Accelerated long-term forgetting in children with temporal lobe epilepsy
45
Accelerated Long-Term Forgetting in TLE 1 Full title: Accelerated Long-Term Forgetting in Children with Temporal Lobe 1 Epilepsy 2 Authors: Michael B. Gascoigne a,e , Mary Lou Smith b , Belinda Barton c , Richard 3 Webster d , Deepak Gill d , & Suncica Lah a,e 4 Author affiliations: a School of Psychology, The University of Sydney, Australia; b The 5 University of Toronto and The Hospital for Sick Children, Toronto, Canada; 6 c Children’s Hospital Education Research Institute, The Children’s Hospital at 7 Westmead and Discipline of Paediatrics and Child Health, Faculty of Medicine, 8 University of Sydney, Australia; d T.Y. Nelson Department of Neurology and 9 Neurosurgery, The Children’s Hospital at Westmead, Sydney, Australia; e ARC Centre 10 of Excellence in Cognition and its Disorders 11 12 Corresponding author: Dr. Suncica Sunny Lah 13 Contact information: Dr. Suncica Sunny Lah, School of Psychology, The University 14 of Sydney, NSW 2006, Australia. Phone: +61 2 9351 2648, Fax: +61 2 9036 5223, 15 Email: [email protected] 16 17
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Accelerated long-term forgetting in children with temporal lobe epilepsy
Accelerated Long-Term Forgetting in TLE
1
Full title: Accelerated Long-Term Forgetting in Children with Temporal Lobe 1
Epilepsy 2
Authors: Michael B. Gascoignea,e, Mary Lou Smithb, Belinda Bartonc, Richard 3
Websterd, Deepak Gilld, & Suncica Laha,e 4
Author affiliations: aSchool of Psychology, The University of Sydney, Australia; bThe 5
University of Toronto and The Hospital for Sick Children, Toronto, Canada; 6
cChildren’s Hospital Education Research Institute, The Children’s Hospital at 7
Westmead and Discipline of Paediatrics and Child Health, Faculty of Medicine, 8
University of Sydney, Australia; dT.Y. Nelson Department of Neurology and 9
Neurosurgery, The Children’s Hospital at Westmead, Sydney, Australia; eARC Centre 10
of Excellence in Cognition and its Disorders 11
12
Corresponding author: Dr. Suncica Sunny Lah 13
Contact information: Dr. Suncica Sunny Lah, School of Psychology, The University 14
of Sydney, NSW 2006, Australia. Phone: +61 2 9351 2648, Fax: +61 2 9036 5223, 15
Email: [email protected] 16
17
Accelerated Long-Term Forgetting in TLE
2
Abstract 1
Adults with temporal lobe epilepsy (TLE) have been found to have accelerated long-2
term forgetting, but this phenomenon has not yet been investigated in children. 3
Although deficits in recall of materials after short (20- to 30-minute) delays have been 4
shown to slowly emerge from childhood to adolescence in patients with TLE, it is 5
unknown whether such a trend will also be found in recall of materials after long 6
delays. This study examined the presence of accelerated long-term forgetting in 7
children with TLE and how it relates to chronological age. Twenty-three children with 8
TLE and 58 healthy controls of similar age, sex distribution and socioeconomic status 9
completed a battery of neuropsychological tests, including standardised tests of story 10
recall and design location, as well as two experimental tests requiring the learning of 11
words and design locations to a criterion, both of which assessed recall after short 12
(30-min) and long (7-day) delays. Word recall at the 7-day delay (relative to the 30-13
min recall) was significantly poorer in the TLE group, compared to the control group. 14
The TLE group also exhibited worse 30-min recall performance on a standardised test 15
of story recall. Individual patient analyses revealed dissociation between performance 16
on the experimental and standardised verbal memory tests; children who were 17
impaired on the experimental test (7-day delay) were not impaired on the standardised 18
test (30-min delay). Compared to controls, patients with a left-hemisphere seizure 19
focus recalled fewer words at short and long delays while patients with an abnormal 20
hippocampus recalled fewer words at the long delay. No between-group differences 21
were found with respect to the design location task. Age negatively correlated with 22
the recall of words after short- and long-term delays within the TLE group, where 23
older age was associated with worse memory. This association was not present in the 24
control group. To our knowledge, this is the first study to show evidence of 25
Accelerated Long-Term Forgetting in TLE
3
accelerated long-term forgetting in children with TLE, which could not be explained 1
by poor performance on standardised memory tests. Additionally, these results 2
suggest that the developmental trajectory of long-term memory in children with TLE 3
is similar to that of short-term memory: deficits emerge gradually, therefore older 4
children are more likely to present with long-term memory deficits. 5
Keywords: Temporal Lobe Epilepsy; Accelerated Forgetting; Memory; Recall; 6
Consolidation 7
8
9
Accelerated Long-Term Forgetting in TLE
4
1 Introduction 1
Studies of adults with temporal lobe epilepsy (TLE) have found evidence of 2
anterograde memory deficits, as shown by poor learning and/or recall of materials 3
after short (20- to 30-minute) delays (i.e. Scoville and Milner, 1957; Hermann et al., 4
1987; Frisk and Milner, 1990; Jones-Gotman et al., 1997; Helmstaedter et al., 1998; 5
Bell et al., 2005; Bell, 2006). Furthermore, the memory deficits seem to be material-6
specific (Milner, 1968), related to the side of epilepsy focus. While dominant 7
(typically left hemisphere) TLE has been associated with impaired verbal memory 8
(Sass et al., 1995; Helmstaedter et al., 1997; Hermann et al., 1997; Helmstaedter and 9
Elger, 1998), non-dominant TLE has been linked (albeit less consistently) with 10
impaired visual memory (Helmstaedter et al., 1991; Breier et al., 1996; Barr, 1997; 11
Baxendale et al., 1998; Smith et al., 2011). In addition to the side, the site of epilepsy 12
focus within the temporal lobe was found to be critical for memory. Smaller 13
hippocampal volume was found to correlate with poorer learning and recall of both 14
verbal (Sass et al., 1994; Wilkinson et al., 2012) and visual information (Baxendale et 15
al., 1998) after short (up to 30-minute) delays. 16
17
Long-term memory formation, however, is not completed after short delays. Instead, 18
Classic Consolidation Theory has proposed that long-term memory formation requires 19
further consolidation, which may take days or months to complete (Squire et al., 20
1984). Moreover, consolidation requires interaction between the hippocampus, which 21
is critical for the initial memory formation, and distributed neocortical storage sites 22
(Squire and Alvarez, 1995; Mayes et al., 2003). On completion of consolidation, 23
memories are independent of the hippocampus and stored in the neocortex. It has 24
been proposed that damage to any of the components of the consolidation network, as 25

Accelerated Long-Term Forgetting in TLE
5
well as disruption of the interactions between the medial temporal lobe and temporal 1
neocortex, may compromise consolidation (Mayes et al., 2003). Consistent with 2
Classic Consolidation Theory is a recently described phenomenon of accelerated 3
long-term forgetting (ALF). In its pure form ALF is characterised by abnormally fast 4
forgetting over long delays (i.e. days or weeks) despite normal acquisition and 5
retention of the information over short delays (i.e. 30 minutes). ALF has been found 6
in several studies that involved adults with TLE (Martin et al., 1991; Blake et al., 7
2000; Muhlert et al., 2011; Lah et al., 2014), with some exceptions (Giovagnoli et al., 8
1995; Bell et al., 2005; Bell, 2006). Nevertheless, as patients with TLE have typically 9
shown poor learning and retention of information over short delays, studies 10
examining long-term memory formation in this population offered additional learning 11
trials and/or examined recall of information relative to the last learning trial (Blake et 12
al., 2000; Muhlert et al., 2011; Narayanan et al., 2012; Wilkinson et al., 2012; Lah, et 13
al., 2014). ALF in TLE usually refers to a faster rate of forgetting over long delays 14
(i.e. days or weeks) relative to shorter delays. 15
16
In adults with TLE, a relationship between this long-term memory deficit and seizure 17
frequency has been found (Mameniskiene et al., 2006). However, some seizure-free 18
patients have also exhibited ALF (e.g. Narayanan et al., 2012) and the only study that 19
employed ambulatory EEG monitoring to investigate the relations between epileptic 20
discharges and ALF, found that subclinical epileptiform discharges (rather than yearly 21
seizure frequency) contributed to ALF (Fitzgerald et al., 2013). Nevertheless, 22
material-specific memory impairments have not been consistently found on long 23
delays. For instance, one study found patients with left-TLE recalled significantly 24
fewer story details compared to both patients with right-TLE and control participants 25

Accelerated Long-Term Forgetting in TLE
6
at a one-hour, but not six-week, delay (Wilkinson et al., 2012). In contrast, in another 1
study (Blake et al, 2000), recall of stories at long delay (8 weeks) was significantly 2
worse in patients with left-TLE relative to patients with right-TLE and control 3
participants. 4
5
Studies that examined the role of hippocampal pathology in ALF have provided 6
equivocal results. Recently, Wilkinson and colleagues (2012) found that neither 7
structural hippocampal abnormality nor volume was related to either ALF or recall of 8
information after a long (six-week) delay. Similarly, in a study that tested recall of 9
verbal and visual information following a four-week delay, ALF was evident for both 10
types of material in patients with TLE, even when those with an identifiable 11
hippocampal lesion were removed from the sample (Mameniskiene et al., 2006). 12
Likewise, when patients with TLE were tested on a verbal memory task that used two 13
long delays, ALF was noticed in patients with and without structural hippocampal 14
abnormalities, but at different delays (one and seven days, respectively), suggesting a 15
difference in the temporal pattern of forgetting (Lah et al., 2014). In contrast, Muhlert 16
et al. (2011) reported that a larger number of patients with mesial temporal sclerosis 17
exhibited impaired three-week recall for both stories (4 out of 7 patients) and visual 18
scenes (7 out of 7 patients) than those without mesial temporal sclerosis (1 out of 7 19
patients; visual task only). However, formal statistical analyses could not be 20
performed on this small dataset. Lastly, Narayanan et al. (2012) reported conflicting 21
findings, as TLE patients with hippocampal abnormalities exhibited ALF and those 22
free of hippocampal abnormalities did not; however, correlations between 23
hippocampal volume and ALF were all small and insignificant. 24
25

Accelerated Long-Term Forgetting in TLE
7
Although the above studies appear to give contradictory results, these could be 1
explained by variations in methodology, such as the unequal opportunity for 2
participants to initially learn material. For instance, Wilkinson et al. (2012) provided 3
participants with a maximum of five trials to demonstrate at least 75% recall of a 4
short story, whereas Muhlert et al. (2011) did not employ a learning criterion and only 5
provided between one and three story presentations, depending on the participant’s 6
learning ability. It is also important to highlight that Mameniskiene et al. (2006) did 7
not measure ALF as defined above, as the authors did not attempt to ensure that recall 8
of verbal information following a short delay was equivalent between patients and 9
controls. 10
11
Thus far there has been little work on long-term memory formation in children with 12
epilepsy. This situation represents a major gap, as long-term memory is critical for 13
developmental and academic progression. Importantly, findings of adult epilepsy 14
studies are not directly applicable to children, as the impact of seizures and 15
underlying substrates on cognitive function have been shown to differ between the 16
mature and developing brain (Smith, 2010). First, while material specific memory 17
deficits related to lesion side are often found in adults with TLE (most consistently for 18
verbal materials), findings are inconsistent in children. Several studies have found that 19
verbal memory deficits were comparable in children with left- and right-TLE (Lendt 20
et al., 1999; Mabbott and Smith, 2003; Nolan et al., 2004). Furthermore, material-21
specific memory deficits were more likely to be found for visual (especially face 22
recognition tasks), rather than verbal material (Mabbott and Smith, 2003; Gonzalez et 23
al., 2007). Second, recent studies revealed that memory deficits become more 24
noticeable as children with TLE grow older. For instance, in a longitudinal study, 25

Accelerated Long-Term Forgetting in TLE
8
verbal memory deficits became apparent during adolescence or young adulthood in a 1
sample of patients with left TLE (Gonzalez et al., 2012) who were free of such 2
impairments in childhood (Gonzalez et al., 2007). Similarly, in a large cross-sectional 3
study involving 1000 healthy control subjects (aged 6-80) and 1157 patients with TLE 4
(aged 6-68 years) Helmstaedter and Elger (2009) found that deficits in recall of verbal 5
information following short delays were not evident in children, but became apparent 6
(relative to healthy controls) during teenage years/young adulthood. Moreover, 7
differences in verbal memory between left and right TLE patients also emerged at this 8
age, with the former group exhibiting poorer performance. It is unknown, however, 9
whether long-term memory deficits also increase in a similar fashion over the course 10
of development. Third, while the impact of site of epilepsy focus within the temporal 11
lobe has been shown to be important for the pattern of memory impairment in adults 12
with TLE, in children with TLE the findings are equivocal. One study found that 13
children (mean age 11.4-12.8 years, range 5-16) with lateral temporal lobe lesions 14
displayed intact visual memory and associative learning, relative to normative 15
standards, whereas children with mesial lesions were impaired (Gonzalez et al., 16
2007). In contrast, another study of children (mean age 12.5 years, range 6-18) found 17
that verbal and visual memory performance was not significantly different between 18
children with mesial TLE and those with seizure foci in other areas of the temporal 19
lobe (Nolan et al., 2004). 20
21
Although studies that have found ALF in adults have almost exclusively involved 22
patients with TLE, no study to date has examined ALF in children with TLE. There 23
has been a small amount of research on children with idiopathic generalised epilepsy. 24
In that work, ALF has been attributed to the poor initial learning of material 25
Accelerated Long-Term Forgetting in TLE
9
(Davidson et al., 2007), or to seizure activity disrupting the consolidation process, 1
which is critical for long-term memory formation (Gascoigne et al., 2012). 2
3
In the current study we aimed to examine long-term memory formation in children 4
with TLE, and explore how it relates to deficits in initial learning, epilepsy variables 5
(side and site of epilepsy focus/lesion) and chronological age. Performance of 6
children with TLE was compared with healthy controls on two measures of long-term 7
memory formation: one verbal and one visual. Standardised measures of recall 8
following short (up to 30 min) delays were also included, to determine whether they 9
would relate to deficits in recall following long delays. 10
11
Based on the reviewed literature we hypothesised that, compared to healthy controls, 12
children with TLE would show deficits in long-term memory formation, but that 13
deficits would not be material specific. Moreover, we predicted that for children with 14
TLE, older age would be associated with greater long-term memory difficulties. 15
Finally, we expected children with an abnormal hippocampus (resulting either from 16
pathology or surgical resection) to have more severe long-term memory impairments 17
than those with an intact hippocampus. 18
19
2 Method 20
2.1 Subjects 21
Twenty-three children with TLE (21 with unilateral foci, two with undetermined 22
laterality) and 58 healthy children (the control group) participated. Inclusion criteria 23
were: aged six to 16 years, fluent in English, and Full Scale Intelligence Quotient 24
(FSIQ) ≥ 80. Exclusion criteria were the presence of: (i) a major sensory deficit; (ii) 25
Accelerated Long-Term Forgetting in TLE
10
another neurological disorder, or (iii) significant neurodevelopmental disorder (e.g. 1
autism, but not learning disability or ADHD). Temporal lobe resection had been 2
performed on seven TLE participants. One TLE participant was left-handed and one 3
had a diagnosed specific learning difficulty (dyslexia). 4
5
All TLE participants were recruited through specialised epilepsy services at the 6
Hospital for Sick Children, Toronto, Canada; McMaster Children’s Hospital, 7
Hamilton, Canada or The Children’s Hospital at Westmead (CHW), Sydney, 8
Australia. Potential participants were identified by review of patient files. 9
Electroencephalography (EEG) records, medical history, and imaging data were 10
reviewed by the treating paediatric neurologists, who determined that potential 11
participants met the International League Against Epilepsy criteria for TLE 12
(Commission on Classification and Terminology of the International League Against 13
Epilepsy, 1989). Treating paediatric neurologists conducted a visual inspection of the 14
MRI images and reviewed the accompanying report. Thirty-one TLE participants 15
were approached; 25 (81%) consented. Two TLE participants were excluded: one 16
obtained an FSIQ score < 80 and the other refused to co-operate with the examiner. 17
18
Sixty healthy participants (free of a history of epilepsy) were recruited for the control 19
group via word-of-mouth recruitment (snowball recruitment), through the peer 20
networks of both TLE and other healthy participants in Canada and Australia. Two 21
control participants were excluded as they refused to complete the long-term recall 22
tasks. 23
24
2.2 Materials 25

Accelerated Long-Term Forgetting in TLE
11
2.2.1 Neuropsychological Measures 1
(i) Intelligence. Participants were administered the two-subtest version 2
(Vocabulary and Matrix Reasoning) of the Wechsler Abbreviated Scale of 3
Intelligence (WASI; Wechsler, 1999). The FSIQ was derived (M = 100, SD 4
= 15). 5
(ii) Standard Memory Tests. Two measures which assessed learning (immediate 6
recall) and recall at short (20 to 30-min) delays were included: the Story 7
Memory subtest from the Wide Range Assessment of Memory and Learning: 8
Second Edition (WRAML2; Sheslow and Adams, 2003) and the Dot 9
Location subtest from the Children’s Memory Scale (CMS; Cohen, 1997). 10
Age scaled scores have M = 10, SD = 3. A 7-day memory trial is not part of 11
these standardised tests. 12
(iii) Experimental Measure of Verbal Memory (Word Recall). Participants were 13
administered word lists derived from the California Verbal Learning Test - 14
Children's Version (CVLT-C; Delis et al., 1994). Children < 9 and ≥ 9 years 15
of age were administered a 9-word and 12-word list, respectively. Firstly, 16
this 9- or 12-word list (list A) was read aloud until the participant either 17
recalled the entire list of words (in any order) on two consecutive trials or 18
reached a maximum of 12 learning trials. Secondly, an additional 9- or 12-19
word list (list B, the “interference list”) was read and recalled once. Thirdly, 20
a recall of list A was requested following two short delays of two minutes 21
(after presentation and recall of list B) and 30 minutes, and one long delay 22
(seven days), without forewarning (i.e. no participant was notified in any 23
way in advance of the 7-day delay trial). The testing of long delay recall was 24
conducted over the telephone. The following scores were used in the current 25
Accelerated Long-Term Forgetting in TLE
12
study: (a) learning efficiency: number of learning trials and (b) recall: a 1
percentage of words recalled (max 100%) relative to the last learning trial. 2
(iv) Experimental Measure of Visual Memory (Design Location): This task was 3
modelled on a spatial memory task developed by Hepworth & Smith (2002). 4
Stimuli included abstract designs that were contained within a 6 x 4 grid and 5
presented on a computer screen. Participants were asked to remember the 6
designs and their respective locations. After presentation of each array of 7
designs, the screen showed an empty grid, next to which were the designs, 8
and participants were asked to drag-and-drop the designs to their correct 9
locations. Following each trial, visual feedback was given for five seconds: 10
correctly placed stimuli were highlighted in green with a checkmark, while 11
incorrectly placed stimuli were highlighted in red with an X (see Figure 1). 12
13
This computerised task consisted of practice, learning and two test phases 14
(administered after 30-min and 7-day delays). In each phase participants 15
were presented with the identical 6 x 4 grid. During the practice phase the 16
grid contained three abstract designs and was exposed for ten seconds. If the 17
participant made a design location error during this phase the presentation 18
was repeated (allowing up to a maximum of five attempts). During the 19
learning phase participants were again presented with the grid which now 20
contained ten new abstract designs (i.e. not identical to the practice phase 21
designs), presented for 15 seconds. This phase continued until participants 22
either reached the learning criterion (placing all stimuli correctly on two 23
consecutive trials) or 12 trials had been reached. During the recall test 24
phases (following a 30-min and 7-day delay) participants were presented 25
Accelerated Long-Term Forgetting in TLE
13
with an empty grid and were again asked to place stimuli in the correct 1
locations. However, no on-screen feedback was given during either of the 2
recall test phases. For the 7-day delay test, participants were contacted by 3
phone and asked to complete the task online after accessing it via a link 4
emailed to their parent/guardian. The following scores were used: (a) the 5
number of learning trials (learning efficiency) and (b) the proportion of 6
stimuli correctly placed (max 100%) relative to the last learning trial (recall). 7
8
9

Accelerated Long-Term Forgetting in TLE
14
Figure 1: Example of the presentation of stimuli during the learning phase of the 1 Design Location task and the on-screen feedback for that trial. 2
3
4
2.2.2 Epilepsy Severity 5
Treating neurologists rated epilepsy severity on the Global Assessment of Severity of 6
Epilepsy (GASE) scale (Speechley et al., 2008). This single-item, seven-point rating 7
scale assesses overall epilepsy severity and takes into consideration the frequency and 8
intensity of seizures, injuries during seizures, severity of post-ictal period, number 9
and side-effects of antiepileptic drugs and the interference of epilepsy or drugs with 10

Accelerated Long-Term Forgetting in TLE
15
daily activities. Severity ratings ranged from 1 (Not at all severe) to 7 (Extremely 1
severe). 2
3
2.3 Procedure 4
The study was approved by the ethics committees of all participating institutions. 5
Only children who agreed to participate and whose parents gave informed consent 6
were included in the study. Children were tested individually over one 90-minute 7
session and contacted by telephone seven days later. Tests were administered in the 8
same order to all participants. Information relating to developmental history, 9
socioeconomic status (SES; i.e. parental years of education) and relevant epilepsy 10
variables (i.e. medication taken at the time of assessment) was collected during 11
structured parent interviews. Information about the child’s epilepsy was verified by 12
treating paediatric neurologists and review of the medical records. Neurologists were 13
blind to children’s scores on neuropsychological tests when completing the GASE 14
scale. 15
16
2.4 Statistical analysis 17
All statistical analyses were performed using a standard alpha of 0.05, unless stated 18
otherwise. Data were screened using Kolmogorov-Smirnov tests to check suitability 19
of variables for parametric analyses. Independent t-tests (or Mann-Whitney U tests) 20
and chi-square (χ2, with Bonferroni corrections) tests were used to examine between 21
group differences on continuous and categorical background variables, respectively. 22
Fisher’s exact test was used when chi-square assumptions were not met. 23
24

Accelerated Long-Term Forgetting in TLE
16
Analysis of covariance (ANCOVA) was employed to compare the TLE and control 1
groups on standardised tests. Repeated measures ANCOVA (Group x Delay), 2
followed by Sidak post-hoc tests, investigated main effects of group, delay and 3
interaction on the Word Recall and Design Location tasks (although analyses for the 4
latter task did not include covariates). All covariates were centered before performing 5
the repeated measures ANCOVA. When data normality assumptions were not met, 6
Kruskal-Wallis tests with Mann-Whitney U post-hoc tests (and a Bonferroni adjusted 7
alpha of 0.008) were employed. Pearson’s (or Spearman’s) correlations were used to 8
assess the relationship between age and scores obtained on the Word Recall and 9
Design Location tasks. 10
11
In order to determine the clinical significance of our findings: whether ALF is present 12
in children whose scores on standardised tests of verbal memory were not impaired, 13
patterns of performance on two memory tests were examined in each individual child. 14
Performance of each child on the Word Recall task and WRAML2: Story Memory 15
(delayed recall) was classified as impaired if their score was less than -1.96 z-scores 16
below the control mean, as previously used in an adult study by Muhlert et al., 2011. 17
Moreover, chi-square analysis was used to determine whether there is a between-18
group difference in the number of children who showed impairments on these 19
experimental and standardised tests. 20
21
3 Results 22
TLE participants had been diagnosed with epilepsy at a mean age of 6.4 years (SD = 23
3.8) and had experienced epilepsy for an average of 6.1 years (SD = 4.0). Twenty-one 24
children with TLE were taking anti-epileptic drugs (AED): 14 on mono- and seven on 25

Accelerated Long-Term Forgetting in TLE
17
poly-therapy. Six separate drugs were taken, with Carbamazepine (n = 8) and 1
Levetiracetam (n = 8) being the most frequently used. The mean seizure severity 2
rating (M = 2.6, SD = 1.2) on the GASE scale corresponded to a rating between “A 3
little severe” and “Somewhat severe”. 4
5
Demographic and additional clinical characteristics are presented in Table 1. The TLE 6
and control groups did not differ in age, years of parental education or sex 7
distribution. While the mean FSIQ for both groups was within the average range, it 8
was significantly lower for the TLE group than for the control group. 9
10
Comparisons were also made between TLE patients with either a left-hemisphere (n = 11
15) or right-hemisphere (n = 6) seizure focus and between those with either a normal 12
(NH, n = 11) or abnormal hippocampus (AH, n = 12). Note, however, that it was not 13
possible to determine the laterality of seizure focus in two patients with TLE. 14
15
The left- and right-TLE patient groups did not differ on any epilepsy-related 16
variables. Compared to the control group, Kruskal-Wallis tests found significant 17
between-group differences in FSIQ, but not in any demographic variables. 18
Subsequent pairwise comparisons revealed that the left-TLE (but not right-TLE) 19
group had significantly lower FSIQ (z = -4.9, p < 0.001) scores than the control 20
group. 21
22
No significant differences in any epilepsy-related variables were found between the 23
AH and NH groups, although significantly more participants in AH group had 24
undergone surgery or were receiving polytherapy than those in the NH group. 25
Accelerated Long-Term Forgetting in TLE
18
Compared to the control group, a significant difference was evident in FSIQ, but not 1
in any demographic variables. Pairwise comparisons found indicated that, compared 2
to control participants, FSIQ was significantly lower in both the NH (z = -3.6, p < 3
0.001) and AH groups (z = -3.3, p = 0.001), although mean FSIQ did not differ 4
between the NH and AH groups. 5
Accelerated Long-Term Forgetting in TLE
19
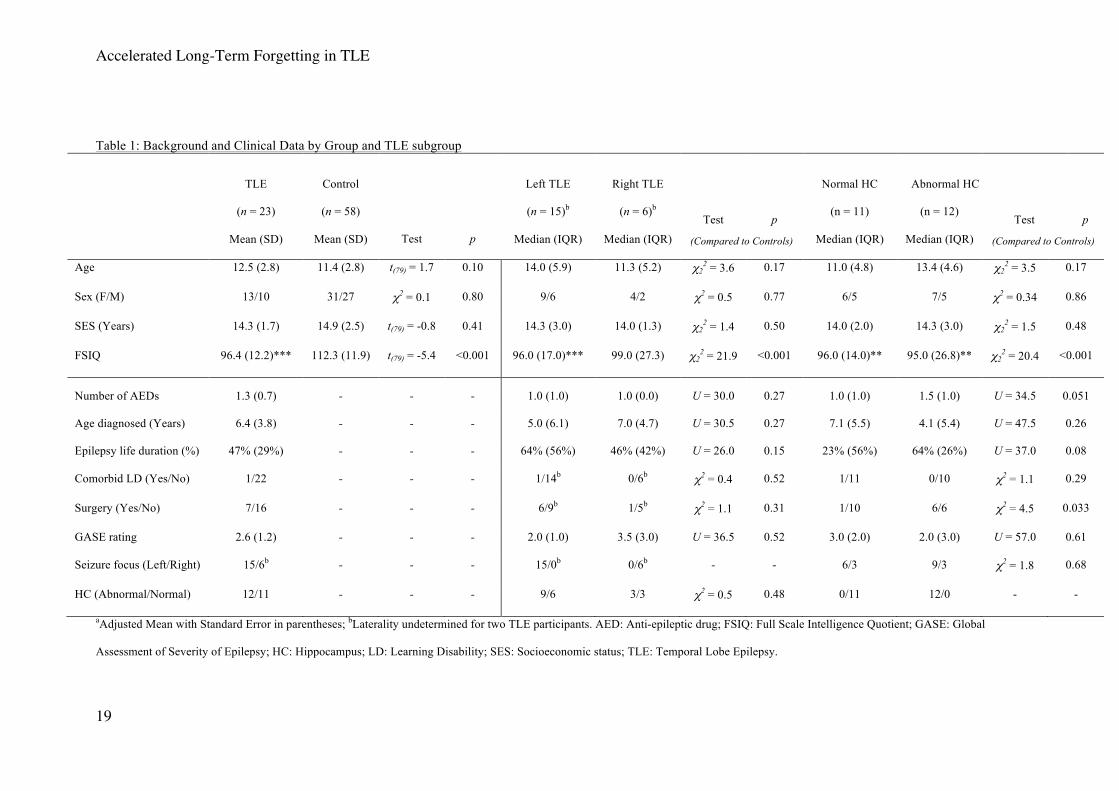
Table 1: Background and Clinical Data by Group and TLE subgroup
TLE
(n = 23)
Mean (SD)
Control
(n = 58)
Mean (SD) Test p
Left TLE
(n = 15)b
Median (IQR)
Right TLE
(n = 6)b
Median (IQR)
Test p
Normal HC
(n = 11)
Median (IQR)
Abnormal HC
(n = 12)
Median (IQR)
Test p
(Compared to Controls) (Compared to Controls)
Age 12.5 (2.8) 11.4 (2.8) t(79) = 1.7 0.10 14.0 (5.9) 11.3 (5.2) χ22 = 3.6 0.17 11.0 (4.8) 13.4 (4.6) χ2
2 = 3.5 0.17
Sex (F/M) 13/10 31/27 χ2 = 0.1 0.80 9/6 4/2 χ2 = 0.5 0.77 6/5 7/5 χ2 = 0.34 0.86
SES (Years) 14.3 (1.7) 14.9 (2.5) t(79) = -0.8 0.41 14.3 (3.0) 14.0 (1.3) χ22 = 1.4 0.50 14.0 (2.0) 14.3 (3.0) χ2
2 = 1.5 0.48
FSIQ 96.4 (12.2)*** 112.3 (11.9) t(79) = -5.4 <0.001 96.0 (17.0)*** 99.0 (27.3) χ22 = 21.9 <0.001 96.0 (14.0)** 95.0 (26.8)** χ2
2 = 20.4 <0.001
Number of AEDs 1.3 (0.7) - - - 1.0 (1.0) 1.0 (0.0) U = 30.0 0.27 1.0 (1.0) 1.5 (1.0) U = 34.5 0.051
Age diagnosed (Years) 6.4 (3.8) - - - 5.0 (6.1) 7.0 (4.7) U = 30.5 0.27 7.1 (5.5) 4.1 (5.4) U = 47.5 0.26
Epilepsy life duration (%) 47% (29%) - - - 64% (56%) 46% (42%) U = 26.0 0.15 23% (56%) 64% (26%) U = 37.0 0.08
Comorbid LD (Yes/No) 1/22 - - - 1/14b 0/6b χ2 = 0.4 0.52 1/11 0/10 χ2 = 1.1 0.29
Surgery (Yes/No) 7/16 - - - 6/9b 1/5b χ2 = 1.1 0.31 1/10 6/6 χ2 = 4.5 0.033
GASE rating 2.6 (1.2) - - - 2.0 (1.0) 3.5 (3.0) U = 36.5 0.52 3.0 (2.0) 2.0 (3.0) U = 57.0 0.61
Seizure focus (Left/Right) 15/6b - - - 15/0b 0/6b - - 6/3 9/3 χ2 = 1.8 0.68
HC (Abnormal/Normal) 12/11 - - - 9/6 3/3 χ2 = 0.5 0.48 0/11 12/0 - -
aAdjusted Mean with Standard Error in parentheses; bLaterality undetermined for two TLE participants. AED: Anti-epileptic drug; FSIQ: Full Scale Intelligence Quotient; GASE: Global
Assessment of Severity of Epilepsy; HC: Hippocampus; LD: Learning Disability; SES: Socioeconomic status; TLE: Temporal Lobe Epilepsy.
Accelerated Long-Term Forgetting in TLE
20
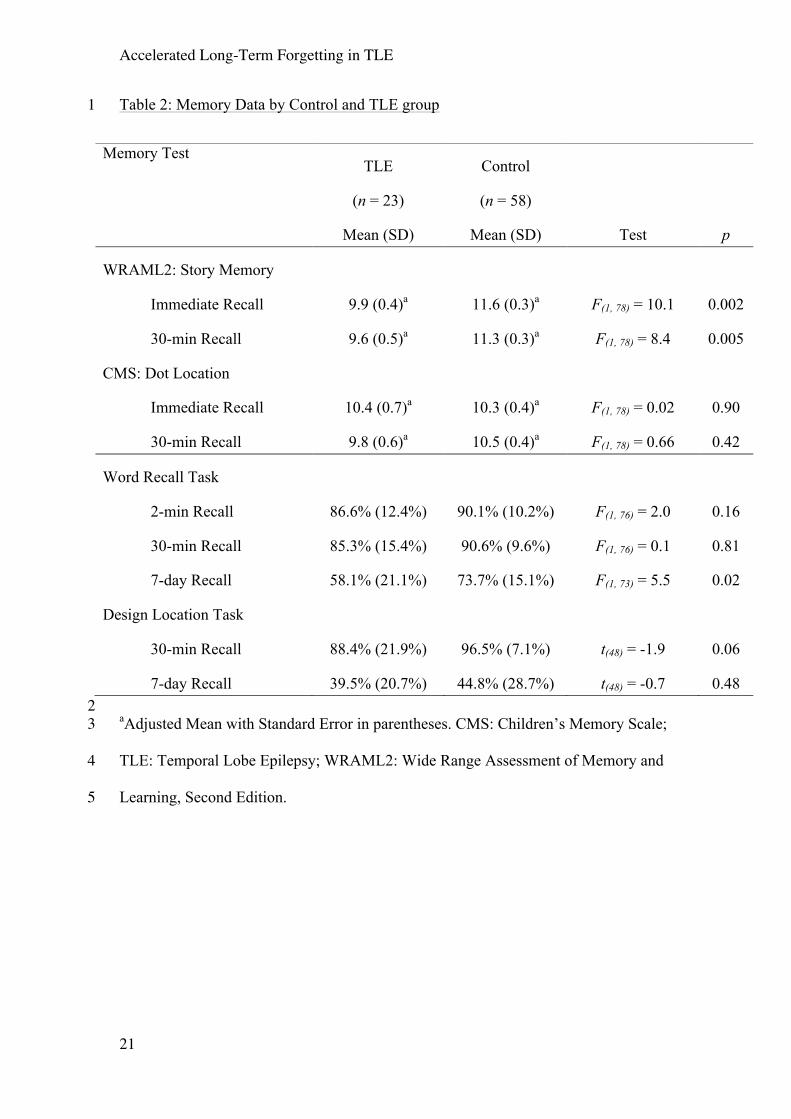
3.1 Analysis 1: Patients versus Controls 1
Scores obtained on standardised and experimental memory tests are summarised in 2
Table 2. After controlling for FSIQ, no significant differences were found between 3
the TLE and control groups on the immediate or short-delay recall of visual material 4
(CMS: Dot Location). However, on the test that demanded recall of verbal materials 5
(WRAML2: Story Memory), the TLE group recalled significantly fewer story details 6
immediately following a presentation and after a short delay compared to the controls. 7
Within the TLE group, the immediate recall of story details was not correlated with 8
Word Recall. However, the short-delay recall of story details correlated with 2-min 9
Word Recall (r = 0.4, p = 0.05), but not 30-min (r = 0.34, p = 0.13) or 7-day recall (r 10
= 0.30, p = 0.17). FSIQ correlated with Word Recall at seven days (r = 0.5, p = 0.03), 11
but not at either 2-min (r = 0.1, p = 0.8) or 30-min delays (r = 0.2, p = 0.4). Because 12
we were interested in recall of information after long delays, FSIQ was included as a 13
covariate in the subsequent ANCOVAs. Delayed recall on CMS: Dot Location did not 14
correlate with either 30-min (r = 0.31, p = 0.19) or 7-day recall (r = 0.21, p = 0.39) on 15
the Design Location task within the TLE group. 16
17
Accelerated Long-Term Forgetting in TLE
21
Table 2: Memory Data by Control and TLE group 1
2 aAdjusted Mean with Standard Error in parentheses. CMS: Children’s Memory Scale; 3
TLE: Temporal Lobe Epilepsy; WRAML2: Wide Range Assessment of Memory and 4
Learning, Second Edition.5
Memory Test TLE
(n = 23)
Mean (SD)
Control
(n = 58)
Mean (SD) Test p
WRAML2: Story Memory
Immediate Recall 9.9 (0.4)a 11.6 (0.3)a F(1, 78) = 10.1 0.002
30-min Recall 9.6 (0.5)a 11.3 (0.3)a F(1, 78) = 8.4 0.005
CMS: Dot Location
Immediate Recall 10.4 (0.7)a 10.3 (0.4)a F(1, 78) = 0.02 0.90
30-min Recall 9.8 (0.6)a 10.5 (0.4)a F(1, 78) = 0.66 0.42
Word Recall Task
2-min Recall 86.6% (12.4%) 90.1% (10.2%) F(1, 76) = 2.0 0.16
30-min Recall 85.3% (15.4%) 90.6% (9.6%) F(1, 76) = 0.1 0.81
7-day Recall 58.1% (21.1%) 73.7% (15.1%) F(1, 73) = 5.5 0.02
Design Location Task
30-min Recall 88.4% (21.9%) 96.5% (7.1%) t(48) = -1.9 0.06
7-day Recall 39.5% (20.7%) 44.8% (28.7%) t(48) = -0.7 0.48

Accelerated Long-Term Forgetting in TLE
22
Figure 2 shows scores obtained on the Word Recall task. A two-way repeated 1
measures ANCOVA found a significant interaction between Group and Delay (F(2, 2
150) = 4.2, p = 0.02). While the between-group differences in the proportion of words 3
recalled following either the 2-min or 30-min delays were not significant, the TLE 4
group recalled significantly fewer words relative to controls at seven days. In 5
addition, a significant main effect of Delay (F(2, 150) = 92.8, p < 0.001) and Group 6
(F(1, 75) = 7.3, p = 0.008) was also found. Post-hoc tests indicated that the number of 7
words recalled at the 7-day delay was significantly less compared to both the 2-min (p 8
< 0.001) and 30-min delays (p < 0.001), but no difference was found between the 2-9
min and 30-min delays (p = 0.89). Across all delays, TLE participants recalled a mean 10
of 9.6% (SE = 3.2%) fewer words than control participants (p = 0.008). 11
12
Figure 2: Recall scores obtained on the Word Recall task by the TLE and control 13 groups covaried for FSIQ (standard error bars). 14
15 16
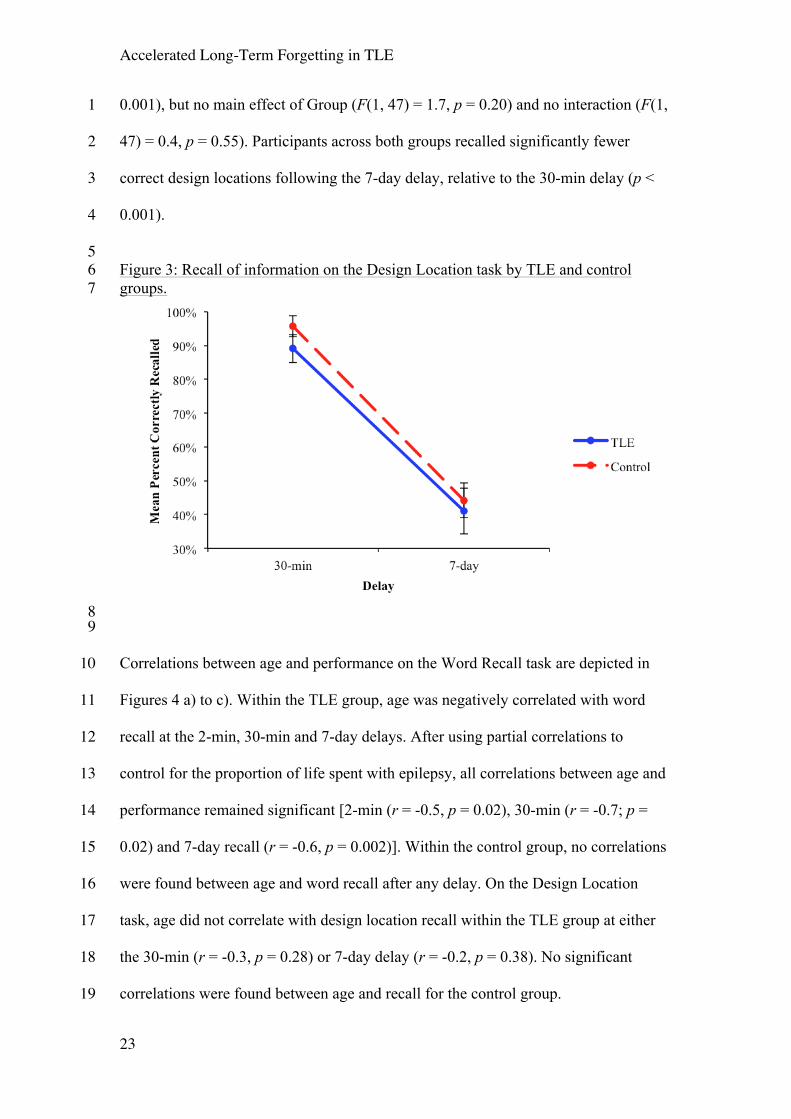
Recall scores obtained on the Design Location task are presented in Figure 3. A two-17
way repeated measures ANOVA found a main effect of Delay (F(1, 47) = 169.9, p < 18
Accelerated Long-Term Forgetting in TLE
23
0.001), but no main effect of Group (F(1, 47) = 1.7, p = 0.20) and no interaction (F(1, 1
47) = 0.4, p = 0.55). Participants across both groups recalled significantly fewer 2
correct design locations following the 7-day delay, relative to the 30-min delay (p < 3
0.001). 4
5 Figure 3: Recall of information on the Design Location task by TLE and control 6 groups. 7
8 9
Correlations between age and performance on the Word Recall task are depicted in 10
Figures 4 a) to c). Within the TLE group, age was negatively correlated with word 11
recall at the 2-min, 30-min and 7-day delays. After using partial correlations to 12
control for the proportion of life spent with epilepsy, all correlations between age and 13
performance remained significant [2-min (r = -0.5, p = 0.02), 30-min (r = -0.7; p = 14
0.02) and 7-day recall (r = -0.6, p = 0.002)]. Within the control group, no correlations 15
were found between age and word recall after any delay. On the Design Location 16
task, age did not correlate with design location recall within the TLE group at either 17
the 30-min (r = -0.3, p = 0.28) or 7-day delay (r = -0.2, p = 0.38). No significant 18
correlations were found between age and recall for the control group. 19

Accelerated Long-Term Forgetting in TLE
24
1 Figure 4: Correlation between participant age with recall following immediate (2-2 min) (A), short (30-min) (B) and long delays (7-day) (C) on the Word Recall task. 3
4 5
Accelerated Long-Term Forgetting in TLE
25
GASE scores did not significantly correlate with 2-min (rs = 0.2; p = 0.5), 30-min (rs 1
= -0.03; p = 0.9) or 7-day word recall (rs = -0.01; p = 0.95), nor with 30-min (rs = -2
0.1; p = 0.66) or 7-day design location recall (rs = -0.2; p = 0.32). 3
4
3.1.1 Individual Analysis 5
To establish whether children who were found to display ALF on the experimental 6
verbal memory task (impaired recall of words at 7 days, but not at 30 min) also 7
exhibited impaired recall on the standardised task of verbal memory (30 min delay), 8
scores on these two tasks were examined for each participant. To determine whether 9
the score was impaired or not, raw scores were converted to z scores. Scores obtained 10
by control participants were used to calculate z scores. A z score of 1.96 or greater 11
below the mean of control participants was considered impaired. 12
13
On the experimental task, a significantly higher proportion of children with TLE 14
(13.0%, n = 3/23; χ2 = 5.0, p = 0.034) exhibited ALF compared to control children 15
(1.7%, n = 1/58). Of these four participants across both groups, none displayed 16
impaired delayed recall performance on the standardised test of verbal memory, 17
WRAML2: Story Memory. 18
19
3.1.2 Assessing the relationship between ALF and incomplete learning 20
On the Word Recall task, significantly more TLE participants (n = 7, 30.4%, Fisher's 21
exact test, p < 0.001) failed to reach the learning criterion compared with the control 22
group (n = 1, 1.7%). All TLE participants who failed to meet this criterion had an 23
abnormal hippocampus; six had a left- and one had a right-hemisphere seizure focus. 24
When only children who reached the learning criterion were examined, an ANCOVA 25

Accelerated Long-Term Forgetting in TLE
26
showed that the TLE and control groups did not differ in the number of learning trials 1
taken [TLE: M = 6.8, SD = 2.4; control: M = 5.9, SD = 2.1; F(1, 74) = 0.5, p = 0.82]. 2
3
In order to determine whether ALF found in the initial analysis was due to incomplete 4
learning, only participants who had met the learning criterion on the Word Recall task 5
were included in the subsequent ANCOVA (with FSIQ as a covariate). A significant 6
Group x Delay interaction (F(2, 132) = 4.4, p = 0.015) was found. No significant 7
between-group difference was evident in the proportion of words recalled at either the 8
2-min (F(1, 69) = 1.2, p = 0.29) or 30-min delay (F(1, 69) = 0.1, p = 0.91); however 9
the TLE group recalled significantly fewer words relative to controls at the 7-day 10
delay (F(1, 66) = 4.4, p = 0.02). Additionally, a main effect of Delay (F(2, 134) = 11
81.2, p < 0.001) and Group (F(1, 67) = 5.1, p = 0.027) was obtained. No difference in 12
the proportion of words recalled was found between the 2-min and 30-min delays (p = 13
0.98), however, significantly fewer words were recalled at the 7-day delay, relative to 14
both 30-min (p < 0.001) and 2-min delays (p < 0.001). Across all delays, the TLE 15
group recalled a mean of 7.7% (SE = 3.4%) fewer words than the control group (p = 16
0.027). 17
18
On the Design Location task significantly more TLE participants (n = 4, 17.4%, 19
Fisher's exact test, p = 0.001) failed to reach the learning criterion, compared to the 20
control group (n = 0). All children who failed to reach criterion had abnormal 21
hippocampi and left-hemisphere seizure foci. Nevertheless, the TLE (M = 7.5, SD = 22
2.3) and control (M = 6.9, SD = 2.6) groups did not differ significantly in the number 23
of learning trials when only those who learned to criterion were considered (t = 0.7, p 24
= 0.46). When only children who reached the Design Location learning criterion were 25

Accelerated Long-Term Forgetting in TLE
27
included in an ANOVA, no interaction effect (F(1, 44) = 0.004, p = 0.95) or main 1
effect of Group (F(1, 44) = 0.04, p = 0.85) was found. However, a main effect of 2
Delay was obtained (F(1, 44) = 173.2, p < 0.001), where participants across both 3
groups recalled significantly fewer correct design locations in the 7-day compared to 4
the 30-min delay (p < 0.001). 5
6
3.1.3 Assessing the relationship between ALF and temporal lobe resection 7
Surgery had been performed on seven children with TLE. In order to determine 8
whether ALF was related to surgery, an ANCOVA (using FSIQ as a covariate) was 9
conducted on only those TLE participants who had not undergone any neurosurgical 10
procedure and wh o had met the learning criterion (n= 12). A significant Group x 11
Delay interaction (F(2, 126) = 3.6, p = 0.03) was found. The TLE group recalled 12
significantly fewer words than the control group following the 7-day delay (F(1, 63) = 13
8.1, p = 0.01), but not at either the 30-min (F(1, 66) = 2.2, p = 0.14) or 2-min delay 14
(F(1, 66) = 1.4, p = 0.25). Main effects of Delay (F(2, 126) = 61.8, p < 0.001) and 15
Group (F(1, 63) = 6.1, p = 0.02) were found. No difference in the proportion of words 16
recalled was found between the 2-min and 30-min delays (p = 0.84), however, 17
significantly fewer words were recalled at the 7-day delay, relative to both 30-min (p 18
< 0.001) and 2-min delays (p < 0.001). Across all delays, the TLE group recalled an 19
average of 9.2% (SE = 3.7%) fewer words than the control group (p = 0.016). 20
21
When these participants were included in an ANOVA related to performance on the 22
Design Location task, no interaction effect (F(1, 37) = 0.48, p = 0.49) or main effect 23
of Group was observed (F(1, 37) = 0.15, p = 0.70). A main effect of Delay was found 24

Accelerated Long-Term Forgetting in TLE
28
(F(1, 37) = 109.8, p < 0.001), as participants across both groups recalled fewer correct 1
design locations from the 30-min to 7-day delay (p < 0.001). 2
3
3.2 Analysis 2: Relationship between side of seizure focus and recall at long delays. 4
Table 3 contains descriptive statistics of the scores obtained by the left-TLE, right-5
TLE and control groups on standardised memory tests that demanded immediate and 6
short-delay recall following presentation. Significant between-group differences were 7
evident on CMS: Dot Location (delayed recall) and WRAML2: Story Memory (both 8
immediate and delayed recall). Pairwise comparisons showed that relative to the 9
control group, the left-TLE group had significantly lower scores on immediate (z = -10
5.1, p < 0.001) and delayed recall (z = -5.1, p < 0.001) on WRAML2: Story Memory 11
and delayed recall (z = -2.5, p < 0.001) on CMS: Dot Location. The right-TLE group 12
did not differ from the control or left-TLE groups on either of these standardised tests. 13
14
When scores were examined on the Word Recall task, significant between-group 15
differences were evident in recall at the 2-min and 7-day delays, with a marginally 16
non-significant difference found at the 30-min delay. Pairwise comparisons revealed 17
that, compared to the control group, the left-TLE group had worse recall of words at 18
the 2-min (z = -2.5, p = 0.01) and 7-day delays (z = -2.7, p = 0.021). The right-TLE 19
group did not differ significantly from either the left TLE or the control groups on 20
word recall. With respect to the Design Location task, no between-group difference 21
was found in the proportion of design locations recalled at either the 30-min or 7-day 22
delays. 23
24
25

Accelerated Long-Term Forgetting in TLE
29
Table 3: Memory Data by Control and TLE Subgroup (Laterality of seizure focus) 1
Control
(n = 58)
Median (IQR)
Left TLE
(n = 15)a
Median (IQR)
Right TLE
(n = 6)a
Median (IQR)
Test p
Post-hoc pairwise
comparison
WRAML2: Story Memory
Immediate Recall 12.0 (3.3) 7.0 (2.3) 9.5 (4.8) χ22 = 26.7 <0.001 L-TLE<NC
30-min Recall 12.0 (3.3) 7.0 (3.0) 9.5 (4.0) χ22 = 27.1 <0.001 L-TLE<NC
CMS: Dot Location
Immediate Recall 11.5 (4.3) 9.0 (6.0) 9.5 (7.8) χ22 = 2.8 0.24 -
30-min Recall 12.0 (5.3) 7.0 (5.5) 9.5 (6.0) χ22 = 6.1 0.048 L-TLE<NC
Word Recall Task
2-min Recall 92.0% (18.0%) 83.0% (15.0%) 92.0% (13.0%) χ22 = 7.0 0.031 L-TLE<NC
30-min Recall 92.0% (18.0%) 82.0% (33.0%) 100.0% (9.0%) χ22 = 5.9 0.054 -
7-day Recall 75.0% (23.0%) 60.0% (34.0%) 75.0% (18.0%) χ22 = 10.5 0.005 L-TLE<NC
Design Location Task
30-min Recall 100% (3.0%) 85.4% (26.0%) 94.0% (9.0%) χ22 = 2.4 0.30 -
7-day Recall 40.0% (32.0%) 35.0% (21.0%) 44.0% (18.0%) χ22 = 0.9 0.64 -
aLaterality undetermined for two TLE participants. CMS: Children’s Memory Scale; IQR: Interquartile 2
Range; NC: Control Group; TLE: Temporal Lobe Epilepsy; WRAML2: Wide Range Assessment of 3
Memory and Learning, Second Edition. 4
5

Accelerated Long-Term Forgetting in TLE
30
3.3 Analysis 3: Recall at long delays in patients with a normal or abnormal 1
hippocampus 2
Scores obtained on memory tests by the AH, NH and control groups are presented in 3
Table 4. When scores obtained on standardised memory tests were compared, 4
significant between-group differences were evident for delayed recall on CMS: Dot 5
Location; the AH group (but not NH group) obtained significantly lower scores for 6
delayed recall (z = -2.5, p = 0.012) relative to the control group. In addition, the 7
groups also differed in immediate and delayed recall on the WRAML2: Story 8
Memory subtest. Compared to the control group, both patient groups recalled 9
significantly fewer details on immediate and delayed recall (NH: z = -3.3, p = 0.001 10
and z = -3.4, p = 0.004, respectively; AH: z = -4.2, p < 0.001 and z = -3.9, p < 0.001, 11
respectively). The AH group also exhibited significantly lower immediate (z = -2.6, p 12
= 0.01) and delayed recall (z = -2.4, p = 0.02) on the WRAML2: Story Memory 13
subtest than the NH group. 14
15
On the Word Recall task, a between-group difference was found in the proportion of 16
words recalled at the 7-day delay, but not at the 2-min or 30-min delays. Pairwise 17
comparisons showed that, compared to the control group, but not the NH group (z = -18
0.8, p = 0.45), the AH group had significantly poorer recall at the 7-day delay (z = -19
2.7, p = 0.023). The difference between NH and control groups was not significant (z 20
= -1.8, p = 0.19). 21
22
A between-group difference was found in the performance on the Design Location 23
task at the 30-min, but not 7-day delay. Pairwise comparisons showed that the AH 24
group had significantly poorer recall of design locations following the 30-min delay, 25

Accelerated Long-Term Forgetting in TLE
31
compared to both the control (z = -2.6, p = 0.025) and NH groups (z = -2.5, p = 1
0.034). 2
3

Accelerated Long-Term Forgetting in TLE
32
Table 4: Memory Data by Control and TLE Subgroup (Presence of Hippocampal 1
Abnormality) 2
Control
(n = 58)
Median (IQR)
Normal HC
(n = 11)
Median (IQR)
Abnormal HC
(n = 12)
Median (IQR) Test p
Post-hoc
pairwise comparison
WRAML2: Story Memory
Immediate Recall 12.0 (3.3) 10.0 (2.0) 7.0 (2.0) χ22 = 25.8 <0.001 AH<NH<NC
30-min Recall 12.0 (3.3) 9.0 (1.0) 7.0 (3.0) χ22 = 24.2 <0.001 AH<NH<NC
CMS: Dot Location
Immediate Recall 11.5 (4.3) 10.0 (7.0) 9.0 (5.0) χ22 = 2.4 0.30 -
30-min Recall 12.0 (5.3) 11.0 (6.0) 7.0 (4.0) χ22 = 6.8 0.03 AH<NC
Word Recall Task
2-min Recall 92.0% (18.0%) 83.0% (25%) 89.0% (18%) χ22 = 4.1 0.13 -
30-min Recall 92.0% (18.0%) 89.0% (25.0%) 87.0% (24.0%) χ22 = 1.8 0.41 -
7-day Recall 75.0% (23.0%) 67.0% (25.0%) 62.0% (44.0%) χ22 = 9.1 0.01 AH<NC
Design Location Task
30-min Recall 100% (3.0%) 100.0% (0%) 85.0% (30.0%) χ22 = 8.4 0.02 AH<NH,NC
7-day Recall 40.0% (32.0%) 40.0% (35.0%) 40.0% (40.0%) χ22 = 1.3 0.51 -
AH: Abnormal Hippocampus; CMS: Children’s Memory Scale; HC: Hippocampus; IQR: Interquartile 3
Range; NH: Normal Hippocampus; TLE: Temporal Lobe Epilepsy; WRAML2: Wide Range 4
Assessment of Memory and Learning, Second Edition. 5

Accelerated Long-Term Forgetting in TLE
33
4 Discussion 1
In this (to our knowledge) first study of long-term memory formation in children with TLE, 2
we found evidence of ALF for verbal, but not visual material. Moreover, ALF was not related 3
to epilepsy variables, such as the side of seizure focus, hippocampal integrity, epilepsy 4
severity or temporal lobe resection. Interestingly, significant negative correlations between 5
age and recall of verbal information were found in the TLE, but not the control group. That 6
is, deficits in recall of verbal information after long, but also short, delays became apparent as 7
children with TLE aged: they appeared to grow into their memory deficits. 8
9
Children with TLE in the present study were found to perform more poorly on a standardised 10
memory test that required recall of short stories immediately after initial hearing and after a 11
30-min delay. Nevertheless, scores obtained on this standardised task did not correlate 12
significantly with the recall of words after a long delay. On the experimental task that 13
demanded recall of verbal information at short and long delays (after learning to a criterion), 14
the group by delay interaction was significant. The between group difference was significant 15
only at long, but not short delays. Furthermore, this between-group interaction remained 16
significant even when those who had not reached the learning criterion were excluded from 17
the analyses. A similar finding was also recently found in children with idiopathic 18
generalised epilepsy (Gascoigne et al., 2012), suggesting that the memory consolidation 19
process can be adversely impacted by seizures, irrespective of whether they are generalised 20
or confined to the temporal lobe. Finally, an additional analysis of individual participants in 21
the present study indicated that a significantly higher proportion of children with TLE 22
displayed impaired 7-day recall, compared to controls. Critically, dissociation was discovered 23
between the experimental and standardised verbal memory tests; children who were impaired 24
on the experimental test (7-day recall) were not impaired on the standardised test (30-min 25

Accelerated Long-Term Forgetting in TLE
34
recall). Together, these findings indicate that ALF is present in some children with TLE in 1
the context of specific experimental learning conditions, which remains undetected on 2
standardised memory tests. 3
4
Of particular interest are the developmental trajectories of verbal memory abilities in children 5
with TLE. Previously, a large-scale cross-sectional study found that recall of verbal 6
information after short (30-min) delays progressively worsened in children with TLE, 7
resulting in an increasing gap between children with TLE and healthy control peers which 8
reached peaks during adolescence/early adulthood (Helmstaedter and Elger, 2009). A similar 9
trend was observed in the current study; a significant negative correlation was found between 10
recall of verbal information after a short delay and age in the TLE group. Nevertheless, our 11
study extends the findings of Helmstaedter and Elger (2009) to recall following long delays. 12
The proportion of verbal information recalled at 7-days, relative to the last learning trial, 13
declined with age within our TLE sample, but not within the control group. This pattern 14
suggests that children with TLE grew into their memory deficits. It is possible that such a 15
phenomenon could be secondary to the cumulative adverse effect of seizures on hippocampal 16
maturation (Mitchell et al., 2003; Sutula et al., 2003). Contrary to such an explanation, 17
however, after accounting for life spent with epilepsy, the relationship between age and 18
verbal recall at short and long delays remained significant in the patient group. Such findings 19
suggest that seizures and verbal memory deficits may represent behavioral manifestations of 20
the same underlying temporal lobe pathology, which may be predominantly long-standing 21
rather than progressive in nature. Nevertheless, as verbal memory is relatively late to mature 22
(Gathercole, 1998), mild deficits in verbal memory may not be detectable at a young age, but 23
become more apparent at a later age. 24
25
Accelerated Long-Term Forgetting in TLE
35
When examining the impact of epilepsy factors on verbal memory, we found that side of 1
seizure focus, presence of hippocampal abnormality and history of surgery were not directly 2
related to recall following long delays. Compared to the control group, patients with left-TLE 3
recalled significantly fewer details on a standardised story memory task and fewer words 4
following short and long delays on the experimental task. However, the recall performance of 5
left-TLE patients did not differ significantly from patients with right-TLE on either of these 6
tasks. Hippocampal integrity appeared to be related to verbal recall deficits following a short 7
delay, as the TLE patient group recalled fewer details on the standardised story memory task 8
than the control group, with a significant difference also being found between those with and 9
without a hippocampal abnormality. On the experimental task, however, no such difference 10
in 7-day word recall was found between patients with a hippocampal abnormality and those 11
without one. 12
13
Although ALF has been previously associated with seizure severity (Mameniskiene et al., 14
2006), seizure frequency (Wilkinson et al., 2012) and even subclinical discharges in adults 15
(Fitzgerald et al., 2013), there was no association between ALF and epilepsy severity in the 16
current study. Future studies could include a more direct measure of seizures, in order to 17
assess their impact on ALF in children. Although the GASE scale used in the current study 18
takes into account the frequency and intensity of seizures, it also considers a variety of other 19
epilepsy-related variables, such as seizure-related injuries and number of prescribed anti-20
epileptic drugs, making it impossible to assess the impact of individual epilepsy-related 21
factors on recall at long delays. 22
23
In contrast to ALF for verbal material, we found no evidence of ALF for visual material. This 24
difference might be due to inadequate sensitivity of the test specifically developed to measure 25
Accelerated Long-Term Forgetting in TLE
36
recall of visual material at long delays. We found no differences between the TLE and 1
control groups in recall of visual information at short or long delays. Nevertheless, when 2
patients were sub-divided, according to the presence or absence of a structural hippocampal 3
abnormality, those with hippocampal abnormality had significantly poorer recall of item 4
locations on the (i) short (but not long) delay of the experimental task relative to those 5
without hippocampal abnormalities and to control children and (ii) short delay of the 6
standardised visual memory task. Also, children with a left (rather than right) hemisphere 7
seizure focus performed poorer on the short delay of the standardised, but not experimental, 8
visual memory test compared to controls. The presence of a 30-minute visual recall deficit in 9
left-TLE patients was unexpected, given that some previous studies have found visual recall 10
deficits to be confined to children with a right-sided temporal lobe seizure focus (e.g. 11
Mabbott and Smith, 2003; Nolan et al., 2004; Gonzalez et al., 2007). However, it should also 12
be noted that it is not unusual for adult left-TLE patients to demonstrate visual memory 13
deficits (e.g. Glosser et al., 2002; Smith et al., 2011). Moreover, the presence of deficits in 14
our left-TLE patients may be partly explained by a comparatively high proportion of children 15
with an abnormal hippocampus in this group. 16
17
Several limitations of the present study should be acknowledged. First, while our analyses 18
suggested that the side of seizure focus and presence of hippocampal structural abnormality 19
were not related to the recall of information after long delays, this non-significant finding 20
should be taken with caution, due to our limited sample size. Nevertheless, it is important to 21
note that such findings are consistent with several adult studies which provided evidence of 22
ALF in patients with TLE, but found that (i) the side of seizure focus was not related to 23
material specific memory deficits at long delays (Martin et al., 1991; Wilkinson et al., 2012) 24
and (ii) recall of information after long delays was not correlated with hippocampal volumes 25
Accelerated Long-Term Forgetting in TLE
37
(Narayanan et al., 2012) or the presence of structural lesions (Mameniskiene et al., 2006; 1
Wilkinson et al., 2012). As this is the first study to examine recall of newly-learned 2
information at long delays in children with TLE, it would be important to conduct large scale 3
studies which use volumetric and/or functional imaging data techniques to validate our 4
findings. Furthermore, instead of relying on visual inspection of clinically-obtained MRI data 5
alone, the use of quantified structural or functional neuroimaging data is likely to allow for a 6
more precise assessment of the relationship between ALF and hippocampal integrity. 7
8
Second, no attempt was made to monitor seizure activity during the retention period in the 9
current study. This lack of information on seizures during this interval is important, as ALF 10
has been associated with the frequency of epileptic seizures (Wilkinson et al, 2012) and with 11
subclinical discharges in a study that used EEG telemetry (Fitzgerald et al., 2013). Therefore 12
seizure activity should be monitored in future studies. Third, while we found consistent 13
evidence of an association between older age and worse recall of verbal information after 14
short and long delays in the TLE group, our study was cross-sectional, rather than 15
longitudinal, and thus only offers indirect evidence about trajectories of verbal memory 16
development in children with TLE. 17
18
Although not without some methodological limitations, our study identified a notable 19
memory deficit in children with TLE and therefore has several significant clinical 20
implications. Importantly, the results of this study suggest that memory deficits following 21
long delays in children with TLE may not be adequately addressed by standardised memory 22
tests. These tests can fail to detect a memory deficit and thereby lead clinicians to the false 23
conclusion that a child's memory is normal. As a consequence, this could potential lead to 24
additional anxiety and lowered self-esteem in children with TLE. Our data also extend 25
Accelerated Long-Term Forgetting in TLE
38
previous findings on the development of memory deficits in children with TLE, suggesting 1
that memory performance may progressively worsen from childhood to adolescence, relative 2
to their healthy control peers. Therefore, the monitoring of memory performance in patients 3
with TLE may be especially important between childhood and teenage years. 4
5
Acknowledgements 6
The authors thank the participants and their family members for their cooperation in this 7
study. We would also like to thank Joe Soliman and Safia Khalil for help in testing the 8
participants, and Drs. Jayne Antony, Cristina Go and Rajesh Ramachandran Nair for helping 9
with the recruitment of TLE patients. This work was supported by the Academy of the Social 10
Sciences in Australia (ASSA) International Science Linkages Scheme (SL and MLS); The 11
University of Sydney Thompson Fellowship (SL); a postgraduate scholarship from The 12
University of Sydney (MG); the Campbell Perry travel scholarship from the School of 13
Psychology, University of Sydney (MG) and a PhD completion scholarship from the 14
Australian Research Council Centre of Excellence in Cognition and its Disorders (MG). 15
16

Accelerated Long-Term Forgetting in TLE
39
References 1
Barr, W. B. (1997). Examining the right temporal lobe's role in nonverbal memory. Brain 2
and Cognition, 35(1), 26-41. 3
Baxendale, S. A., Thompson, P. J., & Paesschen, W. V. (1998). A test of spatial memory and 4
its clinical utility in the pre-surgical investigation of temporal lobe epilepsy patients. 5
Neuropsychologia, 36(7), 591-602. doi: 10.1016/s0028-3932(97)00163-2 6
Bell, B. D. (2006). WMS-III Logical memory performance after a two-week delay in 7
temporal lobe epilepsy and control groups. Journal of Clinical and Experimental 8
Neuropsychology, 28(8), 1435-1443. doi: 10.1080/13803390500434367 9
Bell, B. D., Fine, J., Dow, C., Seidenberg, M., & Hermann, B. P. (2005). Temporal lobe 10
epilepsy and the selective reminding test: The conventional 30-minute delay suffices. 11
Psychological Assessment, 17(1), 103-109. doi: 10.1037/1040-3590.17.1.103 12
Blake, R., Wroe, S., Breen, E., & McCarthy, R. (2000). Accelerated forgetting in patients 13
with epilepsy: evidence for an impairment in memory consolidation. Brain, 123, 472–483. 14
doi: 10.1093/brain/123.3.472 15
Breier, J. I., Plenger, P. M., Castillo, R., Fuchs, K., Wheless, J. W., Thomas, A. B., . . . 16
Papanicolaou, A. (1996). Effects of temporal lobe epilepsy on spatial and figural aspects of 17
memory for a complex geometric figure. Journal of the International Neuropsychological 18
Society, 2(6), 535-540. doi: 10.1017/S1355617700001703 19
Cohen, M. J. (1997). Children's Memory Scale (CMS). San Antonio, TX: The Psychological 20
Corporation. 21
Accelerated Long-Term Forgetting in TLE
40
Commission on Classification and Terminology of the International League Against 1
Epilepsy. (1989). Proposal for revised classification of epilepsies and epileptic syndromes. 2
Epilepsia, 30(4), 389-399. 3
Davidson, M., Dorris, L., O'Regan, M., & Zuberi, S. (2007). Memory consolidation and 4
accelerated forgetting in children with idiopathic generalized epilepsy. Epilepsy & Behavior, 5
11, 394-400. doi: 10.1016/j.yebeh.2007.05.004 6
Delis, D., Kramer, J., Kaplan, E., & Ober, B. (1994). California Verbal Learning Test - 7
Children's Edition. San Antonio, TX: The Psychological Corporation. 8
Fitzgerald, Z., Thayer, Z., Mohamed, A., & Miller, L. A. (2013). Examining factors related to 9
accelerated long-term forgetting in epilepsy using ambulatory EEG monitoring. Epilepsia, 10
54(5), 819-827. doi: 10.1111/epi.12090 11
Frisk, V., & Milner, B. (1990). The role of the left hippocampal region in the acquisition and 12
retention of story content. Neuropsychologia, 28(4), 349-359. doi: 10.1016/0028-13
3932(90)90061-R 14
Gascoigne, M. B., Barton, B., Webster, R., Gill, D., Antony, J., & Lah, S. S. (2012). 15
Accelerated long-term forgetting in children with idiopathic generalized epilepsy. Epilepsia, 16
53(12), 2135-2140. doi: 10.1111/j.1528-1167.2012.03719.x 17
Gathercole, S. E. (1998). The Development of Memory. Journal of Child Psychology and 18
Psychiatry, 39(1), 3-27. doi: 10.1111/1469-7610.00301 19
Giovagnoli, A. R., Casazza, M., & Avanzini, G. (1995). Visual Learning on a Selective 20
Reminding Procedure and Delayed Recall in Patients with Temporal Lobe Epilepsy. 21
Epilepsia, 36(7), 704-711. doi: 10.1111/j.1528-1157.1995.tb01050.x 22
Accelerated Long-Term Forgetting in TLE
41
Glosser, G., Cole, L., Khatri, U., DellaPietra, L., & Kaplan, E. (2002). Assessing nonverbal 1
memory with the Biber Figure Learning Test—Extended in temporal lobe epilepsy patients. 2
Archives of Clinical Neuropsychology, 17(1), 25-35. doi: http://dx.doi.org/10.1016/S0887-3
6177(00)00093-7 4
Gonzalez, L. M., Anderson, V. A., Wood, S. J., Mitchell, L. A., & Harvey, A. S. (2007). The 5
localization and lateralization of memory deficits in children with temporal lobe epilepsy. 6
Epilepsia, 48(1), 124-132. doi: 10.1111/j.1528-1167.2006.00907.x 7
Gonzalez, L. M., Mahdavi, N., Anderson, V. A., & Harvey, A. S. (2012). Changes in 8
memory function in children and young adults with temporal lobe epilepsy: A follow-up 9
study. Epilepsy & Behavior, 23(3), 213-219. doi: 10.1016/j.yebeh.2011.11.017 10
Helmstaedter, C., & Elger, C. E. (1998). Functional plasticity after left anterior temporal 11
lobectomy: Reconstitution and compensation of verbal memory functions. Epilepsia, 39(4), 12
399-406. doi: 10.1111/j.1528-1157.1998.tb01392.x 13
Helmstaedter, C., & Elger, C. E. (2009). Chronic temporal lobe epilepsy: a 14
neurodevelopmental or progressively dementing disease? Brain, 132(10), 2822-2830. doi: 15
10.1093/brain/awp182 16
Helmstaedter, C., Grunwald, T., Lehnertz, K., Gleißner, U., & Elger, C. E. (1997). 17
Differential involvement of left temporolateral and temporomesial structures in verbal 18
declarative learning and memory: evidence from temporal lobe epilepsy. Brain and 19
Cognition, 35(1), 110-131. doi: 10.1006/brcg.1997.0930 20
Helmstaedter, C., Hauff, M., & Elger, C. E. (1998). Ecological validity of list-learning tests 21
and self-reported memory in healthy individuals and those with temporal lobe epilepsy. 22
Accelerated Long-Term Forgetting in TLE
42
Journal of Clinical and Experimental Neuropsychology, 20(3), 365-375. doi: 1
10.1076/jcen.20.3.365.824 2
Helmstaedter, C., Pohl, C., Hufnagel, A., & Elger, C. E. (1991). Visual learning deficits in 3
nonresected patients with right temporal lobe epilepsy. Cortex, 27(4), 547-555. doi: 4
10.1016/S0010-9452(13)80004-4 5
Hepworth, S., & Smith, M. (2002). Learning and recall of story content and spatial location 6
after unilateral temporal-lobe excision in children and adolescents. Child Neuropsychol, 8(1), 7
16-26. doi: 10.1076/chin.8.1.16.8718 8
Hermann, B., Seidenberg, M., Schoenfeld, J., & Davies, K. (1997). Neuropsychological 9
characteristics of the syndrome of mesial temporal lobe epilepsy. Archives of Neurology, 10
54(4), 369-376. doi: 10.1001/archneur.1997.00550160019010 11
Hermann, B. P., Wyler, A. R., Richey, E. T., & Rea, J. M. (1987). Memory function and 12
verbal learning ability in patients with complex partial seizures of temporal lobe origin. 13
Epilepsia, 28(5), 547-554. doi: 10.1111/j.1528-1157.1987.tb03687.x 14
Jones-Gotman, M., Zatorre, R. J., Olivier, A., Andermann, F., Cendes, F., Staunton, H., . . . 15
Wieser, H. G. (1997). Learning and retention of words and designs following excision from 16
medial or lateral temporal-lobe structures. Neuropsychologia, 35(7), 963-973. doi: 17
10.1016/S0028-3932(97)00024-9 18
Lah, S., Mohamed, A., Thayer, Z. Miller, L. & Diamond, K. (2014). Accelerated long-term 19
forgetting of verbal information in unilateral temporal lobe epilepsy: Is it related to structural 20
hippocampal abnormalities and/or incomplete learning? Journal of Clinical and Experimental 21
Neuropsychology, 2, 158-169. doi:10.1080/13803395.2013.874405 22
Accelerated Long-Term Forgetting in TLE
43
Lendt, M., Helmstaedter, C., & Elger, C. E. (1999). Pre- and postoperative 1
neuropsychological profiles in children and adolescents with temporal lobe epilepsy. 2
Epilepsia, 40(11), 1543-1550. doi: 10.1111/j.1528-1157.1999.tb02038.x 3
Mabbott, D., & Smith, M. (2003). Memory in children with temporal or extra-temporal 4
excisions. Neuropsychologia, 41, 995–1007. doi: 10.1016/S0028-3932(02)00318-4 5
Mameniskiene, R., Jatuzis, D., Kaubrys, G., & Budrys, V. (2006). The decay of memory 6
between delayed and long-term recall in patients with temporal lobe epilepsy. Epilepsy & 7
Behavior, 8(1), 278-288. doi: 10.1016/j.yebeh.2005.11.003 8
Martin, R., Loring, D., Meador, K., Lee, G., Thrash, N., & Arena, J. (1991). Impaired long-9
term retention despite normal verbal learning in patients with temporal lobe dysfunction. 10
Neuropsychology, 5, 3–12. doi: 10.1037/0894-4105.5.1.3 11
Mayes, A., Isaac, C., Holdstock, J., Cariga, P., Gummer, A., & Roberts, N. (2003). Long term 12
amnesia: A review and detailed illustrative case study. Cortex, 39, 567-603. doi: 13
10.1016/S0010-9452(08)70855-4 14
Milner, B. (1968). Preface: Material-specific and generalized memory loss. 15
Neuropsychologia, 6(3), 175-179. doi: http://dx.doi.org/10.1016/0028-3932(68)90017-1 16
Mitchell, L. A., Harvey, A. S., Coleman, L. T., Mandelstam, S. A., & Jackson, G. D. (2003). 17
Anterior Temporal Changes on MR Images of Children with Hippocampal Sclerosis: An 18
Effect of Seizures on the Immature Brain? American Journal of Neuroradiology, 24(8), 19
1670-1677. 20
Muhlert, N., Grünewald, R. A., Hunkin, N. M., Reuber, M., Howell, S., Reynders, H., & 21
Isaac, C. L. (2011). Accelerated long-term forgetting in temporal lobe but not idiopathic 22
Accelerated Long-Term Forgetting in TLE
44
generalised epilepsy. Neuropsychologia, 49(9), 2417-2426. doi: 1
10.1016/j.neuropsychologia.2011.04.018 2
Narayanan, J., Duncan, R., Greene, J., Leach, J.-P., Razvi, S., McLean, J., & Evans, J. J. 3
(2012). Accelerated long-term forgetting in temporal lobe epilepsy: Verbal, nonverbal and 4
autobiographical memory. Epilepsy & Behavior, 25(4), 622-630. doi: 5
http://dx.doi.org/10.1016/j.yebeh.2012.06.038 6
Nolan, M. A., Redoblado, M. A., Lah, S., Sabaz, M., Lawson, J. A., Cunningham, A. M., . . . 7
Bye, A. M. E. (2004). Memory function in childhood epilepsy syndromes. Journal of 8
Paediatrics and Child Health, 40(1-2), 20-27. doi: 10.1111/j.1440-1754.2004.00284.x 9
Sass, K. J., Buchanan, C. P., Kraemer, S., Westerveld, M., Kim, J. H., & Spencer, D. D. 10
(1995). Verbal memory impairment resulting from hippocampal neuron loss among epileptic 11
patients with structural lesions. Neurology, 45(12), 2154-2158. doi: 10.1212/wnl.45.12.2154 12
Sass, K. J., Westerveld, M., Buchanan, C. P., Spencer, S. S., Kim, J. H., & Spencer, D. D. 13
(1994). Degree of hippocampal neuron loss determines severity of verbal memory decrease 14
after left anteromesiotemporal lobectomy. Epilepsia, 35(6), 1179-1186. doi: 10.1111/j.1528-15
1157.1994.tb01786.x 16
Scoville, W. B., & Milner, B. (1957). Loss of recent memory after bilateral hippocampal 17
lesions. Journal of Neurology, Neurosurgery and Psychiatry, 20(1), 11-21. 18
Sheslow, D., & Adams, W. (2003). Wide Range Assessment of Memory and Learning 2 19
(WRAML−2). Wilmington, DE: Wide Range, Inc. 20
Smith, M. L. (2010). Neuropsychology in epilepsy: Children are not small adults. Epilepsia, 21
51, 68-69. doi: 10.1111/j.1528-1167.2009.02451.x 22
Accelerated Long-Term Forgetting in TLE
45
Smith, M. L., Bigel, M., & Miller, L. A. (2011). Visual paired-associate learning: in search of 1
material-specific effects in adult patients who have undergone temporal lobectomy. Epilepsy 2
Behav, 20(2), 326-330. doi: 10.1016/j.yebeh.2010.11.019 3
Speechley, K. N., Sang, X., Levin, S., Zou, G. Y., Eliasziw, M., Smith, M. L., . . . Wiebe, S. 4
(2008). Assessing severity of epilepsy in children: preliminary evidence of validity and 5
reliability of a single−item scale. Epilepsy & Behavior, 13(2), 337−342. doi: 6
10.1016/j.yebeh.2008.05.001 7
Squire, L., Cohen, N., & Nadel, L. (1984). The medial temporal region and memory 8
consolidation: a new hypothesis. In H. Weingartner & E. Parker (Eds.), Memory 9
consolidation: psychobiology of cognition (pp. 185-210.). Hillsdale, NJ: Lawrence Elbaum. 10
Squire, L. R., & Alvarez, P. (1995). Retrograde amnesia and memory consolidation: a 11
neurobiological perspective. Current Opinion in Neurobiology, 5(2), 169-177. doi: 12
10.1016/0959-4388(95)80023-9 13
Sutula, T. P., Hagen, J., & Pitkänen, A. (2003). Do epileptic seizures damage the brain? 14
Current Opinion in Neurology, 16(2), 189-195. 15
Wechsler, D. (1999). Wechsler Abbreviated Scale of Intelligence (WASI). San Antonio, TX: 16
Harcourt Assessment. 17
Wilkinson, H., Holdstock, J. S., Baker, G., Herbert, A., Clague, F., & Downes, J. J. (2012). 18
Long-term accelerated forgetting of verbal and non-verbal information in temporal lobe 19
epilepsy. Cortex, 48(3), 317-332. doi: 10.1016/j.cortex.2011.01.002 20