
Association of variation in Fc receptor 3B gene copy number with rheumatoid arthritis in Caucasian...
14
Association of variation in Fcγ receptor 3B gene copy number with rheumatoid arthritis in Caucasian samples Cushla McKinney 1 , Manuela Fanciulli 2 , Marilyn E Merriman 1 , Amanda Phipps-Green 1 , Behrooz Z Alizadeh 3 , Bobby P C Koeleman 3 , Nicola Dalbeth 4 , Peter J Gow 5 , Andrew A Harrison 6 , John Highton 7 , Peter B Jones 4 , Lisa K Stamp 8 , Sophia Steer 9 , Pilar Barrera 10 , Marieke J H Coenen 11 , Barbara Franke 11 , Piet L C M van Riel 10 , Tim J Vyse 12 , Tim J Aitman 2 , Timothy R D J Radstake 10 , and Tony R Merriman 1 1 Department of Biochemistry, University of Otago, Dunedin, New Zealand 2 MRC Clinical Sciences Centre and Division of Medicine, Imperial College London, London, UK 3 Complex Genetics Section, Department of Medical Genetics, University Medical Centre Utrecht, Utrecht, The Netherlands 4 Department of Medicine, University of Auckland, Auckland, New Zealand 5 Department of Rheumatology, Middlemore Hospital, Auckland, New Zealand 6 Department of Medicine, University of Otago, Wellington, New Zealand 7 Department of Medicine, University of Otago, Dunedin, New Zealand 8 Department of Medicine, University of Otago, Christchurch, New Zealand 9 Kings’ College Hospital NHS Foundation Trust, London, UK 10 Department of Rheumatology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands 11 Department of Human Genetics, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands 12 Division of Medicine, Imperial College London, London, UK Abstract Objective—There is increasing evidence that variation in gene copy number (CN) influences clinical phenotype. The low-affinity Fcγ receptor 3B (FCGR3B) located in the FCGR gene cluster is a CN polymorphic gene involved in the recruitment to sites of inflammation and activation of polymorphonuclear neutrophils (PMNs). Given recent evidence that low FCGR3B CN is a risk factor for systemic but not organ-specific autoimmune disease and the potential importance of PMN in the pathophysiology of rheumatoid arthritis (RA), the authors hypothesised that FCGR3B gene dosage influences susceptibility to RA. Methods—FCGR3B CN was measured in 643 cases of RA and 461 controls from New Zealand (NZ), with follow-up analysis in 768 cases and 702 controls from the Netherlands and 250 cases and 211 controls from the UK. All subjects were of Caucasian ancestry. Results—Significant evidence for an association between CN <2 and RA was observed in the Dutch cohort (OR 2.01 (95% CI 1.37 to 2.94), p=3×10–4) but not in the two smaller cohorts (OR 1.45 (95% CI 0.92 to 2.26), p=0.11 and OR 1.33 (95% CI 0.58 to 3.02), p=0.50 for the NZ and UK populations, respectively). The association was evident in a meta-analysis which included a previously published Caucasian sample set (OR 1.67 (95% CI 1.28 to 2.17), p=1.2×10–4). Correspondence to Tony R Merriman, Department of Biochemistry, University of Otago, P O Box 56, Dunedin 9054, New Zealand; [email protected]. Competing interests None. Ethics approval Ethical approval for the study in New Zealand was given by the MultiRegion (cases) and Lower South Ethics Committees (controls), in the UK by the local research ethics committees of Lewisham Hospital and Guy’s and St Thomas’ Hospitals and in The Netherlands by the local ethics committee. All subjects gave written informed consent. Provenance and peer review Not commissioned; externally peer reviewed. Europe PMC Funders Group Author Manuscript Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03. Published in final edited form as: Ann Rheum Dis. 2010 September ; 69(9): 1711–1716. doi:10.1136/ard.2009.123588. Europe PMC Funders Author Manuscripts Europe PMC Funders Author Manuscripts
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Association of variation in Fc receptor 3B gene copy number with rheumatoid arthritis in Caucasian...

Association of variation in Fcγ receptor 3B gene copy numberwith rheumatoid arthritis in Caucasian samples
Cushla McKinney1, Manuela Fanciulli2, Marilyn E Merriman1, Amanda Phipps-Green1,Behrooz Z Alizadeh3, Bobby P C Koeleman3, Nicola Dalbeth4, Peter J Gow5, Andrew AHarrison6, John Highton7, Peter B Jones4, Lisa K Stamp8, Sophia Steer9, Pilar Barrera10,Marieke J H Coenen11, Barbara Franke11, Piet L C M van Riel10, Tim J Vyse12, Tim JAitman2, Timothy R D J Radstake10, and Tony R Merriman1
1Department of Biochemistry, University of Otago, Dunedin, New Zealand 2MRC ClinicalSciences Centre and Division of Medicine, Imperial College London, London, UK 3ComplexGenetics Section, Department of Medical Genetics, University Medical Centre Utrecht, Utrecht,The Netherlands 4Department of Medicine, University of Auckland, Auckland, New Zealand5Department of Rheumatology, Middlemore Hospital, Auckland, New Zealand 6Department ofMedicine, University of Otago, Wellington, New Zealand 7Department of Medicine, University ofOtago, Dunedin, New Zealand 8Department of Medicine, University of Otago, Christchurch, NewZealand 9Kings’ College Hospital NHS Foundation Trust, London, UK 10Department ofRheumatology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands11Department of Human Genetics, Radboud University Nijmegen Medical Centre, Nijmegen, TheNetherlands 12Division of Medicine, Imperial College London, London, UK
AbstractObjective—There is increasing evidence that variation in gene copy number (CN) influencesclinical phenotype. The low-affinity Fcγ receptor 3B (FCGR3B) located in the FCGR gene clusteris a CN polymorphic gene involved in the recruitment to sites of inflammation and activation ofpolymorphonuclear neutrophils (PMNs). Given recent evidence that low FCGR3B CN is a riskfactor for systemic but not organ-specific autoimmune disease and the potential importance ofPMN in the pathophysiology of rheumatoid arthritis (RA), the authors hypothesised that FCGR3Bgene dosage influences susceptibility to RA.
Methods—FCGR3B CN was measured in 643 cases of RA and 461 controls from New Zealand(NZ), with follow-up analysis in 768 cases and 702 controls from the Netherlands and 250 casesand 211 controls from the UK. All subjects were of Caucasian ancestry.
Results—Significant evidence for an association between CN <2 and RA was observed in theDutch cohort (OR 2.01 (95% CI 1.37 to 2.94), p=3×10–4) but not in the two smaller cohorts (OR1.45 (95% CI 0.92 to 2.26), p=0.11 and OR 1.33 (95% CI 0.58 to 3.02), p=0.50 for the NZ andUK populations, respectively). The association was evident in a meta-analysis which included apreviously published Caucasian sample set (OR 1.67 (95% CI 1.28 to 2.17), p=1.2×10–4).
Correspondence to Tony R Merriman, Department of Biochemistry, University of Otago, P O Box 56, Dunedin 9054, New Zealand;[email protected].
Competing interests None.
Ethics approval Ethical approval for the study in New Zealand was given by the MultiRegion (cases) and Lower South EthicsCommittees (controls), in the UK by the local research ethics committees of Lewisham Hospital and Guy’s and St Thomas’ Hospitalsand in The Netherlands by the local ethics committee. All subjects gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Europe PMC Funders GroupAuthor ManuscriptAnn Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Published in final edited form as:Ann Rheum Dis. 2010 September ; 69(9): 1711–1716. doi:10.1136/ard.2009.123588.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

Conclusions—One possible mechanism to explain the association between reduced FCGR3BCN and RA is the reduced clearance of immune complex during infl ammation. However, it is notknown whether the association between RA and FCGR3B CN is aetiological or acts as a proxymarker for another biologically relevant variant. More detailed examination of genetic variationwithin the FCGR gene cluster is required.
INTRODUCTIONCopy number variation (CNV) in immune-response genes has been implicated in severalautoimmune diseases including CCL3L1 involvement in rheumatoid arthritis (RA)1 andsystemic lupus erythematosus (SLE),2 and association of β-defensins with Crohn’s disease3
and psoriasis.4 Recently, CNV in the gene coding for the Fcγ receptor 3B (FCGR3B), themost abundant neutrophil binding site for polymeric IgG and immune complexes, has alsobeen shown to be associated with immune-mediated glomerulonephritis,5 SLE67 and, albeitwith a conflicting nature of association, antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis: CN <2 as risk factor6 or CN >2 as risk factor.7
The Fcγ receptor IIIb is constitutively expressed by polymorphonuclear leucocytes8 and isinvolved in many critical neutrophil functions including recruitment to sites ofinflammation910 and activation.11 In addition, anti-FcγRIIIb antibodies and solubleFcγRIIIb (released from apoptotic polymorphonuclear neutrophils (PMNs) or shed fromactivated PMNs by cleavage of the glycosylphosphatidylinositol anchor) delay neutrophilapoptosis1213 and may compete with IgG for binding sites to perpetuate localinflammation.12 The presence of autoantibodies and accumulation of activated neutrophils atsites of inflammation is a feature of RA and SLE, and there is evidence that these cells arefunctionally abnormal. For example, extended survival of PMN is observed in RA and SLE,which may reflect dysregulation of apoptosis, a major mechanism by which the activity ofneutrophils is controlled.14 The pathogenesis of RA is mediated in part by PMN, whichcompose 80–90% of the cellular infiltrate during active RA.15–17 In addition to releasingproinflammatory cytokines including tumour necrosis factor (TNF), activated PMN producelarge amounts of potentially damaging reactive oxygen species (ROS) (O2, H2O2 andHOCL) and granular enzymes such as proteases and permeability-inducing factors, all ofwhich potentially contribute to tissue damage and joint erosion (see Edwards and Hallett17
for review). FcγRIIIb has been implicated in the release of these toxic products in responseto soluble immune complexes such as those found in RA joints.11 Genetic variation otherthan CN variants in the FCGR locus has already been associated with RA.18 Furthermore,FcγR-mediated production of ROS and apoptosis is impaired in PMN isolated from patientswith RA.1119
There is clinical evidence implicating FcγR in the pathogenesis of RA,14–16 association of ahaplotype encompassing FCGR3B with RA,20 and association of FCGR3B CN with SLEand other systemic but not organ-specific immune-mediated pathology.5–7 RA is a diseasewith both organ-specific and non-specific features which primarily affects the synovialmembrane but also involves a number of other tissues. On this basis, we hypothesised thatFCGR3B CN plays a role in the pathogenesis of RA. This was tested in a multicentre studyby measuring FCGR3B CN in three Caucasian RA case–control cohorts.
METHODSStudy subjects
All study subjects were of European Caucasian descent. The New Zealand (NZ) RA cohortconsisted of 643 patients recruited from outpatient clinics in Auckland, Bay of Plenty,Wellington, Canterbury, Otago and Southland in NZ. The control group (n=461) consisted
McKinney et al. Page 2
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

of healthy subjects recruited from Otago. The UK RA cohort consisted of 250 patients withRA recruited at Lewisham and Guy’s and St Thomas’ Hospitals. One hundred and fifty-nineUK controls were purchased from the European Collection of Cell Cultures (ECACC)(http://www.hpacultures.org.uk/collections/ecacc.jsp) and genotyped by us, with the dataaugmented by a further 52 ECACC control samples genotyped by Hollox et al.21 The Dutchcases (n=768) were recruited from the central and eastern regions of the Netherlands.2223
These were compared to 702 controls recruited from blood donor centres within Utrecht andAmsterdam. All the patients with RA were diagnosed according to the 1987 AmericanCollege of Rheumatology criteria for RA.24 Demographic and clinical information on thecases and controls is given in table 1.
For the NZ and Netherlands cohorts and the UK case cohort, DNA was prepared from wholeblood by chloroform extraction. The ECACC genomic DNA was derived fromlymphoblastoid cell lines. Recruitment and DNA extraction occurred over a period of morethan 5 years for the NZ samples, whereas DNA extraction occurred over a period of lessthan 2 years for the Dutch samples and UK case samples. All TaqMan Real-Time PCR wasdone at the University of Otago in NZ. This necessitated shipping dried samples from theUK and the Netherlands to NZ where they were subsequently resuspended. All aqueousDNA was stored suspended in Tris-EDTA at −20°C.
Each of the three sample sets had ≥95% power (α=0.05) to detect an effect equivalent to thatreported for FCGR3B CN <2 in SLE in a UK sample set (OR 2.21).6 At lower effect sizes,power decreased (eg, at OR 1.5 the power was 75% in the NZ sample set, 86% in theNetherlands sample set and 41% in the UK sample set). The combined sample set, however,was adequately powered to detect effects >1.3 (79% power at OR 1.3).
Measurement of FCGR3B CNAt the FCGR3 locus there are two patterns of CNV that include FCGR3B25—the major onealso encompasses FCGR2C and the minor one also encompasses HSPA7/FCGR2C/FCGR3A/HSPA6 (deviation from CN=2 present in 11.2% and 0.8%, respectively, of ahealthy sample set from the Netherlands25). The exact boundaries of CNV are not known.
FCGR3B CN was measured using TaqMan Real-Time PCR, as described in the onlinesupplement, using an assay based on one previously described for CCL3L1.26 Variations inDNA quality increase the ‘noise’ of the assay system,21 which can prevent clear clusteringof continuous values around whole integers and poor quality DNA increases the risk of falsepositive results.27 All NZ and Netherlands case genomic DNA samples wereelectrophoresed on an agarose gel and integrity scored from 1 (single high molecular weightband) to 4 (most degraded). Samples with scores of 3 and 4 were discarded from analysis.This was not done for the Netherlands control samples because they exhibited discrete CNbins (see fig 4 in online supplement), suggesting no blurring of CN calls owing to DNAdegradation.27 Insufficient genomic DNA was available for the UK samples to enabletesting by agarose gel. To minimise DNA degradation, NZ samples were freshly dilutedfrom 200 μg/ml stock and used within 2 weeks.
Assignation of FCGR3B CNIn order to compensate for differences in mean and variance distribution between cases andcontrols, the a posteriori model fitting CNVtools algorithm28 was used to determine the cut-off CN value between 1 and 2 for each sample set and CN was assigned as described inmore detail in the online supplement.
As additional evaluations of the qPCR assay, 72 NZ controls were first analysed byparalogue ratio testing (PRT)/restriction enzyme digest variant ratio using a previously
McKinney et al. Page 3
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

developed and validated assay.21 Our data demonstrated good agreement between PRT(which has a first-pass error rate of 8%29) and TaqMan assays within the range of 1–3copies (see table 2 in online supplement), and there was strong agreement between theassigned NA type by both methods. Eight of the PRT results differed by one copy comparedwith CNVtools assignment, with the PRT value uncertain for one of the differences. Wethen compared genotypes between the 30 overlapping UK ECACC controls genotyped by usand by Hollox et al21 (see table 3 in online supplement) and achieved 100% concordance inCN assignment.
Association analysisThe distributions of FCGR3B CN between patients and controls after CN assignment byCNVtools were compared using the χ2 test. Logistic regression analysis was used tomeasure the RA-associated risks of low FCGR3B CN as the OR relative to CN ≥2 using theSTATA 7.0 statistical package (StataCorp, College Station, Texas, USA). Because a mixtureof CNVtools fitting models28 were needed for our cohorts, combined (meta-) analysis of allthree cohorts was performed using the Mantel–Haenszel test, comparing CN <2 to ≥2 aftertesting for heterogeneity by the Breslow–Day test.
RESULTSThe distribution of FCGR3B CN as a continuous variable is shown in figure 1. CNassignment showed that 93.6% of the combined control cohort had two or more copies ofFCGR3B and 6.4% carried single copy deletions (table 2). No control individuals lackedboth alleles. One patient in each of the Dutch and NZ case cohorts had a null FCGR3Bgenotype. The FCGR3B CN allele distribution among our controls was very similar to thatobserved previously based on measurement by the multiplex ligand-dependent probeamplification technique in a cohort of 129 healthy individuals of Northern Europeanancestry (CN 0, 0%; 1, 7%; 2, 83%; 3, 10%),24 and similar to that observed using anintegrated ;approach in UK samples (CN 0, 0%; CN 1, 4%; 2, 87%; >3, 9%).21
To test the hypothesis that FCGR3B CN influences susceptibility to RA, the influence ondisease risk of CN <2 of FCGR3B was tested under the prediction that any association ofFCGR3B with RA would be similar to that evident in SLE where CN <2 increases the riskof disease by slowing the rate of immune complex clearance during transientinflammation.5–7 Table 2 shows the disease risk for CN 0–1 relative to CN ≥2. Significantevidence for an association between CN <2 and RA was observed in the Dutch cohort (OR2.01 (95% CI 1.37 to 2.94), p=3×10−4) but not in the two smaller cohorts (OR 1.45 (95% CI0.92 to 2.26), p=0.11 and OR 1.33 (95% CI 0.58 to 3.02), p=0.50 for the NZ and UKpopulations, respectively). In a combined (meta) analysis that included previously publisheddata from a small case–control sample set of Northern European ancestry (table 2; OR 1.31(95% CI 0.51 to 3.34)), there was strong evidence for CN <2 FCGR3B increasing the risk ofdisease (figure 2; OR 1.67 (95% CI 1.28 to 2.17), p=1.2×10−4).
Given that rheumatoid factor (RF) is an anti-FCG, we tested for an association betweenFCGR3B CN and the presence or absence of RF (table 3). There was some evidence for anassociation of low CN with RF-negative RA in the NZ and UK cohorts (p=0.08 and p=0.02,respectively), but not in the Dutch cohort (p=0.69). In the combined cohorts there was noevidence for differential association between FCGR3B CN <2 and RF status, nor was thereany evidence for an association between NA type and RA for NZ and UK samples with CN1 or 2 (see table 4 in online supplement).
McKinney et al. Page 4
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

DISCUSSIONOur results provide evidence that CNV in FCGR3B is associated with RA (combinedanalysis of four Caucasian RA case–control sample sets: OR 1.67 (95% CI 1.28 to 2.17),p=1.2×10−4). While only the largest sample set exhibited a significant association with RA,the other three included in the meta-analysis consistently showed an increased risk for RA(OR >1) in the presence of FCGR3B deletion, and there was no significant intercohortheterogeneity (table 2; p=0.60, Breslow–Day). While the ANCA-associated systemicvasculitis data require further clarification,67 our results are consistent with previous reportsof an association between low CN and systemic autoimmunity in other diseases includingglomerulonephritis and SLE.5–7 This suggests a common pathogenic role for FCGR3B (oran associated variant in the FCGR locus) in systemic autoimmune diseases.
Confirmed genetic associations have defined aberration in the activation, regulation andmigration of T cells as central to the aetiology of RA in Caucasian populations, includingHLA-DRB1,30 protein tyrosine phosphatase N22,31 a locus near the TNF-induced protein 3gene,3233 the signal transducer and activator of transcription 4 gene,34 a locus between theTNF receptor-associated factor 1 and C5 genes3536 and the CD40, chemokine ligand 21,CD122, KIF5A and protein kinase chloroquine genes.3738 The association of FCGR3B CNwith RA reported here still requires further replication in other populations before it can beconsidered confirmed. Nonetheless, if this association is validated, it would implicategenetic regulation of immune complex deposition and clearance in the pathophysiology ofRA. Although there was no association between FCGR3B CN and RF status, we had noinformation on the presence or absence of anti-cyclic citrullinated peptides (anti-CCPs) inall of our populations and therefore could not analyse the relationship between anti-CCP andFCGR3B CN. Antibodies to citrullinated proteins are now considered a more specificmarker of disease than RF status,39 and although there is a large overlap between anti-CCPand the presence/absence of RF, it is possible that FCGR3B deletion is more stronglyassociated with anti-CCP negative RA. This needs to be addressed in future studies.
Although quantitative PCR (qPCR) has been a popular method for measuring CNV owing tosuitability for genotyping a large number of samples, and is a relatively accurate method ofdetecting single-copy deletions and duplications,29 there are a number of factors that caninfluence the accuracy of assays. Because CN is measured relative to a reference gene,variation in amplification efficiency and experimental conditions can alter the ratio of thetwo products and thus apparent CN.28 DNA quality also influences assay efficiency and canintroduce false positives and batch effects when comparing cohorts collected and storedunder different conditions.2728 Because the CN values are (rarely) integer values, arbitrary‘binning’ of samples to whole numbers can introduce false associations if the distribution oftwo populations differs in mean and/or variance.28 To compensate for batch effects andsystematic errors, cases and controls were assayed concurrently. The modelling algorithmCNVtools was used to determine the cut-off between CNs 1 and 2 and those with values±0.05 of the cut-off between CNs 1 and 2 were removed. Independent verification of theqPCR technique was carried out using PRT (see Materials and methods). Because degradedDNA samples can yield spurious CNV results,27 samples exhibiting excessive degradationwere removed from analysis in this study.
Genotyping within the FCGR locus is a complex undertaking owing to the extensivehomology that exists between the FCGR genes. Because there is FCGR3B duplication anddeletion on multiple haplotypes,2125 there are no known single nucleotide polymorphisms(SNPs) that can be used to accurately predict CN.21 A major conclusion from thecomprehensive analysis of the FCGR locus by Hollox et al21 was that direct measurement ofCN by an integrated suite of methods combined with association analysis of SNPs is
McKinney et al. Page 5
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

required to fully evaluate the contribution of FCGR3B to RA. Here we focused on directmeasurement of FCGR3B CN by a single method (TaqMan) that is suited to larger-scalegenotyping. Future work on this locus in RA should include data on association of SNPhaplotypes.
FCGR3B CN correlates with the level of receptor expression (both surface and solubleforms), neutrophil adherence to IgG and internalisation of opsonised particles.7 While ourresults appear counterintuitive to the possibility that FcγRIIIB deletion has a role in RAthrough this process, they highlight the fact that the differential roles of PMN activation andimmune complex clearance in the immune response (and the exact function of FcγRIIIB)require further investigation. It is also relevant to emphasise that our data are consistent withthe findings observed in SLE.67 There are at least three possible explanations for howreduced FcγRIIIb levels could increase the risk of RA.
First, FcγRIIIb can bind intravascular immune complexes in the absence of any otherinflammatory mediators but fails to generate ROS, whereas FcγRIIa (predominantlyexpressed by macrophages and natural killer (NK) cells) is responsible for ROS-mediatedtissue damage.40 The reduced adherence and phagocytic capabilities of PMN in the case oflow FCGR3B CN may delay clearance of immune complexes during episodes of transientinflammation and prolong the inflammatory response either to initial joint damage or to anexogenous infection that subsequently triggers an autoimmune response. This would allowthe development of an inflammatory milieu where FcγRIIa activity predominates, as hasbeen suggested for glomerulonephritis and SLE.6741
Second, changes in FCGR3B CN may alter PMN function indirectly by shifting the balanceof activating receptors and potentially ‘unmasking’ the effects of functional polymorphismsin other FCG receptors. Furthermore, PMN are an important source of proinflammatorychemokines, which are partly mediated through FcγRIIa and FcγRIIIa.8 Both are FCGreceptors that have been implicated in RA and SLE.41
A third possibility is that the increased susceptibility to RA associated with low FCGR3BCN is due not to reduced FCGR3B dosage but to deletion in FCGR2C, since CNV in thesetwo genes is strongly related.2542 FcγRIIc is expressed on macrophages, PMN43 and NKcells44 where it triggers antibody-dependent cellular toxicity (ADCC).45 ADCC may play animportant role in regulating autoimmune responses by lysing autologous immature dendriticcells.4546 Defective NK cell cytotoxicity has been reported in a number of autoimmunedisorders including RA, juvenile RA, SLE and macrophage activation syndrome.4748 AnSNP within exon 5 of FCGR2C is functionally equivalent to a deletion of the gene. The nullallele of this polymorphism occurs more often in patients with RA than in controls andresults in an apparent shift towards increased expression of the inhibitory FcγRIIb.49
Whether this is also the case in the context of FCGR3B/FCGR2C deletion is unknown. Itshould be noted that rare (~1%) deletion events encompassing FCGR3B/FCGR2C/FCGR3Ahave been observed in Caucasian populations.25
In this paper we provide evidence for an association between a low FCGR3B CN andsusceptibility to RA. Whether this is due to biological effects of FcγRIIIb itself or is a proxymarker for another biologically relevant polymorphism will require further study, validationin other sample sets and better characterisation of structural variation within the FCGRlocus.
Supplementary MaterialRefer to Web version on PubMed Central for supplementary material.
McKinney et al. Page 6
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
AcknowledgmentsThe authors would like to thank NZ research nurses Gael Hewett and Sue Yeoman for assistance in recruitingpatients, and Chris Barnes for his assistance with CNVtools.
Funding This work was supported by the Health Research Council of New Zealand, Arthritis New Zealand and theNZ Child Health Research Foundation, Medical Research Council (UK) intramural funding from the ClinicalSciences Centre and Wellcome Trust project grant 083167. BZA was supported by a grant from the NetherlandsOrganization for Health Research and Development (ZonMw; grant number 016.096.121).
REFERENCES1. McKinney C, Merriman ME, Chapman PT, et al. Evidence for an influence of chemokine ligand 3-
like 1 (CCL3L1) gene copy number on susceptibility to rheumatoid arthritis. Ann Rheum Dis. 2008;67:409–13. [PubMed: 17604289]
2. Mamtani M, Rovin B, Brey R, et al. CCL3L1 gene-containing segmental duplications andpolymorphisms in CCR5 affect risk of systemic lupus erythaematosus. Ann Rheum Dis. 2008;67:1076–83. [PubMed: 17971457]
3. Bentley RW, Pearson J, Gearry RB, et al. Association of higher DEFB4 genomic copy number withCrohn’s disease. Am J Gastroenterol. 2010; 105:354–9. [PubMed: 19809410]
4. Hollox EJ, Huffmeier U, Zeeuwen PL, et al. Psoriasis is associated with increased beta-defensingenomic copy number. Nat Genet. 2008; 40:23–5. [PubMed: 18059266]
5. Aitman TJ, Dong R, Vyse TJ, et al. Copy number polymorphism in Fcgr3 predisposes toglomerulonephritis in rats and humans. Nature. 2006; 439:851–5. [PubMed: 16482158]
6. Fanciulli M, Norsworthy PJ, Petretto E, et al. FCGR3B copy number variation is associated withsusceptibility to systemic, but not organ-specific, autoimmunity. Nat Genet. 2007; 39:721–3.[PubMed: 17529978]
7. Willcocks LC, Lyons PA, Clatworthy MR, et al. Copy number of FCGR3B, which is associatedwith systemic lupus erythematosus, correlates with protein expression and immune complex uptake.J Exp Med. 2008; 205:1573–82. [PubMed: 18559452]
8. Fanger MW, Shen L, Graziano RF, et al. Cytotoxicity mediated by human Fc receptors for IgG.Immunol Today. 1989; 10:92–9. [PubMed: 2525910]
9. Kocher M, Siegel ME, Edberg JC, et al. Cross-linking of Fc gamma receptor IIa and Fc gammareceptor IIIb induces different proadhesive phenotypes on human neutrophils. J Immunol. 1997;159:3940–8. [PubMed: 9378982]
10. Coxon A, Cullere X, Knight S, et al. Fc gamma RIII mediates neutrophil recruitment to immunecomplexes. A mechanism for neutrophil accumulation in immune-mediated inflammation.Immunity. 2001; 14:693–704. [PubMed: 11420040]
11. Fossati G, Moots RJ, Bucknall RC, et al. Differential role of neutrophil Fcgamma receptor IIIB(CD16) in phagocytosis, bacterial killing, and responses to immune complexes. Arthritis Rheum.2002; 46:1351–61. [PubMed: 12115243]
12. Durand V, Pers JO, Renaudineau Y, et al. Soluble Fcgamma receptor IIIb alters the function ofpolymorphonuclear neutrophils but extends their survival. Eur J Immunol. 2001; 31:1952–61.[PubMed: 11449347]
13. Youinou P, Durand V, Renaudineau Y, et al. Pathogenic effects of anti-Fc gamma receptor IIIb(CD16) on polymorphonuclear neutrophils in non-organ-specific autoimmune diseases.Autoimmun Rev. 2002; 1:13–19. [PubMed: 12849053]
14. Peng SL. Neutrophil apoptosis in autoimmunity. J Mol Med. 2006; 84:122–5. [PubMed:16362398]
15. Wipke BT, Allen PM. Essential role of neutrophils in the initiation and progression of a murinemodel of rheumatoid arthritis. J Immunol. 2001; 167:1601–8. [PubMed: 11466382]
16. Mandik-Nayak L, Allen PM. Initiation of an autoimmune response: insights from a transgenicmodel of rheumatoid arthritis. Immunol Res. 2005; 32:5–13. [PubMed: 16106055]
17. Edwards SW, Hallett MB. Seeing the wood for the trees: the forgotten role of neutrophils inrheumatoid arthritis. Immunol Today. 1997; 18:320–4. [PubMed: 9238834]
McKinney et al. Page 7
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

18. Lee YH, Ji JD, Song GG. Associations between FCGR3A polymorphisms and susceptibility torheumatoid arthritis: a metaanalysis. J Rheumatol. 2008; 35:2129–35. [PubMed: 18843786]
19. Fairhurst AM, Wallace PK, Jawad AS, et al. Rheumatoid peripheral blood phagocytes are primedfor activation but have impaired Fc-mediated generation of reactive oxygen species. Arthritis ResTher. 2007; 9:R29. [PubMed: 17355628]
20. Morgan AW, Barrett JH, Griffiths B, et al. Analysis of Fcgamma receptor haplotypes inrheumatoid arthritis: FCGR3A remains a major susceptibility gene at this locus, with an additionalcontribution from FCGR3B. Arthritis Res Ther. 2006; 8:R5. [PubMed: 16356189]
21. Hollox EJ, Detering JC, Dehnugara T. An integrated approach for measuring copy numbervariation at the FCGR3 (CD16) locus. Hum Mutat. 2009; 30:477–84. [PubMed: 19143032]
22. Welsing PM, van Riel PL. The Nijmegen inception cohort of early rheumatoid arthritis. JRheumatol Suppl. 2004; 69:14–21. [PubMed: 15053447]
23. Kievit W, Fransen J, Oerlemans AJ, et al. The efficacy of anti-TNF in rheumatoid arthritis, acomparison between randomised controlled trials and clinical practice. Ann Rheum Dis. 2007;66:1473–8. [PubMed: 17426065]
24. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revisedcriteria for the classifi cation of rheumatoid arthritis. Arthritis Rheum. 1988; 31:315–24. [PubMed:3358796]
25. Breunis WB, van Mirre E, Geissler J, et al. Copy number variation at the FCGR locus includesFCGR3A, FCGR2C and FCGR3B but not FCGR2A and FCGR2B. Hum Mutat. 2009; 30:E640–50. [PubMed: 19309690]
26. Gonzalez E, Kulkarni H, Bolivar H, et al. The influence of CCL3L1 genecontaining segmentalduplications on HIV-1/AIDS susceptibility. Science. 2005; 307:1434–40. [PubMed: 15637236]
27. Cukier HN, Pericak-Vance MA, Gilbert JR, et al. Sample degradation leads to false-positive copynumber variation calls in multiplex real-time polymerase chain reaction assays. Anal Biochem.2009; 386:288–90. [PubMed: 19121619]
28. Barnes C, Plagnol V, Fitzgerald T, et al. A robust statistical method for case-control associationtesting with copy number variation. Nat Genet. 2008; 40:1245–52. [PubMed: 18776912]
29. Armour JA, Palla R, Zeeuwen PL, et al. Accurate, high-throughput typing of copy numbervariation using paralogue ratios from dispersed repeats. Nucleic Acids Res. 2007; 35:e19.[PubMed: 17175532]
30. Wordsworth BP, Lanchbury JS, Sakkas LI, et al. HLA-DR4 subtype frequencies in rheumatoidarthritis indicate that DRB1 is the major susceptibility locus within the HLA class II region. ProcNatl Acad Sci USA. 1989; 86:10049–53. [PubMed: 2481309]
31. Lee YH, Rho YH, Choi SJ, et al. The PTPN22 C1858T functional polymorphism and autoimmunediseases – a meta-analysis. Rheumatology (Oxford). 2007; 46:49–56. [PubMed: 16760194]
32. Plenge RM, Cotsapas C, Davies L, et al. Two independent alleles at 6q23 associated with risk ofrheumatoid arthritis. Nat Genet. 2007; 39:1477–82. [PubMed: 17982456]
33. Thomson W, Barton A, Ke X, et al. Rheumatoid arthritis association at 6q23. Nat Genet. 2007;39:1431–3. [PubMed: 17982455]
34. Remmers EF, Plenge RM, Lee AT, et al. STAT4 and the risk of rheumatoid arthritis and systemiclupus erythematosus. N Engl J Med. 2007; 357:977–86. [PubMed: 17804842]
35. Plenge RM, Seielstad M, Padyukov L, et al. TRAF1-C5 as a risk locus for rheumatoid arthritis – agenomewide study. N Engl J Med. 2007; 357:1199–209. [PubMed: 17804836]
36. Kurreeman FA, Rocha D, Houwing-Duistermaat J, et al. Replication of the tumor necrosis factorreceptor-associated factor 1/complement component 5 region as a susceptibility locus forrheumatoid arthritis in a European family-based study. Arthritis Rheum. 2008; 58:2670–4.[PubMed: 18759306]
37. Barton A, Thomson W, Ke X, et al. Rheumatoid arthritis susceptibility loci at chromosomes10p15, 12q13 and 22q13. Nat Genet. 2008; 40:1156–9. [PubMed: 18794857]
38. Raychaudhuri S, Remmers EF, Lee AT, et al. Common variants at CD40 and other loci confer riskof rheumatoid arthritis. Nat Genet. 2008; 40:1216–23. [PubMed: 18794853]
McKinney et al. Page 8
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

39. Nishimura K, Sugiyama D, Kogata Y, et al. Meta-analysis: diagnostic accuracy of anti-cycliccitrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Ann Intern Med.2007; 146:797–808. [PubMed: 17548411]
40. Tsuboi N, Asano K, Lauterbach M, et al. Human neutrophil Fcgamma receptors initiate and playspecialized nonredundant roles in antibody-mediated inflammatory diseases. Immunity. 2008;28:833–46. [PubMed: 18538590]
41. Tsuchiya N, Kyogoku C, Miyashita R, et al. Diversity of human immune system multigenefamilies and its implication in the genetic background of rheumatic diseases. Curr Med Chem.2007; 14:431–9. [PubMed: 17305544]
42. de Haas M, Kleijer M, van Zwieten R, et al. Neutrophil Fc gamma RIIIb deficiency, nature, andclinical consequences: a study of 21 individuals from 14 families. Blood. 1995; 86:2403–13.[PubMed: 7662988]
43. Cassel DL, Keller MA, Surrey S, et al. Differential expression of Fc gamma RIIA, Fc gamma RIIBand Fc gamma RIIC in hematopoietic cells: analysis of transcripts. Mol Immunol. 1993; 30:451–60. [PubMed: 8464427]
44. Metes D, Galatiuc C, Moldovan I, et al. Expression and function of Fc gamma RII on humannatural killer cells. Nat Immun. 1994; 13:289–300. [PubMed: 7894200]
45. Ernst LK, Metes D, Herberman RB, et al. Allelic polymorphisms in the FcgammaRIIC gene caninfluence its function on normal human natural killer cells. J Mol Med. 2002; 80:248–57.[PubMed: 11976734]
46. Pazmany L. Do NK cells regulate human autoimmunity? Cytokine. 2005; 32:76–80. [PubMed:16169244]
47. Dalbeth N, Callan MF. A subset of natural killer cells is greatly expanded within inflamed joints.Arthritis Rheum. 2002; 46:1763–72. [PubMed: 12124859]
48. Villanueva J, Lee S, Giannini EH, et al. Natural killer cell dysfunction is a distinguishing feature ofsystemic onset juvenile rheumatoid arthritis and macrophage activation syndrome. Arthritis ResTher. 2005; 7:R30–7. [PubMed: 15642140]
49. Stewart-Akers AM, Cunningham A, Wasko MC, et al. Fc gamma R expression on NK cellsinfluences disease severity in rheumatoid arthritis. Genes Immun. 2004; 5:521–9. [PubMed:15334114]
McKinney et al. Page 9
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

Figure 1.Distribution of Fcγ receptor 3B copy number (CN) as a continuous variable in the three caseand control cohorts. Data are shown without removal of samples. Boxes and linesencompass samples within 1 and 2 SD from the mean, respectively. Mean (SD) values forthe six sample sets are (from left to right): 2.23 (0.45), 2.04 (0.39), 2.18 (0.25), 1.89 (0.20),2.14 (0.24) and 1.92 (0.26).
McKinney et al. Page 10
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
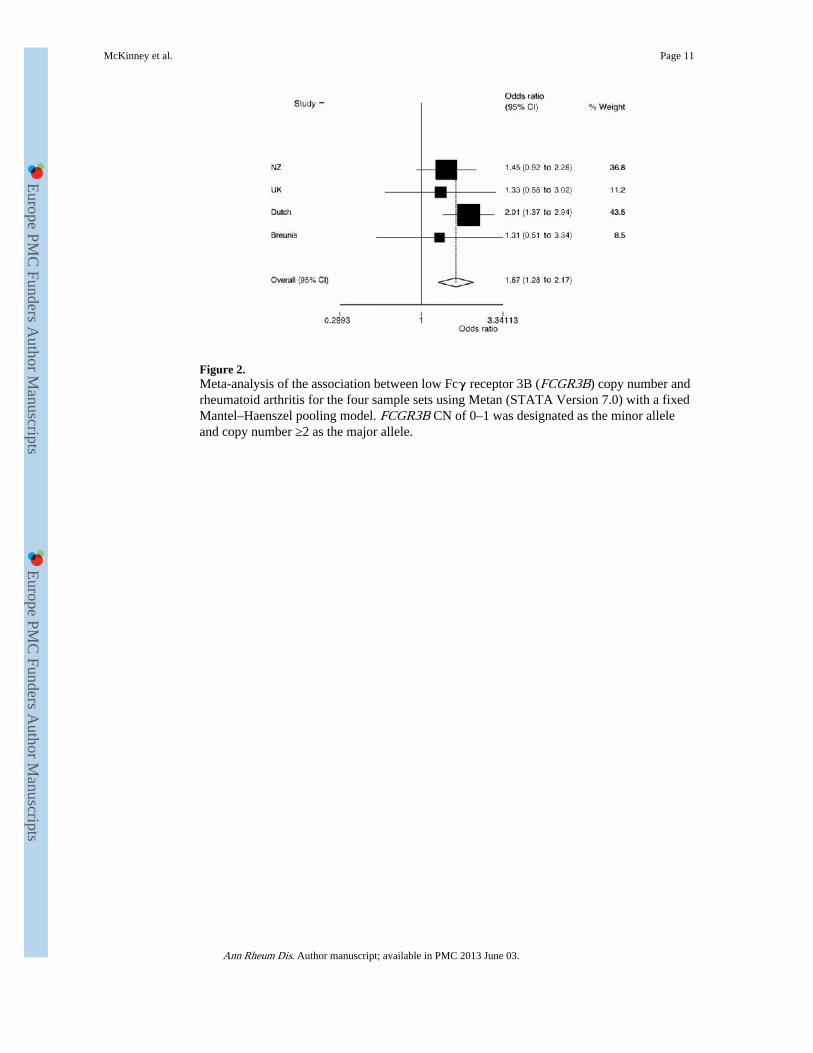
Figure 2.Meta-analysis of the association between low Fcγ receptor 3B (FCGR3B) copy number andrheumatoid arthritis for the four sample sets using Metan (STATA Version 7.0) with a fixedMantel–Haenszel pooling model. FCGR3B CN of 0–1 was designated as the minor alleleand copy number ≥2 as the major allele.
McKinney et al. Page 11
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
McKinney et al. Page 12
Table 1
Demographic and clinical characteristics
Age (mean,range, N*)
Women% (N)
RF% (N)
CCP% (N)
SE positivity% (N)
New Zealand
Cases 65.5, 20–88, 351† 78.8 (643) 82.3 (560) 67.0 (367) 80.1 (626)
Controls 44.6, 17–95, 461† 61.2 (461) – – –
UK
Cases NA 79.3 (241) 63.1 (241) NA 79.1 (239)
Controls NA NA – – –
The Netherlands
Cases 48.7, 4–79, 578‡ 65.5 (586) 78.5 (685) NA NA
Controls NA 49.2 (702) – – –
*N is the number of individuals from which data were available.
†Age at recruitment.
‡Age at disease onset.
CCP, cyclic citrullinated peptide; NA, not available; RF, rheumatoid factor.
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
McKinney et al. Page 13
Table 2
Fcγ receptor 3B (FCGR3B) copy number (CN) and risk for rheumatoid arthritis (RA)
FCGR3B CN Cases, N (frequency) Controls, N (frequency) OR (95% CI) p Value
New Zealand RA <2 60 (0.099) 32 (0.071) 1.45 (0.92 to 2.26) 0.11
≥2 546 (0.901) 421 (0.929) 1.00
UK RA <2 15 (0.062) 10 (0.047) 1.33 (0.58 to 3.02) 0.50
≥2 228 (0.938) 202 (0.953) 1.00
Dutch RA <2 86 (0.116) 43 (0.061) 2.01 (1.37 to 2.94) 3.0×10−4
≥2 655 (0.884) 658 (0.939) 1.00
Breunis RA25 <2 10 (0.089) 9 (0.070) 1.31 (0.51 to 3.34) 0.57
≥2 102 (0.901) 120 (0.930) 1.00
Combined RA* <2 171 (0.100) 94 (0.063) 1.67 (1.28 to 2.17) 1.2×10−4
≥2 1531 (0.900) 1401 (0.937) 1.00
*p=0.60, Breslow–Day.
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
McKinney et al. Page 14
Table 3
Fcγ receptor 3B (FCGR3B) distribution in rheumatoid factor (RF) positive and negative patients
FCGR3B CN RF negative,N (frequency)
RF positive,N (frequency) OR (95% CI) p Value
New Zealand (RA) <2 14 (0.156) 41 (0.094) 0.56 (0.29 to 1.08) 0.08
2 76 (0.844) 396 (0.896) 1.00
UK RA <2 10 (0.115) 5 (0.034) 0.27 (0.09 to 0.82) 0.02
2 77 (0.885) 142 (0.966) 1.00
Dutch RA <2 16 (0.112) 64 (0.124) 1.13 (0.63 to 2.02) 0.69
2 127 (0.888) 451 (0.876) 1.00
Combined RA* <2 40 (0.125) 110 (0.100) 0.78 (0.53 to 1.14) 0.20
2 280 (0.875) 989 (0.900) 1.00
*p=0.055, Breslow–Day.
CN, copy number; RA, rheumatoid arthritis.
Ann Rheum Dis. Author manuscript; available in PMC 2013 June 03.




















