
Abnormalities of auditory event-related potentials in schizophrenia prior to treatment
10
Abnormalities Schizophrenia of Auditory Event-Related Prior to Treatment Potentials in Yoshio Hirayasu, Naohiko Asato, Hirokazu Ohta, Hiroto Hokama, Hajime Arakaki, and Chikara Ogura Background: P300 amplitude reduction is a consistent finding in schizophrenic patients, but it is unclear if this abnormality predates neuroleptic treatment or is present at onset of illness. Methods: Auditory event-related potentials (ERPs), dur- ing a standard oddball paradigm, were ,'ecorded from 45 neuroleptic-naive schizophrenics, 56 drug-free, previously treated schizophrenics, and 73 healthy normal controls. Forty-seven of the schizophrenic subjects had their first episode within the past year. Results: N200 amplitude did not differ among groups. P300 amplitude was significantly smaller in both neuro- leptic-naive and previously treated schizophrenic groups compared to .the control groups. There were no significant differences between the two schizophremc groups in P300 amplitude. N200 and P300 latency were prolonged in previously treated schizophrenics compared to neurolep- tic-naive schizophrenics and normal controls. Conclusions:: The present study suggests that ERP abnor- malities, especially P300 amplitude reduction, are already present prior to the administration of ne,~roleptic medica- tion in the earliest stage of schizophrenia. Biol Psychi- atry 1998;43:244-253 © 1998 Society of Biological Psy- chiatry Key Words: Event-related potentials, schizophrenia, neu- roleptic-naive, first episode, N200, P300 Introduction W hile neurobiological abnormalities are consistently found in chronic-schizophrenia, these measures have most commonly been obtained well after the onset of symptoms and after the introduction of psychopharmaco- logic treatment in the late course of the disease. For From the Departrc~ent of Neuropsychiatry, University of the Ryukyus, Nishihara, Okinawa, Japan. Address reprint re~luests to Yoshio Hirayasu, MD, PhD, Harvard Medical School, Department o1' Psychiatry at Brockton VA Medical (enter (Psychiatry 116A), 940 Belmont Street. Brockton, MA 02401. Received May 24, 1996; revised November 12, 1996; revised March 24, 1997: revised May 5;, 1997; accepted May 15, 1997. example, event-related potentials (ERPs) to auditory stim- uli have been frequently reported to be abnormal in schizophrenia, but there are few data regarding whether this abnormality predates neuroleptic treatment or other changes associated with the onset of schizophrenia. ERPs provide a physiological measure of selective attention and processing of novel stimuli (Donchin and Coles 1988). In clinical studies, ERPs have been most commonly obtained with an "oddball" paradigm in which subjects are asked to count or respond to rare target stimuli that appear ran- domly among frequent nontarget stimuli. Task-relevant auditory stimuli elicit a negative deflection in the electro- encephalogram (EEG) at about 200-300 msec, the N200 component, as well as a positive deflection at 300-600 msec, the P300 component. N200 amplitude reduction has been reported in schizophrenia (Ogura et al 1991; O'Donnell et al 1993; Javitt et al 1995). Many studies have shown a reduction in the auditory P300 amplitude in patients with schizophrenia relative to controls, regardless of medication status (Pritchard 1986; Ogura et al 1987; Pfefferbaum et al 1989; McCarley et al 1991; Ohta et al 1993). In addition, prolongation of P300 latency in schizo- phrenics has been reported by several investigators (Blackwood et al 1987; St Clair et al 1989). From a psychological standpoint, reduction of P300 amplitude and prolongation of latency may reflect a failure to allocate attention resources to a stimulus (Polich 1987; Kramer and Strayer 1988). From a neurobiological perspective, re- duced amplitude may reflect grey matter abnormalities shown on quantitative magnetic resonance imaging (MRI) studies (McCarley et al 1993; O'Donnell et al 1993), and prolonged latency may indicate a neurodegenerative pro- cess (Polich et al 1990; O'Donnell et al 1995). Several methods, such as EEG, computed tomography, magnetic resonance imaging, positron emission tomogra- phy (PET), and single-photon emission computed tomog- raphy (SPECT) have provided evidence of structural and functional abnormalities in first-episode schizophrenics with a short duration of illness (Bogerts et al 1990; DeLisi et al 1991; Ebmeier et al 1993; Sponheim et al 1994; Hirayasu et al 1996). For example, Parellada et al (1994) © 1998 Society of Biological Psychiatry 0006-3223198l$19.00 PII S0006-3223(97)00275-8
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Abnormalities of auditory event-related potentials in schizophrenia prior to treatment
Abnormalities Schizophrenia
of Auditory Event-Related Prior to Treatment
Potentials in
Yoshio Hirayasu, Naohiko Asato, Hirokazu Ohta, Hiroto Hokama, Hajime Arakaki, and Chikara Ogura
Background: P300 amplitude reduction is a consistent finding in schizophrenic patients, but it is unclear if this abnormality predates neuroleptic treatment or is present at onset of illness.
Methods: Auditory event-related potentials (ERPs), dur- ing a standard oddball paradigm, were ,'ecorded from 45 neuroleptic-naive schizophrenics, 56 drug-free, previously treated schizophrenics, and 73 healthy normal controls. Forty-seven of the schizophrenic subjects had their first episode within the past year.
Results: N200 amplitude did not differ among groups. P300 amplitude was significantly smaller in both neuro- leptic-naive and previously treated schizophrenic groups compared to .the control groups. There were no significant differences between the two schizophremc groups in P300 amplitude. N200 and P300 latency were prolonged in previously treated schizophrenics compared to neurolep- tic-naive schizophrenics and normal controls.
Conclusions:: The present study suggests that ERP abnor- malities, especially P300 amplitude reduction, are already present prior to the administration of ne,~roleptic medica- tion in the earliest stage of schizophrenia. Biol Psychi- atry 1998;43:244-253 © 1998 Society of Biological Psy- chiatry
Key Words: Event-related potentials, schizophrenia, neu- roleptic-naive, first episode, N200, P300
Introduct ion
W hile neurobiological abnormalities are consistently found in chronic-schizophrenia, these measures
have most commonly been obtained well after the onset of symptoms and after the introduction of psychopharmaco- logic treatment in the late course of the disease. For
From the Departrc~ent of Neuropsychiatry, University of the Ryukyus, Nishihara, Okinawa, Japan.
Address reprint re~luests to Yoshio Hirayasu, MD, PhD, Harvard Medical School, Department o1' Psychiatry at Brockton VA Medical (enter (Psychiatry 116A), 940 Belmont Street. Brockton, MA 02401.
Received May 24, 1996; revised November 12, 1996; revised March 24, 1997: revised May 5;, 1997; accepted May 15, 1997.
example, event-related potentials (ERPs) to auditory stim- uli have been frequently reported to be abnormal in schizophrenia, but there are few data regarding whether this abnormality predates neuroleptic treatment or other changes associated with the onset of schizophrenia. ERPs provide a physiological measure of selective attention and processing of novel stimuli (Donchin and Coles 1988). In clinical studies, ERPs have been most commonly obtained with an "oddball" paradigm in which subjects are asked to count or respond to rare target stimuli that appear ran- domly among frequent nontarget stimuli. Task-relevant auditory stimuli elicit a negative deflection in the electro- encephalogram (EEG) at about 200-300 msec, the N200 component, as well as a positive deflection at 300-600 msec, the P300 component. N200 amplitude reduction has been reported in schizophrenia (Ogura et al 1991; O'Donnell et al 1993; Javitt et al 1995). Many studies have shown a reduction in the auditory P300 amplitude in patients with schizophrenia relative to controls, regardless of medication status (Pritchard 1986; Ogura et al 1987; Pfefferbaum et al 1989; McCarley et al 1991; Ohta et al 1993). In addition, prolongation of P300 latency in schizo- phrenics has been reported by several investigators (Blackwood et al 1987; St Clair et al 1989). From a psychological standpoint, reduction of P300 amplitude and prolongation of latency may reflect a failure to allocate attention resources to a stimulus (Polich 1987; Kramer and Strayer 1988). From a neurobiological perspective, re- duced amplitude may reflect grey matter abnormalities shown on quantitative magnetic resonance imaging (MRI) studies (McCarley et al 1993; O'Donnell et al 1993), and prolonged latency may indicate a neurodegenerative pro- cess (Polich et al 1990; O'Donnell et al 1995).
Several methods, such as EEG, computed tomography, magnetic resonance imaging, positron emission tomogra- phy (PET), and single-photon emission computed tomog- raphy (SPECT) have provided evidence of structural and functional abnormalities in first-episode schizophrenics with a short duration of illness (Bogerts et al 1990; DeLisi et al 1991; Ebmeier et al 1993; Sponheim et al 1994; Hirayasu et al 1996). For example, Parellada et al (1994)
© 1998 Society of Biological Psychiatry 0006-3223198l$19.00 PII S0006-3223(97)00275-8

ERP in Neuroleptic-Naive Schizophrenics BIOL PSYCHIATRY 245 1998 ;43:244 -253
Table 1. Demographic and Clinical Characteristics in Neuroleptic-Naive and Previously Treated Schizophrenics, and Controls Subjects
Neuroleptic-naive Previously treated Control p value
n 45 56 73 - - Age (years) 25.7 _+ 7.9 27.8 ± 9.2 27.0 _+ 8.7 NS Sex, M/F 32/13 32/24 45/28 - - Subtype, C/D/P/U 0/14/16/15 4/12/22/18 - - Age at onset (years) 23.1 ± 7.1 24.3 ± 8.7 NS Illness duration (years) a 2.7 4.0 NS BPRS, total 36.5 -+ 9.3 31.2 ± 12.4 .02
Values are mean _+ SD; otherwise, data are frequency counts. M, male; F, female; C, catatonic; D, disorganized; P, paranoid; U, undifferentiated; BPRS, Brief Psychiatric Rating Scale.
Illness duration is the average age at recording of ERPs minus age at onset of illness.
measured regional cerebral blood flow with SPECT in neuroleptic-naive acute schizophrenics. Schizophrenics had significantly higher prefrontal blood flow than did controls during resting conditions. PET studies have also revealed high glucose metabolism in the frontal lobe of neuroleptic-naive schizophrenics (Cleghorn et al 1989). These PET findings differ from that of hypofrontali ty reported in chronic patients previously treated with neu- roleptics. In addition, no significant alterations have been found in striatal D2 receptor densitie,; or affinities between the neuroleptic-naive schizophrenics and controls (Hietela et al 1994). On the other hand, previous neuroleptic treatment is known to increase the number of striatal D2 dopamine receptors (Burr et al 1977). One factor that may contribute to the differential results between neuroleptic- naive and chronic schizophrenia in PET studies is the
clinical state. Few ERP studies have included large samples of pa-
tients who have never been exposed to neuroleptic treat- ment. Introduction of neuroleptic and anticholinergic med- ication may influence neurobehavioral, cognitive, memory, and psychomotor perfo~anance (Frith 1984; Medal ia et al 1988; Spohn and Strauss 1989; Cassen et al 1990), and may cause prolonged change in cerebral dopamine-receptor occupancy (Baron et al 1989; Farde et al 1992). Consequently, two decades after the first report of P300 amplitude reduction in schizophrenia (Roth and Cannon 1972), it remains unclear ~hether the psychobio- logical abnormality is an early direct effect of the disease process, or secondary to treatment or other changes associated with chronic mental illness.
It would therefore be of considerable interest to know whether P300 amplitude reductiorL predates neuroleptic treatment and other lifestyle changes that occur after the first episode of schizophrenia. In this study, the auditory ERPs were recorded soon after illness onset from a large sample of schizophrenics who had never taken neuroleptic medication. This sample was compared to patients who had been previously treated, and tc normal controls.
Methods and Materials
Subjects All subjects were dextral as determined by the handedness questionnaire of Raczkowski and Kalat (1974). One hundred forty-four patients were recruited at the University of the Ryukyus Hospital, Okinawa, Japan and five hospitals that are associated with the University of the Ryukyus Hospital. Five patients were excluded due to change in diagnosis. Thirteen patients were excluded from this study due to problems during recording (i.e., movement of body or eyes, or high-frequency noise). Twenty-five of them were excluded due to low counting accuracy with less than 90%. Initial diagnosis was made by attendant psychiatrists at the outpatient clinic. Final diagnosis was made after interview by the authors' group at the Depart- ment of Psychiatry of the University of the Ryukyus Hospital. All patients met the DSM-III-R criteria for schizophrenia of the American Psychiatric Association (1980). The remaining 101 patients (64 male and 37 female) had not been treated with neuroleptic medication for at least 2 weeks prior to the experi- ment. Forty-five patients had never been treated with neurolep- tics, i.e., were neuroleptic-naive (NN), whereas 56 patients had been previously treated (PT). Absence of previous neuroleptic medication was verified during an interview with each patient and members of his/her family. Forty-seven patients (27 neuro- leptic-naive and 20 previously treated) experienced their first episode of psychosis within a year prior to ERP recordings. The descriptive data for the neuroleptic-naive and previously treated schizophrenic groups are presented in Table 1. A normal control group was recruited from the community and hospital staff. No control subjects had psychiatric histories. All the subjects, including the schizophrenic patients, were free of neurological diseases, mental retardation, and physical illnesses that might affect cognitive function or produce hearing loss. Informed consent to the experiment was obtained from the individual subjects.
Procedure Auditory ERPs were obtained using an oddball task. Stimuli consisted of a 1-kHz tone-burst (frequent, nontarget stimulus) and a 2-kHz tone-burst (rare, target stimulus). The respective

246 BIOL PSYCHIATRY Y. Hirayasu et al 1998 ;43:244 -253
probabilities of the rare and frequent stimuli were .2 and .8. Stimuli were presented in random order at 75 dB sound pressure level. Stimulus duration was 90 msec, with rise and fall times of 10 msec. The interstimulus interval was 1.7 ~ 0.1 sec. Forty artifact-free targets were obtained for each s'abject. To familiar- ize the subjects with the task, they were given short practice runs before the ERP recording. Subjects were ins:ructed to count the number of rare tones, and to report their cc,unt after each run; however, if counting accuracy was less than 90%, the subject was excluded from the experiment.
Scalp EEGs were recorded from 16 Ag-AgC1 disk electrodes placed at Fpl, Fp2, F7, F3, Fz, F4, F8, C3, C4, Th, P3, Pz, P4, T6, O1, and 02, according to the International 10/20 system. All the electrodes were referred to linked earlobes. Electrode imped- ance was maintained at less than 5 kfL The electro-oculogram (EOG) was recorded from electrodes placed ~.bove and below the
right eye. Amplifiers had a bandpass of 0.16 (time constant (tc) = 1.0 sec)-30 Hz. The EEGs and EOG were sampled at the rate of 2.4 msec per point with a laboratory computer (NEC- SANEI 7T18 and DPI200, Japan). ERPs were averaged sepa- rately for the rare and frequent stimuli. Trials were automatically rejected if at any point during the averaging epoch the voltage exceeded + 100 IxV in the EOG lead. The averaged potentials were baselined to the mean potential of the 120-msec period preceding them. Subjects were evaluated either in a morning session after breakfast (10-11 AM), or after lunch (1:30-2:30 PM).
Data Analysis
Measures of peak latency and peak amplitude for N200 and P300 were derived from the ERPs of individual subjects to rare target
Fpl
. J ~ L-,-, l
F7 F3 Fz
T5
C3
P3 Pz
Jr, l . .
Fp2
j._ek L_ j
F4
-1 C4
, _ _
P4 T6
O1 02
- - - - T 10/iV __1+
- , " --- 200 ms
Schizophrenics (neuroleptic-naive, N=45) Schizophrenics (previously treated, N=56)
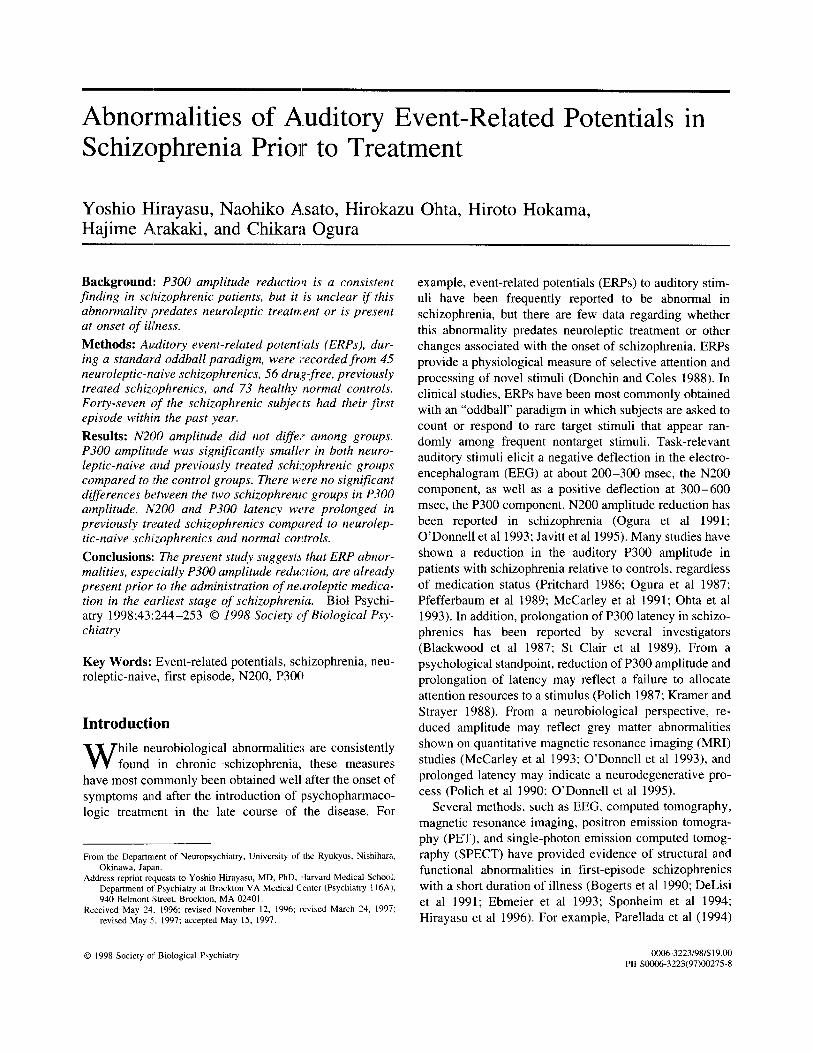
. . . . . Normal controls (N=73) Figure 1. Grand averaged target ERPs from 16 sites in neuroleptic-naive schizophrenics, previously treated schizophrenics, and normal
controls.
ERP in Neuroleptic-Naive Schizophrenics BIOL PSYCHIATRY 247 1998 ;43 :244-253
stimuli. The respective peaks were defined as the maximum negative voltage in the range of 180-290 msec, for N200, and the maximum positive voltage in the range: of 240-450 msec, for P300. To control for type I error, the; Greenhouse-Geisser correction was applied when appropriate to repeated measures (epsilon values are provided). A two-factor mixed [medication (neuroleptic-naive, previously treated, and normal controls)] analysis of variance (ANOVA) was first applied to the N200 and P300 data with midline electrodes (Fz, Pz) as a within factor. A four-factor mixed [medication X hemisphsre (F7, F3, T5, P3/F4, F8, P4, T6) x anterior/posterior (F7, F3, F4, F8/T5, P3, P4, T6) x medial/lateral (F3, F4, P3, P4/F7, F8, 'I'5, T6)] ANOVA was performed on both the N200 and P300 data from these lateral electrode sites. To test whether neuroleptic exposure or chronic- ity affected ERP component, two ANOVAs were applied. In the first ANOVA, four patient groups were constructed with the control group. The four patient groups are NN-first episode (n = 27), NN-multiple episode (n = 18), PT-first episode (n = 20), and PT-multiple episode (n = 36). A two-factor (group x electrode) ANOVA was then applied to the N200 and P300 data from midline electrodes (Fz, Pz). Additionally, a three-factor [medication (naive or previously treated) X episode (first or multiple) × electrode] ANOVA was applied for only the schizophrenic groups to the N200 and P300 data from midline electrodes (Fz, Pz). To test the gender di~Yference, a three-factor [medication x gender (male or female) x electrode] ANOVA was applied to the N200 and P300 latency and amplitude from midline electrodes (Fz, Pz).
Results
Behavioral Results
Counting accuracy across subjects was 98.6 + 2.1% for NN schizophrenics, 98.4 ± 2.4% for PT schizophrenics, and 99.6 --- 0.9% for the controls. These counting accu- racies were significantly different among the three subject groups [ F ( 2 , 1 7 1 ) = 8.4, p < .01] . Post hoc analyses by Tukey indicated that the accuracy of both NN and PT groups was significantly lower than that of normal con- trois (p < .05); however, analysis of covariance (AN- COVA) did not show that the effect of the counting accuracy was an indicator in predicting the ERP latency or amplitude.
ERP Results
Grand mean waveforms of ERPs to target stimuli at 16 electrodes in the two schizophrenic groups and the control group are shown in Figure 1. A negative-going peak can be seen at about 100 msec (NI00), fol lowed by a small positivity at about 175 msec (P200). Between 200 and 300 msec, there is another negative-going component (N200), fol lowed by a large posit ivity peaking at about 300 msec (P300). The waveforms for the patient groups and the control group clearly diverge after about 200 msec.
240
Jm
i
n----n.. . .nu...m_._ u 1-i. . [ 3 .
- - - . o . - ~ C o n t r o l (n=78) ] - - -El- - NN (n=45)
i . . - I - * PT (ri--56)
N=00 la tency ( m u ¢ ) ~ la tency ( m N ¢ )
I |
360 " l . . . . i - " " •
[ ] - - - O . .E l
(
200 320 F7 F3 Fz F4 F8 F7 F3 Fz F4 F8
b ! ,
220: - - - . . o E] 340
I 200 t 320 . - - - ,
T$ P3 Pz P4 T6 1"5 P3 Pz P4 T6
Electrode Electrode
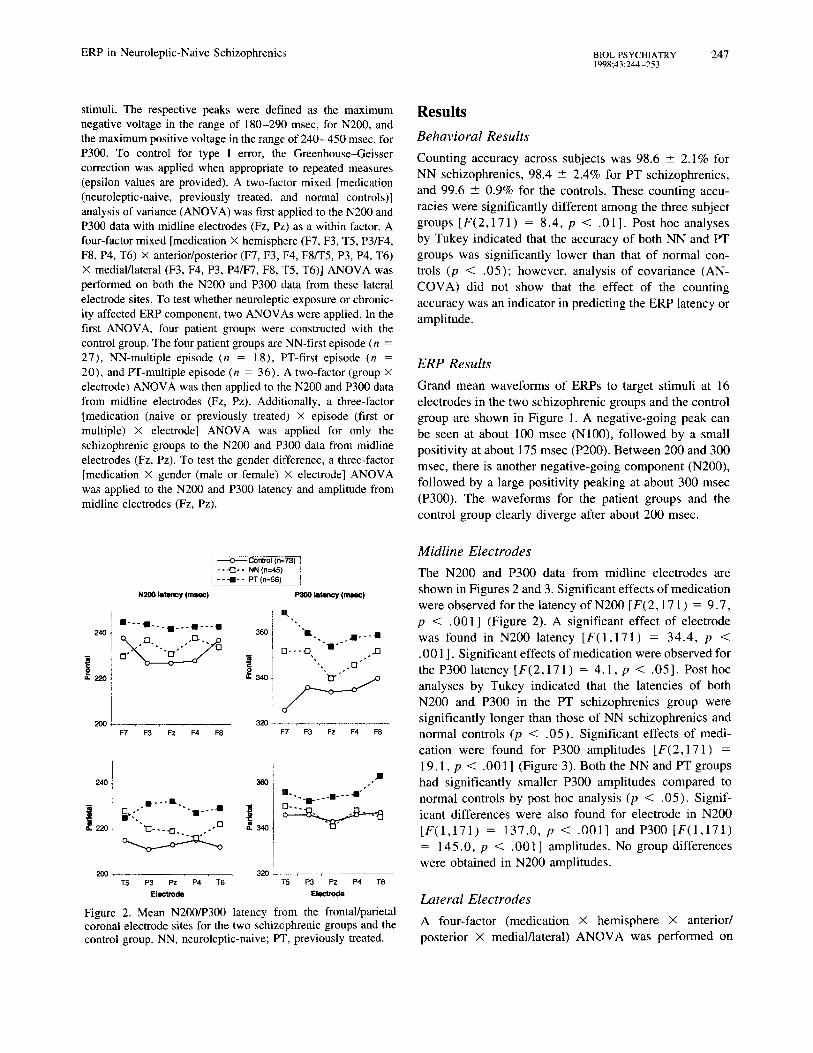
Figure 2. Mean N200/P300 latency from the frontal/parietal coronal electrode sites for the two schizophrenic groups and the control group. NN, neuroleptic-naive; PT, previously treated.
Midline Electrodes
The N200 and P300 data from midline electrodes are shown in Figures 2 and 3. Significant effects of medication were observed for the latency of N200 [ F ( 2 , 1 7 1 ) = 9 .7 , p < .001 ] (Figure 2). A significant effect of electrode was found in N200 latency [ F ( 1 , 1 7 1 ) = 34 .4 , p < .001 ]. Significant effects of medication were observed for the P300 latency [ F ( 2 , 1 7 1 ) = 4 .1 , p < .05 ]. Post hoc analyses by Tukey indicated that the latencies of both N200 and P300 in the PT schizophrenics group were significantly longer than those of NN schizophrenics and normal controls (p < .05) . Significant effects of medi- cation were found for P300 amplitudes [ F ( 2 , 1 7 1 ) = 19.1, p < .001 ] (Figure 3). Both the NN and PT groups had significantly smaller P300 amplitudes compared to normal controls by post hoc analysis (p < .05) . Signif- icant differences were also found for electrode in N200 [ F ( 1 , 1 7 1 ) = 137.0, p < .001] ~mdP300 [ F ( 1 , 1 7 1 ) = 145.0 , p < .001] amplitudes. No group differences
were obtained in N200 amplitudes.
Lateral Electrodes
A four-factor (medication X hemisphere X anterior/ posterior x medial/lateral) A N O V A was performed on

248 BIOL PSYCHIATRY Y. Hirayasu et al 1998;43:244-253
) ---..o---GontJ'ol (n=73) "l - - --(~- - N N ( n = 4 5 ) ;
] - - - I I - - PT (n=56)
N200 ~=rnl~ltude (pV)
15
~ , ~ . . ~ ~=1o . : . . . . / - s
-[3.- . . c3-
0
P3(O amp.rude (pv)
"[3
F7 F 3 Fz F4 F 8 F7 =3 Fz F4 F 8
0 i
/
-5 ~ - - ~ - ~ - ~ 0 1 T5 P3 Pz P4 T6 TM T5 P3 Pz P4 T6
E ! l e c t m d e E l e c t r o d e
Figure 3. Mean NZ00/P300 amplitude from the frontal/parietal coronal sites for the two schizophrenic grcups and the control group. NN, neuroleptic-naive; PT, previously treated.
both N200 and P300 data from the electrode sites shown in Figures 2 ~,nd 3. Significant effect ef medication was obtained for' N200 latency IF(2,171 = 8.1, p < .001 ]. Post hoc analyses indicated that the N200 latency in the PT schizophrenic group was significantly longer than those of NN schizophrenics and norraal controls (p < .05). The frontal leads yielded somewhat longer N200 latency than the posterior leads [F(1,171) = 83.0, p < .001 ]. The. factor of anterior/posteric,r x medial/lateral interacted with the group [F(2,171 ) = 7.2, p < .01]. A significant effect of medication w~,s also obtained in P300 latency [F(2,171) = 7.0, p < .011. Post hoc analyses indicated that the P300 latency in the PT schizo- phrenic group was significantly longer than those of normal controls (p < .05). Significant interactions in medication × anterior/posterior [F(2,171) --- 5.0, p < .01] and medication × hemisphere x anterior/posterior [F(2,171) = 3.5, p < .05] were found for P300 latency. These findings indicated that I'300 latencies in the left frontal electrodes were prolonged in the PT schizo- phrenics compared to normal controls.
No significant main effect of medication was found for N200 amplitude. Significant effects of medication group in N200 amplitude were found for the factors of hemi- sphere [F(1,171) = 5.5, p < .05] and anterior/ posterior electrodes [F(1,171 ) = 45.1, p < .001 ], and there were interactions of hemisphere x anterior/posterior
[F(1,171) = 4.5, p < .05], anterior/posterior X medial/lateral [F(1,171) = 109.5, p < .001], and hemisphere × anterior/posterior × medial/lateral IF( 1,171 ) = 7.2, p < .01 ]. These results indicated that N200 amplitude was larger (more negative) at right front-medial sites compared to other electrode sites; how- ever, none of these factors interacted with the medication group.
A significant main effect of medication was obtained for P300 amplitude [F(2,196) = 26.9, p < .001]. Both the NN and PT groups had significantly smaller P300 amplitudes compared to normal controls by post hoc analysis (p < .05). Significant differences were also found for anterior/posterior sites [F(1,171) = 133.3, p < .001 ] and medial/lateral sites [F( 1,171) = 200.0, p < .001]. The interactions of hemisphere × anterior/ posterior [F(1,171) = 5.6, p < .05], anterior/poste- rior × medial/lateral [F ( I , 171 ) = 15.4, p < .001], and hemisphere X anterior/posterior x medial/lateral [F(1,171) = 5.2, p < .05] were also significant. The data indicated that P300 amplitude at left frontolateral sites are larger (more positive) than those at right fronto- lateral electrode sites; however, these factors did not interact with group.
Normalization of the amplitude (McCarthy and Wood 1985) was applied for both N200 and P300 using the anterior coronal chain (F8, F3, Fz, F4, and F7) and the posterior coronal chain (T5, P3, Pz, P4, and T6), and results are shown in Figure 4. A three-factor (medica- tion X anterior/posterior x coronal chain) analysis of variance was performed with these normalized values. Significant effects of anterior/posterior [F(1,171) = 61.5, p < .001], and coronal chain [F(4,684) = 3.1, p < .05, e = .6], and interactions of anterior/poste- rior × coronal chain [F(4,684) = 57.8, p < .001, ~ = .8] were found for N200 amplitudes. None of them interacted with medication group. Significant effects of anterior/posterior [F(1,171) --- 158.0, p < .001] and coronal chain [F(4,684) = 135.0, p < .001, e = .5], and interactions of anterior/posterior X coronal chain [F(4,684) = 14.4, p < .001, E = .7] were also found for P300 amplitudes. Interactions of medication x anteri- or/posterior [F(2,171) = 5.6, p < .01], and medica- tion × anterior/posterior × coronal chain [F(8,684) = 2.8, p < .05, E = .7] were significant for P300 amplitudes. These findings suggest that distribution of P300 amplitude differed in midline frontal region among subject groups.
First Episode
To test whether neuroleptic exposure or chronicity af- fected the ERP components, two ANOVAs were applied.

ERP in Neuro lep t ic -Naive Schizophren ics BIOL PSYCHIATRY 249 1998;43:244 -253
: ---.o---Canb'ol (n=*~) ] : - - -1:3- - NN (n=45) I [ - - ' l - - PT (n=56)
N200 ampl i tude P300 amplitude 0.2 1 0.6 1
0.4 240 -
, ~ m
-O4
43.6 0 Fi' F3 FZ F4 F8 F7 F3 Fz F4 F8
S-
0.2 ~ 0.6
01 I . ' " " " . ¢' _ ! 0 , i
,'* I -s-
0.2 z -0.4 ~ I /
~ 1 0 I
-0.6 0 l T5 P3 PZ P4 T6 T5 P3 Pz P4 T6
Electrode Electrode
Figure 4. Normalized values from N20(I/P300 amplitude at the frontal/parietal coronal electrode sites for the two schizophrenic groups and the control group. NN, neuroleptic-naive; PT, previ- ously treated.
, - . - - 0 - ~ Control (n=73) j - - -C]- - NN-FE (n=27) I - - - & - * NN-ME (n=18) I - - - I - - PT-FE (n=20)
- - - & - - PT-ME (n--36)
" l
Fz Pz
-°I i i g !
~ 3 4 0 ~
f
32oi
• . . . . . . : : : : : |
Fz Pz
In the first, a two-factor (group X electrode) ANOVA was applied to the N200 and P300 data from midline electrodes (Fz, Pz) as shown in Figure 5. The four patient groups and controls did not differ with respect to age. Demographic information of the four patient groups are summarized in Table 2. Counting accuracies for target tones in the four schizophrenic groups were not different (NN-first episode, 98.6 - 1.9%; NN-muitiple episode, 98.6 +- 2.3%; PT-first episode, 98.4 - 2.1%; and PT-multiple episode, 98.3 -+ 2.6%).
A significant effect of group was found in N200 latency [F(4 ,169) = 8.8, p < .001]. A post hoc test (Tukey) indicated N200 latencies of the PT-first episode patient group were significantly longer than those of other patient groups and normal controls (p < .05). Neither effect of group nor interactions were significant for P300 latency. A significant group effect was also found for P300 amplitude [F(4 ,169) = 10.0, p < .001]. Post hoc test also showed that P300 amplitudes of the four schizophrenic groups were smaller than those of normal controls (p < .05). The N200 amplitude did not differ among groups.
Additionally, a three-factor (medication x episode x electrode) ANOVA was applied for only the schizophrenic groups to the N200 and P300 data from midline electrodes. Significant effects of medication [F(1,97) = 9.9, p < .01] and episode [F(1 ,97) = 5.2, p < .01] were found
15-
A
S ~ 10.
I s .
S ~ ¢- , ;£-
FZ Pz FZ PZ Electrode Eloctmdo
Figure 5. Mean N200/P300 amplitude and latency from the midline electrode sites for the four schizophrenic groups and the control group. NN, neuroleptic-naive; PT, previously treated; FE, first episode; ME, multiple episode.
for latency of N200. A significant interaction of medica- tion × episode was also obtained for N200 latency [F(1 ,97) = 6.5, p < .05]. These findings indicated that N200 latency of PT-first episode schizophrenics was longer than that of the other schizophrenic groups. No significant effect of medication or episode was obtained for P300 latency. Neither medication nor episode effects were found for the amplitude of N200 and P300 among the four schizophrenic groups.
Gender
A three-factor (medication x gender x electrode) ANOVA was applied as shown in Figure 6. The age of the subjects did not differ significantly. Significant effects of medication [F(2 ,168) = 10.2, p < .001] and gender [F(1 ,168) = 4.9, p < .05] and an interaction of medication x gender [F(2 ,168) - 3.1, p < .05] were found for N200 latency. These findings suggested that N200 latency in female subjects was shorter than that of male subjects. A significant effect of medication [F(2 ,168) = 4.2, p < .05] was also found in P300 latency. There was no main effect of gender or interaction of medication and gender for P300 latency. Significant effects of both medication [F(2,168) = 17.1, p < .001] and gender [F(1,168) = 6.8, p < .01] were obtained for P300 amplitude. There was no signi-

250 BIOL PSYCHIATRY Y. Hirayasu et al 1998:43:244 253
Table 2. Demographic and Clinical Characteristics in Four Schizophrenic Groups Divided by Neuroleptic Experience and Episode (First or Multiple)
Neurolept ic-naive Previously treated
First Multiple First Multiple p value
n 27 18 20 36 - -
Age (years) 23.9 + 7.7 28.4 _+ 7.5 25,5 -+ 8.6 29.1 +- 9.4 NS
Sex, M/F 16/11 16/2 11/9 21/15 - -
Subtype, C/D/Pied 0/9/10/8 0/5/6/7 3/5/7/5 1/7/15/13 - -
Age at onset (years) 23.4 _+ 7.5 22.5 _+ 6.2 26.3 _+ 10.7 23.1 _+ 7.3 NS
Illness durat ion (years) ~ 0.4 6.3 0.5 6.0 < . 0 l
BPRS, total 38.0 -+ 10.0 34.3 + 7.8 29.2 -+ 15.3 32.4 _+ 7.8 NS
Values are mean +- SD; otherwise, data are frequency counts. M, male; F, female; C. catatonic; D, disorganized; P, paranoid; U, undifferentiated; BPRS, Brief Psychiatric Rating Scale.
Illness duration is the average age at recording of ERPs minus age at onset of illness.
ficant interaction of medication × gender for P300 amplitude. These data suggested that 13300 amplitude in female subjects was larger than that of male subjects. No significant effect of gender was found for N200 amplitude.
Discussion
In this study, ERPs using the auditory oddball paradigm on neuroleptic-naive schizophrenics, patien:s withdrawn from medication, and normal controls were recorded. P300 amplitude reduction was evident in patients who had never been exposed to neuroleptics, and this reduction was comparable to that of patients who had been treated with neuroleptic medication. Therefore, P300 amplitude reduc- tion in schizophrenia does not appear to result from chronicity, l,ong-term medication, or other changes in lifestyle associated with chronic schizophrenia. Prolonged N200 and P300 latencies in schizophrenics were also found in this study. Post hoc analyses indicated thal the latencies of both N200 and P300 in the previously treated patient group were significantly longer than those of neuroleptic-naive schizophrenics and normal controls at the midline electrodes.
Over the past two decades, overwhehning evidence has accumulated that schizophrenia is assaciated with both physiological and anatomical abnormalities in the brain. Data from the present study suggests that the reduction of P300 amplitude often noted in treated patients is, in fact, present at illness onset. This abnormality may be a traitlike feature of the illness, in that in the present data it is unchanged in patients with slightly longer disease duration who have been treated with neuroleptic medication. Sim- ilarly, other studies have demonstrated that changes in medication status (Ford et al 1994) and age (O'Donnell et al 1995) have little, if any, effect on ?300 amplitude in schizophrenia; however, the studies by Levit et al (1973) and Duncan et al (1987) suggested improvement of P300
amplitude when medication was associated with improved clinical status. Preliminary follow-up studies from our group also suggest that P300 amplitude improved after treatment in schizophrenics. This improved P300 ampli- tude, however, still did not return to the level of normal controls (Asato et al 1996; Hirayasu and Ogura 1996). Therefore, P300 amplitude abnormalities in schizophren- ics could be both a trait- and a state-dependent deficit. Further studies are required to clarify the change of P300 amplitude associated with specific clinical status and treatment.
P300 amplitude reduction is apparent soon after the onset of psychotic symptoms; however, the question of whether it predates illness onset remains unresolved. High-risk studies have not, as yet, provided evidence of P300 amplitude reduction prior to the first psychotic episode (Friedman et al 1988; Schreiber et al 1991; Ogura et al 1994). In conjunction with the present data, such results are consistent with the hypothesis that reduced P300 amplitude may be a marker of the biological changes that initiate psychotic symptoms, rather than a marker of vulnerability. In this respect, findings of P300 amplitude reduction in schizotypal subjects (Salisbury et al 1996) suggest that these individuals may be showing a muted expression of the schizophrenic process, consistent w i t h evidence for the genetic association between schizophre- nia and schizotypal personality disorder.
Although topographic P300 asymmetry in schizophren- ics has been reported, topographic asymmetry for ERP components was not found in neuroleptic-naive schizo- phrenics compared to controls. Electrodes were placed at T5/T6 instead of T3/T4, the location where deficits were most strongly lateralized in prior studies. Hence, different electrode placements may have contributed to the lack of ERP asymmetry in our results. Another influence on P300 topography is performance accuracy. In this study, the counting accuracy for target tones in the schizophrenic groups was significantly lower than for normal controls,

ERP in Neuroleptic-Naive Schizophrenics B1OL PSYCHIATRY 25 l 1998;43:244-253
24O
- - - -O- - -Cont ro l (n--45) - - -El- - NN (n=32} - - -,11- - PT (n=32)
role
O - . . . " ' ' B
180 FZ PZ
360
1 I
32o;
5 - Fz Pz
24O
220-
200- i
180
360-
34O
32O
57
! - - -O-- - -Cont ro l (n--28) i I - - - O - - NN(n=13) I I " " -IB- - PT (n=24)
t3
Fz Pz
• . . . . . . . . . . . •
t .o
Fz Pz
g ! = 0 Q. | | J
-5 - Fz Pz Fz Pz
+o! +o- . : . : . -
. , , ~ o . . + I r * * "-'+
==.si ,.. i i
o ; o~ Fz Pz Fz Pz
F l ~ t m d A Electrode
Figure 6. Mean N200/P300 amplitude and latency from the midline electrode sites for the two schizophrenic groups and the control group according to gender. NN, neuroleptic-naive; PT, previously treated.
although the difference was off by only 1% relative to controls. Error trials could lead to a different P300 topographic distribution than correct trials (Gehring et al 1995); however, an additional ANCOVA failed to show that the counting accuracy effect is an indication in predicting the P300 amplitude in this study.
N200 abnormalities to auditory ~timuli have been re- ported in schizophrenics. In some Sttldies, the amplitude of N200 has been reported to be smaller in schizophrenics (Ogura et al 1991 ; O'Donnell et al 1'993; Javitt et al 1995). N200 amplitude reduction may be a later effect of the
disease process (apparent in chronic patients by O'Donnell et al 1993; Ford et al 1994); however, N200 amplitude was not significantly different in the present study, possibly due to an overlap between N200 and P300. The controls had a large-amplitude P300, which may have reduced the preceding N200; the schizophrenic group showed the reverse effects. This overlap could potentially account for the absence of an N200 amplitude effect in our study.
P300 has been described in terms of stimulus evalua- tion, decision making, context updating, and neuronal reset indexing postdecision closure mechanisms (Donchin et al 1978; Pritchard 1981). Reduction of P300 amplitude may be an indication of diminished capacity to generate probability-based expectancies. The N200 likely reflects both automatic (i.e., mismatch detection) and controlled information processing (i.e., expectancy mismatch), target discrimination and classification (N~i~it~nen and Picton 1986). The present study suggests that N200 and P300 abnormalities predate the administration of neuroleptic medication in the earliest stage of schizophrenia. The ERP abnormalities of neuroleptic-naive schizophrenics imply a deficit of cognitive function before medication. Delayed N200 and P300 latency have typically been associated with aging and dementing illness, and have been inter- preted as a slowing of cognitive processing speed. In this study, both the N200 and the P300 were prolonged in previously treated schizophrenia, which may be related to treatment with neuroleptics.
The authors greatly thank Dr. R.W. McCarley, Dr. B.F. O'Donnell, and Dr. J.E. Anderson of Harvard Medical School for critical reading of the manuscript. We also would like to thank Mrs. Toshiko Tamanaha for technical assistance.
References
American Psychiatric Association (1980): Diagnostic and Sta- tistical Manual of Mental Disorders, 3rd ed rev. Washington, DC: American Psychiatric Press.
Asato N, Hirayasu Y, Ogura C, et al (1996): Are event-related potential abnormalities in schizophrenics trait or state depen- dent? In: Ogura C, Koga Y, Shimokochi M, editors. Recent Advances in Event-Related Brain Potential Research. Am- sterdam: Elsevier, pp 564-567.
Baron JC, Marinot JL, Cambon H, et al (1989): Striatal dopamine receptor occupancy during and following withdrawal from neuroleptic treatment: Correlative evaluation by positron emission tomography and plasma prolactin levels. Psycho- pharmacology 99:463-472.
Blackwood DH, Whalley LJ, Christie JE, Blackburn IM, St Clair D, McInnes A (1987): Changes in auditory P3 event-related potential in schizophrenia and depression. Br J Psychiato, 150:154-160.

252 BIOL PSYCHIATRY Y. Hirayasu et al 1998;43:244-253
Bogerts B, Ashtari M, Degreef G, Alvir JM, Bilder RM, Lieberman JA (1990): Reduced temporal limbic structure volumes on magnetic resonance images in first episode schizophrenia. Psychiatry Res 35:1-13.
Burr DR, Creese I, Snyder SH (1977): Antischizophrenic drugs: Chronic treatment elevates dopamine receptor binding in brain. Science 196:326-328.
Cassen G, Inglis AK, Appelbaum PS, Guthel TG (1990): Neuroleptics: Effects on neuropsychological function in chronic schizophrenic patients. Schizoph~" Bull 16:477-499.
Cleghorn JM, Garnett ES, Nahmias C, et 5.1 (1989): Increased frontal and reduced parietal glucose rrLetabolism in acute untreated schizophrenia. Psychiatry Res 28:119-133.
DeLisi LE, Hoff AL, Schwartz JE, et al (19!}1): Brain morphol- ogy in first-episode schizophreniclike p~,;ychotic patients: A quantitative magnetic resonance imaging study. Biol Psychi- atry 29:15'9 -175.
Donchin E, Coles MGH (1988): Is the P300 component a manifestation of context updating? Behae Brain Sci 11:357- 373.
Donchin E, Ritter W, McCallum WC (19781: Cognitive psycho- physiology: The endogenous componertts of the ERP. In: Callaway E, Tueting P, Koslow S, editors. Event-Related Brain Potentials in Man. New York: Academic Press, pp 349 -442.
Duncan CC, Morihisa J, Fawcett RW, Kirch DG (1987): P300 in schizophrenia: State or trait marker? Psychopharmacol Bull 23:497-513,1.
Ebmeier KP, Blackwood DHR, Murray C, et al (1993): Single- photon emission computed tomography with 99n~Tc-examet- azine in unmedicated schizophrenic patients. Biol Psychiatry 33:487-495.
Farde L, Nordstrom A, Wiesel F, Pauli S, Hallidin C, Sedvall G (1992): Positron emission tomographic aaalysis of central D 1 and D2 dopamine receptor occupancy in patients treated with classical neuroleptics and clozapine. Arch Gen Psychiatry 49:538-544.
Ford JM, White PM, Csernansky JG, Faustman WO, Roth WT, Pfefferbaum A (1994): ERPs in schizophrenia: Effects of antipsychotic medication. Biol Psychiatry 36:153-170.
Friedman D, Cornblatt B, Vaughan HJ, Erlenmeyer KL (1988): Auditory event-related potentials in children at risk for schizophrenia: The complete initial sample. Psychiat~ Res 26:203-221.
Frith CD (1984): Schizophrenia, memory and anticholinergic drugs. J Abnorm Psychol 98:341-356.
Gehring WJ, Coles MGH, Meyer DE, Donclain E (1995): A brain potentials' manifestation of error-related processing. In: Kar- mos G, Molnar M, Csepe V, Czigler I, Desmedt JE, editors. Perspectives of Event-Related Potentials Research (EEG suppl 40). Amsterdam: Elsevier, pp 261-272.
Hietela J, Syvalahti E, Vuorio K, et al (1994): Striatal D2 dopamine receptor characteristics in neuroleptic-naive schizophrenic patients studied with posi'xon emission tomog- raphy. Arch Gen Psychiatry 51:116-123.
Hirayasu Y, Ogura C (1996): Event-related potential (ERP) abnormalities in schizophrenia: Effects of subtype, clinical course, neuroleptic medication and clinical symptoms. In: Ogura C, Koga Y, Shimokochi M, editors. Recent Advances
in Event-Related Brain Potential Research. Amsterdam: Elsevier, pp 922-929.
Hirayasu Y, Shenton ME, Dickey CC, et al (1996): Brain CSF volume in patients with first episode psychosis (abstract). Biol Psychiatry 39:519.
Javitt DC, Doneshka P, Grochowski S, Ritter W (1995): Im- paired mismatch negativity generation reflects widespread dysfunction of working memory in schizophrenia. Arch Gen Psychiatry' 52:550-558.
Kramer AF, Strayer DL (1988): Assessing the development of automatic processing: An application of dual-task and event- related brain potential methodologies. Biol Psychol 26:231- 267.
Levit R, Sutton S, Zubin J (1973): Evoked potential correlates of information processing in psychiatric patients. Psychol Med 3:487-494.
McCarley RW, Faux SF, Shenton ME, Nester PG, Adams J (1991): Event-related potentials in schizophrenia: Their bio- logical and clinical correlates and a new model of schizo- phrenic pathophysiology. Schizophr Res 4:209-231.
McCarley RW, Shenton ME, O'Donnell BF, et al (1993): Auditory P300 abnormalities and left posterior superior tem- poral gyrus volume reduction in schizophrenia. Arch Gen Psychiatry 50:190-197.
McCarthy G, Wood CC (1985): Scalp distributions of event- related potentials: An ambiguity associated with analysis of variance models. Electroencephalogr Clin Neurophysiol 62: 203-208.
Medalia A, Gold J, Merriam A (1988): The effects of neurolep- tics on neuropsychological test results of schizophrenics. Arch Clin NeuropsychoI 3:249-271.
N~i~it~inen R, Picton TW (1986): N2 and automatic vs controlled processes. In: McCallum WC, Zappoli R, Denoth F, editors. Cerebral Psychophysiology: Studies in Event-related Poten- tials (EEG suppl 38). New York: Elsevier, pp 169-178.
O'Donnell BF, Shenton ME, McCarley RW, et al (1993): The auditory N2 component in schizophrenia: Relationship to MRI temporal lobe gray matter and to other ERP abnormal- ities. Biol Psychiatry 34:26-40.
O'Donnell BF, Faux SF, McCarley RW, et al (1995): Increased rate of P300 latency prolongation with age in schizophrenia. Arch Gen Psychiatry 52:544-549.
Ogura C, Nageishi Y, Shimokochi M (1987): Evaluation of event-related potentials in schizophrenia using principal com- ponent analysis. In: Johnson R, editor. Current Trend in Event-Related Potential Research. Amsterdam: Elsevier, pp 733-737.
Ogura C, Nageishi Y, Matsubayashi M, Omura F, Kishimoto A (1991): Abnormalities in event-related potentials, NI00, P200, P300 and slow wave in schizophrenia. Jpn J Psychia- try, Neurol 45:57-65.
Ogura C, Hirano K, Nageishi Y, et al (1994): Deviate P200 and P300 in non-patient college students with high scores on the schizophrenia scale of the Minnesota Multiphasic Personality Inventory (MMPI). Int J Psychophysiol 16:89-97.
Ohta H, Hokama H, Fukao K, Hirano K, Ogura C (1993): Cognitive impairment in schizophrenic patients on event- related potentials component P300. Psychiatr Neurol Jpn 95:439-452.

ERP in Neuroleptic-Naive Schizophrenics BIOL PSYCHIATRY 253 1998;43:244-253
Parellada E, Catafau AM, Bernardo M, Lomena F, Gonzales- Monclus E, Setoain J (1994): Prefrontal dysfunction in young acute neuroleptic-naive schizophrenic patients: A resting and activation SPECT study. Psychiatr Res 55:131-139.
Pfefferbaum A, Ford JM, White PM, Roth WT (1989): P3 in schizophrenia is affected by stimulus modality, response requirements, medication status, ard negative symptoms. Arch Gen Psychiat~ 46:1035-1044.
Polich J (1987): Task difficulty, probability, and inter-stimulus interval as determinants of P300 from auditory stimuli. Electroencephalogr Clin Neurophysiol 68:311-320.
Polich J, Ladish C, Bloom FIE (1990): P300 assessment of early Alzheimer's disease. Electroencephalogr Clin Neurophysiol 77:179-189.
Pritchard WS (1981): Psychophysiologi¢ of P300. Psychol Bull 89:506 -540.
Pritchard WS (1986): Cognitive event-related potential correlates of schizophrenia. Psychol Bull 100:43-66.
Raczkowski D, Kalat JW (1974): Reliability and validity of some handedness questionnaire items. Neuropsychologia 12:43- 47.
Roth WT, Cannon EH (1972): Some features of the auditory evoked response in schizophrenia. Arch Gen Psychiatry 27:466-471.
Salisbury DF, Voglmaier MV, Seidman LJ, McCarley RW (1996): Topographic abnormalities of P3 in schizotypal per- sonality disorder. Biol PsychiatD, 40:165-172.
Schreiber H, Stolz-Born G, Rothmeier J, Kornhuber A, Kornhu- ber HH, Born J (1991): Endogenous event-related brain potentials and psychometric performance in children at risk for schizophrenia. Biol Psychiatry 30:177-189.
Spohn HE, Strauss ME (1989): Relation of neuroleptic and anticholinergic medication to cognitive functions in schizo- phrenia. J Abnorm Psychol 98:367-380.
Sponheim SR, Clementz BA, Iacono WG, Beiser M (1994): Resting EEG in first-episode and chronic schizophrenia. Psychophysiology 31:37-43.
St Clair D, Blackwood D, Muir W (1989): P300 abnormality in schizophrenic subtypes. J Psychiatr Res 23:49-55.




















