
Enhanced GRK2 Expression and Desensitization of βAR Vasodilatation in Hypertensive Patients
Upload
independentCategory
view
0download
0
Renin, Angiotensin and Aldosterone System in Pathogenesis and Management of Hypertensive Vascular Disease
JOHN H. LARAGH, M D.
LESLIE 3AER, M.D.
HANS R. BRUNNER, M.D.
FRITZ R. BUHLER, M.D.
JEAN E. SEALEY, B.S.
E. DARRACOTT VAUGHAN, Jr., M.D.
New York, New York
From the Department of Medicine, College
of Physicians and Surgeons, Columbia-
Presbyterian Medical Center, New York, New York 10032. Requests for reprints
should be addressed to Dr. John H.
Laragh.
The renin angiotensin aldosterone concatenation, via two ef-
fector components, angiotensin II and aldosterone, simultane- ously regulates (1) body sodium and water content, (2) arterial
blood pressure and (3) potassium balance. Renin, secreted in response to stimuli which compromise
kidney perfusion, increases plasma angiotensin and this stimu- lates aldosterone secretion. Vascular tone is regulated by an interaction between angiotensin levels and available (intravas- cular) sodium ions. The two hormones thus restore sodium bal- ance and arterial pressure, thereby turning off renin release. Potassium homeostasis is maintained by two direct but oppos- ing effects of plasma potassium levels on aldosterone and renin secretion.
Derangements of this cybernetic system are involved in the pathogenesis of malignant hypertension, primary and pseudo- primary aldosteronism, renovascular hypertension and oral con- traceptive hypertension.
Subtler abnormalities in the renal adrenal axis occur in es- sential hypertension: Three major subgroups exhibit low (27
per cent), normal (57 per cent) or high plasma renin activity (16 per cent). When aldosterone is included, eight different hormonal profiles have been identified.
Longitudinal studies indicate that, in contrast to groups with normal and high renin activity, patients with low renin essen- tial hypertension appear to be protected from the development of strokes and heart attacks despite similar hypertension and cardiac enlargement and a higher age.
Taken with the observations in malignant hypertension, plasma renin activity emerges as a risk factor predisposing to serious vascular injury. It thus may be a useful guide for de- termining etiology and prognosis.
New therapeutic strategies are also suggested. Patients with low renin activity may not require early treatment whereas it should be diligently applied in those with high renin activity. Moreover, individualized antihypertensive therapy to correct spe- cific derangements in the renin system holds special promise.
In the past twelve years it has become apparent that the
renin-angiotensin-aldosterone system plays a vital role in the
regulation of electrolyte and blood pressure homeostasis in
man. Studies of patients with malignant hypertension in par-
ticular provided a critical clue for identification of this
Volume 52, May 1972 633

RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION-LARAGH ET AL.
‘EFFECTIVE’ BLOOD VOLUME or PRESSURE-
RENAL J.G CELLS I
RENIN
I +
PLASMA SUBSTRATE - ANGIOTENSIN I I
ADRENAL CORTEX c__, ALDOSTERONE
RENAL TIJBULE- No+ RESORPTION
Figure 1. The renin-angiotensin-aldosterone system and the cybernetics of sodium and volume homeostasis.
renal-adrenal hormonal interrelationship [l-3]. It has been shown that derangements of this regula- tory system occur not only in malignant hyperten- sion and in primary aldosteronism [l-5], but also in renal vascular hypertension [6] and in oral con- traceptive hypertension [7a]. These disorders rep- resent the more dlramatic syndromes in which ab- normalities of renin and aldosterone are easily demonstrated. But, altogether they comprise only a small portion of the large hypertensive popula- tion.
In this discussion, the aberrations in the renin- angiotensin-aldosterone system characteristic of these syndromes will be considered in detail in order to elaborate the pathophysiology of the con- ditions and the dynamic behavior of the regula- tory system. With this information in hand, the possibility of a less apparent participation of the renal-adrenal axis in the more common forms and stages of hypertensive vascular disease will be examined. In particular, the question whether or not subtle abnormalities are involved in the large population of hypertensive subjects now subsumed under the. rubric of benign essential hypertension will be considered.
From all of this, a physiologic classification of the spectrum of hypertensive diseases in terms of apparent involvement of the renal-adrenal hor- monal system can be developed. This information ‘may be useful for understanding etiology, deter- mining prognosis and planning treatment of pa- tients with high blood pressure.
THE SYSTEM DEFINED
The renin-angiotensin-aldosterone system appears to regulate sodium balance, fluid volume and blo’od pressure as follows: when, as the result of
such events as helmorrhage, sodium depletion, transudation or alimentary loss, effective blood volume contracts and arterial pressure falls, the kidney’s perfusion is threatened and it secretes renin into the blood stream. Renin acts enzymati- caliy on a plasma globulin to release angiotensin I. Angiotensin I is then rapidly hydrolyzed to angio- tensin II by pulmonary and plasma converting en- zymes. Angiotensin II, in addition to its pressor action, stimulates aldosterone secretion. Aldo- sterone acts on the kidney to cause sodium reten- tion. This positive sodium balance leads to a sec- ondary retention of water and expansion of the extracellular fluids. Thus angiotensin and aldo- sterone together act to raise the blood pressure and restore renal perfusion, thereby compensating the system and shutting off the initial signal to renal renin release (Figure 1).
Arterial blood presure is maintained by a co- ordinated interaction between plasma angiotensin and available sodium ions. The product of this interaction determines vascular tone and pressor responsiveness. This relationship has been char- acterized in normal human subjects receiving an- giotensin infusions [14]. Angiotensin-aldosterone- induced sodium retention was associated with in- creased pressor sensitivity to angiotensin. Con- versely, sodium-depleted subjects exhibited a re- duced pressor responsiven’ess. The low blood pres- sures and the markedly reduced sensitivity of pa- tients with cirrhosis and ascites in the face of large increases in total body sodium content suggest that it is the amount of sodium retained within the vascular bed or in the effective circulation which is important in this relationship [14]. These results describe an internally controlled feedback for hormonal interaction built around the state of sodium balance. More recent studies have dem- onstrated that the binding affinity of angiotensin II vascular receptors is directly related to the state of sodium balance [79].
Simultaneously, the renin-angiotensin system participates in the regulation of potassium homeo- stasis. This activity tends to stabilize plasma po- tassium Ieve,ls and avoid dangerous hyperkalemia which may develop in patients with adrenal in- sufficiency after a meal of high potassium con- tent. Increases in plasma potassium act directly on the adrenal cortex to stimulate aldosterone release. This in turn promotes kaliuresis. As the plas’ma potassium level falls, aldosterone secre- tion is retarded [7b,7c]. At the same time, in- creases in plasma potassium act directly on the kidney to inhibit renin release whereas hypoka-
634 The American Journal of Medicine

RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
lemma is a potent stimulus for renin secretion.
Thus renal conservation 0’ elimination of potas-
sium ions is closeiy related to opposite changes
In both renin anti aldosterone secretion [7d,7e]. Full understanding of these interrelationships re-
quires further study. The ultimate signal indl;cing renin release has
not yet been identified, but it appears to involve
a pressure or stretch sensitive receptor in the renal afferent arterioles, a distal tubular macula densa receptor responsive to changes in sodium delivery, changes in autonomic nerve activity and
changes in potassium balance. Increases in plasma angiotensin levels may “feed back” to retard fur-
ther renin secretion. The renin-angiotensin-aldosterone system has
two effector hormones: angiotensin II and aldo- sterone.
Angiotensin II is an octapeptide with three strik- ing physiologic actions: (1) in constricting the arterioles, it is by weight the most potent pressor substance known; (2) it acts directly on the kidney to cause sodium retention with lower dosages and natriuresis with larger amounts; and (3) it acts on the adrenal cortex to evoke a prompt and sustained increase in aldosterone secretion. The concentra- tion of angiotensin II in human venous plasma normally ranges from 1 to 10 mpg/100 ml.
Aldosterone, the second effector hormone of the system, is an adrenal corticosteroid, unique because of its 18.aldehyde configuration. It acts primarily on the renal tubules to increase the re- absorption of sodium chloride and to promote the elimination of potassium ions. Like angiotensin II, aldosterone is present in relatively minute amounts. Its blood level is approximately l/lO,OOOth of that of cortisol, and in man it
ranges from 1 to 10 m,Lg/lOO ml of venous plasma. Yet, because of its great potency, aldo-
sterone undoubtedly plays a major role in sodium and potassium homeostasis.
The other components of the renin-angiotensin system do not have any known significant physio- logic actions. Thus, renin is a proteolytic enzyme made and secreted primarily, if not exclusively, by the juxtaglomerular cells of the kidney. Renin acts enzymatically on a circulating plasma globu- lin, the renin substrate also called angiotensino- gen, to release the decapeptide angiotensin I. Angiotensin I is hydrolyzed very rapidly by con- verting enzymes present in the lung and more slowly by similar enzymes in plasma, which re-
move the terminal histidyl-leucine liberating into
the circulation the physiologically active octapep-
Volume 52, May 1972
tide, angiotensln II. It has not yet been possible
to measure endogenous plasma angiotensin I.
Howeve<. when converting enzymes are inhibited
in vitro! the quantitation of angiotensin I forma- tion becomes a measure of renin activity.
In this system. both the renin substrate and the converting enzymes are ordinarily present in
sufficient amount so that their concentrations are not physiologically rate-limiting for the forma- tion of angiotensin II. Therefore, a relatively small change in the concentration of renin in plasma is usually the major determinant of the final concentration of circulating angiotensin II. By
changing the plasma concentrations of the effector componen’i-s, angiotensin II and aldosterone, this hormonal interaction simultaneously regulates (1)
body sodium and water content, and thus hydro- static pressures; (2) arterial blood pressure; and (3) potassium balance.
Because the direct measurement of circulating angiotensin II requires methods of great sensi- tivity and because changes in plasma renin usu-
ally closely parallel induced changes in circulat- ing angiotensin II, the measurement of plasma renin “activity” has proved to be a simpler and a most reliable indicator of changes in angiotensin generation. Moreover, since the kidney is the major source of plasma renin, measurements of plasma renin activity are ordinarily a reliable in- dex of renal renin secretion.
For a more detailed review of the hormonal system, the reader is referred to recent mono-
graphs C&91.
STUDY APPROACHES
Patient Material. Patients at the Nephritis Hyperten-
sion Clinic or the Doctor’s Private Office Facilities of the Columbia-Presbyterian Medical Center were studied over a period of fifteen years. Although this institu-
tion accepts referrals from the greater New York area and also from more distant points, the principal catch-
ment area consists of upper parts of Manhattan and the Bronx.
Most of the patients were admitted to the metabolic unit of Presbyterian Hospital, but about 20 per cent were studied as outpatients. Prior to evaluation, all had discontinued taking antihypertensive and diuretic drugs for at least three weeks, and they were given diets con- taining unrestricted amounts of sodium. All were given a complete work-up that included intravenous pyelogra- phy and often renal arteriography.
The renin-angiotensin-aldosterone system was eval- uated on the fifth day of a fixed dietary regimen of known electrolyte content. Most patients were studied in this way at two or more different levels of constant
635

RENIN. ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
sodium intake. Renin activity was measured from plasma samples taken at noon after the patients had been ambulatory for at l’east four hours. Matching twenty-four hour urine samples were saved for the de- termination of aldosterone and sodium excretion.
Procedures necessarily differed for the patients studied as outpatients. Such patients were instructed not to avoid sodium in their diets, and the state of their salt balance was inferred from twenty-four hour urinary sodium excretion. Among them, the rate of sodium ex- cretion ranged from 100 to 250 mEq/day with little intraindividual variation. At these rates, the influence of any dietary inconsistency on renin and aldosterone secretion could be expected to be small. The findings among the outpatients have completely paralleled and reinforced the data obtained under controlled condi- tions in the metabolic unit.
Normal values were defined by submitting normal volunteers to the same dietary regimens utilized for patients. Some of the normal volunteers were studied while housed on the metabolic ward, others were not hospitalized but received a constant dietary regimen, and a third group was allowed unrestricted diets. Analytical fviettiods. Plasma renin activity was mea- sured using a basic incubation procedure followed by either pressor bioassay or radioimmunoassay of angio- tensin I. The methods are accurate and reproducible. The standard deviation of the radioimmunoassay is 11.6 per cent [lo], somewhat lower than the bioassay procedure [lo]. Interchangeability of the results is achieved when a correction factor of 2.2 is applied to bioassay results in order to account for the greater pressor activity per unit weight of angiotensin II com- pared with angiotensin I.
Aldosterone excretion was evaluated by measure- ment of the twenty-four hour urinary excretion rate of the acid-labile conjugate of the hormone. The aldo- sterone, which is reconstituted by acid hydrolysis, can be quantitated with a sensitive, reliable and relatively simple radioimmunoassay [ll] or, in earlier studies, a more laborious method which utilizes instead multiple chromatography, acetylation and a double isotope dilu- tion technic [12]. Complete correlation and identity of the results of the two methods has been demonstrated over a wide range. The standard deviation of the radio- immunoassay is less than 8 per cent and is lower than that of the double isotope dilution method [ll].
It has been our view that the twenty-four hour uri- nary measurement is an integrated reflection of the daily adrenal secretion of aldosterone and thus pro- vides more useful information than a plasma value which can reflect only a single point in time. Twenty- four hour urine collections are ‘essential at any rate, since the interpretation of either plasma renin or plasma aldosterone levels requires that they be related to the state of sodium balance, an evaluation of which is provided by no practical alternative to twenty-four hour urine collections.
CRITERIA FOR EVALUATION OF
HORMONAL ABNORMALITIES
Our own approaches in studying the renin-an-
giotensin-aldosterone system has been fully re-
ported elsewhere [l-4,10-12], but at least one aspect of the methods employed warrants em- phasis in this review of the state of the art for it is critically responsible for some findings we con- sider important. This pertains to the question of relating assay values to the state of salt balance.
It should be obvious at the outset that a system whose physiologic tasks are associated with salt
balance, and is triggered by the effects of changes in salt balance, must be evaluated relative to this feature. Whether a given level of renin, angioten- sin or aldosterone can be considered normal de- pends on its physiologic assignment of the mo- ment, either to maintain a satisfa’ctory electrolyte
equilibrium or to buffer the consequences of an undesirably high or low salt level. This problem
has been given consideration by most workers in the field and generally settled by the practice of setting certain bracketed ranges of normal values for various levels of salt ~intake. Values found in
salt-controlled subjects can then be evaluated against these ranges.
The grossly abnormal levels obtained in the more acute hypertensive states can be assessed against such an index with relative ease. How- ever, when there are subtle abnormalities in the
system these may not be exposed with the use of such brackets. Thus, if the urine sodium level of the sample falls at one extreme of the bracketed range an abnormal value ,m#ight be interpreted as normal because such values would be normal for the other extreme of the bra’cket. This becomes a
problem of some consequence when the intent is to study the renin-angiotensin-aldosterone sys- tem involvement in the more indolent, chronic conditions in which deviations from normal are expectedly of smaller dimension.
Accordingly, we have taken a different approach and have attempted to construct an index of normality whose continuity would reflect t,he linear responsiveness of this system. By subjecting nor- mal volunteers to various levels of salt balance nomograms were constructed giving normal values for renin a,ctivity and aldosterone excretion over a wide range of physiologic variation. As can be seen in Figure 2, the relationship of these values to salt balance is direct, continuous and within rather well defined limits. This index permits a more precise observation of renin-angiotensin-al-
636 The American Journal of Medicine

RENIN. ANGIOTENSIN AND ALDOjTERONE SYSTEM IN HYPERlENSION LARAGH ET A_
Figure 2. Refation of both renin ac-
tivity in plasma samples obtained at
noon and of the corresponding twenty-
four hour urinary excretion of aldoste-
rone to the concurrent daily rate of SO-
dium excretion. For these normal sub-
jects, the data describe a similar dy-
namic hyperbolic relationship between
each hormone and sodium excretion.
Of note is the fact that subjects stud-
ied on random diets outside the hos-
pital exhibited similar relationships, a
finding which validates the use of this
nomogram in studying outpatients or
subjects not receivrng constant diets.
See text.
Norwol Subjects
,. RIahiDOM SAMPLf ,. L_-__. _ -. ..~
8,:
0
0 100 ZOO 300 0 100 200 URINE SODIUM mfR/QaY
dosterone system relationships in essential hyper- tension as will be discussed later.
It also became apparent in practice, by com- parison, that the close association between salt balance and the components of the renin-angio- tensin-aldosterone system was equally well re- flected whether salt balance status was deter- mined on the basis of dfetary control (balance conditions) or on the basis of a random twenty- four hour urine collection. We found with serial daily studies that changes in the renin and aldo- sterone levels closely followed changes in the urinary sodium excretion rate even before equi- librium was achieved. There was often a lag of up to four days before sodium intake was reflected by urinary sodium excretion. During this period the renin and aldosterone values exhibited an appro- priate relationship to sodium excretion but not to
sodium intake. Technically, too, daily sodium out- put is more readily tracked than either dietary in- take or the more laborious and error ridden sodium balance calculations. The approach has the ad- ditional advantage of being applicable to the study elf outpatients on random diets.
Certain theoretic consrderations support the practice. The kidney is normally the major route for sodium elimination, and the rate of sodium excretion reflects the extent to which the kidney
is being directed to retain or release sodium. The hormonal activity is thus related to the target organ response rather than to changes in the homeostatic function which probably is subserved, i.e., sodium balance.
The results in Figure 2 suggest certain guide- lines for classification of patients. Thus, it is ap-
parent that patients with high renin levels may not be detected if studied while adhering to a low salt diet. Also, it is difficult to identify patients with subnormal plasma renin activity when the urinary sodium excretion is above 150 mEq/day. If only one point on the curve is available for
classification of a patient, the ideal range of urinary sodium excretion would be between 40 and 100 mEq/day. In the case of plasma renin ac- tivity, occasional values appear inappropriately high in subjects not under dietary control (Figure 2). However, no subjects eating random diets ex- hibited inappropriately low values. Thus, patients who exhibit borderline high plasma renin activity and those whose values fall on the lower edge of the normal curve should be more definitively categorized under balance conditions.
Pathophysiology of Hypertensive Syndromes with Outstanding Abnormalities of the Renin-Angioten- sin-Aldosterone System
Malignant Hypertension Versus Primary and Pseudoprimary Aldosteronism. The syndrome of malignant hypertension is defined clinically by severe and accelerating hypertension with neuro- retinopathy and evidence of advancing renai dis- ease, and pathologically by necrotizing arterio- litis especially involving the kidney [13]. The con- dition, usually a sequel to various types of benign hypertension, is nearly always fatal within a year if no treatment is applied.
An analysis of the physiologic derangements observed in this syndrome has led to an under- standing of the renin-angiotensin system and its involvement in various other disorders. Thus, an
Volume 52, May 1972 637

RENIN. ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
MALIGNANT HrPERTEMSlO#
2G Patients -43 Oalarminotionr
ALOOSTERONE .
i
A A
SECRETION 600 #glOAY :
600 -
500 -
400 -
300 -
200 -
100 -
4 .
i:
.3 .
. . I A
. OLb”““” 100 1, I I I. 200 300 I LI 0 811 100 200 I
URINARY SODIUM EXCRETION m&q/DAY
early survey of the possible role of increased aldo- sterone secretion in the spectrum of hypertensive diseases revealed that aldosterone secretion was practically always increased not only in primary aldosteronism but also in malignant hypertension [l]. Indeed, the values observed in malignant hypertension were often enormously elevated to levels considerably higher than those observed in primary aldos’teronism (Figure 3). These observations raised a qu’estion: How do these two hypertensive disorders, characterized by oversecretion of aldosterone differ and what do they have in common? Actually, the two con- ditions are quite different. The typical clinical picture of primary aldosteronism is one of benign, often long-standing hypertension. Potassium wast- age is the cardinal physiologic defect. Pathologi- cally, there is little vascular injury. The condition is completely cured by removal of the offending adenoma. Therefore, primary aldosteronism may be viewed as a clinical expression of autonomous oversecretion of aldosterone in an otherwise healthy subject.
On the other hand, malignant hypertension is quite a different disorder both clinically and path- ologically. Adrenal tumors are not the rule so tmhat
638
Figure 3. Aldosterone secretion and sodium excretion in malignant hyper- tension. In all but one instance, marked oversecretion was observed. At the higher levels of sodium excretion in particular, there is no overlap with the normal range. From Laragh et al. 1121.
adrenal oversecretion appears bilateral and there- fore is most likely secondary to an extraneous stimulus. That is, the adrenal involvement is a secondary one. This likelihood is further sup- ported by clinical experience indicating that the hypertensive process is not affected even by total adrenalectomy [1,2]. The renal-adrenal axis and its participation in malignant hypertension: The preceding consider- ations allowed the suspicion that the striking aldo- sterone discharge in malignant hypertension is a secondary response related to stimulation of the adrenals by sources external to them. In search- ing for the stimulus our group decided to study angiotensin to see whether it was the agent re- sponsible for the hyperaldosteronism of malignant hypertension. Even though this material had be- come unpopular, since no role for it had been defined, we suspected that the renal pressor sub- stance might be involved because obviously kidney ‘damage is the cardinal site of pathologic change in m,alignant hypertension. It was possible to dem- onstrate a renal-adrenal hormonal interaction be- cause an infusion of angiotensin II into normal vol- unteers resulted in a ,marked increase in the adre- nal secretion of aldosterone [2]. The effect was
The American Journal of Medicine

RENIN. ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
highly selective because cortisol secretion did not
increase and because the response could not be induced by any other pressor agent [14]. It there-
fore appeared that angiotensin, which is the most powerful pressor substance known, also had a second vital function-as a trophic hormone to call forth the secretion of aldosterone.
This evidence for a kidney-adrenal interaction revived interest in the renal pressor system as a regulator of blood pressure. It also allowed our hypothesis (Figure 4) concerning the mechanisms in malignant hypertension [2,3]. In malignant hy-
pertension, a critical degree of damage has de- veloped in the kidney for initial reasons not al- ways clear. When this critical renal damage de- velops, a sequence is set in motion: renin, se- creted inapproprrately into the blood stream in excessive amount, interacts with the circulating renin substrate to release more angiotensin II.
Angiotensin II, in addition to raising the blood pressure by constricting the arterioles, also stim- ulates the secretion of aldosterone by the adrenal cortex. The aldosterone, in turn, acts on the kid- ney to increase sodium retention in the attempt
to elevate volume and restore renal perfusion. In normal subjects, this feedback loop is closed
by the sodium retention, and the increased renin secretion ceases. However, in those with malig- nant hypertension, a vicious cycle develops. The induced aldosteronism cannot turn off the secre- tion of renin, perhaps partly because it cannot in- duce appropriate sodium retention in the damaged target organ, kidney. A situation results in which there is too much angiotensin and too much aldo- sterone in the blood at the same time. A vicious cycle is initiated, characterized by more renin, more angiotensin and aldosterone, more hyper- tension and more renal damage. We believe that this vicious cycle is crucial to the pathogenesis of the malignant hypertensive syndrome.
Another way of putting it is to say that under normal circumstances the kidney, when its per- fusion is threatened, triggers off a corrective and self-limiting dose of hypertension. But in malig- nant hypertension the kidney is behaving inap- propriately, for the danger to perfusion comes from damage rather than from hypotensive phe- nomena. There is nothing to shut off the process, because the response is irrelevant to the signal. Runaway hypertension results.
There is a good deal of evidence to support this view. First, the early work of Kahn et al. [15] showed excessive angiotensin in the blood of pa-
Figure 4. The renal-adrenal axis involving renin, angio-
fensin and aldosferone in regulation of sodium and po-
tassium balance and blood pressure. The interaction is
depicted as first identified in patients with malignant
hypertension in whom, because of defective feedback, if
becomes involved in pafhogenesis. See text.
tients with malignant hypertension. Somewhat more recent animal experiments by Masson and his associates [16] indicate that in rats injections of either renin or aldosterone alone do not pro- duce any significant pathologic changes, but when
given together, severe and rapidly fatal vasculitis follows. Furthermore, in dogs the malignant syn-
drome can be reproduced in the Goldblatt model by tightening the clamps, and this is accompanied by hyperreninemia and hyperaldosteronism not observed in dogs with the benign form of hyper-
tension [17]. This idea that an excess of renin or angiotensin causes vascular injury is additionally supported by a number of other animal studies [18-211. The contrasting pathophysiology of primary and pseudoprimary aldosteronism: In contrast to the hyperaldosteronism of malignant hyper- tension, primary aldosteronism (adrenal adenoma) and pseudoprimary aldosteronism (diffuse hyper- plasia) are two adrenal cortical disorders char- acterized by seemingly autonomous oversecre- tion of aldosterone with suppressed plasma renin activity. Pseudoprimary aldosteronism differs in that the hormonal abnormalities are quantitatively less marked, and hypo- kalemia is milder or absent [22-241. Also, the hypertension in primary aldosteronism is usually cured by removing the offending adenoma whereas the hypertension of pseudoprimary aldosteronism is not improved by partial or even total adrenalec- tomy [22,23]. Accordingly, although these two adrenal disorders appear to differ from each other
Volume 52, May 1972 639
RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
biologically, they have in common the clinical pre- sentation of benign hypertension with a high aldo- sterone level and suppressed plasma renin ac- tivity.
The benign or milder nature of these two adrenal cortical disorders as contrasted with
malignant hypertension can be attributed to the absence of renin and angiotensin [2-41. Thus,
aldosterone, secreted autonomously and in the
absence of any renal damage, would be expected to suppress renal release of renin and prevent ini- tiation of the vicious cycle which seems essentially related to the pathogenesis of malignant hyperten- sion.
This thesis, developed from observations in these renal and adrenal disorders, relates the vascular injury of hypertension primarily to the excessive or inappropriate secretion of renin. However, it is likely that changes in sodium bal- ance and in aldosterone secretion also can be i,m#portant in the equation. Such an association
seems likely if only from the knowledge that aldo- sterone operates within the system to determine sodium balance which in turn modulates both the secretion of renin [‘25,26] and the action of angio- tensin [14]. Furthermore, it is known that the vasculotoxic effects of renin are best demonstrated in animals fed salt [27]. In the same way too, the experimental vascular disease produced by min- eralocorticoids such as aldosterone requires ade- quate dietary salt [16,28,29]. Indeed, this latter experimental state can at times become “malig- nant” with fibrinoid arteriolitis. Thus, from the animal experiment, it seems possible that in man too, very marked “primary” adrenal oversecretion of aldosterone might ultimately exceed the buffer capacity of the hormonal interaction and induce the vicious cycle of malignant hypertension which apparently is most often initiated by renal damage. However, in only one or two uncertain instances of primary aldosteronism has malignant hyper- tension been described [30,31]. Clinical Implications. The pathophysiologic ab-
errations so far described have implications for understanding normal physiology and for analyz- ing clinical problems exemplified by a whole vari- ety of milder forms of high blood pressure. A large body of evidence has now accumulated to indi- cate that the renal-adrenal hormonal interaction plays a major role in the day to day regulation of salt balance and blood pressure in all of us. Many studies indicate that a low sodium diet in normal subjects produices a high plasma renin level, and
the high renin level caused by the low salt diet is
probably the reason for the hyperaldosteronism and renal sodium conservation that occurs in normal subjects. Conversely, high salt diets in animals or in man will promptly arrest the secre- tion of renin, and then aldosterone secretion falls.
The dynamic responses of these hormones to changes in dietary salt go a long way towards ex- plaining the magnificent constancy of our body
weight despite wide fluctuations in diet. There are also key implications of these observa-
tions for the detection and analysis of renal and adrenal abnormalities in hypertensive patients. Accordingly, if a hypertensive patient has hyper- aldosteronism, the next step is to find out why. If he has hyperaldosteronism and plasma renin is increased, the aldosteronism of the patient is secondary to the release of renin and is related to some sort of renal disturbance. On the other hand, if a patient has hyperaldosteronism or clinical evidence of it (hypokalemia is a very reliable clini-
cal sign) and his plasma renin levels are low, one can then suspect that the adrenal is primarily at fault-an autonomous adenoma of diffuse hyper- plasia operating to increase aldosterone secre- tion, induce the retention of salt and so suppress the kidney’s secretion of renin. Hypokalemia as a Clinical Sign. A most reliable clinical indicator of aldosteronism, whether it is due to a renal or an adrenal disturbance, is the presence of hypokalemia. This is to be expected, since the sodium retaining hormone aldosterone is also a kaliuretic agent. Indeed, under experi- mental conditions, evidence of potassium deple- tion is practically always associated with a physio- logic excess of mineralocorticoid.
It is therefore most relevant to characterize the plasma potassium levels in all hypertensive pa- tients with several measurements, preferably at widely spaced intervals. In so doing, two precau- tions should be taken: (1) the patient should not take any diuretic drugs for at least three weeks, and (2) whenever #possible, the patient should be maintained on an unrestricted or liberal sodium intake since a low sodium diet can mask the kaliuretic effect of aldosterone by reducing distal tubular sodium supply.
In our experience, the greatest degree of hypo- kalemia occurs in primary aldosteronism due to an adenoma. Thus, in twelve of these patients the mean plasma potassium was 2.5 mEq/L [22]. ln eleven patients with pseudoprimary aldosteron- ism (bilateral hyperplasia) the mean value was
640 the American Journal Of Medicine

RENIN. ANGIOTENSIN AND ALDOSTEHONE SYSTEM IN HYPERTENSION -- LARAGH ET AL.
3.6 mEqil_. jnd ;tjme vaI,.ies in this group fell
Into the lower noima: range. The lesser hypoka- iemia in the latter group can be related to an USU-
ally milder degrer: of aldosterone oversecretion. Hypokalernla after occurs in malignant hyperten- i;ion too [l], in c.ur -eport, the mean value was 3.6 mEq/L in sixft:en cases. However, il? this con- dition, the expression of hypokalemia is retarded because of acconepanying renal failure with aci- dosis and azotemL3
Some examples of so-called “normokalemic” primary aldosteronism have been reported [32]. However, with the approaches outlined herein we have not observed this phenomenon, and we be- lieve it to be a rare variant of an uncommon dis-
ease. Such patients might instead represent a variant form of low renin essential hypertension, exhibiting suppressed plasma renin activity with a slightly increased aldosterone secretion [33]. Whatever the case proves to be, since some of these reportedly normokalemic patients may have mild or borderline hypertension, temporization or a program of medical management is probably a reasonable clinical alternative to exploration. Additional Work-up. The work-up of hypertensive patients suspected of having primary or pseudo- primary aldosteronism therefore involves as a first step the characterization of plasma potassium levels under the conditions described. The next step is the demonstration of inappropriately high aldosterone secretion when the urinary sodium excretion is in excess of 100 mEq/day (see nomo- gram, Figure 2) and of an inappropriately low plasma renin activity when the urinary sodium
excretion is somewhere below 40 mEq/day (see nomogram, Figure 2). Ideally, these measure- ments are best obtained under balance con- ditions. However, as indicated, such data can also be reliably obtained in properly instructed out- patients. The patient becomes a possible candi- date for surgery If hyperaldosteronism, hypokale- mia and suppressed renin activity are unequivo- cal with the more flagrant deviations suggesting an adenoma of primary aldosteronism rather than the hyperplasia of pseudoprimary aldosteronism [22-24-j. Since the patient with the latter condi- tion may not benefit from surgery, there is still disagreement about the value of exploration. How- ever, despite the use of various physiologic tests beyond the scope of this discussion, exploration may still be the only truly definitive approach to the differentiation of primary from pseudoprimary aldosteronism.
!X#CT 6 OFFSET OF ORaL CWWRAMPTIVE WPERTFNSION IN A SINGLE PATIENT
MAY 12fhOAY 4th MONTH 9th DAY I MONTH 4 MONTHS 1966 -- I-
Figure 5. Oral contraceptive hypertension in a thirfy- three year old woman in whom hypertension was first discovered after three years of oral contraceptive therapy with Enovid, 5 mg. Hypertension disappeared after drug withdrawal. It reappeared, as shown here, when treat- ment was renewed, and then disappeared again after withdrawal of the drug. The appearance and disappear- ance of hypertension was associated with concomitant increases and decreases in renin, aldosterone, renin substrate and reactivity to renin. The data illustrate that in this patient the observed increase in renin activity was largely due to an increase in renin substrate concenfmra- tion. From Newton et al. [34]
Oral Contraceptive Hypertension: A Role for Renin Substrate. Despite a number of suggestions that hypertension, the most frequent complication of pregnancy, is strongly associated with sodium and water retention and with heightened endogenous estrogen activity, not until recently was the possi- bility explored that administration of exogenous gonadal hormones might duplicate the association.
Following this possibility, in 1967 our group [7] reported that when oral contraceptive therapy was discontinued in eleven hypertensive women, their blood pressure levels fell, in some cases to normal. Moreover, in two patients in whom blood pressure levels returned to normal, rechallenge with an- other oral contraceptive reproduced the hyper- tensive condition.
Figure 5 illustrates the findings in a thirty-three year old woman whose blood pressure was normal prior to starting Enovid@ treatment [34]. Three years later, when she first came to our Center, it was 200/130 mm Hg. A complete work-up in- cluding renal angiography gave negative results. Contraceptive therapy was discontinued, and the blood pressure returned to normal levels in the next sel!eral months. At this point, the hormonal
Volume 52, May 1972 641
RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
Oiiufrd Phma 140
I20
RENIN I00
SUBSTRATE 80 REACTIVITY 6.
nglmlllir 40 !
0 1000 2000 3000
RENIN SUBSTRATE q/ml
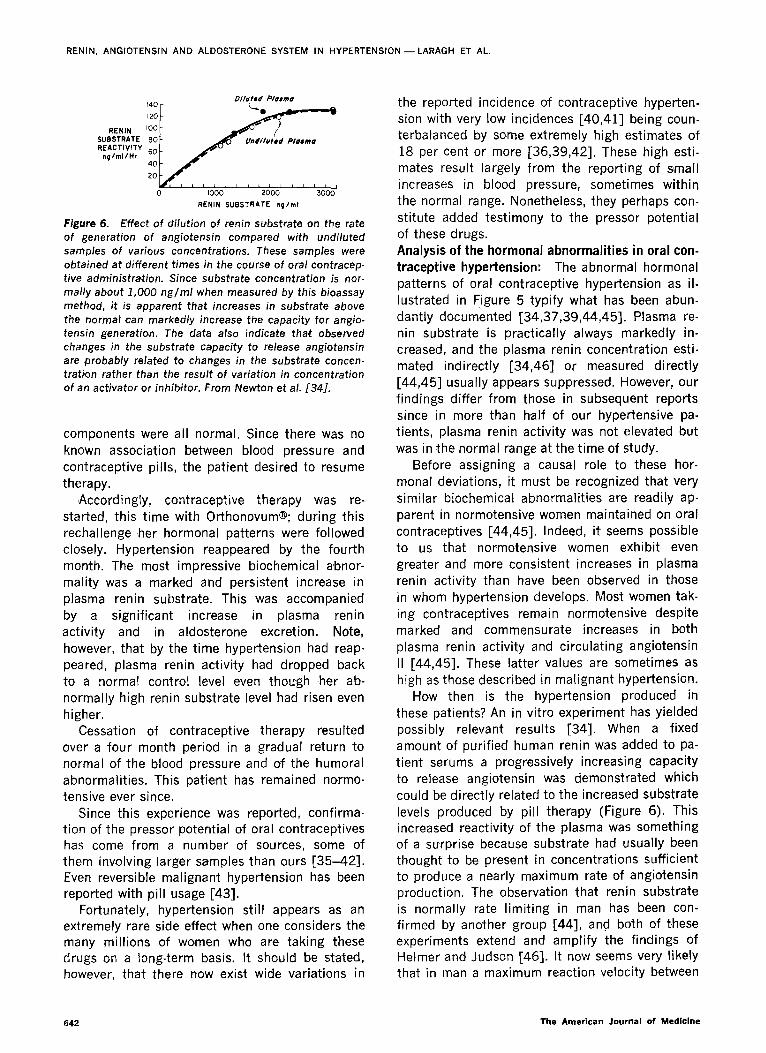
Figure 6. Effect of dilution of renin supbstrate on the rate
of generation of angiotensin compared with undiluted
samples of various concentrations. These samples were
obtained at different times in the course of oral contracep-
tive administration. Since substrate concentration is nor-
mally about 1,000 ng/ml when measured by this bioassay
method, it is apparent that increases in substrate above
the normal can markedly increase the capacity for angio- tensin generatio’n. The data also #indicate that observed
changes in the substrate capacity to release angiotensin are probably related to changes in the substrate concen-
tration rather than the result of variation in concentration
of an activator or inhib,itor. From Newton et al. 1341.
components were all normal. Since there was no known association between blood pressure and contraceptive pills, the patient desired to resume therapy.
Accordingly, contraceptive therapy was re- started, this time with Orthonovum@; during this rechallenge her hormonal patterns were followed closely. Hypertension reappeared by the fourth month. The most impressive biochemical abnor- mality was a m,a.rked and persistent increase in plasma renin substrate. This was acco’mpanied by a significant increase in plasma renin activity and in aldosterone excretion. Note, however, that by the time hypertension had reap- peared, plasma renin activity had dropped back to a normal control level even though ,her ab- normally high renin substrate level had risen even higher.
Cessation of contraceptive therapy resulted over a four month period in a gradual return to normal of the blood pressure and of the humoral abnormalities. This patient has remained normo- tensive ever since.
Since this experience was reported, confirma- tion of the pressor potential of oral contraceptives has come from a number of sources, some of them involving larger samples than ours [35-421. Even reversible malignant hypertension has been reported with pill usage [43].
Fortunately, hypertension still appears as an extremely rare side effect when one considers the many millions of women who are taking these drugs on a long-term basis. It should be stated, however, that there now exist wide variations in
642
the reported incidence of contraceptive hyperten- sion with very low incidences [40,41] being coun- terbalanced by some extremely high estimates of
18 per cent or more [36,39,42]. These high esti- mates result largely from the reporting of small increases in blood pressure, sometimes within the normal range. Nonetheless, they perhaps con-
stitute added testimony to the pressor potential of these drugs.
Analysis of the hormonal abnormalities in oral con- traceptive hypertension: The abnormal hormonal patterns of oral contraceptive hypertension as il- lustrated in Figure 5 typify what has been abun- dantly documented [34,37,39,44,45-j. Plasma re- nin substrate is practically always markedly in- creased, and the plasma renin concentration esti- mated indirectly [34,46] or measured directly [44,45] usually appears suppressed. However, our findings differ from those in subsequent reports since in more than half of our hypertensive pa- tients, plasma renin activity was not elevated but
was in the normal range at the time of study. Before assigning a causal role to these hor-
monal deviations, it must be recognized that very similar biochemical abnormalities are readily ap- parent in normotensive women maintained on oral contraceptives [44,45]. Indeed, it seems possible to us that normotensive women exhibit even greater and more consistent increases in plasma renin activity than have been observed in those in whom hypertension develops. Most women tak- ing contraceptives remain normotensive despite marked and commensurate increases in both plasma renin activity and circulating angiotensin
II [44,45]. These latter values are sometimes as high as those described in malignant hypertension.
Ho’w then is the hypertension produced in these patients? An in vitro experiment has yielded possibly relevant results [34]. When a fixed amount of purified human renin was added to pa- tient serums a progressively increasing capacity to release angiotensin was demonstrated which
could be directly related to the increased substrate
levels produced by pill therapy (Figure 6). This increased reactivity of the plasma was something of a surprise because substrate had usually been thought to be present in concentrations SuffiCient
to produce a nearly maximum rate of angiotensin production. The observation that renin substrate is normally rate limiting in man has been con- firmed by another group [44], and both of these experiments extend and amplify the findings of Helmer and Judson [46]. It now seems very likely that in man a maximum reaction velocity between
The American Journal of Medicine

RENIN, ANGIOTENSIN AND ALDOSTCRONE SYSTEM IN HYPERTENSION -- LARAGH ET AL.
enzyme and subs’rate may not be achieved until
plasma substrate !evels ar? increased by five or
more trmes the normal range.
A priori, one might expect that because of this greater substrate r-eactivity hypertension could re- suit from excessive responses to normal amounts of renin secreted in response to various physio-
logic signals. However, in vivo, with prolonged pill treatment, compensatory homeostatic adjust- ments occur with plasma renin activity tending
to return to normal (Figure 5). Several studies have suggested that this is due to a compensatory fall
in renin concentrations [34,39,44,45]. According
to this sequence of events, one mechanism for hypertension could be failure of renal renin secretion to suppress normally or adequately in
adjusting to the rising substrate concentration. As attractive as this explanation may be, it is not yet
supported by the facts since plasma renin activity was found to be normal in at least half of our hypertensive patients, and some of the values
were lower than those observed in normotensive women on the pill [7]. The hypertension induced in these patients may therefore be affecting the renal baroreceptor to reduce renin secretion. This
sequence is illustrated in Figure 5. Thus, the question still remains u’nsettled as to whether oral contraceptive hypertension is related to an inap-
propriately high renin activity or is caused by an-
other mechanism.
Other factors may be important in the equation.
One is the renal sodium retaining effect of estro-
gens, expressed clinically in the well known ten-
dency for f!urd retention and further supported by
recent studies describing an increased blood vol-
ume and cardiac output in women receiving contrlsceptive therapy [45]. In this context, oral contraceptive hypertension would involve an hy- dremrc effect perhaps similar to that induced by
an excess of mineralocorticoid hormones. Another possibilrty is a direct stimulating effect of estro-
gens on renal renin secretion, which might hamper adequate suppression in the face of hypertension. Evidence for this comes from our observations that
in some patients the increase in plasma renin ac-
tivity was greater than could be accounted for by
the increase in plasma renin substrate [34]. Diagnostic and Therapeutic Implications. It
seems from these studies that the nub of the problem is patient susceptibility. As yet, there are no clear guidelines. Even the obvious parallel be-
tween natural and “plastic” pregnancy offers no clues for we have observed oral contraceptive hy- pertension in a number of women who had un-
eventful pregnancies. However, as one might ex- pect, preexisting or occult renal disease may act
to compromise the buffer capacity of the system
as occurred in two of our patients. Another sensi- tizing factor may be any preexisting tendency to
fluid retention. In the absence of more meaningful data, it is
probably safest for the clinician to administer oral contraceptives with special caution to women with
a prior history of hypertension, excessive weight
Figure 7. Essential hyper- tension: 219 patients. Re- lation of noon plasma renin
activity and of the corre- sponding daily aldosterone excretion to the concurrent daily rate of sodium excre- tion. Triangles = low renin,
open circles = normal renin, squares = high renin es- sential hypertension. From Brunner et al. [52].
n 0
l
Volume 52, May 1972 643

RENIN. ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
gain and edema during menstruation, and a famil- ial tendency to high blood pressure and its conse- quences, hypertensive abnormalities or renal dis- ease in prior pregnancies, or an edematous sen- sitivity to salt.
Fortunately, pill-induced edema and hyperten
sion are reversible by stopping the medication. A woman beginning to take oral contraceptives must be monitored frequently. She should be instructed
to watch her weight carefully, this being one of
the surest and earliest indicators of sodium and water retention. Her blood pressure should be taken no later than two months after starting medi- cation, checked frequently (bimonthly) thereafter
and compared with an adequately established base line. With these simple precautions, the pill may be used as indicated by the clinical situation.
Subtle Abnormalities in the Renin-Angiotensin- Aldosterone System in Essential Hypertension.
Using the approaches and the information just described, let us next consider the problem of
benign essential hypertension. In this category, the role of the renal-adrenal axis remains to be fully clarified. Previous studies, although not al- together in agreement, have most often reported normal aldosterone excretion in these patients. However, certain abnormal features have been described such as an impaired metabolic clearance [47], a failure of normal suppression with sodium loading [48] or a failure of aldosterone to increase normally with sodium deprivation [49,50]. On the other hand, more convincing abnormalities in plasma renin activity have been reported so that
even though this measurement is normal in the majority of these patients, in significant fractions
it may be either subnormal [49-571 or abnormally increased [51,52].
Figure 7 presents a plot of 368 determinations of plasma renin activity and aldosterone excretion in 219 patients with essential hypertension. As for the normal volunteers (Figure 2) the data are re- lated to the concurrent rate of sodium excretion, and normal limits are given by the dotted lines.
The scatter of both renin and aldosterone values is considerably wider for the hypertensive subjects than for the normal volunteers, permitting their classification into high, normal and low cate- gories. In this series, fifty-nine patients (27 per cent) showed reduced plasma renin activity (low renin hypertension); in thirty-six patients (16 per cent) this parameter was abnormally high (high renin hypertension), and in the remaining 124 pa- tients (57 per cent) it fell within the normal range
c521.
MEAN DIASTOLIC
BLOOD PRESSURE
mm Hg
BLOOD UREA
NITROGEN w%
CREATININE CLEARANCE
ml/min
URIC ACID mq 81.
PLASMA
[K+l mEq/L
PLASMA CHOLESTEROL
mq%
RENIN: Low Normal High I n) (59) o- (36)
8 :::.: .::: :x,x $;;;
200
100
0
Figure 8. Mean diastolic blood pressures and clinical bio-
chemical features of the three renin su’btypes of essential
hypertension.
Clinical correlates of renin subgroups: An analy- sis of the clinical features and natural history of these patients with essential hypertension indi- cates that the biochemical deviations have mean- ingful clinical correlates. The mean ages of the patients with low renin (forty-six years) and high renin (forty-three years) hypertension did not dif- fer significantly, but those with normal renin ac-
tivity were significantly younger (37.5 years). There were, however, no differences in the known
duration of the hypertension between any of the groups.
There was a significantly greater incidence of black patients (42 per cent) with low renin ac- tivity compared with only 24 per cent with normal renin activity and 11 per cent with high renin activity. These results tend to confirm the im- pression that low renin hypertension is relatively more common in blacks [53,54].
Figure 8 presents relevant clinical data for the
three subgroups. Of note are the findings that both the mean diastolic pressure and blood urea nitrogen levels were significantly higher and the plasma potassium level was significantly lower in the patients with high renin activity as compared with the other two groups. No significant differ- ences were found in any other routine indicators including plasma uric acid, plasma cholesterol and fasting blood sugar levels (not shown). There were no significant differences in diastolic hyper- tension, the blood urea nitrogen, plasma potas-
644 The American Journal of Medlclne

RENIN, ANGIOTENSIN AND ALDOSTE:RONE SYSTEM IN HYPERTENSION-LARAGH ET AL.
sium or plasma i holestercl levels in the groups
with normal and ow renin activity. However, per-
haps nor unexpectedly, the more severe form of hyperterlslon wittl a tendency to azotemia and hypokalemia rn the group with high renin activity was also accompanied by a greater incidence of grade 2 and 3 retlnopathy and of proteinuria. A further classification to include aldosterone:
Each of the three renin subtypes defined in essen- tial hypertension can in turn be associated with three different patterns of aldosterone excretion as illustrated in Figure 9. Accordingly, nine theo- retically possible hormonal patterns emerge in eight of which patients have been identified. The frequency of occurrence of these eight different patterns as determined from our study of 219 patients is shown in Figure 9 where low and high estimates of frequency are given for each group. The two numbers which provide a range of fre- quency result from the application of two differ- ent sets of criteria, strict and loose, which take into account the fact that a small fraction of the patients are either inconsistent or fall into border- line zones with respect to these traits. This analysis has been described in detail elsewhere [52]. For simplicity, mean values for frequency will form the basis of the present discussion.
The major fraction of these 219 patients (45 per cent) was found to exhibit a normal renin level with a correspondingly normal aldosterone level. Indeed, in only minor fractions of those patients with normal renin levels was there any deviation either up or down from normal aldosterone values. Especially noteworthy is the high incidence of low renin essential hypertension, with a mean of 27 per cent and a range from 19 to 31 per cent. In
high
PLASMA
RENIN normal
ACTIVITY
low normal high
ALDOSTERONE
EXCRETION
Figure 9. Frequency distributkon of various hormonal patterns observed in essential hypertension. The first value in each category is derived from application of “stringent” and the second from less stringent criteria. Whichever criteria are used, the frequency of distribution is not modified appreciably. See text. From Brunner et a/.
[521.
Volume 52, May 1972
these sI.lb]ects aldosterone secretion rates were
usually normal, although in a small and possibly
signiflcEnt portion of them they were reduced. A
rare rinding was increased aldosterone excretion in the p<esence of subnormal renin levels possibly suggest ng occult primary aldosteronism, but the few patients with this pattern had only slightly elevatec aldosterone levels and no hypokalemia.
Since we have not found tumors in similar pa- tients, and since even total adrenalectomy does not cure their hypertension, we do not recommend
exploratory adrenal surgery for such normokalemic patients with mildly excessive aldosterone excre- tion [22]. Renin activity was high in 16 per cent of the group. Among these, the aldosterone excre- tion was either normal or correspondingly elevated. In none of the patients with high renin activity was aldosterone secretion reduced.
Returning to Figures 7 and 9, one might draw the conclusion that in patients with essential hy-
pertension renin activity is more likely to be ab- normal than is aldosterone excretion. However, we cautiously venture the possibility that some of the seemingly “normal” aldosterone values may be in- appropriate to the hormonal interaction. What is normal for normal subjects may not be so for hy- pertensive su’bjects. One example of this might be the 17 per cent (13 to 21 per cent) of patients with normal aldosterone excretion rates but low renin activity; this might in fact represent an ab- normally high aldosterone value for that level of renin activity. A truly “normal” relationship be- tween aldosterone and renin, one in which the adrenoc.ortical response is linearly appropriate to a given renin secretion, is probably the one repre- sented by the three boxes situated on the diagonal, from left lower corner to right upper corner. Amal- gamating these three groups, about 60 per cent of all of the hypertensive patients show an ap- propriate renal-adrenocortical relationship.
Relationship of renin and aldosterone to heart attacks and strokes in the three renin subgroups of essential hypertension: Left ventricular hy- pet-trophy as defined by electrocardiographic and roentgenographic criteria occurred with fairly equal frequency in the three renin subgroups with the incrdences ranging from 15 to 22 per cent. However, a most striking difference emerges from this analysis: Not one occurrence of heart attack or stroke was recorded among the patients with low renin essential hypertension. In contrast, these complications occurred with a frequency of 11 per cent in those with normal renin activity and of 14 per cent in those with high renin activity.
645

RENIN. ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
The complete absence of either strokes or heart attacks in low renin essential hypertension is highly significant statistically, analysis of the re- sults indicating that the highest possible incidence of such events in a low renin hypertensive popula-
tion at large would be 4.9 per cent (5 per cent confidence limits).
These observations may go a long way towards explaining why certain hypertensive patients toler- ate remarkably high blood pressures for prolonged periods of time. Moreover, it should be pointed out that the benign nature of low renin essential hypertension is similar to the usually benign na- ture of primary aldosteronism [l-3], another con- dition in which renin is similarly suppressed
C45,W. In contrast, the high incidence of cardiovascu-
lar complications among hypertensive patients with normal or high renin activity is in keeping
with the vasculotoxic effects of renin which have already been discussed as a mechanism of the severe vasculitis in human malignant hypertension. Implications for Etiology. The various abnormal hormonal patterns observed suggest nonhomo- geneity of the patients and underline the possi-
bility that multiple etiologies exist among patients heretofore classified under the umbrella of benign essential hypertension. Further study is certainly required especially in the minor categories in which very few patients have been identified. Those patients with normal renin and normal aldosterone levels may become the group for whom the term essential hypertension will survive. Diagnostic and Therapeutic Implications. These results indicating biochemical nonhomogeneity of the essential hypertensive population may have im- plications for patient management if they can be confirmed in larger series. First of all, because it has prognostic value, plasma renin activity may help to determine the urgency of antihypertensive therapy. Accordingly, early application of antihy- pertensive therapy may not be appropriate for patients with low renin activity whereas such treat-
ment should be most aggressively applied in es- sential hypertensive patients with high renin ac- tivity. Secondly, further understanding of drug ac- tion may permit the selected use of antihyperten- sive agents which can control abnormalities in renin secretion.
Hypertensive Diseases Exhibiting Inconsistent or Still Uncertain Abnormalities in Renin and Aldo- sterone
Renal Vascular Hypertension. Following the clas- sic experiment of Goldblatt et al. in 1934 [SS]
646
and the demonstration of the pressor agent renin in the renal venous blood of ischemic kidneys [59], it has often been assumed that this agent is the cause of experimental Goldblatt hyperten- sion and its naturally occurring counterparts in man. However, numerous studies of established renovascular hypertension in animals and in man have demonstrated normal or even low plasma renin [6,17,25,60], angiotensin [61-631 and aldosterone [12] levels. In addition, active or pas- sive immunization of animals against the effects of angiotensin II has often failed to prevent or cor- rect the hypertension [64,65].
One possible reason for these inconsistencies has perhaps been the failure to appreciate that there may be more than one mechanism for renal hypertension. Experimental renal hypertension in- duced by ischemia of one kidney with the contra- lateral one untouched differs from that in which
the opposite kidney has been removed. The former model exhibits a higher plasma renin [66] and a lower total body sodium [67] level than the latter. That these findings are pathogenetically meaning- ful is suggested by recent studies in which endog- enous angiotensin II was blocked either by acute antibody injection [68] or by infusion of specific peptide inhibitors [68,69]. Both approaches lowered the blood pressure of the two kidney type to normal but had no effect in the one kidney model. Therefore, it appears that the renin-angio- tensin system might have a causal role in the two kidney form but does not seem to be involved in one kidney renal hypertension. The results of all these animal studies suggest that two different mechanisms may be involved in the development and maintenance of experimental renal hyperten- sion.
Such different ‘mechanisms should be consid- ered in the analysis and evaluation of human reno- vascular hypertension, especially since no clear-cut evide’nce has been provided that renin is the only or the consummate,cause of this condition. Accord- ingly, although an elevated peripheral plasma renin
level supports the possibility of a Goldblatt mecha- nism, a normal or low plasma renin level can also occur in this condition so that this finding per se cannot rule out the diagnosis. Therefore, the measurement of peripheral plasma renin activity has been of limited usefulness as a screening pro- cedure for curable renovascular hypertension 1701.
However, based on the evidence that circulating renin is more apt to be released from the ischemic kidney, evaluation of renin activity in the venous effluent of both kidneys has gained wide usage. A ratio in renal vein renins of 1.5 to 2.0 between the
The American Journal of Medicine

RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL
involved and uninvolved side is considered to pre-
dict curability [71-731. A,lthough this approach
has improved the accuracy of predicting surgical
curability, it is clear that not all patients with sub- sequent cure have exhibited an abnormal ratio. Once again these observations suggest that factors other than renin may be causally involved.
A factor not always taken into account in differ- ential renal vein studies is the fact that circulating
renin is not cleared by the kidney [74,75]. Hence, even if a kidney secretes no renin at all, it contin- ues to deliver into the vein approximately that which entered it from the arterial side. Therefore, arterial input should be subtracted from the renal venous renin content so that the new contribution, i.e., the renin secretion can be evaluated. In our experience, when this correction factor was ap- plied, patients who were subsequently proved to have curable Goldblatt hypertension exhibited a more marked disparity in renin secretion between the two kidneys. Even more important, when this approach was used to analyze patients, in those subsequently cured by surgery net renin secretion from the contralateral kidney was consistently near zero. This finding emphasizes the impor- tance of establishing that the contralateral kidney is uninvolved befo’re advising surgery. A useful
technical refinement in performing these differen- tial renal vein studies has been to utilize a form of renin stimulation such as sodium depletion, tilting [76,77], or controlled hypotension [78] to “un- mask” unilateralization by amplifying the rate of renin release from the involved kidney.
Notwithstanding the possible usefulness of such better differential analysis of renal renin se- cretion, one is still bound to explain the cause of the hypertension in that significant fraction of cur- able patients in whom peripheral circulating
plasma renin levels are normal preoperatively. One must search for more direct and convincing evi- dence for a role for renin. Possibilities worthy of research include increased pressor responsiveness to normal angiotensin levels, i.e., changes in affinity af angiotensin II vascular receptors with subtle changes in sodium balance [79] and im- paired metabolism of the hormones. Alternatively, one must also face the real possibility that renin and angiotensin are not crucially involved in caus- ing renovascular hypertension. Unilateral and Bilateral Renal Parenchymal Dis- eases. The situation with respect to unilateral in- trarenal diseases and their relationship to hyper- tension is even less clear. An earlier review of the experience of this area by Homer Smith [80] re- vealed most disappointing cure rates. There has
Volume 52, May 1972
been little reason to change this impression. in
this category are included such diverse conditions
as pyelonephritis, renal atrophy, infarcts, cysts,
tumors, granulomatous diseases such as tubercu- losis, stones and hydronephrosis. The heterogene- ity of these conditions makes the development of diagnostic criteria to predict cure especially diffi- cult. Accordingly, renal vein renin studies have all too often failed to show unilateralization. Although our understanding of these conditions remains in- complete and ill defined, it does seem that when
severe or malignant hypertension occurs, in this group too, differential renal vein renin determina-
tions may be useful for establishing the extent to which one or both sides are involved and estimat-
ing surgical potential. Further study of this hetero- geneous group may identify specific intrarenal le- sions which are associated with increased renin
secretion. Similarly, there is little information about the
role of the renal-adrenal axis in bilateral renal parenchymal diseases. However, it is theoretically possible that changes in plasma renin activity could prove useful for following variations in ac- tivity of the disease processes, especially in immu- nologically based disorders associated with vascu-
litis. End Stage Kidney Diseases. In contrast to the heterogeneous group with unilateral or bilateral renal parenchymal diseases without marked renal failure, in end stage renal disease the contribution of the renal factor to the hypertensive process has been clarified by the experience with bilateral ne-
phrectomy. In a majority of hypertensive patients with chronic renal failure, regular dialysis satis- factorily controls hypertension [81]. This control is paralleled by decreases in total exchangeable sodium, extracellular fluid volume and cardiac out- put [82,87]. In this group, plasma renin activity
may be normal or even low [83,84]. However, in a small fraction of patients, dialysis
fails to reduce the blood pressure and it even ac- celerates the hypertension. This “uncontrollable” form of hypertension is characterized by a some- times markedly increased plasma renin activity, angiotensin II and aldosterone [83,85-871, by a high total peripheral resistance and by small extra-
cellular volume changes causing drastic changes in blood pressure. Most of these abnormalities are corrected by bilateral nephrectomy suggesting that the kidney may be responsible for this intractable hypertension. In this particular group, demonstra- tion of an elevated plasma renin activity has proved to be a useful guide for advising total nephrec- tomy.
647

RENIN. ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
TABLE I Angiotensin II Generation in Hypertensive Vascular Disease
Low Plasma Renin Activity Normal Plasma Renin Activity
A. Aldosteronism
1. Primary
2. Pseudoprimary
3. Tertiary? 1221
4. Glucocorticoid suppressible [88]
B. Mineralocorticoidism
1. ll-beta hydroxylase deficiency [89]
2. 17-alpha hydroxylase deficiency (90-921
3. Adrenal carcinoma
4. Ectopic ACTH-secreting tumors
5. Excess 18-OH DOC? [93]
C. No clearly demonstrable
adrenal-cortical disease
1. Low renin essential hypertension
2. Parenchymal renal disease*
3. Liddle’s syndrome [94]
4. Gordon’s hyperkalemic patient [95]
5. latrogenic: mineralocorticoid or
licorice ingestion
A. Normal aldosterone secretion
1. Normal renin essential
hypertension
2. Unilateral renal disease*
3. Bilateral renal vascular
or parenchymal disease*
4. Cushing’s syndrome
5. Coarctation of the aorta
6. Pheochromocytoma
High Plasma Renin Activity _~_ _.__
A. Secondary aldosteronism
1. Malignant or severe hypertension
2. Unilateral renal disease with
severe hypertension
3. Bilateral renal vascular or
parenchymal disease*
4. High renin essential hypertension
5. Renin-secreting kidney tumors [96]
6. latrogenic: oral contraceptive use
B. Without secondary aldosteronism
1. Potassium depleted patients with
above disorders
--. * Note that patients with parenchymal or renal vascular (unilateral or bilateral) disease may exhibit low, normal or high circu-
lating plasma renin activity.
A Physiologic Classification of Plasma Renin Ac-
tivity in Hypertensive Diseases. In Table I the spectrum of hypertensive disorders is summarized according to plasma renin activity, and then these conditions are subclassified depending on their associated adrenal cortical behavior. Those condi- tions for which references are cited have not been
discussed since they are either extremely rare or still subject to taxonomic doubts. The clinical nuances of these rare disorders can be obtained from the sources cited.
The normal interaction between renin activity
and aldosterone secretion provides a physiologic
basis for this classification. Accordingly, low plasma renin levels may be induced by antecedent adrenal overactivity and, conversely, high plasma renin levels usually lead to a secondary adrenal overactivity. However, that adrenal overactivity is probably not the only cause for suppressed plasma
TABLE II Antihypertensive Drugs-Pharmacology of Renin Stimulation and Suppression
____- Renin Inhibitors Renin Stimulators
____
Propranolol [97,105] Aldosterone antagonists [102]
Clonidine [98,99] Other diuretics [103,104]
Methyl DOPA [loo] Vasodilators:
Reserpine Nitroprusside [78]
Ganglionic blockers [loll Diazoxide [106]
Guanethidine (?) Hydralazine [107] Guancydine [lOS]
renin activity is well exemplified by the large popu-
lation of patients with low’renin essential hyperten- sion. Another point illustrated by the tabulation is that patients with chronic kidney disease can fall into any one of the three categories. The Renal-Adrenal Axis in Therapeutic Strategy: A Look at the Future. The data here presented de-
scribe the present state of our knowledge of the renal-adrenal axis with respect to its involvement in hypertensive vascular disease, The analysis is by no means intended to exclude the possibly vital participation of other neural, humoral or local tis- sue mechanisms in the pathogenesis of these con-
ditions. However, it does appear that an understanding
of the behavior of renin and aldosterone can pro- vide a basis for specific diagnosis at least in cer- tain forms of renal and adrenal hypertension. The experience further suggests that biochemical pro- filing of patients with respect to the kidney and adrenal hormones may have a broad application in classifying patients with so-called essential hyper- tension. This information could also prove helpful in determining prognosis and planning therapy for these patients.
It is already known from scattered reports that some antihypertensive drugs increase plasma renin activity whereas others ‘markedly reduce it (Table II). It therefore seems possible that in the application of these drugs in treatment, the selec-
648 The American Journal of Medicine
tion of agents that can cortect renin abnormalities
might produce a nore satisfactory blood pressure response and a Letter prognosis. This potentially
promising approai:h could cevelop criteria for more rational drug ther-apy, specifically tailored to cor- rect a particular .3bnormal biochemical profile. In this regard! in a recent study the striking suppres- sion of renin secretion by propranolol was used diagnostically and therapeutically to advantage in renovascular and other renin forms of high blood
pressure [105]. Thus, it might turn out to be pos- sible pharmacologically to mimic the physiologic. naturally occurring protective response that pa- tients with low renin levels are fortunate enough to be able to muster unaided.
It is apparent that diuretics, the mainstay of therapy, usually produce in short-term periods of
observatron_ :lety striking increases II! plasma
rerrirj actrvctj. However, there IS inadequate infor-
mat:c:n aborit the effects of their protracted admin-
istration on reni I and aldosterone secretion. Diu- retie-tnducec hyperreninemia might be undesirable in view of the possible relationship between plasma renin activity and the development of strokes and heart attacks. However, since the vasculotoxic ef-
fects of renin appear to be sodium dependent, the volume depletion associated with diuretic therapy may vitiate or eliminate this hazard. Furthermore, there is also little information about long-term ef-
fects of those antihypertensive drugs known to lower renin levels acutely, and combination drug therapy requires similar long-term studies. All these possibilities should intrigue inquiring physi- cians.
RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION -- LAHAGH ET AL.
REFERENCES
1. Laragh JH, Ulick S, Januszewicz W, Deming QB, Kelly WG, Lieberman S: Aldosterone secretion and primary and malignant hypertension. J Clin Invest 39: 1091, 1960.
2. Laragh JH, Angers M, Kelly WG, Lieberman S: Hy- potensive agents and pressor substances. The effect of epinephrine, norepinephrine, angio- tensin II and others on the secretory rate of ald’osterone in man. JAMA 174: 234, 1960.
3. Laragh JH: The rol’e of aldosterone in man: evi- dence for regulation ‘of electrolyte balance and arterial pressure by ‘renal-adrenal system which may be involved in malignant hypertension. JAMA 174: 293, 1960.
4. Laragh JH, Cannon PJ, Ames RP: Aldosterone se- cretion and various forms of hypertensive vas- cular disease. Ann Intern Med 59: 117, 1963.
5. Conn JW: Plasma renin activity in primary aldo- steronism. Importance in differential diagnosis and in research o’f essential hypertension. JAMA 190: 134, 1964.
6. Dustan HP, Tarazi RC, Frohlich ED: Functional cor- relates of plasma renin activity in hypertensive patients. Circulation 41: 555’. 1970.
7. (aj Laragh JH, Sealey JE, Ledingham JGG, Newton MA: Oral contraceptives. Renin. aldosterone and high blood pressure. JAMA 2011918, 1967.
(b) Laragh JH, Stmoerk HC: A study of the mechan- ism of secretion of the s’odium-retaining ho’r- mone (aldosterune). J Clin Invest 36: 383, 1957.
(c) Cannon PJ, Ames RP, Laragh JH: Relation be- tween potassium balance and ald’o’sterone secre- tion in nsormal subjects and in patients with hy- pertensive or renal iubular disease. J Clin Invest 45: 865, 1966.
(d) Sealey JE, Clark I, Bull MB, Laragh JH: Po,tas- sium balance and the control of renin secretion, J Clin Invest 49: 2119, 1970.
(e) Brunner HR, Baer L, Sealey JE, Ledingham JGG, Laragh JH: The influence of potassium ad- ministration and of potassium deprivation on
8.
9.
10.
11.
12.
13.
14.
15
16.
17.
Kahn JR, Skeggs LT, Shumway NP, Wisenbaugh PE: The assay of hypertensin from the arterial blood of normotensive and hypertensive human beings. J Exp Med 95: 523, 1952.
Masson GMC, Mikasa A, Yasuda H: Experimental vascular disease elicited by aldosterone and renin. Endocrinology 71: 505, 1962.
Carpenter CCJ, Davis JO, Ayers CR: Relation of renin, angimotensin II, and experimental renal hypertension to aldosterone secretion. J Clin Invest 40: 2026, 1961.
18. Giese J: Acute hypertensive vascular disease. Acta
plasma renin in normal and hypertensive sub- jects. J Clin Invest 49: 2128, 1970.
Page IH, McCubbin JW: Renal Hypertension, Chi- cago, Year Book Medical Publishers, 1968.
Lee MR: Renin and Hypertension: A Modern Syn- thesis, London, Lloyd Luke, Ltd., 1968.
Sealey JE, Gerten-Banes J, Laragh JH: Physiologic variation in plasma renin activity, renin substrate concentration and renin substrate reactivity in man measured by either radioimmunoassay or bioassay, Kidney Int 1: 240, 1972.
Sealey JE, Buhler FR, Manning EL, Laragh JH: Physiologic variations in aldosterone excretion measured by either radioimmunoassay or double sotope diluti’on. Circ Res (in press).
Laragh JH, Sealey JE, Sommers SC: Patterns of adrenal secretion and urinary excrebon of al- dosterone and plasma renin activity in normal and hypertensive subjects. Circ Res 19 (suppl I): 158, 1966.
Volhard F, Fahr T: Die Brightsche Nierenkrankheit, Klinik, Pathologie und Atlas, Berlin, Springer- Verlag, 1914.
Ames RP, Borkowski AJ, Sicinski AM, Laragh JH: Prolonged infusions of angiotensin II and nor- epinephrine and blood pressure, electrolyte bal- ance, aldosterone and cortisol secretion in nor- mal man and in cirrhosis with ascites. J Clin Invest 44: 1171, 1965.
Volume 52, May 1972 649

RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Path Microbial Stand 62: 481, 1964. Cuthber-t MF, Peart WS: Studies on the identity of
a vascular permeability factor of ,renal origin. Clin Sci 38: 309, 1970.
Gavras H, Brown JJ, Lever AF, Macadam RF, R’obertson JIS: Acute renal failure, tubular necro- sis and myocardial infarction induced in the rabbit by i’ntrav,enous angiotensin II. Lancet 2: 19, 1971.
Asscher AW, Wnson SG: A vascular permeability factor of renal origin. Nature (London) 198: 1097, 1963.
Baer L, Sommers SC, Krakoff LR, Newton MA, Laragh JH: Pseudo-primary aldostero,nism: an entity distinct from true primary aldosteronism. Circ Res 26, 27 (suppl 1): 203, 1970.
‘Bdglieri EG, Schambelan M, Slato,n PE, Stockigt JR: The intercurrent hypertension of primary aldo- steronism. Circ Res 26, 27 (suppl 1): 195, 1970.
Ferriss JB, Brown JJ, Fraser R, Kay AW, Neville AM, O’Muircheartaigh IG, Robertson JIS, Sym’ington T, Lever AF: Hypertension with aldosterone ex- cess and Cow plasma-renin: preosperative d,istinc- tion between patients with and without adreno- cortical tum,our. Lancet 2: 9951, 1970.
Brown JJ, Davies DL, Lever AF, Robertson JIS: Variations in plasma renin concentration in sev- eral physiological and pathollogical states. Canad Med Ass J: 90: 201, 1964.
Goodwin FJ, Knowlto,n Al, Laragh JH: Absence oif renin suppression by desoxyco’rticosterone ace- tate ,in rats. Amer J Physitol 216: 1476, 1969.
Masson GMC, Kashii C, Matsunaga M, Page IH: Hypertensive vascular d.isease induced by bet- erologous renin. Circ Res 18: 219, 1966b.
Selye H, Stone H, Timiras PS, Schaffenburg C: In- fluenc’e of sodium chlo’ride upon the actio’ns of desoxycorticosteoone acetate. Amer Heart J 37: 1009,1949.
Gross F: Renin und Hypertensin, physi,ologische oder pathol’ogische Wirkstoffe? Klin Wschr 36: 693, 1958.
Kaplan NM: Primary aldosteronism with malig- nant hypertension. New Eng J Med 269: 1282, 1963.
McAllister RG Jr, Van Way CW III, Dayani K, An- derson WJ, Temple E, Michelakis AM, Co’ppage WS Jr, Oates JA: Malignant hypertens~io~n: ,ef- feet of therapy on renin and aldosterone. Circ Res 28, 29 (suppl 2): 160, 1971.
Conn JW, Rovner DR, Cohen EL, Nesbit RM: No,r- mokalemic primary aldosteronism. JAMA 195: 111, 1966.
Baer L, Brurmer HR, Buhler FR, Laragh JH: Pseudo- primary aldosteronism, a variant of Ilo,w-renin essential hypertension, Berlin, Springer-Verlag (in press).
Newto’n MA, Sealey JE, Ledlingham JGG, Laragh JH: High sbllood pressure and oral contraceptives. Changes in plasm,a renin and renin substrate and in aldosterone excretion. Amer J Obstet Gynec 101: 1037, 1968.
Woomds JW: Oral contraceptives and hypertension. Lancet 2: 653, 1967.
Tyson JEA: Oral contraception and elevated blood pressure. Amer J Obstet Gynec 100: 875, 1%8.
Weinberger MH, Collins RD, Dowdy AJ et al.: Hyper- tension induced by oral contraceptives contain- ing lestro,gen and gestagen. Ann Intern Med 71: 891,1969.
38.
39.
40.
41.
42.
43.
44.
45’.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56. Fishman LM, Kuchel 0, Liddle GW, Michelakis AM,
Crane MG: Hypertension, Metab’olic Effects of Go- nadal Hormones and Contraceptive Steroids (Salhanick HA, Kipnis DM, VandeWiele RL, eds), New York, Plenum Press, 1969, p 737.
Saruta T, Saade GA, Kaplan NM: Possible mech- anism for hypertensio,n induced by ‘oral con- traceptives: diminished feedback suppression of renal release. Arch Intern Med (Chicago) 126: 621, 1970.
Goodlin RC, Waechter V: Oral contraceptives and blood pressure. Lancet 1: 1262, 1969.
Kunin CM, McCormack RC, Abernathy JR: Oral oontraceptives and blood pressure. Arch Intern Med (Chicago) 123: 363, 1969.
Weir RJ, Briggs E, Mack A, Taylor L, Browning J, Naismith L, Wilson E: Blood pressure <in women after ‘one year ,of oral contraception. Lancet 1: 467, 1971.
Harris PWR: Malignant hypertension associated with ‘oral co’ntraceptives. Lancet 2: 466, 1969.
Skinner SL, Lumbers EL, Symonds EM: Alteration by oral contraceptives of normal menstrual changes in plasma renin acbvity, concentration and substrate. Clin Sci 36: 36, 1969.
Caine MD, Walters WA, Catt KJ: Effects of oral con- trac.eptive therapy ‘on the srenin-angiotensin sys- tem. J Clin Endocr 33: 671, 1971.
Helmer OM, Judson WE: Influence of high renin substrate levels on renin-angiotensin system in pregnancy. Amer J Obstet Gynec 99: 9, 1967.
Nowaczynski W, Kuchel 0, G,enest J: A decreased metabolic clearance rate of aldosterone in be- nign essential hypertension. J Clin Invest 50: 2184, 1971.
Luetscher JA, Weinberger MH, Dowdy AJ, Nokes GW, Balikian H, Brodie A, Willoughby S: Effects of sodium loadxing, sodium depletion and pos- ture on plasma aldoste,rone concentration and renin activity in hypertensive patients. J Clin Endocr 29: 1310, 1969.
Weinberger MH, Dowdy AJ, Nokes GW, Luetscher JA: Plasma renin activity and aldosterone secre- tion in hypertensive patients during high and low sodium ‘intake and administration of di- uretic. J Clin Endocr 28: 359, 1968.
Williams GH, Rose LI, Dluhy RG, McCaughn D, J’agger IPI, Hickler RB, Lauler DP: Abnlormal re- sponsiveness of the renin ald’osterone system to acute stimulatio,n in patients with essential hy- pertension. Ann Intern Med 72: 317, 1970.
Ledingham JGG, Bull MB, Laragh JH: The meaning of aldosterone in hypertensive disease. Circ Res 20, 21 (suppl 2): 177, 1967.
Brunner HR, Laragh JH, Baer L, Newton MA, Goo’d- win FT, Krakoff LR, Bard RH, Bijhler FR: Essen- tial hypertension: renin and aldosterone, heart attack and stroke. New Eng J Med 286: 441, 1972.
Helmer OM: Renin activity in blood from ,patients with hypertension. Canad Med Ass J 90: 221, 1964.
Creditor MC, Loschky UK: Plasma renin activity in hypertension. Amer J Med 43: 371, 1967.
Jose A, Crout JR, Kaplan NM: Suppressed plasma renin activity in essential hypertension: roles of plasma volume, blolod pressure, and sympa- thetic nervous system. Ann Intern Med 72: 9, 1970.
650 The American Journal of Medicine
RE.NIN, ANGIOTENSIN AND ALDOSERONE SYSTEM IN HYPERTENSION -- LARAGH ET AL.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76
Gordon RD. Chick WT: incidence of primary al- dosteromsm tn uncomplicated “essential” hy- pertension. J4MA 205: C97, 1968.
Kaneko Y, iked,3 T, Takedg T, lnoue G, Tagawa H, Ueda H. Rer,ln release In patients with benign essential h\ pertension Circulation 38: 353, 1968.
Goldblatt t-i, Ly,?ch J, Hanral RF, Summervllle WW: Studies on experlmental hypertension. I. The production c-if persistent elevation Of systolic blood-pressug~e by means of renal ischemia. J Exp Med 59: 347, 1934.
Braun-MenBndez E, Fasciolo JC, Leloir LF, MU~~OZ
JM: The substance causing renal hypertension. J Physlol 98: 283, 1940.
Gross F: The remn-angiotensin system and hy- pertenslon. Ann Intern Med 75: 777, 1971.
Catt KJ, Cran L, Zlmmet PZ et al.: Angiotensin II blood levels In human hypertension. Lancet 1: 459.1971.
Kotchen TA, Lytton B, Morrow LB, Mulrow PJ, Shutkin PM, Stansel HC: Angiotensin and aldo- sterone In renovascular hypertension. Arch Intern Med (Chicago) 125: 265, 1970.
Blair-West JR, Cain MC, Catt KJ et al.: Role of the kidney 111 experimental renovascular hyper- tension. Clrc Res 26, 27 (suppl 2): 149, 1970.
MacDonald GJ LOUIS WJ, Renzini V, Boyd GW, Peart WS: Renal clip hypertension in rabbits im- munized against angiotensin II. Circ Res 27: 197, 1970.
Eide I, Aars H: Renal hypertension in rabbits im- munized wltn angiotensin II. Stand J Clin Lab invest 25: 119, 1970.
Miksche LW, Mlksche U, Gross F: Effect of sodium restriction on renal hypertension and on renin activity in the rat. Circ Res 27: 973, 1970.
Toblan L, Coffee K, McCrea P: C,ontrasting ex- changeable sodium in rats with different types of Goldbiatt hypertensi’on. Amer J Physiol 217: 458, 1969.
Brunner HR, Klrshman DJ, Sealey JE, Laragh JH: Hypertension of renal origin: evidence for two different mechanisms. Science 174: 1344, 1971.
Krieger EM, Salgado HC, Assan CJ, Greene LLJ, Ferreira SH: Potential screening test for detec- tion of overactivity of renin-angiotensin system. Lancet 1: 269, 1971.
del Greco F, Simon NM, Goodman S, Roguska J: Plasma renin activity in primary and secondary hypertension. Medicine 46: 475, 1967.
Bourgoignie J, Kurz S, Catanzaro FJ, Serirat P, Perry HM: Renal venous renin in hypertension, Amer J Med 48: 332, 1970.
Fitz A: Renal venous renin determinations in the diagnosis of surgically correctable hypertension. Circulation 36: 942, 1967.
Winer BM, Lubbe WF, Simo,n M, Williams JA: Renin in the diagnosis of renovascular hypertension. JAMA 202: 139, 1967.
Heacox R, Harvey AM, Vander AJ: Hepatic inactiva- tion of renin. Circ Res 21: 149, 1967.
Schneider EG, Davis JO, Baumber JS, Johnson JA: The hepatic metabolism of renin and aldoste- rone. A review with new observati’ons on the he- patic clearance of renin. Circ Res 26, 27 (suppl 1): 175, 1970.
Pawsey CGK, Vandongen R, Gordon RD: Renal ve- nous renin ratio in the diagnosis of renovascu- lar hypertension: measurement during active
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
sscretlon of renin. Med J Aust 58: 12i, ~971. \ierrnlllion SE, Sheps SG, Strong CG. Harrison EG,
Hunt .iC: Effect of sodium depletion on renin a:tivlty of renal venous plasma in renovascular hypertension. JAMA 208: 2302. 1969.
K.aneko Y, lkeda T, et al.: Renin release during acute reduction of arterial pressure in normo- tenslve subjects and patients with renovascular hypertension. J Clin Invest 46: 705, 1967.
Brunner HR, Chang P, Wallach R et al.: Angioten- s n II vascular receptors: their avidity in rela- tionship to sodium balance, the autonomic ner- vous system and hypertension. J Clin Invest
51: 58, 1972. Smith HW: Hypertension and urologic disease.
Amer J Med 4: 724, 1948. Thomson GE, Waterhouse K, McDonald HP Jr,
Friedman EA: Hemodialysis for chronic renal failure. Arch Intern Med (Chicago) 120: 153, 1967.
Blumberg A, Nelp WB, Hegstrom RM et al.: Ex- tracellular volume in patients with chronic renal disease treated for hypertension by sodium re- striction. Lancet 2: 69, 1967.
Brown JJ. Dtisterdieck G, Fraser R, Lever AF, Rsob- ertson JIS, Tree M, Weir RJ: Hypertension and chronic renal failure. Brit Med Bull 27: 128, 1971.
Weidmann P, Maxwell MH, Lupu AN, Lewin AJ, Massry SG: Plasma renin activity and blood pressure in terminal renal failure. New Eng J Med 285: 757, 1971.
Vertes V, Cangiano JL, Berman LB et al.: Hyper- tension in end-stage renal disease. New Eng J Med 280: 978, 1969.
Gleadle RI, Brown JJ, Curtis JR, Fraser R, Lawson DH, Lever AF, Linton AL, McVeigh S, Robertson JIS, dewardener HE, Wing AJ: Plasma renin con- centrati’on and the control of blood pressure in patients with chronic renal failure: the effect of haemodialysis. Proceedings of the European Transplant Association, Stockholm, June 1969, vol 6 (Kerr DNS, ed), Lond’on, Pitman Medical, p 131.
Onesti G, Swartz C, Ramirez 0 et al.: Bilateral ne- phrectomy for control of hypertension in uremia. Trans Amer Sot Artif intern Organs 14: 361, 1968.
Sutherland DJA, Ruse GL, Laidlaw GC: Hyperten- sion, increased aldosterone secretion and low plasma renin activity, relieved by dexametha- sone. Canad Med Ass J 95: 1109, 1966.
Eberlein WR, Bongiovanni AM: Plasma and urinary corticosteroids in hypertensive form of congeni- tal adrenal hyperplasia. J Biol Chem 223: 85, 1965.
Bigl eri EG, Herron MA, Brust N: 17.hydroxyla- tisn deficiencv in man. J Clin Invest 45: 1946. 1966. _
Golclsmith 0, Solomon DH, Horton R: Hypogo- nadism and mineralocorticoid excess: the 17.hy- droxylase deficiency syndrome. New Eng J Med 277. 673, 1967.
New Ml: Male pseudohermaphroditism due to 17a- hydroxylase deficiency. J Clin Invest 49: 1930, 1970.
Melby JC. Dale SL, Wilson TE: 18.hydroxy-deoxy- corticosterone in human hypertension. Circ Res 28, 29 (suppl 2): 143, 1971.
Liddle GW, Bledsoe R, Coppage WS Jr: A familial
Volume 52, May 1972 651

RENIN, ANGIOTENSIN AND ALDOSTERONE SYSTEM IN HYPERTENSION - LARAGH ET AL.
renal disorder simulating primary aldosteronism but with negligible aldosterone secretion. Trans Ass Amer Physicians 76: 199, 1963.
95. Gordon RD, Geddes RA, Pawsey CGK, O’Halloran MW: Hypertension and severe hyperkalaemia as- sociated with suppression of renin and aldoster- one and oompletely reversed by dietary sodium restriction. Aust Ann Med 19: 287, 1970.
96. Lee MR: Renin-secreting kidney turnouts. A rare but remediable cause ‘of serious hypertension. Lancet 2: 254, 1971.
97. Winer N, Chokshi DS, Yoon MS, Friedman AD: Ad- renergic receptor medsiation and renin secretion. J Clin Endocr 29: 1168, 1969.
98. Baer L, Brunner HR, Buhler FR, Laragh JH: Sup- pression of renin and aldosterone by clonidine. Ann Intern Med 74:830, 1971.
99. Onesti G, Schwartz AB, Kim KE, Pas-Martinez V, Swartz C: Antihypertensive effect of clonidine. Circ Res 28, 29 (suppl 2): 53, 1971.
100. Shakil M, Fasola AF, Priviteria PJ, Lipicky RJ, Martz BL, Gaffney TE: Effect of methyl d’opa on plasma renin a&ivity in man. Circ Res 25: 543, 1969.
101. Kaneko Y, Takeda T, lkeda T, Tagawa H, lshii M, Takabatake Y, Ueda H: Effect of ganglion-block-
ing agents on renin release in hypertensive pa- tients. Circ Res 27: 97, 1970.
102. Bull MB, Laragh JH: Amiloride: a potassium-spar- ing agent. Circulati,on 37: 45, 1968.
103. Tarazi RC, Dustan HP, Frohlich ED: Long-term thiazide therapy in essential hypertension. Circu- lation 41: 709, 1970.
104. Bourgoignie JJ, Catanzaro FJ, Perry HM Jr: Renin- angi,otensin-aldosterone system during chronic thiazide therapy of benign hypertension. Circula- tion 37: 27, 1968.
105. Bi.ihler RF, Baer L, Vaughan ED, Brunner HR, Laragh JH: Inhibition of renin by propranolol. A specific treatment for renal hypertension? Pre- sented at the 64th Annual Meeting of the Ameri- can Society for Clinical Investigation, May 1972, Atlantic City, N.J.
106. Baer L, Goodwin FJ, Laragh JH: Diazoxide-inmduced renin release in man. Dissociatimon from volume changes. J Clin Endocr 29: 1107, 1969.
107. Ueda H, Kaneko Y, Takeda T, lkeda T, Yagi S: Ob- servations on the mechanism of renin release by hydralazine in hypertensive patients. Circ Res 26, 27 (suppl 2): 201, 1970.
108. Baer L: Perso.nal observations.
652 The American Journal of Medicine
Copyright © 2022 FDOKUMEN




















