
Date - - eScholarship
171
MATERNAL ANXIETY, SOMATIC SYMPTOMS, MARITAL ADJUSTMENT, AND FAMILY RELATIONSHIPS IN SECOND PREGNANCY by Lucy Newmark Sammons B.S., Stanford University, l973 M.S., University of California, San Francisco, l979 DISSERTATION Submitted in partial satisfaction of the requirements for the degree of DOCTOR OF NURSING SCIENCE in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA San Francisco Approved: º Committee in Charge Deposited in the Library, University of California, San Francisco Date - - - University Librarian Degree Conferred: . . . SEP 8, 1965 -
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Date - - eScholarship
MATERNAL ANXIETY, SOMATIC SYMPTOMS, MARITAL ADJUSTMENT,
AND FAMILY RELATIONSHIPS IN SECOND PREGNANCY
byLucy Newmark Sammons
B.S., Stanford University, l973M.S., University of California, San Francisco, l979
DISSERTATION
Submitted in partial satisfaction of the requirements for the degree of
DOCTOR OF NURSING SCIENCE
in the
GRADUATE DIVISION
of the
UNIVERSITY OF CALIFORNIA
San Francisco
Approved:º
Committee in Charge
Deposited in the Library, University of California, San Francisco
Date- - -
University Librarian
Degree Conferred: . . . SEP 8, 1965-

(3) Copyright 1985
by
Lucy Newmark Sammons
All Rights Reserved
MATERNAL ANXIETY, SOMATIC SYMPTOMS, MARITAL ADJUSTMENT, AND
FAMILY RELATIONSHIPS IN SECOND PREGNANCY
Lucy Newmark Sammons, R.N., D.N. S.
University of California, San Francisco, 1985
This study described and compared characteristics of maternal health
and perceptions of family relationships throughout the course of second
pregnancy, guided by developmental concepts and propositions from the
psychology of pregnancy literature. Hypotheses predicted that the four
dependent variables of maternal anxiety, somatic symptom levels, marital
adjustment, and maternal concerns about family relationships would be
dynamic over the three antenatal trimesters and the fourth postnatal
trimester; that somatic symptom occurrence would be perceived as more
frequent during second than first pregnancy; and that the dependent
variables would demonstrate intercorrelations.
One hundred and ninety-one obstetrically low risk, partnered women
delivering their second baby through private or prepaid health insurance
plans participated in a passive observational study employing a modified
cross-sectional sequential design. Subjects were recruited into one of
four cross-sectional trimester groups and completed the Spielberger
State—Trait Anxiety Inventory, the Spanier Dyadic Adjustment Scale, an
original Family Relationships Questionnaire, an original Somatic Symptoms
checklist, and a Demographic sheet. The design called for repeated
testing of 135 subjects three months after first testing.
Analysis of variance and two-sample t-test procedures revealed
higher levels of family relationship concerns in the third trimester than
the second trimester, and lower somatic symptom levels in the
midtrimester than in early or late pregnancy. Contrary to study

hypotheses, state anxiety and marital satisfaction were found to be
stable across the four perinatal trimesters. Somatic symptom frequency
was perceived as greater in second pregnancy than previous pregnancy,
with notably greater fatigue. Using correlational statistics, highly
significant associations were demonstrated among all four dependent
variables. Major concerns of secundigravidae antepartally were
anticipated jealousy of the firstborn about the baby, other aspects of
sharing maternal affection and attention between baby and firstborn, and
fear for the expected baby's health after the good fortune of having had
one healthy child. Major postpartal concerns were firstborn misbehavior,
maternal regret at the lack of an exclusive relationship with the new
baby, and firstborn difficulty with sharing maternal affection and
attention.
/– º 29t tº 4 / … / ^ (AX__Lucy Newmark Sammons, Author Ramona T. Mercer, Chair
Acknowledgments
It is my pleasure to take this opportunity to thank the individuals
and agencies who helped with all phases of this project. The essential
relationships I share with the following people are testimony that this
endeavor could not have been undertaken and completed without their
support and assistance.
My Dissertation Chair and Sponsor, Dr. Ramona Mercer, provided
caring, conscientious, and expert assistance throughout my doctoral
education. Dissertation Committee members were Dr. Katharyn May and Dr.
Jacqueline Ventura. Jointly, their guidance and suggestions ably
assisted me in traversing the course from the theoretical underpinings of
this investigation to the realities of research implementation.
Access to subjects was accomplished with the assistance of Ob–Gyn
Nurse Practitioners at Kaiser Permanente Medical Group facilities in
Walnut Creek, Antioch, and Pleasanton. Muriel Giles, Diane Siepel, and
Alicia McAtee made special efforts to provide facility liaison and
maintain recruitment. Susan Gillespie's thorough and energetic
contributions were extraordinary. The participation of Dr. Robert
Marten, Dr. Stephen Weinstein, Dr. Vincent DiMaggio, and Dr. Elwood
Kronick and their staffs is also appreciated. Community-based childbirth
educators Marti Paulson and Rhonda McGrath generously offered their
expertise during the instrument development phase. And to the 191 women
who took time out from their busy lives to participate in this study, I
express my sincere appreciation.
Assistance with data analysis was provided by Dr. Mark Hudes, who
good-naturedly clarified my search for meaning through foot-high piles of
output. Expert guidance and thoughtful counsel regarding all aspects of
iv

computing was graciously provided by Dr. Robert Slaughter.
Colleagues in the UCSF School of Nursing have assisted me both
formally in group seminars and informally through individual contacts
over the years of my doctoral education. The richness and satisfaction
I have derived from these relationships have added immeasurably to the
quality of my doctoral student life. Maternity Seminar members Helen
Dulock, Patricia Mann, Shannon Perry, and Colleen Stainton provided a
forum for discussion and assistance with instrument development. Seminar
members Ellen Olshansky and Brook Randall provided both assistance with
presentation of the research project and findings, as well as humor and
nurturance essential to balancing our lives as novice scholars in and out
of academia.
I am also appreciative of financial support for my doctoral
education and this investigation. I have received support from the
Charles M. Goethe Scholarship Committee; Sierra Pacific Region
Soroptimist International; UCSF Instructional Use of Computing Funds;
UCSF Regents Fellowship; School of Nursing Century Club; UCSF Patent
Funds; National Research Service Award NU–05667–01, DHHS, DN; Stanford
Nurse Alumnae; and California Nurses' Association, Region XI.
I wish to express my gratitude to additional individuals, who,
although they were not formally involved in my dissertation work, have
made significant contribution through their caring. I express
appreciation to my parents, Marion and Milton Maxwell Newmark, who
instilled in me a love of academics and the desire to pursue excellence.
I am grateful to Renee Sheehan and Deanna Bogart, both graduate-prepared
nurses, for helping me keep my family intact and my dissertation on
track, while continuously celebrating the joy of our children. With my

husband, Tim Sammons, I share the relief of this great undertaking now
reaching completion. And to our children, Julie and Andrew, who have
known only a Student–Mom in their young lives, I dedicate this work.
They have enriched my life beyond measure.
San Francisco, California
August, 1985
vi

Table of Contents
Page
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . iv
List of Tables. . . . . . . . . . . . . . . . . . . . . . . . . x
List of Figures . . . . . . . . . . . . . . . . . . . . . . . . xi
Chapter I The Study Problem. . . . . . . . . . . . . . 1
Problem Statement and Study Purpose. . . . . . 2Significance . . . . . . . . . . . . . . . . . . . . . . 3
Chapter II Conceptual Framework and Literature Review. . . . . 6
Introduction . . . . . . . . . . . . . . . . . . . . . . . 6Conceptual Framework . . . . . . . . . . . . . . . . . . . 6
Developmental Psychology of Pregnancy . . . 7Family Development Framework. . . . . . . 9
Maternal Anxiety in Second Pregnancy . . . . . . . . . . . 11
Variables Affecting Anxiety in Second Pregnancy . . . 13
Time . . . . . . . . . . . . . . . . . . . . . . 13Demographic Variables. . . . . . . . . . . . . . 14Experiential and Attitudinal Wariables . . . . . 17
Maternal Concerns during Second Pregnancy . . . . . . 19Maternal Concerns following Second Pregnancy. . . . . 22Conclusions . . . . . . . . . . . . . . . . . . . . . 25
Maternal Perception of Family Relationships in SecondPregnancy . . . . . . . . . . . . . . . . . . . . . . . 26
Marital Relationship . . . . . . . . . . . . . . . . . 29Mother–Baby Relationship. . . . . . . . . . . . . . . 32Father–Baby Relationship . . . . . . . . . . . . . . . 33Mother—Child Relationship . . . . . . . . . . . . . . 34Father—Child Relationship . . . . . . . . . . . . . . 36Child-Baby Relationship . . . . . . . . . . . . . . . 37Variables Affecting Dyadic Family Relationships in
Second Pregnancy . . . . . . . . . . . . . . . . . 38Conclusions . . . . . . . . . . . . . . . . . . . . . 43
Somatic Symptoms in Second Pregnancy . . . . . . . . . . . 45
Introduction. . . . . . . . . . . . . . . . . . . . . 45Prenatal Symptomatology . . . . . . . . . . . . . . . 47Postpartum Symptomatology . . . . . . . . . . . . . . 49Conclusions . . . . . . . . . . . . . . . . . . . . . 50
vii
Interrelationships Between Anxiety, Family Relationships,and Somatic Symptoms in Second Pregnancy. . . . . . . . 51
Anxiety and Family Relationships. . . . . . . . . . . 51Anxiety and Somatic Symptoms. . . . . . . . . . . .Somatic Symptoms and Family Relationships . . . . . . 53Conclusions . . . . . . . . . . . . . . . . . . . . . 54
Definitions and Hypotheses . . . . . . . . . . . . . . . . 55
Definitions . . . . . . . . . . . . . . . . . . . . . 55Hypotheses. . . . . . . . . . . . . . . . . . . . . . 55
Chapter III Methodology. . . . . . . . . . . . . . . . . . . . 56
Introduction . . . . . . . . . . . . . . . . . . . . . . . 56Design . . . . . . . . . . . . . . . . . . . . . . . . . . 56Setting. . . . . . . . . . . . . . . . . . . . . . . . . . 58Sample . . . . . . . . . . . . . . . . . . . . . . . .
-
Data Collection Methods. . . . . . . . . . . . . . . . . . 61
Demographic and Background Data Sheet . . . . . . . . 61Spielberger State-Trait Anxiety Inventory . . . . . . 62Dyadic Adjustment Scale . . . . . . . . . . . . . . . 63Family Relationships Questionnaire. . . . . . . . . . 64Somatic Symptoms Checklist. . . . . . . . . . . . . . 67
Procedure. . . . . . . . . . . . . . . . . . . . . . . . . 69Data Analysis Procedures . . . . . . . . . . . . . . . . . 75Summary. . . . . . . . . . . . . . . . . . . . . . . . . . 78
Chapter IV Results . . . . . . . . . . . . . . . . . . . . . . 79
Introduction . . . . . . . . . . . . . . . . . . . . . . . 79Demographic and Obstetrical Characteristics of the Sample. 79Dependent Variable Measures. . . . . . . . . . . . . . . . 87
Anxiety . . . . . . . . . . . . . . . . . . . . . . . 87Marital Satisfaction. . . . . . . . . . . . . . . . . 90Family Relationships Questionnaire. . . . . . . . . . 91Somatic Symptoms. . . . . . . . . . . . . . . . . . . 95
Interrelationship of Dependent Variables . . . . . . . . . 100Other Findings . . . . . . . . . . . . . . . . . . . . . . 102Hypothesis Testing . . . . . . . . . . . . . . . . . . . . 104Summary. . . . . . . . . . . . . . . . . . . . . . . . . . 106
Chapter V Discussion . . . . . . . . . . . . . . . . . . . . . 108
Relation of Findings to Research Questions . . . . . . . . 108
Change in Dependent Variables by Trimester. . . . . . 108Anxiety. . . . . . . . . . . . . . . . . . . . . 108Marital Satisfaction . . . . . . . . . . . . . . 111
viii

Family Relationship Concerns . . . . . . . . . . 111Somatic Symptoms . . . . . . . . . . . . . . . . 112
Description of Principal Family Relationship Concerns 112Description of Somatic Symptoms . . . . . . . . . . . 114Associations Among Dependent Variables. . . . . . . . 115
Study Limitations. . . . . . . . . . . . . . . . . . . . . 116Significance and Implications for Health Care. . . . . . . 117Recommendations for Future Research. . . . . . . . . . . . 120Summary. . . . . . . . . . . . . . . . . . . . . . . . . . 121
References. . . . . . . . . . . . . . . . . . . . . . . . . . . 123
Appendices
: Cover Sheet for T-1 Packet. . . . . . . . . . . . . . . 140Consent Form. . . . . . . . . . . . . . . . . . . . . . 141Demographic and Background Information Sheet. . . . . . 142Spielberger STAI-State Self-Evaluation Questionnaire. . 144Spielberger STAI-Trait Self-Evaluation Questionnaire. . 145Spanier Dyadic Adjustment Scale . . . . . . . . . . . . 146Family Relationships Questionnaire—Prenatal . . . . . . 149Family Relationships Questionnaire-Postpartum . . . . . 150Symptoms of Pregnancy Checklist . . . . . . . . . . . . 151
: Postpartum Symptoms Checklist . . . . . . . . . . . . . 152Recruitment Flier . . . . . . . . . . . . . . . . . . . 153Comments for T-1 Packet . . . . . . . . . . . . . . . . 154Cover Sheet for T-2 Packet. . . . . . . . . . . . . . . 155Categorization of Antecedent Variables. . . . . . . . . 156
ix

List of Tables
Table Page
3. 1 Dependent Variable Measures Obtained at T-1 and T-2. . . . 76
4.1 Demographic Characteristics of Total Sample and Groups . . 80
4.2. Obstetric Characteristics of Total Sample and Groups . . . 83
4.3 Dependent Variable Measures for Total Sample and Groups:Analysis of Variance. . . . . . . . . . . . . . . . . 88
4.4 Trimester-Related Antecedent Wariables Affecting DependentVariables . . . . . . . . . . . . . . . . . . . . . . 89
4.5 Highest FRQ Item Scores for Total Sample and TrimesterGroups. . . . . . . . . . . . . . . . . . . . . . . . 93
4.6 Change in FRQ-A Item Means by Trimester: Paired tº Tests. . 94
4.7 Trimester Effects on Symptom Antepartal:—Comparative (SXAC)Levels: Two-Way Analysis of Variance. . . . . . . . . 96
4.8 Trimester Effects on Symptom Antepartal–Current (SXAN)Levels: Paired tº Tests. . . . . . . . . 96
4.9 Frequent Somatic Symptoms for Total Sample and TrimesterGroups. . . . . . . . . . . . . . . . . . . . . . . . 97
4. 10 Change in Somatic Symptoms by Trimester: Paired t Tests. . 99
4. 11 Somatic Symptoms in Second vs. First Pregnancy: One-samplet Tests . . . . . . . . . . . . . . . . . . . . . . . 100
4. 12 Association Between Anxiety, Marital Adjustment, SomaticSymptoms and Family Relationship Concerns . . . . . . 101
4.13 Relations of Selected Variables to Maternal Health . . . . 103
5.1 Weeks of Pregnancy by Trimester Group. . . . . . . . . . . 109
List of Figures
Figure Page
2. 1 Changes in Family Dyads in Second Pregnancy. . . . . . . . 28
3. 1 Sample Distribution in Modified Cross-SectionalSequential Design . . . . . . . . . . . . . . . . . . 57
xi

Chapter I
The Study Problem
Over two million women a year in the United States experience a
second or higher order live birth (Monthly Vital Statistics, 1983), yet
the experiences of these women are seriously neglected by multiple
scholarly disciplines and architects of health policy. First births make
up only 42.8% of all live births in this country, but it is upon this
minority group that psychologists, sociologists, and nurses have
traditionally focused their interests.
Second births make up the largest portion of later births. The
birth rate for second pregnancies had increased annually from 1978 to
1980, then demonstrated a slight (1%) decline consistent with overall
birth rates in 1981, the last year for which full statistics are
available. Second order births actually increased in 1981 for 30–34 year
olds (1%) and 35–39 year olds (7%), supporting the pattern for delayed
childbearing that has emerged since the early 1970's.
The extent to which higher order pregnancies (subsequent
pregnancies, or those occurring after the first birth) have been
neglected is pervasive. A federal government program developed in a
House Committee for consideration by the legislature extends Medicaid
coverage to low-income pregnant women only if they are expecting their
first child (House Committee, 1983). Clinicians as well have left those
experiencing a subsequent pregnancy as an underserved population. A
national survey of 25 veteran childbirth educators across the country
concluded that, "Conspicuous for its absence is a multipara class,
despite the special interests of multiparas——interests which frequently
do not include as much instruction in coping with labor and delivery"

(Shearer & Bunnin, 1983, p. 252).
Several dimensions of the second pregnancy experience emerge as
warranting investigation. Recent reviews have determined it is vital for
expansion of the knowledge base of the psychology of pregnancy to
investigate further the experiences of women and families during second
and later pregnancies (Leifer, 1980; Tilden, 1980; Valentine, 1982). Far
from "knowing the ropes," the woman experiencing a subsequent pregnancy
experiences changes in three arenas——the psychological, social and
physical spheres——which warrant attention during pregnancy (Kirkpatrick,
1978; Mercer, 1979; Westbrook, 1978a). The most critical psychological
and social variables for research about pregnancy have been succinctly
identified by Barnard (1981, p. 286), who stated, "The concepts of anxiety
and of supportive relationships have clearly emerged as unavoidable
independent variables in the study of childbearing and childrearing."
She questions whether health care providers can give responsible care
during the perinatal period without collecting information about these
two variables. The third realm of changes during pregnancy, that of
physical changes, impinges upon the woman's experience as subjectively
defined somatic symptoms. Hence, anxiety, family relationships, and
somatic symptoms are identified as three salient variables affecting the
second pregnancy experience.
Problem Statement and Study Purpose
This study aims to expand knowledge about the second pregnancy
experience. A woman experiencing second pregnancy is referred to as a
"secundigravida." Generally stated, answers are sought for the question,
what are the characteristics of maternal health and concerns about family

relationships throughout the course of second pregnancy? Maternal health
is conceptualized as having two dimensions, the psychological dimension
of anxiety and the physical dimension of somatic symptoms. Family
relationship concerns are considered in terms of dyadic, or two-member
relationships, such as husband—wife, or parent-firstborn.
The purpose of the study is to seek answers to the following
research questions:
1. Do maternal health and perceptions of family relationships
change with time through the course of second pregnancy?
2. What are the principal concerns of the secundigravida regarding
dyadic family relationships?
3. What are the most commonly perceived somatic symptoms of second
pregnancy? Do secundigravidae perceive themselves as having symptoms more
of less often than during their previous pregnancy?
4. Are there correlations among levels of the key dependent
variables: maternal anxiety, family relationship concerns, and frequency
of somatic symptoms?
Significance
This study is useful at both a theoretical and an applied level. At
the theoretical level, the investigation adds to the knowledge base
describing psychological and sociological aspects of pregnancy and early
parenting. By answering the research questions, salient properties and
relationships about second pregnancies will be illuminated, thus filling
the gaps that have existed in this area.
At the applied level, each of the three dependent variables has
demonstrated significance regarding health status and family functioning.
The study of anxiety in pregnancy was encouraged in 1959 (Caplan) in

order to make women more comfortable, to direct psychiatric intervention
towards prevention of the development of disturbed maternal-child
relations, and to investigate the potential for reducing complications of
pregnancy. The association between maternal anxiety and medical
complications of pregnancy is supported by prospective studies (Gorsuch &
Key, 1974; McDonald, 1968; Norbeck & Tilden, 1983). Recent technological
and neurobiochemical advances have allowed quantification and
specification of possible mechanisms for the impact of psychological
factors on perinatal outcomes. Direct evidence of the physiologic
effects of anxiety in pregnant humans is now available. Conflicts and
psychological processes including anxiety in pregnancy have been
correlated with anxiety in labor, uterine contractility, length of labor,
fetal heart rate patterns and newborn Apgar scores (Lederman, Lederman,
Work & McCann, 1978a, 1978b, 1981). High levels of anxiety are related
to complications of labor and newborn depression. Hence, increased
knowledge of the magnitude, sources, and patterns of anxiety throughout
second pregnancy may suggest strategies to improve perinatal health.
Perceptions of family dyadic relationships have evident significance
as an integral part of parenting, childrearing, marital stability and
satisfaction, and family integrity in a social context wherein these
family functions are often challenged. The marital relationship is
acknowledged to have major impact on pregnancy and the puerperium in a
variety of theoretical perspectives. Quality of the pregnant woman's
relationship with her husband has repeatedly been found to be one of the
major determinants of maternal adaptation to pregnancy and parenthood in
empirical investigations (Grossman, Eichler & Winickoff, 1980; Lederman,
Weingarten & Lederman, 1981; Westbrook, 1978b; Shereshefsky & Yarrow,
1973). Increased knowledge of the nature and magnitude of a woman's
concerns about the marital and other dyadic relationships provides
direction for therapeutic intervention to reduce anxiety and discord.
Hence, increased knowledge of family relationships during second
pregnancy will have value for providers and policymakers concerned with
maternity and neonatal care, family health care, adult mental health, and
marriage and family therapy.
Increased knowledge of somatic discomforts during second pregnancy
has relevance for providers and planners of health care and education to
maternity clients. A greater knowledge base about somatic symptoms will
facilitate the provision of more accurate anticipatory guidance to
clients. Specific knowledge of the timing of symptoms through the course
of pregnancy may also suggest a sequential plan for health education
about pregnancy symptoms and their management that may increase
opportunities for client self-care. Data-based guidance provided to
pregnant women may reduce unnecessary use of health care services by
clients who have been adequately prepared for normative symptoms such as
common sensations and minor discomforts.
The study of anxiety, perceptions of family relationships and
somatic symptoms during second pregnancy has been identified as an
important area for further study. In the following chapter, the
conceptual perspective guiding this investigation is presented and
relevant literature is reviewed.
Chapter II
Conceptual Framework and Literature Review
Introduction.
In this chapter, a conceptual framework based on individual
developmental changes during pregnancy and family development is
presented. Thereafter, maternal anxiety and concerns, maternal
perception of dyadic family relationships, and somatic symptoms in
second pregnancy are examined. The purpose of this literature review is
to provide a description of the current state of knowledge about the
phenomena of concern, to identify inconsistencies or limitations of
previous studies which indicate refinements needed in further
investigation, to identify variables known to affect the focal phenomena,
to suggest directional relationships guiding hypothesis formation and
research design, and to place the present inquiry within the broader
realm of received theory and existent literature. The chapter concludes
with statements of the research hypotheses.
Conceptual Framework
A developmental framework is appropriate for investigation of human
patterns as they move through time. A synthesis of family development
and life-course analysis is necessary to understand the movement through
time of an individual family member and the family organization itself
(Elder, 1978). Applying this perspective to the second pregnancy
experience requres consideration of the individual, in this case the
pregnant woman, as well as her family. A dual focus on individual and
family change during childbearing was espoused by Caplan (1959), who
described pregnancy as a state of disequilibrium in both the

intrapersonal forces in the pregnant woman and the interpersonal forces
in her family. An eclectic framework based on psychology of pregnancy
and family development concepts guides this investigation.
Developmental Psychology of Pregnancy
In the classic expositions of the developmental psychology of
pregnancy by Rubin (1975), four critical maternal tasks are described:
ensuring safe passage for the infant, ensuring acceptance of the baby by
the family, binding—in to the new child, and giving of oneself. Progress
in completing each task may be monitored throughout the trimesters of
pregnancy (Rubin, 1975). Increasing centration of maternal focus is
described as the pregnant woman turns her attention increasingly inwards.
Cognitive style is similarly observed to trace a developmental
trajectory, as first trimester concern with the question of being
pregnant gives way to midtrimester focus on the child's condition,
yielding to a third trimester characterized by protectiveness and
vulnerability (Rubin, 1970). A developmental perspective is further
applied to attainment of the maternal role antepartally and postpartally
by classification of the processes of taking—in; concern with self system
categories of the ideal image, the self image, and body image; and the
operations of mimicry, role play, fantasy, introjection-projection
rejection (I-P-R), identity, and grief work (Rubin, 1967). Whereas a
sequential ordering of these processes is suggested, with mimicry
occurring earlier in pregnancy, role play and fantasy predominating from
early to middle pregnancy, and I-P-R observed late in pregnancy, Rubin
conceptualizes the ordering of these processes as more cyclical than
straight-line (1967).
Rubin's work provides support for examining the gravida's

psychological status using the three-month interval of a pregnancy
trimester while seeking developmental patterns. However, applicability
of the tasks and processes described by Rubin to contemporary
secundigravidae are challenged for several reasons. First, major changes
in societal attitudes, women's roles, and health care practices since
Rubin's data collection may have altered psychological processes of
pregnancy, just as Martell and Mitchell (1984) suspect puerperal
attitudes and behaviors have changed since Rubin's early landmark works.
Second, Rubin's data are based on intensive interviews and observations of
small samples willing to tolerate such scrutiny. Testing of her
propositions with larger sample sizes is needed to confirm
generalizability of findings. Third, the concepts and processes
presented in Rubin's works are difficult to operationalize and apply to a
culturally diverse population.
A fourth limitation of developmental conceptual frameworks for
pregnancy has been the failure to adequately address second and later
order pregnancies (Tilden, 1980). Rubin (1967) comments that the
processes of maternal role attainment are somewhat modified for
multigravidae compared to first-time mothers. However, her observations
generally included only minor alterations to the processes described for
first-time mothers. She does acknowledge a unique aspect of second
pregnancy by describing grief work as including detachment from the first
child as well as letting go of the mother's former identity, in later
pregnancies.
Whereas changes in the realm of object relations during pregnancy
have focused on the baby, the mate, and the woman's own mother, (Tilden,
1980) theoretical notions including relationships with the firstborn have

been largely neglected. An important expansion to the conceptual view of
the developmental psychology of subsequent pregnancies is provided by
Walz and Rich (1983), who define the principal tasks of taking-on a
second child as adjusting to the new role, providing continued nurturance
to the older child, and establishing and maintaining family
relationships. Behavioral categories derived from their descriptive,
naturalistic study of the neomaternal period are: promoting acceptance of
the baby, particularly with the first child; grieving the loss of an
exclusive dyadic relationship with the first child; planning tasks;
reformulating the relationship with the first child; identifying the
second child by comparison with the first; and assessing self, including
the capability to nuture two children. Although this elaborated view of
the psychological tasks of mothering two children greatly enriches the
conceptual parameters of the psychology of second pregnancy by
illucidating the dynamics of the mother—firstborn relationship, this
contribution is based solely on interview and observation during the
immediate postpartum period spent in the hospital. The pattern of
progression through these tasks during the course of pregnancy is yet to
be revealed.
Family Development Framework
The family developmental framework is an eclectic merging of
concepts from the disciplines of demography, economy, rural sociology,
developmental psychology, interactionist theory, and role theory (Hill
& Rodgers, 1964). The resulting product is a combination of social
systems, structural functionalism, and a social-psychological approach
which recognizes that dynamic persons are individuals and family members
at the same time (Rowe, 1981). The framework is unique in bringing to

10
family study the developmental concepts of family and social time. The
family changes as reciprocal interaction patterns develop to fulfull the
individual's and family's changing needs and desires. A change in one
part of the family affects change in other parts (Rowe, 1981).
The framework incorporates the concept of developmental task which
had previously been applied to the individual by human developmentalists.
While each family member confronts individual tasks, simultaneously the
family is negotiating tasks which may or may not be supportive of the
individual endeavor. According to Duvall's (1977) classic textbook on
family development, the family performs basic tasks essential for
survival and continuity dealing with maintenance of physical needs,
allocation of resources, determination of home management functions,
socialization, establishment of emotive capacities, reproduction,
negotiation with society, and maintenance of morale and motivation.
Developmental tasks specific to a stage in the family life cycle are in
addition to these basic tasks.
The family life cycle is composed of a sequence of stages as the
family expands, contracts and dissolves. Definition of the stage is
determined by childbearing, progress of the oldest child through school,
departure of the youngest child, employment status and death of a spouse
(Duvall, 1977). Successful achievement of family developmental tasks
leads to present satisfaction, approval, and success with later tasks,
while failure leads to family unhappiness, societal disapproval and
difficulty with later family devlopmental tasks. Although the notions of
family developmental tasks and the family life cycle have not withstood
attempts to establish their empirical validity (Magrabi & Marshall, 1965;
Nock, 1979; Spanier, Sauer, & Larzelere, 1979), their usefulness as

11
conceptual tools, illustrative principles, or didactic techniques has
been supported.
The family development conceptual framework recognizes birth of the
first child as a major developmental step, marking transition of the
family into the childbearing stage (Duvall, 1977). Although the most
pronounced transformations of structure and advancements in a family's
system of meanings usually take place with the first occurrence of a
normative event such as addition of a child, there are exceptions. There
may be special intensity in response to a subsequent birth, or the
subsequent event may have special meaning in the family unit (Terkelsen,
1980).
Hence, the addition of a second child to the family, whether viewed
as a crisis or a less stressful normative transition, stimulates change
within the family. Selection of the family development framework
dictates that an attempt be made to look at some aspect of all family
members, as well as to attempt to capture the dynamic qualities of family
interaction through time.
Maternal Anxiety in Second Pregnancy
Study of the psychosocial experience of pregnancy has evolved from a
legacy of psychoanalytic studies based on pathologic cases (Bibring,
1959; Bibring, Dwyer, Huntington, & Valenstein, 1961; Deutsch, 1945) to
empirically based investigations that include large numbers of generally
healthy women (Colman & Colman, 1971; Entwistle & Doering, 1981;
Grossman, Eichler & Winikoff, 1980; Shereshefsky & Yarrow, 1973).
However, with the exception of the work by Grossman, these investigators
generally have limited themselves to examination of first pregnancy. A
12
discussion of the specific psychosocial variable of interest, that of
anxiety in second pregnancy, must therefore draw on a limited number of
studies in which parity is often only an incidental demographic variable
or parity status is mixed, including both first and later pregnancies.
In this section, variables affecting anxiety in second pregnancy
will be described, following comments on the concept and measurement of
anxiety. Then the sources of maternal concern and the level of anxiety
produced in second pregnancy, often as compared to first pregnancy, will
be examined for the prenatal period and then the postpartum period.
Spielberger (1976) presents a conceptualization of anxiety that is
reflective of current usage in anxiety research. Stress is the
objective, consensually validated stimulus property of a situation which
is characterized by either physical or psychological danger. An anxiety
state is characterized by the intensity of subjective feelings of
tension, apprehension, nervousness and worry experienced by an individual
at a particular moment, and by activity of the autonomic nervous system.
Anxiety also refers to a complex psychobiological process involving a
sequence of cognitive, affective, physiological and behavioral events
initiated by external stimuli or cognitions. Anxiety states vary in
intensity and duration, whereas an individual's trait anxiety is a
relatively more stable disposition towards anxiety.
One of the major methodological advances in the study of maternal
psychological stress is the use of standardized questionnaires for the
measurement of anxiety (Yamamoto & Kinney, 1976). When the focus of
investigation is intrapsychic activity at an unconscious level, then
projective tools such as Rorshach Psychodiagnostic Examination, Selected
Thematic Apperception Test Cards, Rotter Sentence Completion Test, and

13
the Draw A Person Test have been used (Bibring, et al., 1961;
Shereshefsky & Yarrow, 1973).
However, when the subjective, consciously perceived feelings of
tension and apprehension are to be measured, other instruments must be
used. The Institute for Personality and Ability Testing—Anxiety (IPAT)
used by Lubin, Gardener, and Roth (1975); the Taylor Manifest Anxiety
Scale (TMAS) used by Davids and DeVault (1962) and McDonald and
Christakos (1963); and the Spielberger State Trait Anxiety Inventory
(STAI) used by Gorsuch and Key (1974), Grossman, Eichler, and Winickoff
(1980), Norbeck and Tilden (1983), and Tilden (1984); have been found to
have interrcorrelations approaching scale reliabilities (Spielberger,
Gorsuch, Lushene, Wagg, & Jacobs, 1983). These intercorrelations permit
consideration of the various instruments as equivalent measures of trait
anxiety. Of these instruments, only the Spielberger STAI (Spielberger,
et al., 1983) allows assessment of both trait anxiety and state anxiety,
the transitory emotional anxiety condition. The ability to assess change
in a key variable through time has theoretical value for an investigation
guided by developmental concepts. Furthermore, the ability to measure
both state and trait anxiety has proven value in pregnancy research,
illustrated by the finding that prenatal trait anxiety was the only
variable predictive of postpartum state anxiety, accounting for 38% of
the variance in a mixed parity sample examined for relationships between
maternal anxiety, personality, attitudes and obstetric complications
(Beck, Siegel, Davidson, Kormeier, Breitenstein, & Hall, 1980).
Variables Affecting Anxiety in Second Pregnancy
Time. The effect of time on anxiety is of major importance when
examining pregnancy from a developmental perspective. Previous

14
longitudinal study of 64 first-time pregnancies revealed changes in
anxiety by trimester (Shereshefsky & Yarrow, 1973). Anxiety levels
assumed a curvilinear pattern, with high first trimester anxiety
subsiding and then rising again in the eighth and ninth months as labor
and delivery approach. Cohen (1978), however, found the drop in anxiety
occurring slightly earlier, noting that confirmation of pregnancy
decreased fears, with a progressive increase in anxieties through
pregnancy in nine primigravid subjects.
This "V"-shaped pattern appears to apply to multigravidae as well.
Lubin, Gardener, and Roth (1975), who followed 44 secundigravidae with no
previous terminations and 14 secundigravidae with previous spontaneous or
therapeutic abortion in a longitudinal study, found anxiety as measured
by the Anxiety Adjective Checklist (AACL) declined second trimester and
rose again third trimester. A rise in anxiety from second to third
trimester was found as well in a sample of 80 black multigravidae
("Anxiety Worse," 1980). Grossman and others (1980) measured anxiety only
during the first and third trimesters. They found anxiety levels were
not significantly different at these two times, but without an
intermediate measure no conclusions can be drawn regarding constancy or
volatility of anxiety. Although Grimm's (1961) sample of 235 normal
pregnant women of mixed parity drawn in groups of 40 from five intervals
spanning late first trimester to late third trimester demonstrated a
significant rise in psychological tension in the second half of the last
trimester, the general level of psychological tension was constant
through pregnancy to that point. Psychological tension was a composite
variable including anxiety, hostility and depression.
Demographic Wariables. Increasing age appears to be related to
15
lower anxiety in pregnant women of varying parity. Burstein, Kinch, and
Stern (1974) found lower anxiety scores with increasing age among their
sample of 61 women of mixed parity, as did Glazer (1980) in her sample of
100 women. Moss (1981) found the greatest number of concerns in her
sample of multiparae among those under 20 years old, and the least
concerns in mother over 30. On the other hand, Lubin and colleagues
(1975) found a slight but significant postive relationship between age
and anxiety in their sample of wives of medical students and staff of
mixed parity.
Socioeconomic status has been related inversely to anxiety in mixed
parity samples (Doty, 1962; Glazer, 1980). Middle-class women had less
emotional disturbance as measured on a Pregnancy Attitude Scale than
their lower class counterparts (Doty, 1967). Maternal education level
has a significant, inverse relationship with anxiety levels during
pregnancy (Glazer, 1980). Moss (1981) found the least concerns among
multiparae with 12 to 14 years of formal education. Amount of formal
education also significantly affected the type of concerns reported by
202 maternity patients questionned postpartally (Light & Fenster, 1974).
Subjects with more than a high school education had greater concerns
about x-rays and birth defects due to medications, while subjects with
less education were more concerned about childbirth, family, subsequent
pregnancies and finances.
Maternal employment status has received only limited attention in
empirical studies of prenatal anxiety, although family theoreticians have
suggested that level of employment positively influences mothers' level
of anxiety (Rollings & Nye, 1979). Nye (1979) proposes that the working
mother who has more and younger children will encounter greater economic

16
costs of childcare, greater opposition by spouse and children, greater
guilt, and greater sanctions from kin and neighbors, than her counterpart
with fewer or older children. In an exploratory study of 40 new mothers
of second-borns, maternal employment was found to increase postpartum
stress (Lynch, 1982). The distinction between employment in a career,
which requires special training and involves movement through an
hierarchy of prestige, compared to employment in a job as a wage-earner,
warrants attention since maintaining both a committment to a profession
and to a family role with children present creates a strain (Aldous,
1982).
Marital status has been found to affect anxiety in a mixed parity
sample (Tilden, 1984). Single women had higher state anxiety scores than
partnered women, who were either legally married or living with a stable
partner. The non-partnered women revealed additional stressors at mid
trimester, such as dealing with decision-making and disclosure issues
(Tilden, 1983). Length of marriage or relationship is also related to
anxiety levels during pregnancy, with shorter relationships associated
with greater anxiety (Glazer, 1980).
The variable exerting the strongest influence on maternal stress in
Lynch's (1982) postpartum investigation of new mothers of second children
was the age of the firstborn. When the firstborn was under two years
old, the child sought attention and struggled with independence issues.
When the firstborn was over six years old, the child's behavior was not
problematic, but stress was created by the greater change in maternal
demands.
The sex of a later-born infant may affect anxiety levels. Moss
(1981) found greater concerns in multiparae who had delivered males.
17
Sumner and Fritsch (1977) report a higher number of concerns expressed by
mothers breastfeeding males compared to females in their mixed parity
sample.
Experiential and Attitudinal Variables. Several aspects of a
woman's reproductive history influence anxiety during second pregnancy.
Olin (1983) found that a previous fertility problem was related to lower
scores on the Spielberger Self–Evaluation Questionnaire for anxiety in
her sample of 68 primigravidae and 77 multigravidae between the ages of
20 and 39. Lower anxiety scores in the third trimester and postpartum
were also found when the current pregnancy was planned (Olin, 1983).
Similarly, Lynch (1982) found an association between high stress
postpartally and unplanned pregnancy.
Previous and current pregnancy and delivery experiences influence
anxiety in secundigravidae. The diagnosis of "high risk pregnancy" in
itself causes uncertainty, guilt, and anxiety (Galloway, 1976). A
previous problematic or traumatic pregnancy or birth experience would be
expected to kindle heightened anxiety as a situation of similar structure
recurs. Antenatal hospitalization at a high risk pregnancy medical
center heightens fears for mother and infant, while imposing concerns
about other dependent children from whom the mothers are separated
(Merkatz, 1978).
Lipson (1984) describes how the woman who has delivered previously
by Cesarean delivery may be confronted with an overwhelming barrage of
diverse opinions due to newly available options for previous surgical
delivery patients. The response to increased responsibility and choice
varies from delight to increased anxiety. In addition, the experience of
having given birth vaginally prior to a Cesarean birth appears to have a

18
positive effect on the mother's emotional status, since multiparous
Cesarean delivery mothers who had experienced a vaginal delivery rated
higher on the Maternal Attitude to Pregnancy Instrument than those who
had never delivered vaginally (Hart, 1980).
Evolving technologies in prenatal diagnosis (Beeson & Douglas, 1983)
may affect the pattern of anxiety in pregnancy. The process of prenatal
diagnosis itself appears to be changing parents' experience of pregnancy
(Beeson, Douglas, & Lunsford, 1983). Anxiety levels increase before
tests and while awaiting results, perhaps in a suspension of commitment to
the pregnancy. Anxiety may decline after favorable results are reported.
Extent of participation in childbirth education classes may be
correlated with maternal anxiety levels. Although attendance at a series
of childbirth education classes did not change anxiety levels in 26
multigravidae reported in 1984 (Walker & Erdman), an earlier study of the
effect of Lamaze childbirth education on anxiety, maternal attitudes to
pregnancy and biomedical parameters of the delivery, did find differences
in pre- and post-class anxiety levels (Zax, Sameroff, & Farnum, 1975).
Class attendance was associated with lower anxiety, as measured by the
Institute for Personality and Ability Testing (IPAT) scale for
experienced, but not first-time, mothers. Moss (1981) found the least
concerns in multiparae who had gone to one series of prenatal classes,
compared to those who took no classes or those who attended multiple
class series. Hence, the relationship between childbirth education class
attendance and anxiety may be complex. Class characteristics of
information—provision and support may reduce anxiety for some women. For
other women, class attendance may not be causally related to anxiety
level changes, but may instead reflect other correlated psychological

19
dimensions manifested as avoidance or attempts at over-preparation.
Life stress was found to account for 21.4% of the variance in emotional
disequilibrium, a construct composed of weighted values for anxiety
(measured by the Spielberger STAI), depression, and self-esteem, in a
sample of 117 normal prenatal patients of mixed parity (Norbeck & Tilden,
1983). Social support, of the emotional type, explained 6.5% of the
variance in emotional disequilibrium. An interactive effect between life
stress and social support was revealed. Olin (1983) found no significant
relationship between stressful events experienced within the preceding 18
months and anxiety levels during pregnancy, using less complex
statistical analyses and a predominantly middle- to upper-middle class
white sample.
Several experiential variables were reported to have no effect on
anxiety levels in pregnancy. Neither birth defects in the family,
complications during the pregnancy or delivery of the woman's mother, nor
the death of the woman's mother significantly affected anxiety levels of
Olin's (1983) 145 subjects measured late in pregnancy.
Maternal Concerns during Second Pregnancy
A concern is defined as "that which busies or occupies one's
thoughts" (McKechnie, 1975, p. 376), while to be concerned is to be
uneasy or anxious, to experience agitation, uneasiness of mind, or a
disturbed state of feeling. Concern and anxiety may be considered
synonomous, or the concerns may be considered the cognitions which
stimulate anxiety. Maternal concerns and maternal anxiety levels during
pregnancy are often investigated concomitantly. The logical relationship
between anxiety levels and number of issues about which a pregnant woman
has concerns has been empirically validated. Glazer (1980) found a

20
significant correlation between the number of concerns indicated by 100
pregnant women of mixed parity and their anxiety level measured by the
Taylor Manifest Anxiety Scale. The types of concerns of pregnant women
also appear to be a function of gestational age. Glazer (1980) describes
how the major concerns shift from self, childbirth and medical care in
the first trimester, to self, childbirth, effects on the baby, finances,
family and subsequent pregnancy by the third trimester when considering
her total sample of first and later pregnancies.
Concerns and anxiety levels in second pregnancy have often been
investigated in comparison to the first pregnancy experience, with
conflicting results. No significant difference in anxiety level by
parity was found using projective measures throughout pregnancy (Grimm,
1961), using the Health Insurance Plan Pregnancy questionnaire on
emotional adjustment and attitudes administered before 16 weeks to assess
worry about the baby (Grimm & Venet, 1966), nor by using the Manifest
Anxiety Scale (Davids, Holden, & Gray, 1963) or the Spielberger STAI
(Olin, 1983) in the third trimester. Despite what might be a common
expectation for decreased fears and conflicts among experienced mothers,
Lederman and Lederman (1979) stressed the importance of their findings
that there were no differences between multiparae and primiparae on
scales for concerns about well-being for self and baby, acceptance of
pregnancy, identification with the motherhood role, feeling prepared for
labor, or fears pertaining to pain, helplessness and loss of control in
their sample of 119 women.
In contrast to these findings, other investigators have reported
differing levels of anxiety and concerns between first-time and
experienced mothers. The secundigravida has been found to be more fearful

21
for the unborn baby (Larsen, 1966), more fearful for herself (Larsen,
1966) including increased mutilation anxiety (Westbrook, 1978a), and more
fearful regarding what childbirth would be like (Norr, Block, Charles, &
Meyering, 1980). In addition, multiparae were less likely to take Lamaze
classes or to receive aid from their husbands during delivery (Norr,
Block, Charles, Meyering, and Meyers, 1977), and more distressed at the
lack of support in labor from nursing personnel (Larsen, 1966).
On the other hand, contradictory reports describe the emotional
burden of first-time mothers as more distressing. Norr and others (1977)
found fewer worries about birth with increasing parity. Burstein, Kinch
& Stern (1974) found greater anxiety and stress in primigravidae when
measured by an original "Pregnancy Anxiety Scale" of 25 items specific to
pregnancy, however they found no significant parity differences using the
Taylor Manifest Anxiety Scale. Primigravidae also reported more fears
about pregnancy and childbirth (Doty, 1967), greater concern about
childbirth pain (Light & Fenster, 1974), greater fear for themselves and
the baby (Erickson, 1976), and greater fear of physical injury (Grossman,
Eichler & Winickoff, 1980).
While weighing the relative contributions of these reports, it is
important to note that all of the investigations documenting increased
anxiety and concern for multigra vidae are based on data collected in the
postpartum period, whereas much of the data describing greater anxiety in
the primigra vidae were actually collected during pregnancy (except Norr
et al., 1977; Light & Fenster, 1974). The length of time between
pregnancy and data collection was as great as seven months (Westbrook,
1978a). The most accurate measurement of a volatile arousal condition
such as state anxiety and its focal concerns is best made during the
22
experience under scrutiny. Retrospective recall allows intervening
events to influence recollection, hence jeopardizing the validity of
purported pregnancy measures.
Maternal Concerns following Second Pregnancy
Postpartum adaptation and parenting concerns are clearly different
in subsequent pregnancies than in first pregnancies. Although the
literature describing prenatal concerns for the secundigravida is
inconsistent, perhaps because there has been a failure to adequately
assess the unique and central issue of bringing a baby into a family
already occupied by a child, clear and long-standing differentiations in
postpartum concerns by parity have been described. A 1967 report of
interviews with 40 mothers of mixed parity (Henning, Martoglio, Quita,
Rembrecht, & Strickland) found multiparae focused on re-establishing
family relationships and a voiding sibling rivalry, needing help in the
home to allow for recovery, and planning for meals; while primiparae
needed guidance and reassurance in planning self care and care of the
baby at home. These themes have been supported in subsequent
investigations to be discussed in this section.
The new first-time mother has concerns about her infant, herself,
and her marital relationship. Primiparae express significantly greater
concerns and needs for information about infant feeding, gastrointestinal
and skin care (Sumner & Fritsch, 1977); about mothering skills, baby
characteristics and behaviors, and anticipatory guidance (Evans, 1968;
Gruis, 1977); and about caring for baby's physical needs and the
responsibilities of mothering (Light & Fenster, 1974; Norr, et al.,
1980) than multiparae. First-time mothers express more concerns about
their own physical care such as discomforts, breast care, rest, sleep,
23
and diet (Evans, 1968; Light & Fenster, 1974). Primiparae are more
worried about how their husbands feel towards them than multiparae (Norr,
et al., 1980). First-time parents undergo a major disruption in the
marital dyad, which researchers speculate explains why adaptation at two
months postpartum was related strongly to a number of general
psychological measures, pregnancy-related characteristics, and marital
satisfaction in early pregnancy for first pregnancies, but not subsequent
pregnancies (Grossman, Eichler, & Winickoff, 1980).
Recently—delivered multiparae express greater concerns focused on
family relationships, external stresses, and time constraints. Gruis
(1977) captured the shift in concerns for experienced mothers in her
finding that the focus in primiparae is the newborn himself, while in the
multipara the focus of concerns is the strain the new child places on the
rest of the family.
Moss (1981) surveyed 56 multiparae, finding that family subjects
were the most often stated major area of concern on the third postpartum
day. Concern about how the children at home will act towards the baby
was nearly universal. Olin (1983) inter viewed a small subset of her
surveyed sample, also finding that multiparae were most concerned about
the effect the new baby would have on their older child or children.
Evans (1968) found greater psychosocial needs in multiparae, a category
encompassing encouragement, nervousness, concerns about visitors, coping
with critical attitudes of family and friends, household help, and
adjustment of older children to the baby.
External stressors reported to increase with parity include the
stress of too much company and interference from relatives and neighbors
(Larsen, 1966) and financial problems (Olin, 1983). Grossman, Eichler &

24
Winickoff (1980) concur that women having subsequent pregnancies are more
vulnerable to external pressures and factors, since socioeconomic status
and recent life stresses were predictors of anxiety and postpartum
depression for them.
Concern with time limitations is reflected in reports of greater
problems with housework and family routines (Larsen, 1966), concern about
enough time to give to each child (Olin, 1983), and a greater concern
with finding time for oneself (Gruis, 1977). Grubb (1980) studied women
in subsequent pregnancies and found mothers had time for their babies'
needs only by depriving themselves. When they had time for their own
needs, it was usually because someone else had assumed some of their
duties. Lynch (1982) concurs that lack of time for self is a source of
stress for the new mother of two. Comparison of social support perceived
by new mothers revealed that primiparae perceive their network members to
be more able to offer tangible aid than do multiparae (Miller, 1984).
The value of a social time framework for study of transition to
parenthood has been illustrated in a case study of a second pregnancy
(LaRossa, 1983).
In addition to increased concerns about their ability to care for
the family, multiparae had greater concerns about having more children
than they wanted and contraception, in a 1974 report (Light & Fenster).
The current importance of this concern may be mitigated by increased
contraceptive options.
Both first-time and repeat mothers share a concern about their
appearance following birth. Return of the figure to normal was the most
common concern of both multiparae and primipare in Gruis' (1977) survey.
Lynch's (1982) sample of 40 new second-time mothers reported their
25
greatest stressor was self-concern about their body figure, self-image,
and change in abdominal muscle tone. The 56 multiparae in Moss's (1981)
study, asked to select from 21 cards describing potential concerns about
their physical or emotional status in the category that evaluated
concerns about self, most often indicated concern about their weight and
return of their figures to normal. Moss (1981) elaborates that the
postpartum concerns related to the mother's body are not discomforts,
such as sore breasts, but concerns about body alterations. Larsen (1966)
found that concern with weight reduction increased with increasing
parity.
Conclusions
A review of the literature describing maternal anxiety in second
pregnancy suggests the direction for future inquiry. Numerous temporal,
demographic, experiential and attitudinal variables have been found to
affect anxiety in pregnancy. The relative weights or contributions of
these variables to anxiety remains unknown. No single study has examined
anxiety through the course of pregnancy with simultaneous monitoring of the
breadth of variables discussed, thus allowing for control of possible
extraneous variance by design or statistical evaluation. Conflicting
reports of the effect of a particular variable on anxiety may be due to
assessment of anxiety using instruments with poor psychometric
properties. An adequate description of anxiety in second pregnancy also
requires strict control of subject parity status, since most of the
previous investigations have grouped together women with varying numbers
of children.
Review of the prenatal and postnatal concerns of secundigravidae
suggest that anxiety levels do not differ consistently from women bearing
26
a first child, but that the foci of concerns for the woman adding a
second child to her family are different. This conclusion is supported
by giving greater credence to investigations which have used standardized
instruments and have measured anxiety and concerns during the time of
interest rather than relying on retrospective recall. The predominant
practice of reporting pregnancy concerns globally, rather than with
specification of the gestational age at which they are manifested, has
failed to reveal any developmental process which may exist.
The study of concerns during second pregnancy has been limited by
assessment in the areas of traditional inquiry for primigra vidae: fear
for baby, fear for self, and fear of childbirth. When open-ended
questionnaires or interview techniques have been used during pregnancy,
multigravidae have indicated that concerns about family relationships are
prominent. Investigators of the postpartum period, however, have
delineated an emphasis on infant, self, and marital concerns for first
time mothers compared to an emphasis on family relationships, external
stresses, and time constraints, as well as body alterations, among
multiparae. A contrast between an internally-oriented first-time mother
with a focus on her baby within, compared to an externally-oriented
second-time mother renegotiating multiple interpersonal relationships is
suggested. Further research, spanning the course of pregnancy, is
required to illucidate these processes. The following section reviews
dyadic relationships in the family of the secundigravida.
Maternal Perception of Family. Relationships in Second Pregnancy
Both prior and ongoing interpersonal relationships have been
acknowledged to exert an influence on pregnancy and parenting. The

27
relationship of the pregnant woman to her own mother has been identified
as crucial to satisfactory assumption of the role of mother to her new
baby in the psychoanalytic literature (Ballou, 1978; Chodorow, 1978;
Deutsch, 1945). Of the ongoing relationships in the nuclear family, the
marital relationship, particularly in first pregnancies, has been found
to have impact on the childbearing experience (Ballou, 1978; Cohen, 1966;
Grossman, et al., 1980; Westbrook, 1978b). However, there is a need for
studies of relationships in pregnancy affected by the presence and
demands of other children (Richardson, 1982).
Examination of relationships within the family context presents
conceptual and methodologic challenges (Cooper, Grote vant, & Condon,
1982; Gilliss, 1983; Miller, Rollins, & Thomas, 1982). Parke, Power,
Tinsley, and Hymel (1979) stress the need to assess the total set of
relationships among family members in order to understand a single dyad,
as exemplified by work on the father-infant relationship and its effect
on the infant's development. Similarly, Lamb (1979) faults previous
parent-infant research for emphasizing a single dyad. With a component
dyad strategy, all dyads are examined to detect direct and indirect
effects on interaction which may be mediated through another person.
Where direct observation is not feasible, maternal perception of other
family member involvement has demonstrated value in the study of parent
child interaction and child development (Eyres, Barnard, & Gray, 1979).
The law of family interaction (Bossard, 1945) mathematically defines
the number of family interactions (dyads) as a function of the number of
people in the family:
Number of Interpersonal Relationships =
( (Number of persons)” – Number of persons) / 2

28
Mother Father"Tw
>]First Child Baby: Fetus/Newborn
Before second pregnancy
After second pregnancy
Figure 2. 1 Changes in Family Dyads in Second Pregnancy
Hence, a family acquiring a fourth member by birth expands from three to
six dyads (See Figure 2.1), changing from a triad to a quadrate.
The only investigator to examine maternal perception of all the
family dyadic relationships of multiparae through the course of pregnancy
is Richardson, who interviewed nine multiparae and five primiparae,
predominantly Mexican-Americans drawn from a lower socioeconomic class
clinic population, at two to seven week intervals starting before 14
weeks gestation (1981; 1983a; 1983b). Subjects listed relationships in
order of impact as 1) husband, 2) a child, 3) parental, and 4) peers,
with husband most important (1981). This reflects the total sample,
however, without consideration of separate rankings by those who have a
child. Relationships were found to be more changing than stable through
pregnancy, underscoring the need for specification of gestational age in
dyadic relationship studies of pregnancy. Relationships with one's
husband and own children were most problematic and most intensely
demanded attention (1981). The composite of relationships appears to
determine the character of the pregnancy experience, since a singular
disturbing relationship only becomes problematic if the woman lacks other
positive supportive relationships or if other relationships are troubled

29
as well (Richardson, 1982).
Each of the six nuclear family dyads during second pregnancy will
next be examined. The purpose of this review is to describe the current
level of knowledge and to identify areas in need of further study.
Marital Relationship
A description of the marital relationship throughout second
pregnancy can only be suggested by combining theoretical notions and
empirical data describing segments of the second childbearing year. In
the psychoanalytic realm, Ballou (1978) describes a vital matrix
involving the husband, mother, and child of the pregnant woman, whose
interrelationships are central to emergence of the woman's sense of the
child as a person. Applicability of this matrix to second pregnancy
is untested. Quality of the pregnant woman's relationship with her
husband has repeatedly been found to be one of the major determinants of
maternal adaptation to pregnancy and parenthood for primiparae in
empirical investigations (Lederman, Weingarten, & Lederman, 1981;
Shereshefsky & Yarrow, 1973), but not for multiparae (Grossman, Eichler,
& Winickoff, 1980). An explanation for the apparently diminished impact
of the marital relationship in later pregnancies has not been
established.
There is a dearth of information about the marital relationship
early in second pregnancy. Richardson (1981) has identified the need for
further study of the marital dyad early in pregnancy through to the
postpartum period. Data collected to develop a pregnancy questionnaire
showed primigravidae have greater satisfaction with their husbands, and
with life in general, than multigravidae among a sample of 124 women
tested at their first antepartal visit, before 16 weeks gestation (Grimm

30
& Venet, 1966). Interview data collected from before 14 weeks gestation
to the end of pregnancy from 14 women of mixed parity yielded findings
that husbands were usually described as the most important significant
other in the women's lives and that changes in affective involvement
dominated task performance (Richardson, 1983b). There was a significant
increase in satisfaction with their marital relationships through the
course of pregnancy for the sample as a whole. However, since only five
of the women were pregnant with their second child (five with first, and
four with third or fourth), two of the women of unspecified parity
separated from their husbands in early pregnancy, and three of the
remaining twelve also shared residences with extended family members, the
generalizability of this finding to secundigra vidae must be considered
limited.
Quality of the marital relationship from middle to late portions of
second pregnancy remains unclear. Rankin and Campbell (1983) were
surprised to find 192 white middle-class Lamaze couples of mixed parity
rate their marital relationships as more satisfactory during the third
trimester than they felt they had been three months earlier. Wagaries of
the instrument or sample characteristics were suspected of countering the
expected decline in satisfaction. Improved marital satisfaction from
from 24–36 weeks of pregnancy to 3–21 days postpartum is reported using
the Interpersonal Conflict Scale (Moore, 1983).
The difficulty in assessing a negative change in the marital
relationship towards the end of pregnancy has been acknowledged by a
leading investigator in the field (Lederman, 1984a). Lower scores for
relationship with husband were recorded for multigravidae compared to
primigravidae late in pregnancy during development of the Relationship

31
with Husband scale (Lederman & Lederman, 1979). The lower scores were
felt to reflect the increased stress between parents with children, or
the greater willingness of multigravidae to acknowledge conflict in
marriage.
Other reports similarly find negative effects of subsequent
childbearing on marital adjustment, reported both as parity comparisons
and as a decline from mid- or late-pregnancy to months and years
following subsequent birth. Feldman's (1971) landmark longitudinal study
revealed that further erosion of the marital relationship occurs as
couples experience second pregnancy compared to those with only one
child. Testing in the fifth month of pregnancy, five weeks postpartum,
and five months postpartum revealed lowered satisfaction in the marriage,
perceived negative personality change in both partners, less satisfaction
with home, more instrumental conversation, more child-centered concerns,
and lowering of sexual satisfaction after childbirth for primipare and
multiparae compared to childless couples. Using a standardized marital
satisfaction instrument, the Spanier Dyadic Adjustment Scale (DAS),
Belsky, Spanier, and Rovine (1983) confirmed significantly lower total
scores and subscale scores for satisfaction, cohesion, and affectional
expression in multiparae compared to primipare. Their contemporary
sample of 72 couples were assessed by interview, questionnaire and
observation, revealing a linear decline from third trimester of pregnancy
through three- and nine-months postpartum. These negative effects of an
additional child appear to be long-lasting, as evidenced by a study of
180 married couples with either no children or children five to thirteen
years old showing an inverse relationship between increasing parity
(none, one, or two children) and marital adjustment measured by the

32
Spanier DAS (Rankin, 1981).
Several explanations for the apparent decrease in marital
satisfaction with increasing numbers of children have been presented.
Harriman's (1983) examination of marital change accompanying parenthood
in a mixed parity sample suggests that changes in the sexual relationship
are central to declining marital satisfaction. Forty-eight subjects of
mixed parity drawn from Lamaze classes completed the Fundamental
Interpersonal Relationships Orientation—Behavior instrument (Griffith,
1976). Their responses suggest that discrepancies in the areas of
affection and inclusion account for incompatability during pregnancy.
Whether the decline in affectional and sexual behaviors causes or results
from decreased marital satisfaction, or whether another element of
marital discord is being reflected in less affectional behavior has not
been determined.
Mother—Baby Relationship
Systematic assessment of the mother-baby relationship during
pregnancy is hampered by instrumentation and methodologic limitations.
Contemporary application of reports of increased negativism during
pregnancy towards second babies compared to first (Wallin & Riley, 1955),
positive correlations between negative maternal attitude and increasing
parity (Laukaran & WandenBerg, 1980), and increasing rejection of
pregnancy with increasing parity (Westbrook, 1978a) is limited due to
retrospective designs, inadequately operationalized concepts, and samples
of limited generalizability.
Cranley (1981a, 1981b) devised a 24-item paper-and-pencil
instrument, with items such as "I can hardly wait to hold the baby," to
measure maternal-fetal attachment. Five subscales are designed to assess

33
role-taking, differentiation of self, giving of self, attributing
characteristics to fetus, and interaction with the fetus. She found no
differences by parity following third trimester administration of the
instrument. A developmental sequence throughout the course of pregnancy
was not reported.
Current lay literature describes the mother-second baby relationship
during pregnancy as problematic or somewhat inferior to the first
experience. A mother described her second experience as marked by less
excitement and drama, reporting that she occasionally forgot she was
pregnant (Mattingly, 1983). Brazelton (1981) described a conflicted
mother who did not feel free to attach to her second baby during
pregnancy until given permission by the pediatrician.
Attempts to assess the mother-baby relationship following delivery
have used observational and self-report techniques. Less time was taken
in affectionate interaction with second-borns than with first-borns at
three months of age in a study by Jacobs and Moss (1976). Second-time
mothers had fewer interactions with their newborns on a maternity ward
than first-time mothers (Norr, et al., 1980), which the authors
cautioned may not mean the affectional bond was less strong, but might be
accounted for by less practice needed in baby care or a more easily
established mothering bond.
Father-Baby Relationship
The limitations restricting generalizability of findings about the
mother—baby relationship during second pregnancy pertain as well to the
father's relationship with his expected second child. Prenatally, Weaver
and Cranely (1983) tested a modified version of Cranley's Maternal-Fetal
Attachment instrument with fathers, but they had too few later child

34
pregnancies in their sample of 100 to make parity comparisons.
Postpartally, husbands of first-time mothers are reported to be more
likely to be doing things with the new baby than husbands of second-time
mothers (Norr, et al., 1980). Experienced clinicians describe maternal
doubts that the father will love the new baby like he does the first
(Jimenez & Jones, 1981). Peterson, Mehl, & Leiderman (1979) suggest
that increasing parity is predictive of decreasing father attachment as
assessed by interview and observation up to six months postpartum. Their
measure of attachment is predominantly care-taking activities.
Mother-Child Relationship
The psychological difficulties of preparing to mother more than one
child are graphically presented in a case study report by Jenkins (1976),
who portrays the secundigravida's feelings of betrayal and guilt as she
anticipates her first child's reaction to the newborn and doubts her
ability to love two children equally. Brazelton (1981) has described the
most difficult thing about having a second baby as the necessary
"desertion" of the first. He states that maternal fear that the older
child will suffer and be damaged by rivalry with the new baby is
universal. Another case study (Ulrich, 1982) describes the intense work
involved in gaining acceptance for a second child, illustrating that
maternal bonds with each family member must be loosened and realigned
(Rubin, 1967a). A parents' childcare manual describes different degrees
of love for the firstborn and new baby (Kelly & Parson, 1975). Mothers
are advised not to be ashamed of the overwhelming love they feel for the
first child compared to the prosaic love for the newborn, while being
reassured that they will find a niche for the newborn after months of
daily care.
35
The quality of the mother—child relationship through the course of
second pregnancy is suggested by findings from Richardson's (1983a)
longitudinal study of nine multigravidae. Based solely on maternal
perceptions, the relationship is typically characterized as good or
positive early in pregnancy, becoming problematic later. A progression
of subtle to dramatic and disruptive child behaviors is noted, with the
majority of mothers ranking the overall relationship as more
unsatisfactory than satisfactory. Children sense very early that their
established role position is in jeopardy. A master clinician concurs
that children are aware early of a change regarding their mother
(Brazelton, 1981). He has observed that the mother unconsciously turns
into herself and subtly withdraws from her other children, so that she
is surprised when the children object.
The nature of the dynamics of the mother—child relationship from the
end of pregnancy to the postpartum period is illucidated by several
short-term longitudinal studies. Both mothers and first-born children
exhibited less emotional warmth towards one another at one to two months
after the birth of a newborn than they exhibited shortly prior to birth
(Taylor & Kogan, 1973). Mothers exhibited decreased attention to the
first-born over the same time span (Dunn & Kendrick, 1980; Kendrick &
Dunn, 1980). Longitudinal evaluation comparing firstborn children who do
and do not acquire siblings supports that "dethronement", or the loss of
the firstborn's exclusive relationship with his parents, is marked by
increased dependency behavior to the mother (Feiring, Lewis, & Jaskir,
1983), with males exhibiting more crying and proximity-seeking while
females show more help-seeking behaviors. A sample of 29 mothers who
received private obstetric care, almost all of whom observed regressive

36
behavioral changes in their toddlers on arrival of their newborns, stated
they believed the regression to be a normal developmental or adaptive
phase, with few expressing concern about such change (Kayiatos, Adams, &
Gilman, 1984).
Additional reports describe maternal perceptions of the mother—child
relationship as problematic in the postpartum period. Multiparae
interviewed weekly postpartum often expressed anger and hostility towards
older children by the third week, due to the child's demands and maternal
frustration (Grubb, 1980). Walz and Rich (1983) elaborated the
additional tasks required of the second time mother induced from their
study of 14 middle-class women hospitalized following normal delivery,
which were discussed previously.
Father-Child Relationship
No empirical investigations have examined maternal perceptions of
the course of paternal-firstborn relations during second pregnancy,
although a few small-scale studies have addressed the status of this dyad
following second pregnancy. Kreppner, Paulsen, and Schuetze (1982)
identify the main problem after the birth of the second child as new
structuring of family—home management, in their hermeneutic longitudinal
study of 16 families. They see the doubling of parental involvement in
child-oriented interactions as generating a specific task for the
parents, that of redistributing their attention for children, creating a
new "economy" of parent—child interactions within the family. The
father's role in intrafamilial dynamics is crucial, because he determines
whether the partition of childcare truly relieves the mother from being
forced to "double" her existence. Three patterns of father involvement
were identified. The parents' roles with both children may be
37
interchangeable, the father may increase care for the first child
allowing the mother greater intimacy with the baby, or the father may
perform more household chores while the mother increases care of both
children.
Other observers have commented on occurrence of the second pattern,
that of increased father—firstborn interaction postpartally. Bryant,
Cordaro, Grace, and Meier (1979) and Jimenez and Jones (1981) describe
fathers as finding themselves closer to their older children in the weeks
after birth, in publications for lay audiences. Exploratory field work
using the grounded theory approach suggests that closer father-child
relationships ease the difficulties of affectional and temporal resource
distribution surrounding subsequent childbearing (Sammons, 1983). In
several families studied by LaRossa and LaRossa (1981), the increased
child care demands following second birth were met by increasing the
father's parental role. This was always by increased father care of the
older child, which the investigators attribute to the less demanding
nature of assisting older children.
Child-Baby Relationship
There is a paucity of rigorously obtained information about the
firstborn-baby relationship during pregnancy. As mentioned earlier, an
expert pediatrician has observed that the child senses pregnancy and its
portent of change even before being told (Brazelton, 1981). Maternal
fear of the older child being damaged by sibling rivalry is considered
universal (Brazelton, 1981).
Attempts to reduce the firstborn's expected suffering caused by the
newborn's arrival form the basis of much of the prenatally- and
intrapartally-focused material relevant to the sibling relationship.
38
Prescriptive advice is given in the nursing literature describing how and
when to prepare older children, and how to deal with their behavior after
delivery (Legg, 1974; Malinowski, 1979; Powell, 1981; Vestal, 1979).
Course content for prenatal classes for children and repeat parents is
delineated (Jimenez, Jones, & Jungman, 1979; Sweet, 1979).
The postpartal behavior of the older member of the sibling dyad has
been described by enumeration of common reactions (Legg, 1974). Kreppner
and associates (1982) describe the ambiguous role of first children as
one of trying to emphasize that they are different from the baby, but
also that they have many of the same needs and wants. Dunn, Kendrick,
and MacNamee (1981) have begun to describe normative firstborn behavior
and sibling interaction, correlating factors associated with the
firstborn's reactions prenatally and postpartally using multivariate
analyses.
Variables Affecting Dyadic Family. Relationships in Second Pregnancy
Variables which have an established or suspected effect on the six
family dyads and how they are perceived by the secundigravida will be
presented. The direction of effect will be included in cases where it is
well established.
Factors exerting an influence on marital quality are reviewed in a
monumental work by Lewis and Spanier (1979), who evaluated several
hundred studies representing virtually all empirical and conceptual
propositions related to marital quality and stability. The influences
described relate to marital satisfaction in general, not specifically to
the period of pregnancy. Premarital predispositions including
personality factors, attitudes and values; social factors; circumstantial
factors; marital expectations; and social maturity level affect marital
39
quality. Among social factors, increased marital quality is related to
homogamy of racial, socioeconomic, religious, intelligence, and age
status between partners. Generally, greater social and personal
resources are related to greater satisfaction. Greater marital
satisfaction from parental models and greater support from significant
others also contribute positively to later marital quality. Following
marriage, social and economic factors affect the relationship. Increased
satisfaction is related to higher socioeconomic status, greater community
embeddedness, and decreased density in household composition. The effect
of wives' employment is complex, apparently related to an aspect of
mutual satisfaction with her degree of workforce participation.
Interpersonal and dyadic factors also relate to marital quality, with
greater positive regard, emotional gratification, communication, role fit
and interaction all correlated with increased satisfaction in marriage.
Multiple factors are considered to affect the parent-infant
relationship. Most attention has been given to the mother-baby dyad. A
theoretical consideration of factors impacting on maternal role
attainment relates enhanced role attainment to positive perceptions of
the birth experience, decreased social stress, increased support systems,
positive self-concept, good maternal and infant health, easy infant
temperament, and types of child-rearing attitudes (Mercer, 1981). The
impact of age is complex, suggesting differing processes among teens,
twenties, and thirty-year olds. Conflicting evidence on early maternal
infant separation has been found. A study of adaptation to motherhood in
20 primiparae revealed that previous experience with infants, and
positive perceptions of help from postpartum nurses and husbands were
additional significant variables (Curry, 1983).

40
While the previous two investigators have focused on the mother
infant dyad for first-time mothers, Kirkpatrick (1978) has developed a
structural model for multiparae distinct from primiparae. In the five
tiered model, the first level includes factors of education, present
income, and number of children; the second level includes childbearing
attitudes, wife's income prior to first and last pregnancy, age at first
parenthood, length of marriage prior to parenthood, and number of
children desired; the third level includes attitudes to pregnancy and
preparation for parenthood; the fourth level is composed of marital
adjustment, concept of the infant, income at time of birth, and spacing;
and the final variable is adjustment to parenthood. Importance of age of
the firstborn is well-supported. Children less than two years old when
their siblings are born are more dependent and have less positive social
behavior than their older counterparts (Feiring, Lewis, & Jaskir; 1983).
Discussion to this point has been limited to the mother-baby dyad
after delivery. Cranley (1981b) examined the relationship between
maternal—fetal attachment in the third trimester and other variables.
She found no differences in attachment scores due to antecedent or
demographic variables, including self-esteem and trait anxiety. Two
situational variables measured in her study were significantly correlated
to fetal attachment, with strong social support (most often provided by
husbands) evidencing a positive influence, and high perception of stress
during pregnancy demonstrating a negative influence. Closely spaced
pregnancies appeared to affect fetal attachment, since multigravidae with
a child 18 months or younger at home had lower attachment scores and
higher perceived stress levels. The effect on fetal attachment of
diagnostic technologies which might give a keener sense of the fetus or

41
knowledge of the sex awaits large-scale testing (Beeson, Douglas, &
Lunsford, 1983). The mother's ordinal position within her family of
origin has no established effect upon mother-baby or mother-child
relationships during pregnancy, but speculatively could arouse empathy
for the similarly placed offspring, since women experience a revival of
early childhood conflicts with siblings and parents during pregnancy
(Caplan, 1957).
The mother-firstborn dyad is affected strongly by the age of the
firstborn. More satisfactory mother—child relationships are reported by
women towards the end of subsequent pregnancy when the child at home is
younger than two or between seven and fourteen years of age (Richardson,
1983a). Postpartally, method of infant feeding may affect the mother's
relationship with both children, as some observers have noted the
greatest amount of jealous behavior at nursing (Kelly & Parson, 1975),
while others have identified bottle-feeding as an additional stressor
(Lynch, 1982).
Interactive effects of variables may influence the mother's
relationships with family members. Both breastfeeding and maternal
employment postpartally lead to problems of role overload in response to
multiple demands (Auerbach, 1984). Results of a study of 105 working and
nonworking primiparae five to nine months postpartum suggest work
involvement should be considered an individual difference variable in
research on new motherhood (Pistrang, 1984). Women for whom work before
pregnancy had high importance, but who found themselves not working
postpartally, reported increased irritability, decreased marital
intimacy, increased costs of motherhood, increased depression, and
decreased self-esteem compared to postpartum non-workers with low pre

42
pregnancy work involvement. Among working mothers, previous work
involvement was unrelated to motherhood experiences.
Factors affecting the father-baby and father-child relationships are
less well established. Future inquiry should monitor those variables
already acknowledged as salient for the parallel maternal dyads. In
addition, there appears to be some basis to the claim that fathers prefer
boys (Parke, Power, Tinsley, & Hymel, 1979), exhibiting a stronger
preference for boys than do mothers, to the extent that couples will have
more children than they originally planned to try for a son (Hoffman,
1977).
Factors affecting the child-baby relationship have been detected by
Dunn, Kendrick, and MacNamee's (1981) multivariate analysis of firstborn
reactions to a newborn among their intensely studied longitudinal
subjects. The temperament of the child is correlated with diverse
reaction patterns. Males exhibit more withdrawal than females, and
younger children demonstrate more clinging than older ones. Maternal
state affects the child's response, with increased maternal tiredness or
depression associated with greater child withdrawal. Bottle feeding was
related to increased irritating behaviors by the child to the baby.
Interactive effects of child's temperament, sex, and mother's state were
found to affect child withdrawal and sleep problems. Postpartally, the
nature of mother—firstborn interactions is correlated with types of
sibling interaction. Increased maternal prohibition to the child is
associated with increased firstborn irritating behaviors towards the
newborn (Dunn, Kendrick, & MacNamee, 1981).
Interrelationships among the family dyads in second pregnancy are
suggested. A strong marital relationship appears to aid the

43
establishment of a positive mother-baby relationship (Richardson, 1981;
Richardson, 1983b; Westbrook, 1979b). A strong father-child relationship
has potential to ease the demands of the mother-baby relationship
(Kreppner, Paulsen, & Schuetze, 1982; Sammons, 1983). Mothers' binding
in to the unborn child may be paralleled by a process of coming to see
one's other children as increasingly separate from oneself (Richardson,
1983a). Mothers with problematic mother—firstborn relationships
particularly withdraw from their children during second pregnancy, while
toddlers and preschoolers frequently reveal new preferences for fathers
or other close family members, and older children become more involved
with peer groups (Richardson, 1983a). The role of the father emerges as
central to facilitating role establishment and renegotiation. Yet he may
find himself virtually unsupported, since the mother focuses on the
mother-child dyad nearly to the exclusion of her relationship with her
husband in her efforts to gain acceptance of the new baby (Walz & Rich,
1983). The mother perceives the mother—child relationship as in jeopardy
and demanding attention, while the marital relationship is regarded as
stable and self-sustaining (Walz & Rich, 1983).
Conclusions
A major thrust among the limited previous investigations of family
relationships in second pregnancy has been to compare the satisfaction or
quality in these relationships to families experiencing addition of the
first child. Where parity differences have been found in such studies,
they uniformly present more negative results for subsequent childbearing.
Family interrelationships are consistently portrayed as highly
conflictual and problematic with the addition of a later-born child.
Therefore, it is appropriate to move the focus of investigation beyond
44
simple parity comparisons to a more indepth examination of the processes
and dynamics of these apparently troublesome relationships.
Measurement problems compromising previous study of family
relationships must be addressed. Relationships are multifaceted,
requiring that the particular aspect of the relationship which is of
interest be specified, while attempting to enhance the validity of
measurement instruments.
Literature review has revealed a multitude of demographic,
attitudinal, and experiential factors which affect the six dyadic
relationships in the secundigravida's family. An attempt should be made
to monitor as many sources of potential extraneous variance as possible
in future investigations, to assist in clarifying relationships between
variables. Re-examination of previous findings is called for,
considering the emergence of new variables such as increased maternal
work—force participation and new prenatal diagnostic modalities.
Previous research on family relationships has failed to reflect
experiences of a broad range of families. Sampling from predominantly
Lamaze class registrants or members of a single socioeconomic status
precludes generalizability to a wider segment of the population. Large
scale, contemporary sampling is indicated.
An adequate description of family relationships during second
pregnancy requires data collection commencing early in pregnancy. With
the notable exception of Richardson's sample of nine multigravidae
(1981), there has been a failure to assess dyadic relationships of
secundigravidae which include the firstborn throughout the course of
pregnancy. Others, such as Dunn and Kendrick (1980), have followed their
subjects from third trimester through the second-born's early childhood.
45
An investigation using the same measures on a sample reflective of
pregnancy from the first trimester to the postpartum period would present
a fuller representation of the childbearing experience.
Somatic Symptoms in Second Pregnancy
Introduction
The meaning and origin of symptoms in pregnancy may be viewed from
one of three perspectives. Symptoms are defined as perceptible changes
in the body or its functions indicating disease (McKechnie, 1975, p.
1849) or dysfunction. The first perspective, derived from the
psychoanalytic tradition, considers symptoms as manifestations of
intrapsychic conflicts. Earlier studies would be expected to express
this viewpoint, which would be consistent with the historical prominence
of the psychoanalytic perspective in the early literature on psychology
of pregnancy. For example, Wallin and Riley (1955) considered nausea and
vomiting (heavily weighted), backache, cramps, and fatigue during
pregnancy to be measures of "acceptance or rejection of the coming
child." As an offshoot of the line of inquiry which seeks to determine
the relationship between psychological attributes during pregnancy and
complications of labor and delivery, Heinstein (1967) examined attitudes,
fears, physical symptoms, and perinatal outcomes of 156 low income clinic
patients of mixed parity. Finding an increase in general physical
discomfort for women during pregnancy compared to before pregnancy, he
acknowledged some contribution from physiological changes, but concluded
that anxiety and fear compounded the difficulties which subjects felt
about pregnancy. A psychiatrist found a group of primigravidae used
symptoms and medical concerns to communicate their emotional states
(Colman, 1969). A relationship between symptom ratings and decreased
46
satisfaction with their bodies, more negative or ambivalent feelings
about pregnancy, and greater menstrual stress among 19 primigravidae led
Leifer (1977) to conclude that the range of somatic distress must be
attributed to personality patterns related to previous psychosocial tasks
and body image.
A second perspective is based on the assumptions of family therapy.
This view holds that individual symptomatology and family interaction are
meaningfully related over time. A study of five mother—father—child
families wherein the child was encopretic demonstrated the relationship
between particular family interaction dimensions and symptoms of
involuntary defecation (Straker & Jacobson, 1979). A moderate but
significant correlational relationship was found between family
developmental crises involving addition or loss of a family member and
onset of symptoms in an individual family member (Hadley, Jacob,
Milliones, Caplan & Spitz (1974). In a study of the addition of a family
member by birth, Ventura (1982) found interactive effects between newborn
infant temperament and parental reports of depression, anxiety, and
somatization.
A third perspective guiding reports of symptoms during pregnancy is
derived from a clinical or physiological orientation. The etiology of
discomforts of pregnancy is perceived as physical sources such as changes
in the musculoskeletal, cardiovascular, and gastrointestinal systems
(Horan, 1984). The goal of such reports is expansion of empirically
based data for improved assessment of pregnancy-related discomforts and
improved therapeutic interventions. Exclusive adoption of a single
perspective is not essential. Horan's (1984) report, which is
physiologically oriented, acknowledged the affects of stress and crises,

47
such as difficult family relationships, in increasing discomfort.
Erickson (1967), reporting on instrument development for symptom
assessment in an era dominated by imputation of psychosomatic
attribution, recognized the practical benefits of identifying "high risk"
patients for therapeutic intervention.
Prenatal Symptomatology
A description of the symptoms of second pregnancy is usually made in
comparison to the first pregnancy. Experienced clinicians list increased
backache, fatigue, varicose veins, and hemorrhoids as distinguishing
symptoms of second pregnancy when writing for the general public
(Hillard, 1983; Jimenez & Jones, 1981). Studies of parity differences in
symptom occurrence present discrepant results. No parity differences
were found when assessed before 16 weeks by Grimm and Venet (1966), or
with cross-sectional evaluation throughout pregnancy by Heinstein (1967).
Kaij, Jacobson, and Nilsson (1967) found multiparae were more often
healthy until delivery and showed lower frequency of onset of slight
psychiatric symptoms during pregnancy, as measured by questionnaires
listing numerous minor physical symptoms mailed postpartally. On the
other hand, multiparae were found less likely to feel very good and more
likely to report greater fatigue during second pregnancy when questioned
postpartally (Norr, et. al., 1980); multiparae scored significantly
higher on irritability and tension, on depression and withdrawal, and on
a Lack of Health During Pregnancy scale administered during all stages of
pregnancy (Erickson, 1976); and to rate higher on a standardized
depression scale in the third trimester (Jarrahi–Zadeh, Kane,
Wandecastle, Lachenbruch, & Ewing, 1969).
Temporal, experiential, and demographic variables have been found to
48
affect symptom occurrence in second pregnancy. Somatic symptoms varied
by trimester as a function of previous pregnancy history in a
longitudinal study by Lubin, Gardener, and Roth (1975). They found
somatic symptoms described a "W" shaped curve for secundigravidae with no
previous abortion (spontaneous or therapeutic), and an inverted “V”
shaped curve in secundigravidae with previous pregnancy termination,
compared to consistent decrease over trimesters for primigravidae. They
attribute the high second trimester score to fear of repeated pregnancy
loss, in a sample where most abortions were spontaneous.
Erickson (1967) devised a checklist assessing the frequency of 31
symptoms which nine primigravidae and 11 multigravidae were to complete
nightly throughout pregnancy. No statistical analyses were attempted on
the small sample, but trends were observed. Symptomatology was not
highly related to trimesters, but groups of symptoms demonstrated trends
through time. Fatigue, depression, irritability, and anxiety were
reported most frequently in the first half and last month of pregnancy.
Backache, increased appetite, tension, and increased sexual desire were
relatively constant through pregnancy. Nausea, vomiting, headache,
decreased sexual desire, and euphoria were generally limited to the first
trimester. Insomnia was problematic throughout pregnancy, increasing the
last month. Swollen limbs, shortness of breath and groin pain were only
problematic the last month.
Increasing socioeconomic status has been found to correlate with
increased physical symptoms (Doty, 1967), while subjects with less than a
high school education recorded significantly more psychosomatic anxiety
than better educated counterparts in another study (Heinstein, 1967).
Incidence of gastrointestinal symptoms of nausea, vomiting or upset

49
stomach was not affected by age, race, education or parity in that study
(Heinstein, 1967). The linkage between somatic symptoms and emotional
status, referred to above, will be discussed further in a later section.
Postpartum Symptomatology
The salience of somatically-oriented topics revealed in studies of
postpartum concerns has been addressed previously in this paper.
Multiparae are concerned with their weight (Larsen, 1966; Lynch, 1982),
body alterations (Moss, 1981), and returning their figures to normal
(Gruis, 1977).
Investigations examining the effect of parity on postpartum
symptomatology reveal slightly more discomforts for multiparae. Fatigue
was the fourth most common concern of the multiparae in Gruis' (1977)
study, reported by 83% of repeat mothers, but was not among the most
highly rated concerns of primipare. On the third postpartum day,
multiparae scored higher on depression, mood change, and fogginess than
primipare (Jarrahi-Zadeh, et al., 1969). While total sample parity
comparisons of 861 Swedish mothers showed no differences in neurotic
symptoms measured by the subjects' own recall of mild somatic symptoms, a
subsample analysis did differentiate by parity (Kaij, Jacobson, &
Nilsson, 1967). Among three-fifths of the sample, increasing occurrence
of "psychiatric symptoms" such as irritability, feeling dyspnea, and
globus was related to increasing number of full-term pregnancies. No
confirmation of the subjects' physical or mental health status
independent of self-administered questionnaire responses is reported.
Analysis of postpartum symptomatology requires consideration of
other factors potentially affecting the woman's discomfort level.
Breastfeeding may produce discomforts and fatigue not experienced by

50
bottle-feeding mothers. The delivery experience may affect postpartum
symptom levels, for example the increased pain resulting from a Cesarean
delivery compared to a vaginal delivery (Frink & Chally, 1984).
Conclusions
Further study is needed to verify and amplify the secundigravida's
experience of somatic symptoms. Synthesis of previous findings is
difficult due to a failure to adopt standardized techniques of
measurement and reporting.
Several aspects of symptom occurrence require clarification. Parity
comarison studies may be misleading if they report no difference between
groups when relying on comparison of simple summation scores. The types
of discomforts experienced may have varied by groups, but such data would
be lost by comparing only number of symptoms. Global reports of symptom
occurrence have less value than reports of particular symptom patterns
(e.g. Erickson, 1967) for clinical applications seeking information for
anticipatory guidance and preventive education. Analysis by comparison
of group means also loses information about individual differences. A
longitudinal study through two pregnancies, examination of meticulous
records maintained through subsequent pregnancies, or measurement of a
gravida's perception of somatic symptoms in comparison to previous
pregnancy would enable evaluation of an individual's comparative
experience of symptoms during pregnancies. Also, a distinction must
be made between whether particular symptoms are scored equally regardless
of the frequency and severity of occurrence, or if symptoms are weighted
according to these parameters. Erickson (1967), for example, proposed a
four-point rating scale based on frequency of occurrence. Criteria for
symptom item inclusion also requires explication.
51
Large sample studies of secundigravidae collecting data
prospectively throughout the course of pregnancy are required. Just as
Heinstein found in 1967, there are still no such studies which provide a
basis for determining what are the normal expectations for physical
complaints during pregnancy.
Interrelationships Between Anxiety, Family Relationships, and Somatic
Symptoms in Second Pregnancy
A review of the interrelationships between the three variables of
interest in second pregnancy leads to consideration of three sets of
paired variables, anxiety and family relationships, anxiety and somatic
symptoms, and somatic symptoms and family relationships.
Anxiety and Family Relationships
Families are units composed of interacting personalities, wherein a
change in one part of the family affects change in other parts (Rowe,
1981). Hence, changes in the anxiety level and behavior of one member
would be expected to influence dyadic family relationships. While no
investigation has systematically assessed such influences on multiple
dyads in second pregnancy, the effect of maternal anxiety on particular
dyads is suggested. The appropriateness of examining the relationship
of individual personality traits or characteristics and the marriage
relationship is supported by Filsinger and Wilson (1983), who found
social anxiety to be negatively correlated with marital adjustment of the
subject, but not the spouse, in a sample of married couples. Davids,
Holden, and Gray (1963) found high maternal anxiety, as measured by the
Taylor MAS in third trimester, related to increased marital conflict and
greater irritability towards the husband. Brown (1984) reported anxiety

52
in a sample of 313 primigravidae to be positively related to satisfaction
with partner support.
While Cranley (1981b) did not find maternal—fetal attachment scores
significantly affected by trait anxiety, she did find a significant
correlation with high perception of stress during pregnancy and lower
scores. Perhaps a measure of maternal transitory state anxiety would
better capture this dynamic. The relationship between anxiety levels and
maternal-baby attachment is complex, as illustrated by Leifer's (1977)
findings based on firsttime mothers. She reported that the focus of
anxiety during pregnancy must be specified, since high anxiety about the
fetus reflected attachment, but high self-concern occurred in women with
minimal attachment to the unborn baby.
The effects of prenatal maternal anxiety on the mother-baby
relationship postpartally are identified by Davids, Raymond, and Gray
(1963), who found high prenatal anxiety scores related to greater
dissatisfaction with the role of being a mother and greater irritability
with children. Whether increased maternal anxiety would cause similar
disaffection between the father and baby, via modeling, or whether the
father would adopt compensatory affectional behaviors is not determined.
Increased maternal anxiety would be expected to strain the mother
firstborn relationship, particularly postpartally, when the mother is
susceptible to external stressors (Grossman, Eichler, & Winickoff, 1980),
the mother—firstborn dyad is problematic (Richardson, 1983a), and
pressure is exhibited as anger and hostility towards the child (Grubb,
1980). Again, response to maternal anxiety in the father—child dyad is
not know. Dunn, Kendrick, and MacNamee (1981) established the
relationship between the mother's depression and negative mood and the

53
firstborn's response to the newborn, but they did not measure maternal
anxiety.
Anxiety and Somatic Symptoms
A positive relationship appears to exist between maternal anxiety
and somatic symptom levels in subsequent pregnancy. Previously discussed
studies found positive correlations between anxiety and fears and
reported symptoms in first and later pregnancies (Colman, 1969;
Heinstein, 1967). Entwistle and Doering (1981) also found that their
primiparous subjects with the most symptoms reported the most anxiety.
Doty (1967) found a correlation between anxiety measured by the Taylor
MAS and physical symptom levels in a third trimester sample of mixed
parity. Lubin, Gardener, and Roth (1975) found a positive significant
correlation between anxiety, measured by both the IPAT and AACL, and
somatic symptoms over the three trimesters of pregnancy, in their sample
of mixed parity. Heinstein (1967) found that women of mixed parity who
were more fearful for themselves or the baby experienced greater
depression, psychosomatic anxiety, and sleep disturbance in a cross
sectional sample from each trimester.
Somatic Symptoms and Family Relationships
Tentative relationships between somatic symptom levels and selected
family dyads are suggested. Positive correlations were found between an
aspect of marital quality, women's satisfaction with partner support, and
levels of emotional and physical symptoms in Brown's (1984) primiparous
sample. Correlation between maternal symptoms and the mother-baby
relationship is suggested by Heinstein's (1967) findings that pregnant
women who expressed positive attitudes and feelings about pregnancy also
reported fewer physical complaints, in a mixed parity sample of 156 women

54
drawn from each trimester. Attitudes towards the condition of pregnancy
cannot be equated with feelings towards the new baby, however. The
mother—firstborn dyad may also be influenced by maternal physical
symptoms, as the mother's fatigue and discomfort add to a relationship
already described as problematic towards the end of pregnancy and into
the postpartum period (Richardson, 1983a; Dunn & Kendrick, 1980).
Conclusions
In conclusion, it appears that the three variables of anxiety,
family relationships, and somatic symptoms during second pregnancy are
interrelated. Statements describing causal linkages between correlated
variables cannot be made.
Anxiety levels are related to family relationships in two regards.
On the one hand, maintenance and renegotiation of each family dyadic
relationship may be a focus of anxiety and a source of concern to the
secundigravida. On the other hand, maternal anxiety levels may affect
the dynamics of the three dyads of which she is a member, and the three
dyads upon which she exerts an indirect influence.
Maternal anxiety levels during pregnancy and levels of somatic
symptoms also appear to be related. Whether this correlation exists in a
sample of women all experiencing second pregnancy and evaluated
throughout pregnancy has not been determined.
The degree of somatic symptoms experienced by the secundigravida is
logically related to the character of the three family dyads of which she
is a member. Whether somatic symptoms are construed as reflective of
emotional and psychological processes or simply as physiologically based
alterations affecting one's feeling of well-being, they can be expected
to influence some aspect of the pregnant woman's interactions and

55
emotional involvement with her mate, her firstborn, and her new baby.
The relationships between these variables have not yet been
systematically investigated in second pregnancy.
Definitions and Hypotheses
Definitions
Second pregnancy is defined as pregnancy in anticipation or
delivered of a second live birth, acknowledging that additional
pregnancies may have terminated in spontaneous or therapeutic abortion
prior to 20 weeks gestation. Fourth trimester and the postpartum period
are used interchangeably to designate the first three months following
delivery. Anxiety is the subjective, consciously perceived feeling of
tension and apprehension composed of both state and trait dimensions
(Spielberger, 1976). Concerns are the cognitions which stimulate anxiety.
Hypotheses
The following hypotheses related to study research questions were
tested among women experiencing second pregnancy:
Hypothesis 1: Second trimester maternal state anxiety and somatic
symptom frequency will be lower than first or third trimester reports.
Hypothesis 2: The number of family relationship concerns of the
mother in third trimester will be greater than first or second trimester.
Hypothesis 3: Marital satisfaction will decline from second
trimester to fourth trimester.
Hypothesis 4: Somatic symptom occurrence will be perceived as higher
during second pregnancy than during first pregnancy.
Hypothesis 5: Maternal anxiety, somatic symptom frequency, and
level of family relationship concerns will be positively related to each
other and inversely related to marital satisfaction.

56
Chapter III
Methodology
Introduction
This chapter describes the research design, research settings,
sample size and selection criteria employed in this investigation. Data
collection instruments and procedures which were chosen for investigating
the research questions and testing the hypotheses are also discussed.
Design
The investigation took the form of a passive observational study
(Cook & Campbell, 1979), since there was no true manipulation of an
independent variable in order to observe causal effects on dependent
variables. In a developmental study such as this one, age is considered
to be an "index variable" (Baltes, Reese, & Nesselroade, 1977) that
provides a clear ordering of events.
A modified cross-sectional sequential design was conducted to
examine the levels and inter-relationships of maternal anxiety, somatic
symptoms, marital satisfaction, and family relationship concerns through
the course of second pregnancy. Sequential designs arise from the three
dimensional analyses of development conceptualized by Schaie (1965),
wherein time, age, and generation are components of development which may
be confounded in any combination. Goldstein (1979) has subsequently
argued that the design is adequately conceptualized by two dimensions,
age and time. In this study, the age dimension is represented by
increasing gestational age, or progression through the three trimesters
of pregnancy and the postpartum period (Ages A-1, A-2, A-3, and A-4). The
time dimension is represented by the interval of three months between the
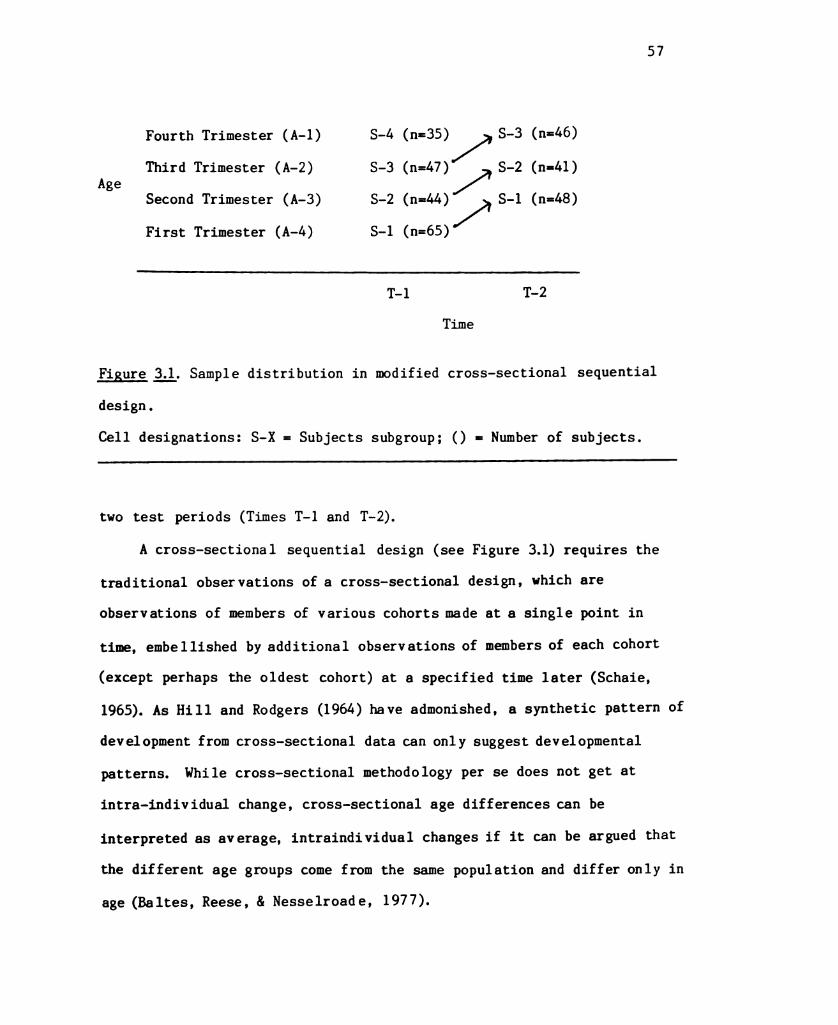
57
Fourth Trimester (A-1) S-4 (n=35) S—3 (n=46)
Third Trimester (A-2) S–3 (n=47) S–2 (n=41)Age 2
Second Trimester (A-3) S–2º S-1 (n=48)First Trimester (A-4) S-1 (n=65)
T–1 T–2
Time
Figure 3.1, Sample distribution in modified cross-sectional sequential
design.
Cell designations: S-X = Subjects subgroup; () = Number of subjects.
two test periods (Times T-1 and T-2).
A cross-sectional sequential design (see Figure 3.1) requires the
traditional observations of a cross-sectional design, which are
observations of members of various cohorts made at a single point in
time, embellished by additional observations of members of each cohort
(except perhaps the oldest cohort) at a specified time later (Schaie,
1965). As Hill and Rodgers (1964) have admonished, a synthetic pattern of
development from cross-sectional data can only suggest developmental
patterns. While cross-sectional methodology per se does not get at
intra-individual change, cross-sectional age differences can be
interpreted as average, intraindividual changes if it can be argued that
the different age groups come from the same population and differ only in
age (Baltes, Reese, & Nesselroad e, 1977).

58
A cross-sectional sequential design provides advantages over either
a simple cross-sectional or simple longitudinal design. The repeated
testing of the same subjects constitutes a "segmented longitudinal study"
(Hill & Rodgers, 1964), or a "one-group pretest-posttest segment"
(Campbell & Stanley, 1963). By also testing different aged groups at
each interval, which can be classified as a "static group comparison"
(Campbell & Stanley, 1963), potential problems of strictly longitudinal
studies from the effects of history and test-retest effects are
diminished. Hence, advantages of longitudinal study allowing measurement
of individual change, and advantages of cross-sectional design, allowing
between—cohort observation, are both achieved in a short period of time.
Usage of the label "cross-sectional sequential" design differs
slightly from that specified by Baltes (1968), who intended to designate
independent observations at all cohort and age levels. Independent
longitudinal observations, as would be created by testing only a randomly
selected half of the sample at each of the two observation periods, would
require twice the sample size, hence doubling recruitment costs.
Therefore, the longitudinal observations were repeated testings of the
same subjects, which is compatible with Schaie's (1965) original
conceptualization.
Setting
Subjects were recruited principally from the obstetric clientele
of a large prepaid Health Maintenance Organization (HMO) in the San
Francisco Bay Area. Although random sampling for representativeness was
clearly not feasible, the selected HMO provided an impressionistic modal
setting (Cook & Campbell, 1979, p. 77) for such an investigation.
59
Services at the selected HMO are available to members and their eligible
dependents who participate through employer—sponsored group health plans
offered to a broad occupational range, as well as to independent
subscribers who may be self-employed or retired. Hence, this HMO
clientele is more broadly reflective of the naturally occurring
heterogeneity in socioeconomic status, age, race, and level of obstetric
complications than would be found by sampling solely at alternative sites
such as the county health care facility, a tertiary medical center
facility, or private health care offices.
This HMO serves 30–50% of the population of Northern California,
where it has achieved a high degree of acceptability (Marymee, 1984).
Obstetric clients delivering at the selected site (200–240 deliveries per
month) receive their ambulatory care at either the main medical complex
or one of two satellite clinics. The majority (86.4%) of the 191 study
subjects were recruited from the HMO clientele, with 35.1% receiving care
at the main medical center (Site 1), 35.6% at one satellite clinic (Site
2), and 15.7% from the second satellite clinic (Site 3). In addition, in
order to hasten the timely accrual of an adequate sample, subjects
constituting 13.6% of the study population were recruited from a private
group obstetrical practice (Site 4), which performs deliveries (20–40 per
month) at the private community hospital in the same city.
Sample
One hundred and ninety-one women who met study inclusion criteria
were inducted into one of four subject groups (S-1 to S-4) during a
prenatal or postpartum clinic visit for their second live birth
pregnancy. The inclusion criteria were: 1) pregnant or delivered within
the previous 3 to 12 weeks, 2) history of only one previous pregnancy

60
carried to term with that first child living at home, 3) present
pregnancy medically uncomplicated (i.e., not labelled "high risk" at the
HMO setting, which excluded maternal diabetes, cardiac disease,
hypertension, collagen disease, malignant tumor, multiple gestation, or
onset of labor before 36 weeks gestation), 4) the firstborn, and newborn
if delivered during the subject accrual period, were free of severe acute
or chronic illness, 5) the woman was married to or living with the
father of both children, 6) she read and spoke English, and 7) she
planned to stay in the geographic area for four months if a second
observation of her cohort was required.
The inclusion criteria dictated certain restrictions in family
structure and health status in order to limit sources of extraneous
variance potentially affecting the dependent variables of anxiety, family
relationship concerns, and somatic symptoms. Limitations on the women's
verbal skills and plans for travel from the area were enforced in order to
facilitate completion of research instruments at two time intervals.
The number of subjects (see Figure 3. 1) recruited initially (T-1)
into each group was: S-1 (initially in their first trimester) = 65,
S–2 (initially second trimester) = 44, S-3 (originally in the third
trimester) = 47, and S-4 (in the fourth trimester) = 35. The cross
sectional sequential design (Baltes, 1968) involved a repeated testing of
all cohorts except the inital post-delivery group at the second
observation period three months later (T-2). Having determined through
power analyses, as discussed subsequently, that measurement scores from
30 subjects in each of groups S-1, S-2, and S-3 must be obtained
at T-2, overrecruitment for these groups was undertaken to allow for
occasional incomplete measures and attrition over the ensuing three

61
months. Attrition was minimal. At T-2, 48 subjects from group S-1, 41
subjects from S-2, and 46 subjects from S-3 participated (see Figure 3.1)
The number of T-2 participants from group S-1 is not reflective of
subject mortality rates. When an adequate number of T-2 measures for
that group were obtained, no further subjects were retested. Reasons for
subject loss are described with study procedures.
Power analyses demonstrate the achieved sample size is sufficient to
reveal at least large effects sizes for all planned analyses when o' = .05
and power = .80, performing two-tailed tests. Independent sample measure
comparisons (n=30) detect standardized difference means of d-.75
(Cohen, 1977). Related sample measure comparisons (n=30) detect
standardized difference means of .53 (Cohen, 1977). Correlational
analyses (n=60) detect magnitudes of association corresponding to effect
size nearing a medium range of .30 appropriate for much psychological
investigation (Cohen & Cohen, 1975).
Data Collection Methods
Data were collected through the use of self-administered paper-and
pencil instruments completed by the subjects. A packet, introduced by
instructions and consent forms (Appendices A & B), containing the
instruments described below was delivered to participants.
Demographic and Background Data Sheet
The Demographic and Background Data Sheet (Appendix C) is an
original questionnaire covering personal and family demographic,
experiential and attitudinal variables which have been identified by
literature review and clinical experience as having potential influence
on maternal health and family relationships during second pregnancy.

62
Information was solicited about maternal and paternal age, occupation,
education, race, and religion; about firstborn characteristics,
obstetrical history and attitudes, and perceived health status; and about
delivery and newborn characteristics for women who had already delivered
their second child. Evolution of the form to maximize clarity and
relevance, while minimizing difficulty or bothersome characteristics,
included pilot testing by women meeting study inclusion cirteria,
revision, additional critiquing by secundigra vidae, and further refining.
Additional input from three faculty experts in maternity and family
health was incorporated into the third and final version.
Spielberger State-Trait Anxiety Inventory
The State-Trait Anxiety Inventory Self-Evaluation Questionnaire
(STAI) (Form Y) (Speilberger, et. al., 1983) is a tool with well
established validity and reliability for measurement of anxiety in
research and clinical practice. The S–Anxiety scale, measuring state
anxiety (see Appendix D), is composed of twenty statements reflecting the
respondent's anxiety "right now". This sensitive indicator for
measurement of transitory anxiety is suitable for repeated administration
(Spielberger, 1976). The T-Anxiety scale, measuring trait anxiety (see
Appendix E), uses twenty statements to evaluate the respondent's anxiety
in general. Each statement is rated on a score of 1 to 4 indicating
intensity of tension, apprehension and nervousness.
This recently modified (Form Y) version of the test was revised as a
purer measure of anxiety, discriminating more precisely between anxiety
and depression. Internal consistencies for state and trait scales are
high as measured by alpha coeeficients (.92 and .90 overall median scores
for normative samples) and item—remainder correlations (Spielberger, et
63
al., 1983). In the present study, alpha coefficients for S-Anxiety were
.93 at T-1 (180 cases) and .94 at T-2 (134 cases). Cronbach alpha
reliability for T–Anxiety at T-1 based on 188 cases was .93. In
addition, concurrent, convergent, divergent, and construct validity of
the STAI scales have been established. Although test scores were
normalized on working adults, college students, high school students and
military recruits, the STAI has well-established use in the subpopulation
of pregnant women (see, for example, Lederman et al., 1981a; Norbeck &
Tilden, 1983).
Dyadic Adjustment Scale
To aide in selection of the optimal instrument for assessment of the
marital relationship during second pregnancy, four multiparae were
administered both the DAS (Dyadic Ajustment Scale) (Spanier, 1976), and
another commonly used instrument, the Locke-Wallace Short MaritalAdjustment Scale (Locke & Wallace, 1959). All respondents preferred the
DAS in terms of ease, emotional comfort, validity, and appropriateness for
a contemporary sample. In addition, the parity status of the married
sample on which the DAS was normalized (mean number of children is two)
supports its suitability for use in study of second pregnancy.
The Dyadic Adjustment Scale (DAS), a widely used paper-and-pencil
measure of marital adjustment, was therefore chosen to assess maternal
perception of the marital relationship. The test has 32 items (Appendix
F) reflecting couple agreement, communication, affection, and commitment.
Content, criterion-related, and construct validity have been documented
(Spanier, 1976). Factor analysis has identified four interrelated
components. These four subscales, labelled consensus, satisfaction,
cohesion, and affectional expression, demonstrate adequate factor

64
stability (Spanier & Thompson, 1982).
Total scale reliability has been reported at a level of .96 for both
Cronbach's Alpha and Spearman–Brown formulas for internal consistency.
(Spanier, 1976). Reported subscale Cronbach alpha values range from .73
to .94. The alpha reliabilities for 173 cases at T-1 and 123 cases at T
2 in this study were: total .93, .89; consensus .82, .80; cohesion .78,
.73; affection .62, .63; and satisfaction .89, . 83.
Family. Relationships Questionnaire
An original instrument for assessment of maternal concerns about
dyadic relationships in a family experiencing second pregnancy was
developed. Because a suitable standardized instrument was available only
for evaluation of the marital relationship, the new instrument was
designed to evaluate maternal perception of the five remaining dyads in a
family adding a second child.
The instrument, the Family Relationships Questionnaire (FRO), was
constructed using an inductive approach. Protection of the rights of
human subjects during instrument development was supervised by the
Committee on Human Research, Univerity of California, San Francisco,
under approval #933416–01.
Statements reflecting maternal perception of concerns about the
mother-baby, father-baby, mother—firstborn, father—firstborn, and
firstborn-baby dyads were collected via an open-ended questionnaire
survey distributed to a convenience sample of 20 women pregnant with or
recently delivered of their second child. This approach for item
generation was selected to provide empirical grounding to material
gathered from literature review and the investigator's clinical
experience and previous field study (Sammons, 1981). The sample of 20

65
was recruited from prenatal "refresher" multigravid Lamaze class
registrants, women known to the investigator socially and their
acquaintances, and patients of the private obstetric practice where the
investigator was affiliated as a Nurse Practitioner.
The questionnaire, composed of questions focusing on each dyad
during the present pregnancy and the previous pregnancy, plus two global
questions requesting comparison between the woman's first and second
pregnancies, was personally distributed or mailed to 29 women. A sample
question asked, "What do you think about most these days regarding your
husband's relationship to your older child?" Twenty questionnaires (69%)
were returned, with seven from first trimester subjects, five from women
in the second trimester, four from those in the third trimester, and four
from women who were six to eight weeks postpartum. Time required to
complete the questionnaire ranged from 10 to 90 minutes.
Questionnaire responses were collated by dyad. For each of the
dyads, the following number of statements were recorded: Mother-baby
41, Father—baby 36, Mother—firstborn 38, Father—firstborn 34, and
Firstborn-baby 47. From the raw responses, three to eight statements were
constructed for each dyad and assembled as Preliminary FRO's. Parallel
versions were created to reflect prenatal and postpartum concerns.
Statements were intended to reflect concerns that were common and which
would be sensitive to and discriminating of varying levels of concern.
Theoretical considerations also guided item selection. An earlier field
study by the investigator suggested that critical dimensions in family
response to arrival of a newborn were affectional, temporal, spatial, and
informational resources (Sammons, 1983). An attempt was made to include
statements for each dyad reflecting these dimensions.

66
The instrument was constructed so that respondents indicated their
level of agreement (1=Strongly agree to 5=strongly disagree) on a five
point Likert-type scale to statements such as, "I want my husband to give
more attention to our older child now." Structural soundness of dyadic
items was reviewed by a doctorally prepared faculty member with expertise
in behavioral science instrument construction.
The Preliminary FRO's were administered to five women, pregnant with
or recently delivered of their second child. Critiques on instrument
clarity, pertinence, awkwardness, redundancy, and comprehensiveness were
considered when making revisions to final versions of the FR0–Prenatal
(see Appendix G) and FRQ-Postpartum (see Appendix H).
The FRO-Prenatal consists of 25 statements. Five statements reflect
maternal perception of the mother-baby relationships (items
#2R, 7R, 11R, 13R,23R); five items reflect perception of the father-baby dyad
(5, 16R, 18R,22R,25R); eight relate to the mother—firstborn dyad
(1,4R,6,10R, 14R, 17R, 19R,20); four pertain to the father—firstborn dyad
(3,8R,21,24); and three address the firstborn-baby dyad (9,12R, 15). The
FRO-Postpartum is composed of 22 statements. Five items reflect maternal
perception of the mother-baby relationship (#2R,6R,10R, 15,19); four are
about the father-baby dyad (4R, 8, 12R, 17); six about mother—firstborn
relations (1,9R, 14R, 16R, 20R, 22R); four about the father-firstborn dyad
(3,7,22, 21R); and three about perceptions of the firstborn-baby dyad
(5R, 13, 18R). Scoring is accomplished by summing the points indicated
from one to five for a total score. Since statements are presented in
either a concern—present or concern—absent manner, some statements
require point reversal before summing. These items are indicated in the
preceeding listing by the letter "R". The resultant possible range of

67
scores is 25 to 125 on the prenatal version and 22 to 110 on the
postpartum version.
For these newly developed instruments, content validity of the items
was determined through expert review and critique by five
maternity/family health care nurse scholars and clinicians. Internal
reliability was determined by computing Cronbach's alha values.
Coefficient alpha for the FRO–Prenatal was .76 with 148 T-1 cases and .78
with 87 T-2 cases. FRO-Postpartum Cronbach alpha values were .75 with 34
T-1 cases and .78 with 45 cases at T-2. These values approach the .80
level of acceptability suggested by Carmines and Zeller (1979). While it
would have been desireable to find high reliability values for each of
the dyad subscales, only the mother-child subscale, with coefficient
alphas .63 to .75, and the postpartum child-baby subscale, with
coefficient al phas of .62 and .63, tended toward internal reliability at
both test periods.
Somatic Symptoms Checklist
The instrument for reporting symptomatology during pregnancy devised
for longitudinal study by Erickson (1967) was modified for use in this
investigation. The original instrument consisted of a list of 31
symptoms, to which the subject responded how frequently the symptom or
feeling was experienced daily on a four point scale ranging from often to
never. For this investigation, several items were deleted, such as
"chills," which did not, in isolation, seem to be common symptoms of
pregnancy or the postpartum period. Other new items, such as "varicose
veins," were added. Preliminary instruments were tested by three
subjects. After revisions for clarity of format and instructions, the
instruments were piloted on an additional six subjects and further
68
refined. The revised instruments contained 29 items on the prenatal form
(Appendix I) and 23 items on the postpartum form (Appendix J).
The tool was modified additionally to assess how the magnitude of
discomfort for a particular complaint relates to the woman's recollected
experience at the same trimester in her previous pregnancy on a three
point scale from less to more frequently experienced presently. This is
in essence comparison by means of retrospective estimates (Schaie, 1973).
While the proposed design offers no group of women pregnant for the first
time for a statistical comparison, the perceived differences are
qualitatively valuable in themselves.
Scoring was accomplished by summing the frequency of symptoms,
providing a range of 0–87 (prenatal) and 0–69 (postpartum). Direct
comparability on this scale between pregnancy and post-delivery is not
expected, since the nature of post-delivery discomfort is often related
to delivery procedures, involutional processes, and lactation. Ranges
for comparative symptom scores are the same as the respective current
symptom version ranges.
Content validity was determined by expert review by three nurse
scholars with extensive clinical and research experience in maternity
health care. Further support for face validity is provided by the
similarity between these instruments and the prenatal symptom list used
by Entwistle and Doering (1981), which was sufficiently sensitive to
detect variations in somatic complaints by trimester in a group of 120
Maryland primigra vidae, and the postpartum feelings and health status
reported most frequently by 264 primiparae investigated by Mercer,
Hackley, and Bostrom (1982). Assessment of internal reliability is
inappropriate, since the instrument measures frequencies of the

69
occurrence of diverse symptoms, which lack theoretical relatedness.
Procedure
All 191 subjects were recruited and inducted into the study from
October 15, 1984, to January 8, 1985. The 135 subjects involved in
repeated testing completed their second questionnaire packets between
January 16 and March 27, 1985. Human Subjects protective assurances were
observed under approval of the Committee on Human Research, University of
California, San Francisco (#933921–01).
Nursing and medical staff involvement in and orientation to the
study project took place in the year proceeding actual data collection.
Site liaison activities, facilitated by the senior Nurse Practitioners
(NPs) at each site, consisted of assistance with: obtaining approval from
nursing, medical, and administrative departments; formulation of
recruitment strategies consistent with local patient flow, logistics, and
time constraints; and fostering staff acceptance.
Recruitment procedures varied by site, dependent upon facilities and
staff commitment to the project. Although later analyses indicated that
there were no differences in the occurrence of the dependent variables
based on site of subject induction, recruitment techniques are discussed
in relation to the four sites to provide an indication of the magnitude
of subjects recruited with minimal bias compared to those subjects who
were more self-selected.
At the site contributing the most (68) subjects, Site 2, prenatal
records of all clinic registrants were reviewed by staff nursing
personnel, due to the high level of commitement of the sole clinic NP.
Potential subjects were then informed of the study on their next prenatal
visit or by telephone. All potential subjects at this site then

70
completed the response card (see "Second Baby Pregnancy" card, Appendix
K) indicating interest in the study. This comprehensive approach
introduced no bias into subject selection.
At Site 1, the clinic held at the HMO medical center itself, 68
subjects were recruited. Here, all new obstetric registrants receiving their
initial obstetric packet information and laboratory forms, at either the
prenatal orientation class or individually, were given the study flier
with detachable response card (Appendix K) from either the investigator
attending the prenatal class or from staff nursing personnel. Once this
system was established, dissemination of recruitment materials to new
registrants, largely in their first trimester, proceeded without any
observable bias. Again, all potential subjects from this source did
return response cards indicating interest in the study.
Recruitment at Site 1 by other methods was less comprehensive.
Collectively, the five NP's at this site see approximately 75% of all
obstetric patients, which excludes high risk obstetric patients, staff
wives, and patients preferring to see only physicians. An attempt was
made to have fliers handed out to all potential subjects seen by the
NP's. However, NP cooperation varied from placement of fliers on all
pertinent obstetric charts seen by all NP's and MD's using a common
nursing station, to lack of involvement in recruitment.
Recruitment at Site 3, where 30 subjects were inducted, was hampered
by difficulties in coordinating with three part-time NP's. After weeks
of poor recruitment, the investigator gained permission to review all
prenatal records for obstetric inclusion criteria. This resulted in the
placement of 100 fliers in eligible charts towards the end of the

71
recruitment period. Since prenatal recruitment ended shortly thereafter,
staff later pulled the unneeded fliers from charts.
At the private obstetric office, Site 4, nursing assistants
introduced the study flier. Twenty-six subjects were recruited from this
site. It appeared that staff here selected subjects who were past the
early months of pregnancy, when staff felt they were still vulnerable to
early pregnancy loss.
An additional method used at all four sites was the prominent
placement of fliers at the obstetric check-in area, where the drop box
for response cards was also located. This technique would tend to favor
inclusion of subjects more highly motivated to actively seek out
involvement in a study, who may be either more comfortable with
themselves or more adamantly concerned about their situation than those
who would not respond to such a general solicitation.
Recruitment for second and third trimester subjects ended November
12, 1984. Since recruitment procedures were integrated into the prenatal
clinic routines, and not the postpartum visit routines, recruitment for
fourth trimester subjects continued on, as well as recruitment for the
additional first trimester subjects required by the design and higher
potential subject mortality of that group.
The recruitment flier briefly described the study goals and
participant requirements. Women were encouraged to deposit a detachable
card in a conveniently located drop-box on the premises, indicating
whether they wished to be contacted for further details. The investigator
collected response cards from each site at least semi-weekly. Potential
subjects were contacted by telephone, informed of the nature of the
study, and given an opportunity to ask questions.

72
Although a minority of subjects had met the investigator at the
clinics or had known the investigator from her prior affiliation with the
private obstetric office, for most subjects this telephone conversation
constituted the only personal contact. The cooperation, commitment, and
candor subsequently demonstrated by participants is remarkable in light
of this minimal relationship. Contributing factors may be the
investigator's identification of herself as a Nurse Practitioner, an
established supportive role for most subjects; an attempt to convey an
accommodating, warm, and respectful attitude; characteristics of the
psychology of pregnancy conducive to sharing the emotional experience;
payment of $5 for each instrument packet completed; and the apparent need
for further information about second pregnancies which these women had
confronted and wished to remedy for others in the future.
Of all response cards received by the investigator, only four
indicated they were not interested in completing questionnaires. One
indicated as a reason the temporariness of her stay in the area; the
other three gave no reason. Additional information about these anonymous
respondants is not available. Women who had completed response cards
were contacted by telephone by the investigator until sufficient numbers
for each trimester group were obtained. During this telephone contact,
additional screening for eligibility was performed. Twenty interested
women were not inducted into the study at this point for the following
reasons: one had a spontaneous abortion since completing the card; two
were medically high-risk patients; eight had firstborn children by a
partner other than the father of the second child; two were separated
from the children's father; one had a second born older than 13 weeks of
age; and six had stepchildren of their husbands' living in or frequently

73
visiting the home. This last group was excluded due to the focus of the
study on introduction of the second child into the family system.
Following explanation of the study by telephone, remarkably, all
women agreed to participate. A packet of questionnaires (see Appendices
A through J, L) was then mailed for the woman to complete at her
convenience at home within the following week. The initial packet
contained a cover letter of instructions, a copy of the consent form to
be retained and one to be returned, the Demographic and Background Data
Sheet, both the state and trait forms of the Spielberger Self-Evaluation
Questionnaire, either the prenatal or postpartum Symptom Checklist
followed by the appropriate version of the Family Relationship
Questionnaire, the Spanier Dyadic Adjustment Scale, and a sheet for
additional comments. Return of the packet was requested in an addressed,
postage-paid envelope which was included.
Three potential subjects had changes before completing the packets
that caused them to no longer fall within the inclusion criteria: one
spontaneous abortion, one marital separation, and one medical high risk
condition. Additional subjects were recruited to fill their places.
Ninety-two percent of the completed packets were returned within three
weeks of being mailed out. Follow-up of delinquent packets consisted of
no more than three telephone or mail contacts. Thirteen of the 15 late
respondents did return packets after the follow-up contacts. Only two
(1%) of the 191 eligible participants were lost to the study for failure
to complete the instruments, one who decided not to participate for
unspecified reasons and one who continually found her schedule too hectic
to find time to fill out the forms. These two were replaced, providing
191 participants at T-1. An additional 59 women who had deposited cards
74
in the drop-boxes were notified that no additional participants were
required.
Three months after completing the first packet, subjects in all but
the initial postpartum group were mailed T-2 packets. The T-2
packets contained a cover sheet (see Appendix M) with questions to update
experiential data that may have changed since T-1 (e.g. route of delivery
if previous packet completed in the third trimester), the appropriate
Symptoms Checklist and FRQ, the Dyadic Adjustment Scale, the state
anxiety version only of the Spielberger Self—Evaluation Questionnaire,
and a return mail envelope. Subjects were compensated $5 for
each packet completed. Payment for initial packet completion was
included in the second packet. Payment for the final packet was
mailed separately within four weeks.
More subjects required follow-up contacts for delinquent return of
packets at T-2 than at T-1. Whereas only 8% of the subjects needed
to be called during the first test administration period, 24% of the
those who eventually did return completed T-2 packets required follow-up
contact for late materials.
Subject loss from T-1 to T-2 was minimal (see Figure 3.1). Of the
47 members of group S-3, who went from third to fourth trimester, only
one subject did not complete her second packet. She gave reasons of
English as a second language making reading difficult, as well as illness
among family members. Of the 44 members of group S-2, who went from
second to third trimester, three subjects did not return their second
packets. One declined participation due to much stress after the-
premature delivery of an infant with hydrocephalus, and two women who
could not be contacted later by telephone failed to respond to written
75
follow-up, after initially indicating continued interest at the second
test period. In order to collect 48 responses from the S-1 group at T-2,
it was not necessary to contact all the original 65 women. Only three
contacted subjects withdrew, two because of spontaneous abortions and one
who reported her husband said the information was too personal. They
were replaced with the next consecutive subjects based on when completed
T-1 packets had been returned. Fourteen members of the original first
trimester group were informed they would not be retested.
In sum, only 7 of the 142 subjects receiving T-2 packets did not
participate, producing an attrition rate of 5% over the three month
period. The 135 participants at T-2 exceeded the sample size demands of
the proposed design and analyses. Due to cases where attrition was known
to result from medical complications, the study sample is reflective of
women experiencing medically uncomplicated pregnancies, which is
consistent with the original intent.
Data Analysis Procedures
Pursuit of answers to the research questions required employment of
descriptive, comparative, and correlational statistics. Data were
analyzed using SPSS-X, version 2.0 (SPSS Inc., 1983).
To determine whether the four dependent variables of maternal
anxiety, marital satisfaction, level of family relationship concerns, and
somatic symptomatology change with time for secundigra vidae, comparisons
were made between measurements taken from subjects in the first, second,
third, and fourth trimesters. Preliminary analyses were performed
to identify potentially confounding variables by examining the
relationships of antecedent variables (demographic and background
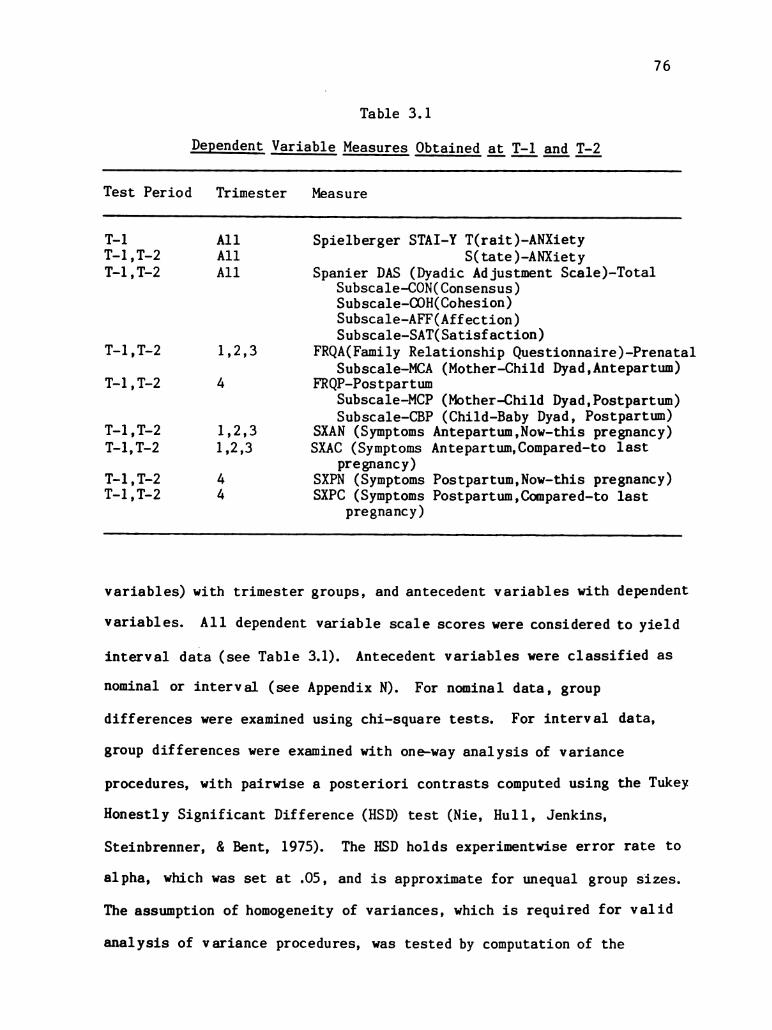
76
Table 3. 1
Dependent. Variable Measures. Obtained at T-1 and T-2
Test Period Trimester Measure
T–1 All Spielberger STAI-Y T(rait)–ANXietyT-1, T-2 All S(tate)—ANXietyT-1, T-2 All Spanier DAS (Dyadic Adjustment Scale)-Total
Subscale—CONCConsensus)Subscale-COH(Cohesion)Subscale-AFF (Affection)Subscale—SAT(Satisfaction)
T-1, T-2 1,2,3 FROA(Family Relationship Questionnaire)-PrenatalSubscale—MCA (Mother—Child Dyad, Antepartum)
T-1, T-2 4 FROP-PostpartumSubscale—MCP (Mother—Child Dyad, Postpartum)Subscale—CBP (Child-Baby Dyad, Postpartum)
T-1, T-2 1, 2, 3 SXAN (Symptoms Antepartum, Now—this pregnancy)T-1, T-2 1,2,3 SXAC (Symptoms Antepartum, Compared-to last
pregnancy)T-1, T-2 4 SXPN (Symptoms Postpartum, Now—this pregnancy)T-1, T-2 4 SXPC (Symptoms Postpartum, Compared—to last
pregnancy)
variables) with trimester groups, and antecedent variables with dependent
variables. All dependent variable scale scores were considered to yield
interval data (see Table 3.1). Antecedent variables were classified as
nominal or interval (see Appendix N). For nominal data, group
differences were examined using chi-square tests. For interval data,
group differences were examined with one-way analysis of variance
procedures, with pairwise a posteriori contrasts computed using the Tukey
Honestly Significant Difference (HSD) test (Nie, Hull, Jenkins,
Steinbrenner, & Bent, 1975). The HSD holds experimentwise error rate to
alpha, which was set at .05, and is approximate for unequal group sizes.
The assumption of homogeneity of variances, which is required for valid
analysis of variance procedures, was tested by computation of the

77
Barlett-Box F statistic, selecting a significance level of p = .05 as
acceptable. The assumption of the absence of covariate-by-factor
interaction in analysis of variance was accepted without testing. In the
search for possible significant relationships between dependent variables
and antecedent variables, the Pearson product moment correlation
coeeficient was computed for antecedent variables. Dichotomous nominal
antecedent variables were examined in relation to dependent variables
using independent t tests, with selection of the Student's t or the
approximation to t as the test statistic based on, respectively, the
presence or absence of equal variances (Nie, et al., 1975.) Nominal
variables with more than two categories were examined in relation to
dependent variables using one-way analysis of variance as described above.
The effect of trimester group membership on the dependent variables
was then examined by two approaches. The effect of trimester on
independent (cross-sectional) samples was determined by performance of
one-way analysis of variance, with control for potential confounding
variables as indicated. The effect of trimester on dependent variables
in related (longitudinal) samples was tested by performing the paired t
test. Computation of correlated t followed assurance that the
correlation between the paired measures was positive (Nie, et al.,
1975). The matched sample comparisons proved to be superior for
detecting change between trimester groups due to removal of the subject
to-subject variability.
Dependent variable scale reliabilities were computed using the
Cronbach alpha measure of internal reliability. To test
interrelationships among dependent variables, the Pearson product moment
correlation coefficient was computed.
78
Analysis of individual item characteristics of FRO and Somatic
Symptom measures was obtained by manual ordering and examination of
descriptive statistics generated for each instrument item and by
performance of one-way analysis of variance procedures. For assessment of
somatic symptoms regarding comparison to the previous pregnancy, one
sample t tests were performed between obtained scores and an assigned
value of "2", which would indicate no difference between perception of
present and previous symptom occurrence on the original instrument scale
employed in this study.
Summary
This chapter explained the modified cross-sectional sequential
design employed to examine the research questions. One hundred and
ninety-one secundigravidae were administered paper-and-pencil
questionnaires assessing their perceptions of anxiety, somatic symptoms,
family relationship concerns, and marital satisfaction. Three months
later, a subsample of 135 subjects underwent repeated testing of the same
measures. Subject recruitment settings and procedures, sample inclusion
criteria, measurement instrument characteristics, and data collection and
analytic procedures were described.
79
Chapter IV
Results
Introduction
Study findings are presented in this chapter. Sample
characteristics of the total sample and comparison groups are first
presented. In the next section, statistical characteristics of the four
dependent variable measures are described. Then, data relevant to the
interrelationships of the four dependent variables are examined.
Finally, statistical analyses in relation to hypothesis testing are
addressed.
Demographic and Obstetrical Characteristics of the Sample
Demographic and obstetrical characteristics of the sample were
examined for the total study sample, as well as analyzed for differences
in occurrence between trimester groups. Among demographic variables, no
significant differences between trimester groups were found for the
variables of maternal or paternal age, race, years of school, or
occupational rank; nor for family religion, marital status, socioeconomic
level, or age of the firstborn (See Table 4.1).
With the exceptions of one 16-year-old and one 17-year-old, the age
range of women participating in the study was 19 to 38 years, with a mean
age of 27.44 and a modal age of 27. Fathers were slightly older, with an
average age of 30.21 years. Most of the study subjects were white, not
of Hispanic origin (86.4% of the participants and 84.8% of their
partners). Fifteen women (7.9%) were Hispanic, seven were Asian/Pacific
Islanders, two were Black, one was an American Indian, and one
categorized herself as belonging to another unspecified group.

80
Table 4.1
Demographic Characteristics of Total Sample and Groups
Variable Trimester Trimester Trimester Trimester Total Test (df)1 2 3 4 Walue
n=65 n=44 n=47 n=35 n=191 p.
Maternal AgeMean 28.08 26.84 27.34 27.15 27.44 F(3,185)SD 4.25 4.28 3. 89 4.42 4.20 .86Range 20–37 16–38 19–37 17–37 16–38 .46
Paternal AgeMean 30.46 29. 67 30.28 30.29 30.21 F(3, 186)SD 5.24 4. 78 4.71 5.58 5.05 T22Range 20–41 22–41 22–42 18–45 18–45 .88
Maternal Race – categories combined for analysisWhite, not Hispanic
59 38 40 28 165 X*(3)Hispanic) 4 5 3 3 15 2.34Other ) 2 1 4 4 11 . 50
Paternal Race – categories combined for analysisWhite, not Hispanic
60 37 37 28 162 X’ (3)Hispanic) 3 7 6 3 19 4.84Other ) 2 O 4 4 10 . 18
Religion – missing values=3Protestant
19 17 12 11 59 X” (9)Catholic 19 15 16 8 58 9.81None 11 2 8 10 31 . 37Other 15 9 10 6 40
Maternal Years of EducationMean 13.86 13. 72 14.24 14. 14 13.97 F(3,185)SD 2. 10 1.94 2.01 1.88 2.00 .64Range 10–19 11–19 12–18 11–18 10–19 .59
Socioeconomic Level – Hollingshead Four-Factor ScaleMean 45.36 42.38 44.23 41.77 43.74 F(3,185)SD 12. 27 9.78 12.25 10.96 11.50 1.00Range 21–66 22–63 27–66 21.5–66 21–66 .39
Age of firstborn (months)Mean 31.26 28.59 32.87 34. 28 31.60 F(3,187)SD 17. 52 14. 55 21.95 14.74 17. 63 .. 79Range 4–84 7–67 12–117 14–74 4–117 .50

81
The two most commonly identified religious affiliations were
Protestant (30.9%) and Roman Catholic (30.4%). A large segment (16.2%)
indicated no preference regarding religion. Other religions indicated
were Church of Later Day Saints (5.2%) and Jewish (2.6%). Twenty-five
additional women wrote in a specific affiliation, such as Christian or
Baptist, which they felt did not fit into the other categories.
All subjects were partnered, as this was requisite for inclusion in
the study. All women were married except four: one in the second
trimester group, two inducted into the third trimester, and one in the
fourth trimester group.
Socioeconomic status (SES) was calculated using the Hollingshead
(1975) Four Factor Index of Social Status. Weighted values are given to
occupation and years of schooling of both partners, if they are involved
in the work force, to obtain a family score between 8 and 66. The
occupations of both employed mothers and fathers in the study sample were
codified according to rankings from one (farm laborers/menial service
workers) to nine (higher executives, proprietors of large businesses, and
major professionals). Women in the sample were almost evenly divided
between those who considered themselves housewives (49.2%) and those who
worked outside the home. Among the 95 women who were employed, the modal
category (27 women) was six (technicians, semiprofessionals, and small
business owners), followed by category five (clerical and sales workers,
small farm and business owners). Women were involved in the entire range
of nine categories. The range of occupations filled by fathers also
spanned the nine categories. Their modal value (59 fathers) was category
four (smaller business owners, skilled manual workers, craftsmen, and
tenant farmers); their mean value was 5.65.

82
Education of the employed partners is also considered in social
status determination. Fathers' schooling ranged from nine to twenty
years, with a sample mean of 14.43 years. This approximated mothers'
education, which spanned ten to nineteen years, with a mean of 13.97
years. Computation of the Hollinghead SES score produced a range of 21
to 66, with a mean of 43.74. This places the average study family in the
lower end of the social stratum labelled "medium business, minor
professional, technical", just above "skilled craftsmen, clerical, sales
workers."
All study families had one healthy child living at home, as this
also was a criterion for study inclusion. The range of ages of
firstborns was 4 to 117 months, with a sample mean of 31.6 months.
Calculations were performed to create a variable called Spacing,
indicative of the age of the firstborn at time of birth of the second
child. The range of spacing was 11 to 118 months, with a mean value of
35.0 months.
Obstetric characteristics of the study sample were examined
to obtain a description of the total sample and to determine if
differences between comparison groups existed (see Table 4.2). No
differences were found between trimester groups regarding the number of
previous spontaneous or therapeutic abortions. The total sample range
was from zero to three miscarriages or abortions, with about one in five
women having experienced miscarriage and about one in three having
experienced an induced abortion.
Women's global recollection of their previous pregnancy and delivery
experience ranged from very easy and comfortable to extremely difficult
and uncomfortable. When examining for between group differences using

83
Table 4.2
Obstetric Characteristics of Total Sample and Groups
Variable Trimester Trimester Trimester Trimester Total Test (df)1 2 3 4 Value
P.
MiscarriagesMean .24 . 12 . 14 .40 .21 F(3,164)SD . 58 . 51 .41 . 72 .56 T. 79Range 0–2 0–3 0–2 0–3 0–3 . 15
Abortions
Mean . 37 .24 .40 .47 . 37 F(3,165)SD . 65 . 58 . 72 . 73 . 67 -
Range 0–2 0–2 0–3 0–2 0–3 .53
Base & Comfort in First Pregnancy/DeliveryVery Easy 10 8 16 8 42 X” (9)Mod Easy 24 17 14 8 63 17.43Somewhat .04Difficult 13 13 3 8 37
Very Diff 14 4 9 10 37
Previous DeliveryWaginal 49 43 40 32 164 X” (3)C/Section 16 1 7 3 27 11.9
.01
Intendedness of Pregnancy- missing values = 3No/Not now 10 18 18 10 56 X? (3)Yes 54 26 29 23 132 10. 37
.02Months Attempting Conception
Mean 3.08 1.86 2.08 2.42 2.43 F(3,180)SD 2.09 2.14 2.14 2.23 2.18 3.36Range 0–8 0–8 0–8 0–8 0–8 .02
Had Prenatal Diagnostic Test – missing values = 2Yes 10 20 19 23 72 X” (3)No 55 24 28 10 117 29.31
.00
Future Prenatal Diagnostic Test Planned – missing values = 16Yes 50 36 43 25 154 X’ (3)No 12 6 1 2 21 7.87
.05
Attend Childbearing Class – missing values = 4Yes 26 19 10 13 68 X*(3)No 39 25 37 18 119 6.29

84
the chi square statistic, it was necessary to collapse categories to
limit the occurrence of cells with expected frequencies less than five.
The forced choice questionnaire format had not allowed expression of a
childbirth experience in which the pregnancy was easy, but the delivery
was difficult. Eleven women had written in such a description, and their
responses were lost in the collapsed cell group comparison. Intergroup
differences were found (X” (9)= 17.43, p = .04; Cramer's V=. 03). In the
third trimester group, more women recalled their previous experience as
being very easy and less recalled it as somewhat difficult, than would be
expected statistically. In the second trimester, more women described
their first experience as somewhat difficult, while fewer women described
it as very difficult, than would be expected. Followup comparison
between just second and third trimester groups revealed second trimester
members had more uncomfortable/moderately difficult experiences than the
third trimester group (X’ (3) = 11.13, p = .01; Cramer's W = . 132).
Most of the study participants (86%) experienced vaginal delivery
with their first pregnancy. Of the 24 women who had had operative
deliveries previously, equal numbers planned repeat Cesareans and vaginal
birth after Cesarean this time. Examination for group differences
revealed more Cesarean births than expected in the first trimester, and
fewer than expected in the second trimester group (X*(3)=11.90, p = .01).
The intendedness of the current pregnancy was assessed by asking
women to respond if the pregnancy was planned: no; yes, but not now; or
yes, now. In this sample of women, the vast majority of whom had access
to prepaid health care, an impressive 29% had not intended to get
pregnant at this time. Testing for group differences after combining
the two categories of respondents not intending to get pregnant at

85
present revealed fewer women in first trimester had unintended
pregnancies than would be expected, while there were more unintended
pregnancies second trimester than expected (X’(3) = 10.37, p = .02).
Comparison groups also differed with the same pattern regarding a
related variable, the number of months women were attempting to conceive
(F(3,180) = 3.36, p = .02). Followup with the Tukey-HSD procedurerevealed that the first trimester group mean score (3.08) was
significatly higher than the second trimester group (M = 1.86) score.
This variable is subject to interpretation in two ways. The value "O"
represented not trying to conceive. Increasing numbers were codes for
incremental numbers of months trying to conceive, with the value "8"
indicating 24 months or more. Hence, one interpretation is that high
values indicate greater difficulty in becoming pregnant, although only
18% reported trying longer than six months. The other interpretation is
that low values indicate less wantedness or intendedness of pregnancy.
Since this question was not evaluated at the second test period, it
cannot be determined whether recollections of intent to conceive vary
through pregnancy, or if this represents a chance mal distribution of the
variable among subjects.
Trimester groups also lacked homogeneity regarding completion of
prental diagnostic tests. Fewer women in their first trimester and more
women in their fourth trimester had undergone diagnostic tests than would
have been randomly expected. This is a reasonable finding, considering
that most of the 62 tests experienced were sonograms, which were
performed largely throughout the second and third trimesters. Consistent
with these findings were group differences in the numbers of women
expecting prenatal tests in the future (X*(3)=7.87, p = .05). More women

86
in the first trimester, and fewer women in the third trimester, planned
future diagnostic tests than expected statistically.
Postpartum characteristics of the sample are summarized for
descriptive purposes. The following figures represent both the 35
women in the fourth trimester at T-1 and the 46 women in the fourth
trimester at T-2. More male (58%) than female infants were born. Most
mothers (72%) selected breastfeeding as the predominant feeding method.
Fathers attended the delivery in all but five (6%) of the cases.
Additional obstetric experiential and attitudinal variables were
monitored. No differences by trimester group were found for number of
children desired by mother, number of children desired by father,
discrepancy between parents in the number of children wanted, maternal or
infant illness, or planned attendance at childbearing classes. Variables
related to family background were also examined. No differences between
comparison groups were found for length of marriage/relationship, sex of
the firstborn, number of sibling in the mother's family of origin, nor
the mother's own birth order.
Trimester groups were also found to be comparable regarding maternal
employment variables. There were no group differences in the mothers'
classifications of selves as housewife or employed person, or hours spent
apart from the firstborn. Among the employed, no group differences were
found between job vs. career classification, or hours spent at work.
In summary, the sample can be characterized as predominantly white,
married women, in their twenties and early thirties, with access to
private or prepaid health care. The women, who typically had two
years of post-high school education, were equally divided between
housewives and those employed outside the home. The average family fell

87
into the social stratum composed of medium business, minor professional,
and technical categories. The typical firstborn child was two and a half
years old.
In addition to demographic variables, a variety of obstetrical,
family, and maternal characteristics were monitored. Group differences
among the comparison trimester groups were found only for the variables
of comfort in first childbearing (COMFORT1), delivery mode for first
birth (DELIVER1), intendedness of second pregnancy (INTEND2), months
trying to conceive (CONCEPTN), and prenatal diagnostic tests experienced
(TEST) or expected (TSTFUTR). Where interactive effects of these
variables with the dependent variables might introduce bias, statistical
controls were instituted.
Dependent Wariable Measures
In this section, the four dependent variables of maternal anxiety,
marital satisfaction, perception of family relationship concerns, and
somatic symptoms will be discussed. For each variable, both descriptive
information about the total sample and comparative information about
trimester groups will be provided.
Anxiety
Both trait and state anxiety measures were obtained (see Table 4.3).
Subject scores for trait anxiety (T-ANX) covered virtually the entire
instrument range. The total sample mean score for T–ANX of 35.01 fell
between published norms of female working adults (34.79) and female
college students (40.40) (Spielberger, et al., 1983). State anxiety (S-
ANX) scores evidenced a slightly more restricted range, with absence of
extremely high anxiety scores noted for the second test administration.
The means for S-ANX scores at both test periods (33.18 and 33.57) were

88
Table 4.3
Dependent Wariable Measures for Total Sample and Groups:Analysis of Variance
Variable Trimester Trimester Trimester Trimester Total Test(df)1 2 3 4 Value
P.
Trait-Anxiet T–1
Mean 34.70 36.49 33.75 35.43 35.01 F(3,187)SD 9.96 11.56 8.23 9.87 9.92 .62Range 20–78 22–68 20–55 24–61 20–78 . 60
State–Anxiety (T-1Mean 32.62 35. 35 31.83 33.31 33.18 F(3,187)SD 10.62 11.93 9.73 10. 20 10.65 . 92Range 20–76 20–64 20–66 20–60 20–76 .43
State-Anxiety (T-2Mean DNA 35. 22 34.68 30.87 33.57 F(2,132)SD DNA 10.42 11.09 8. 74 10.21 2.53Range DNA 20–59 20–62 20–56 20–62 .08
Marital Satisfaction: DAS
Mean 111.67 110.84 117.06 113.62 113.14 F(3, 186)SD 15. 72 15. 29 15. 37 15. 66 15.59 1.51Range 51–144 50–131 56–144 67–139 50–144 .21
Family Relationships Questionnaire - Antepartum (FRQA)Mean 55.91 57.20 54.72 DNA 55.92 F(2,153)SD 10.30 11.41 11. 49 DNA 10.95 . 57Range 35–86 41–90 33–88 DN 33–90 .57
Symptoms, Antepartum – Now (SXAN)Mean 25.38 24. 18 24.89 DNA 24.90 F(2,153)SD 7. 74 11. 32 9.07 DNA 9.22 .22Range 11-48 5–57 7–41 DNA 5–57 .80
Symptoms, Antepartum - Comparative (SXAC).Mean 59.91 58.46 61.17 DNA 59.89 F(2,147)SD 5.41 5.25 5.30 DNA 5.40 2.76Range 47–73 40–70 47–70 DNA 40–73 .07
below reported means
students (38.76).
for female working adults (35.20) and college
One-sample t tests were performed to compare study
sample anxiety scores with the norms for working adult women, revealing
no differences in T-ANX scores (t(190)=.31, p = .76). However, study

89
Table 4.4
Trimester-Related Antecedent Variables Affecting Dependent Variables
Dependent Wariable Antecedent Wariable Test value (df or n), p
State Anxiety COMFORT1 F(3,175)=4.20, p = .0067INTEND2 t(76.01)=4.05, p = .000CONCEPTN r(n=184)=–. 18, p = .014
Marital DAS COMFORT1 F(3,174)=2.55, p = . O575INTEND2 t(73.18)=-3. 37, p = .008
FRQ-Antepartal COMFORT1 F(3,141)=.70, p = . 5548CONCEPTN r(n-153)=–.22, p = .007INTEND2 t(68.08)=2.81, p = .007
Symptoms Antepartal—Now COMFORT1 F(3,141)=4.58, p = .0043
Symptoms Antepartal–ComparativeCOMFORT1 F(3,136)=3.32, p = .0218
sample S–ANX scores were significantly lower than normative data
(t(190) = -2.62, p = .01).
The effect of pregnancy trimester on state anxiety was evaluated by
cross-sectional and longitudinal examinations of S-ANX scores. In the
one-way analysis of variance, no differences were found between the four
trimester group scores at T-1 or T-2 (see Table 4.3). Three of the six
antecedent variables previously identified which were not evenly
distributed across trimester groups demonstrated relationships with
S–ANX. These variables (see Table 4.4) indicated higher anxiety among
women who recalled a difficult, rather than easy, previous pregnancy; who
were not intending this pregnancy; and who were trying fewer months to
conceive. The three variables were were entered into a three-way
analysis of covariance, in which trimester of first test administration
(TRIM1), COMFORT1, and INTEND2 served as non-metric factors, and CONCEPTN
was the covariate with S-ANX. No trimester main effects with S-ANX were

90
found (F(3,140) = .22, p = .88).
Longitudinal evaluation of patterns of state anxiety throughout
pregnancy was made through repeated measures tests in related samples.
Paired t-test scores of the 135 subjects tested at T-2 (see Figure 3.1)
were examined by trimester group. No differences in S-ANX scores between
the two administrations were found for Subjects group S-1, t{47) = -1.68,
p = . 10; group S-2, tC40) = .21, p = .84; or group S-3, t(45) = .25,
p = .81.
Marital Satisfaction
Marital satisfaction was measured with the Spanier Dyadic Adjustment
Scale (DAS) (see Table 4.3). Obtained scores ranged from 50 to 144, on a
scale with a theoretical range of 0 to 151 (Spanier, 1976). Although
high and low score cut-off points are not provided in the literature, the
mean scores for married (114.8) and divorced (70.7) couples used in
instrument development (Spanier, 1976) are available for comparison. The
study mean of 113.1 approximates the married sample score from that
report. However, the total and trimester group scores are considerably
higher than the 97.2 mean reported in another study for contemporary
multiparous couples tested in the third trimester, and three and nine
months postpartum (Belsky, Spanier, & Rovine, 1983). Examination of the
component subscale scores reveals that it is the subscale for
Satisfaction which is considerably higher (39.63 vs. 28.2) in the current
study than in the 1983 report.
No differences by trimester group membership were demonstrated
through one-way analysis of variance procedures (F(3, 186) = 1.51,
p = .21). Two-way analysis of covariance was then performed to control
for potentially confounding variables COMFORT1 and INTEND2. Marital

91
satisfaction scores had been found to be higher in women reporting an
easy/comfortable previous childbearing and positive intendedness of
current pregnancy (see Table 4.4). No main effects for trimester were
found (F(3,144) = 1.56, p = .20).
Marital satisfaction was reported as stable, rather than dynamic,
through related sample measures as well. Paired t tests failed to
demonstrate differences from T-1 to T-2 for Subject group S-1,
t(47) = −.88, p = .38; S-2, tC40) = −.62, p = .54; or S-3, t(45) = 1.00,
p = .32.
Family Relationships Questionnaire
The Family Relationships Questionnaire (FRO) will be discussed first
in terms of the total scale, and second in terms of individual items.
The FRO-A was administered to subjects in the first three trimesters,
while the FRO-P was administered only to subjects in the fourth
trimester. Scores on the FRO—A ranged from 33 to 99, with a mean of
55.92, out of a theoretical range of 25 to 125. Higher scores represent
a higher cummulative level of maternal concern about family
relationships. FRO-P scores varied from 29 to 73, with a theoretical
range of 22 to 110. Because this investigation represents the first use
of the FRO's, there are no normative data for comparative analyses.
Cross-sectional analyses involving the three prenatal trimesters
in one-way analyses of variance failed to reveal trimester group
differences in the level of maternal concerns about family relationships,
where F(2,153) = .57, p = .57 (see Table 4.3). The only dyadic prena tal
subscale demonstrating internal consistency, as reported earlier, was the
mother—child antepartum (MCA) subscale. No cross-sectional group
differences were detected with this subscale either, with F(2,153) = .56,

92
p = .57.
Two trimester-related antecedent variables were related to FRO-A
scores at either T-1 or T-2 (see Table 4.4). Levels of family
relationship concerns were negatively correlated with number of months
trying to conceive (r. = −.22, p = .007). Also, women not intending to
become pregnant reported higher levels of concern. Because COMFORT1 had
demonstrated a strong relationship with many maternal health variables,
it was included in the followup analysis as well. Therefore, a three-way
analysis of covariance including TRIM1, COMFORT1, INTEND2, and CONCEPTN
was performed. No main effects for TRIM1 were found, with F(2,118) =
1.075, p = .345).
The dependent sample longitudinal comparisons revealed no
differences in FRQ-A or MCA scores between first and second trimester
measures. However, Subjects group S-2, which was in the second trimester
at T-1 and the third trimester at T-2, demonstrated significant increases
in both scores. Mean FRQ-A scores increased from 56.58 to 61.36, t|40) =
–2.98, p = .005. Mean MCA scores increased from 17.70 in the second
trimester to 19.44 in the third trimester, tC40) = -2.51, p = .016.
Individual items on the FRO instruments were also examined. The
range of response for an individual item was from one to five. Following
reversal of concern—present item scores, high scores represent greater
maternal concern. The descriptive information which follows is based on
the T-1 administration. On the antepartum version, all 25 items elicited
the full range of responses, except four items (#9, 14, 15, 24) which
produced ranges of one to four. On the postpartum version, the range of
responses was not used as fully, with 15 items spanning 1–5, 6 items
ranging from 1–4, and one item (#7) eliciting only responses 1-2.
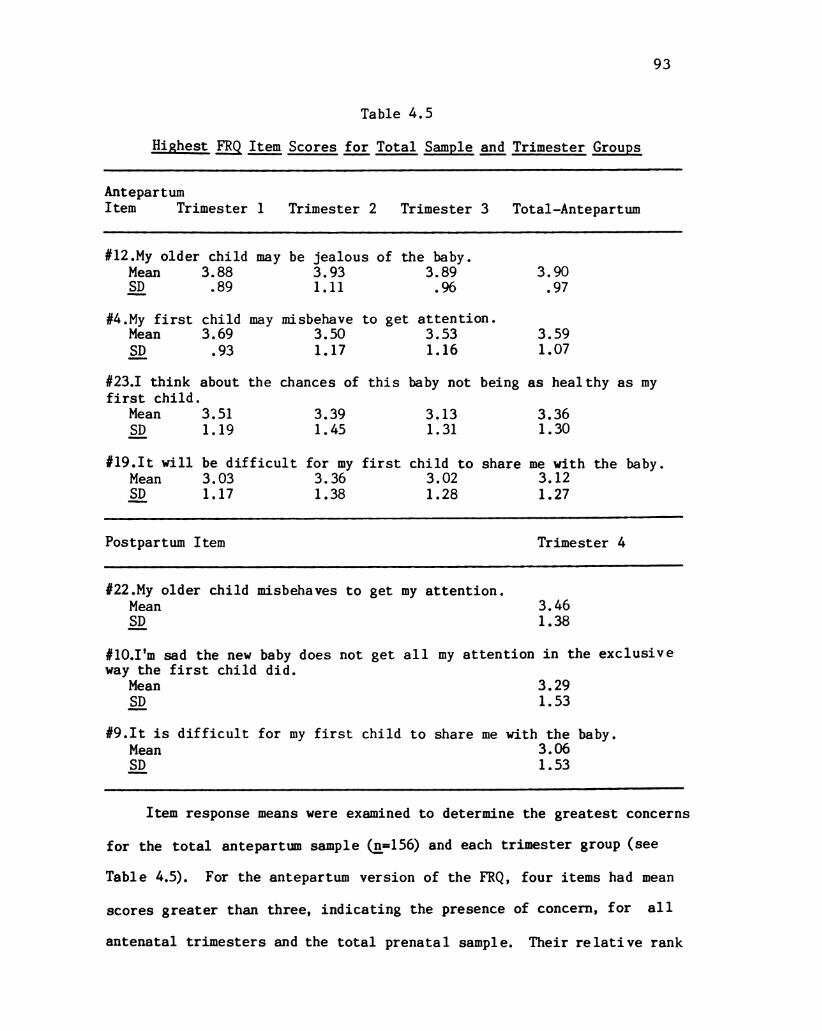
93
Table 4.5
Highest FRQ Item Scores for Total Sample and Trimester Groups
AntepartumItem Trimester 1 Trimester 2 Trimester 3 Total—Antepartum
#12.My older child may be jealous of the baby.Mean 3. 88 3.93 3. 89 3.90SD . 89 1.11 .96 .97
#4. My first child may misbehave to get attention.Mean 3. 69 3.50 3.53 3.59
SD .93 1. 17 1.16 1.07
#23.I think about the chances of this baby not being as healthy as myfirst child.
Mean 3.51 3.39 3.13 3.36SD 1. 19 1.45 1. 31 1. 30
#19. It will be difficult for my first child to share me with the baby.Mean 3.03 3. 36 3.02 3. 12SD 1. 17 1. 38 1.28 1.27
Postpartum Item Trimester 4
#22.My older child misbehaves to get my attention.Mean 3.46SD 1. 38
#10.I'm sad the new baby does not get all my attention in the exclusiveway the first child did.
Mean 3.29SD 1.53
#9. It is difficult for my first child to share me with the baby.Mean 3.06SD 1. 53
Item response means were examined to determine the greatest concerns
for the total antepartum sample (n=156) and each trimester group (see
Table 4.5). For the antepartum version of the FRO, four items had mean
scores greater than three, indicating the presence of concern, for all
antenatal trimesters and the total prenatal sample. Their relative rank

94
Table 4.6
Change in FRQ-A Item Means by Trimester: Paired T-tests
Item Mean (1) Mean (2) (df)t, p.
Subject Group S-1, Trimester 1 vs Trimester 2
#21 1. 792 2. 188 (47) –2.22, .031
Subject Group S-2, Trimester 2 vs Trimester 3
#2 2. 317 2.756 (40) –2.37, .022#4 3.415 3. 878 (40) -2.60, .013#7 1. 717 2. 122 (40) –2.59, .013#8 2.951 3.537 (40) —2.76, .009#17 2. 175 2. 750 (39) –2.89, .006#18 2.415 3. 195 (40) —4.61, .000
remained constant throughout trimesters. Three items dealt with
distribution of affection and attention within the mother—firstborn-baby
triad. The fourth dealt with maternal health concerns for the new baby.
Average scores of three items from the postpartum FRO were greater than
three. These items reflected themes of responses by the firstborn or the
mother to the finite resources of affection and attention.
Potential patterns of individual maternal concerns through pregnancy
were examined from both cross-sectional and longitudinal perspectives.
Oneway analyses of variance of the 25 FRO-A items through the three
prenatal trimesters revealed change by trimester in only one item,
F(2,153) = 4.40, p = .014. A posteriori contrasts revealed that women in
the second trimester were more concerned about their husbands spending
enough time with the firstborn (#21, mean = 2.43) than were women in the
third trimester (mean = 1.77).
Data from longitudinal measurements demonstrated changes in the
levels of several maternal concerns by trimester (see Table 4.6). From

95
first to second trimester, the mean of only one item changed, in an upward
direction. From second trimester to third trimester, six item means
changed, all in the direction indicating greater maternal concerns in
third trimester. The nature of the increasing concerns address paternal
(#18) and maternal (#2) preference about the baby's sex; decreased
maternal pleasure with the pregnancy due to the firstborn (#17);
increased desire for the husband to attend to the firstborn (#8);
increasing concern about ability to love the newborn as the firstborn
(#7); and greater concerns about firstborn misbehavior (#4).
Somatic Symptoms
The levels of somatic symptoms experienced by secundigravidae were
assessed with antenatal and postpartal instruments for both the current
pregnancy (SXAN and SXPN), and as compared to the same trimester of the
previous pregnancy (SXAC and SXPC). Higher scores indicate greater
frequency of symptoms now. The obtained range of current antepartum
symptom scores spanned from 5 to 57, while comparative antepartum scores
varied from 47 to 73, both out of a theoretical range of 0 to 87 (see
Table 4.3). Current postpartum scores occupied the lower end of the
possible range, varying from 2 to 38, while comparative postpartum scores
went from 44 to 60, out of a possible range of 0 to 69.
One-way analysis of variance failed to reveal trimester effects on
either current or comparative somatic symptom levels (see Table 4.3).
However, comfort of first childbearing was related to both trimester and
symptomatology (see Table 4.4). Followup a posteriori contrasts
demonstrated that women who recollected their previous childbearing as
very easy had current symptom level mean scores (20.93) significantly
lower than either women with somewhat difficult (mean = 27.61) or very
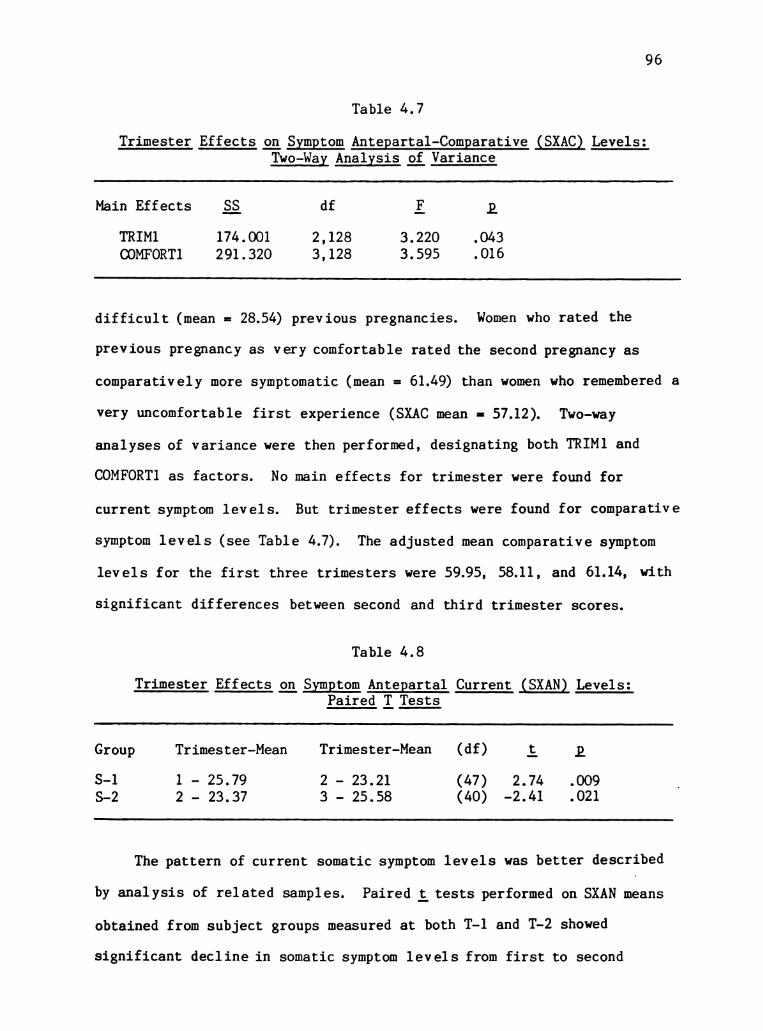
96
Table 4.7
Trimester Effects on Symptom Antepartal-Comparative (SXAC) Levels:Two-Way Analysis of Variance
Main Effects SS df F. P.
TRIM1 174.001 2, 128 3.220 .043COMFORT1 291. 320 3, 128 3.595 .016
difficult (mean = 28.54) previous pregnancies. Women who rated the
previous pregnancy as very comfortable rated the second pregnancy as
comparatively more symptomatic (mean = 61.49) than women who remembered a
very uncomfortable first experience (SXAC mean = 57.12). Two-way
analyses of variance were then performed, designating both TRIM1 and
COMFORT1 as factors. No main effects for trimester were found for
current symptom levels. But trimester effects were found for comparative
symptom levels (see Table 4.7). The adjusted mean comparative symptom
levels for the first three trimesters were 59.95, 58.11, and 61.14, with
significant differences between second and third trimester scores.
Table 4.8
Trimester Effects on Symptom Antepartal Current (SXAN). Levels:Paired T Tests
Group Trimester–Mean Trimester–Mean (df) t P
S-1 1 – 25.79 2 — 23.21 (47) 2.74 .009S–2 2 – 23. 37 3 – 25.58 (40) —2.41 .021
The pattern of current somatic symptom levels was better described
by analysis of related samples. Paired t tests performed on SXAN means
obtained from subject groups measured at both T-1 and T-2 showed
significant decline in somatic symptom levels from first to second

trimester, and an increase in symptom levels from second to third
trimester (see Table 4.8).
Table 4.9
Frequent Somatic Symptoms for Total Sample and Trimester Groups
AntepartalSymptom Total—Antepartum Trimester 1 Trimester 2 Trimester 3
TirednessMean 2.03 2.25 1.77 1.96SD .80 . 75 .94 .63
Frequent UrinatingMean 1.99 1.94 2.00 2.04SD .84 . 85 . 75 .91
IrritabilityMean 1.26 1.29 1.27 1.22SD . 85 . 74 .95 . 92
Trouble SleepingMean 1.21 1. 11 .95 1.57
SD 1.02 .99 .96 1.04
NauseaMean 1. 20 1.83 . 89 .62SD 1. O7 .98 .95 .82
Postpartum Symptom Trimester 4
TirednessMean 2.06SD . 87
OverweightMean 1.87SD 1.13
Breast discomfortMean 1. 31
SD 1.02
IrritabilityMean 1.26SD .85
98
Data about individual symptoms were also examined. To determine
which symptoms occurred with greatest frequency, mean scores for each
symptom were rank ordered by magnitude within total antepartal sample and
trimester groups. Respondents ranked frequency of symptom occurrence
from 0 = rare/none, to 3 = constant, so scores greater than 1.5 are above
the scale midpoint. Although the most frequent symptoms for the total
antepartum period, in descending order, were tiredness, frequent
urinating, irritability, trouble sleeping, and nausea, this order did not
persist by trimester grouping (Table 4.9). Most frequent postpartum
somatic symptoms were tiredness, overweight, breast discomfort, and
irritability, followed by backache and constipation.
As would be expected due to the differential rank ordering of
symptoms by antepartal trimester, multiple symptoms demonstrated
significant differences in frequency by trimester group. Repeated
measures from subjects obtained at T-1 and T-2 revealed that frequency of
12 of the 29 symptoms evaluated differed between first and second
trimesters (see Table 4.10). Decreases occurred in frequency of
dizziness, appetite loss, nausea, tiredness, vomiting, weakness, cold
hands/feet, and breast discomfort; while increases in backache, shortness
of breath, swollen legs/hands, and groin/pelvic pain/pressure were
detected. The subjects who moved from second to third trimester
experienced decreases in nausea, increased appetite, headache, and breast
discomfort; as well as increased frequency of backache, trouble sleeping,
painful intercourse, shortness of breath, and groin/pelvic pain/pressure.
Data allowing comparison between somatic symptom frequency during
the present and previous pregnancy (SXAC and SXPC) took the form of
ratings on a three-point scale evaluating the current symptom frequency

99
Table 4.10
Change in Somatic Symptoms by Trimester: Paired T-test
Symptom Mean (1) Mean (2) (df) to p
Subject Group S-1, Trimester 1 vs. Trimester 2
5. Dizziness . 625 .333 (47) 3. 10, .00310. Appetite loss . 979 . 417 (47) 5.07, .00011. Nausea 2.000 .521 (47) 11.40, .00015. Tiredness 2. 271 1. 646 (47) 4.23, .00016. Vomiting . 833 . 229 (47) 4.82, .00017. Weakness . 936 . 638 (46) 3.72, .00120. Cold hands/feet . 936 . 596 (46) 2.07, .04428. Breast discomfort 1.333 . 771 (47) 3.71, .001
1. Backache . 872 1. 319 (46) –3.48, .00113. Shortness of breath . 521 . 896 (47) –2.65, .01114. Swollen legs/hands . 146 .521 (47) –3.54, .00129. Groin/pelvic pain . 750 1. 250 (47) —3.23, .002
Subject Group S-2, Trimester 2 vs. Trimester 3
11. Nausea . 829 .463 (40) 2.49, .01723. Increased appetite 1. 171 . 829 (40) 3.00, .00527. Headache 1.146 . 658 (40) 3.48, .00129. Breast discomfort 1. 131 . 610 (40) 4.11, .000
1. Backache 1.073 1.415 (40) –2.65, .0117. Trouble sleeping . 902 1. 780 (40) -5.60, .00012. Painful intercourse .564 . 769 (38) —2.08, .04413. Shortness of breath . 658 1. 146 (40) -3.86, .00029. Groin/pelvic pain . 878 1.658 (40) —4. 19, .000
as 1=now less, 2=now the same, or 3=now more, than the same trimester of
the previous pregnancy. One-sample t-test comparisons of SXAC and SXPC
item means to a value of "2" allowed determination of which symptoms were
perceived as having different frequency in second pregnancy. Fourteen
symptoms were experienced differently for secundigravidae (see Table
4.11), with seven symptom comparisons producing p < .001. Three symptoms
were perceived as occurring less often in second pregnancy, while 11
symptoms were experienced more often for secundigravidae. Postpartal

100
Table 4.11
Somatic Symptoms in Second vs. First Pregnancy: One-sample t Test
Antepartal Symptom Mean T-test comparison to 2.00: (df)t, p
Backache 2. 18 (154) 3.46, .001Trouble sleeping 2.25 (152) 5.67, .000Depression 2. 12 (150) 2.65, .009Shortness of breath 2.14 (153) 3.20, .002Tiredness 2.40 (154) 7.65, .000Weakness 2.19 (150) 5.03, .000Frequent urinating 2. 15 (154) 3.77, .000Irritability 2.21 (153) 4.37, .000Heartpounding 2.13 (146) 3.22, .002Headache 2. 12 (151) 2.61, .010Groin/pelvic pain 2.19 (150) 3.81, .000
Swollen legs/hands 1.76 (152) —5.69, .000Rapid weight gain 1. 87 (155) –2.57, .011Increased appetite 1.90 (153) —2.04, .043
comparative symptom measures produced no significant differences from the
first pregnancy, based on only 30 – 35 values per symptom. Postpartal
comparative symptom means which varied the most from 2.00 were tiredness
(M = 2.23, tC34) = 1.85, p = .07) and trouble sleeping (M = 2. 18,
t(33) = 1.79, p = .08).
Interrelationship of Dependent Variables
Association among the dependent variables was examined by
computation of Pearson product-moment correlation coeeficients (r). The
strength and direction of the identified associations for dependent
variable measures for the total sample at T-1 are presented in Table
4.12. The resultant matrix presents as a highly enmeshed set of
variables describing maternal health. All the prenatal dependent
measures demonstrated highly significant correlations in the expected

101
Table 4. 12
Association Between Anxiety, Marital AdjustmentSomatic Symptoms, and Family Relationship Concerns
Variables S–ANX
Pearson's r (n), P
T—ANX DAS SXAN SXPN FRO—A FRO–P
State Anxiety(S–ANX)
Trait Anxiety .832(T-ANX) (191)
.000%
Marital -.559(DAS) (190)
.000%
Symptoms . 537Ante-Now (156)(SXAN) .0003%
Symptoms —. 023Post–Now ( 35)(SXPN) . 897
Family Concern .477Ante (156)(FRO–A) .000+
Family Concern .406Post ( 35)(FRO–P) .016
*p < .001
—. 601(190). OOO%
.473 – .334(156) (155).000+ .000+
. 148 .048 DNA( 35) ( 35). 395 . 785
.492 – .433 .261 DNA(156) (155) (156).0003% . 000+ .001
. 492 –. 366 DNA .089 DNA( 35) ( 35) ( 35).044 .031 . 610
directions, with high anxiety, low marital satisfaction, high levels of
somatic symptoms, and high levels of family relationship concerns
significantly related (p & .001). The two postpartum measures
were dependent upon a more limited sample size of 35. Postpartum level
of maternal family relationship concerns nonetheless evidenced

102
significant associations with anxiety and marital satisfaction. Only
postpartum symptom levels failed to demonstrate association with other
dependent variables at T-1.
The association among measures obtained at T-2 was examined in a
similar manner. All measures except T-ANX were obtained at the second
test period. S-ANX and FRQ—A continued to demonstrate strong
associations with antenatal variables. Postpartum variables demonstrated
stronger association to other measures, with postpartum group size of 46
at T-2. FRQ-P was related to S-ANX, r =.473, p = .001; to DAS, r=-.489,
p = .001; and approached a significant relationship to SXPN, ra.196,
p = .053. SXPN demonstrated a strong relationship to S-ANX, ra.459, p =
.001. The absence of association between postpartum symptom levels and
marital satisfaction persisted, and the association between antepartum
symptoms and marital satisfaction was not significant at T-2.
Other Findings
Incidental to analyses undertaken to answer the study research
questions, relationships between a variety of antecedent variables and
the dependent variables of maternal health were observed. Those
demographic and background variables related to more than one dependent
variable are summarized in Table 4.13. All relationships refer to data
obtained at T-1 unless otherwise specified.
Maternal age was negatively correlated with state and trait anxiety,
and current somatic symptom levels both before and after delivery.
Socioeconomic status was related to those same four variables, as well as
being positively correlated with marital adjustment. The number of
miscarriages experienced was positively related to state anxiety, but not
to trait anxiety. This suggests that women who have had a miscarriage
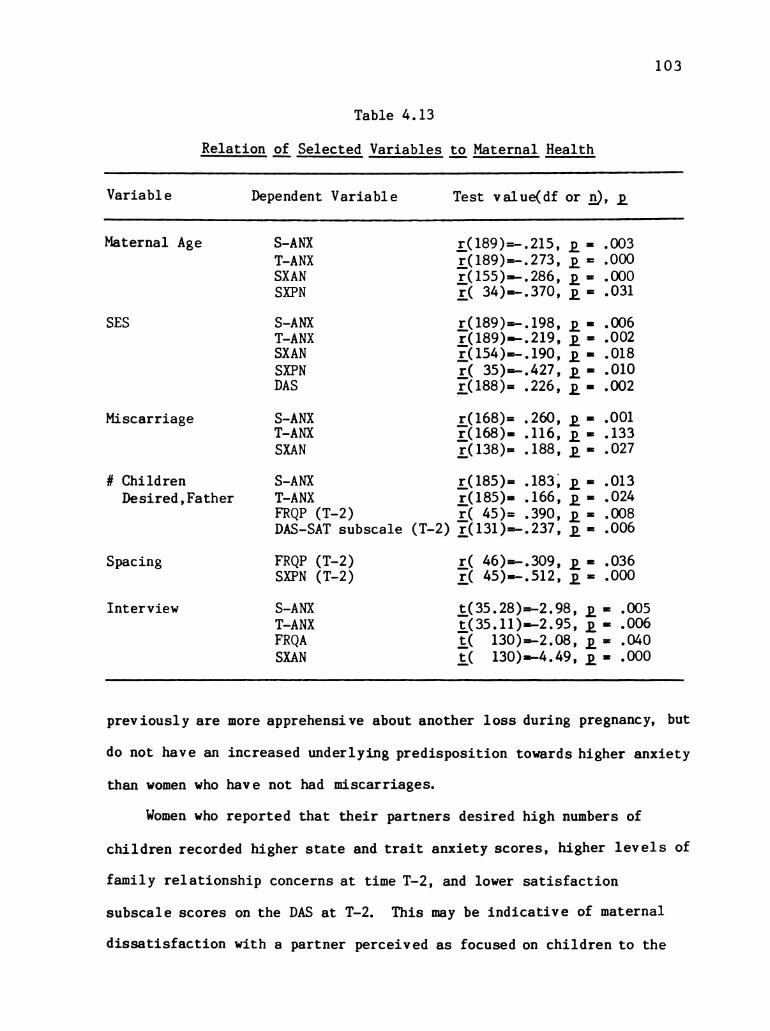
103
Table 4.13
Relation of Selected Variables to Maternal Health
Variable Dependent Wariable Test value(df or n), p.
Maternal Age S–ANX r (189)=–.215, p = .003T—ANX r(189)=–.273, p = .000SXAN r (155)=–.286, p = .000SXPN r( 34)=–.370, p = .031
SES S–ANX r (189)=–. 198, p = .006T–ANX r(189)=–.219, p = .002SXAN r(154)=–. 190, p = .018SXPN r( 35)=–.427, p = .010DAS r(188)= .226, p = .002
Miscarriage S–ANX r(168)= .260, p = .001T-ANX r(168)= . 116, p = . 133SXAN r(138)= . 188, p = .027
# Children S–ANX r (185)= . 183, p = .013Desired, Father T–ANX r(185)= . 166, p = .024
FROP (T-2) r( 45)= .390, p = .008DAS–SAT subscale (T-2) r(131)=–.237, p = .006
Spacing FROP (T-2) r( 46)=–.309, p = .036SXPN (T-2) r( 45)=-.512, p = .000
Interview S–ANX t(35.28)=–2.98, p = .005T—ANX t(35.11)=–2.95, p = .006FROA |t( 130)=–2.08, p = .040SXAN t( 130)=–4.49, p = .000
previously are more apprehensive about another loss during pregnancy, but
do not have an increased underlying predisposition towards higher anxiety
than women who have not had miscarriages.
Women who reported that their partners desired high numbers of
children recorded higher state and trait anxiety scores, higher levels of
family relationship concerns at time T-2, and lower satisfaction
subscale scores on the DAS at T-2. This may be indicative of maternal
dissatisfaction with a partner perceived as focused on children to the

104
detriment of the marital dyad. Alternatively, since some male partners
had children by previous marriages not living in their current home, the
relationship between subjects' emotional discomfort and higher numbers of
children desired by their partner may, speculatively, reflect stresses of
remarriage with stepchildren in some cases.
The number of months of spacing between first and second children
was negatively correlated postpartally with both levels of family
relationship concerns and current symptoms, as measured at T-2. These
selected variables contribute to a profile of the secundigravida at risk
for poor health. High anxiety, high symptom levels, high levels of
postpartum concerns, and lower marital adjustment scores were associated
with low age, low SES, a history of spontaneous abortions, a partner's
high fertility desires, and closely spaced children.
A methodologic finding is also noteworthy. Initially interviews
were planned, although they were not conducted due to the adequacy of the
quantitative data. At the time written consent was obtained from
subjects, women were asked to indicate whether they would agree to being
interviewed later for one hour, at a time and 1 ocation of their choice.
The consent further stated that if respondents said "yes" now, they may
change their mind later. About 1 in 12 study participants would be
involved. The 29 subjects who declined potential interviews were more
anxious, had higher levels of antepartal family relationship concerns,
and had more antepartal somatic symptoms than the 130 women who agreed
they could be contacted for interview.
Hypothesis Testing
The first hypothesis, that midtrimester state anxiety and somatic
symptom frequency would be lower than first or third trimester levels,

105
was partially supported. No differences between trimester groups in
anxiety levels were found. Lower somatic symptom levels for second
trimester were found in comparison to first and third trimester scores in
repeated testing of longitudinal subjects.
The second hypothesis, that the level of maternal family
relationship concerns would be higher in third trimester than first or
second trimester was also partially supported. Dependent sample testing
demonstrated higher scores for both the total family relationship scale
and the maternal-child subscale in the third trimester compared to the
second trimester. The cross-sectional independent sample testing showed
no differences between the three trimester groups. The design did not
permit comparison of first and third trimester groups between dependent
samples.
The third hypothesis, that marital satisfaction will decline from
second trimester to fourth trimester, was not accepted. No group
differences were found through either cross-sectional or longitudinal
analyses.
The fourth hypothesis, that perceived frequency of somatic symptom
occurrence will be higher in second pregnancy than in first pregnancy,
was accepted. Of fourteen symptoms perceived differentially between the
two pregnancies, eleven were experienced more frequently the second time.
The fifth hypothesis, predicting the interrelationships between
maternal anxiety, somatic symptom frequency, level of family relationship
concerns, and marital satisfaction, was accepted. The matrix created by
the interrelationships of the dependent variables, including their
alternate versions, includes 17 cells. Of these, 13 demonstrated
significant associations based on the first test administration. Those

106
cells were reexamined with data from the second test period, which
altered trimester group distribution. Of four variable relationships not
significantly associated at T-1, one involving trait anxiety was not
examined; one demonstrated highly significant association; one
association approached significance; and one, postpartum symptom levels
and marital satisfaction, remained unrelated. A11 associations were in
the predicted direction.
Summary
Data analytic procedures and study findings were presented in this
chapter. Sample characteristics of the total sample and comparison
groups were described. The sample can be characterized as obstetrically
low risk, white, married women in their twenties and early thirties,
delivering their second baby through private or prepaid health insurance
plans. Differences betwen trimester comparison groups were found only
for comfort and delivery mode of previous childbearing, intendedness of
and months trying to conceive the current pregnancy, and prenatal
diagnostic tests experienced or expected.
Statistical analyses required to answer the research questions were
performed with the four study dependent variables. Testing of hypotheses
related to the effect of trimester on maternal health variables revealed
higher levels of family relationship concerns in the third trimester than
the second trimester, and lower somatic symptom levels in the
midtrimester than in early or late pregnancy. Contrary to study
hypotheses, both state anxiety and marital satisfaction were found to be
stable across the four trimesters of pregnancy and the postpartum period.
Somatic symptom frequency was found to be greater during second pregnancy

107
compared to recollections of the previous pregnancy, as predicted. The
hypothesis regarding interrelationships between maternal anxiety, somatic
symptom frequency, level of family relationship concerns, and marital
satisfaction was supported. In addition, information describing
frequency and trimester distribution of specific family relationship
concerns and somatic symptoms was provided.

108
Chapter V
Discussion
In this chapter, the meaning of study findings are discussed in
relation to the research questions. Limitations of this investigation
are presented. The significance of the study and implications for
nursing and health care are discussed. The chapter concludes by
addressing directions for future research suggested by outcomes of this
investigation.
Relation of Findings to Research Questions
Change in Dependent Variables by Trimester
The first research question sought the answer to whether maternal
health and perceptions of family relationships change with time through
the course of second pregnancy. Study findings will be discussed in
relation to each dependent variable.
Anxiety. Study findings failed to support the hypothesis that
midtrimester anxiety would be lower than anxiety in the first or third
trimesters. Several factors may account for why the current study
results differ from those of Lubin, Gardener, and Roth (1975), who
identified the "W" shaped pattern of anxiety among primiparae and
multiparae. Differences in demographic characteristics between Lubin's
work and this study do not appear to account for discrepant results,
since samples appear comparable regarding race, age, education, and SES.
However, the status of Lubin's subjects regarding other factors with an
identified effect on anxiety in secundigravidae, such as comfort of
previous childbearing and intentedness of pregnancy, are not known.

109
Table 5.1
Weeks of Pregnancy by Trimester Group
Trimester 1 Trimester 2 Trimester 3 Trimester 4 Total
Range 6 – 14 15 – 27 28 – 39 43 – 50 6 – 50Mode 11 22 35 43/44 11Mean 10.74 20.09 33. 74 46.00 25.02SD 2.01 3.41 3.68 2.40 13.55
The construct of anxiety was measured with different instruments.
Lubin and others used the Anxiety Adjective Check List (AACL). The
instrument used for anxiety measurement in this study was the Spielberger
STAI. Although Spielberger and others (1983) did not address inter
instrument correlations for state anxiety tools, he reported having found
high correlations between his instrument and several other measures of
trait anxiety. He found only moderate correlations with the AACL,
suggesting that that scale is apparently less adequate as a measure of
trait anxiety.
Failure of this study to detect higher levels of anxiety in the
first trimester may be due to failure to take measurements at intervals
adequately representing the trimester distinctions. While administration
of first trimester test packets varied from 6 to 14 weeks, the modal test
time was 11 weeks and the mean was 10.74 weeks (see Table 5.1). Lubin (1975)
reports that his first test administration was at two months. It may be
that subjects in this study had already passed the weeks of ambivalence
and fear of miscarriage that accounted for high anxiety in other reports.
Consideration of sample anxiety scores in relation to established
norms is also valuable in interpreting study findings. Anxiety trait
scores were consistent with norms for working adult women, indicating

1 10
study subjects were within population parameters for the underlying
predisposition towards apprehension and tension. However, scores for the
transitory feelings of state anxiety were lower for study subjects than
for the normative group. Grossman and others (1980) similarly found
scores on the Spielberger STAI-State to be below normative levels, with
values of 33.1 first trimester and 33.68 in the third trimester
(comparable to values in this study of 32.6 and 33.18). Since Grossman
did not obtain a midtrimester measure, no conclusions from that study can
be made about a pattern of state anxiety across all three trimesters.
But among women with initially low state anxiety scores, it may be that
further reduction of anxiety would not occur. Further research is needed
to determine if a midtrimester decline in anxiety would occur among women
with high trait anxiety, or among women with high state anxiety during
pregnancy. Women in this study, perhaps in concert with their relatively
stable lifestyle, the financial provider's employment status, and
assurance of adequate health care, which were all indirectly inclusion
criteria, reacted to second pregnancy with less anxiety than their
normative, non-pregnant counterparts were experiencing.
The methodologic rigor employed in studying anxiety in pregnancy
meets the standards recently explicated by Lederman (1984a). In a
thoughtful review of the measurement of anxiety in pregnancy, she calls
for consideration of age, education, parity, gravidity, socioeconomic
status, previous obstetrical experience, health and health history,
marital status and relationship, trimester of pregnancy, gravida's coping
experiences, social desirability, design, instrumentation, and state and
trait anxiety. The current study succeeded in attending to the majority
of these elements.

111
Marital Satisfaction. Marital satisfaction was also found to be
stable across the four trimesters of pregnancy. Hence, incongruencies in
the literature between reports of increasing satisfaction in late
pregnancy (Rankin & Campbell, 1983; Richardson, 1983b) and into the
postpartum period (Moore, 1983), compared to reports of declining
satisfaction (Belsky, Spanier, & Rovine, 1983; Feldman, 1971) are not
resolved.
The failure to find differences between third and fourth trimester
reports of marital satisfaction was inconsistent with the findings of
Belsky and others (1983), who found declining satisfaction using the same
instrument on a contemporary sample of comparable race, education, and
SES. This discrepancy may be clarified by consideration of data
collection times. Data collection points for paper-and-pencil measures
in the Belsky study were the last trimester of pregnancy and three months
postpartum. Combined with data from the Miller and Sollie (1980) report,
which identified a "baby honeymoon" interval postpartally followed by
stressful effects of the newborn, the boundaries of the honeymoon period
can be defined as extending through the first month and ending by the
third postpartal month. The average time of postpartum data collection
in this study was six weeks (see Table 5.1), too early to detect marital
dissatisfaction that may follow. It is difficult to interpret why
average DAS scores among the study subjects were considerably higher than
the scores obtained by participants in the Belsky study, who were self
selected volunteers recruited individually and through public
solicitations.
Family. Relationship Concerns. As hypothesized, the level of family
relationship concerns increased in the third trimester. Both FRQ total
112
and FRQ Mother–Child Antepartal scores increased. These findings are
consistent with Richardson's (1983a) observations of the increasingly
problematic nature of the mother-child relationship through subsequent
pregnancy.
Somatic Symptoms. Change in somatic symptom levels across the three
antepartal trimesters assumed the hypothesized pattern of lower frequency
midtrimester than in first or third trimester. This is consistent with
the pattern for secundigravidae found by Lubin and others (1975), and
with widely held conceptions of the midtrimester as the comfortable,
benign portion of pregnancy marked by feelings of well-being (Rubin,
1984).
Description of Principal Family. Relationship Concerns
The second research question was exploratory in nature, asking for
descriptors of the most common family relationship concerns of
secundigravidae. The same four items were ranked the highest by all
antenatal trimester groups, underscoring their prominence to the
secundigravidae. The most salient concern throughout pregnancy involves
jealousy of the firstborn about the baby. Two of the other most common
concerns also deal with sharing affection and attention among the
firstborn and the baby. Rubin (1984) speaks to the uniquely human
problem of simultaneously managing two or more ongoing maternal-child
relationships. Mothers are bound in by a history of mutual and
reciprocal experiences with older children. Rubin observes that the
secundigravida in particular, influenced by guilt in bringing another
child into the time and space previously occupied by the firstborn alone,
attempts to maintain ties to the firstborn with time, companionship, and
interest.

113
Of 25 items on the prenatal FRO, the statement indicative of the
third highest level of concern through each trimester and the total
antepartal sample was, "I think about the chances of this baby not being
as healthy as my first child." The predominance of this issue throughout
pregnancy appears to indicate more than the task of ensuring safe
passage, which Rubin (1984) describes as evolving towards the end of
second trimester. Clinical experience and data collected during FR0
instrument development support that multigravidae have a keen sense of
limited fortune. Study participants all had one healthy child living at
home. By virtue of having already experienced the good fortune of the
firstborn's good health, there is a sense of fear of having used up part
of one's quota from the finite pool of healthy babies.
Three items from the postpartal FRO indicated high levels of
concerns by mothers. These items dealt with responses by the firstborn
or the mother to distribution of affection and attention. The concerns
of women in the study, who had been home from three to ten weeks, vary
somewhat from the observations of hospitalized women which led to Walz
and Rich's (1983) identification of tasks of taking on a second child.
The highest rated item, "My older child misbehaves to get my attention,"
reveals a recognition of negative behavior by of the firstborn. Based on
their hospitalized sample, Walz and Rich discussed the task of Promoting
Acceptance, but observed that mothers failed to report firstborn's
negative responses, either due to refusal to accept them or denial of
their existence. Data from this study demonstrate that such thorough
denial of firstborn misbehavior is no longer operable after several weeks
at home postpartally.

114
The second rated FRQ-P item, "I'm sad the new baby does not get all
my attention in the exclusive way the first child did," indicates
grieving over the absence of a "first time" experience with the second
born. Walz and Rich did not identify this task among newly delivered
mothers. The task of Grieving which they identified pertained solely to
the loss of a pre-existing exclusive relationship with the firstborn.
The third rated FRQ-P item fits into Walz and Rich's task of
Reformulating a Relationship, referring to the maternal—firstborn dyad.
Hence, a shift can be discerned between previously reported
descriptions of maternal concerns about family relationships of the
secundigravida in the first three days following birth and the concerns
after several weeks at home. An initial "honeymoon" period with the
firstborn during hospitalization appears to have passed by three to six
weeks postpartum. During later weeks, feelings towards the firstborn are
less benign, and the interests of the newborn are more prominent.
Description of Somatic Symptoms
The third research question had both descriptive and comparative
aspects, inquiring about the description of common somatic symptoms
during second pregnancy, and about their occurrence compared to the first
pregnancy. The symptoms identified as occurring most frequently during
the three trimesters of second pregnancy are similar to those described
by Erickson (1967), who studied 9 primigravidae and 11 multigravidae
longitudinally. It appears that the symptoms women experience in each
trimester of second pregnancy are the same ones which would be expected
during first pregnancy, with fatigue, frequent urination, and nausea most
frequent first trimester; frequent urination and fatigue predominating in
115
the mid trimester; and the two lead symptoms followed by trouble sleeping,
and groin/pelvic pressure in the third trimester.
However, approximately half of the 29 symptoms evaluated were
perceived as being experienced differently during the second pregnancy
than during first childbearing. Only three symptoms were perceived as
occurring less often in the second pregnancy; while eleven symptoms were
reported more frequently (see Table 4.11, p.100). Of the three symptoms
with reports of lower frequency in second pregnancy, one may be
attributable to measurement techniques. Seasonal effects may have
influenced the reported reduction in swelling, since data were collected
in Fall and Winter, when summer heat would not be a factor in increased
swelling. Therefore, a distinction which may clarify reported
discrepancies discussed earlier between symptoms among primigravidae vs.
multigravidae may be based on what is being assessed. The types of
symptoms which are felt appear to be common to women of varying parity.
The frequency with which these symptoms are felt differs markedly, with
the greater frequency preponderantly occurring during the second
pregnancy.
Associations Among Dependent Variables
The fourth research question asked if correlations existed between
the dependent variables. Highly significant associations were found
between maternal anxiety, family relationships concerns, marital
adjustment, and somatic symptom frequency levels. Although pairs of
study dependent variables had been linked in reports discussed earlier,
this study demonstrated a robust relationship among this cluster of
variables elaborating maternal health in second pregnancy.
116
Study Limitations
Recruitment of the majority of study participants appeared to take
place without systematic bias. However, the health care settings
selected as research sites and the homogeneous communities from which
subjects were drawn produced a sample which is limited to women with
Private or prepaid health insurance and limited in racial diversity.
Data collection was limited to a mono method approach.
Complementing paper-and-pencil self-report instruments with other methods
such as interview or observation may have provided validity checks to
data obtained. However, that may be accomplished at the cost of
decreased external validity, based on the data collected which
demonstrated that women willing to participate in more personal or
invasive methods such as interviews represent a sample which is
significantly skewed toward less anxious, less concerned, more
comfortable subjects.
Assessment of phenomena within families is problematic and
challenging (Gilliss, 1983). Assessment of family relationships from a
sole respondent in this study is legitimized by a focus on maternal
health, and the growing body of literature linking maternal perceptions
and concerns to perinatal outcomes and maternal well-being. However,
the boundaries of knowledge related to young family formation, parenting
roles, and sibling relations could be expanded by obtaining data from
multiple respondents.
Lacking tools with established psychometrics for the assessment of
maternal perception of family relationship concerns, it was necessary to
develop an original instrument. Refinement of the FRO and exploration of
its psychometric properties would enhance its value in later analyses of

11 7
the present data set, as well as in future applications. Similarly, the
somatic symptom checklist, particularly the postpartum version, would
benefit from refinement including deletion of underutilized items.
Seasonal effects referred to previously warrant consideration.
Significance and Implications for Health Care
Findings from the study yield both theoretical and practicalcontributions. At the theoretical level, a matrix associating aspects of
maternal physical health, maternal emotional health, marital dyadic
adjustment, and perceptions of family relationship concerns at the time
of addition of the secondborn child has been identified. Further
exploration of the interrelationship of these variables is required to
attempt predictive modeling. Knowledge of the occurrence of this cluster
of variables is also of practical value to maternity and family service
practitioners. The different factors vary in the degree to which they
may be easily, rapidly, or accurately assessed. The variables also
differ in their amenability to therapeutic intervention. Knowledge of
the strong association of the variables prepares the practitioner to be
alert for other co-occurring factors once one has been identified, and to
support the pregnanct woman and her family in the multiple dimensions
suggested by this variable matrix.
The knowledge that contemporary women, many involved in multiple
roles during subsequent childbearing, experience less state anxiety
during pregnancy than their non-pregnant normative counterparts, despite
normative trait anxiety levels, bodes well for perinatal health.
Multigravidae were found to experience lower perinatal complications than
primigravidae, in a study examining psychological and social factors in
complications of pregnancy (Norbeck & Tilden, 1983). Further knowledge

118
of the mechanism which mediates the accommodation in multigravidae,
whether it be social, psychological, or hormonal, would be of value in
extending the benefits of reduced perinatal anxiety to high risk groups.
Although trimester of pregnancy was found to be an important factor
only in the incidence of symptomatology and family relationship concerns,
additional variables related to multiple maternal health variables were
identified. Many of these, such as maternal age, SES, number of
miscarriages, spacing of children, comfort of previous childbearing, and
intendedness of current pregnancy, are easily assessable. Preventive
services to support physical, emotional, and family health can be
directed to target populations with identifiable high-risk
characteristics.
Information obtained about two easily assessable maternal background
variables in particular suggests directions for emphasis in providing
health care to childbearing women. The relationship between low
intendedness of second pregnancy and poor maternal health scores
indicates a need for assistance with contraceptive vigilance from women's
health care providers. This need is particularly impressive in light of
unintended pregnancies among almost one-third of this adult study
population with access to largely prepaid health care. The salience of
perceptions of the comfort of first childbearing highlights the need for
maternity care providers to facilitate resolution of feelings regarding
prior childbirth.
Increased knowledge of the nature and dynamics of somatic symptom
occurrence and family relationship concerns throughout the course of
pregnancy provides nurses with important information for planning and
providing maternal and family services. The timing of informational and
119
support services can be guided by knowledge of when symptoms are most
frequent or when family relationships are most conflictual. The content
of material for anticipatory guidance is dictated by a systematically
obtained data base. For example, secundigravidae should be informed of
the comparative increase in fatigue they are likely to experience, and
encouraged to set realistic goals and make adequate preparations.
Of methodologic interest is the consistent superiority of
longitudinally obtained data over cross-sectional data in detecting
differences in dependent variables, despite meticulous monitoring of a
breadth of confounding variables. Longitudinal investigations, despite
their costs and complexities, provide accuracy in assessment not
otherwise possible in perinatal health research, where confounding
variables may be unquantifiable or as yet unidentified, due to the
decrease in subject-to-subject variability in dependent samples.
The strengths of this investigation include population sampling,
design characteristics, and analytic procedures. Recruitment strategies
were effective in obtaining a study sample that is more diversified than
the upper-middle class subjects with more advanced education who
frequently constitute samples in childbearing and family formation
studies. Mothers' education varied from 10 to 19 years, with the average
schooling being two years of post-high school education. Fathers,
similarly, averaged two years of trade or post-secondary education.
The carefully conceived design is another strength of the
investigation. The prospective, short-term panel longitudinal design
lends itself effectively to assessment of developmental phenomena in
individuals and families. The cross-sectional sequential design in
particular demonstrated value in detecting developmental patterns with

120
great efficiency and economy of investigator and participant resources.
Observations pertaining to the entire childbearing year were obtained
without encountering problems of prolonged subject retention, biased
subject mortality, extensive retesting, or commitment of investigator
resources to a more extended data collection schedule. Data analysis
procedures were also carefully conceived and appropriately implemented.
Intervening variables were carefully monitored and controlled for through
statistical procedures. Further research using this type of design is
warranted.
Recommendations for Future Research
One direction for future research based on the findings of this
study involves refinement of the original measurement instrument, the
Family Relationships Questionnaire. Factor analytic studies would reveal
an underlying factor structure, which could be used in secondary analysis
of the existing data and in subsequent studies to explicate maternal
concerns and psychological processes through pregnancy and the addition
of a second child into the family.
Further data analytic procedures applied to the cluster of dependent
variables which were found to be strongly interrelated would provide
valuable knowledge of maternal health and family relationships. Causal
modeling would permit predictive statements elucidating the relationships
such as that between marital dissatisfaction and high maternal anxiety.
Following development of patient education materials based on the
descriptive information about somatic symptoms and common family
relationship concerns, effects of the information on both the perinatal
client and the health care system could be evaluated. Maternal health,

1.21
comfort, and satisfaction variables could be monitored. Utilization of
health care facilities could be assessed as well, to determine if
preventive educational strategies affected consumption of health care
services.
Nursing intervention research could be directed to assess the
effects of preventive and supportive services provided to women
identified through demographic and obstetrical background factors as
being at high risk for maternal health and troublesome family
relationships when pregnant with a second child. A team approach would
make available the abilities of a clinically expert women's health
clinical specialist and a family care specialist, versed in family
dynamics and therapeutics.
Summary
This concluding chapter addressed the meaning of study findings in
relation to research questions and congruent and incongruent reports in
the literature. Anxiety and marital relationship scores were found to be
stable across the four pregnancy trimesters. In the case of anxiety,
this stability may be accounted for as 1) an accurate assessment with the
instrument used, or 2) a valid representation of anxiety in a low
anxiety population, or 3) a distortion due to failure to adequately
represent trimester groups by date of test administration. The stability
in marital relationship measures also appears to be due to the early
portion of the postpartum period assessed. Family relationship concerns
and somatic symptom levels both rose from second to third trimester. All
four dependent variables demonstrated strong associations.
Descriptive data derived from the FRO revealed themes of concern
over the baby's health based on fear of limited good fortune, and greater

122
negative attribution to the firstborn at home postpartally than is
reflected in data obtained in the hospital postpartally. Comparable
symptoms appear to occur with second and earlier pregnancy, although many
symptoms are experienced with different frequency from one pregnancy to
the other. The majority of symptoms perceived with differing frequency
are experienced more frequently in the subsequent childbearing.
Perception of increased tiredness was a prominent finding. Study
limitations, significance and implications for nursing care, and
directions for future research were also discussed.
123
References
Aldous, J. (Ed.). (1982). Two paychecks: Life in dual-earner families.
Beverly Hills: Sage.
Anxiety worse near term despite previous pregnancy. (1980, January 15).
Ob Gyn News. 15(2), p. 19.
Auerbach, K. (1984). Employed breastfeeding mothers: Problems they
encounter. Birth, 11, 17–20.
Ballou, J. W. (1978). The Psychology of Pregnancy. Lexington, Mass:
Lexington Books.
Baltes, P. B. (1968). Longitudinal and cross-sectional sequences in the
study of age and generation effects. Human Development, 11, 145–171.
Baltes, P. B., Reese, H. W., & Nesselroade, J. R. (1977). Life-span
developmental psychology: Introduction to research methods. Monterey,
CA: Brooks/Cole.
Barnard, K. (1981). Closing. Birth defects: Original articles series,
17(6), 285–288.
Beck, N. C., Siegel, L. J., Davidson, N. P., Kormeier, S., Breitenstein,
A., & Hall, D. (1980). The prediction of pregnancy outcome: Maternal
preparation, anxiety, and attitudinal sets. Journal of Psychosomatic
Research, 24, 343–351.
Beeson, D., & Douglas, R. (1983). Prenatal diagnosis of fetal disorders,
Part I: Technological capabilities. Birth, 10, 227-232.
Beeson, D., Douglas, R., & Lunsford, T. F. (1983). Prenatal diagnosis of
fetal disorders, Part II: Issues and implications. Birth, 10, 233-241.
Belsky, J., Spanier, G. B., & Rovine, M. (1983). Stability and change in
marriage across the transition to parenthood. Journal of Marriage and
124
the Family, 45, 567-577.
Bibring, G. (1959). Some considerations of the psychological processes in
pregnancy. The Psychoanalytic Study of the Child. 16, 113–121.
Bibring, G., Dwyer, T., Huntington, D., & Valenstein, A. (1961). A study
of the psychological processes in pregnancy and of the earliest
mother-child relationship. The Psychoanalytic Study of the Child, 16,
9–71.
Bossard, J. H. (1945). The law of family interaction. American Journal of
Sociology, 50, 292-294.
Brazelton, T. B. (1981). On Becoming a Family. New York: Delacorte Press.
Brown, M. A. (1984, May). Support, health, and stress in expectant
mothers and fathers. Paper presented at the Seventeenth Annual
Communicating Nursing Research Conference, Western Council on Higher
Education for Nursing, San Francisco.
Bryant, N., Cordaro, K., Grace, B., & Meier, E. P. (1979). We're All
Having the Baby, (rev. ed). Pittsburgh, PA: New World Complex.
Burstein, I., Kinch, R. A. H., & Stern, L. (1974). Anxiety, pregnancy,
labor and the neonate. American Journal of Obstetrics and Gynecology,
118(2), 195-199.
Campbell, D. T., & Stanley, J. C. (1963). Experimental and quasi
experimental designs for research. Chicago: Rand McNally.
Caplan, G. (1957). Psychological aspects of maternity care. American
Journal of Public Health, 47, 25–31.
Caplan, G. (1959). Concepts of Mental Health and Consultation.
Washington, DC: U. S. Government Printing Office.
Carmines, E. G., & Zeller, R. A. (1979). Reliability and validity
assessment. Beverly Hills: Sage.
125
Chodorow, N. (1978). The reproduction of mothering. Berkeley: University
of California Press.
Cohen, D. S. (1978). Fears during pregnancy. In K. A. Knafl & H. K. Grace
(Eds.) Families across the life cycle (pp. 166-180). Boston: Little,
Brown.
Cohen, J. (1977). Statistical power analysis for the behavioral sciences
(rev. ed.). New York: Academic Press.
Cohen, J., & Cohen, P. (1975). Applied multiple regression/correlation
analysis for the behavioral sciences. New York: John Wiley and Sons.
Cohen, R. L. (1966). Pregnancy stress and maternal perceptions of infant
endowment. Journal of Mental Subnormality, 12(22), 18–23.
Colman, A. D. (1969). Psychological state during first pregnancy.
American Journal of Orthopsychiatry, 39. 788-797.
Colman, A., & Colman, L. (1971). Pregnancy: The Psychological Experience.
New York: Herdes and Herdes.
Cook, T. D., & Campbell, D. T. (1979). Quasi-experimentation: Design and
analysis issues for field settings. Chicago: Rand McNally.
Cooper, C. R., Grotevant, H. D., & Condon, S. M. (1982). Methodological
challenges of selectivity in family interaction: Assessing temporal
patterns of individuation. Journal of Marriage and the Family, 44,
749–754.
Cranley, M. S. (1981a). Development of a tool for the measurement of
maternal attachment during pregnancy. Nursing Research, 30, 281–284.
Cranley, M. S. (1981b). Roots of attachment: The relationship of parents
with their unborn. Birth Defects: Original Article Series, 17, 59-83.
Curry, M. A. (1983). Variables related to adaptation to motherhood in
"normal" primiparous women. JOGN Nursing, 12, 115-121.

126
Davids, A., & DeVault, S. (1962). Maternal anxiety during pregnancy and
childbirth abnormalities. Psychosomatic Medicine, 24, 464–470.
Davids, A., Holden, R., & Gray, G. (1963). Maternal anxiety during
pregnancy and adequacy of mother and child adjustment eight months
following childbirth. Child Development, 34, 993-1002.
Peutsch, H. (1945). The Psychology of Women, Vol II: Motherhood. New
York: Grune and Stratton.
Doty, B. A. (1967). Relationships among attitudes in pregnancy and other
maternal characteristics. Journal of Genetic Psychology, lll, 203–217.
Dunn, J. & Kendrick, C. (1980). The arrival of a sibling: Changes in
patterns of interaction between mother and first-born child. Journal
of Child Psychology and Psychiatry, 21, 119-132.
Dunn, J., Kendrick, C., & MacNamee, R. (1981). The reaction of firstborn
children to the birth of a sibling: Mother's reports. Journal of Child
Psychology and Psychiatry, 22, 1-18.
Duvall, E. M. (1977). Marriage and Family Development, (5th ed.). New
York: J. B. Lippincott.
Elder, G. H., Jr. (1978). Approaches to social change and the family.
American Journal of Sociology, 84, Sl-S38.
Entwistle, D. R., & Doering, S. G. (1981). The first birth: A family
turning point. Baltimore: The Johns Hopkins University Press.
Erickson, M. T. (1967). Method for frequent assessment of symptomatology
during pregnancy. Psychological Reports, 20, 447-450.
Erickson, M. T. (1976). The influence of health factors on psychological
variables predicting complications of pregnancy, labor, and delivery.
Journal of Psychosomatic Research, 20, 21–24.

127
Evans, R. (1968). Needs identified among breast-feeding mothers. ANA
Clinical Sessions (pp. 162–171). New York: Appleton—Century—Crofts.
Eyres, S. J., Barnard, K. E., & Gray, C. A. (1979). Child health
assessment, Part III, 2–4 years: Final report Grant NU-00559.
Washington DC: DHEW, Division of Nursing.
Feiring, C., Lewis, M., & Jaskir, J. (1983). Birth of a sibling: Effect
on mother-firstborn child interaction. Journal of Developmental and
Behavioral Pediatrics, 4, 190-195.
Feldman, H. (1971). The effects of children on the family. In A. Michele
(Ed.), Family. Issues of Employed Women in Europe and America (pp. 107–
125). Leiden, The Netherlands: Brill.
Filsinger, E. E., & Wilson, M. R. (1983). Social anxiety and marital
adjustment. Family. Relations, 32, 513–519.
Frink, B. B., & Chally, P. (1984). Managing pain responses to Cesarean
childbirth. MCN-The American Journal of Maternal-Child Nursing. 2,
270–272.
Galloway, K. (1976). The uncertainty and stress of high risk pregnancy.
MCN-The American Journal of Maternal Child Nursing 1, 294–299.
Gilliss, C. L. (1983). The family as a unit of analysis: Strategies for
the nurse researcher. Advances in Nursing Science, 5(3), 50–59.
Glazer, G. (1980). Anxiety levels and concerns among pregnant women.
Research in Nursing and Health, 3, 107-113.
Goldstein, H. (1979). The design and analysis of longitudinal studies.
London: Academic Press.
Gorsuch, R. L., & Key, M. K. (1974). Abnormalities of pregnancy as a
function of anxiety and life stress. Psychosomatic Medicine, 26, 352
362.

128
Griffith, S. (1976). Pregnancy as an event with crisis potential for
marital partners: A study of interpersonal needs. JOGN Nursing, 5(6),
35–38.
Grimm, E. R. (1961). Psychological tension in pregnancy. Psychosomatic
Medicine, 23, 520–525.
Grimm, E. R., & Venet, W. R. (1966). The relationship of emotional
adjustment and attitudes to the course and outcome of pregnancy.
Psychosomatic Medicine, 28, 34-49.
Grossman, F. K., Eichler, L. S., & Winickoff, S. A. (1980). Pregnancy.
Birth, and Parenthood. San Francisco: Jossey-Bass.
Grubb, C. A. (1980). Perceptions of time by multiparous women in relation
to themselves and others during the first postpartal month. Maternal
Child Nursing Journal, 9, 225–331.
Gruis, M. (1977). Beyond maternity: Postpartum concerns of mothers. MCN
The American Journal of Maternal-Child Nursing, 2, 182-18°.
Hadley, T., Jacob, T., Milliones, J., Caplan, J., & Spitz, D. (1974). The
relationship between family developmental crisis and the appearance of
symptoms in a family member. Family Process, 13, 207-214.
Harriman, L. C. (1983). Personal and marital changes accompanying
parenthood. Family. Relations, 32, 387–394.
Hart, G. (1980). Maternal attitudes in prepared and unprepared Cesarean
deliveries. JOGN Nursing, 9, 243–245.
Heinstein, M. I. (1967). Expressed attitudes and feelings of pregnant
women and their relations to physical complications of pregnancy.
Merrill-Palmer Quarterly, 13, 217-236.
Henning, E., Martoglio, G., Quita, M., Reinbrecht, J., & Strickland, M.
(1967). A dynamic nursing appraisal of the puerperium. In N. Lytle
129
(Ed.), Maternal health nursing (pp. 153–163). Dubuque, IA: William 9.
Brown.
Hill, R., & Rodger, R. H. (1964). The developmental approach. In H. I.
Christensen (Ed.), Handbook of marriage and the family (PP. 171–211).
Chicago: Rand McNally.
Hillard, P. A. (1983, June). The second time around. Parents, pp. 76–78.
Hoffman, L. W. (1977). Changes in family roles, socialization, and sex
differences. American Psychologist, 32, 644–658.
Hollingshead, A. B. (1975). Four factor index of social status. Working
paper. Yale University.
Horan, M. (1984). Discomfort and pain during pregnancy. MCN-The American
Journal of Maternal-Child Nursing, 9, 267-269.
House Committee measure extends MCH coverage. (1983, November–December).
American Nurse, P. 2.
Jacobs, B. S., . & Moss, H. A. (1976). Birth order and sex of sibling as
determinants of mother-infant interaction. Child Development, 47, 315
322.
Jarrahi–Zadeh, A., Kane, F. J., Wandecastle, R. L., Lachenbruch, P. A., &
Ewing, J. A. (1969). Emotional and cognitive changes in pregnancy and
early puerperium. British Journal of Psychiatry, 115, 797-805.
Jenkins, P. (1976). Conflicts of a secundigravida. Maternal-Child Nursing
Journal, 5, 117-126.
Jimenez, S. L. M., & Jones, L. C. (1981). Pregnancy the second time
around. American Baby, 42, pp. 34, 48, 49.
Jimenez, S. M., Jones, L. C., & Jungman, R. G. (1979). Prenatal classes
for repeat parents: A distinct need. MCN-The American Journal cf.
Maternal-Child Nursing, 4, 305-308.

130
Kaij, L. Jacobson, L., & Nilsson, A. (1967). Postpartum mental disorder
in an unselected sample: The influence of parity. Journal of
Psychosomatic Research, 10, 317-322.
Kayiatos, R., Adams, J., & Gilman, B. (1984). The arrival of a rival:
Maternal perceptions of a sibling. Journal of Nurse-Midwifery, 29,
205–213.
Kelly, M., & Parsons, E. (1975). The mother's almanac. New York:
Doubleday.
Kendrick, C. & Dunn, J. (1980). Caring for a second baby: Effects on
interaction between mother and firstborn. Developmental Psychology,
16, 303–311.
Kirkpatrick, W. (1978). Adjustment to parenthood: A structural model.
Genetic Psychology Monographs, 98, 51-82.
Kreppner, K., Paulsen, S., & Schuetze, Y. (1982). Infant and family
development: From triads to tetrads. Human Development, 25, 373-391.
Lamb, M.E. (1979). The effects of the social context on dyadic social
interaction. In M. E. Lamb, S. J. Suomi, & G. R. Stephenson (Eds.),
Social Interaction Analysis. Madison: University of Wisconsin Press.
LaRossa, R. (1983). The transition to parenthood and the social reality
of time. Journal of Marriage and the Family, 45, 579–589.
LaRossa, R. & LaRossa, M. M. (1981). Transition to parenthood-how infants
change families. Beverly Hills: Sage.
Larsen, W. L. (1966). Stresses of the childbearing year. American Journal
cf. Public Health, 56(1), 32–36.
Laukaran, W. H., & Vanden Berg, B. J. (1980). The relationship of maternal
attitude to pregnancy outcomes and obstetric complications. American
Journal of Obstetrics and Gynecology, 136, 374-379.
131
Lederman, E., Lederman, R. P., Work, B. A., & McCann, D. S. (1981).
Maternal psychological and physiologic correlates of fetal-newborn
health status. American Journal of Obstetrics and Gynecology, 132,956–959.
Lederman, R. P. (1984a). Anxiety and conflict in pregnancy: Relationship
to maternal health status. In H. H. Werley & J. J. Fitzpatrick (Eds.),
Annual review of nursing research: Vol. 2 (pp. 28–61). New York:
Springer.
Lederman, R. P. (1984b). Psychosocial Adaptation in Pregnancy. New York:
Prentice-Hall.
Lederman, R., & Lederman, E. (1977, December). The development of a
prenatal self-evaluation questionnaire for the measurement of seven
psychological dimensions. Paper presented at the meeting of the
Council of Nurse Researchers, San Antonio, TX.
Lederman, R. P., Lederman, E., Work, B. A., & McCann, D. S. (1978a). The
relationship of maternal anxiety, plasma catecholamines, and plasma
cortisol to progress in labor. American Journal of Obstetrics and
Gynecology, 132, 495-501.
Lederman, R., Lederman, E., Work, B. A., & McCann, D. S. (1978b).
Relationship of psychological factors in pregnancy to progress in
labor. Nursing Research, 28, 94-97.
Lederman, R. P., Lederman, E., Work, B. A., & McCann, D. S. (1981). The
relationship of maternal prenatal development to progress in 1abor and
fetal-newborn health. Birth Defects: Original Articles Series, 17(6),
5–28.
Lederman, R. P., Weingarten, C. T., & Lederman, E. (1981). Postpartum
self-evaluation questionnaire: Measures of maternal adaptation. In

132
Birth Defects: Original Articles Series, 17(6), 201-231.
Legg, C., Sherick, I., & Wadland, W. (1974). Reaction of preschool
children to the birth of a sibling. Child Psychiatry and Human
Development, 5(1), 3–39.
Leifer, M. (1977). Psychological changes accompanying pregnancy and
motherhood. Genetic Psychology. Monographs, 95, 55-96.
Leifer, M. (1980). Pregnancy. Signs: Journal of Women in Culture and
Society, 5, 754–765.
Lewis, R. A., & Spanier, G. B. (1979). Theorizing about the quality and
stability of marriage. In W. R. Burr, R. Hill, F. I. Nye, & I. L.
Reiss (Eds.) Contemporary theories about the family, Vol. 1 (pp. 268–
294). New York: The Free Press.
Light, H. K., & Fenster, C. (1974). Maternal concerns during pregnancy.
American Journal of Obstetrics and Gynecology, 118(1), 46–50.
Lipson, J. G. (1984). Repeat Cesarean births: Social and psychological
issues. JOGN Nursing, 13, 157–162.
Locke, H. J., & Wallace, K. M. (1959). Marital-adjustment and predication
tests: Their reliability and validity. Marriage and Family Living, 21,
251–255.
Lubin, B., Gardener, S. H., & Roth, A. (1975). Mood and somatic symptoms
during pregnancy. Psychomatic Medicine, 37, 136-146.
Lynch, A. (1982). Maternal stress following the birth of a second child.
In M. H. Klaus, & M. D. Robertson (Eds.), Birth, Interaction, and
Attachment (pp 61-66). Skillman, NJ: Johnson and Johnson.
Malinowski, J. S. (1979). Answering a child's questions about sex and a
new baby. American Journal of Nursing, 79, 1965–1968.

133
Magrabi, F. M., & Marshall, W. H. (1965). Family developmental tasks: A
research model. Journal of Marriage and the Family, 27, 454-461.
Martell, L. K., & Mitchell, S. K. (1984). Rubin's "puerperal change"
reconsidered. JOGN Nursing, 13, 145-149.
Marymee, M. (1984, February 5). Kaiser foresees its biggest growth
outside already saturated Bay Area. The Herald (Available from Sparks
Newspapers, Danville, CA), p. 35.
Mattingly, E. B. (1983, October). Motherhood the second time around.
American Baby, pp. 18, 23.
McDonald, R. (1968). The role of emotional factors in obstetric
complications: A review. Psychosomatic Medicine, 30, 222-237.
McDonald, R. L., & Christakos, A. C. (1963). Relationship of emotional
adjustment during pregnancy to obstetric complications. American
Sournal of Obstetrics and Gynecology, 86, 341-348.
McKechnie, J. L. (Ed.) (1975). Webster's new twentieth century dictionary
(2nd ed.). Springfield, MA: G. & C. Merriam.
Mercer, R. T. (1979). She's a multip...she knows the ropes. MCN-The
American Journal of Maternal-Child Nursing, 4, 301-304.
Mercer, R. T. (1981). A theoretical framework for studying factors that
impact on the maternal role. Nursing Research, 30, 73–77.
Mercer, R. T., Hackley, K. C., & Bostrom, A. (1982). Factors having an
impact on maternal role attainment the first year of motherhood Grant
MC-R-060435–03. Unpublished data. Rockville, MD: DHHS, Bureau of
Community Health Services.
Merkatz, R. (1978). Prolonged hospitalization of pregnant women: The
effects on the family. Birth and the Family. Journal, 5, 204-206.
134
Miller, B. C., Rollins, B. C., & Thomas, D. L. (1982). On methods of
studying marriages and families. Journal of Marriage and the Family,
44, 851–873.
Miller, B. C., & Sollie, D. L. (1980). Normal stresses during the
transition to parenthood. Family Relations, 29, 459–465.
Miller, S. (1984, May). Change in the social support network during role
transition: A study of child-bearing women. Poster session Presented
at the Seventeenth Annual Communicating Nursing Research Conference,
Western Council on Higher Education for Nursing, San Francisco.
Monthly Vital Statistics Report. (1983, December 29). 32(Suppl. 9), 1-40.
Moore, D. S. (1983). Prepared childbirth and marital satisfaction during
the antepartum and postpartum periods. Nursing Research, 32, 73–79.
Moss, J. R. (1981). Concerns of multiparas on the third postpartum day.
JOGN Nursing, 10, 421-424.
Nie, N. H., Hull, C. H., Jenkins, J. G., Steinbrenner, K., & Bent, D.
(1975). S. P. S.S. (2nd ed.). New York: McGraw-Hill.
Nock, S. L. (1979). The family life cycle: Empirical or conceptual tool?
Journal of Marriage and the Family, 41. 15–26.
Norbeck, J. S., & Tilden, W. P. (1983). Psychological and social factors
in complications of pregnancy: A prospective multivariate approach.
Journal of Health and Social Behavior, 24, 30–46.
Norr, K. L., Block, C. R., Charles, A. G., & Meyering, S. (1980). The
second time around: Parity and birth experience. JOGN Nursing, 9, 30–
36.
Norr, K., Block, C., Charles, A., Meyering, S., & Meyers, E. (1977).
Explaining pain and enjoyment in childbirth. Journal of Health and
Social Behavior, 18, 260–275.

135
Nye, F. I. (1979). Choice, exchange, and the family. In W. R. Burr, R.
Hill, F. I. Nye, & I. L. Reiss (Eds.), Contemporary theories about the
family: Vol II. (pp. 1–41). New York: Free Press.
Olin, L. (1983). Anxiety in pregnancy: A comparison of primiparas and
multiparas. Dissertation Abstracts International, 44, 2256B.
(University Microfilms No. DA8326147.)
Parke, R. D., Power, T. G., Tinsley, B. R., & Hymel, S. (1979). The
father's role in the family system. Seminars in Perinatology, 3, 25
33.
Peterson, G. H., Mehl, L. S., & Leiderman, P. H. (1979). The role of some
birth-related variables in father attachment. American Journal of
Orthopsychiatry, 49, 330–338.
Pistrang, N. (1984). Women's work involvement and experience of new
motherhood. Journal of Marriage and the Family, 46, 433–447.
Powell, M. L. (1981). Parental management of sibling interactions. In
Assessment and Management of Developmental Changes and Problems in
Children (2nd ed). St. Louis: C. W. Mosby.
Rankin, D. J. (1981). Marital adjustment of couples with zero, one, or
two children. Dissertation Abstracts International, 42, 139–B.
(University Microfilms No. 81 14146).
Rankin, E. A. D., & Campbell, N. D. (1983). Perception of relationship
changes during third trimester of pregnancy. Issues in Health Care of
Women, 6, 351–359.
Richardson, P. (1981). Women's perceptions of their important dyadic
relationships during pregnancy. Maternal-Child Nursing Journal, 10,
159–174.
136
Richardson, P. (1982). Significant relationships and their impact on
childbearing: A review. Maternal-Child Nursing Journal, 11, 17-40.
Richardson, P. (1983a). Women's perceptions of change in relationships
shared with children during pregnancy. Maternal-Child Nursing Journal,
12, 75–88.
Richardson, P. (1983b). Women's perceptions of change in relationships
shared with their husbands during pregnancy. Maternal-Child Nursing
sjournal, 12, 1-19.
Rollings, E. M., & Nye, F. I. (1979). Wife—mother employment, family, and
society. In W. R. Burr, R. Hill, F. I. Nye, & I. L. Reiss (Eds.),
Contemporary theories about the family: Vol I (pp. 203–226). New York:
The Free Press.
Rowe, G. P. (1981). The developmental conceptual framework to the study
of the family. In F. I. Nye, & F. M. Berardo (Eds.), Emerging
Conceptual Frameworks in Family. Analysis (pp. 198-222). New York:
Praeger.
Rubin, R. (1967). Attainment of the maternal role, Parts I & II.Nursing
Research, 16, 237-245, 342–345.
Rubin, R. (1970). Cognitive style in pregnancy. American Journal of
Nursing, 70, 502-508.
Rubin, R. (1975). Maternal tasks in pregnancy. Maternal-Child Nursing
Journal, 4, 143-153.
Rubin, R. (1984). Maternal identity and the maternal experience. New
York: Springer.
Sammons, L. N. (1981). Use of field work method to examine the impact of
the newborn on older siblings. Unpublished manuscript, University of
California, School of Nursing, San Francisco.
137
Sammons, L. N. (1983). Factors affecting perceived impact of newborns on
older siblings. Networking (Available from P.O.B. 619, Bowie, MD
20715), 1(4), 1.
Schaie, K. W. (1965). A general model for the study of developmental
problems. Psychological Bulletin, 64, 92–107.
Schaie, K. W. (1973). Methodological problems in descriptive
developmental research on adulthood and aging. In J. R. Nesselroade, &
H. W. Reese (Eds.), Life-span developmental psychology: Methodological
issues. New York: Academic Press.
Shearer, M. H., & Bunnin, N. (1983). Childbirth educators in the 1980's:
A survey of 25 veterans. Birth, 10, 251-258.
Shereshefsky, M. P., & Yarrow, L. (1973). Psychological aspects of a
first pregnancy and early postnatal adaptation. New York: Raven Press.
Spanier, G. (1976). Measuring dyadic adjustment: New scales for assessing
the quality of marriage and similar dyads. Journal of Marriage and the
Family, 2, 15–28.
Spanier, G., Sauer, W., & Larzelere, R. (1979). An empirical evaluation
of the family life cycle. Journal of Marriage and the Family, 41, 27
38.
Spanier, G. B., & Thompson, L. (1982). A confirmatory analysis of the
Dyadic Adjustment Scale. Journal of Marriage and the Family. A4, 731–
738.
Spielberger, C. D. (1976). The nature and measurement of anxiety. In C.
D. Spielberger, & R. Diaz-Guerrero (Eds.), Cross-cultural anxiety. New
York: John Wiley and Sons.
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Wagg, P. R., & Jacobs,
G. A. (1983). Manual for the State-Trait Anxiety. Inventory (Form Y).

138
Palo Alto, CA: Consulting Psychologists Press.
SPSS Inc. (1983). SPSS-X User's Guide. Chicago: McGraw-Hill.
Straker, G., & Jacobson, R. (1979). A study of the relationship betwen
family interaction and individual symptomatology over time. Family
Process, 18, 443–450.
Summner, G., & Fritsch, J. (1977). Postnatal parental concerns: The first
six weeks of life. JOGN Nursing, 6, 27–32.
Sweet, P. (1979). Prenatal classes for children. MCN-The American Journal
of Maternal-Child Nursing, 4, 82-83.
Taylor, M . K., & Kogan, K. L. (1973). Effects of birth of a sibling on
mother-child interactions. Child Psychiatry and Human Development. 4,
53–58.
Terkelsen, K. G. (1980). Toward a theory of the family life cycle. In E.
A. Carter, & M. McGoldrick (Eds.) The Family Life Cycle: A Framework
for Family. Therapy. New York: Gardner Press.
Tilden, W. P. (1980). A developmental conceptual framework for the
maturational crisis of pregnancy. Western Journal of Nursing Research,
2, 667–682.
Tilden, W. P. (1984). The relation of selected psychosocial variables to
single status of adult women during pregnancy. Nursing Research, 33,
102–107.
Ulrich, S. C. (1982). Psychosocial work of a secundigravida in relation
to acceptance of her baby. Maternal-Child Nursing Journal, ll 1-9.
Valentine, D. P. (1982). The experience of pregnancy: A developmental
process. Family. Relations, 31, 243-248.
Ventura, J. N. (1982). Parent coping behaviors, parent functioning, and
infant temperament characteristics. Nursing Research, 31, 269–273.

139
Westal, K. W. (1979). Siblings: Adapting to accommodate the neonate.
Issues in Health Care of Women, 1(4), 15–25.
Walker, B., & Erdman, A. (1984). Childbirth education programs: The
relationship between confidence and knowledge. Birth, 11, 103–108.
Wallin, P., & Riley, R. P. (1955). Reactions of mothers to pregnancy and
adjustment of offspring in infancy. In M. B. Sussman (Ed.), Marriage
and the Family (pp. 139–144). Cambridge: Houghton Mifflin.
Walz, B., & Rich, 0. J. (1983). Maternal tasks of taking—on a second
child in the postpartum period. Maternal-Child Nursing Journal, 12,
185–216.
Weaver, R. H., & Cranley, M. S. (1983). An exploration of paternal—fetal
attachment behavior. Nursing Research, 32, 68–72.
Westbrook, M. T. (1978a). The effect of the order of birth on a women's
experience of childbearing. Journal of Marriage and the Family, 40,
165–172.
Westbrook, M. T. (1978b). The reactions to child-bearing and early
maternal experience of women with differing marital relationships.
British Journal of Medical Psychology, 51, 191-199.
Yamamoto, K, & Kinney, D. (1976). Pregnant women's ratings of different
factors influencing psychological stress during pregnancy.
Psychological Reports, 39, 203-214.
Zax, M., Sameroff, A. J., & Farnum, J. E. (1975). Childbirth education,
maternal attitudes, and delivery. The American Journal of Obstetrics
and Gynecology, 123, 185-190.

Appendix A
Cover Sheet for T–l Packet
ºSECOND BABY PREGNANCY STUDY
PACKET #1
1. Please read and sign the top "Consent" form and place it in thereturn en velope. (You retain the Consent form labelle d "This is foryour records.")
2. Complete this packet of questionnaires within one week, if possible.Make sure you have checked both front and back sides of each page |Please d is regard extra lines and numbers in the far columns used foranalyzing results.
3. Return the packet, with one consent form, in the prepaid envelope.
4. You will receive a check for $5.00 with you r next packet in a bout 3months (or with in 4 weeks if you have a 1 ready del i v ere d or if you werein the group that only fills out only one set of forms.)
5. Question n aire s of ten don't let you t e l l the who le story, so pleasefeel free to make a d di ti on a 1 comments a long the way or a t the end thatclarify the way you feel. A page at the end is provided for thispurpose.
6. If you would like a copy of the results of the study when a vailable(around mid 1985) complete the form on the back page.
7. If you no longer wish to participate in this project, please checkhe re and return this sheet to me in the prepaid en v e l'ope. Pleasein dicate why you wish to withdraw:
Otherwise, I will be looking forward to your responses within a week orSO .
Thank you again for your most valuable help with this project
Lorrie Sammons, RN, NPDoctoral Candidate,University of California, San Franciscoc/o 2608 Campeche CourtSan Ramon, CA 94.583

Appendix B 141
UNIVERSITY OF CALIFORNIA, SAN FRANCISCO
BERKELEY - DAVIS • IRVINE • LOS ANCELES • RIVERSIDE • SAN DIECO - SAN FRANCISCO SANTA BARBARA • SANTA CRUZ
SCHOOL OF NURSING SAN FRANCISCO, CA LIFOR NIA 941 4 3
Department of Family Health Care NursingStudy No. 9334 21–01
CONSENT TO BE A RESEARCH SUBJECT
A) Lorrie Sammons, RN, NP, a nurse in the UCSF Graduate Nursing program, isstudying women during and after pregnancy with a second baby. I have beeninvited to be in this study.
B) If I agree to be in the study,1) I will fill out 1 or 2 sets of forms about my background, my feelings, andmy family relationships. These forms take less than an hour to complete athome. If I forget to complete them, I will receive a phone call and/or aletter as a reminder.2) A few (about 1 in 12) of the women completing questionnaires will be askedby telephone if they would agree to being interviewed for one hour, at a timeand location of their choice. The inter view is about the feelings, symptoms,and family relationships during second pregnancy. If I am asked, I agree tobe inter viewed (Please check) Yes; No. If I say "yes" now, I may changemy mind later.3) Mrs. Sammons may also review my medical records.
C) There should be no risk to me unless some of the items in the questionnaires make me feel upset or concerned about emotional or family changes. IfI feel upset, I can a) contact my regular Obstetrical doctor or nurse, or b)contact Mrs. Sammons (666–4695) to discuss these feelings. I may choose not toanswer any questions I do not want to answer.
My privacy will be protected by separating names from responses. Confidentiality will be protected as far as possible under the law.
D) There will be no direct benefit to me from participating in this study. Itis hoped this study will improve understanding of the emotional, physical andfamily changes of second pregnancy so that clinicians can be more helpful tofamilies in the future.
E) I will receive $5 for each packet of questionnaires or interview.
F) I have talked with Lorrie Sammons, RN, about this study, who has offered toanswer any questions I may have at 666–4695. In addition, I may contact theCommittee on Human Research, which is concerned with the protection of volunteers in research projects between 8 and 5, Monday–Friday at (415) 666–1814.
G) I have received a copy of this form to keep. My participation is voluntaryand I have the right to decline to participate or withdraw at any pointwithout jeopardy to my health care.
Signature of participant Date
This copy is to be returned with completed questionnaires.

142Appendix C
BACKGROUND INFORMATION In O :
T- z- 3- tº- 5- 6
Today's date: Baby due date /delivery date: —■-
— —9.9Your age 10, 11
Check your occupation category (do not count the 3 months before& after delivery if different from your usual activity).
A. House wife: O I.B. Work outside home (either full or part-time) _12
If "B": do you consider employment to be "Job" or "Career" ? - 13Nature of work: T T14, 15Number of hours spent at employment-related work, preparation &commute in typical recent week: 16, 17If you usually have outside employment, do you plan to return towork 2 No . Yes , when 2 . Completely undecided . 18
19Your number of years of schooling (High school = 12): — —20, 21
Circle which comes closest to describing your race or ethnicgroup : 0. Hispanic 1. American Indian or Alaskan Native
2. Black 3. Asian or Pacific Islander4. White, not of Hispanic origin5. Other. Please describe —22
Circle your religious preference: 0. Roman Catholic 1. Jewish2. Pro testant 3. LDS 4. Jehovah's Witness 5. No preference6. Other: Please describe _23
Number of brothers & sisters in your own family besides yourself: _24If oldest child = #1, what is the number of your birth order?_ —25
Number of previous pregnancies: _ 26, 27Misc arriages: Abortions: 28, 29
Age of your child living at home : Years +Months _ _30, 31
Sex of your older child : Male Female —32
Number of hours first born away from mother in typical week (includeall separations, e.g. child's school, child's activities,child visiting relatives, child care, etc.): _33
Relationship with children's father : Married Not married _34
Length of marriage/relationship in years:-
_35, 36
Total number of children desired by you :_ — 37by your husband : I38
I39Number of people living in household besides you, spouse, first born l!0. ly(and newborn , if arrived): Describe relationship :
- -0, 141
Husband's age:-
_42,43
Husband's racial/ethnic group0. Hispanic 1. American Indian or Alaskan Native
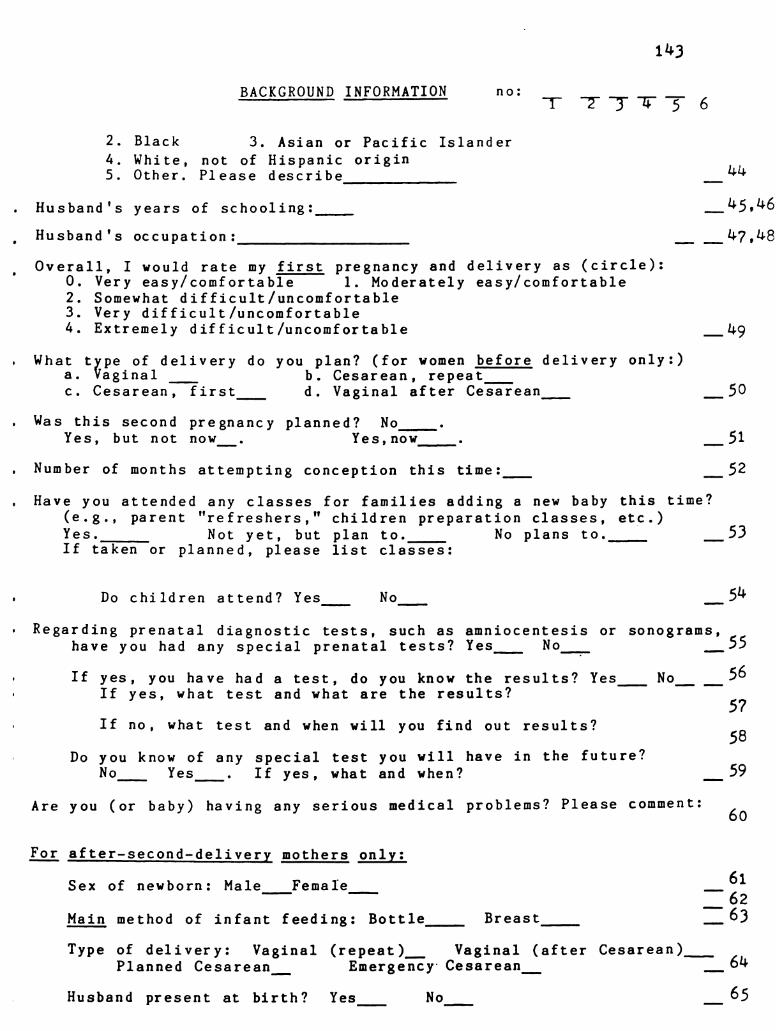
1143
BACKGROUND INFORMATION n O : -
+ -■ - -3 + -■ - 6
2. Black 3. Asian or Pacific Island er4. White, not of Hispanic origin5. Other. Please describe _ !!!,
Husband's years of school ing: _45,46
Husband's occupation : — — 47,48
Overall, I would rate my first pregnancy and delivery as (circle) :0. Very easy/comfor table 1. Moderately easy/comfortable2. Somewhat difficult/un comfortable3. Very difficult /uncomfortable4. Extremely difficult/uncomfor table — 49
What *WP: of delivery do you plan? (for women before delivery only : )a . Vaginal b. Cesarea n, repeatc. Cesar ean , first d. Vaginal after Cesare an — 50
Was this second pregnancy planne d ? No-
Yes, but not now . Yes, now-
— 51
Number of months at tempting conception this time: — 52
Have you at tended any classes for families a da ing a new baby this time?(e.g., parent "re freshers," children preparation classes, etc.)Yes. Not yet, but plan to . No plans to . 53If taken or planned, please list classes:
Do children at tend ? Yes No _54
Regarding prenatal diagnostic tests, such as amniocentesis or sonograms,have you had any special pre natal tests 2 Yes No _55
If yes, you have had a test, do you know the results 2 Yes No 3%If yes, what test and what are the results 2 57
If no , what test and when will you find out results 7 58Do you know of any special test you will have in the future?
No Yes . If yes, what and when 2 _59
Are you ( or baby) having any serious medical problems ? Please comment: 60
For after-second-delivery mothers only:
Sex of new born : Male Female –;Main method of infant feeding : Bottle Breast T 63
Type of delivery: Vaginal (repeat)_ Waginal (after Cesarean)Planned Cesare an Emergency Cesare an T 64
Husband present at birth 2 Yes No 65

Appendix D
SELF-EVALUATION QUESTIONNAIRE
DIRECTIONS: A number of statements which people have used todescribe themselves are given below. Read each statement and then '', /.
blacken in the appropriate circle to the right of the Statement to indi- 12. K. °, ^*,cate how you feel right now, that is, at this moment. There are no right * . , 72, '',or wrong answers. Do not spend too much time on any one statement ”, °, %, ^2,but give the answer which seems to describe your present feelings best. 2 *, *, *.
!. I feel calm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . j\ } @ 3
2. I feel secure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . T 3, 3, 3
3. I am tense . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3) @ 3) 3,
4. I feel strained . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 : 3 7
5. I feel at case . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $ 3 5, 2
6. I feel upset . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . © 3, § 3
7. I am presently worrying over possible misfortunes . . . . . . . . . . . . . . () (? 3) 3
8. I feel satisfied . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . © $ 3, 3.
9. I feel frightened . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3) 3 3, 3
10. I feel comfortable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . T. G. 3, 7.
ll. I feel self-confident . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 (?) 3, 2
12. I feel nervous . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . @ 3, 3) (3)
13. I am jittery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . o a 3 &14. I feel indecisive . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3) (? 3) (3)
15. I am relaxed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . G) @ 3) (3)
16. I feel content . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . G.) (3) 3) (3)
17. I am worried . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . G) (?) G) (3)
18. I feel confused . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Q) @ G) 3)
19. I feel steady . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Q) @ 3) (3)
20. I feel pleasant . . . . . . . . . . . . . . . . . . . . . . . . . . * . . . . . . . . . . . . . . . . . . . . . () () (3) (3)
@ Consulting Psychologists Press577 College Avenue, Palo Alto, California 94306
Reproduced by special permission of the Publisher, ConsultingPsychologists Press, Inc., Palo Alto, CA 94.306 from the STAI-yby Charles Spielberger and Associates Copyright 1983. Furtherreproduction is prohibited without the Publisher's consent.

11:5Appendix E
SELF-EVALUATION QUESTIONNAIRESTAI Form Y-2
DIRECTIONS: A number of statements which people have used to
describe themselves are given below. Read each statement and then º, º,blacken in the appropriate circle to the right of the statement to in- º, W. %,dicate how you generally feel. There are no right or wrong answers. Do 5. 1. %. f_ ‘.not spend too much time on any one statement but give the answer *1, %. *z, ”,which seems to describe how you generally feel. 4 *■ , *. 1. 'j.
21. I feel pleasant . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (i) (? (3, 3.
22. I feel nervous and restless . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (Ö (2, 3, 2
23. I feel satisfied with myself . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (i) (? 3, 2.
24. I wish I could be as happy as others seem to be . . . . . . . . . . . . . . . . . 1 *, 3, 2
25. I feel like a failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 : 2 3 (3.
26. I feel rested . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1, 2 3, 2
27. I am “calm, Cool, and collected” . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (i) 2. 3. 2.
28. I feel that difficulties are piling up so that I cannot overcome them (i) 3, 3 (3)
29. I worry too much over something that really doesn't matter . . . . . . © 3, 3. 2.
30. I am happy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . © (? 3 3
31. I have disturbing thoughts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . () (? 3, 3)
32. I lack self-confidence . . . . . . . . . . . . . . . . . . . . . .- - - - - - - - - - - - - - - - -
@ 3, 3, 2)
33. I feel secure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (i) @ 3 (3)
34. I make decisions casily . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . © (?) 3 (3)
35. I feel inadequate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3) 3, 3) (3)
36. I am content . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 (?) 3 (3)
37. Some unimportant thought runs through my mind and bothers me 3) (?) 3 (3)
38. I take disappointments so keenly that I can't put them out of my
mind . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . @ 3 3, 3)
39. I am a steady person . . . . . . . . . . . . . . . . . . . . . . . . . . . . . * - - - - - - - - - - - - 3) 3 3) (3)
40. I get in a state of tension or turmoil as I think over my recent concerns
and interests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . G) @ (3, 3)
Reproduced by special permission of the Publisher, ConsultingPsychologists Press, Inc., Palo Alto, CA 94.306 from the STAI-Yby Charles spielberger and Associates Copyright 1983. Furtherreproduction is prohibited without the Publisher's consent.

146
Appendix F
Spanier Dyadic Adjustment Scale
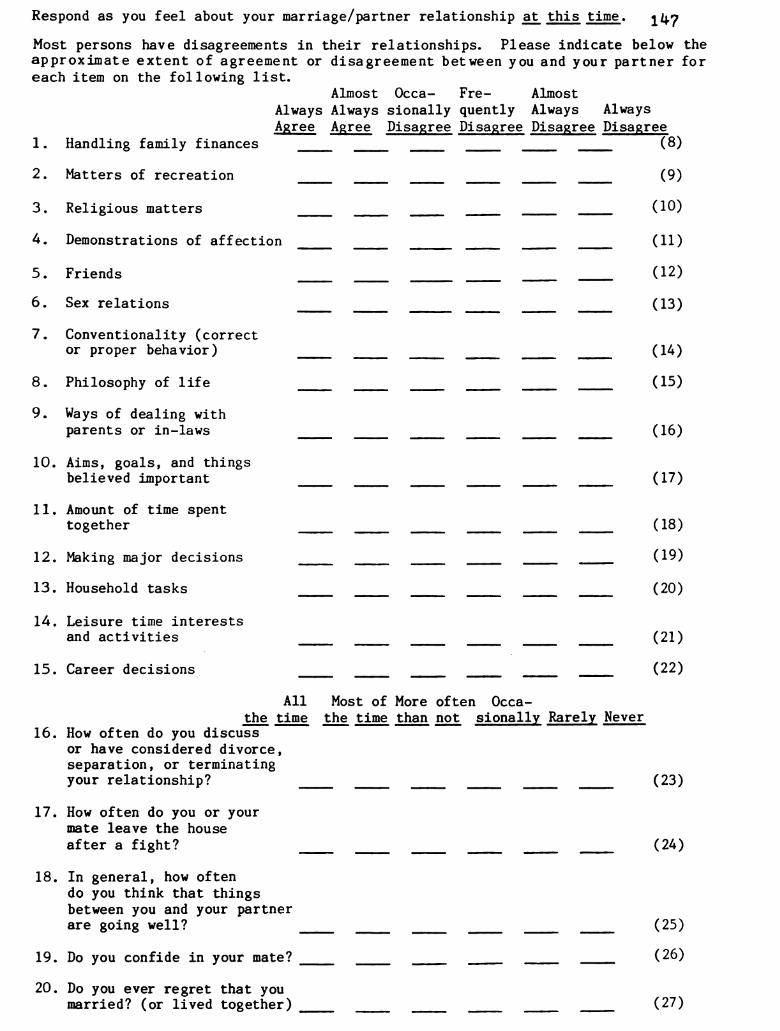
Respond as you feel about your marriage/partner relationship at this time. 1 l;7
Most persons have disagreements in their relationships. Please indicate below theapproximate extent of agreement or disagreement between you and your partner foreach item on the following list.
Almost Occa— Fre— Almost
Always Always sionally quently Always AlwaysAgree Agree Disagree Disagree Disagree Disagree
1. Handling family finances (8)
2. Matters of recreation (9)
3. Religious matters (10)
4. Demonstrations of affection (11)
5. Friends (12)
6. Sex relations (13)
7. Conventionality (corrector proper behavior) (14)
8. Philosophy of life (15)
9. Ways of dealing withparents or in-laws (16)
10. Aims, goals, and thingsbelieved important (17)
11. Amount of time spenttogether (18)
12. Making major decisions (19)
13. Household tasks (20)
14. Leisure time interestsand activities (21)
15. Career decisions (22)
All Most of More often 0ccathe time the time than not sidnally Rarely Never
16. How often do you discussor have considered divorce,separation, or terminatingyour relationship? (23)
17. How often do you or yourmate leave the house
after a fight? (24)
18. In general, how oftendo you think that thingsbetween you and your partnerare going well? (25)
19. Do you confide in your mate? (26)
20. Do you ever regret that youmarried? (or lived together) (27)

All Most of More often Occathe time the time than not sionally Rarely Never
21. How often do you and your 1 l;8partner quarrel? (28)
22. How often do you and your mate"get on each other's nerves?" (29)
Every Almost OccaDay Every Day sionally Rarely Never
23. Do you kiss your mate? (30)
All of Most of Some of Very few None ofthem them them of them them
24. Do you and your mate engage inoutside interests together? (31)
How often would you say the following events occur between you and your mate?Less than Once or Once or
once a twice a twice a Once a MoreNever month month week day often
25. Have a stimulatingexchange of ideas (32)
26. Laugh together (33)
27. Calmly discuss something (34)
28. Work together on a project (35)
These are some things about which couples sometimes agree and sometime disagree.Indicate if either item below caused differences of opinions or were problems inyour relationship during the past few weeks. (Check yes or no)
Yes. No.29. Being too tired for sex. (36)
30. Not showing love. (37)
31. The dots on the following line represent different degrees of happiness in yourrelationship. The middle point, "happy," represents the degree of happiness ofmost relationships. Please circle the dot which best describes the degree ofhappiness, all things considered, of your relationship.
1 2 3 4 5 6O O O o o o ©
Extremely Fairly A Little Happy Very Extremely PerfectUnhappy Unhappy Unhappy Happy Happy (38)
32. Which of the following statements best describes how you feel about the futureof your relationship?
I want desperately for my relationship to succeed and would go to almost anylength to see that it does.
that it does.- - - -
I want very much for my relationship to succeed, and will do my fair share tosee that it does.
It would be nice if my relationship succeeded, but I can't do much more thanI am doing now to help it succeed.It would be nice if it succeeded, but I refuse to do any more than I am doingnow to keep the relationship going.My relationship can never succeed, and there is no more than I can do to keepthe relationship going. (39)
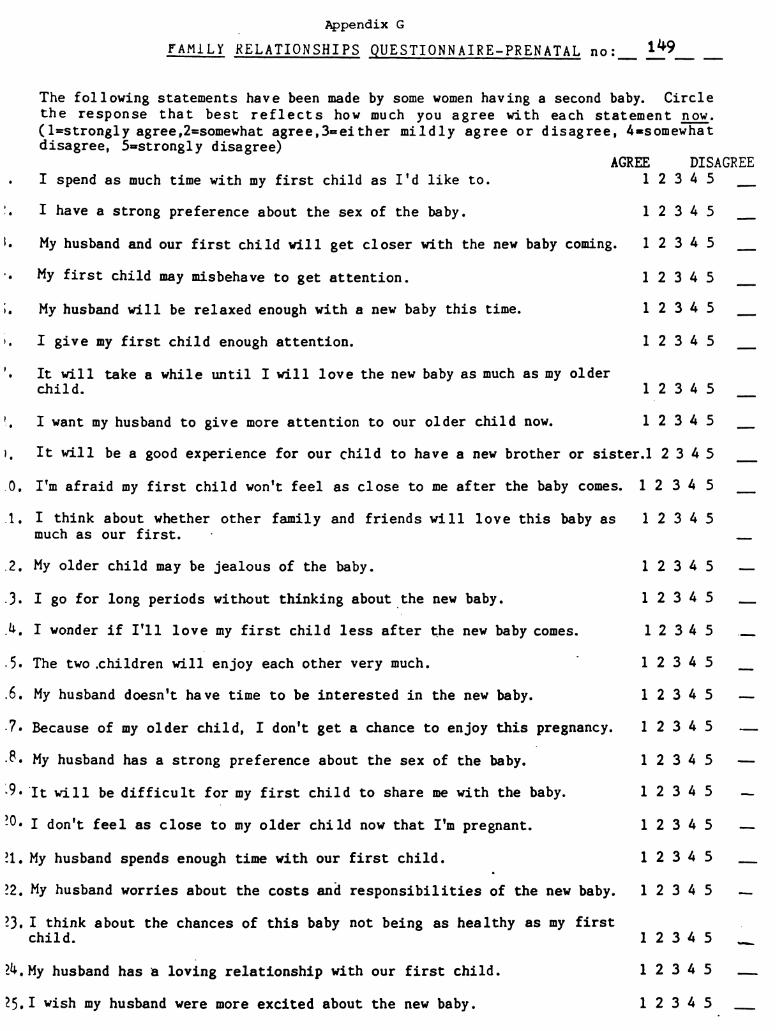
21.
22.
23.
Appendix G
Family RELATIONSHIPS QUESTIONNAIRE-PRENATAL no: ***
The following statements have been made by some women having a second baby.
disagree, 5=strongly disagree)
Circle
the response that best reflects how much you agree with each statement now.(1=Strongly agree,2=somewhat agree, 3= either mildly agree or disagree, 4=somewhat
AGREE
I spend as much time with my first child as I'd like to. 1 2
I have a strong preference about the sex of the baby. 1 2
My husband and our first child will get closer with the new baby coming. 1 2
My first child may misbehave to get attention. 1 2
My husband will be relaxed enough with a new baby this time. 1 2
I give my first child enough attention. 1 2
It will take a while until I will love the new baby as much as my olderchild. 1 2
1 2I want my husband to give more attention to our older child now.
DISAGREE3 4
3 4
3 4
3 4
3 4
5
It will be a good experience for our child to have a new brother or sister.1 2 3 4 5
I'm afraid my first child won't feel as close to me after the baby comes.
I think about whether other family and friends will love this baby asmuch as our first.
My older child may be jealous of the baby.
I go for long periods without thinking about the new baby.
I wonder if I'll love my first child less after the new baby comes.
The two children will enjoy each other very much.
My husband doesn't have time to be interested in the new baby.
Because of my older child, I don't get a chance to enjoy this pregnancy.
My husband has a strong preference about the sex of the baby.
It will be difficult for my first child to share me with the baby.
I don't feel as close to my older child now that I'm pregnant.
My husband spends enough time with our first child.
My husband worries about the costs and responsibilities of the new baby.
I think about the chances of this baby not being as healthy as my firstchild.
24. My husband has a loving relationship with our first child.
25. I wish my husband were more excited about the new baby.
1 2 3 4 5
1 2 3 4 5
1 2
1 2
3 4
3 4
3 4

Appendix H 150
FAMILY RELATIONSHIPS QUESTIONNAIRE-POSTPARTUM In O
The following statements have been made by some women who have had a second baby.Circle the response that best reflects how much you agree with each statement now.(1=Strongly agree,2=somewhat agree, 3=either mildly agree or disagree, 4=somewhatdisagree, 5=strongly disagree)
AGREE DISAGREE
! . I spend as much time with my first child as I would like to. 1 2 3 4 5
2. I think about whether other family and friends love this baby asmuch as our first. 1 2 3 4 5
3. My husband and our first child are getting closer now that the newbaby is here. 1 2 3 4 5
4. My husband doesn't seem to have time to spend with the new baby. 1 2 3 4 5
5. My older child is jealous of the baby. 1 2 3 4 5
5. It will take more time until I love the new baby as much as myolder child. 1 2 3 4 5
7. My husband has a loving relationship with our first child. 1 2 3 4 5
3. My husband is very excited about the new baby. 1 2 3 4 5
9. It is difficult for my first child to share me with the baby. 1 2 3 4 5
10. I'm sad the new baby does not get all my attention in the exclusiveway the first child did. 1 2 3 4 5
11. My husband spends enough time with our first child. 1 2 3 4 5
12. My husband worries about the costs and responsibilities of the newbaby. 1 2 3 4 5
13. Our older child acts in a very caring way towards the baby.-
1 2 3 4 5
1". My older child doesn't let me enjoy the baby. 1 2 3 4 5
15. I can handle the time demands of my new baby. 1 2 3 4 5
16. I don't feel as close to my older child now that the new baby is here. 1 2 3 4 5
17. My husband pays a lot of attention to the new baby. 1 2 3 4 5
18. My older child is enjoying being a big brother/sister. 1 2 3 4 5
19. I don't get enough time with the new baby. 1 2 3 4 5
20. My older child acts as though I don't love her/him as much as I usedto. 1 2 3 4 5
21. I want my husband to give more attention to our older child now. 1 2 3 4 5
22. My older child misbehaves to get my attention. 1 2 3 4 5
3) L. N. Sammors, 1984

Appendix I
SYMPTOM'S OF PREGNANCY CHECKLIST no ; – — — — — —
The following are sensations or discomforts of pregnancy sometimes described bywomen. Indicate how often you have experienced each item recently by circling thenumber that best reflects your experience: 0=rarely or not at all; 1=occasionally;2=fairly often; 3= very often to constantly. Use a ruler if needed.
Then, compare to last time. Indicate if you are experiencing the item more orless often than you did at the same month of your previous pregnancy, to the best ofyour memory: A=less than before; B– the same; C=more than before.
THIS PREGNANCY NOW COMPARED TO LAST PREGNANCYRARE/NONE CONSTANT NOW LESS SAME NOW MORE
backache O 1 2 3 A B C — — 9, 10
varicose veins 0 l 2 3 A B C — — 11 - 12
constipation O 1 2 3 A B C — — 13.1%diarrhea 0 1 2 3 A B C — — 15, 16dizziness O l 2 3 A B C — — 17, 18heartburn O l 2 3 A B C — — 19, 20
trouble sleeping 0 l 2 3 A B C- -
21, 22
bleeding O 1 2 3 A B C — — 23, 24depression O 1 2 3 A B C — — 25, 26appetite loss O 1 2 3 A B C _ _ 27, 28I■ lau Sea O l 2 3 A B C _ _ 29, 30painful intercourse 0 1 2 3 A B C
- -31, 32
shortness of breath 0 1 2 3 A B C - -33, 34
swollen legs/hands 0 l 2 3 A B C- -
35, 36tiredness O l 2 3 A B C _ _ 37, 38vomiting 0 1 2 3 A B C _ _ 39,40weakness O l 2 3 A B C — — 41,42
flushed feeling 0 1 2 3 A B C _ _ 43,44frequent urinating 0 l 2 3 A B C
- -l; 5, 196
cold hands/feet 0 1 2 3 A B C __ 47,48irritability 0 1 2 3 A B C _ _ 49, 50rapid weight gain 0 , 1 2 3 A B C _ _ 51, 52increased appetite 0 l 2 3 A B C - -
53,514heartpounding O 1 2 3 A B C - -
55, 56hemorrhoids O 1 2 3 A B C _ _ 57, 58anxiety 0 1 2 3 A B C __ 59,60headache 0 1 2 3 A B C __ 61.62breast discomfort 0 l 2 3 A B C - -
63,614groin/pelvic pain 0 1 2 3 A B C - -
65,66or pressure
If you are feelido vo: reve any i
ng symptoms differently than at this month of your last pregnanºdeas as to why? Please comment below or on the inside back cover.
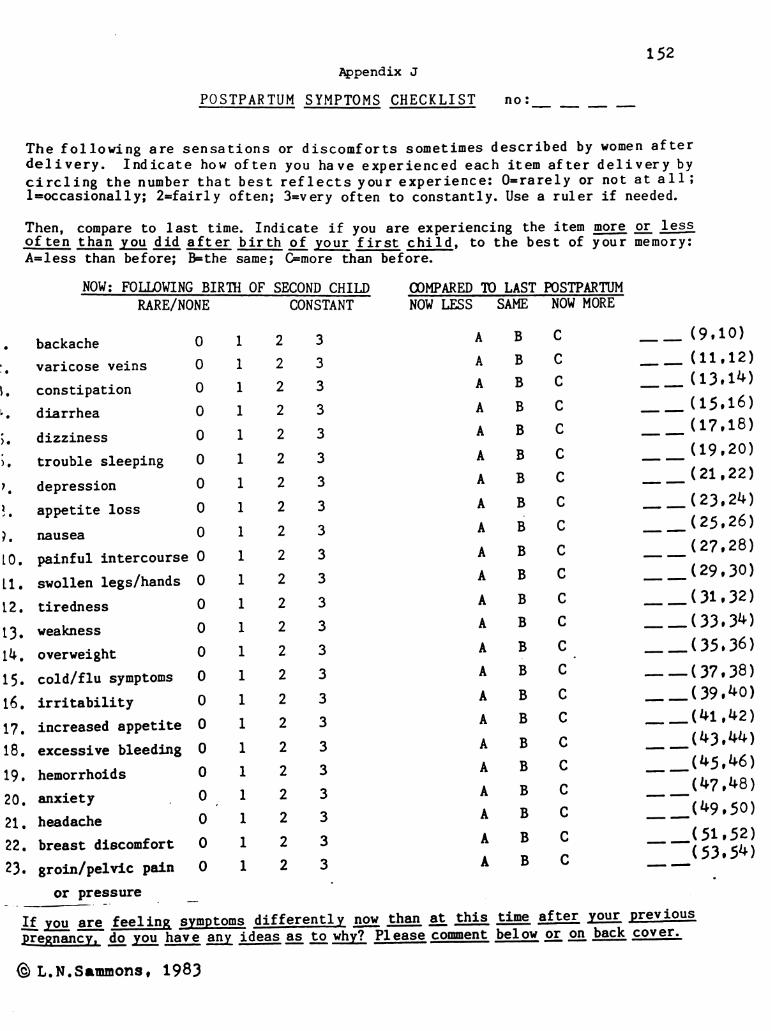
152
11.
13.
19.
20.
21.
22.
23.
If you are feeling symptoms differently n2g than at this time after your Previous
Appendix J
POSTPARTUM SYMPTOM'S CHECKLIST In O :
The following are sensations or discomforts sometimes described by women afterdelivery. Indicate how of ten you have experienced each item after delivery bycircling the number that best reflects your experience: 0= rarely or not at all ;1=occasionally; 2-fairly often; 3=very often to constantly. Use a ruler if needed.
º tº: to last time. Indicate if you are experiencing the item more ori lessen than you did after birth of your first child, to the best of your memory:A=less than before; B– the same; C=more than before.
NOW: FOLLOWING BIRTH OF SECOND CHILD COMPARED TO LAST POSTPARTUMRARE/NONE CONSTANT NOW LESS SAME NOW MORE
backache 0 1 2 3 A B C _ _ (9,10)varicose veins O l 2 3 A B C — — (11.12)
constipation O 1 2 3 A B C __ (13.1%)diarrhea 0 1 2 3 A B C __ (15,16)dizziness O l 2 3 A B C _ _ (17, 18)trouble sleeping O l 2 3 A B C _ _ (19.20)depression O 1 2 3 A B C __ (21, 22)appetite loss O l 2 3 A B C __ (23.2%)Ilau Sea O l 2 3 A B C __ (25,26)painful intercourse 0 l 2 3 A B C __ (27, 28)swollen legs/hands 0 l 2 3 A B C _ _ (29, 30)tiredness O 1 2 3 A B C — — (31 - 32)weakness O l 2 3 A B C — — (33.3%)
overweight O l 2 3 A B c __ (35, 36)cold/flu symptoms 0 l 2 3 A B C — — (37,38)irritability O l 2 3 A B C _ _ (39, 40)increased appetite 0 l 2 3 A B C _ _ (41,42)excessive bleeding 0 l 2 3 A B C __(43,44)hemorrhoids 0 1 2 3 A B C __(45,46)anxiety 0 1 2 3 A B C __(47,48)headache 0 1 2 3 A B C __(49.50)breast discomfort 0 1 2 3 A B C __(51, 52)groin/pelvic pain 0 1 2 3 A B C
-—' 53, 54)
or pressure
pregnancy, do you have any ideas as to why? Please comment below or on back cover:
(3) L. N. Sammons, 1983

Appendix K153
Recruitment Flier
HAVING ASECOND BABY? JUST DELIVERED YOUR SECOND?
You are invited to take part in a study of the emotions, symptoms andrelationships during second pregnancy.
What to do:
Complete a set of questionnaires in about 45 minutes at your convenience at homenow and again in 3 months. (All responses are treated anonymously and confidentially.)
What you will receive:1. $5.00 per set of questionnaires, in appreciation of the accommodation to your
your schedule.2. A summary of the results, if desired.
How to get more information:Complete the “Second Baby” card (attached, or available on drop-box at appt. desk)and place it in the yellow drop-box by the OB appointment desk or phone-in area.You will be contacted within a week.
If you are interested, DROP OFF THE CARD TODAY. Women in each month of pregnancy and first3 months after delivery are needed NOW.
Study conducted by Lorrie Sammons, RN, NP, Doctoral candidate, School of Nursing, University ofCalifornia, San Francisco (666-4695). Correspondence address: 2608 Campeche Court, San Ramon,California 94583.
T-“SECOND BABY PREGNANCY” card–,
ALL women who are pregnant with thier second baby or who delivered within 3 months are asked to respond. PLEASE COMPLETE
Would you be interested in completing a set of- -questionnaires about
the second pregnancy experience? THIS CARD
- - IDNO, because (please indicate why; you will NOT be contacted). . . TODAY!
DYES, My name:Baby due date/date delivered:Phone number(s) where I can be reached:Best times to call:
- t!
Address:
Q(GºDROPIN YELLOW Box by OB appointment desk or by phone-inarea TODAY or mail to Lorrie Sammons, RN, NP, 2608 CampecheCt., San Ramon CA 94583.

Appendix L- - - - -
Comments for T–l Packet
Is the re any thing you would like to comment on a bout emotions,physical sensations, or family relationships when having a secondb a by ?
Is there anything that you felt might be having a particularinfluence on you and your family during/after this pregnancy?
Are there any reactions to this set of question n aires you wouldlike to share 2
Please feel free to use the following space for any comments:
Thank you.
Complete the following only if you would like a copy of theresults of this study around mid 1985.
Name:Address:

155
Appendix M
Cover Sheet for T-2 Packet()
SECOND BABY PREGN ANC Y STUDY
PACKET #2
Thank you for completing the first packet of questionnaires. I am happy to be ableto enclose $5 in appreciation for your assistance.
Please complete this questionnaire this week and return it to me in the envelopeprovided. You should receive another $5 within four weeks. Please indicate if youhave a new address:
1. Today's date: Baby due date/delivery date: _(7)— (8.9)
2. Have their been any major changes in your lives in the last 3 months that mightaffect your emotions, symptoms, and family relationships other than pregnancy/delivery itself? If yes, please comment (use reverse if needed): (10)
3. Has there been any serious illness or complication for you or the baby? Ifyes, please comment here or on the reverse side: (11)
4. Did you attend any pregnancy related classes since completing the last packet?Yes No . (12)
If yes, did your first child attend? Yes No_. T(13)
5. Regarding prenatal diagnostic tests (e.g. amniocentesis, sonogram), did you haveany tests since completing the last packet? Yes No_. If yes, what kind? (14)
6. Did you get the results of any prenatal tests since completing the last packet?Yes_ No_. If yes, what kind of test and what were the results? _(15)
If you have delivered since completing packet #1, please indicate:
7. Sex of newborn : Male Female _(16)
8. Main method of infant feeding: Bottle Breast_ _(17)
9. Delivery type: Vaginal (repeat)_ Waginal (after Cesarean)_Planned Cesarean_ Emergency Cesarean_ (18)
10. Husband present at birth? Yes_ No_ _(19)
andIf you no longer wish to participate in this project, please check herereturn this sheet to me in the prepaid envelope. Please indicate why you wish towithdraw:
Lorrie Sam mons, RN, NP; 2608 Campeche Ct. , San Ramon, CA 94.583
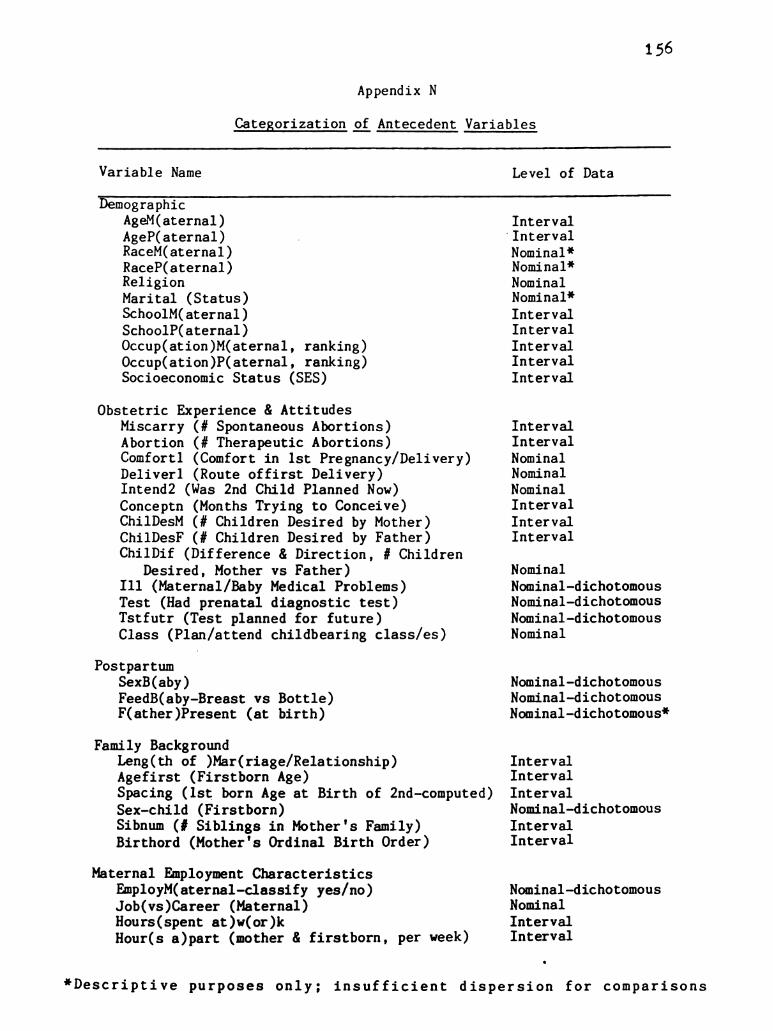
156
Appendix N
Categorization of Antecedent Variables
Variable Name Level of Data
DemographicAgeM(aternal) IntervalAgeP(aternal)
-Interval
RaceM(aternal) Nominal *RaceP(aternal) Nominal”Religion NominalMarital (Status) Nominal”SchoolM(aternal) IntervalSchool P(aternal) IntervalOccup(ation)M(aternal, ranking) IntervalOccup(ation)P(aternal, ranking) IntervalSocioeconomic Status (SES) Interval
Obstetric Experience & AttitudesMiscarry (# Spontaneous Abortions) IntervalAbortion (# Therapeutic Abortions) IntervalComfortl (Comfort in 1st Pregnancy/Delivery) NominalDeliver 1 (Route of first Delivery) NominalIntend 2 (Was 2nd Child Planned Now) NominalConceptn (Months Trying to Conceive) IntervalChilBesM (# Children Desired by Mother) IntervalChilDesR (# Children Desired by Father) IntervalChilBif (Difference & Direction, # Children
Desired, Mother vs Father) NominalIll (Maternal/Baby Medical Problems) Nominal—dichotomousTest (Had prenatal diagnostic test) Nominal—dichotomousTstfutr (Test planned for future) Nominal—dichotomousClass (Plan/attend childbearing class/es) Nominal
PostpartumSex B(aby) Nominal-dichotomousFeedB(aby-Breast vs Bottle) Nominal—dichotomousF(ather)Present (at birth) Nominal—dichotomous”
Family BackgroundLeng (th of )Mar(riage/Relationship) IntervalAge first (Firstborn Age) IntervalSpacing (1st born Age at Birth of 2nd-computed) IntervalSex-child (Firstborn) Nominal—dichotomousSibnum (# Siblings in Mother's Family) IntervalBirthord (Mother's Ordinal Birth Order) Interval
Maternal Employment CharacteristicsEmployM(aternal-classify yes/no) Nominal—dichotomousJob (vs)Career (Maternal) NominalHours (spent at) w(or)k IntervalHour(s a) part (mother & firstborn, per week) Interval
*Descriptive purposes only; insufficient dispersion for comparisons
º JJ)7.91/11/ / /l/º/ º -\ -: º J.J.'■ 1/fºlk / //º 2.* ----
Jº y 4/ l/#/(J S tº cºuncisco Sº & 0.01.1, +/ º sº c) tº ii,'---- -
3. sº ºr.-12 ~ 1.
-º O/le sº
––”, L! B RA R_Y s
—r-º O/2 - _º ”, L. G. RA■ ,ºlº ■ º ■ º... º. º. ºn ■ º
(/C & sº ºvºi g in * -- * - C * - sº ºvugin ºf º % c2. Nº-º, sº 12 sº 74.
* º cºlº■ ? "( - 2.s. --~~~~ ** Q}''J//?' I ■ º/º (J 2ºutcº sº,º !/? º, c) ■ ºutcº sº. " ºulº/” º
- º º -º O) sº º LI B R A. R_Y º
-
º O/2 sº ºBRARY & L. º, l 3. º […] º, º -º r- º, ~ º […]| || 9 º, […] sº –– º, L. J S- | | | *. [...] sº ---
> * - ~ * º * º- - --- ~/C *-s ºvugin º-' s - C -- ºg
*. - ** -o--
S- -
º, -º- * 42 sº 7' 51/?? / / /* 12 º' C■ .
-
*S* 2,731/4"-º, cºnciº º, " ºpiº. º sº, º/rºw º * º/d
st- w º- * tº 22- -- tº tº 2.
-
-*.~ -
>-
ºº
s
J. sº & O--
■ wººd in º L. J sº -: (C º [...] sº sººn” -- sº º (C * […]-
2 º O- -
sº. Cº■■ inci■ co ºOle sº-º. Lières sº-º. Ole sº tie Rare sº
* […]” * [] Tº. * []S
* ~.º ºf Cº■■ o sº.
*-
& so ---, -º Çe & --rºl º
[T]_s Jºvº■ J 17 * -- sº ~/C º I sºon” -- sº º/C* sº *... sº *... sº ”, sº-º 11/ / /l/?? 2.<s * ~~ %.S Nº. 1 ■ º * >
----ºut º & 42 a■ º/ºncºco ■ º. * !/? S & 1//, /77 ■ ºsº 1, Sº ºt- > * > Sº 't-- ■ º -º- f- º *o
~sº - A
I º, O■ lº sº L■ B RARY Cs Cº. J/2 - sº […] ”, L■ B R A■Q- º ---- •o -- rº & Q- -
[T] º --- º --r-7/C *. Cºlº sºariº Hºls - C -- ºvug■ * --_ º, sº yºu gº 74 & ~ º, sº *
º/? º 42.sº■ ºnC.C.O. º º, cºlº■ ºpSº º, C■ .1//, /.!/?■ , ■ o s º1. your. *S sºº º / sº ºo *-- sº ºº O/ 2– º ºBRARY Sº º, O 2– º […]”. LIBRARY & L. J º, sº ■ º
p" L. J ‘o. [...] -& –– º ---ºr- lsº ‘o.-
[T- º - - -Fºlsº ºc º■ - ºgº ºld ºc º■ - ºutº, sº
*. a*S* * w %2 º' C■ . … *s ºfº, Sºnº, º º■ º º cºncºs º º■
º o Z- º-
f
º - -9. -- - - º
[-º, LIBRARY º L. º, O)2– ~gº ■ º, L1B RARY is LC º, ..) AO & * >
-* , -ºr- & C- [...]
-+. | || & º […] sº 7\t c º, L. º -- *... lu.
■ vº■ g in º º ~/C * . º 9 IT º, sº * (IC ~
º 1. º -2.s C■ . ©■ º
*gº º/º 2.S.sº ”, 7//771/1■ t, ■ co sº º, sº º
-º
Cº.
Nº, sº 7 sº4. ** -- *
º, *º, Cº.//ºncº so,* - sº º *--
c º, e c ()
J/2 . º Hº. L! B RARY & º, O) º […] ”, LIBRARY sº |~C■ ”, L. o > L. %. [T] * cº --- º, --r-
[…] + * * º º L l!-- ºgº º º■ C ºr ºvugº ººº
*
&-
!
º, º -º, sº+, -
tº C■ º ■ ºº
- Sº %, sº 4
* Sº gº.) º/” to ºs ..., ºs pººl/11///p\Ogº ºn!/?Sº is a C º/ºutcº º 4.-
º/” º3 * Sº tº Sº 'º - S "- *~- * 0/1 ºr -º, Library sºr-■ º 0/2 sº, º Lie Rºº[ ] *, sº [...] 'º * [] "... . sº [...] º
-> *-i- ■ o re-r-, “ º, tº ■ ºr
TAC * [I] sº sºon * -- - C - Tº sººn L-w*-* -
y º *º º º4.s + !, --
- 72 … -- -y ºt - 1.
--º gº!/?". º %.S. c) * * *---------- º gº / º º■ ºme (■ º is a
-is *. º ■ ºutcº s */
-"J -º º! -
-S º -S- J.- tº .* º -* tº a
º º /2 - & - ■ y * *. )/2 . º- -ºr Linº, O & º, L. BRARY sº [-r] ". . is ■ º—r--- sº Q- [...] –8. --- º sº L. Q- º *
º cº ** r ~ º ºº º, tº 1–J S __º -- ** º, L. ~. c- º N- -Lºlº º■ C ºl ºvuginº -- s (((' … [I]. ºvºi &”. -y ºp & o - - º §
-> º º
- 42 º º **/?
+ ^2 sº Q º, Sº ~, º ■-
Fººd º cºlº/”C 2: º Aº, cº, º cºlº■ ,
» JJ)7.21/? -■ / 4/2" ( J. z -- -- ~~ ** U.J.) 1.9l ºn f 'º', ' 2. “ * * * *f, *-*- : * * *-* * *
º wºulº/ *S § 4. ºwn, Kºo sº. *Sº * cº fººd* º º -º- * - ** º
2- * *. in - * º, * } *
º ...) 4- sº ■ º- º, L. BRARY is U º, ..) le sº [...] * L. BRARY isl ”. sº - * * , - r º º […] º --- * * , Lºl º
-* * ~ r - - * * - r sº
* * ■ - sº ºvug in º -- ~/C * -- sº ºvº gº º----" º .** !/ S.
-º .* º, º
12. Nº y A/º % Sº *, --> º * A fºº º, sº -tº gº, *olº■ ?Sº 2 cºncº gº º■ º | Sºº * - - --- - *~ tº º, s -º- º
* * … * > * , • * º y n • º* R_Y & [...] º, ..) 4–2 ...sº ■ º- º, Li B R ARY sº ■ º, 4.// 4–2 lº º, L.
-
º *o * –4 _* * A- - --''.
~ * *... […] º---
º ºr- _* º, […] º-----l s º/C º,
--- s Aºivºj g in %, L– ~ * - C º, * -- º Aºvº 3 in º- * º
sº C■ .- *
º, sº Rº: º º, º-- *
º S’ 0.] }} y !/?" º , --,cºncisco gº tº */ Sº gº c ºntº º, º/º*.* º *
- -
º, Lºs Rare sº- º, Ols sº Fº, L. BRARY sº [...] º, O■ lº s-
L. J º - * "…
~,
-
-º, L. | º *. […]
- - -
o, sº º, º º
j G |T| º, º *T/C º,-
s Aºvº g tº °, º cºC º-
º A.■ º º, sº C■ º º, sº oº: o "...sº º - *** cºsº *. *- º/rancisco sº *.º
y * * * * & ■ ºwrº■■ o sº º,( )
- 4
º s º * O■ ) º 9, º º*—2 lº º, L. BRARY & [...] “. . /*-2 s. º, Leº, sº tººC Q *- 4- C - * * *- --- * gº -* - º -- *- e
*-
-O ---r- * *
[...] 3 O L …” º- ACTS vºl 3 in º, L. s *T/C %. º Aºvº. 9 in %. _S -C º,- ºº º,
- º 12 *-- fºr.
-12, Nº. 3. * ºr * * * * *z, *
-
- .7//?? A ■ º 2.* ... … *.* {}}}'}.} º/º 2. Sº ■ º.Ø 0.33% */º SS & Sººn, ■ º J. y- % { º ! ■ l 'S s * C .1/7, 7", º■ t !º O
º O) sº % sº ". o f sº °o. Fºo|º. le s Hº, tºº sº. 2. le s Hº Leºº, As
- -* - º, ** [...] º, […] º --- º, -r ºº * * - -
| | º
2* º [I] s Aºivºj 3 in º, […] - ■ C ”, ---- s Aºvº G in ºr2 .**
*.S- 4- º
* 42"...s º ~ *s < ºpiº t ■ º ”, sº *
- ... • f * * * - -* if: - - -- *
ºf CºCJ & dºout/?ºy sº C■■ n./rºci ■ º & Cº.-
Sº - *. c).* s' %2. *
/2 sº ** *- * s" %. / is ºARY Sº [-r-, “º ..) A-2 Sº º, LIBRARY Sº [. º, ..) le Sº ■ º * L
_º [] º, sº | –4 | `o-
_* [...] º, tº ---- * ,
– sº º/C º […] sº sºon * –– º *T/C º Cº ºvº an º- s c Sº t
...tº "...º º, sº * > ºº/”
-
~ a º-
y 2 < - **** * S l/?'—■ ■ º ºC■ .&/ºncºco º º g: cy.º/rºncºs º º 'Sº sº *. Sº tº & -
} 1- Tº
^ (x / →a- *,- º, L! B RA R_Y º [...] °. 0/2_ sº F- º, L! B ºº º r- º
C L.y t * º -
*o --- º > Q 3 Q- _*-
| | [. T ~-
| | & sººn º º■ c *-s ºvºgº º' --C -2. w ~ - w
~, ”, “S” º, sº ~, '4. Sº-
º, ºr yº, Nº …, xN º gº * * *
º 2 S-
*.* cºlº/”º 2.s S. -*.*.*.*.*.*. * * ººwº sº tº cº lºcºco so
->
S º *. CY4.& 7mºc.ººd S 6,ºº *2. * º O.
- -**.
2– s […] * L. BRARY sº º, J/2 - s ■ º º, Li BRARY- sº ---- * --- As L. J *.. º ----- º, ■ -r- J _º º,r * ----, -º - * - * º * --
– ºvºgri º Lºl's - ■ º º'-' cºvy an *. º -y *T/C *
* *
Z
* J.
**y * ºº % -
- * --: ; ; – "º- ºg - !, **
**- º %2 . ; ; ; ; ; ; ; ; ; ;... rif fººt.
-
º/º } % S 7.*º wºup. º º ; : } s: !". A ■ ºl/, y sº, c)º 7-i/■ cº
)/2 . tº sº.9.º, º .** 2.■ º. 2's sº 4- ºr--º, tºº * He room -- ~ … […] sº
- cº ~ NOT TO BE TAKEN FROM T * . . . * *(' * [I] s *RVto 12
*::: – sº ºvº gº º –-º
º, sº car. Nr. º
ºf CºCº is* *
N **--º
*
< gºº/* / cºpiº. º º -\,:Çe- º -
sº º 4
, ºr
*g, *, * *:…
sº, cº 77-incºo ss º is a C*º, *
-º- 4. " - &-ºn-º. O/lº sº, º, Li *-*. O/l, sº ºARY & L. º, º ■ º ”, LIBRARY sº [-r] *, * // 4–2 lº […] º, L
* - * - *- *- wº-- wº- C- -S °o ºr- sº Q- cº
- -l º º º, [. | & º L. J sº º, [. Sº-
ºis º■ º'-' ºvºgº º-'s º■ C 2. – º Aº V8 g in ºsº * %. Sº ”, -> *4, sº
- -
A sº º + */º
-
Sº ■ º, ºs cºlº■■ ºvo ºf W., 7.…, º cºn■ ºo

- -
-
- - - -
-
- -
-
- -
-
--
-
-
-
-
-
-
-
-
-
-
-
-
-




















