
Have talent? Have Internet? Wait no more. Get set for webbing ...
Upload
independentCategory
view
3download
0
ORIGINAL ARTICLE
David E. Spaner Æ Caitlin Hammond Æ Jenny Mena
Cindy Foden Æ Andrea Deabreu
A phase I/II trial of oxidized autologous tumor vaccines during the‘‘watch and wait’’ phase of chronic lymphocytic leukemia
Received: 7 June 2004 / Accepted: 21 September 2004 / Published online: 17 December 2004� Springer-Verlag 2004
Abstract Based on their activity in patients with ad-vanced stage chronic lymphocytic leukemia (CLL), aphase I/II study was designed to evaluate the feasibility,safety, and efficacy of autologous vaccines made fromoxidized tumor cells in patients with earlier stage CLL,and to determine an optimal schedule of injections.Eighteen patients (at risk for disease progression andwith white blood cell counts between 15 and100·106 cells/ml) were injected intramuscularly with10 ml of oxidized autologous blood (composed mainlyof CLL cells) either 12 times over 6 weeks (group 1), 12times over 16 days (group 2), or 4 times over 6 weeks(group 3). Fourteen out of eighteen patients had Raistage 0–II disease, while 4/18 had stage III–IV diseasebut did not require conventional treatment. Partialclinical responses, associated with enhanced anti-tumorT cell activity in vitro, were observed in 5/18 patients ofwhom three were in group 2. Stable disease was observedin six patients while disease progression appeared not tobe affected in the remaining patients. Toxicity wasminimal. Vaccination with oxidized autologous tumorcells appears worthy of further investigation and may bea potential alternative to a ‘‘watch and wait’’ strategy forselected CLL patients.
Keywords Human Æ Cancer vaccines Æ Tumorimmunity Æ Chronic lymphocytic leukemia ÆCostimulatory molecules
Abbreviations APC: Antigen presenting cell Æ CLL:Chronic lymphocytic leukemia Æ WBC: White bloodcell Æ PHA: Phytohemagglutinin Æ PWM:Pokeweed mitogen Æ IFN: Interferon Æ 2-ME:2-Mercaptoethanol Æ MLR:Mixed lymphocyte response ÆCR: Complete response Æ PR: Partial response Æ PD:Progressive disease Æ SD: Stable disease Æ pt: Patient Æ SE:Standard error Æ Ig: Immunoglobulin Æ
Introduction
Chronic lymphocytic leukemia (CLL) is the most com-mon form of leukemia in the Western World [1]. Sinceconventional chemotherapy does not cure this disease, a‘‘watch and wait’’ policy is employed (before and afterchemotherapy) until patients become symptomatic froma high tumor burden [2]. This policy is based on thefailure to demonstrate a survival benefit for treatmentwith cytotoxic agents before the onset of symptoms, butis clearly not satisfactory for patients who will inevitablydevelop progressive disease (PD). Moreover, the besttime to make a therapeutic maneuver that will have ameaningful impact on patient survival is likely to bewhen the disease burden is low.
A number of clinical observations (such as spontane-ous remissions associated with increased immune activityduring infections [3], responses to immunomodulatorycytokines [4], and a graft-versus-leukemia effect afterallogeneic stem cell transplantation [5]) suggest that CLLcells may be subject to T cell-mediated immunothera-peutic approaches. Tumor-reactive T cells can be found inmany patients [6] but inherent weak immunogenicity ofCLL cells may allow them to escape natural T cell-medi-ated controls. Vaccines may be able to present CLLantigens in an immunogenic manner and cause these
D. E. Spaner (&) Æ C. Hammond Æ J. MenaDivision of Molecular and Cellular Biology,Research Institute, Sunnybrook and Women’s CollegeHealth Sciences Center, S-116A, Research Building,2075 Bayview Avenue, Toronto, ON, Canada, M4N 3M5E-mail: [email protected].: +416-480-6100-2510Fax: +416-480-5737
D. E. Spaner Æ C. Foden Æ A. DeabreuToronto-Sunnybrook Regional Cancer Center,Toronto, Canada, M4N 3M5
D. E. SpanerDepartment of Medicine, University of Toronto,Toronto, Canada, M5G 2C4
D. E. Spaner Æ C. HammondDepartment of Medical Biophysics,University of Toronto, Toronto, Canada, M5G 2M9
Cancer Immunol Immunother (2005) 54: 635–646DOI 10.1007/s00262-004-0626-5

CLL-reactive T cells to acquire a cytotoxic effector func-tion for sufficient time to clear tumor cells [5]. Such vac-cines could offer a meaningful therapeutic maneuver inthe ‘‘watch and wait’’ phase of management.
With the possible exception of the immunoglobulinidiotype, specific CLL target antigens have not been welldescribed [7]. This absence of defined antigens may beobviated by using cancer vaccines made from autolo-gous tumor cells that have been modified to make themmore immunogenic [8]. These vaccines should be able toactivate a broad range of tumor-reactive T cells, even ifthe specific antigens to which the T cells are respondingare unknown.
Chronic lymphocytic leukemia cells can be mademore immunogenic (and, consequently, used as autolo-gous vaccines) by activating them in vitro through CD40[9] or with CpG-oligodeoxynucleotides and cytokines[10], or by transfecting them with CD40L [11]. However,the cell processing required to make such vaccines is notgenerally available and can be cumbersome, inefficient,expensive, and even dangerous [12].
In contrast, simple treatment of tumor cells withoxidizing radiation also makes them more immunogenic[13]. For example, vaccines made from irradiatedautologous tumor cell lines improve disease control insome melanoma patients [14]. CLL is unique amongimmunologically susceptible cancers in that the periph-eral blood of patients is highly enriched in tumor cellsand can potentially be used directly to make patient-specific vaccines. These considerations led us tohypothesize that blood from CLL patients, subjected tomultiple oxidative stressors, could form the basis of anautologous vaccine strategy for the treatment of thiscancer [6]. Indeed, we observed a transient clinical re-sponse (along with an increase in CLL-reactive T cellnumbers) in one of two advanced-stage patients whowere treated with 12 injections of their own oxidizedtumor cells over a 6-week period [6]. Although the exactmechanism of action is unknown, it is thought that theoxidized CLL cells released heat shock proteins (whichmay present tumor-specific antigens [15]) and intracel-lular ‘‘danger signals’’ (such as free radicals, uric acid[16], and HMGB-1 [17]) that engaged the patient’s im-mune system, and led to the activation of tumor-reactiveT cells [13]. On the basis of these findings, we developeda phase I/II clinical trial to further explore the feasibility,safety, and efficacy of this approach.
An additional aim of the trial was to determine anoptimal injection schedule. The original schedule [6] wasadopted from previous trials of oxidized blood as a vac-cine for autoimmune disorders [18]. However, the kineticsof antigen delivery and total antigen dose can profoundlyaffect the type of immunity that results from vaccination[19]. Altering the number and frequency of injections offixed volumes of oxidized blood can potentially changethe delivery of antigen sufficiently to promote type 1 (orcell-mediated) immunity, which is thought to be desiredfor effective anti-tumor responses [20]. Preliminaryexperiments in mice suggested that oxidized cells (that
have been injected subcutaneously) are cleared in drain-ing lymph nodes, within 24 h (D. Spaner, unpublishedobservations). Accordingly, daily injections of oxidizedblood should provide a sustained level of antigenic stimuli(associated with induction of cytotoxic T cells [21]) whileinjections of oxidized blood every couple of weeks shouldprovide short-lived antigenic pulses that might also leadto type 1 immune responses [22].
Methods
Patients and eligibility criteria
Eligible patients were required to have a diagnosis ofCLL on the basis of a persistent absolute lymphocytosis(>5,000 mature-appearing lymphocytes/ll), with thepredominant cell population having low-density surfaceimmunoglobulin (Ig) expression, monoclonal expressionof k or j light chains, and sharing the B-cell markers,CD19, CD20, and CD23 with the CD5 antigen (in theabsence of other pan-T-cell markers) [2]. Patients withany Rai stage [23] were potentially eligible for the study.However, some Rai stage 0 patients may have an indolentdisease that never progresses or requires treatment (incontrast to patients with higher Rai stage who often re-quire treatment at some point in the course of their dis-ease) [24]. At the time the study was initiated, biologicalprognostic markers [25] were not used to exclude patientswho might have indolent disease [24]. To exclude suchRai stage 0 patients, a white blood cell (WBC) countbetween 15 and 40·106 cells/ml must have increased by aleast 15% within the previous 12 months, or the bonemarrow must have been involved diffusely with CLL.Examination of the bone marrow was otherwise not arequirement for study entry. Patients who had beentreated previously with chemotherapy or radiation musthave finished the treatment at least 1 year before entryinto the study. Patients were required to be older than18 years and have an ECOGperformance status of 0 or 1.Patients with WBC counts >100·106 cells/ml were ex-cluded, because of potential cell concentration-dependenteffects of the oxidizing agents. No patient had clinicalsigns of infection, or symptoms related to CLL that re-quired treatment with conventional chemotherapy, at thetime of the study. All patients gave informed and writtenconsent, and approval for the study was obtained fromboth the ethics committee of the Sunnybrook and Wo-men’s College Health Sciences Center and the CanadianHealth Protection Branch. The trial began in June 2001and the last follow-up visit was in January 2003.
Treatment
Patients were recruited sequentially into three groups(consisting of six patients each) that received differenttreatment schedules:
636

Group 1: 12 injections over 6 weeks (two injections perweek)Group 2: 12 injections over 16 days (five injections perweek)Group 3: four injections over 6 weeks (on days 1, 2, 21,and 38)
Patients were seen before each injection, at 4 and7 weeks following the first treatment, and at 3 and6 months following the last treatment, to evaluate tox-icity and clinical response. Patients who were judged tohave responded to the treatments at the 7-week post-first-treatment evaluation (on the basis of changes inperipheral blood lymphocyte counts) were offeredadditional monthly treatments. A total of five patients(pts. 2, 8, 10, 18, and 11) received these additionalinjections.
Response criteria
The criteria of Cheson et al. [2] were used to assess re-sponses. Complete response (CR) required the absenceof CLL cells, as measured by bone marrow examinationand standard complete blood counts, along with noevidence of tumor masses on physical examination,confirmed by radiologic investigations. Partial response(PR) was defined as ‡50% decrease in peripheral bloodlymphocyte count from the pretreatment baseline leveland ‡50% reduction in the size of the liver and/orspleen, and of lymphadenopathy (sum of the products ofthe diameters, in two planes, of cervical, axillary, supr-aclavicular, inguinal, and femoral lymph nodes), alongwith either normal or ‡50% improvement in granulo-cyte, platelet, and hemoglobin numbers, that weremaintained for at least 2 months [2]. The majority ofpatients in this study had Rai stage 0 or I disease, andCT scans or ultrasounds to document changes inlymphadenopathy or hepatosplenomegaly, were notperformed routinely. Accordingly, a PR in this study isessentially a ‡50% decrease in peripheral blood lym-phocyte count from the pretreatment baseline levelmaintained for at least 2 months. PD was defined by‡50% increase in hepatosplenomegaly, circulating lym-phocytes, or sum of the products of at least two lymphnodes, appearance of new nodes, or transformation to amore aggressive histology. Patients who did not achievea CR or PR, or who did not exhibit PD, were consideredto have stable disease (SD).
Oxidized autologous CLL cell vaccines
Blood (10 ml) was collected into 2 ml of sodium citrateand transferred immediately to a sterile, disposable, low-density polyethylene vessel (Model VC7002) for ex vivotreatment. The cells were then subjected to a combina-tion of oxidative physicochemical stressors under strictlycontrolled conditions in a VC7001 blood treatment unit
(Vasogen, Mississauga, ON), as described previously [6].Briefly, the blood sample was exposed to heat(42.5±1.0�C), a mixture of medical grade oxygen con-taining 14.5±1.0 lg/ml of ozone at standard tempera-ture and pressure, and UV-C light at a wavelength of253.7 nm with a total energy of 2.0 J/cm2. At the end ofthe 20 min treatment, the cells were allowed to settle for7 min, transferred immediately to a sterile syringe, andinjected intramuscularly into the gluteal region of thepatient, along with a local anesthetic (l ml of 2%Lidocaine).
The treatment caused lysis of many erythrocytes.Immediate viability of mononuclear cells (measured bytrypan blue exclusion) was >75%, although >90% ofcells died when cultured for >24 h (data not shown).The purity of CD5+ CD19+ B-CLL cells in the oxidizedcell vaccines was the percentage of CLL cells in theperipheral blood and ranged from 70% to 90%(depending on the total WBC count), but was notmeasured routinely.
Reagents
Phycoerythrin-labeled or FITC-labeled CD80 (B7-1),CD86 (B7-2), CD54 (ICAM-1), and CD83 were pur-chased from Pharmingen (San Francisco, CA, USA).Phorbol dibutyrate (PDB) was from Sigma ChemicalCo. (St. Louis, MO, USA). Stock solutions of PDB(5 mg/ml) were made in DMSO. Clinical grade IL-2(Chiron Corporation, San Francisco, CA, USA) waspurchased from the hospital pharmacy. Phytohemag-glutinin (PHA), pokeweed mitogen (PWM), and humanAB serum were from Sigma.
Flow cytometry and clinical immunological monitoring
Cell staining was performed as described [6], using hu-man intravenous gamma globulin (10 lg) (Bayer Corp.,Elkhart, IND) to block non-specific binding to Fc-receptors. Fluorescence from specifically reacting anti-bodies was measured on a FACScan flow cytometer(Becton Dickinson Labware, Franklin Lake, NJ, USA).At least 10,000 events were analyzed in each experiment.CD38 expression on CLL cells was determined in theclinical flow cytometry laboratory of the PathologyDepartment at the Sunnybrook and Women’s CollegeHealth Sciences Center. Complete blood counts wereobtained from the hospital clinical hematology labora-tory. Serum immunoglobulin and rheumatoid factorlevels were determined according to routine clinicallaboratory procedures.
Cell purification
Chronic lymphocytic leukemia and T cells were isolatedimmediately from blood by negative selection (Rosette-
637

Sep, StemCell Technologies, Vancouver, BC) accordingto the manufacturer’s instructions. Briefly, 75% of theplasma was first removed to concentrate peripheralblood mononuclear cells, increase cell yield, and mini-mize the required antibodies. T cells (>96% purity)were obtained with antibodies against CD16, CD19,CD36, CD56, and glycophorin A. CLL cells were iso-lated with antibodies against CD2, CD3, CD14, CD16,CD56, and glycophorin A. The resulting purity ofCD19+ CD5+ cells was >96% with <0.1% con-tamination by CD3+ cells. Cells were then cryopre-served so that subsequent T cell cultures could beperformed simultaneously under the same conditions.
Activation of CLL cells for mixed lymphocyte responses(MLRs)
Effective vaccination with autologous tumor vaccinesshould increase T cell responses to CLL antigens [20]. Inthe absence of defined CLL-specific antigens, an autol-ogous MLR was used to measure tumor-reactive T cellresponses. This assay had been shown, previously, tocorrelate with a whole cell ELISPOT assay for T cellsthat produced interferon (IFN)-c in response to antigenson CD40-activated CLL cells [6]. The latter assay wasused to demonstrate increases in anti-CLL T cell reac-tivity in a patient who was injected with oxidizedautologous tumor cells before initiation of the presenttrial [6]. Note that CLL cells, themselves, are poor directstimulators of T cells in vitro and require activation tomake them good antigen presenting cells (APCs) [11].
To increase their T cell-stimulatory capabilities,purified CLL cells (1.5·106 cells/ml) were cultured inserum-free AIM-V medium (GibcoBRL, Grand Island,NY, USA) plus 2-mercaptoethanol (2-ME) (Sigma)(5·10�5 M) in 24-well plates (Becton Dickinson Lab-ware) for 4 days at 37�C in 5% CO2. PDB, IL-2, andserum were added at 100 ng/ml, 5,000 U/ml, and 10%final concentrations, respectively, at the beginning of theculture period. Results of others [10, 26] and ourselves[27] were used to justify the use of these reagents toincrease the immunogenicity of CLL cells for use asstimulators in MLRs.
CLL-reactive T cell responses in MLRs
Cryopreserved T cells were thawed, washed, restedovernight in culture, and then re-suspended at1·106 cells/ml in AIM-V medium. Activated CLL cellswere washed at least four times (to remove residualimmunomodulators), irradiated (2,500 cGy), and sus-pended at 2.5·105 cells/ml in AIM-V. Responders andstimulators were then mixed in a 1:1 (vol:vol) ratio(determined to give optimal stimulation in preliminaryexperiments) and cultured in 96-well round bottomplates (Becton Dickinson Labware) without additionalcytokines or serum. Proliferation was measured 6 days
later using a colorimetric assay [6]. Alamar blue (Bio-source International, Camarillo, CA, USA) (20 ll) wasadded to each well and absorbances were determined,24 h later, at wavelengths of 540 nm (reduced state) and595 nm (oxidized state) in an optical density colorimetermicroplate reader (Molecular Devices, Menlo Park, CA,USA). Alamar blue is reduced from the oxidized indigoblue form to the fluorescent pink state by the increasedratios of NADPH/NADP, FADH/FAD, FMNH/FMN, and NADH/NAD in the reducing environmentof metabolically active cells [28].
Assay background was assessed in wells that wereincubated with responder T cells in the presence of CLLcells that had been thawed and cultured, but not acti-vated otherwise. As a measure of anti-CLL T cell pro-liferation at each time point, the average and standarderror (SE) were calculated from the results of triplicatewells. Since patient samples were limited, the assays wereperformed only once, in most cases. However, for pts. 1,8, 11, and 14, the assays were repeated independentlyand gave similar results.
Mitogen responses
T cells (200 ll of a 7.5·105 cells/ml suspension in AIM-V medium plus 2-ME) were cultured with PHA (10 lg/ml) or PWM (2.5 lg/ml) in 96-well flat-bottomed plates(Becton Dickenson Labware) for 5 days before addingAlamar blue.
Statistical analysis
The Student t-test was used to determine p-values fordifferences between sample means. Differences with a p-value of <0.05 were considered to be significant.
Results
Hematologic response
The clinical characteristics of the 18 patients enrolled inthe study are shown in Table 1. The majority (14/18patients) had relatively early stage disease (Rai stage 0–II) [23] and 4/18 had stage III or IV disease withoutclinical symptoms to necessitate treatment with chemo-therapy. The individual clinical courses over the 6-month study period are shown in Fig. 1. No CRs de-fined as absence of detectable disease [2] were observedin any patient. However, the circulating WBC count(made up mainly of neoplastic lymphocytes) decreasedby approximately 50% for at least 2 months in five pa-tients (pts. 2, 7, 8, 10, and 18) and, thus, met therequirements for PR [2]. In six patients (pts. 1, 4, 6, 11,12, and 13), the WBC count remained relatively un-changed throughout the study period and these patientswere classed as having SD [2]. Even among these
638

patients, however, several (pts. 1, 6, 11, and 13) ap-peared to have had a minor response to the vaccines; inthat their WBC count decreased around 25% at the endof the active period of treatment before increasing to thepretreatment values.
Of the patients classed as ‘‘partial responders’’ (pts. 2,7, 8, 10, and 18), pts. 2 and 8 have been treated subse-quently with chlorambucil and splenic irradiation, 1 and2 years after completing the 6-month response evalua-tion, respectively. The remaining ‘‘partial responders’’and the patients classed as having ‘‘SD’’ (except pt. 13,who died of a myocardial infarction) have not requiredadditional treatment for their CLL for at least18 months after the 6-month response evaluation peri-od. However, since these patients did not require treat-ment before entering the study, it is not possible toattribute their subsequent lack of need for conventionaltherapy to the vaccinations.
In the remaining seven patients, the WBC count atthe end of the study period was greater than 50% higherthan at the beginning, and these patients were classed ashaving PD [2]. Patient 9 was also included in this cate-gory, although his final WBC was not quite 50% higherthan his initial WBC (Fig. 1). Of these latter patients, pt.3 was found to have developed transformation to a largecell lymphoma and subsequently went on to receive anallogeneic bone marrow transplant. This patient had arapid lymphocyte doubling time [29] (after a course ofchlorambucil) that appeared to be unaffected by theexperimental injections (Fig. 1). Patient 14 (who hadpreviously received local radiation therapy) requiredtreatment with Fludarabine for symptomatic CLLbeginning 13 months after entering the study protocol.
None of the other patients who were classed as devel-oping PD have required institution of chemotherapy,with the longest period of follow-up being 26 months.
No substantial changes in erythrocyte or plateletcounts (except for pt. 3) were observed. Serum IgG levelsdid not change significantly in any patient. In pt. 6, IgMlevels (which were initially low to normal (Table 3)) in-creased from 0.18 g/l to 0.27 g/l (normal 0.4–2.5 g/l) atthe end of the active treatment period but returned tothe starting values several months later.
In an attempt to enhance the apparent responses seenimmediately upon completion of the scheduled injec-tions, monthly maintenance injections were adminis-tered to pts. 2, 8, 10, 11, and 18. These ‘‘booster’’injections did not turn PRs into CRs but the patientswho received them (except pt. 2) continued to have lowerWBC counts at the end of the study period than theirstarting values.
In summary, 28% of the patients (5/18) exhibited aPR to their oxidized cell vaccines, while 33% (6/18) hadSD, and 39% (7/18) had disease progression (Table 2).Of the five patients who had PRs, three were injectedaccording to the more intense group 2 schedule.
Effect of tumor burden and hypogammaglobulinemiaon clinical outcome
A number of parameters were examined for their rela-tionships to the clinical outcome of the injections. Age(Table 1) did not seem to be of major importance. Twoof the patients who had PRs after vaccination (pts. 8 and10) were 75 and 77 years old, respectively.
Table 1 Patient clinical characteristics
Patienta Group Age (years) Sex Diseaseduration (years)
Rai stage Previoustherapy
WBCb CD38 (%) Vaccineeffect
1 1 39 F 7 I None 36 25 S2 1 50 M 1 I None 31 NA R3 1 52 F 4 IV C 20 14 P4 1 64 M 5 I None 34 5 S5 1 69 M 2 II None 35 1 P6 1 48 F 11 IV None 80 2 S7 2 62 M 1 0 None 22 9 R8 2 77 F 4 I C 37 46 R9 2 64 M 7 II None 91 2 P10 2 75 F 6 II None 52 8 R11 2 60 M 4 I C 42 3 S12 2 55 F 7 I None 98 1 S13 3 76 M 23 IV IVIG 81 3 S14 3 57 M 6 III R 87 32 P15 3 63 M 6 II None 52 5 P16 3 60 F 1 I None 31 11 P17 3 48 F 1 I None 21 10 P18 3 50 F 7 I None 45 8 R
0 lymphocytosis, I with adenopathy, II with hepatosplenomegaly,III with anemia, IV with thrombocytopenia [2], C chlorambucil orother alkylators, Rads local radiation, IVIG immunoglobulinreplacement, R partial response, S stable disease, P progressivedisease
aCorresponding patient numbers are maintained throughout thisarticlebWhite blood cell count (·106 cells/ml) at the beginning of thevaccine protocol
639
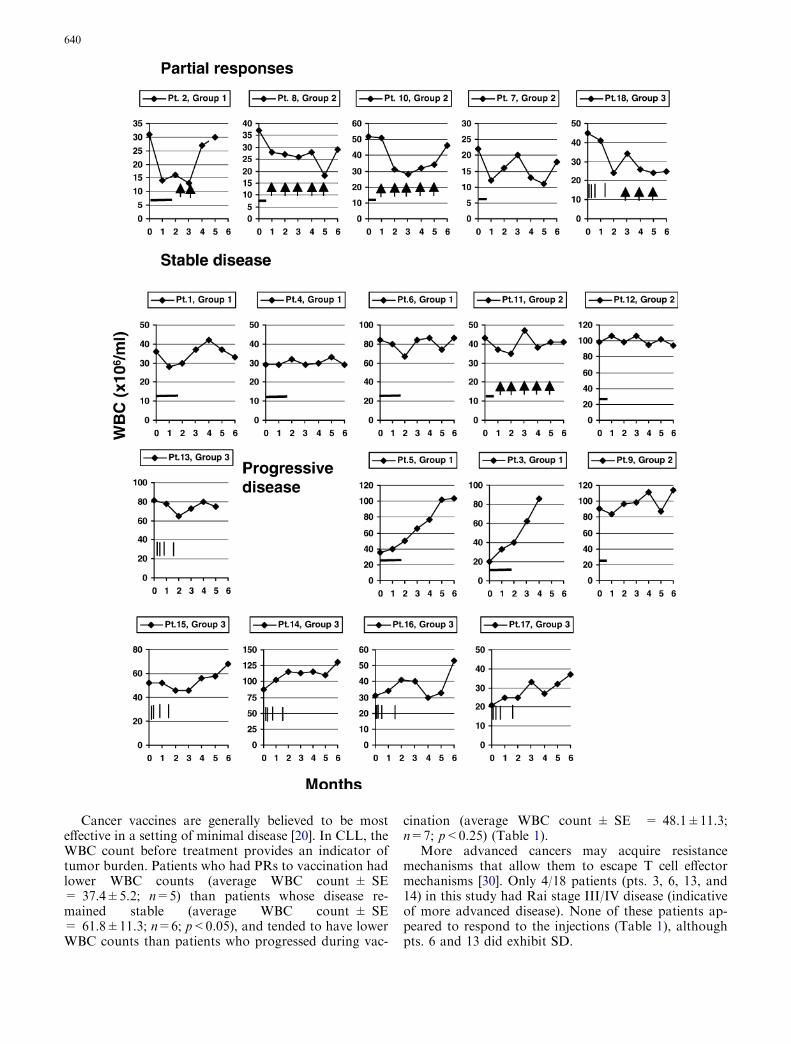
Cancer vaccines are generally believed to be mosteffective in a setting of minimal disease [20]. In CLL, theWBC count before treatment provides an indicator oftumor burden. Patients who had PRs to vaccination hadlower WBC counts (average WBC count ± SE= 37.4±5.2; n=5) than patients whose disease re-mained stable (average WBC count ± SE= 61.8±11.3; n=6; p<0.05), and tended to have lowerWBC counts than patients who progressed during vac-
cination (average WBC count ± SE = 48.1±11.3;n=7; p<0.25) (Table 1).
More advanced cancers may acquire resistancemechanisms that allow them to escape T cell effectormechanisms [30]. Only 4/18 patients (pts. 3, 6, 13, and14) in this study had Rai stage III/IV disease (indicativeof more advanced disease). None of these patients ap-peared to respond to the injections (Table 1), althoughpts. 6 and 13 did exhibit SD.
640

Chronic lymphocytic leukemia is associated with thedevelopment of a state of hypogammaglobulinemia [31].The cause of this humoral immunodeficiency is multi-factorial and thought to reflect partly a T cell deficiencystate. Somewhat surprisingly, patients whose diseaseresponded partially (average IgM ± SE = 0.51±0.2;n=5), or remained stable (average IgM ± SE= 0.13±0.04; n=6), after vaccination tended to havelower levels of serum IgM than patients whose diseaseprogressed over the course of the study (average Ig-M ± SE = 2.02±1.3; n=7) (Table 3), but again theserelationships were not statistically significant (p<0.25and p<0.10 for patients with responses and SD, re-spectively).
Toxicity and adverse events
The injections were generally well tolerated. Severalpatients (pts. 4, 8, 9, and 10) reported an improved senseof well-being during, and after, the period of activetreatment. The major toxicity consisted of local pain atthe injection site, which was transient and not consid-ered serious. Three patients, injected on the group 2injection schedule, reported a syndrome described as‘‘generalized burning’’ after the third or fourth injec-tions, which lasted for several hours, was not associatedwith fever or rash, and disappeared during the secondweek of injections. In pt. 6, rheumatoid factor activity
Table 2 Summary of trial results
No. ofpatients
Partialresponsesa
Stabledisease
Progressivedisease
Group 1 6 1 3 2Group 2 6 3 2 1Group 3 6 1 1 4Total 18 5 6 7
aPartial response is a ‡50% decrease in peripheral blood lympho-cytes, lymphadenopathy, and splenomegaly for at least 2 months.Progressive disease is a ‡50% increase in circulating lymphocytesor transformation to a more aggressive histology. Complete re-sponse is the absence of detectable leukemia cells. Stable disease iseverything else [2]
Table 3 Patient immunological characteristics
Patient Vaccineeffect
CD80 (%)a CD86 (%) IgM (g/l)b Initial anti-CLLresponsec
(A545–590 nm)
Peak increasein anti-CLLresponsed (A545–590 nm)
Final anti-CLLresponsee
(A545–590 nm)
2 R 4* 8 <0.05 0.112±0.006 0.054±0.003 0.166±0.0087 R 8 26 0.65 0.091±0.005 0.334±0.047 0.154±0.0088 R 8 40 0.51 0.002±0.000 0.076±0.004 0.002±0.00010 R 17 34 1.19 �0.037±0.002 0.252±0.010 0.130±0.00118 R 17 13 0.19 0.16±0.002 0.217±0.003 0.377±0.0084 S 1 11 0.18 �0.006±0.000 0.032±0.001 0.012±0.0011 S 3 7 0.07 0.058±0.000 0.052±0.001 0.093±0.0016 S 26 15 0.18 0.177±0.007 0.072±0.004 �0.023±0.00111 S 7* 5 0.07 0.08±0.001 0.012±0.001 0.046±0.00212 S 1 79 0.25 �0.017±0.000 0.021±0.001 �0.017±0.00113 S 48* 3 <0.05 0.386±0.019 0.037±0.002 0.370±0.0183 P 2* 6 1.19 0.062±0.014 0.046±0.012 0.121±0.0345 P 1 14 0.29 0.177±0.001 �0.112±0.003 0.021±0.0019 P 16 33 1.5 NA NA NA14 P 3 42 9.7 0.065±0.002 0.043±0.003 0.108±0.01115 P 9 30 0.27 0.148±0.001 0.006±0.001 0.067±0.00116 P 4 31 0.06 0.193±0.006 0.082±0.002 0.177±0.00717 P 4 17 1.1 0.165±0.003 0.022±0.001 0.162±0.008
R partial response, S stable disease, P progressive disease, NA notavailableaThe percentages of CD80+ and CD86+ circulating CLL cells weredetermined by flow cytometry. For the values marked by a ‘‘*’’, theCD80 and CD86 expression were determined on CLL cells that hadbeen cultured in vitro for 4 days for use as control stimulator cellsin proliferation assays, as described in the Materials and methodsbThe normal range for serum IgM is 0.4–2.5 g/lcT cells purified from the patients’ blood before commencing thevaccination protocol were stimulated with irradiated, activated
autologous CLL cells. After 6 days of culture, proliferation wasmeasured in a colorimetric assay, as described in the Materials andmethods. The average and standard error of the results from trip-licate wells are reporteddThe peak increase in anti-CLL response is the difference betweenthe maximum proliferative response at any time after vaccinationand the initial anti-CLL responseeThe final anti-CLL response is the response at the time of the lastfollow-up visit. The average and standard error of the results fromtriplicate wells are reported
Fig. 1 Clinical course of individual patients. The clinical responseto vaccination is shown for each patient during the 6-month periodof monitoring while on the study. The WBC counts beforevaccination (time 0) and each month during the follow-up periodare shown on the x-axis. The schedule of injections for group 1 isindicated by the long horizontal bar (12 injections over 6 weeks).The schedule for group 2 is indicated by the short horizontal bar (12injections over 16 days) and the schedule for group 3 is indicated bythe four vertical bars (four injections on days 1, 2, 21, and 38). Thelines with arrowheads indicate booster injections given at monthlyinjections to patients who appeared to respond to their prescribedinjections. The patients are grouped according to their apparentresponses to vaccination
b
641

increased from 19 IU/ml to 114 IU/ml (normal<40 IU/ml) around the time of the last injection, butdecreased to 23 IU/ml over the following 3 months.
Immunological responses
T cells were collected from each patient before com-mencing the injections and at regular intervals after-wards. CLL cells that had been cryopreserved at thebeginning of the trial were used as stimulators, sinceCLL cells taken later on might have been subject toselective immunological pressures resulting in theemergence of antigen-loss variants [14]. For each pa-tient, proliferation assays with the stored T cell sampleswere performed simultaneously to allow a meaningfulcomparison of anti-CLL responses at the different timepoints. As a control the differences in proliferative re-sponses to CLL cells were not simply a result of artifactsassociated with freezing and thawing, the quality of thethawed T cells was indicated by also measuring theirability to proliferate in response to the mitogens, PHA,and PWM.
As shown in Table 3 (column 6), responsiveness of Tcells to (unknown) autologous CLL antigens beforevaccination was variable. For example, pts. 4, 8, 10, 11,and 12 did not appear to have CLL-reactive T cells inthis assay. However, there appeared to be no correlationof a pre-existing anti-CLL proliferative response withthe subsequent clinical response to vaccination.
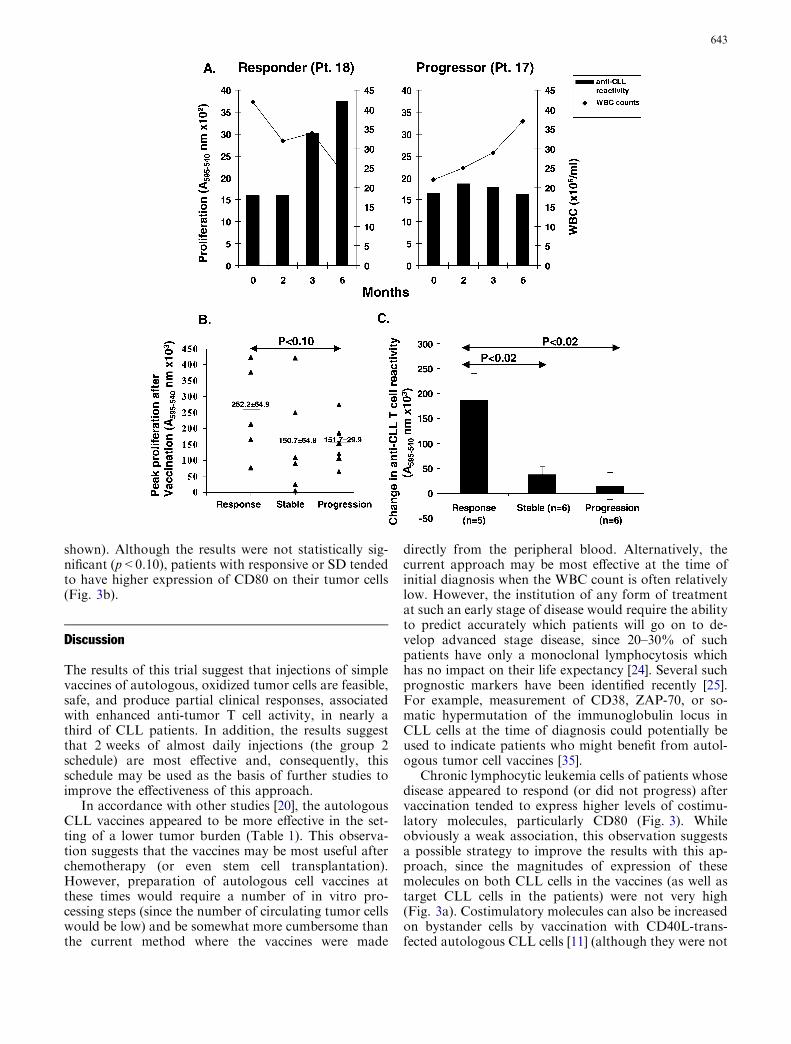
T cell responses after vaccination were also highlypatient-specific (Table 3, column 7). In some cases, therewas a clear increase in the proliferative response at somepoint (more than three standard deviations above theinitial average response from the triplicate wells, or(more conservatively) >0.050 absorbance units higherthan before the injections), as exemplified by pt. 18(Fig. 2a) and pts. 1, 2, 6, 7, 8, 10, and 16 (Table 3,column 7). In others, increased CLL-reactive T cell re-sponses could not be demonstrated with this assay (e.g.,pt. 17, see Fig. 2a). On an individual basis, pts. 1 and 6had SD and pt. 16 had disease progression, despite anapparent increase in anti-CLL T cell reactivity inducedby the vaccines. In general, the absolute peak prolifer-ative response after vaccination was higher in the pa-tients who appeared to have PRs to the vaccines(Fig. 2b). Moreover, when the change from baselinereactivity was calculated, there was a statistically sig-nificant increase in T cell reactivity to CLL antigens inthe patients who responded clinically to the injections(p<0.02), compared with patients whose disease eitherremained stable or progressed (Fig. 2c).
In five patients (pts. 2, 3, 7, 10, and 18), the prolif-erative T cell response at the end of the study was>0.050 absorbance units higher than before entering thestudy (Table 3, column 8). Note that pts. 2, 8, 10, 11,and 18 received monthly maintenance injections forsome, or all, of the follow-up period after completing theactive injection protocol. Of the patients who exhibited
an increased anti-CLL T cell response in vitro at the endof the study, four had PRs to vaccination. Most of theremaining 12 evaluable patients (without increased anti-CLL T cell reactivity in vitro at the end of the study) hadeither PD or SD.
Costimulatory molecule expression on CLL cells
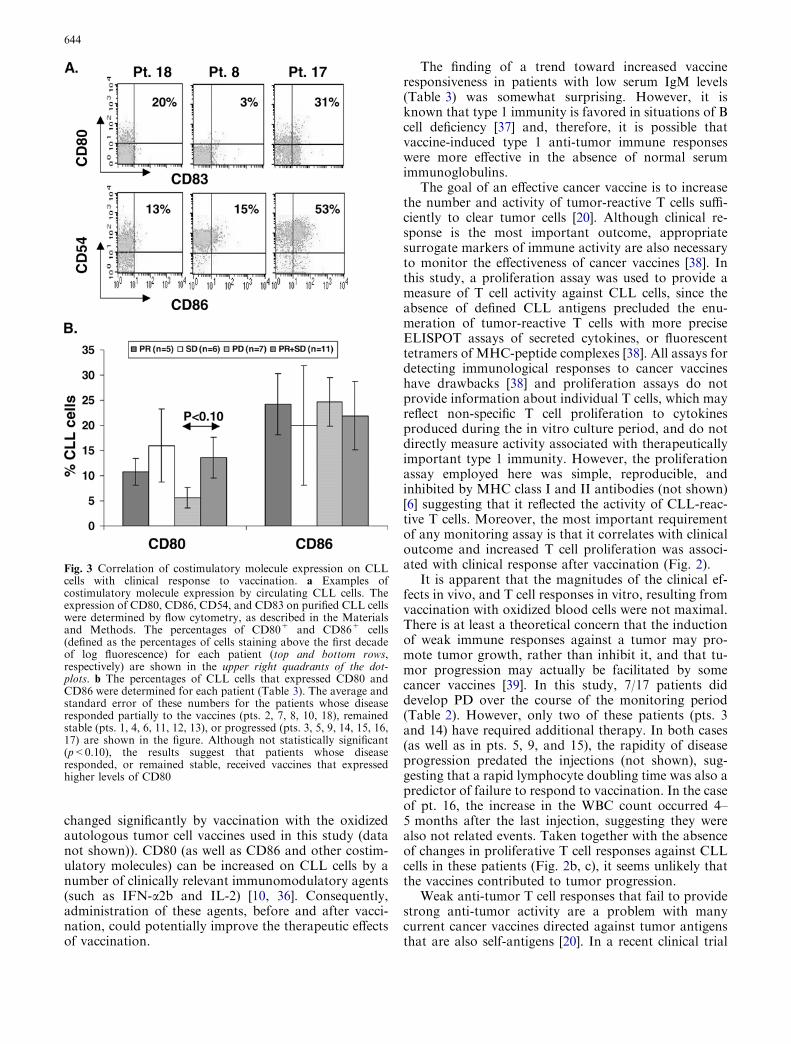
We anticipated that tumor-reactive T cells would bestimulated in draining lymph nodes directly by oxidizedtumor cells, as well as by CLL antigens shed from theoxidized cells and presented indirectly by professionalAPCs, such as dendritic cells [32]. Costimulatory mole-cules (including members of the B7-family, such asCD80 and CD86), adhesion molecules (such as CD54),and other molecules (such as CD83) expressed on APCsare important for strong activation of T cells [33].Moreover, once an anti-tumor response has been initi-ated by a vaccine, costimulatory molecules on the targettumor cells may be important for maintaining strongcytotoxic T cell effector function [34]. Accordingly, weexamined the expression of CD80, CD86, CD54, andCD83 on the CLL cells of the study patients (Fig. 3).CD80 and CD86 expression, especially, were found to behighly variable, as shown by the examples in Fig. 3a anddid not change significantly in the short time betweenoxidation and injection into the patient (data not
Fig. 2 Correlation of clinical responses with changes in anti-CLL Tcell reactivity. Blood was taken before and after the vaccinationprotocol. T cells were isolated as described in the Materials andmethods and then cryopreserved. As a measure of anti-CLL T cellreactivity, an aliquot of pretreatment CLL cells was thawed andactivated with phorbol esters and IL-2 in order to make them intoefficient APCs, as described in the Materials and methods. After4 days, the activated CLL cells were washed, irradiated, and usedto stimulate the T cells from the different time-points (after theyhad been thawed simultaneously and washed). Subsequent T cellproliferation was measured in a colorimetric assay, 7 days later. aCharacteristic results are shown for pt. 18 (who exhibited a PR tothe vaccine protocol) and pt. 17 (who did not). T cell proliferationand corresponding WBC counts at the different time points areshown. As a control to ensure that apparent increases in anti-CLLresponses were not simply an artifact of freezing conditions at thattime point, the ability of the thawed T cells to respond to mitogenswas measured (at the time that the anti-CLL assays were set up) bya colorimetric assay after 5 days of stimulation. For pt. 18, thePHA responses at 0, 2, 3, and 6 months were 0.014, 0.007, 0.129,and 0.034, respectively. For pt. 17, these PHA responses were0.011, 0.070, 0.042, and 0.070, respectively. b The absolute value ofthe peak T cell proliferation response to CLL cells after vaccinationis shown for each patient. The average and standard error was thendetermined for patients whose disease responded, stabilized, orprogressed after the vaccines (as described in Tables 1, 2, andFig. 1). A response to vaccination tended to correlate with a higherT cell reactivity against CLL cells (approaching statistical signif-icance; p<0.10). c For each patient, the initial anti-CLL T cellproliferative response before vaccination was subtracted from thepeak response at any time during the study period (Table 3). Theaverage and standard error of these differences were thendetermined according to the clinical outcome. The results showthat a response to vaccination correlated with a significant increase(p<0.02) in T cell reactivity against CLL cells
c
642
shown). Although the results were not statistically sig-nificant (p<0.10), patients with responsive or SD tendedto have higher expression of CD80 on their tumor cells(Fig. 3b).
Discussion
The results of this trial suggest that injections of simplevaccines of autologous, oxidized tumor cells are feasible,safe, and produce partial clinical responses, associatedwith enhanced anti-tumor T cell activity, in nearly athird of CLL patients. In addition, the results suggestthat 2 weeks of almost daily injections (the group 2schedule) are most effective and, consequently, thisschedule may be used as the basis of further studies toimprove the effectiveness of this approach.
In accordance with other studies [20], the autologousCLL vaccines appeared to be more effective in the set-ting of a lower tumor burden (Table 1). This observa-tion suggests that the vaccines may be most useful afterchemotherapy (or even stem cell transplantation).However, preparation of autologous cell vaccines atthese times would require a number of in vitro pro-cessing steps (since the number of circulating tumor cellswould be low) and be somewhat more cumbersome thanthe current method where the vaccines were made
directly from the peripheral blood. Alternatively, thecurrent approach may be most effective at the time ofinitial diagnosis when the WBC count is often relativelylow. However, the institution of any form of treatmentat such an early stage of disease would require the abilityto predict accurately which patients will go on to de-velop advanced stage disease, since 20–30% of suchpatients have only a monoclonal lymphocytosis whichhas no impact on their life expectancy [24]. Several suchprognostic markers have been identified recently [25].For example, measurement of CD38, ZAP-70, or so-matic hypermutation of the immunoglobulin locus inCLL cells at the time of diagnosis could potentially beused to indicate patients who might benefit from autol-ogous tumor cell vaccines [35].
Chronic lymphocytic leukemia cells of patients whosedisease appeared to respond (or did not progress) aftervaccination tended to express higher levels of costimu-latory molecules, particularly CD80 (Fig. 3). Whileobviously a weak association, this observation suggestsa possible strategy to improve the results with this ap-proach, since the magnitudes of expression of thesemolecules on both CLL cells in the vaccines (as well astarget CLL cells in the patients) were not very high(Fig. 3a). Costimulatory molecules can also be increasedon bystander cells by vaccination with CD40L-trans-fected autologous CLL cells [11] (although they were not
643
changed significantly by vaccination with the oxidizedautologous tumor cell vaccines used in this study (datanot shown)). CD80 (as well as CD86 and other costim-ulatory molecules) can be increased on CLL cells by anumber of clinically relevant immunomodulatory agents(such as IFN-a2b and IL-2) [10, 36]. Consequently,administration of these agents, before and after vacci-nation, could potentially improve the therapeutic effectsof vaccination.
The finding of a trend toward increased vaccineresponsiveness in patients with low serum IgM levels(Table 3) was somewhat surprising. However, it isknown that type 1 immunity is favored in situations of Bcell deficiency [37] and, therefore, it is possible thatvaccine-induced type 1 anti-tumor immune responseswere more effective in the absence of normal serumimmunoglobulins.
The goal of an effective cancer vaccine is to increasethe number and activity of tumor-reactive T cells suffi-ciently to clear tumor cells [20]. Although clinical re-sponse is the most important outcome, appropriatesurrogate markers of immune activity are also necessaryto monitor the effectiveness of cancer vaccines [38]. Inthis study, a proliferation assay was used to provide ameasure of T cell activity against CLL cells, since theabsence of defined CLL antigens precluded the enu-meration of tumor-reactive T cells with more preciseELISPOT assays of secreted cytokines, or fluorescenttetramers of MHC-peptide complexes [38]. All assays fordetecting immunological responses to cancer vaccineshave drawbacks [38] and proliferation assays do notprovide information about individual T cells, which mayreflect non-specific T cell proliferation to cytokinesproduced during the in vitro culture period, and do notdirectly measure activity associated with therapeuticallyimportant type 1 immunity. However, the proliferationassay employed here was simple, reproducible, andinhibited by MHC class I and II antibodies (not shown)[6] suggesting that it reflected the activity of CLL-reac-tive T cells. Moreover, the most important requirementof any monitoring assay is that it correlates with clinicaloutcome and increased T cell proliferation was associ-ated with clinical response after vaccination (Fig. 2).
It is apparent that the magnitudes of the clinical ef-fects in vivo, and T cell responses in vitro, resulting fromvaccination with oxidized blood cells were not maximal.There is at least a theoretical concern that the inductionof weak immune responses against a tumor may pro-mote tumor growth, rather than inhibit it, and that tu-mor progression may actually be facilitated by somecancer vaccines [39]. In this study, 7/17 patients diddevelop PD over the course of the monitoring period(Table 2). However, only two of these patients (pts. 3and 14) have required additional therapy. In both cases(as well as in pts. 5, 9, and 15), the rapidity of diseaseprogression predated the injections (not shown), sug-gesting that a rapid lymphocyte doubling time was also apredictor of failure to respond to vaccination. In the caseof pt. 16, the increase in the WBC count occurred 4–5 months after the last injection, suggesting they werealso not related events. Taken together with the absenceof changes in proliferative T cell responses against CLLcells in these patients (Fig. 2b, c), it seems unlikely thatthe vaccines contributed to tumor progression.
Weak anti-tumor T cell responses that fail to providestrong anti-tumor activity are a problem with manycurrent cancer vaccines directed against tumor antigensthat are also self-antigens [20]. In a recent clinical trial
Fig. 3 Correlation of costimulatory molecule expression on CLLcells with clinical response to vaccination. a Examples ofcostimulatory molecule expression by circulating CLL cells. Theexpression of CD80, CD86, CD54, and CD83 on purified CLL cellswere determined by flow cytometry, as described in the Materialsand Methods. The percentages of CD80+ and CD86+ cells(defined as the percentages of cells staining above the first decadeof log fluorescence) for each patient (top and bottom rows,respectively) are shown in the upper right quadrants of the dot-plots. b The percentages of CLL cells that expressed CD80 andCD86 were determined for each patient (Table 3). The average andstandard error of these numbers for the patients whose diseaseresponded partially to the vaccines (pts. 2, 7, 8, 10, 18), remainedstable (pts. 1, 4, 6, 11, 12, 13), or progressed (pts. 3, 5, 9, 14, 15, 16,17) are shown in the figure. Although not statistically significant(p<0.10), the results suggest that patients whose diseaseresponded, or remained stable, received vaccines that expressedhigher levels of CD80
644
involving melanoma patients, we observed similartransient anti-tumor responses after vaccines composedof the defined tumor antigen, gp100 [40]. More profoundtherapeutic responses were seen when high doses ofIFN-a2b were administered subsequently to these pa-tients [40]. These results suggest an important thera-peutic synergy between tumor vaccines and IFN-a2b,since single agent therapy with either modality has onlymodest effects on metastatic melanoma [41]. If thissynergy applies to CLL, the use of oxidized tumor cellvaccines followed by IFN-a2b may be an effectivetreatment strategy for this hematologic malignancy.
Regardless of these considerations, the results ob-tained in this study suggest that oxidized autologoustumor vaccines (with or without additional immuno-modulatory agents) may offer a potential alternative tothe traditional ‘‘watch and wait’’ strategy for selectedCLL patients. Even if disease stabilization only (whichmight still prolong the time to institution of chemo-therapy and have an impact on overall survival) isachieved, this approach appears to merit further clinicalinvestigation.
Acknowledgements Supported by grants from the Leukemia Re-search Fund of Canada, the Ontario Cancer Research Network(OCRN), and from Vasogen, Inc.
References
1. Caligaris-Cappio F, Hamblin TJ (1999) B-cell chronic lym-phocytic leukemia: a bird of a different feather. J Clin Oncol17:399
2. Cheson BD, Bennett JM, Grever M, Kay N, Keating MJ,O’Brien S, Rai KR (1996) National Cancer Institute-sponsoredworking group guidelines for chronic lymphocytic leukemia:revised guidelines for diagnosis and treatment. Blood 87:4990
3. Ribera JM, Vinolas N, Urbano-Ispizua A, Gallart T, Mont-serrat E, Rozman C (1987) ‘‘Spontaneous’’ complete remissionsin chronic lymphocytic leukemia: report of three cases and re-view of the literature. Blood Cells 12:471
4. Ziegler-Heitbrock HW, Schlag R, Flieger D, Thiel E (1989)Favorable response of early stage B CLL patients to treatmentwith IFN-alpha 2. Blood 73:1426
5. Schetelig J, Thiede C, Bornhauser M, Schwerdtfeger R, KiehlM, Beyer J, Sayer HG, Kroger N, Hensel M, Scheffold C, HeldTK, Hoffken K, Ho AD, Kienast J, Neubauer A, Zander AR,Fauser AA, Ehninger G, Siegert W (2003) Evidence of a graft-versus-leukemia effect in chronic lymphocytic leukemia afterreduced-intensity conditioning and allogeneic stem-cell trans-plantation: the Cooperative German Transplant Study Group.J Clin Oncol 21:2747
6. Gitelson E, Hammond C, Mena J, Lorenzo M, Buckstein R,Berinstein N, Imrie K, Spaner DE (2003) Chronic lymphocyticleukemia-reactive T cells during tumor progression and afteroxidized autologous tumor cell vaccines. Clin Can Res 9:1656
7. Krackhardt AM, Witzens M, Harig S, Hodi FS, Zauls AJ,Chessia M, Barrett P, Gribben JG (2002) Identification of tu-mor-associated antigens in chronic lymphocytic leukemia bySEREX. Blood 100:2123
8. Ward S, Casey D, Labarthe MC, Whelan M, Dalgleish A,Pandha H, Todryk S (2002) Immunotherapeutic potential ofwhole tumour cells. Cancer Immunol Immunother 51:351
9. Schultze JL, Michalak S, Seamon MJ, Dranoff G, Jung K,Daley J, Delgado JC, Gribben JG, Nadler LM (1997) CD40-activated human B cells: an alternative source of highly efficient
antigen presenting cells to generate autologous antigen-specificT cells for adoptive immunotherapy. J Clin Invest 100:2757
10. Decker T, Schneller F, Kronschnabl M, Dechow T, LipfordGB, Wagner H, Peschel C (2000) Immunostimulatory CpG-oligonucleotides induce functional high affinity IL-2 receptorson B-CLL cells: costimulation with IL-2 results in a highlyimmunogenic phenotype. Exp Hematol 28:558
11. Wierda WG, Cantwell MJ, Woods SJ, Rassenti LZ, PrussakCE, Kipps TJ (2000) CD40-ligand (CD154) gene therapy forchronic lymphocytic leukemia. Blood 96:2917
12. Chuah MK, Collen D, VandenDriessche T (2003) Biosafety ofadenoviral vectors. Curr Gene Ther 3:527
13. Demaria S, Ng B, Devitt ML, Babb JS, Kawashima N, LiebesL, Formenti SC (2004) Ionizing radiation inhibition of distantuntreated tumors (abscopal effect) is immune mediated. Int JRadiat Oncol Biol Phys 58:862
14. Baurain JF, Colau D, van Baren N, Landry C, Martelange V,Vikkula M, Boon T, Coulie PG (2000) High frequency ofautologous anti-melanoma CTL directed against an antigengenerated by a point mutation in a new helicase gene. JImmunol 164:6057
15. Castelli C, Rivoltini L, Rini F, Belli F, Testori A, Maio M,Mazzaferro V, Coppa J, Srivastava PK, Parmiani G (2004)Heat shock proteins: biological functions and clinical applica-tion as personalized vaccines for human cancer. CancerImmunol Immunother 53:227
16. Shi Y, Evans JE, Rock KL (2003) Molecular identification of adanger signal that alerts the immune system to dying cells.Nature 425:516
17. Scaffidi P, Misteli T, Bianchi ME (2002) Release of chromatinprotein HMGB1 by necrotic cells triggers inflammation. Nat-ure 418:191
18. Cooke ED, Pockley AG, Tucker AT, Kirby JD, Bolton AE(1997) Treatment of severe Raynaud’s syndrome by injectionof autologous blood pretreated by heating, ozonation andexposure to ultraviolet light (H-O-U) therapy. Int Angiol16:250
19. Bretscher P (2004) Living with the ups and downs of the twosignal model. Immunol Cell Biol 82:141
20. Berzofsky JA, Terabe M, Oh S, Belyakov IM, Ahlers JD, JanikJE, Morris JC (2004) Progress on new vaccine strategies for theimmunotherapy and prevention of cancer. J Clin Invest113:1515
21. Kundig TM, Shahinian A, Kawai K, Mittrucker HW, SebzdaE, Bachmann MF, Mak TW, Ohashi PS (1996) Duration ofTCR stimulation determines costimulatory requirement of Tcells. Immunity 5:41
22. Parish CR (1996) Immune deviation: a historical perspective.Immunol Cell Biol 74:449
23. Rai KR, Sawitsky A, Cronkite EP, Chanana AD, Levy RN,Pasternack BS (1975) Clinical staging of chronic lymphocyticleukemia. Blood 46:219
24. Guarini A, Gaidano G, Mauro FR, Capello D, Mancini F, DePropris MS, Mancini M, Orsini E, Gentile M, Breccia M,Cuneo A, Castoldi G, Foa R (2003) Chronic lymphocyticleukemia patients with highly stable and indolent disease showdistinctive phenotypic and genotypic features. Blood 102:1035
25. Kay NE, Jelinek DF (2002) B-CLL: is the enigma of diseaseheterogeneity about to be revealed? Blood 100:1110
26. Okamura J, Letarte M, Stein LD, Sigal NH, Gelfand EW(1982) Modulation of chronic lymphocytic leukemia cells byphorbol ester: increase in Ia expression, IgM secretion andMLR stimulatory capacity. J Immunol 128:2276
27. Hammond C, Shi Y, Mena J, Tomic Y, Cervi D, He L, de-Benedette M, Schuh A, Wender P, Radvanyi L, Spaner D(2004) Effect of serum and anti-oxidants on the immunoge-nicity of protein kinase C-activated chronic lymphocytic leu-kemia cells. J Immunother 27:(in press)
28. Ahmed SA, Gogal RMJ, Walsh JE (1994) A new rapid andsimple non-radioactive assay to monitor and determine theproliferation of lymphocytes: an alternative to [3H]thymidineincorporation assay. J Immunol Methods 170:211
645

29. Montserrat E, Sanchez-Bisono J, Vinolas N, Rozman C (1986)Lymphocyte doubling time in chronic lymphocytic leukaemia:analysis of its prognostic significance. Br J Haematol 62:567
30. Ellem KA, Schmidt CW, Li CL, Misko I, Kelso A, Sing G,Macdonald G, O’Rourke MG (1998) The labyrinthine ways ofcancer immunotherapy—T cell, tumor cell encounter: ‘‘how doI lose thee? Let me count the ways’’. Adv Cancer Res 75:203
31. Cantwell M, Hua T, Pappas J, Kipps TJ (1997) AcquiredCD40-ligand deficiency in chronic lymphocytic leukemia. NatMed 3:984
32. Ochsenbein AF, Sierro S, Odermatt B, Pericin M, Karrer U,Hermans J, Hemmi S, Hengartner H, Zinkernagel RM (2001)Roles of tumour localization, second signals and cross primingin cytotoxic T-cell induction. Nature 411:1058
33. Hart DN (1997) Dendritic cells: unique leukocyte populationswhich control the primary immune response. Blood 90:3245
34. Allison J, Stephens LA, Kay TW, Kurts C, Heath WR, MillerJF, Krummel MF (1998) The threshold for autoimmune T cellkilling is influenced by B7-1. Eur J Immunol 28:949
35. Crespo M, Bosch F, Villamor N, Bellosillo B, Colomer D,Rozman M, Marce S, Lopez-Guillermo A, Campo E, Mont-serrat E (2003) ZAP-70 expression as a surrogate for immu-noglobulin-variable-region mutations in chronic lymphocyticleukemia. N Engl J Med 348:1764
36. Spaner DE, Hammond C, Mena J, Shi Y (2004) Effect of IL-2Rbeta-binding cytokines on costimulatory properties of CLLcells: implications for immunotherapy. Br J Haematol 127:531
37. Qin Z, Richter G, Schuler T, Ibe S, Cao X, Blankenstein T(1998) B cells inhibit induction of T cell-dependent tumorimmunity. Nat Med 4:627
38. Keilholz U, Weber J, Finke JH, Gabrilovich DI, Kast WM,Disis ML, Kirkwood JM, Scheibenbogen C, Schlom J, MainoVC, Lyerly HK, Lee PP, Storkus W, Marincola F, Worobec A,Atkins MB (2002) Immunologic monitoring of cancer vaccinetherapy: results of a workshop sponsored by the Society forBiological Therapy. J Immunother 25:97
39. Prehn RT (1993) Tumor immunogenicity: how far can it bepushed? Proc Natl Acad Sci USA 90:4332
40. Astsaturov I, Petrella T, Bagriacik EU, de Benedette M, UgerR, Lumber G, Berinstein N, Elias I, Iscoe N, Hammond C,Hamilton P, Spaner DE (2003) Amplification of virus-inducedantimelanoma T-cell reactivity by high-dose interferon-al-pha2b: implications for cancer vaccines. Clin Cancer Res9:4347
41. Kirkwood JM, Ibrahim JG, Sondak VK, Richards J, FlahertyLE, Ernstoff MS, Smith TJ, Rao U, Steele M, Blum RH (2000)High- and low-dose interferon alfa-2b in high-risk melanoma:first analysis of intergroup trial E1690/S9111/C9190. J ClinOncol 18:2444
646
Copyright © 2022 FDOKUMEN




















