A genome-wide scan for loci influencing adolescent cannabis dependence symptoms: Evidence for...
10
ORIGINAL ARTICLE A Genome-Wide Search for Quantitative Trait Loci That Influence Antisocial Drug Dependence in Adolescence Michael C. Stallings, PhD; Robin P. Corley, PhD; Briana Dennehey, PhD; John K. Hewitt, PhD; Kenneth S. Krauter, PhD; Jeffrey M. Lessem, PhD; Susan K. Mikulich-Gilbertson, PhD; Soo Hyun Rhee, PhD; Andrew Smolen, PhD; Susan E. Young, PhD; Thomas J. Crowley, MD Background: Among adolescents, externalizing prob- lem behavior and substance use disorders are often co- morbid. Familial influences, including shared genetic risk factors, may account for part of this comorbidity. Previ- ously we reported 2 chromosomal regions (3q24-3q25 and 9q34) likely to contain genes that influence sub- stance dependence vulnerability (DV) in adolescence. Objectives: To identify quantitative trait loci (QTLs) that influence externalizing problem behavior in adoles- cence and to determine whether any identified QTL over- lap chromosomal regions that influence DV. Design: Regression-based QTL mapping procedures de- signed for selected sibling pair samples. Setting: Patient probands were drawn from consecu- tive admissions to residential and outpatient (milieu- type) treatment facilities for substance abuse and deli- quency operated by the University of Colorado; most of these patients were referred for treatment by juvenile jus- tice or social service agencies. Patients: A total of 249 proband-sibling pairs from 191 families were selected for the study. Patient probands were 13 to 19 years of age; siblings of the probands ranged in age from 12 to 25 years. Main Outcome Measures: A community-based sample of 4493 adolescents and young adults was used to de- fine clinically significant, heritable, age- and sex- normed indexes of DV, conduct disorder symptoms (CDS), and a composite index of antisocial substance de- pendence (DV CDS). Siblings and parents were geno- typed for 374 microsatellite markers distributed across the 22 autosomes (mean intermarker distance, 9.2 cen- timorgans). Results: For both DV and CDS, there was evidence of linkage to the same region on chromosome 9q34, as well as to 3q24-3q25 for DV, and a novel region on chromo- some 17q12 for CDS. Our composite index (DV CDS) yielded the strongest evidence for linkage (logarithm of odds = 2.65) to the chromosome 9q34 region. Conclusion: These results provide the first evidence of a potential molecular genetic basis for the comorbidity between DV and antisocial behavior. Arch Gen Psychiatry. 2005;62:1042-1051 A MONG ADOLESCENTS, CON- duct disorder (CD) and substance use disorders (SUDs) are frequently co- morbid in both clinical 1-7 and general population samples. 8-11 A re- cent meta-analysis of 51 twin and adop- tion studies suggests that approximately 40% of the variation in adolescent and adult antisocial behavior can be ac- counted for by genetic factors, 12 and large- scale twin studies have estimated the heri- tability of CD at 24% to 74% 13 and 70%. 14 Family, twin, and adoption studies sug- gest that genetic variation influences the risk of abuse and dependence on alcohol and nicotine, 15-25 and studies of illicit drug abuse and dependence also suggest im- portant genetic and familial contribu- tions to risk for the development of illicit SUDs. 26-35 Although the etiologic mechanisms un- derlying the co-occurrence of CD and SUDs remain unclear, support is increasing for the hypothesis that common genetic risks may explain part of their comorbidity. 36-39 More- over, this common risk may extend to a broader array of disinhibitory psychopatho- logic features in general. 40-53 Because of the strong comorbidity and the evidence that genetic risks contribute to both CD and SUDs, we have hypoth- esized that common genetic influences may contribute to these disorders. Our analytical approach requires probands who are highly selected for our phenotypes of interest (ie, extreme scoring). We have spe- cifically recruited a selected sample of ado- Author Affiliations: Institute for Behavioral Genetics (Drs Stallings, Corley, Hewitt, Lessem, Rhee, Smolen, and Young) and Department of Molecular, Cellular, and Developmental Biology (Drs Dennehey and Krauter), University of Colorado, Boulder; and Division of Substance Dependence, University of Colorado School of Medicine, Denver (Drs Mikulich-Gilbertson and Crowley). (REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM 1042 ©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.com Downloaded from
Transcript of A genome-wide scan for loci influencing adolescent cannabis dependence symptoms: Evidence for...

ORIGINAL ARTICLE
A Genome-Wide Search for Quantitative Trait LociThat Influence Antisocial Drug Dependencein AdolescenceMichael C. Stallings, PhD; Robin P. Corley, PhD; Briana Dennehey, PhD; John K. Hewitt, PhD; Kenneth S. Krauter, PhD;Jeffrey M. Lessem, PhD; Susan K. Mikulich-Gilbertson, PhD; Soo Hyun Rhee, PhD; Andrew Smolen, PhD;Susan E. Young, PhD; Thomas J. Crowley, MD
Background: Among adolescents, externalizing prob-lem behavior and substance use disorders are often co-morbid. Familial influences, including shared genetic riskfactors, may account for part of this comorbidity. Previ-ously we reported 2 chromosomal regions (3q24-3q25and 9q34) likely to contain genes that influence sub-stance dependence vulnerability (DV) in adolescence.
Objectives: To identify quantitative trait loci (QTLs)that influence externalizing problem behavior in adoles-cence and to determine whether any identified QTL over-lap chromosomal regions that influence DV.
Design: Regression-based QTL mapping procedures de-signed for selected sibling pair samples.
Setting: Patient probands were drawn from consecu-tive admissions to residential and outpatient (milieu-type) treatment facilities for substance abuse and deli-quency operated by the University of Colorado; most ofthese patients were referred for treatment by juvenile jus-tice or social service agencies.
Patients: A total of 249 proband-sibling pairs from 191families were selected for the study. Patient probands were
13 to 19 years of age; siblings of the probands ranged inage from 12 to 25 years.
Main Outcome Measures: A community-based sampleof 4493 adolescents and young adults was used to de-fine clinically significant, heritable, age- and sex-normed indexes of DV, conduct disorder symptoms(CDS), and a composite index of antisocial substance de-pendence (DV � CDS). Siblings and parents were geno-typed for 374 microsatellite markers distributed acrossthe 22 autosomes (mean intermarker distance,9.2 cen-timorgans).
Results: For both DV and CDS, there was evidence oflinkage to the same region on chromosome 9q34, as wellas to 3q24-3q25 for DV, and a novel region on chromo-some 17q12 for CDS. Our composite index (DV � CDS)yielded the strongest evidence for linkage (logarithm ofodds=2.65) to the chromosome 9q34 region.
Conclusion: These results provide the first evidence ofa potential molecular genetic basis for the comorbiditybetween DV and antisocial behavior.
Arch Gen Psychiatry. 2005;62:1042-1051
A MONG ADOLESCENTS, CON-duct disorder (CD) andsubstance use disorders(SUDs) are frequently co-morbid in both clinical1-7
and general population samples.8-11 A re-cent meta-analysis of 51 twin and adop-tion studies suggests that approximately40% of the variation in adolescent andadult antisocial behavior can be ac-counted for by genetic factors,12 and large-scale twin studies have estimated the heri-tability of CD at 24% to 74%13 and 70%.14
Family, twin, and adoption studies sug-gest that genetic variation influences therisk of abuse and dependence on alcoholand nicotine,15-25 and studies of illicit drugabuse and dependence also suggest im-portant genetic and familial contribu-
tions to risk for the development of illicitSUDs.26-35
Although the etiologic mechanisms un-derlying the co-occurrence of CD and SUDsremain unclear, support is increasing for thehypothesis that common genetic risks mayexplain part of their comorbidity.36-39 More-over, this common risk may extend to abroader array of disinhibitory psychopatho-logic features in general.40-53
Because of the strong comorbidity andthe evidence that genetic risks contributeto both CD and SUDs, we have hypoth-esized that common genetic influencesmay contribute to these disorders. Ouranalytical approach requires probands whoare highly selected for our phenotypes ofinterest (ie, extreme scoring). We have spe-cifically recruited a selected sample of ado-
Author Affiliations: Institutefor Behavioral Genetics(Drs Stallings, Corley, Hewitt,Lessem, Rhee, Smolen, andYoung) and Department ofMolecular, Cellular, andDevelopmental Biology(Drs Dennehey and Krauter),University of Colorado,Boulder; and Division ofSubstance Dependence,University of Colorado Schoolof Medicine, Denver(Drs Mikulich-Gilbertson andCrowley).
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1042
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

lescent patient probands and their families (including sib-ling pairs) from consecutive admissions to treatmentprograms that specialize in the treatment of adolescentswith SUDs and comorbid antisocial behavioral prob-lems. In a recent genome-wide search for quantitative traitloci (QTLs) underlying substance dependence vulner-ability (DV),54 we reported regions on chromosome 3q24-3q25 and chromosome 9q34 that may confer risk for sub-stance dependence. In the same adolescent sample we nowextend this work, searching for chromosomal regions thatmay be involved in comorbid SUDs and CD. Specifi-cally, the gene-mapping goals of the present study wereto identify QTLs that influence adolescent CD and to de-termine whether there are overlapping chromosomal re-gions likely to contain genes that influence comorbid risk.Indication of shared chromosomal regions would pro-vide the first evidence of a molecular genetic basis forthe comorbidity between these common disorders.
METHODS
ASCERTAINMENT OF CLINICAL ANDCOMMUNITY SAMPLES
Details regarding sample ascertainment and inclusion and ex-clusion criteria for the adolescent clinical and community sampleshave been described previously.54 Patient probands were drawnfrom consecutive admissions to residential and outpatient (milieu-type) treatment facilities for substance abuse and deliquency op-erated by the University of Colorado; most of these patients werereferred for treatment by juvenile justice or social service agen-cies. The clinical sample included 249 proband-sibling pairs from191 families. Probands were 13 to 19 years of age (mean±SD age,15.9±1.3 years) at the time of assessment. The ethnicity distri-bution was 7.8% African American, 36.5% Hispanic, 52.1% white,and 3.6% other. The community sample included 4493 indi-viduals 12 to 25 years of age (mean±SD age, 15.9±2.1 years)drawn from the Colorado Twin Registry,55 the Colorado Adop-tion Project,56 and the Colorado Adolescent Substance Abuse fam-ily study.57 The ethnicity distribution of the community samplewas 81.6% white, 12.1% Hispanic, 2.3% African American, and4% of mixed or unknown ethnicity. We have previously re-ported55 that substance use patterns and prevalence rates in thecommunity sample are comparable to those reported in na-tional studies.58,59
ASSESSMENT
Participants were administered an extensive battery of cogni-tive, psychiatric, and sociodemographic assessments that in-cluded structured diagnostic interviews and self-report ques-tionnaires in the treatment facilities (probands) or homes(siblings) as described previously.54 All participants who wereat least 18 years of age gave informed written consent to par-ticipate. For juveniles, a parent or legal guardian gave writtenconsent for participation, and assent was obtained from all ju-veniles. All research protocols and consent forms were ap-proved by the institutional review boards of the University ofColorado, Denver (for proband assessment), and the Univer-sity of Colorado, Boulder (for assessments of all other rela-tives), and all subjects were paid for participation.
Substance use data were obtained using the Composite In-ternational Diagnostic Interview-Substance Abuse Module(CIDI-SAM).54,60 Conduct disorder was assessed using the Di-agnostic Interview Schedule for Children (DISC) for all pa-
tient probands. Conduct disorder for siblings younger than 19years was assessed using the DISC, whereas siblings 19 yearsor older were assessed using the Diagnostic Interview Sched-ule (DIS). Participants recruited between 1993 and 1997 wereassessed with DSM-III-R versions of the DISC61 and DIS.62 Par-ticipants recruited between 1998 and 2001 were assessed us-ing DSM-IV versions of the DISC63 and DIS,64 modified for scor-ing both DSM-III-R and DSM-IV symptoms and diagnoses.Adjustments for potential instrument effects are described herein.
PHENOTYPE DEFINITIONS
We used DSM criterion (symptom) counts to create 3 quantita-tive phenotypes to assess DV, CD symptoms (CDS), and a com-posite index of antisocial substance dependence (DV�CDS). Themean number of DSM-IV dependence symptoms (ie, total symp-tom count across all classes of substances divided by the num-ber of substances used repeatedly) was used as our index of DV(see Stallings et al54 for details regarding the validity of this in-dex), and the total number of DSM-III-R CD symptoms was usedas our quantitative measure of CDS. (DSM-III-R criteria were usedfor CDS because DSM-IV versions of the DISC and DIS assess-ments were unavailable at the outset of the study; the version ofthe CIDI-SAM that was used provided DSM-IV symptom countsfor substance dependence.)
Because of marked age trends on these indexes in our com-munity sample, the measures were age and sex corrected us-ing standard regression procedures and then standardized withinsex groups to express scores in our selected (clinical) siblingsample in relation to the population means and variability foradolescents and young adults. In addition, CDS scores were ob-tained from the DISC for probands and younger siblings butfrom the DIS for older siblings, and 2 versions of the DISC andDIS assessments were used. To account for any instrument ef-fects that may not have been corrected for by our age adjust-ments, interview type was dummy coded and used to obtainresidual CDS scores. (Instrument type accounted for only 1.2%of the variance in our age- and sex-corrected CDS scores in thecommunity sample.)
Standardized DV and CDS scores were summed to form acomposite index of antisocial substance dependence(DV�CDS). This index was then subsequently restandard-ized so that the metric of the composite (sum) index was thesame as for our individual measures of DV and CDS (ie, meansof 0 and SDs of 1 in our community sample).
DNA COLLECTION AND GENOTYPING
The methods used for preparation of genomic DNA and geno-typing of the 374 microsatellite markers (ABI PRISM LMS2-MD10 panels; PE Biosystems, Foster City, Calif ) have been de-scribed previously.54 For 47% of the families, genotypes wereavailable from both parents; 49% included genotypes from 1parent, and for 4% of the sibships, no parental genotypes wereavailable. Sibships included 147 pairs, 35 trios, 7 sibships of 4,and 3 sibships of 5. Sex-averaged marker maps were obtainedfrom the Marshfield Center for Medical Genetics database (http://research.marshfieldclinic.org/genetics), and allele frequen-cies were estimated from the full sample using Merlin.65 Table1gives marker information for each chromosome and meansacross the 22 autosomes.
VALIDATION OF GENOTYPES ANDRELATIONSHIP STATUS
Validation of genotypes and family relationships was per-formed with the Graphical Relationship Representation pro-gram,66 Pedstats,67 and Merlin.65 Details are described in our
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1043
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

previous communication.54 Genetic analysis indicated 28individuals in whom paternity and/or full-sibling status wasquestioned. In addition, 1 proband did not have completeCIDI-SAM and DISC assessments, and 11 individuals weregenotyped for less than 50% of the markers. These individualswere removed from the sample before linkage analysis, result-ing in a final sample of 249 sibling pairs. Twelve markers wereomitted for low call rates; the mean call rate for the markersused was approximately 85%. Estimated marker haplotypesfrom Merlin indicated no evidence for excessive recombinationevents, and few genotypes (0.07%) were flagged as highlyunlikely. Genotypes flagged as unlikely were not concentratedamong certain markers, individuals, or families, and analysesthat removed unlikely genotypes yielded essentially identicalresults to full-sample analyses, so these genotypes wereretained. Identity-by-descent (IBD) sharing for all sibpairs wasestimated at 1-centimorgan (cM) intervals (and also at eachmarker for single-point analyses) across the genome (auto-somes) using Merlin.
STATISTICAL ANALYSIS
The regression-based sibpair linkage method that we used wasproposed by Fulker et al68,69 as an extension of the methods origi-nally developed by Fulker, DeFries, and colleagues70 for theanalysis of selected twin data. The rationale of the DeFries-Fulker (DF) linkage analysis for selected sibling samples is thatthe siblings of selected probands should demonstrate differen-tial regression toward the population mean on a quantitativetrait commensurate with the proportion of marker alleles theyshare IBD with the proband, given that a QTL is linked to aparticular chromosomal marker. The following regression modelwas fit to data from 249 proband-sibling pairs:
C=��b1P�b2(�i)=ε,
where C is the quantitative score of the proband’s sibling, P isthe proband’s score, �i is the estimated mean proportion of al-leles shared IBD for the sibling pair at location (i) in the ge-nome, and � and ε are the regression constant and distur-bance term, respectively. A t test of the significance of the b2
regression coefficient provides a test of linkage, which can beexpressed as an approximate logarithm of odds (LOD) score(t2/[2�natural log of 10]) . We used the DF regression–basedQTL linkage analysis as operationalized in QMS2,71 a series ofintegrated SAS macros available at http://ibgwww.colorado.edu/~lessem/software/qms2.html.
RESULTS
SAMPLE CHARACTERISTICS
The percentages of participants who met the criteria forDSM diagnoses of substance dependence (DSM-IV) andCD (DSM-III-R) are given in Table 2. Note the greaterprevalence of substance dependence in the clinical pro-bands and their siblings compared with community ado-lescents. There is substantial polysubstance use, with morethan half of the clinical probands (56.7%) meeting crite-ria for 2 or more substance dependence diagnoses. Sib-lings of the clinical probands also show substantially higherrates of substance dependence and dependence on mul-tiple substances than community adolescents. Rates of CDare substantially higher among our clinical probands andtheir siblings compared with community adolescents.
Table 1. Marker Information
ChromosomeNo.
No. ofMarkers
MeanDistance,
cM*Mean
Heterozygosity†
MeanMultipoint
Information‡
1 31 9.38 78.26 0.552 30 8.73 79.98 0.573 23 9.84 82.05 0.544 22 9.63 77.84 0.515 22 9.23 79.46 0.566 20 9.52 78.94 0.517 19 9.09 81.74 0.578 14 11.79 76.91 0.539 21 7.70 76.39 0.60
10 19 9.38 78.27 0.5911 17 9.06 74.52 0.5512 18 9.68 79.38 0.5713 14 8.04 76.77 0.5614 13 10.65 74.34 0.5415 13 8.87 79.28 0.5716 13 9.62 77.82 0.5417 15 8.99 76.33 0.5518 13 10.50 78.32 0.5419 12 8.09 79.75 0.5820 13 7.93 79.52 0.5721 5 9.04 68.36 0.4722 7 7.91 76.14 0.52
Total 374 9.24 78.29 0.55
Abbreviation: cM, centimorgans.*Mean intermarker distance for each chromosome.†Mean heterozygosity averaged across the markers on each chromosome.‡Mean multipoint information averaged across 1-cM intervals for each
chromosome from Merlin.
Table 2. Diagnostic Prevalences and Descriptive Statisticsfor Quantitative Measures in the Selected Siblingand Community Samples
Probands SiblingsCommunity
Sample
Prevalence by DSMdiagnosis, %*
Tobacco dependence 56.6 28.1 9.0Alcohol dependence 36.1 9.6 3.9Marijuana dependence 60.7 17.6 4.5Other dependence† 26.7 9.2 1.9�2 Dependence
diagnoses56.7 14.4 5.3
CD 89.5 31.7 10.0Quantitative measures,
mean (SD)DV 2.27 (1.49) 0.53 (1.38) −0.02 (0.96)CDS 3.11 (1.64) 1.06 (1.69) 0 (1)DV � CDS 3.15 (1.49) 0.97 (1.58) 0 (1)
Phenotypic correlation(rDV,CD)
0.31 0.47 0.49
Heritability of DV . . . . . . 0.34Heritability of CDS . . . . . . 0.38Genetic correlation
(Rg[DV,CDS]). . . . . . 0.47
Abbreviations: CD, conduct disorder; CDS, CD symptoms; DV, dependencevulterability; DV � CDS, composite (sum) index of antisocial substancedependence.
*DSM-IV substance dependence diagnosis and DSM-III-R conductdisorder diagnosis.
†Illicit substance other than marijuana; means are in standard deviationunits standardized for the community adolescent sample.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1044
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

On average, our clinical probands score 2 to 3 SDshigher than community adolescents on our measures ofDV, CDS, and DV�CDS. Siblings of the probands showregression to the population mean but score approxi-mately half an SD higher than community adolescentson DV and nearly 1 SD higher for CDsx and DV�CDS.Means and SDs in the community sample are 0 and 1,respectively, because scores were standardized on thatsample. The mean and SD for DV differ slightly fromthose values because recruitment of the communitysample is ongoing and the community sample is nowlarger (N=4493 vs 3676) than for our previous report.54
For consistency with that investigation, the standardiza-tion of DV was not recalculated for the larger sample.
Our measures of DV and CDsx correlate substan-tially (r=0.49) in our community adolescent sample(Table 2). As expected, this correlation is attenuated inour highly selected clinical probands. Biometrical analy-ses of our community twin sample indicate that thesemeasures are heritable (h2
DV=0.34; h2CDsx=0.38), and the
genetic correlation between them was estimated atRg=0.47.
SINGLE-POINT LINKAGE RESULTS
Table3 gives the 29 chromosomal markers (several con-tiguous) where single-point DF regression analyses re-sulted in a significant t value (P�.05). Reported P val-ues are actual values obtained without adjustment formultiple testing. At 3 marker locations (3q24-3q25, 9q34,and 17q12), single-point LOD scores exceeded 2.0 (cor-responding to t values �3.03 ). Single-point analysis in-cludes only informative sibling pairs at a given markerlocation, so some caution in interpretation is advised giventhat the number of informative pairs varies for each analy-sis. Despite this limitation, an advantage of single-pointresults is that they do not depend on a correct markermap and can be less sensitive to genotyping errors.72
MULTIPOINT RESULTS
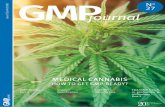
Figure 1 shows LOD score plots from multipoint DFregression analyses performed at 1-cM intervals acrossthe genome (22 autosomes). The advantage of multi-point analyses compared with single-point evaluations
Table 3. Statistically Significant Single-Point Linkage Results (t Values)
ChromosomeNo. Marker Heterozygosity
Position,cM* DV† CDS† DV � CDS†
No. of InformativeSibling Pairs
1 D1S214 79.5 14.04 1.72‡ 482 D2S347 85.2 131.51 1.78‡ 1232 D2S338 82.3 250.54 1.88‡ 1.79‡ 1323 D3S1279 78.1 169.60 2.53§ 1.92‡ 1553 D3S1614 85.4 177.75 3.21� 2.34‡ 3.27� 1644 D4S424 82.5 144.56 1.79‡ 2.01‡ 1615 D5S410 68.1 156.47 1.75‡ 1305 D5S422 86.0 164.19 2.24‡ 1576 D6S446 69.1 189.00 2.10‡ 2.17‡ 1297 D7S661 75.0 155.10 1.76‡ 1609 D9S1826 60.1 159.61 1.89‡ 1.99‡ 2.42§ 1129 D9S1838 89.6 163.84 2.69§ 2.58§ 3.15§ 215
10 D10S189 75.1 19.00 1.80‡ 15411 D11S902 81.5 21.47 2.34‡ 2.06‡ 11611 D11S905 42.9 51.95 2.22‡ 2413 D13S171 68.0 25.08 2.08‡ 10313 D13S159 85.9 79.49 2.08‡ 7915 D15S994 72.3 40.25 1.69‡ 9417 D17S798 56.8 53.41 3.03§ 2.49§ 6117 D17S787 83.7 74.99 1.86‡ 18718 D18S478 59.0 52.86 1.78‡ 12119 D19S209 89.8 10.97 1.85‡ 17419 D19S220 87.4 62.03 1.97‡ 1.88‡ 19619 D19S420 83.2 66.30 1.72‡ 18819 D19S902 84.0 72.72 1.71‡ 18820 D20S112 80.8 39.25 2.52§ 1.86‡ 2.45§ 17820 D20S107 83.1 55.74 2.30‡ 15320 D20S178 77.1 66.16 1.90‡ 2.15‡ 12720 D20S196 87.3 75.01 2.02‡ 1.92‡ 169
Abbreviations: CDS, conduct disorder symptoms; cM, centimorgans; DV, dependence vulnerability; DV � CDS, composite (sum) index of antisocial substancedependence.
*Distance in Kosambi centimorgans from the p-terminus.†Data are t statistics from single-point DeFries-Fulker regression analyses.‡P�.05 (P values are nominal values uncorrected for multiple testing).§P�.01.� P�.001.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1045
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

is that information from all 249 sibling pairs is used foreach linkage test evaluation.
Multipoint mapping results indicated 3 regions withLOD scores greater than 1.0, generally corroborating thesingle-point results. These findings provide support forthe hypothesis that common genes may explain part ofthe comorbidity between DV and CDS. The strongest evi-dence for linkage (LOD=2.65) was found for our com-
posite index of antisocial substance dependence(DV�CDS), suggesting evidence for a QTL that influ-ences both DV and CDS on chromosome 9q34 (nearmarkers D9S1826 and D9S1838). Evidence for QTLs thatprimarily influence DV on chromosome 3q24-3q25 (nearmarkers D3S1279 and D3S1614) and CDS on chromo-some 17q12 (near marker D17S798) was also found. These3 chromosomal regions are shown in greater detail in
3.0
1.5
2.5
2.0
1.0
0.5
0 500 1000 1500 2000 2500 3000
22212019181716151413121110987654321
0
3.0
1.5
2.5
2.0
1.0
0.5
0
3.0
1.5
2.5
2.0
1.0
0.5
0
Cumulative Centimorgans
Chromosome No.
LOD
Scor
e
0 500 1000 1500 2000 2500 3000
22212019181716151413121110987654321
Cumulative Centimorgans
Chromosome No.
LOD
Scor
e
0 500 1000 1500 2000 2500 3000
22212019181716151413121110987654321
Cumulative Centimorgans
Chromosome No.
LOD
Scor
e
A
B
C
Figure 1. Multipoint logarithm of odds (LOD) scores estimated from DeFries-Fulker regression analyses across the genome. A, Dependence vulnerability. B,Conduct disorder symptoms. C, Dependence vulnerability and conduct disorder symptoms.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1046
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

Figures 2, 3, and 4. Descriptive statistics from our DFregression analyses at these locations are given in Table4.
Table 5 gives the sibling means plotted as a func-tion of the estimated mean number of alleles shared IBDwith the proband for our maximum LOD score loca-tions on chromosomes 3q24-3q25, 9q34, and 17q12. Tocompute category means, we collapsed the estimated IBDdistribution into 3 categories: 0% to 25%, more than 25%to 75%, and more than 75% alleles shared IBD at eachlocation. At our 3q24-3q25 peak location, the siblingmeans for DV, CDS, and DV � CDS show approxi-mately half an SD difference between sibpairs with an es-timated IBD of less than 25% compared with sibling pairswith an estimated IBD of greater than 75%. For our 9q34location, the mean difference among these groups for DVis of similar magnitude, whereas mean differences for CDSand DV�CDS are approximately 80% of an SD. As ex-pected from our regression results, mean differences arelower in magnitude at our 17q12 location. The patternof means at the 3q24-3q25 location suggests the possi-bility of a nonadditive QTL, whereas the pattern of meansat the 9q34 location is consistent with an additive QTL.
CHECKS ON ANALYTICAL ASSUMPTIONS
Although the regression-based methods we used are ro-bust to departures from normality, we performed sev-eral tests on the assumptions of our analyses. Plots of re-siduals by predicted values (at the 3 maximum LOD scorelocations) indicated no obvious heteroscedasticity prob-lems. Consistent with expectations, approximately 5%of the absolute values of the standardized residuals ex-ceeded 2.0 and approximately 1% exceeded 3.0 for eachof these analyses. Sensitivity analyses were also con-ducted at these locations, systematically dropping eachsibling pair from the analysis (with replacement) and re-computing regression statistics from the remaining pairs.Evaluation of regression influence statistics indicated noparticularly influential cases or outliers. Nonetheless, tominimize any bias introduced by outliers, we identifiedthe 5% most extreme individuals (2.5% in each direc-tion), truncated their scores to the value of the most ex-treme cases in the remaining 95% of the sample,73 andthen reconducted our regression analyses for each phe-
1.4
0.8
1.2
1.0
0.6
0.4
0.2
0
D17S
849
D17S
831
D17S
938
D17S
1852
D17S
799
D17S
921
D17S
1857
D17S
798
D17S
1868
D17S
787
D17S
944
D17S
949
D17S
785
D17S
784
D17S
928
Markers
LOD
Scor
e
Dependence VulnerabilityConduct Disorder SymptomsCombined
Figure 4. Multipoint logarithm of odds (LOD) scores estimated fromDeFries-Fulker regression analyses for chromosome 17.
Table 4. Peak Chromosomal Regions Yielding LOD ScoresGreater Than 1.0
ChromosomePosition,
cM* t † P Value‡ E(p)§ LOD �
Dependence vulnerability3q24-3q25 173 2.74 .003 .005 1.639q34 161 2.96 .002 .002 1.91
Conduct disorder9q34 162 2.85 .002 .003 1.7617q12 54 2.41 .008 �.001 1.26
Composite index3q24-3q25 175 2.62 .005 .006 1.499q34 161 3.49 �.001 �.001 2.65
Abbreviations: cM, centimorgans; LOD, logarithm of odds.*Distance from the p-terminus for location of maximum LOD score.†Test statistic (t value) from multipoint DeFries-Fulker regression analysis.‡Obtained P value assuming a t distribution.§Empirically derived P value.�t2/2 � natural log of 10.
1.8
0.8
1.6
1.4
1.2
1.0
0.6
0.4
0.2
0
D3S1
297
D3S1
304
D3S2
338
D3S1
263
D3S1
266
D3S1
277
D3S1
289
D3S3
681
D3S1
271
D3S1
278
D3S1
267
D3S1
292
D3S1
569
D3S1
614
D3S1
565
D3S1
311
Markers
Dependence VulnerabilityConduct Disorder SymptomsCombined
LOD
Scor
e
D3S1
300
D3S1
566
D3S1
285
D3S1
279
D3S1
580
D3S1
262
D3S1
601
Figure 2. Multipoint logarithm of odds (LOD) scores estimated fromDeFries-Fulker regression analyses for chromosome 3.
3.0
1.5
2.5
2.0
1.0
0.5
0
D9S2
88D9
S288
D9S2
86D9
S285
D9S1
57D9
S171
D9S1
61
D17S
175
D9S1
67D9
S283
D9S2
87D9
S169
0D9
S167
7D9
S168
2D9
S290
D9S1
838
Markers
Dependence VulnerabilityConduct Disorder SymptomsCombined
LOD
Scor
e
D9S2
73
D9S1
817
D9S1
776
BH10
21D9
S164
D9S1
826
Figure 3. Multipoint logarithm of odds (LOD) scores estimated fromDeFries-Fulker regression analyses for chromosome 9.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1047
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

notype at the 3 maximum LOD score locations. The LODscores for DV, CDS, and DV�CDS at our 9q34 peak lo-cation increased to 1.98, 1.84, and 2.74, respectively; LODscores for the 3 phenotypes at our 3q24-3q25 peak lo-cation were 1.55, 0.77, and 1.57, respectively; and LODscores at the 17q12 peak location were 0.00, 1.25, and0.28, respectively. Comparisons between these results andthose from the full sample given in Table 4 indicate thatour findings are not simply artifacts that result from theundue influence of a few outliers.
EMPIRICAL SIGNIFICANCE LEVELS
We used permutation simulations to derive empirical Pvalues for our obtained results at each of our peak loca-tions. Empirical null distributions were simulated by ran-domly permuting IBD estimates with phenotypic scoresfor a given sibling pair (maintaining the family struc-
tures, phenotypic scores, and IBD estimates from the realdata set). We then conducted our regression analyses on5000 random permutations of our data to obtain empiri-cal P values for the regression test statistics obtained ateach of our maximum LOD score locations (ie, reportedP values are the proportion of times of 5000 simulationsthat we observed t values greater than or equal to the maxi-mum values we obtained at 3q24-3q25, 9q34, and 17q12).Those P values, given in Table 4, are not substantiallydifferent from those assuming a t distribution, again sug-gesting that our results are not unduly biased by viola-tions of the assumptions of our analyses.
QUALITATIVE ANALYSES
To explore these data further, we used a variant of theaffected sibling pair method. We defined affected statusas scoring above a z-score cutoff of 1.96 for each of our3 phenotypic measures. Sibling pairs were considered con-cordant extreme-scoring pairs if they both scored abovethe respective z-score cutoff. When only the proband ex-ceeded the threshold and the sibling did not, the pair wasconsidered a discordant pair. A z score greater than 1.96would include approximately 2.5% of the general popu-lation. By defining affection status this way, we are notsuggesting that many of our sibling pairs are unaffected.This analysis was used to determine whether sibling pairsconcordant for extreme scores on our quantitative phe-notypes also showed increased allele sharing IBD at thelocations suggested by our regression analyses.
Table 6 gives the estimated proportion of allelesshared IBD for siblings defined as concordant high scor-ing and discordant pairs for our peak locations and forthe flanking markers proximal to each of the peak loca-tions. At susceptibility loci, the mean proportion of al-leles that are IBD is expected to be less than 50% for dis-cordant pairs and greater than 50% in concordant pairs(the null expectation for siblings is 50%). In general, thereis a trend for increased allele sharing among extreme-
Table 5. Sibling Means by IBD at Peak LOD Score Locations
Peak LocationIBD Sharing
No. ofSiblingPairs
Phenotypes, Mean (SD)*
DV CDS DV � CDS
3q24-3q25�25% 51 −0.20 (0.15) −0.07 (0.23) −0.16 (0.19)25%-75% 129 −0.11 (0.12) −0.17 (0.14) −0.16 (0.13)�75% 69 0.35 (0.19) 0.36 (0.21) 0.41 (0.20)
9q34�25% 74 −0.29 (0.14) −0.42 (0.16) −0.42 (0.15)25%-75% 110 −0.00 (0.13) 0.04 (0.15) 0.02 (0.14)�75% 65 0.34 (0.19) 0.41 (0.25) 0.43 (0.22)
17q12�25% 59 0.08 (0.20) −0.26 (0.17) −0.12 (0.18)25%-75% 139 −0.04 (0.11) −0.06 (0.14) −0.06 (0.13)�75% 51 0.08 (0.20) 0.48 (0.28) 0.30 (0.25)
Abbreviations: CDS, conduct disorder symptoms; DV, dependencevulnerability; DV � CDS, composite (sum) index of antisocial substancedependence; IBD, identity by descent; LOD, logarithm of odds.
*Means can be interpreted in standard deviation units.
Table 6. Mean Allele Sharing IBD at Peak LOD Locations on C3, C9, and C17 for Concordant High-Scoring Pairsand Discordant Sibling Pairs
Location
Concordant High-Scoring Pairs (z�1.96), Mean (SD)* Discordant Pairs, Mean (SD)†
DV (n = 30) CDS (n = 51) DV � CDS (n = 44) DV (n = 124) CDS (n = 143) DV � CDS (n = 158)
Chromosome 3D3S1279 0.61 (0.05) 0.62 (0.05) 0.59 (0.05) 0.50 (0.03) 0.46 (0.03) 0.49 (0.03)D3S1614 0.57 (0.06) 0.63 (0.05) 0.60 (0.06) 0.54 (0.03) 0.50 (0.03) 0.53 (0.03)Peak LOD score 0.59 (0.05) 0.62 (0.05) 0.59 (0.05) 0.52 (0.03) 0.48 (0.02) 0.51 (0.02)
Chromosome 9D9S1826 0.58 (0.07) 0.60 (0.05) 0.57 (0.05) 0.45 (0.03) 0.45 (0.03) 0.46 (0.03)D9S1838 0.59 (0.07) 0.61 (0.05) 0.58 (0.05) 0.44 (0.03) 0.45 (0.03) 0.46 (0.03)Peak LOD score 0.59 (0.07) 0.60 (0.05) 0.58 (0.05) 0.45 (0.03) 0.45 (0.03) 0.46 (0.03)
Chromosome 17D17S798 0.46 (0.05) 0.55 (0.04) 0.53 (0.04) 0.50 (0.03) 0.45 (0.02) 0.46 (0.02)Peak LOD score 0.46 (0.05) 0.55 (0.04) 0.53 (0.04) 0.50 (0.03) 0.45 (0.02) 0.46 (0.02)
Abbreviations: CDS, conduct disorder symptoms; DV, dependence vulnerability; DV � CDS , composite (sum) index of antisocial substance dependence;IBD, identity by descent; LOD, logarithm of odds.
*Sibling pairs in which both the proband and sibling both score above the z-score cutoff.†Proband score is above threshold but sibling score is not; cell entries are the mean percentage of alleles that shared IBD (from multipoint IBD probability
estimates) at the respective locations; the null expectation for siblings is 50%.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1048
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

scoring sibling pairs for our 3q24-3q25 and 9q34 peakLOD score regions. As expected, this trend is less evi-dent for our 17q12 location, where only our CDS phe-notype yielded an LOD score greater than 1.0. A trendfor decreased allele sharing among discordant sibling pairswas found for all phenotypes at our 9q34 region. Thiswas not found for our 3q24-3q25 region, again suggest-ing the possibility of a nonadditive QTL in this region.
COMMENT
This study extends our initial findings of putative QTLsunderlying DV in adolescence54 by performing addi-tional genome scans for CDS and a composite pheno-type reflecting antisocial substance dependence(DV�CDS) on the same adolescent sample. Our find-ings provide preliminary support for the hypothesis thatcommon genes may influence CD and substance depen-dence vulnerability in adolescence. Single-point analy-ses indicated 29 markers with nominally significant(P�.05) test results for linkage for 1 or more of our mea-sures. Multipoint mapping analyses corroborated 3 lo-cations, with the strongest evidence for QTLs influenc-ing CD and DV detected on chromosome 9q34 (nearmarkers D9S1826 and D9S1838). A QTL more stronglyassociated with DV was detected on chromosome 3q24-3q25 (near markers D3S1279 and D3S1614), and a pu-tative QTL unique to CDS was reported on chromo-some 17q12 (near marker D17S798).
Our maximum LOD score in the region of 9q34 meetscriteria for suggestive linkage (LOD=2.65). The evi-dence for linkage to 3q24-3q25 and 17q12 is less strongbut of sufficient magnitude to warrant further study ofthese regions. Although these locations do not meet thecriteria of Lander and Kruglyak74 for significant linkage,few studies of comparable sample size will individuallyhave sufficient power to identify QTLs at this level of sig-nificance. A strength of our design was the use of a sampleof 249 selected sibling pairs, which provides roughly thesame power as 1000 to 2000 unselected sibling pairs,69
using our analytical methods. Even so, the power to de-tect QTLs of low effect size (�15% heritability) is lim-ited. Clearly, these findings require replication in inde-pendent adolescent samples. However, a series of checkson our current analyses indicate that our linkage resultsare robust to outliers and the phenotypic distributionalproperties of our sample.
Other investigators have suggested QTLs in the vicin-ity of ours for substance-related behaviors. Uhl et al,75 in-vestigating QTLs for polysubstance abuse vulnerability inan adult sample, reported a significant association with aregion on chromosome 3 within 10 cM of our peak loca-tion (173-175 cM). Long et al76 also reported suggestiveevidence for linkage to 3 markers on chromosome 3, span-ning the region 165.3 to 181.1 cM in a genome scan forgenetic linkage to alcohol dependence. Bergen et al77 re-ported a similar region associated with smoking status onchromosome 3 (171.7 cM) and a region close to our peaklocation on chromosome 9 (161 cM). A recent genome scanfor QTLs associated with CD78 did not find the same lo-cations as we did for our CDS measure. The authors did
report a QTL on chromosome 3 (134 cM) near a second-ary peak (LOD=0.80) evident from our genome scan forour DV measure (Figure 2). However, their adult samplewas selected for high-density alcoholism, and CD symp-toms were retrospectively reported. In addition, theirsample was not highly selected for CD (approximately 13%would meet criteria for a diagnosis), so our samples arenot directly comparable.
There are several limitations of our study. First, endo-phenotypes that uniquely represent specific genetic con-tributions to CDS and DV are unknown. Our phenotypeswere constructed from standard psychiatric symptom clus-ters (DSM criteria). These clusters, although useful for guid-ing currently available treatments, generally do not con-sider differences in etiologies.
Second, because CD and SUDs develop over time, weused age- and sex-normed quantitative phenotypes to ex-press CD and DV in our selected sibling sample in rela-tion to the population means and variability for commu-nity adolescents. Although CD and polysubstance use arecharacteristic of our high-risk probands and their sib-lings, not all of our study participants have fully passedthrough the age of risk, and this may limit the validityof our phenotypes.
Finally, our clinical adolescent sample was selected forboth problem substance use and CD; thus, our findingsmay not generalize to broader substance-abusing popu-lations without comorbid antisocial behavior. However,joint selection for both of these phenotypes would not beexpected to lead to the finding of a common QTL in theabsence of pleiotropy or strong linkage disequilibrium.
To explore our results further, we conducted a searchfor candidate genes within ±5 megabases (Mb) of eachof our peak locations79 (http://genome.ucsc.edu). Thesesearches yielded approximately 100 genes within eachregion. We highlight herein some candidates of interest(a full listing of identified genes in these regions can befound on our Web site at http://ibgwww.colorado.edu/cadd/a_center/research). Potential candidates in the re-gion of 3q24-3q25 include the phospholipase D1 gene(PLD1); a serine proteinase inhibitor gene (SERPINI1);claudin 11, an oligodendrocyte transmembrane proteingene (CLDN11); and neuroligin 1 (NLGN1). A notablecandidate near our 9q34 region is the dopamine �-hy-droxylase gene (DBH). However, when we added a SNPmarker within the DBH gene (DBH-1021C→T80) to ourchromosome 9 map, there was no evidence of linkage nearthis marker, suggesting that our putative QTL is distalto the DBH locus. Other potential candidates in the re-gion include GRIN1 (NMDAR1), a gene that codes for asubunit of the N-methyl-D-aspartate receptor; a neuro-blastoma protein gene (AMY); a chloride intracellularchannel gene (CLIC3); and a calcium channel gene(CACNA1B). Candidates within ±5 Mb of our 17q12 peaklocation include the serotonin transporter gene (SLC6A4);a cyclin-dependent kinase 5 regulatory subunit (CDK5R1)that codes for a protein that is a neuron-specific activa-tor of CDK5; and OMG, a gene that codes for an oligo-dendrocyte myelin glycoprotein. Although we re-stricted our systematic search to ±5 Mb, we note withinterest that DARPP-32,81 a dopamine- and cyclic aden-osine monophosphate–regulated phosphoprotein that ap-
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1049
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

pears to be essential for dopaminergic and serotonergicneurotransmission, is located 6.3 Mb from our chromo-some 17 peak. Putative gene function was ascertained fromthe GeneCards82 database (http://bioinfo1.weizmann.ac.il/genecards/).
In summary, CD and SUDs are frequently comorbidin adolescence.1-3,6-11 Although the precise etiologic mecha-nisms that underlie the frequent co-occurrence of theseproblem behaviors remain unclear, the current investi-gation was motivated by increasing evidence that com-mon genetic risks may explain part of the comorbidi-ty.36,37,39-51 The goal of our current program of researchis to extend this biometrical evidence to localize chro-mosomal regions that contain genes that influence boththese disorders. Results of this study provide the first evi-dence of a potential molecular genetic basis for the co-morbidity between drug dependence vulnerability andantisocial behavior in adolescents.
Submitted for Publication: December 12, 2003; final re-vision received March 25, 2005; accepted March 28, 2005.Correspondence: Michael C. Stallings, PhD, Institute forBehavioral Genetics, Campus Box 447, University of Colo-rado, Boulder, CO 80309-0444 ([email protected]).Funding/Support: This research was supported in partby grants DA-05131, DA-11015, and DA-12845 from theNational Institute on Drug Abuse, Bethesda, Md.Acknowledgment: This article is dedicated to the late DavidW. Fulker. We acknowledge Stacey Cherny, PhD, andMarissa Ehringer, PhD, for their statistical and bioinfor-matics consultation and Kristen Ehlers, BA, for data man-agement. Genotyping was performed by Jane Hutchin-son, MS, Liping Liu, MS, and Chinatsu McGeary, BA. Weespecially thank the participants of the clinical, family, twin,and adoption studies of the Center for the Genetics andTreatment of Antisocial Drug Dependence.
REFERENCES
1. Brown SA, Gleghorn A, Schuckit MA, Myers MG, Mott MA. Conduct disorder amongadolescent alcohol and drug abusers. J Stud Alcohol. 1996;57:314-324.
2. Crowley TJ, Riggs PD. Adolescent substance use disorder with conduct disor-der and comorbid conditions. NIDA Res Monogr. 1995;156:49-111.
3. Clark DB, Jacob RG, Mezzich A. Anxiety and conduct disorders in early onsetalcoholism. Ann N Y Acad Sci. 1994;708:181-186.
4. Flory K, Lynam DR. The relation between attention deficit hyperactivity disorderand substance abuse: what role does conduct disorder play? Clin Child Fam Psy-chol Rev. 2003;6:1-16.
5. Moss HB, Lynch KG. Comorbid disruptive behavior disorder symptoms and theirrelationship to adolescent alcohol use disorders. Drug Alcohol Depend. 2001;64:75-83.
6. Myers MG, Brown SA, Mott MA. Preadolescent conduct disorder behaviors pre-dict relapse and progression of addiction for adolescent alcohol and drug abusers.Alcohol Clin Exp Res. 1995;19:1528-1536.
7. Young SE, Mikulich SK, Goodwin MB, Hardy J, Martin CL, Zoccolillo MS, Crow-ley TJ. Treated delinquent boys’ substance use: onset, pattern, relationship toconduct and mood disorders. Drug Alcohol Depend. 1995;37:149-162.
8. Armstrong TD, Costello EJ. Community studies on adolescent substance use,abuse, or dependence and psychiatric comorbidity. J Consult Clin Psychol. 2002;70:1224-1239.
9. Disney ER, Elkins IJ, McGue M, Iacono WG. Effects of ADHD, conduct disorder,and gender on substance use and abuse in adolescence. Am J Psychiatry. 1999;156:1515-1521.
10. Kandel DB, Johnson JG, Bird HR, Weissman MM, Goodman SH, Lahey BB, Re-gier DA, Schwab-Stone ME. Psychiatric comorbidity among adolescents with sub-
stance use disorders: findings from the MECA Study. J Am Acad Child AdolescPsychiatry. 1999;38:693-699.
11. Windle M. Coexisting problems and alcoholic family risk among adolescents. AnnN Y Acad Sci. 1994;708:157-164.
12. Rhee SH, Waldman ID. Genetic and environmental influences on antisocial be-havior: a meta-analysis of twin and adoption studies. Psychol Bull. 2002;128:490-529.
13. Eaves LJ, Silberg JL, Meyer JM, Maes HH, Simonoff E, Pickles A, Rutter M, NealeMC, Reynolds CA, Erikson MT, Heath AC, Loeber R, Truett KR, Hewitt JK.Genetics and developmental psychopathology, 2: the main effects of genes and en-vironment on behavioral problems in the Virginia Twin Study of Adolescent Behav-ioral Development. J Child Psychol Psychiatry. 1997;38:965-980.
14. Slutske WS, Heath AC, Dinwiddie SH, Madden PA, Bucholz KK, Dunne MP, StathamDJ, Martin NG. Modeling genetic and environmental influences in the etiology ofconduct disorder: a study of 2,682 adult twin pairs. J Abnorm Psychol. 1997;106:266-279.
15. Goodwin DW. Alcoholism and genetics: the sins of the fathers. Arch Gen Psychiatry.1985;42:171-174.
16. Heath AC, Meyer J, Jardine R, Martin NG. The inheritance of alcohol consump-tion patterns in a general population twin sample, II: determinants of consump-tion frequency and quantity consumed. J Stud Alcohol. 1991;52:425-433.
17. Heath AC, Bucholz KK, Madden PA, Dinwiddie SH, Slutske WS, Bierut LJ, StathamDJ, Dunne MP, Whitfield JB, Martin NG. Genetic and environmental contribu-tions to alcohol dependence risk in a national twin sample: consistency of find-ings in women and men. Psychol Med. 1997;27:1381-1396.
18. Heath AC, Whitfield JB, Madden PA, Bucholz KK, Dinwiddie SH, Slutske WS, BierutLJ, Statham DB, Martin NG. Towards a molecular epidemiology of alcohol de-pendence: analysing the interplay of genetic and environmental risk factors. BrJ Psychiatry Suppl. 2001;40:S33-S40.
19. Hrubec Z, Omenn GS. Evidence of genetic predisposition to alcoholic cirrhosisand psychosis: twin concordances for alcoholism and its biological end pointsby zygosity among male veterans. Alcohol Clin Exp Res. 1981;5:207-215.
20. McGue M. Mediators and moderators of alcoholism inheritance. In: Turner JR,Cardon LR, Hewitt JK, eds. Behavior Genetic Approaches in Behavioral Medi-cine. New York, NY: Plenum Press; 1995:17-44.
21. McGue M, Iacono WG, Legrand LN, Elkins I. Origins and consequences of age atfirst drink, II: familial risk and heritability. Alcohol Clin Exp Res. 2001;25:1166-1173.
22. Prescott CA, Hewitt JK, Heath AC, Truett KR, Neale MC, Eaves LJ. Environmen-tal and genetic influences on alcohol use in a volunteer sample of older twins.J Stud Alcohol. 1994;55:18-33.
23. Prescott CA, Kendler KS. Genetic and environmental contributions to alcohol abuseand dependence in a population-based sample of male twins. Am J Psychiatry.1999;156:34-40.
24. Rose RJ, Dick DM, Viken RJ, Kaprio J. Gene-environment interaction in pat-terns of adolescent drinking: regional residency moderates longitudinal influ-ences on alcohol use. Alcohol Clin Exp Res. 2001;25:637-643.
25. Tyndale RF. Genetics of alcohol and tobacco use in humans. Ann Med. 2003;35:94-121.
26. Han C, McGue MK, Iacono WG. Lifetime tobacco, alcohol and other substanceuse in adolescent Minnesota twins: univariate and multivariate behavioral ge-netic analyses. Addiction. 1999;94:981-993.
27. Kendler KS, Prescott CA. Cannabis use, abuse, and dependence in a population-based sample of female twins. Am J Psychiatry. 1998;155:1016-1022.
28. Kendler KS, Karkowski LM, Neale MC, Prescott CA. Illicit psychoactive sub-stance use, heavy use, abuse, and dependence in a US population-based sampleof male twins. Arch Gen Psychiatry. 2000;57:261-269.
29. Luthar SS, Rounsaville BJ. Substance misuse and comorbid psychopathologyin a high-risk group: a study of siblings of cocaine misusers. Int J Addict. 1993;28:415-434.
30. Maes HH, Woodard CE, Murrelle L, Meyer JM, Silberg JL, Hewitt JK, Rutter M,Simonoff E, Pickles A, Carbonneau R, Neale MC, Eaves LJ. Tobacco, alcohol anddrug use in eight- to sixteen-year-old twins: the Virginia Twin Study of Adoles-cent Behavioral Development. J Stud Alcohol. 1999;60:293-305.
31. McGue M, Elkins I, Iacono WG. Genetic and environmental influences on ado-lescent substance use and abuse. Am J Med Genet. 2000;96:671-677.
32. Merikangas KR, Avenevoli S. Implications of genetic epidemiology for the pre-vention of substance use disorders. Addict Behav. 2000;25:807-820.
33. Moss HB, Majumder PP, Vanyukov M. Familial resemblance for psychoactivesubstance use disorders: behavioral profile of high risk boys. Addict Behav. 1994;19:199-208.
34. Newlin DB, Miles DR, van den Bree MB, Gupman AE, Pickens RW. Environmen-tal transmission of DSM-IV substance use disdorders in adoptive and step families.Alcohol Clin Exp Res. 2000;24:1785-1794.
35. Rounsaville BJ, Kosten TR, Weissman MM, Prusoff B, Pauls D, Anton SF, Meri-
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1050
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from

kangas K. Psychiatric disorders in relatives of probands with opiate addiction.Arch Gen Psychiatry. 1991;48:33-42.
36. Langbehn DR, Cadoret RJ, Caspers K, Troughton EP, Yucuis R. Genetic and en-vironmental risk factors for the onset of drug use and problems in adoptees. DrugAlcohol Depend. 2003;69:151-167.
37. Miles DR, van den Bree MB, Pickens RW. Sex differences in shared genetic andenvironmental influences between conduct disorder symptoms and marijuanause in adolescents. Am J Med Genet. 2002;114:159-168.
38. Pickens RW, Svikis DS, McGue M, LaBuda MC. Common genetic mechanismsin alcohol, drug, and mental disorder comorbidity. Drug Alcohol Depend. 1995;39:129-138.
39. Slutske WS, Heath AC, Dinwiddie SH, Madden PA, Bucholz KK, Dunne MP, StathamDJ, Martin NG. Common genetic risk factors for conduct disorder and alcoholdependence. J Abnorm Psychol. 1998;107:363-374.
40. Babor TF, Hofmann M, DelBoca FK, Hesselbrock V, Meyer RE, Dolinsky ZS, Roun-saville B. Types of alcoholics, I: evidence for an empirically derived typology basedon indicators of vulnerability and severity. Arch Gen Psychiatry. 1992;49:599-608.
41. Cadoret RJ, Yates WR, Troughton E, Woodworth G, Stewart MA. Adoption studydemonstrating two genetic pathways to drug abuse. Arch Gen Psychiatry. 1995;52:42-52.
42. Cloninger CR, Bohman M, Sigvardsson S. Inheritance of alcohol abuse: cross-fostering analysis of adopted men. Arch Gen Psychiatry. 1981;38:861-868.
43. Cloninger CR. Neurogenetic adaptive mechanisms in alcoholism. Science. 1987;236:410-416.
44. Cloninger CR, Sigvardsson S, Gilligan SB, von Knorring AL, Reich T, BohmanM. Genetic heterogeneity and the classification of alcoholism. Adv Alcohol SubstAbuse. 1988;7:3-16.
45. Hesselbrock V, Meyer R, Hesselbrock M. Psychopathology and addictive disor-ders: the specific case of antisocial personality disorder. Res Publ Assoc ResNerv Ment Dis. 1992;70:179-191.
46. Iacono WG, Carlson SR, Taylor J, Elkins IJ, McGue M. Behavioral disinhibitionand the development of substance-use disorders: findings from the MinnesotaTwin Family Study. Dev Psychopathol. 1999;11:869-900.
47. Jessor R, Donovan JE, Costa FM. Beyond Adolescence: Problem Behavior andYoung Adult Development. Cambridge, England: Cambridge University Press;1991.
48. Krueger RF, Hicks BM, Patrick CJ, Carlson SR, Iacono WG, McGue M. Etiologicconnections among substance dependence, antisocial behavior, and personal-ity: modeling the externalizing spectrum. J Abnorm Psychol. 2002;111:411-424.
49. Moffitt TE, Lynam D Jr. The neuropsychology of conduct disorder and delin-quency: implications for understanding antisocial behavior. Prog Exp Pers Psy-chopathol Res. 1994:233-262.
50. Sher KJ, Trull TJ. Personality and disinhibitory psychopathology: alcoholism andantisocial personality disorder. J Abnorm Psychol. 1994;103:92-102.
51. Young SE, Stallings MC, Corley RP, Krauter KS, Hewitt JK. Genetic and environ-mental influences on behavioral disinhibition. Am J Med Genet. 2000;96:684-695.
52. Iacono WG. Identifying psychophysiological risk for psychopathology: ex-amples from substance abuse and schizophrenia research. Psychophysiology.1998;35:621-637.
53. Iacono WG, Lykken DT, McGue M. Psychophysiological prediction of substanceabuse. NIDA Res Monogr. 1996;159:129-149; discussion 150-160.
54. Stallings MC, Corley RP, Hewitt JK, Krauter KS, Lessem JM, Mikulich SK, RheeSH, Smolen A, Young SE, Crowley TJ. A genome-wide search for quantitativetrait loci influencing substance dependence vulnerability in adolescence. DrugAlcohol Depend. 2003;70:295-307.
55. Young SE, Corley RP, Stallings MC, Rhee SH, Crowley TJ, Hewitt JK. Substanceuse, abuse and dependence in adolescence: prevalence, symptom profiles andcorrelates. Drug Alcohol Depend. 2002;68:309-322.
56. DeFries JC, Plomin R, Fulker DW. Nature and Nurture During Middle Childhood.Oxford, England: Blackwell Publishers; 1994.
57. Miles DR, Stallings MC, Young SE, Hewitt JK, Crowley TJ, Fulker DW. A family his-tory and direct interview study of the familial aggregation of substance abuse: theAdolescent Substance Abuse Study. Drug Alcohol Depend. 1998;49:105-114.
58. Johnston L, Bachman JG, O’Malley PM. Monitoring the Future: National Resultson Adolescent Drug Use: Overview of Key Findings, 1999. Bethesda, Md: Na-tional Institute on Drug Abuse; 2000.
59. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: National Re-sults on Adolescent Drug Use: Overview of Key Findings, 2000. Bethesda, Md:National Institute on Drug Abuse; 2001. NIH publication 01-4923.
60. Robins LN, Cottler LB, Babor TF. WHO-NIH Composite International DiagnosticInterview—Substance Abuse Module. St Louis, Mo: Washington University Schoolof Medicine, Dept of Psychiatry; 1993.
61. Shaffer D, Fisher P, Dulcan MK, Davies M, Piacentini J, Schwab-Stone ME, La-hey BB, Bourdon K, Jensen PS, Bird HR, Canino G, Regier DA. The NIMH Diag-nostic Interview Schedule for Children Version 2.3 (DISC-2.3): description, ac-ceptability, prevalence rates, and performance in the MECA Study. J Am AcadChild Adolesc Psychiatry. 1996;35:865-877.
62. Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental HealthDiagnostic Interview Schedule: its history, characteristics, and validity. Arch GenPsychiatry. 1981;38:381-389.
63. Shaffer D, Fisher P, Lucas C. The Diagnostic Interview Schedule for Children–IV.New York, NY: Ruane Center for Early Diagnosis, Division of Child Psychiatry,Columbia University; 1997.
64. Robins LN, Cottler LB, Bucholz K, Compton W, North CS, Rourke KM. Diagnos-tic Interview Schedule–IV. St Louis, Mo: Washington University School of Medi-cine, Dept of Psychiatry; 1998.
65. Abecasis GR, Cherny SS, Cookson WO, Cardon LR. Merlin–rapid analysis of densegenetic maps using sparse gene flow trees. Nat Genet. 2002;30:97-101.
66. Abecasis GR, Cherny SS, Cookson WO, Cardon LR. GRR: graphical representa-tion of relationship errors. Bioinformatics. 2001;17:742-743.
67. Abecasis GR, Cardon LR, Cookson WO. A general test of association for quan-titative traits in nuclear families. Am J Hum Genet. 2000;66:279-292.
68. Fulker DW, Cardon LR, DeFries J, Kimberling WJ, Pennington BF, Smith SD.Multiple regression analysis of sib-pair data on reading to detect quantitative traitloci. Reading Writing. 1991;3:299-313.
69. Fulker DW, Cardon LR. A sib-pair approach to interval mapping of quantitativetrait loci. Am J Hum Genet. 1994;54:1092-1103.
70. DeFries JC, Fulker DW. Multiple regression analysis of twin data. Behav Genet.1985;15:467-473.
71. Lessem JL, Cherny SS. DeFries-Fulker multiple regression analysis of sibshipQTL data: a SAS macro. Bioinformatics. 2001;17:371-372.
72. Sullivan PF, Neale BM, Neale MC, van den Oord E, Kendler KS. Multipoint andsingle point non-parametric linkage analysis with imperfect data. Am J Med GenetB Neuropsychiatr Genet. 2003;121:89-94.
73. Fernandez JR, Etzel C, Beasley TM, Shete S, Amos CI, Allison DB. Improving thepower of sib pair quantitative trait loci detection by phenotype winsorization. HumHered. 2002;53:59-67.
74. Lander E, Kruglyak L. Genetic dissection of complex traits: guidelines for inter-preting and reporting linkage results. Nat Genet. 1995;11:241-247.
75. Uhl GR, Liu Q, Walther D, Hess J, Naiman D. Polysubstance abuse-vulnerabilitygenes: genome scans for association, using 1004 subjects and 1494 single-nucleotide polymorphisms. Am J Hum Genet. 2001;69:1290-1300.
76. Long JC, Knowler WC, Hanson RL, Robin RW, Urbanek M, Moore E, BennettPH, Goldman D. Evidence for genetic linkage to alcohol dependence on chro-mosomes 4 and 11 from an autosome-wide scan in an American Indian population.Am J Med Genet. 1998;81:216-221.
77. Bergen AW, Korczak JF, Weissbecker KA, Goldstein AM. A genome-wide searchfor loci contributing to smoking and alcoholism. Genet Epidemiol. 1999;17:S55-S60.
78. Dick DM, Li T-K, Edenberg HJ, Hesselbrock V, Kramer J, Kuperman S, PorjeszB, Bucholz K, Goate A, Nurnberger J Jr, Foroud T. A genome-wide screen forgenes influencing conduct disorder. Mol Psychiatry. 2004;9:81-86.
79. Kent WJ, Sugnet CW, Furey TS, Roskin KM, Pringle TH, Zahler AM, Haussler D.The human genome browser at UCSC. Genome Res. 2002;12:996-1006.
80. Zabetian CP, Anderson GM, Buxbaum SG, Elston RC, Ichinose H, Nagatsu T, KimKS, Kim CH, Malison RT, Gelernter J, Cubells JF. A quantitative-trait analysis ofhuman plasma-dopamine beta-hydroxylase activity: evidence for a major func-tional polymorphism at the DBH locus. Am J Hum Genet. 2001;68:515-522.
81. Greengard P, Allen PB, Nairn AC. Beyond the dopamine receptor: the DARPP-32/protein phosphatase-1 cascade. Neuron. 1999;23:435-447.
82. Rebhan M, Chalifa-Caspi V, Prilusky J, Lancet D. GeneCards: Encyclopedia forGenes, Proteins and Diseases. Weizman Institute of Science, Bioinformatics Unitand Genome Center. Available at: http://bioinformatics.weizman.ac.il/cards. Ac-cessed October 23, 2003.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 62, SEP 2005 WWW.ARCHGENPSYCHIATRY.COM1051
©2005 American Medical Association. All rights reserved. at Univ of Colorado Hlth Sci Ctr, on February 1, 2006 www.archgenpsychiatry.comDownloaded from