
a comparative study of depression, suicidality and quality of
122
i A COMPARATIVE STUDY OF DEPRESSION, SUICIDALITY AND QUALITY OF LIFE AMONG DIABETES MELLITUS AND ESSENTIAL HYPERTENSION PATIENTS IN ENUGU, NIGERIA BY DR IGWE, MONDAY NWITE (MBBS, MPH NIG.) A DISSERTAION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF THE FELLOWSHIP OF THE COLLEGE IN THE FACULTY OF PSYCHIATRY. MAY 2011.
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of a comparative study of depression, suicidality and quality of

i
A COMPARATIVE STUDY OF DEPRESSION, SUICIDALITY AND QUALITY OF
LIFE AMONG DIABETES MELLITUS AND ESSENTIAL HYPERTENSION
PATIENTS IN ENUGU, NIGERIA
BY
DR IGWE, MONDAY NWITE
(MBBS, MPH NIG.)
A DISSERTAION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL
COLLEGE OF NIGERIA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS
FOR THE AWARD OF THE FELLOWSHIP OF THE COLLEGE IN THE FACULTY
OF PSYCHIATRY.
MAY 2011.
ii
DECLARATION
This dissertation is submitted in partial fulfillment for the award of the Fellowship of
the National Postgraduate Medical College of Nigeria. The study reported here is
original and has not been published or presented to any institution for the award of
degree/fellowship.
………………………………
DR M. N. IGWE
MAY 2011.

iii
SUPERVISORS’ CERTIFICATION
We certify that Dr M.N. Igwe of the Department of Psychological Medicine, Ebonyi
State University Teaching Hospital, Abakaliki carried out this study under our
supervision.
Prof. Richard Uwakwe ………………………………………..
Department of Psychiatry
Nnamdi Azikwe University Teaching Hospital
Nnewi, Anambra State
Dr. Gabriel M. Onyeama …………………..…………………..
Department of Psychological Medicine
University of Nigeria Teaching Hospital
Ituku – Ozalla, Enugu State
Dr. Muideen O. Bakare ………………………………………..
Child and Adolescent Psychiatry Unit
Federal Neuropsychiatric Hospital
New Haven, Enugu, Enugu State

iv
H EAD OF DEPARTMENT’S CERTIFICATION
I certify that Dr. M.N. Igwe carried out this study while in the department headed by
me at Ebonyi State University Teaching Hospital, Abakaliki.
………………………………..
DR A. C. AHANOTU
v
DEDICATION
This study is dedicated to the Almighty God who raises the poor out of the dust, lifts
up the beggar from the dunghill to set them among princes and make them inherit
the throne of glory (1 Sam 2:8).

vi
ACKNOWLEDGEMENTS
I am grateful to Almighty God for seeing me through the residency
programme and for making it possible for me to complete this study at this time.
I express my profound gratitude to my supervisor, Professor Richard Uwakwe
who despite his numerous engagements still made out time to guide me through all
the stages of this work. My sincere appreciation also goes to Dr. G. M Onyeama and
Dr. M.O Bakare who were co-supervisors for their accessibility, patience, guidance
and useful comments in the course of this study.
I thank my Head of Department, Dr. A.C Ahanotu for creating an enabling
environment for me to carry out this work. I equally thank Dr. C. Nwigwe, Chairman
Medical Advisory Committee, Ebonyi State University Teaching Hospital, Abakaliki for
his fatherly encouragement while this study lasted.
I also appreciate Dr. K.O Okonkwo and Dr. J.U Achor who played great roles
in my training and were always available whenever I sought their assistance. Dr.
Robsam Ohayi and Dr. N.O.K Obayi were also of immense assistance during the
course of this study. I thank them too.
Finally, I thank my beautiful wife, Nonye and lovely children, Divine, Nneoma,
Ugonna and Chisom for their support, patience, encouragement and prayers during
the period of this study.

vii
ABSTRACT
Background: Diabetes mellitus and essential hypertension are chronic medical
conditions that place a lot of burden on patients. The presence of co-morbid
depression, suicidal behaviour and impaired quality of life may compound the
problems, leading to poor prognosis.
Objective: This study assessed the prevalence of depression, suicidal behaviour,
quality of life and the socio-demographic correlates among subjects with diabetes
mellitus and compared them with subjects with essential hypertension.
Method: A total of 540 subjects, 270 each for diabetes mellitus and essential
hypertension were interviewed. Consecutive and consenting subjects with diabetes
mellitus and essential hypertension that met the inclusion criteria were recruited
from the endocrinology and cardiology clinics in University of Nigeria Teaching
Hospital Enugu. A socio-demographic questionnaire was used to assess the socio-
demographic characteristics. Major depressive episode of Mini-International
Neuropsychiatric Interview (M.I.N.I.) and Beck Depression Inventory were used to
assess depression while the suicidality module of M.I.N.I. was used to assess suicidal
behaviour. The World Health Organization Quality of Life-Bref (WHOQoL-Bref) was
used to assess quality of life.
Results: The prevalence of depression for the subjects with diabetes mellitus was
27.8% and 26.7% for those with essential hypertension. The subjects with diabetes
mellitus had prevalence of 6.3% for suicidal behaviour while those with essential
hypertension had 7.8%. The subjects with diabetes mellitus had been significantly ill
for a longer duration compared to the subjects with essential hypertension. The

viii
subjects with essential hypertension had significantly higher quality of life scores in
physical health, psychological well-being and social relationship domains. Depression
was more likely in subjects with diabetes mellitus if they were not married or had no
formal education while the subjects with essential hypertension were more likely to
have depression if they were not married, had no formal education or not employed.
Suicidal behaviour was more likely in subjects with diabetes mellitus if they had no
formal education while in those with essential hypertension suicidal behaviour was
more likely in females, those not married and those not educated. Males, married,
educated and employed subjects with diabetes mellitus scored higher on the
WHOQoL-Bref while males, married and educated subjects with essential
hypertension had higher scores.
Conclusion: Depression, suicidal behaviour and impaired quality of life may co-
occur with diabetes mellitus and essential hypertension. The negative impact of
these co-occurrences on achieving good glycaemic and blood pressure control calls
for screening for these conditions when indicated. This may enhance early detection
and treatment.

ix
TABLE OF CONTENTS
Title page - - - - - - - - - i
Declaration page - - - - - - - - - ii
Supervisor’s certification - - - - - - - - iii
Head of Department’s certification - - - - - - iv
Dedication - - - - - - - - - v
Acknowledgements - - - - - - - - - vi
Abstract - - - - - - - - - vii
Chapter One
Introduction - - - - - - - - - 1
Chapter Two
Literature Review - - - - - - - - - 4
2.1 Definition of concepts - - - - - - - 5
2.2 Depression and diabetes mellitus - - - - - - 7
2.3 Suicidal behaviour in diabetes mellitus - - - - - 9
2.4 Quality of life in diabetes mellitus - - - - - 10
2.5 Depression and Hypertension - - - - - - 12
2.6 Quality of life and suicidal behavioural in hypertension - - 12
2.7 Nigerian Studies - - - - - - - - 13
Chapter Three
Aims and Objectives - - - - - - - - 16
3.1 Specific Objectives - - - - - - - - 16
3.2 Hypotheses - - - - - - - - 16
x
Chapter Four
Methodology
4.1 study setting - - - - - - - - 18
4.2 Eligibility Criteria - - - - - - - - 19
4.3 Sample size determination - - - - - - 20
4.4 Ethical Issues - - - - - - - - 20
4.5 Instruments - - - - - - - - - 21
4.6 Translation of the study instruments - - - - - 28
4.7 Formal training on the use of instruments - - - - 29
4.8 Pilot study - - - - - - - - - 29
4.9 Procedure - - - - - - - - - 30
4.10 Statistical analysis - - - - - - - - 32
Chapter Five
Results
5.1.1 Socio-demographic variables of the subjects with diabetes mellitus
and Subject with essential hypertension - - - - - 33
5.2 The rates of depression (current episode) among the subject with
diabetes mellitus and essential hypertension - - - - 37
5.3 Suicidal behaviour among the subjects with diabetes mellitus
and essential hypertension - - - - - - - 39
5.4 Quality of life scores among the subjects with diabetes mellitus
and essential hypertension. - - - - - - 43
5.5 Association between depression and socio-demographic variables - 45

xi
5.6 Association between suicidal behaviour (suicidal ideation, plan
and attempt) and socio-demographic variables - - - - 51
5.7 Association between quality of life (QoL) scores and
socio-demographic variables - - - - - - 57
Chapter Six
Discussion - - - - - - - - - - 65
6.1 Socio-demographic characteristics of the subjects - - - 65
6.2 Rates of depression (current episode) - - - - - 65
6.3 Suicidal behaviour (ideation, plan and attempt) - - - 66
6.4 Quality of life - - - - - - - - 67
6.5 Correlates of depression - - - - - - - 68
6.6 Correlates of suicidal behaviour - - - - - - 70
6.7 Correlates of quality of life scores - - - - - 70
6.8 Relevance of the study to the practice of psychiatry - - - 71
6.9 Limitations of the study - - - - - - - 71
6.10 Recommendations - - - - - - - 72
6.11 Conclusion - - - - - - - - 72
References - - - - - - - - 73
Appendix 1: Socio-Demographic Questionnaire- - - - - 80
Appendix 2: Beck Depression Inventory - - - - - 81
Appendix 3: Mini-International Neuropsychiatric Interview - - 90
Appendix 4: The World Organization Quality of Life (WHOQoL)-Bref - 95
Appendix 5: Consent Form - - - - - - 107
xii
CHAPTER ONE
INTRODUCTION
Many chronic medical conditions are complicated by emotional and
psychological disorders and yet the emotional dimensions of such chronic medical
conditions are often overlooked when medical care is considered (Turner & Kelly,
2000). Patients with chronic medical conditions often have to adjust their
aspirations, lifestyle, and employment. Many grieve about their predicament before
adjusting to it. But others have protracted distress and may develop psychiatric
disorders, most commonly depression and anxiety (Turner & Kelly, 2000).
Depressive and anxiety disorders are the commonest psychiatric conditions occurring
in the context of chronic medical illnesses, including diabetes mellitus where
prevalence of affective disorders was reported as 20-25% (Turner & Kelly, 2000).
Emotional and psychological disorders may affect the quality of life of the
patients and may have deleterious concomitants like suicidal ideation and behaviour.
The prevalence of suicidal ideation complicating depressive disorders related to
medical illnesses has been studied empirically. The risk of suicide is greater among
patients with physical illnesses than among the general population with a prevalence
estimate of 22 – 60% (Kishi, et al 2001, Shah, et al 2000).
Depressive symptoms and syndromes are common in the medically ill,
although they are frequently unrecognized and untreated (Rodin & Voshart, 1986).
Diabetes is one of such chronic medical conditions that could be associated with
depressive syndromes. Diabetes mellitus is a group of metabolic diseases
characterized by hyperglycemia resulting from defects in insulin secretion, insulin
action, or both. The chronic hyperglycemia of diabetes is associated
xiii
with long-term damage, dysfunction, and failure of various organs, especially the
eyes, kidneys, nerves, heart, and blood vessels (American Diabetes Association,
2004).
Diabetes mellitus is a chronic and debilitating medical condition that
constitutes a source of stress to sufferers and, as such, affects their quality of life
and usually presents a difficult medical condition to live and cope with (Aldwin &
Revenson, 1987). Adaptation to chronic diseases like diabetes mellitus is a difficult
and complex process. This may necessitate several adjustments in the patient's
lifestyle (Brannon & Feist, 1997). Social relationships may also be severely affected
and commonly emotional responses like withdrawal, loneliness, guilt feelings,
hopelessness and suicidal ideation have been noted. (Mosaku, et al 2008).
Previous research work has shown that a relationship exists between
depression and diabetes mellitus (Anderson, et al 2001). Depression has been
associated with hyperglycemia, diabetes-related complications, perceived functional
limitations of patients with diabetes mellitus, socioeconomic status, marital status,
obesity and smoking habits (de Groot, et al 2001, Everson, et al 2002).
Related to the foregoing, other medical conditions like hypertension can also
co-exist with depressive disorders. Hypertension (high blood pressure) is defined as
a repeatedly elevated blood pressure exceeding 140mmHg systolic and 90 mmHg
diastolic (Devereux, et al 1993). Essential hypertension accounts for 95% of all cases
of hypertension with unknown etiology (Carretero & Oparil, 2000). Hypertension has
been noted to be associated with increased prevalence of depression (Rabkin, et al
1983). Presence of co-morbid depression in patients with hypertension adversely
affects the management and worsens the prognosis in such patients (Simonsick, et

xiv
al 1995). Depression has also been associated with higher risk of stroke in the
elderly with hypertension (Oshira, et al 2001). Hopelessness has also been reported
to be an important factor in cardiovascular disorders, including hypertension
(Everson, et al 2000).
Most of the studies that have assessed depression and quality of life in
chronic medical conditions in Nigeria have been done in the South-western geo-
political part of the country. It seems that studies comparing depression, suicidal
behaviour and quality of life among the patients who have diabetes mellitus and
essential hypertension are scanty in Nigeria. Understanding these interactions in the
setting of consultant clinics in South-eastern Nigeria is relevant to the practice of
psychiatry. Such a comparative data will help expand our knowledge about co-
morbidity of depression and suicidal behaviour in diabetes mellitus and essential
hypertension in addition to assessing the impact of such conditions on the quality of
life of the affected patients.
This study is designed to determine the interrelationship between depression,
suicidal behaviour and quality of life of patients who have diabetes mellitus, and to
compare these with patients that are diagnosed with essential hypertension.

xv
CHAPTER TWO
LITERATURE REVIEW
Untreated psychiatric illness is associated with increased morbidity, a longer
hospital stay and ultimately, increased costs of care (Gomez, 1987). This often leads
to wasteful, costly and inefficient use of medical services and complications of the
disorders and treatments among these patients (Musisi & Tugumisirize, 2001).
Therefore, early detection and treatment of mental disorders, is essential. This is
especially necessary since symptoms of such mental disorders are frequently not
recognized when co-morbid with chronic medical conditions (Turner & Kelly, 2000).
Diagnosis of depression in the medically ill can be difficult and challenging as
doctors may be well equipped for the biomedical aspects of care but not for the
challenges of understanding the psychological, social, and cultural dimensions of
illness and health, yet diagnosis and treatment are essential (Turner & Kelly, 2000).
The possibility that a significant proportion of the patients attending a medical
outpatient health facility may have unrecognized mental disorders suggests that
psychiatric conditions need to be recognized and managed appropriately (Ndetei, et
al 2009). In Nigeria, there are only about 110 working psychiatrists (World Health
Organization, 2005), 110 resident doctors training in psychiatry (Ayonrinde, et al.
2004) serving a population of approximately 140 million people (National Population
Commission, 2006). This translates to inadequate psychiatric services to the
population.

xvi
2.1 Definition of Concepts
i). Depression
The term depression can variously define an affect, mood state, a disorder,
symptom, syndrome or a specific entity (Gelder, et al 2003). Depressive disorders
are affective (mood) disorders characterized by depressed mood, loss of interest or
pleasure, feelings of worthlessness or inappropriate guilt, recurrent thoughts of
death or suicidal ideation, weight changes, sleep disturbances, fatigue, impaired
concentration and psychomotor disturbance. A positive diagnosis requires five or
more of the nine with evidence of functional impairment and a minimum duration of
two weeks (American Psychiatric Association, 1994).
ii) Suicidality
Suicidal behaviour or suicidality can be conceptualized as a continuum ranging
from suicidal ideation, making plans to suicide attempts and completed suicide
(Gelder, et al 2003). Ideation includes thinking that one is better off dead or wishes
one were dead, wanting to harm oneself or to hurt or injure oneself, think about
suicide and having a suicide plan, while making a suicide attempt involves taking
active steps to prepare to injure oneself with expectations to die and deliberately
injuring oneself without intention of dying (Sheehan, et al 1998).
(iii) Quality of life
The concept of quality of life has received considerable attention as an inclusive
notion of health and as a basis for health interventions (Hendry & McVittie, 2004).
Quality of life has been defined in multiple ways and mean different things

xvii
to different people. The concept has been described as a person’s sense of well-
being that stems from satisfaction or dissatisfaction with the areas of life that are
important to him/her (Ferrans, 1990). It can also be defined as the degree of need
for satisfaction within the areas of the physical, psychological, social, activity,
material and structural areas (Hørnquist, 1990). It has also been defined as a
measure of happiness and satisfaction with life, or goal achievement, or social utility
(Dedhiya & Kong, 1995).
A mathematical approach was brought to quality of life when it was defined
as utility scores that reflect preferences for the health states and allow morbidity and
mortality improvements to be combined into a single weighted measure; quality-
adjusted life years (Revicki & Kaplan, 1993).
A more encompassing view regards quality of life as the individuals’
perceptions of their position in life, in the context of the cultural and value systems
in which they live and in relation to their goals, expectations, standards and
concerns (World Health Organization, 1996). Based on this definition, the World
Health Organization quality of life-100 was developed by the World Health
Organization quality of life Group with fifteen international field centres,
simultaneously, in an attempt to develop a quality of life assessment that would be
applicable cross-culturally (WHO, 1996).
Most researchers are of the opinion that quality of life is complex and
composed of multiple dimensions (Bowling 1995, Ferrans, 1996, Spilker, 1996).
These perspectives of quality of life have been proposed: sociological, economic,
psychological, philosophical and ethical but health has emerged as an important and
distinct perspective (Taylor, et al 2008). World Health Organization quality of

xviii
life-bref (WHOQoL-Bref) which was used in this study has four domains- physical
health, psychological, social relationships and environment.
2.2 Depression and diabetes mellitus
There is a bidirectional association between depression and diabetes. The
presence of diabetes doubles the odds of co morbid depressive disorder (Pompili, et
al 2009). Similarly, the presence of depressive symptoms makes the afflicted
individual more vulnerable to becoming diabetic. In a study of 6,814 men and
women, aged 45 to 84 years, patients diagnosed with diabetes were 54% more
likely to develop depression than patients who were not. Patients with depressive
symptoms were 42% more likely to develop diabetes (Brownlee, 2008). Indeed,
patients who have diabetes mellitus, diagnosed with co morbid depression have an
elevated risk of death from both causes, greater than that of depression or diabetes
alone. (Egede, et al 2005). Furthermore, studies suggest that in patients with
diabetes mellitus who have depression, the severity of depression is correlated with
the severity of diabetes-related complications, independent of the type of diabetes
(Pompili, et al 2009). Depression has also been noted as a modifiable risk factor
whose treatment could improve glycaemic control and health outcomes in patients
with diabetes mellitus (Gendelman, et al 2009).
Katon, et al (2004) in a population-based mail survey study reported that
independent factors that were associated with a significantly higher likelihood of
meeting criteria for major depressive disorder among patients with diabetes mellitus
included younger age, female sex, less education, single status, basal metabolic
index ≥ 30 kg/m2, smoking, higher non- diabetic medical co morbidity, higher

xix
numbers of diabetes complications in men, treatment with insulin, and higher HbA1c
levels in patients ≤ 65 years of age.
In another study, where 506 patients who have diabetes mellitus were
assessed for depressive disorders and depressive symptoms using a structured
interview (Composite International Diagnostic Interview [CIDI]), and a questionnaire
for depressive symptoms (Center for Epidemiological Studies Depression Scale
[CESD], it was reported that the prevalence of depressive symptoms was 22% while
9.9% met a CIDI diagnosis of major depressive disorder (Fisher, et al 2007).
Similarly, the levels of depression were self-rated by using the Hospital
Anxiety and Depression scale in a controlled study of 60,869 individuals with and
without diabetes mellitus. Several factors were correlated with depression in types 1
and 2 diabetes. However, these factors were not different from those of the non-
diabetic population. Co-morbid chronic somatic diseases were associated with
depression in type 2 but not type 1 diabetes mellitus. In type 2 diabetes mellitus,
those without co morbidity had the same odds of depression as the non-diabetic
population with no chronic somatic diseases. No significant associations were found
for hyperglycemia in relation to depression in type 1 and type 2 diabetes mellitus
(Engum, et al 2005).
A research work involving 458 participants with diabetes and 546 without
diabetes and using Beck Depression Inventory-II, reported findings showing that
compared with non-diabetic participants, adults with type 1 diabetes report more
symptoms of depression and more antidepressant medication usage. Mean BDI-II
score, adjusted for age and sex, was significantly higher in participants with type 1
diabetes than in non-diabetic participants and participants reporting diabetes

xx
complications had higher mean BDI-II scores than those without complications
(Gendelman, 2009).
Anderson, et al (2001) in a meta-analysis involving 42 studies, reported that
the odds of depression in the group with diabetes mellitus were twice that of those
without diabetes mellitus. The prevalence of co-morbid depression was significantly
higher in diabetic women (28%) than in diabetic men (18%). Prevalence of
depression in the uncontrolled population was 30% while in the controlled studies it
was 21%. Prevalence of depression in clinical samples was 32% and in community
studies was 20%. Prevalence when assessed by self-report questionnaires was 31%
but by standardized diagnostic interviews it was 11%.
2.3 Suicidal behaviour in diabetes mellitus
Pompili, et al (2009) examined the role of diabetes in suicide ideation and
attempt, independent of mood disorders or the side effects of psychotropic drugs
and found that patients with diabetes, compared to a control group, scored higher
on two subscales of the Beck Hopelessness Scale: Loss of Motivation and Future
Expectations, which are significantly related to suicidality. Patients with diabetes
mellitus also registered higher for suicidality on the Suicide Score Scale and showed
significantly lower self-efficacy than the control group
Adolescents with diabetes mellitus displayed higher than expected rates of
suicidal ideation, but relatively few attempted suicide over the follow-up period.
Among those who did attempt suicide, diabetes-related methods commonly used
were potentially lethal doses of insulin which were easily available to them. Suicidal

xxi
ideation shortly after insulin dependent diabetes mellitus onset was related only to
concurrent severity of depressive symptoms. Also, it has been noted that suicidal
ideation and not complying with medical regimen are strongly associated among
teenagers with diabetes mellitus (Goldston, et al 1994).
Patients with diabetes undergoing polytherapy (the use of multiple
medications or treatments) are at a higher risk for suicide ideation and attempt.
Type of diabetes mellitus is not thought to be a significant risk factor, but rather, the
severity of the symptoms and the inconvenience of the treatment are thought to be
more relevant. Patients with combined treatments tend to score higher on several
measures in the Beck Hopelessness Scale. These deficiencies which may lead to a
poorer quality of life, more depression and nervousness, and more reporting of
hardships due to physical or emotional problems. Patients suffering diabetes mellitus
who are above 50 years of age are at a higher risk for suicide ideation and attempt
(Pompili, et al 2009).
2.4 Quality of life in diabetes mellitus
Patients with a chronic medical illness sometimes report a surprisingly high
level of satisfaction with their quality of life (Cassileth, 1984), but clinicians often
underestimate the quality of life of these patients (Uhlmann, 1991).
Diabetes mellitus has a profound effect on the quality of life and on the
physical and emotional health of the individual, with patients suffering type 1
diabetes mellitus generally reporting a worse quality of life than patients with type 2
diabetes (Pompili, et al 2009).
Some demographic variables are associated with low quality of life in

xxii
people with diabetes mellitus. These variables include female sex, increasing age,
low or no formal education and generally people with diabetes mellitus report worse
quality of life compared to the general population (Rubin, 2000).
Patients who had diabetes mellitus were predominantly dissatisfied with their
life circumstances and patients with type 1 had lower quality of life scores relative to
the control group. However, having additional medical problems, having diminished
sexual desire, being young, unemployed and single were significantly associated with
poor quality of life, but illness duration was not (Awadalla, et al 2006).
A study conducted among patients with type 2 in Portugal, showed that
female subjects had poorer quality-of-life ratings than male subjects. Patients were
more likely to regard diabetes mellitus and the consequent changes resulting
because of the illness as a threat rather than as a challenge. A greater proportion of
the patients who have diabetes used avoidance coping mechanisms, which were
related to worse quality of life. Coping style was significantly correlated with several
dimensions of quality of life of these patients with type 2 diabetes mellitus (Coelho,
et al 2003).
Role limitations, the severity of the diabetes symptoms and the
inconveniences of the treatment lead to a poorer quality of life (Pompili, et al 2009).
Empirical studies suggest that the self-perception of poor health is associated
with a significantly increased risk of suicidal ideation among general medical
patients, even in the absence of common mental and physical disorders (Goodwin &
Olfson, 2002). Perceived good quality of life is associated with reduced suicide risk
and higher self-efficacy. Self-efficacy is a major predictor of strong mental health
and positive feelings of fitness, both of which serve protective functions.

xxiii
2.5 Depression and hypertension
Association between major depression and cardiovascular disease has been
established and hypertension is significantly associated with symptoms of depression
(Scherrer, et al 2003). These authors reported that men who have cardiovascular
disease were significantly more likely to have depressive symptoms.
Assessing prevalence of depression in patients with hypertension has received
some considerable attention. Rabkin, et al (1983) reported that major depression
was three times more common among patients with hypertension even when known
cardiac risk factors were taken into account and mild depressive symptoms were
present in 20% of patients with hypertension (Bonnet, et al 2005).
2.6 Quality of life and suicidal behaviour in hypertension
Individuals’ perception of quality of life may be affected by their illness and
also by their therapy. This is the case with patients who have hypertension (Cote, et
al 2004). Although many patients who have mild to moderate hypertension may
have no symptoms (Lawrence, et al 1996), antihypertensive drug therapies are often
associated with many unpleasant adverse effects that may impact negatively on
many aspects pertaining to the quality of life of the patients (Hill, et al 1985).
Patients with pulmonary arterial hypertension have substantial functional and
emotional limitations that adversely affect their health related quality of life
(Shafazard, et al 2004).
In a cross-sectional survey aimed at determining the relationship between
symptoms and health-related quality of life in patients receiving drug therapy

xxiv
for hypertension, it was reported that symptoms have a greater impact on health-
related quality of life than patient’s characteristics, blood pressure or drug related
factors (Erickson, et al 2004).
Hopelessness was associated with increased incidence of hypertension in 616
Finish men, who had normal blood pressure initially, in a 4-year follow-up
prospective study. Participants who had high levels of hopelessness at baseline were
3 times more likely to become hypertensive than those who were not hopeless, after
adjustments for age, body mass index, baseline resting blood pressure, physical
activity, smoking, alcohol consumption, education, and parental history of
hypertension (Everson, et al 2000).
2.7 Nigerian studies
Depression is a common disorder that is widely distributed in the population
(Kessler, et al 2003). In a two phase community based cross sectional study carried
out in Oyo state, using 1105 participants with multistage sampling technique, the
prevalence of depression was found to be 5%. Depression was found to be more
prevalent among women than men - 6% and 5% respectively. The adolescent
population had a prevalence of 10% (Amoran, et al 2007).
A study that aimed at assessing the psychological condition of a group of
Nigerians having diabetes mellitus, reported a prevalence rate of 25% for depression
(Akinlade, et al 1996) whereas Coker et al (2000) reported a prevalence of
depression as 4% among attendees of a general hospital department. Both studies
concluded that psychiatric symptomatology was associated with low occupational
status, duration of diabetes and sexual dysfunction.

xxv
A recent study conducted at Ife, among patients with diabetes mellitus, using
patients with asthma and apparently healthy individuals as controls, recorded the
prevalence of depression as 20% compared to that in asthma (12%). Predictors of
depression included age of the patient, poor glycemic control and duration of
diabetes mellitus. Factors that correlated significantly with diabetic general well-
being include depression, anxiety and fasting blood glucose level. Depression and
the presence of co-morbid medical conditions significantly predicted a low quality of
life (Mosaku, et al 2008).
Clinical depression has been documented to be a common problem among
patients who have diabetes mellitus in Nigeria and those with co-morbid depression
tend to have higher health care costs (Agbir, et al 2010). The prevalence rate of
major depressive episode was 19.4% and depression was significantly correlated
with sex, with a female to male ration of 3:1 and was also significantly associated
with unmarried patients and those who had a poor relationship with their partners.
There was no significant association between depression and respondents’ age,
educational qualifications, employment status, place of residence, household
composition and monthly income (Agbir, et al 2010).
Depression is not only highly co-morbid with diabetes mellitus but also affects
treatment goals negatively (James, et al 2010). This study, recently conducted at the
University of Benin Teaching Hospital, Nigeria reported a prevalence of clinical
depression as 30% among those who have diabetes mellitus compared with 9.5% in
the apparently healthy control group. Having a smaller income and more children
were significantly correlated with higher depression symptoms on Beck depression
inventory.
xxvi
Most Nigerians who have diabetes mellitus have been noted to perform fairly
well on World Health Organization quality of life instrument, short version and poor
quality of life was particularly associated with some physical complications of
diabetes mellitus, lower income, lower educational status, low-rated employment
and type 2 diabetes mellitus (Issa & Baiyewu, 2006).
Overall health related quality of life has been documented to be better in the
group of patients who have hypertension with good control of blood pressure.
Increasing blood pressure, physical symptoms, the presence of stroke, and visual
impairment were significant negative predictors of the overall health-related quality
of life among patients with hypertension (Ogunlana, et al 2009).

xxvii
CHAPTER THREE
AIMS AND OBJECTIVES
The general aim of this study was to determine the prevalence of depressive
symptoms, suicidal behaviour and assess quality of life among the subjects with
diabetes mellitus and to compare these with the subjects who have essential
hypertension at the University of Nigeria Teaching Hospital Enugu, Nigeria.
3.1 Specific Objectives
1. To determine and compare the prevalence of depression among the subjects
with diabetes mellitus and those with essential hypertension at the University
of Nigeria Teaching Hospital Enugu.
2. To determine and compare the prevalence of suicidal behaviour among the
subjects with diabetes mellitus and those with essential hypertension.
3. To determine and compare the quality of life of the subjects with diabetes
mellitus and those that have essential hypertension.
4. To relate depression, suicidal behaviour and quality of life scores of the
subjects with diabetes mellitus and essential hypertension to clinical and
socio-demographic variables.
3.2 Hypotheses
The study proposed the following hypotheses:
1 That depression and depressive symptoms would be more prevalent in the
subjects with diabetes mellitus than those with essential hypertension.
2 That suicidal risk would be higher in the subjects with diabetes

xxviii
mellitus than those with essential hypertension.
3 That quality of life in the subjects with diabetes mellitus would be lower
compared to those with essential hypertension.
4 Socio-demographic variables - female sex, lower educational status, low-rated
employment and lower income would be associated with increased prevalence
of depression, suicidal risk and poor quality of life in the subjects with
diabetes mellitus and essential hypertension.
CHAPTER FOUR
xxix
METHODOLOGY
4.1 Study Setting.
This study was carried out at the endocrinology and cardiology clinics of
University of Nigeria Teaching Hospital Enugu. The hospital began as a General
Hospital for Africans at a temporary site in Ogbete area of Enugu metropolis.
At the end of the Nigerian civil war in 1970, the then government of East
Central State converted it to a specialist hospital with effect from July 01, 1970. The
Federal Government by virtue of decree 23 of 1974 took over the Hospital and
consequently approved the construction of a new permanent site at Ituku-Ozalla.
Presently this new site is functional and located 21 kilometers from Enugu city along
the Enugu-Port Harcourt express way. All services hitherto rendered at the old site
have since been moved to the permanent site with effect from 8th January, 2007.
The Hospital site covers an area of 200 acres with the entire parcel of land
measuring about 747 acres.
There are 41 main departments with three outpost comprehensive health
centers at Obukpa (Enugu State), Abagana (Anambra State) and Isuochi (Abia
State). The Hospital has nine institutions for training of nurses, midwives, laboratory
scientists, medical records officers etc. The bed capacity is 702 with average daily
bed occupancy being 500. The hospital offers 24- hour emergency service as well as
outpatient clinics that include diabetic and cardiology units. There is also a wide
range of laboratory and radiological services. University of Nigeria Teaching Hospital
has many consultants in various medical specialties, 377 resident doctors, nurses,
pharmacists and other paramedical staff. There are also non-medical staffs that run
the daily administrative activities of the Hospital.
xxx
The services of the Hospital are highly subsidized by the Federal Government of
Nigeria. Patients from south- east, south-south and north-central geo-political zones
of Nigeria receive care in this tertiary referral centre.
4.2 Eligibility criteria
a. Inclusion criteria
i. Established diagnosis of type 1 or type 2 diabetes mellitus by a
consultant endocrinologist.
ii. Subjects diagnosed to have essential hypertension by a consultant
cardiologist.
iii. Subjects aged 18 - 64 years.
iv. Willingness to give informed consent.
v. Established disease for at least 1 year and stable without need for
hospital admission for 3 months prior to assessment.
b. Exclusion Criteria
i. Subjects aged<18 years or older than 64 years.
ii. Not willing to give informed consent.
iii. Subjects with severe cognitive impairment
iv. Co-morbid diabetes mellitus and hypertension in one subject.
v. Subjects who have hypertension secondary to another identifiable disease
vi. Unconscious patients and those too ill to participate in the study.
vii. History of mental illness, head injury or substance abuse.
4.3 Sample size determination
The sample size for the study was calculated using the formula

xxxi
N = z2pq/d2 (Araoye, 2003).
Where N = sample size
z2 = confidence interval (a constant) which is 1.96
p = prevalence of the problem determined from a previous study done in
Nigeria- 20% (a recent study in patients with diabetes at Obafemi Awolowo
University Teaching Hospital Ile-Ife, Nigeria reported elevated depressive symptoms
based on use of depression-rating scales (Mosaku, et al. 2008).
q = 100-p
d = level of confidence (5%).
Therefore, the sample was calculated as;
N = z2pq d2
= 1.96x1.96x20x80 5x5
= 246
To make allowance for attrition, a 10% increase was made by adding 24. This
gave a minimum sample size of approximately 270 each for the subjects with
diabetes mellitus and essential hypertension respectively. In essence 540
participants took part in the study.
4.4 Ethical Issues
Approval for this study was obtained from Ethics Committee of University of
Nigeria Teaching Hospital, Enugu Nigeria. All participants gave informed consent
before recruitment into the study. The study did not involve any procedure that was
detrimental to the subjects. It was explained to them that non-

xxxii
participation in the study would not in any way attract any form of penalty or affect
the service they received at the hospital. Subjects were free to withdraw from the
study at any time, even after having initially consented. The subjects found to have
clinically significant depression or high suicidal risk, were advised and subsequently
referred for appropriate care.
4.5 Instruments
4.5.1 Socio-demographic Questionnaire
This questionnaire was designed to provide information about the
respondents’ age, gender, marital status, occupation, level of education, ethnic
background, religion, age of onset of diabetes mellitus/essential hypertension,
duration of illness, type of diabetes mellitus and present drug regimen. The socio-
demographic questionnaire is included as appendix 1.
4.5.2 Beck Depression Inventory
The Beck Depression Inventory (Beck et al, 1988) developed by Dr. Aaron T.
Beck in 1961, is a 21-question multiple-choice self-report inventory about how the
subject has been feeling in the past two weeks. It is one of the most widely used
instruments for measuring the severity of depression. Questions on the Beck
Depression Inventory (BDI) assess mood, pessimism, and sense of failure, self-
dissatisfaction, guilt, punishment, self-dislike, self-accusation, suicidal ideas, crying,
irritability, social withdrawal, body image, work difficulties, insomnia, fatigue,
appetite, weight loss, bodily preoccupation, and loss of libido.

xxxiii
Internal consistency studies demonstrated a correlation coefficient of 0.86 for
the test items, and the Spearman-Brown correlation for the reliability of the BDI
yielded a coefficient of 0.93. Content validity is high since the BDI evaluates quite
well a wide variety of symptoms and attitudes associated with depression.
Beck reported a study in which coefficients of 0.65 and 0.67 were obtained in
comparing results of the BDI with psychiatrists’ ratings of patients (Beck, 1988).
When the test is scored, a value of 0 to 3 is assigned for each answer and the scores
are summed to determine the severity of the depression. Higher total scores indicate
more severe depressive symptoms.
The total score is calculated by adding up the scores for all 21 items to give a range
of 0-63. The scores of 0-9 indicates absence of depression, 10-15 mild depression,
16-19 borderline clinical depression, 20-29 moderate depression, and 30-63 severe
depression.
The BDI suffers from the same problems as other self-report inventories
(Bowling, 2005), in that its scores can be easily exaggerated or minimized by the
person completing them. Like all questionnaires, the way the instrument is
administered can have an effect on the final score. If a patient is asked to fill out the
form in front of other people in a clinical environment, for instance, social
expectations might elicit a different response compared to administration via a postal
survey.
Another serious limitation is that in participants with concomitant physical
illness, it has been suggested that the BDI's reliance on physical symptoms such as
fatigue might artificially inflate scores due to symptoms of the illness, rather than of
depression (Moore, 1998).

xxxiv
BDI has been used in various studies in Nigeria by Akinawo, (1993) and
Adewuya, et al (2007). The BDI is presented as appendix 2.
4.5.3 The Mini-International Neuropsychiatric Interview
The Mini-International Neuropsychiatric Interview (M.I.N.I.) is a short
structured diagnostic interview, developed jointly by psychiatrists and clinicians in
the United States and Europe in 1990 for DSM-IV and ICD-10 psychiatric disorders.
With an administration time of approximately 15 minutes, it was designed to meet
the need for a short but accurate structured psychiatric interview for multicenter
clinical trials and epidemiology studies and is expected to be used as a first step in
outcome tracking in non-research clinical settings (Sheehan, 1998).
It is a widely used instrument by health professionals and organizations with
translations into many languages (Otsubo, et al 2005). It can be used by clinicians
after a brief training session while lay interviewers require more extensive training.
Validation and reliability studies have been done comparing the M.I.N.I. to the
Structured Clinical Interview (SCID-P) for DSM-III-R and the Composite International
Diagnostic Interview (CIDI), a structured interview developed by the World Health
Organization for lay interviewers based on ICD-10 criteria. The results of these
studies showed that the M.I.N.I. has acceptably high validity and reliability scores
(Sheehan, et al 1998). The advantage over other diagnostic instruments like SCID-P
and CIDI is its brevity and that it can be administered in a much shorter period of
time.
xxxv
There are many modules for diagnostic categories but only the major
depressive episode and suicidality modules were used in this research.
Mini-International Neuropsychiatric Interview (M.I.N.I.) has been used in Nigeria by
Adewuya, (2006), Adewuya & Mosaku, et al (2006) and Adewuya & Oginni, et al
(2006).
i) Major depressive episode (MDE) of M.I.N.I.
Major Depressive Episode module of MINI which is grouped as A-module has
six sections A1to A6.
Questions A1 to A3 assessed Current Major Depressive Episode.
Question A4 assessed Recurrent Major Depressive Episode, while question A5 to A6
assessed Major depressive episode with melancholia.
In this study questions A1 to A3 were used since the study assessed major
depressive episode (current).
All questions were coded with YES or NO answers.
Question A1 assessed depressed mood in the past 2 weeks.
Question A2 asked about interests and enjoyments of most of the things the
respondents used to experience in the past.
Question A3 was sub-divided into a to g. The questions here assessed other
parameters when the respondent was depressed or uninterested. For instance, sub-
question 3a asked for level of appetite and weight and 3b asked for sleeping
difficulty, waking up in the middle of the night, early morning wakefulness, or
excessive sleeps.
Question 3c assessed reduced speech and movement, being fidgety,

xxxvi
restlessness, or having trouble sitting still, while sub-question 3d assessed frequency
of tiredness or no energy. Sub-question 3e assessed the frequency of feeling of
worthlessness or guilt, while question 3g asked about hurting self, feeling suicidal, or
wishes for death.
The overall score for major depressive episodes, current was 5 or more yes codes in
questions A1 to A3.
The Major Depressive Episode module of M.I.N.I. is included as appendix 3a.
ii Suicidality module of M.I.N.I.
The Suicidality module of this instrument which is grouped as C Module was
used for this study. There were nine questions in this module labeled C1 to C9.
Questions C1 to C8 assessed events in the past one month while question C9
assessed for suicide attempt in a patient’s lifetime.
C1 asked about suffering any accident and was divided into C1a and C1b. Question
C1a assessed plan or intention to hurt oneself in the accident either passively or
actively while C1b assessed for intention to die as a result of the accident. Scores of
zero were ascribed to C1, C1a and C1b respectively.
C2 assessed for thoughts of being better off dead or wishing for death with a score
of 1 point for yes response.
C3 assessed wanting to harm oneself or to hurt or to injure oneself. This had a score
of 2 points.
C4 asked about thinking of suicide with a score of 6 while C5 assessed for suicide
plan with a score of 8. C6 asked about taking any active steps to prepare to injure

xxxvii
oneself or to prepare for a suicide attempt in which he/she expected or intended to
die and has a score of 9.
C7 assessed deliberately injuring oneself without intending to kill himself/herself with
a score of 4 points. C8 assessed suicide attempt with a score of 10 points.
Each question had a response of either YES or NO with various numerical points
ascribed. For those whose responses were coded yes except C1, summation of the
points specified the level of suicide risk. Scores 1-8 points indicated low suicidal risk,
9-16 moderate and ≥ 17 points as high suicide risk respectively. The Suicidality
module of M.I.N.I. is included as appendix 3b.
4.5.4 World Health Organization Quality of Life-Bref (WHOQoL-Bref)
The World Health Organization quality of life (WHOQoL) project was initiated
in 1991 and aimed at developing an international cross-culturally comparable quality
of life assessment instrument. It assesses the individual's perceptions in the context
of their culture and value systems, and their personal goals, standards and concerns.
WHOQoL instruments were developed collaboratively in a number of centers
worldwide, and have been widely field-tested (WHO, 1996). The WHOQoL-Bref is a
26-item self-administered generic questionnaire, being a shorter version of the
original WHOQoL-100 scale. It is more convenient for use in large research studies
or clinical trials (Murphy, et al 2000).
WHOQOL-Bref instrument emphasizes the subjective responses of patients
rather than objective conditions. It was developed in a wide range of languages for
use in different cultural settings (including Sub-Saharan Africa), and yields
comparable scores across cultures. Together with other measures, the
xxxviii
WHOQoL-Bref enables health professionals to assess changes in quality of life over
the course of treatment and it is anticipated that in future the WHOQoL-Bref will
prove useful in health policy research and will make up an important aspect of the
routine auditing of health and social services (WHO, 1996).
The instrument is made up of four domains or dimensions and sub domains or
facets. The broad domains are physical health, psychological health, social
relationships, and environment.
Three of the four domains of the WHOQoL-Bref (physical, psychological and
environment domains) have been established to demonstrate satisfactory reliability
and validity. However, the social relationships domain exhibited poor validity
(Naumann & Byrne, 2004).
The WHOQoL-Bref produces a quality of life profile. Each of the 26 items has
5 options to which the patient is expected to respond on a 5-point Likert type scale.
It is possible to derive four domain scores. There are also two items that are
examined separately: question 1 asks about an individual’s overall perception of
quality of life and question 2 asks about an individual’s overall perception of their
health. The four domain scores denote an individual’s perception of quality of life in
each particular domain. Domain scores are scaled in a positive direction (i.e. higher
scores denote higher quality of life).
The raw scores for each domain of WHOQoL-Bref were calculated by adding
values of single items according to instructions given at the end of the questionnaire
(WHO, 1996). These raw scores were transformed on the scale ranging from 0 to
100 where 0 was the lowest and 100 was the highest related quality of life scores
respectively. The negatively worded items have reversed scores (Odili,

xxxix
Ugboka, Oparah 2010). The method for calculating raw scores and subsequent
conversion to transformed scores is shown in appendix 4.
Alternatively, the mean score of items within each domain can used to
calculate the domain score. A score of mean ± 1 standard deviation (SD) on each
domain is graded fair, a score of < mean – 1SD is poor and a score of > mean +
1SD is good (Olusina & Ohaeri, 2003).
The World Health Organisation quality of life instrument, short version has
been used in Nigeria by Olusina & Ohaeri (2003), Makanjuola, et al (2005), Issa &
Baiyewu (2006), Fatoye, et al. (2006), Ohaeri, et al (2006). The WHOQoL-Bref is
included as appendix 4.
4.6 Translation of the study instruments
Major depressive episode and suicidality modules of Mini-International
Neuropsychiatric Interview, Beck’s Depression Inventory and the World Health
Organization Quality of Life (WHOQoL-Bref were translated into igbo language which
is the predominantly spoken language in the study area. These instruments were
first translated from English to Igbo language and then back translated from Igbo to
English. The English to Igbo translation was done by an experienced teacher of Igbo
language in Ishiagu Girls’ Secondary School Ebonyi State. She holds a university
degree in Igbo language too and has been involved in other translation works in the
past. The back translation from Igbo to English was done by an Igbo newscaster in
Radio Nigeria FM Abakaliki who speaks both English and Igbo Languages fluently in
addition to possession of a degree in English/Igbo language Education.

xl
Subjects who did not understand English language were interviewed with
Igbo versions of the study instruments.
4.7 Formal training on the use of instruments
The author received a formal training in the use of the instruments for this
study. One of the supervisors (RU) trained the author on the use of Beck Depression
Inventory, Mini-International Neuropsychiatry Interview and World Health
Organization Quality of Life -Bref. The author observed the supervisor administer
these instruments to 10 subjects who met the inclusion criteria for this study.
Thereafter, the author was observed by the supervisor as he administered the
questionnaires. This continued till the supervisor was satisfied that the author was
conversant and properly trained to administer all the instruments required for this
study.
4.8 Pilot Study
A pilot study was conducted at the endocrinology outpatient clinic and
cardiology clinic of University of Nigeria Teaching Hospital Enugu. This pilot test was
done among ten subjects with diabetes mellitus at the endocrinology clinic and
another ten subjects with essential hypertension at the cardiology clinic to determine
the clarity, acceptability, ease of administration of the instruments and identify
logistical problems. The twenty subjects selected met the inclusion criteria for the
study and were consecutive attendees at the endocrinology or cardiology clinic. This
was to ensure that the pilot samples were representative of the original samples for
the study. The subjects who participated in the pilot study were not part of the
xli
main study. The pilot study was done in August, 2010 before the commencement of
the main study under the supervision of one of the supervisors (RU).
4.9 Procedure
Subjects with hypertension were largely seen at the cardiology clinics, which
held three days every week (Monday, Wednesday and Friday). Similarly the subjects
with diabetes mellitus were seen at the endocrinology clinic which held once a week
(every wednesday). The subjects for the study were recruited from the two clinics.
Consecutive attendees who met the inclusion criteria were recruited into the study
until the required sample size was attained. The study was carried out over 6
months period (between August, 2010 and January, 2011).
Subjects diagnosed as having diabetes mellitus or essential hypertension were
initially identified. After confirming that a subject met the inclusion criteria, voluntary
informed consent was obtained. Information about the subject such as age, sex,
religious affiliation, marital status, ethnic group, occupation, age of onset of diabetes
mellitus or essential hypertension, duration of illness and type of diabetes mellitus
were extracted from the subject’s case note and coded into the proforma. Where
applicable, other pieces of information were obtained directly from the patient.
Thereafter, the researcher personally administered all the three instruments to the
participants: Beck Depression Inventory (Appendix 2), Major Depressive Episode and
suicidality modules of Mini-International Neuropsychiatric Interview (Appendix 3) and
The World Health Organization Quality of Life (WHOQoL)-Bref (Appendix 4) one
after the other. Any participant who did not understand English language was
interviewed with Igbo versions of the study instruments by the researcher,
xlii
who is of Igbo extraction with a good command of the written and spoken language.
Problems experienced during the pilot study were noted and necessary
adjustments made which were then applied to the main study. The author observed
that self-administration of the instruments was not feasible because many of the
subjects were not literate and those who were literate had varied levels of
education. The author therefore administered the instruments to the subjects by
reading the questions and options out to them. The subjects chose the options most
applicable to them after ensuring that they understood the questions. Responses by
the participants were recorded and this eliminated the likelihood of not responding
to some questions.
All the instruments were therefore interviewer administered. It has been
shown that these instruments can be validly administered by the interviewer
especially in our environment with different levels of literacy (Issa, Baiyewu 2006,
Odili, Ugboka, Oparah 2010).
This procedure was followed until 270 consecutive attendees who meet the
inclusion criteria at the endocrinology outpatient clinic were recruited for the
subjects with diabetes mellitus. The same number of subjects with essential
hypertension was interviewed at the cardiology clinic. It took an average of 45
minutes to administer all the questionnaires for the study to a subject. Efforts were
made to match closely the subjects who had diabetes mellitus with those who had
essential hypertension in terms of age (± 5years) and sex.
4.10 Statistical analysis
Analysis was done with the Statistical Package for Social Sciences

xliii
(SPSS version 16). Frequency counts and chi-square (x2) test were used for
categorical variables while continuous variables were analyzed using the student t-
test. All statistical values were set at 5% level of significance (p < 0.05).
CHAPTER FIVE
RESULTS

xliv
5.1.1 Socio-demographic variables of the subjects with diabetes mellitus
and subjects with essential hypertension
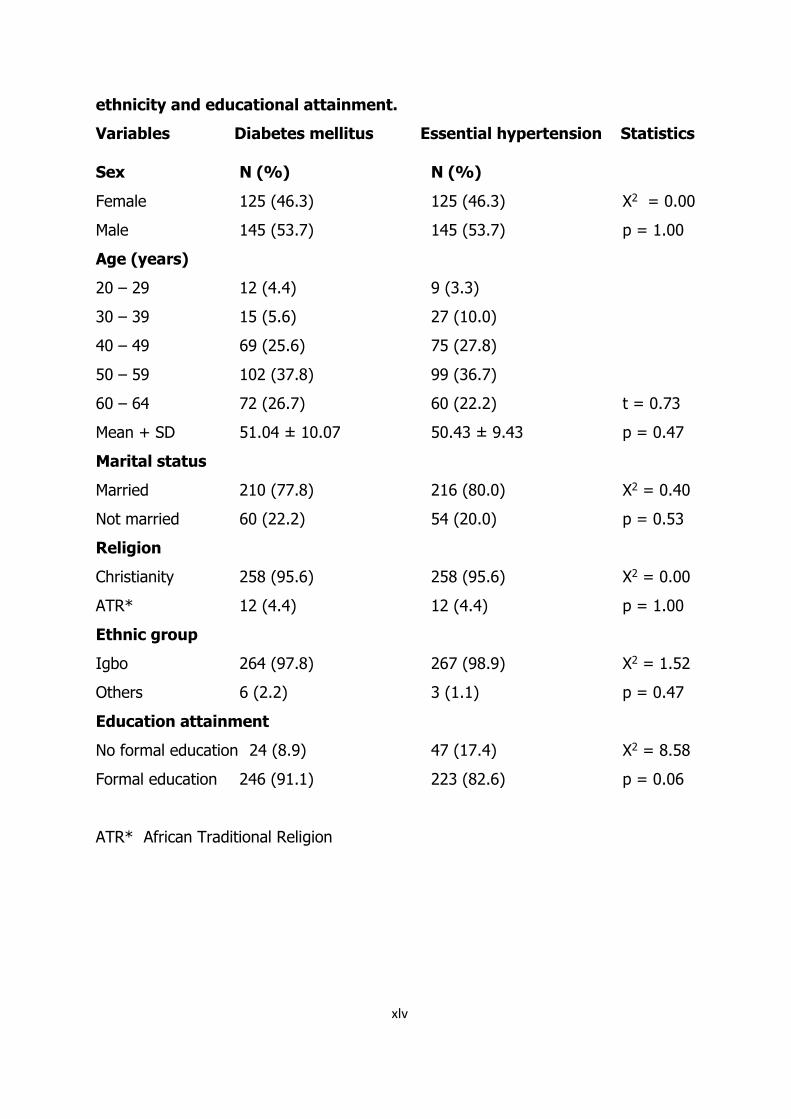
Table 5.1.1 shows the socio-demographic variables of the subjects separated
(i.e. subjects with diabetes mellitus and subjects with essential hypertension). In
each group, 125 (46.3%) were females and 145 (53.7%) were males (X2 = 0.00, p
= 1.00) The mean age for the subjects with diabetes mellitus was 51.0 ± 10.1 years
and this did not significantly differ from 50.4 ± 9.4 years for the subjects with
essential hypertension (t = 0.73, p = 0.47). Amongst the subjects with diabetes
mellitus, 210 (77.8%) were married while for the subjects with essential
hypertension, 216 (80%) were married (X2 = 0.40, p = 0.53). Twenty four (8.9%) of
the subjects with diabetes mellitus had no formal education while among the group
with essential hypertension, forty seven (17.4%) had no formal education (X2 =
8.58, p = 0.06).
Table 5.1.1 Distribution of the subjects with diabetes mellitus and
essential hypertension according to gender, age, marital status, religion,
xlv
ethnicity and educational attainment.
Variables Diabetes mellitus Essential hypertension Statistics
Sex N (%) N (%)
Female 125 (46.3) 125 (46.3) X2 = 0.00
Male 145 (53.7) 145 (53.7) p = 1.00
Age (years)
20 – 29 12 (4.4) 9 (3.3)
30 – 39 15 (5.6) 27 (10.0)
40 – 49 69 (25.6) 75 (27.8)
50 – 59 102 (37.8) 99 (36.7)
60 – 64 72 (26.7) 60 (22.2) t = 0.73
Mean + SD 51.04 ± 10.07 50.43 ± 9.43 p = 0.47
Marital status
Married 210 (77.8) 216 (80.0) X2 = 0.40
Not married 60 (22.2) 54 (20.0) p = 0.53
Religion
Christianity 258 (95.6) 258 (95.6) X2 = 0.00
ATR* 12 (4.4) 12 (4.4) p = 1.00
Ethnic group
Igbo 264 (97.8) 267 (98.9) X2 = 1.52
Others 6 (2.2) 3 (1.1) p = 0.47
Education attainment
No formal education 24 (8.9) 47 (17.4) X2 = 8.58
Formal education 246 (91.1) 223 (82.6) p = 0.06
ATR* African Traditional Religion

xlvi
5.1.2 Distribution of the subjects with diabetes mellitus and essential
hypertension according to employment status, occupation and
duration of illness.
Table 5.1.2 shows the distribution of the two groups of subjects (diabetes
mellitus and essential hypertension) according to employment status, occupation
and duration of illness. The subjects with hypertension were statistically significantly
more likely to be employed, compared to those with diabetes mellitus (X2 = 9.4, p <
0.001). The subjects with diabetes mellitus had a significantly higher illness duration
(mean 7.0 ± 6.3 years), than those with essential hypertension (mean 5.5 ± 5.5
years), (t = 3.06, p < 0.001).

xlvii
Table 5.1.2 Distribution of the subjects with diabetes mellitus and
essential hypertension according to employment status, occupation and
duration of illness.
Diabetes mellitus Essential hypertension Statistics
Employment status N (%) N (%)
Employed 186 (68.9) 217 (80.4) X2 = 9.40
Not employed 84 (31.1) 53 (19.6) p < 0.001
Occupation
Professional/Senior officer/Manager 20 (7.4) 30 (11.1)
Skilled/Service/Associate professionals 48 (17.8) 45 (16.7)
Craft-related/Semi-skilled/clerks 18 (6.7) 18(6.7)
Farmers/ Elementary occupations 184 (68.1) 177 (65.6)
Years of illness
Below 5 years 138 (51.1) 192 (71.1)
5 years and above 132 (48.9) 78 (28.9)
Mean + SD 7.02 ± 6.27 5.47 ± 5.52 t = 3.06
Range 2 – 32 2 – 30 p < 0.001

xlviii
5.2 The rates of depression (current episode) among the subjects with
diabetes mellitus and essential hypertension
Table 5.2 shows the rates of depression (current episode) among the subjects
with diabetes mellitus and essential hypertension. On the Beck Depression
Inventory, the rate of depression among the subjects with diabetes mellitus was
30% and this did not significantly differ from the subjects with essential
hypertension who had 28.5% (X2 = 0.14, p = 0.71). This was also true of the
depression rate using the Mini-International Neuropsychiatric Interview (X2 = 0.08, p
= 0.77).

xlix
Table 5.2 The rates of depression (current episode) among the subjects
with diabetes mellitus and essential hypertension
Diabetes mellitus Essential hypertension
Instrument N (%) N (%)
BDI 81 (30.0) 77 (28.5)
M.I.N.I 75 (27.8) 72 (26.7)

l
5.3.1. Suicidal behaviour among the subjects with diabetes mellitus and
essential hypertension
Table 5.3.1 shows the distribution of the subjects with diabetes mellitus and
essential hypertension according to suicidal behaviour (ideation, plans and attempt).
Subjects with essential hypertension were more likely to exhibit suicidal behaviour
than the subjects with diabetes mellitus but this was not statistically significant (X2 =
0.45, p = 0.50).

li
Table 5.3.1 Suicidal behaviour among the subjects with diabetes mellitus
and essential hypertension
Diabetes mellitus Essential hypertension
Suicidal behaviour N (%) N (%)
Yes 17 (6.3) 21 (7.8)
No 253 (93.7) 249 (92.2)

lii
5.3.2 Suicidal risk among the subjects with diabetes mellitus and
essential hypertension.
Table 5.3.2 shows the suicidal risk among the subjects with diabetes
mellitus and essential hypertension. Subjects with diabetes mellitus were
more likely to score high on the suicidality module of M.I.N.I. compared to
the subjects with essential hypertension (X2 = 7.5, p = 0.06).

liii
Table 5.3.2 Suicidal risk among the subjects with diabetes mellitus and
essential hypertension.
Diabetes mellitus Essential hypertension
Suicidal risk N (%) N (%)
Low - moderate 14 (5.2) 21 (7.8)
High 3 (1.1) 0 (0)
liv
5.4 Quality of life scores among the subjects with diabetes
mellitus and essential hypertension.
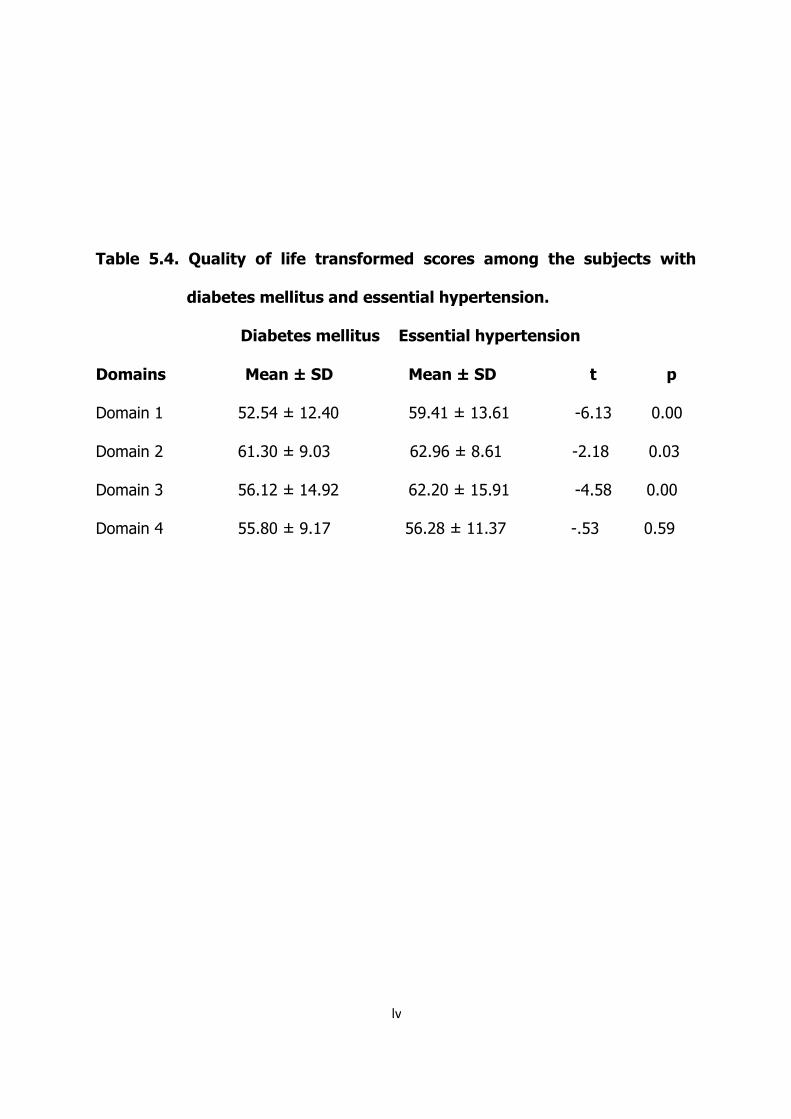
Table 5.4 shows the quality of life (QoL) transformed scores among the subjects
with diabetes mellitus and essential hypertension. Subjects with essential
hypertension were more likely to have higher scores in domain 1 (t = -6.13, p <
0.001), domain 2 (t = -2.18, p = 0.03) and domain 3 (t = -4.58, p < 0.001)
compared to the subjects with diabetes mellitus.
lv
Table 5.4. Quality of life transformed scores among the subjects with
diabetes mellitus and essential hypertension.
Diabetes mellitus Essential hypertension
Domains Mean ± SD Mean ± SD t p
Domain 1 52.54 ± 12.40 59.41 ± 13.61 -6.13 0.00
Domain 2 61.30 ± 9.03 62.96 ± 8.61 -2.18 0.03
Domain 3 56.12 ± 14.92 62.20 ± 15.91 -4.58 0.00
Domain 4 55.80 ± 9.17 56.28 ± 11.37 -.53 0.59
lvi
5.5 Association between depression and socio-demographic
variables
5.5.1 Association between depression and marital status among the
subjects with diabetes mellitus and essential hypertension.
Table 5.5.1 shows the distribution of depression according to marital status among
the subjects with diabetes mellitus and essential hypertension. Two hundred and ten
subjects with diabetes mellitus were married and 48 (22.9%) of them had
depression. The non-married subjects were more likely to have depression than
those who were married (X2 = 11.41, p < 0.001).
Similarly, Fifty four subjects with essential hypertension were not married
(single, widowed, divorced or separated) and 24 (44.4%) of them had depression.
Significantly more non-married subjects were likely to have depression compared to
those who were married among the subjects with essential hypertension (X2 =
10.91, p < 0.001).

lvii
Table 5.5.1 Distribution of depression according to marital status among the
subjects with diabetes mellitus and essential hypertension.
Marital status N Yes Percent (%)
DM
Married 210 48 22.9
Not married 60 27 45
HPTN
Married 216 48 22.2
Not married 54 24 44.4
*DM Diabetes mellitus
* HPTN Essential hypertension

lviii
5.5.2 Association between depression and educational status among
the subjects with diabetes mellitus and essential hypertension.
Table 5.5.2 shows the distribution of depression according to educational status
among the subjects with diabetes mellitus and essential hypertension. Twenty four
patients with diabetes mellitus had no formal education and 13 (54.2%) of them had
depression. The subjects with no formal education were more likely to have
depression compared to those with formal education (X2 = 14.51, p < 0.001).
Depression was higher among the subjects with essential hypertension
without formal education compared to those with formal education (X2 = 17.32, p <
0.001).

lix
Table 5.5.2 Distribution of depression according to educational status among
the subjects with diabetes mellitus and essential hypertension.
Educational status N Yes Percent (%)
DM
No formal education 24 13 54.2
Formal education 246 69 28
HPTN
No formal education 47 24 51.1
Formal education 223 48 21.5

lx
5.5.3 Association between depression and employment status among
the subjects with diabetes mellitus and essential hypertension.
Table 5.5.3 shows the distribution of depression according to employment
status among the subjects with diabetes mellitus and essential hypertension. One
hundred and eighty six of the subjects with diabetes mellitus were employed and 45
(24.2%) had depression. Eighty four patients were not employed, 30 (35.7%) of
whom had depression.
Two hundred and seventeen of the subjects with essential hypertension were
employed and 51 (23.5%) of them had depression. Depression was more likely in
patients with no jobs (X2 = 5.67, p = 0.02).

lxi
Table 5.5.3 Distribution of depression according to employment status
among the subjects with diabetes mellitus and essential hypetension.
Employment status N Yes Percent (%)
DM
Employed 186 45 24.2
Unemployed 84 30 35.7
HPTN
Employed 217 51 23.5
Not employed 53 21 39.6

lxii
5.6 Association between suicidal behaviour (suicidal ideation, plan and
attempt) and socio-demographic variables.
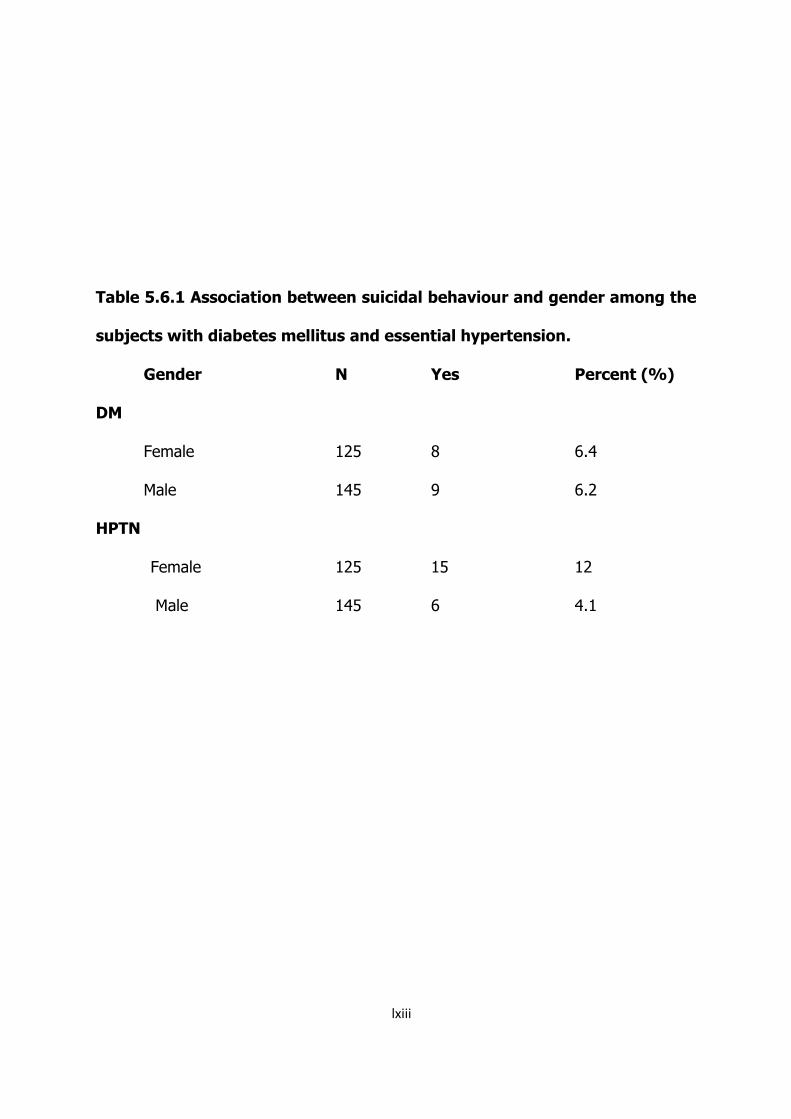
5.6.1 Association between suicidal behaviour and gender among the
subjects with diabetes mellitus and essential hypertension.
Table 5.6.1 shows the distribution of suicidal behaviour according to gender
among the subjects with diabetes mellitus and essential hypertension. Eight females
(6.4%) had suicidal behaviour and this did not significantly differ from the 9 (6.2%)
males with diabetes mellitus who had suicidal behaviour (X2 = 0.00, p = 0.95).
Female subjects with essential hypertension were more likely to have suicidal
behaviour (X2 = 5.79, p = 0.02).
lxiii
Table 5.6.1 Association between suicidal behaviour and gender among the
subjects with diabetes mellitus and essential hypertension.
Gender N Yes Percent (%)
DM
Female 125 8 6.4
Male 145 9 6.2
HPTN
Female 125 15 12
Male 145 6 4.1

lxiv
5.6.2 Association between suicidal behaviour and marital status among
the subjects with diabetes mellitus and essential hypertension.
Table 5.6.2 shows the distribution of suicidal behaviour according to marital
status among the subjects with diabetes mellitus and essential hypertension. Five
(8.3%) of the subjects with diabetes mellitus who were single (never married,
widowed, divorced or separated), exhibited suicidal ideation, plans or attempts
compared to 12 (5.7%) married subjects who had suicidal behaviour.
However, subjects with essential hypertension who were single (never
married, widowed, separated or divorced) were more likely to have suicidal ideation,
plans or attempt (X2 = 19.63, p < 0.001).

lxv
Table 5.6.2 Distribution of suicidal behaviour according to marital status
among the subjects with diabetes mellitus.
Marital status N Yes Percent (%)
DM
Married 210 12 5.7
Not married 60 5 8.3
HPTN
Married 216 9 4.2
Not Married 54 12 22.2

lxvi
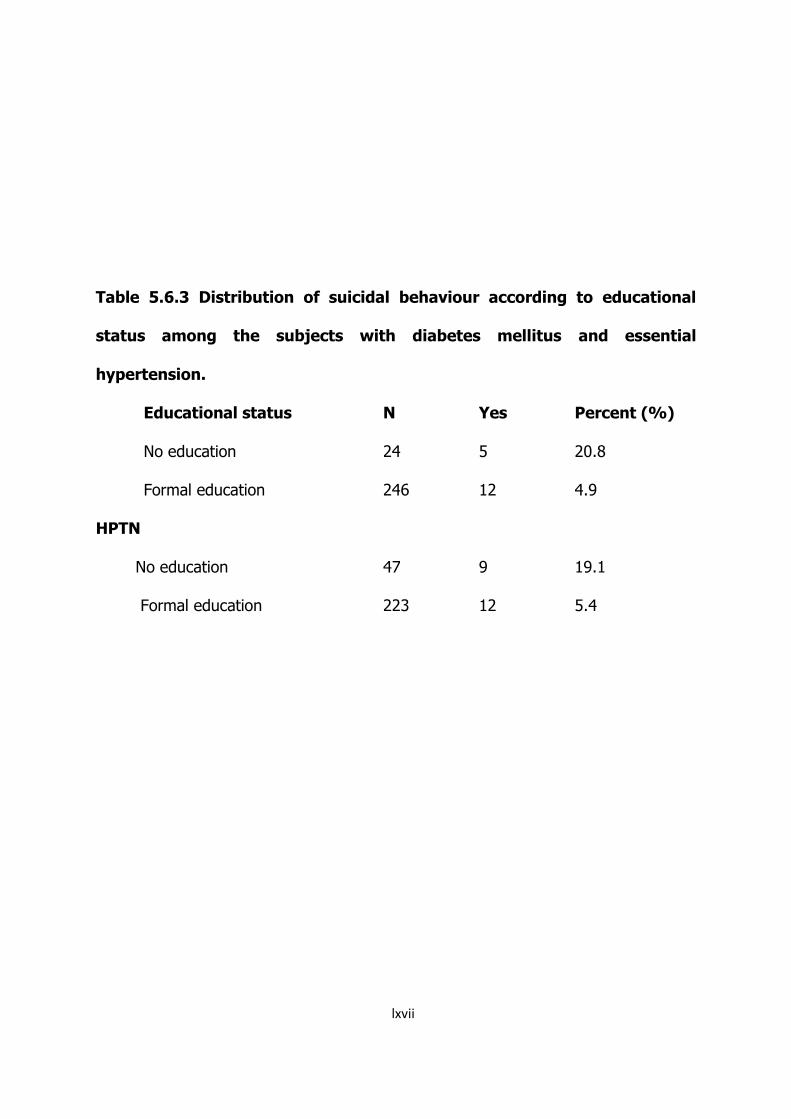
5.6.3 Association between suicidal behaviour and educational
status among the subjects with diabetes mellitus and
essential hypertension.
Table 5.6.3 shows the distribution of suicidal behaviour according to educational
status among the subjects with diabetes mellitus and essential hypertension.
Subjects with diabetes mellitus having no formal education were more likely to
exhibit suicidal ideation, plans and attempts. Twenty four subjects with diabetes
mellitus had no formal education and 5 (20.8%) of them had suicidal behaviour
compared to 12 (4.9%) who had formal education and also had suicidal behaviour
(X2 = 9.44, p < 0.001).
Subjects with essential hypertension who had no formal education were more
likely to exhibit suicidal behaviour compared to the subjects who had formal
education. Nine (19.1%) of the subjects who had no formal education had suicidal
behaviour while 12 (5.4%) of the subjects who had formal education (primary,
secondary or tertiary) had suicidal behaviour (X2 = 10.26, p < 0.001).
lxvii
Table 5.6.3 Distribution of suicidal behaviour according to educational
status among the subjects with diabetes mellitus and essential
hypertension.
Educational status N Yes Percent (%)
No education 24 5 20.8
Formal education 246 12 4.9
HPTN
No education 47 9 19.1
Formal education 223 12 5.4

lxviii
5.7 Association between quality of life (QoL) scores and socio-
demographic variables.
5.7.1 Association between QoL scores and gender among the subjects
with diabetes mellitus and essential hypertension.
Table 5.7.1 shows the distribution of QoL scores with gender among the
subjects with diabetes mellitus and essential hypertension. Male subjects with
diabetes mellitus scored significantly higher in domain 1 (t = -3.72, p < 0.001) and
domain 2 (t = 2.57, p = 0.01).
Male subjects with essential hypertension scored higher than the female
subjects in all the four domains. Males had statistically significant higher scores than
females in domain 2 (t = 2.09, p = 0.04) and domain 3 (t = -2.54, p = 0.01).

lxix
Table 5.7.1 Distribution of QoL scores and gender among the subjects with
diabetes mellitus and essential hypertension.
Gender Domain 1 Domain 2 Domain 3 Domain 4
DM
Female 53.62 ± 9.09 60.00 ± 9.55 57.17 ± 14.52 52.78 ± 11.70
Male 57.68 ± 8.85 62.81 ± 8.17 55.22 ± 15.26 52.34 ± 13.01
HPTN
Female 55.09 ± 12.07 61.94 ± 9.44 59.58 ± 17.13 59.08 ± 11.77
Male 57.30 ± 10.67 64.13 ± 7.42 64.46 ± 14.46 59.70 ± 13.52

lxx
5.7.2 Association between QoL scores and marital status among the
subjects with diabetes mellitus and essential hypertension
Table 5.7.2 shows the distribution of QoL scores and marital status among
the subjects with diabetes mellitus and essential hypertension. Married subjects with
diabetes mellitus had higher QoL scores in domain 1, domain 3 and domain 4 but
this difference was statistically significant in only domain 3 (t = 2.69, p = 0.01).
Subjects with essential hypertension who were married were more likely to
have higher QoL scores. The scores differed significantly in domain 1 (t = 2.19, p =
0.03) and domain 3 (t = 2.07, p = 0.04).

lxxi
Table 5.7.2 Distribution of QoL scores and marital status among and the
subjects with diabetes mellitus and essential hypertension
Marital status Domain 1 Domain 2 Domain 3 Domain 4
DM
Married 56.09 ± 9.43 61.41 ± 7.87 57.41 ± 14.41 52.89 ± 12.73
Unmarried 54.80 ± 8.20 61.60 ± 12.33 51.60 ± 15.90 51.35 ± 11.17
HPTN
Married 57.01 ± 11.50 63.25 ± 8.73 63.13 ± 16.25 58.75 ± 13.29
Unmarried 53.24 ± 10.48 61.95 ± 8.23 58.15 ± 13.83 61.74 ± 14.69

lxxii
5.7.3 Association between QoL scores and educational status among the
subjects with diabetes mellitus and essential hypertension
Table 5.7.3 shows the distribution of QoL scores and educational status
among the subjects with diabetes mellitus and essential hypertension. The subjects
with diabetes mellitus who had formal education had higher QoL scores in all the
four domains but the scores differed significantly in only domain 4 (t = 3.01, p <
0.001).
The subjects with essential hypertension who had formal education had
higher QoL scores in the four domains but the scores differed significantly in domain
1 (t = 3.03, p < 0.001) domain 3 (t = 2.91, p < 0.001) and domain 4 (t = 4.28, p <
0.001).
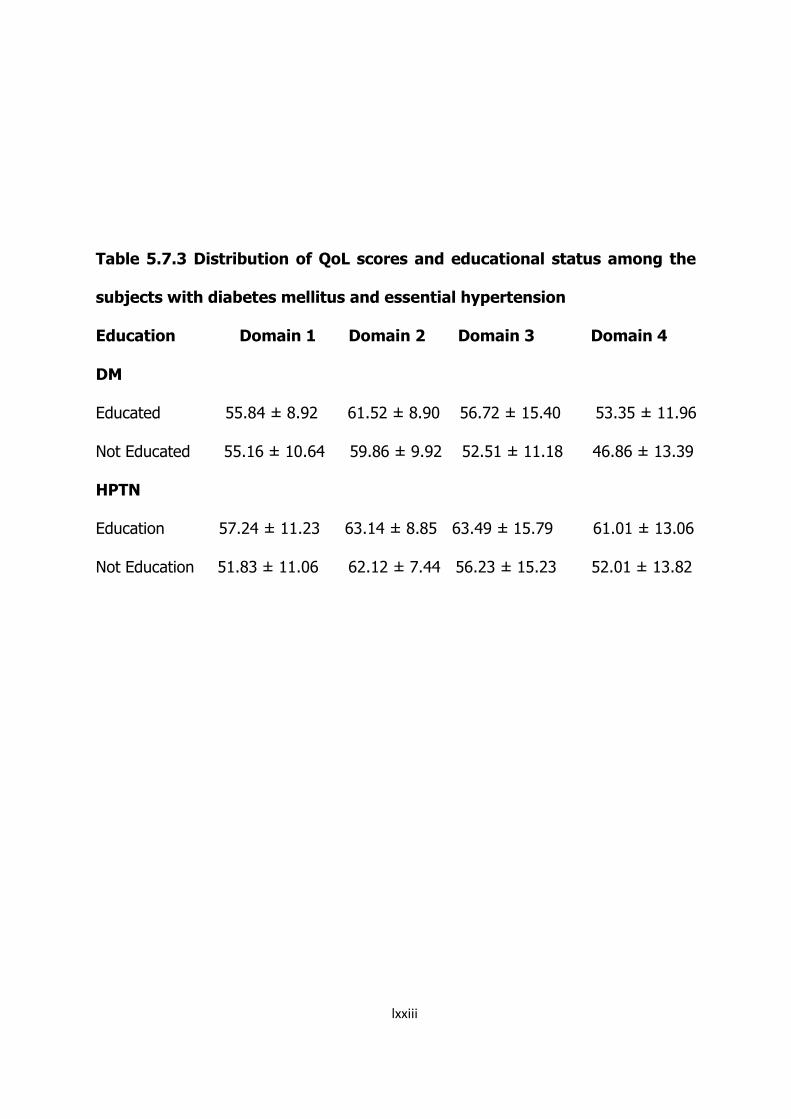
lxxiii
Table 5.7.3 Distribution of QoL scores and educational status among the
subjects with diabetes mellitus and essential hypertension
Education Domain 1 Domain 2 Domain 3 Domain 4
DM
Educated 55.84 ± 8.92 61.52 ± 8.90 56.72 ± 15.40 53.35 ± 11.96
Not Educated 55.16 ± 10.64 59.86 ± 9.92 52.51 ± 11.18 46.86 ± 13.39
HPTN
Education 57.24 ± 11.23 63.14 ± 8.85 63.49 ± 15.79 61.01 ± 13.06
Not Education 51.83 ± 11.06 62.12 ± 7.44 56.23 ± 15.23 52.01 ± 13.82

lxxiv
5.7.4 Association between QoL scores and employment status among the
subjects with diabetes mellitus and essential hypertension
Table 5.7.4 shows the distribution of QoL scores and employment status
among the subjects with diabetes mellitus and essential hypertension. Subjects with
diabetes mellitus who were employed had higher QoL scores in domain 1, domain 2,
domain 3 and differed significantly in domain 1 (t = 3.07, p < 0.001). The subjects
who were not employment scored higher in domain 4 but the difference was not
statistically significant (t= -1.27, p = 0.21).
The QoL scores by the subjects with essential hypertension who were
employed did not significantly differ in any of the four domains compared to the
scores by those who had no jobs.

lxxv
Table 5.7.4 Distribution of QoL scores and employment status among the
subjects with diabetes mellitus and essential hypertension
Employment Domain 1 Domain 2 Domain 3 Domain 4
DM
Employed 56.94 ± 8.30 61.66 ± 8.10 56.66 ± 13.99 51.90 ± 10.67
Not employed 53.29 ± 10.48 60.50 ± 10.83 54.93 ± 16.82 53.96 ± 15.55
HPTN
Employed 56.24 ± 11.43 63.33 ± 8.55 62.83 ± 16.07 59.10 ± 13.26
Not employed 56.44 ± 11.22 61.46 ± 8.80 59.69 ± 15.13 60.65 ± 15.02

lxxvi
CHAPTER SIX
DISCUSSION
6.1 Socio-demographic characteristics of the subjects.
The mean age of the subjects with diabetes mellitus was 51.04 ± 10.07 years
and was similar to 54.65 ± 9.5 years reported in a study that comparatively assessed
depression, anxiety and quality of life among patients with diabetes mellitus (Mosaku
et al, 2008).
It is not surprising that majority of the subjects were of Igbo ethnic
extraction, being the dominant ethnic group in the study site. In the diabetes mellitus
group, 88.9% were married, 95.6% were Christians, and 68.9% were employed. This
was in agreement with results from previous work (James et al, 2010).
A significant proportion of the subjects with diabetes mellitus were not
employed (31.1%) compared to the subjects with essential hypertension (19.6%).
One reason may perhaps be that diabetes mellitus is a chronic and debilitating
medical condition that constitutes a source of stress to the subjects and also affects
their quality of life (Aldwin & Revenson, 1987).
The years of illness ranged from 2 to 32 years for the subjects with diabetes
mellitus and 2 to 30 years for the subjects with essential hypertension. The mean
duration of illness for the subjects with diabetes was 7.0 ± 6.3 years while for the

lxxvii
subjects with essential hypertension, it was 5.5 ± 5.5 years ( t = 3.06, p < 0.001).
6.2 Rates of depression (current episode)
On the Beck Depression Inventory (BDI), the rate of depression among the
subjects with diabetes mellitus was 30% and did not significantly differ from the
subjects with essential hypertension who had a rate of 28.5% (p = 0.71). This was
also true of the depression rate using Mini-International Neuropsychiatric Interview
(M.I.N.I.) where the subjects with diabetes mellitus had 27.8% and the subjects
with essential hypertension had 26.7% (p = 0.77).
The finding was in agreement with an earlier hospital based study conducted at a
teaching hospital in Benin, Nigeria among patients with diabetes mellitus. The study
employed similar methodology with the present study and reported a 30%
prevalence of clinical depression among the subjects with diabetes mellitus using the
depression module of the Schedule for the Clinical Assessment in Neuropsychiatry
(James et al, 2010).
Furthermore, the prevalence of depressive symptoms using a cut-off score of
10 and above on the BDI was 30% among the subjects with diabetes and this was
close to the 25% reported in another study in Western Nigeria that employed the
use of a rating scale among a cohort of Nigerians with diabetes mellitus (Akinlade et
al, 1996), but much higher than the 20% reported in a different study which also
used a rating scale among the subjects with diabetes mellitus (Mosaku et al, 2008).
The finding of prevalence of 26.7% of depression among the subjects with
essential hypertension was similar to a previously reported 20% in a study that
assessed depressive symptoms and association with unhealthy lifestyles in

lxxviii
subjects with hypertension (Bonnet et, al 2005).
6.3 Suicidal behaviour (ideation, plan and attempt)
The findings from this study showed that proportionally, subjects with
essential hypertension were more likely to exhibit suicidal ideation, plan and attempt
(7.8%), compared to the subjects with diabetes mellitus (6.3%). However, suicidal
risk was higher in patients with diabetes mellitus. Three (1.1%) patients with
diabetes mellitus scored high on the suicidality module of M.I.N.I.
These findings were in agreement with a previous Italian study of quality of
life and suicidal risk in subjects with diabetes mellitus (Pompili et, al 2009). The
authors reported that subjects with diabetes mellitus showed greater hopelessness
and suicidal ideation (7.4%) than internal medicine outpatients (6.5%).
The present finding is however in contrast to that reported in a US study (Druss &
Pincus, 2000). The authors examined the association between the presence of a
general medical illness and suicidality in a representative sample of US young adults
and reported that 25.2% of those with a general medical illness had suicidal ideation
and 8.9% had made suicide attempts at a point in their lives. The reason for the
high figures may be because the US study assessed lifetime prevalence of suicidal
behaviour while the present study assessed only suicidal behaviour over the last one
month prior to the interview.
Moreover, majority of the subjects were predominantly Christians (95.6% for
subjects with diabetes mellitus and 95.6% for subjects with essential hypertension).
Suicide is intolerable among Christians and considered a sin of disobedience against
God (The Holy Bible, 2004).

lxxix
6.4 Quality of life
Subjects with diabetes mellitus had statistically lower quality of life scores in
three of the four domains (physical health, psychological and social relationships)
compared with patients who had essential hypertension. This lower mean scores
may perhaps be attributed to the burden that diabetes mellitus places on the
subjects as a result of its demanding nature in management and potential
debilitating complications. Similar scoring pattern was reported in a study that
assessed the impact of diabetes mellitus on the health-related quality of life of
Nigerians. The study compared 112 subjects with diabetes mellitus and 81 healthy
controls (Odili et, al 2010).
Domain 4 (environmental domain) assesses physical safety, financial well-
being, condition of physical environment and living place. There was no significant
difference in the mean scores by subjects with diabetes mellitus and those with
essential hypertension. It could be reasoned that the environment affected the
quality of life of those with diabetes mellitus and essential hypertension equally.
Inclusion criteria for the subjects in this study had been those who were medically
stable for at least 3 months prior to the study. Previous study had reported a similar
finding that when subjects with diabetes mellitus are compared with apparently
healthy control group, the health-related quality of life of the subjects with diabetes
mellitus was lower in all the domains except the environmental domain (Odili et al,
2010).
6.5 Correlates of depression.

lxxx
This study found a significant association between not being married and
having no formal education and having diagnosis of depression among patients with
diabetes mellitus. Depression was more likely in patients with essential hypertension
if the subjects were not married, not educated and not employed. Marriage offers
caregiving and social supports to subjects with diabetes mellitus or essential
hypertension. It has been shown that the family is a major source of support for
psychological adjustments of patients to disease (Bloom &Spiegel, 1984). Such may
not be available to subjects who were single, divorced or widowed.
Having no formal education was associated with depression in this study. Lack
of education is a strong impediment to understanding the dynamics of chronic
medical conditions and complexities involved in good glycaemic control for the
subjects with diabetes mellitus. This finding was in agreement with a previous study
that reported less number of years of formal education as significantly associated
with depression among subjects with diabetes (Mier et al, 2008).
By extrapolation, subjects with less education or no formal education may
earn less as they are likely to get poorly paid jobs. Subjects with low earning power
face the burden of maintaining life style changes that could sustain cost of
medication adherence and dietary restrictions necessary for good glycaemic control
in diabetes mellitus. The relationship between earning power and depression in
diabetes mellitus has been reported in a similar cross-sectional study of 200 subjects
with diabetes mellitus at the University of Benin Teaching Hospital, Nigeria. The
authors used the depression module of Schedule for the Clinical Assessment in
Neuropsychiatry (SCAN) to diagnose depression and Beck Depression Inventory to
assess depression and its severity. (James et al, 2010).

lxxxi
Although female subjects and those not employed with diabetes mellitus were
more likely to have depression, this study found no statistically significant
associations. This agreed with another study which reported no significant
associations between female gender and depression among subjects with diabetes
(James et al, 2010). However, this contrasts with a report of another study that
found significant associations between female and depression among the subjects
with diabetes mellitus. (Mier et, al 2008).
6.6 Correlates of suicidal behaviour.
Suicidal behaviour (ideation, plans and attempts) was likely in subjects with
diabetes mellitus if they had no formal education while in patients with essential
hypertension suicidal behaviour was likely in females, those not married and those
not educated. Diabetes mellitus may have profound effects on physical health,
emotional health and quality of life (Pompili et al, 2009). Having no formal education
may predispose to low self-esteem and lead to feelings of hopelessness as the
patient battles with understanding the dynamics of the disease. Presence of the
disease in a subject with no education is therefore a double burden.
6.7 Correlates of quality of life scores.
Lower quality of life scores were likely in females, those not married,
those not educated and unemployed subjects among those with diabetes
mellitus while lower scores were likely in females, those not married and
those non-educated subjects in those with essential hypertension. Lower
income, lower education and low- rated employment had been reported
lxxxii
to adversely affect the quality of life of subjects with diabetes mellitus in a
cross-sectional study of 251 patients with diabetes mellitus attending the
University of Ilorin Teaching Hospital, Nigeria. (Issa & Baiyewu, 2006). Like
the present study, the authors administered a socio-demographic
questionnaire and World Health Organization quality of life instrument, short
version to the subjects. The findings of the present study concur with this
6.8 Relevance of the study to the practice of psychiatry
Diabetes mellitus and essential hypertension are two chronic medical
conditions that place a lot of burden on patients, health care resources utilization,
work productivity and quality of life. The presence of co-morbid depressive
symptoms, suicidal behaviour and impaired quality of life may compound the
problems, leading to a poorer prognosis in both diabetes mellitus and hypertension.
The identification of the presence of depressive symptoms, suicidal behaviour
and changes in functioning may enhance health workers’ effectiveness in helping
patients maintain adherent behaviour with drug and non-drug interventions in
diabetes mellitus and essential hypertension. This will ultimately become beneficial
to patients with diabetes mellitus and essential hypertension who may have co-
morbid depressive symptoms, suicidal behaviour or impaired quality of life.
6.9 Limitations of the study
1. This study was a cross-sectional based non-population representative
study. Its results cannot be generalized to the entire population.

lxxxiii
2. No causal links or directions can be inferred in a cross-sectional survey of
this nature.
Despite these caveats, the findings from this study should serve as a
baseline data for comparison in future studies especially in South-eastern
Nigeria.
6.10 Recommendations
In view of the findings from this study, the following recommendations will be useful
to caregivers, policy makers and patients.
1. Future studies should address the deficiencies of the present investigation.
More specifically, studies that will establish the cause of depression,
suicidal behaviour and impaired quality of life in subjects with diabetes
mellitus and essential hypertension should be the area of focus.
2. It is possible that collaboration between psychiatrists and internists who
manage diabetes mellitus and essential hypertension may be helpful. This
could be explored.
3. Intervention programmes to raise the quality of life and reduce depression
in diabetes mellitus and essential hypertension may be necessary.
6.11 Conclusion
The findings of this study have shown that depression, suicidal behaviour and
impaired quality of life may co-occur with diabetes mellitus and essential
hypertension. The negative impact of these co-occurrences on achieving good
glycaemic and blood pressure control calls for screening for these conditions when
indicated. This may enhance early detection and treatment.

lxxxiv
REFERENCES
Adewuya A.O. (2006). Prevalence of major depressive disorders in Nigerian college students with alcohol-related problems. General Hospital Psychiatry. 28(2): 169-173.
Adewuya A.O., Ola B.A., Aloba O.O. (2007). Prevalence of major depressive
disorders and a validation of the Beck depression inventory among Nigerian adolescents. European Child and Adolescent Psychiatry. 16(5): 287-292.
Adewuya A.O., Ola B.A., Aloba O.O., Ajayi O.E., Oyedeji A.O., Balogun M.O,
Mosaku S.K. (2006). Prevalence and correlates of major depressive disorders in Nigerian outpatients with heart failure. Psychosomatics. 47: 479-485.
Adewuya A.O., Ola B.A., Aloba O.O., Mapayi B.M., Oginni O.O. (2006).
Depression among Nigerian university students: prevalence and socio-demographic correlates. Social Psychiatry & Psychiatric Epidemiology. 4(8): 674-678.
Agbir T.M., Audu M.D., Adebowale T.O., Goar S.G. (2010). Depression among
medical outpatients with diabetes: A cross-sectional study at Jos University Teaching Hospital, Jos, Nigeria. Ann Afr Med.9:5-10.
Akinawo E.O. (1993). Prevalence of Psychopathological Symptoms in a Nigerian
Prison. Psychopathologie De Africaine XXV(i): 93-104. Akinlade K.S., Ohaeri J.U., Suberu M.A. (1996). The psychological condition of
a cohort of Nigerian diabetic subjects. Afr J Med Med Sci. 25(1): 61-67. Aldwin C.M, Revenson T. (1987). Does coping help? a re-examination of the
relation between coping and mental health. J Pers Soc Psychol 53: 337-348. American Diabetes Association (2004). Diagnosis and classification of diabetes
mellitus. Diabetes Care 27: no. suppl 1 s5-s10 American Psychiatric Association (1994). Diagnostic and statistical manual of
mental disorders, 4th edition (DSM-IV). Washington DC.
lxxxv
Amoran O., Lawoyin T., Lasebikan V. (2007). Prevalence of depression among adults in Oyo state, Nigeria: a comparactive study of rural and urban communities. Aust J Rural Health. 15(3): 211-5.
Anderson R.J., Freedland K.E., Clouse R.E., Lustman P. (2001). The
prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care. 24: 1069–1078.
Araoye A.O. (2003). Research Methodology with Statistics for Health Sciences. 1st
edition, Ilorin, Nigeria. 120-125. Awadalla A.W., Ohaeri J.U., Tawfiq A.M., Al-Awadi S.A. (2006). Subjective
quality of life of outpatients with diabetes: comparison with family caregivers' impressions and control group. J Natl Med Assoc. 98(5): 737–745.
Ayonrinde O., Gureje O., Lawal R. (2004). Psychiatric research in Nigeria:
bridging tradition and modernization. The British Journal of Psychiatry. 184: 536-538.
Beck A.T., Ward C.H., Mendelson M., Mock J., Erbaugh J. (1961). An
inventory for measuring depression. Arch. Gen. Psychiatry 4: 561–71. Bergner M., Bobbitt R.A., Carter W.B., Gilson B.S. (1981). The sickness
impact profile: Development and final revision of a health status measure. Medical Care 19: 787-805.
Bloom J., Spiegel D. (1984). The effects of two dimensions of social support in
the psychological well-being and social functioning of women with advanced breast cancer. Soc Sci Med 19:831-837.
Bonnet F., Irving K., Terra J.L., Nony P., Berthezene F., Moulin P. (2005).
Depressive symptoms are associated with unhealthy lifestyles in hypertensive patients with the metabolic syndrome. J Hypertens. 23: 611–617.
Bowling A. (2005). Mode of questionnaire administration can have serious effects
on data quality. Journal of public health 27 (3): 281–91. Bowling A. (1995). What things are important to people’s lives? A survey of the
public’s judgments to inform scales of health related quality of life. Social Science and Medicine. 41: 1447-1462.
Brannon L., Feist J. (1997). Living with chronic illness, in Health Psychology: An
Introduction to Behavior and Health. Pacific Grove, Calif, Brooks/Cole, pp 265-300.
Brownlee C. (2008). Depression and Diabetes Are Fellow Travelers, Researchers Say. The JHU Gazette 37(40), 1-2.
Carretero O.A., Oparil S. (2000). Essential hypertension: definition and etiology.
Circulation. 101: 329-335.
lxxxvi
Cassileth B.R, Lusk E.J., Strouse T.B., Miller D.S, Brown L.L., Cross P.A.,
Tenaglia A.N. (1984). Psychosocial status in chronic illness. N Engl J Med 311: 506-511
Coelho R., Amorim I., Prata J. (2003). Coping styles and quality of life in
patients with non-insulin-dependent diabetes mellitus. Psychosomatics 44: 312-318.
Coker A.O., Ohaeri J.U., Lawal R.A., Orija O.B. (2000). Specific psychiatric
morbidity among diabetics at a Nigerian General Hospital. East Afr Med J. 77(1): 42-45.
Cote I., Gregoire J., Moisan J., Chabot I. (2004). Quality of life in hypertension: The SF-12 compared to the SF-36. Can J Clin Pharmacol 11(2): 232-238
Dedhiya S., Kong S. X. (1995). Quality of life: an overview of the concept and
measures. Pharmacy World and Science. 17(5): 141-148. de Groot M., Anderson R., Freedland K.E., Clouse R.E, Lustman P.J. (2001).
Association of depression and diabetes complications: a meta-analysis. Psychosom Med 63: 619–630.
Devereux R.B., James G.D., Pickering T.G. (1993). What is normal blood
pressure? Comparison of ambulatory pressure level and variability in patients with normal or abnormal left ventricular geometry. Am J Hypertens 6:211-2115.
Druss B., Pincus H. (2000). Suicidal ideation and suicide attempts in general
medical illnesses. Arch Intern Med. 160:1522 – 1526. Egede L., Nietert P., Zheng D. (2005). Depression and All-Cause and Coronary
Heart Disease Mortality Among Adults With and Without Diabetes. Diabetes Care. 28(6): 1339-1345.
Engum A., Mykletun A., Midthjell K., Holen A., Dahl A.A. (2005). Depression
and Diabetes; A large population-based study of socio-demographic, lifestyle, and clinical factors associated with depression in type 1 and type 2 diabetes. Diabetes Care. 28(8): 1904-1909.
Erickson S.R., William B.C., Gruppen L.D. (2004). Relationship between
symptoms and health-related quality of life in patients treated for hypertension. Pharmacotherapy 24(3): 344-50.
Everson A.S., Kaplan G.A, Goldberg D.E., Salomen J.T. (2000). Hypertension
Incidence Is Predicted by High Levels of Hopelessness in Finish Men. Hypertension 34(2): 561-567.

lxxxvii
Everson A.S., Maty S.C, Lynch J.W., Kaplan G.A. (2002). Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J Psychosom Res 53: 891–895.
Fatoye F.O., Komolafe M.A., Adewuya A.O., Fatoye G.K. (2006). Emotional
distress and self-reported quality of life among primary caregivers of stroke survivors in Nigeria. East Afr Med J. 83: 271-279.
Ferrans C. E. (1990). Development of a quality of life index for patients with
cancer. Oncology Nursing Forum. 17(3): 15-19. Ferrans C. E. (1996). A concept analysis of quality of life. Journal of Orthopaedic
Nursing. 9 (1): 12-18. Fisher L., Skaff M.M., Mullan J.T., Arean P., Mohr D., Masharani U. Glasgow
R., Laurencin G. ( 2007). Clinical depression versus distress among patients with type 2 diabetes; not just a question of semantics. Diabetes Care 30: 542–548.
Gelder M.G., Lopez-Ibor Jr J.J., Andreasen N.C. (2003). New Oxford textbook
of Psychiatry. Oxford University Press, UK. Gendelman N., Snell-Bergeon J.K., McFann K., Kinney G., Wadwa R.P.
Bishop F., Rewers M. (2009). Prevalence and correlates of depression in individuals with and without type 1 diabetes. Diabetes Care 32 (4) 575-579.
Goldston D. B., Kovacs M., Ho V. Y., Parrone P.L. M.S., Stiffler L. (1994).
Suicidal ideation and suicide attempts among youth with insulin-dependent diabetes mellitus. Journal of the American Academy of Child and Adolescent Psychiatry. 33(2): 240-246.
Gomez J. (1987). Liaison psychiatry: mental health problems in the general
hospital. Croom and Helm Publications. Beckenham, UK. Goodwin R., Olfon M. (2002). Self-perception of poor health and suicidal ideation
in medical patients. Psychological Medicine. 32(7): 1293-1299 Hendry F., McVittie C. (2004). Is quality of life a health concept? Measuring and
understanding life experiences of older people. Qualitative Health Research 14 (7): 961-975.
Hill J.F., Bulpitt C.J., Fletcher A.E. (1985). Angiotensin converting enzyme
inhibitors and quality of life: the European trial. J Hypertens Suppl. 3: S91-94.
Hørnquist J.O. (1990). Quality of life: concept and assessment. Scand J Public Health. 18: 69-79.
Issa B.A., Baiyewu O. (2006). Quality of life of patients with diabetes

lxxxviii
mellitus in a Nigerian teaching hospital. Hong Kong J Psychiatry. 16: 27-33.
James B.O., Omoaregba J.O., Eze G., Morakinyo O. (2010). Depression among patients with diabetes mellitus in Nigerian Teaching Hospital. South African Journal of Psychiatry. 16:2
Katon W., Von Korff M., Ciechanowski P., Russo J., Lin E., Simon G., Ludman E., Walker E., Bush T., Young B. (2004). Behavioral and clinical factors associated with depression among individuals with diabetes. Diabetes Care 27: 914–920.
Kessler R.C., Berglund P., Demler O.,Jin R., Koretz D., Merikangas K.R., Rush A.J., Waters E.E.,Wang P. (2003). The epidemiology of major depressive disorder. JAMA. 289: 3095-3105.
Kishi Y., Robinson R.G., Kosier J.T. (2001). Suicidal ideation among patients with acute life – threatening physical illness. Psychosomatics. 42: 382-390.
Lawrence W.F., Fryback D.G., Martin P.A., et al (1996). Health status and
hypertension: A population-based study. J Clin Epidemiol. 49: 1239-1245. Makanjuola A.B., Adeponle A.B., Obembe A.O. (2005). Quality of life in
patients with schizophrenia in Nigeria. Nigeria Med Pract. 48: 36-42. Mier N., Bocanegra-Alonso A, Zhan D, et al. (2008). Depression and diabetes
in bi-national border population. J Am Board Fam Med 21:224-233. Moore M.J., Moore P.B., Shaw P.J. (1998). Mood disturbances in motor neurone
disease. Journal of the neurological sciences 160 Suppl 1: S53–6. Mosaku K., Kolawole B., Mume C., Ikem R. (2008). Depression, Anxiety and
Quality of Life among Diabetic Patients: A Comparative Study. Journal of the National Medical Association. 100(1): 73-78.
Murphy B., Herrman H., Hawthorne G., Pinzone T., Evert H. (2000).
Australian WHOQoL instruments: User’s manual and interpretation guide. Australian WHOQoL Field Study Centre, Melbourne, Australia.
Musisi S., Tugumisirize J. (2001). Psychiatric consultation liaison at Mulago
Hospital. Makerere Univ Med School J. 35: 4–11. National Population Commission (2006). Population census of the Federal
Republic of Nigeria. Abuja, Nigeria. Naumann V.J., Byrne G.J.A . (2004). WHOQOL-BREF as a measure of quality of
life in older patients with depression. International Psychogeriatrics. 16(2): 159-173.

lxxxix
Ndetei D., Khasakhala L., Kuria M., Kokonya D., Mutiso V. (2009). The prevalence of mental disorders in adults in different level general medical facilities in Kenya: a cross-sectional study. Ann Gen Psychiatry 8: 1.
Odili U.O., Ugboka L.U., Oparah A.C. (2010). Quality of life of people with
diabetes in Benin City as measured with WHOQoL-Bref. The internet journal of Law, Healthcare and Ethics 6:2.
Ogunlana M.O., Adedokun B.,Dairo M.D., Odunaiya N.A. (2009). Profile and
predictor of health-related quality of life among hypertensive patients in south-western Nigeria. BMC Cardiovasc Disord 17(9): 25.
Ohaeri J.U., Olusina A.K., Al-Abassi A.M. (2006). Path analytical study of the
short version of the WHOQOL instrument. Psychopathology 39: 243-247. Olusina A.K., Ohaeri J.U. (2003). Subjective quality of life recently discharged
Nigerian psychiatric patients. Soc Psychiatry & Psychiatr Epidemiol. 38: 707-714
Oshira T, Iso H, Satoh S, Sankai T, Tanigawa T, Ogawa Y., Imano H., Sato
S., Kitamura A., Shimamoto T. (2001). Prospective study of depressive symptoms and risk of stroke among Japanese. Stroke. 32(4): 903-7.
Otsubo T., Tanaka K., Koda R., Shinoda J., Sano N., Tanaka S., Aoyama H.,
Mimura M., Kamijima K . (2005). Reliability and validity of Japanese version of the Mini-International Neuropsychiatric Interview. Psychiatry Clin Neurosci. 59 (5): 517-26.
Pompili M., Lester D., Innamorati, M., DePisa E., Amore, M., Ferrara C.,
Tatarelli R., Girardi P. (2009). Quality of life and suicide risk in patients with diabetes mellitus. Psychosomatics. 50(1): 16-23.
Rabkin J., Charles E., Kass F. (1983). Hypertension and DSM-III depression in
psychiatric outpatients. Am J Psychiatry 140(8): 1072-1074. Revicki D.A., Kaplan R.M. (1993). Relationship between psychometric and utility-
based approaches to the measurement of health-related quality of life. Quality of Life Research. 2: 477-487.
Rodin G., Voshart K. (1986). Depression in the medically ill: an overview. Am J
Psychiatry. 143: 696-705. Rubin R.R. (2000). Diabetes and quality of life. Diabetes Spectrum. 13(1): 21-23 Scherrer J.F., Xian H., Bucholz K.K., Eisen S.A., Lyons M.J., Goldberg
J.,Tsuang M., True W.R. (2003). A twin study of depression symptoms, hypertension, and heart disease in middle-aged men. Psychosom Med. 65(4): 548-57

xc
Shafazand S., GoldsteinM.K., Doyle R.L., Hlatky M.A., Gould M.K. (2004).
Health-related quality of life in patients with pulmonary arterial hypertension Chest .126: 1452-1459.
Shah A., Hoxey A., Mayadunne V. (2000). Suicidal ideation in acutely medically
ill elderly inpatients: prevalence, correlates and longitudinal stability. International Journal of Geriatric Psychiatry. 15(2): 162-169.
Sheehan D.V., Lecrubier Y., Sheehan K.H, Amorim P., Janavs J., Weiller E.,
Hergueta T., Baker R., Dunbar G. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 59 Suppl 20: 22-33.
Simonsick E., Wallace R., Blazer D., Berkman L. (1995). Depressive
symptomatology and hypertension-associated morbidity and mortality in older adults. Psychosom Med. 57(5): 427-35.
Spilker B. (1996). Quality Of Life And Pharmacoeconomics In Clinical Trials. Lippincott Williams & Wilkins, USA.
Taylor R.M., Gibson F., Franck L.S. (2008). A concept analysis of health-related quality of life in young people with chronic illness. Journal of Clinical Nursing. 17(14): 1823-1833
The Bible League (2004). The Holy Bible, New Living Translation. Chicago,
USA. Turner J., Kelly B. (2000). Emotional dimensions of chronic disease. West J Med.
17(2): 124-128. Uhlmann R.F., Pearlman R.A. (1991). Perceived quality of life and preferences
for life-sustaining treatments in older adults. Arch Intern Med 141: 495-497. World Health Organization (2005) Atlas: Country Profiles on Mental Health
Resources. WHO, Geneva. World Health Organization (1996). WHOQOL-BREF: Introduction,
administration, scoring and generic version of the assessment. Field version, WHO, Geneva.
xci
APPENDIX 1
Socio-Demographic Questionnaire
This is to obtain some information about you Please kindly answer the
questions as much as you can They are for research purposes and measures have
been put in place to ensure confidentiality of the data. Thanks for your time.
1. Age in years__________________
2. Gender: (a) Male [ ] (b) Female [ ]
3. Religious Affiliation: (a) Christianity [ ] (b) Islam [ ]
(c) African Traditional Religion [ ] (d) Others (Specify) [ ]
4. Marital Status: (a) Married [ ] (b) Single [ ]
(c) Separated [ ] (d) Divorced [ ] (e) Widowed [ ]
5. Ethnic Group: (a) Igbo [ ] (b) Yoruba [ ]
(c) Hausa [ ] (d) Others (Specify) [ ]
6. Level of education: (a) No formal education [ ]
(b) Primary [ ] (c) Secondary [ ] (d) Tertiary [ ]
7. Occupation
8. Employment status:
(a) Student [ ] (b) Not employed [ ] (c) Employed [ ]
9. Age of onset of diabetes/hypertension.

xcii
10. Duration of illness……………….
11. Type of diabetes: (a) Type1[ ] (b) Type 2 [ ]
12. Present drug regimen.
xciii
APPENDIX 2
Beck Depression Inventory
Name: ____________________ Marital status: ________ Age: _____________ Sex:
__________ Occupation: _______________________
Education:_____________________________
Instructions: This questionnaire consists of 21 groups of statements. Please read
reach each group of statements carefully, and then pick out the one statement in
each group that best describes the way you have been feeling during the past two
weeks, including today. Circle the number beside the statement you have picked. If
several statements in the group seem to apply equally well, circle the highest
number for that group. Be sure that you do not choose more than one statement for
any group, including Item 16 (Changes in Sleeping Pattern) or Item 18 (Changes in
Appetite).
1. Sadness
0. I do not feel sad
1. I feel sad much of the time
2. I am sad all the time
3. I am so sad or unhappy that I can’t stand it
2. Pessimism
0. I am not discouraged about my future
1. I feel more discouraged about my future than I used to be
2. I do not expect things to work out for me
3. I feel my future is hopeless and will only get worse
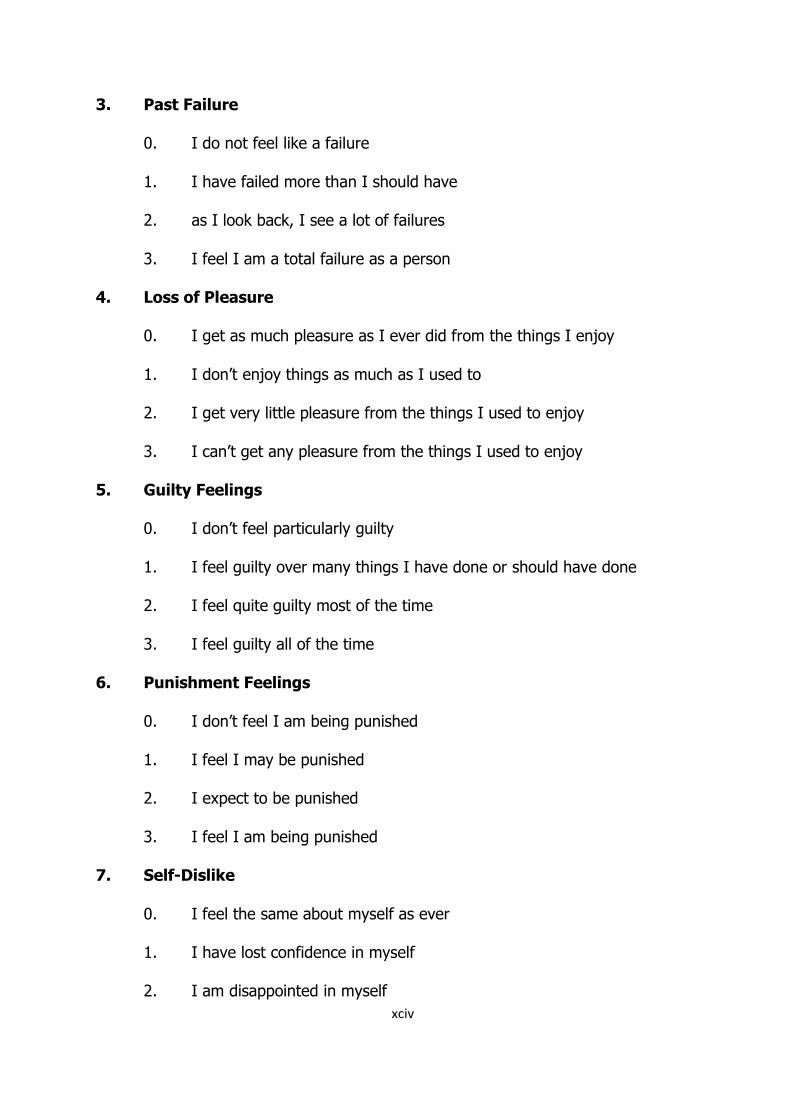
xciv
3. Past Failure
0. I do not feel like a failure
1. I have failed more than I should have
2. as I look back, I see a lot of failures
3. I feel I am a total failure as a person
4. Loss of Pleasure
0. I get as much pleasure as I ever did from the things I enjoy
1. I don’t enjoy things as much as I used to
2. I get very little pleasure from the things I used to enjoy
3. I can’t get any pleasure from the things I used to enjoy
5. Guilty Feelings
0. I don’t feel particularly guilty
1. I feel guilty over many things I have done or should have done
2. I feel quite guilty most of the time
3. I feel guilty all of the time
6. Punishment Feelings
0. I don’t feel I am being punished
1. I feel I may be punished
2. I expect to be punished
3. I feel I am being punished
7. Self-Dislike
0. I feel the same about myself as ever
1. I have lost confidence in myself
2. I am disappointed in myself

xcv
3. I dislike myself
8. Self-Criticalness
0. I don’t criticize or blame myself more than usual
1. I am more critical of myself than I used to be
2. I criticize myself for all of my faults
3. I blame myself for everything bad that happens
9. Suicidal Thoughts or Wishes
0. I don’t have any thoughts of killing myself
1. I have thoughts of killing myself, but I would not carry them out
2. I would like to kill myself
3. I would kill myself if I had the chance
10. Crying
0. I don’t cry anymore than I used to
1. I cry more than I used to
2. I cry over every little thing
3. I feel like crying, but I cant
11. Agitation
0. I am no more restless or wound up than usual
1. I feel more restless or wound up than usual
2. I am so restless or agitated that it’s hard to stay still
3. I am so restless or agitated that I have to keep moving or doing
something
12. Loss of Interest
0. I have not lost interest in other people or activities

xcvi
1. I am less interested in other people or things than before
2. I have lost most of my interest in other people or things
3. it’s hard to get interested in anything
13. Indecisiveness
0. I make decisions about as well as ever
1. I find it more difficult to make decisions than usual
2. I have much greater difficulty in making decisions than I used to
3. I have trouble making any decisions
14. Worthlessness
0. I do not feel I am worthless
1. I don’t consider myself as worthwhile and useful as I used to
2. I feel more worthless as compared to other people
3. I feel utterly worthless
15. Loss of Energy
0. I have as much energy as ever
1. I have less energy than I used to have
2. I don’t have enough energy to do very much
3. I don’t have enough energy to do anything
16. Changes in Sleeping Pattern
0. I have not experienced any change in my sleeping pattern
1a. I sleep somewhat more than usual
1b. I sleep somewhat less than usual
2a. I sleep a lot more than usual
2b. I sleep a lot more than usual

xcvii
3a. I sleep most of the day
3b. I wake up 1-2 hours early and can’t get back to sleep
17. Irritability
0. I am no more irritable than usual
1. I am more irritable than usual
2. I am much more irritable than usual
3. I am irritable all the time
18. Changes in Appetite
0. I have not experienced any change in my appetite
1a. My appetite is somewhat less than usual
1b. My appetite is somewhat greater than usual
2a. My appetite is much less than before
2b. My appetite is much greater than usual
3a. I have no appetite at all
3b. I crave food all the time
19. Concentration Difficulty
0. I can concentrate as well as ever
1. I can’t concentrate as well as usual
2. it’s hard to keep my mind on anything for very long
3. I find I can’t concentrate on anything
20. Tiredness or Fatigue
0. I am no more tired or fatigued than usual
1. I get more tired or fatigued more easily than usual

xcviii
2. I am too tired or fatigued to do a lot of the things I used to do
3. I am too tired or fatigued to do most of the things I used to do
21. Loss of Interest in Sex
0. I have not noticed any recent change in my interest in sex
1. I am less interested in sex than I used to be
2. I am much less interested in sex now
3. I have lost interest in sex completely
Becks Depression Inventory -----Igbo version
N’me ihe ndi a e deputara, horo nke kacha wee metuta gi n’ime izu uka abuo
gara aga.
1. 0 Anaghi m enwe obi mwute.
1. Anam enwe obi mwute kwa mgbe kwa mgbe.
2. Anam enwe obi mwute oge obula.
3. Anam enwe obi mwute nke na mgaghi ebuli ya.
2. 0. Enwerem olileanya maka odinihu.
1. Obi esighi m ike maka odinihu otum si enwebu.
2. Echeghim na ihe ga agaram nke oma.
3. O di m ka olileanya adighi tinyere na ihe ga aka njo no odinihu.
3. 0. Echeghi m na anaghim eme nke oma.
1. Adagom karia kam kwesiri ida.
2. O buru na m leghachi anya na azu na ndum, ihe m na ahu nani bu
emeghi nke oma.
3. Dika mmadu, ana m ahu onwe m dika onye n’ emeghi nke oma

xcix
ma ncha na ndu.
4. 0. Ana m enwe afo ojuju n’ ihe dika m si enwe na mbu.
1. Ihe anaghi atokwa m uto dika o si atom na mbu.
2. Anam enweta obere afo ojuju n’ ihe ndi natabum uto
3. Anaghim enwetazi afo ojuju obula n’ihe ndi natobum uto.
5. 0. Obi m anaghi ama m ikpe.
1. Obi m na-ama m ikpe banyere ihe ufodu mmere ma obu mkwesiri ime.
2. Obi m na- ama m ikpe otutu oge.
3. Obi m na-ama m ikpe oge obula.
6. 0. Anaghim eche na a na-ata m ahuhu.
1. O di m ka e nwere ike ita m ahuhu.
2. Ana m atu anya na a ga-ata m ahuhu.
3. O di m ka a na-ata m ahuhu.
7. 0. E nwerem ntukwasi obi n’ onwem
1. E nweghim ntukwasi obi n’ onwem.
2. Onwe m adighizi m mma.
3. A kporom onwem asi.
8. 0. Adighim akwa onwem emu ma obu ita onwem uta karia kam si emebu.
1. Anam akwazi onwem emu karia kam si emebu.
2. Anam akwa onwem emu mgbe obula maka ihe ndi m n’emetachaghi.
3. Ana m ata onwe m uta maka ihe ojoo obula mere.
9. 0. A naghi m eche uche obula maka igbu onwe m.
1. Uche igbu onwem dim n’obi mana enweghi m ike ime nke a.
2 Oga amasim igbu onwe m.

c
3. M nwee ohere nga egbu onwe m.
10. 0. Anaghi m ebe akwa karia ka m si ebe na mbu.
1. Ana m ebezi akwa ugbua karia ka m si ebe na mbu.
2. Ana m ebe akwa nihe ntakiri obula.
3. Ona amasim ibe akwa ma enweghim ike.
11. 0. O dighi m ka m na enwe mgbakasi ahu karia ka m si enwe bu.
1. Ana m enwetu ngbakasi ahu karia ka m si enwebu.
2. Ana m enwe mgbakasi ahu nke nam aghaghi I nonwu otu ebe.
3. Ana m enwe mgbakasi ahu ruo nam ga nagaghari.
12. 0. Enwere m mmasi n’ebe ndi ozo no.
1. Mmasi m na-enwe n’ebe ndi mmadu no gbadatara nwaobere.
2. Mmasi m na-enwezi n’ebe ndi mmadu no pere nnukwu mpe
3. Enweghizim mmasi obula gbasara ihe obula.
13. 0. Ana m enwe mkpebi nke oma dika m si enwebu na mbu.
1. Ona esirim ike inwe mkpebi karia ka m si enwe na mbu.
2. Ana m enwezi nnukwu nsogbu inwe mkpebi karia ka m si enwe na mbu
3. Anaghi m enwezi mkpebi obula ma ncha.
14. 0. Anaghi ahu onwe m dika onye nabaghi uru.
1. Odim ka mabazi uru ruo otu mdi na mbu.
2. Odim ka uru mbara gbadara nnuku ma atunyere ndi ozi.
3. Odim ka enwezi uru m bara ma oli.
15. 0. E nwere m ike igaghari dika m si emebu na mbu
1. Ike m gbada karia ka odi na mbu.
2. Enwezim ike ime ihe nke ukwu.

ci
3. Ike adighim iru oru obula ma ncha.
16. 0. E nwere m ike irahu ura nke oma dika m si arahu na mbu.
1. Anaghi m arahu ura nke oma dika m si arahu na mbu.
2. Anaghi m arahu ura ebe odikarisiri nta karia ka m si arahu na mbu
3. Ana meteta ura n’oge otutu awa karia ka m si eteta na mbu ma
agaghim arahu ozo.
17. 0. Anaghim ewe iwe karia ka m si ewebu.
1. Anam ewezi iwe ugbua karia ka m si ewebu.
2. Iwe na ewekarizi m ugbu karia ka m si ewebu.
3. Iwe na ewezi m oge obula.
18. 0. O nweghi mgbanwe na ka m si eri bu nri.
1. Ka m si eri ihe adighizi ka o si adibu na mbu.
2. Ka m si eri ihe joro nnukwu njo ugbua.
3. Aguu anaghizi agu m ma ncha.
19. 0. Anam esogide ihe dika otu m si emebu.
1. Anaghim esogide ihe dika otu m si emebu. .
2. O narazim ahu isogide ihe ogologo oge.
3. Enwezim ike isogide ihe obula.
20. 0. Ike adighi agwum karia otu odi na mbu.
1. Ike n’agwuzim karia otu odi na mbu.
2. Ike n’agwuzim ugbua ime ihe m na emebu na mbu.
3. Ike n’agwuzim ugbua ime otutu ihe m na emebu na mbu.
21. 0. Onwebeghi mgbanwe m choputara nso nso a maka mmasi m n’ebe mmeko
nwoke na nwanyi no.
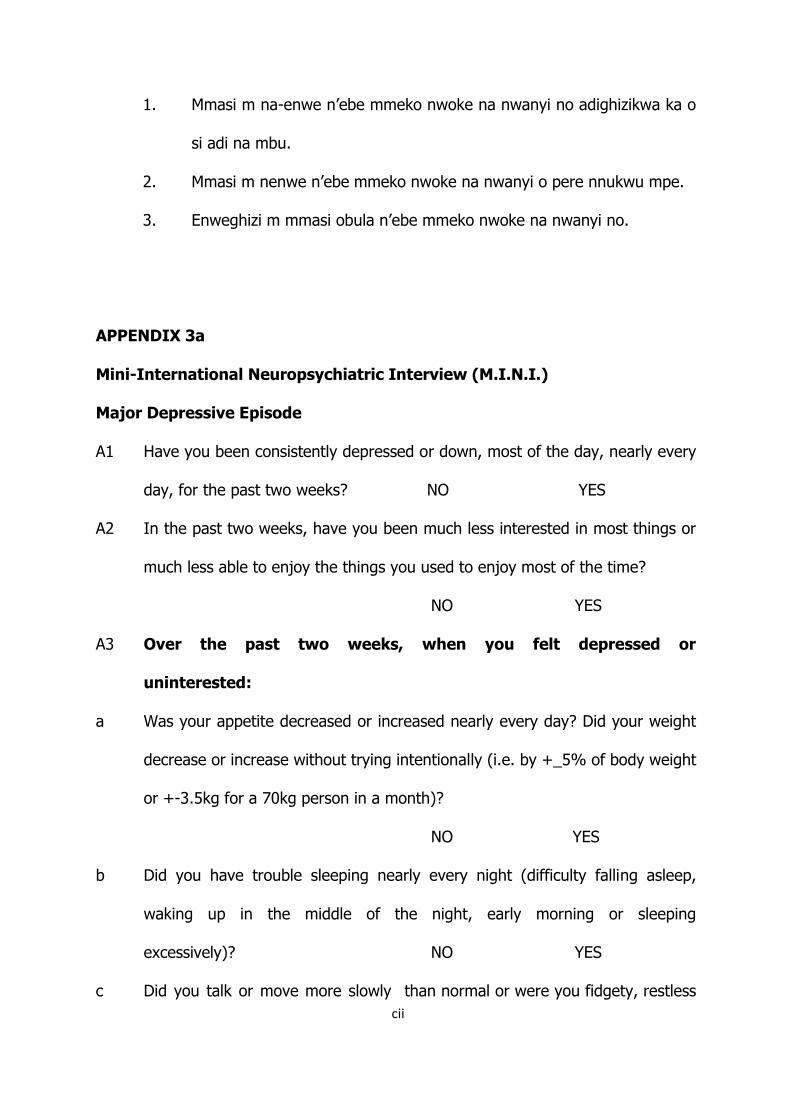
cii
1. Mmasi m na-enwe n’ebe mmeko nwoke na nwanyi no adighizikwa ka o
si adi na mbu.
2. Mmasi m nenwe n’ebe mmeko nwoke na nwanyi o pere nnukwu mpe.
3. Enweghizi m mmasi obula n’ebe mmeko nwoke na nwanyi no.
APPENDIX 3a
Mini-International Neuropsychiatric Interview (M.I.N.I.)
Major Depressive Episode
A1 Have you been consistently depressed or down, most of the day, nearly every
day, for the past two weeks? NO YES
A2 In the past two weeks, have you been much less interested in most things or
much less able to enjoy the things you used to enjoy most of the time?
NO YES
A3 Over the past two weeks, when you felt depressed or
uninterested:
a Was your appetite decreased or increased nearly every day? Did your weight
decrease or increase without trying intentionally (i.e. by +_5% of body weight
or +-3.5kg for a 70kg person in a month)?
NO YES
b Did you have trouble sleeping nearly every night (difficulty falling asleep,
waking up in the middle of the night, early morning or sleeping
excessively)? NO YES
c Did you talk or move more slowly than normal or were you fidgety, restless

ciii
or having trouble sitting still almost every day? NO YES
d Did you feel tired or without energy almost every day? NO YES
e Did you feel worthless or guilty almost every day? NO YES
f Did you have difficulty concentrating or making decisions almost every day?
NO YES
g Did you repeatedly consider hurting yourself, feel suicidal or wish that you
were dead? NO YES
A4 a During your lifetime, did you have other episodes of two weeks or more
when you felt depressed or uninterested in most things, and had most of the
problems we just talked about? NO YES
b In between 2 episodes of depression, did you ever have an interval of at
least 2 months, without any depression and any loss of interest?
NO YES
M.I.N.I Major Depressive Episode-----Igbo version
A1 N’ ime izuuka abuo gara aga I na-enwe obi idamba otutu oge?
Ee Mba
A2 N’ ime izuuka abuo gara aga o na emetuta gi nke na I naghi enwe mmasi
n’otutu ihe I na-nwebu mmasi na ha maobu na ihe na-atobu gi uto abughizi
ihe I na-enwe mmasi na ha? Ee Mba
A3 N’ime izuka abuo gara aga mgbe I nwere obi idamba:
a). Ka I si eri nri o gbagoro ka ogbadara ?. I chere na aru gi ogbagoro maobu
gbadaa n’esiteghi n’igbambo nke gi n’ ihe dika pasenti ise?
Ee Mba
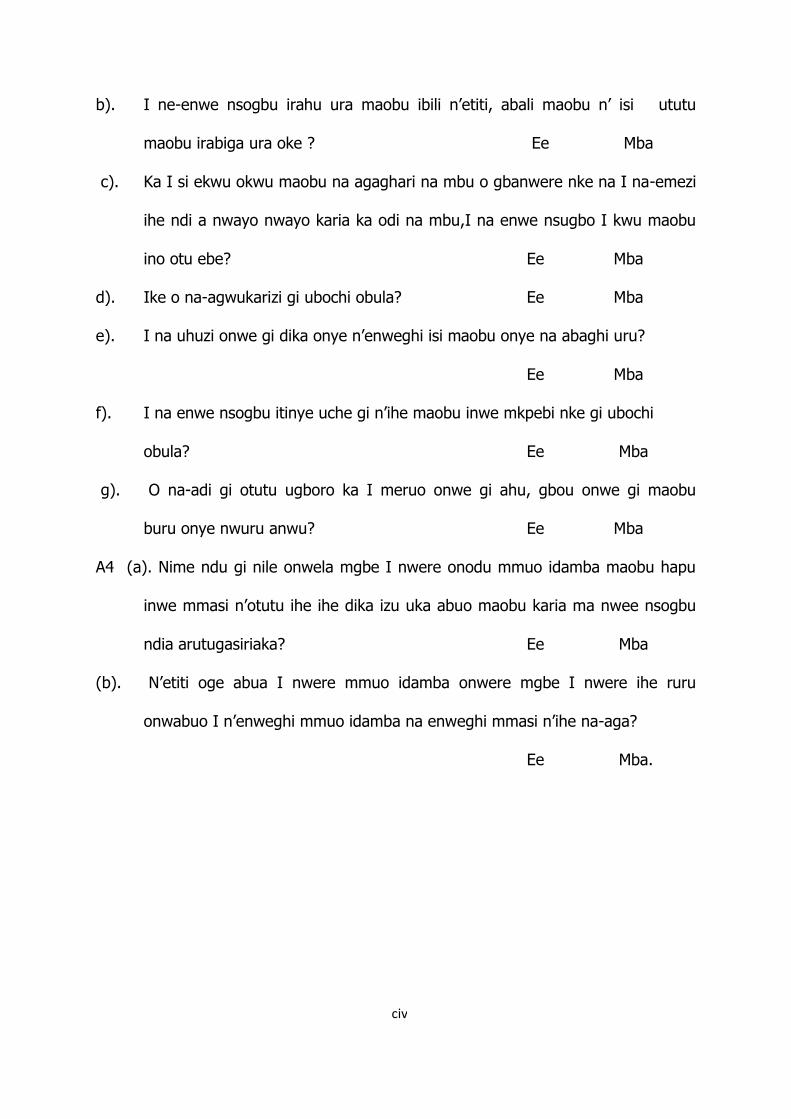
civ
b). I ne-enwe nsogbu irahu ura maobu ibili n’etiti, abali maobu n’ isi ututu
maobu irabiga ura oke ? Ee Mba
c). Ka I si ekwu okwu maobu na agaghari na mbu o gbanwere nke na I na-emezi
ihe ndi a nwayo nwayo karia ka odi na mbu,I na enwe nsugbo I kwu maobu
ino otu ebe? Ee Mba
d). Ike o na-agwukarizi gi ubochi obula? Ee Mba
e). I na uhuzi onwe gi dika onye n’enweghi isi maobu onye na abaghi uru?
Ee Mba
f). I na enwe nsogbu itinye uche gi n’ihe maobu inwe mkpebi nke gi ubochi
obula? Ee Mba
g). O na-adi gi otutu ugboro ka I meruo onwe gi ahu, gbou onwe gi maobu
buru onye nwuru anwu? Ee Mba
A4 (a). Nime ndu gi nile onwela mgbe I nwere onodu mmuo idamba maobu hapu
inwe mmasi n’otutu ihe ihe dika izu uka abuo maobu karia ma nwee nsogbu
ndia arutugasiriaka? Ee Mba
(b). N’etiti oge abua I nwere mmuo idamba onwere mgbe I nwere ihe ruru
onwabuo I n’enweghi mmuo idamba na enweghi mmasi n’ihe na-aga?
Ee Mba.

cv
APPENDIX 3b
Mini-International Neuropsychiatric Interview- Suicidality Module
In the past month did you:
C1. Suffer any accident? NO YES
C1a. Plan or intend to hurt yourself in that accident either passively or actively?
NO YES
C1b Did you intend to die as a result of this accident? NO YES
C2 Think that you would be better off dead or wish you were dead?
NO YES
C3 Want to harm yourself or to hurt or to injure yourself? NO YES
C4 Think about suicide? NO YES
C5 Have a suicide plan? NO YES
C6 Take any active steps to prepare to injure yourself or to prepare for a
suicide attempt in which you expected or intended to die? NO YES
C7 Deliberately injure yourself without intending to kill yourself? NO YES
C8 Attempt suicide? NO YES
In your lifetime:
C9 Did you ever make a suicide attempt? NO YES
M.I.N.I. Suicidality Module-----Igbo version
N’onwa gara aga:
C1. I nwere ihe mberede o bula? Mba Ee

cvi
C1a. I ji aka gi cho I meru onwe gi ahu n’ihe mberede ahu? Mba Ee
C1b. Ebum nobi gi o bu ka I nwuo n’ihi ihe mberede ahu? Mba Ee
C2. I chere na o kara ika gi mma ma o buru na I nwuru n’ihe mberede ahu?
Mba Ee
C3. I choro imeru onwe gi ahu? Mba Ee
C4. I chere echiche Igbu onwe gi? Mba Ee
C5. I metula nkwado maka igbu Onwe gi? Mba Ee
C6. O nwetula mgbe I kwadoro I ga I meru Mba Ee
C7. I matula uma meruo onwe gi ahu n’ebughi n’obi igbu onwe gi?
Mba Ee
C8. I gatula igbu onwe gi? Mba Ee
Na ndu gi n’ile
C9. E nwela mgbe I choro igbu onwe gi? Mba Ee
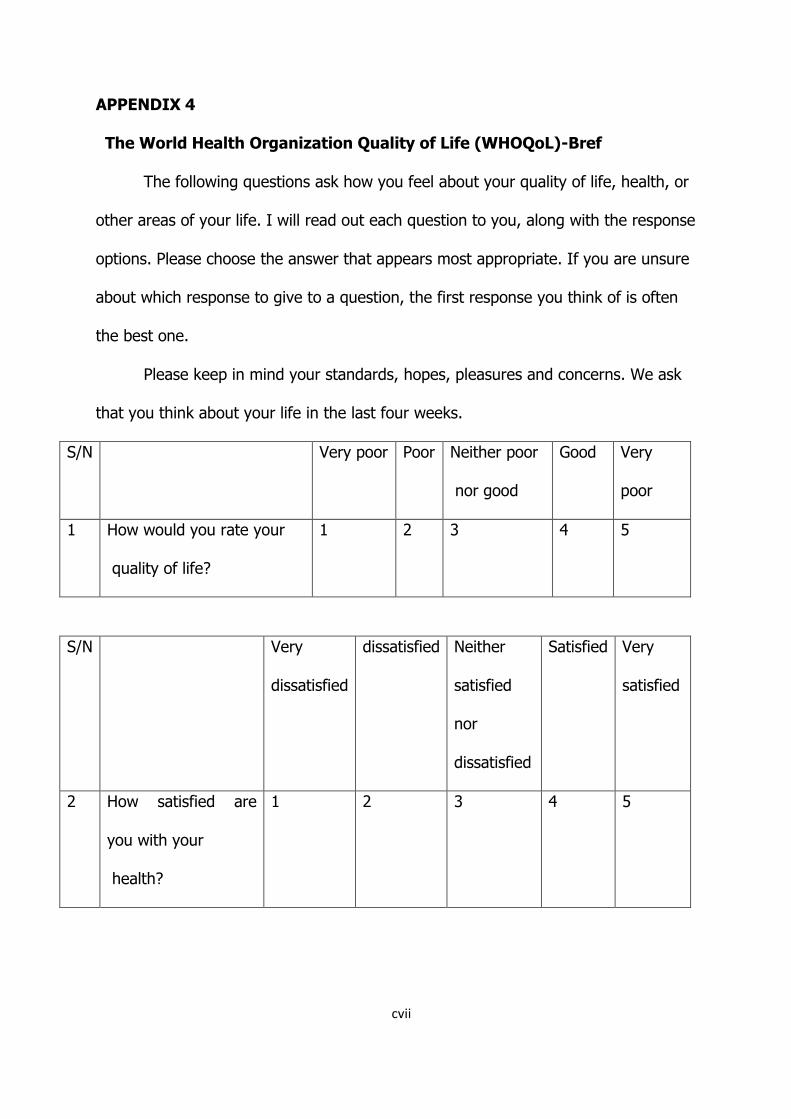
cvii
APPENDIX 4
The World Health Organization Quality of Life (WHOQoL)-Bref
The following questions ask how you feel about your quality of life, health, or
other areas of your life. I will read out each question to you, along with the response
options. Please choose the answer that appears most appropriate. If you are unsure
about which response to give to a question, the first response you think of is often
the best one.
Please keep in mind your standards, hopes, pleasures and concerns. We ask
that you think about your life in the last four weeks.
S/N Very poor Poor Neither poor
nor good
Good Very
poor
1 How would you rate your
quality of life?
1 2 3 4 5
S/N Very
dissatisfied
dissatisfied Neither
satisfied
nor
dissatisfied
Satisfied Very
satisfied
2 How satisfied are
you with your
health?
1 2 3 4 5

cviii
The following questions ask about how much you have experienced certain things in
the last four weeks.
S/N Not at all A little A moderate amount
Very much
An extreme amount
3 To what extent do you feel
that physical pain prevents
you from doing what you
need to do?
1 2 3 4 5
4. How much do you need any
medical treatment to
function in your daily life?
1 2 3 4 5
5. How much do you enjoy
life?
1 2 3 4 5
6 To what extent do you feel
your life to be meaningful?
1 2 3 4 5
S/N Not at all A little A moderate amount
Very much
Extremely
7 How well are you able to
concentrate?
1 2 3 4 5
8 How safe do you feel in
your daily life?
1 2 3 4 5

cix
9 How healthy is your
physical environment?
1 2 3 4 5
S/N Not at all A little moderate Mostly Completely
10 Do you have enough
energy for every day life?
1 2 3 4 5
11 Are you able to accept your
bodily appearance?
1 2 3 4 5
12 Have you enough money to
meet your needs?
1 2 3 4 5
13 How available to you is
information that you need
in your day-to-day life?
1 2 3 4 5
14 To what extent do you
have the opportunity for
leisure activities?
1 2 3 4 5
S/N Very poor Poor Neither
poor
nor good
Good Very poor
15 How well are you able to
get around?
1 2 3 4 5

cx

cxi
S/N Very dissatisfied
dissatisfied Neither satisfied nor dissatisfied
Satisfied Very satisfied
16 How satisfied are
you with your sleep?
1 2 3 4 5
17. How satisfied are
you with your ability
to perform your
daily living activities?
1 2 3 4 5
18 How satisfied are
you with your
capacity for work?
1 2 3 4 5
19 How satisfied are
you with yourself?
1 2 3 4 5
20 How satisfied are
you with your
personal
relationships?
1 2 3 4 5
21 How satisfied are
you with your sex
life?
1 2 3 4 5

cxii
22 How satisfied are
you with the support
you get from
your friends?
1 2 3 4 5
23
How satisfied are
you with the
conditions of your
living place?
1 2 3 4 5
24 How satisfied are
you with your
access to health
services?
1 2 3 4 5
25. How satisfied are
you with your
transport?
1 2 3 4 5
The following question refers to how often you have felt or experienced certain
things in the last four weeks.
S/N Never Seldom Quite often Very
often
Always

cxiii
26 How often do you have
negative feelings such as
blue mood, despair,
anxiety, depression?
5 4 3 2 1

cxiv
Do you have any comments about the assessment?
Calculating transformed domain scores
Raw domain scores are calculated by straight forward summative scaling of
constituent items. Three negatively-worded items need to be reverse-scored (Q3, Q4
and Q26), as shown in the formulae (WHO, 1996).
The raw domain scores are calculated as follows:
Physical health = (6-Q3) + (6-Q4) + Q10 + Q15 + Q16 + Q17 + Q18
Psychological health = Q5 + Q6 + Q7 + Q11 + Q19 + (6-Q26)
Social relationships = Q20 + Q21 + Q22
Environment = Q8 + Q9 + Q12 + Q13 + Q14 + Q23 + Q24 + Q25
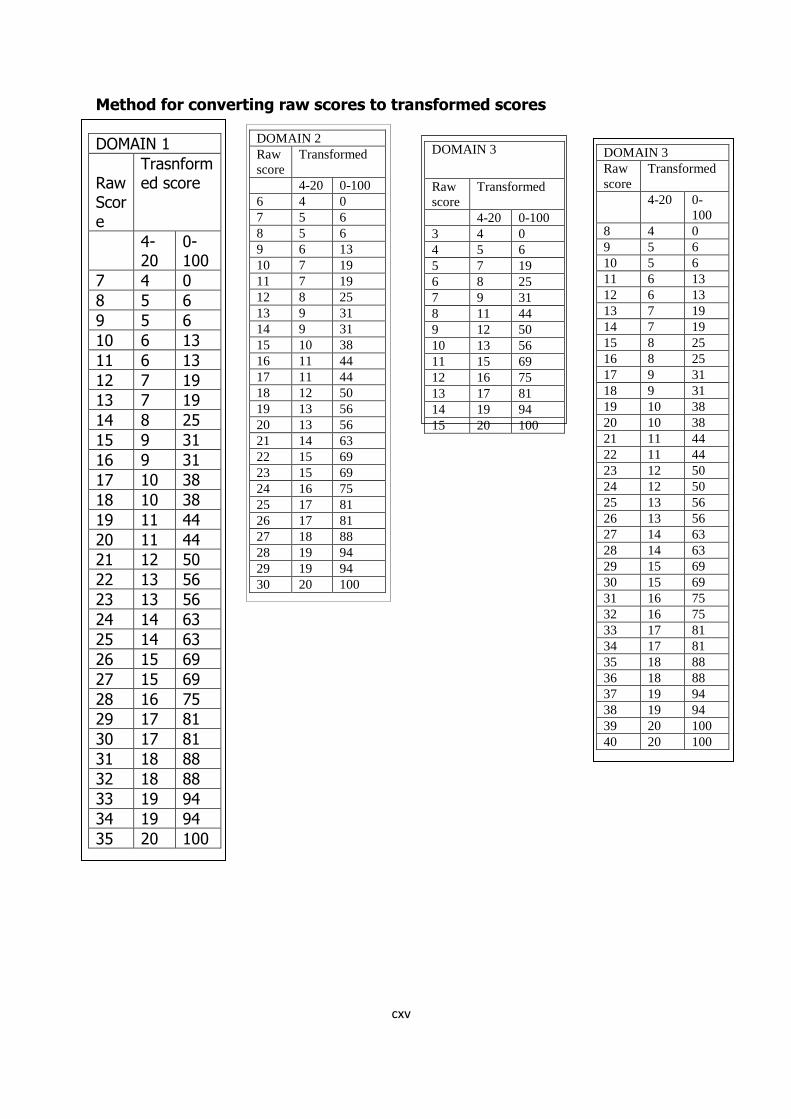
cxv
Method for converting raw scores to transformed scores
DOMAIN 1
Raw Score
Trasnformed score
4-20
0-100
7 4 0
8 5 6
9 5 6
10 6 13
11 6 13
12 7 19
13 7 19
14 8 25
15 9 31
16 9 31
17 10 38
18 10 38
19 11 44
20 11 44
21 12 50
22 13 56
23 13 56
24 14 63
25 14 63
26 15 69
27 15 69
28 16 75
29 17 81
30 17 81
31 18 88
32 18 88
33 19 94
34 19 94
35 20 100
DOMAIN 2
Raw
score
Transformed
4-20 0-100
6 4 0
7 5 6
8 5 6
9 6 13
10 7 19
11 7 19
12 8 25
13 9 31
14 9 31
15 10 38
16 11 44
17 11 44
18 12 50
19 13 56
20 13 56
21 14 63
22 15 69
23 15 69
24 16 75
25 17 81
26 17 81
27 18 88
28 19 94
29 19 94
30 20 100
DOMAIN 3
Raw
score
Transformed
4-20 0-100
3 4 0
4 5 6
5 7 19
6 8 25
7 9 31
8 11 44
9 12 50
10 13 56
11 15 69
12 16 75
13 17 81
14 19 94
15 20 100
DOMAIN 3
Raw
score
Transformed
4-20 0-
100
8 4 0
9 5 6
10 5 6
11 6 13
12 6 13
13 7 19
14 7 19
15 8 25
16 8 25
17 9 31
18 9 31
19 10 38
20 10 38
21 11 44
22 11 44
23 12 50
24 12 50
25 13 56
26 13 56
27 14 63
28 14 63
29 15 69
30 15 69
31 16 75
32 16 75
33 17 81
34 17 81
35 18 88
36 18 88
37 19 94
38 19 94
39 20 100
40 20 100

cxvi
Igbo Version of WHOQoL-Bref
Ajuju ndi a bu maka i mata etu i si ahuta ndu gi, ahu gi nakwa ihe ndi ozo gbasara
ndu gi. M ga aguputara gi ajuju o bula tinyekwuoro aziza ya. Biko horo aziza nke
dabara adaba. Ya buru na o gbagwo-juru gi anya bu osisa nke i ga enye, nke mbu
ahu batara gi n’obi na-abukari nke dabara adaba.
Biko buru n’obi maka udi mmadu i bu, olile-anya gi na ihe na-enye gi obi uto. Anyi
na-aju ka i chee maka etu i si bie ndu n’izu uka ano gara aga.
O joro njo O
rigughi
afo
O dighi mma, o
dighikwanu nfo
Odi
mma
O di ezigbo
mma
1 Kedu etu i si huta
ndu gi?
1 2 3 4 5
O rijugi
afo ma otu
O jugi
afo
O bughi na o
juru afo o bughi
kwanu na o jughi
afo
O
juru
afo
O juru ezigbo
afo
2. Kedu etu ndu gi si
judebe gi afo?
1 2 3 4 5
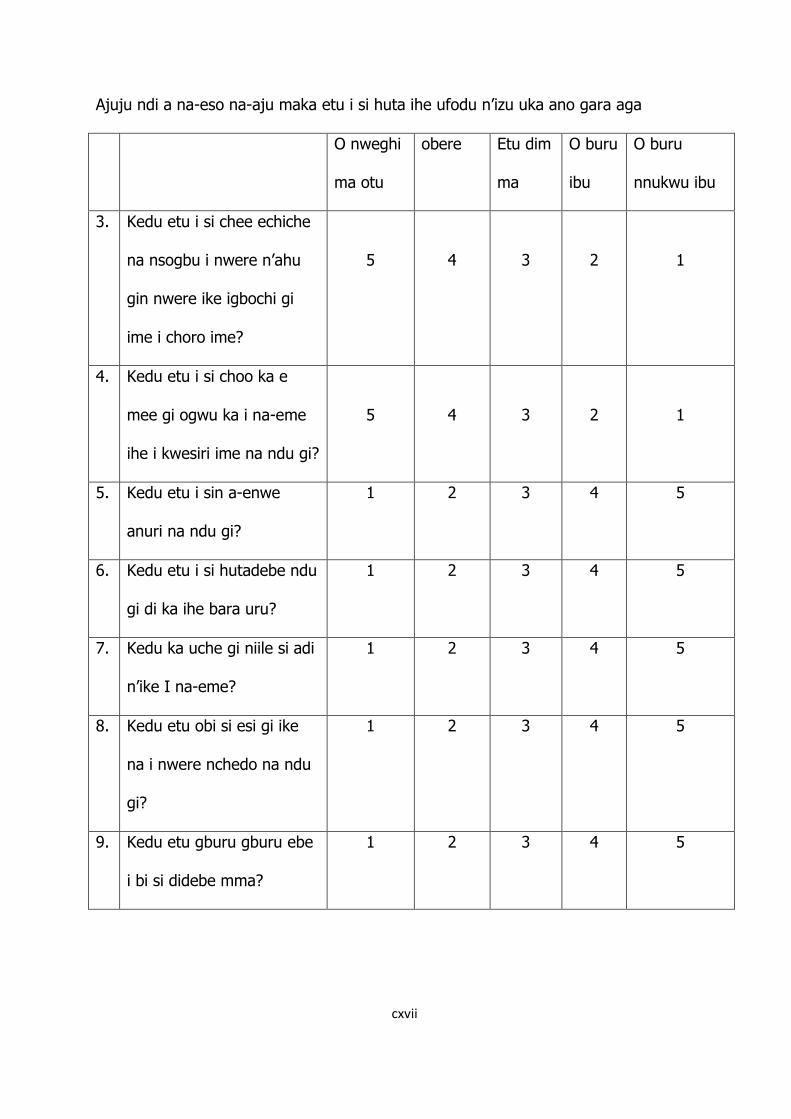
cxvii
Ajuju ndi a na-eso na-aju maka etu i si huta ihe ufodu n’izu uka ano gara aga
O nweghi
ma otu
obere Etu dim
ma
O buru
ibu
O buru
nnukwu ibu
3. Kedu etu i si chee echiche
na nsogbu i nwere n’ahu
gin nwere ike igbochi gi
ime i choro ime?
5
4
3
2
1
4. Kedu etu i si choo ka e
mee gi ogwu ka i na-eme
ihe i kwesiri ime na ndu gi?
5
4
3
2
1
5. Kedu etu i sin a-enwe
anuri na ndu gi?
1 2 3 4 5
6. Kedu etu i si hutadebe ndu
gi di ka ihe bara uru?
1 2 3 4 5
7. Kedu ka uche gi niile si adi
n’ike I na-eme?
1 2 3 4 5
8. Kedu etu obi si esi gi ike
na i nwere nchedo na ndu
gi?
1 2 3 4 5
9. Kedu etu gburu gburu ebe
i bi si didebe mma?
1 2 3 4 5

cxviii
Ajuju ndi a na-eso na-aju maka etu i si huta ma o bu menwuo ihe ufodu n’izu uka
ano gara aga
O nweghi
ma otu
obere Etu dim
ma
O
buru
ibu
O buru
nnukwu ibu
10. I na-enwe ume zuru oke
ubochi niile nke ndu gi?
1
2
3
4
5
11. I nabatara etu ahu gi di?
12 I nwere ego ga-ezuru gi ime
ih
1
2
3
4
5
13 Kedu etu ozi obula i choro i
nu si eru gi nti
1
2
3
4
5
14 Kedu etu i si enwedebe
ohere ime ihe o bula na-
enye gi onwu?
1
2
3
4
5
O juru
njo
O
rigughi
afo
O dighi
mma, o
dighikwanu
njo
O dim
ma
O di
ezigbo
mma
15. Kedu etu i na-esi agagharitu 1 2 3 4 5
16. Kedu etu i si e nwedebe afo
ojuju n’ihi ura gi?
1 2 3 4 5
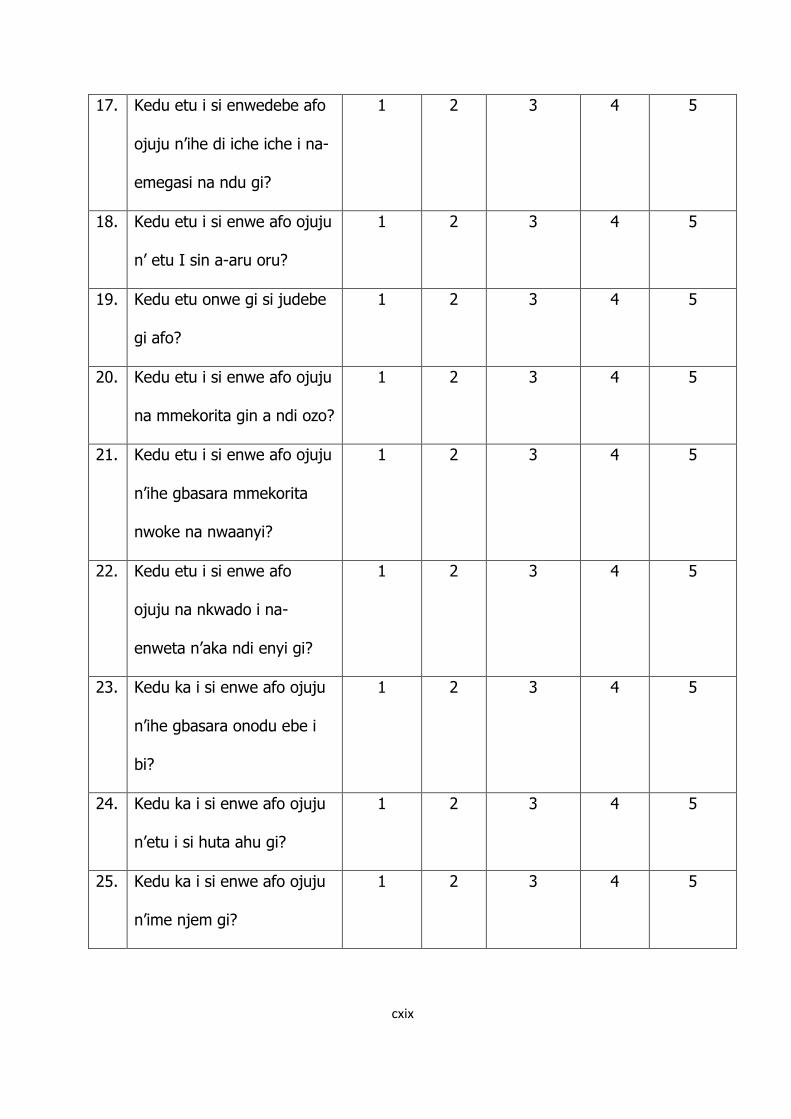
cxix
17. Kedu etu i si enwedebe afo
ojuju n’ihe di iche iche i na-
emegasi na ndu gi?
1 2 3 4 5
18. Kedu etu i si enwe afo ojuju
n’ etu I sin a-aru oru?
1 2 3 4 5
19. Kedu etu onwe gi si judebe
gi afo?
1 2 3 4 5
20. Kedu etu i si enwe afo ojuju
na mmekorita gin a ndi ozo?
1 2 3 4 5
21. Kedu etu i si enwe afo ojuju
n’ihe gbasara mmekorita
nwoke na nwaanyi?
1 2 3 4 5
22. Kedu etu i si enwe afo
ojuju na nkwado i na-
enweta n’aka ndi enyi gi?
1 2 3 4 5
23. Kedu ka i si enwe afo ojuju
n’ihe gbasara onodu ebe i
bi?
1 2 3 4 5
24. Kedu ka i si enwe afo ojuju
n’etu i si huta ahu gi?
1 2 3 4 5
25. Kedu ka i si enwe afo ojuju
n’ime njem gi?
1 2 3 4 5
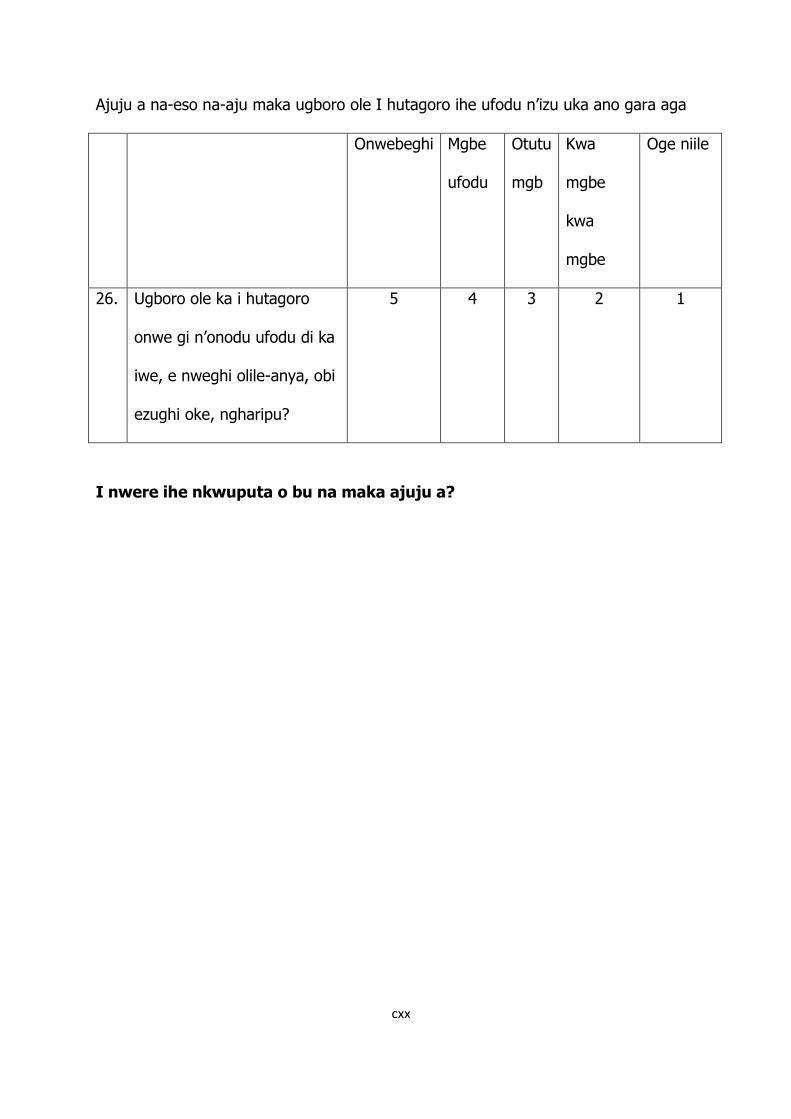
cxx
Ajuju a na-eso na-aju maka ugboro ole I hutagoro ihe ufodu n’izu uka ano gara aga
Onwebeghi Mgbe
ufodu
Otutu
mgb
Kwa
mgbe
kwa
mgbe
Oge niile
26. Ugboro ole ka i hutagoro
onwe gi n’onodu ufodu di ka
iwe, e nweghi olile-anya, obi
ezughi oke, ngharipu?
5 4 3 2 1
I nwere ihe nkwuputa o bu na maka ajuju a?

cxxi
APPENDIX 5
Consent Form
Introduction
You have been selected to participate in a study aimed at assessing depressive
symptoms, suicidal behavior and quality of life among patients with diabetes mellitus
and essential hypertension in a teaching hospital in Enugu, Nigeria.
Voluntary nature of participation: Participation in this study is completely
voluntary. Though selected for this exercise, you are free to accept or reject. If you
decide to participate, you are free to withdraw from the study any time you deem fit.
You are not required to do any investigations or undergo any invasive procedures.
Objection or participation in this study will not in any way influence the services you
receive in this hospital.
Study procedure: You will be asked questions about your age, religion, marital
status, level of education as well as presence of depressed mood in the past two
weeks, plans to harm or kill yourself and how you feel about your quality of life,
health or other areas of your life. Please give the most appropriate responses to the
questions.
Risks: There are no expected risks as no invasive procedures are involved.
Confidentiality: All information provided will be treated with confidentiality. Any
data emanating from this research will not in any way reveal information about
individual participant.
Feedback: The researcher will be available at any time to answer questions you
may have concerning this project. You can reach him on 08033116952 or through
the Department of Psychological Medicine, UNTH Enugu.
cxxii
Response: I have read though and understood the above information. I fully
understand the nature, risks, benefits of the study and hereby consent willingly and
fully to take part in it.
-------------------------------------------- ---------------------------------------------
Name/signature of Respondent Name/signature of Researcher
Date Date
---------------------------------------------
Name/signature of witness
Date




















