
&al º (Zºp - eScholarship
353
VALIDATION OF A PATIENT CLASSIFICATION INSTRUMENT FOR PSYCHIATRIC PATIENTS BASED ON THE JOHNSON MODEL FOR NURSING by Vivien Dee DISSERTATION Submitted in partial satisfaction of the requirements for the degree of DOCTOR OF NURSING SCIENCE in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA San Francisco Approved: &al º (Zºp Committee in Charge Deposited in the Library, University of California, San Francisco Date - - - - - - - - - - - - - - - - University Librarian - SEP 07 1986 Degree Conferred: - - - - - - - -
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of &al º (Zºp - eScholarship

VALIDATION OF A PATIENT CLASSIFICATION INSTRUMENT FOR PSYCHIATRIC PATIENTS
BASED ON THE JOHNSON MODEL FOR NURSING
by
Vivien Dee
DISSERTATION
Submitted in partial satisfaction of the requirements for the degree of
DOCTOR OF NURSING SCIENCE
in the
GRADUATE DIVISION
of the
UNIVERSITY OF CALIFORNIA
San Francisco
Approved:
&al º (ZºpCommittee in Charge
Deposited in the Library, University of California, San Francisco
Date- - - - - - - - - - - - - - - -
University Librarian-
SEP 07 1986Degree Conferred:
- - - - - - - -

Copyright G) 1986
by
Vivien Dee
ii

VALIDATION OF A PATIENT CLASSIFICATION INSTRUMENT
FOR PSYCHIATRIC PATIENTS BASED ON THE
JOHNSON MODEL FOR NURSING
Vivien Dee, R.N., D.N.Sc.
University of California, San Francisco, 1986
The purpose of this research was to assess the reliability and validity of a
patient classification instrument for psychiatric patients (NPH-PCI) based on the
Johnson Model for Nursing. Equivalence reliability and criterion-related validity
were the two specific psychometric properties investigated.
Data were collected by direct observation of patient behaviors at the UCLA
Neuropsychiatric Hospital from August, 1982, through November, 1984. A
purposive sample was selected from four child inpatient units for four-hour
observations by three independent raters (staff, shift coordinator and observer). At
the completion of each observational period, the Behavior Criteria Checklist--
comprised of a patient behavior checklist, subsystem category rating scale and
system category rating scale--was completed.
Mean inter-rater agreements, computed on tº 51 patient observations with
respect to patient behaviors for three comparison paired groups (staff, shift
coordinator and observer) exceeded the 60% criterion for inter-rater reliability.
Mean inter-rater agreements ranged from 67% to 84%. Mean inter-rater
agreements of staff and shift coordinator pairs were above the 60% criterion for
iii

* * * * - - - - - - - - - - - * * * ** - * - - - * * * - - - - º -
* - - - - - - - - - - - - - - - - - -
- - - * * - - - - - -
* * * * - - - - - -
~ * - * - . . .- - - - - * - - s * * * *
- - - - . - * - - ... • - - -
-tº . . . . . . .
- -* . . .
- • * * * * * *
- * * - - º - - . . . .
- * - - - - - - - -
- - - - • * * *
- -
* - - - * -
º º - - -
- - - º
- * - - - - - - - -
. . . . . . . - -
-- - - * * * - -
".-
. . . . .- * * * º -
- . . . . . . . . . . . . . . . . * * * * * . . .
* - - - - • * - - -
- * * * * * - - - - -
- * -- - - - -
- - - , - * * -
- - e.
* - - - - - - - - - -" – * - tº i º - - *-* * - . * -
- . . w ; : *-
- * * - *- - - -

the system category ratings (67%) and most subsystems' category ratings (60% for
dependency to 68% for eliminative), with the exception of sexual (57%) and
aggressive-protective (57%) subsystems.
Findings showed that all R2 values for subsystems categories (ranging from
.08 for sexual to .36 for achievement) had low to moderate explanatory power; but
that the R2 value for the system category (.52) had good explanatory power. The
moderate R2 values for the subsystem categories suggest that further work is
needed to identify additional relevant patient behaviors for inclusion within each
subsystem.
Findings also indicated that the system category was generalizable across
inpatient units, age and sex groups. Affiliative and dependency subsystems
categories were also generalizable across these same groups and units.
In conclusion, the NPH-PCI appears promising for further development. It is
anticipated that additional studies will provide further support for the reliability
x/2” a.a. S-4×4,424 /24. 2).and validity of the NPH-PCI.
iv

--

Dedication
To my mother, Ivy Marie W. Dee, whose courage, integrity and optimism have
guided me throughout my life.


Acknowledgement
This dissertation represents not only the culmination of a course of academic
study at the University of California, San Francisco (UCSF), but also the
continuation of research begun in 1978 with the development of a patient
classification system for the UCLA Neuropsychiatric Hospital (NPH-PCS) at
Los Angeles.
It is impossible to acknowledge in these few paragraphs the direct and
indirect contributions of all my colleagues to the NPH-PCS project and their
support during my doctoral studies. However, certain individuals stand out and
therefore deserve special recognition.
I am most thankful to Mrs. Bertha Unger, Associate Administrator and
Director of Nursing Services at the UCLA Neuropsychiatric Hospital, for my initial
introduction to the concept of patient classification systems and their value to
nursing administration. For her continuing and unfailing support during the many
phases of the patient classification project and throughout the course of my
doctoral studies, I am grateful.
I also wish to thank Dr. Jeanine Auger, my longtime colleague at the UCLA
Neuropsychiatric Hospital. Her ideas were instrumental in shaping the evolution of
the Johnson Model and in translating its theoretical framework into clinical
application. She also provided me with constructive criticism of the manuscript.
I also wish to thank Dean Margretta Styles and Dr. Jane Norbeck, my
graduate advisors at USCF, for their guidance, inspiration and support throughout
my years of academic coursework. I wish to express my sincere appreciation to the
members of my doctoral committee: Dr. Sandra Ferketich, Chair; Dr. Nancy
vi

→··
----|-••----
*
a··
|-·■·*•|-
·
----
|-··
.*
----
-*·
----
--------
--■■
··----
--------*
*···
*
•••**••*h
----
■ |-|----------
•
•----*…··
|-------

Lovejoy and Dr. Charlene Harrington. They provided me with constructive
criticism, sharpened my ideas and challenged me to further develop my thoughts
and to refine the focus of this manuscript.
I also wish to acknowledge the following individuals for their assistance:
Dr. Peter Christensen of UCLA Hospital Computing Services for statistical
analyses of the data and Mr. Bruce Schwagerl of UCLA Neuropsychiatric Hospital,
Nursing Services, for typing the manuscript in its final form.
Finally, I wish to express my appreciation to my husband and friend, John
Robert Smith. He gave me the space and time in which to create and participated
actively in the writing process by asking numerous questions, challenging my ideas
and reviewing the manuscript extensively. I am deeply grateful for his love,
patience, support and understanding.
vii


Table of Contents
ABSTRACT
LIST OF TABLES
LIST OF ILLUSTRATIONS
CHAPTER I: THE STUDY PROBLEM
Introduction
Statement of the problemPurpose of the studySignificance of the study
CHAPTER II: CONCEPTUAL FRAMEWORK AND LITERATURE REVIEW
Conceptual frameworkJohnson Behavioral System Model
Conceptualization of the modelAmplifications of the modelApplications of the modelImplications of the model
Literature review
Patient classification systemsDefinition
Types of patient classification systemsLevels of categoriesIndicators of care
Early developments (1940s-1960s)Current developments (1970s-1980s)Reliability of patient classification systemsValidity of patient classification systemsGeneralizability of patient classification systems
UCLA Neuropsychiatric Hospital Patient Classification SystemDevelopment of instrumentWalidity and reliability of instrument
CHAPTER III: METHODOLOGY
Research designResearch strategies
Equivalence reliabilityCriterion-related validity
Page
iii
xi
xiv
:1010
1 l;2022
21;2424242!262729313233363637
l;3lil;lil;l;6
viii

·
·----··--
|-··*|-·
·
·
···
·|-
**·*
...•------
■-
~~~----T••…*<■ --***wº-|-
,■(v''----
\■,
…•■■»
**
----

Table of Contents – continued
Research questionsStudy definitionsDescription of research settingSampleData collectors
ObserversStaff and shift coordinators
Instrument
Research proceduresObservational proceduresScheduling of patient observationsData collection proceduresPretesting
Data analyses
CHAPTER IV: RESEARCH RESULTS
Introduction
Sample description of patient observationsProfile of data collectors
Results related to equivalence reliabilityPatient behaviors
Subsystems categoriesSystem categories
Results related to criterion-related validityImpact of patient behaviors on subsystem categoriesImpact of subsystem categories on system category
Examination of residualsZero mean
HomoscedasticityNormal distribution
IndependenceResults related to generalization
Across inpatient unitsAcross sex groupsAcross age groups
Summary of Results
CHAPTER V: DISCUSSION
Interpretation of resultsInterpretation of results related to equivalence reliabilityInterpretation of results related to criterion-related reliabilityInterpretation of results related to generalizability
64646576768085858699
1031031031031031081081 101 101 10
1 121 12116120
ix

f º-
*
-
-
-:ºf
*
***
*
-
º

Table of Contents - continued
Research issues limiting study findingsSample selectionPatient observation schedules
Study periodObservational procedures
Directions for future research
Instrument developmentResearch design
Implications of findings for nursing
REFERENCES
APPENDIX A: NPH Patient Classification System
APPENDIX B; Subsystems Behaviors
APPENDIX C: Behavioral Criteria Checklist
APPENDIX D: Summary Statistics on Independent Variables
Page
12212312312!125126126129130
1.33
1 l;2
152
161
168


Table 1
Table 2
Table 3
Table l;
Table 5
Table 6
Table 7
Table 8
Table 9
Table 10
Table 11
Table 12
Table 13
Table 1 l;
Table 15
Table 16
Table 17
Table 18
List of Tables
A Comparison of Behavioral Subsystems' Functions
Definition and Behavioral Characteristics of Subsystems
General Framework for Categorization of Patient Behaviors
Timetable for Observer Recruitment, Training and DataCollection
Number of Patient Observations Completed and Included inFinal Data Base
Number of Patient Observations Included in Final Data Baseon Each Unit
Number of Patient Observations Included in Final Data Base
by Categories and Time Periods (A-West)
Number of Patient Observations Included in Final Data Base
by Categories and Time Periods (A-South)
Number of Patient Observations Included in Final Data Base
by Categories and Time Periods (5–West)
Number of Patient Observations Included in Final Data Base
by Categories and Time Periods (6-West)
Number and Sex of Patients for All Categories on Each Unit
Number of Patients by Age Groups
Number of Patients by Psychiatric Categories Per Unit
Number and Classification on Staff on Each Unit
Number and Classification of Shift Coordinators on EachUnit
Educational Preparation of Staff and Shift Coordinators
Mean Inter-rater Agreements for Three Paired Groups OnPatient Behaviors for Each Subsystem
Percentage of Patient Behaviors Observed
l;0
57
66
67
68
69
70
71
72
73
7t;
75
77
78
79
81
xi

- - - -
- - - * * -
- - - -
- - . . - -
... • - - - - **
* * -- - -t -
-
- - -
- * * * - -
r * ... - * -
s - - - * - * -
- * - . -
t - - * -
- - i ... * * - -
- - - - . - -
- - - - s - - - -
- - - - - - 1 - - -
- - t - - - - -
* - - . . - -
- *- - - * * -
- - t - - - - -
- -
- º * *
- - . . . . . . - - - a .
- 4 - - - * - - -
- - - * - - . 1
- - -1 - - a . . "
- . - *::
- - - * * *-
. . . . . cº" - . . " ... "

Table 19
Table 20
Table 21
Table 22
Table 23
Table 24
Table 25
Table 26
Table 27
Table 28
Table 29
Table 30
Table 31
Table 32
Table 33
List of Tables - continued
Inter-rater Agreement on Subsystems for Three PairedGroups
Inter-rater Agreement Between Staff and Observer GroupsOn Subsystems by Categories
Inter-rater Agreement Between Shift Coordinators andObserver Groups on Subsystems by Categories
Patient Behaviors as Predictors of Subsystem Category
Patient Behaviors as Predictors of Ingestive SubsystemCategory
Patient Behaviors as Predictors of Eliminative SubsystemCategory
Patient Behaviors as Predictors of Affiliative SubsystemCategory
Patient Behaviors as Predictors of Dependency SubsystemCategory
Patient Behaviors as Predictors of Sexual SubsystemCategory
Patient Behaviors as Predictors of Aggressive-ProtectiveSubsystem Category
Patient Behaviors as Predictors of Achievement SubsystemCategory
Patient Behaviors as Predictors of Restorative SubsystemCategory
Comparison of Full and Reduced Equations of PatientBehaviors as Predictors of Subsystem Category
Significance Tests on Full and Reduced Equations ofPatient Behaviors as Predictors of Subsystem Category
Subsystem Categories as Predictors of System Category
Page
82
83
84
87
88
89
90
91
92
93
9t;
95
98
100
101
xii

º
* -
-s t v - -
.*
-
- * ,
* *
- - - - -. . . … -- -
* -
* - -
- t
* * * * , ,
, r c. * *
. . * : *
- - * - *e - -
- * -- -
-. . . " º
* .
1 .- * * - --
- * *
º º
-
- - -
* -
* -
s - - -
*
- -
- * -
-
* .º - *
* -º - a
- *~~
f : -
* * * *
*
- -
º -
- *
*.
. . . . .
- - * :
--
- -

List of Tables – continued
Page
Table 34 Results of Chi-Square Goodness of Fit Tests for Distribution 105of Residuals from Patient Behaviors and Subsystems Regressions
Table 35 Tests on Model Consistency Across Units, Sex and Age Groups 109
xiii


Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
List of Illustrations
Johnson Behavioral System Model
Patient Behaviors as Predictors of Subsystem Category(Reduced Equation)
Subsystems Categories as Predictors of System Category(Reduced Equation)
Plot of Standardized Residuals Against Self-Care Activities
Histogram of Standardized Residuals for Sexual Subsystem
Histogram of Standardized Residuals for AggressiveProtective Subsystem
102
10 l;
106
107
xiv


CHAPTER I
The Study Problem
Introduction
Health care expenditures in the United States increased 344% between 1973
and 1983, from $103 billion to $355 billion, and are continuing to outpace inflation
with an annual growth rate exceeding 9%. Current projections indicate that by
1990, health care expenditures will surge to $660 billion and represent over 11% of
the gross national product (Arnett, Cowell, Davidoff & Freeland, 1985).
The primary factors that have contributed directly or indirectly to rising
health care costs are increases in: (1) price of basic materials and services
required (i.e., food, equipment, energy, minimum wage increase), responsible for
approximately 58% of the rise; (2) specialization and greater use of technological
resources, responsible for almost 35% of the rise; and (3) life expectancy, resulting
in an increase of resource utilization and intensity of services, accounting for
approximately 10% of the rise (Davis, 1983). The third party payors' cost-based
retrospective reimbursement schemes have inhibited competition among providers
of care resulting in higher health care costs and ultimately higher insurance
premiums for the consumer of health care (Davis, 1983). All of these factors have
played a significant part in sustaining a continued high level of growth for health
care expenditures.

j: ºf■ º
|-··-----*
,|-----**-
*|-·|-•
•|---
--------•!*··-·-*
…
~~----|-…*---
----…*··|--
-,-
«…»----**...
•
-·•-----··■···
·-,··--------
••

Acute care hospitals have been under increasing scrutiny and attack from
both state and federal governments for the past decade with regard to their part in
the ever-increasing costs of health care. For example, the Social Security
Amendment of 1983 (PL 98-21) mandated that hospitals reimbursed by Medicare be
paid a fixed amount for each case based on Diagnostic Related Group (DRG)
categories. This legislation culminates a series of reimbursement reforms and cost
containment measures that were initiated decades ago as part of efforts to alter
health care delivery (Shafer, 1983).
Nursing, as the hospital's largest department, has been particularly vulnerable
to cost containment policies (Walker, 1982). Staffing costs have been estimated to
be approximately 70% of the nursing department's budget (Simms, 1982) and
represent approximately 30% of all hospital costs (Smits, Fetter & McMahan,
1984).
As a result of the federal government's decision to pay hospitals
prospectively by DRGs, nursing costs must be measured in a reliable and valid way
to demonstrate the intensity of nursing care that patients require and the relation
between nursing costs and DRG classification (Piper, 1983; Joel, 1983; Riley &
Schaefers, 1984; Mitchell, Miller, Welcher & Walker, 1984; Lagona & Stritzel,
1984). The need to provide maximum nursing care in the most cost-effective
manner has given impetus to the resurgence of patient classification systems (PCS)
within nursing service settings not only for staff allocation purposes but also as a
foundation for fiscal management in the identification of nursing care costs per
patient (Nyberg & Wolff, 1984). Approximately 5,000 of the 7,000 short-term,
acute care facilities accredited by the Joint Commission on Accreditation of
Hospitals (JCAH) now utilize some form of patient classification system to classify

----·--- ----·|-|-|-|-|--
|------· ·|-----*…***·-
----·
.*--------|------------■ -----
--------·----|---------|-|-----»*
-|-·-----|-----|-|-|-*-•.----|-------------••
•|-*-*-|-,-
*■
··----|------ |-••|-·---------→
·-*-
|-*-|-|-·**· |-··|-••·-→•
•
·----|-*|-----|-,■ ----·|--|-----·
--------|--|-·
*|-----|-*-*-
-
*•-
-----|-·-
·-|---.*|-••-----··-…
·|-
·•-|-----···
*|--
-------|-|-→···
-----,|-*,·|-*-|-→·|-|-·*
----■-|-----|-.**+
*··· -----***|-•
•|---·
----|-•----|-|--|-·---- ·|-----·*-*|-
·|-·→·
|---…*■ .·
|
------•■ |-·|-•
----*--■ -|-*|-|----- |-------•|-- ··--|-----·,
-----•·-|-|---------|-----|-|-|--|-|-·|-••
|-
-,-|--''-|-|-|--
·|-----|-*|-·-*•----|-·,■ -------- -**----■ |-·
••
·
*|---------*·-
·|-·· ----*|-·-****|-+··--|-· ··•••|-----
-
|-·-
-----|-*…--------•-|-----|-|-•
•*|----------|-
----•·*■4--------· |-•----|--|-*--,·→··----|-*,|-·-|----- |-|-----------·-
-
-**-■-•
•·•· ·|-■±----·|---
----·----••.→|-|--|-,■
|-|--|---------*|-|-·
-|---------•|-- |-|-•|-**|--|-----|-
--------|-----*…|---|-
----••*…*--------|----- ----|-|-----•••|-----· ----·|-|------|-
----
|----------*
-,’-■ ••-~.-----
-·-**….*------------··*
…
-|-·*.|--|-
·----■-----···*
----------------■**~^-ae■ ~
ae-„**-|--*
ae-|-|--"------→·|-|-*-*|-|- ·|-·-----
-
|-------|-|-
→
·--------•*·*…*----|-· ·----|--
,
-----|- •·•••-*|-|-
·----
•·-----|-■
±**----|-■-|-
→.'|-·---- -----*-*…|-••|-|- --------
|-*…|-|-|-■■■
■ º·----|-|-------|- ----*.----|-·----|-|-
|-----|-|------* |-tº|-■ |-----|-*-r--|-
|-
|-*----*|-••
•*,■ ----·----·|---·-----
·-·----------■*----·
----·
------·|-·**·
----•*----·|-----,■ ·----- ·----·|-----→·**··→••|*-*- ----------·*•-,·*■ ••-----|-·
------·*--|-…’|-|-----·|-----
-----→·|---------|----- •…
--•·--------··*
---*-»----·|-----· -+→|-|-|-|-----|- ·*·*|-|-|-------

patients according to patient care requirements for staffing purposes (Alward,
1983). These systems provide ways of identifying patients' needs for nursing
service and corresponding ways in which these needs may be met (Giovanetti,
1979).
The purpose of classification systems is to categorize patients according to
the magnitude of their need for nursing care. However, problems of defining and
quantifying psychiatric patient needs and required nursing actions have presented
major difficulties in the development of patient classification systems which can
be applied to the psychiatric setting. One possible approach to resolving this
problem is to utilize a model of nursing (Dee & Auger, 1981; Auger & Dee, 1982a;
Dee & Auger, 1983b).
The value of models of nursing as a theoretical basis for educational
programs has been widely accepted within academic nursing circles; most, if not
all, theoreticians have been predominantly identified with education rather than
service. Several advantages for using nursing models in clinical practice have been
proposed, including: (1) allowing nurses to describe, explain, predict and control
clinical phenomena for the purpose of achieving desired patient outcomes; and (2)
changing the way nurses comprehend and process information so that nursing
actions can be more purposeful at all levels (Chinn & Jacobs, 1983).
Preliminary to exploring the problem of defining and quantifying patient
needs, a patient classification instrument based on the Johnson Behavioral System
Model of Nursing was developed at the UCLA Neuropsychiatric Hospital to define
and describe patient behaviors. It was assumed that utilization of a single model
would: (1) provide a frame of reference for systematic assessment of patient
behaviors, (2) enhance communication and agreement among staff regarding

■
■ |-…~~
~--
-
-|-•
•■ ~· ·|-|- |-|-*…* ··-…••
|-|-…•
•~~----·■■ --··|-|-~~-|- ----|--
|-••|-----|-----*·
|-|-----»
----|-•|----- |---*~~,---------→·*…|-----
·•|-|-|-→· ·→·|-
··----|---ae
·
------■■ •-, |-*----|-
*,
----t-··|-----|- -
-|--■ ------ *-·|-·-…•.•→·
|-
|-••|-|-*…
-
-*-
■ -■ --|-··ae|- ----|---,|-••
--------|-•· ·•|-|-|--
-••|-|------
-|-----|-·■■ •• ■
-**…
----*·
|-
·|×|-|-* ·«“|-----*
*|-|-|--·*•
•----·····:
•••
•·---
|-·|- *----…|-*…--|-|- *----|-
|-
•
•·|-*--------- ·|- -
-*•·--· •-*→----··,■
■
----|-·---------
-**
-----·*•••--------••|-* ----*&·---**
-|-
·••■ ----|-----|----------·■
··
-→·•-
-----·■ *…*---- |-|---------*|-|-
~~------- ··-|-●----|-ae|----- |-|-••-|-*----|- |-•-|-
--------→
·•·----••
----*-----|- ·--------* ----|-|-*|-→
·|-----*------ ·■
-•
•••*|-~L
----|-|-···|-*-
·-
-·|-→
·|-■-
|-|-*-
|-|-- |-·-

identified problems, and (3) integrate knowledge concerning significant bio-psycho
socio-cultural factors related to complex patient behaviors (Auger & Dee, 1983).
Statement of the Problem
As stated previously, the purpose of classification systems is to categorize
patients according to the magnitude of their need for nursing care, but the
problems of defining and quantifying patient needs have continued to present major
difficulties in the development of systems which can predict nursing care needs.
The primary use for most patient classification systems has been for staffing
purposes. The majority of patient classification systems found in the literature
have been designed for use in medical surgical settings. To date, there have been
two published articles describing the use of PCS in the clinical setting of
psychiatry. In addition to the PCS developed for UCLA Neuropsychiatric Hospital
in Los Angeles, California (Auger & Dee, 1983), one was developed for C. F.
Menninger Memorial Hospital in Topeka, Kansas (Schroeder & Washington, 1983).
The major difference between the PCS designed for medical and surgical
settings and those designed for psychiatric settings are the critical indicators
chosen for patient care. PCS designed for medical and surgical settings emphasize
physical and physiological indicators of care, while those designed for psychiatric
settings emphasize psychosocial patient care indicators (Auger & Dee, 1983).
Generally, the psychiatric patient is able to provide his or her daily physical care
requirements in contrast to the medical-surgical patient. The focus of psychiatric

-- -
* *
º
*-
-
■
*
■
* *
º -- º
* *
- s-
* -
t* ,
- * ,* - -
* *- º
-- e.
w :
* * *
--
*
- - - - - ** - * . . . .
* º,º º - -
- - • - * * * - - -( : - * * * * * * * * -
* -
.* * . . . . . - . . .-
* . . . . - -; . . . . . . . . • , ,
. . . . . * -- - - . .
* - -- * ~ * - . . . -
. . . . . . . . . • * * * * *
-- -- * → t - - - - -
-■ , " , , , ■ : • * * - -
- . . . . . . - - -
-. . . . . . . . . . . . . . .
* - - * * - * * ... "2. * * * l - * - 1 =
- e - -- - . . .
. -- * * * .
- - . º - - - - - -
* , * - - - - - * : -
- • . --> *- : , . . . . . . . . . . . .
• * ... • 1 * . . * . . .* º
* * - . . . . . . . . . .
. . . . * . . . . ; -- - *-
- - - - * * * ** - -
, - - - - --
- - - - - -
- - - - . . . .

care falls in the areas of behavioral management, for example, establishing limits,
environmental safety, verbal interactions and behavior modification.
Since patient census has not been shown to be a sensitive predictor of nursing
resource utilization (Pardee, 1968; Poland, English, Thornton & Owens, 1970;
Meyer, 1978; Thompson, 1984), the majority of PCS now categorize patients
according to predetermined descriptors of care such as daily living activities,
treatment, nursing procedures and so forth, based on an analysis of current
practice within an institution. A limitation of these systems is that nursing care
may be based on available staffing and budgetary constraints rather than on
clinical decisions based on patient characteristics/behaviors. Another limitation is
that the classification systems based on current institutional practices are
restricted in their application to other institutions where the standards of practice
may differ.
In contrast, the PCS developed for the UCLA Neuropsychiatric Hospital
(NPH) at Los Angeles, California, was designed to address the relationship between
patient characteristics/behaviors and the corresponding nursing care
action/interventions (Auger & Dee, 1983). It was an assumption of this PCS that
patient behaviors provide a more accurate indicator of patient's need for service
than the provision of nursing care based on available staffing.
A major limitation of PCS is the lack of reliability and validity of most
systems. Although Fray (1984), Auger and Dee (1983) and Grant, Bellinger and
Sweda (1982) have begun to address the issue of content validity and the
significance of establishing inter-rater reliability of patient classification systems,
these two areas remain frequently ignored. Many developers and users of PCS have
indicated that the lack of staff sophistication in the use of statistical methods, the

r
••
|- …
•|-· ·*--
■ -••
~
|----- -,*---- -•·*
*
----- *,
· ~■
-,
·
|- ·|-|-
|-·* |-· *-
·
·

institution's budgetary constraints and the lack of specific guidelines in which to
conduct validity and reliability studies have been contributing factors for the
continuing failure to address the issue of validity and reliability of PCS (Finlayson,
1976; Georgette, 1970; Fray, 1984; Schroeder, Rhodes & Shields, 1984; Alward,
1983).
The lack of published literature on the application of nursing models in
clinical settings is an indication that the practical usefulness of nursing models has
not been fully explored. To date, only three articles have been published that
discuss the application of the following nursing models within nursing service
settings: (1) Roy Adaptation Model on an 18-bed orthopedic unit at the National
Hospital in Arlington, Virginia (Mastal, Hammond & Roberts, 1982); (2) Johnson
Model on the Child Inpatient Service at the Neuropsychiatric Hospital in Los
Angeles, California (Dee & Auger, 1983a); and (3) Neuman Systems Model on a 27
bed surgical unit at Mercy Catholic Medical Center in Darby, Pennsylvania
(Capers, O'Brien, Kelly & Fenerty, 1985).
In summary, the following conclusions can be drawn:
1. The majority of PCS have been designed for use in medical surgical
settings. Consequently, lists of patient care activities are specific to
the physical and physiological care needs rather than the psychological
and psychosocial patient care needs specific for psychiatric settings.
2. The descriptors of care for most PCS have been developed based on
institutional practices and may therefore be restricted in their
application to other institutions where standards of practice differ.
3. The lack of validity and reliability of most PCS have limited the
generalization of these systems to other patient care settings.

•••*----■ |-■
-,|-*…----
----
·
…
•
■ ----|-*.
----→·
----|-}----|-|-|-
*«
|-·|-*…•|-
·
·|-·,■
|-··■
|-·

4. The practical usefulness of nursing models in clinical settings has not
been fully explored and demonstrated.
Purpose of the Study
The primary objective of this study was to assess the reliability and validity
of the patient classification instrument developed for UCLA Neuropsychiatric
Hospital (NPH-PCI). Validation was conducted through empirical investigation and
the use of statistical analyses.
For this study, the following research questions were posed:
1. What is the reliability estimate of the NPH-PCI when patient
behaviors in each of the eight subsystems are observed and
categorized independently by different observers?
2. Which of the patient behaviors in each subsystem are the best
predictors of the subsystem rating?
3. Which subsystems are the best predictors of the system rating?
Significance of the Study
Because of the dearth of literature in the following areas: (1) reliability and
validity of patient classification systems in general, (2) reliability and validity of
PCS designed for use in psychiatric settings in particular, (3) generalization of
patient classification systems, and (4) application of nursing models in patient care

·
----|--
·
|---------|-----·|-'.----'--|---
-
-|-
----
|---
|-|-|--|-|-·|-----·----|-
·|-|-|-
--}·
--
->
f : … I rº2 . . ;vº 3

settings as basis for clinical practice, this research marks the beginning effort to
establish a reliable and valid classification instrument based on the Johnson Model.
The potential advantages of utilizing a reliable and valid patient
classification instrument based on a model of nursing as a theoretical framework
are:
1.
3.
4.
5.
Provides a frame of reference for systematic assessment of patient
behaviors,
Enhances communication and agreement among staff regarding
identified problems,
Provides a basis for the evolution of new knowledge,
Allows for the provision of nursing care based on assessed patient
behaviors, and
Allows for the development of patient outcome criteria.
Furthermore, it is anticipated that a reliable and valid patient classification
instrument has the capability for generalization to other patient care settings. A
patient classification instrument which identifies patient characteristics or
behaviors can more adequately explain the variable intensity of nursing care
required by each patient than patient census as a criteria. Such an instrument can
then serve to:
1.
3.
Estimate nursing workload based on patient care needs as opposed to
patient census, medical diagnoses or DRG classification as a single
criteria for staffing,
Identify nursing care costs for fiscal management and the development
of management and budgetary models for nursing services,
Provide a mechanism for quality care audits, and

|-·*•
*---·
·
|-
----|-·•
•----
|--·----·|-----•·•----·|-•|-----
|-·|-·-----|-----|-|-·|-|-·--------*-|-|-·|------••
•|-|--…|-|-·-----*|-·
|-
|-|-*-
*-"
·|-
|-→·|-----·■ ----|-----|-*
*----|-
·|--|-
-*|-|--·|-~~··|-|-|-·
|-*·
|-
----·-■ |---
---|-·*----·
|--
-·|-|-··--|-|-|-|---------→·
|-··|-·|-|-----|-■ *,----
----|-|-------
-·
·|-|-·-- -
-|-
·----|-*
*…-
|-
----··|-
·
----··|-·|---·*
-|-----•-·--------|-|-|-·|-
|---|-
·
*-*·|-
|---
·|-|-··*----··**,..…
|--,----|-----·*----|-
·
|-··
|-••-
*...~~
*
·|-··----••••----------
----•■ -*■
------…•|-·••
·•
•--------■■ |-|-
.**-
·-·*
•
•·· |-····
→
·-→
·--·*
→•----…º·
·*
··…*
-,

4. Develop nursing practice domains and nursing intervention strategies.
In summary, this chapter has presented the rationale for the development of
the study and objective for the study. Numerous implications for a reliable and
valid patient classification instrument based on a model of nursing were also
presented.


CHAPTER II
Conceptual Framework
Johnson Behavioral System Model
Conceptualization of the Model
The concept of behavior is basic to the Johnson Behavioral System Model
(Johnson Model) for nursing. Behavior, like any other discrete phenomenon, can be
isolated for study apart from all other human qualities as an operational system.
The assumption is that "what a human does is more important than what he is and
that behavior is one of the central problems of existence" (Johnson, 1977, p. 3).
The focus then is on how a person interacts with other people and, more
specifically, the particular forms of behavior that have been shown to have major
adaptive significance (Johnson, 1977; Johnson, 1980).
The Johnson Model is constructed on the following assumptions about man as
a behavioral system (Johnson, 1968; Johnson, 1977; Johnson, 1980):
1. Man strives continually to maintain behavioral system balance which
reflects behavioral adjustments or adaptations that have been
successful. These observed behaviors, however, may or may not
always coincide with the cultural norms for acceptable or healthy
behaviors.
- 10 -

*,
-
*--
******
-
**
->
**
-
*-
***
--*...?-***
-*-***
*-
*,».

2. Behavioral systems balance or some degree of regularity and
constancy in behavior is essential to man.
3. Man actively seeks new experiences which may disturb his behavioral
system balance temporarily. Behavioral modifications may be
required to re-establish balance.
Johnson (1968) defines a behavioral system as constituting a complex of
observable features or actions that determines and limits the interaction of an
individual and his environment. The behavioral system establishes the relation of
the person to the objective events and situations in his environment. Behavior
functions as a response modality and serves as a mechanism for communication
between the person and the surrounding environment. These actions and/or
response modes are basic groupings of behavior that can be distinguished in terms
of the purpose or function of the behavior. These groupings of behavior, referred
to as subsystems of behavior, are conceived as forming an organized and integrated
whole, the behavioral system (Johnson, 1968).
The subsystems identified by Johnson (1968 & 1980) are affiliation,
aggression, dependence, achievement, ingestion, elimination and sex. An eighth
subsystem of restoration was subsequently added (Grubbs, 1980; Auger, 1976).
Each subsystem is "'comprised of a set of behavioral responses or responsive
tendencies which seem to share a common drive or goal'." (Johnson, 1968, p.3).
Figure 1 depicts the Johnson Behavioral System Model as illustrated by Auger
(1976).
These behavioral responses are made up of a number of related behavioral
acts which are functional in achieving the goal of the subsystem. Although these
responses are developed and modified through maturation and experience, they are
- 11 -

••
|× ·
----
·|-|-|-|-*
*
|-·|-→ ·|-|----- |---*
|-|-*
---------
|-· ••----|-■-
|-e
*---- |-----· |-· *·------
-→·
-■ |-~ |-*·
|-
|-· -----|-· -·----|-· ·|- |----- ----|----- |-· ·
----•----•• |-→-■ -- ----→
·

Figure 1
Johnson Behavioral System Model
From Behavioral System and Nursing, J. R. Auger, 1976, p.37. Reprinted with
permission.
BEHAVIORAL SYSTEM
|NGESTIVE
RESTORATIVE ELIMINATIVE
ACHIEVEMENT AFFILIATIVE
AGGRESSIVE DEPENDENCYPROTECTIVE
SEXUAL
- 12 -


determined developmentally and are continuously governed by a multitude of
biological, psychological and social factors that operate in a complex interlocking
fashion (Johnson, 1968; Johnson, 1980).
These subsystems are linked and open: a disturbance in one is likely to affect
others. Each subsystem has certain functional requirements that must be met for
continued viability, development and growth. These functional requirements are:
(1) protection, (2) nurturance and (3) stimulation. Each subsystem must be
protected from noxious influences with which the system cannot cope, nurtured
through appropriate supplies from the environment and stimulated to enhance
growth and prevent stagnation (Johnson, 1968; Johnson, 1980).
Each subsystem is made up of at least four structural components:
1. Goal - is defined as that which is sought. The manifest goal is the
immediate intention of the behavior, while the latent goal must be
inferred. For example, in the ingestive subsystem, the manifest goal
is appetite satisfaction and the latent goal is biological survival
(Johnson, 1977). Although goals for each of the subsystems may be the
same for all individuals, the goals may vary according to the value
placed on goal attainment (Johnson, 1977; Johnson, 1980).
Set - means the individual's predisposition to act. Through maturation,
experience and learning, an individual uses preferred ways of behaving
under particular circumstances with selected individuals (Johnson,
1977; Johnson, 1980).
Choice - is defined as the entirety of the behavioral repertoire
available to the individual for the achievement of a particular goal. In
other words, choice constitutes the scope of action alternatives from
which an individual can choose (Johnson, 1977; Johnson, 1980).
- 13 -


4. Action - is the individual's actual behavior that is observable (Johnson,
1977; Johnson, 1980).
These four structural components interact with one another to create an
overall goal or function for the subsystem. Although each subsystem has a
specialized function, the system as a whole is dependent upon an integrated
performance. The integrity of the system is maintained when: (1) conditions in the
internal and external environment of the system remain orderly and predictable
and (2) functional requirements of the subsystem as a whole are met through the
individual's own efforts or through an external regulatory force for the purpose of
restoring, maintaining and attaining stability at the highest possible level for the
individual (Johnson, 1980).
Johnson (1980) asserts that the goal of nursing actions in each case is to
restore, maintain or attain behavioral system balance for the individual. Johnson's
assertion is based on the following assumptions about nursing: (1) nursing's
traditional concern for the person who is ill and (2) nursing's primary goal to assist
the person in achieving and maintaining behavioral system balance and dynamic
stability (Johnson, 1968). Nursing, therefore, acts as an external regulatory force:
(1) by changing the structural components of the individual's behavioral subsystems
or (2) through the fulfillment of the functional requirements of the subsystems, to
preserve the organization and integration of the patient's behavior at an optimal
level.
Amplifications of the Model
A most notable difference between the Johnson Model as originally conceived
by Johnson and that as presented by Grubbs and Auger is the inclusion of an eighth
– 14 –


behavioral subsystem, the restorative subsystem. The rationale for the inclusion of
this additional behavioral subsystem was not, however, stated in either author's
writings. According to J. Grubbs (personal communication, April 4, 1985), eight
subsystems (restorative subsystem included) were taught by Johnson in 1966 when
she was a graduate student of Johnson's. J. Auger (personal communication,
April 11, 1985) states that her writings on the Johnson Model were based on class
papers presented to her by faculty while she was instructor of the undergraduate
course "Basic Nursing Science" at University of California, Los Angeles.
It was Johnson's rationale that the relief of fatigue was more a function of
the aggressive-protective subsystem than the restorative subsystem (Lovejoy,
1981). J. Auger (personal correspondence, April 18, 1985), however, states that the
"restorative subsystem, in and of itself, contains goals that define the subsystem
apart from all other subsystems. It is a most important subsystem to the survival
of the organism as a viable entity."
Although Grubbs and Auger had similar interpretations of the function of the
restorative subsystem, Auger's interpretation of the ingestive and eliminative
subsystems differs from that of Grubbs. According to Auger, (1976), the functions
of the ingestive subsystem include the "'taking-in'" (p. 35) of substances; for
example, food and fluids, as well as the "'taking-in'" (p. 35) of sensory
information. Sensory information (perception, sight and knowledge) enables the
individual to initiate required compensatory responses in order to maintain a state
of psychophysiological equilibrium with changes in the external environment.
Auger (1976) further states that "it is through this ingestive activity that the
individual is able to differentiate himself as a separate entity from all other
objects and persons existing in the outer world" (p. 53).
- 15 -


Grubbs considers communication as an input and output mechanism that
serves the same purpose for all subsystems; consequently, the "'taking-in'" (p. 228)
of information cannot be classified as ingestive behavior (Grubbs, 1980). Grubbs
(1980) concurs with Johnson (1980) that the function of the ingestive subsystem is
specific to the appetitive pleasures.
Grubbs (1980) views the function of the eliminative subsystem as primarily
that of expelling biologic wastes and bodily secretions. Auger is of the opinion that
eliminative behaviors also include such acts as speech, nonverbal gestures,
expression of affective states (crying, laughing, yelling) and other actions that
serve to communicate the general state of the individual to the environment
(Auger, 1976). A comparison of the subsystems' functions as defined by Johnson
(1980), Auger (1976) and Grubbs (1980) is shown in Table 1.
Although the concept of environment and its role as a regulator of behavioral
system activity was not addressed by Johnson (1968, 1977, 1980) in any detail, it
was given significant attention by Auger (1976). Environment as described by
Auger (1976) consists of both the external and internal environments. The external
environment includes all those persons, objects and phenomena that can potentially
permeate the boundary (sensory thresholds) of the individual. The external
environment surrounding an individual contains a wide variety of sources of
information; for example, climatic and seasonal changes, societal rules and values,
educational systems and religious beliefs, are forms of input into the behavioral
system. The internal environment is also an equally important source of input. It
originates from within an individual in the form of emotions, motivations, thoughts,
fantasies, attitudes and reflexive responses. The process by which the individual
comprehends and evaluates these complex stimuli for their meaning and intent is
– 16 -

:

Table 1
A Comparison of Behavioral Subsystems' Functions
JOHNSON (1980) AUGER (1976) GRUBBS (1980)
Affiliative: Security,Social inclusion,intimacy andformulation of strongbonds.
Ingestive: Appetitesatisfaction.
Dependency: Approval,attention, recognitionand physical assistance.
Eliminative: Excretionof wastes.
Affiliative: To belongor be associated withothers in some form of
specific relationship.This goal includes theprocess of interaction.
Ingestive: To bringinto the individual a
substancé, object orinformation that the
individual perceives ordetermines to be
lacking. This goal oftaking-in may be forpleasure, gratificatio■ ,relief of pain, safetyand knowledge.
Dependency: To seekhelp, to obtain anothergoal, or to seekassistance in a task
related activity.
Eliminative: To release,let gö, get rid of wasteproducts; excess ornonfunctional matter
within the system. Itmay be viewed as a goalof tension-reduction.
Affiliative: To relate
or belong to somethingor someone other thanoneself to achieve
intimacy and inclusion.
Ingestive: To take inneeded resources fromthe environment to
maintain the integrityof the organism toachieve a state of
pleasure; to internalizethe externalenvironment.
Dependency: To maintain environmentalresources needed for
obtaining help,assistance, attentio■ ,permission, reassuranceor security; to gaintrust and reliance.
Eliminative: To expelbiologic wastes; toexternalize theinternal environment.
– 17 -

- - - - - - -
- - - - - - - -* - - - - - - -
- - - * - -- - - - -
* * * * ~ * - - -
- -
- - . º
- - - t
- - - - - - " * - - . .* - -- - - - - - - - -
- - - - - - -
- - -
* -
- -
-
* * - - i. -
- º - -
f - -
-. . . . .
-. . . . .
- - - - - - - - - - - - - - - -
* - - - - - - - -
* . - - - -
- - - - -
* * -- . . .
- - - -
- . . . . - - - - - * - -- - - * * - : - - e -
- * * * .*, */ - * - - - .
* - - -
- - - - -• * , - . - -
- *
* * - - -

Table 1 (continued)
A Comparison of Behavioral Subsystems' Functions
JOHNSON (1980) AUGER (1976) GRUBBS (1980)
Aggressive: Selfprotection andpreservation.
Sexual: Courting,procreation andgratification, genderrole identity.
Achievement:
Exploration, masteryand/or control of selfand environment.
Aggressive-Protective;To protect oneself,others or property fromreal or imagined harm,or threat of harm inin the form of attack.
Sexual: To procreateand ensure survival of
collective individuals,or to obtain pleasurefrom sexual activities.
This goal includes thedevelopment andmaintenance of an
adaptive sexual identityfor the purposes ofseeking or attracting alove object.
Achievement: Tomaster or controloneself and theenvironment in such a
way as to obtain adesired object, positionor need.
Restorative: To
maintain energybalance throughout thesystem throughtransformation andredistribution of the
available energythroughout the system,in accordance with thedemands of the various
subsystems.
Aggressive-Protective;To protect oneself orothers from real or
imagined threateningobjects, persons orideas; to achieve selfprotection and selfassertion.
Sexual: To procreate,to gratify or attract,fulfill expectationsassociated with one's
sex; to care for othersand be cared about bythem.
Achievement: Tomaster or controloneself or one's
environment; toachieve mastery orControl.
Restorative: To relieve
fatigue and/or achievea state of equilibriumby reestablishing orreplenishing the energydistribution among theother subsystems; toredistribute energy.
- 18 -


referred to as the perceptual process. Perception is controlled by sensory
receptors and selectively regulates the nature and amount of stimuli allowed to
penetrate the system boundary. Perception is considered to be a major
determinant of how an individual will behave. However, this evaluative process
also involves the activity of the biologic, psychologic, social and cultural regulators
and their contribution to the transformation and differentiation of the stimulus
into an internal event (Auger, 1976).
Grubbs (1980) identified several "'variables'" (p. 236) that encompassed the
biological, psychological, social and cultural factors outside the boundary of the
behavioral system and have the capacity to alter or change behavior within the
system. These "'variables'" (p. 236) are considered by Grubbs to be synonymous
with the concept of environment. They are:
1. Developmental - abilities that are modified by experience or acquired
skills,
2. Ecological – the environment of a person's upbringing,
3. Level of Wellness - responses in relation to the health and illness
Continuum,
4. Cultural - factors affecting attitudes, beliefs and behaviors learned
through education, discipline and training,
5. Familial - those persons of common ancestry,
6. Pathological – anatomic and physiologic changes from the norm,
7. Sociological – expectations related to one's role based on rank, status
or position in society,
8. Psychological - factors relating to internal psychic processes,
including cognitive functioning, and
- 19 -


9. Biological - capacities based on maturation and growth that are
dependent on anatomic and physiological functioning.
Auger (1976) also identified a list of factors that regulate and influence
behavioral responses, namely: (1) genetic inheritance, (2) intelligence, (3) age, (4)
sex, (5) attitudes, values and beliefs, (6) creative and problem-solving abilities and
(9) self-concept. According to Auger, although some of these regulating factors
are enduring traits and are relatively stable such as sex and body height, other
factors including social class, role expectations, values and beliefs develop from an
interaction with the environment. All of these regulators, however, share the
ability to influence the goals, set, choice and acts associated with each of the
behavioral subsystems as well as to the system as a whole (Auger, 1976).
According to Auger (1976) and Grubbs (1980), the biological, psychological,
social and cultural factors represent the major regulators of ongoing behavioral
responses. They exist to guide and limit behavior and to monitor and coordinate
the inter-relationships between the subsystems.
Applications of the Model
The major utility of the model is in the assessment phase of the nursing
process. The model provides nursing with a framework in which to describe patient
behaviors. Although the delineation of the behavioral subsystems was made and
functions for each of the subsystems were provided, the model, as conceptualized
by Johnson (1968, 1977, 1980) was not operationalized for direct applicability to
the clinical setting. This limitation is actually a strength, as it allows the nursing
practitioner to describe behaviors specific to the patient population she serves and
– 20 -

----· ·* ··*
*
…•• *…
•-- •••
•■
·
----*…• ---- →·
|-ae·
*·- →
·--

offers a systematic approach with which to evaluate behavior and to provide a
basis for determining what is needed for protection, nurturance and stimulation.
With the increasing acceptance of nursing theory, the model has been utilized
by nurse practitioners to guide their work with mentally retarded adolescents
(Holaday, 1980), patients with hepatitis (Damus, 1980), visually impaired children
(Small, 1980), patients on hemodialysis (Broncatello, 1980), patients with accidental
injury (Rawls, 1980), patients with asthma (Lovejoy, 1981) and patients with
ventricular tachycardia (McCauley, Choromanski & Liu, 1984). Auger and Dee
(1983) used the model as a framework for the development of patient classification
system with the capability to establish staffing levels based on patients' needs.
Several researchers have utilized the Johnson Model as a theoretical
framework for describing patient behaviors, and for the development of assessment
tools. Holaday (1981 & 1982) conducted two research studies in relation to the
affiliative subsystem of behavior. These studies were conducted to determine the
effect of a chronically ill infant's cry on the development of maternal response
patterns. The potential benefit of these studies is the development of nursing
intervention strategies, in which the nurse can assist the mother in interpreting the
meaning of the infant's cry and in developing a broader choice of maternal response
patterns.
Derderian (1983) and Derderian and Forsythe (1983) utilized the Johnson
Model as a comprehensive framework for the development of the Derderian
Behavioral System Model instrument. This instrument resulted in the
categorization of 193 items representing each subsystem of the behavior. It was
designed to assess the perceived behavioral changes of cancer patients. According
– 21 -


to Derderian (1983), the instrument provides a system for describing and
documenting patient behavioral changes as to their existence, direction, quality
and importance, and the illness effects associated with them. This systematic
documentation of patient behaviors renders nursing data potentially more fruitful
for clinical nursing research.
Lovejoy (1983) also based the construction of a 47-item projective assessment
tool on the Johnson Model. The projective assessment tool was designed to
measure the perceptions of family members of children with leukemia. With
further refinements and testing, this tool may be used by nurses to assess family
members' behavioral patterns that might adversely affect the growth and
development of the child with leukemia. Other research studies have also been
conducted to determine the specific characteristics of oncology patients (Newlin,
1976) as well as patients who have been isolated from others because of illness
(Fawzy, 1979).
Implications of the Model in Nursing Practice
The behavioral analysis approach provides a comprehensive framework in
which various types of data can be organized into a cohesive structure. Knowledge
of the relationship between current and past behavior facilitates the identification
of problem areas; the nurse can then assist the patient in developing adaptive and
functional behaviors. In addition, this knowledge provides a frame of reference for
establishing realistic goals for recovery based on an appraisal of the patient
behaviors prior to the onset of illness.
In summary, this section has presented the conceptualization and
amplification of the Johnson Behavioral System Model. The model's application as
- 22 -

*
ae
•
•· |-• |-----■- -
-••••
· ·
!■
-…"
-
-■ ”■
5|-*
•·••
•----→·
*--
--·
----~|- *·
- *…■
--------*
-eº
|-|---
-*-*
----
*-
·|- ··----
r----- --------:
•■-
•----*-■ …
■ ••ae
«.
·
•*→
•• * ~~ |---º *…|- ----··
----■-
*-
----**. ••
→· *&-

a theoretical base for the development of nursing assessment tools and implication
for nursing practice were described.
- 23 –

Literature Review
Patient Classification Systems (PCS)
Definition
A patient classification system refers to the identification and classification
of patients into groups of care categories and to the quantification of these
categories as a measure of nursing care required (Giovanetti, 1979). All patient
classification systems have in common the goal of categorizing patients according
to pre-established criteria for the purpose of determining the need for nursing care
resourceS.
Types of Patient Classification Systems
The two major types of patient classification systems identified by Abdellah
and Levine (1965) are: (1) Prototype evaluation and (2) Factor evaluation.
Characteristics of patients typical to each category of care are described in
prototype evaluation while indicators or descriptors of direct nursing care are
described in factor evaluation.
Levels of Categories
Both factor and prototype evaluation classification systems include
categories for rating patient's nursing care requirement ranging from little
assistance (Category I) to great need for assistance (Category IV). The PCS
developed by the University Hospital in Seattle, Washington (Pardee, 1968) provides
an example of a 3-category system based on the patient's ability to care for
- 24 -

-***•****-***,,,----y;:-,,)------,-..;-**-*--r.ri
..........;A...---......."r*........-.......
--*:--****.-
.....................................
•**:*,***-***-***:-*~*";,,--*--**.........*■ º:................
---..-------
.......................................
-•tº,---.............■ o.2.........
r*-,-"";:y:*r-•****************-*.........*-....
-...-*.......
--f:...2....................................... -........*-2-.........*-,---------
--I--....***…•**,,-....*,,f*****-,-
****.*-*--•*::-*-**-**
--***,.-"-----------
...........…,2×...........!........
T.").TºGº*>..ºfsº,,,,12 ...........ºff:.22.ºfC.2....
-y2
--------------*
1.)>,–.........;r...*......º*
-----*--
-1*,,,2J.....-*)...)|2|...-
--**----------
--.........;)i■■ º.J...............
º-----s--------?--*-
..........*,....-
....;......
r---------------
.....................................".
5...Iºf2:1
-----------—−-,--------------------->........*i■...;;;,;;;;2(,,;)
ºff:;;;;;;,;;,

himself: for example, Category I - refers to patients requiring a minimal amount
of nursing care; Category II - refers to patients requiring a moderate amount of
care; and Category III - refers to patients requiring the most care.
Kingston General Hospital in Ontario, Canada utilized a 4-category PCS
based on Jelinek, Haussmann, Hegy vary and Neuman's work (1974) at the Medicus
Systems Corporation (Plummer, 1976). Several other PCS, such as those at
Presbyterian-Saint Luke's Medical Center in Denver, Colorado (Reinert and Grant,
1981) and Medical Center Hospital of Vermont at Burlington, Vermont (Dale &
Mable, 1983) have also utilized a k-category system. However, none of these
authors provided reasons for their selection of a 4-category system. Fray (1984)
selected a 4-category system on the basis that change on the number of categories
might result in problems with user compliance. Auger and Dee (1983) added a
fourth category to the original 3-category system to account for patients that
require continuous one-to-one intensive nursing care.
PCS at the William Beaumont Hospital in Troy, Michigan (Grant, Bellinger &
Sweda, 1982) provides an example of a 6-category system for rating nursing care
requirements. Since the primary objective of the article describing this system
was to measure productivity in staffing units and to make budgetary projections,
the authors did not describe the distinctive differences between the six category
levels.
The Medicus Systems Corporation recommended four levels of categories as
the most accurate classification of patients. Jelinek, Haussmann, Hegyvary and
Neuman (1974) found that the variance within a 3-category system was too large
and that the statistical probability of error was higher within a 5-category system.
The additional categories did not yield a significant increase in discrimination
- 25 -

|-··----
----
----- ·
|-*…
·~----→··-
…
|-•→·
·----|- ·----- |-|-----•
•*-
*…*|-|- -*|----- ·------»
------------ |-*--
*
…|- |-----•• |-••·* ----
|-··|-
|-*-*
*··|- --------·*··
|-----
·
*-----
·→·|- |-··■
·-
••*••
■
-··|-- |-··
----! ----~•
•|-
----*·
*-
-→• *··
•••*-----→·
----••
·,---
→
·→|- -----*|-*…
*→·
■
*-
-|-
|-••·*----|-•
--------|-----
·|-
*a----
·
-→·
----|-·
----,■
----••• ----·-
·
----•••"
|-· -----· ----•••|- ae,••• ----·----*
*••·•
•-----
*•*----
*. *· • *· ·---- *→·
·
|-• ·
→·
·· |-·→·
+→
·· -------- |-*|- •
----- |-|-----
,
■ • ••·••
----*· •• _
•----→
·*…**-
·
|-|-|- •••
*|-· ·
----|-·
·•----
·
*
|-·
**
|-*+
·----*- ·· •+·
·
|-
----→----
|-·…
*· ·
-*
|- ·|-----|- …
** →|- |-|-----
|-·----* |-|-→
·
·|-·
·
-
---- ·----|- --------* ■-
*
•■ ---- |--· :•+*

among patient types. The authors, however, did not provide statistical data or
further explanation to support their recommendation.
Indicators of Care
Indicators of care found in the prototype evaluation system include
statements that attest to the capabilities of the patient to care for
himself/herself; for example, his ability to ambulate, to feed himself, to bathe
himself and to care for his own eliminative needs. Indicators of care found in
factor evaluation system are those that include requirements for specific nursing
activities such as: taking wound culture, performing pre-operative scrub, doing
daily weights, and so forth.
A certain degree of rater subjectivity is inherent in both the prototype
evaluation and the factor evaluation systems. However, since the factor
evaluation system is based on quantitative observable variables, it has been
considered to be more objective than the prototype evaluation system.
Staff are usually more receptive to a prototype evaluation system because it
allows for simple explanation and understanding and does not increase paperwork or
time away from patient care (Roehrl, 1979; Schroeder, Rhodes & Shields, 1984). A
criticism of prototype evaluation design is that it may be difficult to monitor the
accuracy of ratings because of observer bias between individuals responsible for
classifying the patient (Reinert & Grant, 1981). Such results are often not distinct
enough to accurately predict the staffing required for a given acuity mix of
patients (Vaughn & McLeod, 1980). Auger and Dee (1983) recommended that staff
consistently identify and discuss their observations to develop a common frame of
reference and achieve a higher degree of agreement.
- 26 -

º

Early Developments (1940s through 1960s)
Patient classification systems have been in existence for many years. The
history of patient classification dates back to the period of Florence Nightingale,
when an intuitively-based information system was used. In this system, the most
seriously ill patients were placed closest to the ward sister's office in order to
facilitate observation while the less seriously ill patients who could take care of
themselves were placed at the far end of the ward to indicate their decreased
dependency on the nursing staff. A limitation of this approach is that its
application allows for differing views to surface as to the nature of high or low
dependency.
A major effort was made to classify patients according to intensity of nursing
care requirements in the late 1940s with the emergence of rising health care costs
and severe personnel shortages. The National League of Nursing in its Study of
Pediatric Nursing in 1947 published a patient classification system in which
patients were rated on a 3-category scale of intensity on each of four factors: (1)
degree of illness, (2) activity, (3) adjustment and (4) number and complexity of
procedures and treatments (Abdellah & Levine, 1965). Although an attempt was
made to relate the amount of required nursing time to patient classification, it was
done in global terms and therefore did not provide a sensitive tool for the planning
and allocation of staffing resources.
During the 1950s, the concept of patient classification shifted to a much
broader base. The patient classification system was used to determine the type of
facilities needed, the amount and kind of nursing services required, and the proper
allocation of patients. The development of the patient classification system began
by recording all services provided to the patient. Based on the assessment of over
– 27 —

* *

100 items of information collected on each patient, the patients were then grouped
into four categories: (1) critical, (2) intensive, (3) standard and (4) minimal
(Aydelotte, 1973).
In the early 1960s, the format for the development of patient classification
systems shifted beyond the assignment of patients to an estimate of nursing time
requirements for patients. Conner's work at Johns Hopkins Hospital served as a
model for the work of others. Conner, an industrial engineer, drew upon factors
associated with nursing problems such as mobility, consciousness, disturbance,
inadequate vision and isolation rather than the usual variables of census, age,
medical diagnosis and sex. Based on continuous observation of direct care provided
to patients presenting these problems, Conner developed a patient classification
system, isolating patients into discrete categories (Conner, 1961).
In 1963, a large group of Southern California hospitals under the guidance of
the Hospital Council of Southern California and Blue Cross of Southern California
established the Commission for Administrative Services in Hospital (CASH). The
first major effort of CASH was an in-depth survey of nursing services. With the
professional guidance of a nursing advisory committee consisting of four directors
of nursing appointed through the cooperation of the Hospital Council and California
Nurses Association, the CASH staff conducted work sampling studies involving six
hospitals. In each of the six hospitals, one nursing unit was selected for the study.
The primary objective of these studies was to determine an equitable workload for
staff between various shifts. Levels of categories were designated as low, average
and high. Twenty-eight nursing activities were identified; for example, back rub,
diet, meds-preparation, bath, report and meds-administration. These activities
were recorded by staff each hour over a 24-hour period. Analysis of this data
– 28 -


resulted in significant redistribution of peak hours of work and staff workload
assignments were then based on the amount of nursing care that patients required.
This approach resulted in an average reduction of 1.35 nursing care hours per
patient day on the test units (Edgecumbe, 1965).
The indicators of care found in most of these earlier PCS were bathing,
feeding, toileting, back rub and so forth. The attention given to these activities,
which were involved in ministering to the basic human needs of patients, attest to
nursing's traditional role and its distinct contribution to patient care which is not
shared by other health care providers (Kruetter, 1957).
A criticism of these earlier patient classification systems was that the
elements for classifying patients according to patient care requirements were
relatively limited in scope and complexity. The critical indicators of care were
primarily pathophysiological in nature and did not consider the sociopsychological
behavior of patient care requirements (Aydelotte, 1973). Emotional support and
patient teaching, two indicators of care viewed by nurses to have significant
clinical value to nursing, were not addressed (Hanson, 1979). The measurement of
time devoted to the nursing process was also not addressed (Thompson, 1984).
Current Developments (1970s through 1980s)
The PETO system was developed in the early 1970s by Poland, English,
Thornton and Owens (1970) for Eugene Talmadge Memorial Hospital in Augusta,
Georgia. Utilizing the factor evaluation design, all elements of direct nursing care
in the PETO system were denoted by points. A higher point value indicated more
nursing attention. The point values were obtained from time studies conducted on
the hospital's 32-bed pediatric unit.
– 29 -

----·…"→·
*--------••
---*,
■ →·
|----**-
-"
|-·----
.*|-→·
••--
·
■■■
+
·■--------·----·.*
-·----••*=
----·----•***
*---------·|-…--
|------
-·**
·→→·
•
■
·
----→·••-----
*•*********•----
**.*, ■ º **

Based on the investigators' literature review, seven major elements were
found to be representative of a large measure of physical nursing care provided at
the study site. The seven major elements were: (1) diet, (2) toileting, (3) vital
signs and measurement, (4) respiratory aids, (5) suction, (6) cleanliness and (7)
turning. In addition to these seven major elements, there were five subcategories
included for diet: (1) feeds self without supervision, (2) feeds self with supervision,
(3) feeds self but needs constant presence of staff or gastrostomy feeding every
four hours, (4) total feeding by personnel and (5) tube feeding.
From the observation of all personnel over several days, average time periods
were obtained for each subcategory. Numerical values corresponding to five
intensities of care were developed; that is, services requiring 7.5, 15, 30, 60 or 90
minutes each. A two-point value assigned to the subcategory of 'feeds self' could
then be translated into 15 minutes of nursing care required. Based on the total
point value assessed and designated for each level of category, a category number,
i.e., Category I, II, III was then assigned to the patient.
The Grasp system developed for Grace Hospital in Morgantown, North
Carolina, (Meyer, 1973) is similar to the PETO system with the exception of two
modifications: (1) point values equivalent to six minutes each were assigned and (2)
emotional support and patient teaching were included as critical indicators of care.
The inclusion of emotional support and patient teaching were based on extensive
time studies showing that 14.5 minutes were required for each patient per shift.
The author did not provide a rationale for a change in the point value. Barham and
Schneider (1980) also found that depending on the levels of categories into which
the patients were classified, a range of six minutes to 20 minutes per patient were
required per shift for emotional support and patient teaching respectively.
– 30 -

*

In contrast to earlier PCS that failed to include emotional support and
patient teaching, recent PCS developed for Kaiser Permanente Centers in Northern
California (Barham & Schneider, 1980) and Presbyterian-Saint Luke's Medical
Center in Denver, Colorado (Reinert & Grant, 1981) have included emotional
support and patient teaching as critical indicators of care.
Reliability of Patient Classification Systems
A most important aspect of reliability in a PCS relates to inter-rater
reliability, or consistency of the classification tool in obtaining the same results
when used by different raters (Giovanetti, 1979). However, it is an area frequently
ignored by developers of PCS.
Grant, Bellinger and Sweda (1982) reported that reliability of PCS was
investigated by using intraclass correlation. Three raters made independent
observations of the same patients for three consecutive days and rated the care
provided for these patients. Findings showed that the intraclass correlation was
0.97 for items pertaining to activities of daily living, 0.89 for emotional cognitive
needs of patients and 0.91 for monitoring elimination.
Fray (1984) reported that reliability was investigated by utilizing paired
classifiers, consisting of the staff nurse caring for the patient and an observer.
One set of paired classifiers categorized 50 patients during the day shift while a
second set of paired classifiers, using the same methodology, categorized the same
patients during the evening shift. A total of 16 staff nurses and two observers
completed the classifications, utilizing different nursing units. Pearson product
moment correlation for the day and evening shifts were 0.983 and 0.924,
respectively.
- 31 -

*
*-*-
·
·
·*
|-*•
•·••
----·→·|-
*-----
→
·--
|-|--…
----{•
•··.
● *·
*
*■ ----
·
|-•----
·-· *…
*··
*-*
----
•
„••
••|- +*■
· ·
·- ·-
* /*
|-
- ·
----
+*
----
·
·|-·
*-
·

According to Abdellah and Levine (1965), a reliable classification system
required a 90 to 95% intraobserver and inter-rater reliability. This type of
reliability can be achieved only when the criteria for patient classification are
precise, specific and accurate and when there is sufficient time for observer
selection and training, staff orientation to practice using the tool and adequate
monitoring procedures.
Walidity of Patient Classification Systems
According to Williams (1977), a patient classification system can only
measure a portion of nursing care--those direct care activities that can be
observed and quantified. Consequently, it is questionable whether validity of
patient classification instruments can ever be shown satisfactorily in terms of
actual patient need (Giovanetti, 1979).
The literature describing the validity of PCS is scant. Fray (1984) reported
that content validity was established by a panel of 34 nurses representing
administration, management, inservice educators, staff nurses and clinical
coordinators. The panel was given detailed guidelines for arriving at the patient's
classification. An agreement rate of 89% was obtained from the panel's responses.
Conner, Flagle, Hsieh, Preston and Singer (1961) conducted two studies to
determine the predictive validity of the PCS. Utilizing work sampling techniques,
the first study was conducted to develop: (1) criteria for levels of categories, such
as self-care, partial care and total care; (2) critical indicators of care such as
ambulation, bathing, feeding, intravenous therapy; and (3) a specified number of
nursing care hours for each level of category. The second study was conducted to
test the predictive validity of the first study by utilizing similar work sampling
- 32

-… i■
-:--
*---------→
·*·
------
-…--
•---- *---- ·|-|- |-■ -------- |-|--
-|-••
··•• •|-*
*
•---
·*
·· -·••
·
••- |-|- →|-• ----|- …|-·
|-· -----
*… -
------|- ----- -----· -*-------■■ |- ·- -
----- |-----→
··---- |-|-*
a*

techniques. Patients observed were classified according to three levels of category
prior to, and thus independently of, the observation of nursing care provided. The
nursing staff was not aware of the patient classification. This study verified
original conclusions about the amount of time nursing staff spent with patients for
each category. Findings from this study showed that patients classified in
Category I (self-care) received 27 minutes of direct care per shift. Patients in
Category II (partial care) received 53 minutes and patients in Category III (total
care) received 137 minutes. These time values were in agreement with those in the
first study.
Generalization of Patient Classification Systems
Few studies have been conducted to establish the reliability and validity of
PCS. Consequently, most PCS have been limited in their generalization to other
patient care settings.
Two studies were conducted to compare patient classification systems (PCS)
for their reliability in determining workload. Findings from the first study
conducted at the Medical Center of Vermont (Roehrl, 1979) showed a significant
correlation among the three patient classification systems selected for the study.
The patient classification systems selected were: (1) Tool A - PCS developed at
the Medical Center Hospital of Vermont, (2) Tool B - PCS developed by Hospital
System Study Group at University of Saskatchewan, Saskatoon, Canada, and (3)
Tool C - PCS developed by Hanson and adopted by San Joaquin Hospital in
Stockton, California.
Tool A addressed six overall items of patient care: (a) diet, (b) hygiene, (c)
mobility, (d) medications and intravenous therapy, (e) behavior and special
- 33 -

- - * * - - - t*
- - º -
- - - - - - * * *-
* ,
t - º : - - * *
- * c \, , . . .
. . . - -
* - - * * - -
-" * -
. .------------
- - - * - - *
t s * . .
. . . . . . . . . . .
- * ~ * . . . . * * -
- - - - - *
. . . . .
-, * t .- - . . . . . . . . . "
-
* * . . . ; : . * * * ...
- * * *
-- ‘. . . . . . "
- * - - " - -* - - * ~ * : " . . * * .
-
* * *.
- . . . . - -
- * * -: - . . . . . - I &
- - - -* * * , ( ; , ;
; : : -
- - *
- - * * *
-. . . .
* : * * * * *
- - - -
- * * ~ *
- - . . .- º - *
- - - :-- * * *
* . .- * . -
-• * * ,
- - * - " - - -
-*. * -- **
: . . . . . .
- - * * *
- -* , ,
* - - - . . .* - - - * *
- -- e- ** - - -
- - -. . . . . . ; : :
- - * * *. . * * * *
- - * *- - - - - - - -
- -
t - * -... " - -
‘. . . . . .• . . . .
- - - - - -* * - -
* * . . * *
* *
.
. . . .
• *
, -
* * *

emotional concerns and (f) physiological state. In addition to these patient care
indicators, three phases of hospitalization were also included: admission, discharge
and transfer of patients. Tool B identified four major components of care as
indicators of the patient's overall requirements: (a) personal care, (b) feeding, (c)
observation and (d) ambulation. Each of these major components was broken down
into individual determinants representing the patient's degree of dependency on
nursing care. These determinants were: (a) incontinence and (b) surgery. Tool C
utilized a checklist of parameters such as: (a) activity, (b) position, (c) intravenous
therapy and (d) observation. All three PCS are examples of the factor evaluation
design utilizing four category levels.
The study was conducted over a 9-week period and divided into three phases:
Phase I was from week 1 through 3, Phase II was from week l; through 6 and
Phase III was from week 7 through 9. All patients on the medical and surgical units
were classified daily between 2:00 p.m. and 7:00 p.m. using each of the three tools.
The classification of patients according to four levels of categories was done by
the registered nurse. Each of the nurses used a different tool for a 3-week period.
The finding showed that 34% of the time there was complete agreement
among the three tools. An additional 30% of the time, there was 99% correlation
between Tools B and C. The data indicated that 64% of the time there was
agreement between Tools B and C. The least amount of correlation occurred
between Tools A and C. One advantage of Tool A was its thoroughness; however, it
took significantly longer to complete. In contrast, Tool C took significantly less
time to complete but failed to address behavioral problems of patients. The
authors did not provide an explanation for the selection of the period of the day for
- 34 -

* *- - -º* , , , ,
*----
••--º- * =
----*•
----•"…•
|-·
+*
·
----·■
•
•
·
*
---------
→·--
----|-·»
+--
----
·*·.
"·*→
··*•■·
·
*|-■
|-
•
•----•
·~}----*
·|-••
·
|-•·*-
-*…*••
■ -----,
-■ |-■
»····
*
··*

the study or indicate the degree of inter-rater agreement among the three
registered nurses. These factors may have affected the study results.
A second study was conducted at Malcolm Medical Center in Washington,
D.C. for the purpose of evaluating two existing PCS and selecting one system that
would most meet the following criteria: (1) be able to recognize the intensity of
care, (2) be measurable and quantifiable, (3) be able to match nursing resources to
patient care requirements, (4) be economical and convenient to report and use, (5)
be directly related to time and effort spent on the activity, (6) be open to audit, (7)
be readily understood by those who plan, schedule and control the workload and (8)
be adaptable to changing requirements (Schroeder, Rhodes & Shields, 1984).
The two PCS evaluated were the CASH system, an example of the prototype
evaluation design and the Grasp system, an example of the factor evaluation design
which was designed for Grace Hospital at Morgantown, North Carolina. The study
was conducted over a 30-day period. Three inpatient units were finally selected as
test sites; (1) medical, (2) obstetrics, and (3) surgical. The charge nurse for each
unit was instructed on how to complete the sheets for the two systems. To prevent
any attempts to bias study results, charge nurses were not told of the purpose for
completing the forms and the forms were not totaled until the end of the 30-day
period. The results of the study showed that both CASH and Grasp systems
reflected similar staffing requirements and demonstrated generalization of these
two systems to patient care settings other than the institutions where these
systems were derived.
In summary, this section has presented an overview of patient classification
systems and examples of PCS in use by acute care hospitals for the past four
decades. Studies on the reliability and validity of PCS were also described.
– 35 -

----■
■ ……
→·
•*.*
|-*- …■ -
--* ----…•
•… .*----**
•----…
|---»* |-·-
■
-••|-
■ · ··----·-
*
••---- ·-·
-*-º
■ ----•
•·*.
•,-----
-+→|- •· |-|-
*
,|-■■
•
•----*
…·
|-·|---------*…----
…·-* ----··
|-••_^,■
|-:-- ••
•••---- ----*…••
•---- ----* -*-|- ·*…-|- -----•,|-*
·-,- ----|× ·*--"
*- ••
|-|-|- ■
··|-----
t■·
•
,|-·■-
|-,■
----:•|- -
-· -----* ·|-|- |-----|-
*
-*••
|--*-----,■
·_•~→·
|-· ·■-
|-|-· ·· ·--------
…
-+*
*|-
----*•
*-|-|-
----
.*
·|- ·· ·|------■ --|-· |-*·
•■ ■
±----- **|- -•--*
*----- ·*·
----
-
-…*
*-
•
•|---------…º |-----*|- |-----·
·
•
•|-|- ·*-*-*
*|- ·|-
·--|-· -----**
----|-----••· ·•,■
----|-·---- ■ •----
|-· ·•|- ·|-· *
…•
~|- |-·---- …"·*
*---- ·|-

UCLA Neuropsychiatric Hospital - Patient Classification System (NPH-PCS)
The NPH-PCS incorporates both the prototype evaluation and factor
evaluation designs; therefore it consists of two parts. The first component lists
behaviors representing varying degrees of adaptiveness from adaptive behaviors
(actions that are meaningful and functional to the situation) to maladaptive
behaviors (actions that lack apparent relationship to events transpiring in the
environment). The second component lists nursing care activities based on the
amount of care the patient requires from minimal care to continuous one-to-one
care (see Appendix A, General Framework). The two component classification
system facilitates correlating patient behavior and need for nursing care.
Development of Patient Classification Instrument (NPH-PCI)
The first component of the NPH-PCS is referred to as the NPH-PCI. This
instrument was based on the Johnson Behavioral System Model as a theoretical
framework for three primary reasons (Auger & Dee, 1983):
1. The model focused on behaviors,
2. The model could be readily coordinated with existing treatment
programs based on social learning principles which emphasize
behavior, and
3. Universal patterns of behavior could be identified for applicability to
all individuals regardless of age.
The model addressed eight subsystems of behavior that are universal and of
primary significance to all persons. The eight subsystems are: ingestive,
eliminative, dependency, affiliative, aggressive-protective, achievement, sexual
– 36 -

-*-º
--"...***--*----?--------
''......,..............-:"................
---------.-"--,-**-*-*-*º..--*....."
;:..........:eºº*,.......+......
+=****-**--**-...*:---*--*-
---tº**-
-**-,º-
.."****:•*º-...•s---*-*----*---
";,.•**-
-** .......
**-•*>.I-----,-...":-'n--:1*:*>*>---*-a.-.........----
---*---....-º:;-*****--,-----*---
,,""-----*..-º***-
*----.:*>.....'.º
---*,•.-*****----
--------*~*-
:;;.........**........r--*****
----------
.....*.*;*-----****---.
------------,-------------,-,--------,-,-º-;;–-------*******------. ,,,,,;;;;;;;;;;;;;;;122tº....):i,;2■ tºn...'
*t-,t<*,."-i.*•*:***--r*.i=i:- ......
-*-i..;:*~**D--".---
*---j.......-*----;:............
******----I-
--****-:
-----*-------
...*------2:".,--2.---...--•****
º1*~y:,,,,,;;;;;....,,,
*.............................
---*-º--º------
.........J....."'".........---*
-----*-**-
***.............-**"....-
..*."
*--****-**t***--s----*----
!...*.------..---***..
--.....--
...........--
........."..."-

and restorative (Johnson, 1968; Johnson, 1977; Johnson, 1980; Auger, 1976; Grubbs,
1980).
The NPH-PCI was operationalized in terms of critical adaptive and
maladaptive behaviors for eight behavior subsystems as defined by Auger and
Grubbs (see Table 1). These behaviors represent the total spectrum of emotional
and behavioral disturbances and developmental disabilities from a wide age range
of patients admitted to the adult and child psychiatric inpatient services. Table 2
presents the operational definitions and characteristics for each behavior
subsystem (Auger & Dee, 1983). The behaviors were designed to meet four
criteria: measurable, observable, relevant to the clinical setting and specific to
the behavior subsystems. These behaviors were ordered into three categories based
on their degree of adaptiveness. The complete list of behaviors for the eight
subsystems and ordered into the three categories is shown in Appendix A (Auger &
Dee, 1985). A fourth category was added to include behaviors of acute intensity
and frequency as well as behaviors that may result in self-injury or injury to others.
Table 3 presents the criteria for the four categories (Auger & Dee, 1983).
Walidity and Reliability of Instrument
Content validity is defined as "representativeness or sampling adequacy of
the content of a measuring instrument" (Kerlinger, 1983, p. 458). It is guided by
the question--is the content representative of the universe of content of the
property being measured? As was previously described in this section, the
behaviors represent the total spectrum of emotional and behavioral disturbances
and developmental disabilities from a wide age range of patients. Content validity
was established through a panel of experts (clinical nurse specialists, nursing
- 37


Table 2
Definitions and Behavioral Characteristics of Subsystems
Critical Behavioral
Subsystem Definition Characteristics
Ingestive Behaviors associated with the intake Food/fluid intake;of needed resources from the sensory perception.external environment, includingfood, information, and objects forthe purpose of establishing aneffective relationship with theenvironment.
Eliminative Behaviors associated with the Bowel/bladder patterns;release of physical waste products. hygiene.
Affiliative Behaviors associated with the Attachment behaviors;development and maintenance of interpersonalinterpersonal relationships with relationships;parents, peers, authority figures; communication skills.establishes a sense of relatedness
and belonging to others.
Dependency Behaviors associated with obtaining Basic self-care skills,assistance from others in the emotional security.environment for completing tasksand/or emotional support; includesseeking of attention, approval,recognition.
Sexual Behaviors associated with specific Knowledge andgender identify for the purpose of behavior congruentpleasure and procreation. with biological sex.
Aggressive- Behaviors associated with real or Protection of selfProtective potential threats in the environment through direct or
for the purpose of ensuring survival. indirect acts;identification of
potential danger.
- 38 -

t-
! . .
* *
-
- *º
sº
-
* - - - - * * * - - -* - - . . . . ( * -
t
* -
– '' .º
t* *
- 1
- - . .
. * -
--
i.
--
-,
- -, -
e
*
-
º
- -
. . ;4.
*s
* -
- -
* -
.
- - -
. . . . ;º
* *
- " - .- - -
- - - -
-- " - - - - .
- - * - e - - •. -
- - ... •* - - - - “. . . * : w
. . . . . . . . -
f : ■ ,
. . . . . . . . . " ■ -
- - - *- - * - - a
•- - • * *
. . ---- - - .
* - - - ** -. . . . . . . . . . .
. . . * . . . * , , .
. . . . . . . . . .
- -c. , t i-, ... [ .
* , , * * . . . . - -- : * ~ *, * c 1 -* - - a +
- * * * * * - -
- !
- *.
. . . . . . . . . . . .
- - , t → -
- -
- . . . . - - º
* : - -
- . . : - * - r
- - * - * : - -
* - - - -
* . . . - * * * *
* : - - -
- - - - * * * .- - - * ~ * - - * . . .
. . . . . . * * * - º -

Table 2 (continued)
Definitions and Behavioral Characteristics of Subsystems
Critical Behavioral
Subsystem Definition Characteristics
Achievement Behaviors associated with mastery Problem-solvingof oneself and one's environment for activities; knowledge ofthe purpose of producing a desired personal strengths andeffect. weaknesses.
Restorative Behaviors associated with Sleep behaviors;maintaining or restoring energy leisure/recreationalequilibrium; relief from fatigue, activities; sick role.recovery from illness.
- 39 –

*: : * > . . r -21, r i■ ■ º : , T = 1. I
. . . . . . . . . 2, 223: . . . . . . ºf . . . . iv. . . . . . . . . . . . . . i.
. . . . . . . . . . .
º . . . (, , , , , \ .-
- . . . . . .
… . º * * * w -. . . -
- - - * - -. . . . . . . . . . . . . . . . .• * .
. . . . . . . . . . . . . . . . . . . . . .* - - - - - - , :
- - - - - - - - - - -
• , . . . . . . . . . .

Table 3
General Framework for Categorization of Patient Behaviors
Category I Behaviors that are healthy; appropriate to developmental
stage and adaptive to the environment.
Category II Behaviors that are inconsistent; in the process of being
learned; may or may not be appropriate to the developmental
stage and maladaptive to the environment.
Category III Behaviors that are severely maladaptive to the environment
and inappropriate to developmental stage.
Category IV Behaviors in one or more subsystems of acute intensity and/or
frequency; includes self-destructive acts and aggressiontoward others.
- l;0 -

- * - - -† : " : * >'', \ . . . . . . . . . . . .
* * - - - º - - - * . .
. . . . - *- * , . . . . . . . * .
- - - - s * - -. . . . . -- - - - a • *
* - - - - - - * - - -
- - . . . . . . * . . . . . . . . . . * * * *
t * . . . . . . . - * ■ , , ºr . . . . . . . . "- -
* . . - - - t t -
. . . . . . . . . " - * * w " . . . . ■ . . . . . . . .
* - ... • - : ... r - - - . . . ... r-. . . . . . . . . . . . . . . . . . . . v . . . . . . - * * * * a
- t -* -* - - - -" . : . . . . - -º ... • . . .
* . . * . . . . . . (, : " . . . * * * * * ■ & s \ . . . ... " *
. . . . . . : , . . . . . . .-- - -"
- - - *
... . . . . . . . . . . .

coordinators and nursing administrators) representing both the adult and child
inpatient services. Each panel member independently evaluated each of the
behavioral indices for compliance according to four criteria: (1) measurable, (2)
observable, (3) relevant to the clinical setting of psychiatry and (4) specific to the
subsystem (Auger & Dee, 1983). The panel of experts also arrived at a general
consensus on the ordering of the behaviors according to the criteria specified in
Table 3. Essentially, content validation consists of judgment. Other types of
validity, including criterion-related validity and construct validity, were not
tested.
A pilot study was conducted to determine inter-rater reliability. A total
sample of 28 registered nurses (14 pairs of data collectors) were selected from
seven psychiatric inpatient units. Using a checklist, each pair of data collectors
identified behaviors of patients that were observed in each of the eight subsystems:
ingestive, eliminative, dependency, affiliative, achievement, sexual, aggressive
protective and restorative. The data collectors then rated a subsystem category
for each of the eight subsystems and a system category using the values of 1, 2, 3
or 4. These values were based on criteria specified for each category (Table 3).
Results showed that staff agreement on independent ratings of patient
behavior significantly exceeded chance, and that inter-rater agreements were all
within five percentage points of each other. Levels of agreement involving
assessment of behaviors that required a low level of observer inference were
highest; for example, such behaviors as handwashing, frequency of bowel
movements and clothes associated with specific gender. Levels of agreement
involving assessment of behaviors that required a high level of observer inference
— l;1 -


were lowest, for example, awareness of personal space, attachment and expression
of feelings (Auger & Dee, 1983).
In summary, the development of the NPH-PCI, including operational
definitions of the Johnson Model, criteria for four categories, content validity and
inter-rater reliability was described in this section.
— l;2 –

CHAPTER III
Methodology
Research Design
This predictive research study was designed to assess the reliability and
validity of the patient classification instrument developed for the UCLA
Neuropsychiatric Hospital (NPH-PCI). The data used in this study was derived
from an observational study designed under the auspices of the UCLA
Neuropsychiatric Hospital, Nursing Services. The observational study was
conducted on four child and adolescent inpatient units at the UCLA
Neuropsychiatric Hospital (NPH) in Los Angeles, California, from August, 1982, to
September, 1984. The objectives of the observational study were fivefold (Auger &
Dee, 1982b):
1. To assess the reliability of staff ratings of patient behaviors as
described in the NPH-PCI,
2. To examine the relationship between ratings of behavioral subsystem
categories and rating of system category,
3. To determine the relationship between patient behaviors and
corresponding levels of nursing care as defined in the NPH-PCS,
4. To measure the number of direct and indirect nursing care hours, and
- l;3 –

* * * * * , -
- - - 1 - I -
t - * : " - º - - - - - " - . - - . . .- - - -
t - - * * * * * * ~ * • * * * - * - * ~ * * -
* - * s - - - -- - - - - - -
- - ( , , , , - V - . : . . . . . . . . . . . . . . . . . . . . . . . . . . . .- º -
. . - * - - - -- - - a - - - - * * * *- * * * - t . . . . . * , - - - : . . * * - - - , , , ;
-- * * : . . .
- - . . . . • * , ! . . . v . .-
- * - - - - - - , - - - - - º - - i – f = i - * * * : " .
- - . . -- - -- " - - - - * * * - -
* - . . . . . . . . . * * * * . . . . - *
* * - - * * * , - " - " * - - * . . . * * . - " . .- *- - • . . . . . . * * * - * * , . . . . . . . . . . .
- - , - . -- " . . . . . . . .” - , , , * . . . . . * . . . . - - - * - * * *tº - * ... • - * * * - - - - - - - * * • * * - -
, ,-
* - - - t t - , - - - * -: - * : - " - - : . * * * - * -. * * * * * - -
* * * * : * ~ * - - - - - i = 1 - - - - t - * * a * * v- * * - - -
- - -
- -
- - . . . . + * . . - - " " . . . . " : - * * * * -. . . . . . . . . . . . . . . . . . . . . . a . . . . . . . . . . . . . . . . . . . . .
- * * - * - -- - . . . . * -- * * *
* . . . . - * * : . - - - - - 1 - . . . ". . . . . . . . . . * * * * * : . . . . - - - . . . . . . . -- * * . . . . . . ( . --
- - * * * - - - - * * * - * * *& " " . . . * . . . . . . - ! . . . . . . ■ .
• - * - . * - - ? - - - - - - *
. . . : ; ; , . . . . . . . . . . . . . . . . . . . . . . .- - - I ‘. . . . [. **
- - - - • *. - - - . * - t - -- - - - - -
º - - . . . . . . . . . "- * * * * * * * * * : # * ** -
-- - -
- * * - * - - - * * * º - - - - - - - * - - - - - **. . . . . . . . . . . . ; * - - - . . . . . . C. . . . . . . . . . . . . . . . . .

5. To determine the number of nursing care hours required to provide
nursing care to patients categorized according to the NPH-PCS.
More specifically, this study addressed two of the five objectives of the
observational study: (1) to assess the reliability of staff ratings of patient
behaviors as described in the NPH-PCI and (2) to examine the relationship between
ratings of behavior subsystems' categories and rating of subsystem category.
Research strategies, procedures and data analyses related to these objectives are
described in this section.
Research Strategies
For an instrument to be used with confidence, the issues of reliability and
validity must be addressed. Equivalence reliability and criterion-related validity
were the two psychometric properties selected for investigation in this study.
Equivalence Reliability
The equivalence approach is utilized when one of the following circumstances
exists: (1) when different observers are using the same instrument to measure the
same phenomena at the same time or (2) when two parallel instruments are
administered to individuals at about the same time (Kerlinger, 1973). A basic
limitation of the latter method is the difficulty of constructing alternative forms
that are parallel (Carmines & Zeller, 1979).
Zeller and Carmines (1980) identified two additional measures of equivalence:
(1) split-half methods and (2) measures of internal consistency. In the split-half
- lºli –


method, the total number of items in the instrument is divided into two halves and
the correlation between the two halves is used to provide an estimate of the
reliability of the full set of items. A criticism of the split-half method is that the
different ways in which items can be grouped into halves have resulted in different
reliability estimates even though the same items are administered to the same
individuals at the same time. In contrast, measures of internal consistency do not
require the splitting or repeating of items. Reliability estimates can be obtained
by using statistical procedures to account for all the variance and covariance of
the items. The most popular of these reliability estimates is given by Cronbach's
alpha (Carmines & Zeller, 1979). However, the following conditions must exist: (1)
the items that make up the composite are homogenous in their relation to each
other; and (2) there is a large number of items (Zeller & Carmines, 1980).
For this study, the alternative form method, split-half methods and measures
of internal consistency were not selected for the following specific reasons:
1. The alternate form method was not selected because there was no
known parallel instrument available.
2. The split-half method was not selected because the nature of the
instrument is such that it could not be divided into parallel halves.
3. Measures of internal consistency was not selected because the items in
the NPH-PCI were not expected to show homogeneity.
Consequently, the method of utilizing different observers to observe and
categorize patients was the logical approach selected for this study. Reliability
estimates, in this instance, refer to the degree of agreement among different
observers when patient behaviors are observed and categorized independently using
the same instrument for the same period of time.
- l;5 -

*** •■

Criterion-Related Walidity
Criterion-related validity is determined by the degree of correspondence
between a measure and its criterion. Essentially, there are two types of criterion
related validity: (1) concurrent validity, which is assessed by correlating a measure
with its criterion at the same point in time and (2) predictive validity, which is
assessed when a future criterion is correlated with the relevant measure (Zeller &
Carmines, 1980). According to Nunnally (1978), criterion-related validity is
predictive validity, and in each case, a predictor measure is related to a criterion
measure. Predictive validity is at issue when the instrument is used to estimate
some important form of behavior that is external to the measuring instrument
itself, the latter being referred to as the criterion. Knapp (1985), however,
cautioned that criterion and predictor measures should be of the same construct.
The degree of correspondence between these two measures, therefore, determines
the predictive validity.
This study proposes that: (1) ratings of patient behavior indicators in each of
the eight subsystems will be positively associated with subsystem category ratings
and (2) subsystem category ratings will be positively associated with system
category ratings. In other words, patient behavior indicators are predictive
measures for subsystem category ratings and subsystem category ratings are
predictive measures for system category ratings. Subsystem category (in the first
instance) and system category (in the latter instance) are criterion measures.
- 46 –

~ ~ *- A. •• º· *→
----·••
|-.»
·-… ----|-*
--
·
-→·- ----*…■ |- -|- ----→··· ----<■ --|-
*----*··|- ----|-|-••·|---
|-
|-* |-* |-|-~|-·
·
----
·
*|-· *-*- -*----*…·
•
…|- …*-→·|- •
■ |-
-■·
*…
--------*--
-"•*----|-* -----...•----•×
|-|--·
■
-*- ·-----i
•|-·ae
•
----→·
|-
·|-·*----•
ae|-|-|-
----
•
•··
*
*-
,■ ·
··*
|-,■ →--
º· |-+*
----
t
■ |--|-
|-·••
·
→
·|-*…
----→·
·- *
·---- ·|-■ ” *|- *|-|-|-
•
■ |-
:
·---- |-·,■
*
|-|-|-*…

Research Questions
Research questions were posed to address reliability, validity and
generalization of the NPH-PCI. Specifically, these questions were:
1.
2.
4.
What is the percentage of agreement between staff, shift coordinator
and observer groups with respect to:
– observed patient behavior indicators?
- ratings of subsystem categories?
- ratings of system categories?
Which patient behavior indicators in each subsystem have the greatest
impact on subsystem category?
Which of the eight subsystem category ratings have the greatest
impact on system category ratings?
Does the model of NPH-PCI predict across age groups, sexes and
inpatient units?
Study Definition
For the purposes of this study, the following general definitions were used:
1. Patient behaviors - Direct observable non-verbal and verbal actions of
the patient. These behaviors represented the total spectrum of
emotional and behavioral disturbances and developmental disabilities
from a wide age range of psychiatric patients. These behaviors were
- l;7 -

* | * * * * : . 1 * * * : *------------------------------
. . - - - - - - - * . . . . - - -
-- . . . . . . . . . ( . . . . . . . . . * - . . º
- - * - + - º - - - º •. -. . . . . . . . . . . . . . . . . . * - - - - - - - - - - - -
- - c . - * * - - - - º - - - * 1- - -
… + . . . * -- *** * * * - ** * - -- - - * * * * * * , I -
- - * * - º * - - - - - - * - . . .c. * s - * * ! . . . . . . . ... " - * ~ * -
- a ... * * * : . . . . . . . . . ;-
r - -*. + * -
* . * : - * * . * * * -
- * - - - - • , - " - " - - - - - -
* . . . . . . - * . . . . . . . s - . . . . . . .-
!-- ", , -",--
- - -- * . - - -. 1 * : . . . . . . . . . . . . .
* , * → - - - - - - - - - . -
- -- . . . . . . . . . . . . . . .
-~ * ( ; ; , , - - - - - - -- -
- " * - . * - - , ,* * - - * * * - * > . . .
- - - - - - - * - * - - * . . - - -
f : . . . . . . * - . . . . . . . . . . . . . . . .
* - . . . . . ■ .
- - - - - - - - - --■ : 3 ºf . . . . . . . . . .
- * - - - - * . . . º - - . . . . . * -
: : - . . . . . . . . . . . - - - . . . . . . . . . ." . . . . . .
- " - - - - - * * * : - " . . . * - -• * *- : * > . . . . . . . . . .- - - -- * - - - -
-, - - - - - - - - - - - - -. . . . . . ! . . .
- - " . . . . . - - . . - - -
-. . . . . . . . . . . . . . . * - - - * . . . . . . . . . . . . . . -
- - - - - - - - - - - - * - . . . -, - .
- * * * *- - - - * - * - - - - - - - - - - - t * - - - -

2.
6.
ordered into the first three categories according to the general
framework shown in Table 3.
Adaptive behaviors - Actions that are meaningful and functional to the
situation. Adaptive responses are characterized as appropriate to the
eliciting stimuli in the environment.
Maladaptive behaviors - Actions that lack apparent relationship to
events transpiring in the environment. Responses may be different or
excessive to the environmental event.
Environment – The social, cultural and physical factors contained
within the hospital setting, such as treatments, philosophy and patient
mix that influence and limit the behavior of the patient.
Subsystem category - Represents the data collectors' ratings on the
overall adaptiveness of a group of contrasting behaviors for the
Subsystem, which may include a mixture of adaptive and maladaptive
behaviors as well as divergent behavioral characteristics. For
example, in the ingestive subsystem, the patient may demonstrate
Category I adaptive behavior for food and fluid intake and Category III
maladaptive behavior in awareness of social and physical environment.
Rating values range from 1 to 4 based on the general framework shown
in Table 3.
System category - Represents the data Collectors' ratings of the
degree of nursing care required by the patient based on the overall
level of behavioral adaptiveness for all eight subsystems. The rating
values for care requirements ranged from 1 – 4. A value of 1
represents minimal nursing care designed to maintain and support
- l;8 -


7.
8.
9.
adaptive behaviors. A value of 2 represents moderate nursing care
designed to structure the environment for the purpose of reinforcing
newly learned adaptive behaviors and modifying maladaptive
behaviors. A value of 3 represents intensive nursing care designed to
structure the environment for the purpose of teaching new adaptive
behaviors and modifying severely maladaptive behaviors. A value of 4
represents one-to-one nursing care management of severely
maladaptive behaviors for the protection of the patient. A detailed
general framework for nursing care requirements is found in
Appendix A.
Shift coordinators - Persons assigned to a specific unit with primary
administrative responsibility for staffing and patient care for a given
8-hour shift (Administrative Nurse I). Relief shift coordinators were
those with primary administrative responsibility in the absence of shift
Coordinators and included Clinical Nurse I, II, III, Administrative Nurse
IV and Per Diem RN.
Observers - Master prepared staff who were recruited specifically for
the observational study and were randomly assigned to any of the four
inpatient study sites. Those recruited were knowledgeable about the
Johnson Model or had prior clinical experience working with patients
in the psychiatric/developmental disabilities settings.
Staff - Part-time and full-time professional and nonprofessional
persons identified as the patient's primary caregiver for a given 8-hour
shift during the observation period. These include Clinical Nurse I, II,
III and IV, Administrative Nurse I and IV, Per Diem RN, Float RN,
- l;9 -

------»------|••---------|,'|-:----|------|---------*n--------****|-•
•*-■-----||-·--→,
--|--,!--
|---------…º*·|-!1••
-·■ ·----■ *•
•*,*|--·„*|---|-|-·----|-
----·■■ -|-|-------------■
-
~:***■,·•*.»|-'.
|-----r-•----•--*|-…;·*•
•+-+·!•••--»----|---·----*.-
-----|-1----·
-••--*-|-••
•------|-|-••|-
*
…*-|-|-*·
|-|-|-→·-··*."
|-|-|-|-→·|-----·----·,■ ·*----|-·|--·|-
·|-|-|-|-*----·
·■1|-|-|---|-··|-→--·•··
|-·*|-|-■ ”
→·
·|-■ |------|-·-…·-----
-
-|-|-·-.
'----|-·|------·•·-----*----|-----|-*
•|---|-|-……|-→·-----*•·-
-
|-→·------*----··-*|-•·
-
----|-----|---------·|-·-|-|-|-----·----|--
-|-----|-·
-·|-----■ -----|--*··→--|-·|-
·
|-----··•----·…•--·•·----
…
•<■ -----···|-·-·|-----|---------…*
→--|-|-
----
…
■
4|–|-----·|-··|--
--------··*••
|-•
•|-|-----|---
|-|-}|-|-----•·■ '■|-~^,-*,·|-*■ |-----
--------|-*|-|-■ |---------→· |-
→
·|-|-•
•|-*••|-----|-+→|-…------------→|-------------|---------·|-|-·
·
--
-*→·
*
-|--
*|-|-~----|-----·|-|-
----··
----|-**|---|---|--·|--…*
|------
|----------|--
·|-*--------|-|-·-·----···•--→
•
•|-:|-·-----
-|-----·

Mental Health Practitioner and Psychiatric Technician, Senior Nurses
Aide, and Nurse Interim Permittee assigned to a specific inpatient
unit.
Description of Research Setting
This research was conducted at NPH, a 209-bed tertiary care hospital and
major teaching medical center of the University of California at Los Angeles which
consists of the following inpatient units: two adult psychiatry, one geropsychiatry,
one neurology, one telemetry, two child psychiatry and two adolescent psychiatry.
Specifically, the research setting selected consisted of the Child Psychiatry/Mental
Retardation Division of the NPH: (1) A-West, a 19-bed unit for children aged
5 - 11 with emotional and behavioral problems, (2) A-South, a 19-bed unit for
adolescents aged 12 - 17 with emotional and behavioral problems, (3) 5-West, a 17
bed unit for children aged 2 - 11 with developmental disabilities and (4) 6-West, a
19-bed unit for adolescents and young adults aged 12 - 23 with developmental
disabilities. The average length of hospital stay on all four inpatient units is
approximately 2 to 3 months. The percent of occupancy on all four inpatient units
is approximately 63 to 78%.
Primary nursing is utilized on all four child and adolescent inpatient units.
The registered nurse (RN) as the patient's primary staff is responsible and
accountable for the planning, supervision and evaluation of all nursing care. An RN
or a non-RN; e.g., licensed psychiatric technician or mental health practitioner is
- 50 -

Aºr
*■
*
* |-|- •----*
••|-→·|-
■
1…-- ·
*·*-
|-|- |-••
|-•*-
-|--…•••
-----rº·→
·*-
----~~…>;
•----,■'
■ |------
·* *---- *· <■ ------••
• ·
·
·
→· •---- ·
·-|-
…•
·«»
----
*----*-
•
•*…
*
*|-*
,-- *
|-* ----
■*
•
•*…· ·
*
----*+* ·
-·*-
-"·ae
■-
•• -
-|- ----*√.
·• |-----.* *
*|-*-
---- ••
**
;:,; ****

the patient's associate staff and participates in the assessment, planning, provision
and evaluation of patient care.
Each inpatient unit maintains a multidisciplinary treatment team composed
of psychiatrists, social workers, nurses, occupational and recreational therapists,
special education teachers and dentists. The treatment approach is eclectic and
consists of individual therapy, milieu therapy, behavioral and psychopharmacologic
interventions, group therapy and family therapy.
Sample
Major consideration was given to two factors in order to increase the power
of the analysis: (1) the selection of a large sample size and (2) determination of
the criteria for sample selection to increase variances in the variables under study
and to decrease variance in extraneous variables (Kerlinger, 1973).
The sample consisted of 683 patient observations on the four selected
inpatient units with each patient observation serving as the unit of analysis. A
purposive sample consisting of patients who met the criteria for each system
category was selected from four inpatient units for observation in order to have an
adequate representation of each category in the sample.
– 51 -

-
4.
* *- - *
- :- - - - -
- - - - :
-- - -
--f
• * ~ *
1 - .
< *; i. ■ .
- º -
* : « . . . .
º - -( . . "
* - -
-* - s
. . .
. . .
. . . . .
* , "
". . . .
ºz º.
ºf
. . .
. . . .
*
- -
º -s
- - - -
: . ( . . .
* *
- - ( : - -
t ... "* * . . .
. . . - * *
. . . .
2 . . . . .
* ** * * * ~ *
". . . . . . .
- . .
s -
* - a -
- º - -
- . -
- ~ * * *
. . . .-
*
*

Data Collectors
Observers
Of the eight observers, seven had a Masters degree in Nursing and one was a
graduate student in Nursing. Five observers were former clinical nurse specialists
on the child inpatient units; their mean nursing experience was 15 years.
Training for the observers consisted of: (1) a 4-hour long course on the
concepts of patient classification systems, basic theoretical concepts of the
Johnson Model and an examination of patient behavior indicators for each of the
behavioral subsystems per category, (2) a 4-hour long pen and paper testing of
inter-rater reliability in rating patient behavior indicators and subsystem
categories based on taped series of patient situations and brief on-unit observations
and (3) a 10-day period of 20 hours on-unit observations in pairs. The inter-rater
agreements of observers ranged from 90 to 95% for patient behavior indicators and
subsystems categories.
Staff and Shift Coordinators
Since the patient classification instrument had already been utilized as a
clinical tool for patient assessment, nursing care planning, intervention and
evaluation of patient progress on the four child and adolescent inpatient units
beginning in April, 1981 (Dee & Auger, 1983a), staff and shift coordinators did not
receive additional training prior to the commencement of the study in August,
1982. However, subsequent new employees were given an hour-long orientation on
the purposes of the patient classification system as a clinical tool and as an
- 52


administrative tool for staffing. A videotape representing examples of three levels
of patient behaviors was shown to facilitate staff understanding.
Staff who had primary responsibility for the care of the patients observed
were the data collectors. Shift coordinators who had administrative
responsibilities for a given 8-hour shift during the observational period were also
data collectors.
Instrument
The Behavior Criteria Checklist is composed of three parts: Part A -
objective measure consists of lists of patient behaviors, Part B – subjective
measure consists of a rating scale for subsystem categories and Part C – subjective
measure consists of a rating scale for system categories. The Behavior Criteria
Checklist is shown in Appendix C.
In designing the Behavior Criteria Checklist, consideration was given to ease
of use. A simple check for each observed behavior would indicate the presence of
the behavior. A total of 61 behavior indicators were identified for the eight
subsystems (see Appendix B). Behavior indicators for each subsystem were
determined to have different variations. For example, limited awareness of
physical and social environment is an example of a Category II behavior while lack
of awareness of physical and social environment is an example of Category III
behavior. Both behavioral statements are variations of awareness of physical and
social environment which is an example of a Category I behavior of the ingestive
- 53 -


subsystem. A total of 166 patient behaviors of different variations were identified
to represent the 61 patient behavior indicators.
To control for internal validity (Cook and Campbell, 1979), these 166 patient
behaviors were listed in random order in the checklist. Category I indicators were
assigned values of 1. Category II indicators were assigned values of 2, and those
indicators that met the criteria for Category III were assigned values of 3.
Behavior indicators that were not observed or were absent were given values of
zero. A detailed discussion of the instrument's development, content validity and
inter-rater reliability is found in Chapter II.
Research Procedures
Observational Procedures
The primary data collection method utilized was direct observation of patient
behaviors by staff, shift coordinators and observers. Four-hour observational
periods were scheduled between the hours of 0700 and 2300 for all days of the
week. Observation on the night shift was not included for two reasons: (1) most of
the patients on the units were asleep and (2) the cost of night observation was
prohibitive. A 4-hour observational period was selected for two primary reasons:
(1) a 2-hour period would present a scheduling problem for observers who had to
report on duty for short periods of time and (2) a more than 4-hour long observation
may result in observer fatigue.
- 54 -


Scheduling of Patient Observations
The patients selected for observations were based on the shift coordinators'
best estimate of patients who met the criteria for each system category at the
beginning of the shift. Category I patients were those who required minimal
nursing care. Category II patients were those who required moderate nursing care.
Category III patients were those who required intensive care and those who
required one-to-one nursing care were Category IV patients.
Observers were randomly assigned for patient observations on the four
inpatient units while staff and shift coordinators remained on their assigned work
units. Scheduling of observations on all four inpatient units was arranged based on
the availability of each observer's work schedule and the availability of patients
who met the specified criteria during the specified H-hour time periods. External
validity was controlled for assignment of sampling by setting (inpatient units), by
time periods and according to criteria specified for system category.
Data Collection Procedures
At the completion of each of the H-hour periods, the shift coordinator,
observer and staff were asked to independently complete a Behavior Criteria
Checklist on each patient observed, identifying those behaviors present during the
observational period for each of the behavioral subsystems. Staff, shift
coordinator and observer also independently categorized each subsystem based on
observed behavior indicators for degree of adaptiveness using criteria specified in
Table 3. The rating values ranged from 1 (adaptive) to 4 (maladaptive). Based on
these eight estimates of subsystems' adaptiveness, raters also estimated the degree
- 55 -

-
... "
• *
e
º
• *
* :
---
. . . . .
* -
-
a "
* * *- -
- * *
... "-
. . . . .
* | - ,
t -
* * * * .
. . . . .* * * * * *
. . . .
- * → -- * - -
* ,
* * *. .
- .
- - -- - - - - - -
■ : : - - - -, * * i■ ºf
* s. . . e -
- . . . . º * * * ,
º - • . . * - -
º t -- : : * = - - -
- . • * : . . . .-
- - - - - - - - - - - - - ~
- - - * * - -
" . . . . . . . . . . . --
* : . . . . . . . . . . . . . . . . . . . .-
* * - - - - - -: * *- -
| * = r -
- º - - - * e| i * , - - t
- - * * -
. . . . . . . . .- . . "
* - - * - - - , - ; : -
* - - * - 2 a v = -
- . 1–1 . . . . . . . . .- º * .
- . - - * * * - - - - --
* * * , : . . . . . . . . .
- - s
a 1. v . ; : . . . . . . . . . . ". . .
**
- **
, - .* -
* *- -
* -
* - ". . .
* -
* - - -
- - - -
* * - *
- - *
* - r
t . .
-
: \ . .
- * , -* a
*

of nursing care required by each patient using the categories described in
Appendix A (1 = minimal care and 4 = one-to-one nursing care).
Pretesting Period
A 10-day period of observer training on the inpatient units was considered as
the pretesting phase. This period allowed patients to become familiar with the
presence of the observers on the units. Table 4 presents the timetable for observer
recruitment, training and data collection.
Data Analysis
The following statistical procedures were used to answer each research
question:
1. What is the degree of inter-rater agreement between staff, shift
coordinator and observer groups with respect to:
– observed patient behavior indicators in each of eight subsystems?
- ratings of subsystem categories?
– ratings of system categories?
A procedure to compute reliability as a function of agreements is to use the
following equation (Kerlinger, 1979):
Inter-rater number of agreementsagreement =
-number of agreements + disagreements
Inter-rater agreement for the three paired groups; e.g. (1) staff versus shift
coordinator groups, (2) staff versus observer groups and (3) shift coordinator versus
- 56 -

. . .
* * *
* -
- * * *- I - , ,
- - - -
! . . ;
º
º

Table l;
Timetable for Observer Recruitment, Training and Data Collection
DATES ACTIVITIES
June 15, 1982
July 13, 1982
July 20, 1982
July 20, 1982–
July 30, 1982
August 9, 1982
December 13, 1982
July 14, 1983
September 7, 1984
Recruitment of observers begins.
Four-hour long training seminar forobservers.
Pen and paper reliability testing forobservers.
A ten-day pretesting phase on inpatient units.
First scheduled patient observation onA-West.
Follow-up meetings with team leaders of
each inpatient unit.
Follow-up meetings with team leaders of
each inpatient unit.
Last scheduled patient observation on
A-South.
- 57 -

*-y-•-*
-,-...**----*-".......**,*--,,
.............;-
-.**--....:-***-****t*."........*-.
=~*---
,,,;,,-
** -*--***---Tº-*2.,-.-.-2º -*---yº--.--,--}{
*-*-
•,,,,-**--º-
------a***** º-->-t............;■
>**r--
-*-*
--***"--**:*-*-------,-******~**:*~*- -:*>º,!...A)".…....--*..:;;;
-
-***--;:j:,"....-5■:*--*
-**---•**--,..****-
>2..•
•.t**-
******;:-e*.-
-*--~*-º-----
-*--*----t-tn*
--*-----*
-,*---r-.--!..
***** J............

observer groups was computed for each patient behavior (total of 166), four
categories for eight subsystems (total of 32) and system categories (total of 4).
According to Polit and Hungler (1983), inter-rater agreement in the vicinity of .70
or even .60 is sufficient for making group-level comparisons. Abdellah and Levine
(1965) suggested that inter-rater agreements for a patient classification instrument
must be in the vicinity of .90 or better. However, this criteria was established for
patient classification instruments which focused on objective nursing care
activities and not subjective estimates. Because of the diversity in educational
preparation, length of clinical experience, work classification and methodological
limitations of the observational procedure, inter-rater agreement of .60 was
determined to be acceptable for this study.
2. Which of the patient behaviors in each of the subsystems have the
greatest impact on subsystem category?
Prior to regression analysis, a correlation matrix was generated and examined
for redundancy and multicollinearity of the independent variables (Gordon, 1968).
According to Lewis-Beck (1980), for multiple regression to produce the " 'best
linear unbiased estimates'" (p. 58), none of the independent variables should be
perfectly correlated with another independent variable. Although independent
variables are almost always intercorrelated in nonexperimental social science data,
an extreme condition of multicollinearity can render the parameter estimates
unreliable. An estimated regression coefficient may also be unstable and fail to
achieve statistical significance. However, multicollinearity is not a problem when
bivariate correlations of independent variables are found to be less than .80 (Lewis
Beck, 1980). Consequently, for this study, a correlation coefficient of less than .80
was considered acceptable.
- 58 -

|-
•
■ |-----
-*…
·--
|---·*
,--
-·*
•|-
••
----•→--------
·
·}•}
-·•----→
·•"|-··
·
··
→·
|--■--
-••·
|-·-
-*-•
·
·*-
·`-|-··,
■ -**•
*****
■1
----••--
----•}·--------·■ +→**-•••••·*----
v
•v_"…-
■ ”*ae----w
w--
·*-->
**,
••
•·w
i~----
----
*
*,sw|-|-··
·
•*…|---~„*••
→
·*|-----
·
*********----|-----••------------••
------«
••••■ !
w
w~·----*----··
~•*|-
·
**,*,
----|-*…■■----
··■
■■ ----·
·•■
•
••|-|-----|-·
ºi.

Multiple regression analysis using the stepwise selection procedure was
utilized to determine the contribution of independent variables to the dependent
variable (Pedhazur, 1982). In this instance, patient behavior indicators in each
subsystem observed by shift coordinators were treated as independent variables and
served as predictor measures for subsystem category ratings. Each of the eight
subsystem category ratings by observers was treated as a dependent variable and
served as criterion measure for behavior ratings.
In order to ensure the reliability of the regression statistics, Pedhazur (1982)
recommended that the ratio of independent variables (patient behavior indicators)
to sample size (patient observation) be at least 30 per variable. Since patient
behavior indicators for each subsystem ranged from 5 to 11 and a total of 331
patient observations were completed by the shift coordinators, the sample size
obtained for this study met the necessary requirement for regression analysis.
Full equations using all independent variables (observed patient behaviors for
each subsystem) were analyzed for their effectiveness in explaining subsystem
category. The squared multiple correlation coefficient (R2) was used extensively
in data analysis to measure the proportion of total variation in the subsystem
category ratings explained by the regression. Once the effectiveness of the full
equation in explaining subsystem category ratings was investigated, reduced
equations were made which consisted of those patient behaviors with an F ratio
significant at p < .05 and a beta weight significantly different from zero at p < .05
(Pedhazur, 1982). This procedure assumed that the reduced equation would yield an
R2 statistically as effective in explaining subsystem category as the full equation.
It was desirable that the final instrument be parsimonious and yet remain effective
in explaining the subsystem category.
– 59 -

•"
*|-·
|-·*
…*
→·
·
■
■ ----…
--|- ----|- ■ -----·
→--
|-* ·-•
*
-■ |-·

A statistically significant relationship among the variables would mean that
the relationship exists in the universe from which the data have come and that such
a relationship does not occur by chance. According to Gold (1969), a substantively
significant relationship among the variables is equally important for it to be
meaningful in the practical situation. However, the magnitude of the relationship
required for substantive significance is a matter of subjective judgment based on
the nature of the problem.
To determine the criterion for significance as an explained variance for
subsystem category ratings (dependent variable), two factors were considered: (1)
most data which attempt to investigate social phenomena yield low R2 values often
below .50 (Werran and Ferketich, 1984) and (2) an R2 value of .70 would be an
acceptable criterion for a well-developed instrument (Verran, 1982).
Consequently, the criterion for statistical significance was set as an
explained variance for subsystem category ratings at a conservative R2 value of
.50 for two reasons: (1) data used in this analysis is derived from an observational
study on patient behaviors, and thus can be considered as social data and (2) data
used in this analysis is considered as an initial step toward a series of validation
studies for a well-developed instrument.
Although multiple regression is a robust statistical technique (Bohrnstedt and
Carter, 1971), violations of a combination of assumptions may lead to serious doubt
and a lack of confidence in the results of the regression analysis (Hey, 1974).
Verran and Ferketich (1984) suggest that the regression assumptions of zero mean,
homoscedasticity, independence and normal distribution can be examined directly
with residual analysis.
– 60 —

----·→·
* -- * * º
•••

For this study, residual analysis using the reduced equations of patient
behaviors was performed to test the assumptions of the regression model. The
following approaches were used for the examination of residuals: (1) frequency
distributions of unstandardized residuals were examined for zero mean; (2) plots of
standardized residuals against predicted dependent variables in the equation were
examined for homoscedasticity; (3) plots of standardized residuals against all
independent variables in the equation were examined for independence; and (4)
histograms of the frequency distribution of categorized residuals and Chi-square
goodness of fit statistical test were used to examine for a normal distribution. It
was expected that all plots would show an equal spread around the zero line, that
the mean would be zero or contained within a 95% confidence interval about zero
and that visual and statistical tests would show no significant difference from the
expected normal distribution (Werran & Ferketich, 1984; Pedhazur, 1982; Shavelson,
1981; Draper & Smith, 1981).
3. Which of the eight subsystems have the greatest impact on system
category?
Multiple regression using the stepwise procedure was also utilized to
determine the contribution of the eight subsystems to system category. In this
instance, the eight subsystems as rated by shift coordinators were treated as
independent variables and served as the predictor measures for system category. A
system category as rated by observers was treated as the dependent variable and
served as the criterion measure. Values for subsystem and system categories
ranged from 1 to 4 and were based on criteria specified in Table 3.
A full equation using all eight subsystems was analyzed for effectiveness in
explaining system category. The squared multiple correlation coefficient (R2) Was
- 61 -

*
- - -
- *
- * :
- *
*. . . ! . . . .
- .
* ... . . .
-. . . "
in: j : 1 . . .
- ' ' ". . . .
- -
* * *
- * * • *
s - -
- -
, a * * * *- * * * *
-
* -
- * *
* *
- * : **
- - *
- * * * * -
* . . .
-
º
* * -
- * =
-- " -
- - * -
* * *- * * *
- - -
* . .: . .
º -
* * . . .
* * • ** - • .
: -" - .
- - - -
. . --- * * *
- * *- - -
- * ** * *
- -
* - - -
º
-
- - -
. . .* -
** *
r**

also used in this data analysis to measure the proportion of total variation in the
system category explained by the regression. Once the effectiveness of the full
equation in explaining system category was investigated, a reduced equation was
made which consisted of those subsystems with an F ratio significant at p < .05 and
a beta weight significantly different from zero at p3.05. This procedure assumed
that a reduced equation would yield an R2 statistically as effective in explaining
system category as the full equation. The criterion for statistical significance was
set as an explained variance for the dependent variable (system category) at 50%.
Residual analysis using the reduced equation was also performed to test the
assumptions of the regression model. An examination of residuals was done
through the use of plots, graphs and statistical tests.
4. Does the model of NPH-PCI predict across age groups, sexes and inpatient
units?
Data analysis to investigate the instruments's generalizability was conducted
by the examination of residuals. If the instrument's explanatory power worked
equally well across all units, age and sex groups, certain visual examination could
be completed to assess this assumption (Ferketich, 1982). Residual analysis, using
the reduced equation for patient behaviors and the reduced equation for
subsystems, was performed. Residuals from the equation were sorted by unit, age
and sex groups and plotted. It was expected that they would be evenly distributed
across age, sex and inpatient units. A Chi-square goodness of fit test was
performed to determine if the residuals tended to be especially high or low for
subsets within age, sex and inpatient units.
In summary, this chapter has presented a description of the research setting
and delineated research procedures and data analysis to investigate and answer
– 62 -

----·*|-
|-·*-+.*|-•|--- ·
·→·-
*••|-·
w
-|-*…*--
-·|--•
•*»|-*
■ •■ |-----|-&
··|-**,-------■••|-|-
*
*----→·
•-·~|-|-
■ |-•------------
*
*|---------|-·|-·
w.
••••
*…*|-----•
"|---
----*•
--
-----·*,
**|-··
*
·|-------w
w*…
·→*
■ *…••
--·-…
~----|-|--
,■
----→·
w
w|--*|-...º|-■ |-|-|-
■
±----|-|-***|-*
v|-·|-****-----
■ -*
-|-|-··
••vr.-**------|-·----·•----|-
•
•·|-

each of the research questions posed. The issues of equivalence reliability,
criterion-related validity and generalization of the instrument were also addressed.
- 63 –

→·•■

CHAPTER IV
Research Results
This chapter presents the results of an observational study conducted to
assess the reliability and validity of the NPH-PCI. This study extended over a 25
month period. The first actual patient observation occurred on August 9, 1982, and
the last patient observation was September 7, 1984. The gradual decrease in
patients who met the criteria for system Category I and the infrequent admission
of patients who met the criteria for system Category IV contributed both to the
duration of the study period and the final decision to terminate the study.
The first section of this chapter presents the sample description of patient
observations sets included in the final data base and a profile of data collectors
who participated in the observational study. Results which relate to the
equivalence reliability, criterion-related validity and generalization are also
presented in this chapter.
Sample Description of Patient Observations
A total of 683 patient observation sets were completed in the course of the
study. However, to control for response bias in ratings, three criteria for the
inclusion of each patient observation set in the final data base were established:
- 64 -

! - c : -*
*
··|-·|---
»••
•
•|-*
*·|-·
••
----------*-·|-
**
----|-*----··
→·
----*■*
·
·
|→·
·
·
•
•*---
·*,
t
:|-*…
•
■ |-*---****|-■º■
*…
»|-*
··--
••|-→·
••
•|-·
*•**

(1) a complete set of different raters; (2) a two-week time lapse between
observations of the same patient in the same system category; and (3) repeat
observation of the same patient in a different system category. A total of 451
patient observation sets (66%) met all three criteria and were therefore included in
the final data base. Table 5 presents the total number of patient observation sets
for all categories on all four inpatient units and those included in the final data
base. Table 6 presents the total number of patient observation sets on each unit
that were included in the final data base. A-South had the least number of patient
observation sets (86) while 6-West had the most patient observation sets (138)
included in the final data base. Tables 7 through 10 represent the number of
patient observation sets on each unit by categories and time periods. Patient
observation sets on 5–West and 6-West accounted for 59% of the total patient
observation sets for Category II and 60% of total patient observation sets for
Category III. Patients by age groups and sex are shown in Tables 11 and 12. Of the
229 patients observed, 189 (83%) were included in the final data base. A majority
of these patients (66%) were male and 89% were between 8 and 19 years old.
These patients represented 18 major psychiatric categories; 19% were found to
have major affective disorders and 20% had conduct disorders (see Table 13).
Profile of Data Collectors
A total of 112 staff, 42 shift coordinators and 8 observers participated in the
observational study, but the final data were drawn from ratings of 86 staff, 40 shift
coordinators and 8 observers. Table 14 presents the number of staff by
- 65 -

4.
*º * -
* - *
* * *1.
* - -
- -
• *
* *
- * --
w
. ( – c.
* - * … "
. . . . . .
- -
* * *
.
* . -
-
... t → * *
-- * ,
* - * * *
- * -
& .
. . . .
. .-
- * * ---
- - - - - -
- - - -
af
: * * *
- - - - - -

Table 5
Number of Patient Observation Sets Completed and Included in Final Data Base
Patient Observation Sets
Completed Included Percent
Category I 153 88 58
Category II 186 132 71
Category III 180 13t; 7t;
Category IV 16% —27. –22
N = 633 N = 451 66
Note. Percent represents the number of included sets divided by the number of
completed sets.
– 66 -


Table 6
Number of Patient Observation Sets Included in Final Data Base on Each Unit
Number Percent
Unit of Sets of N
A-West (A-W) 98 22.0
Child Psychiatry Unit
A-South (A-S) 86 19.0
Adolescent Psychiatry Unit
5-West (5–W) 129 28.5
Child Developmental Disabilities Unit
6-West (6–W) 138 30.2
Adolescent Developmental Disabilities Unit
N = 451 100.0
– 67 –

* , a . . . . . . . . . * -- - * * * * * * * ~ -
+
- -
- -- -
* . . . . -
- - - - -
-- - -
- - s -
- - - * ~ * * ‘. . . . .
- - * - -
- - - - *
- - - . . . - t . .-
- - - - - - - * - " - -
• * *
- - - - - *
-: - ■ : t - -- - * * * - 4. - - - - -
- - -
- * -

Table 7
Number of Patient Observation Sets Included in Final Data Base by Categories and
Time Periods for A-West (Child Psychiatry)
Time Periods
1 2 3 l;
Percent
(0700-1100) (1100–1500) (1500–1900) (1900–2300) of N
Category I 7 5 5 7 24.5
Category II 9 8 6 3 26. 5
Category III 6 8 l; 6 24.5
Category IV 6 7 6 5 24. 5
N = 98 100.0
- 68 -

* - - t ---
- * *
-
º
-
! -------- ºr 'i “ . . . . . . . . . . . . . . . . . ;
* - * -
* . --* . . - -
* * • . .
- - - - *
*. -
- - - * ** * * -

Table 3
Number of Patient Observation Sets Included in Final Data Base by Categories and
Time Periods for A–South (Adolescent Psychiatry)
Time Periods
l 2 3 l;
Percent
(0700-1100) (1100–1500) (1500–1900) (1900–2300) of N
Category I l; 6 3 2 17
Category II 5 7 6 10 33
Category III 5 9 7 9 35
Category IV 2 l 5 5 15
N = 86 100
– 69 –

* -- - -
- -
* * * * *- *-----
º ! f-
- - - - - - t * * *
- º - - - ... --
- -
*- * , .
-*-
º - - - - -* sº -
- - - -

Table 9
Number of Patient Observation Sets Included in Final Data Base by Categories and
Time Periods for 5–West (Child Developmental Disabilities)
Time Periods
l 2 3 l;
Percent
(0700-1100) (1100–1500) (1500–1900) (1900–2300) of N
Category I 5 6 6 5 17
Category II 7 10 10 12 30
Category III 8 9 11 10 30
Category IV 8 9 6 7 23
N = 129 100
- 70 -


Table 10
Number of Patient Observation Sets Included in Final Data Base by Categories and
Time Periods for 6–West (Adolescent Developmental Disabilities)
Time Periods
l 2 3 l;
Percent
(0700-1100) (1100–1500) (1500–1900) (1900–2300) of N
Category I 3 10 6 8 20
Category II 9 12 10 8 28
Category III 9 12 12 9 30
Category IV 9 7 6 8 22
N = 138 100
- 71 -

-- - - - - - - - - . . . . - - - * - - -, i < * : * * * - -
; : :------ ---------------------- - - -- -- - - - -
. . - - * . . . . * * * * * --- - - - - - - - --
, - * . . . . . . . . . . . . . . . --> * > * - * . .- - ------------------ - ----
- * *- - " -
-* * * * - -
* - -

Table 11
Number and Sex of Patients for All Categories on Each Unit
Percent
A-W A-S 5–W 6–W n of N
Male l;5 20 29 30 12! 66
Female 11 18 17 12 62 _34
Total 56 38 l;6 l;9 189 100
N = 189
– 72 –


Table 12
Number of Patients by Age Groups
Percent
Groups Ages In of N
l l; – 7 Years 21 11
2 8 - 1 1 Years 70 37
3 12 – 15 Years l;5 24
l; 16 – 19 Years 52 28
5 20 – 23 Years —k –4
N = 189 100
- 73 -


Table 13
Number of Patients by Psychiatric Category per Unit
Percent
Psychiatric Categories A-W A-S 5–W 6-W of N
Organic Mental Disorder l 3 1 3 l;
Schizophrenic Disorder 5 l; 1 8 10
Major Affective Disorder 10 8 2 15 19
Psychotic Disorder Not Elsewhere 1 3 1 l; 5
Classified
Pervasive Developmental Disorder 1 O 6 2 5
Somatoform Disorder l O O O 1
Anxiety Disorder 2 1 O O 2
Personality Disorder 2 2 2 2 l;
Eating Disorder 3 7 O 2 6
Stereotyped Movement Disorder O 0 O 1 1
Other Disorder of Physical Manifestation O 0 0 l 1
Anxiety Disorder of Childhood/Adolescence l; 0 8 l 6
Conduct Disorder 16 7 8 6 20
Other Disorder of Infancy and Childhood 2 0 0 O 1
Attention Deficit 8 3 3 1 7
Mental Retardation O O 12 2 7
Specific Developmental Disorder O 0 2 l l
N = 189
- 74 –

* .

Table 14
Number of Staff by Classification on Each Unit
Percent
Classification A-W A-S 5–W 6–W of N
Senior Nurses Aide 0 O 0 1 1
Nurse Interim Permittee O O 1 O 1
Clinical Nurse II 11 8 9 7 l;1
Clinical Nurse III 1 3 1 2 8
Clinical Nurse IV O l O O 1
Administrative Nurse I l l 2 1 6
Per Diem RN O l O 1 2
Float RN O O 1 O 1
Mental Health Practitioner l; 2 2 2 12
Senior Mental Health Practitioner 0 l l 1 3
Psychiatric Technician 3 3 2 3 13
Senior Psychiatric Technician O 1 l 2 5
Registry Psychiatric Technician 1 1 2 O 5
Float PT –4 —% —% —k —k
Total 21 22 22 21 100
86N –
- 75 -


classification who observed on each unit. Of these 86, Clinical Nurse II was the
largest group (41%) followed by Psychiatric Technician (13%) and Mental Health
Practitioner (12%). In the staff group, nurses completed 54% of the total patient
observations, psychiatric technicians completed 27% and mental health
practitioners completed 19% of the total patient observations. Table 15 presents
the number and classification of shift coordinators on each unit. Of these, Clinical
Nurse II was the largest group (55%), followed by Administrative Nurse I (28%).
However, 331 patient observations (73%) were completed by the Administrative
Nurse I group. A total of 31 data collectors participated in both staff and shift
coordinator groups. The educational preparation of all staff and shift coordinators
is shown in Table 16. Of these 85 staff and shift coordinators, l;9% had Bachelor
Degrees and 19% had Masters Degrees.
Results Related to Equivalence Reliability
The issue of reliability was addressed by using the equivalence approach.
Inter-rater agreements were computed for staff, shift coordinator and observer
groups with respect to ratings of: (1) observed patient behavior, (2) subsystem
categories and (3) system categories.
Patient Behaviors
Table 17 shows that the mean inter-rater agreements for the three paired
groups with respect to patient behavior ratings for each subsystem were all above
the 60% pre-established criterion for inter-rater reliability. Agreements were
- 76 -

- - - * * * * * * - - - - -
- - * ‘. . . • * * * - - - ; : \ . . . . . . . . . . . . . . . . . . .
- - - - - - - - º -1 * ~ * * - - * - - r• ‘ - - - -
, * * * ~ * *. - C. . . . . . * -
- - - - . . --
-• - * - . . . . . - . . . . . . . . . . . . . . . . . .
- s - -z • *-
. . . . . . . . . * * * * * -
- - - - -... " . . . . . 2 ºf * * * . . . . . . . . . . . . . . .
-
- t - - - - - - - -
- - º, . . . " * * - - º - * ! . . .
t - - * - -. . . . * - - *
- - - - - - r * - - * - - - - - - - º
- - - - - - - - - - e * - -- - ! . . - - - - - - - - - *
- - -
- - - - -- * * * * - - * * * * * * : a * * * -
- * * * - - - w. . . . . . . . . . . . . . *
- * - - - - - * * • . - - s - - - -
* * - - - * * * - - - - - - - * - - - - * - * . . . . . * *
- . - - - -, ... • " * - - - - - - - - - -
* - - - - - - º - - - - - * - - - -- -
- - - - * - * . . . . : * * *
- * * º - - * ~ * * * * * * * ~ * - - - - * - - i * - - - - -
- * * * * -- - * *-- - - * - - ? º -
* * : * * * : * : * ~ *
- - - - - - - - -
-- - , , , . " - : - - - - . . . .
- - - * - - - -
- - ... • - - - " . . . . . " - - -- - *
* * * . . . . ; - - - - ". . . . . . . . . . . . * , .*
- - - - - - - - - - - - - - - - - - - * * - - -- * \ . . . . . . * * * .* * : - * * *
- - - - *
. . . . . . . . . . . . . . . . . . . . .- - -
- . - - - " * - - - -- - - - ... - º -". . . . . . . . . . . . . . . - * * * - - - * * ! . . . . . . . . . . . .
- *-
; : - - * - - - * - - - - - - - - * - - * * * - - - -
* - - - - - - -. . . . . . . . . . . . - * * * - - - - - - - º - - -
* - -
* - . . . - - - - - - - - - * - . . . . . . "- - -
- - - - - - - * - * * - -- - - - - - - º . . . . . . . .- - -
- e.

Table 15
Number of Shift Coordinators by Classification on Each Unit
Percent
Classification A-W A-S 5–W 6–W of N
Clinical Nurse II 7 3 7 5 55
Clinical Nurse III 2 2 1 l 15
Administrative Nurse I 3 3 2 28
Administrative Nurse IV —% —% —% —k —é
Total 12 8 11 9 100
N = 40
- 77 –


Table 16
Educational Preparation of Staff and Shift Coordinators
Number Percent
Education of Staff of N
RN: Diploma in Nursing 7 8
RN: BA/BS 33 l;0
RN: MA/MS/MPH/MN 9 | 1
RN: AA 6 7
Undergraduate AA 1 1
PT: License 14 16
PT: BA/BS 1 l
PT: MA/MS 1 1
BA/BS 7 8
MA/MS —é –4
N = 85 100
Note. Staff who participated in the observational study on more than one unit
were counted once.
– 78 -

--- - - - - - - - ** • ** * - -, " * - - - * -- . . . . * *
2- : ; ; ; i■ ■ º. 334 of . . . . . . . . . i*i; ;
. -
. . .
- - * - --
º e
; ! - º
- * * * * * •- - - -
* *
- -
- - . . .-- - -
- - - * *
t
. . . . . . . . . . . . . . . . . . . . . . . " ; : . . . . . . .
º - - -
º , , . . . . . . . * * * *

Table 17
Mean Inter-Rater Agreement (%) for Three Paired Groups on Patient Behaviors for
Each Subsystem
Staff and Shift Staff and Shift Coordinator
Subsystem Coordinator Observer and Observer
Ingestive 82 79 80
Eliminative 84 80 81
Affiliative 73 67 68
Dependency 78 74 7t;
Sexual 84 83 84
Aggressive-Protective 81 79 82
Achievement 77 71 72
Restorative 81 76 77
- 79 -

- - - - - - - * - - - • * -ºf ºf T ºf tº ■ —- 3 f : .
. . . . . .
* * … . . * * f : . . . .
* -vº * -
s v . . . .
- * - - - - - -
- * * - \ . . . . .
- º-
. . . . .
- s º - -
- * - !,- -
º º - -* :
-
- ~ * - - * * > . . .
- -3 : … . • *- - * * ~ *
- - - " - - -
e * * * - - * *

within four percentage points of each other. Agreements were highest for the
staff and shift coordinator groups as compared to the remaining two comparison
paired groups. Agreements ranged from 73% on affiliative behaviors to 84% on
eliminative and sexual behaviors. Table 18 shows that the observer group noted
significantly more adaptive behaviors and significantly fewer severely maladaptive
behaviors than either of the two groups.
Subsystems Categories
A comparison of inter-rater agreements on subsystems (all categories) for the
three paired groups was consistently highest for staff and shift coordinator groups
as compared to the two remaining comparison paired groups (see Table 19).
Agreements on eliminative subsystem were consistently highest (66% - 68%) while
agreements on aggressive-protective subsystem were the lowest for all three
paired groups (37% - 57%). Agreements for staff and shift coordinator groups were
above the 60% pre-established criterion for inter-rater reliability on most
subsystems with the exception of sexual and aggressive-protective subsystems. A
breakdown of inter-rater agreements for subsystems by categories showed that
Category I ratings were consistently highest on all eight subsystems. Agreements
ranged from 59% for affiliative subsystem to 94% for eliminative subsystem
between staff and observer groups and 77% for affiliative subsystem to 96% for
ingestive subsystem between shift coordinator and observer groups (see Tables 20
and 21).
- 80 -

…
•■-|-·~!|-|-|-~!
•*••·-•.*
*
-§|·|-|-•-····→·
·*…~----------»ae
…
*----.*----·*•-••,
!·|-|-·--
-*…*|-•;----
•
•|---------|-■!----
|-··|-•|---------
-·*·|-•
•
•·~••·----
•••
+
·→·
•|-|-·
*-----…
*----·*•
•-,--
…·|-*…*·|-
----·*
--
-|-*-,
*|------
'
+■--------|-|-■-
···••
••
•·--
--------*
*--------
·
**-|-*|-
··•→
|-••→
·----|-*·,'
--------~~·|-r---------·

Table 18
Percentage (%) of Patient Behaviors Observed (N = 437 Possible Responses)
Severely
Adaptive Maladaptive Maladaptive
Observer lili 22 16
Shift Coordinator 31 20 26
Staff 24 21 26
- 81 -

º : ‘.
* -
. . . . . . . .",*
—-----' ------
- - - -
- - - * * -
- a º - I -
* - -
* * ~ *

Table 19
Inter-Rater Agreement (%) on Subsystems for Three Paired Groups
Staff and Shift Staff and Shift Coordinator
Subsystem Coordinator Observer and Observer
Ingestive 64 53 5l.
Eliminative 68 66 66
Affiliative 61 lili l; 5
Dependency 60 t! 3 l;0
Sexual 57 51 52
Aggressive-Protective 57 l;0 37
Achievement 64 t;5 l;6
Restorative 61 52 58
- 82 -

Q ', 1.
- * t - r - - º ... • - - e* * * * . . * * * : * ( ; ; ; ; • *.*, * is 3 --, * g :- - - *– --
- - - * ‘. . .• * º J J 1 ( , , .
- - - -
w * * * - I - - - - : 3 . . .
* - - -
: \ , , : .--
- - -
º ‘. . . . . . . .
** - - • * *- - - s * . . . .
* , * * . . º
- - - - - - - - *
* - e - -!
- - - , - * - - ... --> -
º . . . -: , , ,-
, -
"a -† : - . . . . . . .
- * * -: , , , , it -

Table 20
Inter-Rater Agreement (%). Between Staff and Observer Groups on Subsystems by
Category
Category Category Category Category
Subsystem I II III IV
Ingestive 90 17 l;3 3
Eliminative 9t; 15 25 0
Affiliative 59 51 l;0 13
Dependency 75 l;8 27 7
Sexual 92 12 15 O
Aggressive-Protective 78 33 21; 5
Achievement 78 l;2 35 0
Restorative 84 31 28 8
– 83 –

* : . . . 2, … - - , , . . . . . . . . . . . . . . . . . . . . . . . . .2-, ºf --, 3, .- -------- - --- --------- * - - - - - --------------------------- ----------- - - - ----------------- ---------
- - - * * * -
* * * ~ * -
- - º - * - -* - * -
- - - - " - - i- * - * * *
- - - -* \ . . . .
- -
*- - - - º
* º -
- - - * s, a
- - - * * ~" . . " -* - . . . . . . - \ . . . . . .
- - - a : ". . . . . .
* - ** * - " - - * * * *- * - - - - - - - - *

Table 21
Inter-Rater Agreement (%) Between Shift Coordinators and Observer Groups on
Subsystems by Categories
Category Category Category Category
Subsystem I II III IV
Ingestive 96 23 36 2
Eliminative 93 15 20 O
Affiliative 77 5l; 38 12
Dependency 81 l;6 24 8
Sexual 95 10 20 0
Aggressive-Protective 86 37 23 7
Achievement 85 l;3 35 6
Restorative 88 33 30 10
– 84 -

-- - - - - * *! . . . . ; ; ; ; ; , , , ; ; ; ; ; ; ; ; ; . . . . .” -- * : *- - - - - - - - - - - - - - - - - - - - - - - - - --------------------
:- -* * - -2 * : * * * * -
-------------- - - - - - ----------- - ------- -
* * - e - * *-
* ... v - - * *
* , *
- -
- - e. - . *- - * . . . . . .
* - - + -
* - - ‘. ** * * -
º -• * , • , - -
.* -
- - º -
•. * * - *. - - -
* * -- - - - - -
º * - - * * * - * - - - * * * * * *
- t - * * . . . .
- -- - - - -*
- - - º * - - * - ºr

System Categories
A comparison of the inter-rater agreements on system categories for the
three paired groups was highest for the staff and shift coordinator groups as
compared to the two remaining comparison paired groups. Agreements (67%) for
staff and shift coordinator groups met the 60% pre-established criterion for inter
rater reliability. Agreements for the remaining paired groups were 51% for staff
and observer groups and 52% for shift coordinator and observer groups.
Agreements for the latter two paired groups did not meet the 60% criterion. A
breakdown of inter-rater agreements for system by categories also showed that
Category I ratings were consistently higher than ratings for Categories II, III and
IV. Agreements between staff and observer groups for Category I ratings were
83% and 89% between shift coordinator and observer groups. Agreements for
Category II – IV ranged from 38% to 48% for the two paired groups.
Results Related to Criterion-Related Walidity
The issue of validity was addressed by determining the relationship between
the predictor measures and the criterion measure. In this study, the following
relationships were determined: (1) patient behaviors as predictor measures and
subsystems categories as criterion measures and (2) subsystems categories as
predictor measures and system category as the criterion measure. Ratings by the
shift coordinators were used as predictors while ratings by observers were used as
the criterion.
- 85 -

-
- -
*
4 -
--
- -
* - *
* - -
* *
. . . .- * *
-
*
-
* *~ *
*.
**.
* * *
t :
* - - -
e-
- -
* -
-, * * *
* *
* ,
º
--
* *
-
• -- -
. .
■ . "
* * *
**e
.
■ st
-
-
* ~ *
- - -
* -- -
* *
". . . . . . v c : , , ; ; ; ;
". . . . . . . " -■ ( ; , , , ;", " ( ; ; , ; ; ; , T 2: ; ; z < .
s - - : . -- … - - - -- " ' -. . . . . . . " tº a º' . . . . v.
- - - - - , , , * - - . . - - - - - - -
. . . . . . . . . . - - - - - : it , , j ■ - ‘
- - - - - . . . - • . * * * * -
(, . . . . . . . . . c. . . . . . . .
- - - * - - - - * - a - - - - -
- i. . . . . . . . * - - * -- i t . . . . . . . . .
-a - * - - ** - - -
* - - * . * - - - . * - º
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ;
- -
- - -
, - - - - -
- * * - * -- -- -
. . . . . . . . .
. . ."* - - * * * * -
. . . . .-
-
* . . . . . . . . .- * ~ * -
- - - - --- " . . ;
. . . . . . . . .
- -
* f * - t
j . . . . º
* - -
a * *
-
* * *
1: .
•
* - *- * -
-- -
* * * :* - . .
- *- - -
- - .- * - *
- *
-,
* , . I
-

As stated in Chapter III, a correlation matrix was generated to examine for
redundancy and multicollinearity of the independent variables. It was found that
all of the bivariate correlations of independent variables had a correlation
coefficient below .80 which was acceptable for this study. Summary statistics are
given for the independent variables in the regression in Appendix D. The standard
deviation ranged from .30 to 1.40 among the independent variables. Note that the
coefficient of variation, which measures the standard deviation as a percentage of
the mean, was moderately large for all variables (greater than 62%). Thus, there
was sufficient variation in each independent variable to apply standard regression
techniques.
Impact of Patient Behaviors on Subsystems Categories
The computed R2 values and significant levels of patient behaviors as
predictors of subsystems category ratings are shown in Table 22. The computed R2
values and significant levels of patient behaviors as predictors for each subsystem
are shown in Tables 23 through 30. These values are for the full equations, and
therefore include all possible independent variables. Reduced equations were made
which consisted of those patient behaviors with an F ratio significant at p < .05 and
a beta weight significantly different from zero at p < .05. Results for the reduced
equations of patient behaviors as predictors for each subsystem category ratings
are illustrated in Figure 2. Table 31 presents a comparison of the computed R2
values for the full and reduced equations. There were no significant differences
(range of one to three percentage points) noted in the R2 values computed for
either of these two equations. The R2 values for all subsystems categories ratings
were below the accepted criteria of .50, suggesting a substantial proportion of
- 86 -

·------·■■ ·|---,·→■■ -·→·
-…|--|-----*|--■ -■ -*----·---|-----|-·-|------|-|-••|-·••----■ ··
|-|-----·----|-·|-----|-|-----■4··----·-----------|-
|-|-|-·*,***|---
·|-···--
|-·|-…--|-·|-|-·----·*|-·-*-··
----|×---------
-·|-·|-*-----|--*
,|-·■
1*|-·*…→••--
-----~----·|-~~-----';·••-----···|-*■
*----*••|-■-·~~•■ |-----→
·|-·--→·-----|-****--
--
…-|-|-----|--
→|-
·|-••-------|-*…|---------•→
-
-|-··-*…|-•·-------------
------··*••••*|-----*■ |-----·
·→·■"-|-
-
-·|-,--|-----|-
•
|-----|-*……----*-----…*-·|---*|---|--•■
}|-+*·|-------+*|-
|--
-------------|*•|--|-|-|-----|-→·|--|-→·---------·-·--
|-*--|--|---|-|-|---·---------->-|-----*
*----|-|-·-
-·|-------------·|-·----■
--|--
---------•×---
|-|-----••,■ ·------|------•••"
…·■ ·.»*…*··--|-----|-■ ·*
---------|-|-■·|-----ae|-·-|---------→·--·-|-*----·-----
****•
•----·----|-|-→
·----··.--------|-·
----|-*----|-|-|-|--•
■ ·•••••…--º|--…
*"
--|-.*|-■ ·•→----|---|-*----------*--|-|-----·|-·----|-••,
-•.·■ ••.
.*■ |-■ ·|--|·· -
-·|-----i····|-|-|-|-------*,■■
|-*…*·-**--*→·|-|------
----|-•
→|-----··-----•×|-|-----|-----
|-|-~----------****----·|--|-|-|-·…··*,-|-
|-*-----------|-
-|-------··…•■ ·••··* ----
|-|---
*|-|-|-*|-•.|-----*•
·•·*----|-
--------|-|-+|---**
--------••----|--*:*|-
••
|-|-•|-|-----|-----|--■ |-----|-·
|-|-•-
-„**|-----|-----•
•----|-|-------|-----
*•*•~!|-·
·----|-*-"·
-
-→·----|-·-
-----|-----•••*-|-|-----•
•|-----·--------|----·--------•----··*·••
--------|-|-|---------■ ··|---------••----|-·----|-|-|--→·:--------------■!|-·|-|-«
…→·
|--·|-----|-*|-|-·|-·|---**■ ~,|-|-----·*…*■ ·|-|-|-
|-|-|---»----
-·|-••|-
:|-*·-*------|-----
·|-·|-|-------*…••------ -
---------·-|-|-~---
-|-|-----·|--
-|-·--------|--→·
·
|-·|---|-------·
·-|--*-|---*··*|-|-|---|-
----
--|----*·-----|-|--■■ --•|-··----------|---|-|-*…··|-|-|-■ ••
|--*|---·*----
-----|---------·*
•----*|-|-|--·…•|--*■ |-·
-
----|--|-|-·----|--■ ·**|-----·|-|-|--|-|-,■ ·|-|-
-·----|-·-*--|·--,
-a-•|-|--*…|--■-!\■ ·|-·
■ --------···--------|------|-J'
,|-------|-----→------|-*■ →·→·----
-~*|-|-·----·----|----*-----

Table 22
Patient Behaviors as Predictors of Subsystem Category (Full Equation)
Number of
Subsystem Variables in
Category Equations R2
Ingestive 11 . 33
Eliminative 5 .21
Affiliative 7 . 27
Dependency 9 .24
Sexual 6 .08
Aggressive-Protective 7 .23
Achievement 10 . 36
Restorative 6 . 32
Note. All values significant at p < .0001.
– 87 -

** . . . . . . . . . . . . . . . . "------------ - 1: * -------- ; ºf . , , f'. . . . . . . * * *
º º * * * º
- - , ,- - - - * -
- -: - - - , *
- * . . . . -
- * →-
* - - * * º * *
-. . . . . . .
- * * * * * * * * *
- . . . .
* , -
- - * * *
- - *. . .” -- . . . . . . .
* * * - . . . .- * . . . ! --
- - ... v . . . . . . . . .
- * - * -- " - - t -. . . . . " . i■ . . . . . . . . • ‘- * -------

Table 23
Patient Behaviors as Predictors of Ingestive Subsystem Category
(Full Equation, R2 = .33)
Patient Behaviors in Equations
By Entry Order Beta
Interpretation of Events . 1 3 +
Awareness of Social/Physical Environment . 13+
Distinguishing of Events - 12 +
Awareness of Social/Physical Boundaries .08
Food Choices .09
Sensory Perception . 16
Ingestion of Food/Fluids at Intervals .0l;
Ingestion of Substances .05
Sufficiency of Intake .03
Eating and Drinking Skills .02
Frequency of Intake .01
*Values significant at p < .05.
- 88 -

•***,'!
--------«-----
*
,••
*****·
■
1*…*<■ --·------
…-------------•~----**…|-**…··*·--
•
^••·-|-----|-■±·----·|-•
•|-■ ·|-·*|--……--
*…*■ •·----|-→··|-----·;--*…----!-·•·…------••---------·*----•■ →·*|-*
■ æ
æ----|------|-→·-------
|-|-v·
■ i
■ ·--------,-·•*----*·--------~~
ae**-*•!■
3*----|-*…■•-→-----£€----*----|-----••';|-****--------···
*·…----•...
•!±-.*---
-
-|-.--·*·
···
·----*-|-|-·~~
!*…*|-|-**.·
*
•→------r■
…
····*•-----"|-|-|------ae•■ --------~·----*•----■-****|-·|-|-|-·|-·----|-■!·*~]•|-|---|-|-•••------·|-----→----·--.-----••·|-
-
----|--*----→·•
*
•|-•·ae■
----------|-·|-•|-
…
****----···
·••----.*|-–
!•"----·----■ v•}-|------
-→··*,
----••----·*
,-------•■
!*|-|-----•*.-■
■ *-|-·;-*-
**-------·----·*
·*|-|-|-----
|-·•
*|-··|-----
·*!|*|*
------------*-·•·•···--------••~
~^<■ ------…º···|-·
*|+·

Table 24
Patient Behaviors as Predictors of Eliminative Subsystem Category
(Full Equation, R2 = .21)
Patient Behaviors in Equations
By Entry Order Beta
Bladder Control .25 +
Hygiene Care . 12 +
Disposal of Body Wastes ... 10 +
Bowel Control - . 14 *
Pattern of Elimination -.08
*Values significant at p < .05.
- 89 -

- • * * * * -
- -
- - I - - - -
- * -
- - -
- - - - - - - - * -
- * - - *- - * - - - * -
- - - - -
- * - - - - - - - * - - -
- --- " " " - - . - -
. - - i * -- a - -- - - - - - -

Table 25
Patient Behaviors as Predictors of Affiliative Subsystem Category
(Full Equation, R2 = .27)
Patient Behaviors in Equations
By Entry Order Beta
Communication of Ideas: Verbally, .23 +
Nonverbally and in Writing
Awareness of Personal Space .09 +
Emotional Attachments .08 +
Interpersonal Relationships with Groups .05
Interpersonal Relationships with Individuals .05
Expression of Feelings -.04
Adaptation to Change .01
*Values significant at p < .05.
– 90 -

*-i-º-º-º-º-º-º-º-º-º-º-º-º:
- - -. . . . . . . . . . . . . . . . - - - -
* * -
*. *-
s . . " - * *
º• * , : : J . . . . . . . . . . . ■ . ■ r.
- - - - ? -
. . . . . . • *- … • -
. . . . . . . . . . . . . . . . . . . .
* - - s -
º - fºr . . . . . . .
- - • * * - -- -
-. . . . . . . . . . . . . . . . . . . . .
- - - * * - * - - - -
* - * * I 1 º. . . … I
- • -- " - - ---
* * * ( , ; ; ; , .* - *
. . . . . . . . . . . . . .

Table 26
Patient Behaviors as Predictors of Dependency Subsystem Category
(Full Equation, R2 = .24)
Patient Behaviors in Equations
By Entry Order Beta
Self-Care Activities . 1 l; +
Decision-Making Ability . 1 1 +
Seeking of Assistance .09%
Separation with Ease . 07
Engages in Situational Attention-Seeking .0l;
Behaviors
Care of Personal Belongings .06
Relies on Own Resources .0l;
Feelings of Hopelessness and Helplessness .0l;
Questions Decision of Authority .01
*Values significant at p < .05.
– 91 -

. . . -* - -
- - * - - *
-* --
- - - * * * * , -
- * - * * * - -
* - * * - * * * --- -
-. . . - -
- * - - - . . * * *
- - * - - -- -* - - - * * ( . . . . ."
-
- * → ... -- -
* * * - * --. - a . . - ** - -
- - -
- ? i - - * *- . . ( * - -
.* -- - * - * ** ~ * * * - * * *
- t - -- - º - -
* - - - - * * t * - - -
- - . . . . . . . . . . . * *

Table 27
Patient Behaviors as Predictors of Sexual Subsystem Category
(Full Equation, R2 = .08)
Patient Behaviors in Equations
By Entry Order Beta
Distinguishes Between Sexual/Nonsexual . 12 +
Approach Behaviors
Engages in Socially Acceptable Behaviors .06 +
Acceptance of Gender Role . 07
Comfort with Body/Physical Changes .03
Distinguishes Between Males and Females -.03
Knowledge of Own Anatomy and Physiology .01
*Values significant at p < .05.
- 92 -

* . . . . . . . ; 2: . . . . . . . . . . . . . . c : . . . . . . . . . . . . . . . . . . . . . . ."------------------------- --- ----- - ----------- -----
- * - --
- - * * * * * * * = . *
- - -** ----- * . . º
- - - ** * * - - - * * - – f : . .
- - -*
- * * * - - * * - " - -
- * . . . “- I , * . - * * * * • * * -
* * * - -
- - - - - . . .
- - - - - - - • . -
-. . . . . . . . . . . . . . . . . c. * - * - *
º - - - -- -
-* ' ', r. º. . . . . . . .
- - * * - •. - -
- * - - - t . . . .- -
■ . . . . . . . .
t a - * . - - •, : . .- ** a * - - * . . . . . * * * : * ~. . . . ■ - 2
'' ... v.- - - º - . . . " , -
- . . . . . . . . - * ■ ( - . . - - - -
* - - - - - - - ---- * ~ * * : * * *
- * -

Table 28
Patient Behaviors as Predictors of Aggressive-Protective Subsystem Category
(Full Equation, R2 = .23)
Patient Behaviors in Equations
By Entry Order Beta
Identifies/Avoids Hazardous Situations ... 10 +
Engages in Acting Out Behaviors ... 10 +
Separation from Group ... 10 +
Ability to Maintain Control Over Stress .06
Selects Response to Threat/Dangerous .06Situations
Phobic Behavior -.05
Response to Threat with Self-Injury .02
*Values significant at p < .05.
– 93 -

. . . . . . . . .
- * - ■ - * * * * º - --
* , - - -
- - * -
-- - - - - - w - - - -
- - - ... ( . - • * * * * * • - -
- - - * * - - - - - . .
- - -- . * * - - * - -- - * * º s - - -
-- - - - - 4 - > * * * *
* * - - . . . * - - -
- ** * * * - - - - º -
- - * - , , " ; -; : . . . .
-
* - *
- - . " - - -* * * * * * * - * *
: - - -, - * * * -- º- - - - - * * * -
- - * . . . * : * I - - - - - * , . . . . . . . .* * s
- - - - - - ... t . .”- - - - . . . * * * * * - -
--- -

Table 29
Patient Behaviors as Predictors of Achievement Subsystem Category
(Full Equation, R2 = .36)
Patient Behaviors in Equations
By Entry Order Beta
Attention Span . 1 l; +
Initiates and Completes Tasks ... 10 +
Selects Goals from Alternatives .08 +
Utilizes Cognitive Abilities .09%
Experiences Successes and Failures - .08 +
Organizes Groups -.20
Identifies, Accepts Strengths and Weaknesses .0l;
Chooses Alternatives -.03
Utilizes Problem-Solving Skills .01
Accepts Direction -.01
*Values significant at p < .05.
– 94 –

* - ? .( . . . . .
- - - *, ** - - --> *‘. . . . . . ; tº j : " : , "t 3 ■ : ; * * * 3 ■ : i:--------- -- - - ----------- -
* *
*.*
- [ _ " - " - . . . . . . . . .
- - - -
.* . . - *- - -
. . . . . . . .
. . * - * . . . . .
- - . . . . . . . * * 1 * * - . .
: . . . . . . . . ‘. . . . . . * . . . . . .
- * - - -* - - -
- - - * - - - ! . . . . . . . . . . . . . . . . . . . .
* - * * . . . . . . . . . . .
- * " . - - - * . ... • - - -
* * * . . . . . . . . . . . . . . . . . . . of , ºf º
- - • . - - * *- ** - . . . . . . . . . . C
- -* 1: ... " . . . . . . . . . . . . . . . . .
! -- f : . . • J
* . • * : - -
- f : . . . . . . . . . . . . .- * º

Table 30
Patient Behaviors as Predictors of Restorative Subsystem Category
(Full Equation, R2 = .32)
Patient Behaviors in Equations
By Entry Order Beta
Engages in Recreational Activities .17%
Participates in Organized Social Group -. 36 +
Sleep Patterns . 12%
Involvement in Range of Activities ... 10 +
Participates in Treatment Regime .09%
Regulates Activities According to Physical .03
Requirements
*Values significant at p < .05.
– 95 -

:
-|*·••••·–''
s:* * *
|
·----·
|-.ae
·----
·
--------
*
----·
-----

Figure 2
Patient Behaviors as Predictors of Subsystem Category (Reduced Equation)
Independent Variables/Patient Variables (Standardized Betas)
Interpretation of Events (.31)Awareness of Social/Physical Environment (.21)
Distinguishing Events (.18)
Bladder Control (.34)
Disposal of Body Wastes (.18)Bowel Control (-.18)
Hygiene Care (.15)
Communication Ideas: Verbally, Nonverbally
and in Writing (.36)Awareness of Personal Space (.18)Emotional Attachments (. 13)
Self-Care Activities (.24)
Decision-Making Ability (.21)Seeks Assistance (.19)
R2 = .30Ingestive
R2 = .21Eliminative
R2 = .26Affiliative
R2 = .22Dependency
– 96 -

7
-******----...............
º
y**--*-
******-*******-----.....;...**....º
**-**--f:****** -----....■ .32(,!----
--
*-----*~*~*-,***** !...............t-***
--*-------------
..........22y---.....
*------------
•**********-----
----.---
º-*-I-r→*>-r*r*****~* ............2:,D'........|
----
**>...-ººjº,....
----*-
**********-ar**;;;;;, -...r.º.-**--
-***------------
----------** ...................-,
--****,,,-.... -:*----**:*~*
------
**************--*...*--
-----***-
-----------
..;,...;...........---
-....-i----
....!............
-----------------------------
--.....;***-,--,-s•*,
--------***--º
-------------------------------------------------------------->-----------→----- •*:*~*>r*--..------------------------•...f.\!2".22..........2....................................

Figure 2 (continued)
Patient Behaviors as Predictors of Subsystem Category (Reduced Equation)
Independent Variables/Patient Variables (Standardized Betas)
Engages in Socially Acceptable Behaviors (. 13)
Distinguishes Between Sexual and Nonsexual > R2 = .07Behaviors (.20) Sexual
Identifies/Avoids Hazardous Situations (.22) R? = .21
Engages in Acting Out Behaviors (.25) > AggressiveSeparates from Group (.18) Protective
Attention Span (.29)Selects Goals from Alternatives (.17)
Experiences Successes and Failures (-.13) > R2 = .35Initiates and Completes Tasks (.18) Achievement
Utilizes Cognitive Abilities (.15)
Engages in Recreational Activities (.26)Participates in Organized Social Group (.24)
Sleep Patterns (.16) N- R2 = .32Participates in Treatment Regime (.11) 27 Restorative
Involvement in Range of Activities (.14)
- 97 -


Table 31
Comparison of Full and Reduced Equations of Patient Behaviors as Predictors of
Subsystem Category
Full Equation Reduced Equation
Subsystem Category R2 R2
Ingestive . 33 . 30
Eliminative .21 .21
Affiliative . 27 .26
Dependency .24 .22
Sexual .08 . 07
Aggressive-Protective .23 .21
Achievement . 36 . 35
Restorative . 32 . 32
– 98 -

* c 1 { . . . . . . .------- - ----------------
* - - - - -* * -
* * * . -
- - - - - - - -
- -- - *
*- - - - - * -
* -- - - * * * * * *
- - - " . . . . . .- -
- - - -
- - - -
- - : . . . . . . -- " . . . . .
- - - * * * * -
* * * * - \ . .-
* * * - . . . .- - - * * * - - -

unexplained variance for each subsystem category. Table 32 presents the results of
the significance tests to see if a full equation predicts significantly better than the
reduced equation. Results of these significance tests show that full equations do
not give significantly better prediction than the reduced equation. Therefore, the
more parsimonious reduced equations were substantially as effective as the full
equations.
Impact of Subsystems Categories on System Category
The computed R? values and significant levels of subsystems categories on
system category are shown in Table 33. These values are for the full equation and
therefore include all possible independent variables/subsystems categories in the
equation. A reduced equation was made which consisted of those subsystems
categories with an F ratio significant at p < .05 and a beta weight significantly
different from zero at p3.05. Results of the reduced equation for subsystems
categories are illustrated in Figure 3. Only three variables were significant in
influencing the system category and accounted for 51% of the variance. The
variables were: ingestive subsystem category, B = .28, p = .0001; restorative
subsystem category, B = .26, p = .0001 and achievement subsystem category,
B = .28, p = .0001. There was a slight decrease in the R2 values computed for the
reduced equation (.51) over the full equation (.52). Both of these R2 values met the
accepted criteria of 50% explained variance for the system category. Results of
significance tests show that the full equation does not give significantly better
prediction that the reduced equation. Again, the more parsimonious reduced
equation was substantially as effective as the full equation.
- 99 -


Table 32
Significance Tests on Full and Reduced Equations of Patient Behaviors as
Predictors of Subsystem Category
Differences
Subsystem in Number of
Category Variables F Ratio F Critical p Value
Ingestive 8 1.70 1.9l; 0.10
Eliminative 1 2.60 3.84 0.11
Affiliative l; 1.78 2. 37 0.13
Dependency 6 2.01 2. 10 0.06
Sexual l; 1.23 2. 37 0.30
Aggressive-Protective 3 2. 37 2.60 0.07
Achievement 5 1. 14 2.21 0.34
Restorative l . 57 3. 83 0. l;5
- 100 –


Table 33
Subsystems Categories as Predictors of System Category (Full Equation, R2 = .52)
Subsystems in Equation
By Entry Order Beta
Restorative . 2822 +
Ingestive . 2641 +
Achievement . 1953 +
Dependency . 1259
Sexual -.065!
Eliminative . Ol' 55
Aggressive-Protective .0239
Affiliative . 0133
* Values significant at p < .05.
- 101 -

* - º ~ : -1, ... " -- - - - - - -, * Z.” * - . . . -** - - - - * . - - -— — & lººk tº ºf fººl ºf ■ º, ■ º tº ºr
. . . . . * L.
*.
- - -: \ . . . . . . . . .
. . . . - . . . .
- * - ‘. . . . . . . .
. f : . .
- º
* * * * ‘
- * ~ * * . . . .
* - - : . . . - . . . . .
r- - º
- * * * \ . . .-
• * * ~ *- : - . . . . . . . -*

Figure 3
Subsystems Categories as Predictors of System Category (Reduced Equation)
Independent Variables/Subsystems (Standardized Betas)
Ingestive Subsystem Category.28
Restorative Subsystem Category .26 R2 = .51
28 System Category
Achievement Subsystem Category
- 102 -


Examination of Residuals for Violations of Regression Assumptions
Zero Mean. Examination of residuals from the reduced equation for all
patient behaviors and subsystems indicated, as expected, that when a constant
term is included in the equation the residual sets all have a mean equal to zero.
Homoscedasticity. Examination of plots for all standardized residuals against
predicted subsystem and system values indicated that variance was equal in all
regressions. Figure 4 provides an example of a plot for standardized residuals
against the predicted values of self-care activities in the dependency subsystem.
The broad band which the horizontal line cuts in half provides evidence for equal
variance (homoscedasticity).
Normal Distribution. The results of Chi-square goodness of fit tests for
distribution of residuals for patient behaviors and subsystems' regressions are
shown in Table 34. All residuals from the reduced equations of patient behaviors
and subsystems were not normally distributed. All observed Chi-square values
exceeded x2 critical (2, N = 331) = 5.99, p.<.05. However, violation of the
normality assumption was minor since F ratios are fairly robust to nonnormality
when there is no evidence of heteroscedasticity (Verran and Ferketich, 1984).
Histograms depicting categorized standardized residuals in groups according to
their distance from the mean are illustrated in Figure 5 for sexual subsystem (X2-
203.52) and Figure 6 for aggressive-protective subsystem (X2 = 9.97). The
histogram for the sexual subsystem appears to be the most nonnormal. However, it
is still unimodal, meeting the essential assumption for regression analysis (Neter,
Wasserman and Whitmore, 1982).
Independence. Residuals from the reduced equations for all patient behaviors
and subsystems were examined. Results from the plots indicated that there was no
- 103 -

f r
t -
º
*
t *
* -
- * .
- - - * -
- - - _º - a -
- - * .-- - - -
* . . . º ( -
-
- * - - * -s - -
- - - - - -
- - . . . -
º - - * - * * *- - * → - - -
- - -
- - * -
- • * * - - - -
- * - - - - * -- - - - - - - * *
. . . . * * * e
º - * * * * - - - - - - - -
* -
- º - - - - - -
- e. º - - e
* * - - - - * - - - -
- - • * * - - -
º º - * * * * - - -
- * : ... - - .* . . . . . . - * . . .
* . . . " +
-
- -
!
-
*
º
- *- º
* * *
* -
t
* -
- *
-
-
-
-
* -
*
-
* *
-
t - -
- - - -
- - - º
- - - - -
- º * * **-
- - - - .* * * * –
- - - * * * --
- - . . -". a - -
- - -. . . .
-* , * * *- . . . . . . . . . .
- - - -- º --
- - -
- - - - ** > * ~ * * =
- - - - -~ *
. . . . .
- - - *- * : * * : ■ .- --- - ---------
- * * * * *
-- - - - * - . .

Figure 4
iestiviPlot of Standardized Residuals Against Self-Care Act
•…u---+-----«
------••••vº■ -■z<b■c)-~uuuo
-------••…
----oocoquaeuw--
-■■■
>■■…oco-
■ ------>o
•v••r-•••roo
--·-o--~
·|-dxuuqo--©><-uvo
--------
3.4o
A C T I W i t i E SC A R ES E L F
2, etc.BNOTE: A=1;
- 104 –

; : -; it-
, , " * - -, - . . . - - . . . . . * : * : *

Table 3!,
Results of Chi-Squared Goodness of Fit Tests for Distribution of Residuals from
Patient Behaviors and Subsystems Regressions
Residuals X2 Observed
Subsystem Categories
Sexual 203. 52
Eliminative 127. 85
Dependency l;9. l;2
Restorative 33. 22
Ingestive 19.79
Affiliative 1 l; .. 32
Achievement 1 li. 11
Aggressive-Protective 9.97
System Category 16.80
X? critical (2, N = 331) = 5.99, p < .05.
- 105 -

; C-2 * *
* - - - - - - - - `- a r < … . . . . . . . . . .- * - . . . . . ; ; ; ; ; *ç i \ . . . . . . .- - - - -------
** I - -
, : . . . . . . . .
* - -
- - -
- - i , , , ,
• * . . . . .
- * -
- - * - - *
- . . . . . . .*-
º : . . . . . . . * *- - - * = * * * -
* * , , • ,- - - - - - - -
. : , , ; ; ; ; ; – " . . . . .
** *, * - . . . .-
- e - - - - - .*
- r = - - * * * * * * ** * - - . . . . . . . .
- - - t - – ‘ ---

Figure 5
Histogram of Standardized Residuals for Sexual Subsystem
FREQUENCY
240 +
||t4.2 to
180 +
12o +
3o
Residuals - Sexual Subsystem
x? = 203.52
- 106 -

:

Figure 6
Histogram of Standardized Residuals for Aggressive-Protective Subsystem
FREQUENCY
too +
Residuals - Aggressive-Protective Subsystem
- 107 -


evidence that the assumption of independence had been violated. All plots showed
an equal spread of residuals about the zero line.
Results Related to Generalization
The results of model consistency across inpatient units, sex and age groups
are shown in Table 35. If the NPH-PCI was generalizable, residuals from patient
behaviors and subsystem categories should be evenly distributed across age, sex and
inpatient units (p X.05).
Across Inpatient Units
Using the Chi-square goodness of fit statistical test, it was found that the
model of NPH-PCI tended to underestimate the maladaptive behaviors in the
ingestive subsystem (p = .03) for the child psychiatry inpatient unit (A-West), and
underestimate the maladaptive behaviors in the eliminative subsystem (p = .001)
for the adolescent developmental disabilities inpatient unit (6-West). It was also
found that the model tended to underestimate the maladaptive behaviors in the
sexual subsystem (p = .03) for all inpatient units, although this was less so for the
adolescent psychiatry unit (A-South). Note that the R2 value for the sexual
subsystem (.07) was exceptionally low (Figure 2). There was no evidence of
differences in model predictive ability among the four units for affiliative,
dependency, aggressive-protective, achievement or restorative subsystems
categories or for the system category.
- 108 -

º
tt
*
‘. . . -- * -
- - - º * - - ºI C - * * * * ~ * . . . . . . .
- * - - - * - - - - - -
- t º * - . .-
- **2 * .
... • - - * -
- º - = r - -
" . - • * * * * * * * * * *
t - - - - - . . .
• - * - * * - * *-*. -
º
-* * * - - -
- - -
--- - - I - , ,
* - - - - -* I - . . . . - - *
- * - - * *• . . .
- . . * * - •
- * , - . -. . . . - - - - - - - - - - * -
* . . - - - - - - - -- - * - - - - - * * * - - - -
* . - * --
- * * * * - - - - - - * -
- - -. * * * * º - -
* * * - - * = - - - - - - *--- -
• . . . .- - - - * . . * -
… " - - . . . .-
* * - - - - - - - - - -* -- , * = * * * * * - - - - -
* . . . . . . - * -- - - - -
* - . . "- -
- - - - * - • * ~ * - *
* - - - - - - - - .

Table 35
Tests on Model Consistency Across Units, Sex and Age Groups
Unit Sex Age
p Value p Value p Value
Subsystems Categories
Ingestive .03 .84 ... l;7
Eliminative .0001 . 39 .03
Affiliative .06 .21 . 16
Dependency .9l; .08 . 11
Sexual .03 . 07 . 50
Aggressive-Protective .08 .01 .04
Achievement ... 10 .03 .08
Restorative .26 .01 .25
System Category ... l;3 ..!!! . 12
Note. X2 test performed for lack of fit on the assumption that the frequency of
positive and negative residuals is constant across units, age groups or sex.
- 109 -

* - … " -‘. . . - * * * *
* * - -
-
-*.
* .- -
t -
-* . . . . ;
* * s
- - . . . . . . ! -
- * : * ~ *- - º *** , , , ; ; ;
* * * - ºf -
: … "- - - -
- - v -- \ . . . . . . .
- * - - - -- º a . - * * * * ~ *
- - - - * - * - - -
* - - -- - - *
- - - * * . . .-
- *** - - - * , - - * , . * - - º -, * *-> - - - : - - - - - - * * - - - * - -
- - - -
* - - ... -- - . . , -. . . . . . t * - - - • . . . . . . . . . -
:

Across Sex Groups
Results show that the model of NPH-PCI tended to underestimate the level
of maladaptive behaviors for females in the achievement (p = .03), aggressive
protective (p = .01) and restorative (p = .01) subsystems. There was no evidence of
differences in model predictive ability among the sexes for ingestive, eliminative,
affiliative or dependency subsystems categories or for the system category.
Across Age Groups
For the purpose of this analysis, patients in Groups l; and 5 were combined
(Group 5 had only 1 patient). It was found that the model of NPH-PCI tended to
underestimate the level of maladaptive behaviors in the aggressive-protective
(p = .0%) and eliminative (p = .03) subsystems for patients 16 to 19 years old
(Group 4). However, there was no evidence of differences in model predictive
ability among the remaining age groups for ingestive, affiliative, dependency,
sexual, achievement or restorative subsystems categories or for the system
category.
Summary of Results
This chapter has presented the results of this study to validate a patient
classification instrument for psychiatric patients based on the Johnson Model for
Nursing. The results were presented in terms of the equivalence reliability,
criterion-related validity and generalizability of the instrument across inpatient
units, sex and age groups.
– 110 –

|-{·
·*
·
*|-
--------·|-■
----·|-·|-■■
■
·-++|-|-•-----
…
…----
•
•··

Equivalence reliability was investigated by computing inter-rater agreements
with respect to patient behaviors, subsystems categories and system categories by
staff, shift coordinator and observer groups. Data indicated that agreement on
patient behavior ratings for the three paired comparison groups far exceeded the
60% criterion pre-established for inter-rater reliability. Ratings for subsystem
category on ingestivé, eliminative, affiliative, dependency, achievement and
restorative subsystems and system category were above the 60% criterion for staff
and shift coordinator paired groups but ratings for subsystems categories and
system category were below the 60% criterion for the two remaining paired groups.
Criterion-related validity was evaluated through the regression of subsystems
category ratings on patient behaviors and through the regression of system
category ratings on subsystems category ratings. Findings showed that the R2
values for all subsystems categories were below the 50% criterion pre-established
for criterion-related validity but that R2 values for system categories were above
the 50% criterion pre-established for criterion-related validity.
The results indicated that 28 patient behavior indicators were as effective as
the 61 patient behavior indicators identified for the eight subsystems in predicting
subsystems categories. The results also indicated that ratings for three subsystems
categories (ingestivé, achievement and restorative) were as effective as ratings for
eight subsystems categories in predicting system category.
The generalizability of the instrument's consistency across inpatient units,
sex and age groups was examined by an analysis of residuals from regression
equations. Data indicated that system category ratings were generalizable across
inpatient units, sex and age groups but that subsystem category ratings for only
two subsystems (affiliative and dependency) were similarly generalizable.
– 11 1 –


CHAPTER V
Discussion
The purpose of this research was to validate a patient classification
instrument for psychiatric patients based on the Johnson Model for Nursing.
Walidation was conducted through empirical investigation and hypothesis testing
using multiple regression. Equivalence reliability and criterion-related validity
were the two psychometric properties investigated in this study.
The results of the research were presented in the previous chapter. The
interpretation of these results, research issues limiting study findings, directions
for future research and implications of findings for nursing practice, theory
development and research are presented in this chapter.
Interpretation of Results
Interpretation of Results Related to Equivalence Reliability
Results of mean inter-rater agreements on patient behaviors for the three
paired groups exceeded the accepted criteria of 60% for equivalence reliability
(see Table 17). Mean inter-rater agreements were within four percentage points of
each other, suggesting that assessment of patient behaviors using the NPH-PCI will
yield clinically similar results when used by different individuals. These results
- 1 12

is
■*
*|-·■--------|-·----·
·|-••-
-••
.
*
·
→
·**a-
*~…••
•·*
•|---»
*…----|-·|×
•|-----
·*
*
→
·----º■

were within the range (.5 to .8) of reliability coefficients obtained in most
behavioral research (Pedhazur, 1982).
Results also showed that the eliminative and sexual subsystems had the
highest inter-rater agreements (see Table 17). These subsystems involve the
assessment of behaviors that require a low level of inference on the part of the
data collectors; for example, patient behaviors such as hand washing, disposal of
body wastes and clothing associated with specific gender. These behaviors are
readily identified and tend to be relatively stable over time. As expected,
affiliative, dependency and achievement behaviors were found to have lower levels
of inter-rater agreements. These behaviors, being associated with emotional
attachments, expression of feelings, and decision-making, require a higher level of
inference on the part of data collectors. These results were similar to earlier
preliminary findings by Auger and Dee (1983).
Results further showed that the staff and shift coordinator groups
consistently achieved higher inter-rater agreements on patient behaviors than the
remaining comparison paired groups. There are two possible reasons for this
finding. First, the staff and shift coordinator paired group was more homogenous
than the two remaining paired groups. Clinical Nurse IIs composed 41% of the
staff group and 55% of the shift coordinator group (Tables 14 and 15). Fifty-one
percent of these nurses had similar educational preparation (see Table 16). Second,
staff and shift coordinator group had more prior knowledge about the patient than
the observer group because they were members of the multidisciplinary team and
Consequently participated in patient care conferences.
Although data collectors completed the Behavior Criteria Checklist
independently, prior discussion of patient problems during patient care conferences
– 113 -


may have promoted uniform observation. Additionally, staff and shift coordinators
cared for patients over a longer period of time interval than observers, which
might facilitate drawing inferences about the meaning of behaviors. Examples of
behaviors which might be influenced by length of time exposed to patients
included: (1) comfort with body and physical changes, distinguishes between male
and female, and knowledge about own anatomy and physiology (sexual subsystem);
(2) established pattern of elimination (eliminative subsystem); and (3) feelings of
hopelessness and helplessness (dependency subsystem).
Interestingly, the observer group reported noting significantly more adaptive
behaviors and less severely maladaptive behaviors than the staff and shift
coordinator groups (see Table 18). These results suggest that staff and shift
Coordinator groups, although having more knowledge about patients' conditions,
were more likely to focus on pathology while the observer group, having less
knowledge about patients' conditions, were more likely to focus on a wider range of
possible behaviors, including those that were adaptive. The focus on adaptive
behaviors permits the use of patient strengths in the development of treatment
strategies (Dee & Auger, 1983a).
Inspection of inter-rater agreements between the two paired groups for
subsystems by categories (Tables 20 and 21) showed that there was lower
agreement between categories II, III and IV (0%–54%). The lack of agreement in
these categories most likely affected the results of the overall inter-rater
agreements for subsystems categories. Agreements ranged from 37% - 66%
(Table 19). These results indicated that data collectors had difficulty in
determining the degree of adaptiveness of the observed behaviors. One reason for
this difficulty is that criteria for rating categories II, III and IV lacked descriptive
– 114 –

adequacy and specificity. For example, there were no operational definitions for
Category IV "behaviors of acute intensity and frequency" (see Appendix A) to assist
the data collectors. A second reason is the inclusion of behaviors requiring
different levels of inference within a subsystem. For example: (1) ingestion of
food and interpretation of events in the ingestive subsystem and (2) basic self-care
skills and emotional security in the dependency subsystem. Theoretical or
mathematical weights for concrete and inferential behaviors were not determined
for this study nor were they available in published literature. Because of the
subjective nature of the behavior indicators, data collectors may have evaluated
the behaviors differently.
Results also showed that staff and shift coordinator groups achieved higher
inter-rater agreements for subsystem categories than the two remaining paired
groups (Table 19). As previously stated, staff and shift coordinator groups had
more knowledge about the overall condition of the patient than the observer group.
Ratings of varying degrees of overall subsystem adaptiveness may have been biased
by prior knowledge about the patient's background. According to Johnson (1980),
regulatory factors are assumed to influence the behavioral responses of the
individual. These factors include; for example, sociological background (external
regulator) or motivations (internal regulator) (Auger, 1976). It is therefore
reasonable to expect that information pertaining to such factors about the patient
may have facilitated agreements on ratings of subsystem categories.
A comparison of the results found in Tables 17 and 19 show that inter-rater
agreements for the three paired groups were significantly higher for the degree of
adaptiveness exhibited by individual patient behaviors than for observed behaviors
in subsystems. A possible reason for this difference is that the ratings for patient
– 115 -


behaviors involved indicating the presence or absence of behaviors that were
pre-specified for degree of adaptiveness or maladaptiveness. In contrast, ratings
of subsystems categories allowed the data collectors ample room for making
inferences and exercising judgements on the degree of subsystems' adaptiveness.
There were also lower inter-rater agreements between staff and observer
paired groups and shift coordinator and observer paired groups for system ratings in
Categories II, III and IV (38% - 48%) indicating that they had difficulty estimating
the level of nursing care required by the patient. These results may have been
caused by the lack of standardization in nursing care. The lack of agreement of
these categories most likely affected the results of the overall inter-rater
agreements of system categories since both inter-rater agreements were below the
60% criterion pre-established for inter-rater reliability.
Staff and shift coordinator groups achieved higher inter-rater agreements on
system categories than the two remaining paired groups probably because staff and
shift coordinators were patient's caregivers and were more knowledgeable about
the range (complexity and intensity) of nursing interventions provided in the
clinical setting and were also more familiar with the patient's nursing care plans
than the observers. It is reasonable to postulate that staff and shift coordinator's
estimation of nursing care required by the patient were most likely based on the
"usual" care received by the patient.
Interpretation of Results Related to Criterion-Related Validity
R2 values computed for the full (inclusion of all independent variables) and
reduced (inclusion of independent variables with an F ratio significant at p .05
and a beta weight significantly different from zero at p .05) equations on all
- 1 16


subsystems were below the 50% criterion for explained variance. The R2 values
ranged from .08 for sexual subsystem to .36 for achievement subsystem (full
equations) and .07 for sexual subsystem to .35 for achievement subsystem (reduced
equations) (Table 31).
Most research data from attempts to investigate social phenomena yield low
R2 values, often well below .50 (Verran & Ferketich, 1984). According to Cohen
(1977), R2 values of .10 would be considered by most researchers in the social
sciences as meaningful and being of medium magnitude. The low to moderate R2
values for all of the subsystems may be due to factors that relate to specification
errors, namely:
1. Subsystems may be inadequately defined, suggesting that patient
behaviors included in the model may not be adequately describing the
subsystems;
2. Subsystems may be incompletely defined, suggesting that relevant
patient behaviors may have been excluded from the model; or
3. Subsystems may be incorrectly defined, suggesting that irrelevant
patient behaviors may have been included in the model.
Errors of measurement--for example, low inter-rater agreements on
subsystems categories--will also lead to an underestimation of the regression
coefficient (Pedhazur, 1982). Note that the inter-rater agreements between shift
coordinator and observer groups for seven of the eight subsystems categories were
substantially below the 60% criterion for inter-rater reliability ranging from 37%
for the aggressive-protective subsystem category to 66% for the eliminative
subsystem category. Cochran (1970), commenting on studies in which complex
- 117 -

>
--
---
-*
-**
*-
•*--
...
-***
**
-
-*
*-
-
;:-.
....2
r-
>,
tº,j:
-
º
*
-*******-
-*-,,...”*....º.
--*-"..-...•
,,,--!..***-
--...!.-*-
--•***--º
~;s*-et*.--
----*--
*--***-:
*-::,
-*--*--***-.......;:....
--:-*,}-**
wy-r-
----,-.**
-*---
–,,,--
*r*,*.....
****-,-."--
..-*-*..
º--*--ºº-
----
-......
-!-
*•****-
****----*--
J

human behaviors were measured, maintained that errors of measurement are
largely the result of data from disinterested data collectors.
Despite the lower than expected R2 values obtained, of particular interest in
this study were the results for the ingestive subsystem. Three of 11 ingestive
behavior indicators were predictors of the ingestive subsystem category rating. All
three of these behavior indicators are behavioral segments describing the concept
of sensory perception, one of two critical behavioral characteristics of the
ingestive subsystem. Auger (1976) argues that the functions of the ingestive
subsystem include not only the " 'taking-in'" (p. 35) of substances, such as food and
fluids, but also the " 'taking-in'" (p. 35) of sensory information, for example,
perception. Sensory information, according to Auger (1976), enables the individual
to initiate required compensatory responses in order to maintain a state of
psychophysiological equilibrium with changes in the external environment, and that
it is through the ingestive activity that the individual is able to differentiate
himself as a separate entity from all other objects and persons existing in the outer
world. This finding shows the relative importance of sensory perception of
psychiatric patients and partially supports the conceptual perspective of Auger
(1976).
Interestingly, ingestive behavior indicators describing food/fluid intake were
not shown to be predictors of the ingestive subsystem category ratings. It is
reasonable to expect that data collectors' ratings may have been biased by timing
of observations and frequency of behaviors associated with food and fluid intake.
These behaviors would most likely be confined primarily to mealtime periods. In
contrast, maladaptive behaviors associated with sensory perception most likely
- 1 18

•••
* *
* ,
••
·■■
·
----••.*
-----|-|-
*…
---…··
·
-
*··
·-

occurred throughout the observational period, thus contributing more significantly
to the overall adaptiveness of the behavioral subsystem.
The low to moderate R2 values indicate that subsystems categories had low
to moderate explanatory power. Further work is needed to identify additional
relevant patient behaviors for inclusion within each subsystem.
The computed R2 values for the full and reduced equations for system
categories were all above the pre-established criterion of .50 for explained
variance. The reduced equation showed that subsystems categories for ingestive,
achievement and restorative were the predictors for ratings of system category.
These results were surprising for two reasons: First, it was the clinical notion that
behaviors for the subsystems of dependency, affiliative, achievement and
aggressive-protective were most often maladaptive in the psychiatric population.
With the exception of the achievement subsystem, these subsystems were not the
same as those shown to predict the system category ratings of nursing care
requirements. One plausible conclusion is that although aggressive-protective,
achievement, dependency, and affiliative subsystems may have been descriptors of
clinical problems of psychiatric patients, these subsystems (with the exception of
achievement) may not necessarily impact/predict the level of nursing care required
over time. For example, in the aggressive-protective subsystem, behavior such as
"acting-out" often required periodic immediate and intensive nursing interventions
of 10 – 15 minutes to provide "limit-setting" on the behavior, while behavior such
as "perceptual distortion of the environment" in the ingestive subsystem often
requires continuous nursing intervention to provide reality testing, orientation and
redirection. It is reasonable, then, to expect that behaviors such as those requiring
nursing interventions consistently over a span of time would be predictors of the
- 1 19

•
■ ••
----.."--------|-··|-|-|-:|-
|---------··--------*-|-,■ |-
|-·|-*
■ ----|-■■ |-----•ae••----*·…•----:■ ·!
|-■ |-|-*…*·**--I|-7.··•
•
•·…*·
|-■ :----|--***|-■ ·**-->-·|-■ -
*•
*|---
--------|-|-----…*----|-|--|-|-:|-·-|-
|-•
¶··|-·----•----|-----|-|-·-
-----|-----|-----|-~^|-·----|-·----
}→·º.-
*•■ ·•|-→·|-
|--|-…•*…*·
·
·|-·
·■ ·|-|-|-*a·*·|-|-----•-*·*-----■|-|--
…--|-----
|-|--|-···■±|-·|-■
*|-
··*···|-
·|-----|-|-|-·-*•*
-----|-<>·|-|-*-…
•----••■-•-
**|-·|-ae■ ----■"*-
----··■ …■
--------*-,-
|-…•**·|-*--|----- |-*…»·
•,--------·,
!·|-••--,----·|-----*…*■■-_-|-|-|-·-|-·|-·
|-|-|->→-■ ----
|-|--··----·*→·} |-*
|- •
•·|-·----
|-…*·|--|-|-··|-|-*…|--…"|--·-----|-·
·|-*…|-|---
-|-*
•|-|-|-|-*-----•••---------•
!----*-**|-■ |-|-·-|--·-·|-|-|-~
}-----·|----------···---------->→
|-·.**----
·
·■■-·→··|-|-
·-·,-·----·-•••
•|-→·
|---·---|-
|-
----··■
|--··----·|--
-|-••…--|-→|-|-----|-
-
-|-|---■■ |-·|-,■-
-|
–·----|-*v---*
*---•*----|-----•i|-
|----------·*…*|-·*•|-
----•---------·--------|-----*-,----■ --→|---
----
----.*|-|-
|---|-----*••→·
|--*-|-|-··*
■ --------
|-·-
-|-*-·----<|-|-----|-
-*·--'•••-••|-}---------
--------·----|---■ |-|-*…*|------|-
-·--------|-|---------·|-••-+→
·|-|-*.|-|---|-·|-*-
|--·-----}·|------|--*
---
--…--|-- ----*…----••·|---|-----|-••|-|-
|-
|-•----■-|-|-|--*,|-··-----·
•
"•
•·----·■ *-→··
-|-|- *--»-……--*,----
·-·|-*·-
-
|-*--
----|--
-·■ ~|-|-·*…------------→→·
|-·|-
|-·|----------|-----|-|-|-|-|---------·--------*|-*•---------|--···|-|-·→·
------|-|-*-,■|-·---- |------|------|---
-·|-*•|-
|---------·----→-|-·*|--
-
----·|-|-----|-|-----|-·|-·-
-|-|-·*|-→·|-|-|-|-|-|-~■ ·|--*---
·•,■ •º
|-·----|-…----|--|-.*···|-•s----|-
|-|-…·→
···|-•*;|-|-----*|-|-·|-|-|-•→----·-…----
*
*·----|-|-
•*••-••-----|-|-·•*•|-|-----|-·*
-•
••■

level of nursing care required: for example, those behaviors associated with
attention span, ability to initiate and complete tasks (achievement subsystems)
ability to engage in recreational activities, and participation in treatment regime
(restorative subsystem). It should be pointed out that although sexual and
eliminative subsystems were not statistically significant, they were clinically
meaningful to the practitioner in the planning of care.
Second, the model as originally conceived by Johnson included seven
subsystems. An eighth restorative subsystem was later added to the model. As
was previously discussed in Chapter II, Johnson argues against the inclusion of the
restorative subsystem in the model. It was her belief that the relief of fatigue was
more a function of the aggressive-protective subsystem than the restorative
subsystem (Lovejoy, 1981). Auger strongly supported the inclusion of the
restorative subsystem in the model. She states that the "restorative subsystem, in
and of itself, contains goals that define the subsystem apart from all other
subsystems. It is a most important subsystem to the survival of the organism as a
viable entity" (J. Auger, personal correspondence, April 18, 1985). The results of
this study support Auger's supposition of the importance of the restorative
subsystem relative to overall behavioral system functioning.
Results of this study support the criterion-related validity of system
category. These results indicate that the ratings of subsystems categories based on
the general framework of the NPH-PCI can be used with confidence to predict the
level of care the patient requires.
- 120 –

1-a "----
··--------|-··*-■ *
**
•
•|-|-•~--------|-----·|-■
,|-|-|-|-→··|-----|-**→·-|-|-•----|-·■
,|-|-
·
*-|--·|-~,■
-
-·-----·*·|-*a·|-·|--
--|-|-|-----
-|-~,~~~*|--
------|-----→·rº•**----|-
|---------→
··-|-------|-*
•■ ··_|-----|-----*-
-*
*|-|-----*|-–■
------·----*----*--*·*|------
,■·|-|-•·-----
----••**…··--ae■
------------…|--
-*…*----·----|-|-·.*J|-*…-----«■■ .*••-,--*…-
*|-----*-*■ ----|-·*---------·|-··*···.*------...•|-·
·
·:~-
-·|-|-|-
-----→··••*e*·*■
|-|-ae…|-----→·----|-|---··|→*·*·|---·
·---------|-|-|-···|------·*----·------------··|--|-----••••|-|-·····-----|-·*-----•.|-
**,•,----|--|-~--··
*----*----|-→|-|-··*-|-|-→
·■ ·|-·--------|-*,|-•*•----|-·--------|-*----·------·|-*|-·|-----|-|-|------·|-----
-
|--|-|-«…*·v•--------·--·---■
-
-|---------*-|-·----|-|--|-·
–
■ ------------→--
|-|-•|-·|-----|-·----··-● |-----|-|--·-
-•|---------*--------|-|-
•••|-•
•----|-·----|-----••|-|-
*
~^-|-·-----·---
-···----·•|-|-••
•-,|-|-
|-----+|-|-----|--··■ ',|-|-*a|-→«»|-·---------·~|-|-··|-·----------|-|-|-----•|-------|-|-----*
·
·
*·-----,·|-*-…|-
·|-*·------|-|--
-·|-|-|-------------|-•••·
|-·*● |-|-----·|-
*
.|-■»|–----|-**--------|-|---------|-|-|-
·→|-------·|-|-|-·|-----|-----|-*•·|-·
··----|-------------·
·
··|-
*|---|-|-|-----••----*-|-
|-
·-,--------·|-·-|-
----|-|-*·■ ••|-
|-
|-|-|----------→|-|-|-•
•|-|-••|-|-|-|--·-…“'.-|--
-|-|-|--…•
•|-|-·
|-·–■ ·----|-
·|-|-·--|-
|-
|-*·*→·|-
|-|-|-|-*|-|-·--|-·|-----
|-·--··--------|-----|-·|-|-|-----·-...~~~|--
-*|-|-|--------*
|-|-·→----|-|-|--→
•*a--|-|-|---|-|------*·|-|-·
------·
·}|-|-···----
|-|-|-|-|-|--·|-
|-··----|-
-|-·|-·•|-
|----…»|-|-
-|--|--|-·--|-|-|-|-----**~|-→-
-
·|-→--•|-----|-----·|-|-·-…|-**→→·*-ae
|-|-|-··----
*

Interpretation of Results Related to Generalizability
It was found that the model of NPH-PCI tended to underestimate the
maladaptive behaviors in the ingestive subsystem for the child psychiatry unit.
This underestimation may be due to: (1) absence of maladaptive ingestive
behaviors specific to the patient population; (2) lack of theoretical weights for the
two distinctively different behavioral characteristics in the ingestive subsystem;
and (3) lack of heterogeneity of sample. There was a disproportionately large
number of patients (n = 34, 40%) with conduct disorders, major affective disorders
and attention deficits on the child psychiatry unit (Table 13).
Results also showed that the model of NPH-PCI tended to underestimate the
maladaptive behaviors in the eliminative subsystem for the adolescent
developmental disabilities unit. This underestimation may be due to the inadequate
representation of maladaptive eliminative behaviors specific to this population in
the model or a lack of heterogeneity of sample. There was also a
disproportionately large number of patients (n = 29, 35%) with conduct disorders,
major affective disorders and schizophrenic disorders on the adolescent
developmental disabilities unit (Table 13).
The model of NPH-PCI also underestimated the maladaptive behaviors in the
sexual subsystems for all inpatient units. These results may be explained by the
exceptionally low R2 values for the sexual subsystem (.07). This lack of
generalizability and the low R2 values indicate that new behaviors in the sexual
subsystem must be developed, redefined and refined.
Results indicated that patient behavior indicators for ingestive, eliminative,
affiliative and dependency subsystems can be used to predict subsystem categories
for male and female. However, it was found that the model of NPH-PCI tended to
- 121 –

*

underestimate the maladaptive behaviors for females in the aggressive-protective,
achievement, and restorative subsystems, suggesting that female behaviors for
these subsystems may differ from those of males and that new achievement,
restorative and aggressive-protective behaviors specific to the female population
may need to be developed.
Results showed that patient behavior indicators for the ingestive, affiliative,
dependency, sexual, achievement and restorative subsystems can be used to predict
subsystem categories for patients tº to 15 years old. However, the model of
NPH-PCI tended to underestimate maladaptive aggressive-protective and
eliminative subsystems for patients 16 to 19 years old. These results suggest that
maladaptive eliminative and aggressive-protective behaviors of older adolescents
may differ from those of young children, latency-aged children and young
adolescents.
There was no evidence of differences in model predictability for the system
across the four inpatient units, four age groups ranging in ages from 4 to 23 years
old and between male and female. These results suggest that the model can be
used to predict levels of nursing care across inpatient units, age and sex groups.
Research Issues Limiting Study Findings
The limitations of this study were related to the research methodology;
specifically, certain aspects of the sample selection, patient observation schedules,
study period and observational procedures.
- 122 -


Sample Selection
As stated previously, the purposive sample consisted of patients who met the
criteria for system category. It was assumed that the large sample size and the
assignment of sampling by inpatient units (child and adolescent psychiatry; child
and adolescent developmental disabilities) would allow for an adequate
representation of patients by age, sex and psychiatric diagnosis. However, in
actuality the sample had a predominance of males (66%) and a predominance of
patients with conduct disorders (20%), major affective disorders (19%) and
schizophrenic disorders (10%). Young children aged 4 - 7 were underrepresented
(11%) in the sample. Greater attention given to these factors might have increased
the heterogeneity of the sample, thus increasing the generalizability of the
findings.
The issue of multiple observations of the same patient was addressed by the
control for dependence of subjects. Patient observations that did not meet the
following criteria were excluded from the sample: (1) a two-week time lapse
between observations of the same patient in the same system category and (2)
repeat observation of the same patient in a different system category. Evidence
from the study showed that the assumption of independence had not been violated.
Patient Observation Schedules
As was previously stated, the assignment of patient observations was based
on the observer's work schedule. Staff and shift coordinators who had primary
patient and administrative responsibilities for a given 8-hour shift, participated as
data collectors. The data collectors were not paired according to comparable skills
- 123 –

f
- * - - * -
º, . . . . . .-
. . . . . . . . . . . . .
* - - * ~ * -
- * * * - -- - -
- - - s - *- - * * - - - - * -
-
- * - " * * * -
- - - -! -
* - * - " . . . . -
º * - - . . . . . . . . . "
- * -- - -
- -... ." . . . . . . . . . . .
- - - - - -
* - * • , , . . . . . . *
- . . - *. - - - - * -- . . . . ‘. . . . . . . . . * , ". -
- * -
* :
* . . - - - - - - - . . .- * - i - * - :
- - - - - - - * * - -
- - - : * i. - - * * - - -
- - - - - - * - - - - - . . :* * - -- i.e. , - * * * * * * - - -
--
- - -” -" . . . . . - * = -
- ar - 3 & . . . . . . . . .-
. . . . .- -
- - - * - - - -- * - - -- ... -! ºf * : . . . . . . . . . . . * r * * *
- s * - - - - - - - * * - - -; , ; ; ; , tº º ■ ix i: , , , . . . . . . . . .
* : * , , , . - * - --- -
- * - - * -
º ‘. . . .( ' '.' ' ~ * * -
* . . * \ . . . . . . . . .
-

or clinical expertise. Consequently, this procedure of assignment resulted in
greater variability in skills and clinical expertise among the raters.
Furthermore, observers were randomly assigned to the four inpatient units
for patient observations while staff and shift coordinators remained on their
primary work unit. Therefore, staff and shift coordinators were more
knowledgeable about the patient and his or her nursing care than the observer.
Higher inter-rater agreements may have been achieved if all data collectors were
paired according to their comparable skills and clinical expertise as well as the
assignment to a specific inpatient unit where they were most knowledgeable.
Study Period
The difficulty of obtaining a large sample size to represent each system
category resulted in an extended study period. The lengthy study period posed
several threats to the internal validity of the study. Specifically, the threats to
internal validity were:
1. History - With the passage of time, change in attitudes of data
collectors about the observational study may have occurred;
2. Maturation - Data collectors may have increased their knowledge
about the Johnson Model as well as skills in data collection;
3. Selection - Subjective estimation of the criteria for system category
may have changed, thus influencing the selection of subjects; and
H. Mortality - There was a gradual decrease in patients who met the
criteria for system Categories I and IV, thus affecting (although
minimally) the selection of a purposive sample.
- 124 –

**.
→·
*
·
·
----…º•¶
** -
*…º-*…*··
*|-~
·-•••·----|---------
|-·--»
•*■■·|--*·----
·
*
-----|-·→••|-

Because of the lengthy study period, observer training should have included
frequent retraining and reclarification of rating criteria to maintain the prestudy
level of inter-rater reliability. Data collected at initial and final phases of the
study should have been compared for reliability and validity. Again, greater
attention given to these factors may have reduced any threats to the internal
validity of the study.
Observational Procedures
A potential weakness of the observational data collection procedure is the
fallibility of the observer. Human perceptual biases are inherent in observational
procedures, the most common of which are expectations and attitudes of the
observers. For this study, subjective measures (rating scales) were used to rate
subsystems and system categories. Several types of errors may have been induced
by the use of rating scales. Raters could be influenced by nonrelated patient
characteristics, or the tendency to rate too positively or too harshly. The
importance of adequate observer training and inter-rater reliability cannot be
overstressed.
Despite the potential weakness of the observational procedure, the greatest
strength of direct observation is that it allows for the collection of data that would
otherwise be impossible to obtain. With this approach, important information
about behavioral patterns are described (Polit & Hungler, 1983).
- 125 -


Directions for Further Research
Despite the methodological limitations, this study has provided valuable
results that can be strengthened through further research. Clearly, there are
several measures that can be taken to increase the reliability, validity and
generalizability of the NPH-PCI. The directions for further research may be
divided into two major areas: (1) Instrument Development and (2) Research Design.
Instrument Development
As stated, the issues of reliability and validity must be favorably resolved for
an instrument to be used with confidence. Although reliability is a necessary but
not sufficient feature of an instrument, it is the basis of all other assessments that
occur. The validity of an instrument is established over time by examining results
across many related studies.
The reliability and validity of an instrument are not totally independent
qualities. Although high reliability provides no evidence of an instrument's
validity, low reliability is evidence of low validity (Polit and Hungler, 1983).
Further refinement of the NPH-PCI should result in higher reliability and
validity coefficients. A panel of experts (including those from a variety of
psychiatric settings) knowledgeable about the Johnson Model can be used to judge
the preciseness and completeness of the behavior indicators. The ways in which
the measurement of patient behaviors can be improved include:
1. Eliminating ambiguous items, such as those behaviors which are not
readily observable; for example, pattern of elimination, feelings of
- 126 -


hopelessness and helplessness, comfort with the body and physical
changes;
2. Decreasing the degree of observer inference by taking smaller
segments of behaviors as units of observation; such behaviors as
emotional attachments, expression of feelings and decision-making;
and
3. Adding relevant patient behavior indicators within each subsystem.
Kerlinger (1973), however, warns that categories which are too specific—
while reducing ambiguity-–tend to be inflexible, rigid and perhaps trivial as well.
Consequently, data collected may become less useful in behavioral research.
The identification of new behaviors can be accomplished by a thorough
review of literature, a review of the patient's medical record and by participant
observation. A panel of experts can also be used to judge the descriptive adequacy
of the subsystems:
1. Are the subsystems completely defined so that relevant behaviors
describing the subsystem are not excluded from the model?
2. Are the subsystems adequately defined so that behaviors included in
the model are describing the subsystem?
3. Should two distinctively different behavior characteristics be included
in the model to describe the same subsystem?
Once these steps have been taken, variations of behaviors can be ordered into
different categories. The influence of regulatory factors such as age, sex,
cognitive thinking, beliefs, values, physiological states, and so forth should also be
investigated in detail in regard to their influences on behavioral responses.
- 127 –

*
------------|-••*
**|-|-■----ae|-----••----|-----*··
-----|-·t.
-
-·→→*
*·|-----
-
■ ----•|-----
----·----•••·|---
·*------------•--------
-•|-|-|-*.·|-------·|-|-----·*
•--------
|-
|-|-*…·|-|-
→•
•|-*|-■ --------
---------*ae·
|-→|---------··--------…
*
·|-----
|-|-|-·|-|-----|-|-|----------,
----*-----··|-----|-----|------*|-
~v:|-
----|-|-|-|--~·,■ *•••-·-----
- -
-•}·
**,→·-----
-|-|-·|--|-|-----•"----••■|-|-·--*
*
-->|-|-|-·--·*|-■----••|-*·|-→·
··|-…»|-
-----|-----|------…
--→·----
-|-*…*|--|-·-
·----|--*
----|-.*·-|-·••.
-------------+*
|-,--*,|-•
-
-----|-*
*|-·--·--
|-*----••-•
!
|----- |-----|-|-|--■
•
!|-|-·|-----■ |-|-|-·
·|-••••|-••
■·
* *

Based on study results, smaller studies can be designed to compare behaviors
of subgroups, for example: (1) male patients, aged 9 – 12 with conduct disorders
and male patients, aged 9 – 12 with schizophrenic disorders, or (2) female patients,
aged 16 - 19 with major affective disorders from intact families and female
patients, aged 16 - 19 with major affective disorders from divorced families. Data
from these studies will provide further information about the variations of
behaviors as well as those behaviors that are common for these subgroups. Criteria
for subsystem categories can then be established with greater accuracy, adequacy
and specificity.
System category, as reflected in the concept of nursing care, also deserves
investigation in detail. Further work in this area should be directed toward the
delineation of nursing care activities in terms of: (1) complexity - the skill
necessary to carry out the task, and (2) intensity - the amount of time required to
complete the task. Earlier work done by Auger and Dee (Appendix A) has provided
a beginning taxonomy of activity categories which can be substantiated through
further research by comparing: (1) different skill levels of staff required to
perform the task, and (2) amount of time required by different skill levels of staff
for task completion. These tasks should include the components of the nursing
process (assessment, intervention and evaluation). Substantiation of the
complexity and intensity of nursing care will provide further data to establish
levels of nursing care with greater accuracy, adequacy and specificity. Levels of
nursing care can then be used for the cost-effective allocation of resources.
Studies should also be done to investigate whether specific demographic
attributes such as age and sex have an impact on system category (level of nursing
care) other than subsystems' categories (behavioral adaptiveness) themselves.
- 128 -

..............
------*:*r***-
...--*--*-
!..º,*.
**-----
*,-J,,**
**----a**.
-!..
-*-...•
**-*º*-**--
-*-*----- ...'"*>..”!",!:.....*-
2-:'',".,I-....
º*-***--*-
-*-º
--*-r-
".....-....
-..*---
j-
•,,-.....
---------:
..":).........-
**.....
‘................
.º*º
---***---
*--*-*..
--*--J-
*-**********--
...--*:****
----:..”.....
--..*...--
--------
-*.----
***-"----...-...-
*.--------
*."
*-,-’s----
--*.....*:*> -*-
********-*-
----..-
**
--
-º*-**
**
*-
****
---
.
.....-
,,-"
‘...•--,-
z\
-
...
....
***
-...•
***
-****
t
-
•*:
r...•
--
-**
s
"..2
-*
-
***
-
-
**
*
....”**
t
-*
*
****-----
t
***
*
-
*
*

Further work is also needed in evaluating the completeness of specific subsystems
in determining overall behavioral system functioning; for example, is the system
completely defined so that relevant subsystems describing the system are not
excluded from the model? Cost benefit analysis can then be done to determine the
relationship between levels of nursing care and patient outcomes based on an
analysis of behavioral adaptiveness.
Ways to decrease observer bias associated with the use of subjective
measures such as rating scales for subsystems and system categories should be
explored. For example, should mathematical weights be used for each patient
behavior shown to be a predictor of subsystem category and likewise, for each
subsystem shown to be a predictor of system category? The development of these
and other new methods and strategies will ultimately enhance the objectivity,
precision, accuracy and sensitivity of the NPH-PCI.
Research Design
As previously stated, human perceptual biases are inherent in observational
procedures. The training of observers in nursing research utilizing observational
methods deserves attention. Consideration should be given to the selection of
observers as well as the cost of observer training. In studies where there is a large
group of observer participants, costs can become prohibitive.
The research methodology for this observational study has required extensive
resources. A possible approach to decreasing the recruitment and training cost of
observers for further research is to utilize a resident nurse expert—-ideally, a
clinical nurse specialist where feasible, or shift coordinator/primary nurse--as the
data collector. There are several advantages of having the resident nurse expert
- 129 –


serve as the data collector. First, the availability of a resident nurse expert on
site reduces scheduling problems. Second, a well-coordinated schedule can result
in a shorter time study period and control of threats to internal validity such as
history, maturation, selection and mortality. Third, training efforts are minimal
for the resident nurse expert who already has the expert knowledge about patient
conditions for a specified patient population and knowledge about a full range of
nursing interventions for these patients. Lastly, an existing staff member is more
likely to remain in the study setting upon the completion of the study while a
recruited observer is more likely to leave upon the completion of the study.
Implications of Findings for Nursing
This research is a pioneering effort to quantify patient behaviors using an
amplified version of the Johnson Model for Nursing. The results of this study have
important implications for practice, theory development and research.
First are the implications that relate to the primary objective of this study:
to assess the reliability and validity of the NPH-PCI. The problems of defining and
quantifying psychiatric patient needs and required nursing care are ones that are
continuously faced by nursing administrators. The solution to these problems can
be optimized with data provided by patient classification systems that are well
tested for reliability and validity. However, to date there has been no comparable
research found which provides a classification system for psychiatric patients that
addresses the relationship between patient attributes/behaviors and the level of
nursing care the patient requires.
- 130 –


Although parts of the NPH-PCI are not yet fully developed, the value of the
NPH-PCI as a clinical tool to assess patient behaviors for the purpose of planning
nursing care is clear. It has provided practitioners with a framework to describe
clinical phenomena and to evolve domains for nursing practice. The utilization of a
single model of nursing has enhanced staff communication and agreement regarding
identified patient problems. It has immeasurably increased the systematic
assessment of patient behaviors by both professional and nonprofessional staff of
diverse educational backgrounds and clinical experiences.
The further development of the NPH-PCI is dependent upon the refinement
and testing of theoretical concepts of Auger-Grubbs interpretation of the Johnson
Model. With further research, the NPH-PCI will enhance its position as a valuable
administrative tool to quantify patient behaviors and accurately predict the level
of care each patient will require. Such an instrument will have direct benefits for
hospital administration in general and nursing administration in particular. The
most important of these benefits are: (1) the development of nursing interventions
based on patient outcome criteria; (2) the development of nursing workload indices
based on patient care needs; and (3) the identification of nursing care costs for
fiscal management.
Second are the implications that relate to the value of testing theory to
determine whether there is congruence between the idea of reality which the
theory suggests and the empirical evidence of that reality. The building of a
scientific knowledge base occurs through repeated testing of theories to
substantiate professional practice.
The major utility of the Johnson Model thus far has been in the assessment
phase of the nursing process; to date, there has been no research found that
- 131 –

--
·
+
+••
----··|-·*
·••
|-**
*·
·
·---- ----
••
■
■ ·-*
*
*--------
·■
----
!
*·
··
-…+→
-
-----…
•
×·|-■·
·•·*
■
|-■··
*•
·*

addresses the predictive elements of the Johnson Model for determining levels of
nursing care. With further development and research, it is anticipated that the
NPH-PCI based on the Johnson Model will achieve a higher degree of reliability
and validity. The validation of this model for nursing has direct benefits for
practice. The model will provide nurses with a framework not only to describe
phenomena, but also to explain, predict and control clinical phenomena for the
purpose of achieving desired patient outcomes. Levels of nursing care provided for
the patient can then be more purposeful, and nursing practice more meaningful to
the practitioner.
Finally, there are the implications that relate to the availability of sound
measures used to test the theoretical formulations underlying nursing practice and
methods that promote the study of complex behaviors. The emphasis for nursing
research should be on the systematic method of inquiry, the use of advanced
quantitative data analysis techniques for theoretical model testing and the
development of new methods and strategies to increase the precision, accuracy and
sensitivity of measurement systems.
- 132 –


References
Abdellah, F., & Levine, E. (1965). Better patient care through nursing research.
New York: McMillan and Company.
Alward, R. (1983). Patient classification systems: ideal vs. reality. Journal of
Nursing Administration, 13(2), 14-18.
Arnett, R., Cowell, C., Davidoff, L., & Freeland, M. (1985). Health spending trends
in the 1980's: Adjusting to financial incentives. Health Care Financing Review,
6(3), 1.
Auger, J. (1976). Behavioral systems and nursing. New Jersey: Prentice-Hall, Inc.
Auger, J., & Dee, W. (1982a, November). Can a model of nursing be translated into
clinical practice? Paper presented at Nursing Research Conference, Stanford
University, San Francisco, California.
Auger, J., & Dee, V. (1982b). Patient classification evaluation study. Unpublished
manuscript, UCLA Neuropsychiatric Hospital, Los Angeles.
Auger, J., & Dee, W. (1983). A patient classification system based on the
behavioral system model of nursing: Part 1. Journal of Nursing Administration,
13(4), 38-l;3.
Auger, J., & Dee, V. (Eds.) (1985). Patient classification instrument: patient
behaviors/nursing interventions. Available from UCLA Neuropsychiatric
Hospital, 760 Westwood Plaza, Los Angeles, California, 90024.
- 133 –

------------------------------------
--—-
····…----·*
■ -·
→·
*-
·
·
|-|-·*
··*
••
•----«
·
……
|--*|-·|-·•
■
■ |-|---·*|-
...*
•
··|-,■
·
----·
·•■
*|-*-->
…º··|-··*
* *
----

Aydelotte, M. (1973). Nursing staffing methodology: a review and critique of
selected literature (DHEW NO NIH 73-433). Washington, DC: U.S.
Government Printing Office.
Barham, W., & Schneider, W. (1980). Matrix: a unique patient classification
system. Journal of Nursing Administration, 10(12), 15–31.
Bohrnstedt, G. & Carter, M. (1971). Robustness in regression analysis. In
Costner, H. (Ed.). Sociological Methodology. San Francisco: Jossey Bass.
Broncatello, K. (1980). Auger in action: application of the models. Advances in
Nursing Science, 2(2), 13–23.
Capers, C., O'Brien, C., Quinn, R., Kelly, R., & Fenerty, A. (1985). The Newman
Systems Model in practice. Journal of Nursing Administration, 15(5), 29–38.
Carmines, E., & Zeller, R. (1979). Reliability and validity assessment. Beverly
Hills: Sage Publications.
Chinn, P., & Jacobs, M. (1983). Theory and nursing: a systematic approach. St.
Louis: The C. V. Mosby Company.
Cochran, W. G. (1970). Some effects of errors of measurement on multiple
correlation. Journal of the American Statistical Association, 63(1), 22-24.
Cohen, J. (1977). Statistical power analysis for the behavioral sciences (rev. ed.).
New York: Academic Press.
Conner, R. (1961). A work sampling of variations in nursing workload. Hospitals,
35(9), 40-41, 111.
Conner, R., Flagle, C., Hsieh, R. Preston, R. & Singer, S. (1961). Effective use of
nursing resources. Hospitals, 35(9), 30-39.
Cook, T., & Campbell, D. (1979). Quasi-experimentation. Boston: Houghton
Mifflin Company.
- 134 –

-***--
-s---
-
•*-*------z'sº-
º!---.---*,
---------*
--*.-*
***•*...y**>-**•*~*,5*-º
-*-i---*~*--*--....
*x--,,,-
--a-
-------- ,-.*-------**..."s**-**--eº
---*.--i.**.....---
--**:------
*--..."-----------------
-----—. -*--.º-*-*....•.*......."
-***---,T...-**
-----:)-2:-*-.*.*-*------**
“...-----....-->-!...
-....---**-**-
------º-
*--------------------------------------------------------º-----s-a--
-*=-...•--
--*----
....**-º
---------------------------------------- *,,a**---*,-e
-s*------*----
•,*-,..*-...-------------------——---—-----
.-"."--
->***--,,--***,•*•*º**-----º
--------...--
------------------,-º--
-•*:*-*--------
;,»**...--—------––*,-a*2**
s---*-i.-*-4--
*-***-*--***s
-.----------------------------,-.--
-----.--*-
•****:*--**.."**
º-----**- ;:■,...
--------
*---------------------------------------------------------------------r---**-*
--------

Dale, R., & Mable, R. (1983). Nursing classification system: foundation for
personnel planning and control. Journal of Nursing Administration, 13(2),
10-13.
Damus, K. (1980). An application of the Johnson Behavioral Systeml Model for
nursing practice. In J. Riehl & C. Roy (Eds.), Conceptual models for nursing
practice (2nd ed.). New York: Appleton-Century Crofts.
Davis, C., (1983). The federal role in changing health care financing. Nursing
Economics, 1(1), 10-17.
Dee, V., & Auger, J. (1981, October). The assessment of behavior of
developmentally disabled children and adolescents based on a model of nursing:
implications for administrative decision making and clinical practice. Paper
presented at the American Association on Mental Deficiency, Detroit,
Michigan.
Dee, W., & Auger, J. (1983a). A patient classification system based on the
behavioral system model of nursing: Part 2. Journal of Nursing Administration,
13(5), 18–23.
Dee, V., & Auger, J. (1983b). Effects of a nursing model on the assessment process
of patient behaviors in the clinical setting of psychiatry. Paper presented at
the American Association on Mental Deficiency, Dallas, Texas.
Derderian, A. (1983). Instrument for theory and research development using the
behavioral system model for nursing: the cancer patient: Part 1. Nursing
Research, 32(4), 196-200.
Derderian, A., & Forsythe, A. B. (1983). Instrument for theory and research
development using the behavioral system model for nursing: the cancer patient:
Part 2. Nursing Research, 32(5), 260–266.
– 135 —


Draper, N., & Smith, H. (1981). Applied regression analysis (2nd ed.). New York:
John Wiley & Sons.
Edgecumbe, R. (1965). The CASH approach to hospital management engineering.
Hospitals, 39(3), 70-74.
Fawzy, N. (1979). Development of a methodology and examination of
characteristics of isolation patient. Unpublished master's thesis, University of
California, Los Angeles.
Ferketich, S. (1982). Model development of a patient classification system using
graphic residual analysis. Unpublished doctoral dissertation, University of
Arizona.
Finlayson, H. (1976). The NUMBRS approach to nursing management. Dimension
in Health Services, 53(5), 39-44.
Fray, C. (1984). An accountability classification instrument for orthopedic
patients. Journal of Nursing Administration, 14(7), 32-39.
Georgette, J. (1970). Staffing by patient classification. Nursing Clinics of North
America, 5(2), 329-339.
Giovanetti, P. (1979). Understanding patient classification system. Journal of
Nursing Administration, 9(2), 4-9.
Gold, R. (1969). Statistical tests and substantive significance. The American
Sociologist, 4(1), 42–46.
Gordon, R. (1968). Issues in multiple regression. American Journal of Sociology,
73(5), 592-616.
Grant, S., Bellinger, A., & Sweda, B. (1982). Measuring productivity through
patient classification system. Nursing Administration Quarterly, 6(3), 77-83.
– 136 –

-
- s
- -- -
* - - -
º * 1: ... " “. . . .
• * f
º -- -

Grubbs, J. (1980). An interpretation of the Johnson Behavioral System Model for
nursing practice. In J. Riehl & C. Roy (Eds.), Conceptual models for nursing
practice (2nd ed.). New York: Appleton-Century Crofts.
Hanson, R. (1979). Issues and methodological problems in nursing staffing research.
Communicating Nursing Research, 12: 51-56.
Hey, J. (1974). Statistics in Economics. London: Martin Robertson and Company.
Holaday, B. (1980). Implementing the Johnson Model for nursing practice. In
Riehl, J. and Roy, C. (Eds.), Conceptual models for nursing practice (2nd ed.).
New York: Appleton-Century Crofts.
Holaday, B. (1981). Maternal response to their chronically ill infant attachment
behavior of cry. Nursing Research, 30(6), 343-347.
Holaday, B. (1982). Maternal conceptual set development: identifying patterns of
maternal response to chronically ill infant Cry. Maternal Child Nursing Journal,
11(1), 47-58.
Jelinek, R., Haussmann, R., Hegyvary, S., & Neuman, J. (1974). A method for
monitoring quality nursing care (HEW Publication No. 76-25). Washington, DC:
U.S. Department of Health, Education and Welfare.
Joel, L. (1983). DRGs: The state of the art of reimbursement for nursing services.
Nursing & Health Care, 4(10), 560-563.
Johnson, D., (1968). One conceptual model of nursing. Paper presented at
Vanderbilt University. Nashville, Tennessee.
Johnson, D. (1977). The behavioral system model of nursing. Paper presented at
the University of Delaware, Newark, Delaware.
- 137 –

º
º
- - -
-
- ->
s -
- * - * - -
- * * * * -

Johnson, D. (1980). The behavioral system model of nursing. In J. Riehl and C.
Roy (Eds.), Conceptual models for nursing practice (2nd ed.). New York:
Appleton-Century Crofts.
Kerlinger, F. (1973). Foundations of behavioral research (2nd ed.). New York:
Holt, Rinehart and WInston, Inc.
Kerlinger, F. (1979). Behavioral Research. New York: Holt, Rinehart and
Winston.
Knapp, (1985). Walidity, reliability, and neither. Nursing Research, 34(3), 189-192.
Kreutter, F. (1957). What is good nursing care? Nursing Outlook, 5(5), 302-394.
Lagona, T., & Stritzel, M. (1984). Nursing care requirements as measured by DRG.
Journal of Nursing Administration, 14(3), 15-18.
Lewis-Beck, M. (1980). Applied regression. Beverly Hills: Sage Publications.
Lovejoy, N. (1981). An empirical verification of the Johnson Behavioral System
Model for nursing. Unpublished doctoral dissertation. University of
Birmingham, Alabama.
Lovejoy, N. (1983). The leukemic child's perception of family behaviors. Oncology
Nursing Forum, 10(4), 21-25.
Mastal, M., Hammond, H., & Roberts, P. (1982). Theory into hospital practice: a
pilot implementation. Journal of Nursing Administration, 12(6), 9-15.
McCauley, K., Choromanski, J., Wallinger, C., & Liu, K. (1984). Learning to live
with controlled ventricular tachycardia: utilizing the Johnson Model. Heart &
Lung, 13(4), 38–43.
Meyer, D. (1978). Workload management system ensures stable nurse-patient ratio.
Hospitals, 52(5), 81-85.
- 138 -


Mitchell, M., Miller, J., Welches, L., & Walker, D. (1984). Determining cost of
direct nursing care by DRGs. Nursing Management, 15(4), 29–32.
Neter, J., Wasserman, W., & Whitmore, G. (1982). Applied statistics (2nd ed.).
Boston: Allyn and Bacon, Inc.
Newlin, N. (1976). Development of a methodology and examination of
characteristics of oncology patient utilizing the Johnson nursing model.
Unpublished master's thesis, University of California, Los Angeles.
Nunnally, J. (1978). Psychometric theory (2nd ed.). New York: McGraw Hill BOok
Company.
Nyberg, J., & Wolff, N. (1984). DRG panic. Journal of Nursing Administration,
14(4), 17-21.
Pardee, G. (1968). Classifying patients to predict staffing requirements. American
Journal of Nursing, 68(3), 517-520.
Pedhazur, E. (1982). Multiple regression in behavioral research (2nd ed.). New
York: Holt, Rinehart and Winston.
Piper, L. (1983). Accounting for nursing functions in DRGs. Nursing Management,
14(11), 46-48.
Plummer, J. (1976). Patient classification proves staffing needs. Dimension in
Health Services, 53(5), 36-38.
Poland, M., English, N., Thornton, N., & Owens, D. (1970). PETO: a system for
assessing and meeting patient care needs. American Journal of Nursing, 700Z),
1479–1 l;82.
Polit, D., & Hungler, B. (1983). Nursing research: principles and methods (2nd ed.).
Philadelphia: J. B. Lippincott Company.
- 139 –


Rawls, A. (1980). Evaluation of the Johnson Behavioral System Model in clinical
practice. Image, 12(1), 13-16.
Reinert, P., & Grant, D. (1981). A patient classification system to meet today's
needs. Journal of Nursing Administration, 11(1), 21-25.
Riley, W., & Schaefers, W. (1983). Costing nursing services. Nursing Management,
14(12), 40–43.
Roehrl, P. (1979). Patient classification system: a pilot test. Supervising Nurse,
10(2), 21-27.
Schroeder, R., Rhodes, A., & Shields, R. (1984). Nurse acuity systems: CASH vs.
GRASP. Nursing Forum, 21(2), 72-77.
Schroeder, P., & Washington, P. (1981). Administrative decision-making: staff
patient ratios. Perspectives in Psychiatric Care, 2003), 111-123.
Shafer, F. (1983). DRGs: history and overview. Nursing and Health Care, 4(7),
388-396.
Shavelson, R. (1981). Statistical reasoning for the behavioral sciences. Boston:
Allyn and Bacon, Inc.
Simms, S. (1982). Chapter 27: Cost effectiveness. In A. Marriner (Ed.),
Contemporary Nursing Management. St. Louis: Mosby and Company.
Small, B. (1980). Nursing visually impaired children with Johnson's Model as a
conceptual framework. In J. Riehl and C. Roy (Eds.), Conceptual Models for
Nursing Practice (2nd ed.). New York: Appleton-Century Crofts.
Smits, H., Fetter, R., & McMahon, L. (1984). Variation in resource use within
diagnosis-related groups: the severity issue. Health Care Financing Review,
Annual Supplement, 71–78.
– 140 –


Thompson, J. (1984). The measurement of nursing intensity. Health Care
Financing Review, Annual Supplement, 47–78.
Vaughn, R., & McLeod, W. (1980). Nursing staffing studies: no need to reinvent the
wheels. Journal of Nursing Administration, 10(3), 9-15.
Verran, J. (1982). Development of the ambulatory care client classification
instrument. Unpublished doctoral dissertation, University of Arizona.
Verran, J., & Ferketich, S. (1984). Residual analysis for statistical assumptions of
regression equations. Western Journal of Nursing Research, 6(1), 26-39.
Walker, D. (1982). The cost of nursing care in hospitals. In L. Aiken (Ed.), Nursing
in the 80s: Crises, opportunitites and challenges. Philadelphia:
J. B. Lippincott Company.
Williams, M. (1977). Quantification of direct nursing care activities. Journal of
Nursing Administration, 7(8), 15-18.
Zeller, R. and Carmines, E. (1980). Measurement in the social sciences. New
York: Cambridge University Press.
- 141 –


Appendix A
NPH-Patient Classification System
- 142 -

;|!*

UCLA NEUROPsyc++iatric Institute HospitaLa CLINKCs
nursing service
criteria For categorization of NURSING CARE REQUIREMENTS
Patient Ber-viors Nursing interventions
Behaviors that are:
a. Appropriate to developmentalstage;
b. Adaptive to environment.
Maintain and support healthy, develop-entally appropriate behaviors.
Reinforce independent behaviors inadaptive areas.
e tºes. The Regents of the University of Caniornia
Provide general supervision.Behavioral Subsystems that are currently inactive.
Physical Health status: Normal/orchronic health problem to which patientis fully adjusted.
Behaviors that are: Provide moderate/periodic supervision.
a. Inconsistent; Maintain behavioral programs/treatmentplans designed to modify maladaptive
b. In process of being learned; behaviors and maintain new adaptivebehaviors.
c. May or may not be appropriateto developmental stage; structure environment as needed to pro
I. vide limits on behavior.d. Maladaptive to the environment.
Provide care in the context of groupPhysical Health status: Chronic or settings.acute health problem of minor significance: e.g. cold. Provide nursing care appropriate to
illnesses and handicaps.
Implement medical treatment regime.
Behaviors that are: provide direct supervision.
a. Severely maladaptive to the Imple-ent behavioral programs/treat-entenviron-ent; plans to modify maladaptive behaviors.
b. Not appropriate to developmental Initiate teaching of new behaviors.stage.
Reinforce adaptive behaviors.Physical Health Status: Chronic or acutehealth problem of major significance: III structure environment to provide limite.g. seizures. on behaviors.
I-ple-ent medical treat-ent regime.
Provide intensive nursing care appropriate to illnesses and handicaps.
Critical activities: new admissions,Seclusion & Restraint, Ect.
Care provided on a 1:1 basis basedCategory III behaviors in one or more on category III patient behaviors ofsubsystems of acute intensity, duration acute intensity, frequency and/orand/or frequency. ºv duration.destructive acts and aggression towardother-. Care provided on a 1:1 basis for the
protection of patient.
Auger/De- 12/83 Page 1
– 143 –

$US$YSTEM: INGESTIVE
(FOOD/FLUID NTAKE, SENSORY INPUT: PERCEPTION)
PATIENT DEHAMORS MURSING INTERVENTIONS
1. Ingests sufficient food/fluids to maintain body weight within 10% of normal.
2. Ingests food/fluids at regular intervals.
3. Uses eating/drinking skills consistently.
4. Selects appropriate foods:a. Based on nutritional requirements;b. 8ise of portions.
5. Aware of physical/social environments:a. Maintains acceptable distance from
others;b. Orientation to time and place;c. Utilises visual/auditory attending
skills.
1. General supervision at meal times.2. Provide food/fluids between meals on
request.Provide alternative settings for ingestive activities: e.g. parks,beach.
Encourage participation in food preparation activities with general supervision.
5. Provide enriched physical, emotionaland social milieuta. Privacy and personal space;b. Leisure time materials;c. Cultural and current events.
3
4.
1. Ingests insufficient food/fluids resultins in body weight losséloz of normal.
2. Ingests food/fluids resulting in bodyweight gain?lor of normal.
3. Ingests food/fluids at irregular intervals.
4. Uses eating/drinking skills inconsistently: e.g. incorrect use of utensils.
5. Restricted/limited food choices.6. Interprets significance of events
inconsistently and inaccurately.7. Difficulty in distinguishing between
events happening in mind/dreams asopposed to external reality.
8. Difficulty in maintaining social andphysical boundaries as distinct fromthose of other people.
1. Refuses or fails to ingest food/fluids,2. Ingests insufficient food/fluids result
ing in body weight loss,”0% of normal.3. Ingests food/fluids resulting in body
weight gain;"zoz of normal.4. Unable or fails to use eating/drinking
skills: e.g. chewing or swallowingproblems.
5. Unaware of physical/social environments:e.g. self-stimulation behavior.
6. Ingests substances potentially harmfulto health: alcohol, drugs, laxatives.
7. Unable to interpret significance ofevents.
8. Unable to distinguish between eventshappening in mind/dreams as opposed toexternal reality.
9. Unable to maintain social and physicalboundaries as distinct from those ofother people.
10. Lack of awareness of personal space.
One or more Category III behaviors ofacute intensity, frequency and/orduration.
IV
1. Periodic supervision at meal times.2. Periodic verbal/physical reinforce
ment for specific eating/drinkingskills.
3. Monitor food selection and consumption.4. Supervise in alternative settings for
eating activities.5. Allow limited participation in food
preparation activities.6. Periodic orientation to staff, daily
activities and unit routine.7. Provide emotional support, counseling
during and following stressful situations.
8. Periodic verbal/physical reinforcementto assist in establishment of socialand physical boundaries.
9. Clarify interactions with others.10. Administer medication as prescribed.
1 Direct supervision & teaching at mealtimes to develop adaptive behaviors.
2. Assist with food/fluid intake betweenmeals.
3. Direct supervision in alternativesettings.
4. Implement treatment plan to developattending skills: e.g. eye contact.
5. Provide frequent orientation to time,place and daily activities.
6. Monitor environment for potentiallyharmful substances/objects.
7. Provide emotional support and counseling to assist in interpretation ofevents.
8. Provide emotional support during andfollowing stressful situations including removal from immediate situations.
9. Provide direction, reality orientation,and support when unable to distinguishreality.
10. Structure environment to provide verbal and physical limits on maladaptivebehaviors.
11. Administer medication as prescribed.
Level III care provided on a 1 : 1 basis.
t 1985 The Regents of the University of CaliforniaPage 2
– 14! -

$US$YSTEM, EUMINATIVE(PATTERN OF ELMINATION: HYGENECARE)
Partent GEMAvtoRº NURGING INTERVENTIONS
1. Total bowel and bladder control. 1. General supervision of elimination and2. Established pattern of elimination. hygiene activities.3. Disposes of body wastes in sanitary 2. Monitor pattern of elimination and
way: e.g. disposal of feces, urine, menstruation.menstrual pad/tampons, nasal 3. Observe for potential disruption indischarge, saliva, perspiration. pattern of elimination.
4. Washes hands following eliminativeactivities.
º
1. Partial/periodic bowel control. 1. Periodic verbal/physical reinforcements2. Partial/periodic bladder control. for elimination.3. Disruption of established pattern 2. Periodic verbal/physical reinforcements
of elimination resulting from and assistance for specific hygieneacute illness, poor eating habits tasks: e.g. handwashing, menstrualor excessive use of laxatives. care,
4. Disposes of body wastes incon- 3. Reinforce successful elimination.sistently: 4. Provide medications as prescribed bya. Fails to flush toilet; physician to alleviate eliminationb. Fails to wipe self following B.M. problems: e.g. antacids, analgesics
5. Lacks adequate knowledge of hygiene º for menstrual cramps.and menstrual care. 5. Monitor disrupted elimination patterns;
e.g. intake and output.6. Implement treatment plan to maintain/
reinforce established pattern of elimination: e.g. toileting schedules.
7. Provide minimal teaching of hygienec-re.
8. Administer medication as prescribed.
1. Absence of bowel control. 1. Implement treatment plan to establish2. Absence of bladder control. pattern of elimination: e.g. toilet3. Severe disruption of established training.
pattern resulting in potential 2. Total care of eliminative needs; e.g.dehydration: e.g. vomiting, diaper care, colostomy care, drains.diarrhea, diaphoresis. 3. Teach self-care, independent skills
4. Fails to dispose of body wastes in related to hygiene, eliminative tasks.sanitary manner: e.g. fecal 4. Direct supervision of hygiene care.smearing. 5. Attend closely to changes in elimina
tion pattern for signs and symptomsII. of physical problems.
6. Administer medication as prescribed.
One or more Category III behaviors Level III care provided on a 1:1 basis.of acute intensity, frequency IVand/or duration.
Page 3*** The Regents of the University of California
- 145 -

SUBSYSTEM: DEPENDENCY
(BASIC SELF-CARE, EMOTIONAL SECURITY)
PATIENT BEHaviors Nursing interventioxº
1. Performs own self-care activities: 1. Provide environment to facilitate in
e.g. bathing, hair washing, oral dependent performance of hygiene,hygiene. grooming activities and maintenance
2. Performs own self-care within a of personal belongings.reasonable length of time. 2. Provide assistance when requested.
3. Maintains personal belongings: e.g. 3. Reinforce independent behaviors.clothing, toiletries. 4. Provide information/explanations in
4. Seeks assistance when needed. preparation for separation related to5. Adjusts to separation from signifi- I hospitalization or placement.
cant others with ease. 5. Provide information regarding impend6. Makes decisions with comfort. ing changes in the milieu.7. Relies on own resources when appro
priate.8. Questions decisions of others when
indicated.
9. Engages in appropriate situationalattention seeking behaviors.
10. Adapts to change in milieu.
1. Requires assistance with bathing, 1. Assist in hygiene/grooming activities:hair washing, and/or oral hygiene. a. Provide periodic verbal/physical
2. Requires assistance with maintenance reinforcements;of personal belongings. b. teach area(s) of deficit.
3. Requires assistance with grooming 2. Provide or limit assistance when indiactivities. cated.
4. Does not seek assistance when needed. 3. Assist in identifying areas where help5. Seeks istance when not needed. is needed.
6. Separates from significant others with 4. Encourage discussion of loss/separadifficulty: e.g. whining, clinging. tion and assist in resolution.
7. Verbalises feelings of hopelessness 5. Periodic verbal/physical reinforceand helplessness. I. ments for independent decision making.
8. Relies periodically on others for 6. Maintain treatment plan to reduce ordecision making. extinguish persistent help seeking/
9. Reluctant to act without directives. attention seeking behaviors.10. Questions or rejects decisions of 7. Promote adaptation to change by:
others in authority frequently. a. Structuring environment;ll. Engages in appropriate situational b. Allowing participation in small
attention seeking behaviors inconsis- group meetings.tently.
12. Experiences difficulty in adaptingto change within milieu.
1. Unable to perform self-care activities: 1. Provide total assistance in self-caree.g. bathing, hair washing, oral activities that cannot be performedhygiene. independently.
2. Unable to complete own grooming/dressing. 2. Teach requisite skills.3. Unable to care for personal belongings. 3. Provide supervision and directives in4. Lack of awareness of need for assistance. area(s) of deficit.5. Experiences excessive difficulty when 4. Assist in identification and recogni
separating from others, or fails to tion of need for assistance in:respond to separation from others. a. Area(s) of skill/knowledge deficit;
6. Preoccupied with feelings of hope- b. Acute/chronic/progressive disabililessness and helplessne | ties.7. Questions or rejects decisions of 5. Provide structured activities toothers in authority constantly. encourage expression of feelings re
8. Relies on others for decision making garding separation, hopelessness, helpexclusivelyt e.g. with adults & peers. lessness: e.g. music, art, drama, etc.
9. Refuses to act without directives. 6. Implement treatment plan to develop10. Engages in negative attention independent decision making.
seeking behaviors. 7. Implement treatment plan to reduce or11. Resistant to change in milieu. extinguish negative attention seeking
behaviors.8. Promote adaptation to change by plan
ning and limiting number of changes.
One or more Category III behaviors of Level III care provided on a 111 basis.acute intensity, frequency and/or IVduration.
Page 4c 1965 The Regents of the University of California
- 146 –

$UCSYSTEM}: ACC00 V LM INT
(MASTERY OF SELF AND ENVIRONMENT)
Selects goals from alternative possibilities.
and completes tasks.Utilises problem-solving abilitiesto initiate and/or complete goaldirected activities.Organises group activities of asocial and/or work oriented nature.
4.
1. Provide opportunity for, and reinforee independent decision making.
2. Maintain abilities to acquire skillsand knowledge by providing challenging learning experieeces.
3. Provide environmental conditionsfor initiation and completion of goaldirected activities.
© 1965 The Regents of the University of California
5. Identifies and accepts strengths and [. 4. Provide opportunity for participationweaknesses in self and others; con- in competitive and cooperative actiºpetes according to these personal vities.factors. 5. Support efforts to improve area(s) of
weakness and maintain strengths.
1. Identifies available alternatives 1. Promote decision making by limitingbut unable to select a goal. number of alternatives.
2. Unable to identify realistic goals. 2. Provide direction in sequisition of3. Selects choices from limited range skill/knowledge.
of alternatives: e.g. two choices. 3. Provide direction for task completion4. Attention span limited: easily dis- by establishing specific steps and/or
tracted. time frames for completion.5. Utilises problem-solving skills in- 4. Structure competitive and cooperative
consistently. activities to permit experience of6. Initiates achievement activities success and provide support when
but fails to complete tasks or coa- EU failure occurs.pletes without optimal use of 5. Promote acceptance of success/failure
| problem-solving skills. of others.7. Limited awareness of strengths and 6. Give simple directions to facilitate
weaknesses of self and others. comprehension of instructions.8. Follows simple directions.
1. Unable to determine goals or identify 1. Provide direct supervision for taskalternatives. completion and assist in problem
2. Does not utilise cognitive abilities solving process.to acquire knowledge. 2. Select alternatives and identify
3. Does not accept direction from goals.others. 3. Identify strengths and weaknesses and
4. Lack of problem-solving skills: e.g. provide opportunity for utilisingengages in repetitive, rote tasks. acquired skills.
5. Lack of awareness of strengths and 4. Limit experiences of failure; provideweaknesses of self and others. opportunity for successful
6. Seeks unrealistic modes of competi- | experiences.tions with repeated experience of 5. Give instructions on very basic level.failure. 6. Assist in completion of tasks: e.g.
7. Limits self to experiences/tasks homework, projects.with guaranteed success. 7. Implement treatment plan to promote
8. Unable to accept responsibility for development of achievement skills.failure. 8. Assist in examining causes for failure
9. Fails to complete tasks. and resolution of feelings.10. Unable to perform tasks/skills appro
priate to developmental stage.
One or more Category III behaviors of Level III care provided on a 1:1 basis.acute intensity, frequency and/or IVduration.
Page 5
– 147 –

sussystEM, AFFILiarivº(DEVELOPMENT OF RELATIONSHIPS, COMMUNICATION SKILLS)
PATENT LENAMORS
1. Establishes and maintains emotional
attachments with significant others.2. Establishes and maintains interper
sonal relationships on an individualbasis with staff and/or peers.
3. Establishes and maintains interpersonal relationships in groupsettings.
1. Maintain effective communication,including spontaneous/plannedinteractions.
2. Encourage expression of feelings.3. Provide opportunities for individual/
group interactions with a variety ofpersons.
4. Support development and maintenance
e 1985 The Regents of the University of Cantornia
4. Communicates effectively: verbal, l of friendships and familynon-verbal, in writing. relationships.
5. Expresses positive and negativefeelings with comfort and as appropriate.
6. Affect congruent with content.
1. Difficulty in forming emotional 1. Provide specific time for establishingattachments to significant others. staff/peer relationships.
2. Establishes and/or maintains 2. Maintain treatment plan to facilitatelimited relationships with staff group participation.and/or peers. 3. Provide periodic prompts/reinforce
3. Relates in superficial or inappro- ment of effective patient communicapriate manner: e.g. teasing, inter- tion.rupting. 4. Maintain treatment plan to facilitate
4. Establishes and maintains limited interactions of patient with familyrelationships in group settings/ and significant others.activities. |
5. Difficulty in communicating ideasand feelings: verbal, non-verbalwritten.
6. Initiates and maintains communication infrequently and/orineffectively.
1. Absence of emotional attachment with 1. Provide regular, intensive 1 1 1 interothers; or excessive, intense actions to establish relationship.attachments. 2. Implement treatment plan to increase
2. Fails to establish or maintain rela- frequency of interactions with staff/tionships on an individual basis. peers.
3. Fails to establish or maintain rela- 3. Implement treatment plan to increasetionships in group interactions. participation in group activities.
4. Fails to initiate/maintain effective 4. Limit contact with family when indicacommunication: verbal, non-verbal ted; provide information regardingor in writing. denial of rights.
5. Indiscriminate attachment to others. | 5. Implement treatment plan to develop6. Unable to express positive/negative basic communication skills and role
feeling states in direct manner: e.g. model interactional techniques.denial of feelings. 6. Assist in identification and expres
sion of positive/negative feelings.
|
One or more Category III behaviors of Level III care provided on a 1 11acute intensity, frequency and/or V basis.duration.
Page 6
– 148 -

$USSYSTEMI; AGGRESSIVE-PROTECTIVE
(PROTECTION OF SELF FROM POTENTVAL/REAL HARM)
Pºrtºn GEMAMMOR$ NURSING INTERVENTIONS
I Identifies and avoids potentialhasardous/dangerous situations inenvironment to self and others.
. Create and maintain a safe environment.Monitor environment for potentiallyhazardous situations.
2. Selects appropriate verbal/ 3. Assess and reinforce adaptive copingnonverbal response to potentially strategies for identifying and avoidhazardous or dangerous situations. ing potentially hazardous and dangerous
3. Maintains control over actions in situations.
stress-producing situation. 4. Provide support when indicated.4. Elicits support from others if
needed.
1. Identifies obvious dangers but not 1. Assist in identifying subtle environsubtle cues of potential harm. mental/internal cues associated with
2. Fails to anticipate dangerous situa- potentially dangerous situations.tions. May be involved in frequent 2. Teach alternative methods for protectaccidents. ing/defending self; includes assertion
3. Selects indirect verbal/nonverbal training, self defense techniques.response to threat. 3. Continuously reinforce coping strate
4. Selects response to threat that ‘gies when present.contains potential for self injury 4. Establish environmental controls whenof minor magnitude. necessary to protect or defend patient.
5. Unable to consistently identify or I 5. Teach identification of, and verbalcontrol one's reactions to stress. expression of anger/frustration.
6. Wanders away from unit or group. 6. Administer medication as prescribed.
1. Lack of awareness of potentially 1. Provide environmental controls to prohasardous situations, or per- tect/defend patient from dangerousceives many situations as situations by:dangerous. a) Medications:
2. Engages in intense/frequent act- b) Locked door;
3. *: behaviors. 1 f d § Seclusion;. Fails to protect self in danger- D) Restraints.ous situations. 2. Closely monitor patient/environment
4. Demonstrates phobic behavior(s). for potentially hasardous situations:5. Selects inappropriate/inadequate e.g. sharp objects, toxic substances.
response to threat. 3. Implement treatment plan to assist in6. Lack of awareness of cause and II. development of internal controls.
effect. 4. Provide direct supervision to assist7. Refuses to remain on unit or with in selecting appropriate response to
group: e.g. elopement (AWOL) threat.8. Selects response to threat that 5. Administer medication as prescribed.
contains potential for self injuryof major magnitude.
One or more Category III behaviors Level III care provided on a 1:1of acute intensity, frequency IV basis.and/or duration.
Page 7c 1965 The Regents of the University of California
– 149 –

$ULSYSTEMI; $EXUAL
(KNOWLEDGE: BEHAVIOR)
PATIENT SEMAMMOR8 NURSING INTERVENTIONS
1. Verbalizes knowledge of one's ownanatomy and physiology.
2. Distinguishes between males andfemales in regards to:a) Self:b) Others.
3. Engages in socially accepted formsof sexual behavior; masturbates inprivate.
1. Model appropriate sex-role behaviors.2. Reinforce socially adaptive sex-role
behaviors.
3. Provide privacy.4. Clarify information and explore feel
ings regarding sexual behavior.
4. Werbalizes and demonstrates comfort Iwith own body and physical changes:a) Body posture:b) Grooming, dress.
5. Accepts own gender identity asexpressed in body movements,clothing and gestures.
1. Lacks adequate knowledge of anatomy/ 1. Clarify misconceptions and providephysiology; or has misconceptions. information to correct area(s) of
2. Discriminates own sexual identity deficient/absent knowledge. Teachbut not that of others (or vice in group setting.versa). 2. Teach alternative ways of dealing
3. Aware of, but fails to use socially with sexual approaches.acceptable forms of sexual behavior: 3. Periodic reinforcement of sociallye.g. exploring, touching others, adaptive behaviors.dressing provocatively. 4. Instruct in use of privacy.
4. Expresses verbally and nonverbally 5. Encourage expression of feelings offeelings of discomfort with body | discomfort/acceptance of one's body.and physical changes, include diet 6. Teach new materials through use ofrestriction to prevent body change. films, lectures, books.
5. Aware of gender identity difference 7. Identify body changes and assist inbut does not demonstrate acceptance process of adjustment.of gender identity in gesture ordress.
6. Unable to discriminate betweensexual and non-sexual approachbehaviors. -
1. Minimal or no knowledge of own 1. Comprehensive teaching to deal withanatomy and/or physiology. fantasies, fears and lack of knowledge.
2. Unable to discriminate between 2. Intensive emotional support/counselingmales and females. regarding sexual behavior/experiences
3. Fails to engage in socially of self and others.accepted sexual behavior: e.g. 3. Implement treatment plan to modify spetouching others excessively, cific sexual behavior including use ofexposing genitals and mastur- privacy.bating in public. 4. Provide feedback and assist in accept
4. Denies body change. ance of body changes.5. Fails or refuses to accept own BLE 5. Establish limits for sexual behavior
gender identity by engaging in and assist in identification of inactivities associated with appropriate behavior.opposite gender: e.g. dresses inclothing of opposite sex,verbalizes incorrect genderidentity.
6. Provokes sexual contact withinappropriate partner.
One or more Category III behaviors Level III care provided on a lilof acute intensity, frequency IV basis.and/or duration.
Page 8© 1985 The Regents of the University of California
- 150 -

$US$YSTEM; RESTORATIVE
(SLEEPBEHAVIOR; RECREATION, RESPONSE TO LLNESS)
Pºrtºn GEMAMMORS
1. Mormal sleep patterns, includingease of onset, maintenance ofsleep for adequate rest.
2. Engages in balanced variety ofphysical/mental recreational
. General supervision at bedtime.Arrange for a balanced variety ofrecreational activities.
. Observe and monitor daily patternsof activity.
activities. 4. Illness:
3. Participates in organized social a) Provide safe physical environment:groups. s b) Support selection of activities
4. Regulates patterns of activity appropriate to health status:according to physical/mental c) Provide medication/supplies/requirements. treatment as prescribed by
5. Participates in prescribed physician;treatment regime. d) Monitor physical status including
height, weight and immunisations.
1. Abnormal sleep pattern, including 1. Structure nighttime routine toperiodic awakenings at night; facilitate settling down.settling difficulties. 2. Monitor sleep patterns for nighttime
2. Engages in limited number and/or awakenings.range of recreational activities: 3. Periodic reinforcement of participae.g. all sedentary activities; tion in group activities.solitary play. 4. Provide environmental structure and
3. Engages in inconsistent pattern direction to regulate patterns ofof activities. activity; provide rest time when
4. Experiences difficulty in adapting º needed.activity level to limitations. 5. Periodic supervision, direction
5. Participates inconsistently in required for basic health behaviors.prescribed treatment regime. 6. Provide physical interventions for
injuries/minor illnesses.7. Administer medication as prescribed.
1. Sleep disruptions and disturb- 1. Direct supervision/close observationances resulting in minimal hours of sleep patterns throughout night.of sleep. 2. Direct supervision of recreational
2. Fails to engage in recreational activity patterns.activities. 3. Initiate activities for patient
3. Sleeps during waking hours: e.g. participation.daytime. 4. Structure daily routine to allow for
4. Participates in activity to a variety of activities throughout day.excessive degree, resulting in 5. Establish limits regarding selectionphysical exhaustion and fatigue. of possible activities.
5. Preoccupied with one form of 6. Close observation of physical healthactivity to exclusion of all status.
others. III 7. Provide complex/frequent physical in6. Does not adapt, or chooses to terventions for major illness/injuries:
ignore limitations imposed by e.g. tube feedings.illness or handicaps. 8. Provide extensive, complex teaching
7. Refuses to participate in pre- program for health problems: e.g.scribed treatment regime. diabetes, seizures.
9. Administer medication as prescribed.
One or more Category III behaviors Level III care provided on a 1:1of acute intensity, frequency IV basis.and/or duration.
Page 9& 1985 The Regents of the University of California
- 151 -

Appendix B
Subsystem Behaviors
- 152 –


Ingestive Behaviors
1.
4.
10.
11.
Eating and drinking skillsa. Consistentb. Inconsistentc. Unable/absence
Ingestion of food and fluids at intervalsa. Regularb. Irregular
Food choices
a. Appropriateb. Restricted
Awareness of social/physical environmenta. Normal awarenessb. Limited awarenessC. Lack of awareness
Sensory perceptiona. Normal
Ingestion of substancesa. Harmful
Interpretation of eventsa. Limited abilityb. Unable to interpret
Awareness of social/physical boundariesa. Limited abilityb. Unable to sense
Distinguishing of eventsa. Limited abilityb. Unable to distinguish
Frequency of intakea. Adequateb. FrequentC. Continuous
Sufficiency of intakea. Adequateb. Inadequatec. Insufficientd. Absence
- 153 -
Appendix CBehavior Criteria
Category Checklistof Corresponding
Behavior Item #
I 21;II 17III 1 l;
I 16II | 1
I 23II 3
I 22II 19III 15
I l
III 9
II 21III 18
II l;III 7
II 10III 25
I 13II 20III 5
I 6II 12II 8III 2

*.- -

Eliminative Behaviors
Bowel controla. Totalb. Partialc. Absence
Bladder controla. Totalb. Partialc. Absence
Pattern of eliminationa. Established
b. Disruptedc. Absence
Disposal of body wastesa. Sanitaryb. Inconsistent
C. Unsanitary
Hygiene Carea. Washes self
b. Lacks adequate knowledge
Appendix CBehavior Criteria
Category Checklistof Corresponding
Behavior Item #
I 11II 3III l;
I 11II 14III 2
I 5II lIII 12
I 10II 13III 6
I 7II 9
- 154 –

t
*
* -
º

Affiliative Behaviors
1.
5.
6.
7.
Emotional attachments
a. Appropriateb. Delayed abilityc. Indiscriminated. Absence
Interpersonal relationships with individualsa. Appropriateb. Limitedc. Fail to establish
Interpersonal relationships with groupsa. Appropriateb. Limitedc. Failure to establish
Adaptation to changea. Able to adaptb. Difficulty in adaptingc. Resistant to change
Communicating ideas: verbally, nonverbally andin writinga. Effective
b. Limited abilityC. Engage infrequentlyd. Fail to initiate
Expresses feelingsa. Appropriateb. Superficialc. Unable to express
Awareness of personal spacea. Appropriateb. Lack of awareness
Appendix CBehavior Criteria
Category ChecklistOf Corresponding
Behavior Item #
I 18II 14III lIII 3
I 13II 9III 19
I l;II 8III 17
I | 1II 15III 12
I 21II 10II 20III 6
I 7II 16III 22
I 2III 5
- 155 -

*
- *
-
º
-
*
* *
tº v i ■ º.
- -
* - * *
- -
. . . . . . . *
- - -
- - : --
º - - •
- -
•- *
. . . - -. . . . . . . . . . -
* . .
* * -
. . . .
: . -
* * . . . . . . .
- - " - -- t = - - * - - -
- - -
* ... ( . .-
-
- 1 - - -
[ . . . . . . .º - * - -
º ! . . . - -
- - , + .- - . . . . . . . . .
. . . ., - 3 a
* * - * -
t - * -- * ‘. . . . . . .
-* - -
* > * > * -* . . . . . . . . . .
* -* *
t
t. . . . .
-* -
: , 3 ■ il
* *
* *
* * *
is

Dependency BehaviorsAppendix C
Behavior Criteria
Category Checklistof Corresponding
Behavior Item #
1. Self-care activities
a. Able to perform I 14b. Performs in reasonable time I 16
c. Requires assistance with bathing II 20d. Requires assistance with grooming II 17e. Unable to perform III 5f. Unable to complete III 8
2. Care of personal belongingsa. Able to care I 18
b. Requires assistance II 19c. Unable to care III 6
3. Seeks assistance
a. Appropriate I 28b. Seeks when not needed II 27c. Fails to seek II ld. Lack of awareness of need III 24
4. Relies on own resources
a. Appropriate I 7b. Reluctance II 11c. Refuses to act III 12
5. Decision-making abilitya. Appropriate I 29b. Periodic reliance on others II 26c. Exclusive reliance on others III 3
6. Separation with easea. Able to adjust I 23b. Separates with difficulty II 21c. Extreme difficulty with separation III 2
7. Feelings of hopelessness/helplessnessa. Verbalizes II 13
b. Preoccupied III l;
8. Questions decision of authoritya. Occasional I 22
b. Frequently II 9c. Constantly III 25
9. Engages in situational attention seeking behaviorsa. Appropriate I 15b. Inconsistent II 10
c. Inappropriate III 30
- 156 -

*
*
-
- -
* *
* *
*
*
º
- *
* -
º* *
*-
zºic iv i■
* . . . . . . . . .
s . . . . - * * *
. . . . . . . . .
-- " - - - - - -
* - * * * * - - - - -
4.
- . . . . . . . . . . "
* . ., , : * . ( .-
-
* . . . . -- |º * * * - - -
- : -- * * *
- . . . . . . . . . .
- - - , , , ,
. . ! --
* * -
- - -- - *-
* * - .- - -
* - -
. . . . . . . . . . . .
* - ". * ~ * * *
- - º - -* * * - - * -
- ! - º e
-, -- - -
‘. .- - *
: . . . . .
- * - -
* - 4 - * * * *
- * : * • -. . - . . . .
-
- * *
* - I - - - * -
- * * . . - * * *‘. . . . . . . . . . . . . . .
. . . ; - -- * - - - - - * -
- -- - -
- * * - - -
. . . . . . . . . .* , - - - - - *
. . . . ~ 1 a - * º - -
- *
f : : * . . . . . .
. . . . . .
-- - -
* * . . . - -
º . . . * * * *
t - -
-- * * - - -
* * * - -. -
-
* * * -
t - - " .*
- * - * ~ * * * - .* - * ---- - * *
* * *
-* - " - -
* * - c : , -
* : * *- -
* -

Sexual Behaviors
1.
5.
Knowledge of own anatomy/physiologya. Verbalizes
b. Lacks knowledgec. Minimal/no knowledge
Distinguishes between males and femalesa. Able to distinguishb. Distinguish self but not othersc. Unable to discriminate
Engages in socially acceptable behaviora. Appropriateb. Aware, but fail to engageC. Inappropriate
Comfort with body/physical changesa. Appropriateb. Expresses discomfortc. Denies changes
Acceptance of gender rolea. Appropriateb. Aware, but fails to demonstratec. Refuses to accept
Distinguish between sexual/nonsexual approachbehavior
a. Inability to discriminateb. Provokes sexual contact
Appendix CBehavior Criteria
Category Checklistof Corresponding
Behavior Item #
I 12II 8III 2
I 17II 6III 1 l;
I 13II lIII 3
I 5II 9III 7
I 11II 16III l;
II 10III 15
- 157 -

--
tº \ . . .
- . . . .
* *- * *
- * - - • *-
. . -
- * * * * --
º- * - - * *
* . --
- -
:
- * * -
º
rº
-
~ *
d :
!
º
- - -
-
* -
- - * = --
-
* * - --
* * --
* - - -
* -- { - - *
* - - **
º - * -
- - - -
. . . . .
. . . . . .

Aggressive-Protective Behaviors
3.
4.
7.
Identifies/avoids hazardous situationsa. Avoids potential hazardsb. Identifies obvious hazards
c. Fails to anticipated. Lack of awareness
e. Unable to protect self
Selects response to threat/dangerous situationsa. Appropriateb. Inappropriatec. Unable to control
Response to threat with self-injurya. Minor injuryb. Major injury
Engages in acting out behaviorsa. Intense acting out
Ability to maintain controla. Appropriateb. Inconsistent
Phobic behaviora. Demonstrates
Separation from groupa. Wanders awayb. Elopes
Appendix CBehavior Criteria
Category Checklistof Corresponding
Behavior Item #
I 11II 6II 1 l;III l;III 7
I 9II 10III 2
II 13III 17
III 3
I 1II 12
III 8
II 5III 16
– 158 -

-
-
*
■ )·■ •*
,-~}
·
·■ --|-!±••
•■ *••••¶----|-→
→→→
→**
*··
-----*„*----·■ -----*-•
×|-|-·-|-!|-.*■ -|-*----
i'
•••••*
*~~
~*•
•-------
--
***|-----|--
→…--···
·•••',
-
|••^■ ·••••••
|-----····
-~|~~■ ;,■■,
…--
-|-|-*,,
º|-…»·--
--|-*··„*·*
,••••
•-----...•
•
■ -……*|-·--·---------·…
**··------------·•••----|--•
•*.*----|-·
··•••
•,--...•
•••–----
…»|-••
•·*•••
•••
•|-|-*…*|-*
|-
,
■ ·|-**-
sv.•••
•|-··
|--"|-■----→···----…■-…***··
-|-}…
---*!·*
-*
*|-------
|-|-!|-|-…**••
······
-|-·*
----·--- -*

Achievement Behaviors
1.
3.
5.
10.
Experiences success and failuresa. Repeated failuresb. Limits self to guaranteed successesc. Unable to accept failure
Chooses alternatives
a. Limited range
Selects goals from alternativesa. Able to select
b. Identifies, but not selectc. Unable to identifyd. Unable to identify or select
Initiates and completes tasksa. Able to initiate and completeb. Initiates, but does not completec. Fails to completed. Unable to perform
Utilizes problem-solving skillsa. Appropriateb. Inconsistent
c. Lack of problem-solving skills
Identifies, accepts strengths and weaknessesa. Able to acceptb. Limited abilityC. Lack of awareness
Attention spana. Limited abilityb. Short span
Organizes groupsa. Able to
Accepts directionsa. Does not acceptb. Follows simple directions
Utilizes cognitive abilitiesa. Does not use to acquire knowledge
Appendix CBehavior Criteria
Category Checklistof Corresponding
Behavior Item #
III 23III 13III 5
II 21
I 6II 17II 22III 19
I 12II | 1III 9III 15
I 18II lIII 16
I 10II 8III 20
II 7III 3
I l;
I 2II 1 l;
III 21;
- 159 -

- * -
* { i \ . . . ■ - ,
. . . . . - - -
- . . . " * * -
* - - - ... • -
- • . - -
- - - - - - - - - - -
- 1 * * * - - s -
- - - -- - - - * -
* - * :- - - - - - -
s - * * - -
- - - - * *
- " - - * - * : . -
c - - * - - . . . . . -
... " - t- - - - * *
- - -
. . . . • * - - -
!- - * - --
* - * * * - * * * * * * * * * t. . * ~ * C - - - t s - * * --
- - - - - ... •* * * * * * * - * . - - -
- + - - - - - --* - - - - - - º
*
. . . -
- - s - - - -- : • - . . . ." --
- * . * . .- - - - - + -
* * * - - - -
- - - - - - - **
º * - -
- - * *º
. . * * * * -
- * * * - - - - - * -- - t -. - - * --
* * * - - . . . . . . . . . - - --
- - * -
- - * - -
- -
- - - . . . .-
- : - -
• * - * * -
* - - --
* * * * -
* → - • * -
* * * * - * → *º
- - - -
- - - - - --
- - * * -
- - - - - * *-
* . . . * * . . . . .
t - * *- - * → - - - --

Restorative Behaviors
3.
4.
5.
Sleep patternsa. Normal
b. Periodic awakeningsc. Sleeps during daytimed. Sleep disruptions
Engages in recreational activitiesa. Balanced recreational activities
b. Engages inconsistentlyc. Fails to engaged. Engages excessively
Involvement in range of activitiesa. Limited
b. Exclusive preoccupation
Participates in treatment regimea. Appropriateb. Inconsistentc. Refuses
Regulates activity according to physicalrequirementsa. Appropriateb. Experiences difficultyc. Ignores limitations
Participates in organized social groupa. Appropriate
Appendix CBehavior Criteria
Category Checklistof Corresponding
Behavior Item #
I 11II 9III 2III 8
I 7II 12III 16III 13
II 14III 5
I 10II 6III l;
I lII 15III 3
I 17
- 160 —

- -- -
-- -
- - s
- - * - -
- -* - *
- -
- - - ,
* - -- - - -
. . .
- " - -
* : * - - - -*-
-
º
• *
-
* *

Appendix C
Behavior Criteria Checklist
- 161 –


BEHAVIORAL CRITERIA CHECKLIST
NAME OFRESPONDENT CLASS/OBSERVER
DATE UNIT TIME COMPLETED
INGESTIVE SUBSYSTEM
1 Normal sensory perception.2. Absence of food/fluid intake. Refusal or failure to eat.3. Restricted/limited food choices.4. Limited ability to sense mental and physical boundaries as distinct from those
of other people.5. Continuous eating/drinking resulting in weight gain 220% normal weight.6. Adequate food/fluid intake to maintain weight within 10% of normal body
weight.7. Unable to sense mental and physical boundaries as distinct from those of other
people.8. Insufficient food/fluid intake resulting in weight lossº 20% normal weight.9. Ingestion of substances potentially harmful to health: drugs, laxatives,etc.
10. Limited ability to distinguish between events happening in mind/dreams asopposed to external reality.
11. Food/fluid intake at irregular intervals.12. Inadequate food/fluid intake resulting in weight loss? 10% of normal body
weight.13. Meals are completed.
Absence of eating/drinking skills; e.g. chewing and swallowing problems.15. Lack of awareness of physical/social environment: self-stimulation behavior.16. Food/fluid intake at regular intervals.
Inconsistent use of eating/drinking skills: e.g. incorrect use of utensils.. Unable to interpret significance of an event; perceptual distortion.
Limited awareness of physical/social environments.20. Frequent intake resulting in weight gain = 10% normal body weight.21. Limited ability to interpret significance of event; perceptual distortions
elicited mainly in emotionally stressful circumstances.22. Awareness of physical/social environment: self in relation to others;
orientation to time & place; utilizes visual/auditory attending skills.23. Selection of appropriate food based on nutritional requirements & size of
portions.24. Consistent use of eating/drinking skills.25. Unable to distinguish between events happening in mind/dreams as opposed
to external reality.
E.-T1 :4.
ELIMINATIVE SUBSYSTEM
1. Disruption of established pattern of elimination due to acute illness, pooreating habits, excessive use of laxatives.
2. Absence of bladder control.3. Partial/periodic bowel control.4. Absence of bowel control.
5. Established pattern of elimination.
- 162 –

BEHAVIORAL CRITERIA CHECKLIST - continued
l
: .
:
6.7.8.9.
10.
ll.12.
I 3.
4.
;
: .10.
1 I -
17.
: ; :20.21.22.
Failure to dispose of body wastes in sanitary manner; e.g. fecal smearing.Washes hands following eliminative activities.Excessive diaphoresis.Lacks adequate knowledge of hygiene and menstrual care.Disposes of body wastes in sanitary way: disposal of feces, urine, menstrualpads/tampons, nasal discharge, saliva, perspiration,etc.Total bowel and bladder control.
Absence of established pattern of elimination; or disruption of establishedpattern resulting in dehydration.Inconsistent disposal of body wastes: failure to flush toilet; and failure towipe following bowel movement.Partial/periodic bladder control.
AFFILIATIVE SUBSYSTEM
Indiscriminate attachment to others.
Maintains acceptable distance from others.Absence of emotional attachment with others, or excessive, intense attachments.
Establishes and maintains interpersonal relationships in group settings.Lack of awareness of personal space.Failure to initiate/maintain effective communication: verbal, non-verbal andin writing.Expresses positive and negative feelings with comfort and as appropriate.Establishes and maintains limited relationships in group activities.Establishes and/or maintains limited relationships with staff and peers.Limited ability to communicate ideas and feelings: verbally, non-verbally andin writing.Ability to adapt to change in milieu.Resistant to change in milieu or daily routine.Establishes and maintains interpersonal relationships on an individual basis:includes relationships with staff and peers.Unstable, delayed ability to form emotional attachments to significant others.Experiences difficulty in adapting to change within the milieu.Relates in superficial or inappropriate manner: e.g. teasing, interrupting,etc.Failure to establish and maintain relationships in group interactions.Establishes and maintains emotional attachments with significant others.Failure to establish or maintain relationships on an individual basis. 2Initiates and maintains communication infrequently and/or ineffectively.Communicates effectively: verbally, non-verbally and in writing.Unable to express positive/negative feeling states in direct way: denial offeelings.
– 163 –

BEHAVIORAL CRITERIA CHECKLIST - continued
}.
–
: :
10.
; } .13.
19.2 O21.2 223.2 {} º
25.26.27.28.29.
6.
8.
DEPENDENCY SUBSYSTEM
Does not seek assistance when needed.Excessive difficulty when separating from others; or, lack of response toseparation from others.Exclusive reliance on others for decision-making-e-g- adults, peers.Preoccupied with feelings of hopelessness and helplessness.Unable to perform self-care activities: bathing, hair washing, oral hygiene.Unable to take care of personal belongings.Relies on own resources when appropriate.Unable to complete own grooming/dressing.Frequently questions or rejects decisions of others in authority.Engages inconsistently in appropriate situational attention seeking behaviors.Reluctance to act without directives.Refuses to act without directives.
Verbalizes feelings of hopelessness and helplessness.Performs own self-care activities: e.g. bathing, hair washing, oral hygiene.Engages in appropriate situational attention seeking behaviors.Performs own self-care within a reasonable length of time.Requires assistance with bathing, hair washing and / or oral hygiene.Maintains personal belongings: e.g. toys, clothings, toiletries.Requires assistance with maintenance of personal belongings.
. Requires assistance with grooming activities.Separates from significant others with apparent difficulty: whining, clinging.
. Occasionally questions decisions of others.Adjusts to separation from significant others with ease.Lack of awareness of need for assistance.Constantly questions or rejects decisions of others in authority.Periodic reliance on others for decision-making.Seeks assistance when not needed.Seeks assistance when needed.Able to make decisions.
SEXUAL SUBSYSTEM
Aware of, but fails to use socially acceptable forms of sexual behaviors;exploring, touching others; sexually provocative gestures and clothing.Has minimal or no knowledge of own anatomy/physiology.Failure to engage in socially accepted sexual behaviors: excessive touching ofothers; exposing genitals, masturbation in public.Failure or refusal to accept own gender identity by engaging in activitiesassociated with opposite gender: dressing in clothing of opposite sex; verbalizes incorrect gender identity.Verbalizes and behaviorally manifests comfort with own body and physicalchanges in body posture and grooming/dress.Can discriminate own sexual identity but not that of others(or vice versa).Denial of body changes.Lacks adequate knowledge of anatomy/physiology, or has misconceptions.
- 164 -

BEHAWIORAL CRITERIA CHECKLIST - continued
9.
10.ll.
12.13.
= 14.15.16.
l l -
7.
12.13.
4.1
15.16.
=1.2.3.4.5.
Expresses feeling of discomfort verbally and non-verbally with body andphysical changes: includes restricted diet to prevent body changes; avoidanceof dressing in communal setting.
-
Inability to discriminate between sexual and non-sexual approach behavior.Acceptance of own gender identity as expressed in body movements, clothing& gestures.Knowledge of one's own anatomy/physiology.Engages in socially accepted forms of sexual behavior; masturbates in privacy.Unable to discriminate between males and females.Provokes sexual contact with inappropriate partner.Awareness of gender identity difference but does not behaviorally demonstrateacceptance of gender identity.Able to distinguish between males and females in regard to self and others.
AGGRESSIVE-PROTECTIVE SUBSYSTEM
Maintains control over actions in stress producing situations and elicits supportfrom others if needed.Unable to control response to threat.Engages in intense/frequent acting-out behaviors.Lack of awareness of potentially hazardous situations or perceives many situations as dangerous.Wanders away from unit or group.Able to identify obvious dangers, but not subtle cues of potential harm.Unable to protect self in dangerous situations.Development of phobic behavior.Able to select appropriate verbal/non-verbal action in potentially hazardous ordangerous situation: direct response to threat; neutralizes source of threat;withdrawal; protecting oneself, or others.
-
Selects verbal/nonverbal action for response to threat in indirect way; actionnot directed toward source of threat.
Able to identify and avoid potential hazardous/dangerous situations in environment to: self and others.
Unable to consistently identify or control one's reactions to stress.Selects response to threat that contains potential for self-injury of minormagnitude.Unable to predict potential danger beforehand, but able to do so once insituation. May be involved in frequent accidents.Lack of awareness of cause/effect.Refuses to remain on unit or with group:e.g. elopement risk.
ACHIEVEMENT SUBSYSTEM
Utilizes problem-solving abilities inconsistently.Does not accept direction from others.Short attention span.Organizes group activities of a social and.or work oriented nature.Unable to accept failure.
– 165 –

BEHAVIORAL CRITERIA CHECKLIST - Continued
17.
Able to select goals{identify and select from alternative possibilities).Attention span limited: easily distracted.Limited awareness of strengths and weaknesses of self and others.Fails to complete tasks.
-
Able to identify and accept strengths and weaknesses in self and others andcompete according to these personal factors.Utilizes skills to initiate achievement behaviors, but either fails to completetask or completes without optimal use of problem-solving skills.Able to initiate and complete tasks.Limits self to experience/tasks with guaranteed success.Follows simple directions.
-
Unable to perform tasks/skills appropriate to developmental stage.Lack of problem-solving skills. Engages in repetitive, rote tasks.Able to identify available alternatives but cannot select one goal.Utilizes problem-solving abilities to initiate and/or complete goal-directedactivities.
Unable to determine goals or identify alternatives.Lack of awareness of strengths and weaknesses of self and others.Able to make choice from limited range of alternatives: e.g. two choices.Unable to identify realistic goals.Seeks unrealistic modes of competition with repeated experience of failure.Does not utilize cognitive abilities to acquire knowledge.
RESTORATIVE SUBSYSTEM
Able to regulate patterns of activity according to physical and mental requirements.Sleeps during daytime.
-
Does not adapt to or chooses to ignore limitations imposed by illness orhandicaps.Refuses to participate in prescribed treatment regime.Exclusive preoccupation with one form of activity to exclusion of all others.Inconsistent participation in prescribed treatment regime.Engages in a balanced variety of physical/mental/ recreational activities.Sleep disruptions and disturbances resulting in minimal hours of sleep.Abnormal sleep pattern, including periodic wakenings at night; settling difficulties.
Participates in prescribed treatment regime.Normal sleep patterns, including ease of onset, maintenance of sleep foradequate rest.Inconsistent pattern of activities.
. Participates in activity to excessive degree resulting in physical exhaustion/fatigue.Engages in limited number of recreational activities; may also be a limitedrange of activities such as all sedentary activities; solitary play.Difficulty in adapting activity level to limitations.Fails to engage in recreational activities.Participates in organized social groups.
- 166 -

BEHAVIORAL CRITERIA CHECKLIST- continued
II. RATE THE OBSERVED LEVEL OF PATIENT BEHAVIOR FOR EACH OF THESUBSYSTEMS LISTED BELOW.
-
1. INGESTIVE 5.SEXUAL
2. ELIMINATIVE 6-AGGRESSIVE-PROTECTIVE
3. AFFILIATIVE 7.ACHIEVEMENT
4. DEPENDENCY 3.RESTORATIVE
OVERALL LEVEL OF PATIENT BEHAVIOR
- *-
- 167 -

Appendix D
Summary Statistics of Patient Behaviors
- 168 -

tº is tº i■ . . is cºiºit 12 tº

Standard Coefficient of
Patient Behaviors Mean Deviation Variation (%)
IngestiveEating and drinking skills .63 .76 120
Ingestion of food and fluids at intervals .42 .64 150
Food choices . 5l; .82 151
Awareness of social/physical environment 1.02 1.04 102
Sensory perception ... l;7 . 50 105
Ingestion of substances .08 ... l;9 599
Interpretation of events .95 1. 30 136
Awareness of social/physical boundaries .76 1. 16 153
Distinguishing of events . 50 1.01 201;
Frequency of intake .61 .67 109
Sufficiency of intake ... l;9 .72 1 l;7
Eliminative
Bowel control .73 .66 90
Bladder control .75 .68 90
Pattern of elimination .73 . 59 80
Disposal of body wastes .68 .96 1 l;0
Hygiene care . 52 .79 152
Affiliative
Emotional attachments 1. l;9 1. 38 91
Interpersonal relationships with individuals 1. 50 1. 17 78
Interpersonal relationships with groups 1.73 1.08 62
Adaptation to change 1. 52 1.25 83
Communicating ideas 1.65 1. 17 71
Expression of feelings 1.82 1. 32 73
Awareness of personal space 1.27 1.25 98
- 169 –


Standard Coefficient of
Patient Behaviors Mean Deviation Variation (%)
DependencySelf-care activities 1. 35 .98 72
Care of personal belongings 1. 17 1.08 92
Seeks assistance 1. 39 1. 30 93
Relies on own resources 1.0l; 1.0l; 100
Decision-making ability 1. 10 1. 20 108
Separation with ease . 55 1.05 192
Feelings of hopelessness/helplessness . 36 .96 262
Questions decision of authority . 92 1.05 115
Engages in situational attention-seeking 1. 39 1. 29 92behaviors
Knowledge of own anatomy/physiology . 89 1. 10 125
Distinguishes between male and female .7l; .6l; 86
Engages in socially acceptable behavior ..!!! .85 196
Comfort with body/physical changes . 58 .79 136
Acceptance of gender role .48 . 59 119
Distinguishes between sexual/nonsexual . 31 .78 255approach behavior
Aggressive-ProtectiveIdentifies/avoids hazardous situations 1. 36 1. 30 96
Selects response to threat/dangerous 1. 16 1.28 1 11situations
Response to threat with self-injury . 53 1.04 197
Engages in acting out behaviors .62 1.22 196
Ability to maintain control 1. 53 1. 17 77
Phobic behavior . 14 .62 l;60
Separation from group .5l; 1.07 200
- 170 -

-----—-
* ... " " - " - - - - - :- - - * ~ * → - -
t º * - - *
- - - * *
e - .- - - - * - -
- - - -
- - º - - - º - * * º
º - - : - - - - -
- - * * - --- - -
* - - - -
- - - * * - - - - - - - -
-* . . . . . . e - - -
- - a t + * * * * * * - * * *- - - -
- - * * - - - - -
- * - - - - º * * * - t- -- - - - - º . -
- - - -- a * - * * * - - -
- -- * * -
n -
- - s * -
w - * - -- - * - - - - - - - - - * - * * - - * * -
* - - -
- - * - - - - - - - - º
- " ... I -- - . . . - - -
- - - - - -• * : * > . . . * - * * * -
- - -
- - • - * - - * * - - - -- -
r s - * . - * * *
- - - - - * - - . . . -
- - - * - -
- - - - - - - º- - º - - - - * * * - * - * * - - * * * *
- - - . . "
* - - - - - " -
- - * - * - * * -
*- - - - - - - - - - * - - - - - - - -
- - - - - - - - - - - - - - s- - - - - * * - - * - - - - * --- - * *
* - =
- - - - - - - - - - * * *- - e * * * - *
* - - - * - -
- - * * * : . . . . . . . . . . . . . . .-
- - - - - - - * -
- - - - - - - - * . .
- - - * - -
- * * -
* * * - - - - - -- -

Standard Coefficient of
Patient Behaviors Mean Deviation Variation (%)
Achievement
Experiences successes and failures .78 1. 32 169
Chooses alternatives . 32 .73 230
Selects goals from alternatives 1.20 1. 30 108
Initiates and completes tasks 1. 35 1.27 95
Utilizing problem-solving skills 1.51 1. 18 78
Identifies, accepts strengths/weaknesses 1.72 1.28 75
Attention span 1.25 1. l;0 112
Organizes groups . 11 . 31 292
Accepts directions 1. 16 .9l; 81
Utilizes cognitive abilities . 52 1. 13 220
Restorative
Sleep patterns .73 1.01 137
Engages in recreational activities 1. 12 1. 10 97
Involvement in range of activities .60 1.06 176
Participates in treatment regime 1. 18 1.00 85
Regulates activity according to physical .67 .90 135requirements
Participates in organized social group .41 ... l;9 121
■ º
!,'!'...
– 171 –


ºiºº■ Cºvºigiºiº––º º--º,S.-7-S-Coºv*-
ºt■■ ºa\º3.º■ ººciºco*2*cºlº/”-*S*),7//z--
-A-Nº.Atº***º-*&º/7ºncºco n:)sººsºº***ev,,•Tººtº4-tº-tº º,cº
-~--sº•o•*------
º7. 2.^>ºº--~
.,&Cº*//º'(-*.*º*
42Sºcº/º5*>~y***sºº,C.ºncºcoNº42,*
º,ºwº----º &Q.ºººOsº ~ºcº** &L.%,L
J/2-sº[…]º,L![3RAR_YºLC°,J/2sºº,L![3
ºO^c*&•o[…]ocº[…]o,■
-72-
cºlºº >-
-7--
42ºny--42sº \ººcºsº,dººr.ººº,cº77/10/■ co.*o&4.Sºº L■0.RARYsº—r-º,O/.3.s[…]º,LIBRARYgº%,O/2&
12o****
-
°sºnA/),º,sºº sº,Cº/ranci■ co**,-
º/”ºsºcº77/7C■ ,■ coººecQ.sºº sº[…]%,LiBRAR_Ysº|||ºO/!-sº[…]º,L■BRAR_Ysº|||º
wCº.&Osºo,**~~
--º*+~C.Co
N-*-->º2
-sºº,i■ /■ ,11/7C/■ .()sº*
-
Sºsºº-
º/ºncº-
O/les[…]º,LIBRARYsº°,O)2–tº&[...]º
Cº.~CºLIBRARYºr -Ocº| n&--9O& º[…]ºJºvº■J17º[...]sº-/C°,[…]ºA8vº;JITºL.&’c
º**...sº4.Sº%.A(%.Sºn1º*>C■ .
-2Sº7%ºf,7/17-*,* ºNº.
-s&Cº/*anCºcosº,dº/”.º3.C■ .7//, --
/2º*.LIBRARYisº-O)º1.º
~y---2º
-
sº[…]*.ºf||*)A-2º[-º,cL.Q.
ºwoO->■ ººwº º|*>
º-:,z-º,||sºº,**º,~S»L I/OºsººvariºLºls-,*.~*C,~5~~ºN.z -yºrsoC/Cº,Jº■ vº■G17 wzº.
sº*, -7.----
-!~"-~ºº
*\,://,/7-7ºr,-,-,-2º'ºf//º*Sº**2Nºº º1/14■ cosºcººl,º/”ºsºcºcºº,*/º
x^~*/-S4.--
--> LIBRARY&-*TºO)p3-º,L■B■ ººQ.nº--
º*)***A-2º'”,\ARYsº-°...)/~2º L..*[…]-L||“...■º'',
C. º,-**>7•or[…]**ººrº~s
-
(,~c-~&~ºf~*f-ºN.º--zcº-º127*
LC(■ (º'-'ºvºgºº-'s(/(º,DTºnO-
*º,º +->ºº%,sºC■ .
~nº1:*2.NºS*-
*Y,Z/7,fºrºfCº0.247.01/11////?*--
2Stºº.|º°,&/ºncºº*
--&2.Odº/777/7cºrd-*./.../
*°oS4.-
*wºº*
º[…]º,L![3RARYs|]°,..)/2.sº[-º,º,LD.RARYº-r-º,tº
~%,----||-
~
O-zº-&O.&
rsº-r--rº AvºgiiºLºlº~/C…[Tsººvuginº--sTAC*[
*2,
Z
-*
º
4-Sº2.
Sºº,-
*sº-º*º “.
*-->º**º-
º----- *>C■ .-
%-sºf*/º-,*z,*:-**,----------
J.J.J.7//?"////(Cºs---
O)sºcºncºº%,-
'yººcº771//■ º
Cºº*cºº ºº-ºOOsº6. .*[…]º,L.BRARYsº[-r]”,/~ºº,LIBRARYºr -
QesºLºlº,~[~!Q.ºL Jº-
º[...]ARºfgin*2.[...]sºº/C%.[…]ºvº■J17º[...]*–
>~,'e,39º~-------
-4. ºcºlº/”*Oº
sººt-S-
º->
wO-
º*:Sº*º,_- º:cººfcº-2.sCº.ºº^-N.-
º,12.7,1170■ ,■ oNº.%_S&*),Z7,*~4.
-!,
~º-
--*,-º-º:-~ >F-r-ºO)n--***o^
s|º-
sº|T”,LIBRARYº||º,//>sºT-º,||3||
O~---o-_*-~ *-*.,7.*T~*…[Tril-C•or——S-
O.--

--
.*-
º,tº RARY * I jº .)/2 sº Hº. Li B R A R_Y ■ º ./] sºro, ■ - sº *. * - - - - * | sº º, ■ º º
- .
;In º L. º - C % tº sº ºvº. 9 in *. _s cº- (C % -- sº ºvº.* 2,-
-> * tl (,ºs O * º -
º... sºº 0.25)./1/11//º º ”.S%
-* *E. o ºs C■ .
- ºJ º *. ºutcº
*-C.
º*.º
t º *
*- .**S. º º O/2 sº. . .”
~ º […] º, L. BRARY sº | r- | º, t º º,• 2 -
- O
* } º
º *...* Jºjº- * * * * *
C 17//, ºlº■■ , U. º cº, *** -f-*~ S’ º
* I ■ º RA R_Y sº---
º&
O) *| || 9.*- y
^c […]* —s --- º - r = º- -y* - º, Lºl s
( :
* - *-
*.- -
■ ºsº A.
-c-r , , , 7. ■ º
+, sº Tºvº; g in º, -> ((( º
º, sº ºutº■ ººQ *2. º -S,
-sº º Jº sº. Cº■ /ºckºoº O) 2– º ‘’, L º º, }) º º º *~~ * * sº
-º, t sº […] 4, | E3 RA R_Y º' [] ”, …'' 4–2 sº [. º, R. RA R_Y lº
* *
^c, […] _º —--- º, ºr º º, […] sº -- º, - r- º |--º! — sº ■ ºvº. 9 in * -- º■ C º' -- ºgº º L– -
S- *-
g* ºn º º, sº ºf ºn ~ *, sº o –* -, - .* - - - * - * * ~ *- * . 75'.7/?? / / //?? (J
-
|Cººl S &,-
Nº º, º 17//{ A■ . U. -S 4 0.7% 7. //? \ y & -\º ■ ºº sº- "… -
º-- º
\Y sº | | º, ..)/ le
ºº --
º,
Vo sº* •r o
º ºvºi g in * Lºl s**cºlº/” > * > C■ .
-
-
-S ”,*
17@■ º A/C Jº J>
sº!
º -
º ->
* , //
… º
º ". º &- '... *-y º º -& - * ,
■ º- º, L. BRARY sº [] º, ..) le s º, L. B R AC- ~& -- -- º-
C * } * * | -->| |- O r s º C * - º
-
/ ~y º & ºvº gº º L– sº - (º º ■ T is ~s wº * | |
-
C º, sº T º, _S / º,-
& A-Tºv \{ } {T ... --* A.
- -y 4. ~ ^*. º---
* * * - * Z, Sº *** º *// ºf 12, N * 12. Sº
º º ºli■ t■ , ■ o % 0.2% put º º º C■ .ºA. 17C■ , ■ o º1º, L. BRARY
-sº
-
.*
Cºl/11/ º2. ~~ º
º
-S- 4- º º t- *-º * º ( ) C ar º
S --- * )/ º ~. Y ~$ * ) ºtcº L. º, t- le sº […] º, Li BRARY is [] º, t
le* - - -
o, —r- sº º Q-C. º ------ o, --- sº º,~ > - - -
t º, L.-
| | L. J º | | - *
|- 2 <> - /C % --- Aº Vº g ■ º %, sº I /(' * sº ºvº;º º ~- - ty ->f ºº !, sº
-º! x- ºn ~. º ~
- *
■ º ºs & ºnctºo gº tºº/º 2 º' ... º.º. o.º.º.º.º sº, º/7′■ tºo sº
ºsº tº CYº/7 tº Cº■■ o is a --
* sº "… - * *. ºf- A / .
4. *
*-
• cº […] º, L■ B RARY In º, O)le s ■ º- *. L. B RARY sº Lºl º,
>*
*- •o —r- > C. º-
>&
-f | o {- * º r ~
* A 8vº, J in º, s º ■ (y *2. ºº Aºvº. 9 in º sº cº
C-
* * *
-s * () * -> l■ ºº
º,”, 72 ** ~y -
* º, * -
º --- *12. Sº * ~,
ºf 71/1. º 2.< .S.- - - - - º gºl/11º/ º S º º
* ºw sº. *- SS * º º il//. 1■ º º °4.-
y / / * Q- '4, cºncº ºº
*
* -
º
* º %, *- * º, * , º
_* -*- *o & ■ ) c ---- * - --º ,-
s' cº, º [...] & ‘c, | º” ". r ~ .*
sº ºvº gº º * -/C * - sº ºvºgri * -- * - /- ~ *º º º º º º * ~" t * º12. N º, sº *1 = * -->
ºf Co º gºº º C).2//, //, //º -- * --> º/º > ºs S.sº//
>‘Jº º %. sº ". *- i. ■ ." i■■ '■ L\t sº 4. sº º, *- º / .”.
• * ~ * O º O ( ) º ** O- ty* Sº […]”. . /2- º […] º, Lib RARY sº [...] ". . 77– sº ■ º * Lºº.
-º sº- º, […] cº -------
º, -- r - 9 º º º------ •o L
- º º º ~ º, - º- r r- /C * - sº ºvºgº º Lºl s TAC º,
-* -ºvug in º
: ~y. "…sº '4 º'-
1 º' ~, * -ºngº, º º■ ºvo º ºn Fºº, º º■ ºvo ºcyºncisco º, ºº *Sº c)da. A.*cº º */º ºº - º - ! *~ - 4- - . .) C º ** * * º 9. º */
- * * ".- 2, s º {} * I tº D A ■ y * º, º
-
º, L! B RA R_Y sº J. Y º l ºt-) 2
º■ º
- -º-
* T ** ---
º, ■ º sº Lºl For REFERENCE Lºlº, TºLC º c- Sº cº- C. ~
º º sº (/C & (/(' º * - s ... Tº º"Sº Sº ■ ºmeº-
º “a 7///7.1/10,O
*, *.*º, sº gº. A*}.7/7, fººtºº *
a *- - * J. NOT TO BE TAKEN FROM THE ROOM Q-2' & 7.///■ Jº -S ºº & º L■ º §§ car. No. 23 n1z **to -: º Tºº, BRARY *::: …, L. BRARY
-> ■º º,
* [ ] 'ºv. a. A- - *- *
-—l (). º * --> -- * º * * sº * -
- º º * * -
J- c -ººº L. Jº º'-º', ºvºun * Sº cº-, , ,
-*/ ...”
º /C º, sº 9, sº (■ (- * -y
4 tº }//º 'A' %. º Ç* … -- º - ~ '4 ~-
'-'. J. - º z - * º - , , , ,-, -- º Jºy'■ 71/11/ / l/?" - 2.< * - --
1 Sº Sº * *- º/7 ºn ■ º U Nº. 2, 4. º º <- 4. º 7.7/7, ■ º ºº * 9, lsº ! *~
*
--
-º 1 *~ - 3.
.# --> - º * º º-
* . O)) * º' -– ’2. I 1 ■ º ■ º. A tº ~ º *... f º- º º, tº tº a tº ~~



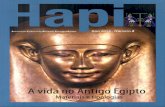


![º]äõ]õ ĪÉéEō +ÉĄėō jÉÉīÉhÉEōÉäŪú - Moneycontrol](https://static.fdokumen.com/doc/165x107/6312276bd43a2591a90546fc/oaeoo-ieeeo-eaeo-jeeieheeoeaeuu-moneycontrol.jpg)
![Áö¼Ó º¸°í¼ PDF[ENG] - Amazon AWS](https://static.fdokumen.com/doc/165x107/6319c7fb0255356abc08699d/aoeo-oi-pdfeng-amazon-aws.jpg)













