A mobile instrumentation platform to distinguish airway disorders
10
A mobile instrumentation platform to distinguish airway disorders This article has been downloaded from IOPscience. Please scroll down to see the full text article. 2013 J. Breath Res. 7 017113 (http://iopscience.iop.org/1752-7163/7/1/017113) Download details: IP Address: 169.237.108.225 The article was downloaded on 28/02/2013 at 02:08 Please note that terms and conditions apply. View the table of contents for this issue, or go to the journal homepage for more Home Search Collections Journals About Contact us My IOPscience
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of A mobile instrumentation platform to distinguish airway disorders

A mobile instrumentation platform to distinguish airway disorders
This article has been downloaded from IOPscience. Please scroll down to see the full text article.
2013 J. Breath Res. 7 017113
(http://iopscience.iop.org/1752-7163/7/1/017113)
Download details:IP Address: 169.237.108.225The article was downloaded on 28/02/2013 at 02:08
Please note that terms and conditions apply.
View the table of contents for this issue, or go to the journal homepage for more
Home Search Collections Journals About Contact us My IOPscience

IOP PUBLISHING JOURNAL OF BREATH RESEARCH
J. Breath Res. 7 (2013) 017113 (9pp) doi:10.1088/1752-7155/7/1/017113
A mobile instrumentation platform todistinguish airway disordersMichael Schivo1, Felicia Seichter2, Alexander A Aksenov3,Alberto Pasamontes3, Daniel J Peirano3, Boris Mizaikoff2,Nicholas J Kenyon1 and Cristina E Davis3
1 Division of Pulmonary, Critical Care, and Sleep Medicine, Center for Comparative Respiratory Biologyand Medicine, University of California, Davis, CA 95616, USA2 Institute of Analytical and Bioanalytical Chemistry, University of Ulm, Germany3 Department of Mechanical and Aerospace Engineering, University of California, Davis, CA 95616,USA
E-mail: [email protected]
Received 31 August 2012Accepted for publication 28 January 2013Published 27 February 2013Online at stacks.iop.org/JBR/7/017113
AbstractAsthma and chronic obstructive pulmonary disease (COPD) are distinct but clinicallyoverlapping airway disorders which often create diagnostic and therapeutic dilemmas. Currentstrategies to discriminate these diseases are limited by insensitivity and poor performance dueto biologic variability. We tested the hypothesis that a gas chromatograph/differential mobilityspectrometer (GC/DMS) sensor could distinguish between clinically well-defined groups withairway disorders based on the volatile organic compounds (VOCs) obtained from exhaledbreath. After comparing VOC profiles obtained from 13 asthma, 5 COPD and 13 healthycontrol subjects, we found that VOC profiles distinguished asthma from healthy controls andalso a subgroup of asthmatics taking the drug omalizumab from healthy controls. The VOCprofiles could not distinguish between COPD and any of the other groups. Our results show apotential application of the GC/DMS for non-invasive and bedside diagnostics of asthma andasthma therapy monitoring. Future studies will focus on larger sample sizes and patientcohorts.
1. Introduction
Asthma and chronic obstructive pulmonary disease (COPD)are common and important respiratory disorders that leadto substantial morbidity and lung dysfunction. While theovert manifestation of these disorders is breathlessness, theunderlying physiologic mechanisms and treatment paradigmsare different. For example, asthma is often characterizedby increased levels of allergen-mediated immunoglobulinE (IgE) production, which leads to mast cell release ofbronchoconstrictive and pro-inflammatory mediators. For asubset of difficult-to-control asthmatics, treatment with ananti-IgE monoclonal antibody, omalizumab, may improvesymptoms and reduce asthma flares over time (Rodrigoet al 2011). In contrast, COPD is characterized byprogressive breathlessness with exertion often due to dynamichyperinflation and fixed airflow obstruction. Therefore,
treatment with long-acting bronchodilators is a front-linetherapy in COPD (Karner and Cates 2012, Decramer et al2009, Qaseem et al 2011). However, the reality is thatapproximately 50% of patients who present to primary carephysicians and specialists have clinical features suggestive ofboth asthma and COPD (Zeki et al 2011).
Current strategies to differentiate asthma from COPDinclude measurements of lung function, a prolonged smokinghistory in COPD, the presence of daily sputum production inCOPD, and exhaled biomarkers including exhaled nitric oxide(eNO), which is classically elevated in asthma and normal inCOPD (Barnes et al 2010, Dweik et al 2011). However, eNOmay not correctly classify patients as evidenced by normallevels of eNO in nonallergic asthma (Dweik et al 2010) andvariable eNO levels in COPD (Gelb et al 2012).
Similarities in clinical presentation, limited discrimina-tory power of conventional diagnostic tool and a limited
1752-7155/13/017113+09$33.00 1 © 2013 IOP Publishing Ltd Printed in the UK & the USA

J. Breath Res. 7 (2013) 017113 M Schivo et al
armamentarium of validated biomarkers create bothdiagnostic and therapeutic dilemmas. This confusion canresult in inappropriate therapies such as monotherapy withlong-acting bronchodilators in asthma leading to an excess ofasthma-related deaths (Nelson et al 2006) or monotherapy withinhaled steroids in COPD leading to an excess of pneumonias(Yang et al 2012).
Complimentary diagnostic modalities to properlycharacterize asthma and COPD include the assessment ofvolatile organic compounds (VOCs) from exhaled breath.Several clinical studies have assessed VOCs in asthma andCOPD, however, with certain limitations. Some clinicalstudies analyzing VOCs have used chemical sensors designedto detect but not identify VOCs (Fens et al 2009, 2011,Montuschi et al 2010, Dragonieri et al 2007). The resultsled to acceptable disease classification, but no furtheranalysis including the specific VOC identification and eventualbiomarker discovery was possible. Alternative studies usedgas chromatography/mass spectrometry (GC/MS) which isconsidered the gold standard for VOC identification but doesnot provide an instrumental platform for bedside or office use(Caldeira et al 2012, Ibrahim et al 2011, Van Berkel et al2010).
Additional studies used portable diagnostic platformsincluding ion mobility spectrometry (IMS) methods withpromising results. Westhoff et al were able to differentiate97 cases of COPD from 35 healthy control subjects usingIMS coupled with a multi-capillary column (MCC) analysisof 10 mL exhaled breath (Westhoff et al 2010, 2011). Inthis study, the investigators identified a single compound,cyclohexanone, which classified COPD from healthy controlswith 91% specificity and 95% predictive value. A similarstudy using IMS looked at 13 COPD patients and 33 healthycontrols (Bessa et al 2011). The investigators found 1 out of98 peaks which significantly separated the clinical groups.Although they did not overtly identify this peak, the authorssuggest that the peak identification was benzofuran, phenol, 4-methylanisol or 1,2,4-trimethylbenzol. A third study looked atCOPD patients with and without alpha-1-antitrypsin (A1AT), aprotective enzyme found in the blood and lungs (Koczulla et al2011). This study identified 5 of 22 peaks which separated 17A1AT-deficient COPD subjects from 8 A1AT-sufficient COPDsubjects.
Basanta et al used differential mobility spectrometry(DMS) to analyze exhaled breath from 20 COPD subjectsand 6 healthy controls who smoke cigarettes (Basanta et al2010). Using a validated exhaled breath collection method,the authors were able to separate the clinical groups based onpartial least-squares discriminant analysis of the datasets withgood reproducibility, a 19% type I error rate (false positive,FP), and 12.4% type II error rate (false negative, FN). Onecharacteristic not addressed in this study was that all 6 healthycontrols were active smokers, while only 2 of the 20 COPDsubjects were active smokers. This fact could have introducedconfounders.
Given the difficulties in accurate diagnosis and thepotential for harmful therapy, there remains an urgent needfor improved diagnostic tools to classify asthma and COPD.
Despite a number of illuminating studies, there is not acomprehensive understanding of the correlation of VOCsbetween asthma and COPD. Therefore, it is important topursue further research efforts in these very common lungdiseases with the ultimate goal of developing a protocol usinga suitable analytical method that can be used for bedsidediagnostics.
As in the Basanta study, our lab has experience with DMSwhich is a highly miniaturized (i.e. micromachined), portablesensor for VOC detection. DMS (also known as high fieldasymmetric waveform ion mobility spectrometry [FAIMS])(Shvartsburg et al 2006, Guevremont 2004, Eiceman et al2002, Borsdorf and Eiceman 2006) is commonly applied for awide variety of analytic purposes, including, but not limited to,explosive detection (Perr et al 2005, Guerra-Diaz et al 2010,Buxton and Harrington 2003), drug detection (Gryniewiczet al 2009, Dunn et al 2011, Jafari et al 2009), bacteriadetection (Shnayderman et al 2005) and VOC detection inhuman samples (Molina et al 2008, Krebs et al 2006).
DMS may be used as an ion-filtering device incombination with MS or liquid chromatography/massspectrometry (LC/MS), or it can function as a stand-alonesensor. The latter renders DMS a suitable technology for VOCdetection in breath diagnostics as it is small and portable,highly sensitive, and consumes little power. The analyticalsignal in DMS is generated from the differences in ion mobilityat low and high electric field conditions. Each chemical speciesis characterized by a unique dependence of its mobility withinan electric field; therefore, the differences in ion mobility maybe used to identify and differentiate VOCs. An additionaldirect current (DC) voltage, called a ‘compensation voltage’(CV), is applied to compensate for the ion drift at differentialfield conditions and to enable a particular chemical species topropagate through the device. The value of the CV is relatedto the ion’s structure and, therefore, is specific for each ionspecies. In combination with GC, DMS is highly suitable toprofile complex VOC distributions.
In this study, we performed proof-of-concept experimentsto explore the feasibility of the GC/DMS-based chemicalsensing to discriminate between VOC profiles from subjectswith asthma, COPD and healthy controls using exhaled breathcondensate (EBC). The DMS device provides orthogonalinformation to drift-time (DT) IMS methods in that in DMSthe ion mobility-related parameter CV only weakly correlateswith ion size (Aksenov et al 2012), unlike in DT IMSwhere ion DT is essentially linear with the ion cross-section(Borsdorf and Eiceman 2006, Eiceman and Karpas 2005). Bythis, DMS could differentiate two ions which are structurallydifferent but have the same or similar mass and charge such asisomers and isobars. Although DT IMS is an excellent portablediagnostic instrument, we chose to use DMS because of ourexperience and for future studies where precise ion speciesidentification is paramount. In addition to the differentialmobility parameter, CV, another dimension of separation canbe achieved through a scan of radiofrequency (RF) waveformamplitude (Basanta et al 2007). This may enable furtherexpansion of information achievable in DMS measurements.The ultimate goal of this work is to identify VOC combinations
2

J. Breath Res. 7 (2013) 017113 M Schivo et al
which will improve diagnostic accuracy and differentiation ofasthma and COPD, in addition to existing diagnostic tools. Itis further anticipated that advanced VOC analysis may leadto the specific identification of exhaled biomarkers of diseaseand inform future mechanistic studies.
2. Materials and methods
2.1. Subject selection
We performed a cross-sectional observational study in subjectswith asthma and COPD, and in healthy control subjects.All subjects provided informed consent prior to enrollment.The UC Davis institutional review board approved all studyactivities including subject recruitment, methods and informedconsent documents. We used standard American ThoracicSociety (ATS) and Global Initiative for Chronic ObstructiveLung Disease (GOLD) definitions to define asthma and COPD(American Thoracic Society 1987, Rabe et al 2007, Miller et al2005). The inclusion criteria for asthma were a subject havinga clinical diagnosis of asthma by a lung specialist, compatiblesymptoms by history (e.g. episodic chest tightness, wheezingand shortness of breath), a <10 pack-year smoking history,and partially or completely reversible airflow obstruction onspirometry or a positive response to a bronchoprovocationchallenge (a reduction in the forced expiratory volume at 1 s[FEV1] by >20% after inhaling <8 mg/dL of methocholine).COPD subjects were defined as having a clinical diagnosis ofCOPD by a lung specialist, compatible symptoms by history(chronic shortness of breath with or without intermittentexacerbations), a smoking history of >10 pack-years andpredominantly fixed airflow obstruction on spirometry withan FEV1 to forced vital capacity ratio (FEV1/FVC) of <0.7.Healthy control subjects could not smoke, could not have anypulmonary disease, and required normal spirometry.
Medication use was not restricted, but subjects neededto be free of asthma or COPD exacerbation for the preceding28 days. All subjects were adults >18 years. Exclusion criteriawere pregnancy, active asthma or COPD exacerbations, andan inability to provide consent. Additionally, all subjects wereasked to refrain from eating or drinking at least 4 h prior to thestudy to minimize dietary confounding factors.
2.2. Study measurements
Anthropomorphic measurements as well as a brief history andphysical exam were obtained. Subjects provided spirometry(if not done in the preceding six months) via an SDI SpirolabII spirometer (Easton, MA) and two exhaled nitric oxide(eNO) samples. The eNO samples were obtained by blowinginto Mylar bags per ATS standards (American Thoracic andEuropean Respiratory 2005). These were then analyzed on aSievers 280i NO Analyzer (Boulder, CO).
2.3. Exhaled breath condensate collection
Subjects rinsed their mouths with tap water and placed onnoseclips to minimize oral and nasopharyngeal contamination.EBC was provided by breathing into a commercially
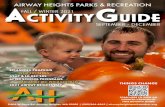
Figure 1. Schematic representation of the GC/DMS instrumentsetup. The volatile compounds collected from headspace of EBC areintroduced into gas chromatograph (GC) column forchromatographic separation. The sample eluting from GC column isionized with a 63Ni ion source prior to entering the DMS sensor. Thefiltered ions are detected at their corresponding compensationvoltage values. El: low-field electric field strength, tl: duration of thelow-field portion of the waveform ; Eh: high-field electric fieldstrength; th: duration of the high-field portion of the Rf waveform;Vc: compensation voltage.
available RTubeTM EBC collector (Respiratory Research,Charlottesville, VA). We chose this modality at the time ofstudy because of the RTube’sTM portability and ease of use. Asleeve cooled to between !40 "C and !50 "C by dry ice wasplaced over the RTubeTM prior to collection. Subjects breathedbetween 10 and 15 min of tidal volume into the RTubeTM.The EBC was collected by sterile pipette and placed into anEppendorf tube for storage at !80 "C.
2.4. GC/DMS analysis
A 500 µL to 1 mL aliquot of EBC was placed into a borosilicatevial and capped with a silicon septum. The vial was placedin a water bath, heated to 90 "C, and the headspace overthe EBC was sampled using a polyacrylate (PA) solid phasemicroextractionfiber (SPME, Supelco, Inc., Bellefonte, PA) topromote extraction of polar compounds from the sample headspace. For extraction, the SPME fiber was inserted through aseptum and kept above the sample for 1 h without EBC sampleagitation. This was performed to optimize VOC collection onthe SPME fiber according to previously published work in thisarea (Snow 2000a, Davis et al 2010). The sorbed chemicalswere then analyzed using a GC/DMS method described below.
The operational principles and design specifications theDMS sensor are described elsewhere (Kolakowski and Mester2007) (Anderson et al 2008). A schematic representationof the system is shown in figure 1. For this study weutilized the microDMX sensor, manufactured by Sionex(Waltham, MA). The detailed design specifications andperformance descriptions are given elsewhere (Petinarideset al 2005, Coy et al 2008, Miller et al 2006). Specifically,the DMS device is comprised of two parallel electrodeswith 0.5 mm gap. The GC column eluent in helium at the1 mL min!1 flow rate was mixed with ultra high purity nitrogencarrier gas (Airgas, Sacramento, CA) and passed at the flowrate of 300 mL min!1 through the DMS device. The analytewas ionized with the 63Ni ionization source prior to enteringthe DMS device. The water content in the carrier gas was
3

J. Breath Res. 7 (2013) 017113 M Schivo et al
Table 1. Subject baseline characteristics.
Healthy Asthma COPD
n 13 13 5Age in yrs (range)a b c 33 (23–66) 50 (18–69) 70.5 (48–89)Sex, M/F (n/n) 11/12 7/14 13/5BMI (range)d c 24.2 (18.2–30.9) 30.9 (20–53.4) 25.2 (18.6–34.5)Spirometryd b c
FEV1 ± SD, prebronchodilator (L) 3.53 ± 0.68 2.13 ± 0.93 1.21 ± 0.57FEV1/FVC ± SD (% predicted) 82 ± 8.2 69 ± 13 49 ± 14
NO ± SD (ppb)e 16 ± 11 24 ± 22 25 ± 12Omalizumab use 0 9 0a p < 0.05.b p < 0.001 Normal-COPD.c p < 0.01 Asthma-COPD.d p < 0.001 Normal-Asthma.e p < 0.05.
below 1 ppm, as reported by the manufacturer. The DMSunit was operated under the following conditions: asymmetricwaveform amplitude 1000 V (in the gap of 0.5 mm, thiscorresponds to the electric field of 20 V cm!1, #80 Td);RF 1.196 MHz with the asymmetric waveform about 34%high field and 66% low field; and the CV scan range !43to +15 V. The CV range of 60 V was scanned with 0.6 V stepat 10 ms per step, corresponding to 100 steps and 1 s totalCV scan time. The wavefunction generator employed in thisstudy can produce waveform with the maximum amplitude of1500 V. However, due to the presence of helium in the carriergas from the GC column eluent, we chose to operate at thelower dispersion voltage of 1000 V to avoid possible electricalbreakdown.
2.5. Statistical analysis
All demographic patient characteristics were comparedbetween clinical groups using the Student’s t-test or WilsonRank Sum test where appropriate in STATISTICA (StatSoft,Tulsa, OK). DMS data analysis performed using MATLABR2011a (Mathworks, Torrence, CA) and PLS Toolbox 6.7.1(Eigenvector Research Inc, Wenatchee, WA).
3. Results
3.1. Subjects
A total of 31 subject samples were screened. Theclinical groups differed significantly in their baselinecharacteristics including age, body mass index, pre-bronchodilator spirometry and eNO levels (see table 1). Thesedifferences were expected as patients with asthma tend to beyounger, have better lung function, and a higher BMI thanpatients with COPD. There was an unanticipated similaritybetween eNO levels in the asthma and COPD groups; however,our subjects reflect patients often encountered in practice ratherthan an artificially selected cohort.
3.2. Algorithm for sample selection for analysis
Figure 2 delineates the algorithm for EBC VOC data sampleselection used during multivariate data analysis.
Figure 2. Algorithm for DMS dataset selection. The raw data isassessed for analytic suitability by applying principal componentanalysis (PCA); the prediction model is built after multiway partialleast-squares analysis (N-PLS); the data are validated; and aconfusion matrix is created.
To select the DMS datasets which display high-qualityinformation, the data were subject to several evaluationtechniques. Initially, all datasets were preprocessed withbaseline correction and smoothing (Savitzky and Golay 1964)to facilitate data comparison. Principal component analysis(PCA) was used to reduce dimensionality (Wold et al 1987).This enables composite data analysis, outlier detection andselection of data fitting within an acceptable range for furtheranalysis. Following the selection of datasets from PCA, weused multiway partial least-squares (N-PLS) regression to findthe relation between X (cube of data) and Y (labels) data spacesin order to model the covariance structures (Bro 1996).
4

J. Breath Res. 7 (2013) 017113 M Schivo et al
(a)
(b)
Figure 3. (a) and (b) Representations of quality DMS plots from ourasthma data. Figure 3(a) (top) shows a three-dimensional plot withcompensation voltage (CV) on the x-axis, retention time on they-axis and ion count (IC) on the z-axis. Each VOC has a unique RTand CV which can be used to ultimately identify the VOC.Figure 3(b) (bottom) shows a typical 2-dimensional output view ofthe three-dimensional graph in 3(a).
An N-PLS model attempts to determine the multidimen-sional direction in the X space that explains the maximummultidimensional variance direction in the Y space. A repre-sentative sample dataset from the asthma group is displayedin figures 3(a) and (b).
3.3. Group separation based on GC/DMS data
After processing the DMS datasets to select appropriate setsto analyze, we performed a validation based on previouslypublished methods (Westerhuis et al 2008). Briefly, the datacube was divided into a ‘test set’ containing 10% of data
and a model set containing 90% of data. The test set was thenintroduced into the model as quasi-unknown data resulting in aclassification output. This output was compared to the a prioriknown classification of the datapoints (i.e. asthma, control orCOPD) resulting in a correct classification (true positive, TP,or true negative, TN) or an incorrect classification (FP or FN).This process was repeated several times in iterations called‘loops’ in order to identify the performance of the establishedmodel.
Figures 4(a) and (b) represent the confusion matricesproduced from such multiple loops. The best levels ofclassification resulted from the asthma versus control groupsand from the subjects taking omalizumab versus healthypatients not on this medication. The results show the meanpercent classification for TP and FP for each group fromall performed loops (20 for asthma versus control, 40 foromalizumab versus none), with each mean assigned a standarderror.
4. Discussion
4.1. Interpretation of the results
In this study, we demonstrated that clinically relevant groupsmay in part be classified and identified using the GC/DMSanalysis of the VOCs from EBC and using appropriatemultivariate data analysis strategies. After executing 20classification optimization loops on the asthma-control groups,we were able to correctly classify asthma subjects 75% ofthe time. While this number is certainly lower than desiredfor a diagnostic test, the potential of the proposed analyticaltechnique is readily demonstrated. With improvements in oursmall sample size, the classification may be further enhanced.Similarly, we were able to correctly discriminate subjectstaking omalizumab from subjects not taking this medication70% of the time after executing 40 loops.
Our study differs from previous efforts in the field ofmobile high-dimensional breath diagnostics in several keyways. First, no study using DMS technology to discriminatebetween asthma and COPD populations has been conductedto date. Second, our study used EBC rather than single-breath capture. EBC theoretically contains a higher abundanceof VOCs and non-volatile compounds, is easier to pre-concentrate, and may be easier to standardize, though dataon this are lacking. Ultimate breath diagnostic methods willideally use single breath capture; however, in our study we
(a) (b)
Figure 4. (a) and (b). Confusion matrices describing the performance of the models to classify asthma from controls (figure 4(a), left) andsubjects taking omalizumab from those not taking this medication (figure 4(b), right). The left graph shows the mean results of 20 executedloops of the dataset. The right graph shows the results of 40 loops.
5

J. Breath Res. 7 (2013) 017113 M Schivo et al
aimed to maximize the quantity of VOCs. Last, our studydesign included a mixed cohort of patients reflective of thosecommonly encountered in clinical practice. The intent wasto present a potential real-world application of the DMStechnology, though our groups may have been more similarbiochemically than different (see section 4.2 below). Futurestudies of this nature will need to utilize highly selectedgroups (i.e. COPD with advanced fixed airflow obstructionand radiographic emphysema).
The ability to classify asthma from non-asthmatic patientsis of high clinical relevance. For example, a condition calledvocal cord dysfunction may mimic the symptoms of asthma,yet it is entirely different in clinical course and therapy(Benninger et al 2011). Hence, correctly classifying a patientas not having asthma if confusing symptoms are present mayprompt an appropriate evaluation and, consequently, effectivetherapy. Although the model established herein does nothave sufficient discriminatory power for a diagnostic test tocorrectly differentiate asthma from non-asthma, the results arepromising and future studies with larger numbers of subjectsand more samples per case should provide significantlyimproved classification models.
The determination of significant differences in VOCprofiles between subjects taking omalizumab and healthycontrols not taking the medication is interesting. Asthmaticswho take omalizumab often have moderate to severe disease,and they may represent a distinct biological group from thosepatients with mild asthma. Asthma severity may engendermore robust VOC metabolites and, thus, severe asthmatics maybe a good patient cohort to study with respect to non-invasivediagnosis. An alternative hypothesis is that omalizumab itselfmay yield a set of distinct VOCs after being metabolized,and this may contribute to the observed differences. Finally,omalizumab produces a host of pharmacological effects to helpbring down the inflammatory status in the omalizumab-treatedpatients. This, in turn, may ultimately manifest in alterationof the VOC profile. While to date there is little knowledge onthe secondary effects of medication on VOC production andpresence in exhaled breath, a noteworthy contribution may besuspected and will be subject to future studies.
While the initial aim of this study was differentiatingasthma from COPD as the clinically most interesting goal, thelimitations of the currently available dataset did not supportthis classification. This is most likely a result of the limitedsample size (see below); yet the quality of the obtaineddata clearly indicates that with a larger group of subjects aseparation between asthma and COPD is very likely. Also,in the course of the study it turned out that the asthma andCOPD groups may have been biologically more related ratherthan different, which reflects in the elevated eNO levels ofboth groups when they should have been significantly lowerin the COPD group (see figure 5). Elevated eNO levels inthe COPD cohort suggest a significant amount of allergicdisease, and future studies will need to identify and excludesuch overlapping populations (Zeki et al 2011) when tryingto validate novel diagnostics. However, the DMS system wasable to distinguish between the control and asthma groups,which had significantly different eNO levels after removingoutliers.
Figure 5. Box-whisker plot of exhaled nitric oxide (eNO) levels bygroup. Though there were no statistical eNO differences betweenthe asthma and COPD groups, there is a clear separation betweenthe control and asthma groups after appropriate removal of threeoutliers from each group (p < 0.001, unpaired Student’s t-test). Thisshows that the selected control group was biologically different thanthe asthma group, as detected by the DMS system. The similar eNOlevels between the asthma and COPD groups indicates a biologicsimilarity between these groups.
4.2. Limitations
While this feasibility study clearly demonstrates the utility ofGC/DMS for exhaled breath VOC analysis to discriminateclinically well-defined patient groups, several limitations ofthe current experimental design and analysis are recognized.
Most evident is that the small number of subjects withinthe clinical groups is insufficient for establishing robustpredictive models, as reflected in the standard errors. In theinvestigated patient cohort, several of the COPD subjectswere of the emphysema subtype, and thus produced onlysmall volumes of EBC. This resulted in inadequate EBCsamples for analysis from many subjects and further limitedthe available sample size. In addition, the GC/DMS analysisand sampling methodologies could be further optimized. Atpresent, there is little a priori knowledge of defined chemicalconstituents that are distinctive within the exhaled breathof asthma or COPD populations. Once such information isavailable, sorbent matrices may specifically be selected toenhance the recovery of specific VOCs of interest from theEBC headspace while simultaneously minimizing the matrixbackground. Finally, given the fact that this was a feasibilitystudy, the recruitment numbers were expectedly low. Yet,demonstrating the potential of the method should significantlyincrease the number of subjects available to future extendedstudies. Nevertheless, it is evident that the between-groupdifferences determined herein would likely be significantlymore pronounced if the sample sizes per case were larger,thus advancing the discriminatory power of the developedpredictive models.
During this study, the RTubeTM was used to collectEBC. Alternative breath collection devices may yield differentquantities and qualities of EBC, although reliable data on this
6

J. Breath Res. 7 (2013) 017113 M Schivo et al
matter are disparate (Huttmann et al 2011, Davidsson andSchmekel 2010, Koczulla et al 2009). Based on recent studiesof our laboratory and others (Loyola et al 2008, Czebe et al2008, Horvath et al 2005, Liu et al 2007), it is anticipated thatconducting a similar clinical trial using continuously cooledEBC collection devices may yield more robust VOC data andfurther enhance the between-group differences.
The SPME headspace sample extraction procedureemployed in this work, though guided by the previous studies(Davis et al 2010, Snow 2000b) and directly utilizing protocolssuggested by the SPME manufacturers, may not be specificallyoptimized for the cohort of subjects included in this study.We have conducted the extraction from the sample heatedto 90 "C as suggested by the manufacturer as a possiblemean to promote SPME headspace extraction (Sigma-Aldrich,LLC 2012). This temperature is at the upper portion of therecommended temperature range, and we recognize that someVOC loss may occur into the septum using this protocol.
During future studies, several adaptations may furtherenhance the discriminatory power with the most substantialimpact possibly achieved via concerted MS studies for reliablyestablishing the chemical identities of asthma and COPD VOCbiomarkers. Apart from the optimization of sampling methods,DMS measurements may also be improved. The ionizationof analyte occurs according to the basicity distributions inproton transfer reactions or according to dissociation energiesin charge transfer reactions. Thus, they differ in efficiency foreach individual chemical moiety. Therefore, it is possible thatthe analytes of interest are suppressed by matrix interferencesor are not efficiently ionized. Both scenarios lead to suppresseduseful analytical signals, and thus to impaired diagnosticresults. For example, if the analytes of interest include aliphatichydrocarbons, then the 63Ni source used in this study wouldnot efficiently ionize these species. However, it has beenreported that alkanes are highly relevant biomarkers indicativeof oxidative stress associated with inflammation processes(Phillips et al 2010). Further advancements may be achievedby modification of the carrier gas. In this study, predominantly(dry) nitrogen was used. Addition of up to 50% of Hewould lead to a significant increase of DMS separation space(McCooeye et al 2001), and may thus enable better resolvingsignals from biomarkers species that are clinically important.While the DMS device used herein was interfaced to aconventional bench-top GC system, the potential of GC/DMStechnology for bed-side monitoring could be fully unlockedupon further miniaturization of the GC component.
Last, an analyte diagnostic library does not currently existfor the DMS system in spite of the parameters which couldbe used for species identification. In this study, comparison ofthe GC/DMS data to GC/MS data would have greatly helpedwith species identification. Future studies may need to obtainboth GC/DMS and GC/MS data from the same subjects untila suitable DMS library exists.
Despite these shortcomings, this proof-of-principle studyshows the potential of DMS sensing in combination with GCproviding potentially valuable diagnostic information on VOCbiomarker panels in exhaled breath for non-invasive diseasediagnostics and disease discrimination.
5. Conclusion
Asthma and COPD represent two airway disorders whichare difficult to accurately diagnose and treat. Consequently,improved diagnostic strategies are needed which are sensitive,portable and complementary to available diagnostic tools.DMS is such a platform, and this study demonstrates thatanalysis of DMS VOC spectra can recognize differencesbetween clinically well-defined groups. Although this studydiscriminated asthma from healthy controls as well as thesubgroup of asthmatics taking omalizumab from healthycontrols, the DMS technology can be applied to many otherrespiratory disorders. DMS has implications for both officediagnostics and as a research tool to ultimately identify specificVOCs which may function in the pathobiology of respiratorydiseases. Further clinical studies should focus on larger subjectrecruitment numbers, improved EBC collection and improvedDMS (or other FAIMS technology) analyte measurements.
Acknowledgments
This work was generously and partially supported byseveral funding agencies. The content of this work is solelythe responsibility of the authors and does not necessarilyrepresent the official view of these agencies. Partial supportis acknowledged from the following: UL1 RR024146 fromthe National Center for Research Resources (NCRR), acomponent of the National Institutes of Health (NIH),and NIH Roadmap for Medical Research (CED, NJK);NIH #HL 105573 (NJK); Gilead Sciences, Inc.(CED); theDefense Advanced Research Projects Agency (DARPA)(CED); Department of the Army (CED), The HartwellFoundation (CED, NJK); NIH #T32-HL007013 and #T32-ES007059 (MS); UC Davis School of Medicine and NIH#8KL2TR000134-07 K12 mentored training award (MS); theGerman Academic Exchange Services (DAAD) (FS); USDepartment of Veterans Affairs, Post-9/11 GI-Bill (DJP).
References
Aksenov A A, Kapron J and Davis C E 2012 Predictingcompensation voltage for singly-charged ions in high-fieldasymmetric waveform ion mobility spectrometry (FAIMS)J. Am. Soc. Mass Spectrom. 23 1794–8
American Thoracic Society 1987 Standardization ofspirometry–1987 update: official statement of AmericanThoracic Society Respir. Care 32 1039–60
American Thoracic Society and European Respiratory Society 2005ATS/ERS recommendations for standardized procedures forthe online and offline measurement of exhaled lowerrespiratory nitric oxide and nasal nitric oxide, 2005 Am. J.Respir. Crit. Care Med. 171 912–30
Anderson A G et al 2008 DMS-IMS2, GC-DMS, DMS-MS: DMShybrid devices combining orthogonal principles of separationfor challenging applications Proc. SPIE 6954 69540H
Barnes P J et al 2010 Exhaled nitric oxide in pulmonary diseases: acomprehensive review Chest 138 682–92
Basanta M, Jarvis R M, Xu Y, Blackburn G, Tal-Singer R,Woodcock A, Singh D, Goodacre R, Thomas C Land Fowler S J 2010 Non-invasive metabolomic analysis ofbreath using differential mobility spectrometry in patients with
7

J. Breath Res. 7 (2013) 017113 M Schivo et al
chronic obstructive pulmonary disease and healthy smokersAnalyst 135 315–20
Basanta M, Singh D, Fowler S, Wilson I, Dennis R andThomas C L 2007 Increasing analytical space in gaschromatography-differential mobility spectrometry withdispersion field amplitude programming J. Chromatogr. A1173 129–38
Benninger C, Parsons J P and Mastronarde J G 2011 Vocal corddysfunction and asthma Curr. Opin. Pulm. Med. 17 45–9
Bessa V, Darwiche K, Teschler H, Sommerwerck U, Rabis T,Baumbach J I and Freitag L 2011 Detection of volatile organiccompounds (VOCs) in exhaled breath of patients with chronicobstructive pulmonary disease (COPD) by ion mobilityspectrometry Int. J. Ion Mobility Spectrom. 14 7–13
Borsdorf H and Eiceman G A 2006 Ion mobility spectrometry:principles and applications Appl. Spectrosc. Rev. 41 323–75
Bro R 1996 Multiway calibration. Multilinear PLS J. Chemom.10 47–61
Buxton T L and Harrington P B 2003 Trace explosive detection inaqueous samples by solid-phase extraction ion mobilityspectrometry (SPE-IMS) Appl. Spectrosc. 57 223–32
Caldeira M, Perestrelo R, Barros A S, Bilelo M J, Morete A,Camara J S and Rocha S M 2012 Allergic asthma exhaledbreath metabolome: a challenge for comprehensivetwo-dimensional gas chromatography J. Chromatogr. A1254 87–97
Coy S L, Krylov E V and Nazarov E G 2008 DMS-prefiltered massspectrometry for the detection of biomarkers Proc. SPIE6954 695411
Czebe K, Barta I, Antus B, Valyon M., Horvath I and Kullmann T2008 Influence of condensing equipment and temperature onexhaled breath condensate pH, total protein and leukotrieneconcentrations Respir. Med. 102 720–5
Davidsson A and Schmekel B 2010 Efficacy of two breathcondensers J. Clin. Lab. Anal. 24 219–23
Davis C E et al 2010 Analysis of volatile and non-volatilebiomarkers in human breath using differential mobilityspectrometry (DMS) IEEE Sensor J. 10 114–122
Decramer M, Celli B, Kesten S, Lystig T, Mehra S, Tashkin D Pand Investigators U 2009 Effect of tiotropium on outcomes inpatients with moderate chronic obstructive pulmonary disease(UPLIFT): a prespecified subgroup analysis of a randomisedcontrolled trial Lancet 374 1171–8
Dragonieri S et al 2007 An electronic nose in the discrimination ofpatients with asthma and controls J. Allergy Clin. Immunol.120 856–62
Dunn J D, Gryniewicz-Ruzicka C M, Kauffman J F,Westenberger B J and Buhse L F 2011 Using a portable ionmobility spectrometer to screen dietary supplements forsibutramine J. Pharm. Biomed. Anal. 54 469–74
Dweik R A, Boggs P B, Erzurum S C, Irvin C G, Leigh M W,Lundberg J O, Olin A C, Plummer A L andTaylor D R (American Thoracic Society Committee onInterpretation of Exhaled Nitric Oxide Levels forClinical Applications) 2011 An official ATS clinical practiceguideline: interpretation of exhaled nitric oxide levels (FENO)for clinical applications Am. J. Respir. Crit. Care Med.184 602–15
Dweik R A et al (National Heart, Lung, and Blood Institute SevereAsthma Research, Program) 2010 Use of exhaled nitric oxidemeasurement to identify a reactive, at-risk phenotype amongpatients with asthma Am. J. Respir. Crit. Care Med.181 1033–41
Eiceman G A and Karpas Z 2005 Ion Mobility Spectrometry2nd edn (Boca Raton, FL: CRC Press)
Eiceman G A, Nazarov E G, Miller R A, Krylov E Vand Zapata A M 2002 Micro-machined planar field asymmetricion mobility spectrometer as a gas chromatographic detectorAnalyst 127 466–71
Fens N, Roldaan A C, van der Schee M P, Boksem R J,Zwinderman A H, Bel E H and Sterk P J 2011 Externalvalidation of exhaled breath profiling using an electronic nosein the discrimination of asthma with fixed airways obstructionand chronic obstructive pulmonary disease Clin. Exp. Allergy41 1371–8
Fens N, Zwinderman A H, Van Der Schee M P, De Nijs S B,Dijkers E, Roldaan A C, Cheung D, Bel E H and Sterk P J2009 Exhaled breath profiling enables discrimination ofchronic obstructive pulmonary disease and asthma Am. J.Respir. Crit. Care Med. 180 1076–82
Gelb A F, Barnes P J, George S C, Ricciardolo F L, Dimaria Gand Zamel N 2012 Review of exhaled nitric oxide in chronicobstructive pulmonary disease J. Breath Res. 6 047101
Gryniewicz C M, Reepmeyer J C, Kauffman J F and Buhse L F2009 Detection of undeclared erectile dysfunction drugs andanalogues in dietary supplements by ion mobility spectrometryJ. Pharm. Biomed. Anal. 49 601–6
Guerra-Diaz P, Gura S and Almirall J R 2010 Dynamic planar solidphase microextraction-ion mobility spectrometry for rapid fieldair sampling and analysis of illicit drugs and explosives Anal.Chem. 82 2826–35
Guevremont R 2004 High-field asymmetric waveform ion mobilityspectrometry: a new tool for mass spectrometry J. Chromatogr.A 1058 3–19
Horvath I et al 2005 Exhaled breath condensate: methodologicalrecommendations and unresolved questions Eur. Respir. J.26 523–48
Huttmann E M et al 2011 Comparison of two devices and twobreathing patterns for exhaled breath condensate samplingPLoS One 6 e27467
Ibrahim B, Basanta M, Cadden P, Singh D, Douce D, Woodcock Aand Fowler S J 2011 Non-invasive phenotyping using exhaledvolatile organic compounds in asthma Thorax 66 804–9
Jafari M T, Rezaei B and Zaker B 2009 Ion mobility spectrometryas a detector for molecular imprinted polymer separation andmetronidazole determination in pharmaceutical and humanserum samples Anal. Chem. 81 3585–91
Karner C and Cates C J 2012 Long-acting beta(2)-agonist inaddition to tiotropium versus either tiotropium or long-actingbeta(2)-agonist alone for chronic obstructive pulmonarydisease Cochrane Database Syst. Rev. 4 CD008989
Kikowatz A, Becher G, Dietze S, Steinhausser W and Beck E 2009Differential ion mobility spectroscopy: non-invasive real-timediagnostics and therapy control in metabolic diseases Eur. J.Med. Res. 14 (Suppl. 4) 121–5
Koczulla R, Dragonieri S, Schot R, Bals R, Gauw S A,Vogelmeier C, Rabe K F, Sterk P J and Hiemstra P S 2009Comparison of exhaled breath condensate pH using twocommercially available devices in healthy controls, asthma andCOPD patients Respir. Res. 10 78
Koczulla R, Hattesohl A, Schmid S, Boedeker B, Maddula Sand Baumbach J I 2011 MCC/IMS as potential noninvasivetechnique in the diagnosis of patients with COPD with andwithout alpha 1-antitrypsin deficiency Int. J. Ion MobilitySpectrom. 14 177–85
Kolakowski B M and Mester Z 2007 Review of applications ofhigh-field asymmetric waveform ion mobile spectrometry(faims) and differential mobile spectrometry (dms) The Analyst132 842–64
Krebs M D, Mansfield B, Yip P, Cohen S J, Sonenshein A L,Hitt B A and Davis C E 2006 Novel technology for rapidspecies-specific detection of Bacillus spores Biomol. Eng.23 119–27
Liu J, Conrad D H, Chow S, Tran V H, Yates D H and Thomas P S2007 Collection devices influence the constituents of exhaledbreath condensate Eur. Respir. J. 30 807–8
Loyola B R, Bhushan A, Schivo M, Kenyon N J and Davis C E2008 Temperature changes in exhaled breath condensate
8

J. Breath Res. 7 (2013) 017113 M Schivo et al
collection devices affect observed acetone concentrationsJ. Breath Res. 2 037005
McCooeye M A, Ells B, Barnett D A, Purves R Wand Guevremont R 2001 Quantitation of morphine and codeinein human urine using high-field asymmetric waveform ionmobility spectrometry (FAIMS) with mass spectrometricdetection J. Anal. Toxicol. 25 81–7
Miller M R et al 2005 Standardisation of spirometry Eur. Respir. J.26 319–38
Miller R A, Nazarov E, Coy S L and Krylov E 2006 Miniaturedifferential mobility spectrometer as a pre-filter foratmospheric-pressure mass spectrometry Int. J. Ion MobilitySpectrom. 9 35–39
Molina M A, Zhao W, Sankaran S, Schivo M, Kenyon N Jand Davis C E 2008 Design-of-experiment optimization ofexhaled breath condensate analysis using a miniaturedifferential mobility spectrometer (DMS) Anal. Chim. Acta628 155–61
Montuschi P et al 2010 Diagnostic performance of an electronicnose, fractional exhaled nitric oxide, and lung function testingin asthma Chest 137 790–6
Nelson H S, Weiss S T, Bleecker E R, Yancey S Wand Dorinsky P M 2006 The Salmeterol Multicenter AsthmaResearch Trial: a comparison of usual pharmacotherapy forasthma or usual pharmacotherapy plus salmeterol Chest129 15–26
Perr J M, Furton K G and Almirall J R 2005 Solid phasemicroextraction ion mobility spectrometer interface forexplosive and taggant detection J. Sep. Sci. 28 177–83
Petinarides J, Griffin M T, Miller R A, Nazarov E Gand Bashall A D 2005 Implementation of a new technology forpoint detection Proc. SPIE 5795 65–74
Phillips M, Cataneo R N, Chaturvedi A, Danaher P J, Devadiga A,Legendre D A, Nail K L, Schmitt P and Wai J 2010 Effect ofinfluenza vaccination on oxidative stress products in breathJ. Breath Res. 4 026001
Qaseem A et al (American College Of Chest Physicians, AmericanThoracic Society and European Respiratory Society) 2011Diagnosis and management of stable chronic obstructivepulmonary disease: a clinical practice guideline update fromthe American College of Physicians, American College ofChest Physicians, American Thoracic Society, and EuropeanRespiratory Society Ann. Intern. Med. 155 179–91
Rabe K F et al (Global Initiative For Chronic Obstructive Lung,Diseases) 2007 Global strategy for the diagnosis, management,and prevention of chronic obstructive pulmonary disease:GOLD executive summary Am. J. Respir. Crit. Care Med.176 532–55
Rodrigo G J, Neffen H and Castro-Rodriguez J A 2011 Efficacy andsafety of subcutaneous omalizumab versus placebo as add-ontherapy to corticosteroids for children and adults with asthma:a systematic review Chest 139 28–35
Savitzky A and Golay M J E 1964 Smoothing + differentiation ofdata by simplified least squares procedures Anal. Chem.36 1627–39
Shnayderman M et al 2005 Species-specific bacteria identificationusing differential mobility spectrometry and bioinformaticspattern recognition Anal. Chem. 77 5930–7
Shvartsburg A A, Mashkevich S V and Smith R D 2006 Feasibilityof higher-order differential ion mobility separations using newasymmetric waveforms J. Phys. Chem. A 110 2663–73
Sigma-Aldrich, LLC 2012 Solid Phase Microextraction (SPME):Sample Preparation and Purificationhttp://www.sigmaaldrich.com/analytical-chromatography/sample-preparation/spme/faq.html
Snow N H 2000a Solid-phase micro-extraction of drugs frombiological matrices J. Chromatogr. A 885 445–55
Snow N H 2000b Solid-phase micro-extraction of drugs frombiological matrices J. Chromatogr. A 885 445–55
Van Berkel J J B N, Dallinga J W, Moller G M, Godschalk R W L,Moonen E J, Wouters E F M and Van Schooten F J 2010 Aprofile of volatile organic compounds in breath discriminatesCOPD patients from controls Respir. Med. 104 557–63
Westerhuis J A, Hoefsloot H C J, Smit S, Vis D J, Smilde A K, VanVelzen E J J, Van Duijnhoven J P M and Van Dorsten F A 2008Assessment of PLSDA cross validation Metabolomics4 81–9
Westhoff M, Litterst P, Freitag L and Baumbach J I 2007 Ionmobility spectrometry in the diagnosis of sarcoidosis: results ofa feasibility study J. Physiol. Pharmacol. 58 (Suppl. 5) 739–51
Westhoff M, Litterst P, Freitag L, Urfer W, Bader Sand Baumbach J I 2009 Ion mobility spectrometry for thedetection of volatile organic compounds in exhaled breath ofpatients with lung cancer: results of a pilot study Thorax64 744–8
Westhoff M, Litterst P, Maddula S, Boedeker B and Baumbach J I2011 Statistical and bioinformatical methods to differentiatechronic obstructive pulmonary disease (COPD) includinglung cancer from healthy control by breath analysis usingion mobility spectrometry Int. J. Ion Mobility Spectrom.14 139–49
Westhoff M, Litterst P, Maddula S, Boedeker B, Rahmann S,Davies A N and Baumbach J I 2010 Differentiation of chronicobstructive pulmonary disease (COPD) including lung cancerfrom healthy control group by breath analysis using ionmobility spectrometry Int. J. Ion Mobility Spectrom. 13 131–9
Wold S, Esbensen K and Geladi P 1987 Principal componentanalysis Chemometr. Intell. Lab. Syst. 2 37–52
Yang I A, Clarke M S, Sim E H and Fong K M 2012 Inhaledcorticosteroids for stable chronic obstructive pulmonarydisease Cochrane Database Syst. Rev. 7 CD002991
Zeki A A, Schivo M, Chan A, Albertson T E and Louie S 2011 Theasthma-COPD overlap syndrome: a common clinical problemin the elderly J. Allergy 2011 861926
9