Molecular Mechanisms of Drug Resistance in Clinical Candida Species Isolated from Tunisian Hospitals
Upload
telecom-paristechCategory
view
1download
0
Journal of Autoimmunity 23 (2004) 75e80
www.elsevier.com/locate/issn/08968411
Analysis of MHC genes in a Tunisian isolate with autoimmunethyroid diseases: implication of TNF �308 gene polymorphism
Noura Bougacha-Elleucha, Ahmed Rebaib, Mouna Mnif c, Hafedh Maknia,d,Mohamed Bellassouadc, Jomaa Jouidae, Mohamed Abidc, A. Hammadia,)
aLaboratoire de Genetique Moleculaire Humaine Faculte de Medecine, Avenue Majida Boulila, 3029 Sfax, TunisiabCentre de Biotechnologie Sfax, Tunisia
cService Endocrinologie, CHU Hedi Chaker, Sfax, TunisiadLaboratoire d’Histocompatibilite, CHU Hedi Chaker, Sfax, Tunisia
eDispensaire Bir Hfaı, Sidi Bouzid, Tunisia
Received 2 December 2003; revised 11 March 2004; accepted 26 March 2004
Abstract
Autoimmune thyroid diseases (AITDs), which include Hashimoto thyroiditis (HT), Graves’ disease (GD) and primary idiopathicmyxoedema (PIM), are recognized as multifactorial diseases. In this study, we have examined single and haplotypic genetic variation
across the major histocompatibility complex (MHC) in a Tunisian isolate with a high prevalence of AITDs (62 patients: 32 with GD,9 with HT and 21 with PIM). Genotyping was performed for HLA class I and II alleles as well as polymorphisms within tumornecrosis factor (TNF), lymphotoxin a (TLa) and heat shock protein (HSP70-02 and HSP70-hom) genes. Our results showedassociation of HLA-A2-B50-TNF 2 haplotype with AITDs ( p ¼ 0:045). Linkage analysis using Simwalk2 program has shown
significant result with TNF �308 gene polymorphism ( p ¼ 0:03). The FBAT has given evidence for genetic association with TNF�308 and HLA-DR gene polymorphisms. TNF 2 allele was associated with GD ( p ¼ 0:0011), whereas TNF 1, HLA-DR11 andDR12 ( p ¼ 0:0039, p ¼ 0:00089 and p ¼ 0:0056, respectively) were rather implicated in HT pathogenesis. Results found by
TDTeSTDT have confirmed the involvement of the TNF �308 gene polymorphism in AITD pathogenesis ( p! 10�9).� 2004 Elsevier Ltd. All rights reserved.
Keywords: MHC; Autoimmune thyroid diseases; TNF �308
1. Introduction
Autoimmune thyroid diseases (AITDs), which in-clude Hashimoto thyroiditis (HT), Graves’ disease (GD)and primary idiopathic myxoedema (PIM), are recog-nized as multifactorial diseases, arising from interactionsof environmental factors with multiple genes. In GD,the autoimmune process results in the production ofthyroid-stimulating antibodies and leads to hyperthy-roidism, whereas in HT, the end result is destruction ofthyroid cells and hypothyroidism. The search for
) Corresponding author. Tel.: +216-74-241-888; fax: +216-74-246-
946.
E-mail address: [email protected] (A. Hammadi).
0896-8411/$ - see front matter � 2004 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jaut.2004.03.011
susceptibility genes involves two major approaches,genome-wide screenings and association studies for can-didate genes. Genome-wide scans have identified manyregions linked to AITDs on different chromosomes[1e3]. Linkage or linkage disequilibrium of GD to themajor histocompatibility complex (MHC) has also beenreported in some populations [4e7]. However, evidencefor linkage was not strong enough to be replicated inother samples or populations [8e10]. This suggests thatdifferent MHC susceptibility loci exist between differentethnic groups and more than one gene was involved inthe genetic susceptibility to AITDs. Indeed, this regionharbors an important number of genes involved in manyautoimmune diseases (AID) [11]. The second approachhas also provided a great deal of information that manycandidate genes involved either in thyroid physiology

76 N. Bougacha-Elleuch et al. / Journal of Autoimmunity 23 (2004) 75e80
[12e16] or in immune response [6,17e19] are conciselyassociated with AITDs. Associations between AITDsand MHC have long been recognized in different popu-lations. GD is associated with the HLA haplotypeA*01-B*0801-DRB1*0301-DQA1*0501-DQB1*0201 [4e5,20e22], whereas autoimmune hypothyroidism has beenweakly associated with HLA-DRB1*03, *04 and *11/*12alleles [23e26]. However, the presence of important im-munoregulatory genes (TNF, HSP70, LMP, TAP) withinthe MHC raises the possibility that HLA associationsseen in AITDs are primarily due to genetic variation inthese immunoregulatory genes which harbor the majorsusceptibility locus. The entireMHCregionwhich has notbeen extensively investigated [23,27], would providemorepower in detecting susceptibility genes.
In order to analyze theMHC region in a rare Tunisianisolate (Akr), with a high prevalence of AITDs, we havegenotyped 134 Akr DNAs for HLA class I and II allelesand polymorphisms within TNF, LTa, HSP70-02 andHSP70-hom genes. Our results have given evidence forgenetic association with TNF �308 gene polymorphism.
2. Patients and methods
2.1. Subjects
Subjects were recruited from a geographic isolate insouth Tunisia named Akr with a high prevalence ofAITDs [28]. Regular clinical follow-up of this isolatesince 1992 has permitted an update of the pedigree. Thispedigree consists in 10 generations of 391 members in-cluding 62 patients subdivided into 32 patients affectedwith GD, 9 patients with HT and 21 patients with PIM(Table 1).
2.2. Clinical assessment
The diagnosis of GD was based on the presence ofbiochemical hyperthyroidism as indicated by a decreaseof TSH, an increase of T4 levels and positive TSHreceptor antibody, in association with diffuse goiter orthe presence of exophthalmos. The diagnosis of HT wasbased on the presence of thyroid hormone replacedprimary hypothyroidism, defined as a TSH level abovethe upper limits associated with positive titers of thyroidantibodies (anti-thyroid peroxidase, or anti-thyroglobu-lin) and a palpable goiter. PIM was diagnosed by thepresence of hypothyroidism requiring T3 or T4 replace-ment. Patients with PIM have an atrophic gland.
2.3. Genotyping methods
Genomic DNA was extracted from 10 ml of pe-ripheral blood lymphocyte (PBL) of Akr patients and
healthy Akr-related controls using standard methods[29]. Subjects were then genotyped for HLA class I andII, TNF �308 A/G, TNFe, TNFc, HSP70-02 andHSP70-hom gene polymorphisms. The location of thesegenes with respect to the HLA gene complex is shown inFig. 1. Genotyping of TNFe and TNFc was performedby PCR technique using specific primers [30]. Screeningfor TNF �308 A/G, HSP70-02 (C1267 A/G) andHSP70-hom (C2437 T/C) was performed by PCR-RFLP technique as previously described [31e32].
HLA class I and II DNA typing was performedby PCR-single standard polymorphism (PCR-SSP)strategy using commercial one lamda micro SSP�HLA class I A and class I B and generic HLA class IIDNA typing tray.
Table 1
Distribution of 62 AITDs patients from the Akr isolate in different
categories with regard to their disease status and clinical parameters
GD (n ¼ 32) HT (n ¼ 9) PIM (n ¼ 21)
Males 16 3 4
Females 16 6 17
Agea 40.48 (20e81) 45 (23e58) 57.15 (30e81)
Age of onseta 28.31 (13e70) 30 (7e50) 45.4 (40e65)
Associated diseases IDDM/
SGS/Addisson
IDDM/NGS Vitiligo
Goiter
Yes 21 5 1
No 11 4 20
Ophthalmopathy
Yes 22 5 0
No 10 4 21
Anti-Tg status
Positive 12 2 7
Negative 20 4 10
Unknown e 3 4
Anti-Tpo status
Positive 16 4 10
Negative 15 2 6
Unknown 1 3 5
a Mean age with the age range between parentheses.
DP EC G F
DMLMP2
TAP1LMP7
TAP2 C4C2 2 1 Hom LTβ TNF LTα
HSP70
Centromere Telomere
DQ DR B A
Fig. 1. Schematic representation showing the main genetic regions of
the human major histocompatibility complex. Polymorphisms within
genes shaded grey have been genotyped in this study.
77N. Bougacha-Elleuch et al. / Journal of Autoimmunity 23 (2004) 75e80
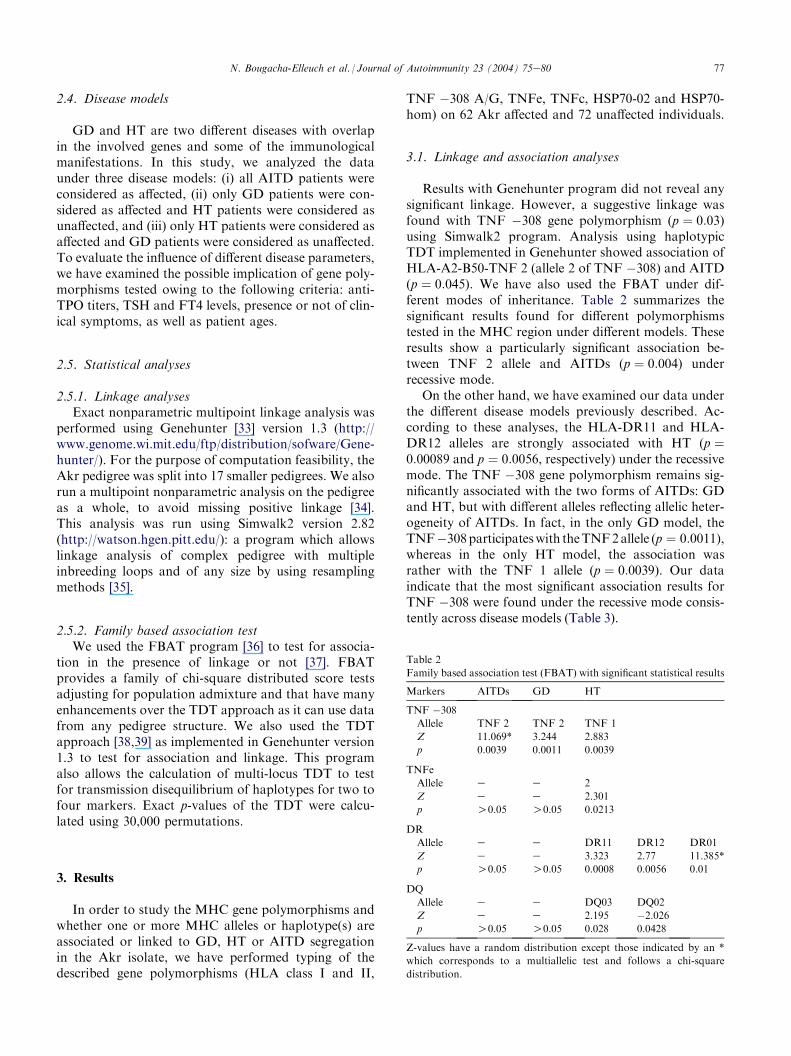
2.4. Disease models
GD and HT are two different diseases with overlapin the involved genes and some of the immunologicalmanifestations. In this study, we analyzed the dataunder three disease models: (i) all AITD patients wereconsidered as affected, (ii) only GD patients were con-sidered as affected and HT patients were considered asunaffected, and (iii) only HT patients were considered asaffected and GD patients were considered as unaffected.To evaluate the influence of different disease parameters,we have examined the possible implication of gene poly-morphisms tested owing to the following criteria: anti-TPO titers, TSH and FT4 levels, presence or not of clin-ical symptoms, as well as patient ages.
2.5. Statistical analyses
2.5.1. Linkage analysesExact nonparametric multipoint linkage analysis was
performed using Genehunter [33] version 1.3 (http://www.genome.wi.mit.edu/ftp/distribution/sofware/Gene-hunter/). For the purpose of computation feasibility, theAkr pedigree was split into 17 smaller pedigrees. We alsorun a multipoint nonparametric analysis on the pedigreeas a whole, to avoid missing positive linkage [34].This analysis was run using Simwalk2 version 2.82(http://watson.hgen.pitt.edu/): a program which allowslinkage analysis of complex pedigree with multipleinbreeding loops and of any size by using resamplingmethods [35].
2.5.2. Family based association testWe used the FBAT program [36] to test for associa-
tion in the presence of linkage or not [37]. FBATprovides a family of chi-square distributed score testsadjusting for population admixture and that have manyenhancements over the TDT approach as it can use datafrom any pedigree structure. We also used the TDTapproach [38,39] as implemented in Genehunter version1.3 to test for association and linkage. This programalso allows the calculation of multi-locus TDT to testfor transmission disequilibrium of haplotypes for two tofour markers. Exact p-values of the TDT were calcu-lated using 30,000 permutations.
3. Results
In order to study the MHC gene polymorphisms andwhether one or more MHC alleles or haplotype(s) areassociated or linked to GD, HT or AITD segregationin the Akr isolate, we have performed typing of thedescribed gene polymorphisms (HLA class I and II,
TNF �308 A/G, TNFe, TNFc, HSP70-02 and HSP70-hom) on 62 Akr affected and 72 unaffected individuals.
3.1. Linkage and association analyses
Results with Genehunter program did not reveal anysignificant linkage. However, a suggestive linkage wasfound with TNF �308 gene polymorphism (p ¼ 0:03)using Simwalk2 program. Analysis using haplotypicTDT implemented in Genehunter showed association ofHLA-A2-B50-TNF 2 (allele 2 of TNF �308) and AITD(p ¼ 0:045). We have also used the FBAT under dif-ferent modes of inheritance. Table 2 summarizes thesignificant results found for different polymorphismstested in the MHC region under different models. Theseresults show a particularly significant association be-tween TNF 2 allele and AITDs (p ¼ 0:004) underrecessive mode.
On the other hand, we have examined our data underthe different disease models previously described. Ac-cording to these analyses, the HLA-DR11 and HLA-DR12 alleles are strongly associated with HT (p ¼0:00089 and p ¼ 0:0056, respectively) under the recessivemode. The TNF �308 gene polymorphism remains sig-nificantly associated with the two forms of AITDs: GDand HT, but with different alleles reflecting allelic heter-ogeneity of AITDs. In fact, in the only GD model, theTNF�308participateswith theTNF2allele (p ¼ 0:0011),whereas in the only HT model, the association wasrather with the TNF 1 allele (p ¼ 0:0039). Our dataindicate that the most significant association results forTNF �308 were found under the recessive mode consis-tently across disease models (Table 3).
Table 2
Family based association test (FBAT) with significant statistical results
Markers AITDs GD HT
TNF �308
Allele TNF 2 TNF 2 TNF 1
Z 11.069* 3.244 2.883
p 0.0039 0.0011 0.0039
TNFe
Allele e e 2
Z e e 2.301
p O0.05 O0.05 0.0213
DR
Allele e e DR11 DR12 DR01
Z e e 3.323 2.77 11.385*
p O0.05 O0.05 0.0008 0.0056 0.01
DQ
Allele e e DQ03 DQ02
Z e e 2.195 �2.026
p O0.05 O0.05 0.028 0.0428
Z-values have a random distribution except those indicated by an *
which corresponds to a multiallelic test and follows a chi-square
distribution.

78 N. Bougacha-Elleuch et al. / Journal of Autoimmunity 23 (2004) 75e80
Table 3
Significant values found with TNF-308 under different models and recessive mode
Markers AITDs GD HT Susceptibility class Anti-TPo TSH FT4 Clinical symptoms
TNF �308
Allele TNF 2 TNF 2 TNF 1 TNF 2 TNF 2 TNF 1 TNF 2 TNF 2
Z 2.251 3.244 2.883 3.244 12.356* 2.519 2.896 8.552*
p 0.024 0.0011 0.0039 0.0011 0.002 0.0117 0.0037 0.0138
Z-values have a random distribution except those indicated by an * which corresponds to a multiallelic test and follows a chi-square distribution.
4. Discussion
Genetic predisposition in AITDs is most likely due tointeractions between several genes and is influenced byso-far unknown non-genetic factors. In order to mini-mize genetic heterogeneity, we have targeted our studyto a rare large multigenerational isolate with high pre-valence of AITDs from South of Tunisia. In this isolate,AITDs appear in association with five other AID(Table 1). This observation is well documented andconfirms again the existence of common susceptibilitygenes for AID as it was already reported [40].
The studied isolate has been used in a genome screenand a maximum lod score was found at marker D2S171in 2p21 [2]. Many candidate genes (IgVH, Cb TCR andCTLA-4) [41e42] were excluded for possible implicationin AITDs pathogenesis in this isolate. Moreover, wehave analyzed six microsatellite markers (D6S299,D6S285, HLA DQB1 CAR1/CAR2, D6S273, TNFaIR2/IR4 and D6S291) in 16 cM spanning the MHCregion and negative lod scores were found (unpublisheddata). Due to the complexity and the high polymor-phism of the MHC and its known implication in theAID susceptibility, we have undertaken a detailed anal-ysis spanning 1.51 cM of the MHC chromosomal region.
In our study, we have found evidence for associationbetween HT and three different DR alleles (HLA-DR11,DR12 and DR01) with varying degrees of contribution(Table 2). This can be explained by intrafamilial heter-ogeneity. Indeed, each allele was associated with manynuclear families belonging to Akr pedigree and not withothers. Family based association test has also shown anassociation between AITDs and TNF �308 gene poly-morphism (p ¼ 0:004).
Linkage analyses using Genehunter program havefailed to detect any linkage with MHC gene polymor-phisms in Akr isolate split into 17 smaller pedigrees.However, Simwalk2 program, which is able to analyzecomplex pedigree with multiple inbreeding loops of anysize, was more powerful and has revealed linkage ofAITDs with TNF �308 gene polymorphism (p ¼ 0:03).This finding is in good agreement with previous findingsthat positive linkage could be missed when notanalyzing the pedigree as a whole [34].
The TNFa gene polymorphism and expression havebeen found to be involved in many AID [43e48]. On the
other hand, few studies which have investigated thispolymorphism in GD pathogenesis have reportedpositive association with TNF 2 allele in Polish andCaucasian populations (p! 0:0001, OR ¼ 4:38; p ¼3! 10�5, OR ¼ 2:2, respectively) [49,23].
There are two allelic forms in the TNF �308 genepolymorphism, referred to as TNF 1 (G) and TNF 2 (A).In the studied isolate, the A allele was associated withGD, whereas the G allele was rather associated with HT.The TNF 2 allele (A) was reported to be associated withhigh constitutive and inducible levels of the TNFa chain[50]. The promoter region of TNFA, in reporter genesystems, showed that the TNF 2 allele creates a promotersequence which is a more potent transcriptional activatorthan the TNF 1 allele [51e52]. However, conflicting datawere found concerning the transcriptional capacity ofthis allele [53e54]. It has also been demonstrated that inGD, thyrocytes express ‘‘de novo’’ HLA-DR antigensfollowing stimulation by TNF, TSH and INFg [55].This ‘‘de novo’’ expression could be implicated in thedevelopment of the autoimmune process in AITDs.
This study has assessed the relative contribution ofvarious immunomodulatory genes within the MHC tosusceptibility to AITDs in an isolate with high preva-lence of AITDs. Even in the absence of a confirmeddirect functional effect for TNF �308 gene polymor-phism, our genetic data clearly identify the latter asa marker of susceptibility to AITDs: the TNF 2 allelewas associated with GD, whereas the TNF 1 and DR11alleles were rather associated with HT. The associationdata alone do not help to understand the pathologicalmechanism of these genes. Functional analysis of TNFand HLA genes should be investigated to better under-stand their role in AITDs pathogenesis. Moreover,sequencing of HLA alleles found in the associatedhaplotype (HLA-A2-B50-TNF 2) will be of great interestmainly if we will find particular alleles.
Acknowledgements
Thisworkwas supportedby theMinisterede laRecher-che Scientifique et de la Technologie (MRST) (Tunisia)and the International Centre for Engineering and Bio-technology (ICGEB) (Italy). We thank Mr AbdelmajidDammak for his helpful review of the manuscript.

79N. Bougacha-Elleuch et al. / Journal of Autoimmunity 23 (2004) 75e80
References
[1] Vaidya B, Kendall-Taylor P, Pearce SHS. Genetics of endocrine
disease. The genetics of autoimmune thyroid disease. J Clin
Endocrinol Metab 2002;87(12):5385e97.[2] Maalej A, Makni H, Ayadi F, Bellassouad M, Jouida J, Bougacha
N, et al. A full genome screening in a large Tunisian family
affected with thyroid autoimmune disorders. Genes Immun 2001;
2:71e5.[3] Tomer Y, Ban Y, Concepcion E, Barbesino G, Villanueva R,
Greenberg DA, et al. Common and unique susceptibility loci
in Graves and Hashimoto diseases: results of whole-genome
screening in a data set of 102 multiplex families. Am J Hum Genet
2003;73(4):736e47.
[4] Vaidya B, Imrie H, Perros P, Young ET, Kelly WF, Carr D, et al.
The cytotoxic T lymphocyte antigen-4 is a major Graves’ disease
locus. Hum Mol Genet 1999;8(Jul (7)):1195e9.[5] Heward JM, Allahabadia A, Daykin J, Carr-Smith J, Daly A,
Armitage M, et al. Linkage disequilibrium between the human
leukocyte antigen class II region of the major histocompatibility
complex and Graves’ disease: replication using a population case
control and family-based study. J Clin Endocrinol Metab 1998;83:
3394e7.
[6] Uno H, Sasazuki T, Tamai H, Matsumoto H. Two major genes,
linked to HLA and Gm, control susceptibility to Graves’ disease.
Nature 1981;292:768e70.
[7] Shields DC, Ratanachaiyavong S, McGregor AM, Collins A,
Morton NE. Combined segregation and linkage analysis of
Graves’ disease with a thyroid autoantibody diathesis. Am J
Hum Genet 1994;55:540e54.
[8] Tomer Y, Barbesino G, Keddache M, Greenberg DA, Davies TF.
Mapping of a major susceptibility locus for Graves’ disease
(GD-1) to chromosome 14q31. J Clin Endocrinol Metab 1997;82:
1645e8.
[9] Roman SH, Greenberg D, Rubinstein P, Wallenstein S, Davies
TF. Genetics of autoimmune thyroid disease: lack of evidence for
linkage to HLA within families. J Clin Endocrinol Metab 1992;74:
496e503.
[10] Ban Y, Davies TF, Greenberg DA, Concepcion ES, Tomer Y.
The influence of human leukocyte antigen (HLA) genes on
autoimmune thyroid disease (AITD): results of studies in
HLA-DR3 positive AITD families. Clin Endocrinol (Oxf) 2002;
57(1):81e8.
[11] Mungall AJ, Palmer SA, Sims SK, Edwards CA, Ashurst JL,
Wilming L, et al. The DNA sequence and analysis of human
chromosome 6. Nature 2003;425:805e11.[12] Cuddihy RM, Dutton CM, Bahn RS. A polymorphism in the
extra cellular domain of the thyrotropin receptor is highly
associated with autoimmune thyroid disease in females. Thyroid
1995;5:89e95.[13] Pirro MT, De Filippis V, Di Cerbo A, Scillitani A, Liuzzi A, Tassi
V. Thyroperoxydase microsatellite polymorphism in thyroid
diseases. Thyroid 1995;5:461e4.
[14] Tomer Y, Greenberg DA, Concepcion E, Ban Y, Davies TF.
Thyroglobulin is a thyroid specific gene for the familial autoim-
mune thyroid diseases. J Clin Endocrinol Metab 2002;87:404e7.
[15] Kotsa KD, Watson PF, Weetman AP. No association between
a thyrotropin receptor gene polymorphism and Graves’ disease in
the female population. Thyroid 1997;7:31e3.
[16] Hadj Kacem H, Rebai A, Kaffel N, Masmoudi S, Abid M, Ayadi
H. PDS is a new susceptibility gene to autoimmune thyroid
diseases: association and linkage study. J Clin Endocrinol Metab
2003;88(May (5)):2274e80.
[17] Balkemore AI, Watson PF, Weetman AP, Duff GW. Association
of Graves’ disease with an allele of the interleukin-1 receptor
antagonist gene. J Clin Endocrinol Metab 1995;80:111e5.
[18] Cuddihy RM, Bahn RS. Lack of an association between alleles of
intereleukin-1 alpha and interleukin-1 receptor antagonist genes
and Graves’ disease in a North American Caucasian population.
J Clin Endocrinol Metab 1996;81:4476e8.
[19] Demaine A, Welsh KI, Hawe BS, Farid NR. Polymorphism of the
T cell receptor beta-chain in Graves’ disease. J Clin Endocrinol
Metab 1987;65:643e6.
[20] Stenszky V, Kozma L, Balazs C, Rochlitz S, Bear JC, Farid NR.
The genetics of Graves’ disease: HLA and disease susceptibility.
J Clin Endocrinol Metab 1985;61:735e40.
[21] Payami H, Joe S, Farid NR, Stenszky V, Chan SH, Yeo PP, et al.
Relative predispositional effects (RPEs) of marker alleles with
disease: HLA-DR alleles and Graves’ disease. Am J Hum Genet
1989;45:541e6.
[22] Yanagawa T, Mangklabruks A, Chang YB, Okamoto Y, Fifalen
ME, Curran PG, et al. Human histocompatibility leukocyte
antigen-DQ-A1*0501 allele associated with genetic susceptibility
to Graves’ disease in a Caucasian population. J Clin Endocrinol
Metab 1993;76:1569e74.[23] Hunt PJ, Marshall SE, Weetman AP, Bunce M, Bell JI, Wass JA,
et al. Histocompatibility leukocyte antigens and closely linked
immunomodulatory genes in autoimmune thyroid disease. Clin
Endocrinol (Oxf) 2001;55(Oct (4)):491e9.[24] Moens H, Farid NR, Sampson L, Noel EP, Barnard JM.
Hashimoto’s thyroiditis is associated with HLA-DRw3. N Engl
J Med 1978;299:133e4.
[25] Farid NR, Sampson L, Moens H, Barnard JM. The association of
goitrous autoimmune thyroiditis with HLA-DR5. Tissue Antigens
1981;17:265e8.
[26] Thompson C, Farid NR. Post-partum thyroiditis and goitrous
(Hashimoto’s) thyroiditis are associated with HLA-DR4. Immu-
nol Lett 1985;11:301e3.
[27] Heward JM, Allahabadia A, Sheppard MC, Barnett AH,
Franklyn JA, Gough SC. Associaton of the large multifunc-
tional proteasome (LMP2) gene with Graves’ disease is a result
of linkage disequilibrium with the HLA haplotype
DRB1*0304-DQB1*02-DQA1*0501. Clin Endocrinol 1999;
51(1):115e8.[28] Makni H, Maalej A, Ayadi F, Abid M, Jouida J, Ayadi H. Suivi
clinique et biologique d’une famille a haute prevalence de maladies
auto-immunes thyroidiennes. La Tunisie Medicale 1996;74(10):
433e8.[29] Kawazaki E. Sample preparation from blood, cells and other
fluids. In: Innis M, Gelffand D, Snisky G, White T, editors. PCR
protocols. A guide to methods and application. San Diego:
Academic Press; 1990. p. 146e52.
[30] Udalova IA, Nedospasov SA, Webb GC, Chaplin DD, Tur-
etskaya RL. Highly informative typing of the human TNF locus
using six adjacent polymorphic markers. Genomics 1993;16(Apr
(1)):180e6.
[31] Wilson AG, di Giovine FS, Balkemore AIF, Duff GW. Single
base polymorphism in the human tumor necrosis factor alpha
(TNFa) gene detectable by NcoI restriction of PCR product.
Hum Mol Genet 1993;1:353e9.
[32] Milner CM, Campell RD. Polymorphic analysis of the three
MHC-linked HSP70 genes. Immunogenetics 1992;36:357e62.[33] Kruglyak L, Daly MJ, Reeve-Daly MP, Lander ES. Parametric
and nonparametric linkage analysis: a unified multipoint ap-
proach. Am J Hum Genet 1996;58(Jun (6)):1347e63.
[34] Garner C, McInnes LA, Service SK, Spesny M, Fournier E, Leon
P, et al. Linkage analysis of a complex pedigree with severe
bipolar disorder, using a Markov chain Monte Carlo method. Am
J Hum Genet 2001;68(Apr (4)):1061e4.
[35] Sobel E, Lange K. Descent graphs in pedigree analysis:
applications to haplotyping, location scores, and marker-sharing
statistics. Am J Hum Genet 1996;58(Jun (6)):1323e37.

80 N. Bougacha-Elleuch et al. / Journal of Autoimmunity 23 (2004) 75e80
[36] Laird NM, Horvath S, Xu X. Implementing a unified approach
to family based tests of association. Genet Epidemiol 2000;
19(Suppl 1):36e42.
[37] Lake SL, Blacker D, Laird NM. Family based tests of association
in the presence of linkage. Am J Hum Genet 2000;67:1515e25.
[38] Spielman RS, McGinnis RE, Ewens WJ. Transmission test for
linkage disequilibrium: the insulin gene region and insulin-
dependent diabetes mellitus (IDDM). Am J Hum Genet 1993;
52:506e16.
[39] Curtis D, Sham PC. A note on the application of transmission
disequilibrium test when a parent is missing. Am J Hum Genet
1995;56:811e2.[40] Alkhateeb A, Steller GL, Old W, Talbert J, Uhlhorn C, Taylor M,
et al. Mapping of an autoimmunity susceptibility locus (AIS1) to
chromosome 1p31.3-p32.3. Hum Mol Genet 2002;11(6):661e7.[41] Fakhfakh F, Maalej A, Makni H, Abid M, Jouida J, Zouali M,
et al. Analysis of immunoglobulin VH and TCR Cb polymor-
phisms in a large family with thyroid autoimmune disorder. Exp
Clin Immunogenet 1999;16:185e91.[42] Maalej A, Bougacha N, Rebai A, BellassouadM, Ayadi-Makni F,
Abid M, et al. Lack of linkage and association between auto-
immune thyroid diseases and the CTLA-4 gene in a large Tunisian
family. Hum Immunol 2001;62:1245e50.[43] Yoon JW, Jun HS. Cellular and molecular pathogenic mecha-
nisms of insulin-dependent diabetes mellitus. Ann N Y Acad Sci
2001;928(Apr):200e11.
[44] Matsuno H, Yudoh K, Katayama R, Nakazawa F, Uzuki M,
Sawai T, et al. The role of TNF-alpha in the pathogenesis of
inflammation and joint destruction in rheumatoid arthritis (RA):
a study using a human RA/SCID mouse chimera. Rheumatology
(Oxf) 2002;41(Mar (3)):329e37.
[45] Romas E, Gillespie MT, Martin TJ. Involvement of receptor
activator of NFkappaB ligand and tumor necrosis factor-alpha in
bone destruction in rheumatoid arthritis. Bone 2002;30(Feb (2)):
340e6.
[46] Zuniga J, Vargas-Alrcion G, Hernandez-Pacheco G, Portal-
Celhay C, Yamamoto-Furusho JK, Granados J. Tumor necrosis
factor-alpha promoter polymorphisms in Mexican patients with
systemic lupus erythematosus (SLE). Genes Immun 2001;
2(Nov (7)):363e6.
[47] Mycko M, Kowalski W, Kwinkowski M, Buenafe AC, Szyman-
ska B, Tronczynska E, et al. Multiple sclerosis: the frequency of
allelic forms of tumor necrosis factor and lymphotoxin-alpha.
J Neuroimmunol 1998;84(Apr 15 (2)):198e206.
[48] Arias AI, Giles B, Eiermann TH, Sterry W, Pandey JP. Tumor
necrosis factor-alpha gene polymorphism in psoriasis. Exp Clin
Immunogenet 1997;14(2):118e22.
[49] Kula D, Jurecka-Tuleja B, Gubala E, Krawczyk A, Szpak S,
Jarzab M. Association of polymorphism of LTa and TNF genes
with Graves’ disease. Folia Histochem Cytobiol 2001;39(Suppl 2):
77e8.
[50] Wilson AG, Symons JA, Mc Dowell TL, di Giovani FS, Duff
GW. Effects of a tumor necrosis factor (TNFa) promotor base
transition on transcriptional activity. Br J Rheumatol 1994;33:
89e97.
[51] Kroeger KM, Carville KS, Abraham LJ. The �308 tumor
necrosis factor-alpha promoter polymorphism affects transcrip-
tion. Mol Immunol 1997;34:391e9.
[52] Wilson AG, Symons JA, McDowell TL, McDevitt HO, Duff GW.
Effects of apolymorphism in the human tumor necrosis factor
a promoter on transcriptional activation. Proc Natl Acad Sci
USA 1997;94:3195e9.
[53] Brinkman BM, Zuijdgeest D, Kaijzel EL, Breedved FC, Verweij
CL. Relevance of the tumor necrosis factor a (TNFa)-308
promoter polymorphism in TNFa gene regulation. J Inflamm
1996;46:32e41.
[54] Stuber F, Udalova IA, Book M, Drutskaya LN, Kuprash DV,
Turetskaya RL, et al. �308 tumor necrosis factor (TNF) poly-
morphism is not associated with survival in severe sepsis and is
unrelated to lipopolysaccharide inducibility of the human TNF
promoter. J Inflamm 1996;46(1):42e50.
[55] Kissonerghis AM, Grubeck-loebenstein B, Pirich K, Feldmann
M, Londei M. Tumor necrosis factor synergises with gamma
interferon on the induction of mRNA for DR alpha chain on
thyrocytes from Graves’ disesase and no toxic goitre. Autoimmu-
nity 1989;4(4):255e66.
Copyright © 2022 FDOKUMEN