
Finite element analysis of actively controlled smart plate with patched actuators and sensors
Upload
teknologimalaysiaCategory
view
1download
0
0016-5107/91/3703-0299$03.00GASTROINTESTINAL ENDOSCOPYCopyright © 1991 by the American Society for Gastrointestinal Endoscopy
A randomized comparative study of laserphotocoagulation, heater probe, and bipolarelectrocoagulation in the treatment ofactively bleeding ulcers
W. M. Hui, MD, M. M. T. Ng, MBBSA. S. F. Lok, MBBS, C. L. Lai, MBBS
Y. N. Lau, MBBS, S. K. Lam, MDHong Kong
A randomized study was performed to compare the efficacy of Nd:YAG laser,heater probe, and bipolar electrocoagulation in the treatment of active bleedingfrom peptic ulcers. Nine hundred and forty-eight consecutive patients with uppergastrointestinal bleeding underwent endoscopy and 91 patients with activebleeding from peptic ulcer were randomized to receive laser (N =30), heaterprobe (N =31), and bipolar electrocoagulation (N =30). The angulation of theprobe to the ulcer base was assessed at endoscopy. The three treatment groupswere comparable in their clinical and endoscopic characteristics. There was nosignificant difference among patients treated with laser, heater probe, and bipolarelectrocoagulation in the rate of re-bleeding (10%, 19.4%, and 10%), duration ofhospital stay (4, 4, and 5 days), and proportion requiring emergency surgery (7%,13%, and 7%), but the cost per patient was higher with laser than heater probeand bipolar electrocoagulation. The angulation of the probe to the ulcer base didnot affect the re-bleeding rate. No complication was reported. We conclude thatthe three modalities were equally effective and safe in endoscopic hemostasisbut because bipolar electrocoagulation and heater probe were cheaper, they wererecommended for use. (Gastrointest Endosc 1991;37:299-304)
Gastrointestinal bleeding complicating peptic ulcerremains a major clinical problem. 1, 2 Despite the development of multiple therapeutic agents that promote ulcer healing, the incidence of emergency surgeryfrom bleeding ulcers has not declined significantly.3In recent years, randomized controlled trials havedemonstrated the efficacy of laser photocoagulation,4,5
bipolar electrocoagulation,6,7 and heater probes in thetreatment of gastrointestinal bleeding from peptic ulcer. These measures reduce re-bleeding and the needfor emergency surgery which is associated with a 25%mortality rate compared with 3% when surgery forpeptic ulcer is performed electively.9 It has generallybeen agreed that endoscopic therapy is indicated in
Received July 2, 1990. For revision November 1, 1990. AcceptedFebruary 25, 1991.From the Department of Medicine, University of Hong Kong, QueenMary Hospital, Hong Kong. Reprint requests: W. M. Hui, MD,Department of Medicine, University of Hong Kong, Queen MaryHospital, Pokfulam Road, Hong Kong.
VOLUME 37, NO. 3, 1991
patients with actively bleeding ulcers. lO However, randomized comparisons between the three modalitieshave not been performed in patients with active bleeding from peptic ulcers. It is known that variability inentry criteria hampered the comparability betweenvarious trials and thus comparison of the three modalities should ideally be conducted in one center. Weundertook the following randomized study to assessthe efficacy of these three modalities in the treatmentof actively bleeding ulcers. Previous studies have indicated that the use of firm pressure is important inthe control of bleeding from lesions in experimentalbleeding ulcersY The angulation of the probe to theulcer base, which is directly related to the pressureapplied, was prospectively evaluated in the study presented here.
METHODS
Patients admitted to the University Medical Unit, QueenMary Hospital, for emergency gastrointestinal bleeding were
299

recruited into the study after active resuscitation. Endoscopywas performed within 24 hours of admission. The possibilityof therapeutic intervention was explained to the patientand/or their relatives and consent for therapeutic intervention obtained before endoscopy. Endoscopy was performedwith Olympus GIF-2TlO end-viewing endoscopes with twochannels (2.8, 3.8 mm) to allow for suction/flushing via onechannel and therapeutic intervention via the other channel.Patients were included in the study if they had activebleeding from the ulcer at the time of endoscopy. Theseincluded arterial spurters and oozing from the ulcer basewith and without visible vessels. Visible vessel was definedas a raised red or black spot on the ulcer base. Clots on topof oozing visible vessels were washed vigorously with coldsaline to allow therapeutic coagulation of the bleeding visiblevessels. When the clot could not be removed after repeatedflushing, the probes were applied to the rim of the base ofthe bleeding point. Patients were excluded from the study ifthey were younger than 18 years of age, did not or could notgive consent, or had multiple ulcers or superficial lesionsless than 5 mm. Gastric ulcers which were malignant onbiopsy were also excluded. After admission, the patientswere actively resuscitated with intravenous plasma andblood transfusion and the vital signs closely monitored. Theywere randomized to receive laser photocoagulation, heaterprobe, and bipolar electrocoagulation. Randomization wasperformed during endoscopy and this was done by drawinglots from sealed envelopes. Equal number of lots for eachtreatment, in series of 10 patients for each group, wereincluded in the envelopes.
The study was approved by the Ethics Committee, University of Hong Kong.
Patients
The characteristics of the patients were prospectivelyobtained. These included symptomatology, e.g., history ofpain, past medical diseases, onset of gastrointestinal bleeding (time between first detecting hematemesis/melena andendoscopy); personal history including smoking and analgesic intake; and vital signs on admission, hemoglobin level,and serum renal and liver biochemistries. Patients wererecorded as chronic analgesic users if standard doses ofanalgesic were used at least once per week in the previous 6months and acute analgesic users if drugs were taken 48hours before the onset of bleeding. Presence of shock wasdefined in this study as systolic blood pressure less than 100mm Hg and/or pulse >100/min.
In addition the following characteristics were noted onendoscopy. The visibility of the field, as indicated by thedegrees of interference with the visual field by the presenceof blood, mucus, and movement of the stomach, was gradedgood, satisfactory, or poor. The degree of cooperation of thepatient was also graded good, satisfactory, or poor. Thesefactors theoretically may affect the endoscopic techniqueand therefore the success of treatment.
Laser treatment
The Cooper Lasersonics 8000 system delivered Nd:YAGlaser energy with continuous wave infrared wave length of1064 nm with a maximum power of 150 watts. The powerwas transmitted through a flexible fiber introduced through
300
one of the biopsy channels of the endoscope. The fiber washeld 1 cm from the ulcer base and the power setting used inthe present trial was 70 watts with 0.5-sec pulses. Photocoagulation was carried out around the vessel and subsequentlyon the vessel itself, aiming at stopping the bleeding withwhitening of the coagulation spot. Careful brushing andwashing of the tip was performed between applications ifthere was tissue stuck to the tip of the fiber.
Bipolar electrocoagulation
A 50-watt BlCAP'" unit (ACMI, Stanford, Conn.) wasused at a setting of 7 and bursts of 2 sec were used. Thelarge BICAP'" probe was used (3.2 mm). Firm pressure wasapplied to the visible vessel at the ulcer base to stop bleeding,and electrocoagulation started from the area immediatelysurrounding the vessel followed by the vessel itself. Whenbleeding stopped, one additional burst was applied afterwhitening of the tissue.
Heater probe
The Olympus heater probe HPU unit (Olympus Co.,Tokyo, Japan) was used. The large probe with a diameter of3.2 mm was used. The coagulation thermal tip was a brasscylinder with a small electric coil which can be heated to2500C when electric current is passed. The cylindrical tip iscoated with Teflon to avoid sticking to the coagulated tissue.The energy setting used in the present study was 25 J /pulseand each pulse of energy was delivered over 3 to 5 sec.Careful cleansing of the tip was performed between applications if tissue was found sticking to its surface, as this willaffect the energy delivered. Similar to the technique employed with BlCAP'", firm pressure was applied and thermocoagulation applied in the same manner.
The angulation of the laser, heater, and BICAP'" probesto the ulcer base and the duration of therapy (time afterclearing the field and washing off the blood clot, if any, tothe end of coagulation) were recorded.
Experience of endoscopists
The procedure was conducted by endoscopists with atleast 5 years of experience in upper endoscopy and whounderwent a run-in period of 6 months before the trial toget acquainted with the three endoscopic modalities to minimize the issue of a learning phase.
Monitoring
After coagulation treatment the ulcer was observed for 5min for evidence of further bleeding. The patients weremanaged in general medical wards by other physicians whowere unaware of the mode of coagulation treatment given.All patients received 50 mg of ranitidine intravenously ateight hourly intervals or 150 mg of ranitidine twice dailywhen oral diet was resumed and blood transfusion was givenas required. The vital signs including blood pressure andpulse, and urine output and hemoglobin level were closelymonitored. Patients were discharged from the hospital whenthe vital signs and hemoglobin level remained stable for 3consecutive days. Re-bleeding was suspected if there washematemesis, fresh melena, drop in blood pressure, risingpulse, or continuous drop in hemoglobin level. This wasconfirmed by repeating the endoscopic examination. Pa-
GASTROINTESTINAL ENDOSCOPY
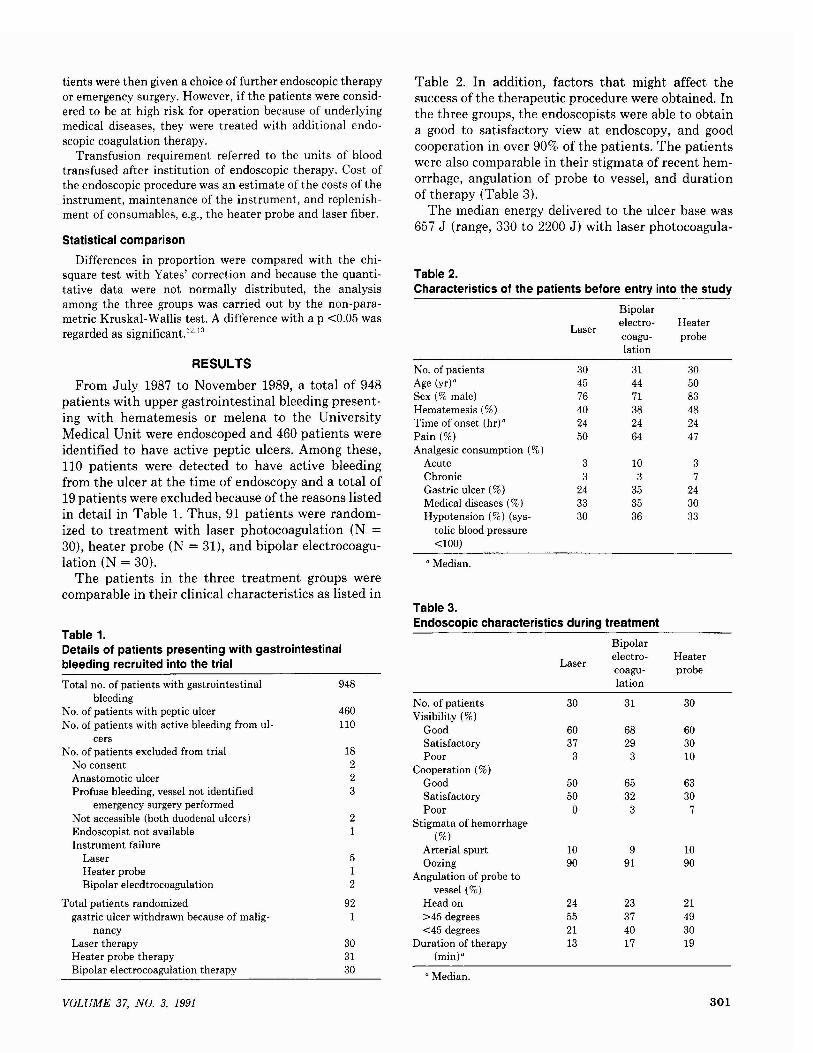
Table 1.Details of patients presenting with gastrointestinalbleeding recruited into the trial
Statistical comparison
Differences in proportion were compared with the chisquare test with Yates' correction and because the quantitative data were not normally distributed, the analysisamong the three groups was carried out by the non-parametric Kruskal-Wallis test. A difference with a p <0.05 wasregarded as significant.12.1~
tients were then given a choice of further endoscopic therapyor emergency surgery. However, ifthe patients were considered to be at high risk for operation because of underlyingmedical diseases, they were treated with additional endoscopic coagulation therapy.
Transfusion requirement referred to the units of bloodtransfused after institution of endoscopic therapy. Cost ofthe endoscopic procedure was an estimate of the costs of theinstrument, maintenance of the instrument, and replenishment of consumables, e.g., the heater probe and laser fiber.
RESULTS
From July 1987 to November 1989, a total of 948patients with upper gastrointestinal bleeding presenting with hematemesis or melena to the UniversityMedical Unit were endoscoped and 460 patients wereidentified to have active peptic ulcers. Among these,110 patients were detected to have active bleedingfrom the ulcer at the time of endoscopy and a total of19 patients were excluded because ofthe reasons listedin detail in Table 1. Thus, 91 patients were randomized to treatment with laser photocoagulation (N =30), heater probe (N = 31), and bipolar electrocoagulation (N = 30).
The patients in the three treatment groups werecomparable in their clinical characteristics as listed in
Table 2. In addition, factors that might affect thesuccess of the therapeutic procedure were obtained. Inthe three groups, the endoscopists were able to obtaina good to satisfactory view at endoscopy, and goodcooperation in over 90% of the patients. The patientswere also comparable in their stigmata of recent hemorrhage, angulation of probe to vessel, and durationof therapy (Table 3).
The median energy delivered to the ulcer base was657 J (range, 330 to 2200 J) with laser photocoagula-
Table 2.Characteristics of the patients before entry into the study
Bipolar
Laserelectro- Heatercoagu- probelation
No. of patients 30 31 30Age (yr)" 45 44 50Sex (% male) 76 71 83Hematemesis (%) 40 38 48Time of onset (hr)" 24 24 24Pain (%) 50 64 47Analgesic consumption (%)
Acute 3 10 3Chronic 3 3 7Gastric ulcer (%) 24 35 24Medical diseases (%) 33 35 30Hypotension (%) (sys- 30 36 33
tolic blood pressure<100)
" Median.
Bipolar
Laserelectro- Heatercoagu- probelation
No. of patients 30 31 30Visibility (%)
Good 60 68 60Satisfactory 37 29 30Poor 3 3 10
Cooperation (%)Good 50 65 63Satisfactory 50 32 30Poor 0 3 7
Stigmata of hemorrhage(%)
Arterial spurt 10 9 10Oozing 90 91 90
Angulation of probe tovessel (%)
Head on 24 23 21>45 degrees 55 37 49<45 degrees 21 40 30
Duration of therapy 13 17 19(min)"
" Median.
Table 3.Endoscopic characteristics during treatment
21
512
921
303130
18223
948
460110
Total no. of patients with gastrointestinalbleeding
No. of patients with peptic ulcerNo. of patients with active bleeding from ul
cersNo. of patients excluded from trial
No consentAnastomotic ulcerProfuse bleeding, vessel not identified
emergency surgery performedNot accessible (both duodenal ulcers)Endoscopist not availableInstrument failure
LaserHeater probeBipolar elecdtrocoagulation
Total patients randomizedgastric ulcer withdrawn because of malig-
nancyLaser therapyHeater probe therapyBipolar electrocoagulation therapy
VOLUME 37, NO.3, 1991 301

tion and 175 J with the heater probe (range, 125 to400 J). The median number of bursts of bipolar electrocoagulation (7 setting X 2 sec) delivered to the ulcerbase was 12 (range, 8 to 20 sec).
The success rate of immediate hemostasis was similar (93% for laser and bipolar electrocoagulation, 94%for heater probe, p < 0.5). The re-bleeding rate, unitsof blood transfused, number of days in hospital, andmortality among the three groups were similar (Table4).
Among the three patients who re-bled after lasertreatment, one patient received laser therapy againand bleeding stopped. The other two patients hademergency surgery. Six patients re-bled in the heaterprobe group. Two patients had emergency surgery,four were given further heater probe treatment buttwo continued to bleed and had surgery. Three patients re-bled after bipolar electrocoagulation. Onepatient stopped bleeding after a second attempt atbipolar electrocoagulation; the other two patients required emergency surgery. There was no significantdifference in the rate of emergency surgery among thethree groups (p < 0.5).
Two patients died during the study. Both were inthe bipolar electrocoagulation group. The first patientwas a 74-year-old man with a history of ischemic heartdisease. Gastrointestinal bleeding stopped after electrocoagulation, but he died on day 5 from myocardialinfarction. There was no clinical evidence of re-bleeding. The second patient was a 78-year-old man withcirrhosis of liver, Child's grade C. He re-bled 2 daysafter bipolar electrocoagulation treatment, and bleeding was controlled with further bipolar electrocoagu-
lation. However, he died on day 5 from hepatic failure.The cost of endoscopic therapy per patient was estimated to be higher with laser therapy than heaterprobe and bipolar electrocoagulation, taking into account installation, recurrent cost for the probes andmaintenance of the instruments (Table 4). None ofthe patients had complications arising from the threeforms of treatment.
Angulation of the probe and re-bleeding
With laser, heater probe, and bipolar electrode there-bleeding rate was similar whether the probes wereapplied head on, at angles between 45 and 90 degrees,or less than 45 degrees to the bleeding visible vessels(Table 5).
Re-bleeding in relation to type of bleeding andlocation of ulcer
Since re-bleeding rates did not differ among thethree treatment groups, they were considered as a
Table 5.Relationship between angle of the probes to the ulcerbase and rate of re-bleeding
Head on>45 <45
Re-bleeding (%) degrees degrees p(%) (%)
Laser 13 7 17 0.7(1/8) (1/15) (1/7)
Heater probe 13 27 18 0.8(1/8) (3/11) (2/12)
Bipolar electroco- 16 7 20 0.2agulation (1/6) (1/15) (2/9)
Bipolar
Laserelectro-
Heater probecoagu-
p
lation
30 30 31
100 (3/3) 67 (2/3) 100 (3/3)93 (25/27) 93 (26/27) 96 (25/27) 0.593 93 94 0.5
33 (1/3) 0(0/3) 33 (1/3)7 (2/27) 13 (3/27) 18 (5/28) 0.2
10 10 19.4 0.21.0 2.0 2.0 0.84 5 4 0.66.7 6.7 12.9 0.50 6.7 0
200 70 50
Table 4.Outcome in laser-treated, bipolar electrocoagulation-treated, and heater-probetreated patients
No. of patientsSuccessfulImmediateHemostasis
Arterial spurt (%)Oozing (%)Total (%)
Re-bleeding rateArterial spurt (%)Oozing (%)All(%)
Transfusion units"Hospital stay (days)"Emergency surgery (%)Mortality (%)Treatment cost/patient
(U.S. $)
"Median.
302 GASTROINTESTINAL ENDOSCOPY

group and the results are shown in Table 6. There wasno significant difference in the re-bleeding rates between the arterial spurters and oozing visible vessels.The re-bleeding rates were higher in patients withgastric ulcer (24%) than those with duodenal ulcer(9%), but the difference was not statistically significant.
DISCUSSION
Patients with stigmata of recent hemorrhage belongto a high risk group. Active bleeding and visible vesselsare impJrtant endoscopic predictors of persistent orrecurrent bleeding. 14,I;; It is recommended that endoscopic treatment should be given to patients withactively bleeding ulcers. lO These therapeutic modalities include Nd:YAG laser, bipolar electrocoagulation,and heater probe.
The present study compared the efficacy of thelaser, bipolar electrocoagulation, and heater probe inthe treatment of actively bleeding ulcers. Care wastaken to exclude patients with minor stigmata ofbleeding since in most of these patients bleeding willsubside spontaneously.16 Furthermore, the experienceof the endoscopist can affect the results of endoscopictherapy.6 The incorporation of experienced endoscopists with a run-in period of 6 months to get acquaintedwith the three endoscopic modalities before the trialhas helped to reduce this problem. The fact that there-bleeding rate among the three endoscopists did notdiffer significantly indicates that their techniqueswere comparable (data not shown). We also consideredfactors like symptoms, blood pressure, and pulse rate,which were known to have prognostic significance,17,18and these were comparable among the three groups.In addition, the importance of a clear endoscopic field
Table 6.Relationship between rate of re-bleeding, type ofbleeding, and location of the ulcer
Type of bleedersArterial spurtOozing visible vessel
Location of the ulcerDuodenal ulcerGastric ulcer
Duodenal ulcerAnteriorPosteriorFloorRoof
Gastric ulcerIncisuralPre-pyloricCorpus (excluding inci
sura)
Re-bleeding rate(%)
22 (2/9)12 (10/82)
9 (6/66)24 (6/25)
6 (2/36)20 (2/10)8 (1/14)
17 (1/6)
23 (3/13)0(0/4)
38 (3/8)
p
>0.1
0.1
0.4
0.4
and a cooperative patient during endoscopy, whichhave not been emphasized previously, were also comparable.
The present study demonstrated that the three modalities were equally effective in achieving endoscopichemostasis, as reflected by the similar re-bleedingrates. Our results have further demonstrated that thetransfusion requirement, number of days in hospital,and the rate of emergency surgery were similar in thethree groups. In the present study two patients died.Both belonged to the bipolar electrocoagulation group.However, in both patients, the cause of death was notdue to uncontrolled bleeding. No therapeutic complications were observed in the present series of patients.
The pressure effect on the vessel contributes tohemostasis by bipolar electrocoagulation and heaterprobe. ll The ability to apply firm pressure depends onthe angle of the probe to the ulcer base. Poor angulation occurs when the ulcer is situated on the highlesser curve in cases of gastric ulcer or in cases withmarked duodenal deformity in duodenal ulcer. In thepresent study, in approximately 30% of the patientsthe angulation of the probes was less than 45 degreesto the vessel, which theoretically would mean lessforce applied to the vessel. However, our resultsshowed that angle of the probe did not affect endoscopic hemostasis by heater probe or bipolar electrocoagulation, as reflected by the rate of re-bleeding.This may be related to the fact that adequate forcehad already been exerted in all patients, thus makingthe angulation of the probe an insignificant determining factor. An alternative explanation may be relatedto the compensatory effect of increased contact whenthe bipolar/heater probe was applied tangentially. Thepresent study showed that the location of the ulcerdid not affect the re-bleeding rate. Lin et al. 19 reportedsimilar re-bleeding rates with non-bleeding visible vessels for duodenal ulcer (39%) and gastric ulcer (48%)without endoscopic treatment. They further reportedthat re-bleeding rates after treatment with heaterprobe were similar in patients with duodenal ulcersand gastric ulcers.20
A number of studies have been performed on theuse of laser photocoagulation in the treatment ofgastrointestinal bleeding. Swain et al.4 and Matthewson et al.5 reported a significant reduction in rebleeding rate (11 to 20% with laser) and requirementfor emergency surgery, but the study by Krejs et al.21
failed to confirm this. This discrepancy is probablyrelated to differences in the entry criteria in thesestudies. Krejs et al. 21 included patients with low riskof re-bleeding as evidenced by the low re-bleeding ratein the control group (13%). Most investigators reported that patients with major stigmata of bleedinghad a re-bleeding rate of approximately 50%.14,15
Laine,? by including only patients with severe bleeding
VOLUME 37, NO.3, 1991 303

and using more bursts of electrocoagulation and firmpressure, demonstrated that bipolar electrocoagulation could reduce the re-bleeding rate (10 to 17%) andthe need for emergency surgery as compared with notreatment, although earlier studies failed to demonstrate any significant difference. 22
,23 Similarly, Jensenet al.8 demonstrated the effectiveness of heater probe.The re-bleeding rates of 10%, 20%, and 10%, respectively, with laser, heater probe, and bipolar electrocoagulation in the present study were similar to thosereported in the controlled studies.4
,5,7,8
Since the present study demonstrated that all threemodalities were equally effective in the reduction ofre-bleeding, the other factor that needed to be considered was the cost. The cost estimated per patient forlaser was higher than that for bipolar electrocoagulation and heater probe. The laser machine is not portable and cannot be applied to critically ill patients inthe Intensive Care Unit. Moreover, in five of eightinstances of instrument failure, the laser machine wasat fault. Therefore, we recommend that bipolar electrocoagulation and heater probe be used for patientswith active gastrointestinal bleeding. Provided adequate pressure and coagulation are given, angulationof the probe does not affect the success of hemostasis.
ACKNOWLEDGMENTS
This study ws supported by the Peptic Ulcer Research Fund (311/041/0372), University of HongKong. The authors are grateful for the assistance ofM. Chong, I. Man, H. Li, Dr. A. Kung, A. Poon, andA. Wong.
REFERENCES1. Johnson SJ, Jones PF, Jyle J, Needham CD. Epidemiology and
cause of gastrointestinal haemorrhage in North-East Scotland.Br Med J 1973;3:655-60.
2. Silverstein FE, Gilbert DA, Tedesco FJ, Buenger NK, PersingJ. The National A/S/G/E Survey on upper gastrointestinalbleeding. Gastrointest Endosc 1981;27:80-93.
3. Gustavsson S, Kelly KA, Melton LJ III, Zinsmeister AR. Trendsin peptic ulcer surgery: a population-based study in Rochester,Minnesota, 1956-1985. Gastroenterology 1988;94:688-94.
4. Swain CP, Kirkham JS, Salmon PR, et al. Controlled trial ofNd:YAG laser photocoagulation in bleeding peptic ulcers. Lancet 1986;1113-6.
304
5. Matthewson KG, Swain CP, Bland M, Kirkham JS, Bown SG,Northfield TC. Randomized comparison Nd:YAG laser, heaterprobe, and no endoscopic therapy for bleeding peptic ulcers.Gastroenterology 1990;98:1239-44.
6. O'Brien JD, Day SJ, Burnham WR. Controlled trial of smallbipolar probe in bleeding peptic ulcers. Lancet 1986;1:464-7.
7. Laine L. Multipolar electrocoagulation in the treatment ofactive upper gastrointestinal tract haemorrhage. A prospectivecontrolled trial. N Engl J Med 1987;316:1613-7.
8. Jensen DM, Machicado GA, Kovacs TOG, et al. Controlledrandomized study of heater probe and BICAP for hemostasisof severe ulcer bleeding [Abstract]. Gastroenterology 1988;94:208.
9. Dronfield MW, Atkinson M, Langman MJS. Effect of differentoperation policies on mortality from bleeding peptic ulcer.Lancet 1979;1:1126-34.
10. Therapeutic endoscopy and bleeding ulcers-NIH Consensusconference. JAMA 1989;262:1369-72.
11. Johnston JH, Jensen DM, Auth D. Experimental comparisonof endoscopic YAG laser, electrosurgery, and heater probe forcanine gut arterial coagulation: importance of compression andavoidance of erosion. Gastroenterology 1987;92:1101-8.
12. Fleiss JL. Statistical methods for rates and proportions. NewYork: John Wiley, 1973.
13. Snedecor GW, Cochran WG. Statistical methods. Ames, Iowa:Iowa State University Press, 1967.
14. Storey DW, Bown SG, Swain CP, et al. Endoscopic predictionof recurrent bleeding in peptic ulcers. N Engl J Med1981;305:915-7.
15. Griffith WJ, Neumann DA, Welsh JD. The visible vessel as anindicator of uncontrolled or recurrent gastrointestinal hemorrhage. N Engl J Med 1979;300:1411-3.
16. Fleischer D. Etiology and prevalence of severe persistent uppergastrointestinal bleeding. Gastroenterology 1983;84:538-43.
17. Bornman P, Theodorou NA, Shuttleworth RD, Essel HP,Marks IN. Importance of hypovolaemic shock and endoscopicsigns in predicting recurrent haemorrhage from peptic ulceration: a prospective evaluation. Br Med J 1985;291:245-7.
18. De Dombal FT, Clarke JR, Clamp SE, Malizia G, Kotwal MR,Morgan AG. Prognostic factors in upper G.I. bleeding. Endoscopy 1986;18(suppl 2):6-10.
19. Lin HJ, Lee FY, Tsai YT, Lee SD, Lee CH. What kind ofnonbleeding visible vessel in a peptic ulcer needs aggressivetherapy? Endoscopy 1990;22:8-11.
20. Lin HJ, Tsai YT, Lee SD, et al. A prospectively randomizedtrial of heat probe thermocoagulation versus pure alcohol injection in nonvariceal peptic ulcer hemorrhage. Gut 1990;31:7537.
21. Krejs GJ, Little KH, Westergaard H, Hamilton JK, Polter DE.Laser photocoagulation for the treatment of acute peptic ulcerbleeding: a randomized controlled clinical trial. N Engl J Med1987;316:1618-21.
22. Kernohan RM, Anderson JR, McKelvey S, et al. Controlledtrial of bipolar electrocoagulation in patients with upper gastrointestinal bleeding. Br J Surg 1984;25:A1185.
23. Goudie BM, Mitchell KG, Birnie GG, et al. Controlled trial ofendoscopic bipolar electrocoagulation in the treatment of bleeding peptic ulcers. Gut 1984;25:A1185.
GASTROINTESTINAL ENDOSCOPY
Copyright © 2022 FDOKUMEN




















