
Tissue CA19.9 content in colorectal adenomas and its value in the assesment of dysplasia
Upload
independentCategory
view
3download
0
AJH 1995; 8:884-893
Alterations of Calcium Metabolism and of Parathyroid Function in Primary Aldosteronism, and Their Reversal by Spironolactone or by Surgical Removal of Aldosterone-Producing Adenomas Ermanno Rossi, Carlo Sani, Franco Perazzoli, Maria Cristina Casoli, Aurelio Negro, and Claudio Dotti
In order to investigate the possible existence of abnormal calcium metabolism and parathyroid function in primary aldosteronism (PA), we have compared the calcium/parathyroid hormone (PTH) profile of patients with PA with the profile of healthy normotensive subjects and of patients with essential hypertension (EH). Furthermore, we have evaluated the effects of spironolactone and the sur- gical removal of aldosterone-producing adenomas on the calcium/PTH profile in the PA patients.
Four groups of 10 subjects each participated in the study: 1) hypertensive patients with PA, 2) pa- tients with low-renin EH (LREH), 3) patients with normal-renin EH (NREH), 4) normotensive healthy subjects (NS). The four groups were well-matched for age, sex, body mass index, and renal function. The three hypertensive groups were also matched closely for blood pressure values and for duration of hypertension. In all subjects, after 1 week of a controlled intake of Na and K, the following pa- rameters were measured: urine excretion of Na, K, Ca, Mg, and P, plasma levels of K, Mg, inorganic P, total calcium and ionized calcium, and plasma renin activity, aldosterone concentration, and in- tact PTH. Blood pressure and laboratory parame-
ters were determined again in all the PA patients after 1 month of 100 mg daily spironolactone ad- ministration, and in four out of the 10 PA patients 2 months after surgical removal of aldosterone-pro- ducing adenomas. All of these subjects had under- gone the same controlled intake of Na and K indi- cated above. Serum intact PTH was higher in PA patients than in the other three groups (P K .01), and serum ionized calcium was significantly higher in normotensive subjects than in the three hypertensive groups (v PA P ~ .01, v LREH and v NREH P ~ .05). An increase in serum ionized cal- cium and a decrease in PTH level were associated with both spironolactone administration (P ~ .001) and surgical treatment (P ~ .05). These results sug- gest the presence of calcium metabolism alterations in both PA and EH patients, but that these alter- ations are more exaggerated in PA, so that higher PTH levels are needed for maintaining low-normal levels of serum ionized calcium. Am J Hypertens 1995;8:884--893
KEY WORDS: Intact parathyroid hormone, serum ion- ized calcium, primary aldosteronism, essential hypertension.
Received December 30, 1994. Accepted April 17, 1995. From the fourth Department of Internal Medicine, S. Maria
Nuova Hospital, Reggio Emilia, Italy (RE, SC, PF, CMC, NA), Laboratory of Endocrinology, S. Maria Nuova Hospital, Reggio Emilia, Italy (DC).
Address correspondence and reprint requests to Dr. Ermanno Rossi, IV Divisione di Medicina Interna, Ospedale S. Maria Nuova, Padiglione L. Spallanzani, Viale Umberto I, N.50, 42100 Reggio Emilia, Italy.
© 1995 by the American Journal off Hypertet~sion, Ltd. 0895-7061/95/$9.50 0895-7061 (95)00182-0

AJH-SEPTEMBER 1995-VOL. 8, NO. 9 CALCIUM AND PARATHYROID HORMONE IN PRIMARY ALDOSTERONISM 885
W hile calcium metabolism and parathy- roid function have been repeatedly studied in essential hypertension (EH), they have only occasionally been ex-
plored in patients with primary aldosteronism (PA).1 Increased concentration of cytosolic free calcium ion in various types of cells, ~5 reduced level of serum ionized calcium (Ca2+), 6-8 increased urinary calcium excretion (UcaV), 9-11 and augmented intestinal cal- cium absorption 12 have been reported separately or in various combinations in groups of subjects with EH when compared with normotensive healthy sub- jects. Appropriately elevated circulating levels of parathyroid hormone (PTH) 9"13 15 and 1,25-(OH)2- vitamin D 15'16 associated with these alterations have also been found. However, these results have not been confirmed by other observations. 17 Further- more, neither the mechanism nor the contribution of these alterations to blood pressure elevation itself has been clearly defined, though their close connection with abnormalities of Na metabolism and with NaC1 sensitivity seems highly probable, ls'19
The evaluation of calcium metabolism in PA, apart from defining it more completely, can help clarify the observed alterations of calcium metabolism in EH, insofar as PA represents a natural model of volume- dependen t and NaCl-sensitive hyper tension with functional similarities to NaCl-sensitive and Iow- renin EH. In the present study, we have examined some aspects of calcium metabolism and parathyroid function in a group of patients with PA who were compared to normotensive healthy subjects and to two subgroups of patients with EH distinguished on the basis of their renin/Na excretion profile. The ef- fects of the aldosterone antagonist spironolactone on serum Ca 2+ and intact (1-84)-PTH levels were also examined in the same subjects with PA. Finally, in the PA patients submitted to adrenal adenoma re- moval, serum CaZ + and intact (1-84)-PTH levels were again measured 2 months postoperatively.
S U B J E C T S A N D M E T H O D S
Four groups of white subjects were included in the study. Of these, group A consisted of 10 consecutive patients with PA, age 32 to 72 years; group B con- sisted of 10 patients with LREH, age 36 to 70 years; group C consisted of 10 patients with normal-renin essential hypertension (NREH), age 33 to 66 years; and, group D consisted of 10 normotensive healthy subjects (NS), age 32 to 68 years. Each PA patient was matched with one subject of each other group for age, sex, body mass index, creatinine clearance, and, in the case of groups B and C, also for blood pressure values and for duration of hypertension (Table 1).
Primary aldosteronism was defined by the pres- ence of each of the following criteria: a plasma aldo- sterone (in nanograms/decil i ter)/renin activity (in nanograms/milliliter/hour) ratio >50 in the sitting po- sition and on three consecutive occasions; a plasma renin activity (PRA) < 1 ng/mL/h in the upright pos- ture for 2 h, after 5 days of a sodium restricted diet (Na intake <40 mmol/L/day); a plasma aldosterone level <7.5 ng/dL at the end of an intravenous infu- sion of 2 L of isotonic saline at a rate of 500 mL/h; and an upright plasma aldosterone level >5 ng/dL after 5 days of fludrocortisone acetate administration (0.1 mg every 6 h).
Glucocorticoid-suppressible aldosteronism was ex- cluded by an upright plasma aldosterone above 2 ng/ dL after 5 days of dexamethasone administration (0.5 mg every 6 h).
Adrenal lesions were assessed by high-resolution, thin section computer tomographic scanning and dexamethasone-suppressed scintigraphy with 131I-6- [3-iodomethyl-norcholesterol. Unilateral adrenal ade- noma was diagnosed in five patients. Bilateral hyper- plasia was presumed on the basis of a symmetrical uptake in scintigraphic scanning in one patient, and of the absence of a unilateral lesion in both computer tomographic and scintigraphic scanning in the other
TABLE 1. CHARACTERISTICS OF THE STUDY GROUPS
NS PA LREH (N = 10) (N -- 10) (N = 10)
NREH (N = 10)
Age (years) Sex ratio (male/female) BMI (kg/m 2) DH (months) SBP (mm Hg) DBP (ram Hg) CrC1 (mL/min/1.72 m R)
48 _+ 12.7 52.4 -+ 12.9 45.6 + 9.1 46.4 + 5.1 5/5 5/5 5/5 5/5
24.3 -+ 1.5 23.1 -+ 0.8 24.8 -+ 1.2 23.4 + 0.9 31.6 z 15.2 35.5 + 15.3 34.3 + 14.7
122.5 +- 14.2 170.3 -+- 17.8" 166.0 --- 17.9" 165.6 + 13.6" 75.5 -+ 7.6 102.2 -+ 3.6* 103.5 ± 4.1" 105.0 + 7.5*
108.9 -+ 24.9 98.3 -+ 16.9 96.0 +- 39.4 113.0 ± 23.2
BMI, Body mass index; DH, duration of hypertension; SBP, systolic blood pressure; DBP, diastolic blood pressure; CrCI, creatinine clearance; NS, normotensive subjects; PA, primary aldosteronism: LREH, low-renin essential hypertension; NREH, normal-renin essential hypertension.
*P < .001 v NS.

886 ROSSI ET AL AJH-SEPTEMBER 1995-VOL. 8, NO. 9
four patients. Adrenocortical adenomas have been confirmed in the four patients so far submitted to unilateral adrenalectomy.
Essential hypertension was established after exclu- sion of secondary hypertension on the basis of ap- propriate clinical and laboratory evaluation, includ- ing a plasma aldosterone/renin activity ratio <30. The definition of low- and normal-renin essential hyper- tension was based on the PRA/Na excretion profile, as described by Brunner, Laragh, et al. 2°
All antihypertensive medications were discontin- ued 4 weeks before the beginning of the study. No hypertensive patient had previously been treated with diuretics, spironolactone, or other potassium sparing drugs. No other drug had been taken by the subjects participating in the study.
For the purpose of matching, the individual sys- tolic and diastolic blood pressures were the average of six office measurements in the seated position on three different visits, 1 week apart in the 3 weeks before the beginning of the study. In the same pe- riod, endogenous creatinine clearance was measured in all subjects. All PA patients had diastolic blood pressure (DBP) >90 mm Hg, and DBP >90 mm Hg was used for the selection of the patients with essen- tial hypertension. Blood pressure levels under 140/90 mm Hg were considered normal in the selection of the control subjects.
After matching, all subjects were placed on a diet containing 40 mmol/day of sodium and 65 mmol/day of potassium, supplemented with common salt (NaC1 100%) given twice daily (at lunch and dinner) in 2-g packets, for a total Na intake of approximately 110 mmol/day. For this purpose, the subjects received specific dietary instructions on how to select and pre- pare their food, and dietary counselling was given every other day in outpatient visits. Compliance with the diet was assessed by detailed food records. On the seventh day all subjects collected a 24-h urine sample. At the end of the urine collection, at 8:00 AM following an overnight fast, blood pressure was mea- sured after 10 min of sitting rest. The individual blood pressures were the mean of three recordings 3 min apart.
Afterwards venous blood was obtained from each subject in the seated position. The 24-h urinary ex- cretion of calcium, magnesium, phosphorus, sodium, and potassium were measured. Blood samples were used to measure serum total calcium, magnesium, potassium, inorganic phosphorus, ionized calcium, PRA, aldosterone, and intact (1-84)-PTH.
After urine and blood collection, the 10 PA patients received 100 mg spironolactone once daily, without discontinuing the controlled intake of sodium (110 mmol/day) and potassium (65 mmol/day). On the 30th day of spironolactone treatment, urine and
blood samples were collected in each PA patient, and blood pressure was measured again, in the same con- ditions as indicated above. The 24-h urinary excretion of Na and K was determined. Venous blood was used to measure serum potassium, serum ionized calcium, PRA, plasma aldosterone, and intact (1-84)-PTH.
Four patients with PA were subsequently submit- ted to unilateral adrenalectomy for adenoma re- moval. In these patients, spironolactone administra- tion was discontinued immediately before surgery. At 2 months postoperatively and after I week of con- trolled intake of sodium (110 mmol/day) and of po- tassium (65 mmol/day), blood pressure and the same laboratory parameters measured at 1 month of spi- ronolactone treatment were measured again. All sub- jects attended our department throughout the study only on the days in which diet counselling, blood pressure measurement, and blood sampling were performed. All subjects gave their informed consent before the beginning of the study, which was ap- proved by the ethical committee of our hospital.
Blood pressure was measured with a standard mer- cury sphygmomanometer, using Korotkoff phase V for diastolic blood pressure. Serum ionized calcium was measured with an ion-selective electrode, with values adjusted to pH 7.4. PRA was evaluated by quantitative determination of angiotensin I, using ra- dioimmunoassay kits obtained from Sorin Biomedica (Saluggia, Italy). Plasma aldosterone was measured using radioimmunoassay kits purchased from Diag- nostic System Laboratories (Webster, TX). Intact se- rum PTH (PTH 1-84) was measured using radiometric assay kits obtained from Diagnostic Products Corpo- ration (Los Angeles, CA).
All other laboratory measurements were carried out by standard analytical techniques.
Statistical Analysis Serum and urinary variables approached a normal distribution (Kolmogorov- Smirnov test). Data are reported as means + standard deviation. The significance of changes induced by spironolactone treatment and comparisons between baseline and 2 months after unilateral adrenalectomy in the patients with primary aldosteronism were an- alyzed by paired t test. Comparisons between groups were made using one-way analysis of variance (ANOVA) followed by Scheff6's F test when signifi- cant. Bivariate correlations among variables were ex- amined with Pearson's correlation coefficients. Step- wise multiple linear regressions were used to exam- ine multiple correlations among variables and to examine the individual contribution of different fac- tors on PTH and Ca 2 + serum levels.
All computations were performed using SPSS/ PC+. A P < .05 was used to establish significant differences or correlations.

AJH-SEPTEMBER 1995-VOL. 8, NO. 9 CALCIUM AND PARATHYROID HORMONE IN PRIMARY ALDOSTERONISM 8 8 7
R E S U L T S
At the end of the matching , age, sex ratio, body mass index and renal funct ion (creatinine clearance) were similar in the four groups . The three hyper t ens ive g roups were also closely ma tched for dura t ion of hy- pe r tens ion and blood pressure values (Table 1).
As s h o w n in Table 2, after 1 week of controlled Na and K intake, b lood pressure values were again com- parable in the three hype r t ens ive g roups and obvi- ously higher than in the control g roup (P < .001). Se rum total calcium, se rum m a g n e s i u m , and se rum inorganic p h o s p h o r u s did not differ be tween the four g roups . S e r u m ion ized ca lc ium was s ignif icant ly higher in no rmo tens ive control subjects (1.25 ± 0.05 mmol/L) than in the three hyper tens ive g roups (1.17 - 0.07 mmol /L for PA, P < .01; 1.19 + 0.04 mmol /L for LREH, P < .05; 1.20 -+ 0.02 mmol /L for NREH, P < .05). Se rum intact (1-84)-PTH was higher in PA pat ients (70 +- 24 pg/mL) than in the o ther three g roups (41 + 15 pg /mL for NS, P < .01; 35 -+ 21 pg/mL for LREH, P < .01; 36 ± 10 p g / m L for NREH, P < .01).
No significant d i f ferences b e t w e e n g roups were found for ur inary excretion of Na and K, which re- flects the control led intake of these cations. U r i n a ~ excretion of calcium t ended to be higher in PA pa- tients, bu t the difference was not statistically signifi- cant. Ur inary excret ion of m a g n e s i u m and p h o s p h o - rus did not differ significantly be t ween groups. A sig- n i f i c an t c o r r e l a t i o n w a s f o u n d b e t w e e n s e r u m ionized calcium and se rum potass ium, both in PA
pat ient (r = 0.74, P < .01; Figure 1A) and in the three g roups of hyper t ens ive as a whole (r = 0.57, P < .001; Figure 1B). In the subjects wi th essent ial hyper - tension as a whole, a significant l inear re la t ionship be tween p lasma intact PTH and a ldos te rone levels was found (r = 0.66, P < .0001).
No o ther significant corre la t ion b e t w e e n s e r u m ionized calcium or PTH level and other pa r ame te r s was found.
Table 3 shows the effects of sp i ronolac tone treat- m e n t in PA pa t ien ts . S e r u m ion ized ca lc ium in- creased f rom 1.17 ± 0.07 mmol /L to 1.26 ±- 0.06 mmol /L (P < .001), while PTH decreased f rom 70 -+ 24 pg/mL to 39 ± 15 pg /mL (P < .0001). Individual changes of s e rum levels of ionized calcium and of intact PTH are s h o w n in Figure 2.
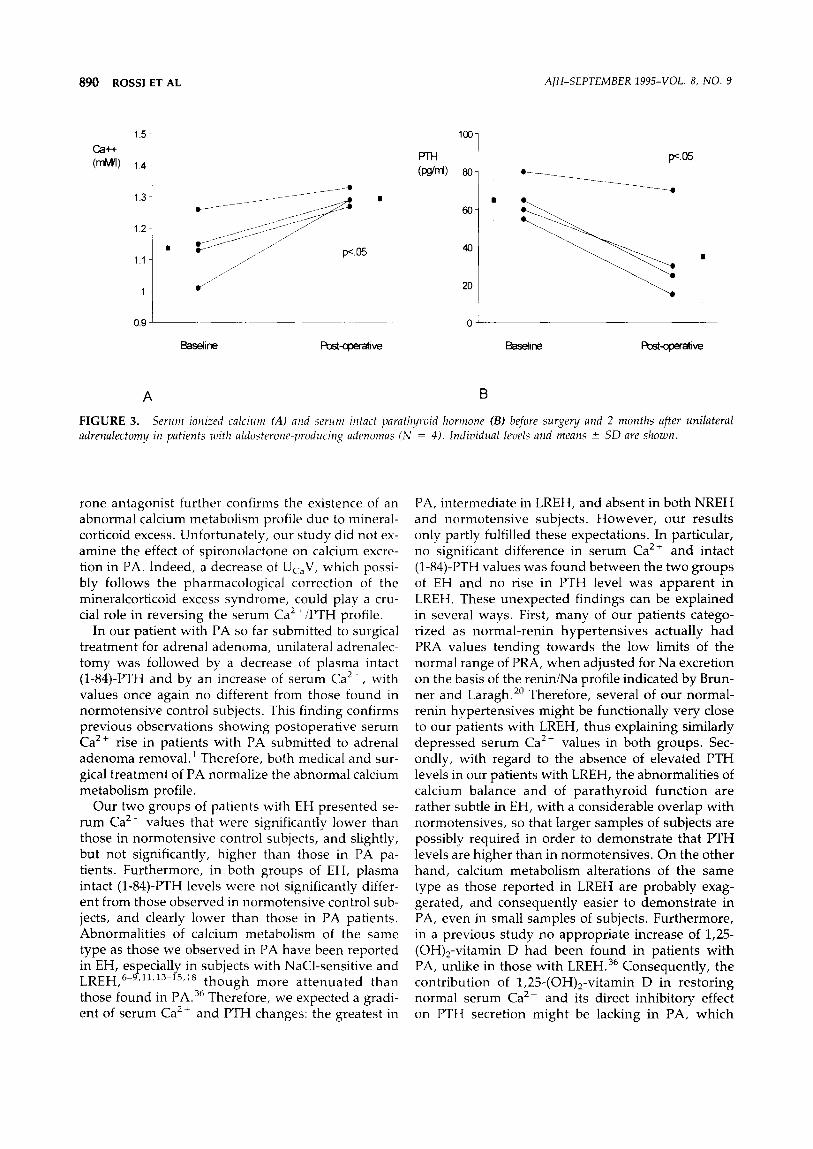
Table 4 shows the effects of unilateral adrenalecto- my on the four PA pat ients so far submi t t ed to sur- gical t r ea tmen t . S e r u m ionized ca lc ium inc reased f rom 1.14 ± 0.1 mmol /L to 1.29 ± 0.02 mmol /L (P < .05), and intact PTH decreased f rom 65 + 11 to 35 ± 24 pg/mL (P < .05). Individual changes in s e rum ion- ized calcium and in PTH are s h o w n in Figure 3.
Serum levels of ionized calcium and of intact PTH, both dur ing spi ronolactone t r ea tment and after sur- gical t rea tment , did not differ f rom those found in the no rmotens ive control subjects at the beg inn ing of the study.
D I S C U S S I O N
Our pat ients with PA had a m e a n s e rum level of in- tact (1-84)-PTH that was significantly h igher than that
TABLE 2. B L O O D P R E S S U R E A N D L A B O R A T O R Y V A L U E S IN THE S T U D Y G R O U P S
N S PA LREH N R E H (N = 10) (N = 10) (N = 10) (N = 10)
Blood pressure SBP (mm Hg) DBP (mm Hg)
Serum measurements PRA (ng/mL/h) ALDO (ng/dL) PTH (pg/mL) Total Ca (mg/dL) Ionized Ca 2 + (mmol/L) K + (retool/L) Mg (mg/dL) P (mg/dL)
Urinary measurements Ca (rag/24 h) Mg (mg/24 h) P (mg/24 h) Na (mmol/24 h) K (mmol/24 h)
121 ± 12.2 168.4 + 15.3~ 163 ± 14.6~ 164.5 ± 13.1~ 72.3 ± 5.3 102.7 ± 2.5~ 101.5 ± 3.8~ 103.4 ± 4.6~
1.28 ± 0.96 0.10 ± 0.02~ 0.29 ± 0.14#t 1.44 ± 0.41tt 19.3 ± 10 37.2 = l l .4 t 18.8 ± 9.3** 22.9 ± 8.6**
41 ± 15 70 ± 24t 35 ± 21"* 36 ± 10"* 8.86 z 0.30 8.94 ± 0.31 8.83 ± 0.39 8.93 ± 0.54 1.25 ± 0.05 1.17 ± 0.07t 1.19 ± 0.04§ 1.20 ± 0.02§ 3.85 ± 0.30 3.25 ± 0.64t 3.72 ± 0.15" 3.84 Z 0.48** 1.83 ± 0.12 1.84 ± 0.26 1.75 ~ 0.12 1.76 ± 0.12 2.77 ± 0.36 2.99 + 0.44 2.74 ± 0.46 2.63 ± 0.67
182 ± 80 206 ± 91 179 ± 61 195 ± 115 83.4 ± 27.0 58.5 ± 39.0 73.9 ± 13.0 76.6 ±34.8 692 ± 247 759 ± 455 695 ± 157 783 ± 255 105 ± 19 108 ± 25 100 ± 25 99 ± 19
70.2 ± 26.1 63.7 ± 14.4 76 ± 20.6 68 ~ 18.4
NS, Control subjects; PA, primary aldosteronism: LREH, low-renin essential hypertension; NREH, normal-renin essential hypertension.
~P < .05, ~-P < .01, ~:P < .001 v NS. *P < .05, **P < .01, f f P < .001 v PA. # P < .001 v NREH.

888 ROSSI ET AL AJH-SEPTEMBER 1995-VOL. 8, NO. 9
~3- A
C a + +
(raM/I)
1 2 - -
0
1 1 - -
13, r
2C
~3 B C a + +
(raM/U)
12
25 20 35 40 4§
K+ (raM/I)
O • O" 0
10
20 25 ~0 ~5 40
K+ (raM/I)
FIGURE 1. Relationship between serum ionized calcium (Ca 2 +) and serum potassium ( K - ) in the group of patients with primary aldosteronism (A), r = 0.74, P < .01, and in the 3 groups of hypertensive patients as a whole (B), r = 0.57, P < .001.
found in both heal thy normotens ive subjects and pa- tients with low- or normal- ren in EH. The greater para thyroid activity, as reflected by the higher serum intact (1-84)-PTH level, was associated with a mean serum Ca 2÷ that was significantly lower than that found in heal thy control subjects. Our results agree with previous findings concerning patients with PA who exhibited elevated PTH levels.] However , in that s tudy PTH was measured with C-terminal radioim- munoassay , which is not very sensitive or specific, above all in the presence of renal impairment . This renal impai rment cannot be ruled out in those pa- tients since renal function was exclusively evaluated th rough blood urea ni t rogen determinat ion.
Mean Uca V was not significantly higher in our pa- tients with PA compared with the other groups of subjects. However , in our s tudy, calcium intake, an impor tant factor affecting calcium excretion, was not
control led, so a significantly h igher UcaV wi th a given dietary intake of calcium cannot be excluded in PA compared to normotens ive control subjects. In- deed, an increase of UcaV after mineralcort icoid ad- ministrat ion has been observed in bo th animals 21 and humans . 22 Also, at an elevated Na intake, h igher UcaV has been repor ted in patients wi th PA com- pared with heal thy normotens ive subjects. 23 This el- evated UcaV needs vo lume expansion and the conse- quent "escape p h e n o m e n o n , " since, w h e n Na intake is very low, animals submit ted to chronic mineralcor- ticoid administrat ion 2] or h u m an s with PA 23 do not exhibit either elevated UcaV or higher UcaV than that found in control subjects. So a ldosterone per se does not seem to be responsible for increased UcaV.
Increased UcaV in PA may be due to reduced re- absorpt ion of calcium following a reduced reabsorp- tion of Na in aldosterone-insensi t ive tubular sites, where Na reabsorpt ion is closely connec ted wi th that of calcium. These tubular sites could be the target for natriuretic factors partly responsible for the "escape p h e n o m e n o n . " The increased Uc~V would cause a reduction of serum Ca 2÷ and consequent ly an appro- priate increase of PTH secretion, such as those we observed in our PA patients. Therefore, the extracel- lular vo lume expans ion fol lowing mineralcort icoid excess should be the prerequisi te for the increased Ca excretion in PA.
The reduct ion of serum Ca 2 . responsible for the increased para thyroid funct ion could be due alterna- tively to an abnormal distribution of calcium be tween extracellular and intracellular compar tments , with a surfeit of cytosolic free calcium coming f rom the ex- tracellular side. This would be similar to Resnick's
TABLE 3. CLINICAL A N D LABORATORY FEATURES OF THE PATIENTS WITH PRIMARY
ALDOSTERONISM BEFORE A N D DURING SPIRONOLACTONE TREATMENT
Spironolactone Baseline Treatment
SBP, mm Hg 168.4 -+ 15.3 139 + 12t DBP, mm Hg 102.7 -+ 2.5 85 -+ 9t K ÷, mmol/L 3.25 -+ 0.64 4.27 + 0.28t Ca 2÷ mmol/L 1.17 -+ 0.07 1.26 + 0.06t PRA, ngAI/mL/h 0.10 + 0.02 0.87 + 1.33" ALDO, ng/dL 37.2 + 11.4 42.1 -+ 16 PTH, pg/mL 70 -+ 24 39 + 15:~ UNaV, mrnol/24 h 108 -+ 25 115 + 26 UKV, mmol/24 h 63.7 -+ 14.4 66.8 + 18
SBP, Systolic blood pressure; DBP, diastolic blood pressure; K +, serum potassium; Ca 2+, serum ionized calcium; PRA, plasma renin activity; ALDO, plasma aldosterone; PTH, plasma parathyroid hormone; U,,,,~V, urinary sodium excretion; UKV, urina~ potassium excretion.
*P < .05; tP < .00I, CP < .0001.

AJH-SEPTEMBER 1995-VOL. 8, NO. 9 CALCIUM AND PARATHYROID HORMONE IN PRIMARY ALDOSTERONISM 889
Ca++ (mM/I)
1,5
1 4
1 3
1,2 -
11
1
0 . 9 - - - -
l (poj~) ~2o
l p< .001 • ~. •
/ /
B j / / p<.O01 I q t , - ~ _
o I
Baseline Spironolactone Baseline SpiroP~actone treatment treatment
A B
F I G U R E 2. Serum ionized calcium (,4) and serum intact parathyroid hormone (B) before and during spironolactone treatment in patients with primary aldosteronism (N = 10). Individual levels and means +_ SD are shown.
h y p o t h e s i s r e g a r d i n g the l o w - r e n i n a n d NaC1- sensit ive type of EH. 18
If this were the case, low se rum Ca 2 * could not closely d e p e n d on increased calcium excretion, thus explaining the absence of significantly higher Uc~V in our pa t i en t s w i th PA. H o w e v e r , this poss ib i l i ty sharp ly contras ts wi th recent f indings of u n c h a n g e d platelet cytosolic free calcium concentra t ion in pa- tients wi th PA, c o m p a r e d to the higher platelet con- centrat ion in pat ients wi th EH. 24
Other possible explanat ions of the al tered calcium metabo l i sm profile in PA cannot be ruled out. In our pat ients wi th PA, as well as in all hyper tens ive sub- jects, the se rum Ca 2 + level was posi t ively correlated wi th s e rum K + concentra t ion. This result indicates a possible pa thogen ic link be t ween po ta s s ium metabo- lism al terat ions and the abnormal i t ies of calcium me- tabolism in PA.
Indeed, the reduct ion of s e rum K ~ level following po ta s s ium depr iva t ion is associated with increased calcium excretion in both no rmotens ive heal thy sub- jects 25 and in pat ients wi th EH, in w h o m a rise of p lasma PTH level has also been found. 26 However , these changes too could be media ted by extracellular vo lume expans ion , since K deplet ion causes Na re- tent ion, desp i te the s u p p r e s s i o n of a ldos terone . 27 L ikewise , p o t a s s i u m d e p l e t i o n cou ld e x a g g e r a t e Na re tent ion and the consequen t increase in UcaV in PA, desp i t e an a t t enua t i on of the a ldos t e rone hypersecre t ion .
The rela t ionship be t ween para thyro id funct ion and PA is fur ther compl ica ted by some repor ts of hyper - calcemic p r i m a r y h y p e r p a r a t h y r o i d i s m assoc ia ted wi th PA. 28-35 Some of the repor ted cases may repre- sent a chance coexistence, while others seem to fall
within mult iple endocr ine neoplas ia type 1. 32 Some cases, however , could result f rom chronic pa ra thy- roid s t imulat ion caused by the low s e r u m Ca 2+ asso- ciated with PA progress ing to a u t o n o m o u s hyper - para thyro id i sm, as has been sugges ted by Resnick and Laragh. 1 In any case, none of our pat ients wi th PA presen ted biochemical features of p r ima ry hype r - para thyro id ism, or, in particular, h igh s e r u m Ca 2+ levels.
In our pat ients wi th PA, spi ronolactone t r ea tmen t was associated with an increase of s e r u m Ca 2 ÷ and a decrease of p la sma intact (1-84)-PTH level, wi th val- ues no different f rom those found in n o r m o t e n s i v e control subjects. This reversal induced by an aldoste-
TABLE 4. C L I N I C A L A N D L A B O R A T O R Y F E A T U R E S OF THE P A T I E N T S W I T H
A L D O S T E R O N E - P R O D U C I N G A D E N O M A S (N = 4) BEFORE S U R G E R Y A N D 2 M O N T H S AFTER
U N I L A T E R A L A D R E N A L E C T O M Y
Baseline Postoperative
SBP, mm Hg 179 +-+ 14 131 -+ 8* DBP, mm Hg 105 ± 2 82 + 3* K ÷, mmol/L 2.72 +- 0.65 3.97 --- 0.26* Ca 2÷ mmo|/L 1.14 ± 0.10 1.29 + 0.02* PRA, ngA1/mL/h 0.11 +- 0.02 1.96 ± 1.25" ALDO, ng/dL 39.6 + 16.9 10.9 + 6.5* PTH, pg/rnL 65 -+ 11 35 --+ 24* UNaV, mmol/24 h 107 + 11 110 -+ 14 UKV, mmol/24 h 64.2 + 7.5 68 + 12.3
SBP, Systolic blood pressure; DBP, diastolic blood pressure; K +, serum potassium; Ca 2 ~, serum ionized calcium; PRA, plasma renin activity; ALDO, plasma aldosterone; PTH, plasma parathyroid hormone; UN~V, urinary sodium excretion; UKV, urinary potassium excretion.
*P < .05.
890 ROSSI ET AL AJH-SEPTEMBER 1995-VOL. 8, NO. 9
C~-t-t-
(rr~)
151 1,4
1.3-
1.2 1" 1.1
0.
p<.05
1001 PTH (r~rrt) 8O
60
40
20
~.C)5
@
--...,
Baseline Post-operative Baseline Pos t~a t i ve
A B
FIGURE 3. Serum ionized calcium (A) and serum intact parathyroid hormone (B) before surgery and 2 months after unilateral adrenalectomy in patients with aldosterone-producing adenomas (N = 4). Individual levels and means + SD are shown.
rone antagonist further confirms the existence of an abnormal calcium metabolism profile due to mineral- corticoid excess. Unfortunately, our study did not ex- amine the effect of spironolactone on calcium excre- tion in PA. Indeed, a decrease of Uc~V, which possi- bly follows the pharmacological correction of the mineralcorticoid excess syndrome, could play a cru- cial role in reversing the serum Ca 2 +/PTH profile.
In our patient with PA so far submitted to surgical treatment for adrenal adenoma, unilateral adrenalec- tomy was followed by a decrease of plasma intact (1-84)-PTH and by an increase of serum Ca 2+, with values once again no different from those found in normotensive control subjects. This finding confirms previous observations showing postoperative serum Ca 2+ rise in patients with PA submitted to adrenal adenoma removal.1 Therefore, both medical and sur- gical treatment of PA normalize the abnormal calcium metabolism profile.
Our two groups of patients with EH presented se- rum Ca 2- values that were significantly lower than those in normotensive control subjects, and slightly, but not significantly, higher than those in PA pa- tients. Furthermore, in both groups of EH, plasma intact (1-84)-PTH levels were not significantly differ- ent from those observed in normotensive control sub- jects, and clearly lower than those in PA patients. Abnormalities of calcium metabolism of the same type as those we observed in PA have been reported in EH, especially in subjects with NaCl-sensitive and LREH, 6-9'11'13-15A8 though more at tenuated than those found in PA. 36 Therefore, we expected a gradi- ent of serum Ca 2+ and PTH changes: the greatest in
PA, intermediate in LREH, and absent in both NREH and normotensive subjects. However, our results only partly fulfilled these expectations. In particular, no significant difference in serum Ca 2-- and intact (1-84)-PTH values was found between the two groups of EH and no rise in PTH level was apparent in LREH. These unexpected findings can be explained in several ways. First, many of our patients catego- rized as normal-renin hypertensives actually had PRA values tending towards the low limits of the normal range of PRA, when adjusted for Na excretion on the basis of the renin/Na profile indicated by Brun- ner and Laragh. 2° Therefore, several of our normal- renin hypertensives might be functionally very close to our patients with LREH, thus explaining similarly depressed serum Ca 2+ values in both groups. Sec- ondly, with regard to the absence of elevated PTH levels in our patients with LREH, the abnormalities of calcium balance and of parathyroid function are rather subtle in EH, with a considerable overlap with normotensives, so that larger samples of subjects are possibly required in order to demonstrate that PTH levels are higher than in normotensives. On the other hand, calcium metabolism alterations of the same type as those reported in LREH are probably exag- gerated, and consequently easier to demonstrate in PA, even in small samples of subjects. Furthermore, in a previous study no appropriate increase of 1,25- (OH)2-vitamin D had been found in patients with PA, unlike in those with LREH. 36 Consequently, the contribution of 1,25-(OH)2-vitamin D in restoring normal serum Ca 2+ and its direct inhibitory effect on PTH secretion might be lacking in PA, which

AJH-SEPTEMBER 1995-VOL. 8, NO. 9 C AL C IUM A N D P A R A T H Y R O I D H O R M O N E IN PRIMARY A L D O S T E R O N I S M 891
partly explains the higher plasma PTH levels needed for maintaining normal or low-normal serum Ca 2- concentrat ion.
Therefore, our pat ients with EH seem to present more a t tenuated alterations of calcium/PTH profile, but of the same type as those we observed in PA. Fur thermore , the positive correlation be tween PTH and aldosterone levels that we have observed in the patients with EH is consistent with a common under- lying mechanism, possibly Na retention, that is re- spons ib le for the e n h a n c e d p a r a t h y r o i d act ivi ty th rough an altered calcium metabolism.
A possible contr ibut ion of altered para thyroid func- tion to the hyper t ens ion itself in PA cannot be ex- cluded. Hyper t ens ion is f requent ly associated with pr imary hyperpara thyro id i sm. 37 39 Fur thermore , in animal models of hyper tens ion , surgical removal of para thyroid glands prevents or at tenuates hyper ten- sion development . 4°~2
A role for PTH in itself seems unlikely, however , considering its wel l -known vasodilatory effects. 4>45 Nevertheless , high PTH levels can stimulate the syn- thesis of 1,25-(OH)x-vitamin D , 46'47 whose propert ies on calcium uptake and growth and contractile force of vascular smooth muscle make it a likely candidate for a contr ibution to hyper tens ion . 4s On the other hand, unlike LREH, where 1,23-(OH)2-vitamin D level is raised, 15"16 PA is apparent ly characterized by both a relatively suppressed 1,25-(OH)2-vitamin D and an inverse relat ionship be tween 1,25-(OH)2-vitamin D and PTH. 36
Evidence indicating the existence of a hyper tens ive substance of para thyroid origin both in some animal models of hyper t ens ion 49-51 and in humans with low- renin and salt-sensitive EH s2'53 has accumulated. In- t e res t ing ly , this p a r a t h y r o i d h y p e r t e n s i v e factor (PHF) has been found in the plasma of DOCA-salt hyper tens ive rats, an animal model of mineralcorti- cold hyper tens ion , but not in r en in -dependen t two- kidney, one-clip hyper tens ive rats. 51 Likewise, PHF could also be elevated in PA patients as a result of para thyroid stimulation and hyperfunct ion.
Our findings might disclose new therapeutic per- spectives and allow greater unders tand ing of the ef- fects of calcium channel blockers in PA. In fact, cal- cium supplementa t ion and calcium channel blockers seem to be more effective in patients with low-renin and NaCl-sens i t ive EH. 54 58 F u r t h e r m o r e , in the same subgroups of EH the effects of calcium supple- menta t ion and calcium channel blockers on blood pressure are apparent ly correlated to pre t rea tment Ca2+/PTH alterations of the same type we have ob- served in PA. ss-s8 Moreover , calcium supplementa- tion both a t tenuates the blood pressure increase and inhibits the expression of PHF in DOCA-salt rats. -~9 So we may hypothes ize analogous effects of calcium
supplementa t ion in patients with PA. Finally, the ef- fects of calcium channel antagonists on blood pres- sure in PA, besides being the result of r educed aldo- s terone secretion, 6° could part ly d e p e n d on the rever- sal or a t tenuat ion of calcium metabol ism changes.
REFERENCES
1. Resnick LM, Laragh JH: Calcium metabolism and parathyroid function in primary aldosteronism. Am J Med 1985;78:385-390.
2. Postnov YV, Orlov SN, Pokudin NI: Alterations of intracellular calcium distribution in the adipose tissue of human patients with essential hypertension. Pfl/igers Arch 1980;388:89-91.
3. Zidek W, Vetter H, Dorst KG, et al: Intracellular Na + a n d Ca 2 + activities in essential hypertension. Clin Sci 1982;63:413435.
4. Erne P, Bolli P, Burgisser E, et al: Correlation of plate- let calcium with blood pressure. Effect of antihyper- tensive therapy. N Engl J Med 1984;310:1084-1088.
5. Bruschi G, Bruschi ME, Caroppo M, et al: Cytoplasmic free [Ca 2~ ] is increased in the platelets of spontane- ously hypertensive rats and essential hypertensive pa- tients. Clin Sci 1985;68:179-184.
6. McCarron DA: Low serum concentrations of ionized calcium in patients with hypertension. N Engl J Med 1982;307:226-228.
7. Resnick LM, Laragh JH, Sealey JE, et al: Divalent cat- ions in essential hypertension: relations between se- rum ionized calcium, magnesium, and plasma renin activity. N Engl J Med 1983;309:888-891.
8. Ljunghall S, Hvarfner A, Lind L: Clinical studies of calcium metabolism in essential hypertension. Eur Heart J 1987;8(suppl B):37-44.
9. McCarron DA, Pingree PA, Rubin RJ, et al: Enhanced parathyroid function in essential hypertension: a ho- meostatic response to a urinary calcium leak. Hyper- tension 1980;2:162-168.
10. Strazzullo P, Nunziata V, Cirillo M, et al: Abnormali- ties of calcium metabolism in essential hypertension. Clin Sci 1983;65:137-141.
11. Strazzullo P, Galletti F, Cirillo M, et al: Altered extra- cellular calcium homeostasis in essential hyperten- sion: a consequence of abnormal cell calcium han- dling. Clin Sci 1986;71:239-244.
12. Gadallah M, Massry SG, Bigazzi R, et al: Intestinal absorption of calcium and calcium metabolism in pa- tients with essential hypertension and normal renal function. Am J Hypertens 1991;4:404-409.
13. Gennari C, Nami R, Bianchini C, et al: Renal excretion of calcium in human hypertension. Am J Nephrol 1986;6(suppl 1):124-127.
14. Grobbee DE, Hackeng WHL, Birkenh/iger JC, et al: Intact parathyroid hormone (1-84) in primary hyper- tension. Clin Exp Hypertens 1986;8:299-308.
15. Resnick LM, Muller FB, Laragh JH: Calcium regulat- ing hormones in essential hypertension: relation to plasma renin activity and sodium metabolism. Ann Intern Med 1986;105:649-654.

892 ROSSI ET AL AJH-SEPTEMBER 1995-VOL. 8, NO. 9
16. Brickman AS, Nyby MD, Von Hungen K, et ah Cal- ciotropic hormones, platelet calcium and blood pres- sure in essential hypertension. Hypertension 1990;16: 515-522.
17. Hughes GS, Jr., Oexmann MJ, Margolius HS, et ah Normal vitamin D and mineral metabolism in essen- tial hypertension. Am J Med Sci 1988;296:252-259.
18. Resnick LM: Cellular calcium and magnesium metab- olism in the pathophysiology and treatment of hyper- tension and related metabolic disorders. Am J Med 1992;93(suppl 2A):11S-20S.
19. Galletti F, Ferrara I, Stinga F, et al: Effect of intrave- nous sodium chloride on renal sodium and calcium handling in hypertensive patients with different sen- sitivities to sodium chloride. J Hyper tens 1993; 11(suppl 5):$194-S195.
20. Brunner HR, Laragh JH, Baer L, et ah Essential hyper- tension: renin and aldosterone, heart attack and stroke. N Engl J Med 1972;286:'441-449.
21. Suki WN, Schwettmann RS, Rector FC, et al: Effect of chronic mineralcorticoid administration on calcium ex- cretion in the rat. Am J Physiol 1968;215:71-74.
22. Cappuccio FP, Markandu ND, Mac Gregor GA: Renal handling of calcium and phosphate during mineral- corticoid administration in normal subjects. Nephron 1988;48:280-283.
23. Rastegar A, Agus Z, Connor TB, et al: Renal handling of calcium and phosphate during mineralcorticoid "escape" in man. Kidney Int 1972;2:279-286.
24. Oh-hashi S, Takata M, Ueno H, et al: Cytosolic free calcium concentrations in platelets in patients with re- novascular hypertension and primary aldosteronism. J Human Hypertens 1992;6:71-74.
25. Lemann J, Jr., Pleuss JA, Gray RW, et ah Potassium administration reduces and potassium deprivation in- creases urinary calcium excretion in healthy adults. Kidney Int 1991;39:973-983.
26. Krishna GG, Kapoor SC: Potassium depletion exacer- bates essential hypertension. Ann Intern Med 1991; 115:77-83.
27. Krishna GG, Chusid P, Hoeldtke RD: Mild potassium depletion provokes renal sodium retention. J Lab Clin Med 1987;109:724-730.
28. Strauch G, Vallotton MB, Touitou Y, et al: The renin- angiotensin-aldosterone system in normotensive and hypertensive patients with acromegaly. N Engl J Med 1972;287:795-799.
29. Ferris JB, Brown JJ, Cumming AMM, et al: Primary hyperparathyroidism associated with primary hyper- aldosteronism. Acta Endocrinol 1983;103:365-370.
30. Herd GW: A case of primary hyperparathyroidism, primary hyperaldosteronism and Cushing's disease. Acta Endocrinol 1984;107:371-374.
31. Hellman DE, Kartchner M, Komar N, et ah Hyper- a ldosteronism, hyperpara thyro id i sm, medul lary sponge kidneys, and hypertension. JAMA 1980;244: 1351-1353.
32. Beckers A, Abs R, Willems PJ, et ah Aldosterone- secreting adrenal adenoma as part of multiple endo- crine neoplasia type 1 (MEN 1): loss of heterozygosity for polymorphic chromosome 11 deoxyribonucleic
acid markers, including the MEN 1 locus. J Clin En- docrinol Metab 1992;75:564-570.
33. Ballards HS, Frame B, Hartsock RJ: Familial multiple endocrine adenoma-peptic ulcer complex. Medicine 1964;43:481-516.
34. Madhavan T, Frame B, Block MA: Influence of surgi- cal correction of primary hyperparathyroidism on as- sociated hypertension. Arch Surg 1970;100:212-214.
35. Fertig A, Webley M, Lynn JA: Primary hyperparathy- roidism in a patient with Conn's syndrome. Postgrad Med J 1980;56:45-47.
36. Resnick LM, Gertner JM, Laragh JH: Abnormal vita- min D metabolism in primary aldosteronism and ex- perimental mineralcorticoid excess. J Hyper tens 1987;5(suppl 5):$99-$101.
37. Hellstrom J, Birke G, Edvall CA: Hypertension in hy- perparathyroidism. Br J Urol 1958;30:13-24.
38. Rosenthal FD, Roy S: Hyper tens ion and hyper- parathyroidism. Br Med J 1972;4:396-397.
39. Lueg MC: Hypertension and primary hyperparathy- roidism: a five year case review. South Med J 1982;146: 1709-1712.
40. Berthelot A, Gairard A: Parathyroid hormone and deoxycorticosterone acetate induced hypertension in the rat. Clin Sci 1980;58:365-371.
41. Gairard A, Berthelot A, Schleiffer R, et al: Parathyroid- ectomy significantly decreases hypertension in spon- taneously hypertensive and deoxycorticosterone plus saline treated rats. Can J Physiol Pharmacol 1982;60: 208-212.
42. Mann JFE, WieceK A, Bommer J, et al: Effects of para- thyroidectomy on blood pressure in spontaneously hypertensive rats. Nephron 1987;45:46-52.
43. Pang PKT, Janssen HF, Yee JA: Effects of synthetic parathyroid hormone on vascular beds of dogs. Phar- macology 1980;21:213--222.
44. Pang PKT, Uang MCM, Kautmann HT, et al: Structure activity relationship of parathyroid hormone: separa- tion of the hypotensive and the hypercalcemic prop- erties. Endocrinology 1983;112:284-289.
45. McCarron DA, Ellison DH, Anderson S: Vasodilation mediated by human PTH 1-34 in the spontaneously hypertensive rat. Am J Physiol 1984;246:F96-F100.
46. Ambrecht HJ, Wongsurawat N, Zenser TW, et al: Ef- fect of PTH and 1,25 (OH)2-D 3 on renal 25 (OH)D 3 metabolism, adenylate cyclase, and protein kinase. Am ] Physiol 1984;246:E102-E107.
47. Haussler MR, Mc Cain TA: Basic and clinical concepts related to vitamin D metabolism and action. N Engl J Med 1977;297:974-983.
48. Bukoski RD, Kremer D: Calcium-regulating hormones in hypertension: vascular actions. Am J Clin Nutr 1991;54:220S-226S.
49. Pang PKT, Lewanczuk RZ: Parathyroid origin of a new circulating hypertensive factor in spontaneously hypertensive rats. Am J Hypertens 1989;2:549-552.
50. Lewanczuk RZ, Wang J, Zhang ZR, et al: Effects of spontaneously hypertensive rat plasma on blood pres- sure and tail artery calcium uptake in normotensive rats. Am J Hypertens 1989;2:26-31.

AJH-SEPTEMBER 1995-VOL. 8, NO. 9 CALCIUM AND PARATHYROID HORMONE IN PRIMARY ALDOSTERONISM 893
51. Lewanczuk RZ, Pang PKT: Parathyroid hypertensive factor is present in DOCA-salt but not two kidney-one clip hypertensive rats. Am J Hypertens 1991;4:802- 805.
52. Lewanczuk RZ, Resnick LM, Blumenfeld JD, et al: A new circulating hypertensive factor in the plasma of essential hypertensive subjects. J Hypertens 1990;8: 105-108.
53. Resnick LM, Lewanczuk RZ, Laragh JH, et al: Para- thyroid hypertensive factor-like activity in human es- sential hypertension: relationship to piasma renin ac- tivity and dietary salt sensitivity. J Hypertens 1993;11: 1235-1241.
54. Weinberger MH, Wagner UL, Fineberg NS: The blood pressure effects of calcium supplementation in hu- mans of known sodium responsiveness. Am J Hyper- tens 1993;6:799-805.
55. Resnick LM, Sealey JE, Laragh JH: Short and long- term oral calcium alters blood pressure (BP) in essen- tial hypertension (abst). Fed Proc 1983;42:300.
56. Resnick LM, Nicholson JP, Laragh JH: Outpatient therapy of essential hypertension with dietary calcium supplementation (abst). J Am Coll Cardiol 1984;3:616.
57. Resnick LM, Nicholson JP, Laragh JH: Calcium, the renin-angiotensin system, and the hypotensive re- sponse to nifedipine. Hypertension 1987;10:254-258.
58. Resnick LM, Nicholson JP, Laragh JH: The effects of calcium channel blockade on blood pressure and cal- cium metabolism. Am J Hypertens 1989;2:927-930.
59. Lin C, Saito K, Tosjino T, et al: Calcium supplemen- tation inhibits the expression of parathyroid hyperten- sive factor in DOCA-salt hypertensive rats. Am J Hy- pertens 1994;7:201-204.
60. Nadler JL, Hseuh W, Horton R: Therapeutic effect of calcium channel blockade in primary aldosteronism. J Clin Endocrinol Metab 1985;60:896-899.
Copyright © 2022 FDOKUMEN




















