Age-Related Changes in Temporal Allocation of Visual Attention: Evidence From the Rapid Serial...
12
Is the impairment in temporal allocation of visual attention in children with ADHD related to a developmental delay or a structural cognitive deficit? Sophie Donnadieu a,b, *, Carole Berger a,b , Marie Lallier c , Christian Marendaz a,d , Annie Laurent e a Laboratoire de Psychologie et Neurocognition, CNRS UMR-5105, Grenoble, France b Universite ´ de Savoie, BP 1104, 73011 Chambe ´ry Cedex, France c Basque Center on Cognition Brain and Language, Donostia-San Sebastian, Spain d Universite ´ Pierre Mende `s France, BP 47, 38040 Grenoble Cedex 9, France e CHU de Grenoble, De ´partement de Psychiatrie, 38000 Grenoble, France 1. Introduction Attention-deficit/hyperactivity disorder (ADHD) affects between 3 and 7% of school-age children (Barkley, 1990; Szatmari, 1992), with boys being over-represented. The disorder is not usually detected before school age. It persists into adolescence in 50–80% of cases clinically diagnosed in childhood and even persists into adulthood in 30–50% of cases (Barkley, Fischer, Edelbrock, & Smallish, 1990; Klein & Mannuzza, 1991; Weiss & Hechtman, 1993). According to the Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition (DSM-5; American Psychiatric Association, 2013), ADHD is characterized by the presence of six or more symptoms of inattention and/or six or more symptoms of hyperactivity–impulsivity before the age of 7 in two or more contexts. On the basis of these three symptom dimensions, the DSM-5 defines three subtypes: ADHD-I (predominantly inattentive type), ADHD-H (predominantly hyperactive-impulsive Research in Developmental Disabilities 36 (2015) 384–395 ARTICLE INFO Article history: Received 20 June 2014 Received in revised form 3 October 2014 Accepted 10 October 2014 Available online Keywords: ADHD Development Selective visual attention Attentional blink Inhibitory process ABSTRACT We investigated the temporal allocation of visual attention in 11-year-old children with attention-deficit/hyperactivity disorder (ADHD) by comparing their attentional blink (AB) parameters (duration, amplitude and minimum performance) with those observed in three groups of healthy control participants (8-year-olds, 11-year-olds and adults). The AB is a marker of impaired ability to detect a second target following the identification of a first target when both appear randomly within a rapid sequence of distractor items. Our results showed developmental effects; with age, the AB duration decreased and the AB minimum moved to shorter lag times. Importantly, 11-year old children with ADHD presented much the same similar AB patterns (in terms of duration and minimum position) as the healthy 8-year-old controls. Our results support the hypothesis whereby impaired allocation of temporal selective attention in children with ADHD is due to a developmental delay and not a specific cognitive deficit. ß 2014 Elsevier Ltd. All rights reserved. * Corresponding author at: Universite ´ de Savoie (Chambe ´ ry), Laboratoire de Psychologie et Neurocognition (UMR 5105), U.F.R. Lettres, Langues et Sciences de l’Homme, De ´ partement de Psychologie, Route du Sergent Revel, Jacob-Bellecombette, BP 1104, F-73011 Chambery Cedex, France. Tel.: +33 479 758 582. E-mail address: [email protected] (S. Donnadieu). Contents lists available at ScienceDirect Research in Developmental Disabilities http://dx.doi.org/10.1016/j.ridd.2014.10.014 0891-4222/ß 2014 Elsevier Ltd. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Age-Related Changes in Temporal Allocation of Visual Attention: Evidence From the Rapid Serial...

Research in Developmental Disabilities 36 (2015) 384–395
Contents lists available at ScienceDirect
Research in Developmental Disabilities
Is the impairment in temporal allocation of visual attention in
children with ADHD related to a developmental delay or astructural cognitive deficit?Sophie Donnadieu a,b,*, Carole Berger a,b, Marie Lallier c, Christian Marendaz a,d,Annie Laurent e
a Laboratoire de Psychologie et Neurocognition, CNRS UMR-5105, Grenoble, Franceb Universite de Savoie, BP 1104, 73011 Chambery Cedex, Francec Basque Center on Cognition Brain and Language, Donostia-San Sebastian, Spaind Universite Pierre Mendes France, BP 47, 38040 Grenoble Cedex 9, Francee CHU de Grenoble, Departement de Psychiatrie, 38000 Grenoble, France
A R T I C L E I N F O
Article history:
Received 20 June 2014
Received in revised form 3 October 2014
Accepted 10 October 2014
Available online
Keywords:
ADHD
Development
Selective visual attention
Attentional blink
Inhibitory process
A B S T R A C T
We investigated the temporal allocation of visual attention in 11-year-old children with
attention-deficit/hyperactivity disorder (ADHD) by comparing their attentional blink (AB)
parameters (duration, amplitude and minimum performance) with those observed in
three groups of healthy control participants (8-year-olds, 11-year-olds and adults). The AB
is a marker of impaired ability to detect a second target following the identification of a
first target when both appear randomly within a rapid sequence of distractor items. Our
results showed developmental effects; with age, the AB duration decreased and the AB
minimum moved to shorter lag times. Importantly, 11-year old children with ADHD
presented much the same similar AB patterns (in terms of duration and minimum
position) as the healthy 8-year-old controls. Our results support the hypothesis whereby
impaired allocation of temporal selective attention in children with ADHD is due to a
developmental delay and not a specific cognitive deficit.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Attention-deficit/hyperactivity disorder (ADHD) affects between 3 and 7% of school-age children (Barkley, 1990;Szatmari, 1992), with boys being over-represented. The disorder is not usually detected before school age. It persists intoadolescence in 50–80% of cases clinically diagnosed in childhood and even persists into adulthood in 30–50% of cases(Barkley, Fischer, Edelbrock, & Smallish, 1990; Klein & Mannuzza, 1991; Weiss & Hechtman, 1993). According to theDiagnostic and Statistical Manual of Mental Disorders – Fifth Edition (DSM-5; American Psychiatric Association, 2013),ADHD is characterized by the presence of six or more symptoms of inattention and/or six or more symptoms ofhyperactivity–impulsivity before the age of 7 in two or more contexts. On the basis of these three symptom dimensions, theDSM-5 defines three subtypes: ADHD-I (predominantly inattentive type), ADHD-H (predominantly hyperactive-impulsive
* Corresponding author at: Universite de Savoie (Chambery), Laboratoire de Psychologie et Neurocognition (UMR 5105), U.F.R. Lettres, Langues et
Sciences de l’Homme, Departement de Psychologie, Route du Sergent Revel, Jacob-Bellecombette, BP 1104, F-73011 Chambery Cedex, France.
Tel.: +33 479 758 582.
E-mail address: [email protected] (S. Donnadieu).
http://dx.doi.org/10.1016/j.ridd.2014.10.014
0891-4222/� 2014 Elsevier Ltd. All rights reserved.

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395 385
type) or ADHD-C (combined type). Studies of the academic achievements of children with ADHD imply that they are morelikely to obtain lower grades in standard measures (reading and maths, for example; see Barkley et al., 1990) than controlchildren of equivalent intelligence. Aggression and conduct problems and depressive or anxiety disorders are oftenassociated with a diagnosis of ADHD (Babinski, Hartsough, & Lambert, 1999; Beauchaine, Hinshaw, & Pang, 2010; Biedermanet al., 2014; Halldorsdottir & Ollendick, 2014).
1.1. Temporal selective attention deficits in ADHD
In view of the obvious importance of attention in ADHD, many studies have tried to elucidate the mechanism underlyingattention deficits. However, the results have been divergent (Blondis, Snow, & Accardo, 1999). Most studies differentiatedbetween two main attentional processes: sustained attention and selective attention. A sustained attention deficit is definedas a gradual decline over time in the attention resources allocated to a given task. A selective attention deficit corresponds todifficulties in focusing on a relevant target while ignoring irrelevant information. Even though this topic has been hotlydebated (for a review, see Wilding, 2005), previous research has indicated that children with ADHD suffer from sustainedattention deficits more than they do from spatial selective attention deficits (Booth et al., 2005; Hazell et al., 1999; Karatekin& Asarnow, 1998; Mason, Humphreys, & Kent, 2003; Tsal, Shalev, & Mevorach, 2005; Van der Meere & Sergeant, 1988).Spatial selective attention has been studied through the application of visual search paradigms, in which participants areasked to detect the presence of a target among simultaneously presented distractors (Treisman & Gelade, 1980; Wolfe,1998). The results of these studies showed that the time taken to correctly detect the target varies as a function of thenumber of distracters to be ignored. Other complementary studies have considered temporal aspects of selective attentionby examining how the allocation of processing resources at one point in time might affect the processing of a subsequentevent. Rapid serial visual presentation (RSVP) paradigms have been widely used to explore the temporal characteristics ofinformation processing (Broadbent & Broadbent, 1987; Chun & Potter, 1995; Raymond, Shapiro, & Arnell, 1992; Reeves &Sperling, 1986; Shapiro, Raymond, & Arnell, 1994; Ward & Duncan, 1996; Weichselgartner & Sperling, 1987; for a review, seeShapiro, Arnell, & Raymond, 1997). Fig. 1a shows an example of an RSVP paradigm used to measure the attentional blink (AB)phenomenon. A participant’s ability to detect a target (T2) in a control (single-target) condition is compared with his/herability to detect the same target after already having identified a first target T1 (i.e. in a two-target condition). After thepresentation of T1, the ability to detect T2 drops for a few hundred milliseconds; this phenomenon is referred to as the AB(Fig. 1b). Several explanatory models have been suggested (Chun & Potter, 1995; Raymond, Shapiro, & Arnell, 1995). The ABmay occur because attention demands for the identification of T1 prevent (for a short period of time) the allocation ofattentional resources to T2, which then become vulnerable to decay or overwriting by subsequent stimuli.
However, when T2 appears immediately after T1 (typically within 100 ms), its detection is not subject to an AB. This so-called ‘‘lag-1 sparing effect’’ (see Fig. 1b) has been ascribed to the dynamic functioning of an attentional gate (Chun & Potter,1995; Shapiro & Raymond, 1994). The attentional gate may open rapidly when T1 is presented (in order to allocate attentionto it) but may take some time to close and disengage attentional resources for T1. Sluggish closing may thus enableprocessing resources to access T2 at the same time as T1. In such a case, T1 and T2 will fall within a single attentional windowlasting for at least 150–200 ms (Sperling & Weichselgartner, 1995). In addition to the lag-1 sparing effect, the AB ischaracterized by three other parameters (as defined by Cousineau, Charbonneau, & Jolicoeur, 2006; Fig. 1b). The amplitude of
[(Fig._1)TD$FIG]
Fig. 1. (a) An illustration of the RSVP paradigm. In this behavioural task, a series of stimuli (letters, in this case) are presented in rapid succession. In the
single-target condition, participants have to detect the presence of a target T2 (e.g. the letter ‘‘X’’). In the two-target condition, participants have to identify
an initial target T1 (e.g. the letter ‘‘S’’) and then detect T2 (e.g. the letter ‘‘X’’ from the single-target condition). (b) Typical AB curves for the detection of T2 in
the single-target condition (filled circles) and the two-target condition (open circles). The vertical axis represent the accuracy of detection of T2 (i) in the
single-target target condition (filled circles) and (ii) in the two-target condition (open circles) when T1 was successfully reported. The horizontal axis is the
lag between the two targets (often a multiple of 100 ms).
Adapted from Cousineau et al. (2006).

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395386
the AB corresponds to the difference between the best and worst performances for T2 detection in the two-target condition.The AB duration corresponds to the number of lag positions in which T2 detection in the two-target condition is impaired(relative to the single-target condition). Increases in AB amplitude and duration are generally thought to reflect a lack ofattentional resources for processing T1 and the following stimuli (Chun & Potter, 1995; Li, Lin, Chang, & Hung, 2004). The ABminimum is the time point (lag) at which T2 detection is worst (see Fig. 1b). The position of the AB minimum may reflect theinstant at which the attentional gate has been closed (in order to process T1).
The reported characteristics of RSVP task performance in ADHD participants vary from one study to another. Someresearchers have reported a specific AB pattern in adults with ADHD – suggesting the existence of a deficit in temporalselective attention in this population (Armstrong & Munuz, 2003; Hollingsworth, McAuliffe, & Knowlton, 2001). Moreexactly, these authors found that the AB in ADHD patients exhibited a greater amplitude and duration (relative to healthyadult participants). In contrast, Carr, Nigg, and Henderson (2006) found that the AB recovery rate was slightly (but notsignificantly) delayed in ADHD groups. They suggested that methodological differences in sample characterization (such asthe nature of individual ADHD subtypes) or the experimental paradigm might account for discrepancies with previousfindings. Mason, Humphreys, and Kent (2005) reported that the AB was longer in children with ADHD than in childrenwithout ADHD. Lastly, Li et al. (2004) observed that the AB occurred later in time in children with ADHD than in controlchildren. A small proportion of participants with ADHD had an AB with a normal amplitude but a later minimum position.These results were replicated in adolescents with a high impulsivity level (Li, Chen, Lin, & Yang, 2005). Li et al.’s two studiestherefore indicate that AB amplitude and/or duration can vary independently of the AB minimum position.
Li et al. (2004) therefore proposed an ‘‘attention-gating model’’ that sought to account for both the longer, more ample ABand the isolated minimum position displacement in individuals with ADHD. This constituted an extension of the varioustwo-stage bottleneck models (e.g. Chun & Potter, 1995; Giesbrecht & Di Lollo, 1998; Jolicoeur & Dell’Acqua, 1998) in whichstimuli are pre-centrally processed before being centrally processed in a second, limited-capacity step. Consolidation andresponse planning may occur during this second stage. Accordingly, if a second target (T2) is displayed while a first target(T1) is being centrally processed, it may be pre-centrally (but not centrally) encoded in memory. The attention-gatingmodel’’ focuses on how information flows from the pre-central (perceptual) buffer to the central processing step. This flowmight be controlled by an attention gate that allows only a certain amount of information to access the central stage at agiven time. According to Li et al. (2004), the dynamics of the attention gate are affected in children with ADHD. More exactly,Li et al. suggested that the gate closes and re-opens more slowly in children with ADHD than in healthy children. In such acase, T2 stimuli (presented after T1) will then access the central stage (in addition to T1), leading to two possible scenarios:(i) if attentional resources are insufficient, the post-T1 stimuli will not be efficiently processed – resulting in a more ample,longer AB; (ii) if attentional resources are sufficient (as it is the case for some children with ADHD), the AB would have anormal amplitude but a later minimum position (see Fig. 1b).
It is noteworthy that the above-mentioned attentional gating mechanisms have been linked to inhibitory processes (seeOlivers & Watson, 2006). According to Raymond et al. (1992), temporal inhibition of post-T1 items is required to protect T1 frominterference during RSVP tasks. This inhibition mechanism may well correspond to closure of the attentional gate (as describedby Li et al., 2004): once the gate has been closed, items displayed several milliseconds after T1 would not be allocated withprocessing resources. The AB would therefore occur when T2 is displayed within the short post-T1 time window.
1.2. Is the temporal selective attention deficit in ADHD related to a developmental delay or a cognitive deficit?
The impaired temporal information processing involved in the AB may have an important role in the deficits observed inADHD (Toplack, Dockstader, & Tannock, 2006). Indeed, selective temporal attention and inhibitory process are crucial fortemporal processing and involve similar frontal cortex networks (Lutcke, Gevensleben, Albrecht, & Frahm, 2009; Smith,Taylor, Lidzba, & Rubia, 2003). Time processing, selective attention and inhibition efficiency all improve with age (Chevalier,2010; Cragg & Nation, 2008; Huang-Pollock, Carr, & Nigg, 2002; Pennequin, Nanty, & Khomsi, 2004; Wright, Waterman,Prescott, & Murdoch-Eaton, 2003;), thus paralleling executive functions and frontal cortex maturation (Halperin & Schulz,2006). It is therefore essential to screen for putative developmental effects in these general executive functions by comparingperformance levels in children with ADHD and younger and age-matched healthy children (Kipp, 2005). Addressing the issueof development is particularly relevant because a recent study showed that ADHD is characterized by a delay in corticalmaturation (Gonon, Guile, & Cohen, 2010; Shaw et al., 2007). The electroencephalography studies have helped finding theneural mechanisms underlying the phenomenon of the AB. Many studies showed that the amplitude of the P3 component iseither reduced or absent for the duration of the AB (Craston, Wyble, Chennu, & Bowman, 2008; Giesbrecht, Sy, & Elliott, 2007;Jolicoeur, Sessa, Dell’Acqua, & Robitaille, 2006; Kranczioch, Debener, & Engel, 2003; McArthur, Budd, & Michie, 1999;Sergent, Baillet, and Dehaene (2005); Sessa, Luria, Verleger, & Dell’Acqua, 2007; Vogel, Luck, & Shapiro, 1998). This resultsuggests that this component would be the neural signature of the treatment performed on the first stimulus during the AB.The attention would be captured by the first stimulus and would cause a lower quality processing of the second stimulus thatappeared just after the first one. The fact that the amplitude of this wave is further reduced in subjects with ADHD suggeststhat the attentional cost in these patients is higher than in control subjects.
The idea that ADHD is related to a developmental delay (rather than a ‘‘structural’’, cognitive deficit in selective attentionand/or inhibition) is supported by the findings of recent studies by Valko et al. (2009) and Doehnert, Brandeis, Imhof,Drechsler, and Steinhausen (2010). These researchers observed developmental differences in neurophysiological markers of

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395 387
inhibition processes and temporal processing deficits in children with ADHD. More precisely, Valko et al. (2009) observedthat the electrophysiological P300 component has a lower amplitude in subjects with ADHD than in controls but alsodepends on developmental effects. It is therefore important to determine whether age-related changes in AB patterns can beobserved in healthy participants. If so, the low-efficiency of gating mechanisms and/or attentional resources described inADHD (see Li et al., 2004) might result in an AB similar to that observed in younger, healthy children.
1.3. Study objectives and hypotheses
The primary objective of the present study was to provide a clear description of the temporal selective attentional deficitin children with ADHD. To that end, we first sought to determine whether this deficit is related to a specific cognitiveimpairment or, in contrast, correspond to a developmental delay. We also sought to determine whether the temporalselective attentional deficit was related to processing resources and/or inhibitory mechanisms. We assessed a putativedevelopmental delay by comparing a group of 11-year-old children with ADHD with a group of healthy, younger (8-year-old)children, a group of healthy age-matched controls and a group of adult controls. In order clarifying the possible involvementof processing resources and/or inhibitory processes, we analyze the four AB parameters:
(a) T
he duration of the lag-1 sparing effect provides information on the amount of attentional resources available and/or thespeed of attentional gate closure. If developmental effects are present, we should observe a lag-sparing effect in the adultgroup but not necessarily in healthy children. According to the developmental hypothesis, we expected to observe a lagsparing effect for children with ADHD if attentional resources are sufficient (Li et al., 2004). These attentional resourceswere evaluated by comparing the respective AB amplitudes in children with and without ADHD, see (d) below.(b) T
he duration of the AB (i.e. the number of lag positions at which performance in the two-target condition was worse thanin the single-target condition) provides information on both the dynamics of gating mechanisms (the speed ofreopening) and the amount of attentional resources available. According to the developmental hypothesis, we expected(i) the AB to be longer in healthy 8-year-olds than in healthy 11-year-olds and longer in older healthy 11-year-oldchildren than in healthy adults (see Garrad-Cole, Shapiro, & Thierry, 2011); and (ii) a similar AB duration in 11-year-oldchildren with ADHD and healthy 8-year-old children.(c) T
he timing of the AB minimum (i.e. the moment at which T2 detection is worst). This parameter time providesinformation on the dynamics of gating. If gate closure is slow, the lag in the minimum should be greater (Li et al., 2004). Ifthe deficit in temporal selective attention presented by children with ADHD corresponds to a developmental delay, wewould expect (i) the AB minimum to be later in healthy 8-year-olds than in healthy 11-year-olds and later in healthy 11-year-olds than in healthy adults; and (ii) similar AB minimum positions in 11-year-old children with ADHD and healthy8-year-old children.(d) T
he amplitude of the AB (i.e. the difference between performances in the single-target condition and the two-targetcondition) provides information on the amount of attentional resources available. We expected (i) the AB amplitude to begreater in healthy 8-year-olds than in healthy 11-year-olds and greater in healthy 11-year-olds than in adults (revealingthe development of attentional resources with age); and (ii) similar AB amplitudes in children with ADHD and healthy8-year-olds.2. Method
2.1. Participants
All participants had normal or corrected-to-normal vision. Prior to inclusion, participants (and their parents, for under-18s) were provided with comprehensive information on the study’s objectives and procedures. All participants (and theirparents, for under-18s) provided their written informed consent to participation.
2.1.1. Control groups
Twenty healthy adults (mean age: 20.05 years, SD = 1.39) took part in the present study. All were psychology studentsattending the University of Savoie (Chambery, France). Furthermore, 40 healthy children were recruited from local schoolsand divided into a group of 20 older children (10 boys and 10 girls with a mean age of 10.93 years, SD = 0.90) and a group of 20younger children (12 boys and 8 girls with a mean age of 7.95 years, SD = 0.34). An analysis of variance (ANOVA) wasperformed on chronological age, with group (healthy 11-year-olds, healthy 8-year-olds and adults) as a between-subjectfactor. As expected, the control group of 11-year-olds was significantly younger than the group of adults, F(1, 76) = 835.57,p< 0.01, and significantly older than the control group of 8-year-olds, F(1, 76) = 89.49, p< 0.01.
We checked for the presence of reading disorders, since children with these disorders are reportedly impaired in RSVPtasks (Hari & Renvall, 2001; Lallier, Donnadieu, Berger, & Valdois, 2010; Lallier, Donnadieu, & Valdois, 2010). The AlouetteReading Test (Lefavrais, 1967) was used to estimate the reading age of each child prior to the AB tasks. Children with areading delay of more than 18 months were excluded from the study. As expected, the mean lexical age was significantlylower, F(1, 57) = 18.79, p< 0.01, in the group of 8-year-old children (mean age: 8.38 years, SD = 0.73) than in the group of11 year-old children (mean age 10.06 years, SD = 1.34).
S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395388
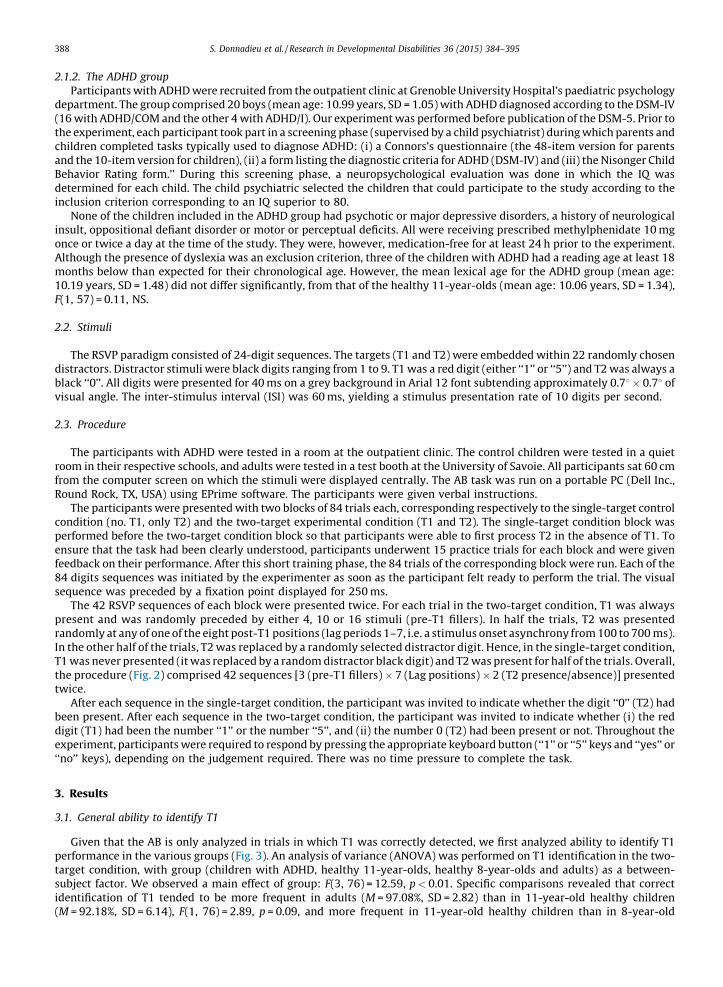
2.1.2. The ADHD group
Participants with ADHD were recruited from the outpatient clinic at Grenoble University Hospital’s paediatric psychologydepartment. The group comprised 20 boys (mean age: 10.99 years, SD = 1.05) with ADHD diagnosed according to the DSM-IV(16 with ADHD/COM and the other 4 with ADHD/I). Our experiment was performed before publication of the DSM-5. Prior tothe experiment, each participant took part in a screening phase (supervised by a child psychiatrist) during which parents andchildren completed tasks typically used to diagnose ADHD: (i) a Connors’s questionnaire (the 48-item version for parentsand the 10-item version for children), (ii) a form listing the diagnostic criteria for ADHD (DSM-IV) and (iii) the Nisonger ChildBehavior Rating form.’’ During this screening phase, a neuropsychological evaluation was done in which the IQ wasdetermined for each child. The child psychiatric selected the children that could participate to the study according to theinclusion criterion corresponding to an IQ superior to 80.
None of the children included in the ADHD group had psychotic or major depressive disorders, a history of neurologicalinsult, oppositional defiant disorder or motor or perceptual deficits. All were receiving prescribed methylphenidate 10 mgonce or twice a day at the time of the study. They were, however, medication-free for at least 24 h prior to the experiment.Although the presence of dyslexia was an exclusion criterion, three of the children with ADHD had a reading age at least 18months below than expected for their chronological age. However, the mean lexical age for the ADHD group (mean age:10.19 years, SD = 1.48) did not differ significantly, from that of the healthy 11-year-olds (mean age: 10.06 years, SD = 1.34),F(1, 57) = 0.11, NS.
2.2. Stimuli
The RSVP paradigm consisted of 24-digit sequences. The targets (T1 and T2) were embedded within 22 randomly chosendistractors. Distractor stimuli were black digits ranging from 1 to 9. T1 was a red digit (either ‘‘1’’ or ‘‘5’’) and T2 was always ablack ‘‘0’’. All digits were presented for 40 ms on a grey background in Arial 12 font subtending approximately 0.78� 0.78 ofvisual angle. The inter-stimulus interval (ISI) was 60 ms, yielding a stimulus presentation rate of 10 digits per second.
2.3. Procedure
The participants with ADHD were tested in a room at the outpatient clinic. The control children were tested in a quietroom in their respective schools, and adults were tested in a test booth at the University of Savoie. All participants sat 60 cmfrom the computer screen on which the stimuli were displayed centrally. The AB task was run on a portable PC (Dell Inc.,Round Rock, TX, USA) using EPrime software. The participants were given verbal instructions.
The participants were presented with two blocks of 84 trials each, corresponding respectively to the single-target controlcondition (no. T1, only T2) and the two-target experimental condition (T1 and T2). The single-target condition block wasperformed before the two-target condition block so that participants were able to first process T2 in the absence of T1. Toensure that the task had been clearly understood, participants underwent 15 practice trials for each block and were givenfeedback on their performance. After this short training phase, the 84 trials of the corresponding block were run. Each of the84 digits sequences was initiated by the experimenter as soon as the participant felt ready to perform the trial. The visualsequence was preceded by a fixation point displayed for 250 ms.
The 42 RSVP sequences of each block were presented twice. For each trial in the two-target condition, T1 was alwayspresent and was randomly preceded by either 4, 10 or 16 stimuli (pre-T1 fillers). In half the trials, T2 was presentedrandomly at any of one of the eight post-T1 positions (lag periods 1–7, i.e. a stimulus onset asynchrony from 100 to 700 ms).In the other half of the trials, T2 was replaced by a randomly selected distractor digit. Hence, in the single-target condition,T1 was never presented (it was replaced by a random distractor black digit) and T2 was present for half of the trials. Overall,the procedure (Fig. 2) comprised 42 sequences [3 (pre-T1 fillers)� 7 (Lag positions)� 2 (T2 presence/absence)] presentedtwice.
After each sequence in the single-target condition, the participant was invited to indicate whether the digit ‘‘0’’ (T2) hadbeen present. After each sequence in the two-target condition, the participant was invited to indicate whether (i) the reddigit (T1) had been the number ‘‘1’’ or the number ‘‘5’’, and (ii) the number 0 (T2) had been present or not. Throughout theexperiment, participants were required to respond by pressing the appropriate keyboard button (‘‘1’’ or ‘‘5’’ keys and ‘‘yes’’ or‘‘no’’ keys), depending on the judgement required. There was no time pressure to complete the task.
3. Results
3.1. General ability to identify T1
Given that the AB is only analyzed in trials in which T1 was correctly detected, we first analyzed ability to identify T1performance in the various groups (Fig. 3). An analysis of variance (ANOVA) was performed on T1 identification in the two-target condition, with group (children with ADHD, healthy 11-year-olds, healthy 8-year-olds and adults) as a between-subject factor. We observed a main effect of group: F(3, 76) = 12.59, p< 0.01. Specific comparisons revealed that correctidentification of T1 tended to be more frequent in adults (M = 97.08%, SD = 2.82) than in 11-year-old healthy children(M = 92.18%, SD = 6.14), F(1, 76) = 2.89, p = 0.09, and more frequent in 11-year-old healthy children than in 8-year-old

[(Fig._2)TD$FIG]
Fig. 2. Representation of the RSVP paradigm used in the present study. Each sequence of single-digit numbers was preceded by a fixation point (presented
for 250 ms). The digit numbers were each presented for 40 ms, with an interstimulus interval (ISI) of 60 ms. In the single-target condition, participants had
to detect the presence of the black digit ‘‘0’’, which was present in half of the trials. In the two-target condition, participants had to identify the target T1 (a
red ‘‘1’’ or ‘‘5’’) and then detect the target T2 (again, a black ‘‘0’’). T1 was be preceded by either 4, 10 or 16 distractors and T2 target could appear in one of
seven possible lag positions after the presentation of T1.
S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395 389
children (M = 85%, SD = 12.62), F(1, 76) = 6.24, p< 0.05, or children with ADHD (M = 80.94%, SD = 11.23), F(1, 76) = 15.29,p< 0.01. However, the ability to identify T1 was similar in children with ADHD and healthy 8-year-olds: F(1, 76) = 1.99, NS.
It is noteworthy that the T1 identification rates were high (>80%) in all groups. Hence, T1 appears to be correctlyprocessed before T2 is presented. This observation suggests that all four groups had adequately engaged their attention inthe two-target task, which validates our subsequent comparison of T2 detection in the single-target and two-targetconditions (i.e. comparison of the AB).
3.2. Ability to detect T2
We calculated the T2 detection sensitivity rate for each participant at each lag time and in each of the two conditions. Hitrates (number of correct detections of T2 when it was present) and false alarm rates (number of reported detections when itwas absent) were computed for each participant. From these rates, the perceptual sensitivity was computed according to the‘‘Signal Detection Theory’’ (Macmillan & Creelman, 1991).
In the two-target condition, T2 sensitivity was computed for trials in which T1 had been correctly identified (e.g. Shapiroet al., 1994). Table 1 presents the mean T2 detection sensitivity rates under the two conditions, for the seven time lags and foreach group of participants. Fig. 4 plots the performance observed for the four groups in each condition (single-target andtwo-target conditions).
[(Fig._3)TD$FIG]Fig. 3. Percent of correct T1 identifications in the two-target condition for adults, healthy 11-year-olds, healthy 8-year-olds and 11-year-old children with
ADHD.

Table 1
Mean (standard deviation) T2 detection sensitivity in the one and two-target conditions in the four groups (adults, healthy 11-year-olds, healthy 8-year-
olds and 11-year-olds with ADHD) and for each of the seven lags.
Adults 11-year-olds 8-year-olds 11-year-olds with ADHD
One-target Two-target One-target Two-target One-target Two-target One-target Two-target
1 0.89 (0.20) 0.77 (0.17) 0.8 (0.20) 0.58 (0.27) 0.68 (0.17) 0.38 (0.27) 0.55 (0.22) 0.35 (0.41)
2 0.94(0.09) 0.56 (0.41) 0.84 (0.19) 0.46 (0.27) 0.64 (0.22) 0.39 (0.25) 0.63 (0.23) 0.22 (0.31)
3 0.90 (0.14) 0.62 (0.34) 0.81 (0.20) 0.43 (0.30) 0.64 (0.24) 0.36 (0.35) 0.72 (0.24) 0.20 (0.46)
4 0.88 (0.18) 0.69 (0.26) 0.87 (0.17) 0.50 (0.30) 0.73 (0.19) 0.28 (0.28) 0.70 (0.29) 0.13 (0.34)
5 0.89 (0.12) 0.77 (0.27) 0.78 (0.16) 0.55 (0.29) 0.74 (0.25) 0.28 (0.28) 0.68 (0.27) 0.21 (0.36)
6 0.94 (0.15) 0.84 (0.15) 0.81 (0.17) 0.64 (0.30) 0.73 (0.21) 0.46 (0.37) 0.61 (0.23) 0.21 (0.36)
7 0.90 (0.15) 0.88 (0.13) 0.73 (0.19) 0.69 (0.31) 0.70 (0.20) 0.40 (0.45) 0.69 (0.21) 0.28 (0.40)
Mean SD 0.91 (0.09) 0.73 (0.17) 0.81 (0.08) 0.55 (0.16) 0.70 (0.11) 0.38 (0.21) 0.65 (0.62) 0.23 (0.24)
S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395390
An ANOVA was performed on T2 detection sensitivity with condition (single-target, two-target) and lag (1–7) as within-subject factors, and group (children with ADHD, healthy 11-year-olds, healthy 8-year-olds and adults) as a between-subjectfactor.
We observed a main effect of group: F(3, 76) = 32.85, p< 0.01. Specific comparisons were made in order to provide clear-cut information on group effects driven by either developmental differences (i.e. a developmental delay) or structuraldifferences (i.e. a cognitive pathology). Overall T2 detection sensitivity was higher in adults (M = 0.82, SD = 0.10) than in 11-year-old healthy children (M = 0.68, SD = 0.1), F(1, 76) = 11.90, p< 0.01, and higher in 11-year-old healthy children than inhealthy 8-year-old children (M = 0.54, SD = 10.14): F(1, 76) = 12.31, p< 0.01. The sensitivity score (M = 0.44, SD = 0.17) waslower in children with ADHD than in healthy 11-year-olds, F(1, 76) = 33.63, p< 0.01, and healthy 8-year-olds: F(1,76) = 5.24, p< 0.05. In the single-target condition, the score was higher for the adult group (M = 0.91, SD = 0.09) than for the11-year-olds (M = 0.81, SD = 0.09), F(1, 76) = 7.15, p< 0.01, and higher for the healthy 11-year-olds than healthy 8-year-oldchildren (M = 0.70, SD = 0.1): F(1, 76) = 8.38, p< 0.01. The score for the ADHD group (M = 0.65, SD = 0.17) was lower thanthat in the control group of 11-year-olds: F(1, 76) = 16.47, p< 0.01, but similar to that in the group of healthy 8-year-olds:F(1, 76) = 1.35, NS. In the two-target condition, the adults performed better than the healthy 11-year-olds (M = 0.73,SD = 0.17, and M = 0.55, SD = 0.16, respectively): F(1, 76) = 8.53, p< 0.01. The healthy 11-year-olds performed better thanhealthy 8-year-old children (M = 0.38, SD = 0.21): F(1, 76) = 8.20, p< 0.01. Lastly, the children with ADHD (M = 0.24,SD = 0.24) had a lower score than the healthy 11-year-olds, F(1, 76) = 26.74, p< 0.01, and the healthy 8-year-olds: F(1,76) = 5.32, p< 0.05.
We observed a significant main effect of condition, F(1, 76) = 177.84, p< 0.01, with better T2 detection in the single-targetcondition (M = 0.77, SD = 0.15) than in the two-target condition (M = 0.48, SD = 0.27). The condition� lag interaction wassignificant, F(6, 456) = 4.72, p< 0.01, as was the group� condition interaction: F(3, 76) = 5.84, p< 0.01. Lastly, thecondition� lag� group interaction showed a trend towards significance: F(18, 456) = 1.48, p = 0.09.
[(Fig._4)TD$FIG]
Fig. 4. T2 detection sensitivity in the single-target condition (filled circles) and the two-target condition (open circles) in the four groups, as a function of the
seven lag times.

[(Fig._5)TD$FIG]
Fig. 5. The mean absolute difference in T2 detection sensitivity between the single-target and two-target conditions for the four groups.
S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395 391
3.3. Intergroup differences in AB parameters
To determine intergroup differences in AB parameters, we examined each of the four parameters (lag sparing, duration,minimum and amplitude) according to the model proposed by Cousineau et al. (2006).
3.3.1. Duration and lag sparing effect
Post-hoc comparisons (using Newman–Keuls post-hoc tests) were performed (see Fig. 4) in order to compareperformance levels under single-target and two-target conditions for each group and at each lag. In adults, a significant effectof condition was observed at lags 2 and 3 (p< 0.05), leading to a 200 ms AB and a lag-1 sparing effect. In healthy 11-year-oldchildren, performance was significantly better in the single-target condition than in the two-target one for lags 2, 3 and 4(p< 0.05); this resulted in a 300 ms AB duration and a lag-1 sparing effect. A significant effect of condition was observed forlags 1–7 in healthy 8-year-old children and for lags 2–7 in 11-year-old children with ADHD (p< 0.05). This resulted in a600 ms AB and a lag-1 sparing effect for children with ADHD but not for healthy 8-year-old children.
3.3.2. Amplitude and minimum
The presence of a significant group� condition interaction prompted us to determine whether the AB amplitude variedfrom one group to another. We evaluated the AB amplitude by subtracting the T2 detection rate in the single-target conditionfrom the T2 detection rate in the two-target condition (e.g. Berger, Donnadieu, Lallier, & Valdois, 2014).
An ANOVA was performed on AB amplitude, with group as a between-subject factor. Significant effects of group, F(3,76) = 8.08, p< 0.01, and lag, F(6, 76) = 4.57, p< 0.01, were observed. Specific comparisons revealed a non-significant trendtowards a lower AB amplitude in adults than in healthy 11-year-old children: F(1, 76) = 3.11, p = 0.08. The AB amplitude wassimilar in healthy 11-year-olds and healthy 8-year-olds: F(1, 76) = 1.16, NS. In children with ADHD, the AB amplitude wassignificantly higher than in age-matched (11-year-old) children, F(1,76) = 9.23, p< 0.01, and showed a non-significant trendtowards higher values than in younger (8-year-old) children: F(1, 76) = 3.84, p = 0.053.
The minimum was positioned at lags 2–4 for adults, 11-year-olds and 8-year-olds, respectively. In children with ADHD,the minimum was positioned at lag 4 (see Fig. 4).
In summary, an AB was observed in all four groups of participants. In healthy participants, the AB was longer for 8-year-olds than for 11-year-olds and longer for 11-year-olds than for adults. The position of the AB minimum differed from onegroup to another: the younger the participants, the later the minimum position. Moreover, the AB amplitude tended to belower in adults than in healthy 11-year-olds but was much the same in healthy 11-year-olds and healthy 8-year-olds. Inchildren with ADHD, the AB was longer and later than in age-matched healthy children (i.e. with a minimum at lag 4 insteadof lag 3). Hence, 11-year-old children with ADHD and healthy 8-year-old children have similar AB duration and minimumpatterns. There was a non-significant trend towards greater AB amplitude in children with ADHD than in healthy 8-year-olds(Fig. 5).
4. Discussion
The present study examined the AB in healthy participants of different ages and in children with ADHD. The objective wasto determine whether the visual temporal selective attention impairment observed in children with ADHD corresponded to adevelopmental delay or a structural deficit in cognitive processes. We shall first discuss developmental aspects of the study

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395392
(i.e. comparisons between healthy children and adults) and then discuss the developmental and structural hypotheses inADHD by focusing on the comparison between the children with ADHD and the two groups of healthy children.
4.1. Comparisons between healthy children and adult participants
In the present study, an AB was observed in adults. The AB minimum was located 200 ms after T1 presentation. This resultis consistent with previous literature data on the visual AB in adults (Reeves & Sperling, 1986; Weichselgartner & Sperling,1987; Ward & Duncan, 1996; for a review, see Shapiro et al., 1997). In healthy children, an AB was also observed but theminimum was located at 300 ms in the group of 11-year-olds and at 400 ms in the group of 8-year-olds. Our data on the timecourse of the AB are consistent with the view that the dynamics of the attentional gate (Li et al., 2004) change with age. Morespecifically, the respective AB minimum positions suggest that the attentional gate closes more slowly in 8-year-olds than in11-year-old children and more slowly in 11-year-olds than in adults. Our present results study the hypothesis whereby theefficiency of gating mechanisms that tap into inhibitory processes increases with age.
A second important result concerns the age-related increment in the AB duration. The AB was longer in healthy 8-year-olds (lags 1–7) than in healthy 11-year-old children (lags 2–4) and adults (lags 2–3). In the literature, it has been assumedthat the AB duration reflects the speed of attentional disengagement speed, i.e. the time needed to re-open the gate. Ourpresent results provide evidence of age-related differences in the speed of visual attention disengagement. In many studiesof the AB, groups of children have been broadly assessed as controls in order to highlight AB impairments in childrensuffering from pathologies such as dyslexia or ADHD (Li et al., 2004; Mason et al., 2005; Visser, Boden, & Giaschi, 2004). Tothe best of our knowledge, only three studies have focused on the developmental time course of visual attention in healthychildren (Dye & Bavelier, 2010; Garrad-Cole et al., 2011; Shapiro & Garrad-Cole, 2003). Our results are in line with thesestudies, which show that the AB shortens with age (when comparing 7-year-olds and 12-year-olds in the study by Garrad-Cole et al., 2011, for example).
Lastly, and in agreement with the literature data (for a review, see Visser, Bischol, & Di Lollo, 1999), a lag-1 sparing effectwas observed in the adult group. Importantly, a lag-1 sparing effect was observed in healthy 11-year-old children but not inhealthy 8-year-olds. The sparing effect provides information on the quantity of attentional resources available for targetprocessing over time. As pointed out by Li et al. (2004), a lag-1 sparing effect is only present if the attentional resources thathave entered the gate are sufficient. If attentional resources are insufficient, slow gate closure might result in a greater lag inthe AB minimum. The absence of a lag sparing effect in 8-year-olds thus suggests that these children’s difficulties stem from alack of attentional resources. However, this conclusion must be considered with a degree of caution, since the AB amplitudewas much the same in 8-year-old children and the older age groups. There was a non-significant trend towards adevelopment effect (i.e. a greater AB amplitude in healthy 11-year-old children than adults). In view of these results, futureresearch must seek to characterize processing limitations that may affect younger children’s temporal attention.
In summary, our present results highlighted age-related differences in the AB in healthy participants. Thesedevelopmental differences were reflected by (i) a greater time lag in the AB minimum in younger participants, (ii) longer ABsin adults than in 11-year-olds and longer ABs in 11-year-olds than in 8-year-olds, and (iii) a trend towards greater ABamplitudes in 11-year-olds than in adults. Overall, these differences may reflect a progressive increase in the efficiency ofselective temporal attention mechanisms with age.
4.2. Comparisons between children with ADHD and age-matched controls
Firstly, the AB minimum occurred later in children with ADHD (at lag 4) than in healthy 11-year-olds (lag 3). This resultsuggests that the dynamics of the attentional gate (i.e., inhibitory processes) are slower in children with ADHD than in age-matched control participants.
The AB was also longer and deeper in children with ADHD than in age-matched healthy children. This result supportsHollingsworth et al.’s (2001) findings in adults with ADHD and Li et al.’s (2004) findings in children with ADHD. It isusually considered that this longer, deeper AB reflects the time and resources required for consolidation of arepresentation of T1 in short-term memory (Chun & Potter, 1995; Jolicoeur, Tombu, Oriet, & Stevanovski, 2002). In Chunand Potter’s (1995) two-stage model, stimuli are detected at stage 1 and consolidated serially at stage 2 (a capacity-limited stage in which the relevant stimuli candidate for processing, T1 and T2, are fully identified and registered inmemory). After this consolidation phase (required for T1 identification), the attentional focus would have to disengagefrom T1 before it could process T2. In children with ADHD, stage 2 processing might be slower (lead to a longer AB) andmight require more attentional resources for consolidation of the target in short term memory (leading to a deeper AB).This is consistent with Barkley’s claim that children with ADHD have problems in encoding and maintaining informationin working memory.
The attention gating model (Li et al., 2004) provides another possible interpretation of the longer, deeper AB in childrenwith ADHD. It suggests that the attentional gate re-opens more slowly for subsequent processing of relevant stimuli (i.e. T2);hence, stimuli that appear when the gate is still closed would be ‘‘blinked out’’. This interpretation is particularly interestingin two respects. Firstly, it is consistent with a potential difficulty in the re-engagement temporal attention to T2 afteridentification of T1. Secondly, this interpretation is coherent with the greater lag in the AB minimum in children with ADHDobserved in the present study. This observation supports the hypothesis whereby the overall functioning of the attentional

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395 393
gate is slower in children with ADHD. When combined with the absence of sufficient attentional resources, this slow-downwould lead to a deeper, longer AB.
4.3. Is the attentional disorder in ADHD related to a developmental delay or a specific cognitive deficit?
In view of our developmental hypotheses, we looked at whether the efficiency of the attentional gate was age-dependant.Our results suggest that this is indeed the case (as exemplified by our comparison between healthy children and adults). Thisdevelopmental effect provides a novel interpretation of literature observations in children with ADHD. The central questionwas whether the specific RSVP task performance pattern observed in children with ADHD resulted from a developmentaldelay in attention maturation or a specific structural dysfunction in the attentional processes.
Our results support the former explanation, since the AB’s duration and minimum position were equivalent in 11-year-old children with ADHD and healthy 8-year-old children. There were also developmental differences between the 8-year-oldchildren, the 11-year-old children and adults. In children with ADHD, the AB minimum occurred at lag 4 (as in healthy 8-year-old children), rather than at lag 3 (as in healthy 11-year-old children). This result suggests that the dynamics of theattentional gate (i.e. the inhibitory processes) are slower in children with ADHD than in healthy age-matched children andslower in healthy younger children than in healthy older children.
We propose then that the peak efficiency of the attentional gating mechanisms (required to engage and disengage theattention needed for this type of task) occurs later in children with ADHD than in healthy children of the same age. However,our results also provide evidence of specific, disease-related effects. Indeed, the AB was deeper in children with ADHD than inage-matched children and showed a non-significant trend toward being deeper than in the 8-year-old children. This resultsuggests that attentional resources in children with ADHD correspond to structural deficit rather than a developmentaldelay. Nevertheless, the absence of developmental difference between the 11-year-olds and the 8-year-olds prevents usfrom concluding as to the presence of a structural deficit. Future research must address this hypothesis.
5. Limitations and conclusions
A atypical patterns of AB amplitude and/or duration have already been reported in previous studies of patients presentingvarious pathologies (such as dyslexia, schizophrenia, and depression) or focal brain lesions (Hari, Valta, & Uutela, 1999;Husain, Shapiro, Martin, & Kennard, 1997; Lallier, Donnadieu, Berger, et al., 2010; Lallier, Donnadieu, & Valdois, 2010; Li et al.,2002; Rizzo, Akutsu, & Dawson, 2001; Rokke, Atmel, Koch, & Andrews, 2002). Hence, these AB deficits may not be specific toADHD patients. Our present study supports the earlier suggestion (Li et al., 2004) that a greater lag in the AB minimum isspecific to ADHD populations. Indeed, Li et al. (2004) considered that the gating deficit (i.e. time needed to close or re-openthe gate) may be critical in the attention impairment observed in children with ADHD. Taken as a whole, Li et al.’s findingsand our present results clarify the origin of the deficit in ADHD (i.e. a developmental delay potentially combined with specificimpairments).
Importantly, we did not look at individual profiles and the attention impairment subtypes of the children with ADHD inthe present study. However, the presence of specific attention impairments for ADHD subtypes has not yet been clearlyevidenced (Carr et al., 2006). Furthermore, the influence of different ADHD subtypes on performance appears to concernperformance in tasks that involve the posterior attentional network rather than the anterior attentional network (for areview, see Nigg, 2006). Overall, we showed that an RSVP task is a useful tool for describing attentional impairments inchildren with ADHD. Restricting the investigation to meaningful AB parameters in the ADHD population might help toclarifying the exact nature of the deficit. Lastly, further research should establish whether use of the RSVP task can shed lighton attentional deficits as a function of the ADHD subtype (i.e. ADHD-COM and ADHD-I).
Our study is important in terms of clinical practice. ADHD is most often assessed using indirect measurements such as theConnors’ questionnaire. It is important to develop objective measures (i.e., quantitative measures of the attentional deficit)that help determining the magnitude of the disorder. A characterization of the deficit using the AB parameter can then beparticularly useful for providing a reliable diagnosis. This allows to focus remediation on key aspects (which will be differentdepending on whether the patient have sustained attention deficits, selective attention deficits, attentional engagementretardation, etc.).
Acknowledgments
This research was funded by the HyperSupers TDAH France charity (http://www.tdah-france.fr/Le-prix-Ribot-Dugas.html). Marie Lallier received a PhD fellowship from the Ministere de l’Education Nationale, de la Recherche et dela Technologie. We also thank the participants and their families for their time and commitment. Lastly, we thank Dr DavidFraser (Biotech Communication SARL, Damery, France) for medical writing support.
References
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: APA.

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395394
Armstrong, I. T., & Munoz, D. P. (2003). Attentional blink in adults with attention-deficit hyperactivity disorder. Influence of eye movements. Experimental BrainResearch, 152, 243–250.
Babinski, L. M., Hartsough, C. S., & Lambert, N. M. (1999). Childhood conduct problems, hyperactivity–impulsivity, and inattention as predictors of adult criminalactivity. Journal of Child Psychology and Psychiatry, 40(3), 347–355.
Barkely, R. A. (1990). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford Press.Barkley, R. A., Fischer, M., Edelbrock, C. S., & Smallish, L. (1990). The adolescent outcome of hyperactive children diagnosed by research criteria: I. An 8-year
prospective follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry, 29, 546–557.Beauchaine, T. P., Hinshaw, S. P., & Pang, K. C. (2010). Comorbidity of attention-deficit/hyperactivity disorder and conduct disorder: Biological, environmental, and
developmental mechanisms. Clinical Psychology: Science and Practice, 17, 327–336.Berger, C., Donnadieu, S., Lallier, M., & Valdois, S. (2014). Age-related changes in temporal allocation of visual attention: Evidence from the rapid visual serial
presentation (RVSP) paradigm. Journal of Cognition and Development (in press).Biederman, J., Wozniak, J., Tarko, L., Serra, G., Hernandez, M., McDermott, K., et al. (2014). Re-examining the risk for switch from unipolar to bipolar major
depressive disorder in youth with ADHD: A long term prospective longitudinal controlled study. Journal of Affective Disorders, 152-154, 347–351.Blondis, T. A., Snow, J. H., & Accardo, P. J. (1999). Methods of measuring attention deficits with or without hyperactivity–impulsivity. In P. J. Accardo, T. A. Blondis,
B. Y. Whitman, & M. A. Stein (Eds.), Attention deficits and hyperactivity in children and adults (pp. 163–187). New York: Marcel Dekker Inc.Booth, J. R., Burman, D. D., Meyer, J. R., Lei, Z., Trommer, B. L., Davenport, N. D., et al. (2005). Larger deficits in brain networks for response inhibition than for visual
selective attention in attention deficit hyperactivity disorder (ADHD). Journal of Child Psychology and Psychiatry, 46(1), 94–111.Broadbent, D. E., & Broadbent, M. H. P. (1987). From detection to identification: Response to multiple targets in rapid serial visual presentation. Perception &
Psychophysics, 42, 105–113.Carr, L. A., Nigg, J. T., & Henderson, J. M. (2006). Attentional versus motor inhibition in adults with attention-deficit/hyperactivity disorder. Neuropsychology, 20(4),
430–441.Chevalier, N. (2010). Les fonctions executives chez l’enfant: Concepts et developpement. Canadian Psychology, 51(3), 149–163.Chun, M. M., & Potter, M. C. (1995). A two-stage model for multiple target detection in rapid serial visual presentation. Journal of Experimental Psychology: Human
Perception and Performance, 21, 109–127.Cousineau, D., Charbonneau, D., & Jolicoeur, P. (2006). Parameterizing the attentional blink effect. Canadian Journal of Experimental Psychology, 60, 175–189.Cragg, L., & Nation, K. (2008). Go or no go? Developmental improvements in the efficiency of response inhibition in mid-childhood. Development Science, 11,
819–827.Craston, P., Wyble, B., Chennu, S., & Bowman, H. (2008). The attentional blink reveals serial working memory encoding: Evidence from virtual and human event-
related potentials. Journal of Cognitive Neuroscience, 21, 550–566.Doehnert, M., Brandeis, D., Imhof, K., Drechsler, R., & Steinhausen, H. C. (2010). Mapping attention-deficit/hyperactivity disorder (ADHD) from childhood to
adolescence – No neurophysiological evidence for a developmental lag of attention but some for inhibition. Biological Psychiatry, 67, 608–616.Dye, M. W. G., & Bavelier, D. (2010). Differential development of visual attention skills in school-age children. Vision Research, 50, 452–459.Garrad-Cole, F., Shapiro, K. L., & Thierry, G. (2011). Developmental aspects of temporal and spatial visual attention: Insights from the attentional blink and visual
search tasks. Child Neuropsychology, 17(2), 118–137.Giesbrecht, B. L., & Di Lollo, V. (1998). Beyond the attentional blink: Visual masking by item substitution. Journal of Experimental Psychology: Human Perception and
Performance, 24, 1454–1466.Giesbrecht, B. L., Sy, J. L., & Elliott, J. C. (2007). Electrophysiological evidence for both perceptual and postperceptual selection during the attentional blink. Journal
of Cognitive Neuroscience, 19, 2005–2018.Gonon, F., Guile, J.-M., & Cohen, D. (2010). Le trouble deficitaire de l’attention avec hyperactivite: Donnees recentes des neurosciences et de l’experience nord-
americaine. Neuropsychiatrie de l’enfance et de l’adolescence, 58, 273–281.Halldorsdottir, T., & Ollendick, T. H. (2014). Comorbid ADHD: Implications for the treatment of anxiety disorders in children and adolescents. Cognitive and
Behavioral Practice, 21(3), 310–322.Halperin, J. M., & Schulz, K. P. (2006). Revisiting the role of the prefrontal cortex in the pathophysiology of attention-deficit/hyperactivity disorder. Psychological
Bulletin, 132, 560–581.Hari, R., & Renvall, H. (2001). Impaired processing of rapid stimulus sequences in dyslexia. Trends in Cognitive Sciences, 5, 525–532.Hari, R., Valta, M., & Uutela, K. (1999). Prolonged attentional dwell time in dyslexic adults. Neuroscience Letters, 271, 202–204.Hazell, P. L., Carr, V. J., Lewin, T. J., Dewis, S., Heathcote, D. M., & Brucki, B. M. (1999). Effortful and automatic processing in boys with ADHD and specific learning
disorders. Journal of Child Psychology and Psychiatry, 40, 275–286.Hollingsworth, D. E., McAuliffe, S. P., & nowlton, K. B. l. (2001). Temporal allocation of visual attention in adult attention deficit hyperactivity disorder. Journal of
Cognitive Neuroscience, 13, 298–305.Huang-Pollock, C. L., Carr, T. H., & Nigg, J. T. (2002). Development of selective attention: Perceptual load influences early versus late attentional selection in
children and adults. Developmental Psychology, 38(3), 363–375.Husain, M., Shapiro, K., Martin, J., & Kennard, C. (1997). Abnormal temporal dynamics of visual attention in spatial neglect patients. Nature, 385, 154–156.Jolicoeur, P., & Dell’ Acqua, R. (1998). The demonstration of short-term consolidation. Cognitive Psychology, 36, 138–202.Jolicoeur, P., Sessa, P., Dell’Acqua, R., & Robitaille, N. (2006). Attentional control and capture in the attentional blink paradigm: Evidence from human
electrophysiology. European Journal of Cognitive Psychology, 18, 560–578.Jolicoeur, P., Tombu, M., Oriet, C., & Stevanovski, B. (2002). From perception to action: Making the connection – A tutorial. In W. Prinz & B. Hommel (Eds.), Attention
and Performance XIX: Common mechanisms of perception and action. Oxford: University Press.Karatekin, C., & Asarnow, R. F. (1998). Components of visual search in childhood onset schizophrenia and attention deficit hyperactivity disorder. Journal of
Abnormal Child Psychology, 26, 367–380.Kipp, K. (2005). A developmental perspective on the measurement of cognitive deficits in attention-deficit/hyperactivity disorder. Biological Psychiatry, 57,
1256–1260.Klein, R., & Mannuza, S. (1991). Long term outcome of hyperactive children: A review. Journal of the American Academy of Child and Adolescent Psychiatry, 30,
383–387.Kranczioch, C., Debener, S., & Engel, A. K. (2003). Event-related potential correlates of the attentional blink phenomenon. Cognitive Brain Research, 17, 177–187.Lallier, M., Donnadieu, S., Berger, C., & Valdois, S. (2010). A case study of developmental phonological dyslexia: Is the attentional deficit in the perception of rapid
stimuli sequences amodal? Cortex, 46, 231–241.Lallier, M., Donnadieu, S., & Valdois, S. (2010). Visual attentional blink in dyslexie children: Parameterizing the deficit. Vision Research, 50, 1855–1861.Lefavrais, P. (1967). Test de l’Alouette. Paris: Editions du centre de psychologie appliquee.Li, C-S.R., Chen, S.-H., Lin, W.-H., & Yang, Y.-Y. (2005). Attentional blink in adolescents with varying levels of impulsivity. Journal of Psychiatric Research, 39,
197–205.Li, C.-S.R., Lin, W.-H., Chang, H.-L., & Hung, Y.-W. (2004). A psychophysical measure of attention deficit in children with attention deficit hyperactivity disorder.
Journal of Abnormal Psychology, 113(2), 228–236.Li, C.-S.R., Lin, W. H., Yang, Y. Y., Huang, C. C., Chen, Y. C., & Chen, T. W. (2002). Impairment of temporal attention in patients with schizophrenia. NeuroReport, 13,
1427–1430.Lutcke, H., Gevensleben, H., Albrecht, B., & Frahm, J. (2009). Brain networks involved in early versus late response anticipation and their relation to conflict
processing. Journal of Cognitive Neuroscience, 21, 2172–2184.Macmillan, N. A., & Creelman, C. D. (1991). Detection Theory: A user’s guide. London: Lawrence Erlbaum Associates.Mason, D. J., Humphreys, G. W., & Kent, L. S. (2003). Exploring selective attention in ADHD: Visual search through space and time. Journal of Child Psychology and
Psychiatry, 44, 1158–1176.

S. Donnadieu et al. / Research in Developmental Disabilities 36 (2015) 384–395 395
Mason, D. J., Humphreys, G. W., & Kent, L. (2005). Insights into the control of attentional set in ADHD using the attentional blink paradigm. Journal of ChildPsychology and Psychiatric, 46(12), 1345–1353.
McArthur, G., Budd, T., & Michie, P. (1999). The attentional blink and P300. Neuroreport, 10, 3691–3695.Nigg, J.-T. (2006). What causes ADHD: Understanding what goes wrong and why. New York: Guilford Press.Olivers, C. N. L., & Watson, D. G. (2006). Input control process in rapid serial visual presentations: Target selection and distractor. Journal of Experimental
Psychology: Human Perception and Performance, 32(5), 1083–1092.Pennequin, V., Nanty, I., & Khomsi, A. (2004). Mesurer la resistance a l’interference chez l’enfant: Elaboration d’un nouveau test a effet Stroop. L’annee
Psychologique, 104, 203–226.Raymond, J. E., Shapiro, K. L., & Arnell, K. M. (1992). Temporary suppression of visual processing in an RSVP task: An attentional blink? Journal of Experimental
Psychology: Human Perception and Performance, 18, 849–860.Raymond, J. E., Shapiro, K. L., & Arnell, K. M. (1995). Similarity determines the attentional blink. Journal of Experimental Psychology: Human Perception and
Performance, 21, 653–662.Reeves, A., & Sperling, G. (1986). Attention gating in short-term visual memory. Psychological Review, 93, 180–206.Rizzo, M., Akutsu, H., & Dawson, J. (2001). Increased attentional blink after focal cerebral lesions. Neurology, 57, 795–800.Rokke, P. D., Atmel, K. M., Koch, M. D., & Andrews, J. T. (2002). Dual-task attention deficits in dysphoric mood. Journal of Abnormal Psychology, 111, 370–379.Sergent, C., Baillet, S., & Dehaene, S. (2005). Timing of the brain events underlying access to consciousness during the attentional blink. Nature Neuroscience, 8,
1391–1400.Sessa, P., Luria, R., Verleger, R., & Dell’Acqua, R. (2007). P3 latency shifts in the attentional blink: Further evidence for second target processing postponement. Brain
Research, 1137, 131–139.Shapiro, K. L., Arnell, K. M., & Raymond, J. E. (1997). The attentional blink. Trends in Cognitive Science, 1, 291–296.Shapiro, K. L., & Garrad-Cole, F. (2003). Age-related deficits and involvement of frontal cortical areas as revealed by the attentional blink task. Journal of Vision,
3, 726a.Shapiro, K. L., & Raymond, J. E. (1994). Temporal allocation of visual attention: Inhibition or interference? In D. Dagenbach & T. H. Carr (Eds.), Inhibitory mechanisms
in attention, memory and language (pp. 151–187). San Diego, CA: Academic Press.Shapiro, K. L., Raymond, J. E., & Arnell, K. M. (1994). Attention to visual pattern information produces the attentional blink in rapid serial visual presentation.
Journal of Experimental Psychology: Human Perception and Performance, 20, 357–371.Shaw, P., Eckstrand, K., Sharp, W., Blumenthal, J., Lerch, J. P., & Greenstein, D. (2007). Attention-deficit/hyperactivity disorder is characterized by a delay in cortical
maturation. Proceedings of the National Academy of Sciences of the United States of America, 104, 19649–19654.Smith, A. B., Taylor, E., Lidzba, K., & Rubia, K. (2003). A right hemispheric frontocerebellar network for time discrimination of several hundreds of milliseconds.
NeuroImage, 20(1), 344–350.Sperling, G., & Weichselgartner, E. (1995). Episodic theory of the dynamics of spatial attention. Psychological Review, 102, 503–532.Szatmari, P. (1992). The epidemiology of attention-deficit hyperactivity disorders. In G. Weiss (Ed.), Child and adolescent psychiatry clinics of North America:
Attention deficit disorder (pp. 361–372). Philadelphia: W.B. Saunders.Toplack, M. E., Dockstader, C., & Tannock, R. (2006). Temporal information processing in ADHD: Findings to date and new methods. Journal of Neuroscience
Methods, 151, 15–29.Treisman, A. M., & Gelade, G. A. (1980). Feature-integration theory of attention. Cognitive Psychology, 12, 97–136.Tsal, Y., Shalev, L., & Mevorach, C. (2005). The diversity of attention deficits in ADHD: The prevalence of four cognitive factors in ADHD versus controls. Journal of
Learning Disabilities, 38(2), 142–157.Valko, L., Doehnert, M., Muller, U. C., Schneider, G., Albrecht, B., Drechsler, R., et al. (2009). Differences in neurophysiological markers of inhibitory and temporal
processing deficits in children and adults with ADHD. Journal of Psychophysiology, 23(4), 235–246.Van der Meere, J., & Sergeant, J. (1988). Focused attention in pervasively hyperactive children. Journal of Abnormal Child Psychology, 16, 627–639.Visser, T. A. W., Bischol, W. F., & Di Lollo, V. (1999). Attentional switching in spatial and nonspatial domains: Evidence from the attentional blink. Psychological
Bulletin, 125(4), 458–469.Visser, T. A. W., Boden, C., & Giaschi, D. E. (2004). Children with dyslexia: Evidence for visual attention deficits in perception of rapid sequences of objects. Vision
Research, 44, 2521–2535.Vogel, E. K., Luck, S. J., & Shapiro, K. L. (1998). Electrophysiological evidence for a postperceptual locus of suppression during the attentional blink. Journal of
Experimental Psychology: Human Perception and Performance, 24, 1656–1674.Ward, R., & Duncan, J. (1996). The slow time-course of visual attention. Cognitive Psychology, 30, 79–109.Weichselgartner, E., & Sperling, G. (1987). Dynamics of automatic and controlled visual attention. Science, 238, 778–780.Weiss, G., & Hechtman, L. (1993). Hyperactive children grown up (2nd ed.). New York: Guilford Press.Wilding, J. (2005). Is attention impaired in ADHD? British Journal of Developmental Psychology, 23, 487–505.Wolfe, J. M. (1998). Visual search. In H. Pashler (Ed.), Attention (pp. 13–73). Hove, East Sussex: Psychology Press.Wright, I., Waterman, M., Prescott, H., & Murdoch-Eaton, D. (2003). A new Stroop-like measure of inhibitory function development: Typical development trends.
Journal of Child Psychology and Psychiatry, 44, 561–575.














![Yackety yack [serial] - Internet Archive](https://static.fdokumen.com/doc/165x107/63276564e491bcb36c0b431c/yackety-yack-serial-internet-archive.jpg)
![The Chanticleer [serial]](https://static.fdokumen.com/doc/165x107/632863a3051fac18490eb46f/the-chanticleer-serial.jpg)

![North Carolina register [serial] - NC OAH](https://static.fdokumen.com/doc/165x107/633bb631a24651471c0221d8/north-carolina-register-serial-nc-oah.jpg)

