
Corticosteroids in Pregnancy. When and How.
42
Conflict Of Interest Statement • The author declares that he has no competing interests or any significant financial interest from pharmaceutical industries, companies or individuals that could directly and significantly affect the design, conduct, or reporting of this presentation.
Transcript of Corticosteroids in Pregnancy. When and How.

Conflict Of Interest Statement
•The author declares that he has no competing interests or any significant financial interest from pharmaceutical industries, companies or individuals that could directly and significantly affect the design, conduct, or reporting of this presentation.

Vasileios S. TsapanosProfessor
Obstetrics-Gynecology – Maternal-Fetal Medicine
University of Patras-Greece

COMMON USE OF CORTICOSTEROIDSDURING PREGNANCY
To Treat Maternal Illness(reduce the immune response in
allergic or inflammatory diseases)
• Inhaled (Respiratory, Nasal)– Asthma
• Topical (Skin, Eye, Mucous)– PUPPP (Pruritic
Urticarial Papules And Plaques Of Pregnancy)
• Systemic (Oral, IM, IV)
–Rheumatoid Arthritis
–Multiple Sclerosis
–Lupus–HELLP Syndrome–In CSs-treated
•Patients stress doses for labor and delivery
To Promote Fetal Lung Maturity
(Management of Preterm Birth)
• Efficacy of treatment• Efficacy in special populations– Multiple gestations– Obese women– IUFGR– Very Early Preterm– Late Preterm
• Safety of treatment• Choice of CSs• Timing of effectiveness• Timing of administration
– Multiple courses– Rescue course
• Guidelines of Major Societies– RCOG– EBCOG– ACOG– ΕΕΠΙ (Hellenic SPM)
• Summary – Future Research
• Infant suffering from neonatal lupus-associated carditis
To Treat An In Utero Infant(Betamethasone and Dexamethasone)

Corticosteroids During Pregnancy
Treating the mother(do not cross the placenta -
metabolized)
• Prednisone– Chrocort*
• Prednisolone– Prezolon
• Methylprednisolone– Medrol
Treating the fetus(enter the fetal circulation)
• Betamethasone– Celestone
• Dexamethasone– Decadron
• Hydrocortisone– Solucortef

1.Inhaled Glucocorticoids During Pregnancy
• Tegethoff M, Greene N, Olsen J, Schaffner E, Meinlschmidt G. Inhaled glucocorticoids during pregnancy and offspring pediatric diseases: a national cohort study (Danish National Birth Cohort ). Am J Respir Crit Care Med. 2012 Mar 1;185(5):557-63. doi: 10.1164/rccm.201108-1482OC. Epub 2011 Dec 28. Source; Division of Clinical Psychology and Psychiatry, Department of Psychology, University of Basel, Switzerland
•Glucocorticoid inhalation during pregnancy may be a risk factor for offspring endocrine and metabolic disturbances–In a line with animal data – it should be considered further.
• Ernst P, Suissa S. Systemic effects of inhaled corticosteroids. Curr Opin Pulm Med. 2012 Jan;18(1):85-9. Source: Centre for Clinical Epidemiology, Lady Davis Research Institute, Jewish General Hospital, 3755 Côte-Ste.-Catherine, Montreal, Quebec, Canada. [email protected]
•Use of even high doses of inhaled CoSt during pregnancy does not appear to affect foetal adrenal function.
Data are reassuring and supporting inhaled CoSt use in pregnancy

Asthma in pregnancy.ACOG practice bulletin; no. 90; 2008 Feb 1,
8 p. Step Therapy Medical Management of Asthma
During PregnancyMild Intermittent Asthma
No daily medications, albuterol as needed
Mild Persistent AsthmaPreferred – Low-dose inhaled corticosteroid
Alternative – Cromolyn, leukotriene receptor antagonist, or theophylline (serum level 5 to 12 mcg/mL)
Moderate Persistent AsthmaPreferred – Low-dose inhaled corticosteroid and salmeterol or medium-dose inhaled corticosteroid or (if needed) medium-dose inhaled corticosteroid and salmeterol
Alternative – Low-dose or (if needed) medium-dose inhaled corticosteroid and either leukotriene receptor antagonist or theophylline (serum level 5 to 12 mcg/mL)
Severe Persistent AsthmaPreferred – High-dose inhaled corticosteroid and salmeterol and (if needed) oral corticosteroid
Alternative – High-dose inhaled corticosteroid and theophylline (serum level 5 to 12 mcg/mL) and oral corticosteroid if needed
Recommentations and Conclusions Level C
•Asthma self-management skills, including self-monitoring, correct use of inhalers, and following a plan for long-term management of asthma and promptly handling signs of worsening asthma, enhance asthma control.•For pulmonary function assessment of patients during outpatient visits, spirometry is preferable, but peak expiratory flow measurement with a peak flow meter also is sufficient.•Ultrasound examinations and antenatal fetal testing should be considered for women who have moderate or severe asthma during pregnancy.•Pregnant patients with asthma, even those with mild or well-controlled disease, need to be monitored with peak expiratory flow rate (PEFR) and forced expiratory volume in the first second of expiration (FEV1) testing as well as by observing their symptoms during pregnancy.•Routine evaluation of pulmonary function in pregnant women with persistent asthma is recommended.•Because pulmonary function and asthma severity may change during the course of pregnancy, routine evaluation of pulmonary function in pregnant women with persistent asthma is recommended.
•It is safer for pregnant women with asthma to be treated with asthma medications than it is for them to have asthma symptoms and exacerbations.
•Clinical evaluation of asthma includes subjective assessments and pulmonary function tests.
•The ultimate goal of asthma therapy in pregnancy is maintaining adequate oxygenation of the fetus by preventing hypoxic episodes in the mother.
•The step-care therapeutic approach (see box below) increases the number and dosage of medications with increasing asthma severity.
•Inhaled corticosteroids are first-line controller therapy for persistent asthma during pregnancy.
•Budesonide is the preferred inhaled corticosteroid for use during pregnancy.
•Inhaled albuterol is recommended rescue therapy for pregnant women with asthma.
•Identifying and controlling or avoiding factors such as allergens and irritants, particularly tobacco smoke, can lead to improved maternal well-being with less need for medication.
•Continuation of immunotherapy is recommended in patients who are at or near a maintenance dose, not experiencing adverse reactions to the injections, and apparently deriving clinical benefit.
•Use of prednisone, theophylline, antihistamines, inhaled corticosteroids, beta2-agonists, and cromolyn is not contraindicated for breastfeeding.
Recommendations and Conclusions Level B

2.Topical Corticosteroids
• C.-C. Chi et.al.Evidence-based (S3) guideline on topical corticosteroids in pregnancy.
British Journal of Dermatology. Volume 165, Issue 5, pages 943–952, November 2011[European Dermatology Forum (guideline subcommittee).
Cohort study on 84 133 pregnant women from the U.K. General Practice Research Database.]• Fatoumah Alabdulrazzaq and Gideon Koren.
Topical corticosteroid use during pregnancy.Canadian Family Physician June 2012 vol. 58 no. 6 643-644
MATERNAL EXPOSURE TO TOPICAL CoSt FETOTOXICITY
IUFGR
Preterm DeliveryOrofacial
CleftFetal Death
Potent-to-Very Potent Significant association
Mild-to-Moderate No association
Any Potency No association

Topical Steroid Potency Comparison
Potency and Product Compares to Potency and Product Compares to
Superhigh Potency I Medium Potency VBetamethasone Dipropionate Gel & Ointment USP (Augmented 0.05%) Diprolene® Betamethasone Dipropionate Lotion
USP 0.05%Diprosone
®Diflorasone Diacetate Ointment USP 0.05% Psorcon® Betamethasone Valerate Cream USP
0.1% Valisone®
Clobetasol Propionate Cream, Ointment, Solution, Emollient & Gel USP 0.05% Temovate® Fluocinolone Acetonide Cream USP
0.025% Synalar®
Halobetasol Propionate Cream/Ointment 0.05% Ultravate® Flurandrenolide Cream USP 0.05% Cordran®
High Potency II Hydrocortisone Butyrate Cream USP 0.1% Locoid®
Amcinonide Cream and Ointment USP 0.1% Cyclocort® Hydrocortisone Valerate Cream USP 0.2% Westcort®
Betamethasone Dipropionate Ointment USP 0.1% Diprosone® Prednicarbate Emollient Cream USP
0.1% Dermatop®
Desoximetasone Cream & Ointment USP 0.25%, Gel 0.05% Topicort® Triamcinolone Acetonide Cream/Lotion
USP 0.1% Kenalog®
Diflorasone Diacetate Cream & Ointment USP 0.05% Florone® Low Potency VI
Fluocinonide Cream, Ointment, Gel & Solution USP 0.05% Lidex® Alclometasone Dipropionate
Cream/Oint. USP 0.05% Aclovate®
Halcinonide Cream 0.1% Halog® Triamcinolone Acetonide Cream USP 0.1%
Aristocort®
Medium Potency III Desonide Lotion USP 0.05% DesOwen®Amcinonide Lotion 0.1% Cyclocort® Fluocinolone Acetonide Cream &
Topical Solution USP 0.01% Synalar®Betamethasone Valerate Ointment USP 0.01% Valisone® Desonide Cream USP 0.05% Tridesilo
n®
Diflorasone Diacetate Cream USP 0.05% Florone®,Maxiflor®
Betamethasone Valerate Lotion USP 0.1% Valisone®
Mometasone Furoate Ointment USP 0.1% Elocon® Low Potency IIITriamcinolone Acetonide Cream USP 0.5% Aristocort® Hydrocortisone Cream, Ointment &
Lot. USP 1% & 2.5% Hytone®Medium Potency IV
Creams, Ointments, Gels , Solutions,
Lotions , Emollients, Drops
Desoximetasone Cream USP 0.05% Topicort® LP
Fluocinolone Acetonide Cream USP 0.2% Synalar® HPFluocinolone Acetonide Ointment USP 0.025% Synalar®
Flurandrenolide Ointment USP 0.05% Cordran®
Triamcinolone Acetonide Ointment USP 0.1%
Aristocort®,
Kenalog®

Comparative Steroid Potencies
Name Glucocorticoidpotency
Mineralocorticoid potency
Duration of action
(t1/2 in hours)Hydrocortisone (cortisol) 1 1 8
Cortisone 0.8 0.8 oral 8, intramuscular 18+
Prednisone 3.5-5 0.8 16-36Prednisolone 4 0.8 16-36Methylprednisolone 5-7.5 0.5 18-40
Dexamethasone 25-80 0 36-54Betamethasone 25-30 0 36-54Triamcinolone 5 0 12-36
Beclometasone
8 puffs 4 times a day
equals 14 mg oralprednisone once a day [clarification needed]
- -
Fludrocortisone acetate 15 200 24
Deoxycorticosterone acetate (DOCA) 0 20 -
Aldosterone 0.3 200-1000 -

Topical Corticosteroids In Pregnancy.
Recommendations• Prefer mild/moderate potency topical CoSt to more potent CoSt during pregnancy.
• Keep potent/very potent topical CoSt as second-line therapy, for as short a time as possible.
• Avoid use on high-absorption areas (eyelids, genitals, flexures).– The risk of adverse events is theoretically increased.
• Currently, there are no data to determine the fetal safety of the newer potent lipophilic topical corticosteroids (mometasone, fluticasone, methylprednisolone) and whether they are associated with less risk of fetal growth restriction.

3. Systemic Corticosteroids In Pregnancy(Oral, IM, IV)
Should not be used in preference(grade of recommendation: B)
•They have the same side effects and benefits in pregnant and non pregnant women•Very little corticosteroid ingested by the mother enters her breast milk•They are not teratogenic (usual doses of prednisone and methylprednisolone)•But compared with topical corticosteroids they have a greater potential for fetotoxicity (as having greater bioavailability than topical corticosteroids)•reduction in fetal birth weight•increase in preterm delivery (PROM)
•Lockshin MD, Sammaritano LR. Corticosteroids during pregnancy. Scand J Rheumatol Suppl. 1998;107:136-8. Source:Cornell University Medical College, Barbara Volcker Center for Women and Rheumatic Disease, Hospital for Special Surgery, New York, NY 10021, USA•Park-Wyllie L, Mazzotta P, Pastuszak A et al. Birth defects after maternal exposure to corticosteroids: prospective cohort study and metaanalysis of
epidemiological studies. Teratology 2000; 62:385–92.•Gur C, Diav-Citrin O, Shechtman S et al. Pregnancy outcome after first trimester exposure to corticosteroids: a prospective controlled study. Reprod Toxicol 2004; 18:93–101.

Corticosteroids In Rheumatoid Arthritis During Pregnancy
• Corticosteroids may be used throughout pregnancy in the lowest effective dose– Makol A, Wright K, Amin S. Rheumatoid arthritis and pregnancy: safety considerations in pharmacological
management. Drugs. 2011 Oct 22;71(15):1973-87. doi: 10.2165/11596240-000000000-00000. Source:Department of Medicine, Mayo Clinic, Rochester, MN 55905, USA
• Corticosteroids may be safely used during pregnancy– Partlett R, Roussou E. The treatment of rheumatoid arthritis during pregnancy. Rheumatol Int. 2011
Apr;31(4):445-9. doi: 10.1007/s00296-010-1643-7. Epub 2010 Dec 1.Source:Bart's and The London School of Medicine and Dentistry, University of London, London, UK

Corticosteroids in Multiple Sclerosis During Pregnancy
• Women who use steroids for acute MS exacerbations may continue to use them during pregnancy
• The use of prednisone in a woman who is breastfeeding should be carefully monitored.

Corticosteroids in Lupus During Pregnancy
•Cortisol = Antiinflammatory hormone
•In use:– Prednisone– Prednisolone– Methylprednisolone (Medrol)
•If CoSt are contraindicated or therapy fails, use Azathioprine

CoSt For HELLP Syndrome In Pregnancy
(HELLP = Hemolysis, Elevated Liver Enzymes, Low Platelets)•Supporting the inclusion of antenatal corticosteroids in the
standard therapy for HELLP syndrome:–Insufficient evidence•Effect on substantive clinical outcomes for the mother and the baby:–No clear evidence•Effect on secondary outcomes (platelet count (DMS>BMS), aspartate transaminase, alanine transaminase, lactate dehydrogenase, and urinary output)–Positive effect•The use of corticosteroids may be justified in clinical situations in which increased rate of recovery in platelet count is considered clinically worthwhile.
• Woudstra DM, Chandra S, Hofmeyr GJ, Dowswell T. Corticosteroids for HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome in pregnancy.
Cochrane Database of Systematic Reviews 2010, Issue 9. Art. No.: D008148. DOI: 10.1002/14651858.CD008148.pub2
• Amorim M, Katz L.Corticosteroids for HELLP (haemolysis, elevated liver enzymes, low platelets) syndrome in pregnancy: RHL commentary (last revised: 1 May 2011).
The WHO Reproductive Health Library; Geneva: World Health Organization.

COMMON USE OF CORTICOSTEROIDSDURING PREGNANCY
To Treat Maternal Illness(reduce the immune response in
allergic or inflammatory diseases)
• Inhaled (Respiratory, Nasal)– Asthma
• Topical (Skin, Eye, Mucous)– PUPPP (Pruritic
Urticarial Papules And Plaques Of Pregnancy)
• Systemic (Oral, IM, IV)
–Rheumatoid Arthritis
–Multiple Sclerosis
–Lupus–HELLP Syndrome–In CSs-treated
•Patients stress doses for labor and delivery
To Promote Fetal Lung Maturity
(Management of Preterm Birth)
• Efficacy of treatment• Efficacy in special populations– Multiple gestations– Obese women– IUFGR– Very Early Preterm– Late Preterm
• Safety of treatment• Choice of CSs• Timing of effectiveness• Timing of administration
– Multiple courses– Rescue course
• Guidelines of Major Societies– RCOG– EBCOG– ACOG– ΕΕΠΙ (Hellenic SPM)
• Summary – Future Research
• Infant suffering from neonatal lupus-associated carditis
To Treat An In Utero Infant(Betamethasone and Dexamethasone)

Efficacy Of Antenatal Corticosteroid Treatment
Introduction Efficacy in special patient populations
Multiple Gestations Obese Women IUGR (IUFGR) Very Early Preterm Late Preterm

Efficacy Of Antenatal CoSs• Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for
women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19;(3):CD004454. Review. – 21 studies, 3885 patients, 4269 infants– Betamethazone, Dexamethazone, Hydrocortizone / Placebo,
No treatment– A single course decreased the risk for:
• Neonatal Death - 31%• RDS – 34%• IVH – 46%• NEC – 54%• Infection in the first 48h – 44%• Need for respiratory support• Admission to NICU • Developmental delay in childhood• Children having cerebral palsy
• A single course of antenatal CoSt should be considered routine for preterm delivery– [....there is no need for further trials...]

Efficacy In Multiple Gestations
• Blickstein I, Shinwell ES, Lusky A, Reichman B; Plurality-dependent risk of respiratory distress syndrome among very-low-birth-weight infants and antepartum corticosteroid treatment. Israel Neonatal Network. Am J Obstet Gynecol. 2005 Feb;192(2):360-4. – The effect of corticosteroids decreased with increasing
plurality– A complete course of antenatal CoSt did reduce the risk of
RDS compared to no steroid treatment in both twin and triplet pregnancies
• Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19;(3):CD004454. Review – Evidence does not confirm the efficacy of CoSt in MG….
• ….because there are no large prospective trials comparing CSs treatment versus no treatment
– Yet, guidelines advocate for CoSt administration• ….because of the weight of the evidence in singleton gestations
• Bibbo C, Deluca L, Gibbs KA, Saltzman DH, Rebarber A, Green RS, Fox NS. Rescue corticosteroids in twin pregnancies and short-term neonatal outcomes. BJOG. 2013 Jan;120(1):58-63. doi: 10.1111/1471-0528.12021. Epub 2012 Nov 2. Source:Department of Obstetrics, Gynecology and Reproductive Science, Mount Sinai School of Medicine, New York, NY, USA – In twins born before 34 weeks of gestation, exposure to
rescue corticosteroids may be associated with improved neonatal outcomes.

Efficacy In Obese Women• Theoretical Concern:
– The effectiveness is influenced by differences in tissue distribution and drug elimination.
• Hashima and coll. The effect of maternal body mass index on neonatal outcome in women receiving a single course of antenatal corticosteroids. Am J Obstet Gynecol. 2010 Mar;202(3):263.e1-5. doi: 10.1016/j.ajog.2009.10.859. Epub 2009 Dec 22
– BMI did not influence neonatal outcome in women receiving a single course of antenatal CoSt.
– Despite theoretical concerns, there is no current evidence supporting an alternative antenatal corticosteroid regimen based upon maternal BMI

Efficacy In IUGR (IUFGR)
• There is a degree of uncertainty about the efficacy– Conflicting literature, no randomized studies, evidence from observational and retrospective trials
• There is also some concern about the safety of use– IUGR is associated with alterations in cardiovascular function to maintain adequate blood flow to vital organs.
– GCoSt are regulators of vascular tone •Effect on brain development and long term function•Adverse effects on placental function and fetoplacental dynamics
•Adverse neurological outcomes

Efficacy In Very Early Preterm
• The decisions surrounding the “threshold of viability” are exceedingly difficult.
• Despite the lack of randomized data on efficacy of CoSs in the very preterm period, the suggestion of benefit for these preterm infants seems sufficient to recommend their use.
• Bonanno C, Wapner RJ. Antenatal corticosteroids in the management of preterm birth: are we back where we started? Obstet Gynecol Clin North Am. 2012 Mar;39(1):47-63. doi: 10.1016/j.ogc.2011.12.006. Source: Division of Maternal Fetal Medicine,
Department of Obstetrics and Gynecology, Columbia University College of Physicians and Surgeons, 161 West 168th Street, New York, NY 10032, USA. [email protected]

Efficacy In Late Preterm
• Late Preterm = 340/7 – 366/7
• Low risk, rare morbidity• But CoSt may also be effective at these gestational ages….– …not because of an increase in surfactant production from type II alveolar cells or acceleration in lung structural development
– ….but by increasing expression of epithelial sodium channels (ENaCs) that allow the alveoli to convert from active fluid secretion to sodium and fluid absorption with subsequent reduction of fetal lung fluid accumulated after a lung injury (RCT/MatFetMedUnNet running).
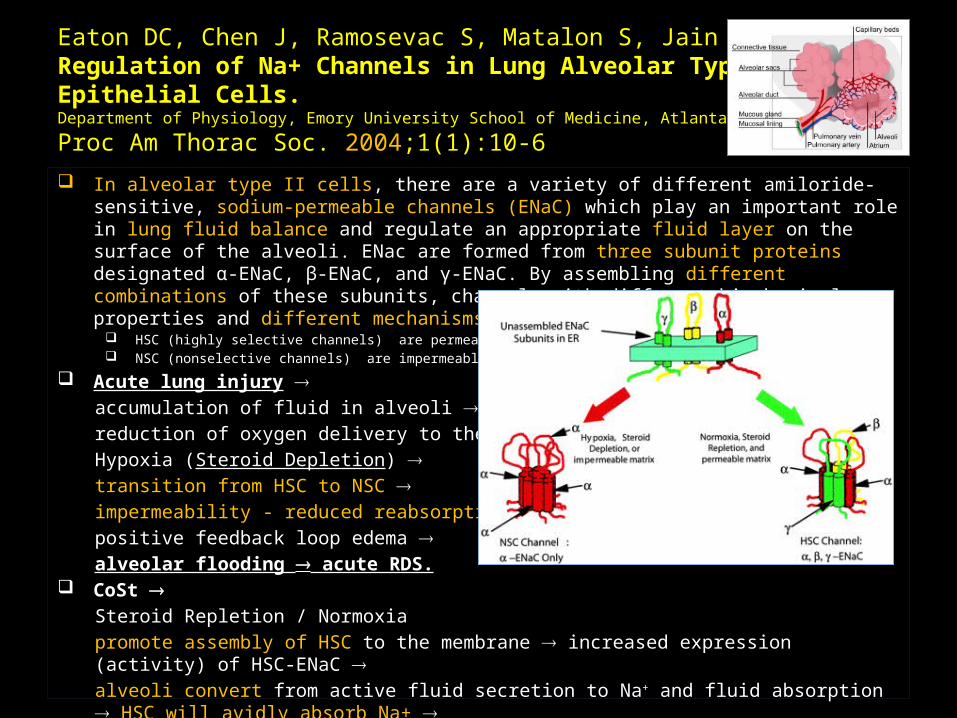
Eaton DC, Chen J, Ramosevac S, Matalon S, Jain L.Regulation of Na+ Channels in Lung Alveolar Type II Epithelial Cells.Department of Physiology, Emory University School of Medicine, Atlanta, GA, USAProc Am Thorac Soc. 2004;1(1):10-6 In alveolar type II cells, there are a variety of different amiloride-
sensitive, sodium-permeable channels (ENaC) which play an important role in lung fluid balance and regulate an appropriate fluid layer on the surface of the alveoli. ENac are formed from three subunit proteins designated α-ENaC, β-ENaC, and γ-ENaC. By assembling different combinations of these subunits, channels with different biophysical properties and different mechanisms for regulation are formed.
HSC (highly selective channels) are permeable NSC (nonselective channels) are impermeable
Acute lung injury accumulation of fluid in alveoli reduction of oxygen delivery to the ATII cells Hypoxia (Steroid Depletion) transition from HSC to NSC impermeability - reduced reabsorption of fluid positive feedback loop edema alveolar flooding acute RDS.
CoSt Steroid Repletion / Normoxiapromote assembly of HSC to the membrane increased expression (activity) of HSC-ENaC alveoli convert from active fluid secretion to Na+ and fluid absorption HSC will avidly absorb Na+ reduction of fetal lung fluid

Safety Of Antenatal Corticosteroid
Treatment

Single Course – Intact Membranes
No association with any significant short term fetal or neonatal adverse effects.
• Fetal death• Birthweight• Hypothalamic-Pituitary axis function
• Incidence of proven infection while in ICU
• RCTs through early adulthood shows no apparent adverse neurologic or cognitive effects
No specific contraindications.
• Active Tuberculosis ?– Immunosuppress
ion from CoSt • exacerbation of systemic infection
• activation of a latent disease
No serious maternal complications.
• No difference in the rate of chorioamnionitis(Cochrane)
• Increase in hyperglycemia in pregestational and gestational diabetes
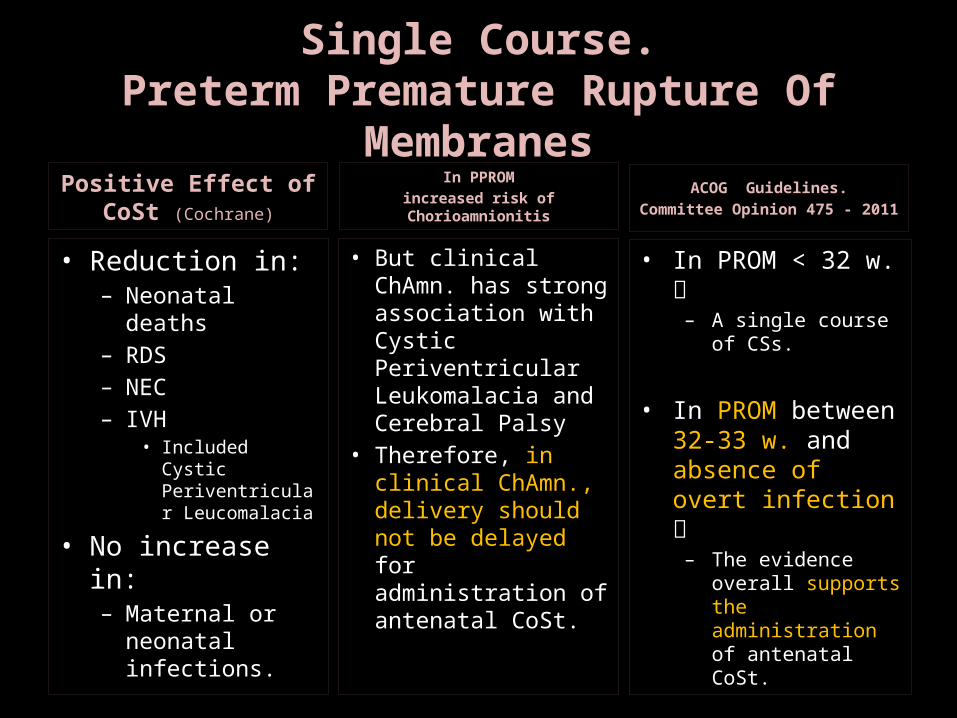
Single Course.Preterm Premature Rupture Of
MembranesPositive Effect of
CoSt (Cochrane)
• Reduction in:– Neonatal deaths
– RDS– NEC– IVH
• Included Cystic Periventricular Leucomalacia
• No increase in:– Maternal or neonatal infections.
ACOG Guidelines.Committee Opinion 475 - 2011
• In PROM < 32 w. – A single course
of CSs.
• In PROM between 32-33 w. and absence of overt infection – The evidence
overall supports the administration of antenatal CoSt.
In PPROMincreased risk of Chorioamnionitis
• But clinical ChAmn. has strong association with Cystic Periventricular Leukomalacia and Cerebral Palsy
• Therefore, in clinical ChAmn., delivery should not be delayed for administration of antenatal CoSt.
Choice Of Antenatal Corticosteroid

Betamethasone
(sodium phosphate + acetate)
Dexamethasone
(sodium phosphate)
Regimen 12 mg/d 2d, IM 6 mg 2/d 2d, IM
Similarities
• Structure• Minimal mineralocorticoid activity
• Week immunosuppressive activity
• Similar high affinities for the GC receptor
• Comparable genomic potencies
Differences
• BMS has longer half-life• DMS has stronger non-genomic effects
Comparison
• Different effects• Different drugs

Lee BH, Stoll BJ, McDonald SA, Higgins RD;National Institute of Child Health and Human
Development Neonatal Research Network. Adverse neonatal outcomes associated with antenatal dexamethasone versus antenatal
betamethasone. Pediatrics. 2006 May;117(5):1503-10
• BMS risk for neonatal death
• Trends of risk for other adverse neonatal outcomes
BMS
Roberts D, Dalziel S.Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev.
2006 Jul 19;(3):CD004454. Review
• BMS grater reduction in RDS than DMS
• DMS puerperal sepsis
BMS
Elimian A, Garry D, Figueroa R, Spitzer A, Wiencek V, Quirk JG.
Antenatal betamethasone compared with dexamethasone (betacode trial): a randomized
controlled trial. Obstet Gynecol. 2007 Jul;110(1):26-30.
• No difference in:• Neonatal mortality• RDS• NEC• Sepsis
• BMS rate of IVH
DMS
Brownfoot FC, Crowther CA, Middleton P. Different corticosteroids and
regimens for accelerating fetal lung maturation for women at risk of preterm
birth. Cochrane Database Syst Rev. 2008 Oct 8;(4):
• DMS IVH compared with BMS (the effect of these two preparations on various prematurity complications)
DMS
Conclusions:
• The conclusions are inconsistent Additional RTCs necessary to determine the preferable agent and the optimal treatment regimen.
•ACOC: Both medications are acceptable

Timing Of Effectiveness.Timing Of Administration

Timing Of Effectiveness• NIH consensus panel 1994
– Optimal benefit = 24h – 7d after initiation of treatment.
• Further studies have shown that effectiveness of antenatal CoSt declines after 7 days.– But the subgroup analyses of these data were strictly criticized in other studies.
– The decline in the effectiveness may not be static across all gestational ages or birth weights.

Timing Of Administration.Multiple Courses – Repeat Doses.
• Crowther CA, McKinlay CJ, Middleton P, Harding JE. Repeat doses of prenatal corticosteroids for women at risk of preterm birth for improving neonatal health outcomes. Cochrane Database Syst Rev. 2011 Jun 15;(6):CD003935. doi: 10.1002/14651858.CD003935.pub3. Review
– 10 RCTs, 4730 women, 5650 neonates– Infant morbidity (death, RDS, IVH, PVL, NEC)– Early childhood follow- up (death, survival free of any disability even major, composite serious outcome)
– Short-term benefits support the use of repeat doses after 7 days• But there is no proof of long-term benefit• In addition, there are no data on overall health, neurodevelopment, and cardiovascular and metabolic function later in childhood or in adulhood after exposure to repeat dose(s).
• MFMU Network Trial :
– After 4 or more courses Cerebral Palsies were shown :• 6 in the repeat CSs group, 1 in the control group
– It suggests caution in prescribing multiple courses of antenatal CoSt.

Timing Of Administration.Rescue Course.
• When to give ?– After 7 days, 14 days or longer ?– No supporting data
• Should this interval change depending on the timing of the initial course ?
• Should it be given routinely ?• Should it be given if PTB is again imminent ?
• There is increasing data that the Rescue approach might be both effective and safe.

Guidelines By Major Societies
RCOGEBCOGACOGΕΕΠΙ

Antenatal Corticosteroids to Reduce Neonatal Morbidity and Mortality
RCOG Green-top Guideline No. 7October 2010
(The Guideline review process will commence in 2013 unless evidence requires earlier review)
1. For women at risk of PTD….. reccomends– For all between 240/7 and 346/7 weeks– If between 230/7 and 236/7 weeks ….
• ....as long as this decision is “made at a senior level, taking all clinical aspects into consideration”.
2. For whom an elective cesarean section is planed prior to 386/7 weeks– (RT the rate of admissions for RDS)
• Rescue Course “should only be considered with caution in these pregnancies where the first course was given at less than 260/7 weeks of gestation and another obstetric indication arises later in pregnancy.”

European Board and Collegeof the Obstetrics and
Gynaecology•Statements by EBCOG regarding various topics will be published (here) soon.

Antenatal Corticosteroid Therapy for Fetal MaturationACOG Committee Opinion 475
A single course At risk of PTD within 7 days Between 24 and 34 weeks’ gestation
Not recommended before 24th w.g. (sparse evidence in this population)
A single Rescue Course, if: The antecedent treatment was given more than 2 weeks prior, and
GA < 326/7, and The patient is deemed likely to give birth within the next week
Obstet Gynecol 2011;117:422-4

Hellenic Society of Perinatal Medicine
ΠΡΟΓΕΝΝΗΤΙΚΗ ΧΟΡΗΓΗΣΗ ΚΟΡΤΙΚΟΣΤΕΡΟΕΙΔΩΝ
ΘΕΣΣΑΛΟΝΙΚΗ 2009
–Τ. ΣιαχανίδουΕπίκουρη Καθηγήτρια Παιδιατρικής-Νεογνολογίας, Πανεπιστημίου ΑθηνώνΜέλος Δ.Σ. της Ε.Ε.Π.Ι.
–Ν. ΠλαχούραςΔ/ντής Ε.Σ.Υ. Μ/Γ Κλινική, Γ.Ν.ΙωαννίνωνΜέλος Ε.Ε.Π.Ι.
Summary.Future Research.

• What is clear:– The benefit of a single course of antenatal CoSt for women
at risk of preterm birth between 24 and 34 weeks
• There are limitations in the current evidence :– On the safety and efficacy of antenatal CoSt– For all of the specific patient populations
• RTCs needed but exceedingly difficult to conduct because of the routine use of antenatal CoSt in these populations
• Remain questions about:– The best dose
• Individual Patient Data Meta-analysis (Caroline Growther – University of Adelaide) = Study to determine the efficacy and safety of various repeat dosing approaches.
– The best preparation– The length of effectiveness– The need for, and timing of repeat dose
• Bonanno C, Wapner RJ. Antenatal corticosteroids in the management of preterm birth: are we back where we started?
Obstet Gynecol Clin North Am. 2012 Mar;39(1):47-63. doi: 10.1016/j.ogc.2011.12.006.Source: Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, Columbia University College of Physicians and Surgeons, 161 West 168th Street, New York, NY 10032, USA. [email protected]





















