
A Combination of Therapies in Conjunction with Physical Activity for Adolescents with Major...
45
Running Head: MULTIFACETED THERAPY 1 YORKVILLE UNIVERSITY A Combination of Therapies in Conjunction with Physical Activity for Adolescents with Major Depressive Disorder and Generalized Anxiety Disorder Traits: A Case Study Hugh Watkins A MASTER’S CASE PRESENTATION SUBMITTED TO THE FACULTY OF BEHAVIOURAL SCIENCES IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS IN COUNSELLING PSYCHOLOGY Fredericton, New Brunswick December 27, 2012
-
Upload
yorkvilleu -
Category
Documents
-
view
0 -
download
0
Transcript of A Combination of Therapies in Conjunction with Physical Activity for Adolescents with Major...

Running Head: MULTIFACETED THERAPY 1
YORKVILLE UNIVERSITY
A Combination of Therapies in Conjunction with Physical Activity for Adolescents with Major
Depressive Disorder and Generalized Anxiety Disorder Traits: A Case Study
Hugh Watkins
A MASTER’S CASE PRESENTATION
SUBMITTED TO THE FACULTY OF BEHAVIOURAL SCIENCES IN PARTIAL
FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
MASTER OF ARTS IN COUNSELLING PSYCHOLOGY
Fredericton, New Brunswick
December 27, 2012
MULTIFACETED THERAPY 2
Abstract
The following case study describes the assessment, case formulation, literature review,
diagnosis, treatment planning, and treatment sessions for a 16-year-old male adolescent with a
diagnosis of major depressive disorder and comorbid features of generalized anxiety disorder.
This client had been referred for counselling by his family doctor because of his longstanding
history of excessive worry, depressive episodes, emotional lability, and withdrawal from social
situations, as well as somatic symptoms of anxiety.
The treatment intervention for this client consisted of a combination of Cognitive-
Behavioural Therapy methods and Pharmacotherapy which addressed: mood charting,
depression, stigma, medication, and wellness. Six individual sessions utilized treatment strategies
chosen to target specific client problems. These sessions involved various treatment methods
including solution-based brief therapy, mindfulness-based, and strengths-based therapy, as well
as exercise therapy. Treatment goals included a decrease in depressive and anxiety
symptomatology, stronger boundaries, increased self-esteem, and increased distress tolerance.
Carefully tailoring treatment sessions to target specific goals identified by the client proved to be
an effective treatment strategy, which yielded a reduction in problematic symptoms.
MULTIFACETED THERAPY 3
Acknowledgments
I would like to express my gratitude towards the entire team at the Brooklin Medical Centre, and
special appreciation to my supervisor, Dr. Roya Firouzabadi-Dashti, for stepping up in a crisis
moment when my previous practicum site had fallen through. Though being very busy in your
own practice and commitments to your patients, you were always willing to offer guidance and
modelled a work ethic that was admirable. You never saw me as a distraction and truly went out
of your way to treat me as a fellow colleague. As I look back on some of the earlier periods in
my practicum, in many ways you’ve been a life saver and an encouragement to me when all
seemed confusing and sometimes overwhelming. Thank you for being my compass as you took
the time to familiarize me with the clinic, fellow doctors, administrative and support staff. In no
time, with your investment, I was able to learn and use formal medical documents and navigate
my way through the medical software; “JonokeMED”.
To Dr. Gary Hughes, my Yorkville University practicum director, and Mrs. Eve Mills-
Nash, Yorkville University Assistant Director, words cannot express my appreciation for you
both, again at a time when I was frustrated and lost during the period when my prior practicum
site collapsed on me at the last minute. Your rapid correspondence, heartfelt words over the
phone, and calming emails were always what I needed at the right moment. Thanks for
bestowing upon me your wisdom and suggestions with all my questions and concerns, and for
creating an opportunity for me to get started on my practicum while facing some timing
challenges.
To my brother, Karl Harding and his lovely wife, thank you for being my voice of hope;
to my parents and mother-in-law, many thanks for your heartfelt prayers and for being my
biggest fans.

MULTIFACETED THERAPY 4
To my darling wife, Stacy, and my greatest treasures, my children Kyle and Chantel, I
thank you for your patience, love and support. After more than twenty years of not being in a
structured learning environment and remembering back to my previous graduation ceremony
uttering those words, “Thank you, God, but never again”, you all stood with me and encouraged
me through this long journey, while letting me know that I can accomplish anything I put my
mind to. “I love you all to infinity and beyond!”
MULTIFACETED THERAPY 5
Contents
Page
Title Page .........................................................................................................................................1
Abstract ............................................................................................................................................2
Acknowledgements ..........................................................................................................................3
Introduction ......................................................................................................................................8
Case Information ..............................................................................................................................8
Presenting Problem ..............................................................................................................8
Social and Educational History ............................................................................................8
Family History .....................................................................................................................9
Social Supports ....................................................................................................................9
Psychiatric History ...............................................................................................................9
Current Situation ................................................................................................................10
Medications ........................................................................................................................10
Client Strengths and Challenges ........................................................................................11
Mental Status .....................................................................................................................11
Risk Assessment ................................................................................................................11
Literature Review...........................................................................................................................12
Diagnosing Major Depressive Disorder.............................................................................12
Major Depressive Disorder and Generalized Anxiety Disorder ........................................15
MULTIFACETED THERAPY 6
Treatment of Major Depressive Disorder ..........................................................................16
Cognitive Behavioural Therapy .............................................................................17
Solution Focused Brief Therapy ............................................................................18
Strengths-Based Cognitive Behavioural Therapy ..................................................19
Physical Activity ....................................................................................................20
Pharmacological Treatments ..................................................................................21
Combination Treatments ........................................................................................21
Treatment Consideration for Generalized Anxiety Disorder Traits ......................22
Assessing Counselling Progress and Outcomes ....................................................22
Case Formulation ...........................................................................................................................23
Case Analysis .....................................................................................................................23
Treatment Plan ...................................................................................................................24
Treatment Summaries ....................................................................................................................26
Week 1 ...............................................................................................................................26
Week 2 ...............................................................................................................................27
Week 3 ...............................................................................................................................29
Week 4 ...............................................................................................................................31
Week 5 ...............................................................................................................................32
Week 6 ...............................................................................................................................33
Results ............................................................................................................................................34
MULTIFACETED THERAPY 7
Discussion ......................................................................................................................................35
References ......................................................................................................................................37
MULTIFACETED THERAPY 8
Combination Therapies in Conjunction with Physical Activity for Adolescents
Blake1
is a regular patient at the Brooklin Medical Centre who was referred to me by his
family doctor at a time when he was struggling with a variety of issues and was desperate for
some assistance to deal with symptoms that were plaguing him. This 16-year-old teenager had a
past diagnosis of major depressive disorder, with generalized anxiety disorder traits and ADHD.
He was currently in a depressed phase with suicidal ideation. During an intake appointment with
me he was assessed and was placed on a waitlist until he was added to my caseload.
Case Information
Reviewing Blake’s prior medical assessments and obtaining his personal history enabled
me to produce a thorough client assessment.
Presenting Problem
This client presented with complaints of depression, excessive worrying, low self-esteem,
poorly established boundaries, and suicidal ideation. His moods had been managed with
medication for about two years prior to his referral and his medical history and low moods were
well documented in his past assessments.
Social and Educational History
Blake reported having challenges focusing on his school work and meeting course
requirements at school. He stated that he had been overwhelmed by his frequent low moods,
often stayed awake at night plagued by suicidal thoughts, and had no desire to get out of bed.
Blake described his social history as rather tumultuous. Typically, while in a positive
mood, he functioned like many other athletic teenagers. He had been actively involved in
organized sports, was often the life of any party, and enjoyed spending time with his childhood
1 Client names and other information have been changed to protect confidentiality.
MULTIFACETED THERAPY 9
friends. However, he often had lingering periods where he felt crippled, not wanting to do
anything or be around anyone. This client was aware of and expressed concerns about the
instabilities in his life. During his assessment he described himself as going through a “loner
period” by his own choice.
Family History
Blake explained that he grew up in a very stable home, with loving parents and a pretty
cool sister who is five years older. He lived in the same home all of his life, which he is grateful
for. His mother is a well established lawyer with her own law practice in the community; he
described her as somewhat of a militant disciplinarian. Blake also stated that his mom was often
away from the home due to the demands of her job. His father had held management duties in
larger companies, but is currently unemployed. His father had some previous struggles with a
mood disorder similar to Blake’s, but had not had difficulties in years. Blake described his
relationship with his sister as typical, generally being good to each other, but definitely noting
that they have had their moments of sibling rivalry. Blake’s sister is currently attending
university and has always been a straight “A” student. His parents often celebrated her
achievements, which heightened the pressure on him as he felt he was a disappointment to his
parents because of his struggles to obtain good grades in school.
Social Supports
Blake described his parents, sister, and three childhood buddies as his main supports. He
also expressed a strong bond between him and his rugby team.
Psychiatric History
Blake did not recall any formal psychiatric treatment, but did recall going through
psychological assessments in grade eight when his family doctor diagnosed him with ADHD and

MULTIFACETED THERAPY 10
proceeded to prescribe mild mood stabilizers. Blake attempted suicide two times, once while in
grade eight and again during the summer of 2011. The first was an attempted overdose and the
second involved holding a loaded weapon to his temple. Blake came to the conclusion that he
would not commit suicide as this would bring devastation to his family.
The course of Blake’s illness has been plagued with depressive phases. However, he did
describe recent instances of intense worrying, accompanied by a decreased need for sleep.
Current Situation
Blake indicated in our session that he has managed to function relatively well and
attributed this to the help of his medication. One of his biggest challenges was lack of sleep and
what he calls “excessive sadness.” At our first assessment, he indicated that he had not
experienced any breakthrough in his depression and suffered unrelenting low self-esteem. His
score on the Beck Depression Inventory II (BDI-II) (Beck, Steer, & Brown, 1996) was 22, which
placed him in the range of moderate depression. With the challenges before him, he emphasized
an inability to manage his responsibilities at school and expressed a lack of desire to continue
playing on his rugby team (which he had always enjoyed). Furthermore, Blake described himself
as a failure. When he looks into his future he becomes overwhelmed with the notion that he does
not have the attributes and skills necessary to succeed. He constantly worried that he was letting
down his family. This client denied any substance abuse or use of alcohol.
Medications
Blake noted that, in the past, he had been on some medication to help him sleep.
Currently he is taking Concerta 75mg once daily and has been on this medication for the past
two years. He wishes to stop using medication and hopes that counselling will be the answer.
MULTIFACETED THERAPY 11
Client Strengths and Challenges
Blake described himself as having the following strengths: friendly, sociable, courteous,
trusting of others, respectful, athletic, and a deep thinker. Areas that Blake felt were challenges
included: low self-esteem which he associated with his depressive episodes, lack of optimism
towards the future, and academics.
Blake performed a Value in Action Inventory of Strengths (VIA-IS) (Peterson &
Seligman, 2004) and his top five character strengths were: love, kindness, fairness, equity and
justice, forgiveness and mercy, and gratitude. His weaknesses from the same assessment were:
spirituality (including a sense of purpose), judgement (including critical thinking and open-
mindedness), zest, enthusiasm, and energy.
Mental Status
Blake attended his first session appropriately dressed and groomed. He appeared to be a
well-mannered youth in great physical health. He was articulate, though at times seemed to be
struggling in thought. At times he maintained good eye-contact and was very accommodating,
but occasionally appeared distracted and would tend to look away. It became clear to me that my
client was lacking sleep, based upon his physical demeanour at the time of the session. He spoke
slowly but his volume and tone of voice were both appropriate. His thinking was logical and,
though he spoke of having thoughts of self-harm, he insisted that he would never carry it out.
Risk Assessment
As previously noted, Blake’s history indicated two past suicide attempts; one involved an
overdose of medication and the other involved holding a gun to his temple almost pulling the
trigger. He continues to express suicidal ideation. He informed me that his family owns several
guns at home that were easily accessible and agreed that, though he has not shared his last
MULTIFACETED THERAPY 12
attempt with anyone, his mother needed to be informed so that the guns could be properly stored.
He insisted that such episodes were “passing thoughts” and that his love for his family was much
more powerful than any fleeting thoughts of ending his life. The suicidality item completed on
the BDI-II (Beck et al., 1996) indicated that Blake had experienced no thoughts of ending his life
in the past two weeks prior to completing the assessment. After further consultation between our
Assistant Director at Yorkville University and my practicum supervisor, we deemed his risk of
suicide to be low.
Literature Review
Diagnosing Major Depressive Disorder
Major Depressive Disorder (MDD) is recognized as one of the most common mental
disorders and it is related to significant disability and death (Glenn et al., 2012). The World
Health Organization states that this widespread disorder has plagued approximately 121 million
people around the world (Clasen, Wells, Ellis, & Beevers, 2012). MDD can be detected at the
early stages of childhood and at various stages of adulthood, although the pinnacle of its
prevalence is in the young adulthood populous (Kessler et al., 2005). A longitudinal study of
high school students between the ages 17 to 31 identified six predictors of first onset of MDD in
young adulthood: female gender, family history of mood disorders, evidence of childhood sexual
abuse, anxiety disorder in childhood, adolescents with self-reported health problems, and
subthreshold depressive symptoms. Prior studies have also identified the following variables as
predictors of first onset (MDD) with comparable effects for gender: family history of depression
(Zimmerman et al., 2010), childhood mistreatment (Jaffee et al., 2002; Smit et al., 2004), anxiety
disorder (Eaton et al., 2008; Grant et al., 2009; Smit et al., 2004), health complications (Smit et
al., 2004), and subthreshold depression (DeGraaf et al., 2002; Glenn et al., 2012; Horwath et
al.,1992).
MULTIFACETED THERAPY 13
Kessler and Walters (1998) note that the impact of MDD is significant for its sufferers
and those in their sphere of influence and can result in greater interpersonal complications,
unemployment, substance abuse, delinquency, and high risk for suicide (Zimmerman, et al.,
2010). MDD is characterized as an emotional disorder that disrupts a person’s mood, motivation,
sleep, eating, concentration, self-worth, and productivity (American Psychiatric Association
[APA], 2000).Specific diagnostic criteria for MDD according to the American Psychiatric
Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) include the
existence of at least five symptoms from a list of nine and one of those symptoms must either be
low mood or loss of interest or pleasure in all, or nearly all, regular activities (APA, 2000).
This persisting sad mood encompasses feeling miserable, low, depressed, or “blue” for
the majority of the day, and a continuation of these symptoms every day for duration of two
weeks or longer (APA, 2000). This symptom plays a hallmark role in the disorder, and nagging
frustration regarding the mechanisms that perpetuate the mood persistence in MDD and the lack
of a clear understanding of what is involved often makes it difficult to ensure an effective
treatment resulting in a positive outcome (Clasen, Wells, Ellis, & Beevers, 2012). Beck (1967),
Ingram (1984), and Teasdale (1988) suggest that cognitive theories of depression recognize that
biases in which depressed individuals rationalize emotional information help propagate the
depressive symptoms. Such biases would involve a tendency to embrace mood-congruent
information in their surroundings (Clasen et al., 2012). Gotlib and Joormann (2010) explain that
cognitive theories further suggest that episodes that prompt sad mood intermingle with these
predispositions to manipulate a vast amount of pre-existing negative thoughts and feelings that
perpetuate sadness. There has been a growing body of studies that confirm these predispositions
to distort emotional information, as well as attentional biases (Clasen et al., 2012).
MULTIFACETED THERAPY 14
Wells and Beevers (2010) performed a study to look at whether attentional biases for
emotional information are related to distorted mood recovery followed by a period of sad mood
among people with and without MDD. Results indicated that as mood reactivity elevated, these
individuals did not exhibit a matching level of mood recovery. However, elevated levels of mood
reactivity did indeed match with greater mood recovery for individuals exhibiting lower levels of
attentional bias for sad stimuli (Clasen, et al., 2012). Wells and Beevers (2010) suggest that such
findings indicate that more severely depressed individuals exhibit impairments in mood recovery
that are matched with attentional biases, specifically when they are exposed to greater mood
activity (Clasen et al., 2012).
Another clinical distinction that is unique to MDD is a chronic course that impairs
psychosocial functioning. Widiger and Smith (2008) examined interpersonal pathoplasticity in
the course of individuals suffering from MDD. Pathoplasticity is recognized by a nonetiological
relationship between psychopathology and personality. Widiger and Smith (2008) suggest that
psychopathology and personality influence the expression of each other, but neither is solely
responsible for the other.
The DSM-IV-TR notes that both children and adolescents have commonly made reference
to irritability as a symptom of MDD, but does not list irritability as a symptom of MDD in the
adult population, despite the fact that in clinical samples of adults, irritability has also been a
symptom of MDD (Fava, Sampson, Walters, Kessler, & Hwang, 2010). A study of 2,307
individuals with MDD found that 1,067 (46%) reported irritability as frequent as being present
half of the time during the preceding week. Of the 46%, most were female, younger, suffered
severe depression and anxiety, mentioned a poor quality of life, and had a history of suicide
attempts and suicide ideation (Perlis et al., 2009). These researchers also found that although
MULTIFACETED THERAPY 15
irritability related depression cannot be labelled as a distinct subtype of MDD, it has a significant
influence on overall severity, anxiety, comorbidity, and suicidality (Perlis et al., 2009).
Finally, it is clear that depression is linked with reduced sleep stability and, though not a
distinct subtype of MDD, Sateia and Nowell (2004) posit that insomnia is a regular symptom
comorbid with major depressive disorder. Results of cardiopulmonary coupling analysis (CPC)
by Sateia and Nowell (2004) indicated that 1) reduced stable sleep and increased unstable sleep
and wakeful/REM conditions were more frequently observed in depressed patients in
comparison to those without depression, 2) medicated patients exhibited a degree of
improvement of stable sleep latency through the use of hypnotics, and 3) some CPC indices
revealed a connection with subjective sleep quality and the severity of depression/insomnia
(Sateia & Nowell, 2004). Sateia and Nowell (2004) state that such an exclusive prospective on
sleep stability in the context of cardiovascular physiology and the easily repeated ECG-based
procedure can, in fact, prove advantageous in the evaluation of insomnia in depression, and
could also help to facilitate treatment effects.
Major Depressive Disorder and Generalized Anxiety Disorder
Traditionally, researchers and clinicians have observed the relationship and overlap
between MDD and generalized anxiety disorder (GAD) in their shared diagnostic features and
their common coupling genetic diathesis. Despite their resemblances, the DSM-IV-TR indicates
that GAD should not be diagnosed if it is evident exclusively during MDD or a different mood
disorder (APA, 2000). The present diagnostic hierarchy rule represents an age-old dispute
regarding GAD’s status as an independent diagnosis (Lawrence, Liverant, Rosellini, & Brown,
2009). In the DSM-III (American Psychiatric Association, 1980) GAD was classified as a
residual category. A clinician was only able to assign the diagnosis as long as the patient in

MULTIFACETED THERAPY 16
question unsuccessfully met the criteria for another anxiety disorder. In the revised DSM-III-R
(American Psychiatric Association, 1987) there were significant alterations where GAD was
established as an independent category, even though the hierarchy rule was introduced to
promote diagnostic parsimony. The DSM-IV-TR states that in GAD a patient’s worries could be
extreme, feel uncontrollable, and also are followed by three of six associated symptoms (APA,
2000). This revision of the definition of GAD has been important for clinicians in that it has
produced an improved diagnostic reliability and also helped to bring clarity to relationships
between GAD and other emotional disorders (Lawrence et al., 2009).
Lawrence et al. (2009) found that high rates of comorbidity between MDD and GAD
were consistent with other studies of structural correlations between anxiety and mood disorders
and behavioural genetics (Lawrence et al., 2009). Lawrence et al. (2009) state that the hierarchy
rule contends that both MDD and GAD must be preserved independently and cannot be
considered as one factor, which again lends support for considering GAD and MDD as separate
constructs (Lawrence, et al., 2009).
Treatment of Major Depressive Disorder
There have been numerous interventions that have been recognized as being efficient in
treating youth suffering from MDD. Some of the more common interventions are comprised of
particular psychotherapies; for example, cognitive behavioural therapy and interpersonal therapy,
pharmacotherapy and a blend of both cognitive behavioural therapy and medication (National
Institute of Mental Health [NIMH], 2006). In 2006, professionals skilled in child and adolescent
depression gathered to examine the status of science related to the treatment of youth depression
and to consider approaches to continued research. They argued that it is essential that all patients
being treated for MDD are clinically monitored for further aggravation of depressive symptoms,

MULTIFACETED THERAPY 17
such as suicidal ideation or other behavioural traits associated with MDD. These experts also
indicated that substantial heterogeneity is evident among adolescents with MDD in respect to
clinical phenomenology, treatment response, and outcome (NIMH, 2006).
Cognitive Behavioural Therapy. Cognitive Behavioural Therapy (CBT) has been
demonstrated to be an effective treatment intervention for reducing symptoms of depression for
youth. Childre and Rozman, (2003) and Kassinove and Tafrate (2002) emphasize the
significance of the client-counsellor relationship as well as the use of open-ended Socratic
questioning to assist clients in reflection and reshaping negative and inaccurate thought
processes. Clients are challenged with homework assignments and psychoeducation. This allows
clients to engage in structured activities that test the validity of cognitions.
Jakobsen, Hansen, Storebo, Simonsen, and Gluud (2011) used meta-analyses and trial
sequential analyses of randomized trials to examine the efficacy of using CBT versus ‘no
intervention’ for MDD. They concluded that although further research was required, there was
evidence that CBT had resulted in considerable improvements in MDD symptoms. However, the
effects of CBT on suicidality, adverse events, and quality of life were vague (Jakobsen et al.,
2011). Evidence has revealed that some depressed youth do not respond to pharmacotherapy or
psychotherapy while others react quite favorably to minimal intervention. It is clear that
attempts to individualize treatment and identify specific treatment goals are needed.
Segal, Williams, and Teasdale (2002) sought to investigate the efficacy of incorporating
mindfulness-based training with cognitive behavioural therapy (MBCT). Kabat-Zinn (1994)
defined “Mindfulness” as intentional, non-judgmental and present-moment awareness. Ma and
Teasdale (2004) and Teasdale et al., (2000) highlighted evidence that MBCT helped to reduce
depressive relapses, where Beautrais, Joyce, Mulder, Fergusson, Deavoll, and Nightingale (1996)
MULTIFACETED THERAPY 18
have indicated that most suicidal behaviour transpires in those depressive relapses. Williams,
Duggan, Crane, and Fennell (2006) posit that many people tend to exhibit periods when they
disregard their habitual coping strategies. Crisis planning and ‘grounding’ meditations have been
implemented to ensure that individuals retain awareness of the tangible present. A recent
research study was conducted with 68 patients in remission or recovery from episodes of
depression, including suicidality. They were selected to participate in a MBCT group or a
waitlist control, with stratification by suicidal history (ideation or attempt) and past depressive
episodes. The outcomes revealed a significant decline of symptoms in the MBCT groups. Results
indicated improvement in mood and cognitive control, and a significant decline in intrusions and
rumination that could possibly result in a decline of motivation to suppress (Hepburn et al.,
2009).
Solution Focused Brief Therapy. Gaining more notoriety in recent years, solution
focused brief therapy (SFBT) stresses swift therapeutic modification and respect for the client’s
perspective, which is reinforced by modern healthcare beliefs. The therapeutic focus is goals
oriented and based on the clients’ expressed future aspirations. The treatment process involves
lines of questioning that engage the client by helping them to visualize their desired outcomes
and discover strengths, resources, and occasions when symptoms are not as evident (Rothwell,
2005). Bor, Gill, Miller, and Parrott (2004) posit that one component that is distinct to SFBT in
contrast to an open-ended intervention is the emphasis on an ending and that ending should be
made clear to the client and regularly articulated throughout the treatment process. They go on to
state that the treatment approach is “ethically driven yet commercially aware” (Bor et al., 2004;
p. 1). Also notable in SFBT is the idea of a contract of between six to ten sessions, with a
specified and realistic goal set at the outset (Lamont, 2012).
MULTIFACETED THERAPY 19
In 1996, De Jong and Hopwood sought to investigate the effectiveness of SFBT through
a case-series sampling of 275 clients observed at the Brief Family Centre in Milwaukee, USA.
The researchers found that 74% of the clients revealed subjective improvement on a 10 point
scale. In addition, at the nine-month follow-up, 77% reported that continued progress had been
evident as a result of therapy and after one year reported an 85% satisfaction rate from the
therapy (DeJong & Hopwood, 1996).
Highlighting an end to the treatment at the early onset of the treatment and throughout
has proven to be a key element in the success of SFBT. Clients who were told treatment would
last 10 sessions started to perform significantly by the eighth and ninth session; those who were
told it would last 5 sessions did so at approximately the fourth session (Battino, 2007). This
approach is based on the premise that, if you as the professional do not have an expectation that
you can help your client, then how can we anticipate that the client will have this expectation?
Battino (2007) posits that the effectiveness of treatment expectation is similar to the
effectiveness of the placebo pill.
Battino (2007) makes further reference to a book Change by Watzlawick, Weakland, and
Fish in 1974 that describes two types of change: First-order change refers to repeating the same
thing over and over within an existing system; and second-order change is external to (or meta)
or not confined to an existing system (irrational, paradoxical, unpredicted). He posits that
effective therapy is characterized as second-order and is processed through reframing. The
process of reframing assists clients to learn alternative perspectives (Battino, 2007).
Strengths-Based Cognitive Behavioural Therapy. The consideration of more
optimistic mental health variables during assessment will result in a brighter clinical picture of a
client’s position than if the practitioner were to focus only on problems and diagnosis. Padesky
MULTIFACETED THERAPY 20
and Mooney (2012) point out that strengths-based CBT does not seek to train clients in new
skills, thoughts, or emotional response, but rather places emphasis on assisting clients in
identifying strengths they already possess and to construct a model of treatment from these
rediscovered strengths. Padesky and Mooney (2012) suggest that individuals already harness
personal strengths that are connected to passionate interests, personal convictions, or patterns of
activities that may help them acquire their desired outcome. The challenge is that most people
are often oblivious to their own strengths and require the assistance from the therapist to extract
those strengths discovered in everyday experiences. Rashid and Ostermann ( 2009) emphasize
that performing a strength-based assessment includes the exploration of both the client’s
strengths and weaknesses which, when taken into account together, can result in effective
treatment strategies. Padesky (2012) adds that, instead of centering on problematic areas with the
client, therapists encourage an in-depth discovery of strengths that exhibit stable activity and are
not connected to problem areas. She further stresses the importance of ensuring a sustained
action is not connected to abnormalities, as CBT researchers have found that individuals are
prone to develop distorted beliefs and maladaptive behaviour patterns in problematic areas rather
than in areas where matters are positive in their life (Padesky & Mooney, 2012).
Physical Activity. Mata et al. (2012) stated that physical activity can be an
advantageous “mood regulator” in individuals with MDD. Reed and Ones (2006) indicate that
researchers have found that light exercise produces positive effect, especially if prior to exercise,
the positive affect was low. Mead et al. (2009) further emphasized that studies of both unselected
and clinical samples have shown that individuals who are prescribed a formal exercise regimen
have been able to drastically decrease levels of depressive symptoms. Mata et al. (2012) noted
that the outcome of exercise was equivalent to those who had engaged in cognitive therapy.
MULTIFACETED THERAPY 21
Bodin and Martinsen (2004) posited that physical activity has been connected to higher self-
efficacy and better self-esteem; Bahrke and Morgan (1978) state its effects as a deterrent of
negative thoughts; and Clark, Milberg, and Ross (1983) note that physical activity improved
retrieval of positive thoughts. From a physiological perspective, exercise has been successful in
stimulating growth of nerve cells and discharging proteins recognized to sustain nerve cells, such
as brain-derived neurotrophic factor (e.g., Cotman & Berchtold, 2002). Considering the effect
that engaging in a structured physical regimen has on depressed individuals, it is likely that it
would prove to be equally advantageous for persons with MDD.
Pharmacological Treatments. Certain pharmaceuticals have shown to be effective in
treating adolescents with both symptoms of depression and anxiety. However, the prescribing
and safety of these medications continue to be a matter of research and development (Williams
& Pearman, 2010). Silva et al. (2005) argue that though there has been a vast variety of
antidepressants available to patients, some results have shown only modest improvement and
remission rates and complaints regarding troubling side effects put limitations on treatment
effectiveness (Papakostas, Cassiello, & Lovieno, 2012). Serotonin reuptake inhibitors (SSRI) are
commonly used in treating depression and anxiety in youth and have been shown to have the
fewest of side effects (Karlsson, Hirvonen, Salminen, & Hietala, 2011). Keeton, Kolos, and
Walkup (2009) state that neither serotonin or epinephrine reuptake inhibitors have demonstrated
to be effective in treating youth with GAD, but further research is merited.
Combination Treatments. Vitello (2009) notes that although there is no concrete
support for the advantages of combining medication and cognitive behavioural therapy treatment
(COMB), two controlled outcome trials have indicated that COMB has been more advantageous
for treating adolescent MDD clients than monotherapy. Vitello’s study compared the
MULTIFACETED THERAPY 22
effectiveness of fluoxetine, CBT, COMB or clinical management with placebo for treating 439
adolescents with MDD. Results revealed that after 12 weeks of treatment, both SSRI and COMB
decreased depression more significantly than with CBT or placebo alone, but also clearly
revealed that COMB is efficient in inducing remission, accomplishing functional recovery, and
decreasing suicidal ideation. It was also noted that after 36 weeks, more suicidal events
transpired in the medication-only group when compared to the CBT only group (Vitello, 2009).
Treatment Consideration for Generalized Anxiety Disorder Traits. Major depressive
disorder (MDD) and generalized anxiety disorder (GAD) share diagnostic features and have
common coupling genetic diatheses. Notwithstanding resemblances, the DSM-IV-TR posits that
GAD’s status is upheld as an independent diagnosis. The diagnostic hierarchy rule dictates that
GAD should not be diagnosed if it is evident exclusively during MDD or a different mood
disorder (APA, 2000). However, given the apparent symptom overlap and similarity, treatments
regarded as efficient for MDD may be equally effective for treating GAD (Lawrence, et al.
2009).
Assessing Counselling Progress and Outcomes. The Beck Depression Inventory II
(BDI-II) (Beck, Steer, & Brown, 1996) is a 21-item self-report scale based upon a two-week time
frame. The items are rated from 0 to 3 on a 4-point likert scale, with higher scores suggestive of
an increased severe symptomology. The total of the scores highlights severity (0 to 13 signifying
minimal depression, 14 to 19 signifying mild depression, 20 to 28 signifying moderate
depression, and 29 to 63 signifying severe depression) (Beck et al., 1996). The assessment tool
monitors the progress of treatment for MDD by administering the self-report at pre- and post-
treatment periods (Ritschel, Cheavens, & Nelson, 2012).
MULTIFACETED THERAPY 23
The Patient Health Questionnaire Generalized Anxiety Disorder (GAD-7) is a 7 item self-
report scale utilized for assessing the severity of the symptoms of anxiety (Spitzer, Kroenke,
Williams, & Lowe, 2006). Like the BDI-II, this assessment tool can be administered to examine
the progression of treatment at both pre- and post-treatment periods. Spitzer et al. (2006) stress
that, although frequently used and strong in validity and reliability, the GAD-7 only suggests a
diagnosis that needs to be confirmed by other diagnostic techniques.
Peterson and Seligman (2004) explain the use of the Values in Action Inventory of
Strengths (VIA-IS) as an apparatus to recognize and rank-order clients on a measure of character
strengths. The VIA-IS is a 240 question survey that is reliable and has promising validity.
Case Formulation
Case Analysis
Blake was referred to me with a current diagnosis of ADHD, major depressive disorder
(MDD) and a noted history indicating features of generalized anxiety disorder (GAD). At the
time of my assessment of Blake, he stated that he had been struggling with his depression over
the past couple of years and made reference to what he described as an unrelenting sad mood. He
continued to state that he felt miserable, low, or “blue” for the majority of the day, lied awake in
bed all night struggling to sleep, did not feel like doing any of his regular activities, and was
often plagued with thoughts of suicide; he recalls having these symptoms every day for durations
of two weeks or longer. His family and friends were aware of a drastic change in Blake’s
behaviour and Blake had gone to his family doctor on a couple of occasions looking for solutions
to his problems. Blake’s symptoms collectively satisfied the criteria for MDD (APA, 2000). His
prolonged and intensifying episodes of sadness were clearly suggestive that his sad mood
MULTIFACETED THERAPY 24
intermingles with his past thought pattern which has the tendency to manipulate pre-existing
negative thoughts and feelings that perpetuate more relenting sadness (Clasen, et al., 2012).
Blake’s presentation and past history did yield evidence for some GAD features as well.
Most notable were his patterns of chronic worrying and his inability to control it, thinking he was
being regarded as a failure to his family, and not believing he had the fortitude within to have a
thriving future.
The dynamics of the case were also influenced by Blake’s poor self-esteem. Low self-
esteem is noted to be rather common in persons with MDD (Kessler & Walters, 1998) and
ramifications can escalate to greater interpersonal complications and high risk for suicide
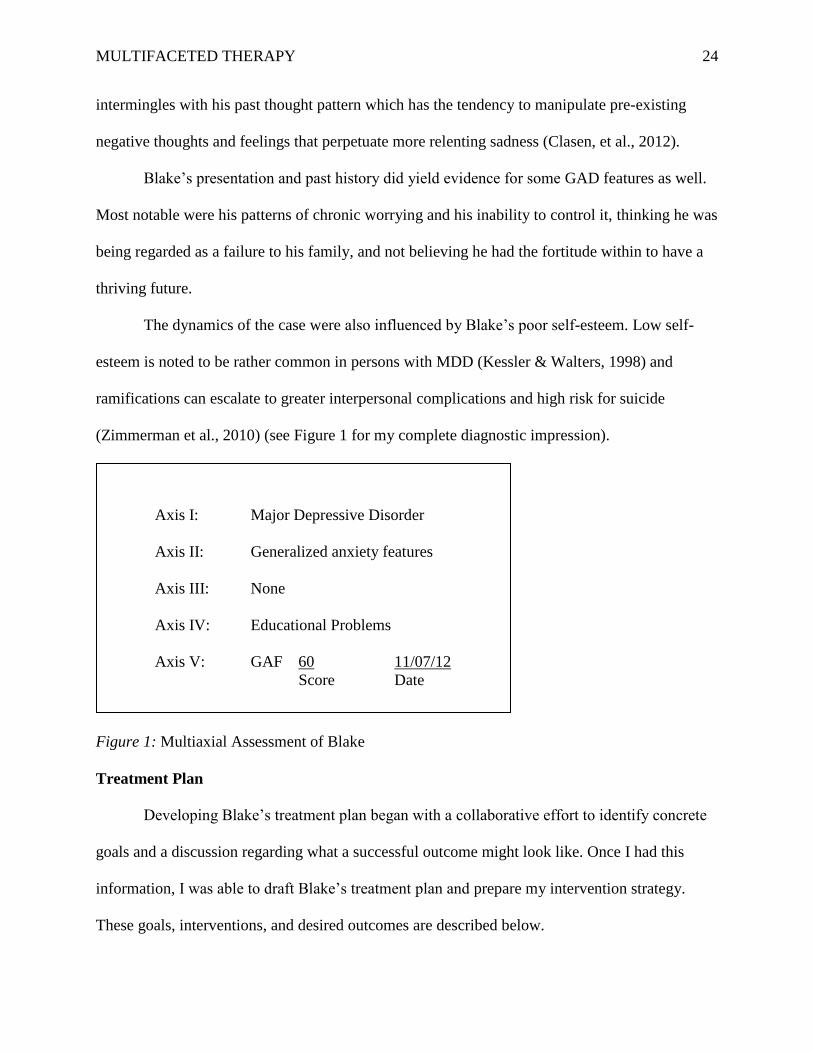
(Zimmerman et al., 2010) (see Figure 1 for my complete diagnostic impression).
Figure 1: Multiaxial Assessment of Blake
Treatment Plan
Developing Blake’s treatment plan began with a collaborative effort to identify concrete
goals and a discussion regarding what a successful outcome might look like. Once I had this
information, I was able to draft Blake’s treatment plan and prepare my intervention strategy.
These goals, interventions, and desired outcomes are described below.
Axis I: Major Depressive Disorder
Axis II: Generalized anxiety features
Axis III: None
Axis IV: Educational Problems
Axis V: GAF 60 11/07/12
Score Date
MULTIFACETED THERAPY 25
Goal #1: Reduce depressive symptoms. Blake found some reduction in his symptoms
of depression as a result of taking his mood stabilizer medication. Given that a vast majority of
his time was spent suffering these depressive symptoms of sadness, feeling miserable, low, or
“blue”, as well as disruptive sleep, offering a means to reduce and prevent future depressive
recurrences was a very significant goal. From the beginning of my assessment, Blake had
indicated that these feelings remained with him all day, every day, consistently for the past two
weeks, if not more.
My planned intervention to help Blake with depressive symptoms was to teach some
basic cognitive behavioural therapy (CBT) strategies such as monitoring thoughts, identifying
think traps, and challenging negative thoughts. Secondly, together we were to establish a regular
exercise routine that could increase endorphins in the brain. Bodin and Martinsen (2004) posit
that physical activity has been connected to higher self-efficacy and better self-esteem. Bahrke
and Morgan (1978) note its effects as a deterrent of negative thoughts.
My plan to measure the outcome of this intervention was to administer the BDI-II (Beck
et al., 1996) both pre- and post-treatment. Also, Blake would evaluate his depressive symptoms
post-treatment and agreed that, if the intervention were effective, he would feel depressed less
than every day.
Goal #2: Coping Behaviours. The formulation of a coping plan is an essential
component of CBT (Williams & Pearman, 2010). By examining Blake’s preferred activities and
safe behaviours, we constructed a list of helpful coping behaviours for Blake to practice. Blake
was taught some breathing and relaxation techniques using art and music. He described a
successful outcome as independent implementation of his coping behaviours.
MULTIFACETED THERAPY 26
Goal #3: Cognitive Restructuring. Changing the way Blake thought about situations
was a key part of his treatment plan. Blake admitted to obsessive negative thought patterns, of
not measuring up, and lack of optimism for a bright and prosperous future; as anxious
adolescents tend to overestimate negative outcomes (Rapee & Heimber, 1997). With the
introduction of solution-based brief therapy, I intended to utilize techniques of reframing as a
way of changing his perspectives. Blake was taught an interesting “as if” instruction to perform
every morning as a means of challenging these negative thoughts (Rothwell, 2005). This was a
way to help Blake discover his personal strengths and begin to explore ways in which he might
utilize them. Blake’s responses on the VIA-IS (Peterson & Seligman, 2004) would be used to
identify his character strengths. This would be accompanied by a collaborative discussion to
understand how he might use them in new behaviours and activities.
Blake described a successful outcome as one that would increase sense of confidence and
heighten his awareness of his personal strengths.
Treatment Summaries
Week 1
I started the session with a check-in to determine how Blake felt about his experience
with the BDI-II and the GAD-7 assessment questionnaires, and how he felt the assessment
process went overall. Blake expressed that he felt the intake and assessment session went very
well, and that it had confirmed for him that things just weren’t right and that the step taken to
seek counselling was a step in the right direction. I revisited the topic of confidentiality and
possible exceptions that include but are not limited to the following situations: child abuse, abuse
of the elderly or disabled, sexual exploitation, criminal prosecutions, and if the client has the
potential to be harmful to himself or to others. He was thankful and stated that he felt that he was
MULTIFACETED THERAPY 27
in a safe place. From there, Blake expressed a concern about not wanting to disappoint me, and
more importantly himself, because he had always struggled to follow through with things. He
talked openly about projects and previous commitments he had made to others and himself, all
which he failed to complete. He felt disappointed and didn’t want counselling to be another
failure. It was here that I encouraged him and introduced a contract of six sessions with a start
and end date clearly identified; outlining the specific and realistic goals we collaboratively
constructed during our assessment (Lamont, 2012). With the brief and clear timeline and an
enthusiastic approach, Blake’s concern was diminished and he seemed determined and
reciprocated enthusiasm.
I introduced mindfulness techniques to Blake during this session, starting off with a
simple breathing exercise. I instructed him to give consideration to the thoughts that come to
him, without judgment, and then to return to focus on his breathing. He enjoyed the exercise and
explained how it had relaxed him. Next, I administered the VIA-IS (Peterson & Seligman, 2004)
to identify strengths that Blake possessed. I explained that examining his strengths would be a
key to his success. He loved the test and looked forward to discussing the results in our next
session.
For his homework, I asked Blake to practice his breathing exercise and to take the time to
write down any project or objective he had, giving it a start and a finish date. He was also to try
and participate in three workouts at the local gym where he held membership.
Week 2
Blake was away on a family vacation for two weeks (which he forgot to inform me about
in our previous visit) and reported that things went okay while he was away. When posed the
question concerning the degree in which he would characterize his depression over the vacation
MULTIFACETED THERAPY 28
period, he indicated the score of 7 out of a possible 10. During extended periods of inactivity,
Blake found that depressive emotions would elevate. He also indicated that, during the vacation
period, he did have one thought of suicide, but quickly dismissed the thought. His sleeping also
continued to be disrupted. He informed me that he practiced mindfulness breathing during his
time away, at least once a day and often two to three times a day for periods of five to seven
minutes each. Many of his thoughts were about feelings of inadequacy, but he did not find it a
struggle to focus back on the breathing. He indicated that the exercise also helped him greatly.
We then had a discussion about the VIA-IS (Peterson & Seligman, 2004) results and
highlighted the fact that his top strengths were love and kindness. This led us into a discussion
about the important role of his family in his life. He went on to talk to me about the bond he had
with his father. “We are exactly alike”, he stated. We also had a brief discussion about the last
attempt he made to commit suicide with the guns in the home; he had opened up to me about this
event during our assessment session. He went on to explain that his love for his family is what
kept him from ever taking his own life. I told him again about my concern that there were so
many weapons in the home and that he had easy access to them. Not wanting to hurt his father or
cause him any undue alarm, we agreed together that we would ensure his mother knew of the
instance and that it would be her duty to properly secure the weapons (which were typically used
for hunting). It was a very emotional session and he was glad to have someone to unload the
weight of such an experience without judgement. For homework, I asked him to practice his
mindfulness breathing daily and also spend some “guy time” with his father, even if it were to
just watch television together. He said they actually had a Saturday fishing day planned, so we
agreed to count that as homework. I also wanted him to spend at least three sessions at the gym.

MULTIFACETED THERAPY 29
Blake seemed quite motivated during this session and agreed to complete his assigned
homework.
Week 3
I started this week with a check-in and, by Blake’s demeanour, he seemed to have
improved quite a bit. He indicated that just by implementing some of the techniques we
discussed in our last session, he was already feeling better about the future and about going back
to school in the fall. He talked about his fishing trip with his dad; what he thought was just going
to be a day trip ended up being a weekend camping expedition. Blake expressed that things went
considerably better than the previous trip. He spent much time canoeing and engaging in other
outdoor activities. He said he had no real depressive episodes and no thoughts of suicide at all.
Overall, he stated that it was a very enjoyable weekend. His sleep patterns were on and off
during the week, but he found that while away in the open air, he slept better. This progress
motivated Blake to book an appointment with his family doctor to discuss discontinuing his
mood stabilizing medication.
In the area of solution-based brief therapy, I introduced a new activity that involved him
imagining that he was granted a miracle, posing the question as described by Battino (2007):
“That as you were sleeping a miracle transpires, and as a result of that miracle, you’ve come to
talk with me today because your problem with depression had been solved. This is a miracle.
You woke up and it indeed came true! What will have changed in your life? What will be
different? How will you know that the miracle has occurred?” (Battino, 2007, p. 22). For the
next 30 to 45 minutes, we engaged in a dialogue, going through every detail about how the
miracle had transformed his life. Blake seemed to gain a significant amount of positive energy
from doing this exercise.
MULTIFACETED THERAPY 30
I also inquired about the amount physical exercise and activity he had engaged in during
the past week. He attempted to stay busy with the family, but noticed that during moments of
inactivity, his negative thoughts would return. He said that he was really fighting hard not to
remain in bed. I told him that I was proud of him for doing this. I emphasized the need to
establish regular activities, such as physical exercise and/or sporting activity, because when he
was idle time seemed to work against him, triggering his negative emotions and depression. For
homework, Blake would continue to practice his mindfulness breathing and try another miracle
exercise. For the following week, when he awoke he was to ask himself, “What would I do
differently today if I was living the first day of the miracle, and am now totally recovered from
this problem”? Of all the things he thought of, he was to choose the easiest concrete thing and
implement it into his daily routine; and every day after, he was to ask himself the same question
and repeat the exercise.
Week 4
I started this session with a check-in, and immediately Blake indicated that he has been
feeling pretty low for the last week and did not know the source of his feelings. He also stated
that the emotions that he was feeling were somewhat different from his usual feelings of
depression. It was not something he recognized as helplessness, but more like boredom. He
found that the last week was uneventful. I replied, “Good news about your keen observation and
that it didn't trigger depression”. He just knew things were different. I encouraged him for
keeping it together, despite the fact that he was going through a low period. Through reflection,
we did identify that he had been staying up quite late a few times over the past couple of weeks
and could be experiencing some fatigue. I introduced some psychoeducation about the
importance of sleep and strategies for getting enough sleep.

MULTIFACETED THERAPY 31
Blake also followed up with me with regard to the discontinuation of his medications. He
and his doctor agreed to the discontinuation of the mood stabilizers as long as he felt the
counselling was making progress. I checked in on his homework assignment, and he stated that
the breathing exercises are becoming a useful coping mechanism and a part of his daily routine.
He was cooperative in doing the “miracle question” exercise. In response to the miracle question
exercise Blake indicated that the activities ranged from hanging out with his buddies to throwing
around the rugby ball with his father, to going on a hike, to working out at the gym, to mixing
beats with his DJ music interface on his computer. He said, “Two weeks have passed since our
last session, during that first week things went well but during the second week, I don’t know
what happened”. I thanked him for all the effort he was making to which he responded that he
was feeling quite optimistic about life.
Collaboratively, we worked on preparing Blake for his return to school the following day.
Going into grade 11 and anticipating the adjustment in course load and degree of difficulty, we
role played hypothetical solutions to employ if he was feeling overwhelmed by certain subjects,
like math which was typically a challenge for him. I chose this approach because if Blake did not
maintain a keen interest in taking charge of his own life, the pressures of the unknown would be
a trigger for his depression. Blake loved the idea of learning the discipline of setting goals and
objectives. In the following week’s session we would evaluate Blake’s first week of school.
Blake indicated an interest in completing The Harrington-O’Shea Career Decision-Making
System Revised (CDM-R) (O'Shea & Feller, 2008). The CDM-R system is a self-scored
assessment that helps students and other career planners identify their occupational interests,
values, and abilities - and match these dimensions to career options. In consideration of both
methods of solution-based brief therapy and strengths-based therapy, I felt this tool would be
MULTIFACETED THERAPY 32
informative and also demonstrate to Blake how the strengths and interests that he already has can
be utilized in numerous areas of vocations and opportunity. For homework, Blake was going to
continue to practice his breathing exercises and work out at the gym three times this week. He
was also eager to do more of the “miracle question” exercise and implement something simple
and concrete into his routine. On the way out, Blake expressed that things in his life have
improved drastically.
Week 5
Blake was excited to see me this session and quickly explained that, in the past week,
starting school had not been as overwhelming as in previous years. He attributed this to the time
we spent in role playing scenarios about classes. He was also sleeping better, although he was
getting to bed late at night. He stated that he believes he has gotten past his feelings of sadness
and has not had any thoughts of suicide for a while (O'Shea & Feller, 2008). Every day, Blake
finds he has been waking up in the morning with a new sense of optimism, knowing that he has
the inner strengths and the support at home to face each day. I took a moment to review some of
the skills we had discussed, particularly those related to goal setting. I emphasised that setting
goals could be a helpful problem-solving strategy and could also assist in the avoidance of
feeling overwhelmed by many tasks, such as school responsibilities.
Together we went over the results of the CDM-R (O'Shea & Feller, 2008), which identified
his career code as ‘Scientific-The Arts’ and his career clusters were ‘math-science, medical-
dental, literary-art’. As we went through his interpretive folder, he was encouraged to see that a
vocational option under life sciences was ‘environmental engineer/environmental
biologist/forester’; all avenues that he always wanted to pursue. He was excited about charting a
course towards his career choices.
MULTIFACETED THERAPY 33
This was our second-to-last session, so I checked in with Blake to see how he was feeling
in regard to our time coming to an end. He expressed sincere gratitude for the opportunity to
undergo one-on-one counselling and appeared optimistic about his future. I encouraged him to
think about questions for our last session and informed him that our last session would not be as
structured and would center primarily on review of what we had talked about in prior sessions. I
also informed him that I would be putting together a resource “gift pack” for his departure.
Week 6
This was my final session with Blake. I administered a check-in to see how he was feeling
about the end of our treatment time together. He indicated that he was a little nervous and that he
would miss our sessions together. He also confirmed that he has remained off of the mood
stabilizing medication and stated that he would continue to do so. He once again told me how
much he appreciated the work we had done together. He indicated that things have continued to
improve both at home and at school. He stated that his thoughts were healthy and expressed no
feelings of sadness; he even played some rugby this past week. Blake has recognized that he is
getting much more sleep than previously. Thoughts of suicide have now become a distant
memory and he looked towards the future with great optimism. Blake went on to tell me that he
met a girl and that there was mutual interest to start dating. I told him I was very excited for him.
I had Blake complete the BDI-II (Beck et al., 1996) during this session and the results
revealed the score had dropped from 22 (moderate depression) to 11 (minimal depression). At
this time, we began to talk about his depressive symptoms in comparison to how he was feeling
now, and we both agreed that the desired outcome identified in his treatment plan was achieved.
Blake indicated that he was feeling sadness less than every day, which was his established
benchmark measuring the success of this intervention.
MULTIFACETED THERAPY 34
In terms of coping behaviours, Blake felt that he has all the tools readily available if and
when symptoms of his depression or anxiety were to come back. Success, as we defined it in the
treatment plan, would have Blake better able to rely on his strengths; through his strengths, he
was able to recognize his family’s love and acceptance towards him and also to see them as a
vital source of support.
Blake was aware of his need to stay active as a means of staying healthy physically,
mentally, and emotionally. Engaging in activities, having a regular exercise regimen, and
acquiring the discipline to set clear goals and objectives with an expected timeline have helped
Blake in tolerance of distress. Although he did confirm he was less easily overwhelmed, he also
acknowledged that it was a work in progress.
Blake felt he had come a long way in his cognitive restructuring. Through mindfulness
breathing and combating negative thoughts by recognizing his strengths and implementing them
into daily routine, he has found a new optimistic approach to living. This, as defined by the
treatment plan, was a success for Blake in that it increased his sense of confidence, as well as
heightened awareness of his personal strengths.
Results
As I reflect on my intervention with Blake, I arrived at the conclusion that it was a great
success. Together we worked on defining treatment goals and carefully considered what a
successful outcome would look like as it related to Blake’s functioning. It was apparent that
Blake had improved in all domains documented in the treatment plan, and it was also understood
that there was room for improvement in terms of his ability to tolerate distress. Through teaching
some basic CBT strategies, Blake was able to monitor his negative thoughts, identify his think
traps, challenge these unhelpful thoughts, and establish a regular exercise regimen. The client
MULTIFACETED THERAPY 35
saw a drastic improvement in his depressive symptoms. Blake found that he was able to identify
and incorporate coping behaviours such as various breathing and relaxation techniques. Blake
also found that he was thinking with greater optimism and confidence as he became more aware
of his personal strengths and had a greater understanding of how they would prove to be
advantageous as he looked towards future career goals and opportunities. Blake also stated he
was feeling depressed less than every day. Blake’s scores on the BDI-II (Beck et al., 1996) pre-
and post-intervention revealed further proof that my intervention with Blake was a success. His
score dropped from a 22, signifying moderate depression, to an 11, suggestive of minimal
depressive symptoms.
Discussion
I believe I was effective in my intervention with Blake, and I appreciate the time I took
prior to regular sessions to carefully devise a treatment plan with my client’s inputs as this
assisted me in maintaining objectivity and effectiveness. I wanted to be authentic in following
my treatment plan, but also felt it was necessary to maintain flexibility and acceptance of where
my client was at during the process. Remaining in this frame of mind, I allowed myself to be
adaptable and willing to change direction if any unexpected circumstances arose. It was
imperative for me to understand that though I can have goals and plans for sessions, the clients
come in with their own ideas and goals. Accepting clients where they are and not where I want
them to be is extremely important in counselling. I also came to understand how important the
celebration of success is for adolescent clients. This encouragement has power in building
rapport and focusing on what the client has accomplished and not just on what needs to be done.
It would be beneficial to re-evaluate Blake’s functioning in approximately two to three
months. My apprehension is that, while he learned and implemented new skills quickly, our short

MULTIFACETED THERAPY 36
time together may not have been sufficient to promote life-long change. During that time, we
would determine whether or not he was continuing his mindfulness practices, thought-
challenging exercises, maintaining his discipline in goal setting, and preserving his heightened
self-esteem. It is imperative to have the assurance that techniques implemented are being
maintained.
Finally, I believe that offering the use of solution-based brief, strengths-based CBT
therapy, and the focus on exercise would be an effective approach for the treatment of major
depressive disorder with generalized anxiety features in youth. I found that it was essential to
send clients home with homework to practice and implement strategies and also provide a
starting point at the commencement of each session. I also found it invaluable to provide the
client with resources prior to the termination of our last session that supported the work in our
sessions in order to increase the likelihood that therapeutic gains would be maintained. It is
apparent to me that multi-faceted therapy can provide clients with an abundance of coping
strategies in a limited amount of time.
MULTIFACETED THERAPY 37
References
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders
(3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders
(3rd ed., rev.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manal of mental disorders
(4th ed., text rev.). Washington, DC: Author.
Bahrke, M. S., & Morgan, W. P. (1978). Anxiety reduction following excercise and meditation.
Cognitive Therapy and Research, 2, 323-333.
Battino, R. (2007). Expectation: Principles and practice of very brief therapy. Contemporary
Hypnosis, 24(1), 19-29.
Beautrais, A., Joyce, P., Mulder, R., Fergusson, D., Deavoll, B., & Nightingale, S. (1996).
Prevalence and comorbidity of mental disorders in persons making serious suicide
attempts: A case control study. American Journal of Psychiatry, 153, 1009-1014.
Beck, A. T. (1988). Depression: Clinical, experimental, and theoretical. New York, NY: Harper
& Row.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clinical
anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology, 56,
893-897.
Beck, A. T., & Steer, R. A. (1993). Beck Anxiety Inventory Manual. San Antonio, TX:
Psychological Corporation.

MULTIFACETED THERAPY 38
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II.
San Antonio, TX: Psychological Corporation.
Beck, A. T., Steer, R. A., & Carbin, M. G. (1988). Psychometric properties of the Beck
Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8,
77-100.
Bodin, T., & Martinsen, E. W. (2004). Mood and self-efficacy during acute excercise in clinical
depression: A randomized, controlled study. Journal of Sport and Exercise Psychology,
26, 623-633.
Bor, R., Gill, S., Miller, R., & Parrott, C. (2004). Doing therapy briefly. London, England:
Palgrave.
Cheavens, J. S., & Heiy, J. (2011). The differential roles of affect and avoidance in major
depressive and borderline personality disorder symptoms. Journal of Social and Clinical
Psychology, 30(5), 441-457.
Childre, D., & Rozman, D. (2003). Transforming Anger: The heartmath solution for letting go of
rage, frustration, and irritation. Oakland, CA: New Harbinger.
Clark, M. S., Milberg, S., & Ross, J. (1983). Arousal cues arousal-related material in memory:
Implications for understanding effects of mood on memory. Journal of Verbal Learning
and Verbal Behavior, 22, 633-649.
Clasen, P. C., Wells, T. T., Ellis, A. J., & Beevers, C. G. (2012, August 6). Attentional biases
and the persistence of sad mood in major depressive disorder. Journal of Abnormal
Psychology. Advance online publication.
MULTIFACETED THERAPY 39
Cotman, C. W., & Berchtold, N. C. (2002). Excercise: A behavioral intervention to enhance
brain health and plasticity. Trends in Neuroscience, 25, 295-301.
DeGraaf, R., Bijl, R. V., Smit, F., & Vollebergh, W. A. (2002). Predictors of first incidence of
DSM-III-R psychiatric disorders in the general population: Findings from the
Netherlands mental health survey and incidence study. Acta Psychiatrica Scandinavica,
106, 303-313.
DeJong, P., & Hopwood, L. E. (1996). Outcome research on treatment conducted at the brief
family therapy center. In S. D. Miller, M. A. Hubble, & B. L. Duncan, Handbook of
solution-focused brief therapy (pp. 272-298). San Francisco, CA: Jossey-Bass.
Eaton, W. W., Shao, H., Nestadt, G., Lee, B. H., Bienvenu, J., & Zandi, P. (2008). Population-
based study of first onset and chronicity in major depressive disorder. Archives of
General Psychiatry, 65, 513-520.
Fava, M., Sampson, N., Walters, E. E., Kessler, R. C., & Hwang, I. (2010). The importance of
irritability as a symptom of major depressive disorder: Results from the national
comorbidity survey replication. Molecular Psychiatry, 15, 856-867.
Glenn, C. R., Kosty, D. B., Seeley, J. R., Rohde, P., Lewinsohn, P. M., & Klein, D. N. (2012).
Predictors of first lifetime onset of major depressive disorder in young adulthood.
Journal of Abnormal Psychology. Advance online publication.
Gotlib, I. H., & Joorman, J. (2010). Cognition and depression: Current status and future
directions. Annual Review of Clinical Psychology, 6, 285-312.
MULTIFACETED THERAPY 40
Grant, B. F., Goldstein, R. B., Chou, S. P., Huang, B., Stinson, F. S., Dawson, D. A., &
Compton, W. M. (2009). Sociodemographic and psychopathologic predictors of first
incidence of DSM-IV substance use, mood and anxiety disorders: Results from the wave
2 national epidemiologic survey on alcohol and related conditions. Molecular Psychiatry,
14, 1051-1066.
Hepburn, S. R., Crane, C., Barnhofer, T., Duggan, D. S., Fennekk, M. J., & Williams, J. M.
(2009). Mindfulness-based cognitive therapy may reduce thought supression in
previously suicidal participants: Findings from a preliminary study. British Journal of
Clinical Psychology, 48, 209-215.
Horwath, E., Johnson, J., Klerman, G. L., & Weissman, M. M. (1992). Depressive symptoms as
relative and attributable risk factors for first onset major depression. Archives of General
Psychiatry, 49, 817-823.
Ingram, R. E. (1984). Toward an information-processing analysis of depression. Cognitive
Therapy and Research, 8, 443-477.
Jaffee, S. R., Moffitt, T. E., Caspi, A., Fombonne, E., Poulton, R., & Martin J. (2002).
Differences in early childhood risk factors for juvenile-onset and adult-onset depression.
Archives of General Psychiatry, 58, 215-222.
Jakobsen, J. C., Hansen, J. L., Storebo, O. J., Simonsen, E., & Gluud, C. (2011). The effects of
cognitive therapy versus "No intervention" for major depressive disorder. PLOS ONE,
6(12), 1-11.
MULTIFACETED THERAPY 41
Kabat-Zinn, J. (1994). Wherever you go, there are you: Mindfulness meditation in everyday life.
New York, NY: Hyperion.
Karlsson, H., Hirvonen, J., Salminen, J., & Hietala, J. (2011). No association between serotonin
5-HT1a receptors and spirituality among patients with major depressive disorders or
healthy volunteers. Molecular Psychiatry, 16, 282-285.
Kassinove, H., & Tafrate, R. C. (2002). Anger management: The complete treatment guidebook
for practitioners. Atascadero, CA: Impact.
Keeton, C. P., Kolos, A. C., & Walkup, J. T. (2009). Pediatric generalized anxiety disorder:
Epidemiology, diagnosis, and management. Pediatric Drugs, 171-183. Retrieved from
http\;//search.ebscohost.com/login.aspx?direct=true&AuthType=url,cookie,ip,uid&db=a9
h&AN=44109990&site=ehost-live
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005).
Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National
Comorbidity Survey Replication. Archives of General Psychiatry, 62, 617-627.
Lamont, N. (2012). The end in sight. Engaging with an existential understanding of time when
working in time-limited practice. Journal of Existential Analysis, 23(1), 89-101.
Lawrence, A. E., Liverant, G. I., Rosellini, A. J., & Brown, T. A. (2009). Gerneralized anxiety
disorder within the course of major depressive disorder: Examining the utility of the
DSM-IV hierarchy rule. Depression and Anxiety, 26, 909-916.
MULTIFACETED THERAPY 42
Ma, H., & Teasdale, J. (2004). Mindfulness-based cognitive therapy for depression: Replication
and exploration of differential relapse prevention effects. Journal of Consulting and
Clinical Psychology, 72, 31.40.
Mata, J., Thompson, R. J., Jaeggi, S. M., Bruschkuehl, M., Jonides, J., & Gotlib, I. H. (2012).
Walk on the bright side: Physical activity and affect in major depressive disorder. Journal
of Abnormal Psychology, 121(2), 297-308.
Mead, G. E., Morley, W., Campbell, P., Greig, C. A., McMurdo, M., Lawlor, D. A., & Dwan, K.
(2009). Exercise for depression. Cochrane Database of Systematic Reviews (7).
National Institute of Mental Health. (2006, February 6-7). Benefits, limitations, and emerging
research needs in treating youth with depression. Retrieved October 28, 2012, from
NIMH: http://www.nimh.nih.gov/research-funding/scientific-meetings/2006/benefits-
limitations-and-emerging-research-intreating-youth-with-
depression/index.shtml[9/6/2011 10:58:19 AM]
O'Shea, A. J., & Feller, R. (2008). The Harrington-O'Shea Career Decision-Making System
Revised, Canadian Edition. Toronto, Ontario, Canada: Pearson.
Padesky, C. A., & Mooney, K. A. (2012). Strengths-based cognitive behavioural therapy: A
four-step model to build resilience. Clinical Psychology & Psychotherapy, 19, 283-290.
Papakostas, G. I., Alpert, J. E., & Fava, M. (2003). S-adenosyl-methionine in depression: A
comprehensive review of the literature. Current Psychiatry Reports, 5(6), 460-466.
MULTIFACETED THERAPY 43
Perlis, R. H., Fava, M., Trivedi, M. H., Alpert, J., Luther, J. F., Wisniewski, S. R., & Rush, A. J.
(2009). Irritability is associated with anxiety and greater severity, but not bipolar
spectrum features, in major depressive disorder. Acta Psychiatrica Scandinavica, 119,
282-289.
Peterson, C., & Seligman, M. E. P. (2004). Character strengths and virtues. New York, NY:
Oxford University Press.
Rapee, R. M., & Heimber, R. G. (1997). A cognitive-behavioral model of anxiety in social
phobia. Behavior Research Therapy, 35, 741-756.
Rashid, T., & Ostermann, R. F. (2009). Strength-based assessment in clinical practice. Journal of
Clinical Psychology, 65, 488-498.
Reed, J., & Ones, D. S. (2006). The effect of acute aerobic excercise on positive activated affect:
A meta-analysis. Psychology of Sport and Exercise, 7, 477-514.
Ritschel, L. A., Cheavens, J. S., & Nelson, J. (2012). Dialectical behavior therapy in an intensive
outpatient program with a mixed-diagnostic sample. Journal of Clinical Psychology,
68(3), 221-235.
Sateia, M. J., & Nowell, P. D. (2004). Insomnia. Lancet, 364, 1959-1973.
Silva, R. R., Alpert, M., Pouget, E., Silva, V., Trosper, S., Reyes, K., & Dummit, S. (2005,
Winter). A rating scale for disruptive behavior disorders, based on the DSM-IV item
pool. Psychiatry Quarterly, 76(4), 327-339.
MULTIFACETED THERAPY 44
Smit, F., Beekman, A., Cuijpers, P., DeGraaf, R., & Vollebergh, W. (2004). Selecting variables
for depression prevention: Results from a population-based prospective longtitudinal
study. Journal of Affective Disorders, 81, 241-249.
Smith, G. T., & John, R. W. (2008). Personality and psychopathology (3rd ed.). New York, NY:
Guilford Press.
Spitzer, R. L., Kroenke, K., Williams, J. B., & Lowe, B. (2006). A brief measure for assessing
generalized anxiety disorder: The Generalized Anxiety Disorder-7. Archives of Internal
Medicine, 166(10), 1092-1097.
Teasdale, J. D. (1988). Cognitive vulnerability to persistent depression. Cognition & Emotion, 2,
247-274.
Teasdale, J., Segal, Z., Williams, J. M., Ridgeway, V., Soulsby, J., & Lau, M. (2000). Prevention
of relapse/recurrence in major depression by mindfulness-based cognitive therapy.
Journal of Consulting and Clinical Psychology, 68, 615-623.
Vitello, B. (2009). Combined cognitive-behavioural therapy and pharmacotherapy for adolescent
depression. CNS Drugs, 23(4), 271-280.
Widiger, T. A., & Smith, G. T. (2008). Personality and psychopathology. In O. P. John, R. W.
Robins, & L. A. Pervin (Eds.), Handbook of personality: Theory and research (3rd ed.,
pp. 743-769) New York, NY: Guilford Press.
Williams, J. M., Duggan, D., Crane, C., & Fennell, M. (2006). Mindfulness-based ccognitive
therapy for prevention of recurrence of suicidal behaviour. Journal of Clinical
Psychology, 62, 201-210.
MULTIFACETED THERAPY 45
Williams, L., & Pearman, C. (2010). Childhood anxiety disorders: Recognition and diagnosis in
the primary care setting. Clinician Reviews, 20(1), 8-12.
Zimmerman, M., Galione, J. N., Chelminski, I., Young, D., Dalrymple, K., & Witt, C. F. (2010).
Validity of a simpler definition of major depressive disorder. Depression and Anxiety, 27,
977-981.

















![In conjunction with Venus [planetary radar astronomy]](https://static.fdokumen.com/doc/165x107/631a4f09bb40f9952b01f2bc/in-conjunction-with-venus-planetary-radar-astronomy.jpg)

