
A latent class analysis of self-reported clinical indicators of psychosocial stability and adherence...
10
Drug and Alcohol Dependence 142 (2014) 46–55 Contents lists available at ScienceDirect Drug and Alcohol Dependence j ourna l ho me pa g e: www.e lsevier.com/locate/druga lcdep A latent class analysis of self-reported clinical indicators of psychosocial stability and adherence among opioid substitution therapy patients: Do stable patients receive more unsupervised doses? Briony Larance a,∗ , Natacha Carragher a , Richard P. Mattick a , Nicholas Lintzeris b,c , Robert Ali d,e , Louisa Degenhardt a,f,g,h a National Drug and Alcohol Research Centre, UNSW Australia, Randwick Campus, 22-32 King Street, Sydney NSW 2052, Australia b The Langton Centre, South Eastern Sydney Local Health District (SESLHD), 591 South Dowling Street, Surry Hills NSW 2010, Australia c Discipline of Addiction Medicine, The University of Sydney, Drug Health Services, Royal Prince Alfred Hospital, Level 6 KGV Building, 83-117 Missenden Road, Camperdown, Sydney NSW 2050, Australia d Discipline of Pharmacology, The University of Adelaide, Medical School South Building, Frome Road, Adelaide SA 5005, Australia e Drug and Alcohol Services South Australia, 161 Greenhill Road, Parkside SA 5063, Australia f School of Population and Global Health, University of Melbourne, Australia g Murdoch Children’s Research Institute, Australia h Department of Global Health, School of Public Health, University of Washington, USA a r t i c l e i n f o Article history: Received 16 June 2013 Received in revised form 21 May 2014 Accepted 21 May 2014 Available online 2 June 2014 Keywords: Methadone Buprenorphine Compliance Supervised dosing Diversion Injection a b s t r a c t Aims: To develop a stability typology among opioid substitution therapy patients using a range of adher- ence indicators derived from clinical guidelines, and determine whether stable patients receive more unsupervised doses. Methods: An interviewer-administered cross-sectional survey was used in opioid substitution therapy programmes in three Australian jurisdictions, totalling 768 patients in their current treatment episode for ≥4 weeks. A structured questionnaire collated data from patients about their demographics, treatment characteristics, past 6-month drug use and medication adherence, psychosocial stability, comorbidity, child welfare concerns and levels of supervised dosing. Latent class analysis (LCA) was used to derive a stability typology. Linear regression models examined predictors of unsupervised dosing in the past month. Results: LCA identified two classes: (i) a higher-adherence group (67%) who had low-moderate probabil- ities of endorsing the opioid substitution therapy stability indicators and (ii) a lower-adherence group (33%) who had moderate-high probabilities of endorsing the stability indicators. There was no associa- tion between adherence profile and the number of unsupervised doses. Significant predictors of receiving larger numbers of unsupervised doses included being older, living in New South Wales or South Australia (vs. Victoria), receiving methadone (vs. mono-buprenorphine), being prescribed in private clinic or gen- eral practice (vs. public clinic), reporting a longer current treatment episode, not receiving a urine drug screen in the past month, being currently employed and not having a prison history. Conclusions: This study suggested that system-level factors and observable indicators of social functioning were more strongly associated with the receipt of less supervised treatment. Future research should examine this issue using prospectively collected data. © 2014 Elsevier Ireland Ltd. All rights reserved. ∗ Corresponding author at: Tel.: +61 2 9385 0241; fax: +61 2 9385 0222. E-mail address: [email protected] (B. Larance). 1. Introduction Opioid substitution therapy is the most effective treatment for opioid dependence, and involves prescribing long-acting opioid medications such as methadone, buprenorphine or buprenorphine–naloxone (Mattick et al., 2009, 2008). Opioid sub- stitution therapy reduces morbidity (Ward et al., 1998), mortality http://dx.doi.org/10.1016/j.drugalcdep.2014.05.018 0376-8716/© 2014 Elsevier Ireland Ltd. All rights reserved.
Transcript of A latent class analysis of self-reported clinical indicators of psychosocial stability and adherence...

Aptd
BRa
b
c
Rd
e
f
g
h
a
ARRAA
KMBCSDI
h0
Drug and Alcohol Dependence 142 (2014) 46–55
Contents lists available at ScienceDirect
Drug and Alcohol Dependence
j ourna l ho me pa g e: www.e l sev ier .com/ locate /druga l cdep
latent class analysis of self-reported clinical indicators ofsychosocial stability and adherence among opioid substitutionherapy patients: Do stable patients receive more unsupervisedoses?
riony Larancea,∗, Natacha Carraghera, Richard P. Matticka, Nicholas Lintzerisb,c,obert Alid,e, Louisa Degenhardta,f,g,h
National Drug and Alcohol Research Centre, UNSW Australia, Randwick Campus, 22-32 King Street, Sydney NSW 2052, AustraliaThe Langton Centre, South Eastern Sydney Local Health District (SESLHD), 591 South Dowling Street, Surry Hills NSW 2010, AustraliaDiscipline of Addiction Medicine, The University of Sydney, Drug Health Services, Royal Prince Alfred Hospital, Level 6 KGV Building, 83-117 Missendenoad, Camperdown, Sydney NSW 2050, AustraliaDiscipline of Pharmacology, The University of Adelaide, Medical School South Building, Frome Road, Adelaide SA 5005, AustraliaDrug and Alcohol Services South Australia, 161 Greenhill Road, Parkside SA 5063, AustraliaSchool of Population and Global Health, University of Melbourne, AustraliaMurdoch Children’s Research Institute, AustraliaDepartment of Global Health, School of Public Health, University of Washington, USA
r t i c l e i n f o
rticle history:eceived 16 June 2013eceived in revised form 21 May 2014ccepted 21 May 2014vailable online 2 June 2014
eywords:ethadone
uprenorphineomplianceupervised dosingiversion
njection
a b s t r a c t
Aims: To develop a stability typology among opioid substitution therapy patients using a range of adher-ence indicators derived from clinical guidelines, and determine whether stable patients receive moreunsupervised doses.Methods: An interviewer-administered cross-sectional survey was used in opioid substitution therapyprogrammes in three Australian jurisdictions, totalling 768 patients in their current treatment episodefor ≥4 weeks. A structured questionnaire collated data from patients about their demographics, treatmentcharacteristics, past 6-month drug use and medication adherence, psychosocial stability, comorbidity,child welfare concerns and levels of supervised dosing. Latent class analysis (LCA) was used to derivea stability typology. Linear regression models examined predictors of unsupervised dosing in the pastmonth.Results: LCA identified two classes: (i) a higher-adherence group (67%) who had low-moderate probabil-ities of endorsing the opioid substitution therapy stability indicators and (ii) a lower-adherence group(33%) who had moderate-high probabilities of endorsing the stability indicators. There was no associa-tion between adherence profile and the number of unsupervised doses. Significant predictors of receivinglarger numbers of unsupervised doses included being older, living in New South Wales or South Australia(vs. Victoria), receiving methadone (vs. mono-buprenorphine), being prescribed in private clinic or gen-
eral practice (vs. public clinic), reporting a longer current treatment episode, not receiving a urine drugscreen in the past month, being currently employed and not having a prison history.Conclusions: This study suggested that system-level factors and observable indicators of social functioningwere more strongly associated with the receipt of less supervised treatment. Future research shouldexamine this issue using prospectively collected data.∗ Corresponding author at: Tel.: +61 2 9385 0241; fax: +61 2 9385 0222.E-mail address: [email protected] (B. Larance).
ttp://dx.doi.org/10.1016/j.drugalcdep.2014.05.018376-8716/© 2014 Elsevier Ireland Ltd. All rights reserved.
© 2014 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Opioid substitution therapy is the most effective treatment
for opioid dependence, and involves prescribing long-actingopioid medications such as methadone, buprenorphine orbuprenorphine–naloxone (Mattick et al., 2009, 2008). Opioid sub-stitution therapy reduces morbidity (Ward et al., 1998), mortality
ohol D
(ceptoiaUpe
sotppafadfi‘2ttomisp
mcmpHuici
ttAmnt(iipAWupiA
vatrpaa
B. Larance et al. / Drug and Alc
Degenhardt et al., 2011), HIV transmission (Gowing et al., 2011),riminality (Hall, 1996), other drug use (Amato et al., 2005; Wardt al., 1998), and substantially improves the quality of life amongeople who are opioid dependent (Padaiga et al., 2007). However,here are significant risks associated with the extra-medical usef the medications used in opioid substitution therapy, includ-ng dependence, injection-related injuries and diseases, overdose,nd mortality (Degenhardt et al., 2008; Strang et al., 2010).nsupervised doses (“take-home medication” or “takeaways”), inarticular, are susceptible to diversion and injection (e.g., Haskewt al., 2008; Ritter and Di Natale, 2005).
The supervised administration of medications in opioid sub-titution therapy, where the dose is consumed under directbservation of a pharmacist/clinician, is recommended in interna-ional guidelines (World Health Organization, 2009) and is standardractice in Australia (Department of Health and Ageing, 2007). Therimary aims of supervised dosing are to maximise both medicationdherence and programmatic adherence (see Larance et al., 2011bor definitions), and minimise the risks, particularly those associ-ted with diversion and injection. However, supervised dosing hasisadvantages; it is labour-intensive and costly, travel may be dif-cult and daily attendance can be counterproductive to leading a
normalised’ life, such as working or having a holiday (Bell et al.,007; Deering et al., 2011; Madden et al., 2008). For these reasons,he provision of some unsupervised dosing is supported interna-ionally (World Health Organization, 2009), but the identificationf patients who are ‘suitable’ for receiving this more flexible treat-ent is crucial. Careful patient selection for unsupervised dosing
s important not only for ensuring the safety and efficacy of opioidubstitution therapy, but also for avoiding criticisms and erosion ofublic and government support for such programmes.
The literature on treatment adherence highlights many ways toeasure medication and programmatic adherence, including pill
ounts, patient self-report, third-party reports, use of electroniconitoring devices, length of treatment episode, and reviews of
rescription records and claims (e.g. Ahn et al., 2008; Dunbar, 1984;ansen et al., 2009; Haynes et al., 2008; Julius et al., 2009). These of multiple rather than single indicators to evaluate adherence
s preferable (Ahn et al., 2008). However, a key challenge facinglinicians and researchers is that it is not always apparent whichndicators are more salient for particular patient groups.
In opioid substitution therapy, ‘stability assessments’ are usedo determine which patients have stabilised on their medica-ion and may therefore be suitable for unsupervised dosing.ssessing patient ‘stability’ involves identifying when a phar-acological equilibrium has been reached (i.e., the patient is
o longer fluctuating between the physical states of intoxica-ion and withdrawal) and examining psychosocial functioningAustralasian Chapter of Addiction Medicine, 2006). Multiplendicators for monitoring treatment progress are recommended,ncluding medication and programmatic adherence, drug use,hysical and psychosocial wellbeing (Australasian Chapter ofddiction Medicine, 2006; Department of Health and Ageing, 2007;orld Health Organization, 2009). The main contraindications to
nsupervised dosing include hazardous use of drugs, injection ofrescribed medication, diversion and/or unsanctioned use of med-
cation, and child welfare concerns (Department of Health andgeing, 2007).
Most guidelines for assessing patient suitability for unsuper-ised dosing are based on indicators of psychosocial stability,dherence and risk defined through clinician consensus. The extento which the assessment domains match the actual practices and
isk profiles of opioid substitution therapy patients has not beenreviously examined in the literature. Therefore, the over-archingims of this study are to: (a) identify a stability typology based oncomprehensive range of adherence indicators spanning drug use,
ependence 142 (2014) 46–55 47
medication and programmatic adherence, psychosocial stability,comorbidity, and child welfare; (b) examine whether this typologypredicts the number of unsupervised doses received by patients,controlling for key demographic and treatment characteristics; and(c) identify the independent predictors of unsupervised dosing.
2. Methods
2.1. Opioid substitution therapy patient sample
Data were derived from the first Australian large-scale post-marketing surveil-lance studies of buprenorphine–naloxone (Larance et al., 2011a). Face-to-faceinterviews were conducted between June 2007 and November 2008 with 768 opi-oid substitution therapy patients in three Australian jurisdictions: South Australia(n = 239), Victoria (n = 277) and New South Wales (n = 252). Further details about thestudy background and methodology are detailed elsewhere (Larance et al., 2011a,b).Briefly, recruitment targeted a range of treatment settings to reflect the mixture ofpublic clinics, private clinics, general practice, and pharmacy dispensers in eachjurisdiction (Australian Institute of Health and Welfare, 2008). There were multiplerecruitment sites in each jurisdiction (>40 recruitment sites in total). To be eligible,participants were enrolled in their current treatment episode for at least one month.Participants were administered a structured questionnaire that examined demo-graphics, treatment characteristics, medication adherence, removal of superviseddoses, diversion of doses, injection of doses and levels of supervised dosing.
2.2. Ethics approval
Ethics approval for the study was obtained from the University of New SouthWales Human Research Ethics Committee (HREC) (Committee A), South Eastern Syd-ney and Illawarra Area Health Service HREC (Northern Hospital Network), SydneySouth West Area Health Service HREC (Western Zone), the University of AdelaideHREC, and the Victorian Department of Human Services HREC.
2.3. Overview of guidelines for assessing patient stability
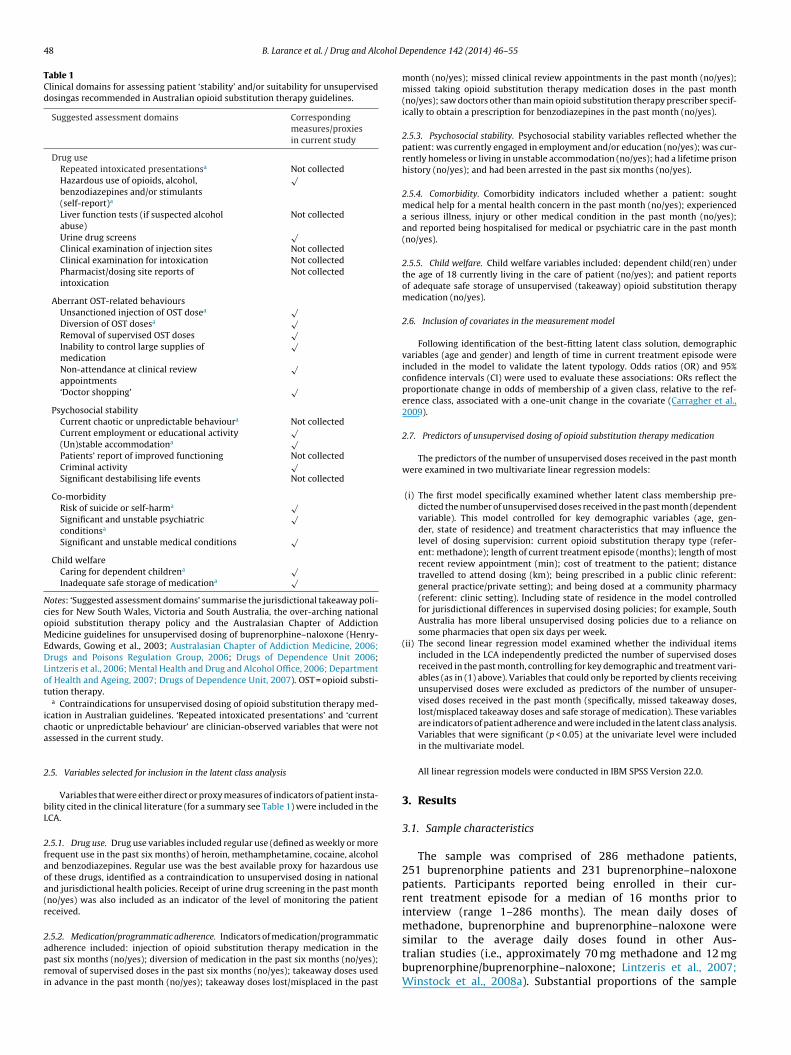
Table 1 summarises the clinical domains for assessing patient stability derivedfrom the national opioid substitution therapy guidelines and the relevant policies inthe three jurisdictions (New South Wales, Victoria and South Australia; Drugs andPoisons Regulation Group, 2006; Drugs of Dependence Unit, 2007; Mental Healthand Drug and Alcohol Office, 2006).
2.4. Overview of latent class analysis
This study uses latent class analysis (LCA) (McCutcheon, 1987) to empiricallyderive a stability typology of opioid substitution therapy patients based on endorse-ment patterns to multiple indicators of psychosocial stability and adherence. LCA isa statistical modelling technique based on the premise that associations among a setof observed categorical variables can be explained by a finite number of mutuallyexclusive classes. LCA is particularly well suited to the aims of this study as: (i) it isexploratory in nature and data-driven, meaning that a priori assumptions are notmade concerning the number of latent classes present; and (ii) it facilitates inclu-sion of multiple measures of adherence without assuming independence among theindicators (Ahn et al., 2008).
Through an iterative process, models with an increasing number of classesare specified. Extraction of latent classes ceases when there is little empirical orsubstantive support for the inclusion of a further class. Model fit is evaluated onthe basis of goodness of fit statistical and parsimony considerations. Statistical fitindices include: the Akaike Information Criterion (AIC) (Akaike, 1974); the BayesianInformation criterion (BIC; (Schwartz, 1978); the sample-size adjusted BIC (SSABIC;Sclove, 1987); the Lo-Mendell–Rubin likelihood ratio test (LMR–LRT; Lo et al., 2001);and an entropy measure (Ramaswamy et al., 1993).
Lower values on the AIC, BIC and SSBAIC indicate better fitting models and,accordingly, extraction of latent classes ceases when these indices reach their low-est values (Nylund et al., 2007). The LMR–LRT evaluates whether a model with kcomponents is a significant improvement over a model with k – 1 components; anon-significant value (i.e., p > 0.05) indicates that the model with one fewer classprovides a more parsimonious fit to the data.
Entropy is based on the posterior probabilities and indicates classification accu-racy; values closer to unity indicate clear classifications and greater precision(Carragher and McWilliams, 2011). Classification accuracy was also evaluated byexamination of the matrix of average conditional or posterior probabilities; highdiagonal and low off-diagonal values reflect good classification quality (Croudaceet al., 2003). Final evaluation of the best-fitting model considered whether the
solution reflected coherent, distinct and conceptually meaningful groups.To avoid the issue of local maxima and to ensure that the LCA model valuesconverged on a global solution, 500 random sets of starting values and 10 final stageoptimisations were specified, and models were checked for replication of the samelog-likelihood value (Muthen and Muthen, 2007).
48 B. Larance et al. / Drug and Alcohol D
Table 1Clinical domains for assessing patient ‘stability’ and/or suitability for unsuperviseddosingas recommended in Australian opioid substitution therapy guidelines.
Suggested assessment domains Correspondingmeasures/proxiesin current study
Drug useRepeated intoxicated presentationsa Not collectedHazardous use of opioids, alcohol,benzodiazepines and/or stimulants(self-report)a
√
Liver function tests (if suspected alcoholabuse)
Not collected
Urine drug screens√
Clinical examination of injection sites Not collectedClinical examination for intoxication Not collectedPharmacist/dosing site reports ofintoxication
Not collected
Aberrant OST-related behavioursUnsanctioned injection of OST dosea √Diversion of OST dosesa √Removal of supervised OST doses
√Inability to control large supplies ofmedication
√
Non-attendance at clinical reviewappointments
√
‘Doctor shopping’√
Psychosocial stabilityCurrent chaotic or unpredictable behavioura Not collectedCurrent employment or educational activity
√(Un)stable accommodationa √Patients’ report of improved functioning Not collectedCriminal activity
√Significant destabilising life events Not collected
Co-morbidityRisk of suicide or self-harma √Significant and unstable psychiatricconditionsa
√
Significant and unstable medical conditions√
Child welfareCaring for dependent childrena √Inadequate safe storage of medicationa √
Notes: ‘Suggested assessment domains’ summarise the jurisdictional takeaway poli-cies for New South Wales, Victoria and South Australia, the over-arching nationalopioid substitution therapy policy and the Australasian Chapter of AddictionMedicine guidelines for unsupervised dosing of buprenorphine–naloxone (Henry-Edwards, Gowing et al., 2003; Australasian Chapter of Addiction Medicine, 2006;Drugs and Poisons Regulation Group, 2006; Drugs of Dependence Unit 2006;Lintzeris et al., 2006; Mental Health and Drug and Alcohol Office, 2006; Departmentof Health and Ageing, 2007; Drugs of Dependence Unit, 2007). OST = opioid substi-tution therapy.
a Contraindications for unsupervised dosing of opioid substitution therapy med-ica
2
bL
2faoa(r
2apri
cation in Australian guidelines. ‘Repeated intoxicated presentations’ and ‘currenthaotic or unpredictable behaviour’ are clinician-observed variables that were notssessed in the current study.
.5. Variables selected for inclusion in the latent class analysis
Variables that were either direct or proxy measures of indicators of patient insta-ility cited in the clinical literature (for a summary see Table 1) were included in theCA.
.5.1. Drug use. Drug use variables included regular use (defined as weekly or morerequent use in the past six months) of heroin, methamphetamine, cocaine, alcoholnd benzodiazepines. Regular use was the best available proxy for hazardous usef these drugs, identified as a contraindication to unsupervised dosing in nationalnd jurisdictional health policies. Receipt of urine drug screening in the past monthno/yes) was also included as an indicator of the level of monitoring the patienteceived.
.5.2. Medication/programmatic adherence. Indicators of medication/programmaticdherence included: injection of opioid substitution therapy medication in theast six months (no/yes); diversion of medication in the past six months (no/yes);emoval of supervised doses in the past six months (no/yes); takeaway doses usedn advance in the past month (no/yes); takeaway doses lost/misplaced in the past
ependence 142 (2014) 46–55
month (no/yes); missed clinical review appointments in the past month (no/yes);missed taking opioid substitution therapy medication doses in the past month(no/yes); saw doctors other than main opioid substitution therapy prescriber specif-ically to obtain a prescription for benzodiazepines in the past month (no/yes).
2.5.3. Psychosocial stability. Psychosocial stability variables reflected whether thepatient: was currently engaged in employment and/or education (no/yes); was cur-rently homeless or living in unstable accommodation (no/yes); had a lifetime prisonhistory (no/yes); and had been arrested in the past six months (no/yes).
2.5.4. Comorbidity. Comorbidity indicators included whether a patient: soughtmedical help for a mental health concern in the past month (no/yes); experienceda serious illness, injury or other medical condition in the past month (no/yes);and reported being hospitalised for medical or psychiatric care in the past month(no/yes).
2.5.5. Child welfare. Child welfare variables included: dependent child(ren) underthe age of 18 currently living in the care of patient (no/yes); and patient reportsof adequate safe storage of unsupervised (takeaway) opioid substitution therapymedication (no/yes).
2.6. Inclusion of covariates in the measurement model
Following identification of the best-fitting latent class solution, demographicvariables (age and gender) and length of time in current treatment episode wereincluded in the model to validate the latent typology. Odds ratios (OR) and 95%confidence intervals (CI) were used to evaluate these associations: ORs reflect theproportionate change in odds of membership of a given class, relative to the ref-erence class, associated with a one-unit change in the covariate (Carragher et al.,2009).
2.7. Predictors of unsupervised dosing of opioid substitution therapy medication
The predictors of the number of unsupervised doses received in the past monthwere examined in two multivariate linear regression models:
(i) The first model specifically examined whether latent class membership pre-dicted the number of unsupervised doses received in the past month (dependentvariable). This model controlled for key demographic variables (age, gen-der, state of residence) and treatment characteristics that may influence thelevel of dosing supervision: current opioid substitution therapy type (refer-ent: methadone); length of current treatment episode (months); length of mostrecent review appointment (min); cost of treatment to the patient; distancetravelled to attend dosing (km); being prescribed in a public clinic referent:general practice/private setting); and being dosed at a community pharmacy(referent: clinic setting). Including state of residence in the model controlledfor jurisdictional differences in supervised dosing policies; for example, SouthAustralia has more liberal unsupervised dosing policies due to a reliance onsome pharmacies that open six days per week.
(ii) The second linear regression model examined whether the individual itemsincluded in the LCA independently predicted the number of supervised dosesreceived in the past month, controlling for key demographic and treatment vari-ables (as in (1) above). Variables that could only be reported by clients receivingunsupervised doses were excluded as predictors of the number of unsuper-vised doses received in the past month (specifically, missed takeaway doses,lost/misplaced takeaway doses and safe storage of medication). These variablesare indicators of patient adherence and were included in the latent class analysis.Variables that were significant (p < 0.05) at the univariate level were includedin the multivariate model.
All linear regression models were conducted in IBM SPSS Version 22.0.
3. Results
3.1. Sample characteristics
The sample was comprised of 286 methadone patients,251 buprenorphine patients and 231 buprenorphine–naloxonepatients. Participants reported being enrolled in their cur-rent treatment episode for a median of 16 months prior tointerview (range 1–286 months). The mean daily doses ofmethadone, buprenorphine and buprenorphine–naloxone were
similar to the average daily doses found in other Aus-tralian studies (i.e., approximately 70 mg methadone and 12 mgbuprenorphine/buprenorphine–naloxone; Lintzeris et al., 2007;Winstock et al., 2008a). Substantial proportions of the sample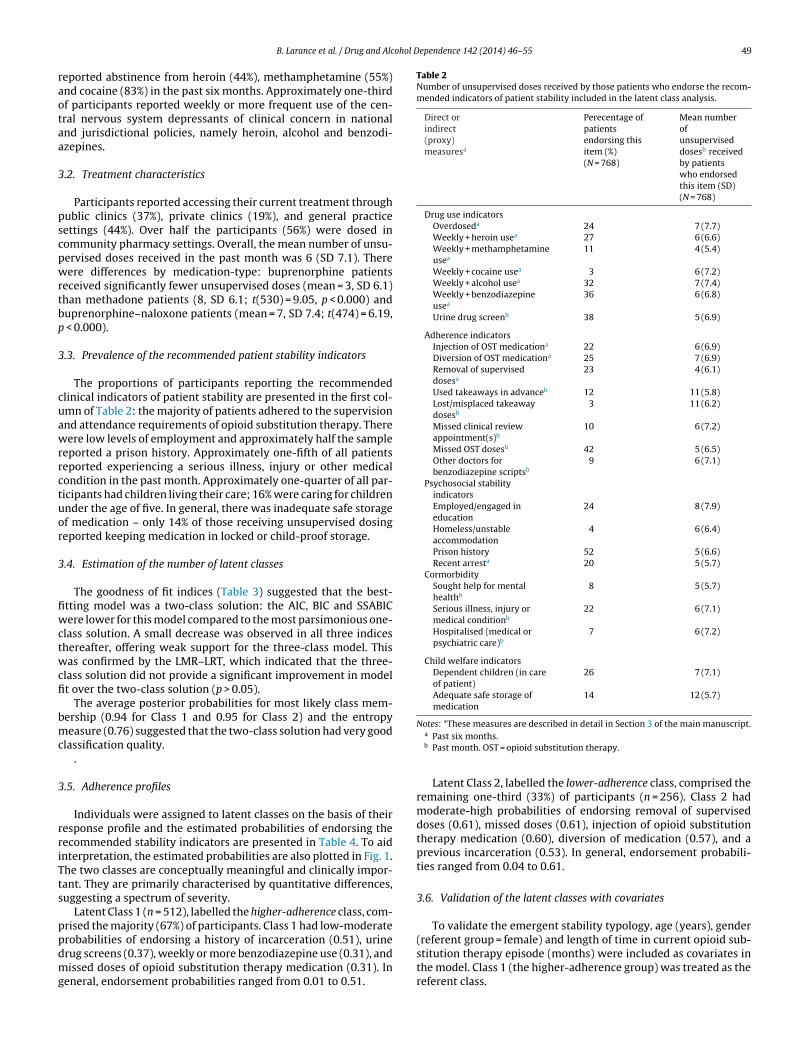
ohol Dependence 142 (2014) 46–55 49
raotaa
3
pscpwrtbp
3
cuawrrctuor
3
fiwctwcfi
bmc
3
rriTts
ppdmg
Table 2Number of unsupervised doses received by those patients who endorse the recom-mended indicators of patient stability included in the latent class analysis.
Direct orindirect(proxy)measuresa
Perecentage ofpatientsendorsing thisitem (%)(N = 768)
Mean numberofunsuperviseddosesb receivedby patientswho endorsedthis item (SD)(N = 768)
Drug use indicatorsOverdoseda 24 7 (7.7)Weekly + heroin usea 27 6 (6.6)Weekly + methamphetamineusea
11 4 (5.4)
Weekly + cocaine usea 3 6 (7.2)Weekly + alcohol usea 32 7 (7.4)Weekly + benzodiazepineusea
36 6 (6.8)
Urine drug screenb 38 5 (6.9)
Adherence indicatorsInjection of OST medicationa 22 6 (6.9)Diversion of OST medicationa 25 7 (6.9)Removal of superviseddosesa
23 4 (6.1)
Used takeaways in advanceb 12 11 (5.8)Lost/misplaced takeawaydosesb
3 11 (6.2)
Missed clinical reviewappointment(s)b
10 6 (7.2)
Missed OST dosesb 42 5 (6.5)Other doctors forbenzodiazepine scriptsb
9 6 (7.1)
Psychosocial stabilityindicatorsEmployed/engaged ineducation
24 8 (7.9)
Homeless/unstableaccommodation
4 6 (6.4)
Prison history 52 5 (6.6)Recent arresta 20 5 (5.7)
CormorbiditySought help for mentalhealthb
8 5 (5.7)
Serious illness, injury ormedical conditionb
22 6 (7.1)
Hospitalised (medical orpsychiatric care)b
7 6 (7.2)
Child welfare indicatorsDependent children (in careof patient)
26 7 (7.1)
Adequate safe storage ofmedication
14 12 (5.7)
Notes: *These measures are described in detail in Section 3 of the main manuscript.
B. Larance et al. / Drug and Alc
eported abstinence from heroin (44%), methamphetamine (55%)nd cocaine (83%) in the past six months. Approximately one-thirdf participants reported weekly or more frequent use of the cen-ral nervous system depressants of clinical concern in nationalnd jurisdictional policies, namely heroin, alcohol and benzodi-zepines.
.2. Treatment characteristics
Participants reported accessing their current treatment throughublic clinics (37%), private clinics (19%), and general practiceettings (44%). Over half the participants (56%) were dosed inommunity pharmacy settings. Overall, the mean number of unsu-ervised doses received in the past month was 6 (SD 7.1). Thereere differences by medication-type: buprenorphine patients
eceived significantly fewer unsupervised doses (mean = 3, SD 6.1)han methadone patients (8, SD 6.1; t(530) = 9.05, p < 0.000) anduprenorphine–naloxone patients (mean = 7, SD 7.4; t(474) = 6.19,
< 0.000).
.3. Prevalence of the recommended patient stability indicators
The proportions of participants reporting the recommendedlinical indicators of patient stability are presented in the first col-mn of Table 2: the majority of patients adhered to the supervisionnd attendance requirements of opioid substitution therapy. Thereere low levels of employment and approximately half the sample
eported a prison history. Approximately one-fifth of all patientseported experiencing a serious illness, injury or other medicalondition in the past month. Approximately one-quarter of all par-icipants had children living their care; 16% were caring for childrennder the age of five. In general, there was inadequate safe storagef medication – only 14% of those receiving unsupervised dosingeported keeping medication in locked or child-proof storage.
.4. Estimation of the number of latent classes
The goodness of fit indices (Table 3) suggested that the best-tting model was a two-class solution: the AIC, BIC and SSABICere lower for this model compared to the most parsimonious one-
lass solution. A small decrease was observed in all three indiceshereafter, offering weak support for the three-class model. Thisas confirmed by the LMR–LRT, which indicated that the three-
lass solution did not provide a significant improvement in modelt over the two-class solution (p > 0.05).
The average posterior probabilities for most likely class mem-ership (0.94 for Class 1 and 0.95 for Class 2) and the entropyeasure (0.76) suggested that the two-class solution had very good
lassification quality..
.5. Adherence profiles
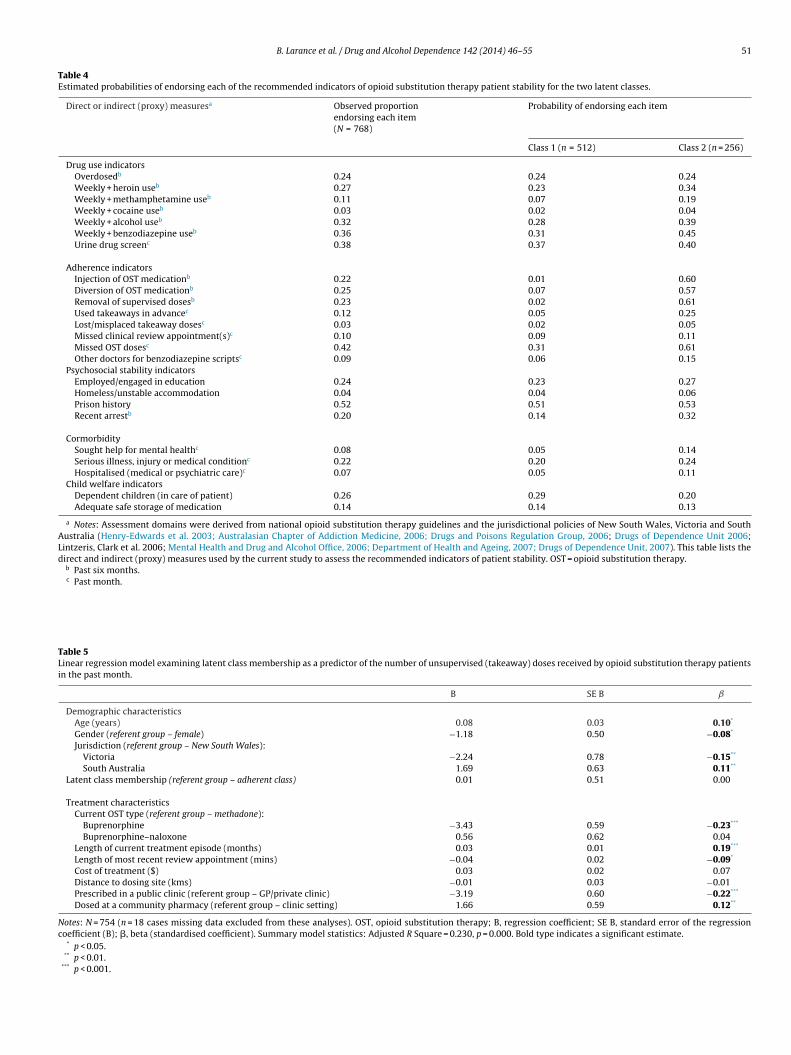
Individuals were assigned to latent classes on the basis of theiresponse profile and the estimated probabilities of endorsing theecommended stability indicators are presented in Table 4. To aidnterpretation, the estimated probabilities are also plotted in Fig. 1.he two classes are conceptually meaningful and clinically impor-ant. They are primarily characterised by quantitative differences,uggesting a spectrum of severity.
Latent Class 1 (n = 512), labelled the higher-adherence class, com-rised the majority (67%) of participants. Class 1 had low-moderate
robabilities of endorsing a history of incarceration (0.51), urinerug screens (0.37), weekly or more benzodiazepine use (0.31), andissed doses of opioid substitution therapy medication (0.31). Ineneral, endorsement probabilities ranged from 0.01 to 0.51.
a Past six months.b Past month. OST = opioid substitution therapy.
Latent Class 2, labelled the lower-adherence class, comprised theremaining one-third (33%) of participants (n = 256). Class 2 hadmoderate-high probabilities of endorsing removal of superviseddoses (0.61), missed doses (0.61), injection of opioid substitutiontherapy medication (0.60), diversion of medication (0.57), and aprevious incarceration (0.53). In general, endorsement probabili-ties ranged from 0.04 to 0.61.
3.6. Validation of the latent classes with covariates
To validate the emergent stability typology, age (years), gender
(referent group = female) and length of time in current opioid sub-stitution therapy episode (months) were included as covariates inthe model. Class 1 (the higher-adherence group) was treated as thereferent class.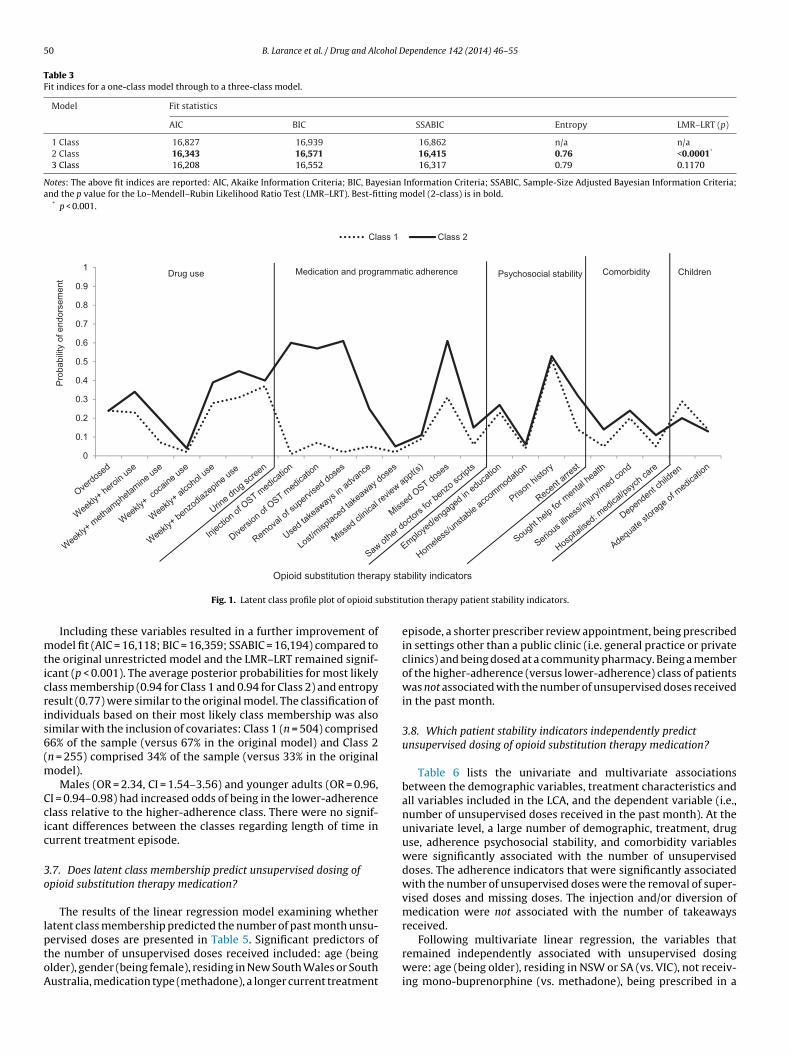
50 B. Larance et al. / Drug and Alcohol Dependence 142 (2014) 46–55
Table 3Fit indices for a one-class model through to a three-class model.
Model Fit statistics
AIC BIC SSABIC Entropy LMR–LRT (p)
1 Class 16,827 16,939 16,862 n/a n/a2 Class 16,343 16,571 16,415 0.76 <0.0001*
3 Class 16,208 16,552 16,317 0.79 0.1170
Notes: The above fit indices are reported: AIC, Akaike Information Criteria; BIC, Bayesian Information Criteria; SSABIC, Sample-Size Adjusted Bayesian Information Criteria;and the p value for the Lo–Mendell–Rubin Likelihood Ratio Test (LMR–LRT). Best-fitting model (2-class) is in bold.
* p < 0.001.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Class 1 Class 2
py sta
Drug use Medication and program matic ad heren ce Psychoso cial stabili ty Children Comorbidity
Pro
babi
lity
of e
ndor
sem
ent
ubstit
mticris6(m
Ccic
3o
lptoA
Opioid substitution thera
Fig. 1. Latent class profile plot of opioid s
Including these variables resulted in a further improvement ofodel fit (AIC = 16,118; BIC = 16,359; SSABIC = 16,194) compared to
he original unrestricted model and the LMR–LRT remained signif-cant (p < 0.001). The average posterior probabilities for most likelylass membership (0.94 for Class 1 and 0.94 for Class 2) and entropyesult (0.77) were similar to the original model. The classification ofndividuals based on their most likely class membership was alsoimilar with the inclusion of covariates: Class 1 (n = 504) comprised6% of the sample (versus 67% in the original model) and Class 2n = 255) comprised 34% of the sample (versus 33% in the original
odel).Males (OR = 2.34, CI = 1.54–3.56) and younger adults (OR = 0.96,
I = 0.94–0.98) had increased odds of being in the lower-adherencelass relative to the higher-adherence class. There were no signif-cant differences between the classes regarding length of time inurrent treatment episode.
.7. Does latent class membership predict unsupervised dosing ofpioid substitution therapy medication?
The results of the linear regression model examining whetheratent class membership predicted the number of past month unsu-
ervised doses are presented in Table 5. Significant predictors ofhe number of unsupervised doses received included: age (beinglder), gender (being female), residing in New South Wales or Southustralia, medication type (methadone), a longer current treatmentbility indicators
ution therapy patient stability indicators.
episode, a shorter prescriber review appointment, being prescribedin settings other than a public clinic (i.e. general practice or privateclinics) and being dosed at a community pharmacy. Being a memberof the higher-adherence (versus lower-adherence) class of patientswas not associated with the number of unsupervised doses receivedin the past month.
3.8. Which patient stability indicators independently predictunsupervised dosing of opioid substitution therapy medication?
Table 6 lists the univariate and multivariate associationsbetween the demographic variables, treatment characteristics andall variables included in the LCA, and the dependent variable (i.e.,number of unsupervised doses received in the past month). At theunivariate level, a large number of demographic, treatment, druguse, adherence psychosocial stability, and comorbidity variableswere significantly associated with the number of unsuperviseddoses. The adherence indicators that were significantly associatedwith the number of unsupervised doses were the removal of super-vised doses and missing doses. The injection and/or diversion ofmedication were not associated with the number of takeawaysreceived.
Following multivariate linear regression, the variables thatremained independently associated with unsupervised dosingwere: age (being older), residing in NSW or SA (vs. VIC), not receiv-ing mono-buprenorphine (vs. methadone), being prescribed in a
B. Larance et al. / Drug and Alcohol Dependence 142 (2014) 46–55 51
Table 4Estimated probabilities of endorsing each of the recommended indicators of opioid substitution therapy patient stability for the two latent classes.
Direct or indirect (proxy) measuresa Observed proportionendorsing each item(N = 768)
Probability of endorsing each item
Class 1 (n = 512) Class 2 (n = 256)
Drug use indicatorsOverdosedb 0.24 0.24 0.24Weekly + heroin useb 0.27 0.23 0.34Weekly + methamphetamine useb 0.11 0.07 0.19Weekly + cocaine useb 0.03 0.02 0.04Weekly + alcohol useb 0.32 0.28 0.39Weekly + benzodiazepine useb 0.36 0.31 0.45Urine drug screenc 0.38 0.37 0.40
Adherence indicatorsInjection of OST medicationb 0.22 0.01 0.60Diversion of OST medicationb 0.25 0.07 0.57Removal of supervised dosesb 0.23 0.02 0.61Used takeaways in advancec 0.12 0.05 0.25Lost/misplaced takeaway dosesc 0.03 0.02 0.05Missed clinical review appointment(s)c 0.10 0.09 0.11Missed OST dosesc 0.42 0.31 0.61Other doctors for benzodiazepine scriptsc 0.09 0.06 0.15
Psychosocial stability indicatorsEmployed/engaged in education 0.24 0.23 0.27Homeless/unstable accommodation 0.04 0.04 0.06Prison history 0.52 0.51 0.53Recent arrestb 0.20 0.14 0.32
CormorbiditySought help for mental healthc 0.08 0.05 0.14Serious illness, injury or medical conditionc 0.22 0.20 0.24Hospitalised (medical or psychiatric care)c 0.07 0.05 0.11
Child welfare indicatorsDependent children (in care of patient) 0.26 0.29 0.20Adequate safe storage of medication 0.14 0.14 0.13
a Notes: Assessment domains were derived from national opioid substitution therapy guidelines and the jurisdictional policies of New South Wales, Victoria and SouthAustralia (Henry-Edwards et al. 2003; Australasian Chapter of Addiction Medicine, 2006; Drugs and Poisons Regulation Group, 2006; Drugs of Dependence Unit 2006;Lintzeris, Clark et al. 2006; Mental Health and Drug and Alcohol Office, 2006; Department of Health and Ageing, 2007; Drugs of Dependence Unit, 2007). This table lists thedirect and indirect (proxy) measures used by the current study to assess the recommended indicators of patient stability. OST = opioid substitution therapy.
b Past six months.c Past month.
Table 5Linear regression model examining latent class membership as a predictor of the number of unsupervised (takeaway) doses received by opioid substitution therapy patientsin the past month.
B SE B ˇ
Demographic characteristicsAge (years) 0.08 0.03 0.10*
Gender (referent group – female) −1.18 0.50 −0.08*
Jurisdiction (referent group – New South Wales):Victoria −2.24 0.78 −0.15**
South Australia 1.69 0.63 0.11**
Latent class membership (referent group – adherent class) 0.01 0.51 0.00
Treatment characteristicsCurrent OST type (referent group – methadone):
Buprenorphine −3.43 0.59 −0.23***
Buprenorphine–naloxone 0.56 0.62 0.04Length of current treatment episode (months) 0.03 0.01 0.19***
Length of most recent review appointment (mins) −0.04 0.02 −0.09*
Cost of treatment ($) 0.03 0.02 0.07Distance to dosing site (kms) −0.01 0.03 −0.01Prescribed in a public clinic (referent group – GP/private clinic) −3.19 0.60 −0.22***
Dosed at a community pharmacy (referent group – clinic setting) 1.66 0.59 0.12**
Notes: N = 754 (n = 18 cases missing data excluded from these analyses). OST, opioid substitution therapy; B, regression coefficient; SE B, standard error of the regressioncoefficient (B); �, beta (standardised coefficient). Summary model statistics: Adjusted R Square = 0.230, p = 0.000. Bold type indicates a significant estimate.
* p < 0.05.** p < 0.01.
*** p < 0.001.

52 B. Larance et al. / Drug and Alcohol Dependence 142 (2014) 46–55
Table 6Linear regression model predicting the number of unsupervised (takeaway) doses received by opioid substitution therapypatients in the past month.
Unadjusted Adjusted
B SE B ̌ B SE B ˇ
Demographic characteristicsAge (years) 0.12 0.03 0.15*** 0.08 0.03 0.10**
Gender (referent group – female) −1.43 0.54 −0.10** −0.77 0.51 −0.05Jurisdiction (referentgroup – New South Wales):
Victoria −0.60 0.54 −0.04** −2.00 0.76 −0.13**
South Australia 2.16 0.55 0.14*** 1.45 0.66 0.09*
Treatment characteristicsCurrent OST type (referent group – methadone):
Buprenorphine −4.51 0.53 −0.30*** −3.74 0.60 −0.25***
Buprenorphine–naloxone 1.15 0.56 0.07* – – –Length of current treatment episode (months) 0.04 0.01 0.26*** 0.03 0.01 0.16***
Length of last review appointment (mins) −0.04 0.02 −0.08* −0.03 0.02 −0.07Cost of treatment ($) 0.08 0.02 0.17*** 0.03 0.02 0.06Distance to dosing site (kms) −0.02 0.04 −0.02 – – –Prescribed in a public clinic (referentgroup – GP/private clinic) −3.22 0.52 −0.22*** −2.85 0.60 −0.19***
Dosed at a community pharmacy (referent group – clinic setting) 1.74 0.51 0.12** 0.86 0.60 0.06
Drug use indicatorsOverdosed1 1.33 0.60 0.08* 1.08 0.56 0.07Weekly + heroin usea −0.77 0.58 −0.05 – – –Weekly + methamphetamine use1 −2.82 0.82 −0.13** −1.25 0.75 −0.06Weekly + cocaine use1 −0.36 1.65 −0.01 – – -Weekly + alcohol use1 1.32 0.55 0.09* 0.48 0.51 0.03Weekly + benzodiazepine usea 0.03 0.54 0.00 – – –Urine drug screenb −1.83 0.53 −0.13** −1.05 0.53 −0.07*
Adherence indicatorsInjection of OST medicationa −0.11 0.62 −0.01 – – –Diversion of OST medicationa 0.94 0.59 0.06 – – –Removal of supervised dosesa −2.88 0.61 −0.17*** −0.81 0.60 −0.05Missed clinical review appointment (s)b −0.25 0.88 −0.01 – – –Missed OST dosesb −1.90 0.52 −0.13*** −0.82 0.48 −0.06Other doctors for benzodiazepine scriptsb −0.27 0.88 −0.01 – – –
Psychosocial stability indicatorsEmployed/engaged in education 2.09 0.60 0.13*** 1.76 0.56 0.11**
Homeless/unstable accommodation −0.39 1.23 −0.01 – – –Prison history −1.73 0.51 −0.12** −1.29 0.50 −0.09*
Recent arresta −1.91 0.65 −0.11** −0.65 0.61 −0.04
ComorbiditySought help for mental healthb −0.60 0.93 −0.02 – – –Serious illness, injury or medical conditionb −0.36 0.62 −0.02 – – –Hospitalised (medical or psychiatric care)b −2.23 0.98 −0.08* −1.31 0.89 −0.05
Child welfare indicatorsDependent children (in care of patient) 0.71 0.59 0.04 – – –
Notes: OST, opioid substitution therapy; N = 739 (n = 33 cases missing data excluded from the linear regression model); B, regression coefficient; SE B, standard error of theregression coefficient; ˇ, beta (standardised coefficient). Summary model statistics for the multivariate linear regression model: Adjusted R Square = 0.269; p = 0.000. Boldtype indicates a significant estimate.
a Past six months.b Past month.
pcth
4
iIpsb
* p < 0.05.** p < 0.01.
*** p < 0.001.
rivate clinic/general practice (vs. public clinic), reporting a longerurrent treatment episode, not receiving a urine drug screen inhe past month, being currently employed and not having a prisonistory.
. Discussion
This study represents the first time LCA has been used to empir-cally examine patterns of adherence and stability among patients.
n addition, the extent to which the clinical guidelines for assessingatient suitability for unsupervised dosing match the self-reportedtability profiles of opioid substitution therapy patients has noteen previously examined in the literature.Two latent classes of patient stability were identified: (i) ahigher-adherence group who had low-moderate probabilities ofendorsing indicators of instability and (ii) a lower-adherence groupwho had moderate-high probabilities of indicators of instabil-ity. Males and younger adults have an increased risk of being inthe lower-adherence class relative to the higher-adherence class.No significant differences emerged between the classes regardinglength of time in current treatment episode.
When using ‘stability assessments’, there is a risk of assum-ing that medication and programmatic adherence are synonymous
with psychosocial stability. In this study, indicators of psychoso-cial stability and comorbidity did not necessarily co-occur withthe main non-adherent practices of concern in opioid substitutiontherapy, specifically diversion, injection and removal of supervised
ohol D
dchnesiniptpd
ooabaphwibrrl‘sie
tburpoAtdtc
teapsepmtsatoadHaous
h
B. Larance et al. / Drug and Alc
oses. This is not to detract from the importance of psychoso-ial stability and comorbidity in terms of individual and publicealth outcomes but, in the present study, these domains didot clearly differentiate those patients who were more adher-nt with the medication or programme requirements of opioidubstitution therapy from those who were less adherent (a lim-tation of assumption-free LCA models). Although our study wasot explicitly designed to evaluate the criteria used by clinicians
n determining eligibility for unsupervised dosing, our analyses ofredictors of the number of unsupervised doses did not supporthe possibility that adherence played a more important role thansychosocial stability in determining suitability for unsupervisedosing.
The current study’s findings suggest there may be groupsf patients who are being prescribed unsupervised dosesf their medication based on system-level factors (suchs jurisdictional differences in levels of methadone versusuprenorphine/buprenorphine–naloxone prescribing or the avail-bility of public clinics and community pharmacy dosing sites), orrescriber heuristics (for example, assumptions that a patient whoas been in opioid substitution therapy for a longer period of timeill be more ‘stable’), rather than actual patient practices. The find-
ng that there was no difference in the levels of unsupervised dosingy latent class membership, despite the higher-adherence groupeporting markedly lower probabilities of diversion, injection andemoval of supervised doses, is important. It highlights the chal-enges in assessing and applying the recommended indicators ofstability’: in a separate study, we found that Australian opioid sub-titution therapy prescribers reported high levels of uncertainty indentifying diversion and injection among their patients (Larancet al., 2011c).
Methadone has been prescribed in Australia sincehe 1970s; buprenorphine was introduced in 2001, anduprenorphine–naloxone in 2006. Other studies have doc-mented buprenorphine/buprenorphine–naloxone patientseceiving higher levels of supervised dosing than methadoneatients (Larance et al., 2011a). The number of unsupervised dosesf buprenorphine–naloxone allowed in jurisdictional policies inustralia is equivalent to that for methadone (and in some jurisdic-
ions, greater numbers of unsupervised buprenorphine–naloxoneoses are permitted). More research is needed to examine whetherhese observed differences in Australian prescribing practicehange over time with increasing experience of the medication(s).
Long-term supervised dosing for stable patients may impedeheir ability to engage in non drug-related activities, such asmployment, especially if extended travel is involved. It is costlynd inconvenient to both patients and clinicians, and may proverohibitive for low and middle income countries where rapidcaling-up of opioid substitution therapy is a priority (Degenhardtt al., 2008; World Health Organization, 2009). On the other hand,rogrammes from which medications are diverted to the blackarket are not beneficial to patients and often not tolerated in
he wider public arena (World Health Organization, 2009). Opioidubstitution therapy programmes will be more sustainable if therere systems to prevent or minimise diversion of opioid substitutionherapy medications, and to monitor the benefits of treatment. Opi-id dependence implies a lack of control over opioid use and therere good theoretical reasons why, at least at the start of treatment,aily supervised dosing may be beneficial (Bell et al., 2008; Worldealth Organization, 2009). Aside from assisting with medicationnd programmatic adherence, it may bring opportunities to providether types of psychosocial support. Careful selection of patients for
nsupervised dosing, therefore remains essential to protecting theafety and integrity of opioid substitution therapy.Only a few studies of supervised versus unsupervised dosingave been conducted (e.g., Bell et al., 2008, 2007; Gerra et al., 2011;
ependence 142 (2014) 46–55 53
Gunderson et al., 2010), and there is a lack of clinical trial data con-ducted with heterogeneous clinical populations. Future research isneeded to establish: (a) whether more opioid substitution therapypatients are suitable for unsupervised dosing of their medicationthan are currently being identified; (b) whether stability changeswhen patients move from supervised to unsupervised dosing; and(c) the individual and public health impacts of expanding unsu-pervised dosing for a larger number of stable patients. This studywas unable to assess whether prescribers give weight to some indi-cators of patient stability and adherence over others in clinicaldecision-making: future research may focus on how prescribersdetermine suitability for unsupervised dosing, and the extent towhich their decisions are influenced by perceived medication risks(e.g., buprenorphine vs. buprenorphine–naloxone in illicit markets)and jurisdictional frameworks.
This study is subject to a number of other limitations. Althoughobjective measures of patient stability (e.g., prescriber reports,results of urine drug screens, liver function tests and other clin-ician/pharmacist reports of patient progress) are recommendedin clinical guidelines, the current study was not able to collectthese and therefore relied on self-report. Other studies of heroinusers, however, have found self-report to be sufficiently reliable tomonitor patterns of drug use (Darke, 1998), and the prevalence ofnon-adherent practices in the current study were consistent withthose found in other studies of opioid substitution therapy patientsin Australia (Winstock and Lea, 2010; Winstock et al., 2008b). Thedata were primarily categorical in nature (i.e., yes/no to any injec-tion of OST medication in last six months) and did not give anindication of how frequently these practices occurred. The time-frames for some adherence indicators included in the LCA varied(e.g., the drug use variables used past six months timeframes, andthe programmatic adherence variables such as missing doses usedpast month timeframes). In addition, the key outcome of interestin the regression model (i.e., number of takeaways) was a ‘pastmonth’ variable – this study has assumed that past six monthsvariables may be associated with current provision of unsuper-vised dosing. These timeframes are typical and used widely toassess these concepts, and are an artefact of the measurementinstrument. The current study included two measures of drug useand three measures of psychosocial stability (see Table 1). Ideally,multiple indicators of a given construct would ensure it is beingadequately measured (including objective measures mentionedabove). Adherence and stability among opioid substitution therapypatients are dynamic and change over time; the extent to whichthe indicators in the current study predict future behaviour andpractices in treatment cannot be determined without longitudinaldata.
Despite these limitations, the present findings offer empiricalsupport for what has previously been based on clinical experi-ence. Overall, the majority of opioid substitution therapy patientsadhered with the conditions of treatment; non-adherent practicesdid occur and some practices were more prevalent than others(e.g., 42% reporting missing doses in the past month). However,the frequency of many of these practices was sporadic. For exam-ple, although 25% of patients reported diverting (selling or givingaway) their opioid substitution therapy medication in the past sixmonths, this equated to less than 5% of the total daily doses dis-pensed to the group as a whole (Larance et al., 2011a). Unsuperviseddosing among patients was not associated with adherence profile,suggesting that at present in Australia, patient adherence does notdrive decisions about levels of supervision. Rather it seems thatsystem-level factors and/or other indicators of social functioning
(such as employment or prison history) determine whether moreflexible models of treatment are provided. The opioid substitutiontherapy programme faces a number of key challenges: agreeingwhether there is an ‘acceptable’ level of diversion and injection (as
5 ohol D
tr
R
aif
C
Av
C
fo(sgaR
A
i#RiPwouooCFt
R
A
A
A
A
A
B
B
C
4 B. Larance et al. / Drug and Alc
hese practices are unlikely to be eliminated entirely) and accu-ately identifying adherent patients.
ole of the funding source
These studies were funded by Reckitt Benckiser by way ofn untied educational grant. This study’s design, conduct andnterpretation of findings are the work of the investigators. Theunder played no role in the conception or writing of this paper.
ontributors
BL undertook the analyses and wrote the first draft of the paper.ll authors contributed to the manuscript and approved the finalersion.
onflict of interest
BL, LD and RPM have received untied educational grantsrom Reckitt Benckiser for the post-marketing surveillancef buprenorphine–naloxone tablets (2006–2008) and film2012–2013), and the development of an opioid-related behaviourcale (2010). NL and RA have also received untied educationalrants from Reckitt Benckiser. All such studies’ design, conductnd interpretation of findings are the work of the investigators;eckitt Benckiser had no role in these.
cknowledgements
BL, LD, and RPM are supported by National Health and Med-cal Research Council (NHMRC) research fellowships (#1073858,1041472, and #1045318). The National Drug and Alcoholesearch Centre at the University of NSW is supported by fund-
ng from the Australian Government under the Substance Misuserevention and Service Improvements Grants Fund. This studyould not have been possible without the generous participation
f people who receive treatment for opioid dependence. This studytilised data collected for the post-marketing surveillance studiesf the diversion and injection of buprenorphine–naloxone carriedut from 2006 to 2008 by the National Drug and Alcohol Researchentre. Special thanks go to Associate Professor Tim Slade and Dr.iona Shand at the National Drug and Alcohol Research Centre forheir comments on an earlier version of this manuscript.
eferences
hn, J., McCoombs, J.S., Jung, C., Croudace, T.J., McDonnell, D., Ascher-Svanum, H.,Edgell, E.T., Shi, L., 2008. Classifying patients by antipsychotic adherence pat-terns using latent class analysis: characteristics of nonadherent groups in theCalifornia Medicaid (Medi-Cal) Program. Value Health 11, 48–56.
kaike, H., 1974. A new look at the statistical model identification. IEEE T. Automat.Control 19, 716–723.
mato, L., Davoli, M., Perucci, C.A., Ferri, M., Faggiano, F., Mattick, R.P., 2005. Anoverview of systematic reviews of the effectiveness of opiate maintenance ther-apies: available evidence to inform clinical practice and research. J. Subst. AbuseTreat. 28, 321–329.
ustralasian Chapter of Addiction Medicine, 2006. Clinical Guidelines: AssessingSuitability for Unsupervised Medication Doses in the Treatment of OpioidDependency. Adult Medicine Division, The Royal Australian College of Physi-cians, Sydney.
ustralian Institute of Health Welfare, 2008. National Opioid PharmacotherapyStatistics Annual Data collection: 2007 Report. AIHW, Canberra.
ell, J., Ryan, A., Mutch, C., Batey, R., Rea, F., 2008. Optimising the benefits of unob-served dose administration for stable opioid maintenance patients: follow-upof a randomised trial. Drug Alcohol Depend. 96, 183–186.
ell, J., Shanahan, M., Mutch, C., Rea, F., Ryan, A., Batey, R., Dunlop, A., Win-
stock, A., 2007. A randomized trial of effectiveness and cost-effectiveness ofobserved versus unobserved administration of buprenorphine–naloxone forheroin dependence. Addiction 102, 1899–1907.arragher, N., Adamson, G., Bunting, B., McCann, S., 2009. Subtypes of depression ina nationally representative sample. J. Affect. Disord. 113, 88–99.
ependence 142 (2014) 46–55
Carragher, N., McWilliams, L.A., 2011. A latent class analysis of DSM-IV criteriafor pathological gambling: Results from the National Epidemiologic Survey onAlcohol and Related Conditions. Psychiatry Res. 187, 185–192.
Croudace, T.J., Jarvelin, M.-R., Wadsworth, M.E.J., Jones, P.B., 2003. Developmentaltypology of trajectories to nighttime bladder control: epidemiologic applicationof longitudinal latent class analysis. Am. J. Epidemiol. 157, 834–842.
Darke, S., 1998. Self-report among injecting drug users: a review. Drug AlcoholDepend. 51, 253–263.
Deering, D.E.A., Sheridan, J., Sellman, J.D., Adamson, S.J., Pooley, S., Robertson, R., Hen-derson, C., 2011. Consumer and treatment provider perspectives on reducingbarriers to opioid substitution treatment and improving treatment attractive-ness. Addict. Behav. 36, 636–642.
Degenhardt, L., Bucello, C., Mathers, B., Briegleb, C., Ali, H., Hickman, M., McLaren,J., 2011. Mortality among regular or dependent users of heroin and other opi-oids: a systematic review and meta-analysis of cohort studies. Addiction 106,32–51.
Degenhardt, L., Larance, B., Mathers, B., Azim, T., Kamarulzaman, A., Mattick, R.P.,Panda, S., Toufik, A., Tyndall, M., Wiessing, L., Wodak, A., 2008. Benefits andRisks of Pharmaceutical Opioids: Essential Treatment and Diverted Medication.A Global Review of Availability, Extra-Medical Use, Injection and the Associa-tion With HIV. Thematic Paper Undertaken On Behalf of the Reference Group tothe United Nations on HIV and Injecting Drug Use National Drug And AlcoholResearch Centre. University of New South Wales, Sydney.
Department of Health and Ageing, 2007. National Pharmacotherapy Policy for PeopleDependent on Opioids. Commonwealth of Australia, Canberra.
Drugs and Poisons Regulation Group, 2006. Policy for Maintainance Pharmacothe-rapy for Opioid Dependence. Drugs Policy and Services Branch. Department ofHuman Sciences, State of Victoria.
Drugs of Dependence Unit, 2006. Policy relating to the use of Suboxone (buprenor-phine and naloxone) and Subutex (buprenorphine) in opioid dependencetreatment programs. Drug and Alcohol Services South Australia, Governmentof South Australia.
Drugs of Dependence Unit, 2007. Policy for Non-supervised Dosing of Methadoneand Buprenorphine in Opioid Dependence Treatment Programs. Drug and Alco-hol Services South Australia, Government of South Australia.
Dunbar, J., 1984. Adherence measures and their utility. Control Clin. Trials 5,515–521.
Gerra, G., Saenz, E., Busse, A., Maremmani, I., Ciccocioppo, R., Zaimovic, A., Gerra,M.L., Amore, M., Manfredini, M., Donnini, C., Somaini, L., 2011. Supervised dailyconsumption, contingent take-home incentive and non-contingent take-homein methadone maintenance. Prog. Neuropsychopharmacol. Biol. Psychiatry 35,483–489.
Gowing, L., Farrell, M., Bornemann, R., Sullivan, L.E., Ali, R., 2011.Oral substitution treatment of injecting drug users for preven-tion of HIV infection. Cochrane Database Syst. Rev. 10, CD004145,http://dx.doi.org/10.1002/14651858.CD004145.pub4.
Gunderson, E.W., Wang, X.-Q., Fiellin, D.A., Bryan, B., Levin, F.R., 2010. Unobservedversus office buprenorphine/naloxone induction: a pilot randomised clinicaltrial. Addict. Behav. 35, 537–540.
Hall, W., 1996. Methadone Maintenance Treatment as a Crime Control Measure,Crime and Justice Bulletin No. 29. NSW Bureau of Crime Statistics and Research,Sydney.
Hansen, R.A., Kim, M.M., Song, L., Tu, W., Wu, J., Murray, M.D., 2009. Comparisonof methods to assess medication adherence and classify nonadherence. Ann.Pharmacother. 43, 413–422.
Haskew, M., Wolff, K., Dunn, J., Bearn, J., 2008. Patterns of adherence to oralmethadone: implications for prescribers. J. Subst. Abuse Treat. 35, 109–115.
Haynes, R.B., Ackloo, E., Sahota, N., McDonald, H.P., Yao, X., 2008. Interventionsfor enhancing medication adherence. Cochrane Database Syst. Rev., CD000011,http://dx.doi.org/10.001002/14651858.CD14000011.pub14651853.
Henry-Edwards, S., Gowing, L., White, J., Ali, R., Bell, J., Brough, R., Lintzeris, N., Ritter,A., Quigley, A., 2003. Clinical guidelines and procedures for the use of methadonein the maintenance treatment of opioids dependence. Australian GovernmentDepartment of Health and Ageing, Commonwealth of Australia.
Julius, R.J., Novitsky, M.A.J., Dubin, W.R., 2009. Medication adherence: a reviewof the literature and implications for clinical practice. J. Psychiatr. Pract. 15,34–44.
Larance, B., Degenhardt, L., Lintzeris, N., Bell, J., Winstock, A., Dietze, P.,Mattick, R., Ali, R., Horyniak, D., 2011a. Post-marketing surveillance ofbuprenorphine–naloxone in Australia: diversion, injection and adherence withsupervised dosing. Drug Alcohol Depend. 118, 265–273.
Larance, B., Degenhardt, L., Lintzeris, N., Winstock, A., Mattick, R., 2011b. Definitionsrelated to the use of pharmaceutical opioids: extramedical use, diversion, non-adherence and aberrant medication-related behaviours. Drug Alcohol Rev. 30,236–245.
Larance, B., Degenhardt, L., O’Brien, S., Lintzeris, N., Winstock, A., Mattick, R.P., Bell, J.,Ali, R., 2011c. Prescribers’ perceptions of the diversion and injection of medica-tion by opioid substitution treatment patients. Drug Alcohol Rev. 30, 613–620.
Lintzeris, N., Clark, N., Winstock, A., Dunlop, A., Gowing, L., Ritter, A., Bell, J., Quigley,A.J., Mattick, R.P., Monheit, B., White, J., 2006. National clinical guidelines andprocedures for the use of buprenorphine in the maintenance treatment of opoid
dependence. Australian Government National Drug Strategy, Commonwealth ofAustralia.Lintzeris, N., Pritchard, E., Sciacchitano, L., 2007. Investigation of Methadone Dosingin Victoria: Factors Influencing Dosing Levels. Turning Point Alcohol and DrugCentre, Melbourne.

ohol D
L
M
M
M
M
M
M
N
P
B. Larance et al. / Drug and Alc
o, Y., Mendell, N., Rubin, D., 2001. Testing the number of components in a normalmixture. Biometrika 88, 767–778.
adden, A., Lea, T., Bath, N., Winstock, A.R., 2008. Satisfaction guaranteed? Whatclients on methadone and buprenorphine think about their treatment. DrugAlcohol Rev. 27, 671–678.
attick, R.P., Breen, C., Kimber, J., Davoli, M., 2009. Methadonemaintenance therapy versus no opioid replacement therapy foropioid dependence. Cochrane Database Syst. Rev. 2, CD002209,http://dx.doi.org/10.1002/14651858.CD002209.pub2.
attick, R.P., Kimber, J., Breen, C., Davoli, M., 2008. Buprenorphine main-tenance versus placebo or methadone maintenance for opioid depend-ence. Cochrane Database Syst. Rev. 2008, CD002207, http://dx.doi.org/10.1002/14651858.CD002207.pub3.
cCutcheon, A.L., 1987. Latent Class Analysis. Cambridge University Press,Cambridge.
ental Health and Drug and Alcohol Office, 2006. New South Wales OpioidTreatment Program: Clinical Guidelines for Methadone and BuprenorphineTreatment of Opioid Dependence. NSW Department of Health, Sydney.
uthen, L.K., Muthen, B.O., 2007. Mplus User’s Guide (1998–2007), fifth ed. Muthén& Muthén, Los Angeles, CA.
ylund, K.L., Asparouhov, T., Muthén, B.O., 2007. Deciding on the number of classes
in latent class analysis and growth mixture modeling: a Monte Carlo simulationstudy. Struct. Equ. Model. 14, 535–569.adaiga, Z., Subata, E., Vanagas, G., 2007. Outpatient methadone maintenancetreatment program. Quality of life and health of opioid-dependent persons inLithuania. Medicina (Kaunas) 43, 235–241.
ependence 142 (2014) 46–55 55
Ramaswamy, V., DeSarbo, W.S., Reibstein, D.J., Robinson, W.T., 1993. An empiri-cal pooling approach for estimating marketing mix elasticities with PIMS data.Market. Sci. 12, 103–124.
Ritter, A., Di Natale, R., 2005. The relationship between take-away methadone poli-cies and methadone diversion. Drug Alcohol Rev. 24, 347–352.
Schwartz, G., 1978. Estimating the dimension of a model. Ann. Statist. 6,461–464.
Sclove, L., 1987. Application of model-selection criteria to some problems in multi-variate analysis. Psychometrika 52, 333–343.
Strang, J., Hall, W., Hickman, M., Bird, S.M., 2010. Impact of supervision of methadoneconsumption on deaths related to methadone overdose (1993–2008): analysesusing OD4 index in England and Scotland. BMJ 341, c4851.
Ward, J., Mattick, R.P., Hall, W., 1998. Methadone Maintenance Treatment and OtherOpioid Replacement Therapies. Harwood Academic Publishers, Amsterdam.
Winstock, A., Lea, T., 2010. Diversion and injection of methadone and buprenorphineamong clients in public opioid treatment clinics in New South Wales, Australia.Subst. Use Misuse 45, 240–252.
Winstock, A., Lea, T., Madden, A., Bath, N., 2008a. Knowledge about buprenorphineand methadone among those receiving treatment for opioid dependence. DrugsEduc. Prev. Pol. 15, 395–409.
Winstock, A., Lea, T., Sheridan, J., 2008b. Prevalence of diversion and injection of
methadone and buprenorphine among clients receiving opioid treatment atcommunity pharmacies in New South Wales, Australia. Int. J. Drug Policy 19,450–458.World Health Organization, 2009. Guidelines For The Psychosocially Assisted Phar-macological Treatment Of Opioid Dependence. WHO Press, Geneva.




















