Acute obstructive pyelonephritis due to pelvic organ prolapse

w¾nqo (Tumour)Definition
According to Acharrya Sushruta,
The large Vegetation of flesh which appears atany part of the body, becomes slightypainful.rounded .immovable and deep- seated andhas its root sunk considerably deep in theaffected part ,and which is due to the vitiationof the flesh and blood by deranged andaggravated doshas (Vayu,Pittam and Kapham ) iscalled an Arvuda or tumour.
The Growth of an Arvuda is oftenfound to be slow and it seldom suppurates. Thecharacteristic symptoms of an Arvuda whichowes its origin to the deranged condition of theVayu,Pittam,Kapham.flesh or fat ,arerespectively identical with those which markcases of Granthis,brought about by the samederanged principles of the body.
Raktaja Arbuda

The deranged doshas(Vayu,Pittam and Kapham)contracting, compressing and drawing thevessels (sira) and blood (of the affectedpart ),raise a slightly suppurated and exudingtunour which is covered with small warts andfleshy tubercles and is called Raktarvuda.Thistumour is rapid in its growth and exudes aconstant flow of (vitiated) blood.Thecomplexion of the patient owing to depletiveactions and other concomitant evils ofheamorrhage becomes pale yellow. The typeshould be considered incurable on account of itshaving its origin in the blood .
Mansarbuda
The flesh of any part of the body hurt by anexternal blow etc.(hurting it with a log ofwood )and vitiated in consequences ,gives riseto a sort of swelling (tumour )which is calledMansarvuda,which originates through the actionof the deranged Vayu.It is glossy ,painless, non–suppurating,hard as astone ,immobile ,and ofthe same colour as the surrounding skin.Such a

tumour appearing in a person addicted to meatdiet becomes deep-seated owing to theconsequent vitiation of an incurabale type.
Prognosis
Even of the aforesaid curable types (suchas the vataja,etc.) the following type ofArbudam (Tumours) should be likewise regardedas incurable, those which appear in thecavity of a srota channel or an artery, orany vulnerable joint of the body and arecharacterized by any sort of secretion andalso immovable ,should be deemed incurable .
An Arbudam (tumour ) cropping up on oneexisting from before is called Adhyarbudam,which should be likewise deemed as incurable.
A couple of contiguous Arbudam (tumour )cropping up simultaneously or one afteranother is called Dviarbudam, which shouldbe held as equally incurable (with one of theforegoing type).
An Arbuda (tumour) of whatsoever type,never suppurates owing to the exuberance ofthe deranged Kapham and Fat as well as inconsequence of the deranged Doshas(Vayu,Pittam and Kapham involved in the

case or out of a specific trait of its ownnature. (Su/Ni/11/6)
Treatment of Arbuda
According to Acharya Sushrutha:
Vataja Arbuda
A poultice composed ofKarkaruka,Erudruka,coconut,Piydla, andCastor seeds ,boiled with milk,water andclarified butter, and mixed withoil,should be applied lukewarm (to thetumour).
As an alternative ,a poultice appliedmade up of boiled meat or Vesa –vara ,should be applied to it.
Formentation of the part in the manner ofa Nadi-Sweda.
The Vitiated blood (of the locality)should be repeatedly cuffed off with ahorn.
Satakuva or trivut boiled with decoctionof the Vayu-suduing drugs and with milkand kanjika ,should be given to patient.
Pittaja arbuda
Application of mild formentation andpoultice (to the affected part) and ofpurgatives are effcacious in PittajaArvuda.
The tumour should be well rubbed with(the rough surface of) the leaves ofthe Goji and it should be plasteredover with the powders of Sarja-rasa,priyangu,pattanga (Red sandalwood),Rodhra,Anjana and Yasti-madhu,mixed with honey.
As an alternative, a plaster composed ofAragvada,Goji,Soma,Vruda dara pastedtogether should be applied to it afterthe secretion Visrava clarifiedbutter ,cooked with Klitaka as a Kalka)and with the decoction ofSyadma,Grikva,Anjanaki

Draksha and saptalika should beprescribed for internal application in acase of a pittaja arvuda .
Kapaja arbuda
Blood should be let out from the affectedpart after the systems of thye patientshas been cleaned (by emetics andpurgatives) then a medicinal plastercomposed of the drugs which areeficacious in correcting the doshas,confined to the upper and lower parts ofthe doshas ,confined to the upper and thelower parts of the organism,should beapplied hot to the tumour.or a plastercomposed of Kansya-nila,suka,langalakyaand kakdani roots and the dung of aKapoli and of paravala pasted togetherwith urine ,or with alkaline watershouled be applied to it.
The kalkas (pastes)ofnishpdva(s’imbi).Pinyaka (oil-cakes ofsesamum)and Kulattha pulse,pasted withcurd-dream and an abundunt quantity offlesh,should be used in plastering the

affected part so that worms and parasitesmay be produced in the ulcer and fliesattracted to it (and so consume the ulcer).
A small portion of the ulcer ,leftunconsumed( un –eaten) by worms andparasites ,etc,should be sacrified andthe ulcer should then be cauterrised withfire.
A comparatively superficial tumour(Arvuda; should be covered with thinleavesof zinc,copper,lead or of iron andcauterrization with fire or with analkali as well an surgical operationshould be carefully and repeatedlyresorted to,so as not to hurt ,nor in anyway injure the body.
The incidental ulcer should be washedwith the decoction of the leaves of theAsphota,Jati and Karvira for the purposeof purification.
A medicated oil ,cooked withBhargi,Vidanga,Patha and Tripala shouldthen be used as a healing remedy.

An experienced physician should treat atumour ,spontaneously suppurating, in themanner of a suppurated ulcer.
Medoja Arbuda (Fat origined tumour)
Should be first fomented and thenincised.
The blood in its inside having beencleansed it should be quickly suturedand then plastered over with a compoundcomposed of Haridra, Grika-dhuma (sootof a room), Rodhra, Pattanga, ManasilandHaridra pounded together and mixed witha proper quantity of honey.
After its purification, thus produced,it should be treated with theapplication of Karanja-Taila.
Even the least particle of doshas(pus ,etc)in a tumour , left unremoved,would lead to a fresh growth of theexcrescence and bring on death just likethe least paricle of an unextinguishedfire.
Hence it should be destroyed in itsentirety.
Ref: (Su/Chi/18/9)
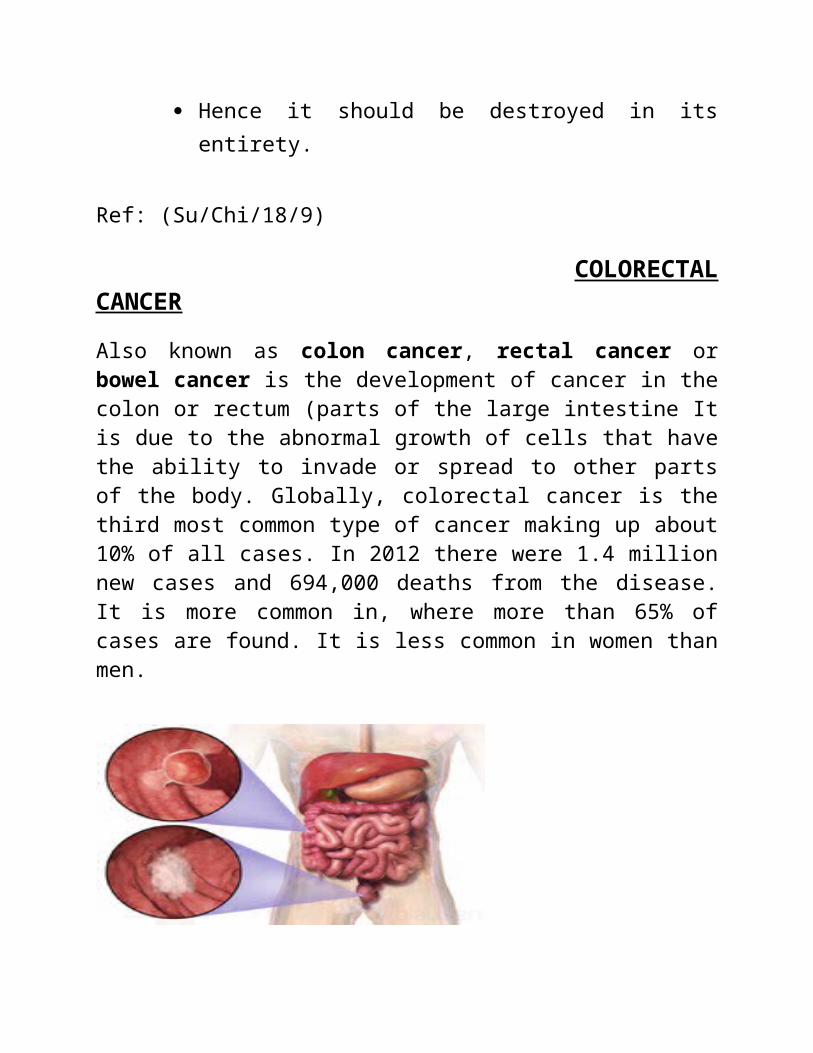
COLORECTALCANCER
Also known as colon cancer, rectal cancer orbowel cancer is the development of cancer in thecolon or rectum (parts of the large intestine Itis due to the abnormal growth of cells that havethe ability to invade or spread to other partsof the body. Globally, colorectal cancer is thethird most common type of cancer making up about10% of all cases. In 2012 there were 1.4 millionnew cases and 694,000 deaths from the disease.It is more common in, where more than 65% ofcases are found. It is less common in women thanmen.

-Location and appearance of twoexample colorectal tumors-
Signs and symptoms
The symptoms and signs of colorectal cancer depend on the location of the tumor in the bowel, and whether it has spread elsewhere in the body (metastasis).
The classic warning signs include:
Worsening constipation. Blood in the stool. Decrease in stool caliber (thickness), Loss of appetite. Loss of weight. Feeling tired all the time. A change in bowel movements Nausea or vomiting in someone over 50 yearsold, While rectal bleeding or anemia arehigh-risk features in those over the age of50.
Other commonly-described symptoms includingweight loss and change in bowel habit aretypically only concerning if associated withbleeding.
Risk factors
Lifestyle.

Older age. Diet. Male gender. Smoking and Alcohol consumers. Lack of physical activities. Family history of colon cancer. Colon polyps. Presence of colon polyps Race. Exposure to radiation. Diabetes. Obesity. A diet high in red and high intake of fat Processed meat while low in fiber increasesthe risk of colorectal cancer.
Inflammatory bowel disease, which includesCrohn's disease and ulcerative colitis, canincrease the risk of colorectal cancer.
Some of the inherited conditions that cancause colorectal cancer include: familialadenomatous polyposis and hereditary non-polyposis colon cancer; however, theserepresent less than 5% of cases. It typicallystarts as a benign tumor, often in the formof a polyp, which over time becomescancerous.
Diagnosis
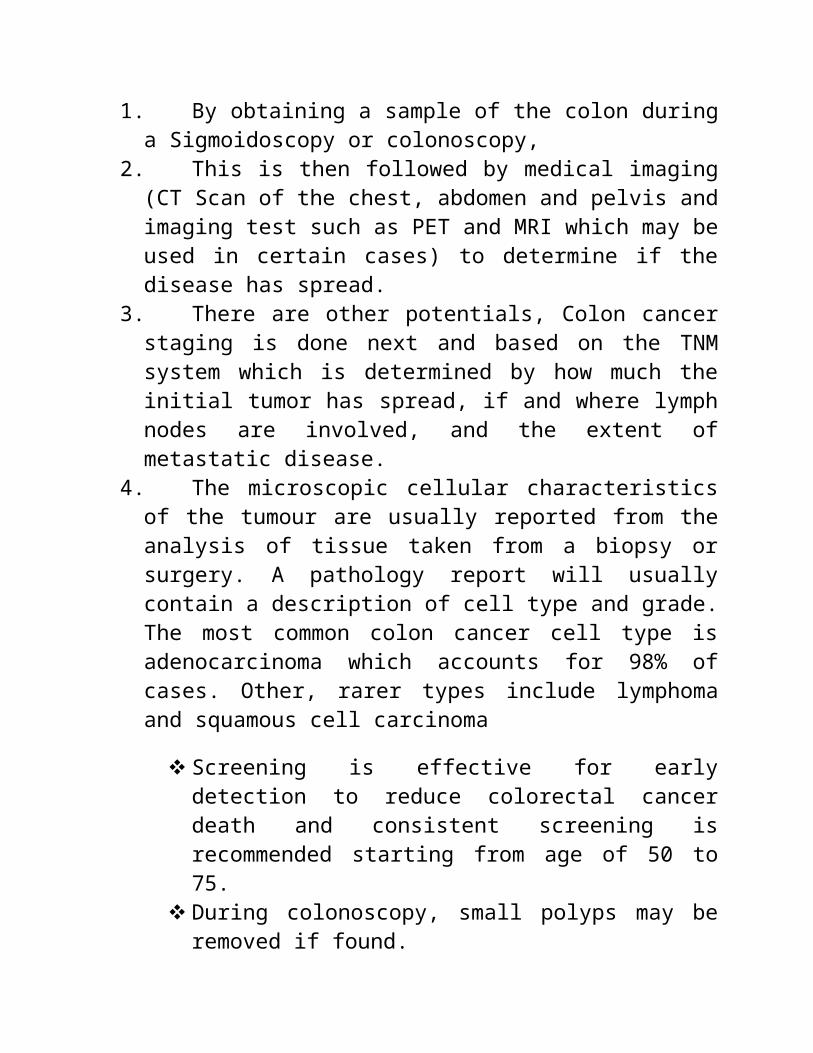
1. By obtaining a sample of the colon duringa Sigmoidoscopy or colonoscopy,
2. This is then followed by medical imaging(CT Scan of the chest, abdomen and pelvis andimaging test such as PET and MRI which may beused in certain cases) to determine if thedisease has spread.
3. There are other potentials, Colon cancerstaging is done next and based on the TNMsystem which is determined by how much theinitial tumor has spread, if and where lymphnodes are involved, and the extent ofmetastatic disease.
4. The microscopic cellular characteristicsof the tumour are usually reported from theanalysis of tissue taken from a biopsy orsurgery. A pathology report will usuallycontain a description of cell type and grade.The most common colon cancer cell type isadenocarcinoma which accounts for 98% ofcases. Other, rarer types include lymphomaand squamous cell carcinoma
Screening is effective for earlydetection to reduce colorectal cancerdeath and consistent screening isrecommended starting from age of 50 to75.
During colonoscopy, small polyps may beremoved if found.

If a large polyp or tumor is found, abiopsy may be performed to check if it iscancerous.
Macroscopica lly
Cancers on the right side of the large intestine(ascending colon and cecum) tend to beexophytic, that is, the tumor grows outwardsfrom one location in the bowel wall. This veryrarely causes obstruction of feces, and presentswith symptoms such as anemia. Left-sided tumourstend to be circumferential, and can obstruct thebowel lumen, much like a napkin ring, andresults in thinner caliber stools.
Macroscopic
Appearance of the inside of the colon showingone invasive colorectal carcinoma (thecrater-like, reddish, irregularly shapedtumor).

Gross appearance of a colectomy specimencontaining two adenomatous polyps (thebrownish oval tumors above the labels,attached to the normal beige lining by astalk) and one invasive colorectal carcinoma(the crater-like, reddish, irregularly shapedtumor located above the label).
Endoscopic image of colon cancer identifiedin sigmoid colon on screening colonoscopy inthe setting of Crohn's disease.
PET/CT of a staging exam of colon carcinoma.Besides the primary tumor a lot of lesionscan be seen. On cursor position: lung nodule
Microscopically
Adenocarcinoma is a malignant epithelial tumor,originating from superficial glandularepithelial cells lining the colon and rectum. Itinvades the wall, infiltrating the muscularis

mucosae layer, the sub mucosa, and then themuscularis propria. Tumor cells describeirregular tubular structures, harboringpluristratification, multiple lumens, reducedstroma ("back to back" aspect). Sometimes, tumorcells are discohesive and secrete mucus, whichinvades the interstitium producing large poolsof mucus/colloid (optically "empty" spaces).This occurs in mucinous (colloid) adenocarcinoma,in which cells are poorly differentiated. If themucus remains inside the tumor cell, it pushesthe nucleus at the periphery. This occurs in"signet-ring cell." Depending on glandulararchitecture, cellular pleomorphism, andmucosecretion of the predominant pattern,adenocarcinoma may present three degrees ofdifferentiation: well, moderately, and poorlydifferentiated.
Micrographs (H&E stain)
Cancer — Invasive adenocarcinoma (the mostcommon type of colorectal cancer). Thecancerous cells are seen in the center and atthe bottom right of the image (blue). Near

normal colon-lining cells are seen at the topright of the image.
Cancer — Histopathologic image of colonic carcinoid.
Precancerous — Tubular adenoma (left ofimage), a type of colonic polyp and aprecursor of colorectal cancer. Normalcolorectal mucosa is seen on the right.
precancerous — Colorectal villous adenoma.
Staging
The colon cancer staging can be made accordingto the TNM staging system from the WHOorganization, the UICC and the AJCC. The Astler-Coller classification (1954) or the Dukesclassification (1932) are now less used.

The T stages of bowel cancer.
Dukes stage A bowel cancer; the cancer is only in the inner lining of the bowel.
Dukes stage B bowel cancer; the cancer has invaded the muscle.
Dukes stage C bowel cancer; the cancer has invaded the nearby lymph nodes.

Dukes stage D bowel cancer; the cancer has metastasized.
Tumour budding
Tumor budding in colorectal cancer is looselydefined by the presence of individual cellsand small clusters of tumor cells at theinvasive front of carcinomas. It has beenpostulated to represent an epithelial–mesenchymal transition (EMT). Tumor budding isa well-established independent marker of apotentially poor outcome in colorectalcarcinoma that may allow for dividing peopleinto risk categories more meaningful thanthose defined by TNM staging, and alsopotentially guide treatment decisions,especially in T1 and T3 N0 (Stage II, Dukes’B) colorectal carcinoma. Unfortunately, itsuniversal acceptance as a reportable factorhas been held back by a lack of definitionaluniformity with respect to both qualitativeand quantitative aspects of tumor budding.
Immunochemistry

Most (50%) colorectal adenomas and (80-90%)colorectal cancer tumors are thought to overexpress the cyclooxygenase-2 (COX-2) enzyme.This enzyme is generally not found in healthycolon tissue, but is thought to fuel abnormalcell growth.
Prognosis
Cancers that are confined within thewall of the colon may be curable withsurgery while cancer that has spreadwidely are usually not curable, withmanagement focusing on improving qualityof life and symptoms.
This, however, depends on how advancedthe cancer is, whether or not all thecancer can be removed with surgery, andthe person's overall health.
Prevention
Life style
Most colorectal cancers should bepreventable, through increased surveillanceand lifestyle change. Life style Currentdietary recommendations to prevent colorectalcancer include increasing the consumption ofwhole grains, fruits and vegetables, and

reducing the intake of red meat. The evidencefor fiber and fruits and vegetables howeveris poor Physical exercise is associated witha modest reduction in colon but not rectalcancer risk. Sitting regularly for prolongedperiods is associated with higher mortalityfrom colon cancer. The risk is not negated byregular exercise, though it is lowered.
Medication
Aspirin and celecoxib appear to decrease therisk of colorectal cancer in those at high riskHowever, it is not recommended in those ataverage risk. There is tentative evidence forcalcium supplementation but it is not sufficientto make a recommendation. Vitamin intake andblood levels are associated with a lower risk ofcolon cancer.
Screening
More than 80% of colorectal cancers arise fromadenomatous polyps making this cancer suitablefor screening. Diagnosis of cases of colorectalcancer through screening tends to occur 2–3years before diagnosis of cases with symptoms.Screening has the potential to reduce colorectalcancer deaths by 60%

The three main screening tests are fecal occultblood testing, flexible sigmoidoscopy, andcolonoscopy Of the three, only sigmoidoscopycannot screen the right side of the colon where42% of malignancies are found Virtualcolonoscopy via a CT scan appears as good asstandard colonoscopy for detecting cancers andlarge adenomas but is expensive, associated withradiation exposure, and cannot remove anydetected abnormal growths like standardcolonoscopy can.
Fecal occult blood testing (FOBT) of the stoolis typically recommended every two years and canbe either guaiac based or immunochemical. Ifabnormal FOBT results are found, participantsare typically referred for a follow-upcolonoscopy examination. Annual to biennial FOBTscreening reduce colorectal cancer mortality by16% and among those participating in screeningcolorectal cancer mortality can be reduced up to23%, although it has not been proven to reduceall-cause mortality. Immunochemical tests arehighly accurate and do not require dietary ormedication changes before testing..
Management

The treatment of colorectal cancer can be aimedat cure or palliation. The decision on which aimto adopt depends on various factors, includingthe person's health and preferences, as well asthe stage of the tumor. When colorectal canceris caught early, surgery can be curative. Whenit is detected at later stages (for whichmetastases are present), this is less likely andtreatment is often directed at palliation, torelieve symptoms caused by the tumour and keepthe person as comfortable as possible.
Treatments
May include some combination of surgery. Radiation therapy. Chemotherapy. Targeted therapy. Aspirin and other non-steroidal anti-inflammatory drugs decrease the risk. Theirgeneral use is not recommended for thispurpose, however, due to side effects.
Surgery
For people with localized cancer, the preferredtreatment is complete surgical removal withadequate margins, with the attempt of achievinga cure. This can either be done by an openlaparotomy or sometimes laparoscopically. Ifthere are only a few metastases in the liver or

lungs they may also be removed. Sometimeschemotherapy is used before surgery to shrinkthe cancer before attempting to remove it. Thetwo most common sites of recurrence ofcolorectal cancer is in the liver and lungs.
A diagram of a local resection of early stage colon cancer
A diagram of local surgery for rectal cancer
Chemotherapy
In both cancer of the colon and rectum,chemotherapy may be used in addition to surgeryin certain cases. The decision to addchemotherapy in management of colon and rectalcancer depends on the stage of the disease.
In Stage I colon cancer, no chemotherapy isoffered, and surgery is the definitivetreatment. The role of chemotherapy in Stage IIcolon cancer is debatable, and is usually notoffered unless risk factors such as T4 tumor orinadequate lymph node sampling is identified. It

is also known that the patients who carryabnormalities of the mismatch repair genes donot benefit from chemotherapy. For stage III andStage IV colon cancer, chemotherapy is anintegral part of treatment.
If cancer has spread to the lymph nodes ordistant organs, which is the case with stage IIIand stage IV colon cancer respectively, addingchemotherapy agents fluorouracil, capecitabineor oxaliplatin increases life expectancy. If thelymph nodes do not contain cancer, the benefitsof chemotherapy are controversial. If the canceris widely metastatic or unresectable, treatmentis then palliative. Typically in this setting, anumber of different chemotherapy medications maybe used. Chemotherapy drugs for this conditionmay include capecitabine, fluorouracil,irinotecan, oxaliplatin and UFT. The drugscapecitabine and fluorouracil areinterchangeable, with capecitabine being an oralmedication while fluorouracil being anintravenous medicine. Antiangiogenic drugs suchas bevacizumab are often added in first linetherapy. Another class of drugs used in thesecond line setting are epidermal growth factorreceptor inhibitors, of which the two FDAapproved ones are cetuximab and panitumumab.

The primary difference in the approach to lowstage rectal cancer is the incorporation ofradiation therapy. Often, it is used inconjunction with chemotherapy in a neoadjuvantfashion to enable surgical resection, so thatultimately as colostomy is not required.However, it may not be possible in low lyingtumors, in which case, a permanent colostomy maybe required. Stage IV rectal cancer is treatedsimilar to stage IV colon cancer.
Radiation therapy
While a combination of radiation andchemotherapy may be useful for rectal cancer,its use in colon cancer is not routine due tothe sensitivity of the bowels to radiation. Justas for chemotherapy, radiotherapy can be used inthe neoadjuvant and adjuvant setting for somestages of rectal cancer.
Palliative care
Palliative care is medical care which focuses ontreatment of symptoms from serious illness, likecancer, and improving quality of life.Palliative care is recommended for any personwho has advanced colon cancer or has significantsymptoms.

Involvement of palliative care may be beneficialto improve the quality of life for both theperson and his or her family, by improvingsymptoms, anxiety and preventing admissions tothe hospital.
In people with incurable colorectal cancer,palliative care can consist of procedures thatrelieve symptoms or complications from thecancer but do not attempt to cure the underlyingcancer, thereby improving quality of life.Surgical options may include non-curativesurgical removal of some of the cancer tissue,bypassing part of the intestines, or stentplacement. These procedures can be considered toimprove symptoms and reduce complications suchas bleeding from the tumor, abdominal pain andintestinal obstruction. Non-operative methods ofsymptomatic treatment include radiation therapyto decrease tumor size as well as painmedications.
Follow-up
The aims of follow-up are to diagnose, in theearliest possible stage, any metastasis ortumors that develop later, but did not originatefrom the original cancer (metachronous lesions).
The U.S. National Comprehensive Cancer Networkand American Society of Clinical Oncology

provide guidelines for the follow-up of coloncancer. A medical history and physicalexamination are recommended every 3 to 6 monthsfor 2 years, then every 6 months for 5 years.Carcinoembryonic antigen blood levelmeasurements follow the same timing, but areonly advised for people with T2 or greaterlesions who are candidates for intervention. ACT-scan of the chest, abdomen and pelvis can beconsidered annually for the first 3 years forpatients who are at high risk of recurrence (forexample, those who had poorly differentiatedtumors or venous or lymphatic invasion) and arecandidates for curative surgery (with the aim tocure). A colonoscopy can be done after 1 year,except if it could not be done during theinitial staging because of an obstructing mass,in which case it should be performed after 3 to6 months. If a villous polyp, a polyp >1centimeter or high grade dysplasia is found, itcan be repeated after 3 years, then every 5years. For other abnormalities, the colonoscopycan be repeated after 1 year.
Routine PET or ultrasound scanning, chest X-rays, complete blood count or liver functiontests are not recommended. These guidelines arebased on recent meta-analyses showing intensivesurveillance and close follow-up can reduce the5-year mortality rate from 37% to 30%.

.=o N%xY (Rectal prolapse)
Definition
According to Acharya Sushrutha, A prolapse or falling out of the anus (due tothe Vayu) in a weak and lean patient throughstraining, urging or flow of stool as indysentery is called Guda-Bhransa or prolapsesani.( su/ni/13/21)
Treatment of Guda-Bhramsa
In a case of Guda-Bhramsa ,the protruded partshould be fomented and lubricated with Sneha.
It should then be gently re-introduced.theregion of the anus should then be bandaged witha piece of hide in the manner of a GophanaBandha.with an opening in it (lying immediatelybelow the anus),so that it may not in any wayinterfere with the emission of Vayu.

The affected part then should be constantly fomented .A quantity of milk ,Maha-Panchamula and the body (flesh) of a mouse bereft of its entrails should be first boiled together (with water ).An oil and Vayu-subduing drugs should beadministered as unguents. By these measures themost difficult cases of Prolapsus ani would becured. (su/chi/20/19)
RECTAL PROLAPSE
WHAT IS RECTAL PROLAPSE?
Rectal prolapse is a condition in which therectum (the last part of the large intestinebefore it exits the anus) loses its normalattachments inside the body, allowing it totelescope out through the anus, thereby turningit “inside out”. While this may beuncomfortable, it rarely results in an emergentmedical problem. However, it can be quite

embarrassing and often has a significantnegative impact on pa Treatment of thiscondition may often require surgery, intendedfor patients with rectal prolapse who areconsidering or have been recommended surgery. Itwill address why surgery may have beenrecommended, what the various treatment optionsare, what it involves and how it may helppatients’ quality of life. Overall, rectal prolapse affects relatively fewpeople (2.5 cases/100,000 people). Thiscondition affects mostly adults, and women over
50 years of age aresix times as likely asmen to develop rectal
prolapse. Most women with rectal prolapse are in

their 60’s, while the few men who developprolapse are much younger, averaging 40 years ofage or less. In these younger patients, thereis higher rate of autism, developmental delay,and psychiatric problems requiring multiplemedications.
Although an operation is not always needed, thedefinitive treatment of rectal prolapse requiressurgery.
RISK FACTORS
While a number of factors have been shown to beassociated with rectal prolapse development,there is no clear cut “cause” of rectalprolapse.
Chronic constipation (infrequent stools orsevere straining) is present in 30-67% ofpatients,
15% experience in Diarrhoea. Some haveassumed that the development of rectal prolapseis a consequence of multiple vaginal deliveries;however, up to 35% of patients with rectalprolapse have never had children.
PRESENTATION
Rectal prolapse tends to present gradually. Initially, the prolapse comes down with a bowel

movement (BM) and then returns to its normalposition. Patients may later describe a mass or“something falling out” that they may have topush back in following a BM. Until the prolapsedrectum goes back in, patients may feel like theyare “sitting on a ball”. Rectal prolapse may beconfused with significant hemorrhoid disease andcan even be confusing at times to physicians notfrequently evaluating and treating this problem.
A = Rectal Prolapse B= Hemorrhoids
Once a prolapse is apparent, fecal incontinence(inability to control gas, liquid or solid BM)occurs in 50-75% of cases and is likely due to anumber of factors. The anal sphincter is astructure made of a number of muscles that allowone to hold on to their stool when the have theurge to move their bowels. When the rectum isprolapsed, it has gone past the anal sphincter,and this allows stool and mucus to pass in an

uncontrolled fashion. Pelvic nerve damage(pudendal nerve) has been shown in many patientswith prolapse. The pudendal nerve contributesto the control of the anal sphincter and damagecan result from direct trauma (birthing injury),chronic diseases such as diabetes, and from backinjury or surgery. The anal sphincter isconstantly stretched by the prolapse itself,adding an additional risk factor forincontinence.
Upwards of 25% to 50% of patients will reportconstipation. Constipation associated withprolapse may result from the bunching up of therectum, creating a blockage that is made worsewith straining, generalized coordinationproblems with the entire pelvic floor, andproblems with the ability of the colon to movestool forward at a normal rate. It is notunusual for some patients to even note bothbouts of constipation and incontinence as well.
Over time, prolapsed rectal mucosa may becomethickened and ulcerated causing significantbleeding. Rarely, the prolapse becomes stuck or“incarcerated” outside the anus – a situationthat could require emergent surgery.
EVALUATION OF PATIENTS WITH PROLAPSE

Before considering surgery, a careful historyand physical examination should be done. Asmentioned above, attention should be focused oncomplaints of constipation, fecal incontinence,and any complaints of urinary incontinence(inability to control urine) or bulging into thevagina.
Direct examination of the anal region isimportant and often reveals low anal sphinctertone (sphincter feels “loose”). The patient maybe asked to squeeze and relax their analsphincter while the doctor has their finger thepatient’s bottom. This helps the doctor get asense of how well the anal sphincter isfunctioning. Formal anal manometry (a test thatdirectly measures the anal sphincter pressures)could be recommended, as low sphincter pressuresmay affect the choice of procedure to repair therectal prolapse.
While a spontaneous prolapse is obvious, it canbe confusing as to whether a patient hassignificant hemorrhoids or rectal prolapse. Todemonstrate a rectal prolapse, the patient maybe asked to strain while being observed whilesquatting, or on a toilet or commode. Whilethis may be somewhat embarrassing for patients,it is very important to make an accurate

diagnosis, as the treatments of hemorrhoids andrectal prolapse are very different.
A colonoscopy will often be necessary to ruleout any associated polyps or cancer prior toconsideration of treatment for rectal prolapse. Colonoscopy is a procedure where a long,flexible, tubular instrument called acolonoscope is used to look at the entire innerlining of the colon (large intestine) and therectum.

WHAT HAPPENS IF PATIENTS CHOOSE TO DO NOTHING ABOUT THEIR RECTAL PROLAPSE?
If a patient has been seen by a colon & rectalsurgeon familiar with the diagnosis andtreatment of rectal prolapse and given adiagnosis of rectal prolapse, they couldpotentially choose to do nothing about it. Patients choosing to do nothing can likelyexpect their amount of prolapse to get largerover time and to have the rectum prolapse moreeasily (may just prolapse with standing). If apatient chooses to delay treatment for aprolonged period of time, they should know thatthe longer a patient goes without having theirprolapse repaired, the greater the chance ofhaving permanent problems with fecalincontinence, as the anal sphincter isrepeatedly stretched out and the chance of nervedamage is increased, too. The length of timethat these changes will occur is widely variableand differs from person to person. In certaincases, the prolapse is very small or the patientis too sick to undergo an operation. In thesecases, supportive garments can help with keepingthe prolapse from coming out all the time.
Untreated, rectal prolapse does not turn intocancer.
SURGERY FOR RECTAL PROLAPSE

There are two general approaches to surgery forrectal prolapse – abdominal operations (throughthe belly) and perineal operations (through “thebottom”). Both approaches aim to stop theprolapse from occurring again and usually resultin a significant improvement in quality of life.
The choice of surgery type depends on bothpatient factors and procedural factors. Patientfactors include the patient’s age, sex, bowelfunction, continence, prior operations, andseverity of associated medical problems. Procedural factors include extent of prolapse,what effect the procedure might have on bowelfunction and incontinence, complication rates ofthe procedure, recurrence rates of the procedureand the individual surgeon’s experience.
Perineal approaches are often better choices forvery elderly patients or patients with verysevere medical conditions in addition to rectalprolapse. Consideration can also be given to aperineal approach in younger males, as there isa small chance (1-2%) of causing sexualdysfunction due to nerve injury during thepelvic dissection that occurs during anabdominal approach. While this is very unusual,it should be considered when making decisionsabout the type of surgery to perform. Youngmales may even want to consider banking sperm

prior to the procedure in the very unlikelyevent they have sexual problems after theprocedure. Operative procedures for rectalprolapse can be performed under a number ofdifferent types of anesthesia. The patient andsurgeon can decide what is appropriate for agiven patient based on their particularcircumstances. Potential options include:General anesthesia (completely asleep with a“breathing tube” in place) Under a spinal block(similar to an epidural injection duringchildbirth)A combination of intravenous relaxingmedications and local anesthesia (numbingmedicine) injected around the anus afterrelaxing medications have been given. This iscalled monitored anesthesia with a perianalblock.
ABDOMINAL APPROACHES
ABDOMINAL RECTOPEXY WITH POSSIBLE BOWEL RESECTION
Most abdominal techniques involve making anincision in the lower abdomen and dividing theloose rectal attachments from the pelvic wallsall the way to the floor of the pelvis. Arectopexy is then performed, whereby the rectumis pulled upwards and secured to the sacrum

(back wall of the pelvis) in a variety of ways. Depending on the surgeon’s preference, therectum may be sutured directly to the sacrumwith stitches or a prosthetic material (mesh)may be included. Regardless of the specifictechnique used, the intent is to hold the rectumin the appropriate position until such a time asscarring occurs to fix the rectum in place. Overall, both of these techniques yield verygood results, with recurrent rectal prolapseoccurring in approximately 2-5% of cases.
When patients complain of a long history ofconstipation, removal of a portion of the colonmay be included in an attempt to improve bowelfunction. The amount of colon removed isdetermined by the severity of constipation andmay involve the use of the previously describedcolonic transit study. Interestingly, inpatients with fecal incontinence prior tosurgery, this symptom improves in about 35%,even with removal of part of the colon. Thisimprovement often occurs within 2 to 3 months.

MINIMALLY INVASIVE RECTOPEXY WITH POSSIBLE BOWELRESECTION
Minimally invasive techniques such aslaparoscopy or robotically, are used in somecenters with equivalent success to traditionalabdominal procedures. Laparoscopy refers to theuse of small incisions through which the surgeon
may place a camera andsurgical instruments,allowing them toperform the sameprocedures describedabove for abdominalapproaches.

Laparoscopic trocars placed for colon surgery.
PERINEAL APPROACHES
It is generally believed that the perinealapproach results in fewer complications andpain, with a reduced length of hospital stay.These advantages have, until recently, beenconsidered to be offset by a higher recurrencerate. Recent data is unclear on this point,however, and a properly executed perinealoperation may yield good long-term results.
PERINEAL RECTOSIGMOIDECTOMY
The most common perineal approach is oftenreferred to as a perineal rectosigmoidectomy oran “Altemeier procedure”, named after thesurgeon who popularized this operation. Thisapproach to the surgical repair of rectalprolapse is done through the anus, with noabdominal incision. In the operating room, therectum is made to intentionally prolapse outsidethe body and is then divided. The excess rectum

and colon is pulled down and out of the body. Afull-thickness excision is done, with theremaining colon pulled down and sewn or stapledto the anus. Lack of an abdominal incision,minimal pain, and a shorter hospital stay makethis procedure an attractive option inappropriate patients.
MUCOSAL SLEEVE RESECTION (DELORME PROCEDURE)
Occasionally, a surgeon may choose to do aperineal procedure slightly less extensive thana perineal rectosigmoidectomy. A Delormeprocedure does not involve a full thicknessresection, as described in the perinealrectosigmoidectomy. Instead, the inner liningof the rectum is stripped away from the muscleand removed. The muscles of the rectum are thenfolded and sewn to themselves (plicate) to

reduce the prolapse. This particular proceduremay be recommended in the setting of a smallprolapse or if the prolapse is full-thicknessbut limited to partial circumference, where aperineal rectosigmoidectomy may be difficult toaccomplish. Incontinence is improved in 40-50%of patients after this procedure.
Complications are quite wide ranging in variousseries (0-76%) and most were due to pre-existingmedical problems. Complications specific to thesurgery include bleeding, leakage of the sewnconnection and stricture development (narrowingof the anal opening). Rates recurrent prolapse(6-26%) are generally felt to be higher thanwith a perineal rectosigmoidectomy.
Copyright © 2022 FDOKUMEN