
Adolescent impulsivity phenotypes characterized by distinct brain networks
Upload
independentCategory
view
2download
0
Atherogenic Vascular and Lipid Phenotypes in Young Type 1 Diabetics are associated with
Diabetes High Risk HLA genotype
Brief title: Diabetes High Risk HLA and early atherosclerosis
Authors:
1Michal Odermarsky, MD, 2Anita Nilsson, MSc, 2Åke Lernmark, MD, PhD, 3Sture Sjöblad, MD, PhD,
1Petru Liuba P, MD, PhD
Affiliation:
Pediatric 1Cardiology and 3Endocrinology, Lund University Hospital, Lund, and 2Department of Clinical
Sciences, University Hospital MAS, Lund University, Malmö, Sweden
Corresponding author:
Petru Liuba, PhD, MD
Division of Cardiology, Department of Paediatrics
Lund University Hospital
SE-22185 Lund, SWEDEN
Tel: +46 46 17 82 67 / Fax: + 46 415 51606 / E-mail: [email protected]
Page 1 of 21
Copyright Information
Articles in PresS. Am J Physiol Heart Circ Physiol (September 28, 2007). doi:10.1152/ajpheart.00795.2007
Copyright © 2007 by the American Physiological Society.
2
ABSTRACT
Background: Expression of human leukocyte antigen (HLA) class II molecules on islet endothelial
cells (EC) is a central vascular event in the pathogenesis of type 1 diabetes. Previous studies
demonstrated the ability of other vascular EC to express HLA and thereby to process islet autoantigens
on their surface. We investigated whether the HLA-DQ2/8 genotype, which confers the highest risk
for type 1 diabetes, is associated with early atherosclerosis in youths with this disease.
Methods: Brachial artery endothelium-dependent, flow-mediated dilation (BA-FMD) and carotid
artery intima-media thickness (CA-IMT), as well as markers of systemic inflammation (C-reactive
protein, fibrinogen, and orosomucoid), HbA1C, LDL, HDL and total cholesterol (TC), were assessed
in 86 children and adolescents with type 1 diabetes (mean age and diabetes duration: 15 and 7 years,
respectively) between 2004 and 2006. HLA genotypes were determined in dried blood spots by an
oligoblot hybridization method.
Results: HLA-DQ2/8 was detected in 34 patients (“DQ2/8”). When this group was compared to the
remaining patients (“non-DQ2/8“, n=52), there were no differences in age, diabetes duration, HbA1C,
body mass index, inflammatory markers, IMT, and TC (p>0.4). In the DQ2/8 group, LDL-to-HDL
ratio was elevated as compared to the non-DQ2/8 group (1.8 vs 1.3, respectively; p=0.001), while
FMD did not significantly differ between the groups (5.3 vs 6.7%, respectively; p=0.08). When
patients were further categorized in relation to CRP (cut-off value 1 mg/l), BA-FMD was significantly
lower (3%, p<0.01), whereas LDL-to-HDL ratio increased further (2.2, p<0.001) in the subgroup of
“DQ2/8”&“CRP>1” patients compared to the remaining three subgroups. These associations remain
significant after adjustment for age, diabetes duration, and HbA1C by ANCOVA. The brachial artery
responses to nitroglycerine were similar in all subgroups.
Conclusion: In conclusion, the diabetes-predisposing HLA-DQ2/8 genotype in children and
adolescents with type 1 diabetes interferes with endothelial and lipid-related mechanisms of early
atherosclerosis, possibly in part through inflammatory pathways.
Key-words: type 1 diabetes; genetics; lipids; vascular function
Page 2 of 21
Copyright Information
3
CONDENSED ABSTRACT
We investigated in 86 children and adolescents with type 1 diabetes whether the HLA-DQ2/8
genotype could influence atherogenic vascular and lipid phenotypes. In the DQ2/8 group, LDL-to-
HDL ratio was significantly elevated (1.8 vs 1.3, p<0.01), while brachial artery`s flow-mediated
dilation (BA-FMD) was only slightly decreased (5.3 vs 6.7%, p=0.08) as compared to the non-DQ2/8
group. When patients were further categorized in relation to CRP (cut-off value 1 mg/l), BA-FMD was
significantly lower (3%, p<0.01) and LDL-to-HDL ratio increased further (3.2, p<0.001) in the
subgroup of “DQ2/8”&”CRP>1” patients compared to the remaining three subgroups.
Page 3 of 21
Copyright Information
4
INTRODUCTION Type 1 diabetes mellitus occurs most frequently in children and adolescents, and is of growing
concern particularly in industrialized countries, including Sweden and the United States, as its
incidence continues to rise (3).
A genetic susceptibility involving class II human leukocyte antigen (HLA) genes
is recognized in more than 80 % of young patients with type 1 diabetes (13). The primary loci of
genetic susceptibility to type 1 diabetes have been mapped to the HLA-DQ region, which is
located on chromosome 6 (23). Two HLA haplotypes DQB1*0302-A1*0301 (DQ8), and
DQB1*0201-A1*0501 (DQ2) appear to confer the highest risk for developing type 1 diabetes
(27), especially when both are present in the genotype (ie, HLA-DQ2/8).
Previous studies suggested that expression of HLA-DQ molecules on the surface of
pancreatic microvascular endothelial cells could be an important vascular pathway in the
autoimmune lymphocyte-mediated reaction that leads to β-cell destruction, the underlying
pathology of type 1 diabetes (26, 17). This process is seemingly not confined to the pancreas
since other organs such as gut and thyroid may be affected as well (1). Recent observation that
aortic vascular endothelial cells also owe the ability to express HLA (6) lends support to this
hypothesis.
An important question is whether the HLA-mediated endotheliopathy could also
occur at the site of the conductance arteries, where atherosclerosis incepts. Type 1 diabetics are at
significant risk for cardiovascular disease in the adult life (2). Early and accelerated
atherosclerosis appears to play an important role in the excess cardiovascular morbidity (2, 5).
In light of the afore-mentioned findings, and given the importance of vascular
endothelial cells throughout the course of atherosclerosis (4) including in diabetes (22), we
investigated whether the diabetes-predisposing HLA genotype DQ2/8 could interfere with lipid
and vascular phenotypes of early atherosclerosis in children and adolescents with type 1 diabetes.
Page 4 of 21
Copyright Information
5
METHODS
A. Study population
Eighty-six children and adolescents aged between 7 – 22 years (mean age 15; 49 males/ 37
females) with type 1 diabetes for at least 6 months (mean duration 7 years) were randomly
recruited from the diabetes outpatient clinic at Children’s Hospital Lund. All patients were on
insulin treatment (Lantus® and Novorapid®). Four patients were on thyroid hormone replacement
therapy (Levaxin®). Exclusion criteria were: familiar hypercholesterolemia, active smoking,
history of premature coronary or cerebrovascular disease among first-degree relatives, and
systemic hypertension. Body weight, height, arterial blood pressure (systolic and diastolic) and
blood glucose were measured upon the ultrasound visit. Data on demographic information,
parental education and current occupation, family and personal history for major cardiovascular
risk factors (primary hypercholesterolemia, hypertension, premature coronary and
cerebrovascular disease) were assessed by questionnaire. Data regarding diabetes duration were
obtained from the registry of the outpatient diabetes clinic.
The study was approved by the ethical committee for human research at the Lund
University. Written consent was obtained from all participants aged 18 years and older or, if
under 18, from their guardians. All participants gave oral consent.
B. HLA typing, inflammatory, and lipid analyses
HLA typing was performed from dried blood spots by DELFIA® method. Briefly, DNA in the
blood was amplified and the presence of the particular alleles was determined by a hybridization
reaction using allele-specific, short oligonucleotides labelled with lanthanide chelates (14).
High-density lipoprotein (HDL), low-density lipoprotein (LDL) and total cholesterol (TC) were
analysed by an enzymatic method (Roche/Hitachi 912, Roche Diagnostics). Plasma high-
sensitivity C-reactive protein (CRP) was measured by enzyme-linked immunoassay using
Page 5 of 21
Copyright Information
6
polyclonal antibodies (DACO Diagnostics, Glostrup, Denmark). Plasma orosomucoid and
fibrinogen were assessed by specific immunoassays.
C. Assessment of endothelium-dependent dilation of the brachial artery
The dilatory responses to hyperaemia (endothelium-dependent agonist) and glycerol trinitrate
(GTN, endothelium-independent) were obtained in 70 patients. Briefly, longitudinal scans of the
brachial artery (nondominant arm) were imaged several centimeters above the antecubital fossa
via a 15-MHz linear ultrasound transducer of an Acuson Sequoia C256 (Siemens AG,
Germany). The ultrasound beam frequency was set at 8 MHz. Once the image was obtained, the
transducer was positioned throughout the ultrasound study with aid of a transducer arm holder
(Great Ormond Street Hospital, London, UK). ECG-gated end-diastolic scans of the artery were
recorded at baseline, and a pressure cuff tourniquet placed around the forearm was thereafter
inflated to 200 mmHg (minimum 50 mmHg over the systolic blood pressure) for 5 minutes. A
new series of frames were taken for 15 seconds before and 120 seconds after cuff deflation.
Arterial flow velocity was obtained prior to and during the first 15 seconds after cuff release by
pulsed Doppler signal at 70° to the vessel with the range gate in the center of the artery. Blood
flow volume was calculated by multiplying the velocity-time integral of Doppler signal by heart
rate and the vessel cross-sectional area. Reactive hyperemia was calculated as percent increase in
flow after cuff release as compared with baseline flow.Following a 10-minute recovery period,
additional frames were taken before and over a 4-minute period after sublingual administration of
400 µg GTN spray. Flow-mediated and GTN-induced dilation of the brachial artery were
expressed as maximum percent dilatation following cuff deflation and GTN administration,
respectively. All scans were taken in a “blind” fashion, with the sonographer being unaware of
the patients` inflammatory and HLA characteristics.
Page 6 of 21
Copyright Information

7
D. Carotid artery ultrasound protocol
The ultrasound system described above was used. The imaging protocol was described in details
previously (16). In short, longitudinal scans in bi-dimensional mode of the 1-cm-long distal end
of the left common carotid artery were imaged so that the lumen-intima and intima-media
interfaces were clearly distinguishable. All scans corresponded to the R-wave on ECG. Four to
six scans from each individual were recorded on videotape for offline analysis of the carotid
artery compliance (CAC), stiffness index (SI), and intima-media thickness (IMT). The mean
carotid IMT of 4 measurements along a 1-cm segment was calculated from each scan. Mean IMT
obtained from all scans from the same subject were averaged, and the resulted mean IMT was
used for statistical analyses.
Statistics
ANOVA was used to assess the differences between the DQ2/8 and non-DQ2/8 groups in age,
BMI, diabetes duration, HbA1C, lipid, inflammatory, and vascular indexes (BA-FMD and CA-
IMT). ANCOVA was used to control the associations of HLA-DQ2/8 genotype with the lipid and
vascular indexes for the possible confounding effects of age, diabetes duration, BMI, and HbA1C.
Simple and multiple regression was used for determining the association between inflammatory,
lipid and vascular indexes. CRP was log-transformed given its skewed distribution. Statistical
significance was set at p<0.05. Data are given as mean±standard errors unless otherwise
specified. StatView for Windows (SAS Institute Inc.®) was employed as statistical software.
RESULTS
Thirty-four patients (39 %, 18 male and 16 female) were positive for the HLA-DQ2/8 genotype.
Among the remaining 52 patients (31 male and 21 female), 15 had one of the two haplotypes
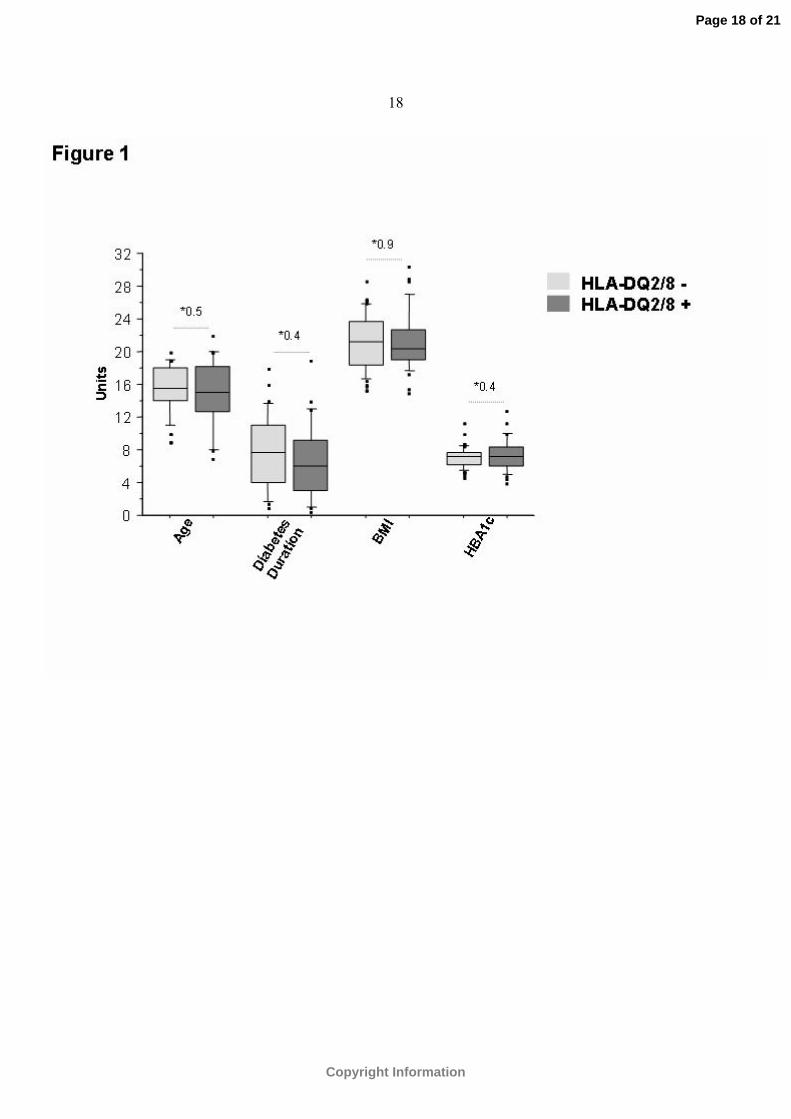
(HLA-DQ2 or DQ8). No differences in age, BMI, diabetes duration, and HbA1C were noted
Page 7 of 21
Copyright Information
8
between the DQ2/8 and non-DQ2/8 groups (p>0.4, Figure 1). Blood glucose was similar in both
groups (8.8 mmol/L in non-DQ2/8 group vs. 8.4 mmol/L in DQ2/8 group, p=0.7).
Lipid and inflammatory profiles
No significant differences in CRP (p>0.4), fibrinogen (p>0.8), and orosomucoid (p>0.7) were
observed between the DQ2/8 and non-DQ2/8 groups.
Lipid data were available in 83 patients. Two patients (one from each group) had HDL
cholesterol below the acceptable level (0.9 mmol/l). LDL cholesterol (acceptable upper limit: 3.3
mmol/l) was abnormally elevated in 5 patients (3 in the non-DQ2/8 group, and 2 in the DQ2/8
group).
When the groups were compared, LDL cholesterol was higher in the DQ2/8 group
(2.5±0.1 mmol/l) than in the non-DQ2/8 group ( 2.1±0.2 mmol/l, p<0.05), whereas HDL
cholesterol did not significantly differ between the DQ2/8 group (1.5±0.07 mmol/l) and the non-
DQ2/8 group (1.7±0.05 mmol/l, p=0.1). Total cholesterol showed a trend toward increased levels
in the DQ2/8 group compared to the non-DQ2/8 group (4.4±0.2 vs 4.1±0.1 mmol/l, p=0.08).
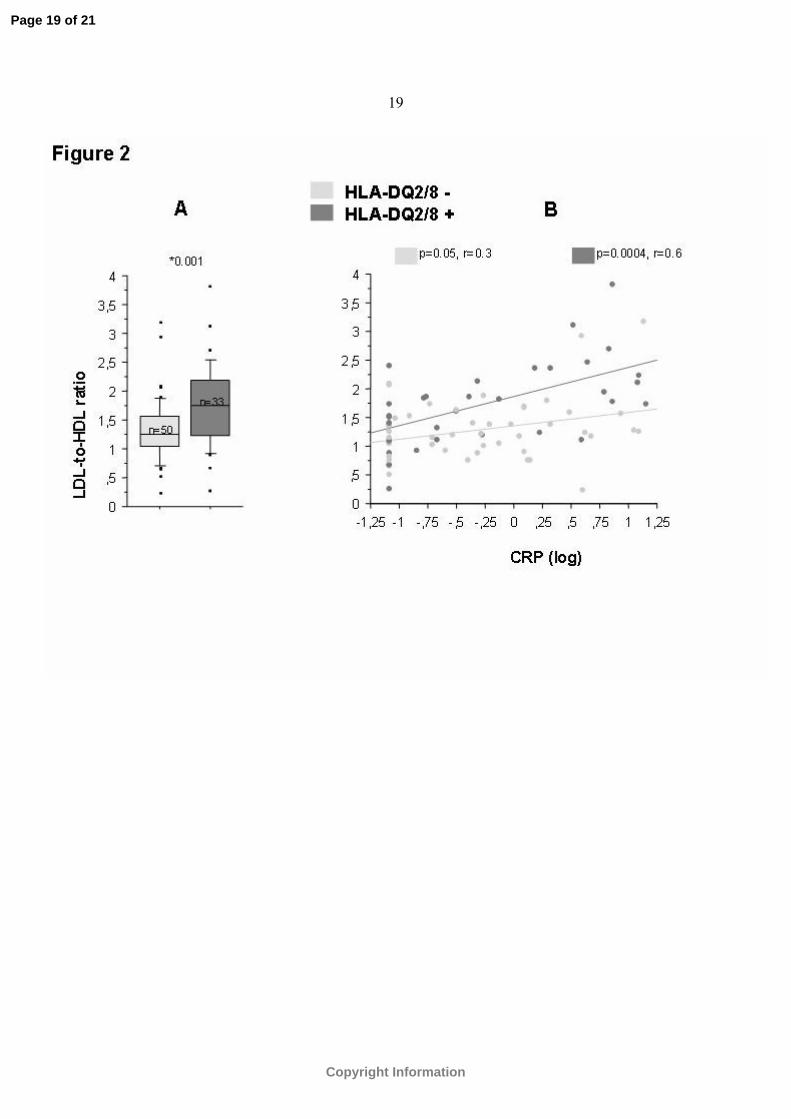
LDL-to-HDL ratio, an important atherogenic lipid index, was significantly higher in
the DQ2/8 group (1.8±0.2) than in the non-DQ2/8 group (1.3±0.2, p<0.01; Figure 2/Panel A).
The difference remained significant after adjustment for age, BMI, diabetes duration, HbA1C, and
CRP (p=0.02 by ANCOVA).
Overall, LDL-to-HDL ratio showed a modest correlation with CRP (r=0.4,
p<0.001) and BMI (r=0.4, p<0.01). When the patients were grouped based on the genotype, the
correlation between CRP and LDL-to-HLD ratio became significant among the DQ2/8 patients
(r=0.6, p<0.001;Figure 2/Panel B). In this group, the association between LDL-to-HDL ratio and
CRP remained significant after adjustment for age, BMI, diabetes duration and HbA1C (p<0.01).
Page 8 of 21
Copyright Information
9
Flow-mediated and GTN-induced dilations of the brachial artery, and intima-media
thickness of the carotid artery
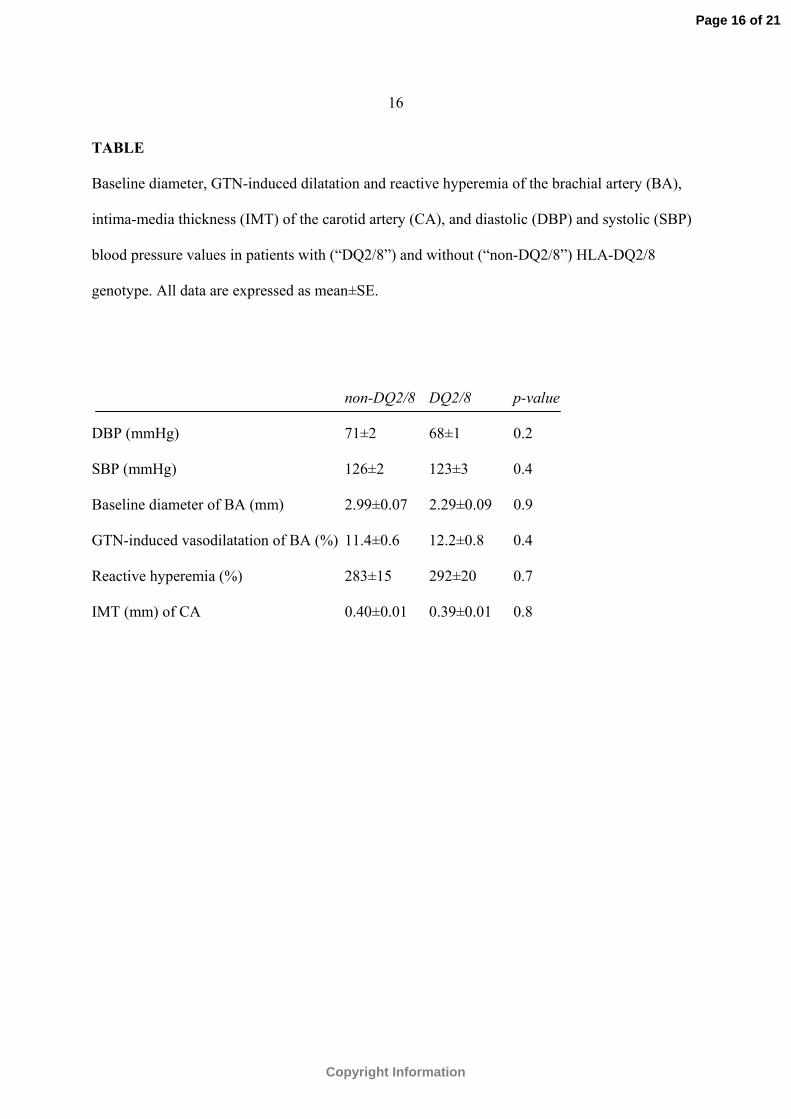
There groups were similar in baseline brachial artery diameter, reactive hyperemia, GTN-induced
dilation and carotid IMT (Table 1).
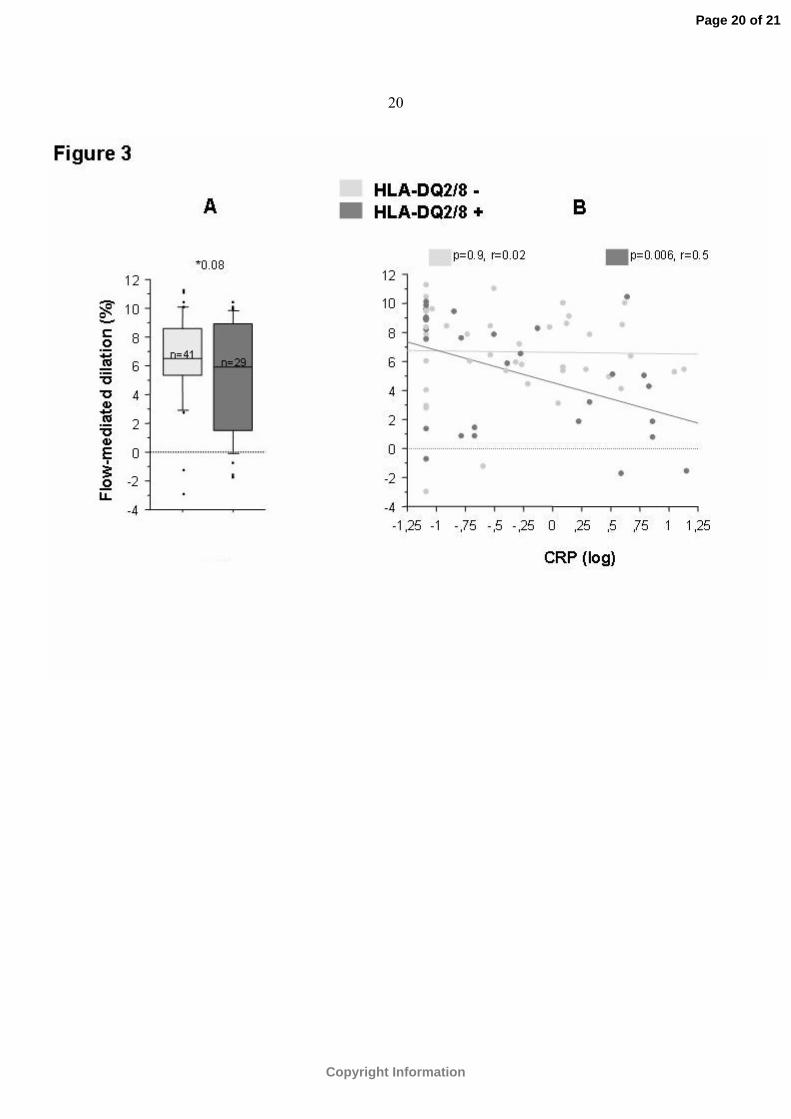
No significant difference was noted between the groups with regard to BA-FMD
(5.3±0.7 in the DQ2/8 group vs 6.7±0.5% in the non-DQ2/8 group, p=0.08; Figure 3/Panel A).
However, in the DQ2/8 group, FMD inversely correlated with CRP (r=0.5, p=0.01), but no such
association was observed in the non-DQ2/8 group (r=0.1, p=0.8; Figure 3/Panel B). FMD did not
correlate with LDL-to-HDL ratio in either groups (p>0.5).
.
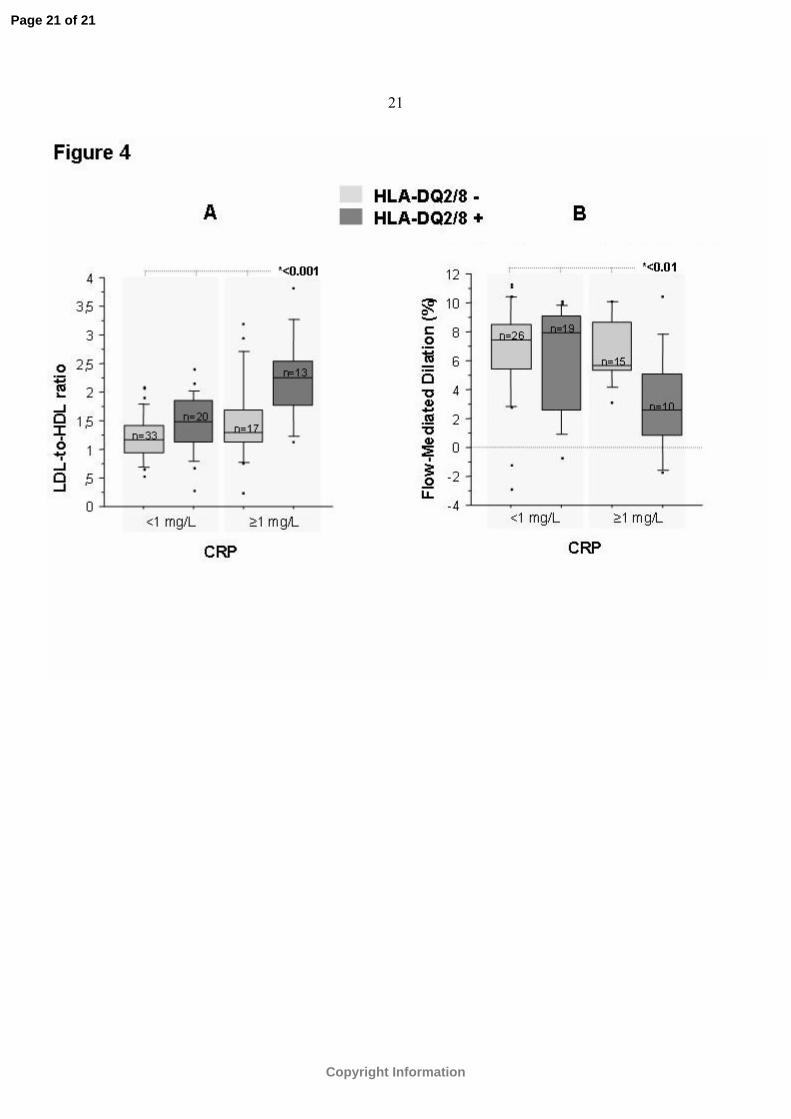
Low-grade inflammation, lipid, and vascular indexes in “DQ2/8+” patients
When the patients were further categorized according to their CRP levels (cut-off value 1 mg/l),
both LDL-to-HDL ratio (Figure 4/Panel A) and FMD (Figure 4/Panel B) showed a shift toward a
more atherogenic profile in the “DQ2/8”&”CRP>1” subgroup (2.2±0.2 and 3±1.1%,
respectively) as compared to the remaining subgroups. The GTN-induced dilatory responses of
the brachial artery and carotid IMT were similar in all subgroups (p>0.3).
DISCUSSION
To the best of our knowledge, this study is the first to suggest that type 1 diabetes children and
adolescents with genotype conferring the highest risk for this disease could be more susceptible
to atherogenic endothelial and lipid phenotypes. Our findings also suggest a possible relationship
between this genetic susceptibility and systemic inflammation.
It is nowadays agreed that type 1 diabetes increases the risk of cardiovascular
disease through inflammatory, oxidative, and glucose-related events that lead to vascular
endothelial damage (11), which is a key-mechanism in atherosclerosis through all of its stages
(4). Mounting evidence points out that a close-to-normal glycemic control in type 1 diabetes
Page 9 of 21
Copyright Information
10
patients is not sufficient to fully prevent the widespread vasculopathy (7), supporting thus the
view that other intrinsic and extrinsic factors are important as well. Although the concept of
heritability of cardiovascular disease has gained increasing attention during the past decade (19),
no study has so far investigated whether genetic factors predisposing for type 1 diabetes could
interfere with atherogenic events in young patients with type 1 diabetes.
Approximately 60% of the familial genetic risk for type 1 diabetes is attributable to
the HLA region (4). HLA DQA1*0301-B1*0302 and DQA1*0501-B1*0201 haplotypes,
especially when both are present in the genotype, have been found to be most strongly associated
with the onset of type 1 diabetes, while other haplotypes, e.g., HLA-DQA1*0102- B1*0602,
confer an age-dependent negative association (27). The precise mechanisms whereby certain
HLA increase diabetes susceptibility are not yet thoroughly clarified, but there is a general
consensus that the HLA DQ molecules exert their effects in part via presentation of peptides from
islet antigens to T cells, which contribute to the destruction of insulin-producing cells (28).
Previous studies (26, 17) have shown that expression of HLA molecules on the endothelial cells
of islet microcirculation goes hand in hand with lymphocyte infiltration, thereby suggesting a
possible pathogenic role of HLA-mediated endothelial vasculopathy in the development of type 1
diabetes. Greening and colleagues (6) demonstrated that both pancreatic and aorta endothelial
cells expressing HLA class II molecules have the ability to process and present the islet
autoantigen GAD65. It is therefore conceivable to assume that endothelial cells of other
peripheral arterial beds migh also owe HLA-mediated antigen presenting capacity in type 1
diabetes (6). Particular HLA-DQ phenotypes, including DQ2/8, appear to facilitate the presence
of potentially pathogenic T cells in the peripheral circulation via thymic selection (10).
Lymphocyte accumulation within the arterial wall is an important mechanistic
component of atherosclerosis development (8), and contributes to endothelial injury (18).
Endothelial injury promotes in turn additional immune events, including release of chemokines
and cytokines, with further endothelial transmigration of immune cells and CRP synthesis via
Page 10 of 21
Copyright Information
11
liver activation by interleukin-6 (15). The increased inflammatory activity leads to alteration of
lipoprotein metabolism characterized in part by increase in LDL and decrease in HDL
cholesterol. Dyslipidemia prevails in type 1 diabetes (12), and has an important role in
endothelial injury and plaque development (24, 25). CRP is slightly, yet significantly elevated in
diabetic children (21). Nevertheless, a slight rise in CRP, ie, over 1 mg/l, appears to be predictive
of the relative risk of future cardiovascular events in apparently healthy adults (20). Järvisalo and
colleagues found that even less plasma concentrations of CRP (ie, 0.7 mg/l) were associated with
decreased endothelial vasodilatory function of the brachial artery (9). How exactly the putative
association of CRP with the endothelial and lipidemic disturbances is amplified in HLA DQ2/8
diabetic patients is difficult to speculate, being to our opinion a tantalizing task for future studies
addressing this topic.
In diabetic children and adolescents, measures of both functional and structural
changes precursive to atherosclerosis seem to be influenced by age and diabetes duration. It is
therefore possible that the observed associations with diabetes-risk HLA might be more
pronounced in older patients or in those with longer disease duration. Also, further studies are
needed to investigate whether a better diabetes control would translate into a lesser impact of the
genotype on atherogenic endothelial and lipid phenotypes. In our study, these associations
remained significant after adjustment for age, diabetes duration, and HbA1c, but a possible
additive effect of these factors on the reported links cannot be ruled out. Whether the genotyping
might be used to identify individuals for whom early lipid management may be warranted is
perhaps an additional important task for future trials given the impact of diabetes dyslipidemia on
cardiovascular risk.
Several limitations need to be considered. The size of the study group is rather
small although invitation to participate was submitted to all diabetic patients registered at our
hospital. Our intention is to recruit additional patients aged 6 to 18 y across the entire part of
Southernmost Sweden (Skåne county). Other HLA genotypes known to predispose to diabetes
Page 11 of 21
Copyright Information
12
will be studied as well. We also intend to include nondiabetic HLA-matched siblings in order to
assess whether the HLA predisposition to diabetes could influence per se the vascular status and
lipid profile in otherwise healthy children. Another limitation resides in the cross-sectional
nature of this study. Follow-up studies over a 2-year period are under way. Finally, even though
flow-mediated dilation of the brachial artery is generally accepted as a surrogate of early
atherosclerosis, it remains uncertain whether it could in time become a clinically useful measure
of cardiovascular risk. Therefore, the precise clinical significance of the observed endothelial
disturbances in relation to HLA-DQ2/8 genotype remains uncertain.
In conclusion, the present study suggests independent associations of HLA-DQ 2/8
genotype, which is known to confer the highest risk for type 1 diabetes, with atherogenic lipid
and vascular endothelial phenotypes in children and adolescents with type 1 diabetes. The
findings warrant large-scale, prospective studies to verify these findings and to assess whether
this and other diabetes-susceptible HLA genotypes could accelerate atherosclerosis already
during the preclinical phase of type 1 diabetes.
Acknowledgements
The study was supported by FAMRI, USA. Additional grants were received from Lund
University, the Swedish Research Council, and the National Institute of Health. We thank Annica
Maxedius, registered nurse, for the excellent technical assistance in ultrasound scanning and
blood sampling throughout the study.
REFERENCES
1. Barker JM. Clinical review: Type 1 diabetes-associated autoimmunity: natural history,
genetic associations, and screening. J Clin Endocrinol Metab 91: 1210-1217, 2006.
Page 12 of 21
Copyright Information
13
2. Creager MA, Lüscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease:
Pathophysiology, clinical consequences, and medical therapy. Circulation 108: 1527-32,
2003.
3. Daneman D. Type 1 diabetes. Lancet 367: 847-858, 2006.
4. Davignon J, Ganz P. Role of endothelial dysfunction in atherosclerosis. Circulation 109:
27-32, 2004.
5. Eckel RH, Wassef M, Chait A, Sobel B, Barrett E, King G, Lopes-Virella M, Reusch J,
Ruderman N, Steiner G, Vlassara H. Prevention Conference VI: Diabetes and
Cardiovascular Disease: Writing Group II: pathogenesis of atherosclerosis in diabetes.
Circulation 105: 138-143, 2002.
6. Greening JE, Tree TI, Kotowicz KT, van Halteren AG, Roep BO, Klein NJ, Peakman M.
Processing and presentation of the islet autoantigen GAD by vascular endothelial cells
promotes transmigration of autoreactive T-cells. Diabetes 52: 717-725, 2003.
7. Goldberg IJ, Dansky HM. Diabetic vascular disease: an experimental objective.
Arterioscler Thromb Vasc Biol 26: 1693-1701, 2006.
8. Hansson GK, Libby P, Schonbeck U, Yan ZQ. Innate and adaptive immunity in the
pathogenesis of atherosclerosis. Circ Res 91: 281-291, 2002.
9. Jarvisalo MJ, Harmoinen A, Hakanen M, Paakkunainen U, Viikari J, Hartiala J,
Lehtimäki T, Simell O, Raitakari OT. Elevated serum C-reactive protein levels and early
arterial changes in healthy children. Arterioscler Thromb Vasc Biol 22: 1323-1328, 2002
10. Jordan MS, Riley MP, von Boehmer H, Caton AJ. Anergy and suppression regulate
CD4(+) T cell responses to a self peptide. Eur J Immunol 30: 136-144, 2000.
11. Joshua IG, Zhang Q, Falcone JC, Bratcher AP, Rodriguez WE, Tyagi SC. Mechanisms of
endothelial dysfunction with development of type 1 diabetes mellitus: role of insulin and
C-peptide. J Cell Biochem 96: 1149-1156, 2005.
Page 13 of 21
Copyright Information
14
12. Kershnar AK, Daniels SR, Imperatore G, Palla SL, Petitti DB, Pettitt DJ, Marcovina S,
Dolan LM, Hamman RF, Liese AD, Pihoker C, Rodriguez BL. Lipid abnormalities are
prevalent in youth with type 1 and type 2 diabetes: the SEARCH for Diabetes in Youth
Study. J Pediatr 149: 314-319, 2006.
13. Lernmark A. Type 1 diabetes as a model for prediction and diagnosis. Autoimmunity 37:
341-345, 2004.
14. Lernmark B, Lynch K, Lernmark A. Cord blood islet autoantibodies are related to stress
in the mother during pregnancy. Ann N Y Acad Sci 1079: 345-349, 2006.
15. Libby P. Inflammation in atherosclerosis. Nature 420: 868-74, 2002.
16. Liuba P, Persson J, Luoma J, Ylä-Herttuala S, Pesonen E. Acute infections in children are
accompanied by oxidative modification of LDL and decrease of HDL cholesterol, and are
followed by thickening of carotid intima-media. Eur Heart J 24: 515-521, 2003.
17. Marelli-Berg FM, Frasca L, Weng L, Lombardi G, Lechler RI. Antigen recognition
influences transendothelial migration of CD4+ T-cells. J Immunol 162: 696-703, 1999.
18. Monaco C, Andreakos E, Kiriakidis S, Feldmann M, Paleolog E. T-cell-mediated
signalling in immune, inflammatory and angiogenic processes: the cascade of events
leading to inflammatory diseases. Curr Drug Targets Inflamm Allergy 3: 35-42, 2004.
19. Nordlie MA, Wold LE, Kloner RA. Genetic contributors toward increased risk for
ischemic heart disease. J Mol Cell Cardiol 39: 667-679, 2005.
20. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, Fadl
YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SC Jr, Taubert K, Tracy RP,
Vinicor F; Centers for Disease Control and Prevention; American Heart Association.
Markers of inflammation and cardiovascular disease: application to clinical and public
health practice: A statement for healthcare professionals from the Centers for Disease
Control and Prevention and the American Heart Association. Circulation 107: 499-511,
2003.
Page 14 of 21
Copyright Information
15
21. Picardi A, Valorani MG, Vespasiani Gentilucci U, Manfrini S, Ciofini O, Cappa M,
Guglielmi C, Pozzilli P; IMDIAB Group. Raised C-reactive protein levels in patients with
recent onset type 1 diabetes. Diabetes Metab Res Rev 23: 211-214, 2007.
22. Raza J, Movahed A. Current concepts of cardiovascular disease in diabetes mellitus. Int J
Cardiol 89: 123-134, 2003.
23. Redondo MJ, Fain PR, Eisenbarth GS. Genetics of type 1 diabetes. Recent Prog Horm
Res 56: 69-89, 2001.
24. Renard CB, Kramer F, Johansson F, Lamharzi N, Tannock LR, von Herrath MG, Chait A,
Bornfeldt KE. Diabetes and diabetes-associated lipid abnormalities have distinct effects
on initiation and progression of atherosclerotic lesions. J Clin Invest 114: 659-668, 2004.
25. Ross R, Aqius L. The process of atherogenesis--cellular and molecular interaction: from
experimental animal models to humans. Diabetologia 35: 34-40, 1992.
26. Savage CO, Brooks CJ, Harcourt GC, Picard JK, King W, Sansom DM, Willcox N.
Human vascular endothelial cells process and present autoantigen to human T-cell lines.
Int Immunol 7: 471-479, 1995.
27. Todd JA. Genetic analysis of type 1 diabetes using whole genome approaches. Proc Natl
Acad Sci U S A 92: 8560-8565, 1995.
28. Tree TI, Duinkerken G, Willemen S, de Vries RR, Roep BO. HLA-DQ-regulated T-cell
responses to islet cell autoantigens insulin and GAD65. Diabetes 53: 1692-1699,
2004.Genetic analysis of type 1 diabetes using whole genome approaches. Proc Natl Acad
Sci U S A 92: 8560-8565, 1995.
Page 15 of 21
Copyright Information
16
TABLE
Baseline diameter, GTN-induced dilatation and reactive hyperemia of the brachial artery (BA),
intima-media thickness (IMT) of the carotid artery (CA), and diastolic (DBP) and systolic (SBP)
blood pressure values in patients with (“DQ2/8”) and without (“non-DQ2/8”) HLA-DQ2/8
genotype. All data are expressed as mean±SE.
non-DQ2/8 DQ2/8 p-value
DBP (mmHg) 71±2 68±1 0.2
SBP (mmHg) 126±2 123±3 0.4
Baseline diameter of BA (mm) 2.99±0.07 2.29±0.09 0.9
GTN-induced vasodilatation of BA (%) 11.4±0.6 12.2±0.8 0.4
Reactive hyperemia (%) 283±15 292±20 0.7
IMT (mm) of CA 0.40±0.01 0.39±0.01 0.8
Page 16 of 21
Copyright Information
17
FIGURE LEGEND
Figure 1: Box plot distribution of age (years), diabetes duration (years), body mass index (BMI,
kg/m2), and glycosylated hemoglobin levels (%) of diabetic patients with (“DQ2/8“n=34) and
without (DQ2/8, n=52) HLA-DQ2/8 genotype. The box plot displays the 25th percentile, median,
and 75th percentile, as well as the 10th and 90th percentiles as horizontal lines outside the box.
* denotes p value.
Figure 2: Panel A-Box plot illustrating the differences in LDL-to-HDL ratio between the DQ2/8
and non-DQ2/8 groups. The box plot displays the 25th percentile, median, and 75th percentile, as
well as the 10th and 90th percentiles as horizontal lines outside the box. Panel B- association of
LDL-to-HDL ratio with CRP in DQ2/8 and non-DQ2/8 patients. * denotes p value, r denotes
correlation coefficient, and n denotes number of patients.
Figure 3: Panel A- Box plot illustrating the differences in brachial artery`s flow mediated
dilation between the DQ2/8 and non-DQ2/8 groups. The box plot displays the 25th percentile,
median, and 75th percentile, as well as the 10th and 90th percentiles as horizontal lines outside the
box. Panel B- Association of brachial artery’s flow-mediated dilation with CRP in in DQ2/8 and
non-DQ2/8 patients. * denotes p value, r denotes correlation coefficient, and n denotes number of
patients.
Figure 4: Box plot distribution of LDL-to-HDL ratio (Panel A) and brachial artery`s flow
mediated dilation (Panel B) in relation to the HLA-DQ2/8 genotype and CRP (cut-point 1 mg/l).
The box plot displays the 25th percentile, median, and 75th percentile, as well as the 10th and 90th
percentiles as horizontal lines outside the box. * denotes p value, and n denotes number of
patients.
Page 17 of 21
Copyright Information
18
Page 18 of 21
Copyright Information
19
Page 19 of 21
Copyright Information
20
Page 20 of 21
Copyright Information
21
Page 21 of 21
Copyright Information
Copyright © 2022 FDOKUMEN




















