and Beta-Thalassemia in Thailand
23
ALPHA- AND BETA-THALASSEMIA IN THAILAND* Prawase Wasi, Supa Na-Nakorn, Sa-nga Pootrakul,? Munsit Sookanek,$ Pensri Disthasongchan,$ Malida Pornpatkul, 1 and Vicharn Panich Division of Hematology. Department of Medicine Siriraj Hospital Medical School. Bangkok, Thailand In Thailand, both a- and P-thalassemia are widespread and there is more than one subtype in each variety. Hemoglobin (Hb) E which is a2, p;6G'u+Lys (Hunt & Ingram, 1959) is remarkably frequent (Na-Nakorn et al., 1956; Sundharagiati et al., 1958, 1959a, 1959b; Flatz et al., 1965; Wasi et al., 1967a), reaching 50 percent in certain areas. These abnormal genes in different combinations result in a spectrum of syndromes ranging from asymptomatic heterozygotes to lethal Hb Bart's hydrops fetalis. Attempts have been made to characterize the various genotypes by clinical, hematologic, biochemical, genetic and cord blood studies. This paper summarizes the manifestations of these syndromes, with particular emphasis on the diseased forms. ALPHA-THALASSEMIA Hb H disease had been known here as inclusion body anemia (Minnich et al., 1954 and 1958) before Hb H was first reported (Rigas et al., 1955 and 1956; Gouttas et al., 1955). As a result of the detection of Hb Bart's (74) in patients with Hb H disease (Ramot et al., 1959; Huehns et al., 1960), the occurrence of Hb H was found to be connected to decreased synthesis of a-chain-a-thalassemia. When the synthesis of a-chains is suppressed, the unconjugated p-dimers polymerize to 04 (Hb H); by means of the same mechanism, Hb Bart's (74) and Hb 64 may occur in Hb H disease (Dance et al., 1963). Usually, Hb H is not detectable in either parent of Hb H patients. One of the parents exhibits findings compatible with a-thalassemia trait, whereas the other parent appears hematologically normal. The genetic mechanism of Hb H disease had been greatly debated (Koler & Rigas, 1961). An immediate question was whether the individuals with Hb H inherited two abnormal genes, or just one a-thalassemia gene, but due to varied expressivity or, alternatively, interaction with certain environmental modifiers, Hb H occurred. Considering the absence of Hb H disease among Negroes despite the presence of a-thalassemia trait, Weatherall (1963) felt that there might be more than one type of a-thalassemia. *This study was supported by United States Public Health Service Grant AM 09805 from the National Institute of Arthritis and Metabolic Diseases. Present addresses: ?Department of Biochemistry, University of British Columbia, Van- couver, B.C. *Department of Medicine, M. D. Anderson Hospital, Texas §Faculty of Medi- cal Technology, University of Medical Sciences, Bangkok 1 Division of Clinical Pathology, Department of Pathology, Siriraj Jospital Medical School, Bangkok, Thailand. 60
Transcript of and Beta-Thalassemia in Thailand
ALPHA- AND BETA-THALASSEMIA IN THAILAND*
Prawase Wasi, Supa Na-Nakorn, Sa-nga Pootrakul,? Munsit Sookanek,$ Pensri Disthasongchan,$ Malida Pornpatkul, 1
and Vicharn Panich
Division of Hematology. Department of Medicine Siriraj Hospital Medical School. Bangkok, Thailand
In Thailand, both a- and P-thalassemia are widespread and there is more than one subtype in each variety. Hemoglobin (Hb) E which is a2, p;6G'u+Lys (Hunt & Ingram, 1959) is remarkably frequent (Na-Nakorn et al . , 1956; Sundharagiati et al., 1958, 1959a, 1959b; Flatz et al., 1965; Wasi et al., 1967a), reaching 50 percent in certain areas. These abnormal genes in different combinations result in a spectrum of syndromes ranging from asymptomatic heterozygotes to lethal H b Bart's hydrops fetalis. Attempts have been made to characterize the various genotypes by clinical, hematologic, biochemical, genetic and cord blood studies. This paper summarizes the manifestations of these syndromes, with particular emphasis on the diseased forms.
ALPHA-THALASSEMIA
H b H disease had been known here as inclusion body anemia (Minnich et al . , 1954 and 1958) before H b H was first reported (Rigas et al., 1955 and 1956; Gouttas et al., 1955). As a result of the detection of H b Bart's ( 7 4 ) in patients with Hb H disease (Ramot et al., 1959; Huehns et al., 1960), the occurrence of H b H was found to be connected to decreased synthesis of a-chain-a-thalassemia. When the synthesis of a-chains is suppressed, the unconjugated p-dimers polymerize to 04 ( H b H); by means of the same mechanism, H b Bart's ( 7 4 ) and H b 6 4 may occur in H b H disease (Dance et al., 1963).
Usually, H b H is not detectable in either parent of H b H patients. One of the parents exhibits findings compatible with a-thalassemia trait, whereas the other parent appears hematologically normal. The genetic mechanism of H b H disease had been greatly debated (Koler & Rigas, 1961). An immediate question was whether the individuals with H b H inherited two abnormal genes, or just one a-thalassemia gene, but due to varied expressivity or, alternatively, interaction with certain environmental modifiers, H b H occurred. Considering the absence of H b H disease among Negroes despite the presence of a-thalassemia trait, Weatherall (1963) felt that there might be more than one type of a-thalassemia.
*This study was supported by United States Public Health Service Grant AM 09805 from the National Institute of Arthritis and Metabolic Diseases.
Present addresses: ?Department of Biochemistry, University of British Columbia, Van- couver, B.C. *Department of Medicine, M . D. Anderson Hospital, Texas §Faculty of Medi- cal Technology, University of Medical Sciences, Bangkok 1 Division of Clinical Pathology, Department of Pathology, Siriraj Jospital Medical School, Bangkok, Thailand.
60

Wasi et al.: Thalassemia in Thai land 61
Segregation of H b H disease among sibs fit well with one-fourth (Wasi et al., 1964). indicating that two abnormal genes are necessary for the development of this disease-the a-thalassemia gene derived from the parent with thalassemia stigmata, and the gene from the apparently normal parent. Because it is either allelic or closely linked to the a-thalassemia gene, and it has a synergistic effect with the classic a-thalassemia gene, the “silent” gene is also believed to be an a-thalassemia gene of a milder type. We have named the classical form of the gene a-thalassemial (a-thall), and the milder form a-thalassemian (a-thalz). Evidence appears to favor this hypothesis. Blood from 30 newborn offspring of H b H pa- tients was examined in our laboratory. H b Bart’s was found in 29 cases, indicating segregation of two a-thalassemia genes, since the presence of H b Bart’s in the new- borns is connected with a-thalassemia. In our laboratory, H b Bart’s was not detectable in the normal cord blood by starch-gel electrophoresis. Furthermore, the findings in these neonates appear to be divided into two groups, one having the definite red-cell stigmata of thalassemia, decreased erythrocytic osmotic fragility and 5-6% H b Bart’s, and another with normal red-cell morphology or minimal thalassemic appearance, with normal erythrocytic osmotic fragility and I-2% H b Bart’s (FIGURE I). They are believed to be carriers for a-thalassemial and a- thalassemiaz, respectively.
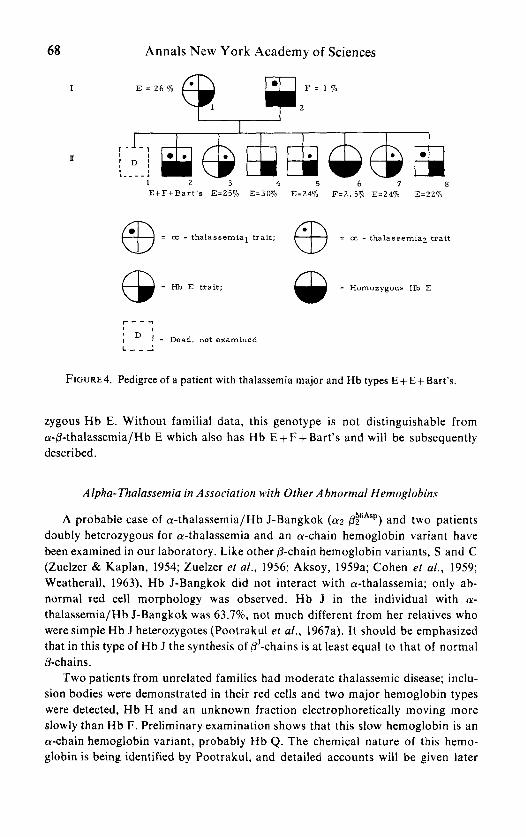
We found that parent-child transmission of H b H was observed in 4 out of 19 families, or 21%; presently, such transmission observed in our laboratory stands at 12/56 or 21.4%. The combined frequency of a-thalassemial and a- thalassemiaz traits should also be around 21%, since a person with Hb H disease can have offspring with the same disease only if the spouse also has a-thalassemia. This expectation is substantiated by our recent finding by starch-gel electrophoresis that 20.45% of 1408 newborns had H b Bart’s in their cord blood. Of these, 9.8% had H b Bart’s a t the 5-6% level, and 10.01% of the newborns had trace or 1-2% H b Bart’s. Taking these two groups as heterozygotes for a-thalassemial and a-thalassemiaz, respectively, a genotype of a-thalassemial/a-thalassemiaz was expected to be found in eight out of 1408 newborns studied. This was ascertained by the finding that seven newborns had H b Bart’s in the vicinity of 25%; five of these seven newborns developed typical H b H disease, and two developed H b A + E + Bart’s disease. The latter (vide infra) also had a-thalassemialla- thalassemiaz genotype and had an H b E gene in addition. Similar cord blood examination in a northern province of Thailand (Na-Nakorn ef al., to be pub- lished) revealed an even higher incidence of H b Bart’s disease.
Hb Bart’s Hydrops Fetalis- Homozygous (Y- Thalassemia 1
This lethal a-thalassemic disease, characterized by the presence of almost or 100 percent H b Bart’s, was first reported by Lie-Injo and Jo (1960) from Indonesia and later by many others, in conjunction with a report of 15 cases from Bangkok by Pootrakul and coworkers (1967b). Recently, Thumasathit and collaborators

62 Annals New York Academy of Sciences
E
(A2) A B a r t ' s 4 4 4
Cord blood, n o r m a l
C o r d blood,Hb E trait
C o r d blood, 570 H 3 B a r t ' s
C o r d blood, 25% Hb B a r t ' s
Cord blood, n o r m a l
C o r d blood, 1.570 Hb B a r t ' s
3. Origin F Anode
FIGURE 1. Starch-gel electrophoresis in Tris-borate-EDTA buffer, pH 8.6, orthodianisi- dine stain.
(1968) reported on 27 subjects with H b Bart's disease from Chiengmai, a northern provinceof Thailand. Most of the cases have been Chinese and Thai, although they include a Greek-Cypriot and a Filipino. Individuals who have this disease either die in utero or soon after birth. They are edematous, with markedly bulging abdomen and slight to moderate jaundice. Placentae are larger than normal and friable. Hepatomegaly is much more pronounced than splenomegaly, in contrast to the finding in hydrops fetalis from blood group isoimmunization. In all of our cases, the lungs failed to expand and remained budlike. The red-cell morphology is that of severe thalassemic disease, but a large mean corpuscular volume is always observed; sickling may also be found in some cases. In starch-gel or cellulose-acetate electrophoresis, only H b Bart's is usually detected. A small amount of hemoglobin may be present a t H b H and H b AF positions. Chromato-

Wasi et al.: Thalassemia in Thai land 63
graphic examination by Kan and colleagues (1967) reveals only 7 4 in a patient with this disease. The fact that inclusion bodies are always evident in a few red cells, however, suggests the presence of H b H (p4).
About one half of the mothers bearing H b Bart’s hydropic fetuses develop toxemia of pregnancy. Unlike H b H disease, both parents of infants with H b Bart’s disease always exhibit the -a-thalassemia trait, indicating homozygosity for a- thalassemial as the cause of this disease. The synthesis of the a-chain is completely suppressed or nearly so in this condition, causing the unconjugated y2 to poly- merize to y4 (Hb Bart’s). It is doubtful whether exchange blood transfusion can save the lives of these babies. Since H b Bart’s has a remarkably high affinity for oxygen without Bohr effect (Benesch et al., 1961; Horton et al., 1962; Benesch & Benesch, 1964), severe anoxemic injury to tissues should occur. If life could be prolonged by successive blood transfusions until such time as &chain synthesis replaces y-chain synthesis, H b /34 would prevail or it would constitute the entire hemoglobin. This hemoglobin is more unstable and has an oxygen affinity similar to that of H b y4. Thus, not much improvement is expected a t this stage.
In spite of the reported 2-7% incidence of H b Bart’s in the blood of the Negro neonates (Schneider & Haggard, 1961; Minnich et al., 1962; Weatherall, 1963) H b Bart’s hydrops fetalis has yet to be found in this race. The discrepancy between the H b Bart’s incidences of 7.1% obtained by Minnich and coworkers (1962) and the 2.0% found by Weatherall (l963), both in United States Negroes, also remains to be explained.
H b H Disease--a- Thalassemial /a- Thalassemias
Evidence for assigning the genotype -a-thalassemial/cY-thalassemia~ to H b H disease has already been discussed. At birth, babies with this disease are mildly anemic, have a more marked alteration of erythrocytes than that usually observed in thalassemia trait, and inclusion bodies are evident in a few red cells. H b Bart’s in the cord blood of these newborns is around 25%. A trace of H b H may be detected in starch-gel electrophoresis. As the infants grow older, H b Bart’s de- creases whereas H b H increases in amount. Typical findings of H b H disease usually develop fully within the first year of life.
The frequency of H b H disease in Bangkok, as estimated from cord blood examination, is 0.0035. To date, 260 patients with H b H disease have been exam- ined in our laboratory (Na-Nakorn et al., to be published); some of our findings are summarized in TABLE 1. It is definitely a milder disease than 0-thalassemia homozygosity and P-thalassemia/Hb E disease. Intraerythrocytic inclusion bodies were evident in every patient but did not always show up in every red cell. The reason for the absence of inclusion bodies (Hb H) in some red cells is not clear. Early precipitation (Fessas & Yataghanas, 1968) and late precipitation of H b @4
(Rigas & Koler, 1961) and the inclusions being “pitted” by the spleen could be one of the explanations. The mean concentration of H b H, as determined by cellu-

64 Annals New York Academy of Sciences
lose acetate electrophoresis (Wasi et al . , 1968a), was 8%. Starch-gel electrophoresis in Tris-borate-EDTA buffer (pH 8.6) revealed H b Bart's in 67 out of 130 cases, its mean relative amount being 4.8%. The mean H b A2 was 1.55% and the alkali- resistant hemoglobin was usually within normal limits. In 16 patients, bands of hemoglobin cathodal to H b Az, a t approximately the positions of H b Gower 1 and Gower 2 (Huehns et al., 1964) were observed (FIGURE 2). These are most likely identical to the slow bands detected in H b A+E+Bart ' s disease (Wasi et al., 1967b), and their chemical natures remain unknown. These slow hemoglobins may not be readily separable from Hb A2 by starch-block electrophoresis, and might have been the reason for the reported increase of Hb A2 in certain cases of H b H disease (Na-Nakorn et al., 1965). This disease was not found to be associated with glucose-6-phosphate dehydrogenase deficiency as would appear from reports by Ramot and coworkers (1959) and Vella (1960). This nonassociation has also been found by Chan and colleagues (1966).
Special mention should be made of the fluctuation of hemoglobin levels and degree of splenomegaly in H b H disease. These reflect environmental effects super- imposing upon genetic defect. Infections and drugs appear to induce increased hemolysis. The amount of iron in the bone marrow of the patients with H b H disease was definitely less than in those with @-thalassemialHb E disease. This is also the case with the amount of iron that is found in other tissues (Bhamarapravati et al., to be published). The reason for this is probably the failure of H b H to be bound by haptoglobin (Nagel & Ranney, 1964). Loss of iron through the urine is thus expected to be greater in H b H disease. Folic acid therapy in thalassemic diseases in the cases studied did not raise the hemoglobin levels. This is probably due to the fact that the Thai diet is already rich in folates and nutritional megalo- blastic anemia is rare in this country. Splenectomy was performed in 50 patients. The levels of hemoglobin were raised 2-3 gm %, because red cells with precipitated H b H are prematurely destroyed in the spleen (Rigas & Koler, 1961; Gabuzda et al., 1965). After splenectomy, naturally-occurring large inclusions were noted in the red cells even without incubation with methylene blue-the so-called post- splenectomy H b H inclusion.
Alpha-thalassemiaz homozygosity should occur in three cases per one thou-
TABLE 1 COMPARISON OF SOME FEATURES OF HEMOGLOBIN H DISEASE
A N D A z - T ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ / H ~ ~ ~ ~ ~ ~ ~ i ~ E DISEASE
Hb H Disease Az-Thalassemia/Hb E Disease Findings ("/.) ("/.)
Defective development I .45 57.4 Mongoloid facies 34.9 81.4 X-ray bone changes 36 92 Hepatomegaly 69 92 SDlenomenaly 79 94 Hemoglobin 7.79 (gm) 6.37 (gm)

Wasi et al.: Thalassemia in Thailand 65
Normal
AZ-thal/Hls E
N o r ma1
Hb H t slow bands
H b H
Cord blood
fl, +r + Origin ? F H Anode
FIGURE 2. Starch-gel electrophoresis in Tris-borate-EDTA buffer, pH 8.6 , benzidine stain, illustrating slow hemoglobin bands in a patient with H b H disease.
sand, as estimated from the gene frequency of 0.056 for a-thalassemiaz. Alpha- thalassemic disease representing a-thalassemiaz homozygosity has not yet been found. It is probable that a-thalassemiaz, even in double dose, is too mild to cause a disease, and may have more or less the same manifestations as a-thalassemial trait.
Alpha-Thalassemia in Association with H b E
H b E and a-thalassemia are often transmitted together from a parent to a child, indicating their independence. This is to be expected, since H b E is a @-chain hemoglobin variant. Alpha-thalassemia and H b E may occur in ten different com- binations, part of which having been identified.

66 Annals New Y ork Academy of Sciences
Alpha-Thalassemial Trait-Hb E Trait and a-Thalassemiaz Trait-Hb E Trait
These genotypes manifest corresponding a-thalassemia traits plus the presence of a reduced amount of H b E. Usually, in simple H b E heterozygotes, the abnormal hemoglobin constitutes 25-3070. In persons doubly heterozygous for H b E and either a-thalassemial or a-thalassemiaz, the amounts of H b E may range between 17 and 25%, but d o not divide sharply into two groups as was originally suggested by Tuchinda and collaborators (1964). The infants whose cord blood contained 5-6% and I-2% H b Bart’s in addition to H b F + A + E are believed to represent a-thalassemia~ H b E and a-thalassemiaz H b E, respectively.
Alpha- Thalassemiaila- Thalassemiaz Hb E Disease
Since 1961, a new thalassemic disease with moderate anemia, characterized by major hemoglobin types of A + E+Bart’s, has been observed in our laboratory (Wasi et al., 1967b). Presently, 32 patients with this disease have been examined. Their clinical manifestations are not different from those of H b H disease. Intra- erythrocytic inclusion bodies were characteristically induced in only a few red cells; the average amount of H b Bart’s was 7.18%, the mean concentration of H b E was 14%, and the mean alkali-resistant value was 3.23%. H b F was always increased by electrophoresis. H b H was observed as a faint band in many patients. Slow hemoglobin bands similar to those observed in H b H disease were noticed. Familial findings were similar to those in H b H disease and, in many instances, both diseases were divided among sibs (FIGURE 3). One parent usually exhibited the characteristics of a-thalassemial trait, and the other had normal hematologic features and was, presumably, the carrier for the a-thalassemiaz trait. H b E was found in a t least one of the parents. These patients with H b A+E+Bart’s are believed to carry the same genes as H b H patients but inherit an H b E gene in addition, thus having the genotype of a-thalassemiallcu-thalassemiaz-Hb E (Hb H/ Hb E). This is further confirmed by the evidence that newborns with H b A + F + E +25% H b Bart’s developed H b A+E+Bart’s disease, whereas neonates with H b A + F + 25% H b Bart’s developed H b H disease. Possible mechanisms for suppres- sion of the expressivity of H b H and H b E in a-thalassemialla-thalassemiaz H b E disease have been discussed (Tuchinda et al., 1964; Wasi et al., 1967b; Fessas, 1968). Experimental evidence indicates that pA-chains compete better than BE- chains for the less available a-chains (Tuchinda ef al., 1967).
Alpha-Thalassemia Trait- Homozygous H b E
In FIGURE 3, all of the offspring of the woman with A+E+Bart’s disease must have inherited either a-thalassemial or a-thalassemiaz from their mother. The father was an H b E heterozygote, and all three offspring had only H b E without H b A. Thus, they were H b E homozygotes with a-thalassemial or a-thalassemiaz. They were not more anemic than cases homozygous for H b E alone. Newborns

Wasi et al.: Thalassemia in Thailand 67
with this genotype were found to have H b E + F , like H b E homozygotes, and a small amount of H b Bart’s in addition. Beyond the neonatal period, it is not presently possible to differentiate between H b E homozygosity and H b E homo- zygosity in association with an a-thalassemia gene.
Normal I H b s A t E
E = 20 !lo
Hba A t E E - 2 5 %
a3
I 2 3 H b s EE EE EE
= a: - thalassemial trait; = cc - thalassemia2 trait
= Hb E trait CD FIGURE 3. Pedigree with hemoglobin H disease and Hb A +E+Bart’s disease among sibs.
Alpha- T h a l u s s e m i a l / a - Thdassemiaz- Homozygous H b E
Patient 11-1 in FIGURE^ had thalassernia major with hemoglobin levels a t about 5 gm %, and his hemoglobin types were consistently E + F + Bart’s in the propor- tions of 84, 13.3 and 2.7 respectively. The mother was H b E trait and the father was homozygous H b E; neither of them was anemic. The lack of H b A in the subject indicates that he inherited the H b E gene from each parent. The presence of H b Bart’s suggests that he also had a-thalassemia. Furthermore, he could not have had just one a-thalassemia gene, because (as described above) homozygous H b E/a-thalassemia trait has the phenotype of H b E homozygosity, and H b Bart’s is not detectable beyond the first few months of life. Thus, in order to have severe thalassemic disease and also H b Bart’s, the patient must have two a-thalassemia genes. The latter should not be both a-thalassernial o r both a-thalassemiaz. For such homozygosities are either too severe or too mild, respectively. Thus, this patient most likely had the genotype of a-thalassemialla-thalassemiaz homo-
68
I
Annals New York Academy of Sciences
I[
1 2 3 4 5 6 7 8 E t F t B a r t ’ s E=25% E=30% E=24% F = 2 . 5 % E=24% E:22%
= oi - thalassemial trait; = oc - thalassemiaz trait
= wb E trait; CD m w = Homozygous Hb E
I - - - - 0 1
i L - - l
1 = Dead, not examined
FIGURE^. Pedigree of a patient with thalassemia major and Hb types E+E+Bart’s.
zygous H b E. Without familial data, this genotype is not distinguishable from a-@-thalassemia/Hb E which also has H b E + F +Bart’s and will be subsequently described.
Alpha-Thalassemia in Association with Other Abnormal Hemoglobins
A probable case of a-thalassernia/Hb J-Bangkok (a2 p~6Asp) and two patients doubly heterozygous for a-thalassemia and an a-chain hemoglobin variant have been examined in our laboratory. Like other @-chain hemoglobin variants, S and C (Zuelzer 8c Kaplan, 1954; Zuelzer et al., 1956; Aksoy, 1959a; Cohen et a f . , 1959: Weatherall, 1963), H b J-Bangkok did not interact with a-thalassemia; only ab- normal red cell morphology was observed. H b J in the individual with a- thalassemia/Hb J-Bangkok was 63.770, not much different from her relatives who were simple H b J heterozygotes (Pootrakul et al., 1967a). It should be emphasized that in this type of H b J the synthesis of /3’-chains is a t least equal to that of normal p-c hai ns .
Two patients from unrelated families had moderate thalassemic disease; inclu- sion bodies were demonstrated in their red cells and two major hemoglobin types were detected, H b H and an unknown fraction electrophoretically moving more slowly than H b F. Preliminary examination shows that this slow hemoglobin is an a-chain hemoglobin variant, probably H b Q . The chemical nature of this hemo- globin is being identified by Pootrakul, and detailed accounts will be given later

Wasi et af.: Thalassemia in Thai land 69
on. Alpha-thalessemia in association with H b Q, an a-chain variant, has been reportedin Chinese and Thai patients (Vella et a/., 1958; Dormandy el ul., 1961; Lie-Injo & Hart, 1963; Lie-Injo et al., 1966). H b Q + H has been observed in such cases; one a-structural gene is converted to aQ, and another a-structural gene is completely suppressed by the a-thalassemia, thereby leading to absence of H b a2 p2 (A) and to polymerization of the unconjugated p2 to p4 (Hb H). However, in a case of a-thalassemia/Hb I (a~6ASP &) in a Negro reported by Atwater and coworkers (1960), there was no significant anemia, no H b H , and H b A was 30%. This discrepancy between the manifestations of a-thalassemia/Hb Q and of a- thalassemia/Hb I illustrates once more the dissimilarity between a-thalassemia in people of the Far East and in American Negroes.
BETA-THALASSEMIA
Several varieties of P-thalassemia, and hereditary persistence of fetal hemo- globin have been found in Thailand. The classic P-thalassemia-A2-thalassemia or P-thalassemia type I (Fessas, 1965) is far more common than others; when un- specified, this type of P-thalassemia is referred to. Although it is unevenly distrib- uted in Thailand, the best overall estimation of classical Az-thalassemia trait is 5%. The heterozygotes are not anemic, have the usual thalassemic red cell morphology, decreased osmotic fragility and elevated H b Az. FIGURE 5 illustrates the relation-
13
12
11
10
9
8
7
6
5
4
3
2
1
% Hb F
r = -0.204
p = . 0 2
. . . . . . .. - .. - -- . : ~. .. *:. . * . . .. :.. f ' . . .... . . ...:.. ,+* . . . :!* p:.. ....< .... - ..........
1 2 3 4 5 6 7
% Hb A Z
F I C U R E 5 . Relationship between the levels of H b A2 and H b F in 131 j3-thalassemia heterozygotes.

70 Annals New York Academy of Sciences
ship between the levels of H b A2 and H b F in 131 P-thalassemia heterozygotes. Two individuals, having 2.81 and 3.07% H b A2 and 8.38 and 13.24% H b F respec- tively, clearly did not belong to the main group; they were heterozygous for F-thalassemia or type I1 (Fessas, 1965)--6/3 thalassemia (Fraser el al., 1964). Exclusive of these two persons, H b A2 was between 3.6 and 7.6%, with a mean of 5.28%. The average alkali-resistant hemoglobin of the 13 1 P-thalassemia hetero- zygotes was 1.6%; in 61 persons H b F was 1% or less, and in no case was it above 6%.
Iron deficiency causes a decrease in H b A2 levels, and in A2-thalassemia trait it may be down to normal (Wasi et al., 1968a). Environmental effects upon expres- sivity of hemoglobin types are less known and deserve more intensive investigation.
E
N o r m a l control
A2 - thal /Hb E
Homozygous Hb E
Unknown genotype
N o r m a l c o r d blood
A+ E control
f Origin F Anode
F ~ G U R E 6. Starch-gel electrophoresis in Tris-borate-EDTA buffer, pH 8.6, orthodianisi- dine stain, illustrating absence of Hb A in classical Az-thalassemia/Hb E disease.

Wasi et a/ . : Thalassemia in Thai land 71
N o r m a l contr 01
A t E control
Mild Az-thal/Hb E
Normal control
Anode T
Origin F
FIGURE 7. Starch-gel electrophoresis in Tris-borate-EDTA buffer, pH 8.6, orthodianisi- dine stain, illustrating presence of Hb A in mild An-thalassemia/Hb E disease.
Upon interaction with H b E, Az-thalassemia may be further divided into two subtypes. Classical An-thalassemia in combination with H b E gene results in a hemoglobin phenotype of E + F without detectable H b A (FIGURE 6). However, ten patients with @-thalassemialHb E disease from four unrelated families clearly had large amounts of H b A, E and F (FIGURE 7). The presence or absence of H b A in P-thalassemialHb E runs in the families, and thus does not appear to be just a matter of different expressivity of the same @-thalassemia gene. The classical or more severe form completely suppresses H b A production, but the milder and

72 Annals New York Academy of Sciences
much rarer form allows some synthesis of H b A. Superficially, heterozygotes for the two subtypes of Az-thalassemia had similar hematologic manifestations. How- ever, the mean H b Az levels obtained by cellulose-acetate electrophoresis in 74 genetically ascertained classical Az-thalassemia heterozygotes was 5.01 % with a standard deviation of 0.6%, whereas the corresponsing values in 14 genetically ascertained mild Az-thalassemia heterozygotes were 4.38% and 0.55%. The dif- ference was significant a t less than 0.001-further evidence for distinction of the two types of An-thalassemia.
Examination of 48 offspring of 19 patients with classic Az-thalassemia/Hb E disease revealed that 26 were AE and the rest were P-thalassemia trait. This indi- cates allelism or close linkage between the two genes. Twenty-five offspring of four women with mild An-thalassemia/Hb E disease married to normal men have also been examined by us; 14 were H b E trait and I I were P-thalassemia trait. This strongly indicates that the mild As-thalassemia gene is also allelic or closely linked to the p-structural cistron as marked by the H b E gene.
Classical Az-ThalassemialHb E Disease
To date, 408 patients with classical Az-thalassemia/Hb E have been examined (Na-Nakorn et al., to be published). Some features are summarized in TABLE 1. Generally P-thalassemialHb E disease is intermediate in severity between H b H disease and typical P-thalassemia homozygosity, although the clinical spectrum overlaps throughout the three. Acid elution staining (Betke & Kleihauer, 1958) consistently showed heterogeneous distribution of H b F. Na-Nakorn and col- leagues (1958) were the first to observe inclusion bodies in this disease, but their significance was not realized prior to the reports of Fessas & Loukopoulos (1964). The inclusion bodies in this disease have the characteristics described by Fessas, and probably are also an aggregation of the unconjugated a-chains. Starch-gel electrophoresis showed only bands of H b E and H b F without H b A. Agar-gel electrophoresis, in citrate buffer a t p H 6.2 (Robinson et al., 1959), which is more sensitive in detecting small amounts of H b A did not reveal H b A. Studies of in vitro hemoglobin synthesis in the reticulocytes of patients with this disease, carried out in conjunction with Weatherall and Clegg, revealed no synthesis of normal P-chains. DEAE-Sephadex-column chromatography and cellulose-acetate electrophoresis according to the techniques described previously (Wasi et al . , 1968a) gave agreeable results on quantities of H b E and H b F; the mean concen- tration of H b F in 132 patients was 48% with a standard deviation of 10.5%, the rest being Hb E. It is unknown how much H b A2 was present in these patients, since H b An and E are indistinguishable short of amino acid analysis. Iron deposit in the bone marrow and in the liver was always heavy, and secondary hemochro- matosis was common. In spite of this cardiac complications, as reported by Engle and coworkers (1964), were not observed (Yipintsoi et a/ . , 1968). Iron deposit in the myocardium was less frequently observed among our patients (Bhamarapravati

Wasi et al.: Thalassemia in Thailand 73
et al., 1967). Splenectomy had been performed in 143 patients, and significant elevation of hemoglobin levels was limited to patients with hypersplenism.
Mild A2-ThalassemialHb E Disease
Ten patients from five different families were found to have thalassemic disease with mild to moderate anemia associated with hemoglobins A + E + F (FIGURE 7). All had palpable splenomegaly and one had definite mongoloid facies. Hemo- globin concentration was 4.5-10.9, averaging 8.2 gm %. By cellulose-acetate elec- trophoresis, the mean values for H b E, F and A respectively were 55, 16, and 29%.
F- Thalassemia (a@ Thalassemia) in Association with Hemoglobin E
Patients I-2,1-3, 11-2 and 11-3 in FIGURE 8 had hepatosplenomegaly, thalassemic red cell morphology, and H b E + F ; H b F was heterogeneously distributed among
I A t E
II
A S E E t F EtF EE EE A t E F=0% F:13% A2=2.8% A2'2.670
= Hb E trait ; @ = p-thalassemia trait @ = Normal 0
FIGURE 8. Pedigree with association between Hb E and Hb F-thalassemia.
the red cells. With the exception of the almost normal hemoglobin level in 1-2, they were just like patients with classical Az-thalassemia/Hb E disease. However, 11-7 and 11-8, children of 1-3 and a normal father, had the findings of thalassemia trait, but their H b A2 was within normal limits and their H b F of 8.38 and 13.24% respectively was clearly higher than the upper limit observed in our Az-thalassemia traits. This suggests that the P-thalassemia gene segregating in this family belongs to the high F-thalassemia category (Zuelzer et al., 1961; Fessas, 1961; Malamos et a/., 1962; Wolff & Ignatov, 1963; Gabuzda et al., 1964). Heterozygotes for F-thalassemia have elevated H b F (6-36%) and a normal amount of H b AT. One

74 Annals New York Academy of Sciences
reported case of homozygosity for this type of thalassemia had neither H b A nor Hb Az (Brancati & Baglioni, 1966). One person doubly heterozygous for F- thalassemia and H b BZ (A$) had no H b Az (Comings & Motulsky, 1966). These indicate that the genetic factor causing F-thalassemia completely inhibits both 6 and @genes in cis position, hence the name 6@ thalassemia (Fraser et al., 1964).
Association between F-thalassemia and @-chain hemoglobin variants have been recorded only in 4 cases, 3 with H b S (Russo & Mollica, 1962; Russo et al., 1963; Stamatoyanopoulos et ai., 1967), and one with C (Silvestroni & Bianco, 1964). This fifth case is the first association with H b E to be observed. H b A was absent in 4 but present in the patient of Russo & Mollica (1962). The latter, i f substan- tiated as F-thalassemia, would indicate heterogeneity of this condition. 1-2 in FIGURE 8 who was doubly heterozygous for F-thalassemia and H b E had 12.7 gm ?6 of hemoglobin, the highest for H b E + F thalassemic disease. The patient with F-thalassemia/Hb S of Stamatoyanopoulos et al. (1967) also had 12 gm % hemo- globin. But the anemia in 1-3, 11-2 and 11-3 (FIGURE 8) suggests varied expressivity.
Cooley’s Anemia (Heterogeneous @- Thalassemic Diseases)
The term Cooky’s anemia as used here is not synonymous with @-thalassemia homozygosity, but refers to @-thalassemic diseases of heterogeneous genotypes, with H b A + F or H b F. The number of patients with Cooky’s anemia seen in our laboratory falls short of the amount anticipated from the gene frequency of @- thalassemia. This is because homozygous @-thalassemia is more severe than @-thalassemia/Hb E and H b H disease and causes death before the patients are old enough to enter the Department of Medicine. Tuchinda in the Pediatrics Depart- ment of this medical school has seen over 100 children with severe Cooky’s anemia (Tuchinda, personal communication).
Altogether only 11 cases of Cooky’s anemia have been examined by us; the findings are summarized in TABLE 2. Except for one case, percentages of H b A:! were at the levels observed in As-thalassemia heterozygotes. In thalassemia major (presumably homozygous p-thalassemia) the relative amount of H b A2 was re- ported as decreased, normal or increased, but in the majority it did not increase (Weatherall, 1965; Silvestroni et al., 1968). Data collected from several sources by Weatherall (1965) show a reciprocal relationship between the percentages of H b AQ and H b F. The absolute amount of H b A2 or of &chain per red cell in thalassemia major has been said to be lower than the normal value of 0.75 ppg, as calculated from the average mean corpuscular hemoglobin concentration and percent of H b A2 (Weatherall, 1965). This is not readily understood considering the fact that one Az-thalassemia gene causes increased production of H b Az by the 6 genes in both cis and trans positions (Cepellini, 1959; Horton et al., 1961; Pearson & Moore, 1965). The above calculation, however, is not satisfactory, since hetero- geneous distribution of H b F in the red cells have not been taken into account.

Wasi et al.: Thalassemia in Thai land 75
Normally synthesis of H b AZ begins near term, and thus should be associated with erythrocytes containing H b A rather than with the older cells containing more Hb F. This idea may also be applicable in thalassemia, i f the fetal red cells occur- ring in this condition represent the process of dedifferentiation. Findings by Gabuzda and colleagues (1963) and Fessas and coworkers (1965) suggest that in thalassemia H b AZ is located in the red cells containing more H b A than those rich in H b F. Synthesis of H b A2 in nonfetal red cells is probably increased in every case of Az-thalassemia major.
Cooley's anemia in adults may not always be the same disease as that seen in pediatric patients. The findings in TABLE 2 illustrate heterogeneous genotypes. Although both parents of Case 6 had elevated H b Az, it is not certain whether the patient was homozygous for classical An-thalassemia or for mild Az-thalassemia or doubly heterozygous for the two types of An-thalassemia. Of patients 8 and 9, one parent had classical Az-thalassemia and the other mild A2-thalassemia, both
TABLE 2 SUMMARY OF FINDINGS IN 1 1 PATIENTS WITH COOLEY'SANEMlA
Age Hb H b F HbAz (yr) (gm %) H b t w e s ("/.I @) Parents 35 7.6 33 7.1 45 8.8 18 6.4 20 6.4 19 7.4 17 7.6 15 8.8 10 8.8
A + F A + F A + F A + F A + F A + F A + F A + F A + F
;q ? 19 33
13 3.4 ? 10 5.7 ? 29 6.8 An-thal x At-thal 23 ?
5 6.8
6 '''1 An-thal x mild Az-thal 3.5 5.7 5 6.1 F 98.3 1.7' An-thal x F-thal
17 6.2 F 92.9 7.1 Az-thal x ?
being ascertained by interaction with H b E (vide supra). Case 10 was doubly heterozygous for Az-thalassemia and F-thalassemia; this combination has been found in only nine cases as summarized by Gabuzda and colleagues (1964); its outstanding feature is that H b F constitutes nearly all of the hemoglobin. The hemoglobin level of 6.1 gm % in our patient illustrates that mild anemia is not as characteristic of Az-thalassemia/F-thalassemia disease as might appear from the literature. It is not known whether some of the patients in TABLE 2 without familial data might represent symptomatic P-thalassemia heterozygotes (Silvestroni & Bianco, 1949; McFarland & Pearson, 1960; Pearson, 1964). However, that much varied expressivity of one P-thalassemia gene has never been observed by us. In view of the remarkable heterogeneity of 0-thalassemia, some forms being very mild (Heller et af., 1966), the studies on symptomatic @-thalassemia heterozygotes and on some weird heterozygotes with very high H b F (Aksoy, 1959b; Aksoy et al . , 1961) deserve reevaluation.

76 Annals New York Academy of Sciences
Hereditary Persistence of Fetal Hemoglobin
Occurrence of hereditary persistence of fetal hemoglobin i n a Thai family has recently been reported by Wasi and colleagues (1968b). Persons doubly hetero- zygous for this gene and the Hb E gene had H b E + F , as in classical A2- thalassemia/Hb E disease, but without anemia. The gene for hereditary persistence of fetal hemoglobin is allelic or closely linked to the Hb E gene.
ALPHA-THAI.ASSEMIA/BETA-THALASSEM I A
Due to heterogeneity in each variety, many types of association occur between a- and P-thalassemia, sometimes including H b E.
Alpha- Thalassemia Trait-P- Thalassemia Trait
Not being allelic, these two genes are not expected to result in more anemia than that usually observed in simple heterozygosities for either gene. However, with H b A2 frequently decreased in a-thalassemia but increased in Az-thalassemia, the a priori expectation of the level of H b A2 in a-thalassemia-P-thalassemia trait (a-P-thalassemia) is not possible.
In FIGURE 9, patients 11-1 and 11-2 were necessarily a-thalassemia trait, since their mother had H b H disease. These two children, who were slightly anemic without hepatosplenomegaly and had elevated H b A2 like their father, must be doubly heterozygous for a- and P-thalassemia. Other instances of double hetero-
I
1 2
A 2 = 5 . 4
A2 = 5 . 6 H b = 11.3 H b = 10.6
A 2 = 6 . 0
= Hb H disease : = a, - thalassemia trait
FIGURE 9. Pedigree with association between a- and 0-thalassernia.

Wasi et al . : Thalassemia in Thailand 77
zygosity for a-thalassemia, either a-thalassemial or a-thalassemiaz, and 0- thalassemia have also been observed to have hematologic findings similar to simple p-thalassemia heterozygotes. Newborns with a-P thalassemia had a small amount of H b Bart’s a t birth; this hemoglobin gradually disappeared as in other patients with a-thalassemia traits, but elevation of Hb Az became apparent approximately three months after birth. Alpha-beta-thalassemia cases had been reported by Fessas (1961, 1965) and by Kan and coworkers (1967); they had the findings of Az-thalassemia trait. Two persons reported as a-P-thalassemia by Pearson (1966) had H b Az of 3.6 and 3.4% respectively, but these two were not genetically man- datory for the said genotype as was the case in the others. If Pearson’s cases truly represented a-P-thalassemia, it would suggest that heterogeneity of a-thalassemia is also expressed through interaction with p-thalassemia. Enough cases have now confirmed that double heterozygosity for a-thalassemia and 6-thalassemia does not cause more anemia than is usually observed in simple heterozygosity for either type of thalassemia. The case with thalassemia major reported by Bernini and coworkers (1962) probably did not belong to this category. The knowledge that any persons with the phenotypes of P-thalassemia heterozygotes may have hidden a-thalassemia provides an explanation for the occurrence of H b Bart’s and/or H b H in children of parents apparently heterozygous for Az-thalassemia
Alpha- Thalassemial / a - Thalassemiaz-@- Thalassemia
Adult patients with thalassemia intermedia with the major hemoglobin types of A+Bart’s have been observed in our laboratory. Their genotype has not been definitely identified. We believe that these patients carry the two a-thalassemia genes as in H b H disease, but that @-chain synthesis is simultaneously inhibited by a certain factor (S). Expressivity of H b 7 4 (Bart’s) in such cases is then more prominent than that of H b P4 (H).
Evidence suggests that the presence of the 0-thalassemia gene may suppress the appearance of H b H in a-thalassemial/a-thalassemiaz genotype.
In FIGURE 10, patients 11-3 and 11-5, both over 20 years old, were anemic, had hepatosplenomegaly and thalassemic facies; in addition to H b A, their blood con- sistently contained H b Bart’s. Their brother, 11-2, had A + E + Bart’s disease and thus the genotype of a-thalassemial/a-thalassemiaz-Hb E as discussed earlier. Patients 11-3 and 11-5 were as anemic as 11-2 and probably also had the two a-thalassemic genes that 11-2 had. 1-3 had An-thalassemia trait. If the deceased father, 1-2, had P-thalassemia gene together with an a-thalassemia and H b E, patients 11-3 and 11-5 then could also have inherited P-thalassemia. The latter would have suppressed P-chain synthesis, and H b 7 4 (Bart’s) instead of H b 04 (H) was thus expressed. Choremis and collaborators (1959) reported a nine-year-old boy who was anemic and had Hb A+Bart’s. Upon reviewing this report, it was found that H b Az in the parents was 3.8 and 4.270, suggesting that the boy might have carried @-thalassemia in addition to a-thalassemia.

78 Annals New York Academy of Sciences
I
A t E P
Normal A + E+ Bar t ’ s A t B a r t ’ s Normal A t Bar t l s
= Hb E t ra i t ; @ = CT - thalassemial t ra i t : = oc - thalassemiaZ t ra i t
: Normal ;
t - + - - - l
i D j = Dead, not examined L - - - - J
FIGURE 10. Pedigree with two patients who had thalassemia intermedia with H b A + Bart’s.
A Ipha- Thalassemia- P - Thalassemial Hb E
A woman with thalassemic disease whose hemoglobin was 6.95 gm % persis- tently showed H b E+F+Bar t ’ s in starch-gel electrophoresis. H b E was 81%, Bart’s 2.28%, the remainder was Hb F. She might have the genotype of a- thalassemial/a-thalassemia2 homozygous H b E (vide supra), but her mother and two of her children had elevated H b A2, indicating that the patient also carried a P-thalassemia gene. The detection of 4.5% of H b Bart’s in the cord blood of her
TABLE 3 CORD BLOOD HEMOGLOBIN PHENOTYPES OF SOME I L L U S T R A T I V E GENOTYPES
H b Types Genotypes Cord Blood
FA Normal FA + 5% Bart’s a-thall/Normal FA + I-2% Bart’s a-thaln/Normal FA + 25% Bart’s a-thall/a-thalz FA + E + 25% Bart’s 100% Bart’s a-thall/a-thall
a-thall/a-thalz-Hb E

Wasi et al.: Thalassemia in Thailand 79
last child further confirmed that the patient also had an a-thalassemial gene. This patient thus inherited at least three abnormal genes, i.e., a-thalassemial, /3- thalassemia, and H b E. Whether she also had a-thalassemiaz is not known. With- out familial examination, this syndrome could not be differentiated from the a- thalassemial /a-thalassemian homozygous H b E described previously. Findings and frequencies of some illustrative or more common syndromes are summarized in TABLES 3and 4.
T A B L E 4 MAJOR HEMOGLOBIN TYPES IN T H E MORE COMMON THALASSEMIC
DISEASES SEEN IN T H A I L A N D
Diseases Major
H b Types Estimated
No. of Patients* 0-thalassemia homozygosity F o r F + A 18,750 0-thalassemialHb E E + F 48,750 H b H A + H 151,986 Hb H / H b E A + E + Bart’s 22,709 H b Bart’s hydrops fetalis Bart’s 80,790
Total = 322.985
*Estimated for the population of 30 million.
REFERENCES
AKSOY, M. 1959a. Abnormal haemoglobins in Turkey. In Abnormal Haemoglobins-A Symposium. J. H. P. Jonxis & J . F. Delafresnaye, Eds. : 216. Blackwell Scientific Publications. Oxford, England.
AKSOY, M. 1959b. Thalassaemia minor with large amount of foetal haemoglobin. Acta Haemat. 22: 188.
AKSOY, M., A. E~R1BozL.v & H. ALPUSTUN. 1961. The thalassaemia syndromes. I : Thalas- saemia minor with large amounts of foetal haemoglobin. Study of a family. Acta Haemat. 26: 136.
ATWATER, J., I. R. SCHWARTZ, A. J. ERSLEV, T. D. MONTGOMERY & L. M. TOCANTINS. 1960. Sickling of erythrocytes in a patient with thalassemia-hemoglobin I disease. New Eng. J. Med. 263: 1215.
BENESCH, R. E., H. M. RANNEY, R. BENESCH & G. M. SMITH. 1961. The chemistry of the Bohr Effect. 11. Some properties of hemoglobin H. J. Biol. Chem. 236 2926.
BENESCH, R. & R. E. BENESCH. 1964. Properties of haemoglobin H and their significance in relation to function of haemoglobin. Nature 202: 773.
BERNINI, L., C. F. COLUCCI, D. D E MICHELE, S . PIOMELLI & M. SINISCALCO. 1962. A possible case of alpha-beta-thalassaemia. Acta Genet. 12: 202.
BETKE, K. & E. KLEIHAUER. 1958. Fetaler und bleibender Blutfarbstoff in Erythrozyten und Erythroblasten von rnenschlichen Feten und Neugeborenen. Blut. 4: 241.
BHAMARAPRAVATI, N., S. NA-NAKORN, P. WASI & S. TUCHINDA. 1967. Pathology of Abnormal Hemoglobin Diseases Seen in Thailand. 1. Pathology of P-thalassemia Hemoglobin E Disease. Amer. J. Clin. Path. 47: 745.
BRANCATI, C. & C. BAGLIONI. 1966. Homozygous PS thalassemia (Phnicrocythaemia). Nature 212 262.
CEPPELLINI, R. 1959. Biochemistry of Human Genetics. Ciba Foundation Symposium. G. E. W. Wolstenholme & C. M. O’Connor, Eds. : 133. Little, Brown and Co. Boston, Mass.

80 Annals New York Academy of Sciences
CHAN, T. K., D. TODD & C. C. WONG. 1966. Erythrocyte glucose-6-phosphate dehydrogen- ase activity in haemoglobin H disease. Nature 209 1147.
CHOREMIS, C., L. ZANNOS-MARIOLEA, J. A. M. AGER & H. LEHMANN. 1959. Persistence of haemoglobin “Bart’s” beyond infancy in a child with thalassaemia. Brit. Med. J. ii: 348.
COHEN, F., W. W. ZEULZER, J. V. NEEL & A. R. RORINSON. 1959. Multiple inherited erythrocyte anomalies in an American Negro family. Hereditary spherocytosis, sickling and thalassemia. Blood 14: 816.
COMINGS, D. E. & A. G. MOTULSKY. 1966. Absence of cis delta chain synthesis in 06 thalassemia (F-thalassemia). Blood 28 54.
DANCE, N., E. R. HUEHNS & G. H. BEAVEN. 1963. The abnormal haemoglobins in haemo- globin H disease. Biochem. J. 87: 240.
DORMANDY, K. M., S. P. LOCK & H. LEHMANN. 1961. Haemoglobin Q alpha-thalassaemia. Brit. Med. J. 1: 1582.
ENGLE, M. A. 1964. Cardiac involvement in Cooley’s anemia. Ann. New York Acad. Sci. 119 694.
FESSAS, PH. 1961. The beta-chain thalassemia. In Haemoglobin Colloquium. H. Lehmann & K. Betke, Eds. : 90. Georg Thieme Verlag. Stuttgart, Germany.
FESSAS, PH. 1965. Forms of thalassaemia. In Abnormal Haemoglobins in Africa. J. H. P. Jonxis, Ed. : 90. Blackwell Scientific Publications. Oxford, England.
FESSAS, PH. 1968. Letter to the editor. Brit. Med. J. k 764. FESSAS, PH. & D. LOUKOPOULOS. 1964. Alpha-chain of human hemoglobin: occurrence
in vivo. Science 143: 590. FESSAS, PH. & X.. YATAGHANAS. 1968. Intraerythroblastic instability of hemoglobin p4
(Hb H). Blood 31: 323. FLATZ, G., C. PIK & S. SRINGAM. 1965. Haemoglobin E and P-thalassaemia: their distribu-
tion in Thailand. Ann. Hum. Genet. 29 151. FRASER, G. R., C. KITSOS, A. G. MOTULSKY, G. STAMATOYANNOPOULOS, D. LOUKOPOULOS,
PH. FESSAS, C. KATTAMIS, B. DEFARANAS, L. ZANNOS-MARIOLEA & C. CHOREMIS. 1964. Thalassemias, abnormal hemoglobins and glucose-6-phosphate dehydrogenase deficiency in the Arta area of Greece. Ann. N.Y. Acad. Sci. 119: 415.
GABUZDA, T. G., D. G. NATHAN & F. H. GARDNER. 1963. The turnover of hemoglobins A, F, and Az in the peripheral blood of three patients with thalassemia. J . Clin. Invest. 42: 1678.
GABUZDA, T. G., D. G. NATHAN & F. H. GARDNER. 1964. Thalassemia trait. Genetic com- binations of increased fetal and AZ hemoglobins. New Eng. J. Med. 270: 1212.
GABUZDA, T. G., D. G. NATHAN & F. H. GARDNER. 1965. The metabolism of the individ- dual C14 labeled hemoglobins in patients with H-thalassemia, with observations on radiochromate binding to the hemoglobins during red cell survival. J. Clin. Invest. 44 315.
GOUTTAS, A,, PH. FESSAS, H. TSEVRENIS & E. XEFTERI. 1955. Description d’une nouvelle vari6t6 d’animie himolytique conginitale. (Etude himatologique, ilectrophoritique et ginitique.) Sang. 26 91 I .
HELLER, P., V. J. YAKULIS, A. I. ROSENZWEIG, C. F. ABILDGAARD & D. L. RUCKNAGEL. 1966. Mild homozygous beta-thalassemia. Further evidence for the heterogeneity of beta-thalassemia genes. Ann. Intern. Med. 64 52.
HORTON, B., R. A. PAYNE, M. T. BRIDGES & T. H. J. HUISMAN. 1961. Studies on an ab- normal minor hemoglobin component (Hb-P2). Clin. Chim. Acta 6 243.
HORTON, B., R. B. THOMPSON, A. DOZY, C. NECHTMAN, E. NICHOLS & T. H. J. HUISMAN. 1962. Inhomogeneity of hemoglobin. VI. The minor hemoglobin components of cord blood. Blood 20 302.
HUEHNS, E. R., F. V. FLYNN, E. A. BUTLER & E. M. SHOOTER. 1960. The occurrence of haemoglobin ‘Bart’s’ in conjunction with haemoglobin H. Brit. J. Haemat. 6: 388.
HUEHNS, E. R., N. DANCE, G. H. BEAVEN, F. HECHT & A. G . MOTULSKY. 1964. Human embryonic hemoglobins. Cold Spring Harbor Sympos. 29 327.
HUNT, J. A. & V. M. INGRAM. 1959. The genetical control of protein structure: the abnormal human haemoglobins. Biochemistry of Human Genetics, a Ciba Foundation Sym- posium: 114. Little, Brown & Co. Boston, Mass.

Wasi et al.: Thalassemia in Thailand 81
KAN, Y. W., A. ALLEN & L. LOWENSTEIN. 1967. Hydrops fetalis with alpha thalassemia.
KOLER, R. D. & D. A. RIGAS. 1961. Genetics of haemoglobin H. Ann. Hum. Genet. 2 5 95. LIE-INJO, L. E. & B. H. Jo. 1960. Hydrops foetalis with a fast-moving haemoglobin. Brit.
LIE-INJO, L. E. & P. L. DE V. HART. 1963. Splenectomy in two cases of haemoglobin Q-H-
New Eng. J. Med. 276 18.
Med. J. ii: 1649.
disease (Hb Q-a-thalassaemia). Acta Haemat. 2 9 358.
disease (Hb Q-a-thalassemia). Blood 28: 830. LOUKOPOULOS, D. & PH. FESSAS. 1965. The distribution of hemoglobin types in thalassemic
erythrocytes. J. Clin. Invest. 44: 231. MALAMOS, B., PH. FESSAS & G. STAMATOYANNOPOULOS. 1962. Types of thalassaemia-trait
carriers as revealed by a study of their incidence in Greece. Brit. J . Haemat. 8: 5. MCFARLAND, W. & H. A. PEARSON. 1960. Thalassemia in “non-Mediterranean” families.
Ann. Intern. Med. 63: 510. MINNICH, V., S. NA-NAKORN, S . TUCHINDA, P. WAS & C. V. MOORE. 1958. Inclusion body
anemia in Thailand (hemoglobin H thalassemia disease). In Proc. Sixth Congr. Internat. SOC. Haemat. : 729. Grune & Stratton, New York, N.Y.
MINNICH, V., J. K. CORDONNIER, W. J. WILLIAMS & c. V. MOORE. 1962. Alpha, beta and gamma hemoglobin polypeptide chains during the neo-natal period with a description of the fetal form of hemoglobin D(st, Louis). Blood 19: 137.
NAGEL, R. L. & H. M. RANNEY. 1964. Haptoglobin binding capacity of certain abnormal hemoglobins. Science 144 1014.
NA-NAKORN, S., V. MINNICH & A. I . CHERNOFF. 1956. Studies on hemoglobin E: 11. The incidence of hemoglobin E in Thailand. J. Lab. Clin. Med. 47: 490.
NA-NAKORN, S., P. WASI & A. SUINGDUMRONG. 1965. Hemoglobin H disease in Thailand: clinical and hematological studies in 138 cases. Israel J. Med. Sci. 1: 762.
PEARSON, H. A. 1964. Thalassemia intermedia. Genetic and biochemical considerations. Ann. N.Y. Acad. Sci. 119 390.
PEARSON, H. A. 1966. Alpha-beta thalassemia disease. New Eng. J. Med. 275: 176. PEARSON, H. A. & M. M. MOORE. 1965. Human hemoglobin gene linkage, report of a
family with hemoglobin @2, hemoglobin S, @-thalassemia, including a probable cross- over between thalassemia and delta loci. Amer. J. Hum. Genet. 17: 125.
POOTRAKUL, S., P. WASI & S . NA-NAKORN. 1967a. Haemoglobin J-Bangkok: A clinical, haematological and genetical study. Brit. J. Haemat. 13: 303.
POOTRAKUL, S., P. WASI & S. NA-NAKORN. 1967b. Haemoglobin Bart’s hydrops foetalis in Thailand. Ann. Hum. Genet. 3 0 293.
RAMOT, B., CH. SHEBA, S . FISHER, J. A. M. AGER & H. LEHMANN. 1959. Haemoglobin H disease with persistent haemoglobin Bart’s in an Oriental Jewess and her daughter. A dual alpha-chain deficiency. Brit. Med. J. 2: 1228.
RIGAS, D. A., R. D. KOLER & E. E. OSGOOD. 1955. New hemoglobin possessing a higher electrophoretic mobility than normal adult hemoglobin. Science 121: 372.
RIGAS, D. A., R. D. KOLER & E. E. OSGOOD. 1956. Hemoglobin H: clinical, laboratory and genetic studies of a family with a previously undescribed hemoglobin. J . Lab. Clin. Med. 4 7 51.
ROBINSON, A. R., M. ROBSON, A. HARRISON & W. W. ZUELZER. 1959. A new technique for differentiation of hemoglobin. J. Lab. Clin. Med. 6 0 745.
Russo, G . & F. MOLLICA. 1962. Sickle cell hemoglobin and two types of thalassemia in the same family. Acta Hemat. 28: 329.
Russo, G., A. LA GRUTTA & F. MOLLICA. 1963. Sulla eterogeneita della thalassemia. Con- tributo casistico ed interpretazione biochimica e genetica. Riv. Ped. Sicil. 18: 239.
SCHNEIDER, R. G & M. E. HAGGARD. 1961. The incidence of hemoglobin variants in Negro and white newborn infants. Amer. J. Dis. Child. 102: 599.
SILVESTRONI, E. & I. BIANCO. 1949. Microcytemia, constitutional microcytic anemia, and Cooley’s anemia. Amer. J. Hum. Genet. 1: 83.
SILVESTRONI, E. & I. BIANCO. 1964. Un caso di malattia microdrepanocitica da Hb S e varieti di microcitemia con quota normale di Hb Az e quota elevata di Hb F (terza varieti di malattia microdrepanocitica). Progr. Med. 2 0 509.
LIE-INJO, L. E., R. P. PlLLAY & V. THURAI-SINGHAM. 1966. Further cases Of Hb Q-H

82 Annals New York Academy of Sciences
SILVESTRONI, E., I. BIANCO & B. GRAZIANI. 1968. The haemoglobin picture in Cooley’s disease. Brit. J. Haemat. 14 303.
STAMATOYANNOPOULOS, G., C. SOFRONIADOU & A. AKRIVAKIS. 1967. Absence of Hemo- globin A in a Double Heterozygote for F-Thalassemia and Hemoglobin S. Blood 30 772.
SUNDHARAGIATI, B. & D. VISESHAKUL. 1958. Paper electrophoretic studies on Hgb E in the people of north east Thailand. J. Med. Serv. Dept. Bangkok 7: 41 1.
SUNDHARAGIATI, B. & D. VISESHAKUL. 1959a. Electrophoretic studies on Hgb E in the people of northern Thailand. J. Med. Serv. Dept. Bangkok 8: 388.
SUNDHARAGIATI, B. & D. VISESHAKUL. 1959b. Electrophoretic studies on Hgb in the people of central Thailand. J. Med. Sew. Dept. Bangkok 8 397.
THUMASATHIT, B., A. NONDASUTA. S. SILPISORNKOSOL, B. LOUSUEBSAKUL, P. UNCHALI- PONGSE & M. MANGKORNKANOK. 1968. Hydrops fetalis associated with Hb Bart’s in northern Thailand. J. Pediat. 73: 132.
TUCHINDA, S., D. L. RUCKNAGEL, V. MINNICH, U. BOONYAPRAKOB, K. BALANKURA & V. SUVATEE. 1964. The coexistence of the genes for hemoglobin E and a-thalassemia in Thais, with resultant suppression of hemoglobin E synthesis. Amer. J. Hum. Genet. 1 6 311.
TUCHINDA, S., D. BEALE & H. LEHMANN. 1967. The suppression of haemoglobin E synthesis when haemoglobin H disease and haemoglobin E trait occur together. Humangenetik 3 312.
VELLA, F. 1960. Experientia 1 6 284 (quoted by Chan ef al., 1966). VELLA, F., R. H. C. WELLS, J. A. M. AGER & H. LEHMANN. 1958. A haemoglobinopathy
involving haemoglobin H and a new (Q) haemoglobin. Brit. Med. J. 1: 752. WASI, P., S. NA-NAKORN & A. SUIKGDUMRONG. 1964. Haemoglobin H disease in Thailand:
a genetical study. Nature 204: 907. WASI, P., S. NA-NAKORN & A. SUINGDUMRONG. 1967a. Study of the distributions of haemo-
globin E, thalassaemias and G-6-PD deficiency in northeastern Thailand. Nature 214: 501.
WASI, P., M. SOOKANEK, S. POOTRAKUL, S. NA-NAKORN & A. SUINGDUMRONG. 1967b. Haemoglobin E and a-thalassaemia. Brit. Med. J. 2: 29.
WASI, P., P. DISTHASONGCHAN & S. NA-NAKORN. 1968a. The effect of iron deficiency on the levels of hemoglobins A2 and E. J. Lab. Clin. Med. 71: 85.
WASI, P., S. POOTRAKUL & S. NA-NAKORN. 1968b. Hereditary persistence of foetal haemo- globin in a Thai family: The first instance in the Mongol race and in association with haemoglobin E. Brit. J. Haemat. 14: 501.
WEATHERALL, D. J. 1963. Abnormal haemoglobins in the neonatal period and their relation- ships to thalassaemia. Brit. J. Haemat. 9 265.
WEATHERALL, D. J. 1965. The Thalassaemia Syndromes. Blackwell Scientific Publications. Oxford, England.
WOLFF, J. A. & V. G. IGNATOV. 1963. Heterogeneity of thalassemia major. Amer. J. Dis. Child. 106: 234.
YIPINTSOI, T., M. HARAPHONGSE, P. WASI & S. NA-NAKORN. 1968. Cardiological examina- tions in hemoglobin E and thalassemia diseases. J. Med. Ass. Thailand. 61: 131.
ZUELZER, W. W. & E. KAPLAN. 1954. Thalassemia hemoglobin C-disease. A new syndrome presumably due to combination of the genes for thalassemia and hemoglobin C. B lood9 1047.
ZUELZER, W. W., J. V. NEEL & A. R. ROBINSON. 1956. Abnormal hemoglobins. In Progress in Hematology. L. M. Tocantins, Ed. : 91. Grune & Stratton. New York, N.Y.
ZUELZER, W. W., A. R. ROBINSON & C. R. BOOKER. 1961. Reciprocal relationship of hemo- globin A2 and F in beta-chain thalassemia, a key to the genetic control of hemoglobin F. Blood 17: 393.