ADDRESSING THE GAPS IN ASSESSMENT AND ... - TSpace
191
ADDRESSING THE GAPS IN ASSESSMENT AND TREATMENT OF THE UPPER EXTREMITY IN REHABILITATION OF INDIVIDUALS WITH NEUROLOGICAL CONDITIONS by Naaz Desai A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Rehabilitation Sciences Institute University of Toronto © Copyright by Naaz Desai 2021
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ADDRESSING THE GAPS IN ASSESSMENT AND ... - TSpace

ADDRESSING THE GAPS IN ASSESSMENT AND TREATMENT OF THE UPPER EXTREMITY IN
REHABILITATION OF INDIVIDUALS WITH NEUROLOGICAL CONDITIONS
by
Naaz Desai
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Rehabilitation Sciences Institute University of Toronto
© Copyright by Naaz Desai 2021
ii
ADDRESSING THE GAPS IN ASSESSMENT AND TREATMENT
OF THE UPPER EXTREMITY IN REHABILITATION OF
INDIVIDUALS WITH NEUROLOGICAL CONDITIONS
Naaz Desai
Doctor of Philosophy
Rehabilitation Sciences Institute
University of Toronto
2021
Abstract
Regaining upper extremity function is critical following stroke and spinal cord injury (SCI). The
objectives of this thesis were to develop and assess the psychometric properties of a 3D printed
version of an upper extremity outcome assessment tool called the Toronto Rehabilitation
Institute-Hand Function Test (TRI-HFT) and to assess the feasibility of stimulating interscapular
muscles using transcutaneous functional electrical stimulation (FES).
The first study explored the feasibility of 3D printing the original TRI-HFT objects and
assessed its inter and intra-rater reliability and convergent validity in chronic stroke. The second
study focused on assessing its psychometric properties in the sub-acute and chronic SCI
populations. We hypothesized that the TRI-HFT could be 3D printed and that the 3D printed test
would have high reliability and validity in stroke and SCI populations. In the third study I
explored the feasibility and benefits of stimulating the Lower Trapezius (LT), Serratus Anterior
(SA) and Upper Trapezius (UT) along with Anterior Deltoid during forward flexion and along
with Middle Deltoid during abduction in able-bodied individuals. The underlying hypothesis was
that it would result in an increased range and more natural reaching movement.

iii
In the first and second study we found that all objects of the TRI-HFT could be
successfully 3D printed with an error margin of less than 10% except for the Paper and the
Sponge objects. The 3D TRI-HFT showed high inter and intra-rater reliability in stroke and SCI.
The 3D TRI-HFT showed strong criterion validity when compared to the Graded Redefined
Assessment of Strength, Sensibility and Prehension test in the SCI population. The 3D TRI-
HFT showed moderate to strong construct validity when compared to the Chedoke-McMaster
Stroke Assessment-Arm and Hand and the Fugl Meyer Assessment-Hand in chronic stroke. In
the third study, the LT, SA and UT could be successfully stimulated using surface FES. The
maximum reach in abduction for FES of middle deltoid along with the interscapular muscles
was 51.77°±17.54° compared to FES for middle deltoid alone which was 43.76°±15.32°.
This work essentially builds on the current state of assessment and FES treatment of the
upper extremity in the rehabilitation domain.
iv
Acknowledgments
“Education is all about being excited about something. Seeing passion and enthusiasm helps
push an educational message.”
-Steve Irwin.
I am forever indebted to my supervisor Dr. Milos R. Popovic who spotted the excitement I felt
by sure virtue of my work. He has been a propelling force in my decision to take on this
challenge of pursuing my PhD. Throughout the course of my PhD, he has been a mentor, a
friend, a colleague lending a listening ear, providing the ever so helpful guidance, perhaps with a
side of humor to keep me going when all seemed to fail. So, to him I say THANK YOU!
I am also grateful to my committee members, Dr. Kristin Musselman and Dr. Rosalie Wang for
agreeing to take the time to help and guide me through this process. I thank them for their
feedback and guidance during the planning and execution of my PhD projects. I would also like
to express my deepest thanks to the faculty at Rehabilitation Sciences Institute, University of
Toronto and my many colleagues at Toronto Rehabilitation Institute-UHN for their intellectual
and supportive words. They knew when I needed them most and always delivered. There is one
other person who has stood by my decision and critically appraised all my work and made me a
better researcher for which I am ever so grateful, Prof. Molly Verrier. Molly, thank you for
believing in me and holding me to high standards.
I am thankful to my two extended families, my own and my husband’s. I am especially grateful
to my late mother who instilled the values of persistence, determination and hard work. My
father and my husband’s parents have believed in me and encouraged my every effort towards
achieving this goal. I am thankful to my brother who has picked up the phone in the middle of
the night halfway across the ocean to hear me relentlessly talk about how my analysis is not
working! I am thankful to my children Aniqa and Arsh (sorry, mummy missed some of our
movie nights!) for their ever reassuring and calming hugs when I needed them the most. Last but
not the least, I am thankful to the love of my life, my husband. Ankur, thank you for being so
understanding, supportive and just being YOU throughout this process when many a times I was
anything but myself.

v
I would also like to acknowledge my funders, the Canadian Institute of Health Research (CIHR
CGS-D award), the Province of Ontario (Ontario Graduate Scholarship), Toronto Rehabilitation
Institute-UHN (TRI graduate scholarship) and the University of Toronto. Finally, I am thankful
to all my study participants for their engagement in my projects.
I dedicate this thesis to my mother Zulekha Kapadia, for she taught me that,
“Education is not preparation for life; education is life itself.”
- John Dewey
vi
Table of Contents
Acknowledgments.......................................................................................................................... iv
Table of Contents ........................................................................................................................... vi
List of Tables ................................................................................................................................. ix
List of Figures ..................................................................................................................................x
List of Appendices ......................................................................................................................... xi
Chapter 1 Introduction .....................................................................................................................1
Chapter 2 Literature Review ............................................................................................................4
2.1 Stroke ...................................................................................................................................4
2.1.1 Epidemiology of Stroke ...........................................................................................4
2.1.2 Pathophysiology and Clinical Presentation .............................................................5
2.1.3 Rehabilitation in Stroke ...........................................................................................7
2.1.4 Summary of Current State of Rehabilitation in Stroke ..........................................15
2.2 Spinal Cord Injury..............................................................................................................18
2.2.1 Epidemiology of Spinal Cord Injury......................................................................18
2.2.2 Pathophysiology and Clinical Presentation ...........................................................19
2.2.3 Rehabilitation in Spinal Cord Injury ......................................................................24
2.2.4 Summary of Current State of Rehabilitation in Spinal Cord Injury ......................30
Chapter 3 Functional Electrical Stimulation Therapy: A Closer Look..........................................33
3.1 History of Functional Electrical Stimulation Therapy (FEST) ..........................................33
3.2 Transcutaneous FES System ..............................................................................................34
3.2.1 FES Hardware ........................................................................................................35
3.2.2 FES Software .........................................................................................................35
3.3 Upper Limb Function in Stroke and Role of FEST ...........................................................36
3.4 Upper Limb Function in Spinal Cord Injury and Role of FEST........................................39

vii
3.5 Our Experiences with Surface FEST to Restore Upper Extremity Function After
Stroke and Spinal Cord Injury ...........................................................................................40
3.6 Limitations and Contraindications for Surface FEST Application ....................................41
Chapter 4 Toronto Rehabilitation Institute-Hand Function Test: Assessment of Gross Motor
Function in Individuals with Spinal Cord Injury ......................................................................42
4.1 Abstract ..............................................................................................................................42
4.2 Introduction ........................................................................................................................43
4.3 Materials and Methods .......................................................................................................58
4.4 Results ................................................................................................................................60
4.5 Discussion ..........................................................................................................................64
4.6 Conclusion .........................................................................................................................68
Chapter 5 Specific Project Aims and Objectives of this Thesis ....................................................69
5.1 Background ........................................................................................................................69
5.2 Specific Project Aims and Objectives of this Thesis .........................................................70
Chapter 6 3-Dimensional Printing in Rehabilitation: Feasibility of Printing an Upper
Extremity Gross Motor Function Assessment Tool ..................................................................72
6.1 Abstract ..............................................................................................................................72
6.2 Introduction ........................................................................................................................73
6.3 Results ................................................................................................................................76
6.4 Discussion ..........................................................................................................................81
6.5 Conclusion .........................................................................................................................84
6.6 Methods..............................................................................................................................84
Chapter 7 Preliminary Evaluation of the Reliability and Validity of the 3D Printed Toronto
Rehabilitation Institute-Hand Function Test in Individuals with Spinal Cord Injury ...............87
7.1 Abstract ..............................................................................................................................87
7.2 Introduction ........................................................................................................................88
7.3 Methods..............................................................................................................................91
7.4 Results ................................................................................................................................93
viii
7.5 Discussion ..........................................................................................................................99
7.6 Conclusion .......................................................................................................................101
Chapter 8 Feasibility and Significance of Stimulating Interscapular Muscles Using
Transcutaneous Functional Electrical Stimulation in Able Bodied Individuals .....................102
8.1 Abstract ............................................................................................................................102
8.2 Introduction ......................................................................................................................103
8.3 Methods............................................................................................................................106
8.4 Results ..............................................................................................................................109
8.5 Discussion ........................................................................................................................112
8.6 Conclusion .......................................................................................................................114
Chapter 9 Discussion and Conclusions ........................................................................................115
9.1 3D TRI-HFT ....................................................................................................................115
9.1.1 Role of 3D Printing in Rehabilitation Science .....................................................115
9.1.2 3D TRI-HFT Objects and Scoring System ..........................................................116
9.1.3 3D TRI-HFT Psychometric Testing .....................................................................118
9.1.4 Limitations ...........................................................................................................118
9.1.5 Strengths and Future Directions for the 3D TRI-HFT .........................................119
9.2 Functional Electrical Stimulation of the Interscapular Muscles ......................................120
9.2.1 Functional Electrical Stimulation of the Interscapular Muscles, Feasibility .......120
9.2.2 FES of Interscapular Muscles Clinical Significance and Future Directions ........121
9.2.3 Limitations ...........................................................................................................121
9.3 Concluding Remarks ........................................................................................................122
References ....................................................................................................................................123
Copyright Acknowledgements.....................................................................................................180

ix
List of Tables
Table 2. 1 Clinical Deficits in Stroke Based on Vascular and Anatomical Localization ........ 6
Table 2. 2 Current Upper Extremity Outcome Measures (Demers et al., 2017) ................... 12
Table 2. 3 American Spinal Cord Association Impairment Scale (AIS)(84)......................... 20
Table 2. 4 Functional Expectations for Patients with SCI (85, 86) ....................................... 22
Table 2. 5 Upper Extremity Outcome Measures in Spinal Cord Injury (92, 97, 98) ............. 27
Table 4. 1 Detailed Description and Rationale for the Items Used in the TRI-HFT ............. 56
Table 4. 2 Intraclass Correlation Coefficients for Inter-rater Reliability for the 10 Objects
and the Wooden Blocks in the TRI-HFT Test .............................................................................. 65
Table 4. 3 Summary of the Mean Test Results for the Control and Intervention Groups at
Baseline (Before) and Upon Completion of the Therapy (After), with Corresponding p Values.65
Table 6. 1 Dimensions of the Original TRI-HFT Objects and the 3D Printed TRI-HFT
Objects…………………………………………………………………………………………...77
Table 6. 2 Time Taken to Complete the 3D TRI-HFT by Individual Study Participant……78
Table 6. 3 Participant Demographics………………………………………………………..78
Table 6. 4 Participants Raw Scores on Upper Extremity Outcome Measures ....................... 79
Table 7. 1 Participant Demographics………………………………………………………..93
Table 7. 2 3D Toronto Rehabilitation Institute-Hand Function Test Scores ......................... 96
Table 7. 3 Graded Redefined Assessment of Strength, Sensibility and Prehension Scores...97
Table 7. 4 Concurrent and Criterion Validity of the 3D TRI-HFT ........................................ 98
Table 7. 5 Time Taken (in minutes) to Complete the 3D TRI-HFT* for B/L Upper
Extremities for All Study Participants ........................................................................................ 101
Table 8. 1 Participant Demographics ................................................................................... 110
Table 8. 2 FES Intensity in Milliamperes (mA) for Individual Muscles for Each Study
Participant………………………………………………………………………………………110
Table 8. 3 Maximum Reach in Degrees Across Ten Trials for Each Experimental Condition for
Individual Study Participant ....................................................................................................... 111

x
List of Figures
Figure 3. 1 NESS H200 ........................................................................................................... 37
Figure 3. 2 MyndMove™ Stimulator ...................................................................................... 38
Figure 3. 3 Compex Motion Stimulator .................................................................................. 39
Figure 4. 1 Itemized Objects Used in the Toronto Rehabilitation Institute-Hand Function
Test……………………………………………………………………………………………….50
Figure 4. 2 Demonstration of How to Manipulate the TRI-HFT ............................................ 52
Figure 4. 3 Demonstration of How to Manipulate the TRI-HFT ......................................... 53
Figure 4. 4 Demonstration of How to Manipulate the TRI-HFT ............................................ 54
Figure 4. 5 Construct Validity of the TRI-HFT Score vs the FIM Self-care Sub-score (Rt.
Hand)……………………………………………………………………………………………..62
Figure 4. 6 Construct Validity of the TRI-HFT Score vs the FIM Self-care Sub-score (Lt.
Hand)……………………………………………………………………………………………..62
Figure 4. 7 Construct Validity of the TRI-HFT Score vs the SCIM Selfcare Sub-score (Rt.
Hand)……………………………………………………………………………………………..63
Figure 4. 8 Construct Validity of the TRI-HFT Score vs the SCIM Selfcare Sub-score (Lt.
Hand)……………………………………………………………………………………………..63
Figure 4. 9 The Relationship between Participant Total Pre- and Post-therapy Scores on TRI-
HFT………………………………………………………………………………………………64
Figure 6. 1 3D Printed Toronto Rehabilitation Institute-Hand Function Test (3D TRI-
HFT)……………………………………………………………………………………………...76
Figure 6. 2 Inter and Intra-rater Reliability of the 3D TRI-HFT ............................................. 80
Figure 7. 1 Inter and Intra-rater Reliability of the 3D TRI-HFT in SCI ................................. 94
Figure 7. 2 Criterion Validity of the 3D TRI-HFT with the GRASSP ................................... 96
Figure 8. 1 Displacement of the Arm in Flexion and Abduction for Study Participant
(SCA18) Across All Experimental Conditions ........................................................................... 112
xi
List of Appendices
Appendix 1 Functional Electrical Stimulation Therapy for Retraining Reaching and Grasping
After Spinal Cord Injury and Stroke…………………………………………………………....141
Appendix 2 3D Toronto Rehabilitation Institute-Hand Function Test (3D TRI-HFT) Scoring
Sheet…………………………………………………………………………………………….151
Appendix 3 Chedoke Arm and Hand Activity Inventory (CAHAI) Scoring Sheet…………154
Appendix 4 Fugl Meyer Assessment-Upper Extremity (FMA-UE) Scoring Sheet…………156
Appendix 5 Chedoke-McMaster Stages of Recovery of the Arm (CMSA-Arm) and Chedoke-
McMaster Stages of Recovery of the Hand (CMSA-Hand) Scoring Sheet…………………….160
Appendix 6 Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP)
Scoring Sheet…………………………………………………………………………………...169
Appendix 7 Functional Independence Measure (FIM) Scoring Sheet…………………...….174
Appendix 8 Spinal Cord Independence Measure (SCIM) Scoring Sheet……………………176
1
Chapter 1 Introduction
Rehabilitation continues to remain center stage in restoring function and independence following
life altering neurological conditions like spinal cord injury (SCI) and stroke. Whereas in the last
2-3 decades rehabilitation scientists have made remarkable advances in the development and
refinement of rehabilitation tools, outcomes post-injury need to be further improved. Just like
any other field in medicine, for the field of rehabilitation to move forward it requires rigorous
testing of technologies/therapies before they can be implemented in clinical practice. In the
research studies presented in this thesis, the goal was to identify and address gaps in upper limb
rehabilitation following stroke and SCI.
In order to validate the use of newer rehabilitation interventions there is a need for
assessment tools that can measure change in function accurately. The first two studies presented
in this thesis discuss the feasibility and psychometric properties of an upper extremity
assessment tool that can be 3D printed and measures function in the activity domain of the
International Classification of Functioning, Disability and Health (ICF) while providing
preliminary information related to body structure and function in both individuals with stroke
and SCI. There are several upper extremity tools currently being used to assess upper extremity
function in the activity domain of the ICF in both stroke and SCI. However, most of these
measures are not developed for and are not validated in the respective populations. Also, these
measures are time based, expensive, not widely or easily available and take more than an hour to
be administered and hence lack clinical utility. This gap in the literature was realized by us ~10
years ago while conducting clinical trials to assess the efficacy of newer rehabilitation therapies
(like functional electrical stimulation and robotics) in individuals with SCI. To address this, our
laboratory developed the Toronto Rehabilitation Institute-Hand Function Test (TRI-HFT). The
TRI-HFT was designed to be simple, quick to administer and yet reliable, valid, and sensitive to
change in individuals with SCI. At the time the scoring was done using a 3-point ordinal scale
(0-2 scale). A score of 0 indicated that the participant was unable to grasp/hold the object in the
given hand position (pronation, neutral position, and supination). A score of 1 indicated that the
participant could grasp the object in the given hand position but was unable to sustain a grip on
the object resulting in a drop after grasping it but prior to completing the task. A score of 2
2
indicated that the participant was capable of performing the test. However, this scoring system
lacked the sensitivity to identify change following therapy and was unable to detect changes in
the reaching component of the upper extremity functional domain. With these limitations in
mind, I re-designed the scoring system of the test and a validation study was conducted to
validate this new scoring system of the TRI-HFT in individuals with SCI. The revised scoring of
the TRI-HFT showed good reliability, validity and sensitivity in SCI. Clinicians and researchers
started inquiring about purchasing the test. Our team realized that we had run into the exact same
issues as the other activity-based assessment tools which is lack of accessibility. Although, the
test object dimensions were published and widely available, self-manufacturing posed the
challenges of repeatability and standardization of the test. Hence, 3D printing of the test seemed
like a logical solution to address these issues. The first and second projects explored the
feasibility of 3D printing the TRI-HFT and evaluated its psychometric properties in individuals
with stroke and SCI.
The focus of the third study was to extend the application of one of the newer and
promising therapies in neurorehabilitation, namely Functional Electrical Stimulation Therapy
(FEST). FEST has gained significant traction as a short-term rehabilitation therapy for improving
function following neurological conditions like stroke, SCI, traumatic brain injury and cervical
myelopathy. Researchers have applied short term FEST to retrain various body functions like
ambulation, reaching, grasping and balance. For the purpose of this thesis, we focused on the use
of surface FEST for retraining upper extremity function in neurological patients. The last two
decades have seen significant work in this field with a few research teams developing and testing
a combination of reaching and grasping protocols including our team, details of which are
discussed in Chapter 3 and 4.
Our team has specifically conducted various clinical trials to assess the efficacy of multi-
channel surface FEST in retraining upper extremity function, and the end product of over 20
years of research is the “MyndMove™” stimulator. The MyndMove™ is a FEST device that is
non-invasive and uses short, low energy electrical pulses to induce muscle contractions. The
device offers a full range of protocols designed specifically to address proximal and distal
impairments of the upper extremity. Up to eight muscle groups can be stimulated during a
protocol. Thirty protocols, of which 17 are for use in stroke and 13 for use in SCI, provide a full

3
range of reaching and grasping movements that are broken down into sub-movements that can be
initiated by the therapist or patient using hand or foot switches. I played a key role in the
development and testing of these stimulation protocols. Upon the commercial clinical launch of
this technology, there was a need realized by clinicians for incorporating interscapular muscles
during upper extremity movements. This gap was identified by several therapists and generated
urgency to address this issue. In my thesis, I addressed this gap by developing and testing upper
extremity protocols that systematically recruit the interscapular muscles along with gleno-
humeral muscles during complex shoulder movements. Thus, the third study presented in this
thesis looks at the feasibility and benefits of stimulating interscapular muscles (Lower Trapezius,
Serratus Anterior and Upper Trapezius) using multi-channel surface FEST. Whereas all FEST
testing was performed in able bodied individuals, the goal is to use these stimulation patterns in
individuals with stroke, SCI, and other neurological conditions where FEST is indicated and
appropriate in order to maximize upper extremity functional gains. At the time of writing this
thesis, the protocols that were developed as part of this effort are fully productized and made
available in the latest version of the MyndMove™ system.
In this thesis I will provide an overview of the current state of the literature related to
upper extremity rehabilitation in individuals with stroke and SCI (Chapter 2) with a detailed
account of FEST and the methodology of its application in individuals with stroke and SCI
(Chapter 3 and 4). Chapter 5 enumerates the specific aims and objectives of my thesis. Chapter
6,7 and 8 discuss the original TRI-HFT and the 3D printed version of the TRI-HFT in both
stroke and SCI populations. Chapter 9 relates to the feasibility of stimulating interscapular
muscles using transcutaneous FES in able bodied individuals and Chapter 10 discusses the
limitations and future directions related to the field of upper extremity rehabilitation.

4
Chapter 2 Literature Review
2.1 Stroke
2.1.1 Epidemiology of Stroke
Stroke or cerebrovascular accident (CVA) is defined as a sudden non convulsive focal
neurologic deficit. Globally, new data from the Global Burden of Disease reports one in four
people will have a stroke in their lifetime (1). In 2013, stroke was the second most common
cause of all deaths (11.8%) (1), behind ischemic heart disease (14.8%) (2). In 2017, the age
standardized mortality rate for stroke was 80.5 per 100,000 population, representing a 13.6%
decline since 2007 (3). The drop-in mortality rate can be attributed, in part, to advancements in
acute stroke care interventions and rapid systems response. However, stroke incidence has not
declined to the same extent.
In North America stroke is the third leading cause of death after heart diseases and
cancers (4-6), and is the most common cause of morbidity and disability in survivors. Every year
in the United States, there are approximately 700,000 cases of stroke — roughly 600,000
ischemic lesions and 100,000 hemorrhages, intracerebral or subarachnoid — with 175,000
fatalities from these causes combined. In Canada, stroke remains a leading cause of adult
disability, with over 400,000 people living with its effects (7). By 2038, the number of Canadians
living with the effects of stroke is expected to increase to between 654,000 and 726,000 (7).
The economic impact of stroke is substantial and the costs of stroke to society are high.
According to a study published by Goeree et al., the Canadian government spends approximately
3% of National healthcare expenditure on stroke and with aging population this percentage is
likely to increase in the near future (8). Stroke-related costs in the US came to nearly $46
billion between 2014 and 2015 (9). This total includes the cost of health care services, medicines
to treat stroke, and missed days of work. A review of economic studies shows a wide range of
per-patient costs from $468 to $146,149 ($US) with few studies examining costs after hospital
discharge. Of all strokes 20% of patients will need medical care and rehabilitation after a CVA
event (4-6).
5
2.1.2 Pathophysiology and Clinical Presentation
Strokes are broadly classified into two types, ischemic and hemorrhagic. Ischemic stroke is due
to brain vessel occlusion (by a thrombus or an emboli) and blockage, and it accounts for 80% of
all strokes (4-6). Ischemic stroke is hence also referred to as a thrombotic or an embolic stroke.
The resultant neurologic syndrome corresponds to the area of the brain that is supplied by one or
more vessels involved. Hemorrhagic stroke is due to blood vessel rupture (intracerebral or
subarachnoid hemorrhage) and accounts for 20% of CVA’s.
There are all gradations of severity, but in all forms of stroke, the essential feature is
abruptness with which the neurologic deficit develops — usually a matter of seconds that stamps
the disorder as vascular. In its most severe form, the patient with a stroke becomes hemiplegic or
even comatosed. In its mildest form, a stroke may consist of a trivial and transient neurologic
disorder insufficient for the patient even to seek medical attention. Most embolic strokes occur
suddenly, and the deficit reaches its peak almost at once. Hemorrhagic strokes tend to evolve
somewhat more slowly over a period of minutes or hours and occasionally days. In cerebral
hemorrhage, also abrupt in onset, the deficit may be virtually static or steadily progressive over a
period of minutes or hours, while sub-arachnoid hemorrhage is almost instantaneous. It follows
that gradual downhill course over a period of several days or weeks. There are, however, many
exceptions, such as the additive effects of multiple vascular occlusions and the progression that
is caused by secondary brain edema surrounding large infarctions and cerebral hemorrhages. At
the other extreme is rapid regression of a focal stroke syndrome that reverses itself entirely and
dramatically over a period of minutes or up to an hour; this defines a Transient Ischemic Attack.
The second essential feature of stroke is its focal presentation. The neurologic deficit reflects
both the location and the size of the infarct or hemorrhage. Hemiplegia stands as the most typical
sign of cerebrovascular diseases, whether in the cerebral hemisphere or brainstem, but there are
many other manifestations, occurring in recognizable combinations. These include paralysis,
numbness, and sensory deficits of many types on one side of the body, aphasia, visual field
defects, diplopia, dizziness, dysarthria, and so forth.
History and physical examination remain the pillars of diagnosing stroke. The most
common historical feature of an ischemic stroke is its acute onset, and the most common

6
physical findings of ischemic stroke are focal weakness and speech disturbance (10). The most
common and reliable symptoms and signs of ischemic stroke are subjective arm weakness,
subjective leg weakness, speech disturbance, arm paresthesia, leg paresthesia, headache, non-
orthostatic dizziness, arm paresis, leg paresis, dysphasia, hemiparetic or ataxic gait, facial
paresis, eye movement abnormality and visual field defect. Reliably distinguishing between
intracerebral hemorrhage and ischemic stroke can only be done through neuroimaging. Both
entities are characterized by acute onset of focal symptoms. Persons with intracerebral
hemorrhage may have gradual worsening of symptoms after the abrupt onset, reflecting an
increasing size of the hematoma. Persons with hemorrhage also may have a decreased level of
consciousness. Subarachnoid hemorrhage presents differently from intracerebral hemorrhage and
ischemic stroke. The most common symptom described by the patient is the “worst headache of
my life.” Symptoms may also include vomiting, seizures, meningismus, and a decreased level of
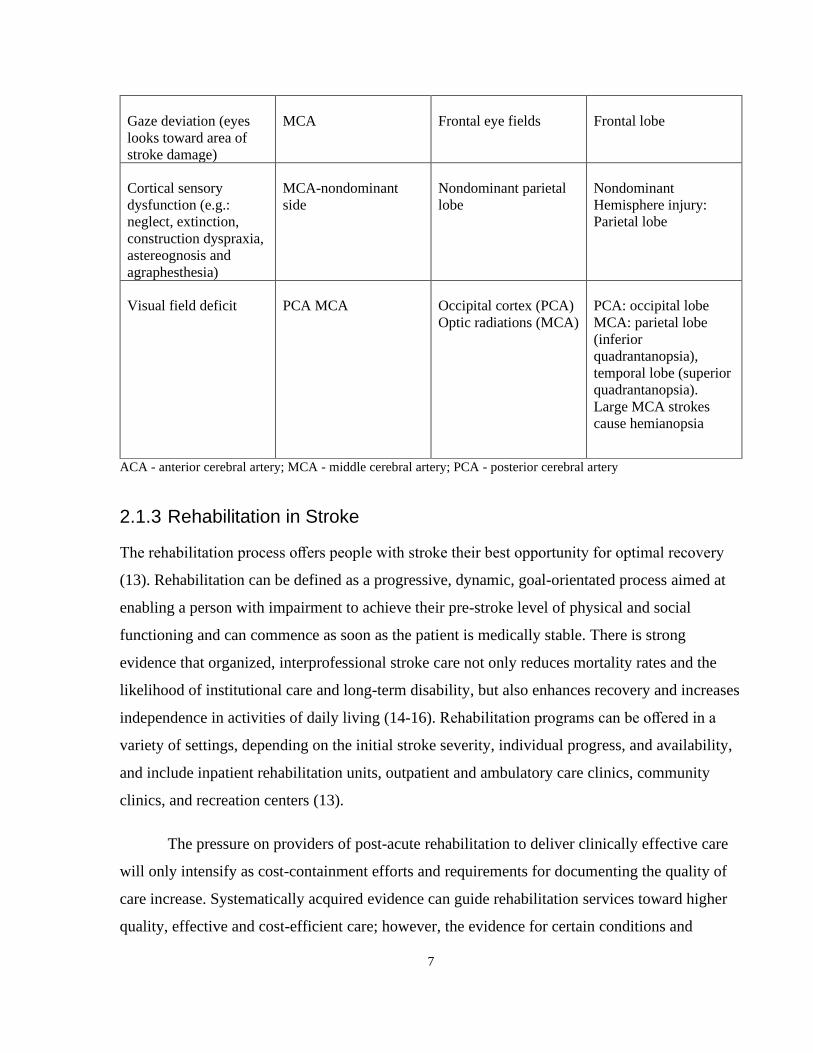
consciousness (11). The specific neurologic deficit will depend on the location of the brain
injury. Table 2.1 provides a brief overview of the common signs and symptoms often
encountered, delineating their corresponding vascular and anatomical localization (12).
Table 2. 1 Clinical Deficits in Stroke Based on Vascular and Anatomical Localization
Clinical deficit Artery Injury location Lobe affected
Unilateral weakness
(affecting face, arm and
leg equally)
Lenticulostriates of the
MCA
Perforating vessels of
the brainstem
Internal capsule
Corticospinal tract
Variable
Unilateral weakness
(affecting face and arm
> leg)
MCA Motor cortex- laterally
affecting face/arm
homunculus
Frontal lobe
Unilateral hemiparesis
(affect leg and trunk)
ACA Motor cortex- medially
affecting leg/trunk
homunculus
Frontal lobe
Aphasia MCA-dominant side Broca’s area (nonfluent
or expressive aphasia)
Wernicke’s area (fluent
or receptive aphasia)
Dominant hemisphere
injury: Broca’s area:
frontal lobe Wernicke’s
area: temporal lobe
7
Gaze deviation (eyes
looks toward area of
stroke damage)
MCA Frontal eye fields Frontal lobe
Cortical sensory
dysfunction (e.g.:
neglect, extinction,
construction dyspraxia,
astereognosis and
agraphesthesia)
MCA-nondominant
side
Nondominant parietal
lobe
Nondominant
Hemisphere injury:
Parietal lobe
Visual field deficit PCA MCA Occipital cortex (PCA)
Optic radiations (MCA)
PCA: occipital lobe
MCA: parietal lobe
(inferior
quadrantanopsia),
temporal lobe (superior
quadrantanopsia).
Large MCA strokes
cause hemianopsia
ACA - anterior cerebral artery; MCA - middle cerebral artery; PCA - posterior cerebral artery
2.1.3 Rehabilitation in Stroke
The rehabilitation process offers people with stroke their best opportunity for optimal recovery
(13). Rehabilitation can be defined as a progressive, dynamic, goal-orientated process aimed at
enabling a person with impairment to achieve their pre-stroke level of physical and social
functioning and can commence as soon as the patient is medically stable. There is strong
evidence that organized, interprofessional stroke care not only reduces mortality rates and the
likelihood of institutional care and long-term disability, but also enhances recovery and increases
independence in activities of daily living (14-16). Rehabilitation programs can be offered in a
variety of settings, depending on the initial stroke severity, individual progress, and availability,
and include inpatient rehabilitation units, outpatient and ambulatory care clinics, community
clinics, and recreation centers (13).
The pressure on providers of post-acute rehabilitation to deliver clinically effective care
will only intensify as cost-containment efforts and requirements for documenting the quality of
care increase. Systematically acquired evidence can guide rehabilitation services toward higher
quality, effective and cost-efficient care; however, the evidence for certain conditions and

rehabilitation settings is better developed than for others. More clearly delineating the evidence
of effectiveness will help determine whether certain post-acute rehabilitation services produce
better outcomes than alternatives. Subsequently, policymakers, health care administrators, and
clinicians might be better informed for making decisions about providing rehabilitation services
that help patients attain functional autonomy and a better quality of life (QOL).
According to the Canadian Stroke Best Practices recommendations all patients with
acute stroke should be assessed to determine the severity of stroke and early rehabilitation needs
(13). Further the guidelines say that initial screening and assessment should ideally be
commenced within 48 hours of admission by rehabilitation professionals in direct contact with
the patient. Assessments of impairment, functional activity limitations, role participation
restrictions and environmental factors should be conducted using standardized, valid assessment
tools. The tools should be adapted for use with patients who have communication differences or
limitations where required. Once a patient with stroke has undergone assessments, a
standardized approach is recommended to determine the appropriate setting for rehabilitation
(inpatient, outpatient, community, and/or home-based settings). All patients with stroke should
receive rehabilitation therapy as early as possible once they are medically stable and able to
participate in active rehabilitation. Individualized rehabilitation plans should include a patient-
centered approach, shared decision-making, culturally appropriate and agreed-upon goals and
preferences of the patient, family, caregivers and the healthcare team.
2.1.3.1 Upper Extremity Rehabilitation in Stroke
Upper limb (i.e., arm, hand and/ or fingers) motor impairments following stroke are often
persistent and disabling (17). Only half of all stroke survivors with an initial plegic (paralyzed)
upper limb regain some useful upper limb function after six months (18), and, of those with
initial arm impairment, 50% have problems with arm function four years post stroke (19).
Activities of daily living (ADLs) largely depend on arm function (20), particularly for personal
activities such as feeding, dressing and grooming. One year after stroke, arm motor impairment
is associated with anxiety (21) and poorer perception of health-related quality of life (22), and
subjective well-being (23). Therefore, improving upper limb function is a core element of
8
9
rehabilitation after stroke to maximize recovery (24). Therapists have developed many diverse
techniques that aim to rehabilitate arm function after stroke.
Rehabilitation interventions for the upper extremity are typically offered by
Physiotherapists or Occupational Therapists (PT/OT’s). Prior to selection of rehabilitation
treatments, clinical assessments including assessments using standardized outcome measures are
done to aid with identifying functional deficits as well as with identifying patient therapy goals.
Standardized outcome measures are typically developed based on the International
Classification of Functioning, Disability and Health (ICF) framework for describing
functioning and disability in relation to a health condition. The ICF focuses on the following
components: body, activities, participation (at individual and societal levels) and contextual
(personal and environmental) (25). In the ICF, functioning and disability are multi-dimensional
concepts, relating to:
• the body functions and structures of people, and impairments thereof (functioning at the
level of the body);
• the activities of people (functioning at the level of the individual) and the activity
limitations they experience;
• the participation or involvement of people in all areas of life, and the participation
restrictions they experience (functioning of a person as a member of society); and
• the environmental factors which affect these experiences (and whether these factors are
facilitators or barriers).
2.1.3.1.1 Outcome Measures in Upper Extremity Rehabilitation Following Stroke
Use of standardized and scientifically sound outcome measures is highly encouraged in clinical
practice and research. A number of guidelines have been developed around the use of upper
extremity outcome measures in stroke (26, 27). However, researchers have identified that with
the development of newer rehabilitation therapies we need technology-supported upper extremity
outcome measures that are easily accessible and can measure change consistently and reliably
(28). The most commonly used upper extremity measures in clinical and research settings for
stroke in the ICF’s body structure and function and activity level domains are the Fugl-Meyer
Assessment Upper Extremity (FMA-UE) (29) and the Action Research Arm Test (ARAT) (30),

10
respectively. The FMA-UE measures the movement, coordination and reflex actions of the
shoulder, elbow, forearm, wrist and hand. The upper extremity motor score ranges from 0 to 66
and items are graded on a 3-point ordinal scale (0 = cannot perform, 1 = performs partially, 2 =
performs fully). The FMA-UE, measures function in the body structure and function domain and
has excellent psychometric properties, however, there are reports in literature related to floor and
ceiling effects (31). The ARAT is an outcome assessment tool that measures upper extremity
function in the activity domain of the ICF. It consists of 19 items that assesses upper extremity
performance (coordination, dexterity and functioning). It is a time-based activity test and is
rated on a 4-point ordinal scale, ranging from 0 (no movement) to 3 (movement performed
normally). Although widely used ARAT has several documented limitations (32).
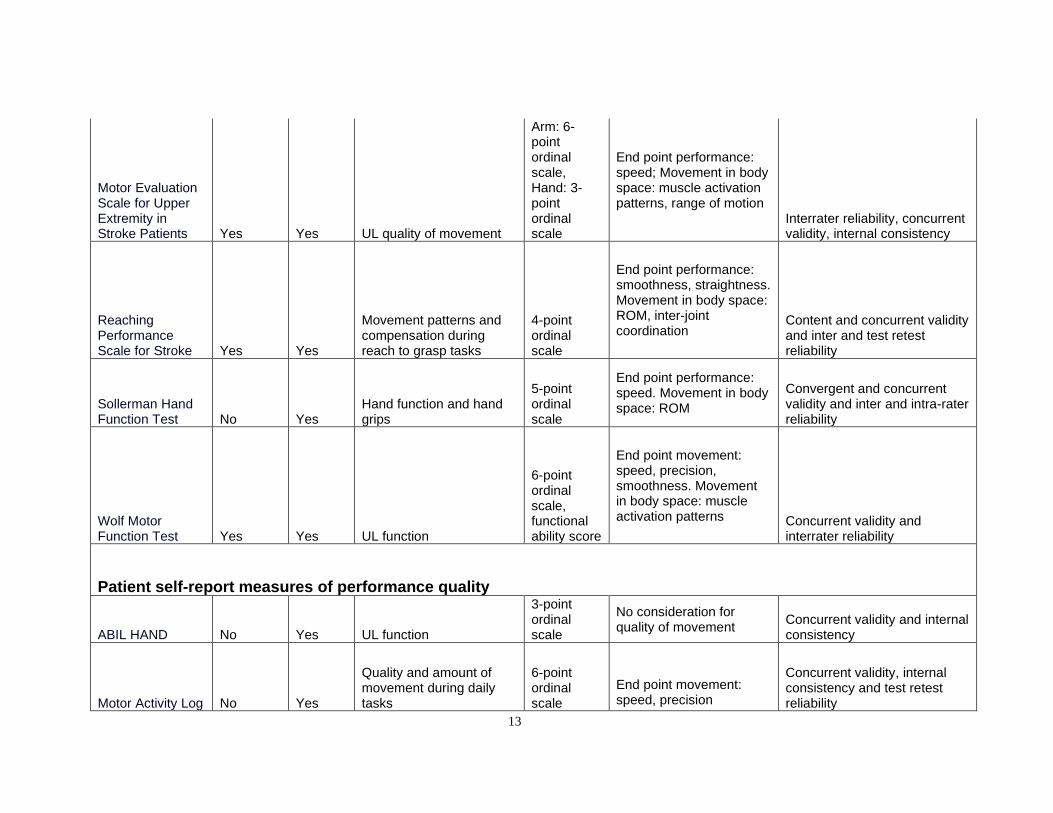
Demers M et al., reviewed 15 upper extremity outcome measures assessing
arm/hand function at the ICF’s activity level recommended by neurological clinical practice
guidelines including the Box and Block test (33), Jebsen Hand function test (34), Nine hole peg
test (35), ARAT(30), Chedoke Arm and Hand Activity Inventory (CAHAI) (36), Arm Motor
ability test (37), Frenchay Arm Test (38), Motor Evaluation Scale for Upper Extremity in Stroke
Patients (39), Reaching Performance Scale for Stroke (40), Test d’Évaluation des Membres
supérieurs des Personnes Âgées (41), Wolf Motor Function Test (42), ABILHAND (43),
Capabilities of the upper extremity (44) and Motor Activity Log (Table 2.2) (45). The review
concluded that current activity measures may not distinguish recovery from compensation and do
not adequately track changes in movement quality over time. Recently with newer rehabilitation
therapies being researched there has been a shift in focus of rehabilitation goals. Although
attaining success at performing functional tasks remains the end goal, therapists are now focused
on retraining correct movement patterns to achieve these goals rather than teaching
compensatory strategies. Secondly, most of the measures are time measures and provide no
information on what components of the movement were accomplished and what components
could not be performed by the patient. The body literature established by researchers and
clinicians in the field of upper extremity rehabilitation places a significant emphasis on
identifying residual neurological integrity. The reason being that the core impairments, and how
they relate to the performance of functional tasks is considered to be a key concept in therapeutic
interventions. Lastly, outcome measures, specifically activity measures like the ARAT and Wolf

11
Motor Function Test (WMFT), require an administration time of more than 20 minutes and
require equipment purchase or construction or copyright payments (27).

12
Table 2. 2 Current Upper Extremity Outcome Measures (Demers et al., 2017) (45)
ICF level of the measure
Outcome Measure
Body Structure/Function Activity Assessed Construct
Main Outcome
Assessment of movement quality
Psychometric Properties evaluated in stroke
Box and Block Test Yes Yes
Unilateral gross manual dexterity
No. of blocks transported in 60 secs
No consideration for quality of movement
Interrater reliability, Test-retest reliability, concurrent validity
Jebsen Hand Function Test No Yes
Fine and gross motor hand function Time
No consideration for quality of movement
Interrater reliability, Test-retest reliability, concurrent validity, internal consistency
Nine Hole Peg Test Yes Yes Fine manual dexterity Time
No consideration for quality of movement
Interrater reliability, Test-retest reliability, concurrent validity, construct validity
Arm Motor Ability Test No Yes UL function time
6-point ordinal scale
End point movement: speed, precision, smoothness. Movement in body space: muscle activation patterns
Interrater reliability, test-retest reliability, concurrent validity, construct validity
Action Research Arm Test Yes Yes UL activity limitation
4-point ordinal scale
End point performance: speed
Interrater reliability, test-retest reliability, concurrent validity, construct validity
Chedoke Arm and Hand Activity Inventory No Yes Arm and hand recovery
7-point ordinal scale
End point performance: speed
Interrater reliability, construct validity
Frenchay Arm Test Yes Yes UL motor function
Pass/Fail on 2-point scale
No consideration for quality of movement Inter and intra-rater reliability
13
Motor Evaluation Scale for Upper Extremity in Stroke Patients Yes Yes UL quality of movement
Arm: 6-point ordinal scale, Hand: 3-point ordinal scale
End point performance: speed; Movement in body space: muscle activation patterns, range of motion
Interrater reliability, concurrent validity, internal consistency
Reaching Performance Scale for Stroke Yes Yes
Movement patterns and compensation during reach to grasp tasks
4-point ordinal scale
End point performance: smoothness, straightness. Movement in body space: ROM, inter-joint coordination
Content and concurrent validity and inter and test retest reliability
Sollerman Hand Function Test No Yes
Hand function and hand grips
5-point ordinal scale
End point performance: speed. Movement in body space: ROM
Convergent and concurrent validity and inter and intra-rater reliability
Wolf Motor Function Test Yes Yes UL function
6-point ordinal scale, functional ability score
End point movement: speed, precision, smoothness. Movement in body space: muscle activation patterns Concurrent validity and
interrater reliability
Patient self-report measures of performance quality
ABIL HAND No Yes UL function
3-point ordinal scale
No consideration for quality of movement
Concurrent validity and internal consistency
Motor Activity Log No Yes
Quality and amount of movement during daily tasks
6-point ordinal scale
End point movement: speed, precision
Concurrent validity, internal consistency and test retest reliability
14
2.1.3.1.2 Rehabilitation Strategies for the Upper Extremity Rehabilitation Following Stroke
Over the past two decades there has been a 10-fold increase in the research being conducted in
the area of upper extremity rehabilitation. Researchers are constantly trying to develop and
improvise therapies to improve outcomes. Traditional therapeutic maneuvers used in the
rehabilitation of the arm include but are not limited to Bobath techniques, neuro-developmental
techniques, strengthening exercises, repetitive task specific training, constraint induced
movement therapy, bilateral arm training, mirror therapy, training for compensatory techniques
using the unaffected upper extremity and many more.
Alongside these long-standing practices there are various newer interventions that are
available or still being researched. Whereas detailed discussion of individual therapies for stroke
is outside the scope of this document, a brief overview follows. The non-invasive rehabilitation
therapies include robot assisted therapies, virtual reality training, Functional Electrical
Stimulation (FES) therapy, Brain computer interface (BCI) -controlled FES therapy, Transcranial
magnetic stimulation therapy (TMS) (46), transcranial direct current stimulation (tDCS) (47)
therapy and many more. Various studies including randomized controlled trials have been
conducted to study the benefits of robot assisted therapy for upper extremity retraining post
stroke (48-50). A recent review by Kwakkel et al., found that robot assisted therapies for the
upper limb allow patients to increase the number of repetitions and hence intensity of practice
poststroke and appears to be a safe therapy (51). Effects on motor control are small and specific
to the joints targeted by the robotic assisted therapy, whereas no generalization is found to
improvements in upper limb capacity (51). Virtual reality interventions have shown some
promising results (52-55) however systematic reviews in this domain state the need for RCT’s
with larger sample sizes and more homogenous outcome assessment tools to allow for
comparison between interventions (56, 57). Whereas BCI-controlled FES therapy, TMS (46) and
tDCS (47) still remain research-based therapies for stroke motor rehabilitation, FEST has gained
significant traction amongst clinicians and is currently in use in both clinical and research
settings. The early application of FEST in stroke was in the form of an orthotic device where the
patient would trigger the FES when a particular function needed to be executed however more
recently FES is being used as a therapeutic modality to retrain function in the hope that after a
certain number of sessions the patient would have regained the ability to perform the targeted

15
activity without the use of FES. Detailed description of the FEST methods and application using
surface stimulation is discussed in Chapter 4.
2.1.4 Summary of Current State of Rehabilitation in Stroke
2.1.4.1 Outcome Measures for Upper Extremity Function
As discussed in detail in Section 2.1.3.1.1 there are various outcome assessment tools that have
been developed to measure upper extremity function in stroke. However, to the best of our
knowledge none of these tools have been clearly identified in the literature as best practice for
assessing upper extremity function. Although, some of these tools like the ARAT have been
successfully validated in the stroke population with good psychometrics, they have limitations
which have contributed to their limited uptake in clinical practice. Besides, with the development
of newer rehabilitation interventions it becomes important to develop assessment tools that are
sensitive to change following these interventions. Also, with an aging population and increased
chances of survival post stroke there is a strain on the healthcare system from a point of view of
rehabilitation providers to patient ratios. Given that rehabilitation remains the mainstay of
treatment post stroke, we need to work towards developing therapies and assessment tools that
are time effective, simple and easy to administer without compromising quality of care. Whereas
we can see that this concept is being incorporated in interventional research with the
development of, for example robotics, such change has not been realized in the rehabilitation
assessment domain. We developed the Toronto Rehabilitation Institute-Hand Function Test
(TRI-HFT) to address this gap in outcome measures (details of this original version of the test
including test development, administration and scoring are discussed in detail in Chapter 6).
Although the TRI-HFT was quick and simple to administer, the issue of accessibility of the test
without compromising standardization (which often becomes a problem with do-it-yourself
manufacturing) restricted its up take by clinicians as well as researchers. The first project of my
thesis aimed to address this issue of accessibility without forsaking standardization. In this
project I explored the feasibility of 3D printing the TRI-HFT and assessed the psychometrics of
the 3D printed test in a small sample of individuals with chronic stroke.
It is important to assess the psychometric properties of an outcome assessment tool as the
quality of information provided by the tool partly depends on this (58). Whereas testing of
16
various psychometric properties is desirable, the often-tested ones are reliability and validity.
The Consensus-based Standards for the selection of health Measurement Instruments
(COSMIN) taxonomy defines reliability as the degree to which the measurement is free from
measurement error (59). There are different types of reliability however for performance-based
measures it is recommended that inter and intra-rater reliability be tested (58). Intra-rater
reliability indicates how consistently a rater administers and scores an outcome measure (58).
Inter-rater reliability indicates how well two raters agree in the way they administer and score
an outcome measure (58). Both the inter and intra-rater reliability of the 3D TRI-HFT were
assessed in stroke population (Chapter 7).
Validity is defined as the degree to which an instrument measures what is intended to be
measured (60). There are different types of validity and as per the COSMIN guidelines the
content and criterion validity are considered important for an outcome to be included in the
core outcome set (COS) (59). A COS is an agreed standardized set of outcomes that should be
measured and reported, as a minimum, in all clinical trials in a specific disease or trial
population (59). Content validity is defined as the degree to which the content of a
measurement instrument is an adequate reflection of the construct to be measured. Criterion
validity is defined as the degree to which the scores of a measurement instrument are an
adequate reflection of a ‘gold standard’(58). Content validity of the original TRI-HFT was
assessed using informal feedback from clinicians in the field (Chapter 10). Due to lack of a
clear ‘gold standard’ for assessment of upper extremity function in stroke, criterion validity in
stroke was not assessed. Instead, construct validity of the 3D TRI-HFT was assessed in stroke.
Construct validity reflects the ability of a test to measure the underlying concept of interest to
the clinician or researcher. The construct validity of the 3D TRI-HFT was assessed by
correlating scores on 3D TRI-HFT with the scores on Chedoke-McMaster Stroke Assessment
(CMSA)-Arm, CMSA-Hand and the Fugl Meyer Assessment-Hand in the stroke population
(Chapter 7).
2.1.4.2 Rehabilitation Therapies for Restoring Upper Extremity Function
Restoring upper extremity function remains a key goal of rehabilitation following stroke.
Whereas various therapeutic modalities are being used to achieve this goal, results following
rehabilitation remain limited. As discussed in the previous section rehabilitation scientists are

17
working hard towards researching therapies that can advance the results post rehabilitation.
Although, therapies like CIMT, mirror therapy, robotics, virtual therapy are being used in some
clinical settings, there is a lack of systematic large scale RCT’s that show the superiority of these
therapies over conventional rehabilitation techniques. Moreover, the recently published Veterans
Affairs (VA) /Department Of Defense (DOD) clinical practice guideline for the management of
stroke rehabilitation provides only weak recommendation for these modalities in motor
rehabilitation (61). To date conventional rehabilitation techniques including but not limited to
activity-based therapy, task specific repetitive movement therapy, strengthening exercises,
weight bearing exercises, stretching and range of motion exercises remain best practice for
restoring function following stroke.
Transcutaneous FEST has been studied over the past several years for its potential to
retrain motor function in stroke (details in chapter 3). Although the DOD guidelines provide
weak recommendation for use of FEST in stroke, the guidelines further state that “The benefits
of using FES intervention (external electrodes) outweigh the harms and could provide improved
function over standard of care. FES/NMES/TENS units are readily available in most clinics and
can be used as an adjunct to task-specific training” (61). We in our laboratory have been
investigating the benefits of FEST in restoring upper extremity function in stroke and spinal cord
injury for the past 15+ years (details in Chapter 4). The results of these studies were very
promising which led to the development of a commercial upper extremity simulator called the
MyndMove™. The details of FES stimulators and their clinical application for upper extremity
rehabilitation including the MyndMove™ is presented in the next two chapters (Chapter 3 and
Chapter 4).
Initially, when the upper extremity protocols were developed for MyndMove™ we
focused on protocols that targeted movements of the shoulder, elbow, wrist and hand. However,
we found a need to expand these to include interscapular muscle stimulation given the
documented evidence of these muscles in shoulder complex movements and during performance
of activities of daily living. This need was strongly voiced by the clinicians using the stimulator
as well. In the third project of my PhD, I expanded on my previously created repertoire of
protocols available for restoring upper extremity function (62). In this project, I assessed the
feasibility of stimulating the Upper Trapezius (UT), Serratus Anterior (SA) and the Lower
18
Trapezius (LT) along with the Anterior or Middle Deltoid during forward flexion and abduction
movements respectively.
2.2 Spinal Cord Injury
2.2.1 Epidemiology of Spinal Cord Injury
The global incidence of acute SCI from 1995 onward suggests a value between 10.4 and 83 cases
per million per annum (63). Half of the injuries are complete (no sensory or motor function is
preserved in the sacral segment S4-S5) and one third result in tetraplegia. The incidence of high
cervical SCI has more than doubled in the United States since the 1970s. The annual incidence of
SCI is approximately 54 cases per one million people in the United States, or about 17,730 new
SCI cases each year (64). The estimated number of people with SCI living in the United States is
approximately 291,000 persons, with a range from 249,000 to 363,000 persons (65). The average
age at injury has increased from 29 years during the 1970s to 43 years recently (66). About 78%
of new SCI cases are male (66). Vehicle crashes are the most recent leading cause of injury,
closely followed by falls. Incomplete tetraplegia is the most frequent neurological category, with
47% of traumatic SCI’s falling in this category (66). The frequency of incomplete and complete
paraplegia is the same. Less than 1% of persons experience complete neurological recovery by
the time of hospital discharge. In Canada, the estimated initial incidence of traumatic spinal cord
injury (tSCI) is 1,785 cases per year, and the discharge incidence is 1,389 (41 per million) (67).
The estimated discharge incidence for non-traumatic spinal cord injury (ntSCI) is 2,286 cases (68
per million). The prevalence of SCI in Canada is estimated to be 85,556 persons (51% tSCI and
49% ntSCI) (67).
The estimated lifetime economic burden associated with a tSCI in Canada ranges from
$1.47 million for a person with incomplete paraplegia to $3.03 million for one with complete
tetraplegia (68). Of the total costs, direct costs represent between 44% and 51% in patients with
paraplegia, and between and 56% and 66% in patients with tetraplegia. Within direct costs, the
most significant cost driver was the cost of attendant care following the injury. These costs alone
ranged from $0.29 million to $1.02 million (38%–60% of direct costs) (68).
19
2.2.2 Pathophysiology and Clinical Presentation
A SCI can be traumatic or non-traumatic in etiology. Traumatic SCI (tSCI) occurs when there is
a sudden, traumatic impact on the spine that compromises the spinal column or fractures or
dislocates vertebrae, subsequently causing damage or compression to the spinal cord (69). The
initial insult is known as the primary injury where frank compression or damage to the spinal
cord occurs (70-72). There are four main characteristic mechanisms of primary injury which
include: 1) Impact plus persistent compression; 2) Impact alone with transient compression; 3)
Distraction; and 4) Laceration/transection (72, 73). Regardless of the form of primary injury,
these forces directly damage ascending and descending pathways in the spinal cord and disrupt
blood vessels and cell membranes, which will cause spinal shock, systemic hypotension,
vasospasm, ischemia, ionic imbalance, and neurotransmitter accumulation otherwise, known as
the secondary injury (73-75). Ultimately the severity of injury is based on how much damage
occurs during the primary injury (76, 77). Overall, the extent of the primary injury determines
the severity of SCI and the severity of injury is the greatest factor in predicting how much
recovery will occur (78, 79).
Non-traumatic SCI (ntSCI) refers to compression of the spinal cord related to a tumor,
infection or degeneration of the spinal column. The mechanism is a gradual compression (slow
SCI) of the cord due to an expanding lesion or progressive degeneration causing increased
compression over time (80-82). Again, the neural tissue does adapt over time, however, once
deficits are significant enough to limit independence and alter function; decompressive measures
are taken. For the period post decompression, we see again a very similar course of recovery as
we do in tSCI. Therefore, there is a window of opportunity to enhance recovery by providing
neurorehabilitation for restoration (83).
Ultimately, all the conditions mentioned above have a presentation of motor and sensory
deficits coupled with functional loss. In other words, they all manifest with a degree of paralysis
or paresis as a result of an upper motor neuron lesion. Over and above the motor and sensory
deficits there are a myriad of other clinical manifestations including initial period of spinal
shock, impaired temperature control, respiratory impairment, spasticity, bladder and bowel
dysfunction, sexual dysfunction and secondary complications like pressure sores, autonomic

20
dysreflexia, postural hypotension, contractures, deep venous thrombosis, osteoporosis and
traumatic pain.
Spinal cord injuries are typically divided into two broad functional categories:
Tetraplegia and Paraplegia. Tetraplegia refers to partial or complete paralysis of all four
extremities and the trunk including the respiratory muscles and results from cervical cord injury.
Paraplegia refers to partial or complete paralysis of all or part of the trunk and both the lower
extremities resulting from lesions of the thoracic or lumbar spinal cord or sacral roots.
The ASIA (American Spinal Injury Association) Impairment Scale (AIS), based on the
Frankel scale, is a clinician-administered scale used to classify the severity (completeness) of
injury in individuals with SCI (Table 2.3). It identifies sensory and motor levels indicative of the
highest spinal level demonstrating “unimpaired” function. Preservation of function in the sacral
segments (S4-S5) is a key for determining the AIS grade.
Table 2. 3 American Spinal Cord Association Impairment Scale (AIS)(84)
AIS level Completeness
of injury
Description
A Complete No sensory or motor function is preserved in the sacral segments S4-S5
B Incomplete Sensory but not motor function is preserved below the neurological level
and includes the sacral segments S4-S5 (light touch, pin prick at S4-S5
or deep anal pressure), AND no motor function is preserved more than
three levels below the motor level on either side of the body.
C Incomplete Motor function is preserved below the neurological level and more than
half of key muscle functions below the single neurological level of
injury (NLI) have a muscle grade less than 3.
D Incomplete Motor function is preserved below the neurological level and at least
half of key muscle functions below the NLI have a muscle grade of 3 or
greater.
E Incomplete If sensation and motor function as tested with the ISNCSCI are graded
as normal in all segments, and the patient had prior deficits, then the AIS

21
grade is E. Someone without an initial SCI does not receive an AIS
grade.
A thorough physical assessment of the patient is carried out to determine respiratory
function, skin condition, sensation, tone and muscle strength. Results assist in determining level
of lesion and identifying general functional expectations. This information is critical for devising
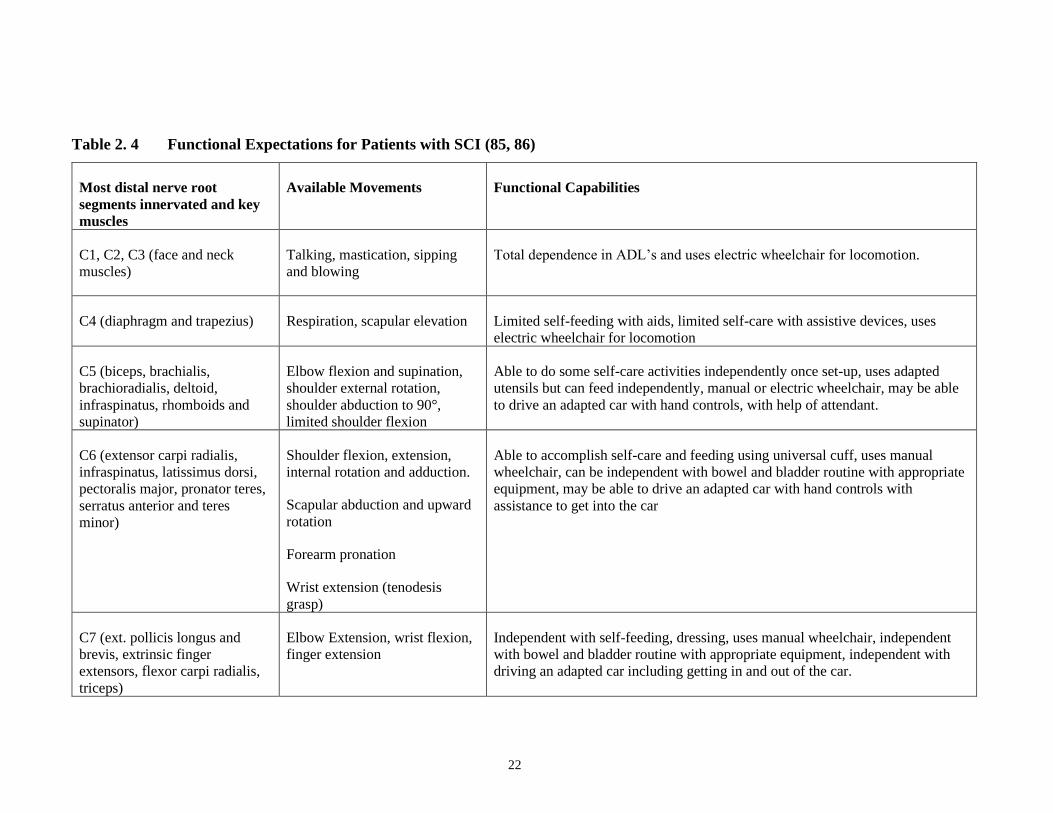
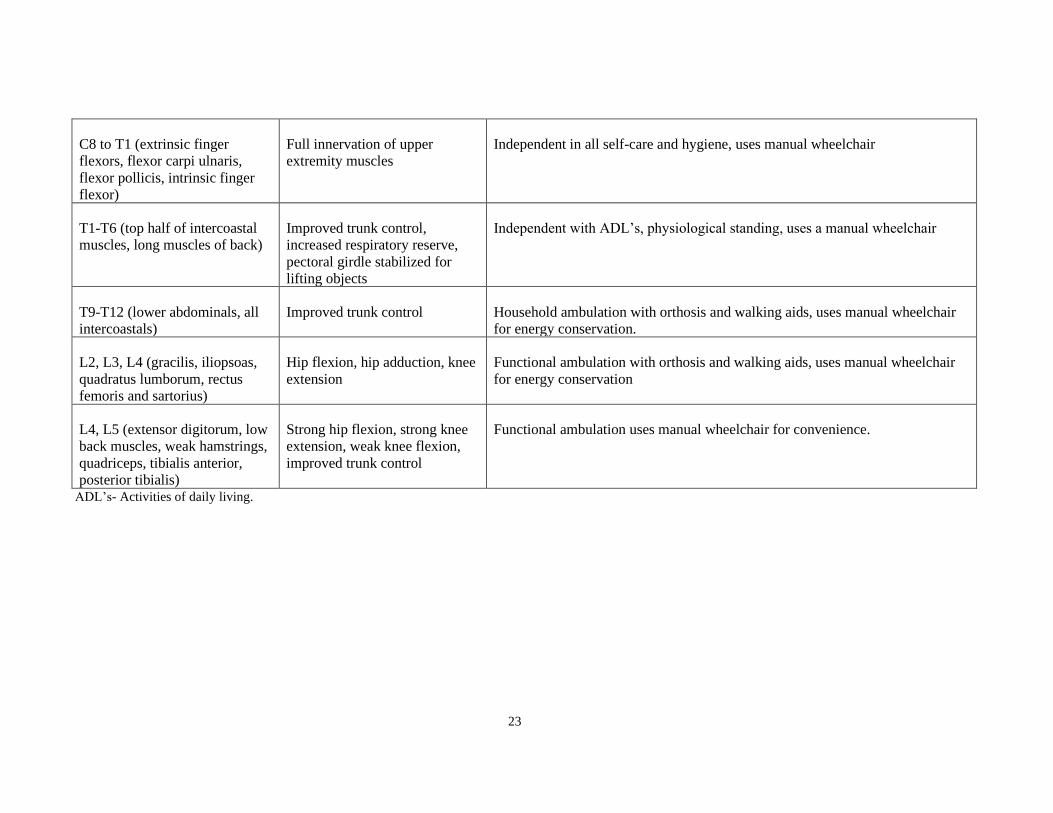
a rehabilitation plan for the patient. The functional abilities to work towards are based on the
level of lesion and are outlined in Table 2.4 (85,86). It is important to note that these are based
on a patient with complete lesion and unimpaired by secondary complications. Individual
variations in presentation exist and patients with incomplete injury may present with functional
capabilities that overlap across multiple levels. The therapy plan is based on individual patient
presentation and will differ from patient to patient.
22
Table 2. 4 Functional Expectations for Patients with SCI (85, 86)
Most distal nerve root
segments innervated and key
muscles
Available Movements Functional Capabilities
C1, C2, C3 (face and neck
muscles)
Talking, mastication, sipping
and blowing
Total dependence in ADL’s and uses electric wheelchair for locomotion.
C4 (diaphragm and trapezius) Respiration, scapular elevation Limited self-feeding with aids, limited self-care with assistive devices, uses
electric wheelchair for locomotion
C5 (biceps, brachialis,
brachioradialis, deltoid,
infraspinatus, rhomboids and
supinator)
Elbow flexion and supination,
shoulder external rotation,
shoulder abduction to 90°,
limited shoulder flexion
Able to do some self-care activities independently once set-up, uses adapted
utensils but can feed independently, manual or electric wheelchair, may be able
to drive an adapted car with hand controls, with help of attendant.
C6 (extensor carpi radialis,
infraspinatus, latissimus dorsi,
pectoralis major, pronator teres,
serratus anterior and teres
minor)
Shoulder flexion, extension,
internal rotation and adduction.
Scapular abduction and upward
rotation
Forearm pronation
Wrist extension (tenodesis
grasp)
Able to accomplish self-care and feeding using universal cuff, uses manual
wheelchair, can be independent with bowel and bladder routine with appropriate
equipment, may be able to drive an adapted car with hand controls with
assistance to get into the car
C7 (ext. pollicis longus and
brevis, extrinsic finger
extensors, flexor carpi radialis,
triceps)
Elbow Extension, wrist flexion,
finger extension
Independent with self-feeding, dressing, uses manual wheelchair, independent
with bowel and bladder routine with appropriate equipment, independent with
driving an adapted car including getting in and out of the car.
23
C8 to T1 (extrinsic finger
flexors, flexor carpi ulnaris,
flexor pollicis, intrinsic finger
flexor)
Full innervation of upper
extremity muscles
Independent in all self-care and hygiene, uses manual wheelchair
T1-T6 (top half of intercoastal
muscles, long muscles of back)
Improved trunk control,
increased respiratory reserve,
pectoral girdle stabilized for
lifting objects
Independent with ADL’s, physiological standing, uses a manual wheelchair
T9-T12 (lower abdominals, all
intercoastals)
Improved trunk control Household ambulation with orthosis and walking aids, uses manual wheelchair
for energy conservation.
L2, L3, L4 (gracilis, iliopsoas,
quadratus lumborum, rectus
femoris and sartorius)
Hip flexion, hip adduction, knee
extension
Functional ambulation with orthosis and walking aids, uses manual wheelchair
for energy conservation
L4, L5 (extensor digitorum, low
back muscles, weak hamstrings,
quadriceps, tibialis anterior,
posterior tibialis)
Strong hip flexion, strong knee
extension, weak knee flexion,
improved trunk control
Functional ambulation uses manual wheelchair for convenience.
ADL’s- Activities of daily living.

24
2.2.3 Rehabilitation in Spinal Cord Injury
Rehabilitation commences once a patient is medically stable and initially may focus on
preventing secondary complications. The overall objectives of rehabilitation include (1) to
improve a patient’s independence in activities of daily living, such as bathing, eating, dressing,
grooming, and wheelchair use; (2) to help a patient accept a new lifestyle with respect to sexual
and recreational activities and housing options; and (3) to aid a patient’s reintegration into
society.
A specialized SCI rehabilitation program provides comprehensive, individualized, and
patient focused rehabilitation services, for inpatient, transitional living, outpatient and follow-up
care, to empower people with SCI and their families to achieve optimal quality of life continuing
into the community (focusing on increasing self-reliance and gaining independence) (87).
Rehabilitation following an SCI typically requires a team approach, with the team comprising of
Physical Medicine and Rehabilitation physicians and allied health professionals including
occupational, speech, physical, respiratory, and recreational therapists; rehabilitation nurses;
psychologists; and social workers. Specialized rehabilitation centers may provide SCI specific
services including custom wheelchair fitting, assistive technology, specialized wound care,
sexuality/reproductive education, etc.
Rehabilitation for patients with SCI has evolved over the years and is undergoing a
paradigm shift. In the past, physical and occupational therapy focused on teaching compensatory
strategies. However, with an increasing understanding of neuroplasticity, goals have shifted
toward neuromuscular re-education and recovery of lost function. During the acute and subacute
phases of treatment, rehabilitation strategies focus on preventing secondary complications,
promoting neuro-recovery and maximizing function (88) . In the chronic phase, compensatory or
assistive approaches are often used, whereas in the acute and subacute phases, there is a greater
emphasis on techniques that address underlying impairments (88) . The optimal management
strategies for patients with acute SCI are difficult to define due to the challenges associated with
rehabilitation research; these include a lack of standardization of interventions, therapeutic doses
and outcome measures, heterogeneous populations, superimposed spontaneous recovery, and
problems with group assignment (89). Despite these challenges, the Paralyzed Veterans
Association developed several guidelines that focus on various components of rehabilitation.

25
Treatment strategies are carefully chosen based on level and extent of injury and functional
expectation based on AIS levels.
2.2.3.1 Upper Extremity Rehabilitation in Spinal Cord Injury
Snoek et al., (2004) surveyed the needs of patients with SCI and found a high impact and high
priority for improvement in hand function in those with tetraplegia comparable to that for
bladder and bowel dysfunction (90). A study by Anderson et al., (2004) found similar results in
which 48.7% of persons with tetraplegia (and 3.3% of persons with paraplegia) reported that
regaining arm and hand function would most improve their quality of life (91). These findings
did not differ by gender or number of years post SCI, which suggests that recovering even partial
arm and hand function may have a significant impact on the independence of many spinal cord
individuals (91). Hence, rehabilitation of the upper limb function following SCI receives a lot of
attention from clinicians and researchers. In a clinical setting, therapies during the acute and sub-
acute phases of recovery typically focus on retraining lost function. Whereas, there are published
guidelines related to goals and potential treatment strategies, almost always therapy is tailored to
individual patient presentation and individual patient goals to be achieved. Clinicians must be
knowledgeable about the change in physical capacity based on level of injury as a prerequisite to
developing optimal rehabilitation programs and for setting realistic individual rehabilitation
goals (87).
2.2.3.1.1 Outcome Measures in Upper Extremity Rehabilitation Following Spinal Cord Injury
Just like with any rehabilitation program, assessment forms the pillar stone of the therapy
program for retraining upper extremity function. In a review conducted by Jones et al., (2018)
the authors discuss the factors that should be considered when using a clinical outcome measure
(92) and presumably the same criteria should apply to the development of clinical outcome
measures as well. The authors state that beyond reliability, validity, and responsiveness of a
clinical outcome measure tool, there are numerous factors that are important to consider. These
considerations include research trial phase and measurement target, whether the outcome
assessment tool is able to distinguish between recovery and compensation, the impact of lower
motor neuron injury, clinical significance of the observed changes, gaps in content, and floor and

26
ceiling effects (92). Although there are numerous upper extremity function assessment tools as
described by Van Tuijl (93) there are reviews that discuss limitations of these tools and hence
advise against their use in SCI population (94-96). Some of the commonly used upper extremity
assessment tools that are validated in SCI and used to assess function in clinical trials are listed
in Table 2.5.

27
Table 2. 5 Upper Extremity Outcome Measures in Spinal Cord Injury (92, 97, 98)
Outcome Measure Primary construct Strengths of the measure
Upper extremity motor scores
(UEMS) derived from ISNCSCI
Upper extremity (UE) strength SCI specific, web based and in person training available through
the American Spinal Injury Association, can be assessed early post injury in all
severities of SCI, Psychometrics established in pediatric and adult
populations, well established, standardized test with normative
data available
Spinal Cord Independence
Measure version III (SCIM III)—
self-care and grooming sub-scale
Independence level in ADLs SCI specific, validated for observation, interview, or self-report, commonly used test
with normative data available, psychometrics established in adults and youths (self-
report)
Capabilities of Upper Extremities
Questionnaire (CUE-Q)
Proximal and distal UE
function
SCI specific, validated in adolescent and adult populations, assesses proximal and
distal function, Items worded in a way to minimize compensation
Jebsen Taylor Hand Function Test hand function Standardized performance-based measure with normative references in healthy
controls, requires mid-line crossing, kit available for purchase
Capabilities of UE function test
(CUE-T)
Proximal and distal UE
function
SCI specific, items designed to reflect requirements of ADLs
compensation not allowed, components of proximal and distal UE function, Assesses
uni- and bi-manual function
Graded Redefined Assessment of
Strength, Sensibility, and
Prehension (GRASSP)
Multidimensional—hand
impairment and function SCI specific, scores reduced with compensation, manual and kit available for purchase,
normative data available
Spinal Cord Injury-Functional
Index (SCI-FI) Computer
Adaptive Testing (CAT) or Short
Form (self-care and fine motor)
Linearized, comprehensive
assessment of function across
multiple domains
SCI specific, large bank of UE items including fine motor, available as short form or
computer adaptive test (two versions: one with use of technology, one does
not allow use of technology), links to pediatric SCI-FI
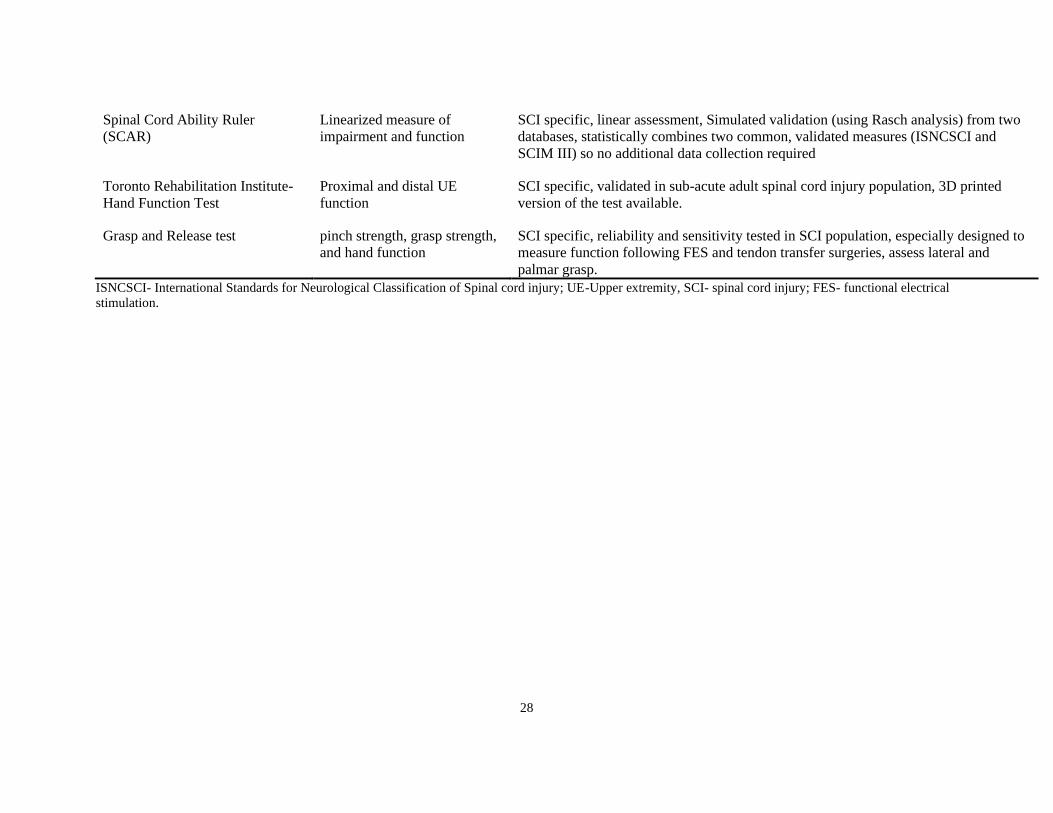
28
Spinal Cord Ability Ruler
(SCAR)
Linearized measure of
impairment and function
SCI specific, linear assessment, Simulated validation (using Rasch analysis) from two
databases, statistically combines two common, validated measures (ISNCSCI and
SCIM III) so no additional data collection required
Toronto Rehabilitation Institute-
Hand Function Test
Proximal and distal UE
function
SCI specific, validated in sub-acute adult spinal cord injury population, 3D printed
version of the test available.
Grasp and Release test pinch strength, grasp strength,
and hand function
SCI specific, reliability and sensitivity tested in SCI population, especially designed to
measure function following FES and tendon transfer surgeries, assess lateral and
palmar grasp.
ISNCSCI- International Standards for Neurological Classification of Spinal cord injury; UE-Upper extremity, SCI- spinal cord injury; FES- functional electrical
stimulation.

29
2.2.3.1.2 Rehabilitation Strategies for The Upper Extremity Following Spinal Cord Injury
The guidelines published by the SCIRE project (87) divides therapies of the upper extremity into
the following categories: (1) Therapy based interventions, (2) Technology based interventions,
(3) Sensorimotor stimulation interventions, (4) Non-invasive brain stimulation interventions, (5)
Surgical interventions, and (6) Complimentary and alternative medicine. Of these 1-3 are
typically delivered by Physiotherapists or Occupational therapists and 4 remains mostly a
research intervention with limited clinical uptake at this time, and 5 and 6 are delivered by
experts in their respective fields and outside the scope of this document.
Therapy based interventions consist of exercise therapy including strength and endurance
training exercises, range of motion exercises, stretching exercises and functional goal-oriented
exercises. Strength training involves isolation and stabilization of muscles through training
protocols involving free weights or machines (99), while functional strength training utilizes
training programs centered around activities of daily living (99). Literature supports the use of
therapies targeting muscle strength and function to improve task performance and quality of life
in individuals with SCI. Range of motion exercises and stretching exercises are used to maintain
joint and muscle integrity and prevent secondary complications like contractures and joint
stiffness.
Technology based interventions in SCI are either used to compensate for lost function
like use of orthotic devices or as therapeutic devices. From a therapeutic perspective, virtual
reality, robotics, FEST, BCI-FEST, and EMG-Biofeedback are some of the non-invasive
techniques that have received a lot of attention from researchers and have found some clinical
acceptance in the developed nations. Most reviews in the field including clinical practice
guidelines concur that it is difficult to draw any definitive conclusions about the efficacy of these
interventions (100).
Sensorimotor interventions include Neuromuscular Electrical Stimulation (NMES) and
Transcutaneous Electrical Stimulation (TENS). Whereas NMES and TENS have been in use for
a while and have shown limited efficacy in restoring motor function (87, 101), FES is a relatively
new therapeutic technique that uses surface stimulation to stimulate the arm and hand muscles in

30
a systematic manner to assist the patient in performing a functional task. What makes FEST
stand apart from the other interventions is its ability to actively engage paralytic muscles in
meaningful ways right from the acute phase of rehabilitation and thus it has the potential to
maximize the effects of neuroplasticity. Details of the FEST intervention and its application in
SCI are discussed in depth in Chapter 4.
2.2.4 Summary of Current State of Rehabilitation in Spinal Cord Injury
2.2.4.1 Outcome Measures for Upper Extremity Function
Amongst the current validated upper extremity activity measures in SCI the main limitations are:
(1) self-fabrication of test objects, which often compromises standardization of the test, or the
test needs to be purchased from a particular supplier (assuming that the supplier does not change
the manufacturing procedure over time, which is almost impossible to assure) to ensure
standardization of test objects; (2) expensive (average cost ~$2,500); (3) takes up to or more than
1 hour to administer ; and (4) requires extensive training on part of the assessor to administer the
test correctly, which means that if the assessment is not used for a longer duration then the
reliability of the test might be questionable. Once again, the original TRI-HFT fulfilled all the
above limitations except for easy accessibility. Hence, the second project of my PhD focused on
assessing the psychometric properties of the 3D printed TRI-HFT in individuals with sub-acute
and chronic SCI. Both the inter and intra-rater reliability of the 3D TRI-HFT were assessed in
SCI population (Chapter 8). Criterion validity of the 3D TRI-HFT was assessed by correlating
the scores on 3D TRI-HFT with the scores on the Graded Redefined Assessment of Strength,
Sensibility and Prehension (GRASSP) as GRASSP is currently considered best practice for
assessment of upper extremity function in SCI in both the body structure and function as well as
the activity domain of the ICF (102). Construct validity of the 3D TRI-HFT was also assessed in
SCI. For this purpose, scores on 3D TRI-HFT were correlated with scores on the Spinal cord
independence measure (SCIM) and the Functional independence measure (FIM).
I have chosen to assess the 3D TRI-HFT in SCI as it addresses all the above four
limitations, namely (1) the 3D printing of the test will ensure that the test is fully standardized;
(2) 3D printing files can be made publicly accessible, which will bring the manufacturing cost to
a minimum; (3) it takes less than 20 min to administer the test; and (4) the test requires no

31
training. Therefore, the goal of the second project is to address the limitations of universal
accessibility as well as limitations related to resources both in terms of cost and personnel in SCI
settings. The details of the 3D printed TRI-HFT test and the psychometrics of the test in SCI are
described in detail in Chapter 8. Chapter 6 provides details on the development and psychometric
testing of the original TRI-HFT.
2.2.4.2 Rehabilitation Therapies for Restoring Upper Extremity Function
Upper extremity rehabilitation remains a top priority for individuals with cervical spinal cord
injury. Whereas there have been improvements in outcomes following rehabilitation, tetraplegic
individuals still live with considerable deficits that compromise their independence and hence
their quality of life. Rehabilitation outcomes depend on multiple factors and there is emerging
evidence to show that volume of therapy is no longer the sole driving variable for improvements
in function and that “what” we do is rather important (103).
Best practice guidelines for rehabilitation following SCI, consider conventional
rehabilitation therapies as an optimal treatment strategy to restore function (87). Conventional
rehabilitation therapies include but are not limited to (a) muscle facilitation exercises; (b) task-
specific, repetitive functional training; (c) strengthening and motor control training using
resistance to available arm motion to increase strength; (d) stretching exercises; (e) electrical
stimulation applied primarily for muscle strengthening; (f) practice of activities of daily living
(ADLs) including self-care where the upper extremities are used as appropriate; and (g)
caregiver training.
There is limited evidence regarding the efficacy of newer rehabilitation strategies like
robotic therapy, EMG biofeedback, BCI controlled FEST, virtual reality and at best these
therapies have been supported as supplement to conventional therapies. FEST has been
researched in this realm as well and when used as an adjunct with conventional rehabilitation
techniques tends to result in better outcomes. A major advantage of the FES therapy is that it is
one of the only therapies that can be incorporated early on in the rehabilitation process to allow
for practice of repetitive task specific activities (104). Also, FES when systematically applied
can recruit muscles in a functional manner to allow for practice based on the principles of

32
activity-based therapy (ABT). Recently, there has been accumulating evidence regarding the
value of ABT in neurorehabilitation (105, 106). One of the gaps in the current application of
FEST for upper extremity retraining is the lack of interscapular muscle involvement despite the
important role that the interscapular muscles play during shoulder complex movements. Health
Canada and FDA approved commercial FES stimulators including the MyndMove™ lack this
important component for functional retraining. In my thesis I attempted to address this gap by
evaluating the feasibility of stimulating interscapular muscles along with shoulder prime movers
during shoulder flexion and abduction movements.
An overview of the current FES and FEST landscape in rehabilitation including its
practical application for upper extremity rehabilitation in SCI is presented in the next two
chapters (Chapter 3 and Chapter 4).

33
Chapter 3 Functional Electrical Stimulation Therapy: A Closer Look
In this chapter the history of FES and the current FES devices used for upper extremity
rehabilitation in stroke and spinal cord injury are described. This Chapter is an excerpt from a
peer reviewed book (107).
Cesar Marquez-Chin, Naaz Kapadia-Desai, and Sukhinder Kalsi-Ryan. Functional Electrical
Stimulation Therapy: A Closer Look. In: Ron Baecker R, Sixsmith A, editors. Brain–Computer
Interfaces Neurorehabilitation of Voluntary Movement after Stroke and Spinal Cord Injury.
Morgan and Claypool; 2021. p. 11-25. doi: 10.2200/S01090ED1V01Y202104ARH017.
3.1 History of Functional Electrical Stimulation Therapy (FEST)
The use of electrical current to manipulate human tissues dates back to several decades. Ever
since Galvani’s demonstration in 1792 that living tissue reacts to electrical currents, the use of
electricity in living tissues has preoccupied the minds of many scientists (108). Amongst its
many uses in medicine one is in the form of functional electrical stimulation therapy (FEST),
which may be defined as the stimulation of neuromuscular units, that are normally under
voluntary control, for rehabilitation purposes (108). Functional electrical stimulation (FES) can
also be defined as a systematic and coordinated application of electrical current to excitable
tissues to supplement or replace function that is lost in neurologically impaired individuals. Both
sensory and motor function can be restored with FES (109). Auditory and visual neuroprostheses
are examples of FES used to restore sensory system functions. Neuroprostheses used for
grasping and walking are examples of FES systems for replacing motor function; a functional
limb movement can be produced by properly coordinating several electrically-activated
muscles (109). The concept is to provide functional restoration through electrical activation of
intact lower motor neurons using electrodes placed on or near the innervating nerve fibers.
Appropriate electrical stimuli can elicit action potentials in the innervating axons, and the
strength of the resultant muscle contraction can be regulated by modulating the stimulus
parameters.

34
FES was first applied back in the 1960’s for retraining gait after stroke (110). Liberson
and his co-workers stimulated the dorsi-flexors of the ankle joint in hemiplegics synchronously
with gait to treat drop foot (110). This successful application gave rise to numerous research
projects, which extended to fundamentally new areas and to the application of a new technology
in rehabilitation. The paradigm was to use it as an orthosis so that the patient would don it when
needed and take it off when the task no longer needed to be done. Around the same time as
Liberson, Long and Masciarelli (111) developed the first FES hand splint which was designed as
a one channel device enabling the patient to control hand opening combined with wrist
extension.
Even back then the technology was realized to have two potential applications (108):
1. As a neuroprosthesis for replacing lost function
2. As a short-term therapeutic device for retraining lost function.
Since the inventions of Liberson and colleagues, FES technology has been researched and
refined significantly and has gained traction amongst rehabilitation specialists for its ability to
restore function and thereby improve quality of life (QOL) of individuals living with the
sequelae of neurological injuries or diseases. Neuroprostheses for replacing lost function have
been mostly in the form of implanted devices. This option is attractive in individuals where
chances of recovery of lost function are minimal. The prosthesis can be implemented in a variety
of ways, such as through stimulation of the spinal cord (112), nerve (113) or muscle (113). This
application has not gained as much attention from the rehabilitation professionals given the
invasive nature of the treatment and several other documented limitations. On the other hand,
short-term therapeutic FES applications for restoring upper and lower extremity motor function
following stroke or SCI (i.e., FEST) are becoming a part of the rehabilitation tool kit in many
rehabilitation hospitals and clinics.
3.2 Transcutaneous FES System
A transcutaneous FES stimulator is non-invasive, and its components can be divided into
hardware and software.
35
3.2.1 FES Hardware
The stimulator hardware consists of three components: (a) the electrical stimulator, (b) the
electrodes used to deliver the stimulation and (c) the user interface. The electrical stimulator is
typically a multi-channel stimulator and may have anywhere from two to twelve stimulation
channels, higher number of channels allow for simultaneous stimulation of multiple muscle or
muscle groups. The electrodes used for transcutaneous stimulation are typically self-adhesive
carbon electrodes. Alternatively, surface electrodes that can be secured using adhesive tape may
also be used. Different stimulators have different types of user interfaces. Neuroprostheses may
accept commercially available accessible switches and, in some cases, it may be possible to
incorporate other specialized sensors allowing individuals with different abilities to command
the device like push buttons, electromyography (EMG)/Biofeedback sensors, sliding
potentiometers etc.
3.2.2 FES Software
The software of the FES system allows one to specify/alter all the stimulation parameters. Based
on individual stimulators the parameters that can be changed are frequency, minimum and
maximum intensity, pulse duration, ramp time, synchronization and order of stimulations, type of
user interactions and number of repetitions. The frequency of stimulation is the rate at which
stimulation pulses are delivered and it affects the strength of the muscle contraction as well as its
quality. The minimum frequency required to induce a tetanic contraction is between 16 and 20
Hz. However, while tetanic contractions can be achieved with a minimum of 20 pulses per
second (114), a pulse frequency of 40 Hz is often needed. Higher pulse frequencies generate
stronger tetanic contractions but they can also result in faster muscle fatigue (115). The pulse
amplitude/intensity refers to the magnitude of the stimulation. It affects directly the type of nerve
fibers that respond to the stimulation with large fibers in close proximity to the stimulation
electrode being recruited first (115). The pulse duration (pulse width) is the time in which the
stimulation pulse is present. The ramp up function augments the electrical charge successively by
prolonging the pulse width from a selected minimum to a chosen maximum value.

36
Typically, prior to a FEST session the sensory, motor, functional and maximum intensity
thresholds are set using the continuous stimulation mode where the stimulation frequency and
pulse duration are pre-set to values of 40Hz and 300 µsec, respectively.
3.3 Upper Limb Function in Stroke and Role of FEST
The therapeutic effects of FEST for restoring upper extremity function are discussed in literature
as early as in 1978. In a study published by L. Vodovnik et al., the authors talk about the
reappearance of functional movements during electrical stimulation as one the major effect of
FES (116). However, up until 1992 use of surface FES was still restricted to stimulation of
muscles of forearm to stimulate hand opening although a great deal of specificity was obtained
using surface stimulation by virtue of use of high-resolution surface electrodes. The next decade
saw exponential work in this field and by 2002 there were various FES grasping systems
available some commercially, some as research devices. In the last 2 decades FES has received
exponential attention from clinical researchers as well as biomedical engineers resulting in
significant refinement of the technique and a much more sophisticated application. Therapeutic
FES (i.e., FEST) developed over the past 10-15 years is based on the premise of activity-based
therapy wherein it aims to accomplish repetitive task-specific practice. FEST has been combined
with various other rehabilitation modalities like mirror therapy, virtual therapy, robotics, tele-
supervised therapy etc. There are a few review articles published in literature that are related to
the efficacy of FES in improving activities of daily living. These articles provide conflicting
evidence in terms of efficacy, but most agree that FEST applied during acute rehabilitation
process results in better outcomes as compared to conventional therapies (117).
The most commonly discussed systems in literature include the Freehand system, NEC
FES Mate system, NESS H200, Bionic Glove, ETHZ-ParaCare neuroprosthesis, the systems
developed by Rebersek and Vodovnik, the Belgrade Grasping–Reaching System and Compex
Motion stimulator. All of these systems were primarily designed and researched in individuals
with SCI except for the NESS H200 and the Compex motion stimulator. Xcite is another multi-
channel FES stimulator. Xcite is a portable system with easy to set up pre-programmed activity
libraries, that deliver sequenced stimulation through up to 12 stimulation channels (118) and is
used both in rehabilitation after stroke and SCI. Compex motion simulator is a 4-channel surface

37
FES device that is fully programmable and allows for designing of stimulation protocols
based on individual patient abilities. The stimulator has been extensively used in research
with positive outcomes for even chronic and severely impaired stroke patients (119, 120),
however this is a research-based stimulator and is no longer widely available. To-date the
only upper extremity surface FES devices that are FDA approved and designed for use in
individuals with stroke are the Handmaster or the Neuromuscular Electrical Stimulation
System (NESS) H200 and the MyndMove™.
NESS H200: The NESS H200 was invented by Roger Nathan and his group in Ben-Gurion
University, Israel. It is a three-channel surface FES device consisting of two parts: the stimulator
and the forearm splint. Control of the device is via a user activated push button (Fig. 3.1). The
stimulator generates electrical impulses that are delivered to the target muscles by hydrated
sponge surface electrodes, held in position by the forearm splint. This device is programmed to
perform three exercise modes and two functional modes. The exercise mode provides repetitive
stimulation to a group of muscles, thereby helping the user to increase muscle strength.
Functional modes, on the other hand, help the user in performing key grip and palmar grasp and,
hence, help them in performing their ADL (121).
Figure 3. 1 NESS H200
MyndMove™: The MyndMove™ stimulator is a FES device that is non-invasive and uses short,
low energy electrical pulses to induce muscle contractions (Fig. 3.2). The device offers a full
range of protocols designed specifically for MyndMove™ therapy to address proximal and distal
impairments of the upper extremity. Up to eight muscle groups can be stimulated during a

38
protocol. Thirty protocols, of which 17 are for use in stroke and 13 for use in SCI, provide a full
range of reaching and grasping movements that are broken down into sub-movements that can be
initiated by the therapist or patient using hand or foot switches. Electrode positioning for
different protocols is facilitated by anatomical illustrations on the device that indicate the desired
location for electrode placement on specific muscle groups. Amplitude for electrical stimulation
of a specific muscle group is adjusted for each user prior to every treatment session (122).
Figure 3. 2 MyndMove™ Stimulator
We in our laboratory have applied FEST to retrain reaching and grasping function in
individuals with both acute and chronic stroke using the 4-channel surface Compex motion
stimulator (Fig 3.3). We have typically used two channels to facilitate proximal shoulder and
elbow movement and two channels to assist with hand opening. Individuals with stroke generally
present with a flexor synergy of the arm with a strong component of finger flexion and thus hand
closing is generally not elicited using FES in this patient population. Although we have not done
a systematic study related to optimal dosing, we have found that it takes a minimum of 20 FEST
sessions to see any change on functional outcome assessments and 40 sessions to see an
improvement in functional status (122, 123).

39
Figure 3. 3 Compex Motion Stimulator
3.4 Upper Limb Function in Spinal Cord Injury and Role of FEST
Despite the publication of various clinical practice guidelines (Consortium for Spinal Cord
Medicine 2005; Consortium for Spinal Cord Medicine, 1999), there is little consensus regarding
the management of the tetraplegic upper limb. This in part is due to the variation in muscle
function after SCI (124). Understanding the diversity of SCI is important in ensuring that therapy
is tailored to each individual and that feedback is elicited from patients regarding their
perceptions of the usefulness of specific interventions. Whereas conventional therapies offer
some customization based on individual abilities, they are limited in being able to engage the
neuromuscular unit in patients with severe paralysis or patients in the acute stages who are still in
a state of flaccid spinal shock. FEST has the ability to overcome this and via stimulation, we are
able to engage the whole neural circuitry in functional movements right from the time patients
are medically stable to be engaged in rehabilitation. Whereas implanted devices require that
patients “plateau” in function, surface FES devices can be used right from day one and because
of the versatile nature of these devices stimulation programs can be modified and customized
based on patient needs throughout the course of rehabilitation.
Amongst the FES devices researched in SCI, except for the Freehand (125) and
NEC FES Mate systems all other neuroprostheses for grasping are FES systems with
surface stimulation electrodes. The NESS H200 (126) , the Bionic glove (127) and the
system developed by Rebersek and Vodovnik (128) are all surface stimulation devices
that enable patients to perform hand opening and closing movements with assistance
40
from FES the only difference being that the Bionic glove is almost exclusively tailored for the
SCI population and enhances the tenodesis grasp in these patients. The Belgrade Grasping and
reaching system (129) is capable of producing not only grasping function but also reaching by
virtue of stimulation of the triceps muscle. The Compex motion stimulator can be programmed
to individual needs based on level and extent of injury and the patient goals to be achieved (130,
131). MyndMove™, remains the state-of-the-art FDA approved transcutaneous stimulator for
SCI with 8 stimulation channels and pre-programmed 13 stimulation protocols that allow for
proximal and distal upper extremity retraining as well as combination protocols that allow more
complex functional movements engaging the whole upper extremity.
3.5 Our Experiences with Surface FEST to Restore Upper Extremity Function After Stroke and Spinal Cord Injury
We have used FEST for over 2 decades in our laboratory to retrain function in individuals with
stroke and SCI. We use a 4-channel surface stimulator that is fully programmable. The
parameters of stimulation used for upper extremity retraining are frequency of 40Hz, pulse width
of 250-400 µsec and intensity between 5mA-40mA. To date, approximately 150 patients with
SCI and 50 patients with stroke have been treated using transcutaneous FEST, ranging from pilot
clinical trials to randomized controlled trials. Our studies have included individuals throughout
the continuum of care as well as with diverse impairment levels. For all of our clinical trials we
have delivered 40 treatment sessions, with 5 sessions a week (1 session/day) or a minimum of 3
sessions per week (1 session/day). Our treatment strategy is to use FES during execution of
functional day-to-day tasks using real objects and in adjunct with conventional strategies as seen
appropriate by the treating therapist. The detailed methods of FES therapy used in the clinical
trials is described in Appendix 1. We have had very promising results treating individuals with
both stroke and SCI (119, 120, 130-134) and this extensive research of ours has led to the
development of a commercial surface FES system that is now in use across several clinics and
rehabilitation hospitals in North America.
41
3.6 Limitations and Contraindications for Surface FEST Application
The target muscles that are intended for FEST treatment have to be accessible for placement of
the stimulation electrodes (134), i.e. surface FES can be applied with a greater level of specificity
when the muscles to be stimulated are more superficial (e.g., Flexor Carpi Ulnaris, Flexor Carpi
Radialis). For muscles that are deeper it might be more challenging to elicit isolated contraction
without stimulating the overlying muscles (e.g., Flexor Digitorum Profundus). In some cases,
such as the Iliopsoas muscle, it may not be possible to stimulate the muscle using surface
electrodes owing to its location. Furthermore, the degree of lower motor neuron injury or nerve-
root damage of the stimulated muscle should not be major. In a number of patients with SCI,
there may be a variable amount of peripheral nerve damage (135) (motoneurons and nerve-roots)
that restricts the application of FES. In addition, the patient must be able to follow the
instructions and actively participate in the therapy process. The patient should not have any
contraindications for FES application including metal implants at the site of stimulation,
pacemaker, open wound or rash at the site of electrode placement, uncontrolled autonomic
dysreflexia, etc.

42
Chapter 4 Toronto Rehabilitation Institute-Hand Function Test: Assessment
of Gross Motor Function in Individuals with Spinal Cord Injury
In this chapter, the results of a pilot study investigating psychometric properties of the original
Toronto Rehabilitation Institute-Hand Function Test in sub-acute spinal cord injury are
presented. This is a peer reviewed publication (please note this manuscript is not a part of the
current thesis projects).
Kapadia N, Zivanovic V, Verrier M, Popovic MR. Toronto Rehabilitation Institute’s Hand
Function Test: Assessment of Gross Motor Function. Top Spinal Cord Inj Rehabil
2012;18(2):167–186.
4.1 Abstract
The objective of this study was to evaluate the inter-rater reliability, construct validity, and
sensitivity of Toronto Rehabilitation Institute–Hand Function Test (TRI-HFT), within an
interventional randomized controlled trial. Twenty- one participants with subacute C4 to C7
spinal cord injury (SCI) were recruited. Based on randomization, participants were allocated to
either the FES therapy group or the conventional occupational therapy group. Baseline and
follow-up assessments of participants were videotaped. For testing inter-rater reliability,
videotaped images were transferred to DVDs that were later observed by 2 observers. Construct
validity was determined by comparing total scores on TRI-HFT to self-care sub-score
components of the Spinal Cord Independence Measure (SCIM) and Functional Independence
Measure (FIM). To establish sensitivity of TRI-HFT, we compared pre- and post-treatment
scores on all 3 measures (i.e. TRI-HFT, FIM, and SCIM). TRI-HFT was found to have high
inter-rater reliability with an intra class correlation coefficient (ICC) of 0.98. Moderate to strong
correlations were found between TRI-HFT total scores and self-care components of FIM and
SCIM for both hands individually post therapy. Due to a floor effect of the FIM and SCIM, there
was weak correlation between pre-therapy scores of the said measures and TRI-HFT. TRI-HFT
was found to be highly sensitive in determining difference in function pre and post therapy. This
study demonstrated that the TRI-HFT is a reliable and sensitive measure to assess unilateral hand
gross motor function in persons with tetraplegia, with moderate to strong construct validity.

43
4.2 Introduction
There has been a growing interest amongst clinicians and researchers in the development of
therapies aimed at restoring upper extremity function, especially in the population of spinal cord
injured individuals, to enhance level of independence and reduce burden of care. Conventional
occupational and physiotherapeutic techniques and other rehabilitation modalities such as FES
and robotic-assisted therapies are focusing on restoring reach and grasp function in individuals
with tetraplegia (123, 134, 136-141). Lateral pinch, pulp pinch, and palmar grasps are the
primary motor hand functions these therapies are trying to improve or restore, as they are
necessary to perform various activities of daily living (ADLs) that may improve independence
and quality of life. With the evolution of new therapies, there has been development of novel
assessment tools to evaluate the efficacy of these therapies (94, 138, 142, 143). Based on
literature review, a need was identified to develop a tool that is user-friendly, evaluates unilateral
gross motor function of the hand to perform power grasp (i.e., palmar grasp) and precision grip
(i.e., lateral pinch and pulp pinch), and that is easy to replicate in clinical settings. This need
resulted in the development of the Toronto Rehabilitation Institute–Hand Function Test (TRI-
HFT). We designed a test to measure palmar grasp, lateral pinch, and pulp pinch, as these are the
most frequently used hand postures in ADLs.
Thus far, a number of attempts have been made to develop different assessment methods
for assessing gross motor hand function in different patient populations (94, 138, 142, 143).
Grasp and Release Test
As early as 1994, Wuolle et al., proposed using the Grasp and Release Test which consisted of 6
different objects to be grasped and released, for patients with tetraplegia (94). Four of the 6 test
objects (e.g., can, peg, block, and videotape) can be easily acquired, because they are objects
commonly used in ADLs (although a videotape is already an obsolete object, as video recorders
are no longer used in many countries). The remaining 2 test objects, the paperweight and the
object used to simulate the use of a fork, were non-standardized objects. The “fork” was a
spring-loaded item that was difficult to manufacture and could not be easily replicated by other
researchers. The paperweight, which had to be manufactured as well, was not described in

44
sufficient detail (i.e., design specifications were not provided). As a result, the feasibility of
using the Grasp and Release Test for measuring hand function in individuals with spinal cord
injury (SCI) was somewhat limited. More importantly, 2 of the 6 tests (peg and block) were not
discriminative with respect to the ability of individuals with C5 to C7 SCI to grasp and release
these objects. Specifically, the individuals with SCI who used a neuroprosthesis for grasping
were able to achieve high scores on these 2 objects with or without the use of a neuroprosthesis
(94, 136).With the small sample size (5 participants) and the inter-rater and intra-rater reliability
not having been fully established, this approach is considered to have many limitations.
Memberg and Cargo developed 2 instrumented objects to quantitatively assess hand
function while using a neuroprosthesis for grasping (142). The 2 objects used were a book-
shaped instrumented object consisting of 2 parallel plates made from a carbon fiber and epoxy
laminate and an instrumented pen/fork made of 2 aluminum beams. The 2 objects recorded force
data and object orientation data throughout palmar and lateral prehension simulated functional
tasks. However, these instrumented objects had design specifications that were difficult to
replicate, limiting the practicality of the test for universal clinical or research applications.
Furthermore, because the objects were manufactured from metal, they did not replicate real life
challenges.
Upper Extremity Function Test
A test proposed by D. Popovic et al., the Upper Extremity Function Test assesses the
participant’s ability to manipulate objects typically used in ADLs (138). It was specifically
designed to assess unilateral gross motor function of the hand in individuals with SCI who were
trained to use a neuroprosthesis for grasping. This test is also a timed test and only takes into
account whether the task is completed or not, as all tasks are scored on an ordinal yes/no scale.
The test protocol has not been standardized, and it requires specific test items that may be
difficult to obtain. This inconsistency, along with limited information about the instrument’s
validity and reliability, limits its practical use.
45
Instrumented Workstation
Gritsenko et al., developed a therapeutic system that consisted of a workstation and an FES
stimulator (144, 145). The workstation included a desk with a number of instrumented objects.
The objects used represented household items. An example is a doorknob and a handle attached
via a cord to a set of weights that are instrumented with potentiometers to monitor the
displacement and velocity of the doorknob and handle. The other objects were 3 rectangular
blocks and a cylinder, which were transferred by the subjects between 2 bays. These were
instrumented with sensors to measure the time required to move the objects between the 2 bays.
This therapeutic system was used on a small sample size (6 participants); yet, its sensitivity has
not been established. In addition, the instrumented objects have design specifications that make
them difficult to replicate, thus limiting the practicality of the test in clinical applications.
Currently, efforts are being made to further simplify and standardize this test (the new
test/therapy device is called “ReJoyce”) and to make it available to the general public (146).
Sollerman Hand Function Test
Wuolle et al., explored standard hand function assessments, unrelated to the use of a
neuroprosthesis for grasping, to ascertain their effectiveness in measuring changes in grasping
function in individuals with an SCI (94). The Sollerman Hand Function Test (SHFT) was one of
the few tools assessed by this team. This test required the participant to perform 20 tasks using 7
grasp styles (143). Wuolle et al., reported that the SHFT was an inappropriate test to evaluate
hand function in individuals with C5 to C7 SCI, as these individuals are often unable to perform
the required 7 grasp strategies and consequently perform poorly with this measurement
instrument (94).
Jebsen Hand Function Test
Wuolle et al., also evaluated the Jebsen Hand Function Test to determine whether it would be an
effective assessment tool to measure hand function change(s) in patients with SCI who were
using a neuroprosthesis for grasping (94, 147). This test evaluates various hand activities using 7
test items: (1) writing; (2) turning over cards that are 7.62 x 12.70 cm (simulated page turning);
(3) picking up small common objects; (4) simulated feeding; (5) stacking checkers; (6) picking
up large objects; and (7) picking up large heavy objects (147, 148). Wuolle et al., found that the

test was inadequate for evaluating the hand function of individuals with SCI, because there were
no guidelines for scoring if they dropped the item(s), substituted a different grasp pattern, or
exceeded the maximum time permitted for completing the task. All these issues are prevalent in
individuals with tetraplegia (94). Wuolle et al., also felt that the manner in which test items were
administered during the test may have had an influence on the score obtained by individuals with
SCI. They reported that poor trunk control and balance have the potential to make it difficult for
these individuals to perform tasks that require crossing the midline to grasp an object, which
would negatively skew the hand function score; the results would not be a true reflection of the
individual’s grasping function.
Minnesota Manual Dexterity Test
This test has been used to measure an individual’s ability to perform simple, but rapid, eye-hand-
finger movements (149-151). It does not differentiate between the size and shape of the objects
that the individual is required to manipulate during the test. Moreover, poor balance and muscle
fatigue, common in the SCI patient populations, may have a negative impact on the Minnesota
Manual Dexterity Test score.
Action Research Arm Test (ARAT)
ARAT was described by Lyle in 1981 as a tool to evaluate upper limb motor function recovery
following a stroke or other brain injuries (32, 152). Nineteen tasks were used to examine both
fine and gross distal and proximal arm motor functions. One of the positive points about ARAT
is that it incorporates reaching within the test; however, it demands reaching without grading it.
The tasks utilized objects that could be readily purchased in a hardware store and required
minimal assembly. Similar to the TRI-HFT, the ARAT is simple to administer and requires
minimal time to complete (5 to 30 minutes). ARAT has been validated in the stroke population,
and the reported inter-rater and intra-rater reliabilities were 0.99 and 0.98, respectively (152).
More recently, the ARAT has been standardized and has shown to be sensitive to functional
motor change in patients who have sustained a stroke or other brain injuries (154). Through use
in research laboratory, the main limitation identified with this tool is the height at which some of
the tasks are performed. Not all tasks are performed at a comfortable height for seated
individuals. Because this test involves upward reaching, the ability to regulate sitting balance
46

47
affects the test scores. For example, many tasks require the participant to grasp and manipulate
objects at shoulder height. Many SCI individuals are unable to perform these maneuvers due to
lack of trunk stability and, as a result, may score poorly on the ARAT, despite the fact that their
gross motor hand function has improved considerably over time. Also, the grading system of the
test is such that if the participant is able to complete the first task, which is labeled as the most
difficult task, then subsequent testing of that subset is not required. If the participant is unable to
complete the first task, then the second task, which is labeled as the easiest task, is attempted. If
the participant is unable to complete that task, then that subset of the test is abandoned, or the
participant is moved on to the next task in that subset. It is our opinion that the difficulty of
performing tasks in the stroke and SCI population is very different due to initial neuropathology.
Also, validity and reliability of the ARAT has not been studied in SCI individuals.
Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP)
GRASSP is one of the more recently developed tests. Based on preliminary work done by Kalsi-
Ryan et al., the items included in the test are (a) sensory assessment of both the dorsal and
palmar surface of the hand using Semmes Weinstein monofilaments; (b) manual muscle testing
for 10 upper extremity muscles; and (c) prehension testing using a modified Sollerman test (6
items instead of 20) (155, 156). The GRASSP takes about 45 to 60 minutes to administer
bilaterally and was developed for assessing subtle changes in the neurological status of the hand
post cervical SCI during different phases post injury (155). Reliability and validity have been
well established and responsiveness is currently being tested (153, 155) The GRASSP is not best
suited for assessing the force generated during unilateral lateral pinch, pulp pinch, and palmar
grasp in individuals with SCI. More specifically, GRASSP prehension components of the tests
[(1) take the bottle and pour the water into the cup, approx. three-fourths full; (2) pull the 9 pegs,
1 by 1, out of the block and place them back into the markings on the opposite side; and (3)
unscrew the lids of the 2 jars and place them on the table] are discriminative with respect to the
FES therapy and neuroprosthesis for grasping, as these 3 tests can show improvement due to
these 2 interventions (i.e., FES therapy and implanted neuroprosthesis). However, GRASSP
prehension components of the tests [(4) take the key from the table, insert it in the lock, and turn
it 90°; (5) pick up the 4 coins, 1 by 1, from the table and drop them through the slot; and (6) pick
up the 4 nuts, 1 by 1, from the table and screw them onto the matching screws] are tests that SCI

48
subjects who took part in the FES therapy for grasping or are using a neuroprosthesis for
grasping, may not necessarily be able to perform, as they require fine finger dexterity. At the
present time, the FES technology (both the FES therapy for grasping and the neuroprosthesis for
grasping) is not developed for fine finger dexterity. Because FES therapy and the use of a
neuroprosthesis for pinch and grasp are the 2 most promising interventions for restoring hand
function in individuals with tetraplegia, a test that specifically evaluates gross motor unilateral
lateral pinch, pulp pinch, and palmar grasp is needed.
AuSpinal
Another recently developed assessment tool is the AuSpinal (157). This tool was developed by
Coates et al., in February 2011and consists of seven different tasks selected from 3 existing hand
function measures – Sollerman Hand Function Test, Rehabilitation Engineering Laboratory
Hand Function Test (Rehabilitation Engineering Laboratory Hand Function Test is identical to
TRI-HFT and is the first name used for TRI-HFT when this test was originally proposed in 2005
(119)), and the Upper Extremity Function Test. This test does address one of the common
limitations of the other tests in that it looks at unilateral gross motor function, however the test
was designed to solely measure function irrespective of type of grasp used and hence is restricted
in terms of guiding therapy progression. Also the psychometric properties of the test require
further investigation (157).
The TRI-HFT is the first clinical assessment tool to measure specifically unilateral gross
motor function focusing on lateral pinch, pulp pinch, and palmar grasp. These 3 prehension
patterns were chosen for mainly 2 reasons. First, they are frequently needed in manipulating day
to day objects. Second, this test was developed with the aim of being able to detect changes in
function secondary to use of FES that is commonly restoring 1 or all 3 of these prehension
patterns. Furthermore, in the last 10+ years, it has been shown that FES is able to induce
neuroplasticity and restore voluntary hand function. Hence, the hope was that TRI-HFT will be
used to help detect improvements in function secondary to neuroplasticity. Recent articles
published by our team suggest that TRI-HFT is very effective in detecting improvements in
function secondary to neuroplasticity (119, 120, 137, 158).

49
The TRI-HFT evaluation requires participants to manipulate (for the purpose of this
article, “manipulate” refers to gross motor function not fine finger movements) standardized
objects, which they may encounter in their daily lives. The objects used in the evaluation tool are
readily available anywhere in the world and require only simple, if any, modifications.
Individuals may or may not use a neuroprosthesis to assist them in manipulating the objects
during the TRI-HFT. The TRI-HFT has been designed to be used to assess the effectiveness of
(a) hand therapies; (b) neuroprosthesis for grasping as an orthosis (i.e., as a permanent assistive
device) in ADLs; (c) FES therapy for restoring voluntary grasping function and (d) surgical
restoration options such as tendon transfer surgeries (123, 136, 159, 160).
The purpose of this study was to establish the reliability, construct validity, and
sensitivity of the TRI-HFT as an evaluation tool for use in patients with SCI and to assess the
unilateral gross motor function of their hand to perform lateral pinch, pulp pinch, and palmar
grasp.
The Toronto Rehabilitation Institute–Hand Function Test
The TRI-HFT consists of 2 parts. The first part of the test assesses the individuals’ ability to
manipulate objects that they may encounter in their daily lives (Figure 4.1, Items 1-11). To
manipulate these objects, they are required to use one of the following: a lateral pinch, a pulp
pinch, or a palmar grasp (Figures 4.2 and 4.3). The second part of the test measures the strength
of their lateral pinch or pulp pinch and palmar grasp (Figure 4.1, Items 12-14). The objects have
been constructed to demonstrate the influence of different weight and texture on performance
and to allow objective measurement of pinch force and circular torque (Figure 4.4).
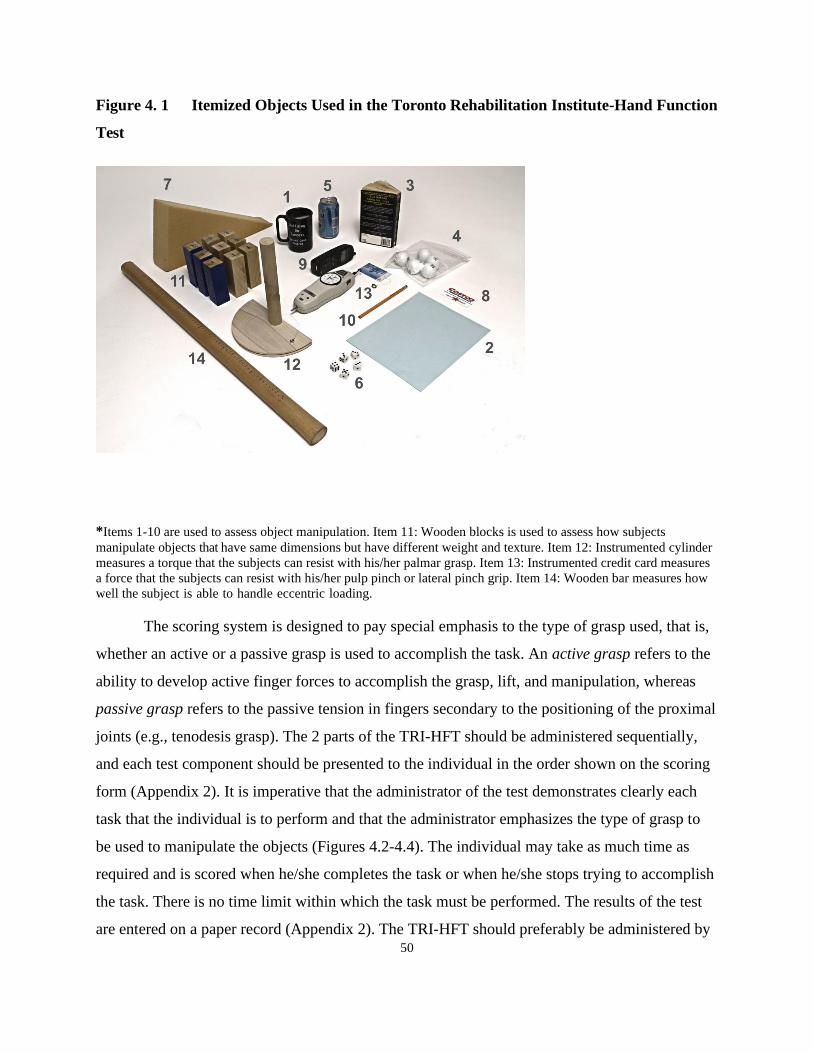
50
Figure 4. 1 Itemized Objects Used in the Toronto Rehabilitation Institute-Hand Function
Test
*Items 1-10 are used to assess object manipulation. Item 11: Wooden blocks is used to assess how subjects
manipulate objects that have same dimensions but have different weight and texture. Item 12: Instrumented cylinder
measures a torque that the subjects can resist with his/her palmar grasp. Item 13: Instrumented credit card measures
a force that the subjects can resist with his/her pulp pinch or lateral pinch grip. Item 14: Wooden bar measures how
well the subject is able to handle eccentric loading.
The scoring system is designed to pay special emphasis to the type of grasp used, that is,
whether an active or a passive grasp is used to accomplish the task. An active grasp refers to the
ability to develop active finger forces to accomplish the grasp, lift, and manipulation, whereas
passive grasp refers to the passive tension in fingers secondary to the positioning of the proximal
joints (e.g., tenodesis grasp). The 2 parts of the TRI-HFT should be administered sequentially,
and each test component should be presented to the individual in the order shown on the scoring
form (Appendix 2). It is imperative that the administrator of the test demonstrates clearly each
task that the individual is to perform and that the administrator emphasizes the type of grasp to
be used to manipulate the objects (Figures 4.2-4.4). The individual may take as much time as
required and is scored when he/she completes the task or when he/she stops trying to accomplish
the task. There is no time limit within which the task must be performed. The results of the test
are entered on a paper record (Appendix 2). The TRI-HFT should preferably be administered by
51
a hand or upper extremity specialist (physiotherapist or occupational therapist). The entire
evaluation for both hands can be completed in less than 30 minutes. When the assessment is to
be recorded on videotape, the camera should be positioned at a 45° angle opposite the involved
upper extremity at 1 m height.
Part 1: Evaluation of object manipulation for lateral or pulp pinch grasp and palmar grasp
The object manipulation subtest was developed to evaluate manual hand dexterity. It
evaluates the ability to use lateral pinch, pulp pinch, and palmar grasp to manipulate common
objects in 3 different gravity-related positions – against gravity (supination), toward gravity
(pronation), and in a gravity-eliminated plane (mid-prone position). A complete description of
the objects used in this test can be found in Table 4.1. Each item is given a score from 0 to 7. To
test the palmar grasp, an individual is presented with the following 5 items: mug, book, soda can,
isosceles triangular sponge, and wireless home telephone (Figure 4.1, Items 1, 3, 5, 7 and 9,
respectively). In spite of the fact that holding a book requires intrinsic muscle activity,
specifically the lumbricals, it was included in the test due to its frequent use in day to day life
and because previous studies using FES have shown an improvement in this type of grip. To test
lateral pinch and precision grip, the individual is presented with the following 5 items: paper
sheet, Ziploc bag filled with 5 golf balls, dice, credit card, and pencil (Figure 4.1, Items 2, 4, 6, 8,
and 10, respectively). To test the strength of the power grasp, the individual is presented with the
following items: 9 rectangular blocks, instrumented cylinder, credit card attached to a
dynamometer, and wooden bar (Figure 4.1, Items 11, 12, 13, and 14, respectively).
With the exception of the instrumented cylinder, credit card attached to a dynamometer, and
wooden bar, all test objects in Figure 4.1 are placed on a desk 20 to 30 cm in front of the
participant, one after another in the order from Item 1 to Item 11. The participant is expected to
pick up the object, lift it completely off the supporting surface, manipulate it, and place it back
down on the table. The exact manner in which the test objects should be presented to an
individual is presented in Figures 4.2, 4.3, and 4.4.

52
Figure 4. 2 Demonstration of How to Manipulate the TRI-HFT
*Items 1, 3, 5, 7, and 9 during the test. These objects are assessing palmar grasp. The numbers in the figure refer to
items in the TRI-HFT and the items in the score sheet (see Appendix 2).
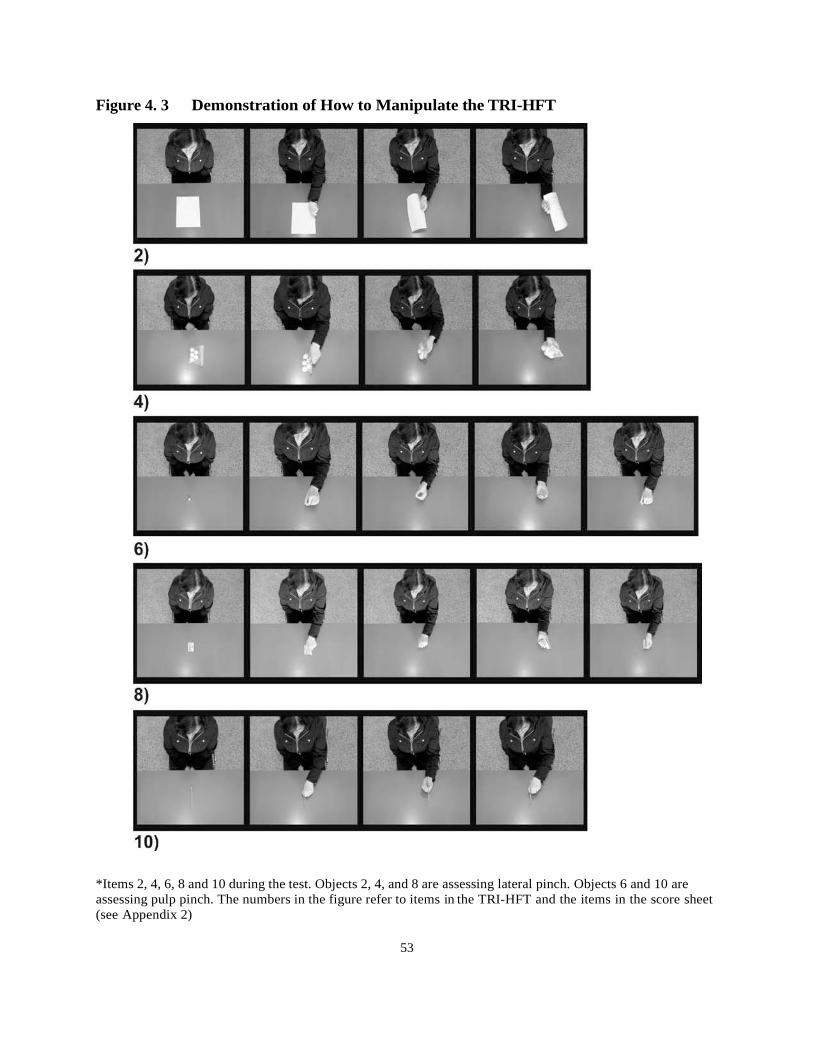
53
Figure 4. 3 Demonstration of How to Manipulate the TRI-HFT
*Items 2, 4, 6, 8 and 10 during the test. Objects 2, 4, and 8 are assessing lateral pinch. Objects 6 and 10 are
assessing pulp pinch. The numbers in the figure refer to items in the TRI-HFT and the items in the score sheet
(see Appendix 2)

54
Figure 4. 4 Demonstration of How to Manipulate the TRI-HFT
*Items 11, 12, 13, and 14 during the test. These objects are assessing strength. The numbers in the figure refer to
items in the TRI-HFT and the items in the score sheet (see Appendix 2).
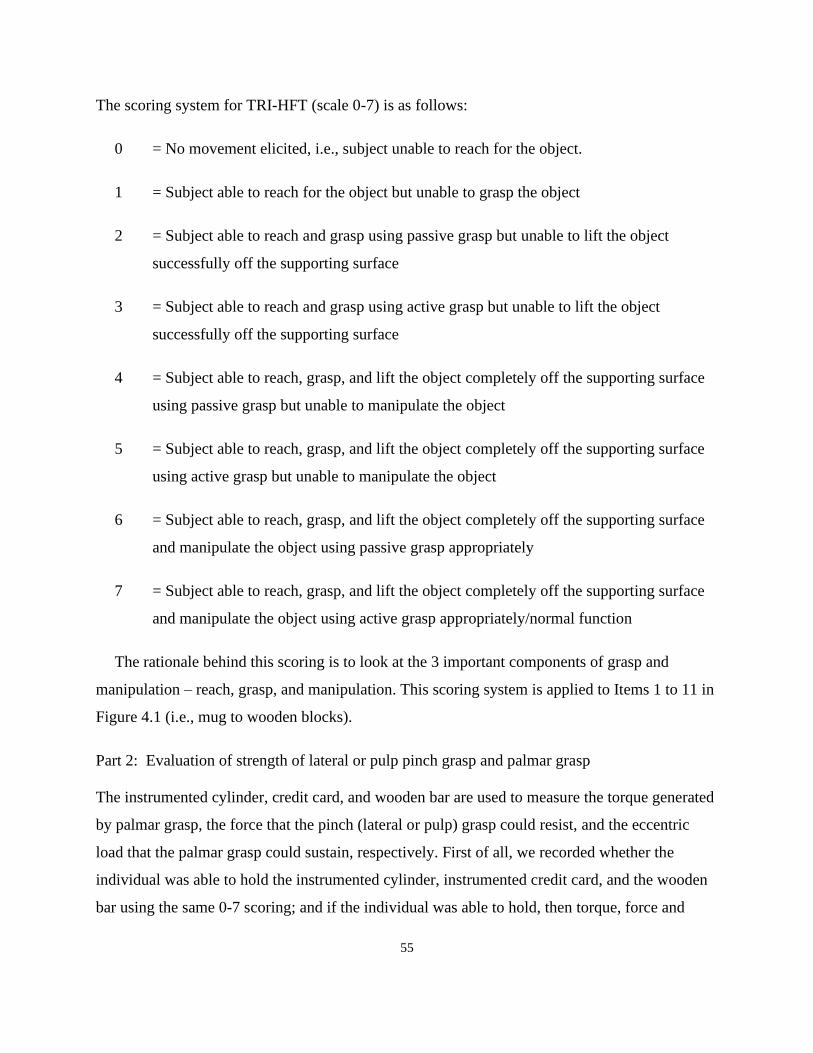
55
The scoring system for TRI-HFT (scale 0-7) is as follows:
0 = No movement elicited, i.e., subject unable to reach for the object.
1 = Subject able to reach for the object but unable to grasp the object
2 = Subject able to reach and grasp using passive grasp but unable to lift the object
successfully off the supporting surface
3 = Subject able to reach and grasp using active grasp but unable to lift the object
successfully off the supporting surface
4 = Subject able to reach, grasp, and lift the object completely off the supporting surface
using passive grasp but unable to manipulate the object
5 = Subject able to reach, grasp, and lift the object completely off the supporting surface
using active grasp but unable to manipulate the object
6 = Subject able to reach, grasp, and lift the object completely off the supporting surface
and manipulate the object using passive grasp appropriately
7 = Subject able to reach, grasp, and lift the object completely off the supporting surface
and manipulate the object using active grasp appropriately/normal function
The rationale behind this scoring is to look at the 3 important components of grasp and
manipulation – reach, grasp, and manipulation. This scoring system is applied to Items 1 to 11 in
Figure 4.1 (i.e., mug to wooden blocks).
Part 2: Evaluation of strength of lateral or pulp pinch grasp and palmar grasp
The instrumented cylinder, credit card, and wooden bar are used to measure the torque generated
by palmar grasp, the force that the pinch (lateral or pulp) grasp could resist, and the eccentric
load that the palmar grasp could sustain, respectively. First of all, we recorded whether the
individual was able to hold the instrumented cylinder, instrumented credit card, and the wooden
bar using the same 0-7 scoring; and if the individual was able to hold, then torque, force and

56
eccentric load were measured respectively. This part of the TRI-HFT is not validated, because
the test results are actual torque, force and displacement measurements.
Table 4. 1 Detailed Description and Rationale for the Items Used in the TRI-HFT
Object Description Rationale
1. Mug A standard mug with a handle
that accommodates at least 3
(preferably 4) of the subjects’
fingers.
Fill the mug with wax until the
total weight is approximately
350-400 g.
The total weight of the mug,
with wax, is approximately 350-
400 g.
Simulates drinking out of a
mug/cup.
The wax simulates the liquid
that would normally be in the
mug. Wax was chosen for safety
in the event that the mug is
dropped.
The weight simulates the
average weight of a mug filled
with coffee.
2. Paper A single sheet of standard 8 ½ x
11 in. or A4 paper.
A typical ADL task.
3. Book A standard paperback book
weighing approximately 200-
300 g (approximately 150-200
pages).
A typical ADL task.
4. Ziploc bag A closed Ziploc bag filled with
5 golf balls.
The bag is approximately 170 x
200 mm. The golf balls are
USGA and R&A regulation
size/weight.
The balls should be allowed to
move freely in the bag. The total
weight of the bag with balls
should be approximately 200 g.
Simulated picking up a bag
filled with popcorn, muffins,
peas, etc.
5. Pop can Use a full pop can (355 mL). Picking up and drinking from a
pop can is a typical ADL task.
6. Dice A standard die for gambling. Picking up a die/sugar cube is a
component of a typical ADL
task.

57
7. Sponge Isosceles triangle with
dimensions: height 40 cm, base
20 cm, thickness 10 cm.
Mimics picking up a soft,
deforming object, such as a
pillow or clothing.
8. Credit card A standard credit card should be
used.
Picking up/using a credit card is
a typical ADL task.
9. Wireless phone A standard mobile phone should
be used.
Approximate weight between
80-100 g.
Picking up and holding a
cellular phone is a typical ADL
task.
10. Pencil A standard HB pencil should be
used.
Picking up a pencil is a
component of a typical ADL
task.
11. Rectangular wooden
blocks
Nine rectangular wooden blocks
(40 x 40 x 120 mm).
Weights: 3 blocks x 100 g; 3
blocks x 200 g; 3 blocks x 300
g.
A hole is drilled into the middle
of each wooden block and metal
rod inserted into the block to
achieve the desired weight.
(Figure 4.1)
The surfaces of each block in
the set of 3 had a different
surface:
Low friction: overhead
transparency sheet
High friction: Dycem nonslip
material
Polished wood: polished wood
surface
To test the strength of palmar
grasp.
To assess the ability of the
participant to manipulate objects
of identical size but varying
weights and surfaces.
12. Instrumented cylinder A polished wooden bar
(diameter 10 mm and length 15
cm) is attached to the top edge
of a wooden cylinder (30 mm in
diameter) so that it protrudes
from the cylinder through its
center and is orthogonal to the
long axis of the cylinder (Figure
4.4). Ten cm from the center of
the cylinder, a string is attached
which fits into a groove of the
side of the semicircle. The other
To test the strength of grasping
torque of the participant’s
palmar grasp.
This activity is required to grasp
and use objects such as a knife,
toothbrush, hairbrush, and
shaver without allowing the
object to slip.
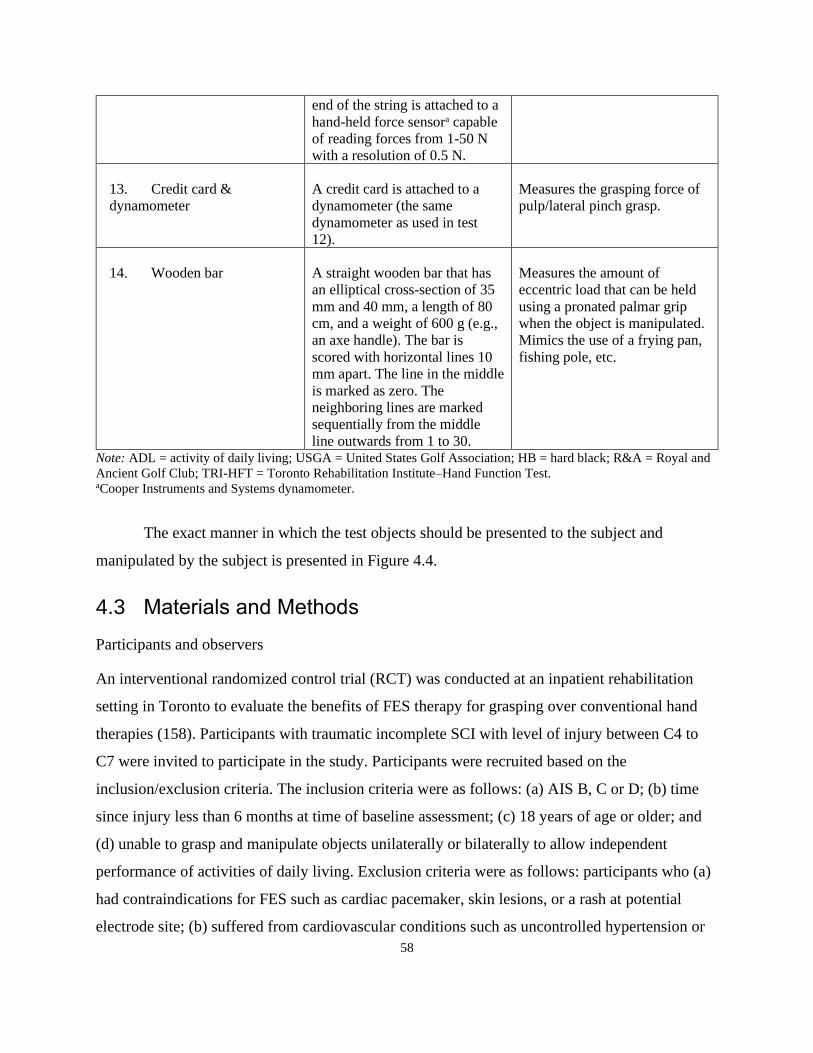
58
end of the string is attached to a
hand-held force sensora capable
of reading forces from 1-50 N
with a resolution of 0.5 N.
13. Credit card &
dynamometer
A credit card is attached to a
dynamometer (the same
dynamometer as used in test
12).
Measures the grasping force of
pulp/lateral pinch grasp.
14. Wooden bar A straight wooden bar that has
an elliptical cross-section of 35
mm and 40 mm, a length of 80
cm, and a weight of 600 g (e.g.,
an axe handle). The bar is
scored with horizontal lines 10
mm apart. The line in the middle
is marked as zero. The
neighboring lines are marked
sequentially from the middle
line outwards from 1 to 30.
Measures the amount of
eccentric load that can be held
using a pronated palmar grip
when the object is manipulated.
Mimics the use of a frying pan,
fishing pole, etc.
Note: ADL = activity of daily living; USGA = United States Golf Association; HB = hard black; R&A = Royal and
Ancient Golf Club; TRI-HFT = Toronto Rehabilitation Institute–Hand Function Test. aCooper Instruments and Systems dynamometer.
The exact manner in which the test objects should be presented to the subject and
manipulated by the subject is presented in Figure 4.4.
4.3 Materials and Methods
Participants and observers
An interventional randomized control trial (RCT) was conducted at an inpatient rehabilitation
setting in Toronto to evaluate the benefits of FES therapy for grasping over conventional hand
therapies (158). Participants with traumatic incomplete SCI with level of injury between C4 to
C7 were invited to participate in the study. Participants were recruited based on the
inclusion/exclusion criteria. The inclusion criteria were as follows: (a) AIS B, C or D; (b) time
since injury less than 6 months at time of baseline assessment; (c) 18 years of age or older; and
(d) unable to grasp and manipulate objects unilaterally or bilaterally to allow independent
performance of activities of daily living. Exclusion criteria were as follows: participants who (a)
had contraindications for FES such as cardiac pacemaker, skin lesions, or a rash at potential
electrode site; (b) suffered from cardiovascular conditions such as uncontrolled hypertension or

59
autonomic dysreflexia requiring medication; or (c) had denervated muscles. The psychometric
properties of the TRI-HFT were studied within this RCT. Gross motor hand function of both
upper extremities was assessed in 21 participants with C4 to C7 SCI using the TRI-HFT. The
other outcome measures used were FIM and SCIM (both total and self-care sub-scores) (161,
162).The mean age of the 21 participants in this study was 43 years of age (range, 16-70). All of
the participants had met the inclusion criteria for participation in the interventional RCT
evaluating the potential benefits of using FES therapy to restore grasping ability (158). In the
RCT, 12 participants received an additional hour of occupational therapy (control group),
whereas 9 participants randomized to the intervention group (FES group) received an additional
hour of FES therapy over and above 1 hour of conventional occupational therapy for grasping
(158). Both groups received 1 hour of therapy 5 days a week for 8 weeks. After 8 weeks of
participation in the therapy program, the TRI-HFT was administered again to the 21 participants.
All of the participants had some degree of impairment with respect to reaching, grasping,
and releasing objects. In particular, all subjects had shown some level of impairment with respect
to performing unilateral gross motor lateral pinch, pulp pinch, and palmar grasp tasks. The
physical impairments involved varying degrees of impairment with voluntary finger flexion and
extension, control of wrist flexion and extension, and forearm pronation and supination. The
TRI-HFT assessment was always completed in 1 session. The total administration time varied
among participants from 10 minutes to 30 minutes based on level of function.
For the purpose of determining inter-rater reliability, each participant’s assessments were
recorded on an encrypted videotape and the data were “de-identified.” Individual copies of a
DVD containing the encrypted videotaped TRI-HFT assessments of the 21 participants,
described above, along with written instructions how TRI-HFT is scored were provided to 2
observers. The observers were 1 physician and 1 physiotherapist, both with expertise in working
with SCI population for over 10 years. The observers were blinded to the participants’ diagnosis,
AIS classification, rehabilitation treatment history, and group allocation.
For assessment of construct validity, the scores on TRI-HFT were compared to the
standardized outcome measures, FIM and SCIM. These outcome measures were administered
within the same session at both baseline and follow-up). The results of the TRI-HFT were

60
compared to those of the self-care components of both FIM and SCIM. The FIM and SCIM are
validated and widely used disability questionnaires in SCI population (161-163).
To determine the sensitivity of the TRI-HFT to detect a change in hand function, the pre
and post scores of the participants were compared following their participation in the
interventional RCT.
Statistical analysis
TRI-HFT construct validity
The construct validity of the TRI-HFT was established by computing Spearman’s correlation
coefficient with the self-care component of the FIM and SCIM. An r value of 0.0 to 0.4 was
considered as weak correlation, 0.4 to 0.7 was considered as moderate correlation, and anything
above 0.7 was considered as strong correlation (164).
Inter-rater reliability
To test the inter-rater reliability of the TRI-HFT, the baseline and follow up scores were
correlated between 2 individuals. All assessments were done individually, and the observers
were not allowed to discuss the video clips or the assigned scores with each other. The intraclass
correlation coefficient and the Spearman’s rank correlation coefficient were calculated using
SPSS version 16 (SPSS, Inc., Chicago, IL).
Tool sensitivity
Using SPSS version 16, the Wilcoxon signed ranks test was used to compare scores before and
after intervention.
For all statistical procedures, P value of significance was set at P < .05.
4.4 Results
Construct validity
The results showed that there was a weak relationship at baseline between FIM self-care sub-
score and TRI-HFT (total object scores Items 1 to 10) (r = 0.13) and between the TRI-HFT and
SCIM self-care sub-score (r = 0.18) for the right hand (Figures 4.5 and 4.7). The scores for the

61
left hand at baseline showed a comparatively moderate correlation between TRI-HFT and FIM
self-care sub-score (r = 0.59) and a weak correlation between TRI-HFT and SCIM self-care sub-
score (r = 0.38) (Figures 4.6 and 4.8). However, stronger correlations were found between the
measures for follow-up data. For the right hand, the correlations between TRI-HFT and FIM
self-care sub-score and between TRI-HFT and the SCIM self-care sub-score were moderately
strong (r = 0.56 and r = 0.48, respectively) (Figures 4.5 and 4.7). For the left hand, the
correlations were moderately strong for associations between TRI-HFT and the FIM self-care
sub-score and between TRI-HFT and the SCIM self-care sub-score (r = 0.73 and r = 0.62,
respectively) (Figures 4.6 and 4.8).
Correlations between TRI-HFT wooden blocks (Item 11) and SCIM and FIM self-care sub-
scores for the right hand at baseline showed weak correlations (r = 0.47 and r = 0.39,
respectively). These scores were even weaker for the left hand (r = 0 and r = 0.35, respectively).
However, the relationships were much stronger at follow-up. For the right hand, the association
between TRI-HFT wooden blocks (Item 11) and FIM self-care sub-score and between TRI-HFT
wooden blocks and SCIM self-care sub-score were moderately strong (r = 0.69 and r = 0.56,
respectively). For the left hand, the association between TRI-HFT wooden blocks (Item 11) and
FIM self-care sub-score and between TRI-HFT wooden blocks and SCIM self-care sub-score
were moderately strong (r = 0.66 and r = 0.56, respectively).
Inter-rater reliability
The inter-rater reliability of the TRI-HFT was examined using the intraclass correlation
coefficient (ICC) and Spearman’s correlation coefficient. ICC for the pretherapy total score of
the right hand was 0.98 and for the left hand was 0.98 (Figure 4.9); the Spearman rho for the
right hand was 0.96 (P < .000) and that for the left hand was 0.98 (P < .000). The ICC for the
posttherapy total score of the right hand was 0.99 (P < .000) and for the left hand was 0.99 (P <
.000); the Spearman rho for the right as well as the left hand was 0.96 (P < .000). The ICC was
also very high for individual task and for the wooden blocks (Table 4.2). Hence, excellent inter-
rater reliability was determined for both the right and left hands.
Sensitivity

62
The baseline scores on TRI-HFT for the 21 participants varied from 0 to 70 on the total object
scores (Items 1 to 10 in Figure 4.1). Post scores also varied from 0 to 70. Irrespective of group
allocation, all participants except 1 showed improvements on all outcome measures including the
TRI-HFT. There were statistically significant differences in scores pre and post therapy for FIM
and SCIM self-care sub-scores and for TRI-HFT object manipulation component (Table 4.3). No
statistically significant differences in change scores between the 2 groups was obtained on the
Figure 4. 5 Construct Validity of the TRI-HFT Score vs the FIM Self-care Sub-score (Rt.
Hand)
*(Items 1-10 in Figure 4.1) for the right hand pre (r = 0.13) and post therapy (r = 0.59). The FIM scores show a
significant floor effect pre therapy.
Figure 4. 6 Construct Validity of the TRI-HFT Score vs the FIM Self-care Sub-score (Lt.
Hand)
0
5
10
15
20
25
30
35
40
0 10 20 30 40 50 60 70
FIM
self
-care
su
bsco
re
TRI-HFT (10 objects)
(Pre- therapy)
0
5
10
15
20
25
30
35
40
0 10 20 30 40 50 60 70
FIM
self
-care
su
bsco
re
TRI-HFT (10 objects)
(Post therapy)
0
5
10
15
20
25
30
35
40
0 20 40 60
FIM
self
-care
su
bsco
re
TRI-HFT (10 objects)
(Pre therapy)
0
5
10
15
20
25
30
35
40
0 20 40 60
FIM
self
care
su
bsco
re
TRI-HFT (10 objects)
(Post therapy)
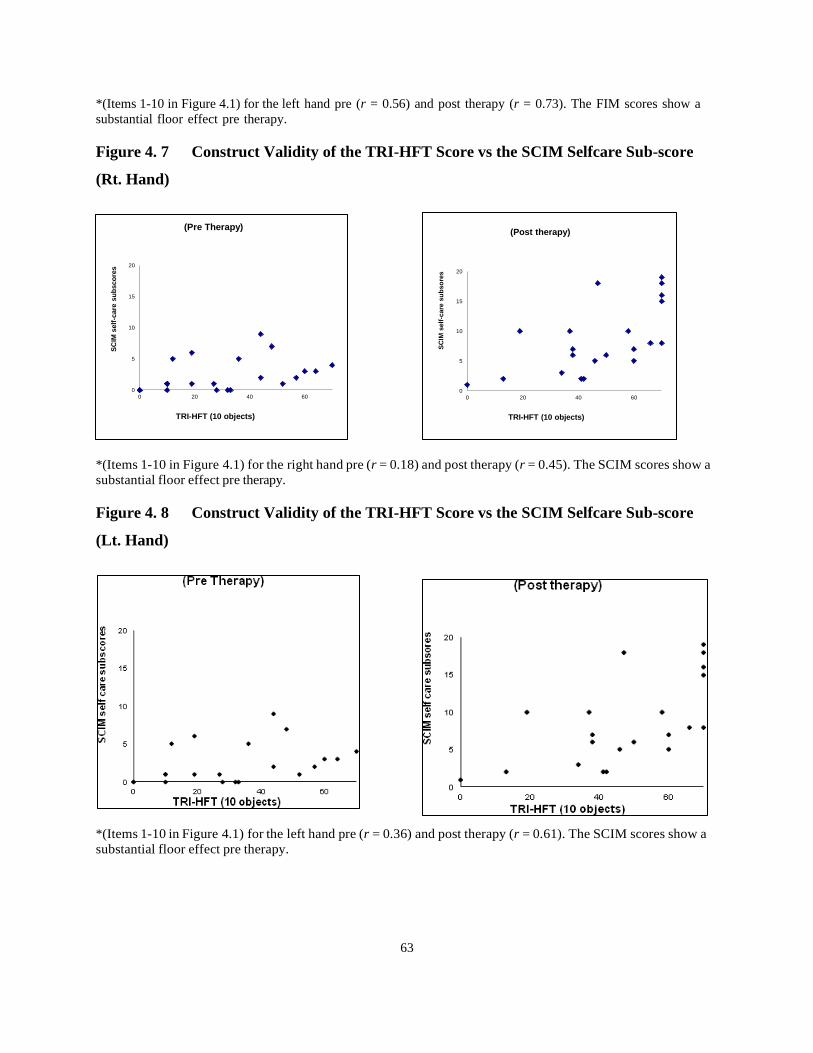
63
*(Items 1-10 in Figure 4.1) for the left hand pre (r = 0.56) and post therapy (r = 0.73). The FIM scores show a
substantial floor effect pre therapy.
Figure 4. 7 Construct Validity of the TRI-HFT Score vs the SCIM Selfcare Sub-score
(Rt. Hand)
*(Items 1-10 in Figure 4.1) for the right hand pre (r = 0.18) and post therapy (r = 0.45). The SCIM scores show a
substantial floor effect pre therapy.
Figure 4. 8 Construct Validity of the TRI-HFT Score vs the SCIM Selfcare Sub-score
(Lt. Hand)
*(Items 1-10 in Figure 4.1) for the left hand pre (r = 0.36) and post therapy (r = 0.61). The SCIM scores show a
substantial floor effect pre therapy.
0
5
10
15
20
0 20 40 60
SC
IM s
elf
-care
su
bsco
res
TRI-HFT (10 objects)
(Pre Therapy)
0
5
10
15
20
0 20 40 60
SC
IM s
elf
-care
su
bso
res
TRI-HFT (10 objects)
(Post therapy)
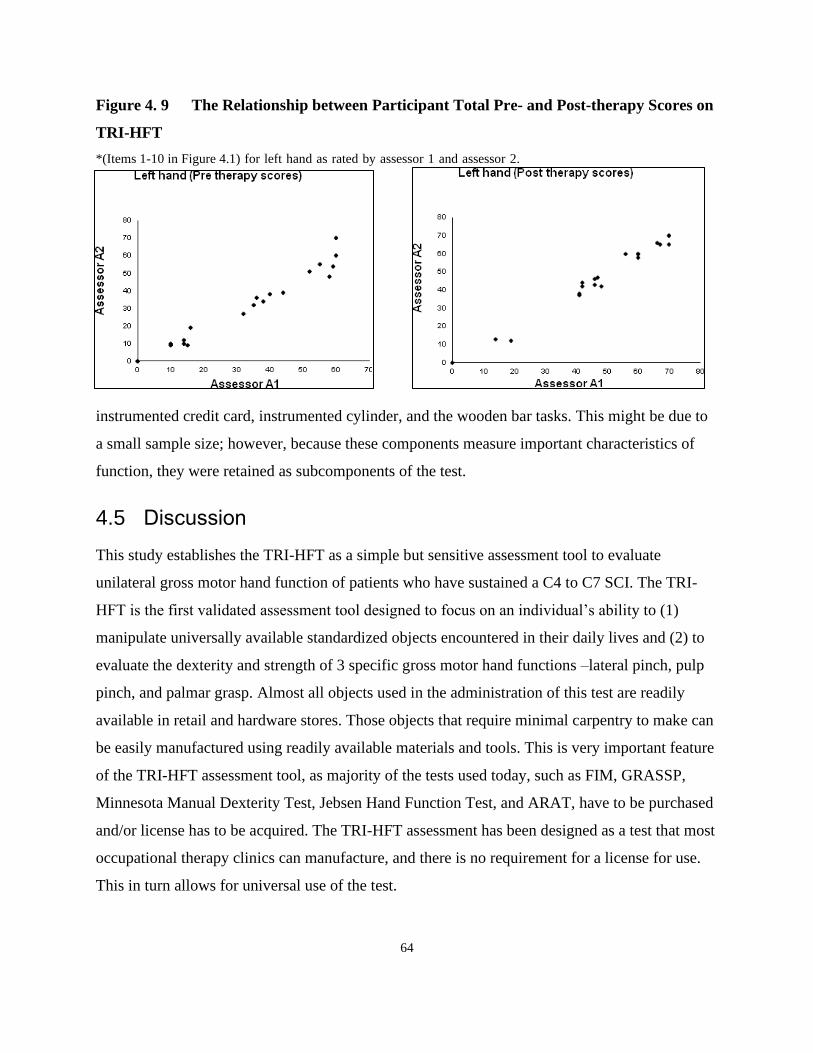
64
Figure 4. 9 The Relationship between Participant Total Pre- and Post-therapy Scores on
TRI-HFT
*(Items 1-10 in Figure 4.1) for left hand as rated by assessor 1 and assessor 2.
instrumented credit card, instrumented cylinder, and the wooden bar tasks. This might be due to
a small sample size; however, because these components measure important characteristics of
function, they were retained as subcomponents of the test.
4.5 Discussion
This study establishes the TRI-HFT as a simple but sensitive assessment tool to evaluate
unilateral gross motor hand function of patients who have sustained a C4 to C7 SCI. The TRI-
HFT is the first validated assessment tool designed to focus on an individual’s ability to (1)
manipulate universally available standardized objects encountered in their daily lives and (2) to
evaluate the dexterity and strength of 3 specific gross motor hand functions –lateral pinch, pulp
pinch, and palmar grasp. Almost all objects used in the administration of this test are readily
available in retail and hardware stores. Those objects that require minimal carpentry to make can
be easily manufactured using readily available materials and tools. This is very important feature
of the TRI-HFT assessment tool, as majority of the tests used today, such as FIM, GRASSP,
Minnesota Manual Dexterity Test, Jebsen Hand Function Test, and ARAT, have to be purchased
and/or license has to be acquired. The TRI-HFT assessment has been designed as a test that most
occupational therapy clinics can manufacture, and there is no requirement for a license for use.
This in turn allows for universal use of the test.

65
Table 4. 2 Intraclass Correlation Coefficients for Inter-rater Reliability for the 10
Objects and the Wooden Blocks in the TRI-HFT Test
Table 4. 3 Summary of the Mean Test Results for the Control and Intervention Groups
at Baseline (Before) and Upon Completion of the Therapy (After), with Corresponding p
Values
Control Group
N=12
Intervention Group
N=9 p values
Before After Before After
FIM self-care sub-score 7.8 17.8 8.1 28.2 0.015 *
SCIM self-care sub-score 3.3 6.4 1.9 12.1 <0.0001*
TRI-HFT Components
• 10 Objects 27.2 38.5 37.1 53.8 0.054*
• Instrumented Cylinder (Able to Hold) 1.9 1.33 1.0 1.7 0.033*
• Instrumented Cylinder
Torque Values (Nm) 0.26 2.59 0.26 1.13 0.4247
• Credit Card (Able to Hold) 1.33 1.41 1.0 1.7 0.035*
• Credit Card
Force Values (N) 2.67 8.76 4.42 12.5 0.422
• Wooden Bar (Able to Hold) 0.63 0.96 0.8 1.5 0.065
• Wooden Bar Thumb Direction
Length Values (cm) 2.88 10.5 1.67 10.94 0.622
• Wooden Bar Little Finger Direction
Length Values (cm) 3.17 11.85 5.56 12.78 0.767
Table 6.2: Intraclass Correlation Coefficients for inter-rater reliability for the 10 objects and the
wooden blocks in the TRI-HFT test (Items 1 to 11 in Figure 6.1)
Objects of the TRI-HFT Left hand Right hand
Pre therapy Post therapy Pre therapy Post therapy
ICC ICC ICC ICC
Mug 0.90 0.90 1.00 0.95
Paper 0.88 0.87 0.95 0.97
Book 0.90 0.95 0.97 0.98
Zip lock bag 0.93 0.96 0.93 0.96
Pop can 0.91 0.99 0.97 0.98
Dice 0.92 0.97 0.95 0.97
Sponge 0.90 1.00 0.95 0.99
Credit card 0.94 0.93 0.96 0.95
Mobile 0.96 1.00 0.97 0.97
Pencil 0.92 1.00 0.91 1.00
Total score (10 objects) 0.98 0.99 0.98 0.99 Wooden Blocks 1.00 1.00 1.00 1.00

66
The results of this study clearly demonstrate the feasibility of the TRI-HFT. It requires
minimal training and does not require a complex instruction manual. When observers viewed
Figures 6.1 to 6.4 and discussed the scoring scheme, they were able to administer and score the
test immediately. Inter-rater reliability for the TRI-HFT was excellent. There was no significant
difference in participant scores between the assessments of the 2 observers.
The correlations for the left-hand paper task were slightly lower (Table 4.2). This may
have been due to the properties of the object. The way the scoring system is developed, grade 2
indicates that the subject is able to reach and grasp the object using a passive grip but is unable to
lift it successfully off the table and grade 4 indicates that the participant is able to reach grasp
and lift the object successfully off the table using a passive grip but is unable to manipulate the
object. Considering the flimsy nature of the paper, the raters found it difficult to judge what
would be considered “off the table.” This was taken into account, and we added the phrase
“completely off the supporting surface” to the scoring system to prevent ambiguity.
The relationship between TRI-HFT and SCIM and FIM self-care sub-scores was lower
for the right hand compared to the left hand. One possible explanation for this finding is that all
the participants were right hand dominant prior to SCI, therefore they may have accommodated
the limitations better on that side. The FIM and SCIM are functional measures and do not take
into account how the task was completed, so participants who scored higher on the FIM and
SCIM may have had lower scores on the TRI-HFT because of the compensatory mechanisms
they used, which the TRI-HFT scoring system takes into account.
The correlations between TRI-HFT and the SCIM and FIM self-care sub-scores were
weak at baseline and the correlations between the same measures were either moderately strong
or strong post therapy. There are a few possible explanations for this. One explanation for this
finding may be that most of our participants had a very low level of function at baseline, and
minor changes in function could not be detected on the FIM and SCIM assessments, owing to a
floor effect. At the same time, the TRI-HFT was able to distinguish slight differences in function
amongst most participants. After therapy, all participants improved their function, even those
participants who scored 0 at baseline improved post therapy, irrespective of their group
allocation. As a result, the floor effect that was prevalent at baseline was eliminated, and we

67
were able to demonstrate stronger relationships between TRI-HFT and FIM and SCIM post
therapy. Another possible explanation for this finding is that SCIM and FIM scores do not take
into account the use of compensatory movements, only the level of independence. Changes in
these scores can therefore reflect training effects (subjects learning to perform tasks within the
constraints of their capabilities) as well as neurological changes, particularly during in-patient
stay in a rehabilitation center. In contrast, the TRI-HFT appears to prevent (take into account) the
use of compensatory movement in order to focus on neurological/motor changes. This inherently
limits the correlations that can be expected between the SCIM/FIM and TRI-HFT.
We found the TRI-HFT to be very sensitive to change in function. The mean change
score on TRI-HFT object manipulation component for the FES group was 16.7 (minimum
change score = 0 and maximum change score = 49) and that for the control group was 11.3
(minimum change score = 0 and maximum change score = 30). This implies that the TRI-HFT is
actually measuring change in terms of function. Also, as shown in Figure 4.5, for some
participants the FIM was unable to demonstrate a change in spite of the TRI-HFT showing a
significant improvement in their function post therapy; this is due in part to the granularity of the
scoring system in the TRI-HFT and in part to the inherent way the health care system is set-up.
Most participants in acute care may not be doing the daily tasks assessed by the FIM and instead
have a caregiver or family member do them. As discussed in the literature review, most of the
tests that are currently being used to assess change in function use “time required to complete the
test” as the sole outcome measure and do not take into account the quality of movement, which is
exactly what the TRI-HFT has been designed to avoid. Moreover, most of the hand function tests
available do not give credit when participants are able to initiate the task but are unable to
complete it successfully. Many of the available hand function tests may not be appropriate to
assess hand function in individuals with SCI: most of the individuals with tetraplegia are able to
initiate tasks but are often unable to complete them successfully, whereas after the therapy
(especially FES therapy), they are able to perform the entire task voluntarily. The TRI-HFT
addresses this granularity of the scoring system and is able to capture subtle but important
changes in hand function before and after the therapy. This feature is of particular importance if
the test were to be used in clinical trial designs, where recovery profiles of hand function are
required.
68
4.6 Conclusion
Our findings indicate that TRI-HFT is a simple, reliable, valid, and sensitive measure to assess
change in unilateral gross motor hand function in individuals with SCI. Furthermore, the TRI-
HFT takes less than 30 minutes to be administered on both upper limbs and can be incorporated
in a clinical setting with ease. Finally, it is a publicly available test. This is a very important
feature, as it creates the potential for significant universal uptake.

69
Chapter 5 Specific Project Aims and Objectives of this Thesis
5.1 Background
This thesis aims to further the field of upper extremity rehabilitation in neurological
population. The first two projects explored the feasibility of developing an upper extremity
assessment tool using the 3D printing technology to overcome accessibility challenges which is
one of the commonly overlooked barriers to clinical uptake of outcome assessment tools. As
summarised in Chapter 2: Section 2.1.4.1 and Section 2.2.4.1, the upper extremity measures
currently used in clinical settings as well as those recommended as core outcome set (For e.g.,
Fugl Meyer-UE and ARAT for stroke) for research have several documented limitations.
From a clinical standpoint the 3D-printed TRI-HFT addresses several of the commonly
listed barriers like insufficient time resources both for outcome measure training as well as
administration, and cost, and accessibility of the measurement tool. The 3D TRI-HFT takes up to
15 mins to be administered bilaterally, administration instructions consist of a two-page self
reading manual and 3D printing allows for clinical set-ups and hospitals with 3D printers to print
their own test (alternatively the test can be bought for CAD $1500). From a research standpoint
accessible, standardised, easy to administer, reliable, and valid outcome measures appropriate to
the patient population and the target intervention are critical for appropriate evaluation of newer
rehabilitation interventions. Chapter 6 and 7 of this thesis discusses the development and
psychometric assessment of the 3D printed Toronto Rehabilitation Institute-Hand Function Test
(3D TRI-HFT). Thus, the 3D TRI-HFT is developed to meet the needs of both clinicians and
researchers keeping in mind the requirements of both these settings (165, 166).
The work on the development of the 3D TRI-HFT was also motivated by the third study
of this thesis that looks to expand the repertoire of existing FES protocols. Whereas, Chapter 8
discusses the feasibility of scapular muscle stimulation using surface FES technology, the end
goal is to apply this in patient population and study the benefits or lack thereof in these target
populations using a standardised outcome assessment tool. Scapular muscle stimulation,
specifically the Upper Trapezius, Lower Trapezius and Serratus Anterior is very important in
both stroke and spinal cord injury population. This is not only for purposes of producing a

70
physiologically correct muscle recruitment pattern during arm elevation but also from the
standpoint of preventing many of the shoulder complications like pain and subluxation that result
from limited ability to actively recruit these muscles during early rehabilitation (167, 168).
This thesis essentially aims to go the full circle by developing newer rehabilitation
interventions and a means to evaluate these interventions using standardised outcome assessment
tools on an ongoing basis, not only in research but also in clinical settings.
Below are the specific aims and objectives related to each of the three studies.
5.2 Specific Project Aims and Objectives of this Thesis
Study 1. 3-Dimensional printing in rehabilitation: Feasibility of printing an upper extremity
gross motor function assessment tool
Objectives:
1. The primary objective of the study was to assess the feasibility of designing and printing
a 3D printed version of the TRI-HFT objects (3D TRI-HFT).
2. The secondary objective was to perform a preliminary analysis of the reliability and
validity of the 3D TRI-HFT in individuals with chronic stroke.
Hypothesis:
1. The TRI-HFT test objects could be successfully 3D printed with minimal modifications
to the test, if any.
2. The 3D TRI-HFT would be a reliable and valid measure to assess upper extremity
function in individuals with stroke as determined by high inter and intra-rater reliability
and moderate to strong construct validity with the CMSA-Arm, CMSA-Hand and FMA-
Hand respectively.
Study 2. Preliminary evaluation of the reliability and validity of the 3D printed Toronto
Rehabilitation Institute-Hand Function Test in individuals with spinal cord injury

71
Objectives:
1. The primary objective was to evaluate the inter-rater and intra-rater reliability; and
criterion and construct validity of the 3D printed Toronto Rehabilitation Institute-Hand
Function Test (3D TRI-HFT) in individuals with sub-acute and chronic SCI.
Hypothesis:
1. The 3D TRI-HFT would be a reliable and valid measure to assess upper extremity
function in individuals with SCI as determined by high inter and intra-rater reliability and
strong criterion validity with the GRASSP respectively.
Study 3. Feasibility and significance of stimulating interscapular muscles using
transcutaneous FES in able bodied individuals.
Objectives:
1. The primary objective was to assess the feasibility of stimulating lower trapezius (LT),
upper trapezius (UT) and serratus anterior (SA) muscles along with anterior or middle
deltoid, in able bodied individuals using surface FES.
2. The secondary objective was to understand the effects of LT, UT and SA stimulation on
maximum arm reach achieved in shoulder flexion and abduction.
Hypothesis:
1. The lower trapezius (LT), upper trapezius (UT) and serratus anterior (SA) muscles could
be stimulated using surface FES in able bodied individuals.
2. The stimulation of the LT, SA and UT along with the Anterior and Middle Deltoid would
result in an increase in maximum arm reach in shoulder flexion and abduction
respectively as measured by the motion capture system.
72
Chapter 6 3-Dimensional Printing in Rehabilitation: Feasibility of Printing an
Upper Extremity Gross Motor Function Assessment Tool
In this chapter, the results of 3D printing the TRI-HFT are presented along with preliminary results
of the psychometric properties of the 3D printed test in individuals with chronic stroke. This
manuscript is published in Biomedical Engineering Online. This manuscript is a part of the current
thesis projects.
Naaz Kapadia, Mathew Myers, Kristin Musselman, Rosalie H. Wang, Aaron Yurkewich and
Milos R. Popovic. 3-Dimensional printing in Rehabilitation: Feasibility of printing an upper
extremity gross motor function assessment tool. Biomed Eng Online. 2021 Jan 5;20(1):2. doi:
10.1186/s12938-020-00839-3. PMID: 33402170.
6.1 Abstract
Background: Use of standardized and scientifically sound outcome measures is encouraged in
clinical practice and research. With the development of newer rehabilitation therapies, we need
technology-supported upper extremity outcome measures that are easily accessible, reliable and
valid. 3-Dimensional printing (3D printing) has recently seen a meteoric rise in interest within
medicine including the field of Physical Medicine and Rehabilitation. The primary objective of
this study was to evaluate the feasibility of designing and constructing a 3D printed version of
the Toronto Rehabilitation Institute-Hand Function Test (TRI-HFT). The TRI-HFT is an upper
extremity gross motor function assessment tool that measures function at the intersection of the
International Classification of Functioning, Disability and Health (ICF) body structure and
function, and activity domain. The secondary objective was to assess the preliminary
psychometrics of this test in individuals with stroke.
Results: 3D design files were created using the measurements of the original TRI-HFT objects.
The 3D printed objects were then compared to the original test objects to ensure that the original
dimensions were preserved. All objects were successfully printed except the sponge and paper
which required some modification. The error margin for weight of the objects was within 10% of
the original TRI-HFT for the rest of the objects. Nine participants underwent the following

73
assessments: the Chedoke Arm and Hand Activity Inventory (CAHAI-Appendix 3), Fugl Meyer
Assessment-Hand (FMA-Hand- Appendix 4), Chedoke-McMaster stages of recovery of the arm
(CMSA-Arm-Appendix 5) and Chedoke-McMaster stages of recovery of the hand (CMSA-
Hand- Appendix 5) and the 3D TRI-HFT (Appendix 2) for assessment of psychometric
properties of the test. The video recorded assessment of the 3D TRI-HFT was used for reliability
testing. Construct validity was assessed by comparing the scores on 3D TRI-HFT with the scores
on CAHAI, CMSA-Arm, CMSA-Hand and FMA-Hand. The 3D TRI-HFT had high inter-rater
reliability (Intra-Class Correlation Co-efficient (ICC) of 0.99; P < 0.001), high intra-rater
reliability (ICC of 0.99; P < 0.000) and moderate-to-strong correlation with the CMSA-Arm,
CMSA-Hand and FMA-Hand scores.
Conclusions: The TRI-HFT could be successfully 3D printed and initial testing indicated that the
test is a reliable and valid measure of upper extremity motor function in individuals with stroke.
6.2 Introduction
Use of standardized and scientifically sound outcome measures is highly encouraged in clinical
practice and research. A number of guidelines have been developed around use of upper
extremity outcome measures in stroke (26, 27). However, researchers have identified that with
the development of newer rehabilitation therapies we need technology-supported upper extremity
outcome measures that are easily accessible and can measure change consistently and
reliably(28). The most commonly used upper extremity measures in clinical and research settings
for stroke in the International Classification of Functioning, Disability and Health (ICF’s) body
structure and function (WHO-Chapter 4) and activity level domains are the Fugl Meyer
Assessment Upper Extremity (FMA-UE) (29) and the Action Research Arm Test (ARAT) (30)
respectively. The ARAT is a time-based activity test and although widely used has several
documented limitations (32). Further, Demers et al., reviewed 15 upper extremity outcome
measures assessing arm/hand function at the ICF’s activity level recommended by neurological
clinical practice guidelines (45). These include the Box and Block test (33), Jebsen Hand
function test (34), Nine hole peg test (35), ARAT(30), Chedoke Arm and Hand Activity
Inventory (CAHAI) (36), Arm Motor ability test (37), Frenchay Arm Test (38) , Motor
Evaluation Scale for Upper Extremity in Stroke Patients (39), Reaching Performance Scale for
74
Stroke (40), Test d’Évaluation des Membres supérieurs des Personnes Âgées (41), Wolf Motor
Function Test (42), ABILHAND (43), Capabilities of the upper extremity (44) and Motor-
Activity Log (45). The review concluded that current activity measures may not distinguish
recovery from compensation and do not adequately track changes in movement quality over
time. Moreover, most of the above stated outcome measures either lack information about
validity, reliability, or responsiveness in the stroke population or require an administration time
of >20 minutes, may require equipment purchase or construction or copyright payment (27).
Thus, there is a need for a tool that can reliably and effectively measure change following
rehabilitation interventions like robot assisted therapies, Functional Electrical Stimulation (FES)
therapy, mirror therapy, brain computer interface-controlled FES therapy and many others. The
tool needs to be (i) universally and easily accessible, (ii) reliable, (iii) valid, (iv) feasible to be
administered within both clinical and research settings, and (v) virtually requiring no training in
order to be used by rehabilitation professionals and research personnel.
We developed the Toronto Rehabilitation Institute-Hand Function Test (TRI-HFT) (98)
an upper extremity gross motor function assessment tool that measures function at the
intersection of the ICF’s body structure and function and activity domain. The TRI-HFT
evaluation requires participants to manipulate everyday objects using only the affected upper
extremity and measures difficulty with manipulation of these objects using the paretic hand. The
scoring differentiates between the use of a physiological grasp versus use of compensatory
strategies during task execution and virtually no training is required to administer the test. The
scoring system requires the participant to reach for the object, grasp it, lift off the supporting
surface and finally manipulate it before replacing it back on the table. The original TRI-HFT test
consists of two parts; 1. Object manipulation and 2. Strength measurement. The object
manipulation part of the test consists of day to day objects that are manipulated using different
types of grip. The test objects include: (1) mug, (2) paper, (3) book, (4) Ziploc bag filled with 5
golf balls , (5) pop can, (6) dice, (7) isosceles triangular sponge, (8) credit card, (9) wireless
home telephone, (10) pencil and (11) 9 rectangular blocks in sets of 3x100g, 3x200g and 3x300g.
Each of the 3 blocks in each weight category of object 11 have surfaces with different levels of
friction. This part of the test is graded on a 0-7 scale where higher scores indicate better

75
performance. The strength measurement part of the test measures the strength of lateral grip and
palmar grasp using three sub-tests i.e. instrumented credit card, instrumented cylinder, and the
wooden bar. It takes approximately 15 minutes to administer the original TRI-HFT, on bilateral
upper extremities, in individuals with spinal cord injury. Administration and scoring of the test
do not require special training and can be administered by reviewing a two-page instruction
sheet. Details on the original test object dimensions and administration are described in Kapadia
et al., (98). The original version of the test was validated in the sub-acute spinal cord injury
population however was not validated in the stroke population.
The original TRI-HFT however failed to see a significant uptake primarily because it was
a challenge to make this test available to interested clinicians and researchers within and outside
of Canada. The original TRI-HFT was fabricated by the researchers and while many of the test
objects were “off the shelf objects” some were manufactured in our laboratory. Although the
original test dimensions are published, we realized that it was challenging for clinicians to
compile the test and besides if the test object dimensions changed then standardization of the test
would become questionable. This limitation became the motivation for exploring the ability to
3D print the test to make it universally accessible.3D-printing has recently seen a meteoric rise in
interest within medicine, and the field of Physical Medicine and Rehabilitation is no exception
(169). Researchers are discovering many medical and dental applications including devices and
implants, biosynthetic and hybrid human tissues including skin, cartilage, and bone and many
more applications (170-172). For the field of physical medicine and rehabilitation 3D printing
has the potential to provide unique solutions to common obstacles related to fabrication and
delivery (169). 3D printing within the rehabilitation world has mostly been explored for
fabricating orthosis, prosthesis and for assistive technologies (173-175).
The primary objective of the current study was to assess the feasibility of designing and
constructing a 3D printed version of the TRI-HFT objects (3D TRI-HFT). It is important to note
that the administration of the 3D TRI-HFT and the scoring system remains the same as the
original TRI-HFT. The secondary objective was to do a preliminary testing of the psychometric
properties of the 3D printed test, specifically the inter and intra-rater reliability of the first part of
the test and construct (convergent) validity of the first and second part of the test in individuals
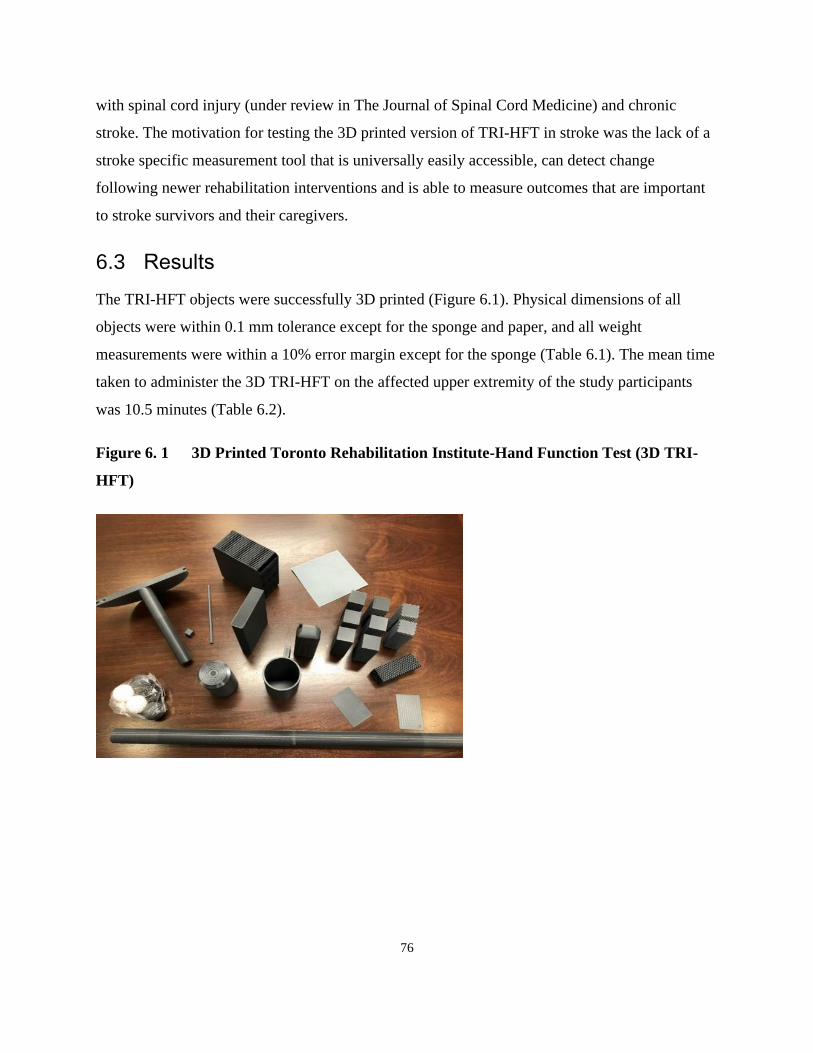
76
with spinal cord injury (under review in The Journal of Spinal Cord Medicine) and chronic
stroke. The motivation for testing the 3D printed version of TRI-HFT in stroke was the lack of a
stroke specific measurement tool that is universally easily accessible, can detect change
following newer rehabilitation interventions and is able to measure outcomes that are important
to stroke survivors and their caregivers.
6.3 Results
The TRI-HFT objects were successfully 3D printed (Figure 6.1). Physical dimensions of all
objects were within 0.1 mm tolerance except for the sponge and paper, and all weight
measurements were within a 10% error margin except for the sponge (Table 6.1). The mean time
taken to administer the 3D TRI-HFT on the affected upper extremity of the study participants
was 10.5 minutes (Table 6.2).
Figure 6. 1 3D Printed Toronto Rehabilitation Institute-Hand Function Test (3D TRI-
HFT)

77
Table 6. 1 Dimensions of the Original TRI-HFT Objects and the 3D Printed TRI-HFT Objects
No. Object
Measurement of original TRI-HFT objects Measurement of 3D TRI-HFT objects
1 MUG Size: 115 x 245 Size: 115 x 250
Weight: 563.98 Weight: 554
2 PAPER Size: 297 x 210 x 0.1 Size: 150 x150 x 0.3
Weight: 0 Weight: 8
3 BOOK Size: 173 x 105 x 26 Size: 175 x 105 x 26
Weight: 315 Weight: 318
4 ZIP LOCK BAG
WITH GOLF BALLS
Size: 170 x 200 Size: 170 x 200
Weight:230 (46 per ball x5 golf balls) Weight:236 (39 per ball x 6 golf balls)
5 POP CAN Size:120 x 61 Size:123 x 66
Weight: 350 Weight: 388
6 DIE Size: 15 x15 x15 Size: 16 x16 x16
Weight: 6 Weight: 4
7 SPONGE
Size: Isosceles triangle with height 400 and
base 200
Weight: 170
Size: Square 142 x142
Weight: 161
8 CREDIT CARD Size: 85 x53 Size: 86 x54 x08
Weight: 0 Weight: 4
9 WIRELESS PHONE
Size: 144 x50 x25
Size: 145 x50 x35
Weight: 223 Weight: 222.3
10 PENCIL Size: 187 x27 Size: 190 x27
Weight: 9 Weight: 6
11 RECTANGULAR
BLOCKS
Size: 115 x35 x35
Weight: 100 /200 /300
Size: 100 x36 x36
Weight: 100 /200 /296
12 INSTRUMENTED
CYLINDER
Size:
Plat Radius:110
Handle length:215
Handle circumference: 95
Weight:300
Size:
Plate radius: 110
Handle length:215
Handle circumference: 95
Weight: 281.49
13 INSTRUMENTED
CREDIT CARD
Size: 85 x53 x0 Size: 86 x54 x08
Weight: 0 Weight: 4
14 ROD
Size:
Length:740
Diameter: 33
Size:
Length:740
Diameter: 33
Weight: 666 Weight: 642
*Size in millimeters and weight in grams.
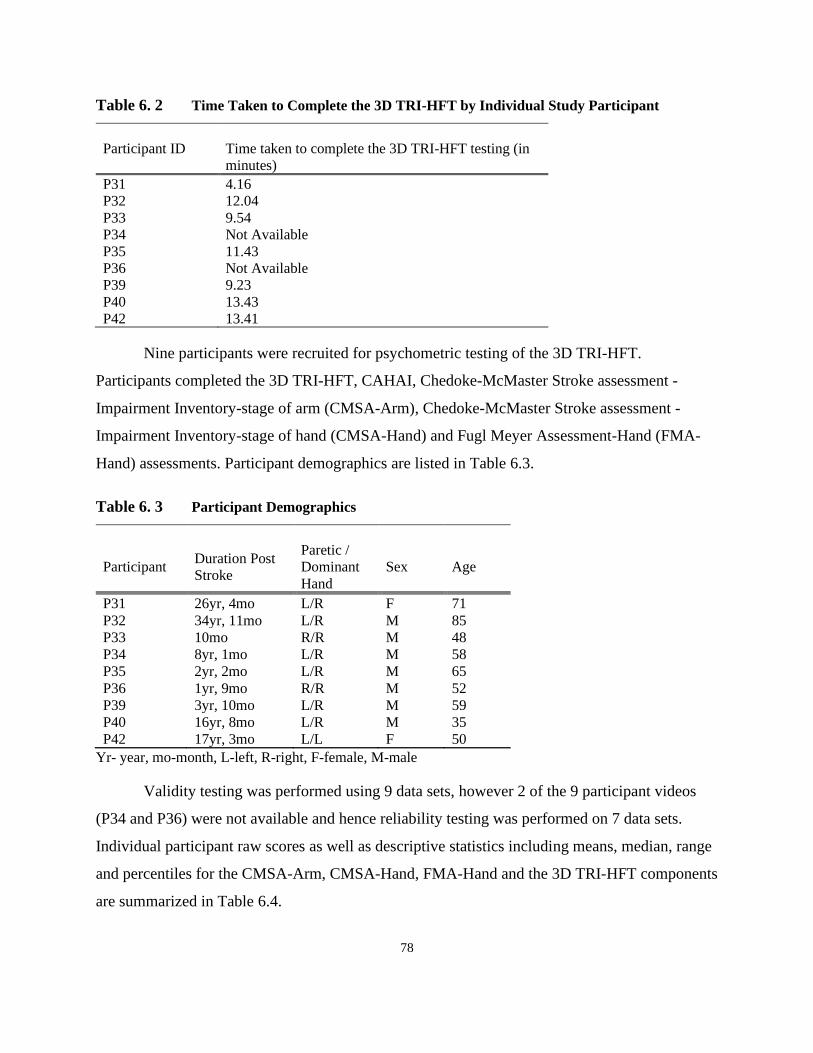
78
Table 6. 2 Time Taken to Complete the 3D TRI-HFT by Individual Study Participant
Participant ID Time taken to complete the 3D TRI-HFT testing (in
minutes)
P31 4.16
P32 12.04
P33 9.54
P34 Not Available
P35 11.43
P36 Not Available
P39 9.23
P40 13.43
P42 13.41
Nine participants were recruited for psychometric testing of the 3D TRI-HFT.
Participants completed the 3D TRI-HFT, CAHAI, Chedoke-McMaster Stroke assessment -
Impairment Inventory-stage of arm (CMSA-Arm), Chedoke-McMaster Stroke assessment -
Impairment Inventory-stage of hand (CMSA-Hand) and Fugl Meyer Assessment-Hand (FMA-
Hand) assessments. Participant demographics are listed in Table 6.3.
Table 6. 3 Participant Demographics
Participant Duration Post
Stroke
Paretic /
Dominant
Hand
Sex Age
P31 26yr, 4mo L/R F 71
P32 34yr, 11mo L/R M 85
P33 10mo R/R M 48
P34 8yr, 1mo L/R M 58
P35 2yr, 2mo L/R M 65
P36 1yr, 9mo R/R M 52
P39 3yr, 10mo L/R M 59
P40 16yr, 8mo L/R M 35
P42 17yr, 3mo L/L F 50
Yr- year, mo-month, L-left, R-right, F-female, M-male
Validity testing was performed using 9 data sets, however 2 of the 9 participant videos
(P34 and P36) were not available and hence reliability testing was performed on 7 data sets.
Individual participant raw scores as well as descriptive statistics including means, median, range
and percentiles for the CMSA-Arm, CMSA-Hand, FMA-Hand and the 3D TRI-HFT components
are summarized in Table 6.4.

79
Table 6. 4 Participants Raw Scores on Upper Extremity Outcome Measures
Participant
CMSA
Arm
Range:
1-7
CMSA
Hand
Range:
1-7
FMA
Hand
Range:
0-14
CAHAI
Range:
13-91
3D TRI-
HFT (No
Blocks)
Range:
0-70
3D TRI-
HFT
(With
Blocks)
Range:
0-133
3D TRI-
HFT
Rod
(Range:
1-30 on
each
side)
3D TRI-HFT
Instrumented
cylinder
[Nm]
Range:
0-50
3D TRI-HFT
Instrumented
credit card
[N]
Range:
0-50
P31 2 2 2 18 10 11 0 0 15
P32 3 3 3 24 41 47 15 21 25
P33 2 2 0 22 10 11 0 0 1
P34 3 3 4 38 60 66 30 12.5 42.5
P35 2 2 2 25 10 11 0 10 35
P36 2 2 2 26 13 14 10 15 37.5
P39 2 2 2 30 10 11 20 29 50
P40 4 3 2 38 26 30 0 5 13
P42 7 2 2 54 45 51 15 8 35
Mean 3 2.33 2.11 30.56 25 28 10.7 11.6 28.2
Median 2 2 2 26 - - - - -
Range 5 1 4 36 - - - - -
25th
percentile
2
2
2
23
- - - - -
50th
percentile
2
2
2
26
- - - - -
75th
percentile
3.5
3
2.5
38
- - - - -
CMSA-Arm: Chedoke-McMaster Stroke Assessment (Impairment Inventory-stage of arm), CMSA-Hand: Chedoke-McMaster Stroke Assessment (Impairment
Inventory-stage of hand), FMA-Hand: Fugl-Meyer Assessment- hand, CAHAI: Chedoke-Arm and Hand Activity Inventory, 3D TRI-HFT: 3D printed Toronto
Rehabilitation institute-Hand Function test *All ranges are for each upper extremity separately except for the CAHAI, which uses bilateral upper extremities to perform test.

80
The inter and intra-rater reliability for the rectangular block’s component of the object
manipulation task could not be assessed as the assessors had difficulty identifying the blocks on
the videos based on their weight and texture.
Intra-rater reliability
There was a high intra-rater reliability for the object manipulation component (objects 1-10) of
the 3D TRI-HFT with an Intra-Class Correlation Co-efficient (ICC) score of 0.99 (95% CI:
0.985-0.999; P < 0.000) (Figure 6.2A).
Inter-rater reliability
The 3D TRI-HFT was found to have a strong inter-rater reliability for the object manipulation
component (object 1-10) of the test (Figure 6.2B). ICC across three assessors (NK, VZ, AY) was
0.998 (95% CI: 0.992-1.0; P < 0.000).
Figure 6. 2 Inter and Intra-rater Reliability of the 3D TRI-HFT
(A) (B)
(a)Scoring at two different time points by the same assessor (i.e. rating 1 and rating 2)
(b)Scoring by three different assessors at a single time point.
Construct Validity
The results showed that there was a statistically significant strong relationship between CMSA-
Arm and the object manipulation part of the 3D TRI-HFT (r = 0.843, p=0.01). A statistically
0
10
20
30
40
50
60
70
0 10 20 30 40 50 60 70
Intra-rater Reliability
0
10
20
30
40
50
60
70
0 1 2 3 4 5 6 7
Inter-rater Reliability Assessor AY
Assessor NK
Assessor VZ
Rating 1
R
ati
ng 2
Participants
3D
TR
I-H
FT
(O
bje
ct

81
significant moderate correlation was found between object manipulation of the 3D TRI-HFT and
FMA-Hand (r= 0.698, p=0.05) and CMSA-Hand (r=0.667, p=0.05). A moderate correlation was
found between object manipulation of the 3D TRI-HFT and CAHAI (r= 0.664, p=0.051),
however this correlation was not statistically significant.
For the strength measurement part of the 3D TRI-HFT test; including the rod, the
instrumented cylinder and the instrumented credit card; no statistically significant relationship
was found with any of the outcome measures i.e. CAHAI, CMSA-Arm, CMSA-Hand or FMA-
Hand. The relationship between the rod and the FMA-Hand approached statistical significance
(r=0.665, p=0.051).
6.4 Discussion
3D printing technology has existed for more than 30 years, but has only recently garnered
increased attention among scientists, engineers, and the public (176). The rise of 3D technology
is attributed to the availability of lower‐cost printers and breakthroughs in techniques and
processing. In the current study we established the feasibility of 3D printing the TRI-HFT. We
found that all objects of the TRI-HFT could be easily printed except for the triangular sponge
and the paper. The discrepancy in dimensions of the paper and sponge are limitations associated
with 3D printing process. However, it is important to note that the “paper” and “sponge” created
using the 3D technology have the look and design of the original objects and that the
modifications are a trade-off that needed to be accepted to make the test universally accessible
and reproducible. The sponge required a new design where it will have the properties of the
“sponge” but is now shaped as a square instead of a triangle. Today the TRI-HFT can be 3D
printed for ~ CAD $ 500. This cost will decline as 3D printers become cheaper. For reference,
the 3D printers costed ~ £175,000 (CAD $300,000) – £250,000 (CAD $ 400,000) in the 1990’s
and currently that price has decreased 10-fold with high end 3D printers costing ~ £10,000 (CAD
$ 20,000) – £35,000 (CAD $ 65,000) (176).
In our convenience sample of 9 individuals with chronic stroke we found that the 3D
printed TRI-HFT had high inter and intra-rater reliability and moderately strong construct
validity when compared to the CMSA and FMA. As seen from the results however it was not
possible to rate the 9 rectangular blocks with different weight and textures from the video

82
assessments. These are now modified (numbered) to have a clear indication of which block is
being manipulated and this indicator can be seen clearly on video recordings allowing for
grading from a video assessment.
Construct validity of the test was assessed as there are no outcome measures identified as
a gold standard for measurement of upper extremity function in the activity or body structure and
function domain of the ICF (58). The object manipulation component of the 3D TRI-HFT
showed a strong correlation with the CMSA-Arm whereas there was a moderately strong
correlation between 3D TRI-HFT and CMSA-Hand and the 3D TRI-HFT and FMA-Hand.
Although the scoring system was initially developed with the spinal cord population in mind, the
granular scoring system allows one to capture function equally effectively in stroke population as
well. Moreover, the test measures function from proximal to distal and allows the assessor to
differentiate between use of physiological versus compensatory grasping patterns. Since most of
the study participants had severe upper extremity impairment, distal function was severely
compromised, and subtle differences went undetected by both the CMSA- hand and the FMA-
Hand. The 3D TRI-HFT however not only successfully captured arm function as seen by the
strong relationship between 3D TRI-HFT and CMSA-Arm but also captured the subtle changes
in hand function.
We found no statistically significant relationship between CAHAI and 3D TRI-HFT. This
is not surprising given that CAHAI is designed to measure bilateral upper extremity function,
whereas 3D TRI-HFT is designed to measure unilateral upper extremity function. In CAHAI,
participants can score points by using the non-paretic hand to stabilize the object to assist the
paretic hand in grasping an object. Participants can also hold objects with both hands to reduce
the gravitational load and use the paretic hand as the supporting hand while the non-paretic hand
performs the accurate arm motions, supinations, and dextrous fine motor skills. Conversely, the
3D TRI-HFT isolates the portions of each task that can be performed unimanually.
We found no statistically significant relationship between the rod, instrumented cylinder
and instrumented credit card of the 3D TRI-HFT with any of the other measures. The rod in the
TRI-HFT is aimed at measuring the participant’s ability to withstand eccentric forces about the
upper extremity joints, the instrumented cylinder and the instrumented credit card are both
83
objective measures and they measure torque and grip strength in Nm and N, respectively using a
dynamometer. The scores on these measures are influenced by the strength of the upper
extremity muscles and neither the CMSA nor the FMA take into account the strength of the
muscles but are focused on synergies and movement isolation.
Existing upper extremity measures like the ARAT and the Fugl Meyer Scale commonly
used in clinical and research settings fail to meet the demands of these environments, which
experience shortages in time and personnel resources. The 3D TRI-HFT takes approximately
~11 mins to be administered on the affected upper extremity and is cost effective. Another
consideration is around importance of the findings of the current assessment tools to patients and
their care givers. Stroke survivors identified the outcomes of ‘Independence, freedom and
autonomy’, ‘Difficulty (with routine tasks)’ and ‘Everyday tasks’ as their three most important
outcomes (177). The objects used in the 3D TRI-HFT are objects commonly used in activities of
daily living. Besides, the scoring system measures the ability to manipulate these objects as they
would be manipulated during activities of daily living and hence the score on the 3D TRI-HFT
provides an objective measure of patient’s independence with these tasks. A recent review
conducted by Miller et al., quoted that though there are a 144 upper extremity outcome measures
being used in individuals with stroke none of these assessments measure what is important
to stroke survivors, their carers and clinicians (177).There are various other review articles in
literature that have looked at existing measures and most have concluded that there is no
consensus amongst clinicians regarding best practices related to use of outcome measures or that
existing tools are not sensitive to change in function and do not capture outcomes that are
important to stroke survivors, carers and clinicians (28, 45, 177-179).
The 3D printed version of the TRI-HFT was pursued to fill this is gap in the literature. 3D
printing technology is becoming increasing accessible, affordable and it ensures standardization
and reproducibility of the outcome assessment tool. As far as we know the TRI-HFT is the first
upper extremity measure that can be 3D printed, and hence can be accessed from anywhere in
the world. This is important for clinicians and researchers as it gives them easy access to a
reliable and valid tool. Further, the objects used in the test are day to day objects that can also be
used as therapy tools by clinicians. From a researcher perspective, having an outcome
assessment tool that is easy to manufacture in-house is important to reduce dependencies on
84
high-cost manufacturing and out of country equipment orders. In a review conducted by Galeoto
et al., the authors concluded that a universal, validated outcome measure is needed to allow
comparisons across practice and recommended that future researchers use a common set of
outcome assessments (180).
There are certain limitations to the study like the small sample size, homogenous study
sample with very limited upper extremity function and lack of gold standard outcome measures
for this population which prevented a more critical comparison of the 3D TRI-HFT. Nonetheless,
this test could be easily 3D printed and was found to be reliable and valid. Future studies will
look at expanding the psychometric testing to the acute and sub-acute stroke population as well
as those with higher levels of upper extremity function.
6.5 Conclusion
Our findings indicate that TRI-HFT is a 3D printable, simple, reliable, open source, and
valid measure that can be accessed from virtually anywhere in the world. The 3D printing of the
test guarantees high repeatability in object manufacturing and makes the test available to all
users with a 3D printer, which are now becoming ubiquitous. The test can be administered with
minimal to no training and produces outcomes that are meaningful not only to the professional
community but also to the patients themselves and their care givers.
6.6 Methods
For the purpose of 3D printing the TRI-HFT, the dimensions of the original test objects were
measured using calipers (precision level 0.01mm) and the weight of the objects were measured
using a kitchen scale (precision level 0.1 gm). These dimensions were used to create 3D printing
design files. Objects were printed on the Stratasys Fortus 450mc in Acrylonitrile Butadiene
Styrene (ABS) plastic with a resolution of 10 thou (~0.254 mm), with the exception of the golf
balls, die, paper, and credit cards, which were printed at a resolution of 5 thou (~0.125 mm).The
rectangular blocks of 200g and 300g were weighted with quarters once printed, in order to reach
the mass of the original objects. The 200g block was weighed with 28 Canadian quarters and the
300g block was weighed with 52 Canadian quarters. All printing files for the 3D TRI-HFT will
be made available at www.kite-uhn.com.

85
Psychometric testing of the 3D TRI-HFT was conducted in both the spinal cord injury
(under review in The Journal of Spinal Cord Medicine) and stroke population. The psychometric
properties of the 3D TRI-HFT were tested within a pilot study aimed at creating a novel and
usable robotic orthosis (MyHero Glove) to improve performance on functional tasks in
individuals with chronic stroke (181). The study was conducted at an outpatient clinic in a
rehabilitation hospital. Research Ethics Board approval for this study was obtained along with
the approval for the pilot study. Individuals greater than seven days post-stroke and with
moderate to severe impairment of hand function were recruited for this pilot study (181). The
inclusion criteria were: (a) stroke survivors greater than seven days post-stroke (b) moderate to
severe Stage of Hand 1 to 4 on the Chedoke-McMaster Stroke Assessment (c) able to understand
and speak English (d) able to give informed consent (e) able to attend at least one session at the
TRI site where they are located (f) passive range of motion of index finger proximal
interphalangeal joint greater than 45 degrees to allow for fitting the robotic glove. The exclusion
criteria were: (a) participants with a severe risk for skin breakdown under applied loads (b)
participants who are not able to verbally respond about their level of pain (c) participants with
severe pain (above 4 on the Pain Rating Scale) in their more affected fingers during massage or
active or passive extension (e.g. arthritis, fracture).
Consenting participants underwent a battery of upper extremity assessments including the
CAHAI (36), FMA-Hand (29), CMSA-Arm, and CMSA-Hand (182) and the 3D TRI-HFT. The
CAHAI is a validated, upper-limb measure that uses a 7-point quantitative scale to score each
item on the scale in order to assess functional recovery of the arm and hand after a stroke and has
demonstrated a high level of measurement quality and clinical utility (28). The total score on
the CAHAI ranges from 13-91. Similarly, the FMA-Hand has also demonstrated a high level
of measurement quality and clinical utility and is recommended for assessment of upper
extremity function in research and clinical practice (28). The CMSA-Arm and CMSA-Hand is
an assessment tool used to measure physical impairment and it assesses stages of recovery
of arm and hand on a 7-point scale.
All participants completed all the above measures in one session with and without the
robotic glove and were rated by the assessor (AY). To address, inter and intra-rater reliability,
and construct validity, participant performance on the first component of the 3D TRI-HFT, i.e.

86
object manipulation without the robotic glove, was video recorded. Prior to the start of the study
the assessor (AY) was introduced to the 3D TRI-HFT and received a one-time 30 min training
session on how to administer and score the test. The 3D TRI-HFT video recorded assessments
were reviewed by two independent assessors (NK- Physiotherapist and VZ- Physician) for
reliability testing. Inter-rater reliability was assessed between all three assessors (NK, VZ, AY).
Construct validity was assessed by comparing scores on the 3D TRI-HFT with the scores on
CAHAI, FMA-Hand and CMSA.
Statistical Analysis:
All statistical procedures were conducted using SPSS version 16 (SPSS, Inc., USA). A p value of
significance was set at < 0.05. The following statistical procedures were used for psychometric
testing:
Inter-rater reliability
For the purpose of inter-rater reliability scores by all three assessors (AY, NK, VZ) were
compared using the ICC (n=7). Two participant videos were not available for testing.
Intra-rater Reliability
For the purpose of intra-rater reliability, assessors NK and VZ reviewed the participant videos
one month apart and re-rated the performance on individual tasks (n=14). The scores from the
two time points were compared using the ICC. Two participant videos were not available for
testing.
Construct validity
The construct validity of the 3D TRI-HFT was established by computing Spearman’s correlation
coefficient with the CAHAI, CMSA-Arm, CMSA-Hand and the FMA-Hand scores (n=9). An r
value of 0.0 to 0.4 was considered as weak correlation, 0.4 to 0.7 was considered as moderate
correlation, and above 0.7 was considered as strong correlation (164).
87
Chapter 7 Preliminary Evaluation of the Reliability and Validity of the 3D Printed Toronto Rehabilitation Institute-Hand Function Test in
Individuals with Spinal Cord Injury
In this chapter, the results of a pilot study investigating the psychometric properties of the 3D
printed Toronto Rehabilitation Institute-Hand Function Test in sub-acute and chronic spinal cord
injury are presented. This manuscript is a part of the current thesis projects.
Naaz Kapadia, Lazar I Jovanovic, Kristin Musselman, Rosalie H. Wang, Cesar Marquez-Chin
and Milos R. Popovic. 3D printed Toronto Rehabilitation Institute-Hand Function Test:
Assessment of Gross Motor Function in Spinal Cord injury. Under review in The Journal of
Spinal Cord Medicine. April 2021.
7.1 Abstract
Objective: The study objective was to evaluate the inter-rater and intra-rater reliability, and
criterion and construct validity of the 3D printed Toronto Rehabilitation Institute-Hand Function
Test (3D TRI-HFT) in individuals with spinal cord injury (SCI).
Design: Single arm interventional study
Setting: Inpatient Rehabilitation Hospital
Participants: 4 individuals with subacute and 3 individuals with chronic SCI
Interventions: Reliability and validity of the 3D TRI-HFT was assessed within two interventional
studies.
Outcome Measures: Participants performed the 3D TRI-HFT, Graded Redefined Assessment of
Strength, Sensibility and Prehension (GRASSP- Appendix 6), Functional Independence Measure
(FIM- Appendix 7) and the Spinal Cord Independence Measure (SCIM- Appendix 8) at baseline,
after 20 and 40 sessions of therapy and at 6 months follow-up from baseline. The 3D TRI-HFT
assessments were video recorded. All assessments were graded at the time of performance and
re-graded from the video recordings for the purpose of reliability testing. Construct validity was

88
tested by comparing the scores on 3D TRI-HFT with the FIM and SCIM self-care sub-scores.
Criterion validity was tested by comparing the scores on 3D TRI-HFT with the scores on various
components of GRASSP.
Results: The 3D TRI-HFT had high intra-rater and inter-rater reliability in sub-acute and chronic
SCI. Moderate to strong correlations were found between the 3D TRI-HFT object manipulation
scores and the FIM and SCIM self-care sub-scores. Strong correlations were found between the
various components of GRASSP and the 3D TRI-HFT.
Conclusions: The 3D TRI-HFT is a reliable and valid measure to assess unilateral hand gross
motor function in individuals with SCI.
7.2 Introduction
Amongst the spinal cord injury (SCI) population, 59.9% have tetraplegia and their highest
priority is to regain upper extremity function (91, 183). Rehabilitation is the mainstay of
treatment for retraining function. To scientifically evaluate novel interventions, researchers need
access to reliable, valid, easy to use and universally accessible clinical outcome assessment tools
that can be administered within reasonable time frames. Although there are many tests of hand
function, few reliable and valid assessments have been developed for SCI (94, 143, 147, 157,
184-186). Hand function tests such as the Action Research Arm Test and the Jebsen Hand
Function test are not recommended for use in the SCI population as they are not specifically
developed for the patterns of grasp impairments present in these individuals. The Grasp and
Release Test is a time-based test and although developed for the SCI population is specifically
recommended in chronic SCI and for studies of upper limb orthoses, FES, and reconstructive
procedures (97). It does not take into account proximal arm function. The first working group of
the International Campaign for Cures of SCI Paralysis aptly recognized that “no SCI therapy will
be considered effective for the treatment of patients unless it improves the ability of patients to
function in their daily routines or activities (187)”. This requires assessments that go beyond
pathophysiology or impairment and are based on the concept of the International Classification
of Functioning, Disability and Health (ICF) (188). In a review done by Jones et al. (92), the
authors identified two outcome measures that are SCI specific upper extremity measures in the

89
activity domain. These measures are the Graded Redefined Assessment of Strength, Sensibility
and Prehension (GRASSP) and the Capabilities of Upper Extremity Function- Test (CUE-T).
The GRASSP is a quantitative impairment measure designed for use in acute and chronic
cervical SCI. It includes five subtests: (i) Strength, (ii) Sensation-Dorsal, (iii) Sensation-Palmar,
(iv) Prehension ability (Qualitative Prehension) and (v) Prehension performance (Quantitative
Prehension) (155) and was developed to address the void in the availability of SCI measures that
detect functional capacity of the hand (156). Sub-tests (i) to (iii) assess function under the body
structure and function domain of the ICF while (iv) and (v) assess function in the activity
domain. The Quantitative Prehension component is a timed test that does not consider proximal
function or quality of movement. The test takes approximately 1-1.5 hour to administer on
bilateral upper extremities and often cannot be tolerated by acute and sub-acute SCI patients
requiring the assessment to be completed over 2 days. It is custom manufactured and difficult to
self fabricate however, can be purchased online for ~ CAD $2,500. There is a 2-day training
module to become certified to perform the test. So, although the psychometric properties of the
test have been established in SCI the above barriers reduce its uptake by clinicians and
researchers.
The CUE-T is intended to evaluate functional limitations as described by Marino RJ
(189) and is validated in SCI. It consists of 19 items, 17 of which are unilateral and test basic
upper limb actions and grasp patterns. It evaluates upper extremity actions such as reaching,
lifting, pulling, and pushing in addition to various grasp patterns. Most items are scored based on
time or number of repetitions in 30 secs and are then scored on a 0-4 scale. The test takes
approximately 1 hour to administer and does not integrate the use of the arm and hand in
activities of daily living. Grasping tasks must be completed using a designated grasp pattern. The
test intends to assess the action, not the task (189).
Amongst the other widely used measures are the Functional Independence Measure
(FIM) (161) and the Spinal Cord Independence Measure (SCIM) (162), both of which have been
validated in the SCI population (162,190). Both these scales measure function in the activity domain.
However, both scales are administered as questionnaires and hence are subjective in nature. It is
important to note that even though the nature of the SCIM-III is subjective, the self-care
90
subcategory provides results which are in very high accordance with the results of an examiner
(191).
In light of the above, we developed the Toronto Rehabilitation Institute-Hand Function
Test (TRI-HFT) in 2012 (98). The TRI-HFT is a test to measure unilateral gross motor function
of the upper extremity and has been validated in individuals with sub-acute SCI (98). It consists
of 2 parts. The first part of the test assesses the individuals’ ability to manipulate the following
objects: (1) mug, (2) book, (3) soda can, (4) isosceles triangular sponge, (5) wireless home
telephone, (6) paper sheet, (7) Ziploc bag filled with 5 golf balls, (8) dice, (9) credit card, (10)
pencil and (11) 9 rectangular blocks in sets of 3x100g, 3x200g and 3x300g. Each of the 3 blocks
in each weight category have surfaces with different levels of friction. The second part measures
the ability to withstand eccentric forces (Rod test), the strength of lateral pinch in Newtons using
a dynamometer (instrumented credit card test) and the strength of palmar grasp in Nm using a
dynamometer (instrumented cylinder). The scoring system for the first part of the test is on a
scale of 0-7, where greater scores indicate better performance. Further details on the original test
objects, administration and scoring are described in Kapadia et al., (98).
While the TRI-HFT has potential for high clinical utility (i.e. low cost, minimal training
required to administer), a limitation to its use has been accessibility. Until now the objects
required for the TRI-HFT had to be acquired from the researchers who developed the measure.
To make it more easily accessible we replicated the test in a 3D printed format. The objects of
the first and second part of the test were successfully printed except for paper and sponge which
needed some modification. For details of the 3D printed version please refer to Kapadia et al.,
2020 (192).
The objective of the current study was to test the psychometric properties of the 3D
printed Toronto Rehabilitation Institute-Hand Function Test (3D TRI-HFT) in individuals with
sub-acute (injury less than 6 months at the time of assessment) and chronic (injury at least 24
months prior to the assessment) SCI. Specifically, we assessed the inter-rater reliability, intra-
rater reliability and construct (convergent) and criterion validity of the 3D TRI-HFT within two
interventional studies.

91
7.3 Methods
The psychometric properties of the 3D TRI-HFT were assessed in the sub-acute and chronic SCI
population, within two single arm interventional studies aimed at assessing the feasibility and
efficacy of EEG-Triggered FES Therapy for upper limb rehabilitation. Inclusion criteria for
study 1 were: (a) traumatic SCI classified as American Spinal Injury Association Impairment
Scale (AIS) B-D, (b) SCI less than 6 months prior to baseline assessment, (c) neurological level
of injury between C4 to C7 and (d) expected length of stay of at least 80 days at the time of study
initiation. The exclusion criteria were (a) history of seizure disorder not effectively managed by
seizure medications, (b) an existing electrical stimulation device (e.g. implantable cardioverter
defibrillator, pacemaker, spinal stimulation), (c) rash or open wound at electrode site, (d)
denervation of the targeted muscles, (e) poorly controlled autonomic dysreflexia, (f) botulinum
toxin injection into affected upper extremity within 3 months prior to the study start, and (g)
currently enrolled in another upper limb study. Inclusion criteria for study 2 were: (a) traumatic
SCI classified as AIS B-D and (b) SCI at least 24 months prior to the baseline assessment. The
exclusion criteria were same as the sub-acute study.
Participants in both studies underwent a battery of assessments at baseline, after 20
sessions of therapy (sessions were carried out 3 to 5 times a week), at discharge (after 40
sessions of therapy) and at 6-months follow-up. These assessments included: (a) FIM (161), (b)
SCIM (162), (c) 3D TRI-HFT and (d) GRASSP (155) and were completed in one session for
both studies. The 3D TRI-HFT was video recorded for assessing inter and intra-rater reliability.
For construct (convergent) validity, scores on the 3D TRI-HFT were correlated with scores on
the self-care sub-scale of the FIM and SCIM. For the assessment of criterion validity, scores on
the 3D TRI-HFT were correlated with scores on the different components of the GRASSP, i.e.
strength, sensation, qualitative and quantitative prehension. The strong psychometric properties
of the GRASSP have led to its use in clinical trials to evaluate primary endpoints related to hand
function (193-196) and this was the reason we choose to use this test for validity testing. The
FIM and SCIM are validated measures in the SCI population (155, 161, 162). For testing
reliability and validity, scores of the left and right upper extremities as well as scores at each
time point were treated as separate independent data points.

92
Assessors: Two assessors with ~10 years of experience doing SCI research were involved
in the psychometric testing of the 3D TRI-HFT. All in-person assessments for both the studies
were carried out by a Research Associate (AB-Physician by training) and all video recorded
assessments were rated by another Research Associate (CD-Physical therapist by training). Both
assessors have 8 years on and off experience with the use of the original version of the TRI-HFT
however they did not receive any additional training for the use of the 3D printed version.
Statistical Analysis was performed as below:
Inter-rater Reliability
The inter-rater reliability of the first component of the test, i.e. object manipulation component
which includes the ten objects and the set of 9 rectangular blocks, was assessed. For inter-rater
reliability, the de-identified video recording from both studies were reviewed by CD and each
task was scored. The scores were then compared to the scores from the original testing
performed by AB. Intraclass correlation coefficient (ICC) were calculated using SPSS version 16
(SPSS, Inc., USA).
Intra-rater Reliability
For the purpose of intra-rater reliability, AB and CD reviewed the participant videos from both
the studies, one month apart and re-rated the participant performance on individual tasks at both
time points. ICC was calculated using SPSS version 16 (SPSS, Inc., USA).
Construct (convergent) and Criterion Validity
The construct (convergent) validity of the 3D TRI-HFT was evaluated by computing Spearman’s
correlation coefficient with the FIM self-care sub-score and the SCIM self-care sub-score. The
criterion validity of the 3D TRI-HFT was established by computing Spearman’s correlation
coefficient’s with the strength, sensation, qualitative prehension and quantitative prehension
scores of the GRASSP. An r value of 0.0 to 0.4 was considered as weak correlation, 0.4 to 0.7
was considered as moderate correlation, and anything above 0.7 was considered as strong
correlation (164). For all statistical procedures, α was set at < 0.05.

93
7.4 Results
For the sub-acute study 4 participants’ data collected at 3 time points in the study, were analyzed.
All 4 participants completed all the outcome assessments at all time points except one participant
who missed one assessment. Inter-rater reliability was determined using 22 datasets (n= (4
participants x3 time points)-1missed appointment X 2 (left and right UE)). For intra-rater
reliability AB and CD re-assessed the participant videos and scored them again (n=44). For
assessing construct validity and criterion validity, scores on the right and left hand as well as at
each time point were treated as independent data points (n=22).
For the chronic study, 3 participants were recruited and assessed at 4 time points except
one participant who missed one assessment. Inter-rater reliability was determined using 22
datasets and intra-rater reliability was determined using 44 datasets (both AB and CD reassessed
the videos). For assessing construct validity and criterion validity scores for the right and left
hand as well as at each time point were treated as independent data points (n=22).
Participant demographics, FIM and SCIM self-care sub-scores for both the studies are
described in Table 7.1 whereas raw scores on the 3D TRI-HFT and GRASSP are presented in
Tables 7.2 and 7.3.
Table 7. 1 Participant Demographics
Participant
ID
Sex Age
Level
of
injury
AIS FIM Self-Care SCIM Self-Care
Baseline Midpoint D F Baseline Midpoint D F
Sub-acute
group
AAOF M 66 C4 C 6 N 18 N 0 N 9 N
AAOG F 72 C4 C 16 23 26 N 5 10 13 N
AAOH M 37 C4 B 6 6 6 N 0 0 0 N
AAOI M 58 C4 D 15 32 35 N 2 16 16 N
AAOJ F 26 C5 B 8 8 N N 2 2 N N
Chronic
group
AAOA M 31 C4 B 6 6 6 6 0 N 0 0
AAOB M 53 C4 C 7 9 10 10 1 2 2 2
AAOC F 31 C4 C 7 7 7 N 1 1 1 N

94
M - male; F - Female; AIS - American Spinal Injury Association Impairment Scale; FIM - Functional Independence
Measure; SCIM - Spinal Cord Independence Measure; D - Discharge; F: Follow-up; AAOJ-data not included in the
analysis as participant dropped out.
Inter-rater Reliability
For both the sub-acute and chronic SCI study, we found a statistically significant strong
correlation between the two assessors for the 10-object manipulation component of the 3D TRI-
HFT with an ICC= 0.994 (95% CI: 0.985-0.998; P < 0.000) (Figure 7.1(a)) and ICC=0.990 (95%
CI:0.976-0.996; P < 0.000) respectively. The inter-rater reliability for the 9 rectangular blocks
could not be assessed for both studies as the assessor had difficulty identifying the blocks based
on their weight and texture from the video recorded assessments.
Intra-rater Reliability
We found statistically significant strong correlation between the first and second rating on the
10-object manipulation component of the TRI-HFT within each assessor. ICC values for the sub-
acute and chronic study are ICC= 0.995 (95% CI: 0.992-0.998; P < 0.000) (Figure 7.1(b)) and
ICC= 0.999 ((95% CI: 0.999-1.00; P < 0.000) respectively.
Figure 7. 1 Inter and Intra-rater Reliability of the 3D TRI-HFT in SCI
(a) (b)
(a) Inter-rater Reliability of the 10-object manipulation component of the 3D TRI-HFT in sub-acute SCI, (b) Intra-
rater Reliability of the 10-object manipulation component of the 3D TRI-HFT in sub-acute SCI.
0
10
20
30
40
50
60
70
0 10 20 30 40 50 60 700
10
20
30
40
50
60
70
0 10 20 30 40 50 60 70
Rater 1
Rat
er 2
Grading 1
Gra
din
g 2

95
Construct and Criterion Validity
Sub-acute SCI Study
The results showed a moderately strong correlation between the FIM selfcare sub-score and the
10-object manipulation component of the 3D TRI-HFT with an r= 0.770 (95% CI: 0.567-0.890,
p=0.01) and the rectangular blocks with an r=0.760 (95% CI: 0.535-0.887, p=0.01). Similarly,
we found a moderately strong correlation between the SCIM self-care sub-score and the 10-
object manipulation component with an r= 0.769 (95% CI: 0.547-0.894, p=0.0) and the
rectangular blocks with an r=0.758, (95% CI: 0.533-0.875, p=0.01).
The 10-object manipulation component showed very strong correlation with the Strength
(r=0.946; 95% CI: 0.830-0.986 p=0.01), Qualitative Prehension (r=0.951; 95% CI: 0.856-0.982
p=0.01) and Quantitative Prehension (r=0.974; 95% CI: 0.0.920-0.991 p=0.01) (Figure 7.2(a))
components of the GRASSP. However, it had a moderate correlation with the Sensation
component of the GRASSP (r=0.523; 95% CI: 0.126-0.740 p=0.05). Similarly, the rectangular
blocks showed a very strong correlation with the Strength (r=0.918; 95% CI: 0.770-0.968,
p=0.01), Qualitative Prehension (r=0.941; 95% CI: 0.854-0.978 p=0.01) and Quantitative
Prehension (r=0.938; 95% CI: 0.830-0.976 p=0.01) components of the GRASSP, but had a
moderate correlation with the Sensation component (r=0.512; 95% CI: 0.115-0.749 p=0.05).The
instrumented cylinder, instrumented credit card and the rod also showed strong to very strong
correlations with all components of the GRASSP except sensation with which it showed only
weak correlations. For correlations with individual test components please refer to Table 7.4.

96
Table 7. 2 3D Toronto Rehabilitation Institute-Hand Function Test Scores
Sub-acute group Chronic group
Participant ID AAOF AAOG AAOH AAOI AAOJ AAOA AAOB AAOC
L R L R L R L R L R L R L R L R
TRI-HFT
Object manipulation
B 10 28 56 24 0 10 0 65 16 16 0 0 10 50 30 0
M N N 68 26 10 18 50 70 N N 0 0 10 58 30 0
D 60 67 68 40 10 24 60 70 20 21 0 0 10 58 42 0
F N N N N N N N N N N 0 0 10 54 N N
Rectangular blocks
B 17 38 50 18 0 9 0 52 18 18 0 0 9 38 22 0
M N N 63 22 9 22 50 63 N N 0 0 9 54 22 0
D 54 54 63 28 9 18 54 63 18 18 0 0 9 54 40 0
F N N N N N N N N N N 0 0 9 54 N N
Instrumented cylinder
B 0 0 2 0 0 0 0 12.5 0 0 0 0 0 8 0 0
M N N 5 1 0 0 0 19 N N 0 0 0 8 0 0
D 4 15 9 0 0 0 6 25 0 0 0 0 0 6 2 0
F N N N N N N N N N N 0 0 0 10 N N
Credit card
B 0 0 1 0 0 0 0 11 0 0 0 0 21 22 0 0
M N N 4 0 0 0 6 38 N N 0 0 0 25 0 0
D 4 14 10 0 0 0 24 50 0 0 0 0 7 42 2 0
F N N N N N N N N N N 0 0 0 24 N N
Rod
B 0 0 15 0 0 0 0 39 0 0 0 0 0 0 0 0
M N N 30 0 0 0 0 60 N N 0 0 0 25 0 0
D 20 48 47 0 0 0 35 60 0 0 0 0 0 17 0 0
F N N N N N N N N N N 0 0 0 38 N N
L = left hand; R = right hand; B = baseline; M = midpoint; D = discharge; F = six month follow up. N – not
available; *AAOJ: data not included in the analysis as participant dropped out and video not available for the
assessment.
Figure 7. 2 Criterion Validity of the 3D TRI-HFT with the GRASSP
(a) (b)
0
10
20
30
0 10 20 30 40 50 60 70
0
10
20
30
0 10 20 30 40 50 60 70
3D TRI-HFT Object Manipulation
GR
AS
SP
- Q
uan
tita
tiv
e P
rehen
sion
3D TRI-HFT Object Manipulation
GR
AS
SP
- Q
uan
tita
tive
Pre
hen
sion
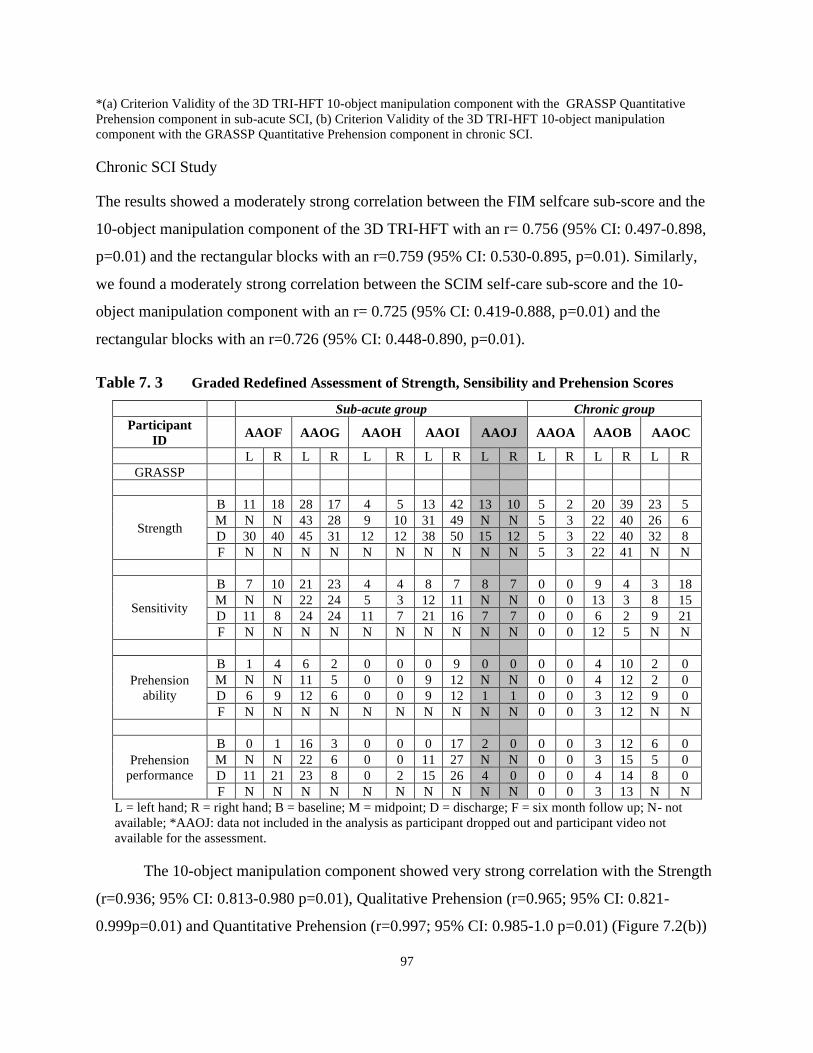
97
*(a) Criterion Validity of the 3D TRI-HFT 10-object manipulation component with the GRASSP Quantitative
Prehension component in sub-acute SCI, (b) Criterion Validity of the 3D TRI-HFT 10-object manipulation
component with the GRASSP Quantitative Prehension component in chronic SCI.
Chronic SCI Study
The results showed a moderately strong correlation between the FIM selfcare sub-score and the
10-object manipulation component of the 3D TRI-HFT with an r= 0.756 (95% CI: 0.497-0.898,
p=0.01) and the rectangular blocks with an r=0.759 (95% CI: 0.530-0.895, p=0.01). Similarly,
we found a moderately strong correlation between the SCIM self-care sub-score and the 10-
object manipulation component with an r= 0.725 (95% CI: 0.419-0.888, p=0.01) and the
rectangular blocks with an r=0.726 (95% CI: 0.448-0.890, p=0.01).
Table 7. 3 Graded Redefined Assessment of Strength, Sensibility and Prehension Scores
Sub-acute group Chronic group
Participant
ID AAOF AAOG AAOH AAOI AAOJ AAOA AAOB AAOC
L R L R L R L R L R L R L R L R
GRASSP
Strength
B 11 18 28 17 4 5 13 42 13 10 5 2 20 39 23 5
M N N 43 28 9 10 31 49 N N 5 3 22 40 26 6
D 30 40 45 31 12 12 38 50 15 12 5 3 22 40 32 8
F N N N N N N N N N N 5 3 22 41 N N
Sensitivity
B 7 10 21 23 4 4 8 7 8 7 0 0 9 4 3 18
M N N 22 24 5 3 12 11 N N 0 0 13 3 8 15
D 11 8 24 24 11 7 21 16 7 7 0 0 6 2 9 21
F N N N N N N N N N N 0 0 12 5 N N
Prehension
ability
B 1 4 6 2 0 0 0 9 0 0 0 0 4 10 2 0
M N N 11 5 0 0 9 12 N N 0 0 4 12 2 0
D 6 9 12 6 0 0 9 12 1 1 0 0 3 12 9 0
F N N N N N N N N N N 0 0 3 12 N N
Prehension
performance
B 0 1 16 3 0 0 0 17 2 0 0 0 3 12 6 0
M N N 22 6 0 0 11 27 N N 0 0 3 15 5 0
D 11 21 23 8 0 2 15 26 4 0 0 0 4 14 8 0
F N N N N N N N N N N 0 0 3 13 N N
L = left hand; R = right hand; B = baseline; M = midpoint; D = discharge; F = six month follow up; N- not
available; *AAOJ: data not included in the analysis as participant dropped out and participant video not
available for the assessment.
The 10-object manipulation component showed very strong correlation with the Strength
(r=0.936; 95% CI: 0.813-0.980 p=0.01), Qualitative Prehension (r=0.965; 95% CI: 0.821-
0.999p=0.01) and Quantitative Prehension (r=0.997; 95% CI: 0.985-1.0 p=0.01) (Figure 7.2(b))
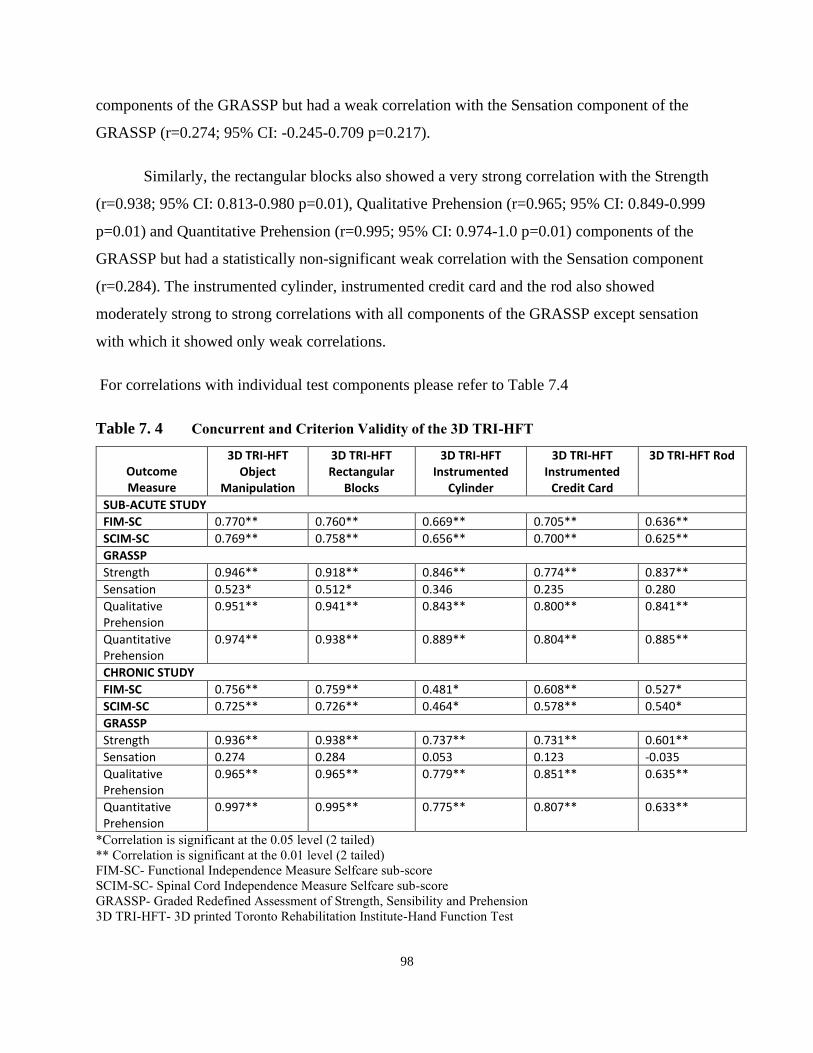
98
components of the GRASSP but had a weak correlation with the Sensation component of the
GRASSP (r=0.274; 95% CI: -0.245-0.709 p=0.217).
Similarly, the rectangular blocks also showed a very strong correlation with the Strength
(r=0.938; 95% CI: 0.813-0.980 p=0.01), Qualitative Prehension (r=0.965; 95% CI: 0.849-0.999
p=0.01) and Quantitative Prehension (r=0.995; 95% CI: 0.974-1.0 p=0.01) components of the
GRASSP but had a statistically non-significant weak correlation with the Sensation component
(r=0.284). The instrumented cylinder, instrumented credit card and the rod also showed
moderately strong to strong correlations with all components of the GRASSP except sensation
with which it showed only weak correlations.
For correlations with individual test components please refer to Table 7.4
Table 7. 4 Concurrent and Criterion Validity of the 3D TRI-HFT
Outcome Measure
3D TRI-HFT Object
Manipulation
3D TRI-HFT Rectangular
Blocks
3D TRI-HFT Instrumented
Cylinder
3D TRI-HFT Instrumented
Credit Card
3D TRI-HFT Rod
SUB-ACUTE STUDY
FIM-SC 0.770** 0.760** 0.669** 0.705** 0.636**
SCIM-SC 0.769** 0.758** 0.656** 0.700** 0.625**
GRASSP
Strength 0.946** 0.918** 0.846** 0.774** 0.837**
Sensation 0.523* 0.512* 0.346 0.235 0.280
Qualitative Prehension
0.951** 0.941** 0.843** 0.800** 0.841**
Quantitative Prehension
0.974** 0.938** 0.889** 0.804** 0.885**
CHRONIC STUDY
FIM-SC 0.756** 0.759** 0.481* 0.608** 0.527*
SCIM-SC 0.725** 0.726** 0.464* 0.578** 0.540*
GRASSP
Strength 0.936** 0.938** 0.737** 0.731** 0.601**
Sensation 0.274 0.284 0.053 0.123 -0.035
Qualitative Prehension
0.965** 0.965** 0.779** 0.851** 0.635**
Quantitative Prehension
0.997** 0.995** 0.775** 0.807** 0.633**
*Correlation is significant at the 0.05 level (2 tailed)
** Correlation is significant at the 0.01 level (2 tailed)
FIM-SC- Functional Independence Measure Selfcare sub-score
SCIM-SC- Spinal Cord Independence Measure Selfcare sub-score
GRASSP- Graded Redefined Assessment of Strength, Sensibility and Prehension
3D TRI-HFT- 3D printed Toronto Rehabilitation Institute-Hand Function Test

99
7.5 Discussion
In this study we assessed the psychometric properties of the 3D TRI-HFT in individuals with
SCI. To the best of our knowledge this is the first validated tool for use in SCI that can be 3D
printed and hence will have universal accessibility. Furthermore, since the test is 3D printed, it
practically eliminates variability related to test manufacturing, which at the present time is
impossible with other hand function tests. In other words, except for the 3D TRI-HFT, other
upper limb tests may have variability in production of the test items, which in turn affects the test
scoring, accuracy and ultimately reproducibility of results (192).
Whilst the 10-object manipulation component of the 3D TRI-HFT showed high inter- and
intra-rater reliability, the reliability of the rectangular blocks could not be assessed as it was
difficult to identify the blocks based on weight and texture on the videos. The 9 blocks are now
numbered for easy identification.
The moderately strong correlations of scores on the 3D TRI-HFT with the FIM and
SCIM selfcare sub-scores is an expected finding given that FIM and SCIM also measure function
at an activity level. In the study by Kalsi-Ryan et al., which looked at the psychometric
properties of the GRASSP, the authors showed similar correlations between scores on the
GRASSP and the FIM and SCIM selfcare sub-scores(102). The FIM and SCIM have
documented floor and ceiling effects (190, 197) and are unable to detect change at either end of
the functional spectrum.
The first part of the 3D TRI-HFT showed strong correlations with the strength,
qualitative and quantitative components of the GRASSP, in both sub-acute and chronic SCI
studies. This finding affirms that it produces the same information about a person’s upper
extremity function as the Qualitative and Quantitative components of the GRASSP. The first part
of the 3D TRI-HFT showed moderate correlations with the sensation component of the GRASSP
in the sub-acute SCI population. This finding is not surprising as the literature has shown poor
correlations between sensory impairment and motor function. These findings are supported by
Kalsi-Ryan et al., as well where the authors showed moderate correlations between International
Standard for Neurological Classification of Spinal Cord Injury-Upper Extremity Motor Scores
(ISNCSCI-UEMS) and sensation (184).
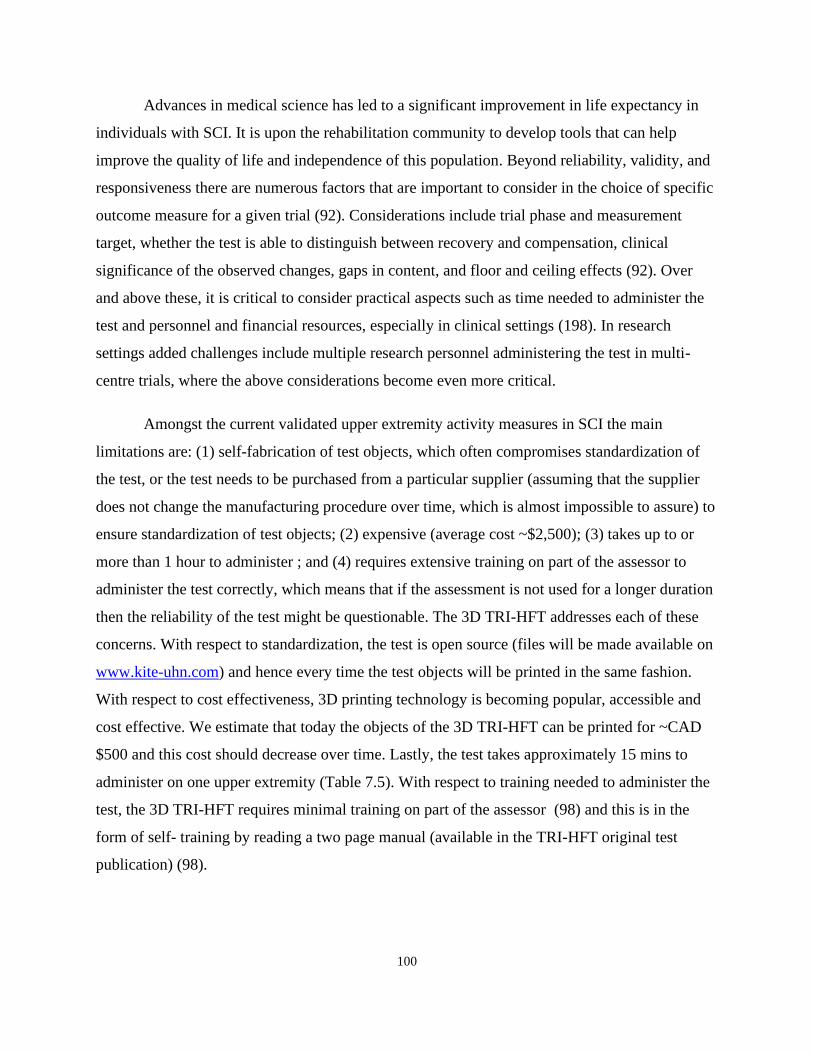
100
Advances in medical science has led to a significant improvement in life expectancy in
individuals with SCI. It is upon the rehabilitation community to develop tools that can help
improve the quality of life and independence of this population. Beyond reliability, validity, and
responsiveness there are numerous factors that are important to consider in the choice of specific
outcome measure for a given trial (92). Considerations include trial phase and measurement
target, whether the test is able to distinguish between recovery and compensation, clinical
significance of the observed changes, gaps in content, and floor and ceiling effects (92). Over
and above these, it is critical to consider practical aspects such as time needed to administer the
test and personnel and financial resources, especially in clinical settings (198). In research
settings added challenges include multiple research personnel administering the test in multi-
centre trials, where the above considerations become even more critical.
Amongst the current validated upper extremity activity measures in SCI the main
limitations are: (1) self-fabrication of test objects, which often compromises standardization of
the test, or the test needs to be purchased from a particular supplier (assuming that the supplier
does not change the manufacturing procedure over time, which is almost impossible to assure) to
ensure standardization of test objects; (2) expensive (average cost ~$2,500); (3) takes up to or
more than 1 hour to administer ; and (4) requires extensive training on part of the assessor to
administer the test correctly, which means that if the assessment is not used for a longer duration
then the reliability of the test might be questionable. The 3D TRI-HFT addresses each of these
concerns. With respect to standardization, the test is open source (files will be made available on
www.kite-uhn.com) and hence every time the test objects will be printed in the same fashion.
With respect to cost effectiveness, 3D printing technology is becoming popular, accessible and
cost effective. We estimate that today the objects of the 3D TRI-HFT can be printed for ~CAD
$500 and this cost should decrease over time. Lastly, the test takes approximately 15 mins to
administer on one upper extremity (Table 7.5). With respect to training needed to administer the
test, the 3D TRI-HFT requires minimal training on part of the assessor (98) and this is in the
form of self- training by reading a two page manual (available in the TRI-HFT original test
publication) (98).
101
Table 7. 5 Time Taken (in minutes) to Complete the 3D TRI-HFT* for B/L Upper Extremities
for All Study Participants
Participant
ID
AAOF AAOG AAOH AAOI AAOJ AAOA AAOB AAOC
Time point
Baseline 14:43 11:38 2:06 11:08 5:25 3:13 18:31 6:21
Mid-point N 13:53 12:10 14:33 N 0:46 16:55 13:51
Discharge 19:07 11:41 11:52 13:33 13:25 0:04 19:00 12:27
Follow-up N N N N N 0:40 18:08 N
*Tasks that were video recorded and timed include 10 object manipulation, 9 rectangular blocks and the
rod test for Bilateral upper extremities.
An added benefit of the 3D TRI-HFT is that since the tasks are routinely used in
everyday life the results of the test are meaningful to the patients and their care providers too. By
successfully completing a component of the 3D TRI-HFT the patient is shown that they can
perform a particular object grasping and manipulation task. The other advantage, specifically in
research settings, is that since it is universally accessible, if used uniformly across clinical trials,
it will enable researchers across the globe to compare interventions that affect upper limb
function and share the data.
7.6 Conclusion
In summary, the 3D TRI-HFT is an open-source test that is simple, reliable, valid and takes up to
15 min to administer. In the context of interventional trials, it may be recommended to be used as
an adjunct measurement to strength and sensibility measurements. It can be easily incorporated
in SCI rehabilitation clinics worldwide with minimal expense to the user and since the objects
are everyday objects they can double-up as therapy tools where appropriate.

102
Chapter 8 Feasibility and Significance of Stimulating Interscapular Muscles Using Transcutaneous Functional Electrical Stimulation in Able
Bodied Individuals
In this chapter, the feasibility of stimulating Lower Trapezius, Upper Trapezius and Serratus
Anterior along with Anterior Deltoid and Middle Deltoid was studied and the influence of
stimulating these interscapular muscles along with shoulder prime movers during shoulder flexion
and shoulder abduction was explored. This manuscript is under review.
Naaz Kapadia, Bastien Moineau, Melissa Marquez-Chin, Mathew Myers, Kai Lon Fok, Kei
Masani and Milos R. Popovic. Feasibility and significance of stimulating interscapular muscles
using transcutaneous functional electrical stimulation in able bodied individuals. Under review in
The Journal of Spinal Cord Medicine. Nov 2020 (Invited manuscript for the JSCM National SCI
2021Special Issue).
8.1 Abstract
Objective: The study objective was to assess the feasibility of stimulating lower trapezius (LT),
upper trapezius (UT) and serratus anterior (SA) muscles along with anterior or middle deltoid,
using surface functional electrical stimulation (FES). The secondary aim was to understand the
effects of LT, UT and SA stimulation on maximum arm reach achieved in shoulder flexion and
abduction.
Design: Single arm interventional study
Setting: Inpatient Rehabilitation Hospital
Participants: Ten healthy volunteers
Intervention: Participants completed 10 trials for each of the 3 conditions in flexion and
abduction, i.e. (1) Active voluntary flexion or abduction, (2) FES for anterior deltoid for flexion
or middle deltoid for abduction, and (3) FES for LT, UT and SA along with anterior deltoid for
flexion or along with middle deltoid for abduction.

103
Outcome Measures: Maximum arm reach and percent angle relative to the voluntary movement
were computed from motion capture data for each condition. Wilcoxon signed rank test was used
to compare the maximum reach between the two FES conditions.
Results: The study results showed that all three of the interscapular muscles can be stimulated
using surface FES. Maximum reach in abduction was greater for FES of middle deltoid along
with the interscapular muscles (51.77°±17.54°) compared to FES for middle deltoid alone
(43.76°±15.32°; Z = -2.701, p = 0.007). Maximum reach in flexion for FES of anterior deltoid
along with interscapular muscles was similar to that during FES of anterior deltoid alone.
Conclusion: Surface FES devices can effectively stimulate interscapular muscles and should be
engaged during upper extremity rehabilitation.
8.2 Introduction
FES for the rehabilitation of upper extremity function was first proposed in 1963 by Long and
Masciarelli (111). The therapeutic benefits of FES were noted as early as 1973, when Rebersek
and Vodovnik developed a simple surface upper extremity orthosis (108, 128) that used position
transducers to trigger hand opening in hemiplegic patients (128). Merletti and colleagues (199) in
1975 developed a two channel surface stimulator with cutaneous electrodes and the same group
tested the feasibility of multi-channel upper extremity FES in hemiplegic patients. They applied
FES to facilitate hand and elbow extension using the nonaffected shoulder i.e. shoulder elevation
and internal rotation were used as control signals for hand opening and elbow extension. They
also successfully applied an additional third channel to stimulate the deltoid muscle.
Transcutaneous FES of the upper extremity has been revolutionized in the last 2-3
decades. There are now transcutaneous commercial systems that serve as orthotic and/or
therapeutic devices. Examples of transcutaneous FES upper extremity systems include the (a)
Neuromuscular Electrical Stimulation System (NESS) H200 or the NESS Handmaster, which
has three stimulation channels that stimulate finger extensors and flexors, and the thumb (115,
126); (b) Bionic Glove which was developed in 1989 and consists of a fingerless glove equipped
with a wrist position sensor and an electrical stimulator (127). It is designed for individuals with
SCI with active wrist flexion and extension; (c) The Belgrade Grasping-Reaching System which

104
can generate palmar and lateral grasps, hand opening and elbow extension, type of grasp is
selected using a button (200); (d) The Compex Motion Neuroprosthesis for Reaching and
Grasping which is a four-channel programmable neuroprosthesis designed specifically to
facilitate reaching and grasping in individuals with SCI and (e) MyndMove™ which is one of
the newest commercially available stimulators and uses FES as a therapeutic intervention to
restore upper limb function after stroke and SCI .
Most of the above systems are multi-channel systems that allow for stimulation of
multiple muscle groups and typically target grasping movements whilst some support additional
reaching movements (e.g., The Belgrade Grasping-Reaching System, Compex Motion and
MyndMove™). The target muscles stimulated are deltoid, biceps brachii, triceps brachii, wrist
and finger extensors and finger flexors. Interestingly, to date none of the transcutaneous FES
systems have targeted the three key interscapular muscles (lower and upper trapezius and
serratus anterior) even though these muscles play a vital role in shoulder movements (109, 122,
144, 201, 202). One study stimulated the upper limb including one of the key interscapular
muscles in patients with chronic stroke for the improvement of reaching movements (203). In
this study the authors used the Compex Motion stimulator with 4 channels and stimulated the
triceps brachii, anterior deltoid, extensor muscles of the wrist, and fingers and lower trapezius
and rhomboid, in two different conditions, i.e. Placebo (low amplitudes that do not produce
muscle contraction) and the FES group (higher amplitudes to produce a motor contraction) (203).
The authors found that participants receiving the FES performed the reaching movements with
less trunk flexion, while shoulder flexion and elbow extension were increased. This study
provides preliminary evidence related to feasibility and potential benefits of stimulating
interscapular muscles using transcutaneous FES.
In our laboratory we have been successfully using transcutaneous FES for retraining
upper extremity function in individuals with stroke and spinal cord injury for over 2 decades
(130, 133, 158, 204, 205). We have used a 4-channel surface stimulator which is fully
programmable (206) and the FES protocols have targeted arm, forearm and hand muscles to
retrain upper extremity function (130, 158). We have used FES triggered task specific functional
arm-hand movements for manipulating real life objects in combination with conventional
rehabilitation techniques. We have attempted to replicate upper extremity movements using FES
105
such that they closely follow the normal physiological movements. This philosophy of
stimulation had to be balanced against the number of stimulation channels available. If the
number of channels were limited and we could not activate all the muscles of interest, then we
would stimulate the prime movers pertinent to the movement performed. Now, with the newer
stimulators having an increased capacity in terms of number of stimulation channels (207), it is
technically possible to stimulate interscapular muscles along with shoulder muscles.
Movement of the scapula on the thorax is essential for normal function of the upper
extremity (208). Amongst the muscles that surround and attach to the scapula, the upper
trapezius (UT), lower trapezius (LT) and the serratus anterior (SA) muscles are believed to be
important for scapulothoracic motion (209). In a study done by Ebaugh et.al, the authors found
that the LT, UT and SA muscles play an important role in producing scapular upward rotation,
especially throughout the mid-range of arm elevation (167).
In upper extremity rehabilitation, clinicians are looking for ways to activate the
interscapular muscles to obtain normal shoulder elevation patterns. Studies looking at the
contributions of scapulothoracic joints in performing activities of daily living like combing hair,
feeding, reaching overhead, washing the back, and washing the contralateral axilla have found
that scapulothoracic upward rotation, and anterior tipping contribute significantly to completion
of these tasks (210). Hence clinicians working with patients who present with difficulty in
accomplishing activities of daily living should consider intervening at these joints specifically.
The limitation of current rehabilitation protocols for retraining upper extremity function is their
inability to engage interscapular muscles in a functional manner especially early on and in
individuals with severely decreased muscle strength. FES has the potential to engage these
scapular muscles in a functional manner irrespective of muscle strength and severity of the
condition.
The primary objective of our study was to test the feasibility of stimulating LT, UT and
SA muscles along with shoulder muscles using transcutaneous FES. We aimed to study the
influence of interscapular muscle FES versus only shoulder muscle FES on shoulder complex
movement in able bodied individuals. To the best of our knowledge this is the first study that will
look at stimulating these muscles using transcutaneous FES. The secondary objective was to

106
explore the effect of FES of LT, SA and UT along with anterior deltoid, and along with middle
deltoid on maximum reach achieved during shoulder flexion and abduction, respectively.
8.3 Methods
Ten able bodied individuals with no history of shoulder injury and with full active and passive
range of shoulder joint movement, were invited to participate in the study. Participants were
recruited from students, volunteers and staff at the hospital. The study was approved by the
Research Ethics Board at University Health Network. Participants were 18 years or older and
provided written consent for participation in the study. Participants recruited to the study took
part in a single two-hour session. The set-up for the experiment consisted of: (a) identifying
motor points for all the muscle groups and securing FES surface self-adhesive electrodes, (b)
determining the sensory, motor, functional and maximum electrical stimulation threshold for all
muscles; and (c) placing reflective markers for collecting the kinematic data.
A 4-channel FES stimulator (Compex Motion, Compex, Switzerland) was used to
stimulate the LT, UT, and SA, along with either the anterior or middle deltoid muscles. Once the
electrodes were secured and amplitude levels for individual muscles adjusted, the stimulator was
operated using a push button either by the study participant or a research assistant on cueing by
the researcher operating the motion capture system. The FES parameters were: stimulation
frequency of 40 Hz, pulse duration of 250µs, and stimulation intensity was determined by the
strength of the contraction and participant tolerance to stimulation (range 20-50 mA, see Table
9.2 for details).
The motor points and electrode positioning for FES for the various muscles were as below:
• Serratus Anterior (SA): Electrode between the latissimus dorsi and the pectoralis major,
on the muscular bulk of the serratus between the 4th and 9th ribs.
• Upper Trapezius (UT): On the superior aspect of the shoulder blade, away from the
supero-medial angle of the scapula to limit stimulation of the levator scapulae muscle.
• Lower Trapezius (LT): Medially and in line with the muscle fibers next to the spine of
T8-T12 below the inferior tip of the scapula, to limit stimulation of the rhomboids.
• Anterior and middle deltoid: on the bulk of the muscle, one proximal and one distal.

107
3-dimensional kinematic data were recorded using Motion Analysis System (Motion Analysis,
USA). The system uses six infra-red cameras connected to the motion analysis data acquisition
system. Calibration was carried out to define X-Y-Z reference for all 6 cameras prior to data
collection. The International Society of Biomechanics’ recommended marker set for the upper
extremity, was used (211). The specific marker locations were as follows:
1. C7: Processus Spinosus (spinous process) of the 7th cervical vertebra
2. T8: Processus Spinosus (spinal process) of the 8th thoracic vertebra
3. IJ: Deepest point of Incisura Jugularis (suprasternal notch)
4. PX: Processus Xiphoideus (xiphoid process), most caudal point on the sternum
5. SC: Most ventral point on the sternoclavicular joint
6. AC: Most dorsal point on the acromioclavicular joint (shared with the scapula)
7. TS: Trigonum Spinae Scapulae (root of the spine), the midpoint of the triangular surface
on the medial border of the scapula in line with the scapular spine
8. AI: Angulus Inferior (inferior angle), most caudal point of the scapula
9. AA: Angulus Acromialis (acromial angle), most laterodorsal point of the scapula
10. PC: Most ventral point of processus coracoideus
11. Anterior GH: Anterior aspect of the head of the Humerus
12. Posterior GH: Posterior aspect of the head of the Humerus
13. EL: Most caudal point on lateral epicondyle
14. EM: Most caudal point on medial epicondyle
15. RS: Most caudal–lateral point on the radial styloid
16. US: Most caudal–medial point on the ulnar styloid
*Please note that for the glenohumeral rotation center which was estimated by either regression or motion
recordings in (211) we determined the same using the anterior and posterior aspects of the head of the Humerus
(markers 11 and 12).
Experimental Conditions: Ten trials for each of the below conditions were performed by each
study participant. For the FES conditions (2,3, 5 and 6), the participants were specifically
instructed not to assist with the movement, i.e. the movement was purely FES elicited movement
carried out upon verbal cueing from the researcher. FES was turned on with the arm in resting
position on a count of 3 by operating a push button. Once maximum range was reached for each
108
of the below conditions, the position was held for about 10 sec, until FES was turned off
(conditions 2, 3, 5, and 6) or until the researcher asked the participant to lower their arm.
1. No FES active flexion (i.e. full range forward flexion movement produced by
participant’s voluntary muscle contraction).
2. FES for only anterior deltoid.
3. FES for anterior deltoid and interscapular muscles (. LT, UT, and SA) simultaneously.
4. No FES active abduction (i.e. full range abduction movement produced by participant’s
voluntary muscle contraction).
5. FES for only middle deltoid.
6. FES for middle deltoid and interscapular muscles (LT, UT, and SA) simultaneously.
Participants were given a 5-minute break between the flexion and abduction trials or in between
trials only if they reported fatigue or requested a break.
The motion capture data were cleaned using Cortex software (Motion Analysis, USA).
Once the motion capture data were visually inspected and correct movement verified then a
template with a marker set was created. Each marker set was labeled using a frame in which all
the markers were clearly visible and in the correct position. The template was used to rectify by
extrapolating it into the remaining frames in the recording. This process was repeated for the first
file of every data set for each participant. Markers in the remaining files were then identified
using the template created. Once all markers were labelled for the entire data set, each individual
file was reviewed to identify gaps which were then corrected using a linear, or cubic
interpolation or a virtual joint function. Selection of the specific technique used to correct the gap
was based on the size of the gap (i.e., number of missing samples) and the expected trajectory of
the maker. Other elements that were corrected manually included mislabeled or swapped
markers, as well as those displaying an unexpected movement.
Data analysis was performed using MATLAB (MathWorks, USA). Marker positions
(X, Y, and Z) for the anterior and posterior shoulder, the medial and lateral humeral epicondyle,
the suprasternal notch, the xiphoid process, T8, and C7, were extracted. Two vectors were
defined: one for the upper arm and one for the thorax. The upper arm vector was defined by the
midpoint between the shoulder’s anterior and posterior markers, and the midpoint between

109
elbow’s medial and lateral epicondyle markers. The thorax vector was defined by the midpoint
between the xiphoid process and T8, and the midpoint between the suprasternal notch and C7.
The angle between the upper arm and thorax vectors was calculated for each frame as the inverse
cosine of the dot product of both vectors divided by the product of the magnitude of both
vectors: 𝑎𝑟𝑐𝑜𝑠(θ) =𝒂∙𝒃
∥𝒂∥∥𝒃∥. The maximum reach of the arm was defined as the maximum angle
achieved. This analysis was performed for all trials of all study participant.
Statistical Analysis: Means for maximum reach across all ten trials for all ten participants for all
conditions were computed. Wilcoxon signed rank test was used to compare the scores between
anterior deltoid and anterior deltoid+ LT+UT+SA as well as between middle deltoid and middle
deltoid+LT+UT+SA conditions. We also calculated the percentage of movement achieved
during all FES conditions relative to the study participants’ voluntary range of motion in both
abduction and flexion. Wilcoxon signed rank test was used to compare the mean percent range of
motion between the middle deltoid and middle deltoid+LT+UT+SA as well as the anterior
deltoid and anterior deltoid+LT+UT+SA.
All analysis was done using SPSS version 26 and an α of 0.05 was considered statistically
significant.
8.4 Results
Ten able bodied participants (Male=9 and Female=1) completed the study. The participants age
ranged from 21 to 31 years (Mean = 25.1, SD=3.47). Their height ranged from 165 to 182 cm
(Mean=174.9, SD =6.22). Their weight ranged from 67.58 to 102.05 kg (Mean= 79.15,
SD=9.92). Nine out of ten participants were right-arm dominant (please refer to Table 8.1 for
individual participant demographics). For all of the study participants we were successfully able
to stimulate LT, UT, SA, anterior deltoid and middle deltoid using surface FES as established by
muscle palpation and visual movement inspection (for FES amplitudes for each participant’s
individual muscles please refer to Table 8.2). No adverse events were reported for any of the
study participants.
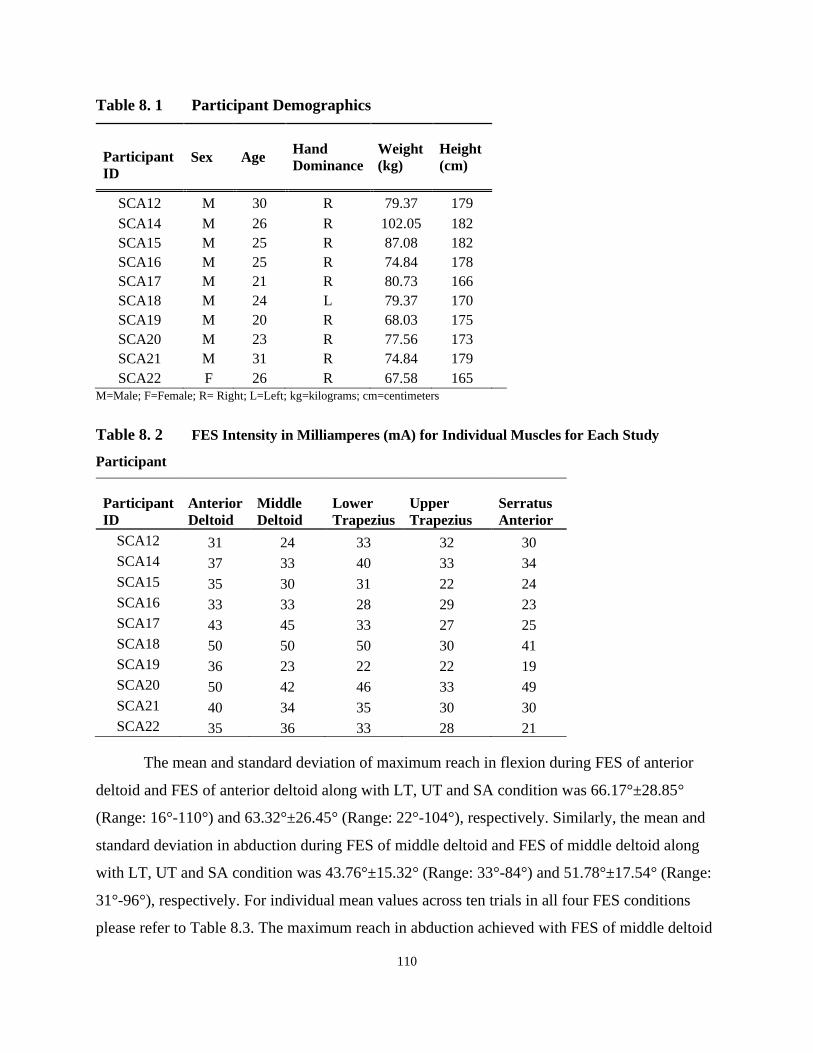
110
Table 8. 1 Participant Demographics
Participant
ID
Sex Age Hand
Dominance
Weight
(kg)
Height
(cm)
SCA12 M 30 R 79.37 179
SCA14 M 26 R 102.05 182
SCA15 M 25 R 87.08 182
SCA16 M 25 R 74.84 178
SCA17 M 21 R 80.73 166
SCA18 M 24 L 79.37 170
SCA19 M 20 R 68.03 175
SCA20 M 23 R 77.56 173
SCA21 M 31 R 74.84 179
SCA22 F 26 R 67.58 165
M=Male; F=Female; R= Right; L=Left; kg=kilograms; cm=centimeters
Table 8. 2 FES Intensity in Milliamperes (mA) for Individual Muscles for Each Study
Participant
Participant
ID
Anterior
Deltoid
Middle
Deltoid
Lower
Trapezius
Upper
Trapezius
Serratus
Anterior
SCA12 31 24 33 32 30
SCA14 37 33 40 33 34
SCA15 35 30 31 22 24
SCA16 33 33 28 29 23
SCA17 43 45 33 27 25
SCA18 50 50 50 30 41
SCA19 36 23 22 22 19
SCA20 50 42 46 33 49
SCA21 40 34 35 30 30
SCA22 35 36 33 28 21
The mean and standard deviation of maximum reach in flexion during FES of anterior
deltoid and FES of anterior deltoid along with LT, UT and SA condition was 66.17°±28.85°
(Range: 16°-110°) and 63.32°±26.45° (Range: 22°-104°), respectively. Similarly, the mean and
standard deviation in abduction during FES of middle deltoid and FES of middle deltoid along
with LT, UT and SA condition was 43.76°±15.32° (Range: 33°-84°) and 51.78°±17.54° (Range:
31°-96°), respectively. For individual mean values across ten trials in all four FES conditions
please refer to Table 8.3. The maximum reach in abduction achieved with FES of middle deltoid

111
along with LT, UT and SA was greater than that achieved with FES of middle deltoid alone in 9
out of 10 participants (Table 8.3). A Wilcoxon Signed-Ranks test indicated that the FES of
middle deltoid along with LT, UT and SA (mean rank = 6) produced a higher maximum reach in
abduction than FES of the middle deltoid alone (mean rank = 1; Z = -2.701, p = 0.007). There
was no significant difference in maximum reach between FES of anterior deltoid and FES of
anterior deltoid along with LT, UT and SA, however 6 out of 10 participants achieved a higher
maximum reach in flexion with interscapular muscle stimulation (Table 8.3).
Displacement of the arm in flexion and abduction for a single participant (SCA18) across
all experimental conditions is presented in Figure 8.1.
Table 8. 3 Maximum Reach in Degrees Across Ten Trials for Each Experimental Condition for
Individual Study Participant
Participant ID AFF AD ADALL AB MD ABALL
SCA12 127.47 46.70 55.85 139.20 34.96 41.97
SCA14 137.23 21.71 16.34 141.37 32.94 30.67
SCA15 125.28 52.02 61.99 136.23 39.49 48.11
SCA16 136.54 79.49 90.86 145.51 84.37 96.09
SCA17 141.04 44.32 46.38 146.02 36.22 41.20
SCA18 134.44 37.70 33.28 131.70 41.97 47.70
SCA19 140.46 76.03 74.04 136.31 33.60 45.95
SCA20 132.12 79.72 83.66 135.34 37.17 50.45
SCA21 122.96 91.33 89.78 137.93 49.33 55.09
SCA22 129.33 104.16 109.54 128.24 47.52 60.459 AFF- active forward flexion; AD - FES of anterior deltoid; ADALL - FES of anterior deltoid along with LT, UT and SA; AB -
active abduction; MD - FES of middle deltoid; ABALL - FES of middle deltoid along with LT, UT and SA

112
Figure 8. 1 Displacement of the Arm in Flexion and Abduction for Study Participant
(SCA18) Across All Experimental Conditions
*X-axis is time in seconds and Y-axis is the displacement of the upper arm in degrees (AFF - Active forward
flexion; AD - FES of anterior deltoid; ADALL- FES of anterior deltoid along with LT, UT and SA; AB - Active
abduction; MD - FES of middle deltoid; ABALL - FES of middle deltoid along with LT, UT and SA).
The mean percent range of motion achieved during flexion for the anterior deltoid
condition was 48.09% and for anterior deltoid along with LT, UT and SA was 50.31% and the
mean percent range of motion achieved during abduction for the middle deltoid condition was
31.70% and for the middle deltoid along with LT, UT and SA condition was 37.57%. The
percent range achieved with the interscapular stimulation was greater for both flexion and
abduction however this difference was statistically significant only in abduction.
8.5 Discussion
Researchers in the past have tried to stimulate certain interscapular muscles noting the
significance of these muscles in normal glenohumeral movement (212, 213). The first evidence
of successful stimulation of the SA muscle to treat winged scapula was reported back in 1953
(212). To the best of our knowledge this is the first study looking at the feasibility of stimulating
all three key interscapular muscles, i.e. lower trapezius (LT), upper trapezius (UT) and serratus
anterior (SA) using transcutaneous FES during shoulder elevation movements. As reported in
our results we were able to successfully stimulate all the target muscles without any adverse
events.

113
It is widely noted in the literature that interscapular muscles play a vital role in
glenohumeral movement specifically the LT, UT and SA. These are critical in the production and
control of scapulothoracic motion which is important for normal function of the upper extremity
(167, 209). For the upper extremity to move through its greatest range of motion, the shoulder
complex must work in a synchronized manner (214). There have been several studies that have
examined three-dimensional (3D) shoulder complex motion while performing activities of daily
living (215-218). Triffitt et al., determined the relationship between active humerothoracic range
of motion (ROM) and completion of 14 activities of daily living in 125 pathologic participants
(217) and they concluded that humerothoracic ROM correlates with the ability to perform
activities of daily living (217). Magermans et al., examined activities of daily living in 24
healthy, female subjects and they found that washing the axilla required the most glenohumeral
flexion (99.6°) reaching overhead required the most glenohumeral abduction (121°) and external
rotation (60.6°), and combing hair required the most scapulothoracic upward rotation (34.4°)
(216). Despite this evidence, in neurorehabilitation there are limited techniques that functionally
recruit the interscapular muscles during task specific training of activities of daily living,
especially in low functioning stroke and cervical spinal cord injury patients who have minimal
voluntary movement.
The current study results showed that stimulating the interscapular muscles resulted in
higher arm reach in abduction however it did not have any significant impact on the range of arm
reach in flexion. Overall, irrespective of the muscles being stimulated, the maximum reach as
well as percent of voluntary movement achieved in flexion was greater than that in abduction.
Since the movement of the arm started with the shoulder in neutral rotation it allowed for
clearance of the greater tubercle under the acromion during forward flexion. However, it may
have restricted its clearance during abduction (214), resulting in decreased range. Secondly, we
found that for abduction the maximum reach achieved with FES of interscapular muscles along
with middle deltoid was greater compared to stimulation of middle deltoid alone. In abduction,
the force of the trapezius is more critical to produce upward rotation of the scapula than the force
of the SA (214), and given the superficial location and size of the trapezius and the fact that there
were a total of four electrodes (two channels) dedicated to the trapezius muscle, all of these
resulted in increased muscle fibre recruitment and hence greater contribution of the muscle

114
towards the movement produced. In contrast, for the flexion trials, the maximum range did not
change with additional stimulation of the interscapular muscles. During flexion, the anterior
orientation of the scapula is important (214) and can be produced only by SA (214). The SA has
a relatively smaller muscle bulk and can be stimulated in isolation along the narrow strip where it
is nestled between the latissimus dorsi and pectoralis major. In our study, it was stimulated using
one channel and lower current amplitudes to prevent radiation of current to the neighbouring
larger abdominal muscles and hence might not have been recruited most optimally to observe its
effect in flexion. Nonetheless, trapezius and SA besides contributing to an increase in range
serve an equally important function as stabilizing synergists for the deltoid acting at the
glenohumeral joint and should be actively engaged during shoulder complex movements.
Some of the limitations of the current study are that it uses a convenience sample of
healthy volunteers; secondly given the wide variation of scapular contributions to glenohumeral
movement the results of the study should be interpreted with caution. Third, it was not possible
to confirm with any certainty that no voluntary effort was used during FES trials.
8.6 Conclusion
In this study we demonstrated that we can successfully recruit the three key interscapular
muscles using surface FES and this provides an avenue for rehabilitation specialists to engage
these muscles during upper extremity rehabilitation.

115
Chapter 9 Discussion and Conclusions
This chapter discusses the key findings and limitations of this thesis and provides future
directions related to optimizing upper extremity rehabilitation in stroke and SCI.
In rehabilitation science, just like any other field, optimal measurement is one of the keys
to the uptake of new therapies in main-stream clinical practice. Outcome is defined as a visible
or practical result (Oxford English Dictionary). Outcome measures are vital to the setting of
standards of care and their measurement, as well as in the assessment of injury severity (219).
The prediction of outcome and the desire to know what the future will bring have led to the
development of more accurate and reliable outcome tools over the years. In general, many of the
outcome measures are based on scoring systems. In most cases there is an advantage gained
between the demands of speed, efficiency, and acceptability to both the clinician and the patient,
and the demands of precision and specificity (219). Most often the criteria for an effective
outcome tool focuses on the assessment being quick, simple to use, reliable, specific to the injury
being assessed, cost-effective, and applicable. However, over and above these one of the key
criteria to wide scale acceptability is accessibility of the measure.
9.1 3D TRI-HFT
9.1.1 Role of 3D Printing in Rehabilitation Science
3D printing technology is gaining increased attention in the health care sector and is quickly and
widely being adapted in various medical fields including orthopedic surgery, dental surgery,
ophthalmology, fabricating hearing aids, for pharmaceutical research etc. However, its
application in physical rehabilitation has been somewhat slow with its use mainly limited to
fabricating of prosthetics, orthotics, splint’s and exoskeletons (169). The business industry
expects 3D printing to become a multibillion-dollar industry in the next 4-5 years, suggesting
that most hospitals and health care sectors in the developed world will own a 3D printer. Thus,
the onus is on us researchers and clinicians in the rehabilitation sector on how best to utilize
technology to improve patient outcomes. In this thesis we established the feasibility of 3D
printing an upper extremity assessment tool. This is a significant milestone as this realizes our
ability to integrate 3D technology in rehabilitation science over and above for the purposes
116
mentioned above. In the literature, there are several review articles that discuss the pitfalls of the
many upper extremity measures. But very seldom in the literature there is a discussion over
accessibility. Lack of accessibility is one of the key takeaways from the fact that there is a wide
discrepancy amongst the outcome measures used in both clinical practice and in rehabilitation
research; and this was the motivation for the first project of this thesis, i.e. feasibility of 3D
printing the TRI-HFT.
9.1.2 3D TRI-HFT Objects and Scoring System
The TRI-HFT test was developed out of a need that was realized when conducting upper
extremity research using newer rehabilitation technologies like robotic therapy and functional
electrical stimulation back in 2012 (98). At the time there were no upper extremity measures
designed for use in SCI specifically and the measures that were being used were not validated in
SCI. Further, we found that they were unable to detect change following therapy using these
newer interventions (98). The framework for the development of the TRI-HFT was based on the
test’s ability to measure function as it relates to the ability to perform activities of daily living in
a barrier free environment. Whilst the primary goal was to measure function, there was a
fundamental need felt to quantify strength as it practically relates to task execution and hence the
grading of active vs passive grasp during task execution. Moreover, in order for the clinician to
plan therapy goals it is important to capture performance on activities of daily living. With this
thought process, we selected the objects that are commonly used in day-to-day life and aimed to
replicate its use in a controlled environment to be able to reliably measure change. The 10
objects of the test are ordinarily used items of day-to-day life. The rectangular blocks with
differing weight and texture were designed to capture the ability to handle objects outside of the
1-10 objects previously tested and also to gain an understanding, if changing the weight or
texture of the objects would have a bearing on the performance. Lastly, Part 2 of the TRI-HFT
was designed as an objective assessment tool that would help with therapy planning and
progression.
The 3D printing process was robust enough to allow for replication of all test objects and
the dimensions of the 3D printed objects was within a 10% error margin of the original objects.
The two objects that could not be replicated in 3D format were the sponge and paper and these
117
were re-designed to comply with the 3D technology. Despite the re-design these two objects
closely simulate the original objects and are able to serve the purpose of their inclusion in the test
object repertoire. Another limitation of the test was that the 9 rectangular blocks could not be
scored from video assessments and hence were not included in the reliability testing as the
assessors had difficulty identifying the different blocks based on weight and texture. This is now
remedied by numbering the blocks such that the numbers are clearly identifiable on camera.
The original scoring system at the time of development of the original test was an ordinal
one with a score of 0-2. A score of 0 indicated that the participant was unable to grasp/hold the
object in the given hand position (pronation, neutral position and supination). A score of 1
indicated that the participant was able to grasp the object in the given hand position but unable to
sustain a grip on the object and dropped the object after grasping it but before completing the
task. A score of 2 indicated that the participant was able to complete the test successfully. This
scoring system was then presented to the clinicians in the field of SCI research for their
feedback. The rehabilitation therapy experts recommended that the scoring scale needs to have
more gradations than the existing three-point ordinal scale to allow for increased instrument
sensitivity and to avoid floor or ceiling effects. They however, commended the use of day-to-day
objects to assess hand function and reported that it significantly enriched the content value of the
results obtained. They also provided positive feedback about the simplified description of task
performance. To address the clinician’s feedback related to scoring, a 7-point scoring system was
developed. The new scoring system was designed to incorporate all the three components of
upper limb function (reach, grasp and manipulation). This was a critical step as the over-arching
goal was to expand the use of the test to the wider neurological population with minimal changes
to the test components if any. This was difficult given the difference in pathophysiology and
presentation of the different conditions. Besides, it was very important to the team to keep the
scoring simple enough that it meant something to the patient and their care givers. The 0-7
system of scoring is designed to record changes in function from proximal to distal and hence
would be applicable to pathologies where recovery profiles are from proximal to distal. The 3D
printed TRI-HFT was evaluated for its psychometric properties in both stroke and SCI albeit in a
small sample. The results nonetheless are promising for both these populations.

118
The ability to 3D-print an outcome assessment tool is a step forward in the application of
technology towards improving health care specifically moving rehabilitation science forward.
The fact that the 3D printed test showed good psychometric properties in our small sample of
SCI and stroke is very encouraging. These two factors combined will give us the ability to
collect data from a larger sample across institutions worldwide to further the results of the
reliability and validity of the test.
9.1.3 3D TRI-HFT Psychometric Testing
The original TRI-HFT was evaluated within an interventional RCT designed to evaluate the
efficacy of FES therapy versus conventional rehabilitation therapy in individuals with sub-acute
SCI. The TRI-HFT was found to have high reliability, validity, and sensitivity in this patient
population. The original test was validated in stroke as well however using the 0-2 scoring
system. 3D printed TRI-HFT assessed in the first and second projects of this thesis has shown
good psychometric properties during the preliminary testing in both stroke and SCI. Whereas,
the 3D printed TRI-HFT showed high reliability and validity in the SCI population, only
moderate correlations of the test were obtained in the stroke population. The 3D TRI-HFT had a
high correlation with the CMSA-Arm but showed only moderate correlations with the hand
specific measures, i.e. the FMA-Hand and the CMSA-Hand. It is important to note that both the
FMA-Hand and the CMSA-Hand are impairment measures. The CAHAI is a functional tool but
allows for bilateral use of the upper extremities and hence the participant may compensate for
the weaker limb by the stronger one.
9.1.4 Limitations
Although the results of the first two projects appear promising, there are certain limitations to
these studies. First and foremost, the sample size used to determine test reliability and test
validity is small and for the stroke study includes participants with minimal upper extremity
function (moderate to Severe Stage of Hand 1 to 4 on the Chedoke-McMaster Stroke
Assessment). Thus, the study results need to be interpreted with caution and might have limited
applicability. Secondly, because of the lack of a gold standard measure to measure activity (ICF
category 4) in stroke we tested convergent validity of the 3D TRI-HFT with the FMA-Hand,
CMSA-Hand and the CAHAI, and we found that the 3D TRI-HFT had moderate correlations

119
with these measures. ARAT is a validated and commonly used measure both in clinical practice
as well as in research for assessing upper extremity function and though the measure has
limitations it might be worthwhile to assess criterion validity of the 3D TRI-HFT with the
ARAT. Also, it is important to mention that responsiveness of the test was not studied as a part
of this thesis.
Another limitation is related to the 3D printing process. All objects were printed using
Acrylonitrile Butadiene Styrene plastic and although the friction level of these objects can be
adjusted (as we did for the 9 rectangular blocks), the sensory feedback may be different from
“real” objects. This is a limitation of the technology, however given the moderate to strong
validity of the test in stroke and SCI in a small sample there is reason to believe that this did not
affect performance significantly. Another limitation of the test is that two of the original objects
needed to be modified significantly to allow them to be 3D printed, these were the paper and the
sponge. This is again a technology limitation, and it might be worthwhile to compare
performance on these objects between the original test and the 3D printed test to see if the
modified design of the objects has any bearing on the manipulation ability.
Lastly although the current projects do not look at the knowledge translation component,
the challenges associated with knowledge translation are widely documented. We have tried to
address many of these in the creation of the 3D printed TRI-HFT namely, making the test simple,
easily accessible, quick to administer, requiring minimal training and designing a scoring system
that is easy and relevant to both clinicians and stakeholders however ascertaining high
psychometrics of the test in the population where it is intended to be used is equally critical. We
discuss the next steps for this in the following subsection related to future directions.
9.1.5 Strengths and Future Directions for the 3D TRI-HFT
Despite the study limitations, the 3D printed test has some strengths too. First and most
importantly the 3D printing process achieves the feat of making an outcome assessment tool
universally accessible (the test files along with the instructions will be made available on our
research institute website). Secondly, because the test objects are functional in nature, in clinical
settings they can be used as therapy objects for training as well. One of the other advantages of
the test is it can be used as a therapy kit that the patient can take home with them and use for

120
training and the same kit translates into an outcome measure that can be scored remotely via tele-
rehabilitation portals (in cases where learnt use is not a contraindication to testing). This has
value where the patient lives remotely and are unable to attend therapy sessions with a
physiotherapist or occupational therapist in person. Another, potential application might be to
instrument these 3D printed objects with force/motion sensors. This can have multiple
applications like recording accurate upper extremity joint movements in 3D space or using these
instrumented objects for playing games while training in virtual reality set-ups.
We are currently conducting a study to explore the reliability and validity of the 3D TRI-
HFT in high functioning chronic stroke and the same collects data on the ARAT as well to
enable us to study criterion validity of the 3D TRI-HFT. A study with a larger sample size to
study reliability and validity in SCI as well is warranted.
9.2 Functional Electrical Stimulation of the Interscapular Muscles
9.2.1 Functional Electrical Stimulation of the Interscapular Muscles, Feasibility
In the third study of this thesis, we explored the ability to stimulate interscapular muscles using
surface FES. There are two things that need to be emphasized, the goal was to engage the
interscapular muscles in a way that they would physiologically work during shoulder complex
movements. Secondly, it was important to be able to do this without stimulating neighboring
muscles and without causing any significant discomfort. As mentioned in Chapters 3 and 4, for
the purpose of this thesis FES refers to the delivery of electrical stimulation in a functional
manner, during execution of task-oriented movements. This is true of interscapular muscles as
well. The intent behind developing FES protocols as a part of this thesis was not strengthening
but retraining.
From a feasibility perspective, it was possible to stimulate the interscapular muscles
using a surface multi-channel stimulator and although this did not result in a significantly greater
range of motion during arm elevation in able bodied individuals, it remains to be seen if it has an
impact on shoulder scapular biomechanics during functional tasks. Another, thing related to
feasibility one needs to keep in mind is that the capabilities of engaging multiple muscle groups
is in part dependent on the available technology i.e., number of channels of stimulation. When

121
there are limited number of channels available then the prime movers should always be the ones
to be targeted.
9.2.2 FES of Interscapular Muscles Clinical Significance and Future Directions
There is strong evidence in the literature related to the clinical importance of interscapular
muscles during shoulder complex movements. In neurological populations, like stroke and SCI,
where the normal joint biomechanics are altered by virtue of either imbalances in muscle tone or
muscle weakness, it is very difficult to engage the interscapular muscles using conventional
rehabilitation strategies, especially early on during therapy. Surface FES provides a viable way
to engage these muscles during task specific training. Given that patients with stroke and SCI are
predisposed to shoulder joint pain and malfunction it becomes even more critical that therapeutic
strategies work towards engaging shoulder complex muscles in as close to a physiological
manner as possible. Using FES early on during rehabilitation provides a means for engaging
these vital muscles during execution of functional tasks thereby not only encouraging normal
joint mechanics but also preventing shoulder pain secondary to altered muscle recruitment
patterns.
One short-term future plan is to study the effects of interscapular muscle stimulation on
the shoulder complex biomechanics of individual study participants as it relates to voluntary
shoulder flexion and abduction movements. In the study presented in this thesis, interscapular
muscles were stimulated along with either anterior deltoid or middle deltoid during shoulder
flexion or abduction movements. Future studies need to look at the influence of stimulating these
muscles specifically during targeted functional tasks like overhead reaching, combing hair,
washing the opposite axilla, raising the arm during donning and doffing of clothes etc. in
individuals with stroke and SCI.
9.2.3 Limitations
Some of the limitations of the current study are its small convenience sample of young able-
bodied adults. Secondly, the study sample consisted predominantly of young males with only
one female participant. Future studies should look at the influence and tolerance of interscapular
muscle stimulation in females. Another limitation of the current study is that FES was applied

122
during conventional flexion and abduction movements and not specifically during a functional
task execution. Future studies are needed to explore how and if interscapular muscle stimulation
affects movement execution during goal-oriented tasks.
9.3 Concluding Remarks
Overall, the goal of this thesis was to advance the field of upper extremity rehabilitation
specifically for individuals with stroke and SCI. In the projects conducted as a part of this thesis,
I attempted to harness the benefits of technology to achieve this. I was able to successfully 3D-
print a hand function assessment tool and establish preliminary reliability and validity in both
stroke and SCI. I also showed that using technology might require some adaptations and one
needs to creatively work around it. For the third project I tried to fill a gap in the literature related
to existing FES upper extremity protocols to include the interscapular muscles. These muscles
are critical for shoulder complex movements and are required to perform activities of daily
living. Whereas this was successfully achieved in young healthy adults it remains to be seen
whether it can be done in patient population and how that might influence upper extremity
rehabilitation using FES.
123
References
1. Lindsay MP, Norrving B, Sacco RL, Brainin M, Hacke W, Martins S, et al. World Stroke
Organization (WSO): Global Stroke Fact Sheet 2019. International journal of stroke : official
journal of the International Stroke Society. 2019;14(8):806-17.
2. Feigin VL, Norrving B, Mensah GA. Global Burden of Stroke. Circulation research.
2017;120(3):439-48.
3. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195
countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease
Study 2017. Lancet (London, England). 2018;392(10159):1736-88.
4. Marx J HR, Walls R. . Rosen's Emergency Medicine. 6th edition ed2006.
5. Ojaghihaghighi S, Vahdati SS, Mikaeilpour A, Ramouz A. Comparison of neurological
clinical manifestation in patients with hemorrhagic and ischemic stroke. World journal of
emergency medicine. 2017;8(1):34-8.
6. Tintinalli JE KG, Stapczynski JS. . Emergency Medicine: A Comprehensive Study
Guide. Sixth Edition ed2004.
7. Krueger H, Koot J, Hall RE, O'Callaghan C, Bayley M, Corbett D. Prevalence of
Individuals Experiencing the Effects of Stroke in Canada: Trends and Projections. Stroke.
2015;46(8):2226-31.
8. Ron Goeree GB, Radmila Petrovic & Suzette Salama Cost of stroke in Canada: a 1-year
prospective study. Journal of Medical Economics.8(1):147-67.
9. Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al.
Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart
Association. Circulation. 2020;141(9):e139-e596.
10. Nor AM, Davis J, Sen B, Shipsey D, Louw SJ, Dyker AG, et al. The Recognition of
Stroke in the Emergency Room (ROSIER) scale: development and validation of a stroke
recognition instrument. The Lancet Neurology. 2005;4(11):727-34.
11. Petridis AK, Kamp MA, Cornelius JF, Beez T, Beseoglu K, Turowski B, et al.
Aneurysmal Subarachnoid Hemorrhage. Deutsches Arzteblatt international. 2017;114(13):226-
36.
12. Stack CA, Cole JW. Ischemic stroke in young adults. Current opinion in cardiology.
2018;33(6):594-604.
13. Teasell R, Salbach NM, Foley N, Mountain A, Cameron JI, Jong A, et al. Canadian
Stroke Best Practice Recommendations: Rehabilitation, Recovery, and Community Participation
following Stroke. Part One: Rehabilitation and Recovery Following Stroke; 6th Edition Update
124
2019. International journal of stroke : official journal of the International Stroke Society.
2020:1747493019897843.
14. Kalra L, Langhorne P. Facilitating recovery: evidence for organized stroke care. Journal
of rehabilitation medicine. 2007;39(2):97-102.
15. Prvu Bettger JA, Stineman MG. Effectiveness of multidisciplinary rehabilitation services
in postacute care: state-of-the-science. A review. Archives of physical medicine and
rehabilitation. 2007;88(11):1526-34.
16. Seiffge DJ, Werring DJ, Paciaroni M, Dawson J, Warach S, Milling TJ, et al. Timing of
anticoagulation after recent ischaemic stroke in patients with atrial fibrillation. The Lancet
Neurology. 2019;18(1):117-26.
17. Lai SM, Studenski S, Duncan PW, Perera S. Persisting consequences of stroke measured
by the Stroke Impact Scale. Stroke. 2002;33(7):1840-4.
18. Kwakkel G, Kollen BJ, van der Grond J, Prevo AJ. Probability of regaining dexterity in
the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke.
2003;34(9):2181-6.
19. Broeks JG, Lankhorst GJ, Rumping K, Prevo AJ. The long-term outcome of arm function
after stroke: results of a follow-up study. Disability and rehabilitation. 1999;21(8):357-64.
20. Sveen U, Bautz-Holter E, Sødring KM, Wyller TB, Laake K. Association between
impairments, self-care ability and social activities 1 year after stroke. Disability and
rehabilitation. 1999;21(8):372-7.
21. Morris JH, van Wijck F, Joice S, Donaghy M. Predicting health related quality of life 6
months after stroke: the role of anxiety and upper limb dysfunction. Disability and rehabilitation.
2013;35(4):291-9.
22. Franceschini M, La Porta F, Agosti M, Massucci M. Is health-related-quality of life of
stroke patients influenced by neurological impairments at one year after stroke? European
journal of physical and rehabilitation medicine. 2010;46(3):389-99.
23. Wyller TB, Sveen U, Sødring KM, Pettersen AM, Bautz-Holter E. Subjective well-being
one year after stroke. Clinical rehabilitation. 1997;11(2):139-45.
24. Langhorne P, Legg L. Evidence behind stroke rehabilitation. Journal of neurology,
neurosurgery, and psychiatry. 2003;74 Suppl 4(Suppl 4):iv18-iv21.
25. C. S, editor Health classifications 1 - An introduction to the ICF. WCPT Keynotes. .
World Confederation for Physical Therapy; 2006.
26. Otterman N, Veerbeek J, Schiemanck S, van der Wees P, Nollet F, Kwakkel G. Selecting
relevant and feasible measurement instruments for the revised Dutch clinical practice guideline
for physical therapy in patients after stroke. Disability and rehabilitation. 2017;39(14):1449-57.

125
27. Sullivan JE, Crowner BE, Kluding PM, Nichols D, Rose DK, Yoshida R, et al. Outcome
measures for individuals with stroke: process and recommendations from the American Physical
Therapy Association neurology section task force. Physical therapy. 2013;93(10):1383-96.
28. Alt Murphy M, Resteghini C, Feys P, Lamers I. An overview of systematic reviews on
upper extremity outcome measures after stroke. BMC neurology. 2015;15:29.
29. Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic
patient. 1. a method for evaluation of physical performance. Scandinavian journal of
rehabilitation medicine. 1975;7(1):13-31.
30. Chen HF, Lin KC, Wu CY, Chen CL. Rasch validation and predictive validity of the
action research arm test in patients receiving stroke rehabilitation. Archives of physical medicine
and rehabilitation. 2012;93(6):1039-45.
31. Gladstone DJ, Danells CJ, Black SE. The fugl-meyer assessment of motor recovery after
stroke: a critical review of its measurement properties. Neurorehabilitation and neural repair.
2002;16(3):232-40.
32. Yozbatiran N, Der-Yeghiaian L, Cramer SC. A standardized approach to performing the
action research arm test. Neurorehabilitation and neural repair. 2008;22(1):78-90.
33. Platz T, Pinkowski C, van Wijck F, Kim IH, di Bella P, Johnson G. Reliability and
validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test,
Action Research Arm Test and Box and Block Test: a multicentre study. Clinical rehabilitation.
2005;19(4):404-11.
34. Sigirtmac IC, Oksuz C. Investigation of reliability, validity, and cutoff value of the
Jebsen-Taylor Hand Function Test. Journal of hand therapy : official journal of the American
Society of Hand Therapists. 2020.
35. Johansson GM, Hager CK. A modified standardized nine hole peg test for valid and
reliable kinematic assessment of dexterity post-stroke. Journal of neuroengineering and
rehabilitation. 2019;16(1):8.
36. Barreca SR, Stratford PW, Lambert CL, Masters LM, Streiner DL. Test-retest reliability,
validity, and sensitivity of the Chedoke arm and hand activity inventory: a new measure of
upper-limb function for survivors of stroke. Archives of physical medicine and rehabilitation.
2005;86(8):1616-22.
37. Fulk G, Martin R, Page SJ. Clinically Important Difference of the Arm Motor Ability
Test in Stroke Survivors. Neurorehabilitation and neural repair. 2017;31(3):272-9.
38. De Souza LH, Hewer RL, Miller S. Assessment of recovery of arm control in hemiplegic
stroke patients. 1. Arm function tests. International rehabilitation medicine. 1980;2(1):3-9.

126
39. Johansson GM, Hager CK. Measurement properties of the Motor Evaluation Scale for
Upper Extremity in Stroke patients (MESUPES). Disability and rehabilitation. 2012;34(4):288-
94.
40. Vianna de Andrade FPP, Padula RS, Binda AC, da Silva ML, Alouche SR. Measurement
properties of the Reaching Performance Scale for Stroke. Disability and rehabilitation. 2019:1-5.
41. Desrosiers J, Hebert R, Bravo G, Dutil E. Upper extremity performance test for the
elderly (TEMPA): normative data and correlates with sensorimotor parameters. Test
d'Evaluation des Membres Superieurs de Personnes Agees. Archives of physical medicine and
rehabilitation. 1995;76(12):1125-9.
42. Berardi A, Dhrami L, Tofani M, Valente D, Sansoni J, Galeoto G. Cross-cultural
adaptation and validation in the Italian population of the wolf motor function test in patients with
stroke. Functional neurology. 2018;33(4):229-53.
43. Ekstrand E, Lindgren I, Lexell J, Brogardh C. Test-retest reliability of the ABILHAND
questionnaire in persons with chronic stroke. PM & R : the journal of injury, function, and
rehabilitation. 2014;6(4):324-31.
44. Marino RJ, Shea JA, Stineman MG. The Capabilities of Upper Extremity instrument:
reliability and validity of a measure of functional limitation in tetraplegia. Archives of physical
medicine and rehabilitation. 1998;79(12):1512-21.
45. Demers M, Levin MF. Do Activity Level Outcome Measures Commonly Used in
Neurological Practice Assess Upper-Limb Movement Quality? Neurorehabilitation and neural
repair. 2017;31(7):623-37.
46. Smith MC, Stinear CM. Transcranial magnetic stimulation (TMS) in stroke: Ready for
clinical practice? Journal of clinical neuroscience : official journal of the Neurosurgical Society
of Australasia. 2016;31:10-4.
47. Pollock A, Farmer SE, Brady MC, Langhorne P, Mead GE, Mehrholz J, et al.
Interventions for improving upper limb function after stroke. The Cochrane database of
systematic reviews. 2014;2014(11):Cd010820.
48. Dehem S, Gilliaux M, Stoquart G, Detrembleur C, Jacquemin G, Palumbo S, et al.
Effectiveness of upper-limb robotic-assisted therapy in the early rehabilitation phase after stroke:
A single-blind, randomised, controlled trial. Annals of physical and rehabilitation medicine.
2019;62(5):313-20.
49. Rodgers H, Shaw L, Bosomworth H, Aird L, Alvarado N, Andole S, et al. Robot Assisted
Training for the Upper Limb after Stroke (RATULS): study protocol for a randomised controlled
trial. Trials. 2017;18(1):340.
50. Taveggia G, Borboni A, Salvi L, Mulé C, Fogliaresi S, Villafañe JH, et al. Efficacy of
robot-assisted rehabilitation for the functional recovery of the upper limb in post-stroke patients:

127
a randomized controlled study. European journal of physical and rehabilitation medicine.
2016;52(6):767-73.
51. Veerbeek JM, Langbroek-Amersfoort AC, van Wegen EE, Meskers CG, Kwakkel G.
Effects of Robot-Assisted Therapy for the Upper Limb After Stroke. Neurorehabilitation and
neural repair. 2017;31(2):107-21.
52. Choi YH, Paik NJ. Mobile Game-based Virtual Reality Program for Upper Extremity
Stroke Rehabilitation. Journal of visualized experiments : JoVE. 2018(133).
53. Ikbali Afsar S, Mirzayev I, Umit Yemisci O, Cosar Saracgil SN. Virtual Reality in Upper
Extremity Rehabilitation of Stroke Patients: A Randomized Controlled Trial. Journal of stroke
and cerebrovascular diseases : the official journal of National Stroke Association.
2018;27(12):3473-8.
54. Lee SH, Lee JY, Kim MY, Jeon YJ, Kim S, Shin JH. Virtual Reality Rehabilitation With
Functional Electrical Stimulation Improves Upper Extremity Function in Patients With Chronic
Stroke: A Pilot Randomized Controlled Study. Archives of physical medicine and rehabilitation.
2018;99(8):1447-53.e1.
55. Yin CW, Sien NY, Ying LA, Chung SF, Tan May Leng D. Virtual reality for upper
extremity rehabilitation in early stroke: a pilot randomized controlled trial. Clinical
rehabilitation. 2014;28(11):1107-14.
56. Laver K, George S, Thomas S, Deutsch JE, Crotty M. Cochrane review: virtual reality for
stroke rehabilitation. European journal of physical and rehabilitation medicine. 2012;48(3):523-
30.
57. Ahn S, Hwang S. Virtual rehabilitation of upper extremity function and independence for
stoke: a meta-analysis. Journal of exercise rehabilitation. 2019;15(3):358-69.
58. Roach KEP, PT Measurement of Health Outcomes: Reliability, Validity and
Responsiveness. JPO Journal of Prosthetics and Orthotics:. January 2006;18(6):8-12.
59. Cecilia AC Prinsen SV, Michael R Rose, Maarten Boers, Peter Tugwell, Mike Clarke,
Paula R Williamson and Caroline B Terwee. Guideline for selecting outcome measurement
instruments for outcomes included in a Core Outcome Set. 2016.
60. Portney LG WM. Foundations of Clinical Research: Applications to Practice. . 2nd ed.
ed. Upper Saddle River, NJ: Prentice Hall, Inc.2000.
61. Sall J, Eapen BC, Tran JE, Bowles AO, Bursaw A, Rodgers ME. The Management of
Stroke Rehabilitation: A Synopsis of the 2019 U.S. Department of Veterans Affairs and U.S.
Department of Defense Clinical Practice Guideline. Annals of internal medicine.
2019;171(12):916-24.

128
62. Bulsen; Abudulkadir DNAaPM, inventor; FDA, assignee. Method for functional
electrical stimulation therapy. USA patent US Provisional Patent Application US 61/664,306
2014.
63. Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord
injury: what learns a worldwide literature survey? Spinal cord. 2006;44(9):523-9.
64. Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O'Connor KC, et al. Traumatic
spinal cord injury in the United States, 1993-2012. Jama. 2015;313(22):2236-43.
65. Lasfargues JE, Custis D, Morrone F, Carswell J, Nguyen T. A model for estimating
spinal cord injury prevalence in the United States. Paraplegia. 1995;33(2):62-8.
66. Facts and figures at a glance. In: Center. NSCIS, editor. 2016.
67. Noonan VK, Fingas M, Farry A, Baxter D, Singh A, Fehlings MG, et al. Incidence and
prevalence of spinal cord injury in Canada: a national perspective. Neuroepidemiology.
2012;38(4):219-26.
68. Krueger H, Noonan VK, Trenaman LM, Joshi P, Rivers CS. The economic burden of
traumatic spinal cord injury in Canada. Chronic diseases and injuries in Canada. 2013;33(3):113-
22.
69. Oyinbo CA. Secondary injury mechanisms in traumatic spinal cord injury: a nugget of
this multiply cascade. Acta neurobiologiae experimentalis. 2011;71(2):281-99.
70. Dumont RJ, Okonkwo DO, Verma S, Hurlbert RJ, Boulos PT, Ellegala DB, et al. Acute
spinal cord injury, part I: pathophysiologic mechanisms. Clinical neuropharmacology.
2001;24(5):254-64.
71. Rowland JW, Hawryluk GW, Kwon B, Fehlings MG. Current status of acute spinal cord
injury pathophysiology and emerging therapies: promise on the horizon. Neurosurgical focus.
2008;25(5):E2.
72. Sekhon LH, Fehlings MG. Epidemiology, demographics, and pathophysiology of acute
spinal cord injury. Spine. 2001;26(24 Suppl):S2-12.
73. Figley SA, Khosravi R, Legasto JM, Tseng YF, Fehlings MG. Characterization of
vascular disruption and blood-spinal cord barrier permeability following traumatic spinal cord
injury. Journal of neurotrauma. 2014;31(6):541-52.
74. Fehlings MG SL. Restoration of spinal cord function. . In: Orthopaedic Knowledge
Update: Spine 2 Am Academy of Orthopaedic Surgeons; 2002. . p. pp, 483-8.
75. Fehlings MG, Vaccaro A, Wilson JR, Singh A, D WC, Harrop JS, et al. Early versus
delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing
in Acute Spinal Cord Injury Study (STASCIS). PloS one. 2012;7(2):e32037.

129
76. Lucas JT, Ducker TB. Motor classification of spinal cord injuries with mobility,
morbidity and recovery indices. The American surgeon. 1979;45(3):151-8.
77. Wilson JR, Hashimoto RE, Dettori JR, Fehlings MG. Spinal cord injury and quality of
life: a systematic review of outcome measures. Evidence-based spine-care journal. 2011;2(1):37-
44.
78. Alizadeh A, Dyck SM, Karimi-Abdolrezaee S. Traumatic Spinal Cord Injury: An
Overview of Pathophysiology, Models and Acute Injury Mechanisms. Front Neurol.
2019;10:282.
79. Khorasanizadeh M, Yousefifard M, Eskian M, Lu Y, Chalangari M, Harrop JS, et al.
Neurological recovery following traumatic spinal cord injury: a systematic review and meta-
analysis. Journal of neurosurgery Spine. 2019:1-17.
80. Kalsi-Ryan S KS, Fehlings MG. . Cervical spondylotic myelopathy: The clinical
phenomenon and the current pathobiology of an increasingly prevalent and devastating disorder.
. The Neuroscientist: A Review Journal Bringing Neurobiology, Neurology and Psychiatry 2013
Aug;;19(4):409-21.
81. Nouri A, Tetreault L, Singh A, Karadimas SK, Fehlings MG. Degenerative Cervical
Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine. 2015;40(12):E675-93.
82. Wilson JR, Fehlings MG, Kalsi-Ryan S, Shamji MF, Tetreault LA, Rhee JM, et al.
Diagnosis, heritability, and outcome assessment in cervical myelopathy: a consensus statement.
Spine. 2013;38(22 Suppl 1):S76-7.
83. Fehlings MG WJ, Kopjar B, Yoon ST, Arnold PM, Massicotte EM, et al. . Efficacy and
safety of surgical decompression in patients with cervical spondylotic myelopathy: Results of the
AOSpine North America prospective multi-center study. . The Journal of Bone and Joint Surgery
American Volume 2013 Sep;95(18):1651-8.
84. Kirshblum SC, Memmo P, Kim N, Campagnolo D, Millis S. Comparison of the revised
2000 American Spinal Injury Association classification standards with the 1996 guidelines.
American journal of physical medicine & rehabilitation. 2002;81(7):502-5.
85. Susan B. O'Sullivan TJS. Physical Rehabilitation Assessment and Treatment. Fourth
Edition ed2001. 897-9 p.
86. Outcomes Following Traumatic Spinal Cord Injury: Clinical Practice Guidelines for
Health-Care Professionals. Paralyzed Veterans of America; July 1999.
87. Amber Harnett ABM, Amanda McIntyre,Ruchi Parikh,James Middleton,Mohit
Arora,Dalton Wolfe and Swati Mehta. Spinal Cord Injury Rehabilitation Practices [Available
from: http://scireproject.com/evidence/rehabilitation-evidence/rehabilitation-practices/key-
points-rehab/.
130
88. Fehlings MG, Tetreault LA, Wilson JR, Kwon BK, Burns AS, Martin AR, et al. A
Clinical Practice Guideline for the Management of Acute Spinal Cord Injury: Introduction,
Rationale, and Scope. Global spine journal. 2017;7(3 Suppl):84s-94s.
89. Dobkin BH. Confounders in rehabilitation trials of task-oriented training: lessons from
the designs of the EXCITE and SCILT multicenter trials. Neurorehabilitation and neural repair.
2007;21(1):3-13.
90. Snoek GJ, MJ IJ, Hermens HJ, Maxwell D, Biering-Sorensen F. Survey of the needs of
patients with spinal cord injury: impact and priority for improvement in hand function in
tetraplegics. Spinal cord. 2004;42(9):526-32.
91. Anderson KD. Targeting recovery: priorities of the spinal cord-injured population.
Journal of neurotrauma. 2004;21(10):1371-83.
92. Jones LAT, Bryden A, Wheeler TL, Tansey KE, Anderson KD, Beattie MS, et al.
Considerations and recommendations for selection and utilization of upper extremity clinical
outcome assessments in human spinal cord injury trials. Spinal cord. 2018;56(5):414-25.
93. van Tuijl JH, Janssen-Potten YJ, Seelen HA. Evaluation of upper extremity motor
function tests in tetraplegics. Spinal cord. 2002;40(2):51-64.
94. Wuolle KS, Van Doren CL, Thrope GB, Keith MW, Peckham PH. Development of a
quantitative hand grasp and release test for patients with tetraplegia using a hand
neuroprosthesis. The Journal of hand surgery. 1994;19(2):209-18.
95. Mulcahey MJ, Betz RR, Smith BT, Weiss AA. A prospective evaluation of upper
extremity tendon transfers in children with cervical spinal cord injury. Journal of pediatric
orthopedics. 1999;19(3):319-28.
96. Bryden AM SA, Mulcahey MJ. . Innovative strategies for improving upper extremity
function in tetraplegia and considerations in measuring functional outcomes. Top Spinal Cord Inj
Rehabil 2005. p. 75-93.
97. Mulcahey MJ, Hutchinson D, Kozin S. Assessment of upper limb in tetraplegia:
considerations in evaluation and outcomes research. Journal of rehabilitation research and
development. 2007;44(1):91-102.
98. Kapadia N, Zivanovic V, Verrier M, Popovic MR. Toronto rehabilitation institute-hand
function test: assessment of gross motor function in individuals with spinal cord injury. Top
Spinal Cord Inj Rehabil. 2012;18(2):167-86.
99. Tomljanović M, Spasić, M., Gabrilo, G., Uljević, O., & Foretić, N. (2011). . Effects of
five weeks of functional vs. traditional resistance training on anthropometric and motor
performance variables. Kinesiology: International journal of fundamental and applied
kinesiology, 2011. p. 145-54.

131
100. Amber Harnett DR, Amanda McIntyre,Swati Mehta,Jerome Iruthayarajah,Brooke
Benton,Robert Teasell,Eldon Loh. Upper Limb Rehabilitation Following Spinal Cord Injury
101. Sheffler LR, Chae J. Neuromuscular electrical stimulation in neurorehabilitation. Muscle
& nerve. 2007;35(5):562-90.
102. Velstra IM, Curt A, Frotzler A, Abel R, Kalsi-Ryan S, Rietman JS, et al. Changes in
Strength, Sensation, and Prehension in Acute Cervical Spinal Cord Injury: European Multicenter
Responsiveness Study of the GRASSP. Neurorehabilitation and neural repair. 2015;29(8):755-
66.
103. Kapadia NM, Bagher S, Popovic MR. Influence of different rehabilitation therapy models
on patient outcomes: Hand function therapy in individuals with incomplete SCI. Journal of
Spinal Cord Medicine. 2014.
104. Patil S, Raza WA, Jamil F, Caley R, O'Connor RJ. Functional electrical stimulation for
the upper limb in tetraplegic spinal cord injury: a systematic review. Journal of medical
engineering & technology. 2014;39(7):419-23.
105. Behrman AL, Ardolino EM, Harkema SJ. Activity-Based Therapy: From Basic Science
to Clinical Application for Recovery After Spinal Cord Injury. Journal of neurologic physical
therapy : JNPT. 2017;41 Suppl 3(Suppl 3 IV STEP Spec Iss):S39-s45.
106. Quel de Oliveira C, Refshauge K, Middleton J, de Jong L, Davis GM. Effects of Activity-
Based Therapy Interventions on Mobility, Independence, and Quality of Life for People with
Spinal Cord Injuries: A Systematic Review and Meta-Analysis. Journal of neurotrauma.
2017;34(9):1726-43.
107. Cesar Marquez-Chin NK-D, and Sukhinder Kalsi-Ryan. . Functional Electrical
Stimulation Therapy: A Closer Look. Ron Baecker R SA, editor: Morgan and Claypool; 2021.
108. Kralj A, Vodovnik L. Functional electrical stimulation of the extremities: part 1. Journal
of medical engineering & technology. 1977;1(1):12-5.
109. Peckham PH, Knutson JS. Functional electrical stimulation for neuromuscular
applications. Annual review of biomedical engineering. 2005;7:327-60.
110. LIBERSON WT, HOLMQUEST HJ, SCOT D, DOW M. Functional electrotherapy:
stimulation of the peroneal nerve synchronized with the swing phase of the gait of hemiplegic
patients. Archives of physical medicine and rehabilitation. 1961.
111. Long C, 2nd. AN ELECTROPHYSIOLOGIC SPLINT FOR THE HAND. Archives of
physical medicine and rehabilitation. 1963;44:499-503.
112. Angeli CA, Edgerton VR, Gerasimenko YP, Harkema SJ. Altering spinal cord
excitability enables voluntary movements after chronic complete paralysis in humans. Brain : a
journal of neurology. 2014;137(Pt 5):1394-409.

132
113. Mortimer JT BN. Peripheral nerve and muscle stimulation. . In: Neuroprosthetics WORLD SCIENTIFIC; Series on Bioengineering and Biomedical Engineering. 2004;2:638-82.
114. Popovic MR, Keller T, Papas IPI, Dietz V, Morari M. Surface-stimulation technology for grasping and walking neuroprostheses. IEEE Engineering in Medicine and Biology Magazine. 2001.
115. Marquez-Chin C, Popovic MR. Functional electrical stimulation therapy for restoration of
motor function after spinal cord injury and stroke: a review. Biomedical engineering online. 2020;19(1):34.
116. Vodovnik L, Kralj A, Stanic U, Acimovic R, Gros N. Recent applications of functional electrical stimulation to stroke patients in Ljubljana. Clinical orthopaedics and related research. 1978(131):64-70.
117. Eraifej J, Clark W, France B, Desando S, Moore D. Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: a systematic review and meta-analysis. Systematic reviews. 2017;6(1):40.
118. Restorative Therapies Baltimore, MD2021 [Available from:
https://restorativetherapies.com/ifes-systems/xcite/.
119. Popovic MR, Thrasher TA, Zivanovic V, Takaki J, Hajek V. Neuroprosthesis for retraining reaching and grasping functions in severe hemiplegic patients. Neuromodulation : journal of the International Neuromodulation Society. 2005;8(1):58-72.
120. Thrasher TA, Zivanovic V, McIlroy W, Popovic MR. Rehabilitation of reaching and grasping function in severe hemiplegic patients using functional electrical stimulation therapy. Neurorehabilitation and neural repair. 2008.
121. Venugopalan L, Taylor PN, Cobb JE, Swain ID. Upper limb functional electrical stimulation devices and their man-machine interfaces. Journal of medical engineering & technology. 2015;39(8):471-9.
122. Hebert DA, Bowen JM, Ho C, Antunes I, O’Reilly DJ, Bayley M. Examining a new functional electrical stimulation therapy with people with severe upper extremity hemiparesis and
chronic stroke: A feasibility study. British Journal of Occupational Therapy. 2017.
123. Popovic MR, Kapadia N, Zivanovic V, Furlan JC, Craven BC, McGillivray C. Functional electrical stimulation therapy of voluntary grasping versus only conventional rehabilitation for patients with subacute incomplete tetraplegia: A randomized clinical trial. Neurorehabilitation and neural repair. 2011;25(5):433-42.
124. Paralyzed Veterans of America Consortium for Spinal Cord Medicine. Preservation of upper limb function following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2005;28(5):434-70.

133
125. Mulcahey MJ, Betz RR, Kozin SH, Smith BT, Hutchinson D, Lutz C. Implantation of the
Freehand System during initial rehabilitation using minimally invasive techniques. Spinal cord.
2004;42(3):146-55.
126. Snoek GJ, MJ IJ, in 't Groen FA, Stoffers TS, Zilvold G. Use of the NESS handmaster to
restore handfunction in tetraplegia: clinical experiences in ten patients. Spinal cord.
2000;38(4):244-9.
127. Prochazka A, Gauthier M, Wieler M, Kenwell Z. The bionic glove: an electrical
stimulator garment that provides controlled grasp and hand opening in quadriplegia. Archives of
physical medicine and rehabilitation. 1997;78(6):608-14.
128. Rebersek S, Vodovnik L. Proportionally controlled functional electrical stimulation of
hand. Archives of physical medicine and rehabilitation. 1973;54(8):378-82.
129. Popovic DB, Popovic MB, Sinkjaer T. Neurorehabilitation of upper extremities in
humans with sensory-motor impairment. Neuromodulation : journal of the International
Neuromodulation Society. 2002;5(1):54-66.
130. Kapadia N, Zivanovic V, Popovic MR. Restoring voluntary grasping function in
individuals with incomplete chronic spinal cord injury: pilot study. Top Spinal Cord Inj Rehabil.
2013;19(4):279-87.
131. Kapadia N, Popovic M. Functional Electrical Stimulation Therapy for Grasping in Spinal
Cord Injury: An Overview. Topics in Spinal Cord Injury Rehabilitation. 2011;17(1):70-6.
132. Kapadia N, Masani K, Craven BC, Giangregorio LM, Hitzig SL, Richards K, et al. A
randomized trial of functional electrical stimulation for walking in incomplete spinal cord injury:
Effects on walking competency. Journal of Spinal Cord Medicine. 2014.
133. Kapadia NM, Nagai MK, Zivanovic V, Bernstein J, Woodhouse J, Rumney P, et al.
Functional electrical stimulation therapy for recovery of reaching and grasping in severe chronic
pediatric stroke patients. Journal of Child Neurology. 2014;29(4):493-9.
134. Popovic MR, Curt A, Keller T, Dietz V. Functional electrical stimulation for grasping
and walking: indications and limitations. Spinal cord. 2001;39(8):403-12.
135. Doherty JG, Burns AS, O'Ferrall DM, Ditunno JF, Jr. Prevalence of upper motor neuron
vs lower motor neuron lesions in complete lower thoracic and lumbar spinal cord injuries. The
journal of spinal cord medicine. 2002;25(4):289-92.
136. Smith B, Peckham PH, Keith MW, Roscoe DD. An externally powered, multichannel,
implantable stimulator for versatile control of paralyzed muscle. IEEE transactions on bio-
medical engineering. 1987;34(7):499-508.
137. Popovic MR, Thrasher TA, Adams ME, Takes V, Zivanovic V, Tonack MI. Functional
electrical therapy: Retraining grasping in spinal cord injury. Spinal cord. 2006;44(3):143-51.

134
138. Popović D, Stojanović A, Pjanović A, Radosavljević S, Popović M, Jović S, et al.
Clinical evaluation of the bionic glove. Archives of physical medicine and rehabilitation.
1999;80(3):299-304.
139. Popovic MR KT. Compex motion: neuroprosthesis for grasping applications. New York:
Elsevier Science Ltd;: MacLachlan M, Gallagher, eds. ; 2004. 197-216. p.
140. Popovic MR TT. Neuroprostheses. New York: Marcel Dekker.2004. 1056-65. p.
141. Popovic M.R. PDB, Keller T. Neuroprostheses for grasping. Neurological research.
2002;24(5):443-52.
142. Memberg WD, Crago PE. Instrumented objects for quantitative evaluation of hand grasp.
Journal of rehabilitation research and development. 1997;34(1):82-90.
143. Sollerman C, Ejeskär A. Sollerman hand function test. A standardised method and its use
in tetraplegic patients. Scandinavian journal of plastic and reconstructive surgery and hand
surgery. 1995;29(2):167-76.
144. Gritsenko V, Prochazka A. A functional electric stimulation-assisted exercise therapy
system for hemiplegic hand function. Archives of physical medicine and rehabilitation.
2004;85(6):881-5.
145. Kowalczewski J, Gritsenko V, Ashworth N, Ellaway P, Prochazka A. Upper-extremity
functional electric stimulation-assisted exercises on a workstation in the subacute phase of stroke
recovery. Archives of physical medicine and rehabilitation. 2007;88(7):833-9.
146. Kowalczewski J, Chong SL, Galea M, Prochazka A. In-home tele-rehabilitation improves
tetraplegic hand function. Neurorehabilitation and neural repair. 2011;25(5):412-22.
147. Jebsen RH, Taylor N, Trieschmann RB, Trotter MJ, Howard LA. An objective and
standardized test of hand function. Archives of physical medicine and rehabilitation.
1969;50(6):311-9.
148. Rudman D, Hannah S. An instrument evaluation framework: description and application
to assessments of hand function. Journal of hand therapy : official journal of the American
Society of Hand Therapists. 1998;11(4):266-77.
149. Agnew PJ. Functional effectiveness of a myo-electric prosthesis compared with a
functional split-hook prosthesis: a single subject experiment. Prosthetics and orthotics
international. 1981;5(2):92-6.
150. Chou FF, Sheen-Chen SM, Leong CP. Neuromuscular recovery after parathyroidectomy
in primary hyperparathyroidism. Surgery. 1995;117(1):18-25.
151. Lourenção MI, Battistella LR, Martins LC, Litvoc J. Analysis of the results of functional
electrical stimulation on hemiplegic patients' upper extremities using the Minnesota manual

135
dexterity test. International journal of rehabilitation research Internationale Zeitschrift fur
Rehabilitationsforschung Revue internationale de recherches de readaptation. 2005;28(1):25-31.
152. Lyle RC. A performance test for assessment of upper limb function in physical
rehabilitation treatment and research. International journal of rehabilitation research
Internationale Zeitschrift fur Rehabilitationsforschung Revue internationale de recherches de
readaptation. 1981;4(4):483-92.
153. Rudhe C, van Hedel HJ. Upper extremity function in persons with tetraplegia:
relationships between strength, capacity, and the spinal cord independence measure.
Neurorehabilitation and neural repair. 2009;23(5):413-21.
154. Lang CE, Wagner JM, Dromerick AW, Edwards DF. Measurement of upper-extremity
function early after stroke: properties of the action research arm test. Archives of physical
medicine and rehabilitation. 2006;87(12):1605-10.
155. Kalsi-Ryan S, Beaton D, Curt A, Duff S, Popovic MR, Rudhe C, et al. The Graded
Redefined Assessment of Strength Sensibility and Prehension: reliability and validity. Journal of
neurotrauma. 2012;29(5):905-14.
156. Kalsi-Ryan S CA, Fehlings MG, Verrier MC. Assessment of the hand in tetraplegia using
the Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP):
impairment versus function. Top Spinal Cord Inj Rehabil 2009;14(4):34-46.
157. Coates SK, Harvey LA, Dunlop SA, Allison GT. The AuSpinal: a test of hand function
for people with tetraplegia. Spinal cord. 2011;49(2):219-29.
158. Popovic MR, Kapadia N, Zivanovic V, Furlan JC, Craven BC, McGillivray C. Functional
electrical stimulation therapy of voluntary grasping versus only conventional rehabilitation for
patients with subacute incomplete tetraplegia: a randomized clinical trial. Neurorehabilitation
and neural repair. 2011;25(5):433-42.
159. Popovic MR, Masani K, Micera S. Functional electrical stimulation therapy: Recovery of
function following spinal cord injury and stroke. Neurorehabilitation Technology, Second
Edition2016.
160. Cizmar I, Zalesak B, Pilny J, Drac P, Fialova J. Possible restorations of the upper
extremity motion in tetraplegic patients - 5-year clinical experience. Biomedical papers of the
Medical Faculty of the University Palacky, Olomouc, Czechoslovakia. 2006;150(2):313-9.
161. Dodds TA, Martin DP, Stolov WC, Deyo RA. A validation of the functional
independence measurement and its performance among rehabilitation inpatients. Archives of
physical medicine and rehabilitation. 1993;74(5):531-6.
162. Catz A, Itzkovich M, Agranov E, Ring H, Tamir A. SCIM--spinal cord independence
measure: a new disability scale for patients with spinal cord lesions. Spinal cord.
1997;35(12):850-6.

136
163. Furlan JC, Noonan V, Singh A, Fehlings MG. Assessment of disability in patients with
acute traumatic spinal cord injury: a systematic review of the literature. Journal of neurotrauma.
2011;28(8):1413-30.
164. Dawson-Saunders B TR. Basic and Clinical Biostatistics. 2nd ed. ed: East Norwalk CT:
Appleton & Lange; 1994.
165. Van Peppen RP, Maissan FJ, Van Genderen FR, Van Dolder R, Van Meeteren NL.
Outcome measures in physiotherapy management of patients with stroke: a survey into self-
reported use, and barriers to and facilitators for use. Physiotherapy research international : the
journal for researchers and clinicians in physical therapy. 2008;13(4):255-70.
166. Braun T, Rieckmann A, Weber F, Grüneberg C. Current use of measurement instruments
by physiotherapists working in Germany: a cross-sectional online survey. BMC health services
research. 2018;18(1):810.
167. Ebaugh DD, McClure PW, Karduna AR. Three-dimensional scapulothoracic motion
during active and passive arm elevation. Clinical biomechanics (Bristol, Avon). 2005;20(7):700-
9.
168. Zhou M, Li F, Lu W, Wu J, Pei S. Efficiency of Neuromuscular Electrical Stimulation
and Transcutaneous Nerve Stimulation on Hemiplegic Shoulder Pain: A Randomized Controlled
Trial. Archives of physical medicine and rehabilitation. 2018;99(9):1730-9.
169. Lunsford C, Grindle G, Salatin B, Dicianno BE. Innovations With 3-Dimensional
Printing in Physical Medicine and Rehabilitation: A Review of the Literature. PM & R : the
journal of injury, function, and rehabilitation. 2016;8(12):1201-12.
170. Banks J. Adding value in additive manufacturing: researchers in the United Kingdom and
Europe look to 3D printing for customization. IEEE pulse. 2013;4(6):22-6.
171. Lee V, Singh G, Trasatti JP, Bjornsson C, Xu X, Tran TN, et al. Design and fabrication
of human skin by three-dimensional bioprinting. Tissue engineering Part C, Methods.
2014;20(6):473-84.
172. Huotilainen E, Paloheimo M, Salmi M, Paloheimo KS, Björkstrand R, Tuomi J, et al.
Imaging requirements for medical applications of additive manufacturing. Acta radiologica
(Stockholm, Sweden : 1987). 2014;55(1):78-85.
173. Telfer S, Munguia J, Pallari J, Dalgarno K, Steultjens M, Woodburn J. Personalized foot
orthoses with embedded temperature sensing: Proof of concept and relationship with activity.
Medical engineering & physics. 2014;36(1):9-15.
174. Gretsch KF, Lather HD, Peddada KV, Deeken CR, Wall LB, Goldfarb CA. Development
of novel 3D-printed robotic prosthetic for transradial amputees. Prosthetics and orthotics
international. 2016;40(3):400-3.
137
175. Medola FO, Fortulan CA, Purquerio Bde M, Elui VM. A new design for an old concept
of wheelchair pushrim. Disability and rehabilitation Assistive technology. 2012;7(3):234-41.
176. Hull C, inventor; Uvp Inc, assignee. Apparatus for production of three‐dimensional
objects by stereolithography. August 8, 1984.
177. Duncan Millar J, van Wijck F, Pollock A, Ali M. Outcome measures in post-stroke arm
rehabilitation trials: do existing measures capture outcomes that are important to stroke
survivors, carers, and clinicians? Clinical rehabilitation. 2019;33(4):737-49.
178. Pandian S, Arya KN. Stroke-related motor outcome measures: do they quantify the
neurophysiological aspects of upper extremity recovery? Journal of bodywork and movement
therapies. 2014;18(3):412-23.
179. Wang S, Hsu CJ, Trent L, Ryan T, Kearns NT, Civillico EF, et al. Evaluation of
Performance-Based Outcome Measures for the Upper Limb: A Comprehensive Narrative
Review. PM & R : the journal of injury, function, and rehabilitation. 2018;10(9):951-62.e3.
180. Galeoto G, Iori F, De Santis R, Santilli V, Mollica R, Marquez MA, et al. The outcome
measures for loss of functionality in the activities of daily living of adults after stroke: a
systematic review. Topics in stroke rehabilitation. 2019;26(3):236-45.
181. Yurkewich A, Kozak IJ, Hebert D, Wang RH, Mihailidis A. Hand Extension Robot
Orthosis (HERO) Grip Glove: enabling independence amongst persons with severe hand
impairments after stroke. Journal of neuroengineering and rehabilitation. 2020;17(1):33.
182. Gowland C, Stratford P, Ward M, Moreland J, Torresin W, Van Hullenaar S, et al.
Measuring physical impairment and disability with the Chedoke-McMaster Stroke Assessment.
Stroke. 1993;24(1):58-63.
183. Simpson LA, Eng JJ, Hsieh JT, Wolfe DL. The health and life priorities of individuals
with spinal cord injury: a systematic review. Journal of neurotrauma. 2012;29(8):1548-55.
184. Kalsi-Ryan S, Beaton D, Curt A, Popovic MR, Verrier MC, Fehlings MG. Outcome of
the upper limb in cervical spinal cord injury: Profiles of recovery and insights for clinical studies.
The journal of spinal cord medicine. 2014;37(5):503-10.
185. Post MW, Van Lieshout G, Seelen HA, Snoek GJ, Ijzerman MJ, Pons C. Measurement
properties of the short version of the Van Lieshout test for arm/hand function of persons with
tetraplegia after spinal cord injury. Spinal cord. 2006;44(12):763-71.
186. Velstra IM, Ballert CS, Cieza A. A systematic literature review of outcome measures for
upper extremity function using the international classification of functioning, disability, and
health as reference. PM & R : the journal of injury, function, and rehabilitation. 2011;3(9):846-
60.
187. Fawcett JW, Curt A, Steeves JD, Coleman WP, Tuszynski MH, Lammertse D, et al.
Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP

138
panel: spontaneous recovery after spinal cord injury and statistical power needed for therapeutic
clinical trials. Spinal cord. 2007;45(3):190-205.
188. Sinnott KA, Dunn JA, Rothwell AG. Use of the ICF conceptual framework to interpret
hand function outcomes following tendon transfer surgery for tetraplegia. Spinal cord.
2004;42(7):396-400.
189. RJ. M. Capabilities of Upper Extremity Test Manual of Administration, . Version 1.1.
ed. Philadelphia:: Thomas Jefferson University; 2016.
190. Hall KM, Cohen ME, Wright J, Call M, Werner P. Characteristics of the Functional
Independence Measure in traumatic spinal cord injury. Archives of physical medicine and
rehabilitation. 1999;80(11):1471-6.
191. Fekete C, Eriks-Hoogland I, Baumberger M, Catz A, Itzkovich M, Lüthi H, et al.
Development and validation of a self-report version of the Spinal Cord Independence Measure
(SCIM III). Spinal cord. 2013;51(1):40-7.
192. Kapadia N, Myers M, Musselman K, Wang RH, Yurkewich A, Popovic MR. 3-
Dimensional printing in rehabilitation: feasibility of printing an upper extremity gross motor
function assessment tool. Biomedical engineering online. 2021;20(1):2.
193. Zariffa J, Kapadia N, Kramer JL, Taylor P, Alizadeh-Meghrazi M, Zivanovic V, et al.
Relationship between clinical assessments of function and measurements from an upper-limb
robotic rehabilitation device in cervical spinal cord injury. IEEE transactions on neural systems
and rehabilitation engineering : a publication of the IEEE Engineering in Medicine and Biology
Society. 2012;20(3):341-50.
194. Zariffa J, Kapadia N, Kramer JL, Taylor P, Alizadeh-Meghrazi M, Zivanovic V, et al.
Feasibility and efficacy of upper limb robotic rehabilitation in a subacute cervical spinal cord
injury population. Spinal cord. 2012;50(3):220-6.
195. Zbogar D, Eng JJ, Miller WC, Krassioukov AV, Verrier MC. Movement repetitions in
physical and occupational therapy during spinal cord injury rehabilitation. Spinal cord.
2017;55(2):172-9.
196. Sinnott KA, Dunn JA, Wangdell J, Johanson ME, Hall AS, Post MW. Measurement of
Outcomes of Upper Limb Reconstructive Surgery for Tetraplegia. Archives of physical medicine
and rehabilitation. 2016;97(6 Suppl):S169-81.
197. Coster WJ, Haley SM, Jette AM. Measuring patient-reported outcomes after discharge
from inpatient rehabilitation settings. Journal of rehabilitation medicine. 2006;38(4):237-42.
198. Tyson S, Connell L. The psychometric properties and clinical utility of measures of
walking and mobility in neurological conditions: a systematic review. Clinical rehabilitation.
2009;23(11):1018-33.

139
199. Merletti R, Acimovic R, Grobelnik S, Cvilak G. Electrophysiological orthosis for the upper extremity in hemiplegia: feasibility study. Archives of physical medicine and rehabilitation.
1975;56(12):507-13.
200. Popović MB. Control of neural prostheses for grasping and reaching. Med Eng Phys. 2003 Jan;25(1):41-50. .
201. Chae J, Bethoux F, Bohine T, Dobos L, Davis T, Friedl A. Neuromuscular stimulation for upper extremity motor and functional recovery in acute hemiplegia. Stroke. 1998;29(5):975-9.
202. Meadmore KL, Exell TA, Hallewell E, Hughes AM, Freeman CT, Kutlu M, et al. The application of precisely controlled functional electrical stimulation to the shoulder, elbow and wrist for upper limb stroke rehabilitation: a feasibility study. Journal of neuroengineering and rehabilitation. 2014;11:105.
203. Cuesta-Gómez A, Carratalá-Tejada M, Molina-Rueda F, Miangolarra-Page JC. Functional
electrical stimulation improves reaching movement in the shoulder and elbow muscles of stroke
patients: A three-dimensional motion analysis. Restorative neurology and neuroscience.
2019;37(3):231-8.
204. Kapadia NM, Zivanovic V, Furlan JC, Craven BC, McGillivray C, Popovic MR. Functional electrical stimulation therapy for grasping in traumatic incomplete spinal cord injury: randomized control trial. Artificial organs. 2011;35(3):212-6.
205. Nagai MK, Marquez-Chin C, Popovic MR. Why is functional electrical stimulation therapy capable of restoring motor function following severe injury to the central nervous system? Translational Neuroscience: Fundamental Approaches for Neurological Disorders2016.
206. Keller T, Popovic MR, Pappas IP, Müller PY. Transcutaneous functional electrical stimulator "Compex Motion". Artificial organs. 2002;26(3):219-23.
207. Hebert DA BJ, Ho C, Antunes I, O’Reilly DJ, Bayley M. . Examining a new functional electrical stimulation therapy with people with severe upper extremity hemiparesis and chronic stroke: a feasibility study. Br J Occup Ther. 2017;80:651-9.
208. Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. The Journal of the American Academy of Orthopaedic Surgeons. 2003;11(2):142-51.
209. Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. The Journal of orthopaedic and sports physical therapy. 1996;24(2):57-65.
210. Rundquist PJ, Obrecht C, Woodruff L. Three-dimensional shoulder kinematics to complete activities of daily living. American journal of physical medicine & rehabilitation. 2009;88(8):623-9.
211. Wu G, van der Helm FC, Veeger HE, Makhsous M, Van Roy P, Anglin C, et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of

140
human joint motion--Part II: shoulder, elbow, wrist and hand. Journal of biomechanics.
2005;38(5):981-92.
212. Rudd JL. Electrical stimulation in serratus anterior paralysis (winged scapula). The Physical therapy review. 1953;33(2):64-7.
213. Bdaiwi AH, Mackenzie TA, Herrington L, Horsley I, Cools AM. Acromiohumeral Distance During Neuromuscular Electrical Stimulation of the Lower Trapezius and Serratus Anterior Muscles in Healthy Participants. Journal of athletic training. 2015;50(7):713-8.
214. Levangie PK Norkin C. Joint Structure and Function: A Comprehensive Analysis,. ed 4
ed: F.A. Davis Company; 2005.
215. Pearl ML, Harris SL, Lippitt SB, Sidles JA, Harryman DT, 2nd, Matsen FA, 3rd. A system for describing positions of the humerus relative to the thorax and its use in the presentation of several functionally important arm positions. Journal of shoulder and elbow surgery. 1992;1(2):113-8.
216. Magermans DJ, Chadwick EK, Veeger HE, van der Helm FC. Requirements for upper extremity motions during activities of daily living. Clinical biomechanics (Bristol, Avon). 2005;20(6):591-9.
217. Triffitt PD. The relationship between motion of the shoulder and the stated ability to perform activities of daily living. The Journal of bone and joint surgery American volume. 1998;80(1):41-6.
218. Doorenbosch CA, Harlaar J, Veeger DH. The globe system: an unambiguous description of shoulder positions in daily life movements. Journal of rehabilitation research and development. 2003;40(2):147-55.
219. Yamamoto L, Magalong E. Outcome measures in stroke. Critical care nursing quarterly. 2003;26(4):283-93; quiz 94-5.

141
Appendix 1 Functional Electrical Stimulation Therapy for Retraining Reaching
and Grasping After Spinal Cord Injury and Stroke

fnins-14-00718 July 7, 2020 Time: 19:34 # 1
METHODSpublished: 09 July 2020
doi: 10.3389/fnins.2020.00718
Edited by:Reinhold Scherer,
University of Essex, United Kingdom
Reviewed by:Jan Fridén,
Swiss Paraplegic Centre, SwitzerlandKevin Lloyd Kilgore,
The MetroHealth System,United States
*Correspondence:Naaz Kapadia
Specialty section:This article was submitted to
Neuroprosthetics,a section of the journal
Frontiers in Neuroscience
Received: 23 January 2020Accepted: 16 June 2020Published: 09 July 2020
Citation:Kapadia N, Moineau B and
Popovic MR (2020) FunctionalElectrical Stimulation Therapy
for Retraining Reaching and GraspingAfter Spinal Cord Injury and Stroke.
Front. Neurosci. 14:718.doi: 10.3389/fnins.2020.00718
Functional Electrical StimulationTherapy for Retraining Reaching andGrasping After Spinal Cord Injury andStrokeNaaz Kapadia1,2,3,4* , Bastien Moineau1,5,6 and Milos R. Popovic2,3,4,5
1 Rehabilitation Engineering Laboratory, The KITE Research Institute, Toronto Rehabilitation Institute-University HealthNetwork, Toronto, ON, Canada, 2 Rehabilitation Sciences Institute, University of Toronto, Toronto, ON, Canada, 3 CRANIA,University Health Network and University of Toronto, Toronto, ON, Canada, 4 The KITE Research Institute, TorontoRehabilitation Institute-University Health Network, Toronto, ON, Canada, 5 Institute of Biomaterials and BiomedicalEngineering, University of Toronto, Toronto, ON, Canada, 6 Myant Inc., Toronto, ON, Canada
Neurological conditions like hemiplegia following stroke or tetraplegia following spinalcord injury, result in a massive compromise in motor function. Each of the two conditionscan leave individuals dependent on caregivers for the rest of their lives. Once medicallystable, rehabilitation is the main stay of treatment. This article will address rehabilitationof upper extremity function. It is long known that moving the affected limb is crucialto recovery following any kind of injury. Overtime, it has also been established thatjust moving the affected extremities does not suffice, and that the movements haveto involve patient’s participation, be as close to physiologic movements as possible,and should ideally stimulate the entire neuromuscular circuitry involved in producing thedesired movement. For over four decades now, functional electrical stimulation (FES) isbeing used to either replace or retrain function. The FES therapy discussed in this articlehas been used to retrain upper extremity function for over 15 years. Published data ofpilot studies and randomized control trials show that FES therapy produces significantchanges in arm and hand function. There are specific principles of the FES therapy asapplied in our studies: (i) stimulation is applied using surface stimulation electrodes, (ii)there is minimum to virtually no pain during application, (iii) each session lasts no morethan 45–60 min, (iv) the technology is quite robust and can make up for specificity to acertain extent, and (v) fine motor function like two finger precision grip can be trained (i.e.,thumb and index finger tip to tip pinch). The FES therapy protocols can be successfullyapplied to individuals with paralysis resulting from stroke or spinal cord injury.
Keywords: functional electrical stimulation, spinal cord injury, stroke, rehabilitation, electrical stimulation,grasping, reaching, arm function
INTRODUCTION
Application of functional electrical stimulation (FES) for therapeutic purposes in rehabilitationsettings dates back to the 1960’s when Liberson et al. (1961) used an FES system to stimulatethe peroneal nerve to correct foot drop by triggering a foot switch, a single-channel electricalstimulation device stimulated the common peroneal nerve via a surface electrode, producing ankledorsiflexion during the swing phase of gait (Liberson et al., 1961). This led to the first commerciallyavailable FES system with surface stimulation electrodes. Since then FES technology has been
Frontiers in Neuroscience | www.frontiersin.org 1 July 2020 | Volume 14 | Article 718

fnins-14-00718 July 7, 2020 Time: 19:34 # 2
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
researched extensively to evaluate its benefits in diverseneurological conditions, and using an array of applicationtechniques (Baldi et al., 1998; Field-Fote, 2001; Popovic et al.,2005, 2011, 2012, 2016; Yan et al., 2005; Frotzler et al., 2008;Griffin et al., 2009; Daly et al., 2011; Kapadia et al., 2011, 2013,2014a; Giangregorio et al., 2012; Maleševic et al., 2012; Martinet al., 2012; Kawashima et al., 2013; Lee et al., 2013; Sadowskyet al., 2013; Ho et al., 2014; Kapadia N. et al., 2014; Popovic,2014; Sharif et al., 2014; Bauer et al., 2015; Howlett et al., 2015;Vafadar et al., 2015; Buick et al., 2016; Cuesta-Gómez et al.,2017; Fu et al., 2019; Straudi et al., 2020). The two commonuses of FES are to replace function (i.e., as an orthotic device)and to retrain function (i.e., as a therapeutic device). In thisarticle we will limit ourselves to the therapeutic applicationof FES.
In the therapeutic application (FES therapy), FES is usedas a short-term treatment modality. The expectation is that,after training with the FES system, the patients will be ableto voluntarily perform the trained activities without FES (i.e.,patients are expected to regain voluntary function). To date, a fewhigh-quality randomized controlled trials have been performed,proving the efficacy of FES therapy over other rehabilitationtechniques (Sharififar et al., 2018; Yen et al., 2019). Thispaucity in multicenter randomized controlled trials and thelimited access to systems that can properly deliver FES therapymight have affected its uptake in clinical settings (Ho et al.,2014; Auchstaetter et al., 2016). Fortunately, both these issuesare being addressed as new FES systems that are specificallydeveloped for FES therapy are being introduced, as well aslarge scale multicenter randomized controlled trials are beingplanned to further confirm the efficacy of this rehabilitationmodality. This article will provide readers with the details onhow transcutaneous multichannel FES therapy for the upperextremity can be applied in clinical trials and as such the samemethodology can be used in clinical practice by physiotherapistsand occupational therapists.
The FES methodology discussed here has been developed withthe intent to be user friendly, robust and to be able to producebetter functional gains than the presently available best-practicerehabilitation techniques. The FES system used in our laboratoryis a surface stimulation system with up to 4 stimulation channelsthat can produce gross motor function as well as precision gripssuch as two finger pinch grip. However, the methodology ofFES application discussed here is pertinent to any multichanneltranscutaneous FES device. We have used transcutaneous FES toretrain reaching and grasping in individuals with both spinal cordinjury and stroke (Thrasher et al., 2008; Kapadia and Popovic,2011; Kapadia et al., 2011, 2013; Popovic et al., 2012; Hebertet al., 2017). The results obtained in both patient populationsindicate functional improvements after 8–14 weeks of therapy(20–48 h of stimulation). Patients showed reduced dependencyon caregivers, and some even became independent in theiractivities of daily living.
This article will extensively detail how FES was applied inthese previously successful clinical trials to retrain reaching andgrasping functions in individuals who sustained a spinal cordinjury or a stroke.
MATERIALS AND EQUIPMENT
The FES system we used was a four channel surface stimulationdevice consisting of a software, a portable stimulator with aprogrammed chip card, self-adhesive stimulation electrodes, andvarious man-machine interfaces, such as push buttons, slidingpotentiometers (Mangold et al., 2005), accelerometers (Widjajaet al., 2011), EMG/biofeedback sensor, joysticks (Sayenkoet al., 2013), foot switches (Popovic et al., 2001b), gait phasedetection system (Pappas et al., 2004) and brain–machineinterface (Márquez-Chin et al., 2009). This FES system has beenextensively used in clinical trials by researchers both in NorthAmerica and in Europe. Its unique capability is the ability toprogram stimulation protocols customized to a patient’s needs inless than 10–15 min.
SoftwareThe software of our FES system allows one to specify/alterall stimulation parameters: frequency, minimum and maximumintensity, pulse duration, ramp time, synchronization andorder of stimulations, type of user interactions and numberof repetitions. The sensory, motor, functional and maximumthresholds are set using the continuous stimulation mode wherethe stimulation frequency and pulse duration are pre-set to valuesof 40 Hz and 200 µs, respectively.
METHODS
Clinical ApplicationsTo date, approximately 150 spinal cord injury and 50 strokepatients have been treated using transcutaneous FES in ourfacilities, ranging from pilot clinical trials to randomizedcontrolled trials. The FES system has been primarily usedas a therapeutic device for retraining reaching and grasping.More recently FES was successfully applied to an individualwith cervical spondylotic myelopathy to retrain upper extremityfunction with very promising results (Popovic et al., 2016).
Neuroprosthesis for Grasping in Spinal Cord InjuryPatients (University Health Network REB # 02-032,REB # 09-007, REB # 09-008)In case of patients with spinal cord injury the upper extremityretraining program is designed based on the level and extentof injury. For example, in C1–C5 cervical incomplete injuriesinitially FES might be used to retrain proximal function and thenonce the patient is able to position their arm in the workingspace then distal function can be trained. The FES protocolsfor retraining proximal function in SCI remain the same asstroke (please refer to the next section on stroke for details). Inpatients with low cervical injury (C6 and below), proximal upperextremity function might be preserved, and FES might then beused to retrain distal function right from the beginning. Also, it isimportant to note that again based on level of injury patient withSCI may have difficulty with both hand closing and opening andwill typically need to be trained for both.
Frontiers in Neuroscience | www.frontiersin.org 2 July 2020 | Volume 14 | Article 718
fnins-14-00718 July 7, 2020 Time: 19:34 # 3
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
Over the years, various grasping protocols have been identifiedand designed allowing for a wide variety of grasping patterns tobe trained with a great deal of fidelity. Currently, the graspingpatterns that can be successfully retrained using a transcutaneousmulti -channel FES system are:
(1) Palmar Grasp (holding a ball)(2) Lateral Grasp (holding a tray)(3) Tripod grip (thumb, index, and middle finger: holding a
pen)(4) Two finger opposition (thumb and index finger: holding a
peg)(5) Lateral Pinch (thumb and index finger: holding a credit
card)(6) Two finger lateral pinch (index and middle finger: smoker’s
grip)(7) Lumbrical grip (all four fingers with the thumb: holding a
closed book).
It is important to mention that FES therapy has the capabilityto help stroke and spinal cord injury patients relearn howto voluntarily perform all of the above grasps bilaterally andsimultaneously, using surface FES system.
We have conducted a number of clinical studies using this FEStechnology the most recent one being a randomized controlledtrial in incomplete cervical SCI patients (Popovic et al., 2011).Individuals allocated to the intervention group in this trialreceived FES stimulation protocols specifically designed for theirupper extremity functional deficits. Individualized stimulationsequences were developed for each patient. The commonlytrained grasping patterns were power and precision grasp wherepower grasp was used mainly to grasp larger everyday objectsand the precision grip was used mainly to manipulate smallerobjects. Power grasp was generated by partly flexing the fingersand the thumb in flexion and slight opposition. Lateral pinchwas generated by fully flexing the fingers followed by the thumbflexion. Muscles that were stimulated during therapy were thefollowing:
• Wrist flexors: flexor carpi radialis and flexor carpi ulnaris;• Wrist extensors: extensor carpi radialis (longus and brevis)
and ulnaris;• Finger flexors: flexor digitorum superficialis and flexor
digitorum profundus;• Finger extensors: extensor digitorum;• Thumb abductors: median nerve, or abductor pollicis brevis
and longus;• Thumb flexors: flexor pollicis brevis and flexor pollicis
longus;• Thumb oppositors: opponens pollicis;• Metacarpophalangeal flexors and interphalangeal joint
extensors: lumbricals.
The FES protocol allowed for individuals with little to novoluntary movement at the wrist and fingers to be able to performsimple tasks while being stimulated with the FES. This is whatdifferentiates FES from other therapies. In the early stages ofFES therapy, all the movements were performed with the help of
FES. The treatment plan and instruction to participants were asfollows:
(1) “Imagine hand opening” (or any movement that thetherapist would like to train).
(2) “Try to perform the movement using your own musclestrength.”
(3) After trying for about 10 s: “Now, try to perform themovement with the help of FES.”
Hence, emphasis was put on participants voluntarilyattempting the movement while being stimulated with theFES. During therapy when the participants started showing anability to voluntarily contract certain muscle groups FES forthose muscle groups was reduced to a minimum and graduallywithdrawn completely. The available channel was then usedon other muscle groups that were still weak and needed to betrained. The order in which muscle groups were sequentially“reactivated” was subject-dependent. FES was always deliveredwhile the participants were performing functional tasks, such asgrasping a mug, pouring water, holding a pen, etc.
The distinctiveness of this intervention is that FES is notprimarily intended for muscle strengthening. Instead, it is usedto retrain the neuromuscular system to execute tasks that itis unable to carry out voluntarily. Movements were performedagainst gravity and sometimes against light manual resistance.The number of repetitions was determined based on individualparticipant’s strength and endurance. In general, all participantsspent 30–45 min out of 1-h session performing activities ofdaily living with FES. The stimulation parameters used werethe following: (a) balanced, biphasic, current regulated electricalpulses; (b) pulse amplitude from 8 to 50 mA (typical values 15–30 mA); (c) pulse width 250 µs; and (d) pulse frequency 40 Hz(Popovic et al., 2011). During the intervention, the therapist, attheir discretion, adjusted the placement of electrodes and guidedthe hand movements. The therapist ensured that the movementswere functional. Occasionally FES would be combined withconventional rehabilitation strategies including strengtheningexercises, stretching exercises, etc.
Neuroprosthesis for Grasping in Stroke Patients(University Health Network REB # 02-032).The most important difference between FES training in spinalcord injury and stroke patients; is that stroke patients havedifficulty opening their hand as they often exhibit flexor synergyand high levels of tone in the finger flexors. In stroke patientstherefore, the focus of the therapy is on hand opening andrelaxing the fingers. In spinal cord injury patient’s the focus of theFES therapy is on finger flexion and grasping tasks as weaknessof the finger flexors is a bigger problem. Below are the methodsof FES application in clinical trials conducted in individuals whosuffered a stroke (Popovic et al., 2005; Thrasher et al., 2008;Kapadia et al., 2013).
For individuals allocated to the FES therapy group, treatmentbegan by proximal shoulder muscle training. The muscles thatwere stimulated were deltoid, biceps, and triceps. Typically,participants would recover proximal function first. As soon asthey gained functional strength in the proximal muscles, FES
Frontiers in Neuroscience | www.frontiersin.org 3 July 2020 | Volume 14 | Article 718

fnins-14-00718 July 7, 2020 Time: 19:34 # 4
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
for those muscles would be discontinued and applied to distalmuscles of the forearm and hand. The most difficult and time-consuming task was to train voluntary extension of the fingers.This is crucial to be able to get one’s hand around the objectsthat need to be manipulated. Once the participants were able tosuccessfully open their hand with FES assistance, low amplitudestimulation of the finger flexors was used to signal hand closing.Stimulation parameters used to stimulate the muscles and nerveswere the same as used for individuals with spinal cord injury(See section on “Neuroprosthesis for Grasping in Spinal CordInjury Patients).
In the early stages of the treatment, the arm/hand tasks wereperformed predominantly with the help of FES. As participantsshowed improvement stimulation was gradually reduced to aminimum and eventually phased out. Typical treatment sessionlasted for about 45 min, including the donning and doffing ofelectrodes. During all FES sessions the physiotherapist guidedthe movements and provided assistance as appropriate tocarry out the intended movement in as close to physiologicalmanner as possible.
Over the years the FES-reaching protocols have expanded tocover various functional reach patterns:
(1) Sideways reaching(2) Sideways reaching with hand opening(3) Forward reaching and retrieving(4) Forward reaching and retrieving with hand opening(5) Reaching over opposite shoulder(6) Reaching over opposite shoulder to forward reaching to
sideways reaching(7) Reaching over opposite knee(8) Hand to mouth
All of these protocols can easily be paired with the FES-grasping protocols for the spinal cord injury population to trainreaching and grasping together.
Practical Considerations for TherapistIn most of the clinical trials, FES sessions of 45–60 min weredelivered 3–5 days a week, for 8–16 weeks, for a total of about40 sessions. In our clinical experience, we found that patientsare able to tolerate a maximum of one 60 min session perday and within the session typically we are able to stimulateone movement pattern for approximately 10–15 repetitionsbefore fatigue sets in, however, it is important to note that thisfrequency is individual based and may vary based on extentof injury, chronicity and status of neuro-muscular system. Self-adhesive surface stimulation electrodes were used during therapy.All the patients were treated by registered physiotherapists oroccupational therapists. In all instances, each phase of the FESwas triggered by the treating Physiotherapist or Occupationaltherapist using a push button. All FES sessions incorporatedfunctional tasks during FES sessions. All FES training was incombination with conventional physiotherapy or occupationaltherapy techniques selected based on individual patient needs.Also, irrespective of the population, patients were required to
concentrate and actively make an attempt to carry out themovement while being assisted by FES, as described above.
The stepwise directions to conduct an upper extremity FEStraining session with a transcutaneous multi-channel FES deviceare as follows:
(1) Identify the functions to be trained (reachingand/or grasping).
(2) Select the order of the tasks to be re-trained: typically,start with gross motor tasks (proximal muscles) in earlystages of therapy followed by fine movement control(distal muscles).
(3) For each task identify the muscles to be stimulated: atany given time either only simple reaching or graspingtasks such as touching mouth or palmar grasp can betrained or more complex tasks such as reaching+ graspingcan be trained based on number of channels availablefor stimulation.
(4) First identify the optimal electrodes positioning: For a givenfunction, find the motor point; the electrode positionwhere a maximal contraction is obtained with minimumstimulation current delivered. We recommend finding themotor point using a smaller electrode, by trying severalpositions on the bulk of the muscles to be stimulated.This allows for finding an electrode position with minimalsecondary and unintentional stimulation of other musclesand/or nerves. Once you find the optimal electrodeposition(s) for a muscle, mark it with a pen/marker, andidentify position(s) for other muscles.
(5) Apply self-adhesive electrodes over the motor points of themuscles identified.Note: In case one has a stimulator that has galvanicallyisolated stimulation channels, one can apply the following:all electrodes on one aspect of the forearm can be“grounded” using a single return/anode electrode, i.e.,all muscles on the palmar aspect of the forearm canbe grounded using one electrode just proximal to theventral aspect of the wrist joint and similarly all electrodeson the dorsal aspect of the forearm can be groundedusing one electrode over the dorsal aspect of the wrist.If the stimulator does not have galvanically isolatedstimulation channels one should not use this “commonground” strategy.If you use non-alternate and asymmetrical pulseswaveform (with the negative depolarizing pulse always onthe same electrode, and the positive balancing pulse at alower amplitude), then you will have an “active” electrodeto be positioned on the motor point, and a “passive” orreturn/anode electrode under which there is no effectivestimulation (setting typically used for smaller muscles). Ifyou use alternate and/or symmetrical pulse waveform, thenboth electrodes are “active” and will trigger contractionssimilarly (setting typically used for larger muscles). Thechoice between one or two active electrode(s) is based onthe muscle size (one active electrode is preferable wherethere is no space on the bulk of the muscle to position twoelectrodes). Also, having a single “active” electrode ensures
Frontiers in Neuroscience | www.frontiersin.org 4 July 2020 | Volume 14 | Article 718

fnins-14-00718 July 7, 2020 Time: 19:34 # 5
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
greater specificity of the muscle and muscle volumethat is stimulated.
(6) Identify and record the different stimulation thresholds:Identify sensory threshold (when the patient feels thecurrent for the first time), motor threshold (when apalpable or a visible contraction is produced), functionalthreshold (when the desired functional movement isproduced) and maximum threshold (beyond which thepatient does not tolerate an increase in current amplitude).Note: It is important to define the thresholds with the samecurrent characteristics (pulse width and frequency) as theone used during FES therapy, because it has an impact onthe comfort and efficiency of the stimulation.
(7) Explain to the patient what to expect when the FES in turnedonExample: “First your hand will close and then it will open.”
(8) Turn on the stimulator and adjust the current intensitiesfor all muscles to the levels determined previously (intensityshould not exceed the determined maximum threshold).Trigger the FES protocol a few times so the patient hasa clear understanding of what to expect with each phaseof FES. Once the patient has a clear understanding of theprotocol, select the functional object to be used duringtraining. If needed, assist the patient to bring their handclose to/around the object to be manipulated.
(9) Instruct the patient that she/he has to make an activeattempt to perform the intended movement.Example: For a grasp/release task, ask the patient to closethe hand to grasp the object and, after the patient hasattempted for about 5–10 s, assist with FES. Once thepatient is able to grasp the object with assistance fromFES, complete the functional task, for example transferobject from point A to point B. Following successfulobject transfer, instruct the patient to release the objectand after about 5–10 s of the patient unsuccessfullyattempting to release the object trigger the FES sequencefor hand opening.
(10) Repeat this protocol 10–15 times. Then, select anotherprotocol and perform the next task for 5–7 min or asappropriate for that task. Execute 3–6 different protocolsin a 1-h session, with active stimulation for 30–40 min(depending on patient’s fatigue and therapist’s expertisewith the system). The 1-h therapy duration includespositioning of the electrodes and all relevant preparationsfor therapy initiation and therapy completion.
(11) Rest time should be given when the patient asks for it and/orwhen muscle fatigue sets in.
(12) When the therapy is completed, turn off the stimulator,remove the electrodes and inspect the skin underneath forany redness.Note: Occasionally redness may be present from theelectrode sticking on the skin, but it should dissipate in lessthan 24 h. Ask patient to monitor area and re-inspect atthe next session.
The selection of stimulation sequences is done based onclinical assessments which typically include use of standardized
assessment tools like Graded Redefined Assessment of Strength,Sensibility and Prehension, Toronto Rehabilitation Institute-Hand Function Test and Spinal Cord Independence MeasureSelf-care Sub-scores in spinal cord injury (Popovic et al., 2011)and Action Research Arm Test and Fugl Meyer assessment –upper extremity scores in stroke (Hebert et al., 2017).
LimitationsThere are certain limitations to this technology. The limb musclesthat are intended for FES treatment have to be accessible forplacement of the stimulation electrodes (Popovic et al., 2001a).There should not be a major degree of lower motor neuron injuryor nerve-root damage of the stimulated muscle. In a number ofpatients with spinal cord injury, there may be a variable amountof peripheral nerve damage (Doherty et al., 2002) (motoneuronsand nerve-roots) that restricts the application of FES. Also, thepatient has to be cognitively able to follow the instructions andactively participate in the therapy process. The patient shouldnot have any contraindications for FES application like metalimplants at the site of stimulation, pace-maker, open wound orrash at the site of electrode placement, uncontrolled autonomicdysreflexia, etc.
Besides, with programmable surface stimulation devices, onewould need an inter-professional team including bio medicalengineers who are proficient in programming the stimulationprotocols. This programming limitation may not apply to themore sophisticated newer FES systems. Presently there arecommercially available FES systems that can deliver FES therapiesdiscussed in this article. The reader is encouraged to find adevice that delivers FES therapies and is approved by the localregulatory body. Systems that do not have neuroplasticity andneuromodulation in their indication for use defined by theregulatory body should be avoided, as these stimulators are formuscle strengthening and improving range of motion, and notfor FES therapy discussed in this article.
RESULTS
To date, in our laboratory transcutaneous FES therapy has beensuccessfully applied to over 200 patients with either stroke orspinal cord injury. Based on the outcomes of these studies, itcan be said that short duration FES therapy combined withconventional occupational therapy and physiotherapy has theability to produce positive changes in these patients (Popovicet al., 2005, 2011, 2016; Thrasher et al., 2008; Kapadia andPopovic, 2011; Kapadia et al., 2013). The underlying mechanismresponsible for these changes include central modulationeffects. Stimulation induces cortical plasticity by modulatingthe ascending pathways through the Ia muscle fiber afferents(Chipchase et al., 2011). Additionally, somatosensory inputs tothe motor cortex are essential for motor learning and control, andplay critical roles in the motor recovery process (Vidoni et al.,2010; Pan et al., 2018). Stimulation above the motor thresholdincreases excitability of corticomotor pathway by activatingsensory axons and recruiting synaptic motoneurons and motorreflex (Chipchase et al., 2011). FES therapy in combination
Frontiers in Neuroscience | www.frontiersin.org 5 July 2020 | Volume 14 | Article 718

fnins-14-00718 July 7, 2020 Time: 19:34 # 6
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
with conventional PT and OT techniques harnesses the benefitsof neuroplasticity thereby improving function and enhancingparticipant independence with activities of daily living.
In the randomized controlled trial carried out in individualswith subacute (<6 months post injury) incomplete traumaticC3–C7 spinal cord injury, it was found that the individuals whoreceived 40 h of FES therapy had far greater improvementson the Self Care Sub-scores of the Functional IndependenceMeasure and Spinal Cord Independence Measure as comparedto individuals who received 40 h of conventional occupationaltherapy (Popovic et al., 2011). These gains were retained, orfurther improvement was observed, in the FES therapy group atthe time of 6 months follow up assessment (Popovic et al., 2011).To date we have obtained similar results in all individuals with
sub-acute incomplete spinal cord injury who received 40 h of FEStherapy (Figure 1).
Similar results were obtained in the randomized controlledtrial carried out in individuals with acute (2–7 weeks post)severe stroke with a total arm and hand score no more than2 on the Chedoke McMaster Stages of Motor Recovery(less than 15 points on Fugl Meyer Assessment UpperLimb Sub-score) (Thrasher et al., 2008; Hebert et al., 2017;Marquez-Chin et al., 2017). The individuals who received12–16 weeks of FES therapy for the arm and hand had statisticallybetter improvement on the Self-care sub-score of the FunctionalIndependence Measure (Figure 2), Fugl Meyer Assessment,Barthel Index, and Chedoke McMaster Stages of MotorRecovery as compared to individuals who received conventional
FIGURE 1 | Self-care Spinal Cord Independence Measure scores for all individuals with incomplete sub-acute spinal cord injury (blue bar indicates score at baselineand red bar indicates gain after 40 × 1 h therapy, treatment group received functional electrical stimulation and control group received conventional PT/OT).
FIGURE 2 | Self-care Functional Independence Measure scores for all individuals with sub-acute stroke (blue bar indicates score at baseline and red bar indicatesgain after 40 × 1 h therapy, treatment group received functional electrical stimulation and control group received conventional PT/OT).
Frontiers in Neuroscience | www.frontiersin.org 6 July 2020 | Volume 14 | Article 718

fnins-14-00718 July 7, 2020 Time: 19:34 # 7
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
occupational therapy and physiotherapy for the same duration.Detailed results of this study are published elsewhere.
In another clinical trial in chronic severe pediatric strokepopulation (Kapadia N. et al., 2014), where all four participantsreceived a total of 48 h of FES therapy, statistically significantimprovements were observed on the Quality of Upper ExtremitySkills Test as well as on various sub components of theRehabilitation Engineering Laboratory Hand Function Test (thisis the Toronto Rehabilitation Institute- Hand Function Test witha scoring system adapted for stroke).
DISCUSSION
Short duration multichannel surface FES is a viable and safetreatment modality that can be successfully applied in patientswith neurological conditions. It is important to note that we didnot formally investigate safety and feasibility in our clinical trialsmainly because transcutaneous FES has been applied in clinicaltrials for over 5 decades now without any reports of major adverseevents. However, given that we have applied FES to over 200patients over the past 15+ years we are able to confidently saythat transcutaneous FES is both safe and feasible. Across all ofour clinical trials we did not encounter any serious adverse eventsand we have been able to successfully retain our study participantsfor the duration of the research therapy. Discussed here is an in-depth application of transcutaneous multi-channel FES therapyof the upper extremity in spinal cord injury and stroke patients.In order to obtain maximum benefits of this therapy there aresome general points to keep in mind.
The goal of this manuscript is not to explore the mechanismof improvement in individuals with stroke and spinal cord injuryfollowing FES as this is a methods paper and as such thesemechanisms have been widely discussed in literature (Quandtand Hummel, 2014; Hara, 2015; Luo et al., 2020; Marquez-Chin and Popovic, 2020). We do, however, recommend somebasic principles of FES application on the widely accepted beliefthat mechanism of improvement with this therapy is basedon the principles of neuroplasticity (Nagai et al., 2016). Firstand foremost it is strongly recommended that therapy shouldbe started as soon as the medical condition of the patientis stabilized, i.e., preferably in the acute or sub-acute phasepost-injury. Secondly, active participation of the patient duringtreatment is critical. Along with the FES, patients have to makean active attempt to execute the target movement. Third, themovements carried out should be functional and should followa physiological pattern as closely as possible (movements similarto those of able-bodied individuals). Fourth, therapy should becombined with conventional rehabilitation modalities (example:stretching and strengthening) to reap maximum benefits. Lastly,while no specific dosing study has been conducted, our grouprecommends delivering at least three 1 h sessions per week.However, our group does not recommend more than one sessionper day, as this often exhausts the patient and prevents themfrom actively participating in the second session. In total, atleast 20 sessions are needed to obtain clinically relevant changes,however, it is often recommended that patients have 40 or more
hours of therapy to maximize outcomes and experience greatergains in function.
It should be noted that, in certain very acute or chronic spinalcord injury cases, a strengthening phase is necessary prior tothe functional training phase because the muscles are minimallyresponsive to stimulation at first (Popovic et al., 2002) due toinitial spinal shock (Galeiras Vázquez et al., 2017) or due tolong-term disuse (Popovic et al., 2002).
It is important to bear in mind that although FES therapyhas not been extensively tested in individuals with cervicalcomplete spinal cord injury, those that have been trained withthe system have shown remarkable improvements that weremuch more profound than those produced with conventionaltherapy (Popovic et al., 2006). This evidence merits conductingmore comprehensive clinical trials with FES therapy in cervicalcomplete spinal cord injury patients.
In conclusion, the most attractive feature of multichannelsurface stimulators is that they are non-invasive, oftenprogrammable and allow for various muscles/muscle groups tobe stimulated simultaneously in physiological patterns. Theyhave a high level of fidelity and are able to produce globalupper-limb motions as well as fine finger movements like twopinch grip (thumb and index finger) and tripod grip (thumb,index, and middle finger) using surface stimulation electrodes.
The specific surface stimulator used in our clinical studies,is not widely available any longer, however, the methodologicalconsiderations discussed above remain the same irrespective ofthe type of stimulation device. Any stimulator that can produceprotocols discussed in this article can be used for FES therapy.Although the new stimulators used for the FES therapy come withguidelines for locating motor points, therapists should be mindfulthat motor points can anatomically vary between individuals. Ifrequired, the first session should be dedicated to finding correctstimulation points, after which these can be marked down forfuture sessions.
As important as it is to assist weak muscles with FES duringexecution of functional tasks, it is equally important that oncefunctional voluntary strength is recovered (at least 3/5 on ManualMuscle Testing), stimulation is withdrawn from those musclesand the patient is encouraged to voluntarily control the musclesthemselves. The available FES channels can then be appliedto other weaker muscle groups that still need retraining. Insome cases, with severe spasticity, manual stretching of the tightmuscles prior to stimulation may yield better results.
DATA AVAILABILITY STATEMENT
The datasets generated for this study are available on request tothe corresponding author.
ETHICS STATEMENT
The studies involving human participants were reviewedand approved by Research Ethics Board, TorontoRehabilitation Institute-University Health Network. Thepatients/participants provided their written informed consent toparticipate in this study.
Frontiers in Neuroscience | www.frontiersin.org 7 July 2020 | Volume 14 | Article 718
fnins-14-00718 July 7, 2020 Time: 19:34 # 8
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
AUTHOR CONTRIBUTIONS
NK, MP, and BM were responsible for the concept andwriting of the manuscript and had read and approved themanuscript. All authors contributed to the article and approvedthe submitted version.
FUNDING
This project was supported by the Christopher & DanaReeve Foundation (TA1-0706-2), Spinal Cord Injury Ontario,
Rick Hansen Institute (SCISN grant 200936), Physician’sServices Incorporated Foundation (PSI Grant #05-06), OntarioNeurotrauma Foundation, Toronto Rehab Foundation, andthrough generous donation of Dean Connor and MarisUffelmann. During his postdoctoral position at TorontoRehabilitation Institute, BM was supported by grants fromSpinal Cord Injury Ontario and Age-Well. NK is a Ph.D.candidate at Rehabilitation Sciences Institute, Universityof Toronto and is supported by the CIHR - FrederickBanting and Charles Best Canada Graduate Scholarship –Doctoral Award.
REFERENCESAuchstaetter, N., Luc, J., Lukye, S., Lynd, K., Schemenauer, S., Whittaker, M., et al.
(2016). Physical Therapists’ use of functional electrical stimulation for clientswith stroke: frequency, barriers, and facilitators. Phys. Ther. 96, 995–1005.doi: 10.2522/ptj.20150464
Baldi, J. C., Jackson, R. D., Moraille, R., and Mysiw, W. J. (1998). Muscleatrophy is prevented in patients with acute spinal cord injury usingfunctional electrical stimulation. Spinal Cord 36, 463–469. doi: 10.1038/sj.sc.3100679
Bauer, P., Krewer, C., Golaszewski, S., Koenig, E., and Müller, F. (2015). Functionalelectrical stimulation-assisted active cycling – therapeutic effects in patientswith hemiparesis from 7 days to 6 months after stroke: a randomized controlledpilot study. Arch. Phys. Med. Rehabil. 96, 188–196. doi: 10.1016/j.apmr.2014.09.033
Buick, A. R., Kowalczewski, J., Carson, R. G., and Prochazka, A. (2016). Tele-supervised FES-assisted exercise for hemiplegic upper limb. IEEE Trans. NeuralSyst. Rehabil. Eng. 24, 79–87. doi: 10.1109/tnsre.2015.2408453
Chipchase, L. S., Schabrun, S. M., and Hodges, P. W. (2011). Peripheral electricalstimulation to induce cortical plasticity: a systematic review of stimulusparameters. Clin. Neurophysiol. 122, 456–463. doi: 10.1016/j.clinph.2010.07.025
Cuesta-Gómez, A., Molina-Rueda, F., Carratala-Tejada, M., Imatz-Ojanguren,E., Torricelli, D., and Miangolarra-Page, J. C. (2017). The use of functionalelectrical stimulation on the upper limb and interscapular muscles of patientswith stroke for the improvement of reaching movements: a feasibility study.Front. Neurol. 8:186. doi: 10.3389/fneur.2017.00186
Daly, J. J., Zimbelman, J., Roenigk, K. L., McCabe, J. P., Rogers, J. M., Butler, K.,et al. (2011). Recovery of coordinated gait: randomized controlled stroke trialof functional electrical stimulation (FES) versus no FES, with weight-supportedtreadmill and over-ground training. Neurorehabil. Neural Repair 25, 588–596.doi: 10.1177/1545968311400092
Doherty, J. G., Burns, A. S., O’Ferrall, D. M., and Ditunno, J. F. Jr. (2002).Prevalence of upper motor neuron vs lower motor neuron lesions in completelower thoracic and lumbar spinal cord injuries. J. Spinal Cord Med. 25, 289–292.doi: 10.1080/10790268.2002.11753630
Field-Fote, E. C. (2001). Combined use of body weight support, functional electricstimulation, and treadmill training to improve walking ability in individualswith chronic incomplete spinal cord injury. Arch. Phys. Med. Rehabil. 82,818–824. doi: 10.1053/apmr.2001.23752
Frotzler, A., Coupaud, S., Perret, C., Kakebeeke, T. H., Hunt, K. J., Donaldson,N. N., et al. (2008). High-volume FES-cycling partially reverses bone loss inpeople with chronic spinal cord injury. Bone 43, 169–176. doi: 10.1016/j.bone.2008.03.004
Fu, M. J., Harley, M. Y., Hisel, T., Busch, R., Wilson, R., Chae, J., et al. (2019). Abilityof people with post-stroke hemiplegia to self-administer FES-assisted handtherapy video games at home: an exploratory case series. J. Rehabil. AssistiveTechnol. Eng. 6:2055668319854000.
Galeiras Vázquez, R., Ferreiro Velasco, M. E., Mourelo Fariña, M., MontotoMarqués, A., and Salvador de la Barrera, S. (2017). Update on traumatic acutespinal cord injury. Part 1. Med. Intensiva 41, 237–247.
Giangregorio, L., Craven, C., Richards, K., Kapadia, N., Hitzig, S. L., Masani, K.,et al. (2012). A randomized trial of functional electrical stimulation for walking
in incomplete spinal cord injury: effects on body composition. J. Spinal CordMed. 35, 351–360. doi: 10.1179/2045772312y.0000000041
Griffin, L., Decker, M. J., Hwang, J. Y., Wang, B., Kitchen, K., Ding, Z., et al. (2009).Functional electrical stimulation cycling improves body composition, metabolicand neural factors in persons with spinal cord injury. J. Electromyogr. Kinesiol.19, 614–622. doi: 10.1016/j.jelekin.2008.03.002
Hara, Y. (2015). Brain plasticity and rehabilitation in stroke patients. J. NipponMed. School Nippon IKA Daigaku Zasshi 82, 4–13. doi: 10.1272/jnms.82.4
Hebert, D. A., Bowen, J. M., Ho, C., Antunes, I., O’Reilly, D. J., and Bayley, M.(2017). Examining a new functional electrical stimulation therapy with peoplewith severe upper extremity hemiparesis and chronic stroke: a feasibility study.Br. J. Occup. Ther. 80, 651–659. doi: 10.1177/0308022617719807
Ho, C. H., Triolo, R. J., Elias, A. L., Kilgore, K. L., DiMarco, A. F., and Bogie, K.(2014). Functional electrical stimulation and Spinal Cord Injury. Phys. Med.Rehabil. Clin. N. Am. 25:631–ix.
Howlett, O. A., Lannin, N. A., Ada, L., and Mckinstry, C. (2015). Functionalelectrical stimulation improves activity after stroke: a systematic review withmeta-analysis. Arch. Phys. Med. Rehabil. 96, 934–943. doi: 10.1016/j.apmr.2015.01.013
Kapadia, N., Masani, K., Craven, B. C., Giangregorio, L. M., Hitzig, S. L., Richards,K., et al. (2014). A randomized trial of functional electrical stimulation forwalking in incomplete spinal cord injury: effects on walking competency.J. Spinal Cord Med. 37, 511–524. doi: 10.1179/2045772314y.0000000263
Kapadia, N., Zivanovic, V., and Popovic, M. R. (2013). Restoring voluntarygrasping function in individuals with incomplete chronic spinal cord injury:pilot study. Top. Spinal Cord Injury Rehabil. 19, 279–287. doi: 10.1310/sci1904-279
Kapadia, N. M., Bagher, S., and Popovic, M. R. (2014a). Influence of differentrehabilitation therapy models on patient outcomes: hand function therapy inindividuals with incomplete SCI. J. Spinal Cord Med. 37, 734–743. doi: 10.1179/2045772314y.0000000203
Kapadia, N. M., Nagai, M. K., Zivanovic, V., Bernstein, J., Woodhouse, J., Rumney,P., et al. (2014b). Functional electrical stimulation therapy for recovery ofreaching and grasping in severe chronic pediatric stroke patients. J. ChildNeurol. 29, 493–499. doi: 10.1177/0883073813484088
Kapadia, N. M., and Popovic, M. R. (2011). Functional electrical stimulationtherapy for grasping in spinal cord injury: an overview. Top. Spinal Cord InjuryRehabil. 17, 70–76. doi: 10.1310/sci1701-70
Kapadia, N. M., Zivanovic, V., Furlan, J., Craven, B. C., Mcgillivray, C., andPopovic, M. R. (2011). Functional electrical stimulation therapy for grasping intraumatic incomplete spinal cord injury: randomized control trial. Artif. Organs35, 212–216. doi: 10.1111/j.1525-1594.2011.01216.x
Kawashima, N., Popovic, M. R., and Zivanovic, V. (2013). Effect of intensivefunctional electrical stimulation therapy on the upper limb motor recovery afterstroke: single case study of a chronic stroke patient, Stroke. Physiother. Can. 65,20–28. doi: 10.3138/ptc.2011-36
Lee, S. Y., Kang, S. Y., Im, S. H., Kim, B. R., Kim, S. M., Yoon, H. M., et al. (2013).The effects of assisted ergometer training with a functional electrical stimulationon exercise capacity and functional ability in subacute stroke patients. Ann.Rehabil. Med. 37, 619–627.
Liberson, W. T., Holmquest, H. J., Scot, D., and Dow, M. (1961). Functionalelectrotherapy: stimulation of the peroneal nerve synchronized with the swingphase of the gait of hemiplegic patients. Arch. Phys. Med. Rehabil. 42, 101–105.
Frontiers in Neuroscience | www.frontiersin.org 8 July 2020 | Volume 14 | Article 718

fnins-14-00718 July 7, 2020 Time: 19:34 # 9
Kapadia et al. Functional Electrical Stimulation in Rehabilitation
Luo, S., Xu, H., Zuo, Y., Liu, X., and All, A. H. (2020). A review of functionalelectrical stimulation treatment in spinal cord injury. Neuromol. Med. doi:10.1007/s12017-019-08589-9 [Epub ahead of print].
Maleševic, N. M., Maneski, L. Z. P., Iliæ, V., Jorgovanoviæ, N., Bijeliæ, G., Keller,T., et al. (2012). A multi-pad electrode based functional electrical stimulationsystem for restoration of grasp. J. NeuroEng. Rehabil. 9:66. doi: 10.1186/1743-0003-9-66
Mangold, S., Keller, T., Curt, A., and Dietz, V. (2005). Transcutaneous functionalelectrical stimulation for grasping in subjects with cervical spinal cord injury.Spinal Cord 43, 1–13. doi: 10.1038/sj.sc.3101644
Marquez-Chin, C., Bagher, S., Zivanovic, V., and Popovic, M. R. (2017). Functionalelectrical stimulation therapy for severe hemiplegia: randomized control trialrevisited. Can. J. Occup. Ther. 84, 87–97. doi: 10.1177/0008417416668370
Marquez-Chin, C., and Popovic, M. R. (2020). Functional electrical stimulationtherapy for restoration of motor function after spinal cord injury and stroke:a review. Biomed. Eng. Online 19:34.
Márquez-Chin, C., Popovic, M. R., Cameron, T., Lozano, A. M., and Chen, R.(2009). Control of a neuroprosthesis for grasping using off-line classificationof electrocorticographic signals: case study. Spinal Cord 47, 802–808. doi:10.1038/sc.2009.41
Martin, R., Sadowsky, C., Obst, K., Meyer, B., and McDonald, J. (2012). Functionalelectrical stimulation in spinal cord injury: from theory to practice. Top. SpinalCord Injury Rehabil. 18, 28–33. doi: 10.1310/sci1801-28
Nagai, M. K., Marquez-Chin, C., and Popovic, M. R. (2016). “Why is functionalelectrical stimulation therapy capable of restoring motor function followingsevere injury to the central nervous system?,” in Translational Neuroscience:Fundamental Approaches for Neurological Disorders, ed. M. Tuszynski (Boston,MA: Springer).
Pan, L. L. H., Yang, W. W., Kao, C. L., Tsai, M. W., Wei, S. H., Fregni, F.,et al. (2018). Effects of 8-week sensory electrical stimulation combined withmotor training on EEG-EMG coherence and motor function in individuals withstroke. Sci. Rep. 8:9217.
Pappas, I. P. I., Keller, T., Mangold, S., Popovic, M. R., Dietz, V., and Morari, M.(2004). A Reliable gyroscope-based gait-phase detection sensor embedded in ashoe insole. IEEE Sensors J. 4, 268–274. doi: 10.1109/jsen.2004.823671
Popoviæ, D. B. (2014). Advances in functional electrical stimulation (FES).J. Electromyogr. Kinesiol. 24, 795–802. doi: 10.1016/j.jelekin.2014.09.008
Popovic, M. R., Curt, A., Keller, T., and Dietz, V. (2001a). Functional electricalstimulation for grasping and walking: indications and limitations. Spinal Cord39, 403–412. doi: 10.1038/sj.sc.3101191
Popovic, M. R., Kapadia, N., Zivanovic, V., Furlan, J. C., Craven, B. C., andMcGillivray, C. (2011). Functional electrical stimulation therapy of voluntarygrasping versus only conventional rehabilitation for patients with subacuteincomplete tetraplegia: a randomized clinical trial. Neurorehabil. Neural Repair25, 433–442. doi: 10.1177/1545968310392924
Popovic, M. R., Keller, T., Papas, I. P. I., Dietz, V., and Morari, M. (2001b). Surface-stimulation technology for grasping and walking neuroprostheses. IEEE Eng.Med. Biol. Magazine 20, 82–93. doi: 10.1109/51.897831
Popovic, M. R., Masani, K., and Micera, S. (2012). “Functional electricalstimulation therapy: recovery of function following spinal cord injury andstroke,” in Neurorehabilitation Technology, eds D. Reinkensmeyer and V. Dietz(Cham: Springer).
Popovic, M. R., Popovic, D. B., and Keller, T. (2002). Neuroprostheses for grasping.Neurol. Res. 24, 443–452. doi: 10.1179/016164102101200311
Popovic, M. R., Thrasher, T. A., Adams, M. E., Takes, V., Zivanovic, V., and Tonack,M. I. (2006). Functional electrical therapy: retraining grasping in spinal cordinjury. Spinal Cord 44, 143–151. doi: 10.1038/sj.sc.3101822
Popovic, M. R., Thrasher, T. A., Zivanovic, V., Takaki, J., and Hajek, V. (2005).Neuroprosthesis for retraining reaching and grasping functions in severehemiplegic patients. Neuromodulation 8, 58–72. doi: 10.1111/j.1094-7159.2005.05221.x
Popovic, M. R., Zivanovic, V., and Valiante, T. A. (2016). Restoration of upperlimb function in an individual with cervical spondylotic myelopathy usingfunctional electrical stimulation therapy: a case study. Front. Neurol. 7:81. doi:10.3389/fneur.2016.00081
Quandt, F., and Hummel, F. C. (2014). The influence of functional electricalstimulation on hand motor recovery in stroke patients: a review. Exp. Transl.Stroke Med. 6:9.
Sadowsky, C. L., Hammond, E. R., Strohl, A. B., Commean, P. K., Eby, S. A.,Damiano, D. L., et al. (2013). Lower extremity functional electrical stimulationcycling promotes physical and functional recovery in chronic spinal cord injury.J. Spinal Cord Med. 36, 623–631. doi: 10.1179/2045772313y.0000000101
Sayenko, D. G., Robinson, M. F., Milosevic, M., Masani, K., and Popovic, M. R.(2013). Video game-based approach in calf muscle training: lessons from pilotstudy. Clin. Res. Foot Ankle 1:110.
Sharif, H., Gammage, K., Chun, S., and Ditor, D. (2014). Effects of FES-ambulationtraining on locomotor function and health-related quality of life in individualswith spinal cord injury. Top. Spinal Cord Injury Rehabil. 20, 58–69. doi: 10.1310/sci2001-58
Sharififar, S., Shuster, J. J., and Bishop, M. D. (2018). Adding electrical stimulationduring standard rehabilitation after stroke to improve motor function.A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 61, 339–344.doi: 10.1016/j.rehab.2018.06.005
Straudi, S., Baroni, A., Mele, S., Craighero, L., Manfredini, F., Lamberti, N., et al.(2020). Effects of a robot-assisted arm training plus hand functional electricalstimulation on recovery after stroke: a randomized clinical trial. Arch. Phys.Med. Rehabil. 101, 309–316. doi: 10.1016/j.apmr.2019.09.016
Thrasher, T. A., Zivanovic, V., McIlroy, W., and Popovic, M. R. (2008).Rehabilitation of reaching and grasping function in severe hemiplegic patientsusing functional electrical stimulation therapy. Neurorehabil. Neural Repair 22,706–714. doi: 10.1177/1545968308317436
Vafadar, A. K., Côté, J. N., and Archambault, P. S. (2015). Effectiveness offunctional electrical stimulation in improving clinical outcomes in the upperarm following stroke: a systematic review and meta-analysis. Biomed. Res. Int.2015:729768.
Vidoni, E. D., Acerra, N. E., Dao, E., Meehan, S. K., and Boyd, L. A. (2010). Role ofthe primary somatosensory cortex in motor learning: an rTMS study. Neurobiol.Learn. Memory 93, 532–539. doi: 10.1016/j.nlm.2010.01.011
Widjaja, F., Shee, C. Y., Au, W. L., Poignet, P., and Ang, W. T. (2011). “Usingelectromechanical delay for real-time anti-phase tremor attenuation systemusing functional electrical stimulation,” in Proceedings of the IEEE InternationalConference on Robotics and Automation, ICRA 2011, Shanghai.
Yan, T., Hui-Chan, C. W. Y., and Li, L. S. W. (2005). Functional electricalstimulation improves motor recovery of the lower extremity and walking abilityof subjects with first acute stroke: a randomized placebo-controlled trial. Stroke36, 80–85. doi: 10.1161/01.str.0000149623.24906.63
Yen, H. C., Chen, W. S., Jeng, J. S., Luh, J. J., Lee, Y. Y., and Pan,G. S. (2019). Standard early rehabilitation and lower limb transcutaneousnerve or neuromuscular electrical stimulation in acute stroke patients: arandomized controlled pilot study. Clin. Rehabil. 33, 1344–1354. doi: 10.1177/0269215519841420
Conflict of Interest: MP is a shareholder in company MyndTec Inc. Technologyand the results presented in the document, except for study “D. A. Hebert, J.M. Bowen, C. Ho, I. Antunes, D. J. O’Reilly, and M. Bayley,” “Examining anew functional electrical stimulation therapy with people with severe upperextremity hemiparesis and chronic stroke: A feasibility study,” “British Journal ofOccupational Therapy, pp:1–10, 2017,” have been produced before the companycreated its first product. MyndTec did not participate in any aspect of datageneration, data acquisition, data processing, data interpretation, manuscriptpreparation and it did not financially support any aspect of this project or thestudies that were discussed in this article. BM is affiliated with Myant Inc., acompany that develops electrical stimulation garments. Myant Inc. was notinvolved in the preparation of this manuscript.
The remaining author declares that the research was conducted in the absence ofany commercial or financial relationships that could be construed as a potentialconflict of interest.
Copyright © 2020 Kapadia, Moineau and Popovic. This is an open-access articledistributed under the terms of the Creative Commons Attribution License (CC BY).The use, distribution or reproduction in other forums is permitted, provided theoriginal author(s) and the copyright owner(s) are credited and that the originalpublication in this journal is cited, in accordance with accepted academic practice.No use, distribution or reproduction is permitted which does not comply withthese terms.
Frontiers in Neuroscience | www.frontiersin.org 9 July 2020 | Volume 14 | Article 718

151
Appendix 2 3D Toronto Rehabilitation Institute-Hand Function Test (3D TRI-
HFT) Scoring Sheet
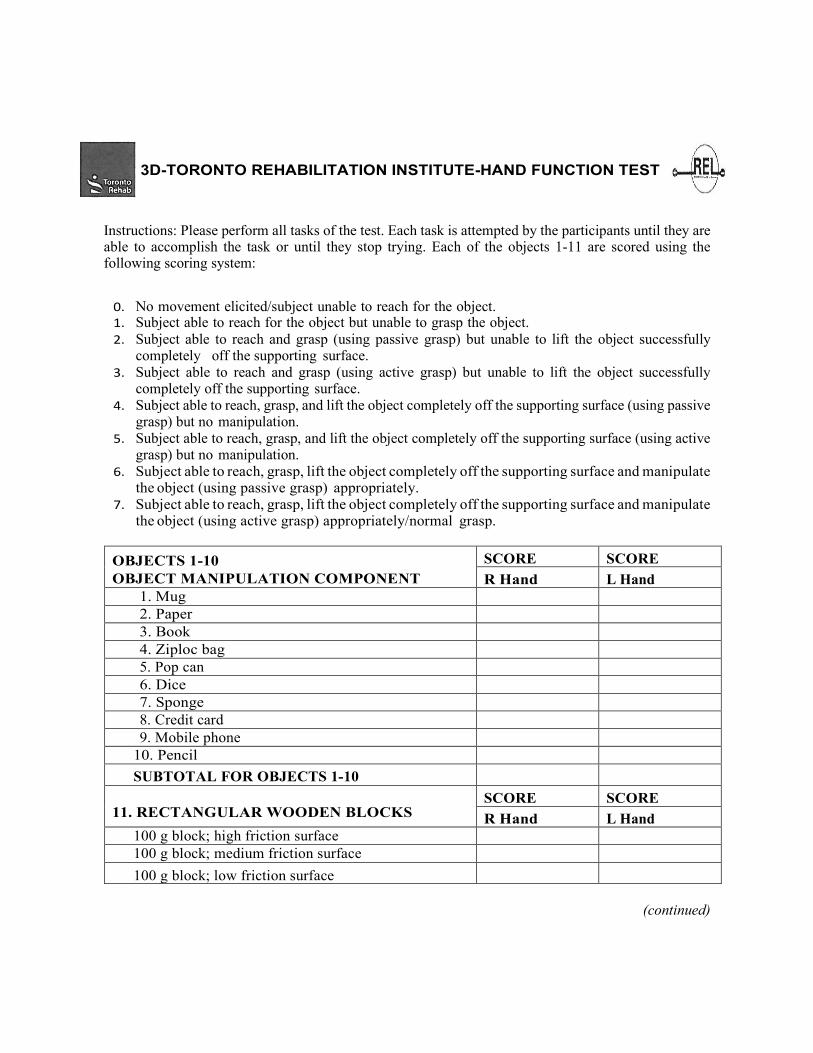
3D-TORONTO REHABILITATION INSTITUTE-HAND FUNCTION TEST
Instructions: Please perform all tasks of the test. Each task is attempted by the participants until they are able to accomplish the task or until they stop trying. Each of the objects 1-11 are scored using the following scoring system:
0. No movement elicited/subject unable to reach for the object. 1. Subject able to reach for the object but unable to grasp the object. 2. Subject able to reach and grasp (using passive grasp) but unable to lift the object successfully
completely off the supporting surface. 3. Subject able to reach and grasp (using active grasp) but unable to lift the object successfully
completely off the supporting surface. 4. Subject able to reach, grasp, and lift the object completely off the supporting surface (using passive
grasp) but no manipulation. 5. Subject able to reach, grasp, and lift the object completely off the supporting surface (using active
grasp) but no manipulation. 6. Subject able to reach, grasp, lift the object completely off the supporting surface and manipulate
the object (using passive grasp) appropriately. 7. Subject able to reach, grasp, lift the object completely off the supporting surface and manipulate
the object (using active grasp) appropriately/normal grasp.
OBJECTS 1-10 OBJECT MANIPULATION COMPONENT
SCORE SCORE R Hand L Hand
1. Mug 2. Paper 3. Book 4. Ziploc bag 5. Pop can 6. Dice 7. Sponge 8. Credit card 9. Mobile phone
10. Pencil SUBTOTAL FOR OBJECTS 1-10
11. RECTANGULAR WOODEN BLOCKS
SCORE SCORE R Hand L Hand
100 g block; high friction surface 100 g block; medium friction surface 100 g block; low friction surface
(continued)

200 g block; high friction surface
200 g block; medium friction surface
200 g block; low friction surface
300 g block; high friction surface
300 g block; medium friction surface
300 g block; low friction surface
SUBTOTAL FOR RECTANGULAR BLOCKS
12. INSTRUMENTED CYLINDER
Cannot hold
Measurement torque (units)
13. INSTRUMENTED CREDIT CARD
Cannot hold
Measurement force (units) 14. ROD
Cannot hold
Bar displacement in thumb direction
Bar displacement in little finger direction
R Hand L Hand
R Hand L Hand
R Hand L Hand

154
Appendix 3 Chedoke Arm and Hand Activity Inventory (CAHAI) Scoring Sheet

35
Chedoke Arm and Hand Activity Inventory: Score Form CAHAI-13 Version
Name: Date:
Activity Scale
1. total assist (weak U/L < 25%) 5. supervision 2. maximal assist (weak U/L = 25-49%) 6. modified independence (device) 3. moderate assist (weak U/L = 50-74%) 7. complete independence (timely, safely) 4. minimal assist (weak U/L > 75%)
Affected Limb: Score
1. Open jar of coffee holds jar
holds lid
2. Call 911
holds receiver
dials phone
3. Draw a line with a ruler holds ruler
holds pen
4. Pour a glass of water holds glass
holds pitcher
5. Wring out washcloth
6. Do up five buttons
7. Dry back with towel
reachs for towel
Grasps towel end
8. Put toothpaste on toothbrush
holds toothpaste
holds brush
9. Cut medium resistance putty holds knife
holds fork
10. Zip up the zipper holds zipper
holds zipper pull
11. Clean a pair of eyeglasses holds glasses
wipes lenses
12. Place container on table
13. Carry bag up the stairs
Total Score /91
Comments
COPY FREELY –DO NOT CHANGE Copyright 2004 Chedoke Arm and Hand Activity Inventory, Hamilton, ON
Funded by The Ontario Ministry of Health and Long Term Care

156
Appendix 4 Fugl Meyer Assessment-Upper Extremity (FMA-UE) Scoring
Sheet
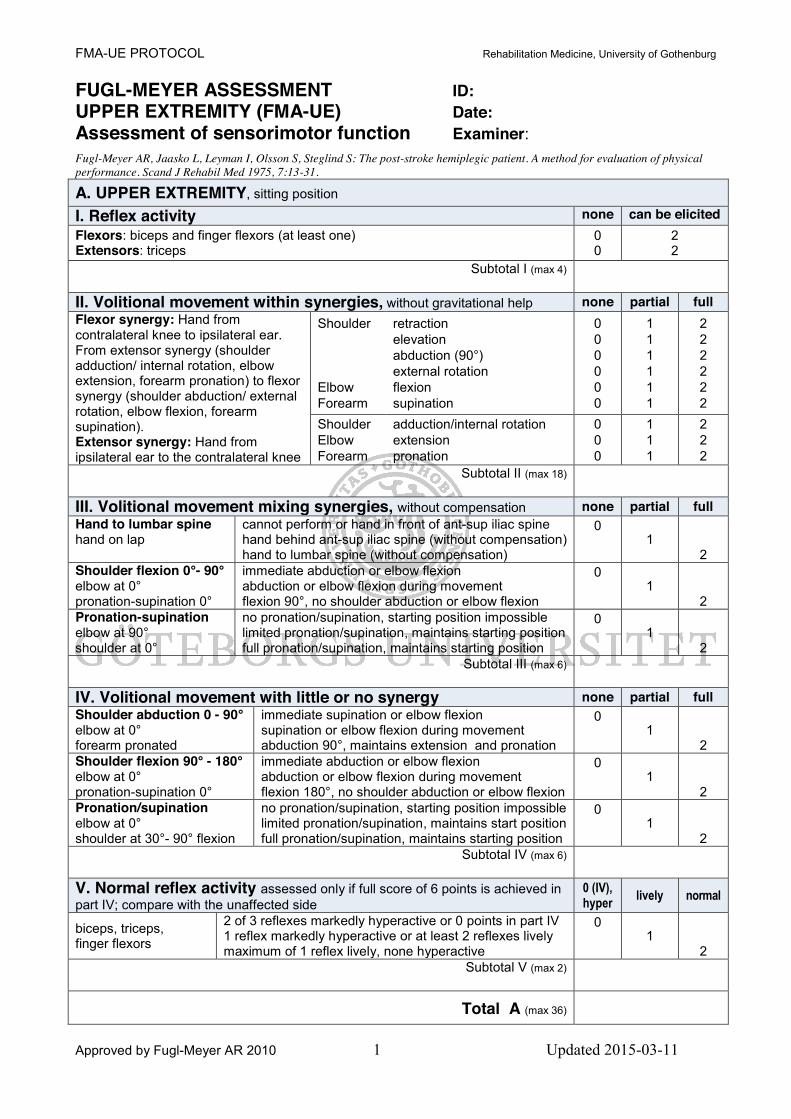
FMA-UE PROTOCOL Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 1 Updated 2015-03-11
FUGL-MEYER ASSESSMENT ID: UPPER EXTREMITY (FMA-UE) Date: Assessment of sensorimotor function Examiner: Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S: The post-stroke hemiplegic patient. A method for evaluation of physical performance. Scand J Rehabil Med 1975, 7:13-31.
A. UPPER EXTREMITY, sitting position
I. Reflex activity none can be elicited Flexors: biceps and finger flexors (at least one) Extensors: triceps
0 0
2 2
Subtotal I (max 4)
II. Volitional movement within synergies, without gravitational help none partial full Flexor synergy: Hand from contralateral knee to ipsilateral ear. From extensor synergy (shoulder adduction/ internal rotation, elbow extension, forearm pronation) to flexor synergy (shoulder abduction/ external rotation, elbow flexion, forearm supination). Extensor synergy: Hand from ipsilateral ear to the contralateral knee
Shoulder Elbow Forearm
retraction elevation abduction (90°) external rotation flexion supination
0 0 0 0 0 0
1 1 1 1 1 1
2 2 2 2 2 2
Shoulder Elbow Forearm
adduction/internal rotation extension pronation
0 0 0
1 1 1
2 2 2
Subtotal II (max 18)
III. Volitional movement mixing synergies, without compensation none partial full Hand to lumbar spine hand on lap
cannot perform or hand in front of ant-sup iliac spine hand behind ant-sup iliac spine (without compensation) hand to lumbar spine (without compensation)
0 1
2
Shoulder flexion 0°- 90° elbow at 0° pronation-supination 0°
immediate abduction or elbow flexion abduction or elbow flexion during movement flexion 90°, no shoulder abduction or elbow flexion
0 1
2
Pronation-supination elbow at 90° shoulder at 0°
no pronation/supination, starting position impossible limited pronation/supination, maintains starting position full pronation/supination, maintains starting position
0 1
2
Subtotal III (max 6)
IV. Volitional movement with little or no synergy none partial full Shoulder abduction 0 - 90° elbow at 0° forearm pronated
immediate supination or elbow flexion supination or elbow flexion during movement abduction 90°, maintains extension and pronation
0 1
2 Shoulder flexion 90° - 180° elbow at 0° pronation-supination 0°
immediate abduction or elbow flexion abduction or elbow flexion during movement flexion 180°, no shoulder abduction or elbow flexion
0 1
2
Pronation/supination elbow at 0° shoulder at 30°- 90° flexion
no pronation/supination, starting position impossible limited pronation/supination, maintains start position full pronation/supination, maintains starting position
0 1
2
Subtotal IV (max 6)
V. Normal reflex activity assessed only if full score of 6 points is achieved in part IV; compare with the unaffected side
0 (IV), hyper lively normal
biceps, triceps, finger flexors
2 of 3 reflexes markedly hyperactive or 0 points in part IV 1 reflex markedly hyperactive or at least 2 reflexes lively maximum of 1 reflex lively, none hyperactive
0 1
2
Subtotal V (max 2)
Total A (max 36)
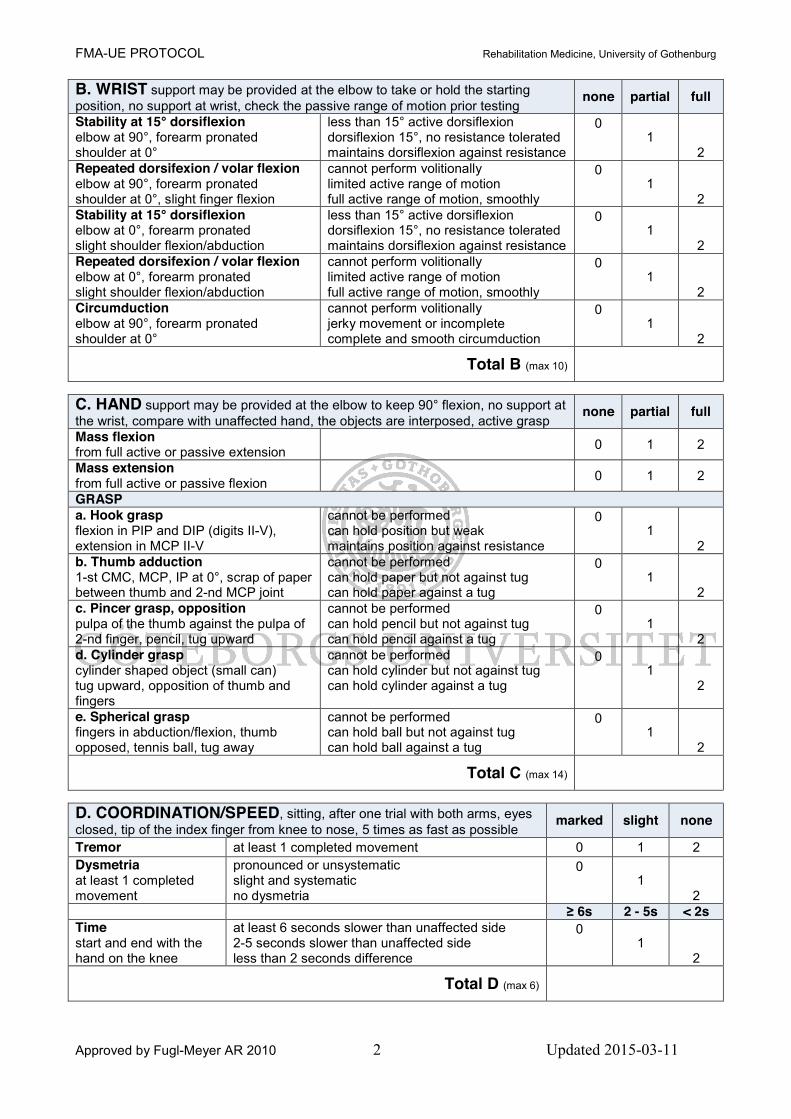
FMA-UE PROTOCOL Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 2 Updated 2015-03-11
B. WRIST support may be provided at the elbow to take or hold the starting position, no support at wrist, check the passive range of motion prior testing
none partial full
Stability at 15° dorsiflexion elbow at 90°, forearm pronated shoulder at 0°
less than 15° active dorsiflexion dorsiflexion 15°, no resistance tolerated maintains dorsiflexion against resistance
0 1
2
Repeated dorsifexion / volar flexion elbow at 90°, forearm pronated shoulder at 0°, slight finger flexion
cannot perform volitionally limited active range of motion full active range of motion, smoothly
0 1
2
Stability at 15° dorsiflexion elbow at 0°, forearm pronated slight shoulder flexion/abduction
less than 15° active dorsiflexion dorsiflexion 15°, no resistance tolerated maintains dorsiflexion against resistance
0 1
2
Repeated dorsifexion / volar flexion elbow at 0°, forearm pronated slight shoulder flexion/abduction
cannot perform volitionally limited active range of motion full active range of motion, smoothly
0 1
2
Circumduction elbow at 90°, forearm pronated shoulder at 0°
cannot perform volitionally jerky movement or incomplete complete and smooth circumduction
0 1
2
Total B (max 10)
C. HAND support may be provided at the elbow to keep 90° flexion, no support at the wrist, compare with unaffected hand, the objects are interposed, active grasp
none partial full
Mass flexion from full active or passive extension 0 1 2
Mass extension from full active or passive flexion 0 1 2
GRASP a. Hook grasp flexion in PIP and DIP (digits II-V), extension in MCP II-V
cannot be performed can hold position but weak maintains position against resistance
0 1
2
b. Thumb adduction 1-st CMC, MCP, IP at 0°, scrap of paper between thumb and 2-nd MCP joint
cannot be performed can hold paper but not against tug can hold paper against a tug
0 1
2
c. Pincer grasp, opposition pulpa of the thumb against the pulpa of 2-nd finger, pencil, tug upward
cannot be performed can hold pencil but not against tug can hold pencil against a tug
0 1
2 d. Cylinder grasp cylinder shaped object (small can) tug upward, opposition of thumb and fingers
cannot be performed can hold cylinder but not against tug can hold cylinder against a tug
0 1
2
e. Spherical grasp fingers in abduction/flexion, thumb opposed, tennis ball, tug away
cannot be performed can hold ball but not against tug can hold ball against a tug
0 1
2
Total C (max 14)
D. COORDINATION/SPEED, sitting, after one trial with both arms, eyes closed, tip of the index finger from knee to nose, 5 times as fast as possible marked slight none
Tremor at least 1 completed movement 0 1 2 Dysmetria at least 1 completed movement
pronounced or unsystematic slight and systematic no dysmetria
0 1
2
≥ 6s 2 - 5s < 2s Time start and end with the hand on the knee
at least 6 seconds slower than unaffected side 2-5 seconds slower than unaffected side less than 2 seconds difference
0 1
2
Total D (max 6)

FMA-UE PROTOCOL Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 3 Updated 2015-03-11
TOTAL A-D (max 66)
H. SENSATION, upper extremity eyes closed, compared with the unaffected side anesthesia hypoesthesia or
dysesthesia normal
Light touch upper arm, forearm palmary surface of the hand
0 0
1 1
2 2
less than 3/4 correct or absence
3/4 correct or considerable
difference
correct 100%, little or no difference
Position small alterations in the position
shoulder elbow wrist thumb (IP-joint)
0 0 0 0
1 1 1 1
2 2 2 2
Total H (max12)
J. PASSIVE JOINT MOTION, upper extremity, sitting position, compare with the unaffected side
J. JOINT PAIN during passive motion, upper extremity
only few degrees (less than 10° in shoulder)
decreased normal
pronounced pain during movement or very marked pain at the end of the movement
some pain
no pain
Shoulder Flexion (0° - 180°) Abduction (0°-90°) External rotation Internal rotation
0 0 0 0
1 1 1 1
2 2 2 2
0 0 0 0
1 1 1 1
2 2 2 2
Elbow Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Forearm Pronation Supination
0 0
1 1
2 2
0 0
1 1
2 2
Wrist Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Fingers Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Total (max 24) Total (max 24)
A. UPPER EXTREMITY /36
B. WRIST /10
C. HAND /14
D. COORDINATION / SPEED / 6
TOTAL A-D (motor function) /66
H. SENSATION /12
J. PASSIVE JOINT MOTION /24
J. JOINT PAIN /24

160
Appendix 5 Chedoke-McMaster Stages of Recovery of the Arm (CMSA-Arm) and Chedoke-McMaster Stages of Recovery of the Hand (CMSA-
Hand) Scoring Sheet

IMPAIRMENT INVENTORY: STAGE OF ARM Score Form Page2
7-15
Standard Starting Position: Sitting with the forearm in the lap or supported on a pillow in the lap in a neutral position, wrist at 0° and fingers slightly flexed. Sitting either unsupported over the side of the bed or plinth, or supported in a chair or wheelchair. Feet should be supported. Encourage good sitting posture during testing (ie. with hips and knees at 90°). Start the assessment at Stage 3.
STAGE 1 Unable to demonstrate at least two of the Stage 2 tasks. STAGE 2 Support the limb as necessary while facilitating the movements. Task 1: Resistance to passive shoulder abduction or elbow extension Position: Standard starting position. Instruction: "Let me move your arm." Method: Choose either a) or b):
a) Abduct and adduct shoulder 5 times with sufficient speed of passive movement to elicit a stretch reflex. Do not exceed 70° of abduction. Feel for resistance to passive movement and watch for active contraction of pectoral muscles. Do with care, respecting pain. b) Flex and extend elbow 5 times with sufficient speed of passive movement to elicit a stretch reflex.
Required: Feel for resistance to passive movement and watch for active contraction of the stretched muscle.
Task 2: Facilitated elbow extension Position: Standard starting position. Instruction: "Straighten your elbow and try to touch your opposite knee." Method: Facilitate a contraction of the elbow extensors. Required: Some observed active elbow extension. Task 3: Facilitated elbow flexion Position: Standard starting position. Instruction: "Bend your elbow." Method: Facilitate a contraction of the elbow flexors. STAGE 3 Task 1: Touch opposite knee Position: Standard starting position. Instruction: "Straighten your elbow and try to touch your opposite knee." Required: Active shoulder adduction and full elbow extension with palm facing down. Permitted: The wrist may be supported in a neutral position so that it does not interfere with
arm extension. Task 2: Touch chin

IMPAIRMENT INVENTORY: STAGE OF ARM Score Form Page2
7-16
Position: Standard starting position. Instruction: "Touch your chin with your hand." Required: Sufficient elbow flexion for any part of the hand to touch the chin. Movement in
synergy is permissible. Not permitted: Flexion of head Task 3: Shoulder shrugging greater than half range Position: Standard starting position. Instruction: "Shrug both shoulders up towards your ears." Required: Active scapular elevation greater than half range. Movement in synergy is
permissible. STAGE 4 Task 1: Extension synergy, then flexion synergy Position: Standard starting position. Instruction: "Reach across and touch your opposite knee with your elbow straight, then
without stopping, touch the ear on your weak side, keeping your elbow up." Required: Shoulder adduction and full elbow extension to touch or pass the top of the
opposite knee with full internal rotation of the shoulder and pronation of the forearm. Then without stopping the shoulder should attain at least 90° of abduction with 0° horizontal flexion and some external rotation when the hand touches the ear. The forearm may be either pronated or supinated.
Don't accept: Prolonged pause between synergies. Task 2: Shoulder flexion to 90° Position: Standard starting position Instruction: "Keep your elbow straight throughout movement, and lift your arm up to shoulder
height." Required: Shoulder flexion to 90˚ with full elbow extension. Forearm may be pronated. Don't accept: Shoulder abduction, scapular elevation or elbow flexion. Task 3: Supination then pronation Position: Elbow at side with 90˚ elbow flexion. Instruction: "Keep your elbow at your side, and turn your palm up and then down." Required: Full supination and full pronation. Elbow remains at side of trunk. Don't accept: Compensatory movement of trunk.
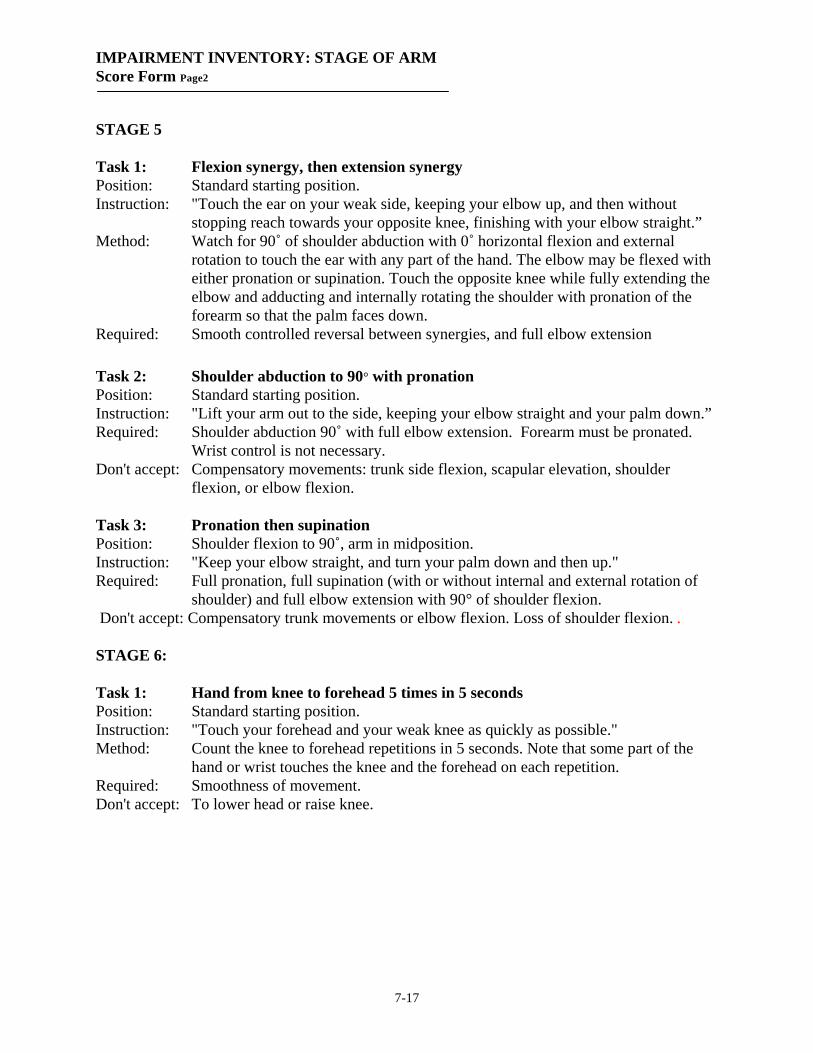
IMPAIRMENT INVENTORY: STAGE OF ARM Score Form Page2
7-17
STAGE 5 Task 1: Flexion synergy, then extension synergy Position: Standard starting position. Instruction: "Touch the ear on your weak side, keeping your elbow up, and then without
stopping reach towards your opposite knee, finishing with your elbow straight.” Method: Watch for 90˚ of shoulder abduction with 0˚ horizontal flexion and external
rotation to touch the ear with any part of the hand. The elbow may be flexed with either pronation or supination. Touch the opposite knee while fully extending the elbow and adducting and internally rotating the shoulder with pronation of the forearm so that the palm faces down.
Required: Smooth controlled reversal between synergies, and full elbow extension
Task 2: Shoulder abduction to 90° with pronation Position: Standard starting position. Instruction: "Lift your arm out to the side, keeping your elbow straight and your palm down.” Required: Shoulder abduction 90˚ with full elbow extension. Forearm must be pronated.
Wrist control is not necessary. Don't accept: Compensatory movements: trunk side flexion, scapular elevation, shoulder
flexion, or elbow flexion. Task 3: Pronation then supination Position: Shoulder flexion to 90˚, arm in midposition. Instruction: "Keep your elbow straight, and turn your palm down and then up." Required: Full pronation, full supination (with or without internal and external rotation of
shoulder) and full elbow extension with 90° of shoulder flexion. Don't accept: Compensatory trunk movements or elbow flexion. Loss of shoulder flexion. . STAGE 6: Task 1: Hand from knee to forehead 5 times in 5 seconds Position: Standard starting position. Instruction: "Touch your forehead and your weak knee as quickly as possible." Method: Count the knee to forehead repetitions in 5 seconds. Note that some part of the
hand or wrist touches the knee and the forehead on each repetition. Required: Smoothness of movement. Don't accept: To lower head or raise knee.
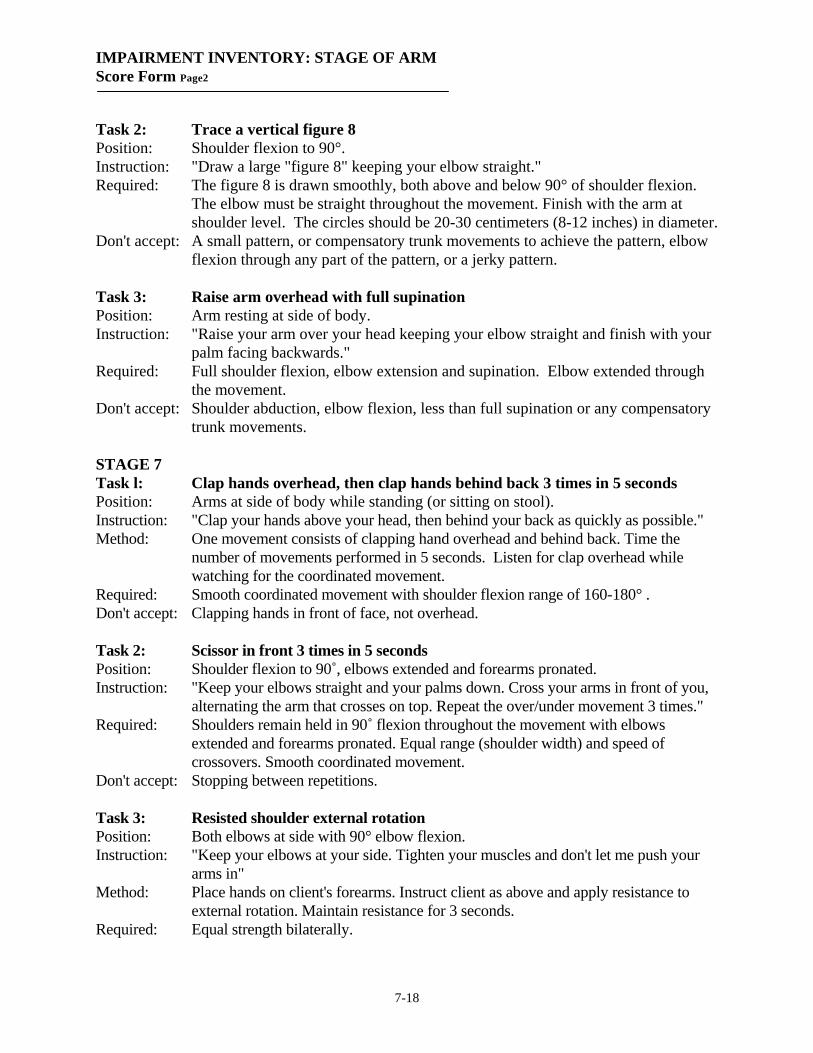
IMPAIRMENT INVENTORY: STAGE OF ARM Score Form Page2
7-18
Task 2: Trace a vertical figure 8 Position: Shoulder flexion to 90°. Instruction: "Draw a large "figure 8" keeping your elbow straight." Required: The figure 8 is drawn smoothly, both above and below 90° of shoulder flexion.
The elbow must be straight throughout the movement. Finish with the arm at shoulder level. The circles should be 20-30 centimeters (8-12 inches) in diameter.
Don't accept: A small pattern, or compensatory trunk movements to achieve the pattern, elbow flexion through any part of the pattern, or a jerky pattern.
Task 3: Raise arm overhead with full supination Position: Arm resting at side of body. Instruction: "Raise your arm over your head keeping your elbow straight and finish with your
palm facing backwards." Required: Full shoulder flexion, elbow extension and supination. Elbow extended through
the movement. Don't accept: Shoulder abduction, elbow flexion, less than full supination or any compensatory
trunk movements. STAGE 7 Task l: Clap hands overhead, then clap hands behind back 3 times in 5 seconds Position: Arms at side of body while standing (or sitting on stool). Instruction: "Clap your hands above your head, then behind your back as quickly as possible." Method: One movement consists of clapping hand overhead and behind back. Time the
number of movements performed in 5 seconds. Listen for clap overhead while watching for the coordinated movement.
Required: Smooth coordinated movement with shoulder flexion range of 160-180° . Don't accept: Clapping hands in front of face, not overhead. Task 2: Scissor in front 3 times in 5 seconds Position: Shoulder flexion to 90˚, elbows extended and forearms pronated. Instruction: "Keep your elbows straight and your palms down. Cross your arms in front of you,
alternating the arm that crosses on top. Repeat the over/under movement 3 times." Required: Shoulders remain held in 90˚ flexion throughout the movement with elbows
extended and forearms pronated. Equal range (shoulder width) and speed of crossovers. Smooth coordinated movement.
Don't accept: Stopping between repetitions. Task 3: Resisted shoulder external rotation Position: Both elbows at side with 90° elbow flexion. Instruction: "Keep your elbows at your side. Tighten your muscles and don't let me push your
arms in" Method: Place hands on client's forearms. Instruct client as above and apply resistance to
external rotation. Maintain resistance for 3 seconds. Required: Equal strength bilaterally.

IMPAIRMENT INVENTORY: STAGE OF HAND Score Form Page2
7-19
Standard sitting position: Sitting with the forearm in the lap, or supported on a pillow, in a neutral position, wrist at 0° and fingers slightly flexed. The client can sit either unsupported on the side of the bed or plinth, or supported in a chair or wheelchair. Feet should be supported. Encourage good sitting posture for testing (ie. with hips and knees at 90°). Start the assessment at Stage 3. STAGE 1 Unable to demonstrate at least two of the Stage 2 tasks. STAGE 2 Support the limb as necessary while facilitating the movements. Task 1: Positive Hoffman Position: Standard starting position. Instruction: "Let me move your fingers." Method: With one hand support the client's middle phalanx of the middle finger. With the
other hand quickly snap the distal phalanx of the middle finger into flexion. A positive response is flexion of the fingers or thumb (or both).
Task 2: Resistance to passive wrist or finger extension Position: Standard starting position. Instruction: "Let me move your hand." Method: Choose either (a) or (b):
a) Extend and flex wrist 5 times with sufficient speed of passive movement to elicit a stretch reflex. Feel for resistance to passive movement and watch for contraction of wrist flexors.
b) Extend and flex fingers 5 times with sufficient speed of passive movement to elicit a stretch reflex. Feel for resistance to passive movement and watch for contraction of finger flexors.
Task 3: Facilitated finger flexion Position: Standard starting position. Instruction: "Bend your fingers." Method: Facilitate a contraction of the finger flexors. Required: Some active finger flexion.
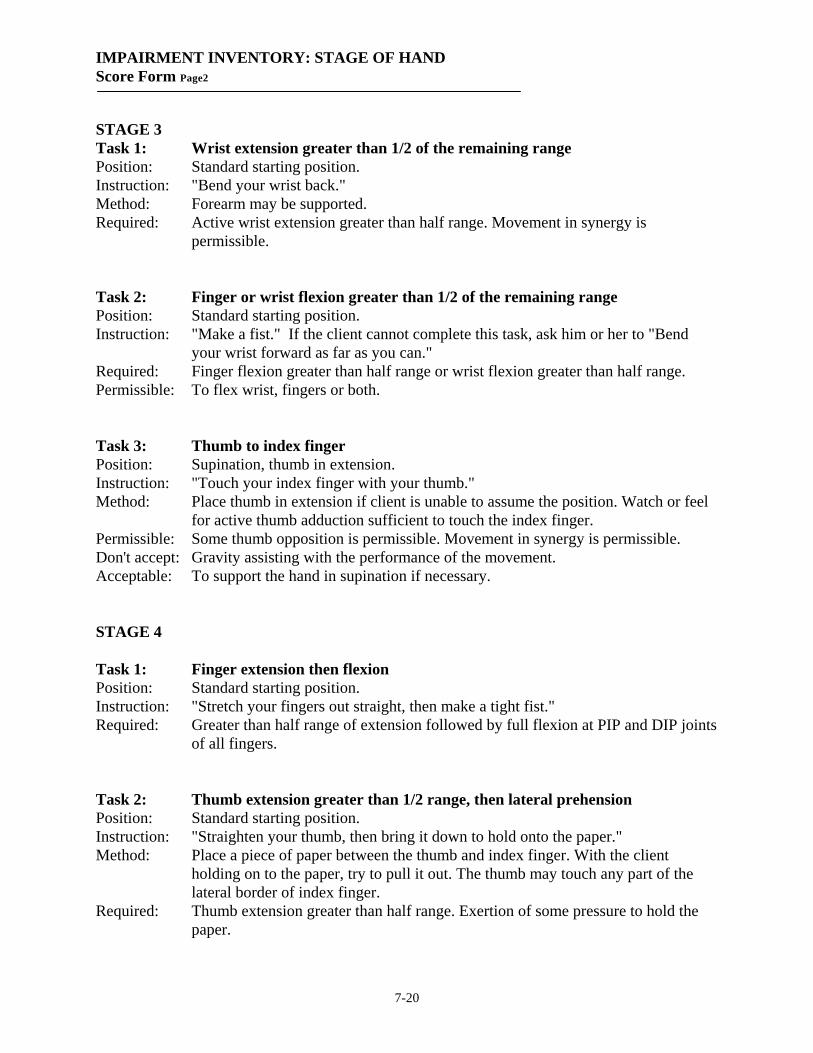
IMPAIRMENT INVENTORY: STAGE OF HAND Score Form Page2
7-20
STAGE 3 Task 1: Wrist extension greater than 1/2 of the remaining range Position: Standard starting position. Instruction: "Bend your wrist back." Method: Forearm may be supported. Required: Active wrist extension greater than half range. Movement in synergy is
permissible. Task 2: Finger or wrist flexion greater than 1/2 of the remaining range Position: Standard starting position. Instruction: "Make a fist." If the client cannot complete this task, ask him or her to "Bend
your wrist forward as far as you can." Required: Finger flexion greater than half range or wrist flexion greater than half range. Permissible: To flex wrist, fingers or both. Task 3: Thumb to index finger Position: Supination, thumb in extension. Instruction: "Touch your index finger with your thumb." Method: Place thumb in extension if client is unable to assume the position. Watch or feel
for active thumb adduction sufficient to touch the index finger. Permissible: Some thumb opposition is permissible. Movement in synergy is permissible. Don't accept: Gravity assisting with the performance of the movement. Acceptable: To support the hand in supination if necessary. STAGE 4 Task 1: Finger extension then flexion Position: Standard starting position. Instruction: "Stretch your fingers out straight, then make a tight fist." Required: Greater than half range of extension followed by full flexion at PIP and DIP joints
of all fingers. Task 2: Thumb extension greater than 1/2 range, then lateral prehension Position: Standard starting position. Instruction: "Straighten your thumb, then bring it down to hold onto the paper." Method: Place a piece of paper between the thumb and index finger. With the client
holding on to the paper, try to pull it out. The thumb may touch any part of the lateral border of index finger.
Required: Thumb extension greater than half range. Exertion of some pressure to hold the paper.

IMPAIRMENT INVENTORY: STAGE OF HAND Score Form Page2
7-21
Task 3: Finger flexion with lateral prehension Position: Standard starting position. Instruction: "Make a tight fist and bring your thumb down to your index finger. Don’t let me
move your thumb.” Method: Test for active lateral prehension (key grip) by trying to move the thumb away
from the index finger. Required: Sufficient finger flexion to bring tips of all fingers to the palm of the hand. Active
thumb flexion, and ability to maintain the prehension position. STAGE 5 Task 1: Finger flexion then extension Position: Standard starting position. Instruction: "Make a tight fist and then straighten your fingers out." Required: Smooth reversal from flexion to extension. Full flexion and full extension of
fingers. Don’t accept: To bend or straighten fingers unevenly. Task 2: Finger abduction Position: Forearm pronated with fingers extended. Instruction: "Spread your fingers apart as far as you can." Required: Full range finger abduction Don't accept: Wrist and finger flexion during movement. Task 3: Opposition of thumb to little finger Position: Hand unsupported (forearm may be supported). Instruction: "Touch the tip of your little finger with the tip of your thumb." Required: Some flexion of MCP, PIP, and DIP joints of the thumb and 5th finger. Don't accept: Wrist flexion. STAGE 6 Task 1: Tap index finger 10 times in 5 seconds Position: Standard starting position with forearm pronated. Instruction: "Keeping your finger straight, tap your index finger as quickly as you can." Required: Active flexion and extension at MCP joint with IP joints in extension, with
smooth movements of equal amplitude. Don't accept: Movement taking place at wrist, or flexion of the IP joints.

IMPAIRMENT INVENTORY: STAGE OF HAND Score Form Page2
7-22
Task 2: Pull trigger, then return Position: Pistol grip, wrist in neutral position, thumb and index finger extended, 3 other
fingers flexed. Instruction: "Bend and straighten your index finger without moving anything else.” Required: Full range flexion and extension of PIP and DIP joints with no movement at the
MCP joint of the index finger. No movement of thumb and other fingers. Don't accept: Any change from the starting position. Task 3: Wrist and finger extension with finger abduction Position: Hand resting on lap or support, forearm pronated. Instruction: "Lift your wrist as far as you can and then stretch your fingers apart." Required: Full range wrist and finger extension with full range of abduction. STAGE 7 Task 1: Thumb to finger tips, then reverse 3 times in 12 seconds Position: Standard starting position with thumb touching the little finger. Instruction: "Starting with the little finger, touch the tip of each finger with your thumb and
then go back to the little finger. Make sure the index and little fingers are touched twice. Do this 3 times."
Required: Smooth, coordinated movement repeated 3 times in 12 seconds. Task 2: Bounce a ball 4 times in succession, then catch it Position: Sitting, holding onto a ball 6.5 centimeters (2.5 inches) in diameter (e.g. a tennis
ball). Instruction: "Bounce the ball 4 times and then catch it." Required: The activity is controlled and the height of the ball (around knee height) is
consistent. It is permissible to bounce ball between the knees or to the outside of weak side.
Don’t accept: Catch and release of the ball. Task 3: Pour 250 ml. from 1 liter pitcher, then reverse Position: Sitting at a table with 250 ml. (1 cup) plastic measuring cup with handle and a
1 liter (1 quart) plastic pitcher on the table. The 1 liter pitcher is three-quarters full. The measuring cup is medial to the pitcher.
Instruction: "With your weak hand, pour the water from the pitcher to the cup. Pick up the cup and pour the water back into the pitcher by turning the palm of your hand up."
Required: The client must pour the water to fill the measuring cup. Task is accomplished without spilling the liquid.
Don’t accept: Pitcher and cup touching, compensatory movements of the trunk or upper limbs or jerky movements.

169
Appendix 6 Graded Redefined Assessment of Strength, Sensibility and
Prehension (GRASSP) Scoring Sheet

Graded Redefined Assessment of Strength Sensibility and Prehension (GRASSP)
GRASSP Copyright 2008 International GRASSP Research and Design Team All Rights Reserved, DO NOT ALTER
1
SCORING SHEETS
1 - Demographics Patients Name Examiner Initials Date of Assessment Age Gender Hand Dominance Pre-injury Post-injury Injury Date Comments
2 - Strength - score 0 to 5 as per instructions in each box, then sum for each side Right Muscles Tested for MMT Left
Anterior Deltoid Elbow Flexors
Elbow Extensors Wrist Extensors
Extensor Digitorum (DIII) Opponens Pollicis
Flexor Pollicis Longus Finger Flexors (DIII)
Finger Abductors First Dorsal Interossei
/50 Total out of 50 for each side /50

Graded Redefined Assessment of Strength Sensibility and Prehension (GRASSP)
GRASSP Copyright 2008 International GRASSP Research and Design Team All Rights Reserved, DO NOT ALTER
2
3 – SensibilitySWM Threshold Scores
Right Hand Left Hand 3.61 (4)
3.61 (4)
3.61 (4)
4.31 (3)
4.56 (2)
6.65 (1)
NR (0) Score Area 3.61 (4)
3.61 (4)
3.61 (4)
4.31 (3)
4.56 (2)
6.65 (1)
NR (0) Score
1 2 3
Dorsal Total /12 Dorsal Total /12
4 5 6
Palmar Total /12 Palmar Total /12
Dorsal Total+Palmar Total=Total SWM /24 Dorsal Total+Palmar Total=Total SWM /24
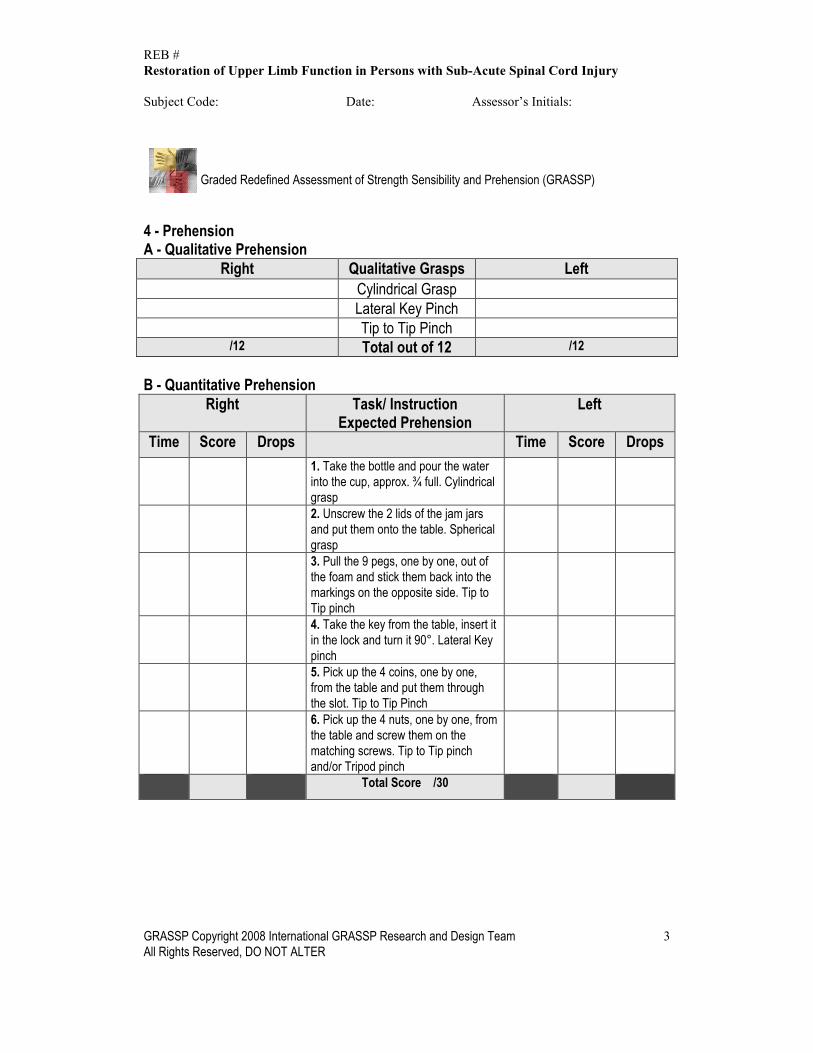
REB # Restoration of Upper Limb Function in Persons with Sub-Acute Spinal Cord Injury
Subject Code: Date: Assessor’s Initials:
Graded Redefined Assessment of Strength Sensibility and Prehension (GRASSP)
GRASSP Copyright 2008 International GRASSP Research and Design Team All Rights Reserved, DO NOT ALTER
3
4 - Prehension A - Qualitative Prehension
Right Qualitative Grasps Left Cylindrical Grasp Lateral Key Pinch Tip to Tip Pinch
/12 Total out of 12 /12
B - Quantitative Prehension Right Task/ Instruction
Expected Prehension Left
Time Score Drops Time Score Drops 1. Take the bottle and pour the waterinto the cup, approx. ¾ full. Cylindricalgrasp2. Unscrew the 2 lids of the jam jarsand put them onto the table. Sphericalgrasp3. Pull the 9 pegs, one by one, out ofthe foam and stick them back into themarkings on the opposite side. Tip toTip pinch4. Take the key from the table, insert itin the lock and turn it 90°. Lateral Keypinch5. Pick up the 4 coins, one by one,from the table and put them throughthe slot. Tip to Tip Pinch6. Pick up the 4 nuts, one by one, fromthe table and screw them on thematching screws. Tip to Tip pinchand/or Tripod pinch
Total Score /30

REB # Restoration of Upper Limb Function in Persons with Sub-Acute Spinal Cord Injury Subject Code: Date: Assessor’s Initials: Graded Redefined Assessment of Strength Sensibility and Prehension (GRASSP)
GRASSP Copyright 2008 International GRASSP Research and Design Team All Rights Reserved, DO NOT ALTER
4
5 – Summary and Total Scores Right Left
STRENGTH-Upper limb (50/50) SWM –DORSAL (12/12) SWM-PALMAR (12/12) PREHENSION – Qualitative (12/12) PREHENSION – Quantitative (30/30) TOTALS /116

174
Appendix 7 Functional Independence Measure (FIM) Scoring Sheet
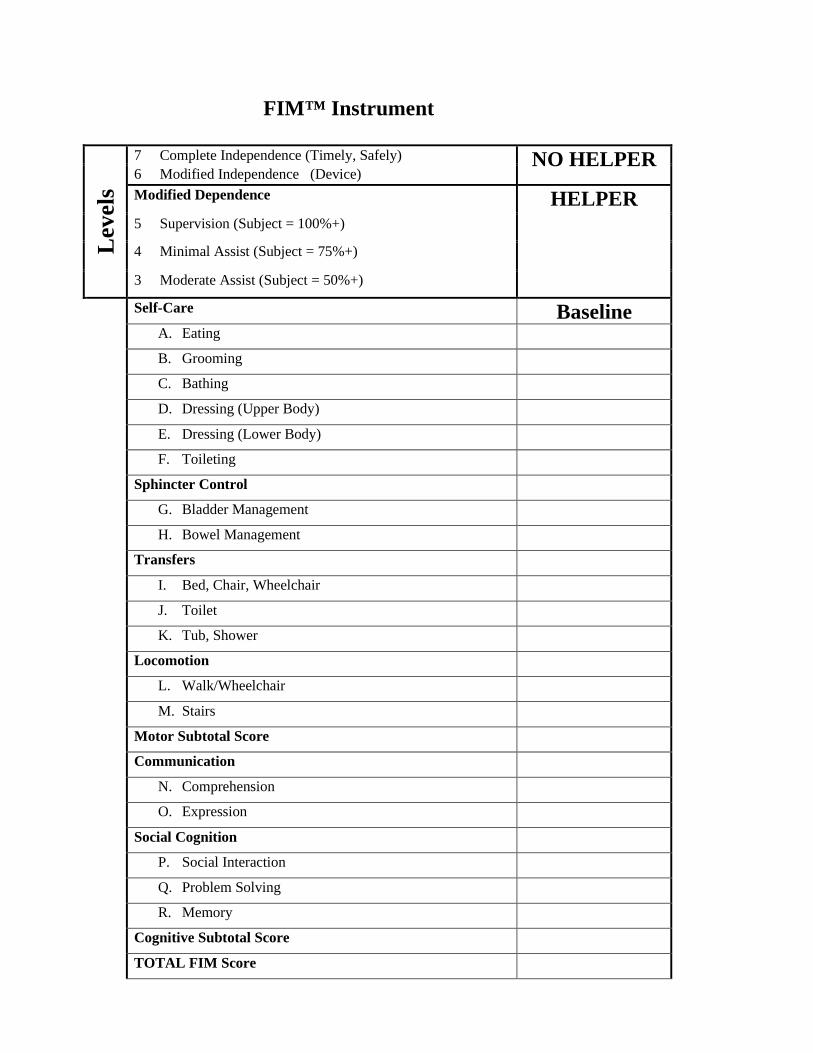
FIM™ Instrument
Lev
els
7 Complete Independence (Timely, Safely) NO HELPER 6 Modified Independence (Device)
Modified Dependence HELPER 5 Supervision (Subject = 100%+) 4 Minimal Assist (Subject = 75%+) 3 Moderate Assist (Subject = 50%+)
Self-Care Baseline A. Eating B. Grooming C. Bathing D. Dressing (Upper Body) E. Dressing (Lower Body) F. Toileting Sphincter Control G. Bladder Management H. Bowel Management Transfers I. Bed, Chair, Wheelchair J. Toilet K. Tub, Shower Locomotion L. Walk/Wheelchair M. Stairs Motor Subtotal Score Communication N. Comprehension O. Expression Social Cognition P. Social Interaction Q. Problem Solving R. Memory Cognitive Subtotal Score TOTAL FIM Score

176
Appendix 8 Spinal Cord Independence Measure (SCIM) Scoring Sheet

Appendix The Spinal Cord Independence Measure, Version III
LOEWENSTEIN HOSPITAL REHABILITATION CENTER Affiliated with the Sackler Faculty of Medicine, Tel-Aviv University
Department IV, Medical Director: Dr. Amiram Catz Tel: 972-9-7709090 Fax: 972-9-7709986 e-mail: [email protected]
Patient Name: ____________________ID:______________ Examiner Name: _________________ (Enter the score for each function in the adjacent square, below the date. The form may be used for up to 6 examinations.)
SCIM-SPINAL CORD INDEPENDENCE MEASURESelf-Care DATE \ \ \ \ \ \ \
1. Feeding (cutting, opening containers, pouring, bringing food to mouth, holding cup with fluid)0. Needs parenteral, gastrostomy, or fully assisted oral feeding1. Needs partial assistance for eating and/or drinking, or for wearing adaptive devices2. Eats independently; needs adaptive devices or assistance only for cutting food and/or pouring and/or opening containers3. Eats and drinks independently; does not require assistance or adaptive devices
2. Bathing (soaping, washing, drying body and head, manipulating water tap). A-upper body; B-lower bodyA. 0. Requires total assistance
1. Requires partial assistance 2. Washes independently with adaptive devices or in a specific setting (e.g., bars, chair)3. Washes independently; does not require adaptive devices or specific setting (not customary for healthy people) (adss)
B. 0. Requires total assistance1. Requires partial assistance2. Washes independently with adaptive devices or in a specific setting (adss)3. Washes independently; does not require adaptive devices (adss) or specific setting
3. Dressing (clothes, shoes, permanent orthoses: dressing, wearing, undressing). A-upper body; B-lower bodyA. 0. Requires total assistance
1. Requires partial assistance with clothes without buttons, zippers or laces (cwobzl)2. Independent with cwobzl; requires adaptive devices and/or specific settings (adss)3. Independent with cwobzl; does not require adss; needs assistance or adss only for bzl4. Dresses (any cloth) independently; does not require adaptive devices or specific setting
B. 0. Requires total assistance 1. Requires partial assistancewith clothes without buttons, zipps or laces (cwobzl)2. Independent with cwobzl; requires adaptive devices and/or specific settings (adss)3. Independent with cwobzl without adss; needs assistance or adss only for bzl4. Dresses (any cloth) independently; does not require adaptive devices or specific setting
4. Grooming (washing hands and face, brushing teeth, combing hair, shaving, applying makeup)0. Requires total assistance 1. Requires partial assistance2. Grooms independently with adaptive devices3. Grooms independently without adaptive devices SUBTOTAL (0-20)
Version III, Sept 14, 2002 EXam 1 2 3 4 5 6
CLALIT
Rasch analysis of SCIM IIIA Catz et al
289
Spinal Cord
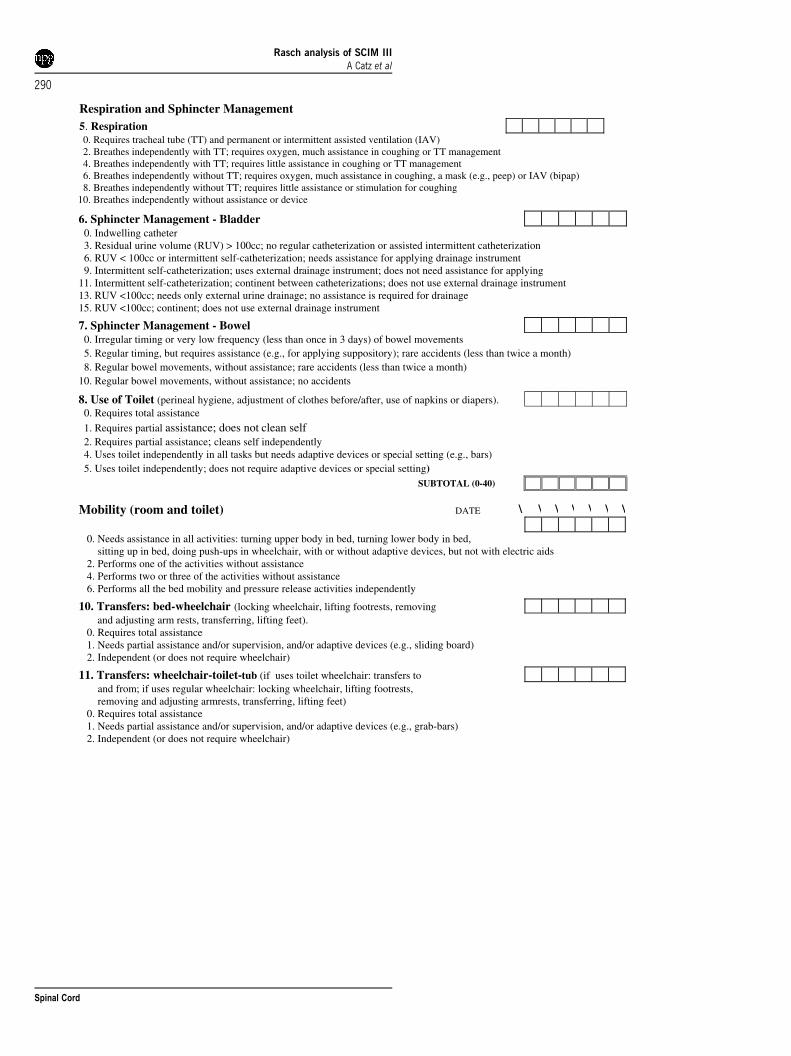
6. Sphincter Management - Bladder 0. Indwelling catheter
3. Residual urine volume (RUV) > 100cc; no regular catheterization or assisted intermittent catheterization 6. RUV < 100cc or intermittent self-catheterization; needs assistance for applying drainage instrument 9. Intermittent self-catheterization; uses external drainage instrument; does not need assistance for applying
11. Intermittent self-catheterization; continent between catheterizations; does not use external drainage instrument 13. RUV <100cc; needs only external urine drainage; no assistance is required for drainage
15. RUV <100cc; continent; does not use external drainage instrument
7. Sphincter Management - Bowel 0. Irregular timing or very low frequency (less than once in 3 days) of bowel movements 5. Regular timing, but requires assistance (e.g., for applying suppository); rare accidents (less than twice a month) 8. Regular bowel movements, without assistance; rare accidents (less than twice a month) 10. Regular bowel movements, without assistance; no accidents
8. Use of Toilet (perineal hygiene, adjustment of clothes before/after, use of napkins or diapers). 0. Requires total assistance 1. Requires partial assistance; does not clean self 2. Requires partial assistance; cleans self independently 4. Uses toilet independently in all tasks but needs adaptive devices or special setting (e.g., bars) 5. Uses toilet independently; does not require adaptive devices or special setting) SUBTOTAL (0-40)
Mobility (room and toilet) DATE \ \ \ \ \ \ \
0. Needs assistance in all activities: turning upper body in bed, turning lower body in bed,
sitting up in bed, doing push-ups in wheelchair, with or without adaptive devices, but not with electric aids
2. Performs one of the activities without assistance
4. Performs two or three of the activities without assistance
6. Performs all the bed mobility and pressure release activities independently
10. Transfers: bed-wheelchair (locking wheelchair, lifting footrests, removing
and adjusting arm rests, transferring, lifting feet).
0. Requires total assistance
1. Needs partial assistance and/or supervision, and/or adaptive devices (e.g., sliding board)
2. Independent (or does not require wheelchair)
11. Transfers: wheelchair-toilet-tub (if uses toilet wheelchair: transfers to
and from; if uses regular wheelchair: locking wheelchair, lifting footrests, removing and adjusting armrests, transferring, lifting feet)
0. Requires total assistance
1. Needs partial assistance and/or supervision, and/or adaptive devices (e.g., grab-bars)
2. Independent (or does not require wheelchair)
Respiration and Sphincter Management 5. Respiration 0. Requires tracheal tube (TT) and permanent or intermittent assisted ventilation (IAV)
2. Breathes independently with TT; requires oxygen, much assistance in coughing or TT management
4. Breathes independently with TT; requires little assistance in coughing or TT management
6. Breathes independently without TT; requires oxygen, much assistance in coughing, a mask (e.g., peep) or IAV (bipap) 8. Breathes independently without TT; requires little assistance or stimulation for coughing
10. Breathes independently without assistance or device
Rasch analysis of SCIM IIIA Catz et al
290
Spinal Cord

13. Mobility for Moderate Distances (10-100 meters)0. Requires total assistance1. Needs electric wheelchair or partial assistance to operate manual wheelchair2. Moves independently in manual wheelchair3. Requires supervision while walking (with or without devices)4. Walks with a walking frame or crutches (swing)5. Walks with crutches or two canes (reciprocal walking)6. Walks with one cane7. Needs leg orthosis only8. Walks without walking aids
14. Mobility Outdoors (more than 100 meters)0. Requires total assistance1. Needs electric wheelchair or partial assistance to operate manual wheelchair2. Moves independently in manual wheelchair3. Requires supervision while walking (with or without devices)4. Walks with a walking frame or crutches (swing)5. Walks with crutches or two canes (reciprocal waking)6. Walks with one cane7. Needs leg orthosis only8. Walks without walking aids
15. Stair Management0. Unable to ascend or descend stairs1. Ascends and descends at least 3 steps with support or supervision of another person2. Ascends and descends at least 3 steps with support of handrail and/or crutch or cane3. Ascends and descends at least 3 steps without any support or supervision
16. Transfers: wheelchair-car (approaching car, locking wheelchair, removing arm-
and footrests, transferring to and from car, bringing wheelchair into and out of car)0. Requires total assistance1. Needs partial assistance and/or supervision and/or adaptive devices2. Transfers independent; does not require adaptive devices (or does not require wheelchair)
17. Transfers: ground-wheelchair
0. Requires assistance1. Transfers independent with or without adaptive devices (or does not require wheelchair)
TOTAL SCIM SCORE (0-100)
SUBTOTAL (0-40)
Mobility (indoors and outdoors, on even surface) 12. Mobility Indoors
0. Requires total assistance1. Needs electric wheelchair or partial assistance to operate manual wheelchair2. Moves independently in manual wheelchair3. Requires supervision while walking (with or without devices)4. Walks with a walking frame or crutches (swing)5. Walks with crutches or two canes (reciprocal walking)6. Walks with one cane7. Needs leg orthosis only8. Walks without walking aids
Rasch analysis of SCIM IIIA Catz et al
291
Spinal Cord
180
Copyright Acknowledgements
Chapter 3 is used with permission from the book,
Cesar Marquez-Chin, Naaz Kapadia-Desai, and Sukhinder Kalsi-Ryan. Functional Electrical
Stimulation Therapy: A Closer Look. In: Ron Baecker R, Sixsmith A, editors. Brain–Computer
Interfaces Neurorehabilitation of Voluntary Movement after Stroke and Spinal Cord Injury.
Morgan and Claypool; 2021. p. 11-25. doi: 10.2200/S01090ED1V01Y202104ARH017.