Bacteria 8
10
L ast year an event doctors had been fearing finally occurred. In three geographically sepa- rate patients, an often deadly bacterium, Staphylococcus aureus, responded poor- ly to a once reliable antidote—the anti- biotic vancomycin. Fortunately, in those patients, the staph microbe remained susceptible to other drugs and was erad- icated. But the appearance of S. aureus not readily cleared by vancomycin fore- shadows trouble. Worldwide, many strains of S. aureus are already resistant to all antibiotics ex- cept vancomycin. Emergence of forms lacking sensitivity to vancomycin sig- nifies that variants untreatable by every known antibiotic are on their way. S. aureus, a major cause of hospital-ac- quired infections, has thus moved one step closer to becoming an unstoppable killer. The looming threat of incurable S. aureus is just the latest twist in an inter- national public health nightmare: in- creasing bacterial resistance to many an- tibiotics that once cured bacterial dis- eases readily. Ever since antibiotics became widely available in the 1940s, they have been hailed as miracle drugs— magic bullets able to eliminate bacteria without doing much harm to the cells of treated individuals. Yet with each passing decade, bacteria that defy not only single but multiple antibiotics—and therefore are extremely difficult to con- trol —have become increasingly common. What is more, strains of at least three bacterial species capable of causing life- threatening illnesses (Enterococcus fae- calis, Mycobacterium tuberculosis and Pseudomonas aeruginosa) already evade every antibiotic in the clinician’s arma- mentarium, a stockpile of more than 100 drugs. In part because of the rise in resistance to antibiotics, the death rates for some communicable diseases (such as tuberculosis) have started to rise again, after having declined in the in- dustrial nations. How did we end up in this worrisome, and worsening, situation? Several inter- acting processes are at fault. Analyses of them point to a number of actions that The Challenge of Antibiotic Resistance The Challenge of Antibiotic Resistance Certain bacterial infections now defy all antibiotics. The resistance problem may be reversible, but only if society begins to consider how the drugs affect “good” bacteria as well as “bad” by Stuart B. Levy Staphylococcus aureus Causes blood poisoning, wound infections and pneumo- nia; in some hospitals, more than 60 percent of strains are resistant to methicillin; some are poised for resistance to all antibiotics (H/C; 1950s) Acinetobacter Causes blood poisoning in patients with compromised immunity (H, 1990s) Enterococcus faecalis Causes blood poisoning and urinary tract and wound infections in patients with compromised immunity; some multidrug-resistant strains are untreatable (H, 1980s) Haemophilus influenzae Causes pneumonia, ear infections and meningitis, especially in children. Now largely preventable by vaccines (C; 1970s) Neisseria gonorrhoeae Causes gonorrhea; multidrug resistance now limits therapy chiefly to cephalosporins (C; 1970s) 46 Scientific American March 1998 OLIVER MECKES Photo Researchers, Inc. CNRI/SPL/PHOTO RESEARCHERS, INC. OLIVER MECKES Photo Researchers, Inc. NIBSC/SPL/PHOTO RESEARCHERS, INC. A. B. DOWSETT SPL/Photo Researchers, Inc. Copyright 1998 Scientific American, Inc.
Transcript of Bacteria 8

Last year an event doctors had been fearing finally occurred. In three geographically sepa-
rate patients, an often deadly bacterium,Staphylococcus aureus, responded poor-ly to a once reliable antidote—the anti-biotic vancomycin. Fortunately, in thosepatients, the staph microbe remainedsusceptible to other drugs and was erad-icated. But the appearance of S. aureusnot readily cleared by vancomycin fore-shadows trouble.
Worldwide, many strains of S. aureusare already resistant to all antibiotics ex-cept vancomycin. Emergence of formslacking sensitivity to vancomycin sig-nifies that variants untreatable by everyknown antibiotic are on their way. S.
aureus, a major cause of hospital-ac-quired infections, has thus moved onestep closer to becoming an unstoppablekiller.
The looming threat of incurable S.aureus is just the latest twist in an inter-national public health nightmare: in-creasing bacterial resistance to many an-tibiotics that once cured bacterial dis-eases readily. Ever since antibioticsbecame widely available in the 1940s,they have been hailed as miracle drugs—magic bullets able to eliminate bacteriawithout doing much harm to the cellsof treated individuals. Yet with eachpassing decade, bacteria that defy notonly single but multiple antibiotics—andtherefore are extremely difficult to con-
trol—have become increasingly common.What is more, strains of at least three
bacterial species capable of causing life-threatening illnesses (Enterococcus fae-calis, Mycobacterium tuberculosis andPseudomonas aeruginosa) already evadeevery antibiotic in the clinician’s arma-mentarium, a stockpile of more than100 drugs. In part because of the rise inresistance to antibiotics, the death ratesfor some communicable diseases (suchas tuberculosis) have started to riseagain, after having declined in the in-dustrial nations.
How did we end up in this worrisome,and worsening, situation? Several inter-acting processes are at fault. Analyses ofthem point to a number of actions that
The Challenge of Antibiotic Resistance
The Challengeof Antibiotic Resistance
Certain bacterial infections now defy all antibiotics. The resistanceproblem may be reversible, but only if society begins to consider how
the drugs affect “good” bacteria as well as “bad”
by Stuart B. Levy
Staphylococcus aureus
Causes blood poisoning,wound infections and pneumo-
nia; in some hospitals, morethan 60 percent of strains areresistant to methicillin; someare poised for resistance to all
antibiotics (H/C; 1950s)
Acinetobacter
Causes blood poisoning in patients with compromised
immunity (H, 1990s)
Enterococcus faecalis
Causes blood poisoning andurinary tract and wound
infections in patients with compromised immunity; somemultidrug-resistant strains are
untreatable (H, 1980s)
Haemophilus influenzae
Causes pneumonia, ear infections and meningitis, especially in children. Now
largely preventable by vaccines (C; 1970s)
Neisseria gonorrhoeae
Causes gonorrhea; multidrug resistance now
limits therapy chiefly tocephalosporins (C; 1970s)
46 Scientific American March 1998
OLI
VER
MEC
KES
Phot
o Re
sear
cher
s, In
c.
CN
RI/S
PL/P
HO
TO R
ESEA
RCH
ERS,
INC
.
OLI
VER
MEC
KES
Phot
o Re
sear
cher
s, In
c.
NIB
SC/S
PL/P
HO
TO R
ESEA
RCH
ERS,
INC
.
A. B
. DO
WSE
TT S
PL/P
hoto
Res
earc
hers
, Inc
.
Copyright 1998 Scientific American, Inc.

could help reverse the trend, if individu-als, businesses and governments aroundthe world can find the will to imple-ment them.
One component of the solution is rec-ognizing that bacteria are a natural, andneeded, part of life. Bacteria, which aremicroscopic, single-cell entities, aboundon inanimate surfaces and on parts ofthe body that make contact with theouter world, including the skin, the mu-cous membranes and the lining of theintestinal tract. Most live blamelessly. Infact, they often protect us from disease,because they compete with, and thuslimit the proliferation of, pathogenicbacteria—the minority of species thatcan multiply aggressively (into the mil-lions) and damage tissues or otherwisecause illness. The benign competitorscan be important allies in the fightagainst antibiotic-resistant pathogens.
People should also realize that al-though antibiotics are needed to controlbacterial infections, they can have broad,undesirable effects on microbial ecolo-gy. That is, they can produce long-lastingchange in the kinds and proportions ofbacteria—and the mix of antibiotic-re-sistant and antibiotic-susceptible types—
not only in the treated individual butalso in the environment and society atlarge. The compounds should thus beused only when they are truly needed,
and they should not be administered forviral infections, over which they have nopower.
A Bad Combination
Although many factors can influence whether bacteria in a person or in
a community will become insensitive toan antibiotic, the two main forces arethe prevalence of resistance genes (whichgive rise to proteins that shield bacteriafrom an antibiotic’s effects) and the ex-tent of antibiotic use. If the collectivebacterial flora in a community have nogenes conferring resistance to a givenantibiotic, the antibiotic will successful-ly eliminate infection caused by any ofthe bacterial species in the collection.On the other hand, if the flora possessresistance genes and the community usesthe drug persistently, bacteria able todefy eradication by the compound willemerge and multiply.
Antibiotic-resistant pathogens are notmore virulent than susceptible ones: thesame numbers of resistant and suscepti-ble bacterial cells are required to pro-duce disease. But the resistant forms areharder to destroy. Those that are slight-ly insensitive to an antibiotic can oftenbe eliminated by using more of thedrug; those that are highly resistant re-quire other therapies.
To understand how resistance genesenable bacteria to survive an attack byan antibiotic, it helps to know exactlywhat antibiotics are and how they harmbacteria. Strictly speaking, the com-pounds are defined as natural substan-ces (made by living organisms) that in-hibit the growth, or proliferation, of bac-teria or kill them directly. In practice,though, most commercial antibioticshave been chemically altered in the lab-oratory to improve their potency or toincrease the range of species they affect.Here I will also use the term to encom-pass completely synthetic medicines,such as quinolones and sulfonamides,which technically fit under the broaderrubric of antimicrobials.
Whatever their monikers, antibiotics,by inhibiting bacterial growth, give ahost’s immune defenses a chance to out-flank the bugs that remain. The drugstypically retard bacterial proliferationby entering the microbes and interfer-ing with the production of componentsneeded to form new bacterial cells. Forinstance, the antibiotic tetracycline bindsto ribosomes (internal structures thatmake new proteins) and, in so doing,impairs protein manufacture; penicillinand vancomycin impede proper synthe-sis of the bacterial cell wall.
Certain resistance genes ward off de-struction by giving rise to enzymes that
The Challenge of Antibiotic Resistance
ROGUE’S GALLERY OF BACTERIA features some types hav-ing variants resistant to multiple antibiotics; multidrug-resistantbacteria are difficult and expensive to treat. Certain strains ofthe species described in red no longer respond to any antibioticsand produce incurable infections. Some of the bacteria cause in-
fections mainly in hospitals (H) or mainly in the community (C);others, in both settings. The decade listed with each entry indi-cates the period when resistance first became a significant prob-lem for patient care. The bacteria, which are microscopic, arehighly magnified in these false-color images.
Mycobacterium tuberculosis
Causes tuberculosis; some multidrug-resistant
strains are untreatable (H/C; 1970s)
Pseudomonas aeruginosa
Causes blood poisoning andpneumonia, especially in
people with cystic fibrosis orcompromised immunity; somemultidrug-resistant strains are
untreatable (H/C; 1960s)
Escherichia coli
Causes urinary tract infections,blood poisoning, diarrhea and
kidney failure; some strains thatcause urinary tract infections
are multidrug-resistant (H/C; 1960s)
Scientific American March 1998 47
Shigella dysenteria
Causes dysentery (bloody diarrhea); resistant strains haveled to epidemics, and some can
be treated only by expensivefluoroquinolones, which are
often unavailable in developingnations (C; 1960s)
CN
RI/S
PL/P
HO
TO R
ESEA
RC
HER
S, IN
C.
OLI
VER
MEC
KES
Phot
o Re
sear
cher
s, In
c.
E. G
RAY
SPL/
Phot
o Re
sear
cher
s, In
c.
CA
MR/
A. B
. DO
WSE
TT S
PL/P
hoto
Res
earc
hers
, Inc
.
Streptococcus pneumoniae
Causes blood poisoning, middle ear infections,
pneumonia and meningitis (C; 1970s)
CN
RI/S
PL/P
HO
TO R
ESEA
RC
HER
S, IN
C.
Copyright 1998 Scientific American, Inc.
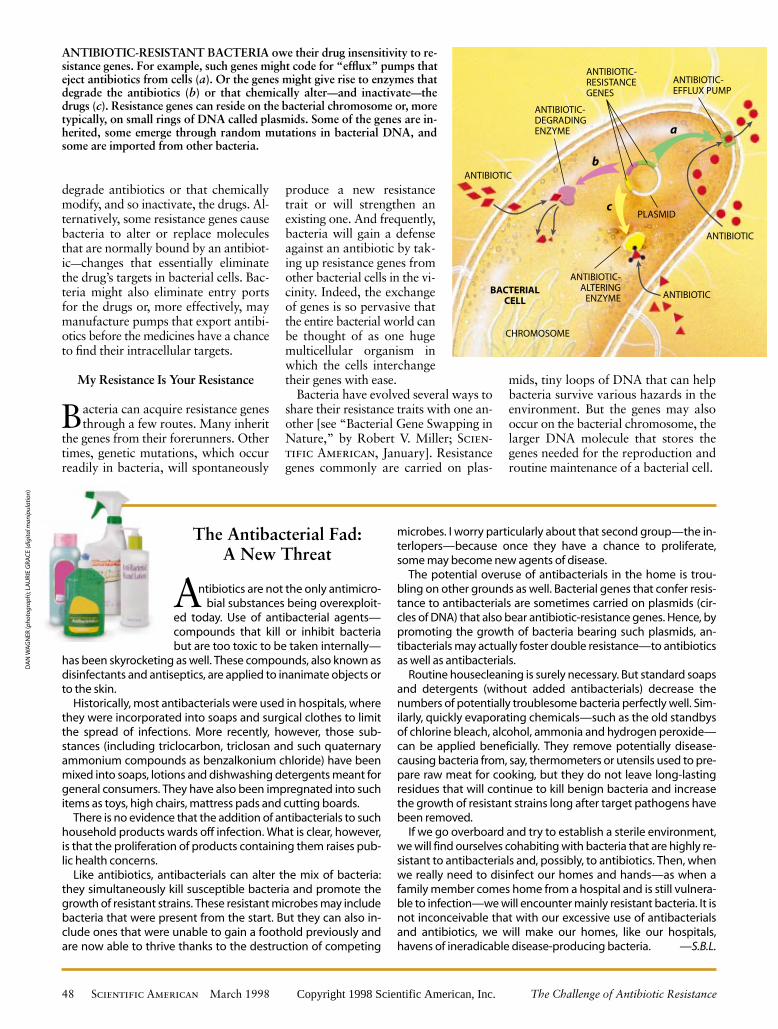
degrade antibiotics or that chemicallymodify, and so inactivate, the drugs. Al-ternatively, some resistance genes causebacteria to alter or replace moleculesthat are normally bound by an antibiot-ic—changes that essentially eliminatethe drug’s targets in bacterial cells. Bac-teria might also eliminate entry portsfor the drugs or, more effectively, maymanufacture pumps that export antibi-otics before the medicines have a chanceto find their intracellular targets.
My Resistance Is Your Resistance
Bacteria can acquire resistance genesthrough a few routes. Many inherit
the genes from their forerunners. Othertimes, genetic mutations, which occurreadily in bacteria, will spontaneously
produce a new resistancetrait or will strengthen anexisting one. And frequently,bacteria will gain a defenseagainst an antibiotic by tak-ing up resistance genes fromother bacterial cells in the vi-cinity. Indeed, the exchangeof genes is so pervasive thatthe entire bacterial world canbe thought of as one hugemulticellular organism inwhich the cells interchangetheir genes with ease.
Bacteria have evolved several ways toshare their resistance traits with one an-other [see “Bacterial Gene Swapping inNature,” by Robert V. Miller; Scien-tific American, January]. Resistancegenes commonly are carried on plas-
mids, tiny loops of DNA that can helpbacteria survive various hazards in theenvironment. But the genes may alsooccur on the bacterial chromosome, thelarger DNA molecule that stores thegenes needed for the reproduction androutine maintenance of a bacterial cell.
48 Scientific American March 1998 The Challenge of Antibiotic Resistance
The Antibacterial Fad: A New Threat
Antibiotics are not the only antimicro-bial substances being overexploit-
ed today. Use of antibacterial agents—compounds that kill or inhibit bacteriabut are too toxic to be taken internally—
has been skyrocketing as well. These compounds, also known asdisinfectants and antiseptics, are applied to inanimate objects orto the skin.
Historically, most antibacterials were used in hospitals, wherethey were incorporated into soaps and surgical clothes to limitthe spread of infections. More recently, however, those sub-stances (including triclocarbon, triclosan and such quaternaryammonium compounds as benzalkonium chloride) have beenmixed into soaps, lotions and dishwashing detergents meant forgeneral consumers. They have also been impregnated into suchitems as toys, high chairs, mattress pads and cutting boards.
There is no evidence that the addition of antibacterials to suchhousehold products wards off infection. What is clear, however,is that the proliferation of products containing them raises pub-lic health concerns.
Like antibiotics, antibacterials can alter the mix of bacteria:they simultaneously kill susceptible bacteria and promote thegrowth of resistant strains. These resistant microbes may includebacteria that were present from the start. But they can also in-clude ones that were unable to gain a foothold previously andare now able to thrive thanks to the destruction of competing
microbes. I worry particularly about that second group—the in-terlopers—because once they have a chance to proliferate,some may become new agents of disease.
The potential overuse of antibacterials in the home is trou-bling on other grounds as well. Bacterial genes that confer resis-tance to antibacterials are sometimes carried on plasmids (cir-cles of DNA) that also bear antibiotic-resistance genes. Hence, bypromoting the growth of bacteria bearing such plasmids, an-tibacterials may actually foster double resistance—to antibioticsas well as antibacterials.
Routine housecleaning is surely necessary. But standard soapsand detergents (without added antibacterials) decrease thenumbers of potentially troublesome bacteria perfectly well. Sim-ilarly, quickly evaporating chemicals—such as the old standbysof chlorine bleach, alcohol, ammonia and hydrogen peroxide—can be applied beneficially. They remove potentially disease-causing bacteria from, say, thermometers or utensils used to pre-pare raw meat for cooking, but they do not leave long-lastingresidues that will continue to kill benign bacteria and increasethe growth of resistant strains long after target pathogens havebeen removed.
If we go overboard and try to establish a sterile environment,we will find ourselves cohabiting with bacteria that are highly re-sistant to antibacterials and, possibly, to antibiotics. Then, whenwe really need to disinfect our homes and hands—as when afamily member comes home from a hospital and is still vulnera-ble to infection—we will encounter mainly resistant bacteria. It isnot inconceivable that with our excessive use of antibacterialsand antibiotics, we will make our homes, like our hospitals,havens of ineradicable disease-producing bacteria. —S.B.L.
ANTIBIOTIC
ANTIBIOTIC
ANTIBIOTIC-RESISTANCEGENES
PLASMID
ANTIBIOTIC
ANTIBIOTIC-ALTERING
ENZYMEBACTERIAL
CELL
CHROMOSOME
ANTIBIOTIC-DEGRADINGENZYME
ANTIBIOTIC-EFFLUX PUMP
b
a
c
ANTIBIOTIC-RESISTANT BACTERIA owe their drug insensitivity to re-sistance genes. For example, such genes might code for “efflux” pumps thateject antibiotics from cells (a). Or the genes might give rise to enzymes thatdegrade the antibiotics (b) or that chemically alter—and inactivate—thedrugs (c). Resistance genes can reside on the bacterial chromosome or, moretypically, on small rings of DNA called plasmids. Some of the genes are in-herited, some emerge through random mutations in bacterial DNA, andsome are imported from other bacteria.
DA
N W
AG
NER
(pho
togr
aph)
; LA
URI
E G
RA
CE
(dig
ital m
anip
ulat
ion)
Copyright 1998 Scientific American, Inc.

Often one bacterium will pass resis-tance traits to others by giving them auseful plasmid. Resistance genes canalso be transferred by viruses that occa-sionally extract a gene from one bacte-rial cell and inject it into a different one.In addition, after a bacterium dies andreleases its contents into the environ-ment, another will occasionally take upa liberated gene for itself.
In the last two situations, the gene willsurvive and provide protection from anantibiotic only if integrated stably intoa plasmid or chromosome. Such inte-gration occurs frequently, though, be-cause resistance genes are often embed-ded in small units of DNA, called trans-posons, that readily hop into other DNAmolecules. In a regrettable twist of fatefor human beings, many bacteria playhost to specialized transposons, termedintegrons, that are like flypaper in theirpropensity for capturing new genes.These integrons can consist of severaldifferent resistance genes, which arepassed to other bacteria as whole regi-ments of antibiotic-defying guerrillas.
Many bacteria possessed resistancegenes even before commercial antibiot-ics came into use. Scientists do not knowexactly why these genes evolved andwere maintained. A logical argumentholds that natural antibiotics were ini-tially elaborated as the result of chancegenetic mutations. Then the compounds,
which turned out to elimi-nate competitors, enabledthe manufacturers to surviveand proliferate—if they werealso lucky enough to possessgenes that protected themfrom their own chemicalweapons. Later, these protec-tive genes found their wayinto other species, some ofwhich were pathogenic.
Regardless of how bacte-ria acquire resistance genes
today, commercial antibiotics can selectfor—promote the survival and propaga-tion of—antibiotic-resistant strains. Inother words, by encouraging the growthof resistant pathogens, an antibiotic canactually contribute to its own undoing.
How Antibiotics Promote Resistance
The selection process is fairly straight-forward. When an antibiotic at-
tacks a group of bacteria, cells that arehighly susceptible to the medicine willdie. But cells that have some resistancefrom the start, or that acquire it later(through mutation or gene exchange),may survive, especially if too little drugis given to overwhelm the cells that arepresent. Those cells, facing reducedcompetition from sus-ceptible bacteria, willthen go on to prolif-erate. When confront-ed with an antibiotic,the most resistant cellsin a group will inevit-ably outcompete allothers.
Promoting resis-tance in known path-ogens is not the onlyself-defeating activityof antibiotics. Whenthe medicines attackdisease-causing bac-
teria, they also affect benign bacteria—
innocent bystanders—in their path. Theyeliminate drug-susceptible bystandersthat could otherwise limit the expansionof pathogens, and they simultaneouslyencourage the growth of resistant by-standers. Propagation of these resistant,nonpathogenic bacteria increases thereservoir of resistance traits in the bac-terial population as a whole and raisesthe odds that such traits will spread topathogens. In addition, sometimes thegrowing populations of bystanders them-selves become agents of disease.
Widespread use of cephalosporin an-tibiotics, for example, has promotedthe proliferation of the once benign in-testinal bacterium E. faecalis, which isnaturally resistant to those drugs. Inmost people, the immune system is ableto check the growth of even multidrug-resistant E. faecalis, so that it does notproduce illness. But in hospitalized pa-tients with compromised immunity, theenterococcus can spread to the heartvalves and other organs and establishdeadly systemic disease.
Moreover, administration of vanco-mycin over the years has turned E. fae-calis into a dangerous reservoir of van-comycin-resistance traits. Recall thatsome strains of the pathogen S. aureus
The Challenge of Antibiotic Resistance Scientific American March 1998 49
DEADBACTERIUM
RESISTANCEGENE
BACTERIUMRECEIVINGRESISTANCE GENES
RESISTANCEGENE
RESISTANCEGENE
PLASMID DONOR PLASMID
Gene goesto plasmid
or tochromosome
VIRUS
BACTERIUMINFECTED
BY A VIRUS
bTRANSFERBY VIRAL DELIVERY
aPLASMIDTRANSFER
cTRANSFEROF FREE DNA
BACTERIA PICK UP RESISTANCE GENES from other bacterial cells inthree main ways. Often they receive whole plasmids bearing one or moresuch genes from a donor cell (a). Other times, a virus will pick up a resis-tance gene from one bacterium and inject it into a different bacterial cell (b).Alternatively, bacteria sometimes scavenge gene-bearing snippets of DNAfrom dead cells in their vicinity (c). Genes obtained through viruses or fromdead cells persist in their new owner if they become incorporated stably intothe recipient’s chromosome or into a plasmid.
SPREAD OF RESISTANT BACTERIA, which occurs readily, canextend quite far. In one example, investigators traced a strain of mul-tidrug-resistant Streptococcus pneumoniae from Spain to Portugal,France, Poland, the U.K., South Africa, the U.S. and Mexico.
ILLU
STR
ATIO
NS
BY
TOM
O N
AR
ASH
IMA
LAU
RIE
GR
AC
E; S
OU
RC
E: C
HRI
STO
PHER
G. D
OW
SON
, TR
AC
EY J
. CO
FFEY
AN
D B
RIA
N G
. SPR
ATT
Uni
vers
ity
of S
usse
x
Copyright 1998 Scientific American, Inc.

BACTERIUM SUSCEPTIBLE TO ANTIBIOTICS
ANTIBIOTIC
SOMEWHAT INSENSITIVEBACTERIUM
SURVIVINGBACTERIUM
BACTERIUMWITH INCREASEDRESISTANCE
DEADBACTERIA
are multidrug-resistant and are respon-sive only to vancomycin. Because vanco-mycin-resistant E. faecalis has becomequite common, public health expertsfear that it will soon deliver strong van-comycin resistance to those S. aureusstrains, making them incurable.
The bystander effect has also enabledmultidrug-resistant strains of Acineto-bacter and Xanthomonas to emerge andbecome agents of potentially fatal blood-borne infections in hospitalized patients.These formerly innocuous microbes werevirtually unheard of just five years ago.
As I noted earlier, antibiotics affect
the mix of resistant and nonresistantbacteria both in the individual beingtreated and in the environment. Whenresistant bacteria arise in treated individ-uals, these microbes, like other bacteria,spread readily to the surrounds and tonew hosts. Investigators have shownthat when one member of a householdchronically takes an antibiotic to treatacne, the concentration of antibiotic-re-sistant bacteria on the skin of familymembers rises. Similarly, heavy use ofantibiotics in such settings as hospitals,day care centers and farms (where thedrugs are often given to livestock fornonmedicinal purposes) increases thelevels of resistant bacteria in people andother organisms who are not being treat-ed—including in individuals who livenear those epicenters of high consump-tion or who pass through the centers.
Given that antibiotics and other anti-microbials, such as fungicides, affect thekinds of bacteria in the environmentand people around the individual beingtreated, I often refer to these substancesas societal drugs—the only class of ther-apeutics that can be so designated. An-ticancer drugs, in contrast, affect onlythe person taking the medicines.
On a larger scale, antibiotic resistancethat emerges in one place can oftenspread far and wide. The ever increasingvolume of international travel has has-tened transfer to the U.S. of multidrug-resistant tuberculosis from other coun-tries. And investigators have document-ed the migration of a strain ofmultidrug-resistant Streptococcus pneu-moniae from Spain to the U.K., theU.S., South Africa and elsewhere. This
bacterium, also known as the pneumo-coccus, is a cause of pneumonia andmeningitis, among other diseases.
Antibiotic Use Is Out of Control
For those who understand that anti-biotic delivery selects for resistance,
it is not surprising that the internationalcommunity currently faces a major pub-lic health crisis. Antibiotic use (and mis-use) has soared since the first commer-cial versions were introduced and nowincludes many nonmedicinal applica-tions. In 1954 two million pounds wereproduced in the U.S.; today the figureexceeds 50 million pounds.
Human treatment accounts for rough-ly half the antibiotics consumed everyyear in the U.S. Perhaps only half thatuse is appropriate, meant to cure bacte-rial infections and administered correct-ly—in ways that do not strongly en-courage resistance.
Notably, many physicians acquiesceto misguided patients who demand an-tibiotics to treat colds and other viralinfections that cannot be cured by thedrugs. Researchers at the Centers forDisease Control and Prevention haveestimated that some 50 million of the150 million outpatient prescriptions forantibiotics every year are unneeded. Ata seminar I conducted, more than 80percent of the physicians present admit-ted to having written antibiotic pre-scriptions on demand against their bet-ter judgment.
In the industrial world, most antibi-otics are available only by prescription,but this restriction does not ensureproper use. People often fail to finishthe full course of treatment. Patientsthen stockpile the leftover doses andmedicate themselves, or their family andfriends, in less than therapeutic amounts.In both circumstances, the improperdosing will fail to eliminate the diseaseagent completely and will, furthermore,
The Challenge of Antibiotic Resistance50 Scientific American March 1998
TOM
O N
AR
ASH
IMA
b
a
c
d
e
Copyright 1998 Scientific American, Inc.

HIGHLY RESISTANTPOPULATION
encourage growth of themost resistant strains, whichmay later produce hard-to-treat disorders.
In the developing world,antibiotic use is even lesscontrolled. Many of thesame drugs marketed in theindustrial nations are avail-able over the counter. Unfor-tunately, when resistance be-comes a clinical problem,those countries, which oftendo not have access to expen-sive drugs, may have no sub-stitutes available.
The same drugs prescribedfor human therapy are wide-ly exploited in animal hus-bandry and agriculture. Morethan 40 percent of the anti-biotics manufactured in the U.S. aregiven to animals. Some of that amountgoes to treating or preventing infection,but the lion’s share is mixed into feed topromote growth. In this last application,amounts too small to combat infectionare delivered for weeks or months at atime. No one is entirely sure how thedrugs support growth. Clearly, though,this long-term exposure to low doses isthe perfect formula for selecting increas-ing numbers of resistant bacteria in thetreated animals—which may then passthe microbes to caretakers and, morebroadly, to people who prepare andconsume undercooked meat.
In agriculture, antibiotics are appliedas aerosols to acres of fruit trees, forcontrolling or preventing bacterial in-fections. High concentrations may killall the bacteria on the trees at the timeof spraying, but lingering antibioticresidues can encourage the growth ofresistant bacteria that later colonize thefruit during processing and shipping.The aerosols also hit more than the tar-geted trees. They can be carried consid-erable distances to other trees and foodplants, where they are too dilute toeliminate full-blown infections but arestill capable of killing off sensitive bac-
teria and thus giving the edge to resis-tant versions. Here, again, resistant bac-teria can make their way into peoplethrough the food chain, finding a homein the intestinal tract after the produceis eaten.
The amount of resistant bacteria peo-ple acquire from food apparently is nottrivial. Denis E. Corpet of the NationalInstitute for Agricultural Research inToulouse, France, showed that when hu-man volunteers went on a diet consist-ing only of bacteria-free foods, the num-ber of resistant bacteria in their fecesdecreased 1,000-fold. This finding sug-gests that we deliver a supply of resistantstrains to our intestinal tract wheneverwe eat raw or undercooked items. Thesebacteria usually are not harmful, butthey could be if by chance a disease-causing type contaminated the food.
The extensive worldwide exploitationof antibiotics in medicine, animal careand agriculture constantly selects forstrains of bacteria that are resistant tothe drugs. Must all antibiotic use be halt-ed to stem the rise of intractable bacte-ria? Certainly not. But if the drugs areto retain their power over pathogens,they have to be used more responsibly.Society can accept some increase in the
fraction of resistant bacteria when adisease needs to be treated; the rise isunacceptable when antibiotic use is notessential.
Reversing Resistance
Anumber of corrective measures can be taken right now. As a start,
farmers should be helped to find inex-pensive alternatives for encouraging an-imal growth and protecting fruit trees.Improved hygiene, for instance, couldgo a long way to enhancing livestockdevelopment.
The public can wash raw fruit andvegetables thoroughly to clear off bothresistant bacteria and possible antibiot-ic residues. When they receive prescrip-tions for antibiotics, they should com-plete the full course of therapy (to en-sure that all the pathogenic bacteria die)and should not “save” any pills for lateruse. Consumers also should refrain fromdemanding antibiotics for colds andother viral infections and might considerseeking nonantibiotic therapies for mi-nor conditions, such as certain cases ofacne. They can continue to put antibi-otic ointments on small cuts, but theyshould think twice about routinely us-
Scientific American March 1998 51
ANTIBIOTIC STOPS
SUSCEPTIBLE BACTERIA IN VICINITY
RESISTANTPOPULATION
DEAD CELLSSUSCEPTIBLEPOPULATION
ANTIBIOTIC USE SELECTS—promotes the evolution and growth of—bacteria thatare insensitive to that drug. When bacteria are exposed to an antibiotic (a), bacterialcells that are susceptible to the drug will die (b), but those with some insensitivity maysurvive and grow (c) if the amount of drug delivered is too low to eliminate every lastcell. As treatment continues, some of the survivors are likely to acquire even strongerresistance (d)—either through a genetic mutation that generates a new resistance traitor through gene exchange with newly arriving bacteria. These resistant cells will thenevade the drug most successfully (e) and will come to predominate (f and g).
TOM
O N
AR
ASH
IMA
ba c d
f g
RESISTANT POPULATION of bacteria will disappear naturally only if susceptible bacteria livein the vicinity. After antibiotic therapy stops (a), resistant bacteria can persist for a while. If sus-ceptible bacteria are nearby, however, they may recolonize the individual (b). In the absence of thedrug, the susceptible bugs will have a slight survival advantage because they do not have to expendenergy maintaining resistance genes. After a time, then, they may outcompete the resistant mi-crobes (c and d). For this reason, protecting susceptible bacteria needs to be a public health priority.
Copyright 1998 Scientific American, Inc.

ing hand lotions and a proliferation ofother products now imbued with an-tibacterial agents. New laboratory find-ings indicate that certain of the bacte-ria-fighting chemicals being incorporat-ed into consumer products can selectfor bacteria resistant both to the an-tibacterial preparations and to antibiot-ic drugs [see box on page 48].
Physicians, for their part, can takesome immediate steps to minimize anyresistance ensuing from required uses ofantibiotics. When possible, they shouldtry to identify the causative pathogenbefore beginning therapy, so they canprescribe an antibiotic targeted specific-ally to that microbe instead of having tochoose a broad-spectrum product.Washing hands after seeing each patientis a major and obvious, but too oftenoverlooked, precaution.
To avoid spreading multidrug-resis-tant infections between hospitalized pa-tients, hospitals place the affected pa-tients in separate rooms, where they areseen by gloved and gowned healthworkers and visitors. This practiceshould continue.
Having new antibiotics could providemore options for treatment. In the 1980spharmaceutical manufacturers, thinkinginfectious diseases were essentially con-quered, cut back severely on searchingfor additional antibiotics. At the time, ifone drug failed, another in the arsenalwould usually work (at least in the in-dustrial nations, where supplies are
plentiful). Now that this happy state ofaffairs is coming to an end, researchersare searching for novel antibiotics again.Regrettably, though, few drugs are like-ly to pass soon all technical and regula-tory hurdles needed to reach the mar-ket. Furthermore, those that are closeto being ready are structurally similarto existing antibiotics; they could easilyencounter bacteria that already havedefenses against them.
With such concerns in mind, scien-tists are also working on strategies thatwill give new life to existing antibiotics.Many bacteria evade penicillin and itsrelatives by switching on an enzyme,penicillinase, that degrades those com-pounds. An antidote already on phar-macy shelves contains an inhibitor ofpenicillinase; it prevents the breakdownof penicillin and so frees the antibioticto work normally. In one of the strate-gies under study, my laboratory at TuftsUniversity is developing a compound tojam a microbial pump that ejects tetra-cycline from bacteria; with the pumpinactivated, tetracycline can penetratebacterial cells effectively.
Considering the Environmental Impact
As exciting as the pharmaceutical re-search is, overall reversal of the
bacterial resistance problem will re-quire public health officials, physicians,farmers and others to think about theeffects of antibiotics in new ways. Each
time an antibiotic is delivered, the frac-tion of resistant bacteria in the treatedindividual and, potentially, in others,increases. These resistant strains endurefor some time—often for weeks—afterthe drug is removed.
The main way resistant strains disap-pear is by squaring off with susceptibleversions that persist in—or enter—atreated person after antibiotic use hasstopped. In the absence of antibiotics,susceptible strains have a slight survivaladvantage, because the resistant bacte-ria have to divert some of their valuableenergy from reproduction to maintain-ing antibiotic-fighting traits. Ultimately,the susceptible microbes will win out, ifthey are available in the first place andare not hit by more of the drug beforethey can prevail.
Correcting a resistance problem, then,requires both improved management ofantibiotic use and restoration of the en-vironmental bacteria susceptible to thesedrugs. If all reservoirs of susceptible bac-teria were eliminated, resistant formswould face no competition for survivaland would persist indefinitely.
In the ideal world, public health offi-cials would know the extent of antibi-otic resistance in both the infectious andbenign bacteria in a community. Totreat a specific pathogen, physicianswould favor an antibiotic most likely toencounter little resistance from any bac-teria in the community. And they woulddeliver enough antibiotic to clear the in-
The Challenge of Antibiotic Resistance52 Scientific American March 1998
NASCENT BACTERIALPROTEIN
ANTIBIOTIC
ANTIBIOTIC-EFFLUX PUMP
PUMP BLOCKER
DRUG BLOCKSPROTEIN SYNTHESIS
BACTERIAL OUTERMEMBRANE
RIBOSOME
a b
TOM
O N
AR
ASH
IMA
ONE PHARMACEUTICAL STRATEGY for overcoming resis-tance capitalizes on the discovery that some bacteria defeat cer-tain antibiotics, such as tetracycline, by pumping out the drugs(a). To combat that ploy, investigators are devising compounds
that would jam the pumps (b), thereby freeing the antibiotics tofunction effectively. In the case of tetracycline, the antibioticworks by interfering with the ribosomes that manufacture bac-terial proteins.
Copyright 1998 Scientific American, Inc.

fection completely but would not pro-long therapy so much as to destroy allsusceptible bystanders in the body.
Prescribers would also take into ac-count the number of other individualsin the setting who are being treated withthe same antibiotic. If many patients ina hospital ward were being given a par-ticular antibiotic, this high density ofuse would strongly select for bacterialstrains unsubmissive to that drug andwould eliminate susceptible strains. Theecological effect on the ward would bebroader than if the total amount of theantibiotic were divided among just afew people. If physicians considered theeffects beyond their individual patients,they might decide to prescribe differentantibiotics for different patients, or indifferent wards, thereby minimizing theselective force for resistance to a singlemedication.
Put another way, prescribers and pub-lic health officials might envision an “an-tibiotic threshold”: a level of antibioticusage able to correct the infections with-in a hospital or community but still fall-ing below a threshold level that would
strongly encourage propagation of re-sistant strains or would eliminate largenumbers of competing, susceptible mi-crobes. Keeping treatment levels belowthe threshold would ensure that theoriginal microbial flora in a person or acommunity could be restored rapidly bysusceptible bacteria in the vicinity aftertreatment ceased.
The problem, of course, is that no oneyet knows how to determine where thatthreshold lies, and most hospitals andcommunities lack detailed data on thenature of their microbial populations.Yet with some dedicated work, research-ers should be able to obtain both kindsof information.
Control of antibiotic resistance on awider, international scale will require co-operation among countries around theglobe and concerted efforts to educatethe world’s populations about drug re-sistance and the impact of improper an-tibiotic use. As a step in this direction,various groups are now attempting totrack the emergence of resistant bacteri-al strains. For example, an internationalorganization, the Alliance for the Pru-
dent Use of Antibiotics (P.O. Box 1372,Boston, MA 02117), has been monitor-ing the worldwide emergence of suchstrains since 1981. The group shares in-formation with members in more than90 countries. It also produces education-al brochures for the public and forhealth professionals.
The time has come for global societyto accept bacteria as normal, generallybeneficial components of the world andnot try to eliminate them—except whenthey give rise to disease. Reversal of re-sistance requires a new awareness of thebroad consequences of antibiotic use—
a perspective that concerns itself notonly with curing bacterial disease at themoment but also with preserving micro-bial communities in the long run, so thatbacteria susceptible to antibiotics willalways be there to outcompete resistantstrains. Similar enlightenment shouldinfluence the use of drugs to combatparasites, fungi and viruses. Now thatconsumption of those medicines has be-gun to rise dramatically, troubling resis-tance to these other microorganismshas begun to climb as well.
The Challenge of Antibiotic Resistance Scientific American March 1998 53
The Author
STUART B. LEVY is professor of molecular biologyand microbiology, professor of medicine and director ofthe Center for Adaptation Genetics and Drug Resistanceat the Tufts University School of Medicine. He is also pres-ident of the Alliance for the Prudent Use of Antibiotics andpresident-elect of the American Society for Microbiology.
Further Reading
The Antibiotic Paradox: How Miracle Drugs Are Destroying theMiracle. S. B. Levy. Plenum Publishers, 1992.
Drug Resistance: The New Apocalypse. Special issue of Trends in Micro-biology, Vol. 2, No. 10, pages 341–425; October 1, 1994.
Antibiotic Resistance: Origins, Evolution, Selection and Spread.Edited by D. J. Chadwick and J. Goode. John Wiley & Sons, 1997.
MIC
K ST
EVEN
S ©
199
8 FR
OM
TH
E N
EW Y
ORK
ER C
OLL
ECTI
ON
, ALL
RIG
HTS
RES
ERV
ED
SA
Some Actions Physicians and Consumers Can Take to Limit Resistance
Physicians• Wash hands thoroughly between patient visits. • Do not accede to patients’ demands for unneeded antibiotics.• When possible, prescribe antibiotics that target only
a narrow range of bacteria.• Isolate hospital patients with multidrug-resistant infections.• Familiarize yourself with local data on antibiotic resistance.
Consumers• Do not demand antibiotics.• When given antibiotics, take them exactly as prescribed and com-
plete the full course of treatment; do not hoard pills for later use.• Wash fruits and vegetables thoroughly; avoid raw eggs
and undercooked meat, especially in ground form.• Use soaps and other products with antibacterial chemicals only
when protecting a sick person whose defenses are weakened.
The easy accessibility to antibiotics parodied in the cartoon is abig contributor to antibiotic resistance. This list suggests some
immediate steps that can help control the problem. —S.B.L.
Copyright 1998 Scientific American, Inc.