
An overview of cardiovascular disease burden in the United States
12
At the Intersection of Health, Health Care and Policy doi: 10.1377/hlthaff.26.1.38 , 26, no.1 (2007):38-48 Health Affairs An Overview Of Cardiovascular Disease Burden In The United States George A. Mensah and David W. Brown Cite this article as: http://content.healthaffairs.org/content/26/1/38.full.html available at: The online version of this article, along with updated information and services, is For Reprints, Links & Permissions: http://healthaffairs.org/1340_reprints.php http://content.healthaffairs.org/subscriptions/etoc.dtl E-mail Alerts : http://content.healthaffairs.org/subscriptions/online.shtml To Subscribe: from the Publisher. All rights reserved. including photocopying or by information storage or retrieval systems, without prior written permission may be reproduced, displayed, or transmitted in any form or by any means, electronic or mechanical, Health Affairs Foundation. As provided by United States copyright law (Title 17, U.S. Code), no part of by Project HOPE - The People-to-People Health 2007 Bethesda, MD 20814-6133. Copyright © is published monthly by Project HOPE at 7500 Old Georgetown Road, Suite 600, Health Affairs Not for commercial use or unauthorized distribution by guest on June 1, 2013 Health Affairs by content.healthaffairs.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of An overview of cardiovascular disease burden in the United States
At the Intersection of Health, Health Care and Policy
doi: 10.1377/hlthaff.26.1.38
, 26, no.1 (2007):38-48Health AffairsAn Overview Of Cardiovascular Disease Burden In The United States
George A. Mensah and David W. BrownCite this article as:
http://content.healthaffairs.org/content/26/1/38.full.html
available at: The online version of this article, along with updated information and services, is
For Reprints, Links & Permissions: http://healthaffairs.org/1340_reprints.php
http://content.healthaffairs.org/subscriptions/etoc.dtlE-mail Alerts : http://content.healthaffairs.org/subscriptions/online.shtmlTo Subscribe:
from the Publisher. All rights reserved.including photocopying or by information storage or retrieval systems, without prior written permission may be reproduced, displayed, or transmitted in any form or by any means, electronic or mechanical,
Health Affairs Foundation. As provided by United States copyright law (Title 17, U.S. Code), no part of by Project HOPE - The People-to-People Health2007Bethesda, MD 20814-6133. Copyright ©
is published monthly by Project HOPE at 7500 Old Georgetown Road, Suite 600,Health Affairs
Not for commercial use or unauthorized distribution
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

An Overview Of CardiovascularDisease Burden In The UnitedStatesData show a growing burden from cardiovascular disease in the U.S.population; now is the time to reverse those trends.
by George A. Mensah and David W. Brown
ABSTRACT: Cardiovascular disease (CVD) is the leading cause of death and a major causeof disability worldwide. In the United States, CVD accounted for 34.4 percent of the 2.4 mil-lion deaths in 2003 and remain a major cause of health disparities and rising health carecosts. In 2006, health care spending and lost productivity from CVD exceeded $400 billion.The aging population, obesity epidemic, underuse of prevention strategies, and suboptimalcontrol of risk factors could exacerbate the future CVD burden. Increased adherence to clin-ical and community-level guidelines and renewed emphasis on policy, environmental, andlifestyle changes will be crucial for its effective prevention and control. [Health Affairs 26,no. 1 (2007): 38–48; 10.1377/hlthaff.26.1.38]
Wo r l d w i d e , c a r d i o va s c u l a r d i s e a s e (CVD) is the leadingcause of death and a major cause of disability and lost productivity inadults.1 In the United States, heart disease and stroke—the principal
components of CVD—rank first and third, respectively, among the leading causesof death.2 The term CVD, as used in this paper, includes rheumatic fever (Interna-tional Classification of Diseases, Tenth Revision [ICD-10] codes I00–I02 and I05–I09);hypertensive diseases (I10–I15); ischemic heart diseases (I20–I25); pulmonaryheart disease and diseases of pulmonary circulation (I26–I28); other forms ofheart disease (I30–I52); cerebrovascular diseases or stroke (I60–I69); diseases ofarteries, arterioles, and capillaries (I70–I79); other diseases of veins, lymphaticvessels, and lymph nodes (I80–I89); other and unspecified disorders of the circula-tory system (I95–I99); and congenital malformations or birth defects of the circu-latory system (Q20–Q28).3
These diseases are common and occur in infants, children, and adults of bothsexes, and they affect people of all races and ethnicities. The lifetime risk for aforty-year-old developing coronary heart disease is roughly 50 percent in men and
3 8 J a n u a r y / F e b r u a r y 2 0 0 7
T r e n d s
DOI 10.1377/hlthaff.26.1.38 ©2007 Project HOPE–The People-to-People Health Foundation, Inc.
George Mensah ([email protected]) is chief medical officer, Office of the Director, National Center for ChronicDisease Prevention and Health Promotion, Centers for Disease Control and Prevention, in Atlanta, Georgia.David Brown is an epidemiologist in the Division of Adult and Community Health in that center.
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

32 percent in women.4 In this paper we present an overview of the CVD burden inthe United States using epidemiologic data on the magnitude and trends of CVDand their implications for policy and program development for cardiovascularhealth promotion and CVD prevention.
The CVD Burden And Trends In The United States� Prevalence and incidence. An estimated one in three U.S. adults (about 71.3
million) have one or more types of CVD.5 The prevalence increases with advancingage and varies within racial, ethnic, geographic, and sociodemographic groups.Among the 71.3 million adults with one or more forms of CVD, the most prevalentconditions are hypertension or high blood pressure (65 million), coronary heart dis-ease (13.2 million), stroke (5.5 million), heart failure (5 million), and congenital heartdefects (1 million).6 Exhibit 1 shows the prevalence of four major CVD categories.
Although advancing age is the most powerful risk factor for CVD, about 62 per-cent of adults living with CVD are younger than age sixty-five. In particular, menand women ages 55–64 are a special concern. In this age group, 52.0 percent ofmen and 56.5 percent of women live with one or more forms of CVD.7 Childrenand young adults also represent an important age group. Although the overall in-cidence of CVD in children and young adults is low (600 cases per year), sudden
U . S . O v e r v i e w
H E A L T H A F F A I R S ~ V o l u m e 2 6 , N u m b e r 1 3 9
EXHIBIT 1Prevalence Of Cardiovascular Diseases In The U.S. Noninstitutionalized CivilianPopulation Age Eighteen And Older, By Race/Ethnicity, 2004
SOURCE: M. Lethbridge-Çejku, D. Rose, and J. Vickerie, “Summary Health Statistics for U.S. Adults: National Health InterviewSurvey, 2004,” 10, no. 228 (2006): Table 2.Vital and Health StatisticsNOTES: Hispanic or Latino may be of any race. Because of small numbers, there is no estimate for Native Hawaiian or otherPacific Islander, other heart disease. CHD is coronary heart disease.
White, non-Hispanic
Black, non-Hispanic
Hispanicor Latino
Asian
Native Hawaiian orother Pacific Islander
American Indianor Alaska Native
0 10 15 20 255Percent
30
Stroke Other heart disease CHD Hypertension
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from
cardiac death accounts for one in five unexpected sudden deaths among childrenages 1–13 and for one in three among those ages 14–21.8 Congenital heart defects, acommon cause of infant death from birth defects, affect thousands of newbornseach year.9
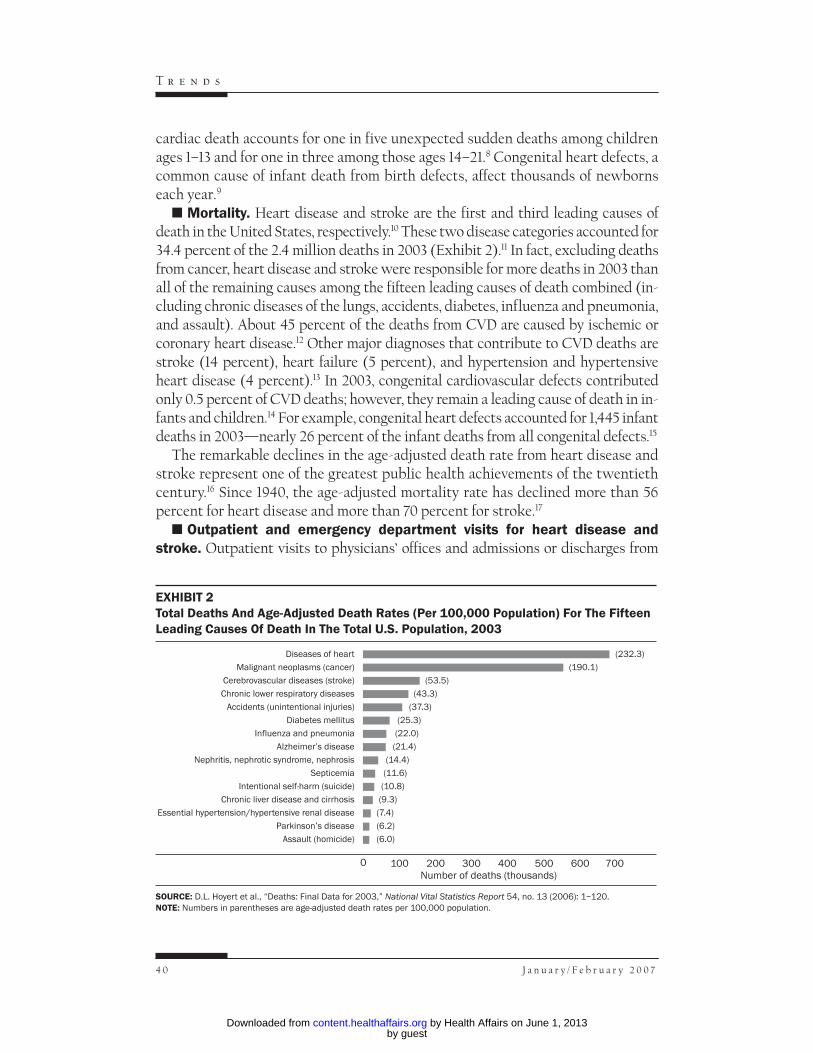
� Mortality. Heart disease and stroke are the first and third leading causes ofdeath in the United States, respectively.10 These two disease categories accounted for34.4 percent of the 2.4 million deaths in 2003 (Exhibit 2).11 In fact, excluding deathsfrom cancer, heart disease and stroke were responsible for more deaths in 2003 thanall of the remaining causes among the fifteen leading causes of death combined (in-cluding chronic diseases of the lungs, accidents, diabetes, influenza and pneumonia,and assault). About 45 percent of the deaths from CVD are caused by ischemic orcoronary heart disease.12 Other major diagnoses that contribute to CVD deaths arestroke (14 percent), heart failure (5 percent), and hypertension and hypertensiveheart disease (4 percent).13 In 2003, congenital cardiovascular defects contributedonly 0.5 percent of CVD deaths; however, they remain a leading cause of death in in-fants and children.14 For example, congenital heart defects accounted for 1,445 infantdeaths in 2003—nearly 26 percent of the infant deaths from all congenital defects.15
The remarkable declines in the age-adjusted death rate from heart disease andstroke represent one of the greatest public health achievements of the twentiethcentury.16 Since 1940, the age-adjusted mortality rate has declined more than 56percent for heart disease and more than 70 percent for stroke.17
� Outpatient and emergency department visits for heart disease andstroke. Outpatient visits to physicians’ offices and admissions or discharges from
4 0 J a n u a r y / F e b r u a r y 2 0 0 7
T r e n d s
EXHIBIT 2Total Deaths And Age-Adjusted Death Rates (Per 100,000 Population) For The FifteenLeading Causes Of Death In The Total U.S. Population, 2003
SOURCE: D.L. Hoyert et al., “Deaths: Final Data for 2003,” 54, no. 13 (2006): 1–120.National Vital Statistics ReportNOTE: Numbers in parentheses are age-adjusted death rates per 100,000 population.
Diseases of heart
Malignant neoplasms (cancer)
Cerebrovascular diseases (stroke)
Chronic lower respiratory diseases
Accidents (unintentional injuries)
Diabetes mellitus
Influenza and pneumonia
Alzheimer’s disease
Nephritis, nephrotic syndrome, nephrosis
Septicemia
Intentional self-harm (suicide)
Chronic liver disease and cirrhosis
Essential hypertension/hypertensive renal disease
Parkinson’s disease
Assault (homicide)
100 300 400 500 600200Number of deaths (thousands)
700
(232.3)
(190.1)
(53.5)
(43.3)
(37.3)
(25.3)
(22.0)
(21.4)
(14.4)
(11.6)
(10.8)
(9.3)
(7.4)
(6.2)
(6.0)
0
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

emergency departments (EDs) represent another important measure of the burdenof CVD. In 2003 alone, there were nearly 70.7 million outpatient physician office vis-its and 4.5 million ED admissions with a primary diagnosis of CVD.18 High bloodpressure, acute and chronic heart failure, and chest pain (that may represent life-threatening conditions such as a heart attack) are among the chief reasons for outpa-tient physician office visits and ED admissions. For example, outpatient and EDdata for 1999–2000 showed that essential hypertension alone accounted for 37.5 mil-lion combined ambulatory care visits and represented the leading cause of outpa-tient visits.19
� Hospitalization for heart disease and stroke. CVD remains a leading causeof admissions or discharges from short-stay hospitals and nursing homes. For exam-ple, in 2003 heart disease as a first-listed diagnosis was the highest-ranked diseasecategory for hospital discharges and represented a 31 percent increase over dis-charges in 1979.20 In fact, analysis of hospital discharge data for 1979–2003 showssizable increases in hospitalization (expressed as a percentage) for major CVD, in-cluding coronary heart disease (16 percent), stroke (29 percent), and chronic heartfailure (174 percent).21 Between 1970 and 2000, the total number of stroke-relatedhospitalizations increased among people age sixty-five or older (372,000 in 1970 ver-sus 711,000 in 2000), although rates of hospitalization remained stable (20.7 per1,000 in 1970 versus 20.4 per 1,000 in 2000).22 Rates were similar for men and womenduring this period, while rates for blacks increased from 14.0 per 1,000 in 1970 to 20.6per 1,000 in 2000 (Exhibit 3).23
� Economic burden of CVD. CVD is the most costly disease in the UnitedStates.24 Using data from multiple sources, the American Heart Association hascompiled a detailed table of 2006 estimates of the direct and indirect costs of heartdiseases, coronary heart disease, stroke, hypertensive heart disease, heart failure,
U . S . O v e r v i e w
H E A L T H A F F A I R S ~ V o l u m e 2 6 , N u m b e r 1 4 1
EXHIBIT 3Age-Adjusted Rates Of Hospital Discharge Per 1,000 Civilian U.S. Residents Age Sixty-Five And Older As A Result Of A Primary Diagnosis Of Cerebrovascular Disease, By SexAnd Race, 1970–2000
SOURCE: A. Ahmed et al., “Cerebrovascular Diseases as Primary Hospital Discharge Diagnoses: National Trend (1970–2000)among Older Adults,” 60, no. 10 (2005): 1328–1332.Journals of Gerontology, Series A: Biological Sciences and Medical SciencesNOTES: Data on race in the National Hospital Discharge Survey data sets have become increasingly incomplete in recent years.For example, incomplete reporting of race was as high as 25 percent of discharges in 2000. Thus, these findings should beinterpreted cautiously.
20
15
10
Discharges per 1,000
1970 1975 1985 1995
25
2000
Whites
Men
1980 1990
Women
Blacks
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from
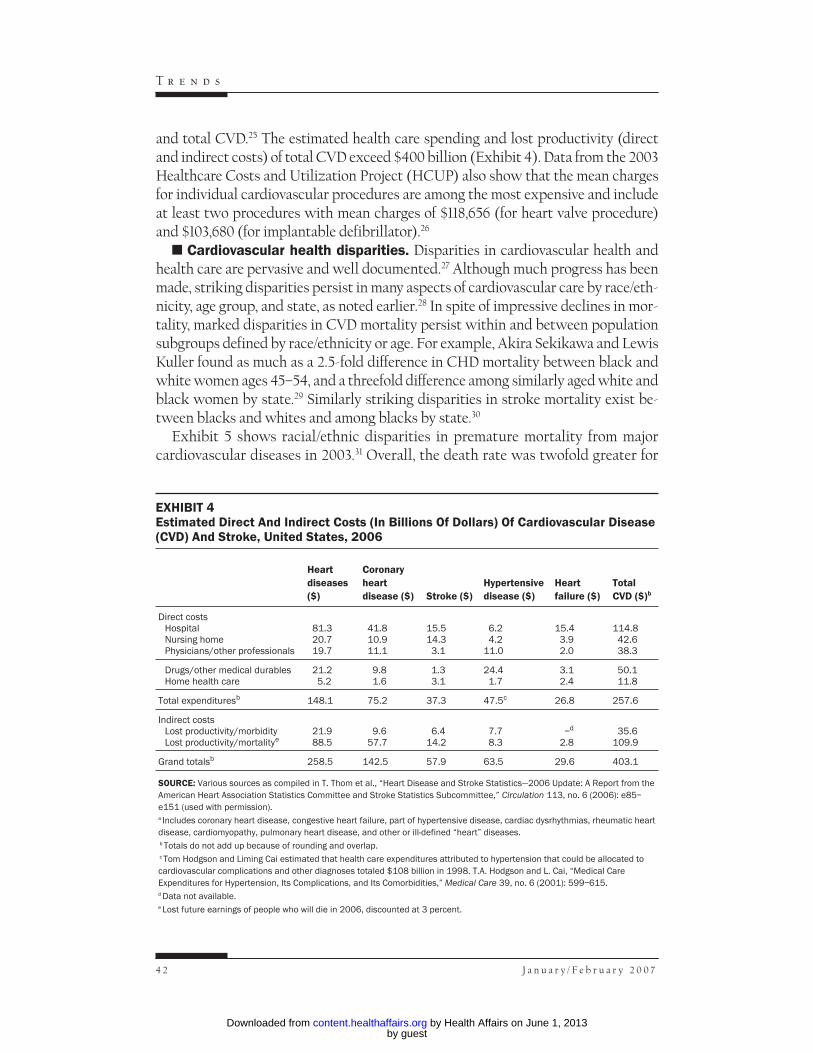
and total CVD.25 The estimated health care spending and lost productivity (directand indirect costs) of total CVD exceed $400 billion (Exhibit 4). Data from the 2003Healthcare Costs and Utilization Project (HCUP) also show that the mean chargesfor individual cardiovascular procedures are among the most expensive and includeat least two procedures with mean charges of $118,656 (for heart valve procedure)and $103,680 (for implantable defibrillator).26
� Cardiovascular health disparities. Disparities in cardiovascular health andhealth care are pervasive and well documented.27 Although much progress has beenmade, striking disparities persist in many aspects of cardiovascular care by race/eth-nicity, age group, and state, as noted earlier.28 In spite of impressive declines in mor-tality, marked disparities in CVD mortality persist within and between populationsubgroups defined by race/ethnicity or age. For example, Akira Sekikawa and LewisKuller found as much as a 2.5-fold difference in CHD mortality between black andwhite women ages 45–54, and a threefold difference among similarly aged white andblack women by state.29 Similarly striking disparities in stroke mortality exist be-tween blacks and whites and among blacks by state.30
Exhibit 5 shows racial/ethnic disparities in premature mortality from majorcardiovascular diseases in 2003.31 Overall, the death rate was twofold greater for
4 2 J a n u a r y / F e b r u a r y 2 0 0 7
T r e n d s
EXHIBIT 4Estimated Direct And Indirect Costs (In Billions Of Dollars) Of Cardiovascular Disease(CVD) And Stroke, United States, 2006
Heartdiseases($)
Coronaryheartdisease ($) Stroke ($)
Hypertensivedisease ($)
Heartfailure ($)
TotalCVD ($)b
Direct costsHospitalNursing homePhysicians/other professionals
81.320.719.7
41.810.911.1
15.514.3
3.1
6.24.2
11.0
15.43.92.0
114.842.638.3
Drugs/other medical durablesHome health care
21.25.2
9.81.6
1.33.1
24.41.7
3.12.4
50.111.8
Total expendituresb 148.1 75.2 37.3 47.5c 26.8 257.6
Indirect costsLost productivity/morbidityLost productivity/mortalitye
21.988.5
9.657.7
6.414.2
7.78.3
–d
2.835.6
109.9
Grand totalsb 258.5 142.5 57.9 63.5 29.6 403.1
SOURCE: Various sources as compiled in T. Thom et al., “Heart Disease and Stroke Statistics—2006 Update: A Report from theAmerican Heart Association Statistics Committee and Stroke Statistics Subcommittee,” Circulation 113, no. 6 (2006): e85–e151 (used with permission).a Includes coronary heart disease, congestive heart failure, part of hypertensive disease, cardiac dysrhythmias, rheumatic heartdisease, cardiomyopathy, pulmonary heart disease, and other or ill-defined “heart” diseases.b Totals do not add up because of rounding and overlap.c Tom Hodgson and Liming Cai estimated that health care expenditures attributed to hypertension that could be allocated tocardiovascular complications and other diagnoses totaled $108 billion in 1998. T.A. Hodgson and L. Cai, “Medical CareExpenditures for Hypertension, Its Complications, and Its Comorbidities,” Medical Care 39, no. 6 (2001): 599–615.d Data not available.e Lost future earnings of people who will die in 2006, discounted at 3 percent.
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

blacks than for whites for each five-year age group for ages 20–64. For coronaryheart disease, 17 percent of the 480,028 deaths in 2003 occurred among people un-der age sixty-five. The proportion of premature deaths from coronary heart dis-ease was greater among blacks (28 percent, number of deaths = 49,274), AmericanIndians (34 percent, 1,905), and Asian or Pacific Islanders (21 percent, 7,367) com-pared with whites (16 percent, 421,482), although some of this difference might beaccounted for by the age distributions of these groups.32
Compared with white adults, hospitalization rates for hypertension in 2000were six times higher among black adults ages 18–44, more than five times higheramong blacks ages 45–64, and nearly three times higher among blacks age sixty-five and older.33 Hospitalization rates for angina and congestive heart failure werealso much higher among blacks than among whites.34 Sex disparities in cardiovas-cular health care and mortality are also pervasive, although recent data show somemajor improvements. For example, Jeffrey Pearcy and Kenneth Keppel have shownthat from 1989 to 1998, disparities in CVD mortality decreased based on sex butwere largely unchanged based on race/ethnicity.35
Cardiovascular Disease And Cause For AlarmSeveral important positive trends have been documented for CVD in the past
century. The dramatic declines in age-adjusted mortality from heart disease,stroke, and total cardiovascular diseases and the major declines in populationmean blood pressure and cholesterol levels represent key examples. Nevertheless,there are many powerful adverse patterns in CVD epidemiology that hold the po-tential for unraveling many of the public health achievements of the past century.Chief among these adverse trends is the graying of America. Advancing age is the
U . S . O v e r v i e w
H E A L T H A F F A I R S ~ V o l u m e 2 6 , N u m b e r 1 4 3
EXHIBIT 5Death Rates From Major Cardiovascular Diseases In Blacks And Whites Ages 20–64,United States, 2003
Death rates per 100,000 population
Age (years) Black White Ratio, black to white
20–2425–2930–34
9.616.129.3
3.75.7
11.0
2.62.82.7
35–3940–4445–49
52.7104.2183.8
21.443.476.1
2.52.42.4
50–5455–5960–64
305.8451.7695.3
124.8203.3333.1
2.52.22.1
SOURCE: National Center for Health Statistics, “Worktable 210R: Death Rates for 113 Selected Causes, Alcohol-InducedCauses, Drug-Induced Causes, and Injury by Firearms, by Five-Year Age Groups, Race, and Sex: United States, 2003,” 22March 2006, http://www.cdc.gov/nchs/data/statab/Mortfinal2003_worktable210f.pdf (accessed 18 October 2006).
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

most powerful risk factor for CVD; therefore, the aging of the U.S. population andthe demographic changes projected for 2020 and beyond will have a major impacton the prevalence of and cost of care for CVD.36
Second, the continuing epidemics of childhood obesity and of obesity and type2 diabetes in adults represent major public health challenges likely to increase themorbidity and mortality from CVD.37 In barely four decades, from 1963–1965 to1999–2002, the prevalence of overweight nearly quadrupled (from 4.6 percent to16.1 percent) in adolescents ages 12–19 and more than tripled (from 4.2 percent to15.8 percent) in children ages 6–11. Among children ages 5–11, data from theBogalusa Heart Study have shown that 27.1 percent now have one or more risk fac-tors for heart disease and that an additional 6.9 percent have two or more risk fac-tors.38 Taken together, these epidemiological findings are great cause for alarm.
Third, the declining prevalence of adults with no known major CVD risk fac-tors is another important concern. Using data from the Behavioral Risk FactorSurveillance System (BRFSS), we demonstrated that the proportion of adultswith no self-reported major CVD risk factors declined from 42 percent in 1991 to36 percent in 2001.39 The decline was noted in both men and women in nearly allstates, racial/ethnic populations, age groups, and education levels.40 In addition,the self-reported prevalence of CVD risk factors (high blood pressure, high choles-terol, diabetes, and obesity) among U.S. adults increased, whereas the prevalenceof smoking remained nearly the same during that decade.41 The recent reports ofincreasing prevalence of metabolic syndrome, a marker of CVD risk-factor cluster-ing, also suggest that the prevalence of low CVD risk factor profiles is decreas-ing.42 The actual prevalence of truly low-risk people (those with favorable levels ofmeasured blood cholesterol and blood pressure who do not smoke and do not havediagnosed diabetes, myocardial infarction, or electrocardiographic abnormalities)has been estimated at about 5–10 percent, much lower than self-reported inBRFSS data and most likely declining.43
Fourth, the increasing use of expensive diagnostic and therapeutic proceduresis another important issue. Over the past two to three decades, the total number ofinpatient diagnostic and therapeutic procedures have increased dramatically. Forexample, from 1979 to 2003, total inpatient operations and procedures for CVD in-creased 470 percent, and the volume of cardiac catheterizations alone increased373 percent.44 The mean charges for these procedures have also increased greatly.45
These trends are highlighted not to suggest impropriety or inappropriate use ofoperations and procedures but to emphasize the potential impact that effectiveprograms for preventing CVD can have on health care costs and resource use.
Epidemiological Evidence For Hope, And The PolicyImplications
The social, environmental, and biological determinants and risk factors forCVD are well established.46 Safe and effective interventions are available for pri-
4 4 J a n u a r y / F e b r u a r y 2 0 0 7
T r e n d s
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

mordial, primary, and secondary prevention and control of CVD. Although adher-ence to established practice guidelines that promote these best practices is sub-optimal, there is evidence that it is improving and that improved adherence has aneffect on survival and quality of life.47 In fact, life-table analyses on the eliminationof specific causes of death suggest that the gains from effective prevention andcontrol of CVD would exceed those of any other cause of death: Life expectancywould rise by almost seven years, but only three years if cancer were eliminated asa cause of death.48 The gains in life expectancy predicted from the elimination ofCVD is not surprising considering the important role that CVD plays as the lead-ing cause of death. A similarly large impact on the reduction and eventual elimina-tion of health disparities might also be seen because CVD contributes greatly tohealth disparities, particularly among people with fewer years of education andamong African Americans.49
The availability of drug and nondrug strategies that could reduce cardiovascu-lar events provides hope that CVD can be eliminated. The prevalence of many car-diovascular risk factors is declining in the United States, although increases insome risk factors are present, particularly among some population subgroups.50
Smoking prevalence continues to decline, and U.S. cigarette sales continue to fall.51
Declines in total cholesterol levels observed between 1960 and the early 1990s andin levels of low-density lipoprotein (LDL) cholesterol from the late 1970s to early1990s in the United States continue.52 These advances are tempered by increases inthe prevalence of hypertension, obesity, and diabetes.53
Although additional evidence is needed, the simultaneous reduction of four car-diovascular risk factors (LDL cholesterol, blood pressure, serum homocysteine,and platelet function) using one combination pill (so-called polypill) adminis-tered to people with existing CVD and everyone age fifty-five and older withoutany screening and without requiring risk factors to be measured has the potentialto reduce ischemic heart disease events and strokes.54 Also, data from one studyusing an evidence-based recipe (Polymeal) that includes wine, fish, dark choco-late, fruits, vegetables, garlic, and almonds suggest the potential to reduce CVDevents and increase life expectancy.55 Although intriguing, these findings andtheir policy implications remain controversial and deserve systematic evaluation.
Nevertheless, the epidemiological data provide support for renewed emphasison both individual level as well as populationwide strategies, including policy andenvironmental changes for cardiovascular health promotion and the aggressiveprevention, treatment, and control of CVD risk factors in all settings includingschools, worksites, health care providers, and the community at large.
U . S . O v e r v i e w
H E A L T H A F F A I R S ~ V o l u m e 2 6 , N u m b e r 1 4 5
“The availability of drug and nondrug strategies that could reducecardiovascular events provides hope that CVD can be eliminated.”
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from

Ca r d i ova s c u l a r d i s e a s e s , principally heart disease and stroke, rankfirst and third, respectively, among the leading causes of death in theUnited States. They are also a leading cause of morbidity and are partly re-
sponsible for persisting and sometimes marked disparities in life expectancy andoverall health. The rising hospitalization rate for major CVD and marked increasein inpatient operations and procedures also contributes greatly to rising healthcare costs. As the U.S. population ages and adverse trends of major risk factors in-cluding the epidemics of obesity and type 2 diabetes continue, CVD will take oneven greater clinical, public health, and economic importance. The time has comefor epidemiological data to play an even greater role in informing the development,implementation, and evaluation of cardiovascular health care policies. Applyingthe best available science through increased adherence to established clinical andcommunity-level guidelines; comprehensive worksite health promotion programs;and renewed emphasis on supportive policy, environmental, and lifestyle changesbeginning in infants, children, and young adults will be crucial for achieving thenational Healthy People 2010 goals for CVD.56
The findings and conclusions in this paper are those of the authors and do not necessarily represent the views of theCenters for Disease Control and Prevention.
NOTES1. A.D. Lopez et al., eds., Global Burden of Disease and Risk Factors (New York: Oxford University Press, 2006);
and C.J.L. Murray and A.D. Lopez, The Global Burden of Disease: A Comparative Assessment of Mortality and Disabil-ity from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020, vol. 1 (Cambridge, Mass.: Harvard Univer-sity Press, 1996).
2. National Center for Health Statistics, Health, United States, 2005, with Chartbook on Trends in the Health of Ameri-cans (Hyattsville, Md.: NCHS, 2005).
3. World Health Organization, International Classification of Diseases and Related Health Problems, Tenth Revision(Geneva: WHO, 1992).
4. D.M. Lloyd-Jones et al., “Lifetime Risk of Developing Coronary Heart Disease,” Lancet 353, no. 9147 (1999):89–92.
5. T. Thom et al., “Heart Disease and Stroke Statistics—2006 Update: A Report from the American Heart As-sociation Statistics Committee and Stroke Statistics Subcommittee,” Circulation 113, no. 6 (2006): e85–e151.
6. Ibid.
7. Ibid.
8. Ibid.
9. Ibid.
10. NCHS, Health, United States, 2005; and D.L. Hoyert et al., “Deaths: Final Data for 2003,” National Vital StatisticsReports 54, no. 13 (2006): 1–120.
11. Ibid.
12. Ibid.
13. Thom et al., “Heart Disease and Stroke Statistics”; and Hoyert et al., “Deaths.”
14. Thom et al., “Heart Disease and Stroke Statistics”; and R.S. Boneva et al., “Mortality Associated with Con-genital Heart Defects in the United States: Trends and Racial Disparities, 1979–1997,” Circulation 103, no. 19(2001): 2376–2381.
15. Thom et al., “Heart Disease and Stroke Statistics.”
16. Centers for Disease Control and Prevention, “Achievements in Public Health, 1900–1999: Decline inDeaths from Heart Disease and Stroke—United States, 1900–1999,” Morbidity and Mortality Weekly Report 48,
4 6 J a n u a r y / F e b r u a r y 2 0 0 7
T r e n d s
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from
no. 30 (1999): 649–656.
17. Ibid.
18. Thom et al., “Heart Disease and Stroke Statistics”; NCHS, National Ambulatory Medical Care Survey: 2003 Sum-mary, Advance Data from Vital and Health Statistics no. 365 (Hyattsville, Md.: NCHS, 2005); and NCHS,National Hospital Ambulatory Medical Care Survey: Emergency Department Summary, 2003, Advance Data from Vitaland Health Statistics no. 358 (Hyattsville, Md.: NCHS, 2005).
19. Thom et al., “Heart Disease and Stroke Statistics.”
20. NCHS, National Hospital Ambulatory Medical Care Survey.
21. Thom et al., “Heart Disease and Stroke Statistics”; and NCHS, “National Hospital Discharge Survey, 2001:Annual Summary with Detailed Diagnosis and Procedure Data,” Vital and Health Statistics 13, no. 156 (2004).
22. A. Ahmed et al., “Cerebrovascular Diseases as Primary Hospital Discharge Diagnoses: National Trend(1970–2000) among Older Adults,” Journals of Gerontology, Series A: Biological Sciences and Medical Sciences 60, no.10 (2005): 1328–1332.
23. Ibid.
24. National Heart, Lung, and Blood Institute, Fact Book, Fiscal Year 2005, http://www.nhlbi.nih.gov/about/05factbk.pdf (accessed 25 August 2006).
25. Thom et al., “Heart Disease and Stroke Statistics.”
26. Ibid.
27. G.A. Mensah, “Eliminating Disparities in Cardiovascular Health: Six Strategic Imperatives and a Frame-work for Action,” Circulation 111, no. 10 (2005): 1332–1336; G.A. Mensah et al., “State of Disparities in Car-diovascular Health in the United States,” Circulation 111, no. 10 (2005): 1233–1241; and V. Vaccarino et al.,“Sex and Racial Differences in the Management of Acute Myocardial Infarction, 1994 through 2002,” NewEngland Journal of Medicine 353, no. 7 (2005): 671–682.
28. A. Sekikawa and L.H. Kuller, “Striking Variation in Coronary Heart Disease Mortality in the United Statesamong Black and White Women Aged 45–54 by State,” Journal of Women’s Health and Gender-Based Medicine 9,no. 5 (2000): 545–558; and G. Howard and V.J. Howard, “Ethnic Disparities in Stroke: The Scope of theProblem,” Ethnicity and Disease 11, no. 4 (2001): 761–768.
29. Sekikawa and Kuller, “Striking Variation.”
30. Howard and Howard, “Ethnic Disparities in Stroke.”
31. “Premature” mortality in this paper refers to the years of potential life lost (YPLL) before age seventy-five.See Table 30 in NCHS, Health, United States, 2005.
32. NCHS, “Table 210F: Deaths from Ischemic Heart Disease by Five-Year Age Group, Race, and Sex,” 22March 2006, http://www.cdc.gov/nchs/data/statab/Mortfinal2003_worktable210f.pdf (accessed 17 Octo-ber 2006).
33. J.S. Holmes et al., “Heart Disease and Prevention: Race and Age Differences in Heart Disease Prevention,Treatment, and Mortality,” Medical Care 43, no. 3 Supp. (2005): I33–I41.
34. Ibid.
35. J.N. Pearcy and K.G. Keppel, “A Summary Measure of Health Disparity,” Public Health Reports 117, no. 3(2002): 273–280.
36. D.K. Foot et al., “Demographics and Cardiology, 1950–2050,” Journal of the American College of Cardiology 35,no. 5, Supp. B (2000): 66B–80B; and R. SoRelle, “Global Epidemic of Cardiovascular Disease Expected bythe Year 2050,” Circulation 100, no. 20 (1999): e101.
37. A.A. Hedley et al., “Prevalence of Overweight and Obesity among U.S. Children, Adolescents, and Adults,1999–2002,” Journal of the American Medical Association 291, no. 23 (2004): 2847–2850; K.M. Flegal et al., “Ex-cess Deaths Associated with Underweight, Overweight, and Obesity,” Journal of the American Medical Associa-tion 293, no. 15 (2005): 1861–1867; and R.H. Eckel et al., “Prevention Conference VII: Obesity, a WorldwideEpidemic Related to Heart Disease and Stroke: Executive Summary,” Circulation 110, no. 18 (2004): 2968–2975.
38. D.S. Freedman et al., “The Relation of Overweight to Cardiovascular Risk Factors among Children andAdolescents: The Bogalusa Heart Study,” Pediatrics 103, no. 6, Part 1 (1999): 1175–1182.
39. N. Paynter et al., “Declining Prevalence of No Known Major Risk Factors for Heart Disease and Strokeamong Adults—United States, 1991–2001,” Morbidity and Mortality Weekly Report 53, no. 1 (2004): 4–7.
40. Ibid.
U . S . O v e r v i e w
H E A L T H A F F A I R S ~ V o l u m e 2 6 , N u m b e r 1 4 7
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from
41. Ibid.
42. E.S. Ford, W.H. Giles, and A.H. Mokdad, “Increasing Prevalence of the Metabolic Syndrome among U.S.Adults,” Diabetes Care 27, no. 10 (2004): 2444–2449; and G.E. Duncan, S.M. Li, and X.H. Zhou, “Prevalenceand Trends of a Metabolic Syndrome Phenotype among U.S. Adolescents, 1999–2000,” Diabetes Care 27, no.10 (2004): 2438–2443.
43. J. Stamler et al., “Low Risk-Factor Profile and Long-Term Cardiovascular and Noncardiovascular Mortal-ity and Life Expectancy: Findings for Five Large Cohorts of Young Adult and Middle-Aged Men andWomen,” Journal of the American Medical Association 282, no. 21 (1999): 2012–2018; and Paynter et al., “Changesin Prevalence of Adults.”
44. Thom et al., “Heart Disease and Stroke Statistics.”
45. Ibid.
46. See, for example, S. Yusuf et al., “Global Burden of Cardiovascular Diseases, Part I: General Considerations,the Epidemiologic Transition, Risk Factors, and Impact of Urbanization,” Circulation 104, no. 22 (2001):2746–2753; S. Yusuf et al., “Global Burden of Cardiovascular Diseases, Part II: Variations in CardiovascularDisease by Specific Ethnic Groups and Geographic Regions and Prevention Strategies,” Circulation 104, no.23 (2001): 2855–2864; and J. Stamler, “Established Major Coronary Risk Factors,” in Coronary Heart DiseaseEpidemiology: From Aetiology to Public Health, ed. M. Marmot and P. Elliott (New York: Oxford UniversityPress, 1992), 35–66.
47. Thom et al., “Heart Disease and Stroke Statistics”; K.A. Eagle et al., “Guideline-Based Standardized Care IsAssociated with Substantially Lower Mortality in Medicare Patients with Acute Myocardial Infarction:The American College of Cardiology’s Guidelines Applied in Practice (GAP) Projects in Michigan,” Journalof the American College of Cardiology 46, no. 7 (2005): 1242–1248; and R.H. Mehta et al., “Enhancing Quality ofCare for Acute Myocardial Infarction: Shifting the Focus of Improvement from Key Indicators to Processof Care and Tool Use: The American College of Cardiology Acute Myocardial Infarction Guidelines Ap-plied in Practice Project in Michigan: Flint and Saginaw Expansion,” Journal of the American College of Cardiol-ogy 43, no. 12 (2004): 2166–2173.
48. R.N. Anderson, U.S. Decennial Life Tables for 1989–91, Volume 1, Number 4: United States Life Tables Eliminating CertainCauses of Death, 1999, http://www.cdc.gov/nchs/data/lifetables/life89_1_4.pdf (accessed 17 October 2006).
49. M.D. Wong et al., “Contribution of Major Diseases to Disparities in Mortality,” New England Journal of Medi-cine 347, no. 20 (2002): 1585–1592.
50. E.W. Gregg et al, “Secular Trends in Cardiovascular Disease Risk Factors According to Body Mass Index inU.S. Adults,” Journal of the American Medical Association 293, no. 15 (2005): 1868–1874.
51. CDC, “Cigarette Smoking among Adults—United States, 2003,” Morbidity and Mortality Weekly Report 54, no.20 (2005): 509–513; and R. Dobson, “U.S. Cigarette Consumption Falls to Lowest Point since 1951,” BritishMedical Journal 332, no. 7543 (2006): 687.
52. M.D. Carroll et al., “Trends in Serum Lipids and Lipoproteins of Adults, 1960–2002,” Journal of the AmericanMedical Association 294, no. 14 (2005): 1773–1781.
53. L.E. Fields et al, “The Burden of Adult Hypertension in the United States 1999 to 2000: A Rising Tide,” Hy-pertension 44, no. 4 (2004): 398–404; A.I. Qureshi et al., “Prevalence and Trends of Prehypertension and Hy-pertension in United States: National Health and Nutrition Examination Surveys 1976 to 2000,” MedicalScience Monitor 11, no. 9 (2005): CR403–CR409; Eckel et al., “Prevention Conference VII”; and J.P. Boyle etal., “Projection of Diabetes Burden through 2050: Impact of Changing Demography and Disease Prevalencein the U.S.,” Diabetes Care 24, no. 11 (2001): 1936–1940.
54. N.J. Wald and M.R. Law, “A Strategy to Reduce Cardiovascular Disease by More than 80 Percent,” BritishMedical Journal 326, no. 7404 (2003): 1419.
55. O.H. Franco et al., “The Polymeal: A More Natural, Safer, and Probably Tastier (than the Polypill) Strategyto Reduce Cardiovascular Disease by More than 75 Percent,” British Medical Journal 329, no. 7480 (2004):1447–1450.
56. U.S. Department of Health and Human Services, Healthy People 2010, 2d ed. (Washington: U.S. GovernmentPrinting Office, 2000).
4 8 J a n u a r y / F e b r u a r y 2 0 0 7
T r e n d s
by guest on June 1, 2013Health Affairs by content.healthaffairs.orgDownloaded from




















