Acid, basic, and neutral peptidases present different profiles in chromophobe renal cell carcinoma...
10
doi:10.1152/ajprenal.00469.2007 294:850-858, 2008. First published Jan 23, 2008; Am J Physiol Renal Physiol Agirregoitia and Adolfo Varona Lorena Blanco, Gorka Larrinaga, Itxaro Pérez, José I. López, Javier Gil, Ekaitz You might find this additional information useful... 31 articles, 6 of which you can access free at: This article cites http://ajprenal.physiology.org/cgi/content/full/294/4/F850#BIBL including high-resolution figures, can be found at: Updated information and services http://ajprenal.physiology.org/cgi/content/full/294/4/F850 can be found at: AJP - Renal Physiology about Additional material and information http://www.the-aps.org/publications/ajprenal This information is current as of April 4, 2008 . http://www.the-aps.org/. American Physiological Society. ISSN: 0363-6127, ESSN: 1522-1466. Visit our website at (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2005 by the respective cells and vasculature, as well as to the control of body fluid volume and composition. It is published 12 times a year publishes original manuscripts on a broad range of subjects relating to the kidney, urinary tract, and their AJP - Renal Physiology on April 4, 2008 ajprenal.physiology.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Acid, basic, and neutral peptidases present different profiles in chromophobe renal cell carcinoma...

doi:10.1152/ajprenal.00469.2007 294:850-858, 2008. First published Jan 23, 2008;Am J Physiol Renal Physiol
Agirregoitia and Adolfo Varona Lorena Blanco, Gorka Larrinaga, Itxaro Pérez, José I. López, Javier Gil, Ekaitz
You might find this additional information useful...
31 articles, 6 of which you can access free at: This article cites http://ajprenal.physiology.org/cgi/content/full/294/4/F850#BIBL
including high-resolution figures, can be found at: Updated information and services http://ajprenal.physiology.org/cgi/content/full/294/4/F850
can be found at: AJP - Renal Physiologyabout Additional material and information http://www.the-aps.org/publications/ajprenal
This information is current as of April 4, 2008 .
http://www.the-aps.org/.American Physiological Society. ISSN: 0363-6127, ESSN: 1522-1466. Visit our website at (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2005 by therespective cells and vasculature, as well as to the control of body fluid volume and composition. It is published 12 times a year
publishes original manuscripts on a broad range of subjects relating to the kidney, urinary tract, and theirAJP - Renal Physiology
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

Acid, basic, and neutral peptidases present different profiles in chromophoberenal cell carcinoma and in oncocytoma
Lorena Blanco,1 Gorka Larrinaga,2 Itxaro Perez,1 Jose I. Lopez,3 Javier Gil,1 Ekaitz Agirregoitia,1
and Adolfo Varona1
1Department of Physiology, Faculty of Medicine and Dentistry, 2Department of Nursing I, Nursing School, and 3Departmentof Anatomical Pathology, Hospital de Cruces, University of the Basque Country, Bilbao, Spain
Submitted 9 October 2007; accepted in final form 16 January 2008
Blanco L, Larrinaga G, Perez I, Lopez JI, Gil J, Agirregoitia E,Varona A. Acid, basic, and neutral peptidases present differentprofiles in chromophobe renal cell carcinoma and in oncocytoma.Am J Physiol Renal Physiol 294: F850–F858, 2008. First publishedJanuary 23, 2008; doi:10.1152/ajprenal.00469.2007.—Renal cell car-cinomas (RCCs) are neoplasias with high prevalence and mortality.We previously reported that several peptidases may be involved in thepathophysiology of clear cell renal cell carcinoma (CCRCC). Now, togain insight into the reasons that lead the various RCC types to behavevery differently with regard to aggressiveness and response to anti-cancer treatments, we analyzed subsets of chromophobe renal cellcarcinoma (ChRCC), and renal oncocytoma (RO), a benign tumor; aswell as different grades and stages of CCRCCs. Particulate APN,APB, and APA activities were decreased in both ChRCC and RO(tumor vs. nontumor tissues). Interestingly, activities were downregu-lated in a tumor-type specific way and the intensities of the decreaseswere stronger in the benign tumor than in the malignant type.Moreover, when two key histopathological parameters for tumorprognosis (high vs. low stage and grade) were analyzed, increases ofactivity were also observed in several of these cell surface peptidases(APN, APB). Some soluble activities (APB, Asp-AP) were alsodownregulated in the RCCs. With respect to genetic expression, PSAand APN were in a positive correlation related to their activities inboth ChRCC and RO; but not APB, Asp-AP, APA, and PGI. Theseresults may suggest an involvement of several peptidases in the patho-physiology of renal cancer, since they presented different patterns ofactivity and expression in tumors with different behaviors.
peptide signaling; renal tumor behavior; chromophobe carcinoma;renal oncocytoma
RENAL CELL CARCINOMAS (RCCs) are neoplasias with high prev-alence and mortality rates. One of the more difficult challengesin treating RCCs involves identifying and distinguishing ag-gressive tumors from those likely to remain indolent with littledetriment to the patient. The clear cell type of carcinoma(CCRCC) is by far the most frequent histological subtype ofRCC, accounting for 70% of cases (27), a prevalence rate thatexplains its intrinsic clinical interest. However, not all kidneytumors are the same and the different histological subtypes ofRCC behave quite differently, both with regard to aggressive-ness in the patient and response to treatment (3, 22). Forexample, when CCRCC is localized, prognosis after surgery isgood, but patients with spread CCRCC have a decidedly worseprognosis (3). The chromophobe subtype of RCC (ChRCC) ismuch less frequent (5% of cases) than CCRCC. On the other
hand, the renal oncocytoma (RO) is also a relatively uncom-mon entity, accounting for only 5% of cases of renal tumors(1). With respect to its clinical interest, ChRCC differs fromCCRCC in its lower rate of metastasis. As a result, surgicalremoval of localized or even locally advanced disease isusually associated with a better prognosis (1, 3). Moreover,although ChRCC and RO are thought to share a commonlineage (1), ChRCC is malignant and RO is benign. As aconsequence, a deeper understanding of the molecular mech-anisms underlying these different renal tumors could be helpfulin gaining insight into renal cancer etiogenesis and clinical.
A wide variety of agents are involved in the development ofrenal neoplasia in experimental animals, but none of them havebeen proven to be an important etiological factor for renalcancer in humans (7). Among the multiple factors involved inneoplastic transformation and tumor progression, peptidasesappear to play a pivotal role. These enzymes are known to havefunctions in growth control, differentiation, and the signaltransduction of many cell systems by modulating the activity ofbioactive peptides, and several cell surface peptidases havebeen characterized as solid tumor markers with different diag-nostic and prognostic rates (17, 30). Renal parenchyma is atissue very rich in both soluble and particulate peptidases (24,31). We previously reported significant alterations in the ac-tivity and the expression profiles of several of the aforemen-tioned enzymes when human samples of primary CCRCC werecompared with their surrounding uninvolved tissue (37). Inter-estingly, with the exception of puromycin-sensitive aminopep-tidase (PSA; EC 3.4.11.14), a soluble activity which increasedin CCRCC, all the peptidases showing alterations of activity intumor cells were downregulated. However, in contrast with theacid (Asp-AP; EC 3.4.11.21), basic (APB; EC 3.4.11.6), andneutral (APN; EC 3.4.11.2) peptidase activities which weredecreased, the tumoral process did not affect either omega(PGI; EC 3.4.19.3) or membrane-bound acid (APA; EC3.4.11.7) peptidase activities. As largely described, alteredpatterns of the expression and catalytic function of theseenzymes may contribute to several disease processes, neoplas-tic transformation, and tumor progression included (4, 10).Many studies describe alterations of peptidases in a broadspectrum of carcinomas, in kidney, and in other organs;however, most of them are performed in animal models orcell cultures. Moreover, since the nature of the aforemen-tioned protein variations used to be contradictory and con-troversial with regard to the different organs and/or tumor
Address for reprint requests and other correspondence: A. Varona, Dept.of Physiology, Faculty of Medicine and Dentistry, Univ. of the BasqueCountry, P.O. Box 699, E-48080 Bilbao, Bizkaia, Spain (e-mail: [email protected]).
The costs of publication of this article were defrayed in part by the paymentof page charges. The article must therefore be hereby marked “advertisement”in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Am J Physiol Renal Physiol 294: F850–F858, 2008.First published January 23, 2008; doi:10.1152/ajprenal.00469.2007.
0363-6127/08 $8.00 Copyright © 2008 the American Physiological Society http://www.ajprenal.orgF850
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

phenotypes, a physiological approaching to the question inthe kidney by establishing first peptidase profiles of alter-ation throughout different RCCs could be helpful in under-standing the clinic of this disease and may be of diagnosticand prognostic interest.
These facts, taken together, make the comparative study ofpeptidase profiles in CCRCC, ChRCC, and RO an interestingmodel to test how the multiple and complex factors interactingin the tumor cells lead to a disease that behaves differently withregard to aggressiveness in the patient and response to treat-ment.
To implement these goals in the present study, we investigatedthe soluble and particulate activities and their mRNA levels ofacid (Asp-AP, APA), basic (APB), neutral (PSA, APN), andomega (PGI) peptidases in ChRCCs and ROs (comparing tumorvs. nontumor tissue). Since a high or low tumor grade and stageare indicators of the tumor aggressiveness potentiality, and tocomplete our previous study, those activities were also ana-lyzed in a CCRCC series comparing these two key histopatho-logical parameters for tumor prognosis. The same peptidaseprofile as in the aformentioned study by our group was selectedfor a better comparison of the results with those in a CCRCCseries, and to cover the complete spectrum of peptide-convert-ing activity.
MATERIALS AND METHODS
The authors declare that all the experiments carried out in this studycomply with current Spanish and European Union laws.
Materials. All the chemicals used were obtained from Sigma (St.Louis, MO).
Renal tissue specimens and sample storage. We analyzed renaltissue in a series from 10 patients with ChRCC (5 males, 5 females,mean age 64 yr, range 46–79), in a series from 8 patients with RO (6males, 2 females, mean age 67 yr, range 44–84), and in a series ofstaged and graded CCRCCs from 73 patients (59 males, 14 females,mean age 62 yr, range 37–84). Profile of grading: G1–G2 � 37,G3–G4 � 36. Profile of staging: T1–T2 � 44, T3–T4 � 29. Patientconsent and Hospital Ethics Committee approval were obtained apriori. Fresh tissue samples were obtained from surgical specimensfrom renal tumor patients. Tumor and nontumor (surrounding unin-volved tissue) areas were obtained for the study in all cases. Tissuesamples were embedded in OCT, frozen in isopentane, and stored at�80°C until the enzyme assays were performed. In addition, selectedtissue samples were formalin-fixed and paraffin-embedded for his-topathological diagnosis following routine methods at the pathologylab. The 2002 TNM Edition was used for tumor staging (33), and theFurhman’s method for grading (15).
Sample preparation. Explanted tissue samples were homogenizedin 10 mM Tris �HCl buffer, pH 7.4, for 30 s at 800 rpm using aHeidolph PZR 50 Selecta homogenizer and ultracentrifuged in aCentrikon T-2070 Kontron Instruments apparatus at 100,000 g for 35min. The resulting supernatants were used to measure soluble enzymeactivities and protein concentrations. To avoid contamination withsoluble enzymes, the resulting pellets were washed three times bysuspension in 10 mM Tris �HCl buffer, pH 7.4. Subsequently, pelletswere homogenized in 10 mM Tris �HCl buffer, pH 7.4, and thencentrifuged at low speed, 1,500 g, for 1 min, to purify sample nuclei.The supernatants thus obtained were used to determine particulateenzyme activities and protein concentrations. All steps were carriedout at 4°C.
Enzyme assays. Peptidase activities were measured by incubatingsamples with a saturating (0.125 mM) concentration of �-naphthyl-amine-derived substrates following the method described by Mantleet al. (24). Alanine aminopeptidase activities (PSA, APN) were
measured using Ala-�-naphthylamide as a substrate. To discriminatebetween PSA and APN forms of total alanine aminopeptidase activity,incubations with the specific PSA inhibitor puromycin (40 �M) wereperformed in parallel. APB and acid aminopeptidase activities (Asp-AP, APA) were quantified with Arg-�-naphthylamide and Asp-�-naphthylamide substrates, respectively. Omega peptidase (PGI) activ-ity was measured fluorimetrically using pGlu-�-naphthylamide as asubstrate. These assays are based on the fluorescence of �-naphthyl-amine generated from the hydrolysis of the substrate by the enzyme.Reactions were initiated by adding 30–50 �l of sample to 1 ml ofappropriate incubation mixture, depending on the enzyme, and sub-strate was analyzed as follows: PSA, APN, APB, and PGI activities(50 mM phosphate buffer, pH 7.4 for PSA, APN, and PGI activities,pH 6.5 for APB, and 0.125 mM aminoacyl-�-naphthylamide); Asp-AP/APA activities (50 mM Tris �HCl buffer, pH 7.4, 1 mM MnCl2,and 0.125 mmol/l aminoacyl-�-naphthylamide). After 30-min incu-bation at 37°C, 1 ml of 0.1 M sodium acetate buffer (pH 4.2) wasadded to the mixture to terminate the reaction. The released �-naphthyl-amine was determined by measuring the fluorescent intensity at 412nm with excitation at 345 nm, in a Shimadzu RF-540 Spectrofluoro-photometer. Blanks were used to determine background fluorescence.Relative fluorescence was converted into picomoles of product usinga standard curve, constructed with increasing concentrations of�-naphthylamine.
Protein determination. Protein concentration was measured intriplicate by the method described by Bradford (8), using 1 mg/mlBSA as the calibrator. The results were recorded as units of peptidase(UP) per milligram of protein. One unit of peptidase activity is theamount of enzyme necessary to release 1 pmol of �-naphthylamineper minute. Fluorogenic assays were linear with respect to hydrolysistime and protein content.
Real-time quantitative PCR analysis. Quantitative RT-PCR fordetecting PSA, APN, APB, Asp-AP, APA, and PGI mRNA wasperformed to determine the transcription levels of these peptidases.The RNA of tumor and nontumor tissue samples from six ChRCCand five RO patients was isolated with the RNeasy Protect kit(Qiagen), including a DNase digestion step using an RNase-freeDNase kit (Qiagen) to exclude possible contamination by genomicDNA.
The Taqman real-time PCR system is based on a three-primermethod. Two of the primers are designed following the traditionalPCR concept (upper and lower primers). The third primer has afluorescent group which, when included in the amplification, increasesfluorescence emission. This system enhances amplification specificity(3 primers are used) and avoids nonspecific double-strand DNAdetection, as the fluorescence is bound to one of the primers. cDNAwas obtained using a Transcriptor reverse transcriptase kit (Roche).Intron spanning Taqman probes were designed following the RocheUniversal Probe Library method (www.roche-applied-science.com).Amplifications were run in a 7900 Real-Time PCR System (AppliedBiosystems). Each value was adjusted by using 18S RNA levels asreference.
The following primers were used: Human PSA: probe human 19;5�-CAGTTGAGGGATTTGCAGTTG-3� (upper primer), 5�-TGAA-GGAGCTGGGTGACTCT-3� (lower primer). Human APN: probehuman 18; 5�-CATCCATCAGAGATGGCAGAC-3� (upper primer),5�-TGCTGAAGAGATCGTTCTGG-3� (lower primer). Human APB:probe human 22; 5�-ACCATGTACGCCCAGAGG-3� (upper primer), 5�-CAGCCTCCAAGCAGGTGTA-3� (lower primer). Human Asp-AP:probe human 64; 5�-AGTCCCTCTCCTTTCCATGC-3� (upperprimer), 5�-TTCCATTTCTCAGTCTCCTTGAG-3� (lower primer).Human APA: probe human 72; 5�-CGGAGAACGGACAAGT-CAAG-3� (upper primer), 5�-GGGCTCATCAAAACAAGGAA-3�(lower primer). Human PGI: probe human 47, 5�-GGGAGAAGCA-CAGTCCACAG-3� (upper primer), 5�-TGTAGCCCTTGTTGT-GTCCA-3� (lower primer).
F851PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

Quantitative data for the mRNA of each peptidase were expressedas relative values with respect to “1”; “1” being the total amount ofmRNA for a specific peptidase detected in the nontumor area of thesample labeled as n � 1.
Statistical analyses. Data were analyzed statistically using SPSS,version 10. Unpaired Student’s t-test was performed to detect differ-ences between uninvolved tissues and tumors, as well as among lowand high grades and stages. Statistically significant differences wereconsidered at P � 0.05.
RESULTS
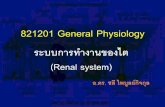
Figure 1 shows the peptidase activities measured in thesoluble and particulate fractions of ChRCC patients. Activity isrecorded as picomoles of product per minute per milligram ofprotein (UP/mg protein) and presented as means � SE for n � 10.
Soluble basic and acid activities (Fig. 1A) decreased signif-icantly in the ChRCC. Thus, APB activity decreased 1.6-foldwhen the tumor compared with nontumor tissue [tumor (t) �6,382 � 823 vs. nontumor (n) � 10,618 � 502 UP/mg prot.;Student’s t-test, P � 0.01], and Asp-AP decreased 4-fold in thesame way (t � 85 � 17 vs. n � 368 � 28 UP/mg prot.;Student’s t-test, P � 0.01). In contrast, neutral (PSA) andomega (PGI) activities in the soluble fraction of the ChRCCwere not significantly altered (PSA: t � 10,269 � 1,052 vs.n � 12,565 � 645 UP/mg prot.; PGI: t � 130 � 22 vs. n �205 � 29 UP/mg prot.).
On the other hand, all the cell surface peptidase activities ofthe ChRCC (Fig. 1B) decreased significantly, with the excep-tion of the PGI, which did not vary significantly (t � 369 � 36
vs. n � 578 � 66 UP/mg prot.). APN/CD13 activity decreased17-fold in the tumor compared with surrounding uninvolvedtissue (t � 2,694 � 1,183 vs. n � 45,637 � 2,432 UP/mg prot.;Student’s t-test, P � 0.001). In the case of APB and APA/gp160 activities, these decreased 12-fold (t � 1,591 � 356 vs.n � 19,306 � 1,324 UP/mg prot.; Student’s t-test, P � 0.001)and 5-fold (t � 158 � 98 vs. n � 813 � 65 UP/mg prot.;Student’s t-test, P � 0.01), respectively.
In Fig. 2, we represent soluble and membrane-bound pepti-dase activities in tumor and unaffected human tissue fromhuman kidney with RO. Activity is recorded as picomoles ofproduct per minute per milligram of protein (UP/mg protein)and presented as means � SE for n � 8.
As shown in Fig. 2A, only the acid activity significantlydecreased (1.5-fold) in the soluble fraction of RO (Asp-AP; t �163 � 17 vs. n � 320 � 21 UP/mg prot.; Student’s t-test, P �0.05). No significant differences were found in soluble PSA,APB, and PGI activities of the human oncocytoma (PSA: t �12,819 � 1,183 vs. n � 8,515 � 853 UP/mg prot.; APB:t � 6,039 � 743 vs. n � 7,757 � 697 UP/mg prot.; PGI: t �262 � 34 vs. n � 334 � 26 UP/mg prot.).
However, as in the case of the ChRCC, most of the mem-brane-bound activities (Fig. 2B) decreased significantly in theRO when compared with the nonpathological surroundingtissue. Again, particulate PGI activity of the RO was the onlyexception (t � 111 � 42 vs. n � 345 � 73 UP/mg prot.).Moreover, we observed that decreases for each peptidaseactivity in the RO were higher than those for the chromophobe
Fig. 1. Soluble (A) and particulate (B) pep-tidase activity profiles in kidney samplesfrom 10 patients with chromophobe cell re-nal cell carcinoma (ChRCC). Columns com-pare neoplastic tissue (ChRCC) with non-tumor surrounding tissue. Values representmeans � SE of peptidase activities recorded aspmol of aminoacyl-�-naphthylamide hydro-lyzed per min (UP) per mg of protein.
F852 PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

tumor. Thus, particulate APN/CD13 activity decreased morethan 30-fold in RO when compared with healthy cells (t �1,265 � 811 vs. n � 38,510 � 2,232 UP/mg prot.; Student’st-test, P � 0.001), APB activity in the membrane-boundfraction of the tumor decreased 16-fold (t � 1,325 � 379 vs.n � 21,319 � 1,582 UP/mg prot.; Student’s t-test, P � 0.001),and cell surface APA/gp160 activity decreased 7.5-fold (t �128 � 53 vs. n � 966 � 78 UP/mg prot.; Student’s t-test,P � 0.01).
The relative expressions of PSA, APN, APB, Asp-AP,APA, and PGI in the tumor and nontumor tissue from humanChRCC (n � 6) and RO kidney samples (n � 5) are shownin Figs. 3 and 4, respectively.
As shown in Fig. 3, in the ChRCC only APN/CD13 (Fig.3B) and PSA (Fig. 3A) expression correlated positively withthe results in enzyme activity. In this sense, the relativeexpression of PSA was slightly but not significantly upregu-lated (1.5-fold) in the tumor, whereas the corresponding cata-lytic activity did not vary significantly. The mRNA for theAPN decreased twofold in the ChRCC, in paralell with thesignificant downregulation observed in its enzymatic activity.In contrast, Asp-AP, APA, APB, and PGI expression in theChRCC were not in correspondence with these activities. Thus,in the tumor-tissue acid peptidases, Asp-AP (Fig. 3C) and APA(Fig. 3D) were 3- and 2.7-fold upexpressed, respectively, APBexpression increased 25% (Fig. 3E), and mRNA of PGI was40% downexpressed.
The expression pattern for peptidases in RO (Fig. 4) wassimilar to that in the chromophobe subtype of renal carci-
noma. The mRNA of PSA (Fig. 4A) increased 10-fold in thetumor, whereas a slight nonsignificant upregulation in itsactivity was observed. APN expression decreased 1.4-foldin the RO when compared with the surrounding unaffectedtissue, which correlated with the results in enzyme activity(Fig. 4B). In contrast to the observed decrease in activity,mRNA for Asp-AP in oncocytic cells was sixfold higherthan mRNA for Asp-AP in nontumor cells (Fig. 4C). APAexpression (Fig. 4D), whose activity was also decreased inRO, did not change in a significant way (20% upexpression)with respect to nontumor expression. Finally, the expressionlevels for APB (Fig. 4E) and PGI (Fig. 4F) were highlyupregulated in RO (APB � 3-fold; PGI � 4.6-fold tumor vs.nontumor).
Table 1 shows the peptidase activity profile throughout lowand high grades and stages in CCRCCs. Low grades (LG)correspond to G1 and G2 phenotypes of the Furhman’s scale,being G3 and G4 the high grades (HG) in that scale. Withrespect to the tumor staging, low stages (LS) were T1 and T2of the 2002 TNM Classification, corresponding T3 and T4 tothe high stages (HS).
All the activities were decreased in the low grade sampleswhen compared with tumors presenting a high grade. Statisti-cally significant decreases were found in PSA (LG vs. HGactivity decreases 2-fold; Student’s t-test, P � 0.001), APN(1.52-fold; Student’s t-test, P � 0.05), Asp-AP (1.44-fold;Student’s t-test, P � 0.05), and membrane-bound PGI (1.43-fold; Student’s t-test, P � 0.05).
Fig. 2. Soluble (A) and particulate (B) pepti-dase activity profiles in kidney samples from 8patients with renal oncocytoma (RCO). Columnscompare tumor tissue (RCO) with nontumor sur-rounding tissue. Values represent means � SE ofpeptidase activities recorded as pmol of amino-acyl-�-naphthylamide hydrolyzed per min (UP)per mg of protein.
F853PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

Fig. 3. Relative PSA (A), APN (B), Asp-AP (C), APA (D),APB (E), and PGI (F) expressions in kidney samples from 6ChRCC patients. Columns compare tumor tissue with sur-rounding nontumor tissue. Scattered diagrams represent mean(black line) � SE of quantified mRNA recorded as valuesrelated to “1”; “1” being the total amount of mRNA for aspecific peptidase detected in the nontumor area of the samplelabeled as n � 1.
F854 PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

In contrast, when CCRCC low and high stages were compared,only particulate APB activity decreased significantly (LS vs. HSactivity decreases 1.45-fold; Student’s t-test, P � 0.05). Slight,but not significant, decreases of activity were found in APN(1.3-fold LS vs. HS) and APA (1.23-fold).
DISCUSSION
According to our results, peptidase-mediated proteolysis inrenal tumors appears to tend toward activity decreases. Weanalyzed peptidase activities and expression and found thatthey were selectively altered by the tumoral process in affectedtissue; moreover, we obtained profiles of activity and relativeexpression that were different with regard to the tumor sub-type.
The major roles of peptidases in the pathobiology of ChRCCand RO seem to be mediated by cell surface forms, since, as wepreviously reported in CCRCC, once again, APN, particulateAPB, and APA activities were strongly decreased in the tumortissue. The main differences between the profiles of cell sur-face activities in ChRCC and those in RO were with regard tothe intensity of the decrease they suffered. Thus, the intensityof APN, particulate APB, and APA activity inhibition wasmuch higher in RO than in ChRCC.
When peptidase activities were compared throughout gradeand stage in the CCRCC, the aforementioned tumor aggres-siveness-related profile of the cell surface peptidases appears tomaintain, since APN, APA, and membrane-bound APB andPGI activities were higher in high grades or stages than in thelow grades and stages of the CCRCC samples.
Our results agree with those in the specialized literature,since peptidases are generally reported to be decreased inRCCs and in different intensities with regard to the subtype.In this sense, Gohring and co-workers (17) also found medium-to-strong downregulation in APN and APA activities whenthey compared several RCC subtypes. Moreover, immunohis-tochemistry assays reported that APA is practically absentfrom the cell surface in oncocytic cells, whereas, althoughthere is a decrease in staining with respect to normal renalcells, this enzyme is strongly expressed in CCRCC (28). Ascell surface APN, APB, and APA were found to be altered ina tumor type-specific way, our results are consistent with otherstudies that involve the aforementioned particulate forms inspecific roles in renal cancer (9, 10, 20, 29).
In contrast with the consensus about the nature of thealterations of peptidase activity in the pathobiology of RCCs,results in the genetic expression are controversial. Both lossand gain of expression have been reported for most peptidases(29). This fact may be partially due to the functional complex-ity of carcinogenic mechanisms. In this sense, our results arenot an exception. Thus, in the ChRCC as well as in the RO,only the relative expression of APN and PSA correlated pos-itively with their activities. However, the mRNA levels ofAsp-AP, APA, APB, and PGI were not in concordance withour data on peptidase activity. We reported a similar pattern ofexpression in our previous study on CCRCC (37).
Despite their uncertain results, these data could be helpful inelucidating whether changes in peptidase activities were due toreal alterations in protein transcription or whether other epige-netic factors may be involved. The positive correlation be-tween alterations of activity and mRNA of PSA and APN thatwere found in both ChRCC and RO tumor subtypes, andpreviously in CCRCC, points to real upregulation of PSA andreal downregulation of APN protein transcription in RCCs.Our results for the relative expression of Asp-AP, APA, APB,and PGI in ChRCC and RO also agree with those we obtainedin CCRCC and may suggest the involvement of genetic muta-
Fig. 4. Relative PSA (A), APN (B), Asp-AP (C), APA (D), APB (E), and PGI(F) expressions in kidney samples from 5 RCO. Columns compare tumortissue with surrounding nontumor tissue. Scattered diagrams represent mean(black line) � SE of quantified mRNA recorded as values related to “1”; “1”being the total amount of mRNA for a specific peptidase detected in thenontumor area of the sample labeled as n � 1.
F855PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

tions or epigenetic cellular factors, different from the regula-tion of gene expression, in the alterations of catalytic activity.Many proteases have functions that are not limited to proteol-ysis (2), while each of the individual peptidases is able toperform several overlapping functions (10). As a result, theexpression of each peptidase must be precisely regulated in atissue- and cell-specific manner, and mRNA levels may notalways reflect the final status of the enzymatic activity in thedisease (19, 21, 36).
On the other hand, our data extend the role of aminopepti-dase activity in renal cancer to include cytosolic forms, sinceseveral soluble peptidases (Asp-AP, soluble APB) were foundto be altered in a tumor-specific way, and with regard to bothhistological subtype and stage/grade. During carcinogenesis,many of the essential alterations which occur in cell physiologyare mediated through extracellular cell signaling pathways thatinteract with intracellular circuits, and so both cell surface andintracellular molecules play pivotal roles in cancer pathobiol-ogy. Thus, not only membrane-bound peptidases but alsosoluble activities may be taking a part in renal cancer. Forexample, it has recently been reported that upregulation ofcertain soluble peptidases induces accelerated growth and re-sistance to apoptosis in the human kidney (34). In agreementwith our results, inhibition of soluble Asp-AP activity was alsodetected in rats with breast cancer induced by N-methyl-nitrosourea (11).
The involvement of peptidases, mainly cell surface forms, inthe pathophysiology of cancer has been widely documented.Most evidences are related to APN (9, 12, 14, 16, 18, 23, 30,31). Although not as frequent as for APN, there is alsoevidence of the involvement of APA (18, 35, 25) and APB (31,32) in cancer pathobiology. Despite the rich variability offunction that peptidases appear to have in cancer, most of thestudies point to an anti-tumor effect, and thus a protective role,when these enzymes are inhibited or downexpressed (31).
Although functions in the pathophysiology of renal cancerhave been described for many cell surface peptidases (10), theultimate mechanisms of action and targets for all these func-tions remain uncertain and in many cases controversial. Thatcontroversy is due, in part, to the multifunctional propertiesand the tissue- or tumor-specific expression of peptidases (2,10). Since peptidases appear to be down- or upregulated in thecancer depending on the affected tissue and the specific type,grade, and stage of the tumor, it is very difficult to reach aconsensus about the specific mechanism of action for a con-
crete enzyme. In addition, several peptidases, such as APN,APB, and APA, may be playing overlapping roles in differentrenal tumors (6, 10). In this sense, the link of the results weobtained in CCRCC, ChRCC, and RO provides a model tostudy how the different and complex cellular and tissue factorsin renal tumors are leading to a disease that behaves quitedifferently with regard to aggressiveness in the patient andresponse to treatment (1, 3, 5). Thus, ROs are benign neo-plasms (5, 26), whereas CCRCCs are strongly aggressive andhave poor prognosis (3, 15). ChRCCs appear to behave moreindolently than the clear cell phenotype (5, 13), and thus,although malignant, they usually manifest a better prognosisthan CCRCCs.
Interestingly, we obtained profiles of APN, APB, and APAactivities in CCRCC (data from Ref. 37), ChRCC, and RO thatwere decreased with respect to normal renal parenchyma in atumor type-dependent manner (Table 2); and in a different waywith regard to aggressiveness due to the different specificbehavior of each type. Thus, when tumor type is benign (RO),the cell surface peptidase activities apparently involved in therenal cancer are found strongly decreased (up to 30-fold withrespect to the nontumor tissue in the case of APN). When thetumor phenotype is malignant (ChRCC), decreases of cellsurface peptidase activities (tumor vs. nontumor tissue) aremuch lower than the aforementioned in the RO (17-fold forAPN). This tumor type-dependent behavior repeats for severalpeptidase activities whose decreases are well-established inthe renal cancer (APN, APB, APA). CCRCC is reported to
Table 1. Peptidase activities in CCRCC in different grades and stages
Peptidase Type Recomended Name EC Number
Grade
P
Stage
PLow (G1–G2) High (G3–G4) Low (T1–T2) High (T3–T4)
Neutral Puromycin-sensitive aminopeptidase (EC 3.4.11.14) 7,980�922 14,378�1,423 �0.001 11,030�1,137 11,654�1,466 n.sAminopeptidase N (EC 3.4.11.2) 4,756�720 7,228�978 �0.05 5,320�828 6,944�943 n.s
Basic Soluble aminopeptidase B (EC 3.4.11.6) 5,078�630 6,713�717 n.s 6,240�719 5,423�543 n.sParticulate aminopeptidase B (EC 3.4.11.6) 1,888�259 2,443�243 n.s 1,847�192 2,683�324 �0.05
Acid Aspartyl aminopeptidase (EC 3.4.11.21) 139�14 200�25 �0.05 163�19 185�27 n.sAminopeptidase A (EC 3.4.11.7) 513�67 656�68 n.s 541�60 664�81 n.s
Omega Soluble pyroglutamyl peptidase I (EC 3.4.19.3) 95�18 188�41 n.s 145�36 142�23 n.sParticulate pyroglutamyl peptidase I (EC 3.4.19.3) 105�12 151�15 �0.05 130�13 125�15 n.s
Values are means � SE of peptidase activities recorded as pmol of aminoacyl-�-naphthylamide hydrolyzed per min (UP) per mg of protein. Profiles of solubleand particulate peptidase activity throughout different histopathological grades (low: G1–G2; high: G3–G4) and stages (low: T1–T2; high: T3–T4) in theevolution of the clear cell renal cell carcinoma (CCRCC). n.s., Not significant.
Table 2. Comparative pattern of APN, APB, and APAactivities throughout the sequence of bad prognostic(CCRCC�ChRCC�RO) in the renal cancer
Intensity of the Activity Decrease (Tumor vs. Normal Parenchyma)
CCRCC ChRCC RCOAPN 25-fold 2217-fold 22230-foldAPB 25-fold 2212-fold 2216-foldAPA 771.16-fold 25-fold 27.5-fold
High malignancy Benign
Profiles of APN, APB, and APA activity throughout tumors of differentaggressiveness: CCRCC, an aggressive carcinoma; chromophobe cell carci-noma (ChRCC), a malignant neoplasm; renal cell oncocytoma (RCO), abenign tumor. Values in the rows represent, for each enzyme and throughoutthe 3 tumor types, how many folds the activity in the tumor tissue weredecreased with respect to the nontumor renal parenchyma. Data for CCRCCare taken from our previous study (Ref. 37).
F856 PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

behave with a worse prognosis than the ChRCC, and so to bemore malignant, and the decreases of the cell surface peptidaseactivities we recorded on it (again comparing CCRCC tumorvs. nontumor) were lower than those we obtained in theChRCC and in the RO (only 5-fold for APN). Thus, when thethree tumor types are compared, it is seen how the peptidaseactivities of the tumor samples behave in an antiparallel waywith regard to the specific malignancy of the tumor (minordecreases when the tumor is more malignant). Moreover, thatantiparallel behavior of the peptidase activity also maintainsalong grading and staging in the CCRCC.
A peptidase-mediated antitumor mechanism in renal cancerconcurs with data in the scientific bibliography. For example,inhibitors of the APN and APB, such as bestatin and puromy-cin, have been reported to induce apoptosis onset in solidtumors (12, 30, 31). Moreover, decreases of mRNA for APNcause inhibition of angiogenesis (16), and APA appears topromote tumor angiogenesis (25). As a result, its inhibitionmay be an antitumor mechanism.
In summary, our data may suggest an involvement of cellsurface peptidases in the pathophysiology of renal cancer.When several peptidases downregulate, it appears to be bene-ficial with respect to tumor evolution. The nature of themechanism still remains speculative. Further studies on otherpeptidases and a new approach to the profile of these enzymesin staged and graded samples of renal cancer will be neccessaryto gain insight into the nature of peptidase actions in renaltumor pathobiology.
ACKNOWLEDGMENTS
We thank A. Carracedo (Universidad Complutense de Madrid) for contri-bution to this study and A. Perez for technical support.
GRANTS
This work was supported by a grant from the Jesus Gangoiti-BarreraFoundation.
REFERENCES
1. Abrahams NA, Tamboli P. Oncocytic renal neoplasms: diagnostic con-siderations. Clin Lab Med 25: 317–339, 2005.
2. Albinston AL, McDowall SG, Matsacos D, Sim P, Clune E, Mustafa T,Lee J, Mendelsohn FA, Simpson RJ, Connolly LM, Chai SY. Evidencethat the angiotensin IV (AT4) receptor is the enzyme insulin regulatedaminopeptidase. J Biol Chem 276: 48263–48266, 2001.
3. Amin MB, Tamboli P, Javidan J, Stricker H, de Peralta Venturina M,Deshpande A, Menon M. Prognostic impact of histologic subtyping ofadult renal epithelial neoplasms: an experience of 405 cases. Am J SurgPathol 26: 281–291, 2002.
4. Antczak C, De Meester I, Bauvois B. Ectopeptidases in pathophysiology.Bioessays 23: 251–260, 2001.
5. Avery AK, Beckstead J, Renshaw AA, Corless CL. Use of antibodies toRCC and CD10 in the differential diagnosis of renal neoplasms. Am J SurgPathol 24: 203–210, 2000.
6. Bank U, Kruger S, Langner J, Roessner A. Review: peptidases andpeptidase inhibitors in the pathogenesis of diseases. Disturbances in theubiquitin-mediated proteolytic system. Protease antiprotease imbalance ininflammatory reactions. Role of cathepsins in tumour progression. AdvExp Med Biol 477: 349–378, 2000.
7. Bannasch P, Zerban H. Animal models and renal carcinogenesis. In:Tumors and Tumorlike Conditions of The Kidneys and Ureters, edited byEble JN. New York: Churchill-Livingstone, 1990.
8. Bradford MM. A rapid and sensitive method for the quantitation ofmicrogram quantities of protein utilizing the principle of protein dyebinding. Anal Biochem 72: 248–254, 1976.
9. Cadel S, Piesse C, Gouzy-Darmon C, Cohen P, Foulon T. Arginylaminopeptidase. In: Aminopeptidases in Biology and Disease, edited byHooper NM and Lendeckel U. New York: Kluwer Academic/Plenum,2004, p. 113–126.
10. Carl-McGrath S, Lendeckel U, Ebert M, Rocken C. Ectopeptidases intumour biology: a review. Histol Histopathol 21: 1339–1353, 2006.
11. Carrera MP, Ramırez-Exposito MJ, Valenzuela MT, Duenas B, GarcıaMJ, Mayas MD, Martınez-Martos JM. Renin-angiotensin system-regulat-ing aminopeptidase activities are modified in the pineal gland of rats withbreast cancer induced by N-methyl-nitrosourea. Cancer Invest 24: 149–153,2006.
12. Cowburn AS, Sobolewski A, Reed BJ, Deighton J, Murray J, Cad-wallader KA, Bradley JR, Chilvers ER. Aminopeptidase N (CD13)regulates tumor necrosis factor-alpha-induced apoptosis in human neutro-phils. J Biol Chem 281: 12458–12467, 2006.
13. Crotty TB, Farrow GM, Lieber MM. Chromophobe cell renal carci-noma: clinicopathological features of 50 cases. J Urol 154: 964–967,1995.
14. Curnis F, Sacchi A, Borgna L, Magni F, Gasparri A, Corti A.Enhancement of tumor necrosis factor alpha antitumor immunotherapeuticproperties by targeted delivery to aminopeptidase N (CD13). Nat Biotech-nol 18: 1185–1190, 2000.
15. Fuhrman SA, Lasky LC, Limas C. Prognostic significance of morpho-logic parameters in renal cell carcinoma. Am J Surg Pathol 6: 655–663,1982.
16. Fukasawa K, Fujii H, Saitoh Y, Koizumi K, Aozuka Y, Sekine K,Yamada M, Saiki I, Nishikawa K. Aminopeptidase N (APN/CD13) isselectively expressed in vascular endothelial cells and plays multiple rolesin angiogenesis. Cancer Lett 243: 135–143, 2006.
17. Gohring B, Holzhausen HJ, Meye A, Heynemann H, Rebmann U,Langner J, Riemann D. Endopeptidase 24.11/CD10 is downregulated inrenal cell cancer. Int J Mol Med 2: 409–414, 1998.
18. Ino K, Shibata K, Kajiyama H, Kikkawa F, Mizutani S. Regulatoryrole of membrane-bound peptidases in the progression of gynecologicmalignancies. Biol Chem 358: 683–690, 2004.
19. Ino K, Uehara C, Kikkawa F, Kajiyama H, Shibata K, Suzuki T, KhinEE, Ito M, Takeuchi M, Itakura A, Mizutani S. Enhancement ofaminopeptidase A expression during angiotensin II-induced choriocarci-noma cell proliferation through AT1 receptor involving protein kinase C-and mitogen-activated protein kinase-dependent signaling pathway. J ClinEndocrinol Metab 88: 3973–3982, 2003.
20. Ishii K, Usui S, Yamamoto H, Sugimura Y, Tatematsu M, Hirano K.Decreases of metallothionein and aminopeptidase N in renal cancertissues. J Biochem (Tokyo) 129: 253–258, 2001.
21. Kehlen A, Gohring B, Langner J, Riemann D. Regulation of theexpression of aminopeptidase A, aminopeptidase N/CD13 and dipepti-dylpeptidase IV/CD26 in renal carcinoma cells and renal tubular epithelialcells by cytokines and cAMP-increasing mediators. Clin Exp Immunol111: 435–441, 1998.
22. Kovacs G, Akhtar M, Beckwith BJ, Bugert P, Cooper CS, DelahuntB, Eble JN, Fleming S, Ljungberg B, Medeiros LJ, Moch H, ReuterVE, Ritz E, Roos G, Schmidt D, Srigley JR, Storkel S, van den BergE, Zbar B. The Heidelberg classification of renal cell tumors. J Pathol183: 131–133, 1997.
23. Luan Y, Xu W. The structure and main functions of aminopeptidase N.Curr Med Chem 14: 639–647, 2007.
24. Mantle D, Lauffart B, McDermott J, Gibson A. Characterization ofaminopeptidases in human kidney soluble fraction. Clin Chim Acta 187:105–113, 1990.
25. Marchio S, Lahdenranta J, Schlingemann RO, Valdembri D, Wessel-ing P, Arap MA, Hajitou A, Ozawa MG, Trepel M, Giordano RJ,Nanus DM, Dijkman HB, Oosterwijk E, Sidman RL, Cooper MD,Bussolino F, Pasqualini R, Arap W. Aminopeptidase A is a functionaltarget in angiogenic blood vessels. Cancer Cell 5: 151–162, 2004.
26. Morra MN, Das S. Renal oncocytoma: a review of histogenesis, histo-pathology, diagnosis and treatment. J Urol 150: 295–302, 1993.
27. Murphy WM, Grignon DJ, Perlman EJ. Tumors of the kidney, bladder,and related urinary structures. AFIP Atlas of Tumor Pathology 4th Series,Fascicle 1, American Registry of Pathology, Washington, DC, 2004;p. 101–240.
28. Nanus DM, Bogenrieder T, Papandreou CN, Finstad CL, Lee A,Vlamis V, Motzer RJ, Bander NH, Albino AP, Reuter VE. Aminopep-tidase A expression and enzymatic activity in primary human renalcancers. Int J Oncol 13: 261–267, 1998.
F857PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from

29. Nanus DM. Of peptides and peptidases: the role of cell surface peptidasesin cancer. Clin Cancer Res 9: 6307–6309, 2003.
30. Petrovic N, Schacke W, Shapiro LH. CD13/Aminopeptidase N in tumorgrowth and angiogenesis. In: Aminopeptidases in Biology and Disease,edited by Hooper NM and Lendeckel U. New York: Kluwer Academic/Plenum, 2004, p. 179–200.
31. Scornik OA, Botbol V. Effects on mammals of the aminopeptidase inhibitorbestatine. In: Aminopeptidases in Biology and Disease, edited by Hooper NMand Lendeckel U. New York: Kluwer Academic/Plenum, 2004, p. 127–143.
32. Sekine K, Fujii H, Abe F, Nishikawa K. Augmentation of dead ligand-induced apoptosis by aminopeptidase inhibitors in human solid tumor celllines. Int J Cancer 94: 485–491, 2001.
33. Sobin LH, Wittekind C. TNM Classification of Malignant Tumours (6th
edition). New York: Wiley-Liss, 2002.
34. Stavropoulou V, Xie J, Henriksson M, Tomkinson B, Imreh S, MasucciMG. Mitotic infidelity and centrosome duplication errors in cells overexpress-ing tripeptidyl-peptidase II. Cancer Res 65: 1361–1368, 2005.
35. Suganuma T, Ino K, Shibata K, Nomura S, Kajiyama H, Kikkawa F,Tsuruoka N, Mizutani S. Regulation of aminopeptidase A expression incervical carcinoma: role of tumor-stromal interaction and vascular endo-thelial growth factor. Lab Invest 84: 639–648, 2004.
36. Tieku S, Hooper NM. Inhibition of aminopeptidases N, A, and W. Are-evaluation of the actions of bestatin and inhibitors of angiotensinconverting enzyme. Biochem Pharmacol 44: 1725–1730, 1992.
37. Varona A, Blanco L, Lopez JI, Gil J, Agirregoitia E, Irazusta J,Larrinaga G. Altered levels of acid, basic, and neutral peptidase activityand expression in human clear cell renal cell carcinoma. Am J PhysiolRenal Physiol 292: F780–F788, 2007.
F858 PEPTIDASES IN DIFFERENT RENAL CELL TUMORS
AJP-Renal Physiol • VOL 294 • APRIL 2008 • www.ajprenal.org
on April 4, 2008
ajprenal.physiology.orgD
ownloaded from