
Addition of immunotherapy with Mycobacterium w vaccine to multi-drug therapy benefits multibacillary...
9
Vaccine, Vol. 13, No. 12. pp. 1102-1110, 1995 Cowrioht 0 1995 Elsevier Science Ltd 0264-410X(94)00033-6 Addition of immunotherapy with Printedl in beat Britain. All rights reserved 0264-410X/95 $lO+O.OO Mycobacterium w vaccine to multi-drug therapy benefits multibacillary leprosy patients S.A. Zaheer*, K.R. Beena*, H.K. Kar’f, A.K. Sharmaf-, R.S. Misral, A. Mukherjees, R. Mukherjee*, H. Kaur*, R.M. Pandey*, R. Walia*, A. Mukhopadhyay” and G.P. Talwarii Immunotherapy with a vaccine consisting of autoclaved Mycobacterium w, was given in addition to standard chemotherapy (multidrug therapy (MDT)) to 93 multibacillary (MB) leprosy patients. One hundred and seven patients with similar types of disease served as controls and received MDT + placebo injections. The study was a double-blind randomised trial. On opening the codes, results obtained were in concordance with those in a single-blind trial which has been extensively reported. Bacteriological clearances were sign$cantIy more rapid in vaccinated patients (~~0.03). Thirty-Jive LL or BL patients with a high bacterial index (BZ) of 6 were completely cleured of acid-fast bacilli (AFB) after eight doses of vaccine. Only 8 patients in the control group became bacteriologically negative in the same time period. They all had BZs <4. Associated with decreasing BZ was accelerated clinical regression of lesions after vaccination and lepromin conversion rates of 100% for BB, 71% for BL and 70% for LL. A signljicant number of immunisedpatients showed histological improvement (p<O.O04). Thirty-six showed a complete disappearance of dermal granulomas and a picture of non-spec$c infiltration. The vaccine did not precipitate neuritis or deformities; episodes were noted in vaccinated patients as were incidences of Type 2 reaction. The overall improvement was reflected by a shorter duration of treatment and faster release of vaccinated patients. Keywords: Combined chemotherapy and immunotherapy: bacteriological clearance; lepromin conversion; histological upgrading; release from treatment (RFT); double blind Leprosy is a chronic, systemic, infectious and debili- tating disease of man caused by Mycobacterium leprae. It is among six priority diseases identified in the WHO Tropical Diseases Research Programme. There are an estimated lo-12 million people suffering from this malady. One-quarter of them are in India alone’. The disease is classified as a spectrum which recog- nises the tuberculoid (TT)/lepromatous (LL) polarity to be, in essence, an indication of the immune status of a patient. In between the two poles: LL and TT are the borderline forms. In the center is the borderline- *National institute of Immunology, New Delhi-l 10067, India. TDepartment of Dermatology, Venereology and Leprology, Dr Ram Manohar Lohia Hospital, New Delhi-l 10001, India. $Department of Dermatology and Leprology, Safdarjung Hospital, New Delhi-l 10029, India. slnstitute of Pathology, Indian Council of Medical Research, Safdarjung Hospital Campus, New Delhi-l 10029, India. IlTo whom correspon- dence should be addressed. (Received 30 June 1993; revised 27 July 1994; accepted 25 October 1994) borderline type (BB) with two subsidiary forms on each side of BB: borderline tuberculoid (BT) and borderline lepromatous (BL)‘. Multibacillary (MB) leprosy encompasses BB, BL or LL forms of leprosy’. These are patients with pronounced deficiency of cell-mediated immune (CMI) responses, bacteriological P ositivity in slit skin smears, and lepromin negativity-. The immunomodulatory effects of boosting CM1 responses by a vaccine can thus be critically assessed in this group of patients. Mvcobacterium w (M. w) vaccine, the immuno- therapeutic effects of which we are assessing, is currently in Phase III clinical trials at two major hospitals in Delhi and in a rural leprosy control community block in Kanpur Dehat along with the National Leprosy Eradi- cation Programme (NLEP) and U.P. Health Director- ate. The vaccine is based on an atypical, cultivable and rapidly growing mycobacterium”J. It resembles bacilli included in Runyon’s group IV, but differs in one respect or another from bacilli presently in that group4.5. The background studies relating to its selection as a 1102 Vaccine 1995 Volume 13 Number 12
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Addition of immunotherapy with Mycobacterium w vaccine to multi-drug therapy benefits multibacillary...

Vaccine, Vol. 13, No. 12. pp. 1102-1110, 1995 Cowrioht 0 1995 Elsevier Science Ltd
0264-410X(94)00033-6
Addition of immunotherapy with
Printedl in beat Britain. All rights reserved 0264-410X/95 $lO+O.OO
Mycobacterium w vaccine to multi-drug therapy benefits multibacillary leprosy patients
S.A. Zaheer*, K.R. Beena*, H.K. Kar’f, A.K. Sharmaf-, R.S. Misral, A. Mukherjees, R. Mukherjee*, H. Kaur*, R.M. Pandey*, R. Walia*, A. Mukhopadhyay” and G.P. Talwarii
Immunotherapy with a vaccine consisting of autoclaved Mycobacterium w, was given in addition to standard chemotherapy (multidrug therapy (MDT)) to 93 multibacillary (MB) leprosy patients. One hundred and seven patients with similar types of disease served as controls and received MDT + placebo injections. The study was a double-blind randomised trial. On opening the codes, results obtained were in concordance with those in a single-blind trial which has been extensively reported. Bacteriological clearances were sign$cantIy more rapid in vaccinated patients (~~0.03). Thirty-Jive LL or BL patients with a high bacterial index (BZ) of 6 were completely cleured of acid-fast bacilli (AFB) after eight doses of vaccine. Only 8 patients in the control group became bacteriologically negative in the same time period. They all had BZs <4. Associated with decreasing BZ was accelerated clinical regression of lesions after vaccination and lepromin conversion rates of 100% for BB, 71% for BL and 70% for LL. A signljicant number of immunisedpatients showed histological improvement (p<O.O04). Thirty-six showed a complete disappearance of dermal granulomas and a picture of non-spec$c infiltration. The vaccine did not precipitate neuritis or deformities; episodes were noted in vaccinated patients as were incidences of Type 2 reaction. The overall improvement was reflected by a shorter duration of treatment and faster release of vaccinated patients.
Keywords: Combined chemotherapy and immunotherapy: bacteriological clearance; lepromin conversion; histological upgrading; release from treatment (RFT); double blind
Leprosy is a chronic, systemic, infectious and debili- tating disease of man caused by Mycobacterium leprae. It is among six priority diseases identified in the WHO Tropical Diseases Research Programme. There are an estimated lo-12 million people suffering from this malady. One-quarter of them are in India alone’.
The disease is classified as a spectrum which recog- nises the tuberculoid (TT)/lepromatous (LL) polarity to be, in essence, an indication of the immune status of a patient. In between the two poles: LL and TT are the borderline forms. In the center is the borderline-
*National institute of Immunology, New Delhi-l 10067, India. TDepartment of Dermatology, Venereology and Leprology, Dr Ram Manohar Lohia Hospital, New Delhi-l 10001, India. $Department of Dermatology and Leprology, Safdarjung Hospital, New Delhi-l 10029, India. slnstitute of Pathology, Indian Council of Medical Research, Safdarjung Hospital Campus, New Delhi-l 10029, India. IlTo whom correspon- dence should be addressed. (Received 30 June 1993; revised 27 July 1994; accepted 25 October 1994)
borderline type (BB) with two subsidiary forms on each side of BB: borderline tuberculoid (BT) and borderline lepromatous (BL)‘.
Multibacillary (MB) leprosy encompasses BB, BL or LL forms of leprosy’. These are patients with pronounced deficiency of cell-mediated immune (CMI) responses, bacteriological
P ositivity in slit skin smears,
and lepromin negativity-. The immunomodulatory effects of boosting CM1 responses by a vaccine can thus be critically assessed in this group of patients.
Mvcobacterium w (M. w) vaccine, the immuno- therapeutic effects of which we are assessing, is currently in Phase III clinical trials at two major hospitals in Delhi and in a rural leprosy control community block in Kanpur Dehat along with the National Leprosy Eradi- cation Programme (NLEP) and U.P. Health Director- ate. The vaccine is based on an atypical, cultivable and rapidly growing mycobacterium”J. It resembles bacilli included in Runyon’s group IV, but differs in one respect or another from bacilli presently in that group4.5. The background studies relating to its selection as a
1102 Vaccine 1995 Volume 13 Number 12

Chemo-immunotherapy in leprosy: S.A. Zaheer et al.
candidate anti-leprosy vaccine have been reported earlier&lo. Recent data, based on the sequence of bases in a polymorphic region of 65 kDa gene, indicate Mycobacterium w is a new species”. Phase I clinical trials conducted in 1983 at Calcutta have been published”.
Phase II/III trials had two series. The initial trial was a single-blind study, where the nature of the vaccine was known to the Head of the clinic but not to the attending Doctors or Investigators. This study had 120 patients. Extensive results on these trials have been published’ 3p20. Similar studies conducted at the Indian Council of Medical Research, JALMA Institute of Leprosy, have confirmed the immunotherapeutic effects of M. w~‘,~~.
The second series of trials was a double-blind one. The codes, which were maintained by the biostatistician, were opened in 1992 and this communication reports results on 200 patients in this study.
In 1990, the vaccine trials were extended to large scale field studies on 414 000 inhabitants in Kanpur Dehat of Uttar Pradesh state of North India. Twenty thousand household contacts and 1100 multibacillary patients have already been enrolled2’. M.w vaccine also forms part of a comparative immunoprophylactic trial being conducted at Chingelput-District (Tamil Nadu State of South India) by the ICMR24. Fifteen thousand subjects of the general population have already been vaccinated with M. w13.
MATERIALS AND METHODS
Vaccine
The vaccine is a suspension of killed Mycobacterium w in physiological saline at 10” bacilli per ml. The details of vaccine preparation have been given previously13. Briefly, M. w from master seed stock was initially grown in Lowenstein-Jensen (L-J) medium. Seed lots were expanded in Middlebrook medium (Difco Laboratories, Detroit, MI) with bovine albumin, dextrose and casein (ADC) enrichment. The bacteria were harvested during the log phase on days 8-9 of culture. The pellet was centrifuged and washed thrice with normal saline (0.085% NaCl). The purity of the preparation was assessed in nutrient agar. The bacilli suspended in saline were autoclaved for 15 min at 15 lb inch - ’ pressure. Complete killing was assessed by lack of growth of the autoclaved specimens in L-J medium after 2 weeks of culture. The sterility of the vaccine preparation was tested in thioglycolate and soya bean casein digest medium. Thiomersal was added to a final concentration of 0.01% as a preservative.
Placebo
One gram of micronised starch (Sarabhai Chemicals, Baroda, India) was dissolved in 100 ml of distilled water. This was autoclaved at 15 lb inch _ ’ pressure for 15 min and dispensed in sterile vials.
Lepromin
Armadillo lepromin containing 40 x lo6 killed bacilli ml-’ was kindly made available by WHO.
Vaccine dose, administration, regimen
The first dose of vaccine was 1 x lo9 autoclaved bacilli in 0.1 ml physiological saline (0.85% NaCl). Subsequent doses contained half the number of bacilli. The vaccine was administered intradermally in the deltoid region. A total of 8 doses were given at 3-month intervals.
Multidrug therapy (MDT)
MDT consisted of 2 weeks of intensive therapy with 600 mg rifampicin, 100 mg clofazimine and 100 mg dapsone daily. Subsequently, theZgatients received for 2 years the WHO recommended regimen of 600 mg rifampicin and 300 mg clofazimine once a month, super- vised, plus 100 mg of dapsone and 50 mg of clofazimine daily, self-administered.
Subjects and design of study
Permission of Drugs Controller of India, Institutional Ethics Committees and consent of subjects enrolled was obtained before initiating the study. Multibacillary patients, belonging to LL, BL or BB forms of leprosy on the basis of clinical status and histopathology were enrolled. All were initially negative to lepromin-A (armadillo-derived). On ethical grounds, the protocol envisaged administration of standard multidrug therapy to all patients. However, one group received, in ad- dition, the vaccine, whereas the other group was given placebo injection of micronised starch.
The study was a double-blind one in which neither the evaluating agency nor the patients were aware of whether the M. w vaccine or micronised starch was injected. Clinical scoring was done by the attending physician and a record of these was maintained in the form of clinical photographs taken at fixed intervals in addition to complete body charts. Furthermore, slit smear examination for BI as well as histopathological examination were carried out by experts, who at no time during the study period had the opportunity to see the patients or know their clinical details. Individual code numbers of patients was the only form of identification provided to the evaluating pathologists.
Clinical scores, bacteriological status, lepromin testing, histological examination
Details have been described13. For purposes of clinical assessment Ramu’s scor-
ing33.34 method was followed. In this system a score of 1 is given to predominantly macular lesions, 2 to diffuse infiltration, 3 to few papules or plaques and 4 to predominantly papulonodular lesions. The body is divided into seven regions, i.e. face, head and neck, right and left upper limbs, chest and abdomen, back and buttock and right and left lower limbs. Each region is scored independently from 1 to 4. The maximum score recordable is 28.
RESULTS
Table I gives the total number of patients belonging to different types of leprosy enrolled in either vaccine or control groups. All patients listed had completed a minimum of 24 months of treatment.
Vaccine 1995 Volume 13 Number 12 1103

Chemo-immunotherapy in leprosy: S.A. Zaheer et al.
Table 1 Changes in clinical scores (mean f S.E.M.)
Type of No. of disease Group patients Initial 6 months 12 months 18 months 24 months
LL Vaccine 53 13.6kO.9 10.3+0.7 7.5kO.6 6.OkO.6 @X0.03) 3.8kO.4 (p.zO.001) Control 68 13.5i0.6 10.8iO.6 8.3kO.5 7.2kO.5 6.3kO.4
BL Vaccine 31 10.9+1.0 7.0i0.8 5.6kO.8 3.8kO.4 2.1 io.3 (~0.001) Control 30 10.4+0.9 7.9i0.6 5.4kO.5 4.6kO.5 4.4i0.6
BB Vaccine 9 8.6k1.7 4.8i0.8 4.6kO.6 3.8zt0.7 2.7k1.2 Q~0.02) Control 9 9.7i0.8 5.8+0.4 5.1il.O 4.6il .l 4.6+1 .O
Statistical analyses were done using Mann-Whitney U-test (non-parametric). For the significant cases, p values are indicated in parentheses
Table 2 Histological changes in patients with LL type leprosy
A. Leprosy type
No. of 12 months
Group patients LL BL BT NSI
24 months
LL BL BB NSI
LL Vaccine Control
53 38 11 2 2 33 11 1 9 68 65 2 - 1 64 3 - 3
B. Leprosy type BL BT Ind NSI BL BT Ind NSI
BL Vaccine Control
31 15 1 2 13 8 - 3 20 30 26 2 - 2 20 1 1 8
C. Leprosy type Histological diagnosis BB BT Ind NSI BB BT Ind NSI
BB Vaccine Ind-1 - 2 1 5 - - 1 7 BT-1 BT/BB-1 BB-5
Control Ind-1 1 1 5 1 1 1 1 5 BT-2
Two patients S-129 and S-159, clinically BB, with macular lesions, showed no histological evidence of leprosy, hence are excluded from analysis. Ind, indeterminate disease. NSI, non-specific infiltration
Local reactions to vaccine
The vaccine was extremely well tolerated. Erythema and induration was seen within a week of vaccination. In the majority of patients, by 2 weeks, there was formation of a well defined ulcer whose size ranged from 3 mm x 3 mm to 9 mm x 9 mm. The ulcer healed spontaneously in 34 weeks with scar formation.
Clinical improvement
As was our experience in the single-blind study’“, patients in the double-blind study receiving the M. w vac- cine showed marked clinical improvement by 6 months. This was evident as rapid regression and flattening of papulonodular lesions and plaques and disappearance of hypopigmented lesions as compared to patients in the control group (Figures 1 and 2). Table I gives the changes in Ramu’s clinical scores (mean & S.E.M.) in the two groups. Decline in scores in BB, BL and LL types of leprosy receiving vaccine was statistically significantly greater than the control group (~~0.02).
Bacteriological changes
Changes in bacterial index (BI) were noted every 3 months. Figure 3a, b, c are bar diagrams depicting mean
BI changes f S.E.M. in the vaccine (93) and control (107) subjects. The fall in BI in LL patients receiving M.w vaccine was significant from 6 months onwards @<O.OOl). This was from 3.64 (& 0.17 S.E.M.) to 1.07 ( f 0.16 S.E.M.) for the vaccine and 4.09 (f 0.13) to 2.46 ( f 0.15 S.E.M.) for the control group. In fact, the decrease in BI after two doses of vaccine (6 months) was lower in the vaccine than that achieved in the control group at 24 months. In BL leprosy patients, initial BIs in the two groups were very similar (Figure 3b) and signifi- cant decreases were seen from 12 months onwards in the vaccine group (pcO.03). The BI at 12 months in the vaccine group (0.771 f 0.16 S.E.M.) was lower than that in the control group at 24 months (0.84 f 0.14 S.E.M.). In BB leprosy patients, all patients receiving M. w became BI=O at 18 months. This was not so in the control group patients (Figure 3~).
Lepromin conversion
At induction all patients were negative in their late reaction (3-4 weeks) to lepromin-A (armadillo- derived). With progressive immunisation, there was a gradual increase in number of patients showing
1104 Vaccine 1995 Volume 13 Number 12
Chemo-immunotherapy in ieprosy: S.A. Zaheer et al.
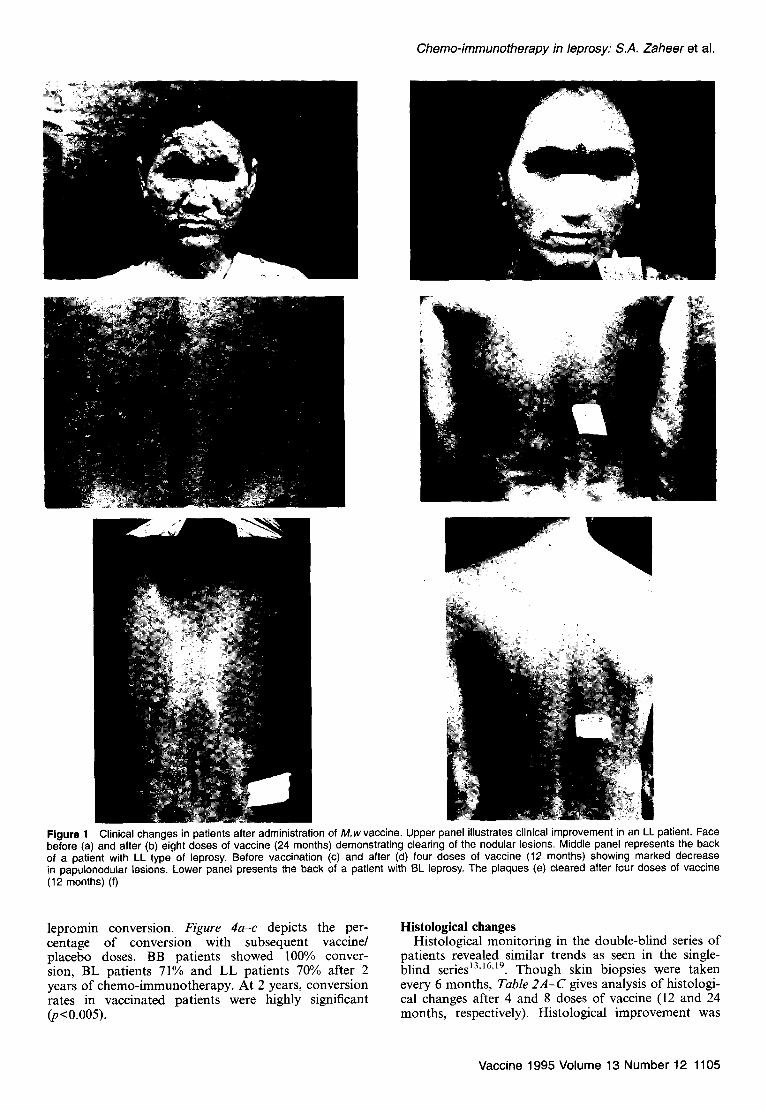
Figure 1 Clinical changes in patients after administration of M.w vaccine. Upper panel illustrates clinical improvement in an LL patient. Face before (a) and after (b) eight doses of vaccine (24 months) demonstrating clearing of the nodular lesions. Middle panel represents the back of a patient with LL type of leprosy. Before vaccination (c) and after (d) four doses of vaccine (12 months) showing marked decrease in papulonodular lesions. Lower panel presents the back of a patient with BL leprosy. The plaques (e) cleared after four doses of vaccine (12 months) (f)
lepromin conversion. Figure 4u-c depicts the per- Histological changes centage of conversion with subsequent vaccine/ Histological monitoring in the double-blind series of placebo doses. BB patients showed 100% conver- patients revealed similar trends as seen in the single- sion, BL patients 71% and LL patients 70% after 2 blind series13,‘6%‘9. Though skin biopsies were taken years of chemo-immunotherapy. At 2 years, conversion every 6 months, Table ZA-C gives analysis of histologi- rates in vaccinated patients were highly significant cal changes after 4 and 8 doses of vaccine (12 and 24 (JKO.005). months, respectively). Histological improvement was
Vaccine 1995 Volume 13 Number 12 1105
Chemo-immunotherapy in leprosy: S.A. i’aheer et al.
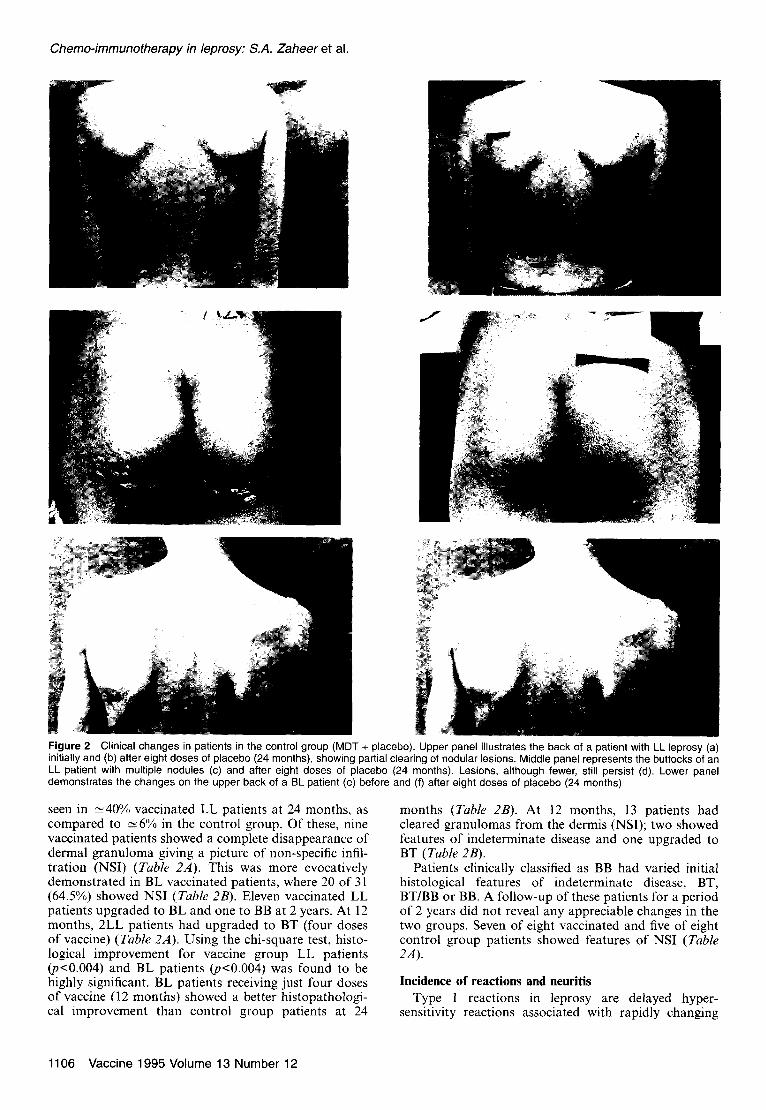
Figure 2 Clinical changes in patients in the control group (MDT + placebo). Upper panel illustrates the back of a patient with LL leprosy (a) initially and (b) after eight doses of placebo (24 months), showing partial clearing of nodular lesions. Middle panel represents the buttocks of an LL patient with multiple nodules (c) and after eight doses of placebo (24 months). Lesions, although fewer, still persist (d). Lower panel demonstrates the changes on the upper back of a BL patient (e) before and (f) after eight doses of placebo (24 months)
seen in -40% vaccinated LL patients at 24 months, as compared to ~6% in the control group. Of these, nine vaccinated patients showed a complete disappearance of dermal granuloma giving a picture of non-specific infil- tration (NSI) (Table ZA). This was more evocatively demonstrated in BL vaccinated patients, where 20 of 31 (64.5%) showed NSI (Tab/e 2B). Eleven vaccinated LL patients upgraded to BL and one to BB at 2 years. At 12 months, 2LL patients had upgraded to BT (four doses of vaccine) (Table 2A). Using the chi-square test, histo- logical improvement for vaccine group LL patients (p~O.004) and BL patients (p<O.O04) was found to be highly significant. BL patients receiving just four doses of vaccine (12 months) showed a better histopathologi- cal improvement than control group patients at 24
months (Table 2s). At 12 months, 13 patients had cleared granulomas from the dermis (NSI); two showed features of indeterminate disease and one upgraded to BT (Table 2B).
Patients clinically classified as BB had varied initial histological features of indeterminate disease, BT, BT/BB or BB. A follow-up of these patients for a period of 2 years did not reveal any appreciable changes in the two groups. Seven of eight vaccinated and five of eight control group patients showed features of NSI (Table 2A).
Incidence of reactions and neuritis
Type 1 reactions in leprosy are delayed hyper- sensitivity reactions associated with rapidly changing
1106 Vaccine 1995 Volume 13 Number 12

Chemo-immunotherapy in leprosy: S.A. Zaheer et al.
I 6
1
i 6
6 I2 18 24 Treatment months
Treatment months Treatment months
n Vaccine q Control n Vaccine 0 Control
n Vaccine 0 Control
(A) W CC)
Figure 3 Changes in BI of leprosy patients in course of treatment with MDT + vaccine or MDT + placebo. (a) Changes in BI of LL patients (53 vaccine; 68 control). Values are mean f S.E.M. The difference between the vaccine and control groups at 6, 12, 18 and 24 months was highly significant, pcO.001. (b) Bacterial Indices in BL patients (31 vaccine; 30 control). Bars give the mean BI + S.E.M. The p value was co.03 between the vaccine and control group at 12 months and ~0.001 at 18 and 24 months. (c) Changes in BI of BB patients. All patients (9) in vaccine group became bacteriologically negative at 18 months
80 t
0 6 12 18 24 Treatment months
- Vaccine - - - Control
@I
Treatment months
- Vaccine - - - Control - Vaccine . - - Control
(4 0
Figure 4 Lepromin conversion in LL (a), BL (b) and BB (c) patients given the vaccine or placebo
cell-mediated immune (CMI) responses”. Type 2 reac- (Table 3A). Using the chi-square test it was revealed tions (ENL or erythema nodosum leprosum) are im- that control group patients had significantly more mune complex reactions associated with deposition of immune complexes at specific target organ sidez5.
episodes of Type 2 reactions (p~O.01). With regards to incidence of neuritis, vaccine group patients had
Higher incidence of upgrading type 1 reactions were less episodes of neuritis than controls (vaccine 68 seen in vaccine (51 episodes in 33 patients) compared episodes in 29 patients; control 91 in 39 patients) to control group (32 episodes in 19 patients). This was (Table 3B). Using the chi-square test it was seen that largely due to the 38 episodes seen in 24 LL patients the control group had significantly more episodes of against only 11 episodes in 7 patients in LL patients neuritis (~~0.04). The ulnar nerve was the most receiving MDT+placebo (Table 3A). Contrary to inci- commonly affected nerve. Fifteen vaccinated dence of Type 1 reactions were incidence of Type 2 patients had deformities during the 2 year follow-up reactions. Only 64 episodes were noted among vacci- against 25 in the control group (Table 3B, Table 4). nated patients vs 109 in the control group. Thirty- Ulnar claw was the commonest deformity followed by seven patients in the vaccine group and 46 in the foot drop. No statistically significant differences were control group showed evidence of Type 2 reactions seen in the two groups.
Vaccine 1995 Volume 13 Number 12 1107

Chemo-immunotherapy in leprosy: S.A. Zaheer et al.
Table 3 DISCUSSION
A. Reactional episodes during treatment
Type I reaction
Group BB BL LL
Type II reaction
BL LL
Vaccine 1 (1) ‘2 (8) 38 (24) 11 (7) 53 (30) Control 5 (3) ‘6 (9) ‘1 (7) 10 (5) 99 (41)
B. Incidence of neuritis and deformities
Group Type of leprosy
No. in study
No. of episodes of neuritis
No. with deformities
Vaccine BB 9 0 1
BL 31 14 (8) LL 53 54 (21) z
Control BB 9 1 (1) 3 BL 30 20 (20) 7 LL 68 70 (70) 15
Figures in parentheses give number of patients experiencing reac- tional episodes (A) or incidence of neuritis (B)
Table 4 Patients released from treatment (RFT) after administra- tion of MDT + M.w vaccine (vaccine group) and MDT + placebo (control group)
No. of Treatment months Type of patients Total
Group leprosy in study 24-26 27-36 37-48 >48 RFT
Vaccine LL 53 19 (35.84) 11 2 - 32 BL 31 23(74.19) 4 - - 27 BB 9 9 (100) - - - 9
Control LL 68 2 (2.94) BL 30 5 (16.66) z BB 9 4 (44.44) 1
Figures in parentheses indicate percent of patients RFT
Release from treatment
Patients were released from treatment (RFT) after the disease became clinically inactive and three consecutive slit smears were negative for acid-fast bacilli (AFB)‘6. At the time of writing, 32 (-60%) of 53 LL patients given vaccine have been RFT; 19 after 2 years of treatment; 11 between 2 and 3 years and 2 beyond 3 years. Fourteen ( 2: 20%) of 68 control group LL patients have been RFT; 2 after 2 years of treatment, 5 between 2 and 3 years and 7 beyond 3 years. Twenty-seven of 31 (2: 87%) (77.4%) patients with BL leprosy, who received M.w vaccine, have been RFT: 23 within 2 years and 4 between 2 and 3 years. In the control BL group, 18 of 30 (60%) have been RFT: 5 within 2 years; 9 between 2 and 3 years and 4 beyond 3 years. In the BB group given vaccine, all 9 patients were released within the mandatory 2 years of treatment. Six of nine control group patients have been RFT: 4 in 2 years; 1 between 2 and 3 years and 1 beyond 3 years (Table 4). Using the chi-square test, the number of patients RFT in BL and LL vaccine group was found to be highly significant (p<O.OOOl) for BL; p<O.OOOl for LL). Fischer’s exact test was used for BB patients as frequencies were small. Patients RFT was again significant for the vaccine group (pcO.04).
Developed in 1 978’7 and currently in advanced Phase III immunotherapeutic trials in Delhi, Mycobacterium w
vaccine has shown definite immunotherapeutic effects in multibacillary (MB) leprosy patients. Reports on results on the first series of patients1”.‘5*‘9 and results reported here on the second series are consistent and in concur- rence with each other. The vaccine has been extremely well tolerated both in hospital-based trials as well as in field trials at several centres.
Attempts are also being made in several laboratories around the world to develop a vaccine for leprosy. These candidate vaccines are at different stages of clinical trials. They are being tested both for immunotherapeutic and immunoprophylactic potential. They are (i) killed M. leprae and live BCG, originally proposed by Convitt e? a1.28; (ii) Indian C ancer Research Centre strain (ICRC)‘9; and (iii) M. vaccae, proposed by Stanford”‘. Two cytokines are also being tested for their immuno- modulatory effects in LL patients. These are gamma interferon3’ and interleukin-23’. Trials with A4.1~ are unique in several respects. They are the first immuno- therapeutic trials where active MB patients have been critically assessed by clinical, immunological, bacterio- logical and histological parameters. These trials have a well matched control group receiving MDT+placebo. Numbers enrolled have been higher than those in any other study, and all patients have received a minimum of 2 years of treatment.
Patients receiving M. w vaccine have shown marked reduction in infiltration and rapid clearing of papulo- nodular lesions. Using Ramu’s clinical scores33.34, vac- cinated patients showed a significant fall in scores in all three forms of leprosy (~~0.02).
With MDT alone, bacterial index (BI) decreases are stated to be between 0.6 and 1 .O units yeai’ (Ref. 35). In our study, rapid BI decreases were seen among vacci- nated patients. Thirty-five BL or LL patients with high BI attained bacteriological negativity within 2628 months of treatment with M.w vaccine + MDT. This was associated with lepromin conversion and/or histo- logical improvement. Two patients with a high BI of 6 (Index Nos 225 and 81) were rendered BI negative in the 2-year time period. This was associated, in both, with a lepromin conversion to positivity status. In the control group, receiving MDT+placebo, only eight BL or LL patients becoming BI=O could be enumerated. Most of them had initial BIs of ~4. It was interesting to note that in all three forms of the disease, BI values in vaccinated patients at 12 months were lower than that achieved by control group patients at 2 years. BI decreases were also statistically significant in vaccinated patients (pcO.03).
Shifts in cell-mediated immune (CMI) status were reflected by the progressive lepromin conversion from negativity to positivity in vaccinated patients. LL and BL patients showed ~70% conversion; BB patients 100% conversion. These are the highest conversion rates attained by any immunomodulator in leprosy.
Histological improvement was significantly more in vaccinated BL and LL patients QcO.04). Forty-four of them showed histological improvement, of which 29 showed a complete disappearance of dermal granuloma resulting in a histological picture of non-specific infiltra- tion (NSI). BB patients, in either vaccine or control
1108 Vaccine 1995 Volume 13 Number 12

groups, histologically did not show any appreciable differences.
That the vaccine upgraded CM1 responses was also evident by the higher incidence of Type 1 reactions in vaccinated patients. In fact, Type 1 reactions are not commonly encountered among LL patients. In our study, we have noted these reactions in 24 patients in vaccine as compared to 7 in the control group. Type 2 reactions occur in the presence of M. leprae antigen?. Far fewer episodes of Type 2 reactions were observed among vaccinated patients (vaccine 64 and control 109), possibly due to rapid clearance of antigen. These obser- vations were also seen in the single-blind series and have been reported18.
It is imperative to monitor incidence of reactions and deformities when using immunomodulators in leprosy. It was reassuring to note that there was a lower inci- dence of neuritis and deformities in the vaccine group and that A4. w vaccine did not aggravate either neuritis or associated motor disturbances. This was also observed histopathologically, where vaccination did not precipi- tate inflammation of dermal nerve twigs16.
The overall clinical, bacteriological and histological improvement among vaccinated patients was reflected by a shorter treatment duration and a significant num- ber being released from treatment (p~O.0001). Thus vaccinated patients had less morbidity, were rendered BI negative faster and ceased to be sources of infection to the community more quickly and there was a reduction in costs of drugs and medical care.
Several studies on Mycobacterium w have shown that it shares a number of B36 and T37 cell epitopes with M. leprae. CD4+ clones from subjects immunised with BCG+M. leprae react with M. w37. Peripheral blood mononuclear cells from TT patients and healthy con- tacts, not previously exposed to M.w proliferate in vitro in response to its antigens38. An immunodominant 28-31 kDa antigen, in M. w, carrying B and T cell determinants, has been reported38. Monoclonal anti- bodies hitherto considered specific to M. leprae or M. tuberculosis react with antigens of Mycobacterium w in Western blots36. Additional studies with this strain have shown that it stimulates T helper-l subsets in murine models with enhanced production of IL-2 and gamma interferon”‘. The vaccine also imparts protection in mice and guinea pigs to challenge with live M. tuberculosis H,,Rv. This effect is seen in both BCG “responder”, and “non-responder” genetic strains of micea.
The precise mechanism of action of the vaccine is difficult to state, however, based on the above studies and results of clinical trials, certain assumptions can be put forward. Talwar” has used the approach of hetero- immunisation, in contrast to the commonly used ap- proach of immunisation with a homologous antigen. The reason is simple. Multibacillary (MB) leprosy patients are devoid of autoregressive potentials as they carry both dead and live acid-fast bacillli AFB for several years and these antigens do not evoke a regres- sive immune response. Moreover, it is our experience (in the control group), that repeated lepromin injections (which are like mini homologous vaccines) do not or rarely alleviate the immune-deficit in polar multi- bacillary patients. Thus there exists a unique situation, in relation to M. leprae and the host, which demands an
Chemo-immunotherapy in leprosy: S.A. Zaheer et al.
overriding of immunological non-responsiveness to the bacillary antigens. Mycobacterium w is able to achieve this by generation of cross reactive T,l type of clones. Gamma interferon seems to be one of the cytokines secreted by antigen stimulated lymphocytes that acti- vates macrophages39. This is associated with enhanced secretion of reactive oxygen intermediates (02 -, H,OJ in the macrophages which leads to a rapid killing and clearance of M. leprae4’. The rapid clearance of AFB from tissues after vaccination, may partially be explained by this mechanism.
Thus, based on our experience with Mycobacterium w vaccine in this study and other studies at several centres, of rapid BI clearance, quicker clinical recovery, shorten- ing of duration of treatment and overall recovery of patients, we would recommend its addition as an adjunct to multidrug therapy in MB leprosy patients.
ACKNOWLEDGEMENTS
The trials are supported from a grant from the Depart- ment of Biotechnology, Government of India (No. BT/ 15/09/006/89 dated 22.10.90). The technical assistance of Mr Dinesh Negi, Mr Amarnath Prasad, Mr Anil Bobin, Mrs Namita Manocha and Mr Kishan Pal is gratefully acknowledged.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
World Health Organization. WHO Expert Committee on leprosy. Sixth report. Tech. Rep. Ser. 1988, 768, 14-15 Jopling, W.H. The disease. In: Handbook of Leprosy (Ed. Jopling, W.H.). William Heinemann Medical, London, 1984, pp. 8-46 Nath, I. Immunology of human leprosy. Current status. Lepr. Rev. 1983, special issue, 31 S-45.S Saxena, V.K., Singh, U.S. and Singh, A.K. Bacteriological study of a rapidly growing strain of mycobacterium. Lepr. lndia 1978, 58588-596 Katoch, V.M. A report on the biochemical analysis of Myco- bacterium w. Lepr. India 1981, 53, 385-389 Mustafa, AS. and Talwar, G.P. Five cultivable mycobacterial strains giving blast transformations and leukocyte migration- inhibition of leukocytes analogous to Mycobacferium teprae. Lepr. India 1978, 50,498-508 Mustafa, A.S. and Talwar, G.P. Delayed hypersensitivity skin reactions to homologous and heterologous antigens in guinea pigs immunized with M. leprae and four selected cultivable mycobacterial strains. Lepr. lndia 1978, 50, 509-519 Fotedar, A., Mehra, N.K., Mustafa, A.S. and Talwar, G.P. Local reactions to intra-dermal instillation of Mycobacterium w and ICRC bacilli in mice. Lepr. India 1978, 50, 520-533 Mustafa, A.S. and Talwar, G.P. Enlargement of draining lymph nodes in mice by four selected cultivable strains of mycobacteria. Lepr. India 1978, 50, 534-538 Mustafa, A.S. and Talwar, G.f? Early and late reactions in tuberculoid and lepromatous leprosy patients with lepromins from Mycobacterium leprae and five selected cultivable myco- bacteria. Lepr. India 1978, 50, 566-571 Reddy, P.P., Amin, A.G., Khandekar, P.S. and Talwar, G.P. Molecular definition of unique species status of Mycobacterium w; a candidate leprosy vaccine strain. ht. J. Lepr. 1994, 84, 229-236 Chaudhuri, S., Fotedar, A. and Talwar, G.P. Lepromin con- version in repeatedly lepromin negative BULL patients after immunization with autoclaved Mycobacterium w. ht. J. Lepr. 1983, 51, 159-168 Talwar, G.P., Zaheer, S.A., Mukherjee, R. et a/. Immunothera- peutic effects of a vaccine based on a saprophytic cultivable mycobacterium, Mycobacterium w, in multibacillary leprosy patients. Vaccine 1990, 8, 121-l 29
Vaccine 1995 Volume 13 Number 12 1109
Chemo-immunotherapy in leprosy: S.A. Zaheer et al.
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
Talwar, G.P., Mukherjee, R., Zaheer, S.A. et al. Present ap- proaches to immunotherapy and immunoprophylaxis in leprosy. In: Progress in Vaccino/ogy(Ed. Talwar, G.P.), Vol. Il. Springer, New York, 1989, pp. 301-311 Talwar, G.P., Zaheer, S.A., Suresh, N.R. et al. Immuno- therapeutic trials with a candidate anti-leprosy vaccine based on Mycobacterium w. Trop. Med. Parasitol. 1991, 41( 369-370 Mukherjee, A., Zaheer, S.A., Sharma, A.K., Misra, R.S., Kar, H.K., Mukherjee, R. and Talwar, G.P. Histopathological monitor- ing of immunotherapeutic trials with Mycobacterium w. ht. J. Lepr. 1992, 60, 28-35 Zaheer, S.A., Suresh, N.R., Kar, H.K., Sharma, A.K., Mukherjee, A., Mukherjee, R. and Talwar, G.P. Immunological upgrading with combined immunotherapy and chemotherapy in an LL patient. A case report. Lepr. Rev. 1991, 61, 297-302 Zaheer, S.A., Misra, R.S., Sharma, A.K. et al. Immunotherapy with Mycobacterium w vaccine decreases the incidence and severity of type 2 (EHL) reactions, Lepr. Rev. 1993, 64, 7-14 Zaheer, S.A., Mukherjee, R., Ram Kumar, B. et al. Combined multidrug and Mycobacterium w vaccine therapy in patients with multibacillary leprosy. J. Infect Dis. 1993, 167, 401-410 Kar, H.K., Sharma, A.K., Misra, R.S. eta/. Induction of lepromin positivity by a candidate anti-leprosy vaccine Mycobacterium w in lepromin negative healthy contacts of multibacillary leprosy patients, lndian J. Lepr. 1992, 64, 495-500 Katoch, K., Natarajan, M., Bagga, A. et a/. lmmunotherapeutic trials using BCG and Mycobacterium strain w along with MDT in highly bacillated BULL cases, Quaderni di Cooperazione Sanitaria. Health Cooperation Papers. 12, 1992, 239-244 Natarajan, M., Katoch, K., Bagga, A.K. and Katoch, V.M. Histological changes with combined chemotherapy and immunotherapy in highly bacillated lepramatous leprosy. Acta Leprologica 1992, 8, 79-86 Walia, R.. Sarathchandra, K.G., Mukherjee, R. et a/. Field trials on the use of Mycobacterium w vaccine in conjunction with multidrug therapy in leprosy patients for immunotherapeutic and immunoprophylactic purposes. Lepr. Rev. 1993, 84, 302- 311 Gupte, M.D. The relevance of future leprosy vaccines to disease control. Lepr. Rev. 1992, 63 (Suppl.), 99S-106s Wemambu, S.N., Turk, J.L., Waters, M.F.R. and Rees, R.J.W. Erythema nodosum leprosum. a clinical manifestation of the Arthus phenomenon. Lancet 1969, ii, 933-935 World Health Organization. Treatment of leprosy. In: A Guide to Leprosy Control. WHO, Geneva, 1980, pp. 23-32 Talwar, G.P. Towards development of a vaccine against leprosy. Lepr. India 1978, 50, 492-497 Convit, J., Aranzazu, N., Pinardi, M.E., Reyes, 0. and Alvarado, J. Immunotherapy with a mixture of Mycobacterium leprae and
29
30
31
32
33
34
35
36
37
38
39
40
41
BCG in different forms of leprosy and in Mitsuda negative contacts. ht. J. Lepr. 1982, 50, 415-424 Deo, M.G., Bapat, C.V., Bhalerao, V., Chaturvedi, R.M., Chulawala, R.G. and Bhatki, W.S. Anti-leprosy potentials of the ICRC vaccine: a study in patients and healthy volunteers. ht. J. Lepr. 1983, 51, 540-549 Stanford, J.L., Rook, G.A.W., Bahr, G.M. eta/. Mycobacterium vaccae in immunoprophylaxis and immunotherapy of leprosy and tuberculosis. Vaccine 1990, 8, 525-530 Kaplan, G., Mathur, N.K., Job, C.K., Nath, I. and Cohn, Z.A. Effect of multiple interferon gamma injections on the disposal of Mycobacterium leprae. Proc. Nat/ Acad. Sci. USA 1989; 86: 8073-8077 Kaplan, G., Britton, W.J., Hancock, G.E. et a/. The systemic influence of recombinant interleukin 2 on the manifestations of lepromatous leprosy. J. Exp. Med. 1991, 173, 993-1006 Ramu, G. and Desikan, K.V. A follow up study of borderline tuberculoid leprosy under sulphone monotherapy. Indian J. Lepr. 1988, 60,26-33 lyer, C.G.S. and Balakrishnan, Ramu G. A comparison of low and conventional dosages of dapsone in the treatment of lepromatous leprosy in India. Lepr. lndia 1977, 49, 372-388 Grosset, J.H. Recent developments in the field of multidrug therapy and future research in chemotherapy of leprosy. Lepr. Rev. 1986, 57, 223-234 Ganju, L., Mukherjee, Ft., Batra, H.V. and Talwar, G.P. Immuno- blot analysis of antigens of Mycobacterium w. A candidate anti- leprosy vaccine using monoclonal antibodies and patients sera. ht. J. Med. Microbial. 1991, 273, 378-385 Mustafa, AS. Identification of T cell activating recombinant antigens shared among three candidate anti-leprosy vaccines, killed M. leprae, M. bovis BCG and Mycobacterium w. ht. J. Lepr. 1988, 56, 265-273 Yadava, A., Suresh, N.R., Zaheer, S.A., Talwar, G.P. and Mukherjee, R. T cell responses to fractionated antigens of Mycobacterium w, a candidate anti-leprosy vaccine, in leprosy patients. Stand. J. Immun. 1991, 34, 23-31 Singh, I.G., Mukherjee, R., Talwar, G.P and Kaufmann, S.H.E. In vitro characteristics of T cells from Mycobacterium w vacci- nated mice. Infect. hmun. 1992,60, 257-263 Singh, LG., Mukherjee, R. and Talwar, G.P. Resistance to intravenous inoculation of Mycobacterium tuberculosis H,, Rv in mice of different inbred strains following immunization with a leprosy vaccine based on Mycobacterium w. Vaccine 1991, 9, 10-14 Kaplan, G., Nathan, C.F., Gandhi, R., Horwitz, M.A., Levis, W.R. and Cohn, Z.A. Effect of interferon gamma on hydrogen peroxide re- leasing capacity of monocytes derived macrophages from patients with lepromatous leprosy. J. Immun. 1986, 137, 983-987
1110 Vaccine 1995 Volume 13 Number 12




















