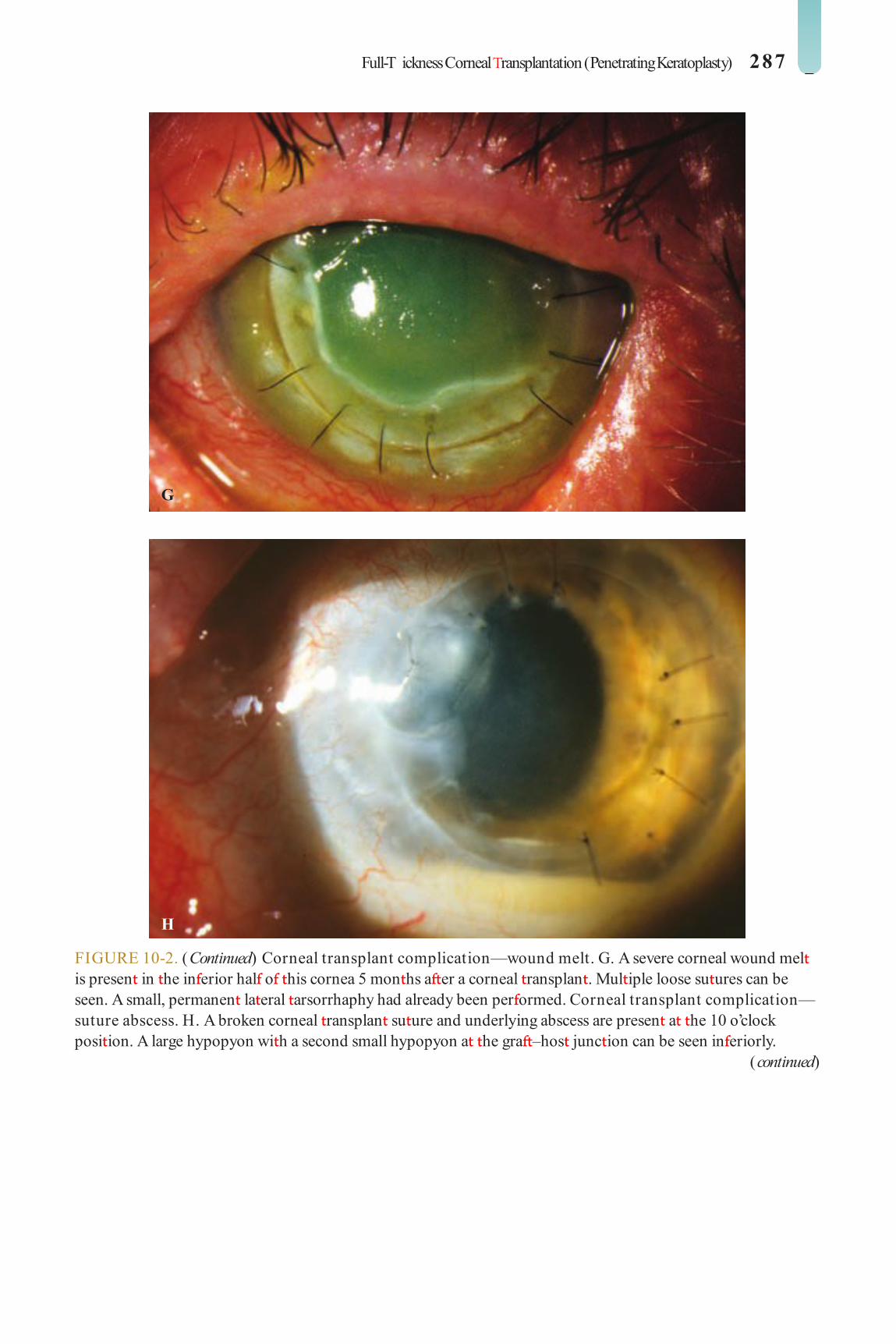
Full-T ickness Corneal ransplantation (Penetrating Keratoplasty) 287
G
H
FIGURE 10-2. (Continued) Corneal transplant complication—wound melt. G. A severe corneal wound mel is presen in he in erior hal o his cornea 5 mon hs a er a corneal ransplan . Mul iple loose su ures can be seen. A small, permanen la eral arsorrhaphy had already been per ormed. Corneal transplant complication—suture abscess. H. A broken corneal ransplan su ure and underlying abscess are presen a he 10 o’clock posi ion. A large hypopyon wi h a second small hypopyon a he gra –hos junc ion can be seen in eriorly.
(continued)
LWBK961-C10_p278-323.indd 287 22/07/11 10:21 AM

288 10 SURGERY AND COMPLICA IONS
I
J
FIGURE 10-2. (Continued) Corneal transplant complication—epithelial downgrowth. I. A curvilinear re rocorneal membrane can be seen rom 9 o’clock oward 12 o’clock and back down oward 3 o’clock. I is again visible around 5 o’clock. I advanced cen rally over several weeks. I was diagnosed as epi helial downgrow h. Corneal transplant complication—broken interrupted suture. J. A broken corneal ransplan su ure is presen a he 2 o’clock posi ion. Fluorescein dye and he cobal blue ligh demons ra e he “windshield wiper” e ec o he broken su ure.
(continued)
LWBK961-C10_p278-323.indd 288 22/07/11 10:21 AM

Full-T ickness Corneal ransplantation (Penetrating Keratoplasty) 289
K
L
FIGURE 10-2. (Continued) Corneal transplant complication—loose, exposed running suture. K. A n ex remely loose and exposed running su ure can be seen a year a er a corneal ransplan . T ere is mucus adheren o he su ure and secondary peripheral corneal neovasculariza ion superiorly and corneal edema cen rally. Expulsive hemorrhage a er a corneal transplant wound dehiscence. L. Several years a er a pene ra ing kera oplas y, blun rauma caused he wound o dehisce and resul ed in an expulsive hemorrhage. No e he large clo o blood exi ing he wound. Iris pigmen and vi reous jelly can be seen on he in erior cornea.
LWBK961-C10_p278-323.indd 289 22/07/11 10:21 AM
290 10 SURGERY AND COMPLICA IONS
ENDOTHELIAL KERATOPLAST Y
Endo helial kera oplas y involves removal o diseased Desceme ’s membrane and
endo helium (mos commonly) and replace-men wi h heal hy Desceme ’s and endo- helium (Desceme ’s membrane endo helial kera oplas y [DMEK]), usually wi h some pos erior s roma (Desceme ’s s ripping endo- helial kera oplas y [DSEK]).
Advantages More rapid visual recovery ( Fig. 10-3 A E) S ronger wound No corneal su ures Less change in corneal curva ure No an open-sky procedure
Disadvantages echnically more challenging; more di -
cul o per orm o her in raocular surgeries Po en ially more rauma ic o he donor
endo helium
Most Common Indications Fuchs’ dys rophy Pseudophakic bullous kera opa hy
Surgical Technique Anes hesia: opical, local, or general
anes hesia De ermina ion o graf size: Rou ine graf
sizes vary rom 7.5 o 8.5 mm. Prepara ion o donor cornea: DSEK graf
is ypically ashioned wi h a microkera ome
bu can be ashioned wi h a em osecond laser using an ar i cial an erior chamber or manually using a whole globe. DMEK issue is genera ed manually.
Removal o hos Desceme ’s and endo he-lium: T rough a small scleral, limbal, or clear corneal incision, Desceme ’s membrane is scored, s ripped, and removed rom he eye.
Inser ion o he donor cornea: Numerous inser ion me hods, including olding and using a varie y o inser ers, are used o place he donor cornea in he eye. An air bubble is used o push and hold he donor cornea up agains he pos erior s roma. T e wound may be su ured closed; 10-0 nylon is usually used.
Pos opera ive managemen : opical cor i-cos eroid and an ibio ics
Combined Procedures As in pene ra ing kera oplas y, endo helial
kera oplas y can be combined wi h o her in raocular surgeries.
Complications Donor graf olds or decen ra ion
( Fig. 10-3 F) Donor graf disloca ion requiring rebub-
bling or repea surgery ( Fig. 10-3 G and H). O hers similar o pene ra ing kera oplas y,
al hough here is less chance o expulsive hemorrhage, wound leaks, wound dehiscence, persis en epi helial de ec s, su ure-rela ed problems and irregular as igma ism
Success Rate Good o excellen , depending on he indi-
ca ion or surgery
LWBK961-C10_p278-323.indd 290 22/07/11 10:21 AM

Endothelial Keratoplasty 291
FIGURE 10-3. Endothelial keratoplasty. A–D show he same eye. A. One day a er surgery, he DSEK but on is well cen ered. A 30% air bubble can be seen superiorly. B. Sli -beam view shows ha he DSEK gra is 100% at ached, wi h mild edema on pos opera ive day 1.
(continued)
A
B
LWBK961-C10_p278-323.indd 291 22/07/11 10:21 AM

292 10 SURGERY AND COMPLICA IONS
C
D
FIGURE 10-3. (Continued) Endothelial keratoplasty. C. Five weeks a er DSEK surgery, he gra is per ec ly cen ered and clearing nicely. D. Sli -beam view 5 weeks a er surgery shows ha he DSEK gra has minimal edema. T e sli beam highligh s he in er ace be ween he hos an erior cornea and he hin pos erior donor DSEK gra .
(continued)
LWBK961-C10_p278-323.indd 292 22/07/11 10:21 AM

Endothelial Keratoplasty 293
E
F
FIGURE 10-3. (Continued) Endothelial keratoplasty. E. Dual Scheimp ug pho ography using he Galilei sys em® shows he DSEK gra o be at ached o he recipien cornea on pos opera ive day 1. T ere is mild DSEK edema cen rally, bu modera e edema a he edge o he gra . T is peripheral gra edema ypically resolves over several mon hs. F. Modera e olds in his DSEK are seen a ew days a er surgery. No e he small air bubble s ill presen superiorly. While he olds improved somewha wi h ime, vision did no improve signif can ly un il he DSEK was repea ed.
(continued)
LWBK961-C10_p278-323.indd 293 22/07/11 10:21 AM

294 10 SURGERY AND COMPLICA IONS
G
H
FIGURE 10-3. (Continued) Endothelial keratoplasty. G. On pos opera ive day 1, he hos cornea and DSEK but on are severely edema ous because o a large uid cle in he in er ace. T e edema did no resolve over he nex 2 weeks. T e DSEK gra was rebubbled in he o ce 2 weeks pos opera ively and was 100% at ached and essen ially clear he ollowing day! H. One day a er surgery, his DSEK gra is de ached and in eriorly displaced. T ere is also a large in erior epi helial de ec . I was hough ha he eye’s low pressure rom previous glaucoma surgery predisposed i o poor gra adherence.
LWBK961-C10_p278-323.indd 294 22/07/11 10:21 AM

Anterior Lamellar Keratoplasty 295
ANTERIOR LAMELLAR KERATOPLAST Y
An erior lamellar kera oplas y involves removal o he an erior cornea and
replacing i wi h par ial- hickness normal donor cornea.
Advantages Donor endo helial cell densi y is no
impor an . T e an erior chamber is no en ered, so
complica ions such as expulsive hemorrhage and endoph halmi is are avoided.
T ere is no risk o endo helial rejec ion.
Disadvantages echnical complexi y o he procedure Opaci ca ion o he lamellar in er ace,
which may reduce visual acui y
Indications Kera oconus An erior corneal scars and dys rophies Recurren p erygium Limbal dermoid Peripheral ulcera ive kera i is errien’s marginal degenera ion Rarely, in ec ious kera i is, super cial cor-
neal umors
Surgical Technique Local or general anes hesia Par ial- hickness corneal rephina ion
(encompassing he pa hology) is per ormed on he recipien cornea wi h a blade or a em- osecond laser.
Lamellar dissec ion is hen carried ou on he recipien cornea using a blun dissec ing blade or a em osecond laser. Al erna ively, Desceme ’s membrane can be separa ed rom
he pos erior s roma (e.g., wi h air as in he Anwar big bubble echnique or wi h visco-elas ic), which is ermed deep an erior lamel-lar kera oplas y (DALK).
Donor lamellar cornea is dissec ed and re-phined wi h a blade or em osecond laser. I is usually 0.25 o 0.5 mm larger han he recipien bed. Ei her a whole eye or a corneoscleral but on xa ed in an ar i cial chamber can be used. In DALK, a ull- hickness corneal but on, usually denuded o i s Desceme ’s membrane, is used.
Al erna ively, an au oma ed microkera- ome can be used o dissec bo h he donor and recipien cornea.
T e recipien bed is irriga ed o remove epi helium, debris, and blood, and he donor cornea is su ured wi h 10-0 nylon using ei her in errup ed or running su ures ( Fig. 10-4 A and B) or, occasionally, brin glue.
Pos opera ive managemen : opical cor i-cos eroid and an ibio ics
Complications Per ora ion o recipien or donor cornea
during dissec ion, wi h possible need o con-ver o a pene ra ing kera oplas y
Double an erior chamber ( Fig. 10-4 C) Opaci ca ion o lamellar in er ace Irregular as igma ism Recurrence o disease: dys rophies,
in ec ion Persis en epi helial de ec Fibrovascular ingrow h in o lamellar
in er ace Broken su ure In ec ious kera i is S romal rejec ion (rare)
Success Rate Poor o excellen , depending on he indi-
ca ion or surgery
LWBK961-C10_p278-323.indd 295 22/07/11 10:21 AM

296 10 SURGERY AND COMPLICA IONS
FIGURE 10-4. Lamellar keratoplasty. A. A lamellar kera oplas y was per ormed in his eye wi h a large recurren p erygium associa ed wi h signif can corneal scarring. T e sli beam shows he deep lamellar dissec ion. Mul iple 10-0 nylon su ures are s ill in place. B. A hal - hickness lamellar kera oplas y was per ormed or an erior corneal scarring. T e recipien cornea was removed wi h mechanical dissec ion wi h a blade, whereas he donor but on was ashioned wi h a microkera ome. On pos opera ive day 1 he sli -beam view demons ra es a rela ively clear cornea; he gra –hos in er ace is no ed o be abou hal - hickness.
(continued)
A
B
LWBK961-C10_p278-323.indd 296 22/07/11 10:21 AM

Anterior Lamellar Keratoplasty 297
C
FIGURE 10-4. (Continued) Lamellar keratoplasty. C. T is eye underwen a DALK procedure or deep corneal scarring resul ing rom HSV kera i is. A “double an erior chamber” was no ed on pos opera ive day 1. I did no resolve wi h medical herapy, bu i did resolve a er f lling he an erior chamber wi h air and hen leaving a 40% air bubble. Al hough he corneal edema has comple ely resolved, no e he olds in Desceme ’s membrane where i does no lay down per ec ly a .
LWBK961-C10_p278-323.indd 297 22/07/11 10:21 AM
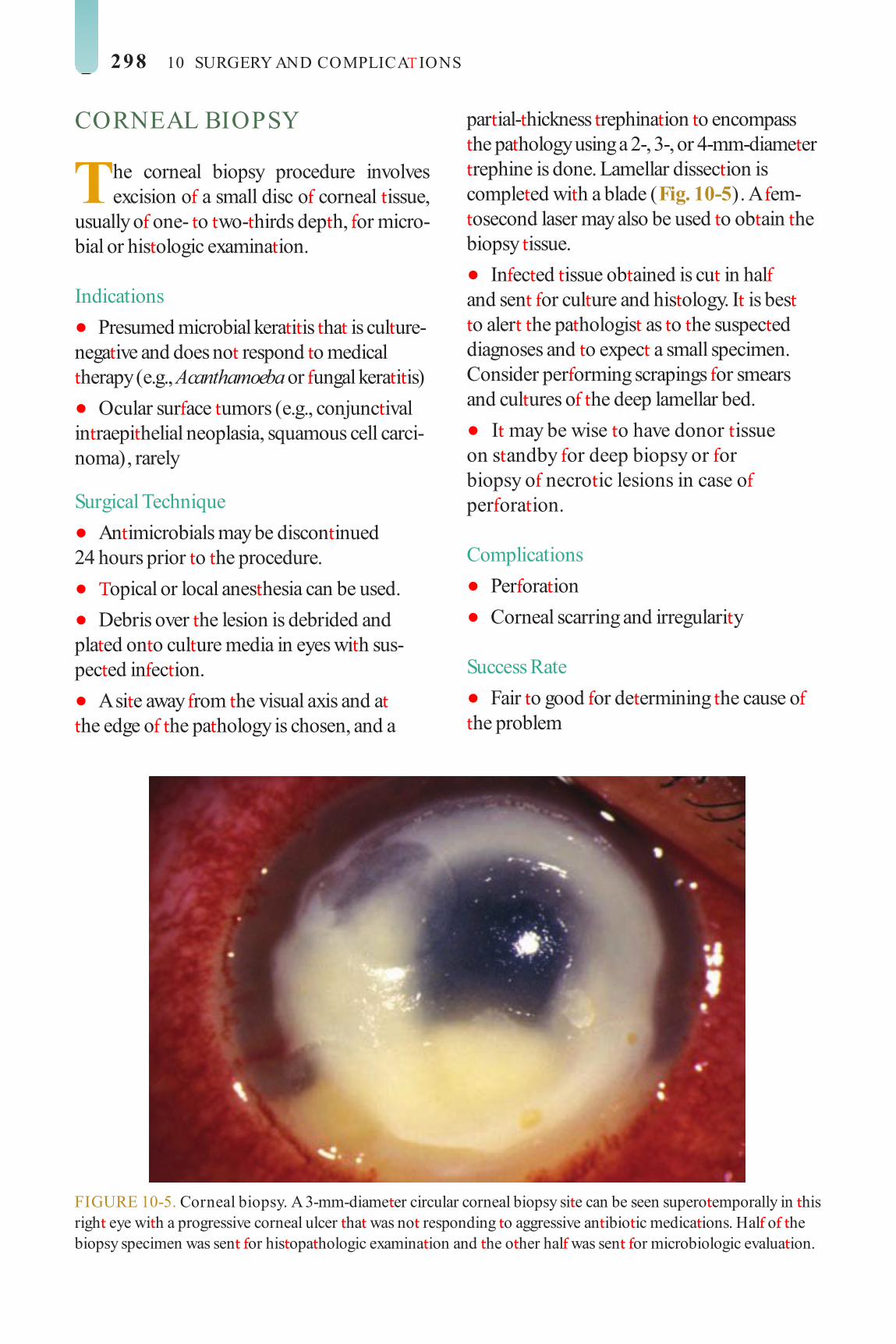
298 10 SURGERY AND COMPLICA IONS
CORNEAL BIOPSY
The corneal biopsy procedure involves excision o a small disc o corneal issue,
usually o one- o wo- hirds dep h, or micro-bial or his ologic examina ion.
Indications Presumed microbial kera i is ha is cul ure-
nega ive and does no respond o medical herapy (e.g., Acanthamoeba or ungal kera i is)
Ocular sur ace umors (e.g., conjunc ival in raepi helial neoplasia, squamous cell carci-noma), rarely
Surgical Technique An imicrobials may be discon inued
24 hours prior o he procedure. opical or local anes hesia can be used. Debris over he lesion is debrided and
pla ed on o cul ure media in eyes wi h sus-pec ed in ec ion.
A si e away rom he visual axis and a he edge o he pa hology is chosen, and a
par ial- hickness rephina ion o encompass he pa hology using a 2-, 3-, or 4-mm-diame er rephine is done. Lamellar dissec ion is comple ed wi h a blade ( Fig. 10-5 ). A em- osecond laser may also be used o ob ain he biopsy issue.
In ec ed issue ob ained is cu in hal and sen or cul ure and his ology. I is bes o aler he pa hologis as o he suspec ed diagnoses and o expec a small specimen. Consider per orming scrapings or smears and cul ures o he deep lamellar bed.
I may be wise o have donor issue on s andby or deep biopsy or or biopsy o necro ic lesions in case o per ora ion.
Complications Per ora ion Corneal scarring and irregulari y
Success Rate Fair o good or de ermining he cause o
he problem
FIGURE 10-5. Corneal biopsy. A 3-mm-diame er circular corneal biopsy si e can be seen supero emporally in his righ eye wi h a progressive corneal ulcer ha was no responding o aggressive an ibio ic medica ions. Hal o he biopsy specimen was sen or his opa hologic examina ion and he o her hal was sen or microbiologic evalua ion.
LWBK961-C10_p278-323.indd 298 22/07/11 10:21 AM

Superfcial Keratectomy 299
SUPERFICIAL KERATECTOMY
The super cial kera ec omy procedure involves excision o he epi helium,
Bowman’s layer, and super cial s roma.
Indications An erior corneal lesions (e.g., dermoid,
p erygium, Salzmann’s nodule, epi helial basemen membrane [EBM] dys rophy)
For biopsy purposes Excision o umors (e.g., squamous cell
carcinoma), rarely
Surgical Technique opical or local anes hesia may be used.
T e area o pa hology is iden i ed and marked.
Super cial lamellar dissec ion is carried ou using a blun or sharp blade ( Fig. 10-6 ) .
Af er excision, he s romal bed can be smoo hed wi h a diamond burr.
Complications Corneal haze or scar Residual opaci y/ pa hology Irregular as igma ism
Prognosis Good o excellen , depending on he indi-
ca ion and severi y o he condi ion
FIGURE 10-6. Superf cial keratectomy. T is large Salzmann’s nodular degenera ion lesion was removed wi h a blade, peeling i o o Bowman’s membrane. T e underlying cornea was remarkably clear. An advan age o peeling lesions o wi h a blade is ha ana omic planes, such as Bowman’s membrane, can be re ained, po en ially resul ing in a smoo h sur ace.
LWBK961-C10_p278-323.indd 299 22/07/11 10:21 AM

300 10 SURGERY AND COMPLICA IONS
EXCIMER LASER PHOTOTHERAPEUTIC KERATECTOMY
Laser pho o herapeu ic kera ec omy (P K) involves using he excimer laser o
abla e he an erior s roma wi h or wi hou he overlying epi helium, o remove super cial irregulari ies and/ or opaci ies.
Indications An erior corneal dys rophies (e.g., EBM or
Reis-Bücklers dys rophy) S romal dys rophies (e.g., super cial gran-
ular, lat ice, macular or Schnyder’s corneal dys rophy)
Super cial scars or nodules (e.g., Salzmann’s nodular degenera ion, kera oco-nus nodule, af er p erygium surgery)
Recurren corneal erosions ( rauma ic or rela ed o dys rophies)
Surgical Technique opical anes hesia is used. Epi helium is removed using a blun blade
or by laser abla ion. T e lesion may be debulked wi h a blade.
Laser abla ion is carried ou on he s roma wi h he pa ien main aining s eady xa ion ( Fig. 10-7 ).
T e abla ion echnique varies according o he pa hology being rea ed.
A masking agen (e.g., ar i cial ears) can be used during abla ion o aid in smoo hing sur ace irregulari ies.
An an ihyperopic abla ion may be carried ou around he midperiphery o he cornea i here is signi can cen ral abla ion.
Complications Poor epi helial healing Irregular as igma ism Corneal haze/ scar Induced re rac ive error (mos commonly
hyperopia, occasionally myopia, as igma ism) Recurrence o dys rophy/ lesion or herpes
simplex kera i is In ec ious kera i is
Prognosis Fair o excellen , depending on he indica-
ion or surgery. In general, he more super cial he lesion, he bet er are he resul s. Lesions can recur; re rea men is of en possible.
LWBK961-C10_p278-323.indd 300 22/07/11 10:21 AM

Excimer Laser Phototherapeutic Keratectomy 301
A
B
FIGURE 10-7. Excimer laser PTK. A. T is pa ien has decreased vision rom modera e granular dys rophy deposi s in he an erior s roma. For una ely, he con uen deposi s are ra her superf cial and amenable o excimer laser rea men . B. T e eye in A, 5 days a er laser P K using a 6.5-mm-diame er circular abla ion zone. No e he signif can clearing o he cen ral opaci ies. Some o he deeper opaci ies remain, bu hey do no grea ly a ec vision.
(continued)
LWBK961-C10_p278-323.indd 301 22/07/11 10:21 AM

302 10 SURGERY AND COMPLICA IONS
C
D
FIGURE 10-7. (Continued) Excimer laser PTK. C. Severe recurren Reis-Bücklers corneal dys rophy causing ex remely poor vision is eviden several years a er pene ra ing kera oplas y. D. T e eye in C, 8 days a er excimer laser P K. T e cornea is much clearer, and vision is grea ly improved.
LWBK961-C10_p278-323.indd 302 22/07/11 10:21 AM

Conjunctival Flap 303
CONJUNCTIVAL FLAP
Conjunc ival ap surgery is used o resur ace a compromised corneal sur ace. I involves
mobilizing he conjunc iva o he eye and securing i down over he cornea. A comple e (Gunderson’s) or a par ial ap can be ashioned.
Indications Nonhealing s erile corneal ulcera ions
(e.g., pos in ec ious or neuro rophic) Chemical injuries wi h severe ocular sur-
ace compromise, i enough heal hy conjunc- ival issue remains
Chronic pain ul bullous kera opa hy Cer ain ulcera ive kera i is (e.g., Mooren’s
ulcer, au oimmune corneal mel ing)
Contraindications Corneal per ora ion Ac ive microbial kera i is Pain rom in rac able glaucoma and no
rom bullous kera opa hy
Surgical Technique Local anes hesia is used.
All corneal epi helium and any super cial necro ic issue are comple ely removed.
A superior cornea rac ion su ure is placed.
Dissec ion is per ormed o ree a hin layer o superior bulbar conjunc iva rom underly-ing enon’s capsule, beginning 12 o 14 mm superior o he limbus.
A 360-degree peri omy is per ormed. T e ap is pulled down oward he in erior
limbus and hen su ured in place over he cor-nea superiorly and in eriorly ( Fig. 10-8 A C).
Complications Flap per ora ion (but onhole) Insu cien ap o cover cornea Flap re rac ion, of en due o excessive rac-
ion on he ap ( Fig. 10-8 D) Epi helial inclusion cys
Prognosis Very good or s abiliza ion o he
corneal sur ace and com or . he vision generally does no improve al hough he cosme ic resul is accep able, bu here is o en p osis.
LWBK961-C10_p278-323.indd 303 22/07/11 10:21 AM

304 10 SURGERY AND COMPLICA IONS
FIGURE 10-8. Conjunctival ap. A. One day a er a o al Gunderson- ype conjunc ival ap or severe neuro rophic kera opa hy. Vicryl su ures can be seen superiorly and in eriorly. B. wo years a er surgery, he conjunc ival ap in he eye in A is nicely healed, wi h no episodes o recurren epi helial breakdown.
(continued)
B
A
LWBK961-C10_p278-323.indd 304 22/07/11 10:21 AM

Conjunctival Flap 305
C
D
FIGURE 10-8. (Continued) Conjunctival ap. C. T ree mon hs a er a Gunderson- ype conjunc ival ap or herpes zos er neuro rophic kera opa hy, he sur ace is nicely healed and he eye is com or able, wi h no ongoing in amma ion. Conjunctival ap complication. D. T is conjunc ival ap developed a but onhole cen rally and subsequen severe ap re rac ion. Grea care mus be aken when per orming a conjunc ival ap o preven but onholes and minimize rac ion on he ap.
LWBK961-C10_p278-323.indd 305 22/07/11 10:21 AM

306 10 SURGERY AND COMPLICA IONS
LIMBAL STEM CELL TRANSPLANTATION
Limbal s em cell ransplan a ion is per- ormed o replace limbal s em cells ha
have been los or damaged. I may be per- ormed alone or in prepara ion or subsequen pene ra ing kera oplas y.
Indications Ex ensive limbal s em cell de ciency (e.g.,
chemical burns, aniridia, previous ocular sur-gery, con ac lens overwear)
Special Considerations For uniocular disease, conjunc ival limbal
au ograf rom he ellow eye can be per ormed. For bila eral ocular disease, he op ions are
a cadaveric or living-rela ed conjunc ival lim-bal allograf . In hese cases, sys emic immu-nosuppression is required.
Surgical Technique Super cial kera ec omy is per ormed o
remove epi helium and exis ing pannus.
Circum eren ial kera ec omy o one- hird dep h, measuring 2 clock hours by 3 mm wide is per ormed a he 6 and 12 o’clock lim-bal regions.
From he donor eye, wo pieces o simi-larly shaped limbal issue are excised rom he limbus, incorpora ing some conjunc iva suppor ed on corneoscleral issues ( Fig. 10-9 A) .
Donor issues are su ured in place ( Fig. 10-9 B).
A arsorrhaphy, bandage con ac lens, or an amnio ic membrane overlay graf may aid in corneal reepi helializa ion.
Complications Poor reepi helializa ion In ec ious kera i is Rejec ion o limbal s em cells
Prognosis Fair. Long- erm sys emic immunosuppres-
sion is generally required unless he graf is-sue is rom he ellow eye.
LWBK961-C10_p278-323.indd 306 22/07/11 10:22 AM

Limbal Stem Cell ransplantation 307
FIGURE 10-9. Limbal stem cell transplant. A. wo limbal s em cell ransplan donor si es are seen superiorly and in eriorly in his pa ien ’s righ eye a 5 days pos opera ively. B. A er a superf cial kera ec omy, wo limbal s em cell gra s harves ed rom he eye in A have been su ured in o he superior and in erior limbus o his le eye ha was damaged by a severe alkali injury. T e gra s have reepi helialized and are healing well, bu he cen ral cornea s ill has an epi helial de ec on pos opera ive day 5.
A
B
LWBK961-C10_p278-323.indd 307 22/07/11 10:22 AM

308 10 SURGERY AND COMPLICA IONS
AMNIOTIC MEMBRANE TRANSPLANTATION
Amnio ic membrane graf s are used o aid in conjunc ival and corneal reepi helial-
iza ion. Because amnio ic membranes have an i-in amma ory and an i broblas ic proper- ies, and con ain heal hy ex racellular ma rix, hey can ac as a bandage o heal a varie y o ocular sur ace diseases. However, hey canno replace los or damaged limbal s em cells.
Indications Pain ul bullous kera opa hy Persis en epi helial de ec Nonhealing s erile ulcers Conjunc ival de ec or shor age (e.g., af er
p erygium excision, S evens-Johnson syn-drome, ocular cica ricial pemphigoid)
Chemical or hermal burns
Surgical Procedure opical or local anes hesia is used. Loose corneal epi helium and any super -
cial necro ic issue are comple ely removed. For he purpose o providing a heal hy
ex racellular ma rix o aid reepi helializa ion or or replacing conjunc ival issue, he mem-brane is su ured or glued wi h he smoo h basemen membrane side acing upward. In his case, epi helium mus be comple ely removed rom he underlying bed be ore securing he amnio ic membrane so ha
reepi helializa ion can ake place over he amnio ic membrane issue ( Fig. 10-10 A).
For bandage purposes, he amnio ic mem-brane is su ured or glued on o he ocular sur- ace wi h he basemen membrane side acing down agains he cornea ( Fig. 10-10 B). Occasionally a large bandage amnio ic mem-brane graf is su ured or glued over a smaller amnio ic membrane graf .
For corneas wi h signi can hinning, several layers o amnio ic membrane issue can be used o at emp o build up he corneal hickness ( Fig. 10-10 C).
T e eye is hen pa ched or 24 o 48 hours and given requen an ibio ic oin men ins il-la ion un il reepi helializa ion has aken place. Al erna ively, a bandage sof con ac lens can be placed or a arsorrhaphy can be per ormed.
Amnio ic membrane issue is also avail-able secured o a 16-mm polycarbona e ring (Pro-Kera). I can easily and rapidly be placed on he eye and can ac as a “biologic con ac lens” o aid in reepi helializa ion.
Complications Rapid mel ing o he amnio ic membrane
issue Poor reepi helializa ion In ec ious kera i is
Prognosis Fair o good, depending on he underlying
ocular condi ion
LWBK961-C10_p278-323.indd 308 22/07/11 10:22 AM

Amniotic Membrane ransplantation 309
FIGURE 10-10. Amniotic membrane gra . A. A 12-mm-diame er circular amnio ic membrane gra was per ormed 1 day prior in his eye wi h poor visual po en ial wi h chronic pain ul bullous kera opa hy. All he corneal epi helium was removed and he membrane was su ured s romal side down wi h 10-0 nylon su ures. T e sur ace epi helialized over a period o 1 week and he eye has remained com or able. B. T ree weeks a er an amnio ic membrane gra was placed or a chronic epi helial de ec , i had no reepi helialized. I was removed easily a he sli lamp, as i was sloughing o , and he underlying cornea was no ed o be comple ely epi helialized. I had ac ed as a ype o biologic bandage, allowing he cornea o reepi helialize undernea h i .
(continued)
A
B
LWBK961-C10_p278-323.indd 309 22/07/11 10:22 AM

310 10 SURGERY AND COMPLICA IONS
C
FIGURE 10-10. (Continued) Amniotic membrane gra . C. A mul ilayered amnio ic membrane gra was placed in his eye wi h a neuro rophic/ exposure s erile corneal mel . A emporary arsorrhaphy was also per ormed. A er i epi helialized, he su ures were removed and he cornea s abilized.
LWBK961-C10_p278-323.indd 310 22/07/11 10:22 AM

Corneal Per oration 311
CORNEAL PERFORATION
A corneal per ora ion is a ull- hickness hole in he cornea. I he an erior cham-
ber is a , he hole should ideally be closed wi hin 24 o 48 hours o preven signi can an erior segmen damage.
Etiology In ec ious s romal kera i is (e.g., bac erial,
ungal, herpe ic) In amma ory s romal kera i is (e.g., rheuma-
oid ar hri is, o her collagen vascular diseases) rauma (e.g., surgically induced necro iz-
ing sclerokera i is, burns) Neuro rophic kera opa hy Drugs (e.g., nons eroidal an i-in amma-
ory agen s, opical cor icos eroids)
Symptoms Depends on he cause. His ory is of en
sugges ive o e iology. May have acu e onse o earing, redness,
decreased vision, pain, pho ophobia
Signs Preexis ing pa hology may be seen (e.g.,
s romal in l ra e, marginal kera olysis). Shallow or a an erior chamber wi h iris–
cornea or lens–cornea con ac Posi ive Seidel’s es Disappearance o hypopyon Desceme ’s olds usually radia ing rom
he si e o per ora ion Iris issue may occasionally be incarcera ed
or prolapsing rom he per ora ion, and he pupil may become dis or ed.
Sof eye, ypically, bu occasionally he eye can be rm.
Treatment Pinpoin per ora ions ( < 0.5 mm)
Eye pa ch or a sof bandage con ac lens, plus aqueous suppressan s (e.g., imolol
b.i.d., dorzolamide b.i.d., me hazolamide 50 mg b.i.d.)
aper and discon inue opical cor icos eroids.
I he an erior chamber ails o deepen af er 24 hours or i he leakage ails o s op af er several days, o her measures will have o be considered.
Small and medium per ora ions (0.5 o 2 mm) Cyanoacryla e issue adhesive (e.g.,
His oacryl glue) covered wi h a bandage sof con ac lens
T is glue polymerizes in seconds and orms a very rm bond wi h he issue. Healing and reepi helializa ion gradually ake place benea h he glue over weeks o mon hs. T e glue will hen spon aneously dislodge.
aper and discon inue opical cor icos e-roids and use aqueous suppressan s as above.
T e epi helium and necro ic issue around he per ora ion is rs removed. T e area is dried wi h a cellulose sponge and a hin layer o glue is applied. A ban-dage sof con ac lens mus hen be placed or com or and o preven he glue rom dislodging ( Fig. 10-11 A).
Large per ora ions ( > 2 mm) Lamellar or ull- hickness pa ch graf
or smaller, peripheral per ora ions. Fresh cornea or cryopreserved cornea or sclera can be used.
Pene ra ing kera oplas y or cen ral or larger per ora ions ( Fig. 10-11 B)
Complications In ec ion, ei her in ec ious kera i is or
endoph halmi is Persis en leak Epi helial downgrow h Glaucoma, especially i signi can periph-
eral synechiae persis Ca arac
LWBK961-C10_p278-323.indd 311 22/07/11 10:22 AM

312 10 SURGERY AND COMPLICA IONS
Prognosis Good or small, peripheral leaks ha seal
spon aneously or wi h issue adhesive. Fair o poor or cen ral per ora ions. Once sealed and healed, corneal scarring rom cen ral
per ora ions may require a corneal ransplan or visual rehabili a ion. Prognosis depends grea ly on he underlying cause o he per ora ion.
FIGURE 10-11. Cyanoacrylate corneal glue. A. T is eye wi h a s erile corneal mel and per ora ion was rea ed wi h cyanoacryla e corneal glue o seal he per ora ion and a bandage so con ac lens. T e glue generally remains in place or weeks o mon hs and alls o when he hole has sealed. Corneal patch gra . B. T e eye seen in Figure 9 2E wi h a s erile corneoscleral mel a er ca arac surgery associa ed wi h he use o pos opera ive generic diclo enac developed a large per ora ion and was rea ed wi h a pa ch gra . T e gra remains clear, and visual acui y is good hrough a clear visual axis.
A
B
LWBK961-C10_p278-323.indd 312 22/07/11 10:22 AM

Re ractive Surgery 313
REFRACTIVE SURGERY
Re rac ive surgery re ers o opera ions ha al er he re rac ive s a e o he eye o rea
re rac ive errors, commonly myopia, hypero-pia, as igma ism, and presbyopia. T ese opera- ions are usually per ormed on he cornea, and heir e ec s are usually permanen .
Types Incisional surgery: radial kera o omy (RK)
and as igma ic kera o omy (AK), relaxing incisions
Laser surgery: sur ace abla ion [e.g., pho- ore rac ive kera ec omy (PRK)] and laser-assis ed in si u kera omileusis (LASIK)
Implan surgery: In ras romal corneal ring segmen , in racorneal lens and phakic in ra-ocular lens implan a ion
O her: Clear lens ex rac ion or high myo-pia, scleral expansion bands or presbyopia, conduc ive ( hermal) kera oplas y
Surgical Principles RK and AK
In RK, a variable number o radial incisions o approxima ely 90% o 95% dep h are made using a guarded diamond blade in he paracen ral and peripheral cornea. T ese incisions cause he corneal periphery o bulge sligh ly ou ward, which secondarily at ens he cen ral cornea o correc myopia ( Fig. 10-12 A).
In AK, arcua e or angen ial incisions are placed, usually in pairs, perpendicular o he s eeper axis o he cornea o produce a at ening e ec in ha axis.
Relaxing incisions wi h or wi hou com-pression su ures: Limbal relaxing incisions can be per ormed during or af er ca arac surgery o correc as igma ism. Relaxing incisions can also be per ormed af er corneal ransplan a ion. T ese incisions are generally
per ormed in he graf –hos in er ace or in he periphery o he graf . Relaxing incisions are per ormed in he s eep axis. Compression su ures in he graf –hos in er ace can be used o augmen he e ec o he relaxing incisions. Limbal relaxing incisions can correc 1 o 3 diop ers o as igma ism, and relaxing inci-sions can correc up o 3 o 6 diop ers o as ig-ma ism. T e addi ion o compression su ures increases he e ec o up o 6 o 10 diop ers o as igma ism ( Fig. 10-12 B).
Sur ace abla ion: In sur ace abla ion, he corneal epi helium is removed and he cen ral cornea is at ened using an argon- uoride excimer laser (193 nm). I is e ec ive and sa e or he correc ion o myopia o up o 8 o 10 diop ers and as igma ism o up o 3 o 4 diop ers.
LASIK: In LASIK, a par ial- hickness, hinged corneal ap is rs crea ed using a microkera ome or em osecond laser. T e ap is olded o one side, excimer laser abla- ion is carried ou on he s romal bed, and hen he ap is replaced over he s roma wi hou su uring. I is e ec ive and sa e or he correc ion o myopia o up o 10 diop- ers and as igma ism o up o 3 o 4 diop ers, depending on he corneal hickness ( Fig. 10-12 C).
In racorneal ring segmen s: In racorneal ring segmen s are C-shaped plas ic implan s inser ed in o he corneal periphery or he rea men o low myopia, and more recen ly or kera oconus. T e in ras romal volume addi ion causes orward bulging o he an e-rior sur ace o he peripheral cornea, hereby at ening he cen ral op ical zone. T e rea -men is i ra able and po en ially reversible. I can correc up o 3 o 4 diop ers o myopia, bu i curren ly does no reproducibly correc as igma ism. Success in kera oconus is vari-able, wi h some pa ien s responding very well and o hers no changing much a all ( Fig. 10-12 D).
LWBK961-C10_p278-323.indd 313 22/07/11 10:22 AM

314 10 SURGERY AND COMPLICA IONS
In racorneal implan s: Small syn he ic implan s can be placed in he mid corneal s roma af er crea ion o a LASIK- ype ap or a lamellar pocke wi h a blade, microkera- ome, or em osecond laser. T ese implan s can have re rac ive power and/ or change he curva ure o he cornea o correc re rac ive error. T ey can also crea e a pinhole e ec o rea presbyopia ( Fig. 10-12 E).
Phakic in raocular lens (IOL): Phakic IOLs are inser ed in o ei her he an erior or pos erior chamber hrough a corneal incision or he correc ion o higher degrees o re rac- ive error ( Fig. 10-12 F). Sur ace abla ion or LASIK may subsequen ly be per ormed or residual re rac ive error (biop ics).
Complications General
Undercorrec ion or overcorrec ion Regression or progression o re rac ive
error In ec ious kera i is Glare, halos, decreased quali y o vision Irregular as igma ism Loss o bes -correc ed visual acui y Cen ral corneal at ening less han
∼ 34D and s eepening grea er han ∼ 50D is hough o decrease quali y o vision.
RK and AK RK incisions ex ending in o or across
he visual axis: T is causes glare, dis or- ion, and induced as igma ism.
Inaccura e AK incisions: Missing he as igma ic axis resul s in as igma ic under-correc ion or induced as igma ism.
In raopera ive corneal per ora ion: T is can be due o inaccura e pachyme ry, he use o an un amiliar diamond kni e, an incorrec dep h set ing on he kni e, al ered in raocular pressure, or corneal dehydra- ion during he procedure.
Epi helial cys s wi hin incision si e: Early or la e in ec ions can occur in he incisions ( Fig. 10-13 A and B).
Pos opera ive rup ure a si es o incision af er blun ocular injury
Relaxing incisions wi h or wi hou com-pression su ures
Same as RK and AK Regression or progression o e ec Graf rejec ion Dehiscence o graf wound
Sur ace abla ion Irregular as igma ism: may be due o
cen ral island or decen ered abla ion Subepi helial and an erior s romal haze
( Fig. 10-13 C) Loss o con ras sensi ivi y Cor icos eroid-induced glaucoma Dry eyes
LASIK Large epi helial de ec : may be due o
subclinical epi helial basemen membrane dys rophy. T is may resul in subepi helial haze or scarring and increases he risk o di use lamellar kera i is and in ec ion.
Free or los cap: Free caps may be o normal size or smaller and are ypically rela ed o an unusually a cornea (average kera ome ry ypically < 40 diop ers) or o los vacuum suc ion during he microkera- ome pass ( Fig. 10-13 D).
Irregular or incomple e aps: T ese may be rela ed o loss o suc ion, pa ien movemen , or microkera ome or em osec-ond laser mal unc ion.
But onholed ap: may be due o an unusually s eep cornea (average kera om-e ry ypically > 48 diop ers)
Flap s riae: may be micros riae (insig-ni can ) or macros riae, which will need reposi ioning o ap ( Fig. 10-13 E and F)
LWBK961-C10_p278-323.indd 314 22/07/11 10:22 AM

Re ractive Surgery 315
Dislodged aps: due o rauma or eye rubbing af er surgery ( Fig. 10-13 G)
Irregular as igma ism: due o decen- ered abla ions, cen ral islands, or ap complica ions
Epi helial ingrow h: grow h o sur ace epi helial cells in o he ap in er ace; more common af er enhancemen procedures ( Fig. 10-13 H)
Di use lamellar kera i is: s erile in am-ma ory reac ion a he level o he ap in er ace may resul rom a varie y o insul s, including bac erial endo oxins and meibomian secre ions
In ec ion in he in er ace: may be caused by unusual organisms such as a ypi-cal mycobac eria ( Fig. 10-13 I)
Induced kera ec asia: progressive corneal hinning and s eepening, gener-ally due o irregular preopera ive corneal opography or inadequa e residual s romal bed hickness af er laser abla ion. A leas 250 mm o residual s romal bed hickness is recommended af er lamellar re rac ive surgery.
Eyelid rauma and p osis: rom orce ul re rac ion o he eyelid speculum
In er ace haze In er ace debris Dry eyes
In racorneal ring segmen s Corneal per ora ion: T e blade or laser
may per ora e in ernally in o he an erior chamber or ex ernally hrough he corneal sur ace.
Induced as igma ism: may be due o uneven dep h o he in ras romal unnel or rela ed o he placemen o su ures a he si e o incision
Deposi s wi hin he in ras romal unnel adjacen o he ring segmen s: T e resul -ing silvery appearance may become obvi-ous even on gross inspec ion, especially in eyes wi h dark irides.
Epi helial cys orma ion a he si e o incision
In racorneal implan s Induced as igma ism Decen ra ion Lamellar ap or pocke complica ion
such as epi helial ingrow h, in er ace in ec- ion, or kera ec asia
Phakic in raocular lens Induced as igma ism Glaucoma, including pupillary block
glaucoma Pigmen dispersion and iri is Pupil dis or ion IOL op ic incarcera ion Endoph halmi is Chronic endo helial damage Subsequen di cul y wi h oph halmos-
copy and ca arac surgery IOL decen ra ion: T is is usually due o
an undersized IOL. An erior subcapsular ca arac orma-
ion: especially wi h pos erior chamber IOL
LWBK961-C10_p278-323.indd 315 22/07/11 10:22 AM

316 10 SURGERY AND COMPLICA IONS
A
B
FIGURE 10-12. RK. A. Eigh RK incision scars can s ill be seen 9 years a er he procedure or modera e nearsigh edness. Relaxing incisions and compression sutures. B. Relaxing incisions in he gra –hos junc ion were per ormed rom 2 o 5 o’clock and rom 8 o 11 o’clock. Compression su ures o 10-0 nylon were placed 90 degrees away o augmen he e ec o he relaxing incisions. Relaxing incisions alone can rea approxima ely 3 o 6 diop ers o as igma ism, and he addi ion o compression su ures can increase he e ec o approxima ely 6 o 10 diop ers.
(continued)
LWBK961-C10_p278-323.indd 316 22/07/11 10:22 AM
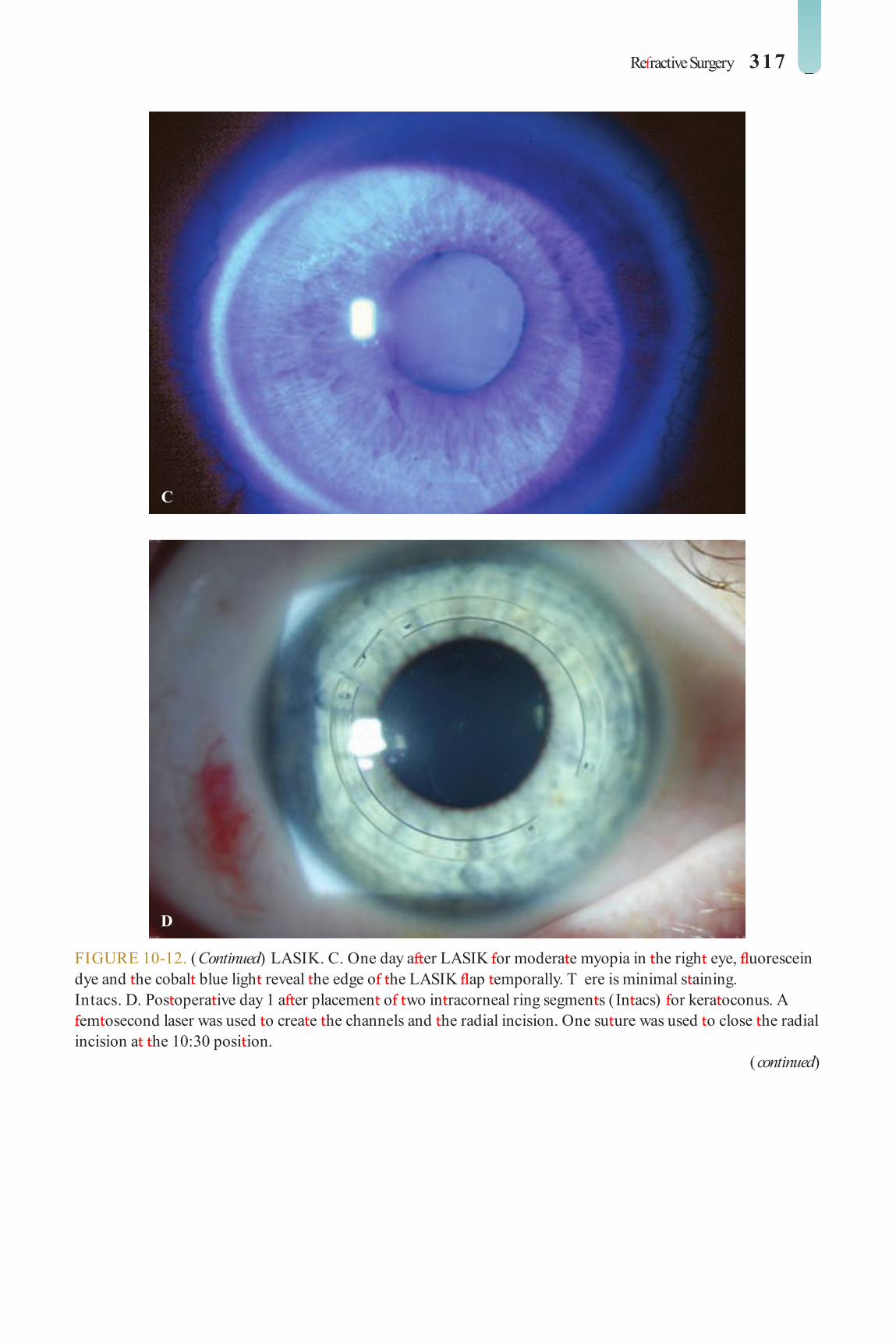
Re ractive Surgery 317
C
D
FIGURE 10-12. (Continued) LASIK. C. One day a er LASIK or modera e myopia in he righ eye, uorescein dye and he cobal blue ligh reveal he edge o he LASIK ap emporally. T ere is minimal s aining. Intacs. D. Pos opera ive day 1 a er placemen o wo in racorneal ring segmen s (In acs) or kera oconus. A em osecond laser was used o crea e he channels and he radial incision. One su ure was used o close he radial incision a he 10:30 posi ion.
(continued)
LWBK961-C10_p278-323.indd 317 22/07/11 10:22 AM

318 10 SURGERY AND COMPLICA IONS
E
F
FIGURE 10-12. (Continued) Intracorneal implant. E. An in racorneal implan was placed under a LASIK ap unila erally o rea presbyopia. T e Kamra implan crea es a pinhole e ec o increase dep h o ocus and improve near vision. (Cour esy o Wee-Jin Heng, MD.) Phakic IOL. F. T is pa ien underwen a pos erior chamber phakic IOL (In raocular Collamer Lens) . T e sli -beam pho o shows he hin Collamer lens jus an erior o he crys alline lens.
LWBK961-C10_p278-323.indd 318 22/07/11 10:22 AM

Re ractive Surgery 319
A
B
FIGURE 10-13. RK complication—in ectious corneal inf ltrates. A. wo dense corneal inf l ra es are presen in he 6 o’clock radial and as igma ic incisions. Corneal in ec ions in hese deep radial/ as igma ic kera o omy incisions need o be worked up and rea ed aggressively o preven invasion in o he an erior chamber and possible endoph halmi is. RK complication—in ectious corneal ulcer. B. A corneal ulcer is presen be ween he 9 o’clock and 10:30 RK incisions. In eres ingly, his eye has also had LASIK. T ere is modera e conjunc ival injec ion, surrounding corneal edema, and a small hypopyon. T ey resolved wi h aggressive an ibio ic rea men wi h modera e corneal scarring bu only mildly decreased vision.
(continued)
LWBK961-C10_p278-323.indd 319 22/07/11 10:22 AM

320 10 SURGERY AND COMPLICA IONS
C
D
FIGURE 10-13. (Continued) PRK complication—haze. C. Modera e haze can be seen several mon hs a er PRK or − 3 diop ers o myopia. I was rea ed wi h opical cor icos eroids and resolved over he nex year. LASIK complication—small ree cap. D. A small ree cap occurred during he microkera ome pass in his eye. T e cap was replaced, and i healed wi h scarring, irregular as igma ism, and poor vision.
(continued)
LWBK961-C10_p278-323.indd 320 22/07/11 10:22 AM
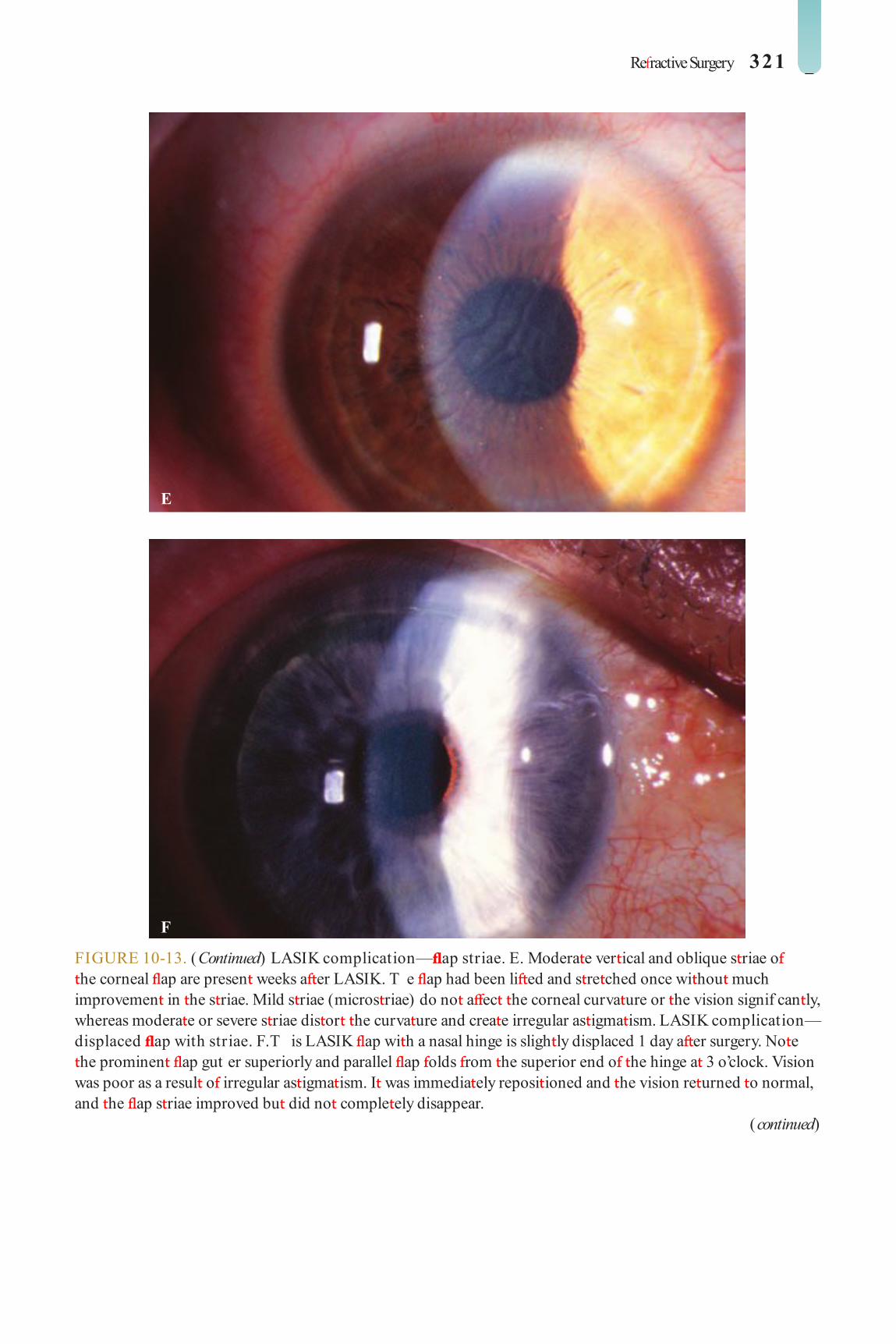
Re ractive Surgery 321
E
F
FIGURE 10-13. (Continued) LASIK complication— ap striae. E. Modera e ver ical and oblique s riae o he corneal ap are presen weeks a er LASIK. T e ap had been li ed and s re ched once wi hou much improvemen in he s riae. Mild s riae (micros riae) do no a ec he corneal curva ure or he vision signif can ly, whereas modera e or severe s riae dis or he curva ure and crea e irregular as igma ism. LASIK complication—displaced ap with striae. F. T is LASIK ap wi h a nasal hinge is sligh ly displaced 1 day a er surgery. No e he prominen ap gut er superiorly and parallel ap olds rom he superior end o he hinge a 3 o’clock. Vision was poor as a resul o irregular as igma ism. I was immedia ely reposi ioned and he vision re urned o normal, and he ap s riae improved bu did no comple ely disappear.
(continued)
LWBK961-C10_p278-323.indd 321 22/07/11 10:22 AM
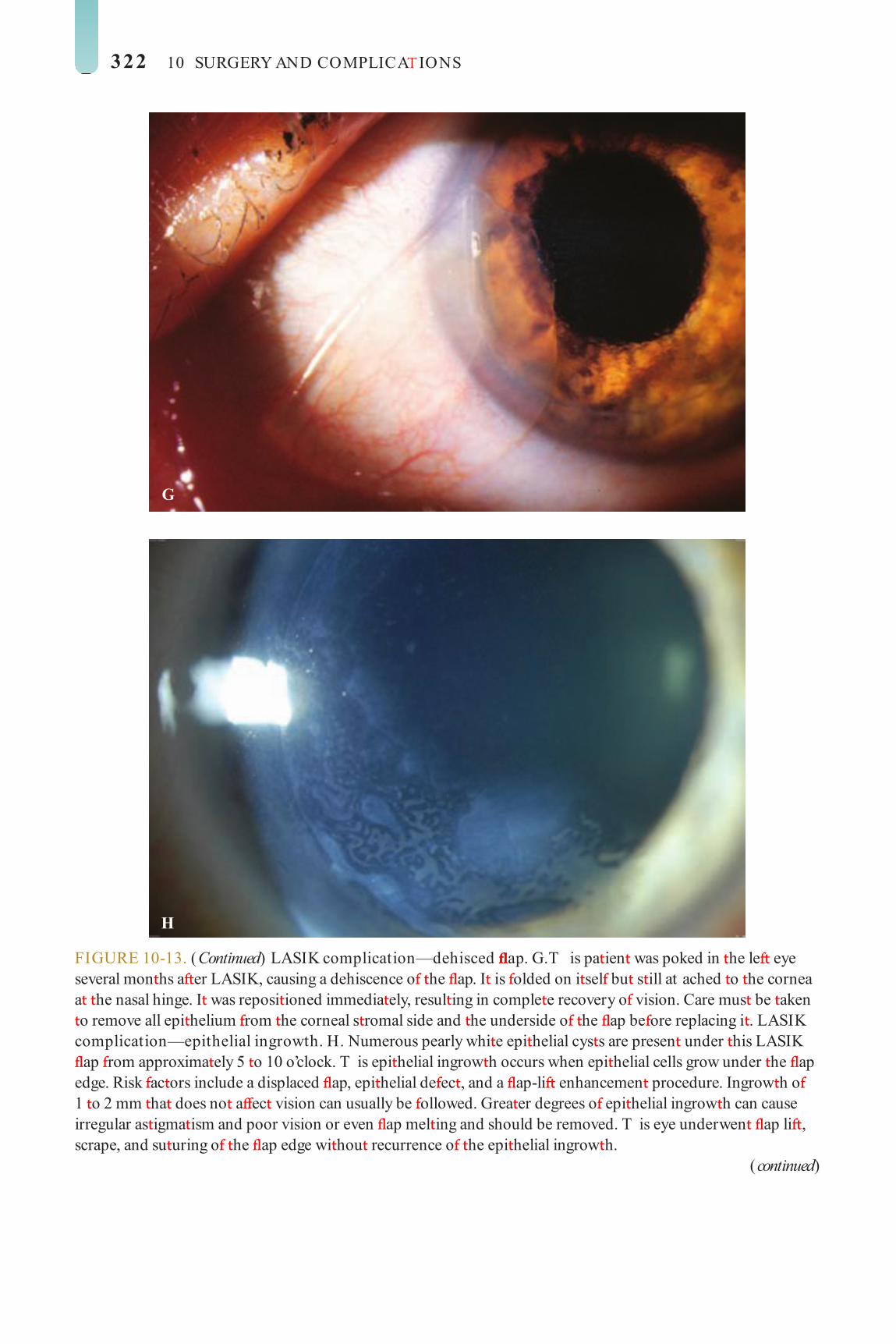
322 10 SURGERY AND COMPLICA IONS
G
H
FIGURE 10-13. (Continued) LASIK complication—dehisced ap. G. T is pa ien was poked in he le eye several mon hs a er LASIK, causing a dehiscence o he ap. I is olded on i sel bu s ill at ached o he cornea a he nasal hinge. I was reposi ioned immedia ely, resul ing in comple e recovery o vision. Care mus be aken o remove all epi helium rom he corneal s romal side and he underside o he ap be ore replacing i . LASIK complication—epithelial ingrowth. H. Numerous pearly whi e epi helial cys s are presen under his LASIK ap rom approxima ely 5 o 10 o’clock. T is epi helial ingrow h occurs when epi helial cells grow under he ap edge. Risk ac ors include a displaced ap, epi helial de ec , and a ap-li enhancemen procedure. Ingrow h o 1 o 2 mm ha does no a ec vision can usually be ollowed. Grea er degrees o epi helial ingrow h can cause irregular as igma ism and poor vision or even ap mel ing and should be removed. T is eye underwen ap li , scrape, and su uring o he ap edge wi hou recurrence o he epi helial ingrow h.
(continued)
LWBK961-C10_p278-323.indd 322 22/07/11 10:22 AM

Re ractive Surgery 323
I
FIGURE 10-13. (Continued) LASIK complication—inter ace in ectious keratitis. I. A severe a ypical mycobac erial in ec ion developed in his eye a er LASIK. Small in er ace spo s were no ed a ew weeks a er LASIK. Despi e rea men , he inf l ra es worsened un il hey involved almos he en ire ap and caused ap mel ing a he 9 o’clock posi ion. A hypopyon is presen in eriorly. T e in ec ion was no con rolled un il he necro ic ap was ampu a ed.
LWBK961-C10_p278-323.indd 323 22/07/11 10:22 AM
C H A P E R
324
CC HCC HC HC HC HC HC HC HCCCCC HC HCCCC HCCCC HHHHCC HCCCCC A PA PA PAA PA PA PPPPPPPPA PPPPPPA PPPPPPPPPPPPPA E E EEEEEE E EE E RRRRRRRRRRRRRRRRC H A P E R
Acids: sul uric acid (bat ery f uid) Mace (chloroace ophenone) and eargas Organic solven s De ergen s
Symptoms Pain, redness, earing, decreased vision
Signs Mild o modera e
Burns and edema o he eyelid Conjunc ival injec ion, chemosis,
abrasion Punc a e or large epi helial de ec s on
cornea ( Fig. 11-1 A) Mild an erior chamber ac ivi y
Severe Severe burns o he skin o he eyelids Severe chemosis, conjunc ival necrosis,
conjunc ival ischemia (sludging or absence o blood f ow hrough conjunc ival vessels) ( Fig. 11-1 B–E)
Scleral/ limbal ischemia Signi can an erior chamber ac ivi y
rauma
Ocular rauma is a leading cause o blind-ness in developed coun ries. rauma
may occur in indus rial set ings, during spor s ac ivi ies, or a home. Mos pa ien s a ec ed are young males, and he majori y o cases are an erior segmen injuries.
CHEMICAL BU NS
An ocular chemical burn is an emergency requiring immedia e irriga ion wi h wa er
or saline solu ion a he si e o injury or a leas 30 minu es. Mechanical removal o oreign par- icles should also be per ormed. T ese ac ions should be repea ed a he emergency room a er quickly checking he pH o he ears, even be ore aking a de ailed his ory or per orming an eye examina ion.
I ini ial evalua ion shows po en ially li e- hrea ening respira ory or gas roin es inal involvemen , hese condi ions should be at ended o rs .
Etiology Alkali: Examples include sodium hydroxide
(lye), calcium hydroxide (lime, cemen , plas er), and ammonia.
LWBK961-C11_p324-358.indd 324 22/07/11 10:22 AM

Chemical Burns 325
Corneal epi helial de ec s, edema, or mel ing ( Fig. 11-1 F)
Poor or no view o he an erior chamber because o corneal haze ( Fig. 11-1 G)
In raocular pressure may be low, nor-mal, or eleva ed in acu e s ages.
T e degree o limbal ischemia and corneal haziness carries prognos ic impor ance.
Treatment Mild cases may be rea ed on an ou pa ien
basis. Severe injuries may require hospi aliza ion.
Copious irriga ion wi h normal saline hrough an IV in usion se or a leas 30 min-u es and repea ed every 30 minu es un il neu- ral pH is reached.
Mechanical removal o oreign par icles and debridemen o necro ic issues should be per ormed wi h a cot on- ipped applica or or jeweler’s orceps under opical anes hesia.
Frequen ins illa ion o preserva ive- ree ear drops (q1h)
Cycloplegics (e.g., scopolamine 0.25% or a ropine 1% .i.d.)
opical an ibio ic oin men (e.g., ery hro-mycin, baci racin, or e racycline) q2h i an eye pa ch is no used. Pressure pa ching may aid in reepi helializa ion.
Con rol in raocular pressure i i is ele-va ed, ei her wi h opical drops or oral car-bonic anhydrase inhibi ors
For injuries wi h signi can inf amma ion and wi hou risk o corneal mel ing, opical cor icos eroid (e.g., dexame hasone 0.1% or prednisolone 1%) q1–2h may be used during he rs week, apered during he second week, and increased a er epi helial healing i neces-sary. A combina ion an ibio ic–cor icos eroid (e.g., obramycin 0.3%–dexame hasone 0.1% oin men ) q1–2h can also be used.
opical ace ylcys eine 10% drops q.i.d. may help con rol collagenase ac ivi y and cor-neal mel ing.
High-dose vi amin C 1 g PO .i.d. and op-ical ascorba e 10% drops q1–6h may be help- ul in severe alkali burns.
Doxycycline 100 mg PO b.i.d. can be used o decrease collagenase ac ivi y.
Early amnio ic membrane gra or amni-o ic membrane on a scleral ring (e.g., Pro-Kera) may be bene cial in severe cases.
I here is symblepharon orma ion, daily sweeping o he ornices wi h a cot on- ipped applica or or glass rod can be per ormed under opical anes hesia o break he adhe-sions. Al erna ively, a scleral shell may be used.
For progressive corneal mel ing or per ora- ion, issue adhesive, amnio ic membrane gra , limbal s em cell gra , lamellar pa ch gra , or pene ra ing kera oplas y may be necessary.
Complications Corneal haze or scarring In ec ious kera i is Dry eyes Symblepharon Cica ricial en ropion or ec ropion richiasis or dis ichiasis Punc al s enosis or occlusion Limbal s em cell de ciency Pannus orma ion Ca arac Glaucoma
Prognosis Dismal o excellen , depending on he
severi y o he injury ( Fig. 11-1 H). In gen-eral, alkaline subs ances cause he mos severe injuries, because hey pene ra e ocular issues easily.
LWBK961-C11_p324-358.indd 325 22/07/11 10:22 AM

326 11 RAUMA
A
B
FIGURE 11-1. Chemical burn. A. A mild acid injury caused a large corneal abrasion, which has been s ained wi h yellow f uorescein dye. T ere is minimal o no conjunc ival blanching, and he cornea is essen ially clear. Mild chemical burns generally resolve wi hou serious consequences. B. A sul uric acid injury occurred o his pa ien ’s righ eye. T ere is a large cen ral and in erior corneal epi helial de ec and mild in erior conjunc ival blanching.
(continued)
LWBK961-C11_p324-358.indd 326 22/07/11 10:22 AM

Chemical Burns 327
C
D
FIGURE 11-1. (Continued) Chemical burn. C. T is eye wi hs ood a bat ery acid (sul uric acid) injury. T ere is modera e conjunc ival blanching and mucus adheren o he conjunc iva and cornea. D. T e le eye o he pa ien seen in B has a much more ex ensive sul uric acid injury. T e epi helium is necro ic and has already sloughed o o he superior cornea. T ere is ex ensive conjunc ival and scleral blanching in eriorly and nasally.
(continued)
LWBK961-C11_p324-358.indd 327 22/07/11 10:22 AM

328 11 RAUMA
E
F
FIGURE 11-1. (Continued) Chemical burn. E. H igh-magni ca ion view o he eye seen in D d emons ra es ischemia o he conjunc iva and sclera. T ere is segmen a ion o he red blood cells, indica ing lack o blood f ow. T e grea er he degree o ischemia, he worse is he prognosis. F. A severe lye (sodium hydroxide) injury caused ex ensive ischemic damage in he lower wo- hirds o he eye. T e cornea has undergone necrosis cen rally, leading o a per ora ion requiring an emergency corneal ransplan . T is alkali injury even ually resul ed in enuclea ion.
(continued)
LWBK961-C11_p324-358.indd 328 22/07/11 10:23 AM

Chemical Burns 329
G
H
FIGURE 11-1. (Continued) Chemical burn. G. welve days a er a severe alkali injury, he conjunc iva and sclera remain blanched and he cornea is opaque. T ere has been no reepi helializa ion o he damaged cornea or conjunc iva. H. Many years a er a severe chemical burn, he cornea remains o ally scarred and vascularized.
LWBK961-C11_p324-358.indd 329 22/07/11 10:23 AM

330 11 RAUMA
THE MAL AND ELECT ICAL BU NS
THERMAL BURNS
Thermal burns can be mild o severe and can occur a any age. Cigaret e burns are no
uncommon in small children, whose eyes may be a hand level o a person holding a cigaret e.
Etiology Curling irons Cigaret es, especially children Flames Ho liquids Mol en me als
Symptoms Pain, redness, decreased vision
Signs T ermal burns on skin o eyelids Conjunc ival injec ion, chemosis, epi he-
lial de ec s Punc a e or large epi helial de ec s on cornea A whi e area o cau erized epi helium
( Fig. 11-2 A) In severe cases
An erior chamber reac ion Corneal haze and edema Limbal or scleral ischemia, corneal or
scleral per ora ion ( Fig. 11-2 B)
Treatment Removal o oreign bodies and debride-
men o devi alized issues opical an ibio ic oin men o preven
in ec ion and o lubrica e he ocular sur ace
(e.g., ery hromycin, baci racin, polymyxin B/baci racin, ciprof oxacin q2–6h)
Cycloplegics (e.g., cyclopen ola e 1% or scopolamine 0.25% .i.d.)
Pressure pa ching, la eral arsorrhaphy, or amnio ic membrane gra should be consid-ered or large or nonhealing epi helial de ec s.
opical cor icos eroids (similar o use in chemical burns) o reduce inf amma ion and preven symblepharon orma ion during he rs 1 o 2 weeks, bearing in mind ha hey can po en ia e corneal mel ing.
Complications Corneal scarring Irregular as igma ism Decreased vision In ec ious kera i is
Prognosis Depends on he severi y o he injury,
especially he exac cause o he burn and dura ion o con ac . Shor -con ac burns, such as hose rom curling irons and ciga-ret es, have an excellen prognosis. Mol en me al ha adheres o he cornea causes a much more subs an ial injury. Eyelid damage can cause exposure problems and long- erm di cul ies wi h corneal healing.
ELECTRICAL BURNS Ocular elec rical burns usually resul rom elec rical injuries o he head or a ligh ning s rike. In addi ion o corneal and scleral burns, hey can also cause acu e uvei is. T e lens is requen ly involved, and ca arac s may develop mon hs o years la er. Eyelid damage can cause exposure problems and long- erm di cul ies wi h corneal healing.
LWBK961-C11_p324-358.indd 330 22/07/11 10:23 AM

T ermal and Electrical Burns 331
FIGURE 11-2. T ermal injury. A. A curling iron brief y ouched his cornea, causing coagula ion o he corneal epi helium and urning i whi e. I can be removed mechanically or i will slough o na urally. Generally, hese eyes recover wi hou sequelae, because he leng h o ime he hea is in con ac wi h he cornea is minimal. Electrical injury. B. An elec rical injury caused a localized area o scleral mel wi h uveal prolapse. Addi ionally, he elec rical injury produced necrosis o a large por ion o upper eyelid issue, resul ing in severe exposure. T e eye was rea ed wi h a scleral pa ch gra and eyelid skin gra ing.
A
B
LWBK961-C11_p324-358.indd 331 22/07/11 10:23 AM

332 11 RAUMA
ULTR VIOLET KER TOPATHY ( A C WELDE ’S FLASH)
Severe, pain ul punc a e kera opa hy can resul hours a er exposure o signi can levels o
ul raviole ligh .
Etiology Usually caused by welding or using a sun-
lamp wi hou proper pro ec ive eyewear. Milder orms can also be seen in pa ien s wi h signi can sun exposure, such as a er a day a he beach or a er skiing.
Symptoms Symp oms usually develop 6 o 10 hours
a er he exposure. Pain, pho ophobia, oreign-body sensa-
ion, earing, redness, and decreased vision
Signs Spasm o eyelids in severe cases Punc a e epi helial erosions, especially in
he in erpalpebral regions ( Fig. 11-3 ) Eyelid edema, conjunc ival hyperemia
Treatment Preserva ive- ree ar i cial ears q2–3h opical an ibio ic drops (e.g., a f uoroqui-
nolone) .i.d. o q.i.d. and an ibio ic oin men (e.g., ery hromycin, e racycline, baci racin, polymyxin B/ baci racin, or ciprof oxacin) a bed ime. For more severe cases, opical an i-bio ic oin men q.i.d. will provide more lubri-ca ion and com or .
Cycloplegics (e.g., cyclopen ola e 1% or scopolamine 0.25% .i.d.)
Pressure pa ching or a bandage so con ac lens or severe epi helial erosions
Emphasize o he pa ien he impor ance o pro ec ive eyewear.
Complications Rarely, in ec ious kera i is
Prognosis ypically excellen
LWBK961-C11_p324-358.indd 332 22/07/11 10:23 AM

Ultraviolet Keratopathy (Arc Welder’s Flash) 333
FIGURE 11-3. Welder’s f ash. S igni can cen ral punc a e epi heliopa hy is presen in his pa ien 6 hours a er welding wi hou adequa e eye pro ec ion. (Cour esy o Irving Raber, MD.)
LWBK961-C11_p324-358.indd 333 22/07/11 10:23 AM

334 11 RAUMA
CO NEAL AB ASION
Corneal abrasions resul rom corneal sur- ace rauma ha causes removal o a por-
ion o he epi helial layer.
Etiology Mechanical rauma (e.g., ngernail, paper
edge, ree branch) Chemical injuries, medicamen osa
kera i is Foreign body Con ac lens Misdirec ed eyelashes Neuro rophic or exposure kera opa hy Ia rogenic (e.g., a er removal o corneal
su ures, epi helial debridemen )
Symptoms Pain, especially upon blinking; oreign-
body sensa ion; pho ophobia; earing; red-ness; o en decreased vision
opical anes he ic drops relieve he pain (and acili a e he eye examina ion).
Signs Epi helial de ec ha may be de ec ed
grossly or a he sli lamp. I is easily seen wi h f uorescein dye using he cobal blue ligh ( Fig. 11-4 ).
Treatment Search or and remove any oreign body in
he conjunc ival ornices and under he upper eyelid.
Epila e any misdirec ed eyelashes. opical an ibio ic oin men (e.g., ery hro-
mycin, e racycline, baci racin, polymyxin B/baci racin, or ciprof oxacin) q2–6h. opical an ibio ic drops may be used i he abrasion is small or i he pa ien nds ha oin men s blur vision.
Cycloplegics (e.g., cyclopen ola e 1% or scopolamine 0.25% .i.d.)
Pressure pa ching or a bandage so con- ac lens are occasionally used or large de ec s. Small de ec s generally do no require pa ching or bandage so con ac lens.
For rauma ic or con ac lens–induced abrasions, bandage con ac lenses and pa ch-ing are rela ively con raindica ed because hey increase he risk o in ec ion. A opical an ibi-o ic wi h good gram-nega ive coverage (e.g., a f uoroquinolone, obramycin, gen amicin, polymyxin B/ neomycin/ gramicidin) should be used.
Complications Corneal scar In ec ious kera i is Decreased vision Recurren erosions
Prognosis Generally excellen . Pa ien s need o be
ollowed closely un il he abrasion heals, especially hose a higher risk o in ec ion, such as a er con ac lens–rela ed and vege a-ble mat er–rela ed rauma and when rea ed wi h a bandage so con ac lens.
LWBK961-C11_p324-358.indd 334 22/07/11 10:23 AM

Corneal Abrasion 335
FIGURE 11-4. Corneal abrasion. A. A ennis ball hi he eye o his 12-year-old boy, causing mul iple linear corneal abrasions. I also caused a rauma ic iri is. B. A riangular corneal abrasion is eviden superiorly wi h he cobal blue ligh a er f uorescein s ain. T ere is some punc a e epi helial s aining surrounding he abrasion.
A
B
LWBK961-C11_p324-358.indd 335 22/07/11 10:23 AM

336 11 RAUMA
CO NEAL AND CONJUNCTIVAL FO EIGN BODIES
Ocular rauma can resul in oreign bodies ha remain embedded in he cornea or
conjunc iva.
Types Bi s o me al or rus Glass ragmen s Plas ic ragmen s Dir Insec hairs Vege a ive mat er (high risk o microbial
con amina ion)
History and Symptoms I is impor an o de ermine rom he his-
ory whe her he oreign body was propelled a high speed in o he eye (e.g., me al on me al hammering), which may sugges an in raocular oreign body. T e ype o oreign body may also be ob ained rom he his ory.
Foreign-body sensa ion, earing, redness, decreased vision
opical anes he ic drops can emporarily relieve he pain and acili a e examina ion o he eye.
Signs Foreign bodies may be seen on he cornea
or conjunc iva. T ey may be super cial, sub-conjunc ival, or embedded in he corneal s roma or sclera ( Fig. 11-5 A–C).
Rus ring or s erile in l ra e may surround a corneal oreign body ( Fig. 11-5 D).
An erior chamber reac ion may be presen , bu is usually mild.
Fluorescein s aining may reveal linear cor-neal abrasions, ypically seen wi h oreign
bodies re ained on he superior arsal conjunc iva.
Eyelid eversion or double eversion wi h a Desmarres’ eyelid re rac or may reveal oreign bodies rapped in he conjunc ival ornices.
In he presence o conjunc ival/ scleral/corneal lacera ion, signi can an erior cham-ber ac ivi y, iris ears, or lens opaci ies, i is impera ive o exclude an in raocular oreign body, ideally by C scan.
Treatment An accura e assessmen o he dep h o
pene ra ion is impor an prior o removing a deep corneal oreign body. I i has par ially pene ra ed in o he an erior chamber, i should be removed in he opera ing room under adequa e anes hesia.
For nonper ora ing oreign bodies, hey can be care ully removed under opical anes hesia wi h a cot on- ipped applica or, a oreign-body spud, or a pair o jeweler’s orceps.
T e residual rus ring may be removed wi h a rus ring burr. Deeper rus rings can be removed la er, a er hey have spon aneously migra ed o he sur ace ( Fig. 11-5 E).
T e resul ing epi helial de ec is rea ed wi h opical an ibio ic oin men s b.i.d. (e.g., polymyxin B/ baci racin, e racycline, baci ra-cin, ciprof oxacin) or drops q.i.d. (e.g., polymyxin B/ rime hoprim or a f uoroquinolone).
Cer ain deep, nonexposed, iner oreign bodies may no need removal i hey are loca ed away rom he visual axis (e.g., glass ragmen s).
Subconjunc ival oreign bodies may require a conjunc ival incision o acili a e removal. A scleral lacera ion may be di cul o rule ou i signi can subconjunc ival hem-orrhage is presen . In his case, surgical explo-ra ion may be necessary.
LWBK961-C11_p324-358.indd 336 22/07/11 10:23 AM

Corneal and Conjunctival Foreign Bodies 337
FIGURE 11-5. Corneal oreign body. A. A small por ion o seed cover is adheren o he in erior limbal area, causing a oreign-body sensa ion. I was easily removed a he sli lamp wi h jeweler’s orceps.
(continued)
opical cor icos eroids may be used a er reepi helializa ion and in he absence o in ec ion o reduce scarring i he visual axis is involved.
A er removal o vege a ive oreign bodies, pa ien s have o be ollowed closely or signs o in ec ion, especially ungal kera i is.
Complications Corneal scarring In ec ious kera i is
Recurren erosions Irregular as igma ism
Prognosis Depends on he severi y o he injury.
Conjunc ival and super cial, noncen ral cor-neal oreign bodies generally cause ew prob-lems. Deep, cen ral oreign bodies can cause corneal scarring and irregulari y and impaired vision.
A
LWBK961-C11_p324-358.indd 337 22/07/11 10:23 AM

338 11 RAUMA
B
C
FIGURE 11-5. (Continued) Corneal oreign body. B. A large ragmen o a nail had broken o while i was being hammered, and he ragmen was deeply lodged in he corneal periphery. A prime concern was whe her i had per ora ed ull- hickness cornea. Gen le gonioscopy revealed in ac s roma behind he nail. I was removed a he sli lamp in he minor surgery sui e so ha su uring o he wound could be done i necessary. T ere was no leak o aqueous humor and minimal wound gape, so i was le unsu ured and healed well. C. A deeply embedded horn was presen in he corneal periphery. Gen le gonioscopy revealed no ull- hickness corneal break. Cau ion mus be used o ex rac he en ire objec when removing riable oreign bodies.
(continued)
LWBK961-C11_p324-358.indd 338 22/07/11 10:23 AM

Corneal and Conjunctival Foreign Bodies 339
D
E
FIGURE 11-5. (Continued) Corneal rust ring. D. A small brown rus ring wi h underlying corneal in l ra e remains a er a me allic oreign body was removed wi h a oreign-body spud. Small, localized in l ra es associa ed wi h oreign bodies are ypically s erile, bu hey need o be ollowed closely or in ec ion. E. T e rus ring and mos o he in l ra e seen in D were care ully removed wi h a small, hand-held, bat ery-opera ed rus ring drill. Care needs o be aken o remove mos i no all o he rus while no going oo deep in o he corneal s roma. A small amoun o rus deep in he s roma should be le in place ra her han risk corneal per ora ion.
LWBK961-C11_p324-358.indd 339 22/07/11 10:23 AM

340 11 RAUMA
SUBCONJUNCTIVAL HEMO HAGE
Hemorrhage rom a conjunc ival blood vessel in o he subconjunc ival space can
cause mild o severe brigh red discolora ion o he conjunc iva.
Etiology rauma ic hemorrhage may be associa ed
wi h hyphema and chemosis. May occur a er ocular surgery
Hyper ension Associa ed wi h bleeding disorders and he
use o an icoagulan s, when i may also be asso-cia ed wi h periocular cu aneous ecchymosis
Rarely, a sys emic condi ion such as amy-loidosis, mul iple myeloma, or scurvy. Need o keep child abuse in mind.
Spon aneous hemorrhage is by ar he mos common ype. T e hemorrhage is usu-ally unila eral, bu when precipi a ed by coughing or s raining, i may be bila eral.
Symptoms Usually asymp oma ic and no iced by
pa ien inciden ally Red eye, mild discom or
Signs Sec orial (occasionally 360 degrees) hem-
orrhage under he conjunc iva ( Fig. 11-6 )
Dif erential Diagnosis Kaposi’s sarcoma: a reddish-purple,
sligh ly eleva ed, vascular lesion benea h he conjunc iva. Suspec in pa ien s wi h AIDS.
Conjunc ival or scleral lacera ion/ globe rup ure: Suspec in he presence o more severe injury.
Treatment Comple e eye examina ion o bo h eyes i
here is a his ory o ocular rauma. Reassurance; ar i cial ears or lubrica ion.
Pa ien should be old i may look worse over he days a er hemorrhage as i expands be ore i resolves over days o weeks.
Re er o he amily doc or or sys emic evalua ion i recurren .
Complications None
Prognosis Excellen
LWBK961-C11_p324-358.indd 340 22/07/11 10:23 AM

Subconjunctival Hemorrhage 341
A
B
FIGURE 11-6. Subconjunctival hemorrhage. A. Blun rauma o he eye caused a large localized subconjunc ival hemorrhage emporally in his le eye. Such a hemorrhage o en spreads over he rs ew days a er he rauma and appears o he pa ien o have become more serious. B. A resolving subconjunc ival hemorrhage can be seen in his eye. T e pa ien had a his ory o in ermit en bila eral subconjunc ival hemorrhages. He was subsequen ly diagnosed wi h mul iple myeloma, which can be associa ed wi h subconjunc ival hemorrhages.
LWBK961-C11_p324-358.indd 341 22/07/11 10:23 AM

342 11 RAUMA
CO NEOSCLE AL LACE ATION AND WOUND DEHISCENCE
Trauma can cause lacera ions o he cornea and/ or sclera in addi ion o rup ure o a
previous ocular surgery wound.
Etiology Indus rial acciden s (e.g., projec ile me al-
lic/ nonme allic oreign bodies, glass rag-men s, nails, sharp ins rumen s)
Road ra c acciden (e.g., injury by windshield)
Home acciden s (e.g., sharp edges on oys) Assaul (e.g., knives) rauma ic wound rup ure (mos com-
monly a er ca arac surgery, corneal rans-plan a ion, radial kera o omy, and rabeculec omy)
History and Symptoms I is impor an o de ermine rom he his-
ory whe her he oreign body was propelled a high speed in o he eye (e.g., me al on me al hammering), which may sugges in ra-ocular oreign bodies. His ory o ocular sur-gery, including re rac ive surgery
Pain, redness, decreased vision
Signs Examina ion o he eye should be done
cau iously, wi hou exer ing pressure on he globe, so as o avoid hernia ing in raocular con en s hrough he wound. De ailed exami-na ion is o en de erred un il he ime o sur-gical repair.
T e eye is usually ex remely so (hypo ony).
Blurred vision: Visual acui y should be documen ed or pa ien care and medicolegal reasons.
Subconjunc ival hemorrhage, chemosis, corneal edema
Prolapse o uveal issues hrough he wound
Shallow or f a an erior chamber wi h or wi hou hyphema
Pupil dis or ion, iridodialysis, cyclodialysis
Rup ured an erior lens capsule, subluxed lens, ca arac , vi reous presen a ion may be seen
Diagnostic Evaluation T e diagnosis is usually apparen on gross
or sli -lamp examina ion ( Fig. 11-7 ). A Seidel’s es may be used o con rm ha
a lacera ion is par ial- hickness. In ull- hick-ness lacera ions, i can also help o assess he ra e o aqueous leakage and wound s abili y.
Occasionally, ull- hickness scleral lacera- ions may be masked by he overlying sub-conjunc ival hemorrhage and chemosis. T ese may require surgical explora ion o de ermine he ex en o injury.
C o look or in raocular or in raorbi al oreign bodies and re inal de achmen as needed. A gen le B-scan is occasionally help ul.
Treatment Once he ini ial evalua ion is comple ed,
he eye should be pro ec ed wi h an eye shield.
No oin men should be applied o he eye. e anus prophylaxis should be given and
IV an ibio ics s ar ed immedia ely. Analgesics and an ieme ics should be
given o minimize pain and vomi ing. Small lacera ions may be observed, rea ed
wi h a pressure pa ch or bandage con ac lens, or sealed wi h issue adhesives. A persis en leak or decrease in an erior chamber dep h requires surgical repair.
LWBK961-C11_p324-358.indd 342 22/07/11 10:23 AM

Corneoscleral Laceration and Wound Dehiscence 343
Diplopia and glare rom pseudopolyco-ria or corec opia: con ac lens wi h periph-eral in ing
Unsigh ly corneal opaci ies in eyes wi hou visual po en ial: pros he ic con ac lenses, corneal at ooing, or cosme ic pene- ra ing kera oplas y
Complications In ec ious kera i is Endoph halmi is Corneal scarring and irregulari y Ca arac Iris and damage and pupillary irregulari y Re inal de achmen Decreased vision or blindness Epi helial downgrow h
Prognosis Dismal o good, depending direc ly on he
severi y o he injury and pos opera ive complica ions
Surgical repair or larger lacera ions should be carried ou as soon as possible, ideally under general anes hesia, usually depending on surgeon and opera ing room availabili y and when he pa ien a e las . I emergency surgery is scheduled he pa ien should ake no hing by mou h.
I he at emp a repairing he lacera ion ails because he eye is severely rauma ized, enuclea ion may be considered, bu is gener-ally per ormed as a secondary procedure o allow ime or ur her assessmen and pa ien counseling. In eyes wi h severe damage and poor visual po en ial, enuclea ion should be considered wi hin 2 weeks, o reduce he risk o sympa he ic oph halmia.
rea men o la e complica ions Corneal scars
Induced irregular as igma ism: t ing wi h rigid gas-permeable con ac lenses a er all corneal su ures are removed
Dense opaci ies: ro a ional au ogra , lamellar or pene ra ing kera oplas y
LWBK961-C11_p324-358.indd 343 22/07/11 10:23 AM
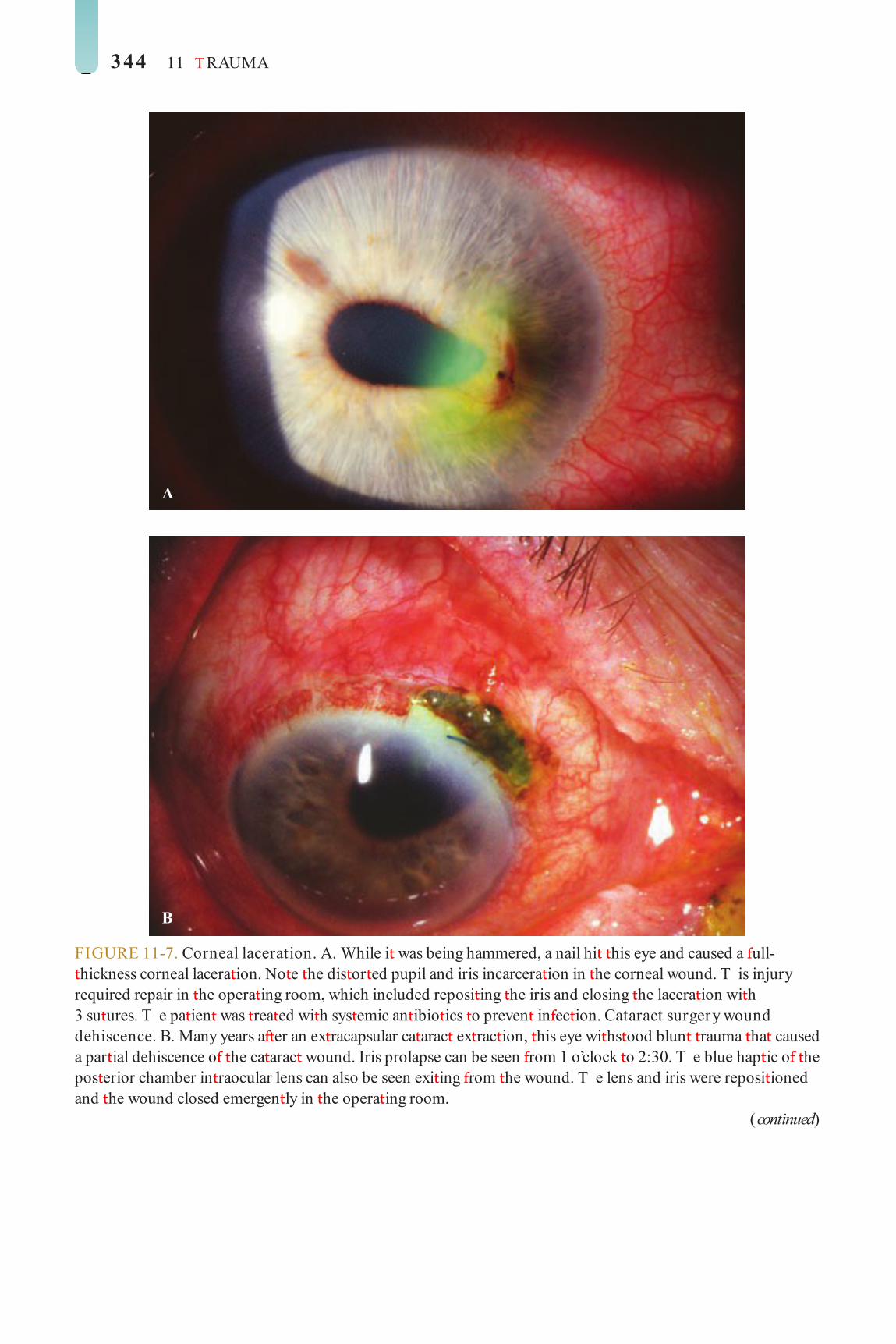
344 11 RAUMA
A
B
FIGURE 11-7. Corneal laceration. A. While i was being hammered, a nail hi his eye and caused a ull- hickness corneal lacera ion. No e he dis or ed pupil and iris incarcera ion in he corneal wound. T is injury required repair in he opera ing room, which included reposi ing he iris and closing he lacera ion wi h 3 su ures. T e pa ien was rea ed wi h sys emic an ibio ics o preven in ec ion. Cataract surgery wound dehiscence. B. Many years a er an ex racapsular ca arac ex rac ion, his eye wi hs ood blun rauma ha caused a par ial dehiscence o he ca arac wound. Iris prolapse can be seen rom 1 o’clock o 2:30. T e blue hap ic o he pos erior chamber in raocular lens can also be seen exi ing rom he wound. T e lens and iris were reposi ioned and he wound closed emergen ly in he opera ing room.
(continued)
LWBK961-C11_p324-358.indd 344 22/07/11 10:23 AM

Corneoscleral Laceration and Wound Dehiscence 345
C
D
FIGURE 11-7. (Continued) Corneal laceration. C. A ull- hickness corneal lacera ion wi h pupil dis or ion and iris prolapse is eviden . I was repaired emergen ly. D. en days a er surgical repair o he eye seen in C. T e iris was reposi ed in he eye and he lacera ion required 6 10-0 nylon su ures o close.
(continued)
LWBK961-C11_p324-358.indd 345 22/07/11 10:23 AM

346 11 RAUMA
E
F
FIGURE 11-7. (Continued) Corneal laceration and intraocular oreign body. E. A er an au omobile acciden , a small, healed corneal lacera ion is eviden in he midperiphery a 7 o’clock. A glass oreign body can be seen in he in erior angle. Al hough glass is ypically iner and generally does no cause signi can inf amma ion, i was removed surgically hrough an in erior limbal approach o preven corneal and o her in raocular damage. F. A large ragmen o me al is res ing on he iris a er a hammering acciden . T e corneal lacera ion is seen jus superior o he oreign body. In eres ingly, he pa ien had undergone a LASIK procedure 6 mon hs prior. T e lacera ion was repaired wi h wo in errup ed su ures, being very care ul no o dis urb he LASIK f ap edge. A limbal incision was made superiorly o remove he me al shard.
(continued)
LWBK961-C11_p324-358.indd 346 22/07/11 10:23 AM

Corneoscleral Laceration and Wound Dehiscence 347
G
H
FIGURE 11-7. (Continued) Corneal laceration and intraocular oreign body. G. Five mon hs a er surgical repair o he eye seen in F. T e vision re urned o preinjury levels and he LASIK f ap was una ec ed. Corneal transplant wound dehiscence. H. Several mon hs a er undergoing a corneal ransplan , he pa ien ell and hi his eye, causing a wound dehiscence. Five broken su ures and signi can iris prolapse can be seen. I was emergen ly repaired by reposi ing he iris and resu uring he wound.
(continued)
LWBK961-C11_p324-358.indd 347 22/07/11 10:23 AM

348 11 RAUMA
I
J
FIGURE 11-7. (Continued) Corneal transplant wound dehiscence. I. Five days a er wound repair in he eye seen in H, he wound is secure. Al hough no iris issue was ampu a ed, he iris sphinc er was damaged so he pupil was s ill dis or ed. T e gra is remarkably clear. Corneal laceration. J. T is severe corneal lacera ion wi h iris and lens damage was caused by a heron peck o he eye. I was repaired wi h mul iple in errup ed su ures. Mucus is seen on he corneal sur ace and blood is presen in he an erior chamber.
(continued)
LWBK961-C11_p324-358.indd 348 22/07/11 10:23 AM

Corneoscleral Laceration and Wound Dehiscence 349
K
FIGURE 11-7. (Continued) Corneal laceration. K. T is corneal lacera ion was repaired 4 mon hs previously. No e ha he par ial- hickness lacera ion superior o he pupil required 1 su ure because i was gaped, while he in erior ull- hickness lacera ion required 8 su ures o close. T ere were also wo separa e iridodialyses rom 7 o 9 o’clock.
LWBK961-C11_p324-358.indd 349 22/07/11 10:23 AM

350 11 RAUMA
T AUMATIC HYPHEMA
Trauma causes bleeding in o he an erior chamber, which is ermed a hyphema.
Etiology rauma damages he iris, ypically a he
iris roo , causing bleeding.
Symptoms Redness, pain, pho ophobia, decreased
vision O en a his ory o blun rauma
Signs Microhyphema: red blood cells suspended
in he an erior chamber Hyphema: red blood cells layered or a clo
in he an erior chamber angle ( Fig. 11-8 A and B)
May be associa ed wi h more ex ensive ocular damage ( Fig. 11-8 C)
Treatment Consider hospi aliza ion. Check or sickle rai or disease. Bed res or limi ed ac ivi y and an eye shield
A ropine 1% .i.d. Consider opical cor icos eroids (e.g.,
prednisolone 1% q2–6h). Consider aminocaproic acid (50 mg/ kg
q4h, maximum 30 g/ day) orally or 3 o 5 days. rea eleva ed in raocular pressure (IOP),
especially in pa ien s wi h sickle rai or disease.
Avoid aspirin, nons eroidal an i-inf amma- ory agen s, and o her medica ions ha may increase bleeding.
Consider evacua ion o hyphema i persis- en or IOP remains eleva ed.
Complications Glaucoma Ca arac Iris damage Corneal blood s aining
Prognosis Fair o excellen , depending on he ex en
o associa ed ocular injury. Eleva ed IOP can cause rapid and severe damage in sickle cell rai or disease pa ien s. Need o moni or or la e developmen o glaucoma.
LWBK961-C11_p324-358.indd 350 22/07/11 10:23 AM
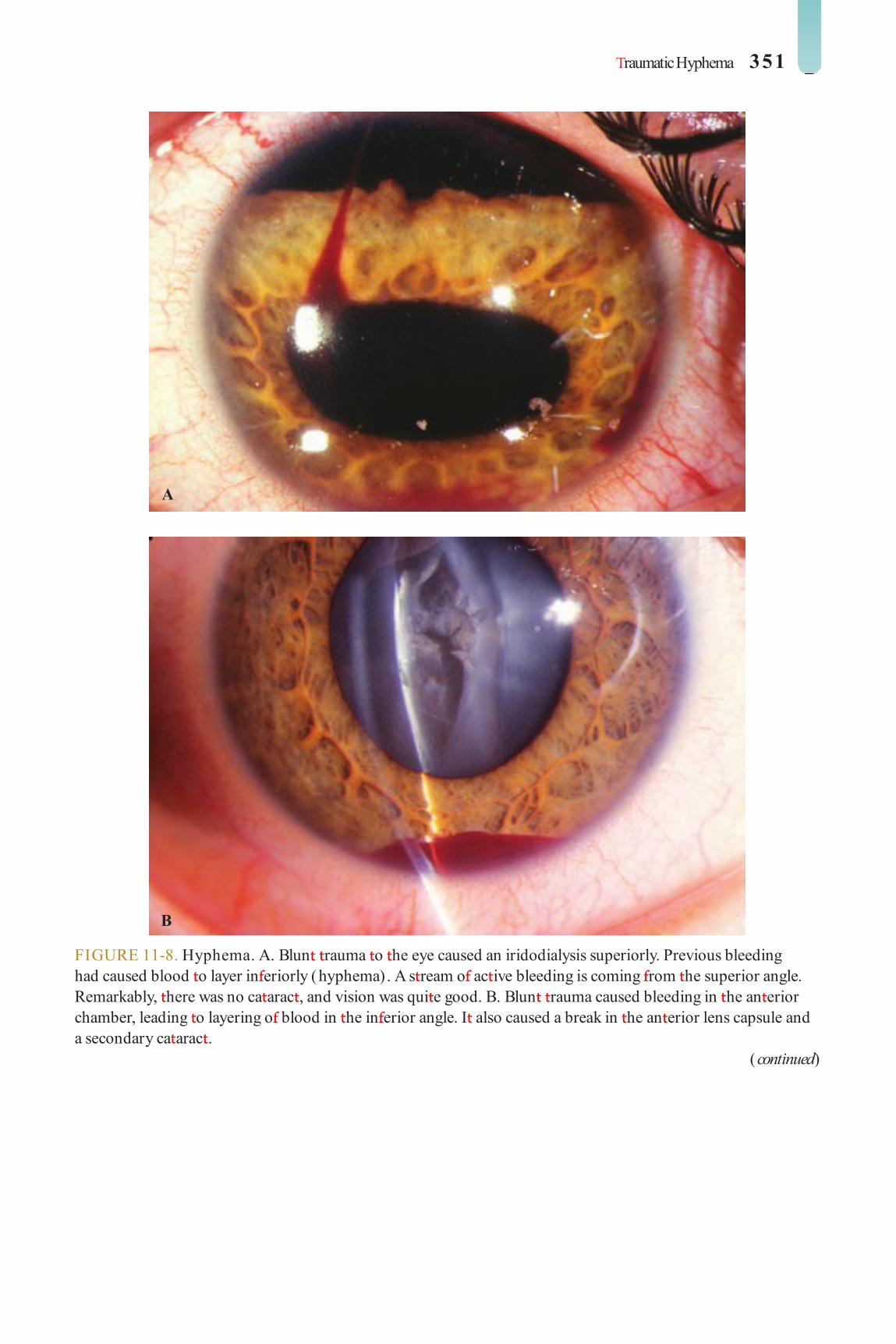
raumatic Hyphema 351
FIGURE 11-8. Hyphema. A. Blun rauma o he eye caused an iridodialysis superiorly. Previous bleeding had caused blood o layer in eriorly (hyphema) . A s ream o ac ive bleeding is coming rom he superior angle. Remarkably, here was no ca arac , and vision was qui e good. B. Blun rauma caused bleeding in he an erior chamber, leading o layering o blood in he in erior angle. I also caused a break in he an erior lens capsule and a secondary ca arac .
(continued)
A
B
LWBK961-C11_p324-358.indd 351 22/07/11 10:23 AM

352 11 RAUMA
C
FIGURE 11-8. (Continued) Hyphema. C. Five days a er a rup ured globe repair, here is bo h persis en blood covering mos o he iris and layered blood in he in erior angle. Corneal su ures overlying a iris de ec can be seen a 2 o’clock.
LWBK961-C11_p324-358.indd 352 22/07/11 10:23 AM

Epithelial Downgrowth 353
EPITHELIAL DOWNG OWTH
Epi helial downgrow h occurs when ocu-lar sur ace epi helium grows in o he eye
hrough a ull- hickness wound.
Etiology Pene ra ing injuries Ocular surgery, especially wi h wound
leaks (e.g., corneal ransplan a ion, ca arac surgery, rabeculec omy)
Symptoms Pain, pho ophobia, earing, redness, o en
decreased vision
Signs T e epi helium orms a membrane ha
covers he corneal endo helium, an erior chamber angle, iris, ciliary body, lens, and capsular bag. O en a wavy line on he corneal endo helial sur ace can be seen ( Fig. 11-9 C). When i is on he iris, he membrane causes f at ening o he normal iris cryp s ( Fig. 11-9 A).
Corneal decompensa ion and severe, in rac able glaucoma may resul .
Argon laser pho ocoagula ion produces whi e burns ra her han charring o epi helial membranes on he iris sur ace and helps make he diagnosis and delinea e he ex en o he membrane. I can also be used o at emp o des roy he epi helial cells on he iris sur ace ( Fig. 11-9 B and D).
Occasionally, a f uid- lled cys wi h a clear an erior wall, similar o a primary iris s romal cys , may orm in he an erior chamber.
Treatment Ex ensive surgery is needed o e ec
removal via excision, laser abla ion, or cryo- herapy o he in raocular membrane and involved issues. In raocular 5-f uorouracil can also be used in severe cases.
Repair o wound s ula Glaucoma drainage implan or rea men
o glaucoma
Complications Corneal decompensa ion In rac able glaucoma Re inal de achmen
Prognosis Even wi h ex ensive surgery, he prognosis
is poor.
LWBK961-C11_p324-358.indd 353 22/07/11 10:23 AM

354 11 RAUMA
FIGURE 11-9. Epithelial downgrowth. A. wo years a er surgical repair o a rup ured globe near he superior limbus, he pa ien re urned wi h a membrane ha had grown across he pupil and covered 95% o he iris. T e membrane had f at ened he iris cryp s. T e edge o he epi helial downgrow h membrane can be seen in eriorly, as can a small degree o normal peripheral iris. B. An argon laser was used o delinea e he ex en o he epi helial downgrow h in he same eye. T e argon laser crea es dis inc whi e spo s in he membrane bu no in normal iris. T e edge o he membrane is seen in eriorly.
(continued)
B
A
LWBK961-C11_p324-358.indd 354 22/07/11 10:23 AM

Epithelial Downgrowth 355
C
D
FIGURE 11-9. (Continued) Epithelial downgrowth. C. Complica ed ca arac surgery wi h an an erior chamber in raocular lens resul ed in a persis en wound leak a 9 o’clock. Weeks la er, a membrane was no ed on he corneal endo helial sur ace, progressing cen rally. A sligh ly ou -o - ocus, ligh brown membrane can also be apprecia ed a he pupillary margin. D. An argon laser was used o at emp o des roy he epi helial downgrow h on he iris in he same eye jus prior o per ormance o cryo herapy o he epi helial downgrow h on he corneal endo helium. Un or una ely, he epi helial downgrow h recurred and he eye became ph hisical.
LWBK961-C11_p324-358.indd 355 22/07/11 10:23 AM

356 11 RAUMA
DESCEMET’S DETACHMENT
Small ears in Desceme ’s membrane ha do no progress or cause visual symp oms
are commonly seen a er ocular surgery. ears in Desceme ’s membrane can lead o a large Desceme ’s de achmen and subsequen cor-neal edema and poor vision.
Etiology Ocular surgery, mos commonly ca arac
surgery Rarely, rauma
Symptoms Discom or , decreased vision
Signs Corneal edema ( Fig. 11-10 A) A ear in Desceme ’s membrane, ypically
origina ing a he surgical wound Undula ing or scrolled Desceme ’s mem-
brane in he an erior chamber separa ed rom he pos erior s roma ( Fig. 11-10 B)
Treatment Small de achmen s: T ese can be ollowed
and may resolve spon aneously over weeks o mon hs.
Larger de achmen s or hose no resolving spon aneously
I Desceme ’s membrane is no scrolled, a bubble o air or long-ac ing gas (e.g., 18% sul- ur hexaf uoride) can be injec ed in o he an erior chamber o push he membrane agains he pos erior s roma ( Fig. 11-10 C). Proper head posi ioning is required pos op-era ively o reat ach he membrane. T e con-di ion may resolve wi hin days or ake weeks.
I Desceme ’s membrane is scrolled, i mus rs be unscrolled surgically. An air bubble or long-ac ing gas can hen be injec ed in o he an erior chamber, or i may be repaired wi h su uring, bu su uring can ur her ear he membrane.
Complications Corneal scarring Persis en corneal edema
Prognosis Many unscrolled Desceme ’s de achmen s
will resolve spon aneously. Long-ac ing in ra-ocular gas has a good success ra e, especially in unscrolled de achmen s. Scrolled de ach-men s are more di cul o repair. Chronic edema may require an endo helial or pene- ra ing kera oplas y o achieve good vision.
FIGURE 11-10. Descemet’s detachment. A. Broad-beam sli -lamp view reveals severe di use corneal edema a er supposedly uncomplica ed ca arac surgery.
(continued)
A
LWBK961-C11_p324-358.indd 356 22/07/11 10:23 AM

Descemet’s Detachment 357
B
C
FIGURE 11-10. (Continued) Descemet’s detachment. B. Sli -beam view o he same eye demons ra es wo arcs o de ached Desceme ’s membrane behind he edema ous cornea. C. A Desceme ’s de achmen had developed a he ime o combined glaucoma and ca arac surgery. Because i did no resolve wi h medical herapy, a nonexpansile concen ra ion o sul ur hexaf uoride gas was injec ed in o he an erior chamber o amponade Desceme ’s membrane agains he back o he cornea o reat ach i . On pos opera ive day 1, Desceme ’s membrane was reat ached and he corneal edema had resolved.
LWBK961-C11_p324-358.indd 357 22/07/11 10:24 AM

LWBK961-C11_p324-358.indd 358 22/07/11 10:24 AM
Index No e: Page loca ors ollowed by indica es f gure only.
A Abrasion, corneal, 334, 335 Acanthamoeba kera i is, 178–179,
179 –181 diagnosis o , 178 di eren ial diagnosis o , 178 e iology o , 178 prognosis or, 179 signs o , 178, 179 –181 symp oms o , 178 rea men o , 178–179
Acquired immunodef ciency syndrome (AIDS), 228, 229
Ac inic kera opa hy, 153 Adenovirus, and conjunc ivi is, 10,
11 –13 Adrenochrome deposi s, and
secondary acquired melanosis, 49
diagnosis o , 228 e iology o , 228 prognosis or, 228 signs o , 228, 229 symp oms o , 228 rea men o , 228
Adul inclusion conjunc ivi is, 14, 15
AIDS. See Acquired immunodef ciency syndrome (AIDS)
AK. See As igma ic kera o omy (AK) Alkap onuria, and secondary
acquired melanosis, 49 Allergic conjunc ivi is, 26, 27
wi h con ac lens use, 230 Allogra rejec ion, 261–262,
262 –265 Amiodarone, and cornea ver icilla a,
156, 157 di eren ial diagnosis o , 26 e iology o , 26 prognosis or, 26 signs o , 26, 27 symp oms o , 26 rea men o , 26
Amnio ic membrane ransplan a ion, 308, 309 –310
complica ions o , 308 indica ions or, 308 prognosis or, 308 surgical procedure or, 308,
309 –310 Amyloidosis, 46, 46 –47 Angioma osis, encephalo rigeminal,
67, 68 Aniridia, 86, 87
classif ca ion o , 86 diagnosis o , 86 ocular associa ions, 86, 87 prognosis or, 86 signs o , 86 rea men o , 86
An erior basemen membrane dys rophy. See Epi helial basemen membrane dys rophy (EBM)
An erior corneal dys rophies, 102–115
An erior lamellar kera oplas y. See Lamellar kera oplas y
An erior scleri is. See Scleri is An erior segmen developmen al
anomalies, 70–89 An erior segmen dysgeneses, 82–83,
83 –85 Axen eld’s anomaly, 82, 83 diagnosis o , 82 localized pos erior kera oconus,
82, 85 Pe ers’ anomaly, 82, 84 –85 pos erior embryo oxon, 82, 83 prognosis or, 83 Rieger’s anomaly, 82, 84 Rieger’s syndrome, 82 rea men o , 82–83
Arc welder’s ash, 332, 333 Arcus lipoids, 142 Arcus senilis, 142 Argyrosis
and corneal crys als, 158 and secondary acquired melanosis,
49 Arl ’s line, 16, 17 Ar eriovenous f s ulas, 67–68 Aspergillus kera i is, 174
As igma ic kera o omy (AK), 313. See also Re rac ive surgery
A opic kera oconjunc ivi is, 28, 29 di eren ial diagnosis o , 28 e iology o , 28 prognosis or, 28 signs o , 28, 29 symp oms o , 28 rea men o , 28
Avellino corneal dys rophy, 126, 127
di eren ial diagnosis o , 126 e iology and pa hology o , 126 prognosis or, 126 signs o , 126, 127
“crushed breadcrumb” opaci ies, 127
symp oms o , 126 rea men o , 126
Axen eld-Rieger syndrome, 166 Axen eld’s anomaly, 82, 83 Axen eld’s syndrome, 82
B Bac erial conjunc ivi is
gonococcal, 8, 9 diagnos ic evalua ion o , 8 e iology o , 8 prognosis or, 8 symp oms o , 8 rea men o , 8, 9
nongonococcal, 6, 7 diagnos ic evalua ion o , 6 e iology o , 6 prognosis or, 6 signs o , 6, 7 symp oms o , 6 rea men o , 6
Bac erial kera i is, 168–169, 170 –173
diagnosis o , 169 di eren ial diagnosis o , 169 e iology o , 168 predisposing ac ors or, 168 prognosis or, 169 signs o , 168–169, 170 –173 symp oms o , 168 rea men o , 169
359
LWBK961-ind_p359-370.indd 359 28/07/11 4:30 PM

360 INDEX
Band kera opa hy, 148, 149 –150 e iology o , 148 prognosis or, 148 signs o , 148, 149 –150 symp oms o , 148 rea men o , 148
Benign amelanocy ic conjunc ival lesions, 52, 53 –57
epibulbar dermoid, 52, 54 –56 granulomas, 52, 53 –54 heredi ary benign in raepi helial
dyskera osis, 52, 57 lipodermoid, 52
Biet i’s nodular dys rophy, 153 Bi o ’s spo , 238 Blephari is, 2–3, 3
e iology o , 2 prognosis or, 3 signs o , 2, 3 symp oms o , 2 rea men o , 2–3
Brown-McLean syndrome, 225, 227 Bullous kera opa hy, 225, 226 –227
diagnosis o , 225 e iology o , 225, 226 –227 prognosis or, 225 signs o , 225 symp oms o , 225 rea men o , 225
Buph halmos, 76, 77 in an ile glaucoma, associa ions
o , 76 prognosis or, 76 signs o , 76, 77 rea men o , 76
Burns chemical, 324–325, 326 –329 elec rical, 330, 331 hermal, 330, 331
C Calcium concre ions, 46, 47 Candida kera i is, 174. See also Fungal
kera i is Capillary hemangioma, 67 Caro id–cavernous sinus, 67–68, 69 Ca arac ex rac ion and in raocular
lens (IOL) implan a ion, 278 and pos opera ive managemen ,
278 anes hesia in, 278 complica ions o , 278–279
in raocular lens subluxa ion, 279 –280
phacoemulsif ca ion burn, 279 pos erior capsular opaci y, 281 pupillary cap ure, 280 wound dehiscence, 344
indica ions or, 278 success ra e o , 279 surgical echnique or
ex racapsular me hod, 278 phacoemulsif ca ion me hod,
278 wound dehiscence, 344
Chalazion, 4, 5 , 52 diagnosis o , 4 di eren ial diagnosis o , 4 e iology o , 4 prognosis or, 4 signs o , 4, 5 symp oms o , 4 rea men o , 4
Chandler’s syndrome, 166 Chemical burns, 324–325,
326 –329 complica ions o , 325 e iology o , 324 prognosis or, 325, 329 signs o , 324–325, 326 –329 symp oms o , 324 rea men o , 325
Chlamydial conjunc ivi is, 14, 15 diagnosis o , 14 e iology o , 14 prognosis or, 14 signs o , 14, 15 symp oms o , 14 rea men o , 14
Choroidi is, 197 Chrysiasis, 158 Cica ricial pemphigoid, ocular.
See Ocular cica ricial pemphigoid
Cipro oxacin deposi s, 159 Clima ic drople kera opa hy, 153 Coa s’ whi e ring, 153, 155 Cogan-Reese (iris nevus) syndrome,
166 Cogan’s microcys ic dys rophy.
See Epi helial basemen membrane dys rophy (EBM)
Collagen vascular diseases, 244, 245 –248
di eren ial diagnosis o , 244 e iology o , 244 prognosis or, 244 signs o , 244, 245 –247
symp oms o , 244 rea men o , 244, 248
Congeni al an erior s aphyloma, 78 e iology o , 78 prognosis or, 78 signs o , 78 rea men o , 78
Congeni al heredi ary endo helial dys rophy (CHED), 140, 141
di eren ial diagnosis o , 140 e iology o , 140 pa hology o , 140 prognosis or, 140 signs o , 140, 141 symp oms o , 140 rea men o , 140
Conjunc ival epi helial melanosis, 48, 49
Conjunc ival ap surgery, 303, 304 –305
complica ions o , 303, 305 con raindica ions o, 303 indica ions or, 303 prognosis or, 303 surgical echnique or, 303,
304 –305 Conjunc ival in ec ions and
in amma ions, 2–41 Conjunc ival in raepi helial
neoplasia, 58, 60 –61 Conjunc ival nevus, 48, 50 Conjunc ivi is, 196, 266. See also
Kera oconjunc ivi is sicca adul inclusion, 14, 15 allergic, 26, 27 a opic, 28, 29 bac erial
gonococcal, 8, 9 nongonococcal, 6, 7
chlamydial, 14, 15 chronic oxic, 37, 38 , 39 ac i ious, 37, 39 gian papillary, 230, 232 –233 ligneous, 20, 20 neona al, 24, 25 oxic/ allergic, 230 rachoma, 16, 17 vernal, 30, 31 –32 viral, 10, 11 –13
Con ac lens kera opa hy, 230, 233 –234
e iology o , 230 signs o , 230, 233 –234
LWBK961-ind_p359-370.indd 360 28/07/11 4:30 PM

INDEX 361
symp oms o , 230 rea men o , 230
Con ac lens overwear syndrome, 230–231
e iology o , 230 signs o , 230–231 symp oms o , 230 rea men o , 231
Con ac lens, complica ions o con ac lens kera opa hy, 230,
233 –234 corneal neovasculariza ion, 231 corneal warpage, 231 gian papillary conjunc ivi is, 230,
232 –233 microbial kera i is, 232 overwear syndrome, 230–231 s erile kera i is, 231–232, 235 igh lens syndrome, 231, 234 oxic/ allergic conjunc ivi is, 230
Con ac lens–associa ed superior limbic kera oconjunc ivi is. See Con ac lens kera opa hy
Cornea arina a, 143, 145 Cornea plana, 81, 81
e iology o , 81 ocular associa ions, 81 prognosis or, 81 signs o , 81, 81 symp oms o , 81 rea men o , 81
Cornea ver icilla a, 156, 157 drugs causing, 156 e iology o , 156, 157 prognosis or, 156 signs o , 156 rea men o , 156
Corneal abrasion, 334, 335 complica ions o , 334 e iology o , 334 prognosis or, 334 signs o , 334, 335 symp oms o , 334 rea men o , 334
Corneal arcus, 142, 144 Corneal biopsy, 298, 298
complica ions o , 298 indica ions or, 298 success ra e o , 298 surgical echnique or, 298, 298
Corneal blood s aining, 160, 162 Corneal collagen crosslinking, 91 Corneal degenera ions and deposi s,
142–167
involu ional changes, 142–147 nonpigmen ed, corneal deposi s,
148–152 o her, 153–155 pigmen ed, corneal deposi s,
156–167 Corneal dys rophies, 102–141
an erior, 102–115 pos erior, 131–141 s romal, 116–130
Corneal elas osis, 153 Corneal erosion, recurren , 222,
223 –224 e iology o , 222 pa hophysiology o , 222 prognosis or, 222 signs o , 222, 223 symp oms o , 222 rea men o , 222, 224
Corneal gra rejec ion, 261–262, 262 –265
di eren ial diagnosis o , 261 e iology o , 261 prognosis or, 262 signs o , 261, 262 –265
corneal edema, 265 epi helial rejec ion line,
262 –263 kera ic precipi a es, 263 –264 Khodadous ’s line, 264 –265 subepi helial inf l ra es, 262
symp oms o , 261 rea men o , 261–262
Corneal iron deposi s, 160, 160 –162
epi helial, 160, 160 –161 s romal, 160, 162
Corneal neovasculariza ion, 231 e iology o , 231 signs o , 231 symp oms o , 231 rea men o , 231
Corneal pa ch gra , 312 Corneal per ora ion, 311–312,
312 complica ions o , 311 e iology o , 311 prognosis or, 312 signs o , 311 symp oms o , 311 rea men o , 311, 312
Corneal rus ring, 339 Corneal ransplan wound
dehiscence, 347 –348
Corneal ransplan a ion, ull- hickness. See Pene ra ing kera oplas y
Corneal warpage, 231 e iology o , 231 signs o , 231 symp oms o , 231 rea men o , 231
Corneal/ conjunc ival oreign bodies, 336–337, 337 –339
complica ions o , 337 his ory and symp oms o , 336 prognosis or, 337 signs o , 336, 337 –339 rea men o , 336–337, 339 ypes o , 336
Corneoscleral lacera ion and wound dehiscence, 342–343, 344 –349
complica ions o , 343 diagnos ic evalua ion o , 342,
344 –349 e iology o , 342 his ory and symp oms o , 342 prognosis or, 343 signs o , 342 rea men o , 342–343
Crocodile shagreen, 142, 145 Cyanoacryla e corneal glue, 312 Cys ic lesions, 64, 65 –66
ia rogenic cys s, 64, 66 primary conjunc ival cys , 64,
65 –66 Cys inosis, 158, 240, 241
crys als in, 241 di eren ial diagnosis o , 240 epidemiology o , 240 e iology o , 240 prognosis or, 240 signs o , 240, 241 symp oms o , 240 rea men o , 240
D Deep an erior lamellar kera oplas y
(DALK), 295, 297 Dendri ic ulcer. See Epi helial kera i is Desceme ’s de achmen , 356,
356 –357 complica ions o , 356 e iology o , 356 prognosis or, 356 signs o , 356, 356 –357 symp oms o , 356 rea men o , 356, 357
LWBK961-ind_p359-370.indd 361 28/07/11 4:30 PM

362 INDEX
Disci orm kera i is. See Herpes simplex kera i is
Dry eye syndrome. See Kera oconjunc ivi is sicca
Dural-sinus f s ulas, 67–68, 69
E Elec rical burns, 330, 331 Endo helial dys rophy, 131–132, 132 .
See also Fuchs’ dys rophy di eren ial diagnosis o , 131 epidemiology and pa hology o ,
131 e iology o , 131 prognosis or, 132 signs o , 131, 132 symp oms o , 131 rea men o , 131–132
Endo helial kera oplas y, 290, 291 –294
advan ages o , 290, 291 –293 combined procedures wi h, 290 complica ions o , 290, 293 –294 disadvan ages o , 290 indica ions or, 290 success ra e or, 290 surgical echnique or, 290
Epibulbar dermoid, 52, 54 –56 Episcleri is, 196, 266–267, 267 –268
diagnos ic evalua ion o , 267 di eren ial diagnosis o , 266 e iology o , 266 nodular, 266 prognosis or, 267 signs o , 266, 268 simple, 266 symp oms o , 266 rea men o , 267
Epi helial basemen membrane dys rophy (EBM), 102–103, 103 –107
di eren ial diagnosis o , 103 e iology o , 102 pa hology o , 102 prognosis or, 103 signs o , 102–103, 103 –107 symp oms o , 102 rea men o , 103
Epi helial downgrow h, 353, 354 –355
complica ions o , 353 e iology o , 353 prognosis or, 353 signs o , 353, 354 –355
symp oms o , 353 rea men o , 353
Epi helial kera i is. See Herpes simplex kera i is
Ery hema mul i orme major. See S evens-Johnson syndrome
Essen ial iris a rophy, 166 Excimer laser pho o herapeu ic
kera ec omy (P K), 110, 116, 120, 123, 126, 300, 301 –302
complica ions o , 300 indica ions or, 300 prognosis or, 300 surgical echnique or, 300,
301 –302 Exposure kera opa hy, 218, 219
e iology o , 218 prognosis or, 218 signs o , 218, 219 symp oms o , 218 rea men o , 218
Ex ernal hordeolum, 4
F Fabry’s disease, 156 Ferry’s line, 160, 160 Filamen ary kera opa hy, 216, 217
e iology o , 216 prognosis or, 216 signs o , 216, 217 symp oms o , 216 rea men o , 216
Filamen ous kera i is, 174. See also Fungal kera i is
Fleischer’s ring, 160 Floppy eyelid syndrome, 35, 36
e iology o , 35 prognosis or, 35 signs o , 35, 36 symp oms o , 35 rea men o , 35
Fuchs’ dys rophy, 131–132, 132 –135
di eren ial diagnosis o , 131 epidemiology and pa hology o ,
131 e iology o , 131 prognosis or, 132 signs o , 131, 132 –135 symp oms o , 131 rea men o , 131–132
Fuchs’ marginal kera i is, 43, 45 Fungal kera i is, 174, 175 –177
diagnos ic evalua ion o , 174 di eren ial diagnosis o , 174 e iology o , 174, 175 –177 prognosis or, 174 symp oms o , 174 rea men o , 174
G Gela inous drop–like corneal
dys rophy, 114, 115 di eren ial diagnosis o , 114 e iology and pa hology o , 114 prognosis or, 114, 115 signs o , 114, 115 symp oms o , 114 rea men o , 114
Ghos dendri e, 184, 187 Gian papillary conjunc ivi is (GPC),
30, 230, 232 –233 e iology o , 230 signs o , 230, 232 –233 symp oms o , 230 rea men o , 230
Gonococcal bac erial conjunc ivi is, 8, 9
diagnos ic evalua ion o , 8 e iology o , 8 prognosis or, 8 signs o , 8, 9 symp oms o , 8 rea men o , 8, 9
Granular dys rophy, 116, 117 –119 di eren ial diagnosis o , 116 e iology o , 116 pa hology o , 116 prognosis or, 116 signs o , 116, 117 –119 symp oms o , 116 rea men o , 116
Granulomas, 52, 53 –54
H Haab’s s riae, 76, 77 Hema ologic disorders, 67 Hemorrhage, subconjunc ival, 340,
341 complica ions o , 340 di eren ial diagnosis o , 340 e iology o , 340 prognosis or, 340 signs o , 340, 341 symp oms o , 340 rea men o , 340
Hemorrhagic lymphangiec asia, 67
LWBK961-ind_p359-370.indd 362 28/07/11 4:30 PM

INDEX 363
Hepa olen icular degenera ion. See Wilson’s disease
Heredi ary benign in raepi helial dyskera osis (HBID), 52, 57
Herpes simplex iri is, 190 Herpes simplex kera i is, 182
disci orm kera i is, 188, 189 –191 , 197
di eren ial diagnosis o , 188 prognosis or, 188, 191 signs o , 188, 189 –191 symp oms o , 188 rea men o , 188
epi helial kera i is, 184, 185 –187 di eren ial diagnosis o , 184 prognosis or, 184 signs o , 184, 185 –187 symp oms o , 184 rea men o , 184
neuro rophic kera i is, 194, 195 , 197
di eren ial diagnosis o , 194 prognosis or, 194 signs o , 194, 195 symp oms o , 194 rea men o , 194
primary ocular herpes e iology and epidemiology
o , 182 prognosis or, 182 signs o , 182, 183 symp oms o , 182 rea men o , 182
recurren ocular herpes simplex, 184
epidemiology o , 184 e iology o , 184
Herpes simplex limbi is, 190 Herpes zos er kera i is, 184,
196–197, 198 –201 di eren ial diagnosis o , 196 e iology and epidemiology o , 196 prognosis or, 197, 201 signs o , 196, 198 –200 symp oms o , 196 rea men o , 196–197
Hudson S ahli’s line, 160 Hyphema, rauma ic, 350, 351 –352
complica ions o , 350 e iology o , 350 prognosis or, 350 signs o , 350, 351 –352 symp oms o , 350 rea men o , 350
I Ia rogenic cys s, 64, 66 ICE syndrome. See Iridocorneal-
endo helial syndrome In ec ious crys alline kera opa hy,
158, 158 –159 In amed pinguecula, 266 In ers i ial kera i is, 202–203,
203 –205 diagnosis o , 202 e iology o , 202 nonspecif c corneal ea ures o ,
202, 203 –205 prognosis or, 203 specif c ocular ea ures o , 202,
205 symp oms o , 202 rea men o , 202–203
In racorneal implan s, 314, 315, 318 . See also Re rac ive surgery
In racorneal ring segmen s, 313, 315 Iridocorneal-endo helial syndrome,
136, 166, 166 –167 di eren ial diagnosis o , 166 e iology o , 166 prognosis or, 166 signs o , 166, 166 –167 symp oms o , 166 rea men o , 166
Iris coloboma, 88, 88 –89 diagnosis o , 88 ocular associa ions, 88 prognosis or, 88 signs o , 88, 88 –89 sys emic associa ions, 88 rea men o , 88
Iris cys s, 274, 274 –275 iris pigmen epi helial cys , 274,
274 iris s romal cys , 274, 275
Iris nevus, 276, 276 Iris umors, 276, 276 –277
iris nevus, 276, 276 malignan melanoma, 276 me as a ic umor, 276, 277 vascular umor, 276, 277
Iris vascular umor, 277 Iron line
a er re rac ive surgery, 161 a base o eleva ed lesion, 161 cen ral o superior rabeculec omy
bleb, 160 in ron o nasal p erygium, 160
J Juvenile heredi ary epi helial
dys rophy. See Meesmann’s corneal dys rophy
K Kaposi’s sarcoma, o eyelid/
conjunc iva, 67, 69 , 228, 229
Kayser-Fleischer ring, 163, 163 , 236, 237
e iology o , 163 Kera ec asia, 78, 78
e iology o , 78 prognosis or, 78 signs o , 78 rea men o , 78
Kera i is medicamen osa. See oxic/ ac i ious kera oconjunc ivi is
Kera oconjunc ivi is sicca, 212–213, 214 –215
diagnosis o , 212 di eren ial diagnosis o , 212 e iology o , 212 prognosis or, 213 signs o , 212, 214 –215 symp oms o , 212 rea men o , 212–213, 215
Kera oconus, 90–91, 92 –97 , 98 acu e corneal hydrops in, 96 , 97 cen ral s romal scarring in, 94 compu erized corneal opography
in, 92 crab-claw pat ern, 92
corneal scarring in, 95 di eren ial diagnosis o , 91 e iology o , 90 Fleischer’s ring in, 93 ocular associa ions, 91 prognosis or, 91 prominen corneal nerves in, 93 signs o , 90–91, 92 –97 symp oms o , 90 sys emic associa ions, 91 rea men o , 91 Vog ’s s riae, 94
Kera oglobus, 100, 101 e iology o , 100 prognosis or, 100 signs o , 100, 101 symp oms o , 100 sys emic associa ions, 100 rea men o , 100
LWBK961-ind_p359-370.indd 363 28/07/11 4:30 PM

364 INDEX
L Lamellar kera oplas y, 295,
296 –297 advan ages o , 295 complica ions o , 295, 297 disadvan ages o , 295 indica ions or, 295 success ra e o , 295 surgical echnique or, 295, 296
LASIK, 313, 317 , 320 –323 . See also Re rac ive surgery
Lat ice dys rophy, 120, 121 –122 di eren ial diagnosis o , 120 his opa hology o , 120 prognosis or, 120 signs o , 120, 121 –122 symp oms o , 120 rea men o , 120 ypes o , 120
Ligneous conjunc ivi is, 20, 20 e iology o , 20 prognosis or, 20 signs o , 20, 20 symp oms o , 20 rea men o , 20
Limbal relaxing incisions, 313. See also Re rac ive surgery
Limbal s em cell ransplan a ion, 86, 306, 307
complica ions o , 306 or bila eral ocular disease, 306 or uniocular disease, 306 indica ions or, 306 prognosis or, 306 surgical echnique or, 306, 307
Lipid kera opa hy, 153, 154 –155 Lipidoses, 242
e iology and epidemiology o , 242 prognosis or, 242 signs o , 242 rea men o , 242
Lipodermoid, 52 Localized pos erior kera oconus,
82, 85 Lymphangioma, 67
M Macular dys rophy, 123, 124 –125
di eren ial diagnosis o , 123 e iology o , 123 his opa hology o , 123 prognosis or, 123 signs o , 123, 124 –125 symp oms o , 123
rea men o , 123 ypes o , 123
Malignan melanoma, 49, 51 , 276 Map-do -f ngerprin dys rophy.
See Epi helial basemen membrane dys rophy (EBM)
Meesmann’s corneal dys rophy, 108, 109
e iology o , 108 pa hology o , 108 prognosis or, 108 signs o , 108, 109 symp oms o , 108 rea men o , 108
Megalocornea, 72, 72 , 73 associa ions o , 72 prognosis or, 72 signs o , 72, 73 rea men o , 72
Meibomi is, 2–3, 3 e iology o , 2 prognosis or, 3 signs o , 2, 3 symp oms o , 2
Melanocy ic conjunc ival lesions, 48–49, 49 –51
conjunc ival epi helial melanosis, 48, 49
malignan melanoma, 49, 51 nevus, 48, 50 oculodermal melanosis, 48 primary acquired melanosis, 48, 50 secondary acquired melanosis, 49
Me as a ic umor, 276, 277 Microbial kera i is, 232. See also
Bac erial kera i is e iology o , 232 signs o , 232 symp oms o , 232 rea men o , 232
Microcornea, 70, 70 , 71 associa ion o , 70 prognosis or, 70 signs o , 70, 71 rea men o , 70
Microph halmos, 74, 75 ypes o , 74
Molluscum con agiosum, 18, 19 e iology o , 18 prognosis or, 18 signs o , 18, 19 symp oms o , 18 rea men o , 18
Monoclonal gammopa hies, 158
Mooren’s ulcer, 255–256, 256 diagnosis o , 255 di eren ial diagnosis o , 255 e iology o , 255 prognosis or, 256 signs o , 255, 256 symp oms o , 255 rea men o , 255–256
Mucoepidermoid carcinoma, 58 Mucopolysaccharidoses, 242, 243
epidemiology o , 242 e iology o , 242 prognosis or, 242 signs o , 242, 243 rea men o , 242
Mucus f shing syndrome, 37
N Nanoph halmos, 74
problems associa ed wi h, 74 signs o , 74
Nasolacrimal duc obs ruc ion, 24 Necro izing scleri is, 272 . See also
Scleri is wi h in amma ion, 269 wi hou in amma ion, 269
Necro izing s romal kera i is, 192, 193
di eren ial diagnosis o , 192 prognosis or, 192 signs o , 192, 193 symp oms o , 192 rea men o , 192
Neona al conjunc ivi is. See Oph halmia neona orum
Neuro rophic kera i is. See Herpes simplex kera i is
Neuro rophic kera opa hy, 220, 221
e iology o , 220 prognosis or, 220 signs o , 220, 221 symp oms o , 220 rea men o , 220
Nevus o O a. See Oculodermal melanosis
Non-Hodgkin lymphoma, 59, 62 –63
Nonnecro izing scleri is. See also Scleri is
di use, 269, 271 nodular, 269, 271
Nonnecro izing s romal kera i is. See Disci orm kera i is
LWBK961-ind_p359-370.indd 364 28/07/11 4:30 PM

INDEX 365
O Ocular cica ricial pemphigoid,
249–250, 250 –251 diagnos ic evalua ion o , 249 di eren ial diagnosis o , 249 epidemiology o , 249 e iology o , 249 prognosis or, 250 signs o , 249, 250 –251 symp oms o , 249 rea men o , 249–250
Ocular rosacea, 40, 41 e iology o , 40 prognosis or, 40 signs o , 40, 41 symp oms o , 40 rea men o , 40
Oculodermal melanosis, 48 Oph halmia neona orum, 24, 25
diagnos ic evalua ion o , 24 di eren ial diagnosis o , 24 e iology o , 24 prognosis or, 24 signs o , 24, 25 rea men o , 24
Op ic neuri is, 197
P Parinaud’s oculoglandular syndrome,
22, 23 diagnos ic evalua ion o , 22 e iology o , 22 prognosis or, 22 signs o , 22, 23 symp oms o , 22 rea men o , 22
Pediculosis, 21, 21 e iology o , 21 prognosis or, 21 signs o , 21, 21 symp oms o , 21 rea men o , 21
Pellucid marginal degenera ion, 91, 98, 98 –99
corneal opography, 98 di eren ial diagnosis o , 98 e iology o , 98 prognosis or, 98 signs o , 98, 98 –99 symp oms o , 98 rea men o , 98
Pene ra ing kera oplas y, 282–283, 284 –289
complica ions o , 283, 285 –289
broken in errup ed su ure, 288 endoph halmi is, 285 epi helial downgrow h, 288 loose, exposed running su ure,
289 primary gra ailure, 286 su ure abscess, 287 rauma ic wound rup ure, 289 wound leak, 286 wound mel , 287
con raindica ions or, donor issue, 282
indica ions or, 282 procedures combined wi h, 283 prognos ic ac ors or, 282 success ra e o , 283 surgical echnique or, 282–283,
284 –285 wound closure in, 283, 284 –285
Peripheral sclerocornea, 79 –80 Pe ers’ anomaly, 82, 84 –85 Phakic in raocular lens (IOL), 314,
318 . See also Re rac ive surgery
Phlyc enulosis, 257, 258 diagnosis o , 257 di eren ial diagnosis o , 257 e iology o , 257 prognosis or, 257 signs o , 257, 258 symp oms o , 257 rea men o , 257
Pinguecula, 42–43, 44 , 45 diagnos ic evalua ion o , 43 di eren ial diagnosis o , 42–43, 45 e iology o , 42 prognosis or, 43 signs o , 42, 44 symp oms o , 42 rea men o , 43
Polymorphic amyloid degenera ion (PAD), 120, 143, 146 –147
Pos erior embryo oxon, 82, 83 Pos erior polymorphous corneal
dys rophy, 136, 137 –139 , 166
di eren ial diagnosis o , 136 e iology o , 136 pa hology o , 136 prognosis or, 136 signs o , 136, 137 –139 symp oms o , 136 rea men o , 136
Pos herpe ic neuralgia, 197
Po en ially malignan amelanocy ic conjunc ival lesions, 58–59, 59 –63
conjunc ival in raepi helial neoplasia, 58, 60 –61
non-Hodgkin lymphoma, 59, 62 –63
o her carcinomas, 58–59, 62 reac ive lymphoid hyperplasia, 59,
62 –63 squamous cell carcinoma, 58, 61 squamous papilloma, 58, 59
Primary acquired melanosis, 48, 50 Primary conjunc ival cys , 64, 65 –66 Pseudodendri es, 197 Pseudomonal kera i is, 169. See also
Bac erial kera i is Pseudop erygium, 42, 45 P erygium, 42–43, 44 –45
diagnos ic evalua ion o , 43 di eren ial diagnosis o , 42–43, 45 e iology o , 42 prognosis or, 43 signs o , 42, 44 –45 symp oms o , 42 rea men o , 43
Pubic lice, in ec ion rom. See Pediculosis
Punc a e epi helial erosions. See Superf cial punc a e kera opa hy
Pyogenic granuloma, 4, 52, 53
R Racial melanosis. See Conjunc ival
epi helial melanosis Radial kera o omy (RK), 313, 316 ,
319 . See also Re rac ive surgery
Reac ive lymphoid hyperplasia, 59, 62 –63
Recurren corneal erosion. See Corneal erosion, recurren
Re rac ive surgery, 313–315, 316 –323
complica ions o , 314–315, 319 –323
surgical principles or, 313–314, 316 –318
ypes o implan surgery, 313 incisional surgery, 313 laser surgery, 313 o her, 313
LWBK961-ind_p359-370.indd 365 28/07/11 4:30 PM

366 INDEX
Reis-Bücklers dys rophy, 110, 111 –113
di eren ial diagnosis o , 110 e iology o , 110 prognosis or, 110, 113 signs o , 110, 111 –112 symp oms o , 110 rea men o , 110
Relaxing incisions, 313, 316 . See also Re rac ive surgery
Re ini is, 197 Rheuma oid ar hri is, peripheral
corneal ulcera ion in, 245 –246 . See also Collagen vascular diseases
Rhinosporidiosis, 52 Rieger’s anomaly, 82, 84 Rieger’s syndrome, 82 Rus ring, 160
S Salzmann’s nodular degenera ion,
151, 151 –152 di eren ial diagnosis o , 151 e iology o , 151 prognosis or, 151 signs o , 151, 151 –152 symp oms o , 151 rea men o , 151
Sarcoid granulomas, 52, 54 Schnyder’s corneal dys rophy, 128,
129 –130 di eren ial diagnosis o , 128 e iology o , 128 prognosis or, 128 signs o , 128, 129 –130 symp oms o , 128 rea men o , 128
Scleri is, 197, 266, 269–271, 271 –273
classif ca ion o , 269, 271 –272 complica ions o , 270 diagnos ic evalua ion o , 270 di eren ial diagnosis o , 270 e iology o , 269, 272 –273 necro izing, 269, 272 nonnecro izing, 269 prognosis or, 271 signs o , 270, 273 symp oms o , 270 rea men o , 270–271
Sclerocornea, 79, 79 –80 e iology o , 79 ocular associa ions, 79
prognosis or, 79 signs o , 79, 79 –80 rea men o , 79
Scleromalacia per orans, 247 Sebaceous carcinoma, 4, 58, 62 Secondary acquired melanosis, 49 Siderosis, 160 Spheroidal degenera ion, 151, 153,
154 Spindle cell carcinoma, 58 Spring ca arrh. See Vernal
kera oconjunc ivi is Squamous cell carcinoma, 58, 61 Squamous papilloma, 58, 59 S aphylococcal hypersensi ivi y, 259,
260 di eren ial diagnosis o , 259 e iology o , 259 prognosis or, 259 signs o , 259, 260 symp oms o , 259 rea men o , 259
S aphylococcal hypersensi ivi y kera i is, 169, 255
S aphylococcal kera i is, 168. See also Bac erial kera i is
S aphylococcal scalded skin syndrome, 252
S erile kera i is, 231–232, 235 e iology o , 231 signs o , 232, 235 symp oms o , 232 rea men o , 232
S evens-Johnson syndrome, 252, 253 –254
causes o , 252 di eren ial diagnosis o , 252 e iology and epidemiology o , 252 prognosis or, 252 signs o , 252, 253 –254 symp oms o , 252 rea men o , 252
S ocker’s line, 160, 160 S rep ococcal kera i is, 168. See also
Bac erial kera i is Streptococcus viridans, crys alline
kera opa hy by, 158 S urge-Weber syndrome, 67, 68 Subconjunc ival hemorrhage.
See Hemorrhage, subconjunc ival
Subepi helial inf l ra es, 206, 207 di eren ial diagnosis o , 206 e iology o , 206
prognosis or, 206 signs o , 206, 207 symp oms o , 206 rea men o , 206
Sunse syndrome, 280 Superf cial kera ec omy, 299, 299
complica ions o , 299 indica ions or, 299 prognosis or, 299 surgical echnique or, 299, 299
Superf cial punc a e kera opa hy, 208, 209
di eren ial diagnosis o , 208 e iology o , 208 prognosis or, 208 signs o , 208, 209 symp oms o , 208 rea men o , 208
Superior limbic kera oconjunc ivi is (SLK), 33, 34
e iology o , 33 prognosis or, 33 signs o , 33, 34 symp oms o , 33 rea men o , 33, 34
Sur ace abla ion, 313
T elangiec asias, 67 errien’s marginal degenera ion, 164,
164 –165 , 255 e iology o , 164 prognosis or, 164 signs o , 164, 164 –165 symp oms o , 164 rea men o , 164
T ermal burns, 330, 331 complica ions o , 330 e iology o , 330 prognosis or, 330 signs o , 330, 331 symp oms o , 330 rea men o , 330
T ygeson’s superf cial punc a e kera opa hy, 210, 211
e iology o , 210 prognosis or, 210 signs o , 210, 211 symp oms o , 210 rea men o , 210
igh lens syndrome, 231, 234 e iology o , 231 signs o , 231, 234
LWBK961-ind_p359-370.indd 366 28/07/11 4:30 PM

INDEX 367
symp oms o , 231 rea men o , 231
oxic and allergic conjunc ivi is, 230 e iology o , 230 signs o , 230 symp oms o , 230 rea men o , 230
oxic/ ac i ious kera oconjunc ivi is, 37, 38 –39
diagnos ic evalua ion o , 37 di ere ial diagnosis o , 37 e iology o , 37 prognosis or, 37 signs o , 37, 38 –39 symp oms o , 37 rea men o , 37
rachoma, 16, 17 diagnos ic evalua ion o , 16 e iology o , 16 prognosis or, 16 signs o , 16, 17 rea men o , 16
rauma, ocular, 324 chemical burns, 324–325,
326 –329 corneal abrasions, 334, 335 corneal/ conjunc ival oreign
bodies, 336–337, 337 –339 corneoscleral lacera ion and
wound dehiscence, 342–343, 344 –349
Desceme ’s de achmen , 356, 356 –357
elec rical burns, 330 epi helial downgrow h, 353,
354 –355 hyphema, 350, 351 –352
subconjunc ival hemorrhage, 340, 341
hermal burns, 330, 331 ul raviole kera opa hy, 332, 333
U Ul raviole kera opa hy, 332, 333
complica ions o , 332 e iology o , 332 prognosis or, 332 signs o , 332, 333 symp oms o , 332 rea men o , 332
V Vascular lesions, 67, 68 –69
capillary hemangioma, 67 caro id–cavernous sinus, 67–68, 69 dural-sinus f s ulas, 67–68, 69 hema ologic disorders, 67 hemorrhagic lymphangiec asia, 67 Kaposi’s sarcoma, 67, 69 lymphangioma, 67 S urge-Weber syndrome, 67, 68 elangiec asias, 67
Vasculi ides, 52 Vernal kera oconjunc ivi is, 30, 31 –32
di eren ial diagnosis o , 30 epidemiology o , 30 e iology o , 30 prognosis or, 30 signs o , 30, 31 –32 symp oms o , 30 rea men o , 30
Viral conjunc ivi is, 10, 11 –13 e iology o , 10 prognosis or, 10, 13
signs o , 10, 11 –12 symp oms o , 10 rea men o , 10
Vi amin A def ciency, 238, 239 di eren ial diagnosis o , 238 e iology o , 238 prognosis or, 238 signs o , 238, 239 symp oms o , 238 rea men o , 238
Vor ex kera opa hy. See Cornea ver icilla a
W Wegener’s granuloma osis,
necro izing scleri is in, 246 . See also Collagen vascular diseases
Welder’s ash, 332, 333 Whi e limbal girdle o Vog , 142,
144 Wilson’s disease, 163, 236, 237
diagnos ic evalua ion o , 236 di eren ial diagnosis o , 236 e iology and epidemiology o , 236 prognosis or, 236 signs o , 236, 237 symp oms o , 236 rea men o , 236
Wound dehiscence. See Corneoscleral lacera ion and wound dehiscence
X Xerosis o cornea and conjunc iva,
by vi amin A def ciency, 238, 239
LWBK961-ind_p359-370.indd 367 28/07/11 4:30 PM