ASSOCIATION OF LEFT VENTRICULAR DIASTOLIC DYSFUNCTION WITH ELEVATED NT-pro-BNP IN GENERAL INTENSIVE...
8
Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited. ASSOCIATION OF LEFT VENTRICULAR DIASTOLIC DYSFUNCTION WITH ELEVATED NTYPRO-BNP IN GENERAL INTENSIVE CARE UNIT PATIENTS WITH PRESERVED EJECTION FRACTION: A COMPLEMENTARY ROLE OF TISSUE DOPPLER IMAGING PARAMETERS AND NTYPRO-BNP LEVELS FOR ADVERSE OUTCOME Ignatios Ikonomidis,* Maria Nikolaou,* Ioanna Dimopoulou, † Ioannis Paraskevaidis,* John Lekakis,* Irini Mavrou, † Marinella Tzanela, ‡ Petros Kopterides, † Iraklis Tsangaris, † Apostolos Armaganidis, † and Dimitrios T.H. Kremastinos* *Second Department of Cardiology and † Second Department of Critical Care Medicine, Attikon Hospital, Medical School, University of Athens, and ‡ Department of Endocrinology, Evangelismos Hospital, Athens, Greece Received 6 Apr 2009; first review completed 21 Apr 2009; accepted in final form 5 May 2009 ABSTRACT—The mechanisms of the N-terminalYproYbrain natriuretic peptide (NTYpro-BNP) release in intensive care unit (ICU) patients with preserved ejection fraction (EF) are unclear. We investigated whether left ventricular (LV) dysfunction, as assessed by tissue Doppler imaging (TDI), is related to NTYpro-BNP levels in ICU patients with preserved EF and has a complementary value to NTYpro-BNP in the determination of in-hospital mortality. We examined 58 mechanically ventilated patients with no history of heart failure (age, 60 T 18 years; EF, 63% T 7%). The systolic (S) and early diastolic (E¶) velocity of the mitral annulus by TDI and the E/E¶ as well as NTYpro-BNP, troponin, lactate acid, blood oxygen (PO 2 /FIO 2 ), sepsis, and ICU mortality were assessed. Systolic, E¶, and E/E¶ correlated with age, PO 2 /FIO 2 , lactate acid, NTYpro-BNP, troponin, history of arterial hypertension, and diabetes (P G 0.05). By multivariate analysis, the determinants of NTYpro-BNP were S (P = 0.024), E/E¶ (P = 0.017), and sepsis (P = 0.015). An NTYpro-BNP greater than 941 pg/mL was a reliable predictor of LV diastolic dysfunction defined as a composite of E¶ less than or equal to 8 cm/s and/or mean E/E greater than or equal to 13 (area under the curve, 75%; P = 0.03). Patients with combined NTYpro-BNP greater than 941 pg/mL and abnormal TDI markers had increased creatinine levels and a lower MAP, PO 2 /FIO 2 , and survival rate than those with abnormal TDI or NTYpro-BNP alone or patients with normal TDI markers and NTYpro-BNP (25%, 60%, 70%, and 84%, respectively; P G 0.05). The addition of abnormal TDI in a model including NTYpro-BNP and sepsis increased the model’s value for in-hospital mortality (P for change = 0.01). In ICU patients with preserved EF, LV diastolic dysfunction and sepsis determine NTYpro-BNP levels. Tissue Doppler imaging markers and NTYpro-BNP have a complementary value for in-hospital mortality. KEYWORDS—Tissue Doppler imaging, diastolic dysfunction, NTYpro-BNP, natriuretic peptides, prognosis, intensive care unit INTRODUCTION Several studies have investigated the use of various clinical and biochemical markers to assess outcome in critically ill patients (1, 2). Recently, the use of natriuretic peptides as prognostic indicators in critical illness has aroused great interest (1Y8). Brain natriuretic peptide (BNP) is a polypeptide neuro- hormone, which is mainly produced and secreted by cardio- myocytes. The main stimuli for its synthesis and release is myocyte stretch because of elevated cardiac pressure and/or volume (2). Thus, increased myocardial wall stress because of hypertension, diabetes and myocardial ischemia, structural myocardial disease such as left ventricular (LV) hypertrophy, and excessive intravascular volume causing myocardial stretch and cardiac dilatation may increase BNP (2, 9). However, inflammation (10), neurohumoral activation, angio- tensine II, stress hormones (2, 11), and hypoxia (12), as well as treatment with inotropic agents and fluids (11), are also considered as triggering factors for BNP production in critically ill patients. The pharmacologic effect of BNP at the cellular level is mediated by increases in cyclic guanosine monophosphate, which lead to relaxation of vascular smooth muscle (2). Brain natriuretic peptide induces vasodilation; inhibits renin, aldosterone, and angiotensin production; increases diuresis; and is thus an important regulator of fluid homeostasis (2). Studies have postulated that the vasodilatory effects of BNP may cause hypotension and impairment of renal function in septic patients (13) or patients with systolic heart failure (14Y16). Brain natriuretic peptide is secreted into the blood as a prohormone, where it is cleaved into active BNP and inactive metabolite N-terminalYpro-BNP (NTYpro- BNP) (2). Brain natriuretic peptide and NTYpro-BNP are produced in equimolar amounts but are removed from the circulation by different mechanisms at different time rates, making the plasma concentration unequal (2). N-TerminalY pro-BNP is mainly excreted by the kidneys, has a longer half- life time, and a better in vitro stability than BNP, which is cleared by specific clearance cell receptors and enzyme 141 SHOCK, Vol. 33, No. 2, pp. 141Y148, 2010 Address reprint requests to Ignatios Ikonomidis, MD, FESC, University of Athens, Attikon Hospital, Perikleous 19, N. Chalkidona, Athens 14343, Greece. E-mail: [email protected]. DOI: 10.1097/SHK.0b013e3181ad31f8 Copyright Ó 2010 by the Shock Society
Transcript of ASSOCIATION OF LEFT VENTRICULAR DIASTOLIC DYSFUNCTION WITH ELEVATED NT-pro-BNP IN GENERAL INTENSIVE...

Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
ASSOCIATION OF LEFT VENTRICULAR DIASTOLIC DYSFUNCTION WITHELEVATED NTYPRO-BNP IN GENERAL INTENSIVE CARE UNIT PATIENTSWITH PRESERVED EJECTION FRACTION: A COMPLEMENTARY ROLE
OF TISSUE DOPPLER IMAGING PARAMETERS AND NTYPRO-BNPLEVELS FOR ADVERSE OUTCOME
Ignatios Ikonomidis,* Maria Nikolaou,* Ioanna Dimopoulou,† IoannisParaskevaidis,* John Lekakis,* Irini Mavrou,† Marinella Tzanela,‡ Petros
Kopterides,† Iraklis Tsangaris,† Apostolos Armaganidis,†
and Dimitrios T.H. Kremastinos**Second Department of Cardiology and †Second Department of Critical Care Medicine, Attikon Hospital,
Medical School, University of Athens, and ‡Department of Endocrinology, EvangelismosHospital, Athens, Greece
Received 6 Apr 2009; first review completed 21 Apr 2009; accepted in final form 5 May 2009
ABSTRACT—The mechanisms of the N-terminalYproYbrain natriuretic peptide (NTYpro-BNP) release in intensive careunit (ICU) patients with preserved ejection fraction (EF) are unclear. We investigated whether left ventricular (LV)dysfunction, as assessed by tissue Doppler imaging (TDI), is related to NTYpro-BNP levels in ICU patients with preservedEF and has a complementary value to NTYpro-BNP in the determination of in-hospital mortality. We examined 58mechanically ventilated patients with no history of heart failure (age, 60 T 18 years; EF, 63% T 7%). The systolic (S) andearly diastolic (E¶) velocity of the mitral annulus by TDI and the E/E¶ as well as NTYpro-BNP, troponin, lactate acid, bloodoxygen (PO2/FIO2), sepsis, and ICU mortality were assessed. Systolic, E¶, and E/E¶ correlated with age, PO2/FIO2, lactateacid, NTYpro-BNP, troponin, history of arterial hypertension, and diabetes (P G 0.05). By multivariate analysis, thedeterminants of NTYpro-BNP were S (P = 0.024), E/E¶ (P = 0.017), and sepsis (P = 0.015). An NTYpro-BNP greater than941 pg/mL was a reliable predictor of LV diastolic dysfunction defined as a composite of E¶ less than or equal to 8 cm/sand/or mean E/E greater than or equal to 13 (area under the curve, 75%; P = 0.03). Patients with combined NTYpro-BNPgreater than 941 pg/mL and abnormal TDI markers had increased creatinine levels and a lower MAP, PO2/FIO2, andsurvival rate than those with abnormal TDI or NTYpro-BNP alone or patients with normal TDI markers and NTYpro-BNP(25%, 60%, 70%, and 84%, respectively; P G 0.05). The addition of abnormal TDI in a model including NTYpro-BNP andsepsis increased the model’s value for in-hospital mortality (P for change = 0.01). In ICU patients with preserved EF, LVdiastolic dysfunction and sepsis determine NTYpro-BNP levels. Tissue Doppler imaging markers and NTYpro-BNP have acomplementary value for in-hospital mortality.
KEYWORDS—Tissue Doppler imaging, diastolic dysfunction, NTYpro-BNP, natriuretic peptides, prognosis, intensive careunit
INTRODUCTION
Several studies have investigated the use of various clinical
and biochemical markers to assess outcome in critically ill
patients (1, 2).
Recently, the use of natriuretic peptides as prognostic
indicators in critical illness has aroused great interest (1Y8).
Brain natriuretic peptide (BNP) is a polypeptide neuro-
hormone, which is mainly produced and secreted by cardio-
myocytes. The main stimuli for its synthesis and release is
myocyte stretch because of elevated cardiac pressure and/or
volume (2). Thus, increased myocardial wall stress because of
hypertension, diabetes and myocardial ischemia, structural
myocardial disease such as left ventricular (LV) hypertrophy,
and excessive intravascular volume causing myocardial
stretch and cardiac dilatation may increase BNP (2, 9).
However, inflammation (10), neurohumoral activation, angio-
tensine II, stress hormones (2, 11), and hypoxia (12), as well
as treatment with inotropic agents and fluids (11), are also
considered as triggering factors for BNP production in
critically ill patients. The pharmacologic effect of BNP at
the cellular level is mediated by increases in cyclic guanosine
monophosphate, which lead to relaxation of vascular smooth
muscle (2). Brain natriuretic peptide induces vasodilation;
inhibits renin, aldosterone, and angiotensin production;
increases diuresis; and is thus an important regulator of fluid
homeostasis (2). Studies have postulated that the vasodilatory
effects of BNP may cause hypotension and impairment of
renal function in septic patients (13) or patients with systolic
heart failure (14Y16). Brain natriuretic peptide is secreted into
the blood as a prohormone, where it is cleaved into active
BNP and inactive metabolite N-terminalYpro-BNP (NTYpro-
BNP) (2). Brain natriuretic peptide and NTYpro-BNP are
produced in equimolar amounts but are removed from the
circulation by different mechanisms at different time rates,
making the plasma concentration unequal (2). N-TerminalYpro-BNP is mainly excreted by the kidneys, has a longer half-
life time, and a better in vitro stability than BNP, which is
cleared by specific clearance cell receptors and enzyme
141
SHOCK, Vol. 33, No. 2, pp. 141Y148, 2010
Address reprint requests to Ignatios Ikonomidis, MD, FESC, University of
Athens, Attikon Hospital, Perikleous 19, N. Chalkidona, Athens 14343, Greece.
E-mail: [email protected].
DOI: 10.1097/SHK.0b013e3181ad31f8
Copyright � 2010 by the Shock Society

Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
neutral endopeptidase (2). Brain natriuretic peptide and
NTYpro-BNP have been widely used as excellent markers in
the diagnosis of LV and prognosis of heart failure patients
(5Y7). In critically ill patients, NTYpro-BNP production may
be triggered by 1) LV dysfunction either preexisting, because
of cardiac disease (9), or acquired, because of hypoxia,
hypoperfusion, and toxic effects of inflammation (11, 12); 2)
renal dysfunction (3); 3) inflammatory mediators released
during infection and/or sepsis (10, 11); 4) elevation of stress
hormones and neurohumoral activation (2, 11) and thus may
be a predictor of adverse outcome.
Traditionally, natriuretic peptides have been used in the
diagnosis and prognosis of systolic and/or diastolic heart
failure (9). Elevated levels of these biomarkers have also been
recognized in noncardiac diseases such as pulmonary embo-
lism, sepsis, chronic obstructive pulmonary disease, and renal
insufficiency (17). The previously discussed noncardiac
causes of elevated NTYpro-BNP are often present in critically
ill patients admitted in a general intensive care unit (ICU).
Tissue Doppler imaging (TDI) indices are able to detect LV
diastolic and/or systolic dysfunction (18Y23) and have been
associated with elevated natriuretic peptide levels during
exercise (24) in patients with suspected diastolic heart failure
despite the presence of a normal ejection fraction (EF).
Furthermore, studies have shown that TDI markers of LV
function bear a prognostic impact on patients with cardiovas-
cular disease (25).
N-TerminalYpro-BNP levels are related with LV diastolic
dysfunction in patients with cardiovascular risk factors such
as hypertension and diabetes or overt cardiac disease (9, 10).
However, the association of LV diastolic dysfunction and
NTYpro-BNP levels in critically ill patients with preserved
EF, no history of chronic heart failure, and a high incidence of
noncardiac causes of elevated NTYpro-BNP during hospital-
ization in a general ICU has not been clearly defined.
In agreement with other investigators, we have previously
shown (3) that nonsurvivors have higher aminoterminal part
of BNP (NTYpro-BNP) levels on admission in ICU than
survivors, and that NTYpro-BNP is an independent predictor
of ICU mortality (3Y8). Furthermore, we have previously
shown that the use of inotropes, renal impairment, sepsis, and
age accounted for nearly 50% of the NTYpro-BNP variation in
ICU patients. However, in our previous study, we did not
investigate whether LV diastolic dysfunction, as assessed by
tissue Doppler echocardiography, is an additional determinant
of elevated NTYpro-BNP levels and whether TDI markers of
LV diastolic dysfunction have an independent and incremen-
tal value to NTYpro-BNP levels in the assessment of the in-
hospital mortality. Thus, in the present study, we hypothesized
that LV diastolic dysfunction is an additional determinant of
increased NTYpro-BNP levels in critically ill patients with
preserved ejection function and no history of heart failure
admitted in a general ICU, and thus, NTYpro-BNP may be a
reliable marker of LV diastolic dysfunction in these patients.
We also hypothesized that elevated NTYpro-BNP and abnor-
mal indices of LV function as assessed by TDI may have a
complementary value in the determination of in-hospital
mortality.
The aim of our study was 1) to investigate whether
NTYpro-BNP levels are independently related to LV diastolic
dysfunction as assessed by TDI in critically ill patients with
preserved ejection function and no history of heart failure
admitted in a general ICU and 2) to examine whether TDI
markers of LV diastolic function and NTYpro-BNP levels
have complementary value in the determination of the in-
hospital mortality in these patients. We have chosen to study
patients with preserved ejection as an association between
systolic cardiac dysfunction, BNP levels, and in-hospital
mortality has been demonstrated in critically ill patients (26).
PATIENTS AND METHODS
PatientsThis prospective single-center study included serial recruitment of
critically ill patients, aged older than 18 years, requiring support withmechanical ventilation, admitted in our general ICU during a 12-monthperiod. The study was approved by the hospital’s ethics committee, andinformed consent was obtained from patients’ relatives. Exclusion criteriaincluded chronic heart failure, defined by known history of hospitalization dueto heart failure decompensation and/or an LV ejection fraction (LVEF) of lessthan 45% on admission echocardiography, atrial fibrillation, and preexistentrenal insufficiency (history of serum creatinine 91.8 mg/dL before ICU entry).Patients’ clinical information included age, sex, reason for admission, diseaseseverity according to the Acute Physiology and Chronic Health Evaluation IIscore, degree of organ dysfunction quantified by the Sequential Organ FailureAssessment (SOFA) score, the presence of sepsis by using widely acceptedguidelines (27), requirement for inotropic agents (norepinephrine, dobut-amine, or dopamine), MAP, and central venous pressure (CVP). Blood gasanalysis, including partial pressure of oxygen (PO2), carbon dioxide (PCO2),and lactate acid, was also available. The ratio of partial pressure of oxygenin blood to the oxygen concentration given during mechanical ventilation(PO2/FIO2) was used as a marker of oxygenation. In-hospital outcome wasdefined as mortality during hospitalization.
EchocardiographyTransthoracic echocardiography was performed on admission using a
Vivid 4 (GE Medical Systems, Horten, Norway) phased array system. Studieswere digitally stored and analyzed by two observers (I.I., M.N.) blinded toclinical and laboratory data using a computerized station (Echopac GE). Allpatients had adequate images for analysis. For the analysis of segmental wallmotion abnormalities, a 16-segment protocol was used (28). Each segmentwas scored as follows: 1 indicates normal; 2, hypokinetic; 3, akinetic; and 4,dyskinetic. A total wall motion score was calculated as the sum of all16 segments. The wall motion score index was defined as the ratio of thenumber of segments with wall motion abnormalities divided by the total of all16 segments (normal value, 1). Patients with wall motion score index greaterthan or equal to 1.125 (corresponding to wall motion abnormalities in at leasttwo segments) were considered to present segmental wall motion abnormal-ities (28). However, none of our patients showed evidence of segmental wallmotion abnormalities. The following parameters were measured from cross-sectional echocardiographic images of the LV: 1) end-diastolic (LVEDD) andend-systolic diameter (in millimeters); 2) interventricular septal (IVS),posterior wall (PW) thickness (in millimeters); 3) relative wall thickness(RWT) as the sum of the IVS and PW thickness divided by the LVEDD; 4)fractional shortening and EF (percentage); and 5) left atrium dimension (inmillimeters). Transmitral pulsed wave Doppler velocities were recorded in thefour-chamber view with the sample volume at the tip of mitral valve leaflets.E and A wave velocities and deceleration time of early transmitral flowvelocity were measured. Myocardial velocities were recorded using color TDIto record low-velocity, high-intensity myocardial signals at a high frame rate(120 MHz). A 5-mm sample volume was placed in septal and lateral corner ofthe mitral annulus in the apical four-chamber views to record the systolicvelocity (S¶), early diastolic velocity (E¶), and late diastolic velocity (A¶). Themean value of the S¶, E¶, and A¶ in the septal and lateral corner was used foranalysis. The ratio of E wave of the mitral inflow measured by pulsed waveDoppler to the E¶ was calculated as an index of LV diastolic filling pressures.All Doppler markers were measured at the end-expiration (29). Interobserverand intraobserver variability of these measurements was 3% and 1.7%,respectively. Patients were stratified into those with or without a composite ofabnormal TDI indices of LV diastolic dysfunction. The composite wasdefined as mean E¶ less than or equal to 8 cm/s and/or septal E¶ younger than
142 SHOCK VOL. 33, NO. 2 IKONOMIDIS ET AL.
Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
40 years less than 9 cm/s, septal E¶ 40 to 60 years less than 7 cm/s, E¶ olderthan 60 years less than 6 cm/s, E/E¶ greater than 12 for the lateral corner, E/E¶greater than 15 for the septal corner of the mitral annulus, mean E/E¶ greaterthan or equal to 13 using previously published cutoff values (9, 18Y23)Furthermore, the patients were also stratified into those with an S less than orequal to 8 cm/s and those with higher S values, suggesting a normal systoliclongitudinal function of the LV (19).
Laboratory measurementsBlood samples were drawn on admission to determine NTYpro-BNP. The
blood was centrifuged and stored at j70-C until assayed. N-TerminalYpro-BNP was measured by the same study-assigned laboratory using commer-cially available kits (NTYpro-BNP; Elecsys 2010, Roche Diagnostics,Mannheim, Germany). The interassay coefficient of variance is less than3.0%. The analytic range is from 20 to 35,000 pg/mL. Patients’ hematologicaland biochemical profile included hemoglobin, white blood cells, platelets,INR creatinine, electrolytes, albumin, bilirubin, and troponin T.
Statistical analysisAll data were tested for normal distribution by the Kolmogorov-Smirnov
test. Results are presented as medians and ranges for parameters with non-normal distribution or mean values and SDs. Group comparisons wereperformed by Mann-Whitney and chi-square tests. Pearson and Spearmancorrelation coefficient assessed the associations between variables. Thelogarithm of the variables with a skewed distribution underwent logarithmictransformation for analysis. By receiver operator characteristic analysis, weassessed the predictive value of NTYpro-BNP for the presence of LV diastolicdysfunction. The area under the receiver operator characteristic curve andcorresponding confidence intervals (CIs), as well as the correspondingsensitivity and specificity, were calculated. Patients’ cohort was also stratifiedas patients with a composite of normal versus abnormal diastolic TDI indices(as previously defined), and the corresponding survival curves were comparedby the log-rank test. The combination of elevated NTYpro-BNP and abnormaldiastolic TDI markers for ICU mortality was also examined by survivalcurves. Univariate Cox regression analysis was used to calculate the relativerisk and CIs of the examined variables for in-hospital mortality. MultivariateCox regression analysis was used to assess the incremental value of thecomposite of abnormal TDI indices over other prognostic factors. The changeof -2LogLikelihood after addition of the composite of abnormal TDI in the
multivariable model was used to assess statistical significance. A P G 0.05was considered statistically significant in all analyses.
RESULTS
Of 75 patients fulfilling the inclusion criteria, 5 had in-
adequate echo image quality due to severe chronic obstructive
pulmonary disease, 5 died on ICU admission and thus did not
have an echo study, and 7 had extensive chest trauma
excluding the feasibility of a transthoracic echo study. Thus,
58 patients (39 men) with a mean age of 60 T 18 years (range,
18Y85 years) under mechanical ventilation were finally
included in the study. Admitting diagnosis was related to
medical (n = 35), surgical (n = 20), or multiple trauma (n = 3)
critical states. Additionally, 39 of 58 patients were diagnosed
to have sepsis, and 5 more had evidence of infection. Of 58
patients, 22 died during hospitalization, yielding an in-
hospital mortality rate of 38%. All patients had preserved
LVEF, with a mean value of 63% T 7%. Echocardiographic
findings are shown in Table 1.
TDI parameters
S, E¶, and E/E¶ correlated with age, NTYpro-BNP, myocar-
dial damage as assessed by troponin levels, PO2/FIO2, lactate
acid, history of hypertension, and RWT (P G 0.05; for all
correlations). Additionally, E¶ and E/E¶ were related with
history of diabetes (P G 0.05) and E¶ with presence of sepsis
(P = 0.04). As assessed by TDI markers, 27 patients (46%)
had a composite of abnormal TDI indices of LV diastolic
function. Of those, 18 patients also had an S less than 8 cm/s.
Patients with a composite of abnormal indices of LV diastolic
function had higher NTYpro-BNP, troponin, lactate acid
levels, incidence of history of hypertension and diabetes,
RWT than patients with normal TDI (P G 0.05; Table 2).
Interestingly, patients with abnormal TDI markers a lower
PO2/FIO2 than patients with normal TDI, suggesting that
elevated LV filling pressures may have caused pulmonary
congestion contributing to hypoxia (P G 0.05; Table 2). MAP
and CVP were similar between patients with abnormal and
normal TDI markers (P = not significant).
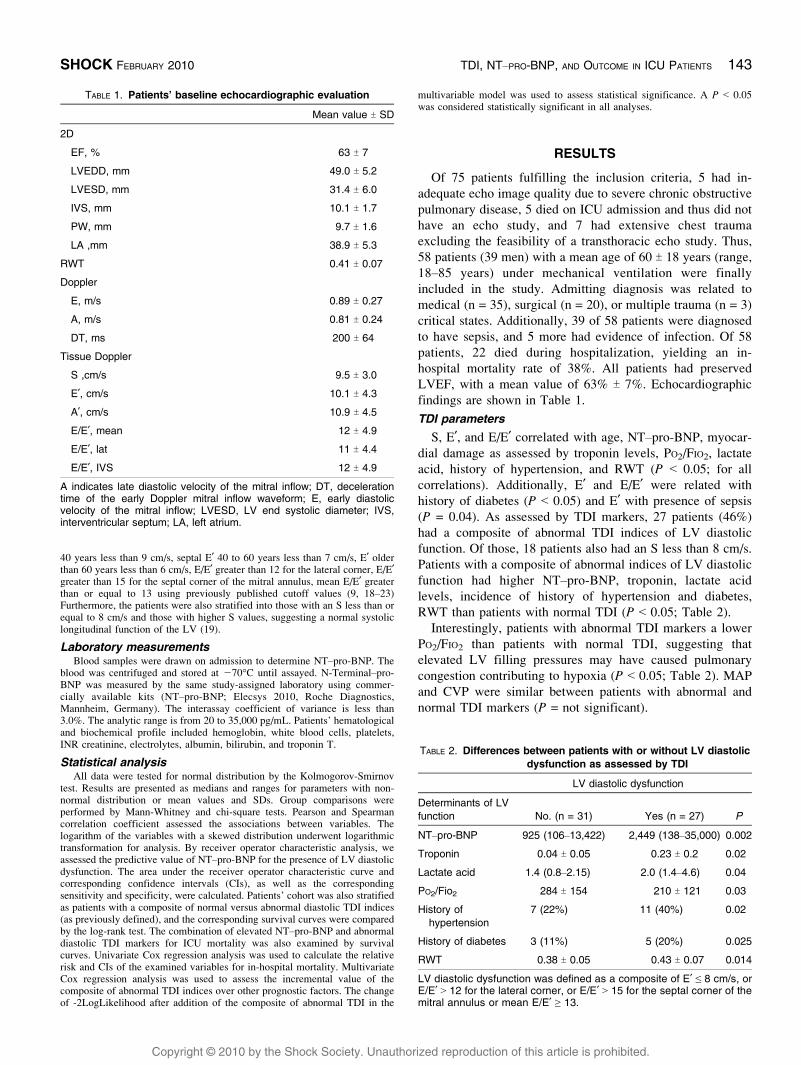
TABLE 1. Patients’ baseline echocardiographic evaluation
Mean value T SD
2D
EF, % 63 T 7
LVEDD, mm 49.0 T 5.2
LVESD, mm 31.4 T 6.0
IVS, mm 10.1 T 1.7
PW, mm 9.7 T 1.6
LA ,mm 38.9 T 5.3
RWT 0.41 T 0.07
Doppler
E, m/s 0.89 T 0.27
A, m/s 0.81 T 0.24
DT, ms 200 T 64
Tissue Doppler
S ,cm/s 9.5 T 3.0
E¶, cm/s 10.1 T 4.3
A¶, cm/s 10.9 T 4.5
E/E¶, mean 12 T 4.9
E/E¶, lat 11 T 4.4
E/E¶, IVS 12 T 4.9
A indicates late diastolic velocity of the mitral inflow; DT, decelerationtime of the early Doppler mitral inflow waveform; E, early diastolicvelocity of the mitral inflow; LVESD, LV end systolic diameter; IVS,interventricular septum; LA, left atrium.
TABLE 2. Differences between patients with or without LV diastolicdysfunction as assessed by TDI
LV diastolic dysfunction
Determinants of LVfunction No. (n = 31) Yes (n = 27) P
NTYpro-BNP 925 (106Y13,422) 2,449 (138Y35,000) 0.002
Troponin 0.04 T 0.05 0.23 T 0.2 0.02
Lactate acid 1.4 (0.8Y2.15) 2.0 (1.4Y4.6) 0.04
PO2/Fio2 284 T 154 210 T 121 0.03
History ofhypertension
7 (22%) 11 (40%) 0.02
History of diabetes 3 (11%) 5 (20%) 0.025
RWT 0.38 T 0.05 0.43 T 0.07 0.014
LV diastolic dysfunction was defined as a composite of E¶ e 8 cm/s, orE/E¶ 9 12 for the lateral corner, or E/E¶ 9 15 for the septal corner of themitral annulus or mean E/E¶ Q 13.
SHOCK FEBRUARY 2010 TDI, NTYPRO-BNP, AND OUTCOME IN ICU PATIENTS 143
Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
N-TerminalYproYbrain natriuretic neptide
In addition to TDI markers, NTYpro-BNP was also as-
sociated with age, myocardial damage as assessed by troponin
levels, RWT, presence of sepsis, inotrope infusion, SOFA
score, and tissue oxygenation as assessed by PO2/FIO2
(P G 0.05 for all correlations) and renal function as assessed
by creatinine levels (regression coefficient b, 0.44; P = 0.02).
In a multivariate linear regression model, including TDI
indices, and univariate determinants of NTYpro-BNP levels
with P less than 0.05 (troponin, age, creatinine, RWT,
presence of sepsis, inotrope infusion, SOFA score, PO2/FIO2)
the most important determinants of NTYpro-BNP levels were
S (regression coefficient b, -0.33; P = 0.024,), E/E¶ ratio
(regression coefficient b, 0.36; P = 0.017), and presence of
sepsis (regression coefficient b, 0.35; P = 0.012). By receiver
operating analysis, an NTYpro-BNP greater than 941 pg/mL
predicted a composite of abnormal TDI markers of LV
diastolic function with 73% sensitivity and 70% specificity
(area under the curve,75%; 95% CI, 68Y94; P = 0.03).
Interestingly, patients with an NTYpro-BNP greater than
941 pg/mL had lower MAP and similar CVP than patients
with lower levels (75 T 11 vs. 84 T 14 mmHg [P = 0.03] and
10.8 T 3.5 vs. 10.9 T 4.0 mmHg [P = 0.83], respectively),
suggesting the presence of a lower BP in the presence of
similar preload or at least similar right atrial Bstretch[ in
patients with increased NTYpro-BNP levels compared with
those with lower levels. Additionally, patients with an
NTYpro-BNP greater than 941 pg/mL had higher creatinine
levels than those with lower levels (1.75 T 1.1 vs. 1.04 T0.5 mg/L; P = 0.03).
Outcome
Of 58 patients, 22 died during hospitalization (59.0 T35 days), yielding a mortality rate of 38%. Survivors had
lower Acute Physiology and Chronic Health Evaluation II
score, troponin, and NTYpro-BNP levels, as well as higher
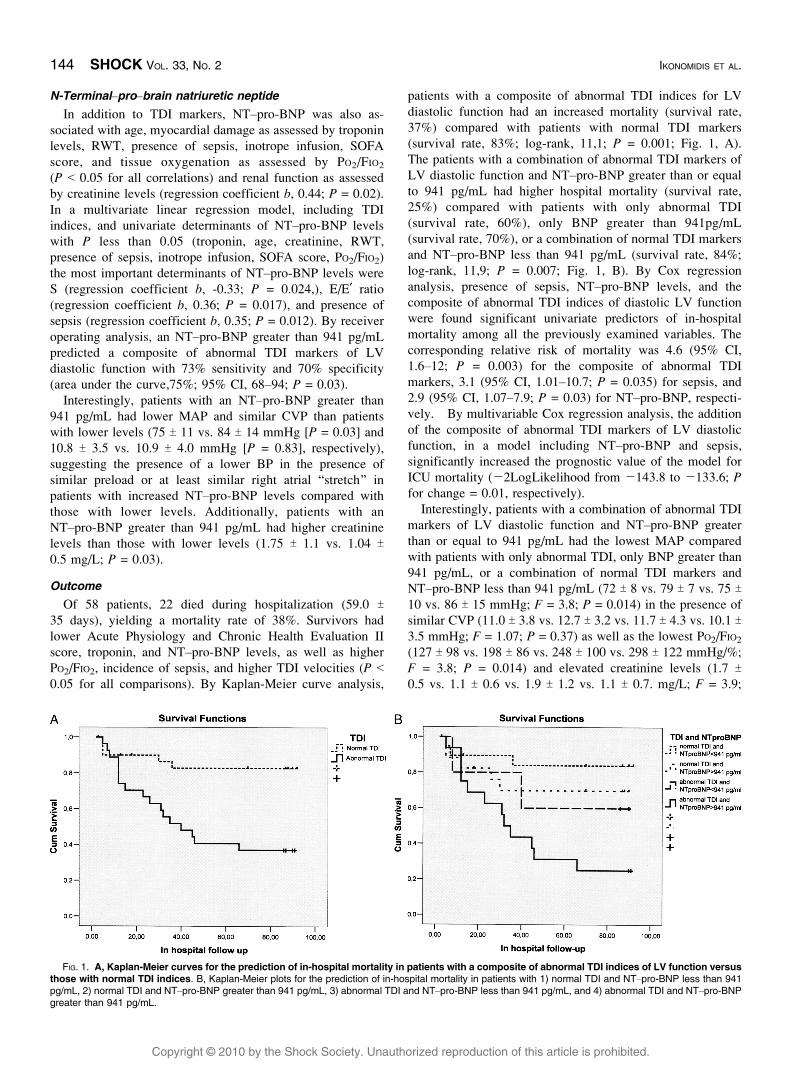
PO2/FIO2, incidence of sepsis, and higher TDI velocities (P G0.05 for all comparisons). By Kaplan-Meier curve analysis,
patients with a composite of abnormal TDI indices for LV
diastolic function had an increased mortality (survival rate,
37%) compared with patients with normal TDI markers
(survival rate, 83%; log-rank, 11,1; P = 0.001; Fig. 1, A).
The patients with a combination of abnormal TDI markers of
LV diastolic function and NTYpro-BNP greater than or equal
to 941 pg/mL had higher hospital mortality (survival rate,
25%) compared with patients with only abnormal TDI
(survival rate, 60%), only BNP greater than 941pg/mL
(survival rate, 70%), or a combination of normal TDI markers
and NTYpro-BNP less than 941 pg/mL (survival rate, 84%;
log-rank, 11,9; P = 0.007; Fig. 1, B). By Cox regression
analysis, presence of sepsis, NTYpro-BNP levels, and the
composite of abnormal TDI indices of diastolic LV function
were found significant univariate predictors of in-hospital
mortality among all the previously examined variables. The
corresponding relative risk of mortality was 4.6 (95% CI,
1.6Y12; P = 0.003) for the composite of abnormal TDI
markers, 3.1 (95% CI, 1.01Y10.7; P = 0.035) for sepsis, and
2.9 (95% CI, 1.07Y7.9; P = 0.03) for NTYpro-BNP, respecti-
vely. By multivariable Cox regression analysis, the addition
of the composite of abnormal TDI markers of LV diastolic
function, in a model including NTYpro-BNP and sepsis,
significantly increased the prognostic value of the model for
ICU mortality (j2LogLikelihood from j143.8 to j133.6; Pfor change = 0.01, respectively).
Interestingly, patients with a combination of abnormal TDI
markers of LV diastolic function and NTYpro-BNP greater
than or equal to 941 pg/mL had the lowest MAP compared
with patients with only abnormal TDI, only BNP greater than
941 pg/mL, or a combination of normal TDI markers and
NTYpro-BNP less than 941 pg/mL (72 T 8 vs. 79 T 7 vs. 75 T10 vs. 86 T 15 mmHg; F = 3.8; P = 0.014) in the presence of
similar CVP (11.0 T 3.8 vs. 12.7 T 3.2 vs. 11.7 T 4.3 vs. 10.1 T3.5 mmHg; F = 1.07; P = 0.37) as well as the lowest PO2/FIO2
(127 T 98 vs. 198 T 86 vs. 248 T 100 vs. 298 T 122 mmHg/%;
F = 3.8; P = 0.014) and elevated creatinine levels (1.7 T0.5 vs. 1.1 T 0.6 vs. 1.9 T 1.2 vs. 1.1 T 0.7. mg/L; F = 3.9;
FIG. 1. A, Kaplan-Meier curves for the prediction of in-hospital mortality in patients with a composite of abnormal TDI indices of LV function versusthose with normal TDI indices. B, Kaplan-Meier plots for the prediction of in-hospital mortality in patients with 1) normal TDI and NTYpro-BNP less than 941pg/mL, 2) normal TDI and NTYpro-BNP greater than 941 pg/mL, 3) abnormal TDI and NTYpro-BNP less than 941 pg/mL, and 4) abnormal TDI and NTYpro-BNPgreater than 941 pg/mL.
144 SHOCK VOL. 33, NO. 2 IKONOMIDIS ET AL.

Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
P = 0.01). Thus, patients with a combination of abnormal TDI
markers and NTYpro-BNP greater than or equal to 941 pg/mL
had the lowest PO2/FIO2 and MAP compared with the
remaining patients, suggesting a greater degree of reduced
blood oxygenation and tissue hypoperfusion.
DISCUSSION
In the present study, we have shown that approximately
half of critically ill patients with Bnormal[ EF and no history
of heart failure had evidence of LV diastolic dysfunction, as
assessed by TDI, and one third of them showed evidence of
impaired longitudinal systolic function. Moreover, this is the
first study that demonstrates the independent association of
elevated NTYpro-BNP levels with LV diastolic dysfunction in
mechanically ventilated, critically ill patients with preserved
EF. Furthermore, we have shown that TDI markers of LV
function and NTYpro-BNP levels are complementary predic-
tors of in-hospital mortality in patients with preserved EF on
admission to a general ICU.
LV diastolic dysfunction in ICU patients
Tissue Doppler imaging of the systolic mitral annulus
motion permits an early detection of the longitudinal systolic
dysfunction even if EF remains Bnormal[ (20, 22, 23).
Furthermore, the advantage of the E¶ over the mitral inflow
Doppler markers of diastolic function is that it behaves as
a relatively preload independent index of LV relaxation
(18, 22). E/E¶ is a widely used marker to assess simply and
accurately LV filling pressures (9, 23). Recently, transthoracic
estimation of the E/E¶ ratio at the end-expiration has been
shown to correlate closely with pulmonary artery occlusion
pressure in mechanically ventilated ICU patients (29). The
reduced TDI velocities of the mitral annulus (S, E¶, E/E¶) have
been shown to predict mortality or cardiovascular events
in patients with heart failure, myocardial infarction, or
hypertension (25).In the present study, we have shown that approximately
half of mechanically ventilated, critically ill patients with
Bnormal[ EF and no history of heart failure have evidence of
LV diastolic dysfunction, as assessed by TDI. Additionally,
31% showed evidence of impaired longitudinal systolic
function as assessed by an S¶less than 8 cm/s in addition to
LV diastolic dysfunction despite the presence of a preserved
EF. A reduced early systolic velocity (S) of the mitral annulus
by TDI has been described in patients with preserved EF and
LV diastolic dysfunction such as patients with hypertension,
coronary artery disease, diabetes, or cardiomyopathies (20).
This finding is thought to reflect an impairment of the LV
longitudinal systolic performance caused by dysfunction of
subendocardial myocardial layers on the ground of hyper-
trophy, fibrosis, elevated filling pressures, and subendocardial
ischemia (20). In our study, there was a close association
between TDI indices of LV diastolic function and age, history
of hypertension or diabetes, and relative wall thickness. It is
known that aging, arterial hypertension, diabetes mellitus, and
increased wall thickness may impair the diastolic properties in
the left ventricle (20Y22, 30). Additionally, in our study,
impaired TDI markers were also related with presence of
sepsis and increased levels of lactate acid. This finding
suggests that acidosis and/or inflammation may play an
additional role in myocardial depression in ICU patients
causing LV diastolic dysfunction. Studies have shown that
lactate acidosis (31) and inflammation (32, 33) are associated
with cardiac systolic or diastolic dysfunction. Therefore, we
may hypothesize that each one of the previously discussed
factors or their combination may worsen the myocardial
diastolic properties and longitudinal systolic function, as
assessed by TDI in critically ill patients with preserved EF.
In support of this hypothesis, TDI markers of LV function
were related with troponin levels, confirming that LV
diastolic dysfunction is related with a new-onset myocardial
damage in critically ill patients with preserved EF on
admission to ICU.In conclusion, LV diastolic dysfunction and impaired
longitudinal systolic function in our ICU patients with
preserved EF may originate from a preexisting increased wall
stress on the grounds of hypertension, diabetes, and increased
wall thickness (9), or may be caused from direct effects of
hypoxia, acidosis, and the release of toxic inflammatory
mediators during infection and/or sepsis on myocardium
(11, 22, 31Y33).
Determinants of NTYpro-BNP levels in ICU
Most studies in ICU patients have focused on LV systolic
dysfunction as assessed by means of an impaired EF and its
impact on natriuretic peptides and mortality (6Y8). The
independent association between NTYpro-BNP and TDI
markers of LV diastolic function found in the present study
suggests that LV diastolic dysfunction is a major determinant
of elevated NTYpro-BNP levels in ICU patients with
preserved EF. Studies have shown that myocyte stretch
because of elevated LV filling pressures may cause BNP
production (2). A further stimulus of NTYpro-BNP release is
tissue hypoxia (12). Thus, reduced blood oxygenation
because of pulmonary congestion on the grounds of LV
diastolic dysfunction may contribute to BNP production. In
our study, an NTYpro-BNP greater than 941 pg/mL was a
reliable predictor of LV diastolic dysfunction with 73%
sensitivity and 70% specificity. In ICU patients, the
myocyte stretch leading to elevated NTYpro-BNP may
originate from the LV filling pressures on the basis of
hypertension, diabetes, and increased wall thickness (9,
24, 34). Supporting this hypothesis, studies have shown that
LV stroke work, as well as pulmonary artery occlusion
pressure assessed after cardiac catheterization, correlated
with NTYpro-BNP in ICU patients (29, 34). However,
increased NTYpro-BNP production may be triggered from
the direct effect of inflammatory mediators during sepsis (10,
11, 13), elevated levels of stress hormones (2, 11), renal
dysfunction (2), or from overtreatment with fluids, vaso-
active medications (11), and positive pressure ventilation in
critically ill patients. Sepsis is associated with high cardiac
output, and therapy includes administration of fluids. It is
possible that cardiac distension occurs, with preserved sys-
tolic function causing elevation of BNP secretion (11, 35). In
agreement with other investigators (4Y8, 10), we have shown
SHOCK FEBRUARY 2010 TDI, NTYPRO-BNP, AND OUTCOME IN ICU PATIENTS 145

Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
in the present study that NTYpro-BNP also correlated with
age, creatinine levels, inotrope infusion, presence of sepsis,
and hypoxia. Furthermore, the independent association, by
multivariate analysis, of NTYpro-BNP levels with S, E/E¶,
and presence of sepsis supports the hypothesis that sepsis
may cause NTYpro-BNP release in critically ill patients in
addition to diastolic LV dysfunction. The interrelation
between sepsis, TDI markers of LV function, and
NTYpro-BNP in our study suggests that the inflammatory
processes and release of inflammatory mediators in septic
conditions may cause LV diastolic dysfunction (10Y22),
leading to elevated NTYpro-BNP levels in ICU patients.
However, sepsis may cause elevated NTYpro-BNP levels
through mechanisms other than myocardial damage such
as renal impairment, increased stress hormones, and
elevated levels of inflammatory cytokines (11) or coex-
istent noncardiac causes of elevated NTYpro-BNP (10). In
summary, elevated NTYpro-BNP may be a marker of
preexisting LV diastolic dysfunction on the grounds of
hypertension diabetes and LV hypertrophy; of acquired LV
diastolic dysfunction because of sepsis, inflammation,
hypoxia, and acidosis; or of the systemic inflammatory
response during infection or sepsis in our critically ill
patients.
Determinants of ICU mortality
In our previous study (3), we have shown that NTYpro-BNP
levels are independent predictors of outcome in a large mixed
ICU population. In the present study, we have demonstrated
that LV diastolic dysfunction may determine NTYpro-BNP
levels in addition to other comorbidities. Furthermore, we
have shown that LV diastolic dysfunction as assessed by TDI
is a prognostic marker for ICU mortality in patients with
preserved EF in addition to elevated NTYpro-BNP levels and
presence of sepsis. In our study, patients with a composite of
abnormal TDI markers of diastolic LV function had a 4-fold
risk of death during hospitalization. Furthermore, the addition
of the composite of abnormal TDI markers of LV diastolic
function, in a model including NTYpro-BNP and sepsis,
significantly increased the prognostic value of the model for
ICU mortality. This finding suggests that in the presence of
low NTYpro-BNP levels or sepsis, TDI markers become
particularly useful in distinguishing patients at a substantially
lower or higher risk of an adverse event.
Additionally, the combination of normal TDI markers and
low NTYpro-BNP was associated with a survival rate of 84%,
whereas the combination of abnormal TDI markers and BNP
has a survival rate of 25%. Thus, the combination of NTYpro-
BNP levels with the TDI parameters of LV function could
discriminate those with an excellent compared with those with
a poor prognosis during ICU hospitalization.
Patients with the combination abnormal TDI markers and
high NTYpro-BNP levels had a lower survival rate compared
with patients with abnormal TDI or NTYpro-BNP alone or to
patients with normal TDI markers and low BNP levels.
Thus, abnormal TDI markers provided additional prognos-
tic information in patients with high NTYpro-BNP levels and
vice versa.
Our results suggest that TDI markers and NTYpro-BNP
levels may be complementary predictors of ICU mortality in
patients in critically ill patients with preserved EF and are in
line with studies demonstrating the independent and incre-
mental prognostic value of TDI markers in cardiovascular
disease (25).
Considering the causal relation of LV diastolic dysfunction
with outcome, LV diastolic dysfunction raises the left atrial
and pulmonary vein pressure (9, 22Y25) and thus causes
pulmonary congestion contributing to reduced blood oxygen-
ation and, consequently, to tissue hypoxia, acidosis, and
multiple organ failure. Indeed, in our study, patients with
LV diastolic dysfunction had a reduced PO2/FIO2 and
increased lactic acid. Additionally, LV diastolic dysfunction
may not permit an adequate increase of stroke volume in the
presence of excessive peripheral vasodilation during sepsis or
under conditions of low output, leading to tissue hypoperfu-
sion (11). In critically ill patients, elevated NTYpro-BNP may
be a cumulative marker of 1) LV diastolic dysfunction either
preexisting, because of cardiac disease, or acquired, because
of hypoxia, hypoperfusion, and toxic effects of inflammation;
2) renal dysfunction, 3) inflammatory process and tissue
hypoxia during infection and/or sepsis; 4) elevation of stress
hormones and neurohumoral activation and thus may be a
valid predictor of adverse outcome (2, 10Y17).
However, BNP is an active hormone that increases the
cellular production of cyclic guanosine monophosphate, lead-
ing to relaxation of vascular smooth muscle cells and renin
inhibition (2). Thus, elevated NTYpro-BNP may cause inap-
propriate vasodilation, especially in septic conditions, leading
to reduced MAP and thus may aggravate tissue hypoperfusion,
renal dysfunction, and multiple organ failure. Brain natriuretic
peptide antagonizes angiotensin IIYinduced efferent arteriolar
vasoconstriction and thus reduces glomerular filtration rate,
leading to increases in creatinine levels (15).
In agreement with this hypothesis, treatment with nesiritide,
a synthetic form of BNP, has been associated with adverse
outcome in patients with heart failure because of hypotension
and deterioration of renal function (14Y16). In the present
study, we have shown that patients with NTYpro-BNP greater
than 941 pg/mL had lower MAP and serum creatinine than
patients with lower NTYpro-BNP. Thus, through these
mechanisms, NTYpro-BNP levels may have a causal associ-
ation with outcome in our critically ill patients. Furthermore,
patients with combination of elevated NTYpro-BNP and
impaired TDI indices had the lowest MAP and PO2/FIO2 in
addition to elevated serum creatinine compared with the
remaining patients. Thus, pulmonary congestion and/or
inadequate increase of stroke volume under conditions of
peripheral vasodilation, because of LV diastolic dysfunction,
combined with a low MAP, because of the vasodilatory
effects of increased BNP, may contribute to reduced blood
oxygenation, tissue hypoperfusion, hypoxia, and further
deterioration of renal function. The previously discussed
mechanisms may at least partially explain the complementary
role of LV diastolic dysfunction and increased NTYpro-BNP
levels in the prediction of adverse outcome in our cohort of
critically ill patients.
146 SHOCK VOL. 33, NO. 2 IKONOMIDIS ET AL.

Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
Study limitations
One of the limitations of our study was the absence of
hemodynamic evaluation of LV filling pressures with a Swan-
Ganz catheter even if the safety and use of these catheters
have been questioned. Furthermore, several studies have
shown a close correlation between elevated E/E¶ and inva-
sively assessed LV filling pressures (9, 18). The relatively
small sample of our patient cohort should also be acknowl-
edged. However, in our study, we have shown that TDI
indices of LV function are a useful prognostic tool, which are
easily performed and readily available by the bedside of
critically ill patients and may discriminate subtle diastolic
abnormalities of the cardiac wall, leading to increased
NTYpro-BNP levels and adverse outcome. Thus, the assess-
ment of TDI velocities of the mitral annulus is a useful tool to
rule out the origin of elevated NTYpro-BNP levels (LV
dysfunction or noncardiac factors) in critically patients with
preserved EF and to stratify more accurately the risk of
adverse outcome on patients’ admission to ICU.
Because patients are admitted into the ICU at varying time
points in the progression of their illness, serial assessment of
TDI markers and NTYpro-BNP over time may be more useful
in the determination of prognosis and the effects of treatment.
In our study, nonsurvivors had reduced oxygenation, a
higher level of acidosis, a higher incidence of sepsis, and
impaired indices of LV diastolic function than survivors. The
close link between adverse outcome and LV diastolic
dysfunction, reduced oxygenation, acidosis, and sepsis in our
study suggests that preexisting diastolic dysfunction may
generate a more Bvulnerable[ myocardium to toxic effects of
hypoxia, acidosis, and sepsis. It should be further investigated
whether prompt treatment of these factors may reverse at least
partly LV diastolic function and, consequently, patients’
prognosis of during ICU hospitalization. In patients with
impaired TDI indices and elevated NTYpro-BNP implying
elevated LV filling pressures, initiation of diuresis, ultra-
filtration, and/or inotropes should be considered individually
according to a patient’s underlying disease, clinical condition,
blood pressure, loading conditions as assessed by CVP, renal
function, and hourly urine volume. However, LV diastolic
dysfunction may also be a marker of increased severity of
illness and thus may not respond to these interventions.
CONCLUSION
In the present study, we have shown that LV diastolic
dysfunction, as assessed by TDI and sepsis, determine
NTYpro-BNP levels in critically ill patients with preserved
EF. Moreover, abnormal TDI indices of LV function and
NTYpro-BNP have a complementary value for in-hospital
mortality.
REFERENCES1. de Rooij SE, Abu-Hanna A, Levi M, de Jonge E: Factors that predict outcome
of intensive care treatment in very elderly patients: a review. Crit Care9:307Y314, 2005.
2. de Lemos JA, McGuire DK: Drazner MHB-type natriuretic peptide in
cardiovascular disease. Lancet 362:316Y322, 2003.
3. Kotanidou A, Karsaliakos P, Tzanela M, Mavrou I, Kopterides P,
Papadomichelakis E, Theodorakopoulou M, Botoula E, Tsangaris I,
Lignos M, et al.: Prognostic importance of increased plasma amino-terminal
proYbrain natriuretic peptide levels in a large mixed intensive care unit
population. Shock 31:342Y347, 2009.4. Januzzi JL, Morss A, Tung R, Pino R, Fifer MA, Thompson BT, Lee-
Lewandrowski E: Natriuretic peptide testing for the evaluation of critically ill
patients with shock in the intensive care unit: a prospective cohort study. CritCare 10:37Y43, 2006.
5. Varpula M, Pulkki K, Karlsson S, Ruokonen E, Pettila V: Predictive value of
N-terminal proYbrain natriuretic peptide in severe sepsis and septic shock. CritCare Med 35:1277Y1283, 2007.
6. Januzzi JL, van Kimmenade R, Lainchbury J, Bayes-Genis A, Ordonez-Llanos
J, Santalo-Bel M, Pinto YM, Richards M: NT-proBNP testing for diagnosis
and short-term prognosis in acute destabilized heart failure: an international
pooled analysis of patients: the International Collaborative of NT-proBNP
Study. Eur Heart J 27:330Y337, 2006.
7. Shah KB, Nolan MM, Rao K, Wang DJ, Christenson RH, Shanholtz CB,
Mehra MR, Gottlieb SS: The characteristics and prognostic importance of NT-
ProBNP concentrations in critically ill patients. Am J Med 120:1071Y1077,
2007.
8. Meyer B, Huelsmann M, Wexberg P, Delle Karth G, Berger R, Moertl D,
Szekeres T, Pacher R, Heinz G: N-terminal pro-B-type natriuretic peptide is an
independent predictor of outcome in an unselected cohort of critically ill
patients. Crit Care Med 35:2268Y2273, 2007.
9. Paulus W, Tsch:pe C, Sanderson J, Rusconi C, Flachskampf F, Rademakers F,
Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, et al.: How to
diagnose diastolic heart failure: a consensus statement on the diagnosis of
heart failure with normal left ventricular ejection fraction by the Heart Failure
and Echocardiography Associations of the European Society of Cardiology.
Eur Heart J 28:2539Y2550, 2007.
10. Ma KK, Ogawa T, de Bold AJ: Selective upregulation of cardiac brain
natriuretic peptide at the transcriptional and translational levels by proin-
flammatory cytokines and by conditioned medium derived from mixed
lymphocyte reactions via p38 MAP kinase. J Mol Cell Cardiol 36:505Y513,
2004.
11. Fried I, Bar-Oz B, Algur N, Fried E, Gavri S, Yatsiv I, MDf, Perles Z, Rein
AJJT, Zonis Z, Bass R, et al.: Comparison of N-terminal pro-B-type natriuretic
peptide levels in critically ill children with sepsis versus acute left ventricular
dysfunction. Pediatrics 118:e1165Ye1168, 2006.
12. Hopkins WE, Chen Z, Fukagawa NK, Hall C, Knot HJ, LeWinter MM:
Increased atrial and brain natriuretic peptides in adults with cyanotic
congenital heart disease: enhanced understanding of the relationship between
hypoxia and natriuretic peptide secretion. Circulation 109:2872Y2877, 2004.
13. Rudiger A, Gasser S, Fischler M, Hornemann T, Von Eckardstein A,
Maggiorini M: Comparable increase of B-type natriuretic peptide and amino-
terminal pro-B-type natriuretic peptide levels in patients with severe sepsis,
septic shock, and acute heart failure. Crit Care Med 34:2140Y2144, 2006.
14. Mills RM, LeJemtel TH, Horton DP, Liang C, Lang R, Silver MA, Lui C,
Chatterjee K: Sustained hemodynamic effects of an infusion of nesiritide
(human b-type natriuretic peptide) in heart failure: a randomized, double-blind,
placebo-controlled clinical trial: Natrecor Study Group. J Am Coll Cardiol34:155Y162, 1999.
15. Sackner-Bernstein JD, Skopicki HA, Aaronson KD: Risk of worsening renal
function with nesiritide in patients with acutely decompensated heart failure.
Circulation 111:1487Y1491, 2005.
16. Sackner-Bernstein JD, Kowalski M, Fox M: Short-term risk of death after
treatment with nesiritide for decompensated heart failure. A pooled analysis of
randomized controlled trials. JAMA 293:1900Y1905, 2005.
17. Zakynthinos E, Kiropoulos T, Gourgoulianis K, Filipatos G: Diagnostic and
prognostic impact of brain natriuretic peptide in cardiac and noncardiac
diseases. Heart Lung 37:275Y285, 2008.
18. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA: Doppler
tissue imaging: a noninvasive technique for evaluation of left ventricular
relaxation and estimation of filling pressures. J Am Coll Cardiol 30:
1527Y1533,1997.
19. Nikitin NP, Witte KK, Thackray SD, de Silva R, Clark AL, Cleland JG:
Longitudinal ventricular function: normal values of atrioventricular annular
and myocardial velocities measured with quantitative two-dimensional color
Doppler tissue imaging. J Am Soc Echocardiogr 16:906Y921, 2003.
20. Yip G, Wang M, Zhang Y, Fung JW, Ho PY, Sanderson JE: Left ventricular
long axis function in diastolic heart failure is reduced in both diastole and
systole: time for a redefinition? Heart 87:121Y125, 2002.
21. Pavlopoulos H, Grapsa J, Stefanadi E, Kamperidis V, Philippou E, Dawson D,
Nihoyannopoulos P: The evolution of diastolic dysfunction in the hypertensive
disease. Eur J Echocardiogr 9:772Y778, 2008.
SHOCK FEBRUARY 2010 TDI, NTYPRO-BNP, AND OUTCOME IN ICU PATIENTS 147

Copyright @ 2010 by the Shock Society. Unauthorized reproduction of this article is prohibited.
22. Mottram PM, Marwick TH: Assessment of diastolic function: what the general
cardiologist needs to know. Heart 91:681Y695, 2005.
23. Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM,
Tajik AJ: Clinical utility of Doppler echocardiography and tissue Doppler
imaging in the estimation of left ventricular filling pressures: a comparative
simultaneous Doppler-catheterization study. Circulation 102:1788Y1794,
2000.
24. Motram P, Haluska B, Marwick T: Response of B-type natriuretic peptide to
exercise in hypertensive patients with suspected diastolic heart failure:
correlation with cardiac function, hemodynamics, and workload. Am Heart J148:365Y370, 2004.
25. Y u CM, Sanderson JE, Marwick TH, Oh JK: Tissue Doppler imaging a new
prognosticator for cardiovascular diseases. J Am Coll Cardiol 49:1903Y1914,
2007.
26. Charpentier J, Luyt CE, Fulla Y, Vinsonneau C, Cariou A, Grabar S, Dhainaut
JF, Mira JP, Chiche JD: Brain natriuretic peptide: a marker of myocardial
dysfunction and prognosis during severe sepsis. Crit Care Med 32:660Y665,
2004.
27. Levy M, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal
SM, Vincent JL, Ramsay G: SCCM/ESICM/ACCP/ATS/SIS international
sepsis definitions conference. Crit Care Med 31:1250Y1256, 2001.
28. Ikonomidis I, Athanassopoulos G, Stamatelopoulos K, Lekakis J, Revela I,
Venetsanou K, Marinou M, Monaco C, Cokkinos DV, Nihoyannopoulos P:
Additive prognostic value of interleukin-6 at peak phase of dobutamine stress
echocardiography in patients with coronary artery disease. A 6-year follow-up
study. Am Heart J 156:269Y276, 2008.29. Combes A, Arnoult F, Trouillet JL: Tissue Doppler imaging estimation of
pulmonary artery occlusion pressure in ICU patients. Intensive Care Med30:75Y81, 2004.
30. Lenzen MJ, Scholte OP, Reimer WJM, Boersma E, Vantrimpont PJMJ, Follath
F, Swedberg K, Cleland J, Komajda M: Differences between patients with a
preserved and a depressed left ventricular function: a report from the
EuroHeart Failure Survey. Eur Heart J 25:1214Y1220, 2004.
31. Teplinsky K, O’Toole M, Olman M,Walley KR, Wood LD: Effect of lactic
acidosis on canine hemodynamics and left ventricular function. Am J Physiol258:H1193YH1199, 1990.
32. Ikonomidis I, Lekakis JP, Nikolaou M, Paraskevaidis I, Andreadou I,
Kaplanoglou T, Katsimbri P, Skarantavos G, Soucacos PN, Kremastinos DT:
Inhibition of interleukin-1 by anakinra improves vascular and left ventricular
function in patients with rheumatoid arthritis. Circulation 117:2662Y2669,
2008.
33. Court O, Kumar A, Parrillo JE, Kumar A: Clinical review: myocardial
depression in sepsis and septic shock. Crit Care 6:500Y508, 2002.
34. Forfia PR, Watkins SP, Rame JE, Stewart KJ, Shapiro EP: Relationship
between B-type natriuretic peptides and pulmonary capillary wedge pressure in
the intensive care unit. J Am Coll Cardiol 45:1667Y1671, 2005.
35. Wolff B, Haase D, Lazarus P, Machill K, Graf B, Lestin HG, Werner D:
Severe septic inflammation as a strong stimulus of myocardial NT-pro brain
natriuretic peptide release. Int J Cardiol 122:131Y136, 2007.
148 SHOCK VOL. 33, NO. 2 IKONOMIDIS ET AL.