
A novel diagnostic criterion for lymph node metastasis in cervical cancer using multi-detector...
7
A novel diagnostic criterion for lymph node metastasis in cervical cancer using multi-detector computed tomography Koji Yamanoi a , Noriomi Matsumura a, ⁎, Aki Kido b , Tsukasa Baba a , Junzo Hamanishi a , Ken Yamaguchi a , Yumiko Yoshioka a , Hisham Abou Taleb a , Kaori Togashi b , Ikuo Konishi a a Department of Gynecology and Obstetrics, Kyoto University, Graduate School of Medicine, Japan b Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University, Graduate School of Medicine, Japan HIGHLIGHTS • Using multi-detector CT, we identified a novel criterion to diagnose lymph node metastasis in a region-by-region manner. • The criterion, 5 mm in a short-axis diameter, helps us precisely assess the lymph node status of cervical cancer patients. • This new criterion should help us develop individualized treatments for cervical cancer patients. abstract article info Article history: Received 21 June 2013 Accepted 12 October 2013 Available online 19 October 2013 Keywords: Cervical cancer Lymph node metastasis Multi-detector computed tomography (MDCT) Neoadjuvant chemotherapy (NAC) Objectives. The sensitivity of the current 10 mm cut-off diameter that is used to diagnose lymph node (LN) metastasis is too low. This is the first study to develop a new criterion to diagnose LN metastasis in a region-by- region manner using multi-detector computed tomography (MDCT). Methods. 1) The short-axis diameter of the LNs in MDCT images from 1-mm slices obtained immediately prior to surgery was compared with the pathological diagnosis in 78 uterine cervical cancer patients undergoing primary surgery. For the region-by-region analysis, we divided para-aortic and pelvic spaces into 13 regions. 2) In 28 cases in which patients received neoadjuvant chemotherapy (NAC) followed by surgery, we compared MDCT images before and after NAC. Results. 1) The optimal cut-off in the region-by-region analysis was 5 mm, yielding 71% sensitivity and 79% specificity. 2) NAC significantly decreased LN size (p b 0.0001). NAC decreased the number of swollen LN regions (N 5 mm) from 51% (81/158) to 26% (41/158). Conclusions. The new criterion developed using MDCT could be effective for accurately assessing LN status. It also facilitates the assessment of NAC efficacy regarding the eradication of LN metastases. © 2013 Elsevier Inc. All rights reserved. Introduction Cervical cancer is the second most common gynecologic malignancy in the world [1]. In addition to surgery and radiotherapy, neoadjuvant chemotherapy (NAC) followed by surgery has been used to treat locally advanced cervical cancer [2]. Because the prognosis of patients with cervical cancer depends largely on lymph node (LN) metastasis [3–5], it is important to assess the LN status accurately before starting treatment. Based on studies comparing the size of the LNs in images and pathological diagnoses, a 10 mm short-axis diameter became the currently accepted cut-off in both clinical practice and clinical trials [6–8]. However, the sensitivity of this conventional criterion has been reported to be as low as 25% [9]. Furthermore, previous studies have generally predicted the presence of LN metastases in the patient without describing the location. In the present study, we conducted a detailed, region-by-region analysis to generate a new criterion that could identify region-specific, swollen LNs. The use of our criterion could lead to the improvement of individualized treatments. In conducting the detailed analysis of LN status, the width of the slices, 7 mm in conventional CT and 5 mm in MRI, was considered to be a key limitation [7]. We therefore used a multi-detector CT (MDCT) scanner, which allowed one mm slice images [10,11]. Using MDCT, we successfully generated a new criterion to diagnose LN metastasis. Using the new criterion, we were able to examine the efficacy of NAC in eradicating LN metastases in a region-by-region manner for the first time. Gynecologic Oncology 131 (2013) 701–707 ⁎ Corresponding author at: 54 Shogoin Kawahara-cho, Sakyo-ku, Kyoto, 606-8507, Japan. Fax: +81 75 761 3967. E-mail address: [email protected] (N. Matsumura). 0090-8258/$ – see front matter © 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ygyno.2013.10.014 Contents lists available at ScienceDirect Gynecologic Oncology journal homepage: www.elsevier.com/locate/ygyno
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A novel diagnostic criterion for lymph node metastasis in cervical cancer using multi-detector...

Gynecologic Oncology 131 (2013) 701–707
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r .com/ locate /ygyno
A novel diagnostic criterion for lymph node metastasis in cervical cancer usingmulti-detector computed tomography
Koji Yamanoi a, Noriomi Matsumura a,⁎, Aki Kido b, Tsukasa Baba a, Junzo Hamanishi a, Ken Yamaguchi a,Yumiko Yoshioka a, Hisham Abou Taleb a, Kaori Togashi b, Ikuo Konishi a
a Department of Gynecology and Obstetrics, Kyoto University, Graduate School of Medicine, Japanb Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University, Graduate School of Medicine, Japan
H I G H L I G H T S
• Using multi-detector CT, we identified a novel criterion to diagnose lymph node metastasis in a region-by-region manner.• The criterion, 5 mm in a short-axis diameter, helps us precisely assess the lymph node status of cervical cancer patients.• This new criterion should help us develop individualized treatments for cervical cancer patients.
⁎ Corresponding author at: 54 Shogoin Kawahara-chJapan. Fax: +81 75 761 3967.
E-mail address: [email protected] (N. Matsu
0090-8258/$ – see front matter © 2013 Elsevier Inc. All rihttp://dx.doi.org/10.1016/j.ygyno.2013.10.014
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 21 June 2013Accepted 12 October 2013Available online 19 October 2013Keywords:Cervical cancerLymph node metastasisMulti-detector computed tomography (MDCT)Neoadjuvant chemotherapy (NAC)
Objectives. The sensitivity of the current 10 mm cut-off diameter that is used to diagnose lymph node (LN)metastasis is too low. This is the first study to develop a new criterion to diagnose LN metastasis in a region-by-region manner using multi-detector computed tomography (MDCT).
Methods.1) The short-axis diameter of the LNs inMDCT images from1-mmslices obtained immediately prior tosurgery was compared with the pathological diagnosis in 78 uterine cervical cancer patients undergoing primarysurgery. For the region-by-region analysis, we divided para-aortic and pelvic spaces into 13 regions. 2) In 28cases in which patients received neoadjuvant chemotherapy (NAC) followed by surgery, we compared MDCTimages before and after NAC.
Results. 1) The optimal cut-off in the region-by-region analysis was 5 mm, yielding 71% sensitivity and 79%
specificity. 2) NAC significantly decreased LN size (p b 0.0001). NAC decreased the number of swollen LN regions(N5mm) from 51% (81/158) to 26% (41/158).Conclusions. ThenewcriteriondevelopedusingMDCTcould be effective for accurately assessing LN status. It alsofacilitates the assessment of NAC efficacy regarding the eradication of LN metastases.
© 2013 Elsevier Inc. All rights reserved.
Introduction
Cervical cancer is the secondmost common gynecologicmalignancyin the world [1]. In addition to surgery and radiotherapy, neoadjuvantchemotherapy (NAC) followed by surgery has been used to treat locallyadvanced cervical cancer [2]. Because the prognosis of patients withcervical cancer depends largely on lymph node (LN) metastasis [3–5],it is important to assess the LN status accurately before startingtreatment.
Based on studies comparing the size of the LNs in images andpathological diagnoses, a 10 mm short-axis diameter became thecurrently accepted cut-off in both clinical practice and clinical trials
o, Sakyo-ku, Kyoto, 606-8507,
mura).
ghts reserved.
[6–8]. However, the sensitivity of this conventional criterion hasbeen reported to be as low as 25% [9]. Furthermore, previous studieshave generally predicted the presence of LN metastases in thepatient without describing the location. In the present study, weconducted a detailed, region-by-region analysis to generate a newcriterion that could identify region-specific, swollen LNs. The useof our criterion could lead to the improvement of individualizedtreatments.
In conducting the detailed analysis of LN status, the width of theslices, 7mm in conventional CT and 5mm in MRI, was considered to bea key limitation [7]. We therefore used a multi-detector CT (MDCT)scanner, which allowed one mm slice images [10,11]. Using MDCT, wesuccessfully generated a new criterion to diagnose LN metastasis. Usingthe new criterion, we were able to examine the efficacy of NAC ineradicating LN metastases in a region-by-region manner for the firsttime.
702 K. Yamanoi et al. / Gynecologic Oncology 131 (2013) 701–707
Materials and methods
Assessment of MDCT images
PatientsPatients with stage IA2 to IIB cervical cancer whowere being treated
in our department were retrospectively analyzed. The staging wasperformed according to the classification of the International Federationof Gynecology and Obstetrics (FIGO, 1994) [12]. With the writtenconsent of each patient, andunder the approval of the ethics committee,we initiated the MDCT study in January 2007: 106 patients underwentMDCT examination within two weeks before surgery; 78 patientsunderwent primary surgery; and the remaining 28 patients receivedNAC followed by surgery. In Table 1, we show the number of patientsarranged according to their cancer stage.
Lymphadenectomy was performed during all of the surgeries, andwe resected LNs separately in a region-by-region manner and madepathological diagnoses for each sample.
NAC regimen and indicationBecause squamous cell carcinoma (SCC) was more sensitive than
adenocarcinoma to chemotherapy in our preliminary analysis, weadministered NAC primarily in stage IB2/IIA/IIB SCC cases (Table 1). Anintravenous infusion of irinotecan (CPT-11) (60mg/m2 on days one andeight) and nedaplatin (NDP) (80mg/m2 on day one) was administered.The cycleswere repeated every 21days. In total, we conducted two cyclesof NAC.
Surgical procedures and the definition of LN locationPelvic lymphadenectomy was conducted in association with type
III radical hysterectomy. The surgical procedure has been reportedpreviously [13].
Para-aortic lymphadenectomy was performed when a metastaticpelvic LN was found after the intraoperative pathological diagnosis offrozen sections or when the surgeon found it necessary. LNs and theirsurrounding tissue were removed from the bifurcation of the commoniliac artery to either the inferior mesenteric artery (IMA) or the levelof the renal vein.
MDCT protocolThe MDCT examination was performed using one of three 64-
detector-row CT scanners (Aquilion, Toshiba Medical Systems, Otawara,Japan) or a 16-detector-row CT scanner (Aquilion, Toshiba MedicalSystems, Otawara, Japan). Patients were placed in the supine position,and the whole abdomen and pelvis were scanned. Image data wereacquired with a 7mm slice thickness, using a 64×0.5mm (64-detector-row CT) or 16 × 1.0 mm (16-detector-row CT) beam collimation, a500ms rotation time, and a 120kVp and 27.5mm (64-detector-row CT)or 14.9 mm (16-detector-row CT) table feed per rotation. The acquiredimages were used to generate images with 1 mm slice thickness. Alldual-phase contrast-enhanced CT images with a single breath-holdwere obtained at 90 s following the intravenous injection of 100 ml of
Table 1Number of patient multi-detector CT image was analyzed.
Stage SCC Non-SCC Total
IA 4 3 7IB1 32 20 52IB2 10 (7) 4 (1) 14 (8)IIA 4 1 5IIB 23 (19) 5 (1) 28 (20)Total 73 (26) 33 (2) 106 (28)
(): NAC cases.
300 or 350 mg/ml non-ionic contrast medium (Iomeron®350, Eisai,Tokyo, Japan; Iopamiron®300, Bayer HealthCare, Osaka, Japan; orOmnipaque®300, Daiichi-Sankyo, Tokyo, Japan) at a rate of 2.5 ml/susing an automatic injector.
Because ourMDCT procedure is the same as previously reported [14],the estimated radiation dose to the whole abdomen was approximately10mSv. The noise of the images with 1mm thickness was greater thanthose with 7 mm thickness. However, there was no difficulty inevaluating the length of LNs, especially in theMDCT imageswith contrastenhancement.
Evaluation of LNs by MDCTThe evaluation of LNs using the MDCT images of 1mm-thick slices
was performed independently by a radiologist (AK) who specializes inthe field of gynecology and by a gynecologic oncologist (KY). The sizeof each LN, measured independently by AK and KY to the first decimalplace, was determined by their consensus.
Region-by-region analysisMost previous studies have been conducted in patient-by-patient
manner. In this study, we aimed to analyze more closely. Because it isunfeasible to compare each LN detected in MDCT images with LNdetected in operation in node-by-node manner, we employed aregion-by-region analysis. In a previous study, the pelvic and para-aortic spaces were divided into five regions prior to conducting aregion-by-region analysis [9]. In the present study, we divided theminto 13 regions (Supplementary Fig. 1) to conduct a more detailedanalysis. We determined the size of the largest LN in each region,termed the regional LN (Reg-LN), and compared it with the pathologicaldiagnosis of LN metastasis in each region. We should note that even ifLNmetastasis existed in a region, the Reg-LNmight not be the involvedLN. Receiver operating characteristic (ROC) curves were drawn todetermine the optimal cut-off size. For the development of the newcriterion, we analyzed only the primary operation cases and excludedthe NAC cases.
Estimate of the efficacy of NAC in eradicating LN metastases using MDCTimages
In patients who received NAC,we performed theMDCT examinationbefore and after NAC and compared the results. Using the new criterionfor determining the swollen Reg-LN,we estimated the efficacy of NAC ineradicating LN metastasis.
Statistical methodsWe used t-tests to compare the parametric values between two
groups and one-way ANOVA for three groups. Paired t-tests were usedfor the paired analysis. To analyze the distribution in a 2 × 2 table, aFisher's exact test was employed. To analyze the distribution in a largertable, the chi-square test was used. We considered a value of pb0.05 tobe a significant difference.
Results
The detection of LNs in 1mm slice images from MDCT
A total of 4765 LNswere pathologically identifiedwithin 980 regionsfrom 106 patients, whereas the total number of visible LNs in theMDCTimages was 800. Thus, the detection rate of LNs byMDCTwas 17% (800/4765). The most difficult LN to detect was the presacral LN (6%),whereas the easiest was the left common iliac LN (46%) (Fig. 1a). Onlyseven of the 800 visible LNs in the MDCT images were over 10mm indiameter.
Among 980 regions from 106 patients, 563 (57%) regions showedone ormore visible LNs in theMDCT images. Metastaseswere identifiedpathologically in 133 LNs within 80 regions from 33 patients. Sixty ofthese 80 (75%) regions showed one or more visible LNs in the MDCT

Fig. 1. Detection of LNs in MDCT images. a) The number of detected LNs by MDCT is indicated by a black box. Pathologically detected LNs are indicated by the sum of the detected andundetected LNs. The distribution was statistically significant (p b 0.0001, chi-square test). PAN: para-aortic LN region; IMA: inferior mesenteric artery; Bif: aortic bifurcation; L: left; R:right. b) The detection rate of Reg-LNs was significantly higher in the involved regions (pN1) than in the uninvolved regions (pN0) (p=0.006).
703K. Yamanoi et al. / Gynecologic Oncology 131 (2013) 701–707
images (Fig. 1b). The detection rate was significantly higher in themetastatic regions than in the non-metastatic regions (p = 0.006)(Fig. 1b). In the following analyses, the largest LN in each region wasdefined as the Reg-LN.
Fig. 2. Region-by-region analysis of LNs. a) Each dot indicates the size of the Reg-LN. Red dotsBlack bar indicates the mean size. Ext: external iliac region; Obt: obturator region; Others: allon the size of the Reg-LN and the presence of the LN metastasis. The gray arrowhead indicatethe black arrowhead is away from the optimal cut-off based on the ROC analysis.
Development of a new criterion to diagnose LN metastasis
We compared the size of the Reg-LN identified by MDCT with thepresence or absence of a pathologically involved LN in 410 regions
indicate size of involved Reg-LNs and tiny black dots indicate size of uninvolved Reg-LNs.other regions. One-way ANOVA was used for the statistical analysis. b) ROC curves baseds the optimal cut-off based on the ROC curves. Note that the 10mm cut-off indicated by
704 K. Yamanoi et al. / Gynecologic Oncology 131 (2013) 701–707
from 71 patients who underwent primary surgery and in whom theReg-LN could be detected in the MDCT images. A statistical analysisusing the ROC curve is difficult when the number of metastasis-positive cases is less than five. Only the external iliac and obturatorregions were positive for metastasis in five or more patients. Thus, weanalyzed the Reg-LNs of the obturator region, external iliac region,and the other regions separately. In all three groups, the size of theReg-LNwas significantly larger in the LN regions containingmetastasesthan in the non-metastatic regions; the mean was 7.9 in the metastaticcase vs. 4.0 mm in the non-metastatic case in the external iliac(p b 0.0001), 6.6 vs. 3.9 mm in the obturator (p b 0.0001), and 5.1 vs.3.8mm in the other regions (p=0.003) (Fig. 2a). The variation in thesize of the Reg-LNs in these three groups was not significant in eithermetastatic or non-metastatic regions (Fig. 2a). The optimal cut-offsizes determined by the ROC curves in the external iliac, obturator,and other regions were 4.9, 5.3, and 5.1 mm, respectively (Fig. 2b).Based on these results, 5 mm was selected as the cut-off size for alltypes of LN regions.
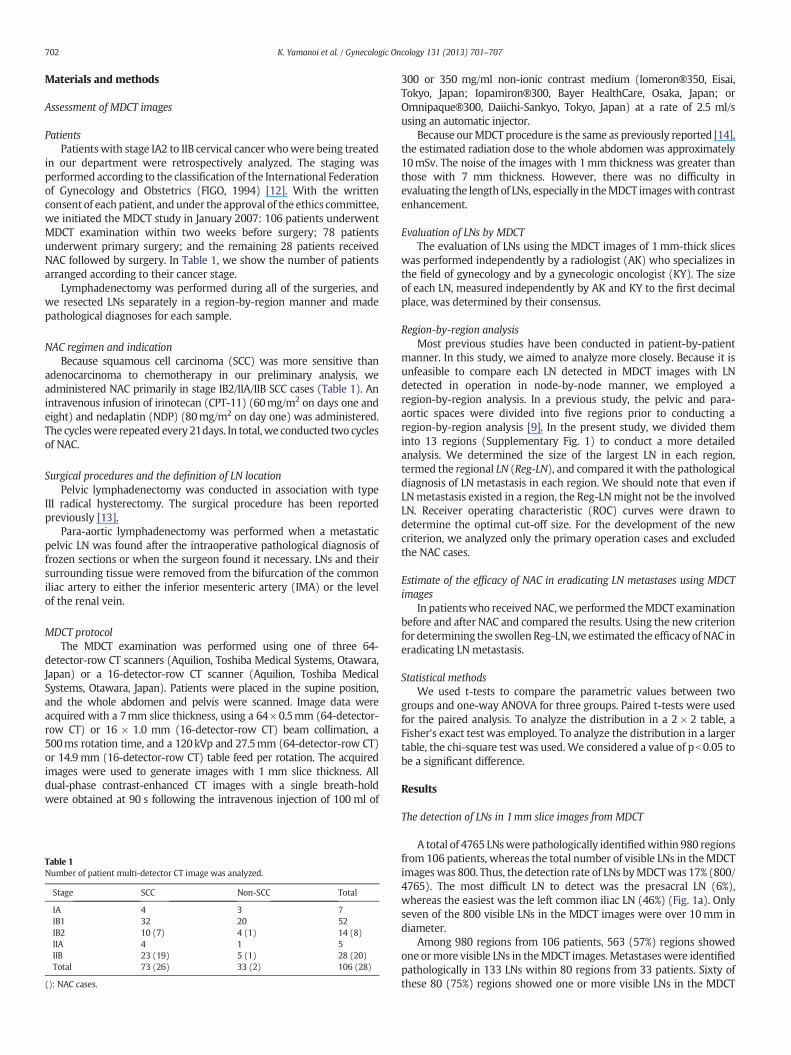
We then analyzed the Reg-LNs from all regions. The size of the Reg-LNs was significantly larger in the LN regions containing metastasesthan in the regions without metastases: mean 6.4 mm vs. 3.9 mm(pb 0.0001) (Fig. 3a). Based on the ROC curve, the optimal cut-off sizeto diagnose a LN metastasis was 4.7 mm (AUC= 0.80, Fig. 3b). In theregion-by-region analysis, we decided the closest whole number,5mm, as the cut-off for clinical use. When the 5mm cut-off was used,the sensitivity, specificity, positive predictive value (PPV), and negativepredictive value were 70, 79, 27, and 96%, respectively.
Next, we divided all cases into SCC and non-SCC to examine theinfluence of histological differences on the detection of LN metastasis.In both SCC and non-SCC patients, the size of the Reg-LN wassignificantly larger in the LN regions with metastases than in the non-metastatic regions: the mean in SCC was 7.1 vs. 4.0 mm and in non-SCC was 6.0 vs. 3.7mm (pb0.0001) (Fig. 3a). The size of the Reg-LN innon-metastatic LN regions was larger in SCC compared with non-SCC,
Fig. 3.Region-by-region analysis of all Reg-LNs among different histological subtypes. a) Each dodots indicate size of uninvolved Reg-LNs. Black bar indicates themean size. To detect the associaway ANOVA was performed. b) ROC curves are based on the size of the Reg-LN and the presendifferent histological subtypes. The gray arrowhead indicates the optimal cut-off based on the Roptimal cut-off based on the ROC analysis.
but the difference was small (Fig. 3a). The optimal cut-off determinedby the ROC curve was 5.4 mm in SCC and 4.7 mm in non-SCC cases(Fig. 3c). Thus, 5 mm, the closest whole number, was again selectedfor use in both histological subtypes.
We also evaluated the conventional 10 mm cut-off. In the primarysurgery cases, only four of all the visible LNs in the MDCT images wereover 10mm in diameter (Fig. 2a). We found that the conventional cut-off of 10mmwas far from the optimal cut-off based on the ROC analyses(Figs. 2b, 3b, c). In addition, we randomly divided our data (primarysurgery cases, region-by-region data) into three groups and conductedROC analyses independently, thus generating cut-off values of 4.9, 5.0and 5.3 (95% CI; 4.55–5.58, data not shown). We therefore concludedthat the conventional 10 mm cut-off is statistically inappropriate inMDCT images.
Assessment of NAC efficacy on metastatic LNs in cervical cancer
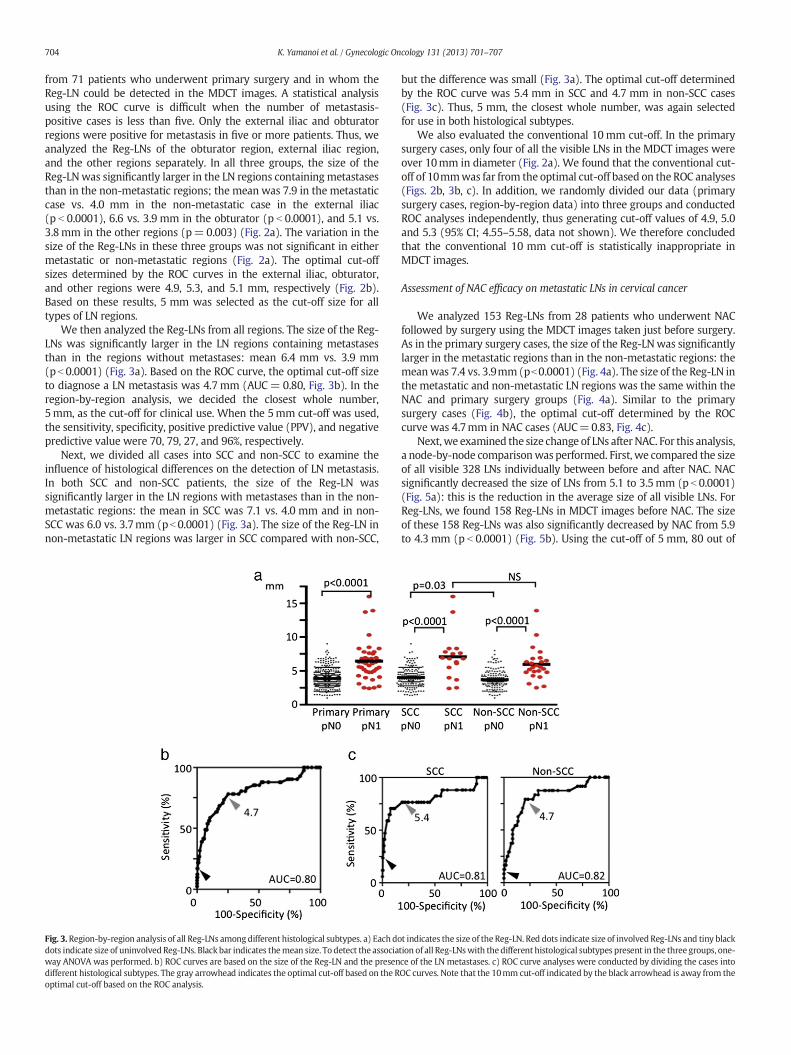
We analyzed 153 Reg-LNs from 28 patients who underwent NACfollowed by surgery using the MDCT images taken just before surgery.As in the primary surgery cases, the size of the Reg-LNwas significantlylarger in the metastatic regions than in the non-metastatic regions: themeanwas 7.4 vs. 3.9mm (pb0.0001) (Fig. 4a). The size of the Reg-LN inthe metastatic and non-metastatic LN regions was the same within theNAC and primary surgery groups (Fig. 4a). Similar to the primarysurgery cases (Fig. 4b), the optimal cut-off determined by the ROCcurve was 4.7mm in NAC cases (AUC=0.83, Fig. 4c).
Next,we examined the size change of LNs afterNAC. For this analysis,a node-by-node comparisonwas performed. First, we compared the sizeof all visible 328 LNs individually between before and after NAC. NACsignificantly decreased the size of LNs from 5.1 to 3.5mm (p b 0.0001)(Fig. 5a): this is the reduction in the average size of all visible LNs. ForReg-LNs, we found 158 Reg-LNs in MDCT images before NAC. The sizeof these 158 Reg-LNs was also significantly decreased by NAC from 5.9to 4.3 mm (p b 0.0001) (Fig. 5b). Using the cut-off of 5 mm, 80 out of
t indicates the size of the Reg-LN. Red dots indicate size of involved Reg-LNs and tiny blacktion of all Reg-LNswith thedifferent histological subtypes present in the three groups, one-ce of the LN metastases. c) ROC curve analyses were conducted by dividing the cases intoOC curves. Note that the 10mm cut-off indicated by the black arrowhead is away from the
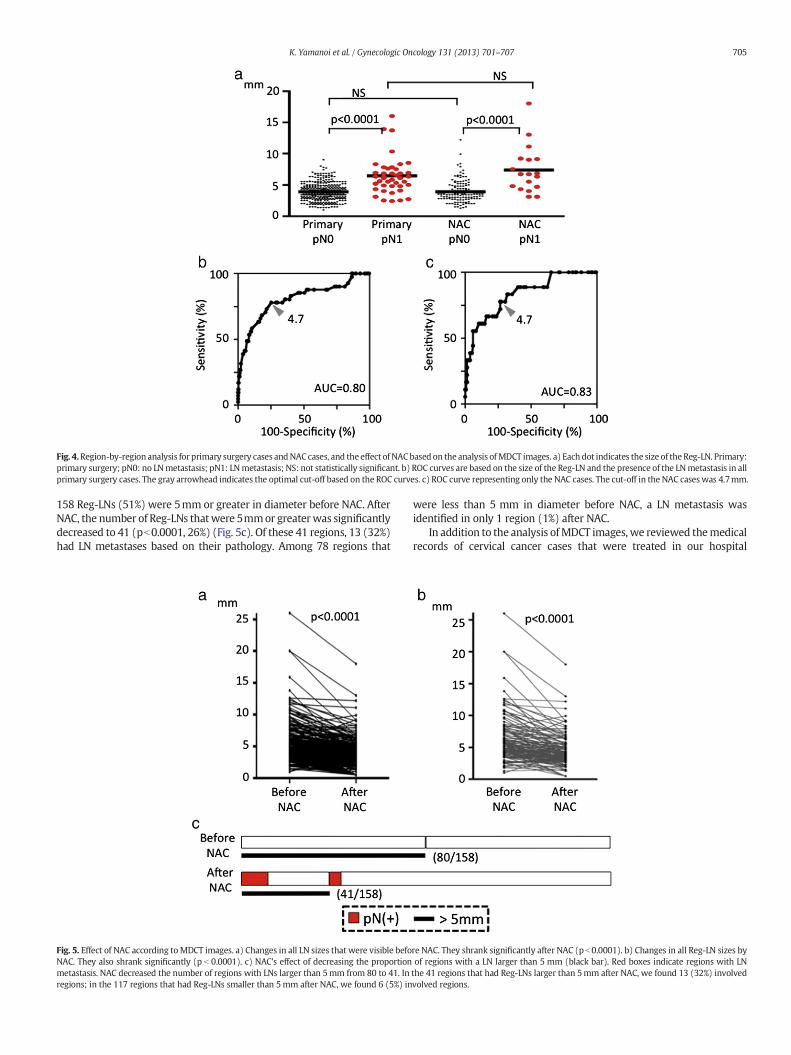
Fig. 4.Region-by-region analysis for primary surgery cases andNAC cases, and the effect of NACbased on the analysis ofMDCT images. a) Each dot indicates the size of theReg-LN. Primary:primary surgery; pN0: no LNmetastasis; pN1: LNmetastasis; NS: not statistically significant. b) ROC curves are based on the size of the Reg-LN and the presence of the LNmetastasis in allprimary surgery cases. The gray arrowhead indicates the optimal cut-off based on the ROC curves. c) ROC curve representing only the NAC cases. The cut-off in the NAC cases was 4.7mm.
705K. Yamanoi et al. / Gynecologic Oncology 131 (2013) 701–707
158 Reg-LNs (51%) were 5mm or greater in diameter before NAC. AfterNAC, the number of Reg-LNs thatwere 5mmor greaterwas significantlydecreased to 41 (pb0.0001, 26%) (Fig. 5c). Of these 41 regions, 13 (32%)had LN metastases based on their pathology. Among 78 regions that
Fig. 5. Effect of NAC according toMDCT images. a) Changes in all LN sizes that were visible befoNAC. They also shrank significantly (p b 0.0001). c) NAC's effect of decreasing the proportionmetastasis. NAC decreased the number of regions with LNs larger than 5mm from 80 to 41. Inregions; in the 117 regions that had Reg-LNs smaller than 5mm after NAC, we found 6 (5%) in
were less than 5 mm in diameter before NAC, a LN metastasis wasidentified in only 1 region (1%) after NAC.
In addition to the analysis ofMDCT images, we reviewed themedicalrecords of cervical cancer cases that were treated in our hospital
re NAC. They shrank significantly after NAC (pb 0.0001). b) Changes in all Reg-LN sizes byof regions with a LN larger than 5 mm (black bar). Red boxes indicate regions with LNthe 41 regions that had Reg-LNs larger than 5mm after NAC, we found 13 (32%) involvedvolved regions.

706 K. Yamanoi et al. / Gynecologic Oncology 131 (2013) 701–707
between1999 and2011. In accordancewith theMDCTanalysis, we foundthat NAC decreased the frequency of LNmetastasis (Supplementary text,Supplementary Fig. 2b).
Discussion
The main objective of this study was to generate a new and morereliable criterion to diagnose LN metastasis pre-operatively. We alsoevaluated the efficacy of NAC in eradicating LN metastasis using thenewly developed criterion because NAC has the potential to eradicateLN and distant metastases [2,15,16].
CT and MRI have been widely used to diagnose LN metastasis[17,18]. In conventional CT or MRI images of 5–7mm slices, 10mm isused as the conventional cut-off for the short-axis diameter in thediagnosis of swollen LNs as potential metastases. However, only sevenof 800 visible LNs in the MDCT images were over 10mm in diameterin this study (data not shown). Therefore, the conventional cut-off of10 mm is not effective in clinical practice. The conventional cut-off isused because of the limitations of conventional CT, which cannotreproducibly measure an object smaller than 10mm in diameter in 5–7mm slices [7].
MDCT is a new form of CT technology and that has an increasedspeed of CT image acquisition [19]. In addition, MDCT provides moreinformation than CT without increasing cost, examination time, orexposure dose depending on how it is protocoled. Although there arereports demonstrating the use of MDCT to diagnose LN metastasis ingastric, esophageal, breast and pancreatic cancer [10,11,20–22], to thebest of our knowledge, this is the first report on the use of MDCT in agynecological cancer.
In previous studies that examined the diagnostic rate for LNmetastasis, a patient-by-patient analysis was used to compare the sizeof the largest LN in a patient with the pathological diagnosis of the LNmetastasis, without describing the location of the LN metastasis.However, to consider individually the extent of the lymphadenectomyand field of radiotherapy, a diagnosis of not only the presence of a LNmetastasis but also the location(s) of the LN metastasis is essential.Accordingly, we determined that the cut-off should be ascertainedusing region-by-region analysis.
Our findings suggested that 5mmwas the most appropriate cut-offfor clinical practice. In addition, a cut-off of 5 mm using MDCT wasreproducible regardless of the location or pathological subtype of thetumor (Figs. 3b, c, 4c). The ROC analyses clearly showed that a cut-offof 10mm is not appropriate.
Using a historical analysis of stage IB2/IIA cases, we found that thefrequency of LN metastasis in NAC cases was significantly lower than inprimary surgery cases (Supplementary Fig. 2b). This result is consistentwith previous reports that the frequency of LN metastasis is lower inpatients who undergo NAC [15,16]. In our analysis, approximately halfof the Reg-LNs that were 5mm or larger shrank to less than 5mm afterNAC (Fig. 5c). Although the shrinkage of LNs does not necessary meananti-tumor effect against involved LNs, this study shows that asubstantial number of involved LNs might have been cured by NAC.Ours is the first study to report the precise change in LN size due toNAC; however, further studies are required to confirm whether NAC iseffective against the LN metastasis of cervical cancer.
In this study, using 1mm slice images, we tried evaluating LN size asclosely as possible in a region-by-regionmanner, but there are still somelimitations. The largest LN in an involved region may not always be theinvolved LN. To compare the preoperative image with the pathologicaldiagnosis in node-by-node manner, data accumulated from image-guided surgery, currently used for gastric or liver cancer [23,24] arenecessary. Although the detection rate of at least one LN in a regionwas increased when involved LNs existed, the detection rate was still75%, not 100% (Fig. 1b). Among operable cervical cancer patients, aPPV of 5mm cut-off was only 27% although PPV is thought to be higher
in advanced cases where operation is impossible and radiotherapy isindicated.
Regardless, the results of our study should have an enormous impacton clinical practice. We consider LNs of 5mm or larger to be potentiallymetastatic. We hope this result would be validated in a prospectivestudy with a large number of cases and node-by-node surgery withimaging analysis.
In conclusion, we suggested an optimal cut-off of 5 mm in MDCTimages for the diagnosis of metastatic LNs within an LN region. Thisnovel diagnostic criterion would improve the individualized treatmentof cervical cancer patients. In the future, clinical trials should beperformed to investigate whether this strategy could improve theprognosis of cervical cancer patients.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ygyno.2013.10.014.
Conflict of interest statement
All authors declare that they have no conflicts of interest.
Acknowledgments
We gratefully thank Dr. Takeshi Kubo for evaluating the radiationdose of MDCT.
References
[1] Rose PG. Chemoradiotherapy: the new standard care for invasive cervical cancer.Drugs 2000;60(6):1239–44.
[2] Matsumura M, Takeshima N, Ota T, Omatsu K, Sakamoto K, Kawamata Y, et al.Neoadjuvant chemotherapy followed by radical hysterectomy plus postoperativechemotherapy but no radiotherapy for Stage IB2-IIB cervical cancer–irinotecan andplatinum chemotherapy. Gynecol Oncol 2010;119(2):212–6.
[3] Tanaka Y, Sawada S, Murata T. Relationship between lymph node metastases andprognosis in patients irradiated postoperatively for carcinoma of the uterine cervix.Acta Radiol Oncol 1984;23(6):455–9.
[4] TakedaN, Sakuragi N, TakedaM, OkamotoK, KuwabaraM, Negishi H, et al.Multivariateanalysis of histopathologic prognostic factors for invasive cervical cancer treated withradical hysterectomy and systematic retroperitoneal lymphadenectomy. Acta ObstetGynecol Scand 2002;81(12):1144–51.
[5] Aoki Y, SasakiM,WatanabeM, Sato T, Tsuneki I, AidaH, et al. High-risk group innode-positive patients with stage IB, IIA, and IIB cervical carcinoma after radicalhysterectomy andpostoperative pelvic irradiation. Gynecol Oncol 2000;77(2):305–9.
[6] Hricak H, Yu KK. Radiology in invasive cervical cancer. AJR Am J Roentgenol1996;167(5):1101–8.
[7] Scheidler J, Hricak H, Yu KK, Subak L, Segal MR. Radiological evaluation oflymph node metastases in patients with cervical cancer. A meta-analysis. JAMA1997;278(13):1096–101.
[8] Schwartz LH, Bogaerts J, Ford R, Shankar L, Therasse P, Gwyther S, et al. Evaluation oflymph nodes with RECIST 1.1. Eur J Cancer 2009;45(2):261–7.
[9] Choi HJ, Roh JW, Seo SS, Lee S, Kim JY, Kim SK, et al. Comparison of the accuracy ofmagnetic resonance imaging and positron emission tomography/computedtomography in the presurgical detection of lymph node metastases in patientswith uterine cervical carcinoma: a prospective study. Cancer 2006;106(4):914–22.
[10] Yan C, Zhu ZG, Yan M, Zhang H, Pan ZL, Chen J, et al. Value of multidetector-rowcomputed tomography in the preoperative T and N staging of gastric carcinoma: alarge-scale Chinese study. J Surg Oncol 2009;100(3):205–14.
[11] Kim AY, Kim HJ, Ha HK. Gastric cancer by multidetector row CT: preoperativestaging. Abdom Imaging 2005;30(4):465–72.
[12] Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan2000. Int J Cancer 2001;94(2):153–6.
[13] Piver MS, Rutledge F, Smith JP. Five classes of extended hysterectomy for womenwith cervical cancer. Obstet Gynecol 1974;44(2):265–72.
[14] TammEP, Rong XJ, CodyDD, Ernst RD, Fitzgerald NE, Kundra V. Quality initiatives: CTradiation dose reduction: how to implement change without sacrificing diagnosticquality. Radiographics 2011;31(7):1823–32.
[15] Rydzewska L, Tierney J, Vale CL, Symonds PR. Neoadjuvant chemotherapy plussurgery versus surgery for cervical cancer. Cochrane Database Syst Rev 2010;1:Cd007406.
[16] Cai HB, Chen HZ, Yin HH. Randomized study of preoperative chemotherapy versusprimary surgery for stage IB cervical cancer. J Obstet Gynaecol Res 2006;32(3):315–23.
[17] Bipat S, Glas AS, van der Velden J, Zwinderman AH, Bossuyt PM, Stoker J. Computedtomography and magnetic resonance imaging in staging of uterine cervicalcarcinoma: a systematic review. Gynecol Oncol 2003;91(1):59–66.
[18] Reinhardt MJ, Ehritt-Braun C, Vogelgesang D, Ihling C, Hogerle S, Mix M, et al.Metastatic lymph nodes in patients with cervical cancer: detection withMR imagingand FDG PET. Radiology 2001;218(3):776–82.

707K. Yamanoi et al. / Gynecologic Oncology 131 (2013) 701–707
[19] Lawler LP, Fishman EK. Multi-detector row CT of thoracic disease with emphasison 3D volume rendering and CT angiography. Radiographics 2001;21(5):1257–73.
[20] Lin H, Chen TW, Li ZL, Zhang XM, Chen XL, Wang LY, et al. Tumor size of resectableoesophageal squamous cell carcinoma measured with multidetector computedtomography for predicting regional lymph node metastasis and N stage. Eur Radiol2012;22(11):2487–93.
[21] Nasu Y, Shikishima H, Miyasaka Y, Nakakubo Y, Ichinokawa K, Kaneko T. A study ofthe assessment of axillary lymph nodes before surgery for breast cancer usingmultidetector-row computed tomography. Surg Today 2010;40(11):1023–6.
[22] Nanashima A, Sakamoto I, Hayashi T, Tobinaga S, Araki M, Kunizaki M, et al.Preoperative diagnosis of lymph nodemetastasis in biliary and pancreatic carcinomas:evaluation of the combination of multi-detector CT and serum CA 19-9 level. Dig DisSci 2010;55(12):3617–26.
[23] Kim YM, Baek SE, Lim JS, Hyung WJ. Clinical application of image-enhancedminimally invasive robotic surgery for gastric cancer: a prospective observationalstudy. J Gastrointest Surg 2013;17(2):304–12.
[24] Chopra SS, Eisele RM, Denecke T, Stockmann M, Lange T, Eulenstein S, et al.Advances in image guided conventional andminimal invasive liver surgery. MinervaChir 2010;65(4):463–78.




















