Zinc-Coated Urea for Enhanced Zinc Biofortification, Nitrogen ...
Upload
independentCategory
view
1download
0
Antibacterial Analysisof a Zinc-based Glass
Polyalkenoate Cement
OWEN CLARKIN
Materials and Surface Science Institute, University of Limerick
Limerick, Republic of Ireland
ANTHONY WREN*Inamori School of Engineering, Alfred University, NY, USA
ROIBEARD THORNTON AND JAKKI COONEY
Department of Life Sciences, University of Limerick, Limerick
Republic of Ireland
MARK TOWLER
Inamori School of Engineering, Alfred University, NY, USA
ABSTRACT: Infection following surgery can result in significant pain andmorbidity for patients undergoing vertebroplasty/kyphoplasty, and often resultsin revision surgery. This study focuses on the development of Al-free glasspolyalkenoate cements (GPCs) based on 0.04SrO–0.12CaO–0.36ZnO–0.48SiO2
glass, with the intent of optimizing their antibacterial efficacy by incorporatinglow–molecular-weight polyacrylic acids (PAA) and trisodium citrate (TSC),and evaluating the resultant GPCs against bacteria relevant to spinal infections,P. aeruginosa and E. coli. Ion-release profiles were determined for theGPC formulation containing E6 PAA (Cement A) and E7 PAA (Cement B), andZn, Na, and Sr release was recorded over 1, 7, and 30 days. Inhibition was found inE. coli at each time period (0–30 days) and this generally decreased with exposuretime in water. The largest GPC inhibition zones were produced by Cement
*Author to whom correspondence should be addressed. E-mail: [email protected] 2, 4 and 6 appear in color online: http://jba.sagepub.com
JOURNAL OF BIOMATERIALS APPLICATIONS Vol. 26 — September 2011 277
0885-3282/11/03 0277–16 $10.00/0 DOI: 10.1177/0885328210364430� The Author(s), 2010. Reprints and permissions:http://www.sagepub.co.uk/journalsPermissions.nav

A (6 mm); however the control material Simplex P þ tobramycin produced muchhigher inhibition zones (11 mm). When testing the GPC against P. aeruginosa,inhibition was only present at the 0-day time period. Simplex Pþ tobramycin wasfound to produce inhibition at each time frame. Analysis of the agar from theinhibition zone of the E. coli test revealed that there is a significant change inZn concentration as compared to a control agar specimen, which suggests thatZn release is responsible for the antibacterial effect of the GPCs.
KEY WORDS: glass polyalkenoate cement, antibacterial, zinc, tobramycin,bone cement.
INTRODUCTION
Bacterial infection is a concern when performing spinal recon-structive surgical procedures such as vertebroplasty and kypho-
plasty [1]. However, attempts have been made to incorporateantimicrobial agents such as gentamycin and tobromycin into acryliccements used for these procedures, which can prevent the spread ofinfection postoperatively [2,3]. This is beneficial as systemic adminis-tration of antimicrobial agents may be compromised due to devascular-ization of bone after the surgical procedure [3]. Acrylic cements arecurrently used for stabilizing vertebral compression fractures (VCFs) inthe spine [1], but have a history of use in total hip replacement (THR)surgery [4]. The addition of antibiotics to these materials can improvetheir antibacterial efficacy; however, there is concern over the bacteria’sability to become resistant to these antibiotics [5,6]. There is alsoconcern relating to the release of antibiotics from acrylic-based cements.Zilberman et al. [7] quote that less than 10% of the trapped drug isactually released from the cement.
In this work, a novel glass polyalkenoate cement (GPC) was developedfor spinal augmentation. Glass polyalkenoate cements (GPCs) wereoriginally formulated for restorative and luting applications in dentistryand are composed of an alumino-silicate-based glass, a polyalkenoic acid(typically polyacrylic acid, PAA) and water [8]. When the componentsare mixed together, hydrogen ions liberated from the PAA chain attackand degrade the surface of the glass particles, which releases metalcations contained within the glass. These cations serve to crosslink thePAA chains resulting in the formation of a cement [9–11]. Attempts touse these materials in skeletal applications have had limited success,mainly due to the inclusion of aluminium (Al3þ) in the glass phase. Al3þ
has been implicated in the pathogenesis of neurological degenerativedisorders such as Alzheimers [12,13] and Parkinsons disease [14], and
278 O. CLARKIN ET AL.

may also inhibit bone metabolism [15]. The cements used in this workcontain zinc (Zn) in place of Al. Zn2þ is a prevalent ion in the body andhas a positive influence on bone metabolism [16–19]. It also exhibitsantibacterial properties [20–22]. This work seeks to expand and improveon previous work by the authors on similar materials by reducing thePAA molecular weight to increase ion release. It also expands on thestrains of bacteria tested as each bacterial species differs in relation totheir virulence [23,24].
For this study, a number of bacteria relevant to infection in the spinewere selected. Pseudomonas aeruginosa is also a common bacterium foundin hip, knee, and spinal infections postoperatively, of which 13.3% ofstrains isolated in the clinical environment were found to be gentamycinresistant [24–26]. P. aeruginosa is commonly found in the blood and incerebral spinal fluid [27]. These infections tend to increase with age, with70% occurring in adults over 55-years old [27]. Escherichia. coli is the mostfrequent gram-negative rod isolated from blood cultures and is commonlyfound in hip, knee, and spinal infections following operations [25,26,28].Boyd et al. showed that an early Zn–GPC composition had antibacterialeffects against two oral bacteria; Streptococcus mutans and Actinomycesviscosus [24]. Wren et al. [23] also showed that similar compositions hadantibacterial effects against E. coli (gram-negative aerobe), Staphlococcusepidermidis (gram-positive, coagulase negative aerobe), and Bacteroidesfragilis (anaerobe). This host of bacteria examined cover the main bacterialstrains found in spinal infection with the exception of P. aeruginosa andStaphlococcus aureus, however antibacterial studies regarding GPCs hasbeen successfully conducted with these particular bacteria [30].
This study builds on the previous work by investigating the use oflower molecular weight acids for GPC formulation and its effects on ionrelease and subsequent antibacterial efficacy. Additional effects oftrisodium citrate (TSC) and the antibiotic tobramycin sulphate (TS)incorporation in the GPCs were also evaluated. TSC has previously beenshown to improve the antibacterial properties and ion-release profiles ofZn–GPCs [23,30], and TS was added in order to compare with thecommercial control Simplex-P þ tobramycin.
MATERIALS AND METHODS
Glass Synthesis
A strontium–calcium–zinc–silicate glass formulation (0.04SrO/0.12CaO/0.36ZnO/0.48SiO2 by mol. fraction) was synthesized by weigh-ing out appropriate amounts of analytical grade reagents
Glass Polyalkenoate Cement 279

(Sigma-Aldrich, Dublin, Ireland) and ball milling them together for 1 h.The mix was then oven dried (1008C, 1 h), fired (14808C, 1 h) in aplatinum crucible, and shock quenched into water. The resulting fritwas dried, ground, and sieved to retrieve a glass powder with amaximum particle size of 45mm.
Polyacrylic Acid
The Polyacrylic Acids (PAAs) used in this study were E6 (Mw – 12,700)and E7 (Mw – 25,700), supplied by Advanced Healthcare Limited (Kent,UK). The PAAs were ground and sieved to retrieve590 mm particles.
Additional Materials
The TSC used in this study was obtained from Reagacon (Shannon,Ireland) and was added to the cement at 10 wt% addition. TobramycinSulphate (TS) (Stryker International, Limerick, Ireland) was added tothe novel GPC at 2.5 wt% additions in order to study antibacterialnature of the antibiotic-loaded cements.
Cement Preparation
Cement formulations (Table 1) were prepared by thoroughly mixingthe glass powder with the PAA and distilled water on a glass plate usinga dental spatula at a powder to liquid (P:L) ratio of 2:1.5. Additions of10 wt% TSC/2.5 wt% TS were also added to the GPC formulation asoutlined in Table 1.
Complete mixing was undertaken within 30 s. Split ring molds werefilled with GPC to produce disks (1.5 mm� 15 mmØ, n¼ 3). Aftermixing, the molds were filled to excess with cement, covered withacetate, and clamped between perspex plates. The clamped specimenswere allowed to set at 378C (1 h) after mixing. Cements were stored indistilled water at 378C and removed for testing after t – 1, 7, and 30 days.
Table 1. Cements formulations used in this study.
Cement Glass PAA Acid wt% TSC % TS %
A BT 101 E6 50 10 –B BT 101 E7 50 10 –BTS BT 101 E7 50 10 2.5
280 O. CLARKIN ET AL.

The quantity of distilled water for incubation of t – 1, 7, and 30 dayspecimens was calculated by using Equation (1):
Vs ¼ Sa10 ð1Þ
where Sa represents the exposed surface area of the cement disc [23].
Ion-release Profiles
The Zinc (Zn), Strontium (Sr), Sodium (Na), and Calcium (Ca)concentrations being released from the cements were determinedfrom water extracts using a Varian SpectrAA-400 atomic absorptionspectrometer (AAS). The optimal working conditions are listed inTable 2.
Standard solutions were used for calibration of the system. NaCl wasadded to Sr and Na while LaCl was added to Ca to inhibit ionization ofthese elements. Three measurements were taken from each aliquot inorder to determine the mean concentration of each element for eachincubation period and all cements were analyzed in triplicate, fromwhich mean and standard deviations were calculated.
Agar Disk-diffusion Test
The antibacterial activity of the cements was evaluated against E. colistrain DH5a, and P. aeruginosa strain PA01 using the agar disk-diffusion method. Luria agar and broth were used for the culture ofE. coli and P. aeruginosa. All organisms were grown at 378C, aerobically,with agitation. Preparation of the agar disk-diffusion plates involvedseeding agar plates with a sterile swab dipped in a 1/50 dilution of theappropriate 16-h culture of bacteria. Three disks of each material wereplaced on the inoculated plates and the plates were cultured for 24 h at378C. Callipers were used to measure zones of inhibition at three
Table 2. Operating parameters for AAS.
Zn Sr Na Ca
Lamp current (mA) 5 10 5 10Fuel Acetylene Acetylene Acetylene AcetyleneSupport Nitrous oxide Nitrous oxide Air Nitrous oxideWavelength (nm) 213.9 460.7 330.2 239.9
Glass Polyalkenoate Cement 281

different diameters for each disk and zone sizes were calculated asfollows:
Inhibition zone ðmmÞ ¼Halo��Disc�
2ð2Þ
All cements were analyzed in triplicate and mean zone sizes� stan-dard deviations were calculated.
Preparation and Analysis of Agar Specimens
Agar strips (3� 14� 5 mm3) were prepared for investigation by EDXfrom the agar diffusion test. The specimens were cut from the assay,extending from the cement disk, through any inhibition zone, out to thebacterial colony. The specimens were then placed on a glass slide andincubated at 378C in an air-assisted oven for 24 h until they were dry.Analysis on the agar specimens was completed using a JEOL JSM-840scanning electron microscope (SEM, SEMTech Solutions, MA, USA)equipped with a Princeton Gamma Tech (PGT) energy dispersive X-ray(EDX) system. All EDX spectra were collected at 20 kV, using a beamcurrent of 0.26 nA. Quantitative EDX converted the collected spectrainto concentration data by using standard reference spectra obtainedfrom pure elements under similar operating parameters, according tostandard procedures.
RESULTS AND DISCUSSION
The first objective of this study was to determine the ion-releaseprofiles from the cements. This gives an indication of the GPCs’ abilityto release antimicrobial ions into an aqueous environment. Cementformulations A and B were examined for their ion release and this wascompared to the molecular weight of the PAA used. Figure 1 showsthe ion-release profiles for Zn, Na, and Sr. This was performed for bothZn–GPC formulations, A (containing E6 PAA) and B (containing E7).
Figure 1(a) and (b) show ion-release profiles for Cement A and B overa period of 30 days. Ca2þ release is negligible and Sr2þ release is low andremains relatively stable throughout the 30 days of incubation. Naþ
release was found to increase in both cements over 1–30 days. Littledifferences were found with Zn2þ from A over 1 (60 ppm) to 30 days(76 ppm). No significant increase is observed between 1 (63 ppm) and 30days (61 ppm) for B. However, a significant drop was found after 7 days(36 ppm).
282 O. CLARKIN ET AL.

The relatively low Sr2þ release results from the low Sr content of theglass phase (0.04SrO). Wren et al. has previously shown that, as a resultof increased TSC content of Zn–GPCs, an increased elution of both Zn2þ
and Naþ is observed; this is likely due to the TSC initially formingsoluble complexes with Ca during setting reaction, thus delaying the set[23]. This may be the cause of the high levels of both ions in solution. Nosignificant difference in Zn2þ ion release is observed between the twoGPCs after 1 day of immersion; however by 30 days, A releasedsignificantly more Zn2þ than B. Similarly, A released more Naþ at eachtime point than B. The reason for the increased ion release from A maybe the reduced binding capacity of the lower molecular weight PAA,subsequently releasing ions into solution instead of binding them intothe polysalt matrix. These ion-release profiles are slightly lower thanthose previously reported by Wren et al. for cements containing 10 wt%TSC; this is contrary to the understanding that increased ion release isassociated with a decreased molecular weight of PAA, as the study byWren et al. considered GPC formulations containing acid with a highermolecular weight [23].
As it can be seen from Figures 2 and 3, Cements A, B, and B containingTobramycin (BTS), alongside the commercial control, exhibited
200Cement A (E6)
(a) (b)
Cement B (E7)
SrZnNa
SrZnNa
175
150
125
100
75Ion
rele
ase
(ppm
)
50
25
0
Time (days)
1 day 7 days 30 days
200
175
150
125
100
75Ion
rele
ase
(ppm
)50
25
0
Time (days)
1 day 7 days 30 days
Figure 1. Sr, Na, and Zn ion release of (a) Cement A and (b) Cement B.
Glass Polyalkenoate Cement 283

16
14
12
10
8
6
4
2
0
Time (days)
0 day 1 day 7 days 30 days
Inhi
bitio
n zo
ne (
mm
)
Figure 3. Inhibition of cements incubated in E.coli from 0 to 30 days.
(a) (b)
(c) (d)
Figure 2. E. coli inhibition of (a) Cement A, (b) Cement B, (c) Cement BTS, and(d) Simplex P-Tobramycin at 0 days.
284 O. CLARKIN ET AL.

inhibition zones in E. coli bacteria when set cements were tested at eachtime frame. As expected, the best-performing GPC, A (inhibition zone,6 mm) contained the lower molecular weight acid (E6) and it performedbest when the cements were immediately incubated without immersionin water. As can be observed from Figure 4, no significant difference ininhibition-zone sizes was observed between the three GPCs at any timeperiod. Inhibition zones of A and B were reduced with time until nosignificant inhibition was observed, after 30 days of immersion in water.For BTS, after 30 days of immersion, the mean inhibition zone increasedbut not significantly. Simplex P-Tobramycin bone cement exhibited asignificantly larger inhibition zone (11.5 mm, 1 day) than any of theGPCs. This reduced after 1 day of immersion, but was still significantlylarger than that for the GPC formulations at all incubation times.
(a) (b)
(c) (d)
Figure 4. P. aeruginosa inhibition of (a) Cement A, (b) Cement B, (c) Cement BTS, and(d) Simplex P-Tobramycin at 0 days.
Glass Polyalkenoate Cement 285

It should be noted that Simplex� P, in the absence of TS, does not inhibitE. coli, S. epidermidis, S. aureus, or P. aeruginosa [23,31].
Studies have shown that Simplex P-Tobramycin can not only releaseantibiotic in an initial burst over the first day of immersion butcontinued release of antibiotic over a 6-week period can also be observed[32]. However, after 6 weeks of immersion, only 0.9% of the antibioticwas released [32], the remainder being trapped in the bulk cement.Release of antibiotics from PMMA cements occur initially from thesurface and subsequently from a network of small cracks and voidswithin the cement mantle. Suggestions have also been made that PMMAswells upon immersion in water resulting in further penetration into thecement matrix which results in gradual antibiotic release [33]. Thus, theamount of antibiotic released is dependent on the available surface areaof cement exposed to water and the release rate is controlled bydiffusion. Penetration of water into the cement matrix and release ofantibiotics is also largely dependent on cement porosity [34,35] androughness, as this affects the surface available for water penetration[36]. These phenomena explain both the large initial antibacterial effectof the cement prior to immersion in water and the ongoing antibacterialeffect to 30 days.
From Figure 5, it can be seen that all GPCs inhibited P. aeruginosabacteria to some degree when freshly set (0 days) but none of theinhibition zones were optically as clear as those of Simplex�
P-Tobramycin. This translucency of the inhibition zone indicates areduction in the growth of bacteria without complete inhibition. As can be
16
No inhibition–A, B, B
No inhibition–A, B, B
No inhibition–A, B,
14
12
10
8
6
4
2
0
Time (days)
0 day 1 day 7 days 30 days
Inhi
bitio
n zo
ne (
mm
)
Figure 5. Inhibition of cements incubated in P. aeruginosa from 0 to 30 days.
286 O. CLARKIN ET AL.
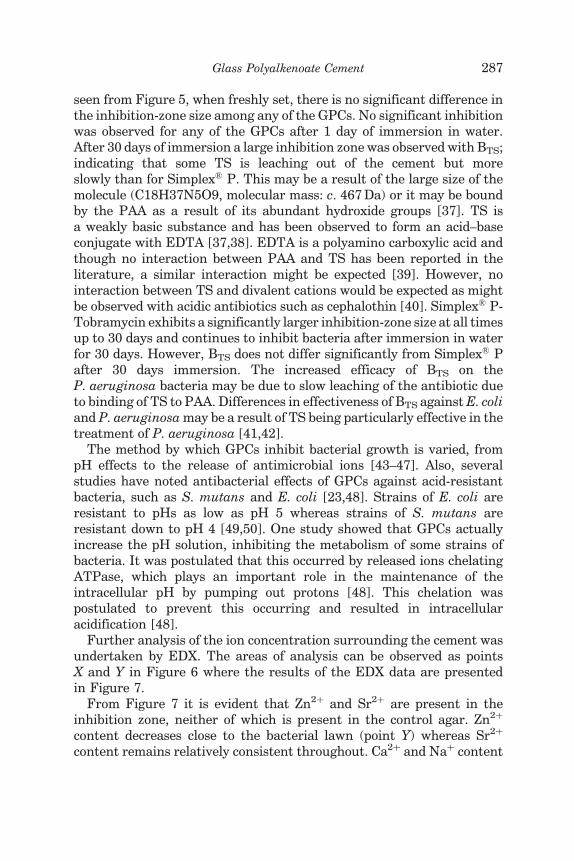
seen from Figure 5, when freshly set, there is no significant difference inthe inhibition-zone size among any of the GPCs. No significant inhibitionwas observed for any of the GPCs after 1 day of immersion in water.After 30 days of immersion a large inhibition zone was observed with BTS;indicating that some TS is leaching out of the cement but moreslowly than for Simplex� P. This may be a result of the large size of themolecule (C18H37N5O9, molecular mass: c. 467 Da) or it may be boundby the PAA as a result of its abundant hydroxide groups [37]. TS isa weakly basic substance and has been observed to form an acid–baseconjugate with EDTA [37,38]. EDTA is a polyamino carboxylic acid andthough no interaction between PAA and TS has been reported in theliterature, a similar interaction might be expected [39]. However, nointeraction between TS and divalent cations would be expected as mightbe observed with acidic antibiotics such as cephalothin [40]. Simplex� P-Tobramycin exhibits a significantly larger inhibition-zone size at all timesup to 30 days and continues to inhibit bacteria after immersion in waterfor 30 days. However, BTS does not differ significantly from Simplex� Pafter 30 days immersion. The increased efficacy of BTS on theP. aeruginosa bacteria may be due to slow leaching of the antibiotic dueto binding of TS to PAA. Differences in effectiveness of BTS against E. coliand P. aeruginosa may be a result of TS being particularly effective in thetreatment of P. aeruginosa [41,42].
The method by which GPCs inhibit bacterial growth is varied, frompH effects to the release of antimicrobial ions [43–47]. Also, severalstudies have noted antibacterial effects of GPCs against acid-resistantbacteria, such as S. mutans and E. coli [23,48]. Strains of E. coli areresistant to pHs as low as pH 5 whereas strains of S. mutans areresistant down to pH 4 [49,50]. One study showed that GPCs actuallyincrease the pH solution, inhibiting the metabolism of some strains ofbacteria. It was postulated that this occurred by released ions chelatingATPase, which plays an important role in the maintenance of theintracellular pH by pumping out protons [48]. This chelation waspostulated to prevent this occurring and resulted in intracellularacidification [48].
Further analysis of the ion concentration surrounding the cement wasundertaken by EDX. The areas of analysis can be observed as pointsX and Y in Figure 6 where the results of the EDX data are presentedin Figure 7.
From Figure 7 it is evident that Zn2þ and Sr2þ are present in theinhibition zone, neither of which is present in the control agar. Zn2þ
content decreases close to the bacterial lawn (point Y) whereas Sr2þ
content remains relatively consistent throughout. Ca2þ and Naþ content
Glass Polyalkenoate Cement 287

as a result of release from the GPC are difficult to determine as they arepresent in large quantities in the control agar. It is likely that Zn2þ andSr2þ ions play a synergistic role in inhibition of bacteria surrounding thecement but that the higher concentration of Zn2þ is most effective in
Figure 6. Image of areas analyzed by EDX; Cement A at t – 0 with E. coli.
60AgarXY
50
40
30
20
10
0Ca Sr Zn Na Cl K P
Nor
m (
wt%
)
Figure 7. EDX of Cement A at 0 days on E. coli.
288 O. CLARKIN ET AL.

inhibiting the bacteria. The method by which Zn ions inhibit bacteria isunknown but could be one of the multiple ways in which it is known toaffect the growth of bacteria (glycolysis, transmembrane protontranslocation, or acid tolerance) [24]. However, TSC is also likely tohave a bacteria-inhibiting effect, as observed in other studies, either byincreasing the Zn2þ released or by direct action of the citrate molecule[23]. The release of citrate from the cement cannot be observed by any ofthe methods undertaken in this study but may have a significant role toplay in the antibacterial nature of the cements.
Though Simplex� P-Tobramycin exhibited superior antibacterialaction against both E. coli and P. aeruginosa, increased usage of TS invarious medical applications may result in bacteria become increasinglyresistant. Consequently, alternative methods for preventing infectionare desirable, particularly by employing ions already prevalent in thebody. Assuming that Zn2þ release is the main mode of action in theantibacterial nature of these cements, it is likely that these formulationswill also inhibit S. epidermidis and B. fragilis, as ion-release profiles ofZn, Na, and Sr compare with previous work by the authors [23].However, this should be confirmed by further analysis of this cementagainst these strains.
REFERENCES
1. Hu, Y.C. and Hart, D.J. Complications of Vertebroplasty and Kyphoplasty,Tech. Region. Anesth. Pain M., 2007: 11: 164–170.
2. Sterling, G.J., Crawford, S., Potter, J.H., Koerbin, G. and Crawford, R. ThePharmokinetics of Simplex-Tobramycin Bone Cement, J. Bone Jt. Surg.,2003: 85: 646–649.
3. Scott, C.P., Higham, P.A. and Dumbleton, J.H. Effectiveness of Bone CementContaining Tobramycin, J. Bone Jt. Surg., 1999: 81: 440–443.
4. Al-Maiyah, M., Hill, D., Bajwa, A. et al. Bacterial Contaminants andAntibiotic Prophylaxis in Total Hip Arthroplasty, J. Bone Jt. Surg., 2005:87(B): 1256–1258.
5. Gillespie, W.J. Prophylaxis against Infection in Orthopaedic Practice, Curr.Orthopaed., 1994: 8: 220–225.
6. Hanssen, A.D. Prophylactic Use of Antibiotic Bone Cement, J. Arthroplasty,2004: 19: 73–77.
7. Zilberman, M. and Elsner, J.J. Antibiotic-eluting Medical Devices for VariousApplications, J. Control. Release, 2008: 130: 202–215.
8. Nicholson, J.W. Adhesive Dental Materials – A Review, Int. J. Adhes. Adhes.,1998: 18: 229–236.
9. Fennell, B. and Hill, R.G. The Influence of Poly(Acrylic) Acid Molar Mass andConcentration on the Properties of Polyalkenoate Cements, J. Mater. Sci.,2001: 36: 5193–5202.
Glass Polyalkenoate Cement 289

10. Nicholson, J.W. Chemistry of Glass Ionomer Cements, Biomaterials, 1998:19: 485–494.
11. Nicholson, J.W. and Wilson, A.D. (1993). Acid–Base Cements – TheirBiomedical and Industrial Applications. Chemistry of Solid State Materials,Cambridge, Cambridge University Press, Vol. 3
12. Bush, A. Aluminium and Alzheimers Disease, Alzheimers Australia, 2004:5: 1–5.
13. Polizzi, S., Pira, E., Ferrara, M. et al. Neurotoxic Effects of Aluminiumamong Foundry Workers and Alzheimers Disease, Neurotoxicology, 2002:23: 761–774.
14. Hoang-Xuan, K., Perrotte, P., Dubas, F., Philippon, J. and Poisson, F.M.Myoclonic Encephalopathy after Exposure to Aluminium, The Lancet, 1996:347: 910–911.
15. Firling, C.E., Hill, T.A. and Severson, A.R. Aluminium Toxicity PerturbsLong Bone Calcification in the Embryonic Chick, Arch Toxicol., 1999:73: 359–366.
16. Yamaguchi, M. and Ma, Z.J. Role of Endogenous Zinc in the Enhancement ofBone Protein Synthesis Associated with Bone Growth of Newborn Rats,J. Bone Miner. Metab., 2001: 19: 38–44.
17. Yamaguchi, M. and Ma, Z.J. Stimulatory Effect of Zinc on DeoxyribonucleicAcid Synthesis in Bone Growth of Newborn Rats: Enhancement with Zincand Insulin Like Growth Factor-I, Calcif. Tiss. Int., 2001: 69: 158–163.
18. Ito, A., Kawamura, H., Otsuka, M. et al. Zinc Releasing Calcium Phosphatefor Stimulating Bone Formation, Mater. Sci. Eng., 2002: 22: 21–25.
19. Rico, H. and Villa, L.F. Zinc, A New Coherent Therapy for Osteoporosis,Calcif. Tiss. Int., 2000: 67: 422–423.
20. Sawai, J. Quantative Evaluation of Antibacterial Activities of Metallic OxidePowders (ZnO, MgO, and CaO) by Conductimetric Assay, J. Microbiol.Meth., 2003: 54: 177–182.
21. Sawai, J., Shinobu, S., Igarashi, H. et al. Hydrogen Peroxide as anAntibacterial Factor in Zinc Oxide Powder Slurry, J. Ferment. Bioeng.,1998: 86: 521–522.
22. Yamamoto, O. Influence of Particle Size on the Antibacterial Activity of ZincOxide, Int. J. Inorg. Mater., 2001: 3: 643–646.
23. Wren, A.W., Boyd, D., Thornton, R., Cooney, J.C. and Towler, M.R.Antibacterial Properties of a Tri-Sodium Citrate Modified GlassPolyalkenoate Cement, J. Biomed. Mater. Res. Part B: Applied Biomater.,2009: 90-B: 700–709.
24. Boyd, D., Li, H., Tanner, D.A., Towler, M.R. and Wall, J.G. TheAntibacterial Effects of Zinc Ion Migration from Zinc-based GlassPolyalkenoate Cements, J. Mater. Sci.: Mater. Med., 2006: 17: 489–494.
25. Perry, J.W., Montgomerie, J.Z., Swank, S., Gilmore, D.S. and Maeder, K.Wound Infections Following Spinal Fusion with Posterior Segmental SpinalInstrumentation, Clin. Inf. Dis., 1997: 24: 558–561.
26. Phillips, J.E., Crane, T.P., Noy, M., Elliott, T.S.J. and Grimer, R.J. TheIncidence of Deep Prosthetic Infections in a Specialist Orthopaedic Hospital:A 15-year Prospective Survey, J. Bone Jt. Surg. (Br), 2006: 88-B: 943–948.
290 O. CLARKIN ET AL.

27. HSPC, Health Protection Surveillance Centre Annual Report. 2007.
28. EARSS, European Antimicrobial Resistance Surveillance System AnnualReport. 2007.
29. Coughlan, A., Boyd, D., Douglas, C. and Towler, M. Antibacterial Coatingsfor Medical Devices Based on Glass Polyalkenoate Cement Chemistry,J. Mater. Sci.: Mater. Med., 2008: 19: 3555–3560.
30. Boyd, D., Clarkin, O.M., Wren, A.W. and Towler, M.R. Zinc-based GlassPolyalkenoate Cements with Improved Setting Times and MechanicalProperties, Acta Biomater., 2007: 4: 425–431.
31. Scott, C.P., Higham, P.A. and Dumbleton, J.H. Effectiveness of BoneCement Containing Tobramycin: An in vitro Susceptibility Study of 99Organisms Found in Infected Joint Arthroplasty, J. Bone Jt. Surg. (Br),1999: 81-B: 440–443.
32. Moojen, D.J.F., Hentenaar, B., Vogely, C.H., Verbout, A.J., Castelein, R.M.and Dhert, W.J.A. In Vitro Release of Antibiotics from CommercialPMMA Beads and Articulating Hip Spacers, J. Arthroplasty, 2008: 23:1152–1156.
33. Hendriks, J.G.E., Van Horn, J.R., Van Der Mei, H.C. and Busscher, H.J.Backgrounds of Antibiotic Loaded Bone Cement and Prosthesis RelatedInfection, Biomaterials, 2004: 25: 545–556.
34. Baker, A.S. and Greenham, L.W. Release of Gentamicin from AcrylicBone Cement. Elution and Diffusion Studies, J. Bone Jt. Surg., 1998: 70:1551–1557.
35. Kuechle, D.K., Landon, G.C., Musher, D.M. and Noble, P.C. Elution ofVancomycin, Daptomycin, and Amikacin from Acrylic Bone Cement, Clin.Orthop. Relat. Res., 1991: 264: 302–308.
36. Van De Belt, H., Neut, D., Uges, D.R.A. et al. Surface Roughness, Porosityand Wettability of Gentamicin-loaded Bone Cements and Their AntibioticRelease, Biomaterials, 2000: 21: 1981–1987.
37. Du, J., Jasti, B. and Vasavada, R.C. Controlled Release of Tobramycinsulfatefrom Poly(Ortho Esters) Implantable Discs for the Treatment ofOsteomyelitis, J. Control. Release, 1997: 43: 223–233.
38. Wang, H. and Tor, Y. Tobramycin-Edta Conjugate: A Noninnocent Affinity-cleaving Reagent, Bioorg. Med. Chem. Lett., 1998: 8: 3665–3670.
39. Blay, G.A., Borjas, R.E., Hughes, S. et al. Polyacrylic Acid (Poly-A) as aChelant and Dispersant, J. Appl. Poly. Sci., 1999: 73: 1097–1115.
40. Stigter, M., Bezemer, J., De Groot, K. and Layrolle, P. Incorporation ofDifferent Antibiotics into Carbonated Hydroxyapatite Coatings on TitaniumImplants, Release and Antibiotic Efficacy, J. Control. Release, 2004: 99:127–137.
41. Masaadeh, H.A. and Jaran, A.S. Incident of Pseudomonas aeruginosa inPost-operative Wound Infection, Amer. J. Inf. Dis., 2009: 5: 1–6.
42. Briedis, D.J. and Robson, H.G. Comparative Activity of Netilmicin,Gentamicin, Amikacin, and Tobramycin against Pseudomonas aeruginosaand Enterobacteriaceae, Antimicrob. Agents Chemo., 1976: 10: 592–597.
43. Vermeersch, G., Leloup, G., Delmee, M. and Vreven, J. AntibacterialActivity of Glass–Ionomer Cements, Compomers and Resin Composites:
Glass Polyalkenoate Cement 291

Relationship between Acidity and Material Setting Phase, J. Oral. Rehab.,2005: 32: 368–374.
44. Deschepper, E.J., Thrasher, M.R. and Thurmond, B.A. Antibacterial Effectsof Light-cured Liners, Amer. J. Dent., 1989: 2: 74–76.
45. Shellis, R.P. and Duckworth, R.M. Studies on the Cariostatic Mechanisms ofFluoride, Int. Dent. J., 1994: 44: 263–273.
46. Scherer, W., Kaim, J., Gottlieb-Schein, E. and Roffe-Bauer, M. Microleakageof Capsulated Glass Ionomer Cements, Amer. J. Dent., 1989: 2: 355–357.
47. Amerongen Willem, E. Dental Caries under Glass Ionomer Restoration,J. Pub. Health Dent., 1996: 56: 150–154.
48. Hayacibara, M.F., Rosa, O.P.S., Koo, H., Torres, S.A., Costa, B. and Cury,J.A. Effects of Fluoride and Aluminum from Ionomeric Materials onS. mutans Biofilm, J. Dent. Res., 2003: 82: 267–271.
49. Smith, H.R., La Ragione, R.M., Woodward, M.J. and Chart, H.An Investigation into the Pathogenic Properties of Escherichia coliStrains BLR, BL21, DH5α and EQ1, J. Appl. Microbiol., 2000:89: 1048–1058.
50. Bender, G.R., Sutton, S.V. and Marquis, R.E. Acid Tolerance, ProtonPermeabilities, and Membrane ATPases of Oral Streptococci, Inf. Imm.,1986: 53: 331–338.
292 O. CLARKIN ET AL.
Copyright © 2022 FDOKUMEN