Anticoagulants in pregnancy
11
CHIEF EDITOR’S NOTE: This article is part of a series of continuing education activities in this Journal through which a total of 36 AMA/PRA category 1 credit hours can be earned in 2006. Instructions for how CME credits can be earned appear on the last page of the Table of Contents. Anticoagulants in Pregnancy Andra H. James, MD, MPH,* David E. Abel, MD,† and Leo R. Brancazio, MD‡ *Assistant Professor, Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina; †Director of Genetics and Staff Perinatologist, Northwest Perinatal Center, Portland, Oregon; and ‡Associate Clinical Professor, Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina Pregnancy is a hypercoagulable state that increases the risk of thromboembolic events. These risks may be further increased in the presence of an acquired or inherited thrombophilia. Throm- bophilias have been associated with both maternal and fetal complications. The use of anticoagu- lants during pregnancy may reduce the risk of maternal thromboses as well as the risk of adverse pregnancy outcomes. The choice of an anticoagulant requires consideration of maternal risks, potential for teratogenicity, the underlying condition necessitating the treatment, and cost. This review examines the options for anticoagulation, the clinical situations that may warrant such treatment, and factors to be considered at delivery and during the postpartum period. Target Audience: Obstetricians & Gynecologists, Family Physicians Learning Objectives: After completion of this article, the reader should be able to describe the roles of acquired and inherited thrombophilia in furthering the hypercoagulable state of pregnancy, identify the potential consequences of using anticoagulants during pregnancy, and summarize the treatment options when anticoagulation is required during pregnancy. Pregnancy confers a fivefold risk of thrombosis (1). This predisposition results from the hypercoagulable state of pregnancy, which has likely evolved to protect women from hemorrhage during miscarriage and child- birth. Among women with thrombophilia, an acquired or inherited predisposition to thrombosis, the risk is even higher, increased from a background risk of one to two per 1000 (2) to as high as one in two (3–5). Not only are women with thrombophilia at a higher risk of thrombosis, they are more likely to experience placental abruption, preeclampsia, fetal growth restriction, still- birth, and possibly recurrent miscarriage (6–8). The goal of anticoagulation is not only to prevent and treat maternal thromboses, but to improve the outcome of pregnancy. In women with a history of thrombosis and thrombophilia, anticoagulants have been shown to re- duce maternal morbidity and mortality (9). In women with the antiphospholipid syndrome (10), an acquired thrombophilia, and recently in women with inherited thrombophilia (11), anticoagulants have been shown to increase the probability of a live birth. The purpose of this article is to review different anticoagulants and their use in pregnancy. CHANGES IN COAGULATION DURING NORMAL PREGNANCY Rudolf Virchow, the 19th-century German pathol- ogist, is credited with describing the three factors that The authors have disclosed that they have no financial relation- ships with or interests in any commercial companies pertaining to this educational activity. The author has disclosed that warfarin, unfractionated heparin, reviparin, tinzaparin, nadroparin, dalteparin, enoxaparin, danap- aroid, recombinant hirudin, fondaparinux, aspirin, dipyridamole, clopidogrel, ticlopidine, abciximab, streptokinase, alteplase, rete- plase and tenecteplase have not been approved by the U.S. Food and Drug Administration for use in pregnancy. Wolters Kluwer Health has identified and resolved all faculty conflicts of interest regarding this educational activity. Reprint requests to: Andra H. James, MD, MPH, Division of Maternal and Fetal Medicine, Box 3967, Duke University Medical Center, Durham, NC 27710. E-mail: [email protected]. CME REVIEWARTICLE Volume 61, Number 1 OBSTETRICAL AND GYNECOLOGICAL SURVEY Copyright © 2005 by Lippincott Williams & Wilkins 3 59
Transcript of Anticoagulants in pregnancy
CHIEF EDITOR’S NOTE: This article is part of a series of continuing education activities in this Journal through which a totalof 36 AMA/PRA category 1 credit hours can be earned in 2006. Instructions for how CME credits can be earned appear onthe last page of the Table of Contents.
Anticoagulants in PregnancyAndra H. James, MD, MPH,* David E. Abel, MD,†
and Leo R. Brancazio, MD‡*Assistant Professor, Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynecology, Duke
University Medical Center, Durham, North Carolina; †Director of Genetics and Staff Perinatologist,Northwest Perinatal Center, Portland, Oregon; and ‡Associate Clinical Professor, Division of Maternal–FetalMedicine, Department of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina
Pregnancy is a hypercoagulable state that increases the risk of thromboembolic events. Theserisks may be further increased in the presence of an acquired or inherited thrombophilia. Throm-bophilias have been associated with both maternal and fetal complications. The use of anticoagu-lants during pregnancy may reduce the risk of maternal thromboses as well as the risk of adversepregnancy outcomes. The choice of an anticoagulant requires consideration of maternal risks,potential for teratogenicity, the underlying condition necessitating the treatment, and cost. Thisreview examines the options for anticoagulation, the clinical situations that may warrant suchtreatment, and factors to be considered at delivery and during the postpartum period.
Target Audience: Obstetricians & Gynecologists, Family PhysiciansLearning Objectives: After completion of this article, the reader should be able to describe the roles of
acquired and inherited thrombophilia in furthering the hypercoagulable state of pregnancy, identify thepotential consequences of using anticoagulants during pregnancy, and summarize the treatment optionswhen anticoagulation is required during pregnancy.
Pregnancy confers a fivefold risk of thrombosis (1).This predisposition results from the hypercoagulablestate of pregnancy, which has likely evolved to protectwomen from hemorrhage during miscarriage and child-birth. Among women with thrombophilia, an acquiredor inherited predisposition to thrombosis, the risk iseven higher, increased from a background risk of one totwo per 1000 (2) to as high as one in two (3–5). Not
only are women with thrombophilia at a higher risk ofthrombosis, they are more likely to experience placentalabruption, preeclampsia, fetal growth restriction, still-birth, and possibly recurrent miscarriage (6–8). Thegoal of anticoagulation is not only to prevent and treatmaternal thromboses, but to improve the outcome ofpregnancy. In women with a history of thrombosis andthrombophilia, anticoagulants have been shown to re-duce maternal morbidity and mortality (9). In womenwith the antiphospholipid syndrome (10), an acquiredthrombophilia, and recently in women with inheritedthrombophilia (11), anticoagulants have been shown toincrease the probability of a live birth. The purpose ofthis article is to review different anticoagulants and theiruse in pregnancy.
CHANGES IN COAGULATION DURINGNORMAL PREGNANCY
Rudolf Virchow, the 19th-century German pathol-ogist, is credited with describing the three factors that
The authors have disclosed that they have no financial relation-ships with or interests in any commercial companies pertaining tothis educational activity.
The author has disclosed that warfarin, unfractionated heparin,reviparin, tinzaparin, nadroparin, dalteparin, enoxaparin, danap-aroid, recombinant hirudin, fondaparinux, aspirin, dipyridamole,clopidogrel, ticlopidine, abciximab, streptokinase, alteplase, rete-plase and tenecteplase have not been approved by the U.S. Foodand Drug Administration for use in pregnancy.
Wolters Kluwer Health has identified and resolved all facultyconflicts of interest regarding this educational activity.
Reprint requests to: Andra H. James, MD, MPH, Division ofMaternal and Fetal Medicine, Box 3967, Duke University MedicalCenter, Durham, NC 27710. E-mail: [email protected].
CME REVIEWARTICLEVolume 61, Number 1OBSTETRICAL AND GYNECOLOGICAL SURVEY
Copyright © 2005by Lippincott Williams & Wilkins 3
59
contribute to thrombosis: hypercoagulability, vascu-lar injury, and stasis (12). Venous stasis is increasedduring pregnancy. Contributing factors are the hor-monally induced increased venous capacitance ofpregnancy (13,14), impaired venous outflow causedby mechanical obstruction from the uterus (15), andpossibly decreased mobility (16–19). Venous stasisand vascular injury (15), however, appear to be lessimportant than hypercoagulability.
Normal pregnancy is accompanied by an in-crease in coagulation factors VII, VIII, X, and vonWillebrand factor and by a pronounced increase infibrinogen (20). Factors II, V, and IX are relativelyunchanged (20). Free protein S, the active, unboundform of protein S, a natural anticoagulant, is de-creased during pregnancy secondary to increased lev-els of its binding protein, the complement componentC4b (20). Plasminogen activator inhibitor type 1(PAI-1) levels are increased fivefold (20). All ofthese changes may contribute to the hypercoagulablestate of pregnancy.
The changes in the coagulation system begin withconception and do not return to baseline until morethan 8 weeks postpartum (20). In a metaanalysisexamining the incidence of deep vein thrombosis(DVT) in pregnancy, 22% of cases were found tooccur in the first trimester (21), and in one series, theproportion of DVT in the first trimester was found tobe as high as 44% (22). Compared with pregnancy,the risk of thrombosis is even higher after delivery(21,22). Over one third of pregnancy-related venousthromboembolism occurs postpartum (21,22).
INDICATIONS FOR ANTICOAGULATION
Despite the increased risk of thrombosis duringpregnancy and postpartum, most women do not re-quire anticoagulation. In most cases, the risks ofanticoagulation outweigh its benefits. The risk ofmaternal bleeding complications with heparin is re-ported to be as high as 2% (23). In addition tomaternal risks, anticoagulants may pose fetal risks,even with the use of agents that do not cross theplacenta. There is a fine balance between hemostaticand thrombotic interactions at the uteroplacental in-terface (24) and, in most women, this balance isachieved with the normal changes of pregnancy.
The exception is women with thrombophilia. In theantiphospholipid syndrome, an acquired thrombophilia,several studies have demonstrated that anticoagulationimproves the outcome of pregnancy (10). In inheritedthrombophilia, until very recently, only case reports andcase series demonstrated the role of anticoagulation in
improving the outcome of pregnancy, but a recent ran-domized trial (11) showed improved outcomes inwomen with inherited thrombophilia and a history of asingle fetal loss greater than 10 weeks gestation. Sixty-nine of 80 women who took 40 mg enoxaparin per dayhad a healthy live birth compared with 23 of 80 whotook a placebo (low-dose aspirin).
Although some experts would recommend throm-boprophylaxis for all pregnant women with inheritedthrombophilia, anticoagulation is not necessary ifthere is no personal history of thromboembolism orpoor pregnancy outcome (25). The exceptions, be-cause of their especially high risk of thrombosis, arewomen with antithrombin deficiency, homozygosityfor the factor V Leiden mutation or the prothrombingene G20210A mutation, or heterozygosity for bothmutations (compound heterozygosity) (26). Althoughthere are no large trials demonstrating the maternal orfetal benefits of anticoagulation in pregnancy, cur-rent indications include the conditions listed subse-quently. Full-dose (adjusted-dose) anticoagulation isrecommended (25,27) for women with:
• Current thrombosis;• A need for lifelong anticoagulation; and• Antiphospholipid syndrome with a history of
thrombosis.
Full dose (adjusted dose) or an intermediate ormoderate dose, as described in 1, is recommended(25,27) for women with:
• Antithrombin deficiency; and• Homozygosity for the factor V Leiden mutation,
the prothrombin gene G20210A mutation, orcompound heterozygosity for both mutations.
Thromboprophylaxis with low-dose anticoagula-tion is recommended (8,25) for women with ahistory of:
• Unprovoked thrombosis;• Antiphospholipid syndrome with a history of
poor pregnancy outcome as the only clinicalcriteria; and
• Thrombophilia and poor pregnancy outcome.
Close observation (assessment of signs and symp-toms of thrombosis at routine prenatal visits) is rec-ommended for women with a history of:
• Thrombosis in the setting of transient risk fac-tors (25); and
• Thrombophilia with no history of thrombosis.
60 Obstetrical and Gynecological Survey

UNIQUE ASPECTS OFANTICOAGULATION IN PREGNANCY
Anticoagulation in pregnancy requires consider-ation of both the mother and fetus. During preg-nancy, there is an increase in blood volume of 40% to50% (13) and an increase in the volume of distribu-tion. An increase in glomerular filtration (13) resultsin increased renal excretion. Additionally, there is inan increase in protein binding of heparin. Agents thatcross the placenta are potentially teratogenic. Be-cause 45% of pregnancies are unintended (28), manywomen do not realize they are pregnant during thecritical period for organogenesis, the fourth to eighthweek postconception (29).
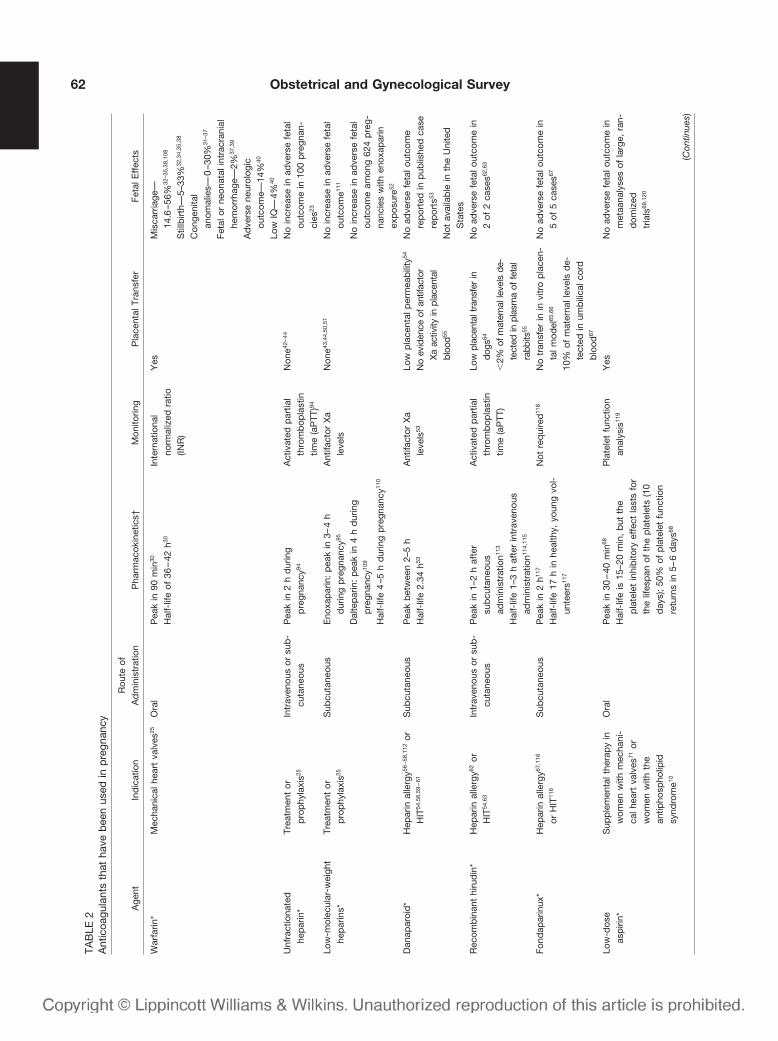
Anticoagulants that have been used in pregnancyare discussed subsequently. Although these medica-tions, including heparin and aspirin, have not beenapproved for use in pregnancy by the U.S. Food andDrug Administration (FDA), they are neverthelesswidely used for the appropriate indications in preg-nancy. Their indications, routes of administration,pharmacokinetics, monitoring, placental transfer, andfetal effects are summarized in Table 2.
WARFARIN
Warfarin is a vitamin K antagonist. The coagulantactivity of factors II, VII, IX, and X requires avitamin K-dependent, posttranslational modification,the addition of a second carboxyl group, to theglutamate residues of the N-terminal regions ofthese proteins. During the process, the reduced formof vitamin K is converted to vitamin K epoxide.Warfarin interferes with the regeneration of the re-
duced form from the epoxide. Treatment with war-farin results in the production of coagulation factorswith reduced coagulant activity. Treatment with war-farin also interferes with the addition of a secondcarboxyl group to the natural anticoagulants, proteinC and protein S. For this reason, patients may ini-tially become hypercoagulable, but ultimately, theanticoagulant effect dominates (30).
Warfarin is generally contraindicated during preg-nancy. Taken during the critical period of organogene-sis, warfarin carries up to a 30% risk of congenitalanomalies (31–37). The reported risk of miscarriageranges from 14.6% to 56% (32,34,35,38). Placentaltransfer of warfarin later in pregnancy can result infetal bleeding (37,39) or stillbirth (32,34,35,38).Long-term neurologic damage has been reportedamong children exposed in utero (40). Consequently,warfarin is rarely prescribed in pregnancy. The ex-ceptional case is the patient at high risk of mortalityfrom thrombosis who may not be sufficiently antico-agulated with either heparin or low-molecular-weightheparin (25). Candidates for warfarin in pregnancyinclude women with mechanical heart valves (25).The current recommendation for the target interna-tional normalized ratio (INR) using adjusted-dosewarfarin in these cases is 2.0 to 3.0 (25).
HEPARIN
Unfractionated heparin (UFH) is a heterogeneousmixture of polysaccharide chains ranging in molec-ular weight from 3000 to 30,000 daltons. Both UFHand low-molecular-weight-heparin (LMWH) exerttheir anticoagulant activity by activating antithrom-
TABLE 1Protocols for thromboprophylaxis in pregnancy
Bates et al, 200425 Duke Protocol
Unfractionated heparinMinidose “low dose” 5000 U subcutaneously every 12 hrs 5000 U subcutaneously every 12 hrs �8 weeksModerate-dose “low dose” Every 12 hrs to target antifactor Xa
level of 0.1–0.3 U/mL7500 U subcutaneously every 12 hrs 8–28 weeks10,000 U subcutaneously every 12 hrs �28
weeksAdjusted-dose “full dose” Every 12 hrs to target midinterval
aPTT in therapeutic rangeEvery 8 or 12 hrs to target midinterval aPTT in
therapeutic rangeLow-molecular-weight heparin
Prophylactic dose “low dose” Enoxaparin 40 mg per dayDalteparin 5000 U per dayTinzaparin 4500 U per day
Enoxaparin 40 mg per day or 30 mg 2 times perday before 28 weeks then Enoxaparin 40 mg 2times per day after 28 weeks
Weight-adjusted dose “full dose” Enoxaparin 1 mg/kg 2 times per dayor 1.5 mg/kg per day
Dalteparin 100 U/kg every 12 hrs or200 U/kg every 24 hrs
Tinzaparin 175 mg U/kg per day
Enoxaparin 1 mg/kg 2 times per day with targetantifactor Xa levelof 0.5–1.0
Anticoagulants in Pregnancy Y CME Review Article 61
TAB
LE2
Ant
icoa
gula
nts
that
have
bee
nus
edin
pre
gnan
cy
Age
ntIn
dic
atio
nR
oute
ofA
dm
inis
trat
ion
Pha
rmac
okin
etic
s†M
onito
ring
Pla
cent
alTr
ansf
erFe
talE
ffec
ts
War
farin
*M
echa
nica
lhea
rtva
lves
25O
ral
Pea
kin
90m
in30
Hal
f-lif
eof
36–
42h30
Inte
rnat
iona
lno
rmal
ized
ratio
(INR
)
Yes
Mis
carr
iage
—14
.6–5
6%32
–35,
38,1
08
Stil
lbirt
h—5–
33%
32,3
4,35
,38
Con
geni
tal
anom
alie
s—0
–30%
31–3
7
Feta
lor
neon
atal
intr
acra
nial
hem
orrh
age—
2%37
,39
Ad
vers
ene
urol
ogic
outc
ome—
14%
40
Low
IQ—
4%40
Unf
ract
iona
ted
hep
arin
*Tr
eatm
ent
orp
rop
hyla
xis25
Intr
aven
ous
orsu
b-
cuta
neou
sP
eak
in2
hd
urin
gp
regn
ancy
94
Act
ivat
edp
artia
lth
rom
bop
last
intim
e(a
PTT
)94
Non
e42–
44N
oin
crea
sein
adve
rse
feta
lou
tcom
ein
100
pre
gnan
-ci
es23
Low
-mol
ecul
ar-w
eigh
the
par
ins*
Trea
tmen
tor
pro
phy
laxi
s25
Sub
cuta
neou
sE
noxa
par
in:
pea
kin
3–4
hd
urin
gp
regn
ancy
95
Ant
ifact
orX
ale
vels
Non
e43,4
4,50
,51
No
incr
ease
inad
vers
efe
tal
outc
ome11
1
Dal
tep
arin
:p
eak
in4
hd
urin
gp
regn
ancy
109
Hal
f-lif
e4
–5h
dur
ing
pre
gnan
cy11
0
No
incr
ease
inad
vers
efe
tal
outc
ome
amon
g62
4p
reg-
nanc
ies
with
enox
apar
inex
pos
ure52
Dan
apar
oid
*H
epar
inal
lerg
y56–5
8,11
2or
HIT
54,5
6,59
–61
Sub
cuta
neou
sP
eak
bet
wee
n2–
5h
Hal
f-lif
e2.
34h53
Ant
ifact
orX
ale
vels
53
Low
pla
cent
alp
erm
eab
ility
54
No
evid
ence
ofan
tifac
tor
Xa
activ
ityin
plac
enta
lbl
ood55
No
adve
rse
feta
lout
com
ere
por
ted
inp
ublis
hed
case
rep
orts
53
Not
avai
lab
lein
the
Uni
ted
Sta
tes
Rec
omb
inan
thi
rud
in*
Hep
arin
alle
rgy62
orH
IT54
,63
Intr
aven
ous
orsu
b-
cuta
neou
sP
eak
in1–
2h
afte
rsu
bcu
tane
ous
adm
inis
trat
ion11
3
Hal
f-lif
e1–
3h
afte
rin
trav
enou
sad
min
istr
atio
n114,
115
Act
ivat
edp
artia
lth
rom
bop
last
intim
e(a
PTT
)
Low
plac
enta
ltra
nsfe
rin
dogs
64
�2%
ofm
ater
nall
evel
sde
-te
cted
inpl
asm
aof
feta
lra
bbits
55
No
adve
rse
feta
lout
com
ein
2of
2ca
ses62
,63
Fond
apar
inux
*H
epar
inal
lerg
y67,1
16
orH
IT11
6
Sub
cuta
neou
sP
eak
in2
h117
Hal
f-lif
e17
hin
heal
thy,
youn
gvo
l-un
teer
s117
Not
req
uire
d11
8N
otr
ansf
erin
invi
tro
pla
cen-
talm
odel
65,6
6
10%
ofm
ater
nall
evel
sd
e-te
cted
inum
bili
calc
ord
blo
od67
No
adve
rse
feta
lout
com
ein
5of
5ca
ses67
Low
-dos
eas
piri
n*S
upp
lem
enta
lthe
rap
yin
wom
enw
ithm
echa
ni-
calh
eart
valv
es71
orw
omen
with
the
antip
hosp
holip
idsy
ndro
me10
Ora
lP
eak
in30
–40
min
68
Hal
f-lif
eis
15–2
0m
in,
but
the
pla
tele
tin
hib
itory
effe
ctla
sts
for
the
lifes
pan
ofth
ep
late
lets
(10
day
s);
50%
ofp
late
let
func
tion
retu
rns
in5–
6d
ays68
Pla
tele
tfu
nctio
nan
alys
is11
9
Yes
No
adve
rse
feta
lout
com
ein
met
aana
lyse
sof
larg
e,ra
n-d
omiz
edtr
ials
69,1
20
(Con
tinue
s)
62 Obstetrical and Gynecological Survey
bin. The active portion of the heparin molecule is aunique five-unit long, saccharide sequence that in-duces a conformational change in antithrombin andaccelerates its interaction with activated factor X(factor Xa), resulting in the inactivation of factor Xa.Thrombin is also inactivated by heparin, but throm-bin’s inactivation requires saccharide sequences thatare 18 units long. Whereas most of the chains of UFHcontain these 18 unit-long sequences, fewer than halfof the chains of LMWH are of sufficient length.Consequently, UFH has activity against both factorXa and thrombin, whereas LMWH has relativelylittle activity against thrombin (41).
Heparins, UFH or LMWH, are the preferred agentsfor anticoagulation in pregnancy (25). The main ad-vantage of heparins over other anticoagulants is thatthere is no transplacental passage (42–44). Disadvan-tages of UFH include the necessity of parenteraladministration, a 2% risk of major bleeding (23),osteoporosis with a 17% to 36% reduction in bonedensity (45,46), a 2% risk of vertebral fracture (47),and a risk of heparin-induced thrombocytopenia(HIT) (25).
There are two types of thrombocytopenia afterheparin administration. One is a benign, self-limitingcondition, noted in 10% to 20% of patients andtypically seen 1 to 4 days after initiation of therapy.There are no thromboembolic or hemorrhagic se-quelae; the platelet count usually remains above100,000 and returns to normal despite continued ad-ministration of heparin (48). The other, HIT, whichresults from the formation of IgG antibodies againsta complex of heparin with platelet factor 4, is sus-pected when the platelet count falls below 100,000,or to 50% of the baseline level, 5 to 15 days after theinitiation of therapy (48). The antibody complexesmay bind to endothelium resulting in life- or limb-threatening thromboses (48). Although the risk of HITis low in pregnancy, and may be lower than in non-pregnant patients (49), the actual risk is unknown (25).
LOW-MOLECULAR-WEIGHT HEPARINS
LMWHs are fragments of unfractionated heparin pro-duced by an enzymatic or chemical depolymerizationprocess that yield chains with a mean molecular weightof approximately 5000 daltons. Compared with UFH,LMWHs have relatively greater activity against fac-tor Xa and are less likely to bind to plasma proteins,endothelial cells, and macrophages. This reduction inbinding increases the bioavailability, half-life, andanticoagulant activity of LMWH relative to UFH (41).TA
BLE
2(C
ontin
ued
)
Age
ntIn
dic
atio
nR
oute
ofA
dm
inis
trat
ion
Pha
rmac
okin
etic
s†M
onito
ring
Pla
cent
alTr
ansf
erFe
talE
ffec
ts
Oth
eran
tipla
tele
tag
ents
*H
isto
ryof
myo
card
ial
infa
rctio
nor
risk
fac-
tors
for
arte
rialt
hrom
-b
osis
Sup
ple
men
talt
hera
py
inw
omen
with
mec
hani
-ca
lhea
rtva
lves
Ora
lD
ipyr
idam
ole:
half-
life
of10
h68
Clo
pid
ogre
l:p
eak
in2
h;ha
lf-lif
e48
h;st
ead
yst
ate
(50
–60
%of
pla
tele
tin
hib
ition
)af
ter
4–7
day
s;68
Ticl
opid
ine:
pea
kp
late
let
inhi
biti
onaf
ter
3–4
day
s121
Ab
cixi
mab
:p
eak
with
inm
inut
es;78
half-
life
30m
inaf
ter
intr
aven
ous
inje
ctio
n68
Pla
tele
tfu
nctio
nan
alys
is12
2–12
5
No
dat
afo
rd
ipyr
idam
ole,
clop
idog
rel,
ticlo
pid
ine.
Asm
alla
mou
ntof
abci
xim
abw
asd
etec
ted
onth
efe
tal
sid
eof
anin
vitr
op
lace
n-ta
lmod
el78
No
adve
rse
feta
lout
com
ew
ithd
i-p
yrid
amol
ein
num
erou
sca
ses
No
adve
rse
feta
lout
com
ew
ithcl
o-p
idog
reli
n2
of2
case
s74,7
5
No
adve
rse
feta
lout
com
ew
ithtic
lop
idin
ein
2of
2ca
ses75
–77
No
adve
rse
feta
lout
com
ew
ithab
-ci
xim
abin
one
case
77
Thro
mb
olyt
ics*
Life
-or
limb
-thr
eate
ning
thro
mb
oem
bol
ism
Intr
aven
ous
Str
epto
kina
se:
half-
life
18–2
3m
in12
6
Alte
pla
se:
half-
life
3–8
min
126
Ret
epla
se:
half-
life
15–1
8m
in12
6
Tene
ctep
lase
:ha
lf-lif
e18
–20
min
126
Non
eN
oFe
tall
oss—
5.8%
91
Hem
orrh
age—
8.1%
91
Mat
erna
lmor
talit
y—1.
2%91
Rep
orts
ofsu
bch
orio
nic
hem
ato-
mas
,89ab
rup
tiop
lace
ntae
84
*Not
app
rove
dfo
rus
ed
urin
gp
regn
ancy
by
the
U.S
.Fe
der
alFo
odan
dD
rug
Ad
min
istr
atio
n.†D
ata
not
spec
ific
top
regn
ancy
unle
ssst
ated
.H
ITin
dic
ates
hep
arin
-ind
uced
thro
mb
ocyt
open
ia.
Anticoagulants in Pregnancy Y CME Review Article 63
There are no large comparative studies in preg-nancy, but in nonpregnant patients, LMWHs havebeen associated with fewer side effects than UFH(25). Although parenteral administration is still re-quired, potential advantages of LMWHs over unfrac-tionated heparin are less bleeding, less bone loss, amore predictable response, a lower risk of HIT, anda longer half-life (25). Like UFH, there is no trans-placental passage (43,44,50,51). The primary disad-vantages of the LMWHs are their cost and longerhalf-life. The latter may increase the risk of bleedingduring the intrapartum period.
The LMWH that has been studied the most isenoxaparin. A Medline search of LMWHs and preg-nancy revealed five articles about reviparin, nineabout tinzaparin, 14 about nadroparin, 37 aboutdalteparin, and 61 about enoxaparin. Both UFH andLMWHs are considered safe in pregnancy (23,52).
DANAPAROID
Danaparoid is a low-molecular-weight heparinoidconsisting of the glycosaminoglycans heparin sul-fate, dermatan sulfate, and chondroitin sulfate (53).Like UFH and LMWH, danaparoid catalyzes theantithrombin-mediated inactivation of factor Xa (53).It is administered intravenously and has low placen-tal permeability (54). No evidence of antifactor Xaactivity has been found in the placental blood ofwomen taking danaparoid (55). It has been consid-ered the drug of choice for cases of heparin allergy(56–58) or HIT in pregnancy (54,56,59–61). In pub-lished cases, no adverse fetal outcomes have been re-ported. Unfortunately, danaparoid is no longer availablein the United States.
RECOMBINANT HIRUDIN
Recombinant hirudin, a direct thrombin inhibitor,is the recombinant version of the medicinal leechprotein. It is administered intravenously or subcuta-neously. There are two published cases of its use inpregnancy, one for heparin allergy (62) and the otherfor HIT (63), neither with adverse fetal outcomes.Placental transfer in humans is not documented, butthere is low transfer in dogs (64) and rabbits (lessthan 2% of maternal levels) (55).
FONDAPARINUX
Fondaparinux, a selective inhibitor of factor Xa, isa pentasaccharide that mimics the active site of hep-
arin that binds to antithrombin. Fondaparinux is ad-ministered subcutaneously. In an in vitro model,there was no placental transfer (65,66), but 10% ofmaternal levels have been detected in umbilical cordblood (67). In the United States, because danaparoidis unavailable, fondaparinux may be the preferredalternative to heparins in the case of heparin allergyor HIT in pregnancy.
ASPIRIN
Aspirin is an antiplatelet drug. Platelets process pros-taglandin H2 (PGH2) to produce thromboxane, whichinduces platelet aggregation and vasoconstriction. As-pirin permanently inactivates cyclooxygenase, the en-zyme necessary for the conversion of arachidonic acidto PGH2, the first step in the process (68).
Aspirin is safe in low doses of 81 mg per day.Large, randomized trials have demonstrated no in-creased risk of miscarriage, congenital anomalies,placental abruption, fetal hemorrhage, or neonatalbleeding (69,70). Although its safety makes it anattractive choice for anticoagulation, 81 mg per dayis insufficient in most cases in which thrombopro-phylaxis is required. In women with either mechan-ical heart valves or the antiphospholipid syndrome,low-dose aspirin may be used in combination withheparins (10,71).
In one study, aspirin alone was shown to comparefavorably with aspirin plus LMWH in the treatmentof women with the antiphospholipid syndrome andno history of thrombosis. The live birth rate was 72%versus 78%, which was not a statistically significantdifference (72). Low-dose aspirin alone may be anacceptable alternative for the woman who has lupus,the lupus anticoagulant, or moderate to high levels ofanticardiolipin antibodies, but no history of throm-bosis or poor pregnancy outcome. In cases of lowlevels of anticardiolipin antibodies, because low lev-els are of questionable significance, no anticoagula-tion is required (73).
OTHER ANTIPLATELET AGENTS
Other antiplatelet agents have been used for throm-boprophylaxis in women with a history of myocardialinfarction, in women with risk factors for arterial throm-bosis and, for supplemental therapy, in women withmechanical heart valves. There are no data for placentaltransfer of dipyridamole, an agent that inhibits plateletsby increasing intraplatelet cyclic AMP, but there arenumerous cases of its use in pregnancy with no adversefetal outcomes reported. There are also no data on
64 Obstetrical and Gynecological Survey
placental transfer of clopidogrel and ticlopidine, whichselectively inhibit ADP-induced platelet aggregation,but there are two cases of the use of clopidogrel (74,75)and two cases of the use of ticlopidine (75,76) with noadverse fetal outcomes. The use of abciximab, whichblocks the platelet glycoprotein IIb/IIIa receptor thatallows platelet aggregation (68), has been reported inthe treatment of one patient with an acute myocardialinfarction during pregnancy with no adverse fetaloutcome (77). A small amount of abciximab wasfound on the fetal side of an in vitro placentalmodel (78).
THROMBOLYSIS
Thrombolysis is indicated for life- or limb-threaten-ing thromboembolism. There are recent reports of itsuse in pregnancy to treat pulmonary embolism (79–83),coronary artery thrombosis (84), massive deep veinthrombosis (81,85,86), cerebral vein thrombosis(87,88), and mechanical valve thrombosis (89,90).Thrombolytic agents such as urokinase, streptokinase,and recombinant tissue plasminogen activator do notcross the placenta (91), but can potentially jeopardizethe fetus if bleeding occurs in the retroplacental space(89) or results in maternal hypovolemia (91). The riskof fetal loss has been estimated to be 5.8% (91) and therisk of maternal mortality to be 1.2% (91).
INITIATING ANTICOAGULATION
Women on lifelong anticoagulation may be con-verted from warfarin to LMWH before pregnancy oras soon as possible after conception. The problemwith conversion before pregnancy is the inconve-nience and discomfort of the parenteral administra-tion of heparins and the risks associated with theirlong-term use. The problem with conversion afterconception is that the half-life of warfarin is 36 to 42hours (30), and it may remain in the maternal circu-lation for several days, increasing the risk of miscar-riage and congenital anomalies.
Women who are not on lifelong anticoagulation,but are candidates for thromboprophylaxis in preg-nancy, should start soon after conception. An excep-tion is women who undergo ovulation induction.Because ovulation induction has been shown to in-crease the risk of thrombosis (92), anticoagulationshould begin when ovulation induction is initiated.
The recommendations for thromboprophylaxis dur-ing pregnancy from the 7th American College of ChestPhysicians Conference on Antithrombotic and Throm-bolytic Therapy (25), as well as the protocol from
Duke University Medical Center, are included inTable 1. The Duke protocol reflects the increasingrequirements for both heparin and LMWH as preg-nancy progresses (93–96).
HEPARIN-INDUCEDTHROMBOCYTOPENIA
Because of the possibility of HIT, the platelet countshould be monitored for the first 2 weeks after start-ing heparin (97). Although platelet counts usuallydrop 10% in pregnancy (98) and thrombocytopeniaaffects up to 10% of all pregnancies (98), HIT is arare but potentially serious complication that must beconsidered in women who develop thrombocytope-nia after starting heparin. HIT is diagnosed when theplatelet count drops by 50% or more after exposureto heparin (usually within 5–10 days) and antiplateletfactor 4 antibodies are detected (99). In women inwhom HIT develops, besides immediate discontinu-ation of heparin or LMWH, the use of an alternativeanticoagulant is required.
PERIPARTUM MANAGEMENT
As a result of the longer half-life of LMWH, con-version to UFH should be considered at 36 to 37weeks gestation or sooner if an earlier delivery isanticipated (ie, multiple gestation, preterm labor,oligohydramnios, fetal growth restriction, or pre-eclampsia are present). Although epidural and spinalhematomas are rare complications of LMWH (100),if LMWH has been administered within 12 to 24hours, anesthesia personnel may be reluctant to pro-vide regional anesthesia. Conversion to the shorter-acting UFH, which clears within 5 hours afteradministration (94), provides the patient with theoption of a regional anesthetic.
Depending on the risk of thrombosis, UFH may beheld for 6 to 24 hours before anticipated delivery.Protamine sulfate, a reversing agent, is rarely necessary.
Although the use of pneumatic compression de-vices for the prevention of peripartum thrombosis hasnot been studied, extrapolation from perioperativedata (101) would suggest benefit. The devices maybe placed in labor after epidural administration orbefore cesarean delivery.
POSTPARTUM MANAGEMENT
The pneumatic compression devices should be leftin place until the patient is ambulatory and untilanticoagulation is restarted. To minimize bleeding
Anticoagulants in Pregnancy Y CME Review Article 65

complications, reinitiation of anticoagulation shouldbe postponed until 12 hours after vaginal delivery, 12hours after epidural catheter removal, or 24 hoursafter cesarean delivery. Unless a woman prefers toremain on UFH or LMWH, she may be bridged towarfarin (continued on UFH or LMWH until a ther-apeutic INR is achieved) and continued on warfarinfor 6 weeks postpartum. Women who had a throm-botic event during pregnancy should be continued onanticoagulation for at least 3 to 6 months. Women onlifelong anticoagulation should be continued on war-farin indefinitely. Although warfarin is contraindi-cated during pregnancy, it is not contraindicatedduring breast feeding. In a study of the transfer ofwarfarin into breast milk, less than 25 ng warfarinwas detected per milliliter (102). The AmericanAcademy of Pediatrics Committee on Drugs supportsbreast feeding for women who take warfarin (103).
CONTRACEPTION
Although contraindicated for the woman who willdiscontinue anticoagulation after the postpartum pe-riod, combined oral contraceptives are acceptable forthe woman who will be on lifelong anticoagulation.For the woman who will not remain on anticoagula-tion, progestin-only contraceptives are probably ac-ceptable. Although progestins may alter the levels ofvarious coagulation factors (104,105) among progestin-only contraceptive users, only a nonsignificant in-crease in the risk of venous thromboembolism hasbeen reported (106). Copper intrauterine devices mayincrease the risk of heavy menstrual bleeding, but thelevonorgestrel intrauterine system reduces menstrualblood flow (107) and may be a good contraceptivechoice for a woman on anticoagulation.
SUMMARY
Pregnancy increases the risk of thrombosis, a riskthat is compounded by the presence of thrombo-philia. Despite the increased risk of thrombosis inpregnancy, anticoagulants are not routinely indicated,because the risks usually outweigh the benefits. Theexception is women on lifelong anticoagulation or cer-tain women with a history of thrombosis or thrombo-philia. In women with thrombophilia, new evidencesuggests that anticoagulants not only decrease therisk of thrombosis, but may reduce the risk of poorpregnancy outcome. Warfarin, although used rou-tinely outside of pregnancy, is potentially harmful tothe fetus and is rarely indicated. Aspirin, in lowdoses, is used primarily as supplemental therapy.
Heparins are the anticoagulants of choice in preg-nancy. LMWH offers the advantages of fewer sideeffects and a longer half-life than UFH. The longerhalf-life, however, may preclude regional anesthesiaso conversion to the shorter-acting UFH should beconsidered in the late third trimester. Becausethe risk of thrombosis is higher immediately afterdelivery, women receiving anticoagulants duringpregnancy should be continued on them postpartum.Although relatively safe, UFH and LMWH are notwithout risks. The clinician must be aware of thepossible side effects and complications of therapy tomanage anticoagulants safely in pregnancy.
REFERENCES
1. Prevention of venous thrombosis and pulmonary embolism.NIH Consensus Development. JAMA 1986;256:744–749.
2. James A, Brancazio L, Jamison M, et al. Peripartum throm-boembolism in the United States 2000–2001: incidence,mortality and risk factors. Am J Obstet Gynecol 2004;191:90S.
3. Pabinger I, Schneider B. Thrombotic risk in hereditary anti-thrombin III, protein C, or protein S deficiency. A cooperative,retrospective study. Gesellschaft fur Thrombose- und Hamo-staseforschung (GTH) Study Group on Natural Inhibitors.Arterioscler Thromb Vasc Biol 1996;16:742–748.
4. Conard J, Horellou MH, Van Dreden P, et al. Thrombosis andpregnancy in congenital deficiencies in AT III, protein C orprotein S: study of 78 women. Thromb Haemost 1990;63:319–320.
5. Hellgren M, Tengborn L, Abildgaard U. Pregnancy in womenwith congenital antithrombin III deficiency: experience oftreatment with heparin and antithrombin. Gynecol ObstetInvest 1982;14:127–141.
6. American College of Obstetricians and Gynecologists. Man-agement of early recurrent pregnancy loss. ACOG PracticeBulletin no. 24. Washington, DC: American College of Ob-stetricians and Gynecologists, February 2001.
7. Alfirevic Z, Roberts D, Martlew V. How strong is the associ-ation between maternal thrombophilia and adverse preg-nancy outcome? A systematic review. Eur J Obstet GynecolReprod Biol 2002;101:6–14.
8. Lockwood CJ. Inherited thrombophilias in pregnant patients:detection and treatment paradigm. Obstet Gynecol 2002;99:333–341.
9. Brill-Edwards P, Ginsberg JS, Gent M, et al. Safety of with-holding heparin in pregnant women with a history of venousthromboembolism. Recurrence of Clot in This PregnancyStudy Group. N Engl J Med 2000;343:1439–1444.
10. Branch DW, Khamashta MA. Antiphospholipid syndrome:obstetric diagnosis, management, and controversies. ObstetGynecol 2003;101:1333–1344.
11. Gris JC, Mercier E, Quere I, et al. Low-molecular-weightheparin versus low-dose aspirin in women with one fetal lossand a constitutional thrombophilic disorder. Blood 2004;103:3695–3699.
12. Dickson B. Venous thrombosis: on the history of Virchow’s Triad.University of Toronto Medical Journal 2004;81:166–171.
13. Gordon M. Maternal physiology in pregnancy. In: Gabbe S,Niebyl J, Simpson J, eds. Normal and Problem Pregnancies,4th ed. New York: Churchill Livingstone, 2002:63–92.
14. Macklon NS, Greer IA, Bowman AW. An ultrasound study ofgestational and postural changes in the deep venous systemof the leg in pregnancy. BJOG 1997;104:191–197.
66 Obstetrical and Gynecological Survey
15. Whitty J, Dombrowski M. Respiratory diseases in pregnancy.In: Gabbe S, Niebyl J, Simpson J, eds. Normal and ProblemPregnancies, 4th ed. New York: Churchill Livingstone, 2002:1033–1064.
16. Danilenko-Dixon DR, Heit JA, Silverstein MD, et al. Riskfactors for deep vein thrombosis and pulmonary embolismduring pregnancy or post partum: a population-based, case–control study. Am J Obstet Gynecol 2001;184:104–110.
17. Sikovanyecz J, Orvos H, Pal A, et al. Leiden mutation, bedrest and infection: simultaneous triggers for maternal deep-vein thrombosis and neonatal intracranial hemorrhage? FetalDiagn Ther 2004;19:275–277.
18. Kovacevich GJ, Gaich SA, Lavin JP, et al. The prevalence ofthromboembolic events among women with extended bedrest prescribed as part of the treatment for premature laboror preterm premature rupture of membranes. Am J ObstetGynecol 182:1089–1092.
19. Carr MH, Towers CV, Eastenson AR, et al. Prolonged bedrestduring pregnancy: does the risk of deep vein thrombosiswarrant the use of routine heparin prophylaxis? J MaternFetal Med 1997;6:264–267.
20. Bremme KA. Haemostatic changes in pregnancy. Best PractRes Clin Haematol 2003;16:153–168.
21. Ray JG, Chan WS. Deep vein thrombosis during pregnancy andthe puerperium: a meta-analysis of the period of risk and the leg ofpresentation. Obstet Gynecol Surv 1999;54:265–271.
22. James AH, Tapson VF, Goldhaber SZ. Thrombosis duringpregnancy and the postpartum period. Am J Obstet Gynecol2005;193:216–219.
23. Ginsberg JS, Kowalchuk G, Hirsh J, et al. Heparin therapyduring pregnancy. Risks to the fetus and mother. Arch InternMed 1989;149:2233–2236.
24. Roberts D, Schwartz RS. Clotting and hemorrhage in theplacenta—a delicate balance. N Engl J Med 2002;347:57–59.
25. Bates SM, Greer IA, Hirsh J, et al. Use of antithromboticagents during pregnancy: the Seventh ACCP Conference onAntithrombotic and Thrombolytic Therapy. Chest 2004;126:627S–644S.
26. James A, Brancazio L, Ortel T. Thrombosis, thrombophiliaand thromboprophylaxis in pregnancy. Clinical Advances inHematology & Oncology 2005;3:187–197.
27. American College of Obstetricians and Gynecologists.Thromboembolism in pregnancy. 2000, ACOG Practice Bul-letin no 19. Washington, DC: American College of Obstetri-cian and Gynecologists, August 2000.
28. Naimi TS, Lipscomb LE, Brewer RD, et al. Binge drinking inthe preconception period and the risk of unintended preg-nancy: implications for women and their children. Pediatrics2003;111:1136–1141.
29. Organogenetic period: the fourth to eighth weeks. In: Moore K,ed. The Developing Human: Clinically Oriented Embryology, 6thed. Philadelphia: WB Saunders Co, 1998:83–106.
30. Ansell J, Hirsh J, Poller L, et al. The pharmacology andmanagement of the vitamin K antagonists: the SeventhACCP Conference on Antithrombotic and ThrombolyticTherapy. Chest 2004;126:204S–233S.
31. Iturbe-Alessio I, Fonseca MC, Mutchinik O, et al. Risks ofanticoagulant therapy in pregnant women with artificial heartvalves. N Engl J Med 1986;315:1390–1393.
32. Sadler L, McCowan L, White H, et al. Pregnancy outcomesand cardiac complications in women with mechanical, bio-prosthetic and homograft valves. BJOG 2000;107:245–253.
33. Chan WS, Anand S, Ginsberg JS. Anticoagulation of preg-nant women with mechanical heart valves: a systematic re-view of the literature. Arch Intern Med 2000;160:191–196.
34. Nassar AH, Hobeika EM, Abd Essamad HM, et al. Pregnancyoutcome in women with prosthetic heart valves. Am J ObstetGynecol 2004;191:1009–1013.
35. Blickstein D, Blickstein I. The risk of fetal loss associated with
warfarin anticoagulation. Int J Gynaecol Obstet 2002;78:221–225.
36. Srivastava AK, Gupta AK, Singh AV, et al. Effect of oralanticoagulant during pregnancy with prosthetic heart valve.Asian Cardiovasc Thorac Ann 2002;10:306–309.
37. Meschengieser SS, Fondevila CG, Santarelli MT, et al. Anti-coagulation in pregnant women with mechanical heart valveprostheses. Heart 1999;82:23–26.
38. Cotrufo M, De Feo M, De Santo LS, et al. Risk of warfarinduring pregnancy with mechanical valve prostheses. ObstetGynecol 2002;99:35–40.
39. Chen WW, Chan CS, Lee PK, et al. Pregnancy in patientswith prosthetic heart valves: an experience with 45 pregnan-cies. QJM 1982;51:358–365.
40. Wesseling J, Van Driel D, Heymans HS, et al. Coumarins duringpregnancy: long-term effects on growth and development ofschool-age children. Thromb Haemost 2001;85:609–613.
41. Weitz JI. Low-molecular-weight heparins. N Engl J Med1997;337:688–698.
42. Flessa HC, Kapstrom AB, Glueck HI, et al. Placental trans-port of heparin. Am J Obstet Gynecol 1965;93:570–573.
43. Harenberg J, Schneider D, Heilmann L, et al. Lack of anti-factor Xa activity in umbilical cord vein samples after subcu-taneous administration of heparin or low molecular massheparin in pregnant women. Haemostasis 1993;23:314–320.
44. Schneider D, Heilmann L, Harenberg J. [Placental transfer oflow-molecular weight heparin.] Geburtshilfe Frauenheilkd1995;55:93–98.
45. Dahlman TC, Sjoberg HE, Ringertz H. Bone mineral densityduring long-term prophylaxis with heparin in pregnancy.Am J Obstet Gynecol 1994;170:1315–1320.
46. Barbour LA, Kick SD, Steiner JF, et al. A prospective study ofheparin-induced osteoporosis in pregnancy using bone den-sitometry. Am J Obstet Gynecol 1994;170:862–869.
47. Dahlman TC. Osteoporotic fractures and the recurrence ofthromboembolism during pregnancy and the puerperium in184 women undergoing thromboprophylaxis with heparin.Am J Obstet Gynecol 1993;168:1265–1270.
48. Warkentin TE, Levine MN, Hirsh J, et al. Heparin-inducedthrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med1995;332:1330–1335.
49. Fausett MB, Vogtlander M, Lee RM, et al. Heparin-inducedthrombocytopenia is rare in pregnancy. Am J Obstet Gy-necol 2001;185:148–152.
50. Dimitrakakis C, Papageorgiou P, Papageorgiou I, et al. Ab-sence of transplacental passage of the low molecular weightheparin enoxaparin. Haemostasis 2000;30:243–248.
51. Melissari E, Parker CJ, Wilson NV, et al. Use of low molecularweight heparin in pregnancy. Thromb Haemost 1992;68:652–656.
52. Lepercq J, Conard J, Borel-Derlon A, et al. Venous throm-boembolism during pregnancy: a retrospective study ofenoxaparin safety in 624 pregnancies. BJOG 2001;108:1134–1140.
53. Ibbotson T, Perry CM. Danaparoid: a review of its use inthromboembolic and coagulation disorders. Drugs 2002;62:2283–2314.
54. Lindhoff-Last E, Bauersachs R. Heparin-induced thrombo-cytopenia-alternative anticoagulation in pregnancy and lac-tation. Semin Thromb Hemost 2002;28:439–446.
55. Dager WE, White RH. Treatment of heparin-induced throm-bocytopenia. Ann Pharmacother 2002;36:489–503.
56. de Saint-Blanquat L, Simon L, Toubas MF, et al. [Treatmentwith danaparoid during pregnancy for a woman with a cuten-ous allergy to low-molecular-weight heparin.] Ann Fr AnesthReanim 2000;19:751–754.
57. Myers B, Westby J, Strong J. Prophylactic use of danaparoidin high-risk pregnancy with heparin-induced thrombocyto-
Anticoagulants in Pregnancy Y CME Review Article 67
paenia-positive skin reaction. Blood Coagul Fibrinolysis2003;14:485–487.
58. Taylor AA. Successful use of heparinoids in a pregnancy compli-cated by allergy to heparin. BJOG 2001;108:1011–1012.
59. Macchi L, Sarfati R, Guicheteau M, et al. Thromboembolicprophylaxis with danaparoid (Orgaran) in a high-thrombosis-risk pregnant woman with a history of heparin-inducedthrombocytopenia (HIT) and Widal’s disease. Clin ApplThromb Hemost 2000;6:187–189.
60. Woo YL, Allard S, Cohen H, et al. Danaparoid thrombopro-phylaxis in pregnant women with heparin-induced thrombo-cytopenia. BJOG 2002;109:466–468.
61. Gill J, Kovacs MJ. Successful use of danaparoid in treatmentof heparin-induced thrombocytopenia during twin preg-nancy. Obstet Gynecol 1997;90:648–650.
62. Aijaz A, Nelson J, Naseer N. Management of heparin allergyin pregnancy. Am J Hematol 2001;67:268–269.
63. Huhle G, Geberth M, Hoffmann U, et al. Management of heparin-associated thrombocytopenia in pregnancy with subcutaneousr-hirudin. Gynecol Obstet Invest 2000;49:67–69.
64. Markwardt F, Fink G, Kaiser B, et al. Pharmacological surveyof recombinant hirudin. Pharmazie 1988;43:202–207.
65. Lagrange F, Brun JL, Vergnes MC, et al. Fondaparinux so-dium does not cross the placental barrier: study using thein-vitro human dually perfused cotyledon model. Clin Phar-macokinet 2002;41:47–49.
66. Lagrange F, Vergnes C, Brun JL, et al. Absence of placentaltransfer of pentasaccharide (Fondaparinux, Arixtra) in thedually perfused human cotyledon in vitro. Thromb Haemost2002;87:831–835.
67. Dempfle CE. Minor transplacental passage of fondaparinuxin vivo. N Engl J Med 2004;350:1914–1915.
68. Patrono C, Coller B, FitzGerald GA, et al. Platelet-activedrugs: the relationships among dose, effectiveness, and sideeffects: the Seventh ACCP Conference on Antithromboticand Thrombolytic Therapy. Chest 2004;126:234S–264S.
69. Duley L, Henderson-Smart D, Knight M, et al. Antiplateletdrugs for prevention of pre-eclampsia and its consequences:systematic review. BMJ 2001;322:329–333.
70. Coomarasamy A, Braunholtz D, Song F, et al. Individualisinguse of aspirin to prevent pre-eclampsia: a framework forclinical decision making. BJOG 2003;110:882–888.
71. Rowan JA, McCowan LM, Raudkivi PJ, et al. Enoxaparintreatment in women with mechanical heart valves duringpregnancy. Am J Obstet Gynecol 2001;185:633–637.
72. Farquharson RG, Quenby S, Greaves M. Antiphospholipidsyndrome in pregnancy: a randomized, controlled trial oftreatment. Obstet Gynecol 2002;100:408–413.
73. Pattison NS, Chamley LW, Birdsall M, et al. Does aspirinhave a role in improving pregnancy outcome for women withthe antiphospholipid syndrome? A randomized controlledtrial. Am J Obstet Gynecol 2000;183:1008–1012.
74. Klinzing P, Markert UR, Liesaus K, et al. Case report: suc-cessful pregnancy and delivery after myocardial infarctionand essential thrombocythemia treated with clopidrogel. ClinExp Obstet Gynecol 2001;28:215–216.
75. Martin M, Romero E, Moris C. [Acute myocardial infarctionduring pregnancy. Treatment with clopidogrel.] Med Clin(Barc) 2003;121:278–279.
76. Ueno M, Masuda H, Nakamura K, et al. Antiplatelet therapyfor a pregnant woman with a mechanical aortic valve: reportof a case. Surg Today 2001;31:1002–1004.
77. Sebastian C, Scherlag M, Kugelmass A, et al. Primary stentimplantation for acute myocardial infarction during preg-nancy: use of abciximab, ticlopidine, and aspirin. CathetCardiovasc Diagn 1998;45:275–279.
78. Miller RK, Mace K, Polliotti B, et al. Marginal transfer ofReoPro (Abciximab) compared with immunoglobulin G(F105), inulin and water in the perfused human placenta invitro. Placenta 2003;24:727–738.
79. Ahearn GS, Hadjiliadis D, Govert JA, et al. Massive pulmo-nary embolism during pregnancy successfully treated withrecombinant tissue plasminogen activator: a case report andreview of treatment options. Arch Intern Med 2002;162:1221–1227.
80. Mazeika PK, Oakley CM. Massive pulmonary embolism inpregnancy treated with streptokinase and percutaneouscatheter fragmentation. Eur Heart J 1994;15:1281–1283.
81. Krishnamurthy P, Martin CB, Kay HH, et al. Catheter-directedthrombolysis for thromboembolic disease during pregnancy: aviable option. J Matern Fetal Med 1999;8:24–27.
82. Kramer WB, Belfort M, Saade GR, et al. Successful uroki-nase treatment of massive pulmonary embolism in preg-nancy. Obstet Gynecol 1995;86:660–662.
83. Walther C, Koestering H. [Therapeutic thrombolysis in theninth week of pregnancy.] Ger Med Mon 1969;14:332.
84. Schumacher B, Belfort MA, Card RJ. Successful treatment ofacute myocardial infarction during pregnancy with tissue plasmin-ogen activator. Am J Obstet Gynecol 1997;176:716–719.
85. Henrich W, Schmider A, Henrich M, et al. Acute iliac veinthrombosis in pregnancy treated successfully by streptoki-nase lysis: a case report. J Perinat Med 2001;29:155–157.
86. Patterson DE, Raviola CA, D’Orazio EA, et al. Thrombolyticand endovascular treatment of peripartum iliac vein throm-bosis: a case report. J Vasc Surg 1996;24:1030–1033.
87. Niwa J, Ohyama H, Matumura S, et al. Treatment of acutesuperior sagittal sinus thrombosis by t-PA infusion viavenography—direct thrombolytic therapy in the acute phase.Surg Neurol 1998;49:425–429.
88. Chow K, Gobin YP, Saver J, et al. Endovascular treatment ofdural sinus thrombosis with rheolytic thrombectomy and in-tra-arterial thrombolysis. Stroke 2000;31:1420–1425.
89. Usta IM, Abdallah M, El-Hajj M, et al. Massive subchorionichematomas following thrombolytic therapy in pregnancy.Obstet Gynecol 2004;103:1079–1082.
90. Fleyfel M, Bourzoufi K, Huin G, et al. Recombinant tissuetype plasminogen activator treatment of thrombosed mitralvalve prosthesis during pregnancy. Can J Anaesth 1997;44:735–738.
91. Turrentine MA, Braems G, Ramirez MM. Use of thrombolyt-ics for the treatment of thromboembolic disease during preg-nancy. Obstet Gynecol Surv 1995;50:534–541.
92. Stewart JA, Hamilton PJ, Murdoch AP. Thromboembolicdisease associated with ovarian stimulation and assistedconception techniques. Hum Reprod 1997;12:2167–2173.
93. Barbour LA, Smith JM, Marlar RA. Heparin levels to guidethromboembolism prophylaxis during pregnancy. Am JObstet Gynecol 1995;173:1869–1873.
94. Brancazio LR, Roperti KA, Stierer R, et al. Pharmacokineticsand pharmacodynamics of subcutaneous heparin during theearly third trimester of pregnancy. Am J Obstet Gynecol1995;173:1240–1245.
95. Casele HL, Laifer SA, Woelkers DA, et al. Changes in thepharmacokinetics of the low-molecular-weight heparinenoxaparin sodium during pregnancy. Am J Obstet Gynecol1999;181:1113–1117.
96. Laifer SA, Casele HL. Puerperal thromboprophylaxis: com-parison of the anti-Xa activity of enoxaparin and unfraction-ated heparin. BJOG 1999;106:614–615.
97. Warkentin TE, Greinacher A. Heparin-induced thrombocyto-penia: recognition, treatment, and prevention: the SeventhACCP Conference on Antithrombotic and ThrombolyticTherapy. Chest 2004;126:311S–337S.
98. McCrae KR, Bussel JB, Mannucci PM, et al. Platelets: anupdate on diagnosis and management of thrombocytopenicdisorders. Hematology Am Soc Hematol Educ Program2001;282–305.
99. Warkentin TE. New approaches to the diagnosis of heparin-induced thrombocytopenia. Chest 2005;127:35S–45S.
68 Obstetrical and Gynecological Survey
100. Horlocker TT. Low molecular weight heparin and neuraxialanesthesia. Thromb Res 2001;101:141–154.
101. Baker WH, Mahler DK, Foldes MS, et al. Pneumatic com-pression devices for prophylaxis of deep venous thrombosis(DVT). Am Surg 1986;52:371–373.
102. Orme ML, Lewis PJ, de Swiet M, et al. May mothers givenwarfarin breast-feed their infants? BMJ 1977;1:1564–1565.
103. Transfer of drugs and other chemicals into human milk.Pediatrics 2001;108:776–789.
104. Beller FK, Ebert C. Effects of oral contraceptives on blood coag-ulation. A review. Obstet Gynecol Surv 1985;40:425–436.
105. Blomback M, Landgren BM, Stiernholm Y, et al. The effect ofprogesterone on the haemostatic mechanism. Thromb Hae-most 1997;77:105–108.
106. Cardiovascular disease and use of oral and injectableprogestogen-only contraceptives and combined injectablecontraceptives. Results of an international, multicenter, ca-se–control study. World Health Organization CollaborativeStudy of Cardiovascular Disease and Steroid Hormone Con-traception. Contraception 1998;57:315–324.
107. Stewart A, Cummins C, Gold L, et al. The effectiveness of thelevonorgestrel-releasing intrauterine system in menorrhagia:a systematic review. BJOG 2001;108:74–86.
108. Vural KM, Ozatik MA, Uncu H, et al. Pregnancy after me-chanical mitral valve replacement. J Heart Valve Dis 2003;12:370–376.
109. Sephton V, Farquharson RG, Topping J, et al. A longitudinalstudy of maternal dose response to low molecular weightheparin in pregnancy. Obstet Gynecol 1307;101:1307–1311.
110. Blomback M, Bremme K, Hellgren M, et al. A pharmacoki-netic study of dalteparin (Fragmin) during late pregnancy.Blood Coagul Fibrinolysis 1998;9:343–350.
111. Sanson BJ, Lensing AW, Prins MH, et al. Safety of low-molecular-weight heparin in pregnancy: a systematic review.Thromb Haemost 1999;81:668–672.
112. Harrison P. Progress in the assessment of platelet function.Br J Haematol 2000;111:733–744.
113. Markwardt F. Hirudin as alternative anticoagulant—a histor-ical review. Semin Thromb Hemost 2002;28:405–414.
114. Markwardt F, Nowak G, Sturzebecher J. Clinical pharmacol-ogy of recombinant hirudin. Haemostasis 1991;1:133–136.
115. Zoldhelyi P, Webster MW, Fuster V, et al. Recombinanthirudin in patients with chronic, stable coronary artery dis-
ease. Safety, half-life, and effect on coagulation parameters.Circulation 1993;88:2015–2022.
116. Parody R, Oliver A, Souto JC, et al. Fondaparinux (ARIXTRA)as an alternative anti-thrombotic prophylaxis when there ishypersensitivity to low molecular weight and unfractionatedheparins. Haematologica 2003;88:ECR32.
117. Donat F, Duret JP, Santoni A, et al. The pharmacokinetics offondaparinux sodium in healthy volunteers. Clin Pharmaco-kinet 2002;41:1–9.
118. Bauer KA. Fondaparinux sodium: a selective inhibitor offactor Xa. Am J Health Syst Pharm 2001;58(suppl 2):S14–17.
119. Feuring M, Haseroth K, Janson CP, et al. Inhibition of plateletaggregation after intake of acetylsalicylic acid detected by aplatelet function analyzer (PFA-100). Int J Clin PharmacolTher 1999;37:584–588.
120. Coomarasamy A, Honest H, Papaioannou S, et al. Aspirin forprevention of preeclampsia in women with historical riskfactors: a systematic review. Obstet Gynecol 2003;101:1319–1332.
121. DiPerri T, Pasini FL, Frigerio C, et al. Pharmacodynamics ofticlopidine in man in relation to plasma and blood cell con-centration. Eur J Clin Pharmacol 1991;41:429–434.
122. Steinhubl SR, Talley JD, Braden GA, et al. Point-of-caremeasured platelet inhibition correlates with a reduced risk ofan adverse cardiac event after percutaneous coronary inter-vention: results of the GOLD (AU-Assessing Ultegra) multi-center study. Circulation 2001;103:2572–2578.
123. Kottke-Marchant K, Powers JB, Brooks L, et al. The effect ofantiplatelet drugs, heparin, and preanalytical variables onplatelet function detected by the platelet function analyzer(PFA-100). Clin Appl Thromb Hemost 1999;5:122–130.
124. Madan M, Berkowitz SD, Christie DJ, et al. Rapid assess-ment of glycoprotein IIb/IIIa blockade with the platelet func-tion analyzer (PFA-100) during percutaneous coronaryintervention. Am Heart J 2001;141:226–233.
125. Grau AJ, Reiners S, Lichy C, et al. Platelet function underaspirin, clopidogrel, and both after ischemic stroke: a case-crossover study. Stroke 2003;34:849–854. Epub Mar 13,2003.
126. Menon V, Harrington RA, Hochman JS, et al. Thrombolysisand adjunctive therapy in acute myocardial infarction: theSeventh ACCP Conference on Antithrombotic and Throm-bolytic Therapy. Chest 2004;126:549S–575S.
Anticoagulants in Pregnancy Y CME Review Article 69