ADAM9 Expression is a Significant and Independent Prognostic Marker of PSA Relapse in Prostate...
12
Prostate Cancer ADAM9 Expression is a Significant and Independent Prognostic Marker of PSA Relapse in Prostate Cancer Florian R. Fritzsche a , Monika Jung b , Angelika To ¨ lle b , Peter Wild c , Arndt Hartmann d , Kirsten Wassermann a , Anja Rabien b , Michael Lein b , Manfred Dietel a , Christian Pilarsky e , Daniela Calvano e , Robert Gru ¨ tzmann e , Klaus Jung b , Glen Kristiansen a,c, * a Institute of Pathology, Charite ´ - Universita ¨ tsmedizin Berlin, Berlin, Germany b Department of Urology, Charite ´ - Universita ¨ tsmedizin Berlin, Berlin, Germany c Institute of Pathology, Universita ¨ tsspital Zu ¨ rich, Zu ¨ rich, Switzerland d Institute of Pathology, University of Regensburg, Regensburg, Germany e Department of Surgery, University Hospital Dresden, Dresden, Germany european urology 54 (2008) 1097–1108 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted November 12, 2007 Published online ahead of print on November 26, 2007 Keywords: ADAM9 Immunohistochemistry qRT-PCR Prognostic marker Prostate cancer Abstract Objectives: A disintegrin and metalloprotease (ADAM) 9 has been impli- cated in tumour progression of prostate cancer. We evaluated the expression of ADAM9 on protein and messenger RNA (mRNA) level in a larger cohort of prostate cancer cases following prostatectomy and correlated the findings with clinicopathological parameters including prostate-specific antigen (PSA) relapse times. Methods: We immunostained 198 clinicopathologically characterised prostate cancer cases for ADAM9. For 25 additional cases, ADAM9 mRNA of microdissected tumour and normal tissue was analysed via quanti- tative reverse transcriptase-polymerase chain reaction. Results: ADAM9 was significantly upregulated in prostate cancer com- pared with normal tissue on mRNA and protein level. ADAM9 protein expression was significantly associated with shortened PSA relapse-free survival in univariate and multivariate analyses, particularly in patients who had received prior androgen ablation. Conclusions: ADAM9 is overexpressed in prostate cancer cases and is an independent prognostic marker of PSA relapse-free survival following radical prostatectomy. Further studies are needed to verify its role as a predictive marker of response to androgen ablation. # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Institute of Surgical Pathology, University Hospital Zurich, Schmelzbergstr. 12, CH-8091 Zurich. Tel. +41 44 2553457; Fax: +41 44 2554416. E-mail address: [email protected] (G. Kristiansen). 0302-2838/$ – see back matter # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2007.11.034
-
Upload
tu-dresden -
Category
Documents
-
view
1 -
download
0
Transcript of ADAM9 Expression is a Significant and Independent Prognostic Marker of PSA Relapse in Prostate...

Prostate Cancer
ADAM9 Expression is a Significant and IndependentPrognostic Marker of PSA Relapse in Prostate Cancer
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 8
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Florian R. Fritzsche a, Monika Jung b, Angelika Tolle b, Peter Wild c, Arndt Hartmann d,Kirsten Wassermann a, Anja Rabien b, Michael Lein b, Manfred Dietel a, Christian Pilarsky e,Daniela Calvano e, Robert Grutzmann e, Klaus Jung b, Glen Kristiansen a,c,*a Institute of Pathology, Charite - Universitatsmedizin Berlin, Berlin, GermanybDepartment of Urology, Charite - Universitatsmedizin Berlin, Berlin, Germanyc Institute of Pathology, Universitatsspital Zurich, Zurich, Switzerlandd Institute of Pathology, University of Regensburg, Regensburg, GermanyeDepartment of Surgery, University Hospital Dresden, Dresden, Germany
Article info
Article history:Accepted November 12, 2007Published online ahead ofprint on November 26, 2007
Keywords:ADAM9ImmunohistochemistryqRT-PCRPrognostic markerProstate cancer
Abstract
Objectives: A disintegrin and metalloprotease (ADAM) 9 has been impli-cated in tumour progression of prostate cancer. We evaluated theexpression of ADAM9 on protein and messenger RNA (mRNA) level ina larger cohort of prostate cancer cases following prostatectomy andcorrelated the findings with clinicopathological parameters includingprostate-specific antigen (PSA) relapse times.Methods: We immunostained 198 clinicopathologically characterisedprostate cancer cases for ADAM9. For 25 additional cases, ADAM9 mRNAof microdissected tumour and normal tissue was analysed via quanti-tative reverse transcriptase-polymerase chain reaction.Results: ADAM9 was significantly upregulated in prostate cancer com-pared with normal tissue on mRNA and protein level. ADAM9 proteinexpression was significantly associated with shortened PSA relapse-freesurvival in univariate and multivariate analyses, particularly in patientswho had received prior androgen ablation.Conclusions: ADAM9 is overexpressed in prostate cancer cases and is an
gnostic marker of PSA relapse-free survival followingtomy. Further studies are needed to verify its role as a
independent proradical prostatec
r of response to androgen ablation.ociation of Urology. Published by Elsevier B.V. All rights reserved.
predictive marke# 2007 European Ass
* Corresponding author. Institute of Surgical Pathology, University Hospital Zurich,Schmelzbergstr. 12, CH-8091 Zurich. Tel. +41 44 2553457; Fax: +41 44 2554416.E-mail address: [email protected] (G. Kristiansen).
0302-2838/$ – see back matter # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2007.11.034

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 81098
1. Introduction
In this study we focused on ADAM9, a member of the‘‘A disintegrin and metalloprotease’’ (ADAM) family,in prostate cancer. This family of proteins isinvolved in different physiological and pathophy-siological functions including cell adhesion, cellmigration, and tissue remodeling [1]. ADAMs aremembrane-anchored glycoproteins that consist of aprotease and an adhesion domain. The interactionsof ADAMs with cell-surface and extracellular matrixproteins could be of relevance to tumour biologybecause these processes are vital for tumourprogression [2–4]. Concordantly, various ADAMshave been shown to represent a potential diagnosticand prognostic marker in human tumours [5].
The type I transmembrane protein ADAM9(synonyms, MDC9, meltrin-g) is a cell adhesionmolecule, found to interact with avb5 integrin, tocleave the insulin B-chain, and to be involved in theectodomain shedding of membrane-anchoredheparin-binding epidermal growth factor (EGF)-likegrowth factor [4,6,7]. In addition, a secreted form ofADAM9 that resulted from alternative splicing wasdescribed [8]. ADAM9 might be essentially involvedin carcinogenesis and tumour progression by med-iating EGF receptor activity and by promoting cancer
Table 1 – Associations (chi-square tests) between the proteinclinicopathological parameters
Total
All cases 198
Age
�62 105
>62 93
Pre-OP PSAb
�9.4 ng/ml 87
>9.4 ng/ml 82
PT status
pT2 110
pT3/4c 88
Gleason sumd
3–6 89
7 56
8–10 52
Residual tumoure
R0 109
R1 87
ADAM9, A disintegrin and metalloprotease 9; Pre-Op PSA, preoperative Pa Dichotomisation was achieved according to the median (100).b Preoperative PSA was not available for 29 cases.c Five cases were pT4.d For one case no Gleason score was given in the report.e Two cases were Rx.
cell invasion via regulation of E-cadherin andintegrins [6,9–15].
In this study we evaluated ADAM9 expression onprotein and transcript level to clarify a diagnostic orprognostic value of ADAM9 in human prostatecancer.
2. Methods
2.1. Patients (reverse transcriptase-polymerase chainreaction)
Twenty-five matched (tumour/normal) prostate samples were
microdissected from frozen sections. Cases used for micro-
dissection and messenger RNA (mRNA) preparation differed
from the cohort used for immunohistochemistry.
2.2. Patients (immunohistochemistry)
One hundred ninety-eight prostatectomy patients were
enclosed in this study. Patient age ranged between 47 and
74 yr (median, 62). Preoperative prostate-specific antigen (PSA)
levels ranged from 0.03 to 150 ng/ml (median, 9.4). Forty-four
patients (22.2%) had received gonadotropin-releasing hor-
mone analogues at the discretion of the referring urologist
prior to surgery (median, 4 wk; range, 2–16 wk). Because this
short-term antiandrogenic therapy did not result in morpho-
logically discernable effects, Gleason score was evaluated as
expression of ADAM9 in prostate cancer and
Low ADAM9a High ADAM9a p value
85 (42.9%) 113 (57.1%)
0.010
36 (34.3%) 69 (65.7%)
49 (52.7%) 44 (47.3%)
0.877
35 (40.2%) 52 (59.8%)
34 (41.5%) 48 (58.5%)
0.471
50 (45.5%) 60 (54.5%)
35 (39.8%) 53 (60.2%)
0.597
40 (44.9%) 49 (55.1%)
24 (42.9%) 32 (57.1%)
21 (40.4%) 31 (59.6%)
0.663
48 (44.0%) 61 (56.0%)
35 (40.2%) 52 (59.8%)
SA; pT status, tumour stage.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 8 1099
usual. Clinical follow-up data, as annually assessed, including
PSA relapse-free survival time were available for all patients.
The median follow-up time of all cases was 46.5 mo (range,
1–180). The median follow-up time of patients without a PSA
relapse was 48 mo (range, 10–180). Sixty-nine patients (34.8%)
experienced a PSA relapse after a median time of 31 mo (range,
3–139). The Gleason scores (GS) in the cohort were distributed
as follows: GS 2–6, 89 (44.9%); GS 7, 56 (28.3%); GS 8–10, 52
(26.3%); missing data, 1 (0.5%) (Table 1).
2.3. Quantitation of ADAM9 mRNA
The total RNA isolation was performed with the use of RNeasy
Micro Kit (Qiagen, Hilden, Germany) from manually micro-
dissected areas of normal prostate tissue, prostatic intrae-
pithelial neoplasia (PIN), and prostate cancer, specified by a
genitourinary pathologist and previously described in detail
[15].
RNA concentrations were measured with the NanoDrop
ND-1000 Spectrophotometer (NanoDrop Technologies, Wil-
mington, DE, USA). The integrity of isolated RNA was assessed
with the use of the RNA 6000 Nano LabChip1 kit and the
Agilent 2100 Bioanalyzer (Agilent Technologies, Palo Alto, CA,
USA). All samples were characterised by an A260/A280 ratio
>1.90 and an RNA integrity value >7.
Complementary DNA (cDNA) synthesis was performed
with the use of the Transcriptor First Strand cDNA Synthesis
Kit (Roche Applied Science, Penzberg, Germany) and a
maximum of 1 mg RNA in reaction. The cDNA volume
amounted to 20 ml.
Real-time polymerase chain reaction (PCR) was performed
with the LightCycler Instrument (Roche Applied Science).
Prediluted (1:5) cDNA was used for the quantification of
reference gene and target gene expression. The PCR reaction
volume was 10 ml including 1 ml diluted cDNA. The PCR run
conditions of the three reference gene quantifications were
the same as described previously [16]. Paired samples of
nonmalignant and malignant tissue areas were measured in
one PCR run. The reaction condition for ADAM9 mRNA and for
its two transcript variants were established separately for
each PCR. The real-time detection of PCR products was
performed with fluorescence dye SYBR green I (QuantiTect
SYBR green PCR Kit; Qiagen); reaction conditions are given in
Table 2. Only one single melting peak was observed for PCR-
specific amplicons. For all genes, calibration curves with
Table 2 – Real-time reverse transcriptase-PCR data with prime
Target gene and transcript variants ACC no.
Total ADAM 9 NM_003816
Transcript variant 1 (transmembrane) NM_003816
Transcript variant 2 (cytosolic) NM_001005845
PCR, polymerase chain reaction; ACC no, GenBank accession number; P
disintegrin and metalloprotease 9.
pooled cDNA were generated. PCR efficiencies were amounted
from cDNA dilution curves of pooled cDNA. Each PCR run
included a cDNA with known expression level and was used as
a standard for quantification of an unknown sample calcu-
lated by LightCycler Software, version 3.5 (Roche Applied
Science). For relative quantification of ADAM9 mRNA and both
transcript variants, the expressions were normalised on
geometric mean of the expression of the three reference
genes hypoxanthine-phosphoribosyl-transferase (HPRT1),
delta aminolevulinate synthase 1 (ALAS1), and K-alpha-1
tubulin (K-ALPHA-1) [16].
2.4. Western blot analysis
Paired tissue samples (cancer/normal) from six prostatect-
omy specimens were used for protein extraction. After
histological control to ascertain the specific histology the
tissue was frozen, minced, and homogenised by an ultra-
sound device in 50 mmol/l Tris-HCl, 10 mmol/l CaCl2, pH 7.5,
with 0.25v/v% Triton1 X-100 (Sigma-Aldrich Chemie GmbH,
Munich, Germany), in the presence of protease inhibitors
(0.1 mmol/l phenylmethylsulphonyl fluoride, 1 mg/ml apro-
tonin, 10 mg/ml soybean trypsin inhibitor). After centrifuga-
tion at 23,000g for 15 min at 4 8C, the supernatants were stored
at �80 8C until analysis. Twenty micrograms of total protein
of each tissue sample were applied for fractionation on an
sodium dodecyl sulphate-polyacrylamide gel electrophoresis
(10% w/v polyacrylamide, reducing conditions) and then
transferred onto a polyvinylidene difluoride membrane
(Millipore Corp, Bedford, MA, USA). The membrane was
incubated with antihuman ADAM9 polyclonal antibody
(0.2 mg/ml; CEDARLANE LABORATORIES Limited, Ontario,
Canada). Actin (anti–b-actin clone AC-74; Sigma-Aldrich
Chemie GmbH) served as a loading control. Horseradish
peroxidase–conjugated goat antirabbit immunoglobulin G
(IgG) and rabbit antimouse IgG (Dako, Hamburg, Germany)
were used as secondary antibodies. The antigen-antibody
reaction was visualised by enhanced chemiluminescence
(Amersham Biosciences, Piscataway, NJ, USA). Intensity of
the detected signals by Western blot was quantified with the
use of Fluor-S MultiImager (Bio-Rad Laboratories, Hercules,
CA, USA).
Specificity of ADAM9 bands were confirmed with the use of
(a) blocking peptide, corresponding to carboxy terminal end of
human ADAM9, at 30-fold concentration excess of the primary
r sequences
Primer sequence 50. . .. . .30 PS (bp) E
F: cag atg gca aaa atc aag ca 151 2.01
R: gat ggg aac tgc tga ggt tg
F: gga tac gga gga agt gtg ga 110 1.91
R: gca cag aca ata agg gga aca
F: gtc atg gac atg gga aat ga 120 1.95
R: ctc cac agt tga tcc ctc ttg
S, PCR product sizes; E, efficiencies of target gene PCRs; ADAM9, A

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 81100
antibody, and (b) control IgG of serum from healthy non-
immunised rabbits (Dako).
2.5. Immunohistochemistry
Formalin-fixed paraffin-embedded tissue was freshly cut
(3 mm), mounted on superfrost slides (Menzel Glaser),
dewaxed with xylene, and gradually hydrated. Antigen
retrieval was achieved by pressure cooking in 0.01 mmol/l
citrate buffer for 5 min. The primary ADAM9 antibody
(primary goat polyclonal antibody, AF949; R&D Systems,
Wiesbaden, Germany) [17] was diluted 1:50 with the use of a
background reducing dilution buffer (Dako) and incubated at
room temperature for 1 h. This antibody (AF949) is specific for
mouse ADAM9 and cross-reacts with human ADAM9. It does
not cross-react with human ADAM8, ADAM10, ADAM15, or
ADAM17/TACE (data not shown). Detection took place by the
conventional labelled-streptavidin-biotin method (LSAB-kit,
Dako) with Fast-Red (Sigma-Aldrich Chemie GmbH) as
chromogen. The slides were counterstained and mounted.
Antibody specificity was confirmed by a blocking experiment,
coincubating the antibody with the corresponding ADAM9
peptide (949-AD, R&D Systems), which abolished immuno-
reactivity. As negative controls we used ADAM9-positive
prostate cancer cases omitting the primary antibody.
2.6. Evaluation of the immunohistochemical stainings
The immunostainings were evaluated by two genitourinary
pathologists. To assess staining intensity and quantity of cells
stained, we applied the H-score separately for prostate cancer,
adjacent normal prostatic tissue (peripheral zone), and PIN.
The staining intensity (including cytoplasmic diffuse and the
polar, luminally accentuated form) was evaluated with a four-
tier grading system (0 = negative, 1 = weak, 2 = moderate, and
3 = strong staining intensity). For each staining intensity
grade, the percentage of tissue stained was multiplied by
the corresponding intensity grade (0–3). Theses values were
summed for each tissue type, resulting in a score between 0
and 300. To delineate between low and high levels of ADAM9
expression, the median H-score was used to dichotomise the
data.
2.7. Statistical analysis
Statistical analysis was performed with SPSS, version 14.0
(SPSS Inc, Chicago, IL, USA). p values < 0.05 were considered
significant.
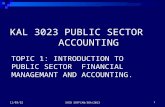
Fig. 1 – ADAM9 messenger RNA (mRNA) expression. (A)
Normalised mRNA expression values of ADAM9. The
columns are means W standard error of the mean.
Significances calculated by paired t tests. (B) Multiple of
normalised prostate cancer (PC) ADAM9 expression to
adjacent normalised prostate tissue (PN) divided according
to the splicing variants (see A). For all splicing variants the
majority of prostate cancers were above the normal tissue
standard. ADAM9, A disintegrin and metalloprotease 9.
3. Results
3.1. Quantitative reverse transcriptase-PCR
The normalised ADAM9 expression was signifi-cantly higher in malignant samples (n = 25) thanin matched nonmalignant samples (both wereevaluated for the total and transmembrane ADAM9),whereas the differences for the secreted form of
ADAM9 remained insignificant (Fig. 1A and B). Stillfor three (12%, total), five (20%, transmembrane),and eight (32%, secreted) samples, ADAM9 expres-sion levels were below those of the correspondingnormal tissue. ADAM9 mRNA expression did notcorrelate with any of the clinicopathological para-meters.
3.2. Western blot
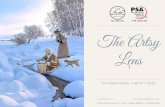
Fig. 2A illustrates a representative blot of ADAM9protein expression in normal and tumour prostatetissue extracts. ADAM9 protein was detectable in alltissue extracts. With the use of Western blotanalysis under reducing conditions, two forms at

Fig. 2 – Western blots and antibody specificity testing. (A) ADAM9 and b-actin in normal (N) and tumour (T) prostate tissue
extracts. (B) Specificity of ADAM9 bands was confirmed with the use of a blocking peptide, corresponding to the carboxy
terminal end of human ADAM9. (C) Peptide blocking of the ADAM9 antibody for immunohistochemistry in corresponding
tissue sections. The figure demonstrates regular ADAM9 expression for the unblocked antibody (left part) and loss of
ADAM9 staining after peptide blocking (right part). ADAM9, A disintegrin and metalloprotease 9.
Table 3 – The amount of ADAM9 protein (Western blot) incancer tissue in relation to normal tissue
Patient Tumour (% density) Tumour (% density)
Total ADAM9(80 + 70 kDa)
80 kDaband
70 kDaband
1 134 183 79
2 84 0 96
3 178 100a 100
4 120 154 89
5 103 37 77
6 118 179 82
Median 119b 127 89
ADAM9, A disintegrin and metalloprotease 9.
Mean values of three independent Western blots. The ADAM9 level
of the normal tissue sample was set to 100%.a In the normal tissue of this patient, the 80 kDa band was absent.b Wilcoxon test (paired samples), p = 0.09.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 8 1101
80 and 70 kDa were detected. In the presence ofexcess blocking peptide, all bands were stronglyreduced (Fig. 2B). In addition, none of these proteinswas visible after immunoblotting with control IgG ofserum from healthy nonimmunised rabbits, demon-strating antibody specificity of the two bands.Relative levels of the 80-kDa protein were increasedin prostate cancer compared with normal tissue (3 of6). The 80-KDa band was absent in two normal tissueextracts. In the cancer sample one of these patientsdisplayed a distinct band at this molecular weight.The expression of the 70-kDa ADAM9-like band wasdecreased in the prostate cancer extracts (3 of 6). Theexpression level of the total ADAM9 protein (80 and70 kDa together) is increased in prostate cancertissue compared with normal prostate tissue (4 of 6)(Table 3).
3.3. ADAM9 immunostaining in prostate tissues
ADAM9 was found in cancerous and normal pro-static epithelia. Of the prostate cancers adjacentnormal prostate tissue, 85.9% (170 of 198) and 88.4%(175 of 198), respectively, showed at least someADAM9 expression. Only 28 (14.1%) prostate cancerswere completely negative. An H-score below that ofthe normal tissue was detected for 50 cases (25.3%),
which is in line with the results from the RNAanalysis. Antibody specificity was confirmed bypeptide blocking (Fig. 2C). In cancerous glands adiffuse cytoplasmic immunoreactivity predomi-nated, whereas a minority of cases (63 cases,31.8%) displayed a luminally accentuated glycoca-lyceal staining pattern, as expected of a transmem-brane protein and as seen in epithelia of benignprostate glands (Fig. 3). Stromal tissue, peripheral

Table 4 – Correlation of ADAM9 protein expression inprostate cancer with conventional clinical or tumourparameters
ADAM9 pTstatus
Gleasonsum
Pre-OPPSA
Age R status
CC 0.039 0.074 �0.047 �0.079 0.007
p 0.585 0.301 0.542 0.270 0.921
N 198 197 169 198 196
ADAM9, A disintegrin and metalloprotease 9; pT status, tumour
stage; Pre-Op PSA, preoperative PSA; R status, residual tumour; CC,
correlation coefficient; p, two-sided significance; N, number of
cases.
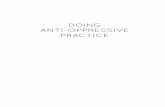
Fig. 3 – Immunohistological expression of ADAM9. (A–C) Glandular prostate cancer tissue displaying weak (A), moderate (B),
and strong (C) ADAM9 protein expression. (D) Prostatic intraepithelial neoplasia (small arrow) surrounded by microglandular
prostate cancer (bold arrows) and an adjacent normal prostatic gland (unfilled arrow). (E and F) Most cases displayed a rather
diffuse cytoplasmic staining for ADAM9 (E, cancer = bold arrow, normal gland = unfilled arrow), but a minority of cases
showed a marked accentuation of a luminally polarised ADAM9 expression (F). ADAM9, A disintegrin and metalloprotease 9.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 81102
nerves, and peripheral vessels were negative forADAM9, whereas skeletal muscle cells as well asganglion cells were positive.
The median H-scores of prostate cancer, PIN(n = 60), and normal tissue were 100, 100, and 90,respectively. The difference in the ADAM9 proteinexpression of tumour and normal tissue was highlysignificant ( p < 0.001). PIN was present in 60 (30.3%)of the 198 cases. ADAM9 expression of PIN wassignificantly higher ( p = 0.001) than in normaltissue but did not differ significantly from theADAM9 expression in the invasive carcinoma( p = 0.645).

Table 5 – Univariate survival analysis (Kaplan-Meier): PSA relapse times of all patients with prostate according toclinicopathological factors and ADAM9 expression
Characteristic No. of cases No. of events 3-year PSA relapse rate (�SE) in % p value
ADAM9 expression 0.003
low 85 19 14.9 � 4.0
high 113 50 28.9 � 4.4
Pre-OP PSA 0.007
�9.4 ng/ml 87 22 22.8 � 4.6
>9.4 ng/ml 82 38 27.3 � 5.1
Age 0.168
�62 yr 105 40 26.1 � 4.4
>62 yr 93 29 19.3 � 4.2
pT status <0.001
pT2 110 27 15.4 � 3.6
pT3/4 88 42 31.8 � 5.1
Gleason sum <0.001
3–6 89 19 11.7 � 3.5
7 56 18 24.7 � 6.0
7–10 52 32 41.1 � 7.1
Residual tumour 0.001
R0 109 29 17.4 � 3.7
R1 87 39 30.0 � 5.0
PSA, prostate-specific antigen; ADAM9, A disintegrin and metalloprotease 9; SE, standard error; Pre-Op PSA, preoperative PSA; pT status,
tumour stage.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 8 1103
3.4. ADAM9 expression, clinicopathological correlations,
and disease-free survival times
In bivariate correlations, the ADAM9 protein expres-sion in prostate cancer did not correlate with any ofthe clinicopathological parameters (Table 4). In thechi-square tests, higher ADAM9 protein expressionwas significantly associated with younger age(Table 1). In univariate survival analysis (Kaplan-Meier) of PSA relapse-free survival times, preopera-tive PSA, pT status (tumour grade), Gleason score,and residual tumour status reached statisticalsignificance (Table 5). Higher ADAM9 expressionin prostate cancer was significantly associated withshortened PSA relapse-free survival times (Fig. 4A,p = 0.003).
To evaluate the influence of the intracellularADAM9 distribution (diffuse cytoplasmic vs. lumin-ally accentuated - polar), we stratified the formeranalysis. The resulting Kaplan-Meier curve (Fig. 4B)revealed a significantly longer PSA relapse-freesurvival for those patients with low ADAM9 andpolar staining pattern. High ADAM9 expressionwas generally unfavourable, but even low ADAM9expression was disadvantageous if diffuse.
After stratification according to antiandrogenicpretreatment, total ADAM9 lost much of its prog-nostic value in patients not pretreated and remaineda significant prognosticator in the group of pre-treated patients only (Fig. 4C). However, when the
ADAM9 distribution patterns were considered,patients with tumours displaying a low polarADAM9 expression had a significantly more favour-able course irrespective of antiandrogen pretreat-ment. We suspected a systemic bias in the group ofpatients who had received antiandrogenic pretreat-ment because this group of patients had (in themedian) higher Gleason scores and higher pT stages.Therefore, a subcohort of patients without pretreat-ment but matching Gleason scores and pT stageswas compiled and subsequently analysed. In thisgroup, no prognostic value of total ADAM9 wasapparent (53 vs. 61 mo, p = 0.455), which suggests afunctional link between androgen ablation andADAM9 expression.
A Cox multivariate analysis over all cases includ-ing pT status, Gleason sum, preoperative PSA level,and residual tumour status further confirmed theindependent prognostic value of total ADAM9(Table 6). This finding was also true for antiandro-gen-pretreated patients in whom ADAM9 was theonly significant parameter for PSA relapse (relativerisk, 3.607; p = 0.031).
4. Discussion
ADAM9 overexpression has been described in awealth of solid tumours including prostate cancer[15,18–21]. In gastric cancer ADAM9 is significantly

Fig. 4 – Prostate-specific antigen (PSA) relapse-free survival curve for ADAM9. The number of events (PSA relapses) in the
specific subgroup is given in brackets. (A) Significantly shorter PSA relapse-free survival times for patients with higher
ADAM9 protein expression. (B) Kaplan-Meier curves for high versus low ADAM9 expression stratified for intracellular
distribution patterns. (C) Kaplan-Meier curve for the subgroup of antiandrogen pretreated patients. ADAM9, A disintegrin
and metalloprotease 9.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 81104
upregulated and ADAM9 inhibition resulted ininhibited cell growth of gastric cancer cell lines[22]. ADAM9 transcript upregulation was found inconditions associated with liver injury [23]. Grutz-mann et al [24] and Alldinger et al [25] discoveredADAM9 mRNA upregulated in pancreatic ductaladenocarcinoma and confirmed an ADAM9 over-
Table 6 – Multivariate survival analysis (Cox regressionmodel) for ADAM9, pT status, Gleason sum, preoperativePSA, and residual tumour status
Variable Relative risk 95%CI p value
ADAM9 1.871 1.030–3.397 0.040
PT status 1.305 0.687–2.479 0.416
Gleason sum 1.719 1.183–2.497 0.004
Pre-OP PSA 1.642 0.959–2.813 0.071
Residual tumour 1.830 0.833–2.702 0.176
ADAM9, A disintegrin and metalloprotease 9; CI, confidence
interval; pT status, tumour stage; Pre-OP PSA, preoperative PSA.
expression in 70% of pancreatic carcinomas byimmunohistochemistry. In a following study of thisgroup, a significant prognostic value of ADAM9expression was demonstrated, which matches ourfindings in prostate cancer [17]. O’Shea et al [19]investigated ADAM9 mRNA and protein expressionin breast cancer, and detected ADAM9 mRNA andthe mature protein significantly upregulated andassociated with a positive nodal status and over-expression of HER-2/neu protein [19]. As there weredifferences in the levels of mature ADAM9 and theprecursor form of the protein between cancer andbenign lesions, an alternative processing of ADAM9in normal and cancerous tissue was suggested.Interestingly, the same study demonstrated ADAM9mRNA in two of two prostate cancer cases [19]. Chinet al [26] analysed genome copy number abnorm-alities in 145 breast cancers and found ADAM9among nine highly amplified genes, which were, onthe basis of supposed protein characteristics [27],

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 8 1105
considered druggable. Overexpression of ADAM9 inlung cancer cell lines resulted in enhanced inva-siveness and was significantly related to brainmetastasis [13]. In melanoma ADAM9 is upregulatedin vivo at the invasion front, further supporting itsrole for tumour progression [28]. Next to thetransmembrane form of ADAM9, a secreted formthat might be relevant for tumour progression hasbeen described [8,29]. We analysed the transmem-brane and the supposedly secreted form of ADAM9by quantitative reverse transcriptase-PCR and couldconfirm the upregulation of total ADAM9. Usingprimers specific for the transmembrane and thesecreted form, we found that both were upregulated,although statistical significance was for only thetransmembrane form, which might be due to oursmall sample size (n = 25).
To our knowledge Karan et al [18] were the first todescribe ADAM9 expression in prostate cancer. Theyfound ADAM9 expression in nine prostate cancercell lines and in eight out of eight histologicalprostate cancer samples, a finding we confirmedpreviously [15]. We found ADAM9 protein signifi-cantly upregulated in cancerous tissue comparedwith adjacent normal tissue, which was alsomirrored by the mRNA results. Still, in up to around30% of tumours, ADAM9 was downregulated.Immunohistochemically we observed different pat-terns of ADAM9 immunoreactivity. In normalprostate glands, we found a luminally polarisedorientation of ADAM9, which was also seen in aminority of tumours, albeit with a higher intensity.However, in most tumours a depolarised diffusecytoplasmic immunoreactivity was noted, whichwas not correlated with Gleason score. The stainingpatterns were not associated with different prog-nostic values, but showed considerable prognosticimpact, if combined with low or high levels ofADAM9 expression. Importantly, patients showing alow polarised ADAM9 expression in their tumours(comparable to the ADAM9 pattern in normalglands) have a comparatively excellent prognosis.Peduto et al [20] found that ADAM9 could cleave andrelease EGF, and observed a positive association ofADAM9 with larger and less well-differentiatedprostate tumours. Although this is a finding thatcould not be verified in our study cohort, our dataclearly show a negative prognostic impact of higherADAM9 levels, indicating a more aggressive disease.This finding is in line with Sung et al [21] whoshowed elevated ADAM9 levels during the transitionfrom androgen-dependent to androgen-indepen-dent and metastatic cancer cells, using a tissuemicroarray (n = 200), which apparently did not allowa detailed survival analysis.
Sung et al [21] also found an inducibility ofADAM9 by oxidative stress and reactive oxygenspecies in prostate cancer cell lines and suggested,in line with Fisher et al [9], that ADAM9 would conferresistance to stress induced injuries. The induci-bility of ADAM9 appeared to be pronounced inandrogen-dependent tumours [30]. This functionaldata might be of relevance to our observations of theprognostic value of ADAM9 in antiandrogenicallypretreated patients. It can be hypothesised thattumour cells that can mediate the stress induced byandrogen ablation by ADAM9 upregulation have asurvival benefit and are thus more aggressive. Itremains to be shown in larger cohorts if ADAM9expression can indeed be used as a predictivemarker of response to antiandrogenic therapy inprostate cancer.
In conclusion our results support the generalnotion of ADAM9 to be associated with moreaggressive tumour behaviour in prostate cancer.ADAM9 protein expression was significantly andindependently associated with shortened PSArelapse-free survival, which suggests its use as aprognostic marker in prostate cancer followingfurther validation.
Conflicts of interest
The authors have nothing to disclose.
Acknowledgements
We are grateful to Britta Beyer for excellent technicalassistance. The support of Ilka Kristiansen and DrMarius Fritzsche is greatly acknowledged.
Appendix A. Supplementary data
Supplementary data associated with this articlecan be found, in the online version, at doi:10.1016/j.eururo.2007.11.034 and via www.europeanurology.com.
References
[1] Nath D, Slocombe PM, Webster A, et al. Meltrin gamma
(ADAM-9) mediates cellular adhesion through alpha(6)-
beta(1)integrin, leading to a marked induction of fibro-
blast cell motility. J Cell Sci 2000;113(pt 12):2319–28.
[2] Iba K, Albrechtsen R, Gilpin BJ, Loechel F, Wewer UM.
Cysteine-rich domain of human ADAM 12 (meltrin alpha)

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 81106
supports tumor cell adhesion. Am J Pathol 1999;154:1489–
501.
[3] Schwettmann L, Tschesche H. Cloning and expression in
Pichia pastoris of metalloprotease domain of ADAM 9
catalytically active against fibronectin. Protein Expr Purif
2001;21:65–70.
[4] Zhou M, Graham R, Russell G, Croucher PI. MDC-9 (ADAM-
9/Meltrin gamma) functions as an adhesion molecule by
binding the alpha(v)beta(5) integrin. Biochem Biophys Res
Commun 2001;280:574–80.
[5] Lendeckel U, Kohl J, Arndt M, et al. Increased expression of
ADAM family members in human breast cancer and
breast cancer cell lines. J Cancer Res Clin Oncol
2005;131:41–8.
[6] Izumi Y, Hirata M, Hasuwa H, et al. A metalloprotease-
disintegrin, MDC9/meltrin-gamma/ADAM9 and PKCdelta
are involved in TPA-induced ectodomain shedding of
membrane-anchored heparin-binding EGF-like growth
factor. EMBO J 1998;17:7260–72.
[7] Roghani M, Becherer JD, Moss ML, et al. Metalloprotease-
disintegrin MDC9: intracellular maturation and catalytic
activity. J Biol Chem 1999;274:3531–40.
[8] Hotoda N, Koike H, Sasagawa N, Ishiura S. A secreted form
of human ADAM9 has an alpha-secretase activity for APP.
Biochem Biophys Res Commun 2002;293:800–5.
[9] Fischer OM, Hart S, Gschwind A, Prenzel N, Ullrich A.
Oxidative and osmotic stress signaling in tumor cells is
mediated by ADAM proteases and heparin-binding epi-
dermal growth factor. Mol Cell Biol 2004;24:5172–83.
[10] Higashiyama S, Nanba D. ADAM-mediated ectodomain
shedding of HB-EGF in receptor cross-talk. Biochim Bio-
phys Acta 2005;1751:110–7.
[11] Hirao T, Nanba D, Tanaka M, et al. Overexpression of
ADAM9 enhances growth factor-mediated recycling of
E-cadherin in human colon cancer cell line HT29 cells.
Exp Cell Res 2006;312:331–9.
[12] Tanida S, Joh T, Itoh K, et al. The mechanism of cleavage
of EGFR ligands induced by inflammatory cytokines in
gastric cancer cells. Gastroenterology 2004;127:559–69.
[13] Shintani Y, Higashiyama S, Ohta M, et al. Overexpression
of ADAM9 in non-small cell lung cancer correlates with
brain metastasis. Cancer Res 2004;64:4190–6.
[14] Mahimkar RM, Visaya O, Pollock AS, Lovett DH. The dis-
integrin domain of ADAM9: a ligand for multiple beta1
renal integrins. Biochem J 2005;385:461–8.
[15] Kristiansen G, Pilarsky C, Wissmann C, et al. Expression
profiling of microdissected matched prostate cancer sam-
ples reveals CD166/MEMD and CD24 as new prognostic
markers for patient survival. J Pathol 2005;205:359–76.
Editorial Comment on: ADAM9 Expression is aSignificant and Independent Prognostic Markerof PSA Relapse in Prostate CancerAlessandra Valentini, Sergio BernardiniDepartment of Internal Medicine, University of Rome‘‘Tor Vergata’’, Rome, [email protected]
[16] Ohl F, Jung M, Xu C, et al. Gene expression studies in
prostate cancer tissue: which reference gene should be
selected for normalization? J Mol Med 2005;83:1014–24.
[17] Grutzmann R, Luttges J, Sipos B, et al. ADAM9 expression
in pancreatic cancer is associated with tumour type and is
a prognostic factor in ductal adenocarcinoma. Br J Cancer
2004;90:1053–8.
[18] Karan D, Lin FC, Bryan M, et al. Expression of ADAMs (a
disintegrin and metalloproteases) and TIMP-3 (tissue
inhibitor of metalloproteinase-3) in human prostatic ade-
nocarcinomas. Int J Oncol 2003;23:1365–71.
[19] O’Shea C, McKie N, Buggy Y, et al. Expression of ADAM-9
mRNA and protein in human breast cancer. Int J Cancer
2003;105:754–61.
[20] Peduto L, Reuter VE, Shaffer DR, Scher HI, Blobel CP.
Critical function for ADAM9 in mouse prostate cancer.
Cancer Res 2005;65:9312–9.
[21] Sung SY, Kubo H, Shigemura K, et al. Oxidative stress
induces ADAM9 protein expression in human prostate
cancer cells. Cancer Res 2006;66:9519–26.
[22] Carl-McGrath S, Lendeckel U, Ebert M, Roessner A, Rocken
C. The disintegrin-metalloproteinases ADAM9, ADAM12,
and ADAM15 are upregulated in gastric cancer. Int J Oncol
2005;26:17–24.
[23] Le Pabic H, Bonnier D, Wewer UM, et al. ADAM12 in
human liver cancers: TGF-beta-regulated expression in
stellate cells is associated with matrix remodeling. Hepa-
tology 2003;37:1056–66.
[24] Grutzmann R, Foerder M, Alldinger I, et al. Gene expres-
sion profiles of microdissected pancreatic ductal adeno-
carcinoma. Virchows Arch 2003;443:508–17.
[25] Alldinger I, Dittert D, Peiper M, et al. Gene expression
analysis of pancreatic cell lines reveals genes overex-
pressed in pancreatic cancer. Pancreatology 2005;5:370–9.
[26] Chin K, DeVries S, Fridlyand J, et al. Genomic and tran-
scriptional aberrations linked to breast cancer pathophy-
siologies. Cancer Cell 2006;10:529–41.
[27] Russ AP, Lampel S. The druggable genome: an update.
Drug Discov Today 2005;10:1607–10.
[28] Zigrino P, Mauch C, Fox JW, Nischt R. Adam-9 expression
and regulation in human skin melanoma and melanoma
cell lines. Int J Cancer 2005;116:853–9.
[29] Mazzocca A, Coppari R, De Franco R, et al. A secreted form
of ADAM9 promotes carcinoma invasion through tumor-
stromal interactions. Cancer Res 2005;65:4728–38.
[30] Shigemura K, Sung SY, Kubo H, et al. Reactive oxygen
species mediate androgen receptor- and serum starva-
tion-elicited downstream signaling of ADAM9 expression
in human prostate cancer cells. Prostate 2007;67:722–31.
Epidermal growth factor, insulin-like growthfactor, and mutations of androgen receptor play arole in the progression of hormone-sensitiveprostate cancer to hormone insensitivity.
Although hormonal therapy is used earlier in thecourse of disease and a primary response rate of80–90% occurs with hormonal ablation, almost all

patients advance to a state of androgen indepen-dence manifested by increasing prostate-specificantigen (PSA) levels and new lesions on bone scans.The median survival time in patients with andro-gen-independent prostate cancer is about 18 moand this condition is also accompanied by theattainment of high resistance to cytotoxic drugs [1].Androgen independence may be an intrinsic, butresting, property of some prostate cancer cells thatare activated in response to androgen deprivation.Only epithelial cells, not basal or stromal cells,undergo apoptosis on androgen withdrawal. Theclonal selection hypothesis relates to the selectivesurvival of preexisting androgen-independent cellswithin the tumour by hormonal deprivation [2].These clonal cells are thought to be poorlydifferentiated and similar to basal or stem cells [3].
Substantial attempts have been expended indescribing the available factors and determiningtheir predictive value for staging, cancer recur-rence, survival, and androgen-independent devel-opment. Interesting observations are constantlybeing made concerning the expression of a widerange of cellular components, including enzymes,structural proteins, ion channels, ligand receptors,gene sequences, among others, that are associatedwith progression of prostate cancer.
Gene products of the A disintegrin and metallo-proteinase (ADAM) family are critically involved incarcinogenesis and tumour progression of varioussolid tumours. It has been described that prostatetumours revealed high levels of ADAM9 mRNA inwell-differentiated carcinomas, but only low orundetectable levels in poorly differentiated carci-nomas. The loss-of-function experiments suggestthat ADAM9 is critical for tumour progression pastthe well-differentiated state, whereas gain-of-function experiments provided additional evi-dence for a causal role of ADAM9 in tumorigenesis.
ADAM9 deficiency delays or prevents prostatetumour progression to advanced states in a mouseprostate cancer model, whereas deregulatedexpression of ADAM9 initially disrupts epithelial
stromal homeostasis in the prostate epithelium,and later leads to prostatic intraepithelial neopla-sia lesions [4]. Interestingly, Fritzsche et al foundthat ADAM9 was significantly up-regulated inprostate cancer in comparison to normal tissueon mRNA and protein levels. ADAM9 proteinexpression was significantly associated with shor-tened PSA relapse-free survival in univariate andmultivariate analyses, particularly in patients whohad received prior androgen ablation [5].
Additionally, the authors hypothesise thatADAM9 is a predictive marker of response toantiandrogenic therapy. Thus, this last hypothesisseems to be more interesting than the single valueof ADAM9 as an independent prognostic factor,to individualise the gene as a molecular markerfor hormone-independent switching of prostatecancer.
References
[1] Yagoda A, Petrylak D. Cytotoxic chemotherapy for
advanced hormone-resistant prostate cancer. Cancer
1993;71(Suppl 3):1098–109.
[2] Isaacs JT, Coffey DS. Adaptation versus selection as the
mechanism responsible for the relapse of prostatic can-
cer to androgen ablation therapy as studied in the Dun-
ning R-3327-H adenocarcinoma. Cancer Res 1981;41:
5070–5.
[3] Rashid MH, Chaudhary UB. Intermittent androgen depri-
vation therapy for prostate cancer. Oncologist 2004;9:
295–301.
[4] Peduto L, Reuter VE, Shaffer DR, Scher HI, Blobel CP.
Critical function for ADAM9 in mouse prostate cancer.
Cancer Res 2005;20:9312–8.
[5] Fritzsche FR, Jung M, Tolle A, et al. ADAM9 expression is
a significant and independent prognostic marker of PSA
relapse in prostate cancer. Eur Urol 2008;54:1097–108.
DOI: 10.1016/j.eururo.2007.11.035
DOI of original article: 10.1016/j.eururo.2007.11.034
Editorial Comment on: ADAM9 Expression is aSignificant and Independent Prognostic Markerof PSA Relapse in Prostate CancerColin CooperInstitute of Cancer Research, Sutton, [email protected]
ADAM9 (a disintegrin and metalloprotease-9) is amembrane-anchored metalloproteinase that playsa key role in the ectodermal shedding of growthfactors. Many growth factors and cytokines, includ-ing all ligands for epidermal growth factor receptor,are synthesized as membrane-anchored proteins.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 8 1107

ADAM9 and other members of this family areresponsible for catalyzing their release from thecell by ectodermal shedding, a process vital for cell-to-cell communication and for cellular homeosta-sis. ADAM9 is also a cell adhesion molecule thatinteracts with the integrin avb5 and that may beinvolved in controlling cell invasion. The elevatedlevels of this protein observed in many commonneoplasms, including prostate, suggests a role forthis protein in the development or progression ofcancer, a view supported by the recent observationthat the ADAM9 gene is both amplified and over-expressed in human breast cancer [1]. In the W10
mouse prostate cancer model knocking out theADAM9 gene made the tumors that develop smallerand more differentiated in appearance, whereas ingain-of-function experiments overexpression ofADAM9 caused the development of prostatic intra-epithelial hyperplasia [2]. In this issue Fritzsche et al[3] provide further compelling evidence for theimportance of ADAM9 overexpression in determin-ing aggression in human prostate cancer. In a studyof 198 prostatectomy cases they showed thatADAM9 expression was significantly associatedwith shortened disease-free relapse. Importantly,in multivariate analyses the expression of ADAM9provided prognostic information in addition to thatobtained from stage, Gleason score, and preopera-tive prostate-specific antigen (PSA) level. Thisassociation still held when the authors consideredonly those patients treated with antiandrogentherapy prior to surgery. It has been shown in otherstudies that ADAM9 levels in prostate cancer cells
are controlled by androgens and by oxidative stressin such a way that induction of ADAM9 expressioncan be completely abrogated by the presence ofantioxidants [4,5]. These results raise the prospectthat the modulation of ADAM9 level or the devel-opment of drugs that directly target its catalyticactivity may be of use in managing prostatecancer.
References
[1] Peduto L, Reuter VE, Shaffer DR, Scher HI, Blobel CP.
Critical function for ADAM9 in mouse prostate cancer.
Cancer Res 2005;65:9312–9.
[2] Sung SY, Kubo H, Shigemura K, et al. Oxidative stress
induces ADAM9 protein expression in human prostate
cancer cells. Cancer Res 2006;66:9519–26.
[3] Fritzsche FR, Jung M, Tolle A, et al. ADAM9 expression is
a significant and independent prognostic marker of PSA
relapse in prostate cancer. Eur Urol 2008;54:1097–108.
[4] Shigemura K, Sung SY, Kubo H, et al. Reactive oxygen
species mediate androgen receptor- and serum starva-
tion-elicited downstream signaling of ADAM9 expres-
sion in human prostate cancer cells. Prostate 2007;67:
722–31.
[5] Chin K, DeVries S, Fridlyand J, et al. Genomic and tran-
scriptional aberrations linked to breast cancer patho-
physiologies. Cancer Cell 2006;10:529–41.
DOI: 10.1016/j.eururo.2007.11.036
DOI of original article: 10.1016/j.eururo.2007.11.034
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 9 7 – 1 1 0 81108