Percutaneous vertebroplasty and kyphoplasty for painful vertebral body fractures in cancer patients
Upload
independentCategory
view
9download
0
JOURNAL OF BONE AND MINERAL RESEARCHVolume 24, Number 7, 2009Published online on February 9, 2009; doi: 10.1359/JBMR.090202� 2009 American Society for Bone and Mineral Research
Advanced Vertebral Fracture Among Newly Diagnosed ChildrenWith Acute Lymphoblastic Leukemia: Results of the Canadian
Steroid-Associated Osteoporosis in the Pediatric Population(STOPP) Research Program
Jacqueline Halton,1 Isabelle Gaboury,1 Ronald Grant,2 Nathalie Alos,3 Elizabeth A. Cummings,4 Maryann Matzinger,1
Nazih Shenouda,1 Brian Lentle,5 Sharon Abish,6 Stephanie Atkinson,7 Elizabeth Cairney,8 David Dix,5
Sara Israels,9 David Stephure,10 Beverly Wilson,11 John Hay,12 David Moher,1 Frank Rauch,6 Kerry Siminoski,11
Leanne M. Ward,1 and the Canadian STOPP Consortium
ABSTRACT: Vertebral compression is a serious complication of childhood acute lymphoblastic leukemia(ALL). The prevalence and pattern of vertebral fractures, as well as their relationship to BMD and otherclinical indices, have not been systematically studied. We evaluated spine health in 186 newly diagnosedchildren (median age, 5.3 yr; 108 boys) with ALL (precursor B cell: N = 167; T cell: N = 19) who were enrolledin a national bone health research program. Patients were assessed within 30 days of diagnosis by lateralthoraco-lumbar spine radiograph, bone age (also used for metacarpal morphometry), and BMD. Vertebralmorphometry was carried out by the Genant semiquantitative method. Twenty-nine patients (16%) had atotal of 75 grade 1 or higher prevalent vertebral compression fractures (53 thoracic, 71%; 22 lumbar). Grade1 fractures as the worst grade were present in 14 children (48%), 9 patients (31%) had grade 2 fractures, and6 children (21%) had grade 3 fractures. The distribution of spine fracture was bimodal, with most occurringin the midthoracic and thoraco-lumbar regions. Children with grade 1 or higher vertebral compression hadreduced lumbar spine (LS) areal BMD Z-scores compared with those without (mean ± SD, 22.1 ± 1.5 versus21.1 ± 1.2; p < 0.001). LS BMD Z-score, second metacarpal percent cortical area Z-score, and back painwere associated with increased odds for fracture. For every 1 SD reduction in LS BMD Z-score, the oddsfor fracture increased by 80% (95% CI: 10–193%); the presence of back pain had an OR of 4.7 (95% CI:1.5–14.5). These results show that vertebral compression is an under-recognized complication of newlydiagnosed ALL. Whether the fractures will resolve through bone growth during or after leukemia chemo-therapy remains to be determined.J Bone Miner Res 2009;24:1326–1334. Published online on February 9, 2009; doi: 10.1359/JBMR.090202
Key words: childhood leukemia, prevalent vertebral fractures
Address correspondence to: Leanne M. Ward, MD, FRCPC, STOPP Principal Investigator and Director, Pediatric BoneHealth Clinical and Research Programs, Children’s Hospital of Eastern Ontario, 401 Smyth Road, Ottawa, Ontario,
Canada K1H 8L1, E-mail: [email protected]
INTRODUCTION
ACUTE LYMPHOBLASTIC LEUKEMIA (ALL), a malignantdisorder of lymphoid progenitor cells, is the most
common form of childhood cancer.(1) Fortunately, contin-ued progress in the development of effective treatmentregimes for ALL has led to a cure rate of >80%.(2) As curerates improve, the sequelae attributed to the disease or itstreatment are increasingly recognized, with skeletal healthhaving emerged as an important short- and long-termconcern for childhood ALL survivors.
Bone morbidity in childhood ALL has long been studiedthrough retrospective review of radiographs and found tobe associated with the leukemic process. Bone lesions havebeen apparent at the time of diagnosis and are purportedlymore frequent in the appendicular than in the axial skele-ton.(3) At appendicular sites, transverse metaphyseal radi-olucencies, lytic and osteosclerotic lesions, and periosteallifting have been observed in numerous reports.(4–7) Ver-tebral fractures have also been reported to occur in chil-dren with newly diagnosed ALL and have typically beenconsidered a rare manifestation of the disease.(8–10) A largeseries of almost 1500 children who were evaluated forvertebral compression on routine chest radiographs at the
1University of Ottawa, Ottawa, Ontario, Canada; 2University of Toronto, Toronto, Ontario, Canada; 3Universite de Montreal,Montreal, Quebec, Canada; 4Dalhousie University, Halifax, Nova Scotia, Canada; 5University of British Columbia, Vancouver, BritishColumbia, Canada; 6McGill University, Montreal, Quebec, Canada; 7McMaster University, Hamilton, Ontario, Canada; 8University ofWestern Ontario, London, Ontario, Canada; 9University of Manitoba, Winnipeg, Manitoba, Canada; 10University of Calgary, Calgary,Alberta, Canada; 11University of Alberta, Edmonton, Alberta, Canada; 12Brock University, St. Catharines, Ontario, Canada.
The authors state that they have no conflicts of interest.
1326

time of ALL diagnosis found a vertebral fracture preva-lence of <2%.(11) However, the specific methodology di-recting the vertebral fracture assessment, the pattern ofvertebral fractures in the lumbar and thoracic spine, andthe relationship between vertebral fractures and otherskeletal parameters such as BMD were not reported.
Therefore, the purpose of this report was to carry out aprospective evaluation of the prevalence, location, sever-ity, and morphology of thoracic and lumbar vertebralfractures in a large, multicenter cohort of children withnewly diagnosed ALL. We further sought to determine therelationship between vertebral fractures and relevantclinical parameters such as the characteristics of the ALL,frequency of back pain, spine BMD, and cortical thickness.
MATERIALS AND METHODS
Patients and study design
Children and adolescents enrolled in the study wererecruited through the Canadian Steroid-Associated Oste-oporosis in the Pediatric Population (STOPP) researchinitiative, a national pediatric bone health research pro-gram funded by the Canadian Institutes of Health Re-search to study bone health and determinants of bonemorbidity in children with chronic illnesses. Patients from1 mo to 17 yr of age were enrolled in the study (N = 186)between January 1, 2005 and December 31, 2007 in 10 par-ticipating tertiary care children’s hospitals across Canada.Patients were studied within 30 days of chemotherapy in-itiation for the treatment of ALL. Children with newlydiagnosed ALL were excluded if the study procedurescould not be carried out within 30 days of chemotherapyinitiation, if they had received prior therapy with medica-tion to treat osteoporosis, if they had received prior treat-ment with calcium and/or vitamin D supplementation thatexceeded the Dietary Reference Intake for age,(12) or ifthey were pregnant or menstruating and unwilling to usea medically approved method of contraception during thecourse of the study. Patients were also excluded from thestudy if they had received, in the 12 mo preceding enroll-ment, intravenous or oral glucocorticoids for >14 consec-utive days before initiation of chemotherapy for thetreatment of the leukemia. The study was approved by theResearch Ethics Boards in each of the participating insti-tutions, and informed consent and/or assent, as appropri-ate, was obtained before study enrollment.
Clinical data
Standard demographic data including age, ethnicity, andALL subdiagnosis (precursor B or T cell) were recorded.All patients were treated according to the Children’s On-cology Group protocols (nine sites) or the Dana FarberCancer Institute protocols (one site). The children wereassigned to a leukemia risk category for relapse (high orstandard risk) as per the National Cancer Institute riskcriteria. Height was measured using a regularly calibratedstadiometer by a pediatric nurse or research associate.Measurements were taken three times, and the averagewas recorded. Infants and children unable to stand were
measured in the supine position; others were measuredstanding. Weight was determined using either a digital ormechanical scale. Height and weight raw values weretransformed into age- and sex-matched Z-scores accordingto the U.S. CDC National Center for Health Statisticsnormative database.(13) Pubertal staging was carried outaccording to the methods of Marshall and Tanner.(14,15)
The presence or absence of back pain at the time of diag-nosis was recorded.
Bone densitometry
BMD was measured in the anterior-posterior directionat the lumbar spine (LS, L1–L4) using either Hologic ma-chines (QDR 4500, three centers; Discovery, two centers;Delphi, one center) or Lunar Prodigy (four centers). Ma-chines were cross-calibrated using a spine phantom thatwas circulated before the study, and measurements wereconverted to Hologic units. LS BMD results were trans-formed to age- and sex-specific Z-scores using the Hologic12.4 normative database. In vivo precision was available in9 of 10 centers and ranged from 0.003 to 0.0173 g/cm2.
Bone age assessment
Radiographs of the left hand and wrist for bone age wereassessed independently by two pediatric radiologists (N.S.,M.M.) according to Greulich and Pyle.(16) If results for thetwo examiners were within 12 mo of each other, the aver-age of the two readings was used. For results that differedby >12 mo (n = 3), a third reader (L.M.W.), blinded to theresults of the first two readings, adjudicated the discrepantreports. The intraclass correlation coefficient, which as-sessed interobserver reliability, was 0.992 (95% CI: 0.989–0.994) between the two initial examiners. The radiographswere also evaluated for the possibility of rickets.
Hand morphometry
From the hand radiographs used for bone age determi-nation, a single observer measured second metacarpallength, midshaft periosteal diameter, and inner diame-ter.(17) From these measurements, the following indiceswere derived: combined cortical thickness, cortical area,percent cortical area, and inner diameter area. Measuredand derived indices were converted into age- and sex-matched Z-scores as previously described.(18) The intra-observer reliability scores assessed by intraclass correlationcoefficient for hand morphometry measurements were asfollows: 1.0 (95% CI: 0.999–1.0), 0.99 (95% CI: 0.986–0.997), and 0.89 (95% CI: 0.777–0.945) for metacarpallength, outer diameter, and inner diameter, respectively.
Vertebral morphometry
Lateral spine radiographs were taken on one or twocassettes, according to the size of the child. Vertebralfracture assessment was carried out independently by tworadiologists (N.S., M.M.) from T4 to L4 according to theGenant semiquantitative(19) method. Discrepancies inspecific vertebral body readings between the first two ra-diologists were resolved by a third expert radiologist(B.L.), who was blinded to the results of the other two. The
VERTEBRAL FRACTURE IN CHILDHOOD ALL 1327
interobserver reliability for the first two readers, as assessedby Cohen’s k, was 0.44 (95% CI: 0.28, 0.59) for fracturedefined as grades 1, 2, or 3 and 0.66 (95% CI: 0.46, 0.87)for fracture defined as grades 2 or 3.
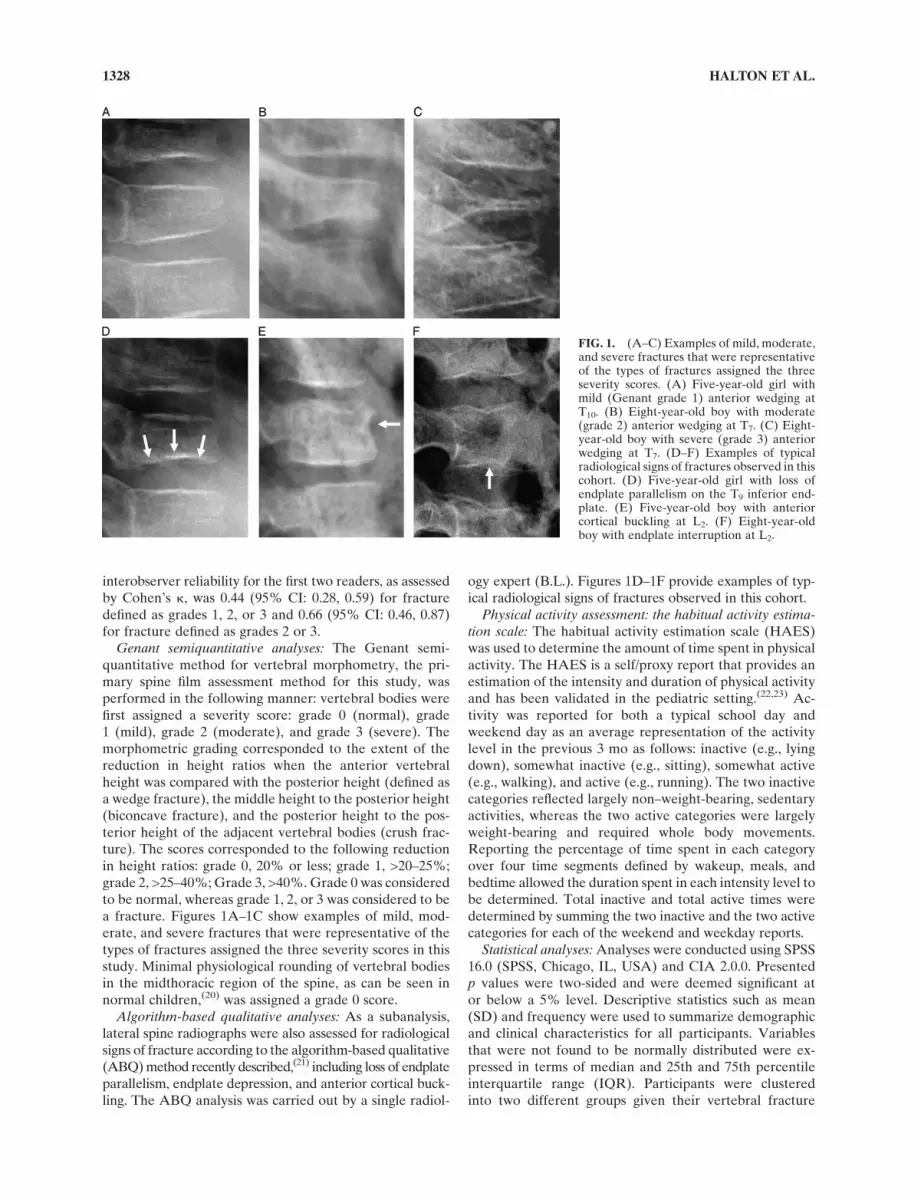
Genant semiquantitative analyses: The Genant semi-quantitative method for vertebral morphometry, the pri-mary spine film assessment method for this study, wasperformed in the following manner: vertebral bodies werefirst assigned a severity score: grade 0 (normal), grade1 (mild), grade 2 (moderate), and grade 3 (severe). Themorphometric grading corresponded to the extent of thereduction in height ratios when the anterior vertebralheight was compared with the posterior height (defined asa wedge fracture), the middle height to the posterior height(biconcave fracture), and the posterior height to the pos-terior height of the adjacent vertebral bodies (crush frac-ture). The scores corresponded to the following reductionin height ratios: grade 0, 20% or less; grade 1, >20–25%;grade 2, >25–40%; Grade 3, >40%. Grade 0 was consideredto be normal, whereas grade 1, 2, or 3 was considered to bea fracture. Figures 1A–1C show examples of mild, mod-erate, and severe fractures that were representative of thetypes of fractures assigned the three severity scores in thisstudy. Minimal physiological rounding of vertebral bodiesin the midthoracic region of the spine, as can be seen innormal children,(20) was assigned a grade 0 score.
Algorithm-based qualitative analyses: As a subanalysis,lateral spine radiographs were also assessed for radiologicalsigns of fracture according to the algorithm-based qualitative(ABQ) method recently described,(21) including loss of endplateparallelism, endplate depression, and anterior cortical buck-ling. The ABQ analysis was carried out by a single radiol-
ogy expert (B.L.). Figures 1D–1F provide examples of typ-ical radiological signs of fractures observed in this cohort.
Physical activity assessment: the habitual activity estima-tion scale: The habitual activity estimation scale (HAES)was used to determine the amount of time spent in physicalactivity. The HAES is a self/proxy report that provides anestimation of the intensity and duration of physical activityand has been validated in the pediatric setting.(22,23) Ac-tivity was reported for both a typical school day andweekend day as an average representation of the activitylevel in the previous 3 mo as follows: inactive (e.g., lyingdown), somewhat inactive (e.g., sitting), somewhat active(e.g., walking), and active (e.g., running). The two inactivecategories reflected largely non–weight-bearing, sedentaryactivities, whereas the two active categories were largelyweight-bearing and required whole body movements.Reporting the percentage of time spent in each categoryover four time segments defined by wakeup, meals, andbedtime allowed the duration spent in each intensity level tobe determined. Total inactive and total active times weredetermined by summing the two inactive and the two activecategories for each of the weekend and weekday reports.
Statistical analyses: Analyses were conducted using SPSS16.0 (SPSS, Chicago, IL, USA) and CIA 2.0.0. Presentedp values were two-sided and were deemed significant ator below a 5% level. Descriptive statistics such as mean(SD) and frequency were used to summarize demographicand clinical characteristics for all participants. Variablesthat were not found to be normally distributed were ex-pressed in terms of median and 25th and 75th percentileinterquartile range (IQR). Participants were clusteredinto two different groups given their vertebral fracture
FIG. 1. (A–C) Examples of mild, moderate,and severe fractures that were representativeof the types of fractures assigned the threeseverity scores. (A) Five-year-old girl withmild (Genant grade 1) anterior wedging atT10. (B) Eight-year-old boy with moderate(grade 2) anterior wedging at T7. (C) Eight-year-old boy with severe (grade 3) anteriorwedging at T7. (D–F) Examples of typicalradiological signs of fractures observed in thiscohort. (D) Five-year-old girl with loss ofendplate parallelism on the T9 inferior end-plate. (E) Five-year-old boy with anteriorcortical buckling at L2. (F) Eight-year-oldboy with endplate interruption at L2.
1328 HALTON ET AL.

status at baseline: fracture (grades 1–3) versus no fracture(grade 0) as assessed by the Genant score. Differencesbetween these two groups in clinical parameters measuredon a continuous scale were assessed using Student’s t-test.A nonparametric approach (Wilcoxon Mann-Whitneytest) was used when required by the shape of the param-eter’s distribution. Sex, leukemia diagnosis, and leukemiarisk category, as well as pubertal stage and presence ofback pain, were compared using x2 test or Fisher’s exacttest, as appropriate.
A logistic regression was performed to identify whetherLS BMD Z-score, percent cortical area Z-score, andpresence of back pain were statistically related to vertebralfracture in the study sample. These variables were chosen apriori based on the parameters that were anticipated to berelevant clinically. ORs along with their 95% CIs werepresented. Differences in LS BMD Z-score between frac-ture severity grades were assessed using a one-way ANOVAand the Scheffe posthoc analysis.
RESULTS
Clinical characteristics
Clinical characteristics of the 186 children with newlydiagnosed ALL are provided in Table 1. Most of the
children were white (75%), precursor B-cell ALL was themost common immunophenotype (90%), and the majorityof subjects were assessed as standard risk ALL (63%).Bone age (median, 5.0 yr) and chronological age (median,5.3 yr) were similar among this largely prepubertal (Tannerstage 1, 78%) cohort. Weight and stature were above av-erage. The LS BMD Z-score was reduced for the entirecohort when determined based on chronological age, withsimilar results when the BMD Z-score was determinedusing bone age instead of chronological age. There were nosigns of rickets on any of the hand and wrist radiographs.
Children were studied for spine BMD at a median of12.5 days (IQR: 4, 22) from chemotherapy initiation andunderwent lateral thoraco-lumbar spine radiograph at a me-dian of 18 days (IQR: 7, 25) from first chemotherapy. Amongthe children with fractures, 10/29 (35%) underwent spineradiographs the day of or before chemotherapy initiation.
Vertebral fracture status
Genant semiquantitative analyses: Twenty-nine patientshad prevalent vertebral fractures (16%). Fifteen pa-tients (52%) had one prevalent vertebral fracture, eightpatients manifested 2–5 fractures (27%) and six patientshad between 6 and 10 fractures (21%). Grade 1 fractureswere present in 14 patients (48%), 9 patients (31%) had a
TABLE 1. Description of the Cohort
Clinical parameters Results
Demographic data
Age (yr) [median (IQR)] 5.3 (3.4, 9.7)
Male [n (%)] 108 (58)
Ethnicity [n (%)]
White 140 (75)
Native/Aboriginal peoples of North America (North American Indian, Metis, Inuit/Eskimo) 12 (7)
South Asian (e.g., East Indian, Pakistani, Punjabi, Sri Lankan) 9 (5)
Black 7 (4)
Other 16(9)
Characteristics of the leukemia
Leukemia diagnosis [n (%)] 186
Pre-B-cell acute lymphoblastic leukemia 167 (90)
T-cell acute lymphoblastic leukemia 19 (10)
Leukemia risk category
Standard risk [n (%)] 117 (63)
High risk [n (%)] 68 (37)
White blood count at diagnosis [n (%)]
�50 27 (15)
<50–20 20 (11)
<20–5 68 (37)
<5 67 (37)
Anthropometry
Height Z-score [mean (SD)] 0.30 (1.2)
Weight Z-score [mean (SD)] 0.43 (1.2)
Pubertal stage [n (%)]
Stage 1 145 (78)
Stage 2–5 41 (22)
Bone age (yr) [median (IQR)], n = 178 5.0 (3.0, 10.0)
Chronological age to bone age difference (yr) [median (IQR)] 20.01 (-0.4, 0.3)
Lumbar spine areal BMD
LS BMD Z-score [mean (SD)] 21.2 (1.3)
LS BMD Z-score for bone age [mean (SD)], n = 178 21.2 (1.3)
VERTEBRAL FRACTURE IN CHILDHOOD ALL 1329
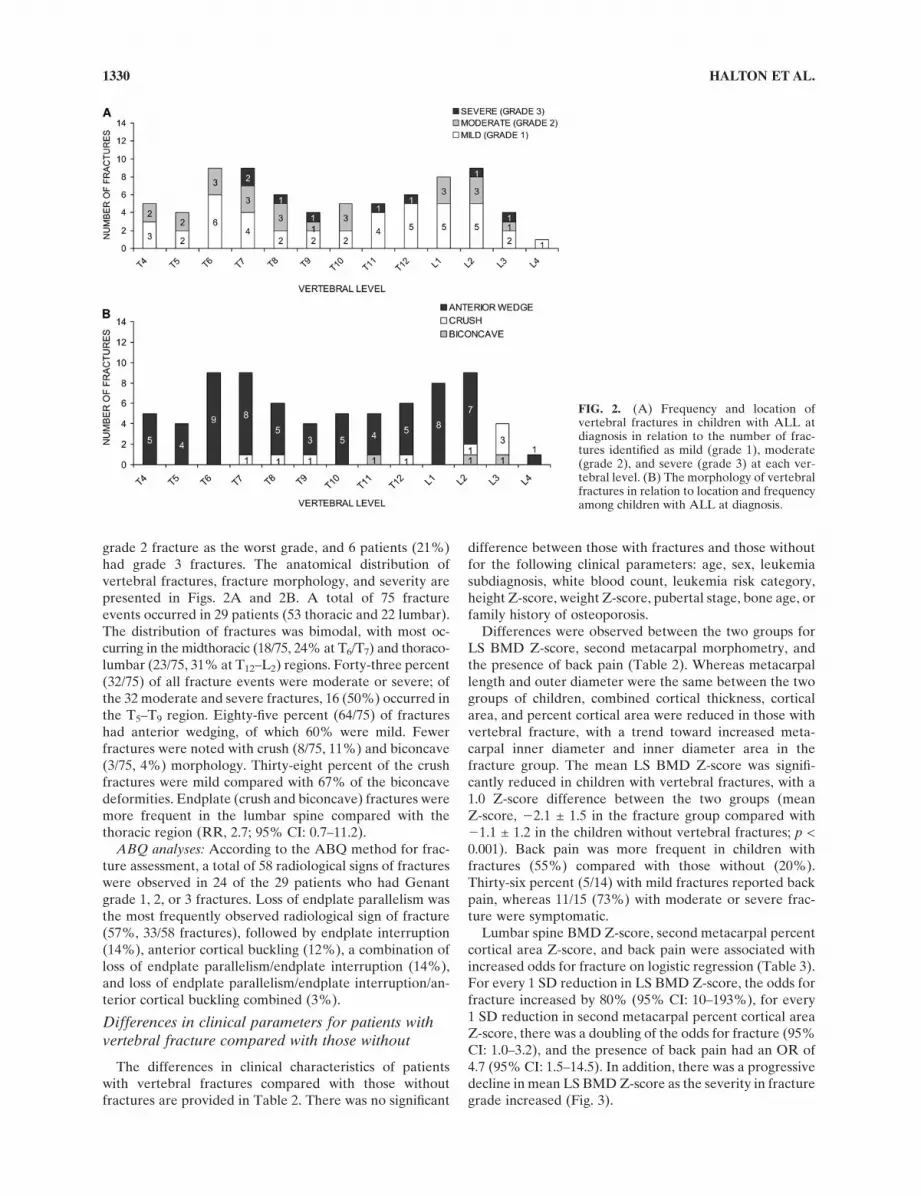
grade 2 fracture as the worst grade, and 6 patients (21%)had grade 3 fractures. The anatomical distribution ofvertebral fractures, fracture morphology, and severity arepresented in Figs. 2A and 2B. A total of 75 fractureevents occurred in 29 patients (53 thoracic and 22 lumbar).The distribution of fractures was bimodal, with most oc-curring in the midthoracic (18/75, 24% at T6/T7) and thoraco-lumbar (23/75, 31% at T12–L2) regions. Forty-three percent(32/75) of all fracture events were moderate or severe; ofthe 32 moderate and severe fractures, 16 (50%) occurred inthe T5–T9 region. Eighty-five percent (64/75) of fractureshad anterior wedging, of which 60% were mild. Fewerfractures were noted with crush (8/75, 11%) and biconcave(3/75, 4%) morphology. Thirty-eight percent of the crushfractures were mild compared with 67% of the biconcavedeformities. Endplate (crush and biconcave) fractures weremore frequent in the lumbar spine compared with thethoracic region (RR, 2.7; 95% CI: 0.7–11.2).
ABQ analyses: According to the ABQ method for frac-ture assessment, a total of 58 radiological signs of fractureswere observed in 24 of the 29 patients who had Genantgrade 1, 2, or 3 fractures. Loss of endplate parallelism wasthe most frequently observed radiological sign of fracture(57%, 33/58 fractures), followed by endplate interruption(14%), anterior cortical buckling (12%), a combination ofloss of endplate parallelism/endplate interruption (14%),and loss of endplate parallelism/endplate interruption/an-terior cortical buckling combined (3%).
Differences in clinical parameters for patients withvertebral fracture compared with those without
The differences in clinical characteristics of patientswith vertebral fractures compared with those withoutfractures are provided in Table 2. There was no significant
difference between those with fractures and those withoutfor the following clinical parameters: age, sex, leukemiasubdiagnosis, white blood count, leukemia risk category,height Z-score, weight Z-score, pubertal stage, bone age, orfamily history of osteoporosis.
Differences were observed between the two groups forLS BMD Z-score, second metacarpal morphometry, andthe presence of back pain (Table 2). Whereas metacarpallength and outer diameter were the same between the twogroups of children, combined cortical thickness, corticalarea, and percent cortical area were reduced in those withvertebral fracture, with a trend toward increased meta-carpal inner diameter and inner diameter area in thefracture group. The mean LS BMD Z-score was signifi-cantly reduced in children with vertebral fractures, with a1.0 Z-score difference between the two groups (meanZ-score, 22.1 ± 1.5 in the fracture group compared with21.1 ± 1.2 in the children without vertebral fractures; p <0.001). Back pain was more frequent in children withfractures (55%) compared with those without (20%).Thirty-six percent (5/14) with mild fractures reported backpain, whereas 11/15 (73%) with moderate or severe frac-ture were symptomatic.
Lumbar spine BMD Z-score, second metacarpal percentcortical area Z-score, and back pain were associated withincreased odds for fracture on logistic regression (Table 3).For every 1 SD reduction in LS BMD Z-score, the odds forfracture increased by 80% (95% CI: 10–193%), for every1 SD reduction in second metacarpal percent cortical areaZ-score, there was a doubling of the odds for fracture (95%CI: 1.0–3.2), and the presence of back pain had an OR of4.7 (95% CI: 1.5–14.5). In addition, there was a progressivedecline in mean LS BMD Z-score as the severity in fracturegrade increased (Fig. 3).
FIG. 2. (A) Frequency and location ofvertebral fractures in children with ALL atdiagnosis in relation to the number of frac-tures identified as mild (grade 1), moderate(grade 2), and severe (grade 3) at each ver-tebral level. (B) The morphology of vertebralfractures in relation to location and frequencyamong children with ALL at diagnosis.
1330 HALTON ET AL.

DISCUSSION
This study highlighted the prevalence (16%) and sever-ity of vertebral fractures as a complication of newlydiagnosed childhood ALL. Whereas back pain occurred in55% of children with vertebral fractures and was highlyassociated with vertebral compression, a significant pro-portion of children nevertheless did not manifest overt
symptoms of their spinal involvement. Children with ALLcan also present with vertebral fractures well after diag-nosis (during chemotherapy)(24,25) and may rebuild spinefractures through bone growth after leukemia treatment.(26)
At the same time, ALL treatment involves glucocorticoidand other potentially osteotoxic therapy that may causefurther deterioration in spine health or inhibit the res-toration process. Our data underscore the importance ofidentification of vertebral fractures at the time of ALL di-agnosis, which will allow children with compromised skele-tal health, whether symptomatic or not, to be monitored forfurther deterioration from the outset of their illness.
Our results, based on prospective radiographic screeningof a large cohort of patients, suggest that vertebral frac-tures around the time of ALL diagnosis are more commonthan previously thought. Most of the related literature inthis area stems from case report documentation of painfulvertebral fractures as an initial presenting symptom of
TABLE 2. Clinical Parameters in Children With Vertebral Compression Compared With Those Without
Clinical parametersCompression
(N = 29)No compression
(N = 157)Difference(95% CI) p
Demographic data
Male [n (%)] 17 (59) 91 (58) 1 (219, 18) 1.0*
Age (yr) [median (IQR)] 6.1 (3.8, 9.9) 5.1 (3.3, 9.6) 20.7 (22.2, 0.5) 0.29†
Diagnosis
Pre-B-cell acute lymphoblastic leukemia [n (%)] 27 (93) 140 (89)4 (212, 12) 0.74*
T-cell acute lymphoblastic leukemia [n (%)] 2 (7) 17 (11)
Leukemia characteristics
White blood count at diagnosis
White blood count [median (IQR)] 5.8 (2.5, 18.1) 7.1 (3.8, 30.2) 1.6 (21.0, 4.0) 0.20†
�50 [n (%)] 4 (14) 23 (15) 21 (212, 16)
0.54*<50–20 [n (%)] 2 (7) 18 (12) 25 (213, 11)
<20–5 [n (%)] 9 (31) 59 (38) 28 (223, 12)
<5 [n (%)] 14 (48) 53 (35) 14 (25, 32)
Leukemia risk assignment
Standard risk [n (%)] 19 (66) 98 (62)3 (217, 19) 0.84*
High risk [n (%)] 10 (34) 58 (37)
Anthropometry
Height Z-score [mean (SD)] 0.2 (1.2) 0.3 (1.2) 20.1 (20.6, 0.3) 0.59‡
Pubertal stage (stage 1) [n (%)] 21 (72) 124 (81)28 (227, 7) 0.33*
Pubertal stage (stages 2–5) [n (%)] 8 (28) 30 (19)
Second metacarpal morphometry
Metacarpal length Z-score [mean (SD)] 0.6 (0.9) 0.4 (0.9) 0.3 (20.2, 0.7) 0.19‡
Inner diameter Z-score [mean (SD)] 0.2 (0.9) 20.2 (0.8) 0.3 (20.1, 0.7) 0.13‡
Outer diameter Z-score [mean (SD)] 0.1 (0.7) 0.2 (0.9) 20.2 (20.6, 0.3) 0.44‡
Combined cortical thickness Z-score [mean (SD)] 20.1 (1.0) 0.5 (0.9) 20.6 (21, 20.1) 0.01‡
Inner diameter area Z-score [mean (SD)] 0.1 (0.9) 20.2 (0.8) 0.3 (20.1, 0.7) 0.12‡
Total area Z-score [mean (SD)] 0.1 (0.8) 0.2 (0.9) 20.2 (20.6, 0.3) 0.42‡
Cortical area Z-score [mean (SD)] 20.01 (0.8) 0.5 (1.0) 20.5 (21.0, 20.1) 0.03‡
Percent cortical area Z-score [mean (SD)] 20.2 (0.9) 0.3 (0.8) 20.5 (20.9, 20.1) 0.02‡
Spine areal BMD
Lumbar spine areal BMD Z-score [mean (SD)] 22.1 (1.5) 21.1 (1.2) 21.1 (21.6, 20.6) <0.001‡
Lumbar spine areal BMD Z-score for bone age [mean (SD)] 22.2 (1.5) 21.04 (1.2) 21.1 (21.6, 20.6) <0.001‡
Back pain
Yes [n (%)] 16 (55) 31 (20) 35 (17, 53) <0.001*
HAES activity levels
Overall relative activity (% to waking hours) [median (IQR)] 19 (8, 42) 26 (7, 49) 22 (213, 7) 0.60†
* Statistical significance determined by x2 test or Fisher’s exact test.† Statistical significance determined by nonparametric test (Mann-Whitney U—two independent samples).‡ Statistical significance determined by independent sample t-tests.
TABLE 3. Clinical Parameters Associated With Increased Oddsfor Fracture
Parameters OR (95% CI) p
Lumbar spine BMD Z-score 1.8 (1.10, 2.9) <0.001
Back pain 4.7 (1.5, 14.5) 0.01
Second metacarpal percent
cortical area Z-score
2.0 (1.0, 3.2) 0.05
Dependent variable: spine fracture (yes or no).
VERTEBRAL FRACTURE IN CHILDHOOD ALL 1331

childhood ALL.(9,10,27) However, previous studies thathave reported on more extensive cohorts of patients haveshown lower fracture prevalence rates. Blatt et al.(8) madecomment during the introduction to a case report that 2 of350 patients presenting with vertebral compression causedby ALL had been identified over a 10-yr period on retro-spective chart review. On the other hand, Baty and Vogt(4)
found vertebral fractures in 2 of 43 patients studied retro-spectively; however, only the results of anterior-posteriorradiographs were presented in that report. The largest caseseries documenting the prevalence of vertebral fracturesamong children with ALL at diagnosis was a retrospectivereview that showed a fracture prevalence of 1.6% in 1466children.(11) These assessments were based on written re-port or review of chest radiographs where, as for the otherreports described above, the specific methodology under-lying the vertebral fracture diagnosis was not reported.Furthermore, this study may have led to an underestimateof the number of fractures at baseline because chest radi-ographs may not be optimal for visualization of vertebralbodies and because most or all of the lumbar vertebrae aretypically not included in images of the chest. Our resultsare unique in this population of newly diagnosed childrenwith ALL, given the prospective design of our study and asystematic and standardized approach to identifying mild,moderate, and severe fractures from T4 to L4 having beenestablished a priori. Of consideration is the fact that ourpatients underwent spine radiographs both before andsoon after chemotherapy initiation. Given the potent os-teotoxicity of glucocorticoids and the paucity of informa-tion available to predict the short-term effect of glucocor-ticoids on spine health in children, we cannot rule out thepossibility that our fracture prevalence rates are slightlyhigher than they would have been if all of the spine radi-ographs had been taken before chemotherapy.
We found a bimodal distribution of fractures, with apredilection for fractures in the midthoracic region and thethoraco-lumbar junction. This distribution of fractures issimilar to what has been consistently reported in adult menand women(28–31) and is proposed to result from the me-chanical stresses on vertebrae induced by the shape of thespine.(32) The thoracic kyphosis is most pronounced at themidthoracic region so that loading in flexion is accentuated.The thoraco-lumbar junction is the site at which the spinetransitions from being more rigidly fixed by ribs to freelymobile, maximizing compression stresses. This bimodalfracture distribution suggests that fractures were appro-priately identified in our cohort of ALL children. Fur-thermore, the association between fractures and clinicallyrelevant parameters such as lower LS BMD Z-score, re-duced second metacarpal percent cortical area Z-score,and back pain lend further support to the fracture assign-ment. We also found that endplate fractures were morecommon in the lumbar spine compared with the thoracicregion, a phenomenon that has also been reported in adultsand is attributed to a more posterior center of gravity inthis region.(32) The fact that wedge deformity was the mostcommon morphological finding is further in keeping withobservations in large populations of adults with vertebralfractures.(32) Another interesting finding was that many ofthe children with vertebral fractures (45%) were asymp-tomatic. This is consistent with data from women withpostmenopausal osteoporosis in whom vertebral compres-sion frequently occurs in the absence of symptoms.(33)
The relationship between clinical parameters and ver-tebral fractures in childhood ALL has been an importanttopic of discussion in the pediatric ALL literature. In thisstudy, we showed that LS BMD, a technique that has beenused in childhood chronic illness for many years despitea paucity of available information on its relationship tobone fragility, is a clinically useful tool. Reductions in LSBMD Z-score were clearly associated with increased oddsfor fracture, with second metacarpal percent cortical areaZ-score also emerging as a relevant clinical correlate (al-though to a lesser extent). Although the relationship be-tween spine BMD and vertebral compression in ALL hasnot been studied previously, the link between the charac-teristics of the leukemia and vertebral compression hasbeen addressed in a number of prior reports, with con-flicting results. Ribeiro et al.(11) found that children withvertebral compression were more likely to manifest favor-able leukemia prognostic features, including a leukocytecount <25 3 109/liter. Other reports have noted that low(8,34)
or normal(35) leukocyte counts tend to be associated withback pain or vertebral compression. Alternatively, Clausenet al.(36) found no relationship between skeletal scintigraphyor radiographic changes and leukemia features. In our study,we did not find a relationship between vertebral fracturesand leukocyte counts, leukemia risk category, or leukemiasubdiagnosis. The discrepancy among findings remains un-clear, but conclusions may be clouded by a lack of systematicdefinition of fractures in previous reports.
The mechanism of the advanced bone morbidity ob-served in childhood ALL around the time of diagnosis hasnot been fully elucidated to date. We observed that spine
FIG. 3. Median LS BMD Z-score for children with ALL at di-agnosis in relation to fracture severity grade (25th and 75th per-centiles). Patients with multiple compression fractures wereclassified according to the highest severity score. ASignificant dif-ference in LS BMD Z-score between children with grade 3 vs.grade 0 compression (p = 0.05). BSignificant difference in LS BMDZ-score between children with grade 2 vs. grade 0 compression(p = 0.001).
1332 HALTON ET AL.

BMD is affected in all children with newly diagnosed ALLregardless of their vertebral fracture status, as evidencedby the fact that the entire cohort showed reductions inspine BMD (mean Z-score, 21.2) despite above-averageheight. Whereas the purpose of our investigation was tostudy the clinical factors associated with spine fracture, andnot to unveil mechanisms per se, the second metacarpalmorphometry measurements do provide insight into thepathophysiological events surrounding the effect of ALLon bone. The normal second metacarpal length and di-ameter in children with vertebral compression but reducedpercent cortical area suggest cortical thinning caused byincreased endosteal resorption (as opposed to reducedperiosteal apposition). One of the prevailing theoriesaround the cause of ALL-induced bone morbidity is theliberation of osteoclast-activating factors by the leukemiccells.(6) Our study supports the suggestion that increasedskeletal resorption is a contributing pathological event.
In conclusion, these results highlight the potential foradvanced spine fractures among children with newly di-agnosed ALL. The potential for rebuilding of the spinethrough bone growth versus further deterioration in theface of bone health threats such as compromised mobilityand medication osteotoxicity remains to be determinedthrough longitudinal study.
ACKNOWLEDGMENTS
This study was primarily funded by an operating grantfrom the Canadian Institutes for Health Research. Addi-tional funding for this work has been provided by the Ca-nadian Institutes for Health Research New InvestigatorProgram (to L.W.), the Canadian Child Health ClinicianScientist Career Enhancement Program (to L.W.), theChildren’s Hospital of Eastern Ontario, and Women andChildren’s Health Research Institute, University ofAlberta. The Canadian STOPP Consortium would like tothank the following individuals: the children and theirfamilies who participated in the study, without whom theSTOPP study would not have been possible. ResearchAssociates who managed the study at the coordinatingcenter (the Children’s Hospital of Eastern Ontario Ottawa,Ontario, Canada): Elizabeth Sykes (STOPP Project Man-ager), Maya Scharke (STOPP Data Analyst and DatabaseManager), Victor Konji (STOPP Publications and Pre-sentations Committee Liaison and hand morphometrymeasurements), Steve Anderson (Children’s Hospital ofEastern Ontario Pediatric Bone Health Program ResearchManager), Catherine Riddell (STOPP National StudyMonitor). Research Associates who took care of the pa-tients from the following institutions: Alberta Children’sHospital, Calgary, Alberta: Eileen Pyra; British ColumbiaChildren’s Hospital, Vancouver, British Columbia: TerryViczko; Children’s Hospital of Eastern Ontario, Ottawa,Ontario: Amanda George, Catherine Riddell; Children’sHospital of Western Ontario, London, Ontario: LeilaMacBean; McMaster Children’s Hospital, Hamilton,Ontario: Susan Docherty-Skippen; IWK Health Centre,Halifax, Nova Scotia: Aleasha Warner; Montreal Chil-dren’s Hospital, Montreal, Quebec: Diane Laforte, Mayito
St-Pierre; Ste. Justine Hospital, Montreal, Quebec: ClaudeBelleville, Stephanie Pellerin, Natacha Gaulin Marion;Stollery Children’s Hospital, Edmonton, Alberta: DeborahOlmstead, Melissa Gabruck, Linda Manasterski; ; TorontoHospital for Sick Children, Toronto, Ontario: Julie Lee,Karen Whitney; Winnipeg Children’s Hospital, Winnipeg,Manitoba: Dan Catte, Erika Bloomfield. The ResearchNurses, Support Staff, and all the STOPP collaboratorsfrom the various Divisions of Nephrology, Oncology,Rheumatology, and Radiology who have contributed tothe care of the children enrolled in the study.
REFERENCES
1. Pui CH, Robison LL, Look AT 2008 Acute lymphoblasticleukaemia. Lancet 371:1030–1043.
2. Pui CH, Evans WE 2006 Treatment of acute lymphoblasticleukemia. N Engl J Med 354:166–178.
3. Willson JKV 1959 Bone lesions in childhood leukemia. Ra-diology 72:672–681.
4. Baty JM, Vogt EC 1935 Bone changes of leukemia in children.AJR Am J Roentgenol 34:310–313.
5. Clark JJ 1936 Unusual bone changes in leukemia. Radiology26:237–242.
6. Halton JM, Atkinson SA, Fraher L, Webber C, Gill GJ,Dawson S, Barr RD 1996 Altered mineral metabolism andbone mass in children during treatment for acute lympho-blastic leukemia. J Bone Miner Res 11:1774–1783.
7. Rogalsky RJ, Black GB, Reed MH 1986 Orthopaedic mani-festations of leukemia in children. J Bone Joint Surg Am68:494–501.
8. Blatt J, Martini SL, Penchansky L 1984 Characteristics ofacute lymphoblastic leukemia in children with osteopenia andvertebral compression fractures. J Pediatr 105:280–282.
9. Samuda GM, Cheng MY, Yeung CY 1987 Back pain and ver-tebral compression: An uncommon presentation of childhoodacute lymphoblastic leukemia. J Pediatr Orthop 7:175–178.
10. Santangelo JR, Thomson JD 1999 Childhood leukemia pre-senting with back pain and vertebral compression fractures.Am J Orthop 28:257–260.
11. Ribeiro RC, Pui CH, Schell MJ 1988 Vertebral compressionfracture as a presenting feature of acute lymphoblastic leu-kemia in children. Cancer 61:589–592.
12. Institute of Medicine 1997 Dietary Reference Intakes forCalcium, Phosphorus, Magnesium, Vitamin D, Fluoride. Na-tional Academy Press, Washington, DC, USA.
13. Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R,Grummer-Strawn LM, Curtin LR, Roche AF, Johnson CL 2002Centers for Disease Control and Prevention 2000 growth chartsfor the United States: Improvements to the 1977 NationalCenter for Health Statistics version. Pediatrics 109:45–60.
14. Marshall WA, Tanner JM 1969 Variations in pattern of pu-bertal changes in girls. Arch Dis Child 44:291–303.
15. Marshall WA, Tanner JM 1970 Variations in the pattern ofpubertal changes in boys. Arch Dis Child 45:13–23.
16. Greulich WW, Pyle SI 1959 Radiographic Atlas of SkeletalDevelopment of the Hand and Wrist, 2nd ed. Stanford Uni-versity Press, Stanford, CA, USA.
17. Spencer RP, Sagel SS, Garn SM 1968 Age changes in fiveparameters of metacarpal growth. Invest Radiol 3:27–34.
18. Garn SM, Poznanski AK, Larson K 1976 Metacarpal lengths,cortical diameters and areas from the 10-state nutrition survey.In: Jaworski ZFG (ed.) Proceedings of the first workshop onbone morphometry. University of Ottawa Press, Ottawa,Canada, pp. 367–391.
19. Genant HK, Wu CY, van Kuijk C, Nevitt MC 1993 Vertebralfracture assessment using a semiquantitative technique. JBone Miner Res 8:1137–1148.
20. Keats TE, Smith TH 1977 An Atlas of Normal DevelopmentalAnatomy. Year Book of Medical Publishers, Chicago, IL, USA.
VERTEBRAL FRACTURE IN CHILDHOOD ALL 1333

21. Jiang G, Eastell R, Barrington NA, Ferrar L 2004 Comparisonof methods for the visual identification of prevalent vertebralfracture in osteoporosis. Osteoporos Int 15:887–896.
22. Hay J 1997 Development and validation of the Habitual ActivityEstimation Scale (HAES). Children Exerc XIX II:125–129.
23. Wells GD, Wilkes DL, Schneiderman-Walker J, Elmi M,Tullis E, Lands LC, Ratjen F, Coates AL 2008 Reliabilityand validity of the habitual activity estimation scale (HAES)in patients with cystic fibrosis. Pediatr Pulmonol 43:345–353.
24. Kakihara T, Watanabe A, Imai C, Hotta H, Tanaka A,Uchiyama M 2002 Chemotherapy-induced multiple vertebralcompression fractures in a boy with acute lymphoblastic leu-kemia. Pediatr Int 44:683–685.
25. Vassilopoulou-Sellin R, Ramirez I 1992 Severe osteopenia andvertebral compression fractures after complete remission in anadolescent with acute leukemia. Am J Hematol 39:142–143.
26. Pandya NA, Meller ST, MacVicar D, Atra AA, Pinkerton CR2001 Vertebral compression fractures in acute lymphoblasticleukaemia and remodelling after treatment. Arch Dis Child85:492–493.
27. Bjerregaard LL, Rosthooj S 2002 Vertebral compression andeosinophilia in a child with acute lymphatic leukemia. J Pe-diatr Hematol Oncol 24:313–315.
28. Rea JA, Chen MB, Li J, Blake GM, Steiger P, Genant HK,Fogelman I 2000 Morphometric X-ray absorptiometry andmorphometric radiography of the spine: A comparison ofprevalent vertebral deformity identification. J Bone Miner Res15:564–574.
29. Vallarta-Ast N, Krueger D, Wrase C, Agrawal S, Binkley N2007 An evaluation of densitometric vertebral fracture as-sessment in men. Osteoporos Int 18:1405–1410.
30. Wu C, van Kuijk C, Li J, Jiang Y, Chan M, Countryman P,Genant HK 2000 Comparison of digitized images with originalradiography for semiquantitative assessment of osteoporoticfractures. Osteoporos Int 11:25–30.
31. Jackson SA, Tenenhouse A, Robertson L 2000 Vertebralfracture definition from population-based data: Preliminaryresults from the Canadian Multicenter Osteoporosis Study(CaMos). Osteoporos Int 11:680–687.
32. Ismail AA, Cooper C, Felsenberg D, Varlow J, Kanis JA,Silman AJ, O’Neill TW 1999 Number and type of vertebraldeformities: Epidemiological characteristics and relation toback pain and height loss. European Vertebral OsteoporosisStudy Group. Osteoporos Int 9:206–213.
33. Dennison E, Cooper C 2000 Epidemiology of osteoporoticfractures. Horm Res 54Suppl 158–63.
34. Newman AJ, Melhorn DK 1973 Vertebral compression inchildhood leukemia. Am J Dis Child 125:863–865.
35. Jonsson OG, Sartain P, Ducore JM, Buchanan GR 1990 Bonepain as an initial symptom of childhood acute lymphoblasticleukemia: Association with nearly normal hematologic in-dexes. J Pediatr 117:233–237.
36. Clausen N, Gotze H, Pedersen A, Riis-Petersen J, Tjalve E 1983Skeletal scintigraphy and radiography at onset of acute lym-phocytic leukemia in children. Med Pediatr Oncol 11:291–296.
Received in original form September 28, 2008; revised formJanuary 8, 2009; accepted February 2, 2009.
APPENDIX: THE CANADIAN STOPPCONSORTIUM (A PAN-CANADIAN,
PEDIATRIC BONE HEALTHWORKING GROUP)
Coordinating center
Children’s Hospital of Eastern Ontario, Ottawa,Ontario: Leanne M. Ward#*x (Study Principal Investiga-tor), Janusz Feber*x (Nephrology), Isabelle Gaboury*x
(Biostatistics, Chalmers Research Group), Jacqueline
Halton*x (Oncology), MaryAnn Matzinger (Radiology,Central Radiograph Analyses), David Moher*x (ResearchMethods, Chalmers Research Group), Johannes Roth(Rheumatology), Nazih Shenoudax (Radiology, CentralRadiograph Analyses)
Participating centers
Alberta Children’s Hospital, Calgary, Alberta: DavidStephure (Site Principal Investigator), Reinhard Kloiber(Radiology), Victor Lewis (Oncology), Julian Midgley(Nephrology), Paivi Miettunen (Rheumatology)
British Columbia Children’s Hospital, Vancouver, Brit-ish Columbia: David Cabral* (Site Principal Investigator),David B. Dix (Oncology), Helen R. Nadel (Radiology),Colin White (Nephrology)
British Columbia Women’s Hospital and Health Sci-ences Center, Vancouver, British Columbia: Brian C.Lentlex (Radiology)
Brock University, Faculty of Applied Health Sciences,St. Catharines, Ontario: John Hayx (Physical ActivityMeasurements)
Children’s Hospital of Western Ontario, London, Ontario:Cheril Clarson (Site Principal Investigator), Elizabeth Cair-ney (Oncology), Guido Filler (Nephrology), Joanne Grim-mer (Nephrology), Keith Sparrow (Radiology)
IWK Health Center, Halifax, Nova Scotia: ElizabethCummings (Site Principal Investigator), Conrad Fernandez(Oncology), Adam M. Huberx (Rheumatology), BiancaLang*x (Rheumatology), Kathy O’Brien (Radiology),Andrew Ross (Radiology)
McMaster Children’s Hospital, Hamilton, Ontario:Stephanie Atkinson*x (Site Principal Investigator), SteveArora (Nephrology), Ronald Barrx (Oncology), CraigCoblentz (Radiology), Peter B. Dent (Rheumatology),Colin Webber* (DXA Methodology)
Montreal Children’s Hospital, Montreal, Quebec: CeliaRoddx (Site Principal Investigator), Sharon Abish (Oncology),LorraineBell (Nephrology),RosieScuccimarri (Rheumatology)
Shriners Hospital for Children, Montreal, Quebec:Frank Rauch*x (Co-Chair, Publications and PresentationsCommittee), Francis Glorieux* (Chair, Ancillary StudiesCommittee)
Ste. Justine Hospital, Montreal, Quebec: Nathalie Alos*(Site Principal Investigator), Josee Dubois (Radiology),Caroline Laverdiere (Oncology), Veronique Phan (Ne-phrology), Claire Saint-Cyr (Rheumatology)
Stollery Children’s Hospital, Edmonton, Alberta: Rob-ert Couch* (Site Principal Investigator), Janet Ellsworth(Rheumatology), Claire LeBlanc (Rheumatology), MauryPinsk (Nephrology), Kerry Siminoskix (Radiology), Bev-erly Wilson (Oncology)
Toronto Hospital for Sick Children, Toronto, Ontario:Ronald Grant* (Site Principal Investigator), MartinCharron (Radiology), Diane Hebert (Nephrology)
Winnipeg Children’s Hospital, Winnipeg, Manitoba:Shayne Tabackx (Site Principal Investigator), Tom Blydt-Hansen (Nephrology), Sara Israels (Oncology), Kiem Oen(Rheumatology), Martin Reed (Radiology)
#Principal Investigator; *Executive Committee Member;xPublications and Presentations Committee Member
1334 HALTON ET AL.
Copyright © 2022 FDOKUMEN