Autologous bone marrow stromal cells loaded onto porous hydroxyapatite ceramic accelerate bone...
10
Autologous bone marrow stromal cells loaded onto porous hydroxyapatite ceramic accelerate bone repair in critical-size defects of sheep long bones E. Kon, 1 A. Muraglia, 2 A. Corsi, 3 P. Bianco, 3 M. Marcacci, 1 I. Martin, 2 A. Boyde, 4 I. Ruspantini, 5 P. Chistolini, 5 M. Rocca, 1 R. Giardino, 1 R. Cancedda, 2,6 R. Quarto 2 1 Istituti Ortopedici Rizzoli, Bologna, Italy 2 Istituto Nazionale per la Ricerca sul Cancro, Centro di Biotecnologie Avanzate, Largo Rosanna Benzi 10, Genova, Italy 3 Dipartimento di Medicina Sperimentale, Universita’ dell’ Aquila, and Universita’ La Sapienza, Roma, Italy 4 Department of Anatomy and Developmental Biology, University College London, London, United Kingdom 5 Laboratorio di Ingegneria Biomedica, Istituto Superiore di Sanita `, Roma, Italy 6 Dipartimento di Oncologia, Biologia e Genetica, Universita’ di Genova, Italy Received 16 February 1999; revised 8 July 1999; accepted 6 August 1999 Abstract: The ability of marrow-derived osteoprogenitor cells to promote repair of critical-size tibial gaps upon au- tologous transplantation on a hydroxyapatite ceramic (HAC) carrier was tested in a sheep model. Conditions for in vitro expansion of sheep bone marrow stromal cells (BMSC) were established and the osteogenic potential of the ex- panded cells was validated. Ectopic implantation of sheep BMSC in immunocompromised mice led to extensive bone formation. When used to repair tibial gaps in sheep, cell- loaded implants (n = 2) conducted a far more extensive bone formation than did cell-free HAC cylinders (n = 2) over a 2-month period. In cell-loaded implants, bone formation was found to occur both within the internal macropore space and around the HAC cylinder while in control cell- free implants, bone formation was limited mostly to the outer surface and was not observed in most of the inner pores. As tested in an indentation assay, the stiffness of the complex HAC–bone material was found to be higher in cell- loaded implants compared to controls. Our pilot study on a limited number of large-sized animals suggests that the use of autologous BMSC in conjunction with HAC-based carri- ers results in faster bone repair compared to HAC alone. Potentially this combination could be used clinically in the treatment of extensive long bone defects. © 2000 John Wiley & Sons, Inc. J Biomed Mater Res, 49, 328–337, 2000. Key words: bone marrow stromal cells; hydroxyapatite; bone reconstruction; orthopedic surgery; tissue engineering INTRODUCTION Multipotent precursor cells able to differentiate along the osteogenic and chondrogenic lineage and to give rise to skeletal tissues are found among the stro- mal cells of the postnatal marrow of mammals. 1 Upon isolation in culture, these cells give rise to discrete colonies of fibroblast-like cells (hence their designa- tion as colony-forming unit-fibroblastic, CFU-f). These cells can be thoroughly expanded and assayed for their osteogenic and chondrogenic potential either in vitro, using appropriate sets of phenotypic markers, or in vivo by means of defined transplantation assays. 2–4 The physiological significance of this unique cell population rests with the multiple pathways of tissue turnover and repair in which they are postulated to be involved, as critical effectors, in the postnatal organ- ism. Hence, their discovery has prompted increasing attention over the past few years as important poten- tial tools for the development of novel therapeutic ap- proaches in a variety of skeletal disorders, including somatic cell and gene therapy. 5–8 In orthopedic sur- gery, a cell-based therapeutic approach could be de- sirable in all instances calling for extensive bone re- construction. Although a number of biomaterial-based approaches have been developed and used with vari- able success to date, 1,9 none has proven ideal so far. Among options attractive in terms of quality of re- sults, cost effectiveness, and risk-benefit balances, hy- Correspondence to: R. Quarto; e-mail: quarto@ermes. cba.unige.it Contract grant sponsor: Associazione Italiana Ricerca sul Cancro Contract grant sponsor: Agenzia Spaziale Italiana Contract grant sponsor: Istituto Superiore di Sanita `, Roma, Italy © 2000 John Wiley & Sons, Inc. CCC 0021-9304/00/030328-10
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Autologous bone marrow stromal cells loaded onto porous hydroxyapatite ceramic accelerate bone...

Autologous bone marrow stromal cells loaded onto poroushydroxyapatite ceramic accelerate bone repair incritical-size defects of sheep long bones
E. Kon,1 A. Muraglia,2 A. Corsi,3 P. Bianco,3 M. Marcacci,1 I. Martin,2 A. Boyde,4 I. Ruspantini,5
P. Chistolini,5 M. Rocca,1 R. Giardino,1 R. Cancedda,2,6 R. Quarto2
1Istituti Ortopedici Rizzoli, Bologna, Italy2Istituto Nazionale per la Ricerca sul Cancro, Centro di Biotecnologie Avanzate, Largo Rosanna Benzi 10, Genova, Italy3Dipartimento di Medicina Sperimentale, Universita’ dell’ Aquila, and Universita’ La Sapienza, Roma, Italy4Department of Anatomy and Developmental Biology, University College London, London, United Kingdom5Laboratorio di Ingegneria Biomedica, Istituto Superiore di Sanita, Roma, Italy6Dipartimento di Oncologia, Biologia e Genetica, Universita’ di Genova, Italy
Received 16 February 1999; revised 8 July 1999; accepted 6 August 1999
Abstract: The ability of marrow-derived osteoprogenitorcells to promote repair of critical-size tibial gaps upon au-tologous transplantation on a hydroxyapatite ceramic(HAC) carrier was tested in a sheep model. Conditions for invitro expansion of sheep bone marrow stromal cells (BMSC)were established and the osteogenic potential of the ex-panded cells was validated. Ectopic implantation of sheepBMSC in immunocompromised mice led to extensive boneformation. When used to repair tibial gaps in sheep, cell-loaded implants (n = 2) conducted a far more extensive boneformation than did cell-free HAC cylinders (n = 2) over a2-month period. In cell-loaded implants, bone formationwas found to occur both within the internal macroporespace and around the HAC cylinder while in control cell-
free implants, bone formation was limited mostly to theouter surface and was not observed in most of the innerpores. As tested in an indentation assay, the stiffness of thecomplex HAC–bone material was found to be higher in cell-loaded implants compared to controls. Our pilot study on alimited number of large-sized animals suggests that the useof autologous BMSC in conjunction with HAC-based carri-ers results in faster bone repair compared to HAC alone.Potentially this combination could be used clinically in thetreatment of extensive long bone defects. © 2000 John Wiley& Sons, Inc. J Biomed Mater Res, 49, 328–337, 2000.
Key words: bone marrow stromal cells; hydroxyapatite;bone reconstruction; orthopedic surgery; tissue engineering
INTRODUCTION
Multipotent precursor cells able to differentiatealong the osteogenic and chondrogenic lineage and togive rise to skeletal tissues are found among the stro-mal cells of the postnatal marrow of mammals.1 Uponisolation in culture, these cells give rise to discretecolonies of fibroblast-like cells (hence their designa-tion as colony-forming unit-fibroblastic, CFU-f). Thesecells can be thoroughly expanded and assayed for
their osteogenic and chondrogenic potential either invitro, using appropriate sets of phenotypic markers, orin vivo by means of defined transplantation assays.2–4
The physiological significance of this unique cellpopulation rests with the multiple pathways of tissueturnover and repair in which they are postulated to beinvolved, as critical effectors, in the postnatal organ-ism. Hence, their discovery has prompted increasingattention over the past few years as important poten-tial tools for the development of novel therapeutic ap-proaches in a variety of skeletal disorders, includingsomatic cell and gene therapy.5–8 In orthopedic sur-gery, a cell-based therapeutic approach could be de-sirable in all instances calling for extensive bone re-construction. Although a number of biomaterial-basedapproaches have been developed and used with vari-able success to date,1,9 none has proven ideal so far.Among options attractive in terms of quality of re-sults, cost effectiveness, and risk-benefit balances, hy-
Correspondence to: R. Quarto; e-mail: [email protected]
Contract grant sponsor: Associazione Italiana Ricerca sulCancro
Contract grant sponsor: Agenzia Spaziale ItalianaContract grant sponsor: Istituto Superiore di Sanita,
Roma, Italy
© 2000 John Wiley & Sons, Inc. CCC 0021-9304/00/030328-10

droxyapatite ceramics (HAC) have gained wide use asbone substitutes for clinical bone reconstruction. Theosteoconductive properties of HAC-based materialscan be improved by manipulating structural charac-teristics of the finished implant device to the desiredanatomical shaping and porosity. We recently haveshown that specific structural features that convey theability of the HAC material to undergo subdivisioninto progressively less massive particles in vivo furtherimprove their osteoconductive performance.1 The useof marrow-derived osteogenic precursor cells in con-junction with high-performance HAC-based materialscan be envisioned as a potential major advance in thedesign of skeletal implant devices.7,8,10–17 We recentlydeveloped a model of critical-size bone defect in sheepin which HAC implants provide satisfactory repair at6 months.9 The present study was designed to verifythat marrow-derived osteoprogenitor cells loadedonto HAC would provide a more effective bone repairover a shorter time compared to cell-free HAC im-plants. A pilot study was designed to verify our hy-pothesis. Two ewes were implanted with cell-loadedHAC cylinders (0.5–1.0 × 108 BMSC/cylinder) andtwo were implanted with cell-free HAC cylinders. Allanimals were sacrificed 60 days after implantation, asin a defined ectopic bone formation model.
MATERIALS AND METHODS
Isolation and culture of sheep BMSC
Four- to five-mL marrow aspirates were harvested inheparin (about 200 units/mL final) from the iliac crest ofewes under total anesthesia. Aspirates were pooled andshipped at 4°C in thermic containers via overnight deliveryto the cell culture facility and processed the following morn-ing. Human BMSC from iliac crest bone marrow aspirateswere prepared, as previously described,3 and used for com-parison.
Marrow samples were washed in phosphate buffer saline(PBS), pH 7.2. Nucleated cells were counted with a nuclearstain (0.1% methyl violet in 0.1M of citric acid), suspended inCoon’s modified Ham’s F12 medium supplemented with10% FCS (Mascia Brunelli, Italy), 1 ng/mL of human recom-binant of fibroblast growth factor 2 (FGF2; Austral Biologi-cals, USA), 100 IU/mL of penicillin, and 100 mg/mL ofstreptomycin (ICN Biomedicals, USA), plated in 100-mmdishes at 0.5–1 × 107 cells per dish, and incubated at 37°C inhumidified atmosphere containing 95% air and 5% CO2.Where indicated, dexamethasone was added to the culturemedium at a concentration of 10−8M. The medium waschanged after 2 days and then twice a week. When culturedishes reached confluence (2 weeks after the original plat-ing), cells were harvested with 0.05% trypsin/0.01% EDTA,counted, and replated in 100-mm dishes at 1 × 105 cells perdish. Colony-forming efficiency (expressed as the ratio be-tween the number of colonies obtained and the number of
cells plated) was evaluated by plating 5 × 105 nucleated bonemarrow cells in 60-mm dishes (∼1.8 × 104/cm2). The me-dium was changed after 2 days and then twice a week. After2 weeks the cells were washed in PBS, fixed with 4% form-aldehyde in 0.1 M of phosphate buffer, pH 7.2, stained with1% methylene blue in borate buffer (10 mM, pH 8.8) for 30min, washed with distilled water, and the colonies counted.
Alkaline phosphatase (ALP) activity was assessed as therate of conversion of p-nytrophenyl phosphate to p-nytrophenol using kit number 104-LL (Sigma, USA). Foreach condition to be tested, 2.5 × 104 cells were plated in four10-mm wells. Two wells were washed with PBS, and 100 mLof 0.01% sodium dodecyl sulphate (SDS) were added. After10 min, 0.5 mL of pre-warmed substrate solution and 0.5 mLof alkaline buffer solution were added in each of the twowells. After 15 min of incubation at 37°C, the contents ofeach well were added to 10 mL of 0.05N NaOH to quenchthe reaction; absorbance was read at 410 nm. The remainingtwo wells were used to perform the Thiazolyl blue (MTT)assay to normalize ALP activity to cell number.3 To evaluatethe number of ALP-positive BMSC colonies, cells werestained for ALP using kit number 86-R following the direc-tions of the manufacturer (Sigma, USA) and the positivecells counted. The dishes then were counterstained with he-matoxylin and the total number of cells were counted andthe percentage of ALP-positive derived.
Validation of sheep BMSC osteogenic potential
The osteogenic potential of sheep versus human BMSCwas evaluated in an in vivo bone formation assay, as de-scribed elsewhere.3 Briefly, after 3–4 weeks of expansion(corresponding to the first passage and approximately 18cell doublings), cells were detached from the dishes with0.05% trypsin/0.01% EDTA, washed in serum-free medium,and resuspended at 2.5 × 105/20 mL of fibrinogen (TIM3Immuno, Italy). Two 10-mL aliquots then were applied ontwo opposite faces of dry ceramic cubes (∼volume: 64 mm3)so that each block was loaded with 2.5 × 105 cells, and 25NIH Units of thrombin (Zimotrombina Baldacci, Italy) wereapplied to achieve fibrin polymerization. The loading vol-ume was based on the average volume that fluid blockscould adsorb. Cell-loaded ceramic blocks then were trans-planted into the subcutis of nude mice.3 After 8 weeks,samples were harvested and routinely processed for histol-ogy. Bone formation was quantitated by image analysistechnique.3 Cell-free HA cubes were used as controls.
Surgical procedures
Four 2-year-old ewes of Italian massese breed were in-volved in this study upon proper approval of ethics com-mittees and legal authorities.
The bioceramic used for in vivo implantation was a highlyporous scaffold based on 100% HA of 70–80% porosity. Poresize distribution was: <10 mm, ∼3% vol.; 10–150 mm, ∼11%vol.; and >150 mm, ∼86% vol. The material was produced
329BONE DEFECT REPAIR BY MARROW STROMAL CELLS

and kindly provided by Fin-Ceramica Faenza (Faenza,Italy). Bioceramic cylinders were cleaned by sonication, ex-tensively rinsed in distilled water, and dry sterilized at200°C for 4 h. BMSC (0.5–1.0 × 108) were resuspended in2.5–3.0 mL of fibrinogen (TIM3 Immuno, Italy). Cylinderswere placed in 50-mL sterile tubes together with the cellsuspension and gently rolled until all the suspension wasadsorbed by the bioceramic pores. One hundred NIH Unitsof thrombin (Zimotrombina Baldacci, Italy) were applied toachieve fibrin polymerization. Fibrin coating was used topreserve the implants from dehydration during surgicalprocedures. Cell-free cylinders were treated with the sameprocedure except cell suspension. The cylinders were deliv-ered by overnight courier to the surgical team and im-planted the following morning. Details of the surgical pro-cedure have been described previously.9 Briefly, 3.5 cm fromthe central third of the left tibia were surgically resected andreplaced with a porous hydroxyapatite (HA) cylinder. Toobtain the required mechanical stability, an external fixator(VM-Jet CiTiEffe, Italy) was applied in all animals.
In two animals the HA implants were loaded with autolo-gous ex vivo expanded bone marrow stromal cells (BMSC).After surgery and every 20 days during the experimentationperiod, the animals were monitored by X-ray. At sacrifice, 2months after surgery, tibial diaphysis specimens, includingthe HA cylinders, were explanted and evaluated by grossexamination, microradiography, histology, and scanningelectron microscopy (SEM).
Evaluation of retrieved implants
Undecalcified specimens were dehydrated in ethanol andembedded in an epoxy resin (Araldite™) or air-dried andused unembedded. One hundred–200-mm thick sectionswere obtained by grinding or by means of a microtomeequipped with a rotating diamond knife (Leica, Germany).Contact microradiographs were prepared using an X-raygenerator XRG 3000 (Ital Structures, Italy) and Kodak high-resolution film. Films developed in Kodak D-19 were fixed,washed, and observed using a Zeiss Axiophot microscope(Zeiss, Germany).
Separate cross sections were used for paraffin or plasticembedding. The macroscopic sections were decalcified in7% nitric acid for 24–48 h or in 10% EDTA in 0.1M of caco-dylate buffer, pH 7.0, for 72 h, post-fixed in 4% formalde-hyde (freshly made from paraformaldehyde) in0.1M, pH 7.2,phosphate buffer for 4 h, and routinely embedded in paraf-fin. Four-mm sections were stained with hematoxylin andeosin (HE). Sections obtained from different macroscopicslices and separated by at least 8 mm along the implant axiswere used for quantitative histology. Bone, soft tissue, andspace vacated by the ceramic dissolved during decalcifica-tion easily were distinguished in HE-stained sections. Mea-surements of bone tissue were made using an interactiveimage analyzer (IAS 2000 Delta System, Italy) and the rel-evant software customized for bone histomorphometry.Measurements were not restricted to internal pore space butalso extended to the substantial amounts of bone formedover the outer aspect of the HAC cylinders. Essentially, ar-
eas occupied by bone were recognized histologically onvideo images captured with a video camera from the micro-scope and measured with a digitizing tablet. The softwareautomatically calculated field size and the percent propor-tion of bone surface to field area. From each histologicalsection, the ratio of bone to non-bone structures (bone vol-ume/total volume: BV/TV %) thus was measured. Each sec-tion was scanned and measured in its entirety. For SEMexamination, dehydrated and polymethylmethacrylate-(PMMA) embedded samples were prepared, polished, andcarbon coated, as described.1 BSE imaging and the density ofmineralization of the bone tissue were evaluated in a digitalSEM (Zeiss DSM 962 with Kontron IBAS external controlcomputer) operating under strictly standardized conditions,as previously described.18–20 QBSE images also allowed fordirect measurements of bone and HAC area in each section.
Biomechanical testing
To investigate potential differences in the biomechanicalcharacteristics of the bone/implant complexes, a compara-tive analysis was performed on samples of both types ofimplant, unimplanted porous HAC scaffolds and ceramic-free bone. As standard mechanical tests can show only mac-roscopic features, and owing to the heterogeneity of thesamples and the porosity of both bone and HA carriers,21 wechose to investigate the inside of the implant by indentationtesting. Indentation is a nondestructive technique where anindentor is driven into a material to test its stiffness. Choos-ing the proper indentor shape and diameter, small homog-enous areas can be tested and the distribution of local stiff-ness obtained. Young’s modulus can be derived from stiff-ness measurements obtained by indentation following themethod proposed by Timoshenko and Goodier.22 Indenta-tion tests were made by other authors on cancellous bone inbovine and canine models.23
We performed preliminary indentation tests on bovinecompact bone to validate the indentation technique, to selectthe optimal indentor, and to establish the testing protocol.On the basis of these preliminary tests, we adopted sometechnical solutions to be used in our study on all samples.Tests were made using a flat-ended, cylindrical, 2.5-mm indiameter steel indentor. We tested an average of 15 sites perside. The distance between any two indentations was 3 mm.Indentation depth was set at 0.35 mm to preserve the com-posite structure and to minimize the effect on the mechani-cal properties of adjacent indentation sites. A preload of 2Nwas applied for 30 s before each indentation test. The inden-tor then was driven into the slice at a constant strain rate of0.1 mm/min. The slope in the linear region of the load-displacement curves relative to each tested site was assumedas a measure of local stiffness for each sample.
For comparison purposes we tested by indentation a3-mm thick slice orthogonally cut out from each tibial di-aphysis in correspondence with the transition portion wherecomposition varies from bone integrated with the ceramic tobone tissue exclusively, an unimplanted porous HAC scaf-fold, and a slab of untreated bone from each tibia.
To determine the variations in stiffness occurring along
330 KON ET AL.

the tibia axis in the transition region between the bony endand the ceramic implant we also prepared and tested six3-mm-thick, 1-mm-apart consecutive slices of a cell-loadedsample. Density values (mass/volume) were derived foreach slab.
RESULTS
In vitro characterization of sheep BMSC
The properties of sheep BMSC in culture and upontransplantation in vivo were characterized by compari-
son with human marrow (colony counts 126 ± 9 vs.41.6 ± 10.1 per million plated nucleated cells). In con-trast with the characteristic heterogeneous morphol-ogy of human BMSC in culture, sheep BMSC colonieswere composed of very homogeneously small, thin,and elongated fibroblast-like cells (not shown). Inter-estingly, while sheep BMSC colonies were consistently
Figure 1. Alkaline phosphatase activity (A) and osteogeniccapacity in vivo (B) of sheep versus human marrow-derivedosteoprogenitor cells. Sheep BMSC do not display ALP ac-tivity at variance with human cells, but do form substantialbone tissue upon transplantation in vivo.
Figure 2. Histology of tissues formed in ectopic transplantsof sheep BMSC in the subcutis of immunocompromisedmice. (A) Bone is extensively formed within the ceramicpores. (B) Only fibrous tissue is found in cell free HAC im-plants. (C) Occasionally, cartilage is observed. Bar = (A, B)100 mm; (C) 25 mm.
331BONE DEFECT REPAIR BY MARROW STROMAL CELLS

negative for ALP, 30–50% of human BMSC colonieswere positive. ALP activity was almost undetectablein sheep BMSC and clearly expressed under basal con-ditions in human BMSC [Fig. 1(A)] Sheep BMSC re-mained ALP negative even when stimulated withdexamethasone; by contrast, ALP activity increased bya significant 60% in human cells upon stimulation bydexamethasone (data not shown).
Tissue formation in ectopic transplants ofsheep BMSC
Transplantation of small HAC cubes loaded withculture-expanded sheep BMSC into the subcutis of im-munocompromised mice resulted in the formation ofprominent amounts of bone at 8 weeks [Fig. 1(B); Fig.2(A)]. Volumes of newly formed bone in transplants ofsheep cells were higher than those obtained in trans-plants of human BMSC (+17%) [Fig. 1(B)]. Hematopoi-etic marrow development in HAC pores lined by thenewly formed bone tissues was regularly observedwith both sheep and human BMSC (not shown). Oc-casionally, transplants of sheep BMSC produced car-tilage, which was never observed in transplants of hu-
mans BMSC [Fig. 2(B)]. Bone, cartilage, and hemato-poietic marrow never were observed in controltransplants of HAC alone [Fig. 2(C)].
Repair of critical-size tibial defects by autologoussheep BMSC
All the animals survived the surgical procedure. Noinfections or extrusions were observed at the implan-tation site. By the second postoperative day, they weremoving normally around their cage, and 1 week laterthey were able to return to their normal environmentand activities.
Callus was established at the interface between thehost bone and the HAC cylinders, either loaded withBMSC or cell-free (Fig. 3). Callus developed aroundthe cortex of the host bone and around the defect in allof the specimens in both groups although it was sig-nificantly more extensive in BMSC-loaded samples.Peri-implant bone formation already was detectable,although discontinuously, at 1 month in animals thathad received the cell-loaded implants but not in con-trol animals. At 2 months, a radiographically moreconspicuous callus was observed in animals receiving
Figure 3. Serial X-rays of the HAC cylinders implanted in the animal tibia. (A,B,C) BMSC-loaded HAC; (D,E,F) cell-freecontrol HAC. (A,D) Post surgery; (B,F) 2 months after transplantation; (C,F) 2 months after transplantation, higher magni-fication. Union was established rapidly at the bone/HAC interface. Callus formation was more extensive in BMSC-loadedsamples.
332 KON ET AL.
cell-loaded HAC implants compared to control ani-mals (Fig. 3).
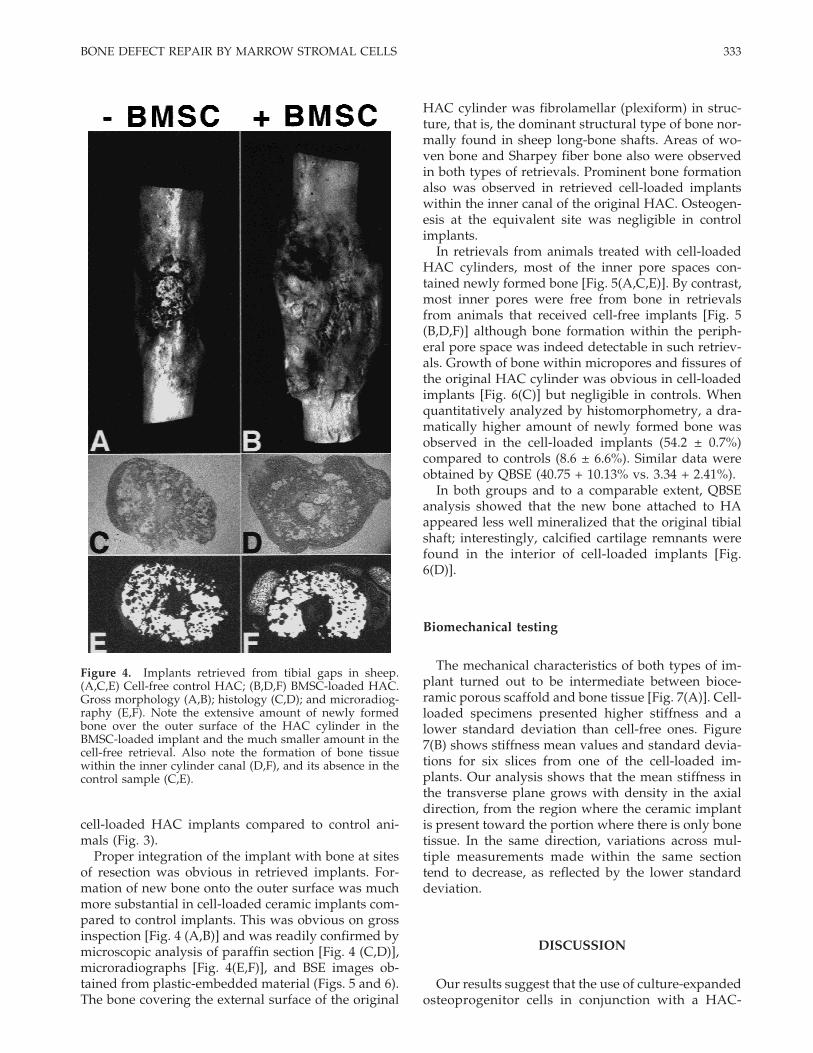
Proper integration of the implant with bone at sitesof resection was obvious in retrieved implants. For-mation of new bone onto the outer surface was muchmore substantial in cell-loaded ceramic implants com-pared to control implants. This was obvious on grossinspection [Fig. 4 (A,B)] and was readily confirmed bymicroscopic analysis of paraffin section [Fig. 4 (C,D)],microradiographs [Fig. 4(E,F)], and BSE images ob-tained from plastic-embedded material (Figs. 5 and 6).The bone covering the external surface of the original
HAC cylinder was fibrolamellar (plexiform) in struc-ture, that is, the dominant structural type of bone nor-mally found in sheep long-bone shafts. Areas of wo-ven bone and Sharpey fiber bone also were observedin both types of retrievals. Prominent bone formationalso was observed in retrieved cell-loaded implantswithin the inner canal of the original HAC. Osteogen-esis at the equivalent site was negligible in controlimplants.
In retrievals from animals treated with cell-loadedHAC cylinders, most of the inner pore spaces con-tained newly formed bone [Fig. 5(A,C,E)]. By contrast,most inner pores were free from bone in retrievalsfrom animals that received cell-free implants [Fig. 5(B,D,F)] although bone formation within the periph-eral pore space was indeed detectable in such retriev-als. Growth of bone within micropores and fissures ofthe original HAC cylinder was obvious in cell-loadedimplants [Fig. 6(C)] but negligible in controls. Whenquantitatively analyzed by histomorphometry, a dra-matically higher amount of newly formed bone wasobserved in the cell-loaded implants (54.2 ± 0.7%)compared to controls (8.6 ± 6.6%). Similar data wereobtained by QBSE (40.75 + 10.13% vs. 3.34 + 2.41%).
In both groups and to a comparable extent, QBSEanalysis showed that the new bone attached to HAappeared less well mineralized that the original tibialshaft; interestingly, calcified cartilage remnants werefound in the interior of cell-loaded implants [Fig.6(D)].
Biomechanical testing
The mechanical characteristics of both types of im-plant turned out to be intermediate between bioce-ramic porous scaffold and bone tissue [Fig. 7(A)]. Cell-loaded specimens presented higher stiffness and alower standard deviation than cell-free ones. Figure7(B) shows stiffness mean values and standard devia-tions for six slices from one of the cell-loaded im-plants. Our analysis shows that the mean stiffness inthe transverse plane grows with density in the axialdirection, from the region where the ceramic implantis present toward the portion where there is only bonetissue. In the same direction, variations across mul-tiple measurements made within the same sectiontend to decrease, as reflected by the lower standarddeviation.
DISCUSSION
Our results suggest that the use of culture-expandedosteoprogenitor cells in conjunction with a HAC-
Figure 4. Implants retrieved from tibial gaps in sheep.(A,C,E) Cell-free control HAC; (B,D,F) BMSC-loaded HAC.Gross morphology (A,B); histology (C,D); and microradiog-raphy (E,F). Note the extensive amount of newly formedbone over the outer surface of the HAC cylinder in theBMSC-loaded implant and the much smaller amount in thecell-free retrieval. Also note the formation of bone tissuewithin the inner cylinder canal (D,F), and its absence in thecontrol sample (C,E).
333BONE DEFECT REPAIR BY MARROW STROMAL CELLS

based material convey a significant improvement inthe repair of critical-size tibial defects in a sheepmodel. Previous data from our laboratory indicatedthat the same material effectively can promote effi-cient repair of identical defects over a 6-month periodwhen used alone.9 Our present data indicate that boththe amount of bone formed onto and within the HACdevice, and the overall stiffness of the HAC/bonecomplex upon retrieval, are improved by their use ofmarrow-derived osteoprogenitor cells loaded onto theHAC cylinder prior to implantation.
In principle, one would expect that the single mostimportant difference in the pattern of new bone for-mation promoted by BMSC loaded onto the HAC ma-terial would rest with the filling of the internal mac-ropore space, with bone formed directly by loaded
cells or their progeny. Indeed, a difference in theamount of bone within the internal pores was ob-served in our study. An interesting finding, however,was the far more prominent amount of bone formedover the external surface and within the inner canal ofthe cell-loaded HAC implant. Potential explanationsfor this pattern include (1) a higher density of loadedcells within the outermost portions of the HAC cylin-der as a result of the distribution of the cells into thematerial; (2) stimulation of resident osteoprogenitorcells within the skeletal tissues of the resection ends bythe implanted cells via a paracrine loop; and (3) com-paratively better survival of loaded cells within theoutermost portions of the HAC cylinder, which areexpected to be vascularized faster and more efficientlythan more internal regions. Further experimentation is
Figure 5. BSE analysis of the pattern of bone formed in the internal macropore spaces in cell-loaded versus cell-freeimplants. Note the extensive lining of HAC surfaces and pore filling in cell-loaded implants (A,C,E) and the low amounts ofbone formed within pores in cell-free implants (B,D,F). BM = bone matrix; HA = hydroxyapatite. Bars = 200 mm.
334 KON ET AL.

needed to address this issue, which would lead tofurther knowledgeable manipulation of the design ofthe cellular–HAC implant device. Interestingly, simi-lar observations recently were made by Bruder andcolleagues.8 However, a notable difference betweentheir study and ours rests with the almost completelack of bone formation, both within pores and over theimplant external surface, in their cell-free implants. Incontrast, we did observe significant osteogenesis inour control implants, in keeping with our previousreports indicating the ability of our HAC materialalone to direct efficient bone repair in the same modelover the long term.9 We consider this a major differ-ence, which may have different explanations. (1) Al-though the surgical model was similar, the animalmodel used was different. (2) The device used toachieve the mechanical stability after the surgery mayhave important implications. In our model we used anexternal fixator while Bruder and colleagues used aninternal plate. The different approach may have con-
sequences on the mechanical stimulation of both im-plant and bone resected ends, perhaps being morestimulated by the use of an external (elastic) fixatorand less or not at all by the use of an internal (rigid)plate. (3) The use of fibrin as a cell sealant in our studymight itself result in the promotion of osteogenesisfrom resident osteogenic cells in our cell-free im-plants.24,25 We showed earlier that long-term events inthe implanted HAC material in vivo include its pro-gressive subdivision into smaller fragments, which re-sults in an increased (osteoconductive) surface.1 Thischange occurs in conjunction with the formation ofbone within native and induced cracks and fissures ofthe original HAC as well as within micropore space.As such, the disintegration of HAC over time is likelya function of the amount of bone formed therein aswell as of mechanical strain in vivo, dissolution ofHAC, and limited amounts of osteoclast-mediated re-sorption. HAC fragmentation and growth of bonewithin micropore space were obvious in the retrieved
Figure 6. Cell-loaded implants. Newly formed bone was found to fill the system of internal fissures (A) and micropore spacecharacteristic of the HAC original (cf. Reference 1). (B) shows areas of Sharpey fiber bone (arrows) within the neocortexformed on the outer surface of the HAC cylinder. (C) shows bone growth within micropore (as opposed to macropore; seeBoyde et al. 19991) space. (D) shows a substantial area of mineralized cartilage. Bars = (A,D) 1 mm; (B) 200 mm; (C) 50 mm.
335BONE DEFECT REPAIR BY MARROW STROMAL CELLS

cell-loaded implants and negligible in controls, likelyreflecting the differences in the extent of bone forma-tion observed. A comparison of the biomechanical re-sults with the structural features observed in the re-trieved implants suggests that osteogenesis withinand around the HAC cylinder leads to an increased
stiffness of the composite HAC–bone material. Cell-loaded implants displayed higher stiffness whensubjected to indentation tests. Taken together, theseobservations suggest that not only do loaded osteo-progenitor cells improve bone formation within theHAC implant, but they also improve mechanical prop-erties as a consequence of greater bone formation andbetter integration/disintegration of HAC itself.
The types of bone tissue formed in the cell-loadedHAC did not differ from those observed in the con-trols and included plexiform bone, predominant in theneocortex, woven, and Sharpey fiber bone.1,26 How-ever, areas of mineralized cartilage merging withnewly formed bone were observed in cell-loaded im-plants. Interestingly, hypertrophic cartilage also wasobserved in ectopic ossicles formed by sheep BMSCupon implantation with HAC carriers in the subcutisof immunocompromised mice. Cartilage formation insuch systems appears to be a characteristic of sheeposteoprogenitor cells and was not observed in im-plants of either human or mouse BMSC. It also isworth mentioning here that in vitro characterization ofsheep BMSC disclosed peculiar biological propertiesof these cells, including their independence on dexa-methasone and lack of expression of ALP activity, thatare worth further study in a general biological context.
The current approach to the treatment of extensivebone gaps that delivers, perhaps, the best performancein terms of functional recovery is the use of vascular-ized autologous bone segments. Still the time neces-sary for the graft to reach complete integration andfull biomechanical strength is very long, ranging be-tween 12 and 18 months. Furthermore, an additionalsignificant lesion is created at the donor site and oftenmore than one surgical procedure is needed. The de-velopment of cell culture technology in conjunctionwith synthetic biomaterials suited for bone substitu-tion may lead to a novel, integrated approach to thedesign and construction of bone substitutes, combin-ing the advantages of biologically boosted osteogen-esis with the osteoconduction intrinsic to the HAC-based ceramics.
References
1. Boyde A, Corsi A, Quarto R, Cancedda R, Bianco P. Osteocon-duction in large macroporous hydroxyapatite ceramic im-plants: Evidence for a complementary integration and disinte-gration mechanism. Bone 1999;24:579–589.
2. Haynesworth SE, Goshima J, Goldberg VM, Caplan AI. Char-acterization of cells with osteogenic potential from humanmarrow Bone 1992;13:81–88.
3. Martin I, Muraglia A, Campanile G, Cancedda R, Quarto R. Fi-broblast growth factor-2 supports ex vivo expansion and main-tenance of osteogenic precursors from human bone marrow.Endocrinology 1997;138:4456–4462.
4. Krebsbach PH, Kuznetsov SA, Satomura K, Emmons RV, Rowe
Figure 7. (A) Mean stiffness values plus standard devia-tion for the HA scaffold (HAC), cell-free implants (Ctr),BMSC-loaded implants (Exp), and bone tissue (Bone). Themechanical properties of bone–ceramic complexes werehalfway between the HAC porous structure and bone.BMSC-loaded implants were stiffer than cell-free implants.The four sample sets yielded higher stiffness values and alower standard deviation as the structure of the materialbecame more compact and the bone phase predominated.(B) Mean stiffness values plus standard deviation and den-sity of the six slabs (A–F) from a BMSC-loaded implant. Inthe axial direction, from the diaphysis—where HAC andbone are integrated—toward the epiphysis—where onlybone tissues is present—(A→F) mean stiffness values for thecross-sections of the bone–HAC aggregate grew while thestandard deviation decreased. Upon a first analysis, stiffnessgrew as sample density grew.
336 KON ET AL.

DW, Robey PG. Bone formation in vivo: Comparison of osteo-genesis by transplanted mouse and human marrow stromalfibroblasts. Transplantation 1997;63:1059–1069.
5. Krebsbach PH, Mankani MH, Satomura K, Kuznetsov SA,Robey PG. Repair of craniotomy defects using bone marrowstromal cells. Transplantation 1998;66:1272–1278.
6. Kadiyala S, Kraus KH, Bruder SP. Canine mesenchymal stemcell-based therapy for the regeneration of bone. Trans TissueEng Soc 1996;1:20.
7. Kadiyala S, Jaiswal N, Bruder SP. Culture-expanded, bonemarrow-derived mesenchymal stem cells can regenerate acritical-sized segmental bone defect. Tissue Eng 1997;3:173–185.
8. Bruder SP, Kraus KH, Goldberg VM, Kadiyala S. The effect ofimplants loaded with autologous mesenchymal stem cells onthe healing of canine segmental bone defects. J Bone Joint Surg1998;80:985–996.
9. Marcacci M, Kon E, Zaffagnini S, Giardino R, Rocca M, CorsiA, Benvenuti A, Bianco P, Quarto R, Martin I, Cancedda R.Reconstruction of extensive long bone defects in sheep usingporous hydroxyapatite sponges. Calcif Tissue Int 1999;64:83–90.
10. Nade S, Armstrong L, McCartney E, Baggalay B. Osteogenesisafter bone and bone marrow transplantation. The ability ofceramic materials to sustain osteogenesis from transplantedbone marrow cells. Preliminary study. Clin Orthop 1983;181:255–263.
11. Ohgushi H, Goldberg VM, Caplan AI. Repair of bone defectswith marrow cells and porous ceramic. Experiments in rat.Acta Orthop Scand 1989;60:334–339.
12. Goshima J, Golberg VM, Caplan AI. The osteogenic potentialof cultured-expanded rat marrow mesenchymal cells assayedin vivo in calcium phosphate ceramic blocks. Clin Orthop 1991;262:298–311.
13. Grundel RE, Chapman MW, Yee T, Moore DC. Autogenic bonemarrow and porous biphasic calcium phosphate ceramic forsegmental bone defects in the canine ulna. Clin Orthop Rel Res1991;26:244–258.
14. Lang H, Mertens T. Porous hydroxylapatite ceramics with ho-mologous osteoblasts from cell cultures for bone replacement.Dtsch Z Mund Kiefer Gesichtschir 1991;15:64–68.
15. Begley CT, Doherty MJ, Hankey DP, Wilson DJ. The culture ofhuman osteoblasts upon bone graft substitutes. Bone 1993;14:661–666.
16. Bruder SP, Fink DJ, Caplan AI. Mesenchymal stem cells inbone development, bone repair, and skeletal regenerationtherapy. J Cell Biochem 1994;56:283–294.
17. Bruder SP, Kurth AA, Shea M, Hayes WC, Kadiyala S. Quan-titative parameters of human mesenchymal stem cell-mediatedbone regeneration in an orthotopic site. Trans Orthop Res Soc1997;22:250.
18. Boyde A, Davy KWM, Jones SJ. Standards for mineral quanti-tation of human bone by analysis of backscattered electronicimages. Scanning 1995;17(V):6–7.
19. Howell PGT, Davy KWM, Boyde A. Mean atomic number andbackscattered electron coefficient for some materials with lowatomic mean number. Scanning 1998;20:35–40.
20. Howell PGT, Boyde A. Monte Carlo simulation of electronbaskscattering from compounds with low mean atomic num-ber. Scanning 1998;20:45–49.
21. Le Huec JC, Schaeverbeke T, Clemnt D, Faber J, Le Rebeller A.Influence of porosity on the mechanical resistance of hydroxy-apatite ceramics under compressive stress. Biomaterials 1995;16:113–118.
22. Timoshenko SP, Goodier JN. Theory of elasticity, 3rd ed. NewYork: McGraw–Hill; 1970. p 380–409.
23. Sumner DR, Willke TL, Berzins A, Turner TM. Distribution ofYoung’s modulus in the cancellous bone of the proximal ca-nine tibia. J Biomech 1994;27:1095–1099.
24. Arnaud E, Morieux C, Wybier M, Devernejoul MC. Potentia-tion of transforming growth factor (TGF-b1) by natural coraland fibrin in a rabbit cranioplasty model. Calcif Tissue Int1994;54:493–498.
25. Fortunato G, Marini E, Valdinucci F, Bonucci E. Long-termresults of hydroxyapatite-fibrin glue implantation in plasticand reconstructive craniofacial surgery. J CraniomaxillofacSurg 1997;25:124–135.
26. Boyde A. Scanning electron microscopy studies of bone. In:Bourne GH, editor. The biochemistry and physiology of bone.Vol 1 e. New York: Academic Press, Inc.; 1976. p 259–310.
337BONE DEFECT REPAIR BY MARROW STROMAL CELLS