childhood emotional maltreatment, depression, and eating
106
CHILDHOOD EMOTIONAL MALTREATMENT, DEPRESSION, AND EATING DISORDER SYMPTOMATOLOGY: EXAMINING THE ROLE OF EARLY MALADAPTIVE SCHEMAS by ERIN ELIZABETH BURNS (Under the Direction of Joan L. Jackson) ABSTRACT The present study examined the role of early maladaptive schemas in the development of depressive and eating disorder (ED) symptoms among college women with a history of emotional maltreatment. Participants were 996 predominately Caucasian female students who completed a questionnaire packet pertaining to the constructs of interest. Structural equation modeling analyses support a model where the relationship between emotional maltreatment and ED symptoms is indirect through the influence of schemas and depression. Although women endorsing a history of emotional maltreatment reported significant associations with multiple schema domains, the strongest association was observed between the Disconnection & Rejection domain. Although preliminary, results support the use of schema therapy with individuals endorsing a history of emotional maltreatment in an effort to ameliorate depressive and ED symptoms. Findings contribute to efforts to understand the sequelae of emotional maltreatment, arguably the most prevalent, yet understudied form of child maltreatment. INDEX WORDS: Emotional maltreatment, Early Maladaptive Schemas, Depression, Eating Disorders
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of childhood emotional maltreatment, depression, and eating
CHILDHOOD EMOTIONAL MALTREATMENT, DEPRESSION, AND EATING
DISORDER SYMPTOMATOLOGY: EXAMINING THE ROLE OF EARLY MALADAPTIVE
SCHEMAS
by
ERIN ELIZABETH BURNS
(Under the Direction of Joan L. Jackson)
ABSTRACT
The present study examined the role of early maladaptive schemas in the development of
depressive and eating disorder (ED) symptoms among college women with a history of
emotional maltreatment. Participants were 996 predominately Caucasian female students who
completed a questionnaire packet pertaining to the constructs of interest. Structural equation
modeling analyses support a model where the relationship between emotional maltreatment and
ED symptoms is indirect through the influence of schemas and depression. Although women
endorsing a history of emotional maltreatment reported significant associations with multiple
schema domains, the strongest association was observed between the Disconnection & Rejection
domain. Although preliminary, results support the use of schema therapy with individuals
endorsing a history of emotional maltreatment in an effort to ameliorate depressive and ED
symptoms. Findings contribute to efforts to understand the sequelae of emotional maltreatment,
arguably the most prevalent, yet understudied form of child maltreatment.
INDEX WORDS: Emotional maltreatment, Early Maladaptive Schemas, Depression, Eating
Disorders

CHILDHOOD EMOTIONAL MALTREATMENT, DEPRESSION, AND EATING
DISORDER SYMPTOMATOLOGY: EXAMINING THE MEDIATING ROLE OF EARLY
MALADAPTIVE SCHEMAS
by
ERIN ELIZABETH BURNS
B.S., James Madison University, 2004
M.S., University of Georgia, 2009
A Dissertation Submitted to the Graduate Faculty of The University of Georgia in Partial
Fulfillment of the Requirements for the Degree
DOCTOR OF PHILOSOPHY
ATHENS, GEORGIA
2012

© 2012
Erin Elizabeth Burns
All Rights Reserved

CHILDHOOD EMOTIONAL MALTREATMENT, DEPRESSION, AND EATING
DISORDER SYMPTOMATOLOGY: EXAMINING THE MEDIATING ROLE OF EARLY
MALADAPTIVE SCHEMAS
by
ERIN ELIZABETH BURNS
Major Professor: Joan L. Jackson
Committee: Sarah Fischer
Anne Shaffer
Electronic Version Approved:
Maureen Grasso
Dean of the Graduate School
The University of Georgia
August 2012

iv
DEDICATION
To my parents, Anna and Edward Burns, whose wisdom, generosity, and enduring
support made this achievement possible. Thank you for planting the seeds not once, but countless
times.
v
ACKNOWLEDGEMENTS
I would like to sincerely thank Dr. Joan Jackson for her support and guidance with this
project. Throughout my graduate studies, her commitment to my development as a researcher
and clinician has been invaluable. She has remained actively engaged as my mentor for more
than five years. Although the frequency of my contact with her will decrease after my
graduation, her influence personally and professionally will remain with me indefinitely. With
respect and gratitude, I wish to extend my heartfelt appreciation. I would also like to recognize
the contribution of my committee members, Dr. Sarah Fischer and Dr. Anne Shaffer, for their
valuable feedback and support on this project and throughout my graduate career.

vi
TABLE OF CONTENTS
Page
ACKNOWLEDGEMENTS......................................................................................................... v
LIST OF TABLES .................................................................................................................. viii
LIST OF FIGURES ................................................................................................................... ix
CHAPTER
1 INTRODUCTION ..................................................................................................... 1
Overview ............................................................................................................. 1
Childhood Emotional Maltreatment ..................................................................... 3
Depression and Eating Disorder Symptomatology ................................................ 8
Child Maltreatment and Eating Disorder Symptomatology ................................. 10
Early Maladaptive Schemas ............................................................................... 17
Summary ........................................................................................................... 28
2 RATIONALE AND HYPOTHESES ....................................................................... 31
Significance ....................................................................................................... 32
Hypothesized Model .......................................................................................... 35
3 METHOD ................................................................................................................ 38
Participants ........................................................................................................ 38
Measures ............................................................................................................ 38
Procedure ........................................................................................................... 42
Data Analytic Plan ............................................................................................. 43

vii
4 RESULTS ............................................................................................................... 50
Sample Characteristics ....................................................................................... 50
Measurement Model .......................................................................................... 53
Structural Models ............................................................................................... 55
5 DISCUSSION.......................................................................................................... 67
REFERENCES ......................................................................................................................... 74
viii
LIST OF TABLES
Page
Table 1: Description of the Young Schema Questionnaire ........................................................ 30
Table 2: Means, Standard Deviations, and Bivariate Correlations of Study Variables ................ 52
Table 3: Summary of Model Fit Indices .................................................................................... 54
ix
LIST OF FIGURES
Page
Figure 1: Hypothesized Structural Model .................................................................................. 37
Figure 2: Measurement Model ................................................................................................... 46
Figure 3: Structural Model 1 ..................................................................................................... 56
Figure 4: Structural Model 2 ..................................................................................................... 58
Figure 5: Structural Model 3 ..................................................................................................... 60
Figure 6: Structural Model 4 ..................................................................................................... 62
Figure 7: Structural Model 5 ..................................................................................................... 64
Figure 8: Structural Model 6 ..................................................................................................... 66

1
CHAPTER 1
INTRODUCTION
Overview
A history of child maltreatment (e.g., child sexual, physical, and emotional abuse, and
neglect) has been associated with increased rates of a variety of psychological and physical
difficulties. Efforts to dissect the multifinality associated with abuse outcomes have initiated a
wave of research focused on examining the underlying mechanisms driving the association
between abuse and subsequent psychopathology. For example, there is evidence that several
factors mediate the relationship between child maltreatment and adult maladjustment, including
negative cognitive style (Gibb et al., 2001; Hankin, 2005), insecure attachment (Hankin, 2005),
emotion dysregulation (Gratz, Bornovalova, Delany-Brumsey, Nick, & Lejeuz, 2007; Burns,
Jackson, Harding, 2010; Tull, Barrett, McMillan, & Roemer, 2007), and experiential avoidance
(Tull, Jakupcak, Paulson, & Gratz,, 2007). Consistent with this research, the current study
investigated the role of early maladaptive schemas (EMS; Young, 1994, 1999; Young, Klosko,
Weishar, 2003) in the development of depressive and eating disorder (ED) symptoms among
college women with a history of emotional maltreatment.
The second objective of the current study was to examine the unique contribution of
emotional maltreatment as it relates to the development of eating disorder (ED) symptoms.
Efforts to elucidate pathways linking early adversity to psychopathology are consistent with
Beck’s content-specificity hypothesis. According to this hypothesis, psychological disorders and
states ought to be “differentiated by the content of their cognitive associates” (Beck, 1976).

2
Given that recent research has provided preliminary evidence for the association between
childhood emotional abuse (CEA) and eating disorder (ED) behavior (Fischer & Hartzell, 2008;
Grilo, Masheb, Brody, Burke-Martindale, & Rothschild, 2005; Kent & Waller, 2000; Kent,
Waller, & Dagnan, 1999; Mazzeo & Espelage, 2002; Messman-Moore & Garrigus, 2007) the
current investigation sought to extend previous findings by investigating the collective impact of
emotional abuse and neglect.
In addition to examining the relationship between emotional maltreatment and ED
symptoms, depressive symptoms were included in the overall model for several reasons. First,
several studies suggest that emotional maltreatment is strongly related to depression, with recent
evidence indicating that emotional maltreatment prospectively predicts the onset of depressive
symptoms (Liu, Alloy, Abramson, Iacoviello, & Whitehouse, 2009). Second, clinical and
epidemiological studies reveal substantial comorbidity across eating and depressive disorders
(Hudson, Hiripi, Pope, & Kessler, 2007). Third, negative affect, also referred to as “associated
mood changes” is included in cognitive behavioral models of bulimia and binge eating as
potential factors that increase propensity for ED behavior (Fairburn, 2008). Lastly, initial
research supports the association between EMS and depressive symptomatology (Lumley &
Harkness, 2007; O’Dougherty Wright, Crawford, & Del Castillo, 2009).
Finally, by examining the predictive value of EMS on the development of ED behaviors,
this study aimed to examine how experiences of emotional maltreatment initiate the development
of specific maladaptive schemas, which perpetuated throughout young adulthood, give rise to
specific maladaptive coping strategies in the form of ED behaviors. Ultimately, by identifying
particular schemas predictive of ED behavior, then efforts to target specific schemas in cognitive
therapy may facilitate treatment with abuse survivors. Finally, a brief literature review of

3
childhood emotional abuse, early maladaptive schemas as they relate to the development of
psychopathology, and of the ED and depression literature particularly as they relate to childhood
maltreatment is included.
Childhood Emotional Maltreatment
Initial research on the enduring effects of child maltreatment has focused almost
exclusively on outcomes associated with child sexual and physical abuse. However, recent
research has responded to the call for studies examining the impact of other forms of abuse,
particularly emotional maltreatment, a term which has been referred to synonymously with labels
such as emotional abuse and/or neglect, psychological battering, verbal abuse, and most
frequently psychological abuse (Glaser, 2002; Hart, Binggeli, & Brassard, 1997; Hart &
Brassard, 1987; Kent & Waller, 2000; O’Hagan, 1995). Although the use of variable
terminology has caused some to argue that using the terms interchangeably may increase
measurement error by falsely presuming that we are examining the same construct (O’Hagan,
1995), deliberate efforts to define study variables appears to have mostly negated this dilemma.
Furthermore, increased reliance on certain measures or “gold standards,” including the
Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998) and the Lifetime Experiences
Questionnaire (LEQ; Rose, Abramson & Kaupie, 2000) has allowed for increased
generalizability across studies.
While an extensive discussion of the different ways in which emotional maltreatment is
defined within the child abuse literature as well across disciplines is beyond the focus of the
current review, some of the more frequently used definitions are worth mentioning. Emotional
abuse has been described as “soul murder” (Garbarino, Guttman, & Seely, 1986), consisting of

4
recurrent parental attacks that serve to devalue, reject, ignore, and undermine a child’s
development and emerging identity. More recent conceptualizations have suggested that
emotional abuse exists on a continuum, highlighting the repetitive nature of the emotional pain
inflicted on the child (e.g. despair, distress, fear, humiliation, dehumanization) as a crucial
component of the definition (Kent & Waller, 2000; O’Hagan, 1995). For the purposes of this
study, emotional maltreatment encompassed both emotional abuse and emotional neglect.
Emotional abuse is defined as “verbal assaults on a child’s sense of worth and well-being, or any
humiliating, demeaning, or threatening behavior directed toward a child by an adult or older
person” (CTQ; Bernstein & Fink, 1998, p.2). Given that this definition refers to acts of
commission or “active” abuse without accounting for emotional damage resulting from the
absence of parental support and responsiveness (i.e., more “passive” maltreatment), this study
also considered the effects of what Bernstein and Fink (1998) refer to as emotional neglect.
Defined as “failure of caretakers to provide a child’s basic psychological and emotional needs,
including love, encouragement, and belonging, and support” (CTQ; Bernstein & Fink, 1998,
p.3), emotional neglect has received increasing attention among researchers (Yates & Wekerle,
2009). Similarly the LEQ (Rose, Abramson & Kaupie, 2000) considers belittling, ridicule,
humiliation, rejection, extortion, and terrorizing as evidence of emotional abuse, while emotional
neglect is conceptualized as instances where the child is ignored, parentified, isolated, or when
caregivers withhold praise, affection, or are psychologically unavailable to the child.
Although studies investigating the enduring impact of emotional maltreatment lag behind
research on childhood sexual and physical abuse (Behl, Conyngham, & May, 2003), compelling
evidence suggests that emotional maltreatment is associated with negative outcomes in early
childhood (Binggeli, Hart, Brassard, & Karlson, 2005; Egeland, 2009), as well as later childhood
5
and adolescence (Hart, Binggeli, & Brassard, 1998; Lumley & Harkness, 2007; Shaffer, Yates,
& Egeland, 2009). In addition to the impact of emotional maltreatment on child and adolescent
development, recent research has confirmed the enduring effect of emotional maltreatment.
Specifically, a history of emotional maltreatment has been associated with a range of adult
psychological difficulties including increased depression (Gibb et al., 2001; Hankin, 2005;
Maciejewski & Mazure, 2006), anxiety (Spertus, Yehuda, Halligan, & Seremetis, 2003),
posttraumatic stress (Burns, Harding, & Jackson, 2010; Spertus et al, 2003), loneliness and social
isolation (Loos & Alexander, 1997), low self-esteem (Briere & Runtz, 1990; Finzi-Dottan &
Karu, 2006; Mullen et al., 1995), substance use severity (Hyman, Garcia, Sinha; 2006), eating
psychopathology (Gerke, Mazzeo, Kliewer, 2006; Mazzeo & Espelage, 2002; Kent & Waller,
2000), and personality disorders (Carr & Francis, 2009; Grilo & Masheb, 2002) as well as
physical health outcomes such as lower self-rated health (Irving & Ferraro, 2006), increased
healthcare utilization (Spertus et al., 2003), and subsequent victimization (Messman-Moore &
Brown, 2004; Rich, Gidycz, Warkentin, Loh,, & Weiland, 2005).
Although there are certainly benefits of examining the impact of multiple forms of
maltreatment simultaneously, understanding the association between specific forms of abuse and
the etiology and development of specific psychological disorders is warranted, particularly as it
relates to prevention and treatment. This may be particularly relevant for understanding the
sequelae of emotional maltreatment given a considerable portion of adults engaging in various
maladaptive behaviors endorse experiences of emotional maltreatment at the exclusion of other
forms of abuse. For example, in a recent study investigating the association of child abuse and
ED symptomatology, 54% of women who endorsed a history of emotional abuse denied a history
of sexual or physical abuse (Messman-Moore & Garrigus, 2007). Similarly, studies investigating

6
the impact of adult retrospective reports of emotional maltreatment suggest that this form of
abuse is alarmingly common, with prevalence rates ranging from 5.6% to 34.8%, depending on
the sample (Messman-Moore & Garrigus, 2007; Mullen, Martin, Anderson, Romans, &
Heribson, 1996; Spertus et al., 2003). In community samples, rates of emotional maltreatment
were approximately 14% for women and 10% for men (Scher, Forde, McQuaid, & Stein, 2004),
while reported prevalence rates among college women from two recent studies ranged from
12.1% to 24.6% (Burns, Jackson, & Harding, 2010; Messman-Moore & Garrigus). A recent
review of empirical studies that exclusively relied on the CTQ to measure emotional abuse and
neglect reported rates as high as 42.2% for emotional abuse and 44.7% (when using a minimum
cut-off of 9 for the emotional abuse subscale and 10 for the emotional neglect subscale) in
community samples (which included several undergraduate samples) (Baker & Maiorino, 2010).
Moreover, rates of emotional maltreatment were significantly higher in the clinical samples than
in the community samples (Baker & Maiorino, 2010). Further evidence of the pervasiveness of
emotional abuse is supported by findings from a study by Mazzeo and Espelage (2002) which
indicated that, in both the validation and cross-validation samples, emotional abuse was the most
frequently endorsed maltreatment experience with nearly two thirds of both samples reporting at
least one item on the CTQ emotional abuse and neglect subscale. Finally, as previously
discussed, our theoretical and empirical understanding of the influence of emotional
maltreatment on the development of maladaptive coping behavior and subsequent psychological
distress is less understood in comparison to sexual and physical abuse.

7
Emotional Maltreatment and Depression
Empirical research investigating the enduring impact of emotional maltreatment has
certainly dispelled the myth that this is an innocuous form of abuse unworthy of attention.
Following the initial wave of research that related emotional maltreatment to a variety of
problematic adult behaviors, several researchers have theorized that emotional maltreatment may
be more strongly associated with depressive symptomatology than sexual and physical abuse
(Gibb et al., 2001; Hankin, 2005; Liu et al., 2009). For example, emotional maltreatment has
been linked to increased rates of depression among college students (O’Dougherty Wright,
Crawford, & Del Castillo, 2009), in a community sample of over 9,000 adult HMO members
(Chapman et al., 2004), as well as in a clinical sample (Kaplan & Klinetob, 2000). Notably,
significantly greater levels of CEA have also been shown to distinguish patients with treatment-
resistant depression and chronic PTSD from patients with treatment responsive depression
(Kaplan & Klinetob, 2000).
According to Rose and Abramson (1992), emotional maltreatment, unlike other forms of
abuse, is characterized by repetitive verbal statements regarding a child’s self-worth and abilities.
These insults often become internalized, subsequently serving as the foundation for the child’s
negative cognitions that contribute to the onset of depression. Although there is evidence that
CSA and CPA are also risk factors for adult depression, it has been hypothesized that the
cognitive schemas that may result from these forms of abuse are less likely to be structured by
explicit, destructive messages directly supplied by the abuser (Rose & Abramson, 1992).
Empirical support for Rose and Abramson’s (1992) theory comes from a study where
participants with high or low cognitive risk for depression (based on the presence or absence of a
negative cognitive style) were followed longitudinally for 2.5 years. Results suggested that

8
childhood emotional, as opposed to physical or sexual, abuse was associated with increased
levels of hopelessness and nonendogenous major depression (NE-MD) as well as hopelessness
depression (HD) at prospective follow-up. Participants who were categorized as evidencing a
high cognitive risk for depression also reported more childhood emotional maltreatment than
individuals with low cognitive risk for depression. Furthermore, results indicated that cognitive
risk fully mediated the relationship between CEA and NE-MD and the relation between CEA
and HD (Gibb et al., 2001).
A recent prospective study explored whether experiences of current emotional
maltreatment predicted the emergence of depression, including major (MD), minor (MiD), and
the subtype of hopelessness depression (HD) in undergraduates (Liu et al., 2009). Findings
revealed that greater emotional maltreatment predicted earlier onset of MD, MiD, an HD
episodes. Furthermore, the authors examined emotional maltreatment perpetrated by peers and
authority figures separately and found that both types predicted shorter time to onset of HD
episodes specifically. In addition to being the first study to provide evidence that current
emotional maltreatment predicts the onset of clinically significant depressive episodes using a
fully prospective design, the authors highlight the importance of targeting experiences of
emotional maltreatment and its appraisal in therapeutic intervention (Liu et al., 2009).
Depression and Eating Disorder Symptomatology
Extensive comorbidity exists between eating disorders (EDs) and depression as
individuals with an ED often report a current or lifetime history of depression (Herzog, Keller,
Sacks, Yeh, & Lavori, 1992; Polivy & Herman, 2002; Wilksch & Wade, 2004). Lifetime
prevalence rates of major depression in ED diagnoses range from 36% to 73% (Halmi, 1995;
9
Hudson, Pope, Jonas, & Yurgelun-Todd, 1983) for bulimia nervosa (BN) with rates as high as
86% for anorexia nervosa (AN) in one study (Rastam, 1992). Increased rates of depression have
also been found in subclinical levels of ED (Cowen, Anderson, & Fairburn, 1992).
Although there are a number of explanations for the link between EDs and depression,
one potential pathway that has received recent empirical support involves brain serotonin levels.
Decreased serotonin levels have been implicated in depression and recent studies suggest that
individuals with bulimia may have lower serotonin levels than normal controls. Although
carbohydrate dense binges tend to alleviate this deficit, the effects are temporary and may
reinforce similar behavior in an effort to experience the “high” associated with increased
serotonin levels (Agras & Apple, 2008). Therefore one function of binge-eating behavior, a
component of the binge-purge subtype of AN, as well as BN and Binge-Eating Disorder (BED),
may be to initially distract from depressive symptoms. Notably, women who are obese as well as
of normal weight report significantly more symptoms of depression than those who do not
endorse binge-eating behavior (Marcus et al., 1990; Webber, 1994). Unfortunately, the very
symptoms that bingeing distracts from are often exacerbated with each subsequent binge as ED
sufferers report feeling powerless against both the ED behavior and the recurrence of negative
mood states (Agras & Apple, 2008, Fairburn, 2008). As a result of the theoretical and empirical
link between depression and disordered eating behaviors, current cognitive models used to
explain this association, including Fairburn’s Cognitive Behavioral Therapy (CBT) model for
bulimia and binge eating (Agras & Apple, 2008; Fairburn, 2008; Fairburn, Marcus, & Wilson,
1993) include negative affect and low self-esteem (two hallmark symptoms of Major
Depression), in addition to loss of control, dieting, and weight and shape concerns as factors
believed to maintain binge eating and purging behavior.

10
Conversely, it is equally important to acknowledge that the relationship between EDs and
depression observed throughout the literature may be the result of common psychological
correlates of both disorders. For example, in a recent study designed to investigate the comorbid
relationship between EDs and unipolar depression, findings revealed that in a regression model
explaining 72.2% of the variance in ED behaviors, depression scores contributed a minimal 1%
of the variance after controlling for self-esteem, social comparison, and body dissatisfaction
(Green et al., 2009). However, before discussing theoretical models linking a history of
emotional maltreatment with the development of EDs, a brief review of the ED literature as it
relates to child maltreatment is necessary.
Child Maltreatment & Eating Disorder Symptomatology
Child abuse was first considered a distal risk factor for eating psychopathology as a result
of research examining the impact of childhood sexual abuse (CSA) specifically. Results of a
recent metal-analysis investigating prevalence rates of sexual abuse among ED samples
suggested that individuals with BN endorsed higher rates of sexual abuse than those without
bulimia (Smolak & Murnen, 2002). Gentile and researchers (2007) included childhood physical
abuse (CPA) in their investigation and found that among ethnically diverse college students, both
physical and sexual abuse independently contributed to increased risk for EDs among women.
Although estimates of prevalence rates of CSA victims with EDs are limited, Johnson and
researchers (2002) reported that 6.6% (or 52 youths) met diagnostic criteria for an ED in their
community-based prospective longitudinal study comprised of 780 mothers and their offspring
with and without an abuse history. Although studies examining this link are limited, initial
research provides preliminary evidence for an association between abuse and EDs, with some

11
researchers proposing that CSA, in particular, may serve as a non-specific risk factor for the
development of eating psychopathology (Smolak & Murnen, 2002).
More recent research has begun to consider the influence of emotional maltreatment in
ED research, with initial findings suggesting that emotional maltreatment may be more strongly
associated with ED behavior than other forms of abuse (Gerke, Mazzeo, Kliewer, 2006; Mazzeo
& Espelage, 2002; Kent & Waller, 2000). For example, Humphrey, Apple, and Kirschenbaum
(1986) found that bulimic and anorexic women report their families as being more belittling and
attacking than non-eating disordered controls. Although this study did not include a specific
measure of emotional maltreatment, a “belittling and attacking” family environment may be
conceptualized as part of the continuum of emotional maltreatment (Kent & Waller, 2000).
In the mid-1990s in response to increased attention to the sequelae of emotional
maltreatment within the extant literature, ED researchers began assessing emotional
maltreatment more directly. Results indicated higher rates of emotional (termed psychological),
physical, and multiple abuse among individuals with bulimia compared to the control group
(Rorty, Yager, & Rossotto, 1994). In only the second study to examine the relationship between
ED symptoms and a range of child abuse experiences including childhood emotional abuse
(CEA), Kent and colleagues (1999) reported that although all forms of child abuse were related
to dysfunctional eating attitudes, CEA emerged as the only form of childhood trauma that
predicted unhealthy adult eating attitudes once covariance between the different forms of abuse
was controlled. Furthermore, results indicated that the association between CEA and unhealthy
adult eating attitudes was perfectly mediated by the women’s level of anxiety and dissociation
(Kent, Waller, & Dagnan, 1999).
12
Shortly thereafter, a review of empirical support for the relationship between CEA and
eating psychopathology, in addition to a proposed theoretical model outlining the potential role
of emotional abuse as a risk factor in the development of eating psychopathology, was published
by the same authors (Kent & Waller, 2000). The model identified several moderating variables,
including age of onset of abuse and gender of the perpetrator, in addition to proposing cognitive-
affective processes (e.g. dissociation, shame, anxiety, and self-esteem) that might act as
mediators. Notably, the author clearly conceptualized CEA as a risk factor for the development
of more general symptomatology, common to both bulimia and anorexia, such as low self-
esteem, body dissatisfaction, and restrictive eating (Briere & Runtz, 1990, Gross & Keller, 1992,
Kent & Waller, 2000), rather than suggesting that emotional maltreatment was uniquely related
to one particular eating disorder. This represented a change from previous literature linking CSA
and CPA to EDs, suggesting that the authors conceptualized the impact of emotional abuse as
having a more generalized impact on disordered eating behavior. Certainly, past research
provides support for this notion, as CSA and CPA appear to better predict bulimic rather than
restrictive symptomatology (e.g. Bushnell, Wells, & Oakley-Browne, 1992, Schmidt, Slone,
Tiller, & Treasure, 1993).
Mazzeo and Espelage (2002) attempted to expand our understanding of the relationship
between emotional abuse and disordered eating by using structural equation modeling (SEM) to
test alexithymia and depression as mediating variables. Results revealed that CPA, CEA, and
physical and emotional neglect were not directly related to disordered eating. Rather, alexithymia
and depression emerged as significant mediators between physical and emotional abuse history
and disordered eating. Although previous research did not find that depression mediated the
relationship between emotional abuse and disordered eating (Kent, Waller, & Dagnan, 1999), it
13
was hypothesized that this may be a result of different statistical analyses, since multiple
regression, unlike SEM, does not identify measurement problems that may influence results
(Mazzeo & Espelage, 2002).
In response to evidence from cross-sectional research linking emotional maltreatment and
eating psychopathology, Johnson and colleagues (2002) conducted a community-based
prospective longitudinal study to examine whether child maltreatment predicts eating and
weight-related problems during adolescence and early adulthood (Johnson, Cohen, Kasen, &
Brook, 2002). Results indicated that a range of childhood adversities were related to increased
risk for disordered eating and weight problems during adolescence and adulthood, even after
statistically controlling for the effects of several confounding variables (e.g. age, challenging
childhood temperaments, childhood eating problems, parental psychopathology, and co-
occurring childhood adversities). Furthermore findings suggest that maladaptive paternal
behavior (e.g. low paternal affection, communication, and time spent with child), a construct that
may be subsumed under the more passive forms of emotional abuse and neglect, was uniquely
associated with risk for eating disorders in offspring (Johnson et al., 2002).
While Johnson and researchers (2002) provide additional support for the relationship
between CEA and disordered eating by examining the relationship in a community sample, Grilo
and colleagues (2005) sought to investigate this relationship in more clinically relevant
population. By examining rates of self-reported childhood maltreatment in extremely obese
bariatric surgery candidates, analyses indicated that CEA was uniquely associated with increased
body dissatisfaction, while emotional abuse and neglect were both related to stronger eating
concerns, elevated depression, and decreased self-esteem after Bonferonni corrections (Grilo,
Masheb, Brody, Toth, Burke-Martindale, & Rothschild, 2005). Although results indicated that

14
child maltreatment in general was not significantly associated with current BMI, binge-eating, or
eating disorder features, bariatric surgery patients reported rates of child maltreatment two to
three times more than those reported in normative samples. In a more recent study from the same
lab, individuals with binge eating disorder (BED) and night eating syndrome (NES) endorsed
increased rates of emotional abuse, but not sexual or physical abuse, when compared to
overweight individuals without an eating disorder diagnosis (Allison, Grilo, Masheb, &
Stunkard, 2007). Again, BMI was not found to relate to abuse, but results provided further
support for the unique association between emotional abuse and depression.
A more recent study continued to investigate these relationships in a sample of treatment
seeking overweight adults who met DSM-IV criteria for Binge Eating Disorder (BED).
Researchers examined the mediating role of self-criticism in the relation between childhood
maltreatment and both depressive symptoms and body dissatisfaction (a variable suspected to
lead to a variety of maladaptive ED behaviors). Path analyses demonstrated that self-criticism
fully mediated the relationship between emotional abuse and depressive symptoms and body
dissatisfaction. The authors highlighted that emotional abuse, unlike sexual abuse, was
associated with greater depressive affect in BED patients providing further support for the
potentially unique association between emotional abuse and depression (Dunkley, Masheb, &
Grilo, 2010).
Impact of Mediating Variables
Although the above studies provide support for the relationship between emotional
maltreatment and eating psychopathology, previous theoretical work in combination with recent
empirical findings propose that this link is not direct (Fischer & Hartzell, 2009; Hund &
15
Espelage, 2006; Mazzeo & Espelage, 2002; Kent & Waller, 2000). Instead, there are likely a
number of psychological and physiological mediators that more fully explain the distal
relationship between emotional maltreatment and the development of ED symptomatology (Kent
& Waller, 2000). Far less research has examined mediators and moderators as they relate to
emotional maltreatment and adult maladjustment (O’Dougherty Wright, Crawford, & Del
Castillo, 2007), let alone examined subsequent eating psychopathology. Two recent studies have
attempted to address this gap in the literature. Hund and Espelage (2006) used structural equation
modeling to test conceptual models relating CEA to disordered eating among undergraduate
females. Results revealed a weak, but significant complex relationship between CEA and
disordered eating that was mediated by alexithymia and general distress (a composite measure of
anxiety and depression) (Hund & Espelage, 2006). In a similar study, Gerke and colleagues
(2006) examined the role of depression and dissociation as possible mediators between
childhood trauma and bulimic symptomatology in a sample of ethnically diverse female
undergraduates. Results indicated that only CEA was correlated with bulimic symptoms and
therefore other forms of trauma were excluded from further analyses. Furthermore, dissociation
was no longer associated with CEA after controlling for depression. Consequently, the final
model indicated that depression mediated the relationship between CEA and bulimic symptoms
(Gerke, Mazzeo, & Kliewer, 2006).
Efforts to increase both our theoretical and empirical understanding of how emotional
maltreatment results in ED behavior has led researchers to propose a number of potential
mechanisms that may impact this relationship. For example, Fischer and Hartzell (2008)
discussed several hypothesized pathways from CEA to the development of subsequent ED
disturbances, including the mediating role of poor interoceptive awareness, dieting, and emotion

16
regulation. Bruch (1973) first identified poor interoceptive awareness, or difficulties with hunger
and satiety cues, resulting from an environment in which a child’s needs are not sufficiently
addressed, as a potential risk factor for disordered eating. Dieting has also been proposed as a
factor that increases binge eating behavior, although the specific way in which restrictive eating
leads to increased binge behavior is still being debated (Fairburn, Marcus, & Wilson, 1993).
Similarly, the way in which emotional abuse may lead to dieting has not been studied, although
low self-esteem (potentially resulting from repetitive emotionally abusive statements) may be
one pathway in which emotional maltreatment initiates attempts to modify weight and shape and
subsequent binge eating (Fischer & Hartzell, 2008).
Finally, recent research has examined what has been referred to as the emotion regulation
hypothesis of binge behavior. Specifically, Heatherton and Baumeister (1991) speculate that the
function of binge eating is to distract from an abstract stimulus (negative thoughts about self;
painful emotions) with a concrete stimulus (food). As previously discussed, binge eating as an
attempt to regulate negative affect has received empirical support within the literature (Fischer,
Smith, Annus, & Hendricks, 2007; Kell, Klump, & Fulkerson, 1997; Stice, 2002) and may be
extended to incorporate emotional maltreatment in that CEA may serve as a risk factor for low
self-esteem. Poor self-esteem may elicit negative affect, which in turn may initiate disordered
eating behavior as an attempt to cope with overwhelming affective states.
In addition to the above mediators, researchers have also considered the role of negative
cognitions or core beliefs in understanding and treating EDs, particularly bulimia (Cooper, 1997;
Fairburn, 1997; Kennedy, 1997; Waller, Ohanian, Meyer, Osman, 2000). Given that emotional
maltreatment encompasses both active and passive attempts to undermine a child’s self-efficacy,
it seems plausible that a child may internalize their abuse experience fostering negative

17
cognitions. While ED researchers have investigated disturbances in cognitions regarding eating,
weight, and shape among women endorsing ED behavior, researchers agree that eating related
cognitions are not sufficient explanatory constructs (Fairburn, Cooper, & Shafran, 2003;
Kennerley, 1996; Waller, Kennerley, & Ohanian, 2007; Waller et al., 2000). Therefore, core
beliefs and subsequent affective experiences (e.g., early maladaptive schemas) that are more
generalized, pervasive, and deeply seated about the self and others may explain more variance in
the development of ED behavior as an effort to manage distress associated with negative
intrusive thoughts.
Early Maladaptive Schemas
Definition
In an effort to further articulate the potential mediating role of core beliefs in the
development of eating disturbances among individuals with a history of emotional maltreatment,
it is necessary to discuss the construct of early maladaptive schemas (EMS) as conceptualized by
Young (see Young, 1994, 1999; Young, Klosko, & Weishar, 2003 ), in further detail. Young and
colleagues developed schema therapy in response to clinical observations that patients with
longstanding difficulties and what he described as “chronic characterological problems” were not
responding to traditional CBT. Dating back to ancient Greek philosophy, the term “schema”
refers to a structure, framework, or outline. Young has expanded the traditional definition to
describe “a broad pervasive theme or pattern comprised of memories, emotions, cognitions, and
bodily sensations” (Young, 1994, 1999; Young, Klosko, & Weishaar, 2003). Young further
explained that schemas incorporate cognitions and emotions of an intrapersonal and
interpersonal nature, that they originate in early childhood or adolescence, and that often they

18
become increasingly elaborate with time and experience. Although positive schemas certainly
exist, Young was most interested in the dysfunctional, self-defeating, and impairing schemas that
he suspected underlie psychopathology and subsequently labeled them early maladaptive
schemas (EMS). Furthermore, EMS are distinguished from the maladaptive behaviors that often
result as a consequence of the distress associated with schema activation. In other words,
behaviors such as substance abuse, inappropriate sexual behavior, and disordered eating are
driven by schemas, but are not part of the schema itself (Young, Klosko, & Weishaar, 2003).
Young suggests that schemas are entrenched, fighting for survival at significant cost to the
individual. In fact, he surmises that individuals are often drawn to situations or people that
trigger their schemas in part due to human nature’s tendency to favor familiarity over change.
Moreover, the more severe or debilitating the schema, the greater the frequency of activation and
the more likely the individual will be to enact various, often maladaptive, coping behaviors.
In an effort to measure the impact of EMS, Young developed the Young Schema
Questionnaire (YSQ: Long Form) comprised of 18 theoretically derived schemas. More recently,
a shorter version yielding 15 schemas has been created (YSQ-SF; Young, 1994) and will be used
in the current study to measure five proposed schema domains (See Table 1). The first domain,
referred to as Disconnection & Rejection, assesses expectations that individual needs for
security, stability, emotional validation, and respect will not be reliably met and includes the
following five schemas: Abandonment/Instability, Mistrust/Abuse, Emotional Deprivation,
Defectiveness/Shame, and Social Isolation/Alienation. Individuals with elevations in this domain
tend to experience coldness, rejection, loneliness, and invalidation in their family of origin, with
more extreme cases reporting abuse experiences. The second domain labeled Impaired Autonomy
& Performance, characterizes people whose expectations about their self and others interferes

19
with their ability to function independently or successfully. This domain includes four schemas:
Dependence/Incompetence, Vulnerability to Harm or Illness, Enmeshment/Undeveloped Self,
and Failure. The third domain measures deficits in internal and external boundary setting,
including inability to honor responsibility to others, in addition to difficulty achieving long-term
goals and is labeled Impaired Limits. The Impaired Limits domain includes two schemas:
Entitlement/Grandiosity and Insufficient Self-Control/Self-Discipline. The fourth domain referred
to as Other-Directedness, includes two schemas: Subjugation and Self-Sacrifice. These schemas
measure an individual’s tendency to focus excessively on the needs and approval of others at the
expense of their own desires. The final schema domain is labeled Overvigilance & Inhibition and
is also comprised of two schemas: Emotional Inhibition and Unrelenting
Standards/Hypercriticalness. Individuals with schema elevations in this domain reportedly
restrict emotion expression and related communication in an effort to avoid disapproval of others
or overwhelming feelings of shame. Additionally, individuals endorse exaggerated expectations
for themselves across a wide range of areas (Young, Klosko, & Weishaar, 2003).
Childhood Maltreatment & Early Maladaptive Schemas
Young proposes that EMS originate primarily from toxic childhood environments,
specifically the child’s nuclear family, although he suggests that they can result from negative
peer or extra-familial relationships. The latter negative experiences, however, are posited to be
less powerful especially if the family environment is a source of strength (Young, Klosko, &
Weishaar, 2003). Young further describes four types of early life experiences that facilitate
schema development. The first is referred to as toxic frustration of needs and results when the
child experiences deficits in basic needs including positive emotions and secure attachment.
20
EMS such as Emotional Deprivation or Abandonment often develop. The second environment is
characterized by traumatic experiences, including exposure to abuse, neglect, or other adverse
child experiences (e.g., loss of a parent or caregiver, physical injury resulting from motor-vehicle
accident or other environmental disaster). Resulting schemas include Mistrust/Abuse,
Defectiveness/Shame, or Vulnerability to Harm. In the third type of family environment, a child
is overindulged and develops schemas such as Dependence/Incompetence or
Entitlement/Grandiosity as a consequence of not learning to appropriately separate from the
familial environment and develop an autonomous self. The fourth environment results when a
child selectively identifies with significant others and internalizes that parent or caregiver’s
thoughts, feelings, and behaviors as their own. The specific schemas that arise from this
environment depend on the type of experiences the child internalizes.
Recent studies have provided empirical support for Young’s primarily theory driven early
environmental typology. EMS have shown associations with childhood adversity and subsequent
maladjustment in adolescents (Lumley & Harkness, 2007) and adults (Harris & Curtin, 2002;
McGinn, Cukor, & Sanderson, 2005; O’Dougherty Wright, Crawford, & Del Castillo, 2009;
Schmidt, Joiner, Young, & Telch, 1995). For example, the EMS of Defectiveness, Insufficient
Self-Control, Incompetence, and Vulnerability were found to partially mediate the association
between maladaptive parenting styles (e.g., low parental care and high parental overprotection)
as measured by the Parental Bonding Instrument (PBI; Parker, Tupling, & Brown, 1979) and
depression severity (Harris & Curtin, 2002). Recently, a significant association was found
between child maltreatment, with the exclusion of childhood physical neglect as measured by the
CTQ, and the Disconnection & Rejection schema domain (apart from the Abandonment
subscale). Contrary to expectations and previous research linking emotional maltreatment to
21
symptoms of Avoidant Personality Disorder (AVPD), the current study did not find support for a
potential mediating pathway from childhood maltreatment and AVPD through the Disconnection
& Rejection domain due to the non significant pathways between child maltreatment and AVPD
as well as between the schema domain and AVPD (Carr & Francis, 2010). EMS have also been
found to distinguish between adolescent perpetrators of sexual abuse and those without a
perpetration history. Richardson (2005) found that the Emotional Inhibition, Social
Isolation/Alienation, and Mistrust/Abuse schemas were most elevated among adolescent
perpetrators and reliably distinguished between adolescent perpetrators with and without a CSA
history. Furthermore, among perpetrators, schema scores were found to differentiate between
adolescents who victimized children versus those who reported acts against peer-aged or adult
females (Richardson, 2005).
In another study of adolescents, Lumley and Harkness (2007) examined the role of
specific EMS in predicting negative mood symptoms among participants with a maltreatment
history. More specifically, they predicted that EMS with themes of danger, (e.g., Mistrust/Abuse
and Vulnerability), which they distinguished based on the content of schemas, would predict
anxious symptomatology among physically maltreated adolescents. Conversely, it was
hypothesized that schemas with themes of loss/worthlessness (e.g., Emotional Deprivation,
Dependency, Defectiveness, Failure, and Social Isolation) would predict anhedonic depression
symptoms among adolescents exposed to emotional maltreatment. Results from the first study to
empirically examine the specificity of Young’s EMS reported mixed support for their
hypotheses. More specifically, the authors did not find specificity in the relationship between
emotional maltreatment and anhedonic depressive symptoms, nor between physical abuse and
anxiety. Instead, both forms of maltreatment predicted anxious and anhedonic symptoms.

22
However, results provided support for schema specificity in predicting subsequent symptoms in
that danger schemas mediated the relationship between general child maltreatment and anxious
symptoms, while loss/worthlessness schemas preferentially mediated the association between
maltreatment and anhedonic symptoms. Notably, specificity emerged exclusively in the
meditational analyses (Lumley & Harkness, 2007).
In addition to providing additional support for Beck’s content- specificity hypothesis
(Beck, 1976), Lumley and Harkness (2007) are some of the first researchers to examine
emotional maltreatment in relation to EMS. Although results did not suggest that emotional
maltreatment preferentially predicted certain schema elevations, the finding that emotional
maltreatment was significantly related to schema elevations provides support for including
emotionally abusive experiences in Young’s conceptualization of the toxic environment that
results in schema development. This is an important development because much of the research
previously relating abuse experiences to schema development and subsequent pathology has
been done exclusively with survivors of sexual and physical abuse.
Early Maladaptive Schemas & Psychopathology
Recent evidence has provided support for Young’s theory that psychological disorders
can be explained by EMS and the problematic ways in which individuals learn to manage them.
Using both long and short versions of the YSQ, results suggest EMS predict adolescent and adult
depression (Harris & Curtin, 2002; Lumley & Harkness, 2007; O’Dougherty Wright, Crawford,
& Del Castillo, 2009; Wang, Halvorsen, Eisemann, & Waterloo, 2010), anxiety (O’Dougherty
Wright, Crawford, & Del Castillo, 2009), social phobia (Pinto-Gouveia, Castilho, Galhardo, &
Cunha, 2006), PTSD (Cockran, Drummond, & Lee, 2010; Price, 2007), ED symptomatology

23
(Dingemans, Spinhoven, & van Furth, 2006; Leung, Waller, & Glyn, 1999; Unoka, Tolgyes, &
Czobor, 2007; Unoka, Tolgyes, Czobor, & Simon, 2010; Waller, Ohanian, Meyer, & Osman,
1999; Waller et al., 2001) personality disorders and subtypes (Carr & Francis, 2010; Petrocelli,
Glaser, Calhoun, & Campbell, 2001; Thimm, 2010), self-harm behaviors (Castille et al., 2007),
attachment difficulties (Mason, Platts, & Tyson, 2005), interpersonal conflict (Messman-Moore
& Coates, 2007) and general psychological (Schmidt & Joiner, 2004) and occupational distress
(Bamber & McMahon, 2008).
In addition to evidence that individuals endorsing a variety of psychological symptoms,
including those who meet full diagnostic criteria for clinical disorders, evidence elevated schema
profiles when compared to normal controls (Carine, 1997), recent studies suggest that particular
schemas may be more predictive of specific symptom presentations (Lumley & Harkness, 2007;
Messman-Moore & Coates, 2007; O’Dougherty Wright, Crawford, & Del Castillo, 2009; Waller
et al., 2000). Although evidence supporting the latter conclusion is preliminary, the findings lend
support to Beck’s content-specificity hypothesis, which indicates that psychological disorders
and states ought to be “differentiated by the content of their cognitive associates” (Beck, 1976).
For example, patients with social phobia evidenced higher levels of EMS in the
Disconnection/Rejection domain compared to patients with other anxiety disorder diagnoses
(Pinto-Gouveia et al., 2006). Further analyses specified that EMS of Mistrust/Abuse, Entitlement,
Emotional Deprivation, Unrelenting Standards, and Social Undesirability/Defectiveness (the
Social Isolation and Defectiveness schemas formed one factor in this study) contributed the most
variance in reported anxiety as it related to social situations and fear of negative evaluation
(Pinto-Gouveia et al., 2006). Lastly, the EMS of Mistrust/Abuse, Emotional Deprivation, Social
Isolation/Alienation, and Insufficient Self-Control/Self-Discipline reliably differentiated

24
individuals engaging in self-harm from those not engaging in self-harm behavior (Castille et al.,
2007). Schema elevations were also able to distinguish between repetitive self-harm and
individuals reporting only one episode of self-harm.
Early Maladaptive Schemas and Depression
As previously described, Lumley and Harkness (2007) found that schemas reflecting
loss/worthlessness (i.e., Emotional Deprivation, Dependency, Defectiveness, Failure, and Social
Isolation) preferentially mediated the association between maltreatment and depressive
symptoms (referred to as anhedonic symptoms) among a sample of 76 depressed adolescent boys
and girls. Similarly, Defectiveness/Shame and Failure (Incompetence/Inferiority) schemas, in
addition to Vulnerability and Insufficient Self-Control/Self-Discipline, were found to partially
mediate the relationship between perceptions of parenting behavior and depressive symptoms
among undergraduates (Harris & Curtin, 2002). In a confirmatory factor analytic study designed
to test the structure of the YSQ domains, the Disconnection & Rejection and Impaired Autonomy
schema domains explained up to 53% of the variance in depression severity in a sample of
clinically depressed (CD), previously depressed (PD), and never depressed (ND) individuals
(Hoffart et al., 2005). In a similar design, CD and PD individuals differed significantly on EMS
profiles compared with ND (Halvorsen et al., 2009). More specifically, YSQ domain scales of
Disconnection & Rejection and Impaired Autonomy emerged as significant predictors of
depression severity replicating previous findings (e.g., Hoffart et al., 2005), in addition to the
Impaired Limits (i.e., Entitlement and Insufficient Self-Control) and Restricted Self-Expression
(Emotional Inhibition, Self-Sacrifice, and Unrelenting Standards). Notably, the Insufficient Self-

25
Control schema was also found to significantly relate to depression in a previous study (e.g.,
Harris & Curtin, 2002).
More recently, efforts to examine the stability of early maladaptive schemas
characterizing individuals vulnerable to depression suggested moderate significant relative
stability for the Disconnection & Rejection and Impaired Limits schema domains, even after
controlling for depression severity in a nine-year follow-up study of depressed patients. Findings
not only highlight the stability of the EMS over time, but underscore the predictive utility of
EMS scales as vulnerability markers for depression (Wang et al., 2010).
In one of the few studies to examine the relationship between emotional maltreatment,
EMS, and depression, hierarchical regression analyses revealed that after controlling for the
effects of gender, income, parental alcohol, and other child abuse experiences, both emotional
abuse and neglect were associated with symptoms of anxiety and depression. Notably, this
association was partially mediated by schemas of Vulnerability to Harm, Shame, and Self-
Sacrifice (O’Dougherty Wright, Crawford, & Del Castillo, 2009).
Early Maladaptive Schemas and Eating Psychopathology
Although researchers have long considered the role of negative cognitions (Kennerley,
1997) in the understanding and treating ED behaviors, empirical work examining the role of
cognitions has been relatively limited. For example, Dobmeyer and Stein (2003) investigated the
role of maladaptive cognitions, in addition to drive for thinness, depressed mood, and low self-
esteem/self-efficacy, in the development of ED symptoms in a 4-year prospective study of
female undergraduates. Findings suggested that initial maladaptive cognitions and drive for
thinness scores were more predictive of later eating pathology than the other factors.

26
More recently ED researchers have begun to investigate more entrenched core beliefs,
that are not related to food, weight, or shape, using Young’s measure of EMS. In the first study
to investigate the relation of EMS to ED behaviors, the authors reported that both anorexic and
bulimic women endorsed significantly higher levels of EMS than control participants. Moreover,
results revealed that the ED groups differed on only one schema, Entitlement, with restrictive
anorexics scoring significantly lower than the bulimic women on this scale (Leung, Waller, &
Thomas, 1999). In another study, examining EMS among women reporting symptoms of
bulimia, results indicated that three schemas (Defectiveness/Shame, Insufficient Self-Control, and
Failure) differentiated women endorsing a history of bulimic behaviors from those without
(Waller et al., 2000). Furthermore, there was evidence that among bulimic women, beliefs
regarding emotional restraint, as measured by the Emotional Inhibition EMS, predicted their
severity of binge behavior, whereas their Defectiveness/Shame beliefs predicted severity of
vomiting.
In the most recent study to examine EMS among ED samples, the authors examined
whether three ED subgroups (i.e., restrictive AN, binge-purging AN, and BN) as defined by the
Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), exhibited specific
profiles of EMS. Additionally, the relationship between body mass index (BMI) and EMS was
examined in each of the ED subgroups. Principle component factor analysis extracted four EMS
factors, which explained 72% of the variance in eating pathology. Findings indicated that the
three ED subgroups differed on EMS factors, and that elevation on Factor 2 (i.e., Defectiveness,
Failure, Dependence, Enmeshment, Subjugation, Approval Seeking) was related to lower BMI
scores (Unoka, Tolgyes, & Czobor, 2007). Additionally, both subgroups of AN evidenced higher
factor loadings on Factor 3 (i.e., Self-Sacrifice, Unrelenting Standards, and Punitiveness). In

27
other words, individuals with AN often prefer to meet the needs of others at the expense of their
own fulfillment, unlike participants diagnosed with BN. Additionally, the anorexic subgroups
endorsed internalized perfectionist standards and beliefs that they should be punished if they do
not achieve their goals according to their endorsement of high levels of the EMS of Unrelenting
Standards and Punitiveness. These results are in accordance with previously held beliefs that
individuals with AN are more perfectionist and rigid than individuals diagnosed with BN (Keel
et al., 2004; Unoka, Tolgyes, & Czobor, 2007). Moreover, findings are consistent with the notion
that maladaptive cognitions play an integral role in the development and maintenance of ED as
well as support the specification of additional ED subtypes. Finally, further support is provided
for the relation of EMS to ED symptomatology, with preliminary evidence for the association
between specific EMS and particular dysfunctional eating behaviors.
Child Maltreatment, Early Maladaptive Schemas, & Eating Psychopathology
Although no studies to date have investigated how EMS may explain the relationship
between emotional maltreatment and disordered eating behaviors, one study has investigated the
mediating role of schemas among bulimic women endorsing a CSA history (Waller, Meyer,
Ohanian, Elliott, Dickson, & Sellings, 2001). Results of regression analyses supported a model
where bulimics’ EMS levels mediate the relationship between CSA and increased ED behaviors,
with evidence that different schemas serve as mediators depending on the symptom under
investigation, thus providing additional support for schema specificity as it relates to ED
symptoms. For example, Abandonment and Mistrust/Abuse EMS acted as a primary mediator,
with depression serving as a secondary mediator in the model depicting the relation between
CSA and frequency of binge behavior. Conversely, Defectiveness/Shame was the primary

28
mediator, and dissociation and depression served as secondary mediators in the model
associating CSA to frequency of vomiting (Waller et al., 2001).
In the only other study to date to examine the role of EMS as mediators in the
relationship between adversity in childhood and eating psychopathology, researchers
investigated the impact of paternal overprotection (as measured by the PBI) on bulimic
psychopathology. Results revealed that the Mistrust/Abuse and Unrelenting Standards schemas
were the only schemas to significantly predict the presence and severity of bulimic behaviors (as
measured by the BITE; Bulimic Investigatory Test, Edinborough). Further analysis revealed that
only the Mistrust/Abuse schema significantly related to paternal overprotection and therefore the
Unrelenting Standards schema was not included in meditational analyses. Findings indicated that
the Mistrust/Abuse schema served as a partial mediator, reducing the predictive power of the
BITE severity to 4.8% from 11% of the variance when included in the model (Meyer & Waller,
2004).
Summary
Recent theoretical and empirical research has provided preliminary evidence for the
impact of emotional maltreatment on the development and etiology of eating psychopathology,
conceptualized as a psychological disorder, but with potentially devastating physical
consequences, including death (Fischer & Hartzell, 2008; Gerke, Mazzeo, Kliewer, 2006; Kent
& Waller, 2000). Further research is necessary to provide additional support for this relationship,
as well as test potential mediating variables that more fully explain the association between
emotional maltreatment and eating psychopathology. Pervasive and dysfunctional core beliefs
about the self and others that develop secondary to abusive environments, conceptualized by

29
Young as EMS, may explain significant variance in this relationship and are therefore worth
investigating given preliminary evidence relating maltreatment to schema development.
Furthermore, EMS represent a modifiable target for treatment and prevention of EDs. Finally,
examining the impact of depression remains important given theoretical and empirical links
between depression and the other constructs of interest in the current study.

30
Table 1: Description of the Young Schema Questionnaire- Short Form (YSQ-SF; Young 1994)
Domains & Schemas Description of Early Maladaptive Schemas
DISCONNECTION &
REJECTION
Expectation that one’s needs for security, safety, stability, empathy,
acceptance, and respect will not be met in a predictable manner.
Family origin is often cold, invalidating, detached, and potentially
abusive.
1. Abandonment/Instability
2. Mistrust/Abuse
3. Emotional Deprivation
4. Defectiveness/Shame
5. Social Isolation/Alienation
1. The belief that it is only a matter of time until close people
will leave or fail to protect me.
2. The expectation that others will hurt, abuse, humiliate, cheat,
lie, manipulate, or take advantage of me.
3. The belief that others will not provide adequate emotional support or nurturance for me.
4. The belief that one is defective or fundamentally flawed.
5. The belief that one is fundamentally different from others
and does not belong.
IMPAIRED AUTONOMY &
PERFORMANCE
Expectations for the environment and self interfere with perceived
ability to function independently or perform successfully. Family
origin is often enmeshed, overprotective, undermining of child
abilities.
6. Dependence/Incompetence
7. Vulnerability to Harm/Illness
8. Enmeshment/Undeveloped Self
9. Failure
6. The belief that one cannot handle everyday responsibilities
competently, without considerable help from others.
7. The belief that catastrophe is imminent and not preventable.
8. A tendency for one’s identity to fused with significant
others, including excessive emotional involvement.
9. The belief that one is inadequate and unsuccessful and
therefore unable to meet important goals.
IMPAIRED LIMITS Difficulties in personal boundaries, responsibilities to others, or goal
orientation often leads to difficulty respecting others, maintaining
commitments, or achieving realistic goals. Family origin is often
overindulgent, permissive, or lacking discipline or direction. 10. Entitlement/Grandiosity
11. Insufficient Self-Control/ Self-
Discipline
10. The belief that one is better than others and is entitled to
different rights and privileges.
11. The belief that one is unable to control one’s impulses
OTHE -DIRECTEDNESS
Excessive focus on the desires, feelings, and behaviors of others, at
the expense of one’s own needs to gain approval and avoid
interpersonal conflict. Family origin is often based on conditional
acceptance and social status is valued over child’s unique needs.
12. Subjugation
13. Self-Sacrifice
12. The belief that others desires take precedent over one’s own
desires
13. A tendency to be focused on meeting the needs of others
Overvigilance & Inhibition Excessive emphasis on suppressing one’s feelings and impulses or
adhering to rigid, internalized rules. Family origin is often,
perfectionist, demanding, and punitive.
14. Emotional Inhibition
15. Unrelenting Standards
14. The tendency to be emotionally restrictive and reluctance to share emotions.
15. The belief that one should strive to meet unattainable levels
of achievement and perfection.

31
CHAPTER 2
RATIONALE AND HYPOTHESES
The purpose of the current study was to investigate the relationships among emotional
maltreatment, maladaptive schemas, depression, and disordered eating behaviors in a sample of
women at high risk for disordered eating behavior. Ultimately, by investigating these
relationships, the study sought to identify specific EMS that serve to mediate the relationship
between early experiences of emotional maltreatment and the development of ED behaviors. By
including a measure of depression in the model, this study aimed to provide further support for
existing theoretical and empirical evidence that, childhood emotional maltreatment is strongly
related to the emergence of depressive symptoms (Liu, et al., 2005, Rose & Abramson, 1992).
Additionally, cognitive behavior models of bulimia and binge eating include the presence of
negative mood symptoms as a potential precursor to engaging in maladaptive eating behaviors
(Agras & Apple, 2008; Fairburn, 2008). Therefore, it was hypothesized that depressive
symptoms would act as a mediator in the current study between emotional maltreatment and ED
symptoms, as in previous studies (see Kong & Bernstein, 2009). Finally, given previous research
suggesting specific EMS predict depressive symptomatology, it was hypothesized that the
current study would find similar associations. Ultimately, by identifying specific schemas
impacting the emergence and maintenance of depression and eating psychopathology among
maltreatment survivors, we move beyond simply recognizing the distal outcomes of emotional
maltreatment and begin to increase our understanding of how emotional maltreatment affects
development.

32
Significance
Considerable research indicates that a history of child maltreatment is associated with a
range of immediate and long-term consequences. Although previous studies have focused almost
exclusively on the outcomes of sexual and physical abuse, efforts to expand and refine our
understanding of childhood emotional maltreatment and its consequences support the association
between emotionally abusive experiences and a variety of negative outcomes. For example, a
history of CEA has been associated with numerous psychological and health-related problems
including increased anxiety, depression, posttraumatic stress, eating psychopathology,
personality disorders, substance abuse, low self-esteem, suicidality, and subsequent victimization
(Briere & Runtz, 1990; Finzi-Dottan & Karu, 2006; Gibb et al., 2001; Glaser, 2002; Hart,
Binggeli, & Brassard, 1998; Kent & Waller, 2000; Messman-Moore & Brown, 2004; Rodgers et
al., 2004; Rich et al., 2005; Sebre et al., 2004; Spertus et al., 2003). Although investigating the
impact of multiple abuse experiences is important, research examining the unique impact of
emotional maltreatment is useful, given that a considerable number of individuals endorse this
form of abuse at the exclusion of other abuse types. For example there is evidence that patients
exclusively endorsing emotional abuse display similar levels of depression, symptomatic
distress, and borderline personality features compared to clients reporting CSA or multiple forms
of abuse (Braver, Bumberry, Green, & Rawson, 1992).
As previously reviewed, there are several studies to date relating emotional maltreatment
and depressive symptomatology. However, of these studies, few have examined potential
mediators that may more fully explain this relationship. Given the pervasiveness of depression
and the myriad consequences including increased mortality (Penninx et al., 2001), decreased
physical health (for reviews see Kiecolt-Glaser, McGuire, Robles, & Glaser, 2002), and given

33
that depression remains the leading cause of disability in the US (The World Health Report,
2004), identification of EMS may serve as modifiable targets for prevention and treatment of
depression.
Conversely, research examining emotional maltreatment and ED symptoms is limited
compared to studies investigating depression as an outcome. Still, understanding the
development and maintenance of EDs is particularly relevant given the frequency of these
behaviors in college women. In a longitudinal incidence study of EDs, results revealed a
continuous linear increase in eating disorder pathology for 15- to 24-year-old females (Lucas,
Crowson, O’Fallon, &Melton, 1999). It is estimated that 1-4% of female college students meet
the full DSM-IV (APA, 1994) criteria for AN or BN, with an additional 35-70% of women
reporting direct and indirect symptoms of disordered eating including loss of appetite control,
periodic use of laxatives, purging or excessive exercise to inhibit weight gain, body image
dissatisfaction and distortion, obsessive monitoring of caloric and fat content, unhealthy weight
fluctuations, excessive weight monitoring, moderate depression, and low self-esteem (Edwards-
Hewitt & Gray, 1993; Heatherton, Nichols, Mahamedi, & Keel, 1995; Nelson, Hughes, Katz, &
Searight, 1999;). Many of the women endorsing subclinical ED symptoms likely fall into the
EDNOS subtype, the most commonly diagnosed subtype with prevalence rates ranging as high
as 50% to 70% of all individuals with eating disorders (Ricca et al., 2001). Although there is
limited research on women with this diagnosis (Fairburn & Bohn, 2005) in part due to the
heterogeneity of this group, ED researchers suggest that in addition to being a common
diagnosis, the distress associated with these ED behaviors may be severe and persistent (Walsh
& Sysko, 2009). Given that a substantial portion of individuals exhibiting maladaptive ED
symptoms do not fit into the current DSM-IV diagnostic categories, as well as the high

34
prevalence of college women endorsing these symptoms, the current study attempted to extend
previous research to address these gaps by investigating ED symptoms (e.g., bingeing, purging,
restricting, and ED related cognitions including eating, weight, and shape concerns) separately,
as they relate to emotional maltreatment.
In addition to providing evidence for the relationship between child maltreatment and
eating psychopathology, particularly the influence of emotional maltreatment, it is important to
increase our understanding of the mechanisms that may more fully explain this distal
relationship. Recently, ED researchers have suggested that although disturbances in cognition
regarding eating, weight, and shape are necessary for understanding EDs, they are not sufficient
explanatory constructs (Fairburn, Cooper, & Shafran, 2003; Waller & Kennerley, 2003; Waller,
2006). Data from a recent study examining maladaptive core beliefs and ED symptoms supports
the idea that distorted cognitions not related to eating disorder psychopathology are present in
ED patients, especially those patients engaging in purging and restricting behaviors (Dingemans,
Spinhoven, van Furth, 2006). Efforts to replicate these results in a larger population of
maltreatment survivors is important. Furthermore, identifying particular schemas that mediate
the association between emotional maltreatment and ED behaviors not only provides additional
support for Young’s EMS taxonomy, but also specific schemata represent potentially modifiable
treatment targets. Effective treatment interventions are particularly necessary given that ED are
widely believed to be one of the most difficult psychological conditions to treat, not to mention
have the highest rate of mortality among mental disorders (Agras, 2001).

35
The Hypothesized Model
The current study proposed a model (see Figure 1) wherein the role of emotional
maltreatment and EMS were examined as they relate to subsequent depressive and ED
symptomatology. The model hypothesized that the presence and severity of emotional
maltreatment in a woman’s childhood and adolescence (i.e., before age 18) would result in
maladaptive schema elevations and subsequent increases in depressive and ED symptomatology.
Based on theoretical and empirical rationale, it was hypothesized that the domains of
Disconnection & Rejection and Impaired Autonomy would be most strongly related to emotional
maltreatment experiences. Although given preliminary findings supporting associations between
schemas in the domains of Other-Directedness and Overvigilance & Inhibition, significant
associations between these domains and emotional maltreatment were also hypothesized.
Similarly, previous studies have suggested that the domains of Disconnection & Rejection,
Impaired Autonomy, and Overvigilance & Inhibition are related to increased symptoms of
depression. Therefore, the current study hypothesized significant relations between these schema
domains and depression. Based on theory and limited empirical research, direct associations
between schemas comprising the Disconnection & Rejection domain, particularly Mistrust/Abuse
and Defectiveness/Shame and binge/purge behavior associated with BN were hypothesized.
Additionally, it was hypothesized that the Overvigilance & Inhibition domain, particularly the
Unrelenting Standards schema, would be related to ED cognitions and restricting behavior (i.e.,
Global Eating Psychopathology construct measured by the EDE-Q). Lastly, besides the final
hypothesis that the Impaired Limits schema domain would evidence the strongest correlation
with ED behaviors, particularly binge eating and purging behavior, additional hypotheses

36
regarding the relationship between EMS and ED symptoms were not made as these analyses
were more exploratory in nature.
In summary, specific direct and indirect effects were hypothesized and modeled in Figure
1. Overall, the current study was designed to test whether the relationship between emotional
maltreatment and depression was indirect through the influence of EMS. In turn, depressive
symptoms were expected to be related to ED symptomatology. Although the model depicts
indirect paths from EMS to ED behaviors via depression, it is certainly plausible that direct
relationships between emotional maltreatment and ED symptoms, as well as between EMS and
ED symptoms exist, although, ultimately, it was hypothesized that including depression would
improve the overall fit of the model

37
Global Eating
Psychopathology
Disconnection &
Rejection
Other
Directedness
Impaired
Autonomy
Impaired Limits
Overvigilance &
Inhibition
Emotional
Maltreatment
Depression
Binge Episodes
Purge Episodes
Figure 1. Hypothesized Structural Model relating emotional maltreatment, EMS, depressive, and ED symptoms. Latent variables are indicated by ellipses,
measured variables by rectangles.

38
CHAPTER 3
METHOD
Participants
Participants were 996 female students recruited from introductory psychology classes
through the research pool during the 2007-2008 academic year. Participation in the current study
fulfilled a research requirement; however, students were also given the opportunity to participate
in library research to fulfill their research requirement.
Measures
Emotional Maltreatment
The Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998) is a 28-item
retrospective self-report questionnaire designed to assess five types of childhood maltreatment
occurring before age 18 including sexual abuse, physical abuse, physical neglect, emotional
abuse, and emotional neglect. For the purposes of this study, only the emotional abuse and
neglect subscales each comprised of five items were used to measure experiences of emotional
maltreatment. Each item begins with the phrase, “When I was growing up,” and is rated on a
five-point Likert scale ranging from “Never true” to “Very often true.” The CTQ has
demonstrated reliability including moderate to high internal consistency reliability coefficients
ranging from α =. 66 to α = .92 across a range of samples, and test-retest reliability coefficients
ranging from .79 to .86 over an average of 4 months (Bernstein et al., 2003; Scher, Stein,

39
Asmundson, McCreary, & Forde, 2001). Alpha’s for the emotional abuse scale have been
reported between .84 and .89 and for the emotional neglect scale between .85 and .91 across both
community and clinical samples (Bernstein et al., 2003). In the present sample, Cronbach’s alpha
was .83 for the emotional abuse subscale and .84 for the emotional neglect subscale. The CTQ’s
validity has been supported by demonstrating convergent validity with ratings of childhood
maltreatment of both clinicians and therapists, and a consistent five-factor structure (Bernstein &
Fink, 1998; Bernstein et al., 2003; Fink et al., 1995; Scher Stein, Asmundson, McCreary, &
Forde, 2001). Clinical cut-off scores offered by the measure’s creator (Bernstein & Fink, 1998)
were used to report descriptive information about the current sample ( 9 and 10 for low to
moderate emotional abuse and neglect respectively; 13 and 15 for moderate to severe
emotional abuse and neglect).
Adverse Child Experiences Study Questionnaire (ACE). Seven additional questions were
used to assess emotional maltreatment. Questions were drawn from a larger questionnaire used in
the Adverse Childhood Experiences (ACE) Study based at Kaiser Permanente’s San Diego
Health Appraisal Clinic and approved by institutional review boards of Kaiser Permanente and
the Office of Protection from Research Risks at the National Institutes of Health. The ACE Study
assessed retrospectively and prospectively, the long-term impact of abuse and household
dysfunction during childhood on a variety of outcomes. Questions were adapted from the
Conflicts Tactics Scale (CTS; Straus, 1990), a commonly used measure in the field of family
violence to assess psychological abuse in childhood. All questions referred to the respondents’
first 18 years of life and assessed both the frequency and perpetrator of the experiences of
emotional abuse and neglect. Sample questions included, “Were you treated in a cold, uncaring
40
way or made to feel like you were not loved,” and “Were you often put down or ridiculed.”
Cronbach’s alpha was .77 in the current sample.
Early Maladaptive Schemas
The Young Schema Questionnaire––short form (YSQ; Young, 1994) contains 75 items
rated on a 6-point scale, ranging from 1 (completely untrue of me) to 6, (describes me perfectly).
These items belong to one of 15 rationally derived categories of EMS (see Table 1). The first
psychometric evaluation of the YSQ (in undergraduate and adult samples) demonstrated
adequate test–retest reliability, (coefficients ranging from .50 to.82) and internal consistency
(alpha coefficients ranging from .83 to .96) (Schmidt et al., 1995). Cronbach’s alpha for the
current sample was .96. A longitudinal psychometric evaluation of the YSQ in a large sample of
adolescents suggests good test–retest reliability for EMS over a 1-year period (retest correlations
from .48 to .69).
Depressive Symptoms
The Beck Depression Inventory-II (BDI-II; Beck, Brown, & Steer, 1988) is a 21-item
self-report measure of the cognitive, affective, motivational, and somatic symptoms of
depression. For each item, participants are asked to rate how they felt during the past week with
higher scores indicating greater severity of current depressive symptoms. Beck and colleagues
(1996) reported a coefficient alpha of .92 for an outpatient sample (n = 500) and a coefficient
alpha of .93 for a college student sample (n = 120). Cronbach’s alpha for the current sample was
.92. Regarding concurrent validity, BDI-II scores are positively correlated with the Scale for
Suicide Ideation (r =. 37), the Beck Hopelessness Scale (r = .68), the Hamilton Psychiatric
Rating Scale for Depression (r =. 71), and the Hamilton Rating Scale for Anxiety (r =. 47).
41
Trauma Symptom Inventory- Depression Subscale (TSI; Briere, 1995). The 13-item
depression subscale of the larger 100-item self-report inventory was used to measure depressive
symptoms. Participants rate the presence of each symptom according to its frequency of
occurrence over the prior six months, using a four-point scale ranging from 0 (never) to 3 (often).
Although the TSI does not generate DSM-IV diagnoses, it is designed to evaluate the severity of
posttraumatic distress, including the presence of depressive symptomatology, both in terms of
mood state and depressive cognitive distortions. The TSI has demonstrated good internal
consistency with mean ranging from 0.84 to 0.87 in a variety of both clinical and nonclinical
samples. Cronbach’s alpha for the depression subscale was .90 in the present sample. The TSI
has been shown to exhibit good convergent, predictive, and incremental validity.
Eating Disorder Symptomatology.
Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994) is a 41-
item self-report measure adapted from the Eating Disorder Examination, a structured interview
to assess eating disorder symptoms (Fairburn, 1993). Although this questionnaire may be used to
make preliminary diagnoses of anorexia nervosa or bulimia nervosa, this measure was not used
for this purpose in the current study. Instead, in an effort to examine a variety of ED behavior,
the four major subscales of the EDE-Q (e.g., Dietary Restraint (DR), Eating Concern (EC),
Weight Concern (WC), and Shape Concern (SC)) are averaged to yield a Global Score, which in
the current study represented the latent construct entitled Global Eating Pathology. Frequencies
of binge eating and compensatory strategies (e.g., self-induced vomiting, laxative and diuretic
misuse) were also assessed in terms of the number of episodes occurring during the past four
weeks and are not included in the Global Score. The four major subscales have demonstrated
excellent internal consistency and test-retest reliability over a two-week time period (Luce &
42
Crowther, 1999). More recently, normative data for undergraduate women indicated internal
consistencies range from .78 for EC to .93 for SC, which was similar to the present sample which
had a Cronbach’s alpha of .93. Test-retest correlations range from .81 to .94 for the four
subscales and from .57 to .70 for the frequency of key behavioral features, including binge
eating, self-induced vomiting, and laxative misuse (Luce, Crowther, & Pole, 2008). Although the
binge and compensatory behaviors appear less reliable, this may be explained by lower
frequencies of these behaviors among non-clinical populations, or potentially a represent a true
change in onset and remission of these behaviors (Luce & Crowther, 1999).
Procedure
As previously indicated, participants were recruited through the research pool. The
researcher began each data collection session with a thorough review of the consent form. In an
effort to maximize honest disclosure regarding sensitive information, students were guaranteed
anonymity. After obtaining informed consent and reinforcing participants’ anonymity and right
to withdraw from the study at any time without penalty, the researcher provided an opportunity
for students to ask any additional questions. After all remaining questions were adequately
answered, surveys were administered.
Once the questionnaire packet was returned to the researcher, the participants were asked
to read a debriefing form explaining the purpose of the study in more detail. Any additional
questions or concerns were addressed at this time. Participants were also given a list of referrals
in the event of future difficulties or distress associated with participation in the current study.
Participants were also encouraged to contact the researcher with additional questions should they
arise.

43
To ensure anonymity, signed consent forms were separated from completed surveys upon
collection and stored in a separate room. The completed surveys did not contain any identifying
information. Lastly, students were granted research credit using the information provided on the
consent form regardless of survey completion.
Data Analytic Plan
Structural equation modeling (SEM) was performed using Analysis of Momentary
Structure 17.0 (AMOS 17.0; Arbuckle, 2009) to examine the proposed model and mediational
hypotheses. SEM was selected because of its several advantages over regression modeling: (1)
use of confirmatory factor analysis to reduce measurement error by utilizing multiple indicators
per latent variable, (2) increased flexibility regarding assumptions (in particular allowing
interpretation in the presence of multicollinearity), (3) the ability to test models with multiple
dependent variables, (4) the ability to compare alternative models to assess relative model fit
with fit indices offered as a measure of how accurately the hypothesized model(s) fit the data
(Kline, 2005).
Sample Size and Power
Several recommendations regarding sample size are provided within the literature in an
effort to ensure adequate power. For example, Mitchell (1993) suggests that there be 10 to 20
times as many cases as variable. Another rule of thumb, based on Stevens (2002), is to have at
least 15 cases per measured variable or indicator. For the current study, which has 41 indicators,
a sample size range of 615 women (based on 15 cases per indicator) to 820 women (based on 20
cases per indicator) are recommended. Notably, a minimum of 861 women is required to
compute the covariance matrix (based on the formula k (k+1)/2 observations, where k is the

44
number of variables). Furthermore, it is recommended that the researcher exceed the minimum
sample size recommendations particularly when data are non-normal (Kline, 2005). Therefore,
the current sample size of over 900 participants appears to exceed current suggestions with
regard to obtaining a modal power level of .8 (Cohen, 1988).
Missing Data
In order to account for missing data, the maximum likelihood (ML) missing data
imputation procedure was used. This method is robust against moderate violations of normality,
however, skewness and kurtosis may lead to an overestimation of the chi-square fit index,
making model rejection more likely (West, Finch, & Curran, 1995). Compared to other methods
available, (e.g., pairwise and listwise deletion), ML estimates are unbiased and have a reduced
likelihood of convergence failure (Enders & Bandalos, 2001; Gold & Bentler, 2000). Notably,
less than 5% of all items were missing and analyses indicated that the data was missing at
random.
Latent Constructs and Corresponding Indicators
A parceling technique was used to create indicators for many of the latent constructs
investigated (See Figure 2). For example, items from the emotional abuse and emotion neglect
subscales of the CTQ were used to create three emotional maltreatment parcels. Items
comprising each scale were assigned randomly to one of the parcels, and item scores were
averaged to compute parcel scores. In addition to the three parcels, the emotional maltreatment
construct was indicated by a frequency count of items endorsed on the ACE questionnaire. Each
of the five schema domains (i.e., Disconnection & Rejection, Impaired Autonomy &
Performance, Impaired Limits, Other Directedness, and Overvigilance & Inhibition) were

45
indicated by five parcels created by randomly assigning individual items from the subscales that
comprise the larger domain (see Table 1 for specific subscale names and descriptions). The latent
construct entitled Global Eating Pathology is indicated by four parcels comprised of items from
the Weight Concern, Shape Concern, and Eating Concern subscales of the EDE-Q as well as the
Dietary Restraint subscale of the EDE-Q. The frequency of Binge Episodes and Purge Episodes
were modeled separately as measured variables because they represent frequency counts of ED
behaviors which are not captured in the EDE-Q Global Score. Finally, depressive
symptomatology is indicated by three parcels of items from the BDI as well as by the depression
subscale of the TSI.
Parceling was used often to increase reliability. The reliability of a parcel of items is
greater than that of a single item, so parcels can serve as more stable indicators of a latent
construct. Additionally, the risk of spurious correlations is reduced, both because fewer
correlations are being estimated and because each estimate is based on more stable indicators.
Finally, parcels have been shown to provide more efficient estimates of latent parameters than do
items (Kline, 2005)
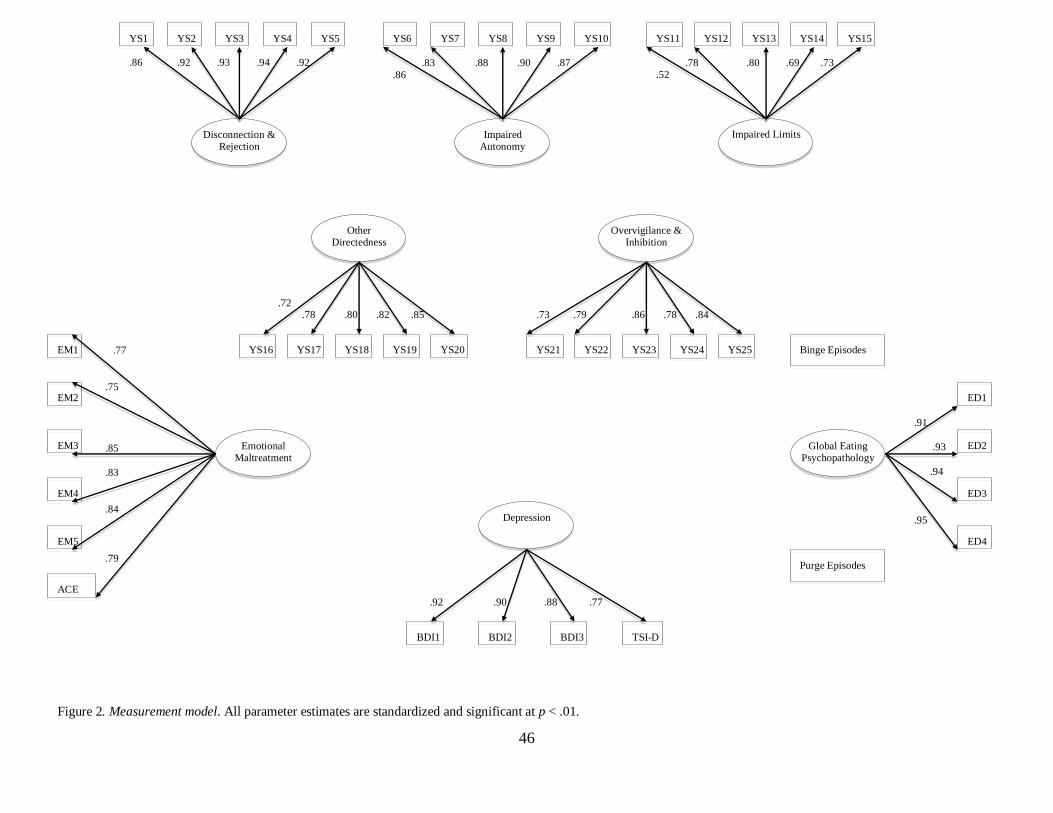
46
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
EM1
EM2
EM3
EM4
EM5
YS1 YS2 YS3 YS4 YS5 YS6 YS7 YS8 YS9 YS15 YS10 YS11 YS12 YS13 YS14
ED1
ED2
ED3
ED4
BDI1 BDI2 BDI3 TSI-D
YS16 YS17 YS18 YS19 YS20 YS21 YS22 YS23
YS24 YS25
ACE
.86 .92 .93 .94 .92
.83 .88 .90 .87
.86
.78 .80 .69 .73 .52
.72 .78 .80 .82 .85
.73 .79 .86 .78 .84
.92 .90 .88 .77
.77
.75
.85
.83
.84
.79
.91
.93
.94
.95
Figure 2. Measurement model. All parameter estimates are standardized and significant at p < .01.
47
Measurement model
Several researchers have argued for a two-step approach to structural equation modeling
where the measurement model is initially tested and, if necessary, respecified before testing the
structural model (See Anderson & Gebing, 1988; Kline, 2005). Confirmatory factor analysis
(CFA) was used to determine if the measurement model (see Figure 2) adequately fit the data by
assessing the relationships between the latent constructs and observed indicators. Of interest is
the factor loading of the observed indicator on the construct of interest, as well as overall model
fit. The proposed measurement model consisted of eight latent variables (i.e., Emotional
Maltreatment, Early Maladaptive Schema Domains, Depression, and Global Eating
Psychopathology), each with four or more indicators, and two measured variables (Binge
Episodes and Purge Episodes).
Specification of CFA model. CFA models must meet necessary standards in order to be
identified. Standard guidelines suggest that CFA models are identified if they contain two or
more factors with at least two indicators, referred to by Bollen (1989) as the two-indicator rule.
Although some researchers suggest that this rule is oversimplified and that models containing
factors with only two indicators are more prone to estimation problems, this appears to be only in
situations where the sample size is small (i.e., less than 200) (See Kline, 2005). As is common
practice in path modeling, measurement errors in the proposed CFA model were assigned a scale
through a unit loading identification (UCI) constraint. Specifically, the unstandardized residual
path coefficient for the direct effect of a measurement error on the corresponding indicator was
fixed to 1.0 (Kline, 2005). Although it was generally expected that indicators would be
correlated with several factors, it is hypothesized that they would demonstrate higher estimated

48
correlations with the factors they are believed to measure (see Graham, Guthrie, & Thompson,
2003; Kline, 2005). Finally, it was anticipated that the proposed CFA model would adequately fit
the data; however, re-specification efforts were utilized as necessary. For example, sometimes
indicators demonstrate poor loadings on the factors to which they were originally assigned.
Inspection of residuals can help identify another factor to which the indicator may be switched.
Similarly, an indicator may have relatively high loadings on multiple factors suggesting the
indicator in question measures more than one construct. This may be dealt with by either
allowing the indicator to load onto multiple factors or by allowing the measurement errors to
covary, as was done in the current study (Kline, 2005).
Consistent with recommendations (See Kline, 2005) multiple fit indices were utilized to
determine if the measurement model effectively accounted for the underlying latent data
structure by converging to adequately reproduce the covariance matrix. First, the chi-square
statistic, the traditional fit index, which reflects the amount of discrepancy between the implied
and observed covariance matrices was computed. A statistically non-significant chi-square fit
index should suggest a well-fitting model and rejection of a model would result from a
statistically significant chi-square. Given that this method is considered stringent and heavily
dependent on sample size resulting in the rejection of adequate fitting models (Bentler & Bonett,
1980), the chi-square statistic was supplemented with additional indexes of fit. The following
indices and cutoffs were used to determine model fit in this study (Marsh, Hau, & Wen, 2004;
Vandenberg & Lance, 2000): root mean square error of approximation (RMSEA; .08 or less
represents acceptable fit; Steiger, 1990), non-normed fit index (NNFI; .90 or higher indicates that
the model cannot likely be significantly improved upon; Bentler & Bonett, 1980) (same as
Tucker-Lewis Index), and the comparative fit index (CFI; .90 or higher represents acceptable fit;

49
Bentler, 1990). These indices differentiate between well-fitting and poor-fitting models by
considering degrees of freedom, model complexity, model misspecifications, sample size, and
potential for replication (see review by Vandenberg & Lance, 2000).
Structural model
Upon specifying the appropriate measurement model, the proposed structural model was
evaluated in order to examine indirect and direct relationships among latent constructs as well as
determine the fit of the model. As indicated above, SEM was used to test the hypothesized
relations between emotional maltreatment, EMS domains, depression, and ED behaviors. The
proposed hypothesized structural model shown in Figure 1 was tested and compared to four
alternative models in an effort to test meditational hypotheses. More specifically, Model 1 (see
Figure 1) depicts the full model with hypothesized paths based on previous theoretical and
empirical findings depicted by arrows. Structural Model 2 and 3 constrained to zero the direct
paths from emotional maltreatment to depression and ED symptoms, respectively. With respect
to emotional maltreatment, these models assessed the mediating role of EMS separately for
depressive and ED symptoms. Structural Model 4 deleted the direct path from EMS to ED
symptoms in order to examine whether the association between maladaptive schemas and eating
psychopathology was mediated by symptoms of depression. In an effort to further examine the
mediating role of depression, pathways to and from the mediator (i.e., from emotional
maltreatment to depression and from depression to ED symptoms) were removed in Structural
Model 5. Finally, Structural Model 6 was tested in which all paths that did not significantly
contribute to the fit of the hypothesized model were removed.

50
CHAPTER 4
RESULTS
Sample Characteristics
Mean age of the 996 participants was 18.98 years (SD = 1.52). Participants were
predominately Caucasian (79.7%; n=794), while 9.43% (n=94) identified as African American,
8.03% (n=80) as Asian, and 2.51% (n=25) as Latina. Over half the sample reported a gross
family income of over $60,000, with 40% of participants (n=352) reporting family income of
over $80,000. With regard to maltreatment history, 240 (24.1%) women endorsed experiences of
emotional abuse, of which 92 (9.2%) women reported moderate to severe emotional abuse.
Experiences of emotional neglect were reported by 204 (20.5%) women, with 46 (4.6%) women
endorsing moderate to severe emotional neglect. See Table 3 for mean, standard deviation, and
bivariate correlations for study variables. Regarding ED symptoms, a potential concern in a
nonclinical, undergraduate sample is the possibility for restricted range in EDE-Q scores.
Previous research has, however, demonstrated that undergraduate women endorse moderate to
high levels of ED pathology (Green et al., 2009), and the current sample appears to be no
exception. Descriptive statistics indicate scores on the EDE-Q ranged from .00 to 5.76, with 25%
of women in the sample obtaining scores above 3.00. These scores are consistent with studies
including undergraduate samples, as well as with larger epidemiological studies (see Green et al.,
2009; Mond, Hay, Rogers, & Owen, 2006) and alleviate EDE-Q restricted range concerns in this
nonclinical sample.

51
Intercorrelations between study variables indicated that emotional abuse and neglect were
significantly correlated with all study variables except frequency of purging. All schema
domains were significantly associated with emotional maltreatment. As hypothesized, the
schema domain of Disconnection & Rejection was more strongly related to indicators of
emotional maltreatment than were other domains. Although the Impaired Autonomy schema
domain was significantly associated with emotional maltreatment, the strength of the association
was to a lesser degree than hypothesized. Schema domains were significantly correlated with
each other, as well as with depression, global ED symptoms, and binge behavior, but not with
frequency of purging. With regard to specific hypotheses, results confirmed that the schema
domains of Disconnection & Rejection and Impaired Autonomy evidenced the strongest
associations to depression. Contrary to expectations, the domain of Impaired Limits showed a
stronger association with depression (as measured by the BDI) than did Overvigilance &
Inhibition. The Disconnection & Rejection domain was most strongly associated with both
global ED symptoms and binge behavior. Meanwhile the Impaired Limits domain, although
significantly correlated to global ED symptoms and binge episodes, did not evidence the strength
of association to ED symptoms predicted, particularly given a non-significant association to
purge behavior. As hypothesized, depressive symptoms as measured by the BDI and TSI
depression subscale were significantly associated with all eating disorder variables.

52
Table 2
Means, Standard Deviations, and Bivariate Correlations of Study Variables
1 2 3 4 5 6 7 8 9 10 11 12 13
1. CEA -- .672** .601** .489** .336** .196** .347** .233** .341** .374** .230** .140** .027
2. CEN -- .450** .548** .363** .197** .301** .223** .344** .352** .137** .148** .065*
3. ACE -- .362** .258** .173** .231** .190** .294** .261** .178** .051 .000
4. D1 -- .718** .464** .558** .510** .615** .644** .315** .196** .050
5. D2 -- .472** .552** .392** .609** .564** .340** .132** .020
6. D3 -- .343** .385** .405** .297** .225** .190** .026
7. D4 -- .453** .471** .558** .282** .152** .060
8. D5 -- .352** .310** .205** .122** .007
9. BDI -- .734** .448** .214** .104**
10. TSI-Dep -- .357** .150** .069*
11. Global ED -- .272** .192**
12. Binge -- .231**
13. Purge --
M 7.39 7.41 .20 43.7 31.3 21.3 23.4 26.8 10.1 6.48 2.05 1.45 .297
SD 3.50 3.20 .40 19.7 12.0 8.13 8.33 8.64 8.66 5.01 1.33 2.97 2.05
Note. D1 = Disconnection Rejection Schema Domain; D2 = Impaired Autonomy & Performance Schema Domain; D3 = Impaired Limits Schema Domain; D4 = Other Directedness Schema
Domain; D5 = Overvigilance & Inhibition Schema Domain. * p < .05; ** p < .01

53
Structural Equation Modeling
A measurement model was first tested for an acceptable fit to the data using confirmatory
factor analysis (Anderson & Gerbing, 1988). Once a measurement model was estimated, a
structural model was tested using the maximum likelihood method in AMOS (version 17.0).
Criteria for acceptable model fit were a comparative fit index (CFI) greater than or equal to .90,
and a root mean square error of approximation (RMSEA) of .08 or less (Hu & Bentler, 1999;
Kline, 2011). See Table 3 for additional fit indices. The chi-square (2) difference test was used
to compare nested models (Steiger, Shapiro, & Browne, 1985).
Measurement Model
As previously described, many of the latent variables were indicated by parcels of items
in an effort to more closely approximate continuous measurement of the latent construct.
Initially, the measurement model (see Figure 2) was tested without allowing the schema domains
and ED variables to correlate (i.e., without allowing schema domain to correlate with other
schemas and binge, purge, and global eating constructs to correlate with each other). This
resulted in a poor fitting model (2 = 6214.8, df = 781; CFI = .843, RMSEA = .084). The second
measurement model, which allowed for the correlation of error terms among variables
theoretically and empirically linked, adequately fit the data (2 = 3980.6, df = 769; CFI = .907,
RMSEA = .065). Fit indices for both measurement models are presented in Table 3. All of the
loadings of the latent and measured variables were significant (p < .001). Hence, all the latent
variables were adequately measured by their respective indicators (See Figure 2). Consequently,
this measurement model was used in subsequent analyses.

54
Table 3
Summary of Model Fit Indices
1. Measurement Model 1 6214.80 781 .084 .825 .843 2. Measurement Model 2 3980.62 769 .065 .888 .907 3. Structural Model 1: 2678.10 750 .051 .924 .944 Full Model
4. Structural Model 2: 2681.58 751 .051 .924 .944 Minus direct path from EM to Depression 5. Structural Model 3: 2679.40 753 .051 .924 .944 Minus direct paths from EM to ED 6. Structural Model 4: 2694.11 755 .051 .924 .944 Minus direct paths from EMS to ED
7. Structural Model 5: 2823.54 754 .053 .920 .940 Minus direct paths from Depression to ED 8. Structural Model 6: 2684.01 758 .051 .924 .944 Minus non-significant paths
Model 2
df RMSEA NFI CFI

55
Structural Models
Structural Model 1: Target model including all hypothesized paths. The first structural
model analyzed was the full model (presented in Figure 3). This model depicts the hypothesized
relationships between emotional maltreatment, schema domains, depression, and ED symptoms
based on previous theoretical and empirical findings. Results indicated that this model provided a
good fit for the data (CFI = .944, RMSEA = .051). See Table 3 for additional fit statistics.
Emotional maltreatment was significantly related to all schema domains hypothesized
(i.e., Disconnection & Rejection, Impaired Autonomy, Other Directedness, and Overvigilance &
Inhibition). Similarly, Disconnection & Rejection and Impaired Autonomy schema domains were
significantly associated to depression as predicted; however, contrary to expectations, the
Overvigilance & Inhibition schema domain was not significantly related to depression or to
global ED symptoms. In fact, the only significant, hypothesized link between schema domains
and ED symptoms existed between Impaired Limits and Binge Episodes ( = .12, p < .05). All
other relationships between schema domains and ED symptoms were indirect through
depression, which was significantly related to all three ED variables but most strongly with
global ED psychopathology ( = .45, p < .05). Although emotional maltreatment was predicted
to be distally related to ED symptomatology, results confirmed that this relationship is not direct,
as emotional maltreatment did not significantly predict global ED symptoms, binge, or purge
behavior.

56
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
.55**
.21**
.36**
.35**
.34**
.38**
.01ns
.16**
.45**
.13*
.04ns
.02ns
-.01ns
.06*
.02ns
-.04ns
.34** .12**
-.02ns
.06ns
Figure 3. Structural Model 1: Target model including all hypothesized paths. Standardized regression weights are presented for the direct paths and indirect
paths hypothesized. Note. *p < .05; **p < .01.
57
Structural Model 2: Test of mediating role of schema domains in the emotional
maltreatment-depression relationship. This model is identical to Structural Model 1, except that
the path from emotional maltreatment to depression was deleted in an effort to test the mediating
role of specific schema domains. The model fit the data well, evidencing identical CFI and
RMSEA values as Structural Model 1 (See Table 3 for additional fit indices). The Overvigilance
& Inhibition schema domain remained a non-significant predictor of depression in this model as
it was in Structural Model 1. The fit of this nested model was compared with the fit of the full
model using the chi-square difference test. Results indicated that the more parsimonious model,
Structural Model 2, was roughly equivalent to Structural Model 1 (2
diff = 3.47, df = 1, p > .05).
Given the non signficant 2
difference value, the direct path from emotional maltreatment to
depressive symptoms does not contribute significantly to model fit. Therefore, findings support
the mediating role of Disconnection & Rejection and Impaired Autonomy schema domains.

58
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
.55**
.21**
.37**
.35**
.34**
.36**
.02ns
.16**
.45**
.13*
.04ns
.02ns
-.01ns
.02ns
-.04ns
.38** .12**
-.02ns
.06ns
Figure 4. Structural Model 2: Test of the mediating role of schema domains in the emotional maltreatment-depression relationship. Standardized regression
weights are presented for the direct paths and indirect paths hypothesized. Note. *p < .05; **p < .01.

59
Structural Model 3: Test of mediating role of schema domains in the emotional
maltreatment-eating symptomatology relationship. Just as the path from emotional maltreatment
to depression was deleted in Structural Model 2, in Structural Model 3, the paths from emotional
maltreatment to ED symptomatology were constrained to zero to test the mediating role of EMS
in the relationship between emotional maltreatment and eating symptomatology. This model fit
the data well, evidencing similar fit indices as the two previous models (CFI = .944, RMSEA =
.051). A non significant 2 difference value (
2diff = 1.30, df = 3, p > .05) suggests that the direct
paths from emotional maltreatment to ED symptoms do not contribute significantly to model fit.
Given that the paths from emotional maltreatment to Global Eating Psychopathology, Binge
Episodes, and Purge Episodes were non-significant in Structural Model 1, it is not surprising that
the impact of constraining these paths to zero was negligible. Findings suggest that the
Disconnection & Rejection schema domain plays a mediating role in the relationship between
emotional maltreatment and both frequency of Binge Episodes and Purge Episodes. Given that
the association between Overvigilance & Inhibition and Global Eating Psychopathology
remained non-significant in this model, mediation was no longer considered.

60
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
.55**
.21**
.36**
.35**
.34**
.38**
.02ns
.16**
.44**
.14*
.06*
.05ns
-.03ns
.34** .12**
-.03ns
.05ns
Figure 5. Structural Model 3: Test of the mediating role of schema domains in the emotional maltreatment-eating symptomatology relationship. Standardized
regression weights are presented for the direct paths and indirect paths hypothesized. Note. *p < .05; **p < .01.

61
Structural Model 4:Test of mediating role of depression in relationships between schema
domains and eating symptomatology. This model is identical to Structural Model 1 except that
the paths from the schema domains (i.e., Disconnection & Rejection and Overvigilance &
Inhibition) to ED symptomatology were removed to test the mediating role of depression in the
relationships between schema domains and eating symptomatology. This model fit the data well
and demonstrated similar fit indices to Structural Model 1 (See Table 3 ). Results from the chi-
square difference test (2
diff = 3.30, df = 3, p > .05) indicated the nested model is equally
acceptable when compared to the full model, albeit more parsimonious. Further, results provide
support for the mediating role of depression. In other words, the relation between schemas and
ED symptomatology appears to be indirect through depression.

62
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
.55**
.21**
.36**
.35**
.38**
.02ns
.17**
.47**
.12*
.04ns
.02ns
.01ns
.06*
.34** .13**
-.04ns
Figure 6. Structural Model 4: Test of mediating role of depression in relationships between schema domains and ED symptomatology. Standardized
regression weights are presented for the direct paths and indirect paths hypothesized. Note. *p < .05; **p < .01.

63
Structural Model 5:Further assessment of the mediating role of depression. In this model,
the pathways to and from the mediator (i.e., from emotional maltreatment to depression and from
depression to ED symptoms) were deleted, as recommended by Holmbeck (1997). This model
was tested in an effort to determine if the removal of these pathways affected the direct
relationship between emotional maltreatment and ED symptoms, which to this point had
remained non-significant in all previous models. Although the relationship between emotional
maltreatment and global ED symptoms was significant in this model ( = .13, p < .05), the chi-
square difference test indicated that the full model, Structural Model 1, was a better fit to the data
(2
diff = 145.4, df = 4, p < .001). The significant chi-square difference test provides further
support for the mediating influence of depression.

64
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
.55**
.21**
.36**
.35**
.34**
.35**
.04ns
.01ns
.04ns
.13
.01ns
.02ns
.39** .12**
-.01ns
.24
Figure 7. Structural Model 5: Further assessment of the mediating role of depression. Standardized regression weights are presented for the direct paths and
indirect paths hypothesized. Note. *p < .05; **p < .01.

65
Structural Model 6:Final model with non-significant paths deleted. The final model
tested removed all non-significant pathways present in the full model (See Figure 4). This model
fit the data well (CFI = .944, RMSEA = .051) and when compared to Structural Model 1, a non-
significant chi-square difference test (2
diff = 5.90, df = 8, p > .05), suggests that this model is an
equally good fit to the data statistically. All paths significant in the full model, Structural Model
1, remained significant in this model and the magnitude of the path coefficients changed
minimally.
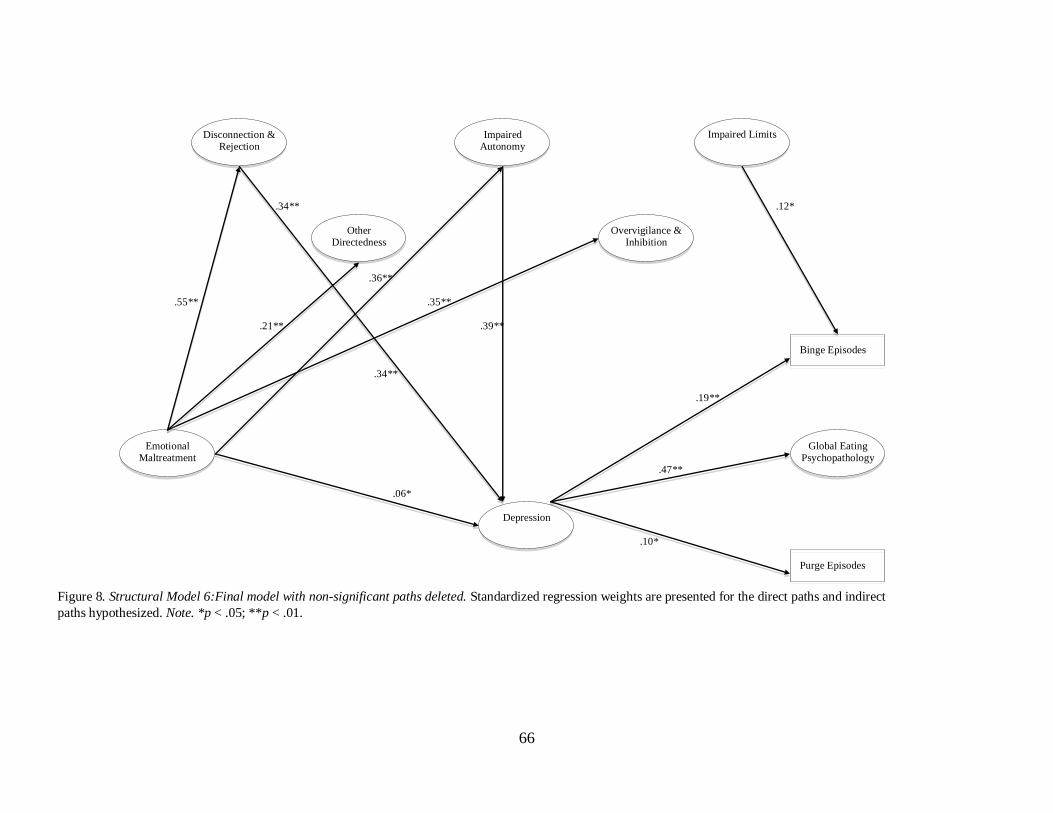
66
Global Eating Psychopathology
Disconnection & Rejection
Other Directedness
Impaired Autonomy
Impaired Limits
Overvigilance & Inhibition
Emotional Maltreatment
Depression
Binge Episodes
Purge Episodes
.55**
.21**
.36**
.35**
.34**
.39**
.19**
.47**
.10*
.06*
.34** .12*
Figure 8. Structural Model 6:Final model with non-significant paths deleted. Standardized regression weights are presented for the direct paths and indirect
paths hypothesized. Note. *p < .05; **p < .01.

67
CHAPTER 5
DISCUSSION
The results of the present study supplement an emerging literature providing evidence for
the enduring effects of emotional maltreatment. In the first study to investigate the relationships
among emotional maltreatment, maladaptive schemas, depression, and disordered eating
behaviors in a sample of women at high risk for ED behavior, results support a model where the
relationship between emotional maltreatment and disordered eating behaviors is indirect through
the influence of schemas and depression. These results, although preliminary, integrate and
expand on previous studies investigating the distal relationship between emotional abuse and
neglect in childhood and adult psychopathology.
Notably, emotional maltreatment did not evidence a direct relationship with any of the
ED outcome variables, except when depression was removed entirely from the model as seen in
Structural Model 5, where a small association was seen between emotional maltreatment and
Global Eating Psychopathology. This finding was consistent with hypotheses regarding the
indirect nature of this potentially distal relationship between emotional maltreatment and ED
symptomatology. Although Kennedy and colleagues (2007) found a direct and unmediated
relationship between emotional abuse and disordered eating, other studies have found not found
support for a direct link (Kent et al., 1999; Mazzeo & Espelage, 2002). Notably, the study that
found a direct link, did so in a sample comprised of both men and women. Results from studies
that have examined the association between emotional maltreatment and ED symptomatology, in
addition to various mediators (e.g., depression, anxiety, dissociation), among women generally

68
point to a weak, but significant indirect relationship. Therefore, it appears that further research is
necessary to better understand the nature of this relationship.
It appears that both explicit statements about a child’s worth in addition to indirect forms
of invalidation become internalized, subsequently serving as the foundation for negative
cognitions that contribute to the onset of depression (Rose & Abramson, 1992). Depressive
symptoms, particularly negative affect and low self-esteem, are then posited to lead to
maladaptive cognitions and behaviors that serve to elicit or maintain weight and shape concerns
as well as drive binge/purge behaviors. Although the link between depression and ED has been
established (Agras & Apple, 2008; Fairburn, 2008; Herzog, Keller, Sacks, Yeh, & Lavori, 1992;
Polivy & Herman, 2002; Wilksch & Wade, 2004), few studies have provided support for the
mediating influence of depression in the relationship between emotional maltreatment and ED
symptoms (Hund & Espelage, 2006; Mazzeo & Espelage, 2002).
Equally noteworthy was the strength of the association between emotional maltreatment
and Disconnection & Rejection. This direct path remained the strongest path across all models
examined. This is important because, although Young theorizes that this domain reflects
individuals where the family of origin is often cold, invalidating, and potentially abusive, limited
empirical evidence exists. To date, only a handful of studies have investigated the relationship
between emotional maltreatment and early maladaptive schemas, of which the majority included
only specific schema subscales such as Mistrust/Abuse, Defectiveness/Shame, and Emotional
Deprivation. Consistent with hypotheses, women endorsing a history of emotional maltreatment
reported significant associations with the schema domains of Impaired Autonomy, Other-
Directedness, and Overvigilance. The finding that emotional maltreatment was significantly
associated with multiple schema domains may suggest that early abuse experiences initiate more
69
pervasive dysfunctional thoughts and emotions represented by multiple schema domains, rather
than demonstrating schema specificity. However, this finding may also be explained by the high
correlations observed between schema domains. Although the majority of research has examined
the influence of particular schema subscales rather than associations present at the domain level,
YSQ validation studies, in addition to a recent study (Roemmele & Messman-Moore, 2011),
report similar intercorrelations between schemas domains as were found in the current study
(Hoffart et al., 2006; Roemmele & Messman-Moore, 2011).
In addition to support for the mediating role of depression, results also suggest that
schemas serve a mediating role in the emotional maltreatment-depression relationship. More
specifically, an indirect relationship through the schema domains of Disconnection & Rejection
and Impaired Autonomy was observed. It is certainly plausible that experiences of emotional
maltreatment would activate the belief that others are not reliable sources of support and
emotional validation, let alone potentially dangerous, leading to further thoughts of one’s own
inadequacy and defectiveness as reflected by the various schema subscales that comprise both of
these domains (e.g., Emotional Deprivation, Defectiveness/Shame, Mistrust/Abuse, Failure,
Vulnerability to Harm). Theoretically, these negative internal attributions and cognitions trigger
symptoms of depressions, as observed in this study as well as in previous research (Harris &
Curtin, 2002; Lumley & Harkness, 2007; O’Dougherty Wright, Crawford, & Del Castillo, 2009).
The association between the schema domains of Disconnection & Rejection and Impaired
Autonomy and depression replicate findings from previous research, particularly a recent study
that examined links between depression and domain-level EMS (see Halvorsen et al., 2009).
However, this is the only study to date to support these domain associations with depression in a
child maltreatment sample.
70
The only significant relationship between any schema domain and ED symptoms was
observed between the Impaired Limits schema domain and Binge Episodes, and it was a small
relationship at that. This was certainly contrary to hypotheses, although it is important to
recognize that only a couple of paths were modeled based on previous literature (i.e., paths were
hypothesized between Disconnection & Rejection and Impaired Limits to both Binge and Purge
Episodes, and from Overvigilance & Inhibition to Global Eating Psychopathology). More
recently, additional support for the relationship between subscales in domains not tested in this
study (i.e., Impaired Autonomy) and ED subgroups has been shown (Unoka, Tolgyes, Czobor, &
Simon, 2010). Although the present sample was not a clinical sample, one- fourth of the sample
endorsed significant eating pathology and was similar to undergraduate samples utilized in
previous studies as indicated above. Still, it is certainly possible that the lack of significant
relationships observed is in part due to the sub-threshold symptoms exhibited by a large portion
of the sample. Furthermore, in addition to using clinical samples, recent studies have examined
the utility of schemas in differentiating between specific ED subtypes (i.e., Anorexia Nervosa-
restricting subtype, Anorexia Nervosa-binge/purge subtype, Bulimia Nervosa), rather than
looking at specific ED behaviors or general cognitions as was done in this study (See Unoka,
Tolgyes, & Czobor, 2007; Unoka et al., 2010). Although these studies extend research
investigating the relation between EMS and eating psychopathology, a recent study provides
evidence that the clinical utility of the DSM-IV Anorexia Nervosa and Bulimia Nervosa
subtypes is questionable given both infrequent subtype use and adequate inter-rater agreement
(Thomas et al., 2010). This finding, coupled with previous research suggesting that emotional
maltreatment may be a risk factor for the development of more general ED symptomatology
(Kent & Waller, 2000), and limited empirical research examining the relationship between EMS

71
and ED behaviors, the current study’s emphasis on ED behaviors rather than diagnostic subtypes
remains a logical first step.
Several limitations of the current study should be noted. First, although the models
examined in this study provided an adequate fit to the data, these findings are preliminary,
require further replication, and do not imply that the model has been “proven” (Kline, 2005).
Given recent evidence that particular schema subscales predict subgroups of ED, further
examination of the schema-ED relationship is necessary, particularly at the schema subscale
level. Given that this was the first study to examine emotional maltreatment, early maladaptive
schemas, depression, and ED symptomatology simultaneously using SEM, specific hypotheses
regarding the influence of specific schema subscales was beyond the scope of the current study.
Although the structural equation modeling results imply the possibility of causality, the design
was cross-sectional and correlational in nature. Therefore, without longitudinal designs,
definitive conclusions about the temporal sequence of variables in the models presented in this
study and the causality of ED behaviors cannot be determined. Additionally, exclusive reliance
on self-report measures, particularly regarding potentially distal events, results in mono-method
and recall bias. Furthermore, given that respondents were asked to report about potentially
difficult experiences and the subsequent use of maladaptive behaviors, it is certainly plausible
that maltreatment and psychological symptoms were underreported. More recently, it has been
suggested that the YSQ-SF measures only the schemas an individual is aware of and therefore
schema avoidance or the coping responses activated by particular schemas may influence
responses (Thimm, 2010). Finally, the multi-collinearity present among the schema domains in
particular, may limit the predictive value of individual variables.

72
In addition to methodological limitations, the external validity of the findings is limited
due to the homogeneity of the present sample. Although it is important to examine these
relationships in a non-clinical sample given the limited empirical support within the literature,
results may not be generalizable to clinical populations, men, or more economically and
ethnically diverse samples.
Despite limitations, the present study attempted to provide a relatively parsimonious
integration of variables that have yet to be examined by previous researchers. Findings provide
preliminary support for the use of schema therapy with individuals endorsing an emotional
maltreatment history in an effort to prevent or reduce depressive and ED symptoms. Waller and
colleagues (2007) have initiated efforts to incorporate schema therapy into existing ED treatment
programs by providing recommendations for addressing the core beliefs that have developed in
response to emotional abuse. Suggestions include focusing on the Mistrust/Abuse and
Abandonment schemas that they theorize result from experiences of emotional maltreatment
(Waller, Corstorphine, & Mountford, 2007). Only one known study to date has attempted to
empirically investigate the use of schema therapy in ED treatment. Findings revealed that at the
end of a 6-month treatment program for individuals with a chronic history of Anorexia, no
significant changes on schemas were observed. Given the sample was limited to eight women,
further research is warranted. Notably, the authors suggested that patients’ ability to identify with
particular schemas (e.g., Unrelenting Standards, Defectiveness/Shame, Emotional Deprivation,
Emotional Inhibition, and Social Isolation) appeared useful is increasing their readiness to
commit to behavioral changes (George, Thorton, Touyz, Waller, & Beumont, 2004). Ultimately,
future research is needed to further clarify the relationship between emotional maltreatment and
ED symptoms in an effort to better examine the utility of incorporating schema therapy into

73
existing ED treatments. Given the chronic nature of eating psychopathology, particularly
Anorexia Nervosa, efforts to develop effective interventions are necessary given the treatment
resistance and relapse inherent in ED populations.

74
REFERENCES
Agras, W. S. (2001). The consequences and costs of the eating disorders. Psychiatric Clinics of
North America, 24(2), 371-379.
Agras, W. S., & Apple, R. F. (2008). Overcoming Eating Disorders: A cognitive-behavioral
therapy approach for bulimia nervosa and binge-eating disorder. New York: Oxford
University Press.
Allison, K. C., Grilo, C. M., Masheb, R. M., Stunkard, A. J. (2007). High self-rated reports of
neglect and emotional abuse by persons with binge eating disorder and night eating
syndrome. Behaviour Research and Therapy, 45(12), 2874-2883.
Arbuckle, J. L. (2009). Amos users’ guide version 17.0. Chicago: Amos Development Company.
Arnow, B., Kennedy, J., & Agras, W. S. (1992). Binge eating among the obese: A descriptive
study. Journal of Behavioral Medicine, 15, 155-170.
Baker, A. J. L., & Maiorino, E. (2010). Assessments of emotional abuse and neglect with the
CTQ: Issues and estimates. Children and Youth Services Review, 32, 740-748.
Bamber, M., & McMahon, R. (2008). Danger-early maladaptive schemas at work! The role of
early maladaptive schemas in career choice and the development of occupational stress in
health workers. Clinical Psychology & Psychotherapy, 15(2), 96-112.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social
psychological research: Conceptual, strategic, and statistical considerations. Journal of
Personality and Social Psychology, 31, 1173-1182.
75
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York: International
Universities Press.
Beck, A. T, Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck
Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8,
77-100.
Behl, L. E., Conyngham, H. A., & May, P. F. (2003). Trends in child maltreatment literature.
Child Abuse & Neglect, 27, 215-229.
Bentler, P. M. (1990). Comparative fit indices in structural models. Psychological Bulletin, 107,
238-246.
Bentler, P. M. & Bonett, D. G. (1980). Significance tests and goodness of fit in the analysis of
covariance structures. Psychological Bulletin, 88, 588-606.
Bernstein, D. P., & Fink, L. (1998). Childhood Trauma Questionnaire manual. San Antonio, TX:
The Psychological Corporation.
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., Zule, W.
(2003). Development and validation of a brief screening version of the childhood trauma
questionnaire. Child Abuse & Neglect, 27, 169-190.
Binggeli, N. J., Hart, S. N., Brassard, M. R., & Karlson, H. C. (2005). Psychological
maltreatment. London: Sage.
Black, D. A., Smith Slep, A. M., & Heyman, R. E. (2001). Risk factors for child psychological
abuse. Aggression and Violent Behavior, 6(2-3), 189-201.
Bolger, K., & Patterson, C. (2001). Pathways from child maltreatment to internalizing problems:
Perceptions of control as mediators and moderators. Development and Psychopathology,
13(4), 913-940.
76
Bollen, K. A., (1989). Structural equations with latent variables. New York: Wiley.
Bondurant, B. (2001). University women’s acknowledgement of rape. Violence Against Women,
7(3), 294-314.
Braver, M., Bumberry, J., Green, K., & Rawson, R. (1992). Childhood abuse and current
psychological functioning in a university counseling center population. Journal of
Counseling Psychology, 39(2), 252-257.
Briere, J. (1995). Trauma Symptom Inventory professional manual. Odessa, FL: Psychological
Assessment Resources.
Briere, J., & Runtz, M. (1990). Differential adult symptomatology associated with three
types of child abuse histories. Child Abuse & Neglect, 14, 357-364.
Browne, A., & Finkelhor, D. (1986). Impact of child sexual abuse: A review of the
research. Psychological Bulletin, 99, 66-77.
Burns, E. E., Jackson, J. L., & Harding, H.H. (2010). Child maltreatment, emotion
regulation, and posttraumatic stress: The impact of emotional abuse. Journal of
Aggression, Maltreatment, & Trauma, 19 (8).
Campos, J. J., Frankel, C. B., & Camras, L. (2004). On the nature of emotion regulation. Child
Development, 75(2), 377-394.
Carr, S. N., & Francis, A. J. P. (2010). Do early maladaptive schemas mediate the relationship
between childhood experiences and avoidant personality disorder features? A preliminary
investigation in a non-clinical sample. Cognitive Therapy and Research, 34, 343-358.
Carter, J. C., Bewell, C., Blackmore, E., & Woodside, D. B. (2006). The impact of child sexual
abuse on anorexia nervosa. Child Abuse & Neglect, 30 (3), 257-269.

77
Castille, K., Prout, M., Marczyk, G., Shmidheiser, M., Yoder, S., & Howlett, B. (2007).
The early maladaptive schemas of self-mutilators: Implications for therapy.
Journal of Cognitive Psychotherapy, 21(1), 58-71.
Cermak, P., & Molidor, C. (1996). Male victims of child sexual abuse. Child & Adolescent
Social Work Journal, 13(5), 385-400.
Chapman, D. P., Whitfield, C. L., Felitti, V. J., Dube, S. R., Edwards, V. J., & Anda, R. F.
(2004). Adverse childhood experiences and the risk of depressive disorders in adulthood.
Journal of Affective Disorders, 82(2), 217-225.
Cicchetti, D., & Lynch, M. (1993) Toward an ecological/transactional model of community
violence and child maltreatment: Consequences for children’s development. Psychiatry
56, 96–118.
Cicchetti, D., & Sroufe, L. (Eds.). (2000). Reflecting on the past and planning for the future of
developmental psychopathology [Special issue]. Developmental and Psychopathology,
12 (3), 255–550.
Cicchetti, D., & White, J. (1990). Emotion and developmental psychopathology. In
N. L. Stein, B. Leventhal, & T. Trabasso (Eds.), Psychological and biological
approaches to emotion (pp. 359-382). Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
Cloitre, M., Cohen, L., & Koenen, K. C. (2006). Treating survivors of childhood abuse:
Psychotherapy for the interrupted life. New York, NY: Guilford Press.
Cloitre, M., Miranda, R., Stovall-Mclough, C., & Han, H. (2005). Beyond PTSD:
Emotion regulation and interpersonal problems as predictors of functional impairment in
survivors of childhood abuse. Behavior Therapy, 36, 119-124.

78
Cockram, D. M., Drummond, P. D., & Lee, C. W. (2010). Role and treatment of early
maladaptive schemas in Vietnam veterans with PTSD. Clinical Psychology and
Psychoptherapy, 17, 165-182.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). New Jersey:
Lawrence Erlbaum.
Dingemans, A. E., Spinhoven, Ph., & van Furth, E. F. (2006). Maladaptive core beliefs and
eating disorder symptoms. Eating Behaviors, 7, 258-265.
Dobmeyer, A. C. &, Stein, D. M. (2003). A prospective analysis of eating disorder risk factors:
Drive for thinness, depressed mood, maladaptive cognitions, and ineffectiveness. Eating
Behaviors, 4(2), 135-147.
Dunkley, D. M., Masheb, R.M., & Grilo, C.M. (2010). Childhood maltreatment, depressive
symptoms, and body dissatisfaction in patients with binge eating disorder: The mediating
role of self-criticism. International Journal of Eating Disorders, 43, 274-281.
Edwards-Hewitt, T., & Gray, J. J. (1993). The prevalence of disordered eating attitudes and
behaviors in Black-American and White-American college women: Ethnic, regional,
class, and media differences. European Eating Disorders Review, 1(1), 41-54.
Enders, C. K., & Bandalos, D. L. (2001). The relative performance of full information
maximization likelihood estimation for missing data in structural equation models.
Structural Equation Modeling, 8, 430-457.
Engeland, B. M. (2009). Taking stock: Childhood emotional maltreatment and developmental
psychopathology. Child Abuse & Neglect, 33(1), 22-26.
79
Fairburn, C. G. (2008). Eating disorders: The transdiagnostic view and the cognitive behavioral
theory. In Fairburn, C. G. (Eds.), Cognitive behavior therapy and eating disorders (pp. 7-
22). New York: NY: Guilford Press.
Fairburn, C. G., & Beglin, S. J. (1994). Assessment of eating disorders: Interview or self-report?
International Journal of Eating Disorders, 16, 363–370.
Fairburn, C. G., & Cooper, Z. (2007). Thinking afresh about the classification of eating
disorders. International Journal on Eating Disorders, 40S, S107-S110.
Fairburn, C. G., Marcus, M. D., & Wilson, G. T. (1993). Cognitive behavioral therapy for binge
eating and bulimia nervosa. In C. G. Fairburn & G. T. Wilson (Eds.), Binge eating:
Nature, assessment, and treatment (12th ed., pp. 361-404). New York: Guilford.
Finzi-Dottan, R., & Karu, T. (2006). From emotional abuse in childhood to psychopathology in
adulthood: A path mediated by immature defense mechanisms and self-esteem. Journal
of Nervous and Mental Disease, 194, 616-621.
Fischer, S., Smith, G. T., Annus, A. M., & Hendricks, M. (2007). The relationship of neuroticism
and urgency to negative consequences of alcohol use in women with bulimic symptoms.
Personality and Individual Differences, 43, 1199-1209.
Fischer, S. & Hartzell, E. (2008) Childhood Emotional Abuse and Binge Eating. In Swain, P.
(Ed.) Binge Eating: Psychological Factors and Treatment. New York: Novascience Press.
Gentile, K., Raghavan, C., Rajah, V., Gates, K. (2007). It doesn’t happen here Eating disorders
in an ethnically diverse sample of economically disadvantaged, urban college students.
Eating Disorders: The Journal of Treatment & Prevention, 15(5), 405-425.
80
Gerke, C.K., Mazzeo, S.E., & Kliewer, W. (2006). The role of depression and dissociation in the
relationship between childhood trauma and bulimic symptoms among ethnically diverse
female undergraduates. Child Abuse & Neglect, 30(10), 1161-1172.
Glaser, D. (2002). Emotional abuse and neglect (psychological maltreatment): A conceptual
framework. Child Abuse & Neglect, 26, 697-714.
Gibb, B. E., Alloy, L. B., Abramson, L. Y., Rose, D. T.,Whitehouse, W. G., Donovan, P.,
Hogan, M. E., et al. (2001). History of childhood maltreatment, depressogenic cognitive
style, and episodes of depression in adulthood. Cognitive Therapy and Research, 24,
425–446.
Gold, M. S., & Bentler, P. M. (2000). Treatments of missing data: A Monte Carlo comparison of
RBHDI; iterative stochastic regression imputation, and expectation-maximization.
Structural Equation Modeling, 7, 319-335.
Graham, J. M., Guthrie, A. C., & Thompson, B. (2003). Consequences of not interpreting
structure coefficients in published CFA research: A reminder. Structural Equation
Modeling, 10, 142-153.
Gratz, K. L., Bornovalova, M. A., Delany-Brumsey, A., Nick, B., & Lejuez, C. W. (2007).
A laboratory-based study of the relationship between childhood abuse and experiential
avoidance among inner-city substance users: The role of emotional nonacceptance.
Behavior Therapy, 38(3), 256-268.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and
dysregulation: Development, factor structure, and initial validation of the difficulties in
emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26,
41-54.

81
Green, M. A., Scott, N. A., Cross, S. E., Liao, K. Y., Hallengren, J. J., Davids, C. M., et al.
(2009). Eating disorder behaviors and depression: A minimal relationship beyond social
comparison, self-esteem, and body dissatisfaction. Journal of Clinical Psychology, 65(9),
989-999.
Grilo, C. M., & Masheb, R. M. (2002). Childhood psychological, physical, and sexual
maltreatment in outpatients with binge eating disorder: Frequency and associations with
gender, obesity, and eating related psychopathology. Obesity Research, 9, 320-325.
Grilo, C. M., Masheb, R. M., Brody, M., Burke-Martindale, C.H., & Rothschild, B.S. (2005).
Binge eating and self-esteem predict body image dissatisfaction among obese men and
women. International Journal of Eating Disorders, 37(4), 347-351.
Gross, A. B., & Keller, H. R. (1992). Long-term consequences of childhood physical and
psychological maltreatment. Aggressive Behavior, 18, 171-185.
Gross, J. J., & Munoz, R. F. (1995). Emotion regulation and mental health. Clinical
Psychology: Science and Practice, 2, 151-164.
Halmi, K. A. (1995). Changing rates of eating disorders: What does it mean? The American
Journal of Psychiatry, 152(9), 1256-1257.
Halvorsen, M., Wang, C. E., Richter, J., Myrland, I., Pedersen, S. K., Eisemann, M., & Waterloo,
K. (2009). Early maladaptive schemas, temperament and character traits in clinical
depressed and previously depressed subjects. Clinical Psychology & Psychotherapy,
16(5), 394-407.
Hankin, B.L. (2005). Childhood maltreatment and psychopathology: Prospective tests of
attachment, cognitive vulnerability, and stress as mediating processes. Cognitive
Therapy and Research, 29(6), 645–671.

82
Harris, A. E., & Curtin, L. (2002). Parental perceptions, early maladaptive schemas, and
depressive symptoms in young adults. Cognitive Therapy and Research, 26, 405–416.
Hart, S. N., Binggeli, N. J., & Brassard, M. R. (1998). Evidence for the effects of psychological
maltreatment. Journal of Emotional Abuse, 1, 27–58.
Hart, S. N., & Brassard, M. R. (1987). A major threat to children’s mental health: Psychological
maltreatment. American Psychologist, 42, 160-165.
Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., & Strosahl, K. (1996).
Experiential avoidance and behavioral disorders: A functional dimensional approach to
diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64, 1152–1168.
Heatherton, T. F., & Baumeister, R. F. (1991). Binge eating as escape from self-awareness.
Psychological Bulletin, 110, 86-108.
Herzog, D. B., Keller, M. B., Sacks, N. R., Yeh, C. J., & Pai, S. (1992). Psychiatric comorbidity
in treatment-seeking anorexics and bulimics. Journal of the American Academy of Child
& Adolescent Psychiatry, 31(5), 810-818.
Hoffart, A., Sexton, H., Hedley, L.M., Wang, C.E., Holthe, H., Haugum, J.A., et al. (2005). The
structure of mal- adaptive schemas: A confirmatory factor analysis and a psychometric
evaluation of factor-derived scales. Cognitive Therapy and Research, 29, 627–644.
Holmbeck, G. N. (1997). Toward terminological, conceptual, and statistical clarity in the study
of mediators and moderators: Examples from the child-clinical and pediatric psychology
literatures. Journal of Consulting and Clinical Psychology, 65, 599-610.
Hudson, J. I., Hiripi, E., Pope, H. G., Kessler, R. C. (2007). The prevalence and correlates of
eating disorders in the national comorbidity survey replication. Biological Psychiatry,
61(3), 348-358.

83
Hudson, J. I., Pope, H. G., Jonas, J. M., & Yurgelun-Todd, D. (1983). Family history study of
anorexia nervosa and bulimia. British Journal of Psychiatry, 142, 133-138.
Humphrey, L. L., Apple, R. F., & Kirschenbaum, D. S. (1986). Differentiating bulimic-anorexic
from normal families using interpersonal and behavioral observational systems. Journal
of Consulting and Clinical Psychology, 54, 190-195.
Hund, A. R. & Espelage, D. L. (2006). Childhood emotional abuse and disordered eating among
undergraduate females: Mediating influence of alexithymia and distress. Child Abuse &
Neglect, 30, 393-407.
Hyman, S. M., Garcia, M., & Sinha, R. (2006). Gender specific associations between types of
childhood maltreatment and onset, escalation, and severity of substance us in cocaine
dependent adults. American Journal of Drug and Alcohol Abuse, 32(4), 655-664.
Irving, S. M., & Ferraro, K. F. (2006). Reports of abusive experiences during childhood
and adult health ratings: Personal control as a pathway? Journal of Aging and Health,
18, 458-485.
Jacobi, C., Hayward, C., & de Zwaan, M. (2004). Coming to terms with risk factors for eating
disorders: Application of risk terminology and suggestions for a general taxonomy.
Psychological Bulletin, 130, 19-65.
Jakupcak, M., Tull, M. T., & Roemer, L. (2005). Masculinity, shame, and fear of emotions as
predictors of men’s expressions of anger and hostility. Psychology of Men and
Masculinity, (6)4, 275-284.
Johnson, J. G., Cohen, P., Kasen, S., & Brook, J. S. (2002). Childhood adversities associated
with risk for eating disorders or weight problems during adolescence or early adulthood.
American Journal of Psychiatry, 159(3), 394-400.

84
Kaplan, M.J., & Klinetob, N.A. (2000). Childhood emotional trauma and chronic
posttraumatic stress disorder in adult outpatients with treatment-resistant depression.
Journal of Nervous and Mental Disease, 189(9), 596-601.
Kiecolt-Glaser, J. K., McGuire, L., Robles, T. F., Glaser, R. (2002). Psychoneuroimmunology:
Psychological influences on immune function and health. Journal of Consulting and
Clinical Psychology, 70(3), 537-547.
Kennedy, A. M., Ip, K., Samra, J., & Gorzalka, B. B. (2007). The role of emotional abuse in
disordered eating. Journal of Emotional Abuse, 7(1), 17-36.
Kennerley, H. (1996). Cognitive therapy of dissociative symptoms associated with trauma.
British Journal of Clinical Psychology, 35, 325–340.
Kent, A., & Waller, G. (2000). Childhood emotional abuse and eating psychopathology.
Clinical Psychology Review, 20, 887-903.
Kent, A., Waller, G., & Dagnan, D. (1999). A greater role of emotional than physical or
sexual abuse in predicting disordered eating attitudes: The role of mediating variables.
International Journal of Eating Disorders, 25, 159-167.
Kline, R. B. (2005). Principles and practice of structural equation modeling. New York:
Guilford Press.
Kong, S., & Bernstein, K. (2009). Childhood trauma as a predictor of eating psychopathology
and its mediating variables in patients with eating disorders. Journal of Clinical Nursing,
18(13), 1897-1907.
Kraus, E. D., Mendelson, T., & Lynch, T. R. (2003). Childhood emotional invalidation and adult
psychological distress: The mediating role or emotional inhibition. Child Abuse &
Neglect, 27, 199-213.

85
Lei, M., & Lomax, R. G. (2005). The effect of varying degrees of nonnormality in structural
equation modeling. Structural Equation Modeling, 12, 1-27.
Leung, N., Waller, G., Thomas, G. (1999). Core beliefs in anorexic and bulimic women. Journal
of Nervous and Mental Disease, 187(12), 736-741.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New
York: The Guilford Press.
Liu, R. T., Alloy, L. B., Abramson, B. M., Iacoviello, B. M., & Whitehouse, W. G. (2009).
Emotional maltreatment and depression: Prospective prediction of depressive episodes.
Depression and Anxiety, 26, 174-181.
Loos, M. E., & Alexander, P.C. (1997). Differential effects associated with self-reported
histories of abuse and neglect in a college sample. Journal of Interpersonal Violence,
12(3), 340-360.
Lucas, A. R., Crowson, C.S., O’Fallon, M. W., & Melton, J.L. (1999). The ups and downs of
anorexia nervosa. International Journal of Eating Disorders, 26, 397-405.
Lumley, M. N., & Harkness, K. L. (2007). Specificity in the relations among childhood diversity,
early maladaptive schemas, and symptom profiles in adolescent depression. Cognitive
Therapy and Research, 31, 639-657.
MacKinnon, D.P., Fairchild, A. J., & Fritz, M. S. (2007). Mediation analysis. Annual Review of
Psychology, 58, 593-614.
MacMillan, H. L., Fleming, J. E., & Streiner, D. L. (2001). Childhood abuse and lifetime
psychopathology in a community sample. American Journal of Psychiatry, 158, 1878-
1883.

86
Maciejewski, P. K., & Mazure, C.M. (2006). Fear of criticism and rejection mediates an
association between childhood emotional abuse and adult onset of major depression.
Cognitive Therapy and Research 30(1), 105-122.
Malinsoky-Rummell, R., & Hansen, D. J. (1993). Long-term consequences of childhood
physical abuse. Psychological Bulletin, 114, 68-79.
Marcus, M. D., Wing, R. R., Ewing, L., Kern, E., Gooding, W., & McDermott, M. (1990).
Psychiatric disorders among obese binge eaters. International Journal of Eating
Disorders, 9(1), 69-77.
Marsh, H. W., Hau, K., & Wen, Z. (2004). In search of the golden rules: Comment on
hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in
overgeneralizing Hu and Bentler’s (1999) findings. Structural Equation Modeling, 11(3),
320-34.
Mason, O., Platts, H., & Tyson, M. (2005). Early maladaptive schemas and adult attachment in a
UK clinical population. Psychology and Psychotherapy: Theory, Research and Practice,
78 (4), 549-564.
Maughan, A, & Cicchetti, D. (2002). The impact of child maltreatment and interadult
violence on children’s emotion regulation abilities. Child Development, 73, 1525–1542.
Mazzeo, S. E. & Espelage, D. L. (2002). Association between childhood physical and emotional
abuse and disordered eating in female undergraduates: An investigation of the mediating
role of alexithymia and depression. Journal of Counseling Psychology, 49(1), 86-100.

87
McGinn, L. K., Cukor, D., & Sanderson, W. C. (2005). The relationship between parenting style,
cognitive style, and anxiety and depression: Does increased early adversity influence
symptom severity through the mediating role of cognitive style? Cognitive Therapy and
Research, 29, 219–242.
Messman-Moore, T. L., & Brown, A. L. (2004). Child maltreatment and perceived family
environment as risk factors for adult rape: is child sexual abuse the most salient
experience. Child Abuse & Neglect, 28, 1019-1034.
Messman-Moore, T. L., & Coates, A.A. (2007). The impact of childhood psychological abuse on
adult interpersonal conflict: The role of early maladaptive schemas and patterns of
interpersonal behavior. Journal of Emotional Abuse, 7, 75-92.
Messman-Moore, T. L. & Garrigus, A.S. (2007). The association of child abuse and eating
disorder symptomatology: The importance of multiple forms of abuse and
revictimization. Journal of Aggression, Maltreatment, & Trauma, 14(3), 51-72.
Merrill, L., Thomsen, C., Sinclair, B., Gold, S., & Milner, J. (2001). Predicting the impact of
child sexual abuse on women: The role of abuse severity, parental support, and coping
strategies. Journal of Consulting and Clinical Psychology, 69(6), 992-1006.
Messman-Moore, T. L., & Coates, A. A. (2007). The impact of childhood psychological abuse
on adult interpersonal conflict: The role of early maladaptive schema patterns of
interpersonal behavior. Journal of Emotional Abuse, 7(2), 75-92.
Messman-Moore, T. L., & Brown, A. L. (2004). Child maltreatment and perceived family
environment as risk factors for adult rape: Is child sexual abuse the most salient
experience. Child Abuse & Neglect, 28, 1019-1034.

88
Meyer, C., & Waller, G. (2000). Subliminal activation of abandonment and eating schemata:
Relationship with eating disordered attitudes in a nonclinical population. International
Journal of Eating Disorders, 27(3), 328-334.
Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., & Herbison, G. P. (1995).
The long-term impact of the physical, emotional, and sexual abuse of children: A
community study. Child Abuse & Neglect, 20, 7-21.
Nelson, W. L., Hughes, H. M., Katz, B., & Searight, H. R. (1999). Anorexic eating attitudes and
behaviors of male and female college students. Adolescence, 34(135), 621-633.
O’Dougherty Wright, M. (2007). The long-term impact of emotional abuse in childhood:
Identifying mediating and moderating processes. Journal of Emotional Abuse, 7, 1-8.
O’Dougherty Wright, M., Crawford, E., & Del Castillo, D. (2009). Childhood emotional
maltreatment and later psychological distress among college students: The mediating role
of maladaptive schemas. Child Abuse & Neglect, 33, 59-68.
O’Hagan, K. P. (1995). Emotional and psychological abuse: Problems of definition.
Child Abuse & Neglect, 19, 449-461.
Penninx, B. W., Beekman, A.T; Honig, A., Deeg, D., Schoevers, R. A., van Eijk, J. T, et al.
(2001). Depression and cardiac mortality: Results from a community-based longitudinal
study. Archives of General Psychiatry, 58(3), 221-227.
Petrocelli, J. V., Glaser, B. A., Calhoun, G. B., & Campbell, L. F. (2001). Personality and affect
characteristics of outpatients with depression. Journal of Personality Assessment, 77 (1),
162-175.
Pinto-Gouveia, J., Castilho, P., Galhardo, A., Cunha, M. (2006). Early maladaptive schemas and
social phobia. Cognitive Therapy and Research, 30(5), 571-584.

89
Polivy, J., & Herman, C. P. (1993). Etiology of binge eating: Psychological mechanisms. In C.
G. Fairburn & G. T. Wilson (Eds.), Binge eating: Nature, assessment, and treatment (pp.
173-205). New York: Guilford Press.
Price, J.P. (2007). Cognitive schemas, defense mechanisms and post-traumatic stress
symptomatology. Psychology and Psychotherapy: Theory, Research and Practice, 80,
343–353.
Rastam, M. (1992). Anorexia nervosa in 51 Swedish adolescents: Premorbid problems and
comorbidity. Journal of the American Academy of Child & Adolescent Psychiatry, 31(5),
819-829.
Rich, C.L., Gidycz, C.A., Warkentin, J. B., Loh, C., & Weiland, P. (2005). Child and
adolescent abuse and subsequent victimization. A prospective study. Child Abuse &
Neglect, 29(12), 1373-1394.
Richardson, G. (2005). Early maladaptive schemas in a sample of British adolescent sexual
abusers: Implications for therapy. Journal of Sexual Aggression, 11(3), 259-276.
Roemmele, M., & Messman-Moore, T. L. (2011). Child abuse, early maladaptive schemas, and
risky sexual behavior in college women. Journal of Child Sexual Abuse, 20, 264-283.
Rorty, M., Yager, J., & Rossotto, E. (1994). Childhood sexual, physical, and psychological
abuse in bulimia nervosa. American Journal of Psychiatry, 151 (8), 1122-1126.
Rose, D. T., & Abramson, L. Y. (1992). Developmental predictors of depressive cognitive
style: Research and theory. In D. Cicchetti & S. L. Toth (Eds.), Developmental
perspectives on depression: Vol. 4. Rochester Symposium on Developmental
Psychopathology (pp. 323–349). Rochester, NY: University of Rochester Press.

90
Rose, D. T., Abramson, L. Y., & Kaupie, L. (2000). The Life Experiences Questionnaire: A
measure of history of emotional, physical, and sexual maltreatment. Unpublished
manuscript, University of Wisconsin-Madison, Madison, WI.
Rosen, L. N., & Martin, L. (1998). Long-term effects of childhood maltreatment history
on gender-related personality characteristics. Child Abuse & Neglect, 22, 197-211.
Roth, S., Newman, E., Pelcovitz, D., van der Kolk, B., & Mandel, F. (1997). Complex PTSD in
victims exposed to sexual and physical abuse: Results from the DSM-IV field trial for
posttraumatic stress disorder. Journal of Traumatic Stress, 10, 539-555.
Saarni, C. (1999). The development of emotional competence. New York: Guilford Press.
Scher, C. D., Forde, D. R., McQuaid, J. R., & Stein, M. B. (2004). Prevalence of demographic
correlates of childhood maltreatment in an adult community sample. Child Abuse &
Neglect, 28, 167-180.
Scher, C. D., Stein, M. B., Asmundson, G. J. G., McCreary, D. R., & Forde, D. R. (2001). The
Childhood Trauma Questionnaire in a community sample: Psychometric properties and
normative data. Journal of Traumatic Stress, 14, 843-857.
Schmidt, N. B., Joiner, T. E., Young, J. E., & Telch, M. J. (1995). The schema questionnaire:
Investigation of psychometric properties and the hierarchical structure of a measure of
maladaptive schemas. Cognitive Therapy and Research, 19, 295–301.
Shaffer, A., Yates, T. M., & Engeland, B. M. (2009). The relation of emotional maltreatment to
early adolescent competence: Developmental processes in a prospective study. Child
Abuse & Neglect 33(1), 36-44.
91
Shields, A., & Cicchetti, D. (1998). Reactive aggression among maltreated children: The
contributions of attention and emotion dysregulation. Journal of Clinical Child
Psychology, 27, 381-395.
Shipman, K., Zeman, J., Penza, S., & Champion, K. (2000). Emotion management skills
in sexually maltreated and nonmaltreated girls: A developmental psychopathology
perspective. Development and Psychopathology, 12, 47-62.
Shipman, K. L., Schneider, R., Fitzgerald, M. M., Sims, C., Swisher, L., & Edwards, E.
(2007). Maternal emotion socialization in maltreating and non-maltreating families:
Implications for children’s emotion regulation. Social Development, 16(2), 268-285.
Smolak, L. & Murnen, S. K. (2002). A meta-analytic examination of the relationship between
child sexual abuse and eating disorders. International Journal of Eating Disorders, 31,
136-150.
Smyth, J. M., Wonderlich, S. A., Heron, K. E., Sliwinski, M. J., Crosby, R. D., Mitchell, J. E., et
al. (2007). Daily and momentary mood and stress are associated with binge eating and
vomiting in Bulimia Nervosa patients in the natural environment. Journal of Consulting
and Clinical Psychology, 75, 629-638.
Sobel, M. E. (1982). Asymptotic confidence intervals for indirect effects in structural equation
models. In S. Leinhardt (Ed.), Sociological methodology 1982 (pp. 290–312).
Washington, DC: American Sociological Association.
Spertus, I. L., Yehuda, R., Wong, C. M., Halligan, S., & Seremetis, S. V. (2003). Childhood
emotional abuse and neglect as predictors of psychological and physical symptoms in
women presenting to a primary care practice. Child Abuse & Neglect 27(11), 1247-1258.
92
Steiger, J. H. (1990). Structural model evaluation and modification: An interval estimation
approach. Multivariate Behavioral Research, 25, 173-180.
Stein, R. I., Kenardy, J., Wiseman, C. V., Dounchis, J. Z., Arnow, B. A., & Wilfley, D. E.
(2007). What's driving the binge in binge eating disorder? A prospective examination of
precursors and consequences. International Journal of Eating Disorders, 40, 195-203.
Stevens, J. (2002). Applied multivariate statistics for the social sciences (4th
ed.). Hillside, NJ:
Erlbaum.
Stice, E. (2002). Risk and maintenance factors for eating pathology: A meta-analytic review.
Psychological Bulletin, 128, 825-848.
Sullivan, T. P., Fehon, D. C., Andres-Hyman, R. C., Lipschitz, D. S., & Grilo, C. M.
(2006). Differential relationships of childhood abuse and neglect subtypes to PTSD
symptom clusters among adolescent inpatients. Journal of Traumatic Stress, 19(2), 229-
239.
Tasca, G. A., Szadkowski, L., Illing, V., Trinneer, A., Grenon, R., Demidenko, N., Krysanski,
V., Balfour, L., & Bissada, H. (2009). Adult attachment, depression, and eating disorder
symptoms: The mediating role of affect regulation strategies. Personality and Individual
Differences, 47, 662-667.
Thelen, M. H., Farmer, J., Wonderlich, S., & Smith, M. (1991). A revision of the bulimia test:
The BULIT-R. Psychological Assessment, 3(1), 119-124.
Thelen, M. H., Mintz, L. B., Vander Wal, J. S. (1996). The bulimia test-revised: Validation with
DSM-IV criteria for bulimia nervosa. Psychological Assessment, 8 (2), 219-221.

93
Thimm, J. C. (2010). Mediation of early maladaptive schemas between perceptions of parental
rearing style and personality disorder symptoms. Journal of Behavior Therapy and
Experimental Psychiatry, 41, 52-59.
Thompson, K. M., & Wonderlich, S. A. (2004). Child sexual abuse and eating disorders. In
Thompson, K. M. (Eds.), Handbook of eating disorders and obesity (pp. 679-694).
Hoboken, New Jersey: John Wiley & Sons.
Thomas, J. J., Delinsky, S. S., St. Germain, S. A., Weigel, T. J., Tangren, C. M., Levendusky, P.
G., & Becker, A. E. (2010). How do eating disorder specialist clinicians apply DSM-IV
diagnostic criteria in routine clinical practice? Implications for enhancing clinical utility
in DSM-5. Psychiatry Research, 178, 511-517.
Tian, P. S. O., & Baranoff, J. (2007). Young schema questionnaire: Review of psychometric and
measurement issues. Australian Journal of Psychology, 59, 78-86.
Tull, M. T., Barrett, H. M., McMillan, E. S., & Roemer, L. (2007). A preliminary investigation
of the relationship between emotion regulation difficulties and posttraumatic symptoms.
Behavior Therapy, 38(3), 303-313.
Tull, M. T., Jakupcak, M., Paulson, A., & Gratz, K. L. (2007). The role of emotional
inexpressivity and experiential avoidance in the relationship between posttraumatic stress
disorder symptom severity and aggressive behavior among men exposed to interpersonal
avoidance. Anxiety, Stress, & Coping, 20(4), 337-351.
Turner, H., & Bryant-Waugh, R. (2004). Eating disorder not otherwise specified (EDNOS):
Profiles of clients presenting at a community eating disorder service. European Eating
Disorders Review, 12, 18-26.

94
Unoka, Z., Tamas, T., & Czobor, P. (2007). Early maladaptive schemas and body mass index in
subgroups of eating disorders. A differential association. Comprehensive Psychiatry, 48,
199-204.
Unoka, Z., Tamas, T., Czobor, P., & Simon, L. (2010). Eating disorder behavior and early
maladaptive schemas in subgroup of eating disorders. Journal of Nervous and Mental
Disease, 198, 425-431.
Vandenberg, R. J., & Lance, C. E. (2000). A review and synthesis of the measurement
invariance literature: Suggestions, practices, and recommendations for organizational
research. Organizational Research Methods, 3(1), 4-69.
Waller, G., Corstorphine, E., & Mountford, V. (2007). The role of emotional abuse in the eating
disorders: Implications for treatment. Eating Disorders, 15, 317-331.
Waller, G., Kennerley, H., & Ohanian, V. (2007). Schema-focused cognitive behavioral therapy
with eating disorders. In L. P. Riso, P. L. du Toit, D. J. Stein, & J. E. Young (Eds.),
Cognitive schemas and core beliefs in psychiatric disorders: A scientist-practitioner
guide (pp. 139–175). New York, NY: American Psychological Association.
Waller, G., Ohanian, V., Meyer, C., & Osman, S. (2000). Cognitive content among bulimic
women: The role of core beliefs. International Journal of Eating Disorders, 28, 235–241.
Walsh, B. T., & Sysko, R. (2009). Broad categories for the diagnosis of eating disorders (BCD-
ED): An alternative system of classification. International Journal of Eating Disorders,
42(8), 754-764.

95
Wang, C. E. A., Halvorsen, M., Eisemann, M., Waterloo, K. (2010). Stability of dysfunctional
attitudes and early maladaptive schemas: A 9-year follow-up study of clinically
depressed subjects. Journal of Behavior Therapy and Experimental Psychiatry, 41, 389-
396.
Webber, E. M. (1994). Psychological correlates of binging and nonbinging obese women.
Journal of Psychology: Interdisciplinary and Applied, 128(3), 339-351.
West, S. G., Finch, J.F., & Curran, P. J. (1995). Structural equation models with nonnormal
variables: Problems and remedies. In Hoyle, R. H. (Eds.), Structural equation modeling:
Concepts, issues, and applications (pp.56-75). Thousand Oaks, CA: Sage Publications.
Whiteside, U., Chen, E., Neighbors, C., Hunter, D., Lo, T., & Larimer, M. (2007). Difficulties
regulating emotions: Do binge eaters have fewer strategies to modulate and tolerate
negative affect? Eating Behaviors, 8, 162-169.
Wilksch, S., & Wade, T. D. (2004). Differences between women with anorexia nervosa and
restrained eaters on shape and weight concerns, self-esteem, and depression.
International Journal of Eating Disorders, 35(4), 571-578.
Wonderlich, S. A., Crosby, R. D., Mitchell, J. E., Roberts, J. A., Haseltine, B., DeMuth, G., et al.
(2000). Relationship of childhood sexual abuse and eating disturbance in children.
Journal of the American Academy of Child and Adolescent Psychiatry, 39(10), 1277-
1283.
Wyatt, G. E., & Newcomb, M. (1990). Internal and external mediators of women’s sexual abuse
in childhood. Journal of Consulting and Clinical Psychology, 58, 758-767.

96
Yates, T. M., & Wekerle, C. (2009). The long-term consequences of childhood emotional
maltreatment on development: (Mal)adaptation in adolescence and young adulthood.
Child Abuse & Neglect, 33 (1), 19-21.
Young, J. E. (1994). Cognitive therapy for personality disorders: A schema-focused approach
(rev. ed.) Sarasota, FL: Professional Resource Press.
Young, J. E. (1999). Cognitive therapy for personality disorders: A schema-focused approach
(3rd ed.). Sarasota, FL: Professional Resource Press.
Young, J. E., Klosko, J. S., & Weishar, M. E. (2003). Schema therapy: A practitioner’s guide.
New York: Guilford Press.