Analgesic efficacy of ultrasound-guided regional anesthesia: a meta-analysis
7
Original contribution Analgesic efficacy of ultrasound-guided regional anesthesia: a meta-analysis ☆ Harold J. Gelfand MD (Fellow), Jean-Pierre P. Ouanes DO (Senior Instructor), Maggie R. Lesley MD (Research Assistant), Phebe S. Ko MD (Research Assistant), Jamie D. Murphy MD (Assistant Professor), Shawn M. Sumida MD (Assistant Professor), Gillian R. Isaac MD, PhD (Assistant Professor), Kanupriya Kumar MD (Assistant Professor), Christopher L. Wu MD (Professor) ⁎ Department of Anesthesiology and Critical Care Medicine, The Johns Hopkins University, Baltimore, MD 21287, USA Received 30 August 2010; revised 3 December 2010; accepted 15 December 2010 Keywords: Meta-analysis; Regional anesthesia; Ultrasonography Abstract Study Objective: To determine if the use of ultrasound guidance (vs non-ultrasound techniques) improves the success rate of nerve blocks. Design: Meta-analysis of randomized controlled trials (RCTs) in the published literature. Setting: University medical center. Measurements: 16 RCTs of patients undergoing elective surgical procedures were studied. Patients underwent ultrasound-guided or non-ultrasound techniques (nerve stimulation, surface landmark) for peripheral nerve blocks. Success rates were measured. Main Results: Ultrasound guidance (vs all non-ultrasound techniques) was associated with a significant increase in the success rate of nerve blocks [relative risk (RR) = 1.11 (95% confidence interval [CI]: 1.06 to 1.17, P b 0.0001]). When compared with nerve stimulator techniques only, ultrasound guidance was still associated with an increase in the success rate (RR = 1.11 [95% CI: 1.05 to 1.17, P = 0.0001]). For specific blocks, ultrasound guidance (vs all non-ultrasound) was associated with a significant increase in successful brachial plexus (all) nerve blocks (RR = 1.11 [95% CI: 1.05 to 1.20, P = 0.0001]), sciatic popliteal nerve block (RR = 1.22 [95% CI: 1.08 to 1.39, P = 0.002]) and brachial plexus axillary nerve block (RR = 1.13 [95% CI: 1.00 to 1.26, P = 0.05]) but not brachial plexus infraclavicular nerve block (RR = 1.25 [95% CI: 0.88 to 1.76, P = 0.22]). Conclusions: Ultrasound-guided peripheral nerve block is associated with an increased overall success rate when compared with nerve stimulation or other methods. Ultrasound-guided techniques also increase the success rate of some specific blocks. © 2011 Elsevier Inc. All rights reserved. 1. Introduction The use of ultrasound-guided peripheral nerve blocks has increased in popularity over the past decade and been reported for many types of peripheral nerve blocks in both ☆ Supported by the Department of Anesthesiology and Critical Care Medicine, The Johns Hopkins University, Baltimore, MD, USA. ⁎ Corresponding author. Tel.: +1 410 955 5608; fax: + 410 614 1796. E-mail address: [email protected] (C.L. Wu). 0952-8180/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.jclinane.2010.12.005 Journal of Clinical Anesthesia (2011) 23, 90–96
Transcript of Analgesic efficacy of ultrasound-guided regional anesthesia: a meta-analysis

Journal of Clinical Anesthesia (2011) 23, 90–96
Original contribution
Analgesic efficacy of ultrasound-guided regionalanesthesia: a meta-analysis☆
Harold J. Gelfand MD (Fellow), Jean-Pierre P. Ouanes DO (Senior Instructor),Maggie R. Lesley MD (Research Assistant), Phebe S. Ko MD (Research Assistant),Jamie D. Murphy MD (Assistant Professor), Shawn M. Sumida MD (Assistant Professor),Gillian R. Isaac MD, PhD (Assistant Professor),Kanupriya Kumar MD (Assistant Professor), Christopher L. Wu MD (Professor)⁎
Department of Anesthesiology and Critical Care Medicine, The Johns Hopkins University, Baltimore, MD 21287, USA
Received 30 August 2010; revised 3 December 2010; accepted 15 December 2010
M
0d
Keywords:Meta-analysis;Regional anesthesia;Ultrasonography
AbstractStudy Objective: To determine if the use of ultrasound guidance (vs non-ultrasound techniques)improves the success rate of nerve blocks.Design: Meta-analysis of randomized controlled trials (RCTs) in the published literature.Setting: University medical center.Measurements: 16 RCTs of patients undergoing elective surgical procedures were studied. Patientsunderwent ultrasound-guided or non-ultrasound techniques (nerve stimulation, surface landmark) forperipheral nerve blocks. Success rates were measured.Main Results: Ultrasound guidance (vs all non-ultrasound techniques) was associated with a significantincrease in the success rate of nerve blocks [relative risk (RR) = 1.11 (95% confidence interval [CI]:1.06 to 1.17, P b 0.0001]). When compared with nerve stimulator techniques only, ultrasound guidancewas still associated with an increase in the success rate (RR = 1.11 [95% CI: 1.05 to 1.17, P = 0.0001]).For specific blocks, ultrasound guidance (vs all non-ultrasound) was associated with a significantincrease in successful brachial plexus (all) nerve blocks (RR = 1.11 [95% CI: 1.05 to 1.20, P = 0.0001]),sciatic popliteal nerve block (RR = 1.22 [95% CI: 1.08 to 1.39, P = 0.002]) and brachial plexus axillarynerve block (RR = 1.13 [95% CI: 1.00 to 1.26, P = 0.05]) but not brachial plexus infraclavicular nerveblock (RR = 1.25 [95% CI: 0.88 to 1.76, P = 0.22]).Conclusions: Ultrasound-guided peripheral nerve block is associated with an increased overall successrate when compared with nerve stimulation or other methods. Ultrasound-guided techniques alsoincrease the success rate of some specific blocks.© 2011 Elsevier Inc. All rights reserved.
☆ Supported by the Department of Anesthesiology and Critical Careedicine, The Johns Hopkins University, Baltimore, MD, USA.⁎ Corresponding author. Tel.: +1 410 955 5608; fax: + 410 614 1796.E-mail address: [email protected] (C.L. Wu).
952-8180/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.jclinane.2010.12.005
1. Introduction
The use of ultrasound-guided peripheral nerve blocks hasincreased in popularity over the past decade and beenreported for many types of peripheral nerve blocks in both

91Meta-analysis of ultrasound-guided blocks
adults and children [1-5]. Although the superior visualizationand localization for injection of local anesthetic provided byultrasound guidance theoretically would result in a reductionin complication rates (eg, neurologic injuries), this has notbeen definitively proven [6,7]. Previous reviews and meta-analyses indicate that ultrasound-guided regional anesthesiamay offer many benefits including a higher block successrate, decreased time to onset of blocks, and possiblyimproved quality of sensory block [8-12]. However, thesemeta-analyses have not examined the analgesic efficacy ofultrasound guidance for specific peripheral nerve blocks. Weundertook a systematic review and meta-analysis to examinethis issue. Our primary outcome measure was the successrate for upper and lower extremity peripheral nerve blocksusing ultrasound-guided (vs non-ultrasound) techniques.
2. Materials and methods
This study qualified for exemption from the JohnsHopkins Institutional Review Board. The National Library
Table 1 Study characteristics
Study Study population Subjects (n) Blo
Casati et al, 2007 [13] M/F adults 30 US/30 C AxiChan et al, 2007 [14] M/F adults 62 US/64 C Axi
Danelli et al, 2009 [15] M/F adults 22 US/22 C PopKapral et al, 2008 [16] M/F adults 80 US/80 C Inte
bracLiu FC et al, 2005 [17] M/F adults 30 US/30 C Axi
Liu SS et al, 2009 [19] M/F adults 115 US/115 C Intebrac
Marhofer et al, 2004 [18] M/F children 20 US/20 C Infrbrac
Macaire et al, 2008 [20] M/F 30 US/30 C Medulna
Oberndorfer et al, 2007 [21] M/F children 23 US/23 C Femscia
Perlas et al, 2008 [22] M/F adults 37 US/37 C Pop
Ponde and Diwan, 2009 [23] M/F children 25 US/25 C Infrbrac
Sauter et al, 2008 [24] M/F adults 40 US/40 C Infrbrac
Sites et al, 2006 [25] M/F adults 28 US/28 C AxiSoeding et al, 2005 [26] M/F adults 20 US/20 C Axi
bracvan Geffen et al, 2009 [27] M/F adults 20 US/20 C PopYu et al, 2007 [28] M/F adults 40 US/40 C Axi
US = ultrasound, C = control, F = female, M = male, Axill brach plex = axillaBupiv = bupivacaine, Lido = lidocaine, epineph = epinephrine, Poplit = poplitealInfraclavic brach plex = infraclavicular brachial plexus, Levobupiv = levobupiva
of Medicine's PUBMED database was searched for the timeperiod 1966 to August 15, 2009, using the textwordsultrasound and nerve block or nerve or interscalene orbrachial plexus or femoral or sciatic or axillary or infra-clavicular or supraclavicular or lumbar plexus or popliteal.These two searches were combined using the usual Booleanmeaning of “AND,” limited to randomized controlled trials(RCTs). Each abstract was then reviewed by one of theauthors for inclusion into the meta-analysis. No minimumsample sizes were invoked for inclusion of studies in theanalysis. Any disputes were resolved by agreement of atleast two reviewers.
For the purposes of this meta-analysis, the primaryoutcome for assessment was the success rate of single-shotperipheral (upper and lower extremity) nerve blocks forsurgical procedures. Success was defined as anesthesiasufficient for surgery without supplementation either withadditional nerve blocks or general anesthesia. Inclusioncriteria included nerve blocks conducted for a surgical pro-cedure and randomized comparison of ultrasound alone to amethod without ultrasound for nerve localization. There wasno age limitation. We excluded any trials that studied the use
ck Control Local anesthetic
ll brach plex Nerve stim Ropiv 0.75% 20 mLll brach plex Nerve stim Bupiv 0.5% + Lido 2% + epineph
1:200K 42 mLlit sciatic Nerve stim Ropiv 0.75% 20 mLrscalh plex
Nerve stim Ropiv 0.75% 20 mL
ll brach plex Nerve stim Lido 1.5% 0.5 mL/kg + epineph5 µg/kg
rscalh plex
Nerve stim Mepiv 1.5% + epineph 1:300K +NaCO3 (1 mEq/10 mL). Pts b 50 kg:45–55 mL. Pts ≥ 50 kg: 55–65 mL
aclavich plex
Nerve stim Ropiv 0.5% 0.5 mL/kg
ian &r nerve
Nerve stim Mepiv 1.5% 4 mL at each nerve
oral &tic nerve
Nerve stim C: Levobupiv 0.5% 0.3 mL/kg U:Levobupiv 0.5% 0.2 [0.06] mL/kg(sciat) 0.15 [0.04] mL/kg (feml)
lit sciatic Nerve stim Lidocaine 1% + 0.25% bupiv +epineph 1:400K 30 mL
aclavich plex
Nerve stim Bupiv 0.5% 0.5 mL/kg
aclavich plex
Nerve stim Mepiv 1.5% + 1:400K epineph0.6 mL/kg
ll brach plex Transarterial Lido 1.5% 30 mLll/interscalh plex
Landmark Ropiv 0.75% 3 mg/kg (interscal)Ropiv 0.6% 3 mg/kg (axill)
lit sciatic Nerve stim Lido 1.5% + epineph 1:200Kllary Nerve stim Ropiv 0.75% + lido 2%
ry brachial plexus, Nerve stim = nerve stimulation, Ropiv = ropivacaine,, Interscal brach plex = interscalene brachial plexus, Mepiv = mepivacaine,caine, sciat = sciatic, feml = femoral.

92 H.J. Gelfand et al.
of ultrasound in conjunction with another method forguidance and those where the purpose of the nerve blockwas not for a surgical procedure (eg, biopsies, positioning).
Relevant data were collected from each article and theresults were recorded. Data were extrapolated from figuresand tables as needed. The primary outcome was overallsuccess rate of peripheral nerve blocks versus those withoutultrasound guidance. Studies were excluded from analysis ifthey reported no comparative information on the magnitudeof the treatment effect. All statistical analyses, includingassessment of heterogeneity, were performed with RevManVersion 5.0. (The Nordic Cochrane Centre, The CochraneCollaboration, Copenhagen, DK, 2008). A random-effectsmodel was used. The level of significance for all tests wasset at an alpha level ≤0.05.
3. Results
Our search resulted in 525 abstracts, of which a total of16 met all inclusion criteria. There were 1,264 subjects in the16 randomized trials used for this meta-analysis. A totalof 508 articles were rejected for the following reasons: 448did not evaluate ultrasound-guided nerve blocks in surgicalprocedures, 30 were not RCTs, 24 did not compareultrasound alone versus control, 5 did not assess upper orlower extremity single-shot nerve blocks, and one did notassess surgical success rate. Table 1 provides a detailedoverview of the studies included in the analysis [13-28].
Fig. 1 Success rate (all blocks): ultrasound versus all non-ultrasound tecguidance on the success rate of peripheral nerve blocks versus all coneach experimental group. “n” = number of patients who had a successfulof RR = 1 (indicating “no difference”), suggesting that nerve blocks guidCI: 1.06 to 1.17), P b 0.0001].
Fig. 1 shows the pooled estimate (meta-analysis)demonstrating the effect of ultrasound guidance onperipheral nerve blocks as compared with all methods ofcontrol. Ultrasound guidance (vs all non-ultrasound) wasassociated with a significant increase in the success rate ofnerve blocks (relative risk [RR] = 1.11 [95% confidenceinterval (CI): 1.06 to 1.17, P b 0.0001]). When comparedwith nerve stimulator techniques only, ultrasound guidancewas still associated with an increase in the success rate(RR = 1.11 [95% CI: 1.05 to 1.17, P = 0.0001]) (Fig. 2).For specific blocks, ultrasound guidance (vs all non-ultrasound) was associated with a significant increase insuccessful brachial plexus nerve block (RR = 1.11 [95%CI: 1.05 to 1.20, P = 0.0001]) (Fig. 3), sciatic poplitealnerve block (RR = 1.22 [95% CI: 1.08 to 1.39, P = 0.002])(Fig. 4) and brachial plexus axillary nerve block (RR = 1.13[95% CI: 1.00 to 1.26, P = 0.05]) (Fig. 5) but not brachialplexus infraclavicular nerve block (RR = 1.25 [95% CI: 0.88to 1.76, P = 0.22]) (Fig. 6).
4. Discussion
When the cumulative data were pooled and analyzed forall blocks, our analysis found a significant increase in theoverall success rate for blocks performed using anultrasound-guided technique versus all non-ultrasoundtechniques. There was a significant increase in the overallsuccess rate for ultrasound-guided technique only when
hniques. The weighted (pooled) estimate for the effect of ultrasoundtrol methods of nerve localization. “N” = number of subjects innerve block. The entire diamond (pooled estimate) lies to the righted by ultrasound are more likely to be successful [RR = 1.11 (95%
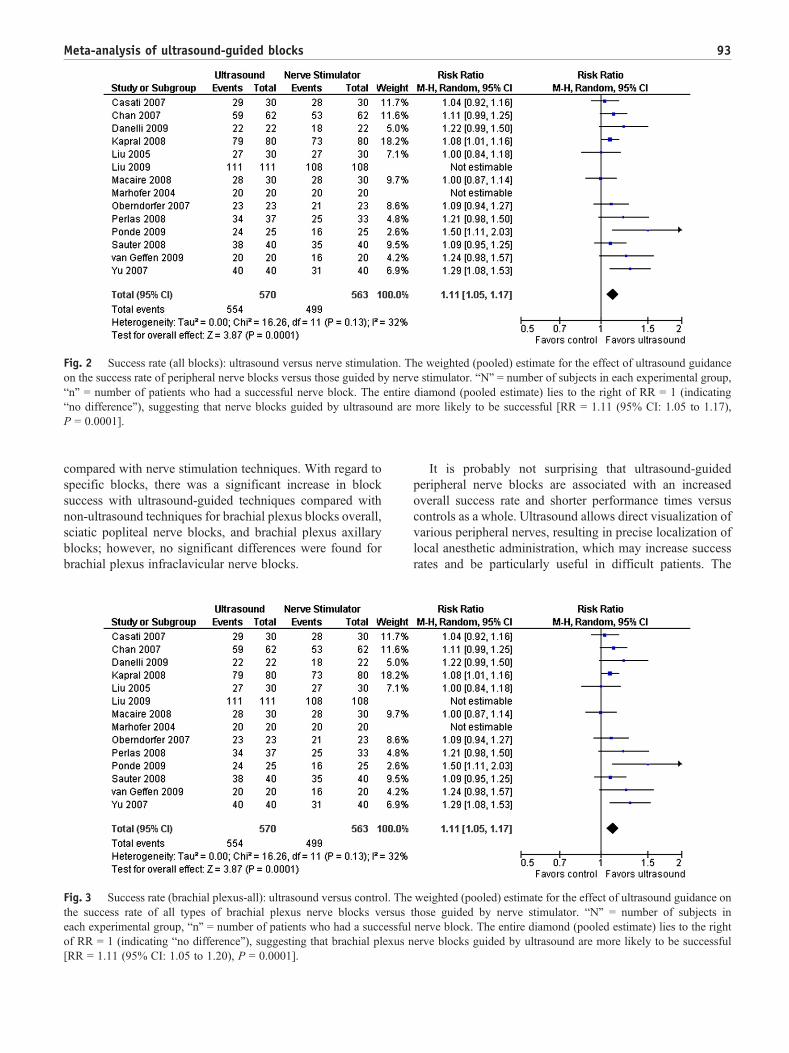
Fig. 2 Success rate (all blocks): ultrasound versus nerve stimulation. The weighted (pooled) estimate for the effect of ultrasound guidanceon the success rate of peripheral nerve blocks versus those guided by nerve stimulator. “N” = number of subjects in each experimental group,“n” = number of patients who had a successful nerve block. The entire diamond (pooled estimate) lies to the right of RR = 1 (indicating“no difference”), suggesting that nerve blocks guided by ultrasound are more likely to be successful [RR = 1.11 (95% CI: 1.05 to 1.17),P = 0.0001].
93Meta-analysis of ultrasound-guided blocks
compared with nerve stimulation techniques. With regard tospecific blocks, there was a significant increase in blocksuccess with ultrasound-guided techniques compared withnon-ultrasound techniques for brachial plexus blocks overall,sciatic popliteal nerve blocks, and brachial plexus axillaryblocks; however, no significant differences were found forbrachial plexus infraclavicular nerve blocks.
Fig. 3 Success rate (brachial plexus-all): ultrasound versus control. Thethe success rate of all types of brachial plexus nerve blocks versuseach experimental group, “n” = number of patients who had a successfulof RR = 1 (indicating “no difference”), suggesting that brachial plexus n[RR = 1.11 (95% CI: 1.05 to 1.20), P = 0.0001].
It is probably not surprising that ultrasound-guidedperipheral nerve blocks are associated with an increasedoverall success rate and shorter performance times versuscontrols as a whole. Ultrasound allows direct visualization ofvarious peripheral nerves, resulting in precise localization oflocal anesthetic administration, which may increase successrates and be particularly useful in difficult patients. The
weighted (pooled) estimate for the effect of ultrasound guidance onthose guided by nerve stimulator. “N” = number of subjects innerve block. The entire diamond (pooled estimate) lies to the righterve blocks guided by ultrasound are more likely to be successful

PP
Fig. 4 Success rate (sciatic popliteal): ultrasound versus control. The weighted (pooled) estimate for the effect of ultrasound guidance on thesuccess rate of sciatic popliteal nerve blocks versus all control methods of nerve localization. “N” = number of subjects in each experimentalgroup, “n” = number of patients who had a successful nerve block. The entire diamond (pooled estimate) lies to the right of RR = 1 (indicating“no difference”), suggesting that sciatic popliteal nerve blocks guided by ultrasound are more likely to be successful [RR = 1.22 (95% CI: 1.08to 1.39), P = 0.002].
94 H.J. Gelfand et al.
ability to directly visualize the target nerve may be associatedwith shorter procedure times (vs traditional techniques) andalso a reduction in block-related complications (presumablyrelated to visualization of needle contact with nerves),despite potential challenges associated with ultrasound-guided regional anesthesia [29].
Our results are similar to those found in previoiussystematic reviews and meta-analyses. A meta-analysis of13 RCTs found that peripheral nerve blocks performed usingultrasound guidance were more likely to be successful [12].Another systematic review of 16 RCTs found that use ofultrasound for upper and lower extremity nerve blocks wasassociated with a better quality of block [11]. Although wedid not assess for outcomes other than block success, otherauthors have noted that the use of ultrasound for nerve blocksis associated with significantly less time to perform blocks,faster onset and longer duration of analgesia, and decreasedthe risk of vascular puncture or hematoma formation duringthe block procedure [10-12].
There are several limitations of our meta-analysis. Theavailable number of subjects for our analysis was relativelysmall, with many studies having b50 subjects in each group.As such, we were unable to determine the efficacy ofultrasound on other outcomes such as “safety” (ie, incidenceof neurological injury). It should be noted that these studies
PP
Fig. 5 Success rate (brachial plexus axillary): ultrasound versus conguidance on the success rate of brachial plexus axillary nerve blocks versuin each experimental group, “n” = number of patients who had a successfuof RR = 1 (indicating “no difference”), suggesting that brachial plexussuccessful [RR = 1.13 (95% CI: 1.00 to 1.26), P = 0.05].
were performed at centers where providers performing theprocedures were likely to be highly skilled in ultrasound-guided techniques; thus, their conclusions may reflect gainshad by the most experienced of providers and these resultsmay or may not be generalizable to other anesthesiologists.In addition, the definition of “success” was somewhatarbitrary and another definition for success may providedifferent results. The process of a meta-analysis requirespooling of different data sources (eg, pediatric and adultpatients, different volumes/doses of local anesthetics) and, assuch, it may be difficult to extrapolate the results of the meta-analysis to a particular patient.
Because of the limited nature of data in the availableRCTs, we were unable to perform any meaningful cost-effeciveness analysis or analysis of patient-oriented outcomessuch as satisfaction. Methodologic quality assessments of theconstituent studies were not performed but the failure tocompletely report method does not necessarily implyinadequacy of a specific study [30]. As it stands, the role ofmethodologic quality indicators is uncertain [3,31,32].Finally, the general limitations of meta-analyses are wellrecognized and have been mentioned elsewhere [33,34].
In summary, our meta-analysis suggests that ultrasound-guided peripheral nerve blocks (vs traditional techniques) areassociated with increased overall success rate, even when
trol. The weighted (pooled) estimate for the effect of ultrasounds all control methods of nerve localization. “N” = number of subjectsl nerve block. The entire diamond (pooled estimate) lies to the rightaxillary nerve blocks guided by ultrasound are more likely to be

PP
Fig. 6 Success rate (brachial plexus infraclavicular): ultrasound versus control. The weighted (pooled) estimate for the effect of ultrasoundguidance on the success rate of brachial plexus infraclavicular nerve blocks versus all control methods of nerve localization. “N” = number ofsubjects in each experimental group. “n” = number of patients who had a successful nerve block. The entire diamond (pooled estimate) crossesRR = 1 (indicating “no difference”), suggesting that brachial plexus infraclavicular nerve blocks guided by ultrasound may not be moresuccessful than other techniques of localization [RR = 1.25 (95% CI: 0.88 to 1.76), P = 0.22].
95Meta-analysis of ultrasound-guided blocks
compared with that by nerve stimulation only. Furthermore,ultrasound-guided techniques increase the success rate ofsome specific blocks (brachial plexus – overall, sciaticpopliteal nerve and brachial plexus axillary nerve blocks) butnot brachial plexus infraclavicular blocks. Many questionsregarding the overall efficacy of ultrasound-guided periph-eral nerve blocks remain unanswered and additional studiesare required to elucidate their role in other aspects of regionalanesthesia [35,36]. Advances in technology, technique, andadditional research may allow for more definitive assessmentof ultrasound as a tool for the successful performance ofperipheral nerve blocks.
Acknowledgment
The authors wish to thank Dr. Shy-Hsien Wu and Tsai-LienWu for their assistance in Mandarin Chinese translation.
References
[1] Salinas FV. Ultrasound and review of evidence for lower extremityperipheral nerve blocks. Reg Anesth Pain Med 2010;35(2 Suppl):S16-25.
[2] McCartney CJ, Lin L, Shastri U. Evidence basis for the use ofultrasound for upper-extremity blocks. Reg Anesth Pain Med 2010;35(2 Suppl):S10-5.
[3] Tsui BC, Pillay JJ. Evidence-based medicine: Assessment ofultrasound imaging for regional anesthesia in infants, children, andadolescents. Reg Anesth Pain Med 2010;35(2 Suppl):S47-54.
[4] Tsui BC, Suresh S. Ultrasound imaging for regional anesthesia ininfants, children, and adolescents: a review of current literature and itsapplication in the practice of neuraxial blocks. Anesthesiology2010;112:719-28.
[5] Tsui B, Suresh S. Ultrasound imaging for regional anesthesia ininfants, children, and adolescents: a review of current literature and itsapplication in the practice of extremity and trunk blocks. Anesthesi-ology 2010;112:473-92.
[6] Neal JM. Ultrasound-guided regional anesthesia and patient safety: anevidence-based analysis. Reg Anesth Pain Med 2010;35(2 Suppl):S59-67.
[7] Barrington MJ, Watts SA, Gledhill SR, et al. Preliminary results of theAustralasian Regional Anaesthesia Collaboration: a prospective auditof more than 7000 peripheral nerve and plexus blocks for neurologicand other complications. Reg Anesth Pain Med 2009;34:534-41.
[8] Liu SS, Ngeow J, John RS. Evidence basis for ultrasound-guided blockcharacteristics: onset, quality, and duration. Reg Anesth Pain Med2010;35(2 Suppl):S26-35.
[9] Neal JM, Brull R, Chan VW, et al. The ASRA evidence-basedmedicine assessment of ultrasound-guided regional anesthesia andpain medicine: executive summary. Reg Anesth Pain Med 2010;35(2Suppl):S1-9.
[10] Walker KJ, McGrattan K, Aas-Eng K, et al. Ultrasound guidance forperipheral nerve blockade. Cochrane Database Syst Rev 2009;4:CD006459.
[11] Liu SS, Ngeow JE, Yadeau JT. Ultrasound-guided regional anesthesiaand analgesia: a qualitative systematic review. Reg Anesth Pain Med2009;34:47-59.
[12] Abrahams MS, Aziz MF, Fu RF, et al. Ultrasound guidance comparedwith electrical neurostimulation for peripheral nerve block: asystematic review and meta-analysis of randomized controlled trials.Br J Anaesth 2009;102:408-17.
[13] Casati A, Danelli G, Baciarello M, et al. A prospective, randomizedcomparison between ultrasound and nerve stimulation guidance formultiple injection axillary brachial plexus block. Anesthesiology2007;106:992-6.
[14] Chan VW, Perlas A, McCartney CJ, et al. Ultrasound guidanceimproves success rate of axillary brachial plexus block. Can J Anaesth2007;54:176-82.
[15] Danelli G, Fanelli A, Ghisi D, et al. Ultrasound vs nerve stimulationmultiple injection technique for posterior popliteal sciatic nerve block.Anaesthesia 2009;64:638-42.
[16] Kapral S, Greher M, Huber G, et al. Ultrasonographic guidanceimproves the success rate of interscalene brachial plexus blockade.Reg Anesth Pain Med 2008;33:253-8.
[17] Liu FC, Liou JT, Tsai YF, et al. Efficacy of ultrasound-guided axillarybrachial plexus block: a comparative study with nerve stimulator-guided method. Chang Gung Med J 2005;28:396-402.
[18] Marhofer P, Sitzwohl C, Greher M, et al. Ultrasound guidance forinfraclavicular brachial plexus anaesthesia in children. Anaesthesia2004;59:642-6.
[19] Liu SS, Zayas VM, Gordon MA, et al. A prospective, randomized,controlled trial comparing ultrasound versus nerve stimulator guidancefor interscalene block for ambulatory shoulder surgery for postoper-ative neurological symptoms. Anesth Analg 2009;109:265-71.
[20] Macaire P, Singelyn F, Narchi P, et al. Ultrasound- or nervestimulation-guided wrist blocks for carpal tunnel release: arandomized prospective comparative study. Reg Anesth Pain Med2008;33:363-8.

96 H.J. Gelfand et al.
[21] Oberndorfer U, Marhofer P, Bösenberg A, et al. Ultrasonographicguidance for sciatic and femoral nerve blocks in children. Br J Anaesth2007;98:797-801.
[22] Perlas A, Brull R, Chan VW, et al. Ultrasound guidance improves thesuccess of sciatic nerve block at the popliteal fossa. Reg Anesth PainMed 2008;33:259-65.
[23] Ponde VC, Diwan S. Does ultrasound guidance improve the successrate of infraclavicular brachial plexus block when compaired withnerve stimulation in children with radial club hands? Anesth Analg2009;108:1967-70.
[24] Sauter AR, Dodgson MS, Stubhaug A, et al. Electrical nervestimulation or ultrasound guidance for lateral sagittal infraclavicularblocks: a randomized, controlled, observer-blinded, comparativestudy. Anesth Analg 2008;106:1910-5.
[25] Sites BD, Beach ML, Spence BC, et al. Ultrasound guidance improvesthe success rate of a perivascular axillary plexus block. ActaAnaesthesiol Scand 2006;50:678-84.
[26] Soeding PE, Sha S, Royse CE, et al. A randomized trial of ultrasound-guided brachial plexus anaesthesia in upper limb surgery. AnaesthIntensive Care 2005;33:719-25.
[27] van Geffen GJ, van den Broek E, Braak GJ, et al. A prospectiverandomised controlled trial of ultrasound guided versus nervestimulation guided distal sciatic nerve block at the popliteal fossa.Anaesth Intensive Care 2009;37:32-7.
[28] Yu W, Xu X, Wu DS, Guo XY, Huang PT. Efficacy of axillaryapproach brachial plexus blocking by ultrasound-guided four points
via one-puncture technique. Zhonghua Yi Xue Za Zhi (Natl Med JChina) 2007;87:740-5.
[29] Chin KJ, Perlas A, Chan VW, et al. Needle visualization in ultrasound-guided regional anesthesia: challenges and solutions. Reg Anesth PainMed 2008;33:532-44.
[30] Juni P, Witschi A, Bloch R, et al. The hazards of scoring the quality ofclinical trials for meta-analysis. JAMA 1999;282:1054-60.
[31] Hueiler-Muntener K, Juni P, Junker C, et al. Quality reporting ofrandomized trials as a measure of methodologic quality. JAMA2002;287:2801-4.
[32] Whiting P, Harbord R, Kleijnen J. No role for quality scores insystematic reviews of diagnostic accuracy studies. BMC Med ResMethodol 2005;5:19.
[33] Hurley RW, Cohen SP, Williams KA, et al. The analgesic effects ofperioperative gabapentin on postoperative pain: a meta-analysis. RegAnesth Pain Med 2006;31:237-47.
[34] Wu CL, Cohen SR, Richman JM, et al. Efficacy of postoperativepatient-controlled and continuous infusion epidural analgesia versusintravenous patient-controlled analgesia with opioids: a meta-analysis.Anesthesiology 2005;103:1079-88.
[35] Saranteas T, Chantzi C, Iatrou C, et al. Ultrasound and regionalanesthesia techniques–is there any limitation? Reg Anesth Pain Med2007;32:546-7.
[36] Harrop-Griffiths AW, Denny NM. Eponymity and the age ofultrasound: how should new blocks be introduced into clinicalpractice? Reg Anesth Pain Med 2006;31:492-5.