A mixed methods investigation of multiple risk exposure and ...
454
A mixed methods investigation of multiple risk exposure and early adolescent girls’ emotional symptoms: Mechanisms, adaptive processes, and lived experience A thesis submitted to the University of Manchester for the degree of Doctor of Philosophy in the Faculty of Humanities 2019 Ola A. Demkowicz School of Environment, Education and Development
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of A mixed methods investigation of multiple risk exposure and ...

Amixedmethodsinvestigationofmultipleriskexposureandearly
adolescentgirls’emotionalsymptoms:Mechanisms,adaptive
processes,andlivedexperience
AthesissubmittedtotheUniversityofManchesterforthedegreeofDoctorof
PhilosophyintheFacultyofHumanities
2019
OlaA.Demkowicz
SchoolofEnvironment,EducationandDevelopment

Blankpage

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
3
Contents
ListofTables...............................................................................................................9
ListofFigures............................................................................................................11
ListofAbbreviations.................................................................................................12
Abstract....................................................................................................................15
Declaration...............................................................................................................16
CopyrightStatement.................................................................................................16
Acknowledgements..................................................................................................17
Chapter1:IntroductionandAims.......................................................................19
1.1ContextoftheStudy...........................................................................................19
1.2TheCurrentStudy...............................................................................................20
1.2.1AimsoftheStudy.........................................................................................21
1.2.2ResearchQuestions.....................................................................................22
1.3GuidingTheoreticalPerspectives........................................................................22
1.4OverviewoftheThesis........................................................................................23
Chapter2:EmotionalSymptomsandEarlyAdolescentGirls...............................25
2.1ChapterOverview...............................................................................................25
2.2DefiningEmotionalSymptoms...........................................................................25
2.3EmotionalSymptoms:TrajectoriesandOutcomes.............................................27
2.4GenderedMentalHealthTrendsandExperiences.............................................28
2.4.1EmotionalSymptomatologyandDisorderamongGirlsandWomen..........28
2.4.2TimeTrendsinEmotionalSymptomsamongAdolescentGirls...................31
2.5LivedExperienceofEmotionalSymptoms..........................................................33
2.6ChapterSummary...............................................................................................34
Chapter3:RiskandResilience............................................................................37
3.1ChapterOverview...............................................................................................37
3.2RiskFactors.........................................................................................................37

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
4
3.2.1YoungRelativeAge......................................................................................38
3.2.2LowAcademicAttainment..........................................................................39
3.2.3HighAcademicAttainment..........................................................................40
3.2.4SpecialEducationalNeeds(SEN).................................................................40
3.2.5LowFamilyIncome......................................................................................42
3.2.6YoungCarerStatus......................................................................................43
3.2.7AdverseChildhoodExperiences(ACEs).......................................................44
3.2.8NeighbourhoodSocioeconomicDeprivation...............................................45
3.3ExposuretoMultipleRiskFactors......................................................................46
3.3.1CumulativeRiskTheoryandResearch.........................................................47
3.3.2MeasurementModelsforMultipleRiskExposure......................................50
3.3.3MechanismsofMultipleRiskEffects...........................................................55
3.4ResilienceandAdaptation..................................................................................58
3.4.1FactorsSupportingPositiveOutcomes........................................................61
3.4.2SocialConnection........................................................................................63
3.4.3ActiveEngagementinHomeandSchoolLife..............................................68
3.4.4EngagementinExtracurricularActivities.....................................................69
3.5MethodologicalApproachesinRiskandResilience...........................................70
3.6ChapterSummary...............................................................................................72
Chapter4:Method.............................................................................................73
4.1ChapterOverview...............................................................................................73
4.2StudyContext.....................................................................................................73
4.2.1HeadStart.....................................................................................................73
4.2.2NationalEvaluationofHeadStart................................................................74
4.2.3IndependenceoftheCurrentStudy............................................................75
4.3EpistemologicalApproach..................................................................................75
4.3.1Pragmatism..................................................................................................76
4.3.2WiderTheoreticalPerspectives...................................................................78
4.4ResearchDesign.................................................................................................82
4.4.1MixedMethodsDesign................................................................................82
MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
5
4.4.2QuantitativeStrand......................................................................................85
4.4.3QualitativeStrand........................................................................................87
4.4.4IntegrationofQuantitativeandQualitativeStrands...................................88
4.5Participants.........................................................................................................89
4.5.1QuantitativeSample....................................................................................89
4.5.2QualitativeSample.......................................................................................93
4.6Materials.............................................................................................................99
4.6.1QuantitativeMaterials.................................................................................99
4.6.2QualitativeMaterials.................................................................................109
4.7Procedure.........................................................................................................112
4.7.1QuantitativeProcedure.............................................................................112
4.7.2QualitativeProcedure................................................................................113
4.8QuantitativeAnalysis........................................................................................115
4.8.1StructuralEquationModelling(SEM)........................................................115
4.8.2Pre-Analysis................................................................................................118
4.8.3MainStatisticalAnalysis.............................................................................119
4.9QualitativeAnalysis...........................................................................................125
4.9.1InterpretativePhenomenologicalAnalysis(IPA)........................................125
4.9.2StagesofIPA..............................................................................................126
4.10MixedMethodsStrategy................................................................................131
4.11QualityandRigour..........................................................................................132
4.11.1QuantitativeStrand.................................................................................132
4.11.2QualitativeStrand....................................................................................133
4.11.3MixedMethods........................................................................................135
4.12EthicalConsiderations....................................................................................135
4.12.1ResponsibilitiestoParticipants................................................................135
4.12.2ResponsibilitiestoSponsorsoftheResearch..........................................138
4.12.3ResponsibilitiestotheCommunityofEducationalResearchers..............138
4.12.4ResponsibilitiestoEducationalProfessionals,Policymakers,andthe
GeneralPublic.....................................................................................................138
4.13ChapterSummary...........................................................................................138

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
6
Chapter5:QuantitativeResults........................................................................139
5.1.ChapterOverview............................................................................................139
5.2PreliminaryAnalyses........................................................................................139
5.3ResearchQuestion1:RiskFactorsandProcesses............................................142
5.3.1RiskFactors................................................................................................142
5.3.2CumulativeRiskEffects.............................................................................146
5.3.3RiskMeasurementModels........................................................................151
5.3.4IndirectEffectsofStress............................................................................158
5.4ResearchQuestion2:FactorsandProcessesforPositiveOutcomes...............162
5.4.1PromotiveFactors.....................................................................................162
5.4.2ProtectiveFactors......................................................................................164
5.5ChapterSummary.............................................................................................175
Chapter6:QualitativeFindings.........................................................................177
6.1ChapterOverview.............................................................................................177
6.2IndividualParticipantThemes..........................................................................177
6.2.1ThemesforAmelia.....................................................................................177
6.2.2 ThemesforJennifer.................................................................................178
6.2.3ThemesforGrace......................................................................................180
6.3MasterThemes.................................................................................................181
6.3.1TheExperienceofSymptoms....................................................................184
6.3.2InternalGrappling......................................................................................190
6.3.3DemandsandControl................................................................................199
6.3.4DrawingonOthers....................................................................................205
6.4ReflexiveAppraisalDiscussion..........................................................................212
6.4.1IdentificationwithParticipants’Experiences............................................212
6.4.2BalancingUniqueandSharedExperiences................................................214
6.4.3WiderKnowledgeofParticipants..............................................................216
6.4.4ContextoftheBroaderStudy....................................................................217
6.5ChapterSummary.............................................................................................219

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
7
Chapter7:Discussion.......................................................................................221
7.1ChapterOverview.............................................................................................221
7.2SummaryofFindings........................................................................................221
7.2.1ResearchQuestion1:RiskFactorsandProcesses.....................................221
7.2.2ResearchQuestion2:FactorsandProcessesforPositiveOutcomes........222
7.2.3ResearchQuestion3:LivedExperience.....................................................224
7.3ResearchQuestion1:RiskFactorsandProcesses............................................225
7.3.1RiskFactors................................................................................................225
7.3.2CumulativeRiskEffects..............................................................................230
7.3.3RiskMeasurementModels........................................................................234
7.3.4IndirectEffectsofStress............................................................................238
7.4ResearchQuestion2:FactorsandProcessesforPositiveOutcomes...............244
7.4.1PromotiveFactors......................................................................................244
7.4.2ProtectiveFactors......................................................................................248
7.5ResearchQuestion3:LivedExperience............................................................255
7.5.1TheExperienceofFeelings........................................................................257
7.5.2InternalGrappling......................................................................................259
7.5.3DemandsandControl................................................................................266
7.5.4DrawingonOthers.....................................................................................274
7.6Meta-InferencesandImplicationsandDirectionsforFutureResearch...........280
7.6.1Meta-InferenceOne:EmotionalSymptomsareEmbeddedinDailyLife..282
7.6.2Meta-InferenceTwo:DemandsandStresscanbePsychologically
Overwhelming.....................................................................................................283
7.6.3Meta-InferenceThree:CloseRelationshipsareCritical.............................287
7.7StrengthsandLimitations.................................................................................290
7.7.1QuantitativeStrand....................................................................................290
7.7.2QualitativeStrand......................................................................................296
7.7.3MixedMethodsDesign..............................................................................299
7.8SummaryandConclusions................................................................................301
References..............................................................................................................303

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
8
Appendices..............................................................................................................387
WORDCOUNT:87,507

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
9
ListofTables
Table Page
4.1 Variablesinthequantitativestrand 88
4.2 Numberofeducationsettingsandparticipantswithineachlocal
authoritypartnershiparea
92
4.3 Proportionsofsamplestatisticscomparativetonationalnorms 93
4.4 Partnershipareas’conceptualisationsofriskusedtoselect
participants
95
4.5 StudentResilienceSurveyadjustedsubscalenamesandrationale 109
5.1 Summaryofdataassumptionreviewacrossthedataset 142
5.2 Descriptivestatisticsforcontinuousvariables 143
5.3 Intraclustercorrelationcoefficientsandbivariatecorrelation
coefficientsforvariablesinRQ1a
145
5.4 Unstandardisedandstandardisedregressionbetacoefficientsand
standarderrorsforhypothesisedriskvariablesaspredictorsof
symptoms
146
5.5 Distributionofthesampleacrossthecumulativeriskindex 149
5.6 Intraclustercorrelationcoefficientsandbivariatecorrelation
coefficientsforvariablesinRQ1b
150
5.7 Unstandardisedandstandardisedregressionbetacoefficientsand
standarderrorsforthecumulativeriskindexasapredictorof
symptoms
152
5.8 Intraclustercorrelationcoefficientsandbivariatecorrelation
coefficientsforvariablesinRQ1c
155
5.9 Unstandardisedandstandardisedfactorloadingsandintracluster
correlationcoefficientsforthelatentriskconstruct
156
5.10 Unstandardisedandstandardisedfactorloadingsforthelatentrisk
constructwithcorrelatedresiduals
156
5.11 Unstandardisedandstandardisedregressionbetacoefficientsand
modelfitindicesforthemultipleriskexposuremodels
158
5.12 Intraclustercorrelationcoefficientsandbivariateandlatent 161

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
10
correlationcoefficientsforvariablesinRQ1d
5.13 Unstandardisedandstandardisedbetacoefficientsfordirect,
indirect,andtotaleffectsofmultipleriskexposure,perceived
distress,andperceivedcopingonemotionalsymptoms
162
5.14 Intraclustercorrelationcoefficientsandbivariateandlatent
correlationcoefficientsforvariablesinRQ2a
164
5.15 Unstandardisedandstandardisedregressionbetacoefficientsand
standarderrorsforhypothesisedpromotivevariablesaspredictors
ofsymptoms
165
5.16 Sixpossiblemoderatorvariableswithsummaryoftheoryandprior
evidenceandregressioncoefficients
168
5.17 Intraclustercorrelationcoefficientsandbivariatecorrelation
coefficientsforvariablesinRQ2b
171
5.18 Unstandardisedandstandardisedbetacoefficientsforspecific
conditionaleffectsforindirecteffectpathways
175
6.1 ThemesforAmelia 180
6.2 ThemesforJennifer 181
6.3 ThemesforGrace 182
6.4 Masterthemesandrepresentationofparticipants 184

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
11
ListofFigures
Figure Page
3.1 Multipleriskexposuremeasurementmodels 52
3.2 Promotiveandprotectiveconceptualmodels 61
4.1 Hierarchyofelementswithinparadigms 78
4.2 Conceptualandstatisticalmoderationmodels 124
4.3 Conceptualandstatisticalconditionalindirecteffectsmodels 125
5.1 Riskfactorsmodel 147
5.2 Linechartforemotionalsymptomsandthecumulativeriskindex 149
5.3 Statisticalmodelforcumulativeriskwithstandardisedregression
betacoefficient
151
5.4 Conceptualmodelforcumulativeriskeffectswithcovariate
model
151
5.5 Multipleriskexposuremeasurementmodels 154
5.6 Statisticalmultipleriskexposuremeasurementmodelswith
standardisedbetacoefficients
159
5.7 Directeffectsandindirecteffectsmodels 163
5.8 Promotivefactorsmodel 166
5.9 Simplifiedstatisticalconditionalindirecteffectsmodel 172
5.10 Indirecteffectsmodel 174
5.11 Specificconditionalindirecteffects 177
7.1 Conceptualrepresentationofthemesfordiscussion 253
7.2 Meta-inferencesacrossthequantitativeandqualitativestrands 278

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
12
ListofAbbreviations
Abbr. Description
ACEs Adversechildhoodexperiences
AFNCCF AnnaFreudNationalCentreforChildrenandFamilies
APA AmericanPsychiatricAssociation
ASD AutisticSpectrumDisorder
CAMHS ChildandAdolescentMentalHealthServices
CBT Cognitivebehaviouraltherapy
CFA Confirmatoryfactoranalysis
CFI ComparativeFitIndex
CIN ChildinNeed
CR Cumulativerisk
DfE DepartmentforEducation
EHC Education,HealthandCare[plan]
FIML Fullinformationmaximumlikelihood
FSM Freeschoolmeals
ICC Intraclustercorrelationcoefficient
IDACI IncomeDeprivationAffectingChildrenIndex
IPA Interpretativephenomenologicalanalysis
MAR Missingatrandom
MCAR Missingcompletelyatrandom
MI Modificationindices
ML Maximumlikelihood
MLR Robustmaximumlikelihood
MNAR Missingnotatrandom
NCLF NationalCommunityLotteryFund
NHS NationalHealthService
NPD NationalPupilDatabase
OCD ObsessiveCompulsiveDisorder
ONS OfficeforNationalStatistics
PSS-4 Four-itemPerceivedStressScale

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
13
RMSEA RootMeanSquareErrorofApproximation
RQ Researchquestion
SATs StatutoryAssessmentTests
SDQ StrengthsandDifficultiesQuestionnaire
SEM Structuralequationmodelling
SEN Specialeducationalneeds
SEPC Standardisedestimatedparameterchange
SES Socioeconomicstatus
SRS StudentResilienceSurvey
TLI Tucker-LewisIndex
UCL UniversityCollegeLondon
UK UnitedKingdom
WHO WorldHealthOrganization
WLSMV Weightedleastsquaremeanandvarianceadjusted
WMF WellbeingMeasurementFramework

14
Blankpage

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
15
Abstract
Rationale:Evidencesuggeststhatfromearlyadolescence,girlsandwomenexperiencegreaterratesofemotionalsymptomsanddisorders,whilerecent
evidenceindicatesincreasedemotionaldistressamongadolescentgirls.The
currentstudysetouttoexaminethefactorsandprocessescontributingtoand
mitigatingemotionalsymptomsamongearlyadolescentgirls,withanemphasison
multipleriskexposure,andtoexplorehowthesephenomenaareexperienced.
Methods:Apragmaticparallelmixedmethodsdesignwasused.Aquantitative
strandincluded8,327girlsaged11–12years,comprisingbothself-reportand
demographicdata,andwasanalysedusingstructuralequationmodelling.A
qualitativestrandexploredthelivedexperienceofthreegirlsaged12years,
analysingaccountsgatheredthroughsemi-structuredinterviewsusing
interpretativephenomenologicalanalysis.QuantitativeResults:Resultsindicated
fourriskfactors:Lowacademicattainment,specialeducationalneeds,lowfamily
income,andcaregivingresponsibilities.Exposuretoagreaternumberofriskfactors
wasassociatedwithincreasedsymptoms,thoughalatentriskconstructincorporatingboththenatureandextentofmultipleriskexposureshowedthe
greatestpredictiveutility.Multipleriskeffectswerefoundtobeassociatedwith
emotionalsymptomsentirelythroughindirecteffectsviacomponentsofstress
appraisalprocesses.Familyadultconnection,schoolpeerconnection,andactiveengagementinhomeandschoollifewereassociatedwithlowerlevelsofemotional
symptoms.Familyadultconnectionandschoolpeerconnectionwerefoundtobe
protectiveinrelationtotheeffectsofmultipleriskexposureuponperceivedstresscomponents.QualitativeFindings:Foursuperordinatethemesweredeveloped:
Theexperienceofsymptoms,whichcapturesthewaysparticipantsconceptualised
andexperiencedthethoughtsandfeelingsassociatedwithsymptoms;internalgrappling,whichexploresparticipants’conflictinunderstandingthesesymptomsin
relationtothemselvesaswellastheouterworld;demandsandcontrol,which
exploresparticipants’experiencesofpersistentdemandsperceivedtobebeyondtheircontrol;anddrawingonothers,exploringthewaysparticipantsmappedout
anddrewonanemotionalsupportnetwork.Meta-Inferences:Quantitativeand
qualitativefindingswereintegratedtodevelopthreemeta-inferences:(1)
Emotionalsymptomsareembeddedindailylife,(2)demandsandstresscanbe
psychologicallyoverwhelming,and(3)closerelationshipsarecritical.Thetheoretical,methodological,andpracticalimplicationsoffindingsareexploredand
directionsforfutureresearcharediscussed.

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
16
Declaration
Noportionoftheworkreferredtointhethesishasbeensubmittedinsupportofan
applicationforanotherdegreeorqualificationofthisoranyotheruniversityor
otherinstituteoflearning.
CopyrightStatement
• Theauthorofthisthesis(includinganyappendicesand/orschedulestothis
thesis)ownscertaincopyrightorrelatedrightsinit(the“Copyright”)ands/he
hasgivenTheUniversityofManchestercertainrightstousesuchCopyright,
includingforadministrativepurposes.
• Copiesofthisthesis,eitherinfullorinextractsandwhetherinhardor
electroniccopy,maybemadeonlyinaccordancewiththeCopyright,Designs
andPatentsAct1988(asamended)andregulationsissuedunderitor,where
appropriate,inaccordancewithlicensingagreementswhichtheUniversityhas
fromtimetotime.Thispagemustformpartofanysuchcopiesmade.
• TheownershipofcertainCopyright,patents,designs,trademarksandother
intellectualproperty(the“IntellectualProperty”)andanyreproductionsof
copyrightworksinthethesis,forexamplegraphsandtables(“Reproductions”),
whichmaybedescribedinthisthesis,maynotbeownedbytheauthorandmay
beownedbythirdparties.SuchIntellectualPropertyandReproductionscannot
andmustnotbemadeavailableforusewithoutthepriorwrittenpermissionof
theowner(s)oftherelevantIntellectualPropertyand/orReproductions.
• Furtherinformationontheconditionsunderwhichdisclosure,publicationand
commercialisationofthisthesis,theCopyrightandanyIntellectualProperty
and/orReproductionsdescribedinitmaytakeplaceisavailableinthe
UniversityIPPolicy(see
http://documents.manchester.ac.uk/DocuInfo.aspx?DocID=24420),inany
relevantThesisrestrictiondeclarationsdepositedintheUniversityLibrary,The
UniversityLibrary’sregulations(see
http://www.library.manchester.ac.uk/about/regulations/)andinThe
University’spolicyonPresentationofTheses

MULTIPLERISKEXPOSUREANDEMOTIONALSYMPTOMSAMONGGIRLS
17
Acknowledgements
Thereareanumberofpeoplewithoutwhomthisthesiswouldnothave
beenpossible.Firstandforemost,Iwishtothankmyprimarysupervisor,Professor
NeilHumphrey,forhissupportandguidancethroughoutthisproject.Neil,youhave
beenatremendoussourceofsupportandawonderfulmentorbothinrelationto
myPhDworkandmywiderdevelopment.Yourfaithinme,andyournever-ending
optimismthateverythingwouldworkoutperfectly,havegivenmethespaceto
figureoutmyowninterestsandvaluesasaresearcherandtodevelopabeliefin
myownjudgement.IamincrediblygratefultohavehadyouasasupervisorandI
owemoretoyouthanIwilleverbeabletoexpress.Enormousthanksarealsodue
tomysecondsupervisor,Dr.MargaritaPanayiotou,forhersupport,kindness,and
friendship.Margarita,Ifeelprivilegedtohavebeenyourfirstdoctoralstudentand
amdeeplygratefulforallofthewisdomyouhavepassedon.Thankyouforyour
infinitepatienceandforpretendingmySEMquestionswereneverdaft,evenwhen
theydefinitelywere.
ThanksareduetoDr.AnnLendrumforsharingherqualitativeexpertiseand
forprovidingmevaluablespaceandtimetoreflectasthisprojecttookshape.Iam
alsogratefultoDr.EmilyStapleyattheAnnaFreudNationalCentreforChildren
andFamiliesforthethoughtfulsupportandguidanceshehasofferedmeasI
developedasaqualitativeresearcher,aswellasfortakingthetimetoreviewdrafts
ofthequalitativesectionsofthisthesis.AdditionalthankstoProfessorJessica
Deightonforherguidanceinthelastthreeyears;Ifeelprivilegedtohaveworked
alongsideher.ThereareanumberofwidercolleaguesintheManchesterInstitute
ofEducationtowhomIoweagreatdeal,forsharingtheirtimeandexpertisewith
meandalsofortheirfriendship.Inparticular,Iwouldliketoextendheartfelt
thankstoDr.EmmaAshworth,forherfriendship,support,andherroleasmyPhD
“bigsister”,andtoDr-to-beTeeMcCaldin,forbeinganall-roundgoodeggandan
eternallypatientsoundingboardandvoiceofreason.
Ofcourse,thisthesiswasonlypossiblethankstothegirlswhosharedtheir
experiences.Ihopethatmyworkhasdonethemjustice.Thankyoualsotoallofthe
educationalsettingsandstaffandlocalauthoritiesinvolvedintheHeadStart

18
programme,whoseworkmadethisresearchpossible.Furthermore,itshouldbe
recognisedthattheNationalLotteryCommunityFundhasfundedtheHeadStart
projectaswellasmyPhD;thisisimportantworkandIamgratefultohavehadthe
opportunitytobeinvolved.IwouldalsoliketoexpressmygratitudetoDr-to-be
MiaEisenstadtandDr.JoshuaHolmesfortakingthetimeandcaretoreviewmy
participantselectionprocesseswithinthequalitativestrandofthisstudy.
Onamorepersonalnote,Iwouldliketoexpressmygratitudetomyfamily
andfriendsfortheirsupportandbeliefinme.Tomymum,Nella,thankyoufor
alwaysteachingmetoexpressmyself,andtomydad,John,thankyoufortelling
metodosousingthebiggestwordsIknow.Inparticular,Dad,thiswouldnothave
beenpossiblewithoutyoufornumerousreasons,andIhopethatyouknowthat.I
wouldalsoliketothankmypartner,Hanson,forhisconsiderablesupportduringmy
PhDandhisunfailingbeliefinme;thankyou,Hanson,foralwaysmakingmelaugh
onthedifficultdaysandcheeringtheloudestonthegoodones.Finally,thanksare
duetoMausforbeingaconsistentsourceofbothcomfortanddistractionduring
thefinalportionofmyPhD.

CHAPTERONE:INTRODUCTIONANDAIMS
19
Chapter1:IntroductionandAims
1.1ContextoftheStudy
Inearlyadolescence,thedevelopmentalperiodbetweentheagesoften
and14(UnitedNationsChildren’sFund,2011),theevidencesuggeststhatgirls
begintoexperiencegreaterlevelsofemotionaldistressthandoboys(Cyranowski
etal.,2000;Kuehner,2017;Nolen-Hoeksema&Girgus,1994;Zahn-Waxleretal.,
2006).Thisgenderdifferencehasbeenshowntopersistthroughoutthelifespan.
Girlsandwomenaretwiceaslikelytoreportdepressivesymptomsanddisorders
comparedtomenfrommid-adolescenceonwards(Cyranowskietal.,2000;Kessler,
2003;Kuehner,2003,2017;Lewinsohnetal.,1998)andareoverallmorelikelyto
experienceanxioussymptomsanddisorders,thoughthisfluctuatesbasedontype
ofanxiety(McLeanetal.,2011;VanOortetal.,2009).Severalstudieshave
reportedasignificantincreaseinemotionaldistressamongadolescentgirlsin
recentyears(Collishawetal.,2010;Finketal.,2015;Lessofetal.,2016).
Accordingly,thereisaneedforresearchthatexploresthefactorscontributingto
theemergenceofsuchdifficultiesforgirlsinearlyadolescence(Finketal.,2015).
Thecurrentstudysetouttoexplorethisphenomenonwithanemphasisonriskand
resilienceprocesses;thatis,thefactorsandprocessescontributingtoemotional
symptomsaswellasthosethatsupportpositiveoutcomes.Itshouldbenotedthat
thecurrentstudyfocuseson“girls”ratherthan“females”inlinewithcurrent
understandingsthatbothbiologicalandwiderpsychosocialandculturalfactors
influencetheemergenceofemotionalsymptomsamongthisgroup,asdiscussedin
ChapterTwo.ConsiderationsaroundthisapproacharepresentedinSection7.7.
Riskfactors,orvariablesassociatedwithincreasedvulnerabilitytonegative
outcomes(Kraemer,Stice,Kazdin,Offord,&Kupfer,2001;TheWorldHealth
Organization[WHO],2005),oftenco-occur,withsomechildrenandyoungpeople
likelytoexperiencemultiplerisks(Flouri&Kallis,2007).Researchhassoughtto
investigatethewayinwhichexposuretomultipleriskfactorsaffectschildand
adolescentoutcomes,includingtheseminalIsleofWightstudy(Rutter,1979),the

CHAPTERONE:INTRODUCTIONANDAIMS
20
RochesterLongitudinalStudy(Sameroffetal.,1993),researchbytheNational
InstituteofChildHealthandHumanDevelopment(Fearon&Belsky,2004),and,
morerecently,theHeadStartprogramme(Deighton,Lereya,etal.,2018),from
whichthecurrentstudydrawsitsdata.Overall,studieshaveshownthatgreater
levelsofriskexposuregenerallycorrespondtoworsenedoutcomes,including
emotionalsymptomsandwiderinternalisingdifficulties(e.g.,Appleyard,Egeland,
Dulmen,&Sroufe,2005;Gerard&Buehler,2004;Horan&Widom,2015;
Panayiotou&Humphrey,2018).Oneofthecentralhypothesesastohowsuch
effectsoccuristhatstressresponsesystemsbecomeoverwhelmedinthefaceof
highlevelsofadversity,negativelyaffectinghealthanddevelopment(Evansetal.,
2013).However,itisimportanttonotethatnotallindividualsexposedtoadversity
willexperiencenegativeoutcomes,necessitatingexaminationofthefactorsthat
supportresilience,orpositiveadaptationincircumstancesofadversityorrisk
exposure(Lutharetal.,2000;Masten,2014b;Ungar,2012).
1.2TheCurrentStudy
Thecurrentstudyoffersamixedmethodsinvestigationofmultiplerisk
exposureandearlyadolescentgirls’emotionalsymptoms.Thestudysetoutto
incorporateandbuildonexistingunderstandingsofmultipleriskexposureandits
relationshipwithearlyadolescentgirls’emotionalsymptoms,including
examinationoftheroleplayedbystressappraisal,ortheextenttowhichone
considerslifestressful(Lazarus,1966;Lazarus&Folkman,1986).Thefactorsand
processescontributingtopositiveoutcomesareexplored,withafocusonfactors
thatmaymitigatethenegativeeffectsofmultipleriskexposure.Thestudyalsoset
outtoexplorelivedexperienceofthesephenomenaamongearlyadolescentgirlsin
ordertounderstandthewaysinwhichgirlsexperienceandmakesenseofthese
areasoftheirlives.Theknowledgegeneratedthroughtheseendeavourscan
contributetoboththeoryandpracticebyfurtheringourunderstandingofthese
phenomenaandmayhaveimplicationsforthesupportandprovisionofferedtoat-
riskadolescentgirls.

CHAPTERONE:INTRODUCTIONANDAIMS
21
1.2.1AimsoftheStudy
Giventheabove,theaimsofthestudyareto:
1. Increaseknowledgeandunderstandingoftheriskfactorsandprocesses
associatedwithemotionalsymptomsamongearlyadolescentgirls,witha
particularfocusonmultipleriskexposure.
Thisaimseekstocontributetotheknowledgebaseregardingtheeffectsofrisk
exposure,andparticularlyexposuretomultipleriskfactors,inrelationtoemotional
symptomsinearlyadolescentgirls.Inexploringdifferentconceptualisationsand
measurementmodelsofmultipleriskexposure,aswellasinvestigatingthestress
hypothesis,thestudywillmakebothconceptualandmethodologicalcontributions
tothisareaofresearch.
2. Assessthefactorsandprocessessupportingpositiveoutcomesinrelationto
emotionalsymptomsamongearlyadolescentgirls.
Inaddressingthisaim,thecurrentstudywilladdtoknowledgeandunderstanding
ofthefactorsthatareassociatedwithloweredemotionaldistressamongearly
adolescentgirls.Byexaminingbothpromotiveandprotectivefactors,thestudywill
furtherunderstandingaroundthefactorsassociatedwithloweredsymptomsfor
earlyadolescentgirlsasawhole,aswellashowaccesstoparticularfactorscan
disruptthenegativeeffectsofmultipleriskexposure.
3. Explorethelivedexperienceofearlyadolescentgirlswhoareexperiencing
emotionalsymptomsinthecontextofriskexposure.
Thefulfilmentofthisaimwillsupportknowledgeandunderstandingofthewayin
whichearlyadolescentgirlsexperienceandmakesenseofemotionalsymptoms
andriskexposureintheirlives.Thiswillcontributetothedevelopmentofamore
in-depthunderstandingofthesesymptomsandexperiencesincontext,which
cannotbeascertainedthroughthequantitativemethodologiesmoretypically
adoptedwithinriskandresilienceresearch.

CHAPTERONE:INTRODUCTIONANDAIMS
22
1.2.2ResearchQuestions
1. Whataretheriskfactorsandprocessesassociatedwithemotionalsymptoms
amongearlyadolescentgirls?
a. Oftherisksidentified,whatisthemagnitudeoftheirassociationwith
earlyadolescentgirls’emotionalsymptoms?
b. Isthereevidenceforacumulativeriskeffectinrelationtoearly
adolescentgirls’emotionalsymptoms?
c. Whichriskmeasurementmodelbestexplainstheeffectsofexposureto
multipleriskfactorsinrelationtoearlyadolescentgirls’emotional
symptoms?
d. Arethereindirecteffectsofperceivedstressintherelationshipbetween
multipleriskexposureandemotionalsymptoms?
2. Whatarethefactorsandprocessesthatsupportpositiveoutcomesin
emotionalsymptomsamongearlyadolescentgirls?
a. Ofthepromotivefactorsidentified,whatisthemagnitudeoftheir
associationwithearlyadolescentgirls’emotionalsymptoms?
b. Towhatextentarethedirectand/orindirectrelationshipsbetween
multipleriskexposure,perceivedstress,andemotionalsymptoms
conditionaluponaccesstoprotectivefactors?
3. Whatisitliketobeanearlyadolescentgirlwhoisexperiencingemotional
symptomsinthecontextofriskexposure?
1.3GuidingTheoreticalPerspectives
Thecurrentstudydrawsonmultipletheoriesinordertoexplorevarying
perspectivesofriskandresilienceinrelationtoearlyadolescentgirls’emotional
symptoms.Firstly,theresearchisguidedbyBronfenbrenner's(1979,1999)
ecologicalsystemstheory,whichpositsthathumandevelopmentoccurswithinthe
contextofmultipleenvironmentsandprocesses.Theresearchisalsoinformedby
cumulativerisktheory,whichpositsthatgreaterriskexposurecorrespondsto

CHAPTERONE:INTRODUCTIONANDAIMS
23
worsenedoutcomesandproposesthatthenumberofriskfactorsismore
importantthanthenatureofthosefactors(Evansetal.,2013;Flouri&Kallis,2007;
Rutter,1979).Explorationofthisprincipleinthestudyisalsounderpinnedby
allostaticloadtheory,ortheconceptthatheighteneddemandoverwhelmsstress
responsesystems(Evans,2003;McEwen,1998;Sterling&Eyer,1988),andbythe
transactionalmodelofstressandcopingoutlinedbyLazarusandcolleagues,
wherebystressoccursthroughaprocessofappraisal(Lazarus,1966;Lazarus&
Folkman,1984).Thestudyisalsoinformedbycurrentunderstandingsofresilience,
whichrecognisesthatadaptationtoadversitydependsuponaccesstoprotective
factorsacrosstheecologythatcancounteractthenegativeeffectsofriskexposure
(Masten,2001,2014b,2014a).Thestudy’sfocusonriskandresilienceisfurther
underpinnedbytheopposingprinciplesofequifinality(therearemultiplepathways
tosingularoutcomes)andmultifinality(similarexperiencescanresultindifferent
outcomes;Cicchetti&Rogosch,1996;Lutharetal.,2000).CicchettiandRogosch
(1996)haveoutlinedthatthesetwoconceptsprovideavaluablelensthrough
whichtoframeriskandresilienceresearchandexploretheparticularfactorsthat
leadtoconvergentordivergentpathwaysacrossindividuals.Finally,thequalitative
strandofthestudyutilisesinterpretativephenomenologicalanalysis(IPA),an
approachconcernedwiththedetailedexplorationoflivedexperience.Assuch,the
numeroustheoreticalperspectivesthatunderpinIPAguidedthecurrentstudy.
Specifically,IPAisgroundedinHusserl's(1927/1971)phenomenology,Heidegger's
(1927/1962)hermeneutic,andanidiographiccommitmenttothein-depth
explorationoftheparticular,asopposedtocreatinggeneralisations(Smith,
Flowers,&Larkin,2009;seeSection4.3.2).
1.4OverviewoftheThesis
ChapterTwooutlinesexistingtheoryandevidencearoundemotional
symptomsandearlyadolescentgirls.Theconceptofemotionalsymptomsis
explored,withconsiderationoftrajectoriesandoutcomes,andanoverviewof
currentevidencerelatingtogenderedmentalhealthtrendsandexperiencesis
presented.ChapterThreeprovidesanoverviewofriskandresilienceresearchand

CHAPTERONE:INTRODUCTIONANDAIMS
24
theapplicationoftheseconceptswithinthecurrentstudy.Thischapteroutlinesthe
particularfactorsinvestigatedinthestudyandexploreshowtheresearch
contributestoknowledgeandunderstandingaroundmultipleriskexposure,the
roleofpsychologicalstress,andadaptiveprocesses.
ChapterFourpresentsthemethodologyandmethodsusedinthestudy.It
outlinesitsepistemologicalstanceanduseofamixedmethodsdesignbefore
comprehensivelydetailingeachstageoftheresearchprocess.ChaptersFiveandSix
presentthequantitativeandqualitativefindingsofthestudy,respectively.Finally,
ChapterSevenpresentsadiscussionofthestudy’sfindings,exploringquantitative
andqualitativefindingsintheirownrightbeforebringingthesetogetherintometa-
inferencesandofferingconclusions.
CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
25
Chapter2:EmotionalSymptomsandEarlyAdolescentGirls
2.1ChapterOverview
Thischapterexploresexistingtheoryandevidencerelatingtoemotional
symptomsandearlyadolescentgirls.Itintroducestheconceptofemotional
symptomsandrelatedtrajectories,beforeoutlininggenderedmentalhealthtrends
andrecentindicationsofincreasedemotionaldistressamongadolescentgirls.
Finally,thechapterexploresthevalueofexamininglivedexperienceofthe
thoughtsandfeelingsassociatedwithemotionalsymptomsandtheuseofthis
approachinthestudy.
2.2DefiningEmotionalSymptoms
MentalhealthisdefinedbytheWHOas“astateofwellbeinginwhichthe
individualrealizeshisorherownabilities,cancopewiththenormalstressesoflife,
canworkproductivelyandfruitfully,andisabletomakeacontributiontohisorher
community”(WHO,2001,p.1).Themostcommonlyreportedformsofmental
healthsymptomsanddisordersamongchildrenandadolescentsinthegeneral
populationcanbebroadlyclassifiedaseitherinternalising(e.g.,anxietyand
depressivesymptomsanddisorders,somaticcomplaints,andsuicidalideationand
behaviours)orexternalising(e.g.,attention-deficithyperactivitydisorder,disruptive
behavioursanddisorders,oppositionaldefiantdisorder,andconductproblemsand
disorders;Kovess-Masfetyetal.,2016;Polanczyk,Salum,Sugaya,Caye,&Rohde,
2015).Thecurrentstudyfocusesonemotionalsymptoms,whichcapturesboth
depressiveandanxioussymptoms(e.g.,sadmoodandworry;alsosometimes
referredtoasemotionalproblems,emotionaldifficulties,oremotionaldistress).
Thedistinctionbetweensymptomanddisordershouldbenotedhere;termssuchas
“symptom”arecommonlyusedtorefertoanobservablestateorbehaviourthat
maybepresenttosomeextentamongthegeneralpopulation,while“disorders”
aretypicallydefinedbynarrowcriteriaspecifyingaparticularcombinationandlevel
ofspecificsymptoms(Friedetal.,2016).Thatis,individualsmayexperiencesome

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
26
levelofagivensymptomatology(e.g.,depressivesymptoms),withoutnecessarily
fulfillingthecriteriaforadiagnosticdisorder(e.g.,MajorDepressiveDisorder;
AmericanPsychiatricAssociation[APA],2013).Thecurrentstudyfocuseson
emotionalsymptoms,ratherthanclassifiedpsychiatricdisorders,foranumberof
reasons.Firstly,asnoted,studieshaveindicatedarisespecificallyinemotional
symptomsamongadolescentgirlsinthegeneralpopulation.Secondly,thestudy
focusesonacommunitysampleratherthanaclinicalsampleandsoisinterestedin
varyinglevelsofsymptomatologyratherthanonlythosefulfillingcriteriafor
disorder.Finally,anumberofstudieshavechallengedthedistinctionbetween
“symptom”and“disorder”,utilisingnetworkanalysistodemonstratethat
symptomsofdepressionandanxietygobeyondthosespecifiedwithinconstricted
diagnosticcriteria,indicatingthatpsychopathologyisnotnarrowlyexpressed
throughdistinctdisorders(Friedetal.,2016;McElroy&Patalay,2019).Thus,the
studysoughttolookbeyonddiagnosticcriteriaandexaminemoregenerallevelsof
symptomatology.Inoutliningfindingsacrossthewiderliterature,however,
evidencerelatingtobothsymptomatologyanddisorderisdrawnupon;insuch
instances,thesetermsareutilisedasappropriatefortransparency.
Researchhasshownthatdepressiveandanxioussymptomsaredistinctbut
stronglyinter-related(Cummingsetal.,2014;Nolen-Hoeksema,2000),with
symptomsoftenidentifiedasintertwined(Friedetal.,2016;McElroy&Patalay,
2019)andhighcomorbidityratesfrequentlyreportedamongadolescents(e.g.,
Angold&Costello,1993;Balázsetal.,2013;Brady&Kendall,1992;Edbrooke-
Childs,Wolpert,Zamperoni,Napoleone,&Bear,2018;WHO,2017).Cummingset
al.(2014)identifiedseveralpossiblehypothesesforthiscomorbidity,including
sharedriskfactors,asequentialassociationinwhichtheexperienceofonesetof
symptomsleadstotheother,andattributiontoasharedunderlyingfactor,suchas
negativeaffectivity.Itshouldadditionallybenotedthatbothdepressiveand
anxioussymptomscanalsobecapturedwithinaglobaldomainof“internalising
difficulties”,whichasnotedalsoencompasseswiderdifficultiessuchassocial
withdrawalandsomaticsymptoms(Achenbach,1966;Fornsetal.,2011).Current
perspectivesholdthatitcanbeusefultoexaminethesevaryinginter-related

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
27
constructsbothindependentlyandinunison,dependingonthestudyaim
(Cummingsetal.,2014;Fornsetal.,2011;Zahn-Waxleretal.,2000).
2.3EmotionalSymptoms:TrajectoriesandOutcomes
Depressionandanxietyareamongthemostcommonmentalhealth
difficultiesacrossthelifespanandposeaglobalpublichealthchallenge(WHO,
2017).Psychopathologyresearchhasconsistentlydemonstratedthatmentalhealth
disorders,includingdepressionandanxiety,oftenhavetheironsetduring
childhoodandadolescence,with75%ofallmentalhealthdisordersoccurringby
theageof24years(Kessleretal.,2005)and50%emergingspecificallyduring
adolescence(Belfer,2008).Thetransitionfromchildhoodintoadolescenceisoften
highlightedasapivotalmomentintrajectoriesofdepressionandanxiety,withthe
typicalage-of-onsetfrequentlyidentifiedasearlyadolescence(e.g.,Costello,
Copeland,&Angold,2011;deLijsteretal.,2016;Jones,2013).Whilelowerratesof
depressionandanxietydisordersareusuallyobservedamongchildrenandyounger
adolescentscomparedtoolderagegroups(WHO,2017),prevalencestudieshave
identifiedworryinglevelsofsymptomatologyanddisorderamongthisgroup.For
instance,onerecentlarge-scalestudy,alsoutilisingHeadStartdata,foundthat
approximatelyoneinfiveadolescentsscoredhigherthanthethresholdtoindicate
abnormallevelsofemotionalsymptoms(Deightonetal.,2019).Anotherrecent
EnglishinvestigationbytheNationalHealthService(NHS)foundthatoneintwelve
childrenandyoungpeopleagedfiveto19wereidentifiedashavinganemotional
disorder,includingdepressiveandanxiousdisorders(NHSDigital,2018).
Emotionalsymptomsinadolescencehaveanumberofshort-andlong-term
implications.Evidenceindicatesassociationswithvariousnegativehealth
behavioursanddisordersincludingeatingdisorders(e.g.,Lewinsohn,Striegel-
Moore,&Seeley,2000;Touchetteetal.,2010)anddrugandalcoholuse(Katonet
al.,2010;McKenzieetal.,2010),aswellascontributingtoloweredschool
attendanceandattainment(Deighton,Humphrey,etal.,2018;Katonetal.,2010;
Owensetal.,2012).Researchhasconsistentlyindicatedthatpersistentemotional
symptomsduringthistimeincreasetheriskofdeliberateself-harm(e.g.,Moranet

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
28
al.,2011;Pattonetal.,2007)andsuicidalideationandbehaviours(e.g.,Kandel,
Raveis,&Davies,1991;Lewinsohn,Rohde,&Seeley,1996;Murphy,2014).Thereis
alsoconsistentevidenceofarelationshipbetweensuchsymptomsinadolescence
andbroadermentalhealthdifficultiesanddisordersinlateryears(e.g.,Kessleret
al.,2005;Roza,Hofstra,VanDerEnde,&Verhulst,2003).Inadulthood,emotional
symptomsareassociatedwithhigherratesofunemploymentandlowered
productivity(Lerner&Henke,2008).Aglobalsystematicreviewidentified
depressivedisordersastheleadingcauseofdisability,withhigherestimatesfor
womenthanmen(Ferrarietal.,2013),whileMathersandLoncar(2006)estimate
thatby2030,depressionwillbealeadingcauseofdiseaseburdeninhighincome
countries.
Suchoutcomeshighlightbothanethicalandeconomicresponsibilityto
understandandsupportmentalhealth(includingemotionalsymptoms)during
adolescence(Kielingetal.,2011).Epidemiologicalresearchhassoughttoestablish
theparticularantecedentsandcorrelatesassociatedwithemotionalsymptoms
acrossthelifespan,whichcansupportearlyidentificationandinterventionfor
thoseatrisk.However,thereisaneedtounderstandthiswithinparticulargroups
andtoexamineunderlyingprocesses.Furthermore,whilethereisawidefieldof
literatureexploringtheantecedentsandimplicationsofemotionalsymptoms,
muchlessiscurrentlyknownregardingthelivedexperiencesofadolescents
managingthesesymptomsorthemeaningoftheseexperienceswithintheirdaily
lives.Thecurrentstudysetouttoexaminethefactorsandprocessesrelatingto
emotionalsymptomsspecificallyamongearlyadolescentgirls,through
identificationofoverarchingpatternsaswellaslivedexperience.
2.4GenderedMentalHealthTrendsandExperiences
2.4.1EmotionalSymptomatologyandDisorderamongGirlsandWomen
Epidemiologicalresearchhasconsistentlyindicatedthatfromearly
adolescenceonwards,girlsandwomenexperiencegreaterratesofdepressiveand
anxioussymptomsanddisordersrelativetomen(Cyranowskietal.,2000;Kuehner,
2017;Nolen-Hoeksema&Girgus,1994;Zahn-Waxleretal.,2006).Frommid-

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
29
adolescenceonwards,approximatelytwiceasmanywomenasmenworldwide
experiencedepression(Cyranowskietal.,2000;Kessler,2003;Kuehner,2003,
2017;Lewinsohnetal.,1998).Whileatageneralleveldepressionwasidentifiedin
2004asthethirdleadingcauseofdiseaseburden,itwasfoundtobetheleading
causeforwomenaged15–44years(WHO,2004).Indeed,thereisalsoevidence
thatdepressiveandanxiousdisordersareassociatedwithgreaterburdenamong
womenthanmen,suggestingthattheyarenotonlymoreprevalentamongwomen,
butcanalsobemoredisabling(McLean,Asnaani,Litz,&Hofmann,2011;WHO,
2004).Priortoadolescence,observedgenderdifferencesfordepressiveand
anxioussymptomsaretypicallysmall(Rozaetal.,2003),withashiftoccurring
betweentheagesof11and13years,whengirlsaretypicallyfoundtobegin
exhibitinggreatersymptomatology(Boretal.,2014;Nolen-Hoeksema,2001;Roza
etal.,2003;Salketal.,2016).Asnotedabove,girlsandwomenareonaverage
twiceaslikelytoexperiencedepressivesymptomsanddisorderscomparedtomen;
thisdisparityhasbeenidentifiedasemergingfromtheageof15yearsonwards
(Cyranowskietal.,2000;Kessler,2003;Kuehner,2003,2017;Lewinsohnetal.,
1998).Thesefindingsappeartobemorestablefordepressivesymptomsand
disordersthanforanxiety.Forinstance,thereisalsoevidencethatgirlsaremore
susceptibletoanxioussymptomsanddisordersevenduringchildhood(McLeanet
al.,2011;VanOortetal.,2009),whiletheage-of-onsetandmagnitudeofgender
differencescanfluctuatebasedontheparticularanxietydisorder(McLeanetal.,
2011).Overall,though,itappearsthatearlyadolescencemaybeapivotaltimein
theemergenceofemotionalsymptomsamonggirls.
Researchershaveattributedsuchgenderdifferencestoawiderangeof
factors.Thisincludespsychologicalandsocioculturalfactorssuchasgirls’and
women’sgreaterruminativecoping(Johnson&Whisman,2013;Nolen-Hoeksema
&Girgus,1994),chronicstrainindailylife(Fredrickson&Roberts,1997;Hammen,
2005;Kuehner,2017;Nolen-Hoeksema,1990,2001;Nolen-Hoeksema&Girgus,
1994),societalobjectificationandharassment(Fredrickson&Roberts,1997;Skoog
etal.,2016),gender-relatedviolencesuchaschildhoodsexualabuse,intimate
physicalandsexualviolence,andrape(Fredrickson&Roberts,1997;Hammen,

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
30
2005;McLean&Anderson,2009;Nolen-Hoeksema,2001),lowself-esteemand
bodydissatisfaction(Bologninietal.,1996;Kostanski&Gullone,1998;Nolen-
Hoeksema,1990;Nolen-Hoeksema&Girgus,1994),emphasisanddependenceon
socialrelationships(Cyranowskietal.,2000),andgreaterempathyskills(Keenan&
Hipwell,2005).Researchershavealsohighlightedanumberofpotentialbiological
andphysiologicalcontributors,includinggreatergeneticpredisposition(Hankinet
al.,2015;McLeanetal.,2011;Merikangasetal.,1985;Steineretal.,2003),
increasedstressreactivityovertime(Compasetal.,1993;Nolen-Hoeksema,2001),
andincreasesinspecificadrenalandovarianhormonesassociatedwithincreased
risk(Albert,2015;Nolen-Hoeksema,2001;Steineretal.,2003).
Nolen-HoeksemaandGirgus(1994)positedthattheemergenceofgender
differencesforemotionalsymptomatologyanddisorderduringearlyadolescenceis
likelynotattributabletoanyonefactor,buttoaninteractionofvarious
contributors.Assuch,theauthorsarguedthatthereisaneedfortheoretical
frameworksthatcanintegratebothbiologicalandpsychosocialfactors,suchas
thoseoutlinedabove.Subsequently,Hyde,Mezulis,andAbramson(2008)outlined
the“ABCmodel”foradolescentdepression,integratingaffective(e.g.,emotional
reactivity),biological(e.g.,pubertalhormones,geneticpredisposition),and
cognitive(e.g.,rumination,objectifiedbodyconsciousness)factors.Hydeetal.
(2008)arguedthatthesearethemajorindividual-leveldomainsthatinteractwith
widersocioculturalfactorstoinfluencedepressivesymptoms.Indeed,researchinto
thisareahasnowproducedcompellingevidencethatbiologicalcomponents,such
asthesexhormonesproducedbyfemalesduringpuberty,caninteractwithwider
individualandinterpersonalstressorsandriskfactorsfordepressiveandanxious
symptomsduringadolescence(Hankinetal.,2015;Kuehner,2017;McLeanetal.,
2011;McLean&Anderson,2009).Thecurrentstudydoesnotseektodirectly
assesstrajectoriesofchangeofgenderdifferencesandwasnotabletoexplore
biologicalfactorsgivenuseofsecondarydata.Nevertheless,thestudycanoffera
numberofcontributionstoknowledgeandunderstandinginthisareagivenits
focusonearlyadolescenceasapivotaldevelopmentalstagefortheemergenceof
emotionaldifficulties.

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
31
2.4.2TimeTrendsinEmotionalSymptomsamongAdolescentGirls
Inrecentyearstherehavebeenindicationsofanincreaseinthelevelsof
emotionalsymptomsexperiencedbyadolescentgirlsintheUnitedKingdom(UK).
Indeed,despitewidespreadconcernsthatchildandadolescentmentalhealthis
worsening,longitudinalresearchhasdemonstratedthatprevalenceratesforother
symptomsanddisordershaveremainedmostlystableacrossrecentdecades
(Collishawetal.,2010;Maughan,Collishaw,Meltzer&Goodman,2008).Onestudy
identifiedanincreaseinthelevelsofself-reportedemotionalsymptomsintwoUK-
basedsamplesofadolescentgirlsaged11–13in2009and2014,achangenot
evidencedinboys’responses,inadditiontoanincreasednumberofgirlsatriskof
disorder(Finketal.,2015).Similarly,Lessofetal.(2016)reportedanincreaseinthe
levelsofemotionalsymptomsreportedbyadolescentgirlsaged14/15inUK-based
samplesbetween2005and2014.Somestudiesfoundnoevidenceofsuchan
increase(Collishawetal.,2010;Greenetal.,2005;Pitchforthetal.,2018),while
recentevidencesupportsincreasedratesofemotionaldisorderamongboth
adolescentgirlsandboys(NHSDigital,2018).
Thoughtherearesomeexceptions,asystematicreviewofinternational
timetrendsinadolescentmentalhealthreportedthatmostoftheincludedstudies
identifiedanincreaseingirls’levelsofself-reportedpsychologicaldistress(Boret
al.,2014).Anumberofmethodologicalexplanationshavebeenposited,including
thoserelatedtothemethodologicalchallengesinassessingcohorttrends,though
testingsuchhypothesesischallengingandassuchtheseexplanationsremain
relativelytheoretical(Collishaw,2015).Forinstance,prevalenceestimatesand
comparisonsofpsychopathologyacrossgroupsusingquestionnairemethodscanbe
sensitivetominordifferencesinitemwording(Goodmanetal.,2007)andcandiffer
acrossinformants(Collishawetal.,2009),suggestingthatthereisapossibilityof
reportingeffectsacrossthisevidencebase(Collishaw,2015).Disparitiescouldalso
berelatedtothetimeatwhichdatawascollected.Forexample,whileCollishawet
al.(2004)foundnoevidenceofthisincreaseacrosssamplesfrom1974,1986,and
1999,alateranalysiscomparingthesamesamplefrom1986alongsideasample

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
32
from2006identifiedasignificantincrease(Collishawetal.,2010).However,recent
findingsfromPitchforthetal.(2018)spannedasimilarlengthoftimebetween
cohorts(1995and2018)andfoundnoevidencetosupportawideninggendergap.
Ithasalsobeenarguedthatgrowingawarenessofmentalhealthhas
contributedtothemedicalizationofeverydayemotionsandstresslevels,which
thusmaybecomeconflatedwithsymptomsanddisorders(Collishaw,2015;
Dowrick&Frances,2013).Intheirsystematicreview,Boretal.(2014)exploredthe
possibilitythatthisgrowingawarenessmayhaveledtoincreasedreadinessto
reportmentalhealthsymptomsamongadolescents.Giventhatincreaseshave
beenobservedspecificallyamonggirls,thishypothesiswarrantsfurtherexplanation
infutureresearch(thoughisbeyondthescopeofthecurrentstudy).Researchhas
demonstratedthatgirlsareoftenmorestronglyencouraged,relativetoboys,to
inspectanddiscusstheiremotionsthroughoutchildhoodandadolescence(Berkeet
al.,2018;Fivush,2007;Root&Denham,2010).Indeed,culturallydominantor
hegemonicmasculinityidealsinWesterncountriescanaffectthewaysinwhich
boysandmenunderstandandrespondtotheirownemotions,potentially
introducingabarrierforexpressingemotions,seekinghelp,andadaptivecoping
behaviours(Cleary,2012;Landstedtetal.,2009;Oransky&Marecek,2009).
However,thoughdifferencesinthewaysthatboysandgirlsaretaughttomanage
andexpressemotionshaslongbeendocumented,thereisnoevidencesuggesting
increasedreadinesstoreportamonggirlsinrecentyears,orindeedatall.Indeed,a
qualitativestudyfocusingonUKadolescentsconcludedthatgirlswerenot
necessarilymorewillingtoreportsymptomscomparedtoboysandfoundthatboth
groupsdescribedsimilarperceivedrepercussionsofdoingso,suchasnegativepeer
reactions(MacLeanetal.,2010).
Ofcourse,itispossiblethatthisevidencereflectsagenuineincreasein
emotionalsymptomsamongrecentcohortsofadolescentgirls.Thisincreaseis
morecommonlyreportedthannot(Boretal.,2014)andhasbeenobservedacross
varyingstagesofadolescence.Aspreviouslyoutlined,genderdifferencesinmental
healthgenerallyemergeduringearlyadolescence,typicallyaroundtheageof12
years(Boretal.,2014;Rozaetal.,2003).Therefore,indicationsofheightened

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
33
prevalenceinthelevelsofemotionalsymptomsamong11-13year-oldgirls(Finket
al.,2015)suggeststhatincreasedlevelsofemotionalsymptomsmaybeoccurring
attheagesuchdifficultiestypicallybecomemorelikelyingirls,ratherthanata
laterstageofadolescence.Suchevidencehighlightsaneedforongoingresearch
examiningfactorsandprocessescontributingtodifficultiesamongthisparticular
agegroup,asitappearstobeapivotalstageingirls’mentalhealthtrajectories.
Althoughitiswellestablishedthattherearegenderdifferencesinmental
healthtrendsacrossthelifespan,asdiscussedearlierinthischapter,thereisno
clarityregardingthecauseofthisapparentincreaseinemotionalsymptomsin
adolescentgirls(Boretal.,2014).Researchershavepositedarangeoffactorsthat
maybecontributingtosuchanincrease,suchassocialmediausage(Finketal.,
2015),increasedsexualisationofadolescentgirls(Boretal.,2014;Finketal.,2015),
increasedacademicpressure(Boretal.,2014;Collishawetal.,2010),andalackof
prioritisationofemotionalsymptomsinschools(Finketal.,2015),thoughsuch
potentialexplanationsremainlargelyspeculative.Itisimportanttonotethatthe
currentstudyisnotfocusedonfactorsthathavecontributedtoanincreaseingirls’
emotionalsymptomsovertimeandinsteadfocusesmoregenerallyonassociated
factorsamongarecentsample.Furthermore,theuseofqualitativeinquiryinthe
proposedstudymaycontributetocurrentunderstandingsofhowemotional
symptomsareperceivedbyearlyadolescentgirlsexperiencingthem.Indeed,when
seekingtounderstandthefactorsthatcontributetooutcomeswithinaparticular
population,itcanbeavaluableexercisetoexplorewhatsuchsymptomsmaymean
tothatpopulationanditsplaceintheirlives(Smithetal.,2009).
2.5LivedExperienceofEmotionalSymptoms
Oneofkeyfacetsofthestudy’squalitativestrandisitsexplorationofhow
emotionalsymptomsareperceivedandexperiencedbyearlyadolescentgirls;that
is,howthesesymptomsactuallyappearandfeeltothosewhohavethem.The
studyofdifficultemotionsandmentalhealthsymptomsanddisordersasfeltand
experiencedsubjectivelybytheindividualisimportantforanumberofreasons.The

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
34
centralityofemotionsandmentalhealthsymptomswithinindividuals’day-to-day
livesisinandofitselfanimportantreasontounderstandhowtheseare
subjectivelyexperiencedandunderstood(Eatough&Smith,2006b).Practically,
greaterinsightintohowindividualsthinkabouttheseexperiencescanfacilitate
moreemotionallysensitiveapproachestosupportandtherapeuticinput,whichis
particularlyimportantinthecontextofadolescencegiventhatthisappearstobea
vulnerableperiodformentalhealthsymptomatologyanddisorder.Todate,there
hasbeenlittledirectexplorationofthewayinwhichvariousmentalhealth
symptoms,includingemotionalsymptoms,arefeltandunderstoodbyadolescents,
despitepersistentinterestintoemotionalandmentalhealthprocessesduringthis
time.Thisapproachisinformedinpartbypastworkfocusedonphenomenological
inquiryintoemotionexperience,orthewayinwhichemotionsarefeltand
constructed,whichaimstoofferinsightintothenuancesofthesephenomenaand
processesandtheroletheyplayinthoughtsandbehaviour.(Eatough&Smith,
2006b;Frijda,2005).Inparticular,thisemphasisonunderstandinghowsymptoms
areexperiencedisguidedbyworkfromEatoughandSmith(2006b,2006a),who
haveusedIPAtoexploreadultwomen’sangerexperiences,highlightingthatIPAis
particularlyvaluableheregivenitsemphasisonmeaningmaking.Thus,here,the
currentstudysoughttobuildaricherunderstandingofemotionalsymptomsamong
earlyadolescentgirlsbyconsideringhowthesedifficultiesandassociatedthoughts
andfeelingsarefeltandpsychologicallyconstructed.Greaterunderstandinginthis
areamaygenerateinsightintothemeaningoftheseexperiencesamongthis
populationaswellashowgirls’understandingsmayinformtheirdecisionsand
responsesinrelationtothesesymptoms.
2.6ChapterSummary
Emotionalsymptomatologyanddisordersoftenhavetheirage-of-onsetin
childhoodandadolescence.Fromearlyadolescence,girlsandwomenexperience
greaterratesofemotionalsymptomatologyanddisorderandevidencesuggestsa
recentincreaseamongadolescentgirls.Thestudysetouttoexplorethefactorsand
processescontributingtosuchdifficultiesamongthisgroup,includingtheroleof

CHAPTERTWO:EMOTIONALSYMPTOMSANDEARLYADOLESCENTGIRLS
35
stress,whichisconsideredtoplayakeyroleintheincreasedratesofsymptoms
observedamongthisgroup.

36
Blankpage

CHAPTERTHREE:RISKANDRESILIENCE
37
Chapter3:RiskandResilience
3.1ChapterOverview
Thischapterprovidesanoverviewofriskandresilienceresearchandthe
applicationoftheseconceptsinthestudy.Itoutlinestheriskvariablesinvestigated
herebeforeexploringtheoryandresearcharoundmultipleriskexposure.Next,the
chapterdiscussestheconceptofresilienceandoutlinesthevariablesassessedhere
inrelationtopositiveoutcomes.Finally,itreflectsonmethodologicaltrendsacross
thisfieldandconsiderstheadvantagesofqualitativeinquiryaspartofamixed
methodsframework.
3.2RiskFactors
Tosomeextent,riskfactorsoftenoperatewithoutagreatdealofspecificity,
withmanyfactorsfunctioningasriskyinrelationtomultipleoutcomesandinthe
contextofvaryingpopulationsandcircumstances(Flouri&Kallis,2007).For
example,povertyandsocialinequalityareshowntohavewide-rangingnegative
effectsacrossthelifespan,includingpoorerphysicalhealth,mentalhealth,child
development,andaccesstoeducation(Brooks-Gunn&Duncan,1997;Reiss,2013).
Nevertheless,theextenttowhichagivenfactorfunctionsasriskycanvary
substantiallydependingonwiderfactors,suchaspopulationcharacteristics(e.g.,
differentialeffectsbasedongenderorethnicity;Lansford,Deater-Deckard,Dodge,
Bates,&Pettit,2004;Leventhal&Brooks-Gunn,2000;McCarty,2008;Panayiotou
&Humphrey,2018)andthenatureoftheriskexposureitself,suchasthetiming,
duration,andchronicityofexposure(Najman,Clavarino,etal.,2010;Reiss,2013;
Wodtke,2013).Thus,itisnecessarytoexaminetheorisedriskfactorsacross
differentpopulationsandcircumstancesinordertounderstandtheirinfluencein
specificcontexts.
Thecurrentstudysetouttocontributetoknowledgeandunderstandingof
theriskfactorsforemotionalsymptomsamongearlyadolescentgirls.Previous

CHAPTERTHREE:RISKANDRESILIENCE
38
researchhasidentifiedawiderangeofriskfactorsassociatedwithemotional
symptomsduringchildhoodandadolescence,spanningmultipledomainswithinthe
developmentalecology.Forinstance,researchhasconsistentlyindicatedthatlow
familyincomeisassociatedwithanincreasedriskofinternalisingdifficulties,
includingemotionalsymptoms(Eamon,2002;Glied&Pine,2002;Morrisonetal.,
2014;Najman,Hayatbakhsh,etal.,2010;Santiagoetal.,2011).Thecurrentstudy
buildsonpreviousresearchbyexaminingmultipleriskfactorsalongsideone
anotheraspartofabroadersetofexplanatoryvariables.Inpreviousstudiesthese
riskfactorshaveoftenbeeninvestigatedinisolation,whichdoesnotcapturethe
naturalco-occurrenceofriskfactorsandsofailstocontrolfortheconfounding
effectsofothercontributingfactors(Evansetal.,2013;Flouri&Kallis,2007;
Sameroffetal.,2003).Thefollowingsubsectionsexplorethehypothesisedrisk
variablesincludedforassessmentinthecurrentstudy,withattentiontofactors
acrossindividual,family,andneighbourhoodlevels,guidedbyBronfenbrenner's
(1979,1999)ecologicalsystemstheory.However,itshouldbenotedthatthe
currentstudycannotofferacomprehensivereviewofallpossibleriskvariables
givenitsuseofsecondarydata.Furthermore,whilethebelowsectionsattimes
considerevidenceofgenderdifferencesrelatingtoagivenriskvariable,thestudy
doesnotdirectlyinvestigatesuchdifferences.Instead,thestudycandevelop
knowledgeoftherelationshipsbetweensuchfactorsandemotionalsymptoms
specificallyamongearlyadolescentgirlsasavulnerablegroup.
3.2.1YoungRelativeAge
Thereismodestevidenceofarelationshipbetweenyoungrelativeageand
emotionalsymptomsduringchildhoodandadolescence,withthosewhoare
youngestrelativetotheirpeersintheiracademicyear(e.g.,thoseborninsummer
monthsinEngland)morelikelytoexperiencedistress.Sucheffectsareunderstood
tobeduetodifferencesinschoolingexperiences,ratherthaneffectsofmonthor
seasonofbirthsuchasincreasedriskofprenatalinfection,andindeedthereis
someempiricalsupportforthishypothesis(Goodman,Gledhill,&Ford,2003).
Threestudieshaveidentifiedanassociationbetweenyoungrelativeageand

CHAPTERTHREE:RISKANDRESILIENCE
39
emotionalsymptomsinchildrenandadolescentsinaUKcontext(Crawford,
Dearden,&Greaves,2013;Goodmanetal.,2003;Patalayetal.,2015).Research
hasreportedtypicallysmall,thoughpracticallymeaningful,effectsizes(Goodman
etal.,2003),includingwithinonestudyfocusedspecificallyonearlyadolescents
(aged11–13years;Patalayetal.,2015)asinthecurrentstudy.
Notably,however,therehasbeenlimitedinvestigationofthisriskfactor
and,furthermore,asmallnumberofstudieshavenotfoundevidenceofan
association(Jeronimusetal.,2015;Lienetal.,2005).However,theseinvestigations
havebeenfocusedonnon-UKsamplesand,asoutlinedabove,relativeageeffects
arethoughttooperatethroughschoolexperiences,whichdifferacrosscountries
(Goodmanetal.,2003).Assuch,effectsmaybespecifictoparticulareducation
systems,warrantingfurtherresearchwithinUKpopulations.
3.2.2LowAcademicAttainment
Researchhasconsistentlyindicatedthatlowacademicattainmentactsasa
riskfactorforinternalisingdifficulties,includingemotionalsymptoms,atvarious
stagesofchildhoodandadolescence(e.g.,Bond,Toumbourou,Thomas,Catalano,
&Patton,2005;Moilanen,Shaw,&Maxwell,2010;Panayiotou&Humphrey,2018).
Studiestypicallyreportsmalltomoderateeffects(e.g.,Bondetal.,2005;Moilanen
etal.,2010;Panayiotou&Humphrey,2018;Weeksetal.,2016).Althoughtheexact
natureofthisrelationshipisnotfullyknown,itisunderstoodthatperceivedfailure
inacademicperformancecanincreasenegativeaffectandself-perceptionsand,
thus,triggerorworseninternalisingdifficulties(Moilanenetal.,2010;Panayiotou&
Humphrey,2018).Notably,thereissomeevidencetosuggestthatthemagnitude
oftheassociationbetweenlowacademicattainmentandinternalisingdifficultiesis
significantlystrongeramonggirlsthanboys(McCarty,2008;Panayiotou&
Humphrey,2018),whichmayreflectthetheorythatgirlsareinclinedtoevaluate
themselvesmorenegativelythanareboys(Pomerantzetal.,2002).Itisimportant
tonotethatalthoughresearchindicatesalongitudinalrelationshipbetweenlow
attainmentandsymptoms(Deighton,Humphrey,etal.,2018;Moilanenetal.,2010;
Panayiotou&Humphrey,2018;Verboom,Sijtsema,Verhulst,Penninx,&Ormel,

CHAPTERTHREE:RISKANDRESILIENCE
40
2014;Weeksetal.,2016),somestudieshavefoundevidenceofbidirectionality
(Deighton,Humphrey,etal.,2018;Verboometal.,2014),necessitatingcautionin
assumingcausalitywithoutlongitudinalanalysiscontrollingforpriorlevelsofboth
variables.
3.2.3HighAcademicAttainment
Alongsideevidencethatlowacademicattainmentisassociatedwith
emotionalsymptoms,thereissomeresearchtosuggestthatthesamemaybetrue
ofhighacademicattainmentandcognitiveability,thoughatpresentevidenceis
scant(Patalay&Fitzimons,2018;Skeltonetal.,2010;J.E.Williams,1996).Ithas
beenhypothesisedthathighattainmentandcorrespondingengagementinmore
challengingacademicworkresultsinincreasedworkloadandpressure,thus
increasingstress,whichinturnleadstoemotionalsymptoms(Suldoetal.,2008).In
feministdiscourseandresearch,ithasbeentheorisedthatacrossthelifespan,high
levelsofsuccessandachievementareparticularlyproblematicforthemental
healthofgirlsandwomeninawaytheyarenotforboysandmen(e.g.,Clance&
Imes,1978).Ithasbeenarguedthatanincreasedfocusontheunderachievement
ofboyshascastgirlsasnaturallyacademicallysuccessfulandnon-problematized
(Jones&Myhill,2004;Renold&Allan,2006;Ringrose,2007;Skeltonetal.,2010).
Thisdiscoursecreatesaninaccuratelypolarisedimageofgenderdifferencesin
schoolfunctioningandmayhaveplacedheightenedpressureongirlstofulfil
genderedexpectationsaroundschooling,includingconsistentlyhighattainment,
whichcouldbeproblematicformentalhealth(Jones&Myhill,2004;Renold&
Allan,2006;Ringrose,2007;Skeltonetal.,2010).Indeed,itcouldalsobeargued
thatsuchissuesmayalsoexplainwhylowacademicattainmentappearsparticularly
problematicforgirls,asexploredintheprevioussubsection.
3.2.4SpecialEducationalNeeds(SEN)
Thereissomeevidencetosuggestthatchildrenandadolescentswhohave
specialeducationalneeds(SEN)experienceincreasedratesofemotionalsymptoms.

CHAPTERTHREE:RISKANDRESILIENCE
41
SENisacollectivetermforvariousadditionalneeds;someofthemostcommonly
recordedtypesofSENinEnglandaremoderatelearningdifficulties,speech,
languageandcommunicationsneeds,andAutisticSpectrumDisorder(ASD;
DepartmentforEducation[DfE]&OfficeforNationalStatistics[ONS],2017a).There
areseveralpossibleexplanationsfortheassociationbetweenSENandemotional
symptoms,whichcannotbeexhaustivelydetailedhere.Onecommonhypothesis,
however,isthatthisrelationshipisduetostresscausedbyproblemsnavigating
educationandpeerrelationships,alongsideotherfactorssuchasloweredself-
esteemandmorenegativeself-judgements(Alexander-Passe,2006;Nelson&
Harwood,2011).IthasalsobeensuggestedthatpupilsdiagnosedwithSENsuchas
learningdisabilitiesmayhavetheiremotionalneedsoverlookedduetoan
increasedfocusontheiracademicneeds(Nelson&Harwood,2011).
Studieshavereportedassociationsbetweeninternalisingsymptomsand
specifictypesofSEN,suchaslearningdifficulties(Emerson,2003;Heiman&
Margalit,1998)anddyslexia(Alexander-Passe,2006;Nelson&Gregg,2012).
Studiestypicallyreportmoderateeffectsizes,asreplicatedinameta-analysisofthe
relationshipbetweenlearningdisabilitiesandanxiety(Nelson&Harwood,2011).
Researchhasevidencedhighratesofdiagnosablepsychiatricconditionsamongthe
SENpopulation,includinganxiousanddepressivedisorders(e.g.,Brereton,Tonge,
&Einfeld,2006;Emerson,2003;Emerson&Hatton,2007;Simonoffetal.,2008).A
smallnumberofstudieshaveindicatedthateffectsoninternalisingdifficultiesin
thispopulationmaybegreaterforgirlsthanforboys,asobservedinsampleswith
ASD(Mandyetal.,2012;Solomonetal.,2012),dyslexia(Nelson&Gregg,2012),
andlearningdisabilities(Emerson&Hatton,2007).
Althoughtherehavebeensomelarge-scaleinvestigations(e.g.,Emerson,
2003;Emerson&Hatton,2007;Heiman&Margalit,1998),researchintothe
relationshipbetweenSENandemotionalsymptomsisoftenreliantonsmallsample
sizesduetolowprevalenceofmanySENconditions.Studiesarefrequently
descriptiveratherthaninferential,limitingtheconclusionsthatcanbedrawn.
Furthermore,considerableheterogeneity,bothwithinspecificSENconditionsand
acrossSENasabroadcategorisation,restrictstheextenttowhichresearchintoany

CHAPTERTHREE:RISKANDRESILIENCE
42
onetypeofSENcanbegeneralisedtootherswiththesameorotherconditions.
Furthermore,childrenandadolescentswithSENappearmorelikelythantheir
peerstobeexposedtoarangeofotherriskfactors,suchasfamilialpoverty(DfE&
ONS,2017b;Emerson,2003;Emerson&Hatton,2007).Indeed,Emersonand
Hatton(2007)foundthataccountingforadditionalriskfactorssubstantially
reducedthevarianceexplainedbyparticipants’learningdisabilities,suggestingthat
effectsinthispopulationmayrelatetothepresenceofmultipleriskexposure.The
currentstudyseekstocontributetocurrentknowledgeandunderstandingofSEN
asariskfactorforemotionalsymptomsbyprovidingalarge-scaleinvestigation
utilisinginferentialstatisticalmethodstooffermorerobustinferencesregarding
thispopulation.
3.2.5LowFamilyIncome
Researchhasconsistentlyindicatedarelationshipbetweenlowfamily
incomeandincreasedemotionalsymptomsduringchildhoodandadolescence(e.g.,
Glied&Pine,2002;Morrisonetal.,2014).Longitudinalresearchhasevidencedthat
theseeffectsoperateovertime,indicatingalevelofcausality(e.g.,Eamon,2002;
Najmanetal.,2010;Santiagoetal.,2011).Thereareseveralexplanatory
hypotheses,thoughthesearenotconsideredmutuallyexclusiveandindeeditis
likelythattherearemultiplepathwaysunderpinningthisassociation(Eamon,2002;
Reiss,2013).Onekeytheoryisthatindividualsandfamilieslivinginpoverty
experiencegreateramountsofstressthathinderstheirmentalhealth,including
stressdirectlycausedbyalackofmoneytomeetneedsandthatcausedby
increasedexposuretootherstressorsanduncontrollablelifeevents(Santiagoetal.,
2011).Indeed,severalstudieshavedemonstratedthatpoverty-relatedstressis
directlyrelatedtoemotionalsymptoms(e.g.,Miech,Caspi,Moffitt,Wright,&Silva,
1999;Santiagoetal.,2011;Wadsworthetal.,2008;Wadsworth&Santiago,2008).
Longitudinalresearchhassuggestedthatlivingwithpovertyaffectsearlybrain
development,whichmayinturnnegativelyaffectemotionandstressregulationin
lateryears,thusnegativelyimpactingmentalhealth(Barchetal.,2016;Lubyetal.,
2013).
CHAPTERTHREE:RISKANDRESILIENCE
43
Investigationsintotherelationshipbetweenlowfamilyincomeand
emotionalsymptomshavereportedrangingeffectsizes,dependingonspecific
populationcharacteristicslikeageandgender(Mendelsonetal.,2008;Reiss,2013).
Indeed,asystematicreviewoftherelationshipbetweenwidersocioeconomic
status(SES)andmentalhealthoutcomesnotedthattherearemixedfindings
regardingwhethergenderdifferencesarepresent(Reiss,2013).Somehave
reportedthatgirlsexperiencedisproportionateeffectsspecificallyfromlowfamily
income(Leveetal.,2005),thoughothershavenotfoundsuchevidence(e.g.,
Mendelsonetal.,2008;Santiagoetal.,2011).
3.2.6YoungCarerStatus
Ayoungcarerisachildoradolescentwhoprovidesongoingcareforafamily
member,mostoftenasiblingoraparent,typicallyduetofactorssuchasdisability,
illness,andalcoholanddrugabuse(Cheesbroughetal.,2017;Hounsell,2013;
Ireland&Pakenham,2010).Asmallnumberofstudieshavefoundincreasedriskof
emotionalsymptomsamongthisgroup(Banksetal.,2001;Shifren&Kachorek,
2003)andaqualitativemeta-synthesisfoundyoungcarersoftendescribedmental
healthsymptomsanddifficulties,includingemotionalsymptoms(Rose&Cohen,
2010).Thereareseveralhypothesesfortheseapparentadverseeffects,including
emotionalneedsbeingoverlooked(Svanbergetal.,2010;Thomasetal.,2003),
interferencewithdevelopmentprocesses(Cox&Pakenham,2014),disruptedor
inconsistentparenting(KennethIPakenhametal.,2012),andanxietyassociated
withthecircumstancenecessitatingcare(Warren,2006).Someresearchhas
indicatedthatyoungcarersaredisproportionatelygirls(ScottishGovernment,
2017;Sharmaetal.,2016),althoughHounsell(2013)concludedthatyoungcarersin
Englandareequallylikelytobegirlsorboys.
Researchwiththispopulationhasbeenhinderedbytherelativelysmall
proportionofyoungcarerswithinthegeneralpopulation,alongsidedifficultiesin
consistentlyidentifyingthisgroupgiventhatschoolsdonotroutinelydocument
youngcarerstatus.Thereisalsoconsiderablescopeforfindingstobesample-
specific,asstudiesfrequentlyfocusoncaregivingaroundspecificconditionsor

CHAPTERTHREE:RISKANDRESILIENCE
44
circumstances.Whereresearchdoesexpandtoawiderfocusongeneralyoung
caregiving,definitionsofwhatconstitutescaregivingstatusvaryacrossbothdata
sourcesandstudies(Banksetal.,2001;Cheesbroughetal.,2017),limitingthe
abilitytogeneralisefindings.Furthermore,severalauthorshaveobservedthatthe
categorisationofyoungcarerstatusasariskfactormayfailtocapturethe
complexityofthiscircumstance(Aldridge,2006;Cox&Pakenham,2014;Newman,
2002),overlookingfactorssuchasthenatureofthecircumstancenecessitatingcare
(Ireland&Pakenham,2010b),thelevelofsupportinplace(Cox&Pakenham,2014;
Olsen&Clarke,2003),andthepossiblebenefitsofcaregiving(Banksetal.,2001).
3.2.7AdverseChildhoodExperiences(ACEs)
Researchhasconsistentlyshownthatadversechildhoodexperiences(ACEs),
whichareexperiencescharacterisedbyfamilydysfunctionandchildhood
maltreatment(Hughesetal.,2017;Youssefetal.,2017),actasariskfactorfor
negativeoutcomesacrossthelifespan,includingemotionalsymptoms(Chapmanet
al.,2004;DeVenter,Demyttenaere,&Bruffaerts,2013;Dubeetal.,2001;Hughes
etal.,2017;Schilling,Aseltine,&Gore,2007;Turner,Finkelhor,&Ormrod,2006;
Youssefetal.,2017).ACEsincludeexperiencesresultingindirectharmtochildren
andadolescents,suchasabuse,andthosethatcauseindirectharm,suchas
exposuretodomesticviolenceorsubstanceabuse(Cavanaugh,Petras,&Martins,
2015;Hughesetal.,2017;Schillingetal.,2007).Itisgenerallyunderstoodthatthe
mechanismunderpinningthenegativeeffectsofACEsisthechronicstresssuch
experiencesplaceonindividuals,impactingneurobiologicalfunctioningand
developmentalprocesseswhich,inturn,leadtonegativeoutcomes(Danese&
McEwen,2012;Hughesetal.,2017).
Inarecentsystematicreviewandmeta-analysis,Hughesetal.(2017)found
thatstudiestypicallyreportlargeeffectsizesintherelationshipbetweenACEsand
adultmentalillhealth,includingemotionalsymptoms.AlthoughACEsisacollective
termcomprisingawiderangeofadverseexperiences,researchhasindicateda
limitedamountofspecificitybetweenparticularexperiencesandmentalhealth
outcomes,withwide-rangingeffectscommonlyobserved(Hughesetal.,2017;

CHAPTERTHREE:RISKANDRESILIENCE
45
Schillingetal.,2007).Indeed,itappearsthatACEsarelikelytoco-occur(Dubeet
al.,2001;Hughesetal.,2017),whilepreviousfindingshavesuggestedadose-
responserelationshipinrelationtodepressivesymptoms,withsymptomatology
increasingasthenumberofACEsonehasbeenexposedtoincreases(Chapmanet
al.,2004;Youssefetal.,2017).Furthermore,thereisgrowingevidencethatACEs
mayhavecumulativeeffectsonadultoutcomes(Hughesetal.,2017),including
specificallyinrelationtoemotionalsymptoms(Schillingetal.,2007;Youssefetal.,
2017).AlthoughpreviousresearchhasexaminedtheeffectsofACEsthroughoutthe
lifespan,studiesarepredominantlyfocusedonadultoutcomes,withonlyasmall
numberofstudiesreportingeffectsamongchildrenandadolescents(Schillingetal.,
2007;Turneretal.,2006).
3.2.8NeighbourhoodSocioeconomicDeprivation
Severalstudieshaveidentifiedanassociation,typicallysmallinsize,
betweenneighbourhoodsocioeconomicdeprivationandemotionalsymptoms
duringchildhoodandadolescence(Flourietal.,2012;Flouri&Sarmadi,2016;Mair
etal.,2008;Schneiders,2003;Sundquistetal.,2015;Xueetal.,2005).
NeighbourhoodsocioeconomicdeprivationisconceptualisedaslowSESatthe
neighbourhoodlevelandcomprisesmultipledimensions,includinglowhousehold
income,receiptofbenefits,lowlevelsofeducation,andovercrowding(e.g.,Denny
etal.,2016;Drukker&vanOs,2003).Ithasbeenhypothesisedthatthis
circumstanceencompassesstressorsthatnegativelyaffecthealth,suchaslackof
resources,inadequatehousing,andviolence,thoughthisprocessisnotfully
understood(Mairetal.,2008).Thereissomeevidencethatlocalarea
characteristicsdisproportionatelyaffectthementalhealthofgirlsandwomen
(Brazil&Clark,2017;Staffordetal.,2005),whichisthoughttobebecausegender
roleexpectationsplacegreateremphasisonsocialandcommunityactivityfor
women(Kavanaghetal.,2006;Staffordetal.,2005).
Thoselivingindeprivedneighbourhoodsaremoreoftenexposedtoa
greaternumberofriskfactorsacrossotherdomains,suchaslowfamilySES,which
canproducecompoundeffects(Boyle&Lipman,2002;Stafford&Marmot,2003;

CHAPTERTHREE:RISKANDRESILIENCE
46
Sundquistetal.,2015);however,neighbourhood-levelvariablesoftenremain
significantaftercontrollingforwiderfactors(Mairetal.,2008;Schneiders,2003;
Stafford&Marmot,2003;Xueetal.,2005).Currently,researchexploringthe
mentalhealtheffectsofneighbourhooddeprivationpredominantlyfocuseson
adults(Sundquistetal.,2015)andisoftenspecifictowiderEuropeancountriesand
AmericaratherthanEngland,limitinggeneralisabilitytoanEnglishadolescent
population.
3.3ExposuretoMultipleRiskFactors
Whilesingleriskfactorsdoappeartobeindividuallyassociatedwith
negativeoutcomes,thereisgrowingevidencethattheyfrequentlydonotoccurin
isolation.Researchhasindicatedthatriskfactorstendtoclusterandsoindividuals
areoftenexposedtoseveral(Flouri&Kallis,2007).Forexample,familialpovertyis
associatedwitharangeofotherriskfactors,suchaslivinginpoorerandmore
dangerousneighbourhoods(Evans,2004;vanHametal.,2011),attendingschools
withfewerresourcesandlessexperiencedteachingstaff(Evans,2004;Gorard,
2016b;Lupton,2005),andbeingidentifiedashavingSEN(DfE&ONS,2017b;
Emerson,2003;Emerson&Hatton,2007).Indeed,EvansandEnglish(2002)found
thatchildrenexposedtofamilialpovertywerelikelytobeexposedtomorerisk
factorsthantheirmoreaffluentpeers.Thisclusteringofriskfactorscaninpartbe
explainedbyBronfenbrenner's(1979,1999)ecologicalsystemstheory,asoutlined
inChapterOne.Thatis,distalfactorslikeclass,race,andculturecanhavewide-
ranginginfluenceovervaryingaspectsanddomainsofanindividual’slife,including
exposuretoriskfactorsacrossmultipledomains,whileinteractionbetweenrisk
factorsislikelytooccur(Evansetal.,2013).
Fromaresearchperspective,suchfindingsfirsthighlighttheneedto
investigatemultipleriskfactorsalongsideoneanother,ratherthaninisolation,so
asnottoover-estimatetheinfluenceofanyonevariable(Sameroffetal.,2003).
Thishasledtoanincreaseintheinvestigationofmultipleriskfactors,often
throughmultipleregressionapproachesthatmoreaccuratelyestimatetheeffects

CHAPTERTHREE:RISKANDRESILIENCE
47
ofeachindividualfactor(Evansetal.,2013).However,thereisagrowing
understandingthatmultipleriskfactorsmayworktogethertocollectivelyinfluence
outcomestoagreaterextentthanwhenexperiencedinisolation,thusbecoming
morethanthesumoftheirparts(Evansetal.,2013;Rutter,1979,1981;Sameroff,
2006;Sameroffetal.,2004).Indeed,thereisevidencetosuggestthatasinglerisk
factorinisolationmaynotexertmeaningfulorlastingeffects,butthatwhenthe
sameriskfactoroccursalongsideothers,theconsequencesmaybemore
substantial(Rutter,1979,1981;Sameroffetal.,2003).Howandwhythismaybe
thecase,however,islesswellunderstood(Evansetal.,2013).Thecurrentstudy
investigatesbothwhetherandhowexposuretomultipleriskfactorsmayaffect
outcomesinthecontextofearlyadolescentgirls’emotionalsymptoms.The
followingsubsectionsexplorekeytheoreticalandmeasurementperspectivesand
previousliteraturerelatingtomultipleriskexposure.
3.3.1CumulativeRiskTheoryandResearch
TheconceptofcumulativeriskstemsfromtheseminalworkofRutter
(1979)duringtheIsleofWightstudiesintochildpsychiatricdisorder,inwhichhe
collatedariskindexofsixfactors,designatingeachparticipantascorerangingfrom
zeroto4+basedontheirlevelofexposure.Rutter(1979)foundevidenceofan
associationbetweenthenumberofriskfactorsandthelikelihoodofchild
psychiatricdisorder.Thoseexposedtooneorzeroriskfactorsexhibitedan
approximatelytwopercentchanceofdisorder;thislikelihoodincreasedwitheach
riskfactorand,attheupperendofthescale,childrenexposedtofourormorerisk
factorsshowedmorethan20%probabilityofdisorder.Furthermore,therewasno
particularcombinationofriskfactorswithgreaterpredictivepower;rather,it
appearedthatthenumberofriskfactorsparticipantswereexposedtowasmore
importantthantheirnature(Rutter,1979).
Cumulativerisktheorybuildsonthisworkandencapsulatestwocore
assumptions.Firstly,the“accumulationprinciple”positsthatthemoreriskfactors
oneisexposedto,thegreaterthenegativeeffectsonagivenoutcome(Evansetal.,

CHAPTERTHREE:RISKANDRESILIENCE
48
2013;Sameroff,2000).Thisisfurtherunderpinnedbythegrowingevidence,as
discussedearlierinthissection,thatriskfactorsmayworktogethertoinfluence
outcomesandthusleadtomoresevereconsequencesthantheindividual
contributionsofanygivenriskfactor,or“massaccumulation”.Secondly,the
“number-over-natureprinciple”holdsthatitisthenumberofriskfactorstowhich
anindividualisexposed,ratherthantheirspecificnature,whichbestpredicts
outcomes(Evansetal.,2013;Sameroff,2000).Thissecondassumptionisgrounded
intheprincipleofequifinality,whereintherearemultiplepathwaystosingular
outcomes(Cicchetti&Curtis,2006;Cicchetti&Rogosch,2002;Lutharetal.,2000).
Assuch,incumulativeriskresearch,riskvariablesaredichotomised(1=risk
present,0=riskabsent)andsummedtocreateanunweightedcompositescoreof
thenumberofriskstowhichanindividualisexposed(Evansetal.,2013;Flouri&
Kallis,2007).Typically,theindexdoesnotcapturethemaximumrangeofrisk
factorsbutinsteadisimposedwithanupperlimitof“xormore”toindicatea
saturationofriskfactors(e.g.,Oldfield,Humphrey,&Hebron,2015;Panayiotou&
Humphrey,2018;Rutter,1979).Thisindexingapproachisconsistentwiththe
understandingthatmanychildrenandadolescentsareexposedtonumerousrisks
andthatthesefrequentlyco-occuracrossmultipledomainsoftheindividual’s
ecology(Evansetal.,2013;Flouri&Kallis,2007).
Todate,researchhaspredominantlyfocusedonidentifyingwhether
cumulativeriskeffectsarepresent;findingsaregenerallyconsistent,withmost
publishedinvestigationsreportingevidenceofeffects(Evansetal.,2013).Several
studieshavefoundanassociationbetweencumulativeriskexposureinchildhood
andadolescenceandemotionalsymptomsandbroaderinternalisingdifficulties,
bothconcurrently(Flouri&Kallis,2007;Jones,Forehand,Brody,&Armistead,
2002;Panayiotou&Humphrey,2018)andlongitudinally(Appleyardetal.,2005;
Gerard&Buehler,2004;Horan&Widom,2015;Panayiotou&Humphrey,2018).
However,intheirsystematicreviewofthecumulativeriskliterature,Evansetal.
(2013)foundthatcumulativeriskeffectsarenotuniform,withanumberof
demographiccharacteristics,includinggender,moderatingsucheffects.Giventhat
riskfactorsthemselvesarealsohighlycontext-specific,suchfindingsdemonstrate

CHAPTERTHREE:RISKANDRESILIENCE
49
theneedtoextendthislineofresearchtospecificoutcomesandgroupsofinterest
inordertounderstandthenatureofmultipleriskeffectsinparticularcontexts.
Thus,thecurrentstudyaimstocontributetoexistingevidencebyexaminingthe
associationbetweencumulativeriskexposureandemotionalsymptomsamong
earlyadolescentgirls,giventhatthisappearstobeapivotalmomentinmental
healthtrajectoriesamonggirlsandwomen.
LimitationsofCumulativeRiskTheoryandResearch
Oneofthecentralfeaturesofcumulativerisktheory,oftenconsideredits
keystrength,couldsimultaneouslybeconsideredaweakness;namely,itsadditive
premiseandindexingapproach.Thistenetreflectsanattempttomirrortheway
riskfactorsnaturallyco-occur,whilethesimplicityofthisapproachmakesthe
conceptparticularlyeasytounderstandfornon-researchers,suchaspolicymakers
(Evansetal.,2013).However,ithasbeenarguedthatthisisanoverlyreductionist
methodforcapturingthewaythatmultiplestressorsoccurandoverlooksthe
complexityofthephenomenonofmultipleriskexposureincontext,aswellasthe
interactionsoccurringacrossecologicaldomains(Belskyetal.,2012;Burchinalet
al.,2000;Halletal.,2010).Ithasbeensuggestedthatwhilethemodelof
cumulativeriskoffersanumberofadvantages,thisreductionismdoesnotlend
itselftounpickingthemorecomplexetiologicalmechanismsunderpinningthe
effectsofmultipleriskexposure(Belskyetal.,2012;Kraemeretal.,2001).The
approachdoesnotallowexplorationordirectmodellingoftheinteractionsthat
occurbetweenriskfactors,whichisoneofthecentralpremisesinhowmultiplerisk
exposureoccursinthefirstinstance(Evansetal.,2013).Inaddition,thenumber-
over-natureprinciple,aswellastheequalweightaffordedtoeachriskfactorin
constructingacumulativeriskindex,isinconsistentwithevidencethattheeffects
ofindividualriskfactorscanvarysubstantially(Halletal.,2010).Methodologically,
ithasbeenarguedthatcollapsingindividualriskfactorinformationintoasingle
compositevariablemaybestatisticallyproblematic,asthelossofinformationmay
reducesensitivityandpredictivepowerinrelationtotheoutcomeofinterest
(Belskyetal.,2012;Evansetal.,2013;Halletal.,2010;Kraemeretal.,2001).

CHAPTERTHREE:RISKANDRESILIENCE
50
Thenumber-over-natureprincipleisalsoatoddswithresearchindicating
thatfactorssuchastiminganddurationofexposureareofimportance(Evansetal.,
2013).Theprocessofdichotomisingindividualriskvariablesinordertocreatea
cumulativeriskindexcancausethelossofmorenuancedriskinformationand,
furthermore,createsasample-specificvariablethatcannotbeassumedtobe
generalisabletothebroaderpopulation(Evansetal.,2013).Indeed,themost
frequentapproachtodichotomisingcontinuousvariablesisdesignatingthoseinthe
sample’supperquartileofexposureas“at-risk”,furthercontributingtosample-
specificity(Evansetal.,2013).Inaddition,thisapproachclassifiesriskbasedon
rarityandisnotsensitivetothethresholdatwhichavariableactuallyconstitutesa
risk(Evansetal.,2013;Kraemeretal.,2005).
3.3.2MeasurementModelsforMultipleRiskExposure
Theconceptualandmethodologicallimitationsofthecumulativeriskmodel
indicateaneedforinvestigationofalternativemeasurementapproaches.
Identificationofthemostappropriaterepresentationofriskexposureisparticularly
necessaryifresearchistomovebeyondestablishingwhethercumulativerisk
effectsoccur,giventhattheyfrequentlyareshowntodoso,andbegintoexplore
theunderlyingmechanismsinordertounderstandwhytheseeffectsoccur(Belsky
etal.,2012).Thecurrentstudysoughttoexploredifferentmeasurementmodelsof
multipleriskexposurewithvaryinglevelsofrepresentationofboththemagnitude
andnatureofriskexposure,giventhatthesefeaturesarecentraltocumulativerisk
theoryandindeedtoitslimitations.Specifically,threemeasurementmodelswere
exploredinrelationtoemotionalsymptomsinthecurrentstudy,asshowninFigure
3.1(overleaf).Itshouldbenotedthattheaimofthisinvestigationisnottooffera
definitiveguideonthemostappropriaterepresentationforfutureresearch;rather,
itistoexplorethesedifferentmodelsinthecontextofearlyadolescentgirls’
emotionalsymptoms,withinonespecificsample.

CHAPTERTHREE:RISKANDRESILIENCE
51
Figure3.1.Multipleriskexposuremeasurementmodels.ModelAshowsamultipleregression
approach,ModelBincludesthecumulativeriskindexasapredictor,andModelCcomprisesalatent
riskconstruct.

CHAPTERTHREE:RISKANDRESILIENCE
52
ThemultipleregressionapproachshowninModelA,whereineachriskfactoracts
asaseparatepredictor,primarilyrepresentsthenatureofeachriskfactor.Asa
modelofmultipleriskexposure,multipleregressionaccountsfortheeffectsofco-
occurringriskfactorstoavoidover-estimationoftheeffectsofanyonevariable.
Thus,thismodelacknowledgesthefrequentco-occurrenceofriskfactors,and
controlsfortheinteractionsthatoccurbetweenthem,butdoesnotdirectlymodel
theeffectsofthisco-occurrence.Assuch,thecumulativeriskmodelshownin
ModelBisoftenconsideredanimprovementuponthisapproachasitdirectly
acknowledgesthewaythatriskfactorscanworktogethercollectivelytoinfluence
outcomesandisthusmoreconsistentwithourunderstandingofriskexposure
(Evansetal.,2013;Flouri&Kallis,2007).Thecumulativeriskindex,then,
representsthenumberofriskfactorsinitsmeasurementofmultipleriskexposure
(Evans&Kim,2013;Flouri&Kallis,2007;Halletal.,2010).
Researchutilisingstructuralequationmodelling(SEM)hasindicatedan
alternativeapproachtounifyingmultipleriskfactorsinanalysiswhileovercoming
someofthelimitationsinherenttocumulativerisktheory,asshowninModelC.
Specifically,asmallnumberofstudieshaveprovidedsupportfora“latentrisk
construct”,whereriskfactorsaretreatedasmanifestindicatorsofalatentmultiple
riskfactor(Belskyetal.,2012;Burchinaletal.,2000;Halletal.,2010;Loukasetal.,
2008).Alatentconstructisonewhichishypotheticalandcannotbedirectly
observed;assuch,itisstatisticallyinferredthroughmultipleproxies(Kline,2016).
Thus,alatentriskconstructallowsriskfactorstobeconvertedintoasingle
predictorvariablewithoutlossofinformationastothenatureofeachindividual
riskfactor(Belskyetal.,2012;Burchinaletal.,2000;Halletal.,2010).Thismay
offeramorenuancedmeasurementofthewayinwhichcombinedriskfactors
operate,incontrasttothesimpleaccumulationapproachincumulativerisktheory,
andmayovercomelimitationsofacumulativeriskindex(Burchinaletal.,2000;Hall
etal.,2010).Specifically,alatentconstructallowsdirectmodellingofthe
interactionsbetweenriskfactors,whichaspreviouslynotedisacentraltheoryasto
howmultipleriskexposureoccursandexertsitsinfluence(Evansetal.,2013).
Ratherthansimplycontrollingfortheseasinthemultipleregressionapproach,a

CHAPTERTHREE:RISKANDRESILIENCE
53
latentapproachdirectlydrawsonthisinformationtoestimatetheunderlying
construct.Inalatentconstruct,factorloadingsofriskfactorsarenotconstrainedto
beequalbutarefreetovary;inotherwords,riskfactorsdonothaveequalweight
asinacumulativeriskindex(Belskyetal.,2012;Burchinaletal.,2000;Halletal.,
2010).Therefore,alatentriskconstructallowsdifferentialrepresentationofeach
riskfactorinrelationtothebroaderconstructofriskexposure,inlinewiththe
strengthsoftheserelationshipsasobservedwithinthedata(Belskyetal.,2012;
Burchinaletal.,2000;Halletal.,2010).Furthermore,retainingindividualriskfactor
informationwithinalatentvariablemayovercomethereducedsensitivityand
predictivepowerassociatedwithcreatingacompositevariableinthecumulative
riskindex(Burchinaletal.,2000;Halletal.,2010).Thismethodalsoprovidesthe
opportunitytoincludeinformationsuchastiminganddurationofriskfactors,
whereavailable(Halletal.,2010).
Overall,then,thelatentriskapproachmayofferamorenuanced
representationofthewaythatriskfactorsinteractandworktogethertoinfluence
outcomes(Burchinaletal.,2000;Halletal.,2010).Furthermore,latentvariables
representtheoreticalconstructsthatarenotdirectlymeasurableandthuscanonly
berealisedthroughmeasurementofacollectionofindicatorvariables(Brown,
2015;Brown&Moore,2012;Kline,2016).Inthisway,alatentriskconstructmore
closelyreflectsourunderstandingofmultipleriskexposureasacomplex
phenomenonoccurringacrossecologicalsystems.Inthissense,exposuretoagiven
setof“riskfactors”cannotentirelycapturethiscomplexity,andinsteadrepresent
markersthatprovideinsightintobroadersystemsofdisadvantagewithinwhich
childrenandyoungpeopleexist.Inthisway,theuseoffactoranalysisinlatent
modellingallowsempiricaltestingofwhethertheriskvariablesofinterestdoinfact
representanassumedoverarchingconstruct.Itisgenerallyconsideredacrucial
steppriortoinferentialanalysistoestablishthatone’sdatasupportsthe
assumptionthatagivensetofvariablesreflectasharedconstruct(Borsboom,
Mellenbergh,&VanHeerden,2003;Brown,2015;Gefen,Rigdon,&Straub,2011).
However,indevelopingacumulativeriskindexthereisnoopportunitytoformally
assessthisassumptionasthereiswithalatentriskconstruct,andthusanyfindings

CHAPTERTHREE:RISKANDRESILIENCE
54
relyonanuntestedassumptionthatthecompositevariabledoesinfactrepresenta
singularandcoherentconstruct.
Todate,veryfewpublishedstudieshavemadeuseofalatentriskconstruct
inthisareaofworkandonlytwostudieshavecomparedsomekindoflatent
representationwithotherapproaches.Burchinaletal.(2000)identifiedthree
distinctriskconstructsthroughexploratoryfactoranalysisandsubsequentlymade
useoffactorscoresaspredictors,whicharevaluesdenotingparticipants’relative
positiononalatentfactor.Theauthorscomparedthiswithmultipleregressionand
acumulativeriskindexaspredictorsofcognitiveandlanguagedevelopmentand
concludedthatthemostappropriaterepresentationofmultipleriskexposuremay
dependuponthestudycontextandsample(Burchinaletal.,2000).Specifically,
theysuggestedthatalatentapproachmaybeusefulinstudieswithfewerrisk
factorsavailable,interestindevelopmentaltrajectories,ormoderatetolarge
samplesizes(Burchinaletal.,2000).Halletal.(2010)extendedthisapproach,
arguingthatitismoreconsistentwithourunderstandingofmultipleriskexposure
asabroadsystemtospecifyonelatentvariablecapturingallriskfactorsofinterest,
ratherthanmultiplelatentfactorsforsubsetsofrisk.Indeed,akeyfeatureofSEM
isthatitisoftenguidedbytheoryratherthandata-drivenandassuchitisgenerally
recommendedtospecifyalatentfactorbasedonexistingtheoryandknowledge.A
moreexploratoryapproachsuchasthatusedbyBurchinaletal.(2000)maybe
moreusefulininstanceswherepoormodelfitisobservedforthehypothesised
factorstructure,whichmayreflectadivergencebetweentheoryandtheparticular
databeingused.InthecaseofHalletal.(2010),asinglelatentconstructwasfound
tohavegoodmodelfit,andtheauthorsfoundthatthisfactorhadgreater
predictivepoweroverchildcognitivedevelopmentthanacumulativeriskindex.
However,inthisstudythefactorwasspecifiedusinganon-traditionalmethod
wherebyindicatorscausethelatentvariable(formativeindicators),ratherthanthe
otherwayaround,asistypicallythecase(reflectiveindicators;Halletal.,2010).
Thisapproachessentiallyactsasafunnelbyunifyingtheindividualeffectsofeach
riskfactor,ratherthandrawingoninteractionsbetweenriskfactorstoinfera

CHAPTERTHREE:RISKANDRESILIENCE
55
broaderconstruct,asisthecasewithtraditionalreflectivefactorindicators(Hallet
al.,2010).
Thecurrentstudybuildsonthesepreviousmethodologicalinvestigationsby
exploringstatisticalrepresentationsofriskspecificallyinthecontextofemotional
symptomsamongearlyadolescentgirls.InlinewithHalletal.(2010),asinglelatent
factorwasexploredtoreflectcurrentunderstandingsofmultipleriskexposureasa
singularbutbroadsystemofdisadvantage,thoughtraditionallatentmodellingwas
utilisedtodirectlymakeuseofthetransactionsbetweenfactors.Alatentvariable
wasused,ratherthangeneratingfactorscoresasusedbyBurchinaletal.(2000),to
facilitatefullinformation.
3.3.3MechanismsofMultipleRiskEffects
Ithasbeenarguedthatriskresearchnowneedstomovebeyondsimply
identifyingwhethermultipleriskeffectsarepresentandinsteadfocuson
understandingthemechanismsofhowsucheffectsoccur(Belskyetal.,2012;Grant
etal.,2003).Giventhatexposuretomultiplerisksinfluencesvaryingaspectsof
healthanddevelopment(Evansetal.,2013;Horan&Widom,2015),itappearsto
bethateffectsoperatethroughbroadermechanismsthatunderpingeneralised
outcomes,ratherthantranslatingdirectlyintonegativeeffectsinanyonearea.
Althougharangeofpathwayshavebeenhypothesisedandinvestigatedfor
individualriskfactors,theunderlyingmechanismsofmultipleriskeffectsareless
wellunderstood,andthereisnotyetastrongexplanationunderlyingtheprinciples
ofcumulativerisktheory(Evansetal.,2013).Threehypotheseshavebeen
identified:(a)Increasedstressandacorrespondingheightenedengagementof
responsesystems;(b)mediationthroughadditionalelementsinthewider
environment,suchasmaternalresponsiveness;and(c)disruptiontointeractions
acrosstheecologicalsystemandthustodevelopmentalprocesses(Evansetal.,
2013).
Thecurrentstudyfocusesontheroleofstress.Whileitisacknowledged
herethattherearelikelymanyco-occurringpathwaysunderlyingtheseeffectsand

CHAPTERTHREE:RISKANDRESILIENCE
56
indeeditwouldbeusefultoexaminethesetogether,thisresearchfocuses
particularlyontheroleofstressforanumberofreasons.Primarily,itshouldbe
notedthatthedatasetunderpinningthisresearchcontainsdataonstress,butdoes
notincludevariablesthatwouldallowexplorationofadditionalhypothesesandas
suchthestudyislimitedtothisinvestigation.However,thereisaclearneedfor
researchthatdoesfocusdistinctlyontheroleofstressinthiscontext.Intermsof
gender,thereisevidencetosuggestthatgirlsandwomenarepronetoreport
higherlevelsofstressthandoboysandmenwithinbothadolescenceand
adulthood(Charbonneauetal.,2009;Hampel&Petermann,2006;Matud,2004),
indicatinganeedtoexaminetheconsequencesofstressspecificallyamongthis
group.Indeed,chronicstressisthoughttobeakeycontributortothehighratesof
emotionalsymptomatologyanddisorderobservedamonggirlsandwomenacross
thelifespanandtoitsemergenceamonggirlsduringearlyadolescence(e.g.,de
Lijsteretal.,2016;Girgus&Yang,2015;Meadowsetal.,2006;Nolen-Hoeksema,
2001).Furthermore,thestresshypothesisiscentraltocumulativerisktheorybut
hasalimitedevidencebaseasitoftenreliesuponmodestsamples,asisdiscussed
below.
Thereisgrowingsupportforthenotionthatstressplaysacentralfactorin
thewaythatriskinfluencesoutcomes.Notably,manyindividualriskfactorsare
theorisedtoexerttheireffectsbyintroducingstressindailylife,buildinginto
chronicstressovertimeandthusaffectingvariousoutcomes.Forinstance,as
discussedearlierinthechapter,stressisakeyhypothesisfortherelationship
betweenemotionalsymptomsandriskfactorsincludingSEN(Alexander-Passe,
2006;Nelson&Harwood,2011),lowfamilyincome(Miechetal.,1999;Santiagoet
al.,2011;Wadsworthetal.,2008;Wadsworth&Santiago,2008),andACEs(Danese
&McEwen,2012;Hughesetal.,2017).Thus,thestresshypothesisinmultiplerisk
exposurebuildsonthisconcept,positingthatasriskfactorsaccumulate,thereis
increaseddemandontheindividual,resultinginheightenedstressand
overwhelmedresponsesystemsthatinturnnegativelyimpacthealthand
development(Evansetal.,2013;Evans&Kim,2013).

CHAPTERTHREE:RISKANDRESILIENCE
57
Muchofthepreviousdiscussionandresearchonthishypothesishasbeen
focusedonallostaticload.Advancesinneurobiologicalresearchhaveindicatedthat
organismscontinuallyadjusttomeetdailyphysicalandsocialdemandsthrougha
dynamicprocesstermedallostasis,whereinvariousbiophysicalandphysiological
systemsworktogethertomaintainaninternalequilibrium,orhomeostasis(Evans,
2003;McEwen,1998;Sterling&Eyer,1988).Thatis,agivendemandmayleadto
aninternalresponse,suchasincreasedcortisollevelsorheightenedblood
pressure.Tomaintainstabilityinthiscontext,threeintegratedsystems,specifically
theneural,neuroendocrine,andimmunesystems,mustdetectboththedemand
andtheinternalresponseandworktoaccordinglyregulateandmediateinternal
responses(Evans,2003;McEwen,1998;Sterling&Eyer,1988).Allostaticload
occurswherethisdemandbecomestoogreatovertime,causingthesesystemsto
eitherbecomeoverworked,failtosufficientlyrespond,orbecomeoverlysensitive,
andleadingtonegativeimplicationsforphysical,emotional,andcognitive
processes(Evans,2003;Hughesetal.,2017;McEwen,1998;Sterling&Eyer,1988).
Theapplicationofthisphenomenontomultipleriskexposure,then,maygo
somewaytoexplainboththeaccumulationeffectsandthenumber-over-nature
principlewithincumulativerisktheory(Evans,2003;Evansetal.,2013).Thatis,
exposuretoseveraldifferentriskfactorsislikelytoresultinachildoradolescent
havingheightenedengagementofthestressandresponsesystems.Indeed,thereis
someevidenceofaconcurrentandlongitudinalassociationbetweenchildhood
cumulativeriskexposureandphysiologicalbiomarkersofallostaticload,including
increasedneuroendocrinestressactivity,restingbloodpressure,andbodyweight
(Brodyetal.,2013;Evans,2003;Evansetal.,2007;Evans&Kim,2012).However,
thesestudieshavenotdirectlyinvestigatedanyformofmediationpathway
throughstressintherelationshipbetweenmultipleriskexposureandnegative
outcomes.Furthermore,priorresearchhasbeenreliantonsomewhatmodest
samplesizesof100–500participants,asmeasuringbiomarkersofallostaticload
systemsusingthemethodsestablishedbyEvans(2003)ishighlydemandingin
termsoftimeandresources.

CHAPTERTHREE:RISKANDRESILIENCE
58
Assuch,thequantitativestrandofthecurrentstudysetouttoempirically
investigatetheroleofstressasanunderlyingmechanisminmultipleriskeffects,in
thecontextofearlyadolescentgirls’emotionalsymptoms.Thestudydoesnot
makeuseofallostaticbiomarkers,inpartbecausetheresearchisconstrainedbyits
secondaryanalysisofadatasetthatincludedself-reporteddataforglobalperceived
stress,ratherthanbiophysicalorphysiologicalvariables.However,therearea
numberofadvantagestothisapproach.Firstly,thisallowstheuseofalargesample
toinvestigatetheserelationshipsonagreaterscalethaninpreviousresearch.
Furthermore,thisapproachgivescredencetothegeneralunderstandingthatstress
isalargelysubjectivephenomenon,withsubstantialindividualdifferencesinthe
extenttowhichagiveneventisconsideredstressful(Lazarus,1966;Lazarus&
Folkman,1984).Theindividualappraisalofagivensituationasstressfulis
consideredtoplayacentralroleintriggeringstressandallostasisresponsesystems
(Burkeetal.,2005;Clarketal.,2007;Logan&Barksdale,2008;Sladeketal.,2016),
whileithasbeensuggestedthatbiophysicalstressresponsesmayincreasethe
perceptionofstress(McEwen,1998).Indeed,asmallnumberofstudieshave
identifiedanassociationbetweenglobalperceivedstress,whichisageneralised
perceptionofstressinday-to-daylife,andarangeofallostaticbiomarkersinboth
adolescentsandadults(e.g.,Oldehinkeletal.,2011;Sladeketal.,2016;Zimmaroet
al.,2016).Thus,thecurrentstudymayprovideinsightbyexaminingwhether
multipleriskexposureresultsinabroadfeelingofstressasappraisedand
experiencedbytheindividual.Thisapproachallowsinvestigationofstressthrough
asimilarlensacrossbothstrandsofthestudy;thatis,thefocusonperceivedstress
withinthequantitativestrandmirrorsthephenomenologicalnatureofthestudy’s
qualitativestrand.
3.4ResilienceandAdaptation
Despiteourunderstandingthattherearefactorsandprocessesthat
increasethelikelihoodofnegativeoutcomes,researchhasshownthatthe
outcomesamongthoseexposedtosuchriskcanvarygreatly(Masten,2001,2014b,
2016).Effortstounderstandwhysomeindividualscanthriveinadverseconditions,
CHAPTERTHREE:RISKANDRESILIENCE
59
whileothersaremorenegativelyimpacted,hasledtoawidebodyofresearch
focusedonthephenomenonofresilience,orpositiveadaptationinthefaceof
adversity(Masten,2001,2014b,2016).Previousinvestigationshaveidentifiedthat
childrenandadolescentsareabletoadapteveninextremecircumstances,suchas
livinginarmedconflictzones(Barber,2013;Nguyen-Gillhametal.,2008).Such
findingschallengedeterministicnotionsthathighlevelsofadversityautomatically
leadtonegativetrajectories,highlightingthatriskisaphenomenongroundedin
probabilityratherthancertainty(Masten,2014b).Thus,whileriskresearchis
underpinnedbyequifinality,theconstructofresilienceisgroundedinmultifinality,
whereinsimilarexperiencescanleadtodifferentoutcomes.Thatis,anindividual’s
functioninginagivencircumstancedependsuponthenatureoftheirindividual
widerecologicalenvironment(Cicchetti&Rogosch,1996;Nolen-Hoeksema&
Watkins,2011;Ungar&Liebenberg,2011).
Masten(2001,2014a,2016)hasoutlinedfour“waves”ofresilienceresearch
todate.Earlyinvestigation,orthe“firstwave”,developedinitialconceptualisations
ofresilienceanditsmeasurement.Initially,itwasbelievedthatresiliencewasa
fixedindividualtrait,withhumanseitherableorunabletoadapttoadverse
circumstances(Masten,2001,2014a,2014b;Rutter,1987;Ungar,2011).Thefield
hasmovedawayfromthisstance,withthesecondwaveofresearchdevelopingan
understandingofresilienceasadynamicandfluidprocessofadaptationthatshifts
overtime,withmanyindividualslikelytoexperiencebothgoodandpoor
functioningwithinarangeofareasacrosstheirlifetime(Barber,2013;Masten,
2001,2014b,2014a;Ungar,2011).Thisresearchdevelopedanunderstandingthat
thispositiveadaptationispromotedthroughinteractionsbetweentheindividual
andelementsoftheirecologicalenvironment,whichthenoperatetomitigatethe
negativeeffectsofrisk(Masten,2014b,2016;Ungar,2011).Theseresourcesthat
canreduceriskeffectsareconceptualisedasprotectivefactors,andasshown
overleafinFigure3.2differfrompromotivefactors,whicharevariablesassociated
withpositiveoutcomesforallindividualsregardlessofriskstatus.

CHAPTERTHREE:RISKANDRESILIENCE
60
Figure3.2.Promotiveandprotectiveconceptualmodels.
However,researchhasindicatedthatthetwooftenoverlap,withthesamefactors
frequentlyidentifiedasbothpromotiveandprotective,suchasapositivefamily
climate.Suchsimilaritieshavedemonstratedthatadaptationtoriskreliesonthe
everydaysystemsencounteredbymostindividuals,ratherthanrequiring
substantiveadditionalefforts(Masten,2001,2014b).Assuch,whileearly
investigationsofresiliencesetouttoidentifywhatmakesspecificindividualsable
toadapt,researchhasinsteadfoundthatresilienceisacommonphenomenonthat
occursacrossthelifespanandissupportedbyeverydayinteractionsandprocesses
(Masten,2001,2014a,2014b;O’DoughertyWright&Masten,2015).Thishasled
Masten(2001,2014b)toconceptualisethephenomenonas“ordinarymagic”.
Thethirdwavebuiltthislearningintoappliedpreventionbyseekingto
increaseaccesstoprotectivefactorsamongat-riskpopulations.Thefourthand
mostrecentwaveofresilienceresearchisprimarilyconcernedwithunderstanding
theunderlyingprocessesofhowsuchfactorsenablepositiveadaptation,drawing
onrecentadvancesinthestudyofneurologicalandbiologicalprocessesandin
statisticalmodelling.Inlinewiththisfourthwave,thequantitativestrandofthe
studysetouttoexploreprotectivefactorsspecificallywithinthecontextofthe
stresshypothesis,tounderstandtherolesuchvariablesplaywithintheunderlying
mechanismsofriskandsymptomatologyinamongearlyadolescentgirls.This
constitutesafocusnotonlyonthefactorsassociatedwithimprovedoutcomesbut
alsoontheadaptiveprocessesbywhichsuchfactorsinfluenceoutcomesMasten
(2001,2014a,2014b)distinguishesbetweenprotectivefactors,orthevariables
associatedwithadaptationtorisk,andadaptiveprocesses,orthespecificsystem

CHAPTERTHREE:RISKANDRESILIENCE
61
throughwhichagivenprotectivefactorinfluencesoutcomes.Ithasbecome
increasinglynotedacrossresilienceresearchthatprotectivefactorsmaywell
functiontoimproveoutcomesbydisruptingunderlyingstressprocesses(Barnes,
2016;Masten,2014b,2018),howevertherehasbeenlimiteddirectinvestigationof
thisprinciple.
3.4.1FactorsSupportingPositiveOutcomes
Thecurrentstudyassessesbothpromotiveandprotectivefactorsinorder
tounderstandwhetherthereisadistinctionbetweenthetwointhecontextof
earlyadolescentgirls’emotionalsymptoms.Itshouldbenotedthatprotective
factorscanoperatepreventatively,actingtodirectlymoderatetheeffectsofrisk
exposure,aswellasretrospectively,supportingrecoveryfromnegativeimpacts
overtime(Masten,2016).Asthecurrentstudyiscross-sectional(seeChapter
Four),itisnotpossibletoisolateherewhetherobservedeffectsserveapreventive
orrecoveryfunction,whichwouldrequiremorecomplexmodellingwithina
longitudinaldesign.Itshouldalsobenotedthattherehasbeendiscussion
regardingwhetherriskandpromotive/protectivefactorscanbeconceptualisedas
distinctfromoneanotheror,alternatively,occurringatoppositeendsofa
continuum.Forinstance,Masten(2018)highlightsthatgoodemotionregulation
skillsareoftenidentifiedasofferingabufferingeffectinthefaceofrisk,butpoor
emotionregulationskillscanexacerbatethewiderrisksassociatedwithcertain
typesofadversity,suchasfamilialpoverty.Thecurrentstudytreatsriskand
promotive/protectivefactorsasdistinctratherthanexaminingeachoneona
spectrum,inordertofacilitatepathwaymodellingexaminingthewayinwhich
theseinteracttoinfluenceoutcomes.However,futureresearchcouldexamine
theseaspartofalargerinteractivenetworkexploringdifferentfactorsasa
continuuminrelationtomentalhealthoutcomesamongadolescents,asrecently
exploredbyFritz,Fried,Goodyer,Wilkinson,andvanHarmelen(2018).
Althoughpreviousresearchhasidentifiedarangeofprotectivefactorsin
relationtoemotionalsymptomsduringadolescence,itcannotbeassumedthat
theseareconsistentacrossallpopulations(Fergus&Zimmerman,2005;Smokowski

CHAPTERTHREE:RISKANDRESILIENCE
62
etal.,2004;Ungar,2011).Thedegreetowhichprotectivefactorsmoderatethe
effectsofriskcanfluctuatebasedongroupcharacteristicssuchasgender(Benzies
&Mychasiuk,2009;Sun&Stewart,2007),age(Sun&Stewart,2007;Ungar,2011),
SES(Benzies&Mychasiuk,2009;Zolkoski&Bullock,2012),andlocalcontext
(Fergus&Zimmerman,2005).Thereisaneed,then,forresearchfocusedon
specificpopulations,outcomes,andcircumstancesinordertounderstandtheway
inwhichresiliencecanoperatefordifferentgroups(Alvord&Grados,2005;
Masten,2014a).Thecurrentstudycontributestounderstandingofthecapacityfor
resilienceinthefaceofmultipleriskexposureandspecificallyinrelationtoearly
adolescentgirls’emotionalsymptoms.However,protectivefactorscanbehighly
context-specificinawaythatcannotalwaysbecapturedstatisticallyinlarge-scale
orheterogeneoussamples.Insomecontexts,factorstypicallycategorisedasrisky
actasatypicalprotectivefactors(Bottrell,2009;Masten,2014b;Ungar,2011).For
instance,withdrawalfromschoolparticipationmaybeprotectiveforanindividual
fromanethnicminoritybackgroundiftheschoolenvironmentfacilitates
marginalisationofthatgroup(Ungar,2011).Similarly,somefactorsmayserveas
bothriskandprotectionsimultaneously,suchasapeernetworkthatprovides
supportbutalsonormalisesriskybehaviourslikedrugabuse,asidentifiedby
Bottrell(2009)inaqualitativestudyofasupportgroupforadolescentmothers.
Thus,whilequantitativeinvestigationcanprovideinsightintothestatistical
interactionsbetweenthesephenomena,itcannotexplorethecomplexitiesofthem
incontext,norprovideinsightintotheexperienceandroleoftheindividualin
theseinteractions,whichnecessitatesqualitativeexploration(Bottrell,2009;Ungar,
2003,2011).Accordingly,thecurrentstudy’smixedmethodsapproachaimedto
offeramorecomprehensiveunderstandingoftheseprocessesincontextwithin
earlyadolescentgirls’emotionalsymptoms.
Thecurrentstudyfocusesexclusivelyonfactorsacrosstheexternal
elementsoftheecologicalsystem,withaparticularfocusontheroleof
interpersonalconnection.Historically,researchhaspredominantlyfocusedon
individual-levelprotectivefactors,resultingincomparablylessevidencerelatingto
externalfactors.Correspondingly,discourseoftenplacesanonusontheindividual

CHAPTERTHREE:RISKANDRESILIENCE
63
toberesponsiblefortheirownresilience,ratherthanonwidersystemicservices
(Burman,2018;Ungar,2012).Thus,thefocushereonexternalfactorscontributes
toabroaderefforttoshifttheonusawayfromtheindividualandontothewider
environment,thuscontributingtodevelopingunderstandingsoftherolethatwider
individualsandsystemscanplay(Burman,2018;Ungar,2012).Thisdecisionwas
furtherunderpinnedbythestudy’suseofsecondarydatameasuredusingthe
StudentResilienceSurvey(SRS;seeSection4.6.1),whichincludedagreaterfocus
uponexternalfactorsandlimitedmeasurementofinternalfactorstheoretically
linkedwithemotionalsymptoms.Inaddition,theresearchplacesaparticular
emphasisontheroleofperceivedinterpersonalconnection,whichisexploredin
greaterdetailinthefollowingsubsection.
3.4.2SocialConnection
Itisgenerallyagreedthathumanshaveacoreneedforsocialconnection
andthatinterpersonalrelationshipsplayakeyroleingeneralhealthand
developmentaswellasresiliencethroughoutthelifespan(Cacioppo&Patrick,
2008;Fritz,deGraaff,etal.,2018;Masten,2014b;Sun&Stewart,2007;Ungar,
2012).Socialrelationshipsandinteractionsaremultifacetedandthequantitative
strandofthestudyfocusesspecificallyonsocialconnection,broadlydefinedas
perceivedinterpersonalclosenesswithindividualsandgroups(Lee,Draper,&Lee,
2001;R.M.Lee&Robbins,1998).Thisisdistinctfrommorespecificbehaviours
suchassocialsupport(Barrera,1986),althoughsuchconstructsaredrawnuponat
timesinthissectionandindeedareexploredmoredirectlyinqualitativeinterviews.
Perceivedconnectionwithothersduringchildhoodandadolescenceisoften
associatedwithreportsoflowerlevelsofinternalisingdifficulties,including
emotionalsymptoms,functioningasbothpromotive(e.g.,Bondetal.,2007;Bovier,
Chamot,&Perneger,2004;EwellFosteretal.,2017;Malaquias,Crespo,&
Francisco,2015)andprotective(e.g.,Bondetal.,2007;Carbonelletal.,2002;
Masten,2014b).Attheotherendofthisconceptualspectrum,feelingsofloneliness
andsocialisolationinchildhoodandadolescencehavebeenshowntopredict
greaterlevelsofemotionalsymptoms,highlightingtheimportanceofperceived

CHAPTERTHREE:RISKANDRESILIENCE
64
socialconnectionforthisoutcome(e.g.,Hall-Landeetal.,2007;Harris,Qualter,&
Robinson,2013;Qualteretal.,2010,2013).Itislikelythattherearemultiple
adaptiveprocessesunderpinningtherelationshipbetweensocialconnectionand
emotionalsymptoms,includingfeelingsofsafetyandsecurity,instillingapositive
senseofself,distractionfromdifficulties,anddirectsupportwithcopingwithand
managingchallenges(Cacioppo&Patrick,2008;Gassetal.,2007;Masten,2014b;
Ungar,2012).Thestressbufferinghypothesis,setoutbyCohenandWills(1985),
suggeststhatsocialrelationshipsfunctiontoimprovewellbeingbylesseningthe
extenttowhichnegativelifeeventsareappraisedasstressful.Severalstudieshave
identifiedanassociationbetweensocialconnectionandloweredstressthroughout
thelifespan,includingbothperceivedstress(Lee,Keough,&Sexton,2002;
Panayiotou&Karekla,2013)andbiomarkers(Evansetal.,2007;Seemanetal.,
2002;Sladek&Doane,2014).However,studieshavetypicallyfocusedupon
moderationofthedirecteffectsofexposuretoadversity,ratherthanexamining
howprotectivefactorsoperatewithinunderlyingstressmechanisms.Morerecent
researchhasbeguntoexpandtoexaminethewaysinwhichstress,adaptation,and
copingprocessesareembeddedwithinwiderecologicalsystems,including
interpersonalinteractionsandrelationships(Skinner&Zimmer-Gembeck,2016).As
such,thecurrentstudysetouttoexaminethefunctionofsocialconnectionsinthe
stressprocessesthatmayunderpinriskeffectsamongearlyadolescentgirls.
Researchexploringtherelationshipbetweeninterpersonalrelationshipsand
mentalhealthhaveoftenfocusedonrelationshipsatagenerallevelorhave
examinedspecificdomains(e.g.,family,peer,orschoollevel)inisolation.More
recentlytherehasbeenanemphasisoninvestigatingmultiplesourcesof
connectednessalongsideoneanother,inordertobetterisolatetheirdifferential
contributionstohealthanddevelopment(EwellFosteretal.,2017;Holt-Lunstadet
al.,2017;Ja&Jose,2017).Assuch,thequantitativestrandofthecurrentstudy
soughttoexaminethefunctionofparticularsourcesofsocialconnection,namely
withinthefamily,school,widercommunity,andpeergroup,inordertosupport
developingknowledgeofthecontributionsmadebytheseconnectionsandtobuild
understandingoftheirroleinstressappraisalprocesses.Researchhasalso

CHAPTERTHREE:RISKANDRESILIENCE
65
suggestedthatthesalienceofparticularsourcesofsocialsupportvariesovertime,
withparentalconnectionbeingimportantduringchildhoodandpeersbecoming
particularlysalientduringadolescence(Umbersonetal.,2010).Thus,the
quantitativestrandofthestudysoughttoinvestigatethecontributionsofdifferent
sourcesofconnectionforgirlsduringearlyadolescenceasapivotalpointinmental
healthdevelopment.Alongsidethis,thequalitativestrandsoughttogobeyondthis
compartmentalisedperspectiveandprovidecomplementaryinsightintohow
relationshipswithothersareseentorelatetotheexperienceofemotional
symptomsandriskexposureandexplorehowgirlsnavigatetheserelationshipsasa
partoftheirlives.
FamilyAdultConnection
Familymembers,particularlyparentsandcarers,areoftenseenasacritical
sourceofinterpersonalconnectionthroughchildhoodandintoadolescence
(Umbersonetal.,2010).Connectionwithfamilymembersduringthistimeis
frequentlyfoundtobeassociatedwithloweredinternalisingandemotional
symptoms(Costelloetal.,2008;Day&Padilla-Walker,2009;Lereyaetal.,2016;
McGrawetal.,2008;Rowe,Zimmer-Gembeck,&Hood,2016;Schulenbergetal.,
2007;Vineretal.,2012;Wille,Bettge,&Ravens-Sieberer,2008).Familyconnection
hasalsobeenfoundtobeinverselyassociatedwithemotionalsymptomswithinat-
riskpopulations(EwellFosteretal.,2017)andtoactasaprotectivefactor
moderatingtheeffectsofrisk(Conger&Conger,2002;Klieweretal.,2004;Li,
Nussbaum,&Richards,2007),includingmultipleriskexposure(Willeetal.,2008).
However,examinationoftheprotectivefunctionoffamilyconnectionfor
emotionalsymptomsremainslimitedoverall,includinginthecontextofmultiple
riskexposure.Thereisalsosomeevidencethatexposuretoeitherpositiveor
negativefamilyinteractionscanaffectgirlsmorestronglythanboys,thoughthis
remainslimited(Telzer&Fuligni,2013).Boththequantitativeandthequalitative
strandofthecurrentstudymayprovidefurtherinsightintotheroleoffamily
connectioningirls’experiencesandoutcomes.
Connectiontoone’sparentstypicallybecomeslesssalientovertime,with
peerconnectionbecomingmoremeaningfulforhealthanddevelopmentoutcomes

CHAPTERTHREE:RISKANDRESILIENCE
66
fromearlyadolescence(Umbersonetal.,2010).Whileparentsactasastressbuffer
inearlychildhood,withobserveddifferencesinindicatorsofstresswhenparents
arepresentoroffersupport,sucheffectsarecomparablylessmeaningfulor
altogetherabsentamongadolescents(Gunnaretal.,2015;Hostinaretal.,2014,
2015).Thefocushereonearlyadolescenceandthestresshypothesisallows
examinationofwhetherandhowfamilyconnectionfunctionsinthecontextofrisk
andperceivedstress,duringaperiodconsideredcriticalforbothgirls’mental
healthandtheroleoftheparent.
SchoolAdultConnection
Asmallnumberofstudieshaveidentifiedanassociationbetweenpositive
teacher-pupilrelationshipsandlowerlevelsofinternalisingsymptoms,including
emotionalsymptoms(Lereyaetal.,2016;Murray&Greenberg,2000;O’Connor,
Collins,&Supplee,2012;Wang,Brinkworth,&Eccles,2013),thoughLongobardi,
Prino,Marengo,andSettanni(2016)foundthataftercontrollingforwider
connectionacrossthefamilyandpeergroups,thisrelationshipofferedno
contributions.Thereremainslimitedresearchexaminingtheprotectivefunctionof
theserelationshipsforemotionalsymptoms.Itmaybethatpositiveconnection
withateacher(orotherschooladult)canfacilitatefeelingsofvalueandbelonging,
orsupportpositiveemotionalandbehaviouraldevelopment(Sointuetal.,2017).
Forindividualswithlimitedpositiverelationshipsathome,apositiverelationship
withaschooladultmightofferacompensatoryresource(Hamre&Pianta,2001).
Notably,accesstoschool-basedrelationshipsfluctuatesduringtimesofeducational
transition,aschildrenandadolescentslosepreviousconnectionswithteachersand
createnewrelationshipsinanewschool,whichcanbechallengingandcanleadto
lowergeneralschoolconnectedness(Loukasetal.,2016).Thecurrentstudy’sfocus
onearlyadolescencereflectsthepointatwhichpupilsinEnglandhaverecently
transitionedfromprimaryschool,wheretheytypicallyhaveonemainclassteacher,
tosecondaryschool,withmultipleteachersacrossthecurriculum.
Researchinthisareaisgenerallylimitedbytheuseofsmallsamplesizes(ca.
150–300)and,crucially,studieshavefrequentlyutilisedsimpleregression
modellingandthusfailedtoaccountforclusteringwithinthedata.Giventhatsuch

CHAPTERTHREE:RISKANDRESILIENCE
67
researchisoftenconductedwithinschools,theremaywellbedifferencesinoverall
levelsofadult-pupilconnectionsbetweenclassesandschoolsthatmayaffectthe
independenceofthedata,necessitatingmorecomplexapproaches.
CommunityAdultConnection
Thecurrentstudyexaminedperceivedconnectionwithanadult“awayfrom
school”,inrecognitionthatparticipantsmaydrawuponrelationshipsandsupport
beyondthefamilyandschoolcontext.Qualitativeresearchhassuggestedthat
adolescentsvaluepositiveandcaringrelationshipswithtrustedadultsregardlessof
theirdomainorrole(Munford&Sanders,2016;Ungar,2004b).Thus,thisfocus
allowsforabroaderscopeofthewayinwhichwiderrelationshipswithadultsmay
contributetoearlyadolescentgirls’emotionalsymptoms,inbothapromotiveand
protectivecapacity.Giventheemphasishereonawidercontext,thespecificityof
thisconnectionisbroadandmaycapturerelationshipswitharangeofpeoplesuch
asgrandparentsandextendedfamily,communityorreligiousleaders,orfamily
friends.
SchoolPeerConnection
Throughoutchildhoodandadolescence,schoolisacentralcontextwithin
whichyoungpeopleengagewithothersonaday-to-daybasis,providingimportant
opportunitiestodevelopsocialskillsandbuildrelationships.Thecurrentstudy
focusesonpeers,whichreferstoanindividual’ssocialgroup;thatis,arelatively
smallgroupsofindividualswithwhomoneinteractsregularly(Jaccardetal.,2005;
A.Ryan,2000;Wilkinson,2010).Thisincludesbutgoesbeyondthenarrower
“friends”,whichcapturesmoreselectiveassociationsthattypicallyofferdifferent
ormorepronouncedqualities,suchasattachment,closeness,andsupport(Jaccard
etal.,2005;Ryan,2000;Wilkinson,2010).
Researchhasconsistentlyindicatedthatpeersareamongthestrongest
socialfactorspredictinghealthbehavioursandoutcomesduringadolescence,as
individualsbecomemoreindependentfromtheirparents(Brown&Larson,2009;
Umbersonetal.,2010).Severalstudieshavefoundthatelementsofpeer
connectionandrelationshipsareassociatedwithloweredlevelsofadolescent

CHAPTERTHREE:RISKANDRESILIENCE
68
internalisingproblems,includingemotionalsymptoms(e.g.,Bosacki,Dane,&
Marini,2007;Lereyaetal.,2016;McGrawetal.,2008;Millingsetal.,2012;Van
Voorheesetal.,2008).Whilethereareindicationsthatpeerconnectioncanprovide
bufferingeffectsinparticularat-riskgroupsinrelationtowideroutcomessuchas
qualityoflife(e.g.,Flaspohleretal.,2009),thereislittledirectexaminationoftheir
protectiveeffectinrelationtoemotionalsymptoms.Therearesomeindicationsof
genderdifferencesintheeffectsofpeerconnection,withgirlsshowinggreater
sensitivitytobothpositiveandnegativepeerexperiences(Bakkeretal.,2010;
Rotenbergetal.,2014),necessitatingfurtherexaminationwithinearlyadolescent
girls.
3.4.3ActiveEngagementinHomeandSchoolLife
Thestudyalsoinvestigatedthepromotiveandprotectivefunctionofthe
extenttowhichparticipantsviewedthemselvesasactivelyengagingintheirhome
andschoollives,inlinewithitsinterestinhowindividualsinteractwiththeexternal
featuresoftheirenvironment.Activeengagementinhomeandschoolliferefers
heretoperceptionsofbeingactivedecision-makersandcontributorsacrossthese
contexts.Duringearlyadolescence,individualsgenerallyexperiencegreater
autonomyanddecision-makinginthehome,particularlysoforgirls(Gutman&
Eccles,2007;Wray-Lakeetal.,2010).Studieshaveindicatedthatchildrenand
adolescentswithgreatercapacityfordecision-makingandcontrolinthehome
generallyreportlowerlevelsofemotionalsymptoms(Beckeretal.,2010;Borelliet
al.,2015;Radziszewskaetal.,1996).Ithasbeensuggestedthatcontributingto
decision-makinginthehomeoffersopportunitiestoidentifyandrespondto
stressorsindailylife,thusdevelopingstressappraisalandcopingcapacities(Becker
etal.,2010;Borellietal.,2015).Intermsofactivecontributionthroughchoresand
otherformsofsupport,researchhasgenerallyfocusedonbroaderoutcomessuch
aspsychologicalwellbeing.Whilesuchcontributionscanpresentchallenges,
potentiallyincreasingburdenandcreatingtension,itisbelievedthatoverallthis
createsasenseofbelongingandsupportssatisfactionandwellbeing(Fuligni&
Pedersen,2002;Fuligni&Telzer,2013;Kavanaughetal.,2015).

CHAPTERTHREE:RISKANDRESILIENCE
69
Activeengagementinschoolisgenerallyexaminedasadimensionof
broaderinstitutionalschoolconnection(e.g.,Bondetal.,2007;EwellFosteretal.,
2017;Loukasetal.,2016),withlimitedresearchexaminingthisnarrowerconstruct
bothgenerallyandinrelationtomentalhealth.Ithasbeenarguedthatthe
developmentalneedsofadolescents,includingthedesireforautonomyand
decision-making,canbeincongruentwiththerulesandsystemsusuallyinplacein
schools,whichareoftenrigidandunamenabletonegotiationwithpupils(Eccleset
al.,1993;Hargreaves,2017;Smetanaetal.,2004).Whileitwouldbeusefulto
examinethedifferentialfunctionsofactiveengagementwithinhomeversusschool
contexts,thesubscaleusedtogatherdataspecifiestheseasasingularconstruct
andsothiswasnotpossible(seeSection4.6.1).Capturedtogether,however,these
insteadofferinsightintotheroleofperceivedactiveengagementindailylife,given
thathomeandschoolarethemajorcontextswithinwhichearlyadolescents
operateonaday-to-daybasis.
3.4.4EngagementinExtracurricularActivities
Finally,thestudyexaminedtheroleofperceivedengagementin
extracurricularactivitiesandhobbies,suchasart,drama,music,sport,andspecial
interestgroupsandclubs.Extracurricularactivitiesareoftendiscussedwithinthe
contextofpositiveyouthdevelopment,whereitisunderstoodthatsuch
engagementcanprovidepositiveopportunitiesforsocialconnectionand
belongingness,aswellassupportingasenseofachievementandpositive
recognitionfromothers(e.g.,Alvord&Grados,2005;Nicholson,Collins,&Holmer,
2004;Schaeferetal.,2011).Thereisalsosomeevidencethatthesebenefitsmaybe
greaterforthosefromlowersocioeconomicbackgrounds(Blomfield&Barber,
2011).Amodestnumberofstudieshaveidentifiedanassociationbetween
extracurricularactivityandlowerlevelsofemotionalsymptomsduringadolescence
(Guèvremontetal.,2014;Lereyaetal.,2016;Molinuevoetal.,2010),thoughthere
isalackofdirectexaminationofitsprotectivefunctioninrelationtoriskeffects.
Notably,extracurricularactivityoftencorrespondstohigherlevelsofconnection
withinthefamily,school,andneighbourhoodcontexts;assuch,effectsshouldbe

CHAPTERTHREE:RISKANDRESILIENCE
70
examinedalongsidethesecontextstoavoidover-estimation(FeldmanFarb&
Matjasko,2012;Kilmeretal.,2010),asisthecaseinthecurrentstudy.
3.5MethodologicalApproachesinRiskandResilience
Theriskandresilienceresearchfieldisprimarilydrivenbyquantitative
inquiry.Thismeansthatthelanguageandconstructstypicallyusedareinherently
statisticalinnature;thatis,thereisadominantfocusonprobabilityand
risk/promotive/protectivefactorsasvariablesassociatedwithincreasedlikelihood
ofparticularpositiveornegativeoutcomes.Asaresult,whilethereisagreatdeal
ofresearchidentifyingcorrelatesandpredictorsofhealthanddevelopment
outcomes,andanincreasedfocusontheeffectsofmultipleriskexposure,there
remainsalimitedunderstandingoflivedexperienceandwhatitmeanstobean
“at-risk”childoradolescent.Whilequantitativeinquiryhasprovidedextensive
evidenceonriskandresiliencebothconceptuallyandinthespecificcontextofchild
andadolescentmentalhealth,therearealsoanumberofadvantagesthat
qualitativeinquirycanoffer.
Atagenerallevel,limitedrepresentationsoflivedexperience,or“whatitis
like”,risksreducingyoungpeopletodatapointsandoverlookingthecomplexity
andmeaningfulnessoftheseexperienceswithintheirdailylivesandlifelong
trajectories(Todres&Wheeler,2001;Yilmaz,2013).Qualitativeresearch,and
particularlyphenomenologicalapproachesasusedinthecurrentstudy,canserve
tohumaniseotherwisedistant“others”inawaythatquantitativeinquirydoesnot
afford,bringingthefocusbackfrompatternsandvariablestopeople(Todres,2007;
Todres&Wheeler,2001).Similarly,suchmethodscanbeparticularlyhelpfulfor
elevatingthevoicesofmarginalisedandunheardgroups(Larkinetal.,2006;Larkin
&Thompson,2012;Pietkiewicz&Smith,2014;Reidetal.,2005),aswithchildren
andyoungpeopleandparticularlythoseexperiencingriskanddisadvantage
(Bottrell,2009).
Qualitativeinquirycanalsoproviderichinsightintothecomplexityof
phenomenaincontext(Johnson&Onwuegbuzie,2004;Mertens,2015),offering

CHAPTERTHREE:RISKANDRESILIENCE
71
thepotentialtowidenthemarginsofthewaywedefineandunderstandthe
phenomenonofinterestbeyondthenarrowedinformationprovidedby
quantitativevariables(Bottrell,2009;Ungar,2003).Indeed,qualitativeresearchled
andpromotedbyUngarandcolleagues(Ungar,2003,2004a;Ungar&Liebenberg,
2011)hasexpandedandchallengedearlierunderstandingsofresilience,
demonstratingthecomplexityandcontextualspecificityofthephenomenon.IPA
hasbeenhighlightedasparticularlyvaluablewhenexaminingcomplexphenomena
(Smith&Osborn,2015a;Wagstaffetal.,2014),whileitsidiographicfocuson
particulargroupsandcontextssupportsthecurrentstudy’saimtounderstand
thesephenomenawithinthespecificcontextofemotionalsymptomsamongearly
adolescentgirls.Finally,qualitativeresearchmaybeparticularlyhelpfulin
addressingenduringquestionsregardingtheunderlyingmechanismsofriskand
resilienceinrelationtomentalhealthoutcomes.Thatis,exploringlivedexperience
ofthesephenomenacanfacilitateagreaterunderstandingofthewaysthat
differentaspectsofanindividual’sliferelatetooneanotherandchangeovertime.
Thislevelofanalysismayelucidateunderlyingprocessessuchastransactionsacross
“riskfactors”,theroleofstress,andtheareasandresourcesthatearlyadolescent
girlsdrawoninnavigatingtheseareasoftheirlives.
Useofqualitativeinquirywithinamixedmethodsstudycanfacilitate
explorationofbothoverarchingpatternsandindividualnuanceandcomplexity,
thusovercomingsomeofthelimitationscommonacrosstheriskandresilience
researchfield.Indeed,Ungar(2019)hasrecentlyhighlightedthattheuseofmixed
methodscanfacilitatebroaderconceptualisationsanddiscoursesaroundriskand
resilienceprocesses,whilealsofacilitatingamorein-depthunderstandingofthese
phenomenathatneitherapproachcouldofferinisolation.Furthermore,itis
notablethatbothstrandsofthecurrentstudyhaveadistinctfocusontheways
thatriskandresilienceprocessesaresubjectivelyexperiencedandunderstood,but
adoptadifferentleveloffocusinthisendeavour.Thatis,thequantitativestrand
focusesonmentalhealthsymptomsthatpredominantlymanifestthemselves
internally(Fredrickson&Roberts,1997;Hammen,2005;Kuehner,2017;Nolen-
Hoeksema,1990,2001;Nolen-Hoeksema&Girgus,1994)andtherolethat
CHAPTERTHREE:RISKANDRESILIENCE
72
subjectivestressappraisalandperceptionsofaccesstoprotectivefactorscanplay,
whilethequalitativestrandseekstoexploreindividualisedsense-makingofthese
phenomena.Thespecificuseofmixedmethodsinthecurrentstudyispresentedin
thefollowingchapterwithconsiderationofhowthequantitativeandqualitative
strandsarebroughttogethertogenerateinsightintoriskandresilienceprocesses
inrelationtoearlyadolescentgirls’emotionalsymptoms.
3.6ChapterSummary
Thestudysetouttoinvestigateeighthypothesisedriskvariablesandto
examinemultipleriskeffectswithattentiontodifferentconceptualisationsand
measurementapproaches,aswellastheroleofstressappraisal.Buildingonthe
conceptofresilience,thestudysoughttoexaminesixhypothesised
promotive/protectivefactors,withanemphasisonexternalfactors.Finally,this
chapterhashighlightedthatmixedmethodsmayfacilitateamorecomprehensive
understandingofthecomplexityandmeaningfulnessoftheseprocesses.

CHAPTERFOUR:METHOD
73
Chapter4:Method
4.1ChapterOverview
Thischapterdetailsandjustifiesthemethodologyandmethodsutilisedin
thecurrentstudy.Itexploresthestudy’scontext,epistemologicalstanceand
influence,anddesign,beforeoutliningeachstageoftheresearchprocess,namely
participants,materials,procedure,andanalyticalstrategy.Finally,effortsforquality
andrigouraredetailedandanoverviewofethicalconsiderationsispresented.
4.2StudyContext
ThedatainthecurrentstudywerecollectedfortheevaluationofHeadStart,
along-termpreventionandpromotionprogrammefocusedonimprovingresilience
andemotionalwellbeingforat-riskyoungpeopleacrosssixareasofEngland.The
projectandevaluationarefundedbytheNationalCommunityLotteryFund(NCLF)
andtheevaluationisbeingcarriedoutbyanAnnaFreudNationalCentrefor
ChildrenandFamilies(AFNCCF)-ledconsortium.
4.2.1HeadStart
HeadStartisalong-termprogrammetriallingarangeofinterventionsand
initiativesaimedatimprovingresilienceandemotionalwellbeingfor10-16year-
olds.Theprogrammeaimsto:
1. Improveemotionalwellbeing;
2. Improveengagementinschoolandacademicattainment;
3. Reducetheonsetofdiagnosablementalhealthdisorders;and
4. Reduceengagementin“risky”behaviour.
HeadStartisbeingdeliveredoverafive-yearperiod(2016–2022)acrosssixlocal
authority-ledareas,specificallyBlackpool,Cornwall,Hull,Kent,Newhamand
Wolverhampton.Theseareaswereselectedforinclusioninthisphaseofthe

CHAPTERFOUR:METHOD
74
programmebasedontheirinvolvementinapreviouspilotingphaseofthe
programme,alongsideconsiderationofdemographiccharacteristicsandlocality.
4.2.2NationalEvaluationofHeadStart
TheevaluationofHeadStartiscurrentlybeingundertakenbyaconsortium
ledbyAFNCCF,involving:
• TheEvidenceBasedPracticeUnit(UniversityCollegeLondon[UCL]and
AFNCCF);
• ChildOutcomesResearchConsortium(AFNCCF);
• TheUniversityofManchesterInstituteofEducation;
• LondonSchoolofEconomics;and
• CommonRoom(aconsultancyorganisationfocusedoninvolvingchildrenand
youngpeopleindevelopingresearch,policy,andpracticerelatingtothem).
Thisevaluationhasthreekeystrands,witharangeofdatautilisedtoaddresseach
one:(a)Quantitativeexplorationofimpact,(b)qualitativeexplorationof
experienceandmechanismsand(c)evidence-basedpracticeanddissemination.
Quantitativedataisgatheredannuallyfrompupilsin114educationsettings
(baselineN=30,843).Thiscomprisesalongitudinalcohortfollowedthroughthe
projectfromYear7(2016/2017)onwards(51%atbaseline),alongsideyear-on-year
snapshotmeasurementsofYear9pupils(2016/2017;49%atbaseline;Deighton,
Lereya,etal.,2018).Thesedataaregatheredeachacademicyearbetween
2016/2017and2021/2022.ParticipantscompletetheWellbeingMeasurement
Framework(WMF),comprisingseveralmeasuresrelatedtowellbeing,mental
health,andresilience(EvidenceBasedPracticeUnit,n.d.).Partnershipareastrack
individuals’engagementwithHeadStartservicesandinterventionsforuseinthe
evaluation.DemographicdataisaccessedfromtheNationalPupilDatabase(NPD).
Qualitativedataisgatheredthroughannualsemi-structuredinterviewswith
childrenandyoungpeople(baselineN=63;Stapley&Deighton,2018),following
onelongitudinalcohortfromYears5and7(2016/2017)onwards.Thesedatawill
begatheredeachacademicyearbetween2016/2017and2021/2022.Further

CHAPTERFOUR:METHOD
75
quantitativeandqualitativedataisgatheredfortheevaluationofprogramme
deliveryandsummativeevaluationsofspecificinterventions;anoverviewofthis
processisnotdescribedhere,asthecurrentstudydoesnotdrawonthisdata.
4.2.3IndependenceoftheCurrentStudy
Thecurrentstudydrawsonquantitativeandqualitativedatagatheredinthe
2016/2017baselinestageofHeadStart.Thecurrentstudyisindependentfromthe
mainevaluationasitfocusesondiscreteaimsandresearchquestionsand
addressesthesethroughseparateanalyses.Thus,itconstitutesanoriginalstudy
thatoffersuniquecontributionstoadolescentmentalhealthresearchand
developmentalpsychopathology.TableA1,AppendixAoutlinesthedifferences
betweenthecurrentstudyandtheevaluationofHeadStart.Itshouldbenotedthat
theauthorofthecurrentstudywasfundedasaresearchassistantforthemain
evaluationandwasinvolvedinthequantitativeandqualitativeevaluationstrands.
4.3EpistemologicalApproach
Itisnecessarywithinsocialresearchtoexplorethebeliefsandassumptions
underpinningtheresearchprocess.Variousconceptualisationshavebeenproposed
tomakesenseofsuchphilosophicalfoundationsandthewayinwhichtheyoperate
toguideresearch.Kuhn(1962)firstintroducedtheideaofparadigms,ordistinct
worldviewsencompassingspecificsetsofbeliefsandassumptions.Lincolnand
Guba(1985)extendedthisbroadconceptualisation,outliningatripartitemodel
withinwhichparadigmscontainedthreespecificbeliefsystems;namely,ontology,
epistemologyandmethodology.However,Crotty(1998)contendedthatontology,
whichcapturesassumptionsregardingthenatureofreality,andepistemology,
whichrelatestothestudyofthisreality,areconceptuallyintertwinedandthus
difficulttoseparate,suggestingthat“totalkoftheconstructionofmeaningisto
talkoftheconstructionofmeaningfulreality”(p.10).Thecurrentstudyapplied
Crotty's(1998)framework,conceptualisingtheresearchprocessasconsistingof
fourkeyelements:(a)Epistemology,orthenatureofknowledgeand,thus,ofthe

CHAPTERFOUR:METHOD
76
relationshipbetweentheresearcherandtheresearch;(b)theoreticalperspective,
orthestanceadoptedbytheresearcher;(c)methodology,ortheresearchdesign;
and(d)methods,orthetoolsandproceduresusedtocollectandanalysedata.
Crotty(1998)outlinedthisasahierarchicalprocess,witheachelementinformedby
theprecedingone(seeFigure4.1).
Figure4.1.Hierarchyofelementswithinparadigms.ReprintedfromThefoundationsofsocial
research:Meaningandperspectiveintheresearchprocess,byM.J.Crotty,(1998),SAGEPublications
Ltd.Copyright1998byMichaelCrotty.
4.3.1Pragmatism
Pragmatismisaphilosophicalschoolofthoughtconcernedwithmeaning
andaction,ratherthanabstractthought,conceptualisingtruthandknowledgeas
provisionalratherthanabsolute(Johnson&Onwuegbuzie,2004;Maxcy,2003).As
aresearchparadigm,pragmatismhasrejectedtraditionallydualistapproachesand
insteademphasisespluralism,whereindifferingtheoriesorperspectivesare
valuablefordevelopingameaningfulunderstandingofaphenomenon(Johnson&
Onwuegbuzie,2004).Hence,pragmatismchallengestheincompatibilitythesis
(Howe,1988),whichcontendsthatquantitativeandqualitativemethodsare
underpinnedbyincompatibleepistemologiesandthusshouldnotbemixed
(Bryman,2008;Johnson&Onwuegbuzie,2004).Quantitativepurists(e.g.,Maxwell
Methods
Methodology
Theoretical
perspective
Epistemology

CHAPTERFOUR:METHOD
77
&Delaney,2004;Popper,1959)havetypicallysubscribedtoa(post)positivist
philosophy,withinwhichanobjectiverealityexistsandmaybemeasured,if
imperfectly,meaningthatestablishinggenerallawsisbothachievableand
desirable(Creswell,2014;Greene,2007;Johnson&Onwuegbuzie,2004).
Contrastingly,qualitativepurists(e.g.,Guba&Lincoln,1989;Schwandt,2000)
generallyadvocateinterpretivismorconstructivism,bothunderpinnedbyabeliefin
multiplesubjectiveconstructionsofreality,meaningbroadgeneralisationsare
neitherdesirablenorachievable(Greene,2007;Guba&Lincoln,1989;Johnson&
Onwuegbuzie,2004).
Bothquantitativeandqualitativepuristsarguethattheseunderlying
paradigmaticdifferencesareinsurmountable(Greene,2007;Johnson&
Onwuegbuzie,2004).Pragmatism,however,eschewssuchmetaphysicalconcerns
andinsteadadoptsa“whatworks”epistemologicalapproach,eitherignoringor
settingasidethesedifferencesinordertofocusonfindingaworkableapproachto
theresearchproblem(Creswell&PlanoClark,2011;Miles&Huberman,1984;
Morgan,2007,2014).Asaresult,pragmatismoffersadvantagesinresearch
concerningthe“realworld”andhasgainedincreasingpopularityacrossthesocial
sciences(Bryman,2008;Morgan,2014).
Inparticular,thecurrentstudyutilisedmixedmethodspragmatisminorder
toaddressitsaims,drawingtogetherbothquantitativeandqualitativeinquiry
throughouttheentireresearchprocess,includingepistemology,datacollection,
analysis,andinferences.Althoughpragmatismisnotcommittedtoanyone
method,itisnowtheprimaryparadigmutilisedwithinmixedmethodsresearch
(Greene,2007,2008;Morgan,2007,2014).Itsemphasisonworkabilityaffords
researcherstheabilitytoblendapproaches(Johnson&Onwuegbuzie,2004;
Morgan,2014).Indeed,theparadigm’sadvocacyofpluralismnotonlyallowssuch
blendingbutactivelyplacesvalueontheuseofmultipleapproachesand,thus,
methods(Morgan,2014).Ontologically,apragmaticpositionassumesthat
knowledgeissubjectivelyconstructedbutisalsogroundedinasharedreality
(Creswell,2014;Johnson&Onwuegbuzie,2004).Recognitionofbothmultipleand
singularrealitiesenablesexplorationofnumerousworldviewswithinonestudy,

CHAPTERFOUR:METHOD
78
evenwheretheseofferdifferentorevenconflictingperspectives(Creswell&Plano
Clark,2011;Miles&Huberman,1984).Inthecurrentstudy,theadoptionof
pragmatismallowsinvestigationofthephenomenaofinterestthroughdifferent
lenses,thusdevelopingamorecomprehensiveunderstanding;these
epistemologicalperspectivesareexploredbelow.
4.3.2WiderTheoreticalPerspectives
Postpositivism
Postpositivismisaschoolofthoughtevolvedfrompositivism,andis
groundedprimarilyintheworkofPopper(1959)andKuhn(1962).Whilepositivism
assumesthatthereisanobjectiverealitythatcanbeobjectivelymeasured,
postpositivismtakesamorecriticalstance,whereinknowledgeofthisrealitycan
onlybeimperfectgiveninherentbiasesandbarrierswithintheresearchprocess
(Creswell,2014).Forexample,withinpostpositivism,aresearchhypothesisis
understoodtobeinformedbytheprevailingconsensusandpreviousresearchand
socannotbeobjective(Kuhn,1962;Popper,1959;Shadishetal.,2002).Inpart,the
rejectionofpositivismarosethroughincreasedempiricalattentiontophenomena
thatcouldnotbedirectlyobserved,includinghumanexperiencessuchasfeeling
andthinking(Mertens,2015),asisofinterestwithinthecurrentstudy.Thus,
postpositivistresearchdoesexploregenerallawsbutfocuseson“theory
falsification”,offeringprobabilisticinferencesratherthanabsolutetruths(Mertens,
2015;Ponterotto,2005;Popper,1959).However,thepursuitoffalsificationmust
itselfberecognisedasfallible(Kuhn,1962;Shadishetal.,2002);theapproach
assumesfirstlythatanycausalhypothesishasbeenperfectlyspecified,whichthe
natureoftheoryrendersimpossible,andsecondlythatthemethodsandmaterials
utilisedprovideanaccuratemeasurementoftheconstructofinterest(Kuhn,1962).
Thisindicatesaneedtoinvestigateahypothesisthroughmultipletheoretical
lenses,acrossheterogeneousconditionsandcontexts,andwithconsiderationof
potentialmediatingandmoderatingfactors(Shadishetal.,2002).

CHAPTERFOUR:METHOD
79
Thecurrentstudyadoptedpostpositivismasalenstoaddressresearch
questions(RQs)1a–dand2a–bastheyseektoaddressspecifichypothesesand
focusoninternalandperceivedprocessesthatcannotbedirectlyobserved.As
such,findingsrepresentprobabilisticclaimsandarecontextuallygroundedwithin
thestudy’ssampleandmethods.Furthermore,conclusionsarenotofferedas
singularfactsbutrepresentacontributiontothebroaderliteratureonrisk
exposure,adaptiveprocesses,andemotionalsymptomswithindifferentcontexts.
InterpretivePhenomenology
Phenomenologyisconcernedwiththewaythatconsciousbeingsinteract
with,andexperience,phenomena.Thus,phenomenologicalresearchseekstolearn
aboutaphenomenonbyaccessinganindividual’slivedexperienceofit(Moran,
2000;Smithetal.,2009).PhenomenologystemsfromtheworkofHusserl
(1927/1971),thoughthereareanumberofmorerecentvariationswhichcanbe
classifiedaseitherdescriptiveorinterpretiveinnature(Mayoh&Onwuegbuzie,
2015;Moran,2000).Descriptivephenomenologicalresearchiscloselyalignedwith
Husserl's(1927/1971)originalapproach,seekingtoexploreanddescribepersonal
experiencesinordertounderstandaphenomenonasitpresentsitself,thusgaining
an“insider’sperspective”(Lopez&Willis,2004;Mayoh&Onwuegbuzie,2015;
Moran,2000).Suchresearchstrivestobepurelydescriptiveandtokeepthevalues,
experiences,andpreconceptionsoftheresearcherfrominfluencingconclusions
(Lopez&Willis,2004;Moran,2000).
Interpretivephenomenologyrealignsthefocustotheindividualthemselves
andthewayinwhichtheymakesenseoftheirexperienceofthephenomenonof
interest(K.A.Lopez&Willis,2004;Smithetal.,2009).Thisapproachstemsfrom
Heidegger(1927/1962),whoexpandedphenomenologybyincorporatingthe
conceptofhermeneutics,orthestudyofmeaningandmeaningfulinterpretation.
Interpretivephenomenologypositsthattheinsider’sperspectivecontains
embeddedmeaningsthattheparticipantmayormaynotbeawareofand,
furthermore,thatareinfluencedbytheirlifeworld;thatis,theperson’sown
individualcontext(Biggerstaff&Thompson,2008;K.A.Lopez&Willis,2004;Smith
etal.,2009).Furthermore,thisformofphenomenologyisgroundedinthenotion

CHAPTERFOUR:METHOD
80
thatinaccessingandexploringanother’sexperience,theresearcherandtheir
worldviewisinherentlyimplicated,thusbringingan“outsider’sperspective”.The
influenceoftheresearcher’svalues,experiences,andpreconceptionsisconsidered
notonlyunavoidablebutalsovaluable,astheresearchermaybeabletogenerate
furtherinsightthroughtheprocessofinterpretation(Larkin&Thompson,2006;
Mayoh&Onwuegbuzie,2015;Pietkiewicz&Smith,2014;Smithetal.,2009).
Thecurrentstudyutilisedonevariationofinterpretivephenomenology,
interpretativephenomenologicalanalysis(IPA),inordertoaddressRQ3.IPAisan
approachconcernedwiththedetailedexplorationofpersonalexperienceand
understandingthewaysinwhichindividualsmakesenseofthisexperience(Smith,
1996,2004,2011a;Smithetal.,2009).Findingsrelatenottothephenomenonof
interestitselfbutrathertotheparticularindividual’sexperiencesand
understandingofthephenomenon(Larkinetal.,2006).Theapproachisshapedby
multipleinfluencesbutisprimarilyunderpinnedbythreekeyphilosophies,drawing
onbothHusserl's(1927/1971)phenomenologyandHeidegger's(1927/1962)
hermeneuticalongsideanidiographiccommitmenttothein-depthexplorationof
theparticular,ratherthanthecreationofgeneralisations(Smithetal.,2009).As
such,IPAattemptstounderstandasmallnumberofparticipants’individual
experiencesofagivenphenomenon,seekingtoidentifyboththatwhichisunique
andthatwhichissharedbetweentheiraccounts(Reidetal.,2005;Smithetal.,
2009).
ThefocusonindividuallivedexperienceinIPAreflectsanontological
assumptionthatthereisnofixedobjectiverealityand,thus,thatitisnecessaryto
accessothers’constructionsofrealityinordertodevelopunderstanding(Mayoh&
Onwuegbuzie,2015;Smithetal.,2009).Indoingso,theinteractionbetweenthe
participants’lifeworldsandtheresearcher’slifeworldisunderstoodtocreatenew
meaningsandinsight(Larkinetal.,2006;Pietkiewicz&Smith,2014).Itisimportant
tonotethattheinterpretationsdrawnfromthisprocessarenotassertedasfacts
butasinherentlycontextualfindings(Reidetal.,2005;Smithetal.,2009).Assuch,
thereisaneedforexplicitreflexivityofthewayinwhichtheresearcher’svalues,
experiencesandpreconceptionsinfluencetheresearchprocessand,thus,how

CHAPTERFOUR:METHOD
81
theseareimplicatedintheresultingfindings(Biggerstaff&Thompson,2008;Smith
etal.,2009;Willig,2013).
UnitingPostpositivismandInterpretivePhenomenologywithinaPragmatic
Approach
Puristswouldarguethattheseapproachescannotbeunitedwithinasingle
studyduetofundamentaldifferencesintheirmetaphysicalassumptions.For
instance,postpositivismassumesanobjectivereality(Creswell,2014;Kuhn,1962;
Popper,1959),whileinterpretivephenomenologypositsthatrealityisindividually
constructed(Mayoh&Onwuegbuzie,2015;Smithetal.,2009).Asnoted,froma
mixedmethodspragmatismperspectiveitisnotonlyacceptablebutevenvaluable
tosetasidethesedifferencesandbringtogethervariedapproachestofacilitatea
fullerunderstandingofagivenphenomenon.However,itcouldbearguedthat
thereareareasofsimilarityacrossthesetwoparadigms,particularlyintheir
applicationinthecurrentstudy.Althoughtheseworldviewsdifferintheir
assumptionsofreality,theyeachrecognisethatdatacannotofferarepresentation
ofasingularreality,giventhatpostpositivismrecognisesthatrealitycannotbe
perfectlymeasured(Creswell,2014).Thisisconsideredparticularlytruewhere
inquiryrelatestointernalhumanprocesses(Mertens,2015),asinthecurrent
study.Indeed,bothstrandsincorporateadistinctfocusonthewayinwhich
participantsperceiveandexperienceparticularphenomena.Thequantitative
strandnotonlyrecognisesthatfindingsinherentlyreflectsubjectiveappraisalsof
realitybutsetouttodosobydesign,givenitsfocusonself-reportedstress
appraisalprocesses,mentalhealthsymptomsthatlargelymanifestthemselves
internally,andtheinfluenceofperceivedaccesstoprotectivefactors.Not
dissimilarly,thequalitativestrandexploresthewayinwhichearlyadolescentgirls
experienceandmakesenseofthesamesymptomsandappraisetheirouterworlds.
Thus,regardlessofbeliefsaboutwhetherrealityitselfisobjectiveorsubjective,
bothsetsofinformationretainanexplicitemphasisonrealityasperceivedand
experiencedattheindividuallevel.Furthermore,ashasbeenexploredhere,
neitherstanceassumestheabilitytoprovideentirelygeneralisablefactsbut
insteadoffershighlycontext-specificinferencesrecognisedtobegroundedwithin

CHAPTERFOUR:METHOD
82
theparticularcircumstancesofthestudy.Inbothcasesthisspecificityextendsto
includeboththeresponsesoftheparticularparticipantsengagedinthestudyas
wellasrecognisingtheinherentinfluenceoftheresearcher’svaluesandbeliefs.
Assuch,theintegrationofbothpostpositivismandinterpretive
phenomenologywithinthecurrentstudyisnotconsideredproblematic.Thestudy
asawholehassoughttodrawtogetherthesedifferingapproachestoexplorea
particularsetofphenomenaasperceivedandexperiencedbyearlyadolescentgirls,
withone(postpositivism)providinganunderstandingofgeneralpatternsatan
overarchinglevelandtheother(interpretivephenomenology)offeringinsightinto
individualisedexperiences.Consistentwiththeuseofmixedmethodspragmatism,
theuseofeachoftheseapproachestogethercandeveloparicherandmore
meaningfulunderstandingoftheseparticularphenomena.Assuch,eachstrandhas
beencarriedoutwithsensitivitytotheparticularphilosophicalassumptionsthat
underpinthem,withattentiontothewayinwhichtheseshouldinformmethods
anddecisions.
4.4ResearchDesign
4.4.1MixedMethodsDesign
Apragmaticparallelmixedmethodsdesignwasutilisedtoaddressthe
researchaims,comprisingbothaquantitativeandaqualitativestrand.Consistent
withtheadoptionofpragmatismasanoverarchinglens,thisdesignwasguidedby
theresearchquestionsandmethodswereselectedtobestaddressthem.The
quantitativestrandaddressedRQs1a–dand2a–bgiventheirfocusonbroad
patterns,whilethequalitativestrandaddressedRQ3duetoitsinterestin
individuallivedexperience.
Greene,CaracelliandGraham(1989)outlinedfivekeypurposesformixed
methodsdesigns:(a)Triangulation,wherethestudyseeksconvergenceoffindings
acrossdifferentmethods;(b)complementarity,wherethestudyseekstoenhance
thefindingsofeachmethodwiththoseoftheother;(c)development,wherethe
findingsfromonemethodinformtheother;(d)initiation,wherethestudyaimsto

CHAPTERFOUR:METHOD
83
discovernewperspectivesorinterpretations;and(e)expansion,wheremixed
methodsareusedtoincreasethebreadthofinquiry.Mixedmethodswereutilised
heretofacilitatecomplementarityacrossfindings.Inacomplementaritydesign,
differentfacetsofthesamephenomenaareinvestigatedinordertodevelopa
morecompleteunderstandingofthephenomena,withtheintegratedstrands
consideredtoadduptomorethanthesumoftheirparts(Bryman,2006;Bryman,
Becker,&Sempik,2008;Greeneetal.,1989).Thisdesignseekstocapitaliseonthe
strengthsofeachmethodinordertooffsettheother’slimitations(Greeneetal.,
1989).Forexample,whilethetypicallydeductivenatureofquantitativemethodsis
usefulwheninvestigatingspecifichypotheses,theuseofinductiveinquirycanbeof
valueinexploringlessestablishedorcomplexphenomena(Johnson&
Onwuegbuzie,2004;Mertens,2015),asinthecurrentstudy.Additionally,different
methodsoffercontrastinglevelsoffocus,aswassoughtinthecurrentstudy;
CreswellandPlanoClark(2011)haveobservedthatquantitativeinquiryfocuseson
themanyandoverlookstheindividual,whilequalitativeinquiryfocusesonthe
individualandthusoverlooksthemany.Assuch,bothmethodswereutilisedto
directlyaddresstheirrespectivelimitationsandthusdevelopamore
comprehensiveunderstandingoftherelationshipbetweenmultipleriskexposure,
adaptiveprocesses,andemotionalsymptomswithinthispopulation.Greeneetal.
(1989)indicatedthatthisdesignmaybeenhancedbytheuseofmethodswithin
similarparadigms;however,theparticularfacetsbeingexploredinthetwostrands
ofthecurrentstudywarrantdifferingparadigmaticperspectivesinordertobest
addresstherespectiveresearchquestions.Thisapproachreflectsthecurrent
study’sadoptionofpragmatismanditsadvocacyforcombiningmultiple
worldviewsinthisway.
Aparallelmixedmethodsdesignencompassesthecollectionofdatafor
bothstrandsconcurrentlyandindependently,asopposedtoasequentialdesignin
whichtheapproachtoonestrandisinformedbyfindingsfromtheother
(Onwuegbuzie&Teddlie,2003;Tashakkori&Teddlie,1998).Thisisconsistentwith
thestudy’suseofmixedmethodstoaddressdifferentresearchquestionsandis
recommendedbyGreeneetal.(1989)forcomplementaritydesigns.Assuch,the

CHAPTERFOUR:METHOD
84
twostrandswereeachundertakenseparatelyandwerethenintegratedfollowing
analysisanddiscussiontocreatemeta-inferencesthatrepresentamore
comprehensiveunderstandingofthephenomenaofinterest(Creswell&Plano
Clark,2011;seeSection4.10fordetailsofintegration).Anequalweightapproach
wasutilised,whereineachstrandistreatedwithequalstatuswithinthe
overarchingstudy(Leech&Onwuegbuzie,2009;Moseholm&Fetters,2017).This
reflectstheequalprioritygiventobothstrandsinthecurrentstudyandthevalue
ofthedifferentinsightseachoffersinbuildingacomprehensiveunderstandingof
thephenomenonbeinginvestigated.Furthermore,ithasbeensuggestedthat
whereonestrandadoptsaphenomenologicallens,anequalweightapproachcan
beparticularlyvaluableincreatingabalancebetweeninductiveanddeductive
inquiry(Hefferon&Gil-Rodriguez,2011;Mayoh&Onwuegbuzie,2015).IPA
methodologistshavearguedthatitisvitaltoplaceequalorgreaterweightonan
IPAcomponentwithinmixedmethodsresearchinordertoreflectitsendeavourto
understandaphenomenonasexperiencedbytheindividual,ratherthanas
understoodbyothersorbytheory(Smith,2011a;Smithetal.,2009).Itshouldbe
notedthatalthoughthereisaproportionatelygreaternumberofresearch
questionsunderpinningthequantitativestrand(RQs1a–dand2a–b),thisisdueto
theirmoredeductivefocusondisaggregatedrelationships,whilethequestion
addressedwithinthequalitativestrand(RQ3)constitutesamoreinductiveinquiry
(seepage22forfullresearchquestions).
Ofcourse,mixedmethodsdesignsencompasssomechallengesand
limitations.Akeychallengeistheheighteneddemand,relativetomono-method
approaches,oftime,resources,andresearcherskills(Doyleetal.,2009),which
JohnsonandOnwuegbuzie(2004)havesuggestedcanbeexacerbatedwithin
concurrentdesigns.However,asbothstrandsinthecurrentstudydrewon
availabledatagatheredaspartoftheevaluationofHeadStart,thislessenedsuch
demandsindatacollectionandsoreducedtheoverallburdenoftheresearch.A
furtherlimitationoftencitedisthedifficultyinproducinganintegrated
representationoffindingsfrombothstrandsthatisaccessibleformixedaudiences

CHAPTERFOUR:METHOD
85
(Sandelowski,2003);efforthasbeentakentoovercomethisinthepresentationof
meta-inferences,asdetailedinSection4.10.
4.4.2QuantitativeStrand
ThequantitativestrandaddressedRQs1a–dand2a–b(aspresentedon
page22)andmadeuseofacross-sectionalobservationaldesign.Observational
researchinvestigatesreal-worldphenomenaandthusexploresinteractions
betweennaturallyoccurringvariables,ratherthanintroducingexperimental
manipulation(Carlson&Morrison,2009;Fife-Schaw,2012;Stroupetal.,2000).This
designisfrequentlyutilisedwithinepidemiologytoexploretheeffectsofexposure
tovariousfactors(vonElmetal.,2008,2014;Woodward,2014),asinthecurrent
study.Inacross-sectionalobservationaldesign,exposureandoutcomedatais
collectedatasingletimepointandprovidesa“snapshot”oftherelationships
betweenvariables(Woodward,2014).Thisdesigndoesnotallowanalysisof
temporalrelationshipsbetweenvariablesandsothereisaneedforcautionin
inferringcausality(Szklo&Nieto,2014;Woodward,2014).
VariablesintheQuantitativeStrand
Table4.1(overleaf)outlinesvariablesalongsidetheirfunctionandpurpose
forinclusion,anddetailsthemeasure,datasourceandmeasurementtype.For
conceptualspecificity,thestudyhasadjustedthelabelsrelatingtotheStudent
ResilienceSurvey(SRS)subscales,whichareutilisedtomeasurepromotiveand
protectivefactors.Examinationofthefacevalidityofthismeasureindicatedthat
theoriginalsubscalenamesdidnotcloselyapproximateitemcontent(seeSection
4.6.1).Similarly,inflatedprevalencelevelsfortheself-reportquestionusedto
assessyoungcarerstatusindicatedthatresponseswerelikelynotrepresentativeof
youngcarersasanarrowcategory.Assuch,forthepurposesofthecurrentstudy
thisvariablewasconsideredtoindicateabroadercategoryofyoungpeoplewho
identifiedashaving“caregivingresponsibilities”tosomeextent;thisisoutlinedand
reflecteduponfurtherinSection4.6.1.

CHAPTERFOUR:METHOD
86
Table4.1
VariablesintheQuantitativeStrand
Variable Function Purpose Measure Data
source
Measurement
type
Relativeage Predictor Riskmodelling Monthofbirth NPD Continuous
Academic
attainment
Predictor Riskmodelling KeyStage2
National
Curriculumtest
results2015/2016
NPD Continuous
SEN Predictor Riskmodelling SENstatus NPD Categorical
Familyincome Predictor Riskmodelling Freeschoolmeal
eligibility
NPD Categorical
Caregiving
responsibilities
Predictor Riskmodelling Youngcarer
statusself-report
question
WMF Categorical
ACEs Predictor Riskmodelling Childinneed
(CIN)status
NPD Categorical
Neighbourhood
socioeconomic
deprivation
Predictor Riskmodelling Income
Deprivation
AffectingChildren
Index(IDACI)
NPD Continuous
Emotional
symptoms
Outcome Outcome,
qualitative
participant
selection
process
Strengthsand
Difficulties
Questionnaire
(SDQ)emotional
symptoms
subscale
WMF Continuous
with
categorical
indicators
Perceived
stress
Mediator
variable
Indirecteffects
modelling
Four-item
PerceivedStress
Scale4(PSS-4)
WMF Continuous
with
categorical
indicators
Familyadult
connection
Predictor
and
moderator
variable
Promotiveand
protective
variable
SRS:Family
support
WMF Continuous
with
categorical
indicators
Schooladult Predictor Promotiveand SRS:School WMF Continuous

CHAPTERFOUR:METHOD
87
connection and
moderator
variable
protective
variable
support with
categorical
indicators
Community
adult
connection
Predictor
and
moderator
variable
Promotiveand
protective
variable
SRS:Community
support
WMF Continuous
with
categorical
indicators
Schoolpeer
connection
Predictor
and
moderator
variable
Promotiveand
protective
variable
SRS:Peersupport WMF Continuous
with
categorical
indicators
Active
engagementin
homeand
schoollife
Predictor
and
moderator
variable
Promotiveand
protective
variable
SRS:Participation
inhomeand
schoollife
WMF Continuous
with
categorical
indicators
Engagementin
extracurricular
activities
Predictor
and
moderator
variable
Promotiveand
protective
variable
SRS:Participation
incommunitylife
WMF Continuous
with
categorical
indicators
School/setting Cluster
variable
Promotiveand
protective
variable
Anonymised
schoolcode
NPD Nominal
Note.NPD=NationalPupilDatabase;SEN=specialeducationalneeds;WMF=WellbeingMeasurementFramework;SRS=StudentResilienceSurvey.
4.4.3QualitativeStrand
Thequalitativestrandofthecurrentstudyadoptedaninterpretive
phenomenologicaldesigntoaddressRQ3(aspresentedonpage22),specifically
guidedbyIPA,whichseekstounderstandthewayinwhichasmallnumberof
individualsmakesenseoftheirexperienceofaparticularphenomenon(Smith,
1996,2004,2011a).IPAisnotonlyananalyticaltechniquebutinsteadoffersan
overarchingframeworktoguidetheresearchprocess(Smithetal.,2009).Thus,use
ofIPAinformedmultipleelementsofthestudy,includingepistemology,
methodologyandmethodsusedtoaddressRQ3.

CHAPTERFOUR:METHOD
88
IPAvaluesdepthratherthanbreadth;ittypicallyutilisesasmallnumberof
participantsinlinewithitsidiographicstanceandseekstodevelopasmallnumber
ofrich,complexthemes(Hefferon&Gil-Rodriguez,2011;Reidetal.,2005).Analysis
focusesonpersonalaccountsoflivedexperience;here,accountsweregenerated
throughinterviews(seeSection4.6.2).Findingsrelatenottothephenomenonof
interestitselfbutrathertotheparticularindividual’sexperiencesand
understandingofthephenomenon(Larkinetal.,2006).Theapproachisinductive
andinvolvesgatheringexpansivedatathatallowstheemergenceofunanticipated
findings;itis,therefore,wellsuitedtoaddressingbroadresearchquestionsrather
thanthoseinvestigatingpreconceivedhypotheses(Larkin&Thompson,2006;
Smith,2004).AnIPAdesignwasdeemedmostappropriateforaddressingRQ3
givenitsfocusondevelopingunderstandingsofgirls’ownexperiencesoflifeinthe
contextofriskexposureandemotionalsymptoms.Furthermore,IPA’sin-depth
approachisconsideredparticularlyusefulwhenexploringcomplexphenomena
(Smith&Osborn,2015b;Wagstaffetal.,2014)andsowasutilisedtoprovidea
complementaryperspectivealongsidethequantitativestrand.
4.4.4IntegrationofQuantitativeandQualitativeStrands
Theintegrationofstrandsisafundamentalstageofmixedmethods
research,asitisthepointatwhichfindingsdoindeedbecome“mixed”(Bryman,
2007;Brymanetal.,2008;Johnson,Onwuegbuzie,&Turner,2007).One
considerationisthestageatwhichintegrationoccurs;asthecurrentstudyutilised
aparalleldesign,thedatafromthequantitativeandqualitativestrandswere
analysedindependentlyandinrelationtotheresearchquestionstheyeach
addressed.Thefindingsfromeachstrandwereeachdocumentedseparatelyand
werethensynthesisedafterinterpretingeachstrandindividuallytodevelopmeta-
inferences,consistentwithguidanceonintegratingconcurrentmixedmethods
(Johnson&Onwuegbuzie,2004;Moseholm&Fetters,2017;Tashakkori&Teddlie,
2003).Thisaimstoalloweachstrandtodevelopfullyandtosubsequentlybuilda
morecomprehensiveunderstandingofthephenomenaofinterest(Creswell,2014;

CHAPTERFOUR:METHOD
89
Creswell&PlanoClark,2011).Furthermore,thisstyleofintegrationisconsistent
withthestudy’suseofmixedmethodstosupportcomplementarity(Brymanetal.,
2008;Greeneetal.,1989).Withinthisdesign,theaimisthatthemeta-inferences
thataredrawnbybringingthetwostrandstogetheroffergreaterinsightintothe
phenomenaofinterestthanwhentheyarepresentedseparately;inotherwords,
togethertheybecomegreaterthanthesumoftheirparts(Brymanetal.,2008;
Creswell&PlanoClark,2011;Greeneetal.,1989).TeddlieandTashakkori(2006)
haveobservedthatalignmentbetweentherationaleforutilisingmixedmethods
andtheactualintegrationproceduresadoptedisakeycomponentofmixed
methodsresearch,asthestatedpurposeshouldactasaclearfunctionofthe
integrationprocess.However,misalignmentbetweenthetwoisacommonissue,
withmanysocialsciencearticlesutilisingacomparativeprocessthatrepresents
triangulationincaseswherethiswasnotthestatedpurpose(Bryman,2006).Given
thecurrentstudy’suseofdifferentmethodstoinvestigatedistinctfacetsofthe
samephenomena,andthuscreatecomplementarityoffindings,thepurposeofthe
integrationstagewasnottoidentifysimilaritiesordivergencesinfindingsasis
prioritisedintriangulationdesigns(Greeneetal.,1989).Instead,theemphasishere
isuponbringingtogetherfindingstocreateamorecomprehensiveunderstanding
ofthesephenomena.Finally,visualrepresentationsofmeta-inferenceswere
utilisedasthisapproachcanincreasetheaccessibilityoffindingstoreaders,
includingresearchersfromvaryingmethodologicalbackgrounds(Mayoh&
Onwuegbuzie,2015;Moseholm&Fetters,2017;Sandelowski,2003).Throughout
theintegrationprocess,thecurrentstudydrewontheinterpretiverigour
componentofTeddlieandTashakkori's(2009)integrativeframework,whichis
concernedwithintegritywithintheprocessofdrawingmeaningfrommixed
methods,tosupportqualityandrigour(seeSection4.11.3).
4.5Participants
4.5.1QuantitativeSample

CHAPTERFOUR:METHOD
90
Thequantitativesamplecomprisedearlyadolescentgirls,aged11–12years
atthetimeofdatacollection(March–July2017).Participantsweredrawnfromthe
largerHeadStartsamplebasedontheirageandrecordedsex(seeSection7.7.1for
reflectionuponsexandgenderinthecurrentstudy).Thetotalpossiblesamplefor
thecurrentstudywas8,327girlsfrom100educationsettingsacrossthesix
partnershipareas(Table4.2).Giventhatthesamplewasselectedfromthesix
HeadStartlocalauthority-ledpartnershipareas,varyingsociodemographic
backgroundswerecaptured;forexample,bothurbanandrurallocalitiesare
representedalongsidevaryingethnicandculturalareaprofiles.Thus,thesample
forthestudyisrepresentativeofarangeofsociodemographiccontextsanditwas
consideredlikelythatsomeparticipantswereexperiencinghighlevelsofrisk.
Educationsettingsincludedmainstreamsecondaryschoolsandasmallernumberof
specialschoolsandalternativeprovisionsettings(e.g.,pupilreferralunits)where
pupilsweredeemedabletoself-report.Thecurrentstudyincludedallgirlsaged
11–12yearsratherthanisolatingthosefromaparticulartypeofeducationsetting,
inlinewiththestudyaims,andeducationsetting-leveldemographicsarenot
exploredasthiswasnotofdirectinterest.However,clusteringiscontrolledforat
theschool/settinglevel(seeSection4.8).Clusteringattheschoollevel,ratherthan
attheclasslevel(i.e.,furtheraccountingforgroupingwithinschools),wastheonly
availableoptiongiventheavailabledatabutwasalsomostappropriategiventhe
focusonsecondaryschool-agedparticipants.Insecondaryschoolgroupingismore
fluidthaninprimaryschool,withpupilsengagingwithawiderangeofpeersand
adultsthroughouttheweek(West,Sweeting,&Young,2010).Assuch,accounting
forclusteringattheschoollevelwasconsideredmostappropriateforthissample.

CHAPTERFOUR:METHOD
91
Table4.2
NumberofEducationSettingsandParticipantswithinEachLocalAuthorityPartnershipArea
Anonymisedpartnership Numberofsettings Numberofparticipants
LA1 31 2,322
LA2 7 740
LA3 11 1,351
LA4 9 469
LA5 35 2,863
LA6 7 582
Note.Partnershipnameshavebeenanonymised.
SampleCharacteristics
Thesociodemographiccharacteristicsofthesamplewereconsidered
alongsidenationalnormsamongthechildandadolescentpopulation,where
available,andarepresentedinTable4.3toaidtransparency.Thesampleshowed
lowerratesofacademicattainment,ethnicminorityidentification,andSENstatus
comparedtothegeneralpopulation.Aslightlyhigherproportionofindividuals
wereeligibleforFSM.Notably,14.7%moreindividualsidentifiedthemselvesas
youngcarerscomparedtothenationalnorm.Thismaybeduetothestudy’suseof
self-reportforthischaracteristic(seeSection4.6.1);theimplicationsofthisinflated
prevalence,bothforthestudyandmorewidely,arediscussedinSections4.6.1and
7.3.1.

CHAPTERFOUR:METHOD
92
Table4.3
ProportionsofSampleStatisticsComparativetoNationalNorms
Characteristic
Sample
proportion
(%)
National
norm
(%)
Differencebetween
sampleandnational
norms(%)
Identifiedasethnicminority 22.2 29.1*a -6.9
IdentifiedasspeakingEnglishasanadditional
language
18.6 18.4*a 0.2
IdentifiedashavingSEN(withorwithouta
statementorEducation,HealthandCarePlan)
8.3 14.4†b -6.1
Currentlyeligibleforfreeschoolmeals 17.2 14.0†a 3.2
Lookedafterbylocalauthority 0.5 0.62†c -.12
Identifiedasayoungcarer 16.8 2.1†d 14.7
Achievedexpectedstandardsorhigheracrossall
testsatKeyStageTwostatutoryassessmenttests
57.0 61.0e,f 4.0
Note.TheethnicgroupnotesutilisedbytheNPD(Asian,Black,Chinese,MixedRace,anyotherethnicgroup)havebeencollapsedintothecategory“ethnicminority”forthepurposesofthistable.*denotesanaveragethatreferstoadolescentsonly;†denotesanaveragethatisrepresentativeofbothchildrenandadolescents.aDfE&ONS(2017).Schools,pupilsandtheircharacteristics:January2017.Nottingham,UnitedKingdom:DfE.bDfE&ONS(2017).SpecialeducationalneedsinEngland:January2017.Nottingham,UnitedKingdom:DfE.cDfE&ONS(2017).ChildrenlookedafterinEngland(includingadoption),yearending31March2017.Nottingham,UnitedKingdom:DfE.dONS(2013).Asummaryofunpaidcareby5to17-yearoldsinEnglandandWales.Retrievedfromhttp://webarchive.nationalarchives.gov.uk/20160107224205/http://www.ons.gov.uk/ons/rel/census/2011-census-analysis/provision-of-unpaid-care-in-england-and-wales--2011/sty-unpaid-care.htmleDfE&ONS(2017).Nationalcurriculumassessmentsatkeystage2inEngland,2017(revised).Nottingham,UnitedKingdom:DfEfThenationalnormutiliseddidnotprovideclearinformationastohowthisstatisticwasreached;specificallywhetherthisfigurereflectedpupils’averageachievementacrossallsubjectsorwhetherthisistheproportionofpupilswhoachievedexpectedstandardsacrosseachindividualsubject.Thecurrentstudyutilisedtheformerapproach.
Giventheuseofacommunitysample,participantsvariedintermsoftheir
levelsofemotionalsymptomsasmeasuredbytheStrengthsandDifficulties
Questionnaire(SDQ)emotionalsymptomssubscale.Ofthetotalsample,68.4%(n=
5,353)reportedexperiencingnormallevelsofsymptoms,10.9%(n=855)reported
borderlinelevels,and19.5%(n=1,621)reportedabnormallevels(inlinewith
guidanceforself-reportedmeasureswhere0–5isnormal,6isborderline,and7–10
isabnormal;SDQInfo,2016).Theremaining6%hadmissingdataacrossallitems(n
=498).Notethattheselevelsofsymptomsarenotablyhigherthantheself-report
normspublishedforthissubscaleinrelationtoBritishgirlsaged11–15,where

CHAPTERFOUR:METHOD
93
86.5%reportednormallevels,6.5%reportedborderlinelevels,and7%reported
abnormallevels(SDQInfo,2000).Ofcourse,thesenormsaredatedandgiven
indicationsofacurrentincreaseinemotionaldistressamongearlyadolescentgirls
maynolongerberepresentativeofcurrentlevelsofsymptomatology.
Nevertheless,thoughthisisnotaclinicalsampleitappearsthattheseare
participantswithelevatedsymptoms,whichisperhapsunsurprisinggiventhat
HeadStartareasareinvolvedduetovaryingtypesoflocaldisadvantage.
4.5.2QualitativeSample
Thequalitativesampleincludedthreegirlsaged12yearsfromtheoriginal
HeadStartqualitativesample,whowereidentifiedasexperiencingemotional
symptomsandrisk.
ThemainHeadStartqualitativesamplecomprised63youngpeopleinthe
baselineyear,ofwhom23identifiedthemselvesasfemaleandaged11–12years.
Eachareainvitedyoungpeoplewithvaryinglevelsof“risk”totakepart;the
partnershipareaseachutiliseddifferentdefinitionsofrisktoselectparticipants,
whichlikelycreatedvariationacrossthewidersample.Assuch,inselectingthe
sampleforthecurrentstudy,possibleparticipantsweresystematicallyassessedfor
risk,ratherthanutilisingpartnershipareas’classifications(seefollowingsection).
Table4.4(overleaf)providesabriefoverviewoftheconceptualisationsofriskinthe
fourareaswhereparticipantswereaged11–12yearsin2016/2017,inorderto
demonstratetheinclusioncriteriafortheHeadStartsample.Participantsintwo
otherHeadStartareaswerenotconsideredforinclusioninthecurrentstudyasthe
sampleinLA6didnotinclude11–12yearoldsandthequalitativeevaluationinLA4
didnotbeginuntilthefollowingyear.Forethicalreasonsitwasnotpossibleto
disclosetheareaeachparticipantinthecurrentstudywasfrom;Table4.4is
includedonlytodetailthecharacteristicsofthelargersample.

CHAPTERFOUR:METHOD
94
Table4.4
PartnershipAreas’ConceptualisationsofRiskusedtoSelectParticipants
Partnership Risklevel Conceptualisation
LA1 High Difficultiesidentified,suchasfamilyadversity,
anxiety,behaviourproblems
Low Nodifficultiespresent
LA2 High Engagedintargetedintervention
Low Nolowriskgroupwasengaged
LA3 High Engagedinintensivetargetedintervention
Medium Engagedinlessintensivetargetedintervention
LA5 High Difficultiesidentified,suchasfamilyadversity,
anxiety,behaviourproblems
Low Nodifficultiespresent
ParticipantSelectionProcess
Thecurrentstudyaimedtoengagethreetofiveparticipantsfromthe
broaderqualitativesample;aflexibleapproachwasadoptedasitwasnotknown
howmanyparticipantswereexperiencingemotionalsymptomsandrisk.Useofa
smallsampleistypicalinIPAduetoitsidiographiccommitmentandtheintensityof
analysis(Reidetal.,2005;Smithetal.,2009).Thissamplesizeisparticularlysmall,
thoughstillconsistentwithguidance,asIPAmethodologistshavehighlightedthat
focusingonaverysmallsampleallowsgreaterdepthinanalysisofeachcaseand
enablesrepresentationofmorenuancedfindings(e.g.,Brocki&Wearden,2006;
Reidetal.,2005;Smith&Osborn,2015).IPArequiresareasonablyhomogeneous
sample,limitedtothosewithsharedcharacteristicsorexperiencesrelevanttothe
researchquestion(Smith&Osborn,2015).Thus,additionalsamplingcriteriawere
utilisedtoselectHeadStartparticipantswithcharacteristicsandexperiences
consistentwiththefocusoftheresearchquestion:
1. Female,aged11-12years;
2. Experiencingemotionalsymptoms;and
3. Experiencingrisk.
CHAPTERFOUR:METHOD
95
Aparticipantselectionprotocolwasdeveloped,withaclearrationaleand
parametersforeachcriterionalongsidestepstoassessthese,andwasutilisedto
guidetheselectionprocess(AppendixB).Duetoethicalconstraints,itwasnot
possibletoaccessdemographicdatatoassessriskthroughavariable-based
cumulativeriskindexsimilartothatusedinthequantitativestrandofthestudy.
However,HeadStartinterviewswerefocusedentirelyonyoungpeople’slivesand
emotions(seeSection5.6.2)anditwasthereforepossibletoassesswhether
participantsmettheseinclusioncriteriausingtheirownaccounts.Thisalloweda
moreinductiveapproach,lessconstrainedbypresuppositionsofwhatconstituted
riskand,additionally,wasnotdependentontheavailabilityofdatarelatingto
specificriskfactorsandemotionalsymptoms.Anoutlineofthisprocess,alongside
themeasurestakentosupportrigour,ispresentedbelow.
Toselecttheparticipantsincludedforassessment,HeadStartinterviewers
utilisedtheprotocolasaguidetonominateHeadStartfemaleparticipantsaged11-
12yearsthattheyfeltdisclosedemotionalsymptomsintheinterview,suchas
feelingsofsadnessorexcessiveworry.Sixparticipantswerenominatedby
interviewers.Theresearcherreviewedthesesixtranscriptsforthesecondcriterion,
“experiencingemotionalsymptoms”,andratedparticipantsontheSDQadult
reportemotionalsymptomssubscale(Goodman,1997),consideringthree
characteristics:(a)Intensityofsymptoms,(b)frequencyofsymptomsasdescribed
bytheparticipant,and(c)frequencyofmentionofsymptomwithintheinterview.A
totalscoreoffiveormorewasconsideredindicativeofborderlinesymptomatology,
consistentwiththeteacherreportthresholdsforUKnorms(SDQInfo,2016).The
researcherthenconsideredthisscorealongsidetheyoungperson’sself-reported
totalscorefromthequantitativedatasettoreachafinaldecisiononwhethera
participantcouldbeconsideredtomeetthiscriterion.
Toreflectthestudy’sfocusonmultipleriskexposure,participantswere
consideredtomeetthethirdcriterion,“experiencingrisk”,iftheydemonstrated
threeormoreindicatorsof“risk”intheirlives.Thiscutoffreflectsindicationswithin
cumulativeriskresearchthatexposuretothreeormoreriskfactorsmayhavea
quadraticeffectonoutcomes(e.g.,Biedermanetal.,1995;Forehand,Biggar,&

CHAPTERFOUR:METHOD
96
Kotchick,1998;Jonesetal.,2002).Toassessthis,theresearcherreviewedeach
transcriptfortwotypesofriskindicators:(a)Mentionofriskfactorsestablishedin
theliteratureand(b)participants’self-perceivedsourcesofstress.
Theavailableevidencefortheinclusioncriteriawasthencollatedand
reviewedforeachparticipant.Itwasanticipatedthattheremaybeinstancesof
discrepanciesbetweendatasources,suchasmisalignmentbetweentheemotional
symptomsscoresgeneratedbytheresearcherandtheparticipant.Thiscouldoccur
forvaryingreasons,includinglimitationsofself-report,timelapsebetweenself-
reportmeasurecompletionandinterviewengagement,ortheresearcher’sown
perspectivesandunderstandingsinfluencingthewayinwhichtheyinterpreted
participants’disclosures.Itwasalsoanticipatedthattheremaybemissingdatafor
theself-reportscore.Assuch,thedecisiontoincludeagivenparticipantwasbased
onasummativejudgementoftheweightofevidence.Tosupportrigourwithinthe
selectionprocedure,theprocesswasdocumentedextensively,withwritten
justificationofhowparticipantsmetinclusioncriteria2and3alongsidesupporting
transcriptquotes(seeAppendixCforanexampledocument).Eachwritten
assessmentwasthenreviewedalongsidetheselectionprotocolbyasecondary
researcherwithknowledgeofriskandmentalhealthandbyanexternalpartywith
clinicaltraining,tosupporttheconfirmabilityofselectiondecisionsfrombotha
theoreticalandapracticalperspective,respectively.
Participants
OfthesixHeadStartparticipantsnominatedbyresearchersforassessment,
threewereidentifiedasmeetingtheinclusioncriteriaforthecurrentstudyandso
wereincludedforanalysis;theremainingthreeparticipantswereexcludedasthey
didnotmeetinclusioncriteria(seeTableD1,AppendixD).Thefollowingsections
presentabriefprofileforeachofthethreeincludedparticipants:Amelia,Jennifer,
andGrace(pseudonyms).
“Amelia”
Atthetimeoftheinterview,Ameliawasaged12yearsandninemonthsand
waslivingwithherparentsandherbrotherinadisadvantagedurbanareain

CHAPTERFOUR:METHOD
97
England.SheidentifiedasWhiteBritish.Ameliadescribedfeelinganxiousonadaily
basisandexplainedthatthisfrequentlycausedhertofeeldistress.Shecommented
severaltimesthatheranxietyseemedtobeworsening.Thesesymptomsappeared
particularlypresentinrelationtospecifictasks,suchasschoolwork,buttheywere
alsoevidentacrosselementsofherdailylife,suchastheappearanceofherclothes.
Ameliafocusedheavilyonheranxietyintheinterviewanddialogueoftenmoved
backtothisarea.BasedonAmelia’sdisclosureofhersymptomsintheinterview,
theresearcherdesignatedaborderlinescoreof5;aself-reportscorewasnot
available,asAmeliadidnotcompletetheWMF.Theresearcheridentifiedthree
knownriskfactorsinAmelia’sinterview:(a)Epilepsy(Daviesetal.,2003;Kariukiet
al.,2016),(b)academicdifficulties(McCarty,2008;Panayiotou&Humphrey,2018)
and(c)ObsessiveCompulsiveDisorder(OCD;NHS,2016).Inaddition,Amelia
describedoneself-perceivedsourceofstress;namely,herparentworkingin
London.
Thesecondaryresearcheragreedwiththeauthor’sjudgementsofAmelia’s
symptomsandrisk.TheclinicalrevieweragreedthatAmeliawasexperiencing
emotionalsymptoms,concludingthatshepresentedas“averytroubledgirlwith
lifelimitingworries.”
“Jennifer”
Atthetimeoftheinterview,Jenniferwasaged12yearsandthreemonths
andwaslivingwithherparentsandtwoyoungersiblingsinadisadvantagedurban
areainEngland.SheidentifiedherselfasAsian.Jenniferdisclosedthatshe
frequentlyhad“negativethoughts”,explainingthatshehaslowself-esteemand
self-confidence,andoftenfeelsdistressedinrelationtothesethoughts.She
describedfrequentanxietyaroundacademicworkandthesesymptomswerealso
presentinwideraspectsofherlife,suchasherfriendships.Jenniferdescribed
cryinginresponsetothesenegativethoughtstoletherfeelingsout.Muchofher
interviewwasfocusedonnegativethoughtsandthedialoguefrequentlymoved
backtothis.BasedonJennifer’sdisclosures,theresearcherdesignatedaborderline
scoreof5.Jennifer’sself-reportscorewas1,whichindicatesnormallevelsof
symptomatology.Asnotedabovethereareseveralpossibleexplanationsforsucha

CHAPTERFOUR:METHOD
98
discrepancy;howeveritshouldalsobenotedthatJenniferexpressedconsiderable
discomfortwithdisclosingfeelingstootherpeopleanditisplausiblethatshedid
notwishtoself-reportthis.Theresearcheridentifiedthreeknownriskfactors:(a)
Increasedacademicdemandsinsecondaryschool(Ryan,Shim,&Makara,2013;
Westetal.,2010),(b)lowself-esteem(Orthetal.,2008;Sowislo&Orth,2013),and
(c)perfectionisticbehaviours(Miloseva&Vukosavljevic-Gvozden,2014;Shafran&
Mansell,2001).Inaddition,Jenniferdescribedoneself-perceivedsourceofstress;
namely,difficultywithsiblingrelationships.
Thesecondaryresearcherwasinagreementwiththeauthor’sjudgements
ofJennifer’ssymptomsandrisk.TheclinicalrevieweragreedthatJenniferwas
experiencing“minorpsychologicalsymptoms”includinganxietyandsuggestedthat
whileshewouldnotmeetthresholdsforChildandAdolescentMentalHealth
Services(CAMHS),shewouldbeconsideredeligibleforschool-basedinterventions.
Givenuseofayoungcommunitysample,thecurrentstudydidnotprioritiseclinical
symptomatologyandinsteadfocusedonparticipantsexhibitingborderline
symptomsorgreater.Thus,Jenniferwasconsideredappropriateforinclusionwith
considerationoftheauthorandreviewers’judgements.
“Grace”
Atthetimeoftheinterview,Gracewasaged12yearsandfourmonthsand
waslivingbetweenherparents’separatehomesinadisadvantagedurbanareain
England,withherfatherashermainguardian.SheidentifiedasWhiteBritish.
Gracedescribedfeelingupsetandanxiousonadailybasis.Shefrequentlytalked
aboutthisinrelationtofeelingunsafeatschoolduetobullyingvictimisation.Grace
describedmultipleincidentsofdistressinherhomelifeduetofamilyconflict.She
disclosedthatshehadrecentlyhadabreakdowninalessonandreportedthatshe
hadoncetriedtoself-harm.Gracetalkedconsistentlyaboutdistressandanxiety
throughouttalkofherfamilyandschoolexperiencesandthisconstitutedalarge
proportionoftheinterview.BasedonGrace’sdisclosures,theresearcher
designatedanabnormalscoreof6;Gracereportedanabnormalscoreof9.The
researcheridentifiedfiveknownriskfactorsinGrace’sinterview:(a)Inter-parental
conflict(Brock&Kochanska,2015;HiuYapetal.,2014),(b)poormaternal

CHAPTERFOUR:METHOD
99
relationship(Branjeetal.,2010;Kim&Cicchetti,2004),(c)lowfamilyincome(Glied
&Pine,2002;Morrisonetal.,2014;Santiagoetal.,2011),(d)maternalalcohol
abuse(Christensen&Bilenberg,2000;McCauleyOhannessian,2012),and(e)
bullyingvictimisation(Bond,Carlin,Thomas,Rubin,&Patton,2001;Menesini,
Modena,&Tani,2016;Stapinski,Araya,Heron,Montgomery,&Stallard,2015).In
addition,Gracedescribedthreeself-perceivedsourcesofstress:(a)Safeguarding
issuesinwiderfamily,(b)argumentsandlackofprivacywithmother’sboyfriend,
and(c)extendedfamilybereavement.
Thesecondaryresearcheragreedwiththeauthor’sjudgementsofGrace’s
symptomsandrisk.TheclinicalrevieweragreedthatGracewasexperiencing
emotionalsymptoms,concludingthat“shedefinitelyhasunderstandableemotional
symptomswhich[cannot]improvewithoutaninterventionathome.”
4.6Materials
4.6.1QuantitativeMaterials
ThestudydrewonquantitativedatacollectedfortheHeadStartevaluation.
Thisincludeddemographicdataforriskmodellingandself-reportdatafromthe
WMFinrelationtoemotionalsymptoms,perceivedstress,andprotectivefactors
(asoutlinedinTable4.1,Section4.4.2).
ProxyRiskFactorIndicators
YoungRelativeAge
Thiswasmeasuredusingmonthofbirth,obtainedfromtheNPDand
expectedtobereliablegiventhatthisisroutinelycollectedandnotsubjectto
changeovertime.Consistentwithpastresearch(Goodmanetal.,2003;Patalayet
al.,2015),participantsweredividedintothreegroupsreflectingEnglishschool
entrydates;thoseborninSeptember–December(eldest),January–April(middle)
andMay–August(youngest).
LowandHighAcademicAttainment

CHAPTERFOUR:METHOD
100
Lowandhighacademicattainmentweremeasuredusingparticipants’
outcomesontheirmostrecentstatutoryassessments,theKeyStageTwoStatutory
AssessmentTests(SATs),completedbypupilsaged10–11yearsinEnglandduring
theirfinalyearinprimaryschool,approximatelyoneacademicyearpriorto
administrationoftheWMF.Thestudyutilisedscaledscores,convertedtestscores
reflectingstandardisedexpectations,whichrangefrom80–120,withascoreof100
orabovesignifyingexpectedstandards(DfE,2016b).Thestudycreatedacomposite
averagepointscore,reflectingoverallattainment;firstthemeanofparticipants’
EnglishreadingandGrammar,punctuationandspellingscoreswascalculatedand
thenthiswascombinedwithMathematicsscoretoobtainanoverallmean,
consistentwithguidance(DfE,2016a).Participantsinthelowestquartileofthe
averagepointscorewereconsideredtohavelowattainmentwhilethoseinthe
upperquartileweredesignatedashavinghighattainment.
SpecialEducationalNeeds(SEN)
SENstatuswasdesignatedforthoseidentifiedbytheNPDashavingSEN
withorwithoutastatementoranEducation,HealthandCare(EHC)plan.Atthe
timeofdatacollection,a“statement”wasaformaldiagnosisofSENinEngland,
whileEHCplanswereutilisedforchildrenandyoungpeopleconsideredtorequirea
greaterlevelofsupportthanthatofferedthroughstandardSENsupportavenues
(UKGovernment,n.d.).Here,SENstatushasbeendesignatedforparticipantsboth
withandwithoutastatementorplan,asindividualscanalsoberecognisedas
requiringSENsupportwithoutbeingformallyrecognisedinthisway(DfE,2018c).
Notethatpoliciesonidentificationandassessmenthavechangedsincethistime,
withallpupilswithastatementbeingtransferredtoEHCplansbyApril2018.
ParticipantswhowereidentifiedbytheNPDashavingSENduetomentalhealth
needswereremovedfromthisclassification(thatis,codedasnothavingSEN)given
thatthiswouldoverlapwiththeoutcomevariable,potentiallydrivinganyobserved
association.DuetothepointatwhichSENassessmentgenerallyoccurs,olderage
groupsaremorelikelytobeidentifiedandassessedashavingSEN,whichismost
prevalentamong11-15yearolds(DfE&ONS,2017).Assuch,itwasexpectedthata
highproportionoftheparticipantsinthecurrentstudywhotrulydohaveSEN

CHAPTERFOUR:METHOD
101
wouldhavebeenidentifiedassuchbythisage.However,itshouldbenotedthat
thisinformationmightnotbeaccurateforallparticipants,assomemayhave
undiagnosedneeds.
LowFamilyIncome
Participantswereidentifiedasbeingoflowfamilyincomeiftheywere
knowntohavebeeneligibleforfreeschoolmeals(FSM)atanypointsinceMay
2011upuntilthemostrecentcensus(Spring2017).PupilsinEnglandareeligibleif
theirparentsareclassifiedashavinglowincome,designatedbasedonthereceipt
ofincome-relatedsupportorreceiptofChildTaxCreditwithanannualincome
lowerthan£16,190(DfE,2012).NotethatFSMisusedasanindicatoroflowfamily
incomeratherthanofbroadersocioeconomicdisadvantageasthisinformation
cannotcapturepupilsexperiencingwiderdisadvantagedespitehigherincome
levels(Ilieetal.,2017;Taylor,2018).Bothcurrentandpreviouseligibilitywere
includedgivenevidenceoflong-termeffects(e.g.,Eamon,2002;Najmanetal.,
2010;Santiagoetal.,2011),thoughitshouldbenotedthateffectscanbemore
profoundforthosecurrentlyinreceiptofFSMrelativetothosepreviouslybutno
longereligible(Gorard,2016a).Here,bothcurrentandprioreligibilitywere
integratedintoasinglebinaryvariable(eligibleatsomepointintheprevioussix
years,ornevereligible)giventhatincumulativeriskresearch,riskisnotweighted
basedonsuchconsiderations.NotethatNPDinformationdenotesonlythosewho
haveclaimedFSM;researchhasestimatedthatanadditionalthreepercentof
pupilsareentitledtoFSMbutdonotclaimitandarethereforenotidentifiedin
censusdataaseligible(DfE,2012).Assuch,itislikelythatthereareasmallnumber
ofparticipantsincorrectlyidentifiedinthisstudyasnoteligibleforFSMand,thus,
notclassifiedasbeingoflowfamilyincome.
CaregivingResponsibilities
Thisriskfactor,initiallyconceptualisedas“youngcarerstatus”,was
measuredusingaself-reportquestionintheWMF.Participantsrespondedtoan
age-appropriatedefinitionofyoungcarerstatus,developedbyHeadStart
evaluatorsandCommonRoomyoungadvisors:“Youngcarersarechildrenand

CHAPTERFOUR:METHOD
102
youngpeopleunder18whoprovideregularorongoingcaretoafamilymember
whohasanillness,disability,mentalhealthconditionordrug/alcoholdependency.
Areyou,orhaveyoueverbeen,ayoungcarer?”Useofadefinitionaimedto
facilitateaccuracy,asitwasanticipatedthatparticipantsmightbeunfamiliarwith
theterm“youngcarer”.Researchsuggeststhatbroadquestionsaboutcaregiving
statusinflatesprevalenceestimates,whilespecifyingadefinitionalongside
examplesofconditionsorcircumstancescanproducestatisticssimilartomore
detailedmeasures(Banksetal.,2001).Thisapproachwaspreferabletolonger
measurestoavoidburdengiventhatyoungcarerstatuswasnotacentralfocus
withintheevaluationofHeadStart.
Here,16.8%ofparticipantsrespondedaffirmatively,substantiallysurpassing
bothconservative(2.1%;ONS,2013)andliberal(ca.8%;BBC,2010)UKprevalence
estimates.Whilesomeofthosewhorespondedaffirmativelymaybeyoungcarers,
andindeedgiventhefocusondisadvantagehigherratesmaybeexpected,it
appearedlikelythatalargeproportionoftheseparticipantsarenottrulyyoung
carersastypicallydefined,butidentifiedwiththedefinitioninsomeway.Given
this,thisvariablewasre-conceptualisedascapturingabroadercategoryof
individualswhoconsideredthemselvesashaving“caregivingresponsibilities”to
someextent.ThiswasalsoinformedbyfieldnotesfromWMFpiloting,asyoung
peoplefrequentlyaskedresearcherswhatconstitutedyoungcarerstatus,including
questioningaboutcaregivingresponsibilitiessuchascaringforsiblingsor
supportingaparentactingasacarer.
AdverseChildhoodExperiences(ACEs)
ACEsweremeasuredusingCINstatus.UnderSection17oftheChildrenAct
(1989),achildoradolescentisconsideredinneedifitisdeemedthat:(a)Theyare
notlikelytoachieveortomaintainreasonablehealthanddevelopmentwithout
localauthorityservicesandsupport,(b)theirhealthanddevelopmentislikelytobe
substantiallyimpairedwithoutlocalauthorityservicesandsupport,or(c)theyhave
adisability.Suchissuesareidentifiedthroughnarrowercriterion;thecategories
recordedintheNPDare(a)Abuseorneglect,(b)child’sdisability/illness,(c)
parentaldisability/illness,(d)familyinacutestress,(e)familydysfunction,(f)
CHAPTERFOUR:METHOD
103
sociallyunacceptablebehaviour,(g)lowincome,(h)absentparenting,(i)cases
otherthanchildreninneedand(j)notstated.Thoughsomeofthesecategories
overlapsomewhatwithotherriskfactorsinthestudy(SEN,lowfamilyincome,and
caregivingresponsibilities),inspectionindicatedlimitedvariableoverlap,indicating
differentialriskgroups.Forexample,of17participantsidentifiedasinneeddueto
childdisability/illness,onlyfourwereidentifiedashavingSEN,suggestingthatCIN
identifiedseparatecircumstances.
CINstatusisdesignatedthroughassessmentbyasocialworker,typically
followingreferralbyaneducation/caresetting,andsoisanescalatedresponse
goingbeyondearlyintervention(Walker,2018).ACINplanisthendeveloped,
detailingservicestobeprovidedforaminimumofthreemonths,andisreviewed
afterthreemonthsandthenatleasteverysixmonthsuntilthechildisnolonger
consideredinneed(ChildLawAdvice,2018;HMGovernment,2015).CINstatusis
recordedannually,withinformationinthecurrentstudyrecordedtoreflect
whetherCINstatuswasinplaceasof31stMarch2017(DfE,2018a,2018b).
ACEsaretypicallymeasuredusingachecklist-stylequestionnairewherein
participantsdisclosureexposuretospecificexperiences,oftenincluding“childhood
physicalabuse”,“householdsubstanceabuse”,“householdmentalillness”,and
“exposuretodomesticviolence”(Hughesetal.,2017).Suchdisaggregated
informationwasnotsoughtasitwasnottheprimaryconcernwithintheevaluation
ofHeadStart;furthermore,suchquestionnairesaretypicallydesignedforadultsor
olderadolescentsandposeethicalissueswithyoungerparticipants.AsACEs
essentiallycaptureparticularelementsoffamilydysfunctionandchildhood
maltreatment(Hughesetal.,2017;Youssefetal.,2017),CINstatuswasconsidered
anappropriateproxy,offeringcurrentinformationratherthanrelyingonrecall
throughhistoricalself-disclosure.
NeighbourhoodSocioeconomicDeprivation
ThiswasmeasuredutilisingIDACIscores,whichmeasurethelocal
proportionofchildrenandyoungpeopleaged0–15yearsinlowincomefamilies,
includingthoseinreceiptofincome-relatedbenefits(DepartmentforCommunities

CHAPTERFOUR:METHOD
104
andLocalGovernment&ONS,2015).Scoresarecalculatedforeachofthe32,844
Lower-LayerSuperOutputAreasinEngland,whicharelocalisedareas
correspondingtopostalcodes(ONS,2012).TheIDACIscorerangesbetweenzero
andone,withgreaterscoresindicatinggreaterneighbourhoodsocioeconomic
deprivation.Thisstatisticisupdatedseveraltimesayear;thecurrentstudyutilised
scoresrecordedinSpring2017,immediatelypriortoadministrationoftheWMF,so
scoreslikelyreflectcompositionatthetimeofsurveycompletion.TheIDACIisa
somewhatnarrowproxyasitmeasuresonlyonedimensionofneighbourhood
socioeconomicdeprivation,howeveritisfrequentlyusedinthiswayforchildand
adolescentresearch(e.g.,Emerson,2012;HowardWilsheretal.,2016;Rasbashet
al.,2010).
Self-ReportMeasurement
Self-reportdatawasdrawnfromHeadStartforparticipants’emotional
symptoms,perceivedstress,andprotectivefactors(measuresareshownin
AppendicesG–I).Thisapproachreflectsgrowinguseofself-reportmeasureswith
childrenandadolescents,givenrecognitionthatthispopulationhasunique
knowledgeoftheirownsymptomsandexperiences(Deightonetal.,2014;Riley,
2004),particularlyforinternalisingdifficulties(e.g.,DeLosReyes&Kazdin,2005;
Kaurin,Egloff,Stringaris,&Wessa,2016).Participantscompletedthesemeasures
aspartofthebroaderWMF,whichincludedanumberofsurveysfocusedon
wellbeing,mentalhealth,andresilience,inlinewiththekeyaimsoftheHeadStart
programmeandevaluation.TheWMFwaspilotedineighteducationsettings(both
mainstreamandalternative)priortoitsrolloutforthemainevaluation,toexplore
recommendationsforimprovementfromyoungpeopleandtoconfirmthevalidity
andreliabilityofmeasures(AppendixEdescribeschangesmadefollowingpiloting).
TheWMFwascompletedinteacher-facilitatedclasses,ausefulapproach
givenindicationsthatclassroomcompletioncanyieldmorevalidprevalence
responsescomparedtoathome(Breneretal.,2006).Supportingmaterialswere
developedtoaidthisprocess,includingashortvideoinwhichyoungpeople
explainedkeyinformationtobeshowntotheclassbeforehand,alongsideguidance
forteacherscontainingkeyinformation,answerstofrequentlyaskedquestions,

CHAPTERFOUR:METHOD
105
andacompletionchecklist(seeAppendixF).TheWMFwascomputer-
administered,offeringgreaterresearchercontrol,collectionoflarge-scaledata,and
reducedhumanerror(Patalayetal.,2016).Participantswererestrictedtoone
responseoptionandcouldaccessdefinitionsofcommonlymisunderstoodwords
(e.g.,optimistic).Anaudioaccompanimentwasavailabletoallowparticipantswith
readingdifficultiestotakepartwithoutsupportfromanadditionalpersonandthus
reduceviolationsofprivacy.Evidencegenerallyindicatessimilarlevelsofsocial
desirabilityacrosscomputer-andpaper-administratedsurveys(Dodou&De
Winter,2014),thoughthisgenerallyrelatestoadultsatpresent.Itremainsunclear
howconsistentpsychometricpropertiesareacrossadministrationmodes(Patalay
etal.,2016);thus,theinternalconsistencyandfactorstructureofeachmeasureis
exploredandpresentedherealongsidepriorevidence.Themeasuresutilisedhere
wereadministeredaspartofawiderinventoryofmeasureswithintheWMF(i.e.,
wellbeingsurvey,widermentalhealthsubscales,emotionregulationscale,and
internalprotectivefactorsubscales).Toreduceordereffects,random
counterbalancingwasimplementedbypresentingthewellbeingsurveyfirstand
protectivefactorquestionslast,orviceversa.Thoseinspecialistprovisionsalways
accessedthewellbeingmeasurefirstforethicalreasons.
Thefollowingsubsectionsoutlinetheself-reportmeasuresusedalongsidea
briefsummaryofexistingevidencefortheirpsychometricproperties,drawingon
guidancefromTerweeetal.(2007).
TheStrengthsandDifficultiesQuestionnaire(SDQ):EmotionalSymptomsSubscale
Emotionalsymptomswereassessedusingthecorrespondingsubscaleofthe
SDQ,a25-itemself-reportmentalhealthmeasurewithafive-factorstructure
comprisingemotionalsymptoms,conductproblems,hyperactivity,peerproblems,
andprosocialbehaviour(Goodman,Meltzer,&Bailey,1998).Theemotional
symptomssubscale(AppendixG)includesfiveitems(e.g.,“Iamoftenunhappy”;
Goodmanetal.,1998).Participantsrespondonathree-pointscaleof“nottrue”,
“somewhattrue”,and“certainlytrue”;thesearescoredas0,1,and2,respectively,
andsummedtocreateatotalscoreof0–10,where10denoteshighlevelsof
emotionalsymptoms.Theself-reportversionisdesignedforadolescentsaged11+

CHAPTERFOUR:METHOD
106
yearsandresearchdemonstratessuitabilityforthisagegroup(e.g.,Goodman,
Ford,Simmons,Gatward,&Meltzer,2000;Muris,Meesters,Eijkelenboom,&
Vincken,2004).
TheSDQsatisfiescriteriaforcontentvaliditysetoutbyTerweeetal.(2007);
itemdevelopmentwasguidedbydiagnosticcriteriaandexistingmentalhealth
measures,andthemeasurehasacleartargetpopulationandcandistinguish
betweencommunityandclinicalsamples(Goodmanetal.,1998).Themeasure
demonstratessatisfactoryconstructvalidity,correlatingwellwithothermental
healthindices(Goodman,2001;VanRoy,Veenstra,&Clench-Aas,2008)and
measuresofpsychopathologyanddisorder(Goodmanetal.,2000;Murisetal.,
2004).Initialresearchshowedsatisfactoryinternalconsistencyfortheemotional
symptomssubscale(α=0.75;Goodmanetal.,1998).
TheFour-ItemPerceivedStressScale(PSS-4)
Perceivedstresswasassessedusingthefour-itemPerceivedStressScale
(PSS-4;AppendixH),aself-reportmeasurecomprisingfouritems(e.g.,“inthelast
month,howoftenhaveyoufeltthatyouwereunabletocontroltheimportant
thingsinyourlife?”;Cohen,Kamarck,&Mermelstein,1983).Participantsrespond
onafive-pointscale,marking0for“never”,1for“almostnever”,2for
“sometimes”,3for“fairlyoften”and4for“veryoften”.Themeasureincludestwo
reverse-wordeditems,withallscoresthencodedadditivelytocreateatotalscore
of0–16,whereahighscoreindicateshigherperceivedstress.ThePSS-4was
designedforadultsbutresearchhasusedlongerversionsofthescalewith
adolescents(e.g.,Martin,Kazarian,&Breiter,1995;Siqueira,Diab,Bodian,&
Rolnitzky,2000).
ThePSS-4isashort-formderivedfromthelonger14-itemPSS,a
unidimensionalglobalmeasureofself-reportedappraisalofnonspecificlifestress
(Cohenetal.,1983).Themeasureshowscontentvalidityasitalignswiththeory
thatthedegreetowhichlifeeventsinfluenceoutcomesfluctuatesbasedonhow
oneperceivestheirstressfulness(Cohenetal.,1983).Arangeofstudieshave
identifiedanassociationbetweenthePSS-4andconcurrentemotionalsymptoms

CHAPTERFOUR:METHOD
107
(e.g.,Herrero&Meneses,2006;Karametal.,2012),indicatingconstructvalidity.
However,findingsregardingthefactorstructureofbothshorterandlongerforms
ofthePSShavebeenmixed,withsomereportingsupportfortwofactors,
“perceiveddistress”and“perceivedcoping”,correspondingtothepositively
wordedandreversedwordeditems,respectively(González-Ramírezetal.,2013;
Leungetal.,2010;Wu&Amtmann,2013).Arecentstudyalsoidentifiedsupport
fora2-factorstructureamonganadolescentcohort(Demkowicz,Panayiotou,
Ashworth,Humphrey,&Deighton,2019).Thoughinitialresearchshowed
satisfactoryinternalconsistency(α=.72;Cohenetal.,1983),researchhasnot
consistentlysupportedthis(Lee,2012).Assuch,thefactorstructureandinternal
consistencyofthismeasurewasassessedpriortothemainanalysistoexamine
whetheraunidimensionalor2-factorstructureshowedbestfittothedata(see
Sections4.8and5.2).
TheStudentResilienceSurvey(SRS)
Hypothesisedpromotiveandprotectivevariableswereassessedusingsix
subscalesfromtheSRS(Sun&Stewart,2007;AppendixI).Theoverallmeasure
showscontentvalidityasitexploresempiricallyestablishedprotectivefactors(Sun
&Stewart,2007),consistentwithcurrentunderstandingsofresilience(Lereyaet
al.,2016;Sun&Stewart,2007).Typically,thisisa47-itemmeasurewitha12-factor
structure;however,toreduceburdenthecommunicationandpro-socialpeers
domainswerenotincludedintheWMFgivenissueswithcontentvalidityand
similaritywithotherdomains.Thecurrentstudywasfocusedonexternalprotective
factorsrelatingtosocialconnectionandactiveengagementanddrewonsubscales
relatingtothesedomainsonly;assuch,theinternallyfocusedself-esteem,empathy
andproblem-solvingsubscaleswerenotutilised.
Assuch,31itemsacrosssixsubscaleswereincludedinthecurrentstudy:
Familyadultconnection,schooladultconnection,communityadultconnection,
schoolpeerconnection,activeengagementinhomeandschoollife,andschoolpeer
support.However,examinationoftheitemsindicatedthattheoriginalsubscale
namesdonotconsistentlyreflectrespectiveitemcontent.Thecurrentstudyhas
thereforeadjustedthenamesofsubscalestomorecloselycapturethenatureof

CHAPTERFOUR:METHOD
108
theitemsthereinandimprovecontentvalidity,achievedthroughongoing
discussionwiththesupervisoryteam(seeTable4.5).
Table4.5
StudentResilienceSurveyAdjustedSubscaleNamesandRationale
Originalname
(Sun&
Stewart,
2007)
Adjusted
name
Itemcontent Rationaleforadjustedname
Family
support
Familyadult
connection
Fouritems(e.g.,“athome,
thereisanadultwho
believesthatIwillbea
success”)
Foritemsacrossfamily,school,and
community,contentgenerally
capturessocialconnectionrather
thanconsistentlyfocusingonactive
supportbehaviours(seeitem
content);givenaconceptual
distinctionbetweentheseconstructs
(Barrera,1986)allnameshavebeen
adjusted.Furthermore,items
specifiedadultsandsonameshave
beenclarifiedtoreflectthis.
School
support
Schooladult
connection
Fouritems(e.g.,“at
school,thereisanadult
wholistenstomewhenI
havesomethingtosay”)
Community
support
Community
adult
connection
Fouritems(e.g.,“away
fromschool,thereisan
adultwhoItrust”)
Peersupport Schoolpeer
connection
Thirteenitems(e.g.,“are
therestudentsatyour
schoolwhowouldinvite
youtotheirhome?”)
Asbefore,itemsrelatetoconnection
ratherthansupportandask
specificallyaboutstudentsatschool
ratherthangeneralpeers(e.g.,
neighbourhoodpeers).
Participation
inhomeand
schoollife
Active
engagement
inhomeand
schoollife
Fouritems(e.g.,“Ihelp
myfamilymake
decisions”)
Thiswasadjustedtoactive
engagementtomorecloselyreflect
itemcontentfocusedonagency,
decision-making,andactive
contributions,thusemphasising
beingactivelyembeddedwithin
theseareasofliferatherthansimply
takingpart.
Participation
incommunity
Engagement
in
Twoitems(“Itakelessons
inmusic,art,sports,or
Itemsdidnotconsistentlycapture
“community”astheyincluded

CHAPTERFOUR:METHOD
109
life extracurricular
activities
haveahobby”) examplespotentiallyrelatingtoone-
to-onelessonsorunaccompanied
hobbies(e.g.,drawing).Thiswasthus
reconceptualisedasengagementin
extracurricularactivities.
Participantsrespondonafive-pointscale,marking1for“never”upto5for
“always”.Subscalesaresummedtogeneratetotalscores,withhigherscores
indicatinggreaterperceivedfactorexposure.TheSRSisdesignedforindividuals
aged11+yearsandevidenceindicatessuitabilityforthisagegroup(Lereyaetal.,
2016;Sun&Stewart,2007).TheSRSshowssatisfactorycontentvalidityasitwas
guidedbytheoryandexistingmeasuresofprotectivefactorsforadolescentsand
underwentpilottestingforitemdevelopment(Sun&Stewart,2007).Themeasure
showsconstructvalidityhavingbeennegativelyassociatedwithemotional
symptoms(Lereyaetal.2016).TheSRShasshownasatisfactorylevelofinternal
consistency,withpaststudiesreportingα=0.92fortheoriginaloverallscale(Sun&
Stewart2007)andalphasrangingfrom0.74to0.93fortheculturallyadapted
subscalesincludedinthecurrentstudy(Lereyaetal.2016).
4.6.2QualitativeMaterials
Interviews
Thestudydrewonqualitativedatacollectedfortheevaluationof
HeadStart.Dataweregatheredthroughin-depthinterviews,inwhichthe
researcherfacilitatesdiscussionoftheparticipants’experiencesandperceptionsof
agivenphenomenontoelicitarichfirst-personaccount(Patton,2015).Interviews
weresemi-structured,whereinresearchersareguidedbyaninterviewschedulebut
areabletoberesponsivetoparticipants’narratives(Brinkmann,2014;Harding,
2013;Langdridge,2007).ThisisthepreferreddatacollectionmethodforIPAasit
facilitatesdetailedandcomprehensiveaccountsofparticipants’livedexperience
(Smithetal.,2009;Smith&Osborn,2015a)andoffersparticipantsgreatercontrol
overthediscussion(Eatough&Smith,2008).Theapproachalsoallowsresearchers
toclarifytheirunderstandingofparticipants’responsesthroughout,whichsupports

CHAPTERFOUR:METHOD
110
thecollectionofhighqualitydata(Brinkmann&Kvale,2015;Britten,1995)andis
particularlyimportantinresearchwithchildrenandyoungpeople(Smith&
Dunworth,2003).However,methodologistshaveidentifiedchallengesacrossthe
method;forinstance,althoughtheflexibilityforresponsivenesstotheparticipant
canbevaluable,thisrequiresahighlevelofskill(Brinkmann&Kvale,2015).Inthe
evaluationofHeadStart,allinterviewershadpriorexperienceofinterviewing
childrenandyoungpeopleandhadundertakenappropriatetraining.Theuseofa
flexibleinterviewschedulecanalsolimitthescopeforcomparisonacross
participants’responses(Patton,2015),thoughthiswasnotproblematicheregiven
theidiographicnatureofIPA.
Allinterviewswerecarriedoutinaone-to-oneformat,asispreferredinIPA
research,asthissupportsrapportandenablesalevelofpersonaldiscussionthat
elicitsrichexperientialdata(Reidetal.,2005).Interviewswereconductedface-to-
faceasthisfacilitatesnaturalnessandtrust,whichisimportantwhenexploring
sensitivetopicssuchasmentalhealth,andcangeneraterichdatabyenabling
nonverbalandparalinguisticcommunication(Irvineetal.,2013),particularlyfor
youngerparticipants(Vogl,2013).
InterviewSchedule
AninterviewschedulewasdevelopedbytheHeadStartevaluationteam
(seeAppendixJ)withsupportfromCommonRoomyoungadvisors.Thekeyaimsof
theinterviewschedulefortheevaluationofHeadStartweretounderstand:
1. Howtheparticipantwasexperiencinglife;
2. Howtheparticipantexperiencedandcopedwithemotions;
3. Howtheparticipantexperiencedandcopedwithproblems;and
4. Theparticipant’sperceptionsandexperiencesofsourcesofsupport.
Theseaimsshapedthetopicsintheinterviewschedule,withquestionsdesignedto
elicitparticipants’perceptionsandexperiencesoftheseareas.Thirteenquestions
weredeveloped,eachwithsuggestedpromptsfortheinterviewer.Questionswere

CHAPTERFOUR:METHOD
111
designedtobeopen-endedandneutral,avoidingassumptivephrasingthatmay
leadtheparticipant(DiCicco-Bloom&Crabtree,2006;King&Horrocks,2010).
Differentkindsofquestionswereutilisedtoelicitdifferenttypesofaccountsand
reflections;(Patton,2015)outlinedsixbroadcategoriesofinterviewquestions,all
ofwhichwereutilisedintheinterviewschedule:(a)Experienceandbehaviour
questionsaimingtoelicitaccountsofbehaviours,actionsandexperiences,(b)
opinionandvaluequestionsfocusingonunderstandingsandinterpretations,(c)
feelingquestionsexploringemotions,(d)knowledgequestionsinquiringabout
knowledgeonagivensubject,(e)sensoryquestionsbuildingonexperienceand
behaviourquestionsbyelicitingaccountsofsensorystimuliand(f)
background/demographicquestionsidentifyingandexploringtheparticipant’s
characteristicsandunderlyingperceptionsofthese.Forexample,a“feelings”
questionthatrelatedtothe“emotions”topicwas“whatsortsoffeelingsor
emotionsdoyouexperiencewhenyouarenotfeelinghappy?”Possibleprompts
hereencouragedtheparticipanttounpacktheemotionbyaskingformoredetail,
orexploringexamples,forinstance“Howdoesthisaffectyourlife/makeyoufeel?”
and“Canyouthinkofanexampleofwhenyouwerefeeling[namedemotion]
recently?Whathappened?”Useofpromptsprovidesadditionalguidanceonthe
typeofinformationthatthequestionseekstoelicitandfacilitatesahighlevelof
detailandcomprehensiveness(King&Horrocks,2010).
Furtherconsiderationwasgiventothesequencingoftopicsandquestions
withintheschedule.Whileuseofasemi-structuredinterviewnecessitatesflexibility
intheorderinwhichtopicsareaddressed,guidancesuggeststhatparticular
elementsshouldremainrelativelyfixedtosupportdataqualityandtoavoidburden
ordistress(Patton,2015).Therefore,thebeginningandendsectionsofthe
scheduleaddressedmoreneutraltopics,whilesensitivetopicswereexploredinthe
middleportionoftheinterview.Toeasetheparticipantintotheprocess,itis
advisabletobeginbyaskingparticipantstodescribearecentactivityorexperience
(Patton,2015);here,thefirstquestionwas“whatdoyoulikeaboutbeingat
school?”Theconcludingquestionaskedtheparticipanttoreflectonwhatadvice
theywouldgivetoafriendexperiencingabroadhypotheticalissue,suchasa

CHAPTERFOUR:METHOD
112
problemathome,toallowparticipantstocreatedistancefromthetopicsjust
discussed.
WhiletheaimsoftheHeadStartqualitativeevaluationdifferfromthatof
thecurrentstudy,thetopicsaddressedininterviewsreflectthefocusofRQ3andit
wasexpectedthatthiswouldgenerateappropriatedataintermsofcontentand
depth.Assuch,participants’overarchingaccountswereutilisedinanalysis,rather
thanisolatingdatafromaspecificsubsetofquestions.Furthermore,theinclusion
ofvaryingtypesofquestionsandtheuseofopen-endedandneutralphrasing
reflectguidancefordesigningascheduleforuseinIPAinterviews(Smithetal.,
2009;Smith&Osborn,2015).Itshouldalsobenotedthattheauthorofthecurrent
studywaspartofthequalitativeevaluationteaminHeadStartandsowasinvolved
inthedevelopmentoftheinterviewschedule.Assuch,therewasongoing
considerationanddiscussionthroughoutthedesignprocessoftheuseofIPAwithin
thecurrentstudyinordertoensurecompatibilitywiththisapproach.
4.7Procedure
4.7.1QuantitativeProcedure
DataCollection
Atleasttwoweekspriortoquantitativedatacollectionparents/carerswere
providedwithaninformationpack(AppendixK)containinganinformationsheet
andanopt-outconsentform(seeSection4.12.1).Participantswerepresentedwith
thisinformationinage-appropriatelanguagepriortobeginningtheWMFandgave
informedassentbytickingaboxtoproceed(AppendixL).
ParticipantscompletedtheWMFinMarch–July2017andsociodemographic
datawasprovidedfromtheNPDinAugust2017(seeSection4.12.1fordetailsof
theconsentprocess).ParticipantscompletedtheWMFthroughasecureonline
systemoncomputersorsimilardigitaldevicesinteacher-facilitatedclassesintheir
educationsettings.Duetothelargesamplesize,itwasnotfeasibleforresearchers
tobepresentforthecompletionofsurveysbut,aspreviouslynoted,education
staffreceivedguidancetoaidtheminfacilitatingcompletion.

CHAPTERFOUR:METHOD
113
DataManagementandPreparation
ParticipantsaccessedtheWMFusingarandomlygeneratedcodeassociated
withparticipants’pupilmatchingreferencenumber,auniqueanonymisedcode
allowingresponsestobelinkedwithdemographicdata.Anonymiseddatawasthen
extractedforthecurrentstudyandpreparedforanalysis;rawitemscoreswere
reversedwhererequired,specificallytwoitemsonthePSS-4,andtotalscoreswere
calculatedforeachscaleorsubscaleused.
4.7.2QualitativeProcedure
InterviewProcedure
HeadStartinterviewparticipantsreceivedanage-appropriateinformation
sheet(AppendixM)andapackforparents/carers(AppendixN)includingan
informationsheetandaparentalconsentformandwereinformedthattheywould
receivea£10shoppingvoucheraftertheinterviewasathankyou(seeSection
4.12.1forethicalconsiderations).BetweenMayandJuly2017,participants
engagedinaone-to-oneinterviewinaprivateandquietspaceintheireducation
setting,carriedoutbyoneofthreeHeadStartresearchers(includingthecurrent
author).Theinterviewerintroducedthemselvesandengagedinsmalltalktobuild
rapportandmaketheparticipantfeelcomfortable,animportantprocessin
interviews(DiCicco-Bloom&Crabtree,2006;Smithetal.,2009).Theinterviewer
reviewedtheinformationsheetwiththeparticipant,checkingunderstandingand
providingopportunitiestoaskquestions,consistentwithguidance(Edmond,2005).
Participantswerethenaskedtogivewrittenassent(AppendixO)iftheywishedto
beinterviewed.
First,theinterviewerreiteratedkeyinformation,detailingthetopictobe
addressed,howdatawouldbeused,areminderthatparticipantsdidnotneedto
answerquestionsandcouldstopatanytime,andareminderofconfidentiality
procedures.AsoutlinedinSection4.6.2,theinterviewbeganwithpreliminary
nonthreateningquestions(e.g.,whatparticipantslikeaboutschool),beforemoving
ontothemainbodyofthescheduleandendingwithneutralquestions.Interviews
CHAPTERFOUR:METHOD
114
lastedapproximately30-45minutes,withamaximumpossibletimeofonehourto
avoiddisruptiontotheschoolday;theinterviewsincludedinthecurrentstudy
rangedfrom40minutestoonehour.Finally,interviewersthankedparticipants,
reiteratedkeyinformation,andprovidedfurtheropportunitiesforquestions.
Participantsthencompletedademographicformdisclosingtheirsex,age,
andethnicbackground(AppendixP).Theywereprovidedwithinformationon
nationalandlocalservicestheymaywishtoaccessafterdiscussingsensitivetopics,
alongsidethenameofamemberofstaffintheirschooltheycouldspeakwith,and
avoucher.Participantswereinvitedtoselectapseudonym,consistentwith
guidanceontreatingyoungpeopleasactiveresearchparticipants(Harcourt&
Conroy,2011).
AdditionalConsiderations
Interviewersutilisedstrategiesthroughoutthisprocesstoprioritise
participants’activeengagementandwellbeing,developedincollaborationwith
CommonRoomyoungadvisors.Giventhepotentiallysensitivenatureofthetopics
discussed,interviewerswereattentivetosignsofdiscomfortanddistressandin
suchinstancesgavetheparticipanttimetocalmdownbeforeaskingwhetherthey
wouldliketoresumetheinterviewand,ifso,howthiscouldbemadeeasier.Adult
colouringsheets,paper,anddrawingequipmentwasavailabletoprovideafocal
pointwhilediscussingdifficulttopicsifnecessary.Interviewerssoughttoverbally
establishseparatenessfromtheschoolandinterventionpractitionerstoreduce
perceptionsoftheinterviewerasanauthorityfigure(Cohen,Manion,&Morrison,
2011;Eder&Fingerson,2003).Interviewerssoughttoconsistentlyreiterateto
participantsthattheirinvolvementwasvalued,conveyingtheirpositionasactive
participants.
DataManagementandPreparation
Withparticipants’permission,interviewswererecordedwithanaudio
deviceforaccuracyandtofacilitatefocusontheparticipant(Patton,2015).Data
weretranscribedverbatimusinganaturalisedapproach,whereinutterancesand
noisessuchaspausesandstutters,nonverbalsoundssuchaslaughterorcoughs,

CHAPTERFOUR:METHOD
115
andnon-standardisedportrayalofparticipants’grammarusageandaccentsare
included(Oliveretal.,2005).Thisapproachwasusedtofacilitateanalytical
interpretationoflanguageusageandverbalandnon-verbalfeaturesaswellas
informationalcontent,asisimportantinIPA(Smithetal.,2009).Transcriptionwas
undertakenbyexternaltranscriptioncompaniesandcheckedforaccuracyby
interviewers.Accountswereanonymised,includingparticipantnamesandthe
namesofanypeopleorplaces;forthecurrentstudy,nameswereanonymised
usingparticipants’selectedpseudonymstopreservethehumanelementafforded
byaname.Audiodataandtranscriptswerestoredelectronicallyonpassword-
protectedcomputerserversaccessibleonlytoHeadStartresearchers.Papercopies
oftranscriptsutilisedinanalysisforthecurrentstudywerestoredinalockedfiling
cabinetaccessibleonlytotheauthor.
4.8QuantitativeAnalysis
4.8.1StructuralEquationModelling(SEM)
SEMisabroadtermdescribingarangeofstatisticalprocedureswherein,
amongotherthings,researcherscanspecifytheory-informeddirectionalpathways
betweenvariablesandexplorehowwellthisfitstheobserveddata(Kline,2016;
Pearl,2012).Thiscapacitytospecifythedirectionandnatureofrelationships
allowsinvestigationoftheunderlyingmechanismsandpossibleadaptiveprocesses
foremotionalsymptoms.SEMalsoenablesmodellingoflatentvariables,consistent
withadistinctionbetweenameasureandtheconstructitseekstocapture,an
advantagenotaffordedinothersmethodssuchasmultipleregression(Kline,2016).
SEMisalignedwiththestudyepistemologicallyasitassumesprobabilistic,not
deterministic,causality,focusingonlikelihoodofeffectsratherthananassumption
ofuniformchange(Kline,2016;Pearl,2012).SEManalysiswascarriedoutusing
Mplusversion8.1andinlaterstages8.3(Muthén&Muthén,1998-2010).
LatentVariableModels
ThedistinctionbetweenmanifestandlatentvariablesiscentraltoSEM;as
discussedinSection3.3.2,alatentvariable(orfactor)cannotbedirectlyobserved

CHAPTERFOUR:METHOD
116
andisinsteadinferredfromseveralmanifestvariables(orindicators)basedon
sharedvarianceamongindicators(Brown,2015;Kline,2016).Itisassumedthata
givenconstructcausesparticipantstorespondinparticularwaystoindicators
capturingassociatedcharacteristics/symptoms,thusprovidinginsightintothe
construct.Here,forexample,theconstructofemotionalsymptomswasnotdirectly
measured;rather,participantsrespondedtoasetofspecificstatementsthat
collectivelyrepresentindicatorsofemotionalsymptoms.SEMalsoestimatesthe
varianceofeachindicatornotexplainedbythelatentvariable(i.e.,common
variance),alsoknownasresidual(measurementerror)oruniquevariance,which
alsorepresentsalatentvariableasitisindirectlyinferred.Accountingforthisoffers
amorereliableformulationofconstructsand,thus,morerobustestimatesof
relationships(Gefenetal.,2011).Here,thestructureofeachlatentfactorandthe
fitoftheoverallmeasurementmodelwereexploredpriortothemainanalysisto
confirmtheirsuitability(seeSection4.8).
Estimators
Inestimatingmodels,theweightedleastsquaremeanandvariance
adjusted(WLSMV)estimatorwasutilised.Thiswasdeemedappropriategivenuse
oflatentfactorsinferredfromcategoricalindicators,asitproduceslessbiased
factorloadingsthanotherrobustestimatorswhereindicatorsareordinalrather
thancontinuous(Brown,2015;Brown&Moore,2012;Flora&Curran,2004;Li,
2016).WLSMVdoesnotassumeindicatornormalitybutinsteadassumeslatent
normaldistribution,thoughsimulationshaveindicatedthatmodestviolationsdo
notgenerallyaffectperformance(Flora&Curran,2004;Liang&Yang,2014).A
drawbackofWLSMVisitsuseoflistwisedeletionwhencovariatesarepresent,
whichislessrobustrelativetoestimatorsusingfullinformationmaximum
likelihood(FIML).Assuch,althoughWLSMVwasconsideredmostappropriategiven
itsadvantagesinmodellingcategoricalvariables,asensitivityanalysiswascarried
outformainanalysismodelsusingmaximumlikelihoodwithrobuststandarderror
(MLR),whichusesFIML.SimilarlytoWLSMV,MLRisabletohandlenon-normality
withinvariablesandthusproducerobustestimates(Wang&Wang,2012).

CHAPTERFOUR:METHOD
117
SensitivityanalysisusingMLRallowedassessmentofwhetherresultsobtained
throughWLSMVwereaffectedbymissingness.
ModelFitIndices
Overallgoodnessoffitwasassessedusingrootmeansquareerrorof
approximation(RMSEA),withvaluesbelow.60andanupper90%confidence
intervalsmallerthan1indicativeofgoodparsimonyfit(D.Hooperetal.,2008;Hu
&Bentler,1999),andComparativeFitIndex(CFI)andTucker-LewisIndex(TLI)
values,comparativefitindicesinwhichvaluesgreaterthan.95indicategoodfit(Hu
&Bentler,1999).Chi-squareisreportedforreferencebutnotconsideredindicative
ofmodelfit,asthisstatisticisstronglyaffectedbysamplesizeandthesizeof
parameterestimates(Brown,2015;Kline,2016).Localisedstrainwasexamined
using(a)Standardisedandnon-standardisedresiduals,withstandardisedvalues
above2.58indicatingpoorfit;(b)theresidualcorrelationmatrix,withvaluesabove
.10indicatingdisagreementbetweentheestimatedmodelandthedata(Kline,
2016);and(c)jointinspectionofmodificationindices(MI)andstandardised
estimatedparameterchange(SEPC),whereMIvaluesgreaterthan10andSEPC
valuesgreaterthan.20indicatethatthecorrespondingparametershouldbefreely
estimated(Wang&Wang,2012;Whittaker,2012).Re-specificationsbasedonpoor
fitweremadeonlywheretherewasatheoreticaljustificationfordoingso,rather
thanbasedpurelyonempiricalinformation,inlinewiththeepistemologicalstance
ofSEM(Brown,2015;Kline,2016).
InterpretingParameters
A.05alphathresholdwasutilisedtoindicatestatisticalsignificance;
however,p-valuethresholdscanbearbitraryandthisvalueissensitivetolarge
samplesize(Durlak,2009;Kline,2016;Sullivan&Feinn,2012).Thus,parameter
significancewasgivencontextualconsiderationalongsidedirectionandmagnitude.
Standardisedfactorloadings(λ)above.40wereconsideredsalient,though
consistentwithguidancethiswasconsideredcontextuallyforeachmodel(Brown,
2015).StandardisedbivariatecorrelationcoefficientsIwereinterpretedusing.10,
.30,and.50asthresholdsforsmall,moderate,andlarge,respectively(Cohen,
1988).FollowingMacKinnon,Lockwood,andWilliams(2004)ininterpreting

CHAPTERFOUR:METHOD
118
standardisedbetaregressioncoefficientpathways(β),.14,.39,and.59were
consideredindicativeofsmall,moderate,andlargeeffectsizesasoutlinedby
Cohen(1988).Itisgenerallyconsideredbetterpracticetointerpretthe
meaningfulnessofaparameterbasedonthemagnitudestypicallyobservedina
givenfield(Keith,2015),howeversuchnormshavenotyetbeenidentifiedwithin
mentalhealthresearchandsothecurrentstudyappliescautionandinsteadmakes
useofthesestandardguidelines.
DataClustering
AsparticipantsengagedwiththeWMFwithineducationsettingsdueto
HeadStartinvolvement,dataclusteringwasanticipatedattheschoollevel,wherein
aportionofvarianceisattributabletosimilaritieswithinthesample.Data
clusteringviolatestheassumptionofdataindependenceandsocanbiasstandard
errors(Hoxetal.,2018).Thedegreeofclusteringcanbeassessedusingthe
intraclustercorrelationcoefficient(ICC).Thedesigneffect(deff)canalsobe
determined,avalueassessinghowmuchclusteringmayaffectstandarderrors
(Kish,1965);however,itscalculationassumesthatclustersareofequalsizeandso
isnotadvisedacrossunequalclusters(Muthén&Satorra,1995).Clustersizeshere
wereunbalancedandrangedfrom1to244(average=83)andthusdeffwasnota
suitableindicator.However,Hoxetal.(2018)havearguedthatregardlessofsuch
statistics,anyexpectedviolationofdataindependenceisproblematicandshould
becontrolledfor.Thus,dataclusteringattheschoollevelwascontrolledforinall
SEManalyses,usingtheType=ComplexcommandinMplus,whichaccountsfor
non-independenceoftheobservationsbyadjustingthestandarderrors(Muthén&
Muthén,1998-2010).
4.8.2Pre-Analysis
DatawerereviewedtoensureconsistencywiththeassumptionsofSEM.
Thefactorstructureofeachmeasurewasexploredthroughconfirmatoryfactor
analysis(CFA),withinspectionofgoodnessoffitindices,areasoflocalisedstrain,
andparameterestimates.InternalconsistencywasinvestigatedusingCronbach’sα

CHAPTERFOUR:METHOD
119
(usingSPSSversion23)andMcDonald’sω(usingMplusversion8.1)toprovidea
balancedevaluation,aseachstatisticpresentslimitations.Cronbach’sαproduces
inflatedvaluesintheabsenceoftau-equivalence(Brown,2015;Cronbach&
Shavelson,2004)andlowervaluesformeasureswithfeweritems(Kline,2016;
Raykov,1997),whileMcDonald’sωcanbeaffectedbynon-normalityor
multidimensionality(Trizano-Hermosilla&Alvarado,2016;Zhang&Yuan,2015).A
cutoffof.70iscommonlyusedforCronbach’sα(e.g.,Terweeetal.,2007),however
thisthresholdisgenerallyindicativeofapproximateadequacyratherthanagold-
standardcutoffandshouldactasguidanceratherthananinclusioncriterion(Dunn
etal.,2014;Kline,2016;Lanceetal.,2006).ThereisnocutoffforMcDonald’sωand
thisisgenerallyreportedfortransparency.
Priortoestimatingstructuralmodelswithmorethanonelatentvariable,a
measurementmodelwasexamined,whichisessentiallythefactorstructureacross
allvariablesunderpinningthestructuralmodelsthatarethemainfocusofanalysis
(Brown,2015;Kline,2016;Muthén&Muthén,1998-2010).Inameasurement
model,alllatentvariablesinter-correlatefreelytoallowinspectionofinter-
relationshipsandensureviability(Brown,2015;Kline,2016;Muthén&Muthén,
1998-2010.;Schreiberetal.,2006).Thisallowsmoreaccuratejudgementsabout
thefitofstructuralmodels,asobservedpoorfitcanbeattributedtoamis-specified
measurementmodel(Brown,2015;Kline,2016).
4.8.3MainStatisticalAnalysis
Thissectiondescribestheanalyticalstrategyforeachresearchquestion.A
sequentialapproachwasadopted,withsomeresultsinformingelementsof
analyticalproceduresforsubsequentquestions;forinstance,riskfactorsidentified
inRQ1ainformtheconstructionofriskconstructsusedinRQs1b–dand2b.
ResearchQuestion1:RiskFactorsandProcesses
RiskFactors

CHAPTERFOUR:METHOD
120
7. Oftherisksidentified,whatisthemagnitudeoftheirassociationwithearly
adolescentgirls’emotionalsymptoms?
AlinearmultipleregressionSEMmodelwasspecifiedwithallhypothesised
riskvariablespredictinglatentemotionalsymptoms.Variableswereclassedas
confirmedriskfactorswheretheirrespectivepathwayontoemotionalsymptoms
wasstatisticallysignificant(p<.05)andintheexpecteddirection.However,as
outlinedintheprevioussection,parametermagnitudewasalsoconsideredin
determiningriskfactorstatus,withparticularlysmallparametervalues(inlinewith
thresholdsof.14,.39,and.59;Cohen,1988)givenadditionalcontextual
consideration.
CumulativeRiskEffects
b.Isthereevidenceforacumulativeriskeffectinrelationtoearlyadolescentgirls’
emotionalsymptoms?
Acumulativeriskindexwascreatedbysummingconfirmedriskfactors,with
eachonecodedas“1=riskpresent”and“0=riskabsent”,tocreateascorefor
eachparticipant.Ifidentifiedforinclusion,thecontinuousvariable,neighbourhood
socioeconomicdeprivation,wouldbedichotomisedusingreceiveroperating
characteristicanalysistoisolatewhereinitsrange“risk”occurs,consistentwith
guidance(Kraemeretal.,2005).
Next,alinearregressionSEMmodelwasspecifiedwiththecumulativerisk
indexpredictinglatentemotionalsymptomstoidentifywhethercumulativerisk
effectswerepresent.Observedeffectswouldbefurtherassessedbyaddingeach
individualconfirmedriskfactorasacovariate,oneatatime,toconfirmeffects
werenotdrivenbyasinglefactorintheindex,consistentwithguidance(Evanset
al.,2013).
RiskMeasurementModels
c.Whichriskmeasurementmodelbestexplainstheeffectsofexposuretomultiple
riskfactorsinrelationtoearlyadolescentgirls’emotionalsymptoms?
Multipleregression,cumulativerisk,andlatentconstructmeasurement
approacheswereexploredaspredictorsofemotionalsymptomsthroughseparate

CHAPTERFOUR:METHOD
121
linearregressionSEMmodels(Figure3.1,Section3.3.2).Modelfitindiceswere
inspectedtoestablishgoodnessoffit,thoughthiswasnotusedtoselectthemost
appropriatemodel,asthefocusisonexplanatorypowerandthereisnowayto
empiricallyusemodelfitindicesformodelcomparisonwhenmodelsarenon-
nested.Toassesswhichmodelshowedthegreatestpredictiveutility,thecentral
interestforthisresearchquestion,regressionbetacoefficientswereinspected
alongsidethevarianceofemotionalsymptomspredictedwithineachmodel.
IndirectEffectsofPerceivedStress
d.Arethereindirecteffectsofperceivedstressintherelationshipbetweenmultiple
riskexposureandemotionalsymptoms?
Amodelwasspecifiedwithbothdirectandindirecteffectsofperceived
stressintherelationshipbetweenmultipleriskexposureandemotionalsymptoms.
ThespecificwayinwhichthePSS-4wasmodelledinthismodel(thatis,as
unidimensionalorasatwo-dimensionalmeasureofperceiveddistressand
perceivedcoping)wasdeterminedbasedontheresultsofCFA,whichare
presentedatthebeginningofChapterFive.Theterm“indirecteffects”isusedhere
ratherthan“mediation”,inlinewithguidanceforinterpretingsuchpathways
withincross-sectionaldata(Kline,2016).Specifyingindirecteffectswithinamodel
resultsinnon-normalityinthedistributionofthesamplealongthesepathways,
necessitatingtheuseofbootstrappingtoovercomeassumptionsofnormality
(Hayes,2013,2017).Here,bias-correctedbootstrapswereutilised,consistentwith
guidance(Hayes,2017),with1,000draws.Thisanalysiswasconductedinthelatest
versionofMplus(8.3),whichallowedbootstrappingwhilealsocontrollingfor
clustering.
ResearchQuestion2:FactorsandProcessesforPositiveOutcomes
PromotiveFactors
7. Ofthepromotivefactorsidentified,whatisthemagnitudeoftheir
associationwithearlyadolescentgirls’emotionalsymptoms?

CHAPTERFOUR:METHOD
122
AlinearmultipleregressionSEMmodelwasspecifiedincludingthesixlatent
SRSsubscalesaspredictorsoflatentemotionalsymptoms.Hypothesisedpromotive
variableswereclassedasconfirmedwheretherespectiveregressionpathwayonto
thelatentemotionalsymptomsoutcomevariablewasstatisticallysignificantatthe
.05alphalevelanddemonstratinganinverserelationship,thoughaswithrisk
factorsparametermagnitudewasalsoassessed(inlinewiththresholdsforβof.14,
.39,and.59;Cohen,1988).
ProtectiveFactors
b.Towhatextentarethedirectand/orindirectrelationshipsbetweenmultiplerisk
exposure,perceivedstress,andemotionalsymptomsconditionaluponaccessto
protectivefactors?
Anindirecteffectmodelwithconditionalpathwayswasinvestigatedto
assesswhetherthenatureofanydirectand/orindirectpathways(asidentifiedin
RQ1d)dependsuponthelevelofone’sperceivedsocialconnectionsandactive
engagement.Notethat“conditionalindirecteffects”canbethoughtofas
conceptuallysimilartomoderatedmediation;however,inmoderatedmediation
theentireunderlyingmechanismismoderated,whileconditionalindirecteffects
focusesonspecificpathwayswithinthatmechanism(Hayes,2017);thecurrent
studyfocusesonthelatter.
Conditionaleffects,ormoderation,occurwhenonevariableaffectsthe
relationshipbetweentwoothervariables;thismoderatorvariablespecifiesthe
conditioninwhichaneffectoccursandcaninfluenceitsstrengthanddirectionality
(Baron&Kenny,1986;Hayes,2013,2017;Holmbeck,1997).Toinvestigateasingle
moderatorinalinearregressionmodel,threecausalpathwayspredictthe
outcome:(a)Thepredictor;(b)themoderator;and(c)theinteractionorproductof
thepredictorandmoderator(Baron&Kenny,1986;seeFigure4.2).Wherethe
interactionisfoundtobestatisticallysignificant,thevariableisidentifiedasa
moderator(Hayes,2013,2017).

CHAPTERFOUR:METHOD
123
Figure4.2.Conceptualandstatisticalmoderationmodels.Theconceptualmodelshowsthe
moderatorinfluencingtherelationshipbetweenpredictorandoutcome.Thestatisticalmodel
presentscausalpathwaysusedtoinvestigatemoderation:(a)Thepredictor,(b)themoderator,and
(c)theinteractionbetweenthetwo.
Inamediationmodel,amoderatorcanbespecifiedalonganystatistically
significantindirectand/ordirectpathway,asdeterminedwithconsiderationof
theory,existingresearch,andone’sresearchquestions(Hayes,2013,2017).Figure
4.3(overleaf)showsconceptualandstatisticaldiagramsforasimpleindirecteffects
modelwithonemoderatormoderatingthefirstpathwayoftheoverarchingindirect
pathway.
Figure4.3.Conceptualandstatisticalconditionalindirecteffectsmodel.Theconceptualmodel
showsonemediator(M),withonemoderator(W)influencingthefirstindirectpathway.The
statisticalmodelpresentsfivecausalpathways:a1andbshowthemediationpathways,c’showsthe
directpathway,a2showstheinfluenceofthemoderatorWonM,anda3showstheeffectsofthe
interactionbetweenthepredictorXandthemoderatorW(XW)onM.Moderationisconsidered
presentwheninteractionpathwaya3issignificant.

CHAPTERFOUR:METHOD
124
Thisdiagramexpressestwoequations,oneforY(theoutcome)andoneforM(the
mediator;Hayes,2013,2017):
Y = b0+ b1M+ c!X
(Equation1)
M = a0+ a1X+ a2W+ a3XW
(Equation2)
Here,moderationwasexaminedforanydirectand/orindirectpathwaysidentified
asstatisticallysignificantinRQ1d,allowingexaminationofwherehypothesised
moderatorvariablesfunctioninrelationtostressmechanisms.Whereanindirect
effectwasobserved,itwasplannedthatmoderationwouldbeexaminedforboth
stagesofindirecteffects,wherethefirststageistheeffectsofriskuponstressand
thesecondstageistheeffectofstressuponemotionalsymptoms.
ThestudydidnotexamineallsixSRSsubscalesaspossiblemoderators,as
thiswouldcreateanunnecessarilycomplexmodel.Thisreflectsthepostpositivist
principleofparsimony,whereinasimplermodel,withfewerparametersandmany
degreesoffreedom,ispreferredwheretheoreticallyplausible(Kline,2016;
Preacher,2006).However,thereisno“ruleofthumb”forthemostappropriate
numberofvariablesorparameterstoincludeinamodelandnoempiricalmethod
toassessthiscontextually.Instead,availableoptionsshouldbereviewedtoidentify
andprioritisethoseexpectedtobemostsalient,withconsiderationoftheoryand
priorempiricalresults(Hayes,2013;Kline,2016).Thus,theoryandpriorresearch
regardingthesixconstructsinrelationtoemotionalsymptomswasexaminedto
identifythosethataremosttheoreticallyrelevant.Thesubscaleswerealsotested
aspredictorsoftheoutcomeandofrelevantmediators(dependingonfindings
fromRQs1d)toassesswhetheramoderationeffectwouldbelikelyinrelationto
eachoftherelevantpathways,asadvisedbyHayes(2013,2017).Thatis,ifa
variableisnotsignificantlyassociatedwiththemediatorsoroutcome,itisunlikely

CHAPTERFOUR:METHOD
125
thatitwouldinteractwithpredictorstomoderateeffects.Finally,with
considerationofboththeoryandtheseempiricalresults,asubsetofvariableswas
selectedforinclusion.TheselectedvariablesarepresentedanddiscussedinSection
5.4.2,inlightoffindingsfromRQ1d.
Totestconditionaleffects,thestudyadaptedexampleMpluscoding
developedbyStride,Gardner,Catley,andThomas(2015),whichhasbeen
configuredbasedonHayes's(2013,2017)theoryandprocedures.Interactions
betweenpredictors/mediatorsandeachofthehypothesisedmoderatorswere
definedasadditionalpredictors,withthemoderatorvariableitselfalsoincludedas
apredictor(asillustratedearlierinFigure4.2).TheMODELCONSTRAINToptionwas
thenutilisedtoassesswhethereffectsvaryasafunctionofthelevelofthe
moderator.Todoso,moderatorvariablesarespecifiedasoccurringatthreevalues
oflow,moderate,andhigh,definedbytheirmean-1SD,mean,andmean+1SD,
respectively(Hayes,2015;Strideetal.,2015).Itshouldbenotedthattofurther
reducethenumberofparameterswithinthismodel,theselectedSRSsubscalesand
PSS-4subscales(wherefoundtobesignificantmediators)weretreatedasmanifest
ratherthanlatent.Assuch,themaximumlikelihood(ML)estimatorwith
bootstrappingwasutilisedforthisanalysisinlinewithuseofcontinuoustotal
scores,giventhattheWLSMVestimatorusedinpreviousanalysesisgenerallymore
robustwheretherearecategoricalindicators(Brown,2015;Brown&Moore,2012;
Flora&Curran,2004;Li,2016).
4.9QualitativeAnalysis
4.9.1InterpretativePhenomenologicalAnalysis(IPA)
ForRQ3,IPAwasutilisedtoexploreparticipants’livedexperienceandthe
waysinwhichtheymakesenseofthisexperience.Aspreviouslydiscussed,inIPA
theresearcherdevelopsaninterpretativeaccountofaparticipant’sexperiential
claimsandconcernsaroundaphenomenon.Analysisisaniterativeandinductive
process,whereintheresearcherenterstheparticipant’s“lifeworld”andengagesin
aclose,systematicanalysisoftheiraccounttodevelopexperientialthemes.Thisis

CHAPTERFOUR:METHOD
126
carriedoutseparatelyforeachparticipantbeforeexploringconvergencesand
divergencesacrossthesample,orcorpusofcases(Smithetal.,2009).Theaimisto
developoverarchingthemescapturingbothanidiographicfocusonthatwhichis
uniquetoeachindividualalongsideawiderfocusonsharedfeatures(Smithetal.,
2009;Smith&Osborn,2015a;Willig,2013).Thefollowingsectionsoutlinespecific
analyticalstagesinmoredetail.
AsdiscussedinSections4.3.2and4.4.3,IPArequiresahermeneutic
interactionbetweentheresearcherandeachparticipant’slifeworldand,thus,both
areconsideredpresentinfindings(Larkin&Thompson,2006;Mayoh&
Onwuegbuzie,2015;Pietkiewicz&Smith,2014;Smithetal.,2009).However,itis
importanttoretainaclosefocusonparticipant’saccounts(Larkinetal.,2006;
Smithetal.,2009;Willig,2013).Thus,thecurrentstudysoughttoembedreflexivity
throughouttheanalyticalprocess;sucheffortsarehighlightedbelowacross
analyticalstagesandalsodiscusseddiscretelyinSections4.11.2and5.4.
4.9.2StagesofIPA
Analysisfollowedthesix-stageframeworkoutlinedbySmithetal.(2009),
withconsiderationofguidancefromarangeofothermethodologicalarticles.
However,IPAguidancedoesnotofferaprescriptiveframeworkastheessenceof
analysisisitsinterpretativefocusandsoresearcherflexibilityisencouraged(Larkin
etal.,2006;Smithetal.,2009;Smith&Osborn,2015a;Smith,2004).Thesixbroad
stagesutilisedwere:
1. Immersion;
2. Initialsystematiccoding;
3. Developmentofemergentthemes;
4. Connectionsacrossemergentthemes;
5. Completionacrosscorpusofcases;and
6. Lookingforpatternsacrosscases.
Thefirstfourstepswerecarriedoutiterativelyforeachparticipantandthisprocess
wasthenrepeatedacrossallcases.Eachtranscriptisapproachedafresh,rather

CHAPTERFOUR:METHOD
127
thanbeinginfluencedbytheanalysisofthepreviouscase,consistentwithIPA’s
idiographicapproach(Smithetal.,2009).Finally,theresearcherreviewedthecases
collectivelyandexploredhowtheyrelatetooneanother.Itshouldbenotedthat
althoughthesestagesaredetailedsequentially,theycompriseacyclicalprocess
andwererevisitedasneededthroughouttheanalyticalprocess.Analysiswas
undertakenbyhandusingpenandpaperratherthansoftware,asthisencourages
closenesswiththedata(Pietkiewicz&Smith,2014;Smithetal.,2009).Eachof
theseanalyticalstepsisdetailedinthefollowingsubsections.Priortobeginningthe
analyticalprocess,theresearcherengagedininspectionoftheirownvaluesand
experiencestoexplorehowthesemightrelatetotheareaofstudyandresearch
questionand,inturn,toreflectonhowthesemayinfluencetheirengagementwith
thedata(seeSection6.4).
StageOne:Immersion
First,theresearcherreadtheparticipant’stranscriptseveraltimesand
listenedtotheaudiorecording.Theaimistobecomeimmersedinthedataand
centrethefocusontheparticipantandtheiraccount,aswellastobecomefamiliar
withthestructureandcontextoftheinterview(Pietkiewicz&Smith,2014;Smithet
al.,2009).Immersionalsofacilitatesexplorationoftheresearcher’spreconceptions
priortosystematicanalysis(Larkin&Thompson,2012).Anyinitialthoughtsthat
arosewerenotedandsetaside(anexampleforAmeliaisshowninAppendixQ).
Thesenotesdonotrepresentformalanalysisandsoarenottakenintoaccountin
laterstages(Smithetal.,2009).
StageTwo:InitialSystematicCoding
Theresearcherthensystematicallycodedthetranscript.Thisisan
exploratoryprocessaimingtoidentifytheexperiencesparticipantsdescribeandthe
waytheymakesenseofthem.Theresearchernotesanythingofinterestwithinthe
data,attendingtobothsemanticcontentandlanguageuse(Reidetal.,2005;Smith
etal.,2009;Willig,2013).Thisistypicallyundertakenincolumns,withdatainone
columnandcodinginaparallelareatoencouragecross-checkingbetweendataand
interpretations(Smithetal.,2009).Multiplecodingcolumnscanbeusedfor
differentkindsofcomments,toencourageattentiontodifferentdatafeaturesand

CHAPTERFOUR:METHOD
128
facilitateseparatenessbetweendescriptivecommentsreflectingdatacontentand
interpretivecommentsthatgobeyondthedataintomoreabstractterritory(Larkin
&Thompson,2012;Smithetal.,2009).Here,columnsfor“content”and“concept”
wereutilisedtoreflectthisdistinction,alongsidea“streamofconsciousness”
columntodocumentmoretentativecomments.Anexamplepageshowingthese
columnsandinitialcodingforAmeliacanbeseeninAppendixR.Inaddition,
decontextualisationstrategieswereutilisedtoencourageattentiontolinguistic
featuresaswellasnarrativeelements,suchasreadingfragmentedlineswithout
considerationofthelargersectionoftext,orreadingthelinesofasectionin
reverse(Smithetal.,2009).
Ongoingreflexivenotesweredocumentedatthebottomofeachpage,to
encourageactivedocumentingofanyinstanceswheredataresonatedinsomeway
orfeltchallengingtointerpretinamorebracketedway.Typicallythiswasnoted
downandreflectedonbrieflyandthensetasidetofocusonanalysis,andreturned
tolatertomoreextensivelyexplorehowthismighthaveinfluencedinterpretation
ofacaseoraproportionofthedata.Thisalsomeantthatanysuchinstanceswere
documentedinthelongterm,sothatinrevisitingdataandcodingatalaterstage
therewereclearnotesshowingwheredatahadresonatedandperhapsbeenmore
substantiallyinfluencedbytheresearcher.
StageThree:DevelopmentofEmergentThemes
Atthisstage,theresearcherdevelopsemergentthemes,consideringboth
thetranscriptandtheinitialcodingjustdeveloped,whicharenowconsideredin
unisonasanexpandeddataset(Smithetal.,2009).Thefocusisprimarilyonthe
initialcodesandsobeginstomoveslightlyawayfromtheparticipant’swords,
thoughtheseshouldstillbeconsideredandindeedshouldbereflectedintheinitial
codinginthefirstinstance(Larkinetal.,2006;Reidetal.,2005;Smithetal.,2009).
Theresearcherbeginsto“zoomout”,consideringlargerfragmentedsectionsof
dataandmovingbeyondthepreviousline-by-lineapproach.Themesarenotedin
thefinalcolumnastheyappearchronologicallyinthetext,thoughthereis
considerationoftheaccountasawholeintermsoftheinterrelationshipsand
connectionsacrossthetranscript(Biggerstaff&Thompson,2008;Smithetal.,

CHAPTERFOUR:METHOD
129
2009).Itisnecessarytoexercisecautioninmovingtoofarfromparticipants’
accounts;inthecurrentstudy,emergentthemeswerecontinuallycheckedagainst
theparticipant’swordstoensurethatinterpretationsweregroundedinthedata.
AnexamplepagefromthisstageofanalysisisinAppendixSforAmelia,showinga
sampleofemergentthemesalongsidedataandcoding.
StageFour:ConnectionsacrossEmergentThemes
Next,theresearcherexploredconnectionsacrosstheparticipant’s
emergentthemes(Smithetal.,2009).Emergentthemesaregroupedtogetherinto
themesordiscardedinlinewiththescopeoftheresearchquestion,andthemes
arethenclusteredtogetherwithinsuperordinatethemes(Biggerstaff&Thompson,
2008;Pietkiewicz&Smith,2014;Smithetal.,2009).Tofacilitatethisprocess,
emergentthemesasidentifiedchronologicallyweretypeduptoallowthemtobe
viewedandexploredsimultaneously.Themeswerefirstlygroupedtogetherbased
onsimilarity,followedbyexplorationofoppositionalconnections,andwerethen
organisedintoastructureofsuperordinatethemes.Variousstrategieswerethen
usedtodevelopthisthematicstructure,includingconsiderationofeachtheme’s
context,frequencyandfunctionwithintheinterview,asrecommendedbySmithet
al.(2009).Suchstrategiesareemployedinunisonratherthanassingulardecision-
makingtools;forexample,athemewouldnotnecessarilyberemovedduetolow
frequencyifitappearedparticularlymeaningfulinaparticipant’slifeworld.To
encouragetheshapingofthemesinaccordancewithparticipants’words,
supportingexcerptsfordevelopingthemeswerecompiledonanongoingbasis,
consistentwithguidance(Pietkiewicz&Smith,2014;Smithetal.,2009;Willig,
2013).Furthermore,theresearcherdevelopedwrittendescriptionsofthemes
duringthisprocesstoencouragefurtherexaminationofhowthemessittogether
withinthethematicstructure(Pietkiewicz&Smith,2014;Smithetal.,2009).Each
participant’sthemesarepresentedatthebeginningofChapterSix,priorto
explorationofthemasterthemesspanningthecorpusasawhole.
StageFive:CompletionacrossCorpus
Stagesonetofourwererepeatedforallthreeparticipants,witheach
transcriptanalysedindividually.Theresearchersoughttobracketanalysisof

CHAPTERFOUR:METHOD
130
previouscasestolimittheirinfluenceoneachindividualaccountasmuchas
possible,inlinewithIPA’semphasisontheidiographic.However,thiscanbe
challengingduetothelevelofimmersionnecessaryinanalysingeachcase(Larkin
etal.,2006;Smithetal.,2009;Wagstaffetal.,2014).Thus,theresearcher
exercisedcautioninthisareaandkeptareflexivecommentaryofthisbracketing
process,alongsideongoingdiscussionwiththesupervisoryteam.
StageSix:LookingforPatternsacrossCases
Finally,thethemesdevelopedforeachcasearebroughttogetherinto
higher-orderthemesrepresentingtheexperiencesandsense-makingofthecorpus
asawhole.Themesshouldcapturebothcommonalitiesanddivergencesacross
cases,tocapturerepresentationofwhatissharedbutalsowhatisdifferentacross
cases(Reidetal.,2005;Smithetal.,2009).Todevelopoverarchingthemes,the
researcherfirstreviewedeachparticipant’sthemesandtherespectivequotes
underpinningthemandnotedinitialthoughtsonpatternsanddifferencesacross
thecases.Severalstrategieswereutilisedtofacilitatethisprocess,suchas
developingavisualdisplayofthemesandcreatingwrittensummariesforemerging
themestoexploreandinspecttheircomposition.Duringthisprocess,the
researcherdevelopedaninitialsetofthemesforthecorpus,retainingasmuch
detailaspossibleatthisearlystage.Asinpreviousphasesofanalysis,themeswere
tentativelyorganisedwithinsuperordinatethemesandthisstructurewasthen
refinedtodevelopamoreunifiedandsynthesisedrepresentationofthecorpus.
Thereisnofixedruleastohowmanythemesshouldbeinthefinalthematic
structure;rather,thegeneralideaisthat“lessismore”and,assuch,asmallerand
moresuccinctsetofthemesispreferred(Pietkiewicz&Smith,2014;Reidetal.,
2005;Smithetal.,2009;Smith&Osborn,2015a).Furthermore,attentiontoboth
uniqueandsharedfeaturesmeansthatnotallparticipantsneedtoberepresented
ineachthemeandindeedathememayincorporatetheexperiencesofjustone
participantwherethiscapturesexperiencesthatappearparticularlysalientintheir
lifeworld.
Theresearcherdocumentedthisprocesscarefullyandengagedinregular
discussionswithmembersoftheresearchsupervisionteamandpeersfamiliarwith

CHAPTERFOUR:METHOD
131
theuseofIPA,inordertobothguidetheprocessandfacilitatereflexivethinking.
Throughoutthisprocess,theresearcherregularlyreviewedthethemesagainstthe
originaltranscriptsandcodingalongwiththeindividualtrackingdocuments
describedinpreviousstagesinanefforttoensurethatthemesweregroundedin
participants’accountsandwords.Themenameswerealsogivenattentionandin
somecaseskeywordsorphrasesfromparticipantswereadoptedaslabelswhere
thesewereconsideredtoencapsulatetheessenceofthetheme;Smith(2011b)
describessuchutterancesinthiscontextas“gems”.Thenuancesandsalient
featuresofthemesareexploredwithinthefinalwrittennarrativeandsowhilethe
thematicstructureshouldfacilitatethiskindofrepresentation,thenuancesand
divergencesdonotnecessarilyneedtobemadeovertinnamingandorganising
themes.Forinstance,oppositionalthemesmaysitalongsideoneanotherandthus
bevisiblesimplyfromtheirnames,butitispossibleforasinglethemeto
encapsulateverydifferentperspectivesorexperiencesandthismaynotbe
immediatelyevidentthroughthethemenamealone.
FinalthemesarepresentedinChapterSixalongsideanindicationofwhich
participantsarerepresentedwithineachtheme,consistentwithguidance(Larkin&
Thompson,2012;Smithetal.,2009).Awrittennarrativedescribesandexplores
eachtheme,notingsalientfeaturesandcommonpatternsaswellasindividual
differencesacrosscases,clarifyingtothereaderwherediscussioniscentredaround
thevoiceoftheparticipantversustheinterpretativevoiceoftheresearcher(Larkin
etal.,2006;Larkin&Thompson,2006;Smithetal.,2009).Findingsarethen
discussedinrelationtopsychologicaltheoryandwiderresearchinChapterSeven,
consideringhowfindingsreflectexistingliteratureaswellaswhatfreshinsightsand
meaningtheyoffer.
4.10MixedMethodsStrategy
InChapterSeven,quantitativeandqualitativefindingsarefirstdiscussed
independentlyofoneanothertoexploretheinferencesofferedbyeachstrand,
consistentwithguidance(Tashakkori&Teddlie,2008a;Teddlie&Tashakkori,

CHAPTERFOUR:METHOD
132
2009).Inferencesandlearningacrossthetwostrandsarethendrawntogetherto
developmeta-inferences,representingamorecomprehensiveunderstandingofthe
phenomena,inlinewithuseofmixedmethodsforcomplementarity(Brymanetal.,
2008;Creswell&PlanoClark,2011;Greeneetal.,1989).Inferencesacrossthe
strandswereconsideredjointlywithattentiontohowfindingsenhancedand
elaboratedupononeanotheraswellasareasofsimilarityandcontrast.This
approachisconsistentwithTashakkoriandTeddlie's(2008)principleofintegrative
efficacy,ortheextenttowhichfindingsareeffectivelyintegratedintotheoretically
coherentmeta-inferences.Avisualrepresentationillustratinghowmeta-inferences
integratelearningacrossthetwostrandsispresentedinChapterSeven,bothto
demonstratethisintegrationtothereaderandtofacilitateaccessibilityfor
audiencesfromvaryingmethodologicalbackgrounds(Mayoh&Onwuegbuzie,
2015;Moseholm&Fetters,2017;Sandelowski,2003).Finally,eachmeta-inference
isdiscussedandexploredwithattentiontoimplicationsanddirectionsforfuture
research.
4.11QualityandRigour
4.11.1QuantitativeStrand
Thequantitativeresearchprocesswasguidedbythepostpositivistprinciples
ofreliability,validity,replicability,andgeneralisability(Mertens,2015)and
attentiontogeneralreportingstandardsfromtheAPAPublicationsand
CommunicationsBoardTaskForce(Appelbaumetal.,2018)andstandardsfor
reportingobservationalepidemiologicalresearch(vonElmetal.,2008,2014).
ReliabilityandValidity
Reliabilityandvalidityreflecttheextenttowhichmeasuresreliablycapture
thespecificconstructofinterest(Mertens,2015).Internalconsistency(both
Cronbach’sαandMcDonald’sω)isreportedforallmeasuresandpreviousevidence
ofvalidityandreliabilityisoutlinedwithattentiontocontentvalidity,construct
validity,andinternalconsistency,inlinewithguidancefromTerweeetal.(2007).
ReplicabilityandGeneralisability

CHAPTERFOUR:METHOD
133
Replicabilityrelatestoprovidingsufficientinformationtoallowresearch
conditionstobere-created,whilegeneralisabilityistheextenttowhichresults
couldbeappliedwithinothersituations,bothofwhichnecessitatetransparent
reporting(Appelbaumetal.,2018;OpenScienceCollaboration,2015).Cleardetails
havebeenprovidedregardingthesample,datacollectionmaterialsand
procedures,andanalyticalprocedures,whileunstandardisedandstandardised
resultsarereportedformainanalysisalongsidesensitivityanalysis.
4.11.2QualitativeStrand
ThequalitativestrandwasguidedbykeyprinciplesfromYardley(2000,
2015),namelysensitivitytocontext,commitmentandrigour,transparencyand
coherence,andimpactandimportance,alongsidespecificIPAguidance(Smith,
2011a;Smithetal.,2009).
SensitivitytoContext
Thisprinciplereflectssensitivitytotheresearchcontext,includingwider
theoryandliterature,thedataandtheirsocioculturalcontext,participants’
perspectives,andethicalconsiderations.Theresearchersoughttoimmerse
themselvesinparticipants’lifeworldsandtoensureinterpretationsandthewritten
narrativewereembeddedwithintheiraccounts(Larkinetal.,2006;Smithetal.,
2009).Illustrativequotesareincludedforeachparticipantincludedinagiven
theme,consistentwithguidanceonIPAstudiesfocusingonthreeorfewer
participants(Smith,2011a).Indiscussingfindingsallpossibleavenuesof
explanationwereexamined,ratherthanadoptingasingletheoreticallensor
narrowlyaligningfindingswithquantitativeresults.
CommitmentandRigour
Thisrelatestocreatinganin-depth,completestudy(Yardley,2000,2015).
Here,stepsweretakentoincludeapurposivesamplewithrichandrelevant
experience.Theresearcherundertookeffortstodevelopcompetenceandskillin
IPAthroughtrainingandpeersupporttoensurecommitmenttothemethod

CHAPTERFOUR:METHOD
134
(Smith,2011a).Theresearcherworkedtoundertakeanin-depth,systematic
analysisthatcouldpushbeyondsurface-levelconclusionsanddevelopmeaningful
themesencompassingbothindividualandsharedexperiences(Larkinetal.,2006;
Smithetal.,2009;Wagstaffetal.,2014).
TransparencyandCoherence
Thisprinciplecapturesclarityandcoherenceinreporting(Yardley,2000,
2015).Effortwastakentodevelopacoherentdesign,withtheresearchquestion
andadoptedepistemologiesinformingtheentireprocess(Yardley,2000,2015).A
cleardescriptionofeachanalyticalstagehasbeenprovidedandarichnarrativeof
findingsispresentedinChapterSix,withclarityindistinguishingdescriptionsof
experiencesfrommoreinterpretivecomments(Smithetal.,2009;Smith,2011a).
Severalstrategieswereutilisedtofacilitatereflexivity,akeyconsiderationwithin
IPA(Larkinetal.,2006;Smithetal.,2009;Wagstaffetal.,2014),throughongoing
documentationofreactionstothedata,useofbracketingtechniquesduring
coding,anddiscussionwiththesupervisorandpeers.Abriefappraisalofthe
reflexivityprocessisofferedinChapterSix.Theanalyticalprocesswas
systematicallydocumentedinamannerthatwouldfacilitateanaudit,whereinan
independentpersoncouldfollowthejourneyfromtherawdatathroughtothefinal
report(Smithetal.,2009;Yin,1989)andthiswasconsistentlysharedanddiscussed
withthemainsupervisortoexplorecredibilityandplausibility.
ImpactandImportance
Thisprincipleemphasisestheneedforfindingstobedeeplyconsideredand
exploredwithconsiderationofimportanceandimpact(Yardley,2000,2015).
DiscussionoffindingsinChapterSevendoesnotsimplyconsiderwhetherfindings
alignwithanexistingmodel,butaspirestoexplorefindingsdeeply,examining
connectionswithwidertheoryandliteratureanddrawingoutnewanduseful
insights(Larkin&Thompson,2012;Pietkiewicz&Smith,2014;Smithetal.,2009).
Tofacilitateimpact,bothpracticalimplicationsandfutureresearchdirectionsare
considered.

CHAPTERFOUR:METHOD
135
4.11.3MixedMethods
Qualityandrigourinmixedmethodsstudiesrelatestothecoherencyofthe
overalldesignandtheextenttowhichmeta-inferencesoffermeaningfulinsight
(Brymanetal.,2008;Tashakkori&Teddlie,2008b).Theparticularmethodsused
areconsistentwiththestudy’saimsandeachoffersinsightintothesamebroad
phenomenawithinthesamepopulation,withconsiderationofeachapproach’s
respectiveepistemologiesthroughout.IntegrationwasguidedbyTashakkoriand
Teddlie's(2008)principleofintegrativeefficacy,withattentiongivento
completeness,elaboration,comparison,andcontrastinbringingtogetherfindings.
Consistentwithguidance,thecontributionsofeachstrandarediscussed
independentlybeforeconsideringwhatthetwostrandsofferjointly(Tashakkori&
Teddlie,2008a;Teddlie&Tashakkori,2009).
4.12EthicalConsiderations
Ethicalconsiderationsarediscussedherewithattentiontoresponsibilities
to(a)Participants,(b)researchsponsors,(c)theeducationalresearchcommunity,
and(d)educationalprofessionals,policymakers,andthegeneralpublic,consistent
withguidancefromtheBritishEducationalResearchAssociation(2011).Ethical
approvalfortheHeadStartevaluation,whichextendstothisstudy,wasgrantedby
theUCLResearchEthicsCommittee,forthequalitativestrandonSeptember30th
2016(ref.7963/002)andforthequantitativestrandonNovember30th2016(ref.
8097/003).
4.12.1ResponsibilitiestoParticipants
VoluntaryInformedConsent
Duetoparticipants’age,parent/carerconsentwassoughtinadditionto
informedassentfromparticipants.Forthequantitativestrand,opt-outconsentwas
utilisedgiventhattheprojectisconsideredapublictaskdesignedtobenefitthe
widerpopulation.Aspreviouslyoutlined,parents/carerswereprovidedwithan

CHAPTERFOUR:METHOD
136
informationpack(AppendixK)containinganinformationsheetoutliningdetailsof
theresearch,thenatureofparticipation,thedatatobeaccessed,datastorageand
usage,andcontactdetails,aswellasanopt-outconsentform.Educationsettings
wererequiredtoissuethisinformationpackatleasttwoweeksbeforedata
collectiontoprovidetimeforreturnofopt-outforms.Priortomeasurecompletion,
participantswerepresentedwithaninformationsheetoutliningthesame
informationinage-appropriatelanguage(AppendixL)andwereaskedtogive
informedassentbytickingaboxtoproceed.
Forthequalitativestrand,opt-inconsentwasused.Parents/carerswere
providedwithaninformationpack(AppendixN)containinganinformationsheet,
outliningtheresearch,thenatureofparticipation,thebenefitsandrisksoftaking
part,datastorageanduse,privacyboundaries,withdrawalinformation,and
contactdetails,alongsideaparentalconsentformtobecompletedandreturned.
Participantswereprovidedwithinformationsheetsoutliningthisinformationin
age-appropriatelanguage(AppendixM).Priortoeachinterview,interviewers
reviewedtheinformationsheetwiththeparticipanttoconfirmunderstandingand
providedopportunitiestoaskquestionsbeforeseekingwrittenassentfrom
participants(AppendixO).
RighttoWithdraw
Participantsmaintainedtherighttowithdrawfromtheresearchatany
time.Thiswasclearlyoutlinedinbothresearchstrandsalongsideassurancethat
participantscouldwithdrawforanyornoreason.
ChildrenandVulnerableYoungPeople
Giventhatparticipantsinthecurrentstudywereaged11–12years,several
measuresweretakentoensureappropriateengagement.Forinstance,all
interviewersheldup-to-dateDisclosureandBarringServiceschecks,age-
appropriateinformationwasprovidedtofacilitateinformedparticipation,and
appropriatedatacollectionmaterialswereusedthroughoutallstagesofthestudy.
Considerationwasalsogiventothesensitivetopicsdiscussedininterviews,
ensuringwellbeinginthisprocessandsignpostingrelevantinformationafterwards,

CHAPTERFOUR:METHOD
137
asdetailedinSection4.7.2.Potentialburdenforquantitativeparticipantswas
minimisedthroughuseofshortformsofmeasureswhereavailableand
appropriate.
Incentives
Qualitativeparticipantsweregivena£10shoppingvoucherfollowing
interviews.Whilethiswasintendedasatokenofthanks,participantswereaware
ofthisbeforetheinterviewandthereforeitcouldbeconsideredanincentive.One
concernisthatafinancialincentivemaycauseyoungpeopletooverlooktherisksof
participation(Seymour,2012),howeverresearchsuggeststhatyoungpeoplecan
viewfinancialincentivesasabonus,ratherthantheirmainreasonforparticipation
(CooperRobbinsetal.,2012).Consistentwithguidelines(CooperRobbinsetal.,
2012;Seymour,2012),this“incentive”wassmallandage-appropriateand
participationremaineddependentonparentalconsent.
Privacy
Dataweretreatedwithconfidentialityandanonymity.Compliantwiththe
DataProtectionAct1998(TheStationeryOffice),participantswereprovidedwith
clearinformationregardingdatastorageandusageandmaintaintherighttoaccess
datarelatingtothem.Researchersstoredelectronicdataonasecurepassword-
protectedserverandwrittenconsentformsinlockedcabinets.Datasetswere
anonymisedpriortousagehere,includingnamesofpeopleorplacesdiscussedby
qualitativeparticipants.
Disclosure
Interviewswerecarriedoutwithadherencetosafeguardingandchild
protectionpoliciesandprocedures.Ifaninterviewerperceivedariskofharmtothe
participantortoothers,thiswassharedwiththesetting’ssafeguardingofficerand
theprincipalinvestigator.Bothparents/carersandparticipantsweremadeaware
ofthisprocedurepriortodatacollection.Whereverpossible,interviewersinformed
participantsofintendeddisclosures.Safeguardingconcernsandactionstakenwere
loggedandstoredsecurely.

CHAPTERFOUR:METHOD
138
4.12.2ResponsibilitiestoSponsorsoftheResearch
Thisresearchwasfacilitatedthroughaccesstodatagatheredforthe
evaluationofHeadStartandtheNCLFarethereforesponsorsofthecurrentstudy.
Thestudyhasbeencompletedinaccordancewiththeagreementsrelatingto
sponsorshipoftheHeadStartevaluationandtheNCLFwillbemadeawareof
findings.
4.12.3ResponsibilitiestotheCommunityofEducationalResearchers
Findingswillbedisseminatedamongtheeducationalresearchcommunity,
tosharecontributionstoknowledgeandfortransparency.
4.12.4ResponsibilitiestoEducationalProfessionals,Policymakers,andthe
GeneralPublic
Findingswillbedisseminatedatvariouslevels,includingeducational
professionals,policymakersandthegeneralpublic.Thiswillbefacilitatedpartly
throughexistingrouteswithinHeadStart,suchasthroughpublicationofevidence
briefingsandpresentationatworkshopswithpartnershipleads,andthrough
publicationstargetingprofessionalsandyoungpeople.
4.13ChapterSummary
Thestudyusedamixedmethodsdesigntodevelopacomprehensive
understandingofemotionalsymptomsamongearlyadolescentgirls.The
quantitativestrandincluded8,327participants,usingSEMtoinvestigateriskeffects
andmechanismsaswellasfactorssupportingpositiveoutcomes.Inthequalitative
strand,IPAwasusedtoexplorethelivedexperienceofthreeearlyadolescentgirls
experiencingemotionalsymptomsinthecontextofriskexposure.Strategieswere
utilisedtofacilitatequalityandrigourandethicalconsiderationshavebeen
addressed.

CHAPTERFIVE:QUANTITATIVERESULTS
139
Chapter5:QuantitativeResults
5.1.ChapterOverview
Thischapterpresentsquantitativeresultspertainingtotheoverarching
researchquestions1and2.Itpresentsanoverviewofpreliminaryanalysesbefore
addressingspecificresearchquestions.Theriskfactorsassociatedwithemotional
symptomsarepresented,followedbyevidencerelatingtomultipleriskeffectsand
indirecteffectsviastressappraisalprocesses.Finally,resultsforpromotiveand
protectivefactorsarepresented.
5.2PreliminaryAnalyses
Preliminaryanalysisinvolvedexploringmissingness,reviewingdataagainst
analyticalassumptionsforSEM,andassessmentofeachmeasure’sfactorstructure
andpsychometricproperties.Abriefsummaryofresultsispresentedhereanda
moredetailedaccountofthisprocesscanbefoundinAppendixT.
Allsurveyitemshadmissingvalues(2.3–5.9%)andalldemographic
variablesexceptCINstatuscontainedmissingvalues(0.4–7.2%).Thisisan
acceptablelevelofmissingnessgivenuseofalargesample(Cheema,2014).32.3%
ofparticipants(N=2,681)hadatleastonemissingvalueacrossitemand
demographicvariables.Little's(1988)missingcompletelyatrandom(MCAR)test
wassignificantatthe.05αlevel(p<.001)andmissingnesswaspredictedby
participantcharacteristicsincludinglowacademicattainment,SEN,ethnicity,
Englishasanadditionallanguage,andneighbourhoodsocioeconomicdeprivation;
thus,missingnesswasassumedtobemissingatrandom(MAR).
Table5.1(overleaf)summarisesresultsfromthereviewofdataagainst
analyticalassumptions(seeAppendixTformoredetailedthresholdandprocedural
details).Thereweresomedeparturesfromnormaldistributionalassumptions,but
thesearelessproblematicinlargersamples(Kline,2016).Furthermore,theWLSMV
estimatorusedformuchofthemainanalysisdoesnotmakedistributional

CHAPTERFIVE:QUANTITATIVERESULTS
140
assumptionsaboutordinalfactorindicators(Li,2016)andtheMLRestimatorused
insensitivityanalysesproducesstandarderrorsrobusttonon-normality(Muthén&
Muthén,1998-2010).
Table5.1
SummaryofDataAssumptionReviewacrosstheDataset
Assumption Summaryofdatareview
Outliers 16SRSitemscores,allfamilyadultconnectionandcommunityadult
connectionitems,andeightschoolconnectionitemsidentifiedasoutliers
Multicollinearity üBivariatecorrelationcoefficientsdidnotexceed.70
Skewness üSkewnessdidnotexceedanabsolutevalueof2
Kurtosis üKurtosisdidnotexceedanabsolutevalueof7
Flooreffects ObservedforallSDQitems(24.2–52.1%),thetwopositively-wordedPSS-4
items(21.1–28.4%),oneschooladultconnectionitem(19.2%),andone
engagementinextracurricularactivitiesitem(26.3%)
Ceilingeffects ObservedforallSDQitems(17.4–42.0%),andallbutoneSRSsubscaleitems
(27.9–87.1%)
Linearity üResidualsclusteredaroundthezerolineinaresidualplot
Homoscedasticity üDatapointswereevenlydistributedaroundthezerolineinaresidualplot
Note.SRS=StudentResilienceScale;SDQ=StrengthsandDifficultiesQuestionnaire
ExplorationofmodelfitandfactorloadingsfortheSDQemotional
symptomssubscaleshowedsupportforaunidimensionalstructurewithfactor
loadingsrangingbetween.51–.78andacceptableinternalconsistency(α=.72;ω=
.80).Resultsalsosupporteda6-domainmultidimensionalstructureacrosstheSRS
withfactorloadingsbetween.66–92andgoodinternalconsistencyforallscales(α
=.71–.93;ω=.81–.96).
ExaminationofthePSS-4showedpoorfitfortheunidimensionalmodel
proposedbyCohenetal.(1983),whereasthe2-factorstructurecomprising
perceiveddistressandperceivedcopingshowedgoodfit.Althoughinternal
consistencyforperceiveddistresswasacceptable(α=.71;ω=.76),lowvalues
wereobservedforperceivedcoping(α=.57;ω=.62),likelybecausethis

CHAPTERFIVE:QUANTITATIVERESULTS
141
multidimensionalstructureappearsinparttobetheresultofreversewording
effects(Demkowiczetal.,2019),indicatinganeedforcautionininferences.
Cautionisalsonecessarygiventhatthesesub-factorscompriseonlytwoitems
each,as2-itemfactorscanbeunstableandproducelessreliableresultsthanthose
comprisedofagreaternumberofitems(Brown,2015;MacCallum,Widaman,
Zhang,&Hong,1999;Raubenheimer,2004).However,thiswasnotwithinthe
controlofthecurrentstudygivenuseofsecondarydata;thus,thestudysoughtto
offeranexploratoryexaminationofthestresshypothesisthatshouldbe
investigatedinfutureworkusingmorerobustmeasurementapproaches.
Finally,Table5.2presentsdescriptivestatisticsforthecontinuousvariables
utilisedacrossanalysis.Thereareveryfewstudiespublishingmeanscoresforthe
SDQemotionalsymptomssubscaleamongrecentcohortsinEngland,particularlyso
whenitcomestodistributionforgirlsspecifically.However,itshouldbenotedthat
themeanscoreinthecurrentstudyexceedsthatsharedbyFinketal.(2015),who
reportedameanscoreof3.49forgirlsina2014sample,whichwasfoundtobe
significantlyhigherthanscoresinapreviouscohortin2009.Assuchitappearsthat
thesampleisperhapsreportingelevatedsymptoms,ashighlightedinSection4.5.1.
Table5.2
DescriptiveStatisticsforContinuousVariables
Variable M SD Scorerange
Emotionalsymptoms(SDQ) 4.28 2.52 0–10
Perceiveddistress(PSS-4items1and4) 2.98 2.13 0–8
Perceivedcoping(PSS-4items2and3) 4.29 1.83 0–8
Familyadultconnection(SRS) 18.02 2.65 4–20
Schooladultconnection(SRS) 15.44 3.80 4–20
Communityadultconnection(SRS) 17.61 3.37 4–20
Schoolpeerconnection(SRS) 54.87 10.53 13–65
Activeengagementinhomeandschoollife(SRS) 13.81 3.57 4–20
Engagementinextracurricularactivities(SRS) 7.24 2.79 2–10
Neighbourhoodsocioeconomicdeprivation(IDACI) .24 .14 .01–.81
Note.SDQ=StrengthsandDifficultiesQuestionnaire;PSS-4=four-itemPerceivedStressScale;SRS=
StudentResilienceSurvey;IDACI=IncomeDeprivationAffectingChildrenIndex.

CHAPTERFIVE:QUANTITATIVERESULTS
142
5.3ResearchQuestion1:RiskFactorsandProcesses
1.Whataretheriskfactorsandprocessesassociatedwithemotionalsymptoms
amongearlyadolescentgirls?
5.3.1RiskFactors
a.Oftherisksidentified,whatisthemagnitudeoftheirassociationwithearly
adolescentgirls’emotionalsymptoms?
StageOne:Pre-Analysis
Table5.3(overleaf)presentsICCvaluesandbivariatecorrelationcoefficients
forvariablesinthisanalysis.

143
Table5.3
IntraclusterCorrelatio
nCo
efficientsa
ndBivariateCorrelatio
nCo
efficientsforVariablesinRQ1a
10
—
Note.IC
C=intraclustercorrelatio
ncoefficient;SEN
=sp
ecialedu
catio
nalneeds;A
CEs=
adversechildho
odexperiences.
*p<.05.**p<.01.***p<.001
.
9 —
.15*
**
8 —
.10*
**
.11*
**
7 —
.15*
**
.21*
**
.37*
**
6 —
.12*
**
.07*
**
.05*
**
.10*
**
5 —
-.13*
**
-.17*
**
-.10*
**
-.07*
**
-.15*
**
4 —
-.32*
**
-.28*
**
-.17*
**
.10*
**
-.07*
**
-.15*
**
3 —
.01
.01
.01
-.01
-.02
-.02
-.01
2 —
-.49*
**
.06*
**
-.08*
**
.03*
*
.00
.03*
.03*
.01
1 —
.01
-.02
.07*
**
-.05*
**
.06*
**
.07*
**
.12*
**
.02*
**
.03*
ICC
.02
.00
.00
.25
.26
.14
.22
.03
.12
.40
Varia
ble
1.Emotiona
lsym
ptom
s
2.You
ngre
lativ
eage(you
ngest)
3.You
ngre
lativ
eage(m
iddle)
4.Low
acade
micattainm
ent
5.Highacad
emicattainm
ent
6.SEN
7.Low
familyincome
8.Caregivingrespon
sibilitie
s
9.ACE
s
10.N
eighbo
urho
od
socioe
cono
micdep
rivation

CHAPTERFIVE:QUANTITATIVERESULTS
144
StageTwo:MainAnalysis
Eachhypothesisedriskvariablewasassessedbasedonthedirection,
statisticalsignificance,andmagnitudeoftheregressionpathwayontoemotional
symptoms.Positivebetaswereexpectedforallpathways.Betaregression
coefficientsareshowninTable5.4(below)andFigure5.1(overleaf).Modelfit
indicesshowedgoodfit:χ2(41)=321.03,p<.001;RMSEA=.03,90%CI[.03,.03],p
=1.00;CFI=.97,TLI=.95.SensitivityanalysisutilisingMLRyieldedsimilarresults.
Table5.4
UnstandardisedandStandardisedRegressionBetaCoefficientsandStandardErrorsforHypothesised
RiskVariablesasPredictorsofSymptoms(n=7,326)
Unstandardised Standardised
Hypothesisedriskfactor B SE β SE
Youngrelativeage(youngest)a -0.01 0.02 -.02 .04
Youngrelativeage(middle)a -0.04 0.02 -.07 .04
Lowacademicattainment 0.06** 0.02 .11** .04
Highacademicattainment -0.01 0.02 -.03 .04
SEN 0.08** 0.02 .15** .05
Lowfamilyincome 0.05** 0.02 .10** .03
Caregivingresponsibilities 0.17*** 0.02 .33*** .04
ACEs 0.01 0.03 .02 .06
Neighbourhoodsocioeconomicdeprivation -0.11* 0.05 -.03* .02
Note.SEN=specialeducationalneeds;ACEs=adversechildhoodexperiences.aEldestyoungrelativeagegroup(bornSeptember–December)utilisedasreferencecategoryfor
dummyvariables.
*p<.05.**p<.01.***p<.001.
Resultsindicatedfourconfirmedriskfactorsthatwerestatisticallysignificant,inthe
expecteddirection,andmeaningfulinsize:(a)Lowacademicattainment,(b)SEN,
(c)lowfamilyincome,and(d)caregivingresponsibilities.Thefirstthreeweresmall
inmagnitude,whileamoderateassociationwasobservedbetweencaregiving
responsibilitiesandemotionalsymptoms.Theseriskfactorsformthebasisfor

CHAPTERFIVE:QUANTITATIVERESULTS
145
subsequentanalysesinresearchquestionsfocusedonriskprocesses(RQs1b–dand
2b).
Onefurtherhypothesisedriskvariable,neighbourhoodsocioeconomic
deprivation,wasfoundtobestatisticallysignificant(p=.04).However,the
parameterestimateshowedthatthiswasintheoppositedirectiontothat
theoreticallyexpectedandwasnearingzeroinsize(β=-.03).Assuch,thiswas
discountedasariskfactor.Theremainingthreehypothesisedriskvariableswere
alsorejectedasriskfactors,astheywerenotstatisticallysignificant:(a)Young
relativeage(bothyoung[p=.58]andmiddle[p=.06]referencegroups);(b)high
academicattainment(p=.41);and(c)ACEs(p=.60).
Figure5.1.Riskfactorsmodel.Standardisedbetacoefficientswithconfirmedriskfactorsinbold
type.SEN=specialeducationalneeds.
*p<.05.**p<.01.***p<.001.

CHAPTERFIVE:QUANTITATIVERESULTS
146
5.3.2CumulativeRiskEffects
b.Isthereevidenceforacumulativeriskeffectinrelationtoearlyadolescentgirls’
emotionalsymptoms?
StageOne:CreationofaCumulativeRiskIndex
ThefourriskfactorsidentifiedinRQ1aweresummedtocreatea
cumulativeriskindex,namelylowacademicattainment,SEN,lowfamilyincome,
andcaregivingresponsibilities.Initially,acumulativeriskindexincludingallfourrisk
factors(0–4)wascreated.Forinstance,aparticipantwithascoreof4isrecorded
asexposedtoallfourriskfactors,whileaparticipantwithascoreof0isrecorded
asexposedtonone.However,lessthanonepercent(n=69)ofparticipantshada
scoreof4.Inspectionofalinechartbetweenthecumulativeriskindexand
emotionalsymptomsindicatedstabilityintheeffectsbetweenthreeandfour
factors(Figure5.2,overleaf).Assuch,theuppertwocategorieswerecollapsedto
captureparticipantsexposedtothreeormoreriskfactors,creatinganindex
spanning0to3+.AsoutlinedinSection3.3.1,thisisconsistentwithapproachesin
previousstudies(e.g.,Oldfieldetal.,2015;Panayiotou&Humphrey,2018;Rutter,
1979)andindicatesthepointatwhichparticipantsareconsideredsaturatedwith
riskfactors.

CHAPTERFIVE:QUANTITATIVERESULTS
147
Figure5.2.Linechartforemotionalsymptomsandthecumulativeriskindex.Emotionalsymptomsis
onthey-axisandtheoriginal0–4cumulativeriskindexisonthex-axis.
Thelargestproportionofthesamplepresentednoriskfactors,withincrementally
fewerparticipantsrepresentedateachlevelofexposure(seeTable5.5).This
distributionisconsistentwithageneralpatternacrosscumulativeriskresearch,
whereinmostindividualswithincommunitysamplesareexposedtoveryfewrisk
factors,ifany,andfewareexposedtothespecificcombinationexaminedinany
onestudy(Evansetal.,2013).
Table5.5
DistributionoftheSampleAcrosstheCumulativeRiskIndex(M=0.82,SD=0.90)
Numberofriskfactors n Proportionofsample(%)
0 3,771 45.3%
1 2,745 33.0%
2 1,304 15.7%
3+ 490 5.9%
Note.Theremaining0.2%(n=17)hadmissingdataacrossallfourriskfactors.
StageTwo:Pre-Analysis
Priortothemainanalysis,theadjustedindexvariablewasreviewedagainst
analyticalassumptionsandwasfoundtobeacceptable.Missingdataacrossthefull

CHAPTERFIVE:QUANTITATIVERESULTS
148
indexwaslow(0.2%),whileskewness(0.84)andkurtosis(-0.23)absolutevalues
werebelowadoptedthresholds.Asistypicalinriskresearch,manyparticipants
werenotexposedtoanyriskfactors,resultinginflooreffects(45.3%)andsothis
variablewastreatedascategoricalratherthancontinuousininterpretingresults,
consistentwithMplusguidance(Muthén,2006).Bivariatecorrelationcoefficients
weregivenparticularattentiontoscreenformulticollinearity,giventhatthe
cumulativeriskindexisacompositevariableconstructedusingriskfactors;
correlationcoefficientswererelativelyhigh(Table5.6),aswouldbeexpected,but
didnotexceed.70.
Table5.6
IntraclusterCorrelationCoefficientsandBivariateCorrelationCoefficientsforVariablesinRQ1b
Variable ICC 1 2 3 4 5 6
1.Emotionalsymptoms .02 —
2.Lowacademicattainment .25 .07 —
3.SEN .14 .06 .28 —
4.Lowfamilyincome .22 .07 .16 .12 —
5.Caregivingresponsibilities .03 .12 .12 .07 .15 —
6.Cumulativeriskindex .12 .13 .66 .47 .69 .55 —
Note.ICC=intraclustercorrelationcoefficient;SEN=specialeducationalneeds.
Allcorrelationcoefficientssignificantatthe.001alphalevel.
StageThree:MainAnalysis
Modelfitindicesindicatedacceptablefit:χ2(9)=430.25,p<.001;RMSEA=
.08,90%CI[.07,.08],p<.001;CFI=.96;TLI=.93.TheTLIvaluewasslightlylower
thanthethresholdof.95;however,theresidualcorrelationmatrixandMIandSEPC
valuesdidnotindicatespecificlocalisedissues.Assuch,thiswasconsidered
acceptablebutprovidedfurtherjustificationforexploringalternativemodelling
approachesinRQ1c.Resultsshowedastatisticallysignificantrelationship(see
Figure5.3andTable5.7,overleaf).

CHAPTERFIVE:QUANTITATIVERESULTS
149
Figure5.3.Statisticalmodelforcumulativeriskwithstandardisedregressionbetacoefficient.
***p<.001.
Consistentwithguidance(Evansetal.,2013),thiswasinvestigatedfurtherto
examinewhetherobservedeffectswereattributabletotheindexor,alternatively,
drivenbyasingleriskfactorcontainedwithinit.Totestthis,thismodelwas
repeatedfourtimeswitheachindividualriskfactoraddedinturn(seeFigure5.4).If
observedeffectswereattributabletoasingleriskfactorratherthantheindex,it
wouldbeexpectedthatincludingthatfactorasacovariatewouldaffectthe
significanceofthispathway.
Figure5.4.Conceptualmodelforcumulativeriskeffectswithcovariatemodel.SEN=special
educationalneeds.
ParameterestimatesforbothmainandcovariateanalysesareshowninTable5.7
(overleaf);sensitivityanalysesusingMLRyieldedsimilarresults.
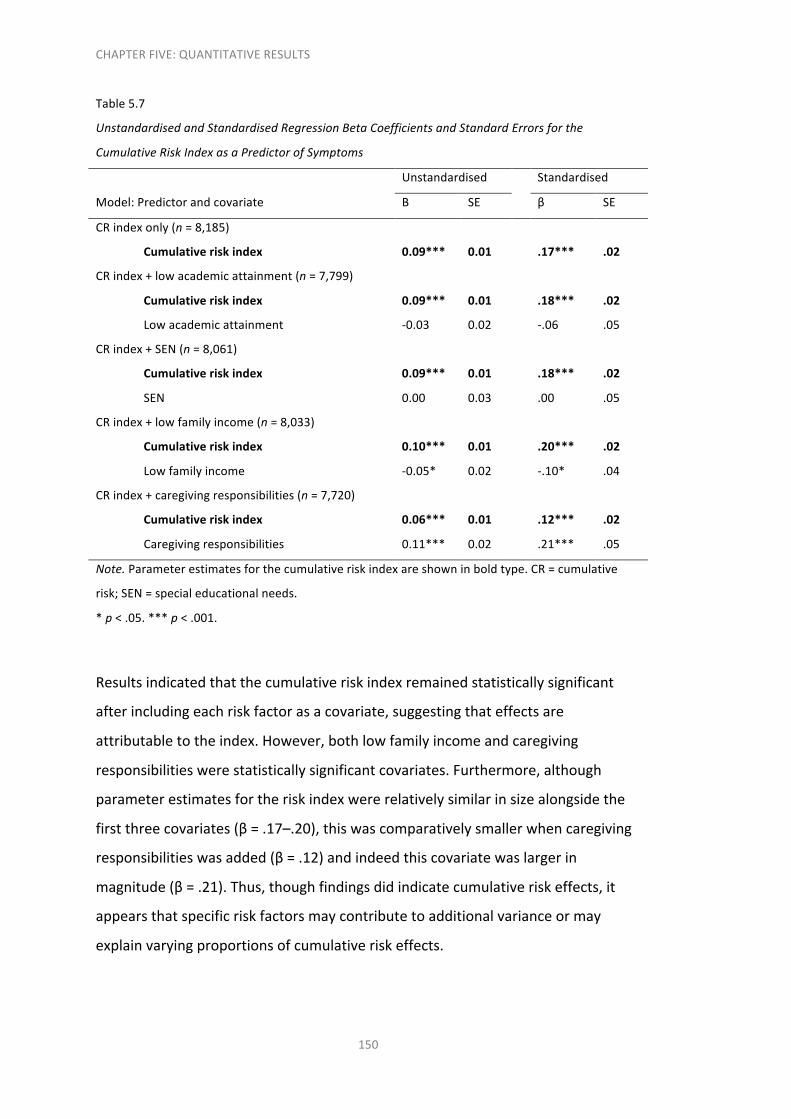
CHAPTERFIVE:QUANTITATIVERESULTS
150
Table5.7
UnstandardisedandStandardisedRegressionBetaCoefficientsandStandardErrorsforthe
CumulativeRiskIndexasaPredictorofSymptoms
Unstandardised Standardised
Model:Predictorandcovariate B SE β SE
CRindexonly(n=8,185)
Cumulativeriskindex 0.09*** 0.01 .17*** .02
CRindex+lowacademicattainment(n=7,799)
Cumulativeriskindex 0.09*** 0.01 .18*** .02
Lowacademicattainment -0.03 0.02 -.06 .05
CRindex+SEN(n=8,061)
Cumulativeriskindex 0.09*** 0.01 .18*** .02
SEN 0.00 0.03 .00 .05
CRindex+lowfamilyincome(n=8,033)
Cumulativeriskindex 0.10*** 0.01 .20*** .02
Lowfamilyincome -0.05* 0.02 -.10* .04
CRindex+caregivingresponsibilities(n=7,720)
Cumulativeriskindex 0.06*** 0.01 .12*** .02
Caregivingresponsibilities 0.11*** 0.02 .21*** .05
Note.Parameterestimatesforthecumulativeriskindexareshowninboldtype.CR=cumulative
risk;SEN=specialeducationalneeds.
*p<.05.***p<.001.
Resultsindicatedthatthecumulativeriskindexremainedstatisticallysignificant
afterincludingeachriskfactorasacovariate,suggestingthateffectsare
attributabletotheindex.However,bothlowfamilyincomeandcaregiving
responsibilitieswerestatisticallysignificantcovariates.Furthermore,although
parameterestimatesfortheriskindexwererelativelysimilarinsizealongsidethe
firstthreecovariates(β=.17–.20),thiswascomparativelysmallerwhencaregiving
responsibilitieswasadded(β=.12)andindeedthiscovariatewaslargerin
magnitude(β=.21).Thus,thoughfindingsdidindicatecumulativeriskeffects,it
appearsthatspecificriskfactorsmaycontributetoadditionalvarianceormay
explainvaryingproportionsofcumulativeriskeffects.
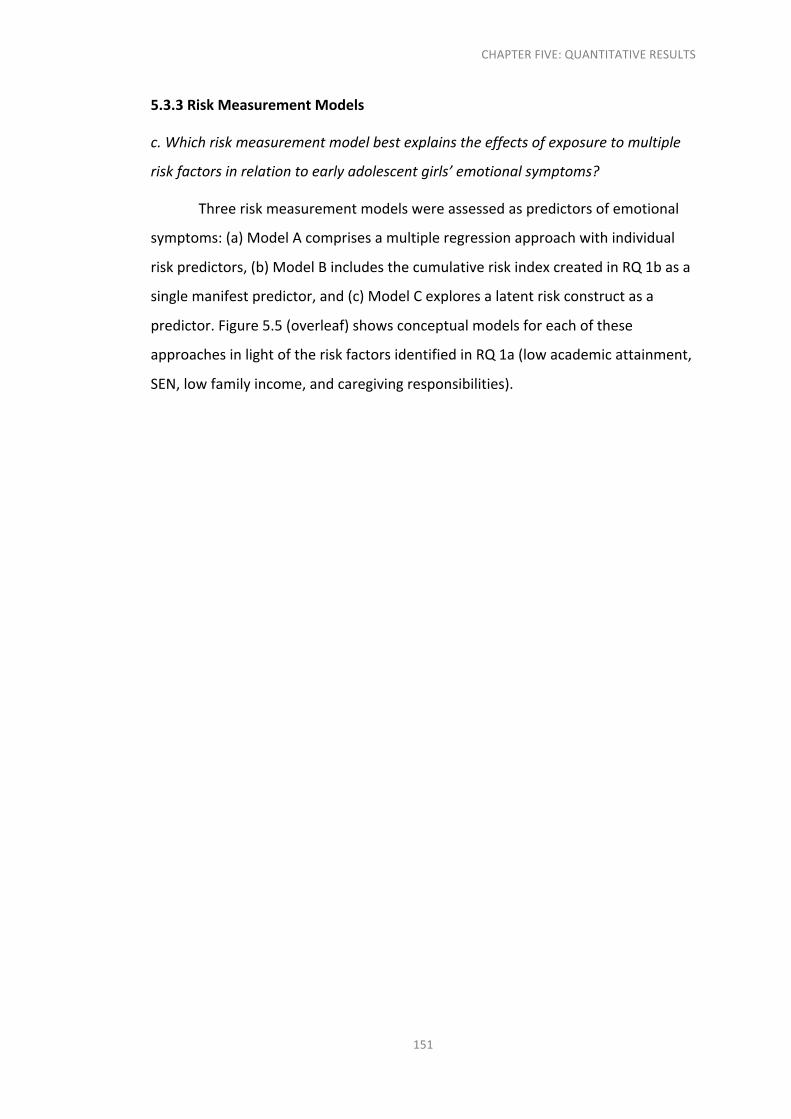
CHAPTERFIVE:QUANTITATIVERESULTS
151
5.3.3RiskMeasurementModels
c.Whichriskmeasurementmodelbestexplainstheeffectsofexposuretomultiple
riskfactorsinrelationtoearlyadolescentgirls’emotionalsymptoms?
Threeriskmeasurementmodelswereassessedaspredictorsofemotional
symptoms:(a)ModelAcomprisesamultipleregressionapproachwithindividual
riskpredictors,(b)ModelBincludesthecumulativeriskindexcreatedinRQ1basa
singlemanifestpredictor,and(c)ModelCexploresalatentriskconstructasa
predictor.Figure5.5(overleaf)showsconceptualmodelsforeachofthese
approachesinlightoftheriskfactorsidentifiedinRQ1a(lowacademicattainment,
SEN,lowfamilyincome,andcaregivingresponsibilities).

CHAPTERFIVE:QUANTITATIVERESULTS
152
Figure5.5.Multipleriskexposuremeasurementmodels.ModelAshowsamultipleregression
approach,ModelBspecifiesthecumulativeriskindexasapredictor,andModelCcomprisesalatent
riskconstruct.SEN=specialeducationalneeds.

CHAPTERFIVE:QUANTITATIVERESULTS
153
StageOne:Pre-Analysis
Table5.8presentsICCvaluesandbivariatecorrelationcoefficientsfor
variablesinthisanalysis.
Table5.8
IntraclusterCorrelationCoefficientsandBivariateCorrelationCoefficientsforVariablesinRQ1c
Variable ICC 1 2 3 4 5 6
1.Emotionalsymptoms .02 —
2.Lowacademicattainment .25 .07 —
3.SEN .14 .06 .28 —
4.Lowfamilyincome .22 .07 .16 .12 —
5.Caregivingresponsibilities .03 .12 .12 .07 .15 —
6.Cumulativeriskindex .12 .13 .66 .47 .69 .55 —
Note.ICC=intraclustercorrelationcoefficient;SEN=specialeducationalneeds.
Allcorrelationcoefficientsaresignificantatthe.001level.
StageTwo:CreationofaLatentRiskConstruct
Priortothemainanalysis,CFAwasusedtoassessthelatentriskconstruct
andameasurementmodelwasexploredforthisfactorandtheemotional
symptomssubscale.Fitindicesdidnotindicateoptimalfit,withtheTLIvalue
substantiallylowerthantheadvised.95:χ2(2)=47.72,p<.001;RMSEA=.05,90%
CI[.04,.07],p=.35;CFI=.94,TLI=.81.MIvaluesexceeding10andSEPCvalues
exceeding.20indicatedthattheresidualcorrelationbetweenlowacademic
attainmentandSENshouldbefreelyestimated,alongsideresidualcorrelations
matrixvaluesexceeding.10.Factorloadingswereunequalandwide-ranging,with
largeloadingsforlowacademicattainmentandSENbutmuchsmallerestimatesfor
lowfamilyincomeandcaregivingresponsibilities(seeTable5.9,overleaf),
suggestingthatthesetwoitemswerebetterrepresentedbythelatentriskfactor.

CHAPTERFIVE:QUANTITATIVERESULTS
154
Table5.9
UnstandardisedandStandardisedFactorLoadingsandIntraclusterCorrelationCoefficientsforthe
LatentRiskConstruct(n=8,310)
λ
Riskindicator Unstandardised Standardised ICC
Lowacademicattainment .76 .76 .25
SEN .71 .71 .14
Lowfamilyincome .44 .44 .22
Caregivingresponsibilities .33 .33 .03
Note.ICC=intraclustercorrelationcoefficient;SEN=specialeducationalneeds.
Allparameterestimatesshownaresignificantatthe.001alphalevel.
Conceptually,thiswasunsurprisinggiventhatpupilswithSENinEnglandgenerally
showloweracademicattainmentthantheirpeers(Humphreyetal.,2013).Assuch,
followingbothpriortheoryandevidence,thefactormodelwasre-specifiedwith
theresidualcorrelationbetweenlowacademicattainmentandSENfreely
estimated,ratherthanconstrainedtozero.Thisadjustmentresultedinexcellentfit;
χ2(1)=1.33,p=.25RMSEA=.01,90%CI[.00,.03],p=1.00;CFI=1.00,TLI=1.00,
withacceptableMI,SEPC,andresidualcorrelationsthresholds.Factorloadings
wereobservedtobemoreconsistentinmagnitude,asshowninTable5.10.As
such,thismodelwasusedinsubsequentanalyses.
Table5.10
UnstandardisedandStandardisedFactorLoadingsfortheLatentRiskConstructwithCorrelated
Residuals(n=8,310)
λ
Riskindicator Unstandardised Standardised
Lowacademicattainment .49 .49
SEN .44 .44
Lowfamilyincome .60 .60
Caregivingresponsibilities .44 .44
Note.Allparameterestimatesshownaresignificantatthe.001alphalevel.

CHAPTERFIVE:QUANTITATIVERESULTS
155
Finally,ameasurementmodelwasspecifiedincludingthelatentrisk
constructandthelatentemotionalsymptomsfactorpriortothemainanalysis(n=
8,324).Fitindicesshowedthatthemeasurementmodelhadgoodfittothedata:χ2
=(25)466.45,p<.001;RMSEA=.05,90%CI[.04,.05],p=.96;CFI=.96,TLI=.94.
ExaminationofmodificationindicesandSEPCvaluesindicatedsomelocalised
strain,howeverasthemodelshowedgoodoverallfitandCFIandTLIvalueswere
generallyacceptable,thesevalueswerenotconsideredtobeproblematicbutwere
noted.Thestandardisedlatentcorrelationbetweenthelatentriskconstructand
emotionalsymptomswas.30(p<.001),whichindicatesamoderateassociationin
theexpecteddirection.Assuch,resultsindicatedthatthemeasurementmodelwas
viableforuseinthesubsequentstructuralmodel(ModelC).
StageThree:MainAnalysis
Thevarianceexplainedbyeachriskmeasurementapproachasapredictor
ofemotionalsymptomsispresentedoverleafinTable5.11alongsidemodelfit
indices,parametercoefficients,andstandarderrors.Figure5.6(overleaf)illustrates
keyinformationinthecontextofeachmodel.Itshouldbenotedthatasensitivity
analysisusingMLRdidnotproducesubstantiallydifferentestimatesthanthose
obtainedusingWLSMV;however,thevarianceexplainedbythelatentrisk
constructwasslightlysmallerinMLR(5.7%)relativetothatproducedinWLSMV
(8.8%).Inspectionofmodelfitindicesindicatedthatallmodelsshowedacceptable
fittothedata,althoughRMSEAvalueswereslightlyhighforModelB.Itshouldbe
notedthatnodirectcomparisonofmodelfitcanbemadeforthesemodelsgiven
thattheyarenon-nested.Thus,inspectionofmodelfitwasinsteadfocusedon
whethereachofthemeasurementmodelscouldbeconsideredanappropriate
representationofriskanditsrelationshipwithemotionalsymptomswithinthis
sample.

156
Table5.11
Unstand
ardisedan
dStan
dardise
dRe
gressio
nBe
taCoefficientsand
Mod
elFitIndicesforth
eMultip
leRisk
ExposureMod
els
Stan
dardise
d SE
.02
.01
.02
.02
.02
.03
Note.M
odelsa
resh
owninboldtype
.R2 =
varianceexplaine
d;SEN
=sp
ecialedu
catio
nalneeds.
**p<.01.***p<.001
.
β .06*
**
.03*
*
.04*
*
.12*
**
.17*
**
.30*
**
Unstand
ardised SE
0.02
0.02
0.02
0.02
0.01
0.01
B 0.08
***
0.07
**
0.05
**
0.17
***
.09*
**
0.16
***
R2
2.8%
2.4%
8.8%
Mod
elfitind
ices
χ2(2
1)=483
.10,p<.001
;RMSEA=.05,90%
CI[.05
,.06
],p=.27;CFI=.95,TLI=.92
χ2 (9)=
430
.25,p<.001
;RMSEA=.08,90%
CI
[.07,.08],p<.001
;CFI=.96,TLI=.93
χ2 (25)=466
.45,p<.001
;RMSEA=.05,90%
CI[.04
,.05
],p=.96;CFI=.96,TLI=.94
Mod
eland
predictors
Mod
elA:M
ultip
lere
gressio
n(n=8,324
)
Low
acade
micattainm
ent
SEN
Low
familyincome
Caregivingrespon
sibilitie
s
Mod
elB:C
umulativerisk(n=8,185
)
Cum
ulativeriskinde
x
Mod
elC:Laten
trisk
con
struct(n
=8,324
)
Laten
trisk
con
struct

CHAPTERFIVE:QUANTITATIVERESULTS
157
Figure5.6.Statisticalmultipleriskexposuremeasurementmodelswithstandardisedbeta
coefficients.SEN=specialeducationalneeds.
**p<.01.***p<.001.

CHAPTERFIVE:QUANTITATIVERESULTS
158
Intermsofexplanatorypower,thecumulativeriskindexinModelBpredictedthe
leastvarianceinemotionalsymptomsacrossthesample(2.4%).Comparatively,the
inclusionofallindividualriskfactorsaspredictorsinModelApredictedaslightly
higheramountofvariance(2.8%).Howeverofthethreemodels,thelatentrisk
constructinModelCpredictedasubstantialamountmorevarianceofemotional
symptoms(8.8%).Itshouldbenoted,however,thatthesearesmallproportionsof
variance;acrosstheliteratureitappearsthatthiscanvarywidely,withsome
studiesfindinglessthantenpercentofvariancebeingpredictedbymultiplerisk
exposureinrelationtochildandadolescentinternalisingoutcomes(Morales&
Guerra,2006)andothersfindinggreateramountssuchas20-30%(Bayeretal.,
2012;Gerard&Buehler,2004;Halletal.,2010)orabove(Patalay&Fitzimons,
2018).However,someofthesestudiesmakeuseoflargernumbersofriskfactors
thanwereavailableinthecurrentstudy.Givenexaminationofsuchsmallfiguresin
predictingvariance,then,theincreasefrom2.8%to8.8%isnotanegligible
increase.Indeed,ofthetwomodelsthatdirectlymodelmultipleriskexposureasa
singularconstruct,ModelB(cumulativerisk)showedasmallassociation(β=.17),
whileModelC(latentconstruct)showedasmalltomoderateassociation(β=.30).
InlightoftheresultsforRQ1c,itwasdeemedappropriatetomakeuseof
thelatentriskconstructinsubsequentanalysesthatincludemultipleriskexposure,
namelyRQs1dand2b,giventhatthisshowedthegreatestpredictivepowerin
relationtoemotionalsymptoms.
5.3.4IndirectEffectsofStress
d.Arethereindirecteffectsofperceivedstressintherelationshipbetweenmultiple
riskexposureandemotionalsymptoms?
Thisresearchquestionfocusesonthedirectandindirectpathways
operatingwithinmultipleriskeffects,focusingonperceivedstress.Givenearlier
CFAresultsthePSS-4wasmodelledusingtwofactors,“perceiveddistress”and
“perceivedcoping”,andthustwoindirectpathwaymechanismswerespecified.

CHAPTERFIVE:QUANTITATIVERESULTS
159
StageOne:Pre-Analysis
Table5.12presentsICCvaluesandbivariate(leftdiagonal)andlatent(right
diagonal)correlationcoefficientsforvariablesinthisanalysis.
Table5.12
IntraclusterCorrelationCoefficientsandBivariate(leftdiagonal)andLatent(rightdiagonalandbold
type)CorrelationCoefficientsforVariablesinRQ1d
Variable ICC 1 2 3 4
1.Emotionalsymptoms .02 — .31 .74 -.56
2.Risktotalscore .11 .13 — .27 -.41
3.Perceiveddistress .01 .52 .11 — -.45
4.Perceivedcoping .01 -.36 -.17 -.29 —
Note.ICC=intraclustercorrelationcoefficients.
Allcorrelationcoefficientsshownaresignificantatthe.001alphalevel.
Ameasurementmodelwascarriedoutforallfourlatentvariablespriortothemain
analysis,whichshowedgoodfittothedata:χ2(58)=885.90,p<.001;RMSEA=.04,
90%CI[.04,.04],p=1.00;CFI=.96,TLI=.95.Resultsindicatedastrongassociation
betweenemotionalsymptomsandperceiveddistress,thoughthiswasbelowthe
suggested.85thresholdforextremecollinearityacrosslatentfactors(Brown,2015)
andsonotconsideredproblematic.
StageTwo:MainAnalysis
Table5.13(overleaf)presentsthedirect,indirect,andtotaleffectsof
multipleriskexposure,perceiveddistress,andperceivedcopingonemotional
symptoms.Modelfitindicesshowedacceptablefit:χ2(58)=885.90,p<.001;
RMSEA=.04,90%CI[.04,.04],p=1.00;CFI=.96,TLI=.95.Notethatthe
relationshipbetweenperceiveddistressandcopingwascontrolledforinthismodel
giventhattheyareconsideredinter-relatedconstructs.

CHAPTERFIVE:QUANTITATIVERESULTS
160
Table5.13
UnstandardisedandStandardisedBetaCoefficientsforDirect,Indirect,andTotalEffectsofMultiple
RiskExposure,PerceivedDistress,andPerceivedCopingonEmotionalSymptoms(n=8,324)
Unstandardised Standardised
Path B SE β SE R2
Totaleffect 0.41*** 0.05 .31*** .03 60.5%
Directeffect 0.05 0.03 .04 .03
Totalindirecteffects 0.36*** 0.04 .27*** .02
Indirectpathway1:Perceiveddistress
Indirecteffects 0.21*** 0.03 .16*** .01
Risk→distress 0.48*** 0.06 .27*** .02 7.2%
Distress→emotional 0.45*** 0.01 .61*** .01
Indirectpathway2:Perceivedcoping
Indirecteffects 0.14*** 0.02 .11*** .01 16.7%
Risk→coping -0.66*** 0.07 -.41*** .03
Coping→emotional -0.22*** 0.02 -.27*** .02
Note.R2=varianceexplained.
***p<.001.
Resultsindicatedthatafteraccountingforindirecteffectstherewasnostatistically
significantdirectassociationbetweenmultipleriskexposureandemotional
symptoms.Statisticallysignificantmoderateeffectswereobservedforbothofthe
indirectpathwaysspecified.Individualdirectpathwaysvariedinsizefrom
moderatetolarge,withthestrongesteffectspresentforthepathwaybetween
perceiveddistressandemotionalsymptoms(β=.61).Thetotalindirecteffects,or
thejointeffectofbothoftheseindirectpathways,wereobservedtobestatistically
significantandsmalltomoderateinsize.Forreference,theindirecteffectsmodelis
illustratedbelowinFigure5.7(overleaf)alongsidetheoriginaldirecteffectsmodel
testedinRQ1c,whereindirectpathwayswerenotincluded.

CHAPTERFIVE:QUANTITATIVERESULTS
161
Figure5.7.Directeffectsandindirecteffectsmodels.Positiveparametersareshowninblocklines,
inverseparametersareshownindashedlines,andnon-significantparametersareshownindotted
lines.UpperandlowercurvedarrowsinModelB(.16and.11)showindirecteffectpathways
betweenriskandemotionalsymptomsviaperceiveddistressandperceivedcoping,respectively.
Notethattheperceiveddistressandperceivedcopingarecorrelatedinthemodeltoaccountfor
theirsharedvariance.
***p<.001.
AsshowninTable5.13,inclusionoftheseindirecteffectpathwaysalsoexplaineda
muchgreaterproportionofthevarianceinemotionalsymptoms(60.5%)compared
tothatexplainedbythelatentriskconstructasasingularpredictorofthisoutcome

CHAPTERFIVE:QUANTITATIVERESULTS
162
asobservedinRQ1c(8.8%).Giventheabove,resultsindicatethatassociations
operateentirelythroughindirectpathwaysviaperceiveddistressandcoping,or
“fullmediation”(Hayes,2017).
5.4ResearchQuestion2:FactorsandProcessesforPositiveOutcomes
1.Whatarethefactorsandprocessesthatsupportpositiveoutcomesinemotional
symptomsamongearlyadolescentgirls?
5.4.1PromotiveFactors
a.Ofthepromotivefactorsidentified,whatisthemagnitudeoftheirassociation
withearlyadolescentgirls’emotionalsymptoms?
StageOne:Pre-Analysis
Table5.14showsICCvaluesandbivariate(leftdiagonal)andlatent(right
diagonal)correlationcoefficientsforvariablesinthisanalysis.
Table5.14
IntraclusterCorrelationCoefficientsandBivariate(leftdiagonal)andLatent(rightdiagonalandbold
type)CorrelationCoefficientsforVariablesinRQ2a
Variable ICC 1 2 3 4 5 6 7
1.Emotionalsymptoms .02 — -.31 -.20 -.26 -.39 -.31 -.17
2.Familyadultconnection .08 -.21 — .52 .64 .50 .40 .53
3.Schooladultconnection .07 -.16 .39 — .50 .40 .53 .18
4.Communityadultconnection .11 -.19 .48 .39 — .52 .54 .34
5.Schoolpeerconnection .06 -.30 .38 .33 .42 — .55 .26
6.Activeengagementinhome
andschoollife
.10 -.24 .44 .42 .41 .45 — .40
7.Engagementinextracurricular
activities
.07 -.13 .20 .14 .24 .19 .29 —
Note.ICC=intraclustercorrelationcoefficient.
Allcorrelationcoefficientsshownweresignificantatthe.001alphalevel.

CHAPTERFIVE:QUANTITATIVERESULTS
163
Ameasurementmodelwithalllatentvariablesshowedacceptablefit:χ2(573)=
4,320.31,p<.001;RMSEA=.03,90%CI[.03,.03],p=1.00,CFI=.98,TLI=.97(see
Table5.14aboveforlatentcorrelations).
StageTwo:Pre-Analysis
Hypothesisedpromotivevariableswereassessedbyspecifyinglinear
regressionpathwaysontoemotionalsymptoms.Pathwayswereassessedbasedon
directionandstatisticalsignificance,withadditionalconsiderationofmagnitude,
withallvariablesexpectedtoshowinverseassociationswithemotionalsymptoms.
Modelfitindicesshowedgoodfit:χ2(573)=4,320.31,p<.001;RMSEA=.03,90%
CI[.03,.03],p=1.00;CFI=.98,TLI=.97(seeTable5.15belowandFigure5.8
overleaf).
Table5.15
UnstandardisedandStandardisedRegressionBetaCoefficientsandStandardErrorsforHypothesised
PromotiveVariablesasPredictorsofSymptoms(n=8,280)
Unstandardised Standardised
Hypothesisedpromotivevariable B SE β SE
Familyadultconnection -0.09*** 0.02 -.14*** .03
Schooladultconnection 0.02 0.01 .03 .02
Communityadultconnection 0.01 0.01 .01 .02
Schoolpeerconnection -0.19*** 0.01 -.28*** .02
Activeengagementinhomeandschoollife -0.06*** 0.02 -.09*** .02
Engagementinextracurricularactivities -0.02 0.01 -.03 .02
Note.***p<.001.
Threeofthesixhypothesisedpromotivevariableswerestatisticallysignificantand
intheexpecteddirection:(a)Familyadultconnection,(b)schoolpeerconnection,
and(c)activeengagementinhomeandschoollife.Betacoefficientsvariedin
magnitude,thoughallweregenerallysmallinsize.Theassociationbetweenschool
peerconnectionandemotionalsymptomswasgreatestinsize,withasmallto
moderateassociation,whileparticipationinhomeandschoollifefellbelowthe

CHAPTERFIVE:QUANTITATIVERESULTS
164
thresholdforasmalleffect.Thethreeremainingvariableswerenotstatistically
significantandwererejectedaspromotivefactors,specifically:(a)Schooladult
connection(p=.25);(b)communityadultconnection(p=.37);and(c)engagement
inextracurricularactivities(p=.09).
Figure5.8.Promotivefactorsmodel.Standardisedbetacoefficientsareshownwithconfirmed
protectivefactorsinboldtype.
***p<.001.
5.4.2ProtectiveFactors
b.Towhatextentarethedirectand/orindirectrelationshipsbetweenmultiplerisk
exposure,perceivedstress,andemotionalsymptomsconditionaluponaccessto
protectivefactors?
Aconditionalindirecteffectsmodelwasinvestigated,withmoderators
modelledontheindirectperceiveddistressandcopingpathwaysidentifiedinRQ

CHAPTERFIVE:QUANTITATIVERESULTS
165
1d.Theaimherewastoassesswhethertheseassociationsweredependentupon
thelevelofone’sperceivedsocialconnectionsandactiveengagement.Conditional
effectswerespecifiedforindirectpathwaysonlygiventhatresultsfromRQ1d
indicatedthatthedirecteffectwasnotsignificant,thusmeaningthereisnoeffect
tobemoderated.
StageOne:IdentificationofVariables
First,thesixSRSsubscaleswerereviewedtoidentifythoseexpectedtobe
mostsalientandthusprioritisedforanalysis.Table5.16(overleaf)presents
considerationsforeachofthesixpossiblemoderatorvariables;first,ashort
summaryoftheoryandpriorresearchisoutlined(basedonthereviewofthe
literaturepresentedinSection3.4.2),alongsidestandardisedparameterestimates
obtainedthroughalinearmultipleregressionmodelwhereinallsubscaleswere
includedaspredictorsofemotionalsymptoms,perceiveddistress,andperceived
coping.Theinclusionstatusofeachvariableasahypothesisedmoderatorisalso
presented.Specifically,fourvariableswereselectedforinclusion,showninbold
typeinTable5.16:(a)Familyadultconnection,(b)schooladultconnection,(c)
schoolpeerconnection,and(d)activeengagementinhomeandschoollife.Two
variableswereexcludedatthisstagegivenlimitedtheoreticalandempirical
support,namely(a)Communityadultconnectionand(b)engagementin
extracurricularactivities.

166
Table5.16
SixPo
ssibleM
oderatorVariableswith
Sum
maryofTheoryan
dPriorE
videncean
dRe
gressio
nCo
efficients(n=6,62
8)
Inclusionstatus
Varia
bleinclud
ed
givenstrong
theo
reticaland
em
piric
alsu
pporta
sa
salientfa
ctorfo
rall
outcom
es
Varia
bleinclud
ed
giventheo
retical
supp
orta
ndgrowing
empiric
alsu
pportin
previousstud
ies,
alon
gsideane
edfo
rexam
inationdu
ring
tran
sition,th
ough
weakem
piric
al
supp
ortw
asobserved
forthe
sample
Varia
bleno
tinclude
dgivenlim
ited
theo
reticalsu
pport
β(SE)
Perceived
coping
.11(.0
1)***
.07(.0
1)***
.03(.0
1)**
Perceived
distress
-.13(.0
2)***
-.05(.0
2)**
-.02(.0
2)
Emotiona
lsymptom
s
-.11(.0
2)***
-.02(.0
2)
-.02(.0
2)
Summaryofth
eoryand
prio
revide
nce
Conn
ectio
nwith
familym
embe
rsinchildho
odand
ado
lescen
ce
isconsidered
critical(U
mbe
rson
eta
l.,201
0)and
isassociated
with
lowerlevelsofinternalisingand
emotiona
lsym
ptom
s(e.g.,Co
stelloeta
l.,200
8;Row
eetal.,201
6),including
protectiv
eeffectsforth
oseexpo
sedtorisk(C
onger&
Con
ger,
2002
;Willeetal.,200
8).
Broa
derschoo
lcon
nected
nesshasfreq
uentlybeenassociated
with
lowered
emotiona
lsym
ptom
s(e.g.,B
ondetal.,200
7;
Costelloeta
l.,200
8)and
ithasbeenargued
thatpositivepup
il-teache
rrelationshipsarecriticallyim
portan
tforpositive
developm
enta
ndoutcomes(Jen
nings&
Green
berg,200
9);
inde
ed,the
reisso
meeviden
ceofa
nassociationbe
tweensuch
relatio
nshipsand
lowered
emotiona
lsym
ptom
s(M
urray&
Green
berg,200
0;W
angetal.,201
3).Thism
aybeaffected
du
ringpe
riodsoftransition
(Lou
kase
tal.,201
6).
Qua
litativeresearchindicatestha
tado
lescen
tsvalue
positive
andcarin
grelatio
nshipswith
trustedad
ultsre
gardlessofthe
irdo
mainorro
le(M
unford&San
ders,201
6;Ungar,200
4b),
Varia
ble
Familyadu
ltconn
ectio
n
Scho
oladu
ltconn
ectio
n
Commun
ity
adult
conn
ectio
n

167
andlackofe
vide
nceof
empiric
allym
eaningful
foro
utcomes
Varia
bleinclud
ed
givenconsisten
ttheo
reticaland
em
piric
alsu
pporta
ssalientacrossa
llou
tcom
es
Varia
bleinclud
edas
thereissome
theo
reticalsu
pport
thatth
ismaybe
meaningful,alon
gside
empiric
alsu
pport
acrossoutcomesinth
esample
Varia
bleno
tinclude
dasth
eoryand
prio
reviden
ceislimite
dan
dthereislittle
empiric
al
supp
ortforth
isas
salientacross
outcom
es
Note.Stand
ardisedpa
rameterestim
atesonlyareshow
nhe
refo
reaseofcom
parison
given
thatth
isissupp
lemen
taryana
lysis
.
P<.01.***p<.001
.
.17(.0
1)***
12.(02
)***
.06(.0
1)***
-.18(.0
2)***
-.08(.0
2)***
.01(.0
1)
-.27(.0
2)***
-.10(.0
2)***
.03(.0
2)
indicatin
gthatth
eremayberelatio
nshipsbeyon
dthefamily
andho
mecontextsth
atarem
eaningful;ho
wever,the
reis
curren
tlylittleempiric
alevide
ncetosu
pportsuch
hypo
thesise
deffects.
Peersa
recon
sistentlyiden
tifiedasth
estrongestsocialfactor
pred
ictin
gad
olescenthealth
beh
avioursa
ndoutcomes(B
rown
&Larson,200
9;Umbe
rson
eta
l.,201
0)and
stud
iess
how
elem
entsofp
eerc
onne
ctioncorrespo
ndto
lowered
internalisingand
emotiona
lsym
ptom
s(Bo
sackieta
l.,200
7;
VanVo
orhe
eseta
l.,200
8)
Childrenan
dad
olescentsw
ithgreatercap
acity
ford
ecision
-makingan
dcontrolintheho
merepo
rtlowerlevelsof
emotiona
lsym
ptom
s(Be
ckereta
l.,201
0;Borellietal.,201
5),
whichm
ayre
lateto
increasedstressapp
raisa
land
cop
ing
capa
citie
s(Be
ckereta
l.,201
0;Borellietal.,201
5).Inascho
ol
contexte
vide
nceislim
itedasth
isisusua
llyexamined
asp
art
ofbroad
ersc
hoolcon
nected
ness.
Thereismod
este
vide
ncetosu
ggesttha
tado
lescen
textracurric
ularactivity
isassociatedwith
loweremotiona
lsymptom
s(Guè
vrem
onte
tal.,201
4;M
olinue
voeta
l.,201
0),
althou
ghth
esestud
iesh
avetypicallynotaccou
nted
forw
ider
form
sofsocialcon
nection,whichisoften
associatedwith
en
gagemen
tand
maycon
flateeffe
cts(Feldm
anFarb&
Matjasko,201
2;Kilm
ereta
l.,201
0).
Scho
olpee
rconn
ectio
n
Activ
een
gagemen
tin
homean
dscho
ollife
Engagemen
tin
extracurric
ular
activ
ities

CHAPTERFIVE:QUANTITATIVERESULTS
168
StageTwo:Pre-Analysis
Table5.17(overleaf)showsICCvaluesandbivariatecorrelationcoefficients
forthevariablesinthisanalysis.
169
Table5.17
IntraclusterCorrelatio
nCo
efficientsa
ndBivariateCorrelatio
nCo
efficientsforVariablesinRQ2b
8 —
Note.IC
C=intraclustercorrelatio
ncoefficient.
*p<.05.***p<.001
.
7 —
.45*
**
6 —
.33*
**
.42*
**
5 —
.39*
**
.38*
**
.44*
**
4 —
-.15*
**
.00
-.11*
**
-.02*
3 —
-.17*
**
.28*
**
.24*
**
.31*
**
.31*
**
2 —
-.29*
**
.11*
**
-.25*
**
-.20*
**
-.28*
**
-.23*
**
1 —
.52*
**
-.36*
**
.13*
**
-.21*
**
-.16*
**
-.30*
**
-.24*
**
ICC
.02
.01
.01
.11
.08
.07
.06
.10
Varia
ble
1.Emotiona
lsym
ptom
s
2.Perceived
distress
3.Perceived
cop
ing
4.Risk
totalscore
5.Fam
ilyadu
ltconn
ectio
n
6.Schoo
ladu
ltconn
ectio
n
7.Schoo
lpeercon
nection
8.Activeen
gagemen
tinho
mean
dscho
ollife

CHAPTERFIVE:QUANTITATIVERESULTS
170
StageThree:MainAnalysis
Figure5.9showsasimplifiedstatisticalmodelwiththeselectedmoderator
variablesmodelledonallindirectpathways,toillustratethewayinwhichthese
factorsandinteractionswithpredictorsaremodelled.
Figure5.9.Simplifiedstatisticalconditionalindirecteffectsmodel.Hypothesisedprotectivefactors
aremoderatingallindirectpathways.Therelationshipbetweenthemoderators,perceiveddistress
andperceivedcoping,iscontrolledfor.Directionality(+/-)isnotassumedgiventhatmoderationcan
influencedirectionality.Foreaseofillustration,parametersarelabelledusingletters,which
correspondtothekeyontherightbottomcornerofthefigure.

CHAPTERFIVE:QUANTITATIVERESULTS
171
Multipleriskexposurewasmodelledhereusingacumulativeriskindex,ratherthan
thelatentapproachsupportedinRQ1c.Theapproachtomodellingresidual
correlationsbetweenindicatorswithinMLrequiresatleastfiveindicatorsforthe
factortobeidentified,meaningMLcouldnotfacilitatecorrelationofresidualsfor
SENandlowacademicattainmentgiveninclusionofonlyfourindicators.While
otherestimatorssuchasWLSMVdonothavethisissue,onlyMLcanspecify
interactionswithalatentvariableasisnecessarytoexamineconditionaleffects
withinthismodel(Muthén&Muthén,1998-2010).Thus,itwasnotpossibleto
utilisethelatentconstruct;theimplicationsofthischallengearereflecteduponin
Section7.3.3.GiventhatearlieranalysisofindirecteffectsinRQ1dmadeuseof
WLSMV,ratherthanML,andutilisedlatentvariablesforriskexposureand
perceiveddistressandcoping,asecondindirecteffectsmodelwasspecifiedusing
MLandmanifestvariablestoreflecttheapproachhere.Thisispresentedbelow
andisnotintendedtoactas“new”resultsregardingindirectstresspathways,but
insteadisshowntofacilitatereadersinobservingthechangesincurredwhen
conditionaleffectsareapplied.Figure5.10(overleaf)showsstandardisedindirect
effectparametersasobtainedwiththisadjustedindirecteffectsmodel.Notethat
thisrepeatedanalysisshowedlowerestimatesfromriskexposureontoperceived
distressandperceivedcopingthanpreviouslyfoundinRQ1d,alongwithlower
indirecteffectsacrossbothpathways.Thesechangesmayinpartbeattributableto
theestimatorbutitisalsolikelythatthisistheresultofusingmanifestvariables
ratherthanlatentfactors,includinguseofacumulativeratherthanlatentrisk
approach.

CHAPTERFIVE:QUANTITATIVERESULTS
172
Figure5.10.Indirecteffectsmodel.Positiveparametersareshowninblocklinesandinverse
parametersareshownindashedlines.ThismodelrepeatsearlieranalysisconductedforRQ1dbut
wasspecifiedwithmanifestvariablesandestimatedusingML,ratherthanWLSMV,tomoredirectly
reflecttheconditionalindirectmodellingapproachandthusfacilitatemoreaccurateassessmentof
changewhereconditionaleffectsareadded.Upperandlowercurvedarrows(.07and.05)show
indirecteffectpathwaysbetweenriskandemotionalsymptomsviaperceiveddistressandperceived
coping,respectively.Notethattheperceiveddistressandperceivedcopingarecorrelatedinthe
modeltoaccountfortheirsharedvariance.
***p<.001.
Table5.18(overleaf)presentsparameterestimatesforthedirectand
indirectpathwayparameters,thecontributionofhypothesisedprotectivefactorsto
distress,coping,andemotionalsymptoms,andconditionaleffectspathways.54
parameterswerespecifiedwithinthismodel,with6,630casesincluded.This
satisfiesguidanceregardingsamplesizeinSEMmodels,whereatleasttwenty
participantsforeachparameterisadvisedinordertoachievebothpowerand
statisticalprecision(Jackson,2003;Kline,2016).

CHAPTERFIVE:QUANTITATIVERESULTS
173
Table5.18
UnstandardisedandStandardisedBetaCoefficientsforSpecificConditionalEffectsforIndirectEffect
Pathways(n=6,630)
Unstandardised Standardised
Path B SE β SE
Directpathwayc’1:Risk→emotional 0.04* 0.02 .03* 0.01
Indirectpathway1:Perceiveddistress
a1:Risk→distress -1.41*** 0.24 -.59*** .10
b1:Distress→emotional 0.20*** 0.05 .40*** 0.10
Indirectpathway2:Perceivedcoping
d1:Risk→coping 0.38* 0.15 .19* .07
e1:Coping→emotional -0.16* 0.07 -.29** .11
ModeratorA:Familyadultconnection
Familyadult→distress -1.46*** 0.18 -.18*** .02
Familyadult→coping 1.00*** 0.14 .14*** .02
Familyadult→emotional 0.04 0.23 .01 .06
Familyadult→a1(risk→distress) 0.48*** 0.14 .36*** .10
Familyadult→b1(distress→emotional) 0.00 0.03 .01 .10
Familyadult→d1(risk→coping) -0.24** 0.09 -.21** .08
Familyadult→e1(coping→emotional) -0.03 0.04 -.12 .14
ModeratorB:Schooladultconnection
Schooladult→distress -0.34** 0.11 -.06** .02
Schooladult→coping 0.35** 0.10 .07** .02
Schooladult→emotional -0.13 0.14 -.05 .05
Schooladult→a1(risk→distress) 0.05 0.05 .04 .06
Schooladult→b1(distress→emotional) 0.03 0.02 .09 .06
Schooladult→d1(risk→coping) 0.06 0.09 .05 .07
Schooladult→e1(coping→emotional) 0.03 0.03 0.09 .08
ModeratorC:Schoolpeerconnection
Schoolpeer→distress -0.41*** 0.04 -.20*** .02
Schoolpeer→coping 0.34*** 0.03 .20*** .02
Schoolpeer→emotional -0.15** 0.05 -.15** .05
Schoolpeer→a1(risk→distress) 0.07* 0.03 .17* .07
Schoolpeer→b1(distress→emotional) 0.00 0.01 -.00 .08
Schoolpeer→d1(risk→coping) -0.06* 0.03 -.16* .07
Schoolpeer→e1(coping→emotional) 0.00 0.01 .02 .12
ModeratorD:Activeengagementinhomeand
schoollife

CHAPTERFIVE:QUANTITATIVERESULTS
174
Engagement→distress -0.64*** 0.11 -.11*** .02
Engagement→coping 0.75*** 0.11 .15*** .02
Engagement→emotional -0.30* 0.15 -.10* .05
Engagement→a1(risk→distress) 0.19 0.10 .11 .06
Engagement→b1(distress→emotional) 0.01 0.02 .03 .06
Engagement→d1(risk→coping) 0.00 0.08 .00 .06
Engagement→e1(coping→emotional) 0.03 0.03 .11 .09
Note.Statisticallysignificantconditionaleffectpathwaysarepresentedinboldtype.
*p<.05.**p<.01.***p<.001.
Inspectionofresultsindicatedthattheeffectsofmultipleriskexposureuponboth
perceiveddistressandperceivedcopingwereconditionaluponlevelsoffamily
adultconnectionandschoolpeerconnection.ConsideredagainstCohen's(1988)
thresholdsof.14,.39,and.59asindicativeofsmall,moderate,andlargeeffect
sizesforstandardisedbetacoefficients,schoolpeerconnectionshowedasmall
effectforbothpathways,whilefamilyadultconnectionshowedamoderateeffect
inrelationtoriskeffectsuponperceiveddistress(a1)andasmalltomoderateeffect
forperceivedcoping(d1).Resultsalsoshowedthatundertheconditionsofgreater
familyadultconnectionandschoolpeerconnection,theeffectsofmultiplerisk
exposureuponthemediatorsarereversedwhencomparedtofindingsfromRQ1d.
Thatis,riskeffectsuponperceiveddistresswereobservedtobeinverseandindeed
werelargeinsize(-.59,comparedto.11withoutconditionaleffects),whileeffects
uponperceivedcopingwereobservedtobepositivebuttostillbesmallinsize(.19,
comparedto-.17withoutconditionaleffects).Figure5.11(overleaf)shows
conditionalindirecteffectsforeaseofinterpretationinrelationtotheresearch
question.
Conditionaleffectswereonlyobservedforthefirststagesofbothindirect
mechanisms;thatis,thepathwaysbetweenmultipleriskexposureandperceived
distressandcoping,respectively.Noconditionaleffectswereobservedinthe
secondstageofindirectmechanisms;thatis,forpathwaysofeitherperceived
distressorperceivedcopinguponemotionalsymptoms.Schooladultconnection
andactiveengagementinhomeandschoollifewerenotfoundtomoderateany
pathwaysacrossthemodel.

CHAPTERFIVE:QUANTITATIVERESULTS
175
Figure5.11.Specificconditionalindirecteffects.Familyadultconnection(FAMILY)andschoolpeer
connection(PEER)areshownmoderatingtheeffectsofmultipleriskexposureuponperceived
distressandperceivedcoping.Positiveparametersareshowninblocklinesandinverseparameters
areshownindashedlines.
*p<.05.**p<.01.***p<.001.
5.5ChapterSummary
Fourriskfactorswereidentified:Lowacademicattainment,SEN,lowfamily
income,andcaregivingresponsibilities.Cumulativeriskeffectswereobserved,
thoughalatentriskconstructshowedgreatestpredictiveutility(butwasnotviable
formorecomplexanalysis).Multipleriskexposurewasassociatedwithemotional
symptomsentirelythroughindirectpathways,viaperceiveddistressandperceived
coping.Threepromotivefactorswereidentified:Familyadultconnection,school
peerconnection,andactiveengagementinhomeandschoollife.Multiplerisk
effectsonperceiveddistressandcopingwereconditionaluponperceivedlevelsof
familyadultconnectionandschoolpeerconnection.

176
Blankpage

CHAPTERSIX:QUALITATIVEFINDINGS
177
Chapter6:QualitativeFindings
6.1ChapterOverview
Thischapterpresentsfindingsfromthequalitativestrandofthecurrent
study.Thechapterfirstoutlinesthethemesdevelopedforeachparticipantbefore
goingontopresentandexplorethemasterthemesdevelopedacrossthecorpus.
Finally,abriefappraisalofthereflexivejourneyispresented.
6.2IndividualParticipantThemes
Itshouldbenotedthatthethemesforeachindividualarenotpresentedas
themainfindingswithinthecurrentstudy.Instead,theyconstituteananalytical
stepaspartofdevelopingthemasterthemesofcentralinterest,whichcapture
perceptionsandexperiencesacrossthesampleasawhole.Thus,individual-level
themesarepresentedheretoestablishtheindividualityofparticipantsandto
illustratethewayinwhichtheseconnectwiththemasterthemespresentedinthe
mainbodyofthischapter.
6.2.1ThemesforAmelia
MuchofAmelia’saccountcentredonher“worries”andthethemes
developedfromhertranscriptreflectthisfocus.Amelia’slifeworldwascentred
aroundherworriesandthesedominatedthewaysheviewedherrelationshipsand
thewaythatshesawherselfasmovingthroughtheworld.Fivesuperordinate
themesweredevelopedforher:(a)Myworries,(b)othershelpme,(c)worriesas
central,(d)powerlessness,and(e)somethingbadwillhappen.Eachofthese
superordinatethemesencapsulatesanumberofsmallerthemes.Table6.1
presentsthesethemes;superordinatethemesareshowninitalics,withrelated
themeslistedbeneaththemalongsidekeywords/phrasesthatillustratetheir
essence.

CHAPTERSIX:QUALITATIVEFINDINGS
178
Table6.1
ThemesforAmelia
Superordinatethemes
Themes
Keyillustrativephrasesfrom
transcripts
Myworries
Worriesastangible
Worriesasseparatefromme
Worriesarepluralandcanmultiply
Worriesareintertwinedwithotherdisorders
myworries
Ihaveaworry
lotsofworries
dizzyoreitherworried
Othersassupportmechanisms
Othershelpme
Sharingemotionsasvaluable
Cumulativesupportnetwork
alotofpeoplehelp
let‘emout
alsohelps
Worriesascentral
Worryiscentralemotion
Worrydefinesrelationships
Worryasdominantthroughoutlife
happynotworried
they’rereallysupportive
worriedalot
Powerlessness
Lackofagency
Passiveemotionalregulation
Rumination
Responsibilityandself-blame
Idon’tknowwhy
takemyworryaway
justlikethinkaboutit
Iforget
Somethingbadwillhappen
Fearofnegativeconsequences
Difficultyconceptualisingthebadthing
Mismatchbetweenexpectationsandreality
somethingbadwillhappen
somethinglikethat
it’snotgonnahappen
6.2.2 ThemesforJennifer
Jennifer’saccountwasstronglydominatedby“negativethoughts”andher
feelingsofnotbeinggoodenough;therewereparticularissuesaroundthe
demandsplacedonherandhermethodsforcopingwiththis.AnalysisofJennifer’s
datawasmorechallengingthanthatoftheotherparticipantsforanumberof
reasons.Aparticulardifficultywasthatsheseemedverydetachedfromherfeelings
andactionsandassuchmuchoftheanalysiswasfocusedonimplicitfeaturesand
themes,requiringahighlevelofreflexivityonthepartoftheresearcher.

CHAPTERSIX:QUALITATIVEFINDINGS
179
Furthermore,manyofthefeaturesinheraccountandtheresultingthemeswere
verycloselyinter-related,whichmeantitwasdifficulttoseparatetheseoutand
explorethemdiscretely;asaresult,someofherthemeshaveverynuanced
differences.FivesuperordinatethemeswereidentifiedforJennifer:(a)Negative
thoughts,(b)notgoodenough,(c)keepingitinside,(d)powerlessness,and(e)
internalconflict.Eachsuperordinatethemecapturesanumberofemergent
themes,whicharepresentedinTable6.2.
Table6.2
ThemesforJennifer
Superordinatethemes
Themes
Keyillustrativephrasesfrom
transcripts
Negativethoughts
Negativethoughtsareaboutme anegativethoughtaboutmyself
Negativethoughtsareacollectivemass getitout
Negativethoughtsblockhappinessandpositivethoughts I’mnotsmiling
Negativethoughtsareirrational Iknowthat’snottrue
Notgoodenough
Idealised“goodness” [grades]says,itall
I’mnotgoodenough I’mnotgoodenough
Relativitytoothers otherpeoplearebetterthanme
Otherpeople’sexpectationsofme they’lljudgeme
Guiltandresponsibility Itrymybest
Keepingitinside
Negativethoughtsareinsideme Ikeepitinside
Negativethoughtsareprivateandsensitive don’twannatell
Lettingoutnegativethoughts speakingout
Unavailabilityofothers myparentsalwayshavework
Powerlessness
Accumulationofdemand alottodealwith
Lackofexternalcontrol Idon’tknowwhattodo
“Productivity”andadaptingtodemand trymybest
Lackofagencyoveremotions itdoesn’thelp
Internalconflict
Detachedfromfeelingsandnegativethoughts Idon’tknowwhy

CHAPTERSIX:QUALITATIVEFINDINGS
180
Detachedfromactions Idon’tlistentomyself
Negativethoughtsasseparatefromidentity notverymyself
6.2.3ThemesforGrace
Grace’saccountwascentredaroundthepeopleinherlifeandsheseemed
toperceiveahighlevelofconflictandthreatintheserelationships,withthemain
exceptionofherdad,whosheviewedasstableandprotectingher.WhileGracedid
describeexperiencingstrongemotions,thiswasnotacentralcomponentinher
accountandshefocusedmorestronglyonrelationshipswithothersand,
interestingly,onherphysicalsafety.ThethemesdevelopedforGracereflectthis
emphasisonherrelationshipswithothersandtheconflictinherlife.Six
superordinatethemesweredevelopedforGrace:(a)Self-careandmyneeds,(b)
whatweoweeachother,(c)feelinglovedandprotected,(d)threat,(e)lackof
control,and(f)lackofrelief.Eachofthesesuperordinatethemescapturesa
numberofemergentthemes,whicharepresentedinTable6.3.
Table6.3
ThemesforGrace
Superordinatethemes
Themes
Keyillustrativephrasesfrom
transcripts
Self-careandmyneeds
Self-protection
Voiceandagency
Hidingandcontrollingemotions
Physicalsafety
trygetaway
stickupformyself
Ikeepitintomyself
amIsafe
Whatweoweeachother
Roleexpectations
Personalresponsibility
likeanothermum
don’twannahurtmymum
Feelinglovedandprotected
Dadasstable
Dadasaprotector
alwaysthereforme
dadwillstepin

CHAPTERSIX:QUALITATIVEFINDINGS
181
Onegoodcancelsoutthebad
Singularsupport
Loveandpriorities
butmydad
theonlyone
allshethinksabout
Threat
OthersareirrationalandIamnot
Othersandsafety
Familysplitaspivotalmoment
Fearofnegativeoutcomes
forgod’ssake
Idon’tfeelsafe
itallstarted
what’sgonnahappen
Lackofcontrol
Voiceunheard
Stuckinthemiddle
Helplessness
shedon’tlistentome
whethertobelieveit
whatshouldIdo
Lackofrelief
Feelingsasanintensestate
Buildingimpactonemotions
Lackofemotionaloutlet
Constantconflict
Breakingpoint
Igetreallyupset
Icouldn’tcope
didn’tknowwhattodo
allthetime
I’vehadenough
6.3MasterThemes
3.Whatisitliketobeanearlyadolescentgirlwhoisexperiencingemotional
symptomsinthecontextofriskexposure?
AsdescribedinSection4.9.2,theindividualthemesacrosstheparticipants
werethenconsideredcollectivelytodevelopasetofmasterthemesacrossthefull
corpus.Thesearepresentedheretoaddressthefinalresearchquestionforthe
currentstudy.Foursuperordinatethemesacrossthethreeparticipantswere
developedthroughthisprocess,namely:
1. Theexperienceoffeelings;
2. Internalgrappling;
3. Demandsandcontrol;and
4. Drawingonothers.

CHAPTERSIX:QUALITATIVEFINDINGS
182
Eachofthesesuperordinatethemescapturesthreetofoursubthemes,whichare
presentedinTable6.4alongsideanoverviewofwhichparticipantsarerepresented
ineachone.Itshouldbenotedthatallindividual-levelthemeswereincorporatedin
thefinalmasterthemes,thoughtovaryingextents;amoredetailedoverviewof
thisintegrationispresentedinTableU1,AppendixU.
Table6.4
MasterThemesandRepresentationofParticipants
Themes Amelia Jennifer Grace
Superordinatetheme1:Theexperienceofsymptoms
Thenatureofsymptoms(objectorstate) Y Y Y
Symptomsareapluralmassthatcangrow Y Y Y
Symptomsascentralanddominantinemotionexperience Y Y N
Superordinatetheme2:Internalgrappling
Symptomsareconnectedtome Y Y Y
Symptomsareseparatefrommyidentity Y Y Y
Passiveexperienceofsymptoms Y Y Y
Mismatchbetweensymptomsandreality Y Y N
Superordinatetheme3:Demandsandcontrol
Demandsandresponsibility Y Y Y
Fearthatsomethingbadwillhappen Y Y Y
Voiceandcontrolovertheworld Y Y Y
Superordinatetheme4:Drawingonothers
Mappingtheemotionalsupportnetwork Y Y Y
Releasingsymptomsthroughtalk Y Y Y
Othersasprotectors N N Y
Thefollowingsectionsoutlineandexploreeachthemeindetail,with
considerationofbothdescriptiveandinterpretivefeatures,nuancesacrossthe
corpus,andinter-thematicconnectionsanddifferences.Thereareseveralfeatures
withinthiswrittennarrativeofwhichthereadershouldbemindful.Firstly,efforts
havebeenmadetobetransparentwherecommentsareinterpretive,throughthe
useoftermssuchas“seemed”or“appeared”whereappropriate.Illustrative
quotesfromparticipantsarepresentedbothtoprovidedirectaccountsoftheir

CHAPTERSIX:QUALITATIVEFINDINGS
183
experiencesandtogroundtheresearcher’sinterpretationswithinparticipants’
wordsandaccounts,inlinewiththesharedcommitmenttobothphenomenology
andthehermeneutic(Larkinetal.,2006;Smithetal.,2009).However,giventhat
IPAshouldinherentlyofferaninterpretativeaccount,thereadershouldnotethat
suchquotesareoftenfeaturedlessheavilyinwrittenaccountsofthemesthanin
otherqualitativeapproaches.Indeed,giventhefocusonthemeaningfulnessof
participants’language,quotescanbeverybriefinsomecases,withsmall
utterancessometimesofferingagreatdealofmeaningandresonanceacrossthe
entirecorpus(Smith,2011b).Itshouldalsobenotedthatparticipants’useof
colloquialisms,suchas“mum”insteadof“mother”,havebeenadoptedwhere
possibletosupportamoreauthenticaccountofparticipants’experiences.
Considerationwasalsogiventoterminologyaroundthefeelingsassociated
withemotionalsymptoms.Theterm“emotionalsymptoms”representsaclinical
constructandthusdoesnotalignwiththefocusonthewayinsuchsymptomsare
experienced,whereinfindingsgobeyondintellectualised“emotions”or
“symptoms”andfocusonsubjectivefeelingsandthoughts.Furthermore,thisterm
wouldnotnaturallypresentitselfinayoungperson’saccount,necessitating
alternativelanguageinlinewiththestudy’sphenomenologicalapproach.However,
eachparticipantmadeuseoftheirownspecifictermsforthesefeelings(e.g.,
Jenniferdescribed“negativethoughts”),renderingitdifficulttodescribecollective
experiencesusingparticipants’ownwords.Whilepreviousemotionresearchhas
drawnonmorecommonlyusedtermslike“anger”(Eatoughetal.,2008;Eatough&
Smith,2006b,2006a),emotionalsymptomscapturesacollectiverangeof
depressiveandanxioussymptomsandhasnocommonwordortermthatcan
encapsulatetheseexperiences.Assuch,participants’owntermsareusedwhere
possibleindiscussingindividualexperience,whilemorecollectiveexperiencesare
describedas“symptoms”and,withinthis,“feelings”and“thoughts”asrelevantto
theparticularlanguageusedbytheindividual.Wherethediscussionreferstowider
emotionalorcognitiveexperiencesbeyondthoseassociatedwithemotional
symptoms(e.g.,happiness),thisismadeclear.

CHAPTERSIX:QUALITATIVEFINDINGS
184
6.3.1TheExperienceofSymptoms
Thissuperordinatethemecapturesthewaythatparticipantsmadesenseof
thethoughtsandfeelingsthatcomprisedtheirsymptoms.Specifically,itexplores
thewaythatparticipantsunderstoodthenatureofthesesymptomsthemselves,
thewaythattheypluralisedthesefeelingsandthoughtsand/orsawthemas
somethingthatcouldgrowandbuild,andhowtheywereseeninrelationtothe
broaderemotionallandscape.
TheNatureofSymptoms(ObjectorState)
Thereweretwomainconceptualisationsacrossthecorpusofwhatexactly
thenatureofthesesymptomsis;namely,eitheratangibleobjectthatcanbehad,
orastatewhichoneenters.Intermsoftheformer,bothAmeliaandJennifer
understoodandpresentedtheirsymptomsasdistinctandtangibleentitiesthat
couldbedefinedandnamed.Firstly,theyeachhadspecificnounsforthesetypesof
feelings,whichtheyusedconsistentlythroughouttheiraccounts.Ameliatalked
abouthaving“aworry”or“worries”,whichweregenerallyunderpinnedbyafear
thatsomethingbadwasgoingtohappen;“aboutmyworries,say,like,willthis
happenorwhatwillhappenifIdothis?”Jenniferinsteaddescribedhaving“a
negativethought”or“negativethoughts”,whichsheexplainedwereoftenabout
her:“Ikindofhavenegativethoughts,like,I’mnotgoingtodowellandstufflike
that[…]IthinkthatI’mnotgoodenough,andlike…that…mmm…yeah,I’mjustnot
goodenough.”Thislabellingofthesymptomssuggeststhattheycouldbedetected
andisolatedasasingularcomponentwithinthebroaderemotionalandcognitive
landscape.Indeed,thislanguageof“aworry”or“athought”offersasensethat
thesearethoughtofascognitionsthatintrusivelypresentthemselvesto
participantsratherthanbeinganaffectivestate.
Thespecificlabelsthattheseparticipantsused,particularlytheuseof
nouns,andthewayinwhichtheyusedthem,gaveasenseofobjectificationof
symptoms.Thatis,acentralfeatureoftheirtalkwasthattheyframedthese
thoughtsassomethingthatthey“have”.Inthisway,theytookonastatusofa
tangiblething;thatis,assomethingthatcanbehad,asopposedtosomethingthat
isfeltorembodied.Thiswasaddedtobythefactthatbothparticipantstalked

CHAPTERSIX:QUALITATIVEFINDINGS
185
aboutthesethoughtsasoccurringbothsingularlyandpluralistically;forinstance,
Jennifertalkedabouthaving“anegativethought”aboutaspecificissuebutalso
talkedmoregenerallyaboutthesecollectivelyasher“negativethoughts”.This
pluralitystrengthenedtheperceptionofanapparentobjectificationofsymptoms
aswellastheideaoftheirbeingcognitionsratherthanaformofaffect.Thatis,it
differsfromthewayinwhichwemightunderstandsadnessoranxietyas
generalisedstates,whicharenottypicallythoughtofasbeingexperienced
singularlyorpluralisticallyinthismanner.
Thisobjectificationofsymptomswasparticularlyclearinthewaythat
Ameliatalkedabouther“worries”.Shedescribedsharingaworrywiththose
aroundherasthoughitwassomethingthatcouldbepassedalongorgivenaway,
withcommentslike“Itexthimaworry”.Thiswasparticularlyevidentwhereshe
explainedacopingstrategyinwhichyou“flick”awayaworry:“Ifit’sonyour
shoulder,like,justflickitoffandthentheworrywillgoaway.”Suchstatementsadd
tothesensethatthesethoughtsareseenastangibleentitiesinaveryrealway,in
thattheycanbepassedalongorquiteliterallyflickedaway.Indeed,this
conceptualisationandparticularlycommentsliketheonesAmeliamakeshere
suggestsomeseparationbetweenthesethoughtsandtheself.Thisapparent
divisionisexploredindetaillaterinthischapterintheinter-connected(though
contradictory)themes“symptomsareconnectedtome”and“symptomsare
separatefrommy“self””.However,thiscertainlyappearstobeanimportant
componentintheconceptualisationofsymptomsbeinghadratherthanfelt,inthat
onecannotfeelsomethingthatispositionedawayfromoneself.
ThisisnottosaythatAmeliaandJenniferexclusivelyusedthislanguage.
Indeed,atsomepointstheydidtalkaboutthesesymptomsasanaffectivestate
thatembodiedthemratherthanatangiblethoughtthattheyhad.Forinstance,
Jennifertalkedaboutgetting“upset”,whileAmeliadescribedtimeswhereshewas
“scared”or“nervous”.However,theseincidentswereanomalieswithinthe
broaderaccountsofbothparticipantsandstoodoutforthisquality,asinalmostall
instancestheyconceptualisedsymptomsasobjectsandmadeuseofcognitive
languageofthoughtsandworries.Grace,however,didnotusethiskindof

CHAPTERSIX:QUALITATIVEFINDINGS
186
languagetodescribehersymptoms,andinsteadtalkedconsistentlyaboutthese
feelingsasastatethatshecouldbeinorcouldbecome,frequentlyreferringto
instanceswhere“Igetreallyupset”.Indeed,almostallcommentsthatGracemade
inregardtothesetypesoffeelingswereeitherintheformofanemotionalstateas
here,orinsomeotherinstancesshedescribedfeelingsomething,suchas“Iwas
feelingstressed”.ThroughthiskindoflanguageitseemedthatGracesawthe
feelingasbeingmuchmoreall-encompassing,saturatingthenatureofherbeingat
thatmomentratherthanhavingamoreseparateandisolatedquality.Thus,Amelia
andJenniferdescribedthoughtsthatwereexternaltothem,whileGracetalkedof
feelingsthatconstitutedadeeperalterationtothestateoftheself.
SymptomsareaPluralMassthatcanGrow
Asnotedinthelasttheme,bothAmeliaandJenniferdescribedhaving
multiple“worries”and“negativethoughts”.Thispluralismspeakstothewayin
whichthetwoparticipantsmadesenseofthesesymptomsasbeingtangibleand
distinct;however,itisalsointerestinghowtheymakesenseofthisasbeing
collective.Throughouttheiraccounts,thetwoparticipantsswitchedbetweenthe
singularconceptualisationof“aworry”and“anegativethought”andpluralised
descriptionsofthesethoughts.Thiscontrastisillustratedwellinthewaythat
Jennifer’sdiscussionofveryspecificnegativethoughtsaboutherself,suchasthat
peopledonotlikeherorthatsheisnotachieving,occursalongsidemoregeneral
commentaryonthesefeelingsasacollectionof“thesenegativethoughts”or
simply“them”.Furthermore,atseveralpointssheswitchestocallingthese
thoughts“it”;forinstance,whenaskedwhethershehasspokentoanyoneelse
aboutthesenegativethoughts,Jenniferreplies“erm…noIkeepitinside.”Thisuse
of“it”suggeststhatthesenegativethoughtsgobeyondsimplybeingacollectionof
multipleconcernsandinsteadactasagreater,singularmasswithinJennifer’slife
world.Inthisway,forbothAmeliaandJennifer,itseemedthatthesesymptoms
werenotsimplyasingularpartoftheirinternallifebutamultitudeofindividual
pointsofdistressorconcern.
ItalsoseemedtobethecaseforbothAmeliaandGracethattheir
symptomscouldbuildandgrow,thougheachofthemunderstoodthisindifferent

CHAPTERSIX:QUALITATIVEFINDINGS
187
ways.ForAmelia,whotalkedaboutherselfassomeonewhohad“lotsofworries”,
thisprocessseemedtohappenthroughanalmostmitosis-likeway,whereinher
thoughtscouldmultiplyifleftunchecked:“Iforgottoflickit[theworry]offthat’s
whymoreworrieskeptoncomingandcoming.”Commentssuchasthesegavea
senseofinternalmultiplicationthatwasbeyondAmelia’scontrol.Similarly,
althoughGracedidnotmakesenseofthesefeelingsasbeingsingularorpluralbut
amoregeneralemotionalstate,shetoodescribedthisfeelingasbuildingwithin
her.OftenforGrace,thisheightenedemotionalstateseemedtobetheresultofan
increaseorpersistenceinthedemandsandstresssheperceivedinherlife.Thus,
whileforAmeliathiswasseenasbeingself-aggravated,witheachworrypotentially
spawningmoreworries,forGraceboththefeelingandtheexternaldemandwould
growtogether,attimesbecomingunmanageable.Forinstance:“Iwaspretty
emotional…andIwasalsobeingbulliedthatday,andIhadabreakdownina
lesson,Icouldn’tcope.”ThereweremultiplepointslikethisinGrace’saccount,
whereshedescribedtryingbutfailingtocopewiththisheightenedemotionalstate
andthedemandsinherexternalworld.Shereflectedthatitoftenbecomes“too
much”or“toohard”todealwith,suggestingthatthisincreasebecomes
overwhelmingandsurpasseshercapacitytocope.Indeed,Gracefrequently
describedthiscombinationasbuildinguntilitreached“acertainpoint”,wherethe
demandsandfeelingsshewasexperiencingwouldbecomeentirelyunmanageable
forhertocopewith.Indeed,sherelayedanumberofeventsinwhichshefeltthat
thishadledtoextremeconsequences,suchashavinga“breakdown”asaboveor,
inoneinstance,cuttingherself:
Iusedtoself-harmmyself,itusedtogetpretty,like…Iusedtogetsobad[…]
Ididn’tknowwhatelsetodo,Iwasjustgettingsomad[…]Iwasfeeling
angry,Iwasfeelingstressed…andlike,Ididn’tknowwhattodoanymore.
Grace’sstatementthat“Ididn’tknowwhattodoanymore”illustratesherfeeling
thatsheisunequippedtomanagethisheightenedlevelofemotionalturmoil.
Indeed,herusehereofseveral“feelings”words–mad,angry,andstressed–gives
afeelingofanintenseemotionalstateandprovidesinsightintohowoverwhelming
thisfeelingcanbeforher.Furthermore,itisnotableherethatGracechangesher

CHAPTERSIX:QUALITATIVEFINDINGS
188
phrasingpartwaythroughthisutterance;sheinitiallyexplains,“itusedtoget”and
thencorrectsherselfto“Iusedtogetsobad”.Thisswitchinlanguagefurtheradds
tothesensethatbothherexternalworldandherinternalworldareboundup
togetherinthisway,assheisnotalwayssurewhetheritistheeventsinherlifeor
heremotionalstatethatisbeyondhercontrol.
SymptomsasCentralandDominantinEmotionExperience
Thewaythatparticipantsmadesenseofthesesymptomswithintheir
broaderemotionallandscapedifferedslightly.ForAmeliaandJennifer,their
“worries”and“negativethoughts”dominatedtheemotionaldiscussionwithintheir
accountsandinsomewayswereseenasdefiningtheotheremotionstheyfelt.
Grace,however,didnotcentralisethesespecificfeelingsinthesamewayand
talkedmorewidelyaboutheremotionalexperience.
ForbothAmeliaandJennifer,therewasastrongsensethroughouttheir
accountsthattheir“worries”and“negativethoughts”werecentraltotheirgeneral
emotionexperience.Firstly,thisdominatedtheiroverallaccounts,withboth
participantsfocusingonthesesymptomsinresponsetoquestionsspecifically
relatingtotheiremotionexperience,aswellasquestionsaroundtheirbroaderday-
to-dayexperiences.Thisfocussuggeststhatthesesymptomsactasasubstantial
componentoftheirdailylives.Wheretalkwithintheinterviewbegantomoveaway
fromthesekindsofthoughtsandfeelings,bothparticipantsquicklymovedbackto
this.ThiswasillustratedwellinanimmediatediversionAmeliatookafterbeing
askedaboutherfamily:
Ilikebeinglike,withmyfamilyonanighttimeandjustrelaxingchilledout
withlikenostressandhomeworkthatI’malsoworriedaboutiflikeIgetit
wrongorifit’slate…because,erm,shallIgiveyouanexampleoflike
homeworkwhenIwasworried?
Indeed,thiskindofdominantfocusonthesesymptomsinparticipants’accountsis
partofthereasonthattheywereselectedforinclusioninthecurrentstudy.As
previouslynoted,theseinterviewswereconductedaspartoftheevaluationof
HeadStartandthustherewasnotnecessarilyanintentiontofocusdistinctlyon

CHAPTERSIX:QUALITATIVEFINDINGS
189
participants’emotionalsymptoms.Rather,discussionofgeneralemotionsfollowed
thefocusandflowoftheparticipantand,thus,thefocushereontheseparticular
kindsoffeelingsandthoughtsacrosstheiraccountsoriginatedfromAmeliaand
Jenniferthemselveswithintheinterviews,ratherthanbeingsoughtattheoutset
bytheinterviewers.Assuch,itisclearintheiraccountsthatthesesymptomswere
asubstantialcomponentoftheirday-to-dayexperiencesandinternallives.
Intermsof“negativeemotions”,neitherAmelianorJenniferfrequently
describedwiderfeelingsoutsideoftheirworriesornegativethoughts,thoughthere
wereveryoccasionalreferencestofeeling“scared”or“angry”.Grace,however,
talkedslightlymorewidelyaboutothernegativeemotionssuchasfeeling“mad”or
“angry”aswellasdiscussionoffeelingupset.Thus,whilethesefeelingswerepart
ofherday-to-daylife,theywerenotnecessarilyseenasthecentreofhernegative
emotionexperienceinthewaytheyseemedtobeforAmeliaandJennifer.Indeed,
forthesetwoparticipants,itseemedthatevenpositiveemotionslikehappinessor
feelingcalmweredefinedquiteliterallyastheabsenceofthesesymptoms,asin
thequotefromAmelia’saccountabove,whichwasaresponsetoaquestionabout
whyspendingtimewithherfamilymadeherfeelhappy.Indeed,whenaskedwhat
itisliketobehappy,Ameliastated,“reallylikehappynotworriedaboutanything”.
Jenniferseemedtoviewthisrelationshipbetweenthesedifferenttypesof
emotionsasthoughhappinesswasabaseline,oratrueself,thatwasinterrupted
bythepresenceofhernegativethoughts:
[Interviewer:Duringtimeswhenyouhaven’tthoughtthatyou’reafailure,
what’s,what’sbeendifferentaboutthosetimes?]Erm,I’mhappy,and…
yeahI’mjust,moremyself
Thus,thereappearstobeoppositionalconceptualisationofthesedifferenttypesof
emotions,inwhichhappinessistheabsenceofa“worry”ora“negativethought”
andcanberemovedordisruptedbythesesymptoms.Inthisway,forthesetwo
participantsthesetypesofemotionsseemtobemutuallyexclusiveandunableto
coexist,resultinginmoredifficultthoughtsandfeelingsdominatingtheiremotional
experiencequiteforcefully.

CHAPTERSIX:QUALITATIVEFINDINGS
190
6.3.2InternalGrappling
Thissuperordinatethemeexplorestheinternaltensionsandconflictsthat
participantswereexperiencinginmakingsenseofthesesymptomsasapartof
them.Firstly,itcapturesthewaythatparticipantslocatedthesesymptomsasbeing
somehowconnectedtothemwhilesimultaneouslybeingseparatefromtheircore
identity.Itexploresthegirls’viewsofthemselvesaspassivewithinboththe
occurrenceandresolutionofthesesymptoms,alongsidetheirapparentbeliefthat
theirthoughtsandfeelingsmaynotberational.Acrossthissuperordinatetheme,
thereisjuxtapositionbetweenabeliefthatthesesymptomsareoccurringinternally
butarenottrulycontrolledbyoneself.
SymptomsareConnectedtoMe
Inallthreecases,participantspresentedthesesymptomstobeconnected
tothemsomehow.Therewasageneralsensethatthesymptomswereconsidered
tooriginateandexistinternally,evenwheretheyaresimultaneouslyseenas
beyondtheparticipants’controlorcausedbyexternalprocesses.Despitetheway
thatAmeliaandJenniferinvokedseparatenessintheirtalkofhavingafeeling,they
stillpresentedthesymptomsasbeingtiedtotheminsomeway.Forboth
participants,therewasaconsistentuseofpossessionlanguage,indicating
ownershipofthesesymptoms.Forinstance,Ameliaestablishedaclearownership
oftheseworriesthroughoutheraccount,referringtothemas“myworries”.Inthis
way,thesethoughtsarethoughtofasbelongingtotheparticipants,evenifthey
arealsomadedistinctthroughtheirconceptualisationasobjects.Thistension
betweenseparationandconnectionwithsymptomsisexploredfurtherthroughout
thissuperordinatethemeasawhole.
Thisnotionofconnectionbetweenthesesymptomsandtheselfisalso
underpinnedbythewaythatallthreeparticipantsdescribedthesesymptomsas
being“inside”,withAmeliaandJennifertalkingspecificallyaboutthembeingin
theirhead:“sometimesIjustlikeforget,like,stillhavemyworriesinmyhead”
(Amelia).BothJenniferandGracediscussedthisinrelationtotheirurgestokeep
thesethoughtsandfeelingshiddenawaywithin;Jenniferexplainedthatthese
thoughtsaresomethingthatshefeelssheshould“keepinsideanddon’twannatell

CHAPTERSIX:QUALITATIVEFINDINGS
191
anyoneelse”.Sucheffortstokeepafeelinginsideindicatethatthisiswhereitis
believedtohaveoriginatedinthefirstinstance,suggestingsomeconnectedness
withtheself.Furthermore,atseveralpointswithinthesetwoaccounts,there
seemedtobeconsiderablediscomfortaroundlettingthesesymptomsout,with
bothparticipantsdescribinginstanceswheretheyhaveattemptedcontrolor
manipulationto“keep”theminside.Forinstance,Gracesawanydemonstrationof
herupsetasamarkerofvulnerabilitytoherbullies,andthusattemptedtocontrol
anyexternalisation:
Well,itdoesgettomequitealot,itishard…butItrynottoletthemsee
that[…]Ihadabreakdowninlesson,Icouldn’tcope,andtheteachersaw…
I,hetookmeoutside,andIwaslike,saying,Iwantedtogohomeandstuff
likethatcauseitwasreallyhard.AndIdidn’t,(sigh),Itriednottoletthe
bullies…seethatIwascrying.
Externalisationofthesesymptomsmaybeseenasuncomfortable,andeven
potentiallywithinone’scontrol,whiletheirinternalexistenceisseenasmore
naturalandlessmalleable.Thus,itseemsthattheyareseenverymuchasprimarily
takingplaceinternally.Thisiseventhecasewhenthefeelingisconsideredtobea
responsetoexternaldemands,andperhapseventheonlyrationalresponse(asis
oftenthecaseforGrace).Thatis,thedemanditselfmaybeexternal,butthefeeling
isaresponsethatisveryfirmlyplacedwithinoneselfandcanpotentiallybekept
there.
Overall,then,therewasanunderlyingfeelingacrossallthreeparticipants
thatthesesymptomsareseenasbeingconnectedtotheself,eitherthrougha
senseofbelongingorthroughabeliefthattheyoccur“inside”oneself.Notably,this
featureclasheswithotheraspectsofthewaythatparticipantstalkedabouttheir
symptoms,particularlywithhowtheyviewedthemasbeingseparatefromtheir
“true”self,asencapsulatedwithinthenexttheme.Thisspeakstothewaythat
differentareasoftheseparticipants’experiencesandsense-makingappearto
directlycontradictoneanother,butalsoreflectsanuancedexperienceintheway
thatthesethoughtsandfeelingscanhappeninsidewithoutdefiningwhatis“me”.

CHAPTERSIX:QUALITATIVEFINDINGS
192
Suchtensionsgiveanimpressionofconsiderableinternalgrapplingthatiscaptured
withinthissuperordinatethemeasawhole.
SymptomsareSeparatefromMyIdentity
Althoughtheparticipantsdiddescribetheirsymptomsasconnectedto
themandtakingplaceinternally,theyalsoestablishedsomelevelofdistancefrom
theircore“self”,oridentity.Onthesurface,itmayappearthatthesetwo
conceptualisationsarediametricallyopposed;however,adistinctionismadehere
betweenrecognisingaconnectionwithafeelingandactivelyincorporatingitinto
one’sidentity.ThewaythatAmeliaandJenniferobjectifiedtheir“worries”and
“negativethoughts”asthingsthatarehad,ratherthanfelt,givesanimmediate
senseofseparateness.Althoughthereareindicationsofpossessionovertheir
symptomsand,therefore,aconnectionwiththem,thisprimaryideaofthemasa
tangibleobjectleavesafundamentalundercurrentofseparation.Beingconnected
toafeelingbecauseitbelongstooneselfisnotthesameasviewingthefeelingasa
partofoneself.Inotherwords,tohaveandownanobjectified“worry”isvery
differentfrombeing“aworriedperson”.Throughthiskindoftalk,thesetwo
participantstookownershipofthesetypesofthoughtsandfeelingswhile
simultaneouslylocatingthemasseparatetothemselves.
Furthermore,allthreeparticipantssawthemselvesassomewhatpassive
withintheprocessofthesesymptoms.Thisnotionisexploredinmoredetailinthe
followingtheme,howeveritalsohasimplicationsinthecontextofidentity.
Specifically,acrossallthreeaccounts,participantsindicatedthatthesesymptoms
wereoperatingindependentlyofthemselves.Thatis,whilethesesymptomsmay
betakingplaceinternally,theparticipantshadnotactivelycreatedorchosenfor
themtotakeplace.Forinstance,Ameliatalkedaboutherworriesas“coming”from
somewhere:“moreworrieskeptoncomingandcoming”.Asaresult,these
thoughtsandfeelingsappearedtocircumventtheparticipantssomehow,meaning
thattheywerenotresponsibleforthethoughtsandfeelingsthemselvesorforthe
actionsthattheytookinresponsetothem;thesethingssimplyoccurred.Thus,
thesesymptomswereexperiencedasanelementoftheirlifeinwhichtheyhadno
activeroleor,indeed,control.Inanalysingandinterpretingthewaythatthese

CHAPTERSIX:QUALITATIVEFINDINGS
193
symptomsfittedintoparticipants’lifeworlds,then,therewasageneralsensethat
theywereunabletoreconcilethesethoughtsandfeelingswiththeircoreself,given
thattheywerebeyondtheirownchoicesandactions.
Therewereseveralwaysinwhichparticipantsdirectlyinvokedaseparation
betweentheirsymptomsandtheirself.Forinstance,Jenniferwasaskedatone
pointwhatwasdifferentaboutthetimeswhenshedidnothavenegativethoughts,
andsheresponded,“I’mhappy,and…yeahI’mjust,moremyself.”Thisparticular
statementwasoneofseveralinwhichJenniferestablishedtheideaof“myself”.
Jennifer’sconceptualisationofthisselfisahappyone;theuseof“just”givesthe
impressionthatthisisseenasafundamentalqualityofhertrueidentity.Assuch,
Jennifer’snegativethoughtsareseenasdisruptingherabilitytofullybethisreal
versionofherself.Inthiswaythereisnotonlyaseparationfromtheself,butsuch
strongimplicationsforfunctioningthatone’sabilitytobeatrue“self”isaffected.
Thisconceptualisationofthesesymptomsasdisruptingtheselfsuggests
thattheyhavenotnecessarilybeenincorporatedintoanewideaofwhattheselfis.
Thatis,whatcomprises“me”isnotchanged,butinsteadisinterruptedbya
separateforce.However,atsomepointsthislackofintegrationseemedtogosofar
astoextendtoadualidentity,inwhichthereisarealself,aswellasanotherself
thatisbeyondcontrol.BothJenniferandGraceconjuredupthisadditionalselfin
theiraccounts;Jennifer,forinstance,talkedabouthowshedidnot“listento
myself”orbelieveinherself.Intheseinstances,Jenniferhadsteppedoutsideofher
realselfandintoasecondselfthatisunreasonableandrefusestorespondtowhat
heroriginalselfisaskingofit.Itcannotlistenorbelieveherandisdrivenbythese
apparentlyirrationalthoughts.Similarly,Gracetalkedaboutanoccasionwhereshe
hadattemptedtohideherfeelingssoasnottoappearvulnerable,butexplained“I
didn’t,(sigh),Itriednot,toletthebullies…seethatIwascrying,butI,Icouldn’t
helpmyself.”Here,Gracealsomakesuseofasecondself.Forher,“I”isa
reasonableselfthatisabletoassessthesituationandattempttoretaincontrol,but
theother“myself”invokedhereislessrestrainedandcannotbecontrolled.Thus,it
appearsthattheexperienceofthesesymptomscancreateaninternaldivide,in
whichthereisarationalselfwithanappropriatesetofactionsandbeliefs,anda

CHAPTERSIX:QUALITATIVEFINDINGS
194
second,moreunreasonable,selfthatisruledbythesesymptomsandgives
unwantedresponses.
Assuch,thereisaconceptualisationacrosstheparticipantsthatthese
symptomsareoccurringwithinthem,butarenottrulyapartoftheircoreidentity.
Thus,althoughthisideaofsimultaneousconnectionandseparationseems
paradoxical,thetwoconceptualisationsdoappeartoco-exist.Theparticipants
appearedtohavesomedifficultymakingsenseofthesesymptomsinrelationto
theiridentityconstructions,andindeedthissimultaneousconnectionand
separationmaynotalwayssithappilytogether.Instancesofinternalconflict,such
astheneedtoformulateadualidentitythatcancapturethesedifferentselfhoods,
suggeststhatthismaynotalwaysbeacomfortablesolution,potentiallyintroducing
furtherdistressthroughaninabilitytoreconcilethesepartsoftheirlifeworlds.
PassiveExperienceofSymptoms
Thistensionbetweenconnectionandseparationwascloselylinkedwiththe
wayinwhichparticipantsviewedtheiragency,orlackthereof,withinthese
symptoms.Allthreegirlspresentedthesethoughtsandfeelingsassomethingthat
operatedindependentlyofthemandsowerebeyondcontrol.Thislackofcontrol
wasmanifestedthroughthewaythatparticipantsexperiencethethoughtorfeeling
inthefirstinstance,aswellasinthewaysthattheymanagethemandtheactions
theytaketoresolvethem.
ForAmeliaandJennifer,therewasastrongsensethattheysawthemselves
aspassivewithintheactualoccurrenceoftheinitialthoughtorfeelings.Bothgirls
repeatedthephrase“Idon’tknowwhy”throughoutdiscussionoftheirsymptoms.
Jennifer’suseofthisphrasewasacentralfeaturewithinherinterview,occurringin
heraccountalmostfiftytimes;forexample,“Idon’tknow.IjustthinkthatI’ma
failure,Idon’tknowwhy.”Forbothgirls,this“Idon’tknow”rhetoricwasthreaded
throughouttheirgeneraltalkintheinterviews,ratherthansolelyoccurringwhen
strugglingtoansweragivenquestionfromtheinterviewer.Thissuggeststhat“not
knowing”isanaturalcomponentofexperiencingthesesymptoms,ratherthan
simplybeingamethodologicalartefact,althoughcertainlyexpressingthese
complexinternalprocessesaloudcouldbeacontributor.Therewerealsoanumber

CHAPTERSIX:QUALITATIVEFINDINGS
195
ofmorenuancedindicationsthatthetwogirlsdidnotseethemselvesashavingan
activerolewithinthesesymptoms.Insomeinstances,forexample,Ameliahad
difficultyarticulatingthesourceofherworriesinthefirstpersonandinstead
expressedthisthroughthevoiceofothers.Forinstance,whilerecallingtheworries
sheexperiencedwhileatathemepark,shehesitatedandswitchedtohermum’s
assessmentofthesituationratherthanherown:“Iwasworried‘causeIdon’tlike…
mymumsaidIdon’tlikethe,d’yaknowtheunknownanddarkrides.”InJennifer’s
account,therewereanumberofoccasionswhereshepausedandwasquietfora
timeasshetriedtoexplainafeelingoranactiontotheinterviewer;oftenwhen
thishappenedshewasnotabletocomeupwiththisexplanation.Onseveral
occasions,sheidentifiedsomedisagreementbetweenherviewofherselfandher
actualexperiences,andintheseinstancessheappearedtoengageinan
uncomfortableattemptatassimilation:
I’mneverreallyhappyeventhoughIgot…high,‘causelike,IgotanAin
Scienceand,stufflikethat[…]Idon’tknow,I’mneverhappy,withmyself.I
meanIambutlike,sometime…I’mneverhappywithlike,thegradethatI
get,Idon’tknow.ButIamhappywithmyself,Iguess.
Jennifer’sdifficultyhereatmatchinguphermismatchedinternalandexternal
worldsindicatesthatshecannotfullycomprehendwhythesethoughtsaretaking
place,giventhattheydonotseemtomakelogicalsensetoher.Asaresult,sheis
leftfeelingunabletoconfidentlyassessherownthoughtsandemotionalstate,
leavingherto“guess”atwhatshethinksandfeels.Theseexperiencessuggestthat
alackofabilitytounderstandwherethesesymptomsarecomingfromorwhythey
donotmatchreality(apointexploredfurtherinthenexttheme)maybeadifficult
andconfusingexperiencewithlittleresolution.
Grace’spassivitywasslightlydifferent.UnlikeAmeliaandJennifer,shehad
lessdifficultyinidentifyingwhereherfeelingscamefrom,drawingdirectlinks
betweenherinternaldistressandthethreatandinstabilitythatshesawinthe
worldaroundher.ToGrace,herfeelingswereanentirelyrationalresponsetothe
behaviourofothers,suchasbulliestargetingherorhermumnotbehavinglikea
parent.Inthisway,herpassivitywasnotinrelationtoanabsenceofunderstanding

CHAPTERSIX:QUALITATIVEFINDINGS
196
ofwherethesefeelingscamefrom,butwasborneoutofalackofcontrolover
thosecauses;sheherselfwasnotchoosingtofeelthisway,itwassimplyan
inevitabilitygiventhevariouschallengesshefaced.
Gracethenalsoseemedtofeelalackofagencyinhowsherespondedto
thesefeelingsoncetheyhadarisen;thisseemedtobethecaseforallthree
participants,astheydidnotconsiderthemselvesabletoactivelyandeffectively
regulateandrespondtothesesymptoms.ForAmeliaandGrace,thisextendedto
makinguseofthosearoundthemtohelpthemmanageandresolvethese
symptoms,astheyseemedtofeelunabletodosoindependently.InAmelia’scase,
thiswasevidencedthroughastrongrelianceonthosearoundhertomanageher
worriesonherbehalf;herdog,familymembers,andfriendswould“make”herfeel
better,or“take”herworryaway:“[mydog]justlike,takemyworryaw-,ermworry
away[…]mydog’sreallyhelpingmenowandjustmakingmelike,notthinkabout
likethenegativethingssoshehelpsalot.”Inthesecomments,Ameliacastsherself
asapassivemediumthroughwhichothersinteractwithandmanageheremotional
landscape,whilesheremainsremovedfromthisprocess.Indeed,whensheis
providedwithstrategiestomanagehersymptomsindependently,shefindsherself
unabletoenactthemanddescribesherthoughtsandfeelingsspirallingoutof
controlandoverwhelmingher:“Iforgottolikeflick[theworry]offthat’swhymore
worrieskeptoncomingandcoming”.Similarly,Gracetalkedaboutkeepinga
feelingwithinheruntilshecouldtalktoatrustedother,usuallyherdad.It
appearedinthiswaythatGracesawherselfasonlyabletocontainandholdthe
feeling,ratherthanactuallydoanythingwithitorresolveit,whichwouldrequire
anotherperson:“Ikeepitintomyselfallday,andthenI’llgohomeandtalktomy
dad.”
Wheretheparticipantsdidtalkaboutthetimestheyhadattemptedtotake
stepstoresolvetheirsymptoms,theydidnotpresentthemselvesasactiveinthese
actions.Theyfounditdifficulttounderstandexactlywhytheydidthesethings,or
feltlikeitwastheonlyoptionavailableratherthanbeinganactualdecisionthey
made.Jennifertalkedabouteatingcomfortfood“forsomereason”,whileGrace
talkedaboutself-harmingbecauseshe“didn’tknowwhattodoanymore”.Inthese

CHAPTERSIX:QUALITATIVEFINDINGS
197
instances,thegirlsdonotseethemselvesasactivelymakingdecisions,asthough
theythemselveshadnottrulychosentodothesethings,theyjusthappened.
Indeed,theyfoundthatthesestrategiesoftendidnotwork,addingtotheirgeneral
senseofhelplessnessinrelationtotheirsymptoms.Whentheinterviewerasked
Jenniferhoweatingcomfortfoodhelped,sheresponded:“N-,itdoesn’thelp,atall,
but,youjustthinkthatitwill,but,itwon’t.Like,eatingcomfortfood,itwon’thelp
you,atall.”Inthisinstance,asinmanyotherpointsinherinterview,Jennifer
switchesfromthefirsttothesecondperson,asthoughtoremoveherselffromany
discussionaroundthispoint.Sheemphaticallymakesthepointherethatthisdoes
nothelp“atall”,indicatingwhatappearstobeatotalrenouncementofthisasa
strategy;yet,itisoneshecontinuestouseinspiteofthisknowledge.Thus,it
seemstherearetimesthatparticipantsmakeuseofstrategiesthatdonotwork,
simplytodosomething,eveniftheydonotbelieveitwillhaveanyeffect.
Therewereseveralways,then,inwhichparticipantssawthemselvesas
passivewithintheoccurrenceandresolutionofthesesymptoms,withthemfeeling
unabletounderstandormanagetheseprocesses.Asaresulttherewasageneral
senseofhelplessnessacrossallthreecases,withparticipantsconsidering
themselvesremovedfromtheseprocessesandonlyabletowatchasthesethings
simplyhappenedwithinthem.
MismatchbetweenSymptomsandReality
Someparticipantsidentifiedamismatchbetweenthenegativeexpectations
thatcomewiththeirsymptomsandtherealityoftheworldaroundthem.Both
AmeliaandJenniferclearlyarticulatedthattheybelievedthattheconcerns
presentedintheirworriesandnegativethoughtswerenotreflectiveofreality.
Ameliatalkedfrequentlyaboutlookingfor“evidence”toprovetoherselfthat
somethingshefearedwouldhappenwasinfactimpossible.Thatis,ifthereisno
evidencethatthiscouldhappen,thentheworryisunfounded:
IfsomethingdoesworrymeI’lljustsaylike,where’stheevidenceaboutit?
Like,andifsomethingdoesh-,like,erm,worrymeI’lljustsaylike,where’s
theevidenceaboutit?LikeIknowit’snotgonnahappen.
CHAPTERSIX:QUALITATIVEFINDINGS
198
Jenniferalsodescribedlookingforevidencetodisproveherparticularconcerns.
Shereflectedthatshehadnegativethoughtsthatnoonelikesher,“but,Iknow
that’snottrue,‘cause,Ihavesomanyfriendshere”,andtalkedabouthowshewas
neverhappywithheracademicachievementeventhoughshecouldseethatshe
alwaysgotthehighestpossiblegrades.Thisactoflookingforexternal
“evidence”todisprovetheirconcernsindicatedthatthegirlsperceivedtheexternal
worldasobjective,whiletheirinnerprocesseswereseenasirrationalandtheir
fearsunfounded.Inthisway,theyappearedtobelievethattheworldaroundthem
providedabarometerofsortsagainstwhichtheycouldcheckandperhapseven
underminetheirfearsandexpectations.
Thisideaofevidencewascoupledwithtalkabout“knowing”thattheirfears
werenottrueordidnotmeasureuptowhattheysawhappeningaroundthem,as
intheexamplesabove.Bothparticipantstalkedconsistentlyabout“knowing”these
things,addingtothesensethattheexternalworldprovidedwhatwasperceivedto
beobjectiveinformationor“evidence”thatcouldfeedintoconcrete“knowledge”.
However,thisalsogaveanimpressionthattheparticipantsveryfirmlybelieved
thattheirinnerconcernsandexpectationsdidnotalignwiththerealitytheysaw.
Thatis,theydidnotsimplythinkorsuspectthatthiswasthecase,theyknewit.
Nevertheless,recognitionofamismatchbetweenexpectationsandreality
didnotseemtobeconsideredparticularlyuseful.Bothgirlsdescribedhowtheir
concernspersistedeveninthefaceofthisunderstandingandevenextendedto
doubtingit.Ameliaseemedtobeabletosayobjectivelythatsheshouldlookfor
evidenceandthatagivenoutcomewouldnothappen,butshewasstillleftwitha
nigglingbeliefthat,inaveryrealway,itcouldhappen.Sheexplainedthatthis
techniquewashelpfulbutthatshewasstillleftwithquestions,“sayingbutwhatif
thereisn’tanyevidenceorwhatifthishappens”.Jennifershowedconsiderable
difficultyandfrustrationaroundthewaythathernegativethoughtsandher
knowledgedidnotmatchup.Shedirectlyexplainedthatanawarenessofthis
mismatchdidnothelp:
IthinkthatI’mnotgoodenough,andlike…that…mmm…yeah,I’mjustnot
goodenough.ButIknowthateveryone’snotperfect.[Interviewer:Doesit

CHAPTERSIX:QUALITATIVEFINDINGS
199
makeadifferenceknowingthat?]NonotreallyI’vealwaysknownthat,but,
yeah.
Thus,abeliefthatone’sconcernsdonotmatchrealitydoesnotnecessarilylessen
thoseconcerns.Anemphasison“knowing”,combinedwithcommentsthatthis
informationdoesnotmakeadifference,suggeststhatthismismatchcanbe
understoodatanobjective,abstractlevel,butdoesnotextendtodeeperthinking
processes.Asaresult,participantswereexperiencinganadditionallayerof
discomfort;firstly,theyweretryingtomakesenseofamismatchbetweentheir
expectationsandreality,withfurtherdifficultyarisingwhenthisknowledgedoes
notchangethewaytheyfeel.Thatis,beingawarethatone’sthoughtsandfeelings
areirrationaldoesnotnecessarilymakethemgoawayandcaninsteadbeafurther
sourceoffrustration.Inattemptingtoexplainthisdisparitybetweenherinnerand
outerworlds,Jenniferexclaimed:“Idon’tknow.It’sabitconfusing.”Thus,notonly
isthisperceivedknowledgefutile,itcanbedirectlydifficulttoincorporateintoan
alreadyconfusinglandscapeofwhatisknownversuswhatisfeltandbelieved.
6.3.3DemandsandControl
Thissuperordinatethemecapturesthewayinwhichparticipantsviewedthe
variousdemandswithintheirworlds.Itexploresthedominanceoftheseperceived
demandswithintheirlifeworldsandtheresponsibilitythatparticipantsfeltto
adapttomeetthem,evenwhenthisadaptationmightbetotheirowndetriment.It
alsocapturesthespeculativefearsthatparticipantshaddevelopedaroundthese
demandsandtheirperceptionofhowmuchcontrolandvoicetheyhaveinfacing
theseissuesintheirexternalworlds.
DemandsandResponsibility
Allthreeparticipantsfeltthattherewerearangeofdemandsonthemin
theirdailyliveswithwhichtheywerestrugglingtocope.Thespecificnatureof
thesedemandswasdifferentforeachparticipant;oftentheywerelocatedwithin
theexternalworld,thoughsomewereinternal.Ameliawasstrugglingwithher
schoolworkandhomeworkandwasdeeplyafraidoftheconsequencesofgetting

CHAPTERSIX:QUALITATIVEFINDINGS
200
thingswrong,whilebattlingherowncompulsivebehavioursand,indeed,worry
aboutherownworry.Jenniferwasalsocopingwithacademicdemandsbut
seeminglyfromtheotherendofthespectrum;shetalkedaboutbeingahigh
achieverwhilealsoexperiencinganunderlyingfearthatshewassomehow“not
goodenough”andanurgetobeconstantly“productive”.Grace’schallengesmostly
relatedtothebehaviourofotherpeople,asshedescribedhavingadifficultandat
timesvolatilerelationshipwithhermumandhermum’sboyfriend,whilealsobeing
persistentlybulliedatschool.
Whilethenatureofthesedemandsdiffersconsiderablyacrossthecorpus,
ineachcasetheyseemedtotakeonanincrediblydominantrolewithinthegirls’
lifeworlds,posingapersistentandoverwhelmingsourceofpressure.Participants
loopedbacktothesamedemandsthroughouttheirinterviewsandpresentedthem
asacentralandconsistentfeatureofday-to-daylife.Thiswasparticularlywell-
illustratedinGrace’suseofabsolutetermsinrelationtothesedemands,which
gavetheimpressionofthemasconstantandunrelenting:“Ialwayssaytohim,
you’renotmydad”;“Igeteverythingblamedonme”;“itneverstopped”[emphasis
added].Indeed,Gracecommented“I’vehaditallmylife”onseveraloccasions,
suggestingthatthesedemandshavebeensuchaconsistentfeatureofherworld
thattheyhavecometobeacceptedasanunavoidable,andindeed
insurmountable,partoflife.Overall,then,thesedemandswerepresentedas
centralwithintheparticipants’livesandindeedappearedtohavebecomethe
subjectofsomefixationwithintheirthinkingprocesses.
Allthreeparticipantsconsistentlydrewdirectlinksbetweenthedemands
placedonthemandthesymptomstheywereexperiencing;forinstance,intalking
aboutthetimeswhenshewasstrugglingtokeepupwithwhatwashappening
duringlessons,Ameliaexplained,“Idon’tlikegettingsomethingwronglikethat’s
whatIworryaboutlike,gettingsomethingwrong[…]ifhegetsmadatmeorgave
meadetentionorsomethinglikethatthat’swhatIworryabout.”Thisjoint
presentationanddiscussionofspecificdemandsandparticipants’symptomsgave
theimpressionthattheseareseenasdeeplyintertwinedcomponentsoftheirlife
worlds.Ashasbeendiscussedearlierinthischapter(inthetheme“Symptomsarea

CHAPTERSIX:QUALITATIVEFINDINGS
201
PluralMassthatcanGrow”),thereweresuggestionsfromsomeparticipantsthatit
wasnotnecessarilyasingledemandthatwasproblematic,butitwaswhenthey
builtupthatthisbecameoverwhelming.Aspreviouslydescribed,Gracetalked
aboutmultipleincidentsbuildinguntiltheeffectsbecamedrastic,likeself-harmor
a“breakdown”.ThiswasalsoaparticularlystrongpatternwithinJennifer’s
account,whodescribedhow“itallpilesup”andbecomes“toomuch”,surpassing
herabilitytomanagethedemandsonher:“It’ssometimesabittoomuch,like,I
can’thandleit‘cause,ImeanI’vegothomeworkfromschoolandthenI’vegota
tutor,andthen…Idon’tknowwhatdosometimes.”
Participantsviewedthemselvesashavingaresponsibilitytokeepupwith
thesedemandsandweretakingeffortstodoso.Jennifer,forinstance,talkedabout
gettingupatfiveo’clockinthemorninginordertokeepupwiththevolumeof
academicworksheneededtocompleteforschoolandhertutoringprogramme.
Sheconsistentlyassertedaresponsibilitytobe“productive”andfeltguiltywhen
shesawherselfasfallingshortofthis:
IjustkindofwasteallthattimethatIhave,like,eveninthemorningsIstill,
goandwatchTVand…yeah,I’llbethereforlike,anhourorso,eventhough
Iwakeuplike,erm...five,halfpastfive…yeah,and,Iwasteallthattime.
Todifferentextents,bothJenniferandGracequestionedwhetherornotthey
shouldinfacthavetokeepupinthisway;thatis,theyappearedtothinkthatthe
demandsbeingplacedonthemwerenotnecessarilyfair.Thiswasparticularly
pronouncedforGrace,whofeltveryintenselythatthewayotherpeoplewere
behavingwasinappropriateandexpressedconsiderablefrustrationaboutthefact
thatthisthenimpactedonher.However,bothgirlsfeltlimitedcontroloveractually
resolvingtheseissues,abeliefthatisexploredindetailinalatertheme;asaresult,
theyfeltthattheyneededtoadapttomeetthesedemands.Forallthree
participants,regardlessofwhethertheyfeltthecircumstancestheyfacedwere
unfair,therewasaclearbeliefthatitwastheirresponsibilitytoadaptandmeet
thesedemands.Eachofthethreegirlsdescribedtakingcleareffortstokeepupand
bendthemselvestoaccommodatethechallengestheywerefacing,asinJennifer’s
excerptabove,evenwhenthisbelievedtobedisruptiveorevenharmfultothem.

CHAPTERSIX:QUALITATIVEFINDINGS
202
Forinstance,Gracewasstrugglingwithadecisionofwhetherornottostop
spendingtimeinhermum’shome,asthiswasseenasavolatileenvironmentand
sheexpressedconcernthatshewasnotsafewhenshewasthere.However,she
wasconflictedinthisdecisionasshewasconcernedaboutupsettinghermum:“I
don’twannahurtmymum,butIdon’twanttobewith…h-,herpartner,‘causehe’s
justdrivingmecrazy.”Thus,theseparticipantsweremakingconsciousdecisions,
sometimesperceivedtobedetrimental,inordertomeetapotentially
overwhelmingsetofperceiveddemandsinfluencingtheirday-to-daylives.
FearthatSomethingBadWillHappen
Eachofthethreeparticipantsdescribedintenseandpervasivefearsthat
somethingbadwasgoingtohappenintheirlives.Aswiththedemandsthey
perceived,thenatureofthisfearwasdifferentforeachparticipant.Jenniferfeared
thatshewouldnotbegoodenoughandthatotherswouldfindoutandjudgeher,
whileGracewasafraidthatsomeonewouldtrytophysicallyhurther.Ameliahada
strongfearthatshewouldgetintroublefornotkeepingupinschool,buttherewas
alsoamoregeneralfearappliedtovariousexperiencesthatshewentthrough,with
anyexperiencesheengagedinseenashavingthepossibilityfornegativeoutcomes.
Ascanbeseen,thespecificfearsthateachgirldescribedwerestronglylinkedto
thenatureofthedemandstheyperceivedaroundthem;forinstance,Grace’sfear
forherphysicalsafetyreflectsherobservationsthatotherpeopleinherhomeand
schoolliferegularlybehaveaggressivelytowardsher.Onseveraloccasions,the
participantstalkedaboutthesefearsdirectlyinrelationtotheirsymptoms.Asin
Amelia’searlierquote,itseemsitisnotalwaysthedemanditself,butthepotential
futureconsequencesthataredistressing;so,forAmelia,itisnotstrugglingwith
schoolworkthatisproblematic,itisthefearthatshewillgetintotroubleforthis.
Althoughthesefearsarerelatedtoparticipants’perceiveddemands,italso
appearedthatthenegativeconsequencestheyfearedhadnotyetcometofruition.
InGrace’saccount,thethreatandverbalaggressioninherschoolandhomelife
hadnotatthispointappearedtohavebecomephysical.Jenniferwasmaintaining
anoutwardimageofbeing“goodenough”andahighachieverandfeltnoonehad
yetrealisedotherwise,whiletheconsequencesAmeliahadactuallyexperiencedin

CHAPTERSIX:QUALITATIVEFINDINGS
203
heracademicdifficultieswererelativelylow-levelcomparedtotheextreme
punishmentsheexpected.Despitethis,thesefearsstillposedaveryrealpossibility
fortheparticipantsandtheywereoftenpresentedasinevitable.Forexample,
Gracefrequentlyused“yet”inhertalkofpossiblephysicalattacks,suchas“she
hasn’tdoneit…yet”,andweighedupduringtheinterviewwhatproofshewouldbe
abletouse“ifanythinghappened”withhermum’sboyfriend.Thefactthatthe
eventstheyfearedwerenotactuallyhappening,atleastnotasofyet,gavethe
impressionthatthegirlsheldanalternativeandhypotheticalworldintheirminds,
filledwithendlessnegativepossibilities.Sometimestheyplayedouthypothetical
scenariostoexplainapointwithoutappearingtohavegiventhisagreatdealof
thought,suggestingthatthesescenariosweresimplyanacceptedpossibilitythat
alreadyexistedintheirmind.Whentryingtoexplainhowshefeltathome,Grace
talkedquitecasuallyaboutwhatwouldhappenifsomeonecameintoherhome
andattackedher.Althoughshebeganthissentencewith“if”toshowits
hypotheticalnature,thelanguageshethenusedexpressesacertaintyratherthana
possibility,presentingthisasafutureeventthat“will”happen,ratherthanas
somethingthatcouldhappen:
IfeelreallysafewhenI’maroundwithmydadandstepmum.‘Causeit’slike,
theywon’ttakeanything.Like…ifsomeonewantstolike,comein,tohurt
me,mydadwillstepinstraightawayorcomeintohurtmystepmum,my
dadwillbeonit.
ThisparticularscenariofromGraceseemedsuchanextremeexample,andwas
presentedassucharealisticpossibility,thatitimmediatelypromptedthe
interviewertoaskwhetherornotGracethoughtthismighthappen.
Indeed,thereweretimesacrossallthreeparticipantswherethepotential
repercussionstheytalkaboutaredramaticandpotentiallycatastrophic.InAmelia’s
account,andtoalesserdegreeforJenniferandGracealso,therewassome
difficultyinconceptualisingwhatthebadthingthatcouldhappenactuallywas.
Ameliatalkedaboutthesefearsthroughoutherinterviewanditwasnotalways
clearwhatshethoughtwouldhappen,simplythatsomethingverywellcouldgo
horriblywrong.Shereferredto“somethinglikethat”andexplainedatonepoint
CHAPTERSIX:QUALITATIVEFINDINGS
204
whenaskedwhatmighthappen:“somethingbadwillhappen.Orsomethinglike
that.”Asaresult,itseemedthatthesepossibleoutcomesthatthegirlsfearedwere
drivenbyanunderlyingfearthattheydidnothavetotalaccessto,giventhatthey
didnotalwaysknowwhatitwastheywereafraidof.Thisabstractnessgavethe
impressionthatperhapstoinspectthesefearstoocloselywassomehow
dangerous,andsoitwasbestnottodoso,orperhapsthatitwasnotevenpossible
toaccessandinspectthem.
VoiceandControlovertheWorld
Asdescribedinanearliertheme,participantsfeltaresponsibilitytoadaptto
meetthedemandsplacedonthem,includingtakingstepsperceivedasdetrimental
tothem.Theimpressionacrossallthreecaseswasthatthiswasunderpinnedbya
beliefthattheyhadeithernorightorabilitytodoanythingaboutthedemand
itself.Notably,thismirrorstheirviewofthemselvesaspassiveinrelationtotheir
symptomsandspeakstoabroadersensethattheparticipantsfeltagenerallackof
controlthroughouttheirlives.
BothAmeliaandJenniferwereexperiencingchallengesinschool,with
AmeliastrugglingtokeepupandJenniferworryingaboutslippinginherstatusasa
highachiever.Ateachturn,itwasclearthattheyperceivedtheonustobeonthem
tomanagethis,withoutquestioningwhetherthesystemtheyweretryingto
navigatehadflawedexpectationsorshouldchange.Instead,theyweretheones
thatwerewrongandnotkeepingup,andtheyweretheonesthatneededtobend
themselvestofit.ThisisillustratedbyJennifer’sperceivedinabilitytotellher
parentsthatshedidnotreallyneedtutors,despitefindingthattheworkshehadto
completefortutoringwasoverwhelmingalongsideherhomework.Shedidnot
believethatshecoulddoanythingtoaddressthisissue,soinsteadshejusttriedto
fiteverythingin:
Wegetsomuchhomeworkand,Ialsohavetutorsso,itgetsabittoomuch,
sometimes[…]Imean,Ialreadyknowthisstuffandlike,I’mjustdoingit
again[…][Interviewer:Wouldyoueverspeaktoyourmumanddadabout
it,doyouthink?]No‘cause,theymightgetmadatme‘causeI,theydidsign
thecontractandIdidagreetoit.

CHAPTERSIX:QUALITATIVEFINDINGS
205
Giventhattheydidnotseeanyrealreasonfortheseexternalfactorstoadaptto
meettheirneeds,thenanychallengesthattheseparticipantsexperienced
constitutedafailureontheirpart.
Gracealsoperceivedalackofcontrolovertheexternalworld,butunlike
AmeliaandJennifersheveryfirmlybelievedthatthethingshappeninginherlife
werewrongandwasfrustratedthattheyaffectedher.Shegenerallyviewedother
peopleasirrationalandconsideredherselfthevoiceofreason.Atseveralpointsin
heraccount,Gracerecountedtimeswhenshehadattemptedtotellotherpeople
thatsomethingwasunfairandhadtriedtocommunicatewhatsheneededinstead.
Forinstance,whentalkingaboutanincidentofwhatsheperceivedtobe
inappropriatebehaviorfromhermum’sboyfriend,Graceexplained,“Iturned
aroundtomymumandsaid,‘allyoudoisbelievehim,youneverbelieveme’.But
heneedstostopdoingthis,butshedon’tlistentome.”Hence,notonlydidGrace
believethechallengesshefacedwereunfair,butshealsobelievedsheshouldbe
abletodosomethingaboutthat.However,herexperiencewasthatthismadelittle
difference,asothersdidnotlistentoherandcontinuedtoignoreherneeds.As
such,althoughGracebelievedthatshehadtherighttovoiceherneeds,thisvoice
hasnotbeenheard;“IsaywhatIwant,tosay,butitjustendsupgoingwrong.”Her
perceivedlackofotheroptionsappearedtohaveleftGraceinasituationof
enforcedhelplessness,whereallshecoulddowastrytoprotectherself.
6.3.4DrawingonOthers
Thisfinalsuperordinatethemeexploresthewaysinwhichtheparticipants
weredrawingonothersastheynavigatedtheirsymptomsandparticulardemands.
Itcapturesthewaysinwhichtheydeterminedwhototurntoforemotional
supportandtheperceivedbenefitsoftalkingtoothersabouttheirthoughtsand
feelings.ThefinalthemefocusesonGrace’sviewofoneparentasherprotector,
boththroughphysicalprotectionandbycompensatingforthehurtcausedby
others.

CHAPTERSIX:QUALITATIVEFINDINGS
206
MappingtheEmotionalSupportNetwork
Thethreeparticipantsappearedtohaveactivelyassessedwhattheywanted
inemotionalsupportandhadidentifiedparticularpeopleintheirworldswhothey
believedcouldfulfiltheseneeds.Thisevaluationandselectivenessgavethe
impressionthattheparticipantswere“mappingout”aneffectiveemotional
supportnetwork.Ameliahadawidersupportnetworkthantheothertwo
participants,thoughtherewasstillevidencethatshewasselectiveinwhoshe
turnedto;thiswaspredominantlyherfamilymembers(includingherdog)anda
smallnumberoffriends,ratherthansimplyanybody.Indeed,ononeoccasionshe
describedhowshetalkedtohersupportworkeraboutthings“inprivate[…]ifI
don’twannatellmyparents”,indicatingthattheremightbetimeswhenitis
necessarytobeselectivewithinthesupportnetwork.GraceandJennifer,onthe
otherhand,hadidentifiedamuchnarrowernetwork,andwerefirmthatthere
werepeopletheywouldnotconsideranappropriatesourceofsupport.Grace
typicallyonlywenttoherdadforhelpwithherfeelingsandrarelyreachedoutto
others.Whenshedid,thiswastypicallyheroldersisterandherstepmum,buteven
intheseinstancesthiswasbecauseherdadwasphysicallyunavailableatthattime,
suchaswhenhewasatwork.Theseindividualsthusservedasatemporarysolution
untilhebecameavailable,orevenasanintermediarywhowouldpassonthe
informationtoherdad,asinthefollowingextract:
Yesterday,itwasjustmeandmystepmum,andthedog.Mydadweren’t[…]
homefromworkyet.And,er…so,ifthathap-,ifthathappensandI’mreally
upsetI’lltalktomystepmum,andthenshe’llliketalktomydadandthen
mydadwilltalktome.
Similarly,Jennifergenerallyfeltitwasmostappropriatetotalktohermumorher
nanabouthernegativethoughts;thoughearlyinherinterviewsheexplainedshe
could“alwaysgoto[her]friends”,shelaterchangedhermindandsaidshewould
onlytalkabouttheseissueswithhermumornan.Indeed,Jenniferseemed
uncomfortablewiththeideaoftalkingtosomeoneelseabouthernegative
thoughts,asexploredinthenextsection,whichmaybewhyshewasinconsistent
inidentifyingwhoshewouldturntoforthistypeofsupport.

CHAPTERSIX:QUALITATIVEFINDINGS
207
Indescribingwhomtheywouldturntoforemotionalsupport,participants
oftenfocusedonparticularqualitiesoftherelationshipstheyhadwiththese
individuals,includingcloseness,trust,andcare.Forinstance,whenaskedwhat
adviceshewouldgivetosomebodystrugglingwiththeirfeelings,Ameliasaidshe
wouldgivethemthesameadvicethat“myfriendsormyparentsoranyonethatI
knowarecloseto[me]willgiveme”.Suchcommentssuggestthattheemotional
supportnetworkcomprisesthosethatcanbeconsideredtohavea“close”
relationship.Jenniferwasconcernedwithwhetherornotsomeonecouldbe
consideredto“genuinely”careforherand,aspartofthis,whetherornotthey
weretrustworthy.Whenaskedhowsheknewshecouldtrustsomeonewiththese
negativethoughts,sheexplained“cause…theywould,really,careforyou,like
genuinelycareforyouandnot,youknow,justfakeit.”Jenniferhighlightedthat
somepeoplewouldofferapoorsourceofsupport,particularlyteachersand
sometimesfriends,astheywouldsaythingstheydidnotmeanortellotherpeople.
Itseems,then,thatforsomeonetobeconsideredaqualitysourceofsupport,
thereneedstobeameaningfulandpersonalrelationshipwiththatindividual.
Anotherconsiderationthatwasmadeinidentifyingwhototurntowasthe
perceivedavailabilityandreliabilityofsupport.BothAmeliaandGracegavethe
impressionthattherewerepeopletheycouldconsistentlyrelyonforemotional
support.Theyemphasisedanobjectiveknowledgethattherewassomeonethey
couldturntowiththesedifficulties,andtrustedthatthiswouldbeanoption;as
Graceemphasisedoften,“IknowIcanrelyonmydad.Iknowthathe’salways
there.”Aspreviouslyexplored,bothoftheseparticipantsreliedstronglyonthose
aroundthemtohelpthemmanagetheirfeelings.Theyviewedthisasaconstant
optionanddrewonitwithouthesitation.Jennifer,ontheotherhand,generallysaw
othersasunavailableforanykindofsupport,particularlyinrelationtohernegative
thoughts,andwasreluctanttoreachouttoothersforhelpwiththis.Mostoften,
thiswasseenasbeingaphysicalabsence;shefrequentlycommentedthather
parents“alwayshavework”andexplainedthatshemightsometimesspeaktoher
mumabouthernegativethoughts,“ifshehastimeoff”.

CHAPTERSIX:QUALITATIVEFINDINGS
208
ReleasingSymptomsthroughTalk
Participantsbelievedthattheirsymptomscouldbereleasedthroughtalking
tothesecarefullyselectedothersintheirlives;thatis,aftersharingagivenfeeling
withanotherperson,itwasnolongerconsidered“inside”them.Forinstance,when
askedwhatpeopleshoulddoiftheywereexperiencingproblemswithworries,
Ameliaexplained,“don’tlike,makeyoufeelshyorhideyourworriesjustlet‘em
outandletpeopleknow.”Thealternative,itseems,istokeepitinside,asin
Jennifer’saccount:
Italktothemalotandlike,sometimesItalktothemaboutthingsthat,erm,
yeahthat…Ikeepinsideanddon’twannatellanyoneelse,but,Italkto
themaboutthataswellanditreallyhelpsme.
Afocusontheinsideand“lettingitout”carriesanimplicitbeliefthattalking
providesaveryliteralrelease.Theemphasishereisongettingthefeelingoutside
ofoneself.Itdoesnotseemtobethatthefeelingisdiminishedorsplitsomehow,
asintheadage“aproblemsharedisaproblemhalved”;rather,thewholefeelingin
itsentiretyisnolongerinsideandhasbeensingularlyreleasedfromtheself.This
addstothesensethatparticipantsviewedthesesymptomsasbothconnectedto
themand,yet,separatefromtheself.
Participantstypicallytalkedaboutreleasingasinglefeelinginthese
interactions;thatis,aparticularworryforAmelia,aspecificnegativethoughtfor
Jennifer,orthestateofupsetthatGracewasinonthatparticularday.Ineachcase,
theirtalkwithothersabouttheirsymptomswashighlyspecifictotheparticular
concernorpointofdistressthattheywereexperiencinginthatmoment,rather
thanbeingaconversationaboutmoregeneraldifficultieswiththesetypesof
thoughtsandfeelings.Forinstance,Gracetalkedabouthowifshebecameupsetat
schoolshewould“keepitinto[herself]allday,andthenI’llgohomeandtalktomy
dad”.Thissuggeststhattheseconversationsaredrivenbywhatisofimmediate
concern,andareusedreactivelytoaddressthespecificthoughtsandfeelingsthat
participantsareexperiencingintheirlivesastheyarise.

CHAPTERSIX:QUALITATIVEFINDINGS
209
Mostly,whatparticipantsappearedtofindmeaningfulaboutsharingtheir
symptomswassimplybeingheard,and“havingsomeonethere”(Jennifer).These
interactionsmadethemfeelcaredforandunderstood;Jennifercommented,“I
trustthem,andliketheyunderstandaswell”,whileAmeliaexplained,“Idotellmy
parentsthoughaboutit…andtheycantellthatIgetworried”.Thereisanemphasis
hereontheinsightthatotherscanhaveintotheseemotionalexperiences,wherein
theycanrecogniseandrelatetothethoughtsandfeelingsexpressed.Theimpetus
wasnotongainingasolutiontoanyproblemthathadfedintothefeeling,with
participantsrarelygivinganyindicationthattheysoughtemotionalsupportasa
meansto“fix”anythingintheirlives.Thiswaspresentoccasionally,butofteninthe
formofadviceorreassurance,ratherthanconcreteaction.Instead,thefocuswas
onthetalkitself:
Interviewer:What’sthefirstthingyoudo[whenyouhaveaworry]?What
doyoudo?
ErmwellboutmyworriesI’dnormallygoandtellmyparentsaboutitand
thenIjustlikechilloutwithmydog(Amelia)
Thismirrorsthewayinwhichparticipantsselectedothersbasedonperceived
qualitiessuchastrustworthinessorrelationshipcharacteristicslikeclosenessand
care,asopposedtochoosingsupportthathasanykindofpowerorabilitytofix
theirperceiveddemands.Inthisway,otherpeopleareabletohelpthemrelease
theiremotionssimplybyprovidingalisteningearand,crucially,showingcareand
understanding.
WhileAmeliaandGraceweregenerallycomfortableaboutsharingtheir
emotionswithothers,Jenniferexperiencedsomediscomfort.Sheviewedher
negativethoughtsasprivateandsensitive,andexplainedthatshewouldpreferto
“keepitinside”.Inspiteofthis,shetoobelievedthattalkingcouldprovidea
releaseforthesethoughts,andshediddescribetalkingtoothersaboutthem“to
justgetitoutofyourhead”.However,itappearedthatshedidsooutofnecessity
ratherthanbecausesheactuallywantedto.Sheseemstohavebeenforcedto
weighupherurgetokeephernegativethoughtsinsideagainstthepotential
benefitsoftalkingtoothers,andhasatleastonsomeoccasionsfoundthatthe

CHAPTERSIX:QUALITATIVEFINDINGS
210
releasetalkingcanofferhaswonout.Hence,itmaybethatevenwhentheactof
talkingaboutthesesymptomsisfelttobeunpleasant,thereleasethatcanbe
achievedmaybesubstantialormeaningfulenoughtooverrideanydiscomfort.
OthersasProtectors
ThisfinalthemeexploresGrace’sbeliefthatherrelationshipwithherdad
couldprotecther,bothinaveryliteral,physicalsenseandbycompensatingforthe
limitsshesawinwhatotherswereofferingher.Thisthemeissolelyunderpinned
byGrace’saccount,asitwasaparticularlysalientandcentralelementofherlife
world.
ItwasevidentthroughoutGrace’saccountthatherrelationshipwithher
dadwasdeeplymeaningfultoher.Shesawhimasaconsistentsourceofsupport
notonlyinrelationtoheremotionsbutalsoinnavigatingherday-to-daylife.In
manyways,thishadtakenonaformofprotection,ofteninaveryliteralphysical
sense.Shetalkedabouthowherdadwas“sostrong”andrelayedincidentsin
whichhehadphysicallykepthersafe,suchaswhenshefellwhilewalking:“causeit
wasrightnexttoaroad,sohejustlikegrabbedholdofme”.Asexploredinan
earliertheme,Graceexpressedconcernsaboutthepossibilityofphysicalharm
fromthepeoplearoundher.However,eveninthesehypotheticalscenariosherdad
washersaviour:
IfeelreallysafewhenI’maroundwithmydadandstepmum.‘Causeit’s,
like,theywon’ttakeanything.Like…ifsomeonewantstolike,comein,to
hurtme,mydadwillstepinstraightawayorcomeintohurtmystepmum,
mydadwillbeonit.
Thus,althoughsheexperiencedongoingfearofphysicalharmfromothers,Grace’s
dad’sstatusastheprotectorprovidedsomecomfort.
Gracewasalsousingherdad’swideractionsasaformofinternal
protection,shieldingherselffromthepaincausedbyherrelationshipwithher
mum.Shesawhermumasfailingtofulfilmotherlybehavioursanddutiesand
appearedhurtbythewaythathershedidnotprioritiseherneeds:

CHAPTERSIX:QUALITATIVEFINDINGS
211
Iturnedtoherandsaid,allyoudoisthinkaboutyourself,‘causethatisall
shedoes.Sh-,allshethinksaboutis,her,allshethinksaboutisher
boyfriend,allshethinksaboutis…money,andbooze,that’sallmymum
thinksabout.
Commentsonhermum’sapparentselfishnesscameupfrequently,carryingan
implicitangerthatGraceherselfisnotfeaturedinhermum’spriorities.However,
shesawloveandcareinherdad’sactions,andthroughoutheraccountshedirectly
drewuponthesewhentalkingabouthermum.Itwasasthoughthethingsthather
daddidforhercouldcompensateforwhathermumdidnot,bothemotionallyand
physically.Inthisway,Gracecouldshieldherselffromthehurtshefeltather
mum’sbehaviourbyremindingherselfthatherdadlovedherandwouldbehave
appropriately.
Gracewouldoftennoteaperceivedfailureonhermum’spartandfollow
thiswith“butmydad”toexplainhowhehaddonesomethingmorehelpful.In
someinstances,theseactsalsoextendedtoaformofphysicalpreservation;Grace
recalledhowasababyherhipshadbeenunformed,andshehadneededtobeina
harnessforseveralhoursadaytoallowthemtodevelop:
Mymum,I(sighs)don’tknowhowtosaythis,but…mymumneverusedto
putmeinit,atalloranything,sheneverusedto…sheneverusedtoreally,I
don’thowtoputitlike,not,likesheneverusedtocareaboutmeor
anything,‘causeIknowsheprobablydid,butsheneverwantedto,like,put
meinit,oranything[…]he[dad]usedtoalwayscomehomeafterareally
longdayandputmeinitallthetime.
Firstly,thisquoteclearlydemonstratestheinnerturmoilthatGracegoesthroughin
tryingtounderstandwhetherornothermum“cares”abouther.Theexcerptalso
illustrateswellthedualrolethatGrace’sdadplayedasherprotector;ontheone
hand,hepreservesherphysically,andontheotherhand,hisloveandcaredirectly
compensatesforthephysicalandemotionaleffectsofhermum’sneglect.This
compensationnotonlyresolvestheissue,butitallowsGracetorecogniseasource
ofcareandloveinherworldthatcanmakeupfortheperceivedlackofit
elsewhere.
CHAPTERSIX:QUALITATIVEFINDINGS
212
6.4ReflexiveAppraisalDiscussion
AsdescribedinChapterFour,stepsweretakenforreflexivitythroughout
thedesign,analysis,andwritingstagesofthequalitativestrand,includinguseofa
researchdiaryanddiscussionwithsupervisorsandpeers.Inthefinalsectionofthis
chapter,keythemesthatarosethroughthisprocessarebrieflyexplored.This
includestheauthor’sownidentificationwithparticipants’experiences,maintaining
abalancebetweenuniqueandsharedexperiences,widerknowledgeof
participantsbeyondtheiraccounts,andtheuseofaconcurrentmixedmethods
design.Thisisnotanexhaustivelistofthereflexivejourney,butisintendedto
provideinsightintocentralaspectsofthisexperienceandeffortstakentomaintain
qualityandrigour.Thissectioniswritteninthefirstpersongivenitsfocuson
understandingthewaysinwhichtheresearcherisimplicatedinthefindings.
6.4.1IdentificationwithParticipants’Experiences
AshighlightedinChapterFour,IPArecognisesthattheinfluenceofthe
researcher’svalues,experiences,andpreconceptionsisconsideredtobenotonly
unavoidablebutalsopotentiallyvaluable,astheresearchermaybeableto
generatefurtherinsight(Larkin&Thompson,2006;Mayoh&Onwuegbuzie,2015;
Pietkiewicz&Smith,2014;Smithetal.,2009).Itcanbeargued,then,thata
researcher’sownpersonalexperiencesofthephenomenonofinterestcanaida
deeperandricherunderstandingofparticipants’sense-makingandexperiences
(Smithetal.,2009).However,itisimportanttoacknowledgesuchinfluencesandto
takeeffortstoensurethatinterpretationsremaingroundedinparticipants’own
accounts,ratherthanbecomingcloudedbytheresearcher’slens.Assuch,carewas
giventhroughouttoexaminingthewaysinwhichImyselfidentifiedwith
participants’experiences.
Primarily,thestudy’sinterestin“whatitislike”tobeanearlyadolescent
girlexperiencingemotionalsymptomsandriskstemsinpartfrommyown
experiencesduringadolescence.Priortobeginninganalysisofdata,Ispenttime
exploringhowmyownvaluesandexperiences,bothpersonalandprofessional,

CHAPTERSIX:QUALITATIVEFINDINGS
213
relatetothefocusofthestudyandthequalitativeresearchquestion,andexplored
howthiscouldinfluencethewayImightinteractwithdata.Idocumentedthese
reflectionsanddiscussedthemwithmysupervisorsandsupportivepeers.During
eachstageofanalysisIsoughttoinspectmyinterpretationsofdatatoexplorethe
extenttowhichtheseweregroundedinthewordsoftheparticipantsthemselves,
asoutlinedinSectionXXtoavoidover-reachingbasedonmyownpreconceptions.
Havingdocumentedmyearlypreconceptionsbeforebeginninganalysis,Iwasable
tolookbacktomyinitialnotesinthisareatohelpmemorerigorouslyexamine
whetherIwasimposingmyownthoughtstoostronglyontheinterpretation.
Furthertothis,therewereanumberofnarrowerareasofparticipant’s
experiencesthatresonatedwithmeinmoreunexpectedways.Jennifer’s
difficultieswithperfectionistictendenciesandproductivityandGrace’sfrustrations
offeelingunheardasanadolescentstronglyresonatedwithme.Whiletheseareas
ofpersonalidentificationmayhavefacilitatedamoremeaningfulinteractionwith
theseaccounts,reflexivebracketingtechniqueswereusedtoensure
interpretationsremainedgroundedinthedataasmuchaspossible.Ikeptongoing
reflexivenotesthroughoutthisprocesswhereverareasofrecognitionarose,
engagedindiscussionwithsupervisorstofacilitatecriticaldiscussionofhowthese
areasdevelopedasthemes,andutiliseddecontextualisationstrategiessuchas
readingfragmentedlines(asdescribedinSection4.9.2).
Tofurthersupportreflexivityinensuringinterpretationsweregroundedin
thecases,afteranalysisofeachindividualcase,Isharedthekeyquotes
underpinningeachthemewithmymainsupervisor.Ithenoutlinedtheprocessof
analysisforthatcase,includingdiscussionofanyparticularpointsthatresonated
withmeorwhereIfeltIhadexperienceddifficultywithbracketing.Mysupervisor
andIreviewedeachthemeinturnwithattentiontothequotesunderpinningitto
explorewhetherthedatapresentedsupportedtheinterpretationsbeingdrawn.I
repeatedthisexerciseafterdevelopingthemesacrossthecorpustoexplore
whetherthecollateddatasupportedeachofthethemesthathadbeencreated.

CHAPTERSIX:QUALITATIVEFINDINGS
214
6.4.2BalancingUniqueandSharedExperiences
AsdescribedinChapterFour,IPAisgroundedinanidiographiccommitment
totheparticular,ratherthantocreatinggeneralisations,andaimstoexploreand
representbothindividualandsharedfindingsacrossthecorpus(Reidetal.,2005;
Smithetal.,2009).Furthermore,theuseofarelativelysmallsampleinthecurrent
studyofferedtheabilitytoexplorecasesingreaterdepth,aswellasformore
nuancedexplorationofexperienceswithinthewrittenaccountsofthemes.Assuch,
ongoingattentionwasgiventoachievinganappropriatebalancebetweenthat
whichisuniqueandthatwhichissharedacrossparticipants’accounts,duringboth
theanalysisandwritingprocesses.
AsnotedinSection4.9.2,breaksweretakenbetweenanalysingindividual
casestocreatedistancefromthepreviousaccountandassociatedthemes.Where
connectionsordifferenceswereidentifiedatthisstage,Inotedthesedownand
inspectedthemtoexaminewhethertheyweregenuinelylocatedwithinthe
separatecasesorwhetherIwascarryingmeaningbetweentheaccounts.I
discussedthisprocesswithsupervisorsandpeersanddocumentedthisclosely.For
instance,JenniferandAmelia’saccountssharedmanycommonfeatures,including
afocusonacademicissues(albeitfromdifferentperspectives),asenseof
powerlessnessandpassivity,andissuesaroundirrationalityintheirthoughtsand
feelings,andsothesenaturallybecameevidentduringanalysisoftheirindividual
cases.TheseappearedquitedifferentfromtheexperiencesofGrace,whowas
facinglargelydifferentchallengesinherlifeandwasmakingsenseofthesein
differentwaysattimes.Forinstance,whileallparticipantsdescribedfeeling
powerlessandadaptingtodemands,AmeliaandJenniferappearedtofeelthat
adaptationwasthemostappropriateaction,whereasGraceviewedthisastheonly
availableresponsegiventhatattemptstoresolvethesechallengeswerenot
successful.
Insuchinstances,Ipausedanalysistospendsometimedocumentingand
appraisingtheseconnectionsandexaminingtheextenttowhichthismighthave
beeninfluencedbymyowninterpretations,orwhetherthisconstitutedthe
emergenceofasharedtheme.Thistypeoffore-structuringofthefinalmaster

CHAPTERSIX:QUALITATIVEFINDINGS
215
themesis,ofcourse,inevitabletosomeextent,butshouldbeinterrogatedclosely
(Smithetal.,2009).Indeed,ithasbeenarguedthatattentiontothewayinwhich
wordsandsense-makingechoacrosscasesallowsbothreflexiveappraisalwhile
alsofacilitatingadeeperinterpretationacrosscases(Goldspink&Engward,2018;
Smithetal.,2009).
Indevelopingmasterthemes,Iexperiencedsomeinitialdiscomfortwherea
themedidnotcaptureexperiencesfromallthreeparticipants,andrealisedthatI
wasattemptingtoreconfigurethesetocaptureexperiencesacrosstheentire
corpus.Indoingso,IfoundthatIwasbeginningto“zoomout”sofarthatitrisked
losingspecificpointsofmeaningandnuance.Inordertochallengethisinstinct,I
spentsometimeexaminingthisdiscomfortandengaginginpeerdiscussion.I
movedbacktoanearlierthematicstructure,whichhadencapsulatedgreater
variabilityacrossparticipants,andlistenedtoeachoftheaudiorecordingsagain
whilereviewingthetrackingofeachcase’sanalysis,inordertorealignmyselfwith
participants’lifeworldsandregainmyfocusontheindividual.Thisallowedmeto
revisitthethemeswitharenewedfocusontheidiographic,andrefinethem
withoutlosingindividualexperienceormeaning.Indeed,inthefinalsetofmaster
themes,therearesomethemeswithonlytwoparticipantsrepresentedandone
themethatcapturedonlyGrace’sexperiences.
Finally,itshouldbenotedthatthethemesandthewayinwhichparticipants
wererepresentedwithinthemchangedthroughthewritingprocess.Themes
sometimescameintosharperfocusthroughdevelopingawrittennarrativeof
them,atwhichpointIrevisitedthedataandearlierstagesofanalysistoassess
thesechangesinjudgement.Insomecases,thismeantrevisitinganalysisofacase;
forexample,throughexplaininghowGracedidnotconceptualisehersymptomsas
objectsbutinsteadasastate,Irealisedthatthishadbeenoverlookedinherinitial
individualthemesandwentbacktoherdatatoreviewthis.Atthisstage,theinitial
theme“symptomsasobjects”became“thenatureofsymptoms(objectorstate)”.

CHAPTERSIX:QUALITATIVEFINDINGS
216
6.4.3WiderKnowledgeofParticipants
AsoutlinedinChapterFour,participantsweredrawnfromthequalitative
baselinesampleintheHeadStartevaluation,whereinparticipantsareinterviewed
annuallyforfiveyearsbymembersoftheresearchteam(includingmyself).As
such,althoughthecurrentstudyfocusedonparticipants’baselineinterviewsin
2017,eachoftheseparticipantstookpartintwofurtherinterviewswhilethis
researchwasbeingconducted,in2018and2019.Specifically,IinterviewedAmelia
atallthreetimepoints(thoughonlyherfirstinterviewfeatureshere),andJennifer
andGracewereinterviewedbyothermembersoftheHeadStartteamandsoIhad
limitedengagementwiththeirlaterinterviews.Thus,myownroleinterviewing
HeadStartparticipantsmeantIsometimeshadaccesstoparticipants’later
experiencesbeyondthedatafocusedonhere.
Firstly,IhaveinterviewedAmeliaatallthreetimepointswithinthe
longitudinalHeadStartprogrammeevaluation,thoughonlyherbaselineinterviewis
utilisedinthecurrentstudy.Toreducetheimpactofthisfurtherengagement,I
analysedthiscasepriortoconductinghersecondinterviewandimmediatelyafter
thisinterviewreflectedondifferencesandsimilaritieswithherpreviousaccount.
Thismeantthatwhileitispossibletoreturntoapreviouslyanalysedcaseandfind
newinterpretationsinIPA,Iwasabletoconsultmynotesfromhersecond
interviewtocross-checkwhetheranynewinsightpossiblyreflectedlater
interactions.IrepeatedthisatthethirdinterviewinApril2019,althoughbythis
stagethequalitativefindingswerefullydevelopedandwrittenup,offeringless
scopeforintrusion.
AlthoughotherresearchersinterviewedJenniferandGrace,Iwasmade
awareofparticularelementsofJenifer’ssecondinterviewthatrelatedtoher
discomfortintalkingtoothers.ThisoccurredduringanalysisofJennifer’scaseand
soitwasimportanttoensurethatthisinformationdidnotimposeitselfonmy
interpretations.Fortunately,thistookplaceafterthesecondstageofanalysingher
accountwascomplete,meaningIhadalreadyrecordedsystematicline-by-line
codingreflectinginterpretationsofthisdata.Thus,indevelopingthemesforthis
caseIutilisedthissystematiccodingtocross-checkmyongoingthinkingtoavoid

CHAPTERSIX:QUALITATIVEFINDINGS
217
introducingnewideasbasedonthiswiderawareness.Beyondthis,IensuredIhad
nofurtherinteractionwiththedataproducedthroughthesecondandthird
interviewswitheitherJenniferorGrace.
Finally,becauseparticipantswereinterviewedbymultipleresearchers,my
knowledgeandinsightintoAmeliaasapersonwasgreaterthanthatofJennifer
andGrace,giventhatIhadmetherandconductedtheinterview.When
participantswerefirstselectedasstudyparticipantsIspokewithJenniferand
Grace’sinterviewerstoexploretheirperspectivesoftheseparticipantsandtheir
interviews.IalsolistenedtoJenniferandGrace’sinterviewaudiorecordingsseveral
timesduringanalysistoretainafocusonthemasindividuals,inordertohelpme
connectmorecloselywiththeirlifeworldsratherthanthroughsimplyinteracting
withwordsonapage.
6.4.4ContextoftheBroaderStudy
Considerationwasgivenheretothecontextoftheanalysiswithinthe
broaderstudy,includingcompletionofotherchaptersandaconcurrent
quantitativestrand.
Duringtheanalyticalprocess,Iwasalsoengaginginwiderreadingand
completingcomponentsofChaptersOne,Two,andThree,exploringandpresenting
thecurrentliteratureintheseareas.Itisofcoursedifficultforresearchersto
separateouttheirwiderknowledgeinagivenareawhencompletinganalysis,and
inthecontextofathesisitisnotalwayspossibletopostponewritingofother
chaptersgiventhevolumeofworktobecompleted.AsaresultIsoughttotake
carethatmyengagementwithdatawasgroundedinthedataitself,ratherthan
drivenbyanyareaoftheliterature.Nevertheless,itshouldbenotedthatSmithet
al.(2009)haveacknowledgedthatexistingconstructswithintheliteraturemaywell
offervalueintheinterpretivecomponentofcodingandmakingsenseofdata,
wherehandledwithcaution.Thereisperhapsadistinctiontobemadebetween
recognisingwiderpsychologicalconstructs(e.g.,“identity”),andlinkingwhatis
observedwithindatatomorenarrowedexistingpiecesoftheoryorliterature(e.g.,
aparticulartheoryofidentityoraspecificfindingpublishedinastudyaround

CHAPTERSIX:QUALITATIVEFINDINGS
218
identity).WhereIobservedthesemorenarrowedparallels,Isoughttopauseand
inspectmythinkingwhyImighthavemadethislink,whichIoftenfoundusefulin
returningtowhatwasofinitialinterestinthedataandmovingoninwithamore
inductivefocus.
Asthetwomixedmethodsstrandsofthecurrentstudywerecarriedout
concurrently,considerationwasgiventhroughouttothewayinwhichelementsof
thequantitativestrandmayinfluencequalitativeprocessesandfindings.This
includesemergingquantitativeresultsaswellasthequantitativestrand’sheavier
focusonnarrowlydefinedconstructsandvariables,suchasriskfactorsand
cumulativerisktheory,thatareinconsistentwiththeinductiveand
phenomenologicalnatureofIPA.AsdescribedinSection4.9.2,theanalyticalsteps
inIPArequiretheresearchertoenterparticipants’lifeworldsandengageinaclose
andsystematicanalysisoftheiraccount.Thisapproachencouragestheresearcher
toconnecttheirthinkingwiththedatainaparticularlyfocusedwayandIfound
thatthiswasusefulinbracketingwiderpreconceptionsbasedonquantitative
hypotheses.Indeed,IfoundthatIcouldsomewhatreadilyidentifysituationswhere
mythinkingwasinfluencedbyelementsofthequantitativestrand,giventhatIwas
activelyanddeliberatelyengagingwiththeseconstructs.Ifeltthiswaslesstruefor
identifyingtheinfluenceofmyownvaluesandpreconceptions,whichareless
easilydefinedandreadilyapparent.
Ialsotookfurtherstepstomanageandwherepossiblelimitthepotential
effectsofcarryingoutquantitativeandqualitativeanalysisconcurrently,including
considerationsoftiming.Thisincludedspacingoutmyengagementwitheither
datasetthroughoutaworkingweek,sothatIalwaystooksometimebetween
completinganygivenanalysis.Forinstance,mostofthetimeItriedtoworkwith
qualitativedataonMondaysandthentoengageinwiderwritingandbroader
departmentalresponsibilitiesonTuesdaysandWednesdays,beforeengagingwith
quantitativeanalysislaterintheweek.Ifeltthisapproachworkedquitewellontwo
counts.Firstly,thismeantIhadsomedistancefromquantitativeanalysisovera
weekendbeforeengagingwithqualitativeanalysisandsodidnothavequantitative
constructsandmodelsattheforefrontofmymindduringanalysis.Secondly,this
CHAPTERSIX:QUALITATIVEFINDINGS
219
approachmeantIhadthespacetoprocessmyreactionsandthoughtsfrom
qualitativeanalysisbeforeengagingwiththequantitativestrandsoasnotto
inadvertently“solve”anylingeringthoughtsaboutacasethroughmyengagement
withstatisticalinformation.ItshouldalsobenotedthatIwaitedtocompletemore
mechanisticcomponentsofanalysis(i.e.,indirecteffectsofperceivedstress
componentsandprotectivefactors)untilIhadidentifiedqualitativethemesacross
thecorpus,insteadfocusingonearlierstagesofanalysis.Ifeltthatthiswas
beneficialasthesemechanismslinkmoreexplicitlywiththeemphasisoninner
processescapturedinthequalitativestrand,whereasidentificationofriskfactors
couldperhapsbelessinfluentialonmythinkingininterpretinggirls’experiences.
Parallelsbetweenthetwosetsoffindingswerecertainlyofinterestgiven
theuseofmixedmethodsandareunavoidablegiventhatbothstrandsfocusonthe
samephenomena.However,Itriedtoensurethatanysimilaritiesorparallelswere
trulylocatedwithinthefindings,ratherthanshapingfindingsinthefirstinstanceby
myownidentificationofsimilarities.WhereIobservedsuchparallels,Inotedthese
separatelytorevisitatalaterstageandmovedoninmyanalysis.Thisapproach
allowedmetodirectlyacknowledgetheseareasinmythinkingandbracketthemas
somethingthatcouldbereturnedtoafterformingamorecompleteimageofthe
qualitativefindings.Thereweresomeinstanceswhenmyinterpretationsofthe
datamoredirectlyreflectedthequantitativestrand,suchasAmelia’sindividualised
theme“cumulativesupportnetwork”mirroring(tosomeextent)cumulativerisk
theory,orGrace’sperceptionofherdadasaprotectorreflectingdiscoursewithin
resilience.Whenthisoccurred,Inotedthesetobracketthemoffduringanalysis,
andreturnedtothematalatertimewhenIcouldinspecttheseinterpretations
closely,discussingthemwithsupervisorsandpeerstoestablishwhethermy
conclusionstrulyreflectedthedataoranimpositionofdiscreteconstructs.
6.5ChapterSummary
IndividualthemesweredevelopedforAmelia,Jennifer,andGraceandfour
superordinatethemesweredevelopedacrossthecorpus:(1)Theexperienceof

CHAPTERSIX:QUALITATIVEFINDINGS
220
symptoms,capturingthewaysparticipantsconceptualisedandexperiencedthe
thoughtsandfeelingsthatcomprisedtheirsymptoms;(2)internalgrappling,
encapsulatingparticipants’conflictinunderstandingthesefeelingsinrelationto
themselvesandtheouterworld;(3)demandsandcontrol,exploringthepersistent
demandsparticipantsexperiencedthattheybelievedtobebeyondtheircontrol;
and(4)drawingonothers,exploringthewaysparticipantsmappedoutanddrew
onanemotionalsupportnetwork.Strategiesforreflexivitywereutilised
throughoutanalysisandkeyareasofthisprocesshavebeenoutlined.

CHAPTERSEVEN:DISCUSSION
221
Chapter7:Discussion
7.1ChapterOverview
Thischapterpresentsadiscussionofthestudy’sfindings.Itbeginsby
summarisingfindingsforeachresearchquestionbeforeexploringtheseingreater
depth,consideringhowexistingtheoryandliteraturemayofferanexplanationand
examininguniquecontributionstoknowledge.Next,findingsacrossthe
quantitativeandqualitativestrandsareintegratedintometa-inferences,whichare
discussedwithconsiderationofimplicationsanddirectionsforfutureresearch.The
chapterthenreflectsonthestudy’sstrengthsandlimitationsand,finally,offers
concludingremarks.
7.2SummaryofFindings
7.2.1ResearchQuestion1:RiskFactorsandProcesses
1.Whataretheriskfactorsandprocessesassociatedwithemotionalsymptoms
amongearlyadolescentgirls?
Thisfirstquestionaimedtoidentifytheriskfactorsassociatedwith
emotionalsymptomsamongearlyadolescentgirls,andtoinvestigatemultiplerisk
effectsandunderlyingprocesses.Analysisidentifiedfourriskfactorssignificantly
associatedwithhigherlevelsofemotionalsymptomswithinthesample,namely
lowacademicattainment,SEN,lowfamilyincome,andcaregivingresponsibilities.
Thefirstthreeoftheseriskfactorsweresmallinmagnitude,whiletheassociation
betweencaregivingresponsibilitiesandemotionalsymptomswasmoderateinsize.
Acumulativeriskscorecomprisingthesefourriskfactorswasfoundtobea
significantpredictorofemotionalsymptoms,providingevidenceforcumulativerisk
effects;thatis,asthenumberofriskfactorsoneisexposedtoincreases,sotoo
doesthereportedlevelofsymptomatology.Assessmentofmeasurementmodels
torepresentmultipleriskexposureindicatedthatalatentriskconstructwasthe
strongestpredictorofemotionalsymptoms,explainingagreaterproportionof

CHAPTERSEVEN:DISCUSSION
222
variancerelativetocumulativeriskscoreandmultipleregressionapproaches.This
latentvariableoffersarepresentationofmultipleriskexposurethatunitesrisk
factorsasasingularconstruct,inlinewithindicationsthatriskstendtocluster
aroundanindividual,whilepreservingthespecificnatureofeachriskfactor,
offeringamorecomplexrepresentationthanisofferedintraditionalcumulative
riskindexing.
Finally,itwasfoundthatmultipleriskexposurewasassociatedwith
emotionalsymptomswithinthesampleentirelythroughindirectpathways,via
perceiveddistressandperceivedcoping.Thatis,greaterlevelsofmultiplerisk
exposurewereassociatedwithgreaterperceiveddistressandloweredperceived
coping,bothofwhichwereassociatedwithgreatersymptoms.Afteraccountingfor
indirecteffects,therewasnoevidenceofastatisticallysignificantdirecteffect
betweenmultipleriskexposureandemotionalsymptoms,indicatingsupportfor
“fullmediation”.Thetotalindirecteffectswerefoundtobesmalltomoderatein
magnitudeandthismodelexplainedasubstantiallylargerproportionofvariance
(60.5%)comparedtothemodelwithonlythelatentconstructasasingular
predictor(8.8%).
7.2.2ResearchQuestion2:FactorsandProcessesforPositiveOutcomes
2.Whatarethefactorsandprocessesthatsupportpositiveoutcomesinemotional
symptomsamongearlyadolescentgirls?
Thisresearchquestionsetouttoidentifythefactorsassociatedwithlower
levelsofemotionalsymptomsamongearlyadolescentgirls(promotiveeffects)and
toinvestigatewhetherexternalfactorsmoderatetheprocessesunderlyingmultiple
riskeffectsamongthispopulation(protectiveeffects).
Analysesfirstidentifiedthreepromotivefactorssignificantlyassociatedwith
lowerlevelsofemotionalsymptomswithinthesample,specificallyfamilyadult
connection,schoolpeerconnection,andactiveengagementinhomeandschool
life.Theseassociationswereallobservedtobesmallinsize,withschoolpeer
connectiondemonstratingthestrongestassociationwithloweredsymptomatology.

CHAPTERSEVEN:DISCUSSION
223
Thefinalmodelexaminedwasaconditionalindirecteffectsmodel,wherein
hypothesisedprotectivefactorsweremodelledasmoderatorsoftheunderlying
distressandcopingmechanismswithintherelationshipbetweenmultiplerisk
exposureandemotionalsymptomsinthesample(Figure5.11,shownagain
overleaf).Inspectionofthismodelindicatedthatpathwaysbetweenriskexposure
andperceiveddistressandcoping,respectively,wereeachmitigatedbygreater
perceivedfamilyadultconnectionandschoolpeerconnection,withfamily
connectiondemonstratingthestrongesteffect.Conditionaleffectswereobserved
onlyforthefirststageofindirecteffects,withthepathwaysfromriskexposureto
bothperceiveddistressandcopingmitigatedbyperceivedconnectiontofamily
adultsandschoolpeers.Thiswasnottrueforthesecondstageoftheindirect
pathways;thatis,parametersfromdistressandcopingtoemotionalsymptoms
unaffectedbyanyoftheprotectivevariablesassessed.Alsoofnotewastheextent
ofthechangeobservedhere.Greaterperceivedconnectiontofamilyadultsand
schoolpeersdidnotsimplylesseneffects,butchangedtheirdirection,sothat
thoseexposedtogreaterlevelsofriskwerelesslikelytoappraisetheirlivesas
stressful(withalargeeffectsize)andmorelikelytoreportagreaterabilitytocope
(withasmalleffectsize).

CHAPTERSEVEN:DISCUSSION
224
Figure5.11.Specificconditionalindirecteffects.Familyadultconnection(FAMILY)andschoolpeer
connection(PEER)areshownmoderatingtheeffectsofmultipleriskexposureuponperceived
distressandperceivedcoping.Positiveparametersareshowninblocklinesandinverseparameters
areshownindashedlines.
7.2.3ResearchQuestion3:LivedExperience
3.Whatisitliketobeanearlyadolescentgirlwhoisexperiencingemotional
symptomsinthecontextofriskexposure?
Thisresearchquestionexploredtheemotionandlivedexperienceof
participants,withafocusonthewayinwhichtheyexperiencedandmadesenseof
theseareasoftheirlives.Findingsweregroundedinfoursuperordinatethemes:
Theexperienceofsymptoms;internalgrappling;demandsandcontrol;anddrawing
onothers.
Ascapturedin“theexperienceofsymptoms”,participantsconceptualised
theirsymptomseitherasobjectifiedcognitiveentitiesthatcouldbehad,or
affectivestatesthatonebecame.Participantsviewedthemasamassthatcould
growandbuild,attimestotheextentthattheywerebeyondtheirowncontrol,
andinsomecasespresentedthesesymptomsasdominantwithintheirbroader
emotionallandscape.Asencapsulatedin“internalgrappling”,participants

CHAPTERSEVEN:DISCUSSION
225
experiencedanumberofinternaltensionsandconflictsinmakingsenseofthese
symptoms,whichtheyappearedtoviewasoccurringwithinthem,butoperating
independentlyofthem.Theyconsideredthesethoughtsandfeelingstobe
connectedtothembutalsoseparatefromtheircoreidentityandpositioned
themselvesaspassivewithinboththeoccurrenceandresolutionofthese
symptoms.Furthermore,insomecasesthesetypesofthoughtsandfeelingswere
seenasirrational,althoughthisbeliefdidnotappeartobehelpfulinchallenging
them.
“Demandsandcontrol”capturedthewaysthatparticipantsmadesenseof
thedifferentdemandsintheirworlds.Theperceiveddemandsthatparticipants
facedwereseenasdominatingtheirlifeworldsandtheyfeltastrongresponsibility
toadapttomeetthesedemands,evenwhenthiswasperceivedtobedetrimental
tothem.Theydescribedintenseandpervasivefearsthatsomethingbadwasgoing
tohappenandbelievedthattheyhadnorightorabilitytodoanythingaboutthe
demandsthattheywerefacing.Finally,“drawingonothers”exploredthewaysthat
participantsdrewonthepeoplearoundthemastheynavigatedtheirsymptoms
andthedemandstheyfaced.Theydescribedaprocessofmappingouttheir
emotionalsupportnetwork,assessingandselectingindividualswhotheyviewedas
abletofulfiltheirsupportneeds,andbelievedthattalkingtoothersabouttheir
symptomscouldbebeneficial.Inthecaseofoneparticipant,otherpeoplecould
alsoactasaprotector,shieldingherfromphysicalharmandcompensatingforthe
hurtcausedbyotherpeopleinherworld.
7.3ResearchQuestion1:RiskFactorsandProcesses
1.Whataretheriskfactorsandprocessesassociatedwithemotionalsymptoms
amongearlyadolescentgirls?
7.3.1RiskFactors
a.Oftherisksidentified,whatisthemagnitudeoftheirassociationwithearly
adolescentgirls’emotionalsymptoms?
CHAPTERSEVEN:DISCUSSION
226
ConfirmedRiskFactors
LowAcademicAttainment
Findingssuggestthatearlyadolescentgirlswithlowacademicattainment
aremorelikelytoreporthigherlevelsofemotionalsymptoms.Thissupportsa
consistenttrendpresentacrosstheliterature,withawealthofstudiesreporting
evidenceofsucharelationship(Bondetal.,2005;Deightonetal.,2018;Panayiotou
&Humphrey,2018).Similarlytopreviousstudies(Bondetal.,2005;Moilanenet
al.,2010;Panayiotou&Humphrey,2018;Weeksetal.,2016),thisassociationwas
observedtobesmallinmagnitudewhenconsideredinlinewithCohen's(1988)
thresholds.
Itshouldbenotedthatpriorevidenceindicatesthattheremaybea
bidirectionalassociationbetweenlowacademicattainmentandemotional
symptoms,withdifficultieswithsuchsymptomspotentiallyinfluencingone’s
achievementlevels(Deighton,Humphrey,etal.,2018;Verboometal.,2014).The
datadrawnuponinthecurrentstudycapturedparticipants’attainment
approximatelyoneyearpriortothecompletionoftheWMF(seeSection4.7.1),
whichprovidesanindicationofalongitudinalassociation;however,asitwasnot
possibletocontrolforprioremotionalsymptoms,bidirectionaleffectscannotbe
ruledout.
SEN
ParticipantswithSENweremorelikelytoreportgreaterlevelsofemotional
symptoms,reflectingpreviousindicationsofincreasedratesamongchildrenand
adolescentswhohaveanSENcondition(e.g.,Emerson,2003;Nelson&Harwood,
2011)aswellasgreaterlevelsofdiagnosablepsychiatricconditions(e.g.,Brereton
etal.,2006;Simonoffetal.,2008).Studieshaveoftenreportedevidenceofa
moderateassociationinrelationtovariousSENconditions(e.g.,Nelson&Harwood,
2011),thoughherethisrelationshipwasfoundtobesmallinsize.However,itis
notablethatthecurrentstudyassessesSENasanoverarchingriskfactorrather
thanfocusingonindividualSENconditionsasinpreviousresearch.AsSENcaptures
considerableheterogeneitybothacrossandwithinconditions(DfE&Department

CHAPTERSEVEN:DISCUSSION
227
ofHealth,2015),suchfindingscannotreasonablybegeneralisedtootherswiththe
sameorotherconditions.Giventhatindividualsaretypicallyidentifiedashaving
SENbecausetheyarerecognisedashavingneedsnoteasilymetwithinusualschool
practices,thecurrentstudyindicatesthatoperatinginaschoolsystemnot
necessarilydesignedtomatchone’sneedsmaybedetrimentalinrelationto
emotionalsymptoms.
LowFamilyIncome
Evidenceofarelationshipbetweenlowfamilyincomeandemotional
symptomsinthecurrentstudywasunsurprising,asthisisoneofthemostwell
establishedriskfactorsacrosspreviousliterature(e.g.,Morrisonetal.,2014;
Santiagoetal.,2011).Thisrelationshipwassmallinsizeandindeedwasthe
weakestcontributoracrosstheconfirmedriskfactors.Mixedfindingsaroundeffect
sizesacrossexistingliterature,rangingfromsmalltomoderate,havebeen
attributedtofluctuationinsamplecharacteristicsincludingageandgender,aswell
asmethodologicalfeaturessuchasmeasurementofincome(Mendelsonetal.,
2008;Reiss,2013).Thecurrentstudyaddstocurrentknowledgeandunderstanding
ofthemagnitudeofthisrelationshipspecificallywithinearlyadolescentgirlsacross
disadvantagedareasofEngland.UseofbothpastandpresentFSMeligibilityto
indicatelowfamilyincomeallowedincorporationofpreviousexposure,inlinewith
evidenceindicatinglong-termeffects(e.g.,Najmanetal.,2010;Santiagoetal.,
2011).However,thestudycouldnotexploreshiftsinthetiming,duration,and
intensityoffamilialpovertyandlowincome,whichcaninfluencetheextentof
effectsuponmentalhealthoutcomes(Reiss,2013).
CaregivingResponsibilities
Participantswhoidentifiedthemselvesashavingsomelevelofcaregiving
responsibilitiesreportedhigherlevelsofemotionalsymptoms.Thereissome
previousevidenceofsuchanassociationamongchildrenandadolescentswith
caregivingresponsibilities(Banksetal.,2001;Kavanaughetal.,2015;Shifren&
Kachorek,2003).However,investigationhasbeenrareandthesestudiesoften
focusonspecificgroupsofcaregivers,suchasthosecaringforadultswitha

CHAPTERSEVEN:DISCUSSION
228
disability,offeringhighlycontextualfindings.Thus,examinationofbroader
caregivingresponsibilitieshereprovidesinsightintopatternsacrossarangeof
circumstances,facilitatinganunderstandingoftheeffectsofdeliveringcareto
othersmoregenerally,ratherthaninthecontextofaspecificneedordisorder,
thusofferinggreatergeneralisability.
AsexploredinChapterFour,thisvariablewasre-definedbasedon
prevalenceestimatesandsoitisimportanttonotethatthisrelatestocaregiving
responsibilitiesatagenerallevelratherthandescribing“youngcarers”.
Nevertheless,thisvariableshowedamoderateassociationwithemotional
symptoms,substantiallylargerthanthatofotherriskfactors.Indeed,thisfinding
suggeststhatgeneralcaregivingresponsibilities,beyondthatreflectedinthe
narrowedcategoryofyoungcarerstatus,maybeparticularlyproblematicfor
emotionalsymptomsduringthisdevelopmentalphase.Qualitativeresearch
exploringyoungcarers’experienceshasindicatedthatcaregivingexperiencesare
markedbypersistentstressinday-to-daylifeandchallengingshiftsinone’sidentity
(Bolasetal.,2007;Earleyetal.,2007;Rose&Cohen,2010).Givenlimited
knowledgeinrelationtohowcaregivingresponsibilitiesmaybeassociatedwith
emotionalsymptoms,findingsindicateaneedtoreplicatethisstudyacrossdiverse
populationsandcontextsandtoundertakefurtherqualitativeexploration.Factors
suchastheextentandtypeofcarethatyoungpeopleareprovidingmayinfluence
themagnitudeofthisassociation,ascouldtherelationshiptothepersonneeding
careorthespecificdifficultynecessitatingcare(Ireland&Pakenham,2010;
Kavanaughetal.,2015).Indeed,givenindicationsthatthecurrentstudyis
capturingawidergroupofindividualsthanthosemoretypicallyidentifiedasyoung
carers,itmaybeimportanttomorefullyunderstandthepointatwhichtheextent
andregularityofcaregivingbecomesproblematicformentalhealthoutcomes.
Asthecurrentstudyfocusesonunderlyingmechanismsandprotective
factorsinthecontextofmultipleriskexposure,suchprocessesarenotdirectly
examinedinrelationtocaregivingresponsibilitiesasanisolatedvariable.Given
currentlimitationsinknowledgeandunderstandingregardingmechanismsand
adaptiveprocessesamongyoungcarers(Kavanaughetal.,2015),alongside

CHAPTERSEVEN:DISCUSSION
229
qualitativeevidencethatyoungcarersreporthighlevelsofstressindailylife(Bolas
etal.,2007;Earleyetal.,2007;Rose&Cohen,2010),futureresearchshouldseekto
directlyexplorethisinrelationtoemotionalsymptoms.Furthermore,the
measurementandprevalenceissuesencounteredhereindicateaneedfor
considerationinthewayinwhichyoungcarerstatusand/orcaregiving
responsibilitiesismeasuredinresearch.Whileapreviousstudyfoundthata
definitionalapproachasadoptedhereyieldedsimilarestimatestomoredetailed
measures(Banksetal.,2001),findingsheresuggestthatthisapproachcouldlead
toinflatedestimates.Itisimportantforresearcherstocarefullyconsiderthe
implicationsoftheirmeasurementapproachandhowopenthismaybeto
interpretationfromparticipants.Furthermore,researchersshouldclarifyfor
readershowmeasurementmayaffectthenatureoftheirdataand,inturn,their
inferences.
ExcludedRiskVariables
Youngrelativeage,highacademicattainment,ACEs,andneighbourhood
socioeconomicdeprivationwerenotfoundtobeassociatedwithincreasedlevelsof
emotionalsymptomshere.Giventhateachofthesevariableswasincludedbased
ontheoreticaland/orempiricalsupportacrosstheliterature,findingsmayoffer
furtherindicationsofthecontextualnatureofrisk.Forinstance,muchofthe
previousevidencearoundACEsandneighbourhoodsocioeconomicdeprivationis
focusedonadults,withlimitedinvestigationofadolescentoutcomes;thus,itmay
bethatthereislittleoveralleffectforearlyadolescentgirls.Similarly,itmaybe
thatthefocusonearlyadolescenceinparticularisrelevant.Forinstance,itmaybe
thatnegativeeffectsinrelationtohighacademicattainmentoccurinlaterstagesof
adolescenceintimesofparticularacademicpressure,suchasGCSEpreparation,
ratherthaninearliereducationalstages.Thefocusongirlscouldalsoberelevant
fortheseriskvariables,asthesefactorscouldperhapsbeproblematicforboysand
thusproduceanassociationifbothgirlsandboyswereanalysedtogether.
Findingsmayalsorelatetothemethodologyused.Asnoted,riskfactorsare
oftenexaminedinisolationratherthaninunison,meaningthatconfoundingeffects
ofotherco-occurringvariablesarenotaccountedfor;thus,itmaybethatthestudy

CHAPTERSEVEN:DISCUSSION
230
offersamorepreciseestimateoftheserelationships.However,itmayalsobethat
themeasurementusedfortheseriskfactorshasinfluencedresults.Forinstance,
useofCINstatusasaproxyforACEsdiffersfromthemoretypicaluseofaself-
reportinventoryspanningnumerousadverseexperiences.Thoughthisovercomes
issuesofrelianceonrecall,itprovidesbinaryinformationratherthanascaled
response(e.g.,cumulativeexposuretoACEs)andmayonlycapturemoreextreme
circumstancesalbeitwithsupportinplace,giventhatdesignationofCINstatus
denotesaneedforprofessionalintervention.
Futureworkisneededtoexplorethesevariablesacrossdifferent
circumstancesandpopulations.Ofcourse,itisalsoimportanttonotethatjust
becauseafactorisnotfoundtofunctionasriskyforagroupasawholedoesnot
meanitisnotproblematicforsomeindividualsorevengroupsofindividualswithin
thatlargergroup.Thisisillustratedwellinthecaseofhighacademicattainment
throughthequalitativeexperiencesofJennifer,whodescribedintensedifficulties
andpressureinrelationtohighattainment.Suchdisparitiesdemonstratetheneed
toretainafocusonindividualexperiencesratherthangeneralpatternsalone,both
inresearchandinpractice.
7.3.2CumulativeRiskEffects
Thecurrentstudyoffersevidenceofsmallcumulativeriskeffectsinrelation
toearlyadolescentgirls’emotionalsymptoms.Specifically,thisfindingprovides
supportfortheaccumulationprinciple,thefirstcoreassumptionofcumulativerisk
theory,whereinincreasedlevelsofriskexposureareassociatedwithworsening
outcomes.Itisalsoconsistentwithageneraltrendacrosspreviouscumulativerisk
investigations,withaccumulationeffectsfoundacrossawiderangeofpopulations
andoutcomes(Evansetal.,2013).Paststudieshaveidentifiedanassociation
betweencumulativeriskexposureandinternalisingdifficulties,includingemotional
symptoms,bothconcurrentlyasinthecurrentstudy(Flouri&Kallis,2007;Jones,
Forehand,Brody,&Armistead,2002;Panayiotou&Humphrey,2018)and
longitudinally(Appleyardetal.,2005;Gerard&Buehler,2004;Horan&Widom,
2015;Panayiotou&Humphrey,2018).Assuch,thisfindingprovidesfurther

CHAPTERSEVEN:DISCUSSION
231
confirmationthatincreasedlevelsofriskexposureappeartonegativelyinfluence
adolescentinternalisingdifficulties.However,thereareindicationsthatcumulative
riskeffectsaremoderatedbyfactorssuchaspopulationcharacteristics,including
gender,andtheoutcomeofinterest(Evansetal.,2013).Giventhatearly
adolescenceappearstobeapivotalmomentingenderedmentalhealthtrajectories
andtheemergenceofgreaterlevelsofdepressiveandanxioussymptomsand
disorderamonggirlsandwomen,itisparticularlyimportanttounderstandthe
contributoryfactorsatthisdevelopmentalstage.Previousstudieshaverarely
focusedexplicitlyonearlyadolescence,insteadspanningwiderdevelopmental
periods,andhaveoftennotfocusedexplicitlyongirlsand/orgenderedpatterns.As
such,thecurrentstudyprovidesfurtherknowledgeandunderstandingspecifically
relatingtocumulativeriskeffectsforemotionalsymptomsatacritical
developmentaljunctureforgirls.
Thesmallrelationshipobservedhereisconsistentwiththemagnitudeof
cumulativeeffectsinpreviousstudiesfocusedoninternalisingdifficultiesincluding
emotionalsymptoms(Gerard&Buehler,2004;M.Panayiotou&Humphrey,2018).
Notably,thereareindicationsthatcumulativeriskeffectsforinternalising
difficultiescouldbeweakerthanthoseobservedforexternalisingdifficultiesand
otheroutcomes.Forinstance,PanayiotouandHumphrey(2018)foundthat
cumulativeriskexposureexertedgreatereffectsforexternalisingdifficultiesthan
internalisingsymptoms(asreportedbyteachers).Thus,itmaybethatcumulative
riskeffectsarenotasprofoundforinternalisingdifficulties,includingemotional
symptoms,relativetoothermentalhealthoutcomes,thoughitremainsunclear
whythismightbethecase.Whiledirectcomparisonofsucheffectsacross
outcomesamongearlyadolescentswasbeyondthescopeofthecurrentstudy,
futureresearchcouldexamineandcomparesuchassociationsfurther.Indeedgiven
indicationsthattheextentandnatureofcumulativeriskeffectscanbeoutcome-
specific(Horan&Widom,2015),futurestudiesshouldexplorewhythismaybethe
case,boththroughqualitativeinquiryandthroughanalyticalmodelsthatcan
examineunderlyingpathwaysforspecificoutcomes.However,giventhatuseofa
latentconstructofferedgreaterpredictivevalidity,asexploredinthefollowing

CHAPTERSEVEN:DISCUSSION
232
section,itcouldbethatafocusonlyontheextentofriskexposureinacumulative
riskindexdoesnotcapturethecomplexityofadversity,whichcouldcontribute
differentiallytodifferentoutcomes.Itcouldalsobethatsuchdisparitiesare
attributabletomeasurementofoutcomes.AlthoughtheSDQsubscaleusedinthe
currentstudyhasshowngoodvalidityandreliability,asoutlinedinChapterFour,it
maybethattheuseofonlyfiveitems,togetherwithathree-pointLikertscale,is
notabletocomprehensivelycapturethecomplexandmultidimensionalconstruct
ofemotionalsymptoms(seeSection7.7.1forareflectiononthemeasuresutilised).
Thereisalsoscopeforfurtheranalysisexamininggenderedcumulativerisk
effectsamonggirlsandwomen.AsexploredinChapterTwo,previousauthorshave
suggestedthatincreasedratesofdepressiveandanxioussymptomatologyand
disorderamonggirlsandwomenarelikelynotattributabletoanysinglefactor,but
rathertoaninteractionofnumerouscontributors(Hydeetal.,2008;Nolen-
Hoeksema&Girgus,1994).Whilesomestudieshaveexaminedinteractions
betweenvaryingstressors,includingbiologicalcomponentsandwiderindividual
andinterpersonalfactors,furtherempiricalexaminationofgender-specifictrends
andpathwaysrelatingtocumulativeriskexposurecouldgenerategreaterinsights.
Thecurrentstudy’suseofsecondarydataanalysismeantthattheriskvariables
assessedwereincludedbasedontheirexistingavailability,ratherthanbeing
selectedbasedonevidencerelatingtothosefactorsconsideredmostproblematic
forgirlsandwomen.Thatis,althoughsomeoftheriskvariablesassessedare
understoodtoexertgreatereffectsforgirlsandwomen(e.g.,lowacademic
attainment,neighbourhoodsocioeconomicdeprivation),thiswasincidental.
Futureresearchshouldseektocollectdatarelatingtoriskfactorsthoughttobe
specificallyproblematicforgirlsandwomeninordertoexplorethewaythat
multipleriskexposuremayfunctionbasedongenderedexperiences.Forinstance,
itcouldbeusefultoassesseffectsinthecontextofacumulativeriskscore
comprisingfactorsunderstoodtodisproportionatelyaffectgirlsandwomen,such
asadrenalandovarianhormones(Albert,2015;Nolen-Hoeksema,2001;Steineret
al.,2003),ruminativecoping(e.g.,Johnson&Whisman,2013;Nolen-Hoeksema&

CHAPTERSEVEN:DISCUSSION
233
Girgus,1994)andgender-relatedviolence(e.g.,Fredrickson&Roberts,1997;
McLean&Anderson,2009).
Itshouldbenotedthattherelativelysmallnumberofhypothesisedrisk
variablestestedinthecurrentstudy,alongwiththeconfirmationofonlyfourrisk
factorsinthissample,precludedinvestigationofsomeofthemorenuanced
aspectsoftheobservedcumulativeriskeffects.Firstly,itwasnotfeasibleto
examinethefunctionalformofthisrelationshiptoassesswhetheralinearor
curvilinearrelationshipwaspresent,ashasbeenexploredinpaststudies(Horan&
Widom,2015;Oldfieldetal.,2015).Pastresearchexaminingthefunctionalformof
cumulativeriskeffectshaveproducedmixedevidence,warrantingongoing
investigation.Multiplestudieshavereportedalinearassociationbetween
cumulativeriskexposureandoutcomes,withincrementalincreasesinnegative
outcomeswitheachadditionalriskfactor,includinginrelationtoemotionaland
internalisingsymptoms(Appleyardetal.,2005;Gerard&Buehler,2004;Horan&
Widom,2015;Ravivetal.,2010).Othershavefoundevidenceofcurvilineareffects,
includingmassaccumulationwithnegativeeffectsbecomingdisproportionateto
thenumberofrisks(Biedermanetal.,1995;Forehandetal.,1998;Jonesetal.,
2002;Oldfieldetal.,2015)andasaturationmodelwherebyeffectsplateauaftera
certainlevelofexposure(Morales&Guerra,2006).However,becausethefinal
cumulativeriskscoreusedinthecurrentstudyconsistedof3+risks,itwasnot
feasibletoassessthefunctionalformofeffectsbecausepaststudieshaveindicated
thatcurvilinearshiftstendtooccurwhenparticipantsareexposedtothreeormore
risks(Biedermanetal.,1995;Forehandetal.,1998;Jonesetal.,2002;Morales&
Guerra,2006).Inparticular,itwouldnothavebeenfeasibletoassesswithcertainty
whetheranycurvilineareffectsobservedatthislevelofriskexposurewouldreflect
agenuineacceleratoryaffect,ortoassessthefunctionalformbeyondthispoint.
Givenmixedfindingsacrosstheliteratureregardingthefunctionalformofrisk
effects,whichmaybeattributabletopopulation-andoutcome-specificity(Horan&
Widom,2015),futurestudiesshouldseektomakeuseofalargerinventoryofrisk
variablestofacilitatesuchanalysisforearlyadolescentgirls’emotionalsymptoms.

CHAPTERSEVEN:DISCUSSION
234
Secondly,itshouldbenotedthatsomestudieshavemadeuseofmultiple
cumulativeriskscoresbygroupingtogetherdomainsoftheoreticallyrelatedrisk
factors.Forinstance,inanexaminationofriskeffectsforpsychopathology,Flouri,
Tzavidis,andKallis(2010)clusteredvariablestogethertocreateadistalfamilyrisk
score(capturingadverseexperiencesinthechild’sfirstyear),aproximalfamilyrisk
score(thoseinthechild’ssecondandthirdyear),andanareariskscore
(encapsulatingneighbourhoodriskfactors).Indeed,Evansetal.(2013)observed
thatstudiesexaminingexposureacrossanumberofdiscretedomainsgenerally
reportlargereffectsizes.Inthecurrentstudy,suchgroupingwasnotpossiblegiven
thesmallnumberofvariablesassessedinthefirstinstance;forexample,hereonly
oneneighbourhood-levelvariablewasavailable.Futurestudiescouldexaminethe
extenttowhichdifferentlevelsofriskexposureacrosstheecologycontributeto
emotionalsymptomsamongearlyadolescentgirls.Nevertheless,thecurrentstudy
alsooffersanumberoffurtheranalysesthatseektoovercomebothconceptual
andmethodologicallimitationswithincumulativerisktheory,inordertodevelop
knowledgeandunderstandingofthisphenomenon,asisexploredinthefollowing
sections.
7.3.3RiskMeasurementModels
Findingssuggestedthatalatentriskvariable,capturingexposureasa
singularconstructwhilepreservinginformationabouteachindividualriskfactor,
showedthegreatestpredictiveutilityforemotionalsymptoms(8.8%).Thus,
unifyingriskexposurewithinasingularpredictorvariablewhilestillretaining
statisticalinformationwassuperiortoapproachesprioritisingoneofthese
features;namely,multipleregression,whichfocusesonthenatureofeachrisk
factor,andacumulativeriskindex,whichcapturesthenumberofriskfactors,with
thesetwoapproachesshowingsimilarlevelsofpredictivepower.Notably,
predictiveutilityacrossallofthesemodelsislowrelativetopreviousstudies
exploringmultipleriskeffectsforinternalisingdifficulties(Bayeretal.,2012;Gerard
&Buehler,2004;Patalay&Fitzimons,2018),howeverthesestudiesdiffer
methodologically,examininglargernumbersofriskfactorsand/orlongitudinal

CHAPTERSEVEN:DISCUSSION
235
associations.Thus,anincreasefrom2.8%to8.8%isnoteworthy.Itisalsoimportant
tohighlightthatevidenceinthecurrentstudyishighlycontext-specificanddoes
notnecessarilyindicatethatalatentriskconstructisthemostappropriate
representationofmultipleriskexposureinallcircumstances.Rather,itsuggests
thatamongthissampleofearlyadolescentgirls,thisparticularsetofriskfactors
reflectedacoherentunderlyingconstructabletopredictthisspecificoutcome.
Firstly,thisisbecausetheviabilityofalatentfactoriscontextuallydetermined
basedontheindicatorsitdrawsuponandinriskresearchstudiesoftendiffer
substantiallyintheamount,type,andmeasurementofriskvariablestheyassess.
Assuch,anygivenstudywouldhaveadifferentcombinationandamountof
indicatorsavailableforlatentfactorformationandexploration.Secondly,existing
researchexamininglatentfactorsforriskeffectsremainslimitedandmostly
constrainedtoevaluationofriskeffectsforcognitiveoutcomes(Belskyetal.,2012;
Burchinaletal.,2000;Halletal.,2010).Itmaybethatthemostappropriate
predictorforagivenoutcomeisdependentuponthenatureoftheavailablerisk
factorsand/orthenatureoftheoutcomeitself.Assuch,thestudydoesnot
concludethatalatentfactormaybethemostsuitableapproachinall
circumstancesandinsteadadvisesthatthisshouldbetestedineachindividualcase
priortoinferentialanalysis.However,thisfindingdoesholdanumberof
methodologicalandconceptualimplications,whichareexploredhere.
Firstly,findingsindicatethatinthemeasurementandmodellingofmultiple
riskexposure,bothunificationandnatureofriskexposuremaybeimportant.This
mirrorsfindingsfrompreviousinvestigationscomparinglatentmodellingwitha
cumulativeriskindexinrelationtocognitiveandlanguagedevelopment(Burchinal
etal.,2000;Halletal.,2010).Thisdifferenceislikelyattributabletothestatistical
advantagesoflatentmodelling,aslatentfactorsaccountformeasurementerror,
offeringmorerobustestimatesofrelationships(Gefenetal.,2011).Ithasalsobeen
highlightedthatcollapsingtogetherriskvariablestocreateacumulativeriskindex
maybestatisticallyproblematicastheresultinglossofinformationmayreduce
sensitivityandpredictivepower(Belskyetal.,2012;Evansetal.,2013;Halletal.,
2010;Kraemeretal.,2001),assupportedbycurrentfindings.Indeed,thoughvery

CHAPTERSEVEN:DISCUSSION
236
fewstudieshaveexploredlatentmodellinginthiscontext,Evansetal.(2013)
reportedintheirsystematicreviewthatof95instanceswherestudieshad
comparedmultipleregressionwithacumulativeriskindex,overhalffoundmultiple
regressiontobesuperiorandonlysevenreportedsupportforacumulativerisk
index(therestofthetime,thesewererelativelyequalinpredictivepower).Thus,
findingsinthecurrentstudyandacrossthewiderliteratureindicatethata
cumulativeriskindexmaynotbethemostusefulwaytomeasuremultiplerisk
exposure,withalatentfactorperhapsofferingamorerobustalternativewith
greaterpredictivepower.
Supportforalatentapproachsuggeststhatitisusefultodrawon
interactionsacrossriskfactors,giventhatwithsomeadjustmenttheseriskfactors
reflectedacoherentunderlyingconstruct.Notably,thisassumptioncannotbe
formallyassessedoraccountedforwithinacumulativeriskindex(Belskyetal.,
2012;Halletal.,2010;Kraemeretal.,2001).Thisprovidessupportforuseof
traditionallatentmodellinginordertodrawupontheseinteractions,ratherthan
thereflectiveapproachundertakenbyHalletal.(2010),whichdoesnotoffer
greaterpredictiveutility.Indeed,thegreaterpredictivepoweraffordedbydrawing
ontheseinteractionsindicatesthatthetransactionsacrossriskfactorsappear
meaningfulforoutcomes,consistentwithRutter's(1979)proposalthattransactions
acrossrisksresultindisproportionateeffects.Nevertheless,thisalsolends
credencetotheargumentthatfocusingonmagnitudeonlymaybeareductionist
waytounderstandacomplexphenomenon,giventhatitdoesnotdirectlydraw
uponthesetransactions(Belskyetal.,2012;Burchinaletal.,2000;Halletal.,2010).
Furthermore,theapproachtakenhereperhapsallowsamorenuanced
representationofriskexposurebyutilisingtheseinteractionstoestimatethe
individualcontributionofeachriskindicator,ratherthanassumingthateachrisk
factorisequallyrepresentativeoftheunderlyingdisadvantageparticipantsface
(Halletal.,2010).
However,itmaybethatthemostappropriatemeasurementmodelfor
multipleriskexposureiscontext-dependent.Hooper,Burchinal,Roberts,Zeisel,
andNeebe(1998)foundthatacumulativeriskindexwassuperiorfor

CHAPTERSEVEN:DISCUSSION
237
communicationbehaviour,butmultipleregressionshowedgreaterpredictiveutility
formentaldevelopmentandreceptivecommunication.Astheseprevious
comparisonshavefocusedoncognitiveandlanguagedomains(Burchinaletal.,
2000;Halletal.,2010),thecurrentstudyprovidesfurthercorroborationanda
uniquecontributionbyexploringthiswithinmentalhealth.Giventhatriskis
context-specificandcanfluctuatebasedontheparticularriskfactors,outcomes,
andpopulationsunderinvestigation,thecurrentstudydoesnotseektoadvocate
forthisasthemostappropriatemethodinallcircumstances.Indeed,Burchinalet
al.(2000)advisethatthespecificmeasurementmodelutilisedmaydependupon
theparticularcontextofeachstudy.Thus,thecurrentstudyprovidesfurther
contextualsupportforBurchinaletal.'s(2000)argumentthatalatentriskconstruct
isparticularlyusefulincasesofarelativelylownumberofriskfactorsandalarge
sample.Thus,researchersexaminingtheeffectsofmultipleriskexposureshould
comparedifferentrepresentationsbeforeundertakingmorecomplexanalyses.
Latentmodellingmayalsobeproblematicwithsmallernumbersofriskfactors,asit
maynotallowforthepost-hocmodificationsnecessarytomakethefactorviable
foranalysis,asfoundherewhencontrollingforresidualcorrelationswasnot
possibleinthefinal,morecomplex,model.Thus,researchersshouldinspect
whethersuchissuesmaybelikelytooccurindeterminingthemostappropriate
analysiswiththeparticularvariablesavailable.
Finally,findingscouldbeconsideredtochallengethenumber-over-nature
principleofcumulativerisktheory,suggestingthatneithertheextentnorthe
natureofriskexposureinisolationyieldsgreaterpredictivepoweroverearly
adolescentgirls’emotionalsymptoms.Directexaminationofthisprinciplehasbeen
modestoverall,withmostpublishedstudiesfocusingonwhetheracumulativerisk
indexispredictiveofoutcomes,andthisassumptionhasnotbeentestedinrelation
toemotionalsymptomsinadolescence.Itisimportanttonote,however,thatthe
currentstudycannotofferadirectconclusionrelatingtothisprinciplegiventhe
focusoncomparingmeasurementmodels.Thatis,itisnotpossibletoascertain
whethertheincreasedpredictivepowerofferedbythelatentriskconstructissolely
theresultofthestatisticaladvantagesitaffords,orwhetherthisisinpartduetoa
CHAPTERSEVEN:DISCUSSION
238
genuineeffect.Onewaytoexplorethisprinciplemoredirectlyisthroughlatent
classanalysis,whichallowsresearcherstoidentifysubgroupsofparticipants
exposedtodifferentcombinationsofriskandthencomparetheeffectsofthese
profilesuponoutcomes(Lanza&Cooper,2016).Severalstudiesadoptingthis
approachhavefoundthattheparticularcombinationsofrisksthatchildrenand
adolescentsexperienceareheterogeneousanddifferinrelationtoimpactupon
outcomes,withsomeriskprofilesassociatedwithgreaternegativeconsequences
acrossparticularareasofhealthanddevelopment(Lanieretal.,2018;Lanzaetal.,
2010;Lanza&Cooper,2016;Rhoadesetal.,2011;A.L.Roy&Raver,2014).This
approachhasindicatedthatriskfactorsdonotappeartocontributeequallyto
outcomesforchildrenandyoungpeopleexperiencinghighlevelsofadversity,
contrarytothenumber-over-natureprinciple.Futurestudiesshouldseektoutilise
thisapproachinrelationtoearlyadolescentgirls’emotionalsymptoms,tomore
directlyidentifytheextenttowhichextentandnatureofexposurecontributesto
outcomes.Thiswouldalsoallowidentificationwhetherthereareparticular
combinationsoffactorsthatcontributetogreatermultipleriskeffectsamongthis
group.
7.3.4IndirectEffectsofStress
Findingssuggestthatindividualsexposedtogreaterlevelsofmultiplerisk
arelikelytoappraisetheirlivesasmorestressfulandtobeexceedingtheircoping
resources,whichinturnareassociatedwithgreaterlevelsofemotionalsymptoms.
Indicationsof“fullmediation”,withtheinclusionofindirectpathwaysnullifyingany
directeffects,indicatethatcomponentsofstressappraisalmayplayasubstantial
roleintheextenttowhichmultipleriskexposureimpactsuponemotional
symptomsinearlyadolescentgirls.Althoughthisconceptofstressasamechanism
forriskeffectsisacentraltenetofcumulativerisktheory,todatenostudieshave
empiricallyexaminedthis.Thus,whilefindingsarecontextuallyspecificto
emotionalsymptomsandearlyadolescentgirls,thestudyoffersnovelempirical
insightintotherolethatstressmayplayinmultipleriskeffects.Futureresearch
shouldexplorethereplicabilityofthisfindingacrossdifferentcontexts,including

CHAPTERSEVEN:DISCUSSION
239
variedpopulationsandoutcomes.Furthermore,althoughthereisevidencethat
multipleriskexposureisalsoassociatedwithheightenedengagementof
physiological,ratherthanpsychological,stress(Brodyetal.,2013;Evans,2003;
Evansetal.,2007;Evans&Kim,2012),thesestudieshavenotfocusedonsuch
associationsasmechanismsformentalhealthoutcomes.Thus,futurestudies
shouldseektoexplorebothpsychologicalandphysiologicalstressresponsesand
theroletheyeachplayintheemergenceofemotionalsymptomsandotherforms
ofmentalhealthsymptomatology,particularlyamongat-riskgroups.
Notably,underlyingindirectpathwaysforbothperceiveddistressand
coping(thatis,effectsspanningbothstagesofthemediationmechanism)were
foundtobemeaningfulandsimilarinmagnitude.Thatis,higherlevelsofrisk
exposurecorrespondtogreaterperceiveddistressandinturnemotional
symptoms;conversely,increasedriskexposureisassociatedwithalower
perceptionofone’sabilitytocopewithstressors,whichalsorelatestoheightened
emotionalsymptoms.Thisindicatesaneedtolookbeyondsimply“stress”in
understandingmechanismsfortheemergenceofmentalhealthsymptomsand
insteadconsidertheextenttowhichadversityisviewedasexceedingone’scoping
capacities.Thisconceptualdistinctionreflectsthetransactionaltheoryofstress
appraisalinitiallypositedbyLazarusandcolleagues,whichincludesboththe
appraisalofstress(distress)andone’sperceivedabilitytomanageorreducethis
potentialharm(coping;Lazarus,1966;Lazarus&Folkman,1984).Whilethisinitial
theoryindicatedasequentialprocessinwhichoneappraisesthreatandthen
assessescopingresourcesandpossibleresponses,thecurrentstudyfocuseson
distressandcopingasinter-relatedphenomena(Cohenetal.,1983).Indeed,ithas
beennotedthattheimmediacyofinteractionsbetweenappraiseddistressand
copingmeansitisdifficulttoempiricallyassesstheseinasequentialfashion,
particularlywhenexploringgeneralappraisalsofliferatherthanparticularstimuli
(Ben-Zur,2019).Nevertheless,researchhasindicatedthatbothdistressandcoping
appraisalsarerelevantforoutcomes,includingmentalhealthsymptoms(Bovieret
al.,2004;Demkowiczetal.,2019;Eppelmannetal.,2016;Suldoetal.,2008).The
distinctrolesthatperceiveddistressandcopingeachplayasunderlying

CHAPTERSEVEN:DISCUSSION
240
mechanismsshouldbeexploredindifferentcontexts.Forinstance,theremaybe
distinctpatternsforinternalisingsymptomatologyanddisordergiventheemphasis
oninternalappraisalofthesecomponents,necessitatinginvestigationofeffectsfor
diversementalhealthoutcomes.Thisfindingalsosuggeststhatitmaybeimportant
toaccountforperceivedcopingcapacitieswithinexplorationsofstressasa
mechanism,regardlessofwhethertheemphasisisonpsychologicalorphysiological
stress.
Indicationsthatperceivedcopingcouldfunctionasadistinctmechanismfor
riskeffectsmayfacilitatepreventionandpromotioneffortstolessenthenegative
impactofadversity.At-riskyoungpeoplefacearangeofpotentiallystressful
experiencesintheirday-to-daylivesanditisgenerallyunlikelythatpractitioners
areabletosubstantiallylessentheextenttowhichthesestressorsoccur.Thus,it
maybemorepragmatictofocusonbolsteringyoungpeople’scopingcapacitiesand
strategies.Indeed,thereisevidencethatpsychoeducationalinterventionsfocused
ondevelopingeffectivecopingbehaviourscanpositivelyimpactperceivedcoping
resourcesamongadolescentexperiencingvariousmentalhealthsymptomsand
difficulties(BevanJonesetal.,2018;Brentetal.,1993;Demasoetal.,2006;M.A.
Lopezetal.,2005).However,itisalsoimportanttoconsiderthatnotallcoping
strategiesaregenerallyconsideredeffectiveorevenpositive(seeSkinneretal.
(2003)foracomprehensivereviewofcopingtaxonomies).Forinstance,reaching
outtoothersforsupportmaybeconsideredanadaptivecopingbehaviour(Skinner
etal.,2003)whileruminationisconsideredmaladaptivegivenassociationswith
depressivesymptoms(Nolen-Hoeksema,2000).Thus,althoughthecurrentstudy
providesinsightintotheextenttowhichparticipantsconsiderthemselvesableto
copewiththeirdailylives,theparticularcopingbehavioursindividualsadoptmay
affecttheextenttowhichthisoffersprotectionagainstnegativeoutcomes.Thus,it
maybehelpfulinfutureresearchtofocusonspecificcopingstrategiesand
behavioursaswellasindividuals’overarchingappraisaloftheirresources,inorder
tomorefullyunderstandhowdifferentapproachesinfluencetherelationship
betweenriskexposureandoutcomes.Inpractice,itmaybehelpfultounderstand

CHAPTERSEVEN:DISCUSSION
241
anindividual’sidiosyncraticcopingstrategiesandtoidentifywherethesemaybe
ineffectiveorharmfulandjointlyexplorealternatives.
Evidenceinthecurrentstudythatmodellingriskexposureinawaythat
unitesriskfactorswhileretainingtheirinformationismeaningfulforoutcomesmay
indicateaneedtoconsiderhowbothmultiplicityandtypeofriskexposuremay
contributetounderlyingstressmechanisms.Discussionoftheallostaticload
hypothesisispredominantlycentredaroundtheoverwhelmingofthebiophysical
stressresponsesystem;however,stressisbothaphysiologicalandapsychological
phenomenon(e.g.,Oldehinkeletal.,2011;Sladeketal.,2016;Zimmaroetal.,
2016).Itmaybethatthenatureofthestressorsbeingfacedisrelevantforthe
appraisalofstress,orthatspecificfactorsmaycontributedifferentiallyto
physiologicalandpsychologicalresponsesystems,warrantingfurtherresearch.This
contributesfurthertocriticismsofcumulativeriskindexingusingaweighted
approachtoriskfactorsasthisassumesallrisksequallycontributetooutcomes,
whichislikelynotthecase(Halletal.,2010).Treatingeachriskfactorasequal
overlooksthefactthatindividualsaremanagingmultiplestressorsthatmaybe
challengingtocopewithindifferentwaysandmayofferdifferentlevelsofmeaning
andrelevancewithinone’slife.Widerfindingsacrossboththequantitativeand
qualitativestrandsofthecurrentstudymayofferfurtherinsightintothese
underlyingprocessesandarediscussedinSection7.6.
Finally,thisfindingisparticularlynotablegiventhestudy’sfocusonearly
adolescentgirls.Chronicstresshasbeenproposedasakeycontributortothehigh
ratesofemotionalsymptomsanddisordersamonggirlsandwomenanditis
thoughtthatthisisparticularlyrelevantduringearlyadolescence,whensuch
symptomsoftenemerge(e.g.,deLijsteretal.,2016;Girgus&Yang,2015;Meadows
etal.,2006;Nolen-Hoeksema,2001).Foranumberofreasons,thecurrentstudy
cannotofferclarityonthistheory;theparticularriskfactorsexaminedarenot
inherentlygendered(comparedto,forinstance,gender-basedviolence),gender
differenceshavenotbeenexploredtoidentifywhetherthisisadistinctpatternfor
girls,andthestudyhasnotinvestigatedtrajectoriestoinferwhetherthisis
particularlymeaningfulfromearlyadolescenceonwards.Nevertheless,indications

CHAPTERSEVEN:DISCUSSION
242
thatstresscomponentsplayakeyroleinthewaythatmultipleriskeffectsrelateto
emotionalsymptomsduringakeyperiodinearlyadolescentgirls’mentalhealth
trajectoriesarenotableandwarrantfurtherattention.
Thereareofcoursesomelimitationstobeawareofwhenconsideringthis
finding.Firstly,thereisaneedtoreflectontheuseofofficiallyrecordedriskdata
viatheNPD(withtheexceptionofcaregivingresponsibilities)asapredictorofself-
reportedperceiveddistressandcoping.Inparticular,theindirecteffectsmodel
assumesthatparticipants’appraisalsoftheirdistressandcopingcapacitiesis,to
someextent,directlyrelatedtotheirlevelofriskexposureasdesignatedviathese
officialrecords.Thoughfindingsdosupportsuchanassociation,thisinherent
assumptionperhapsoverlookswhetherparticipantsactuallyconsiderthese
particularfactors(orcombinationoffactors)ascontributingtotheirstresslevels.
Althoughpastresearchindicatesthatofficiallyrecordedriskdataistypicallymore
reliableandrobustasapredictorofvariousoutcomescomparedtoself-report
methods(e.g.,Brownetal.,1998;Wallace,Stuart,&Smith,2014),wherestudies
focusonstressorotherinternalisedmechanismsself-reportofriskexposuremay
haveaddedvalue.Thatis,itmaybebeneficialtomoredirectlydrawon
participants’self-perceivedexposuretopossiblestressors(e.g.,throughthe
AdolescentStressQuestionnaire)inordertomoredirectlyassesshowday-to-day
challengesinfluenceanindividual’sstressappraisalsand,inturn,theirlevelof
emotionalsymptoms.Thecurrentstudy’suseofofficialdatamayfailto
comprehensivelycapturehowvariousfactorsrelatetostressappraisal
mechanisms,andfutureresearchcouldexplorewhetherdifferentapproachesto
measurementcontributetodifferentialpathwaysinunderlyingstressmechanisms.
Thereisalsoaneedtoconsidertherelationshipbetweenemotional
symptomsandperceivedstresscomponents,bothconceptuallyand
methodologically.Emotionalsymptoms,whichasoutlinedinChapterTwocaptures
bothdepressiveandanxiousfeelings,hassomeconceptualsimilaritywithstress
appraisalprocesses,thoughtheydorepresentconceptuallydistinctconstructs.
Thatis,emotionalsymptomsareessentiallyfeelingsofdistress,worry,and
perceivedlackofcontroloverone’sexternalworld,whichisnotunlikethefeelings

CHAPTERSEVEN:DISCUSSION
243
onewouldexpecttoexperienceifreportinghighlevelsofglobalperceivedstress
(asmeasuredusingthePSS-4).Inthecurrentstudy,althoughdatashowsa
correlationbetweensymptomsandperceiveddistress(r=.52,asshowninFigure
5.12inSection5.3.4)andperceivedcoping(r=.36),respectively,thesecorrelations
arenotsohighastosuggestthattheyareoverlappingconstructs(inlinewiththe
.70thresholdadoptedformulticollinearity;Tabachnick&Fidell,2013).However,it
shouldbeconsideredthatboththeSDQandthePSS-4eachofferalimitednumber
ofitems,withemotionalsymptomscomprisingfiveitems,andperceiveddistress
andcopingeachcomprisingjusttwoitems.AlthoughtheSDQsymptomssubscale
wasdesignedwithattentiontodiagnosticcriteriaandexistingmeasuresatthetime
ofdevelopment(Goodmanetal.,1998),itisnotconsideredadiagnostictooland
reliesuponjustfiveitemstojointlycaptureaverysmallnumberofdepressiveand
anxioussymptomatology.Thus,inferenceofeachconstructisgroundedinlimited
information,whichisperhapsnotidealwhenexploringtherelationshipsbetween
suchinter-relatedconstructs,asthisrelationshipmaybeinflatedifevenasmall
amountofitemsareconceptuallysimilar.Itisimportantthatfutureresearchseeks
toexplorestressasamechanismforemotionalsymptomatologyanddisorderusing
morecomprehensivemeasuresofeachconstructinfutureresearchtofacilitate
morerobustassessmentoftheseunderlyingprocesses.
Indeed,collectionofbothstressandsymptomsdatafromasinglesource
(i.e.,self-report)warrantscautioninthisparticularregard,aswellasforanalysisof
furthermodelsexploringsymptomsandstressinrelationtoprotective/promotive
variables,respectively.Relianceondatafromasinglesourcecaninflate
relationshipsbetweenvariablesgiventhatthisapproachcanincreasetheshared
varianceacrossvariables(Conway&Lance,2010;Doty&Glick,1998).Itisalso
importanttonotethattheuseoflargelycross-sectionaldata,withnoabilityto
controlforpriorlevelsofstress,emotionalsymptoms,orlevelsofconnectionor
engagement,meansthatcausalitycannotbeinferred.Itwillbekeythatthis
mechanismisinvestigatedfurtherusingdatacollectedfrommultipleinformants
(e.g.,self-reportandparent-report)withinalongitudinaldesign,particularlygiven

CHAPTERSEVEN:DISCUSSION
244
theconceptualoverlapbetweenemotionalsymptomsandstress(seeSection7.7
forfurtherreflectiononthestrengthsandlimitationsoftheseapproaches).
7.4ResearchQuestion2:FactorsandProcessesforPositiveOutcomes
2.Whatarethefactorsandprocessesthatsupportpositiveoutcomesinemotional
symptomsamongearlyadolescentgirls?
7.4.1PromotiveFactors
a.Ofthepromotivefactorsidentified,whatisthemagnitudeoftheirassociation
withearlyadolescentgirls’emotionalsymptoms?
ConfirmedPromotiveFactors
FamilyAdultConnection
Greaterperceivedlevelofconnectiontoafamilyadultcorrespondedhere
toloweredlevelsofemotionalsymptoms.Thisreflectslargelyconsistentfindings
acrosspreviousliterature,whereinstrongerconnectionwithfamilymembersis
frequentlyreportedtobeassociatedwithreducedlevelsofinternalisingand
emotionalsymptoms(e.g.,Costelloetal.,2008;Roweetal.,2016;Willeetal.,
2008).Itshouldbenotedthatthescaleusedtomeasurefamilyconnectioninthe
currentstudyfocuseson“anadult”withinthehome.Whilethisdoesnot
necessarilylimitresponsestoparents/carers,itislikelythatthisisthecase,though
forsomethismayencompassextendedfamilymemberswhoalsoresidewithinthe
home.Thus,whilethereisevidencethatconnectiontosiblingscanactasavaluable
resourceforchildrenandadolescents(e.g.,Buist,Deković,&Prinzie,2013;Gasset
al.,2007),suchrelationshipsareunlikelytobecapturedhereunlesssiblingsare
consideredadults.
Giventhatpreviousresearchsuggeststhatone’sparentalconnection
becomeslesssalientduringadolescence,withagreateremphasisonfriends(B.B.
Brown&Larson,2009;Umbersonetal.,2010),itisnotableherethatfamily
connectiondiddemonstrateasmall,thoughmeaningful,association.However,as

CHAPTERSEVEN:DISCUSSION
245
exploredlaterinthefollowingsubsection,connectionwithschoolpeerswasshown
tohaveasmalltomoderaterelationshipwithreducedsymptomatology,thus
providingfurthersupportforapatterninwhichparentsarelessinfluentialfor
healthbehavioursandoutcomesthanarepeers(Brown&Larson,2009;Umberson
etal.,2010).Notably,however,ithasbeenarguedthatfamilyrelationshipsmay
playaparticularlycomplexroleinfunctioningandoutcomesduringadolescence,
operatingthroughindirecteffectsovertimethatcannotbecapturedinexamininga
directrelationship(Roweetal.,2016;Williams&Merten,2014).Furtherfindingsin
thecurrentstudyrelatingtoprotectivefactorsandqualitativeexperiencesmay
offerfurtherinsightintothemeaningfulnessandnatureofsocialconnectionsfor
girlsduringthistime,includingwithfamilymembers,asexploredlaterinthis
chapter.
SchoolPeerConnection
Findingsindicatethatearlyadolescentgirlswhoperceivegreater
connectiontotheirschoolpeersarelikelytoreportlowerlevelsofemotional
symptoms.Previousstudieshaveconsistentlyfoundevidencethatelementsof
peerconnectionandrelationshipsduringadolescenceareassociatedwithlowered
levelsofinternalisingdifficulties,includingemotionalsymptoms(e.g.,Bosackietal.,
2007;Lereyaetal.,2016;McGrawetal.,2008;Millingsetal.,2012;VanVoorhees
etal.,2008).Assuch,thisfindingprovidesfurtherconfirmationthatconnectionto
one’speerscanservetopositivelyinfluencethisaspectofmentalhealthforgirls
duringearlyadolescence.Furthermore,asnotedabove,thisrelationshipwas
showntobemoderateinsizeandindeedwaslargerthantheothervariables
identifiedasservingapromotivefunction,includingfamilyconnection.Thecurrent
studyprovidesfurtherinsightintoearlyadolescenceinparticular,demonstrating
thateveninthisearlystageofadolescence,peersappeartoconstitutean
importantpredictorofmentalhealthoutcomes.Inaddition,itshouldbenotedthat
themeasureusedinthisstudycapturespeers,ratherthanthenarrowercategory
offriends,andalsorelatesparticularlytopeersinaschoolcontextratherthan
capturingwiderpeerrelationships,suchasthoseinone’sneighbourhood.Assuch,
findingsindicatethatconnectiontopeersspecificallywithintheschoolcontextcan

CHAPTERSEVEN:DISCUSSION
246
bemeaningful,whichissomewhatunsurprisinggiventhatschoolservesasa
centralsocialcontextforchildrenandyoungpeople.
ActiveEngagementinHomeandSchoolLife
Participantswithgreaterperceivedactiveengagementintheirhomeand
schoolliveswerelesslikelytoreportexperiencingemotionalsymptoms.This
relationshipwassmall,butstatisticallysignificant.Previousresearchhasnot
directlyexaminedthisrelationshipineitherahomeorschoolcontext,thoughthere
hasbeensomeresearchexaminingrelatedoutcomessuchaspsychological
wellbeing(Fuligni&Pedersen,2002;Fuligni&Telzer,2013;Kavanaughetal.,2015).
Anumberofstudieshaveidentifiedarelationshipbetweeninstitutionalschool
connectionatanoverarchinglevelandemotionalsymptoms(Bondetal.,2007;
Costelloetal.,2008;EwellFosteretal.,2017;Loukasetal.,2016;Pateetal.,2017),
buthavenotgenerallyfocusedonthissub-componentofschoolconnectedness.
Thus,thisfindingoffersanovelcontributiontotheliteratureasitisthefirstto
examinethespecificconstructofactiveengagementacrossthesecontextsin
relationtoemotionalsymptoms.
Thisfindingsuggeststhattheextenttowhichearlyadolescentgirlsperceive
themselvestobeactivedecision-makersandcontributorsintheirday-to-daylifeis
relatedtopositiveoutcomesforemotionalsymptoms.Evidenceofsucha
relationshipwithinearlyadolescenceisnotable,asthisdevelopmentalphaseis
oftenaccompaniedbygreaterautonomyanddecision-makinginthehome,
particularlyamonggirls(Gutman&Eccles,2007;Wray-Lakeetal.,2010).Atthe
sametime,earlyadolescentsarenavigatingthepotentiallychallengingtransitionto
anewandunfamiliarsecondaryschool.Researchhasindicatedthatthereisoften
littleemphasisonthevoiceofyoungpeopleduringthetransitiontosecondary
schoolandindeedthisprocesscanleadtofeelingsofdisengagementforsome(van
Rensetal.,2018).Ithasalsobeenarguedthatinadolescencethereisanincreasing
emphasisonadultcontrolandorderinbothschoolandthehome,whichis
arguablyatoddswiththedevelopmentalneedforgreaterautonomy(Ecclesetal.,
1993;Hargreaves,2017;Smetana,Campione-Barr,&Daddis,2004).Thecurrent
finding,then,providesfurthersupportfortheargumentthatbothschoolsand

CHAPTERSEVEN:DISCUSSION
247
familiesshouldensurethatearlyadolescentsareprovidedwithappropriate
opportunitiestobeactivedecision-makersandcontributors.
ExcludedPromotiveVariables
Perceivedschooladultconnection,communityadultconnection,and
engagementinextracurricularactivitieswerenotfoundtobepromotivefor
emotionalsymptoms.Althoughthepossibilityforthesevariablestobepromotive
wastheoreticallyorempiricallysupportedacrossthewiderliterature,allthreehad
modestevidencebasescomparedtoconnectiontoone’speersandfamilies,which
aremoreestablishedpromotivefactorsforhealthanddevelopment.Thus,the
studyoffersgreaterinsightintothestatusofthesevariablesinrelationtoearly
adolescentgirls’emotionalsymptoms.Itisplausiblethatcontextualfactorssuchas
timingarerelevanthere;forinstance,studiesreportingschooladultconnectionto
bepromotivehavegenerallynotdirectlyfocusedonearlyadolescence(e.g.,Lereya
etal.,2016;O’Connoretal.,2012;Wangetal.,2013),asisthecasehere.Thefirst
yearofsecondaryschoolisatimeoffluctuationinschool-basedrelationshipsand
teacher-pupildynamics(Loukasetal.,2016)anditmaybethatanyperceived
connectiontoschooladultsmaynotyetbemeaningfulinrelationtointernalising
difficultiesatthisearlystage.
Itmaybethatmeasurementofthesevariablesplaysaroleinthesefindings.
Forinstance,themeasureforcommunityadultconnectionfocusesonanadult
“awayfromhomeorschool”,whichcouldreasonablycapturerelationshipswitha
widerangeofindividualsincludinggrandparentsandextendedfamily,community
orreligiousleaders,orfamilyfriends,amongstotherpossibilities.Thenatureof
suchrelationships,andindeedtheirquality,regardlessoftheadult’sroleorrelation
totheparticipant,coulddiffersubstantially,whichmaybemeaningfulformental
healthoutcomes.Similarly,theremaybeparticulartypesofextracurricular
activitiesthataremoremeaningfulforoutcomesthanothers,whichwouldnot
havebeencapturedhere.Notably,thestudy’scross-sectionaldesignwouldnot
offerinsightintolong-termeffects;giventhatthesefactorsaretheorisedtooffer
wideradvantages(e.g.,engagementinextracurricularactivitiesisbelievedto
supportsocialskills;Alvord&Grados,2005;Nicholsonetal.,2004;Schaeferetal.,

CHAPTERSEVEN:DISCUSSION
248
2011),longitudinalanalysisofindirecteffectsmayoffermoreinsight.Finally,itis
notablethatallthreeofthesefactorsmaybemoremeaningfulforthosewith
negativeorlimitedrelationshipsinthefamilyandpeergroup(Hamre&Pianta,
2001);directexaminationofsuchcompensatoryinteractionswasbeyondthescope
ofthecurrentstudybutshouldbeprioritisedinfutureresearch.
7.4.2ProtectiveFactors
b.Towhatextentarethedirectand/orindirectrelationshipsbetweenmultiplerisk
exposure,perceivedstress,andemotionalsymptomsconditionaluponaccessto
protectivefactors?
ProtectiveFactorsandStressAppraisal
Therewereseveralfeaturesofparticularnoteinthewaythatprotective
factorsfunctionedinrelationtoindirecteffects.Firstly,resultsindicatedthatthese
factorsfunctionedonlyonthefirststage,ratherthanthesecondstage,of
underlyingstressmechanisms.Thatis,findingssuggestthatinformalrelationships
withfamilyadultsandschoolpeerscanaffectthewaythatat-riskearlyadolescent
girlsappraisetheirlivesasstressfuloroverwhelminginrelationtotheircoping
resources.Thisofferssupportforthestressbufferinghypothesisasoutlinedin
ChapterThree,whereinsocialrelationshipslessentheextenttowhichnegativelife
eventsareperceivedtobestressful.Thishasbecomeacentralcomponentof
resiliencetheoryandresearch(Barnes,2016;Masten,2014b,2018)andseveral
studieshavefoundthatsocialconnectionmoderatestheeffectsofnegativelife
eventsuponmentalhealthsymptomsanddisorders(e.g.,Anderson,Salk,&Hyde,
2015;Ditzen&Heinrichs,2014;Hazeletal.,2015;Landermanetal.,1989).
However,asnoted,studieshavetypicallyfocuseduponmoderationofthedirect
effectsofexposuretoadversity,ratherthanexamininghowprotectivefactors
operatewithinunderlyingstressmechanisms.Thus,thecurrentstudyprovides
directempiricalevidencetosupportstressbufferinginrelationtomultiplerisk
exposure,inthecontextofearlyadolescentgirls’emotionalsymptoms.

CHAPTERSEVEN:DISCUSSION
249
Resultsalsoindicatethattheseconnectionsappearnottobemeaningfulin
relationtohowappraiseddistressorcopingcapacitiesinfluencesymptoms.Thatis,
onceanearlyadolescentgirlhasappraisedtheirlifetobestressfulorexceeding
theircopingresources,externalfactorsincludingsocialconnectionandactive
engagementindailylifeappearunlikelytolimittheextenttowhichthisevokes
depressiveandanxioussymptoms.Thisoffersclarityontheparticularfunctionof
stressbufferingatthepsychologicallevel,whichisofparticularinterestgiven
growingemphasisonthewaythatprotectivefactorsrelatetostressprocessesin
thecurrent“fourthwave”ofresilienceresearch(Masten,2014b,2016,2018).This
insightemphasisestheneedforsystemsandpractitionerstotakeproactivesteps
toboosttheresourcesofat-riskadolescentgirls,ratherthanprimarilyresponding
reactivelywhereindividualsappeartobe,orreportfeeling,overwhelmed.This
couldbeachievedthroughfacilitatingqualityinformalrelationships;forinstance,
interventionsfocusedonimprovingparentingskillsandqualitycanbebeneficialfor
arangeofchildandadolescentoutcomes,particularlyforthosefromhigh-risk
backgrounds(e.g.,Horwitzetal.,2010;Pattersonetal.,2002;Sanders,2008;Scott,
2012).However,futureresearchcouldalsoseektoidentifywhetherthereare
factorsthatmoderatetheimpactofstressuponoutcomes.Thismaybeparticularly
importantforunderstandingtheapparentphenomenonofskin-deepresilience
observedinstudieswithAfricanAmericanadolescents,whereinupwardlymobile
individualsexposedtomultipleriskfactorswerefoundtohavehighlevelsof
allostaticloadmarkers,buttobemaintaininggenerallypositiveoutcomes(Brodyet
al.,2013;Miller,Cohen,Janicki-Deverts,Brody,&Chen,2016).
Thedegreeoftheconditionaleffectsobservedhereisnotable,withthe
relationshipsbetweenriskexposureandperceiveddistressandcopingentirely
reversedafteraccountingforinteractionswithwiderfactors.Thisfindingappears
toillustratethecontextualambiguityofwhatismeantbyriskandresilience,a
distinctionarguedbyUngar(2011,2012)tobeoverlysimplisticandfailingto
accountforthecomplexsystemswithinwhichindividualsoperate.Theextentto
whichthesefactorschangedthenatureofeffectsthereforedemonstratesthe
valueofcomplexanalysesthatcanincorporatethewiderprocessesand

CHAPTERSEVEN:DISCUSSION
250
transactionsinfluencingoutcomes,ratherthanfocusingonsingularpredictorsas
positiveornegative(Belskyetal.,2012;Ungar,2011,2012).Here,itappearsthat
whereanat-riskgirlconsidersherselftobeembeddedwithinastrongsocial
networkoffamilyadultsandschoolpeers,circumstancesotherwiseconsidered
riskymayservetohelponethrive.Whileitisoftenarguedthatindividualrisk
factorscanhavebenefitswithappropriatesupportinplace,suchascaregiving
responsibilities(Banksetal.,2001;Fraser&Pakenham,2009;Ireland&Pakenham,
2010;KennethIanPakenhametal.,2006,2007),thecurrentstudygoesbeyond
singularpredictorsandindicatespossiblebenefitsevenforthoseexperiencing
greaterlevelsofadversity.
Thisperhapshighlightsthesociallydeterminednatureofadversity,wherein
itisnotaparticularfactorthatleadstoanegativeoutcomebutthewiderstructural
systemsinwhichsuchcircumstancesareembedded(CommissiononSocial
DeterminantsofHealth,2008;Graham&Kelly,2004;Marmot,2005;Vineretal.,
2012).Forinstance,beingafamilyinalowerincomebracketdoesnotinandof
itselfcausestress,butdifficultiesareincurredwhenoneliveswithinasocietythat
doesnotprioritiseequalopportunitiesforhousing,employment,education,
healthcare,andsafety.Thatis,here,thefactorsconsidered“risky”forearly
adolescentgirls’emotionalsymptomsmaynotbeautomaticallyadverseforall
individuals,butmayevenbebeneficialwherethereisappropriatesocialsupportin
place.Conversely,however,itmaybethatyoungpeoplebattlingthemostcomplex
systemsofriskexposurebecome,overtimeand/orwithsocialsupport,more
accustomedtoandpracticedinadaptingtochallengethantheirpeerswithlower
levelsofexposureorlesssupport(orboth).Suchadjustmentscouldleadto“trade-
offs”,ornegativeimpactinotherareas,assuggestedbyMasten(2018)and
indicatedinthecasesofskin-deepresilienceoutlinedabove.Findingshighlightthe
needforresearcherstoinvestigatethecomplexprocessesandinteractionsthat
influenceyoungpeople’soutcomesinthecontextof“adversity”tobetter
understandcontextualnuancesandcomplexities.
Itisimportanttonotethatthesefindingsareconceptuallyspecific.Firstly,
inferencesrelatetoperceivedstressandmaynothavebeenthesamehadthe

CHAPTERSEVEN:DISCUSSION
251
focusbeenonallostaticbiomarkers;futurestudiesshouldexaminetheseprocesses
withattentiontobothpsychologicalandphysiologicalstressresponses.Thestudy
wasalsonotabletoexaminewhethertheseprotectivefactorsaffectedthe
overarchingstresspathwaystoemotionalsymptoms,insteadfocusingondiscrete
pathwayswithinunderlyingmechanisms,asitisnotpossibletodosowhere
continuousmoderatorsaremodelledonbothstages(Hayes,2015).Thatis,the
studyhasfoundthataccesstoparticularfactorsinfluencestheeffectsofrisk
exposureuponperceiveddistressandcoping,buthasnotinvestigatedwhetherthis
lessenstheextenttowhichriskexposureinfluencesemotionalsymptomsviastress
appraisal.Thisisanimportantfeaturethatneedstobeexaminedinfuture
research.Furthermore,onlyexternalfactorswereinvestigated;theremaybe
internalfactors,suchasfacetsofemotionregulationorlocusofcontrol,thatcould
bemeaningfulinmitigatingtheeffectsthatgreaterperceivedstresshasupon
emotionalsymptoms.Futureresearchcouldexplorebothexternalandinternal
factorsinrelationtostressmechanismsformentalhealth.Studiescouldalso
explorethedevelopmentaltimingofsuchinfluences,asadolescentsaremorelikely
thanyoungerchildrentomanagetheirstressmoreinternallythroughregulating
theirresponsesandattemptingtochallengethestressfulsituation(Barnes,2016;
Compasetal.,2001).
Ofcourse,itshouldalsobeconsideredthatthesefindingsmayhavebeen
affectedbytheparticularmethodsemployedhere,includingthetemporalnature
ofthedata.Theriskfactorsutilisedtocreateacompositeriskvariablewere
predominantlymeasuredusinginformationgatheredpriortoparticipants’
completionofmeasures,withtheexceptionofcaregivingresponsibilities.Allother
variablesexaminedinthismodelwerecross-sectional(stressappraisal
components,protectivevariables,andemotionalsymptoms).Thus,itmightbethat
indicationsofconditionaleffectsforthefirststageofthismodelaremorerobust,
whileresultsrelatingtothesecondstageofthemodelmaybeaffectedbytheir
relianceondatacollectedatasingletimepoint.Forinstance,itmightbethat
participants’responsestotheSRSsubscaleitemswereaffectedbytheirlevelsof
distress,coping,andemotionalsymptomsatthatspecifictimepoint,orviceversa.

CHAPTERSEVEN:DISCUSSION
252
Itisimportantthatfutureresearchexaminestheseeffectslongitudinally,firstlyto
overcomeanymeasurementeffectsbutalsobecauseitisunderstoodthat
protectivefactorsaremostpowerfulwhenembeddedinone’slifeovertime
(Barnes,2016;Masten,2014b).
ConfirmedProtectiveFactors:FamilyAdultandSchoolPeerConnection
Findingssuggestthatgreaterperceivedconnectiontofamilyadultsand
schoolpeersbothaffectedtheextenttowhichmultipleriskexposureinfluenced
perceiveddistressandperceivedcoping.Thissectionexplorestheseprotective
factorsjointly,giventhattheyaregenerallyconsideredthemostimportant
informalsocialconnectionsinyoungpeople’sworlds(Brown&Larson,2009;
Umbersonetal.,2010;Umberson&Montez,2010)andinordertofacilitate
discussionoftheirrelativecontributions.
Intermsoffamilyadults,findingsmirrorresultsfrompreviousstudies
indicatingthatparentsandcarerscanplayanimportantroleinbufferingtheeffects
ofnegativeeventsuponstressduringthisdevelopmentalperiod(Andersonetal.,
2015;Gunnaretal.,2015;Hazeletal.,2015;Hostinaretal.,2015,2014).Though
severalstudieshaveidentifiedthatpeerrelationshipspredictlowerlevelsof
internalisingdifficulties(e.g.,Bosackietal.,2007;Lereyaetal.,2016;McGrawetal.,
2008;Millingsetal.,2012;VanVoorheesetal.,2008),therehasbeenlimited
investigationoftheirroleinstressresponses.Wherethishasbeeninvestigated,
studieshavereportedthatpeerrelationshipsand/orfriendshipsdonotshowstress
bufferingqualitiesandmayinfactincreasestressresponsesamongadolescents
(Doometal.,2017;Printzetal.,1999).However,asnoted,theinteractionaleffect
ofbothfamilyandpeerrelationshipswithadversityhasnotpreviouslydirectly
beentestedforunderlyingstressmechanisms,withfindingsgenerallyfocusing
purelyonstressoutcomesoronmentalhealthoutcomes,ratherthanexploring
interactionswithinamorecomplexmodel.
Itisparticularlynotablethatfamilyconnectionwasfoundtoexerta
strongereffectuponriskpathwaysthanconnectiontoone’speers.Researchhas
consistentlyindicatedthatinadolescence,peersmorestronglypredicthealth
outcomesthandoparents,adistinctshiftfromearlierdevelopmentalstages

CHAPTERSEVEN:DISCUSSION
253
(Brown&Larson,2009;Umbersonetal.,2010).Indeed,previousanalysisforRQ2a,
examiningthepromotivefactorsforemotionalsymptoms,foundthatpeer
connectionwasmorestronglyassociatedwithloweredsymptomatology,relativeto
familyadultconnection.Thisshiftsuggeststhatalthoughpeersappearmore
importantforemotionalsymptomsatagenerallevel,familyadultsmayplaya
morevitalroleintheextenttowhichearlyadolescentgirlsexperiencingadversity
appraisetheirlivesasstressful.Priorevidencesuggeststhatthestressbuffering
roleofparentalrelationshipsisoftenweakerorevenabsentamongadolescents,
includingearlyadolescents,relativetochildren(Doometal.,2015;Gunnaretal.,
2015;Hostinaretal.,2014,2015).However,thesestudieshavegenerally
investigatedphysiologicalbiomarkersratherthanpsychologicalstressandhave
beenfocusedonthedirectpresenceofparentswithinexperimentallymanipulated
laboratorystressors.Thus,althoughthecurrentstudydoesnotexamine
trajectoriesorexploredifferentagegroups,findingsprovideimportantinsightinto
therolethatfamilyadultscanplayinthe“realworld”,indicatingthatearly
adolescentgirlsexperiencingmultiplepossiblestressorsonaday-to-daybasis
clearlybenefitfromperceivedrelationshipswithparentsand/orotherfamily
adults.
However,itmaybethatthesefindingsareattributabletotheageof
participants,asearlyadolescencerepresentsthetransitionalperiodbetween
childhoodandadolescence.Futurestudiesshouldseektoexaminethe
developmentaltimingintheextenttowhichfamilyandpeerscontributebothto
generaloutcomesaswellasforstressbuffering.Itshouldalsobeconsideredthat
thesedifferentialcontributionsdependuponthenatureoftheriskoneisexposed
to,asindividualsmayturntodifferentpeopleforsupportorcomfortdependingon
theneedcreatedbytheparticularstressorathand(Barrera,1986;Stapleyetal.,
2019).Althoughthecurrentstudy’semphasisonmultipleriskexposuremeanssuch
effectsrelatetoabroadersystemofadversityratherthansingularfactors,itmay
bethattheparticularfactorsmeasuredhereallhappentobecircumstancesfor
whichparentconnectionisconsideredmoremeaningfulthanpeerconnection.
Futurestudiesshouldseektoexplorestressbufferingeffectsfordifferentrisk

CHAPTERSEVEN:DISCUSSION
254
factorsandprofilesofriskexposuretodeterminewhetherdifferentsourcesof
supportareofgreaterimportanceindifferentcontexts.
ExcludedProtectiveVariables
Perceivedconnectiontoaschooladultandactiveengagementwerenot
observedtofunctionasprotectivefactorsatanystageofunderlyingstress
mechanisms.Thisisnotablegiventhatithaspreviouslybeensuggestedthatthese
factorsmayinfluencestresslevels;forinstance,ithasbeensuggestedthat
contributinginthehomedevelopsstressappraisalandcopingcapacities(Beckeret
al.,2010;Borellietal.,2015).Contextually,itisreasonabletoassumeforschool
connectionandindeedpartiallyforhomeandschoolengagementthatthismay
reflectthetimingofthestudyinrelationtoeducationaltransition.Futureresearch
shouldexploretherolethatdifferenttypesofsocialconnection,includingteacher-
pupilrelationships,mayplayforparticularriskgroupsandoutcomesacross
differentdevelopmentalstagesofchildhoodandadolescence.
Consideredagainstpreviousanalysisofpromotivevariables,itisnotable
thatengagementinhomeandschoollifewasfoundtobepromotiveforsymptoms.
Indeed,intheconditionalindirecteffectsmodelthisvariablewasshowntohavea
smallassociationwithbothloweredperceiveddistressandgreaterperceived
coping.However,thesedidnotoperatetoaffectunderlyingpathways(thatis,
interactionpathwayswerenotstatisticallysignificant).Thus,whileperceptionsof
activeengagementappeargenerallypositiveforearlyadolescentgirls,theyappear
nottofunctiontodisrupttheeffectsofmultipleriskexposureeitherforstress
componentsoremotionalsymptoms.Thesefindingssuggestthatforgirlsexposed
tohighlevelsofriskexposure,theabilitytomakedecisionsandcontributeacross
theirdailylivesmaynotbesufficientlymeaningfultooffsettheextentofthe
demandsbeingplacedonthem.Thus,thoughitmaybebeneficialatagenerallevel
toprovideopportunitiesforearlyadolescentgirlstocontributewithintheirhome
andschoollives,thismaybeunlikelytobebeneficialforreducingsymptomsamong
thoseexperiencingadversityacrossthesedomainsortospecificallycombatthe
extenttowhichtheyfeelstressedorunabletocopeintheirday-to-daylives.

CHAPTERSEVEN:DISCUSSION
255
Ofcourse,theremaybemethodologicalexplanationsforthesefindings.In
measuringhomeandschoolengagement,focusingonbothhomeandschoollife
simultaneouslycouldalsohavemaskedeffectsonlypresentinoneofthese
domains,thoughthisjointfocusdoesofferinsightintotheeffects(orlackthereof)
offeelinglikeanactivememberacrossday-to-daylife.Indeed,thiscorrespondsto
theriskfactorsidentifiedandincludedintheriskexposurevariable,asthesewere
allgenerallylocatedatthefamilyandschoollevels.However,Ifagreaterinventory
ofriskfactorshadbeenavailable,itmighthavebeenpossibletogroupfactors
basedondomain(e.g.,schoolversushome),whichcouldallowanalysisofcontext-
specificprotectiveeffectsforfactorslikeschoolconnection.Itmayalsobethatthe
focusonanadultatschoolatagenerallevelmaynotcapturerelationshipswith
schoolstaffmorededicatedtopastoralsupport,whichmaybemorevaluablefor
thosefacingadversity.
7.5ResearchQuestion3:LivedExperience
Thissectiondiscussesqualitativefindings,exploringhowexistingtheoryand
literaturemayhelptoexplainparticipants’experiencesalongsidetheinsight
generatedinthecurrentstudy.Organisationofthisdiscussionisinformedbythe
masterthemespresentedinChapterSixbutismoreconceptuallyguided;thatis,
overarchingsectionsgenerallycorrespondtosuperordinatethemes,andthe
discussionpointswithinthesemayfocusonasinglethemeorbringtogether
multiplethemes,asillustratedoverleafinFigure7.1.Thisapproachhasbeenused
tofacilitateamorein-depthdiscussionandreflectstheneedforselectivenessin
exploringfindingsachievedthroughIPA,ratherthanexhaustivediscussion,given
therichnessofinformationencapsulatedinthemes(Smithetal.,2009).This
explorationisnotconstrainedtoanyonetheoreticallens,inlinewiththestudy’s
pluralisticapproachandtheuseofIPAasaninductiveprocess,anddiscussionwill
drawontheoryandthewiderliteratureasrelevant.

CHAPTERSEVEN:DISCUSSION
256
Figure7.1.Conceptualrepresentationofthemesfordiscussion.Masterthemesareshownonthe
lefthandside,groupedwithinsuperordinatethemes,andarrowsshowhowthesehavebeen
integratedtofacilitateaconceptualdiscussionofqualitativefindings,asshownontherighthand
side.

CHAPTERSEVEN:DISCUSSION
257
7.5.1TheExperienceofFeelings
ConceptualisationsofSymptoms
Participantsconceptualisedthedifferentfeelingsandthoughtsassociated
withtheirsymptomsindifferentways.Gracetalkedaboutthesefeelingsasastate
ofbeing,recallingtimeswhenshewas“gettingupset”or“feelingstressed”.This
conceptualisationrepresentsamoreimmersiveaffectiveexperience,inwhichthe
emotionisconsideredafeelingstatethatencompassestheself.Ameliaand
Jennifer’stalkwasmorecognitivelyoriented,withafocuson“worries”and
“thoughts”ratherthanonsomethingthatisfelt.Thesedifferentconceptualisations
appeartoreflectboththeaffectiveandcognitiveimpairmentsgenerallyconsidered
centraltobothdepressiveandanxioussymptomatologyanddisorder.Thatis,
depressiveandanxioussymptomscanbeaffective(e.g.,feelingsofsadnessand
fear),cognitive(e.g.,negativethoughtpatternsandinformationprocessingbiases),
andsomatic(i.e.,bodilyalterationssuchasfatigue,headaches,andstiffness;Beck
&Clark,1988;Kapfhammer,2006;Kokanovic,2011;Kovacs&Beck,1979;Stein,
2006).Thus,itappearsthatparticipantsfocusedmoreonparticularcomponentsin
theiraccounts.Suchdistinctionsmayreflectdifferingmanifestationsofparticular
symptoms;thatis,AmeliaandJennifermaybemoregreatlyexperiencingcognitive
symptomsrelativetoGrace,whomaybepredominantlypresentingwithaffective
difficulties.However,itcouldalsobethatthisreflectsdifferentwaysofthinking
aboutandmakingsenseofone’ssymptoms,withafocusoneitherfeelingsor
thoughtssimplyrepresentingdifferentwaysofunderstandingoverarching
difficulties.
Indeed,itisparticularlynotablethatthewayAmeliaandJennifertalked
abouttheirworriesandnegativethoughts,respectively,gaveasensethattheysaw
themnotonlyasthoughtsbutasobjectsthatcanbehadandevengivenaway.
Thus,thisfocusoncognitionmaynotnecessarilybeareflectionofpredominantly
cognitivesymptomatology,butinsteadmayactasawaytorationaliseormaintain
controloverdifficultthoughtsandfeelings.Previousqualitativestudieshavefound
thatadolescentsexperiencingdepressiveandanxioussymptomscanfindthem
confusinganddifficulttocontrol(Dundon,2006;McCannetal.,2012;Midgleyet

CHAPTERSEVEN:DISCUSSION
258
al.,2017;Wisdom&Green,2004).Externalisationandobjectificationofone’s
feelingsastangibleobjectsseparatefromtheselfmayreflectalackofcontrolor,
conversely,couldrepresentpsychologicalattemptstoretaincontrol.Indeed,such
externalizationofone’sdifficultiesisakeycomponentofsometherapeutic
approaches,suchasthenarrativeapproach,asawaytoseparatetheseissuesfrom
theselfandallowthemtobeinterrogatedwithoutself-alienation(White&Epston,
1990).ItmaybethatAmeliaandJenniferhaveindependentlyundertakensuch
thinkingstrategiesasamethodofcontrol.However,theemphasisonindividualised
sense-makingheremeansitisnotpossibletosaywhetherthisexternalisation
processisprotectiveorharmful,orindeedboth,dependingonthecontextand
individual.Thatis,thesemethodsofthinkingcouldhavecontributedto
participants’lowsenseofcontrolovertheirsymptomsbut,conversely,couldbe
protectingthemfromworsenedlevelsofdifficultiesorwiderperceivednegative
consequencessuchasshiftsinidentity(asexploredlaterinthischapter).Itmaybe
importantforpractitionersworkingwithadolescentgirlsexperiencingthese
symptomstounderstandonanindividualbasisthewaythattheyconceptualise
theirsymptoms,andhowtheseconstructionsrelatetowiderbeliefsanddecisions.
EmotionIntensityandCentrality
Participantsdescribedtheirsymptomsandassociatedthoughtsandfeelings
asbeingintenseandbuildingupuntiltheyfeltunmanageable,andinsomecasesas
beingdominantwithintheirwideremotionallandscape.Suchunderstandingsand
experiencessuggestthatemotionalsymptomsactasacentralandpotentially
overwhelmingpartofone’sinnerlife.Themultiplicityandintensitythat
participantsdescribedoffersinsightintothemultifacetedwayinwhichsuch
symptomsmaymanifestandbeunderstoodbyearlyadolescentgirls.Thatis,they
appearedheretobemorethansimplyanoverarchinglowmoodoraheightened
stateofanxiety,andwereinsteadseenascomprisingmanydifferentindividual
pointsofconcernanddistressthatoperatetogethertooverwhelmtheself.Though
therehasbeenlittlequalitativeexplorationofhowadolescentsexperiencethese
difficulties,anotherphenomenologicalstudyreportedsimilarfindings,with
adolescentspresentingtheirdepressionasamultitudeofvariedbutintense“bad

CHAPTERSEVEN:DISCUSSION
259
feelings”(Woodgate,2006).Thisconceptualisationofdifficultthoughtsandfeelings
asbuildinguptosomethingmorethanthesumoftheirparts,andthusbecoming
unmanageable,showshowintenselysuchdifficultiescanbeexperiencedandthe
inherentlossofcontrolthataccompaniesthem.Thisinsightintothecomplex
realityofhowemotionalsymptomsarefeltdemonstratestheneedtosupportearly
adolescentgirlsinexploringandcopingwiththedifferentwaysinwhichsuch
difficultiesmanifestthemselvesacrossdailylife.
Thismanifestationofsymptomsasoverwhelminganddifficulttomanage
mayexplainwhyforsome,thesethoughtsandfeelingscametodominatetheir
wideremotionallandscape.Here,bothAmeliaandJenniferappearedtohave
dividedtheirinnerworldsintothepresenceandabsenceofsymptomatology,with
evenpositiveemotionscomingtobedefinedinthisway.Suchunderstandingsand
experiencesreflectarecognitionthatemotionalsymptomsanddisordersare
definednotonlybythepresenceofdepressiveand/oranxiousfeelingsand
thoughts,butalsobytheirabilitytointrudeuponandlimitwiderareasofemotion
andcognition(AmericanPsychiatricAssociation,2013).Ithasbeenarguedthat
positiveemotionsarecriticalforcopingandadaptationinrelationtomentalhealth,
offeringawayforindividualstomentallyoffsetnegativeexperiencesasaformof
emotionregulation(Gloria&Steinhardt,2016;Tugade,2011;Tugade&
Fredrickson,2004).Here,althoughparticipantsdidnotdescribeaprocessofusing
positiveemotionstomentallyoffsetmoredifficultfeelings,theyhadcordonedoff
thesepositiveemotionsasseparatefromtheirsymptoms.Thatis,happiness
becomesconceptualisedonlyasaspacewherethesedifficultfeelingsandthoughts
areabsent.Thisperhapsindicatestheextenttowhichsuchfeelingsdominate
participants’worlds,giventhattheyconceptualisetheirexperiencesentirely
throughthelensofthepresenceorabsenceofsymptomatology.
7.5.2InternalGrappling
DistancebetweenEmotionalSymptomsandtheSelf
Acrossallthreeaccounts,therewasastrongsensethatparticipantshad
establishedaseparationfromtheirsymptoms,whichtheysawasoperatingwithin

CHAPTERSEVEN:DISCUSSION
260
thembutalsoindependentlyofthem.Theypresentedthemassomethingthat
aroseoftheirownaccordand,oncetheyoccurred,werenoteasilycontrolledand
managed.Indicationsthatparticipantsfeltlittlecontrolovertheactualoccurrence
ofthesesymptomsinthefirstinstanceareunsurprising.Currentperspectiveshold
thatemotionoccurswithinthebrainindependentlyofcognitiveprocesses,andcan
thenbeperceived,interpreted,andregulated(Ledoux,2000;Salzman&Fusi,
2010).Thatis,humanscannotcontrolthearrivalofanemotion,butmaybeableto
cognitivelymodifyandmanageit(Ledoux,2000;Salzman&Fusi,2010).However,it
maybethatperceivedlossofcontrolwhenobservingtheoccurrenceofthese
symptomsiscompoundedwhenonestrugglestomakecausalattributionsfor
them.Here,AmeliaandJenniferexpresseddifficultyinunderstandingwherethese
symptomscamefrom,oftenexpressingalackof“knowing”.Asnotedearlierinthis
chapter,anumberofqualitativestudieshavereportedsimilarfindings,withsome
adolescentsexperiencingsuchsymptomsvoicingasenseofbewildermentand
confusionaboutwheresymptomshavecomefrom(Dundon,2006;McCannetal.,
2012;Midgleyetal.,2017;Wisdom&Green,2004).Midgleyetal.(2017)reflected
thatconfusionregardingtheoccurrenceofsymptomsmayindeedrepresenta
featureorsymptomofdepressioninitsownright,andthatworkingtojointly
inspectone’ssymptomsandattempttounderstandcausaloriginsmaythusbea
usefultherapeuticprocess.Causalattributionsandresponsestoexternaldemands
areexploredingreaterdetaillaterinthischapter,butareworthnotingatthisstage
inregardstohowthismayinfluencesense-makingofsymptomsandassociated
thoughtsandfeelingsthemselves.
Furthertoparticipants’perceivedlossofinternalcontrolinobservingthe
occurrenceoftheseemotions,theyalsoexpressedalackofagencyinregulating
andcontrollingthesesymptomsoncetheyhadarisen.Participantsseemedtofeel
unabletoeffectivelyregulateandrespondtotheiremotionsindependently,
insteadconsistentlyrelyingonexpressingthemtoothers.Whilethereare
understoodtobebenefitsinarticulatingthoughtsandfeelingstoothers,as
exploredlaterinthischapter,thesetwoparticipantsseemedtobelievethiswasthe
onlywaytolessenthesesymptoms,withtheirownrolesimplybeingtoholdontoit

CHAPTERSEVEN:DISCUSSION
261
untilanotherpersonwasavailable.Whereparticipantsdidtalkaboutstepsthey
hadtakentoresolvetheirthoughtsandfeelings,theydidnotgenerallysee
themselvesashavingactivelydecidedtodothosethings;theysimplyhappenedor
wereconsideredtheonlyavailableoptions,suchasself-harmingoreatingjunk
food.
Conceptually,suchexperiencesappeartosuggestlowlevelsofemotional
self-efficacy,whichpertainstohowconfidentindividualsareinrelationtotheir
emotionalabilities,includingcopingwithandmanagingdifficultemotions(Bandura
etal.,1999;Capraraetal.,2008;Kirketal.,2008).Itisimportanttonotethatself-
efficacyrelatestoone’sperceivedratherthanactualability(Bandura,1997),which
herealignswiththefocusonparticipants’subjectiveaccountsratherthanany
assessmentofregulatoryability.Thereisgrowingempiricalevidencethatlowered
emotionalself-efficacyisassociatedwithdepressiveandanxioussymptomsamong
childrenandadolescents(e.g.,Capraraetal.,2008;DiGiuntaetal.,2018;Muriset
al.,2001;Muris,2002;Niditch&Varela,2012).Asnotedabove,qualitativestudies
haveindicatedaperceivedlossofemotionalcontrolamongadolescents
experiencingemotionalsymptomatology(Dundon,2006;McCannetal.,2012;
Midgleyetal.,2017;Wisdom&Green,2004)andsomehavenotedthat
perceptionsofhavingactivecopingstrategiestomanagethesefeelingscan
facilitategreaterperceivedcontrol(Dundon,2006;Wisdom&Green,2004).
Findingsinthecurrentstudyfurtheraugmentunderstandinginthisarea,
suggestingthatexperiencingemotionalsymptomscanbedisempoweringand
confusingforearlyadolescentgirlsandmaybeperceivedasexceedingone’s
emotionalcapacity.Suchfindingsservetoemphasisetheimportanceofclear
emotionalsupportavenues,asexploredlaterinthischapter,butalsohighlightthe
needtobolsterbothregulationskillsandbeliefinsuchabilitieswithinthe
individual.
Thispassivityandlackofcontrolwerealsopartofawidersenseacross
thesecasesthatparticipantshadnotreconciledthesesymptomswiththeirsenseof
whotheywere.Theytalked,forinstance,offeeling“moremyself”whenthese
symptomswereabsent,orrecountedtimeswhentheiractionsdidnotreflectthat

CHAPTERSEVEN:DISCUSSION
262
oftheir“self”(e.g.,“Icouldn’thelpmyself”).Suchreflectionsinvokeasenseof
distancebetweenthesesymptomsandone’strueself;thisselfisperhapsis
considerednottofeelthesetypesofthingsandisabletobehaveinawaythatis
rationalandcontrolled.Thesesymptomsandactions,then,maybeperceivedasa
deviationfromtheconstructedselfinawaythatisdifficulttomakesenseof.Given
thefocushereonearlyadolescence,thisintersectionbetweenidentityandmental
healthisofparticularnote.Identity,broadlydefinedasone’sinternalconstruction
oftheself(Erikson,1959;Marcia,1980,1993;McAdams,1988,2011),isgenerally
consideredtosubstantiallyshiftandchangeinadolescence,asyoungpeople
engageinpersonalandsocialexperimentationandengagemoredeeplywitha
widerrepertoireofvaluesandbeliefs(Bukowskietal.,2011;Marcia,1980).Given
thatmanymentalhealthdisordershavetheirage-of-onsetinadolescence(Kessler
etal.,2005),particularlydepressionandanxiety(e.g.,Costelloetal.,2011;de
Lijsteretal.,2016;Jones,2013),itseemsimportanttoexploreandunderstandhow
suchexperiencesmayinteractwithdevelopingconstructionsoftheself.
Identityandmentalhealthareoftenconsideredascloselyintertwined,with
manydominanttheoriesofmentalhealthanddisorderincorporatingelementsof
identityconstruction(Thoits,2013).Theoristshave,forinstance,attributed
disordertounconsciouspersonalityconflicts(Freud,1933),arrestedidentity
development(Erikson,1963;Freud,1933),threatstoorlossofone’sidentity
(Breakwell,1986;G.W.Brown&Harris,1978),andthreatstoself-esteem
(Abramsonetal.,1989).However,lessattentionhasbeengiventohowthe
experienceofmentalhealthsymptomatologyanddisordermayinfluenceone’s
identityconstruction,ratherthantheotherwayaround.Qualitativestudieshave
highlightedthatthiscanbeaproblematicexperienceinadolescence,withyoung
peopledescribingidentityconfusionorinterruptionastheyexperiencesymptoms
andbehavioursseenasincongruentwiththeirsenseofthemselves(Crossley,2000;
Inderetal.,2008;Kuwabaraetal.,2007;Wilmotsetal.,2019).Findingssuchas
thesemayreflectthepsychodynamicdefencemechanismofsplittingoftheego,a
stateofinnerconflictwhereinanindividualisunabletounifydifferentpartsof
themselvesintoacoherentwhole(Freud,1933,1940).Thisseparationofone’s

CHAPTERSEVEN:DISCUSSION
263
symptomsfromtheselfmayindeedgobeyondalossofcontrolandinsteadreflect
aprotectiveact,meanttopreserveaprimaryconstructionofoneselfashappyand
rational,ratherthandefinedbythesemorenegativethoughtsandfeelingsandthe
actionstheyleadto.Researchhasidentifiedinstancesofyoungpeoplewhoover
timehavecometoseesymptomsanddisordersasacentralcomponentoftheir
identity,perhapstoholdontoasenseofstabilityforthoseexperiencingturbulence
inadolescence(Breenetal.,2013;Shawetal.,2009).Thisintegrationofdisorder
intotheselfcanmeanthattreatmentorchallengescanbeperceivedasathreatto
one’sidentity,promptingreluctancetoengageintherapyorworktowards
recovery(Shawetal.,2009;Warner,2001).Suchfindingsdosuggestthata
separationbetweentheselfandemotionalsymptomscouldbeanimportantactof
self-preservationforsome.Fromatherapeuticperspective,Midgleyetal.(2017)
havesuggestedthatempoweringyoungpeopletoexplorethemeaningoftheir
experiencesandsymptomsmayoffergreaterfeelingsofcontrolandorderand,in
turn,helptheminre-establishingasenseofidentity.
CognitiveDistortions
Participants’beliefsthatsomeoftheirthoughtsdidnotreflectrealityrelate
totheconceptofcognitivedistortion,oranegativebiasederrorininformation
processing,akeytenetofthecognitivemodelofpsychopathology(Beck,1963,
1974;Beck,Rush,Shaw,&Emery,1979).Distortionsoccurautomaticallyand
generallyreflectanindividual’scorebeliefsaboutthemselvesandtheworld(Beck,
1963;Hollon&Kendall,1980).Itisbelievedthatthisisatypicalhumanbehaviour,
butthatmorefrequentorpronouncedcognitivedistortionsbothprecedeand
maintainpsychopathology(Beck,1963,1974;Becketal.,1979).Therehasbeena
particularemphasisontheroleofcognitivedistortioninnegativeaffectivity;such
thinkingpatternsareseentocontributetothedevelopmentofdepressionandare
understoodtoaffectone’sstressappraisalcapacities,thusprovokingheightened
anxiety(Beck,1963,1974;Beck&Clark,1988;Muris&Field,2008).
Researchhasdemonstratedthatchildrenandadolescentsreporting
depressionandanxietyarelikelytoexperienceheightenedand/orfrequent
cognitivedistortions(e.g.,Birhameretal.,1996;Maric,Heyne,VanWidenfelt,&

CHAPTERSEVEN:DISCUSSION
264
Westenberg,2011;Pereira,Barros,&Mendonça,2012;Rudolph&Clark,2001).
Indeed,thereissomeevidencethatincreasedcognitivedistortionmayactasa
mediatorintherelationshipbetweenearlyadversityandadolescentemotional
symptoms(Flouri&Panourgia,2011;Panourgia&Comoretto,2017).Itisperhaps
unsurprisingthatsuchthinkingpatternswerepresentedbythesetwoparticipants,
giventhattheywereeachexperiencingemotionalsymptomsandmultiplerisk
exposure.Cognitivedistortionscanmanifestthemselvesindifferentways;several
typesofdistortionwerereportedbyAmeliaandJennifer.Forinstance,both
describedatypeofdistortionreferredtoasemotionalreasoning,whereinone’s
feelingsandbeliefsareunconditionallyassumedtobecorrect,outweighingmore
rationalisedthinking(Burns,1980).Theyalsodescribedcatastrophizing,where
negativefuturepredictionsaremadebasedonlittletonoevidence,andmental
filtering,wherebynegativeinformationisfocuseduponandpositiveinformationis
devalued(Beck,1963;Burns,1980).
Notably,althoughbothAmeliaandJenniferexpressedexplicitbeliefsthat
thesethoughtsdidnotmatchreality,thisdidnotdiminishthethoughtsoraffect
widerthinkingpatterns.Thus,notonlywerethesethoughtsoccurring
automatically,buttheyweresustainedthroughamoreconsciousinspection.This
mayreflectthedominantviewofinformationprocessingasadualprocess,withan
automaticresponseaswellasamorecontrolled,reflectiveresponse(Gawronski&
Bodenhausen,2006;Shiffrin&Schneider,1977;Strack&Deutsch,2004,2011).
Whilediscussionofcognitivedistortionsgenerallyfocusesontheirstatusas
automatic,itappearsthatthismaybeinterspersedwithamoreconscious
inspectionandacceptanceofsuchthoughts.Thisinabilitytousearecognitionof
distortiontoactivelychallengehasalsobeendescribedbyolderadolescents
experiencingemotionalsymptomsinpreviousqualitativeresearch(Wisdom&
Green,2004),indicatingthatthisdifficultyisnotnecessarilyduetocognitive
capacitiesinearlyadolescence.Cognitive-focusedtreatmentapproachessuchas
cognitivebehaviouraltherapy(CBT)typicallyincludecognitiverestructuring,
whereinapatientistaughttomonitortheirautomaticthoughts,identifyany
possibledistortions,andchallengethesethoughtsthroughexaminingtheevidence

CHAPTERSEVEN:DISCUSSION
265
forandagainstthem(Heninetal.,2016).Notably,AmeliaandJennifer
demonstratedtheabilitytoidentifythesedisparities,buttheiridentification
contradictory“evidence”didnotofferthemanewperspective.Indeed,Amelia’s
frequentquestion“what’stheevidence?”reflectsthetypeofquestioning
encouragedinCBT,suggestingshemayhavepreviouslyengagedinthisapproachin
someway.
Itmaybethatsuchawarenessisnotsufficientlypowerfultocreatechange
unlessexploredactivelywithanotherperson(suchasatherapist)orundertaken
alongsideothermethodsofchallengingfeelingsandbehaviours,asisthecasein
CBT.Indeed,arecentmeta-analysisfoundthatcognitiverestructuringwith
depressedadolescentswaseffectiveonlywhencoupledwithothercomponents,
includingchallengingreactivebehaviours(Oudetal.,2019).However,itmayalso
bethatchallengingone’sautomaticthoughtsdoesnotnecessarilyalterunderlying
beliefsystems;corebeliefsareunderstoodtodevelopininfancyandtobeless
susceptibletochangethanmoreimmediatepatternsofthinkingandbehaviour
(Beck,1995;Fishbein&Ajzen,2005;Wellman,1992).CBTasofferedtochildren
andadolescentswithintheNHSistypicallybriefandsometimescomputerised,
whichmaynotprovidesufficienttimetofacilitatechangeincorebeliefs.Notably,
althoughresearchshowsbothimmediateandlong-termpositiveimpactfor
childrenandyoungpeopleexperiencinganxietyanddepression(e.g.,Marchetal.,
2007;Vigerlandetal.,2017;Wolk,Kendall,&Beidas,2015),suchfindingsfocuson
wholegroupchangeratherthanonindividualimprovementrates.Arecentstudy
foundthattherapeuticservicesforadolescentsexperiencingdepressionand
anxiety,includingbutnotlimitedtoCBT,didnotresultinimprovementforthe
majorityofindividuals(Edbrooke-Childsetal.,2018).Itmaybethatforsome
childrenandadolescents,facilitatinganawarenessofthesethoughtsasdistorted
maynoteffectivelychallengethinkingpatterns,warrantingfurtherattentionin
therapeuticevaluations.

CHAPTERSEVEN:DISCUSSION
266
7.5.3DemandsandControl
PersistentStressors
Understandingtheparticularfeaturesandexperiencesthatparticipants
describeindiscussingstressorsmayprovideinsightintohowtheyareperceivedto
bestressful.Thiscanaidunderstandingofthestressappraisalprocessexplored
earlierinthischapter,whichacknowledgesthatthereareenvironmental
antecedentslikelytopromptstress,butemphasisesthatthisisultimately
dependentonthewayinwhichonemakessenseofandassessestheseexperiences
(Folkman&Moskowitz,2000;Lazarus,1966,1990;Lazarus&Folkman,1984;
Lazarus&Launier,1979;Park&Folkman,1997).Here,participantsdrewattention
toboththemultiplicityofstressorsintheirlivesaswellasthewayinwhichthey
wereembeddedasongoingissues.Thedemandstheyexperiencedwerenot
necessarilytalkedaboutasthoughtheywerestressfulinandofthemselves,but
insteadweredescribedasbuildinguporinteractingwithoneanothertobecome
overwhelming.Gracetalkedaboutmultipleincidentsanddemandsbuildinguntil
theycauseddrasticeffects,likeself-harmora“breakdown”,whileJennifertalked
abouthowdemands“pileup”andbecome“toomuch”tohandle.Furthermore,
althoughthestressorsdescribedtypicallyrelatedtoday-to-dayconcernssuchas
negativeinteractionsoracademicpressures,thesewerenotseenasisolated
incidentsbutwereperceivedasembeddedwithinongoingissues,constituting
chronicstressors(Epeletal.,2018).Forinstance,Grace’sinteractionswithhermum
werestressfultoherassingularincidents,butalsotookongreatermeaningwithin
aninternalnarrativeofhermumas“always”havingoverlookedherneedsand,
indeed,compoundedthisnarrative.
Previousqualitativestudieshavereportedsimilarattributionsamong
childrenandyoungpeopleexperiencingemotionalsymptomsanddisorders,
whereinstressorsaccumulateuntila“breakingpoint”isreached(Dundon,2006;
Midgleyetal.,2017).Suchexperiencesmirrortheconceptoftheallostaticload
hypothesisincumulativerisktheory,whereinstressresponsesystemsbecome
overwhelmedwhentaskedwithrespondingtotoomanydemands(Evans,2003;
McEwen,1998;Sterling&Eyer,1988).However,participants’accountsillustrate

CHAPTERSEVEN:DISCUSSION
267
thisprocessasaconsciouslivedexperienceoffeelingoverwhelmed,ratherthan
simplyhavinganunderlyingphysiologicalresponseinwhichsystemsare
overwhelmed.Seminalliteratureexploringallostaticloadhasgenerallyfocusedon
physiologicalstressprocessesanduseofbiomarkersasawaytoassessthe
phenomenon(e.g.,Evans,2003;McEwen,1998;Sterling&Eyer,1988),but
infrequentlyacknowledgescognitiveappraisalsorpsychologicalstress.Findings
hereandelsewherethatadolescentsfeelcognitivelyandemotionallyoverwhelmed
emphasisesthatone’sabilitytocopewithpsychologicalstresscanalsobecome
overloadedinthefaceofmultipledemands.Indeed,previousworkhasnotonly
demonstratedthatpsychologicalandphysiologicalstresssystemsareinter-related,
buthasalsosuggestedthatitisone’sappraisalofmultiplestressors,ratherthan
thestressorsthemselves,thatbestpredictsallostaticload(Burkeetal.,2005;Clark
etal.,2007;Logan&Barksdale,2008;Sladeketal.,2016).Thus,itmaybe
importanttoconsidertheroleplayedbybothpsychologicalandphysiologicalstress
infutureadolescentmentalhealthresearchinordertocomprehensivelyexplore
stressasamechanismformentalhealthoutcomes.
Indeed,suchfindingscouldbeconsideredtoillustratethecontextualnature
ofmentalhealth.Asarticulatedinthetransactionalmodelofstressandthe
allostaticloadtheory,beingfacedwithconsistentstressorsthatexceedone’s
perceivedabilitytocopeisnaturallygoingtocontributetofeelingsofdistress.It
couldwellbearguedthatallthreeparticipants’feelingsofdistressandanxietyare
anentirelynaturalresponsetothevariouschallengestheyexperienceintheirlives.
Throughthislens,thereisperhapsaneedtoquestionwhetherthecategorisation
ofanyformofemotionaldistressasamentalhealth“symptom”or“difficulty”is
sensitivetothisreality,whereinindividuals’responsesmaybeappropriateoreven
healthy.Forinstance,Grace’sfrustrationanddistressoveradults’failuretohear
herevenassheindicatesthreatstohersafetycouldwellbeconsideredanadaptive
responsetothefailureofotherstosupportherboundaries.Indeed,ithasbeen
arguedthatsuchresponsesmaybehealthybutmayalsobecomeheightenedover
timeinresponsetocontinuedthreateningexperiences,whichcouldovertime
amplifyemotionalresponses(McLaughlin,2016).Suchconsiderationscreate

CHAPTERSEVEN:DISCUSSION
268
questionsaroundthewiderresponsibilitiesofsystemstosupportyoungpeoplein
addressingthesewiderareasofstressratherthanlabellingdifficultiesas
symptoms;thisisexploredingreaterdepthlaterinthischapter.
Indeed,theideathatone’sappraisalofagivensituationcanbeinfluenced
byaninternalnarrativesupportspreviousargumentsthatcumulativestressover
timecanshapethewaythatindividualsperceiveandappraisepotentiallystressful
events(Epeletal.,2018).Thismayalsoprovideinsightintowhygreaterchronicity
anddurationinexposuretostressorsandriskfactorsisseentocontributeto
worsenedmentalhealthoutcomes(Brooks-Gunn&Duncan,1997;Hammen&
Brennan,2003;Najman,Clavarino,etal.,2010;Reiss,2013),particularlygiventhat
stressisconsideredinstrumentalinriskeffectsmoregenerally(Evansetal.,2013).
Takentogetherwithindicationsthatmultipleco-occurringstressorscanbe
particularlystressful,findingsindicatethatinterpretationofagiveneventisnotan
isolatedappraisal,butisinsteadinformedbyone’swidercontextandhistory.This
maybeparticularlypronouncedamongindividualsexperiencingemotional
symptoms,asinthecurrentstudy,giventhatcognitivedistortionsandtendencies
towardsnegativeinformationprocessingcommonlyoccuraspartofthese
difficulties(e.g.,Birhameretal.,1996;Maric,Heyne,VanWidenfelt,&Westenberg,
2011;Pereira,Barros,&Mendonça,2012;Rudolph&Clark,2001).
Findingssuggestthatforadultsofferingsupporttoadolescentsexperiencing
stress,itwouldbeusefultodevelopanunderstandingofthewidercontextand
internalnarrativesthatinformtheirresponses.Thismaybeparticularlyimportant
wherearesponsedoesnotappearproportionatetothesituation,giventhat
prevailingdiscoursesofadolescentsisthattheyareirrationalandpronetomood
swings,whichcanleadtodismissiveadultresponses(Blakemore,2018;Stapleyet
al.,2016).Thismayalsoprovideopportunitiestojointlyreviewandidentity
persistentstressorswithyoungpeopleanddevelopappropriatecopingstrategies
oractiveresponses.Indeedfromaclinicalperspective,ithasbeensuggestedthat
adolescentswhoholdcausalbeliefsaboutexternalfactorscontributingto
symptomsarelikelytobenefitfromexploratorytherapeuticapproaches,suchas

CHAPTERSEVEN:DISCUSSION
269
psychodynamictherapy,tofacilitatethemindirectlyexploringandunderstanding
thesechallenges(Midgleyetal.,2017).
SocialDemandandThreat
Therewereinstanceswherethestressorsthatparticipantsidentifiedwere
orientedaroundspecificpeopleandsocialinteractions.ForAmeliaandJennifer,
thisgenerallyappliedtoteachers,whileforGracehermumandbullieselicited
distress.Thisreflectsadualityinsocialties,whereininteractionscanbepositive
andharmful,dependingonthecircumstances(S.Cohen,2004;Umberson&
Montez,2010).Anevolutionarynecessityforsocialinclusionmeansthatperceived
exclusionorriskcanbeexperiencedprofoundly,promptingstrongemotions(Allen
&Badcock,2003;MacDonald&Leary,2005).Adolescenceisaperiodofhighsocial
stressgivenincreasedcomplexityinrelationshipsalongsidegreateremphasison
peerrelationshipsandautonomyfromparents(Daveyetal.,2008;vanRoekelet
al.,2015).
Ofthenegativeinteractionsdescribedbyparticipants,parentalconflict,
parentalneglect,andbullyingvictimizationarewelldocumentedasproblematicfor
mentalhealth,whichisunsurprisinggiventheimportanceofparentsandpeersin
adolescence(Umbersonetal.,2010).Difficultieswithinparentalrelationshipsare
oftenassociatedwithemotionalsymptomatologyanddisorder,includingpoor
maternalcare(Branjeetal.,2010;Kim&Cicchetti,2004;Rey,1995;Schmidetal.,
2011;vanderVoortetal.,2014)andparent-childconflict(Brock&Kochanska,
2015;HiuYapetal.,2014),whileresearchhasconsistentlyindicatedarelationship
betweenbullyingvictimizationandemotionaldifficulties(e.g.,Bondetal.,2001;
Menesinietal.,2016;Stapinskietal.,2015).Thereislessresearchdirectlyfocused
onteachers.Researchhasshownthatchildrenandadolescentsrecogniseacademic
pressurefromteachers(Akos&Galassi,2004;Gorard&See,2011;Klingeretal.,
2015)andcandistinguishdifferentialteacherbehaviourbasedonpupil
performanceandcharacteristics(e.g.,Babad,2009;Brattesani,Weinstein,&
Marshall,1984;Myhill&Jones,2006).Qualitatively,adultsvividlyrecallnegative
experiencesofteachersperceivedtobehavecruellyorunfairly(e.g.,Díez,2010;
Miller,2015;Miller&Shifflet,2016).Takentogetherwithcurrentfindings,this
CHAPTERSEVEN:DISCUSSION
270
suggeststhatnegativeencounterswithteacherscanbeexperientiallymeaningful
toadolescents.Todate,thereislittlequalitativeexplorationofhowadolescents
viewteachers;asnotedbyBakxetal.(2015),researchtypicallyexploresteachers’
perspectives,whilepupilperspectivesofteacherpracticesareoftenexamined
quantitatively.Thiswarrantsfurtherexploration,includingamongthose
experiencingemotionalsymptoms,asinthecurrentstudy,asitmaybeespecially
importanttolessenanxietiesintheclassroomforthisgroup.Thismaybe
particularlytrueforgirls,givenheightenedpressure(Jones&Myhill,2004;Klinger
etal.,2015;Renold&Allan,2006;Skeltonetal.,2010)andconceptualisationsof
girlsasacademicallynon-problematic(Jones&Myhill,2004;Renold&Allan,2006;
Ringrose,2007;Skeltonetal.,2010).
Negativeinteractionseliciteddistressandfrustrationamongparticipants,
aligningwithevidencethattheyareassociatedwithelevatedstress(Cohen,2004;
DeVries,Glasper,&Detillion,2003)andtheemergenceandmaintenanceof
adolescentemotionalsymptoms(Herres&Kobak,2014;LaGreca&Harrison,2010;
A.Leeetal.,2010;Willetal.,2016).However,symptomsthemselvesmay
contributetothemeaningfulnessofnegativeinteractions,asdepressedindividuals,
includingchildrenandadolescents,oftenseekexcessivereassuranceandgreater
negativefeedbackinsocialinteractions(Evraire&Dozois,2011;Hamesetal.,2013)
andshowattentionalbiastowardsnegativesocialevents(e.g.,Banerjee,2008;
Luebbeetal.,2010;Wrightetal.,2010).Indeed,someofthissocialdistresswas
centredonfuturepredictions.Gracefearedthatherbullieswouldactualisetheir
threatsofphysicalaggression,withsomeindicationsthatshegeneralisedthisto
otherdomains,suchastalkingaboutastrangerassaultingherathome.Indeed,
priorevidenceindicatesthatbullyingvictimizationisachronicstressor,heightening
bothday-to-dayandlong-termanxiety(Carlisle&Rofes,2007;Craig,1998;Zarate-
Garzaetal.,2017).Similarly,AmeliaandGraceexpressedworryaboutpossible
responsesfromteachersiftheywerenotacademicallykeepingup.Thecurrent
studycannotascertaintheextenttowhichsuchissuesaretheresultofnegative
socialinformationprocessingorareasonableextrapolationbasedonexperiences,

CHAPTERSEVEN:DISCUSSION
271
butregardlessofhowcloselythisreflectsreality,theseinteractionsandpredictions
weresufficientlyrealtoparticipantstowarrantdistress.
Finally,itwasnotablethatGraceusedhersupportiverelationshipwithher
dadtocompensateforperceivedshortcomingsfromhermum.Researchexamining
theinteractionbetweenpositiveandnegativesocialinteractionshas
predominantlyexploredthiswithinspecificrelationships(Rossetal.,2019),rather
thanacrossone’ssocialnetwork.Itmaybeusefultoexaminehowdifferenttypes
ofrelationshipsinteractacrossadolescents’socialnetworkstounderstandhow
largelynegativerelationshipscansitalongsidemorepositiveones.Furthermore,
Grace’smentalidentificationofapositiveresourcetooffsetanegativeexperience
mirrorstheconceptofactiveresilience,whereinindividualsactivelymakedecisions
toadapttoadversity(Lerner,Theokas,&Jelicic,2005;Murray,2010;Ungar,2012).
Previousresearchhaslargelyfocusedonspecificbehaviours,suchasavoiding
particularsituations,buthasalsoindicateduseofthinkingstrategies.Murray
(2010)foundthatyoungoffendersengagedintemporalleaps,focusingonfuture
lifetoavoidcriminalactivity,and“othered”offenderstolimittheviewofoneselfas
agroupmember.Suchbehavioursaresimilarto,thoughdistinctfrom,Grace’s
mentalcompensation,whichcloselyelicitstheideaof“protective”functionsin
adversity.Furtherqualitativeresearchcouldexplorehowyoungpeopleperceive
theirownrolewithintheresilienceprocesstogainfurtherinsightintosuch
decision-making.
ControllabilityandVoice
Althoughparticipantsdididentifydemandsacrosstheirday-to-daylives,
theydidnotallconsistentlyattributetheiremotionalsymptomsorassociated
feelingsdirectlytothesestressors.Graceheldafirmbeliefthatthedemands
placedonherwereunreasonableandcausedherfeelingsofupsetandfrustration;
however,AmeliaandJennifergenerallytalkedasthoughtheproblemwasnotthe
demanditself,butrathertheirinabilitytorisetomeetit.Regardless,allthree
participantsdescribedfeelingaresponsibilitytoadapttomeetdemands,even
wheresuchactionswereperceivedtobedetrimentaltothem.Forinstance,
Jenniferdescribedgettingoutofbedatfiveo’clockinthemorninginordertokeep
CHAPTERSEVEN:DISCUSSION
272
upwithacademicwork,whileGracetalkedaboutgoingtohermum’shomedespite
feelingunsafethereasshedidnotwanttohurtherfeelings.Thus,since
participantsbelievedtheycouldnotcontroltheirenvironment,theyinsteadhadto
controltheirownbehavioursandresponses.
Thisdistinctionbetweencontrollingtheworldandcontrollingtheselfis
articulatedinRothbaum,Weisz,andSynder's(1982)two-processmodelof
perceivedcontrol.Thismodelcomprisesprimarycontrol,whereanindividual
attemptstocontroltheirouterworldinlinewiththeirownneeds,andsecondary
control,whereanindividualchangesthemselvestofitwiththedemandsofthe
world.Here,participantslargelyengagedinsecondarycontrol,andthoughGrace
didundertakeeffortstowardsprimarycontrol,thesewerenotperceivedtobe
successful.Asaresult,failurestokeepupwithdemandsareattributedtotheself,
resultinginfurtheradaptationandself-blame.Thisapparentcontradictionbetween
perceiveduncontrollabilityandacontinuedsenseofresponsibilityandself-blame
illustratesthedepressiveparadox,whichhighlightstheillogicalnatureofblaming
oneselfforuncontrollableevents(Abramson&Sackeim,1977).Notably,thereis
evidencethatadolescentgirlsexperiencingemotionalsymptomsanddisordersmay
bemoreinclinedtowardsself-blamefollowingadverseevents,relativetoboys
(e.g.,Bennettetal.,2005;Zlomke&Hahn,2010).
Whileallparticipantsdescribedadaptingtheirownbehavioursand
responses,therewasvariationinbeliefsandactionsaroundeffortstowards
primarycontrol.ThoughAmeliaandJenniferdidnotconsideritappropriatefor
themtoaskotherstochangetheirbehaviour,Gracedescribedconsistentlytelling
othersthatasituationwasunfairandcommunicatingwhatsheneededinstead,but
shegenerallyfoundthatthismadelittledifference.Thus,whileAmeliaandJennifer
appearedtoviewsecondarycontrolattemptsasthemostappropriatecourseof
action,thisappearedtobemoreofanenforcedactforGrace,giventhatherefforts
tocontroltheexternalworldwereperceivedashavingfailed.Thisfeelingofbeing
unheardreflectsawiderissueofeverydaypowerimbalancesbetweenadultsand
youngpeople.Researchhasindicatedthatdespiterecognitionoftheirrighttobe
heardinmattersaffectingthem(UnitedNationsChildren’sFund,1989),children

CHAPTERSEVEN:DISCUSSION
273
andadolescentsoftenfeeltheyarenottrulygivenasayindecisionsandinstead
feel“bossedabout”(Blakemore,2018;Hargreaves,2017;Kilkellyetal.,2005;
Lundy,2007;Morrow,1999).
Anincreasedemphasisonpositiveyouthdevelopmentperspectivesand
approacheshasledtoagrowingbodyofliteratureexploringthebenefitsof
introducingsystemsandapproachesthatcanempoweryoungpeopleandenhance
theirvoice(e.g.,Hazel,2016;Sargeant&Gillett-Swan,2015;Wong,Zimmerman,&
Parker,2010).However,thesestudiesareoftenfocusedonengagementwith
youngpeopleinaneducationalsettingorcommunitysettingssuchasyouthclubs.
Whileeffortstodevelopsharedcontrolandshareddecision-makingwithinsuch
contextsisimportantandindeedmaybevaluableforyoungpeoplelikeAmeliaand
Jennifer,itremainsunclearhowyoungpeoplemanageissuesofvoiceand
empowermentinafamilycontext.Researchhasemphasisedthatitis
developmentallybeneficialforadolescentstobepartofdecisionswithinafamily
contextandindeedthatthismaypromotepositiveoutcomesintermsofemotional
symptoms(e.g.,Beckeretal.,2010;Borellietal.,2015;Radziszewskaetal.,1996).
Yet,thereislittleunderstandingofwhathappenswhentheseneedsareoverlooked
andofhowwidersystemsmightbeinvolvedinfacilitatingyouthvoiceinafamily
context.Thus,whereadolescentsareidentifiedashavingmentalhealthsymptoms,
includingemotionalsymptoms,itmaybeimportantnotonlytoaddresscopingand
emotionregulationskills,butalsotojointlyidentifyareasofdifficultyandstress
acrosstheirworlds,andtoexplorewaystodirectlyaddresstheseandempowerthe
youngperson.
Itisimportanttonotethatparticipants’judgementoftheseparticular
stressorsasbeyondtheirimmediatecontrolisnotunreasonable.Academic
pressure,poorparentalrelationships,andbullyingvictimizationareallissuesthat
arelikelynoteasilyresolvedbyyoungadolescents.Indeed,findingsindicateaneed
toconsiderwhenitisappropriatetoexpectyoungpeopleto“adapt”or“cope”
withadversity,andwhenthereisaneedtofacilitatechangetobettermeettheir
needs.Ithasbeensuggestedpreviouslythattheconceptsofresilienceand
adaptationmaybedangerousinthattheyplacetheonusonanindividualtofit

CHAPTERSEVEN:DISCUSSION
274
withthestatusquo,thuscircumventinganyneedforsystemicchangesthatcould
facilitategreaterequality(Burman,2018;DeVerteuil&Golubchikov,2016;Ungar,
2012).Findingsheresuggestthatadaptationmaybedetrimentalinsomecases,
necessitatingpotentiallyharmfulbehaviours.ItisnotablethatmuchofAmeliaand
Jennifer’sdifficultiesinday-to-dayliferelatedtoacademicpressures,echoing
reflectionsbyMidgleyetal.(2017)thatacademicdemandsareperceivedbyyoung
peopletobeacommonstressorbutarenotgenerallyemphasisedinadversity
literature.Suchdifficultiesarenotablegiventhatyoungpeopleoftendonotfeel
“heard”withineducationsettings(e.g.,Lundy,2007),whichmaybeparticularly
trueforstudentspresentingashavingmentalhealthsymptoms,including
emotionalsymptoms(e.g.,Baker,2016;Cefai&Cooper,2010;Lewis&Burman,
2008).Itmaybeimportantforpolicymakersandpractitionerstocriticallyreflecton
when“resilience”istrulyrequiredandwhenitmayinsteadbenecessarytoadapt
tomeettheneedsofyoungpeoplefromdiversebackgrounds.
7.5.4DrawingonOthers
Help-SeekingBeliefsandBehaviours
Participants’mappingoftheemotionalsupportnetworkalignswith
literaturearoundmentalhealthhelp-seeking,definedbyRickwoodandThomas
(2012)asanadaptivecopingprocesstogainexternalhelpwithmentalhealth.This
includesbothinformalsocialnetworks(e.g.,family,friends)andformalavenues
(e.g.,teachers,psychologists).Participants’relianceonfamilyandfriendsfollows
consistentevidencethatadolescentsoverwhelminglyseekhelpforpersonaland
emotionalissuesfrominformalconnections,ratherthanprofessionals(e.g.,
D’Avanzoetal.,2012;deAnstiss,2009;JacksonWilliams,2012;Rickwoodetal.,
2005;Wilson,Bushnell,&Caputi,2011;Wilson,Rickwood,&Deane,2007).
Researchhaslargelyconcludedthatgirlsandwomenaremorelikelytoseekhelp
thanboysandmen(Barker,2007;Parker&Brotchie,2010;Rickwood&
Braithwaite,1994;Sen,2004);however,thisoverarchingpatternmaskscontext-
dependentvariability.Evidencesuggeststhathelp-seekingamonggirlsandwomen
variesaccordingtocharacteristicssuchasSES(e.g.,Fonseca,Gorayeb,&Canavarro,

CHAPTERSEVEN:DISCUSSION
275
2015)andsexuality(e.g.,McNair&Bush,2016),aswellasthetypeofmental
healthdifficultyforwhichhelpissought,withevidenceofreversedorevenabsent
genderdifferencesinthecontextofdepression(e.g.,Angstetal.,2002;
Zimmerman,2005).Currentfindingsfurtherindicateneedforanuanced
perspectiveofthisissue,asparticipantsshowedvaryinglevelsofdiscomfortin
sharingemotionswithothersandallreportedaccessinglittletonoprofessional
support.Furthermore,youngeradolescents,asofinteresthere,canbemore
reluctanttoseekbothinformalandformalsupport(Boldero&Fallon,1995;Boyd
etal.,2011;Wilson&Deane,2012),whiledepressionandanxietyareassociated
withloweredhelp-seeking,bothinformalandformal(e.g.,Wilsonetal.,2011,
2007;Wilson&Deane,2010).Intersectionalityoftheseissuesamidstcurrent
concernsaroundemotionalsymptomatologyamongearlyadolescentgirlsindicates
theneedtoexplorehelp-seekingtendenciesamongthisgroup.
Findingsalsoprovideinsightintotheinterpretivemeaningattachedto
specificavenuesofsupportandhowthisinformsdecisions.Ithasbeensuggested
thathelp-seekingisanactiveprocess,withindividualslikelyevaluatinghelpsources
contextuallygiventheirissueandthetypeofsupportdesired(Boldero&Fallon,
1995;Rickwood,2015).Currentfindingssupportthis,withparticipantsactively
assessingtheirneedsandidentifyingindividualsperceivedasabletofulfilthese.
Theiremphasisonrelationalqualitiesofcloseness,trust,andcaremayexplainwhy
familyandfriendsareoftenrelieduponforemotionalsupportand,indeed,reflects
qualitiesprioritisedbyadolescentsinpreviousstudies(Gulliver,Griffiths,&
Christensen,2010;Martin,Romas,Medford,Leffert,&Hatcher,2006;Rickwoodet
al.,2005).Perceivedavailabilitywasalsoconsideredmeaningful;AmeliaandGrace
highlighted“knowing”theyhadconsistentandreliablepeopleavailable,while
Jennifersawothersasfrequentlyunavailableforemotionalsupport.Ithas
previouslybeentheorisedthatevenperceivedavailabilityofsocialsupportcan
lessentheextenttowhichaneventisappraisedasstressful,thusbufferingstress
andpreventingnegativeemotionalresponses(Kawachi&Berkman,2001).This
emphasisonavailabilitymayfurtherexplainadolescentrelianceonfamilyand
friends,asinteractionswithsuchindividualsareoftenembeddedacrossdailylife.

CHAPTERSEVEN:DISCUSSION
276
However,thereisaneedtoconsiderthequalityofsupportfromfamilyand
peers.Responsesmaybenegativeorguidedbyindividualisedandculturalvalues
(Barker,2007;Cauceetal.,2002;Guoetal.,2015;Stanton-Salazar&Spina,2005),
whileindividualsmaynotbeequippedtorecogniseorrespondtosignsofmental
healthsymptoms(Barker,2007;Rickwoodetal.,2005;Wilsonetal.,2011)and
indeedmayofferunhealthysolutions(Rickwoodetal.,2005;Schwartz-Mette&
Rose,2012).Arelianceonfamilyandfriends,amongparticipantsandasevidenced
acrossthewiderliterature,demonstratestheimportanceofimprovingknowledge
andskillsamongparentsandyoungpeopletofacilitateeffectivesupport(D’Avanzo
etal.,2012;Rickwoodetal.,2005).However,youngpeoplemaybeselectivewithin
theirinformalnetworks,filteringoutindividualsperceivedasunhelpfulevenwhere
thesecouldtypicallybeconsideredimportantsupportavenues.Here,Grace
perceivedhermumtobeuncaringandsochosenottoshareissueswithher,
thoughofcoursethisdependsuponidentificationofsucharisk.
Therewaslittlediscussionofprofessionalhelp-seekingamongparticipants;
thoughAmeliadiddescribesomeinteractionswithsupportbothinandoutof
schooltheserelationshipsweretreatedasaugmentingthesupportofferedby
familyandfriends.CurrentpolicyinEnglandencompassesagrowingemphasison
schoolsasacontextforpromotingmentalhealth,withteachersconsideredakey
supportsystem(DepartmentofHealthandEducation,2017;Fazeletal.,2014;
Vostanisetal.,2013;Weare,2010).However,participants’talkofteachersdidnot
reflectaviewofthemasanappropriateavenueforhelp-seeking.Amelia
demonstratedconsistentanxietyaroundinteractionswithteachers,Gracenoted
thatsherarelyaskedteachersforhelpandinsteadcalledherdadregarding
problemsinschool,whileJenniferbelievedthatteacherswouldnot“genuinely”
care.Thiscouldbeconsideredpartofabroaderpatterninwhichteachersare
perceivedasusefulonlyinthecontextofschool-relatedissues(e.g.,academic
difficultiesorpeerconflict),whilefamilyandfriendsareconsideredmost
appropriateformorepersonalissuessuchasemotions(Boldero&Fallon,1995;
Bowersetal.,2013;Rickwoodetal.,2005;Stapleyetal.,2019).Ifemphasison
teachersasakeysourceformentalhealthsupportistocontinueineducational

CHAPTERSEVEN:DISCUSSION
277
policy,thereisaneedtoconsiderhowthisavenuecanbemademoreappealingto
youngpeople.Itmayhelptodrawontherelationalqualitieshighlightedhereand
inpriorliterature,providingopportunitiesforadolescentstodeveloptrusting
relationshipswithteachersinwhichtheyfeelcaredforandunderstood,ideally
beforeissuesarise(Rickwoodetal.,2005).Notably,suchqualitiesmirrorthe
featuresoftendiscussedinthecontextoftherapeuticalliance,acriticalcomponent
forchangethatdescribesthequalityandstrengthofacollaborativetherapist-client
relationship(Ackermanetal.,2001;Cooper,2004;Pattison&Bell,2018;Rogers,
1957).Itmaybethattrainingaroundcounsellingandtherapeuticinterpersonal
skillscouldaidteachersincreatingmeaningfulrelationshipsforchangewith
adolescents.
TalkingasaRelease
Participants’centralaimwhenseekinghelpoftenappearedtobesimplyto
sharetheirsymptomsandthoughtsverbally,astheyperceivedthisasaformof
release.Thisisgenerallyconsideredemotionalsupport,whereintrustedothers
offerfeelingsofvalueandcomfortand,inthecontextofmentalhealth,provide
supportforemotionalneedsordistress(Barker,2007;Jacobson,2009).The
perceivedusefulnessofsuchinteractionsreflectsevidencethatemotionalsupport
frombothadultsandpeersisassociatedwithloweredlevelsofemotional
symptomsduringadolescence(e.g.,Boudreault-Bouchardetal.,2013;Slavin&
Rainer,1990),particularlyasabufferagainstadverseevents(e.g.,Desjardins&
Leadbeater,2011;Yeung&Leadbeater,2009;YeungThompson&Leadbeater,
2013).Theemphasisthatparticipantsplacedontalkingwithotherswhen
experiencingadifficulttime,andthereleasethattheydescribed,suggestsa
perceptionthatthisisthemostvaluablemethodofsupportavailableindailylife,
withlittlementionofothersupporttypessuchasinstrumentalsupport(i.e.,direct
supportwithanissue)orinformationalsupport(i.e.,informationaboutanissueor
treatment).Thecurrentstudymaysupportunderstandingofhowtheprocessof
emotionalsupportandtalkingthroughdistresswithclose,trustedotherscanoffer
aneffectivecopingstrategyinthecontextofmentalhealth,asunderlying
mechanismsarenotfullyunderstood(Lakey&Orehek,2011).

CHAPTERSEVEN:DISCUSSION
278
Thereleaseparticipantsemphasisedisofparticularnoteandsoisfocused
uponhere.Theactoftranslatingone’sfeelingsintowords(bothverbalandwritten)
hasrecentlybeenconceptualisedasaffectlabelling,aformofemotionregulation
(Torre&Lieberman,2018).Researchhasshownthataffectlabellingcandiminish
theintensityofanemotion(Fanetal.,2019;Torre&Lieberman,2018)and
neuroimagingstudieshaveconsistentlyfoundthataffectlabellinginresponseto
emotionalstimuliyieldsdecreasedlevelsofamygdalaactivation,alongside
increasedactivationofprefrontalregions(Burklundetal.,2014;Costafredaetal.,
2008;Liebermanetal.,2007).Giventhattheamygdalaisassociatedwiththe
generationofemotion,itisnotablethatsymbolicconversionofemotionappearsto
shifttheonusofprocessingtoanotherregion,perhapssignallingtotheamygdala
thatitsroleiscomplete(Torre&Lieberman,2018;Woodetal.,2016).However,it
remainsunclearexactlywhatunderpinsthisshift.Intheirrecentreview,Torreand
Lieberman(2018)identifiedanumberofplausiblemechanisms;theysuggestthat
(a)Labelsmaysimplybeaproxyforavaluableprocessofself-reflection,(b)that
labellingcouldfacilitatecomprehensionofacomplexemotionalstate,or(c)that
thetranslationoffeelingsintosymbolicmeaningallowscreationofdistancefrom
theself.Thoughthecurrentstudyofcoursedoesnotempiricallytestthesepossible
mechanisms,participants’talkofafeelingbeing“out”ofthemafterarticulatingit
maycontributetounderstandinginthisarea.Thatis,afocusontalkingasawayto
releaseemotionsfromtheself,ratherthansimplylesseningthem,suggeststhat
theactofsymbolicconversionintowordscouldofferasenseofdistancebetween
theselfandthefeeling(Torre&Lieberman,2018).Notably,thisalsoreflects
participants’invocationsofseparatenessfromtheirfeelings,astheseactsof
mentaldistancingmayfurtherfunctiontolessentheirintensity.
Consideringfindingsalongsidethewiderevidence,itappearsthatvoicing
one’sdifficultthoughtsandfeelingsisnotsimplyaformofself-expressionoraway
toelicitemotionalsupport,butpotentiallyanactofemotionregulationinandof
itself.TorreandLieberman(2018)havesuggestedthataffectlabellinglikelyalters
thebehaviouraleffectsofagivenemotion,includingmentalhealthoutcomes.For
instance,onestudyfoundthatparentsreporteddecreasedobservedanxietylevels

CHAPTERSEVEN:DISCUSSION
279
afteradolescentgirlsdocumentedtheiremotionalstatesindiaries(Thomassinet
al.,2012).Thus,thesenseofreleasethatparticipantsdescribedmaynotjust
attenuatemoreimmediatefeelingsbutmayalsofunctiontoreduceassociated
symptomsandbehaviours.Thisoffersarelativelystraightforwardopportunityto
providesupporttoadolescentsexperiencingmentalhealthsymptomatology,
includingemotionalsymptoms,simplythroughlistening.Indeed,articulatingand
workingthroughone’semotionsaloudisgenerallyacentralcomponentinalmost
alltherapeutictreatmentapproaches,foradolescentsandadultsalike(Cooper&
McLeod,2011;Greenberg&Watson,2015;Kegerreis&Midgley,2018;Pascual-
Leone&Greenberg,2007;Southam-Gerow&Kendall,2002).Aconceptual
emphasisonaffectlabellingaseitherspokenorwritten(Torre&Lieberman,2018)
suggestsitcouldbeusefultoofferalternativemethods,suchasdiaryentries,for
individualswhoexperiencediscomfortinsharingemotionswithothersorwhodo
notperceivethemselvestohaveclearsupportavenues,aswithJennifer.
However,itshouldbeconsideredthatthisactoftalkingaboutone’sfeelings
asamethodofemotionregulationmayrequiretheuseofparticularskills,which
notallyoungadolescentsmaypossess.Thatis,theabilitytoidentifyandmake
senseofthespecificfeaturesofone’semotionsandtothenverballyarticulate
themrequiresacertainlevelofemotionalself-awarenessandemotional
vocabulary,whichmayhaveimplicationsforvariousgroups.Attheindividuallevel,
thereareparticularconditionsandSENassociatedwithloweredemotional
awareness,suchasASD(Hilletal.,2004;Hobsonetal.,2006;Silanietal.,2008).
Therearealsopsychosocialfactorsthatmayinfluencesuchskills;forinstance,
parentstypicallyuseagreaternumberandvarietyofemotionwordswhen
engagingwithyoungdaughters,relativetosons(Fivush,2007;Fivushetal.,2000;
Zaman&Fivush,2013).TorreandLieberman(2018)havehighlightedthatitis
unclearwhethertheabilitytoinspectandarticulateone’semotionsinagranular
wayoffersmoreorlessbenefitintermsofaffectlabelling.Futureresearchshould
examinewhethergreateremotionalawarenessandemotionalvocabularyis
advantageousinthisprocess,withparticularattentiontohowthisaffectsgroupsof
individualslikelytoexperiencedifficultiesintheseareas.

CHAPTERSEVEN:DISCUSSION
280
7.6Meta-InferencesandImplicationsandDirectionsforFutureResearch
Havingoutlinedandexploredinferencesthatcanbedrawnfromfindings
acrossboththequantitativeandqualitativestrands,herethislearningisintegrated
tocreatemeta-inferences.AsdiscussedinSection4.4.1,thisapproachisconsistent
withthestudy’suseofmixedmethodstoachievecomplementarityacrossstrands
(Brymanetal.,2008;Greeneetal.,1989).Thesemeta-inferencesrepresentamore
comprehensiveunderstandingofmultipleriskexposureandemotionalsymptoms
amongearlyadolescentgirls,capturingtheinsightgeneratedbyconsideringboth
setsoffindingstogether.Itisimportanttonotethatbecausemeta-inferencesseek
togobeyondsimplydescribingdataandinsteadaimtocapturemeaningful
interpretationsoffindings,theresearcherisimplicatedintheconclusionsoffered
here.
Threemeta-inferencesweredevelopedinlightoftheinsightgenerated
througheachofthesestrands:
1. Emotionalsymptomsareembeddedindailylife;
2. Demandsandstresscanbepsychologicallyoverwhelming;and
3. Closerelationshipsarecritical.
Figure7.2(overleaf)illustrateshoweachofthesemeta-inferenceshasbeen
informedbythelearningandconclusionsdrawnwithineachindividualstrand.To
facilitateaccessibilityformixedaudiences,arecognisedissueinpresenting
integratedfindingsinmixedmethodsresearch(Sandelowski,2003),thisfigure
focusesontheconclusionsandinterpretationsalreadydrawnacrosseachstrand,
ratherthanonrawfindings.Forinstance,theboxesdowntheleft-handsidedonot
presentstatisticalinformationsuchassignificancevaluesorcoefficients,but
insteadpresenttheknowledgegeneratedinaddressingtheresearchquestion.

281
Figu
re7.2.M
eta-inferencesacrossthe
qua
ntita
tivean
dqu
alita
tivestrand
s.Qua
ntita
tiveinferencesaresh
ownon
theleft-han
dsid
ewith
inre
ctan
gularsha
pesa
nd
qualita
tiveinferencesaresh
ownon
therig
ht-han
dsid
ewith
inovalsha
pes,with
relevantre
searchque
stionsindicateddo
wneachside
.Meta-inferencesacrossb
oth
strand
saresh
owninth
ecentreofthe
figurewith
inro
unde
drectan
gularsha
pes,with
arrow
ssho
wingho
wth
eseareinform
edbyinferencesacrossthe
twostrand
s.

CHAPTERSEVEN:DISCUSSION
282
7.6.1Meta-InferenceOne:EmotionalSymptomsareEmbeddedinDailyLife
Bothquantitativeandqualitativefindingssuggestthatemotionalsymptoms
areinterwovenwithinearlyadolescentgirls’day-to-daylives.Experientially,
qualitativeparticipantsunderstoodthesesymptomsasacentralpartoftheirinner
worlds,constitutinganintense,andattimesunmanageable,collectionofintrusive
thoughtsandfeelings.Acrossbothstrandsofthestudy,findingssuggestthatitis
notjustthesymptomsthatarepresentindailylife,however,butalsothe
circumstanceswithwhichsuchsymptomsareintertwined.Thatis,emotional
symptomsareassociatedbothstatisticallyandexperientiallywithchallenges
embeddedinthecontextofdailylife,particularlyacrossfamilyandschoolcontexts.
Thesedailyexperiencespromptongoingfeelingsofstressandasensethatoneis
notabletocopewithorcontroleitherexternaldemandsorone’sownsymptoms
(asdiscussedinthefollowingsection).Takentogether,then,findingsacrossboth
strandsillustratethatemotionalsymptomscanbedeeplyembeddedwithinearly
adolescentgirls’day-to-daylives.
Theextenttowhichthesesymptomsappeartobemanifestedand
intertwinedasapartofdailylifeisworrying.Earlyadolescenceiswidelyconsidered
avulnerableperiodforemotionaldifficultiesamonggirlsandwomen,yetevenat
thisearlystagethereareclearindicationsthatthesesymptomscanbeanintensely
problematicareaofday-to-daylifeforsomegirls.Indeed,thequantitativesample
herewasfoundtohaveelevatedsymptomscomparedtonormsforthemeasure
used,withapproximatelyoneinfivereportingabnormallevelsofsymptomatology
(seeSection4.5.1).Theregularityandintensityofsuchdifficultiestherefore
emphasisesanethicalresponsibilityonthepartofresearchersandpractitionersto
understandandaddresstheseissues,particularlyforgirlsexperiencingadversity.
Asidefromthenegativeshort-andlong-termoutcomesassociatedwithemotional
symptomsinadolescence,thedailynatureoftheseexperiencessignalsathreatto
qualityoflifeamongthisgroup.Attentiontotheseissuesappearsespeciallyurgent
ifemotionalsymptomsanddisordersareindeedrisingamongadolescentgirls,as
theevidencecurrentlysuggests(Boretal.,2014;Collishawetal.,2010;Finketal.,
2015;Lessofetal.,2016;NHSDigital,2018).

CHAPTERSEVEN:DISCUSSION
283
Thus,thereisaneedtoconsiderhowsupportandinterventioncanbe
offeredinamannerthatissensitivetothedailycontextofthesedifficulties,ifwe
aretoeffectivelyworktoreducesymptomatologyandsupportqualityoflifeamong
thisgroup.Targetedinterventionsforadolescentmentalhealthsymptoms(e.g.,
CBTorcounselling)aretypicallydeliveredonaweeklybasis,oftenwithabrief
durationperiodvaryingfromfourto12weeksofregularsessions(e.g.,Dasetal.,
2016;Neufeld,Dunn,Jones,Croudace,&Goodyer,2017).Whilethisapproachcan
facilitatepositiveoutcomesforsomeadolescents(e.g.,Dasetal.,2016;Edbrooke-
Childsetal.,2018;McArthur,Cooper,&Berdondini,2013;Neufeldetal.,2017),
suchtreatmentsmayalsoserveonlyasashort-term“quickfix”thatdoesnot
reflecttheongoingrealityofyoungpeople’smentalhealthandwidercontexts
(Bondetal.,2004;Durham,2007).Thatis,brieftreatmentsmightnotbesufficient
inkeepingupwiththewaythatdifficultiessuchasemotionalsymptomsmanifest
asapartofdailylife,especiallyiftheyarenotdesignedtospecificallyaddressthe
widerongoingcircumstancesthatareoverwhelminganindividualinthefirstplace.
Itmaybethatgreaterdurationandregularityoftreatmentcouldbehelpful,
perhapsparticularlyinthecaseofschool-basedcounsellingwhereavailabilitycould
reasonablybeincreased.However,findingsherealsoemphasisetheneedforany
treatmentmadeavailabletobecoupledwitheffortstodevelopwidersystemsof
informalsupportthataremoreconsistentlyavailableandperhapspreferredfor
day-to-daysupport.Thisisexploredlaterinthischapterinthecontextofmeta-
inferencethree.
7.6.2Meta-InferenceTwo:DemandsandStresscanbePsychologically
Overwhelming
Findingsacrossbothstrandsofthestudyhaveclearlydemonstratedthat
theexperienceofmultipledemandscanbepsychologicallyoverwhelmingforearly
adolescentgirls,promptingstressandexceedingone’ssenseofcontrolandcoping
capacities.Furthermore,suchexperiencesandappraisalsappearlinkedwith
emotionalsymptomsamongthisgroup.Thisisevidentinquantitativeresults
aroundtheindirecteffectsofstressappraisalcomponentsaswellasinqualitative

CHAPTERSEVEN:DISCUSSION
284
findingsthatthedemandsofdailylifeactasapersistentandoverwhelmingsource
ofstress.Atitssimplestlevel,then,thestudyisabletoconcludethatagreaterlevel
ofdemandisoverwhelming,whichappearsrelatedtofeelingsofdepressionand
anxiety,thusofferingsupportforthestresshypothesis.However,therearea
numberofmorecomplexfacetstothisfindingwhenconsideringbothquantitative
andqualitativefindingstogether,raisingconsiderationsaroundthewaythatwe
thinkaboutandaddresstheseissues,bothinthelivesofearlyadolescentgirlsand
moregenerally.
Forinstance,itisimportanttonotethattheemphasisacrossbothstrands
ofthestudywasonpsychologicalstress.Bothstatisticallyandexperientially,
findingsindicatethatthelinkbetweenmultipleriskexposureandemotional
symptomsappearslargelyattributabletoanactive,conscioussenseofbeing
mentallyoverwhelmedandunabletocope.Thiscontrastswiththewiderresearch
landscapearoundmultipleriskexposureandthestresshypothesis,whichrarely
givesdirectconsiderationtothewaysinwhichindividualsperceiveandthinkabout
thesedemands.Cumulativerisktheory’sprioritisationofthenumberofriskfactors
oneisexposedtoreducescomplexexperiencestoequalunitsofmeasurementand,
indoingso,directlyoverlooksthemeaningofagivenfactortotheindividualand
theextenttowhichtheyappraiseittobeproblematic.Inthesameway,discussion
ofthestresshypothesisgenerallyfocusesonallostaticloadand,thus,physiological
stressresponsesystems(Evansetal.,2013),despiteevidenceofassociations
betweenphysiologicalandpsychologicalstress(e.g.,Oldehinkeletal.,2011;Sladek
etal.,2016;Zimmaroetal.,2016).Thus,thesetheoriesappeartofocusupon
underlyingmechanismsasthoughtheyentirelybypassindividualperceptionand
cognition,treatingpeopleasthoughtheysimplyexistpassivelyinriskylandscapes
ratherthanactivelyappraisingandnavigatingtheseexperiences.Thisischallenged
inthecurrentstudynotonlybyindicationsofindirecteffectsviastressappraisal
components,butalsothroughqualitativefindingsdemonstratingthecomplex
meaningsthatindividualsattachtoagivendemand.Here,suchappraisalswerenot
onlyinformedbythesituationathand,butalsobytheindividual’sinterpretationof
thateventwithintheirwidernarrativeovertimeandappraisalsofcontrollability.

CHAPTERSEVEN:DISCUSSION
285
Overall,then,findingsacrossthestudyprovidesupportforagreaterfocuson
psychologicalprocesseswithinriskandstressresearchmovingforward,bothfor
earlyadolescentgirlsandmoregenerally.Thiscouldbeexploredthroughsimilar
modelstothecurrentstudy,byacknowledgingandexploringunderlying
mechanismsofstressappraisal,orcouldperhapsinvolvemorenuanceddata
collectionmethods,suchasself-reportingofone’sappraisalsofspecificstressors
alongsideglobalstress.
Ofcourse,itshouldbenotedthatalthoughthecurrentstudyprovidesan
explorationofthestresshypothesisinmultipleriskexposure,itdoessowithina
highlyspecificcontextandpopulation.Asidefromthespecificityoftheparticular
riskfactorsexploredandthefocusonearlyadolescentgirls,itmayalsobe
particularlyrelevantthattheemphasishereisonemotionalsymptoms,whichtend
tomanifestinternally.AsnotedinChapterThree,thereareseveralother
hypotheses(beyondthestressmechanismexploredhere)astohowmultiplerisk
effectsoperate.Itmustbeconsideredthatthemechanismbywhichriskeffects
operatecouldbedependentupontheoutcomeofinterest.Thatis,feelingsof
distressandanxietyarearguablybynaturelikelytoresultfromfeelingsofbeing
overwhelmed.However,itmaybethatotherdisruptionstohealthand
developmentinthecontextofadversitycanbeattributedtoalternative
mechanisms.Forinstance,studiesshowthatmultipleriskeffectsnegativelyimpact
cognitivedevelopmentamongyoungchildren(Belskyetal.,2012;Burchinaletal.,
2000;Halletal.,2010);itistheoreticallyplausiblethatsucheffectsmightoccurvia
disruptiontoproximalprocessesofdevelopmentratherthansolelyduetostress.
Futurestudiesshouldseektomorecomprehensivelyexploredifferentriskeffect
mechanismsacrossarangeofpopulations,contexts,andoutcomes,todevelopa
morenuancedunderstandingofhowadversityimpactsuponchildrenandyoung
people’soutcomes.
Nevertheless,indicationsthattheexperienceofmultipledemandscanbe
overwhelmingandcanmakeonefeeloutofcontrolandunabletocopewarrants
seriousattentiontohowsuchfeelingscanbealleviatedamongadolescentgirls
experiencingadversity.Theparticularissuesthatyoungpeoplefaceinthecontext

CHAPTERSEVEN:DISCUSSION
286
ofadversityareoftenbeyondtheircontrol,ascanbeconsideredtruefortherisk
factorsfoundinthequantitativestrandandintheexperiencesofparticipantsinthe
qualitativestrand.Bothsetsoffindingsindicatethatearlyadolescentscannot
reasonablybeexpectedtoresolvethepresenceorintensityofagivenstressor,
particularlywhenattemptingtomanagenumerousdifferentchallengesacrosstheir
dailylives.Anyattemptstoallowyoungpeopletosharetheirconcernsorto
facilitatedevelopmentofcopingstrategiesandemotionregulationskillsare
arguablyinsufficientwithouteffortstodirectlyalleviatethepressuresthey
experienceinlife.Forinstance,schoolsmaybeabletoofferadaptationsforthose
experiencingemotionalsymptoms,suchasreducingacademicworkloadand
pressure,orcouldexplorewaystoprovidesupporttofamiliesexperiencingissues
inthehome.Asdiscussedearlierinthischapter,importantconcernshavebeen
raisedaboutimposingexpectationsofresilienceuponyoungpeoplewithout
consideringtheneedforsystemicchangesthatcanfacilitateequalopportunities
(Burman,2018;DeVerteuil&Golubchikov,2016;Ungar,2012).Bothpolicyand
researchneedstobesensitivetosuchissuesifwearetoaddressinequalitiesin
adolescentmentalhealth.
Indeed,thecomplexwaysinwhichthesedemandsareembeddedwithin
one’slifeandareappraisedandnavigatedbyindividualsperhapsalsonecessitates
considerationoftheterminologyanddiscourseof“risk”thatdominatesthe
adversityliterature.Conceptually,“risk”reflectsincreasedlikelihoodofnegative
outcomes,whichdoesneatlyencapsulatethestatisticalwayinwhichthis
phenomenonisexploredand,tosomeextent,emphasisesprobabilityratherthan
determinism(Zolkoski&Bullock,2012).However,thisterminologyperhapscannot
dojusticetothedynamicwayssuchfactorsactuallyoperateincontextandthe
mechanismscontributingtosucheffects.Thatis,inrealitytheeffectsof“risk
factors”arenotsimplyamatterofstatisticallikelihood,wherebyprobablyanearly
adolescentgirlfacingmultipleriskexposurewillspontaneouslybecomedepressed
andanxious.Instead,thesefactorsactaspersistentandaccumulativechallenges
thatthoseexperiencingadversitymustmanageonaday-to-daybasis,likelyfeeling
overwhelmedandattemptingtodrawonsupportfromfamilyandpeersasawayto

CHAPTERSEVEN:DISCUSSION
287
bolsterthemselvesagainstnegativeconsequences.Ithasbeenarguedelsewhere
thatthediscourseofrisk(andindeedresilience)servetolabelandstigmatizeat-
riskgroupswithlittleclearemphasisonactuallyresolvingthechallengesthatcause
themtobeatrisk(seeFollesø,2015;Foster&Spencer,2011).Findingshere
providefurtherindicationsthatthislanguagemayserveasapoorrepresentation
forthecomplicatedanddynamicchallengesthatyoungpeopleareactively
attemptingtocopewith,withlittlerealcapacitytochallengesuchsystems
themselves.Asthefieldmovesforwardwithagreaterfocusonexploringthe
complexetiologicalmechanismscontributingtodifferentialoutcomesamong
particulargroups,wemaywellneedashiftinlanguagethatencouragesinspection
ofwhythesegroupsare“atrisk”.Forinstance,afocuson“demands”,asisfoundin
thephysiologicalstressliterature,maymorecloselymatchtherealitythat“risk
factors”areasourceofdailystrainandchallengethatmaybedifficulttomanage
withoutsupport.Thereareofcourseexceptionstothis,suchasexaminationof
geneticfactors;however,researchfocusedonpsychologicalandsocio-cultural
influencesonhealthanddevelopmentmaybenefitfromgreaterattentiontothe
realityofhowsuchfactorsmanifestasastressfulpartofdailylife.Futureresearch
shouldseektoworktogetherwithyoungpeopleandpolicymakerstodevelopmore
nuancedandinclusivesystemsoflanguagethroughwhichtoexploretheseissues.
7.6.3Meta-InferenceThree:CloseRelationshipsareCritical
Thecurrentstudyhasprovidedclearevidencethatgreaterperceived
connectiontofamilyadultsandpeersplayacriticalroleforearlyadolescentgirls
experiencingadversity.Quantitatively,greaterperceivedconnectioninthese
domainswasassociatedwithloweredsymptomatology(thatis,promotiveforall
individuals)andalsomeantthatthoseexperiencinggreaterlevelsofriskwereless
(ratherthanmore)likelytoappraisetheirlivesasstressfulandexceedingtheir
copingcapacities.Qualitativefindingsrevealedthatearlyadolescentgirlssought
emotionalsupporttoreleasedifficultthoughtsandfeelings,withaparticular
emphasisoninformalavenuesbasedonrelationalqualitiesofcloseness,trust,and
care,aswellasperceivedavailability.

CHAPTERSEVEN:DISCUSSION
288
Takentogether,findingsindicatethatsupportiverelationshipswithclose,
trustedothersarehighlymeaningfulbothforstressappraisalandformanagement
andregulationofsymptoms.Thereare,ofcourse,subtledifferencesacrossthetwo
strandsinrelationtotheprecisecontextandrolethatotherpeopleplay.
Quantitativefindingsfocusonperceivedconnectionasmeaningfulforbothstress
appraisalandsymptoms,whilequalitativefindingsofferedinsightintotheroleof
moredirectivesupportseekingwithintheserelationshipsforalreadypresent
symptoms.AsoutlinedinChapterThree,connectionrelatesmoregenerallyto
interpersonalcloseness,whilesupportisconceptualisedasaspecificbehaviour
(Barrera,1986).Nevertheless,togetherfindingsemphasisethemeaningfulnessof
theserelationships,withparticipants’emphasisonrelationalqualitiesand
availabilityperhapsofferinginsightintowhyinformalrelationshipsappeartoplay
suchakeyroleinstressbuffering.Indeed,insightintotheroleofperceived
connectioninstressappraisalcouldalsobegleanedfromGrace’saccount,wherein
shementallyoffsetthehurtcausedbyhermum’sperceivedactionsbyfocusingon
thepositiverelationshipshehadwithherdad.Thatis,theapparentimportanceof
informalsocialconnectionscouldbeattributabletospecificinteractions,suchas
provisionofemotionalsupport,butcouldalsorelatetotheirroleasapositivepart
ofyoungpeople’slives,compensatingforandoffsettingthechallengestheyface.
Inquantitativemodellingofconditionalindirecteffectsandinqualitative
findings,parents/carers(andotherfamilyadults)appearedtoplaythemost
importantroleforthoseexperiencingdifficulties.Asexploredearlierinthis
chapter,theheightenedimportanceofparentalrelationshipsrelativetopeersis
particularlynotablegiventhatearlyadolescenceisapivotalmomentinsocial
relationships,whereinone’speersbegintobecomemorepredictiveofhealth
outcomes(Brown&Larson,2009;Umbersonetal.,2010).Assuch,findingsindicate
thatatleastinthisearlystageofadolescence,caringandsupportiveparental
relationshipscontinuetobestatisticallyandexperientiallymeaningfulforearly
adolescentgirlsexperiencingadversityand/oremotionalsymptoms.Future
researchshouldexploretrajectoriesacrosschildhoodandadolescencetoexplore

CHAPTERSEVEN:DISCUSSION
289
howindividualsdrawondifferentsocialrelationshipsovertime,withattentionto
whetherthisdiffersbasedonlevelsofadversityandsymptomatology.
Thisemphasisoninformalrelationshipoffersarelativelysimplemethodfor
supportingearlyadolescentgirlsandoffersanumberofimplicationsforhow
resourcescanbefocusedtofacilitatesocialsupportsystemsforthisgroup.Firstly,
inworkingtosupportanindividualfacingmultipledemandsand/orexperiencing
symptoms,itmaybebeneficialtojointlymapouttheirsupportnetworkinorderto
exploretheirperceivedavailabilityandqualityofsourcesofsupportacrossdaily
life.Itwouldalsobebeneficialtoinvolvebothfamiliesandpeersinsuchinstances,
offeringsupporttothemindevelopingtheappropriateknowledgeandskillsto
offereffectivesupport,asrecommendedinpreviousresearch(D’Avanzoetal.,
2012;Rickwoodetal.,2005).Althoughconnectiontoschooladultswasnotfound
tobemeaningfulacrosseitherstrandofthestudy,carefulconsiderationshould
alsobegiventohowmoreformalavenuesofsupportmightbemademore
appealingtoearlyadolescentgirls.Asexploredearlierinthischapter,training
aroundcounsellingandtherapeuticinterpersonalskillscouldaidschoolstaffin
developingrelationshipsthataremoremeaningfulforthisgroup.Itmayalsobe
usefultoensurethatthereareclearlyavailablestaffdedicatedtonon-academic
needs,suchaspastoralsupportandschoolcounsellors,givenindicationsthat
youngpeopledonotalwaysfeelitisateacher’sroletoofferemotionalsupport
(Boldero&Fallon,1995;Bowersetal.,2013;Rickwoodetal.,2005;Stapleyetal.,
2019).Thismaybeparticularlyimportantwherethehomeenvironmentis
consideredriskyorayoungpersonfeelsunabletoturntofamilyadultsforsupport.
Forinstance,inthecurrentstudyGracefirmlyfeltitwouldbeunhelpfultoaskher
mumforsupportandindeedviewedhermumasasubstantialpartofher
difficulties;althoughthisparticipanthadherdadtocompensateforthis,many
youngpeoplemaynothaveaccesstoamorepositivefamilialconnection.Future
researchshouldseektoexplorehowformalisedsupportnetworkscouldbuildon
theparticularqualitiesofferedwithininformalrelationshipsinordertoencourage
suchhelp-seekingbothgenerallyandforthosewithoutaccesstoqualityinformal
relationships.

CHAPTERSEVEN:DISCUSSION
290
7.7StrengthsandLimitations
Thecurrentstudyhasanumberofstrengthsbut,asinanystudy,isnot
withoutlimitations.Thissectionoffersareflectiononthestudydesignand
methodologicalapproachesutilisedhere,exploringhowtheyhavefacilitated
developmentofrobustandmeaningfulconclusionswhilealsoexaminingthe
boundariesofthislearning.Theseareasareexploredinturnforthequantitative
strand,thequalitativestrand,andtheoverarchingmixedmethodsdesign.
7.7.1QuantitativeStrand
StudyDesign
Thestudy’sobservationaldesignhasenabledexplorationofnaturally
occurringrelationshipsandprocesseswithinmultipleriskexposureandemotional
symptomsduringavulnerabledevelopmentalperiodforgirls.However,most
variablesweregatheredatonetimepointthroughtheWMFandthoughalmostall
riskvariablesweremeasuredusingearlierdata,theinabilitytocontrolforprior
levelsoftheoutcomevariablesmeansthistimelagcannotproperlyestablish
causality(A.L.Duckworthetal.,2010;Ployhart&Vandenberg,2010).Thus,
althoughSEMmodelsincludeddirectionalpathwaysspecifiedbasedontheoryand
priorresearch,causalitycannotbeassumedandcarehasbeentakeninpresenting
anddiscussingfindingstobesensitivetothistemporality.Furthermore,thereis
theoryandpriorevidencethatcouldalsosuggestbi-directionalityinthese
relationships.Forinstance,adolescentsexperiencingemotionalsymptomsmay
experiencegreaterdifficultyactivelymanagingdailystressors(P.Westetal.,2010),
whileindecisivenessandimpairmenttosocialfunctioningarerecognisedas
symptomsofdepression(AmericanPsychiatricAssociation,2013).Futurestudies
shouldexaminetheserelationshipsthroughalongitudinalpaneldesigntoexplore
directionalityovertime.
FocusonPatternsamongGirls
Thestudyfocusedongirlsinparticular,ratherthanexploringandcomparing
patternsandprocessesamongbothgirlsandboystoestablishgenderdifferences.

CHAPTERSEVEN:DISCUSSION
291
Consistentevidenceofhighratesofemotionalsymptomatologyanddisorder
amonggirlsandwomen,alongsideindicationsofearlyadolescenceasavulnerable
period,necessitateongoingfocusedinvestigationoftheparticularfactorsand
processescontributingtodifficultiesamongearlyadolescentgirls.Thus,this
approachoffersinsightintoaspecificphenomenonwithinavulnerablegroup,but
doesnotofferadirectcomparisonofthisrelationshipacrossgendergroups.
Findingscanaugmentwhatisalreadyknownacrossthewiderliteratureandfuture
researchcouldtestwhethertherearedifferentialcontributionsaccordingto
genderwithintheserelationshipsandprocesses.
However,itshouldalsobenotedthatthestudy’semphasison“girls”could
beconsideredproblematic,aswouldbetrueofastudyfocusingondifferences
between“girls”and“boys”.Theseapproachesareinherentlyreliantonabinary
conceptualisationofgender,whichimposesspecificexpectationsonotherwise
heterogeneousgroupsofindividualsandfailstoaccountfor(ordirectlyexamine)
individualswhoarenotcisgender.Itisimportanttonotethatthecurrentstudy
focusesonindividualsrecordedwithintheNPDasfemale(i.e.,sexwasusedinstead
ofgender),howevertherewasnoaccessiblerecordofwhethertheseindividuals
wouldallidentifythemselvesasgirls.Inthecurrentstudy,carehasbeentakento
beclearthatfindingsareinherentlyprobabilisticratherthanconclusiveforall
individualsandthusrefertobroadpatternsacrossthisgroup,ratherthanclear
outcomesforall.Here,useofsecondaryanalysismeantitwasnotpossibleto
measuregenderinamoreinclusivewaythatallowedparticipantstoidentify
themselvesas“girls”,butfuturestudiescouldseektodosofollowingthe
recommendationsofBauer,Braimoh,Scheim,andDharma(2017).However,it
shouldbenotedthatthespecificapproachappropriateinanygivenstudyis
perhapsnotstraightforwardinthisarea;thatis,itisarguedthatthereare
biologicalfactorsthatcontributetodifficultiesforfemales(asdiscussedinChapter
Two)aswellaspsychosocialfactorsthoughttoberelatedtogender,ratherthan
biologicalsex.Studiesshouldseektobecontextuallysensitivetosuchissues
dependingonthenatureoftheirresearch.

CHAPTERSEVEN:DISCUSSION
292
SamplingStrategyandSample
Thestudy’suseofdatagatheredprimarilyfortheevaluationofHeadStart
necessitatesconsiderationaboutexternalvalidityandthegeneralisabilityof
findings,giventhelackofrandomsampling.Thisapproachmeantthatparticipants
weredrawnfromlocalitieswhowereengagedinamentalhealthandwellbeing
programmeandhadbecomeinvolvedinthisprojectduetoarecognisedneedfor
additionalprovisionandawidercontextofdisadvantage.Firstly,then,itmustbe
consideredthatparticipantsinthecurrentstudyarelikelyexperiencinggreater
levelsofdisadvantageand,potentially,symptomatology.Indeed,asreportedin
Section4.5.1,thesampleshowedslightlyhigherthanaveragelevelsofFSM
eligibilityaswellaselevatedlevelsofemotionalsymptoms.However,giventhat
thestudyisspecificallyinterestedintheeffectsofmultipleriskexposureupon
symptoms,useofanat-risksampleoffersanappropriaterepresentationofthe
populationofinterest.InrelationtoengagementinHeadStart,thestudyfocused
onbaselinedataandsomostparticipantswerelikelytohaveexperiencedlimited
programmeengagementinthisearlystage.Thoughitwasnotpossibletocontrol
forengagementintheprogrammeintheanalysesundertakenhere,most
educationsettingsinEnglandcurrentlydeliversomeformofwellbeingandmental
healthprovision,tovaryingextents(Brown,2018).
Akeystrengthofthecurrentstudyisitstotalquantitativesampleof8,327
girls,aslargesamplesizesaregenerallyrecommendedwithinepidemiological
researchinordertoensuregreaterprecisioninestimates(Chan&Altman,2005;
Machinetal.,2018;Woodward,2014).Giventhatexistingstudiesintosomeofthe
factorsexploredherehaveoftenbeenlimitedbyuseofsmallersamplesizes,such
asSENandcaregivingresponsibilities,thestudyoffersmorerobustinferencesto
thisexistingknowledgebase.Furthermore,toavoidover-orunder-estimating
relationshipsthattendtooccurwithinlargesamplesizes,suchassmallp-values,
theeffectsizeofparameterswerealsoconsideredgivenunderstandingsthatlarge
effectsizescanaffectsuchvalues.
Measurement

CHAPTERSEVEN:DISCUSSION
293
Itshouldbenotedthatbecausethestudymakesuseofdataprimarily
gatheredfortheevaluationofHeadStart,thescopeandtypeofmeasurement
approacheswerenotdeterminedbytheauthorofthecurrentstudy.
Self-ReportMeasurement
Useofself-reportwasakeystrengthinseveralways.Firstly,current
perspectivesemphasisetheneedforyoungpeopletoreportontheirownmental
healthsymptoms,ratherthanrelyingonwiderinformantssuchasteacherand
parents(A.T.Beck,1963).Thisisparticularlyrelevantforresearchrelatedto
internalisingdifficulties,asstudieshaveshownthattherecanbeinformant
discrepanciesbetweenadolescentsandtheirparentsforsuchsymptoms,thought
tobebecausetheyarelessobservabletoothersrelativetoexternalisingdifficulties
(Fredrickson&Roberts,1997;Hammen,2005;Kuehner,2017;Nolen-Hoeksema,
1990,2001;Nolen-Hoeksema&Girgus,1994).Useofself-reporthasalsofacilitated
afocusonstressappraisal,asthisconstructcannotreasonablybereportedby
anyoneotherthantheindividualthemselves.Giventhatthisisakeycomponentof
stressprocesses(Deightonetal.,2014;Riley,2004),theabilitytoexplorestressas
perceivedbytheindividualhasallowedimportantinsightintotheroleof
psychologicalstressprocesseswithinmultipleriskeffects.Similarly,itisunderstood
thatsocialconnectionandasenseofengagementinareasoflifearemeaningfulfor
outcomesintermsofhowtheyareperceivedbyanindividualratherthanany
objectivemeasurementsystem.Thus,self-reportherehasallowedanoverarching
emphasisonthewayinwhichindividualsperceivetheseareasoftheirworldsand
themeaningthisoffers.
However,itshouldbenotedthatarelianceonasinglesource–here,self-
reportasusedformostvariables–canintroduceaformofcommonmethodsbias
intodataand,inturn,results.Specifically,gatheringthemajorityofdatafroma
singlesourcecanartificiallyheightenthesharedvarianceacrossvariables,
potentiallyinflatingresults(Conway&Lance,2010;Doty&Glick,1998).Itisargued
thatthismaybeheightenedincross-sectionalresearch,whereresponsesare
gatheredfromonesourceatasingletimepoint(Lindell&Whitney,2001).While
thisissueisnotconsideredtoinvalidateresearchresults,itnecessitatesalevelof

CHAPTERSEVEN:DISCUSSION
294
cautionininferringtherelationshipsbetweensuchvariables(Doty&Glick,1998).
Assuch,inthecurrentstudythereisaneedtobecautiousininterpreting
relationshipsbetweenemotionalsymptomsandstresscomponentsand
promotive/protectivevariables,respectively.Futureresearchcouldseektodrawon
multipleinformants,suchasself-reportalongsideparent-report,inordertocreate
integrateddata,preferablywithinalongitudinaldesign,tomorereliablyestablish
theserelationships.
Itisalsoimportanttonotethatthemeasuresutilisedherearenotwithout
limitations.Aparticularissueisthattheuseofa2-factorstructureforthePSS-4is
statisticallyproblematic,as2-itemfactorscanbeunstableandproducelessreliable
resultsrelativetomoreextensivecollectionsofitems(Brown,2015;MacCallumet
al.,1999;Raubenheimer,2004).Assuch,conclusionsrelatingtoperceivedstress
processesareofferedheretentativelyandfuturestudiesshouldseektoreplicate
thisfindingusingmorerobustmeasures.Fromatheoreticalperspective,2-item
measuresmightalsobeinsufficientinfullycapturingtheconstructofinterest.
Furthermore,althoughasoutlinedinSection4.6.1theSDQemotional
symptomssubscalehasgenerallybeenfoundtobereliableandvalid(Goodmanet
al.,1998),thismeasureisimperfect.Someoftheitemsshowedlowreadabilityfor
earlyadolescentsinarecentstudy(Patalayetal.,2018),whichmayhaveaffected
participants’responseshere.Furthermore,theuseofonlyfiveitemsmaynotbe
sufficienttocomprehensivelycaptureacomplexconstructsuchasemotional
symptoms,whichisindeedajointrepresentationofbothdepressiveandanxious
symptomatology.Notwithstandingtheseconsiderations,thissubscaleisgenerally
consideredacceptableandtheSDQwasrecentlynotedbyBentley,Hartley,and
Bucci(2019)asbeingapromisingself-reportmeasureforadolescentmentalhealth.
RiskMeasurement
Withtheexceptionofcaregivingresponsibilities,riskvariableswere
measuredusingproxyinformationfromtheNPD.Overall,thisapproachoffers
relativelyreliableinformation,asitrelatestovariablesthatareroutinelyrecorded
byschoolsandhaveoftenbeendesignatedthroughclearprocedures,suchas

CHAPTERSEVEN:DISCUSSION
295
classificationbyaprofessional(e.g.,SENstatusandCINstatusasaproxyforACEs),
useofsetcriteriaorscales(e.g.,FSMeligibilityforfamilyincome,academic
attainment,andIDACIforneighbourhoodsocioeconomiclevel),orrecordingof
fixedinformation(e.g.,monthofbirthforrelativeage).Nevertheless,itis
importanttonotethattheserepresentproxyvariablesformorecomplex
phenomenathatoftencannotbecomprehensivelycapturedforriskresearch
(Kraemeretal.,2005).Forinstance,participantsherewereconsideredtobeinan
at-riskSENgroupiftheyweredocumentedashavingSEN(withorwithouta
statementorEHCplan).However,asexploredearlierinthischapteritisnot
necessarilythepresenceofaspecialoradditionalneedthatisproblematic,but
insteadhavingcomplexneedswithinaneducationalsystemandwidersocietythat
isoftennotcongruentwiththeseneeds.Thus,theriskvariablesexploredinthe
currentstudyaretreatedasproxyindicatorsofwidersystemsofdailychallenge
andeffortshavebeentakentoensuresensitivitytothisdistinctioninpresenting
anddiscussingresults.
Furthermore,someoftheapproachesutilisedtomeasureparticularrisk
variableswerenotconsideredideal,suchascaregivingresponsibilitiesandACEs(as
discussedearlierinthischapter).Aspreviouslyoutlined,theuseofCINstatusasa
proxyforACEsovercomestherelianceonrecalltypicallyfoundinACEsresearch,
butalsoofferslimitedinformationandlikelyoverlooksmanyindividuals
experiencingACEsgiventhatitfocusesthoseinthemostextremecircumstances.
Indeed,manyoftheriskvariablesexploredherewerebinaryinnature,thus
offeringlimitedinformation;thoughthisisgenerallynotconsideredproblematicin
multipleriskresearchgivenfrequentuseofcumulativeriskindices,supportfor
latentmodellingoffersalternativesthatcouldincorporatemorenuancedrisk
informationinfutureresearch.
AnalyticalFocusandApproach
UseofSEMisaclearstrengthofthequantitativestrand,asthishas
facilitatedrobustexplorationofspecificpathwaysandprocessesaswellas
explorationofalternativemeasurementmodels,offeringinsightintothelimitations
ofthecumulativeriskindex(thoughasnoted,acumulativeriskindexhadtobe

CHAPTERSEVEN:DISCUSSION
296
utilisedinlateranalysesduetodifficultymodellingthelatentconstructinmore
complexmodels).Examinationofmultiplerisk,promotive,andprotectivevariables
simultaneously,respectively,hasenabledmorepreciseestimationoftheirrelative
contributionstoemotionalsymptoms,asseveralofthesefactorshaveoftenbeen
investigatedinisolationdespiteevidencethattheyfrequentlyco-occur.
However,theparticularvariablesandpathwaysexploredheremayhave
overlookedsomemorecomplexfeaturesoftheseprocesses.Forinstance,the
emphasisonsocialconnectionasabroadconstructdoesnotcapturethe
multidimensionalityofrelationshipsandsocannotshowwhetherparticular
relationshipcharacteristicssuchascloseness,conflict,andwarmthmayinfluence
stressbufferingprocesses.Intermsofthepathwaysinvestigated,afocuson
specificdirectionalpathwaysmayhaveoverlookedthepossibilityofmorecomplex
cyclicalrelationshipsamongthesevariables.Forinstance,anindividualmight
appraiseagivensituationasstressfulandsomaydrawactivelyonsocial
connectionstofindwaystomanagethisissue,inturnreducingappraisedstress.
Suchcomplexitiesemphasisetheneedtoincorporatequalitativeinquiryalongside
quantitativeinvestigationsinordertomorefullyunderstandthenuanceswithin
theseprocessesandrelationships.
7.7.2QualitativeStrand
AnalyticalDepth
UseofIPAhasfacilitatedarichandin-depthexplorationofhowearly
adolescentgirlsexperienceandmakesenseoftheiremotionalsymptomsandhow
thisrelatestowiderelementsofdemandandsupportsystems.Giventhatriskand
resilienceprocessesaretypicallyinvestigatedquantitatively,thislevelofdepthisa
particularstrengthofthestudy.Indeed,useofIPAspecificallyhasfacilitatedaclose
andidiographicunderstandingoflivedexperiencethatwouldnothavebeen
affordedbyotherqualitativeapproachesmorefocusedoncapturinggrouped
patternsofexperience,suchasthematicorcontentanalysis.Forinstance,thematic
analysisofthewiderHeadStartqualitativedatasetidentifiedtheparticularsocial

CHAPTERSEVEN:DISCUSSION
297
supportavenuesthatearlyadolescentstypicallyusedandexploredbarriersand
facilitatorstosupport-seeking(Stapleyetal.,2019).Thecurrentstudyexplored
theseexperiencesatamoremicroscopicleveland,indoingso,providedinsight
intothethinkinginformingthesedecisionsamongearlyadolescentgirls(thatis,
throughassessmentofrelationalqualities),aswellascapturingtheimmediate
emotionalbenefitsparticipantsexperiencedintalkingtothesecloseandtrusted
others.
DrawingDatafromWiderProject
Useofdataprimarilygatheredforawiderprojectshouldbeconsidered
here.ThescheduleusedinHeadStartinterviewsaimedtocoverbroadareasof
interestbutwasdesignedtofollowtheparticularexperiencesandareasraisedby
participants.Thisresultedinconsiderableheterogeneityacrossthesampleandthe
currentstudyrepresentsoneofseveralattemptsto“zoomin”andexplore
particularsubsetsofexperienceingreaterdepth.However,thismeantthatthe
specificphenomenaofinterestinthecurrentstudywerenotalwaysdirectly
probedininterviews.Inparticular,participantswerenotaskedwhetherbeingagirl
wasmeaningfultothemintheseparticularareasoftheirlivesandsoitwasnot
possibletoexplorewhethertheseexperiencesareconsideredbythemtobe
gendered.Assuch,itmustbeacknowledgedthatthisapproachhaslimitedthe
fullnesswithwhichRQ3canbeaddressed(i.e.,“Whatisitliketobeanearly
adolescentgirlexperiencingemotionalsymptomsinthecontextofrisk
exposure?”).Thatis,whilethethemesgarneredhereofferclearinsightintothe
waythattheseparticulargirlsmakesenseoftheirsymptomsandtheirouter
worlds,findingscannotbeconsideredtotellusthattheseexperiencesare
specificallyrelatedtotheiridentityas“girls”.Thisisanimportantdistinctionas
findingscannotthereforeofferclarityonperceiveddifferencesinexperiencesthat
mayariseasaresultofgender,whichwouldbeparticularlyusefulgiventhewidely
observedgendergapindepressiveandanxioussymptomatologyanddisorder.
Futureresearchshouldseektodirectlyexploreadolescentperspectivesonthe
influenceofgenderinmentalhealthexperiences,whichmayprovidefurtherinsight

CHAPTERSEVEN:DISCUSSION
298
intowhyearlyadolescenceappearstobeaparticularlyvulnerabletimeforgirlsin
particular(Epeletal.,2018).
Furthermore,itmayreasonablybethattherewereotherHeadStart
participantswhowereexperiencingemotionalsymptomsinthecontextofrisk
exposurebutdidnotdiscusstheseintheirinterview,eitherthroughchoiceorasa
resultofinterviewerquestioning.Hadindividualsbeendirectlyengagedin
interviewsforthepurposeofthecurrentstudy,awiderormorediversesample
maywellhavebeencapturedthroughamoredirectedfocus.
Sampling
Itshouldalsobeconsideredthattheparticularsamplingproceduresutilised
mayhaveoverlookedsomegroupsofindividuals.Participantswereselectedfor
inclusioninHeadStartinterviewsbyschoolstaff,whomayhavebeenbiased
towardsselectingparticulartypesofindividuals.Forinstance,youngpeople
consideredmorearticulatemayhavebeenprioritisedgivenuseofaspoken
interview,thuspotentiallyoverlookinggroupssuchasthosewithSENorlanguage
barriers.Furthermore,althoughtheprocessofselectingparticipantsforthecurrent
studyfromthewidersamplewascarefullymanagedandinvolvedconsultationwith
asecondaryresearcherandaclinicalreviewer,theapproachmayhavefavoured
particularwaysofexpressingandarticulatingemotionalsymptoms.Forinstance,
theremayhavebeenparticipantsexperiencingemotionalsymptomswhofocused
moreonfeelingsofangerorfrustrationintheiraccounts.Indeed,thereisresearch
toindicatethatfeelingsofangermayrepresentacomponentofdepressionamong
adolescents,beyondsimplyfeelingsofsadness(Stapleyetal.,2019).Thus,focusing
onemotionalsymptomsasidentifiedthroughparticularcriteriawithininterviews
maynothavecaptureddiverseexpressionsofemotionalsymptomsandcouldalso
haveoverlookedindividualsexperiencingcomorbidsymptomsanddisorders.
ExperientialFocus
Finally,theuseofexperientialaccountsanalysedthroughIPAnecessitates
sensitivitytotheboundariesofinferences.Anemphasisonperceptionsandsense-
makingisvaluableinunderstandingthewayphenomenaareunderstoodandhow

CHAPTERSEVEN:DISCUSSION
299
thisinformsdecisionsandactions.However,thissimultaneouslylimitsthecapacity
todeterminewhethertheissuesparticipantsdescribearereasonablejudgements
ofothers’actionsoraresultofnegativeinformationprocessing,whichasoutlined
iscommontoemotionalsymptoms.Thissubjectivityisconsistentwiththe
epistemologicalprinciplesofIPAanditsemphasisonunderstandingphenomenaas
theypresentthemselves;indeed,fromthisperspective,itcanbearguedthatthe
rationalityofyoungpeople’sjudgementsisnotofcentralconcern.However,itis
importanttonotethatthestudycannotofferconclusivenessinthisareaanditis
importantthatpractitionersnavigateandexplorethisdistinctiononan
individualisedbasis.Finally,asexploredinChapterFour,theinterpretivenatureof
IPAmeansthatfindingsinherentlycaptureresearcherinterpretations.Thisis
generallyconsideredvaluableastheresearchermaybeabletogeneratefurther
insightandmeaningthroughtheirinterpretationofparticipants’accounts(Larkin&
Thompson,2006;Mayoh&Onwuegbuzie,2015;Pietkiewicz&Smith,2014;Smith
etal.,2009).However,thisparticularfeatureofIPAmeansthatitisimportantfor
readerstokeepinmindthatfindingsandinferencesarenotofferedasasingular
anddefinitiveexplanationforparticipants’experiences,butareinsteadpresented
asonecredibleexplanation.
7.7.3MixedMethodsDesign
Akeystrengthofthecurrentstudyisitsmixedmethodsdesign.Asexplored
inSection4.4.1,thisapproachhasbeenutilisedforcomplementarity,offering
explorationofbothoverarchingpatternsandindividualexperience.Indeed,itcould
bearguedthatthespecificmethodsutilisedhereareparticularlydiverseintheir
levelsoffocus.Thatis,IPAhasahighlyidiographicemphasisnotfoundinall
qualitativeapproaches,whileSEMfitspre-specifiedstructuralmodelstodataand
thusoffersadeductive,variable-focusedapproachtotestingpathways.Theextent
ofthisdifferencemeansthatthestrengthsandlimitationsofeachapproacharein
starkcontrastand,thus,thestrengthsofeachapproachcanoffsettheother’s
limitationsparticularlywell.Forinstance,useofthematicanalysisinsteadofIPA
wouldnothaveencompassedanidiographicapproachorofferedsuchanalytical

CHAPTERSEVEN:DISCUSSION
300
depth,andwouldinsteadhavefocusedmorestronglyonsurface-levelgroup
patterns.Suchanapproach,thoughstillmoreinductivethanSEM,wouldnothave
offeredtheextentofcomplementarityalongsidethequantitativestrandthathas
beenfacilitatedbyuseofIPA.Indeed,asdemonstratedinthemeta-inferences
presentedearlier,integrationofthesediverseapproacheshasfacilitatedan
enrichedinsightthatcouldnothavebeengainedthrougheitheroneofthese
approachesinisolation,asistheaimincomplementarity(Greeneetal.,1989).The
richnessofintegrationofferedherehasalsobeenaidedbytheuseofanequal
weightapproach,withrecognitionthateachstrandoffersequallyrelevant
informationtobeconsideredindevelopingoverarchingconclusions.Furthermore,
ithaspreviouslybeenhighlightedthatuseofmultiplemethodsfor
complementaritycansupportgreatertransferabilityandexternalvalidityacrossthe
researchasawhole(Polit&Beck,2010).
Althoughtheseapproachesarefocallyandmethodologicallydissimilar,
therewasconsiderableoverlapandcomplementarityinrelationtotheway
particularphenomenawereinvestigatedacrossthesestrands,whichhasfacilitated
developmentofmeta-inferences.Boththevariablesusedinthequantitativestrand
andtheinterviewscheduleusedtofacilitatequalitativedatacollectionincludedan
emphasisonthechallengesthatat-riskgirlsface,ontheextenttowhichthey
perceivetheirlivestobestressful,andthewayinwhichsocialrelationshipscanbe
consideredmeaningful.Asaresult,thequantitativestrandhasfacilitatedan
understandingofbroadpatternsamongearlyadolescentgirls,whilequalitative
findingshaveofferedinsightintowhysuchpatternsmightexist.Forinstance,
quantitativeresultsindicatedthatfamilyandpeerrelationshipsaremeaningfulfor
howat-riskgirlsperceivethestressfulnessoftheirlives,whilequalitativefindings
suggestedthismaybebecausegirlspreferinformalsupportavenuesdueto
relationalqualities(asexploredinmeta-inferencethree).
Thestudy’suseofaparallelapproach,inwhicheachstrandisundertaken
concurrentlyandindependently,wasconsistentwithitsadoptionofmixed
methodsfordistinctresearchquestionsanditsemphasisoncomplementarity
(Greeneetal.,1989).Overall,then,thisapproachdidfittheneedsofthestudy;

CHAPTERSEVEN:DISCUSSION
301
however,thereweresomeunanticipatedaspectswithinbothstrandsforwhicha
levelofsequentialcontrolmighthavebeenvaluable.Forinstance,further
quantitativevariablescouldhavebeenincorporatedbasedonareasofqualitative
experiences,suchasacademicpressureorcontrollability.Conversely,itmighthave
beenvaluabletorecruitfurtherqualitativeparticipantswithdirectexperiencesof
relationshipsnotedinthequantitativestrand,suchascaregivingresponsibilitiesas
ariskfactor.Futureresearchcouldseektocarryoutanintegratedsequential
designthatcouldmorefluidlydeveloponanongoingbasis,suchasinvestigating
riskvariablesspecificallyoutlinedbyparticipants,or,conversely,identifying
participantsbasedonstatisticallyidentifiedriskfactorsorprofiles.
7.8SummaryandConclusions
Thecurrentstudysetouttodevelopknowledgeandunderstandingofearly
adolescentgirls’emotionalsymptomsinthecontextofmultipleriskexposure,with
particularattentiontomechanisms,adaptiveprocesses,andlivedexperience.The
study’squantitativestrandhasgeneratedknowledgeofthefactorsandprocesses
associatedwithsymptomsamongthisgroup,demonstratingthatstressappraisal
appearstoplayakeyroleinmultipleriskeffectsandthatinformalrelationshipscan
stronglyinfluencesuchappraisals.Qualitativeexplorationhasrevealedthatgirls
canfindsymptomsintenseandchallengingtomakesenseofandthatthey
experiencepersistentdemandsthatareperceivedtobebeyondtheircontrol,while
carefullyselectingindividualstoturntoforsupport.Takentogether,findingshave
shownthatemotionalsymptomsareanembeddedpartofdailylife,thatthe
demandsandstressearlyadolescentgirlsfacecanbepsychologically
overwhelming,andthatcloseandtrustedothersplayacriticalroleforgirls
experiencingadversity.
Thisresearchoffersanumberoforiginaltheoretical,methodological,and
practicalcontributionstoknowledgeandunderstanding.Thestudyhasrevealed
theinherentcomplexityofmultipleriskexposure,emphasisingtheimportanceof
exploringhowparticularfactorsinteractwithinanindividual’slifeandsuggesting
thatstressappraisalsandthemeaningattachedtotheseeventsplaysanimportant

CHAPTERSEVEN:DISCUSSION
302
role.Suchfindingshaveofferedacriticalperspectiveoncumulativerisktheoryand
highlighttheneedtogobeyondsimplytestingforthepresenceofcumulativerisk
effectsandinsteadexploringwhysucheffectsoccur.Alongsidethis,thestudy
demonstratestheimportanceofexaminingadaptiveprocessesandemphasisesthe
criticalroleofqualitysocialconnectionsamongearlyadolescentgirls’informal
networks.Thestudy’smixedmethodsdesignhasfacilitatedarichandnuanced
understandingoftheseriskandresilienceprocesses,demonstratingthevalueof
bringingtogetherdiverseworldviewsandmethodstodevelopourunderstandingof
theemergenceofemotionalsymptoms.Fundamentally,findingsrevealthatbeing
anearlyadolescentgirlinthecontextofadversitycanbeanintenseanddifficult
experiencewithlittlesenseofcontrol.Itisimperativethatfutureresearchand
practiceexploreswaystoreducetheextentofdemandplacedonadolescents
facingadversityandtofacilitateaccesstoqualitysupportsystems.

REFERENCES
303
References
Abramson,L.Y.,Metalsky,G.I.,&Alloy,L.B.(1989).Hopelessnessdepression:A
theory-basedsubtypeofdepression.PsychologicalReview,96,358–372.
https://doi.org/10.1037/0033-295X.96.2.358
Abramson,L.Y.,&Sackeim,H.A.(1977).Aparadoxindepression:Uncontrollability
andself-blame.PsychologicalBulletin,84,838–851.
Achenbach,T.M.(1966).Theclassificationofchildren’spsychiatricsymptoms:A
factor-analyticstudy.PsychologicalMonographs:GeneralandApplied,80(7),
1–37.https://doi.org/10.1037/h0093906
Ackerman,S.J.,Benjamin,L.S.,Beutler,L.E.,Gelso,C.J.,Goldfried,M.R.,Hill,C.,
Lambert,M.J.,Nocross,J.C.,Orlinsky,D.E.,&Jackson,R.(2001).Empirically
supportedtherapyrelationships:Conclusionsandrecommendationsforthe
Division29TaskForce.Psychotherapy:Theory,Research,Practice,38,495–
497.https://doi.org/10.1037/0033-3204.38.4.495
Aguinis,H.,Gottfredson,R.K.,&Joo,H.(2013).Best-practicerecommendationsfor
defining,identifying,andhandlingoutliers.OrganizationalResearchMethods,
16,270–301.https://doi.org/10.1177/1094428112470848
Akos,P.,&Galassi,J.P.(2004).Middleandhighschooltransitionsasviewedby
students,parents,andteachers.ProfessionalSchoolCounseling,7,212–221.
Albert,P.R.(2015).Whyisdepressionmoreprevalentinwomen?Journalof
PsychiatryandNeuroscience,40,219–221.
https://doi.org/10.1503/jpn.150205
Aldridge,J.(2006).Theexperiencesofchildrenlivingwithandcaringforparents
withmentalillness.ChildAbuseReview,15,79–88.
https://doi.org/10.1002/car.904
Alexander-Passe,N.(2006).Howdyslexicteenagerscope:Aninvestigationofself-
esteem,copinganddepression.Dyslexia,12,256–275.
https://doi.org/10.1002/dys.318
Allen,N.B.,&Badcock,P.B.T.(2003).Thesocialriskhypothesisofdepressed
mood:Evolutionary,psychosocial,andneurobiologicalperspectives.
PsychologicalBulletin,129,887–913.https://doi.org/10.1037/0033-

REFERENCES
304
2909.129.6.887
Alvord,M.K.,&Grados,J.J.(2005).Enhancingresilienceinchildren:Aproactive
approach.ProfessionalPsychology:ResearchandPractice,36,238–245.
https://doi.org/10.1037/0735-7028.36.3.238
AmericanPsychiatricAssociation.(2013).Diagnosticandstatisticalmanualof
mentaldisorders(5thed.).AmericanPsychiatricAssociation.
Anderson,S.F.,Salk,R.H.,&Hyde,J.S.(2015).Stressinromanticrelationshipsand
adolescentdepressivesymptoms:Influenceofparentalsupport.Journalof
FamilyPsychology,29,339–348.https://doi.org/10.1037/fam0000089
Angold,A.,&Costello,E.J.(1993).Depressivecomorbidityinchildrenand
adolescents:Empirical,theoretical,andmethodologicalissues.TheAmerican
JournalofPsychiatry,150,1779–1791.
https://doi.org/10.1176/ajp.150.12.1779
Angst,J.,Gamma,A.,Gastpar,M.,Lépine,J.P.,Mendlewicz,J.,&Tylee,A.(2002).
Genderdifferencesindepression:EpidemiologicalfindingsfromtheEuropean
DEPRESIandIIstudies.EuropeanArchivesofPsychiatryandClinical
Neuroscience,252,201–209.https://doi.org/10.1007/s00406-002-0381-6
Appelbaum,M.,Cooper,H.,Kline,R.B.,Mayo-Wilson,E.,Nezu,A.M.,&Rao,S.M.
(2018).Journalarticlereportingstandardsforquantitativeresearchin
psychology.AmericanPsychologist,73,3–25.
https://doi.org/10.1037/amp0000191
Appleyard,K.,Egeland,B.,Dulmen,M.H.M.Van,&Sroufe,L.A.(2005).When
moreisnotbetter:Theroleofcumulativeriskinchildbehavioroutcomes.
JournalofChildPsychologyandPsychiatry,46,235–245.
https://doi.org/10.1111/j.1469-7610.2004.00351.x
Babad,E.(2009).Thesocialpsychologyoftheclassroom.Routledge.
Baker,P.H.(2016).Managingstudentbehavior:Howreadyareteacherstomeet
thechallenge?AmericanSecondaryEducation,33(3),51–64.
Bakker,M.P.,Ormel,J.,Verhulst,F.C.,&Oldehinkel,A.J.(2010).Peerstressors
andgenderdifferencesinadolescents’mentalhealth:TheTRAILSstudy.
JournalofAdolescentHealth,46,444–450.
https://doi.org/10.1016/j.jadohealth.2009.10.002
REFERENCES
305
Bakx,A.,Koopman,M.,DeKruijf,J.,&DenBrok,P.(2015).Primaryschoolpupils’
viewsofcharacteristicsofgoodprimaryschoolteachers:Anexploratory,open
approachforinvestigatingpupils’perceptions.TeachersandTeaching:Theory
andPractice,21,543–564.https://doi.org/10.1080/13540602.2014.995477
Balázs,J.,Miklõsi,M.,Keresztény,Á.,Hoven,C.W.,Carli,V.,Wasserman,C.,Apter,
A.,Bobes,J.,Brunner,R.,Cosman,D.,Cotter,P.,Haring,C.,Iosue,M.,Kaess,
M.,Kahn,J.P.,Keeley,H.,Marusic,D.,Postuvan,V.,Resch,F.,…Wasserman,
D.(2013).Adolescentsubthreshold-depressionandanxiety:Psychopathology,
functionalimpairmentandincreasedsuiciderisk.JournalofChildPsychology
andPsychiatryandAlliedDisciplines,54,670–677.
https://doi.org/10.1111/jcpp.12016
Bandura,A.(1997).Self-efficacy:Theexerciseofcontrol.W.H.Freemanand
Company.
Bandura,A.,Pastorelli,C.,Barbaranelli,C.,&Caprara,G.V.(1999).Self-efficacy
pathwaystochildhooddepression.JournalofPersonalityandSocial
Psychology,76,258–269.https://doi.org/10.1037/0022-3514.76.2.258
Banerjee,R.A.(2008).Socialcognitionandanxietyinchildren.InC.Sharp,P.
Fonagy,&I.Goodyer(Eds.),Socialcognitionanddevelopmental
psychopathology(pp.239–269).OxfordUniversityPress.
Banks,P.,Cogan,N.,Deeley,S.,Hill,M.,Riddell,S.,&Tisdall,K.(2001).Seeingthe
invisiblechildrenandyoungpeopleaffectedbydisability.Disability&Society,
16,797–814.https://doi.org/10.1080/09687590120083967
Barber,B.K.(2013).Politicalconflictandyouth.Psychologist,26,336–339.
https://doi.org/10.1111/jcpp.12056
Barch,D.,Pagliaccio,D.,Belden,A.,Harms,M.P.,Gaffrey,M.,Sylvester,C.M.,
Tillman,R.,&Luby,J.(2016).Effectofhippocampalandamygdalaconnectivity
ontherelationshipbetweenpreschoolpovertyandschool-agedepression.
AmericanJournalofPsychiatry,173,625–634.
https://doi.org/10.1176/appi.ajp.2015.15081014
Barker,G.(2007).Adolescents,socialsupportandhelp-seekingbehaviour:An
internationalliteraturereviewandprogrammeconsultationwith
recommendationsforaction.WorldHealthOrganization.

REFERENCES
306
Barnes,A.J.(2016).Childhoodstressandresilience.InM.R.Korin(Ed.),Health
PromotionforChildrenandAdolescents(pp.85–98).Springer.
Baron,R.M.,&Kenny,D.A.(1986).Themoderator-mediatorvariabledistinctionin
socialpsychologicalresearch:Conceptual,strategic,andstatistical
considerations.JournalofPersonalityandSocialPsychology,51,1173–1182.
https://doi.org/10.1037/0022-3514.51.6.1173
Barrera,M.J.(1986).Distinctionsbetweensocialsupportconcepts,measures,and
models.AmericanJournalofCommunityPsychology,14,413–446.
https://doi.org/10.1007/BF00922627
Bauer,G.R.,Braimoh,J.,Scheim,A.I.,&Dharma,C.(2017).Transgender-inclusive
measuresofsex/genderforpopulationsurveys:Mixedmethodsevaluation
andrecommendations.PLoSONE,12(5),e0178043.
https://doi.org/10.1371/journal.pone.0178043
Bayer,J.K.,Ukoumunne,O.C.,Mathers,M.,Wake,M.,Abdi,N.,&Hiscock,H.
(2012).Developmentofchildren’sinternalisingandexternalisingproblems
frominfancytofiveyearsofage.AustralianandNewZealandJournalof
Psychiatry,46,659–668.https://doi.org/10.1177/0004867412450076
BBC.(2010,November16).Numberofchildcarers“fourtimespreviousestimate.”
BBCNews.
Beck,A.T.(1963).Thinkinganddepression:I.Idiosyncraticcontentandcognitive
distortions.ArchivesofGeneralPsychiatry,9,324–333.
https://doi.org/10.1001/archpsyc.1963.01720160014002
Beck,A.T.(1974).Cognition,affect,andpsychopathology.InR.E.Nisbett(Ed.),
Thoughtandfeeling:Cognitivealternationoffeelingstates(pp.127–140).
Routledge.
Beck,A.T.,&Clark,D.A.(1988).Anxietyanddepression:Aninformationprocessing
perspective.AnxietyResearch,1,23–36.
https://doi.org/10.1080/10615808808248218
Beck,A.T.,Rush,J.,Shaw,B.F.,&Emery,G.(1979).Cognitivetherapyof
depression.GuilfordPress.
Beck,J.S.(1995).Cognitivetherapy:Basicsandbeyond.GuilfordPress.
Becker,K.D.,Ginsburg,G.S.,Domingues,J.,&Tein,J.Y.(2010).Maternalcontrol

REFERENCES
307
behaviorandlocusofcontrol:Examiningmechanismsintherelationbetween
maternalanxietydisordersandanxietysymptomatologyinchildren.Journalof
AbnormalChildPsychology,38,533–543.https://doi.org/10.1007/s10802-010-
9388-z
Belfer,M.L.(2008).Childandadolescentmentaldisorders:Themagnitudeofthe
problemacrosstheglobe.JournalofChildPsychologyandPsychiatryandAllied
Disciplines,49,226–236.https://doi.org/10.1111/j.1469-7610.2007.01855.x
Belsky,J.,Schlomer,G.L.,&Ellis,B.J.(2012).Beyondcumulativerisk:
Distinguishingharshnessandunpredictabilityasdeterminantsofparenting
andearlylifehistorystrategy.DevelopmentalPsychology,48,662–673.
https://doi.org/10.1037/a0024454
Ben-Zur,H.(2019).Transactionalmodelofstressandcoping.InV.Zeigler-Hill&T.
K.Shackelford(Eds.),Encyclopediaofpersonalityandindividualdifferences.
Springer.https://doi.org/10.1007/978-3-319-28099-8_2128-1
Bennett,D.A.(2001).HowcanIdealwithmissingdatainmystudy?Australianand
NewZealandJournalofPublicHealth,25,464–469.
https://doi.org/10.1111/j.1467-842X.2001.tb00294.x
Bennett,D.S.,Ambrosini,P.J.,Kudes,D.,Metz,C.,&Rabinovich,H.(2005).Gender
differencesinadolescentdepression:Dosymptomsdifferforboysandgirls?
JournalofAffectiveDisorders,89,35–44.
https://doi.org/10.1016/j.jad.2005.05.020
Bentley,N.,Hartley,S.,&Bucci,S.(2019).Systematicreviewofself-report
measuresofgeneralmentalhealthandwellbeinginadolescentmentalhealth.
ClinicalChildandFamilyPsychologyReview,22,225–252.
https://doi.org/10.1007/s10567-018-00273-x
Benzies,K.,&Mychasiuk,R.(2009).Fosteringfamilyresiliency:Areviewofthekey
protectivefactors.ChildandFamilySocialWork,14,103–114.
https://doi.org/10.1111/j.1365-2206.2008.00586.x
Berke,D.S.,Reidy,D.,&Zeichner,A.(2018).Masculinity,emotionregulation,and
psychopathology:Acriticalreviewandintegratedmodel.ClinicalPsychology
Review,66,106–116.https://doi.org/10.1016/j.cpr.2018.01.004
BevanJones,R.,Thapar,A.,Stone,Z.,Thapar,A.,Jones,I.,Smith,D.,&Simpson,S.

REFERENCES
308
(2018).Psychoeducationalinterventionsinadolescentdepression:A
systematicreview.PatientEducationandCounseling,101,804–816.
https://doi.org/10.1016/j.pec.2017.10.015
Biederman,J.,Milberger,S.,Faraone,S.V.,Kiely,K.,Guite,J.,Mick,E.,,Ablon,S.,
Warburton,R.,&Reed,E.(1995).Family-environmentriskfactorsfor
attention-deficithyperactivitydisorder:AtestofRutter’sindicatorsof
adversity.ArchivesofGeneralPsychiatry,52,464–470.
https://doi.org/10.1001/archpsyc.1995.03950180050007
Biggerstaff,D.,&Thompson,A.R.(2008).Interpretativephenomenologicalanalysis
(IPA):Aqualitativemethodologyofchoiceinhealthcareresearch.Qualitative
ResearchinPsychology,5,214–224.
https://doi.org/10.1080/14780880802314304
Birhamer,B.,Ryan,N.D.,Williamson,D.E.,Brent,D.A.,Kaufman,J.,Dahl,R.E.,
Perel,J.,&Nelson,B.(1996).Childhoodandadolescentdepression:Areview
ofthepast10years.PartI.JournaloftheAmericanAcademyofChildand
AdolescentPsychiatry,35,1427–1439.https://doi.org/10.1097/00004583-
199611000-00011
Blakemore,S.J.(2018).Inventingourselves:Thesecretlifeoftheteenagebrain.
PublicAffairsBooks.
Blomfield,C.J.,&Barber,B.L.(2011).Developmentalexperiencesduring
extracurricularactivitiesandAustralianadolescents’self-concept:Particularly
importantforyouthfromdisadvantagedschools.JournalofYouthand
Adolescence,40,582–594.https://doi.org/10.1007/s10964-010-9563-0
Bolas,H.,VanWersch,A.,&Flynn,D.(2007).Thewell-beingofyoungpeoplewho
careforadependentrelative:Aninterpretativephenomenologicalanalysis.
PsychologyandHealth,22,829–850.
https://doi.org/10.1080/14768320601020154
Boldero,J.,&Fallon,B.(1995).Adolescents’help-seeking:Whatdotheygethelp
forandfromwhom?JournalofAdolescence,18,193–209.
https://doi.org/10.1006/jado.1995.1013
Bolognini,M.,Plancherel,B.,Bettschart,W.,&Halfon,O.(1996).Self-esteemand
mentalhealthinearlyadolescence:Developmentandgenderdifferences.

REFERENCES
309
JournalofAdolescence,19,233–245.https://doi.org/10.1006/jado.1996.0022
Bond,L.,Butler,H.,Thomas,L.,Carlin,J.,Glover,S.,Bowes,G.,&Patton,G.(2007).
Socialandschoolconnectednessinearlysecondaryschoolaspredictorsoflate
teenagesubstanceuse,mentalhealth,andacademicoutcomes.Journalof
AdolescentHealth,40,9–18.https://doi.org/10.1016/j.jadohealth.2006.10.013
Bond,L.,Carlin,J.B.,Thomas,L.,Rubin,K.,&Patton,G.(2001).Doesbullyingcause
emotionalproblems?Aprospectivestudyofyoungteenagers.BMJ,323,480–
484.https://doi.org/10.1136/bmj.323.7311.480
Bond,L.,Patton,G.,Glover,S.,Carlin,J.B.,Butler,H.,Thomas,L.,&Bowes,G.
(2004).TheGatehouseProject:Canamultilevelschoolinterventionaffect
emotionalwellbeingandhealthriskbehaviours?JournalofEpidemiologyand
CommunityHealth,58(12),997–1003.
https://doi.org/10.1136/jech.2003.009449
Bond,L.,Toumbourou,J.W.,Thomas,L.,Catalano,R.F.,&Patton,G.(2005).
Individual,family,school,andcommunityriskandprotectivefactorsfor
depressivesymptomsinadolescents:Acomparisonofriskprofilesfor
substanceuseanddepressivesymptoms.PreventionScience,6,73–88.
https://doi.org/10.1007/s11121-005-3407-2
Bor,W.,Dean,A.J.,Najman,J.,&Hayatbakhsh,R.(2014).Arechildandadolescent
mentalhealthproblemsincreasinginthe21stcentury?Asystematicreview.
TheAustralianandNewZealandJournalofPsychiatry,48,606–616.
https://doi.org/10.1177/0004867414533834
Borelli,J.L.,Margolin,G.,&Rasmussen,H.F.(2015).Parentalovercontrolasa
mechanismexplainingthelongitudinalassociationbetweenparentandchild
anxiety.JournalofChildandFamilyStudies,24,1559–1574.
https://doi.org/10.1007/s10826-014-9960-1
Borsboom,D.,Mellenbergh,G.J.,&VanHeerden,J.(2003).Thetheoreticalstatus
oflatentvariables.PsychologicalReview,110,203–219.
https://doi.org/10.1037/0033-295X.110.2.203
Bosacki,S.,Dane,A.,&Marini,Z.(2007).Peerrelationshipsandinternalizing
problemsinadolescents:Mediatingroleofself-esteem.Emotionaland
BehaviouralDifficulties,12,261–282.

REFERENCES
310
https://doi.org/10.1080/13632750701664293
Bottrell,D.(2009).Understanding“marginal”perspectives:Towardsasocialtheory
ofresilience.QualitativeSocialWork,8,321–339.
https://doi.org/10.1177/1473325009337840
Boudreault-Bouchard,A.M.,Dion,J.,Hains,J.,Vandermeerschen,J.,Laberge,L.,&
Perron,M.(2013).Impactofparentalemotionalsupportandcoercivecontrol
onadolescents’self-esteemandpsychologicaldistress:Resultsofafour-year
longitudinalstudy.JournalofAdolescence,36,695–704.
https://doi.org/10.1016/j.adolescence.2013.05.002
Bovier,P.A.,Chamot,E.,&Perneger,T.V.(2004).Perceivedstress,internal
resources,andsocialsupportasdeterminantsofmentalhealthamongyoung
adults.QualityofLifeResearch,13,161–170.
https://doi.org/10.1023/B:QURE.0000015288.43768.e4
Bowers,H.,Manion,I.,Papadopoulos,D.,&Gauvreau,E.(2013).Stigmainschool-
basedmentalhealth:Perceptionsofyoungpeopleandserviceproviders.Child
andAdolescentMentalHealth,18,165–170.https://doi.org/10.1111/j.1475-
3588.2012.00673.x
Boyd,C.P.,Hayes,L.,Nurse,S.,Aisbett,D.,Francis,K.,Newnham,K.,&Sewell,J.
(2011).Preferencesandintentionofruraladolescentstowardseekinghelpfor
mentalhealthproblems.RuralandRemoteHealth,11,1582–1595.
Boyle,M.H.,&Lipman,E.L.(2002).Doplacesmatter?Socioeconomicdisadvantage
andbehavioralproblemsofchildreninCanada.JournalofConsultingand
ClinicalPsychology,70,378–389.https://doi.org/10.1037//0022-
006X.70.2.378
Brady,E.U.,&Kendall,P.C.(1992).Comorbidityofanxietyanddepressionin
childrenandadolescents.PsychologicalBulletin,111,244–255.
https://doi.org/10.1037/0033-2909.111.2.244
Branje,S.J.T.,Hale,W.W.,Frijns,T.,&Meeus,W.H.J.(2010).Longitudinal
associationsbetweenpercievedparent-childrelationshipqualityand
depressivesymptomsinadolescence.JournalofAbnormalChildPsychology,
38,751–763.https://doi.org/10.1007/s10802-010-9401-6
Brattesani,K.A.,Weinstein,R.S.,&Marshall,H.H.(1984).Studentperceptionsof

REFERENCES
311
differentialteachertreatmentasmoderatorsofteacherexpectationeffects.
JournalofEducationalPsychology,1984,236–247.
https://doi.org/10.1037/0022-0663.76.2.236
Brazil,N.,&Clark,W.A.V.(2017).Individualmentalhealth,lifecourseeventsand
dynamicneighbourhoodchangeduringthetransitiontoadulthood.Healthand
Place,45,99–109.https://doi.org/10.1016/j.healthplace.2017.03.007
Breakwell,G.M.(1986).Copingwiththreatenedidentities.Methuen.
Breen,A.V.,Lewis,S.P.,&Sutherland,O.(2013).Briefreport:Non-suicidalself-
injuryinthecontextofselfandidentitydevelopment.JournalofAdult
Development,20,57–62.https://doi.org/10.1007/s10804-013-9156-8
Brener,N.D.,Danice,K.E.,Kann,L.,Grunbaum,J.A.,Gross,L.A.,Kyle,T.M.,&
Ross,J.G.(2006).Theassociationofsurveysettingandmodewithself-
reportedhealthriskbehaviorsamonghighschoolstudents.PublicOpinion
Quarterly,70,354–374.https://doi.org/10.1093/poq/nfl003
Brent,D.A.,Poling,K.,McKain,B.,&Baugher,M.(1993).Apsychoeducational
programforchildrenofaffectivelyillchildrenandadolescents.Journalofthe
AmericanAcademyofChild&AdolescentPsychiatry,32,770–774.
https://doi.org/10.1097/00004583-199307000-00010
Brereton,A.V.,Tonge,B.J.,&Einfeld,S.L.(2006).Psychopathologyinchildrenand
adolescentswithautismcomparedtoyoungpeoplewithintellectualdisability.
JournalofAutismandDevelopmentalDisorders,36,863–870.
https://doi.org/10.1007/s10803-006-0125-y
Brinkmann,S.(2014).Interview.InT.Teo(Ed.),EncyclopediaofCriticalPsychology
(pp.1008–1010).SpringerUS.https://doi.org/10.1007/978-1-4614-5583-7
Brinkmann,S.,&Kvale,S.(2015).Interviews:Learningthecraftofqualitative
researchinterviewing.SAGEPublications.
BritishEducationalResearchAssociation.(2011).Ethicalguidelinesforeducational
research.InBritishEducationalResearchAssociation.
Britten,N.(1995).Qualitativeinterviewsinmedicalresearch.BMJ,311,251–253.
https://doi.org/10.1136/bmj.311.6999.251
Brock,R.L.,&Kochanska,G.(2015).Interparentalconflict,children’ssecuritywith
parents,andlong-termriskofinternalizingproblems:Alongitudinalstudy

REFERENCES
312
fromages2to10.DevelopmentandPsychopathology,28,45–54.
https://doi.org/10.1017/S0954579415000279
Brocki,J.M.,&Wearden,A.J.(2006).Acriticalevaluationoftheuseof
interpretativephenomenologicalanalysis(IPA)inhealthpsychology.
PsychologyandHealth,21,87–108.
https://doi.org/10.1080/14768320500230185
Brody,G.H.,Yu,T.,Chen,E.,Miller,G.E.,Kogan,S.M.,&Beach,S.R.H.(2013).Is
resilienceonlyskindeep?:RuralAfricanAmericans’socioeconomicstatus-
relatedriskandcompetenceinpreadolescenceandpsychologicaladjustment
andallostaticloadatage19.PsychologicalScience,24,1285–1293.
https://doi.org/10.1177/0956797612471954
Bronfenbrenner,U.(1979).Theecologyofhumandevelopment:Experimentsby
natureanddesign.HarvardUniversityPress.
Bronfenbrenner,U.(1999).Environmentsindevelopmentalperspective:
Theoreticalandoperationalmodels.InS.L.Friedman&T.D.Wachs(Eds.),
Measuringenvironmentacrossthelifespan:Emergingmethodsandconcepts
(pp.3–28).PsychologicalAssociationPress.
Brooks-Gunn,J.,&Duncan,G.J.(1997).Theeffectsofpovertyonchildren.The
FutureofChildren,7(2),55–71.https://doi.org/10.2307/1602387
Brown,B.B.,&Larson,J.(2009).Peerrelationshipsinadolescence.InRichardM.
Lerner&L.Steinberg(Eds.),Handbookofadolescentpsychology:VolumeTwo:
Contextualinfluencesonadolescentdevelopment(Vol.2,pp.74–103).John
Wiley&Sons,Inc.
Brown,G.W.,&Harris,T.O.(1978).Socialoriginsofdepression:Astudyof
psychiatricdisorderinwomen.FreePress.
Brown,J.,Cohen,P.,Johnson,J.G.,&Salzinger,S.(1998).Alongitudinalanalysisof
riskfactorsforchildmaltreatment:Findingsofa17-yearprospectivestudyof
officiallyrecordedandself-reportedchildabuseandneglect.ChildAbuse&
Neglect,22,1065–1078.https://doi.org/10.1016/S0145-2134(98)00087-8
Brown,R.(2018).Mentalhealthandwellbeingprovisioninschools.
Brown,T.A.(2015).Confirmatoryfactoranalysisforappliedresearch(2nded.).The
GuilfordPress.

REFERENCES
313
Brown,T.A.,&Moore,M.T.(2012).Confirmatoryfactoranalysis.InRickH.Hoyle
(Ed.),Handbookofstructuralequationmodellng(pp.361–379).TheGuilford
Press.
Bryman,A.(2006).Integratingquantitativeandqualitativeresearch:Howisit
done?QualitativeResearch,6,97–113.
https://doi.org/10.1177/1468794106058877
Bryman,A.(2007).Barrierstointegratingquantitativeandqualitativeresearch.
JournalofMixedMethodsResearch,1,8–22.
https://doi.org/10.1177/2345678906290531
Bryman,A.(2008).Theendoftheparadigmwars?InP.Alasuutari,L.Bickman,&J.
Brannen(Eds.),TheSAGEhandbookofsocialresearchmethods(pp.13–25).
SAGEPublications.
Bryman,A.,Becker,S.,&Sempik,J.(2008).Qualitycriteriaforquantitative,
qualitativeandmixedmethodsresearch:Aviewfromsocialpolicy.
InternationalJournalofSocialResearchMethodology,11,261–276.
https://doi.org/10.1080/13645570701401644
Buist,K.L.,Deković,M.,&Prinzie,P.(2013).Siblingrelationshipqualityand
psychopathologyofchildrenandadolescents:Ameta-analysis.Clinical
PsychologyReview,33,97–106.https://doi.org/10.1016/j.cpr.2012.10.007
Bukowski,W.M.,Bergevin,T.,&Miners,R.(2011).Socialdevelopment.InA.Slater
&G.Bremner(Eds.),Anintroductiontodevelopmentalpsychology(pp.551–
584).BPSBlackwell.
Burchinal,M.R.,Roberts,J.E.,Hooper,S.,&Zeisel,S.A.(2000).Cumulativeriskand
earlycognitivedevelopment:Acomparisonofstatisticalriskmodels.
DevelopmentalPsychology,36,793–807.https://doi.org/10.1037/0012-
1649.36.6.793
Burke,H.M.,Davis,M.C.,Otte,C.,&Mohr,D.C.(2005).Depressionandcortisol
responsestopsychologicalstress:Ameta-analysis.Psychoneuroendocrinology,
30,846–856.https://doi.org/10.1016/j.psyneuen.2005.02.010
Burklund,L.J.,DavidCreswell,J.,Irwin,M.R.,&Lieberman,M.D.(2014).The
commonanddistinctneuralbasesofaffectlabelingandreappraisalinhealthy
adults.FrontiersinPsychology,5,221–230.

REFERENCES
314
https://doi.org/10.3389/fpsyg.2014.00221
Burman,E.(2018).(Re)sourcingthecharacterandresiliencemanifesto:
Suppresionsandslippagesof(re)presentationandselectiveaffectivities.
SociologicalResearchOnline,23,416–437.
https://doi.org/10.1177/1360780418769671
Burns,D.D.(1980).Feelinggood:Thenewmoodtherapy.Signet.
Cacioppo,J.T.,&Patrick,W.(2008).Humannatureandtheneedforsocial
connection.W.W.Norton&Company,Inc.
Caprara,G.V.,DiGiunta,L.,Eisenberg,N.,Gerberino,M.,Pastorelli,C.,&
Tramontano,C.(2008).Assessingregulatoryemotionalself-efficacyinthree
countries.PsychologicalAssessment,32,736–740.
https://doi.org/10.1371/journal.pone.0178059
Carbonell,D.M.,Ph,D.,Reinherz,H.Z.,Sc,D.,Giaconia,R.M.,Stashwick,C.K.,
Paradis,A.D.,&Beardslee,W.R.(2002).Promotingresilienceinyoungadults
atriskfordepression.ChildandAdolescentSocialWorkJournal,19,393–413.
https://doi.org/10.1023/A:1020274531345
Carlisle,N.,&Rofes,E.(2007).Schoolbullying:Doadultsurvivorsperceivelong-
termeffects?Traumatology,13,16–26.
https://doi.org/10.1177/1534765607299911
Carlson,M.D.A.,&Morrison,R.S.(2009).Studydesign,precision,andvalidityin
observationalstudies.JournalofPalliativeMedicine,12,77–82.
https://doi.org/10.1089/jpm.2008.9690
Cauce,A.M.,Domenech-Rodríguez,M.,Paradise,M.,Cochran,B.N.,Shea,J.M.,
Srebnik,D.,&Baydar,N.(2002).Culturalandcontextualinfluencesinmental
healthhelpseeking:Afocusonethnicminorityyouth.JournalofConsulting
andClinicalPsychology,70,44–55.https://doi.org/10.1037/0022-006X.70.1.44
Cavanaugh,C.E.,Petras,H.,&Martins,S.S.(2015).Gender-specificprofilesof
adversechildhoodexperiences,pastyearmentalandsubstanceusedisorders,
andtheirassociationsamonganationalsampleofadultsintheUnitedStates.
SocialPsychiatryandPsychiatricEpidemiology,50,1257–1266.
https://doi.org/10.1007/s00127-015-1024-3
Cefai,C.,&Cooper,P.(2010).Studentswithoutvoices:Theunheardaccountsof

REFERENCES
315
secondaryschoolstudentswithsocial,emotionalandbehaviourdifficulties.
EuropeanJournalofSpecialNeedsEducation,25,183–198.
https://doi.org/10.1080/08856251003658702
Chan,A.-W.,&Altman,D.G.(2005).Epidemologyandreportingofrandomised
trialspublishedinPubMedjournals.TheLancet,365,1159–1162.
https://doi.org/10.1016/S0140-6736(05)71879-1
Chapman,D.P.,Whitfield,C.L.,Felitti,V.J.,Dube,S.R.,Edwards,V.J.,&Anda,R.F.
(2004).Adversechildhoodexperiencesandtheriskofdepressivedisordersin
adulthood.JournalofAffectiveDisorders,82,217–225.
https://doi.org/10.1016/j.jad.2003.12.013
Charbonneau,A.M.,Mezulis,A.H.,&Hyde,J.S.(2009).Stressandemotional
reactivityasexplanationsforgenderdifferencesinadolescents’depressive
symptoms.JournalofYouthandAdolescence,38,1050–1058.
https://doi.org/10.1007/s10964-009-9398-8
Cheema,J.R.(2014).Somegeneralguidelinesforchoosingmissingdatahandling
methodsineducationalresearch.JournalofModernAppliedStatistical
Methods,13(2),53–75.https://doi.org/10.22237/jmasm/1414814520
Cheesbrough,S.,Harding,C.,Webster,H.,Taylor,L.,&Aldridge-Young,J.(2017).
ThelivesofyoungcarersinEngland.DepartmentforEducation.
ChildLawAdvice.(2018).Childinneed.https://childlawadvice.org.uk/information-
pages/child-in-need-services/#What-is-a-child-in-need-plan-
Christensen,H.B.,&Bilenberg,N.(2000).Behaviouralandemotionalproblemsin
childrenofalcoholicmothersandfathers.EuropeanChild&Adolescent
Psychiatry,9,219–226.https://doi.org/10.1007/s007870070046
Cicchetti,D.,&Curtis,W.J.(2006).Thedevelopingbrainandneuralplasticity:
Implicationsfornormality,psychopathology,andresilience.InD.Cicchetti&D.
J.Cohen(Eds.),Developmentalpsychopathology(2nded.,pp.1–64).John
Wiley&Sons,Inc.
Cicchetti,D.,&Rogosch,F.A.(1996).Editorial:Equifinalityandmultifinalityin
developmentalpsychopathology.DevelopmentandPsychopathology,8,597–
600.https://doi.org/10.1017/S0954579400007318
Cicchetti,D.,&Rogosch,F.A.(2002).Adevelopmentalpsychopathology

REFERENCES
316
perspectiveonadolescence.JournalofConsultingandClinicalPsychology,70,
6–20.https://doi.org/10.1037//0022-006X.70.1.6
Clance,P.R.,&Imes,S.A.(1978).Theimposterphenomenoninhighachieving
women:Dynamicsandtherapeuticintervention.Psychotherapy:Theory,
Research&Practice,15,241–247.https://doi.org/10.1037/h0086006
Clark,M.S.,Bond,M.J.,&Hecker,J.R.(2007).Environmentalstress,psychological
stressandallostaticload.Psychology,HealthandMedicine,12,18–30.
https://doi.org/10.1080/13548500500429338
Cleary,A.(2012).Suicidalaction,emotionalexpression,andtheperformanceof
masculinities.SocialScienceandMedicine,74,498–505.
https://doi.org/10.1016/j.socscimed.2011.08.002
Cohen,J.(1988).Statisticalpoweranalysisforthebehavioralsciences(2nded.).
LawrenceErlbaumAssociates.
Cohen,L.,Manion,L.,&Morrison,K.(2011).Researchmethodsineducation.
Routledge.
Cohen,S.(2004).Socialrelationshipsandhealth.AmericanPsychologist,59,676–
684.https://doi.org/10.1037/0003-066X.59.8.676
Cohen,S.,Kamarck,T.,&Mermelstein,R.(1983).Aglobalmeasureofperceived
stress.JournalofHealthandSocialBehavior,24,385–396.
https://doi.org/10.2307/2136404
Cohen,S.,&Wills,T.A.(1985).Stress,socialsupport,andthebufferinghypothesis:
Atheoreticalanalysis.PsychologicalBulletin,98,310–357.
https://doi.org/10.1037/0033-2909.98.2.310
Collishaw,S.(2015).Annualresearchreview:Seculartrendsinchildandadolescent
mentalhealth.JournalofChildPsychologyandPsychiatryandAllied
Disciplines,56,370–393.https://doi.org/10.1111/jcpp.12372
Collishaw,S.,Goodman,R.,Ford,T.,Rabe-Hesketh,S.,&Pickles,A.(2009).Howfar
areassociationsbetweenchild,familyandcommunityfactorsandchild
psychopathologyinformant-specificandinformant-general?JournalofChild
PsychologyandPsychiatryandAlliedDisciplines,50,571–580.
https://doi.org/10.1111/j.1469-7610.2008.02026.x
Collishaw,S.,Maughan,B.,Natarajan,L.,&Pickles,A.(2010).Trendsinadolescent

REFERENCES
317
emotionalproblemsinEngland:Acomparisonoftwonationalcohortstwenty
yearsapart.JournalofChildPsychologyandPsychiatryandAlliedDisciplines,
51,885–894.https://doi.org/10.1111/j.1469-7610.2010.02252.x
CommissiononSocialDeterminantsofHealth.(2008).Closingthegapina
generation:Healthinequitythroughactiononthesocialdeterminantsof
health.FinalreportoftheComissiononSocialDeterminantsofHealth.World
HealthOrganization.
Compas,B.E.,Connor-Smith,J.K.,Saltzman,H.,Thomsen,A.H.,&Wadsworth,M.
E.(2001).Copingwithstressduringchildhoodandadolescence:Problems,
progress,andpotentialintheoryandresearch.PsychologicalBulletin,127,87–
127.https://doi.org/10.1037/0033-2909.127.1.87
Compas,B.E.,Orosan,P.G.,&Grant,K.E.(1993).Adolescentstressandcoping:
Implicationsforpsychopathologyduringadolescence.JournalofAdolescence,
16,331–349.https://doi.org/10.1006/jado.1993.1028
Conger,R.D.,&Conger,K.J.(2002).ResilienceinMidwesternfamilies:Selected
findingsfromthefirstdecadeofaprospective,longitudinalstudy.Journalof
MarriageandFamily,64,361–373.https://doi.org/10.1111/j.1741-
3737.2002.00361.x
Conway,J.M.,&Lance,C.E.(2010).Whatreviewersshouldexpectfromauthors
regardingcommonmethodbiasinorganizationalresearch.JournalofBusiness
andPsychology,25(3),325–334.https://doi.org/10.1007/s10869-010-9181-6
Cooper,M.(2004).Towardsarelationally-orientatedapproachtotherapy:
Empiricalsupportandanalysis.BritishJournalofGuidanceandCounselling,32,
451–460.https://doi.org/10.1080/03069880412331303268
Cooper,M.,&McLeod,J.(2011).Pluralisticcounsellingandpsychotherapy.SAGE
PublicationsLtd.
CooperRobbins,S.C.,Rawsthorne,M.,Paxton,K.,Hawke,C.,RachelSkinner,S.,&
Steinbeck,K.(2012).“Youcanhelppeople”:Adolescents’viewsonengaging
youngpeopleinlongitudinalresearch.JournalofResearchonAdolescence,22,
8–13.https://doi.org/10.1111/j.1532-7795.2011.00759.x
Costafreda,S.G.,Brammer,M.J.,David,A.S.,&Fu,C.H.Y.(2008).Predictorsof
amygdalaactivationduringtheprocessingofemotionalstimuli:Ameta-

REFERENCES
318
analysisof385PETandfMRIstudies.BrainResearchReviews,58,57–70.
https://doi.org/10.1016/j.brainresrev.2007.10.012
Costello,D.M.,Swendsen,J.,Rose,J.S.,&Dierker,L.C.(2008).Riskandprotective
factorsassociatedwithtrajectoriesofdepressedmoodfromadolescenceto
earlyadulthood.JournalofConsultingandClinicalPsychology,49,143–157.
https://doi.org/10.1037/0022-006X.76.2.173.Risk
Costello,E.J.,Copeland,W.,&Angold,A.(2011).Trendsinpsychopathologyacross
theadolescentyears:Whatchangeswhenchildrenbecomeadolescents,and
whenadolescentsbecomeadults?JournalofChildPsychologyandPsychiatry
andAlliedDisciplines,52,1015–1025.https://doi.org/10.1111/j.1469-
7610.2011.02446.x
Cox,S.D.,&Pakenham,K.I.(2014).Confirmatoryfactoranalysisandinvariance
testingoftheYoungCarerofParentsInventory(YCOPI).Rehabilitation
Psychology,59,439–452.https://doi.org/10.1037/a0035860
Craig,W.M.(1998).Therelationshipamongbullying,victimization,depression,
anxiety,andaggressioninelementaryschoolchildren.Personalityand
IndividualDifferences,24,123–130.https://doi.org/10.1016/s0191-
8869(97)00145-1
Crawford,C.,Dearden,L.,&Greaves,E.(2013).Whenyouarebornmatters:
EvidenceforEngland.
Creswell,J.W.(2014).Researchdesign:Qualitative,quantitativeandmixed
methodsapproaches(4thed.).SAGEPublications.
Creswell,J.W.,&PlanoClark,V.L.(2011).Designingandconductingmixed
methodsresearch(2nded.).SAGEPublications.
Cronbach,L.J.,&Shavelson,R.J.(2004).Mycurrentthoughtsoncoefficientalpha
andsuccessorprocedures.EducationalandPsychologicalMeasurement,64,
391–418.https://doi.org/10.1177/0013164404266386
Crossley,M.L.(2000).Introducingnarrativepsychology:Self,traumaandthe
constructionofmeaning.OpenUniversityPress.
Crotty,M.(1998).Thefoundationsofsocialresearch:Meaningandperspectivein
theresearchprocess.SAGEPublications.
Cummings,C.M.,Caporino,N.E.,&Kendall,P.C.(2014).Comorbidityofanxiety

REFERENCES
319
anddepressioninchildrenandadolescents:20yearsafter.Psychological
Bulletin,140,816–845.https://doi.org/10.1037/a0034733
Cyranowski,J.M.,Frank,E.,&Young,E.(2000).Adolescentonsetofthegender
differenceinlifetimeratesofmajordepression:Atheoreticalmodel.Archives
ofGeneralPsychiatry,57,21–27.https://doi.org/10.1001/archpsyc.57.1.21
D’Avanzo,B.,Barbato,A.,Erzegovesi,S.,Lampertico,L.,Rapisarda,F.,&Valsecchi,
L.(2012).Formalandinformalhelp-seekingformentalhealthproblems:A
surveyofpreferencesofItalianstudents.ClinicalPractice&Epidemiologyin
MentalHealth,8,47–51.https://doi.org/10.2174/1745017901208010047
Danese,A.,&McEwen,B.S.(2012).Adversechildhoodexperiences,allostasis,
allostaticload,andage-relateddisease.PhysiologyandBehavior,106,29–39.
https://doi.org/10.1016/j.physbeh.2011.08.019
Das,J.K.,Salam,R.A.,Lassi,Z.S.,Khan,M.N.,Mahmood,W.,Patel,V.,&Bhutta,Z.
A.(2016).Interventionsforadolescentmentalhealth:Anoverviewof
systematicreviews.JournalofAdolescentHealth,59,S49–S60.
https://doi.org/10.1016/j.jadohealth.2016.06.020
Davey,C.G.,Yücel,M.,&Allen,N.B.(2008).Theemergenceofdepressionin
adolescence:Developmentoftheprefrontalcortexandtherepresentationof
reward.NeuroscienceandBiobehavioralReviews,32,1–19.
https://doi.org/10.1016/j.neubiorev.2007.04.016
Davies,S.,Heyman,I.,&Goodman,R.(2003).Apopulationsurveyofmentalhealth
problemsinchildrenwithepilepsy.DevelopmentalMedicineandChild
Neurology,45,292–295.https://doi.org/10.1017/S0012162203000550
Day,R.D.,&Padilla-Walker,L.M.(2009).Motherandfatherconnectednessand
involvementduringearlyadolescence.JournalofFamilyPsychology,23,900–
904.https://doi.org/10.1037/a0016438
deAnstiss,H.(2009).Mentalhealthhelp-seekingandrefugeeadolescents:
Qualitativefindingsfromamixedmethodsinvestigation.Australian
Psychologist,45,29–37.https://doi.org/10.1080/00050060903262387
deLijster,J.M.,Dierckz,B.,Utens,E.M.W.J.,Verhulst,F.C.,Zieldorff,C.,
Dieleman,G.C.,&Legerstee,J.S.(2016).Theageofonsetofanxiety
disorders.TheCanadianJournalofPsychiatry,62,237–246.

REFERENCES
320
https://doi.org/10.1177/0706743716640757
DeLosReyes,A.,&Kazdin,A.E.(2005).Informantdiscrepanciesintheassessment
ofchildhoodpsychopathology:Acriticalreview,theoreticalframework,and
recommendationsforfurtherstudy.PsychologicalBulletin,131,483–509.
https://doi.org/10.1037/0033-2909.131.4.483
DeVenter,M.,Demyttenaere,K.,&Bruffaerts,R.(2013).Therelationshipbetween
adversechildhoodexperiencesandmentalhealthinadulthood:Asystematic
literaturereview.TijdschriftVoorPsychiatrie,55,259–268.
Deighton,J.,Croudace,T.,Fonagy,P.,Brown,J.,Patalay,P.,&Wolpert,M.(2014).
Measuringmentalhealthandwellbeingoutcomesforchildrenandadolescents
toinformpracticeandpolicy:Areviewofchildself-reportmeasures.Childand
AdolescentPsychiatryandMentalHealth,8,14–28.
https://doi.org/10.1186/1753-2000-8-14
Deighton,J.,Humphrey,N.,Belsky,J.,Boehnke,J.,Vostanis,P.,&Patalay,P.(2018).
Longitudinalpathwaysbetweenmentalhealthdifficultiesandacademic
performanceduringmiddlechildhoodandearlyadolescence.BritishJournalof
DevelopmentalPsychology,36,110–126.https://doi.org/10.1111/bjdp.12218
Deighton,J.,Lereya,S.T.,Casey,P.,Patalay,P.,Humphrey,N.,&Wolpert,M.
(2019).Prevalenceofmentalhealthproblemsinschools:Povertyandother
riskfactorsamong28000adolescentsinEngland.TheBritishJournalof
Psychiatry,215,565–567.https://doi.org/10.1192/bjp.2019.19
Deighton,J.,Lereya,S.T.,Patalay,P.,Casey,P.,Humphrey,N.,&Wolpert,M.
(2018).Mentalhealthproblemsin11-14year-olds:Resultsfromthefirst
HeadStartannualsurveyof30,000children.
Demaso,D.R.,Marcus,N.E.,Kinnamon,C.,&Gonzalez-Heydrich,J.(2006).
Depressionexperiencejournal:Acomputer-basedinterventionforfamilies
facingchildhooddepression.JournaloftheAmericanAcademyofChildand
AdolescentPsychiatry,45,158–165.
https://doi.org/10.1097/01.chi.0000190353.98570.fe
Demkowicz,O.,Panayiotou,M.,Ashworth,E.,Humphrey,N.,&Deighton,J.(2019).
Thefactorstructureandpsychometricpropertiesofthefour-itemPerceived
StressScalewithinEnglishadolescents.EuropeanJournalofPsychological

REFERENCES
321
Assessment.https://doi.org/10.1027/1015-5759/a000562
Denny,S.,Lewycka,S.,Utter,J.,Fleming,T.,Peiris-John,R.,Sheridan,J.,Rossen,F.,
Wynd,D.,Teevale,T.,Bullen,P.,&Clark,T.(2016).Theassociationbetween
socioeconomicdeprivationandsecondaryschoolstudents’health:Findings
fromalatentclassanalysisofanationaladolescenthealthsurvey.
InternationalJournalforEquityinHealth,15,109–120.
https://doi.org/10.1186/s12939-016-0398-5
DepartmentforCommunitiesandLocalGovernment,&OfficeforNational
Statistics.(2015).TheEnglishindicesofdeprivation2010.
DepartmentforEducation.(2012).Pupilsnotclaimingfreeschoolmeals.
DepartmentforEducation.(2016a).Primaryprogressmeasures.
DepartmentforEducation.(2016b).Scaledscoresatkeystage2.
https://www.gov.uk/guidance/scaled-scores-at-key-stage-2
DepartmentforEducation.(2018a).Guidance:Childreninneedcensus:Guideto
submittingdata.https://www.gov.uk/guidance/children-in-need-census
DepartmentforEducation.(2018b).Nationalpupildatabase:Userguideand
supportinginformation.
https://www.gov.uk/government/publications/national-pupil-database-user-
guide-and-supporting-information
DepartmentforEducation.(2018c).Specialeducationalneeds:Transferof
statementsofSENtoeducation,healthandcareplans,endMarch2018.Ad
hocnotice.
DepartmentforEducation,&DepartmentofHealth.(2015).Specialeducational
needsanddisabilitycodeofpractice:0to25years.DepartmentforEducation.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads
/attachment_data/file/398815/SEND_Code_of_Practice_January_2015.pdf
DepartmentforEducation,&OfficeforNationalStatistics.(2017a).Special
educationalneedsinEngland:January2017.
DepartmentforEducation,&OfficeforNationalStatistics.(2017b).Statementsof
SENandEHCplans:England,2017.
DepartmentofHealthandEducation.(2017).Transformingchildrenandyoung
people’smentalhealthprovision:agreenpaper.https://doi.org/979-1-5286-
REFERENCES
322
0061-3
Desjardins,T.L.,&Leadbeater,B.J.(2011).Relationalvictimizationanddepressive
symptomsinadolescence:moderatingeffectsofmother,father,andpeer
emotionalsupport.JournalofYouthandAdolescence,40,531–544.
https://doi.org/10.1007/s10964-010-9562-1
DeVerteuil,G.,&Golubchikov,O.(2016).Canresilienceberedeemed?:Resilience
asametaphorforchange,notagainstchange.City,20,143–151.
https://doi.org/10.1080/13604813.2015.1125714
DeVries,A.C.,Glasper,E.R.,&Detillion,C.E.(2003).Socialmodulationofstress
responses.PhysiologyandBehavior,79,399–407.
https://doi.org/10.1016/S0031-9384(03)00152-5
DiGiunta,L.,Iselin,A.M.R.,Lansford,J.E.,Eisenberg,N.,Lunetti,C.,Thartori,E.,
Basili,E.,Pastorelli,C.,Bacchini,D.,UribeTirado,L.M.,&Gerbino,M.(2018).
Parents’andearlyadolescents’self-efficacyaboutangerregulationandearly
adolescents’internalizingandexternalizingproblems:Alongitudinalstudyin
threecountries.JournalofAdolescence,64,124–135.
https://doi.org/10.1016/j.adolescence.2018.01.009
DiCicco-Bloom,B.,&Crabtree,B.F.(2006).Thequalitativeresearchinterview.
MedicalEducation,40,314–321.https://doi.org/10.1111/j.1365-
2929.2006.02418.x
Díez,A.M.(2010).Schoolmemoriesofyoungpeoplewithdisabilities:Ananalysis
ofbarriersandaidstoinclusion.DisabilityandSociety,25,163–175.
https://doi.org/10.1080/09687590903534346
Ditzen,B.,&Heinrichs,M.(2014).Psychobiologyofsocialsupport:Thesocial
dimensionofstressbuffering.RestorativeNeurologyandNeuroscience,32,
149–162.https://doi.org/10.3233/RNN-139008
Dodou,D.,&DeWinter,J.C.F.(2014).Socialdesirabilityisthesameinoffline,
online,andpapersurveys:Ameta-analysis.ComputersinHumanBehavior,36,
487–495.https://doi.org/10.1016/j.chb.2014.04.005
Dong,Y.,&Peng,C.-Y.J.(2013).Principledmissingdatamethodsforresearchers.
SpringerPlus,2,222–239.https://doi.org/10.1186/2193-1801-2-222
Doom,J.R.,Doyle,C.M.,&Gunnar,M.R.(2017).Socialstressbufferingbyfriends

REFERENCES
323
inchildhoodandadolescence:EffectsonHPAandoxytocinactivity.Social
Neuroscience,12,8–21.https://doi.org/10.1080/17470919.2016.1149095
Doom,J.R.,Hostinar,C.E.,VanZomeren-Dohm,A.A.,&Gunnar,M.R.(2015).The
rolesofpubertyandageinexplainingthediminishedeffectivenessofparental
bufferingofHPAreactivityandrecoveryinadolescence.
Psychoneuroendocrinology,59,102–111.
https://doi.org/10.1016/j.psyneuen.2015.04.024
Doty,D.H.,&Glick,W.H.(1998).Commonmethodsbias:Doescommonmethods
variancereallybiasresults?OrganizationalResearchMethods,1(374–406).
https://doi.org/10.1177/109442819814002
Dowrick,C.,&Frances,A.(2013).Medicalisingunhappiness:Newclassificationof
depressionrisksmorepatientsbeingputonadrugtreatmentfromwhichthey
willnotbenefit.BMJ,347,f7140.https://doi.org/10.1136/bmj.f7140
Doyle,L.,Brady,A.M.,&Byrne,G.(2009).Anoverviewofmixedmethodsresearch.
JournalofResearchinNursing,14,175–185.
https://doi.org/10.1177/1744987108093962
Drukker,M.,&vanOs,J.(2003).Mediatorsofneighbourhoodsocioeconomic
deprivationandqualityoflife.SocialPsychiatryandPsychiatricEpidemiology,
38,698–706.https://doi.org/10.1007/s00127-003-0690-8
Dube,S.R.,Anda,R.F.,Felitti,V.J.,Chapman,D.P.,Williamson,D.F.,&Giles,W.H.
(2001).Childhoodabuse,householddysfunction,andtheriskofattempted
suicidethroughoutthelifespan.JournaloftheAmericanMedicalAssociation,
286,3089–3096.https://doi.org/10.1001/jama.286.24.3089
Duckworth,A.L.,Tsukayama,E.,&May,H.(2010).Establishingcausalityusing
longitudinalhierarchicallinearmodeling:Anillustrationpredicting
achievementfromself-control.SocialPsychologicalandPersonalityScience,1,
311–317.https://doi.org/10.1177/1948550609359707
Dundon,E.E.(2006).Adolescentdepression:Ametasynthesis.JournalofPediatric
HealthCare,20,384–392.https://doi.org/10.1016/j.pedhc.2006.02.010
Dunn,T.J.,Baguley,T.,&Brunsden,V.(2014).Fromalphatoomega:Apractical
solutiontothepervasiveproblemofinternalconsistencyestimation.British
JournalofPsychology,105,399–412.https://doi.org/10.1111/bjop.12046

REFERENCES
324
Durham,R.C.(2007).Treatmentofgeneralizedanxietydisorder.Psychiatry,6,183–
187.https://doi.org/10.1016/j.mppsy.2007.03.003
Durlak,J.A.(2009).Howtoselect,calculate,andinterpreteffectsizes.Journalof
PediatricPsychology,34,917–928.https://doi.org/10.1093/jpepsy/jsp004
Eamon,M.K.(2002).Influencesandmediatorsoftheeffectofpovertyonyoung
adolescentdepressivesymptoms.JournalofYouthandAdolescence,31,231–
242.https://doi.org/10.1023/A:1015089304006
Earley,L.,Cushway,D.,&Cassidy,T.(2007).Children’sperceptionsandexperiences
ofcaregiving:Afocusgroupstudy.CounsellingPsychologyQuarterly,20,68–
80.https://doi.org/10.1080/09515070701217830
Eatough,V.,&Smith,J.A.(2006a).Ifeellikeascrambledegginmyhead:An
idiographiccasestudyofmeaningmakingandangerusinginterpretative
phenomenologicalanalysis.PsychologyandPsychotherapy:Theory,Research
andPractice,79,115–135.https://doi.org/10.1348/147608305X41100
Eatough,V.,&Smith,J.A.(2006b).Iwaslikeawildwildperson:Understanding
feelingsofangerusinginterpretativephenomenologicalanalysis.British
JournalofPsychology,97,483–498.
https://doi.org/10.1348/000712606X97831
Eatough,V.,&Smith,J.A.(2008).Interpretativephenomenologicalanalysis.InThe
SAGEHandbookofqualitativeresearchinpsychology(pp.179–194).SAGE
Publications.
Eatough,V.,Smith,J.A.,&Shaw,R.(2008).Women,anger,andaggression.Journal
ofInterpersonalViolence,23,1767–1799.
https://doi.org/10.1177/0886260508314932
Eccles,J.S.,Midgley,C.,Wigfield,A.,Buchanan,C.M.,Reuman,D.,Flanagan,C.,&
MacIver,D.(1993).Developingduringadolescence:Theimpactofstage-
environmentfitonyoungadoloscents’experiencesinschoolsandinfamilies.
AmericanPsychologist,48,90–101.
Edbrooke-Childs,J.,Wolpert,M.,Zamperoni,V.,Napoleone,E.,&Bear,H.(2018).
Evaluationofreliableimprovementratesindepressionandanxietyattheend
oftreatmentinadolescents.BJPsychOpen,4,250–255.
https://doi.org/10.1192/bjo.2018.31

REFERENCES
325
Eder,D.,&Fingerson,L.(2003).Interviewingchildrenandadolescents.InJ.A.
Holstein&J.F.Gubrium(Eds.),Insideinterviewing:newlenses,newconcerns
(pp.32–53).SAGEPublications.
Edmond,R.(2005).Ethnographicresearchmethodswithchildrenandyoung
people.InS.Greene&D.Hogan(Eds.),Researchingchildren’sexperience:
Approachesandmethods(pp.123–140).SAGEPublications.
Emerson,E.(2003).Prevalenceofpsychiatricdisordersinchildrenandadolescents
withandwithoutintellectualdisability.JournalofIntellectualDisability
Research,47,51–58.https://doi.org/10.1111/j.1365-2788.2011.01415.x
Emerson,E.(2012).Deprivation,ethnicityandtheprevalenceofintellectualand
developmentaldisabilities.JournalofEpidemiologyandCommunityHealth,66,
218–224.https://doi.org/10.1136/jech.2010.111773
Emerson,E.,&Hatton,C.(2007).Thementalhealthofchildrenandadolescents
withlearningdisabilitiesinBritain.
Epel,E.S.,Crosswell,A.D.,Mayer,S.E.,Prather,A.A.,Slavich,G.M.,Puterman,E.,
&Mendes,W.B.(2018).Morethanafeeling:Aunifiedviewofstress
measurementforpopulationscience.FrontiersinNeuroendocrinology,49,
146–169.https://doi.org/10.1016/j.yfrne.2018.03.001
Eppelmann,L.,Parzer,P.,Lenzen,C.,Bürger,A.,Haffner,J.,Resch,F.,&Kaess,M.
(2016).Stress,copingandemotionalandbehavioralproblemsamongGerman
highschoolstudents.MentalHealthandPrevention,4,81–87.
https://doi.org/10.1016/j.mhp.2016.03.002
Erikson,E.H.(1959).Identityandthelifecycle.InternationalUniversitiesPress.
Erikson,E.H.(1963).Childhoodandsociety(2nded.).Norton.
Evans,G.W.(2003).Amultimethodologicalanalysisofcumulativeriskandallostatic
loadamongruralchildren.DevelopmentalPsychology,39,924–933.
https://doi.org/10.1037/0012-1649.39.5.924
Evans,G.W.(2004).Theenvironmentofchildhoodpoverty.AmericanPsychologist,
59,77–92.https://doi.org/10.1037/0003-066X.59.2.77
Evans,G.W.,&English,K.(2002).Theenvironmentofpoverty:Multiplestressor
exposure,psychophysiologicalstress,andsocioemotionaladjustment.Child
Development,73,1238–1248.https://doi.org/10.1111/1467-8624.00469

REFERENCES
326
Evans,G.W.,&Kim,P.(2012).Childhoodpovertyandyoungadults’allostaticload:
Themediatingroleofchildhoodcumulativeriskexposure.Psychological
Science,23,979–983.https://doi.org/10.1177/0956797612441218
Evans,G.W.,&Kim,P.(2013).Childhoodpoverty,chronicstress,self-regulation,
andcoping.ChildDevelopmentPerspectives,7,43–48.
https://doi.org/10.1111/cdep.12013
Evans,G.W.,Kim,P.,Ting,A.H.,Tesher,H.B.,&Shannis,D.(2007).Cumulative
risk,maternalresponsiveness,andallostaticloadamongyoungadolescents.
DevelopmentalPsychology,43,341–351.https://doi.org/10.1037/0012-
1649.43.2.341
Evans,G.W.,Li,D.,&Whipple,S.S.(2013).Cumulativeriskandchilddevelopment.
PsychologicalBulletin,139,1342–1396.https://doi.org/10.1037/a0031808
EvidenceBasedPracticeUnit.(n.d.).LearningfromHeadStart:Wellbeing
measurementframeworkforsecondaryschools.EvidenceBasedPracticeUnit.
Evraire,L.E.,&Dozois,D.J.A.(2011).Anintegrativemodelofexcessive
reassuranceseekingandnegativefeedbackseekinginthedevelopmentand
maintenanceofdepression.ClinicalPsychologyReview,31,1291–1303.
https://doi.org/10.1016/j.cpr.2011.07.014
EwellFoster,C.,Horwitz,A.,Thomas,A.,Opperman,K.,Gipson,P.,Burnside,A.,
Stone,D.M.,&King,C.A.(2017).Connectednesstofamily,school,peers,and
communityinsociallyvulnerableadolescents.ChildrenandYouthServices
Review,81,321–331.https://doi.org/10.1016/j.childyouth.2017.08.011
Fan,R.,Varol,O.,Varamesh,A.,Barron,A.,vandeLeemput,I.A.,Scheffer,M.,&
Bollen,J.(2019).Theminute-scaledynamicsofonlineemotionsrevealthe
effectsofaffectlabeling.NatureHumanBehaviour,3,92–100.
https://doi.org/10.1038/s41562-018-0490-5
Fazel,M.,Hoagwood,K.,Stephan,S.,&Ford,T.(2014).Mentalhealthinterventions
inschoolsinhigh-incomecountries.TheLancetPsychiatry,1,377–387.
https://doi.org/10.1016/S2215-0366(14)70312-8
Fearon,R.M.P.,&Belsky,J.(2004).Attachmentandattention:Protectionin
relationtogenderandcumulativesocial-contextualadversity.Child
Development,75,1677–1693.https://doi.org/10.1111/j.1467-

REFERENCES
327
8624.2004.00809.x
FeldmanFarb,A.,&Matjasko,J.L.(2012).Recentadvancesinresearchonschool-
basedextracurricularactivitiesandadolescentdevelopment.Developmental
Review,32,1–48.https://doi.org/10.1016/j.dr.2011.10.001
Fergus,S.,&Zimmerman,M.A.(2005).Adolescentresilience:Aframeworkfor
understandinghealthydevelopmentinthefaceofrisk.AnnualReviewof
PublicHealth,26,399–419.https://doi.org/10.1177/030981689505500103
Ferrari,A.J.,Charlson,F.J.,Norman,R.E.,Patten,S.B.,Freedman,G.,Murray,C.J.
L.,Vos,T.,&Whiteford,H.A.(2013).Burdenofdepressivedisordersby
country,sex,age,andyear:Findingsfromtheglobalburdenofdiseasestudy
2010.PLoSMedicine,10,e1001547.
https://doi.org/10.1371/journal.pmed.1001547
Fife-Schaw,C.(2012).Introductiontoquantitativeresearch.InG.M.Breakwell,J.A.
Smith,&D.B.Wright(Eds.),Researchmethodsinpsychology(pp.17–38).
SAGEPublications.
Fink,E.,Patalay,P.,Sharpe,H.,Holley,S.,Deighton,J.,&Wolpert,M.(2015).
Mentalhealthdifficultiesinearlyadolescence:Acomparisonoftwocross-
sectionalstudiesinEnglandfrom2009to2014.JournalofAdolescentHealth,
56,502–507.https://doi.org/10.1016/j.jadohealth.2015.01.023
Fishbein,M.,&Ajzen,I.(2005).Theory-basedbehaviorchangeinterventions:
CommentsonHobbisandSutton.JournalofHealthPsychology,10,27–31.
https://doi.org/10.1177/1359105305048552
Fivush,R.(2007).Maternalreminiscingstyleandchildren’sdeveloping
understandingofselfandemotion.ClinicalSocialWorkJournal,35,37–46.
https://doi.org/10.1007/s10615-006-0065-1
Fivush,R.,Brotman,M.A.,Buckner,J.P.,&Goodman,S.H.(2000).Gender
differencesinparent-childemotionnarratives.SexRoles,42,233–253.
https://doi.org/10.1023/A:1007091207068
Flaspohler,P.D.,Elfstrom,J.L.,Vanderzee,K.L.,&Sink,H.E.(2009).Standbyme:
Theeffectsofpeerandteachersupportinmitigatingtheimpactofbullyingon
qualityoflife.PsychologyintheSchools,46,636–649.
https://doi.org/10.1002/pits.20404

REFERENCES
328
Flora,D.B.,&Curran,P.J.(2004).Anempiricalevaluationofalternativemethodsof
estimationforconfirmatoryfactoranalysiswithordinaldata.Psychological
Methods,9,466–491.https://doi.org/10.1037/1082-989X.9.4.466
Flouri,E.,&Kallis,C.(2007).Adverselifeeventsandpsychopathologyandprosocial
behaviorinlateadolescence:Testingthetiming,specificity,accumulation,
gradient,andmoderationofcontextualrisk.JournaloftheAmericanAcademy
ofChild&AdolescentPsychiatry,46,1651–1659.
https://doi.org/10.1097/chi.0b013e318156a81a
Flouri,E.,Mavroveli,S.,&Tzavidis,N.(2012).Cognitiveability,neighborhood
deprivation,andyoungchildren’semotionalandbehavioralproblems.Social
PsychiatryandPsychiatricEpidemiology,47,985–992.
https://doi.org/10.1007/s00127-011-0406-4
Flouri,E.,&Panourgia,C.(2011).Genderdifferencesinthepathwayfromadverse
lifeeventstoadolescentemotionalandbehaviouralproblemsvianegative
cognitiveerrors.BritishJournalofDevelopmentalPsychology,29(2),234–252.
https://doi.org/10.1348/0261-510X.002002
Flouri,E.,&Sarmadi,Z.(2016).Prosocialbehaviorandchildhoodtrajectoriesof
internalizingandexternalizingproblems:Theroleofneighborhoodandschool
contexts.DevelopmentalPsychology,52,253–258.
https://doi.org/10.1037/dev0000076
Flouri,E.,Tzavidis,N.,&Kallis,C.(2010).Adverselifeevents,areasocioeconomic
disadvantage,andpsychopathologyandresilienceinyoungchildren:The
importanceofriskfactors’accumulationandprotectivefactors’specificity.
EuropeanChild&AdolescentPsychiatry,19,535–546.
https://doi.org/10.1007/s00787-009-0068-x
Folkman,S.,&Moskowitz,J.T.(2000).Positiveaffectandtheothersideofcoping.
AmericanPsychologist,55,647–654.https://doi.org/10.1037/0003-
066X.55.6.647
Follesø,R.(2015).Youthatriskortermsatrisk?Young,23,240–253.
https://doi.org/10.1177/1103308815584877
Fonseca,A.,Gorayeb,R.,&Canavarro,M.C.(2015).Women’shelp-seeking
behavioursfordepressivesymptomsduringtheperinatalperiod:Socio-

REFERENCES
329
demographicandclinicalcorrelatesandperceivedbarrierstoseeking
professionalhelp.Midwifery,31,1177–1185.
https://doi.org/10.1016/j.midw.2015.09.002
Forehand,R.,Biggar,H.,&Kotchick,B.A.(1998).Cumulativeriskacrossfamily
stressors:Short-andlong-termeffectsforadolescents.JournalofAbnormal
ChildPsychology,26,119–128.https://doi.org/10.1023/A:1022669805492
Forns,A.,Abad,J.,&Kirchner,T.(2011).Internalisingandexternalisingproblems.In
R.J.R.Levesque(Ed.),EncyclopediaofAdolescence(pp.1464–1469).Springer.
Foster,K.R.,&Spencer,D.(2011).Atriskofwhat?possibilitiesoverprobabilitiesin
thestudyofyounglives.JournalofYouthStudies,14,125–143.
https://doi.org/10.1080/13676261.2010.506527
Fraser,E.,&Pakenham,K.I.(2009).Resilienceinchildrenofparentswithmental
illness:Relationsbetweenmentalhealthliteracy,socialconnectednessand
coping,andbothadjustmentandcaregiving.Psychology,HealthandMedicine,
14,573–584.https://doi.org/10.1080/13548500903193820
Fredrickson,B.L.,&Roberts,T.(1997).Objectificationtheory:Toward
understandingwomen’slivedexperiencesandmentalhealthrisks.Psychology
ofWomenQuarterly,21,173–206.https://doi.org/10.1007/978-3-319-33228-
4_643
Freud,S.(1933).Newintroductorylecturesonpsycho-analysis.W.W.Norton.
Freud,S.(1940).Splittingoftheegointheprocessofdefence.Internationaler
ZeitschriftPsychoanaltischerImago.
Fried,E.I.,Epskamp,S.,Nesse,R.M.,Tuerlinckx,F.,&Borsboom,D.(2016).What
are“good”depressionsymptoms?ComparingthecentralityofDSMandnon-
DSMsymptomsofdepressioninanetworkanalysis.JournalofAffective
Disorders,189,314–320.https://doi.org/10.1016/j.jad.2015.09.005
Frijda,N.H.(2005).Emotionexperience.CognitionandEmotion,19,473–497.
https://doi.org/10.1080/02699930441000346
Fritz,J.,deGraaff,A.M.,Caisley,H.,vanHarmelen,A.-L.,&Wilkinson,P.O.(2018).
Asystematicreviewofamenableresiliencefactorsthatmoderateand/or
mediatetherelationshipbetweenchildhoodadversityandmentalhealthin
youngpeople.FrontiersinPsychiatry,9,230.

REFERENCES
330
https://doi.org/10.3389/fpsyt.2018.00230
Fritz,J.,Fried,E.I.,Goodyer,I.M.,Wilkinson,P.O.,&vanHarmelen,A.L.(2018).A
networkmodelofresiliencefactorsforadolescentswithandwithoutexposure
tochildhoodadversity.ScientificReports,8,15774.
https://doi.org/10.1038/s41598-018-34130-2
Fuligni,A.J.,&Pedersen,S.(2002).Familyobligationandthetransitiontoyoung
adulthood.DevelopmentalPsychology,38,856–868.
https://doi.org/10.1037/0012-1649.38.5.856
Fuligni,A.J.,&Telzer,E.H.(2013).Anotherwayfamilycangetintheheadand
undertheskin:Theneurobiologyofhelpingthefamily.ChildDevelopment
Perspectives,7,138–142.https://doi.org/10.1111/cdep.12029
Gass,K.,Jenkins,J.,&Dunn,J.(2007).Aresiblingrelationshipsprotective?A
longitudinalstudy.JournalofChildPsychologyandPsychiatryandAllied
Disciplines,48,167–175.https://doi.org/10.1111/j.1469-7610.2006.01699.x
Gawronski,B.,&Bodenhausen,G.V.(2006).Associativeandpropositional
processesinevaluation:Anintegrativereviewofimplicitandexplicitattitude
change.PsychologicalBulletin,132,692–731.https://doi.org/10.1037/0033-
2909.132.5.692
Gefen,D.,Rigdon,E.E.,&Straub,D.(2011).AnupdateandextensiontoSEM
guidelinesforadministrativeandsocialscienceresearch.MISQuarterly,35,iii–
xiv.https://doi.org/10.2307/23044042
Gerard,J.M.,&Buehler,C.(2004).Cumulativeenvironmentalriskandyouth
maladjustment:Theroleofyouthattributes.ChildDevelopment,75,1832–
1849.https://doi.org/10.1111/j.1467-8624.2004.00820.x
Girgus,J.S.,&Yang,K.(2015).Genderanddepression.CurrentOpinionin
Psychology,4,53–60.https://doi.org/10.1016/j.copsyc.2015.01.019
Glied,S.,&Pine,D.S.(2002).Consequencesandcorrelatesofadolescent
depression.ArchivesofPediatricsandAdolescentMedicine,156,1009–1014.
https://doi.org/10.1001/archpedi.156.10.1009
Gloria,C.T.,&Steinhardt,M.A.(2016).Relationshipsamongpositiveemotions,
coping,resilienceandmentalhealth.StressandHealth,32,145–156.
https://doi.org/10.1002/smi.2589

REFERENCES
331
Goldspink,S.,&Engward,H.(2018).Boomingclangsandwhisperingghosts:
AttendingtothereflexiveechoesinIPAresearch.QualitativeResearchin
Psychology,16,291–304.https://doi.org/10.1080/14780887.2018.1543111
González-Ramírez,M.T.,Rodríguez-Ayán,M.N.,&Hernández,R.L.(2013).The
PerceivedStressScale(PSS):Normativedataandfactorstructureforalarge-
scalesampleinMexico.SpanishJournalofPsychology,16(e47),1–9.
https://doi.org/10.1017/sjp.2013.35
Goodman,R.(1997).TheStrengthsandDifficultiesQuestionnaire:Aresearchnote.
JournalofChildPsychologyandPsychiatry,38,581–586.
https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
Goodman,R.(2001).PsychometricpropertiesoftheStrengthsandDifficulties
Questionnaire.JournaloftheAmericanAcademyofChildandAdolescent
Psychiatry,40,1337–1345.https://doi.org/10.1097/00004583-200111000-
00015
Goodman,R.,Ford,T.,Simmons,H.,Gatward,R.,&Meltzer,H.(2000).Usingthe
StrengthsandDifficultiesQuestionnaire(SDQ)toscreenforchildpsychiatric
disordersinacommunitysample.TheBritishJournalofPsychiatry,177,534–
539.https://doi.org/10.1192/bjp.177.6.534
Goodman,R.,Gledhill,J.,&Ford,T.(2003).Childpsychiatricdisorderandrelative
agewithinschoolyear:Crosssectionalsurveyoflargepopulationsample.BMJ,
327,327–331.https://doi.org/10.1136/bmj.327.7413.472
Goodman,R.,Iervolino,A.C.,Collishaw,S.,Pickles,A.,&Maughan,B.(2007).
Seeminglyminorchangestoaquestionnairecanmakeabigdifferenceto
meanscores:Acautionarytale.SocialPsychiatryandPsychiatricEpidemiology,
42,322–327.https://doi.org/10.1007/s00127-007-0169-0
Goodman,R.,Meltzer,H.,&Bailey,V.(1998).TheStrengthsandDifficulties
Questionnaire:Apilotstudyonthevalidityoftheself-reportversion.
InternationalReviewofPsychiatry,15,173–177.
https://doi.org/10.1080/0954026021000046137
Gorard,S.(2016a).Acautionarynoteonmeasuringthepupilpremiumattainment
gapinEngland.BritishJournalofEducation,Society&BehaviouralScience,
14(2),1–8.https://doi.org/10.9734/BJESBS/2016/23618

REFERENCES
332
Gorard,S.(2016b).Thecomplexdeterminantsofschoolintakecharacteristicsand
segregation,England1989to2014.CambridgeJournalofEducation,46,131–
146.https://doi.org/10.1080/0305764X.2015.1045446
Gorard,S.,&See,B.H.(2011).Howcanweenhanceenjoymentofsecondary
school?Thestudentview.BritishEducationalResearchJournal,37,671–690.
https://doi.org/10.1080/01411926.2010.488718
Graham,H.,&Kelly,M.P.(2004).Healthinequalities:Concepts,frameworksand
policy.
Grant,K.E.,Compas,B.E.,Stuhlmacher,A.F.,Thurm,A.E.,McMahon,S.D.,&
Halpert,J.A.(2003).Stressorsandchildandadolescentpsychopathology:
Movingfrommarkerstomechanismsofrisk.PsychologicalBulletin,129,447–
466.https://doi.org/10.1037/0033-2909.129.3.447
Green,H.,McGinnity,A.,Meltzer,H.,Ford,T.,&Goodman,R.(2005).Mentalhealth
ofchildrenandyoungpeopleinGreatBritain,2004.OfficeforNational
Statistics.
Greenberg,L.S.,&Watson,J.C.(2015).Emotion-focusedtherapy:Coachingclients
toworkthroughtheirfeelings(2nded.).AmericanPsychologicalAssociation.
Greene,J.C.(2007).Mixedmethodsinsocialinquiry.Jossey-Bass.
Greene,J.C.(2008).Ismixedmethodssocialinquiryadistinctivemethodology?
JournalofMixedMethodsResearch,2,7–22.
https://doi.org/10.1177/1558689807309969
Greene,J.C.,Caracelli,V.J.,&Graham,W.F.(1989).Towardaconceptual
frameworkformixed-methodevaluationdesigns.EducationalEvaluationand
PolicyAnalysis,11,255–274.https://doi.org/10.3102/01623737011003255
Groves,R.,Dillman,D.,Eltinge,J.,&Little,R.J.A.(2002).Surveynonresponse.
Wiley.
Guba,E.G.,&Lincoln,Y.S.(1989).Fourthgenerationevaluation.SAGE
Publications.
Guèvremont,A.,Findlay,L.,&Kohen,D.(2014).Organizedextracurricularactivities:
Arein-schoolandout-of-schoolactivitiesassociatedwithdifferentoutcomes
forcanadianyouth?JournalofSchoolHealth,84,317–325.
https://doi.org/10.1111/josh.12154

REFERENCES
333
Gulliver,A.,Griffiths,K.M.,&Christensen,H.(2010).Perceivedbarriersand
facilitatorstomentalhealthhelp-seekinginyoungpeople:Asystematic
review.BMCPsychiatry,10,113–122.https://doi.org/10.1186/1471-244X-10-
113
Gunnar,M.R.,Hostinar,C.E.,Sanchez,M.M.,Tottenham,N.,&Sullivan,R.M.
(2015).Parentalbufferingoffearandstressneurobiology:Reviewingparallels
acrossrodent,monkey,andhumanmodels.SocialNeuroscience,10,474–478.
https://doi.org/10.1080/17470919.2015.1070198
Guo,S.,Nguyen,H.,Weiss,B.,Ngo,V.K.,&Lau,A.S.(2015).Linkagesbetween
mentalhealthneedandhelp-seekingbehavioramongadolescents:
Moderatingroleofethnicityandculturalvalues.JournalofCounseling
Psychology,62,682–693.https://doi.org/10.1037/cou0000094
Gutman,L.M.,&Eccles,J.S.(2007).Stage-environmentfitduringadolescence:
Trajectoriesoffamilyrelationsandadolescentoutcomes.Developmental
Psychology,43,522–537.https://doi.org/10.1037/0012-1649.43.2.522
Hall-Lande,J.A.,Eisenberg,M.E.,Christenson,S.L.,&Neumark-Sztainer,D.(2007).
Socialisolation,psychologicalhealth,andprotectivefactorsinadolescence.
Adolescence,42,265–286.https://doi.org/10.1130/B26151.1
Hall,J.E.,Sammons,P.,Sylva,K.,Melhuish,E.,Taggart,B.,Siraj-Blatchford,I.,&
Smees,R.(2010).Measuringthecombinedrisktoyoungchildren’scognitive
development:Analternativetocumulativeindices.BritishJournalof
DevelopmentalPsychology,28,219–238.
https://doi.org/10.1348/026151008X399925
Hames,J.L.,Hagan,C.R.,&Joiner,T.E.(2013).Interpersonalprocessesin
depression.InterpersonalProcessesinDepression,9,355–377.
https://doi.org/10.1146/annurev-clinpsy-050212-185553
Hammen,C.(2005).Stressanddepression.AnnualReviewofClinicalPsychology,1,
293–319.https://doi.org/10.1146/annurev.clinpsy.1.102803.143938
Hammen,C.,&Brennan,P.(2003).Severity,chronicity,andtimingofmaternal
depressionandriskforadolescentoffspringdiagnosesinacommunitysample.
ArchivesofGeneralPsychiatry,60,253–258.
https://doi.org/10.1001/archpsyc.60.3.253

REFERENCES
334
Hampel,P.,&Petermann,F.(2006).Perceivedstress,coping,andadjustmentin
adolescents.JournalofAdolescentHealth,38,409–415.
https://doi.org/10.1016/j.jadohealth.2005.02.014
Hamre,B.K.,&Pianta,R.C.(2001).Earlyteacher-childrelationshipsandthe
trajectoryofchildren’sschooloutcomesthrougheighthgrade.Child
Development,72,625–638.https://doi.org/10.1111/1467-8624.00301
Hankin,B.L.,Young,J.F.,Abela,J.R.Z.,Smolen,A.,Jenness,J.L.,Gulley,L.D.,
Technow,J.R.,Gottlieb,A.B.,Cohen,J.R.,&Oppenheimer,C.W.(2015).
Depressionfromchildhoodintolateadolescence:Influenceofgender,
development,geneticsusceptibility,andpeerstress.JournalofAbnormal
Psychology,124,803–816.https://doi.org/10.1037/abn0000089
Harcourt,D.,&Conroy,H.(2011).Informedconsent:Processesandproceduresin
seekingresearchpartnershipswithyoungchildren.InD.Harcourt,B.Perry,&
T.Waller(Eds.),Researchingyoungchildren’sperspectives:Debatingtheethics
anddilemmasofeducationalresearchwithchildren(pp.38–51).Routledge.
Harding,J.(2013).Qualitativedataanalysis:Fromstarttofinish.SAGEPublications.
Hargreaves,E.(2017).Children’sexperiencesofclassrooms:Talkingaboutbeing
pupilsintheclassroom.SAGEPublications.
Harris,R.A.,Qualter,P.,&Robinson,S.J.(2013).Lonelinesstrajectoriesfrom
middlechildhoodtopre-adolescence:Impactonperceivedhealthandsleep
disturbance.JournalofAdolescence,36,1295–1304.
https://doi.org/10.1016/j.adolescence.2012.12.009
Hayes,A.F.(2013).Introductiontomediation,moderation,andconditionalprocess
analysis:Aregression-basedapproach.TheGuilfordPress.
Hayes,A.F.(2015).Anindexandtestoflinearmoderatedmediation.Multivariate
BehavioralResearch,50,1–22.
https://doi.org/10.1080/00273171.2014.962683
Hayes,A.F.(2017).Introductiontomediation,moderation,andconditionalprocess
analysis:Aregression-basedapproach(2nded.).GuilfordPress.
Hazel,C.E.(2016).Empoweredlearninginsecondaryschools:Promotingpositive
youthdevelopmentthroughamultitieredsystemofsupports.American
PsychologicalAssociation.

REFERENCES
335
Hazel,N.,Oppenheimer,C.W.,Technow,J.,Young,J.,&Hankin,B.L.(2015).Parent
relationshipqualitybuffersagainsttheeffectofpeerstressorsondepressive
symptomsfrommiddlechildhoodtoadolescence.DevelopmentalPsychology,
50,2115–2123.https://doi.org/10.1037/a0037192
Hefferon,K.,&Gil-Rodriguez,E.(2011).Interpretativephenomenologicalanalysis.
ThePsychologist,24,756–759.https://doi.org/10.1002/9780470776278.ch10
Heidegger,M.(1962).Beingandtime.Blackwell(Originalworkpublished1927).
Heiman,T.,&Margalit,M.(1998).Loneliness,depression,andsocialskillsamong
studentswithmildmentalretardationindifferenteducationalsettings.The
JournalofSpecialEducation,32,154–163.
https://doi.org/10.1177/002246699803200302
Henin,A.,Micco,J.A.,Schoeller,M.,Boudreaux,A.,&Hirshfeld-Becker,D.(2016).
Cognitivebehaviouraltherapywithchildrenandadolescents.InT.E.Petersen,
S.Sprich,&S.Wilhelm(Eds.),TheMassachusetsGeneralHospitalhandbookof
cognitivebehavioraltherapy(pp.259–275).HumanaPress.
Herrero,J.,&Meneses,J.(2006).Shortweb-basedversionsofthePerceivedStress
(PSS)andCenterforEpidemiologicalStudies-Depression(CESD)Scales:A
comparisontopencilandpaperresponsesamonginternetusers.Computersin
HumanBehavior,22,830–846.https://doi.org/10.1016/j.chb.2004.03.007
Herres,J.,&Kobak,R.(2014).Theroleofparent,teacher,andpeereventsin
maintainingdepressivesymptomsduringearlyadolescence.Journalof
AbnormalChildPsychology,43,325–337.https://doi.org/10.1007/s10802-014-
9896-3
Hewitt,P.L.,Flett,G.L.,&Shawn,W.M.(1992).ThePerceivedStressScale:Factor
structureandrelationtodepressionsymptomsinapsychiatricsample.Journal
ofPsychopathologyandBehavioralAssessment,14,247–257.
Hill,E.,Berthoz,S.,&Frith,U.(2004).Briefreport:Cognitiveprocessingofown
emotionsinindividualswithautisticspectrumdisorderandintheirrelatives.
JournalofAutism&DevelopmentalDisorders,34,229–235.
https://doi.org/10.1023/B:JADD.0000022613.41399.14
HiuYap,M.B.,Pilkington,P.D.,Ryan,S.M.,&Jorm,A.F.(2014).Parentalfactors
associatedwithdepressionandanxietyinyoungpeople:Asystematicreview

REFERENCES
336
andmeta-analysis.JournalofAffectiveDisorders,156,8–23.
https://doi.org/10.1016/j.jad.2013.11.007
HMGovernment.(2015).Workingtogethertosafeguardchildren:Aguidetointer-
agencyworkingtosafeguardandpromotethewelfareofchildren.
Hobson,R.P.,Chidambi,G.,Lee,A.,Meyer,J.,Müller,J.I.,Carpendale,M.,Bibok,
M.,&Racine,T.P.(2006).Foundationsforself-awareness:Anexploration
throughautism.MonographsoftheSocietyforResearchinChildDevelopment,
71,vii–166.https://doi.org/10.1111/j.1540-5834.2006.00387.x
Hollon,S.D.,&Kendall,P.C.(1980).Cognitiveself-statementsindepression:
Developmentofanautomaticthoughtsquestionnaire.CognitiveTherapyand
Research,4,383–395.https://doi.org/10.1007/BF01178214
Holmbeck,G.N.(1997).Towardterminological,conceptual,andstatisticalclarityin
thestudyofmediatorsandmoderators:Examplesfromthechild-clinicaland
pediatricpsychologyliteratures.JournalofConsultingandClinicalPsychology,
65,599–610.https://doi.org/10.1037/0022-006X.65.4.599
Holt-Lunstad,J.,Robles,T.,&Sbarra,D.A.(2017).Advancingsocialconnectionasa
publichealthpriorityintheUnitedStates.AmericanPsychologist,72,517–530.
https://doi.org/10.1037/amp0000103
Hooper,D.,Coughlan,J.,&Mullen,M.(2008).Structuralequationmodelling:
Guidelinesfordeterminingmodelfit.ElectronicJournalofBusinessResearch
Methods,6,53–60.https://doi.org/10.1037/1082-989X.12.1.58
Hooper,S.R.,Burchinal,M.R.,Roberts,J.E.,Zeisel,S.,&Neebe,E.C.(1998).Social
andfamilyriskfactorsforinfantdevelopmentatoneyear:Anapplicationof
thecumulativeriskmodel.JournalofAppliedDevelopmentalPsychology,19,
85–96.https://doi.org/10.1016/S0193-3973(99)80029-X
Horan,J.M.,&Widom,C.S.(2015).Cumulativechildhoodriskandadult
functioninginabusedandneglectedchildrengrownup.Developmentand
Psychopathology,27,927–941.https://doi.org/10.1017/S095457941400090X
Horwitz,S.M.,Chamberlain,P.,Landsverk,J.,&Mullican,C.(2010).Improvingthe
mentalhealthofchildreninchildwelfarethroughtheimplementationof
evidence-basedparentinginterventions.AdministrationandPolicyinMental
HealthandMentalHealthServicesResearch,37(1–2),27–39.

REFERENCES
337
https://doi.org/10.1007/s10488-010-0274-3
Hostinar,C.E.,Johnson,A.E.,&Gunnar,M.R.(2015).Parentsupportisless
effectiveinbufferingcortisolstressreactivityforadolescentscomparedto
children.DevelopmentalScience,18,281–297.
https://doi.org/10.1111/desc.12195
Hostinar,C.E.,Sullivan,R.M.,&Gunnar,M.R.(2014).Psychobiological
mechanismsunderlyingthesocialbufferingoftheHPAaxis:Areviewofanimal
modelsandhumanstudiesacrossdevelopment.PsychologicalBulletin,140,
256–282.https://doi.org/10.1037/a0032671
Hounsell,D.(2013).Hiddenfromview:TheexperiencesofyoungcarersinEngland.
HowardWilsher,S.,Harrison,F.,Yamoah,F.,Fearne,A.,&Jones,A.(2016).The
relationshipbetweenunhealthyfoodsales,socio-economicdeprivationand
childhoodweightstatus:Resultsofacross-sectionalstudyinEngland.
InternationalJournalofBehavioralNutritionandPhysicalActivity,13,4–11.
https://doi.org/10.1186/s12966-016-0345-2
Howe,K.R.(1988).Againstthequantitative-qualitativeincompatibilitythesisor
dogmasdiehard.EducationalResearcher,17(8),10–16.
https://doi.org/10.3102/0013189X017008010
Hox,J.J.,Moerbeek,M.,&vandeSchoot,R.(2018).Multilevelanalysis:Techniques
andapplications(3rded.).Taylor&Francis.
Hu,L.T.,&Bentler,P.M.(1999).Cutoffcriteriaforfitindexesincovariance
structureanalysis:Conventionalcriteriaversusnewalternatives.Structural
EquationModeling,6,1–55.https://doi.org/10.1080/10705519909540118
Huber,P.J.(1981).Robuststatistics.JohnWiley.
Hughes,K.,Bellis,M.A.,Hardcastle,K.A.,Sethi,D.,Butchart,A.,Mikton,C.,Jones,
L.,&Dunne,M.P.(2017).Theeffectofmultipleadversechildhood
experiencesonhealth:Asystematicreviewandmeta-analysis.TheLancet
PublicHealth,2,e356–e366.https://doi.org/10.1016/S2468-2667(17)30118-4
Humphrey,N.,Wigelsworth,M.,Barlow,A.,&Squires,G.(2013).Theroleofschool
andindividualdifferencesintheacademicattainmentoflearnerswithspecial
educationalneedsanddisabilities:Amulti-levelanalysis.InternationalJournal
ofInclusiveEducation,17,909–931.

REFERENCES
338
https://doi.org/10.1080/13603116.2012.718373
Husserl,E.(1971).Phenomenology(R.E.Palmer,trans.).JournaloftheBritish
SocietyforPhenomenology,2,77-90(Originalworkpublished1927).
Hyde,J.S.,Mezulis,A.H.,&Abramson,L.Y.(2008).TheABCsofdepression:
Integratingaffective,biological,andcognitivemodelstoexplainthe
emergenceofthegenderdifferenceindepression.PsychologicalReview,115,
291–313.https://doi.org/10.1037/0033-295X.115.2.291
Iglewicz,B.,&Hoaglin,D.C.(1993).Howtodetectandhandleoutliers.ASQC
QualityPress.
Ilie,S.,Sutherland,A.,&Vignoles,A.(2017).Revisitingfreeschoolmealeligibilityas
aproxyforpupilsocio-economigdeprivation.BritishEducationalResearch
Journal,43,253–274.https://doi.org/10.1002/berj.3260
Inder,M.,Crowe,M.,Moor,S.,Luty,S.,Carter,J.,&Joyce,P.(2008).“Iactually
don’tknowwhoIam”:Theimpactofbipolardisorderonthedevelopmentof
self.Psychiatry,71,123–132.https://doi.org/10.1521.psyc.2008.71.2.123
Ireland,M.J.,&Pakenham,K.I.(2010).Youthadjustmenttoparentalillnessor
disability:Theroleofillnesscharacteristics,caregiving,andattachment.
Psychology,HealthandMedicine,15,632–645.
https://doi.org/10.1080/13548506.2010.498891
Irvine,A.,Drew,P.,&Sainsbury,R.(2013).“AmInotansweringyourquestions
properly?”Clarification,adequacyandresponsivenessinsemi-structured
telephoneandface-to-faceinterviews.QualitativeResearch,13,87–106.
https://doi.org/10.1177/1468794112439086
Ja,N.M.,&Jose,P.E.(2017).“Ican’ttakeholdofsomekindofalife”:Theroleof
socialconnectednessinengaging“lost”adolescentswithintheirlives.Journal
ofYouthandAdolescence,46,2028–2046.https://doi.org/10.1007/s10964-
017-0656-x
Jaccard,J.,Blanton,H.,&Dodge,T.(2005).Peerinfluencesonriskbehavior:An
analysisoftheeffectsofaclosefriend.DevelopmentalPsychology,41,135–
147.https://doi.org/10.1037/0012-1649.41.1.135
Jackson,D.L.(2003).Revisitingsamplesizeandnumberofparameterestimates:
SomesupportfortheN:qhypothesis.StructuralEquationModeling,10,128–

REFERENCES
339
141.https://doi.org/10.1207/S15328007SEM1001_6
JacksonWilliams,D.(2012).WheredoJamaicanadolescentsturnforpsychological
help?ChildandYouthCareForum,41,461–477.
https://doi.org/10.1007/s10566-012-9177-7
Jacobson,D.E.(2009).Typesandtimingofsocialsupport.JournalofHealthand
SocialBehavior,27,250–264.https://doi.org/10.2307/2136745
Jennings,P.A.,&Greenberg,M.T.(2009).Theprosocialclassroom:Teachersocial
andemotionalcompetenceinrelationtostudentandclassroomoutcomes.
ReviewofEducationalResearch,79,491–525.
https://doi.org/10.3102/0034654308325693
Jeronimus,B.F.,Stavrakakis,N.,Veenstra,R.,&Oldehinkel,A.J.(2015).Relative
ageeffectsinDutchadolescents:Concurrentandprospectiveanalyses.PLoS
ONE,10,e0128856.https://doi.org/10.1371/journal.pone.0128856
Johnson,D.P.,&Whisman,M.A.(2013).Genderdifferencesinrumination:Ameta-
analysis.PersonalityandIndividualDifferences,55,367–374.
https://doi.org/10.1016/j.paid.2013.03.019
Johnson,R.B.,&Onwuegbuzie,A.J.(2004).Mixedmethodsresearch:Aresearch
paradigmwhosetimehascome.EducationalReseacher,33(7),14–26.
https://doi.org/10.3102/0013189X033007014
Johnson,R.B.,Onwuegbuzie,A.J.,&Turner,L.A.(2007).Towardadefinitionof
mixedmethodsresearch.JournalofMixedMethodsResearch,1,112–133.
https://doi.org/10.1080/17439760.2016.1262619
Jones,D.J.,Forehand,R.,Brody,G.,&Armistead,L.(2002).Psychosocial
adjustmentofAfricanAmericanchildreninsingle-motherfamilies:Atestof
threeriskmodels.JournalofMarriageandtheFamily,64,105–115.
https://doi.org/10.1111/j.1741-3737.2002.00105.x
Jones,P.B.(2013).Adultmentalhealthdisordersandtheirageatonset.British
JournalofPsychiatry,202,s5–s10.https://doi.org/10.1192/bjp.bp.112.119164
Jones,S.,&Myhill,D.(2004).“Troublesomeboys”and“compliantgirls”:Gender
identityandperceptionsofachievementandunderachievement.British
JournalofSociologyofEducation,25,547–561.
https://doi.org/10.1080/0142569042000252044

REFERENCES
340
Kandel,D.B.,Raveis,V.H.,&Davies,M.(1991).Suicidalideationinadolescence:
Depression,substanceuse,andotherriskfactors.JournalofYouthand
Adolescence,20,289–309.https://doi.org/10.1007/BF01537613
Kapfhammer,H.-P.(2006).Somaticsymptomsanddepression.DialoguesinClinical
Neuroscience,29,65–69.
Karam,F.,Bérard,A.,Sheehy,O.,Huneau,M.C.,Briggs,G.,Chambers,C.,Einarson,
A.,Johnson,D.,Kao,K.,Koren,G.,Martin,B.,Polifka,J.E.,Riordan,S.H.,Roth,
M.,Lavigne,S.V.,Wolfe,L.,Braddock,S.,Quinn,D.,Jones,K.L.,…Wisner,K.
(2012).Reliabilityandvalidityofthe4-itemPerceivedStressScaleamong
pregnantwomen:ResultsfromtheOTISantidepressantsstudy.Researchin
NursingandHealth,35,363–375.https://doi.org/10.1002/nur.21482
Kariuki,S.M.,Newton,C.R.J.C.,Prince,M.J.,&Das-Munshi,J.(2016).The
associationbetweenchildhoodseizuresandlaterchildhoodemotionaland
behavioralproblems:Findingsfromanationallyrepresentativebirthcohort.
PsychosomaticMedicine,78,620–628.
https://doi.org/10.1097/PSY.0000000000000305
Katon,W.,Richardson,L.,Russo,J.,C.A.,M.,C.,R.,E.,M.,Richards,J.,&Grossman,
D.C.(2010).Depressivesymptomsinadolescence:Theassociationwith
multiplehealthriskbehaviors.GeneralHospitalPsychiatry,32,233–239.
https://doi.org/10.1016/j.genhosppsych.2010.01.008
Kaurin,A.,Egloff,B.,Stringaris,A.,&Wessa,M.(2016).Onlycomplementaryvoices
tellthetruth:Areevaluationofvalidityinmulti-informantapproachesofchild
andadolescentclinicalassessments.JournalofNeuralTransmission,123,981–
990.https://doi.org/10.1007/s00702-016-1543-4
Kavanagh,A.M.,Bentley,R.,Turrell,G.,Broom,D.H.,&Subramanian,S.V.(2006).
Doesgendermodifyassociationsbetweenselfratedhealthandthesocialand
economiccharacteristicsoflocalenvironments?JournalofEpidemiologyand
CommunityHealth,60,490–495.https://doi.org/10.1136/jech.2005.043562
Kavanaugh,M.S.,Stamatopoulos,V.,Cohen,D.,&Zhang,L.(2015).
Unacknowledgedcaregivers:Ascopingreviewofresearchoncaregivingyouh
intheUnitedStates.AdolescentResearchReview,1,29–49.
https://doi.org/10.1007/s40894-015-0015-7

REFERENCES
341
Kawachi,I.,&Berkman,L.F.(2001).Socialtiesandmentalhealth.JournalofUrban
Health,78,458–467.https://doi.org/10.1093/jurban/78.3.458
Keenan,K.,&Hipwell,A.E.(2005).Preadolescentcluestounderstanding
depressioningirls.ClinicalChildandFamilyPsychologyReview,8,89–105.
https://doi.org/10.1007/s10567-005-4750-3
Kegerreis,S.,&Midgley,N.(2018).Psychodynamicapproachestocounselling
childrenandyoungpeople.InM.Robson&S.Pattison(Eds.),Thehandbookof
counsellingchildrenandyoungpeople(pp.45–58).SAGEPublications.
Keith,T.Z.(2015).Multipleregressionandbeyond:Anintroductiontomultiple
regressionandstructuralequationmodeling(2nded.).Routledge.
Kessler,R.C.(2003).Epidemiologyofwomenanddepression.JournalofAffective
Disorders,74,5–13.https://doi.org/10.1016/S0165-0327(02)00426-3
Kessler,R.C.,Berglund,P.,Demler,O.,Jin,R.,Merikangas,K.R.,&Walters,E.E.
(2005).Lifetimeprevalenceandage-of-onsetdistributionsofDSM-IVdisorders
intheNationalComorbiditySurveyreplication.ArchGenPsychiatry,62,593–
602.https://doi.org/10.1001/archpsyc.62.6.593
Kieling,C.,Baker-Henningham,H.,Belfer,M.,Conti,G.,Ertem,I.,Omigbodun,O.,
Rohde,L.A.,Srinath,S.,Ulkuer,N.,&Rahman,A.(2011).Childandadolescent
mentalhealthworldwide:Evidenceforaction.TheLancet,378,1515–1525.
https://doi.org/10.1016/S0140-6736(11)60827-1
Kilkelly,U.,Kilpatrick,R.,&Lundy,L.(2005).Children’srightsinNorthernIsland.
Kilmer,R.P.,Cook,J.R.,Munsell,E.P.,&Salvador,S.K.(2010).Factorsassociated
withpositiveadjustmentinsiblingsofchildrenwithsevereemotional
disturbance:Theroleoffamilyresourcesandcommunitylife.American
JournalofOrthopsychiatry,80,473–481.https://doi.org/10.1111/j.1939-
0025.2010.01050.x
Kim,J.,&Cicchetti,D.(2004).Alongitudinalstudyofchildmaltreatment,mother-
childrelationshipqualityandmaladjustment:Theroleofself-esteemand
socialcompetence.JournalofAbnormalChildPsychology,32,341–354.
https://doi.org/10.1023/B:JACP.0000030289.17006.5a
King,N.,&Horrocks,C.(2010).Interviewsinqualitativeresearch.SAGE
Publications.

REFERENCES
342
Kirk,B.A.,Schutte,N.S.,&Hine,D.W.(2008).Developmentandpreliminary
validationofanemotionalself-efficacyscale.PersonalityandIndividual
Differences,45,432–436.https://doi.org/10.1016/j.paid.2008.06.010
Kish,L.(1965).Surveysampling.Wiley.
Kliewer,W.,NelsonCunningham,J.,Diehl,R.,AdamsParrish,K.,Walker,J.M.,
Atiyeh,C.,Neace,B.,Duncan,L.,Taylor,K.,&Mejia,R.(2004).Violence
exposureandadjustmentininner-cityyouth:Childandcaregiveremotion
regulationskill,caregiver-childrelationshipquailty,andneighborhood
cohesionasprotectivefactor.JournalofClinicalChildandAdolescent
Psychology,33,477–487.https://doi.org/10.1207/s15374424jccp3303_5
Kline,R.B.(2016).Principlesandpracticeofstructuralequationmodeling(4thed.).
TheGuilfordPress.
Klinger,D.A.,Freeman,J.G.,Bilz,L.,Liiv,K.,Ramelow,D.,Sebok,S.S.,Samdal,O.,
Dür,W.,&Rasmussen,M.(2015).Cross-nationaltrendsinperceivedschool
pressurebygenderandagefrom1994to2010.EuropeanJournalofPublic
Health,25,51–56.https://doi.org/10.1093/eurpub/ckv027
Kokanovic,R.(2011).Thediagnosisofdepressioninaninternationalcontext.InD.
Pilgrim,A.Rogers,&B.Pescosolido(Eds.),TheSAGEhandbookofmental
healthandillness(pp.127–146).SAGEPublications.
Kostanski,M.,&Gullone,E.(1998).Adolescentbodyimagedissatisfaction:
Relationshipswithself-esteem,anxiety,anddepressioncontrollingforbody
mass.JournalofChildPsychologyandPsychiatryandAlliedDisciplines,39,
255–262.https://doi.org/10.1017/S0021963097001807
Kovacs,M.,&Beck,A.T.(1979).Cognitive-affectiveprocessesindepression.InC.E.
Izard(Ed.),EmotionsinPersonalityandPsychopathology(pp.415–422).
Springer.
Kovess-Masfety,V.,Husky,M.M.,Keyes,K.,Hamilton,A.,Pez,O.,Bitfoi,A.,Carta,
M.G.,Goelitz,D.,Kuijpers,R.,Otten,R.,Koc,C.,Lesinskiene,S.,&Mihoav,Z.
(2016).Comparingtheprevalenceofmentalhealthproblemsinchildren6–11
acrossEurope.SocialPsychiatryandPsychiatricEpidemiology,51,1093–1103.
https://doi.org/10.1007/s00127-016-1253-0
Kraemer,H.C.,Lowe,K.K.,&Kupfer,D.J.(2005).Toyourhealth:Howto

REFERENCES
343
understandwhatresearchtellsusaboutrisk.OxfordUniversityPress.
Kraemer,H.C.,Stice,E.,Kazdin,A.,Offord,D.,&Kupfer,D.(2001).Howdorisk
factorsworktogether?Mediators,moderators,andindependent,overlapping,
andproxyriskfactors.AmericanJournalofPsychiatry,158,848–856.
https://doi.org/10.1176/appi.ajp.158.6.848
Kuehner,C.(2003).Genderdifferencesinunipolardepression:Anupdateof
epidemiologicalfindingsandpossibleexplanations.ActaPsychiatrica
Scandinavica,108,163–174.https://doi.org/10.1034/j.1600-
0447.2003.00204.x
Kuehner,C.(2017).Whyisdepressionmorecommonamongwomenthanamong
men?TheLancetPsychiatry,4,146–158.https://doi.org/10.1016/S2215-
0366(16)30263-2
Kuhn,T.S.(1962).Thestructureofscientificrevolutions(2nded.).TheUniversityof
ChicagoPress.
Kuwabara,S.A.,VanVoorhees,B.W.,Gollan,J.K.,&Alexander,G.C.(2007).A
qualitativeexplorationofdepressioninemergingadulthood:disorder,
development,andsocialcontext.GeneralHospitalPsychiatry,29,317–324.
https://doi.org/10.1016/j.genhosppsych.2007.04.001
LaGreca,A.M.,&Harrison,H.M.(2010).Adolescentpeerrelations,friendships,
andromanticrelationships:Dotheypredictsocialanxietyanddepression?
JournalofClinicalChildandAdolescentPsychology,34,49–61.
https://doi.org/10.1207/s15374424jccp3401
Lakey,B.,&Orehek,E.(2011).Relationalregulationtheory:Anewapproachto
explainthelinkbetweenperceivedsocialsupportandmentalhealth.
PsychologicalReview,118,482–495.https://doi.org/10.1037/a0023477
Lance,C.E.,Butts,M.M.,&Michels,L.C.(2006).Thesourcesoffourcommonly
reportedcutoffcriteria:Whatdidtheyreallysay?OrganizationalResearch
Methods,9,202–220.https://doi.org/10.1177/1094428105284919
Landerman,R.,George,L.K.,Campbell,R.T.,&Blazer,D.G.(1989).Alternative
modelsofthestressbufferinghypothesis.AmericanJournalofCommunity
Psychology,17,625–642.https://doi.org/10.1007/BF00922639
Landstedt,E.,Asplund,K.,&GillanderGådin,K.(2009).Understandingadolescent

REFERENCES
344
mentalhealth:Theinfluenceofsocialprocesses,doinggenderandgendered
powerrelations.SociologyofHealthandIllness,31,962–978.
https://doi.org/10.1111/j.1467-9566.2009.01170.x
Langdridge,D.(2007).Phenomenologicalpsychology:Theory,researchandmethod.
PearsonEducation.
Lanier,P.,Maguire-Jack,K.,Lombardi,B.,Frey,J.,&Rose,R.A.(2018).Adverse
childhoodexperiencesandchildhealthoutcomes:Comparingcumulativerisk
andlatentclassapproaches.MaternalandChildHealthJournal,22,288–297.
https://doi.org/10.1007/s10995-017-2365-1
Lansford,J.E.,Deater-Deckard,K.,Dodge,K.A.,Bates,J.E.,&Pettit,G.S.(2004).
Ethnicdifferencesinthelinkbetweenphysicaldisciplineandlateradolescent
externalizingbehaviors.JournalofChildPsychologyandPsychiatryandAllied
Disciplines,45,801–812.https://doi.org/10.1111/j.1469-7610.2004.00273.x
Lanza,S.T.,&Cooper,B.R.(2016).Latentclassanalysisfordevelopmental
research.ChildDevelopmentPerspectives,10,59–64.
https://doi.org/10.1111/cdep.12163
Lanza,S.T.,Rhoades,B.L.,Nix,R.L.,&Greenberg,M.T.(2010).Modelingthe
interplayofmultilevelriskfactorsforfutureacademicandbehaviorproblems:
Aperson-centeredapproach.DevelopmentandPsychopathology,22,313–
335.https://doi.org/10.1017/S0954579410000088
Larkin,M.,&Thompson,A.R.(2006).Interpretativephenomenologicalanalysis.In
A.R.Thompson&D.Harper(Eds.),Qualitativeresearchmethodsinmental
healthandpsychotherapy:Aguideforstudentsandpractitioners(pp.99–116).
JohnWiley&Sons.
Larkin,M.,&Thompson,A.R.(2012).Interpretativephenomenologicalanalysis.In
A.Thompson&D.Harper(Eds.),Qualitativeresearchmethodsinmental
healthandpsychotherapy:Aguideforstudentsandpractitioners(pp.99–116).
JohnWiley&Sons.
Larkin,M.,Watts,S.,&Clifton,E.(2006).Givingvoiceandmakingsensein
interpretativephenomenologicalanalysis.QualitativeResearchinPsychology,
3,102–120.https://doi.org/10.1191/1478088706qp062oa
Lazarus,R.S.(1966).Psychologicalstressandthecopingprocess.McGraw-Hill.

REFERENCES
345
Lazarus,R.S.(1990).Theory-basedstressmeasurement.PsychologicalInquiry,1,3–
13.https://doi.org/10.1007/sl0734-011-9485-0
Lazarus,R.S.,&Folkman,S.(1984).Stress,appraisal,andcoping.Springer
PublishingCompany,Inc.
Lazarus,R.S.,&Folkman,S.(1986).ContrastingtheHasslesScaleandthePerceived
StressScale:Who’sreallymeasuringappraisedstress?AmericanPsychologist,
41,716–718.https://doi.org/10.1037/0003-066X.41.6.716
Lazarus,R.S.,&Launier,R.(1979).Stress-relatedtransactionsbetweenpersonand
environment.InL.A.Pervin&M.Lewis(Eds.),Perspectivesininteractional
psychology(pp.287–327).Springer.
Ledoux,J.E.(2000).Emotioncircuitsinthebrain.AnnualReviewofNeuroscience,
23,155–184.https://doi.org/10.1146/annurev.neuro.23.1.155
Lee,A.,Hankin,B.L.,Mermelstein,R.J.,Lee,A.,Hankin,B.L.,Perceived,R.J.M.,&
Lee,A.(2010).Perceivedsocialcompetence,negativesocialinteractions,and
negativecognitivestylepredictdepressivesymptomsduringadolescence.
JournalofClinicalChildandAdolescentPsychology,39,603–615.
https://doi.org/10.1080/15374416.2010.501284
Lee,E.H.(2012).ReviewofthepsychometricevidenceofthePerceivedStress
Scale.AsianNursingResearch,6,121–127.
https://doi.org/10.1016/j.anr.2012.08.004
Lee,R.M.,Draper,M.,&Lee,S.(2001).Socialconnectedness,dysfunctional
interpersonalbehaviors,andpsychologicaldistress:Testingamediatormodel.
JournalofCounselingPsychology,48,310–318.https://doi.org/10.1037/0022-
0167.48.3.310
Lee,R.M.,Keough,K.A.,&Sexton,J.D.(2002).Socialconnectedness,social
appraisal,andperceivedstressincollegewomenandmen.Journalof
CounselingandDevelopment,80,355–361.https://doi.org/10.1002/j.1556-
6678.2002.tb00200.x
Lee,R.M.,&Robbins,S.B.(1998).Therelationshipbetweensocialconnectedness
andanxiety,self-esteem,andsocialidentity.JournalofCounselingPsychology,
45,338–345.
Leech,N.L.,&Onwuegbuzie,A.J.(2009).Atypologyofmixedmethodsresearch

REFERENCES
346
designs.QualityandQuantity,43,265–275.https://doi.org/10.1007/s11135-
007-9105-3
Lereya,S.T.,Humphrey,N.,Patalay,P.,Wolpert,M.,Böhnke,J.R.,Macdougall,A.,
&Deighton,J.(2016).TheStudentResilienceSurvey:Psychometricvalidation
andassociationswithmentalhealth.ChildandAdolescentPsychiatryand
MentalHealth,10,44–59.https://doi.org/10.1186/s13034-016-0132-5
Lerner,D.,&Henke,R.M.(2008).Whatdoesresearchtellusaboutdepression,job
performance,andworkproductivity?JournalofOccupationaland
EnvironmentalMedicine,50,401–410.
https://doi.org/10.1097/JOM.0b013e31816bae50
Lerner,R.M.,Theokas,C.,&Jelicic,H.(2005).Youthasactiveagentsintheirown
positivedevelopment:Adevelopmentalsystemsperspective.InW.Greve,K.
Rothermund,&D.Wentura(Eds.),Theadaptiveself:Personalcontinuityand
intentionalself-development(pp.31–48).Hogrefe&HuberPublishers.
Lesage,F.X.,Berjot,S.,&Deschamps,F.(2012).Psychometricpropertiesofthe
FrenchversionsofthePerceivedStressScale.InternationalJournalof
OccupationalMedicineandEnvironmentalHealth,25,178–184.
https://doi.org/10.2478/S13382-012-0024-8
Lessof,C.,Ross,A.,Brind,R.,Bell,E.,&Newton,S.(2016).Longitudinalstudyof
youngpeopleinEnglandcohort2:Healthandwellbeingatwave2.
Leung,D.Y.,Lam,T.,&Chan,S.S.(2010).ThreeversionsofPerceivedStressScale:
ValidationinasampleofChinesecardiacpatientswhosmoke.BMCPublic
Health,10,513.https://doi.org/10.1186/1471-2458-10-513
Leve,L.D.,Kim,H.K.,&Pears,K.C.(2005).Childhoodtemperamentandfamily
environmentaspredictorsofinternalizingandexternalizingtrajectoriesfrom
age5toage17.JournalofAbnormalChildPsychology,33,505–520.
Leventhal,T.,&Brooks-Gunn,J.(2000).Theneighborhoodstheylivein:Theeffects
ofneighborhoodresidenceonchildandadolescentoutcomes.Psychological
Bulletin,126,309–337.https://doi.org/10.1037//0033-2909.126.2.309
Lewinsohn,P.M.,Gotlib,I.H.,Lewinsohn,M.,Seeley,J.R.,&Allen,N.B.(1998).
Genderdifferencesinanxietydisordersandanxietysymptomsinadolescents.
JournalofAbnormalPsychology,107,109–117.https://doi.org/10.1037/0021-

REFERENCES
347
843X.107.1.109
Lewinsohn,P.M.,Rohde,P.,&Seeley,J.R.(1996).Adolescentsuicidalideationand
attempts:Prevalence,riskfactors,andclinicalimplications.ClinicalPsychology:
ScienceandPractice,3,25–46.https://doi.org/10.1111/j.1468-
2850.1996.tb00056.x
Lewinsohn,P.M.,Striegel-Moore,R.H.,&Seeley,J.R.(2000).Epidemiologyand
naturalcourseofeatingdisordersinyoungwomenfromadolescencetoyoung
adulthood.JournaloftheAmericanAcademyofChildandAdolescent
Psychiatry,39,1284–1292.https://doi.org/10.1097/00004583-200010000-
00016
Lewis,R.,&Burman,E.(2008).Providingforstudentvoiceinclassroom
management:Teachers’views.InternationalJournalofInclusiveEducation,
12(2),151–167.https://doi.org/10.1080/13603110600790605
Li,C.H.(2016).Confirmatoryfactoranalysiswithordinaldata:Comparingrobust
maximumlikelihoodanddiagonallyweightedleastsquares.BehaviorResearch
Methods,48,936–949.https://doi.org/10.3758/s13428-015-0619-7
Li,S.T.,Nussbaum,K.M.,&Richards,M.H.(2007).Riskandprotectivefactorsfor
urbanAfrican-Americanyouth.AmericanJournalofCommunityPsychology,
39,21–35.https://doi.org/10.1007/s10464-007-9088-1
Liang,X.,&Yang,Y.(2014).AnevaluationofWLSMVandBayesianmethodsfor
confirmatoryfactoranalysiswithcategoricalindicators.InternationalJournal
ofQuantitativeResearchinEducation,2,17.
https://doi.org/10.1504/IJQRE.2014.060972
Lieberman,M.D.,Eisenberger,N.I.,Crockett,M.J.,Tom,S.M.,Pfeifer,J.H.,&
Way,B.M.(2007).Puttingfeelingsintowords:Affectlabelingdisrupts
amygdalaactivityinresponsetoaffectivestimuli.PsychologicalScience,18(5),
421–428.https://doi.org/10.1111/j.1467-9280.2007.01916.x
Lien,L.,Tambs,K.,Oppedal,B.,Heyerdahl,S.,&Bjertness,E.(2005).Isrelatively
youngagewithinaschoolyearariskfactorformentalhealthproblemsand
poorschoolperformance?Apopulation-basedcross-sectionalstudyof
adolescentsinOslo,Norway.BMCPublicHealth,5,102–110.
https://doi.org/10.1186/1471-2458-5-102

REFERENCES
348
Lincoln,Y.S.,&Guba,E.G.(1985).Naturalisticinquiry.SAGEPublications.
Lindell,M.K.,&Whitney,D.J.(2001).Accountingforcommonmethodvariancein
cross-sectionalresearchdesigns.JournalofAppliedPsychology,86(1),114–
121.https://doi.org/10.1037/0021-9010.86.1.114
Little,R.J.A.(1988).Atestofmissingcompletelyatrandomformultivariatedata
withmissingvalues.JournalofTheAmericanStatisticalAssociation,83,1198–
1202.
Little,R.J.A.,&Rubin,D.B.(1987).Statisticalanalysiswithmissingdata.John
Wiley&Sons.
Little,R.J.A.,&Rubin,D.B.(2002).Statisticalanalysiswithmissingdata(2nded.).
JohnWiley&Sons.
Liu,J.,Chen,X.,&Lewis,G.(2011).Childhoodinternalizingbehaviour:Analysisand
implications.JournalofPsychiatricandMentalHealthNursing,18,884–894.
https://doi.org/10.1111/j.1365-2850.2011.0173.x
Logan,J.G.,&Barksdale,D.J.(2008).Allostasisandallostaticload:Expandingthe
discourseonstressandcardiovasculardisease.JournalofClinicalNursing,17,
201–208.https://doi.org/10.1111/j.1365-2702.2008.02347.x
Longobardi,C.,Prino,L.E.,Marengo,D.,&Settanni,M.(2016).Student-teacher
relationshipsasaprotectivefactorforschooladjustmentduringthetransition
frommiddletohighschool.FrontiersinPsychology,7,1988.
https://doi.org/10.3389/fpsyg.2016.01988
Lopez,K.A.,&Willis,D.G.(2004).Descriptiveversusinterpretivephenomenology:
Theircontributionstonursingknowledge.QualitativeHealthResearch,14,
726–735.https://doi.org/10.1177/1049732304263638
Lopez,M.A.,Toprac,M.G.,Crismon,M.L.,Boemer,C.,&Baumgartner,J.(2005).A
psychoeducationalprogramforchildrenwithADHDordepressionandtheir
families:ResultsfromtheCMAPfeasibilitystudy.CommunityMentalHealth
Journal,41(1),51–66.https://doi.org/10.1007/s10597-005-2599-z
Loukas,A.,Cance,J.D.,&Batanova,M.(2016).Trajectoriesofschool
connectednessacrossthemiddleschoolyears:Examiningtherolesof
adolescens’internalizingandexternalizingproblems.Youth&Society,48,557–
576.https://doi.org/10.1177/0044118X13504419

REFERENCES
349
Loukas,A.,Prelow,H.M.,Suizzo,M.A.,&Allua,S.(2008).Motheringandpeer
associationsmediatecumulativeriskeffectsforlatinoyouth.Journalof
MarriageandFamily,70,76–85.https://doi.org/10.1111/j.1741-
3737.2007.00462.x
Luby,J.,Belden,A.,Botteron,K.,Marrus,N.,Harms,M.P.,Babb,C.,Nishino,T.,&
Barch,D.(2013).Theeffectsofpovertyonchildhoodbraindevelopment:The
mediatingeffectofcaregivingandstressfullifeevents.JAMAPediatrics,167,
1135–1142.https://doi.org/10.1001/jamapediatrics.2013.3139
Luebbe,A.M.,Bell,D.J.,Allwood,M.A.,Swenson,L.P.,&Early,M.C.(2010).Social
informationprocessinginchildren:Specificrelationstoanxiety,depression,
andaffect.JournalofClinicalChildandAdolescentPsychology,39,386–399.
https://doi.org/10.1080/15374411003691685
Lundy,L.(2007).“Voice”isnotenough:conceptualisingArticle12oftheUnited
NationsConventionontheRightsoftheChild.BritishEducationalResearch
Journal,33,927–942.https://doi.org/10.1080/01411920701657033
Lupton,R.(2005).Socialjusticeandschoolimprovement:Improvingthequalityof
schoolinginthepoorestneighbourhoods.BritishEducationalResearchJournal,
31,589–604.https://doi.org/10.1080/01411920500240759
Luthar,S.S.,Cicchetti,D.,&Becker,B.(2000).Theconstructofresilience:Acritical
evaluationandguidelinesforfuturework.ChildDevelopment,71,543–562.
https://doi.org/10.1111/1467-8624.00164
MacCallum,R.C.,Widaman,K.F.,Zhang,S.B.,&Hong,S.H.(1999).Samplesizein
factoranalysis.PsychologicalMethods,4,84–99.
https://doi.org/10.1037/1082-989x.4.1.84
MacDonald,G.,&Leary,M.R.(2005).Whydoessocialexclusionhurt?The
relationshipbetweensocialandphysicalpain.PsychologicalBulletin,131,202–
223.https://doi.org/10.1037/0033-2909.131.2.202
Machin,D.,Campbell,M.J.,Tan,S.B.,&Tan,S.H.(2018).Samplesizesforclinical,
laboratoryandepidemiologystudies(4thed.).WileyBlackwell.
MacKinnon,D.P.,Lockwood,C.,&Williams,J.(2004).Confidencelimitsforthe
indirecteffect:Distributionoftheproductandresamplingmethods.
MultivariateBehavioralResearch,39,99–128.

REFERENCES
350
https://doi.org/10.1207/s15327906mbr3901
MacLean,A.,Sweeting,H.,&Hunt,K.(2010).“Rules”forboys,“guidelines”forgirls:
Genderdifferencesinsymptomreportingduringchildhoodandadolescence.
SocialScienceandMedicine,70,597–604.
https://doi.org/10.1016/j.socscimed.2009.10.042
Mair,C.,DiezRoux,A.V.,&Galea,S.(2008).Areneighbourhoodcharacteristics
associatedwithdepressivesymptoms?Areviewofevidence.Journalof
EpidemiologyandCommunityHealth,62,940–946.
https://doi.org/10.1136/jech.2007.066605
Malaquias,S.,Crespo,C.,&Francisco,R.(2015).Howdoadolescentsbenefitfrom
familyrituals?Linkstosocialconnectedness,depressionandanxiety.Journal
ofChildandFamilyStudies,24,3009–3017.https://doi.org/10.1007/s10826-
014-0104-4
Mandy,W.,Chilvers,R.,Chowdhury,U.,Salter,G.,Seigal,A.,&Skuse,D.(2012).Sex
differencesinautismspectrumdisorder:Evidencefromalargesampleof
childrenandadolescents.JournalofAutismandDevelopmentalDisorders,42,
1304–1313.https://doi.org/10.1007/s10803-011-1356-0
March,J.S.,Silva,S.,Petrycki,S.,Curry,J.,Wells,K.,Fairbank,J.,Burns,B.,Domino,
M.,McNulty,S.,Vitiello,B.,Severe,J.,Casta,C.,&Kennard,B.(2007).The
treatmentforadolescentswithdepressionstudy(TADS):Long-term
effectivenessandsafetyoutcomes.PsychiatryandBehavioralSciences,64,
1132–1144.https://doi.org/10.1001/archpsyc.64.10.1132
Marcia,J.E.(1980).Identityinadolescence.InJ.Adelson(Ed.),Handbookof
adolescentpsychology(pp.159–187).Wiley.
Marcia,J.E.(1993).Theegoidentitystatusapproachtoegoidentity.InJ.E.Marcia,
A.S.Waterman,D.R.Matteson,S.L.Archer,&J.L.Orlofsky(Eds.),Ego
Identity(pp.3–21).Springer-Verlag.
Maric,M.,Heyne,D.A.,VanWidenfelt,B.M.,&Westenberg,P.M.(2011).
Distortedcognitiveprocessinginyouth:Thestructureofnegativecognitive
errorsandtheirassociationswithanxiety.CognitiveTherapyandResearch,35,
11–20.https://doi.org/10.1007/s10608-009-9285-3
Marmot,M.(2005).Socialdeterminantsofpublichealth.Lancet,365,1099–1104.

REFERENCES
351
https://doi.org/10.1016/S0140-6736(05)71146-6
Martin,J.,Romas,M.,Medford,M.,Leffert,N.,&Hatcher,S.L.(2006).Adult
helpingqualitiespreferredbyadolescents.Adolescence,41,127–140.
Martin,R.A.,Kazarian,S.S.,&Breiter,H.J.(1995).Perceivedstress,lifeevents,
dysfunctionalattitudes,anddepressioninadolescentpsychiatricinpatients.
JournalofPsychopathologyandBehavioralAssessment,17,81–95.
https://doi.org/10.1007/BF02229205
Masten,A.S.(2001).Ordinarymagic:Resilienceprocessesindevelopment.
AmericanPsychologist,56,227–238.https://doi.org/10.1037//0003-
066X.56.3.227
Masten,A.S.(2014a).Globalperspectivesonresilienceinchildrenandyouth.Child
Development,85,6–20.https://doi.org/10.1111/cdev.12205
Masten,A.S.(2014b).Ordinarymagic:Resilienceindevelopment.TheGuilford
Press.
Masten,A.S.(2016).Resilienceindevelopingsystems:Progressandpromiseasthe
fourthwaverises.EuropeanJournalofDevelopmentalPsychology,13,297–
312.https://doi.org/10.1080/17405629.2016.1147344
Masten,A.S.(2018).Resiliencetheoryandresearchonchildrenandfamilies:Past,
present,andpromise.JournalofFamilyTheoryandReview,10,12–31.
https://doi.org/10.1111/jftr.12255
Mathers,C.D.,&Loncar,D.(2006).Projectionsofglobalmortalityandburdenof
diseasefrom2002to2030.PLoSMedicine,3,2011–2030.
https://doi.org/10.1371/journal.pmed.0030442
Matud,M.P.(2004).Genderdifferencesinstressandcopingstyles.Personalityand
IndividualDifferences,37,1401–1415.
https://doi.org/10.1016/j.paid.2004.01.010
Maxcy,S.J.(2003).Pragmaticthreadsinmixedmethodsresearchinthesocial
sciences:Thesearchformultiplemodesofinquiryandtheendofthe
philosophyofformalism.InA.Tashakkori&C.Teddlie(Eds.),Handbookof
mixedmethodsinsocialandbehavioralresearch(pp.51–90).SAGE
Publications.
Maxwell,S.E.,&Delaney,H.D.(2004).Designingexperimentsandanalyzingdata.

REFERENCES
352
LawrenceErlbaum.
Mayoh,J.,&Onwuegbuzie,A.J.(2015).Towardaconceptualizationofmixed
methodsphenomenologicalresearch.JournalofMixedMethodsResearch,9,
91–107.https://doi.org/10.1177/1558689813505358
McAdams,D.P.(1988).Power,intimacy,andthelifestory:Personologicalinquiries
intoidentity.TheGuilfordPress.
McAdams,D.P.(2011).Narrativeidentity.InS.Schwartz,K.Luyckx,&V.Vignoles
(Eds.),Handbookofidentitytheoryandresearch(pp.99–115).Springer.
McArthur,K.,Cooper,M.,&Berdondini,L.(2013).School-basedhumanistic
counselingforpsychologicaldistressinyoungpeople:Pilotrandomized
controlledtrial.PsychotherapyResearch,23,355–365.
https://doi.org/10.1080/10503307.2012.726750
McCann,T.V.,Lubman,D.I.,&Clark,E.(2012).Theexperienceofyoungpeople
withdepression:Aqualitativestudy.JournalofPsychiatricandMentalHealth
Nursing,19,334–340.https://doi.org/10.1111/j.1365-2850.2011.01783.x
McCarty,C.A.(2008).Adolescentschoolfailurepredictsdepressionamonggirls.
JournalofAdolescentHealth,43,180–187.
https://doi.org/10.1016/j.neuron.2009.10.017.A
McCauleyOhannessian,C.(2012).Parentalproblemdrinkingandadolescent
psychosocialadjustment:Themediatingroleofadolescent-parent
communication.JournalofResearchonAdolescence,22,498–511.
https://doi.org/10.1111/j.1532-7795.2012.00791.x
McElroy,E.,&Patalay,P.(2019).Insearchofdisorders:Internalizingsymptom
networksinalargeclinicalsample.JournalofChildPsychologyandPsychiatry
andAlliedDisciplines,Advanceonlinepublication.
https://doi.org/10.1111/jcpp.13044
McEwen,B.S.(1998).Stress,adaptation,anddisease.JournalofExperimental
Psychology:General,136,23–42.
McGraw,K.,Moore,S.,Fuller,A.,&Bates,G.(2008).Family,peerandschool
connectednessinfinalyearsecondaryschoolstudents.Australian
Psychologist,43,27–37.https://doi.org/10.1080/00050060701668637
McKenzie,M.,Olsson,C.A.,Jorm,A.F.,Romaniuk,H.,&Patton,G.C.(2010).

REFERENCES
353
Associationofadolescentsymptomsofdepressionandanxietywithdaily
smokingandnicotinedependenceinyoungadulthood:Findingsfroma10-
yearlongitudinalstudy.Addiction,105,1652–1659.
https://doi.org/10.1111/j.1360-0443.2010.03002.x
McLaughlin,K.A.(2016).Futuredirectionsinchildhoodadversityandyouth
psychopathology.JournalofClinicalChildandAdolescentPsychology,45,361–
382.https://doi.org/10.1080/15374416.2015.1110823
McLean,C.P.,&Anderson,E.R.(2009).Bravemenandtimidwomen?Areviewof
thegenderdifferencesinfearandanxiety.ClinicalPsychologyReview,29,
496–505.https://doi.org/10.1016/j.cpr.2009.05.003
McLean,C.P.,Asnaani,A.,Litz,B.T.,&Hofmann,S.G.(2011).Genderdifferencesin
anxietydisorders:Prevalence,courseofillness,comorbidityandburdenof
illness.JournalofPsychiatricResearch,45,1027–1035.
https://doi.org/10.1016/j.jpsychires.2011.03.006
McNair,R.P.,&Bush,R.(2016).Mentalhealthhelpseekingpatternsand
associationsamongAustraliansamesexattractedwomen,transandgender
diversepeople:Asurvey-basedstudy.BMCPsychiatry,16,209–224.
https://doi.org/10.1186/s12888-016-0916-4
Meadows,S.O.,Brown,J.S.,&Elder,G.H.(2006).Depressivesymptoms,stress,
andsupport:Genderedtrajectoriesfromadolescencetoyoungadulthood.
JournalofYouthandAdolescence,35,99–103.
https://doi.org/10.1007/s10964-005-9021-6
Mendelson,T.,Kubzansky,L.D.,Datta,G.D.,&Buka,S.L.(2008).Relationof
femalegenderandlowsocioeconomicstatustointernalizingsymptomsamong
adolescents:Acaseofdoublejeopardy?SocialScienceandMedicine,66,
1284–1296.https://doi.org/10.1016/j.socscimed.2007.11.033
Menesini,E.,Modena,M.,&Tani,F.(2016).Bullyingandvictimizationin
adolescence:Concurrentandstablerolesandpsychologicalhealthsymptoms.
TheJournalofGeneticPsychology,1325,115–134.
https://doi.org/10.3200/GNTP.170.2.115-134
Merikangas,K.R.,Weissman,M.M.,&Pauls,D.L.(1985).Geneticfactorsinthesex
ratioofmajordepression.PsychologicalMedicine,15,63–69.

REFERENCES
354
https://doi.org/10.1017/s0033291700020936
Mertens,D.M.(2015).Researchandevaluationineducationandpsychology(4th
ed.).SAGEPublications.
Mertler,C.A.,&Reinhart,R.V.(2017).Advancedandmultivariatestatistical
methods:Practicalapplicationandinterpretation(6thed.).Routledge.
Midgley,N.,Parkinson,S.,Holmes,J.,Stapley,E.,Eatough,V.,&Target,M.(2017).
“DidIbringitonmyself?”Anexploratorystudyofthebeliefsthatadolescents
referredtomentalhealthserviceshaveaboutthecausesoftheirdepression.
EuropeanChildandAdolescentPsychiatry,26,25–34.
https://doi.org/10.1007/s00787-016-0868-8
Miech,R.A.,Caspi,A.,Moffitt,T.E.,Wright,B.R.E.,&Silva,P.A.(1999).Low
socioeconomicstatusandmentaldisorders:Alongitudinalstudyofselection
andcausationduringyoungadulthood.AmericanJournalofSociology,104(4),
1096–1131.https://doi.org/10.1086/210137
Miles,M.B.,&Huberman,A.M.(1984).Qualitativedataanalysis:Asourcebookof
newmethods.SAGEPublications.
Miller,G.E.,Cohen,S.,Janicki-Deverts,D.,Brody,G.H.,&Chen,E.(2016).Viral
challengerevealsfurtherevidenceofskin-deepresilienceinAfricanAmericans
fromdisadvantagedbackgrounds.HealthPsychology,35,1225–1234.
https://doi.org/10.1037/hea0000398
Miller,K.(2015).Frompasttopresent:Howmemoriesofschoolshapeparental
viewsofchildren’sschooling.InternationalJournalofEarlyYearsEducation,
23,153–171.https://doi.org/10.1080/09669760.2014.992869
Miller,K.,&Shifflet,R.(2016).Howmemoriesofschoolinformpreserviceteachers’
fearedanddesiredselvesasteachers.TeachingandTeacherEducation,53,
20–29.https://doi.org/10.1016/j.tate.2015.10.002
Millings,A.,Buck,R.,Montgomery,A.,Spears,M.,&Stallard,P.(2012).School
connectedness,peerattachment,andself-esteemaspredictorsofadolescent
depression.JournalofAdolescence,35,1061–1067.
https://doi.org/10.1016/j.adolescence.2012.02.015
Miloseva,L.,&Vukosavljevic-Gvozden,T.(2014).Perfectionismdimensionsin
children:Associationwithanxietyanddepression.Procedia-Socialand

REFERENCES
355
BehavioralSciences,159,78–81.https://doi.org/10.1016/j.sbspro.2014.12.332
Mitchell,A.M.,Crane,P.A.,&Kim,Y.(2008).Perceivedstressinsurvivorsof
suicide:PsychometricpropertiesofthePerceivedStressScale.Researchin
NursingandHealth,31,576–585.https://doi.org/10.1002/nur.20284
Moilanen,K.,Shaw,D.S.,&Maxwell,K.L.(2010).Developmentalcascades:
Externalizing,internalizing,andacademiccompetencefrommiddlechildhood
toearlyadolescence.DevelopmentalPsychopathology,22,635–653.
https://doi.org/10.1017/S0954579410000337
Molinuevo,B.,Bonillo,A.,Pardo,Y.,Doval,E.,&Torrubia,R.(2010).Participationin
extracurricularactivitiesandemotionalandbehavioraladjustmentinmiddle
childhoodinSpanishboysandgirls.JournalofCommunityPsychology,38,
842–857.https://doi.org/10.1002/jcop.20399
Morales,J.R.,&Guerra,N.G.(2006).Effectsofmultiplecontextandcumulative
stressonurbanchildren’sadjustmentinelementaryschool.Child
Development,77,907–923.https://doi.org/10.1111/j.1467-8624.2006.00910.x
Moran,D.(2000).Introductiontophenomenology.Routledge.
Moran,P.,Coffey,C.,Romaniuk,H.,Olsson,C.A.,Borschmann,R.,Carlin,J.B.,&
Patton,G.C.(2011).Thenaturalhistoryofself-harmfromadolescenceto
youngadulthood:Apopulation-basedcohortstudy.Lakartidningen,108,
2709–2710.https://doi.org/10.1016/S0140-6736(11)61141-0
Morgan,D.L.(2007).Paradigmslostandpragmatismregained.JournalofMixed
MethodsResearch,1,48–76.https://doi.org/10.1177/2345678906292462
Morgan,D.L.(2014).Pragmatismasaparadigmforsocialresearch.Qualitative
Inquiry,20,1045–1053.https://doi.org/10.1177/1077800413513733
Morrison,K.M.,Shin,S.,Tarnopolsky,M.,&Taylor,V.H.(2014).Associationof
depressionandhealthrelatedqualityoflifewithbodycompositioninchildren
andyouthwithobesity.JournalofAffectiveDisorders,172,18–23.
https://doi.org/10.1016/j.jad.2014.09.014
Morrow,V.(1999).“Wearepeopletoo”:Children’sandyoungpeople’s
perspectivesonchildren’srightsanddecision-makinginEngland.International
JournalofChildren’sRights,7,149–170.
https://doi.org/10.1163/15718189920494318

REFERENCES
356
Moseholm,E.,&Fetters,M.D.(2017).Conceptualmodelstoguideintegration
duringanalysisinconvergentmixedmethodsstudies.Methodological
Innovations,10(2),1–11.https://doi.org/10.1177/2059799117703118
Munford,R.,&Sanders,J.(2016).Findingmeaningfulsupport:Youngpeople’s
experiencesof“risky”environments.AustralianSocialWork,69,229–240.
https://doi.org/10.1080/0312407X.2015.1133682
Muris,P,Meesters,C.,Eijkelenboom,A.,&Vincken,M.(2004).Theself-report
versionoftheStrengthsandDifficultiesQuestionnaire:Itspsychometric
propertiesin8-to13-year-oldnon-clinicalchildren.TheBritishJournalof
ClinicalPsychology,43,437–448.https://doi.org/10.1348/0144665042388982
Muris,Peter.(2002).Relationshipsbetweenself-efficacyandsymptomsofanxiety
disordersanddepressioninanormaladolescentsample.Personalityand
IndividualDifferences,32,337–348.https://doi.org/10.1016/S0191-
8869(01)00027-7
Muris,Peter,&Field,A.P.(2008).Distortedcognitionandpathologicalanxietyin
childrenandadolescents.CognitionandEmotion,22,395–421.
https://doi.org/10.1080/02699930701843450
Muris,Peter,Schmidt,H.,Merckelbach,H.,&Schouten,E.(2001).Thestructureof
negativeemotionsinadolescents.JournalofAbnormalChildPsychology,29,
331–337.https://doi.org/10.1023/A:1010361913186
Murphy,S.M.(2014).Determinantsofadolescentsuicidalideation:ruralversus
urban.TheJournalofRuralHealth,30,175–185.
https://doi.org/10.1111/jrh.12042
Murray,C.(2010a).Conceptualizingyoungpeople’sstrategiesofresistanceto
offendingas“activeresilience.”BritishJournalofSocialWork,40,115–132.
https://doi.org/10.1093/bjsw/bcn115
Murray,C.(2010b).Conceptualizingyoungpeople’sstrategiesofresistanceto
offendingas“activeresilience.”BritishJournalofSocialWork,40(1),115–132.
https://doi.org/10.1093/bjsw/bcn115
Murray,C.J.L.,&Greenberg,M.T.(2000).Children’srelationshipwithteachers
andbondswithschool:Aninvestigationofpatternsandcorrelatesinmiddle
childhood.JournalofSchoolPsychology,38,432–445.

REFERENCES
357
https://doi.org/10.1016/S0022-4405(00)00034-0
Muthén,B.O.(2006).Censoredandnonnormaldata.Www.Statmodel.Com.
http://www.statmodel.com/discussion/messages/11/144.html?1519671449
Muthén,B.O.,&Satorra,A.(1995).Complexsampledatainstructuralequation
modeling.SociologicalMethodology,25,267–316.
https://doi.org/10.2307/271070
Muthén,L.K.,&Muthén,B.O.(n.d.).Mplususer’sguide(6thed.).Muthén&
Muthén.
Myhill,D.,&Jones,S.(2006).“Shedoesn’tshoutatnogirls”:Pupils’perceptionsof
genderequityintheclassroom.CambridgeJournalofEducation,36,99–113.
https://doi.org/10.1080/03057640500491054
Najman,J.M.,Clavarino,A.,McGee,T.R.,Bor,W.,Williams,G.M.,&Hayatbakhsh,
M.R.(2010).Timingandchronicityoffamilypovertyanddevelopmentof
unhealthybehaviorsinchildren:Alongitudinalstudy.JournalofAdolescent
Health,46,538–544.https://doi.org/10.1016/j.jadohealth.2009.12.001
Najman,J.M.,Hayatbakhsh,M.R.,Clavarino,A.,Bor,W.,O’Callaghan,M.J.,&
Williams,G.M.(2010).Familypovertyovertheearlylifecourseandrecurrent
adolescentandyoungadultanxietyanddepression:Alongitudinalstudy.
AmericanJournalofPublicHealth,100,1719–1723.
https://doi.org/10.2105/AJPH.2009.180943
Nelson,J.M.,&Gregg,N.(2012).Depressionandanxietyamongtransitioning
adolescentsandcollegestudentswithADHD,dyslexia,orcomorbid
ADHD/dyslexia.JournalofAttentionDisorders,16,244–254.
https://doi.org/10.1177/1087054710385783
Nelson,J.M.,&Harwood,H.(2011).Learningdisabilitiesandanxiety:Ameta-
analysis.JournalofLearningDisabilities,44,3–17.
https://doi.org/10.1177/0022219409359939
Neufeld,S.A.S.,Dunn,V.J.,Jones,P.B.,Croudace,T.J.,&Goodyer,I.M.(2017).
Reductioninadolescentdepressionaftercontactwithmentalhealthservices:
alongitudinalcohortstudyintheUK.TheLancetPsychiatry,4,120–127.
https://doi.org/10.1016/S2215-0366(17)30002-0
Newman,T.(2002).“Youngcarers”anddisabledparents:Timeforachangeof

REFERENCES
358
direction?DisabilityandSociety,17,613–625.
https://doi.org/10.1080/0968759022000010407
Nguyen-Gillham,V.,Giacaman,R.,Naser,G.,&Boyce,W.(2008).Normalisingthe
abnormal:Palestinianyouthandthecontradictionsofresilienceinprotracted
conflict.HealthandSocialCareintheCommunity,16,291–298.
https://doi.org/10.1111/j.1365-2524.2008.00767.x
NHS.(2016).ObsessiveCompulsiveDisorder(OCD):Symptoms.
https://www.nhs.uk/conditions/obsessive-compulsive-disorder-
ocd/symptoms/
NHSDigital.(2018).MentalhealthofchildrenandyoungpeopleinEngland,2017:
Summaryofkeyfindings.
Nicholson,H.J.,Collins,C.,&Holmer,H.(2004).Youthaspeople:Theprotective
aspectsofyouthdevelopmentinafter-schoolsettings.AnnalsoftheAmerican
AcademyofPoliticalandSocialScience,591,55–71.
https://doi.org/10.1177/0002716203260081
Niditch,L.A.,&Varela,R.E.(2012).Perceptionsofparenting,emotionalself-
efficacy,andanxietyinyouth:Testofamediationmodel.ChildandYouthCare
Forum,41,21–35.https://doi.org/10.1007/s10566-011-9150-x
Nolen-Hoeksema,S.(1990).Sexdifferencesindepression.StanfordUniversityPress.
Nolen-Hoeksema,S.(2000).Theroleofruminationindepressivedisordersand
mixedanxiety/depressivesymptoms.JournalofAbnormalPsychology,109,
504–511.https://doi.org/10.1037/0021-843X.109.3.504
Nolen-Hoeksema,S.(2001).Genderdifferencesindepression.JournalofPsychiatric
Research,33,243–250.https://doi.org/10.1016/s0022-3956(98)00064-8
Nolen-Hoeksema,S.,&Girgus,J.S.(1994).Theemergenceofgenderdifferencesin
depressionduringadolescence.PsychologicalBulletin,115,424–443.
https://doi.org/10.1037/0033-2909.115.3.424
Nolen-Hoeksema,S.,&Watkins,E.R.(2011).Aheuristicfordeveloping
transdiagnosticmodelsofpsychopathology:Explainingmultifinalityand
divergenttrajectories.PerspectivesonPsychologicalScience,6,589–609.
https://doi.org/10.1177/1745691611419672
O’Connor,E.E.,Collins,B.A.,&Supplee,L.(2012).Behaviorproblemsinlate

REFERENCES
359
childhood:Therolesofearlymaternalattachmentandteacher-child
relationshiptrajectories.AttachmentandHumanDevelopment,14,265–288.
https://doi.org/10.1080/14616734.2012.672280
O’DoughertyWright,M.,&Masten,A.S.(2015).Pathwaystoresilienceincontext.
InL.C.Theron,L.Liebenberg,&M.Ungar(Eds.),Youthresilienceandculture:
Commonalitiesandcomplexities(pp.3–22).Springer.
OfficeforNationalStatistics.(2012).2011census:Populationandhousehold
estimatesforsmallareasinEnglandandWales,March2011.
OfficeforNationalStatistics.(2013).Asummaryofunpaidcareby5to17-yearolds
inEnglandandWales.
Oldehinkel,A.J.,Ormel,J.,Bosch,N.M.,Bouma,E.M.C.,VanRoon,A.M.,
Rosmalen,J.G.M.,&Riese,H.(2011).Stressedout?Associationsbetween
perceivedandphysiologicalstressresponsesinadolescents:TheTRAILSstudy.
Psychophysiology,48,441–452.https://doi.org/10.1111/j.1469-
8986.2010.01118.x
Oldfield,J.,Humphrey,N.,&Hebron,J.(2015).Cumulativeriskeffectsforthe
developmentofbehaviourdifficultiesinchildrenandadolescentswithspecial
educationalneedsanddisabilities.ResearchinDevelopmentalDisabilities,21,
66–75.https://doi.org/10.1016/j.ridd.2015.05.010
Oliver,D.G.,Serovich,J.M.,&Mason,T.L.(2005).Constraintsandopportunities
withinterviewtranscription:Towardsreflectioninqualitativeresearch.Social
Forces,84,1273–1289.https://doi.org/10.1353/sof.2006.0023
Olsen,R.,&Clarke,H.(2003).Parentinganddisability:Disabledparents’
experiencesofraisingchildren.ThePolicyPress.
Onwuegbuzie,A.J.,&Teddlie,C.(2003).Aframeworkforanalyzingdatainmixed
methodsresearch.InA.Tashakkori&C.Teddlie(Eds.),Handbookofmixed
methodsinsocialandbehavioralresearch(pp.351–384).SAGEPublications.
OpenScienceCollaboration.(2015).Estimatingthereproducibilityofpsychological
science.Science,349,aac4716.https://doi.org/10.1126/science.aac4716
Oransky,M.,&Marecek,J.(2009).“I’mnotgoingtobeagirl”:Masculinityand
emotionsinboys’friendshipsandpeergroups.JournalofAdolescentResearch,
24,218–241.https://doi.org/10.1177/0743558408329951

REFERENCES
360
Orth,U.,Robins,R.W.,&Roberts,B.W.(2008).Lowself-esteemprospectively
predictsdepressioninadolescenceandyoungadulthood.Journalof
PersonalityandSocialPsychology,95,695–708.https://doi.org/10.1037/0022-
3514.95.3.695
Oud,M.,Winter,L.De,Vermeulen-smit,E.,Bodden,D.,Nauta,M.,Stone,L.,
Heuvel,M.VanDen,Al,R.,Graaf,I.De,Kendall,T.,Engels,R.,&Stikkelbroek,
Y.(2019).EffectivenessofCBTforchildrenandadolescentswithdepression :A
systematicreviewandmeta-regressionanalysis.EuropeanPsychiatry,57,33–
45.https://doi.org/10.1016/j.eurpsy.2018.12.008
Owens,M.,Stevenson,J.,Hadwin,J.A.,&Norgate,R.(2012).Anxietyand
depressioninacademicperformance:Anexplorationofthemediatingfactors
ofworryandworkingmemory.SchoolPsychologyInternational,33,433–449.
https://doi.org/10.1177/0143034311427433
Pakenham,KennethI,Tilling,J.,&Cretchley,J.(2012).Parentingdifficultiesand
resources:Theperspectivesofparentswithmultiplesclerosisandtheir
partners.RehabilitationPsychology,57,52–60.
https://doi.org/10.1037/a0026995
Pakenham,KennethIan,Bursnall,S.,Chiu,J.,Cannon,T.,&Okochi,M.(2006).The
psychosocialimpactofcaregivingonyoungpeoplewhohaveaparentwithan
illnessordisability:Comparisonsbetweenyoungcaregiversandnoncaregivers.
RehabilitationPsychology,51,113–126.https://doi.org/10.1037/0090-
5550.51.2.113
Pakenham,KennethIan,Chiu,J.,Bursnall,S.,&Cannon,T.(2007).Relations
betweensocialsupport,appraisalandcopingandbothpositiveandnegative
outcomesinyoungcarers.JournalofHealthPsychology,12,89–102.
https://doi.org/10.1177/1359105307071743
Panayiotou,G.,&Karekla,M.(2013).Perceivedsocialsupporthelps,butdoesnot
bufferthenegativeimpactofanxietydisordersonqualityoflifeandperceived
stress.SocialPsychiatryandPsychiatricEpidemiology,48,283–294.
https://doi.org/10.1007/s00127-012-0533-6
Panayiotou,M.,&Humphrey,N.(2018).Mentalhealthdifficultiesandacademic
attainment:Evidenceforgender-specificdevelopmentalcascadesinmiddle

REFERENCES
361
childhood.DevelopmentandPsychopathology,30,523–538.
https://doi.org/10.1017/S095457941700102X
Panourgia,C.,&Comoretto,A.(2017).Docognitivedistortionsexplainthe
longitudinalrelationshipbetweenlifeadversityandemotionalandbehavioural
problemsinsecondaryschoolchildren?StressandHealth,33,590–599.
https://doi.org/10.1002/smi.2743
Park,C.L.,&Folkman,S.(1997).Meaninginthecontextofstressandcoping.
ReviewofGeneralPsychology,1,115–144.https://doi.org/10.1037/1089-
2680.1.2.115
Parker,G.,&Brotchie,H.(2010).Genderdifferencesindepression.International
ReviewofPsychiatry,22,429–436.
https://doi.org/10.3109/09540261.2010.492391
Pascual-Leone,A.,&Greenberg,L.S.(2007).Emotionalprocessinginexperiential
therapy:Why“theonlywayoutisthrough.”JournalofConsultingandClinical
Psychology,75,875–887.https://doi.org/10.1037/0022-006X.75.6.875
Patalay,P.,Belsky,J.,Fonagy,P.,Vostanis,P.,Humphrey,N.,Deighton,J.,&
Wolpert,M.(2015).Theextentandspecificityofrelativeageeffectsonmental
healthandfunctioninginearlyadolescence.JournalofAdolescentHealth,57,
475–481.https://doi.org/10.1016/j.jadohealth.2015.07.012
Patalay,P.,&Fitzimons,E.(2018).Mentalill-healthandwellbeingatage14:Initial
findingsfromtheMilleniumCohortStudyAge14Survey.
Patalay,P.,Hayes,D.,Deighton,J.,&Wolpert,M.(2016).Acomparisonofpaper
andcomputeradministeredStrengthsandDifficultiesQuestionnaire.Journal
ofPsychopathologyandBehavioralAssessment,38,242–250.
https://doi.org/10.1007/s10862-015-9507-9
Patalay,P.,Hayes,D.,&Wolpert,M.(2018).Assessingthereadabilityoftheself-
reportedStrengthsandDifficultiesQuestionnaire.BJPsychOpen,4,55–57.
https://doi.org/10.1192/bjo.2017.13
Pate,C.M.,Maras,M.A.,Whitney,S.D.,&Bradshaw,C.P.(2017).Exploring
psychosocialmechanismsandinteractions:Linksbetweenadolescent
emotionaldistress,schoolconnectedness,andeducationalachievement.
SchoolMentalHealth,9,28–43.https://doi.org/10.1007/s12310-016-9202-3

REFERENCES
362
Patel,V.,Flisher,A.J.,Hetrick,S.,&McGorry,P.(2007).Mentalhealthofyoung
people:aglobalpublic-healthchallenge.Lancet,369,1302–1313.
https://doi.org/10.1016/S0140-6736(07)60368-7
Patterson,J.,Barlow,J.,Mockford,C.,Klimes,I.,Pyper,C.,&Stewart-Brown,S.
(2002).Improvingmentalhealththroughparentingprogrammes:Block
randomisedcontrolledtrial.ArchivesofDiseaseinChildhood,87,472–477.
https://doi.org/10.1136/adc.87.6.472
Pattison,S.,&Bell,S.(2018).Thetherapeuticallianceincounsellingprocess.InM.
Robson&S.Pattison(Eds.),Thehandbookofcounsellingchildrenandyoung
people(pp.169–182).SAGEPublications.
Patton,G.C.,Hemphill,S.A.,Beyers,J.M.,Bond,L.M.,Toumbourou,J.W.,
McMorris,B.J.,&Catalano,R.F.(2007).Pubertalstageanddeliberateself-
harminadolescents.JournaloftheAmericanAcademyofChildandAdolescent
Psychiatry,46,509–514.https://doi.org/10.1097/chi.0b013e31803065c7
Patton,M.(2015).Qualitativeresearchandevaluationmethods(4thed.).SAGE
Publications.
Pearl,J.(2012).Thecausalfoundationsofstructuralequationmodeling.InR.H.
Hoyle(Ed.),Handbookofstructuralequationmodeling(pp.68–91).Guilford
Press.
Peng,C.-Y.J.,Harwell,M.,Liou,S.-M.,&Ehman,L.H.(2007).Advancesinmissing
datamethodsandimplicationsforeducationalresearch.InS.S.Sawilosky
(Ed.),Realdataanalysis(pp.21–30).InformationAgePublishing,Inc.
Pereira,A.I.F.,Barros,L.,&Mendonça,D.(2012).Cognitiveerrorsandanxietyin
schoolagedchildren.Psicologia:ReflexãoeCrítica,25.
https://doi.org/10.1590/S0102-79722012000400022
Peugh,J.L.,&Enders,C.K.(2004).Missingdataineducationalresearch:Areview
ofreportingpracticesandsuggestionsforimprovement.ReviewofEducational
Research,74,525–556.https://doi.org/10.3102/00346543074004525
Pietkiewicz,I.,&Smith,J.A.(2014).Apracticalguidetousinginterpretative
phenomenologicalanalysisinqualitativeresearchpsychology.Czasopismo
PsychologicznePsychologicalJournal,20,7–14.
https://doi.org/10.14691/CPPJ.20.1.7

REFERENCES
363
Pitchforth,J.,Fahy,K.,Ford,T.,Wolpert,M.,Viner,R.M.,&Hargreaves,D.S.
(2018).Mentalhealthandwell-beingtrendsamongchildrenandyoungpeople
intheUK,1995–2014:Analysisofrepeatedcross-sectionalnationalhealth
surveys.PsychologicalMedicine,49,1275–1285.
https://doi.org/10.1017/s0033291718001757
Ployhart,R.E.,&Vandenberg,R.J.(2010).Longitudinalresearch:Thetheory,
design,andanalysisofchange.JournalofManagement,36,94–120.
https://doi.org/10.1177/0149206309352110
Polanczyk,G.V,Salum,G.A.,Sugaya,L.S.,Caye,A.,&Rohde,L.A.(2015).Annual
researchreview:Ameta-analysisoftheworldwideprevalenceofmental
disordersinchildrenandadolescents.TheJournalofChildPsychologyand
Psychiatry,3,345–365.https://doi.org/10.1111/jcpp.12381
Polit,D.F.,&Beck,C.T.(2010).Generalizationinquantitativeandqualitative
research:Mythsandstrategies.InternationalJournalofNursingStudies,
47(11),1451–1458.https://doi.org/10.1016/j.ijnurstu.2010.06.004
Pomerantz,E.M.,Altermatt,E.R.,&Saxon,J.L.(2002).Makingthegradebut
feelingdistressed:Genderdifferencesinacademicperformanceandinternal
distress.JournalofEducationalPsychology,94,396–404.
https://doi.org/10.1037/0022-0663.94.2.396
Ponterotto,J.G.(2005).Qualitativeresearchincounselingpsychology:Aprimeron
researchparadigmsandphilosophyofscience.JournalofCounseling
Psychology,52,126–136.https://doi.org/10.1037/0022-0167.52.2.126
Popper,K.(1959).Thelogicofscientificdiscovery.Hutchinson&Co.(Originalwork
published1935).
Preacher,K.J.(2006).Quantifyingparsimonyinstructuralequationmodeling.
MultivariateBehavioralResearch,41,227–259.
https://doi.org/10.1207/s15327906mbr4103_1
Printz,B.L.,Shermis,M.D.,&Webb,P.M.(1999).Stress-bufferingfactorsrelated
toadolescentcoping:Apathanalysis.Adolescence,34,715–734.
Qualter,P.,Brown,S.L.,Rotenberg,K.J.,Vanhalst,J.,Harris,R.A.,Goossens,L.,
Bangee,M.,&Munn,P.(2013).Trajectoriesoflonelinessduringchildhoodand
adolescence:Predictorsandhealthoutcomes.JournalofAdolescence,36,

REFERENCES
364
1283–1293.https://doi.org/10.1016/j.adolescence.2013.01.005
Qualter,Pamela,Brown,S.L.,Munn,P.,&Rotenberg,K.J.(2010).Childhood
lonelinessasapredictorofadolescentdepressivesymptoms:An8-year
longitudinalstudy.EuropeanChildandAdolescentPsychiatry,19,493–501.
https://doi.org/10.1007/s00787-009-0059-y
Radziszewska,B.,Richardson,J.L.,Dent,C.W.,&Flay,B.R.(1996).Parentingstyle
andadolescentdepressivesymptoms,smoking,andacademicachievement:
Ethnic,gender,andSESdifferences.JournalofBehavioralMedicine,19,289–
305.https://doi.org/10.1007/BF01857770
Rasbash,J.,Leckie,G.,Pillinger,R.,&Jenkins,J.(2010).Children’seducational
progress:Partitioningfamily,schoolandareaeffects.JournaloftheRoyal
StatisticalSociety,173,657–682.https://doi.org/10.1111/j.1467-
985X.2010.00642.x
Raubenheimer,J.E.(2004).Anitemselectionproceduretomaximisescale
reliabilityandvalidity.SAJournalofIndustrialPsychology,30(4),59–64.
https://doi.org/10.4102/sajip.v30i4.168
Raviv,T.,Taussig,H.N.,Culhane,S.E.,&Garrido,E.F.(2010).Cumulativerisk
exposureandmentalhealthsymptomsamongmaltreatedyouthplacedinout-
of-homecare.ChildAbuseandNeglect,34(10),742–751.
https://doi.org/10.1016/j.chiabu.2010.02.011
Raykov,T.(1997).Scalereliability,Cronbach’scoefficientalpha,andviolationsof
essentialtau-equivalencewithfixedcongenericcomponents.Multivariate
BehavioralResearch,32,329–353.
https://doi.org/10.1207/s15327906mbr3204
Reid,K.,Flowers,P.,&Larkin,M.(2005).Exploringlivedexperience.Psychologist,
18,20–23.
Reiss,F.(2013).Socioeconomicinequalitiesandmentalhealthproblemsinchildren
andadolescents:Asystematicreview.SocialScienceandMedicine,90,24–31.
https://doi.org/10.1016/j.socscimed.2013.04.026
Renold,E.,&Allan,A.(2006).Brightandbeautiful:Highachievinggirls,ambivalent
femininities,andthefeminizationofsuccessintheprimaryschool.Discourse,
27,457–473.https://doi.org/10.1080/01596300600988606

REFERENCES
365
Rey,J.M.(1995).Perceptionsofpoormaternalcareareassociatedwithadolescent
depression.JournalofAffectiveDisorders,34,95–100.
https://doi.org/10.1016/0165-0327(95)00005-8
Rhoades,B.L.,Greenberg,M.T.,Lanza,S.T.,&Blair,C.(2011).Demographicand
familialpredictorsofearlyexecutivefunctiondevelopment:Contributionofa
person-centeredperspective.JournalofExperimentalChildPsychology,108,
638–662.https://doi.org/10.1016/j.jecp.2010.08.004
Rickwood,D.J.(2015).Respondingeffectivelytosupportthementalhealthand
well-beingofyoungpeople.InJ.Wyn&H.Cahill(Eds.),Handbookofchildren
andyouthstudies(pp.139–154).Springer.https://doi.org/10.1007/978-981-
4451-15-4
Rickwood,D.J.,&Braithwaite,V.A.(1994).Social-psychologicalfactorsaffecting
help-seekingforemotionalproblems.SocialScience&Medicine,39,563–572.
https://doi.org/10.1016/0277-9536(94)90099-X
Rickwood,D.J.,Deane,F.P.,Wilson,C.J.,&Ciarrochi,J.(2005).Youngpeople’s
help-seekingformentalhealthproblems.AustralianE-Journalforthe
AdvancementofMentalHealth,4,218–251.
https://doi.org/10.5172/jamh.4.3.218
Rickwood,D.J.,&Thomas,K.(2012).Conceptualmeasurementframeworkfor
help-seekingformentalhealthproblems.PsychologyResearchandBehavior
Management,5,173–183.https://doi.org/10.2147/PRBM.S38707
Riley,A.W.(2004).Evidencethatschool-agechildrencanself-reportontheir
health.AmbulatoryPediatrics,4,371–376.https://doi.org/10.1367/A03-
178R.1
Ringrose,J.(2007).Successfulgirls?Complicatingpost-feminist,neoliberal
discoursesofeducationalachievementandgenderequality.Genderand
Education,19,471–489.https://doi.org/10.1080/09540250701442666
Rogers,C.R.(1957).Thenecessaryandsufficientconditionsoftherapeutic
personalitychange.JournalofConsultingPsychology,21,95–103.
https://doi.org/10.1037/h0045357
Root,A.K.,&Denham,S.A.(2010).Theroleofgenderinthesocializationof
emotion:Keyconceptsandcriticalissues.NewDirectionsforChildand

REFERENCES
366
AdolescentDevelopment,2010(128),1–9.https://doi.org/10.1002/cd.265
Rose,H.D.,&Cohen,K.(2010).Theexperiencesofyoungcarers:Ameta-synthesis
ofqualitativefindings.JournalofYouthStudies,13,473–487.
https://doi.org/10.1080/13676261003801739
Ross,K.M.,Rook,K.,Winczewski,L.,Collins,N.,&DunkelSchetter,C.(2019).Close
relationshipsandhealth:Theinteractiveeffectofpositiveandnegative
aspects.SocialandPersonalityPsychologyCompass,13(6),1–19.
https://doi.org/10.1111/spc3.12468
Rotenberg,K.J.,Qualter,P.,Holt,N.L.,Harris,R.A.,Henzi,P.,&Barrett,L.(2014).
Whentrustfails:Therelationbetweenchildren’strustbeliefsinpeersand
theirpeerinteractionsinanaturalsetting.JournalofAbnormalChild
Psychology,42,967–980.https://doi.org/10.1007/s10802-013-9835-8
Rothbaum,F.,Weisz,J.R.,&Synder,S.S.(1982).Changingtheworldandchanging
theself:Atwo-processmodelofperceivedcontrol.JournalofPersonalityand
SocialPsychology,42,5–37.https://doi.org/10.1037/0022-3514.42.1.5
Rowe,S.L.,Zimmer-Gembeck,M.J.,&Hood,M.(2016).Fromthechildtothe
neighbourhood:Longitudinalecologicalcorrelatesofyoungadolescents’
emotional,social,conduct,andacademicdifficulties.JournalofAdolescence,
49,218–231.https://doi.org/10.1016/j.adolescence.2016.04.001
Roy,A.L.,&Raver,C.C.(2014).Areallrisksequal?Earlyexperiencesofpoverty-
relatedriskandchildren’sfunctioning.JournalofFamilyPsychology,28,391–
400.https://doi.org/10.1037/a0036683
Roza,S.J.,Hofstra,M.B.,VanDerEnde,J.,&Verhulst,F.C.(2003).Stable
predictionofmoodandanxietydisordersbasedonbehavioralandemotional
problemsinchildhood:A14-yearfollow-upduringchildhood,adolescence,
andyoungadulthood.AmericanJournalofPsychiatry,160,2116–2121.
https://doi.org/10.1176/appi.ajp.160.12.2116
Rudolph,K.D.,&Clark,A.G.(2001).Conceptsofrelationshipsinchildrenwith
depressiveandaggressivesymptoms:Social-cognitivedistortionorreality?
JournalofAbnormalChildPsychology,29,41–56.
https://doi.org/10.1023/A:1005299429060
Rutter,M.(1979).Fifteenthousandhours:Secondaryschoolsandtheireffectson

REFERENCES
367
children.PaulChapmanPublishingLtd.
Rutter,M.(1981).Stress,copinganddevelopment:Someissuesandsome
questions.JournalofChildPsychologyandPsychiatry,22,323–356.
https://doi.org/10.1111/j.1469-7610.1981.tb00560.x
Rutter,M.(1987).Psychosocialresilienceandprotectivemechanisms.American
JournalofOrthopsychiatry,57,316–331.https://doi.org/10.1111/j.1939-
0025.1987.tb03541.x
Ryan,A.(2000).Peergroupsasacontextforthesocializationofadolescents’
motivation,engagement,andachievementinschool.EducationalPsychologist,
35,101–111.https://doi.org/10.1207/S15326985EP3502_4
Ryan,A.M.,Shim,S.S.,&Makara,K.A.(2013).Changesinacademicadjustment
andrelationalself-worthacrossthetransitiontomiddleschool.Journalof
YouthandAdolescence,42,1372–1384.https://doi.org/10.1007/s10964-013-
9984-7
Salk,R.H.,Petersen,J.L.,Abramson,L.Y.,&Hyde,J.S.(2016).Thecontemporary
faceofgenderdifferencesandsimilaritiesindepressionthroughout
adolescence:Developmentandchronicity.JournalofAffectiveDisorders,205,
28–35.https://doi.org/10.1016/j.jad.2016.03.071
Salzman,C.D.,&Fusi,S.(2010).Emotion,cognition,andmentalstate
representationinamygdalaandprefrontalcortex.AnnualReviewof
Neuroscience,33,173–202.
https://doi.org/10.1146/annurev.neuro.051508.135256
Sameroff,A.J.(2000).Developmentalsystemsandpsychopathology.Development
andPsychopathology,12,297–312.
https://doi.org/10.1017/S0954579400003035
Sameroff,A.J.(2006).Identifyingriskandprotectivefactorsforhealthychild
development.InA.Clarke-Stewart&J.Dunn(Eds.),Familiescount:Effectson
childandadolescentdevelopment(pp.53–76).CambridgeUniversityPress.
Sameroff,A.J.,Gutman,L.M.,&Peck,S.C.(2003).Adaptationamongyouthfacing
multiplerisks:Prospectiveresearchfindings.InS.S.Luthar(Ed.),Resilienceand
vulnerability:Adaptationinthecontextofchildhoodadversities(pp.364–391).
CambridgeUniversityPress.

REFERENCES
368
Sameroff,A.J.,Seifer,R.,Baldwin,A.,&Baldwin,C.(1993).Stabilityofintelligence
frompreschooltoadolescence:Theinfluenceofsocialandfamilyriskfactors.
ChildDevelopment,64,80–97.https://doi.org/10.1111/j.1467-
8624.1993.tb02896.x
Sameroff,A.J.,Seifer,R.,&McDonough,S.C.(2004).Contextualcontributorsto
theassessmentofinfantmentalhealth.InR.DelCarmen-Wiggins&A.Carter
(Eds.),Handbookofinfant,toddlerandpreschoolmentalhealthassessment
(pp.61–76).OxfordUniversityPress.
Sandelowski,M.(2003).Tablesortableaux?Thechallengesofwritingandreading
mixedmethodsstudies.InA.Tashakkori&C.Teddlie(Eds.),Handbookof
mixedmethodsinsocialandbehavioralresearch(pp.321–350).SAGE
Publications.
Sanders,M.R.(2008).TripleP-PositiveParentingProgramasapublichealth
approachtostrengtheningparenting.JournalofFamilyPsychology,22,506–
517.https://doi.org/10.1037/0893-3200.22.3.506
Santiago,C.D.C.,Wadsworth,M.E.,&Stump,J.(2011).Socioeconomicstatus,
neighborhooddisadvantage,andpoverty-relatedstress:Prospectiveeffectson
psychologicalsyndromesamongdiverselow-incomefamilies.Journalof
EconomicPsychology,32,218–230.
https://doi.org/10.1016/j.joep.2009.10.008
Sargeant,J.,&Gillett-Swan,J.K.(2015).Empoweringthedisempoweredthrough
voice-inclusivepractice:Children’sviewsonadult-centriceducational
provision.EuropeanEducationalResearchJournal,14,177–191.
https://doi.org/10.1177/1474904115571800
Schaefer,D.R.,Simpkins,S.D.,Vest,A.E.,&Price,C.D.(2011).Thecontributionof
extracurricularactivitiestoadolescentfriendships:Newinsightsthroughsocial
networkanalysis.DevelopmentalPsychology,47,1141–1152.
https://doi.org/10.1037/a0024091
Schafer,J.L.,&Graham,J.W.(2002).Missingdata:Ourviewofthestateoftheart.
PsychologicalMethods,7,147–177.https://doi.org/10.1037//1082-
989X.7.2.147
Schilling,E.A.,Aseltine,R.H.,&Gore,S.(2007).Adversechildhoodexperiencesand

REFERENCES
369
mentalhealthinyoungadults:Alongitudinalsurvey.BMCPublicHealth,7,30–
40.https://doi.org/10.1186/1471-2458-7-30
Schmid,B.,Blomeyer,D.,Buchmann,A.F.,Trautmann-Villalba,P.,Zimmermann,U.
S.,Schmidt,M.H.,Esser,G.,Banaschewski,T.,&Laucht,M.(2011).Qualityof
earlymother-childinteractionassociatedwithdepressivepsychopathologyin
theoffspring:Aprospectivestudyfrominfancytoadulthood.Journalof
PsychiatricResearch,45(10),1387–1394.
https://doi.org/10.1016/j.jpsychires.2011.05.010
Schneiders,J.(2003).Neighbourhoodsocioeconomicdisadvantageandbehavioural
problemsfromlatechildhoodintoearlyadolescence.JournalofEpidemiology
&CommunityHealth,57,699–703.https://doi.org/10.1136/jech.57.9.699
Schreiber,J.B.,Nora,A.,Stage,F.K.,Barlow,E.A.,King,J.,Nora,A.,&Barlow,E.A.
(2006).Reportingstructuralequationmodelingandconfirmatoryfactor
analysisresults:Areview.TheJournalofEducationalResearch,99,232–338.
https://doi.org/10.3200/JOER.99.6.323-338
Schulenberg,J.,Theokas,C.,Curry,L.,Youngblade,L.M.,Huang,I.-C.,&Novak,M.
(2007).Riskandpromotivefactorsinfamilies,schools,andcommunities:A
contextualmodelofpositiveyouthdevelopmentinadolescence.Pediatrics,
119,S47–S53.https://doi.org/10.1542/peds.2006-2089h
Schwandt,T.A.(2000).Threeepistemologicalstancesforqualitativeinquiry:
Interpretivism,hermeneutics,andsocialconstructionism.InN.K.Denzin&Y.
S.Lincoln(Eds.),Handbookofqualitativeresearch(pp.189–213).SAGE
Publications.
Schwartz-Mette,R.A.,&Rose,A.J.(2012).Co-ruminationmediatescontagionof
internalizingsymptomswithinyouths’friendships.DevelopmentalPsychology,
48,1355–1365.https://doi.org/10.1038/jid.2014.371
Scott,S.(2012).Parentingqualityandchildren’smentalhealth:Biological
mechanismsandpsychologicalinterventions.CurrentOpinioninPsychiatry,25,
301–306.https://doi.org/10.1097/YCO.0b013e328354a1c5
ScottishGovernment.(2017).Youngcarers:Reviewofresearchanddata.
SDQInfo.(2000).SDQfrequencydistributionsforBritish11-15yearoldgirls.
http://sdqinfo.com/norms/UKNorm12.pdf

REFERENCES
370
SDQInfo.(2016).ScoringtheStrengthsandDifficultiesQuestionnaireforage4-17
or18+.http://www.sdqinfo.com/py/sdqinfo/c0.py
Seeman,T.E.,Singer,B.H.,Ryff,C.D.,DienbergLove,G.,&Levy-Storms,L.(2002).
Socialrelationships,gender,andallostaticloadacrosstwoagecohorts.
PsychosomaticMedicine,64,395–406.https://doi.org/10.1097/00006842-
200205000-00004
Sen,B.(2004).Adolescentpropensityfordepressedmoodandhelpseeking:Race
andgenderdifferences.JournalofMentalHealthPolicyandEconomics,7,
133–145.
Seymour,K.(2012).Usingincentives:Encouragingandrecognisingparticipationin
youthresearch.YouthStudiesAustralia,31(3),51–59.
https://doi.org/10072/48522/80893
Shadish,W.,Cook,T.,&Campbell,T.(2002).Experimentsandgeneralizedcausal
inference.HoughtonMifflinCompany.
Shafran,R.,&Mansell,W.(2001).Perfectionismandpsychopathology:Areviewof
researchandtreatment.ClinicalPsychologyReview,21,879–906.
https://doi.org/10.1016/S0272-7358(00)00072-6
Sharma,N.,Chakrabarti,S.,&Grover,S.(2016).Genderdifferencesincaregiving
amongfamily:Caregiversofpeoplewithmentalillnesses.WorldJournalof
Psychiatry,6,7–17.https://doi.org/10.5498/wjp.v6.i1.7
Shaw,S.K.,Dallos,R.,&Shoebridge,P.(2009).Depressioninfemaleadolescents:
AnIPAanalysis.ClinicalChildPsychologyandPsychiatry,14,167–181.
https://doi.org/10.1177/1359104508100882
Shiffrin,R.M.,&Schneider,W.(1977).Controlledandautomatichuman
informationprocessing:II.Perceptualleaning,automaticattending,anda
generaltheory.PsychologicalReview,84,127–190.
https://doi.org/10.1037/0033-295X.84.2.127
Shifren,K.,&Kachorek,L.V.(2003).Doesearlycaregivingmatter?Theeffectson
youngcaregivers’adultmentalhealth.InternationalJournalofBehavioral
Development,27,338–346.https://doi.org/10.1080/01650250244000371
Silani,G.,Bird,G.,Brindley,R.,Singer,T.,Frith,C.,&Frith,U.(2008).Levelsof
emotionalawarenessandautism:AnfMRIstudy.SocialNeuroscience,3,97–

REFERENCES
371
112.https://doi.org/10.1080/17470910701577020
Simonoff,E.,Pickles,A.,Charman,T.,Chandler,S.,Loucas,T.,&Baird,G.(2008).
Psychiatricdisordersinchildrenwithautismspectrumdisorders:Prevalence,
comorbidity,andassociatedfactorsinapopulation-derivedsample.Journalof
theAmericanAcademyofChildandAdolescentPsychiatry,47,921–929.
https://doi.org/10.1097/CHI.0b013e318179964f
Siqueira,L.,Diab,M.,Bodian,C.,&Rolnitzky,L.(2000).Adolescentsbecoming
smokers:Therolesofstressandcopingmethods.JournalofAdolescentHealth,
27,399–408.https://doi.org/10.1016/S1054-139X(00)00167-1
Skelton,C.,Francis,B.,&Read,B.(2010).“Brainsbefore‘beauty’?”Highachieving
girls,schoolandgenderidentities.EducationalStudies,36,185–194.
https://doi.org/10.1080/03055690903162366
Skinner,E.A.,Edge,K.,Altman,J.,&Sherwood,H.(2003).Searchingforthe
structureofcoping:Areviewandcritiqueofcategorysystemsforclassifying
waysofcoping.PsychologicalBulletin,129,216–269.
https://doi.org/10.1037/0033-2909.129.2.216
Skinner,E.A.,&Zimmer-Gembeck,M.J.(2016).Thedevelopmentofcoping:Stress,
neurophysiology,socialrelationships,andresilienceduringchildhoodand
adolescence.SpringerInternationalPublishing.
Skoog,T.,Özdemir,S.B.,&Stattin,H.(2016).Understandingthelinkbetween
pubertaltimingingirlsandthedevelopmentofdepressivesymptoms:Therole
ofsexualharassment.JournalofYouthandAdolescence,45,316–327.
https://doi.org/10.1007/s10964-015-0292-2
Sladek,M.R.,&Doane,L.D.(2014).Dailydiaryreportsofsocialconnection,
objectivesleep,andthecortisolawakeningresponseduringadolescents’first
yearofcollege.JournalofYouthandAdolescence,44,298–316.
https://doi.org/10.1007/s10964-014-0244-2
Sladek,M.R.,Doane,L.D.,Luecken,L.J.,&Eisenberg,N.(2016).Perceivedstress,
coping,andcortisolreactivityindailylife:Astudyofadolescentsduringthe
firstyearofcollege.BiologicalPsychology,117,8–15.
https://doi.org/10.1016/j.biopsycho.2016.02.003
Slavin,L.A.,&Rainer,K.L.(1990).Genderdifferencesinemotionalsupportand

REFERENCES
372
depressivesymptomsamongadolescents:Aprospectiveanalysis.American
JournalofCommunityPsychology,18,407–421.
https://doi.org/10.1007/BF00938115
Smetana,J.G.,Campione-Barr,N.,&Daddis,C.(2004).Longitudinaldevelopment
offamilydecisionmaking:Defininghealthbehavioralautonomyformiddle-
classAfricanAmericanadolescents.ChildDevelopment,75,1418–1434.
https://doi.org/10.1111/j.1467-8624.2004.00749.x
Smith,J.A.(1996).Beyondthedividebetweencognitionanddiscourse:Using
interpretativephenomenologicalanalysisinhealthpsychology.Psychologyand
Health,11,261–271.https://doi.org/10.1080/08870449608400256
Smith,J.A.(2004).Reflectingonthedevelopmentofinterpretative
phenomenologicalanalysisanditscontributiontoqualitativeresearchin
psychology.QualitativeResearchinPsychology,1,39–54.
https://doi.org/10.1191/1478088704qp004oa
Smith,J.A.(2011a).Evaluatingthecontributionofinterpretativephenomenological
analysis.HealthPsychologyReview,5,9–27.
https://doi.org/10.1080/17437199.2010.510659
Smith,J.A.(2011b).“Wecouldbedivingforpearls”:Thevalueofthegemin
experientialqualitativepsychology.QualitativeMethodsinPsychology
Bulletin,12,6–15.
Smith,J.A.,&Dunworth,F.(2003).Qualitativemethodology.InJ.Valsiner&K.
Connolly(Eds.),Handbookofdevelopmentalpsychology(pp.603–621).SAGE
Publications.
Smith,J.A.,Flowers,P.,&Larkin,M.(2009).Interpretativephenomenological
analysis:Theory,methodandresearch.SAGEPublications.
Smith,J.A.,&Osborn,M.(2015a).Interpretativephenomenologicalanalysis.In
Qualitativepsychology:Apracticalguidetoresearchmethods(2nded.,pp.
25–52).SAGEPublications.
Smith,J.A.,&Osborn,M.(2015b).Interpretativephenomenologicalanalysisasa
usefulmethodologyforresearchonthelivedexperienceofpain.British
JournalofPain,9,41–42.https://doi.org/10.1177/2049463714541642
Smokowski,P.R.,Mann,E.A.,Reynolds,A.J.,&Fraser,M.W.(2004).Childhood

REFERENCES
373
riskandprotectivefactorsandlateadolescentadjustmentininnercity
minorityyouth.ChildrenandYouthServicesReview,26,63–91.
https://doi.org/10.1016/j.childyouth.2003.11.003
Sointu,E.T.,Savolainen,H.,Lappalainen,K.,&Lambert,M.C.(2017).Longitudinal
associationsofstudent–teacherrelationshipsandbehaviouralandemotional
strengthsonacademicachievement.EducationalPsychology,37,457–467.
https://doi.org/10.1080/01443410.2016.1165796
Solomon,M.,Miller,M.,Taylor,S.L.,Hinshaw,S.P.,&Carter,C.S.(2012).Autism
symptomsandinternalizingpsychopathologyingirlsandboyswithautism
spectrumdisorders.JournalofAutismandDevelopmentalDisorders,42,48–
59.https://doi.org/10.1007/s10803-011-1215-z
Southam-Gerow,M.A.,&Kendall,P.C.(2002).Emotionregulationand
understanding:Implicationsforchildpsychopathologyandtherapy.Clinical
PsychologyReview,22,189–222.https://doi.org/10.1016/S0272-
7358(01)00087-3
Sowislo,J.F.,&Orth,U.(2013).Doeslowself-esteempredictdepressionand
anxiety?Ameta-analysisoflongitudinalstudies.PsychologicalBulletin,139,
213–240.https://doi.org/10.1037/a0028931
Stafford,M.,Cummins,S.,Macintyre,S.,Ellaway,A.,&Marmot,M.(2005).Gender
differencesintheassociationsbetweenhealthandneighbourhood
environment.SocialScienceandMedicine,60,1681–1692.
https://doi.org/10.1016/j.socscimed.2004.08.028
Stafford,M.,&Marmot,M.(2003).Neighbourhooddeprivationandhealth:Doesit
affectusallequally?InternationalJournalofEpidemiology,32,357–366.
https://doi.org/10.1093/ije/dyg084
Stanton-Salazar,R.D.,&Spina,S.U.(2005).Adolescentpeernetworksasacontext
forsocialandemotionalsupport.YouthandSociety,36,379–417.
https://doi.org/10.1177/0044118X04267814
Stapinski,L.A.,Araya,R.,Heron,J.,Montgomery,A.A.,&Stallard,P.(2015).Peer
victimizationduringadolescence:concurrentandprospectiveimpacton
symptomsofdepressionandanxiety.Anxiety,StressandCoping,28,105–120.
https://doi.org/10.1080/10615806.2014.962023

REFERENCES
374
Stapley,E.,&Deighton,J.(2018).HeadStartyear1:Nationalqualitativeevaluation
findings:Youngpeople’sperspectives.CAMHSPress.
Stapley,E.,Demkowicz,O.,Eisenstadt,M.,Wolpert,M.,&Deighton,J.(2019).
CopingwiththestressesofdailylifeinEngland:Aqualitativestudyofself-care
strategiesandsocialandprofessionalsupportinearlyadolescence.Journalof
EarlyAdolescence,Advanceonlinepublication.
https://doi.org/10.1177/0272431619858420
Stapley,E.,Midgley,N.,&Target,M.(2016).Theexperienceofbeingtheparentof
anadolescentwithadiagnosisofdepression.JournalofChildandFamily
Studies,25,618–630.https://doi.org/10.1007/s10826-015-0237-0
Stein,D.J.(2006).Advancesinunderstandingtheanxietydisorders:Thecognitive-
affectiveneuroscienceof“falsealarms.”AnnalsofClinicalPsychiatry,18,176–
182.https://doi.org/10.1080/10401230600801192
Steiner,M.,Dunn,E.,&Born,L.(2003).Hormonesandmood:Frommenarcheto
menopauseandbeyond.JournalofAffectiveDisorders,74,67–83.
https://doi.org/10.1016/S0165-0327(02)00432-9
Sterling,P.,&Eyer,J.(1988).Allostasis:Anewparadigmtoexplainarousal
pathology.InD.Duckworth(Ed.),Handbookoflifestress,cognitionandhealth
(pp.629–649).JohnWiley&Sons.
Strack,F.,&Deutsch,R.(2004).Reflectiveandimpulsivedeterminantsofsocial
behavior.PersonalityandSocialPsychologyReview,8,220–247.
https://doi.org/10.1207/s15327957pspr0803_1
Strack,F.,&Deutsch,R.(2011).Thetwosidesofsocialbehavior:Modernclassics
andoverlookedgemsontheinterplayofautomaticandcontrolledprocesses.
PsychologicalInquiry,14,209–215.
https://doi.org/10.1080/1047840X.2003.9682881
Stride,C.B.,Gardner,S.,Catley,N.,&Thomas,F.(2015).Mpluscodeformediation,
moderation,andmoderatedmediationmodels.
http://www.offbeat.group.shef.ac.uk/FIO/mplusmedmod.htm
Stroup,D.F.,Berlin,J.A.,Morton,S.C.,Olkin,I.,Williamson,G.D.,Rennie,D.,
Moher,D.,Becker,B.J.,Sipe,T.A.,&Thacker,S.B.(2000).Meta-analysisof
observationalstudiesinepidemiology:Aproposalforreporting.JAMA,283,

REFERENCES
375
2008–2012.https://doi.org/10.1001/jama.283.15.2008
Suldo,S.M.,Shaunessy,E.,&Hardesty,R.(2008).Relationshipsamongstress,
copingandmentalhealthinhigh-achievinghighschoolstudents.Psychologyin
theSchools,45,273–290.https://doi.org/10.1002/pits.20300
Sullivan,G.M.,&Feinn,R.(2012).Usingeffectsize-orwhythepvalueisnot
enough.JournalofGraduateMedicalEducation,4,279–282.
https://doi.org/10.4300/JGME-D-12-00156.1
Sun,J.,&Stewart,D.(2007).Developmentofpopulation-basedresiliencemeasures
intheprimaryschoolsetting.HealthEducation,107,575–599.
https://doi.org/10.1108/MBE-09-2016-0047
Sundquist,J.,Li,X.,Ohlsson,H.,Råystam,M.,Winkleby,M.,Sundquist,K.,Kendler,
K.S.,&Crump,C.(2015).Familialandneighborhoodeffectsonpsychiatric
disordersinchildhoodandadolescence.JournalofPsychiatricResearch,66–
67,7–15.https://doi.org/10.1016/j.jpsychires.2015.03.019
Svanberg,E.,Stott,J.,&Spector,A.(2010).“Justhelping”:Childrenlivingwitha
parentwithyoungonsetdementia.AgingandMentalHealth,14,740–751.
https://doi.org/10.1080/13607861003713174
Szklo,M.,&Nieto,F.J.(2014).Epidemiology:Beyondthebasics(3rded.).Jones&
BartlettLearning.
Tabachnick,B.G.,&Fidell,L.S.(2013).Usingmultivariatestatistics(6thed.).
PearsonEducationLimited.
Tashakkori,A.,&Teddlie,C.(1998).Mixedmethodology:Combiningqualitativeand
quantitativeapproaches.SAGEPublications.
Tashakkori,A.,&Teddlie,C.(2003).Thepastandfutureofmixedmethods
research:Fromdatatriangulationtomixedmodeldesigns.InA.Tashakkori&
C.Teddlie(Eds.),Handbookofmixedmethodsinsocialandbehavioralresearch
(pp.671–702).SAGEPublications.
Tashakkori,A.,&Teddlie,C.(2008a).Qualityofinferencesinmixedmethods
research:Callingforanintegrativeframework.InM.M.Bergman(Ed.),
Advancesinmixedmethodsresearch:Theoriesandapplications(pp.109–119).
SAGEPublications.https://doi.org/101-119
Tashakkori,A.,&Teddlie,C.(2008b).Qualityofinferencesinmixedmethods

REFERENCES
376
research:Callingforanintegrativeframework.InM.M.Bergman(Ed.),
Advancesinmixedmethodsresearch:Theoriesandapplications(pp.101–119).
SAGEPublications.https://doi.org/101-119
Taylor,C.(2018).Thereliabilityoffreeschoolmealeligibilityasameasureofsocio-
economicdisadvantage:EvidencefromtheMillenniumCohortStudyinWales.
BritishJournalofEducationalStudies,66,29–51.
https://doi.org/10.1080/00071005.2017.1330464
Teddlie,C.,&Tashakkori,A.(2006).Ageneraltypologyofresearchdesigns
featuringmixedmethods.ResearchintheSchools,13,12–28.
Teddlie,C.,&Tashakkori,A.(2009).Foundationsofmixedmethodsresearch:
Integratingquantitativeandqualitativeapproachesinthesocialand
behavioralsciences.SAGEPublications.
Telzer,E.H.,&Fuligni,A.J.(2013).Positivedailyfamilyinteractionseliminate
genderdifferencesininternalizingsymptomsamongadolescents.Journalof
YouthandAdolescence,42,1498–1511.https://doi.org/10.1007/s10964-013-
9964-y
Terwee,C.B.,Bot,S.D.M.,deBoer,M.R.,vanderWindt,D.A.W.M.,Knol,D.L.,
Dekker,J.,Bouter,L.M.,&deVet,H.C.W.(2007).Qualitycriteriawere
proposedformeasurementpropertiesofhealthstatusquestionnaires.Journal
ofClinicalEpidemiology,60,34–42.
https://doi.org/10.1016/j.jclinepi.2006.03.012
DataProtectionAct1998,(1998)(testimonyofTheStationeryOffice).
TheWorldHealthOrganization.(2005).Childandadolescentmentalhealthpolicies
andplans.https://doi.org/10.3109/10398562.2011.603329
Thoits,P.A.(2013).Self,identity,stress,andmentalhealth.InC.S.Aneshensel,J.C.
Phelan,&A.Bierman(Eds.),Handbookofthesociologyofmentalhealth(pp.
357–377).Springer.
Thomas,N.,Stainton,T.,Jackson,So.,Cheung,W.Y.,Doubtfire,S.,&Webb,A.
(2003).“Yourfriendsdon’tunderstand”:Invisibilityandunmetneedinthe
livesof“youngcarers.”ChildandFamilySocialWork,8,35–46.
https://doi.org/10.1046/j.1365-2206.2003.00266.x
Thomassin,K.,Morelen,D.,&Suveg,C.(2012).Emotionreportingusingelectronic

REFERENCES
377
diariesreducesanxietysymptomsingirlswithemotiondysregulation.Journal
ofContemporaryPsychotherapy,42,207–213.
https://doi.org/10.1007/s10879-012-9205-9
Todres,L.(2007).Embodiedenquiry:Phenomenologicaltouchstonesforresearch,
psychotherapyandspirituality.PalgraveMacmillan.
Todres,L.,&Wheeler,S.(2001).Thecomplementarityofphenomenology,
hermeneuticsandexistentialismasaphilosophicalperspectivefornursing
research.InternationalJournalofNursingStudies,38,1–8.
https://doi.org/10.1016/S0020-7489(00)00047-X
Torre,J.B.,&Lieberman,M.D.(2018).Puttingfeelingsintowords:Affectlabeling
asimplicitemotionregulation.EmotionReview,10,116–124.
https://doi.org/10.1177/1754073917742706
Touchette,E.,Henegar,A.,Godart,N.T.,Pryor,L.,Falissard,B.,Tremblay,R.E.,&
Côté,S.M.(2010).Subclinicaleatingdisordersandtheircomorbiditywith
moodandanxietydisordersinadolescentgirls.PsychiatryResearch,185,185–
192.https://doi.org/10.1016/j.psychres.2010.04.005
Trizano-Hermosilla,I.,&Alvarado,J.M.(2016).BestalternativestoCronbach’s
alphareliabilityinrealisticconditions:Congenericandasymmetrical
measurements.FrontiersinPsychology,7,769–777.
https://doi.org/10.3389/fpsyg.2016.00769
Tugade,M.M.(2011).Positiveemotionsandcoping:Examiningdual-process
modelsofresilience.InS.Folkman(Ed.),TheOxfordhandbookofstress,
health,andcoping(pp.186–109).OxfordUniversityPress.
Tugade,M.M.,&Fredrickson,B.L.(2004).Resilientindividualsusepositive
emotionstobouncebackfromnegativeemotionalexperiences.Journalof
PersonalityandSocialPsychology,86,320–333.https://doi.org/10.1037/0022-
3514.86.2.320
Turner,H.A.,Finkelhor,D.,&Ormrod,R.(2006).Theeffectoflifetimevictimization
onthementalhealthofchildrenandadolescents.SocialScienceandMedicine,
62,13–27.https://doi.org/10.1016/j.socscimed.2005.05.030
UKGovernment.(n.d.).Childrenwithspecialeducationalneedsanddisabilities
(SEND).RetrievedAugust27,2019,fromhttps://www.gov.uk/children-with-

REFERENCES
378
special-educational-needs/extra-SEN-help
ChildrenAct,(1989).
Umberson,D.,Crosnoe,R.,&Reczek,C.(2010).Socialrelationshipsandhealth
behavioracrosslifecourse.AnnualReviewofSociology,36,139–157.
https://doi.org/10.1146/annurev-soc-070308-120011.Social
Umberson,D.,&Montez,J.K.(2010).Socialrelationshipsandhealth:Aflashpoint
forhealthpolicy.JournalofHealthandSocialBehavior,51,S54–S66.
https://doi.org/10.1177/0022146510383501
Ungar,M.(2003).Qualitativecontributionstoresilienceresearch.QualitativeSocial
Work:ResearchandPractice,2,85–102.
https://doi.org/10.1177/1473325003002001123
Ungar,M.(2004a).Aconstructionistdiscourseonresilience:Multiplecontexts,
multiplerealitiesamongat-riskchidrenandyouth.Youth&Society,35,341–
365.https://doi.org/10.1177/0044118x03257030
Ungar,M.(2004b).Theimportanceofparentsandothercaregiverstotheresilience
ofhigh-riskadolescents.FamilyProcess,43,23–41.
https://doi.org/10.1111/j.1545-5300.2004.04301004.x
Ungar,M.(2011).Thesocialecologyofresilience:Addressingcontextualand
culturalambiguityofanascentconstruct.AmericanJournalof
Orthopsychiatry,81,1–17.https://doi.org/10.1111/j.1939-0025.2010.01067.x
Ungar,M.(2012).Socialecologiesandtheircontributiontoresilience.InM.Ungar
(Ed.),Thesocialecologyofresilience:Ahandbookoftheoryandpractice(pp.
13–31).Springer.
Ungar,M.(2019).Designingresilienceresearch:Usingmultiplemethodsto
investigateriskexposure,promotiveandprotectiveprocesses,and
contextuallyrelevantoutcomesforchildrenandyouth.ChildAbuse&Neglect,
96,104098.https://doi.org/10.1016/j.chiabu.2019.104098
Ungar,M.,&Liebenberg,L.(2011).Assessingresilienceacrossculturesusingmixed
methods:ConstructionoftheChildandYouthResilienceMeasure.Journalof
MixedMethodsResearch,5,126–149.
https://doi.org/10.1177/1558689811400607
UnitedNationsChildren’sFund.(1989).TheUnitedNationsConventiononthe

REFERENCES
379
RightsoftheChild.
UnitedNationsChildren’sFund.(2011).Adolescence:Anageofopportunity.
vanderVoort,A.,Linting,M.,Juffer,F.,Bakermans-Kranenburg,M.J.,
Schoenmaker,C.,&vanIJzendoorn,M.H.(2014).Thedevelopmentof
adolescents’internalizingbehavior:Longitudinaleffectsofmaternalsensitivity
andchildinhibition.JournalofYouthandAdolescence,43,528–540.
https://doi.org/10.1007/s10964-013-9976-7
vanHam,M.,Manley,D.,Bailey,N.,Simpson,L.,&Maclennan,D.(2011).
Neighbourhoodeffectsresearch:Newperspectives.Springer.
VanOort,F.V.A.,Greaves-Lord,K.,Verhulst,F.C.,Ormel,J.,&Huizink,A.C.(2009).
Thedevelopmentalcourseofanxietysymptomsduringadolescence:The
TRAILSstudy.JournalofChildPsychologyandPsychiatryandAlliedDisciplines,
50,1209–1217.https://doi.org/10.1111/j.1469-7610.2009.02092.x
vanRens,M.,Haelermans,C.,Groot,W.,&vandenBrink,H.M.(2018).Facilitating
asuccessfultransitiontosecondaryschool:(How)doesitwork?Asystematic
literaturereview.AdolescentResearchReview,3,43–56.
https://doi.org/10.1007/s40894-017-0063-2
vanRoekel,E.,Ha,T.,Verhagen,M.,Kuntsche,E.,Scholte,R.H.J.,&Engels,R.C.M.
E.(2015).Socialstressinearlyadolescents’dailylives:Associationswithaffect
andloneliness.JournalofAdolescence,45,274–283.
https://doi.org/10.1016/j.adolescence.2015.10.012
VanRoy,B.,Veenstra,M.,&Clench-Aas,J.(2008).Constructvalidityofthefive-
factorStrengthsandDifficultiesQuestionnaire(SDQ)inpre-,early,andlate
adolescence.JournalofChildPsychologyandPsychiatry,andAlliedDisciplines,
49,1304–1312.https://doi.org/10.1111/j.1469-7610.2008.01942.x
VanVoorhees,B.W.,Paunesku,D.,Kuwabara,S.A.,Basu,A.,Gollan,J.,Hankin,B.
L.,Melkonian,S.,&Reinecke,M.(2008).Protectiveandvulnerabilityfactors
predictingnew-onsetdepressiveepisodeinarepresentativeofU.S.
adolescents.JournalofAdolescentHealth,42,605–616.
https://doi.org/10.1016/j.jadohealth.2007.11.135
Verboom,C.E.,Sijtsema,J.J.,Verhulst,F.C.,Penninx,B.W.J.H.,&Ormel,J.
(2014).Longitudinalassociationsbetweendepressiveproblems,academic

REFERENCES
380
performance,andsocialfunctioninginadolescentboysandgirls.
DevelopmentalPsychology,50,247–257.https://doi.org/10.1037/a0032547
Vigerland,S.,Serlachius,E.,Thulin,U.,Andersson,G.,Larsson,J.O.,&Ljótsson,B.
(2017).Long-termoutcomesandpredictorsofinternet-deliveredcognitive
behavioraltherapyforchildhoodanxietydisorders.BehaviourResearchand
Therapy,90,67–75.https://doi.org/10.1016/j.brat.2016.12.008
Viner,R.M.,Ozer,E.M.,Denny,S.,Marmot,M.,Resnick,M.,Fatusi,A.,&Currie,C.
(2012).Adolescenceandthesocialdeterminantsofhealth.TheLancet,379,
1641–1652.https://doi.org/10.1016/s0140-6736(12)60149-4
Vogl,S.(2013).Telephoneversusface-to-faceinterviews:Modeeffecton
semistructuredinterviewswithchildren.SociologicalMethodology,43,133–
177.https://doi.org/10.1177/0081175012465967
vonElm,E.,Altman,D.G.,Egger,M.,Pocock,S.J.,Gøtzsche,P.C.,&
Vandenbroucke,J.P.(2008).TheStrengtheningtheReportingofObservational
StudiesinEpidemiology(STROBE)statement:Guidelinesforreporting
observationalstudies.JournalofClinicalEpidemiology,61,344–349.
https://doi.org/10.1016/j.jclinepi.2007.11.008
vonElm,E.,Altman,D.G.,Egger,M.,Pocock,S.J.,Gøtzsche,P.C.,&
Vandenbroucke,J.P.(2014).TheStrengtheningtheReportingofObservational
StudiesinEpidemiology(STROBE)statement:Guidelinesforreporting
observationalstudies.InternationalJournalofSurgery,12,1495–1499.
https://doi.org/10.1016/j.ijsu.2014.07.013
Vostanis,P.,Humphrey,N.,Fitzgerald,N.,Deighton,J.,&Wolpert,M.(2013).How
doschoolspromoteemotionalwell-beingamongtheirpupils?Findingsfroma
nationalscopingsurveyofmentalhealthprovisioninEnglishschools.Childand
AdolescentMentalHealth,18,151–157.https://doi.org/10.1111/j.1475-
3588.2012.00677.x
Wadsworth,M.E.,Raviv,T.,Reinhard,C.,Wolff,B.,DeCarloSantiago,C.,&Einhorn,
L.(2008).Anindirecteffectsmodeloftheassociationbetweenpovertyand
childfunctioning:Theroleofchildren’spoverty-relatedstress.JournalofLoss
andTrauma,13,156–185.https://doi.org/10.1080/15325020701742185
Wadsworth,M.E.,&Santiago,C.D.C.(2008).Riskandresiliencyprocessesin

REFERENCES
381
ethnicallydiversefamiliesinpoverty.JournalofFamilyPsychology,22,399–
410.https://doi.org/10.1037/0893-3200.22.3.399
Wagstaff,C.,Jeong,H.,Nolan,M.,Wilson,T.,Tweedlie,J.,Phillips,E.,Senu,H.,&
Holland,F.(2014).Theaccordionandthedeepbowlofspaghetti:Eight
researchers’experiencesofusingIPAasamethodology.TheQualitative
Report,19,1–15.
Walker,G.(2018).Workingtogetherforchildren:Acriticalintroductiontomulti-
agencyworking(2nded.).BloomsburyAcademic.
Wallace,E.,Stuart,E.,&Smith,S.M.(2014).Riskpredictionmodelstopredict
emergencyhospitaladmissionincommunity-dwellingadults:Asystematic
review.MedicalCare,52(751–765).
Wang,J.,&Wang,X.(2012).Structuralequationmodeling:Applicationsusing
Mplus.JohnWiley&SonsLtd.
Wang,M.-T.,Brinkworth,M.,&Eccles,J.(2013).Moderatingeffectsofteacher-
studentrelationshipinadolescenttrajectoriesofemotionalandbehavioral
adjustment.DevelopmentalPsychology,49,690–705.
https://doi.org/10.1037/a0027916
Warner,S.(2001).Disruptingidentitythroughvisibletherapy:Afeminist
poststructuralapproachtoworkingwithwomenwhohaveexperiencedchild
abuse.FeministReview,68,115–139.
https://doi.org/10.1080/01417780110042437
Warren,J.(2006).Youngcarers:Conventionalorexaggeratedlevelsofinvolvement
indomesticandcaringtasks?ChildrenandSociety,21,136–146.
https://doi.org/10.1111/j.1099-0860.2006.00038.x
Weare,K.(2010).Promotingmentalhealththroughschools.InP.Aggleton,C.
Dennison,&W.Ian(Eds.),Promotinghealthandwellbeingthroughschools.
Routledge.
Weeks,M.,Ploubidis,G.B.,Cairney,J.,Wild,T.C.,Naicker,K.,&Colman,I.(2016).
Developmentalpathwayslinkingchildhoodandadolescentinternalizing,
externalizing,academiccompetence,andadolescentdepression.Journalof
Adolescence,51,30–40.https://doi.org/10.1016/j.adolescence.2016.05.009
Wellman,H.,&Gelman,S.A.(1992).Cognitivedevelopment:Foundationaltheories

REFERENCES
382
ofcoredomains.AnnualReviewofPsychology,43,337–375.
https://doi.org/10.1146/annurev.psych.43.1.337
West,P.,Sweeting,H.,&Young,R.(2010).Transitionmatters:Pupils’experiences
oftheprimary-secondaryschooltransitionintheWestofScotlandand
consequencesforwell-beingandattainment.ResearchPapersinEducation,
25,21–50.https://doi.org/10.1080/02671520802308677
West,S.G.,Finch,J.F.,&Curran,P.J.(1995).Structuralequationmodelswith
nonnormalvariables:Problemsandremedies.InR.H.Hoyle(Ed.),Structural
equationmodeling:Concepts,issuesandapplications(pp.56–75).SAGE
Publications.
White,M.,&Epston,D.(1990).Narrativemeanstotherapeuticends.Norton.
Whittaker,T.A.(2012).Usingthemodificationindexandstandardizedexpected
parameterchangeformodelmodification.JournalofExperimentalEducation,
80,26–44.https://doi.org/10.1080/00220973.2010.531299
Wilkinson,R.B.(2010).Bestfriendattachmentversuspeerattachmentinthe
predictionofadolescentpsychologicaladjustment.JournalofAdolescence,33,
709–717.https://doi.org/10.1016/j.adolescence.2009.10.013
Will,G.,Lier,P.A.C.Van,Crone,E.A.,&Güro,B.(2016).Chronicchildhoodpeer
rejectionisassociatedwithheightenedneuralresponsestosocialexclusion
duringadolescence.JournalofAbnormalChildPsychology,44,43–55.
https://doi.org/10.1007/s10802-015-9983-0
Wille,N.,Bettge,S.,&Ravens-Sieberer,U.(2008).Riskandprotectivefactorsfor
children’sandadolescents’mentalhealth:ResultsoftheBELLAstudy.
EuropeanChildandAdolescentPsychiatry,17,133–147.
https://doi.org/10.1007/s00787-008-1015-y
Williams,A.L.,&Merten,M.J.(2014).Linkingcommunity,parenting,and
depressivesymptomtrajectories:Testingresiliencemodelsofadolescent
agencybasedonrace/ethnicityandgender.EmpiricalResearch,43,1563–
1575.https://doi.org/10.1007/s10964-014-0141-8
Williams,J.E.(1996).Gender-relatedworryandemotionalitytestanxietyforhigh-
achievingstudents.PsychologyintheSchools,33,159–162.
https://doi.org/10.1002/(SICI)1520-6807(199604)33:2<159::AID-

REFERENCES
383
PITS9>3.0.CO;2-M
Willig,C.(2013).Introducingqualitativeresearchinpsychology(3rded.).Open
UniversityPress.
Wilmots,E.,Midgley,N.,Thackeray,L.,Reynolds,S.,&Loades,M.(2019).The
therapeuticrelationshipinCognitiveBehaviourTherapywithdepressed
adolescents:Aqualitativestudyofgood-outcomecases.Psychologyand
Psychotherapy:Theory,ResearchandPractice,Advanceonlinepublication.
https://doi.org/10.1111/papt.12232
Wilson,C.J.,Bushnell,J.A.,&Caputi,P.(2011).Earlyaccessandhelpseeking:
Practiceimplicationsandnewinitiatives.EarlyInterventioninPsychiatry,5,
34–39.https://doi.org/10.1111/j.1751-7893.2010.00238.x
Wilson,C.J.,&Deane,F.P.(2010).Help-negationandsuicidalideation:Theroleof
depression,anxietyandhopelessness.JournalofYouthandAdolescence,39,
291–305.https://doi.org/10.1007/s10964-009-9487-8
Wilson,C.J.,&Deane,F.P.(2012).Briefreport:Needforautonomyandother
perceivedbarriersrelatingtoadolescents’intentionstoseekprofessional
mentalhealthcare.JournalofAdolescence,35,233–237.
https://doi.org/10.1016/j.adolescence.2010.06.011
Wilson,C.J.,Rickwood,D.J.,&Deane,F.P.(2007).Depressivesymptomsandhelp-
seekingintentionsinyoungpeople.ClinicalPsychologist,11,98–107.
https://doi.org/10.1080/13284200701870954
Wisdom,J.P.,&Green,C.A.(2004).“Beinginafunk”:Teens’effortstounderstand
theirdepressiveexperiences.QualitativeHealthResearch,14,1227–1238.
https://doi.org/10.1177/1049732304268657
Wodtke,G.T.(2013).Durationandtimingofexposuretoneighborhoodpoverty
andtheriskofadolescentparenthood.Demography,50,1765–1788.
https://doi.org/10.1007/s13524-013-0219-z
Wolk,C.B.,Kendall,P.C.,&Beidas,R.S.(2015).Cognitive-behavioraltherapyfor
childanxietyconferslong-termprotectionfromsuicidality.Journalofthe
AmericanAcademyofChildandAdolescentPsychiatry,54,175–179.
https://doi.org/10.1016/j.jaac.2014.12.004
Wong,N.T.,Zimmerman,M.A.,&Parker,E.A.(2010).Atypologyofyouth

REFERENCES
384
participationandempowermentforchildandadolescenthealthpromotion.
AmericanJournalofCommunityPsychology,46,100–114.
https://doi.org/10.1007/s10464-010-9330-0
Wood,A.,Lupyan,G.,&Niedenthal,P.(2016).Whydoweneedemotionwordsin
thefirstplace?CommentaryonLakoff(2015).EmotionReview,8,274–275.
https://doi.org/10.1177/1754073915595103
Woodgate,R.L.(2006).Livingintheshadowoffear:Adolescents’livedexperience
ofdepression.JournalofAdvancedNursing,56,261–269.
https://doi.org/10.1111/j.1365-2648.2006.04020.x
Woodward,M.(2014).Epidemiology:Studydesignanddataanalysis(3rded.).CRC
Press.
WorldHealthOrganization.(2001).Strengtheningmentalhealthpromotion.
WorldHealthOrganization.(2004).Theglobalburdenofdisease2004.
https://doi.org/10.1038/npp.2011.85
WorldHealthOrganization.(2017).Depressionandothercommonmental
disorders:Globalhealthestimates.
Wray-Lake,L.,Crouter,A.C.,&McHale,S.M.(2010).Developmentalpatternsin
decision-makingautonomyacrossmiddlechildhoodandadolescence:
Europeanamericanparents’perspectives.ChildDevelopment,81,636–651.
https://doi.org/10.1111/j.1467-8624.2009.01420.x
Wright,M.,Banerjee,R.,Hoek,W.,Rieffe,C.,&Novin,S.(2010).Depressionand
socialanxietyinchildren:Differentiallinkswithcopingstrategies.Journalof
AbnormalChildPsychology,38,405–419.https://doi.org/10.1007/s10802-009-
9375-4
Wu,S.,&Amtmann,D.(2013).PsychometricevaluationofthePerceivedStress
Scaleinmultiplesclerosis.ISRNRehabilitation,2013,1–9.
https://doi.org/10.1155/2013/608356
Xue,Y.G.,Leventhal,T.,Brooks-Gunn,J.,&Earls,F.J.(2005).Neighborhood
residenceandmentalhealthproblemsof5-to11-year-olds.Archivesof
GeneralPsychiatry,62,554–563.https://doi.org/10.1001/Archpsyc.62.5.554
Yardley,L.(2000).Dilemmasinqualitativehealthresearch.PsychologyandHealth,
15,215–228.https://doi.org/10.1080/08870440008400302

REFERENCES
385
Yardley,L.(2015).Demonstratingvalidityinqualitativepsychology.InJ.A.Smith
(Ed.),Qualitativepsychology:Apracticalguidetoresearchmethods(3rded.,
pp.257–272).SAGEPublicationsLtd.
Yeung,R.,&Leadbeater,B.(2009).Adultsmakeadifference:Theprotectiveeffects
ofparentandteacheremotionalsupportonemotionalandbehavioral
problemsofpeer-victimizedadolescents.JournalofCommunityPsychology,
38,80–98.https://doi.org/10.1002/jcop.20353
YeungThompson,R.S.,&Leadbeater,B.J.(2013).Peervictimizationand
internalizingsymptomsfromadolescenceintoyoungadulthood:Building
strengththroughemotionalsupport.JournalofResearchonAdolescence,23,
290–303.https://doi.org/10.1111/j.1532-7795.2012.00827.x
Yilmaz,K.(2013).ComparisonofquantitativeandqualitativerResearchtraditions:
Epistemological,theoretical.EuropeanJournalofEducation,48,311–325.
https://doi.org/10.1111/jppi.12086
Yin,R.(1989).Casestudyresearch:Designandmethods(2nded.).SAGE
Publications.
Youssef,N.A.,Belew,D.,Hao,G.,Wang,X.,Treiber,F.A.,Stefanek,M.,Yassa,M.,
Boswell,E.,McCall,W.V.,&Su,S.(2017).Racial/ethnicdifferencesinthe
associationofchildhoodadversitieswithdepressionandtheroleofresilience.
JournalofAffectiveDisorders,208,577–581.
https://doi.org/10.1016/j.jad.2016.10.024
Zahn-Waxler,C.,Crick,N.R.,Shirtcliff,E.A.,&Woods,K.E.(2006).Theoriginsand
developmentofpsychopathologyinfemalesandmales.InD.Cicchetti&D.J.
Cohen(Eds.),Developmentalpsychopathology:Volumeone:Theoryand
method(2nded.,pp.76–138).JohnWiley&Sons,Inc.
Zahn-Waxler,C.,Klimes-Dougan,B.,&Slattery,M.J.(2000).Internalizingproblems
ofchildhoodandadolescence:Prospects,pitfalls,andprogressin
understandingthedevelopmentofanxietyanddepression.Developmentand
Psychopathology,12,443–466.https://doi.org/10.1017/S0954579400003102
Zaman,W.,&Fivush,R.(2013).Genderdifferencesinelaborativeparent-child
emotionandplaynarratives.SexRoles,68,591–604.
https://doi.org/10.1007/s11199-013-0270-7
REFERENCES
386
Zarate-Garza,P.P.,Biggs,B.K.,Croarkin,P.,Morath,B.,Leffler,J.,Cuellar-Barboza,
A.,&Tye,S.J.(2017).Howwelldoweunderstandthelong-termhealth
implicationsofchildhoodbullying?HarvardReviewofPsychiatry,25,89–95.
https://doi.org/10.1097/HRP.0000000000000137
Zhang,Z.,&Yuan,K.H.(2015).Robustcoefficientsalphaandomegaand
confidenceintervalswithoutlyingobservationsandmissingdata:Methods
andsoftware.EducationalandPsychologicalMeasurement,76,387–411.
https://doi.org/10.1177/0013164415594658
Zimmaro,L.A.,Salmon,P.,Naidu,H.,Rowe,J.,Phillips,K.,Rebholz,W.N.,Giese-
Davis,J.,Cash,E.,Dreeben,S.J.,Bayley-Veloso,R.,Jablonski,M.E.,Hicks,A.,
Siwik,C.,&Sephton,S.E.(2016).Associationofdispositionalmindfulnesswith
stress,cotrisol,andwell-beingamonguniversityundergraduatestudents.
Mindfulness,7,874–885.https://doi.org/10.1007/s12671-016-0526-8
Zimmerman,F.J.(2005).Socialandeconomicdeterminantsofdisparitiesin
professionalhelp-seekingforchildmentalhealthproblems:Evidencefroma
nationalsample.HealthServicesResearch,40,1514–1533.
https://doi.org/10.1111/j.1475-6773.2005.00411.x
Zlomke,K.R.,&Hahn,K.S.(2010).Cognitiveemotionregulationstrategies:Gender
differencesandassociationstoworry.PersonalityandIndividualDifferences,
48,408–413.https://doi.org/10.1016/j.paid.2009.11.007
Zolkoski,S.M.,&Bullock,L.M.(2012).Resilienceinchildrenandyouth:Areview.
ChildrenandYouthServicesReview,34,2295–2303.
https://doi.org/10.1016/j.childyouth.2012.08.009

APPENDICES
387
Appendices
Appendix Page
A DifferencesbetweenthecurrentstudyandtheevaluationofHeadStart 388
B Qualitativeparticipantselectionprotocol 390
C Examplequalitativeparticipantselectionoverview(Amelia) 397
D QualitativeHeadStartparticipantsnominatedfor,butnotincludedin,the
currentstudy
401
E ChangesmadeafterpilotingoftheWellbeingMeasurementFramework
(WMF)
402
F Guidanceprovidedtoteacherstofacilitatesurveyadministration 403
G StrengthsandDifficultiesQuestionnaire(SDQ)emotionalsymptomssubscale 413
H Four-itemPerceivedStressScale(PSS-4) 414
I StudentResilienceSurveysubscales 415
J Qualitativeinterviewschedule 417
K Quantitativeinformationpackforparents/carers 421
L Quantitativeparticipantinformationforyoungpeople 427
M Qualitativeparticipantinformationsheetforyoungpeople 429
N Qualitativeinformationpackforparents/carers 432
O Qualitativeparticipantassentform 437
P Demographicformforqualitativeparticipants 438
Q Exampleofinitialthoughtsdocumentedinstageoneofqualitativeanalysis
(Amelia)
439
R Analyticalcodingcolumnsandexampleofinitialcodinginstagetwoof
qualitativeanalysis(Amelia)
441
S Exampleofemergentthemesalongsidedataandcodinginstagethreeof
qualitativeanalysis(Amelia)
442
T Detailedaccountofpreliminaryanalysisresults 443
U Integrationofindividual-levelthemesintomasterthemes 452

APPENDICES
388
AppendixA:DifferencesbetweentheCurrentStudyandtheEvaluationofHeadStart
TableA1
DifferencesBetweentheCurrentStudyandtheHeadStartEvaluation
Feature Currentstudy HeadStartevaluation
Type Studycompletedforsubmissionasa
PhDthesis
Fundedevaluationofanational
mentalhealthprogramme
Staffing Individualthesisauthor,withinput
fromsupervisors
Largeresearchteamacrossmultiple
partnerships
Aim1 Increaseknowledgeand
understandingoftheriskfactorsand
processesassociatedwithemotional
symptomsamongearlyadolescent
girls,withaparticularfocuson
multipleriskexposure
Helpservicesconsiderthemeasurable
impactoftheirinterventionsby
analysingtheinteractionbetween
specificmodifiablefeaturesand
qualitiesoftheinterventionsprovided
andrelevantindicatorsofchangesin
resilienceandwellbeing
Aim2 Assessthefactorsandprocesses
supportingpositiveoutcomesin
relationtoemotionalsymptoms
amongearlyadolescentgirls
Examineexperienceandpossible
mechanismsunderpinningHeadStart
Aim3 Explorethelivedexperienceofearly
adolescentgirlswhoare
experiencingemotionalsymptomsin
thecontextofriskexposure
Considerevidence-basedpracticeand
disseminationtoaidlearningand
development
Temporality Cross-sectional Longitudinal,cross-sectional
Design Parallelmixedmethodsdesign;
observational
Parallelmixedmethodsdesign;quasi-
experimentalandlongitudinal
Populationof
interest
Earlyadolescentgirlsaged11-12
years
Youngpeopleaged10-16years
Quantitative
sample
Earlyadolescentgirlsaged11-12
years(Year7,2016/2017)atthetime
oftheWMFbaseline
Youngpeopleaged11-12yearsatthe
timeoftheWMFbaseline(Year7,
2016/2017)andyoungpeopleaged
13-14years(Year9,2016/2017)atthe
timeofeachannualcompletionofthe
WMF(2017-2022)
Qualitative Girlsaged11-12yearsatbaseline Youngpeopleaged9-12yearsat

APPENDICES
389
sample interviews,experiencingemotional
symptomsandmultipleriskexposure
baselineinterviews;deliveryagents;
andpartnershipleads
Quantitative
analysis
SEM Descriptiveanalysis,multilevel
analysis,SEM
Qualitative
analysis
Interpretativephenomenological
analysis
Thematicanalysisandidealtype
analysis
Outcomevariable Emotionalsymptoms Wellbeing;mentalhealthdifficulties;
mechanisms
Targetaudience Academiccommunity;mentalhealth
andeducationalprofessionals;and
youngpeople
TheNCLF;HeadStartpartnership
areas;mentalhealthandeducational
professionals;youngpeople;and
academiccommunity

APPENDICES
390
AppendixB:QualitativeParticipantSelectionProtocol
Thisdocumentdetailstheparticipantselectionprotocolforthequalitative
strandofamixedmethodsPhDthesisfocusedonthemultipleriskexposureand
earlyadolescentgirls’emotionalsymptoms,withattentiontomechanisms,
adaptiveprocesses,andlivedexperience.Thequalitativestrandseekstoaddress
thefollowingresearchquestion:
Whatisitliketobeanearlyadolescentgirlexperiencingemotional
symptomsinthecontextofriskexposure?
Theresearchquestionaimstoexploreearlyadolescentgirls’livedexperienceto
provideinsightintothecomplexitiesofthesephenomenaincontextandtheir
meaningtogirlsthemselves.Inordertoaddressthisresearchquestion,uptofive
participantswillbesoughtfromanexistingqualitativesamplewhohavetakenpart
inin-depthinterviewsaspartoftheevaluationofHeadStart.Participantinterviews
thatmeettheinclusioncriteriaforthecurrentstudywillbeanalysedusing
interpretativephenomenologicalanalysis(IPA).Thisdocumentoutlinesthe
inclusioncriteriaandtherationaleforeachcriterion,beforedetailingtheselection
process,specificallycriteriaassessmentsteps,rigourstepsandtheexpected
timeframe.
Inclusioncriteria
1. Female,aged11-12years
Rationale:thisstudyisfocusedongirlsasalthoughresearchhasshownthat
overalltheprevalenceofchildandadolescentmentalhealthdifficultieshasbeen
relativelystableinrecentdecades,severalstudieshavereportedarecentincrease
inemotionaldistressamongadolescentgirls(Boretal.,2014;Collishawetal.,2010;
Finketal.,2015;Lessofetal.,2016).Thestudyseekstoutiliseparticipantsaged11-
12yearsasthisageappearstorepresentsapivotalstageinthedevelopmentof
mentalhealthdifficulties,wherebyemotionalsymptomsbecomemoreprevalentin
girls,particularlyrelativetotheirmalepeers(Boretal.,2014;Rozaetal.,2003).As
such,thecurrentstudyseekstobroadencurrentunderstandingsofthefactorsthat

APPENDICES
391
contributetosuchdifficultiesforgirlsduringthisdevelopmentalphase,alongside
factorsthatmaylessensuchnegativeeffects.
2. Experiencingemotionalsymptoms
Rationale:theresearchisfocusedonemotionalsymptomsdueto
indicationsthatlevelsofemotionaldistressappeartohaveincreasedingirlsin
recentcohorts,asoutlinedabove.‘Emotionalsymptoms’arebroadlydefinedas
feelingsofdepressionandanxiety.AstheHeadStartqualitativeevaluationutilisesa
communitysample,highproportionsofparticipantswithabnormal/clinicallevelsof
symptomatologyarenotanticipated.Assuch,thecurrentstudydrawson
emotionalsymptomsascharacterisedwithinthecorrespondingsubscaleofthe
StrengthsandDifficultiesQuestionnaire(SDQ;Goodman,1997;Goodmanetal.,
1998)asalenstocharacteriseandassesssymptoms(seecriteriaassessment
below),asthisisappropriateforuseinacommunitysample.
3. Experiencingrisk
Rationale:thequalitativestrandseekstounderstandexperienceofriskas
partofthestudy’sbroaderfocusonmultipleriskexposure,specificallythe
cumulativemodelofrisk.Assuch,thestudyseekstoutiliseparticipantswhoare
experiencingmultipleriskexposureaspartoftheirlives.Thestudyseeksto
considerparticipants’ownaccountsof‘risk’intheirlivesalongsideconsiderationof
establishedriskfactors(seecriteriaassessmentbelow).
CriteriaAssessment
Thefollowingsectionoutlinestheassessmentprocessfortheinclusion
criteria.Whileundertakingthisprocess,theresearcherwilldocumentthisprocess
infullandprovidewrittenjustificationsofeachstageforallparticipantsreviewed,
withsupportingquotes/excerptsfromtranscriptstosupportdecisions.
1. Female,aged11-12years
TheinitialstageofselectionfromtheoverallHeadStartqualitativesample
willidentifyparticipantsthatarefemaleandaged11–12yearsaccordingtothe
demographicinformationtheyprovidedaspartoftheinterviewprocess.

APPENDICES
392
2. Experiencingemotionalsymptoms
HeadStartparticipantswillbeidentifiedasmeetingthiscriterionthrough
twostages.Firstly,interviewerswillnominateHeadStartparticipantsthattheyfeel
disclosedemotionalsymptomsintheinterviewprocess,withthisdocumentacting
asaguide.
Thesenominatedparticipantswillthenundergosystematicassessmentfor
disclosureofemotionalsymptomsthroughthestagesdescribedbelow.
Theresearcherwillassesseachtranscript,consideringparticipants’accounts
inrelationtotheSDQadultreport‘emotionalsymptoms’subscaleitemsoutlinedin
Table1(Goodman,1997).AscanbeseeninTable1,itemsarescoredonascaleof
0-2,where0=nottrue,1=somewhattrue,and2=certainlytrue.Indetermining
theappropriatescoreforeachsymptom,theresearcherwillconsiderarangeof
factors,specificallyfrequencyofsymptomsasdescribedbyparticipants,intensityof
symptomsasdescribedbyparticipants,andfrequencyofmentionofsymptoms
withininterviews.Atotalscoreof4onthesubscalewillbeconsideredindicativeof
borderlinesymptomatology,consistentwithguidelinesoutlinedbySDQInfo(2016),
thoughthiswillactasaguideratherthanacutoff.Wheretheresearcheridentifies
thatasymptomcouldbeconsidered‘certainlytrue’butisoccurringinisolation,
thiswillbeconsideredonacase-by-casebasis,astheextentofthesymptommay
aloneindicateanappropriatelevelofsymptomatology.Forexample,ifa
participantdescribedfrequentlyfeelingextremelyunhappy,down-heartedor
tearful,butdidnotdescribeothersymptoms,thisalonemayindicatean
appropriatelevelofemotionaldistress.Itshouldbenotedthatthisexcludes
‘headaches,stomach-achesorsickness’ifoccurringinisolationasthismaybe
relatedtowiderphysicalissues.

APPENDICES
393
Table1:Teacher/parentSDQemotionalsymptomssubscale
Not
True(0)
Somewhat
True(1)
Certainly
True(2)
Oftencomplainsofheadaches,stomach-achesorsickness ☐ ☐ ☐Manyworries,oftenseemsworried ☐ ☐ ☐Oftenunhappy,down-heartedortearful ☐ ☐ ☐Nervousorclingyinnewsituations,easilyloses
confidence
☐ ☐ ☐
Manyfears,easilyscared ☐ ☐ ☐
Theresearcherwillreviewtheirownassessmentagainsttheparticipant’sownself-
reportedSDQscore,basedontheitemsshowninAppendixG.Ascoreof6willbe
consideredtoindicateborderlinesymptomatology,consistentwithguidelines
outlinedbySDQInfo(2016).Again,thiswillnotrepresentacutoffandwillinstead
beconsideredinconjunctionwithassessmentfromstage(i).Itshouldbenoted
thatthismaynotbeavailableforallparticipantsasthiswascompletedaspartof
thequantitativestrandofHeadStart,ratherthanaspartoftheinterviewprocess.
Table2:Self-reportSDQemotionalsymptomssubscale
Not
True(0)
Somewhat
True(1)
Certainly
True(2)
Igetalotofheadaches,stomach-achesorsickness ☐ ☐ ☐Iworryalot ☐ ☐ ☐Iamoftenunhappy,down-heartedortearful ☐ ☐ ☐Iamnervousinnewsituations;Ieasilyloseconfidence ☐ ☐ ☐Ihavemanyfears,Iameasilyscared ☐ ☐ ☐
Foreachparticipant,theresearcherwillmakeafinaldecisionutilisingthe
informationgatheredthroughthesestepsandwilldocumentjustificationforthis.It
shouldbenotedthatitisnotanticipatedthatthesubscalescoresgeneratedbythe
researcherandtheparticipantwillbeinagreement.Thisisforarangeofreasons,
suchasthefactthattheparticipantcompletedtheirself-reportsubscaleona

APPENDICES
394
separateoccasionratherthanonthedayoftheinterview,thepotentialthat
participantsdidnotdisclosesymptomsduringtheinterview,andthatthe
researcher’sownperspectivesandunderstandingsislikelytoinfluencethewayin
whichtheymakesenseofparticipants’disclosures.Assuch,theresearcherwill
considerbothsourcesofinformationtoreachafinaldecisionandwilldocument
thisprocessclearly.
3. Experiencingrisk
Toreflectthestudy’sfocusonmultipleriskexposure,participantswillbe
consideredtomeetthiscriterioniftheydemonstratemultipleindicatorsof‘risk’in
theirlives.Namely,aminimumofthreeormoreindicatorsofriskshouldbe
identifiedacrossthetwostagesoutlinedbelow,asarangeofstudieshave
indicatedthatexposuretothreeormoreriskfactorsoftenaffectsoutcomes
disproportionately(e.g.,Jonesetal.,2002;Morales&Guerra,2006;Rutter,1979).
Thiscriterionwillbeassessedusingtwomethods:
a. Transcriptsofparticipantsidentifiedasexperiencingemotionalsymptomswill
bereviewedformentionofknownriskfactors,i.e.thosewithfactors
identifiedinpreviousresearchasincreasingthelikelihoodofemotional
symptomsinadolescence(e.g.lowacademicattainment,lowfamilyincome).
Writtenjustificationwillincludereferencestoappropriateliteratureand
researchunderpinningclassificationasariskfactor.
b. Thesetranscriptswillthenbereviewedforparticipants’owndescriptionsof
self-perceivedsourcesofstress.Forthisstage,theresearcherwillutilise
bracketingstrategies,wherebytheresearcherseekstosetasidetheirexisting
understandingofthephenomenon/conceptsandoftheexistingresearchin
thisarea.Arangeofbracketingstrategieswillbeused,including:
i. Keepingmemosofdecisionsandtheunderpinningrationaleswithina
reflexivejournal;
ii. Ongoingconsiderationandreviewingofthesedecisions;
iii. Discussingthesereflectionswithanexternalparty(i.e.,PhDsupervisor);
iv. Consideringownresponsestointerviewers’questionsinorderto
positionselfinrelationtointerpretationofparticipants’feedback;and

APPENDICES
395
v. Consideringresponsesinisolationfromtherestofthetextinorderto
decontextualiseresponses(Smithetal.,2009).
RigourSteps
Arangeofmeasureswillbetakentosupportrigourwithintheparticipant
selectionprocess,namely:
a. Thefullprocesswillbedocumentedextensivelybytheresearcher,with
writtenjustificationofhowparticipantsmeetinclusioncriteria2and3and
supportingquotes/excerptsfromtranscriptstosupportdecisions.The
researcherwillalsodocumenttheparticipantsnotidentifiedasmeetingthe
inclusioncriteriaalongsidejustificationofthesedecisions.Theprocesswill
alsobedocumentedinthereflexivejournalkeptaspartofthebroader
study.TheresearcherwillengageinreflexivediscussionwiththePhD
supervisoraspartofthisprocesstodevelopandrefinedecisions.
b. Theselectedparticipantswillbereviewedbyasecondaryresearcherwith
knowledgeofriskandmentalhealth.Thepurposeofthisstepistosupport
theconfirmabilityofselectiondecisionsandtheprocesscanbeconsidered
similartoanauditasisrecommendedinqualitativeanalysis(Smithetal.,
2009;Yin,1989)
c. Thesecondaryresearcherwillbeprovidedwiththepresentdocumentasa
guide,alongsidethewrittenjustificationdocumentedforeachselected
participantcompletedaspartofstage(a).Thesecondaryresearcherwillbe
invitedtoconfirmtheselectionofeachparticipantandprovidecommentsif
appropriate.Thesecondaryresearcher’sfeedbackwillthenbeincorporated
beforethefinalsampleisidentified.
d. Theselectedparticipantswillthenbereviewedbyanexternalpartywitha
clinicalorcounsellingbackground.Thepurposeofthisstepisalsoto
supporttheconfirmabilityofselectiondecisionsandagaincanbelikenedto
anaudit;however,thisreviewdiffersfromthepreviousstageasaclinical
reviewermayofferaperspectivethatisgroundedinpracticalexperience
withtheadolescentpopulation,ratherthanatatheoreticallevel.

APPENDICES
396
e. Thereviewerwillbeprovidedwiththepresentdocumentasaguide,
alongsidethewrittenjustificationdocumentedforeachselectedparticipant
completedaspartofstage(a).Thereviewerwillbeinvitedtoconfirmthe
selectionofeachparticipantandprovidecommentsifappropriate.The
reviewer’sfeedbackwillthenbeincorporatedbeforethefinalsampleis
identified.

APPENDICES
397
AppendixC:ExampleQualitativeParticipantSelectionOverview(Amelia)
“Amelia”
Age:12years,9months
1. Emotionalsymptoms
Ameliawasincludedforreviewastheinterviewer(inthiscasethecurrent
author)identifiedherashavingdisclosedemotionalsymptoms.Takingintoaccount
researcherjudgementsbasedonAmelia’sinterview,Ameliahasbeenidentifiedas
experiencingemotionalsymptoms.
InterviewerNominationComments
Giventhatinthisinstancetheinterviewwascarriedoutbytheauthorofthe
currentstudy,thesenotesaretheinitialimpressionsoutlinedfollowingthe
interview.
• Disclosedhighlevelsofanxietyinmostareasoflife
• Specificanxietyinrelationtoacademicwork
• Frequentfeelingsofstressandfrustration,oftenarisingfromanxiety
• Difficultyusingstrategiesprovidedbysupportworker
• DisclosedObsessiveCompulsiveDisorder(OCD)
ResearcherAssessment
IntensityofSymptoms.Ameliadescribedfeelingworriedas“upsetand
stressedout,andabitlike,likeconfusedsayinglike“ohwhat,shouldIdothisorwill
thishappen?””Shecommentedseveraltimesthatheranxietyseemedtobe
worsening;“(mum)saidthatmyworrieskeepongettinglikebiggerandbigger”and
heranxietyappearedtopreventherfromdoingthings,suchasgoingonrideson
holiday,oraskingforhelpinlessons“Idon’treallyputmyhandup[…]sometimes,
erm,Ijustseewhattheotherperson’sdoing”.Shecommentedthatsherepeats
sometasks;“itmakesmefeellikestressedoutcauseifintperfectthenI’llhaveto
doitagain.”Ameliaexplainedthatsheaccessessupportinrelationtoheranxiety

APPENDICES
398
butthatshestrugglestousethestrategiesshe’sgiven;“Istillfeelreallyworriedand
anxiousIjustlikesometimeslikeIforgettheadvice”.
FrequencyofSymptoms.Ameliadescribedfeelinganxiousonadailybasis.
Thiswasparticularlypresentindiscussionofherschoolwork,forexample“Idon’t
likegettingsomethingwronglikethat’swhatIworryabout,likegettingsomething
wrong[…]if(teacher)getsmadatmeorgavemeadetentionorsomethinglike
that,that’swhatIworryabout”.Ameliaalsodescribedsymptomsinotherareasof
herdailylife,suchas“forexampleifmytieintrightor,it’slikeeverythinghastobe
perfect[…]itstillgetsmeworried”,aswellasinmorespecificcircumstancessuch
asonholiday;“whenIwasonholidaytoDisneyworldandIwasworriedcauseI
don’tlike[…]theunknownandthedarkrides[…]IsaidIwon’tgoonitanywaybutI
wasstillreallyworriedaboutit”.
FrequencyofMentionwithinInterview.Ameliafocusedheavilyonher
anxietyintheinterviewandoftenthedialoguemovedbacktothisarea.For
example,whenaskedwhatmadeherhappy,Ameliadescribedthisinrelationto
theabsenceofworry“Iwouldbesmilingandcheery…andyeahI’lljustbereallylike
happynotworriedaboutanything.”
SDQResearcherReport.BasedonAmelia’sdisclosureofhersymptoms
withintheinterview,theresearcherdesignatedascoreof5(seeTable1foritem
scores).
Table1:Teacher/parentSDQemotionalsymptomssubscale
Not
True(0)
Somewhat
True(1)
Certainly
True(2)
Oftencomplainsofheadaches,stomach-achesorsickness þ ☐ ☐
Manyworries,oftenseemsworried ☐ ☐ þ
Oftenunhappy,down-heartedortearful þ ☐ ☐
Nervousorclingyinnewsituations,easilylosesconfidence ☐ þ ☐
Manyfears,easilyscared ☐ ☐ þ

APPENDICES
399
Self-ReportofSymptoms
Ameliadidnotcompletethequantitativesurveyandsotherewasnoself-
reportofhersymptomsavailable.
2. Risk
Theresearcheridentifiedthreeknown/empiricalriskfactorsinAmelia’s
interviewandoneadditionalself-perceivedsourceofstress.Thisindicatesthat
Ameliaisexperiencinganappropriatelevelofriskforinclusioninthecurrentstudy.
a. Knownriskfactors:
i. Epilepsy:Ameliadisclosedthatshehasepilepsy.Researchhasconsistently
indicatedthatchildrenandadolescentswithepilepsyareatanincreased
riskofemotionalsymptoms(e.g.,Davies,Heyman,&Goodman,2003;
Kariuki,Newton,Prince,&Das-Munshi,2016).
ii. Academicdifficulties:Ameliadescribedstrugglingwithacademicwork,
explainingthatshestrugglestofocusontasksa,explainingthatshe
strugglestofocusontasksandfindstheclassroomstressful.Lowacademic
attainmentandacademicdifficultieshavepreviouslybeenidentifiedasa
riskfactorforemotionalsymptomsinadolescence,specificallyforgirls(e.g.,
McCarty,2008;Panayiotou&Humphrey,2018).
iii. OCD:AmeliadisclosedthatshehasOCDandexplainedthatthisaffectsher
dailybehaviour.ThoughanxietyasasymptomofOCDisoftenexperienced
inrelationtospecificobsessions,itoftenco-occursalongsidemore
generalisedanxiety(NHS,2016),asisindicatedinAmelia’sinterview.
b. Additionalself-perceivedsourcesofstress:
i. ParentworkinginLondon:Ameliadescribedhavingworriesabouther
fatherandhisjobasheworksinLondon,andthatifheisstressedorupset
shealsobecomesstressedorupset.
3. Review
Secondaryresearcherreviewcomments:

APPENDICES
400
Iagreethatjudgementsofemotionalsymptomsandthelevelofriskthat
Ameliaisexperiencingarereasonableforinclusioninthecurrentstudy,having
reviewedAmelia'sfulltranscript,listenedtotheaudiofile,andtheassessment
document.
(MiaEisenstadt,AFNCCF)
Clinicalreviewcomments:
Ameliacomesacrossasquiteconfusedandnotknowingherownmindvery
well.Shetalksaboutperfectionism,andthisextendstoherfearsaroundhowgood
atherapypatientsheis(worryingshe’llforgetthestrategiesshe’sbeengiven).She
mayhavesomeOCD.ThefearaboutridesatDisneylandwasextremelyinteresting
andmademewonderifshehasnightmares.Shealsoshowshowvulnerableher
mindisintakinghertoafrighteningplaceasevenimaginingwherethedarkand
unknownrideswouldtakeherwasbadenough.Isuspectshebroughtthisup
becausesheisawarethatherworriesarelimitingherownexplorationandability
tohavefunandwantshelp.Thefactthatshedidn’tcompletedtheSDQmakesme
thinkabouthelplessnessagainaswellasnotknowingherownmind.Shecame
acrossasaverytroubledgirlwithlifelimitingworries.Ialsofeltsheseemedquite
lostandscaredasIreadheranswers,almostlikeshedidn’tknowwhatwas
happening,asensationIdidn’thavewiththeothertwoparticipants.
(JoshuaHolmes,AFNCCFandNHS)

APPENDICES
401
AppendixD:QualitativeHeadStartParticipantsNominatedfor,butnotIncludedin,theCurrentStudy
TableD1
OverviewandRationaleforExclusionofNominatedHeadStartParticipants
Code Emotionalsymptoms Risk Rationaleforexclusion
YP1 YP1describedfeelinganxious
andpanickedinherdailylife.
YP1identifiedasingleself-
perceivedsourceofstress;
i. Livinginmultiple
houses
YP1wasexperiencing
emotionalsymptomsbut
didnotdisclosea
sufficientlevelofriskfor
inclusioninthestudy.
YP2 YP2becamebrieflytearfulin
theinterviewwhendiscussing
bullyingvictimisationbutdid
nototherwisedemonstrateor
disclosesymptoms.However,
emotionswerenotdirectly
discussedintheinterviewas
thispartoftheschedulewas
notaddressed,andsoitwas
notpossibletoassessYP2’s
emotionalsymptoms.
YPidentifiedtwoknown
riskfactors;
i. Bullyingvictimisation
ii. Fatheranger
Itwasnotpossibleto
assessYP2’semotional
symptomsasthe
questionsaround
emotionswerenotasked
intheinterview.
Furthermore,YP2wasnot
experiencingasufficient
levelofriskforinclusion.
YP3 YP3disclosedsomeissues
withangerandsomedistress
insocialsituations.However,
thesesymptomswere
infrequentlydiscussedinthe
interviewandthispartofthe
schedulewasnotaddressed;
assuchitwasnotpossibleto
reachaclearconclusionon
thelevelofheremotional
symptoms.
YP2disclosedthreeknown
riskfactors;
i. Bullyingvictimisation
ii. Studentmobility
iii. Inter-parentalviolence
YP3wasexperiencingan
appropriatelevelofrisk,
butitwasnotpossibleto
reachaclearconclusion
onheremotional
symptoms,asthe
questionsinthispartof
theinterviewschedule
werenotasked.

APPENDICES
402
AppendixE:ChangesMadeAfterPilotingoftheWellbeingMeasurementFramework(WMF)
EightmainchangesweremadetotheWMFfollowingpilotingwithineight
educationsettings:
1. Informationwasaddedtotheparticipantinformationsheet,includingan
assurancethatquestionscouldbeskippedandaninstructiontoaskateacherif
anythingwasunclear(AppendixF);
2. Anestimatedcompletiontimeof20-40minuteswasaddedtotheinformation
sheet;
3. Rolloverbuttonswerehighlightedincolourandunderlinedtoincreasevisibility;
4. Additionaldefinitionswereaddedforcommonlymisunderstoodwords,
including“nervous”(SDQemotionalsymptoms)and“partner”(SRSschoolpeer
connection);
5. Counterbalancingoftheinitialandfinalmeasureswasimplementeddueto
observeddeclinesinconcentration;
6. Theyoungcarerquestionwaspresentedsooner,asitwasinitiallypresentedat
theendandresearchersobservedthatpupilsoftenaccidentallyoverlookedthis
question;
7. Aprogressionbarwasaddedforeachpage(e.g.page4/14);and
8. Guidanceforteacherswasdevelopedbasedonobservationsandfocusgroup
feedback.

APPENDICES
403
AppendixF:GuidanceProvidedtoTeacherstoFacilitateSurveyAdministration
Checklist
Thepointsbelowprovideaquickchecklistofimportantconsiderationsforteachers
beforepupilsbeginthesurvey.Eachpointiscoveredinmoredetailinthecribsheet
thatfollows,whichwestronglyencourageyoutoread.
Haveyou:
• Readthroughthecribsheet?
• Printedoutacopyofthecribsheetinordertointroducethesurveytothe
studentsonthesurveyday?
• ViewedtheshortWMFintroductoryvideo,andarrangedforittobeshownto
pupils?
• Trialledthesurveyyourself?
• Madeotherarrangementsforthepupilswhohavebeenoptedoutofthesurvey
bytheirparents,andforthosewhofinishearly?
• Ensurethatyouhavecorrectsurveypasswordsforyourclass,foreachpupil
whoispermittedtocompletethesurvey?
• Setupthesurveyonschoolcomputers?E.g.makingthesurveylinkavailableas
ashortcutonstudents’desktopsorasalinkontheschool’sintranet.
• Madesurethosepupilswhousuallyhaveadditionalassistanceintheclassroom
havethisinplaceforthesurvey(e.g.theirteachingassistant).

APPENDICES
404
CribSheetforTeachers
Backgroundandgeneralguidance
ThankyouverymuchforbeinginvolvedintheHeadStartevaluation.Thisstudy
aimstoinvestigatethebestwaystosupportyoungpeople’semotionalwellbeing
andtheirabilitytomanagewhenexperiencingdifficulties.Tohelpyouintroduce
thesurveytoeachclass,wehaveprovidedacribsheetbelow.
Thesurveywilltakeabout30-40minutesbutsomestudentsmayfinishitmuch
earlier(i.e.within10-15minutes).Becauseofthis,itwouldgreatifyoucouldthink
ofpossibleactivitiesthattheearlyfinisherscandoinadvance.Thesemayinclude
(butarenotlimitedto):readingabook,designingaposter,orlookingatspecific
websites.Ifthesurveytakesplaceawayfromaregularlesson,itmaybeacaseof
simplysendingtheearlyfinishersbacktotheirregularclassroom.
Ontheotherhand,somestudentsmayfindithardertounderstandthesurvey
questionshencetakealittlelonger.Itisimportantthatyouallowthemtimeand
spacetounderstandthequestionsandofferahelpinghandonlywhenasked.More
importantly,pleaseavoidlookingatthestudents’answersastheyareconfidential.
Sometimesstudentsmayfindsomeofthesurveyquestionsabstractandstruggleto
imaginesuchscenarios.Tohelpwiththis,wehaveprovidedasectionon
‘frequentlyaskedquestions’attheendofthisdocument.Youmayalsofindit
usefultogiveexamplesthatmightbefamiliartothestudent(i.e.Imagineyoucame
outfromclasslateandyouarealone,willxxaskyoutojoinin?).
Somestudentsmayfindithardtounderstandtheresponseoptions,ifsoplease
remindthemthattheresponseoptionsrangeinseverity(i.e.fromdisagreeto
agreeorfromnevertoalways).
Somechildrenmayhavedifficultyreadingtheitemsduetothefontsize,ifso
pleaseremindthemthattheycanzoominbypressing“Ctrl+Plussign”andzoom
outbypressing“Ctrl+Minussign”.
Tohelpstudentswithreadingdifficultiesorspecialeducationneedsyoumaywant
tohaveaprintoutofthesurveyandreadthequestionsforthem(orhavea

APPENDICES
405
teachingassistantorlearningmentordothiswiththem).Ifthisisthechosen
option,pleasesupportstudentsinunderstandingthequestionbutmakesurethey
aregivenspacetoselecttheiranswerprivately(e.g.,lookawayormoveaway).
TohelpstudentswhoarestrugglingwithEnglish,pleaseconsiderhaving
translators.Pleasealsonotethatoneofthequestionnaires,theStrengthsand
DifficultiesQuestionnaire(SDQ),isavailableinanumberofdifferentlanguages
whichyoucandownloadfromtheSDQwebsite:
http://www.sdqinfo.com/py/sdqinfo/b0.py
Ifthereisanytechnicalproblemwiththewebsite(i.e.ifthewebsitestops
responding),pleasedirectthestudentsbacktothepasswordpageandallowthem
toputtheirpasswordsagain.Bypressingthe“next”button,theycangetbackto
wheretheywere.

APPENDICES
406
IntroducingchildrentotheWellbeingMeasurementFramework(WMF):Acrib
sheetforschoolsstaffintroducingthesurvey
Thissectiongivesanintroductiontothesurveycoveringsomeofthekeydetails.We
havealsocreatedashortvideotointroducepupilstothesurvey(2minutes50
secondslong),whichcanbefoundontheHeadStartLearningwebsite.Thisvideowas
createdbyyoungpeopleforotherswhomaycompletethesurvey,andassuchcanbe
helpfulinexplainingthesurveytopupils.
Youcanalsousethesuggesteddescriptionbelowverbatimorasageneralguideofthe
pointstocover.Thestudentswillalsoseeaversionofthisinformationonthescreen
beforetheyagreetoparticipate.
“OurschoolistakingpartinabigprojectcalledMeasuringWellbeinginSchoolswith
lotsofotherschoolsacrossthecountry.Wearedoingthistotryandimprovesupport
giventoallchildrenandyoungpeopletoimprovetheirwellbeingandalsotosupport
thosewhomayneedsomeextrahelpcopingwithdifficulties.
Onthecomputer,youwillbeaskedtocompleteaquestionnaireaboutyourfeelings,
friendships,homelifeandschoollife.Pleasedonotrush.Someofyoumayfinishthe
questionnairein10minutesandsomecantakeupto30-40minutes.
Ifyoufinishabitearly,please[pleaseinsertanactivityforstudentswhofinishearlyto
do].Pleasedonottalkanddisturbothers.
Youranswerswillbekeptprivatebythepeoplerunningtheproject.Yourparentsand
yourteacherhavebeentoldthatyouareansweringquestionsbuttheywillnotseeyour
answers.
Ifyoudonotwanttotakepartthat’sabsolutelyfine,youdon’thavetodoit.Justletme
knowthatyoudon’twanttotakepartbeforewestart.
Orifyoustarttotakepartandthenchangeyourmind,that’sfineaswell.Justletme
knowthatyoudon’twanttocarryon.

APPENDICES
407
Whileothersarecompletingthesurvey,youcando[pleaseinsertanactivityfor
studentswhowillnottakepart,thismightbethesameactivityasforstudentswho
finishearly].
Inthesurvey,somewordsarehighlightedingreenandunderlined.Thatmeansyoucan
hoveryourmouseoveritandseeanexplanationoftheword.Ifyoudonotunderstand
anyofthequestions,pleaseraiseyourhandandI/wewilltrytoexplainitasmuchas
possible.Itisnotatestandtherearenorightorwronganswers.Thatmeansthatall
theanswersarepersonaltoyou,soIwouldpleaseaskyoutobequietandfocuson
yourownscreen.Ifthereareanyquestionsyoudon’tfeelhappyansweringyoudon’t
havetoanswerthem,justleavethemblank.
Ifcompletingthequestionsmakesyouthinkyoumightneedsomesupportaboutthe
kindsofthingsthesurveycovers,pleasespeakto[pleaseinsertanappropriatecontact
name(e.g.me,schoolnurse,SENCo,counselloretc.]
Tostartthesurvey,pleaseinsertyouruniquepasswordwhereitsays“Password”and
clicknext.Nowreadthefirstpageofthesurveyandifyouarehappytoanswerthe
surveytick“Ihavereadtheaboveandconsenttotakepartinthissurvey”.
Ifyoudonotwanttotakepartinthesurvey,pleaseraiseyourhand.”
Attheendofthesurveyyoumightalsowanttoreiteratethepointaboutthe
supportthat’savailablewithintheschool:
“Thanksfortakingthetimetotakepartinthesurvey.AsIsaidbeforeyoustarted,if
completingthequestionshasmadeyouthinkyoumightneedsomesupport,please
speakto[pleaseinsertanappropriatecontactname(e.g.me,schoolnurse,SENCo,
counselloretc.]”

APPENDICES
408
Glossaryoffrequentlyaskedsurveyquestions
• Accusedof-“Iamoftenaccusedoflyingorcheating”àBeingtoldthatyoudid
somethingwhichyouhaven’t.
• “Atschool,Idecidethingslikeclassactivitiesorrules”àAsateacher,youmay
bebetterplacedtogiveexamples.Ifastudentstrugglestounderstandthis
question,pleaseprovideexamplesfromyourclass.
• Attention-“IfinishtheworkI'mdoing.Myattentionisgood”àBeingableto
sticktoonetask.
• ConcentrationàBeingabletofocus.
• Feelingcloseto-“I’vebeenfeelingclosetootherpeople”àHavinggood
relationshipwithothers.Thismightincludefriendshipsorrelationshipswith
yourfamily.
• Fidgetingorsquirming-“Iamconstantlyfidgetingorsquirming”àMove
aroundalot.
• HomelifeàFamilylife.
• “Idothingsathomethatmakeadifference(i.e.makethingsbetter)”àDo
anythingtoimprovethingsathome,suchashelpingaroundthehouse,helping
afamilymemberetc.
• “Idothingsthatmakeadifference(i.e.makethingsbetter)”àHelpothers.
• “Ihavegoalsandplansforthefuture”àAsateacher,youmaybebetter
placedtogiveexamples.Ifastudentstrugglestounderstandthisquestion,
pleaseprovideexampleswherethestudentmighthavesetgoals,pleaseallow
themtothinkoflong-termgoals.
• “I’vebeenabletomakeupmyownmindaboutthings”àIcanmakedecisions
formyself.
• “I’vebeendealingwithproblemswell”àIhavebeenmanagingmyproblems
well.
• “Inthelastmonth,howoftenhaveyoufeltconfidentaboutyourabilityto
handleyourpersonalproblems?ӈInthelastmonth,howoftenhavethought
thatyouareabletoworkthroughyourproblems?

APPENDICES
409
• “Inthelastmonth,howoftenhaveyoufeltthatthingsweregoingyourway?”
àInthelastmonth,howoftenhaveyoufeltthatthingsweregoingasyou
wantthemtogo?
• “Inthelastmonth,howoftenhaveyoufeltthatyouwereunabletocontrolthe
importantthingsinyourlife?ӈInthelastmonth,howoftenhaveyoufound
youhavenopoweroverthingsgoingoninyourlife?
• LeisureactivitiesàHobbies.
• Minor/definite/severe-(responseoptionsononeofthequestionnaire)àLow
/medium/high.
• “…missyouifyouweren’tinschool”àWonderwhereyouareand/orbe
disappointedifyouarenotthere.
• Nervous-“Iamnervousinnewsituations.Ieasilyloseconfidence”àFeeling
anxious.
• Optimistic-“I’vebeenfeelingoptimisticaboutthefuture”àHopeful.
• Partner-“…pickyouforapartner”àPickyoutobepartofateamoragroup.
• PilingUp-“Inthelastmonth,howoftenhaveyoufeltdifficultieswerepilingup
sohighthatyoucouldnotovercomethem?ӈhowoftenhaveyoufeltthat
youhadsomanyproblemsthatyoucouldnotovercomethem.
• Restless–“Iamrestless,Icannotstaystillforlong”àunabletostaystill.
• “…sharethingswithyou”àSharebothphysicalthings(i.e.pencil,book)and
information.
• “SometimesIgetinvolvedinthingslaterIwishIcouldgetoutof”àSometimes
IregretthingsthatIdo.
• Somewhattrue-(responseoptionononeofthequestionnaire)àPartlytrue,
partlynottrue.
• Thinkingclearly-“I’vebeenthinkingclearly”àBeingabletofocusonthoughts.
• Useful–“I’vebeenfeelinguseful”àHelpful.
• Volunteer–“Ioftenvolunteertohelpothers(parents,teachers,children)”à
Offertohelpotherswithoutbeingasked.
• Youngcarer-Youngcarerischildrenandyoungpersonsunder18whoprovide
orintendtoprovidecare,assistanceorsupporttoanotherfamilymember.

APPENDICES
410
Theycarryout,oftenonaregularbasis,significantorsubstantialcaringtasks
andassumealevelofresponsibilitywhichwouldusuallybeassociatedwithan
adult.Thepersonreceivingcareisoftenaparentbutcanbeasibling,
grandparentorotherrelativewhoisdisabled,hassomechronicillness,mental
healthproblemorotherconditionconnectedwithaneedforcare,supportor
supervision.

APPENDICES
411
Frequentlyaskedquestionsbythechildren
1) WhyamIbeingaskedtofillinthissurvey?
Thiswillhelpustolearnaboutyoungpeople’smentalhealthandemotional
wellbeing.Itwillhelpyourschooltofindoutthebestwaysofhelpingyoungpeople
tohavegoodmentalhealthandemotionalwellbeing.
2) WhowillseetheanswersIgive?
Thesurveyisanonymous.Thismeansnooneatyourschoolwillseetheanswers
yougive.Youranswersgototheresearchteam.Theyputallchildrenandyoung
people’sanswerstogethersothattheycanlearnabouthowchildrenandyoung
peoplearefeelingacrossthewholeschool.
Asnooneinyourschoolwillseeyouranswers,ifyouneedtotalktosomeone
aboutyourfeelings,youneedtospeaktoateacheroranotheradultyoutrustin
school.
3) Istheprojectjustforkidswithproblemsorforeveryone?
Thisprojectisforallchildrenandyoungpeople.Weallneedtolookafterour
mentalandemotionalhealth,justlikeweneedtolookafterourphysicalhealth.
4) Willthesurveyaffectus?
Answeringthesurveywon’thaveimmediateeffectsonyou.But,wehopethatthe
surveywillhelpyourschooltolearnabouthowtobettersupportchildrenand
youngpeople’semotionalwellbeing.
5) Whydoyouhavetheyoungcarerquestion?Whatdoyouwanttoknow?
Wewanttomakesureweunderstandthefeelingsoflotsofdifferentchildrenand
youngpeople.Somechildrenandyoungpeopleareyoungcarersthismeansthey
provideregularorongoingcaretoafamilymemberwhohasanillness,disability,
mentalhealthconditionordrug/alcoholdependency.Wewanttomakesurewe
understandhowyoungcarersfeelsowecanlearnwhathelpandsupportthey
mightneed.

APPENDICES
412
6) Someofthequestionsareverysimilar–isthatatrick?
Somequestionsmaysoundverysimilar,butit’snotatrick.Somequestionsmayask
thesamethingindifferentwayssothatwecanmakesurewereallyunderstand
howchildrenandyoungpeoplearefeeling.
7) Isthisatest?
No,thisisn’tatest.Therearenorightorwronganswers.Thesurveyisjust
interestedinlearningaboutyourthoughtsandfeelings.
8) DoIhavetoanswereveryquestion?
Ifyoudon’twanttoansweraquestion,that’sok.It’syourchoicewhichquestions
youanswer.Ifyoudon’twanttoansweraquestion,justleaveitblankandmove
ontothenextone.
9) HowwilltheHeadStartprogrammehelpotherpeopleinthefuture?
TheHeadStartprogrammeistryingtofindthebestwaytohelpchildrenstay
mentallyhealthy,managestressandworries,dowellatschool,avoidgetting
involvedinriskybehaviour(suchasdruguse,drinkingtoomuchalcoholoranti-
socialbehaviour)andenjoylife.

APPENDICES
413
AppendixG:StrengthsandDifficultiesQuestionnaire(SDQ)EmotionalSymptomsSubscale(Goodmanetal.,1998)
Foreachitem,pleasemarktheboxforNotTrue,SomewhatTrueorCertainlyTrue.
Itwouldhelpusifyouansweredallitemsasbestyoucanevenifyouarenot
absolutelycertainortheitemseemsdaft!Pleasegiveyouranswersonthebasisof
howthingshavebeenforyouoverthelastsixmonths.
Not
TrueSomewhat
TrueCertainlyTrue
Igetalotofheadaches,stomach-achesorsickness � � � Iworryalot � � � Iamoftenunhappy,down-heartedortearful � � � Iamnervousinnewsituations;Ieasilyloseconfidence � � � Ihavemanyfears,Iameasilyscared � � �

APPENDICES
414
AppendixH:Four-ItemPerceivedStressScale(PSS-4)(S.Cohenetal.,1983)Thequestionsinthisscaleaskyouaboutyourfeelingsandthoughtsduringthelast
month.Ineachcase,pleaseindicatewithacheckhowoftenyoufeltorthoughta
certainway.
0
never1
almostnever
2sometimes
3fairlyoften
4veryoften
Inthelastmonth,howoftenhaveyoufeltthatyouwereunabletocontroltheimportantthingsinyourlife?
� � � � �
Inthelastmonth,howoftenhaveyoufeltthatyouwereunabletocontroltheimportantthingsinyourlife?
� � � � �
Inthelastmonth,howoftenhaveyoufeltthatthingsweregoingyourway?
� � � � �
Inthelastmonth,howoftenhaveyoufeltdifficultieswerepilingupsohighthatyoucouldnotovercomethem?
� � � � �

APPENDICES
415
AppendixI:StudentResilienceSurveysubscales(Sun&Stewart,2007)Subscale Never Always
Familyadultconnection
Athome,thereisanadultwho… � � � � �
Isinterestedinmyschoolwork � � � � � BelievesthatIwillbeasuccess � � � � �
Wantsmetodomybest � � � � �
ListenstomewhenIhavesomethingtosay � � � � �
Schooladultconnection
Atschool,thereisanadultwho… � � � � � Reallycaresaboutme � � � � �
TellsmewhenIdoagoodjob � � � � �
ListenstomewhenIhavesomethingtosay � � � � �
BelievesthatIwillbeasuccess � � � � �
Communityadultconnection
Awayfromschool,thereisanadultwho… � � � � � Reallycaresaboutme � � � � �
TellsmewhenIdoagoodjob � � � � �
BelievesthatIwillbeasuccess � � � � � Itrust � � � � �
Schoolpeerconnection
Aretherestudentsatyourschoolwhowould…
� � � � �
Chooseyouontheirteamatschool � � � � �
Tellyouyou’regoodatdoingthings � � � � �
Explaintherulesofagameifyoudidn’tunderstandthem
� � � � �
Inviteyoutotheirhome � � � � � Sharethingswithyou � � � � �
Helpyouifyouhurtyourself � � � � �
Missyouifyouweren’tatschool � � � � �
Makeyoufeelbetterifsomethingisbotheringyou
� � � � �
Pickyouforapartner � � � � � Helpyouifotherstudentsarebeingmeantoyou
� � � � �
Tellyouyou’retheirfriend � � � � �
Askyoutojoininwhenyouareallalone � � � � �
Tellyousecrets � � � � �
Activeengagementinhomeandschoollife
Idothingsathomethatmakeadifference(i.e.makethingsbetter)
� � � � �
Ihelpmyfamilymakedecisions � � � � � Atschool,Ihelpdecidethingslikeclassactivitiesorrules
� � � � �

APPENDICES
416
Idothingsatmyschoolthatmakeadifference(i.e.makethingsbetter)
� � � � �
Engagementinextra-curricularactivities
Awayfromschool… � � � � � Iamamemberofaclub,sportsteam,churchgroup,orothergroup
� � � � �
Itakelessonsinmusic,art,sports,orhaveahobby
� � � � �

APPENDICES
417
AppendixJ:QualitativeInterviewScheduleIntroduction:“Thankyousomuchfordoingthisinterviewwithme.Ihaveafew
questionsthatI’dliketoaskyouaboutyourunderstandingandexperiencesof
copingordealingwithdifficulttimes,suchaswithdifferentfeelingsandemotions
orinsituationsatschoolorathome.Ifyoudon’twanttoansweraquestionorif
it’sunclearthenjusttellmeandwecanskipit,orIcanexplainit.Wewillwriteup
whatwefindfromallofourinterviewswithyoungpeopleyourageupanddown
thecountryandwewillsendyouacopyofourfindings.Everythingthatwetalk
abouttodayisprivateorconfidentialunlessI’mworriedthatanyharmordangeris
goingtocometoyouortoanyoneelse,inwhichcasethenIwouldneedtospeakto
mysupervisor,whosenameisJess,and[nameofschoolsafeguardingofficer],butI
wouldtellyouifIwasworriedinthiswayfirst.Youarewelcometostopthe
interviewatanytimeorskipaquestionifyouwantto”
Talkingaboutlife:1. Whatdoyoulike/notlikeaboutbeingatschool?
Possibleprompts:o Favourite/leastfavouritesubjects?o Whatdoyoulike/notlikeaboutthis?Why?o Howdoyouhandlethis?
2. Canyoutellmeabouttheareathatyoulivein?Whatisyourareawhereyou
livelike?Possibleprompts:o Yourstreet?o Thingstodo/placestogonearwhereyoulive?o Whatdoyoulike/notlikeaboutlivinghere?Whatdoyoulike/notlike
aboutthis?Why?o Howdoyouhandlethis?
3. Canyoutellmeaboutwhatlifeislikeforyouathome?
Possibleprompts:o Whodoyoulivewithathome?

APPENDICES
418
o Whatdoyoulikeaboutbeingathome?Whatdoyoulikedoingwithyourparents/brothersorsisters/pets?Aretherearethingsthatyoudoaltogetherasafamily?Whatdoyoulikeaboutthis?Why?
o Isthereanythingthatyoudon’tlikesomuchaboutbeingathome?Whatdoyounotlikeaboutthis?Why?Howdoyouhandlethis?
4. Canyoutellmeaboutyourfriendships?Possibleprompts:o Doyouhavefriendsinschool?Friendsoutofschool?o Whatdoyoulikedoingwithyourfriends?Whatdoyoulikeaboutthis?
Why?o Isthereanythingthatyoudon’tlikesomuchaboutspendingtimewith
yourfriends?Whatdoyounotlikeaboutthis?Why?Howdoyouhandlethis?
Talkingaboutemotions:
5. Whatkindsofthings(e.g.activities,places,orpeople)canmakeyoufeelhappy?
Possibleprompts:o Howdoyouliketohavefun?o Howdoesthisconnect/leadtoyoufeelinghappy?o Canyouthinkofanexampleofwhenyouwerefeelinghappyrecently?
Whathappened?
6. Beinghappycanlookorfeeldifferentforeveryone,soIwaswonderingwhatthislookslikeorfeelslikeforyou?
Possibleprompts:o WhatwouldIsee/noticeifyouwerefeelinghappy?o Whatwouldyoubefeeling/doing?
7. Whatkindsofthings(e.g.activities,places,orpeople)canmakeitharderor
moredifficultforyoutofeelhappy?Possibleprompts:o Howdoesthisconnect/leadtoyoufeelingthisway?
8. Whatsortsoffeelingsoremotionsdoyouexperiencewhenyouarenotfeeling
happy?(Remembertounpackandexploredifferentfeelings/emotionsastheyarementioned,e.g.‘Beingsadcanlookorfeeldifferentforeveryone,soIwas

APPENDICES
419
wonderingwhatthislookslikeorfeelslikeforyou?’,‘Whattypesofthingsdoyouworryabout?’)
Possibleprompts:o Howdoesthisaffectyourlife/makeyoufeel?o CanyouthinkofanexampleofwhenyouwerefeelingXrecently?What
happened?
9. Whenyouarenotfeelinghappyorhavingahardtime,whatdoyoudotofeelbetter?Whatdoyoudowhenyouhaveproblems/difficultiesinyourlife?
Possibleprompts:o Howdoyouhandleit?o Who/whathelps/makesyoufeelbetter?Wheredoyougoforhelp/
support?Whatcheersyouup?Whatdotheydo?o Howdoesthishelpyou?o Doesthisvary/changedependingonhowyouarefeeling?Why?o Isthereanythingthatisunhelpfulforyouorthatmakesyoufeelworse?o Isthereanyonethatyoudefinitelywouldn’ttalktowhenyouarefeeling
thisway?Why?
10. Haveyoueverreceivedanyhelporsupportinrelationtofeelinglikethis(i.e.unhappy)?
Ifyes,o Whatdidthisinvolve?Whatdidyoudo?Whodidyoumeetwith?o Canyoutellmeabouthowyoucametoreceivethishelporsupport?o Comparedtobeforeyoureceivedthishelporsupport,howdidyoufeel
afterwards?Didanythingimprove/getworse?What?Wasthiswhatyouexpected?
o Whatwashelpfulaboutthishelporsupport?o Wasthereanythingthatwasunhelpful?What?o Wasthereanythingthatyouwouldhavelikedtohavebeendifferent
aboutthehelporsupport?What?
Ifno,
o Wouldyouliketoreceiveanyhelporsupport?What?
TalkingaboutHeadStart:(ifHeadStarthasnotalreadybeendiscussed)
11. HaveyouheardofsomethingcalledHeadStart?Ifyes,canyoutellmeaboutwhatHeadStartis?Ifno,explainwhatHeadStartisinthatarea.

APPENDICES
420
12. HaveyoubeeninvolvedinanyactivitiesorlessonsaspartofHeadStart?Ifyes:o Whatdidthisinvolve?Whatdidyoudo?Whohaveyoumetwith?What
happens?Whendoyoudoit?Howoften?o CanyoutellmeabouthowyoucametobeinvolvedinHeadStart?o ComparedtobeforeyougotinvolvedinHeadStart,howhaveyoubeen
feeling?Hasanythingimproved/gotworse?What?Wasthiswhatyouexpected?
o WhathaveyoufoundhelpfulaboutbeinginvolvedinHeadStart?Hastherebeenanythingthatyouhavefoundunhelpful?What?
o Wasthereanythingthatyouwouldhavelikedtohavebeendifferentabouttheactivities/lessons?What?
o Haveyouevertakenpart/beeninvolvedinanythinglikethisbefore?What?
o WouldyourecommendHeadStarttoanyofyourfriends?DoanyofyourfriendsparticipateinHeadStart?
Givingsuggestions/advice:13. Whatadviceorhelpwouldyougivesomeoneyourageiftheywere
experiencingaproblemwith:o Theirfriendships?o Theirfamily?o School?o Theirfeelingsoremotions?
Possibleprompts:o Wheredoyouthinktheyshouldgo?Whodoyouthinktheyshould
speakto?o Isthisadvicethatyouwouldfollowyourselfifyouwereexperiencing
this?Why/whynot?
Conclusion:“Thanksverymuchagainfordoingthisinterviewwithmetoday;it’s
beensohelpfultospeaktoyou.Doyouhaveanyquestionsformenowthatwe’ve
finishedtheinterview?Wearegoingtousetheseinterviewstohelpustoworkout
howbesttohelpyoungpeopleyouragewhentheyareexperiencingdifficult
situationsorfeelings.Wewillgetbackintouchwithyouaroundthistimenextyear
toseewhetheryou’rehappytospeakwithusagainabouthowthingsareandwhat
mayhavechangedsincewelastsawyou.Wouldyouliketochooseapseudonym
forwhenwewriteupourfindings?Thisisanothernamethatwewilluseforyouin
ourwrite-uptohelpensurethatotherpeopledon’trecogniseyou”

APPENDICES
421
AppendixK:QuantitativeInformationPackforParents/Carers
DearParents/GuardiansofYear7students,
Wearewritingtoyoubecausewewouldliketogainabetterunderstandingofyoungpeoples’wellbeingsothoseworkingwiththemcanimprovethesupportthatisprovided.
Todothiswewanttocollectviewsfromallchildrenintherelevantyeargroupsatparticipatingschools.Wewilldothisbyusingonlinesurveysonceayear(forfiveyears),starting2017.
Weareaskingyoutohelpbyallowingyourchildtoparticipate.
Beforeyouandyourchilddecidewhetheryouwouldliketotakepart,itisimportantforyoutoknowwhatitwillinvolve.Pleasetaketimetoreadtheattachedinformationsheetcarefullyanddiscussitwithothersifyouwish.Ifthereisanythingthatisnotclear,orifyouwouldlikemoreinformation,pleasedonothesitatetocontactus.
Thenextfewpages:
1)Tellyouabitabouttheresearchandwhatitinvolvesforyouandyourchild.
2)Asksyouifyouarehappyforyourchildtoparticipate.
3)Givesyouareplysliptofillinandsendbacktousifyoudonotwantyourchildtotakepart.
Ifyouarehappyforyourchildtobeinvolvedintheresearch,youdonotneedtotakeanyfurtheraction.IfyouDONOTwantyourchildtobeinvolvedintheresearch,theattachedsheettellsyouwhattodo.
IfyouhaveanyquestionspleaseemailusonHeadStart@annafreud.orgorcalluson02074432294.
Anypersonalinformationwillbetreatedconfidentially.TheinformationwillbetreatedasstrictlyconfidentialandhandledinaccordancewiththeprovisionsoftheDataProtectionAct1998.
Thankyoufortakingthetimetoreadaboutourresearch.
Yoursfaithfully,
DrJessicaDeightonEvidenceBasedPracticeUnit(EBPU)UniversityCollegeLondonandtheAnnaFreudCentreJordanHouse47BrunswickPlaceLondon,N16EB

APPENDICES
422
InformationSheetforParents/Carers
Whatisthestudyfor?
Thisstudytriestogainabetterunderstandingofourstudents’wellbeingsothat
improvementscanbemadetosupportthem.
Whatisthedurationoftheresearch?
TheresearchitselfrunsfromSeptember2016untiltheendof2023.Thesurveys
willtakeplaceyearly.
Whatwillparents/guardiansbeaskedtodo?
Weareaskingforyourpermissionforyourchildtocompleteasurveyonceayear
foruptofiveyears(thefinaltimewouldbewhenyourchildisinYear11).The
surveyasksquestionsabouttheirschool,friends,themselvesandisnotexpectedto
takelongerthan40minutestocomplete.
Whoisbeingaskedtotakepart?
Allchildrenatyourchild’sschoolinyears7and9willbeaskedtotakepartinthis
research.
Whatwillyourchildbeaskedtodo?
Thestudywillinvolveyourchildcompletingashortsurvey.Thesurveyasks
questionsabouttheirschool,friends,andthemselves,andisnotexpectedtotake
longerthan40minutestocomplete.Beforeyourchildtakespartinthe
questionnaires,theirclassteacherwillreadaloudinformationabouttheresearch
andyourchildwillbeaskedtotickaboxiftheyarehappytotakepartinthe
research.Wewillnotaskanyidentifiableinformation(suchasnames,addresses
etc.).
Theschoolwillalsogiveusinformationaboutpupilcharacteristicssuchasspecial
educationneedsanddeprivation.

APPENDICES
423
Whatarethepossiblerisks/disadvantagesoftakingpart?
Therearenoknownrisks/disadvantagestotakingpartinthisquestionnaire.Ifany
risksordisadvantagesbecomeknownduringtheresearch,youandyourchildwill
beinformedstraightaway.Youcanalsogetindependentsupportandadvicefroma
charitycalledYoungMinds.Theirparenthelplinenumberis08088025544.
Ifyoueverwishtomakeaformalcomplaintabouttheconductoftheresearchyou
shouldcontactDr.JessicaDeighton,EvidenceBasedPracticeUnit(EBPU),UCLand
theAnnaFreudCentre,JordanHouse,47BrunswickPlace,London,N16EB.
Whohasreviewedtheresearch?
Allresearchislookedatbyanindependentgroupofpeople,calledaResearch
EthicsCommittee,toprotectyourinterests.Thisresearchhasbeenapprovedby
theUCLResearchEthicscommittee(UCLEthicsnumber:8097/003).
Whatarethepossiblebenefitsoftakingpart?
Thereisnoguaranteedbenefitintakingpart.Mostpeoplefindtakingpartin
researchrewarding,astheycontributetothedevelopmentofknowledgethatmay
benefitotherpeopleinthefuture.
Whatdataistheresearchusing?
Theresearchwillcombinechildself-reportdataanddatafromothersources.Child
self-reportdatawillbeusedtounderstandhowchildrenandyoungpeoplefeel
abouttheirschool,friends,andthemselves.Self-reportdatamaybelinkedwith
datafromothersourcessuchashealthdataordataheldbythelocalauthority.It
mayalsobelinkedtoinformationaboutwhetherstudenthasreceivedany
additionalsupportorservicesforresilienceoremotionalwell-being.Thiswillbe
usedtounderstandmoreaboutdifferentcharacteristicsofyoungpeople
completingthesurveyandunderstandwhethersupportprovidedtochildrenand
youngpeoplehelpthemfeelbetter.NONEOFTHESEDATAWILLBEUSEDTO
IDENTIFYINDIVIDUALCHILDREN.

APPENDICES
424
Howwillmychild’sdatabestoredandwhowillhaveaccesstoit?
• Allinformationwillbetreatedstrictlyconfidentially.Theresearchteamwill
ensurethatthehigheststandardsofconfidentialityaremaintained
throughout.
• Amemberoftheresearchteamandadesignateddataleadatthe
participatinglocalauthoritywillhaveaccesstotheidentifiabledata.
• Identifiabledatawillonlybeusedtolinkdifferentdatasources.Itwon’tbe
usedtoidentifyindividualchildren.
• Thewebsitethathousesthesurveywillbecompletelysecureandpassword
protected.Allsurveydatawillbestoredonasecureandpassword
protectedservertowhichonlyseniormembersoftheresearchteamhave
access.
• Oncethedataislinked,itwillbeanonymizedandtheanalysiswillbecarried
outontheanonymizeddata.
• AlldatawillbecollectedandstoredinaccordancewiththeDataProtection
Act1998.
• Theinformationmaybepresentedatconferencesorusedaspartof
academicpublicationsandastudentproject.Noinformationpresentedwill
identifyanyindividualsinvolved.
Contactforfurtherinformation
Forgeneralqueries: Fortechnicalqueries:JessicaDeighton LawrenceWoEvidenceBasedPracticeUnit(EBPU) SchoolofEducationUCLandtheAnnaFreudCentre UniversityofManchesterJordanHouse OxfordRoad47BrunswickPlaceLondon,N16EB
Manchester,M139PL
Email:[email protected] Email:[email protected],pleaseseeourwebsiteforfurtherdetailsabouttheresearchandteam.Thewebsitecanbefoundat:www.headstartlearning.info
Thankyoufortakingthetimetoreadthisinformationsheet.Yourhelpmakesourresearchpossible!

APPENDICES
425
Agreeingforyourchildtobepartofthisresearch
• Wehopeyouwillallowyourchildtotakepartinthisresearch.
• Ifyoudonotwantyourchildtoparticipateinthisresearch,youneedtolet
usknowbefore<InsertDate>.Pleasecompletetheformbelow,usethe
freepostcodebelowandreturnitto:
FREEPOST(RLYU-KAAB-AXRC)
LawrenceWo
SchoolofEducation,
B4.10EllenWilkinsonBuilding,
UniversityofManchester,
OxfordRoad,
Manchester,
M139PL
Alternatively,LawrenceWocanbecontactedbytelephoneon01612753415or
Itwillbemadecleartoallchildrenwhentheyaregiventhequestionnairesthat
theydonothavetoansweranyquestionsthattheydon’twanttoandtheydonot
havetotakepartatalliftheydon’twantto.
Pleaseseenextpageforareplysliptofillinandsendifyoudonotwantyourchild
totakepartintheresearch.
Youonlyneedtocompleteandreturnthisslipifyoudonotwishyourchildtotake
part.
Ifyouarehappyforyourchildtotakepartthenyoudonotneedtodoanything.

APPENDICES
426
Iwishtowithdrawmychildfromtakingpartintheresearch.Mydetailsareas
follows:
Child’sname:
Parentorcarer’sname:
YearGroup:
Nameofmychild’sschool:
Signature: Date:
[Responserequiredby<insertdate>]

APPENDICES
427
AppendixL:QuantitativeParticipantInformationforYoungPeopleWethankyouforconsideringparticipatinginthissurvey.Belowweexplainwhat
thisinvolvesandifyouchoosetoparticipateyouwillthenbedirectedtothe
survey.
Whatisthestudyfor?
ThisresearchisanevaluationofaprogrammecalledHeadStartwhichishappening
inschoolsinEnglandacross6areas.TheaimofHeadStartistoprovidesupportto
childrenandyoungpeopletoimprovetheirwellbeingandalsotosupportthose
whomayneedsomeadditionalsupportcopingwithdifficulties.
Whatareyouaskedtodo?
Youwillbeaskedtocompletesomequestionsaboutyourfeelings,friendshipsand
schoollife.Thequestionswilltake20-40minutes.Itisnotatestandthereareno
rightorwronganswers.
Whoisbeingaskedtotakepart?
Allchildreninyouryeargroupatyourschoolwillbeaskedtotakepartinthisstudy.
Whichdataisbeingusedinthestudy?
Thestudymaycombineyourquestionnairedata(thesurveythatyouareaboutto
fillin)andinformationcollectedfromothersourcessuchasyourage,whetheryou
havespecialeducationalneedsyourschoolattendance,informationaboutyour
health,contactwithservicesandwhetheryouarereceivinganysupportfor
resilienceoremotionalwellbeing.NONEOFTHISINFORMATIONWILLBEUSEDTO
IDENTIFYYOU.
Howwillthedatabestoredandwhowillhaveaccesstoit?
Allofthesurveyswillbeconfidential.Youranswerswillbekeptsecretbythe
peoplewhoputthequestionsonthecomputer.Theydonotworkatyourschoolor
knowwhoyouare.Yourparentsandyourteacherhavebeentoldthatyouare

APPENDICES
428
answeringquestionsbuttheywillnotseeyouranswers.Amemberoftheresearch
teamandadesignateddataleadatyourlocalauthoritywillhaveaccesstoyour
databuttheywillnotuseittoidentifyyouinanyway.Yourpersonalinformation
willonlybeusedtolinkinformationfromdifferentdatasources.Onceallthedata
islinkedyourpersonalinformationwillbetakenout.Alldatawillbecollectedand
storedinaccordancewiththeDataProtectionAct1998.
DoIhavetotakepart?
No!Itisuptoyouwhetherornotyoutakepartinthisstudy.Ifyoudecidenow,or
atalaterdate,thatyoudonotwishtoparticipateinthisresearchyouarefreeto
stopatanytime,withoutgivingareason.
Ifyouchoosenottotakepartyouwillnotgetintrouble.Evenifyoustarttotake
partandthenchangeyourmindthatisalsookay.
Ifyoustartthequestionnaire,youarefreetoskipquestionsthatyoudonotwant
toanswer.
Ifyouhaveanyquestionsaboutthissurveyorwhatyouwillbeaskedtodothen
askyourteacher.
Thankyouforthinkingabouttakingpartinourproject.
Whathappensnow?
Ifyouarehappytotakepart,pleaseticktheboxbelowandyoucanthenaccessthe
survey.
<onlinetickboxhere>

APPENDICES
429
AppendixM:QualitativeParticipantInformationSheetforYoungPeople
InformationSheetforYoungPeople
Whatistheresearchabout?ThisresearchislookingataprogrammecalledHeadStart,whichishappeninginsixareasacrossEngland.TheaimofHeadStartistogivesupporttoyoungpeopletoimprovetheirwellbeingandhelpthemtocopewithdifficultsituationsthattheymightfacenoworinthefuture.Thispartoftheresearchaimstofindoutmoreaboutthesupportbeingofferedtoyoungpeopleinthesesixareas.Itaimstofindoutwhathashelpedandwhathasbeenlesshelpful,inordertolearnforthefutureabouthowtoimprovesupportthataimstoincreaseyoungpeople’swellbeing.Whoarewespeakingto?WearespeakingtoyoungpeoplewhomayhavehadsupportfromHeadStart(orwhomayreceivesupportinthefuture),andstaffwhodeliverthissupport.Weareaskingdifferentgroupsofpeoplesothatwecanbuildupagoodpictureovertimeofwhatthissupporthasbeenlike,whoithashelped,andhowitcanbeimprovedinthefuture.WewouldliketoinviteyoutotakepartinthisresearchprojectbecauseyourschoolhassuggestedthatyouandotheryoungpeopleinyourschoolmayhavesomeexperienceofHeadStartsupportnoworinthefuture.Whatdoesthisinvolve?Takingpartinthisprojectmeansagreeingtobeinterviewedonceayearforuptofiveyears(thefinaltimewouldbewhenyouareinYear11).Youwillreceivea£10Love2Shopvoucheraftereachinterviewasathankyoufromtheresearchteamfortakingpart.Withyourpermission,wewillre-contactyoueachyeartoarrangeyourinterview.Thiswillbeaninterviewwithjustyouandaresearcher.Theresearcherwillaskyouafewquestionsaboutyourunderstandingofcopingindifficulttimes,andabouttheservicesorsupportthatyoumayhavereceived.Theresearcherwillaskaboutyourviews,opinions,andexperiences.Theconversationcanlastforaslongasyouwanttotalk(uptoamaximumof1hour),butwillusuallylastfor30to45minutes.Yourinterviewcantakeplaceinaprivateroomatyourschool,atyourhouse,orinalocalcommunitybuilding.Theresearcherwilltalktoyouaboutthequestionsthattheyaregoingtoaskyouatthebeginningoftheinterviewsothatyouwillknowwhattoexpect.Theinterviewwillbeaudio-recordedsothatwecan
Titleofproject:HeadStartQualitativeEvaluationThisstudyhasbeenapprovedbytheUCLResearchEthicsCommittee(ProjectIDNumber):7963/002

APPENDICES
430
writedownwhatyousaidafterwards,sothatwedon’tforget.Thewrittenversionoftheinterviewiscalleda‘transcript’.Whatarethebenefitsoftakingpart?Youtakingpartinthisprojectmayhelpustounderstandmoreaboutwhathelpstoincreaseyoungpeople’swellbeingandsomayhelptoimproveservicesforyoungpeople.Thismaybenefitotheryoungpeopleinthefuture.Somepeoplefindthattakingpartinresearchlikethiscanbeapositiveandinterestingexperience.Ifyouwouldliketoseewhatwefindfromthisresearch,youcantelltheresearcherthatyoumeetwithandwewillsendthistoyouattheendoftheproject(in2023).Whataretherisksoftakingpart?Therearefewriskstotakingpart.Occasionally,someonemayfeelupsetaboutsomethingthattheyaretalkingabout.Theresearchersthinkthatitisveryimportantthatyouarecomfortableintheinterviewandthatyouonlytalkaboutwhatyouwantto.Ifthereisanythingthatyoudon’twanttotalkaboutthenjustlettheresearcherknowandtheywilldefinitelynotpressureyoutodoso.If,aftertheinterview,youfeelupsetandwanttotalktosomeonefurther,theresearcherwillhavegivenyoualistofpeopleinyourlocalareathatyoucanspeakwith.Willinformationaboutmebekeptconfidential?Yourinterviewwillbekeptstrictlyconfidentialorprivate.Theonlytimethatwemightneedtobreakthisruleisifyoutellussomethingthatmakesusthinkthatyou,orsomeoneelse,isindanger.Inthatcase,wewillhavetotellsomeonewhocanstopthatdangerfromhappening.Audiorecordingswillbekeptinapassword-protectedcomputerfolderandwillonlybeaccessedbyresearchersinvolvedwiththisproject.Whentherecordingsaretypedupastranscripts,anydetailsthatcanidentifyyouasanindividualwillbetakenout.Thismeansthatyournamewillbechanged,aswellasthenamesofothersorplacesthatyoumaymention.Wemaywriteupsomeofthethingsthatyousayinreports,whichwillbereadbypeopleoutsideofthisresearch,butotherpeoplewon’tbeabletorecognisethatit’syouinthereports.Wewillkeepaudiorecordingsupuntiltheendoftheproject(May2023),whentheywillbedeleted.WhathappensifIchangemymind?Youcanchangeyourmindabouttakingpartinthisresearch,atanytime.Youdonothavetotellusareasonforthis.Ifyoudowishtoleavethestudy,yourinterviewaudiorecordingandtranscriptwillbedeleted.Oncewehavewrittenthereportsofthefindings(4-6monthsaftertheinterviews),itwillnotbepossibletowithdrawyourcontributions,soitisbesttotellusassoonaspossibleifyoudochangeyourmind.Youcanalsostoptheinterviewatanypoint–justtellthe

APPENDICES
431
researcherinterviewingyouthatyounolongerwishtotakepart.Leavingthestudyatanystagewillnotaffecthowanyonetreatsyouandwillnotaffecttheservicesthatyoumayreceive.Itwillnotdisadvantageyouinanyway.Whathappensnext?Pleasediscusstheinformationabovewithothersoraskusifthereisanythingthatisnotclearorifyouwouldlikemoreinformation.Youcankeepthisinformationsheettolookatwheneveryouneedto.Ifyoudecidethatyouwouldliketotakepart,youcantellyourparent/guardianandgiveyourassent(onawrittenform).Yourparent/guardianmustalsogivetheirconsent(onawrittenform)inorderfortheinterviewtogoahead.Thenyouandyourparent/guardiancanreturntheformstousandwewillarrangeatime,atyourconvenience,tointerviewyou.Alldatawillbecollectedandstoredinaccordancewithprevailingdataprotectionlegislation.
Researchercontactdetails:Name:EmilyStapleyContactdetails:Ifyouhaveanyquestions,[email protected]

APPENDICES
432
AppendixN:QualitativeInformationPackforParents/Carers(coverletter,informationletter,andconsentform)
DearParent/Carer,
Thisletterisaboutaresearchproject,ledbytheAnnaFreudNationalCentreforChildrenandFamilies,toevaluateaprogrammecalledHeadStart.HeadStartisa5-yearprogrammeaimingtoincreaseresilienceandwellbeingin10-16yearoldsinsixareasacrossEngland,ofwhich[nameofpartnership]isone.
Allyoungpeopleexperiencedifficulttimesatonepointoranother.Thisprojectisareallyexcitingandone-of-a-kindopportunityforustolearnvaluableinformationaboutyoungpeople’sperspectivesoncopingindifficulttimes,thesupportthattheymayreceiveinrelationtotheirwellbeing,andhowthismaychangeovertime.
Weareaskingyoutohelpbyallowingyourchildtoparticipateinthisstudy.Thenextfewpages:
Tellyouabitabouttheprojectandwhatitinvolvesforyourchild
Askyouifyouarehappyforyourchildtoparticipateinthisproject
Giveyouaconsentformtosignandsendbacktoyourchild’sschoolifyouarehappyforyourchildtotakepart
Beforeyouandyourchilddecidewhetheryourchildwouldliketotakepartinthisresearchproject,itisimportantforyoutoknowwhatthiswillinvolve.Pleasetaketimetoreadtheattachedinformationsheetcarefullyanddiscussitwithothersifyouwish.Ifthereisanythingthatisnotclear,orifyouwouldlikemoreinformation,pleasedonothesitatetocontactus.
Ifyouhaveanyquestions,[email protected].
Anypersonalinformationwillbetreatedconfidentiallyandwillnotbesharedbeyondtheresearchteam.TheinformationwillbehandledinaccordancewiththeprovisionsoftheDataProtectionAct1998.
Thankyoufortakingthetimetoreadaboutourproject.Wemaynotbeabletointervieweveryone,butifyouarehappyforyourchildtotakepart,pleasesignandreturntheattachedconsentformto[nameofstaffmemberatyourchild’sschool].
Yoursfaithfully,
DrEmilyStapley
EvidenceBasedPracticeUnit(EBPU),UniversityCollegeLondonandAnnaFreudNationalCentreforChildrenandFamilies,4-8RodneyStreet,London,N19JH

APPENDICES
433
InformationSheetforParents/Carers
Whatistheresearchabout?ThisresearchislookingataprogrammecalledHeadStart,whichishappeninginsixareasacrossEngland.TheaimofHeadStartistoprovidesupporttoyoungpeopletoimprovetheirwellbeingandhelpthemtocopewithdifficultsituationsthattheymaybefacingnoworthattheymayfaceinthefuture.Thispartoftheresearchaimstofindoutmoreabouttheservicesthatarebeingofferedtoyoungpeopleinthesesixareastodothis.Itaimstofindoutwhathashelpedandwhathasbeenlesshelpful,inordertolearnforthefutureabouthowtoimproveservicesthataimtoincreaseyoungpeople’swellbeing.Whoarewespeakingto?WearespeakingtoyoungpeoplewhomayhavereceivedormayinfuturereceivesupportorservicesfromHeadStart,andstaffwhohaveorganisedtheservices.Weareaskingdifferentgroupsofpeoplesothatwecanbuildupagoodpictureovertimeofwhattheseserviceshavebeenlike,whotheyhavehelped,andhowtheycanbeimprovedinthefuture.WewouldliketoinviteyourchildtotakepartinthisresearchprojectbecausetheymayhaverecentlyusedaHeadStartservice.Whatdoesthisinvolve?Takingpartinthisprojectmeansagreeingforyourchildtobeinterviewedonceayearforuptofiveyears(thefinaltimewouldbewhenyourchildisinYear11).Yourchildwillreceivea£10Love2Shopvoucheraftereachinterviewasathankyoufromtheresearchteamfortakingpart.Withyourchild’spermission,wewillre-contactyourchildeachyeartoarrangetheirinterview.Thiswillbeaninterviewwithjustyourchildandaresearcher.Theresearcherwillaskyourchildsomequestionsabouttheirunderstandingofcopingindifficulttimes,andaboutthesupportorservicesthatyourchildmayhavereceived.Theresearcherwillaskaboutyourchild’sviews,opinions,andexperiences.Theconversationcanlastforaslongasyourchildwantstotalk(uptoamaximumof1hour),butwillusuallylastfor30to45minutes.Yourchild’sinterviewcantakeplaceinaprivateroomatyourchild’sschool,atyourhouse,orinalocalcommunitybuilding–whereverismoreconvenientforyouandyourchild.Theresearcherwilltalktoyourchildaboutthequestionsthattheyaregoingtoaskyourchildatthebeginningoftheinterviewsothatyourchildwillknowwhattoexpect.Theinterviewwillbeaudio-recordedsothatwecanwritedownwhatyourchildsaidafterwards,sothatwedon’tforget.Thewrittenversionoftheinterviewiscalleda‘transcript’.Whatarethebenefitsoftakingpart?Yourchildtakingpartinthisprojectmayhelpustounderstandmoreaboutwhathelpstoincreaseyoungpeople’swellbeingandsomayhelptoimproveservicesfor

APPENDICES
434
youngpeople.Thismaybenefitotheryoungpeopleinthefuture.Somepeoplefindthattakingpartinresearchlikethiscanbearewardingandinterestingexperience.Whataretherisksoftakingpart?Therearefewriskstotakingpart.Occasionally,someonemayfeelupsetaboutsomethingthattheyaretalkingabout.Theresearcherswillensurethatyourchildiscomfortableintheirinterviewandthatyourchildonlydiscusseswhattheyfeelabletotalkabout.Theresearcherswillaskyourchildtotellthemifthereisanythingthattheydon’twanttotalkaboutandtheywilldefinitelynotpressureyourchildtodoso.If,intheunlikelyeventyourchildfeelsupsetaftertheirinterviewandwantstotalktosomeonefurther,theresearcherwillhavegivenyourchildalistofpeopleinyourlocalareathattheycanspeakwith.Willinformationaboutmeandmychildbekeptconfidential?Yourchild’sinterviewwillbekeptstrictlyconfidentialorprivate.Theonlytimethatwemightneedtobreakthisruleisifyourchildtellsussomethingthatmakesusthinkthatyourchild,orsomeoneelse,isindanger.Inthatcase,wewillhavetotellsomeonewhocanstopthatdangerfromhappening.Audiorecordingswillbekeptinapassword-protectedcomputerfolderandwillonlybeaccessedbyresearchersinvolvedwiththisproject.Whentherecordingsaretypedupastranscripts,anydetailsthatcanidentifyyourchildasanindividualwillbetakenout.Thismeansthatyourchild’snamewillbechanged,aswellasthenamesofothersorplacesthatyourchildmaymention.Wemayusequotesfromyourchild’sinterviewwhenwewriteupreports,butitwillnotbepossibletoidentifyyourchildfromthequotes.Wewillkeepaudiorecordingsupuntiltheendoftheproject(May2023),whentheywillbedeleted.WhathappensifIchangemymind?Youand/oryourchildcanchangeyourmindsabouttakingpartinthisresearch,atanytime.Youdonothavetotellusareasonforthis.Ifyouand/oryourchilddowishtoleavethestudy,yourchild’sinterviewaudiorecordingandtranscriptwillbedeleted.Oncewehavewrittenthereportsofthefindings(4-6monthsaftertheinterviews),itwillnotbepossibletowithdrawyourchild’scontributions,soitisbesttotellusassoonaspossibleifyoudochangeyourmind.Yourchildcanalsostoptheinterviewatanypointandtheresearcherwillletthemknowatthestartoftheirinterviewthattheyjustneedtotelltheresearcherinterviewingthematanypointthattheynolongerwishtotakepart.Leavingthestudyatanystagewillnotaffecthowanyonetreatsyouoryourchildandwillnotaffecttheservicesthatyouoryourchildmayreceive.Itwillnotdisadvantageyouinanyway.Whathappensnext?

APPENDICES
435
Pleasediscusstheinformationabovewithothersoraskusifthereisanythingthatisnotclearorifyouwouldlikemoreinformation.Youcankeepthisinformationsheettolookatwheneveryouneedto.Ifyoudecidethatyouwouldlikeyourchildtotakepart,youwillneedtogiveyourconsent(onawrittenform).Yourchildmustalsogivetheirassent(onawrittenform)totakepartinorderfortheinterviewtogoahead.Thenyouandyourchildcanreturntheformstousandwewillarrangeatime,atyourconvenience,tointerviewyourchild.AlldatawillbecollectedandstoredinaccordancewiththeDataProtectionAct1998.Researchercontactdetails:Name:EmilyStapleyContactdetails:Ifyouhaveanyquestions,[email protected]

APPENDICES
436
InformedConsentFormforParents/Carers(AboutTheirChild)
Pleasecompletethisformafteryouhavereadtheinformationsheetand/orlistenedtoanexplanationabouttheresearch.TitleofProject:HeadStartQualitativeEvaluationThisstudyhasbeenapprovedbytheUCLResearchEthicsCommittee(ProjectIDNumber):7963/002Ifyouhaveanyquestionscomingfromtheinformationsheet,oranyotherquestionsabouttheresearchstudy,pleaseasktheresearcherbeforeyoudecidewhetherornotyougiveconsentforthechildoryoungpersonthatyouareresponsiblefortojoinin.Participant’sStatementI
• havereadthenoteswrittenaboveandtheinformationsheet,andunderstandwhatthestudyinvolves
• understandthatifIormychilddecideatanytimethatwenolongerwishtotakepartinthisproject,Icantelltheresearchersandleavethestudystraightaway.IunderstandthatIdonothavetogiveareasonforthisandthattheresearcherswon’texpectmeormychildto.IunderstandthatwithdrawingfromthestudywillnotaffectanyservicesthatwereceivefromHeadStartoranywhereelse
• understandthatmychild’sinterviewswillbeaudio-recordedandIagreetothisaudiorecording
• consenttotheinformationthatIandmychildgivebeingusedaspartofthisresearchstudy
• understandthatsuchinformationwillbetreatedasstrictlyconfidential,andhandledinlinewiththeDataProtectionAct1998
• understandthatthethingsthatmychildsaysmaybeusedinreportsalongwiththeresponsesofotherparticipantsinthestudy,butwillnotbeidentifiable
• consenttomychildbeingre-contactedbytheresearchteamonceayearoverthenextfiveyears
• agreethattheresearchprojectnamedabovehasbeenexplainedenoughtomeandIagreeformychildtotakepartinthisstudy
Signed Date:

APPENDICES
437
AppendixO:QualitativeParticipantAssentFormYouareagreeingthat:• Youarehappytobeinterviewed• Wewillaudiorecordtoday’sconversationandtypeitupasatranscript• Wemaywriteupyourviewsinreports,whichwillbereadbypeopleoutsideof
thisresearch,butotherpeoplewon’tbeabletorecognisethatit’syouinthereports
• Youarehappyforustore-contactyounextyearaboutarranginganotherinterviewwithyou
Weareagreeingthat:• Thisformwillbekeptinalockedfilingcabinet• Theaudiorecordingandtranscriptofyourinterviewwillonlybeaccessedby
researchersinvolvedwiththisproject
Pleasecircletheanswersbelow:
Hassomebodyelseexplainedthisresearchtoyou? Yes/No
Doyouunderstandwhatthisresearchisabout? Yes/No
Haveyouaskedallthequestionsyouwant? Yes/No
Haveyouhadyourquestionsansweredinawayyouunderstand? Yes/No
Doyouunderstandit’sOKtostoptakingpartatanytime? Yes/No
Areyouhappytotakepart? Yes/No
Ifanyanswersare‘no’oryoudon’twanttotakepart,don’tsignyourname!Ifyoudowanttotakepart,youcanwriteyournamebelow:
________________ ________________Myname Date________________ ________________ ________________Nameofresearcher Date Signaturetakingconsent

APPENDICES
438
AppendixP:DemographicFormforQualitativeParticipantsAboutMe
Iam:(age)………years………monthsIam:(pleasetick)Male☐Female☐Other☐Pleasespecify:Prefernottodisclose☐Iam:(pleasetick)WhiteBritish☐Irish☐AnyotherWhitebackground☐AsianorAsianBritishIndian☐Pakistani☐Bangladeshi☐Chinese☐AnyotherAsianbackground☐MixedWhiteandBlackAfrican☐WhiteandBlackCaribbean☐WhiteandAsian☐OtherAnyotherethnicgroup☐Pleasespecify:…………………Prefernottodisclose☐ParticipantIDnumber:

APPENDICES
439
AppendixQ:ExampleofInitialThoughtsDocumentedinStageOneofQualitativeAnalysis(Amelia)
• WorryisacentralelementofAmelia’slife• Sheplacesclearvalueonothersknowingherdifficultiesandbeingawareofherneeds
–otherpeopleareimportanttoher• Dogisimportantalso,seemstiedinwithfeelings• Worryaboutpossiblenegativeoutcomes–whatwillhappen,willthishappen?• Worriesasatangiblething–‘myworries’likeaphysicalcarry-ablethingalmost?
Separatetoher?• Mistakes,gettingsomethingwrong–tiedintoOCDanxiety?• ‘Where’stheevidence’–pastCBT?CBTelements?DoesAmeliaactuallyusethis
techniqueorisitalearntmantraofsorts?Thisisunclear.• ‘Idecidedtosit’–respondingtoneeds;agency• Whendogisscared,doesthisreflectpartofAmelia?Isshereassuredbythis?Also
describeshappinesswhendogisnotscared.Seemstoreflectherinnerprocesses(andpotentialforlesseningofthese?)
• Family=important,centralpartoflife• Happyistheabsenceofworry;discussionof‘happy’frequentlyreturnstoworrytalk• Schoolandhomeworkandacademicexpectationscreatealotofstressandworryfor
Amelia• ‘Xhelpsme’often!• ‘Mummy’–seemsaveryyoungwordforage,reflectfamilydynamic?• ‘Idon’tknowwhy’–I’mnotincontrolofthis,Idon’tunderstand• Thingsbeingphysicallyperfect–tie,clothingetc.,aswellasperformance,i.e.academic
workandhomework• Laterininterviewsomeofthetalkaroundmumshifts–mumasfrustrated,mad,stop
makingproblembiggeretc.(isAmeliadisappointedpeopleinhereyes?)• ‘Soundweird’–concernoverwhatotherswillthink• Couldthephysicalityof‘myworries’comefromvisualisationexercisewithsupport?P.
15• Supportworkerprovidesanotheravenueoutsideofparents• Epilepsyfeedsworryandstress• Worryandstress–sameordifferent?• Somethingisherearoundtheongoingnessofherworriesbeingherfault–Iforgotto
flickitaway,I’mfeedingthem,sometimesIforget–anelementofblameratherthanresponsibility,maybe?
• Difficultyexplainingwhatthe‘badthing’is–isitunknown?• MumprioritisingschooloverSMASH;Ameliadoesn’tseemtoagree• Emotionalcontagion:dadstressed=Igetstressed• Talkingisgood• SchooladviceseemstobewhatothersaretellingAmeliabutshestrugglestoenactthis• Elementsofpowerlessness?Difficultyusingstrategyplusmuminfluence?

APPENDICES
440
• Issheanxiousintheinterview?Shehashistorynext,thiscouldbefeedingintotheconsistencyofworriesascentral
• Relativityinacademicdifficulty?IfeveryoneelseisokaybutI’mstruggling…he’llgetmad
• Worryseemsexcessivearoundparticularthingsbutalsogenerally‘justdosomethingwrongingeneral’
• Worriesaffectdailylifeandstopherhavingexperiences–again,elementsofpowerlessness
• ‘Doyouwant,like’–effortstomakesureshe’sfollowingtheinterviewer,seemsalittlenervous
• What’sthedifferencebetweenremovingworriesanddistraction?P.26• Dodgeball–thingsaremyfault.ShouldIbetryingharder?• Reroutesbackto‘helpsme’frequently• ‘AmIdoingitright’–fearofmistakes,doesthislinkwithhercheckinginwiththe
interviewerandseekingpermission• HedoeshelpmebutIstillhavetodoit• Privateconversations–SMASHandsupport–seemvalued• ‘Somethingbadwillhappen’–fearofpossibleconsequences,worstcasescenario,fear
ofunknown

APPENDICES
441
AppendixR:AnalyticalCodingColumnsandExampleofInitialCodinginStageTwoofQualitativeAnalysis(Amelia)
Th
emes
REFLEX
IVE:linkwith
thisasbeingexplicitlype
rfectio
nistm
ayre
flectm
yow
niss
uesw
ithth
is
Concep
t
Rumination
It’sm
yrespon
sibility
tonotm
akeitbigger,
but,Iamm
akingit
bigger,I’m
notin
controlofit
“Ihaveaworry”
again,re
peated
useof
phrase,w
orryasa
thingthatIha
ve
Rumination
Othersk
nowingmy
need
s(even
thedo
g)
isrelevantand
valuab
le
Itmakesm
yworrygo
away–ta
ngible,
passive
Alleviatesso
mebu
tno
tall
Limitsof‘eviden
ce’–
wha
tifthe
reisn’t
any?The
nwha
t?Fear
ofunkno
wnne
gativ
econseq
uences–wha
tifsalways
unde
rpinne
dby
outcom
ebe
inga
negativ
eon
e“Idon
’tknow
why”–
passive,notincon
trol
ofinne
rprocesses
Ikno
wworryisn’t
accuratebutth
isdo
esn’th
elp
Conten
t
“it’snotgon
na
happ
en”–
mism
atch
Mum
tellingm
eI’m
makingthe
prob
lembigger
Mydo
gisattune
dtom
ymoo
dan
dknow
swhe
nI’m
worrie
d
Isitan
dthinkab
out
it
Shecantellan
dshe
respon
ds,brin
gs
meatoy
“inmyhe
ad”
myworrygoe
saw
ay–butnot
entirely,Istillhave
questio
ns–only“a
bit”
“Wha
tif,wha
tif”–
wha
tmight
happ
en?
Everythinghasto
be
perfect
“Idon
’tknow
why”
–mymum
saysX
butI’m
stillworrie
d(doe
sn’the
lp)
Stream
“aworry”versus
“myworrie
s”as
elsewhe
re–iseach
onedistinct?
Perfectio
nistic
tend
encies?Note–
laterm
entio
nof
OCD
?
I:Aretherean
yothe
rexamples,erm
…ofo
f,thingsliketh
at,o
fbitsofe
vide
nce
thatyou
kindofth
inkab
out?
P:Yeah,whe
nlike,likeagainwhe
nIh
aveaworryorsom
ething,m
ymum
sayslike
whe
re’sth
eeviden
ce,you
kno
w,it’snotgon
nahap
pensolikestop
makingthe
prob
lembiggera
nderm
,mydo
gcantellwhe
nI’m
worrie
daswellcau
senormally
Iplaywith
herbutIjustsitd
ownlikeIsaidlikeearlieronan
djustliketh
inkab
out
itan
dsheno
rmallyjustlikecom
eswith
ato
yorso
mething,soshealsohelpsm
ea
lotb
ecau
sesh
ecantellifI’m
upsetorsom
ething…so
shehe
lpsa
lot.
I:Okay…
doyo
ufin
dithe
lpfultothinkab
outthe
…you
kno
w,w
onde
ringab
out
theeviden
ce?How
doe
sthat,w
henyo
uthinkofwha
t’sth
eeviden
cefo
rthis,
howdoe
s,how
doyo
uthinkthathelps?
P:W
ellIth
inkithe
lpslikeabitb
ecau
seitm
akeslikem
yworrygoaw
aybutstill
likeinm
yhe
adth
ere’slikequ
estio
nssa
yingbutwha
tifthe
reisn’ta
nyevide
nceor
wha
tifthish
appe
nsor…
likefo
rexampleifmytie
intrightor,it’slikeeverything
hastobe
perfect,Idon
’tknow
whybut,ith
asto
bepe
rfecttolike,butm
ymum
saidnoon
e’sp
erfect,b
utitstillgetsm
eworrie
d.It’sjusthow
…
I:So
isth
atafe
elingyo
uha
ve,the
n,th
atsom
ething
abo
utwan
tingthingsto
be…

APPENDICES
442
AppendixS:ExampleofEmergentThemesAlongsideDataandCodinginStageThreeofQualitativeAnalysis(Amelia)
Them
es
Worrie
sas
tangible
Rumination
Others
know
ingmy
need
s,
supp
ort
Passive
Worryas
tangible
Lackof
control
Spira
lling
Ane
edto
be
perfect
Fallibilityof
strategy
Passive“I
don’tk
now
REFLEX
IVE:linkwith
thisasbeingexplicitlype
rfectio
nistm
ayre
flectm
yow
niss
uesw
ithth
is
Concep
t
Rumination
It’sm
yrespon
sibility
tonotm
akeitbigger,
but,Iamm
akingit
bigger,I’m
notin
controlofit
“Ihaveaworry”
again,re
peated
useof
phrase,w
orryasa
thingthatIha
ve
Rumination
Othersk
nowingmy
need
s(even
thedo
g)
isrelevantand
valuab
le
Itmakesm
yworrygo
away–ta
ngible,
passive
Alleviatesso
mebu
tno
tall
Limitsof‘eviden
ce’–
wha
tifthe
reisn’t
any?The
nwha
t?Fear
ofunkno
wnne
gativ
econseq
uences–wha
tifsalways
unde
rpinne
dby
outcom
ebe
inga
negativ
eon
e“Idon
’tknow
why”–
passive,notincon
trol
ofinne
rprocesses
Ikno
wworryisn’t
accuratebutth
isdo
esn’th
elp
Conten
t
“it’snotgon
na
happ
en”–
mism
atch
Mum
tellingm
eI’m
makingthe
prob
lembigger
Mydo
gisattune
dtom
ymoo
dan
dknow
swhe
nI’m
worrie
d
Isitan
dthinkab
out
it
Shecantellan
dshe
respon
ds,brin
gs
meatoy
“inmyhe
ad”
myworrygoe
saw
ay–butnot
entirely,Istillhave
questio
ns–only“a
bit”
“Wha
tif,wha
tif”–
wha
tmight
happ
en?
Everythinghasto
be
perfect
“Idon
’tknow
why”
–mymum
saysX
butI’m
stillworrie
d(doe
sn’the
lp)
Stream
“aworry”versus
“myworrie
s”as
elsewhe
re–iseach
onedistinct?
Perfectio
nistic
tend
encies?Note–
laterm
entio
nof
OCD
?
I:Aretherean
yothe
rexamples,erm
…ofo
f,thingsliketh
at,o
fbitsofe
vide
nce
thatyou
kindofth
inkab
out?
P:Yeah,whe
nlike,likeagainwhe
nIh
aveaworryorsom
ething,m
ymum
sayslike
whe
re’sth
eeviden
ce,you
kno
w,it’snotgon
nahap
pensolikestop
makingthe
prob
lembiggera
nderm
,mydo
gcantellwhe
nI’m
worrie
daswellcau
senormally
Iplaywith
herbutIjustsitd
ownlikeIsaidlikeearlieronan
djustliketh
inkab
out
itan
dsheno
rmallyjustlikecom
eswith
ato
yorso
mething,soshealsohelpsm
ea
lotb
ecau
sesh
ecantellifI’m
upsetorsom
ething…so
shehe
lpsa
lot.
I:Okay…
doyo
ufin
dithe
lpfultothinkab
outthe
…you
kno
w,w
onde
ringab
out
theeviden
ce?How
doe
sthat,w
henyo
uthinkofwha
t’sth
eeviden
cefo
rthis,
howdoe
s,how
doyo
uthinkthathelps?
P:W
ellIth
inkithe
lpslikeabitb
ecau
seitm
akeslikem
yworrygoaw
aybutstill
likeinm
yhe
adth
ere’slikequ
estio
nssa
yingbutwha
tifthe
reisn’ta
nyevide
nceor
wha
tifthish
appe
nsor…
likefo
rexampleifmytie
intrightor,it’slikeeverything
hastobe
perfect,Idon
’tknow
whybut,ith
asto
bepe
rfecttolike,butm
ymum
saidnoon
e’sp
erfect,b
utitstillgetsm
eworrie
d.It’sjusthow
…
I:So
isth
atafe
elingyo
uha
ve,the
n,th
atsom
ething
abo
utwan
tingthingsto
be…

APPENDICES
443
AppendixT:DetailedAccountofPreliminaryAnalysisResultsMissingness
Missingvaluesarecommoninquantitativeinquiry,particularlyin
educationalandpsychologicalresearch(Pengetal.,2007;Peugh&Enders,2004),
andcanoccurforvariousreasonsincludingsystemerrorsanditemnonresponse
(Little&Rubin,2002).Analyticaleffectsvarycontextuallyduetofactorsincluding
samplesize,patternsofmissingness,anddatalossmechanism;thus,thereisno
establishedcutoffforacceptablelevelsofmissingness(Dong&Peng,2013;
Tabachnick&Fidell,2013).Bennett(2001)indicatestenpercentaspotentially
problematic,whilePengetal.(2007)advisetwentypercent.TabachnickandFidell
(2013)conservativelysuggestthatinalargedatasetwithrandomlyoccurring
missingness,belowfivepercentcanbeacceptable,thoughtheyemphasisethatthis
dependsondatasetcharacteristics,whileCheema(2014)advisessomemissingness
inalargesampleisnon-problematic.
Itisusefultoexaminethepatternofmissingness,asmissingvaluescan
occurwithinisolatedvariables,acrossrandomunrelatedvariables,oracrossrelated
variables(Dong&Peng,2013;Schafer&Graham,2002);thelatteroftenoccursdue
tosurveynonresponsewhendemographicinformationisobtainedseparately
(Grovesetal.,2002;Schafer&Graham,2002),asinthecurrentstudy.Littleand
Rubin(1987,2002)outlinedthreemechanismsformissingness:(a)MCAR,where
missingnessisrandom;(b)MAR,wheremissingnessispredictedbyothermeasured
variables;and(c)notmissingatrandom(NMAR),wheremissingnessisassociated
withthevariableitself.MCARistestedusingamultivariateanalysisoutlinedby
Little(1988).MARisexploredbyinvestigatingtherelationshipbetween
missingnessandothervariables,suchasparticipantcharacteristics(Kline,2016;
Tabachnick&Fidell,2013).NMARischallengingtoassess,asverifyingwhether
missingnessonavariableiscausedbythevariableitselfrequiresknowledgeofthe
missingvalues(Kline,2016;Little&Rubin,2002;Peugh&Enders,2004).AsNMAR
cannotberejected,MARcannotbefullyacceptedandisinsteadexploredfor
transparency(Little&Rubin,2002;Peugh&Enders,2004).

APPENDICES
444
Here,allsurveyitemscontainedmissingdata(2.3–5.9%).Alldemographic
variablesexceptchildinneedstatuscontainedmissingvalues(0.4–7.2%).32.3%(N
=2,681)hadatleastonemissingvalueacrossitemanddemographicvariables.
Little's(1988)MCARtestwassignificantatthe.05αlevel(p<.001)andsoMCAR
wasrejected.Alogisticmultipleregressionwithallparticipantcharacteristics
indicatedthat:(a)lowacademicattainmentpredictednonresponseonallbuttwo
surveyitems;(b)SENpredictedmissingnessforthreeSDQitems,oneSRSschool
adultconnectionitem,andseveralSRSpeerconnectionitems;and(c)ethnicgroup,
speakingEnglishasanadditionallanguage,andlowneighbourhoodsocioeconomic
statuswerefrequentpredictorsofmissingnessonitemsacrosstheSRSsubscales(p
<.05).Thus,missingitem-leveldatawasassumedtobeMAR,thoughtentativelyas
NMARcannotbeexamined.
DataAssumptions
Datawerereviewedagainstanalyticalassumptions,namelyoutliers,
multicollinearity,skewnessandkurtosis,floorandceilingeffects,andlinearityand
homoscedasticity(seeTableT1overleaf).Therewereconsistentinstancesofceiling
effectsandoutliersacrossSRSitems.ThisdistributionreflectstheParetoprinciple,
wherebythemajorityofapopulationislikelytorespondinaparticularwayand
thusonlyaminorityresponddifferently(Aguinisetal.,2013).Here,thislikely
reflectsuseofacommunitysample,whereinitisunsurprisingthatmost
participantsreportedhigherSRSscores.However,departuresfromnormal
distributionassumptions,asobservedhere,canbelessproblematicwithinlarger
samples(Kline,2016)andsoarenotexpectedtobesubstantiallyinfluentialhere.
Furthermore,theWLSMVestimatorusedinmainanalysisdoesnotmake
distributionalassumptionsaboutfactorindicatorswheretheyaretreatedasordinal
ratherthancontinuous(Li,2016)andasensitivityanalysiswasundertakenusing
theMLRestimator,whichproducesstandarderrorsrobusttonon-normality
(Muthén&Muthén,1998-2010).

APPENDICES
445
TableT1
SummaryofDataAssumptions,AdoptedThresholds,andResultsacrosstheDataset
Assumption Threshold Result
Outliers Themedianabsolute
deviation(MAD)should
notexceed2.24(Huber,
1981)orwherethe
mediancapturesmore
than50%ofcasesa
modifiedz-scoreestimate
shouldnotexceed3.5
(Iglewicz&Hoaglin,1993)
16SRSitemscoresshowedamodifiedz-score
exceeding3.5,fourfamilyadultconnectionitems,
fourcommunityadultconnectionsubscaleitems,
andeightschoolpeerconnectionsubscales;
outliersweregenerallyclusteredonavalueof
one,or‘never’
Multicollinearity Bivariatecorrelations
shouldnotexceed.70
(Tabachnick&Fidell,
2013)
ü
Skewness Skewnessshouldnot
exceedanabsolutevalue
of2,giventhelarge
samplesize(West,Finch,
&Curran,1995)
ü
Kurtosis Kurtosisshouldnotexceed
anabsolutevalueof7
(Westetal.,1995)
ü
Flooreffects Thelowestpossibleitem
valuecapture<15%of
responses(Terweeetal.,
2007)
FlooreffectsobservedforallSDQitems(24.2-
52.1%),thetwopositively-wordedPSS-4items
(21.1-28.4%),oneschooladultconnectionitem
(19.2%),andoneengagementinextracurricular
activitiesitem(26.3%)
Ceilingeffects Thehighestpossibleitem
valueshouldcapture<15%
ofresponses(Terweeet
al.,2007)
CeilingeffectsobservedforfourSDQitems(17.4-
42.0%),andallbutoneSRSsubscaleitems(27.9-
87.1%)
Linearity Residualsshouldcluster
aroundthezerolineina
residualplot,ratherthan
curving(Mertler&
ü

APPENDICES
446
Reinhart,2017)
Homoscedasticity Datapointsshouldbe
evenlydistributedaround
thezerolineinaresidual
plot(Mertler&Reinhart,
2017;Tabachnick&Fidell,
2013)
ü
FactorStructureandPsychometricPropertiesofMeasures
FactorStructure
SDQEmotionalSymptomsSubscale.Inlinewithoriginalconstructionofthe
SDQ(Goodmanetal.,1998),aunidimensionalstructurewasassessedforthe
emotionalsymptomssubscale.Fitindicesindicatedacceptablefitwithacceptable
factorloadings(TableT2):χ2(5)=255.28,p<.001;RMSEA=.08,90%CI[.07,.09],
p<.001;CFI=.98,TLI=.95.
TableT2
StandardisedFactorLoadingsandIntraclusterCorrelationCoefficientsforSDQEmotionalSymptoms
Subscale
Items λ ICC
Igetaloadofheadaches,stomach-achesorsickness .51*** .02
Iworryalot .78*** .02
Iamoftenunhappy,downheartedortearful .72*** .01
Iamnervousinnewsituations.Ieasilyloseconfidence .62*** .02
Ihavemanyfears,Iameasilyscared .66*** .01
Note.λ=standardisedfactorloadings;SDQ=StrengthsandDifficultiesQuestionnaire=;ICC=
intraclustercorrelationcoefficient.
***p<.001.
PSS-4UnidimensionalandMultifactorialExploration.Twostructureswere
investigatedforthePSS-4:aone-factormodelinlinewiththeoriginalmeasure
(Cohenetal.,1983),anda2-factormodelcomprisingperceiveddistressand

APPENDICES
447
perceivedcoping,givenprevioussupportforbothaunidimensional(Lesageetal.,
2012;Mitchelletal.,2008)anda2-dimensionalstructure(Demkowiczetal.,2019;
Leungetal.,2010;seeTableT3).
Theone-factorstructureshowedpoorfit:χ2(2)=1,182.44,p<.001;RMSEA
=.27,90%CI[.29,.30],p<.001;CFI=.86,TLI=.58.ExaminationofMIandSEPC
statisticssuggestedthatresidualcorrelationsbetweenthefirstandfourthitems
(positively-worded)andthesecondandthirditems(negatively-worded)shouldbe
freelyestimated,whileallresidualcorrelationmatrixvaluesexceeded.10.The2-
factorstructureshowedgoodfit:χ2(1)=20.99,p<.001;RMSEA=.05,90%CI[.03,
.07],p=.46;CFI=1.00,TLI=.99,withimprovedMIandSEPCvaluesandacceptable
residualcorrelations.Examinationofa2-factorstructurewaspre-determinedand
theoreticallygroundedandthesevaluesprovidedempiricalsupportforre-
specification.Thus,CFAindicatedsupportforthe2-factorstructureofthePSS-4
andassuchthisstructureisutilisedwithinthecurrentstudy.Notethatinanalysis,
theperceivedcopingfactoritemsarenolongerreverse-codedastheycomprisea
distinctfactorandsoneednotvaryinthesamedirectionastheitemsforming
perceiveddistress.Furthermore,thesefactorsarecorrelatedinanymodelwhere
bothareusedasamoderatetolargelatentcorrelationof.46(p<.001)was
observed.SeeTableT3forfactorloadings.
TableT3StandardisedFactorLoadingsandIntraclusterCorrelationCoefficientsforPSS-4UnidimensionalandMultidimensionalStructures Standardisedfactorloadings 2-factorstructure(λ) Items
Onefactorstructure(λ)
Perceiveddistress
Perceivedcoping
ICC
Inthelastmonth,howoftenhaveyoufeltthatyouwereunabletocontroltheimportantthingsinyourlife?
.66 .68 – .01
Inthelastmonth,howoftenhaveyoufeltconfidentaboutyourabilitytohandleyourpersonalproblems?
.44 – .61 .01
Inthelastmonth,howoftenhaveyoufeltthatthingsweregoingyourway?
.51 – .73 .01

APPENDICES
448
Inthelastmonth,howoftenhaveyoufeltdifficultieswerepilingupsohighthatyoucouldnotovercomethem?
.83 .91 – .01
Note.λ=standardisedfactorloadings;CFA=ConfirmatoryFactorAnalysis;PSS-4=four-itemPerceivedStressScale;ICC=intraclustercorrelationcoefficient.Allparameterestimatesshownaresignificantatthe.001level.
SRSsubscales.ConsistentwiththeoriginalconstructionoftheSRS(Sun&
Stewart,2007),a6-domainmultidimensionalstructurewasassessed.Results
indicatedgoodfit:χ2(419)=3,853.581,p<.001;RMSEA=.032,90%CI[.031,.033],
p=1.00;CFI=0.98,TLI=0.98(seeTableT4forfactorloadingsandICCs).
TableT4StandardisedFactorLoadingsandIntraclusterCorrelationCoefficientsforStudentResilienceSurveySubscaleItemsSubscales Items λ ICCFamilyadultconnection
Athome,thereisanadultwho…
Isinterestedinmyschoolwork .77 .02 BelievesthatIwillbeasuccess .84 .01 Wantsmetodomybest .81 .04 ListenstomewhenIhavesomethingtosay .81 .01Schooladultconnection
Atschool,thereisanadultwho…
Reallycaresaboutme .78 .03 TellsmewhenIdoagoodjob .85 .02 ListenstomewhenIhavesomethingtosay .81 .02 BelievesthatIwillbeasuccess .85 .02Communityadultconnection
Awayfromschool,thereisanadultwho…
Reallycaresaboutme .87 .02 TellsmewhenIdoagoodjob .90 .01 BelievesthatIwillbeasuccess .92 .01 Itrust .81 .02Peersupport Aretherestudentsatyourschoolwhowould… Chooseyouonyourteamatschool .75 .01 Tellyouyou’regoodatdoingthings .78 .02 Explaintherulesofagameifyoudidn’t
understandthem.73 .02
Inviteyoutotheirhome .71 .03 Sharethingswithyou .82 .01 Helpyouifyouhurtyourself .83 .02 Missyouifyouweren’tatschool .82 .01

APPENDICES
449
Makeyoufeelbetterifsomethingisbotheringyou .83 .01 Pickyouforapartner .82 .00 Helpyouifotherstudentsarebeingmeantoyou .85 .01 Tellyouyou’retheirfriend .86 .01 Askyoutojoininwhenyouareallalone .86 .01 Tellyousecrets .71 .01Activeengagementinhomeandschoollife
Idothingsathomethatmakeadifference(i.e.makethingsbetter)
.73 .01
Ihelpmyfamilymakedecisions .73 .01 Atschool,Ihelpdecidethingslikeclassactivitiesor
rules.66 .01
Idothingsatmyschoolthatmakeadifference(i.e.makethingsbetter)
.77 .01
Engagementinextracurricularactivities
Awayfromschool…
Iamamemberofaclub,sportsteam,churchgroup,orothergroup
.79 .08
Itakelessonsinmusic,art,sports,orhaveahobby .86 .06Note.λ=standardisedfactorloadings;ICC=intraclustercorrelationcoefficient.Allparameterestimatesshownaresignificantatthe.001level.
TableT5presentslatentcorrelationsacrosssubscales;thesearesimilarin
magnitudetoresultsfromLereyaetal.(2016).
TableT5LatentCorrelationsbetweenStudentResilienceSurveySubscalesFactor 1 2 3 4 5 61.Familyadultconnection — 2.Schooladultconnection .52 — 3.Communityadultconnection .64 .50 — 4.Schoolpeerconnection .50 .40 .51 — 5.Activeengagementinhomeandschoollife
.60 .53 .54 .55 —
6.Engagementinextracurricularactivities
.30 .18 .34 .26 .40 —
Note.Alllatentcorrelationcoefficientsshownaresignificantatthe.001level.
InternalConsistency
AnalysisindicatedthattheSDQemotionalsymptomssubscaleandallSRS
subscalesshowedagoodlevelofinternalconsistency(TableT6).Givensupportfor

APPENDICES
450
a2-factorstructureforthePSS-4,scalereliabilitywasassessedatboththeone-
factorandthe2-factorlevel.Fortheone-factorstructure,bothCronbach’sαand
McDonald’sωvalueswererelativelylow.Whilebothstatisticsshowcomparatively
highervaluesforthe2-itemperceiveddistressfactor,lowervalueswereobserved
forperceivedcoping.Itisplausiblethatthisdiscrepancyispartiallyduetothelow
numberofitems(Kline,2016;Raykov,1997),althoughthevaluesforperceived
distressweremorefavourable.Thus,valuesforperceivedcopingmayindicatethat
thissub-factorisdefinedonthebasisofreversewordingeffects,asindicated
previously(Demkowiczetal.,2019),ratherthanduetoahighlevelofagreementin
theconstruct.
TableT6ReliabilityCoefficientsMeasure No.ofitems Cronbach’sα McDonald’sωSDQemotionalsymptoms 5 .72 .80PSS-4perceivedstress(allitems) 4 .63 .72PSS-4perceiveddistress(items1and4) 2 .71 .76PSS-4perceivedcoping(items2and3) 2 .57 .62SRSfamilyadultconnection 4 .77 .88SRSschooladultconnection 4 .86 .89SRScommunityadultconnection 4 .88 .93SRSschoolpeersupport 13 .93 .96SRSactiveengagementinhomeandschoollife
4 .77 .81
SRSengagementinextracurricularactivities
2 .71 .87
Note.SDQ=StrengthsandDifficultiesQuestionnaire;PSS-4=four-itemPerceivedStressScale;SRS=StudentResilienceSurvey.
SummaryofPsychometricProperties
ResultsindicatethattheSDQemotionalsymptomssubscaleandallSRS
subscalesarerobustforuseinthestudy.Findingssuggestthatitwouldbe
appropriatetoutilisea2-factorstructureforthePSS-4,ratherthanthe
unidimensionalformatproposedinitsoriginalconstruction.However,thelow
internalconsistencyfortheperceivedcopingsub-factorandpreviousindications
thatthisstructureislikelytheresultofreversewordingeffects(Demkowiczetal.,

APPENDICES
451
2019),indicatinganeedforcautionininferences.Thus,findingsinrelationtothis
measurearepresentedtentatively.

APPENDICES
452
AppendixU:IntegrationofIndividual-LevelThemesintoMasterThemesTableU1Integrationofthemes:individualthemetrackingParticipantandindividualtheme CorpusthemeAmelia Worriesastangible (1.1)Thenatureofsymptoms(objectorstate)
(2.2)SymptomsareseparatefrommyidentityWorriesasseparatefromme (2.2)SymptomsareseparatefrommyidentityWorriesarepluralandcanmultiply (1.2)SymptomsareapluralmassthatcangrowWorriesareintertwinedwithotherdisorders (1.1)Thenatureofsymptoms(objectorstate)Othershelpme (4.1)MappingtheemotionalsupportnetworkSharingemotionsisvaluable (4.2)ReleasingsymptomsthroughtalkCumulativesupportnetwork (4.1)MappingtheemotionalsupportnetworkWorryiscentralemotion (1.2)Symptomsascentralanddominantinemotion
experienceWorrydefinesrelationships (1.3)Symptomsascentralanddominantinemotion
experience(4.1)Mappingtheemotionalsupportnetwork
Worryasdominantthroughoutlife (1.3)Symptomsascentralanddominantinemotionexperience(3.2)Fearthatsomethingbadwillhappen
Lackofagency (2.3)Passiveexperienceofsymptoms(3.3Voiceandcontrolovertheworld
Passiveemotionalregulation (2.3)PassiveexperienceofsymptomsRumination (2.1)Symptomsascentralanddominantinemotion
experienceResponsibilityandself-blame (2.3)Passiveexperienceofsymptoms
(3.1)Demandsandresponsibility(3.3)Voiceandcontrolovertheworld
Fearofnegativeconsequences (3.1)Demandsandresponsibility(3.2)Fearthatsomethingbadwillhappen(3.3)Voiceandcontrolovertheworld
Difficultyconceptualisingthebadthing (3.2)FearthatsomethingbadwillhappenMismatchbetweenexpectationsandreality (2.4)Mismatchbetweensymptomsandreality Jennifer Negativethoughtsareaboutme (1.1)Thenatureofsymptoms(objectorstate)Negativethoughtsareacollectivemass (1.2)SymptomsareapluralmassthatcangrowNegativethoughtsblockhappinessandpositivethoughts
(1.3)Symptomsascentralanddominantinemotionexperience
Negativethoughtsareirrational (2.4)MismatchbetweensymptomsandrealityIdealised‘goodness’ (3.1)DemandsandresponsibilityI’mnotgoodenough (3.1)DemandsandresponsibilityRelativitytoothers (3.1)DemandsandresponsibilityOtherpeople’sexpectationsofme (3.1)Demandsandresponsibility
(3.2)FearthatsomethingbadwillhappenGuiltandresponsibility (3.1)Demandsandresponsibility
(3.3)Voiceandcontrolovertheworld

APPENDICES
453
Negativethoughtsareinsideme (2.1)SymptomsareconnectedtomeNegativethoughtsareprivateandsensitive (2.1)Symptomsareconnectedtome
(4.2)ReleasingsymptomsthroughtalkLettingoutnegativethoughts (2.1)Feelingsareinsideme(andmayneedtocome
out)(4.2)Releasingsymptomsthroughtalk
Unavailabilityofothers (4.1)MappingtheemotionalsupportnetworkAccumulationofdemand (3.1)DemandsandresponsibilityLackofexternalcontrol (3.3)Voiceandcontrolovertheworld“Productivity”andadaptingtodemand (3.1)Demandsandresponsibility
(3.3)VoiceandcontrolovertheworldLackofagencyoveremotions (2.3)PassiveexperienceofsymptomsDetachedfromfeelingsandnegativethoughts
(2.2)Symptomsareseparatefrommyidentity(2.3)Passiveexperienceofsymptoms
Detachedfromactions (2.2)Symptomsareseparatefrommyidentity(2.2)Passiveemotionexperience
Negativethoughtsasseparatefromidentity (2.2)Symptomsareseparatefrommyidentity Grace Self-protection (3.1)Demandsandresponsibility
(3.2)Fearthatsomethingbadwillhappen(3.3)Voiceandcontrolovertheworld
Voiceandagency (3.3)VoiceandcontrolovertheworldHidingandcontrollingemotions (2.1)Symptomsareconnectedtome
(2.3)PassiveexperienceofsymptomsPhysicalsafety (3.2)FearthatsomethingbadwillhappenRoleexpectations (3.1)Demandsandresponsibility
(4.1)Mappingtheemotionalsupportnetwork (4.3)OthersasprotectorsPersonalresponsibility (3.1)DemandsandresponsibilityDadasstable (4.1)Mappingtheemotionalsupportnetwork
(4.3)OthersasprotectorsDadasaprotector (4.3)OthersasprotectorsOnegoodcancelsoutthebad (4.3)OthersasprotectorsSingularsupport (4.1)Mappingouttheemotionalsupportnetwork
(4.2)ReleasingsymptomsthroughtalkLoveandpriorities (4.1)Mappingtheemotionalsupportnetwork
(4.3)OthersasprotectorsOthersareirrationalandIamnot (2.4)Mismatchbetweensymptomsandreality
(3.1)Demandsandresponsibility(3.3)Voiceandcontrolovertheworld
Othersandsafety (3.2)Fearthatsomethingbadwillhappen(4.3)Othersasprotectors
Familysplitaspivotalmoment (3.3)VoiceandcontrolovertheworldFearofnegativeoutcomes (3.2)FearthatsomethingbadwillhappenVoiceunheard (3.3)VoiceandcontrolovertheworldStuckinthemiddle (3.1)Demandsandresponsibility
(3.3)VoiceandcontrolovertheworldHelplessness (3.3)Voiceandcontrolovertheworld

APPENDICES
454
Feelingsasanintensestate (1.1)Thenatureofsymptoms(objectorstate)(1.2)Symptomsareapluralmassthatcangrow
Buildingimpactonemotions (1.3)SymptomsareapluralmassthatcangrowLackofemotionaloutlet (2.3)PassiveexperienceofsymptomsConstantconflict (3.1)DemandsandresponsibilityBreakingpoint (1.3)Symptomsareapluralmassthatcangrow
(3.1)Demandsandresponsibility