What Do We Know About Suicidality in Autism Spectrum Disorders? A Systematic Review
15
What Do We Know About Suicidality in Autism Spectrum Disorders? A Systematic Review Magali Segers and Jennine Rawana Suicidality is a common and concerning issue across development, and there is a plethora of research on this topic among typically developing children and youth. Very little is known, however, about the nature of suicidality among individuals with autism spectrum disorders (ASDs). The purpose of the current study was to undertake a systematic literature review to assess the current state of the research literature to examine the prevalence of suicidality among individuals with ASD, related demographic and clinical profiles, and associated risk and protective factors. A literature search using key terms related to suicidality and ASD yielded 10 topical studies that were evaluated for the study objectives. Suicidality was present in 10.9–50% of the ASD samples identified in the systematic review. Further, several large-scale studies found that individuals with ASD comprised 7.3–15% of suicidal populations, a substantial subgroup. Risk factors were identified and included peer victimization, behavioral problems, being Black or Hispanic, being male, lower socioeconomic status, and lower level of education. Only one study reported on protective factors, and this is identified as a significant gap in the literature. Several methodological weaknesses were present in the current literature, such as lack of appropriate comparison groups and little to no use of empirically validated measures for ASD diagnosis and suicide assessment. Additional research is necessary to understand better how this unique population experiences and expresses suicidal tendencies. Recommendations for future research are discussed. Autism Res 2014, 7: 507–521. © 2014 International Society for Autism Research, Wiley Periodicals, Inc. Keywords: autism spectrum disorders; suicide; suicidality; prevalence; risk factors; protective factors Introduction Autism spectrum disorders (ASD) are common neuro- developmental disorders characterized by persistent defi- cits in social communication and social interaction and restricted, repetitive patterns of behavior, interest, and activities [American Psychiatric Association, 2013]. The most current estimate for prevalence rates of ASD is 1 in 94 children in Canada (Ouellette-Kuntz et al., 2012) and 1 in 88 in the United States [Centers for Disease Control and Prevention, 2012]. Changes in societal awareness and diagnostic guidelines and practices have highlighted the importance of increasing our understanding of the com- plexities of the disorder. It is increasingly important for clinicians and researchers alike to be aware of the clinical and mental health issues associated with ASD and how they may present differently from typical development. Indeed, the most severe and life-threatening mental health issues are behaviors related to suicidality [Hawton, Saunders, & O’Connor, 2012]. As understanding and awareness of ASD continues to grow, it is critical to examine how suicidal thoughts and behaviors are expressed among individuals with this unique clinical profile. High rates of comorbidity with a range of psychiatric disorders are seen in ASD, particularly with mood and anxiety disorders [Ghaziuddin & Greden, 1998; Hedley & Young, 2006; Munesue et al., 2008]. The connection between mood disorders and suicidal behaviors in typical development is relatively well understood and well researched [Kasper, Schindler, & Neumeister, 1996; Rao, Weissman, Martin, & Hammond, 1993]; however, we know very little about suicidal behaviors in ASD. Con- sidering the high rates of mood and anxiety disorders in ASD [Strang et al., 2012; White, Oswald, Ollendick, & Scahill, 2009] and the established link between depres- sive symptoms such as hopelessness and suicidal behav- iors in typical development [Saltz & Marsh, 1990], it is a critical next step to examine this link in ASD. In the current article, a very broad definition of suicidality was adopted and included ideation (e.g., thoughts of death, thoughts of harming oneself, planning a suicide), self- harm behaviors (e.g., cutting, burning), attempts (e.g., drug overdose, poisoning, jumping), and completed suicide. Suicidality in ASD needs to be examined sepa- rately from typical development to appreciate the complex interplay of ASD-specific traits on factors con- tributing to the onset and recurrence of suicidality. Indi- From the Department of Psychology, York University, ON, Canada Received September 05, 2013; accepted for publication March 18, 2014 Address for correspondence and reprints: Jennine S. Rawana, PhD,131 Behavioural Sciences Building, York University, 4700 Keele St., Toronto, ON, Canada, M3J 1P3, Phone: 416 736 2100 Ext. 20771. E-mail: [email protected] Published online 5 May 2014 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/aur.1375 © 2014 International Society for Autism Research, Wiley Periodicals, Inc. LITERATURE REVIEW INSAR 507 Autism Research 7: 507–521, 2014
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of What Do We Know About Suicidality in Autism Spectrum Disorders? A Systematic Review

What Do We Know About Suicidality in Autism Spectrum Disorders?A Systematic ReviewMagali Segers and Jennine Rawana
Suicidality is a common and concerning issue across development, and there is a plethora of research on this topicamong typically developing children and youth. Very little is known, however, about the nature of suicidality amongindividuals with autism spectrum disorders (ASDs). The purpose of the current study was to undertake a systematicliterature review to assess the current state of the research literature to examine the prevalence of suicidality amongindividuals with ASD, related demographic and clinical profiles, and associated risk and protective factors. A literaturesearch using key terms related to suicidality and ASD yielded 10 topical studies that were evaluated for the studyobjectives. Suicidality was present in 10.9–50% of the ASD samples identified in the systematic review. Further, severallarge-scale studies found that individuals with ASD comprised 7.3–15% of suicidal populations, a substantial subgroup.Risk factors were identified and included peer victimization, behavioral problems, being Black or Hispanic, being male,lower socioeconomic status, and lower level of education. Only one study reported on protective factors, and this isidentified as a significant gap in the literature. Several methodological weaknesses were present in the current literature,such as lack of appropriate comparison groups and little to no use of empirically validated measures for ASD diagnosisand suicide assessment. Additional research is necessary to understand better how this unique population experiencesand expresses suicidal tendencies. Recommendations for future research are discussed. Autism Res 2014, 7: 507–521.© 2014 International Society for Autism Research, Wiley Periodicals, Inc.
Keywords: autism spectrum disorders; suicide; suicidality; prevalence; risk factors; protective factors
Introduction
Autism spectrum disorders (ASD) are common neuro-developmental disorders characterized by persistent defi-cits in social communication and social interaction andrestricted, repetitive patterns of behavior, interest, andactivities [American Psychiatric Association, 2013]. Themost current estimate for prevalence rates of ASD is 1 in94 children in Canada (Ouellette-Kuntz et al., 2012) and1 in 88 in the United States [Centers for Disease Controland Prevention, 2012]. Changes in societal awareness anddiagnostic guidelines and practices have highlighted theimportance of increasing our understanding of the com-plexities of the disorder. It is increasingly important forclinicians and researchers alike to be aware of the clinicaland mental health issues associated with ASD and howthey may present differently from typical development.Indeed, the most severe and life-threatening mentalhealth issues are behaviors related to suicidality [Hawton,Saunders, & O’Connor, 2012]. As understanding andawareness of ASD continues to grow, it is critical toexamine how suicidal thoughts and behaviors areexpressed among individuals with this unique clinicalprofile.
High rates of comorbidity with a range of psychiatricdisorders are seen in ASD, particularly with mood andanxiety disorders [Ghaziuddin & Greden, 1998; Hedley &Young, 2006; Munesue et al., 2008]. The connectionbetween mood disorders and suicidal behaviors in typicaldevelopment is relatively well understood and wellresearched [Kasper, Schindler, & Neumeister, 1996; Rao,Weissman, Martin, & Hammond, 1993]; however, weknow very little about suicidal behaviors in ASD. Con-sidering the high rates of mood and anxiety disorders inASD [Strang et al., 2012; White, Oswald, Ollendick, &Scahill, 2009] and the established link between depres-sive symptoms such as hopelessness and suicidal behav-iors in typical development [Saltz & Marsh, 1990], it is acritical next step to examine this link in ASD. In thecurrent article, a very broad definition of suicidality wasadopted and included ideation (e.g., thoughts of death,thoughts of harming oneself, planning a suicide), self-harm behaviors (e.g., cutting, burning), attempts (e.g.,drug overdose, poisoning, jumping), and completedsuicide. Suicidality in ASD needs to be examined sepa-rately from typical development to appreciate thecomplex interplay of ASD-specific traits on factors con-tributing to the onset and recurrence of suicidality. Indi-
From the Department of Psychology, York University, ON, CanadaReceived September 05, 2013; accepted for publication March 18, 2014Address for correspondence and reprints: Jennine S. Rawana, PhD,131 Behavioural Sciences Building, York University, 4700 Keele St., Toronto, ON,
Canada, M3J 1P3, Phone: 416 736 2100 Ext. 20771. E-mail: [email protected] online 5 May 2014 in Wiley Online Library (wileyonlinelibrary.com)DOI: 10.1002/aur.1375© 2014 International Society for Autism Research, Wiley Periodicals, Inc.
LITERATURE REVIEW
INSAR 507Autism Research 7: 507–521, 2014

viduals with ASD experience the world differentlycompared with typically developing individuals, frombasic information processing to social perspectives andnavigating the social world [Frith, 1989]. As such, indi-viduals with ASD may exhibit and express suicidal ten-dencies and behaviors in ways that deviate from thetrajectory observed in typical development. Most impor-tantly, increasing our understanding of how suicidalbehaviors are characterized in ASD will inform how theymay be managed, treated, and prevented.
The current review is focused on research in which theintent of the study was to examine behaviors related tosuicide. It is important to note that there are a number ofother types of self-injurious behaviors that are sometimesobserved in ASD, such as stereotypic movements andnon-suicidal self-injury. Stereotyped motor movementsinclude behaviors such as head banging, face slapping,biting, or sucking [APA, 2013], and are more typicallyobserved in individuals with ASD with lower intelligencequotient (IQs) [Weiss, 2002]. These stereotypic move-ments are often repetitive, seemingly purposeless, andshow no clear intention to harm oneself [Weiss, 2002].Non-suicidal self-injury includes inflicting pain or injury tooneself, often for the purposes of reducing negativeemotion or to solve an interpersonal difficulty [APA,2013]. Non-suicidal self-injury is, however, highly predic-tive of suicide and attempted suicide. Therefore, thecurrent review will focus specifically on suicide attemptand non-fatal self-harm behavior in which an individualinflicts pain on his or her body in efforts to reduce nega-tive emotions and not stereotyped self-injurious behav-iors oftentimes associated with ASD.
Despite the limited research on the topic of suicide inASD to date, a systematic review to ascertain the currentstate of the literature is both timely and appropriate.Conducting a systematic synthesis of high qualityresearch to date is useful as it allows for a more relevant,empirically derived understanding than a more informalreview would offer. Considering the seriousness andprevalence of suicidality, as the second most commoncause of death in young people worldwide [Hawton et al.,2012], it is imperative to keep research in this fieldcurrent and reflective of shifts in culture and societalvalues and norms (e.g., impact of the Internet). Further-more, suicidal behaviors such as non-fatal self-harm aredeemed as critical behaviors to monitor, as they are asso-ciated with an increased risk of suicide in both youth andadults [Bergen et al., 2012; Hawton et al., 2012; Skegg,2005]. The studies conducted to date, however prelimi-nary, offer valuable insight to what is currently knownabout suicide among individuals with ASD. The broadaim of the current review is to gather evidence fromempirical, peer-reviewed research that examines suicidalbehavior in individuals with ASD. Specific research ques-tions included:
1. What is the prevalence of suicidal behaviors in ASD?2. How likely is a diagnosis of ASD among suicidal
individuals?3. What is the demographic and clinical profile of the
groups studied?4. What are the risk and protective factors for suicide in
ASD? Are any of these ASD specific?5. How are these studies being conducted methodologi-
cally? Is there consistency across studies?
It is the aim that by answering the above questions, asolid understanding of the status of the research in thisarea can be gained, including acknowledging existingareas of strength and weakness. Furthermore, capturingand synthesizing extant research will help inform futureresearch directions and theoretical approaches.
Methods
A literature search was performed on November 11th,2013 using PsychINFO, Web of Science, and Medline(OVID) databases. An initial search was performed usingthe following terms: “autism,” “autism spectrum disor-ders,” “Asperger syndrome,” and “pervasive developmen-tal disorder.” This search was combined with a secondsearch using the following terms: “suicide,” “suicidal,”“suicidality,” “suicidal ideation,” “suicide attempts,”“self-harm,” and “suicide prevalence.” To streamline hitsto the most appropriate and relevant articles, terms weresearched under “subject headings” or “topic” in all data-bases. This search yielded a list of 22 articles. A number ofarticles were subsequently discarded from the analysisbecause the examination of suicidality in ASD was notcentral to the theme or purpose of the paper (n = 4) or thearticle was not available in English (n = 2). The remaining16 articles were then categorized by article type: Letters tothe Editor (n = 1), Editorial (n = 1), Theoretical (n = 1),Case Studies (n = 3), and Clinical Study (n = 10). Refer-ence lists for the 10 clinical studies were inspected foradditional relevant articles of which one additionalarticle was included. Because the focus of the currentstudy was to gain an appreciation and an understandingof the prevalence, risk factors, and comorbidities associ-ated with suicidal behavior in ASD, only clinical studieswere included in the analyses (n = 11). To keep the focuson representative groups of individuals, opinion piecesand theoretical articles were excluded (n = 3). Casestudies (n = 3) were evaluated for anecdotal informationrelevant to the experience of suicidality.
Interestingly, suicidal behavior in ASD is a relativelycontemporary research topic with the majority ofresearch in the area conducted within the last 7 years(2007–2013) and one earlier study in 1999. A majority ofthe research is published in clinically focused medicaljournals (e.g., psychiatry, nursing; n = 6), with a small
INSAR508 Segers and Rawana/Systematic review of suicidality in ASD

number of studies published in psychology or develop-mentally based journals (n = 4) or broader social sciencejournals (n = 1). The majority of published studies wereconducted in the Unites States of America (n = 4), fol-lowed by European countries (n = 3; United Kingdom,Italy, Sweden), Japan (n = 2), and Turkey (n = 1).
ResultsCharacteristics of Research Samples
In the currently reviewed studies, there was a relativelyeven divide between the age groups studied; 40% hadadult participants, 40% had child participants (3–10years), 50% adolescent participants (11–17 years), and20% conducted research with emerging adults [18–29years; Arnett, 2007]. Despite a slightly heavier emphasison adults (including emerging adults), all of the majordevelopmental periods were identified in the review,although given the small number of studies available; theinformation on suicidal behavior in ASD across ages isstill very limited. All of the studies were cross-sectional innature, with no study following participants for anyextended period of time.
To gain an accurate sense of how suicidal behaviorsmight be unique to ASD, it is important to make referenceto a comparison sample. Of the studies examined here,four did not use a comparison sample, two used typicallydeveloping individuals without psychiatric issues, andfive used psychiatric, developmentally delayed, orsuicidal patients without ASD (see Table 1). It is relevantto note that the majority of samples had anoverrepresentation of male participants. With the excep-tion of the study by [Rydén, Rydén, & Hetta, 2008] whopurposefully included only female participants and thestudy by Mikami et al. [2009] who had comparablegender ratios, the other samples had men and boys com-prise at least 77% of the sample. Given that ASD is four tofive times more likely to occur in boys than in girls [CDC,2012], the gender disparity observed here might be rep-resentative of the population. However, care should betaken, when possible, not to overshadow the experiencesof women and girls with ASD, which may prove to bequalitatively different from the male experience [Rivet &Matson, 2011]. Furthermore, if gender ratios are notsimilar across clinical and control groups, the compari-sons drawn from the study may be limited because of apossible gender confound.
There was some variety in the type of settings in whichstudies were conducted that may influence the nature ofthe findings. For example, research settings included hos-pitals (40%), community clinics (30%), universities(10%), mail-based questionnaires (10%), and web-basedinterfaces (10%). Data collected from hospitals tend to bebased on patients who required psychiatric treatment forsevere injuries resulting from a suicidal attempt. Thus,
research being conducted in hospitals represent suicidalbehaviors of a far more severe degree (e.g., physical harmresulting from a suicide attempt), whereas, studies occur-ring in community clinics or online may be accessingindividuals with milder symptoms (e.g., ideation).Finally, while country in which the research was con-ducted was recorded for evaluative purposes, there didnot appear to be any systematic differences in results orcharacteristics of research samples.
Suicidal Behaviors in ASD
Only three studies measured suicidal attempt separatelyfrom ideation or other suicidal behaviors; in these cases,reported attempts ranged from 7.2 to 15%. Reported ratesof suicidal ideation and behaviors had a much broaderrange of incidence from 10.7 to 50%. Mayes, Gorman,Hillwig-Garcia, and Syed [2013] looked at suicidalattempt and suicidal ideation separately in children. It isinteresting to note that there was only a small differencebetween the percentage of children who attemptedsuicide (7.2%) and those who displayed suicidal ideation[10.9%; Mayes et al., 2013]. Raja, Azzoni, and Frustaci[2011] also examined suicidal ideation and attempts sepa-rately among adults and found a slightly larger differencebetween percentage of individuals who experienced sui-cidal thoughts (31%) and those who actually attemptedsuicide (7.7%). Interestingly, Balfe and Tantam [2010]found a proportionally similar disparity between ideation(40%) and attempts (15%) across a wide age range (13–64), although their percentages where slightly higherthan those reported by Raja et al. [2011] and were notseparated by age group due to small sample size (n = 42).Mukaddes and Fateh [2010] found that while none of thechildren (aged 6–11 years) displayed suicidal behaviors,close to half (42%) of adolescents (aged 12–20 years) inthe sample did, indicating a substantial increase of sui-cidal behaviors from childhood to adolescence. Generallyspeaking, with the exception the Mukaddes and Fateh[2010] study, rates of suicidal behaviors were loweramong children and adolescents (0–12.8%) comparedwith adult samples. In samples of emerging adults andadults, suicidal ideation in ASD was reported to bebetween 31–50% [Raja et al., 2011; Shtayermman, 2007,2008]. Raja et al. [2011] were the only researchers toreport on incidence of completed suicide in an ASDsample (7.7%).
Prevalence of ASD in Suicidal Populations
Four studies examined the occurrence of ASD in largersuicidal adult populations; the rates ranged from 7.3 to15%, highlighting the fact that as a subgroup, individualswith an ASD diagnosis made up a substantial portion ofindividuals who engage in suicidal behaviors [Kato et al.,
509Segers and Rawana/Systematic review of suicidality in ASDINSAR

Tabl
e1.
Basi
cSt
udy
Info
rmat
ion
Incl
udin
gDe
mog
raph
ican
dSa
mpl
eIn
form
atio
n
Refe
renc
eLo
cati
onBr
ief
desc
ript
ion/
stud
ypu
rpos
eRe
sear
chse
ttin
gAS
Dsa
mpl
ede
scri
ptio
nan
dN
ASD
sam
ple
age
(in
year
s)M
(SD)
ASD
sam
ple
gend
er(m
ale
%)
Com
pari
son
sam
ple
desc
ript
ion
and
NCo
mpa
riso
nsa
mpl
eag
e(i
nye
ars)
M(S
D)Co
mpa
riso
nsa
mpl
ege
nder
(mal
e%)
Har
dan
&Sa
hl,
1999
USA
Toex
amin
esu
icid
alit
yin
acl
inic
ally
refe
rred
sam
ple
(inp
atie
ntan
dou
tpat
ient
)of
child
ren
and
adol
esce
nts
wit
hde
velo
pmen
tald
isab
iliti
es(o
fw
hich
indi
vidu
als
wit
hAS
Dm
ake
upa
subs
ampl
e).
Hos
pita
l(m
edic
alce
nter
)Au
tist
ic(3
6);
PDD-
NOS
(27)
63
Child
ren
and
adol
esce
ntsb
Not
repo
rted
Child
ren
and
adol
esce
nts
wit
hde
velo
pmen
tal
diso
rder
san
dco
mor
bid
psyc
hiat
ric
diso
rder
s.
Child
ren
and
Adol
esce
nts
9.5
(ran
ge:
3–19
)c
72%
(of
enti
resa
mpl
e,in
clud
ing
ASD
grou
p)
Shta
yerm
man
,20
07,
2008
USA
Toex
amin
eth
ele
velo
fsu
icid
alid
eati
onan
dco
mor
bid
diso
rder
sam
ong
adol
esce
nts
and
youn
gad
ults
wit
hAs
perg
ers
synd
rom
e.
Mai
l-an
dw
eb-b
ased
,se
lf-re
port
Aspe
rger
s10
Emer
ging
adul
ts19
.7(3
.0)
90%
––
–
Rydé
n,et
al,
2008
Swed
enEx
amin
esth
elin
kbe
twee
nAS
Dan
dbo
rder
line
pers
onal
ity
diso
rder
inw
omen
and
com
pare
acro
sscl
inic
alm
easu
res.
Clin
ic(t
reat
men
tce
nter
)As
perg
ers
orPD
D-NO
S6
Adul
ts31
.2(8
.89)
0%a
Bord
erlin
epe
rson
alit
ydi
sord
erw
itho
utAS
D35
Adul
ts28
.6(8
.17)
0%a
Mik
ami,
etal
.,20
09Ja
pan
Toex
amin
eth
efr
eque
ncy
and
clin
ical
feat
ures
ofad
oles
cent
sw
ith
perv
asiv
ede
velo
pmen
tald
isor
der
rela
tive
tosu
icid
eat
tem
pts.
Hos
pita
l(A
dvan
ced
crit
ical
care
cent
er)
Aspe
rger
s(6
)PD
D-NO
S(6
)12
Adol
esce
nt17
.1(1
.6)
41.7
%Ty
pica
llyde
velo
ping
82Ad
oles
cent
16.9
(1.6
)11
.3%
Balfe
&Ta
ntam
,20
10U
nite
dKi
ngdo
mTo
desc
ribe
the
livin
g,em
ploy
men
tan
dps
ycho
-soc
ials
itua
tion
ofa
com
mun
ity
sam
ple
ofad
ults
and
adol
esce
nts
wit
hAS
.
Mai
l-ba
sed
self-
repo
rtqu
esti
onna
ires
Aspe
rger
sor
HFA
42Ad
oles
cent
san
dad
ults
26.2
(11.
9)
88%
––
–
Muk
adde
san
dFa
teh
[201
0]Tu
rkey
Repo
rton
the
rate
sof
com
orbi
dity
ofps
ychi
atri
cdi
sord
ers
inin
divi
dual
sw
ith
Aspe
rger
sdi
sord
er.
Clin
ic(p
riva
teps
ychi
atry
)As
perg
ers
37Ch
ildre
n,ad
oles
cent
s,em
ergi
ngad
ults
10.9
(4.5
)
86.4
%–
––
Raja
etal
.,20
11It
aly
Care
fule
xam
inat
ion
ofsu
icid
alid
eati
onan
dbe
havi
orin
adul
tps
ychi
atri
cpa
tien
tsw
ith
ASD.
Hos
pita
l(p
sych
iatr
icin
tens
ive
care
unit
)
Aspe
rger
s(1
6),
Auti
sm(5
),PD
D-NO
S(5
)26
Adul
ts30
.2(9
.8)
96.2
%Ps
ychi
atri
cpa
tien
tsw
itho
utan
ASD
2495
Adul
ts42
.7(1
4.9)
45.4
%
Kato
,et
al.,
2012
Japa
nTo
exam
ine
the
freq
uenc
yan
dcl
inic
alfe
atur
esof
suic
ide
atte
mpt
sin
adul
tsw
ith
ASD.
Emer
genc
yro
om/h
ospi
tal
(adv
ance
dcr
itic
alca
rece
nter
)
ASD
43Ad
ults
33.7
(12.
6)81
.4%
Suic
idal
pati
ents
wit
hout
anAS
D54
4Ad
ults
42.5
(17.
0)30
.3%
May
es,
etal
.,20
13U
SAEx
amin
atio
nof
the
freq
uenc
yof
suic
idal
idea
tion
and
atte
mpt
sin
child
ren
wit
hAS
D.
Clin
ic(p
sych
iatr
ydi
agno
stic
)H
FA(5
37),
LFA
(254
)79
1Ch
ildre
n6.
6(3
.1)
84.1
%Ty
pica
ldev
elop
men
tw
ith
maj
orde
pres
sive
diso
rder
(35)
and
wit
hout
(186
)
Child
ren
depr
essi
onsa
mpl
e13
.0(2
.3)
typi
cals
ampl
e8.
7(1
.7)
Depr
essi
onsa
mpl
e(2
5.7%
);ty
pica
lsa
mpl
e(4
3.5%
)
Stor
chet
al.,
2013
USA
Toex
amin
eth
eph
enom
enol
ogy
and
clin
ical
corr
elat
esof
suic
idal
thou
ghts
and
beha
vior
sin
yout
hw
ith
ASD.
Uni
vers
ity
Auti
sm(2
8),
Aspe
rger
s(3
9),
PDD-
NOS
(35)
102
Child
ren
and
adol
esce
nts
10.5
5(2
.31)
77%
––
–
ASD,
auti
smsp
ectr
umdi
sord
ers;
HFA
,hi
gh-f
unct
ioni
ngau
tism
;LF
A,lo
w-f
unct
ioni
ngau
tism
;PD
D-NO
S,pe
rvas
ive
deve
lopm
enta
ldis
orde
r—no
tot
herw
ise
spec
ifie
d.a O
nly
fem
ale
parti
cipan
tswe
rein
clude
din
this
stud
y.b S
epar
ate
mea
nfo
rASD
sam
ple
notr
epor
ted.
c SD
notr
epor
ted.
INSAR510 Segers and Rawana/Systematic review of suicidality in ASD

2013; Mikami et al., 2009; Rydén et al., 2008]. Twostudies recorded the specific method of attempt by indi-viduals with ASD and how that compared with othersuicidal patients [Kato et al., 2013; Mikami et al., 2009]. Itis notable that adults with ASD who were hospitalized forsuicidal behaviors tended to use more aggressive andlethal means (i.e., cutting, stabbing, carbon monoxidepoisoning), resulting in greater bodily harm and longerhospital stays compared with the rest of the sample [Katoet al., 2013]. Mikami et al. [2009] reported that the ASDsample were less likely than the typically developingsample to use drug overdose as a method (58 vs. 79%) andalso used other methods such as jumping and poisoning.According to Kato et al. [2013], individuals with ASDwere less likely to make a suicide attempt based on pre-cipitating events occurring within the last 24 hours,whereas this was the case for almost half of the typicallydeveloping sample. Individuals with ASD hospitalized forsuicide attempts also tend to have a more limited historyof psychiatric treatment than comparison groups[Mikami et al., 2009]. Hardan and Sahl (1999) examineda number of characteristics related to suicidality in adevelopmentally delayed sample of which ASD com-prised 14.8%. They did not examine characteristics sepa-rately for the ASD sample, however, they did find higherreports of more violent suicide methods such as hanging(15%), stabbing (19%), and jumping off a bridge or infront of a moving vehicle (13%) compared with lessviolent methods, such as drowning (4%) or overdose(4%).
Psychiatric Comorbidities in Suicidal Individualswith an ASD
Reporting on comorbidities was not a key focus of thecurrent study as this area has been relatively wellresearched [Ghaziuddin & Greden, 1998; Hedley &Young, 2006; Munesue et al., 2008]. However, given thestrong relationship between certain psychiatric diagnoses(e.g., major depressive disorder) and suicidal behavior, itis worth commenting on these rates in the context of thecurrent review. Mood disorders (e.g., major depressivedisorder, bipolar disorder) were reported to be present in13.7–37% of individuals, and anxiety disorders (e.g., gen-eralized anxiety disorder, social anxiety, obsessive com-pulsive disorder, specific phobia) were present in 7.7–74.5% of the samples reported here [Mayes et al., 2013;Mukaddes & Fateh, 2010; Shtayermman, 2007, 2008;Storch et al., 2013]. Balfe and Tantam [2010] also reportedhigh rates of depression (35%) and anxiety (51%);however, these figures were taken from single items froma questionnaire and were not validated by other means(see Table 2). The presence of adjustment disorders wasextremely high among adults, estimated to be present in70–83% of adults in hospital settings [Kato et al., 2013;
Mikami et al., 2009]; in comparison, a much lower inci-dence was reported in youth with developmental disabili-ties (15%; Hardan & Sahl, 1999). Other psychiatricconditions that were reported to be comorbid with ASDwere disruptive behavior disorder (56.8%; Storch et al.,2013), post-traumatic stress disorder (5.8%; Storch et al.,2013), borderline personality disorder [Rydén et al.,2008], tic disorders (18%), and schizophrenia [62%; Rajaet al., 2011]. The high estimate of schizophrenia (62%) inthe Raja et al. [2011] study is likely related to the sampleof patients who were seen in the psychiatric care unit ofa hospital and thus is likely not representative ofcomorbidity with ASD more generally. While Hardan andSahl (1999) did not report comorbidities specific to theirASD subsample, they report relatively high rates of oppo-sitional defiant disorder (59.5%), attention deficit hyper-activity disorder (45%), and post-traumatic stress disorder(6%) among children and adolescents with developmen-tal disabilities.
Risk Factors Associated with Suicide in ASD
Risk factors are a combination of individual, relational,community, and societal factors that are associated withsuicidality [CDC, 2012]. Risk factors were reported here ifthe authors of the study conducted regression analysesidentifying certain factors as predictors of suicidality or ifthey explicitly stated that certain factors put individualswith ASD at a higher risk for suicidal behaviors. Peervictimization occurred in a large percentage (38–75%) ofthe samples reported here and anecdotally was a triggerfor suicidal behaviors in many individuals with ASD[Mayes et al., 2013; Mikami et al., 2009; Shtayermman,2007, 2008]. Considering that social impairment is a corefeature of the diagnosis of an ASD, it is not surprising thatit is a significant contributor to the difficulties experi-enced by this population. Storch et al. (2013) found thatin a small sample (n = 11), youth with an autism diagno-sis were more likely to have suicidal thoughts or behav-iors compared with youth with a diagnosis of Asperger’ssyndrome. Other characteristics that appear to be associ-ated with individuals at a higher risk of suicidal behaviorsare substance abuse [7.7%; Raja et al., 2011], behavioralproblems, and taking psychotropic medications [Mayeset al., 2013]. Demographic factors such as being male,being older than 10 years, being single, being Black orHispanic, and having a lower socioeconomic status werealso associated with suicidal behavior in ASD (seeTable 2). Hardan and Sahl (1999) found that being male,being an inpatient (vs. outpatient) and a higher level ofcognitive functioning in individuals who were develop-mentally delayed were associated with an increase insuicidal behaviors; however, given that these were find-ings for the entire sample (of which individuals with ASD
511Segers and Rawana/Systematic review of suicidality in ASDINSAR

Tabl
e2.
Suic
idal
Beha
vior
san
dRe
late
dFa
ctor
sin
ASD
Refe
renc
eSu
icid
albe
havi
orm
easu
red
inst
udy
Prev
alen
ceof
suic
idal
beha
vior
inAS
Dsa
mpl
ePr
eval
ence
ofAS
Din
suic
idal
sam
ple
Iden
tifi
edco
mor
bidi
ties
/psy
chia
tric
char
acte
rist
ics
Risk
fact
ors
orpr
edic
tors
ofsu
icid
albe
havi
ors
Prot
ecti
vefa
ctor
s
Har
dan
&Sa
hl,
1999
Suic
idal
idea
tion
/ges
ture
s/at
tem
pt,
met
hod
used
/con
side
red,
leth
alit
yof
met
hods
,fr
eque
ncy
ofsu
icid
ility
,pe
rvas
iven
ess
ofsu
icid
albe
havi
ors,
past
expo
sure
tosu
icid
e,un
ders
tand
ing
ofth
eco
ncep
tof
deat
h
11%
14.8
%OD
D(5
9.5%
);AD
HD
(45%
);de
pres
sive
diso
rder
s(3
0%);
adju
stm
ent
diso
rder
s(1
5%);
PTSD
(6%
)
Mal
e(7
2%)
inpa
tien
t(v
s.ou
tpat
ient
);hi
gher
func
tion
ing
indi
vidu
als
–
Shta
yerm
man
,20
07,
2008
Idea
tion
;As
sess
edus
ing
the
Suic
idal
Idea
tion
Ques
tion
nair
eth
atm
easu
res
num
ber
and
freq
uenc
yof
suic
idal
thou
ghts
.
Suic
idal
idea
tion
(47–
50%
)–
MDD
(20%
);GA
D(3
0%);
Addi
tion
alps
ychi
atri
cdi
agno
ses
(67%
)Pe
erVi
ctim
izat
ion
(38%
)–
Rydé
n,et
al,
2008
Atte
mpt
and
self-
harm
asse
ssed
from
med
ical
reco
rds.
Suic
ide
risk
asse
ssed
bysc
ores
onSu
icid
eAs
sess
men
tSc
ale
–15
%Bo
rder
line
pers
onal
ity
diso
rder
Bord
erlin
epe
rson
alit
ydi
sord
er–
Mik
ami,
etal
.,20
09At
tem
pt;
Emer
genc
yro
ompa
tien
tsw
hoin
flict
edse
riou
sse
lf-ha
rmw
ith
suic
idal
idea
tion
.–
12.8
%M
ood
diso
rder
(8.3
%),
anxi
ety
diso
rder
(8.3
%)
adju
stm
ent
diso
rder
(83%
)
Mal
e,pe
ervi
ctim
izat
ion
(75%
)–
Balfe
&Ta
ntam
,20
10Su
icid
alth
ough
ts,
aske
dpa
rtic
ipan
tsw
heth
erth
eyha
dev
erth
ough
tab
out
killi
ngth
emse
lves
;At
tem
pt,
aske
dpa
rtic
ipan
tsw
heth
erth
eyha
dev
ertr
ied
toki
llth
emse
lves
.
Suic
idal
thou
ghts
(40%
);su
icid
eat
tem
pt(1
5%)
–De
pres
sion
(“Do
you
feel
depr
esse
d?”;
35%
),an
xiet
y(“
Doyo
ufe
elan
xiou
s?”;
51%
)
––
Muk
adde
s&
Fate
h,20
10Be
havi
ors;
not
clea
rlyde
fine
d,pr
esum
ably
info
rmat
ion
gath
ered
from
psyc
hiat
ric
inte
rvie
w.
Suic
idal
beha
vior
s(1
6%to
tals
ampl
e;42
%of
adol
esce
nts
age
12–2
0;0%
inch
ildre
n)
–An
xiet
yDi
sord
ers
(OCD
and
spec
ific
phob
ia;
54%
),Di
srup
tive
Beha
vior
diso
rder
s(A
DHD,
ODD,
CD;
48%
),M
ood
diso
rder
s(M
DDan
dBP
;37
%),
Tic
Diso
rder
s(1
8%)
––
Raja
,et
al.,
2011
Idea
tion
,as
ked
pati
ents
whe
ther
they
wis
hed
todi
e,th
ough
tab
out
suic
ide
orpo
ssib
lem
etho
ds;
Atte
mpt
,as
ked
pati
ents
whe
ther
they
had
atte
mpt
edsu
icid
eor
self-
harm
edin
any
way
;Co
mpl
eted
suic
ide,
reco
rded
met
hod
Com
plet
edsu
icid
e(7
.7%
),su
icid
eid
eati
on(3
1%),
suic
ide
atte
mpt
(7.7
%)
–Sc
hizo
phre
nia
(61.
5%);
moo
ddi
sord
er(2
3.1%
);OC
D(7
.7%
);su
bsta
nce
abus
edi
sord
er(1
5.4%
)
––
Kato
,et
al.,
2012
Atte
mpt
;Pa
tien
tsad
mit
ted
toth
eem
erge
ncy
room
due
tose
riou
sph
ysic
alha
rmre
sult
ing
from
asu
icid
eat
tem
pt.
–7.
3%Ad
just
men
tdi
sord
er(7
0%);
moo
ddi
sord
er(1
8.6%
);an
xiet
ydi
sord
er(1
6.3%
);su
bsta
nce-
rela
ted
diso
rder
(2.3
%)
Youn
ger,
sing
le(u
nmar
ried
),lo
wer
educ
atio
n–
May
es,
etal
.,20
13Id
eation
(“ta
lks
abou
tha
rmor
killi
ngse
lf”)
and
Atte
mpt
s(“
delib
erat
ely
harm
son
esel
for
atte
mpt
ssu
icid
e”)
asra
ted
bym
othe
rson
the
Pedi
atri
cBe
havi
orSc
ale.
Suic
ide
atte
mpt
(7.2
%),
suic
idal
idea
tion
(10.
9%)
–M
DD(2
6.4%
)De
pres
sion
,be
havi
orpr
oble
ms,
peer
vict
imiz
atio
n,m
ale,
low
erSE
S,Bl
ack/
His
pani
c,ol
der
than
10ye
ars
Fem
ale,
Whi
te/A
sian
,hi
gher
SES,
noim
puls
iven
ess,
moo
ddy
sreg
ulat
ion,
orbe
havi
orpr
oble
ms;
Youn
ger
than
10ye
ars;
pare
ntw
ith
prof
essi
onal
orm
anag
eria
locc
upat
ion
Stor
che
al.,
2013
Idea
tion
(“th
ough
tsof
deat
hor
dyin
g”;
“tho
ught
abou
tki
lling
him
/her
self”
;“t
houg
htof
aw
ayto
kill
him
/her
self”
and
Atte
mpt
(“tr
ied
toki
llhi
m/h
erse
lf”)
asra
ted
bych
ildre
nan
dth
eir
care
give
rs.
Suic
idal
thou
ghts
/be
havi
ors
(10.
7%)
–So
cial
phob
ia(8
6.3%
);GA
D(7
4.5%
);sp
ecif
icph
obia
(62.
7%);
sepa
rati
onan
xiet
ydi
sord
er(4
1.2%
);OC
D(3
5.2%
);PT
SD(5
.8%
);M
DD/d
ysth
ymia
(13.
7%);
DBD
(56.
8%)
Auti
smdi
agno
sis
(com
pare
dw
ith
Aspe
rger
);M
DD/
dyst
hym
ia;
PTSD
–
Note
.M
easu
res
desc
ribe
din
Tabl
e3.
ADH
D,at
tent
ion-
defi
cit
hype
ract
ivit
ydi
sord
er;
ASD,
auti
smsp
ectr
umdi
sord
er;
BP,
bipo
lar
diso
rder
;CD
,co
nduc
tdi
sord
er;
DBD,
disr
upti
vebe
havi
ordi
sord
er;
GAD,
gene
raliz
edan
xiet
ydi
sord
er;
MDD
,m
ajor
depr
essi
vedi
sord
er;
OCD,
obse
ssiv
eco
mpu
lsiv
edi
sord
er;
ODD,
oppo
siti
onal
defi
ant
diso
rder
;PT
SD,
post
-tra
umat
icst
ress
diso
rder
;SE
S,so
cioe
cono
mic
stat
us.
a Rep
orte
dfo
rent
irede
velo
pmen
tally
dela
yed
sam
ple/
notA
SDsp
ecifi
c.
INSAR512 Segers and Rawana/Systematic review of suicidality in ASD

comprise 27%) it cannot be concluded that these findingsapply to individuals with ASD.
Protective Factors Associated with Suicide in ASD
Surprisingly, despite the increasing importance of adopt-ing a positive or strength-based approach when under-standing mental health issues among young people[Cheon, 2008; Norrish & Vella-Brodrick, 2009], only onestudy made any mention of factors that may buffer orprotect against suicidality among individuals with ASD.Mayes et al. [2013] noted that being female, White,Asian, and having a higher socioeconomic status weredemographic factors related to an absence of any suicidalbehaviors. Additionally, children who did not demon-strate impulsiveness, behavioral problems, or mooddysregulation were also at a much lower risk of develop-ing suicidal behaviors [Mayes et al., 2013].
Assessing ASD
A major issue concerning all research in ASD is ensuringthat every individual included in the sample in questiondoes, in fact, present with ASD by consistent and reliablestandards. In other words, if consistent and reliable mea-sures are employed, researcher bias is less likely to influ-ence inclusion into a diagnostic category. Measures used toconfirm ASD varied considerably (see Table 3). Only twostudies in this review used the recommended “gold-standard” measures in their assessment of ASD (for detailson the “gold standard” in ASD measures, see Discussion).Balfe and Tantam [2010] used the Autism DiagnosticInterview-Revised (ADI-R) with a subset of their partici-pants (40%) and commented on the difficulty of complet-ing this measure with adult participants’ parents; however,Storch et al. (2013) reported that all of their participantswere assessed using both the Autism Diagnostic Observa-tion Schedule (ADOS) and the ADI-R in combination withDSM-IV criteria. Two studies [Kato et al., 2013; Mikamiet al., 2009] used the Autism-Spectrum Quotient (AQ)—Japanese version [Baron-Cohen, Wheelwright, Skinner,Martin, & Clubley, 2001; Kurita, Koyama, & Osada, 2005]in combination with the DSM-IV diagnostic criteria. Someof the other measures employed included the Krug Asper-ger’s Disorder Index [Krug & Arick, 2003], Asperger Syn-drome Diagnostic Interview for Adolescents [Gillberg,Gillberg, Råstam, & Wentz, 2001], psychiatric telephoneinterview with parents for screening of childhoodautism—tics, attention-deficit hyperactivity disorder andother comorbidities [Hansson et al., 2005], and the Check-list for Autism Spectrum Disorder [Mayes, 2012]. The mostconsistent method used to assess the presence of an ASDacross the studies was clinical judgment based on psychi-atric interviewing and criteria from the Diagnostic and
Statistical Manual of Mental Disorders (DSM) third orfourth edition.
Assessing Suicidal Behaviors
As in the ASD assessment, methods for assessing the pres-ence of suicidal behaviors were heterogeneous and hadless of a reliance on structured instruments (see Table 3),this was most likely a significant contributing factor tothe large range of suicidal behaviors reported acrossstudies (10.7–50%). The most consistently used methodwas an assessment of the participant’s medical records(e.g., length of hospital stay, attempted method, psychi-atric history) followed by psychiatric interview witheither the individual themselves or a parent. For example,Hardan and Sahl (1999) assessed participants’ medicalrecords using a “Suicidality Data Form” for the purpose ofcollecting data on methods used/considered, the lethalityof methods, frequency of suicidal thoughts and/or behav-iors, pervasiveness of suicidal behaviors (duration ofsymptom and whether the incident was episodic, con-tinuous, or isolated), past exposure to suicide, and under-standing of the concept of death. Several studies basedsuicidal behaviors on participant responses to direct ques-tions regarding whether they thought about killing them-selves, whether they had thought about a plan forsuicide, and whether they had attempted self-harm orsuicide in the past [Balfe & Tantam, 2010; Raja et al.,2011]. Specific instruments used to assess suicidal behav-iors included: the Suicidal Ideation Questionnaire[Reynolds, 1991], the Suicide Assessment Scale [Nimeus,Alsen, & Träskman-Bendz, 2000], the Schedule for Affec-tive Disorders and Schizophrenia for School AgeChildren—Present and Lifetime Version [K-SADS-PL;Kaufman et al., 1997], Anxiety Disorder InterviewSchedule—Child and Parent Versions (Silverman &Albano, 1996) and the Pediatric Behavior Scale [Lindgren& Koeppl, 1987]. It should be highlighted that in general,suicidality was poorly defined and varied significantlyfrom study to study. Many studies used single items fromnon-suicide-specific measures, which limits the reliabilityand utility of the data collected. For example, the Mayeset al. [2013] study used only two items from the PediatricBehavior Scale, and Mukaddes and Fateh [2010] do notexplicitly define their measurement of suicidal behaviors,yet indicate use of psychiatric interview and theK-SADS-PL [Kaufman et al., 1997].
Assessing Intelligence
Given the high rates of co-occurring intellectual disabilitywith ASD, it is important to assess intelligence. An accu-rate assessment of intelligence makes comparisons withother populations (e.g., typical developing, individualswith schizophrenia) more meaningful and can protect
513Segers and Rawana/Systematic review of suicidality in ASDINSAR
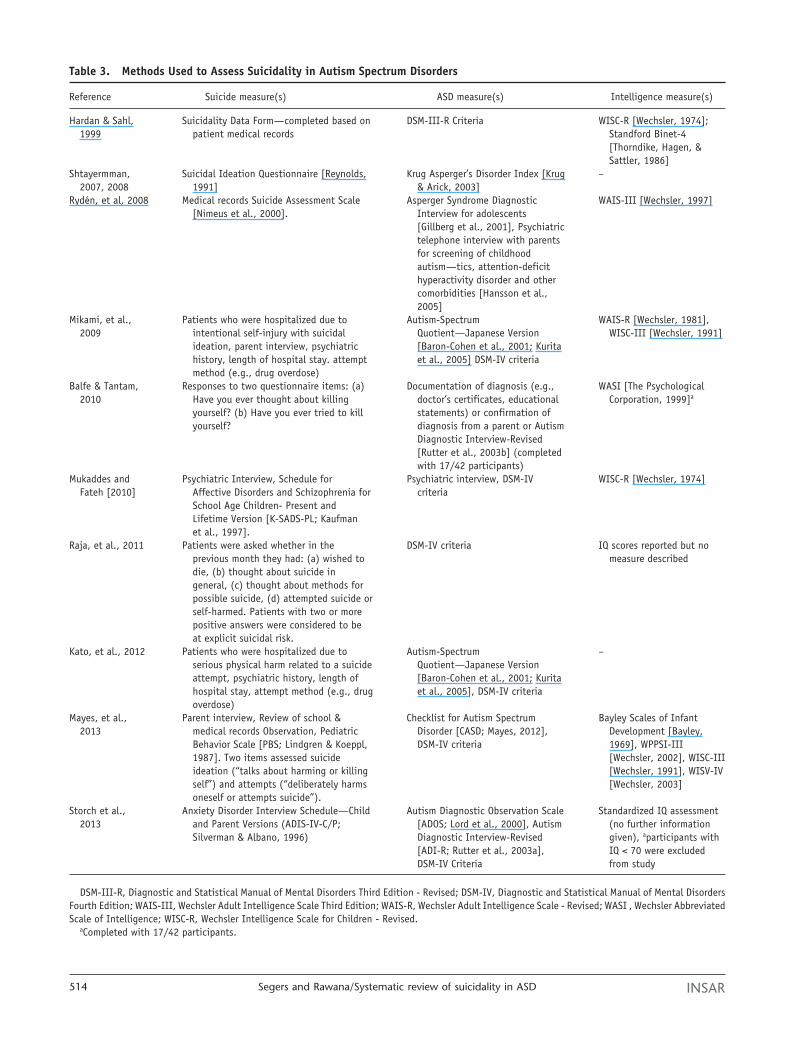
Table 3. Methods Used to Assess Suicidality in Autism Spectrum Disorders
Reference Suicide measure(s) ASD measure(s) Intelligence measure(s)
Hardan & Sahl,1999
Suicidality Data Form—completed based onpatient medical records
DSM-III-R Criteria WISC-R [Wechsler, 1974];Standford Binet-4[Thorndike, Hagen, &Sattler, 1986]
Shtayermman,2007, 2008
Suicidal Ideation Questionnaire [Reynolds,1991]
Krug Asperger’s Disorder Index [Krug& Arick, 2003]
–
Rydén, et al, 2008 Medical records Suicide Assessment Scale[Nimeus et al., 2000].
Asperger Syndrome DiagnosticInterview for adolescents[Gillberg et al., 2001], Psychiatrictelephone interview with parentsfor screening of childhoodautism—tics, attention-deficithyperactivity disorder and othercomorbidities [Hansson et al.,2005]
WAIS-III [Wechsler, 1997]
Mikami, et al.,2009
Patients who were hospitalized due tointentional self-injury with suicidalideation, parent interview, psychiatrichistory, length of hospital stay. attemptmethod (e.g., drug overdose)
Autism-SpectrumQuotient—Japanese Version[Baron-Cohen et al., 2001; Kuritaet al., 2005] DSM-IV criteria
WAIS-R [Wechsler, 1981],WISC-III [Wechsler, 1991]
Balfe & Tantam,2010
Responses to two questionnaire items: (a)Have you ever thought about killingyourself? (b) Have you ever tried to killyourself?
Documentation of diagnosis (e.g.,doctor’s certificates, educationalstatements) or confirmation ofdiagnosis from a parent or AutismDiagnostic Interview-Revised[Rutter et al., 2003b] (completedwith 17/42 participants)
WASI [The PsychologicalCorporation, 1999]a
Mukaddes andFateh [2010]
Psychiatric Interview, Schedule forAffective Disorders and Schizophrenia forSchool Age Children- Present andLifetime Version [K-SADS-PL; Kaufmanet al., 1997].
Psychiatric interview, DSM-IVcriteria
WISC-R [Wechsler, 1974]
Raja, et al., 2011 Patients were asked whether in theprevious month they had: (a) wished todie, (b) thought about suicide ingeneral, (c) thought about methods forpossible suicide, (d) attempted suicide orself-harmed. Patients with two or morepositive answers were considered to beat explicit suicidal risk.
DSM-IV criteria IQ scores reported but nomeasure described
Kato, et al., 2012 Patients who were hospitalized due toserious physical harm related to a suicideattempt, psychiatric history, length ofhospital stay, attempt method (e.g., drugoverdose)
Autism-SpectrumQuotient—Japanese Version[Baron-Cohen et al., 2001; Kuritaet al., 2005], DSM-IV criteria
–
Mayes, et al.,2013
Parent interview, Review of school &medical records Observation, PediatricBehavior Scale [PBS; Lindgren & Koeppl,1987]. Two items assessed suicideideation (“talks about harming or killingself”) and attempts (“deliberately harmsoneself or attempts suicide”).
Checklist for Autism SpectrumDisorder [CASD; Mayes, 2012],DSM-IV criteria
Bayley Scales of InfantDevelopment [Bayley,1969], WPPSI-III[Wechsler, 2002], WISC-III[Wechsler, 1991], WISV-IV[Wechsler, 2003]
Storch et al.,2013
Anxiety Disorder Interview Schedule—Childand Parent Versions (ADIS-IV-C/P;Silverman & Albano, 1996)
Autism Diagnostic Observation Scale[ADOS; Lord et al., 2000], AutismDiagnostic Interview-Revised[ADI-R; Rutter et al., 2003a],DSM-IV Criteria
Standardized IQ assessment(no further informationgiven), aparticipants withIQ < 70 were excludedfrom study
DSM-III-R, Diagnostic and Statistical Manual of Mental Disorders Third Edition - Revised; DSM-IV, Diagnostic and Statistical Manual of Mental DisordersFourth Edition; WAIS-III, Wechsler Adult Intelligence Scale Third Edition; WAIS-R, Wechsler Adult Intelligence Scale - Revised; WASI , Wechsler AbbreviatedScale of Intelligence; WISC-R, Wechsler Intelligence Scale for Children - Revised.
aCompleted with 17/42 participants.
INSAR514 Segers and Rawana/Systematic review of suicidality in ASD

against confounds. It should be clear what characteristicsare unique to ASD and what traits may be present in allindividuals with intellectual disability. The majority ofstudies (70%) did make use of intelligence measures tocharacterize and describe their samples with the excep-tion of the web-based study [Shtayermman, 2007, 2008]and one hospital study [Kato et al., 2013]. Furthermore,most studies used some format of the well-standardizedWechsler tests (i.e., Wechsler Adult Intelligence Scale,Wechsler Intelligence Scale for Children, Wechsler Abbre-viated Scale of Intelligence, or Wechsler Preschool andPrimary Scale of Intelligence) depending on the age ofparticipants.
Case Studies
A small number of case studies (n = 3) were reviewed (seeTable 4) to gauge whether similar trends were reportedanecdotally in case studies as were observed in clinicalstudies. Not surprisingly, all of the individuals in thereported case studies were male; two adults (Hare, 1997;Spencer et al., 2011) and one child of elementary schoolage (Schmid, Truog, & Damian, 2011). In terms of suicidalbehaviors, all of the participants either threatened orengaged in self-harm/suicide attempts using knives (e.g.,hunting knife, butcher knife) or sharp objects (i.e., brokenglass). Both adults described in the case studies used exces-sive alcohol consumption related to or in conjunctionwith their suicidal behaviors. Individuals in each of thecases had additional psychiatric diagnoses includingschizophrenia, major depressive disorder, and impulsecontrol disorder. Furthermore, each case report describedinterpersonal issues triggered suicidal acts. For instance,Hare (1997) describes a 26-year-old male who experienced
particular low mood after visits with his mother and whoexperienced internalizing issues after social interactionswith females, including his mother. Spencer et al. (2011)account the suicidal acts of a man, who attempted suicidefollowing interpersonal conflicts at his place of employ-ment. Finally, the case report of a school-aged child detailssuicidal ideation related to being bullied at school (Schmidet al., 2011). Three important points are highlightedwithin these case reports: (a) methods used by individualswith ASD involve potentially lethal means (e.g., sharpobjects and alcohol); (b) all cases had psychiatric diagno-ses in addition to ASD, and (c) interpersonal issues appearto act as a trigger in the suicidal acts of individuals withASD.
DiscussionKey Findings
The current literature review revealed a dearth of articlesstemming from a variety of disciplines (e.g., psychiatry,nursing, psychology) and research settings (e.g., hospi-tals, clinics, universities, web based) that have set thestage for examining suicidal behaviors in ASD. Consider-ing that only 10 separate studies and 3 case reports wereconsidered appropriate for this review, there is significantroom for continued investigation in this line of research.The opportunity to compare and contrast between theavailable studies, however, allows for a clearer picture ofareas that are better understood and areas in which infor-mation is lacking. It also allows for a commentary onmethodological approaches and considerations particularto studying suicidal behaviors in ASD.
This review highlighted that suicidal behaviors are asignificant issue for individuals with ASD and have been
Table 4. Case Studies
ReferenceASD diagnosis;
diagnostic measure
Participant characteristics(age, gender, relationship
status; IQ)Suicidal behaviors described
and assessment measure
Identifiedcomorbidities/psychiatric
characteristicsAdditional clinical
information
Hare, 1997 Aspergersyndrome; nomeasurereported
26 years; male;single, low-averageIQ (WAIS-R)
Cutting (using broken glass);excessive alcoholconsumption, BeckDepression Inventory[BDI; Beck et al., 1987]
Schizophrenia Poor relationship withmother; social anxiety
Spencer et al.,2011
Autism spectrumdisorder; nomeasurereported
44 years; male;married; no IQreported butparticipant haduniversity degree
Cutting (using knives);excessive alcoholconsumption; two knownsuicide attempts
Major depressivedisorder;impulse controldisorder;
Violence towards others(coworkers)
Schmid, 2011 Aspergersyndrome; nomeasurereported
Elementary schoolage; male; no IQlevel reported
Used knife in suicide attempt Depression Participant was bullied inschool; subject wasrefusing schoolattendance; aggressivebehavior towards objects
IQ, Intelligence Quotient; WAIS-R, Wechsler Adult Intelligence Scale-Revised.
515Segers and Rawana/Systematic review of suicidality in ASDINSAR

observed to be present in 10.7–50% of samples. A numberof factors may have contributed to the variability in theincidence of suicidal behaviors. These include age groupstudied (prevalence increases with age), research setting(e.g., hospital vs. community clinic), and inconsistency inthe measures used to assess suicide. Several factors suggestthat individuals with ASD may be particularly vulnerableto suicidal thoughts and behaviors because of characteris-tics related to the disorder itself and its social implications(e.g., isolation, difficulties communicating with others,peer victimization). While the focus of this review was onthe status of research and empirical knowledge, the resultshave both theoretical and practical implications. Forexample, clinicians should be aware of the importance forscreening for depression and other mental health issues inindividuals with ASD, particularly when suicidal behav-iors are present. Furthermore, the knowledge that suicidalbehaviors are a valid and significant concern for individu-als with ASD also contributes to our theoretical under-standing of the presentation of the disorder. Kato et al.[2013] found that individuals with ASD who attemptedsuicide (a) had persistent rather than spontaneous stress-ors, (b) used more lethal means, and (c) were less con-nected to psychiatric services. These troublesome factssuggest that individuals with ASD may actually be morelikely to succeed in their first suicide attempt and there-fore, should be taken extremely seriously when suicidalbehaviors are present [Kato et al., 2013]. The higher inci-dence of males, compared with females, with the disordershould also be considered when assessing risk in individu-als with ASD. Research with typically developing popula-tions has indicated that males use more lethal means andare more successful in completing suicide than females[Hawton et al., 2012], which may account for the greaterseverity of physical harm and increase in the use of lethalmeans observed [Kato et al., 2013; Mikami et al., 2009].These results were mirrored in case study reports in whichsuicidal behaviors reported involved sharp objects, as wellas excessive alcohol consumption. Despite males making agreater proportion of the ASD population than females, itis important that researchers expand their efforts to studyhow females may differ in their presentation (e.g., possiblyhigher rates of attempts or lower rates of completion) andexpression of suicidal behaviors, give that we know this tobe the case in typically developing youth [Hawton et al.,2012]. Future research should clarify and separate the roleof gender and ASD symptoms on suicidal behaviors.
A strength of the literature looking at suicidality in ASDis that while some of the studies have considerably smallsample sizes, at least a few had medium and large [e.g.,N = 791; Mayes et al., 2013] samples, which strengthensthe generalizability of the results. Furthermore, the bodyof literature reviewed here covers an adequate represen-tation of developmental periods. Even though morestudies tended to use adult participants, efforts were
made to conduct research on children, adolescents, andemerging adults. Having equal representation across agegroups allows for comparisons in the development andpresence of suicidal behaviors across the life span. It isrecommended that future research should attempt tofollow a cohort across an extended period of time tocapture and characterize the developmental trajectory ofsuicidal behaviors in ASD. For example, such an analysismay find that youth with ASD who have suicidal behav-iors display them at a later stage than typically develop-ing youth, perhaps linked with delayed development ofindependence and/or social skills. This type of informa-tion will have important clinical utility for working withyouth with ASD.
While the majority of studies reported on here includecomparison groups, a significant percentage (40%) didnot. The inclusion of representative and appropriatecomparison groups is critical when making comparisonswith normative development. The type of comparisongroup selected will guide the questions to be asked andthe meaning that can be drawn from the comparison.There is unique value and motivation to comparingsuicidality in ASD to both typically developing “healthy”populations as well as to typically developing popula-tions with psychiatric diagnoses and issues.
Assessment Measures
This review provides aggregated data on the measuresused to assess ASD, suicidal behaviors, and IQ in thesestudies. Diagnostic measures are critical to confirm truepresence of an ASD and to ensure that researchers studyand report accurately on the population they intend to.The majority of studies did not use “gold-standard” mea-sures for ASD diagnosis, which limits the reliability andaccuracy of the ASD research samples described here. Ingeneral, the current literature falls short on its use ofwell-validated diagnostic measures and instead relies onclinical impression and DSM criteria to confirm diagno-ses. A possible explanation for the decreased use of psy-chological measurement tools is that a good number ofthe studies reported here originate from the medical com-munity where there may be less knowledge and/or train-ing in the use of diagnostic measures.
There are an abundance of available measures, devel-oped in recent years, for screening and diagnosis of ASD;however, not all of these measures have been well evalu-ated or validated [see for comprehensive overview andguidelines: Campbell, 2005; Carpenter, 2012; Filipek et al.,1999; Khouzam, El-Gabalawi, Pirwani, & Priest, 2004]. Theresearch and clinical diagnostic “gold standard” for assess-ing ASD [Charman & Gotham, 2013; Filipek et al., 1999] istypically comprised of two instruments: ADOS [Lord et al.,2000] and ADI-R [Rutter, Le Couteur, & Lord, 2003b].The ADOS, an observational measure, and the ADI-R, a
INSAR516 Segers and Rawana/Systematic review of suicidality in ASD

caregiver interview, are both widely used instruments anddemonstrate good reliability and specificity for diagnosingan ASD, particularly when used in combination [Charman& Gotham, 2013; de Bildt et al., 2004]. Other instrumentssuch as the Diagnostic Interview for Social and Com-munication Disorders [Wing, Leekam, Libby, Gould, &Larcombe, 2002] and the Developmental, Dimensionaland Diagnostic Interview [Skuse et al., 2004] can also beused as diagnostic tools, although these measures are notas well validated as the ADOS and the ADI-R [Charman &Gotham, 2013]. Rating scales can also be used in conjunc-tion with other measures to assist in confirming ordisconfirming the presence of an ASD. Two of the mostwidely used and best-validated rating scales availablefor use with children and adolescents are the SocialCommunication Questionnaire [SCQ; Rutter, Bailey, &Lord, 2003a] and the Social Responsiveness Scale [SRS;Constantino & Gruber, 2002]. The SCQ has the additionaladvantage of being based on the ADI-R and DSM criteria.The AQ [Baron-Cohen et al., 2001] is currently the onlywell-validated self-report measure of autism-like symp-toms in adults and has been translated into many differentlanguages and now also has child and adolescent versions[Auyeung, Baron-Cohen, Wheelwright, & Allison, 2008;Baron-Cohen, Hoekstra, Knickmeyer, & Wheelwright,2006].
The degree of inconsistency with the tools used formeasuring suicidal behavior makes it difficult to makevalid comparisons between studies or draw meaningfulconclusions. Differences in how “suicidality” as a con-struct was measured may account for the large ranges inreported rates of suicidal behavior. Only two formal,suicide-specific measures were used in the current review:the Suicidal Ideation Questionnaire [Reynolds, 1991] andthe Suicide Assessment Scale [Nimeus et al., 2000]. Fur-thermore, because of the inconsistency in how“suicidality” was assessed, there is also variability in howthe concept was defined. For the purposes of this review,suicidal behaviors was defined in its broadest sense,which included suicidal ideation, self-harm behaviors,suicidal attempt, and completed suicide. Researchersshould consider teasing apart these constructs and mea-suring them as separate entities to better understand thecomplex issue of suicide.
Bryan and Rudd [2006] have put forth guidelines inthe assessment of suicide risk in clinical settings;however, their suggestions are important considerationswhen assessing suicide in a research context. Forexample, they stress the importance of using accurateterminology, categorizing level of risk, and assessingmultiple areas of functioning to aid in explicit andcareful identification of suicidality. A comprehensiveassessment of suicidality should include predispositionto suicidal behavior, precipitants or stressors, symptom-atic presentation, presence of hopelessness, the nature
of suicidal thinking (e.g., availability or lethality ofmeans), previous suicidal behavior, impulsivity and self-control, and protective factors [Bryan & Rudd, 2006].Gutierrez’s [2006] reviewed guidelines for assessing riskand protective factors of adolescent suicide and high-lighted self-report measures as economical, valid, anduseful research tools. Gutierrez [2006] recommends apackage of measures, which address the necessary ele-ments of a suicide assessment: suicidal thoughts [Sui-cidal Ideation Questionnaire; Reynolds, 1987], suicidalbehaviors [Self-Harm Behavior Questionnaire; Gutierrez,Osman, Barrios, & Kopper, 2001], depression [ReynoldsAdolescent Depression Scale 2; Reynolds, 2002], andprotective factors [Reasons for Living Inventory for Ado-lescents; Osman et al., 1998].
Risk and Protective Factors
Assessment of risk and protective factors did not receiveadequate attention in the studies in the current review.Understanding the factors that may increase or decreaselikelihood of suicide are critical in working toward effec-tive screening, prevention, and treatment. Risk factorsmay include demographic information, personal orfamily history of suicidal behavior, life stressors such asillness or loss, other psychiatric conditions, and hopeless-ness and impulsivity, to name only a few. A number ofrisk factors related to suicide in typical populations havebeen identified and include being male, being an adoles-cent or young adult, depression, drug and alcohol abuse,family history of suicide, family history of psychiatricdisorders, and previous history of self-harm and suicideattempt [Hawton, Casañas, Comabella, Haw, & Saunders,2013]. Protective factors were nearly completely over-looked in studies reviewed here. For clinicians, beingaware of protective factors can be particularly helpful insuicide assessment and clinicians may want to emphasizeand bolster these factors and skills in their clients. Someof the protective factors that researchers may include arepresence of social support, problem-solving skills, copingskills, active participation in treatment, presence of hope-fulness, children present in the home, pregnancy, reli-gious commitment, life satisfaction, intact reality testing,fear of social disapproval, and fear of suicide or death[Bryan & Rudd, 2006]. A few of the protective factors thathave been found to buffer suicidal behaviors in typicaldeveloping populations include having supportive rela-tionships, religious beliefs, and being the caregiver foryoung children [Hawton & van Heeringen, 2009]. Clini-cians should assess individuals with ASD for suicidal ide-ation and behaviors with special consideration of thesocial circumstances that may act as protective (e.g., care-givers, support systems) or risk factors (e.g., social isola-tion, peer victimization).
517Segers and Rawana/Systematic review of suicidality in ASDINSAR

Conclusion
The current study set out to characterize the current stateof extant literature on ASD and suicidality. We sought outinformation regarding prevalence rates of suicidal behav-iors in ASD as well as the prevalence of ASD in largersuicidal populations. We were interested in the demo-graphic and clinical profile of participant groups andwhat risk and protective factors were associated with sui-cidal behaviors. Finally, we wanted to know how thesestudies were being conducted methodologically, in termsof design, measurement tools, comparison groups, and soforth. Despite a small sample of articles, the currentreview offers a meaningful picture of our current under-standing of suicidality in ASD and provides useful guide-lines and recommendations for researchers movingforward. Recommendations provided here are not meantto be exhaustive; rather, they should be thought of asguidelines and considerations for those preparing toconduct similar studies in the future. In sum, futurestudies should make efforts to:
1. Operationally define the construct of suicidality.Clearly specify the aspect of suicidality being examined(e.g., ideation, self-harm, attempt, prevalence, etc.)
2. Examine prevalence rates of completed suicide in ASD;information regarding accurate estimates of com-pleted suicide is needed, including factors associatedwith completed suicides that may inform suicide pre-vention programs (e.g., number of previous attempts,access to suicide/crises services).
3. Make use of longitudinal design to inform a develop-mental trajectory of suicidality in ASD. Becausesuicidality disproportionally affects adolescents andyouth, studies should be designed to capture this criti-cal period (e.g., 11–25 years). However, the develop-mental periods preceding and following this periodshould also be examined to characterize enduring andtemporary factors that contribute and protect againstsuicidality.
4. Include the use of well-validated measures of ASDdiagnosis and suicidal behaviors.a. In settings where time and resources are limited,
researchers may choose to use rating scales andquestionnaires that are based on or correlate highlywith more comprehensive interviews or observa-tional tools. For example, third-party rating scalessuch as the SCQ and the SRS require a minimalamount of time to complete and do not require theextensive training needed to administer an ADI-R oran ADOS.
b. If an ADOS or ADI-R are not possible, researchersshould consider using multiple sources and tools toconfirm an ASD diagnosis. For a younger child, anycombination of the following can be utilized:
parent report, teacher report, diagnostic reportfrom a trusted health professional, observation, andDSM criteria. For adults, the inclusion of a self-report of ASD symptoms and characteristics (e.g.,AQ) is strongly advised.
c. Brief versions of well-validated measures can be usedwhen time is limited and if available. For example,the autism spectrum [Baron-Cohen et al., 2001] hasa 10-item version that displays good sensitivity,specificity, and predictive value compared with fullversions [Allison, Auyeung, & Baron-Cohen, 2012].
5. Make use of appropriate comparison groups. The typeof comparison group used will depend on the researchquestion. In most instances, when the study aims tounderstand and identify qualities unique to ASD, typi-cally developing participants without known historyof neurological impairment is likely most appropriate.In other cases, specific constructs (e.g., suicidal ide-ation) may be compared and contrasted betweenseveral childhood disorders (e.g., ASD, attentiondeficit hyperactivity disorder, Tourette’s syndrome,etc.). While studies lacking comparison groups candescribe the sample in question, it is often difficult toplace their findings into a broader developmentalcontext or draw meaningful conclusions beyond whatwas true for that particular group.
6. Include girls and women in samples and analyze sepa-rately from boys and men to understand gender dif-ferences in the expression of suicidal behaviors inASD.
7. Include individuals with intellectual impairments asparticipants in research studies to ensure that findingsare representative of the broader ASD population; themajority of individuals with ASD also have an intel-lectual disability [70%; Fombonne, 2005].
8. Explore cultural factors that may contribute to under-standing suicidality among individuals with ASD.Future studies could build upon existing researchexamining psychiatric comorbidity with suicidalityamong culturally diverse populations [Kato et al.,2013; Mikami et al., 2009].
9. Measure and analyze the role of protective and riskfactors (see Discussion for examples) in the expressionof suicidal behaviors in ASD.a. Studies should be designed to allow for comparison
between identified risk (e.g., depression, males,family history of suicide; [Hawton et al., 2013] andprotective factors [e.g., supportive relationships,religious beliefs, parental support; Hawton & vanHeeringen, 2009; McDonald, Bowker, Rubin,Laursen, & Duchene, 2010] in typically developingpopulations compared with those found in ASD.This would include screening for depression,anxiety, and other mental health issues associatedwith suicidality.
INSAR518 Segers and Rawana/Systematic review of suicidality in ASD

b. Researchers may also examine specific characteris-tics or factors affected by ASD symptoms. Forexample, this review has identified that peer rela-tions likely play in role in the mental and emotionalwell-being of individuals with ASD, as in typicallydeveloping youth. However, given that socialimpairment is a core tenet of ASD and the high ratesof peer victimization in this population, peer/socialsupport will be an important factor to examine inrelation to suicidality in this population.
In conclusion, suicidal behaviors have been shown tobe a legitimate concern in individuals with ASD. Clini-cians and researchers should be aware that individualswith ASD may use more lethal means that may increasethe probability of a successful first attempt. While thisreview was helpful in determining the prevalence,comorbidities, and risk factors of suicide, continuedresearch is needed to identify and clarify factors that willhave a protective and preventative influence on individu-als with ASD. In turn, further research on suicide amongindividuals with ASD can lead to best practice clinicalguidelines on this topic that have yet to be established.
References
Allison, C., Auyeung, B., & Baron-Cohen, S. (2012). Toward brief“red flags” for autism screening: The short Autism-SpectrumQuotient and the Short Quantitative Checklist in 1000 casesand 3000 controls. Journal of the American Academy ofChild & Adolescent Psychiatry, 51, 202–212.
American Psychiatric Association. (2013). Diagnostic and statis-tical manual of mental disorders (5th ed.). Washington, DC:American Psychiatric Association.
Arnett, J.J. (2007). Socialization in emerging adulthood. In J.E.Grusec & P.D. Hastings (Eds.), Handbook of socialization:Theory and research (pp. 208–231). New York, NY: GuilfordPress.
Auyeung, B., Baron-Cohen, S., Wheelwright, S., & Allison, C.(2008). The Autism-Spectrum Quotient: Children’s Version(AQ-Child). Journal of Autism and Developmental Disorders,38, 1230–1240.
Balfe, M., & Tantam, D. (2010). A descriptive social and healthprofile of a community sample of adults and adolescents withAsperger syndrome. BMC research notes, 3, 300.
Baron-Cohen, S., Hoekstra, R.A., Knickmeyer, R., &Wheelwright, S. (2006). The Autism-Spectrum Quotient(AQ)—Adolescent Version. Journal of Autism and Develop-mental Disorders, 36, 343–350.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., &Clubley, E. (2001). The Autism-Spectrum Quotient (AQ): Evi-dence from Asperger syndrome/high-functioning autism,males and females, scientists and mathematicians. Journal ofAutism and Developmental Disorders, 31, 5–17.
Bayley, N. (1969). Bayley Scales of Infant Development. NewYork, NY: The Psychological Corporation.
Beck, A.T., & Steer, R.A. (1987). BDI, Beck depression inventory:manual. New York: The Psychological Corporation.
Bergen, H., Hawton, K., Waters, K., Ness, J., Cooper, J., et al.(2012). How do methods of non-fatal self-harm relate toeventual suicide? Journal of Affective Disorders, 136, 526–533.
Bryan, C.J., & Rudd, M.D. (2006). Advances in the assessment ofsuicide risk. Journal of Clinical Psychology, 62, 185–200.
Campbell, J.M. (2005). Diagnostic assessment of Asperger’s dis-order: A review of five third-party rating scales. Journal ofAutism and Developmental Disorders, 35, 25–35.
Carpenter, P. (2012). Diagnosis and assessment in autism spec-trum disorders. Advances in Mental Health and IntellectualDisabilities, 6, 121–129.
Centers for Disease Control and Prevention. (2012). Prevalenceof autism spectrum disorders autism and developmental dis-abilities monitoring network, 14 Sites, United States, 2008.MMWR Surveillance Summaries, 61, 1–19.
Charman, T., & Gotham, K. (2013). Measurement issues: Screen-ing and diagnostic instruments for autism spectrumdisorders–lessons from research and practise. Child and Ado-lescent Mental Health. 18, 52–64. doi:10.1111/j.1475-3588.2012.00664.x
Cheon, J.W. (2008). Convergence of a strengths perspective andyouth development toward youth promotion practice.Advances in Social Work, 9, 176–190.
Constantino, J.N., & Gruber, C.P. (2002). The Social Responsive-ness Scale. Los Angeles, CA: Western Psychological Services.
de Bildt, A., Sytema, S., Ketelaars, C., Kraijer, D., Mulder, E., et al.(2004). Interrelationship between Autism Diagnostic Obser-vation Schedule-generic (ADOS-G), Autism DiagnosticInterview-Revised (ADI-R), and the Diagnostic and StatisticalManual of Mental Disorders (DSM-IV-TR) classification inchildren and adolescents with mental retardation. Journal ofAutism and Developmental Disorders, 34, 129–137.
Filipek, P.A., Accardo, P.J., Baranek, G.T., Cooks, E.H. Jr., Dawson,G., et al. (1999). The screening and diagnosis of autistic spec-trum disorders. Journal of Autism and Developmental Disor-ders, 29, 439–484.
Fombonne, E. (2005). The changing epidemiology of Autism.Journal of Applied Research in Intellectual Disabilities, 18,281–294.
Frith, U. (1989). Autism: Explaining the enigma. Oxford, UK:Blackwell Scientific Publications.
Ghaziuddin, M., & Greden, J. (1998). Depression in childrenwith autism/pervasive developmental disorders: A case-control family history study. Journal of Autism and Develop-mental Disorders, 28, 111–115.
Gillberg, C., Gillberg, C., Råstam, M., & Wentz, E. (2001). TheAsperger syndrome (and high-functioning autism) diagnosticinterview (ASDI): A preliminary study of a new structuredclinical interview. Autism: The International Journal ofResearch and Practice, 5, 57–66.
Gutierrez, P.M. (2006). Integratively assessing risk and protectivefactors for adolescent suicide. Suicide and Life-ThreateningBehavior, 36, 129–135.
Gutierrez, P.M., Osman, A., Barrios, F.X., & Kopper, B.A. (2001).Development and initial validation of the self-harm behaviorquestionnaire. Journal of Personality Assessment, 77, 475–490.
519Segers and Rawana/Systematic review of suicidality in ASDINSAR

Hansson, S.L., Röjvall, A.S., Rastam, M., Gillberg, C., Gillberg, C.,& Anckarsäter, H. (2005). Psychiatric telephone interviewwith parents for screening of childhood autism–tics,attention-deficit hyperactivity disorder and othercomorbidities (A–TAC) preliminary reliability and validity.The British Journal of Psychiatry, 187, 262–267.
Hardan, A., & Sahl, R. (1999). Suicidal behavior in children andadolescents with developmental disorders. Research in Devel-opmental Disabilities, 20, 287–296.
Hare, D.J. (1997). The Use of Cognitive-Behavioural Therapywith People with Asperger Syndrome: A Case Study. Autism,1, 215–225.
Hawton, K., Casañas I., Comabella, C., Haw, C., & Saunders, K.(2013). Risk factors for suicide in individuals with depression:A systematic review. Journal of Affective Disorders 147,17–28.
Hawton, K., Saunders, K.E., & O’Connor, R.C. (2012). Self-harmand suicide in adolescents. The Lancet, 379, 2373–2382.
Hawton, K., & van Heeringen, K. (2009). Suicide. The Lancet,373, 1372–1381.
Hedley, D., & Young, R. (2006). Social comparison processes anddepressive symptoms in children and adolescents withAsperger syndrome. Autism: The International Journal ofResearch and Practice, 10, 139–153.
Kasper, S., Schindler, S., & Neumeister, A. (1996). Risk of suicidein depression and its implication for psychopharmacologicaltreatment. International Clinical Psychopharmacology, 11,71–79.
Kato, K., Mikami, K., Akama, F., Yamada, K., Maehara, M., et al.(2013). Clinical features of suicide attempts in adults withautism spectrum disorders. General Hospital Psychiatry, 35,50–53.
Kaufman, J., Birmaher, B., Brent, D., Rao, U.M.A., Flynn, C., et al.(1997). Schedule for Affective Disorders and Schizophreniafor School-Age Children-Present and Lifetime Version(K-SADS-PL): Initial reliability and validity data. Journal ofthe American Academy of Child & Adolescent Psychiatry, 36,980–988.
Khouzam, H.R., El-Gabalawi, F., Pirwani, N., & Priest, F. (2004).Asperger’s disorder: A review of its diagnosis and treatment.Comprehensive Psychiatry, 45, 184–191.
Krug, D.A., & Arick, J.R. (2003). Krug Asperger’s Disorder Index.Austin, TX: Pro-Ed Inc.
Kurita, H., Koyama, T., & Osada, H. (2005). Autism-SpectrumQuotient–Japanese Version and its short forms for screeningnormally intelligent persons with pervasive developmentaldisorders. Psychiatry and Clinical Neurosciences, 59, 490–496.
Lindgren, S.D., & Koeppl, G.K. (1987). Assessing child behaviorproblems in a medical setting: development of the PediatricBehavior Scale. Advances in Behavioral Assessment of Chil-dren and Families, 3, 57–90.
Lord, C., Risi, S., Lambrecht, L., Cook, E.H., Jr., Leventhal, B.L.,et al. (2000). The Autism Diagnostic Observation Schedule—generic: A standard measure of social and communicationdeficits associated with the spectrum of autism. Journal ofAutism and Developmental Disorders, 30, 205–223.
Mayes, S.D. (2012). Checklist for Autism Spectrum Disorder.Wood Dale, IL: Stoelting.
Mayes, S.D., Gorman, A.A., Hillwig-Garcia, J., & Syed, E. (2013).Suicide ideation and attempts in children with autism.Research in Autism Spectrum Disorders, 7, 109–119.doi:10.1016/j.rasd.2012.07.009
McDonald, K.L., Bowker, J.C., Rubin, K.H., Laursen, B., &Duchene, M.S. (2010). Interactions between rejection sensi-tivity and supportive relationships in the prediction of ado-lescents’ internalizing difficulties. Journal of Youth andAdolescence, 39, 563–574. doi:10.1007/s10964-010-9519-4
Mikami, K., Inomata, S., Hayakawa, N., Ohnishi, Y., Enseki, Y.,et al. (2009). Frequency and clinical features of pervasivedevelopmental disorder in adolescent suicide attempts.General Hospital Psychiatry, 31, 163–166.
Mukaddes, N.M., & Fateh, R. (2010). High rates of psychiatricco-morbidity in individuals with Asperger’s disorder. WorldJournal of Biological Psychiatry, 11, 486–492.
Munesue, T., Ono, Y., Mutoh, K., Shimoda, K., Nakatani, H., &Kikuchi, M. (2008). High prevalence of bipolar disordercomorbidity in adolescents and young adults with high-functioning autism spectrum disorder: A preliminary study of44 outpatients. Journal of Affective Disorders, 111, 170–175.
Nimeus, A., Alsen, M., & Träskman-Bendz, L. (2000). The SuicideAssessment Scale: An instrument assessing suicide risk ofsuicide attempters. European Psychiatry, 15, 416–423.
Norrish, J.M., & Vella-Brodrick, D.A. (2009). Positive psychologyand adolescents: Where are we now? Where to from here?Australian Psychologist, 4, 270–278.
Osman, A., Downs, W.R., Kopper, B.A., Barrios, F.X., Baker, M.T.,et al. (1998). The Reasons for Living Inventory for Adoles-cents (RFL-A): Development and psychometric properties.Journal of Clinical Psychology, 54, 1063–1078.
Ouellette-Kuntz, H., Coo, H., Yu, C.T., Lewis, M.E., Dewey, D.,Hennessey, P.E., . . . & Holden, J.J. (2012). Status reportNational epidemiologic Database for the Study of Autism inCanada (NeDSAC). Chronic Diseases and Injuries in Canada,32, 84–89.
Raja, M., Azzoni, A., & Frustaci, A. (2011). Autism spectrumdisorders and suicidality. Clinical Practice and Epidemiologyin Mental Health, 7, 97–105. doi: 10.2174/1745017901107010097
Rao, U., Weissman, M.M., Martin, J.A., & Hammond, R.W.(1993). Childhood depression and risk of suicide: A prelimi-nary report of a longitudinal study. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 32, 21–27.
Reynolds, W.M. (1987). Suicidal Ideation Questionnaire (SIQ).Odessa, FL: Psychological Assessment Resources.
Reynolds, W.M. (1991). Psychometric characteristics of the adultSuicidal Ideation Questionnaire in college students. Journalof Personality Assessment, 56, 289–307.
Reynolds, W.M. (2002). Reynolds Adolescent Depression Scale.Lutz, FL: Psychological Assessment Resources.
Rivet, T.T., & Matson, J.L. (2011). Review of gender differences incore symptomatology in autism spectrum disorders. Researchin Autism Spectrum Disorders, 5, 957–976. doi: 10.1016/j.rasd.2010.12.003
Rutter, M., Bailey, A., & Lord, C. (2003a). The Social Communi-cation Questionnaire: Manual. Los Angeles: Western Psycho-logical Services.
INSAR520 Segers and Rawana/Systematic review of suicidality in ASD

Rutter, M., Le Couteur, A., & Lord, C. (2003b). Autism DiagnosticInterview-Revised. Los Angeles, CA: Western PsychologicalServices.
Rydén, G., Rydén, E., & Hetta, J. (2008). Borderline personalitydisorder and autism spectrum disorder in females: A cross-sectional study. Clinical Neuropsychiatry: Journal of Treat-ment Evaluation, 5, 22–30.
Saltz, A., & Marsh, S. (1990). Relationship between hopelessnessand ultimate suicide: A replication with psychiatric outpa-tients. American Journal of Psychiatry, 147, 190–195.
Schmid, A.M., Truog, A.W., & Damian, F.J. (2011). Care of thesuicidal pediatric patient in the ED: A case study. The Ameri-can Journal of Nursing, 111, 34–43.
Shtayermman, O. (2007). Peer victimization in adolescents andyoung adults diagnosed with Asperger’s syndrome: A link todepressive symptomatology, anxiety symptomatology andsuicidal ideation. Issues in Comprehensive PediatricNursing, 30, 87–107. doi: 10.1080/01460860701525089
Shtayermman, O. (2008). Suicidal ideation and comorbid disor-ders in adolescents and young adults diagnosed with Asper-ger’s syndrome: A population at risk. Journal of HumanBehavior in the Social Environment, 18, 301–328. doi:10.1080/10911350802427548
Silverman, W.K., & Albano, A.M. (1996). Anxiety Disorders Inter-view Schedule for DSM-IV.: Parent interview schedule (Vol.1). Oxford University Press.
Skegg, K. (2005). Self-harm. The Lancet, 366, 1471–1483.Skuse, D., Warrington, R., Bishop, D., Chowdhury, U., Lau, J.,
et al. (2004). The developmental, dimensional and diagnosticinterview (3Di): A novel computerized assessment for autismspectrum disorders. Journal of the American Academy ofChild & Adolescent Psychiatry, 43, 548–558.
Spencer, L., Lyketsos, C.G., Samstad, E., Dokey, A., Rostov, D., &Chisolm, M.S. (2011). A suicidal adult in crisis: An unex-pected diagnosis of autism spectrum disorder. AmericanJournal of Psychiatry, 168, 890–892.
Storch, E.A., Sulkowski, M.L., Nadeau, J., Lewin, A.B., Arnold,E.B., Mutch, P.J., . . . & Murphy, T.K. (2013). The
phenomenology and clinical correlates of suicidal thoughtsand behaviors in youth with autism spectrum disorders.Journal of Autism and Developmental Disorders, 43, 2450–2459.
Strang, J.F., Kenworthy, L., Daniolos, P., Case, L., Wills, M.C.,et al. (2012). Depression and anxiety symptoms in childrenand adolescents with autism spectrum disorders withoutintellectual disability. Research in Autism SpectrumDisorders, 6, 406–412. doi: 10.1016/j.rasd.2011.06.015
The Psychological Corporation (1999). Wechsler AbbreviatedScale of Intelligence. San Antonio, TX: Author.
Thorndike, R.L., Hagen, E.P., & Sattler, J.M., (1986). TheStanford–Binet Intelligence Scale: Fourth edition. Chicago,IL: Riverside.
Wechsler, D. (1974). Wechsler Intelligence Scale for children—Revised. New York, NY: The Psychological Corporation.
Wechsler, D. (1981). Wechsler Adult Intelligence Scale—Revised.San Antonio, TX: The Psychological Corporation.
Wechsler, D. (1991). Wechsler Intelligence Scale for Children—Third edition. San Antonio, TX: The PsychologicalCorporation.
Wechsler, D. (1997). Wechsler Adult Intelligence Scale—Thirdedition. San Antonio,TX: The Psychological Corporation.
Wechsler, D. (2002). Wechsler Preschool and Primary Scale ofintelligence—Third edition. San Antonio, TX: The Psycho-logical Corporation.
Wechsler, D. (2003). Wechsler Intellectual Scale for Children–Fourth edition (WISC-IV). San Antonio, TX: The Psychologi-cal Corporation.
Weiss, J. (2002). Self-injurious behaviours in autism: A literaturereview. Journal on Developmental Disabilities, 9, 127–144.
White, S.W., Oswald, D., Ollendick, T., & Scahill, L. (2009).Anxiety in children and adolescents with autism spectrumdisorders. Clinical Psychology Review, 29, 216–229.
Wing, L., Leekam, S.R., Libby, S.J., Gould, J., & Larcombe, M.(2002). The diagnostic interview for social and communica-tion disorders: Background, inter-rater reliability and clinicaluse. Journal of Child Psychology and Psychiatry, 43, 307–325.
521Segers and Rawana/Systematic review of suicidality in ASDINSAR