
Avian influenza: virology, diagnosis and surveillance
19
Author Proof 10.2217/FMB.13.81 © 2013 Future Medicine Ltd ISSN 1746-0913 Future Microbiol. (2013) 8(9), 1–19 part of 1 Avian influenza (AI) is an acute avian respira- tory disease caused by AI viruses (AIVs) that affect many species of domestic and wild birds and can also infect other animal species. In poultry, AI is characterized by marked varia- tion in morbidity and mortality. The notifiable form of AI (NAI) describes an outbreak of AI in poultry due to any H5 or H7 subtype of influenza A virus (IAV) or an infection by any AIV resulting in an intravenous pathogenicity index >1.2 or causing at least 75% mortality [1] . HPNAI is a ‘list A’ notifiable disease (BOX 1) of the World Organization for Animal Health (OIE), which describes serious transmissible diseases that can potentially spread very rapidly between countries and are of major significance for the international trade of animals and animal prod- ucts, and so have severe socioeconomic or public health costs [1] . LPNAI includes all IAVs of H5 and H7 subtype that are not HPNAI viruses. Low pathogenicity avian influenza (LPAI) refers to all infections caused by AIVs that are not NAI viruses and include H1-H4, H6, and H8-H16 LPAI [2, 201] . The HPAI viruses are restricted to subtypes H5 and H7, although not all H5 and H7 viruses cause HPAI. The risk from AI is generally low in most people, as AIVs do not usually infect humans. However, there have been several cases of conjunctivitis in humans related to LPAI. AIV has been transmitted to humans (e.g., H1N1 in 1976, 1986 and 1988; H3N2 in 1993; H7N7 in 1996; and H9N2 in 1998, 1999 and 2003) inducing mild, severe or fatal infections [3,4] . While it has been suggested that aerosolized droplets or direct contact with virus in poultry feces can lead to infections in humans [5] , poul- try-to-human transmission of IAVs is unlikely to cause pandemic influenza. This requires the emergence of viral subtypes with human-to- human transmissibility arising from mutations, genetic rearrangement of viral RNA segments or genetic reassortment between different strains of virus [6,7] in a permissive host [8] , with pigs being the probable ‘mixing vessel’ [9] . Several examples of human-adapted IAVs exist that have initiated a number of pandemics in the last century [10] . The emergence of the Asian- based HPAI H5N1 virus, in particular, high- lights the continuing public health concerns over human fatalities and its potential emergence as a future pandemic virus. This implicates AI as one of the most threatening trans-boundary diseases facing humans [11] , highlights the potential risk IAV poses to human health and economy [12–14] and strongly emphasizes the urgent requirement for continued high levels of awareness and sur- veillance programs to monitor for emerging AIVs [15] . Accordingly, the WHO has complemented its human surveillance network with a program Avian influenza: virology, diagnosis and surveillance Mohamed E El Zowalaty* 1,2,3 , Stephen A Bustin 1 , Mohamed I Husseiny 3,4 & Hossam M Ashour* 5,6 1 Postgraduate Medical Institute, Faculty of Health, Social Care & Education, Anglia Ruskin University, Chelmsford, Essex, UK 2 Faculty of Public Health & Tropical Medicine, Jazan University, Jazan, Saudi Arabia 3 Department of Microbiology & Immunology, Faculty of Pharmacy, Zagazig University, Zagazig, Egypt 4 Beckman Research Institute at City of Hope, Duarte, CA, USA 5 Department of Pharmacy Practice, Eugene Applebaum College of Pharmacy & Health Sciences, Wayne State University, Detroit, MI, USA 6 Department of Microbiology & Immunology, Faculty of Pharmacy, Cairo University, Cairo, Egypt *Authors for correspondence: [email protected] n [email protected] Avian influenza virus (AIV) is the causative agent of a zoonotic disease that affects populations worldwide with often devastating economic and health consequences. Most AIV subtypes cause little or no disease in waterfowl, but outbreaks in poultry can be associated with high mortality. Although transmission of AIV to humans occurs rarely and is strain dependent, the virus has the ability to mutate or reassort into a form that triggers a life-threatening infection. The constant emergence of new influenza strains makes it particularly challenging to predict the behavior, spread, virulence or potential for human-to-human transmission. Because it is difficult to anticipate which viral strain or what location will initiate the next pandemic, it is difficult to prepare for that event. However, rigorous implementation of biosecurity, vaccination and education programs can minimize the threat of AIV. Global surveillance programs help record and identify newly evolving and potentially pandemic strains harbored by the reservoir host. Keywords n avian influenza n diagnosis n real-time PCR n surveillance n vaccines n virus isolation n waterfowl Review Future Microbiology
Transcript of Avian influenza: virology, diagnosis and surveillance

Author Pro
of
10.2217/FMB.13.81 © 2013 Future Medicine Ltd ISSN 1746-0913Future Microbiol. (2013) 8(9), 1–19
part of
1
Avian influenza (AI) is an acute avian respira-tory disease caused by AI viruses (AIVs) that affect many species of domestic and wild birds and can also infect other animal species. In poultry, AI is characterized by marked varia-tion in morbidity and mortality. The notifiable form of AI (NAI) describes an outbreak of AI in poultry due to any H5 or H7 subtype of influenza A virus (IAV) or an infection by any AIV resulting in an intravenous pathogenicity index >1.2 or causing at least 75% mortality [1]. HPNAI is a ‘list A’ notifiable disease (Box 1) of the World Organization for Animal Health (OIE), which describes serious transmissible diseases that can potentially spread very rapidly between countries and are of major significance for the international trade of animals and animal prod-ucts, and so have severe socioeconomic or public health costs [1]. LPNAI includes all IAVs of H5 and H7 subtype that are not HPNAI viruses. Low pathogenicity avian influenza (LPAI) refers to all infections caused by AIVs that are not NAI viruses and include H1-H4, H6, and H8-H16 LPAI [2, 201].
The HPAI viruses are restricted to subtypes H5 and H7, although not all H5 and H7 viruses cause HPAI. The risk from AI is generally low in most people, as AIVs do not usually infect humans. However, there have been several cases of conjunctivitis in humans related to LPAI. AIV
has been transmitted to humans (e.g., H1N1 in 1976, 1986 and 1988; H3N2 in 1993; H7N7 in 1996; and H9N2 in 1998, 1999 and 2003) inducing mild, severe or fatal infections [3,4]. While it has been suggested that aerosolized droplets or direct contact with virus in poultry feces can lead to infections in humans [5], poul-try-to-human transmission of IAVs is unlikely to cause pandemic influenza. This requires the emergence of viral subtypes with human-to-human transmissibility arising from mutations, genetic rearrangement of viral RNA segments or genetic reassortment between different strains of virus [6,7] in a permissive host [8], with pigs being the probable ‘mixing vessel’ [9].
Several examples of human-adapted IAVs exist that have initiated a number of pandemics in the last century [10]. The emergence of the Asian-based HPAI H5N1 virus, in particular, high-lights the continuing public health concerns over human fatalities and its potential emergence as a future pandemic virus. This implicates AI as one of the most threatening trans-boundary diseases facing humans [11], highlights the potential risk IAV poses to human health and economy [12–14] and strongly emphasizes the urgent requirement for continued high levels of awareness and sur-veillance programs to monitor for emerging AIVs [15]. Accordingly, the WHO has complemented its human surveillance network with a program
Avian influenza: virology, diagnosis and surveillance
Mohamed E El Zowalaty*1,2,3, Stephen A Bustin1, Mohamed I Husseiny3,4 & Hossam M Ashour*5,6
1Postgraduate Medical Institute, Faculty of Health, Social Care & Education, Anglia Ruskin University, Chelmsford, Essex, UK 2Faculty of Public Health & Tropical Medicine, Jazan University, Jazan, Saudi Arabia 3Department of Microbiology & Immunology, Faculty of Pharmacy, Zagazig University, Zagazig, Egypt 4Beckman Research Institute at City of Hope, Duarte, CA, USA 5Department of Pharmacy Practice, Eugene Applebaum College of Pharmacy & Health Sciences, Wayne State University, Detroit, MI, USA 6Department of Microbiology & Immunology, Faculty of Pharmacy, Cairo University, Cairo, Egypt�*Authors for correspondence: [email protected] n [email protected]
Avian influenza virus (AIV) is the causative agent of a zoonotic disease that affects populations worldwide with often devastating economic and health consequences. Most AIV subtypes cause little or no disease in waterfowl, but outbreaks in poultry can be associated with high mortality. Although transmission of AIV to humans occurs rarely and is strain dependent, the virus has the ability to mutate or reassort into a form that triggers a life-threatening infection. The constant emergence of new influenza strains makes it particularly challenging to predict the behavior, spread, virulence or potential for human-to-human transmission. Because it is difficult to anticipate which viral strain or what location will initiate the next pandemic, it is difficult to prepare for that event. However, rigorous implementation of biosecurity, vaccination and education programs can minimize the threat of AIV. Global surveillance programs help record and identify newly evolving and potentially pandemic strains harbored by the reservoir host.
Keywords
n avian influenza n diagnosis n real-time PCR n surveillance n vaccines n virus isolation n waterfowl
Revie
wFu
ture
Mic
rob
iolo
gy

Author Pro
of
Future Microbiol. (2013) 8(9)2 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
focusing on the ecology and surveillance of influenza viruses in wild animals [16,17].
Human influenza pandemicsThe three worldwide influenza outbreaks (pan-demics) in the 20th century occurred in 1918, 1957 and 1968 [18]. Each pandemic caused significant social and economic upheaval. The rapid spread, combined with high morbidity and mortality, gave rise to intense levels of anxiety and fear among the public. The ‘Spanish flu’ (1918–1919) was caused by direct transmission of the H1N1 virus from birds [19] and is consid-ered to be the ‘mother of all pandemics’ [20]. It spread across the entire world within 3 months, infecting 50% of the world’s population and resulting in an estimated 30–50 million deaths [21]. The ‘Asian flu’ (1957–1958) was caused by genetic reassortment between human H1N1 and avian H2N2 influenza viruses. This pan-demic spread across the world in approximately 6 months and, together with a second wave of infections, affected approximately 40–50% of the world’s population, killing approximately 1 million people [22]. The ‘Hong-Kong f lu’ (1968–1969) pandemic was caused by a H3N2 virus, which resulted from reassortment of cir-culating human H2N2 and avian H3 virus in
China, spreading to Hong Kong and the rest of the world, and causing the deaths of a few million individuals [22].
In February 2009, a new swine-origin influ-enza A (H1N1) virus emerged in Mexico from multiple reassortment events involving a unique combination of gene segments from human, swine and avian type A viruses [23–27], result-ing in the first influenza pandemic of the 21st century [28,29]. By mid-April, it had reached the USA via human-to-human transmission, leading the WHO to raise its pandemic alert successively to phases 4 (27 April), 5 (29 April) and 6 (11 June) [24]. Although now in the post-pandemic phase, the H1N1 (2009) virus is one of the seasonal influenza viruses in global circulation and continues to be a major challenge to public health.
History of HPAIIn 1878, a contagious disease of poultry asso-ciated with high mortality was first described in Italy and named ‘fowl plague’. In 1955, the causative agent was identified as an IAV, based on the presence of A type-specific ribonucleo-protein. This resulted in the term fowl plague being replaced by the more suitable term HPAI [17, 30–32]. In 1961, a high proportion of deaths in common terns (Sterna hirundo) in South Africa was attributed to the HP A/H5N3 virus, which was the first demonstration of a HPAI virus in wild birds before the HP A/H5N1 [33]. The 1997 outbreak of respiratory disease in humans in Hong Kong caused by H5N1, which was previ-ously known to infect only avian species, raised serious concerns about the potential for another pandemic in humans [34,35]. The H5N1 virus seems to have emerged in southeast China dur-ing 1996 [36], where it reassorted with viruses circulating in other avian species and emerged as a new H5N1 virus in Hong Kong. After an initial major outbreak of HPAI in chickens and other birds, it was unexpectedly transmitted to humans [37], and in May 1997 a 3-year-old boy became the first human to die of a respira-tory illness related to an H5N1 virus infection [38]. An additional 17 cases were diagnosed in November and December of the same year [17]. A few years later, the virus spread to several Asian countries, infecting humans for the second time in February 2003 [39].
Since late 2003 until the present day, the world has witnessed the deadliest outbreak in the history of HPAI in birds. In addition, the transmission of A/H5N1 virus to humans is on the increase in Asia, southeast Asia, Africa and
Box 1. Notifiable avian influenza.
�n List A notifiable diseases of the World Organization for Animal Health are defined as transmissible diseases that have the potential for very serious and rapid spread, irrespective of national borders, are of serious socioeconomic or public health consequence and are of major importance in the international trade of animals and animal products.
�n Notifiable avian influenza (AI) is defined as an infection of poultry caused by any influenza A virus of the H5 or H7 subtypes or by any AI virus with an intravenous pathogenicity index in chickens of greater than 1.2 (or, as an alternative, at least 75% mortality). AI can be categorized into highly pathogenic notifiable avian influenza, including high-pathogenicity H5 and H7 subtypes, low-pathogenicity avian influenza (LPAI), which includes all H5 and H7 LPAI subtypes, and all other LPAIs, which are not notifiable to the World Organization for Animal Health, including H1–H4, H6 and H8–H16 LPAIs.
Box 2. Antigenic drift versus antigenic shift.
�n Antigenic drift is defined as the process whereby small changes or mutations accumulate in the virus, mainly in the surface glycoproteins (predominantly hemagglutinin [HA]), which happen continually over time. The new virus strains thus produced have different antigenic profiles and may not be recognized by antibodies against the older strains, thereby making the individual susceptible to infection with the new strains.
�n Antigenic shift is an abrupt, major change in the HA and/or neuraminidase (NA) proteins of the virus that occurs when surface HA and NA segments reassort between different viruses, resulting in the emergence of a new subtype. Alternatively, the new HA and NA combination may have emerged from an animal population that is so different from the same subtype in humans that most people do not have immunity to the new virus.

Author Pro
of
www.futuremedicine.com 3future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
the Middle East. Between 1997 and April 2013, HPAI A/H5N1 infection has been identified in 628 human cases, with 374 deaths confirmed in 15 countries, resulting in a fatality rate of 59.55%; the highest numbers of cases/deaths were reported in Indonesia, Egypt, Vietnam and China, respectively [202]. Although A/H5N1 originated in China, it is still unclear why the number of cases is not the highest in its originat-ing location. So far, there has been no evidence of sustained human-to-human transmission of AIV. However, if the virus mutates or rearranges deliberately or spontaneously into a form that is more easily transmissible between humans, it will have the potential to kill millions in a pandemic.
The concurrent A/H5N1 virus possesses three of the four properties necessary to cause a pandemic: it infects people, most people are immunologically naive and it is highly lethal. However, it lacks the capacity for sustained human-to-human transmission [18,40]. Although that capacity may require only a single genetic reassortment or mutation, up until now, most infected people have been infected through direct contact with infected poultry [41]. While there have been extensive efforts by the WHO to report all cases, the numbers might not reflect the real picture, especially in developing countries, since not all cases are being admitted to hospitals or reported by governments. In developed coun-tries, the strict implementation of biosecurity and preventive procedures in poultry farms helps guard against the spread of AIV. Annual surveil-lance programs among waterfowl have also been implemented in the USA and Europe.
In the spring of 2013, another ongoing out-break of novel avian A/H7N9 virus that origi-nated from multiple reassortment events has again emerged in China, where H7N9 has so far caused infection in 131 laboratory-confirmed human cases, including 36 deaths [42,43]. The recent A/H7N9 could potentially produce a human pandemic since the virus is more humanized in traits and could increase human-to-human transmission, if transmitted among poultry or pigs, raising public health concerns of a looming pandemic influenza in human [44,45].
In addition to AIV, other influenza viruses exist and can cause influenza epizootics among various animal species [5]. In some species, the disease mimics human influenza, while in others, there are no signs of disease. Since the demonstration of swine influenza (Hsw1N1) in 1930 and later in 1955, and with the identifica-tion of influenza viruses in horses and ducks, transmission to other animals has become more
evident and has attracted the attention of influ-enza researchers. Influenza A/H3N2 viruses dis-covered in horses were also found in pigs, cattle, chickens, dogs and other species throughout the world [46]. An outbreak of severe respiratory dis-ease in a pack of English foxhounds in the UK in September 2002 was caused by an equine A/H3N8 virus [47]. H3N8 and H3N2 canine influ-enza viruses have been reported in racing canine populations in the USA [48].
Aquatic birds have been revealed as the source of influenza viruses in sea mammals, such as seals (H4N5, H7N7) and whales (H13N2, H13N9, H1N3) [5]. In this context, it is worth noting the concerns expressed about the use of ferrets as a model. Ferrets are considered to be the best model for IAV because of their high suscepti-bility and the fact that IAV infection in ferrets closely resembles that in humans with respect to clinical signs, pathogenesis and immunity. Indeed, recent studies in ferrets have shown that IAV can acquire the capacity for airborne trans-mission between mammals without recombina-tion in an intermediate host, and therefore con-stitute a high risk for human pandemic influenza [49,50]. The ability to produce such an infection raises both biosecurity and biosafety concerns and could even lead to a human pandemic [51].
Genome & virology of AIVInfluenza viruses are members of the family
Orthomyxoviridae (orthos, Greek for straight; myxa, Greek for mucus) which belongs to group V (negative-polarity ssRNA) of the Bal-timore system of virus classification [52]. There are five genera: influenza virus A, B and C, Isavirus and Thogotovirus [53,54]. Each genus includes only one species of IAV, influenza B virus and influenza C virus. Influenza A and C viruses infect multiple species, while influenza B viruses almost exclusively infect humans [55]. IAVs include avian, swine, equine and canine influenza viruses, as well as human IAVs.
The structure of IAVs has been extensively studied and reported [56]. The genome of IAVs comprises eight negative-sense, viral ssRNA seg-ments that are numbered in order of decreasing length, as summarized in TaBle 1. The two main surface glycoproteins of influenza viruses as shown in Figure 1 are the hemagglutinin (HA) and neuraminidase (NA) proteins, which function in the attachment and release of the virion to and from cells. They are major antigenic determi-nants and so are major targets for the immune response to which neutralizing antibodies are made [57]. Theoretically, different combinations

Author Pro
of
Future Microbiol. (2013) 8(9)4 future science group
Review El Zowalaty, Bustin, Husseiny & AshourTa
ble
1. T
he
gen
om
ic s
egm
ents
of
infl
uen
za A
vir
us
and
th
eir
enco
ded
pro
tein
s an
d f
un
ctio
ns.
RN
A
seg
men
t n
um
ber
RN
A s
egm
ent
(mR
NA
† )
len
gth
in
nu
cleo
tid
es
Gen
e p
rod
uct
ion
d
escr
ipti
on
Enco
ded
p
rote
in(s
)‡
Loca
lizat
ion
an
d f
eatu
res
Nas
cen
t p
rote
in
len
gth
§ in
am
ino
ac
ids
Ap
pro
xim
ate
nu
mb
er o
f
mo
lecu
les
per
vir
ion
Pro
po
sed
pro
tein
fu
nct
ion
(s)
123
41 (2
320
)PB
1Po
lym
eras
e ba
sic
1, 8
7 kD
aV
irion
inte
rior,
infe
cted
cel
l nu
clei
757
30–6
0H
eter
otrim
eric
P c
ompl
ex a
ssoc
iate
d w
ith N
P an
d vi
rion
RNA
, RN
A t
rans
crip
tion
and
the
repl
icat
ion
com
pone
nt o
f RN
A p
olym
eras
e (p
olym
eras
e su
buni
t); i
nitia
tion
of
tran
scrip
tion,
RN
A t
rans
crip
tase
, RN
A e
long
atio
n an
d en
donu
clea
se a
ctiv
ity
PB1-
F287
Proa
popt
otic
act
ivit
y
223
41 (2
320
)PB
2Po
lym
eras
e ba
sic
2, 9
6 kD
aV
irion
inte
rior,
infe
cted
cel
l nu
clei
759
30–6
0Po
lym
eras
e su
buni
t; R
NA
tra
nscr
ipta
se, h
ost
cell
mRN
A c
ap
reco
gniti
on a
nd v
irule
nce
322
33 (2
211)
PAPo
lym
eras
e ac
idic
, 85
.5 k
Da
Viri
on in
terio
r, in
fect
ed c
ell
nucl
ei71
630
–60
Poly
mer
ase
subu
nit;
RN
A t
rans
crip
tase
and
pro
teas
e
417
78 (1
757)
HA
Hem
aggl
utin
in,
220
kDa
hom
otrim
er
Glo
bula
r he
ad b
ears
an
tigen
ic s
ites
and
rece
ptor
bi
ndin
g si
te; s
tem
; tr
ansm
embr
ane
span
; cy
topl
asm
ic t
ail
550
500
Surf
ace
glyc
opro
tein
, viru
s bi
ndin
g to
sia
lic a
cid-
cont
aini
ng
rece
ptor
s on
hos
t ce
ll; p
enet
ratio
n of
viru
s ge
nom
e in
to
host
cel
l cyt
opla
sm b
y fu
sion
of
viru
s an
d ho
st c
ell
mem
bran
es (a
ttac
hmen
t to
cel
l mem
bran
es a
nd r
ecep
tor
bind
ing
) and
maj
or a
ntig
enic
det
erm
inan
t
515
65 (1
540
)N
PN
ucle
opro
tein
, 55
kD
aV
irion
inte
rior,
asso
ciat
ed
with
P c
ompl
ex a
nd v
iral R
NA
498
100
0En
casi
date
s RN
A; R
NA
syn
thes
is a
nd R
NA
nuc
lear
impo
rt
regu
latio
n; in
tera
cts
with
RN
As
and
poly
mer
ase
prot
eins
as
a m
ajor
com
pone
nt o
f th
e nu
cleo
caps
id; r
ole
in v
RNA
re
plic
atio
n; r
ole
in v
irus
mat
urat
ion
and
pack
agin
g
614
13 (1
392)
NA
Neu
ram
inid
ase,
24
0 kD
a ho
mot
etra
mer
Viri
on e
nvel
ope,
infe
cted
cel
l su
rfac
e, c
ytop
lasm
ic t
ail;
tran
smem
bran
e sp
an;
extr
acel
lula
r st
alk;
glo
bula
r he
ad b
ears
ant
igen
ic s
ites
and
enzy
me
activ
e si
te
454
100
Surf
ace
glyc
opro
tein
; ant
igen
ic d
eter
min
ant,
sia
lidas
e (n
eura
min
idas
e)-c
atal
yzin
g cl
eava
ge o
f te
rmin
al s
ialic
aci
d re
sidu
es f
rom
gly
coco
njug
ates
, the
reby
dig
estin
g m
ucin
to
enab
le t
he v
irus
to r
each
its
targ
et e
pith
eliu
m a
nd
faci
litat
ing
rele
ase
of in
fect
ious
pro
geny
viru
s
† Ded
uced
fro
m R
NA
seq
uenc
e, e
xclu
ding
pol
y-A
tra
ct. T
otal
RN
A n
ucle
otid
e se
quen
ce le
ngth
is 1
3,58
8.
‡ Det
erm
ined
by
bioc
hem
ical
and
gen
etic
app
roac
hes.
§D
eter
min
ed b
y nu
cleo
tide
sequ
ence
ana
lysi
s an
d pr
otei
n se
quen
cing
.P
com
plex
: Pol
ymer
ase
prot
ein
com
plex
; RN
P: R
ibon
ucle
opro
tein
; vRN
P: V
iral r
ibon
ucle
opro
tein
. D
ata
take
n fr
om [1
94].

Author Pro
of
www.futuremedicine.com 5future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
Tab
le 1
. Th
e g
eno
mic
seg
men
ts o
f in
flu
enza
A v
iru
s an
d t
hei
r en
cod
ed p
rote
ins
and
fu
nct
ion
s (c
on
t.).
RN
A
seg
men
t n
um
ber
RN
A s
egm
ent
(mR
NA
† )
len
gth
in
nu
cleo
tid
es
Gen
e p
rod
uct
ion
d
escr
ipti
on
Enco
ded
p
rote
in(s
)‡
Loca
lizat
ion
an
d f
eatu
res
Nas
cen
t p
rote
in
len
gth
§ in
am
ino
ac
ids
Ap
pro
xim
ate
nu
mb
er o
f
mo
lecu
les
per
vir
ion
Pro
po
sed
pro
tein
fu
nct
ion
(s)
710
27 (1
005
)M
1M
1, 2
8 kD
aBe
neat
h lip
id b
ilaye
r of
viri
on
enve
lope
; ass
ocia
tes
with
vR
NPs
in m
atur
e vi
rion
to
form
nuc
leoc
apsi
d
252
300
0C
entr
al r
ole
in r
eplic
atio
n an
d vi
rus
asse
mbl
y, m
odul
atin
g nu
clea
r tr
ansp
ort
of v
RNP;
ear
ly in
fect
ion:
bou
nd t
o vR
NP
prio
r to
RN
P tr
ansp
ort
to n
ucle
us; l
ate
infe
ctio
n: b
inds
RN
P,
sign
alin
g RN
P tr
ansp
ort
from
nuc
leus
to
cell
surf
ace,
m
edia
tes
asso
ciat
ion
of R
NP
with
hem
aggl
utin
in a
nd
neur
amin
idas
e at
the
cel
l mem
bran
e, p
rom
otin
g vi
rion
form
atio
n an
d bu
ddin
g
M2
M2,
15
kDa
hom
otet
ram
erV
irion
env
elop
e, in
fect
ed c
ell
surf
ace
(abu
ndan
t);
extr
acel
lula
r re
gion
; tr
ansm
embr
ane
span
; cy
topl
asm
ic t
ail;
tetr
amer
s fo
rm c
atio
n-se
lect
ive
chan
nel
9730
00
Mem
bran
e ca
tion
chan
nel a
ctiv
ity;
viru
s un
coat
ing
and
asse
mbl
y; in
fect
ed c
ell:
spec
ifica
lly r
aise
s pH
of
Gol
gi t
o pr
otec
t pH
-sen
sitiv
e he
mag
glut
inin
; viri
on: m
ay p
erm
it ac
idifi
catio
n of
viru
s in
terio
r du
ring
pass
age
thro
ugh
endo
som
al p
athw
ay in
ord
er t
o di
ssoc
iate
vRN
P fr
om M
1
889
0 (8
68)
NS1
NS1
, 25
kDa
dim
erIn
fect
ed c
ell n
ucle
i23
0M
ultif
unct
iona
l pro
tein
and
vira
l int
erfe
ron
anta
goni
st
prot
ein;
reg
ulat
ion
of h
ost
gene
exp
ress
ion;
bin
ds R
NA
, th
ereb
y in
hibi
ting
host
mRN
A t
rans
latio
n, r
egul
atin
g vi
ral
pre-
mRN
A s
plic
ing
and
tran
slat
ion
and
vira
l pol
ymer
ase
activ
ity,
and
dow
nreg
ulat
ing
dsRN
A-in
duce
d an
tivira
l re
spon
ses
NEP
/NS2
NS2
, 14
kDa
Ass
ocia
ted
with
cor
e co
mpo
nent
s of
viri
on;
cyto
plas
m o
f in
fect
ed c
ells
121
Med
iate
s nu
clea
r ex
port
of
vRN
Ps
† Ded
uced
fro
m R
NA
seq
uenc
e, e
xclu
ding
pol
y-A
tra
ct. T
otal
RN
A n
ucle
otid
e se
quen
ce le
ngth
is 1
3,58
8.
‡ Det
erm
ined
by
bioc
hem
ical
and
gen
etic
app
roac
hes.
§D
eter
min
ed b
y nu
cleo
tide
sequ
ence
ana
lysi
s an
d pr
otei
n se
quen
cing
.P
com
plex
: Pol
ymer
ase
prot
ein
com
plex
; RN
P: R
ibon
ucle
opro
tein
; vRN
P: V
iral r
ibon
ucle
opro
tein
. D
ata
take
n fr
om [1
94].

Author Pro
of
Future Microbiol. (2013) 8(9)6 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
from the 17 HA and ten NA subtypes [58,59] can be found, and each subtype may contain several subtypes. Mutations can introduce additional variability, and so the number of AIV strains is indefinite.
In 1972, the WHO recommended a new sys-tem for influenza nomenclature and classifica-tion of influenza viruses into genetically distinct subtypes based on their NA and HA antigens [60,61]. The nomenclature consists of two parts: a strain designation and a description of the NA and HA antigens [60,62]. To date, only three HA (H1, H2 and H3) and two NA (N1 and N2) sub-types have caused human epidemics, as defined by sustained and widespread person-to-person transmission [8]. Nevertheless, the recent discov-ery of the highly divergent IAV subtype H17N10 in bats from Guatemala in South America rein-forces the importance of surveillance for moni-toring the evolution of influenza viruses among different animal populations. Thus far, this new
distinct H17N10 virus is the only subtype that is not found in an avian species [58,59].
Epidemiology of AI The evolutionary success of IAV is a prototypic example of the ability of microbes to adapt to their many hosts. Influenza is fundamentally a recurring background disease that re-emerges slightly differently each year due to the con-tinuously evolving nature of their surface gly-coproteins, referred to as antigenic drift [63]. At unpredictable time periods, influenza presents a newly emerging disease caused by viruses with completely different surface antigens, termed antigenic shift (Box 2), infecting humans with little or no immunity against these strains [57]. This antigenic variability of AIVs is due to their highly error-prone replication process [64] that, together with viral genome assortment, allows influenza viruses to adapt to their host, thus acquiring a pandemic potential [65].
Hemagglutinin
Neuraminidase
M2 ion channel
RNP
Figure 1. Molecular structure representation of influenza A virus showing two surface glycoproteins (hemagglutinin and neuraminidase), the major antigenic determinants of the virus. The hemagglutinin protein is responsible for binding to sialic acid receptors on host cells. Human influenza A viruses preferentially bind to sialic acids in an a2,6 conformation, while those from avian species bind mostly to sialic acids in an a2,3 conformation. RNP: Ribonucleoprotein. Image was reproduced from the Centers for Diseases Control and Prevention (CDC), Atlanta, Georgia, USA [206] with permission.

Author Pro
of
www.futuremedicine.com 7future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
The ecology and epidemiology of AI have changed substantially in the last two decades [66]. AI infections due to LP A/H9N2 subtype have become widespread in Asia, whereas the HP A/H5N1 subtype has been the causative agent of widespread infections in poultry across other areas of the world, resulting in a modified eco-epidemiology and zoonotic potential [67].
As shown in Figure 2, the primary difference between LPAI and HPAI virus is local versus systemic replication, respectively. One of the key determinants of virulence is the ability of the host to proteolytically cleave the HA precursor HA0 into HA1 and HA2 subunits, an essen-tial requirement for binding to the cell surface receptors and fusion of the viral envelope with the endosomal membrane. An analysis of HA subtypes that circulate in aquatic birds, as well as HAs representative of the subtypes that have infected the human population, indicates that the cleavage efficiency can vary significantly for different HA subtypes and some display strin-gent selectivity for specific proteases [68]. The HA of mammalian viruses contains only a sin-gle arginine and, rarely, a single lysine, at the cleavage site and is cleaved extracellularly, limit-ing their spread in mammalian hosts to tissues that express the appropriate proteases. Similarly,
LPAI viruses have an HA cleavage site with one basic arginine or lysine residue that is cleaved only by proteases with monobasic specificity. As a result, LPAI infection in birds is restricted to the digestive or respiratory tracts and results in milder illness or no disease at all. By contrast, HPAI viruses are invariably HA subtypes H5 or H7 with a polybasic cleavage site, introduced either as a result of insertion or substitution [69–71]. This polybasic cleavage site is susceptible to the protease furin, which is ubiquitous in cells [72]. The factors that cause mutation from LPAI to HPAI, which occurs only in birds, are not known, but it seems that the wider the circula-tion of LPAI in poultry, the higher the chance that mutation into HPAI will occur [73]. It is important to remember, however, that acquisi-tion of a polybasic HA cleavage site is the only necessary step for the evolution of LPAI strains into HPAI viruses, since not all H5 or H7 sub-types are hypervirulent. There are additional virulence determinants within the HA itself [74,75] and in other viral proteins, suggesting that virulence is under polygenic control [73,76,77].
Persistence of AIV in the environmentLPAI viruses are ubiquitous [16] and approxi-mately 90 species from some 12 of the 50 orders
Avian strains isolated from human H5N1 (1997 HK)
Avirulent avian isolate H5
Cleavage site
–C
–C–C
N–
N–N–
LPAI: proteases localized inrespiratory and intestinal organs
HPAI: ubiquitous proteases
GRETR
KXR
RKRKKR
KKRKKR
RERRRKKR
RSSR
KRRRR
RRKKR
G
G
G
G
G
G
G
Avirulent avian isolate H7
Virulent avian isolate H7
Virulent avian isolate H5
Avian strains isolated from human H9N2 (1999 HK)
Avian strains isolated from human H7N7 (2003 NL)
Avian strains isolated from human H5N1 (2004 Asia)
S–S
TMHA2HA1
HA0 TM
Figure 2. Schematic representation of the protease cleavage site in influenza A viruses hemagglutinin. HA0 is cleaved into disulfide linked subunits HA1 and HA2 at a specific cleavage site shown in red (single letter amino acid code is used to identify the amino acid sequence at the hemagglutinin cleavage site). The hemagglutinins of LPAI viruses are cleaved by proteases that are localized in respiratory and intestinal organs, resulting in mild localized infections, whereas the hemagglutinins of HAI viruses have multiple basic amino acids, which are cleaved by ubiquitous proteases in a wide range of organs, resulting in lethal systemic infection. Most human isolates of avian strains also possess polybasic cleavage sites. The TM domain is shown in orange. HK: Hong Kong; HPAI: High-pathogenicity avian influenza; LPAI: Low-pathogenicity avian influenza; NL: The Netherlands; TM: Transmembrane.

Author Pro
of
Future Microbiol. (2013) 8(9)8 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
of birds carry all strains of influenza, with birds inhabiting wetland and aquatic environments showing the highest rates of influenza infection [78]. Mixed infections with different influenza subtypes among waterfowl are also common [12,13,79]. Carriers are mainly of the orders Anseri-formes (especially the families Anatidae [ducks, geese, and swans], Charadriiformes [terns and waders] and Procellariiformes [shorebirds, gulls and seabirds]) and thus act as a reservoir for the virus [80]. The migratory nature of many of these species and the persistence of influenza in these populations facilitates the dissemination of influenza viruses worldwide [81]. Influenza viruses infect different species and have become very successful parasites in their avian hosts, causing mostly silent or asymptomatic infections while creating the opportunity to infect other immunologically naive hosts [5].
Interspecies barriers and the host species speci-ficity mechanisms, such as receptor preference and host factors interacting with HA, NA, viral polymerase and other internal genes, are impor-tant molecular constraints and determinants for their transmissibility of AIVs among different species [82,83]. IAV particles bind their target cells through interaction between their HA molecules and the sialic acid-containing cell-surface recep-tors on the host cells. Human influenza viruses bind preferentially to N-acetylneuraminic acid (sialic acid), which is attached to a galactose molecule by an a2,6 linkage (SAa2,6Gal), while AIVs mostly bind to silalic acid with an a2,3 linkage [84]. In human tracheal epithelial cells, a2,6 linkages predominate, while a2,3-linkages are more common in duck gut epi-thelial cells [83]. Recently, it was indicated that epithelial cells of the human lower respiratory tract contain both SAa2,3Gal and SAa2,6Gal but with different distributions [85]. In humans, a2,3 linkages are also present in respiratory epi-thelial cells, but their presence is less abundant than a2,6 linkages [86]. This explains the low infectivity but high pathogenicity of some AI strains in mammalian species [56]. AIVs do not generally replicate well in humans and vice versa [87,88], so it is possible that reassortment took place in an intermediate host. Pig populations have been proposed as a potential mixing vessel where reassortment takes place, since both avian and human strains can infect and replicate in pigs [89]. This is attributed to the fact that tra-cheal cells of pigs, where influenza replication occurs, contain a2,3-linked sialic acid receptors preferred by avian viruses, as well as those with the a2,6-linkage favored by human strains [89].
The mechanisms by which influenza viruses pass from one bird to another and cause infec-tion are not fully understood, but may be due to combinations of factors that include strain of virus, species of bird and environmental factors. In wild ducks, for example, influenza viruses rep-licate preferentially in the cells lining the intesti-nal tract and are excreted in high concentrations in the feces. Contamination of water supplies by infective feces and fomites that contain concen-trations as high as 107 infectious particles/g [5] is one obvious route of infection [5,90]. This has led to the assessment of ducks being the ‘Trojan horses’ of H5N1 in their surreptitious spread of viruses because they do not show symptoms after HP H5N1 infection [91]. Influenza viruses have coevolved with ducks over a very long period of time, allowing the establishment of equilibria between hosts and viruses so that neither suffers a significant loss of biological fitness. Hence, it is important to determine whether antigenic diver-sity is driven naturally in ducks or whether it is it the consequence of vaccine usage. Furthermore, it will be necessary to determine the genomic characteristics of ducks that are associated with natural resistance in some species and ascertain what dose of vaccine antigen is required to pre-vent transmissible levels of virus excretion by ducks of different species [91].
Clearly, the natural reservoir of IAVs could be the source of the next human influenza pan-demic [92] and so the routine surveillance and early detection of these viruses [93,94], their hosts and their migratory patterns [95], as well as the study of the impact of environmental and social factors on their interactions [97], are key to the control, management and eradication of the disease [97]. One consequence of this has been the formulation in the USA of an interagency strategic plan by a group of federal and state resource, as well as science agencies, to conduct surveillance in wild birds in order to determine the possible pathways of entry [98].
In addition to carrying mixed populations of AIVs, waterfowl can host additional viruses, especially the avian paramyxoviruses (APMVs) [99,100]. Several studies have demonstrated the circulation of influenza virus with APMV-1 (also known as Newcastle disease virus [NDV]), APMV-2, APMV-4 and APMV-6 [101–105]. The coexistence of NDV with AIV in field samples might present a diagnostic problem when it is desired to isolate and characterize only AIVs for surveillance and epidemiological purposes. The overwhelming growth of NDV may inhibit AIV growth, which in turn will decrease the chance

Author Pro
of
www.futuremedicine.com 9future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
of detection of AI subtypes. In several AIV surveillance studies, if a sample is found to be positive for NDV, it is not processed for AIV detection; only if a sample is found to be negative for NDV it is screened for AIV [106]. In a recent report, it was found that treatment of the sample with NDV polyclonal antiserum facilitates the isolation of AI from samples containing both AIVs and NDV [102].
Diagnosis of AI An effective strategy for understanding the ecology and epidemiology of the virus, and thus controlling the spread of influenza viruses, depends on the availability of reliable laboratory techniques permitting accurate and sensitive detection of AIVs in waterfowl [107,108]. Clinical diagnosis of AIV in birds is performed by the isolation and characterization of the virus, which varies with species and type of infection [109] and can be either presumptive or definitive. Clinical symptoms can be a valuable tool for presump-tive diagnosis of HPAI, whereas LPAI infection is asymptomatic [110]. Definitive diagnosis of AIV depends on specific laboratory methods, including the indirect evidence of infection by serological methods, which detect anti-influenza antibodies, and direct detection methods for live virus, viral antigen or viral nucleic acid [111].
Specimen collectionClinical specimens for AIV diagnosis in birds can be obtained from either live or dead birds. Wild birds in surveillance programs of migrating waterfowl are usually trapped using night light-ing, rocket netting and hunter harvesting tech-niques [203,204]. Samples from live birds should include both tracheal and cloacal swabs, since it has been shown that the analysis of both oro-pharyngeal and cloacal swabs provides an accu-rate snapshot of AIV status in birds [79,112–114]. If this is not possible, the collection of fresh feces may also serve as an alternative [115].
Samples should be placed in an isotonic phos-phate-buffered saline or viral transfer medium consisting of brain–heart infusion medium con-taining several antibiotics to eliminate any bacte-ria that may interfere with subsequent diagnostic procedures [116]. Although diagnostic samples can be stored temporarily at 40°C, it is recom-mended that all samples be kept at -800°C until tested, especially if prolonged storage is antici-pated [117]. In addition, field samples should be maintained under strict cold chain conditions from the moment of acquisition and should not be subjected to frequent freeze–thaw cycles, as
this results in significantly decreased virus titers [79]. In addition, technical details such as the use of dry or wet swabs, the pH of viral transfer medium and the time taken to transport sam-ples to the testing laboratory play a crucial role in the successful isolation of AIVs from field samples [114].
Serological methodsSerological methods for the diagnosis of AI in birds play an important role in monitoring the disease in populations and can provide an accurate method for the detection of influenza infection [118]. Serological diagnosis is important in case of LPAI to ensure freedom of infection for commercial purposes. Conversely, in cases of HPAI, serological methods are of little value since birds die before producing antibodies [111]. Serological methods are thus useful epidemio-logically for strain surveillance, but cannot be used for rapid diagnosis, which would allow therapeutic intervention [119]. Common serologic tests for AIV include hemagglutination inhibi-tion (HI), NA inhibition, agar gel precipitation (also known as agar gel immunodiffusion), virus neutralization, complement fixation (CF), enzyme immunoassay and indirect immunofluo-rescence [120,121]. These tests are based on the presence of influenza-specific antibodies that first appear approximately 2 weeks after initial infection and peak at 4–7 weeks after initial infection [121]. HI and NA inhibition assays are labor-intensive and time-consuming and require several controls for standardization. However, they are inexpensive, use readily available rea-gents and display high specificity in identifying strains [122]. HI is more specific in differentiating between HA subtypes [123]. The agar gel immu-nodiffusion test detects IgM and some IgG and is type-specific [124]. Although CF tests have been used for the identification of influenza iso-lates [119], the Canadian Public Health Labora-tories stopped offering this test in 2009 because influenza CF serology does not provide a reliable indicator of immunity or response to vaccination and is not recommended for the diagnosis of acute influenza infection [205].
Virus isolationInfluenza virus was first isolated in 1933, by inoculation of specimens into the amniotic cav-ity of 10–12-day-old embryonating chicken eggs (ECEs) [125], where permissive infection occurs in the cells lining the amniotic and allantoic cavities [119]. This method, using either spe-cific pathogen-free chicken eggs or specific

Author Pro
of
Future Microbiol. (2013) 8(9)10 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
antibody-negative eggs [126], continues to be the gold standard technique for AIV diagnosis and remains the most sensitive method for generat-ing very high titers of all but one AIV [120]. The exception is the recently discovered bat virus A/H17N10; to date, all attempts to propagate this virus in cell cultures or chicken embryos have failed [59]. Although commercial non-specific pathogen-free eggs have been used for AIV propagation and isolation, their vaccination history should be carefully checked to confirm the absence of other pathogens that might affect AIV isolation [13].
Allantoic fluids negative for virus can be passaged into ECEs for up to three passages and retested for HA before being recorded as negative. However, AIV isolation in ECEs requires a readily available continuous supply of fertilized chicken eggs and special incuba-tors [127]. It can take days to weeks to achieve high titers, the method is labor- and resource-intensive and there is a mandatory requirement of a high level of biosecurity facilities (generally biosafety level 3) if HPAI is suspected. Hence, it is not widely used for the routine diagnosis of influenza infection. On the other hand, egg isolation provides high quantities of live infec-tious virus and reference laboratories therefore utilize this culture system to ensure high sensi-tivity and for biological characterization, full-length sequence analysis and antiviral resistance studies [111,128]. This method also enables the production of virus stocks for epidemiological monitoring and vaccine updating, which is a critical requirement for the diagnosis of AI in the index cases.
The technique of conventional culture of influenza viruses in a cell culture was introduced in 1940s [121] and provides a useful method for the primary isolation of some human or swine influenza isolates that do not grow well in ECEs [118,129]. Since viral culture amplifies the inocu-lum, it is more sensitive than direct methods of detection [13]. Cell cultures can be monitored for the development of cytopathic effects, the manifestation of hemadsorption after the addi-tion of erythrocytes or for the presence of influ-enza antigens [121]. Various mammalian and bird cell lines have been used to isolate influ-enza viruses. The most commonly used cells are: primary rhesus monkey kidney and rhe-sus monkey kidney (LLC MK2) cells, African green monkey kidney cells, mink lung epithelial cell line (Mv1Lu), buffalo green monkey kid-ney, Madin–Darby canine kidney, green mon-key continuous cell line (Vero), human lung
embryonating cells (MRC-5), CACO-2 cell lines, CCL-141 (duck embryo) cells, CCL-169 (goose embryonic kidney) cells, duck embryo fibroblast cells and chicken embryo fibroblast cells [130–135].
Alternatively, since viruses are released slowly from the cell surface of virus-infected cells, hemadsorption results in erythrocytes adher-ing directly to these infected cells, which can be observed microscopically [119]. In addition to ECEs, Madin–Darby canine kidney cells are now considered a valuable system for the isola-tion of influenza viruses. However, since AIVs have different host and in vitro growth proper-ties depending on the strain [136,137] and not all host cells are universally permissive to all AIV subtypes, virus isolation is effective only when the cell culture is sensitive to the inoculated virus [138]. In addition, this method requires the rapid transport of specimens to the laboratory, since delays may lead to inactivation of the virus and hence failure to isolate any infectious agent [139].
Although conventional cell culture takes up to 2 weeks to generate results, it is very sensi-tive. Cytopathic effects such as intracytoplasmic basophilic inclusion bodies are observed. The presence of influenza virus can be ascertained using either hemadsorption with guinea pig red blood cells [108] or immunofluorescence on cul-tured cells. Immunofluorescence has the twin advantages of higher sensitivity in the detection of positive cultures and can also be used to type the isolated virus.
Another useful technique for the culture of AIVs is the rapid shell vial culture, which uses single or mixed cell lines using monolayers of two different cell types in a single vial [121]. This technique has the advantage of enhancing sensitivity and shortening the time to detection through enhancing the viral infectivity of the cells by centrifugation (time to diagnosis: 24 h vs 13 days postinoculation) [140,141]. Sensitivity is equivalent to that of conventional tube cul-tures and greater than that of direct fluorescent-antibody tests [142].
Molecular methods Molecular methods, also known as nucleic acid tests, detect viral nucleic acid (i.e., RNA) and promise to shorten the turnaround time for the laboratory diagnosis of AIV. There is a range of different types of molecular diagnostic tests. Until recently, the most commonly used was reverse transcription PCR (RT-PCR), where purified RNA of the virus, isolated from chicken eggs, cell cultures or from clinical specimens, is

Author Pro
of
www.futuremedicine.com 11future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
reverse transcribed into cDNA, which is then exponentially amplified using AIV-specific oli-gonucleotide primers [143–148]. Conventional RT-PCR is an end point assay, where the PCR product is analyzed on agarose gel after eth-idium bromide staining to separate the PCR product according to molecular weight, which allows presumptive identification [128,146,149]. Its main disadvantage is the ease with which the assay can be contaminated and the tedi-ous amount of work involved in running and visualizing gels.
Other nucleic acid test methods include the use of RT-PCR with detection by ELISA [150], nucleic acid sequence-based amplification [151] and H5 RT-loop-mediated isothermal amplifica-tion [152]. However, none of these can compete with quantitative real-time PCR (RT-qPCR), which is a homogeneous assay requiring minimal hands-on time and no post-PCR processing [153]. RT-qPCR typically uses a fluorescently labeled probe to detect the increase in PCR product while the test is being performed and the results are reported in real-time. All these methods have the potential to provide rapid and sensitive diag-nostic results.
RNA is most commonly extracted from AIVs using phenol-guanidinium thiocyanate [154] or one of the recently developed commercially avail-able kits that depend on the adsorption of RNA to silica gel-based columns. These methods for the detection of influenza are highly sensitive, specific and versatile [155], with the column-based methods having the advantage in terms of the reliable generation of intact RNA [156]. Once the viral RNA is extracted, it can be used not only to identify the isolate as AIV, but also to fur-ther determine the subtype and even the strain by sequence ana lysis utilizing an array of several influenza-specific primers. The viral genotype can be determined by sequencing some or all of the AIV genes, although some level of virus amplification in ECEs or cell culture is required for full-length sequence ana lysis [121]. Molecular methods are rapid, of acceptable sensitivity, and provide results within a relatively short time for targeted treatment and limitation of the spread of infection. This is crucial in situations in which rapid diagnosis is necessary, such as in epidemics and in patients with specific medical conditions [120,157].
There are several concerns with molecular diagnostic methods. Foremost is the techni-cal problem associated with the viral sequence that gives rise to both genetic drift and shift. The exquisite specificity of PCR can suddenly
become a liability if the sequence change or reassortment includes primer binding sites and the assay no longer amplifies the altered target sequences. Consequently, nucleic acid-based testing requires routine updating of the primers [13]. Another is the potential for obtaining false-negative results that may occur due to the pres-ence of inhibitors (which are concentrated along with pathogens during sample processing), low virus titers, degradation of target RNA before amplification and errors in setting up a reaction [158,159]. The problem of RNA quality, in par-ticular, is a critical issue, as these tests require RNA samples to be of good quality and the use of degraded RNA or inefficient PCR reac-tions can make these methods unreliable and may yield inaccurate results [13,107]. Hence, it is important to follow a rigid quality assessment program and, taking the example of RT-qPCR, there is a requirement to report the protocols accurately and comprehensively using the mini-mum information for publication of quantitative real-time PCR experiments (MIQE) guidelines [160]. Even then, the conversion of mRNA to cDNA is highly variable, and RT-qPCR results can vary considerably with the choice of reverse transcriptase.
mRNA molecules are not linear molecules, but instead form secondary structures through extensive intrastrand base pairing. This results in numerous stem-loop structures consisting of sin-gle-stranded loops and double-stranded hairpin structures of varying length. The efficiency of the RT step depends heavily on the primers used for cDNA synthesis not targeting the hairpin structures, since the intermolecular (i.e., primer to mRNA) hybridization kinetics are infavour-able compared with intramolecular (i.e., mRNA to itself) hybridization. Hence, it is important to choose suitable RT primers that target the loops, rather than the stems. Similarly, it is important to ensure that the amplicon itself is free from secondary structures at the PCR primer binding sites, as extensive secondary structures there can give rise to significantly different results. It must be noted that assays only determine total patho-gen number and do not provide information as to whether a pathogen has the ability to establish an infection or not. Hence, a positive result may not necessarily pose a public health threat, and so there is a requirement for additional assays that can determine viability.
None of the diagnostic tests discussed so far are easily carried out in the field, and none can provide virtually instant results. Rapid point-of-care diagnosis is critical for the control and

Author Pro
of
Future Microbiol. (2013) 8(9)12 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
management of influenza infection in humans, as it enables the fast administration of appro-priate antiviral therapy within the first 2 days of illness [161], reduces the length of in-patient hospital stay and minimizes the unnecessary use of antibiotics [162]. Rapid antigen capture immu-noassay tests can provide results within 30 min or less and are easy to perform [163]. They are based on an immunochromatographic reaction that uses a monoclonal antibody targeted to a specific antigen of influenza, usually the nucleo-protein. They can therefore detect any AIV [164–
167] and include tests such as the Directigen™ Flu A and Directigen Flu A and B tests (Becton Dickinson Diagnostic Systems, MD, USA) and the BinaxNow® influenza A and B test (Binax, Inc., ME, USA) [163].
VaccinesVaccination in poultry can minimize the threat of AI. Vaccines against AI are important tools for protecting the poultry industry and humans, since vaccines help increase resistance to infec-tion, prevent illness and death, reduce virus replication and reduce viral transmission to birds and mammals, including humans. DNA vaccination could provide protective immunity in animal models against different infectious diseases. The basic principle of DNA vaccina-tion is the induction of an immune response by intramuscular injection or the use of a ‘gene gun’ of naked DNA (plasmid) encoding the targeted gene into the host cells [168]. The restrictions of DNA vaccination are vaccine cost, problems with delivery into birds, low efficiency in birds and its requirement of large amounts of puri-fied plasmids [169]. The reason DNA vaccines are not suitable in the poultry industry include their time-consuming application, expenses and undue stress to the chickens.
DNA delivery technologies are effective and essential for inducing a strong and long-lasting immune response that is required to induce high and continued levels of antigen production at proper target sites. A variety of intracellular bac-teria have been utilized as live carriers for effi-cient delivery of either DNA vaccine constructs or vaccine antigens [170] directly into professional APCs [171]. This strategy can elicit humoral and cellular responses against the pathogens from which the target genes are derived [172–175].
Live oral attenuated Salmonella typhimurium is a well-known, useful carrier for the expres-sion and delivery of heterologous antigens to mucosal lymphoid tissue, including the HA of AIV [176]. The viable bacteria multiply inside the
Salmonella-containing vacuole and deliver the recombinant antigen into the host cell cytosol [177,178]. DNA vaccines delivered by attenuated S. typhimurium SL7207 and boosted with a con-ventional killed vaccine confer protection on chickens against infection with the H9 subtype of AIV [179]. Another approach is the utiliza-tion of SPI2-encoded type III secretion system [180] for antigen expression and delivery into the cytoplasm of APCs, which increases safety and efficacy. Such vaccines have been shown to be very effective in eliciting both CD8+ and CD4+ T-cell-mediated immune responses in models of infectious diseases and cancer [178,181–184].
Interestingly, the development of an immune response to HA glycoprotein is important for the protection of chickens against challenge with the AIV infection [185]. Accordingly, a wide variety of vaccines against AIV has been developed and tested in experimental conditions, but only inac-tivated whole AIV vaccines and live recombinant fowlpox virus vectors expressing HA vaccines have been licensed and widely used in various countries [186].
Future perspectiveThe recent outbreak in humans of a novel influenza A/H7N9 in China in March 2013 shed light on the importance of surveillance efforts to alleviate public health concerns of AI. Extensive global surveillance programs are urgently required to help predict the circulating AI strains that may produce potential pandem-ics in humans. Vaccines and molecular immu-nology approaches are currently the subject of extensive research efforts aimed at minimiz-ing the threat of AI. These are complemented by surveillance programs that are essential for monitoring the AI dynamics in their recognized reservoirs. The outcome of active surveillance for AIVs in different parts of the world, including Malaysia, will fill the gap in knowledge regard-ing the true disease status in Malaysia, Egypt and several countries in southeast Asia. Similar to many countries in southeast Asia, Malaysia is endemic for NDV, but its current AI dis-ease status is unknown. Outbreaks of HP A/H5N1 were reported in 2004, 2006 and 2007 in poultry, although none have been reported since. The country borders Indonesia, which is endemic for A/H5N1, and Thailand, which has also had outbreaks of HP A/H5N1 AI. In addi-tion, in countries such as Thailand, Indonesia, and China where pigs are not fully protected from acquiring infection with any possible avian influenza viruses, the generation of pandemic

Author Pro
of
www.futuremedicine.com 13future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
influenza strains is a possibility. It was recently reported that the unprotected transport of pigs and the breach of biosecurity measures could facilitate the mixed infection of humans and pigs with avian viruses and the generation of newer strains of greater pandemic potential [187, 188]. This could also explain the emergence of influ-enza A strains of pandemic potential in China and southeast Asia. Because of the lack of active surveillance, particularly in duck populations, the true disease status in such regions remains undetermined.
Although the use of influenza vaccines to protect the poultry industry and humans is an effective procedure to control the disease, the current use of vaccination encounters several challenges [189]. A major hurdle is the increased chance of having asymptomatically infected poultry spreading the virus. In addition, poor administration is the most common cause of vaccine failure in poultry making the available AI vaccines are not efficient to elicit protective
immune responses, thus, search for new AI vac-cine delivery mechanisms should be advocated such as nanovaccines. Another drawback of cur-rently applied vaccines used in poultry is the low antigen stability in the vaccines and the short duration of immunity. Worryingly, it has been recently reported that independent recombina-tion events between distinct attenuated infec-tious laryngotracheitis virus vaccine strains can result in virulent recombinant viruses [190]. This prospect might arise in AIVs as well. Although the use of nanotechnology to deliver AI vaccines may improve vaccine efficacy and overcome the recombination challenges [191,192], for now, we advocate strict biosecurity procedures coupled with the implementation of worldwide intera-gency surveillance efforts modeled on those of the USA and Europe in high-risk regions, such as in developing countries, to identify potentially pandemic strains [193–195]. Surveillance and diag-nosis of AI in humans and birds are not similar and involve different techniques. Thus, AIV
Executive summary
Background & history�n Avian influenza virus (AIV), which is closely related to human influenza virus, appeared nearly 150 years go and has recently re-
emerged, causing grave concern among certain populations.�n Several pandemics of AIV have afflicted human populations with devastating impact.�n The recently emerged viruses, mainly A/H5N1 and A/H7N9, arose from several reassortment events in different hosts and pose a
significant threat to human public health.
Genome & virology of AIV�n Although the structure of AIV has been fully elucidated, it remains difficult to predict when the next pandemic will occur. �n Hemagglutinin and neuraminidase are the major antigenic determinants of influenza A viruses.�n Acquisition of a polybasic hemagglutinin cleavage site is not the only necessary step for the evolution of low-pathogenicity avian
influenza strains into high-pathogenicity avian influenza viruses. There are other factors that are also required.
Epidemiology of AIV�n AIVs are natural inhabitants of waterfowl, mainly migratory ducks.�n Several interspecies barriers determine the transmissibility of AIVs among different species and, finally, to humans.�n Surveillance is of importance in order to monitor the current status of avian influenza in populations and to update vaccine databases.�n Global programmed surveillance programs in Asia, a potential origin of the next pandemic, should be promptly initiated.
Diagnosis of AIV�n Diagnosis of avian influenza infection in waterfowl is different from diagnosis in humans.�n Suitable and reliable diagnostic techniques in real time will guard against severe infection in humans and allow monitoring of AIVs
spreading in their natural reservoirs.�n Virus isolation in embryonating chicken eggs should be advocated as the cornerstone diagnostic technique of isolation of live AIVs for
subsequent characterization and updating of vaccine databases.�n Nucleic acid-based tests are useful techniques for the screening of AIVs during surveillance studies.�n The specificity of quantitative PCR is subject to several factors, such as the primers, RNA extraction method, RNA integrity and presence
of inhibitors, among others.�n Virologic and serological techniques, along with rapid molecular methods (e.g., quantitative PCR), will provide information and suitable
intervention strategies to limit the pandemic potential of avian influenza in humans and poultry.
Vaccines�n Vaccines are useful tools to minimize the threat of avian influenza in poultry, but a concern that is associated with the use of vaccines in
poultry is that vaccines could increase the chance of having asymptomatically infected poultry spreading the virus.�n DNA vaccines and nanovaccines are promising tools to improve currently applied avian influenza vaccines in poultry.

Author Pro
of
Future Microbiol. (2013) 8(9)14 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
surveillance in AIV’s natural reservoirs of wild birds is of high importance in order to monitor the silent circulating strains and protect poultry from being infected with LPAI strains, as well as HPAI. Biosecurity measures, environmental pro-tection and handling of poultry in at-risk farms or locations of endemic infections will limit and control the spread of the disease in humans and will minimize poultry-to-human transmission. Virologic and serological monitoring, along with the use of rapid molecular methods (e.g., quantitative PCR), will provide information in real time in order to enable suitable intervention strategies to limit the AI pandemic and disease potential in humans and poultry. Finally, it is
advisable to use complementary methods for the identification of AIV, since this approach is most likely to yield a reliable and comprehensive evaluation of circulating viruses [13,107].
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the sub-ject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
ReferencesPapers of special note have been highlighted as:n of interestnn of considerable interest
1. World Organization for Animal Health. Avian influenza. In: Manual of Diagnostic Tests and Vaccines for Terrestrial Animals: Mammals, Birds, and Bees. (6th Edition, Volume 1). Office International des Epizooties, France, 465–481 (2008).
2. Swayne DE. The global nature of avian influenza. In: Avian Influenza. Wiley-Blackwell, NJ, USA, 126–127 (2009).
3. Kurtz J, Manvell RJ, Banks J. Avian influenza virus isolated from a woman with conjunctivitis. Lancet 348(9031), 901–902 (1996).
4. Webster RG, Geraci J, Petursson G, Skirnisson K. Conjunctivitis in human beings caused by influenza A virus of seals. N. Engl. J. Med. 304(15), 911 (1981).
5. Webster RG, Bean WJ, Gorman OT, Chambers TM, Kawaoka Y. Evolution and ecology of influenza A viruses. Microbiol. Mol. Biol. Rev. 56(1), 152–179 (1992).
6. Kilbourne ED. Influenza immunity: new insights from old studies. J. Infect. Dis. 193(1), 7–8 (2006).
7. Lindstrom S, Cox N, Klimov A. Genetic analysis of human H2N2 and early H3N2 influenza viruses, 1957–1972: evidence for genetic divergence and multiple reassortment events. Virology 328(1), 101–119 (2004).
8. Palese P Shaw ML Orthomyxoviridae: the viruses and their replication. In: Fields’ Virology. Knipe DM, Howley PM, Griffin DM, Lamb RA, Martin MA (Eds). Lippincott, Williams & Wilkins, PA, USA, 1647–1689 (2007).
9. Capua I, Alexander DJ. Avian influenza and human health. Acta Tropica 83(1), 1–6 (2002).
10. Saif YM. Diseases of Poultry. Iowa State Press, IA, USA (2003).
11. Arzt J, White W, Thomsen B, Brown C. Agricultural diseases on the move early in the third millennium. Vet. Pathol. 47(1), 15–27 (2010).
12. El Zowalaty ME, Abin M, Chander Y, Redig PT, Goyal SM. Isolation of H5 avian influenza viruses from waterfowl in the upper midwest region of the United States. Avian Dis. 55(2), 259–262 (2011).
13. El Zowalaty ME, Abin M, Raju S et al. Isolation of avian influenza virus from polymerase chain reaction-negative cloacal samples of waterfowl. J. Vet. Diagn. Invest. 23(1), 87–90 (2011).
n� First comprehensive study in literature on the isolation of AI viruses from waterfowl after passage in embryonating chicken eggs and prior to rapid RT-qPCR to improve the detection and isolation of live influenza viruses for further characterization. It is imperative to perform virus isolation during AI surveillance efforts to obtain a clear picture on the circulating AIV and to understand that depending solely on qRT-PCR may yield spurious results.
14. Garten RJ, Davis CT, Russell CA et al. Antigenic and genetic characteristics of swine-origin 2009 A(H1N1) influenza viruses circulating in humans. Science 325(5937), 197–201 (2009).
15. Mounts AW, Kwong H, Izurieta HS et al. Case–control study of risk factors for avian influenza A (H5N1) disease, Hong Kong, 1997. J. Infect. Dis. 180(2), 505–508 (1999).
16. Alexander DJ. Avian influenza: historical aspects. Avian Dis. 47, 4–13 (2003).
17. Lupiani B, Reddy SM. The history of avian influenza. Comp. Immunol. Microbiol. Infect. Dis. 32(4), 311–323 (2009).
18. Nichols JE, Leduc JW. Influenza. In: Vaccines for Biodefense and Emerging and Neglected Diseases. Barrett AT, Stanberry LR (Eds). Academic Press, Waltham, MA, USA, 497-525 (2008).
19. Taubenberger JK, Reid AH, Krafft AE, Bijwaard KE, Fanning TG. Initial genetic characterization of the 1918 ‘Spanish’ influenza virus. Science 275(5307), 1793–1796 (1997).
20. Taubenberger J, Morens D. 1918 Influenza: the mother of all pandemics. Emerg. Infect. Dis. 12(1), 15–22 (2006).
21. Cox NJ, Tamblyn SE, Tam T. Influenza pandemic planning. Vaccine 21(16), 1801–1803 (2003).
22. Hehme N, Engelmann H, Künzel W, Neumeier E, Sänger R. Pandemic preparedness: lessons learnt from H2N2 and H9N2 candidate vaccines. Med. Microbiol. Immunol. 191(3–4), 203–208 (2002).
23. Newcastle disease. In: Manual of Standards for Diagnostic Tests and Vaccines. Office International des Epizooties, France, 161–169 (1996).
24. Garten RJ, Davis CT, Russell CA et al. Antigenic and genetic characteristics of swine-origin 2009 A (H1N1) influenza viruses circulating in humans. Science 325(5937), 197–201 (2009).
25. Igarashi M, Ito K, Yoshida R, Tomabechi D, Kida H, Takada A. Predicting the antigenic structure of the pandemic (H1N1) 2009 influenza virus hemagglutinin. PLoS ONE 5(1), e8553 (2010).
26. Smith GJ, Vijaykrishna D, Bahl J et al. Origins and evolutionary genomics of the 2009 swine-origin H1N1 influenza A epidemic. Nature 459(7250), 1122–1125 (2009).
27. Zhang W, Qi J, Shi Y et al. Crystal structure of the swine-origin A (H1N1)-2009 influenza

Author Pro
of
www.futuremedicine.com 15future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
A virus hemagglutinin (HA) reveals similar antigenicity to that of the 1918 pandemic virus. Protein Cell 1(5), 459–467 (2010).
28. Perez-Padilla R. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N. Engl. J. Med. 361(7), 680 (2009).
29. Smith GJ, Vijaykrishna D, Bahl J et al. Origins and evolutionary genomics of the 2009 swine-origin H1N1 influenza A epidemic. Nature 459(7250), 1122–1125 (2009).
30. Centanni ESE. La peste aviaria I & II. Communicazione fatta all’accademia delle scienze mediche e naturali de Ferrara. (1901).
31. Stubs EL, Biester HE, Devries L. Fowl pest. In: Diseases of Poultry. Iowa State Press, IA, USA, 493–502 (1952).
32. Perroncito E. Epizoozia tifoide nei gallinacei. Ann. Accad. Agric. Torino. 126, 21–87 (1878).
33. Becker WB. The isolation and classification of tern virus: influenza virus A/tern/South Africa/1961. J. Hyg. (Lond.) 64(3), 309–320 (1966).
34. Subbarao K, Klimov A, Katz J et al. Characterization of an avian influenza A (H5N1) virus isolated from a child with a fatal respiratory illness. Science 279(5349), 393–396 (1998).
35. Webster RG. Predictions for future human influenza pandemics. J. Infect. Dis. 176(Suppl. 1), S14–S19 (1997).
36. Guo Y, Xu X, Wan X. [Genetic characterization of an avian influenza A (H5N1) virus isolated from a sick goose in China]. Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi 12(4), 322–325 (1998).
37. Claas EC, Osterhaus AD, van Beek R et al. Human influenza A H5N1 virus related to a highly pathogenic avian influenza virus. Lancet 351(9101), 472–477 (1998).
38. Mounts AW, Kwong H, Izurieta HS et al. Case–control study of risk factors for avian influenza A (H5N1) disease, Hong Kong, 1997. J. Infect. Dis. 180(2), 505–508 (1999).
39. Peiris JS, Yu WC, Leung CW et al. Re-emergence of fatal human influenza A subtype H5N1 disease. Lancet 363(9409), 617–619 (2004).
40. Banner D, Kelvin AA. The current state of H5N1 vaccines and the use of the ferret model for influenza therapeutic and prophylactic development. J. Infect. Dev. Ctries 6(06), 465–469 (2012).
41. Bartlett JG. Planning for avian influenza. Ann. Intern. Med. 145(2), 141–144 (2006).
42. Li Q, Zhou L, Zhou M et al. Preliminary report. epidemiology of the avian influenza A
(H7N9) outbreak in China. N. Engl. J. Med. doi:10.1056/NEJMoa1304617 (2013) (Epub ahead of print).
43. Liu D, Shi W, Shi Y et al. Origin and diversity of novel avian influenza A H7N9 viruses causing human infection: phylogenetic, structural, and coalescent analyses. Lancet 381(9881), 1926–1932 (2013).
44. Zhu H WD, Kelvin Dj, Li L et al. Infectivity, transmission, and pathology of human H7N9 influenza in ferrets and pigs. Science 341(6142), 183–186 (2013).
nn� Recent outbreaks caused by avian H7N9 influenza viruses could be the beginning of a human avain influenza pandemic with possible human-to-human spread. The finding that efficient transmissibility of H7N9 viruses in ferrets by direct contact raises grave public health concerns.
45. Uyeki TM, Cox NJ. Global concerns regarding novel influenza A (H7N9) virus infections. N. Engl. J. Med. 368(20), 1862–1864 (2013).
46. Easterday BC. Animals in the influenza world. Phil. Trans. R. Soc. Lond. 288(1029), 433–437 (1980).
47. Daly JM, Blunden AS, Macrae S et al. Transmission of equine influenza virus to English foxhounds. Emerg. Infect. Dis. 14(3), 461–464 (2008).
48. Song D, Kang B, Lee C et al. Transmission of avian influenza virus (H3N2) to dogs. Emerg. Infect. Dis. 14(5), 741–746 (2008).
49. Herfst S, Schrauwen EJ, Linster M et al. Airborne transmission of influenza A/H5N1 virus between ferrets. Science 336(6088), 1534–1541 (2012).
50. Imai M, Watanabe T, Hatta M et al. Experimental adaptation of an influenza H5 HA confers respiratory droplet transmission to a reassortant H5 HA/H1N1 virus in ferrets. Nature 486(7403), 420–428 (2012).
51. Berns KI, Casadevall A, Cohen ML et al. Adaptations of avian flu virus are a cause for concern. Science 335(6069), 660–661 (2012).
52. Baltimore D. Expression of animal virus genomes. Bacteriol. Rev. 35(3), 235–241 (1971).
53. Virology Division International Union of Microbiologival Societies. Virus Taxonomy. Eighth Report of the International Committee on the Taxonomy of Viruses. Fauquet CM, Mayo MA, Maniloff J, Desselberger, Ball LA (Eds). Academic Press, MA, USA (2005).
54. MacLachlan NJ, Dubovi EJ. Orthomyxoviridae. In: Fenner’s Veterinary Virology (4th Edition). Academic Press, MA, USA, 353–370 (2011).
55. Hay AJ, Gregory V, Douglas AR, Lin YP. The evolution of human influenza viruses. Phil. Trans. R. Soc. Lond. 356(1416), 1861–1870 (2001).
56. Bouvier NM, Palese P. The biology of influenza viruses. Vaccine 26, D49–D53 (2008).
57. Steinhauer D, Skehel J. Genetics of influenza viruses. Annu. Rev. Genet. 36, 305–332 (2002).
58. García-Sastre A. The neuraminidase of bat influenza viruses is not a neuraminidase. Proc. Natl Acad. Sci. USA 109(46), 18635–18636 (2012).
59. Tong S, Li Y, Rivailler P et al. A distinct lineage of influenza A virus from bats. Proc. Natl Acad. Sci. USA 109(11), 4269–4274 (2012).
60. A revision of the system of nomenclature for influenza viruses: a WHO memorandum. Bull. World Health Organ. 58(4), 585–591 (1980).
61. Fouchier RA, Munster V, Wallensten A et al. Characterization of a novel influenza A virus hemagglutinin subtype (H16) obtained from black-headed gulls. J. Virol. 79(5), 2814–2822 (2005).
62. [A revised system of nomenclature for influenza A viruses: WHO report]. Bull. World Health Organ. 57(4), 611–617 (1979).
63. Fauci AS. Emerging and re-emerging infectious diseases: influenza as a prototype of the host–pathogen balancing act. Cell 124(4), 665–670 (2006).
64. Zambon MC. Epidemiology and pathogenesis of influenza. J. Antimicrob. Chemother. 44(Suppl. B), 3–9 (1999).
65. Desselberger U, Nakajima K, Alfino P et al. Biochemical evidence that new influenza virus strains in nature may arise by recombination (reassortment). Proc. Natl Acad. Sci. USA 75(7), 3341–3345 (1978).
66. Olsen B, Munster VJ, Wallensten A, Waldenström J, Osterhaus AD, Fouchier RA. Global patterns of influenza A virus in wild birds. Science 312(5772), 384–388 (2006).
67. Capua I, Alexander DJ. Avian influenza infections in birds a moving target. Influenza Other Respi. Viruses 1(1), 11–18 (2007).
68. Galloway SE, Reed ML, Russell CJ, Steinhauer DA. Influenza HA subtypes demonstrate divergent phenotypes for cleavage activation and pH of fusion: implications for host range and adaptation. PLoS Pathog. 9(2), e1003151 (2013).
69. Senne DA, Panigrahy B, Kawaoka Y et al. Survey of the hemagglutinin (HA) cleavage site sequence of H5 and H7 avian influenza viruses: amino acid sequence at the HA

Author Pro
of
Future Microbiol. (2013) 8(9)16 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
cleavage site as a marker of pathogenicity potential. Avian Dis. 40(2), 425–437 (1996).
70. Vey M, Orlich M, Adler S, Klenk HD, Rott R, Garten W. Hemagglutinin activation of pathogenic avian influenza viruses of serotype H7 requires the protease recognition motif R-X-K/R-R. Virology 188(1), 408–413 (1992).
71. Wood GW, McCauley JW, Bashiruddin JB, Alexander DJ. Deduced amino acid sequences at the haemagglutinin cleavage site of avian influenza A viruses of H 5 and H 7 subtypes. Arch. Virol. 130(1–2), 209–217 (1993).
72. Stieneke-Gröber A, Vey M, Angliker H. Influenza virus hemagglutinin with multibasic cleavage site is activated by furin, a subtilisin-like endoprotease. EMBO J. 11(7), 2407–2414 (1992).
73. Alexander DJ. An overview of the epidemiology of avian influenza. Vaccine 25(30), 5637–5644 (2007).
74. Bogs J, Veits J, Gohrbandt S et al. Highly pathogenic H5N1 influenza viruses carry virulence determinants beyond the polybasic hemagglutinin cleavage site. PLoS ONE 5(7), e11826 (2010).
75. Gohrbandt S, Veits J, Hundt J et al. Amino acids adjacent to the haemagglutinin cleavage site are relevant for virulence of avian influenza viruses of subtype H5. J. Gen. Virol. 92(1), 51–59 (2011).
76. Hatta M, Kawaoka Y. The NB protein of influenza B virus is not necessary for virus replication in vitro. J. Virol. 77(10), 6050–6054 (2003).
77. Seo SH, Hoffmann E, Webster RG. Lethal H5N1 influenza viruses escape host anti-viral cytokine responses. Nat. Med. 8(9), 950–954 (2002).
78. Hinshaw VS, Webster RG, Turner B. The perpetuation of orthomyxoviruses and paramyxoviruses in Canadian waterfowl. Can. J. Microbiol. 26(5), 622–629 (1980).
79. El Zowalaty ME, Abin M, Chander Y, Redig PT, Goyal SM. Improved method for the isolation and sub-typing of avian influenza viruses from oropharyngeal samples of ducks. Avian Dis. 55(3), 439–442 (2011).
80. Stallknecht DE. Ecology and epidemiology of avian influenza viruses in wild bird populations: waterfowl, shorebirds, pelicans, cormorants, etc. Avian Dis. 47(Special issue), 61–69 (2003).
81. Charlton B, Crossley B, Hietala S. Conventional and future diagnostics for avian influenza. Comp. Immunol. Microbiol. Infect. Dis. 32(4), 341–350 (2009).
82. Peiris JM, de Jong MD, Guan Y. Avian influenza virus (H5N1): a threat to human
health. Clin. Microbiol. Rev. 20(2), 243–267 (2007).
83. Webby R, Hoffmann E, Webster R. Molecular constraints to interspecies transmission of viral pathogens. Nat. Med. 10, S77–S81 (2004).
84. Couceiro J, Paulson JC, Baum LG. Influenza virus strains selectively recognize sialyloligosaccharides on human respiratory epithelium; the role of the host cell in selection of hemagglutinin receptor specificity. Virus Res. 29(2), 155–165 (1993).
85. Shinya K, Ebina M, Yamada S, Ono M, Kasai N, Kawaoka Y. Avian flu: influenza virus receptors in the human airway. Nature 440(7083), 435–436 (2006).
86. Matrosovich M, Zhou N, Kawaoka Y, Webster R. The surface glycoproteins of H5 influenza viruses isolated from humans, chickens, and wild aquatic birds have distinguishable properties. J. Virol. 73(2), 1146–1155 (1999).
87. Beare AS. Replication of avian influenza viruses in humans. Arch. Virol. 119(1–2), 37 (1991).
88. Hinshaw VS, Webster RG, Naeve CW, Murphy BR. Altered tissue tropism of human–avian reassortant influenza viruses. Virology 128(1), 260–263 (1983).
89. Ito T, Couceiro JN, Kelm S et al. Molecular basis for the generation in pigs of influenza A viruses with pandemic potential. J. Virol. 72(9), 7367–7373 (1998).
90. Slemons RD, Easterday BC. Virus replication in the digestive tract of ducks exposed by aerosol to type-A influenza. Avian Dis. 22(3), 367–377 (1978).
91. Kim JK, Negovetich NJ, Forrest HL, Webster RG. Ducks: the trojan horses of H5N1 influenza. Influenza Other Respi. Viruses 3(4), 121–128 (2009).
92. Janies D, Hill AW, Guralnick R, Habib F, Waltari E, Wheeler WC. Genomic analysis and geographic visualization of the spread of avian influenza (H5N1). Syst. Biol. 56(2), 321–329 (2007).
93. Ollier L, Caramella A, Giordanengo V, Lefebvre JC. High permissivity of human HepG2 hepatoma cells for influenza viruses. J. Clin. Microbiol. 42(12), 5861–5865 (2004).
94. Perez DR, Sorrell EM, Donis RO. Avian influenza: an omnipresent pandemic threat. Pediatr. Infect. Dis. J. 24(11 Suppl.), S208–S216 (2005).
95. Ferro PJ, El-Attrache J, Fang X et al. Avian influenza surveillance in hunter-harvested waterfowl from the gulf coast of Texas (November 2005–January 2006). J. Wildl. Dis. 44(2), 434–439 (2008).
96. Furuse Y, Suzuki A, Kamigaki T, Oshitani H. Evolution of the M gene of the influenza A
virus in different host species: large-scale sequence analysis. Virol. J. 6, 67 (2009).
97. Munster VJ, Fouchier RA. Avian influenza virus: of virus and bird ecology. Vaccine 27(45), 6340–6344 (2009).
98. Pedersen K, Swafford SR, Deliberto TJ. Low pathogenicity avian influenza subtypes isolated from wild birds in the United States, 2006–2008. Avian Dis. 54(1 Suppl.), 405–410 (2010).
99. Hua YP, Chai HL, Yang SY, Zeng XW, Sun Y. Primary survey of avian influenza virus and Newcastle disease virus infection in wild birds in some areas of Heilongjiang Province, China. J. Vet. Sci. 6(4), 311–315 (2005).
100. Stallknecht DE, Shane SM, Zwank PJ, Senne DA, Kearney MT. Avian influenza viruses from migratory and resident ducks of coastal Louisiana. Avian Dis. 34(2), 398–405 (1990).
101. Douglas KO, Lavoie MC, Kim LM, Afonso CL, Suarez DL. Isolation and genetic characterization of avian influenza viruses and a Newcastle disease virus from wild birds in Barbados: 2003–2004. Avian Dis. 51(3), 781–787 (2007).
102. El Zowalaty ME, Chander Y, Redig PT, El Latif HKA, El Sayed MA, Goyal SM. Selective isolation of Avian influenza virus (AIV) from cloacal samples containing AIV and Newcastle disease virus. J. Vet. Diagn. Invest. 23(2), 330–332 (2011).
103. Hinshaw VS, Wood JM, Webster RG, Deibel R, Turner B. Circulation of influenza viruses and paramyxoviruses in waterfowl originating from two different areas of North America. Bull. World Health Organ. 63(4), 711–719 (1985).
104. Jahangir A, Ruenphet S, Ueda S et al. Avian influenza and Newcastle disease viruses from northern pintail in Japan: isolation, characterization and inter-annual comparisons during 2006–2008. Virus Res. 143(1), 44–52 (2009).
105. Slemons RD, Johnson DC, Osborn JS, Hayes F. Type-A influenza viruses isolated from wild free-flying ducks in California. Avian Dis. 18(1), 119–124 (1974).
106. Slemons RD, Shieldcastle MC, Heyman LD, Bednarik KE, Senne DA. Type A influenza viruses in waterfowl in Ohio and implications for domestic turkeys. Avian Dis. 35(1), 165–173 (1991).
107. Lira J, Moresco KA, Stallknecht DE, Swayne DE, Fisher DS. Single and combination diagnostic test efficiency and cost analysis for detection and isolation of avian influenza virus from wild bird cloacal swabs. Avian Dis. 54(Suppl. 1), 606–612 (2010).
108. Weinberg A, Mettenbrink CJ, Ye D, Yang CF. Sensitivity of diagnostic tests for influenza

Author Pro
of
www.futuremedicine.com 17future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
varies with the circulating strains. J. Clin. Virol. 33(2), 172–175 (2005).
109. Philippa JD. Avian influenza. In: Zoo and Wild Animal Medicine Current Therapy (6th Edition). Fowler ME (Ed.). Saunders, PA, USA, 79–87 (2008).
110. Swayne DE, Suarez DL. Highly pathogenic avian influenza. Rev. Sci. Tech. 19(2), 463–482 (2000).
111. Suarez DL, Das A, Ellis E. Review of rapid molecular diagnostic tools for avian influenza virus. Avian Dis. 51(1 Suppl.), 201–208 (2007).
112. Ellström P, Latorre-Margalef N, Griekspoor P et al. Sampling for low-pathogenic avian influenza A virus in wild mallard ducks: oropharyngeal versus cloacal swabbing. Vaccine 26(35), 4414–4416 (2008).
113. Jindal N, De Abin M, Primus AE et al. Comparison of cloacal and oropharyngeal samples for the detection of avian influenza virus in wild birds. Avian Dis. 54(1), 115–119 (2010).
114. Roelandt S, Outtrim L, Browning C, Alexander DJ, Brown IH, Irvine RM. Evaluation of two different swab transport systems in the detection of avian influenza virus excretion from infected pekin ducks Anas platyrhynchos. J. Virol. Methods 184(1–2), 8–14 (2012).
115. WHO. Laboratory procedures. In: WHO Manual on Animal Influenza Diagnosis and Surveillance. WHO Press, Switzerland, 98, 15–19 (2002).
116. Docherty DE, Slota PG. Use of muscovy duck embryo fibroblasts for the isolation of viruses from wild birds. Methods Cell Sci. 11(3), 165–170 (1988).
117. Taubenberger JK, Layne SP. Diagnosis of influenza virus: coming to grips with the molecular era. Mol. Diagn. 6(4), 291–305 (2001).
118. Potter C, Zuckerman AJ, Banatvala JE, Pattison JR. Influenza. In: Principles and Practice of Clinical Virology. Wiley, NY, USA, 199–223 (1987).
119. Newton DW, Treanor JJ, Menegus MA. Clinical and laboratory diagnosis of influenza virus infections. Am. J. Manag. Care 6(Suppl. 5), S265–S275 (2000).
120. Petric M, Comanor L, Petti CA. Role of the laboratory in diagnosis of influenza during seasonal epidemics and potential pandemics. J. Infect. Dis. 194(Suppl. 2), S98–S110 (2006).
121. Prince HE, Leber AL. Comparison of complement fixation and hemagglutination inhibition assays for detecting antibody responses following influenza virus
vaccination. Clin. Vaccine Immunol. 10(3), 481–482 (2003).
122. Julkunen I, Pyhala R, Hovi T. Enzyme immunoassay, complement fixation and hemagglutination inhibition tests in the diagnosis of influenza A and B virus infections. Purified hemagglutinin in subtype-specific diagnosis. J. Virol. Methods 10(1), 75–84 (1985).
123. Pearson JE, Senne DA. Diagnostic procedures for avian influenza. Avian Dis. 47, 222–227 (2003).
124. Smith W, Andrewes CH, Laidlaw PP. A virus from influenza patients. Lancet 2, 66 (1933).
125. Swayne DE, Senne DA, Suarez DL. Avian influenza. In: A Laboratory Manual for the Isolation, Identification, and Characterization of Avian Pathogens. Dufour-Zavala L (Ed.). American Association of Avian Pathologists, GA, USA, 128–134 (2008).
n� Diagnsotic principles followed in the identification and characcterization of avian influenza viruses as well as other avian pathogens.
126. Cattoli G, Drago A, Maniero S et al. Comparison of three rapid detection systems for type A influenza virus on tracheal swabs of experimentally and naturally infected birds. Avian Pathol. 33(4), 432–437 (2004).
127. Cattoli G, Capua I. Molecular diagnosis of avian influenza during an outbreak. Dev. Biol. (Basel) 124, 99–105 (2006).
128. Carman S, Stansfield C, Weber J, Bildfell R, Van Dreumel T. H3N2 influenza A virus recovered from a neonatal pig in Ontario – 1997. Can. Vet. J. 40(12), 889–890 (1999).
129. Clavijo A, Tresnan DB, Jolie R, Zhou EM. Comparison of embryonated chicken eggs with MDCK cell culture for the isolation of swine influenza virus. Can. Vet. J. 66(2), 117–121 (2002).
130. Lee CW, Jung K, Jadhao S, Suarez D. Evaluation of chicken-origin (DF-1) and quail-origin (QT-6) fibroblast cell lines for replication of avian influenza viruses. J. Virol. Methods 153(1), 22–28 (2008).
131. Moresco KA, Stallknecht DE, Swayne DE. Evaluation and attempted optimization of avian embryos and cell culture methods for efficient isolation and propagation of low pathogenicity avian influenza viruses. Avian Dis. 54(1 Suppl.), 622–626 (2010).
132. Munster VJ, Baas C, Lexmond P et al. Practical considerations for high-throughput influenza A virus surveillance studies of wild birds by use of molecular diagnostic tests. J. Clin. Microbiol. 47(3), 666–673 (2009).
133. Reina J, Fernandez-Baca V, Blanco I, Munar M. Comparison of Madin–Darby canine kidney cells (MDCK) with a green monkey
continuous cell line (Vero) and human lung embryonated cells (MRC-5) in the isolation of influenza A virus from nasopharyngeal aspirates by shell vial culture. J. Clin. Microbiol. 35(7), 1900–1901 (1997).
134. Schultz-Cherry S, Dybdahl-Sissoko N, McGregor M, Hinshaw VS. Mink lung epithelial cells: unique cell line that supports influenza A and B virus replication. J. Clin. Microbiol. 36(12), 3718–3720 (1998).
135. Shope RE. Swine influenza : III. Filtration experiments and etiology. J. Exp. Med. 54(3), 373–385 (1931).
136. Webster RG. Influenza virus: transmission between species and relevance to emergence of the next human pandemic. Arch. Virol. 13, 105–113 (1997).
137. Fouchier RA, Bestebroer TM, Herfst S, van der Kemp L, Rimmelzwaan GF, Osterhaus AD. Detection of influenza A viruses from different species by PCR amplification of conserved sequences in the matrix gene. J. Clin. Microbiol. 38(11), 4096–4101 (2000).
138. Allwinn R, Preiser W, Rabenau H, Buxbaum S, Stürmer M, Doerr HW. Laboratory diagnosis of influenza – virology or serology? Med. Microbiol. Immunol. 191(3–4), 157–160 (2002).
139. Espy MJ, Smith TF, Harmon MW, Kendal AP. Rapid detection of influenza virus by shell vial assay with monoclonal antibodies. J. Clin. Microbiol. 24(4), 677–679 (1986).
140. Stokes CE, Bernstein JM, Kyger SA, Hayden FG. Rapid diagnosis of influenza A and B by 24-h fluorescent focus assays. J. Clin. Microbiol. 26(7), 1263–1266 (1988).
141. Dunn JJ, Gordon C, Kelley C, Carroll KC. Comparison of the Denka-Seiken INFLU A.B-Quick and BD Directigen Flu A+B kits with direct fluorescent-antibody staining and shell vial culture methods for rapid detection of influenza viruses. J. Clin. Microbiol. 41(5), 2180–2183 (2003).
142. Chander Y, Jindal N, Stallknecht DE, Sreevatsan S, Goyal SM. Full length sequencing of all nine subtypes of the neuraminidase gene of influenza A viruses using subtype specific primer sets. J. Virol. Methods 165(1), 116–120 (2010).
143. Hoffmann E, Stech J, Guan Y, Webster RG, Perez DR. Universal primer set for the full length amplification of all influenza A viruses. Arch. Virol. 146(12), 2275–2289 (2001).
144. Jindal N, Chander Y, de Abin M et al. Amplification of four genes of influenza A viruses using a degenerate primer set in a one step RT-PCR method. J. Virol. Methods 160(1–2), 163–166 (2009).
145. Lee MS. Identification and subtyping of avian influenza viruses by reverse transcription-

Author Pro
of
Future Microbiol. (2013) 8(9)18 future science group
Review El Zowalaty, Bustin, Husseiny & Ashour
PCR. J. Virol. Methods 97(1–2), 13–22 (2001).
146. Bustin SA. Quantification of mRNA using real-time reverse transcription PCR (RT-PCR): trends and problems. J. Mol. Endocrinol. 29(1), 23–39 (2002).
147. Wacker MJ, Godard MP. Analysis of one-step and two-step real-time RT-PCR using SuperScript III. J. Biomol. Tech. 16(3), 266–271 (2005).
148. Munch M, Nielsen LP, Handberg KJ, Jorgensen PH. Detection and subtyping (H5 and H7) of avian type A influenza virus by reverse transcription-PCR and PCR-ELISA. Arch. Virol. 146(1), 87–97 (2001).
149. Dybkær K, Munch M, Handberg KJ, Jørgensen PH. Application and evaluation of RT-PCR-ELISA for the nucleoprotein and RT-PCR for detection of low-pathogenic H5 and H7 subtypes of avian influenza virus. J. Vet. Diagn. Invest. 16(1), 51–56 (2004).
150. Collins RA, Ko LS, So KL, Ellis T, Lau LT, Yu AC. Detection of highly pathogenic and low pathogenic avian influenza subtype H5 (Eurasian lineage) using NASBA. J. Virol. Methods 103(2), 213–225 (2002).
151. Imai M, Ninomiya A, Minekawa H et al. Development of H5-RT-LAMP (loop-mediated isothermal amplification) system for rapid diagnosis of H5 avian influenza virus infection. Vaccine 24(44–46), 6679–6682 (2006).
152. Spackman E, Senne DA, Myers TJ et al. Development of a real-time reverse transcriptase PCR assay for type A influenza virus and the avian H5 and H7 hemagglutinin subtypes. J. Clin. Microbiol. 40(9), 3256–3260 (2002).
153. Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal. Biochem. 162(1), 156–159 (1987).
154. Song DS, Lee YJ, Jeong OM et al. Evaluation of a competitive ELISA for antibody detection against avian influenza virus. J. Vet. Sci. 10(4), 323–329 (2009).
155. Muyal JP, Muyal V, Kaistha BP, Seifart C, Fehrenbach H. Systematic comparison of RNA extraction techniques from frozen and fresh lung tissues: checkpoint towards gene expression studies. Diagn. Pathol. 4(1), 9 (2009).
156. van Elden LJ, van Kraaij MG, Nijhuis M et al. Polymerase chain reaction is more sensitive than viral culture and antigen testing for the detection of respiratory viruses in adults with hematological cancer and pneumonia. Clin. Infect. Dis. 34(2), 177–183 (2002).
157. Borm SV, Steensels M, Ferreira H et al. A universal avian endogenous real-time reverse
transcriptase-polymerase chain reaction control and its application to avian influenza diagnosis and quantification. Avian Dis. 51(s1), 213–220 (2007).
158. Das A, Spackman E, Senne D, Pedersen J, Suarez DL. Development of an internal positive control for rapid diagnosis of avian influenza virus infections by real-time reverse transcription-PCR with lyophilized reagents. J. Clin. Microbiol. 44(9), 3065–3073 (2006).
159. Bustin SA, Benes V, Garson JA et al. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 55(4), 611–622 (2009).
nn� Comprehensive set of guidelines that describe the minimum information necessary for evaluating qPCR experiments to encourage better experimental practice, allowing more reliable and unequivocal interpretation of qPCR results.
160. Couch RB. Prevention and treatment of influenza. N. Engl. J. Med. 343(24), 1778–1787 (2000).
161. Barenfanger J. Clinical and financial benefits of rapid detection of respiratory viruses: an outcomes study. J. Clin. Microbiol. 38(8), 2824–2828 (2000).
162. Rahman M, Vandermause MF, Kieke BA, Belongia EA. Performance of Binax NOW Flu A and B and direct fluorescent assay in comparison with a composite of viral culture or reverse transcription polymerase chain reaction for detection of influenza infection during the 2006 to 2007 season. Diagn. Microbiol. Infect. Dis. 62(2), 162–166 (2008).
163. Chua TH, Ellis TM, Wong CW et al. Performance evaluation of five detection tests for avian influenza antigen with various avian samples. Avian Dis. 51(1), 96–105 (2007).
164. Cui S, Tong G. A chromatographic strip test for rapid detection of one lineage of the H5 subtype of highly pathogenic avian influenza. J. Vet. Diagn. Invest. 20(5), 567–571 (2008).
165. Ho HT, Qian HL, He F et al. Rapid detection of H5N1 subtype influenza viruses by antigen capture enzyme-linked immunosorbent assay using H5- and N1-specific monoclonal antibodies. Clin. Vaccine Immunol. 16(5), 726–732 (2009).
166. Wada A, Sakoda Y, Oyamada T, Kida H. Development of a highly sensitive immunochromatographic detection kit for H5 influenza virus hemagglutinin using silver amplification. J. Virol. Methods 178(1), 82–86 (2011).
167. Wolff JA, Malone RW, Williams P et al. Direct gene transfer into mouse muscle in vivo. Science 247(4949 Pt 1), 1465–1468 (1990).
168. Lai WC, Bennett M. DNA vaccines. Crit. Rev. Immunol. 18(5), 449–484 (1998).
169. Gentschev I, Dietrich G, Spreng S et al. Recombinant attenuated bacteria for the delivery of subunit vaccines. Vaccine 19(17–19), 2621–2628 (2001).
170. Mollenkopf H, Dietrich G, Kaufmann SH. Intracellular bacteria as targets and carriers for vaccination. Biol. Chem. 382(4), 521–532 (2001).
171. Husseiny MI, Hensel M. Evaluation of an intracellular-activated promoter for the generation of live Salmonella recombinant vaccines. Vaccine 23(20), 2580–2590 (2005).
172. Husseiny MI, Hensel M. Rapid method for the construction of Salmonella enterica serovar Typhimurium vaccine carrier strains. Infect. Immun. 73(3), 1598–1605 (2005).
173. Li L, Fang W, Li J, Huang Y, Yu L. Oral DNA vaccination with the polyprotein gene of infectious bursal disease virus (IBDV) delivered by the attenuated Salmonella elicits protective immune responses in chickens. Vaccine 24(33–34), 5919–5927 (2006).
174. Michael A, Stratford R, Khan S, Dalgleish A, Pandha H. Novel strains of Salmonella typhimurium as potential vectors for gene delivery. FEMS Microbiol. Lett. 238(2), 345–351 (2004).
175. Liljebjelke KA, Petkov DI, Kapczynski DR. Mucosal vaccination with a codon-optimized hemagglutinin gene expressed by attenuated Salmonella elicits a protective immune response in chickens against highly pathogenic avian influenza. Vaccine 28(27), 4430–4437 (2010).
176. Husseiny MI, Hensel M. Evaluation of Salmonella live vaccines with chromosomal expression cassettes for translocated fusion proteins. Vaccine 27(28), 3780–3787 (2009).
177. Husseiny MI, Wartha F, Hensel M. Recombinant vaccines based on translocated effector proteins of Salmonella pathogenicity island 2. Vaccine 25(1), 185–193 (2007).
178. Pan Z, Zhang X, Geng S et al. Priming with a DNA vaccine delivered by attenuated Salmonella typhimurium and boosting with a killed vaccine confers protection of chickens against infection with the H9 subtype of avian influenza virus. Vaccine 27(7), 1018–1023 (2009).
179. Russmann H, Shams H, Poblete F, Fu Y, Galan JE, Donis RO. Delivery of epitopes by the Salmonella type III secretion system for vaccine development. Science 281(5376), 565–568 (1998).
180. Evans DT, Chen LM, Gillis J et al. Mucosal priming of simian immunodeficiency virus-specific cytotoxic T-lymphocyte responses in rhesus macaques by the Salmonella type III

Author Pro
of
www.futuremedicine.com 19future science group
Avian influenza viruses: virology, diagnosis & surveillance Review
secretion antigen delivery system. J. Virol. 77(4), 2400–2409 (2003).
181. Nishikawa H, Sato E, Briones G et al. In vivo antigen delivery by a Salmonella typhimurium type III secretion system for therapeutic cancer vaccines. J. Clin. Investig. 116(7), 1946–1954 (2006).
182. Xiong G, Husseiny MI, Song L et al. Novel cancer vaccine based on genes of Salmonella pathogenicity island 2. Int. J. Cancer 126(11), 2622–2634 (2010).
183. Xu X, Husseiny MI, Goldwich A, Hensel M. Efficacy of intracellular activated promoters for generation of Salmonella-based vaccines. Infect. Immun. 78(11), 4828–4838 (2010).
184. Swayne DE, Kapczynski D. Strategies and challenges for eliciting immunity against avian influenza virus in birds. Immunol. Rev. 225(1), 314–331 (2008).
nn� Comprehensive review of AI vaccines and vaccination techniques to maximize immune responses in poultry with future prospectives to imporve the efficiency of available AI vaccines.
185. Swayne DE. Avian influenza vaccines and therapies for poultry. Comp. Immunol. Microbiol. Infect. Dis. 32(4), 351–363 (2009).
186. 187. Wuethrich B: Chasing the fickle swine flu. Science 299(5612), 1502-1505 (2003).
187. 188. Zhu Y, Qi X, Cui L, Zhou M, Wang H: Human co-infection with novel avian influenza A H7N9 and influenza A H3N2 viruses in Jiangsu province, China. The Lancet 381(9883), 2134 (2013).
n� First reprot on the dual infection of human with both avian and seasonal influenza viruses suggesting a potential
source for virus reassortment between a human and an avian influenza viral strain might lead to the generation of a pandemic strain.
188. Lee CW, Suarez DL. Avian influenza virus: prospects for prevention and control by vaccination. Anim. Health Res. Rev. 6(1), 1–15 (2005).
189. Lee SW, Markham PF, Coppo MJC et al. Attenuated vaccines can recombine to form virulent field viruses. Science 337(6091), 188–188.
190. Fernando GJ, Chen X, Prow TW et al. Potent immunity to low doses of influenza vaccine by probabilistic guided micro-targeted skin delivery in a mouse model. PLoS ONE 5(4), e10266 (2010).
191. Poinern GREJ, Le XT, Shan S et al. Ultrasonic synthetic technique to manufacture a pHEMA nanopolymeric-based vaccine against the H6N2 avian influenza virus: a preliminary investigation. Int. J. Nanomed. 6, 2167–2174 (2011).
192. Comin A, Stegeman J, Klinkenberg D, Busani L, Marangon S. Design and results of an intensive monitoring programme for avian influenza in meat-type turkey flocks during four epidemics in northern Italy. Zoonoses Public Health 58(4), 244–251 (2012).
193. Kelvin AA, Meloni D, Sansonetti P et al. Influenza monitoring in Sardinia, Italy identifies H3 subtype in Mediterranean wild migratory birds. J. Infect. Dev. Ctries 6(11), 786–797 (2012).
194. Lebarbenchon C, Chang C-M, van der Werf S et al. Influenza A virus in birds during spring migration in the Camargue, France. J. Wildl. Dis. 43(4), 789–793 (2007).
195. Lamb RA, Choppin PW. The gene structure
and replication of influenza virus. Annu. Rev. Biochem. 52(1), 467–506 (1983).
Websites201. World Organization for Animal Health
(OIE). Infection with viruses of notifiable avian influenza. Terrestrial Animal Health Code Chapter 10.4. www.oie.int/fileadmin/Home/eng/Internationa_Standard_Setting/docs/pdf/A_TAHSC_Feb_2012_Part_A.pdf (Accessed 22 May 2012)
202. WHO. Cumulative number of confirmed human cases of avian influenza A (H5N1) reported to WHO. www.who.int/influenza/human_animal_interface/HAI_Risk_Assessment/en/index.html (Accessed 5 May 2013)
203. US Interagency Working Group. An early detection system for highly pathogenic H5N1 avian influenza in wild migratory birds: US Interagency Strategic Plan. Washington, DC, USA (2006). www.nwhc.usgs.gov/publications/other/aisurveillanceplan.pdf (Accessed 5 September 2012)
204. US Department of the Interior and US Geological Survey. Surveillance plan for the early detection of H5N1 highly pathogenic avian influenza virus in migratory birds in the United States: surveillance year 2009 (Edited by Brand CJ) (2009). http://pubs.usgs.gov/gip/92/pdf/gip-92.pdf (Accessed 24 September 2012)
205. London Laboratory Services Group (2013). www.lhsc.on.ca/lab/labstracts_llsg.htm (Accessed 18 May 2012)
206. www.cdc.gov/ H1N1flu/images.htm (Accessed 5 May 2013)





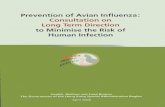

![[Session: Detection and Diagnostics] Improved Diagnostic Tests for Avian Influenza Surveillance](https://static.fdokumen.com/doc/165x107/631244f28f84754bd30a49f3/session-detection-and-diagnostics-improved-diagnostic-tests-for-avian-influenza.jpg)












