Emotional abuse
28
This article was downloaded by: [Computing & Library Services, University of Huddersfield] On: 02 October 2011, At: 10:19 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Aggression, Maltreatment & Trauma Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wamt20 Sticks and Stones May Break My Bones: The Effects of Emotional Abuse Helen Gavin a a Division of Psychology & Counselling, University of Huddersfield, Huddersfield, United Kingdom Available online: 09 Aug 2011 To cite this article: Helen Gavin (2011): Sticks and Stones May Break My Bones: The Effects of Emotional Abuse, Journal of Aggression, Maltreatment & Trauma, 20:5, 503-529 To link to this article: http://dx.doi.org/10.1080/10926771.2011.592179 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Emotional abuse

This article was downloaded by: [Computing & Library Services, University of Huddersfield]On: 02 October 2011, At: 10:19Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Aggression, Maltreatment &TraumaPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wamt20
Sticks and Stones May Break My Bones:The Effects of Emotional AbuseHelen Gavin aa Division of Psychology & Counselling, University of Huddersfield,Huddersfield, United Kingdom
Available online: 09 Aug 2011
To cite this article: Helen Gavin (2011): Sticks and Stones May Break My Bones: The Effects ofEmotional Abuse, Journal of Aggression, Maltreatment & Trauma, 20:5, 503-529
To link to this article: http://dx.doi.org/10.1080/10926771.2011.592179
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date. The accuracy of anyinstructions, formulae, and drug doses should be independently verified with primarysources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.

Journal of Aggression, Maltreatment & Trauma, 20:503–529, 2011Copyright © Taylor & Francis Group, LLCISSN: 1092-6771 print/1545-083X onlineDOI: 10.1080/10926771.2011.592179
Sticks and Stones May Break My Bones:The Effects of Emotional Abuse
HELEN GAVINDivision of Psychology & Counselling, University of Huddersfield, Huddersfield,
United Kingdom
The relationship between psychological maltreatment in child-hood and adult well-being has previously been established viathe statistical modeling of psychometric data. This study exam-ines a set of statistical data regarding abuse alongside personalaccounts. A group of 165 participants completed several psycho-metric scales, including a measure of childhood emotional abuse.Several participants were then invited to participate in interviewsexploring issues in more depth. Statistical analysis supported pre-vious findings, but the interviews exposed themes pertinent to theexamination of long-term effects of emotional abuse, such asacknowledgment of abuse. The findings support the use of a mixedmethodology, as statistical measurements alone did not revealsome detail. The implications of this finding for psychologicalresearch and practice are discussed.
KEYWORDS cumulative disadvantage, emotional abuse, mixedmethodology
If your child has been called names, how do you comfort her? The saying“Sticks and stones may break my bones, but words will never hurt me” is onethat dates back to at least the 19th century, and is possibly much older thanthat (Northall, 1894). However, the efficacy of this axiom for someone who issuffering verbal abuse is questionable; the reassurance that taunts and insultscannot hurt does not make the pain go away. It is generally thought thatthere is a distinction between physical pain and emotional or social pain;
Submitted 17 April 2010; revised 2 July 2010; accepted 31 August 2010.Address correspondence to Helen Gavin, Division of Psychology & Counselling,
University of Huddersfield, Queensgate, Huddersfield HD1 3DH, UK. E-mail: [email protected]
503
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

504 H. Gavin
physical hurt is seen as more damaging. This might not be the case, andignoring the pain can be hazardous. James (1890/1950) suggested that thosewho experience social ostracism or emotional mistreatment find it moredisturbing than physical punishment. Chen, Williams, Fitness, and Newton(2008) also discovered that social pain is remembered long after physicalpain has faded in memory, and it appears to have far-reaching consequencesfor mental health, relationships, and adaptation to change. Moreover, socialor emotional pain, embarrassment, or ostracism can be relived time aftertime, whereas it is difficult to mentally re-create physical pain. This articleexamines current thinking about the potential consequences of nonphysicalpain experienced in childhood and reports on empirical research exploringthese consequences as well as the recollections of nonphysical pain in agroup of adults.
NONPHYSICAL PAIN AND ITS OUTCOMES
Physical or sexual abuse in childhood is an established risk factor for adulthealth problems (Clark, de Bellis, Lynch, Cornelius, & Martin, 2003; Kendall-Hackett, 2002). A particular form of nonphysical abuse, childhood emotionalabuse, might have even more far-reaching consequences due to its insidiousand unremitting nature. Abuse is any behavior that is designed to controland subjugate another human being through the use of fear, humiliation, orverbal or physical assaults. Emotional abuse is any kind of abuse that is psy-chological rather than physical in nature, including verbal abuse, constantcriticism, intimidation, manipulation, and a refusal to be pleased. Riggs andKaminski (2010) asserted that “the notion that emotional abuse harms chil-dren is unequivocal” (p. 6), and suggested that it is responsible for some ofthe lasting effects of sexual and physical abuse as well as being destructivein its own right. Examinations of how these effects manifest themselves inadults who do and who do not report such childhood abuse is therefore avalid objective.
Irving and Ferraro (2006) demonstrated that abusive experience duringchildhood affected self-rated health, with emotional abuse by parents hav-ing the largest negative contribution to perceived adult health. This findingwas irrespective of the sex of the participant, but the largest single predictorof low health ratings in women was emotional abuse by the mother. Thismight go some way to explaining the findings of Long and Mullen (1994),who reported on a study of women who abused alcohol and explored fac-tors they perceived as being contributory to their behavior. They found thatemotional pain was a major factor in female alcohol abuse, with emotionalabuse by parents contributing to that pain in over 34% of those interviewed.As this study did not make comparisons to men who abuse alcohol, it is diffi-cult to determine the precise contribution of sex, but it is clear that emotionalpain is a major factor of concern for later health and perceived health.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 505
Other mental health issues can also be affected by early experience.Gibb, Benas, Crossett, and Uhrlass (2007) found a relationship among emo-tional abuse, verbal victimization by peers (bullying), and the likelihoodof adult depression. Depression is experienced by large numbers of peo-ple and is characterized by sadness, loss of interest or pleasure, feelings ofguilt or low self-worth, disturbed sleep or appetite, low energy, and poorconcentration (World Health Organization, 2008). In adulthood, twice asmany women receive a diagnosis of or treatment for depression than men(Hyde, Mezulis, & Abramson, 2008). This gender discrepancy starts to showitself in puberty and reaches adult levels of difference at around 15 yearsof age. Similarly, some anxiety disorders, such as phobias and social anx-iety, affect women disproportionately to men (Halbreich & Kahn, 2007).Other physical conditions with a psychological element that we are onlyjust beginning to understand (e.g., idiopathic headache, fibromyalgia, andirritable bowel syndrome) are also suffered predominantly by women andare clearly linked to psychosocial risk factors (Ali et al., 2000; Walker et al.,1997). Some researchers, such as Ferraro and Nuriddin (2006), suggest thatwomen are more likely to suffer health-related consequences due to expe-riencing childhood psychological stress than men, including higher risk forboth physical and mental illnesses. Due to such sex differences, biologicaland genetic models of all the preceding conditions are compellingly con-vincing. However, biology alone does not account for these differences, asthey would be much larger if there was a solely gender-based etiology. Inaddition, depression and anxiety would respond to gender-based educationand therapy. The medical field is moving toward more integrative theoriesand models, suggesting that the differences among patients emerge due toa set of factors that include hormonal, genetic, and psychological factors.
It is also proposed that negative life events have more impact on thosewith a predisposition to depression or anxiety. For example, Maciejewskiand Mazure (2006) suggest that there are particular cognitive styles, suchas fear of criticism and rejection, that predict adult onset of major depres-sion and are associated with emotional abuse. What does not appear to beexplained is why such factors might be present or why such styles might beadopted, what these negative life events might be, or why women and girlsmight be more vulnerable. Integrative explanations such as that proposedby Hyde et al. (2008) are valuable but ignore the individualistic nature ofdevelopment and the robustness of some individuals who experience suchfactors but who do not develop difficulties. This is one element this studyseeks to address by examining the accounts of people who do report suchabuse in their childhood and comparing them with those who do not.
Emotional abuse does not, of course, only happen in isolation fromother forms of maltreatment. Survivors of sexual abuse also report that, inaddition to any long-lasting physical effects of the abuse itself, the betrayaland loss of innocence has a profound consequence for later life. Such effects
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

506 H. Gavin
might extend to other forms of abuse. Irving and Ferraro (2006) found thatreported emotional abuse experiences in childhood were associated withlower personal control, which, in turn, leads to lower ratings of adult health.The major period for development of personal control is during childhoodand early adolescence, when the individual should begin to feel empow-ered and to have influence over his or her own life events (Zimmerman,1995). Irving and Ferraro suggest that abuse during this age period alters thisdevelopment and is subsequently reinforced by, and makes one more sus-ceptible to, negative experience in later adolescence and adulthood. Theirfindings imply that this adverse effect can result in poorer health, or atthe very least, a perception of poor health. There is also a clear relation-ship between childhood abuse and the probability of being exposed tolater trauma, thus compounding the effects (Classen, Palesh, & Aggarwal,2005). Surviving abuse can therefore mean not only recovery from abusiveepisodes, but also continuing to experience disadvantage in terms of psy-chological adjustment and adaptation in later life. This effect is described inthe cumulative disadvantage theory, which has broad implications for healthresearch as well as social and criminological outcomes.
CUMULATIVE DISADVANTAGE THEORY
The impact of one set of negative experiences is not just immediate, butcompounds throughout the life course, as individuals subjected to early dis-advantage are more likely to have developmental issues, encounter negativeexperiences, or perceive events in a negative light. Hence, a person who isabused in childhood will tend to choose relationships that are themselvesabusive in nature. Indeed, emotionally abused individuals are more likelyto exhibit mistrust and high rejection expectancy toward new people thanthose who have experienced little or no abuse (Berenson & Anderson, 2006).This viewpoint has had a major impact on health-related issues and on thestudy of individual characteristics that might be involved in the developmentof ill health or the maintenance of good health. Ferraro and Nuriddin (2006)found a sex difference in poor health outcomes due to emotional distressand attributed it to the possibility that men and women might experience dif-ferent forms of disadvantage through the life course. Criminological researchalso suggests that childhood delinquency can indicate feelings of anger thatcan translate into problems such as depression or alcohol abuse later in life(Hagan & Foster, 2003). Hence, the disadvantage of growing up in an envi-ronment where delinquency is the norm accumulates due to the adverseeffects of the early experiences. Therapies that lead the individual to higherpersonal control and empowerment could therefore be more effective inseveral situations, but such efficacy has yet to be fully explored (Carbone,2010). Such models also link the accumulation of negative experience to the
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 507
development of learned helplessness, which in turn is linked to the like-lihood of depression even in young children (Cole et al., 2007). It wouldbe pertinent to suggest then that any examination of how childhood emo-tional abuse affects the adult should address the individual’s propensity foradaptation or coping compared to those who do not develop such strategies.
WHAT IS EMOTIONAL ABUSE?
As mentioned earlier, emotional abuse is any kind of behavior that isdesigned to psychologically subjugate, control, or harm the recipient. Assuch, it can erode self-confidence, sense of self-worth, and self-concept. Itis insidious, as perpetrators might disguise it as advice or guidance, butconstant berating and belittling leads to the loss of personal value, leavingvictims with deep and long-lasting (although invisible) scars (Glaser, 2002).Emotional abuse does not have the same visibility as sexual or physicalabuse (Rees, 2010), but clinicians agree that it is a core element of both andmight even be more damaging. Emotional abuse also manifests itself in sev-eral guises, such as aggressing, denying, and minimizing. Aggressive formsof abuse include insults, threats, blaming, and ordering, all of which under-mine the equality and autonomy of the victim. However, aggression can alsobe indirect, taking the form of criticism, advice, or help, but with the intentto belittle and control the recipient. Denying is a potent aspect of the abuseand can result in the recipient’s perception of his or her world becomingdistorted or invalidated. For example, a victim might confront the abuserwith an example of his or her aggressive behavior but the abuser refuses toacknowledge the event or the victim’s account of it. Another form of denialis to withhold (e.g., the abuser refuses to listen or communicate) or to failto acknowledge that the victim has any valid viewpoint or feeling beyondthe abuser’s own. Minimizing is a less extreme form of denial and consistsof countering the accusation of abuse with attempts to question the victim’sexperience as exaggeration or oversensitivity, or trivializing the experienceof the victim (Jantz & McMurray, 2009).
If such behavior takes place in a child’s relationship with an adult,when the child becomes an adult he or she might find that his or herrelationships mirror or expand on his or her own victimization. If therehas been little opportunity to set personal standards, develop viewpoints,and validate feelings and perceptions, the developing child experiencesthe abusive environment as normal. Therefore, even destructive relation-ships might feel familiar or comfortable to the victim. Victims of emotionalabuse often struggle with feelings of powerlessness, hurt, fear, and angerand might interpret even positive interactions in negative ways (Iwaniec,Larkin, & Higgins, 2006). For example, a woman who always encounteredcriticism of her appearance in childhood might interpret her friends’ or
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

508 H. Gavin
partner’s compliments as sarcastic or, alternatively, might continually seekreassurance.
Negative impact on adult relationships is only one outcome of expe-riencing childhood emotional abuse. Hund and Espelage (2006) proposeda model that linked childhood emotional abuse to alexithymia, general dis-tress, and disordered eating. The results of their study of a nonclinical sampleof 588 women illustrated a complex relationship between emotional abuseand alexithymia, depression, anxiety, and disorder eating. They concludedthat childhood emotional abuse could have a severe negative impact onsurvivors. This was supported by Kennedy, Ip, Samra, and Gorzalka (2007),who found a direct effect of childhood emotional abuse on eating pathol-ogy in nonclinical participants even when taking into account self-esteem,depression, anxiety, and other forms of abuse. They went on to suggestthat any examination of health issues in terms of abuse outcomes would beincomplete without considering emotional abuse as a factor.
The studies just detailed all suggest that the events of childhood form alasting impression throughout the life course and have major consequencesfor adult physical and mental health. There are some underlying implicationsin the literature that require examination. Some studies give the impressionthat there is a difference between men and women in terms of outcomes ofchildhood experience, with women being at higher risk of developing prob-lems such as alcoholism (Long & Mullen, 1994) or eating disorders (Hund &Espelage, 2006) if they were subjected to psychological maltreatment as chil-dren. However, many studies demonstrating the effect of abuse on womendo not include direct comparisons with male participants.
A second demographic factor to consider is that, because cumulativedisadvantage is a life course issue and negative events have a compoundingeffect, age is a contributory factor in that more negative events will havebeen experienced by an older person. This is bolstered by a stereotype ofolder people being more concerned about their health and exhibiting healthanxiety (Boston & Merrick, 2010). There is evidence to suggest that researchhas irrevocably linked cumulative disadvantage to age, but, according toDannefer (2003), only in gerontological research that examines differencesrobustness in older people. Although many studies affirm that the life courseperspective is an important one, none have addressed this directly by exam-ining whether age has a mediating effect other than for people who areover 65 years of age. If age is a contributing factor, it might be expectedthat older people would demonstrate more disparity in health or perceivedhealth as a consequence of differences in positive and negative experiencesand their accumulated effects. Thus, any such research should include ageas a variable.
A further point to note is that great deal of the research has beenbased on predominantly quantitative methodology in that it makes infer-ences from the examination of relationships in data drawn from measures ofhealth and abuse. Previous quantitative research typically used samples of
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
Sticks and Stones May Break My Bones 509
thousands, although studies linking childhood emotional abuse to specificphysical outcomes, such as fibromyalgia, or psychological well-being such asthe propensity for depression, use much smaller samples (e.g., Walker et al.,1997). Additionally, some studies have concentrated on female participantsonly or on specific professions, a methodological limitation acknowledgedclearly in the literature (see Reyome, Ward, & Witkiewitz, 2010). It is pos-sible, therefore, that some issues are being overlooked. In the same waythat we assume it is inevitable that survivors of sexual abuse will themselvesbecome abusers, we are in danger of assuming that childhood emotionalabuse will result in an unhealthy and abusive adult. There seems to be littleemphasis in the literature on individuals who survive abuse but do not goon to abuse others or experience abusive relationships. The points raisedare therefore the basis for this study.
OBJECTIVES OF THIS STUDY
This study was designed to attempt to discover whether there are any factorsthat can mitigate the nonclinical negative impacts of childhood events out-side of the clinical arena. Identifying adults with reported childhood abusewhose scores on adult health, well-being, and personal control scales arehigh and comparing those with lower scores, together with adults who donot score highly on the abuse scales, would seem to be a fruitful course totake. Observed differences between adults who report emotional (or other)abuse, but are robust enough to have positive adult experiences, and adultswho have experienced abuse and are lacking in adult positive experiencesmight help in identifying the psychological adjustments (and hence the ther-apeutic process) that could help current and future survivors of abuse copewith their abusive experiences and go on to have healthy adult experi-ences. This study utilized a mixed methodological format: a psychometricapproach to profiling participants with high or low levels of abuse and dif-ferentially reported difficulties in adulthood, and an analysis of personalaccounts.
The major objectives for this study were to identify adult men andwomen with and without reported childhood emotional abuse and to mea-sure variables in which emotional abuse is implicated as leading to loweractual or perceived health. Statistical analysis of the scores on these mea-sures comparing variables in terms of sex of the participants and levelsof reported abuse will determine whether this sample demonstrates theexpected relationship between childhood emotional abuse and adult healthand adaptation. Once this relationship was observed, participants were cat-egorized into high and low abuse and high and low health outcomes.A subsample was drawn to provide a detailed examination of the adults’reported accounts. In this way, a mixed methodological approach was usedand evaluated for efficacy in the examination of these issues.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

510 H. Gavin
METHOD
Ethics
All research protocols adhered to British Psychological Society codes of con-duct with respect to research with human participants. Participants weregiven information about the study at all points of data collection and wereasked to sign a consent form indicating they were providing permissionto use the data collected for the purpose of the study. Participants wereassured that personal information would remain confidential and that onlythe researcher had access to any of the data. Participants were also informedthat they could withdraw from the study at any time (up to disseminationof findings) without explanation or consequence. Data were coded to pro-vide anonymity and identification codes were kept in secured files storedseparately from the data file. Sources of support were offered to partici-pants in case they wished to discuss issues raised by the questionnaires orinterviews.
Participants
Participant recruitment was conducted via a poster campaign on a universitycampus and in nearby residential suburban areas. This broadened the par-ticipant pool but did not allow recruitment to extend to areas beyond whatmight be identified as a reasonably affluent district. The posters advertisedthe study as examining childhood experiences and the effect they have onadult outlook. There were no exclusion criteria other than a minimum ageof 18.
Thirty-five men and 130 women ranging in age from 22 to 45 (M =31.77) answered the advertisements. None of these potential participantswere excluded from this study. Each participant completed several question-naires designed to elicit information about experiences of childhood abuse,personal control levels, and current perceived health. Participants were notrecruited on the basis of any other criteria, such as mental health issuesor stress-related illnesses, although these factors appear in the literature.Therefore, some participants might have had such problems, but this studydid not make comparisons between groups on these factors.
Participants were also asked to indicate whether they would be willingto engage in a second stage of the study, which involved interviews withthe researcher. All participants indicated they were willing to be interviewed.Once the psychometric scale scores were entered into the data file and initialdescriptive statistics were compiled, participants were categorized on thebasis of their sex and whether their abuse was high or low. The randomselection of participants for the second stage of the study was carried outusing these classifications (see data plan later).
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 511
Instruments
The Child Abuse and Trauma Scale (CATS; Sanders & Becker-Lausen, 1995)is a 38-item scale measuring severity of sexual abuse, negative home envi-ronment and neglect, and punishment. It has high internal consistency(Cronbach’s α = .63–.90) and test–retest reliability (r = .71–.91). Kent andWaller (1998) further extracted a fourth construct—emotional abuse—thathas high internal consistency (α = .9) with the other subscales. The scoresfor this construct range from 0 to 28.
The Health Perceptions Questionnaire (Ware, 1976) has subscales forcurrent health (scored 9–45), prior health (3–15), susceptibility/resistance(4–20), health outlook (4–20), health worry (4–20), sickness orientation(2–10), rejection of the sick role (4–20), and attitude toward going tothe doctor (2–10). The subscales have internal consistency, with alpharanging from .90 (current health) to .45 (health worry), and good test–retest reliability (r = .59–.86). Ware also reports high construct validityfor measurement of past and present health, future health, and sick rolepropensity.
The Internal Control Index (ICI; Duttweiler, 1984) is an indicator of cog-nitive processing, autonomy, resistance to social influence, self-confidence,and delay of gratification. It has high reliability (α = .85) and there is a strongprincipal component, two replicable factors, and evidence for convergentvalidity. It has been used to measure the relationship between perceivedcontrol and recovery from traumatic events such as rape (Regehr, Cadell, &Jansen, 1999). Scores can range from 28 to 140, with higher sores indicatinghigher internal locus of control.
The Satisfaction With Life Scale (SWLS; Diener, Emmons, Larsen, &Griffin, 1985) measures self-reported level of satisfaction in general termsand is not related to any specific aspect. Satisfaction with life is one factorof the construct of subjective well-being and is distinguished from affectiveappraisal as it is cognitively, not emotionally, driven. Internal consistencyand alpha coefficients are above .8 and test–retest reliability was reportedas .82. Construct validity demonstrates an expected change over time anddistinctions between groups as predicted. The scale is scored from 7 to 35,with higher scores denoting higher satisfaction.
Participant Profile
Using the scoring on the various scales and subscales, participants wereprofiled in terms of negative and positive childhood experiences and therelationship of those experiences on reported satisfaction with life, percep-tion of health, and level of internalized control. Along with the completionof scales, participants were asked to indicate if they would be willing toparticipate in further interviews with the researcher and were told these
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

512 H. Gavin
interviews would include questions about childhood, current relationships,and the effects childhood experiences might have had on adult life.
Scales that showed correlation with emotional abuse scores were exam-ined to choose which participants would be included in the interview stage.Scores on the emotional abuse scales and those that were correlated withit were separated into upper and lower quartiles. Hence, participants withscores indicating high or low levels of emotional abuse and high or lowscores on other scales of interest were included in the next stage. The inten-tion was to divide participants into four categories representing the upperand lower quartiles. The categories were as follows: (a) high emotionalabuse plus high scores on other scales; (b) high emotional abuse plus lowscores on other scales; (c) low emotional abuse plus high scores on otherscales; and (d) low emotional abuse plus low scores on other scales.
The selection criteria for this stage included measurements of low andhigh emotional abuse, as the study objectives were to identify any disparitiesbetween participants in these groups in terms of adult levels of health (seedata analysis). These participants were then interviewed by the researcher,who followed a semistructured interview schedule incorporating questionsas previously outlined. Of the participants who agreed to participate ininterviews, four men and four women were selected on the basis of theirprofiles.
Interview Schedule
The interview schedule was developed by combining the questions from theemotional abuse construct of the CATS with other issues derived from the lit-erature around relationships and adaptability. Each interviewee was given awritten list of these questions and the interviewer asked him or her if theissues indicated in the questions had occurred and whether they had indi-cated as much during the questionnaire stage of the study. The followingtopics were also discussed: (a) How would you describe your relationshipwith your parents (caregivers or stepparents) now? What do you think youmight have learned from these relationships; (b) Is there anything in thoserelationships that you try to emulate or avoid in relationships with your ownchildren or partner; and (c) How do you view your health? The interviewwas interviewee-led, meaning the interviewee was allowed to speak freelyabout the topics but was guided back to these questions if necessary.
Interview Procedure
The interview started with neutral questions, then moved onto questionsabout relationships with parents and caregivers when a child, eliciting exam-ples of interactions to illustrate the subject being discussed. The interview
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 513
then moved on to current and recent relationships with parents and theeffect that relationship might have had. If appropriate, the interviewee wasasked if he or she thought there was anything about the parental rela-tionship that affected current situations. As stated earlier, the interviewwas interviewee-led, with some probes being prepared if necessary. Theinterviewee’s comfort related to speaking about these subjects was care-fully monitored. If there were any signs of distress, the line of questioningwas paused or abandoned. A pause in interviewing only occurred with oneinterviewee, who chose to carry on with the interview after a short break.
Data Analysis
The study was conducted in two parts: a quantitative design using severalpsychometric scales and a qualitative interview stage. Once participants hadbeen given information and a consent form to sign, they were asked tocomplete the four scales and to indicate if they were willing to participantin Stage 2. Data analysis was conducted using SPSS (IBM, New York) todetermine several pieces of information:
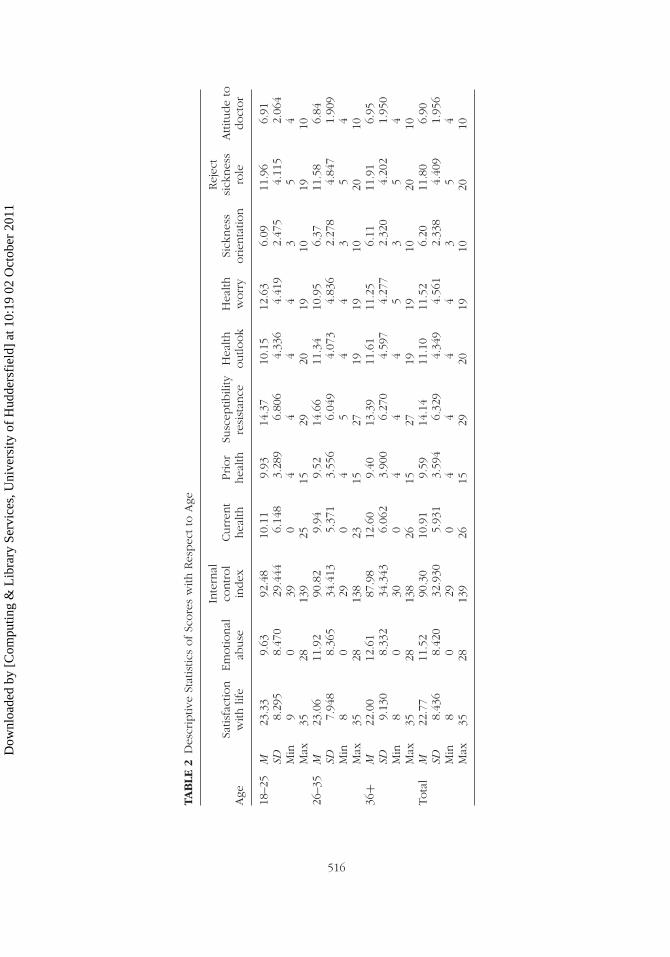
1. Descriptive statistics were compiled for all of the score variables withrespect to sex and age of the participant. Although the reviewed litera-ture did not directly examine any effect of age on the health outcomes,there is evidence to suggest that the effects of negative experiencesaccumulate over the life course (Dannefer, 2003). It is also thought thatconcern for health increases and the perception of good health decreaseswith age, although this is only seen in older adults (Boston & Merrick,2010). This sample only contained young and middle-aged adults, but theopportunity to explore any mediating effect of age was seen as important.
2. Correlational analysis of all the variables was carried out to determine thestrength and direction, if any, of the relationship between the measuredvariables. To determine any effect of the demographic variables, partialcorrelation was also carried out.
3. As the literature reviewed indicated clear sex differences in both the inci-dence of health concerns and the response to emotional abuse (Ferraro& Nuriddin, 2006), sex differences were computed using independent ttests to identify any such differences in this sample.
4. The descriptive statistics implied that there might be an effect of age;therefore, one-way analyses of variance (ANOVAs; with three categoriesof age) were performed on the scores.
5. A correlation matrix of all bivariate Pearson correlation coefficients wasproduced to determine the relationships among the measures. The samematrix was produced controlling for sex, as age had been shown to haveno significant effect or covariation effect.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

514 H. Gavin
6. An examination of these analyses allowed a participant profile to bedrawn up to select interviewees for the next stage of the study. Interviewtranscripts were analyzed using thematic analysis (see below).
RESULTS
Quantitative Results and Selection of Interviewees
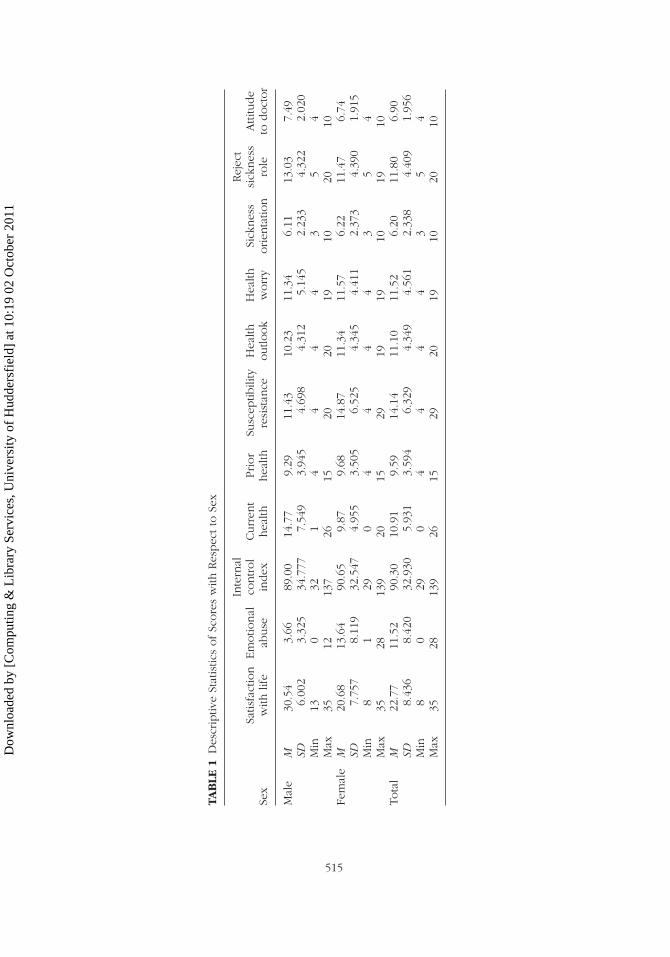
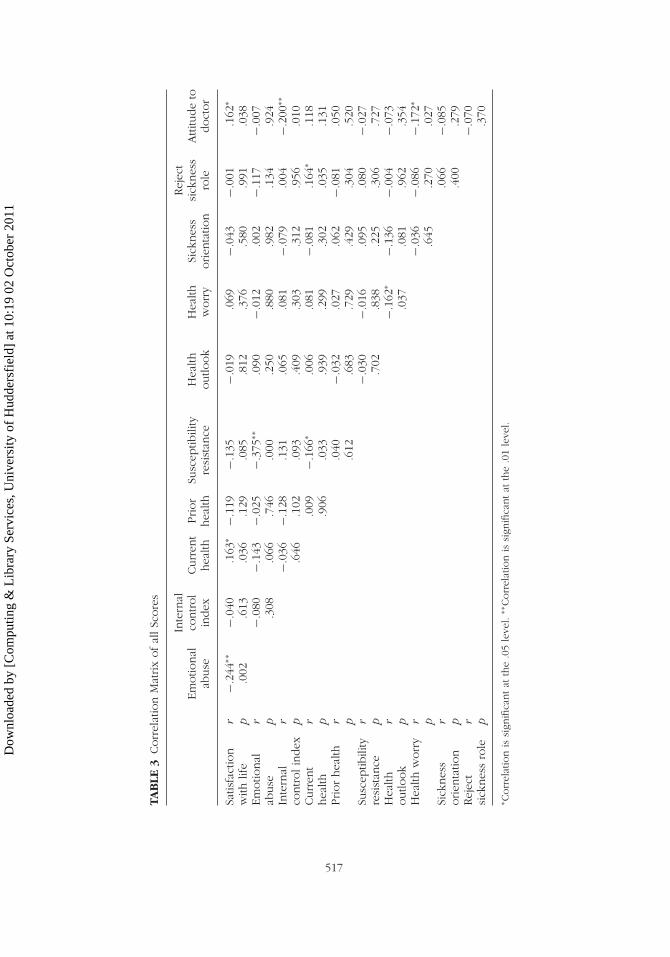
As already described in analysis Stage 1, scale scores were examined viadescriptive statistics and a correlation matrix. Table 1 shows the descriptivestatistics for all scale scores with respect to sex. Table 2 shows descriptivestatistics of all scale scores with respect to age. Table 3 shows a correlationmatrix of all scores.
Significant (p < .01) negative correlations were observed betweenemotional abuse and satisfaction with life (r = −.244) and susceptibility/
resistance to ill health (r = −.375). Susceptibility/resistance and currenthealth were significantly (p < .05) negatively correlated (r = −.166), aswere ICI and attitude to going to doctor (r = −.200), health outlook andhealth worry (r = −.162), and health worry and attitude to going to doc-tor (r = −.172). Significant (p < .05) positive correlations were observedbetween satisfaction with life and current health (r = .163), satisfactionwith life and attitude going to doctor (r = .162), and current health andrejection of sickness role (r = .640). However, most of these correlationsbecame nonsignificant when partial correlation controlling for sex was per-formed. Performing a correlation matrix on just the female participantsshowed that there were clear negative correlations between emotional abuseand susceptibility/resistance (r = −.625, p < .01) and internal control andattitude to going to the doctor (r = −.244, p < .01).
One major issue highlighted in the literature is that women appear to bemore susceptible to the influences of negative life events. To determine if thiswas reflected in the sample, the scale scores were subjected to independentsamples t tests for samples with unequal variances (due to the disparity insample sizes). Significant differences were found between men and womenon the following variables. Table 4 shows the t-test results on the scalescores for differences between men and women.
Univariate ANOVAs were then carried out to determine the effect of ageon all scale scores. The only variable to be affected by age was perceivedcurrent health, F(2, 162) = 3.681, p < .05, MSE = 34.063. There were nointeraction effects between age and sex for any of the scale scores.
It appears then that the only variable to systematically affect scores onany of the scales is sex, although this finding must be treated with cautiondue to the disparity in numbers of men and women in the sample. However,this substantiated the decision to interview both men and women in moredepth. As age did not appear to be a contributory or distinguishing factor,
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
TAB
LE1
Des
crip
tive
Stat
istic
sofSc
ore
sw
ithRes
pec
tto
Sex
Sex
Satis
fact
ion
with
life
Em
otio
nal
abuse
Inte
rnal
control
index
Curr
ent
hea
lthPrior
hea
lthSu
scep
tibili
tyre
sist
ance
Hea
lthoutlo
ok
Hea
lthw
orr
ySi
cknes
sorien
tatio
n
Rej
ect
sick
nes
sro
leA
ttitu
de
todoct
or
Mal
eM
30.5
43.
6689
.00
14.7
79.
2911
.43
10.2
311
.34
6.11
13.0
37.
49SD
6.00
23.
325
34.7
777.
549
3.94
54.
698
4.31
25.
145
2.23
34.
322
2.02
0M
in13
032
14
44
43
54
Max
3512
137
2615
2020
1910
2010
Fem
ale
M20
.68
13.6
490
.65
9.87
9.68
14.8
711
.34
11.5
76.
2211
.47
6.74
SD7.
757
8.11
932
.547
4.95
53.
505
6.52
54.
345
4.41
12.
373
4.39
01.
915
Min
81
290
44
44
35
4M
ax35
2813
920
1529
1919
1019
10To
tal
M22
.77
11.5
290
.30
10.9
19.
5914
.14
11.1
011
.52
6.20
11.8
06.
90SD
8.43
68.
420
32.9
305.
931
3.59
46.
329
4.34
94.
561
2.33
84.
409
1.95
6M
in8
029
04
44
43
54
Max
3528
139
2615
2920
1910
2010
515
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
TAB
LE2
Des
crip
tive
Stat
istic
sofSc
ore
sw
ithRes
pec
tto
Age
Age
Satis
fact
ion
with
life
Em
otio
nal
abuse
Inte
rnal
control
index
Curr
ent
hea
lthPrior
hea
lthSu
scep
tibili
tyre
sist
ance
Hea
lthoutlo
ok
Hea
lthw
orr
ySi
cknes
sorien
tatio
n
Rej
ect
sick
nes
sro
leA
ttitu
de
todoct
or
18–2
5M
23.3
39.
6392
.48
10.1
19.
9314
.37
10.1
512
.63
6.09
11.9
66.
91SD
8.29
58.
470
29.4
446.
148
3.28
96.
806
4.33
64.
419
2.47
54.
115
2.06
4M
in9
039
04
44
43
54
Max
3528
139
2515
2920
1910
1910
26–3
5M
23.0
611
.92
90.8
29.
949.
5214
.66
11.3
410
.95
6.37
11.5
86.
84SD
7.94
88.
365
34.4
135.
371
3.55
66.
049
4.07
34.
836
2.27
84.
847
1.90
9M
in8
029
04
54
43
54
Max
3528
138
2315
2719
1910
2010
36+
M22
.00
12.6
187
.98
12.6
09.
4013
.39
11.6
111
.25
6.11
11.9
16.
95SD
9.13
08.
332
34.3
436.
062
3.90
06.
270
4.59
74.
277
2.32
04.
202
1.95
0M
in8
030
04
44
53
54
Max
3528
138
2615
2719
1910
2010
Tota
lM
22.7
711
.52
90.3
010
.91
9.59
14.1
411
.10
11.5
26.
2011
.80
6.90
SD8.
436
8.42
032
.930
5.93
13.
594
6.32
94.
349
4.56
12.
338
4.40
91.
956
Min
80
290
44
44
35
4M
ax35
2813
926
1529
2019
1020
10
516
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
TAB
LE3
Corr
elat
ion
Mat
rix
ofal
lSc
ore
s
Em
otio
nal
abuse
Inte
rnal
control
index
Curr
ent
hea
lthPrior
hea
lthSu
scep
tibili
tyre
sist
ance
Hea
lthoutlo
ok
Hea
lthw
orr
ySi
cknes
sorien
tatio
n
Rej
ect
sick
nes
sro
leA
ttitu
de
todoct
or
Satis
fact
ion
with
life
r−.
244∗∗
−.04
0.1
63∗
−.11
9−.
135
−.01
9.0
69−.
043
−.00
1.1
62∗
p.0
02.6
13.0
36.1
29.0
85.8
12.3
76.5
80.9
91.0
38Em
otio
nal
abuse
r−.
080
−.14
3−.
025
−.37
5∗∗.0
90−.
012
.002
−.11
7−.
007
p.3
08.0
66.7
46.0
00.2
50.8
80.9
82.1
34.9
24In
tern
alco
ntrolin
dex
r−.
036
−.12
8.1
31.0
65.0
81−.
079
.004
−.20
0∗∗
p.6
46.1
02.0
93.4
09.3
03.3
12.9
56.0
10Curr
ent
hea
lthr
.009
−.16
6∗.0
06.0
81−.
081
.164
∗.1
18p
.906
.033
.939
.299
.302
.035
.131
Prior
hea
lthr
.040
−.03
2.0
27.0
62−.
081
.050
p.6
12.6
83.7
29.4
29.3
04.5
20Su
scep
tibili
tyre
sist
ance
r−.
030
−.01
6.0
95.0
80−.
027
p.7
02.8
38.2
25.3
06.7
27H
ealth
outlo
ok
r−.
162∗
−.13
6−.
004
−.07
3p
.037
.081
.962
.354
Hea
lthw
orr
yr
−.03
6−.
086
−.17
2∗
p.6
45.2
70.0
27Si
cknes
sorien
tatio
nr
.066
−.08
5p
.400
.279
Rej
ect
sick
nes
sro
ler
−.07
0p
.370
∗ Corr
elat
ion
issi
gnifi
cantat
the
.05
leve
l.∗∗
Corr
elat
ion
issi
gnifi
cantat
the
.01
leve
l.
517
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

518 H. Gavin
TABLE 4 Significant Mean Differences between Men andWomen on Scale Scores
Measure t (p<.01) Mean difference
Emotional abuse 11.003a 9.981b
Satisfaction With Life Scale 8.077a 9.866Perceived current health 3.640a 4.907Susceptibility resistance 3.515a 3.441b
aIndicates that the difference between the means is statistically signif-icant. bIndicates that the mean score on that measure was higher forwomen.
TABLE 5 Upper and Lower Quartiles (and Min/Max) forEmotional Abuse and Satisfaction with Life
Emotional abuseSatisfaction with
life
M 11.66 (male) 22.7713.64 (female) 30.54 (male)
20.68 (female)Min 0 (male) 13 (male)
1 (female) 8 (female)Max 12 (male) 35 (both)
28 (female)Percentiles 25 1 (male) 26 (male)
6 (female) 14 (female)75 5 (male) 35 (male)
20 (female) 26.25 (female)
the selection of participants for interviews was not based on age but simplytheir sex and scores on the scales of interest (i.e., those shown as havingsignificant mean differences in the t test results).
Once all the preceding analyses had been performed, the participantsample was categorized on the basis of sex and scores on two variables:emotional abuse and SWLS. The latter was chosen as the scores showedsignificant negative correlation with emotional abuse. Each of the score vari-ables was split into quartiles and participants who fell into the combinationof top and bottom quartiles of the two scores were considered for inclusion.Table 5 shows the upper and lower quartiles (and minima/maxima) for thescores for emotional abuse and satisfaction with life.
A random number corresponding to the participant number in the filewas then generated and that participant contacted. Four male and fourfemale participants were selected for interview, and all agreed to partici-pate. Table 6 shows the ranges within which the criteria for selection mustlie and the scores on the measures for participants selected for the interviewphase.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 519
TABLE 6 Interviewees and Selection Criteria
Sex
Emotionalabuse (EA)
rangeSatisfaction withlife (SWLS) range Category
Selected participants(EA score/SWLS
score)
M 0 – 1 35 Low abuse/high satisfaction M1 (0/35)M 0 – 1 13–26 Low abuse/ low satisfaction M2 (1/13)M 5 – 12 35 High abuse/high
satisfactionM3 (11/35)
M 5 – 12 13–26 High abuse/low satisfaction M4 (12/35)F 1 – 6 8–26 Low abuse/high satisfaction F1 (1/33)F 1 – 6 8–26 Low abuse/low satisfaction F2 (2/9)F 20 – 28 26.25–35 High abuse/high
satisfactionF3 (28/14)
F 20 – 28 26.25–35 High abuse/low satisfaction F4 (28/31)
Participants were assured that all data were treated with confidentialityand anonymity and that only the interviewer would know their identity.Some participants expressed concern at being selected for the interviewphase, but they were reassured that this was simply a research procedureand that it had no bearing on any mental or physical health aspect. Eachparticipant was assigned a code to identify his or her transcript and to allowany quotes used as evidentiary information to be linked to the characteristicof interest.
Interviews
The interviews were transcribed verbatim and examined using a thematicanalytical approach (Gavin, 2008). Thematic analysis is a process of makingexplicit the structures and meanings that the participant or reader embodiesin a text. The transcripts were subjected to analysis by two readers whonoted regularly occurring themes, atypical themes, or both. This resulted ina thematic overview in which each reader had identified types of responses.These were exchanged and each read the other’s commentary, indicatingagreement or otherwise. This process went on in several iterative instancesuntil consensus was achieved. In this way, a set of overarching themes withsubsidiary themes was identified. Confirmatory or exclusionary evidence wassought across all transcripts.
Interpretation
Psychometric examination of childhood emotional abuse and adult per-ceptions of personal control, health, and well-being was carried out. Thestatistical analysis suggests that there is a contributory relationship betweenrecollected levels and type of abuse in childhood and adult health and
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

520 H. Gavin
adaptation as measured by personal control and ratings of perceived health.This supports the previous findings from the relevant research literature.There also seems to be a clear sex difference in the experience of abuse.However, interpretation of these results should be treated with caution dueto the small sample size. It should also be noted that the scales were primar-ily used to check that this sample could be compared to previous researchand to profile and identify suitable participants for inclusion in the interviewportion of the study.
Interview Themes
Several themes emerged from the transcribed interviews. After iterativechecking and refinement from the two judges’ notations, the following pri-mary themes were identified: (a) memory (memories of abuse or lack ofabuse); (b) rejection (of abused state); (c) responses (recollected responsesto abusive episodes); and (d) replication (of behavior).
Each of the themes had relationships with the others depending on thecharacteristics of the interviewees (see later). However, there were itemsthat did not appear across all participants, and further iterative examina-tion exposed secondary themes: (a) abuse (type); (b) child (happiness inchildhood); (c) adult (happiness in adulthood); (d) intensity (of abuse); (e)vulnerability; and (f) resilience.
MEMORIES OF ABUSE OR LACK OF ABUSE
According to the scale scores, four of the interviewees (M3/M4/F3/F4) hadexperienced emotional abuse; the other four (M1/M2/F1/F2) had not orindicated very low levels. The interviewees with higher levels of abuserecalled several instances in which a parent or caregiver (in this case allrecalled examples involving the mother or stepmother) had performed oneor more of the actions described in the emotional abuse construct of theCATS, but many also recalled accompanying physical chastisement. Thissuggests a link between memory for abuse and abuse type, identified as asecondary theme. The following statements were made in response to ques-tions about parents getting angry with the interviewee as a child or blamingthe child:
F4: She (mother) used shout at me a lot, usually because I wasn’t doingsomething the way she wanted it done, but it was always accompaniedby a slap.
M3: We learned pretty quickly to recognize when she (stepmother) wasin a bad mood. It wasn’t difficult, and we’d just stay out of the way.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
Sticks and Stones May Break My Bones 521
It is noteworthy that the interviewees who did not record emotional abusedid recall actions that could be interpreted as emotionally abusive accordingto Jantz and McMurray’s (2009) descriptions, but the interviewees viewedthem as appropriate punishment or behavior. For example, when askedabout parental ridiculing, one interviewee said:
M1: Well, my mum used to always try and embarrass me in front ofrelatives, or even my school friends. She did it to my brother, too. Heused to wet the bed and she nicknamed him “Soppy” and told everyonewhat it meant. I was glad she didn’t do anything like that to me!
Although this could be interpreted as humiliation, the interviewee remem-bered this as an example of his mother being funny and outgoing.Additionally, when discussing the question of parental dislike, one inter-viewee showed how a parent’s disinterest in the child’s accomplishmentscan affect the child:
F1: My parents were always a bit dismissive about things that they didn’tthink important. I once got the lead in the school play . . . but my mumjust said they wouldn’t be coming to see me in it; it was a waste of time,because I’d make a mess of it.
Blame was also mentioned by several interviewees, although all insistedthis was not abusive but simply represented mistakes on the parent’s partor a sibling trying to shift blame. All interviewees reiterated that they werenot abused in any way and that any punishment received was merited. Theyalso suggested that punishment was an acceptable form of control in dealingwith children. For example, one participant stated, “I think that parents don’tpunish kids enough. I see little brats are rude and noisy, and the parents letthem run riot.”
Memory of abuse then is never clear-cut for these interviewees; theyrecall incidents that are possibly aggressive, humiliating, dismissive, or deny-ing, but do not acknowledge them as such. This supports Glaser’s (2002)assertion that the abuser is adept at hiding behavior in another form andthat the scars of emotional abuse are often invisible even to the victim.
REJECTION (OF ABUSED STATE)
The lack of memories of abuse appeared to be linked to a rejection ofan abused state; participants who scored low on emotional abuse but whowere relating episodes of identified actions rejected any suggestion that theyhad been abused. There appears to be a disparity between how differentparticipants viewed the incidents of this nature, which is independent ofany of the other constructs examined.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
522 H. Gavin
F2: No, I wouldn’t say we were abused, just she (mother) was a bit strict,but you have to be with kids don’t you?
F4: I must have been a horrible kid. I never did anything right for her,and I expect I deserved everything she (mother) dished out.
M3: We ran riot after my dad remarried, it can’t have been easy on her(stepmother) taking five kids on. We learned quickly that if she wasgrouchy we’d get what we deserved.
Such statements demonstrate reflection on the interviewees’ own behaviorwithout an acceptance of the parent as abuser. Rejection is not simply a lackof recall about incidents, as the preceding section shows that intervieweesdo remember interactions of this nature. This is unmistakably a refutation ofany abused state. This then begs the question: Is our definition of emotionalabuse at fault, or is there some rationalizing function happening with respectto recall of a childhood experience? Perhaps a productive strategy would beto consider what the responses to the parental behavior were.
RESPONSES (RECOLLECTED RESPONSES TO ABUSIVE EPISODES)
Interviewees were asked to recall what their response had been when theyrecounted abusive episodes, irrespective of whether they defined them assuch. Most indicated that they responded by avoiding the behavior that ledto the episode or avoiding the abusive parent.
M2: I never knew what would set her (mother) off so I just stayed out ofher way as much as possible.
M4: I just avoided being alone with her (mother).
Such reactions appear to be avoidant in nature. Where such a strategy wasnot possible, the described action is despondent (e.g., F3: “I tried as hard asI could to be good, do all the things she [mother] wanted, but it was neverenough, she always criticized everything”).
This seems to be indicative of learned helplessness, which is closelyimplicated in the development of depression and other illnesses (Cole et al.,2007) and associated with the accumulation of negative developmentalexperiences (Evans, Gonnella, Marcynyszyn, Gentile, & Salpekar, 2005).
REPLICATION (OF BEHAVIOR)
Some interviewees, particularly those who scored high on emotional abuse,suggested that their adult behavior was affected by the memory of childhoodexperience.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 523
F4: Both me and my sister have no kids. I know I decided fairly early thatI wouldn’t have any, as I wouldn’t want to be responsible for putting akid through that, you know. And I feel I wouldn’t be able to stop myself.
M1: Well, no one behaves the same way with their own kids as theirparents did, do they?
Secondary themes emerged, linked to the primary themes discussedearlier. Abuse type and rejection of abused state were clearly expressed inrelation to memory of abuse. Although interviewees were distinguished onthe basis of whether they had experienced abuse or not and whether theyidentified behavior as abusive, another distinction appears to be the intensityof the abuse. Those who reported high levels of abuse were divided onwhether these happened frequently or not and whether they were consistentbehaviors. This is defined here as intensity. Female participants reportedregular episodes but also stated that there appeared to be little consistencyin what would trigger the abuse, or reported that abuse was a constantexperience. Male participants did not express their recollections in this way.For example, see the contrast between a female and male interviewee onthis point:
F3: I think something like that happened every day or so, but I can’treally say so, because sometimes I’d get punished, and sometimes she(mother) didn’t bother with me.
M4: I generally knew what would set her (mother) off, so learned toavoid her.
Parents’ behavior clearly impacted on whether participants recalledbeing happy as children and whether they declared themselves happy now.Some of this was related to the impact parental behavior had on childhoodfriendships:
F4: I didn’t bring friends home, they were deemed either too young forme, or older, and therefore “boy mad” [interviewer question]. I was about8 or 9 when I realized that I shouldn’t, or rather couldn’t, have friends.
F4: Happy? Oh no, I wasn’t a happy kid. [Probe] I spent my childhoodbeing afraid, I never wanted to go home after school, but there wasnowhere else to go.
For some interviewees the impact went further than childhood. In addi-tion to distancing themselves from the abusive parent or deciding not toperpetuate abusive behavior, some participants suggested that they blamedthe parent for negative feelings in adulthood (e.g., F3: “I still can’t relax if
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

524 H. Gavin
I’m doing something she [mother] would have disapproved of, like stayingout late”).
A major issue in the literature was the impact that childhood abuse hadon the perceived health in the adult child. Although no interviewee madedirect links between abuse and health, there were references to the way inwhich individuals approached their own health, interpreted as vulnerabilityand resilience:
F3: She (mother) used to say we were attention seeking if we tried tosay we were ill. My sister once had a bad cough and was slapped everytime she made a noise. She ended up being diagnosed with asthma. I’malways worried that if I ignore something small I’ll end up really ill.
M3: I don’t worry about my health, which is odd, because we’d getshipped off to the doctor if we had the slightest sniffle. I tend todownplay things like that as I hate having to go to the GP.
One group of participants of particular interest were those who hadreported high levels of childhood emotional abuse but who were also highscorers on scales indicating a healthy adaptation to adult life. These individ-uals were M4 and F4. Although not necessarily typical of the population ofpeople in these circumstances, a further analysis of their answers was con-ducted. It was interesting that they talked about the abuse in very detachedterms. M4 in particular described his response to his abusive parent asavoidance, in that he learned to keep out of his mother’s way. F4, con-versely, reported that she felt trapped (“nowhere else to go”) but also thatshe had made explicit adjustments, such as choosing not to have childrenand not making friends. Later in the interview, she stated that she had sev-ered ties with her family and felt better for it. These strategies were, for theseparticipants, healthy adjustments.
Interviewees who reported that they had experienced no abuse or lowlevels of abuse (M1/M2/F1/F2) were also of interest in terms of adaptation.Although they recorded no episodes of emotional abuse in the questionnaireresponses and during the interviews denied that any abuse had taken place,their interviews did expose recollections of behavior that were abusive.The current health and personal control scores for two of these intervie-wees (M2/F2) were as low as their high abuse counterparts, suggesting thatacknowledgment of abuse might be a factor in its effect; in what way it isan effect is not yet clear.
DISCUSSION
Statistical analysis of the measures collected from this sample supportedsome of the literature concerning childhood experience of emotional abuse
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 525
and its long-lasting effects. Irving and Ferraro (2006) suggest that there is aclear link, possibly a causal relationship, between emotional abuse and latermaladjustment in adult life. Such adjustments seem to be poor levels of per-sonal control and high levels of susceptibility to illness. Riggs and Kaminski(2010) have even asserted that it might be the emotionally abusive com-ponents of physical and sexual abuse that are responsible for long-lastingnegative consequences into adulthood. The sample examined here showedsignificant negative relationships between emotional abuse and satisfactionwith life and resistance to illness, suggesting that abuse has effects through-out the life course. However, the link between abuse and personal controlwas not exhibited by this sample.
There is a case for sex differences in the experience and consequencesof emotional abuse. The sex disparity for anxiety disorders might be dueto differential experience of emotional abuse. Halbreich and Kahn (2007)and Hyde et al. (2008) propose the same for depression. No measurementof such illnesses was made in this sample, but there are clear sex differ-ences in experience of abuse and its relationship to adult characteristics.Interpretations must be cautious due to the sample size, but women weremore likely to report having experienced abusive episodes, were more sus-ceptible to illness, reported lower levels of satisfaction with life, and hadmore negative perceptions of their current health.
Interview analysis showed several themes emerging in terms of howinterviewees recalled childhood experiences, their response to them, andtheir current perceived health. There were differences in how intervieweesremembered the experiences, as some denied that they had been abuseddespite the fact that some of their recounted episodes could have beeninterpreted as abusive. This position was interpreted as a rejection or denialof the abused state. The interviewees in this category clearly did not thinkthey had been abused, but they also did not show as healthy an adaptationto adult life as either of the nonabused individuals or the abused but healthyindividuals.
An interesting outcome appears to be that even if an individual doesnot recall his or her childhood as being abusive, there are events that couldbe interpreted as such. It appears that this might still have the potential fora negative effect, as these individuals (M2/F2) did show a profile of lowerhealth perceptions and internal control. In interviews, these two participantsdescribed incidents that did appear to be abusive but expressed no blametoward the abusive parent. The converse is also of note, as those who hadexperienced abuse but who had a healthy adult life appeared to use the strat-egy of distance and avoidance in adulthood, even if this was not explicitlyacknowledged.
This does have implications for an application of cumulative disadvan-tage theory to emotional abuse. The premise that experiencing childhoodabuse will lead to an accumulation of more negative experiences as a result
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

526 H. Gavin
of maladaptations does not appear to hold for individuals who adopt familyavoidant strategies. The reverse is true for people who do not acknowledgetheir childhood events as abusive, and they might indeed experience anaccumulation of disadvantageous encounters and outcomes. If the cumu-lative disadvantage theory and hypotheses generated from it are to be ofpractical use in research and practice, the possibility of unacknowledgedabuse will need to be taken into account. A state of denial in a client isone of the first barriers encountered by psychotherapists (Mearns & Thorne,2007). Additionally, adult survivors of childhood physical and sexual abuseoften assert that the emotional aspects of the abuse, such as betrayal, are asimportant as any other (Willows, 2009).
Limitations of the Study
The mixed methodological approach to the research questions appears tohave been appropriate in that previous research findings were confirmedand extended and also used as the basis for selection of interviewees andconstruction of an interview schedule. However, the sample included in thequantitative stage was relatively small, and a wider range of experiencesmight have been captured with a larger sample. Additionally, although thequalitative stage of the study exposed rich and detailed material, it is stillunclear whether this sample of eight provides a typical depiction of a widerset of experiences. Having established a process of research and analysis, itis proposed that a similar study be carried out with larger samples.
There are further items to be considered in future research. For exam-ple, the sex difference in the quantitative measures was not evident in theinterviews. Including more men in the first stage might garner participantswith more extreme scores, leading to a wider range of experiences to beexamined.
A second issue that emerged during analysis, but that is yet to be fullyexplored, is that the recollected abuse for this sample was in each instancecarried out by the female parent (i.e., mothers or stepmothers). This mightnot be surprising, as women still bear the primary responsibility for childcare and the episodes recalled appear to fall within that category of interac-tion. However, the question of differences in the sex of the parent in termsof emotional abuse would bear scrutiny.
CONCLUSION
This study used both statistical analysis of psychometric scores and interpre-tive analysis of semistructured interviews, leading to a rich data set. Statisticalanalysis of scores on various measures demonstrated that the link betweenabuse and adaptation was present in the research sample. Further discussion
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 527
of elements contained in the emotional abuse construct revealed themes per-tinent to the long-term effects of a virtually invisible form of maltreatment.These effects include, first, the likelihood of family avoidant strategies beingof use to those who experience childhood abuse but develop into healthyadults, and second, of the long-term detrimental effect of unacknowledgedabuse.
Findings from this relatively small sample suggest that there is a widerrange of effects that determine how childhood experiences contributeto accumulated psychological disadvantages throughout the life course.Implications for adjustment to adult life have been proposed. As such, thestudy’s objectives have been met and further examination of the issues raisedis proposed.
REFERENCES
Ali, A., Toner, B. B., Stuckless, N., Gallop, R., Diamant, N. E., Gould, M. I., et al.(2000). Emotional abuse, self-blame, and self-silencing in women with irritablebowel syndrome. Psychosomatic Medicine, 62, 76–82.
Berenson, K. R., & Anderson, S. M. (2006). Childhood physical and emotional abuseby a parent: Transference effects in adult interpersonal relations. Personalityand Social Psychology Bulletin, 32, 1509–1522.
Boston, A., & Merrick, P. (2010). Health anxiety among older people: An exploratorystudy of health anxiety and safety behaviors in a cohort of older adults in NewZealand. International Psychogeriatrics, 22, 549–558.
Carbone, D. J. (2010). Using cognitive therapies to treat unstable attachment patternsin adults with childhood histories of social rejection. Journal of Aggression,Maltreatment & Trauma, 19(1), 105–134.
Chen, Z., Williams, K., Fitness, J., & Newton, N. (2008). When hurt will not heal:Exploring the capacity to relive social and physical pain. Psychological Science,19, 789–795.
Clark, D. B., de Bellis, M. D., Lynch, K. G., Cornelius, J., & Martin, C. S. (2003).Physical and sexual abuse, depression and alcohol use disorders in adolescents:Onsets and outcomes. Drug and Alcohol Dependence, 69, 51–60.
Classen, C. C., Palesh, O. G., & Aggarwal, R. (2005). Sexual revictimization: A reviewof the empirical literature. Trauma, Violence, and Abuse, 6 , 103–129.
Cole, D., Warren, D., Dallaire, D., Lagrange, B., Travis, R., & Ciesla, J. (2007).Early predictors of helpless thoughts and behaviors in children: Developmentalprecursors to depressive cognitions. Clinical Child Psychology and Psychiatry,12(2), 295–312.
Dannefer, D. (2003). Cumulative advantage/disadvantage and the life course: Cross-fertilizing age and social science theory. The Journals of Gerontology, Series B:Psychological Sciences, 58, 327–337.
Diener, E., Emmons, R., Larsen, J., & Griffin, S. (1985). The Satisfaction with LifeScale. Journal of Personality Assessment, 49(1), 71–75.
Duttweiler, P. C. (1984). The Internal Control Index: A newly developed measure oflocus of control. Educational and Psychological Measurement, 44, 209–221.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011
528 H. Gavin
Evans, G., Gonnella, C., Marcynyszyn, L., Gentile, L., & Salpekar, N. (2005). The roleof chaos in poverty and children’s socioemotional adjustment. PsychologicalScience, 16(7), 560–565.
Ferraro, K., & Nuriddin, T. (2006). Psychological distress and mortality: Are womenmore vulnerable? Journal of Health and Social Behavior, 47(3), 227–241.
Gavin, H. (2008). Understanding research methods and statistics in psychology.London: Sage.
Gibb, B., Benas, J., Crossett, S., & Uhrlass, D. (2007). Emotional maltreatment andverbal victimization in childhood: Relation to adults’ depressive cognitions andsymptoms. Journal of Emotional Abuse, 7(2), 59–73.
Glaser, D. (2002). Emotional abuse and neglect (psychological maltreatment):A conceptual framework. Child Abuse and Neglect, 26 , 697–714.
Hagan, J., & Foster, H. (2003). S/he’s a rebel: Towards a sequential stress theory ofdelinquency and gendered pathways to disadvantage to emerging adulthood.Social Forces, 82(1), 53–86.
Halbreich, U., & Kahn, L. (2007). Atypical depression, somatic depression and anx-ious depression in women: Are they gender-preferred phenotypes? Journal ofAffective Disorders, 102(1), 245–258.
Hund, A., & Espelage, D. (2006). Childhood emotional abuse and disordered eatingamong undergraduate females: Mediating influence of alexithymia and distress.Child Abuse and Neglect, 30(4), 393–407.
Hyde, J., Mezulis, A. H., & Abramson, L. (2008). The ABCs of depression:Integrating affective, biological, and cognitive models to explain the emer-gence of the gender difference in depression. Psychological Review, 115(2),291–313.
Irving, S. M., & Ferraro, K. F. (2006). Reports of abusive experiences during child-hood and adult health ratings: Personal control as a pathway? Journal of AgingHealth, 18, 458–485.
Iwaniec, D., Larkin, E., & Higgins, S. (2006). Research review: Risk and resilience incases of emotional abuse. Child and Family Social Work, 11, 73–82.
James, W. (1950). The principles of psychology (Vol. 1). New York: Dover. (Originalwork published 1890)
Jantz, G., & McMurray, A. (2009). Healing the scars of emotional abuse (Rev. andupdated ed.). Ada, MI: Revell Books.
Kendall-Hackett, K. A. (2002). The health effects of childhood abuse: Four path-ways by which abuse can influence health. Child Abuse and Neglect, 26(6/7),715–729.
Kennedy, M. A., Ip, K., Samra, J., & Gorzalka, B. B. (2007). The moderating role ofchildhood emotional abuse in disordered eating. Journal of Emotional Abuse,7(1), 17–36.
Kent, A., & Waller, G. (1998). The impact of childhood emotional abuse: An exten-sion of the child abuse and trauma scale. Child Abuse and Neglect, 22(5),393–399.
Long, A., & Mullen, B. (1994). An exploration of women’s perceptions of the majorfactors that contributed to their alcohol abuse. Journal of Advanced Nursing,19, 623–639.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011

Sticks and Stones May Break My Bones 529
Maciejewski, P. K., & Mazure, C. M. (2006). Fear of criticism and rejection mediatesan association between childhood emotional abuse and adult onset of majordepression. Cognitive Therapy and Research, 30(1), 105–122.
Mearns, D., & Thorne, B. (2007). Person centred counselling in action. London:Sage.
Northall, G. F. (1894). Folk phrases of four counties. Oxford, England: OxfordUniversity Press.
Rees, C. (2010). Understanding emotional abuse. Archives of Disease in Childhood,95(1), 59–67.
Regehr, C., Cadell, S., & Jansen, K. (1999). Perceptions of control and long-termrecovery from rape. American Journal of Orthopsychiatry, 69(1), 110–115.
Reyome, N. D., Ward, K., & Witkiewitz, K. (2010). Psychosocial variables asmediators of the relationship between childhood history of emotional maltreat-ment, codependency, and self-silencing. Journal of Aggression, Maltreatment &Trauma, 19,159–179.
Riggs, S. A., & Kaminski, P. (2010). Childhood emotional abuse, adult attach-ment, and depression as predictors of relational adjustment and psychologicalaggression. Journal of Aggression, Maltreatment & Trauma, 19, 75–104.
Sanders, B., & Becker-Lausen, E. (1995). The measurement of psychological mal-treatment: Early data on the child abuse and trauma scale. Child Abuse andNeglect, 19, 315–323.
Walker, E. A., Keegan, D., Gardner, G., Sullivan, M., Bernstein, D., & Katon, W.(1997). Psychosocial factors in fibromyalgia compared with rheumatoid arthritis:II. Sexual, physical, and emotional abuse and neglect. Psychosomatic Medicine,59, 572–577.
Ware, J. E., Jr. (1976). Scales for measuring general health perceptions. Health ServiceResearch, 11(4), 396–415.
Willows, J. (2009). Moving on after childhood sexual abuse: Understanding the effectsand preparing for therapy. New York: Routledge.
World Health Organization. (2008). Health topics. Retrieved from http://www.who.int/topics/en/ retrieved 12.1.2010
Zimmerman, M. A. (1995). Psychological empowerment: Issues and Illustrations.American Journal of Community Psychology, 23, 581–599.
Dow
nloa
ded
by [
Com
putin
g &
Lib
rary
Ser
vice
s, U
nive
rsity
of
Hud
ders
fiel
d] a
t 10:
19 0
2 O
ctob
er 2
011