Allostatic load in an environmental riskscape: The role of stressors and gender
21
Allostatic Load in an Environmental Riskscape: The Role of Stressors and Gender Christine A. Mair a , Malcolm P. Cutchin b , and M. Kristen Peek c a Department of Sociology and Anthropology, University of Maryland, Baltimore County, 1000 Hilltop Circle, Baltimore, MD 21250-0002 b Department of Allied Health Sciences, University of North Carolina, CB #7122, Bondurant Hall, Suite 2050, Chapel Hill, NC 27599-7122 c Department of Preventive Medicine and Community Health, University of Texas Medical Branch, 301 University Blvd, Galveston, TX 77555-1153 Abstract Stressors are theorized to be associated with higher allostatic load (AL), a concept of physiological wear measured as a composite of physical biomarkers. Risk of high AL may vary by gender and may be intensified in places with significant environmental risks, otherwise known as ‘environmental riskscapes’. Yet, no study has examined the relationship between stressors, gender, and allostatic load in an environmental riskscape. Using primary data collected in a sample (N=1072) exposed to various environmental and social stressors, we find that long-term residence in Texas City (more than 30 years), residential proximity to petrochemical plants, perceived poor neighborhood conditions, and daily hassles are associated with higher allostatic load components. Variation in AL differs by gender and the types of biomarkers examined. Gender moderates the effect of length of residence in Texas City on cardiovascular health risk. We discuss our findings in light of current research on stressors, gender, allostatic load, and double jeopardy within environmental riskscapes. Keywords allostatic load; stressors; gender; environmental riskscapes; health disparities Introduction Conceptually, allostatic load (AL) refers to the body's ability to adjust physiologically to stressors. Operationalized as a measure of physiological homeostasis (Sterling and Eyer, 1988), AL is measured through a diverse set of biomarkers collected from blood, saliva, and other clinical means that reflect cardiovascular, metabolic, inflammatory, neuroendocrine, and immune-related risk (McEwen, 1998; McEwen and Seeman, 1999; Seeman et al., 2001). As the body adapts to its environment, it undergoes “wear and tear” that can accumulate, leading to systemic dysregulation manifested as higher AL (Dowd et al., 2009; Ganzel et al., 2010; Glei et al., 2007; Seeman et al., 1997). Although women report more stressors and © 2011 Elsevier Ltd. All rights reserved. Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. NIH Public Access Author Manuscript Health Place. Author manuscript; available in PMC 2012 July 1. Published in final edited form as: Health Place. 2011 July ; 17(4): 978–987. doi:10.1016/j.healthplace.2011.03.009. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Transcript of Allostatic load in an environmental riskscape: The role of stressors and gender
Allostatic Load in an Environmental Riskscape: The Role ofStressors and Gender
Christine A. Maira, Malcolm P. Cutchinb, and M. Kristen Peekc
aDepartment of Sociology and Anthropology, University of Maryland, Baltimore County, 1000Hilltop Circle, Baltimore, MD 21250-0002bDepartment of Allied Health Sciences, University of North Carolina, CB #7122, Bondurant Hall,Suite 2050, Chapel Hill, NC 27599-7122cDepartment of Preventive Medicine and Community Health, University of Texas Medical Branch,301 University Blvd, Galveston, TX 77555-1153
AbstractStressors are theorized to be associated with higher allostatic load (AL), a concept of physiologicalwear measured as a composite of physical biomarkers. Risk of high AL may vary by gender andmay be intensified in places with significant environmental risks, otherwise known as‘environmental riskscapes’. Yet, no study has examined the relationship between stressors, gender,and allostatic load in an environmental riskscape. Using primary data collected in a sample(N=1072) exposed to various environmental and social stressors, we find that long-term residencein Texas City (more than 30 years), residential proximity to petrochemical plants, perceived poorneighborhood conditions, and daily hassles are associated with higher allostatic load components.Variation in AL differs by gender and the types of biomarkers examined. Gender moderates theeffect of length of residence in Texas City on cardiovascular health risk. We discuss our findingsin light of current research on stressors, gender, allostatic load, and double jeopardy withinenvironmental riskscapes.
Keywordsallostatic load; stressors; gender; environmental riskscapes; health disparities
IntroductionConceptually, allostatic load (AL) refers to the body's ability to adjust physiologically tostressors. Operationalized as a measure of physiological homeostasis (Sterling and Eyer,1988), AL is measured through a diverse set of biomarkers collected from blood, saliva, andother clinical means that reflect cardiovascular, metabolic, inflammatory, neuroendocrine,and immune-related risk (McEwen, 1998; McEwen and Seeman, 1999; Seeman et al., 2001).As the body adapts to its environment, it undergoes “wear and tear” that can accumulate,leading to systemic dysregulation manifested as higher AL (Dowd et al., 2009; Ganzel et al.,2010; Glei et al., 2007; Seeman et al., 1997). Although women report more stressors and
© 2011 Elsevier Ltd. All rights reserved.Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to ourcustomers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review ofthe resulting proof before it is published in its final citable form. Please note that during the production process errors may bediscovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptHealth Place. Author manuscript; available in PMC 2012 July 1.
Published in final edited form as:Health Place. 2011 July ; 17(4): 978–987. doi:10.1016/j.healthplace.2011.03.009.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

higher perceived stress, no study has examined the relationship between stressors, gender,and AL. Further, we know little about how stressors and gender shape AL within anenvironmental riskscape— such as an area with substantial environmental health risks orpoor neighborhood conditions (Morello-Frosch and Shenassa, 2006; Simandan, 2010). Thus,this study is one of the first to assess the relationship between stressors, gender, and AL inthe context of an environmental riskscape. After describing further context for the study,methods, and findings, we discuss how our study supports a new understanding of themechanisms that contribute to health disparity.
Stress Processes and Allostatic Load RiskStressful environments get “under the skin” to cause health problems (Taylor et al., 1997),yet there is still much unknown about how that process may work and how particularexposure to contextual conditions may shape the process. Chronic and acute exposure tostressors may yield long-term health consequences (Ganzel et al., 2010; McEwen, 1998).Stressors are theorized to be associated with neuroendocrine responses, which can havecascading effects on other systems of the body by increasing blood pressure, immune-responses, cancer, etc. (McEwen, 1998; Taylor et al., 1997). Theoretically, stressors such asdangerous situations, social instability, living in an “unpleasant neighborhood,” negative lifeevents, and daily hassles may be linked to elevated allostatic load (McEwen, 1998; McEwenand Seeman, 1999). In addition, health disparities literature posits gender differences in thestress process. Thus, there may be gender differences in AL and its components as well asgender differences in the association between stressors and AL.
In terms of the physical environment, stressors such as environmental hazards or poor-quality built environments, may be chronic or acute and are theoretically linked to poorhealth (Cutchin, 2007; Hill et al., 2009; Pearlin et al., 2005; Stronegger at al., 2010).Specifically, living in close proximity to an environmental hazard or having a high level ofperceived exposure to environmental threats is associated with increased stress (Burby andStrong, 1997; Hallman and Wandersman, 1992; Luginaah et al., 2000; Yang and Matthews,2010). Stress resulting from these types of environmental stressors may be associated withnegative physiological outcomes. For example, a study of Three Mile Island in Pennsylvaniafinds elevated physiological risk factors, such as lower lymphocytes, higher cortisol, andhigher levels of herpes simplex reactivation among residents living near the damagednuclear reactor (McKinnon et al., 1989). In addition to environmental hazards, neighborhoodconditions may operate as stressors. Evans (2003) reports that physical aspects of theneighborhood (household crowding, quality) are associated with elevated AL among ruralchildren. These studies provide preliminary empirical evidence of a link betweenenvironmental stressors and risk of elevated AL. Yet, it is unknown if exposure toenvironmental hazards, perceived risk from those hazards, or poor quality neighborhoods areassociated with elevated AL.
Stressors that are more psychosocial in origin—such as negative life events (e.g., divorce ordeath of a loved one) and daily hassles (e.g., family or financial worries)—are also theorizedto be associated with AL (McEwen, 1998). Yet, the few studies to test the relationshipbetween negative life events and AL or physiological dysregulation find little to noassociation (Clark et al., 2007; Glei et al., 2007). Further, no study has tested the linkbetween daily hassles and AL. Daily hassles are weakly associated with poor immuneflexibility (Peters et al., 2003), chest pain (Lau et al., 1996), and outpatient health careutilization (Williams et al., 1992)—all of which may indirectly reflect physiologicaldysregulation.
In addition to stressors per se, clinical classifications of high risk AL differ for men andwomen (Seeman et al., 2002), although no studies examine gender differences in stressors
Mair et al. Page 2
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

and AL. Women are typically classified as a disadvantaged group, yet this disadvantagedoes not always translate into poorer health (Macintyre et al., 1996; Rieker and Bird, 2005).Theoretical examinations of gender health disparities suggest that differences in the effectsof stressors may not necessarily indicate that men and women are differentially susceptibleto stressors (Aneshensel et al., 1991). Women may have more exposure to stressors (Riekerand Bird, 2005). Indeed, women report more negative life events (Turner and Avison, 2003)and higher stress levels (McDonough and Walters, 2001). However, some studies find thatstressor exposure does not account for gender differences (McDonough and Walters, 2001;Turner and Avison, 2003). A study exploring concern over environmental risk reports thatwomen have higher concern about risk than men in high quality neighborhoods but not in“stressed” neighborhoods (Greenberg and Schneider, 1995). Few studies, however, examinegender differences in the relationship between stressors and health in environmentalriskscapes. Thus, it is unknown whether stressful environments get “under the skin” morefor women than for men.
Stressors and Allostatic Load in Environmental RiskscapesOverlapping risk factors may leave individuals vulnerable to double jeopardy. Morello-Frosch and Shenassa (2006) incorporate the concept of double jeopardy in a manner thanconsiders local context and AL. The authors propose a framework that incorporates builtenvironment, social environment, and psychosocial stressors as fundamental risks associatedwith allostatic load. They suggest that the combination of community-level and individual-level stressors creates a unique form of double jeopardy that can lead to health disparities,particularly among already disadvantaged groups such as women. This ‘riskscape’framework explicitly suggests a strong relationship between place and physiological wear,as indicated by A. What the literature lacks, however, are studies that combine variouscommunity and individual-level measures of stressors together with gender to betterunderstand place-based jeopardy for higher allostatic load.
Although the environmental riskscape is “driven by the distribution of power, privilege andeconomic resources” (Morello-Frosch and Shenassa, 2006, p. 1152), Morello-Frosch andShenassa do not suggest processes that shape such distributions in particular places oridentify analytical perspectives through which to recognize them. In contrast, Cutchin(2007) argues that there are several intertwined geographical processes at work in such riskyand unequal places. Specifically, he describes historical and cultural processes materializedin the landscape of Texas City, Texas as a way to illuminate the agents and power that createunequal risk. Cutchin (2007) also invokes political ecology and territoriality perspectives tounderstand the intertwined local, state, national, and global scale processes that emerge inthe local landscape and neighborhoods of Texas City. Those processes differentiate the riskexperienced by various groups in Texas City. Other work by Cutchin and colleagues (2008)argues that at a smaller scale, the transactional process of stress and coping, theorized byLazarus (1991; 1999), is relevant to understanding risky environments and individuals'relationship with them—a relationship that, in turn, influences health.
By taking these perspectives as a group and integrating them with allostatic load theory, wecan begin to more thoroughly theorize an important health process—stressor exposure andthe bodily response to it. The benefit of this approach is that it allows us to analyticallycombine processes at various scales of analysis. Therefore, these processes can beconsidered either upstream (more distal) or direct (more proximal) causes of AL and thepoor health it indicates. Broader scale foci, such as the global reach and power of oilcorporations, go well beyond the meso-scale conceptualizations of Ganzel et al., (2010) andMorello-Frosch and Shenassa (2006). Yet, those meso-scale understandings are essential tounderstand risk and health in particular places, particularly when combined withtransactional stress and coping theory. Allostatic load theory completes the picture. The
Mair et al. Page 3
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
allostatic load perspective implicates specific physiological processes that reflectindividuals' exposures and experiences within those broader geographical scales. Thistheoretical integration of allostatic load and geographical theory marks an initial step towardSimandan's (2010) recent call for allostatic load research that would unify explanationacross geographical scales, ranging from the body to the global political economy.Moreover, this combined perspective stretches the understanding of a riskscape toencompass a broader range of processes. Although not all components of this integratedview can be included in this study, an awareness of a more holistic geographicalunderstanding of process, place, and health facilitates an enhanced position for inference andexplanation.
HypothesesIn accordance with the allostatic load and health geography literature, we hypothesized thatstressors are associated with higher overall AL and AL components. Drawing from genderand health literature, we hypothesized that the predictive power of stressors varies by genderand by the type of allostatic outcome examined. Finally, we hypothesized that gendermoderates the relationship between stressors and AL, suggesting different processes bygender.
Data and MethodsData
We analyzed data from the Texas City Stress and Health Study collected between 2004 and2006 in Texas City, Texas, a small urban setting in close proximity to a large complex ofpetrochemical plants (Cutchin, 2007; Cutchin et al., 2008; Meyler et al., 2007; Peek et al.,2008; Peek at al., 2009a). The dataset was designed to study sociobiological stress andhealth in a representative sample of individuals from multiple ethnic/race groups (N=2706).These data are particularly suited to the study of stressors, gender, and AL for two primaryreasons. First, this dataset contains an unusually diverse collection of stressor measures.Second, the study collected numerous AL biomarkers from a large subsample of respondents(N=1457).
Texas City residents were surveyed in three stages: (a) All households in a 12 mile2 areanear the oil refineries were contacted and classified into three groups (Hispanics 25-64years, Hispanics 65+ years, and non-Hispanics); (b) Each Hispanic household and 1/8 of allnon-Hispanic households were selected; (c) Of Hispanics 25-64 years and non-Hispanics,one adult in each household was randomly selected as eligible for interview and allHispanics aged 65+ were deemed eligible for interview. This sampling design yielded threestrata: (a) 1/8 of all non-Hispanic households; (b) a majority of Hispanic households withone respondent aged 25-64; and (c) a full census of Hispanics aged 65+ from the study area.Households with at least one Hispanic adult present were classified as “Hispanic”.
The study utilized U.S. Census Bureau Current Population Survey methods for listing,enumeration, and interviewing—yielding a response rate of 80 percent. Respondents wereasked to provide a blood sample and 54 percent (N=1457) complied. A trained phlebotomistdrew blood in a clinic or in the subject's home between 8 and 11 AM after fasting. Bloodsamples were centrifuged to obtain plasma, which was stored at −70°C until testing. Plasmalevels of IL-6, IL-10, CRP, and TNF-alpha were analyzed using standard ELISA methods.Samples were batch analyzed to minimize interassay variation. Anti-viral antibody titerswere determined by indirect immunofluorescence (Stowe et al., 2001; Tingate et al., 1997).Commercially-prepared substrate slides and control sera (Microgen Laboratories, LaMarque, TX, and Bion Enterprises, Park Ridge, IL) were used for determining antibody
Mair et al. Page 4
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
titers to EBV-VCA, EBV-EA, EBNA, and HSV-1. All specimens were batch analyzed andread blind-coded. Detailed information on the blood collection protocol is availableelsewhere (Peek et al., 2009a, 2009b; Stowe et al., 2010a, 2010b). The institutional reviewboard at University of Texas Medical Branch approved the study protocol, and informedconsent was obtained from all participants.
Because the “other” race/ethnicity category composed a small proportion of the biomarkersubsample (N=15) and because Hispanics not of Mexican origin in the subsample were adiverse group (N=82), we excluded those individuals. From this biomarker subsample, weincluded cases with full data on all 16 biomarkers (N=1192). After listwise deletion, ouranalytical sample included 1072 respondents.
MeasuresDependent variables included total allostatic load and four components of AL(cardiovascular, metabolic, inflammatory, and immune-related; see Table 1). Traditionalcomposite measures of AL identify “high risk” cut-offs for each biomarker and sum theresulting binary scores, similar to a checklist. This approach, however, reduces variation andmay not capture the full range of AL (Loucks et al., 2008). Therefore, we opted for a z-scoremeasure of AL to utilize the interval scores and their variation. Results from this z-scoredsummation variable creation method did not differ significantly from results using thedichotomous summation method. Before stratifying the sample by gender, we constructed z-scores (mean=0, S.D.=1) for each of the 16 biomarkers. We then created a summation scorefor total AL as well as cardiovascular, metabolic, inflammatory, and immune-relatedcomponents of AL.
Consistent with previous studies, we included age, age squared, and race/ethnicity in ourmodels (Crimmins et al., 2003; Geronimus et al., 2006). For specific operationalization ofvariables, see Table 1. Age was a continuous variable. We constructed an age squared termto account for non-linear effects. Race/ethnicity was derived from self-identified race/ethnicity and nativity status. Our analysis included non-Hispanic Whites, non-HispanicBlacks and individuals of Mexican origin. For individuals of Mexican origin, we distinguishbetween “foreign-born” and “US-born” (Crimmins et al., 2007; Kaestner et al., 2009; Peeket al., 2009b).
Our key independent variables were gender and stressors. Because thresholds of biomarker“high risk” differ by gender, we controlled for gender in analyses of the total sample(1=female) and also stratified the sample by gender. Measures of stressors includedexposure to petrochemical plants, concern about petrochemical health risks, neighborhoodperception, negative life events, and daily hassles. Exposure to the plants was measured bytwo variables: length of time residing in Texas City and residential distance from thepetrochemical plants' fence line in meters. Because our theoretical scope includes an interestin chronic, long-term environmental stressors and to be consistent with previous literature(Cutchin et al., 2008), we categorized length of residence in Texas City as less than 15years, 15 to 30 years, and more than 30 years (reference category=less than 15 years).Concern about petrochemical health risk (CAPHRS; Cutchin et al., 2008) was a summationscore of four items measuring respondents' subjective assessments of exposure concern.Neighborhood perception was measured with the perceived neighborhood scale, whichincluded subscales for social embeddedness, sense of community, satisfaction withneighborhood, and perceived crime (Martinez et al., 2002). Higher neighborhood perceptionscores indicate a more positive perception. Negative life events were measured by 27 itemsto indicate whether or not respondents or an immediate family member experienced negativelife events (such as injuries, accidents, deaths, crime, family issues, and financial/job/schooltroubles) in the past year (Turner et al., 1995). Higher scores indicate more negative life
Mair et al. Page 5
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

events. Daily hassles were measured as a summation score of 18 items on a scale of 0 to 3,which asked respondents how bothered they were by responsibilities, time/moneyconstraints, family/friend issues, and neighborhood/environment concerns. Increasing valuesindicate more daily hassles (Kanner et al., 1981).
We also included the following potential confounding factors: married; Medical OutcomesStudy (MOS) Social Support Scale (Sherbourne and Stewart, 1991); high school degree;income; smoking and exercise behaviors; perceived stress (Cohen and Williamson, 1988);sum of chronic health conditions; and health insurance status (Table 1).
AnalysisWe began our analysis by addressing missing data. Missing data on neighborhoodperception items ranged from 0.7 percent (N=20) to 8 percent (N=202). Summing theseitems yielded 22 percent of cases with at least one missing item for the scale (N=604).Income contained 11 percent missing cases (N=296). Missing data analysis determined thatthese items were missing at random. Therefore, we imputed these measures with an EMestimation algorithm (PSAW 18; Garson, 2008). In addition, we removed eight items fromthe daily hassles scale and two from the negative life events scale due to missing data. Inboth cases, removing these items reduced missing data and improved reliability estimates(Cronbach's alpha). We also conducted multivariate outlier analysis and identified 11outliers. Because sensitivity tests determined that these outliers did not change the results,these cases were not removed.
All analyses were performed for the total sample, for men, and for women. We conducteddescriptive analysis (Table 2) and ordinal least squares (OLS) regression analysis (Tables 3and 4). For OLS models predicting total AL, Model 1 included sociodemographic variables:age, age squared, and race/ethnicity, and female (for the total sample). Model 2 addedstressors to the model and Model 3 added all control variables. Model 3 (full model) wasused in analyses predicting components of AL (Table 4). Models predicting theinflammatory component were not statistically significant as a whole and thus are notpresented in Table 4. To examine the potential moderating effect of gender, we testedinteraction effects between gender and stressors for AL and its subcomponents (Newsom etal., 2003). Because there was a statistically significant interaction between gender and a keystressor measure (residing in Texas City for more than 30 years) when predictingcardiovascular AL, we present all results for the total sample, as well as stratified by genderin order to explore the explanatory power of stressors and the role of Texas City residencefor women and men separately.
ResultsDescriptive statistics revealed differences in AL and stressors by gender (Table 2). Men hadhigher total, cardiovascular, and metabolic AL. Women possessed higher immune-relatedAL. For the total sample, age ranged from 25 to 90 years, 60 percent of respondents werefemale (N=627), 40 percent were non-Hispanic White (N=426), 11 percent were non-Hispanic Black (N=116), 37 percent were US-born Mexican American (N=400), and 12percent were foreign-born Mexicans (N=130). Nearly 65 percent of the sample resided inTexas City for at least fifteen years with a larger proportion of men spending thirty or moreyears in the community, although this difference was not statistically significant. Meandistance from the plants was 1755 meters. Mean distance did not vary significantly bygender. The average CAPHRS score was 14. Women had slightly higher concern (15) thanmen (14). Men reported more positive neighborhood perception (80, compared to 73 forwomen), fewer negative life events (just under 2, compared to over 2 for women), and fewerdaily hassles (10, compared to 14 for women). Men in our sample were more likely to be
Mair et al. Page 6
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

older, married, earn higher income, smoke, exercise moderately, have health insurance, andreport fewer health conditions.
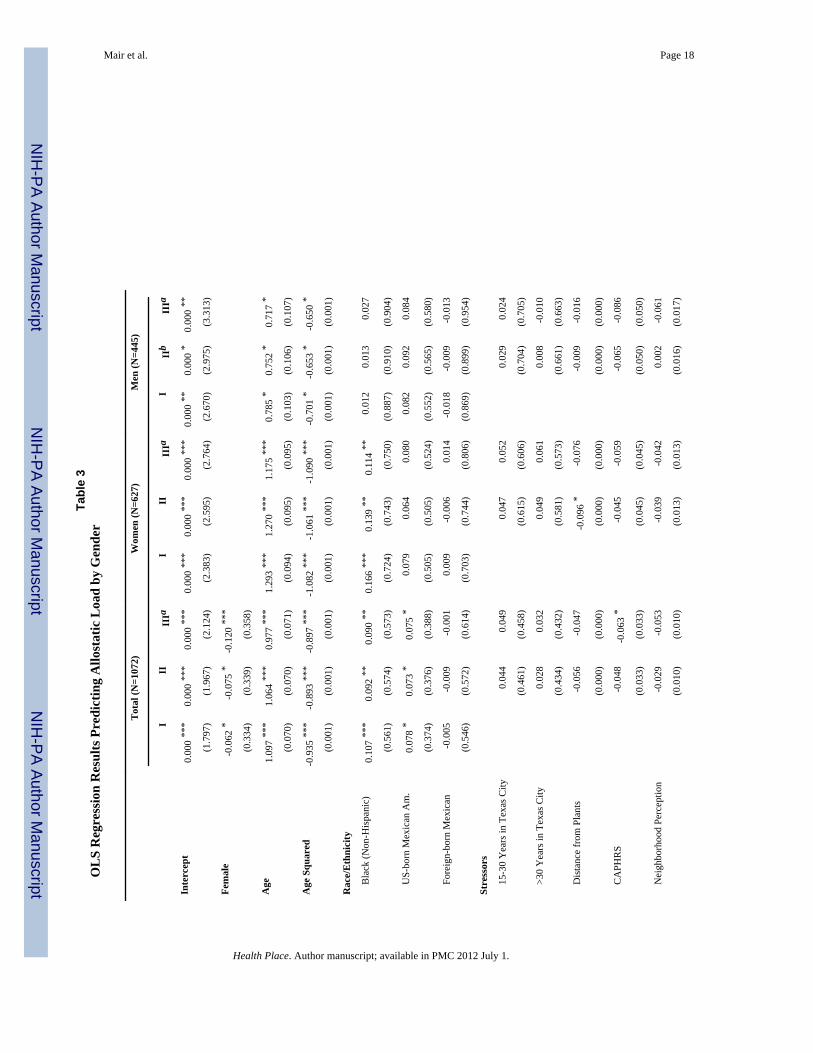
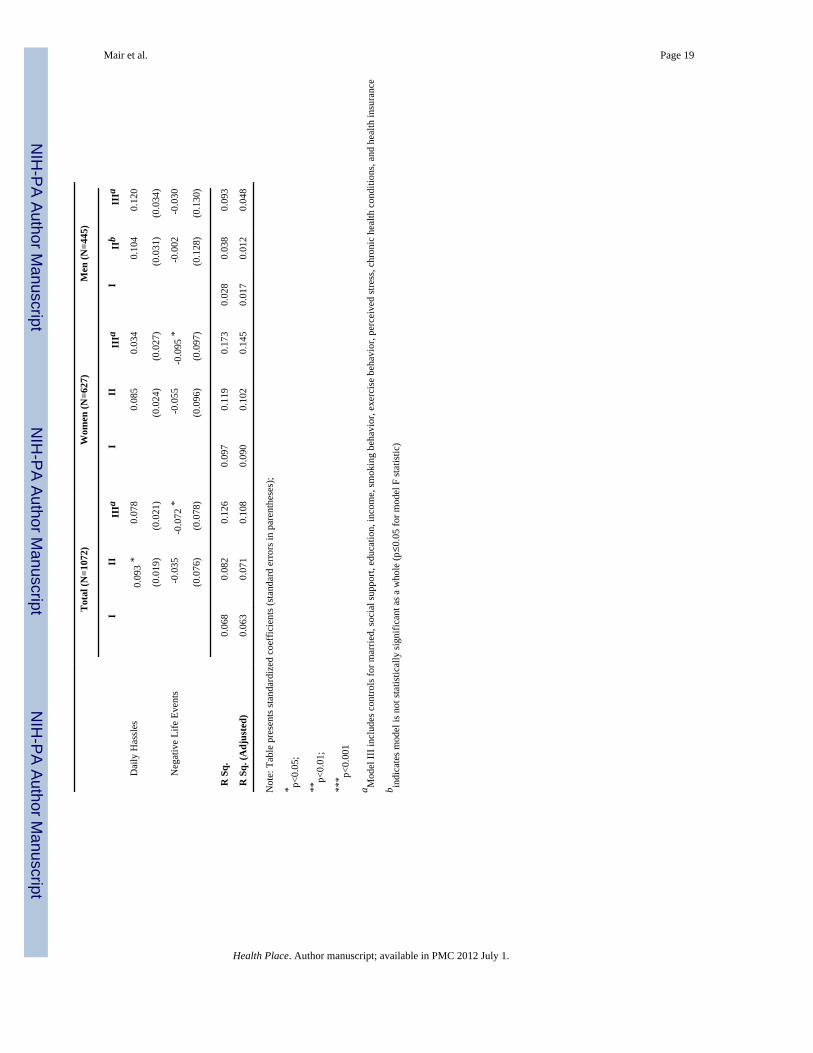
In multivariate analyses predicting total AL (Table 3), Model 1 explained six percent of thevariation (adjusted R2=.063), Model 2 explained seven percent after adding stressors(adjusted R2=.071), and Model 3 with controls explained 11 percent (adjusted R2=.108).Comparing model fit for the full sample, stressors added little explanatory power and onlymarginally improved the fit of the model. For AL components in the total sample (Table 4),the full model explained the most variation in cardiovascular AL (adjusted R2=.131). In thefull sample predicting total AL, the daily hassles score was associated with AL in thepredicted direction before controls were added (Table 3, Model 2, β=.093, p=.012). In Table4 predicting AL components for the total sample, living in Texas City for more than 30years was linked to higher cardiovascular AL (Table 4, β=.084, p=.028) and more dailyhassles predicted higher metabolic AL (Table 4, β=.088, p=.034), net of all controls. Greaterdistance from the petrochemical plants was associated with lower immune-related AL (β=-.065, p=.046) and positive neighborhood perception was associated with lower metabolic AL(β=-.080, p=.022).
In terms of basic gender differences, women had lower total AL (Table 3, Model 3, β=-.120,p=<.001; Table 4), cardiovascular AL, and metabolic AL, but higher immune-related AL.Yet, non-Hispanic Black women had higher cardiovascular and immune-related ALcompared to non-Hispanic white women. Our ability to explain variation in AL andcomponents differed by gender. Women's models explained more variation in allostatic load.Although Model 1 (Table 3) explained nine percent of variation in total AL for women(adjusted R2=.090), Model 3 explained as much as 15 percent (adjusted R2=.145). For men,Model 1 (Table 3) explained two percent of the variation in total AL (adjusted R2=.017) andModel 3 explained five percent (adjusted R2=.048). For women (Table 4), the modelexplained the largest amount of variance in cardiovascular AL (adjusted R2=.192), followedby metabolic (adjusted R2=.076), and then immune-related (adjusted R2=.055). For men(Table 4), we see a different trend. The full model explained the largest amount of variationin men's metabolic AL (adjusted R2=.067), followed by cardiovascular AL (adjusted R2=.036), then immune-related AL (adjusted R2=.031).
Turning to the role of stressors and gender, greater geographic distance from thepetrochemical plants was linked to lower total AL for women before controls were added(Table 3, Model 2, β=-.096, p=.019). More negative life events were associated with lowertotal AL for women in the final model (Model 3, β=-.095, p=.027). As with the full sample,however, adding stressors did not improve the overall fit of the model. Stressors did notsignificantly predict total AL for men in this sample. Examining components of AL (Table4), residing in Texas City for more than 30 years predicting higher cardiovascular AL forwomen (β=-.104, p=.031). Greater geographic distance from the petrochemical plants wasassociated with lower cardiovascular AL for women (β=-.088, p=.031) and lower immune-related AL for men (β=-.107, p=.036). Finally, greater CAPHRS was linked to lowercardiovascular AL for men (β=-.136, p=.012). Because of the significant interaction betweenstressors and gender for cardiovascular AL (gender and residing in Texas City for more than30 years; β=.558, p=.020), gender moderates the relationship between Texas City residenceand cardiovascular AL. In other words, living in Texas City for more than 30 years wasrelated to higher cardiovascular health risk for women but not men (Table 4).
Mair et al. Page 7
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

DiscussionStressors and Allostatic Load
We found partial support for our first hypothesis that stressors predict higher AL. Fourstressors were linked to elevated AL or AL components: long-term residence in Texas City,proximity to the petrochemical plants, poor neighborhood perception, and more dailyhassles. These factors represent distinct processes. Texas City-related stressors aremechanisms of allostatic strain through their roles as environmental health threats. Not onlydo the plants produce smells, noise, and visible emissions, but residents are aware of ahistory of health risk and dangerous explosions, one of which occurred during datacollection (Cutchin et al., 2008).1 Poor neighborhood perception is a less diffuse mechanismthan Texas City-specific causes because neighborhood conditions are more immediatelyexperienced by residents, regardless of location. Neighborhood perception also represents asocial dimension of the environment (e.g., crime perception and social embeddedness).Daily hassles are more directly experienced, as they vary by individual more so than plantproximity and neighborhood perception. All four stressors can be considered chronicstressors that should be associated with AL, a process of dysregulation that occurs slowlyover time (thus the associated term ‘weathering’). Therefore, it is particularly noteworthythat although the linkages between chronic stressors and AL are not consistent across allmodels, they all predict some component of AL in our sample.
Gender and Allostatic LoadWhile the stress process literature discusses chronic, life-long stressors and AL, healthdisparities research may offer some insight into how chronic stressors may be captured inother variables such as gender. In support of our second hypothesis, there were genderdifferences in the explanatory power of our models and this effect varied by the type of ALoutcome assessed. Our ability to predict AL through exposure to stressors was substantiallygreater for the sample of women compared to men. For men, very few of the variablesexamined offered insight into AL risk. Thus, not only are men in Texas City at risk due totheir elevated AL, but we also know very little about the mechanisms that contribute toelevated AL for men. This insight reveals men's potential health risk. For women, we areable to pinpoint specific probable causes of elevated AL, such as long-term residence inTexas City or being non-Hispanic Black. Interactions between gender and race/ethnicity,however, were not statistically significant, indicating that race/ethnicity is not necessarilymore important for women than it is for men. Further, men and women in our sample did nothave significant descriptive differences in terms of Texas City-related stressors or racial/ethnic composition. Rather, gender differences in our ability to predict AL may indicate thatmen and women manifest strain differently. This finding is consistent with health disparitiesliterature, which notes that differential exposure to stressors is not necessarily linked todifferences in actual stress and that health disparities should be evaluated using multiplehealth outcomes (McDonough and Walters, 2001; Turner and Avison, 2003). Future studiesshould continue to assess AL and AL components separately in order to assess a variety ofphysiological manifestations of stress for men and women.
1To ensure that exposure to the explosion did not bias results, the authors conducted sensitivity analyses for the subsample ofindividuals with full data on allostatic load components as well as full data on their experiences regarding the explosion (N=142).Although previous work found that exposure to this explosion was associated with poorer perceptions of health (Peek et al., 2008) andmore concern about plant-related health risk (Cutchin et al., 2008), whether or not a respondent was exposed to the explosion did notaffect allostatic load
Mair et al. Page 8
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Place Processes and Allostatic LoadIn addition to the direct effect of stressors and the explanatory power of stressors by gender,we found partial support for our final hypothesis that gender moderates the relationshipbetween stressors and AL. Specifically, long-term residence in Texas City is significantlylinked to higher cardiovascular risk for women only. This important gender differenceallows us to explore an interesting new view of allostatic health risk through the concept ofoverlapping disadvantages, or “double jeopardy.” Chronic stressors may influence ALthrough less obvious mechanisms, such as being a lifelong member of a disadvantagedgroup (e.g., being a woman) while experiencing prolonged exposure to an environmentalriskscape (e.g., long-term residence in Texas City). The consequences of this enduring riskmay be best understood when compared to the effects of shorter-term stressors.Neighborhood perception and daily hassles, for example, were poor predictors of AL. Inaddition, concern about petrochemical health risk and negative life events were actuallyassociated with lower AL. If we interpret these results as non-spurious, it may be that thesemeasures reflect acute stressors, which are less likely to manifest as physiological risk (AL),compared to chronic stressors.
Because environmental riskscape exposure appears to have the most consistent relationshipto elevated AL in our analysis, it implies that broader geographical processes shaping theTexas City riskscape are implicated in the story of allostatic load. By extending allostaticload theory and riskscape concepts, we are able to include broader and more historicalprocesses of political power and territoriality. Risk exposure in the city as a whole(represented by years in the city) and in particular parts of the city (represented by distanceto the plants and neighborhood conditions) have a role in understanding AL in the TexasCity sample (Cutchin, 2007). By combining a consideration of chronic stressors anddisadvantaged group membership in our analysis, along with the integrated perspectives ofvarious geographical scales and processes, we are able, if only indirectly, to view the role ofbroader processes of inequality (e.g., global corporations, state apparatuses, and localagents) in enhanced AL risk in certain individuals. Moreover, the potential lesson learned isthat it is not simply disadvantaged group membership that is related to AL. AL health risk isconnected to broader powers that create risky urban environments, chronic stressors,unequal neighborhoods, and limited opportunities for particular groups.
Therefore, the concept of an environmental riskscape encompasses more than simplyphysical exposure to an environmentally-compromised space. Riskscapes themselves areinherently systems of ‘double jeopardy,’ as the individuals living within them are deeplyintertwined in unequal geographical processes at multiple levels. This complex system ofinfluences also creates additional inequalities such as the inability to relocate fromenvironmental threats (Cutchin, 2007). Such inequalities, in turn, are accentuated forindividuals who are members of more than one disadvantaged group (e.g., minority women).Overlapping sources of jeopardy may become too much to cope with, especially without theresources or the power to counter the underlying macro-level causes of inequality. Althoughsensitivity tests of race/ethnicity interactions indicate that the effects of gender and stressorsdo not differ significantly by race/ethnicity in Texas City, minority women residing in otherenvironmental riskscapes may be at risk for ‘triple jeopardy’ and thus vulnerable to poorhealth outcomes such as elevated AL. Indeed, studies in the US have found extensiveevidence of the health risks associated with racial/ethnic spatial inequality (Massey, 2004;Williams and Collins, 2001), particularly in environmental riskscapes (Hipp and Lakon,2010; Pastor et al., 2005). Therefore, the role of race/ethnicity in the broader story ofstressors, gender, and allostatic load deserves continued attention in future work exploringhealth disparities in environmental riskscapes.
Mair et al. Page 9
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Before concluding this study, we first review a few limitations. First, these data are cross-sectional. In the absence of longitudinal data, we are conservative in our discussion ofcausality. Second, although the environmentally-compromised nature of Texas City allowsus to explore the concept of riskscapes, the dataset is not nationally representative and thusour ability to generalize findings to other locales is limited. Finally, we did not examineneuroendocrine components of AL in our analysis so the results of this study cannot bedirectly compared to Seeman et al.'s (2002) study of gender and AL.
ConclusionDespite limitations, this study is the first known examination of stressors, gender, and ALwithin an environmental riskscape and thus provides important contributions. First, ouranalysis provides one of the most comprehensive tests of stressors and AL by exploring arange of chronic and acute stressors through diverse measures such as exposure toenvironmental threat, subjective assessments of risk and neighborhoods, and daily hassles/negative life events. Second, although most studies of AL immediately stratify samples bygender without theoretically or empirically addressing the role of gender in health risk, ourstudy specifically outlines a theoretical argument for gendered health disparities and offersan empirical test of the direct and moderating influences of gender. Finally, this studyexamines allostatic load within the context of an environmental riskscape and proposes amodel in which geopolitical mechanisms intertwine to create a landscape wheredisadvantaged individuals experience heightened health risk (allostatic load).
In conclusion, our study suggests that chronic stressors, such as residential proximity topetrochemical plants, prolonged residence in Texas City, negative neighborhood perception,and daily hassles may be linked to elevated AL or AL components. Although women in oursample were exposed to more chronic stressors, they fared better than men in terms of AL.Women, however, are at cardiovascular risk for ‘double jeopardy’ when living in anenvironmentally-compromised landscape for a prolonged period of time while men are not.This combination of chronic stressor and gender considerations is a potential new directionfor future research on stress, AL, and health disparities. Furthermore, our findings should beinterpreted in the wider context of geographical processes theorized to be related to thecreation of environmental riskscapes and to AL. Knowledge of disparities and increased riskis not sufficient to understand ultimate causes of allostatic load. Rather, it is essential to lookacross geographical scales at processes that shape risk and eventually the physiologicalresponse to stress from risk. By considering stressors, gender, and AL in the framework of ariskscape, we develop a more integrative understanding about how place is central to health.
AcknowledgmentsThe authors wish to thank James S. Goodwin and two anonymous reviewers for their helpful comments andsuggestions. This work was supported by Grant P50 CA10563 from the National Cancer Institute which funded theUTMB Center for Population Health and Health Disparities as well as the Texas City Stress and Health Study.
ReferencesAneshensel CS, Rutter CM, Lachenbruch PA. Social-structure, stress, and mental-health: Competing
conceptual and analytic models. American Sociological Review. 1991; 56:166–178.Burby RJ, Strong DE. Coping with chemicals: Blacks, Whites, planners, and industrial pollution.
Journal of the American Planning Association. 1997; 63:469–480.Clark MS, Bond MJ, Hecker JR. Environmental stress, psychological stress and allostatic load.
Psychology, Health & Medicine. 2007; 12:18–30.
Mair et al. Page 10
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Cohen, S.; Williamson, G. Perceived Stress in a Probability Sample of the US. In: Spacapam, S.;Oskamp, S., editors. The Social Psychology of Health: Claremont Symposium on Applied SocialPsychology. Sage; Newbury Park: 1988. p. 31-67.
Crimmins EM, Johnston M, Hayward M, Seeman T. Age differences in allostatic load: an index ofphysiological dysregulation. Experimental Gerontology. 2003; 38:731–734. [PubMed: 12855278]
Crimmins EM, Kim JK, Alley DE, Karlamangla A, Seeman T. Hispanic paradox in biological riskprofiles. American Journal of Public Health. 2007; 97:1305–1310. [PubMed: 17538054]
Cutchin MP. The need for the “new health geography” in epidemiologic studies of environment andhealth. Health & Place. 2007; 13:725–742. [PubMed: 17208033]
Cutchin MP, Martin KR, Owen SV, Goodwin JS. Concerns about petrochemical health risk before andafter a refinery explosion. Risk Analysis. 2008; 28:589–601. [PubMed: 18643817]
Dowd JB, Simanek AM, Aiello AE. Socio-economic status, cortisol and allostatic load: a review of theliterature. International Journal of Epidemiology. 2009; 38:1297–1309. [PubMed: 19720725]
Evans GW. A multimethodological analysis of cumulative risk and allostatic load among ruralchildren. Developmental Psychology. 2003; 39:924–933. [PubMed: 12952404]
Ganzel BL, Morris PA, Wethington E. Allostasis and the human brain: Integrating models of stressfrom the social and life sciences. Psychological Review. 2010; 117:134–174. [PubMed: 20063966]
Garson, GD. Data Imputation for Missing Values. Statnotes: Topics in Multivariate Analysis. 2008.Retrieved 1 March 2010, from http://faculty.chass.ncsu.edu/garson/pa765/statnote.htm
Geronimus AT, Hicken M, Keene D, Bound J. “Weathering” and age patterns of allostatic load scoresamong blacks and whites in the United States. American Journal of Public Health. 2006; 96:826–833. [PubMed: 16380565]
Glei DA, Goldman N, Chuang YL, Weinstein M. Do chronic stressors lead to physiologicaldysregulation? Testing the theory of allostatic load. Psychosomatic Medicine. 2007; 69:769–776.[PubMed: 17942833]
Greenberg MR, Schneider DF. Gender differences in risk perception: Effects differ in stressed vs. non-stressed environments. Risk Analysis. 1995; 15:503–511. [PubMed: 7480950]
Hallman WK, Wandersman AH. Attribution of responsibility and individual and collective copingwith environmental threats. Journal of Social Issues. 1992; 48:101–118.
Hill TD, Burdette AM, Hale L. Neighborhood disorder, sleep quality, and psychological distress:Testing a model of structural amplification. Health & Place. 2009; 15:1006–1013. [PubMed:19447667]
Hipp JR, Lakon CM. Social disparities in health: Disproportionate toxicity proximity in minoritycommunities over a decade. Health & Place. 2010; 16:674–683. [PubMed: 20227324]
Kaestner R, Pearson JA, Keene D, Geronimus AT. Stress, allostatic load, and health of Mexicanimmigrants. Social Science Quarterly. 2009; 90:1089–1111. [PubMed: 21165158]
Kanner AD, Coyne JC, Schaefer C, Lazarus RS. Comparison of two modes of stress measurement:Daily hassles and uplifts versus major life events. Journal of Behavioral Medicine. 1981; 4:1–39.[PubMed: 7288876]
Lau G, Hui KK, Lam SK. Life events and daily hassles in patients with atypical chest pain. AmericanJournal of Gastroenterology. 1996; 91:2157–2162. [PubMed: 8855740]
Lazarus, RS. Emotion and Adaptation. Oxford: Oxford University Press; 1991.Lazarus, RS. Stress and Emotion: A New Synthesis. New York: Springer Publishing; 1999.Loucks EB, Juster RP, Pruessner JC. Neuroendocrine biomarkers, allostatic load, and the challenge of
measurement: A commentary on Gersten. Social Science & Medicine. 2008; 66:525–530.Luginaah IN, Taylor SM, Elliott SJ, Eyles JD. A longitudinal study of the health impacts of a
petroleum refinery. Social Science & Medicine. 2000; 50:1155–1166. [PubMed: 10714934]Macintyre S, Hunt K, Sweeting H. Gender differences in health: Are things really as simple as they
seem? Social Science & Medicine. 1996; 42:617–624. [PubMed: 8643986]Martinez ML, Black M, Starr RH. Factorial structure of the Perceived Neighborhood Scale (PNS): A
test of longitudinal invariance. Journal of Community Psychology. 2002; 30:23–43.Massey DS. Segregation and stratification: A biosocial perspective. Du Bois Review. 2004; 1:7–25.
Mair et al. Page 11
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

McKinnon W, Weisse CS, Reynolds CP, Bowles CA, Baum A. Chronic stress, leukocytesubpopulations, and humoral response to latent viruses. Health Psychology. 1989; 8:389–402.[PubMed: 2555149]
McDonough P, Walters V. Gender and health: reassessing patterns and explanations. Social Science &Medicine. 2001; 52:547–559. [PubMed: 11206652]
McEwen BS. Protective and damaging effects of stress mediators. New England Journal of Medicine.1998; 338:171–179. [PubMed: 9428819]
McEwen BS, Seeman T. Protective and damaging effects of mediators of stress - Elaborating andtesting the concepts of allostasis and allostatic load. Annals of the New York Academy ofSciences. 1999; 896:30–47. [PubMed: 10681886]
Meyler D, Stimpson JP, Cutchin MP. Landscapes of risk - Texas City and the petrochemical industry.Organization & Environment. 2007; 20:204–212.
Morello-Frosch R, Shenassa ED. The environmental “Riskscape” and social inequality: Implicationsfor explaining maternal and child health disparities. Environmental Health Perspectives. 2006;114:1150–1153. [PubMed: 16882517]
Newsom JT, Prigerson HG, Schulz R, Reynolds CF. Investigating moderator hypotheses in agingresearch: Statistical, methodological, and conceptual difficulties with comparing separateregressions. International Journal of Aging & Human Development. 2003; 57:119–150. [PubMed:15151187]
Pastor M, Morello-Frosch R, Sadd JL. The air is always cleaner on the other side: Race, space, andambient air toxics exposures in California. Journal of Urban Affairs. 2005; 27:127–148.
Pearlin LI, Schieman S, Fazio EM, Meersman SC. Stress, health, and the life course: Some conceptualperspectives. Journal of Health and Social Behavior. 2005; 46:205–219. [PubMed: 16028458]
Peek MK, Cutchin MP, Freeman DH, Perez NA, Goodwin JS. Perceived health change in theaftermath of a petrochemical accident: an examination of pre-accident, within-accident, and post-accident variables. Journal of Epidemiology and Community Health. 2008; 62:106–112. [PubMed:18192597]
Peek MK, Cutchin MP, Freeman D, Stowe RP, Goodwin JS. Environmental hazards and stress:evidence from the Texas City Stress and Health Study. Journal of Epidemiology and CommunityHealth. 2009a; 63:792–798. [PubMed: 19282316]
Peek MK, Cutchin MP, Salinas JJ, Sheffield KM, Eschbach K, Stowe RP, Goodwin JS. Allostatic loadamong non-Hispanic whites, non-Hispanic blacks, and people of Mexican origin: Effects ofethnicity, nativity, and acculturation. American Journal of Public Health. 2009b; 99:1–7.
Peters ML, Godaert GLR, Ballieux RE, Heijnen CJ. Moderation of physiological stress responses bypersonality traits and daily hassles: less flexibility of immune system responses. BiologicalPsychology. 2003; 65:21–48. [PubMed: 14638287]
Rieker PP, Bird CE. Rethinking gender differences in health: Why we need to integrate social andbiological perspectives. Journals of Gerontology Series B-Psychological Sciences and SocialSciences. 2005; 60:40–47.
Seeman TE, Singer BH, Rowe JW, Horwitz RI, McEwen BS. Price of adaptation - Allostatic load andits health consequences - MacArthur studies of successful aging. Archives of Internal Medicine.1997; 157:2259–2268. [PubMed: 9343003]
Seeman TE, Singer BH, Ryff CD, Love GD, Levy-Storms L. Social relationships, gender, andallostatic load across two age cohorts. Psychosomatic Medicine. 2002; 64:395–406. [PubMed:12021414]
Seeman TE, McEwen B, Rowe J, Singer BH. Allostatic load as a marker of cumulative biological risk:MacArthur studies of successful aging. Proceedings of the National Academy of Science. 2001;98:4770–4775.
Sherbourne CD, Stewart AL. The MOS Social Support Survey. Social Science & Medicine. 1991;32:705–714. [PubMed: 2035047]
Simandan D. On how much one can take: relocating exploitation and exclusion within the broaderframework of allostatic load theory. Health & Place. 2010; 16:1291–1293. [PubMed: 20813575]
Mair et al. Page 12
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Sterling, P.; Eyer, J. Allostasis: A new paradigm to explain arousal pathology. In: Fisher, S.; Reason,J., editors. Handbook of Life Stress, Cognition and Health. John Wiley & Sons; New York: 1998.p. 629-649.
Stowe RP, Mehta SK, Ferrando AA, Feeback DL, Pierson DL. Immune responses and latentherpesvirus reactivation in spaceflight. Aviation, Space, and Environmental Medicine. 2001;72:884–891.
Stowe RP, Peek MK, Cutchin MP, Goodwin JS. Plasma cytokine levels in a population-based study:Relation to age and ethnicity. Journals of Gerontology Series a-Biological Sciences and MedicalSciences. 2010a; 65:429–433.
Stowe RP, Peek MK, Perez NA, Yetman DL, Cutchin MP, Goodwin JS. Herpesvirus reactivation andsocioeconomic position: A community-based study. Journal of Epidemiology and CommunityHealth. 2010b; 64:666–671. [PubMed: 19825788]
Stronegger WJ, Titze S, Oja P. Perceived characteristics of the neighborhood and its association withphysical activity behavior and self-rated health. Health & Place. 2010; 16:736–743. [PubMed:20378392]
Taylor SE, Repetti RL, Seeman T. Health psychology: What is an unhealthy environment and howdoes it get under the skin? Annual Review of Psychology. 1997; 48:411–447.
Tingate TR, Desmond JL, Muller HK, Stowe RP, Pierson DL. Antarctic isolation: immune and viralstudies. Immunology and Cell Biology. 1997; 75:275–283. [PubMed: 9243293]
Turner RJ, Avison WR. Status variations in stress exposure: Implications for the interpretation ofresearch on race, socioeconomic status, and gender. Journal of Health and Social Behavior. 2003;44:488–505. [PubMed: 15038145]
Turner RJ, Wheaton B, Lloyd DA. The epidemiology of social stress. American Sociological Review.1995; 60:104–125.
Williams DR, Collins C. Racial residential segregation: A fundamental cause of racial disparities inhealth. Public Health Reports. 2001; 116:404–416. [PubMed: 12042604]
Williams R, Zyzanski SJ, Wright AL. Life events and daily hassles and uplifts as predictors ofhospitalization and outpatient visitation. Social Science & Medicine. 1992; 34:763–768. [PubMed:1604370]
Yang TC, Matthews SA. The role of social and built environments in predicting self-rated stress: Amultilevel analysis in Philadelphia. Health & Place. 2010; 16:803–810. [PubMed: 20434389]
Mair et al. Page 13
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 14
Tabl
e 1
Des
crip
tion
of V
aria
bles
Var
iabl
eD
escr
iptio
n
Allo
stat
ic L
oad
Tota
l AL
= Su
m o
f 16
biom
arke
rs, z
-sco
red
(mea
n=0;
S.D
.=1)
Su
b-C
ompo
nent
sC
ardi
ovas
cula
r = 1
) Dia
stol
ic b
lood
pre
ssur
e, m
mH
g +
2) S
ysto
lic b
lood
pre
ssur
e, m
mH
g
Met
abol
ic =
3) R
atio
of T
otal
/HD
L ch
oles
tero
l + 4
) Gly
cate
d he
mog
lobi
n, %
+ 5
) BM
I kg/
m2 +
6) T
rigly
cerid
es, m
g/dL
- 7)
HD
L ch
oles
tero
l, m
g/dL
Infla
mm
ator
y =
8) C
-rea
ctiv
e pr
otei
n, m
g/dL
+ 9
) Int
erle
ukin
-6, p
g/m
L +
10) T
umor
nec
rosi
s fac
tor α
, μg/
L +
11) I
nter
leuk
in-1
, pg/
mL
-12)
Inte
rleuk
in-1
0, p
g/m
L
Imm
une-
Rela
ted
= 13
) Lat
ent E
BV
-cap
sid
antig
en (V
CA
) + 1
4) E
arly
ant
igen
(EA
) + 1
5) E
BV
nuc
lear
ant
igen
(EB
NA
) + 1
6) H
SV-1
Fem
ale
1=Fe
mal
e
Age
Age
(con
tinuo
us)
Age
Squ
ared
(Age
)2
Rac
e/E
thni
city
W
hite
(Non
-His
pani
c)Re
fere
nce
Cat
egor
y
B
lack
(Non
-His
pani
c)1=
Bla
ck (N
on-H
ispa
nic)
U
S-bo
rn M
exic
an A
mer
ican
1=U
S-bo
rn o
f Mex
ican
orig
in
Fo
reig
n-bo
rn M
exic
an1=
Fore
ign-
born
of M
exic
an o
rigin
Stre
ssor
s
Y
ears
in T
exas
City
Res
pond
ent h
as re
side
d in
Tex
as C
ity fo
r les
s tha
n 15
yea
rs (r
efer
ence
cat
egor
y), 1
5-30
yea
rs (1
=15-
30 y
ears
), or
mor
e th
an 3
0 ye
ars (
1= >
30 y
ears
)
D
ista
nce
from
Pla
nts
Res
iden
tial d
ista
nce
from
pet
roch
emic
al c
ompl
ex (c
alcu
late
d us
ing
geog
raph
ical
info
rmat
ion
syst
em so
ftwar
e an
d an
alg
orith
m d
eter
min
ing
the
shor
test
dis
tanc
e fr
omre
spon
dent
's ho
me
and
the
boun
dary
of t
he p
etro
chem
ical
com
plex
in m
eter
s.)
C
APH
RS
Con
cern
Abo
ut P
etro
chem
ical
Hea
lth R
isk;
Cro
nbac
h's A
lpha
=0.
970
How
con
cern
ed a
re y
ou th
at…
(1=N
ot a
t all
Con
cern
ed…
5=E
xtre
mel
y C
once
rned
)
1. P
ollu
tion
from
the
oil a
nd c
hem
ical
pla
nts m
ight
har
m y
our h
ealth
or y
our f
amily
's he
alth
?
2. A
ccid
ents
, suc
h as
exp
losi
ons o
r spi
lls, f
rom
the
oil a
nd c
hem
ical
pla
nts m
ight
har
m y
our h
ealth
or y
our f
amily
's he
alth
?
3. S
tore
d w
aste
from
the
oil a
nd c
hem
ical
pla
nts m
ight
har
m y
our h
ealth
or y
our f
amily
's he
alth
?
4. T
he o
il an
d ch
emic
al p
lant
s mig
ht c
ause
hea
lth p
robl
ems o
r dis
ease
in y
ou o
r you
r fam
ily?
N
eigh
borh
ood
Perc
eptio
nPe
rcei
ved
Nei
ghbo
rhoo
d Sc
ale
(Mar
tinez
et a
l., 2
002)
; Cro
nbac
h's A
lpha
=0.
915
D
aily
Has
sles
Dai
ly H
assl
es S
cale
(Kan
ner e
t al.,
198
1), t
runc
ated
with
eig
ht it
ems (
such
as j
ob-r
elat
ed) d
ropp
ed d
ue to
mis
sing
dat
a; C
ronb
ach'
s Alp
ha=
0.90
3
N
egat
ive
Life
Eve
nts
Life
Eve
nts S
tress
or S
cale
(Tur
ner e
t al.,
199
5), t
wo
item
s dro
pped
due
to m
issi
ng d
ata;
Cro
nbac
h's A
lpha
=0.
716
Health Place. Author manuscript; available in PMC 2012 July 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 15
Var
iabl
eD
escr
iptio
n
Con
trol
Var
iabl
es
M
arrie
d1=
Mar
ried
So
cial
Sup
port
MO
S So
cial
Sup
port
Surv
ey (S
herb
ourn
e &
Ste
war
t, 19
91);
Cro
nbac
h's A
lpha
=0.
970
H
igh
Scho
ol D
egre
e1=
Has
hig
h sc
hool
deg
ree
In
com
e1=
<$10
,000
; 2=$
10,0
00- <
$15,
000;
3=$
15,0
00 to
<20
,000
; 4=$
20,0
00 to
<$2
5,00
0; 5
=$25
,000
to <
$35,
000;
6=$
35,0
00 to
<$5
0,00
0; 7
=$50
,000
to <
$75,
000;
8=
$75,
000+
Sm
okin
g B
ehav
ior
1=H
as sm
oked
100
+ ci
gare
ttes i
n lif
e
Ex
erci
se B
ehav
ior
1=H
as e
xerc
ised
3-7
day
s ove
r las
t wee
k
Pe
rcei
ved
Stre
ssPe
rcei
ved
Stre
ss S
cale
(Coh
en &
Will
iam
son,
198
8); C
ronb
ach'
s Alp
ha=
0.88
2
C
hron
ic H
ealth
Con
ditio
nsSu
m o
f doc
tor-
diag
nose
d ch
roni
c he
alth
con
ditio
ns (s
troke
/bra
in h
emor
rhag
e, c
ance
r, di
abet
es, o
verw
eigh
t, ch
roni
c re
spira
tory
pro
blem
s, ar
thrit
is, a
nxie
ty, h
eart
atta
ck,
skin
pro
blem
s, ga
ll bl
adde
r dis
ease
)
H
ealth
Insu
ranc
e1=
Has
hea
lth in
sura
nce
Health Place. Author manuscript; available in PMC 2012 July 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 16
Tabl
e 2
Des
crip
tive
Stat
istic
s by
Gen
der
Tot
al (N
=107
2)W
omen
(N=6
27)
Men
(N=4
45)
Mea
n or
% (M
in, M
ax)/(
N=)
Mea
n or
% (M
in, M
ax)/(
N=)
Mea
n or
% (M
in, M
ax)/(
N=)
Allo
stat
ic L
oad
-0.1
27 (-
30, 3
0)-0
.517
(-30
, 30)
0.42
1 (-
14, 2
3)*
C
ardi
ovas
cula
r-0
.016
(-6,
7)
-0.2
41 (-
6, 7
)0.
302
(-5,
7)
***
M
etab
olic
-0.0
16 (-
12, 1
5)-0
.358
(-12
, 15)
0.46
6 (-
8, 1
5)**
*
In
flam
mat
ory
-0.0
10 (-
30, 2
6)-0
.021
(-30
, 26)
0.00
6 (-
3, 2
4)
Im
mun
e-R
elat
ed-0
.084
(-4,
11)
0.10
5 (-
4, 1
1)-0
.353
(-3,
10)
***
Fem
ale
58.4
89%
(N=6
27)
Age
51.6
21 (2
5, 9
0)49
.931
(25,
90)
54.0
01 (2
5, 8
8)**
*
Rac
e/E
thni
city
W
hite
(Non
-His
pani
c)39
.739
% (N
=426
)37
.799
% (N
=237
)42
.472
% (N
=189
)
B
lack
(Non
-His
pani
c)10
.821
% (N
=116
)11
.802
% (N
=74)
9.43
8% (N
=42)
U
S-bo
rn M
exic
an A
mer
ican
37.3
13%
(N=4
00)
36.8
42%
(N=2
31)
37.9
78%
(N=1
69)
Fo
reig
n-bo
rn M
exic
an12
.127
% (N
=130
)13
.557
% (N
=85)
10.1
12%
(N=4
5)
Stre
ssor
s
15
-30
Yea
rs in
Tex
as C
ity20
.990
% (N
=225
)19
.300
% (N
=121
)23
.370
% (N
=104
)
>3
0 Y
ears
in T
exas
City
44.1
20%
(N=4
73)
41.7
90%
(N=2
62)
47.4
20%
(N=2
11)
D
ista
nce
from
Pla
nts
1754
.746
(23,
474
7)17
01.5
16 (4
0, 4
747)
1829
.748
(23,
471
5)
C
APH
RS
14.1
81 (4
, 20)
14.5
98 (4
, 20)
13.5
93 (4
, 20)
**
N
eigh
borh
ood
Perc
eptio
n75
.664
(7, 1
08)
72.9
62 (7
, 107
)79
.472
(23,
108
)**
*
D
aily
Has
sles
12.6
39 (0
, 51)
14.3
08 (0
, 51)
10.2
88 (0
, 39)
***
N
egat
ive
Life
Eve
nts
2.10
2 (0
, 15)
2.27
4 (0
, 15)
1.85
8 (0
, 13)
**
Con
trol
Var
iabl
es
M
arrie
d58
.209
% (N
=624
)50
.080
% (N
=314
)69
.663
% (N
=310
)**
*
So
cial
Sup
port
64.6
82 (0
, 76)
64.8
53 (0
, 76)
64.4
40 (0
, 76)
H
igh
Scho
ol D
egre
e65
.112
% (N
=698
)64
.593
% (N
=405
)65
.843
% (N
=293
)
In
com
e4.
807
(1, 8
)4.
497
(1, 8
)5.
245
(1, 8
)**
*
Sm
okin
g B
ehav
ior
51.0
26%
(N=5
47)
42.1
05%
(N=2
64)
63.5
96%
(N=2
83)
***
Ex
erci
se B
ehav
ior
40.0
19%
(N=4
29)
34.7
69%
(N=2
18)
47.4
16%
(N=2
11)
***
Health Place. Author manuscript; available in PMC 2012 July 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 17
Tot
al (N
=107
2)W
omen
(N=6
27)
Men
(N=4
45)
Mea
n or
% (M
in, M
ax)/(
N=)
Mea
n or
% (M
in, M
ax)/(
N=)
Mea
n or
% (M
in, M
ax)/(
N=)
Pe
rcei
ved
Stre
ss13
.301
(0, 3
9)14
.515
(0, 3
9)11
.591
(0, 3
0)**
*
C
hron
ic H
ealth
Con
ditio
ns1.
976
(0, 1
0)2.
104
(0, 8
)1.
796
(0, 1
0)**
H
ealth
Insu
ranc
e62
.220
% (N
=667
)58
.054
% (N
=364
)68
.090
% (N
=303
)**
*
Not
e:
* p<0.
05;
**p<
0.01
;
*** p<
0.00
1
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 18
Tabl
e 3
OL
S R
egre
ssio
n R
esul
ts P
redi
ctin
g A
llost
atic
Loa
d by
Gen
der
Tot
al (N
=107
2)W
omen
(N=6
27)
Men
(N=4
45)
III
IIIa
III
IIIa
III
bII
Ia
Inte
rcep
t0.
000
***
0.00
0 **
*0.
000
***
0.00
0 **
*0.
000
***
0.00
0 **
*0.
000
**0.
000
*0.
000
**
(1.7
97)
(1.9
67)
(2.1
24)
(2.3
83)
(2.5
95)
(2.7
64)
(2.6
70)
(2.9
75)
(3.3
13)
Fem
ale
-0.0
62 *
-0.0
75 *
-0.1
20 *
**
(0.3
34)
(0.3
39)
(0.3
58)
Age
1.09
7 **
*1.
064
***
0.97
7 **
*1.
293
***
1.27
0 **
*1.
175
***
0.78
5 *
0.75
2 *
0.71
7 *
(0.0
70)
(0.0
70)
(0.0
71)
(0.0
94)
(0.0
95)
(0.0
95)
(0.1
03)
(0.1
06)
(0.1
07)
Age
Squ
ared
-0.9
35 *
**-0
.893
***
-0.8
97 *
**-1
.082
***
-1.0
61 *
**-1
.090
***
-0.7
01 *
-0.6
53 *
-0.6
50 *
(0.0
01)
(0.0
01)
(0.0
01)
(0.0
01)
(0.0
01)
(0.0
01)
(0.0
01)
(0.0
01)
(0.0
01)
Rac
e/E
thni
city
B
lack
(Non
-His
pani
c)0.
107
***
0.09
2 **
0.09
0 **
0.16
6 **
*0.
139
**0.
114
**0.
012
0.01
30.
027
(0.5
61)
(0.5
74)
(0.5
73)
(0.7
24)
(0.7
43)
(0.7
50)
(0.8
87)
(0.9
10)
(0.9
04)
U
S-bo
rn M
exic
an A
m.
0.07
8 *
0.07
3 *
0.07
5 *
0.07
90.
064
0.08
00.
082
0.09
20.
084
(0.3
74)
(0.3
76)
(0.3
88)
(0.5
05)
(0.5
05)
(0.5
24)
(0.5
52)
(0.5
65)
(0.5
80)
Fo
reig
n-bo
rn M
exic
an-0
.005
-0.0
09-0
.001
0.00
9-0
.006
0.01
4-0
.018
-0.0
09-0
.013
(0.5
46)
(0.5
72)
(0.6
14)
(0.7
03)
(0.7
44)
(0.8
06)
(0.8
69)
(0.8
99)
(0.9
54)
Stre
ssor
s
15
-30
Yea
rs in
Tex
as C
ity0.
044
0.04
90.
047
0.05
20.
029
0.02
4
(0.4
61)
(0.4
58)
(0.6
15)
(0.6
06)
(0.7
04)
(0.7
05)
>3
0 Y
ears
in T
exas
City
0.02
80.
032
0.04
90.
061
0.00
8-0
.010
(0.4
34)
(0.4
32)
(0.5
81)
(0.5
73)
(0.6
61)
(0.6
63)
D
ista
nce
from
Pla
nts
-0.0
56-0
.047
-0.0
96 *
-0.0
76-0
.009
-0.0
16
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
C
APH
RS
-0.0
48-0
.063
*-0
.045
-0.0
59-0
.065
-0.0
86
(0.0
33)
(0.0
33)
(0.0
45)
(0.0
45)
(0.0
50)
(0.0
50)
N
eigh
borh
ood
Perc
eptio
n-0
.029
-0.0
53-0
.039
-0.0
420.
002
-0.0
61
(0.0
10)
(0.0
10)
(0.0
13)
(0.0
13)
(0.0
16)
(0.0
17)
Health Place. Author manuscript; available in PMC 2012 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 19
Tot
al (N
=107
2)W
omen
(N=6
27)
Men
(N=4
45)
III
IIIa
III
IIIa
III
bII
Ia
D
aily
Has
sles
0.09
3 *
0.07
80.
085
0.03
40.
104
0.12
0
(0.0
19)
(0.0
21)
(0.0
24)
(0.0
27)
(0.0
31)
(0.0
34)
N
egat
ive
Life
Eve
nts
-0.0
35-0
.072
*-0
.055
-0.0
95 *
-0.0
02-0
.030
(0.0
76)
(0.0
78)
(0.0
96)
(0.0
97)
(0.1
28)
(0.1
30)
R S
q.0.
068
0.08
20.
126
0.09
70.
119
0.17
30.
028
0.03
80.
093
R S
q. (A
djus
ted)
0.06
30.
071
0.10
80.
090
0.10
20.
145
0.01
70.
012
0.04
8
Not
e: T
able
pre
sent
s sta
ndar
dize
d co
effic
ient
s (st
anda
rd e
rror
s in
pare
nthe
ses)
;
* p<0.
05;
**p<
0.01
;
*** p<
0.00
1
a Mod
el II
I inc
lude
s con
trols
for m
arrie
d, so
cial
supp
ort,
educ
atio
n, in
com
e, sm
okin
g be
havi
or, e
xerc
ise
beha
vior
, per
ceiv
ed st
ress
, chr
onic
hea
lth c
ondi
tions
, and
hea
lth in
sura
nce
b indi
cate
s mod
el is
not
stat
istic
ally
sign
ifica
nt a
s a w
hole
(p≤0
.05
for m
odel
F st
atis
tic)
Health Place. Author manuscript; available in PMC 2012 July 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 20
Tabl
e 4
OL
S R
egre
ssio
n R
esul
ts P
redi
ctin
g C
ompo
nent
s of A
llost
atic
Loa
d by
Gen
dera
Tot
al (N
=107
2)W
omen
(N=6
27)
Men
(N=4
45)
Car
dio.
Met
ab.
Imm
une
Car
dio.
Met
ab.
Imm
une
Car
dio.
Met
ab.
Imm
une
Inte
rcep
t0.
000
***
0.00
0 *
0.00
0 *
0.00
0 **
*0.
000
0.00
00.
000
**0.
000
*0.
000
(0.6
80)
(1.2
25)
(0.8
66)
(0.8
60)
(1.5
46)
(1.1
46)
(1.0
80)
(1.9
85)
(1.3
42)
Fem
ale
-0.1
54 *
**-0
.176
***
0.10
7 **
(0.1
14)
(0.2
06)
(0.1
46)
Age
1.31
2 **
*0.
640
**0.
322
1.37
5 **
*0.
749
**0.
467
1.19
4 **
0.56
40.
151
(0.0
23)
(0.0
41)
(0.0
29)
(0.0
30)
(0.0
53)
(0.0
39)
(0.0
35)
(0.0
64)
(0.0
43)
Age
Squ
ared
-1.1
73 *
**-0
.702
***
-0.1
61-1
.138
***
-0.8
41 *
*-0
.300
-1.1
76 *
*-0
.589
0.01
7
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
01)
(0.0
00)
(0.0
00)
(0.0
01)
(0.0
00)
Rac
e/E
thni
city
B
lack
(Non
-His
pani
c)0.
115
***
-0.0
180.
121
***
0.14
6 **
*-0
.047
0.14
7 **
0.06
4-0
.017
0.07
6
(0.1
83)
(0.3
31)
(0.2
34)
(0.2
33)
(0.4
20)
(0.3
11)
(0.2
95)
(0.5
42)
(0.3
66)
U
S-bo
rn M
exic
an A
m.
-0.0
060.
088
*0.
088
*-0
.005
0.06
90.
125
**0.
019
0.12
7 *
0.04
4
(0.1
24)
(0.2
24)
(0.1
58)
(0.1
63)
(0.2
93)
(0.2
17)
(0.1
89)
(0.3
48)
(0.2
35)
Fo
reig
n-bo
rn M
exic
an-0
.058
0.04
40.
050
-0.0
460.
026
0.04
4-0
.066
0.06
70.
062
(0.1
96)
(0.3
54)
(0.2
50)
(0.2
51)
(0.4
51)
(0.3
34)
(0.3
11)
(0.5
72)
(0.3
87)
Stre
ssor
s
15
-30
Yea
rs in
Tex
as C
ity0.
056
-0.0
060.
000
0.07
4-0
.024
-0.0
100.
004
0.01
10.
007
(0.1
46)
(0.2
64)
(0.1
87)
(0.1
89)
(0.3
39)
(0.2
51)
(0.2
30)
(0.4
22)
(0.2
86)
>3
0 Y
ears
in T
exas
City
0.08
4 *
0.00
90.
013
0.10
4 *
0.04
30.
001
0.04
0-0
.027
0.02
3
(0.1
38)
(0.2
49)
(0.1
76)
(0.1
78)
(0.3
20)
(0.2
37)
(0.2
16)
(0.3
97)
(0.2
69)
D
ista
nce
from
Pla
nts
-0.0
440.
016
-0.0
65 *
-0.0
88 *
-0.0
47-0
.036
0.00
90.
087
-0.1
07 *
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
(0.0
00)
C
APH
RS
-0.0
37-0
.044
-0.0
210.
013
-0.0
28-0
.026
-0.1
36 *
-0.0
69-0
.012
(0.0
11)
(0.0
19)
(0.0
14)
(0.0
14)
(0.0
25)
(0.0
19)
(0.0
16)
(0.0
30)
(0.0
20)
N
eigh
borh
ood
Perc
eptio
n-0
.018
-0.0
80 *
-0.0
11-0
.003
-0.0
680.
005
-0.0
23-0
.095
-0.0
38
Health Place. Author manuscript; available in PMC 2012 July 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mair et al. Page 21
Tot
al (N
=107
2)W
omen
(N=6
27)
Men
(N=4
45)
Car
dio.
Met
ab.
Imm
une
Car
dio.
Met
ab.
Imm
une
Car
dio.
Met
ab.
Imm
une
(0.0
03)
(0.0
06)
(0.0
04)
(0.0
04)
(0.0
07)
(0.0
05)
(0.0
05)
(0.0
10)
(0.0
07)
D
aily
Has
sles
0.01
90.
088
*0.
055
-0.0
060.
084
0.03
30.
088
0.05
20.
082
(0.0
07)
(0.0
12)
(0.0
09)
(0.0
08)
(0.0
15)
(0.0
11)
(0.0
11)
(0.0
21)
(0.0
14)
N
egat
ive
Life
Eve
nts
-0.0
30-0
.047
-0.0
52-0
.051
-0.0
81-0
.045
0.00
90.
001
-0.0
55
(0.0
25)
(0.0
45)
(0.0
32)
(0.0
30)
(0.0
54)
(0.0
40)
(0.0
42)
(0.0
78)
(0.0
53)
R S
q.0.
149
0.09
60.
083
0.22
00.
107
0.08
70.
081
0.11
10.
077
R S
q. (A
djus
ted)
0.13
10.
077
0.06
30.
192
0.07
60.
055
0.03
60.
067
0.03
1
Not
e: T
able
pre
sent
s sta
ndar
dize
d co
effic
ient
s (st
anda
rd e
rror
s in
pare
nthe
ses)
;
* p<0.
05;
**p<
0.01
;
*** p<
0.00
1
a All
mod
els i
nclu
de c
ontro
ls fo
r mar
ried,
soci
al su
ppor
t, ed
ucat
ion,
inco
me,
smok
ing
beha
vior
, exe
rcis
e be
havi
or, p
erce
ived
stre
ss, c
hron
ic h
ealth
con
ditio
ns, a
nd h
ealth
insu
ranc
e
Health Place. Author manuscript; available in PMC 2012 July 1.