
300106912ramya.pdf - EPrints@Tamil Nadu Dr MGR Medical ...
58
A STUDY TO EVALUATE THE EFFECTIVENESS OF VIDEO ASSISTED PROGRAMME ON KNOWLEDGE AND ATTITUDE REGARDING PREVENTION OF RESPIRATORY PROBLEMS AMONG COTTON MILL WORKERS IN SELECTED COTTON MILLS, MADURAI- 2011. A DISSERTATION SUBMITTED TO THE TAMILNADU DR. M.G.R.MEDICAL UNIVERSITY, CHENNAI. IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE IN NURSING APRIL - 2012
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of 300106912ramya.pdf - EPrints@Tamil Nadu Dr MGR Medical ...

A STUDY TO EVALUATE THE EFFECTIVENESS OF VIDEO
ASSISTED PROGRAMME ON KNOWLEDGE AND ATTITUDE
REGARDING PREVENTION OF RESPIRATORY PROBLEMS AMONG
COTTON MILL WORKERS IN SELECTED COTTON MILLS,
MADURAI- 2011.
A DISSERTATION SUBMITTED TO
THE TAMILNADU DR. M.G.R.MEDICAL UNIVERSITY, CHENNAI.
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS
FOR THE DEGREE OF
MASTER OF SCIENCE IN NURSING
APRIL - 2012

ACKNOWLEDGEMENT
“I can do all things through christ who strenghtens me”
Philipians 4:13
I praise and thank God almighty for his blessing and abundant grace that
enriched me throughout the study.
It is my pleasure to express my heartfelt gratitude and sincere thanks to
Dr.Mrs.C. Jothi Sophia M.Sc., (N), Ph.D., Principal , CSI Jeyaraj Annapackiam
College of Nursing, for her expert guidance, encouragement and motivation and
valuable suggestion not only in the study but also throughout the academic career
which helped to lay down a strong foundation for this study.
I would like to express my sincere gratitude to Prof.Mrs. Merlin Jeyapal,
M.Sc (N), Ph.D, Vice Principal, for constant support to this study.
I wish to express my deepest sense of gratitude to my esteemed guide Prof.
Mrs. G. Jaya Thanga Selvi, M.Sc(N), Ph.D, Head of the Department, Medical
Surgical Nursing, C.S.I. Jeyaraj Annapackiam College of Nursing, for her guidance,
support, encouragement and patience corrections, keen interest in the conception,
planning, and execution of the present study which has continuously motivated me for
the successful completion of this dissertation.
I extend my sincere thanks to Panel of experts for their valuable suggestions
to conduct this study.
I express my sincere thanks to Mrs. Anbu Roselin, M.Sc (N) RN.RM,
Mrs.Jeya Jothi M.Sc (N) RN.RM, and MS.Sobia Gnana Mary M.Sc (N) RN.RM,
Lecturers of CSI Jeyaraj Annapackiam college of Nursing for their individual
guidance and valuable suggestions to conduct this study.
I extend my sincere thanks to the Panel of judges in the dissertation
committee for their valuable suggestion throughout this study.
I extend my special thanks to the Managing directors who have permitted
this study to conduct in their esteemed companies and made it successful one.

I would like to express my grateful thanks to Mr. Mani, M.Sc., M.Phil,
Statistician for this excellent advice and support in analyzing and interpreting the
data.
I am also grateful to Mrs. Angelin Mannova, Librarian, CSI Jeyaraj
Annapackiam College of Nursing, for the help in availing the library facility.
I extend my sincere thanks to my classmates “THE GLITTERING
GLADIOLUS”, for their co-operation, prayers and help throughout this study.
I extend my sincere thanks to my beloved family members for their prayers,
support and encouragement throughout this Master programme.

ABSTRACT
Introduction
Respiratory problems associated with exposure to cotton dust have been
studied by many researchers and studies have proved the long term consequences for
disability and mortality of former cotton textile workers.
Statement of the problem
“A study to evaluate the effectiveness of Video Assisted Programme on
knowledge and attitude regarding prevention of respiratory problems among cotton
mill workers in selected Cotton Mills, Madurai.”
Objectives
1. To assess the existing level of knowledge and attitude on prevention of
respiratory problems among selected cotton mill workers, Madurai.
2. To assess the post test level of knowledge, attitude and practice on
prevention of respiratory problems among selected cotton mill workers,
Madurai.
3. To find out the difference between pretest and post –test level of knowledge
and attitude on prevention of respiratory problems among selected cotton
mill workers, Madurai.
4. To find out the association between post tests level of knowledge and
attitude on prevention of respiratory problems among selected cotton mill
workers with the selected demographic variables.
Review of literature
A Review of literature of the study was prepared relevant to the study related
to respiratory problems of cotton mill workers, knowledge and attitude respiratory
problems of cotton mill workers.

Conceptual Framework
The conceptual framework was based on Nola J. Pender, Health promotion
model. Areas of focus were Individual characteristics and experiences, Behavior-
specific cognitions and affect and Behavioral outcomes.
Methodology
Research design
In this chapter the investigator discusses the chosen research approach and the
rationale. An experimental approach was used to assess the Effectiveness of video
assisted programme. Pre experimental design was adopted with one group pre test and
post test design.
Setting of the study
The setting of the study is selected cotton mills, Madurai.
Sample size
The sample size for the study is 60 .Samples for this study were selected
through non probability - purposive sampling.
Results
Results shows that majority of workers had adequate knowledge (66%) and
favourable attitude (75%) on respiratory problems. The obtained paired‘t’ value for
pre and posttest regarding knowledge and attitude regarding prevention of respiratory
problems among cotton mill workers were 7.353 and 11.409, which was highly
significant.
Conclusion
The investigator hopes that the video teaching program could increase the
knowledge and attitude among cotton mill workers.

1
CHAPTER-I
INTRODUCTION
“Safety is like a lock - But you are the key.
Be alert, be aware, and be alive.
Know safety - No problem, No safety - Know problem.”
An "environment" is the whole of surrounding things. Surroundings are
defined by a central entity. Generally, environment refers to the biological, physical
and social things on the earth or in inhabitable space outside the earth's atmosphere.
Every human being spends their 1/3rd of the time daily in his working area. And while
thinking about the working area, how healthy it is? Is it safety to the employees?
Actually the healthy and safety environment is the right of the workers. Higher the
healthy environment maintained higher the productivity.
Occupational diseases reflect health hazards brought on by exposure within
the work environment. Due to lack of education, unaware of hazards of their
occupations, general backwardness in the sanitation, poor nutrition and climatic
proneness of this geographic region to epidemics aggravate their health hazards from
work environment (Wang et al., 2003).
In 1956, an epidemiological study in the cotton industry in the UK
documented the occurrence of respiratory problems like byssinosis (Schilling, 1956)
Worldwide, India is the second largest producer of textile goods, which account for
20% of the national industrial output. Twenty million workers are employed in 1175
cotton mills across the country, representing a major occupational group (Datt and
Sundaram, 1998).
Exposure to cotton dust has long been associated with adverse respiratory
effects and diminished lung function, which is most evident as byssinosis, a chest
tightness experienced by workers on the first day back after a weekend or vacation
break (Schilling, 1956; Roach and Schilling, 1960 and Berry et al., 1973). Most

2
studies indicate that adverse respiratory effects are more closely associated with
cotton fiber dust (Castellan et al., 1984, 1987; Kennedy et al., 1987).
The reported rates vary from 3% in the UK versus 30–50% in countries like
Indonesia, Sudanand India [3–9]. In our country, the prevalence of byssinosis in the
cotton industry has been found to be as high as 46.0% in the studies done since
1966.Respiratory problems have been reported from most countries with a textile
industry. A high prevalence (63% in men and 48% in women) in cardroom workers of
Lancashire cotton mills processing coarse cotton.
Among cardroom workers, El Batawi reported a prevalence of 27% in Egypt
and Belin et al a prevalence of25-60% in Sweden.23 Prevalences of 21% and 88%
were reported by Valic and Zuskin for Yugoslavia,45 11% by Tuypens for Belgium,6
and 11%, 26%, and 38 4% by Bouhuys et al7 and Merchant et al8 for the United
States. In a recent report from the United Kingdom, only 23 new cases of byssinosis
were reported in 2101 cases of occupational respiratory diseases in 1989. In the
United States strict hygiene standards were enforced in 1978, and these have also
reduced the incidence of this disease.
In developing countries, however, byssinosis is still found in a high
percentage of textile workers, as the following summary indicates: India Three recent
studies in different places suggest a high prevalence of byssinosis. The first study was
carried out at Ahmedabad by Parikh et all' in three textile mills processing a medium
variety of cotton where 929 workers from the spinning department were examined.
The results showed a mean prevalence of 30% in blowrooms and 38% in cardrooms.
The cotton dust concentrations (dust after removal of fly) measured by cone samplers
were 6-8 times higher than the permissible concentrations recommended by the
British Occupational Hygiene Society.
This higher prevalence of byssinosis compared with earlier Indian studies
showed that if correct methods are not used in epidemiological surveys, the
investigators are likely to report a low prevalence of the disease. The second study
carried out by Gupta and Gupta in Delhi in a mill processing a coarse variety of cotton
found the following prevalences: blowroom 37%, cardroom 47%, spinning 17%,

3
weaving 22%, and finishing 7%. The study used only questionnaires to detect cases
and neither pulmonary function tests nor dust measurements were included.
The third study was carried out in Kishangarh, Rajasthan, in a mill processing
coarse and synthetic yarn. Among 616 workers examined the prevalence of byssinosis
found was blow room 28%, card room 30%, draw frame 26%, ring frame 20%, and
winding 25%. The higher prevalence rates reported in sections other than in
blowrooms and cardrooms in the second and third study could have been due to the
coarse variety of cotton or the closeness of these sections to cardrooms.
In India, only a limited number studies have been conducted to highlight
occupational hazards in cotton mills. Tirupur being a textile city in Coimbatore
district have 18 ginning factories employing 1,50,00 labours.
There are about 17 cotton mills around Madurai. There are numerous textile
and chemical industries operating in the area, including Thiagarajar Mills (one of the
largest manufacturer and exporter of 100% Indian cotton yarn), Kasim Textile Mills,
Sundaram Textiles, Weaves India, and Vaigai Group.
Working in textile industry hours together, months and years together creates
many health problems earning bread on one side and also neglecting the risk factors
during work can cause many diseases and disabilities. We can prevent those
occupational diseases if we adapt certain precautions and preventive measures.
Byssinosis
(Due to exposure of cotton dust) it is respiratory disease. The most commonly
affected system in the body due to exposure of cotton dust is respiratory problem. It is
also commonly known as brown lung disease; Byssinosis is an occupational disease
caused by inhalation of cotton dust in textile industry. Different name for Byssinosis
are “brown lung disease”, “cotton workers lung,” & “Mill fever, “cotton bract
disease”.

4
Riskfactors of byssinosis
Byssinosis most commonly affect textile workers who work in a
manufacturing process where cotton, flax: hemp, yarn, thread, fabric and rope making
activities are performed.
Signs and symptoms of byssinosis
Byssinosis symptoms may appear as quickly as a couple of hours after
exposure and diminish when leaving the manufacturing environment. However, after
long periods of exposure, symptoms may last for days or even weeks after leaving the
manufacturing environment. Long term exposure to cotton, flax hemp or jute
fibers/dust may cause permanent scarring of lungs and airways, leading to debilitating
lung disease Persons with byssinosis generally experience the following symptoms
throughout the work week.
- Wheezing
- Tightness of chest
- Coughing
- Symptoms of byssinosis are more severe during humid weather
People who smoke suffer the most severe impairment from byssinosis. The
combination of dust/ fiber and smoke both aggravate the lungs and airway.
Diagnosis of byssinosis
Chest x-ray and pulmonary function test can be used to diagnosis byssinosis.
PFTs will show a decrease in lung capacity as the day progresses and the exposure
continued.
Treatment of Byssinosis
There is cure of byssinosis it is treated immediately.
Prevention of byssinosis
It can be prevented by using exhaust hoods and face mask, improving ventilation
during manufacturing activities and using wetting producer which help to control the
level of dust caused by the textile.
• Pre- employment screening – To detect hyper reactivity and sensitivity to
textile dust.

5
• Smoking cessation is important as it worsen the condition.
• Transfer of person from work place for few days also reduces the risk of
relapse.
• Maintain highly ventilated, good lighting and hygienic environment
• Intake of balanced diet
• Avoid smoking and tobacco chewing
• Adequate rest and sleep
Awareness is very important because awareness regarding occupational health
contributes lot in prevention of disease in workers, healthy worker and healthy work
environment increase the productivity of work as were as contribute progress in
national development.
SIGNIFICANCE AND NEED FOR THE STUDY
In recent days the number of industries on the increase. In India there are
approximately 60 million workers over the age of 16, are involved in various kind of
industrial works. Textile industries are the oldest occupation in India, thousands of
workers are involved in textile manufacturing. A review of textile industry quotes that
it is the largest manufacturing sector in India, accounting for around 20% of India’s
industrial output and 37% of total exports.
Textile manufacturing goes under several process of knitting; winding;
spinning ; dying; etc. Exposure to these processes for years together are causing major
health problems among textile workers. As it is mentioned earlier that healthy
workers and healthy work environment helps to increase the production. The health
impact of work is an important aspect of most clients for whom the community health
nurses provides care. At least one third of average adult life is spent at work;
therefore, the workplace has a significant potential influences on individuals health
and is a primary site for the delivery of preventive health care.
Occupation is the one in which person not only earn his daily bread but also
spent one third of average adult life. These industries have also contributed in
increasing the occupational hazards among workers. The protections of health of
working population in these are primary concern of occupational nurse.

6
According to recent estimate, the cost of work related heat loss and associated
productivity loss may amount to several percent of the total gross national product of
country. In India there are about 1.07 million workers are engaged in the manufacture
of cotton textile. 20 million workers are involved in textile industry, in which
byssinosis, hypertension, noise induced hearing loss, dermatitis and risk of cancer due
to various chemicals and dyes are common occupational diseases found among
weavers. A study done by NGO, in 1995 byssinotic condition was first recorded in
Indian history of 150 years. Maximum number of byssinosis cases reported in the
cotton textile industry as it is one of the largest industries in the world.
If well educated, motivated, reinforced supervised and guided properly, then
will became asset to the organization, society and the nation by the large. So far our
knowledge is concerned, however very less studies conducted in India to find out
occupational health problems of cotton mill workers.
Training and education to these workers is an essential component of
occupational health. It is extremely important to make people aware and concerned
about work place. Hence responsibility of community health nurse lies in imparting
knowledge related to specific measure in preventing occupational hazards.
Community health nurse plays an important role in preventing and controlling
occupational hazards. She functions independently and carries responsibility for better
health of workers.
During the community posting, the investigator found many clients visiting
Community health centre with respiratory problems. The investigator was curious to
know the reason and found that it is because of the exposure to cotton dust mainly
who are working in cotton mill. Hence, the investigator decided to give awareness to
prevent the respiratory problem among cotton mill workers.

7
STATEMENT OF THE PROBLEM
A study to evaluate the effectiveness of video assisted programme on
knowledge and attitude regarding prevention of respiratory problems among cotton
mill workers in selected Cotton Mills at Madurai.
OBJECTIVES
1. To assess the existing level of knowledge and attitude on prevention of
respiratory problems among selected cotton mill workers at Madurai.
2. To assess the post test level of knowledge and attitude on prevention of
respiratory problems among selected cotton mill workers at Madurai.
3. To find out the difference between pretest and post –test level of knowledge
and attitude on prevention of respiratory problems among selected cotton mill
workers at Madurai
4. To find out the association between post tests level of knowledge and attitude
on prevention of respiratory problems among selected cotton mill workers
with the selected demographic variables.
NULL HYPOTHESIS
HO1: There will not be a significant difference in the knowledge and attitude
on prevention of respiratory problems among selected cotton mill workers after
video assisted programme.
HO2: There will not be a significant association between post test level of
knowledge and attitude on prevention of respiratory problems and selected
demographic variables.

8
OPERATIONAL DEFINITIONS
Effectiveness
In this study it refers that the outcome of video Assisted Programme as
evaluated by the help of significant mean difference between pretest and post test
scores on knowledge and attitude regarding prevention of respiratory problems among
cotton mill workers.
Video assisted teaching programme
In this study it refers that a well planned structured instruction with the use of
LCD helps to internalize the importance of prevention of respiratory problems among
cotton mill workers.
The aspects included were, definition of respiratory problem, route of
transmission, symptoms, preventive measures and to minimize the chance of
incidences of respiratory problems among cotton mill workers.
Knowledge
In this study it refers that the level of understanding on prevention of
respiratory problems by the cotton mill workers as expressed through written response
as measured by structured knowledge questionnaires.
Attitude
In this study it refers that the way of thinking, beliefs and feelings regarding
prevention of respiratory problems as expressed in the form of statements as measured
by 3 point Likert scale.
Prevention of respiratory problem
In this study it refers that the measures like teaching on stopping the
occurrence of respiratory problem by improving the practice of protective measures
for those who are in the risk to develop respiratory problems like byssinosis, allergic
rhinitis, chronic bronchitis and bronchial asthma due to the exposure of cotton dust.

9
Cotton mill workers
In this study it refers that the employees who work in a cotton mills under the
risk to develop respiratory problems.
ASSUMPTIONS
The knowledge and attitude on prevention of respiratory problems among
cotton mill workers are lacking. Cotton mill workers may have some knowledge and
attitude on prevention of respiratory problems. Nurses have their role in prevention of
occupational hazards.Video assisted programme will help to enhance the knowledge
and attitude of cotton mill workers in the prevention of respiratory problems.
DELIMITATIONS
Study is limited to,
- Workers those who are exposed to cotton dust and are at risk of developing
respiratory problems.
- The data collection took place for only six weeks; therefore it has limitations
in terms of evaluating the attitude
- Data collection done by interview and structured questionnaire
PROJECTED OUTCOME
The findings of the study would help to
- identify the respiratory problem
- create awareness to cotton mill workers
- develop a teaching module
- identify the effectiveness of video assisting programme
It improves the knowledge and attitude on prevention of respiratory problems
among cotton mill workers.
It would be useful contribution for improving the practice of protective measures
during the working period.

10
CHAPTER – II
REVIEW OF LITERATURE
In this study, the review of literature has been presented as per the available
research studies and relevant literature from with the strength of the study was drawn
as follows:
Studies related to respiratory problems of cotton mill workers
Studies related to knowledge on respiratory problems among cotton
mill workers
Studies related to attitude respiratory problems of cotton mill workers
STUDIES RELATED TO RESPIRATORY PROBLEMS OF COTTON MILL
WORKERS
Ajeet jaiswal (2011) done a study on the occupational health function among
female textile workers mainly in the reduction of respiratory function. It is aimed to
find the factors associated with the deterioration of respiratory function among female
textile workers. The sample consisted of 243 men above the age of 20 years who had
worked for at least 3 months years in a textile factory and 235 female non textile
workers of same area were studied. All the respondents were interviewed by a
pretested questionnaire to gather information regarding the chest symptoms, certain
personal characteristics and occupational history. Statistical analyses like Chi-square
and odds ratio was done to determine the significant difference between female textile
workers and female non textile workers. Univariate analysis of the factors for
symptomatic byssinosis showed that dusty worksites, heavy smoking and duration of
service years were significant. Logistic regression analysis showed that working in the
scouring (odds ratio 11.0), spinning (odds ratio 4.7) and weaving sections (odds ratio
2.6), heavy smoking (odds ratio 12.4) and more than 10 years of service to discourage
smoking among textile workers need to be strengthened to minimize the risk of
developing byssinosis.

11
Joseph mberikunashe1, et all (2006) studied on the Prevalence and risk factors
for obstructive respiratory conditions among textile industry workers in Zimbabwe,
Workers in the cotton processing industries risk developing obstructive respiratory
conditions due to prolonged exposure to cotton dust. They conducted a cross sectional
analytic study. Workers were randomly sampled and data was collected using
interviewer-administered questionnaires. Respiratory function was assessed using
spirometry and chest auscultation. A walk through survey was conducted and a
checklist was used to capture hazards and control measures in the work place. A total
of 194 workers participated. The prevalence of severe respiratory obstruction was
27.8%. It was 50.0% among the blowers, 35.3% in waste recovery, 32.5% in carders,
15.0% in spinners and 7.5% among weavers. The mean years of exposure between the
affected and the nonaffected were significantly different (T =2.20; p< 0.05). Working
in the blowing department was significantly associated with developing respiratory
obstruction (OR=3.53; 95% CI= 1.61- 7.79) but working in the weaving department
was significantly protective (OR 0.16; CI 0.04- 0.59).Working in a department for
less than 10 years was protective (OR =0.94; 95% CI= 0.48- 1.85), but not significant.
Obstructive respiratory conditions are common among textile workers, with those in
blowing and waste recovery sections being the most affected. They recommended
worker rotation every six months, regular spirometric screening employment of a
medical officer.
R-s koskela, et all (2005) conducted a study on Respiratory disease and
cardiovascular morbidity .Work related dust exposure is a risk factor for acute and
chronic respiratory irritation and inflammation. The study comprised 6022 dust
exposed (granite, foundry, cotton mill, iron foundry, metal product, and electrical)
workers hired in 1940–76 and followed until the end of 1992. National mortality and
morbidity registers and questionnaires were used. The statistical methods were
person-year analysis and Cox regression. Co-morbidity from cardiovascular and
respiratory diseases ranged from 17% to 35%. In at least 60% of the co-morbidity
cases a respiratory disease preceded a cardiovascular disease. Chronic bronchitis,
pneumonia, and upper respiratory tract infections predicted IHD in granite workers
(rate ratio (RR)�=�1.9; 95% CI 1.38 to 2.72), foundry workers (2.1; 1.48 to 2.93),
and iron foundry workers (1.7; 1.16 to 2.35). Dust exposure was not a significant

12
predictor of IHD or other CVD in any group. Dust exposure was related to respiratory
morbidity. Thus, some respiratory diseases appeared to act as intermediate variables
in the association of dust exposure with IHD. Dust exposure had only a small direct
effect on IHD and other CVD. IHD morbidity was associated with preceding
respiratory morbidity. A chronic infectious respiratory tract disease appeared to play
an independent role in the development of IHD.
X-r wang, et all (2003), motivated to determine chronic effects of long term
exposure to cotton dust and endotoxin on incidence of respiratory symptoms and the
effect of cessation of exposure. Respiratory health in 429 Chinese cotton textile
workers (study group) and 449 silk textile workers (control group) was followed
prospectively from 1981 to 1996. Byssinosis, chest tightness, and non-specific
respiratory symptoms were assessed by means of identical standardised
questionnaires at four time points. Exposures to cotton dust and endotoxin were
estimated using area samples collected at each survey. Incidence and persistence of
symptoms were examined in relation to cumulative exposure and exposure cessation
using generalised estimating equations (GEE). Among cotton workers, the
cumulative incidence of byssinosis and chest tightness was 24% and 23%,
respectively, and was significantly more common in smokers than in non-smokers. A
high proportion of symptoms were found to be intermittent, rather than persistent.
Multivariate analysis indicated a trend for higher cumulative exposure to endotoxin in
relation to a higher risk for byssinosis. Chronic exposure to cotton dust is related to
both work specific and non-specific respiratory symptoms. Byssinosis is more
strongly associated with exposure to endotoxin than to dust. Cessation of exposure
may improve the respiratory health of cotton textile workers; the improvement
appears to increase with time since last exposure.
Maunder lR (2003), conducted a study with one hundred and sixty-nine and
175 cotton textile workers were enrolled in the first (1991) and second (1996) surveys
to investigate the prevalence of byssinosis. The synergistic effect of smoking on
cotton dust exposure was also evaluated although the difference in second study
(38.9%) was not statistically significant; smoke had significantly higher frequency
than non smokers in both surveys. The frequency of respiratory symptoms and the
prevalence of severe byssinosis in the second survey were (14.9%and 12.6%)

13
respectively. The reduction of symptoms was due to remodeling of this old cotton
mill. The prevalence’s higher than in non- smokers only found in first survey, but not
found in the second survey. These results indicate that smoking potentate’s
byssinosis. The second study reveals high prevalence of byssinosis still smoking was
found to show an additive effect on cotton dust exposure.
Thoreia Mohamed Mahmoud et all (2001) done a study of occupational health
hazards among spinning factory workers.. The aims of the work are study the
occupational health hazards among the workers in Assiut Spinning Factory and to
assess the different protective measures used during working day to prevent the
different hazards.The total number of the studied sample was 550 workers out of 650
who worked in the productive and repair sectors. A questionnaire was constructed
include two parts, one to assess the industrial hazards and their preventive measures
and the second one included the information from the health record of the worker in
Health Insurance included pre-placement examination and periodic medical
examination. The data collection took about 6 months (from July to the end of
December 2001). Study revealed that the vast majority of workers (96.9%) were
males. About two thirds (65.8%) of workers have experience of work for 20-30 years
(mean was 20.5+5.3). 67.3% of the Workers were mentioned that the mask is
available and only 41.6% from them using it during work. 99.5% of workers
mentioned about the availability of the emergency equipments. Moreover 99.3% of
workers mentioned that there are no health education programs. The workers in the
blending and picking department, carding and spinning department and combing and
twisting department suffer from cough (68.3%, 60.2% and 73.7% respectively), chest
pain (68.3%, 57.6%, and 64.9% respectively), and dyspnea (70.7%, 68.1% and 71.9%
respectively). The difference from other departments was statistically significant. Ear
disease and ear secretion were common symptoms among more than half of the
workers in the above mentioned departments in addition to winding and doubling
departments and the differences from other departments were statistically significant
(P<0.05). Only 63.8% of workers were performed periodic medical examination. It
was found that 13.4%, 11.1% and 2.3% were suffering from chronic bronchitis,
chronic bronchitis with emphysema and bronchial asthma respectively. 13.4% of
workers have sensory deafness while 9.9% have sensory conductive deafness. The

14
study recommend with improving of worker’s health through: Periodic medical
examination should be performed to all workers in the factory. Periodic inspection of
working environment by industrial hygienist through regularmeasurement of noise
level, illumination, ventilation and cotton dust concentration. Training and health
education programs should be provided to all workers from the start of work.
Emphasizing the correct use of personal protective measures. If possible, the factory
should look into the possibility of replacing the old machines with new ones, which is
less noisy.
STUDIES RELATED TO KNOWLEDGE ON RESPIRATORY PROBLEMS
AMONG COTTON MILL WORKERS
MS. A.Arockia Mary 2010 Done a Non experimental descriptive correlational
study to assess the Knowledge and Attitude regarding Occupational Hazards among
cotton mill workers in a selected textile industry, Bangalore. Sample size was 60.The
objectives are to assess the knowledge regarding Occupational Hazards among cotton
mill workers to assess the attitude regarding Occupational Hazards among cotton mill
workers, to correlate between the knowledge and attitude regarding Occupational
Hazards among cotton mill workers, to associate the knowledge and attitude
Occupational Hazards among cotton mill workers. The study will be conducted at the
selected textile industry; Bangalore. Correlation coefficient will be to analyze
correlation between the knowledge and attitude. Chi-square test will be used to
analyze association. The researcher further recommended that same study can be
conducted in a large scale.
Mr. Basavaraj S. July 2010“A Quasi experimental study to evaluate the
effectiveness of structured teaching programme regarding knowledge on respiratory
problems (bagassosis) and its prevention among the workers of gyanba sugars and
developers limited, doddabathi, the main objective is to assess the effectiveness of
structured teaching programme on prevention of respiratory tract problems
(Bagassosis) through post test knowledge. The total study sample consists of 80
workers. Simple random sampling technique and lottery method was used. The data
was analysed by using appropriate statistical methods.

15
A quasi-experimental experimental study conducted in 2007 by Jessica S Kale
in Belgaum, Karnataka, with an objective to assess the knowledge and practice of
preventing occupational health hazards among textile weavers with a sample size of
55 through implementing planned teaching program. Result showed that 11% (6) had
good knowledge during pre test, has improved to 100% (55) during post test. The
researcher further recommended that same study can be conducted in a different
setting.
R. Altina S.et all (2000) done a 15 year follow up observation of the
prevalence of byssinosis is decreasing in industrialized countries and persists at high
levels in developing countries, this prevalence is remaining constant in Turkey. In
order to determine the effects of past cotton dust exposure on the respiratory tract, a
total of 223 persons working in a cotton mill were included in this study. A
questionnaire was used to inquire about respiratory symptoms. Participants underwent
several spirometric measurements, which were performed on the 1st, 3rd and 5th day
of the working week. Cotton dust measurements were performed in different divisions
of the factory. The most common respiratory symptom was chest tightness (20.3%).
The prevalence of byssinosis was 14.2% in cotton- processing workers. Among these
cases, 28.6% had symptoms on the 1st day of the week, and 71.4% had symptoms on
all days of the week. An acute effect was seen in 53.6% of the workers with
byssinosis. Mean respirable dust levels were between 0.095 and 0.413 mg/ m3. In
spite of technological improvements, respirable dust concentrations are still above the
permissible limits, and thus the risk of byssinosis remains. Workers in the cotton
industry where obsolete technology is used and standardized protection measures are
not applied should be followed for byssinosis.
Mentesinot Woldeyohannes, et all (1991) studied to investigate the prevalence
of respiratory problems, in particular byssinosis, and to explore factors associated
with their occurrence among a group of 595 randomly selected workers representing
40-5% of those exposed to dusty operations in a typical Ethiopian cotton textile mill.
A standard questionnaire on respiration was administered and pre and post shift
forced vital capacity (FVC) and forced expiratory volume in one second (FEVI) were
determined for each worker; workers found to have byssinosis and other respiratory
diseases were compared with workers having no respiratory diseases in terms of the

16
level and duration of exposure to cotton dust and other variables. Multiple area air
samples from different sections were analysed for elutriated cotton dust
concentrations (086-3 52 mg/im3). The prevalence of byssinosis was 43-2% among
blowers and 37-5% in carders in comparison with four to 24% among workers in
other sections. Prevalence of chronic bronchitis ranged from 17-6 to 47 7% and
bronchial asthma from 8'5 to 20'5% across all sections. Significant across shift
decrements in FEV, and FVC were seen in those workers with respiratory tract
diseases compared with those workers without such diseases. A significant dose
response relation for pulmonary function and respiratory illnesses was also found by
regression analysis. Department of Community Health, Faculty of Medicine, Addis
Ababa University, Ministry of Health, Addis Ababa, People's Democratic Preventive
measures are proposed. Further research including a nationwide survey of textile mills
is suggested. This is the first epidemiological study of the textile industry in Ethiopia.
R-S Koskela et all (1990) conducted a study regarding The mortality and
disability of cotton mill workers in five Finnish cotton mills. The population under
study comprised all 1065 women exposed to raw cotton dust who had been hired
between 1950 and 1971. The minimum exposure period was five years. For the study
on disability, the cohort was followed up until the end of 1981. The follow up period
for the mortality analysis was from 1950 to 1985. At the end of 1981 the observed
number of prevalent disability pensions for respiratory disease was 15, whereas 3 9
were expected (p < 0 01) on the basis of the national figures for women. There were
46 musculoskeletal diseases (27-7 expected p < 0-01), of which 24 were osteoarthritis
(14-5 expected) and 13 rheumatoid arthritis (6-6 expected). The incidence rates of
disability pensions were calculated for the period 1969-81. Comparison of incidence
rates between cotton mill workers and the Finnish female population showed
excessive rates for both respiratory diseases (p < 0 001) and musculoskeletal diseases
(p < 0-01), with an excess of new cases of rheumatoid arthritis (p < 0-05). By the end
of 1985 the number of person-years was 31 678 and the number of deaths 95. The
standardized mortality ratios for the total period of follow up (1950-85) showed no
excess for respiratory diseases. Mortality from cardiovascular diseases was also lower
than expected. The observed number of tumours was 33, the corresponding expected
number 32-0. Thirteen tumours were in the digestive organs (6-6 expected, p < 0-05)

17
and three were lung cancers (19 expected). Five workers had died from renal disease;
the expected number was 1-5 (p < 0-05).
STUDIES RELATED TO ATTITUDE RESPIRATORY PROBLEMS OF
COTTON MILL WORKERS
A 25-Year Follow-up Study on Long-term Effects of Work Cessation on
Respiratory Health of Textile Workers was conducted by Jing Shiet all,(2009)1Civil
and Environment Engineering School, University of Science and Technology,
Beijing, Rationale: The degree to which chronic respiratory health effects caused by
exposures to cotton dust and endotoxin is reversible after cessation of textile work is
unknown. Objectives: To investigate changes in lung function and respiratory
symptoms after cessation of textile work and to determine whether past exposure to
cotton dust and endotoxin or smoking history modify the associations. Methods: We
performed a prospective cohort study consisting of 447 cotton textile workers exposed
to cotton dust and 472 unexposed silk textile workers, with a 25-year follow-up.
Spirometry testing and respiratory questionnaires were conducted at 5-year intervals.
Generalized estimated equations were used to model the average 5-year change in
FEV1 and odds ratios of respiratory symptom prevalence. Measurements and Main
Results: Years since cessation of textile work was positively associated with 11.3
ml/yr and 5.6 ml/yr gains in 5-year FEV1 change for cotton and silk workers,
respectively. Among male cotton workers, smokers gained more FEV1 per year after
cessation of exposure than did nonsmokers, and the risk of symptoms of chronic
bronchitis and byssinosis was larger for smoking than for nonsmoking male cotton
workers. Conclusions: Cessation of textile work was significantly associated with
improvement in lung function and respiratory symptoms. The positive effect of work
cessation was greater for cotton workers than for silk workers. For cotton workers, the
improvement in lung function loss after cessation of textile work was greater among
smokers, but no differences were observed for silk workers.

18
Mr.Sateesh Satawaji (2007 ) done a Study To Assess The Knowledge And
Practice On Prevention Of Respiratory Problems Among The Workers Of Cotton
Industry In Selected Area At Bijapur, Karnataka After the study, the investigator finds
the level of knowledge and practices regarding the prevention of respiratory problems
among the workers at cotton industry. Based on the findings the investigator
developed the teaching model to the workers of selected cotton industry.
Yih-Ming SU1, et all (2003) done a study on Additive Effect of Smoking and
Cotton Dust Exposure on Respiratory Symptoms and Pulmonary Function of Cotton
Textile February 13, One hundred and sixty-nine and 175 cotton textile workers
(CTWs) were enrolled in the first (1991) and second (1996) surveys to investigate the
prevalence of byssinosis. The synergistic effect of smoking on cotton dust exposure
was also evaluated. Although the difference in prevalence of abnormal pulmonary
function between the first (38.5%) and second study (38.9%) was not statistically
significant, smokers had significantly higher frequency than nonsmokers in both
surveys. A significant trend existed between the cotton dust levels and the frequency
of abnormal lung function. The significant trend was also noted in both smokers and
nonsmokers. The frequency of respiratory symptoms and the prevalence of severe
byssinosis in the second survey (14.9% and 12.6%, respectively) were significantly
lower than that in the first survey (39.7% and 21.9%, respectively). The reduction of
symptoms was due to remodeling of this old cotton mill. The prevalences of
respiratory symptoms and byssinosis in smokers being significantly higher than in
nonsmokers only found in the first survey, but not found in the second survey. These
results indicate that smoking potentiates the effect of cotton dust exposure on
respiratory symptoms and byssinosis. The second study reveals high prevalence of
byssinosis still existed in Taiwanese cotton mill, although the prevalence was
declining. Smoking was found to show an additive effect on cotton dust exposure.
Anti-smoking campaign, occupational health program to reduce the dust exposure,
and periodical medical examination are measures to prevent from byssinosis.
A survey done by Vasantha Kandaswamy (2003) on occupational hazard in
textile industries reveals that most of the workers and family members at Coimbatore
(Tamilnadu) India, suffer from either asthma, allergy, TB or from frequent attacks of
cold. Only few or negligible people suffered from cancer. Another strange ailment

19
were nose block, throat infection, which were also a frequent problem faced by them,
future it is also found that the number of weavers who suffered from skin problem
was less than the number of weavers who faced with respiratory problems, thus the
major occupational health hazards faced by weavers was respiratory problem.
An epidemiological survey B. Lammers, 1963 of 414 English and 980 Dutch
male cotton workers was undertaken to determine the prevalence of byssinosis and
respiratory symptoms, and to compare the ventilatory capacities in the two
populations, with particular reference to the influence of air pollution. The English
workers were employed in six mills in Lancashire and the Dutch workers in three
mills in Almelo spinning similar grades of cotton. The methods used included a
questionnaire on respiratory symptoms and illnesses, the collection and examination
of sputum and the measurement of the forced expiratory volume over 0 75 sec. The
crude rates for byssinosis were similar, 13-5 % and 17% respectively in the English
and Dutch card and blow rooms, and 1-5 % and 1 6% respectively in the spinning
rooms. The English workers had significantly higher prevalence of persistent cough
and persistent phlegm and significantly lower indirect maximum breathing capacities.
Nearly twice as many English produced specimens, and the mean volume of sputum
was greater for the English workers. The prevalence of bronchitis, defined as
persistent phlegm and at least one chest illness during the past three years, causing
absence from work, was higher in the English than in the Dutch workers in both types
of work room, but not significantly so after standardizing for differences in age. Since
there are important differences in the social security systems of the two countries,
which may encourage more absence from illness among the Dutch, a comparison of
bronchitis thus defined is likely to be invalid. The higher prevalence of respiratory
symptoms and lower ventilator capacities in the English are unlikely to be due to
observer error. They are discussed in relation to smoking habits, exposure to cotton
dust, and air pollution. The most likely explanation of the unfavourable picture
presented by the English workers is the much higher level of air pollution in
Lancashire.

20
Richards. F. Schilling (1964) done epidemiological studies of chronic
respiratory disease among cotton operatives. Compared with chronic diseases like
cancer, coronary heart disease, and rheumatism, it is a very small public health
problem. Nevertheless, it illustrates in microcosm the difficulties of finding the extent
and causes of a chronic disease in a community. It is easy to misinterpret the etiology
and misjudge the importance of a disease using traditional methods of analyzing
mortality and morbidity data and investigating patients in hospital. Instead, a
relatively new type of epidemiology is required-one that studies groups of people and
the environmental and personal factors that together may cause a disease and
influence its course. Clinical epidemiology demands a different approach from
hospital medicine since the unit of study is the group or family rather than the
individual patient, and clinical skills have to be used rather differently. In hospitals
most patients have unequivocal evidence of disease, and diagnosis seldom depends on
a single examination. In field surveys, subjects are often examined only once and
many are found to be normal or to have only early manifestations of disease. This
necessitates more precise definition of the indices of disease than is usually required
in Byssinosis among cotton operative’s schilling hospital practice, as well as
standardization of the techniques of measurement. In the investigation of chronic
respiratory disease, clinical epidemiologists have devoted considerable efforts to the
standardization of questionnaires on chest symptoms, lung function tests, and
radiological films.
L. Belin et all From the Departments of Allergology and Clinical Physiology,
Sahlgrenska (1964) studied The prevalence of byssinosis and chronic respiratory
symptoms in 117 workers in four Swedish cotton mills. Changes of forced expiratory
volume in 0-75 sec. (F.E.V.0.75) duringa Monday and a Wednesday were assessed in
64 male workers in four cardrooms in these mills.Dust sampling was performed with
weighed millipore filters.Prevalences of byssinosis as judged from the workers'
histories were 68 %, 55 %, 44 %, and 25 %in the four mills; the lowest prevalence of
25 % was found in a mill spinning both high grade cotton yarn and rayon. Among 67
workers in the mills having a byssinosis prevalence of 68 % and 55 %, 60% were
non-smokers, 70% had chronic cough, and 27% had chronic dyspnoea. The
F.E.V.0.75decreased on Monday in workers who gave a history of Monday dyspnoea,

21
and to a lesser degree, but still significantly, in those who did not. In spite of marked
differences in fine dust (i.e., dust smaller than 2 mm. diameter) concentrationsin the
four cardrooms, no significant relations between dust content, byssinosis prevalence,
andF.E.V.0.75 changes on Monday could be demonstrated. The prevention and
treatment of byssinosis is discussed. Workers at risk should receive a periodical
medical examination including at least a spirographical pulmonary function test
atintervals of one year or less.
I. Dingwall-Fordyce and J. G. O'sullivan from the Department of Occupational
Health, University of Manchester done a study to determine whether byssinosis
occurred among workers in the waste cotton industry. It was undertaken in 1950 at the
instigation of the Minister of National Insurance. Twenty-two mills, representative of
the industry, were surveyed. All the men in these mills, who were over 35 years of
age and with at least 11 years' exposure to cotton dust, were seen. The investigations
included a work history, a clinical examination, an assessment of effort dyspnoea, and
a chest radiograph. There were I40 men who had never been exposed to any dust
hazard other than waste cotton. In this group were found seven (5%) men with
disabling byssinosis and 35 (25%) men with lesser degrees of the same disease. There
were also I5 (11%) men with bronchitis or emphysema without byssinosis. Thus it
was established that byssinosis did occur in the waste cotton industry. Insurance
cover, under the National Insurance (Industrial Injuries) Act, I946, was subsequently
extended to workers in the waste cotton industry. The survey provided no evidence
that either the type of waste cotton processed or an admixture of raw cotton played a
significant part in the aetiology or incidence of the disease.
K.Priya et all conducted a Cross-sectional study study on respiratory problems
in cotton mill workersThey found Cotton industry workers sometimes face a chronic
debilitating disease known as Byssinossis. Health status of workers of Vijaya mohini
Mills Trivandrum City was assessed in this context.the objectives are to assess the
level of awareness about the health hazards in cotton industry among cotton mill
workers and to find the prevalence of respiration diseases among them.Seventy
workers on the evening shift of Vijayamohini mill were included in the study. Semi
structured Questionnaire was used to collect the data. Data analysis was done using

22
proportions.All of the workers were aware that they belonged to a high risk group
related to respiratory illness. They knew tact Cotton dust causes pulmonary
diseases.None of them were satisfied with the existing safety practices.47% of
workers are not using mask either due to inadequacy or due to discomfort it
creates.Only one third of the workers were getting information from sources other
than their colleagues.40% of the workers had respiratory problem.Among them 70%
were with more than forty years experience.47% of the smokers are affected and 30%
of the non smokers are affected.Periodic medical examination were absent at the
setting.

26
CHAPTER-III
METHODOLOGY
RESEARCH METHODOLOGY
In this chapter the investigator discusses the chosen research approach and the
rationale. A detailed account of study preparatory and planning phase was discussed
as well as how the research was conducted and how data was analyzed. Steps to
address rigour, ethical considerations and management issues such as time scale and
financial implications are also discussed.
RESEARCH APPROACH
An experimental approach was used to assess the Effectiveness of video
assisted programme
RESEARCH DESIGN
Pre experimental design was adopted with one group pre test and post test
design.
SETTING OF THE STUDY
The setting of the study is selected cotton mills, Madurai. They are private
limited industries. Total strength of the mills are 30, 20, 20 respectively. They have
separate departments for each processing. Totally 4 departments namely, blow room,
carding, spinning and cone winding. There were many workers having more than
three years experience. The investigator chose setting due to availability of samples,
co-operation of authorities, and feasibility in terms of time, money and material and
language convenience.
VARIABLES
Dependent Variable: knowledge and attitude.
Independent Variable: video assisted programme.

27
POPULATION
The target population: All the cotton mill workers working in cotton mill at
Madurai
Accessible population: Cotton mill workers those who are exposed to cotton
dust in selected cotton mills at Madurai.
SAMPLE
Workers those who are employed in the selected cotton mills exposed to
cotton dust during the study and fulfil the inclusion criteria were selected as a sample.
SAMPLE SIZE
The sample size for the study is 60 cotton mill workers in selected cotton mills
,Madurai.
SAMPLING TECHNIQUE
Samples for this study were selected through non probability - purposive
sampling. These samples are those that use whatever subjects are available rather than
following a specific subject selection process. In the present study purposive sampling
technique used to select the cotton mill workers, samples were selected based on
sampling criteria.
CRITERIA FOR SAMPLE SELECTION
Inclusion criteria
Workers who are,
between 21 to 60 years of age.
able to read Tamil.
both gender
available during the data collection time.
willing to participate in this study.
Exclusion criteria
Workers who are
not exposed to cotton dust in the mill.

28
DESCRIPTION OF THE INSTRUMENT
The instrument was developed by the investigator with the guidance of
experts. The tool consist of three parts.The structured questionnaire was prepared to
assess the knowledge and attitude on respiratory problems
Part I- base line data
Part II- knowledge on respiratory problem and its prevention
Part III- attitude on respiratory problems
Part I
It consists of 10 baseline data such as age, sex, and educational status, duration
of work, habit of exercise, and personal habits of person.
Part II
It consists of structured knowledge questionnaire with 20 multiple choice
questions. Each question has 4 responses with one right answer on knowledge among
adult patients regarding respiratory problems on the basis of introduction, causes,
symptoms, prevention.
Part III
It consists of ten positive statements and ten negative statements to assess the
attitude among cotton mill workers. The scale used in this study is 3 Point Likert
scale. The options included were agree, uncertain and disagree.
SCORING PROCEDURE
Part II
The multiple choice questions have four responses each with one right answer,
which is allotted a score of one and every wrong answer was given a score of zero.
The total attainable score of knowledge questionnaire was 20. The total score was
converted into percentage and the resulting score was ranged as follows:
15-20 - Adequate knowledge
8-14 - Moderately adequate knowledge
Below7 - Inadequate knowledge

29
Part III
It consists of 3 Point Likert scale of ten statements to assess the attitude on
respiratory problems. The options included were agree, uncertain, and disagree. The
maximum score for measuring the attitude was 60. A score of one was given for
disagree, score of two was given for uncertain, score of three was given for agree for
each positive statements. A score of one was given for agree, score of two was given
for uncertain, score of three was given for disagree for each negative statements.
Attitude score was interpreted as follows:
41-60 - Favourable attitude
20-40 - Unfavourable attitude
VALIDITY AND RELIABILITY OF THE TOOL
The content validity of an instrument is essentially based on the adequate
coverage of the subject matter. In the present study 12 experts including 1 pulmonary
physician, 10 nursing experts and one community health nursing professor, validated
the entire section of the tool. The experts were requested to check the relevance of the
items in the tools. Based on the recommendations, few items were modified. The tool
was first drafted in English, Tamil translation was done and drafted by Tamil experts
and checked for language validity.
The reliability of an instrument is the degree of consistence with which it
measures the attribute it is supposed to be measuring over a period of Time. The
reliability of interview schedule was established by using split half method. The
second test was conducted 7 days after the first test to the same group of workers.
Then the scores obtained were correlated. Reliability was computed using Karl
Pearson’s correlation co-efficient and it was found to be 0.96 for knowledge and 0.96
for attitude,which was highly, positively correlated. The tool was found to be reliable.
DATA COLLECTION PROCEDURE
The data was collected among workers who are working in selected cotton
mill workers, Madurai. Written permission was sought and obtained from the
authorities concerned. The period of data collection was 6 weeks. 60 workers were
selected as per above mentioned criteria with prior informed verbal consent to
participate in the study. Initially good rapport was maintained with the adult patients
and the purpose of the study was explained to them. Workers were made comfortable

30
and privacy was provided. Data was collected through the structured questionnaire to
assess the knowledge and attitude among cotton mill workers. Video teaching
regarding the respiratory problems and its prevention was given on the first day. It
was followed by the post test after 7 days. Same procedure was followed for the other
two cotton mills also.
DATA COLLECTION SCHEDULE
Week Cotton mill Pretest and video
teaching Post test
1 1 1st day 8th day
2 2 1st day 8th day
3 3 1st day 8th day
PILOT STUDY
The pilot study was conducted among 6 workers in cotton mill in Tanakkankulam,
Madurai after obtaining formal permission from authorities before the main study to
achieve the following puposes.
- To understand and handle the difficulties that may be encountered in the actual
study.
- To become familiar with the use of the study tool
- To find out the feasibility and application of the tool
- To find out the sensitivity of the tool.
Structured questionnaire which consists of 20 questions was used to assess the risk
factors and 20 questions was used for data collection to assess the existing knowledge
and Likert 3 Point attitude scale to assess the attitude among Cotton mill workers.
This time taken to complete the tool was found to be satisfactory in terms of
simplicity and clarity. Based on the time taken for collecting the data, arbitrary
decision was taken to keep the sample size to 60.

31
PROTECTION OF HUMAN RIGHTS
The proposed study was conducted after the approval of dissertation
committee of the college. Permission was obtained from the concern persons in each
cotton mill. Each individual client was informed about the purpose of the study and
confidentiality was promised and ensured. Informed consent was obtained from each
individual. The patient had the freedom to leave the study at his/ her wish without
assigning any reason. Thus the ethical issues were ensured in this study.

32
CHAPTER – IV ANALYSIS AND INTERPRETATION
This chapter deals with the description of the sample analysis and
interpretation of the data collected among cotton mill workers to interpret the
knowledge and attitude on prevention of respiratory problem. The data collected were
tabulated, analyzed and presented based on the objectives.
The findings were organized and presented in the following sections:
1. Distribution of cotton mill workers based on the demographic variables.
2. Distribution of pre test and post test Level of Knowledge among cotton
mill workers on respiratory problems.
3. Distribution of pre test and post Level of Attitude among cotton mill
workers on respiratory problems.
4. Difference of pre test, post test level of knowledge and attitude.
5. Association of knowledge with the selected demographic variables on
prevention of respiratory problems among cotton mill workers
6. Association of attitude with the selected demographic variables on
prevention of respiratory problems among cotton mill workers

33
TABLE 1.a
DISTRIBUTION OF COTTON MILL WORKERS BASED ON THE
DEMOGRAPHIC VARIABLES N=60
S.No Demographic Variables Frequency Percentage
1 Age in years
21-30 15 25
31-40 16 27
41-50 20 33
51-60 9 15
2 Sex
Male 24 40
Female 36 60
3 Educational status
Educated 18 30
Uneducated 42 70
4 Occupation (in year)
1-10 years 25 42
11-20 years 26 43
>20 years 9 15
5 Overtime work
Some times 16 26
Regularly 27 45
Often 10 17
Never 7 12
Table 1.a reveals that among 60 cotton mill workers majority 20 (33%) of
workers were between 41-50 years. Regarding Sex, majority 36 (60%) is Females.
With regard to educational status, majority 42(70%) were uneducated. In connection
with occupational experience majority 26 (43%) were 11-20years experience. With
regard to Overtime work majority 27(45%) are regularly doing the overtime.

34
TABLE 1.b
DISTRIBUTION OF COTTON MILL WORKERS BASED ON THE
DEMOGRAPHIC VARIABLES
N=60
S.No Demographic Variables Frequency Percentage
6 Place of work
Blow room 12 20
Carding 19 32
Drawing 9 15
Spinning 9 15
Cone winding 11 18
7 Exercise
Walking/Running 14 23
Yoga 3 5
Any other 14 23
Not at all 29 49
8 Habits
Smoking 9 15
Consuming alcohol 14 23
Tobacco chewing 15 25
Any other 12 20
None of the above 10 17
Table 1.b reveals that among 60 cotton mill workers majority 19(32%) are
working in carding department. In connection to habits Majority 15(25%) are having
tobacco chewing habits.

35
TABLE 1.c
DISTRIBUTION OF COTTON MILL WORKERS BASED ON THE
DEMOGRAPHIC VARIABLES
N=60
S.No Demographic Variables Frequency Percentage
9 Disease
Allergic disorders 7 12
Pulmonary tuberculosis 19 32
Bronchial asthma 19 32
Other respiratory problems 7 12
None of the above 8 13
10 Symptoms
Persistent cough 11 18
Fever 22 37
Loss of weight 7 12
Chest tightness 8 13
Shortness of breath 7 12
None of the above 5 8
Table 1.c reveals that among 60 cotton mill workers majority majority 19
(32%) are suffering from pulmonary tuberculosis and bronchial asthma. Regarding
Symptoms majority 22(37%) are having fever.

36
FIGURE 2
DISTRIBUTION OF PRE TEST AND POST TEST LEVEL OF KNOWLEDGE
AMONG COTTON MILL WORKERS ON RESPIRATORY PROBLEMS
The above figure reveals that pre test knowledge majority 40(66%) had
inadequate knowledge. The post test knowledge revealed majority36 (60%) had
adequate knowledge and 16(27%) had moderately adequate knowledge. It is inferred
that there is a significant difference between pre and post – test level of knowledge of
respiratory problems among cotton mill workers.
37
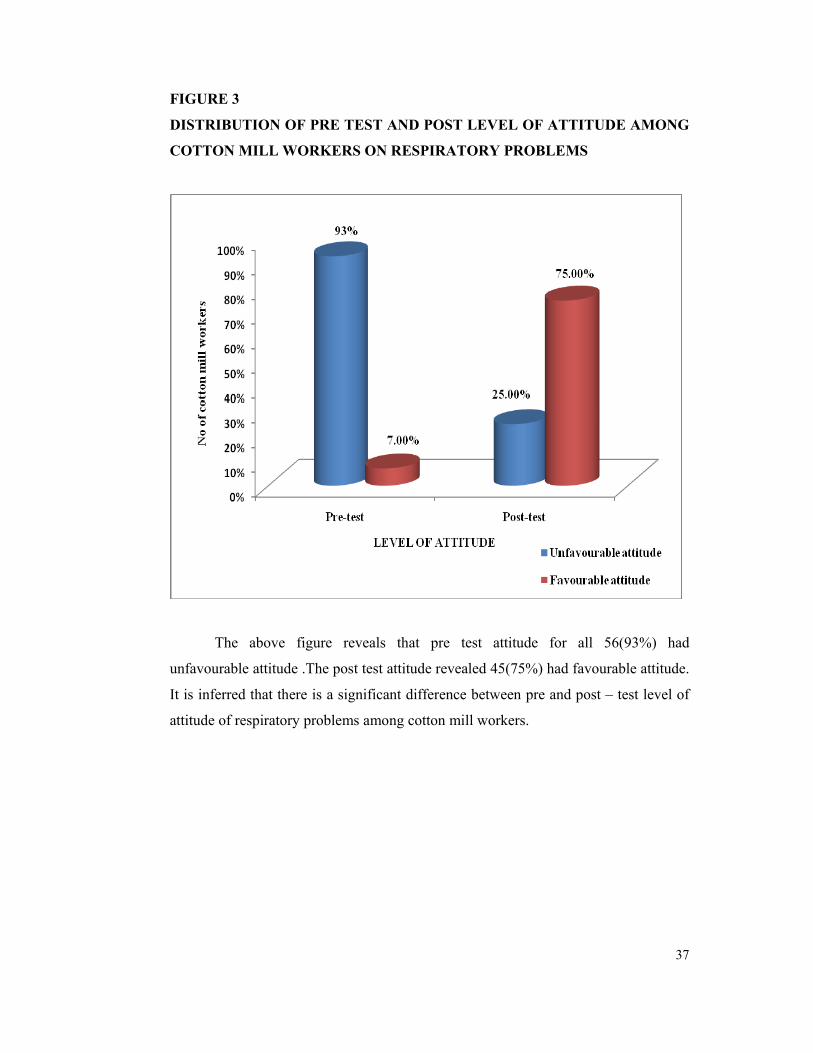
FIGURE 3
DISTRIBUTION OF PRE TEST AND POST LEVEL OF ATTITUDE AMONG
COTTON MILL WORKERS ON RESPIRATORY PROBLEMS
The above figure reveals that pre test attitude for all 56(93%) had
unfavourable attitude .The post test attitude revealed 45(75%) had favourable attitude.
It is inferred that there is a significant difference between pre and post – test level of
attitude of respiratory problems among cotton mill workers.

38
TABLE 2
DIFFERENCE OF PRETEST; POST TEST LEVEL OF KNOWLEDGE
AND ATTITUDE
Max Pre test scores Post test scores
‘t’ value Area score Mean SD
Mean
% Mean SD
Mean
%
Knowledge 20 10.52 3.61 53 15.45 3.96 77 7.353***
Attitude 60 29 7.06 48 46.95 10.97 78 11.409***
(p<0.001 highly significant)
The above table reveals the obtained knowledge of pre-test and post test. The
pretest mean score was 10.52 with a standard deviation of 3.93; post-test mean score
was 15.45 with a standard deviation of 3.96 and the paried‘t’ score on knowledge was
7.353 (p<0.001) was highly significant and the obtained attitude pretest mean score
was 29 with a standard deviation of 7.06 .The mean difference of post test was 46.95
with a standard deviation of 10 and the obtained paired‘t’ score was 11.409 (p<0.001)
was highly significant. It is inferred that there is a significant difference between pre
and post –test level of knowledge and attitude on respiratory problems among cotton
mill workers. Therefore video teaching programme brings improvement in their
knowledge and attitude among cotton mill workers. Thereby the research hypothesis
was accepted.

39
TABLE 3.a
ASSOCIATION OF KNOWLEDGE WITH THE SELECTED
DEMOGRAPHIC VARIABLES
N = 60
Demographic variable In-
adequate moderate Adequate
χ2
value
p-
value
Age
21-30yrs
1
3
11
31-40 yrs 2 4 10
41-50 yrs 4 6 10 2.53# 0.87
51-60yrs 1 3 5
Overtime
work
Some times
3 4 9
Regularly 2 6 19
Often 2 3 5 3.38# 0.76
Never 1 3 3
Occupational
experience in
years
1-10 yrs
4 5 16
11-20 yrs 3 8 15 1.08# 0.9
>20 yrs 1 3 5
# Not significant at 0.05% level.
Table 3.a presents the association between post test level of knowledge with
demographic variables among cotton mill workers. Regarding age, the χ2 was
2.53(p<0.05) which was not significant. Regarding Occupational experience, the χ2
was 1.079(p<0.05) which was also not significant. Regarding overtime work the χ2
was 3.378 (p<0.05) which was not significant.

40
TABLE 3.b
ASSOCIATION OF KNOWLEDGE WITH THE SELECTED
DEMOGRAPHIC VARIABLES
N=60
Demographic variable In-
adequate Moderate Adequate χ2 value
p-
value
Place
of
work
Blow room
2
4
6
Carding 2 9 8
Drawing 1 1 7
Spinning 0 2 7 12.578# 0.127
Cone winding 3 0 8
Habits
Smoking
1
3
5
Consuming
alcohol
3 5 6
Tobacco Chewing 1 3 11 6.815# 0.557
Any other 3 3 6
None of the
above
0 2 8
# Not significant at 0.05% level.
Table 3.b presents the association between post test levels of knowledge with
demographic variables among cotton mill workers. Regarding Place of work, the χ2
was 12.578 (p<0.05) which was not significant. Regarding habits the χ2 was 3.13
(p<0.05) which was not significant.

41
TABLE 4.a
ASSOCIATION OF ATTITUDE WITH THE SELECTED DEMOGRAPHIC
VARIABLES
N = 60
Demographic variable Un
favourable
attitude
Favourable
attitude Chi
square
value
p-
value
Age
21-30
4
11
31-40 3 13
41-50 6 14 0.659# 0.883
51-60 2 7
Occupational
experience in
years
1-10 9 16
11-20 4 22 2.93# 0.23
>20 2 7
Place of work
Below room 4 8
Carding 4 15
Drawing 3 6 2.756# 0.6
Spinning 3 6
Cone
winding
1 10
# Not significant at 0.05% level.
Table 4.a presents the association between post test levels of attitude with
demographic variables among cotton mill workers. Regarding age, the χ2 was
0.659(p<0.05) which was not significant. Regarding Occupational experience, the χ2
was 2.93(p<0.05) which was also not significant. Regarding Place of work, the χ2 was
2.756 (p<0.05) which was not significant.

42
TABLE 4.b
ASSOCIATION OF ATTITUDE WITH THE SELECTED DEMOGRAPHIC
VARIABLES N = 60
Demographic
variable
Un
favourable
attitude
Favourable
attitude χ2
P value
Overtime work
• Some times 4 12
• Regularly 7 20
• Often 4 6 3.456# 0.315
• Never 0 7
• Not at all 2 4
• Smoking 2 7
Habits
• Consuming
alcohol 3 11
• Tobacco
Chewing 6 9 3.13# 0.536
• Any other 3 9
• None of the
above 1 9
# Not significant at 0.05% level.
Table 4.b presents the association between post test levels of attitude with
demographic variables among cotton mill workers.Regarding overtime work the χ2
was 3.456 (p<0.05) which was not significant. Regarding habits the χ2 was 6.815
(p<0.05) which was not significant.

43
CHAPTER- V DISCUSSION
The study was conducted to evaluate the effectiveness of video assisted
programme on knowledge and attitude regarding prevention of respiratory problems
among cotton mill workers in selected cotton mills, Madurai. This chapter deals with
the discussion and interpretation of the findings to assess the Knowledge and Attitude
on respiratory problems among cotton mill workers.
This study was conducted by pre experimental design. Subjects were selected
by purposive sampling method. The sample size was 60.
A questionnaire and checklist was used to find out the knowledge and
attitude among cotton mill workers regarding respiratory problems. The response
were analysed through preexperimental measures (mean, frequency, percentage,
standard deviation) and inferential statistics (chi-square,‘t’ test).
The discussion was based on the objectives specified in this study.
The first objective of this study was to assess the existing level of knowledge and
attitude on prevention of respiratory problems among selected cotton mill
workers.
Pretest knowledge revealed 40 (66%) had inadequate knowledge and10
(15%) had moderately adequate knowledge. And the pretest attitude for all56 (93%)
had unfavourable attitude. The pretest knowledge (mean=10.52, SD=3.62). The
pretest attitude (Mean=29, SD= 7.06). These findings were consistent with the study
done by K.Priya et all found the existing knowledge of using safety practices of the
sample were not satisfactory. They identified that before teaching the knowledge and
attitude among cotton mill workers are lacking. Thus teaching programme will
improve their knowledge and brings changes in their attitude.

44
The second objective of this study was to assess the post test level of knowledge,
attitude and practice on prevention of respiratory problems among selected
cotton mill workers.
The post test knowledge revealed 36(60%) had adequate knowledge and
16 (27%) had moderately adequate knowledge, the post test attitude revealed 45(75%)
had favourable attitude. The post test knowledge (Mean= 15.45, SD= 3.96) the post
test attitude (Mean=46.95, SD=10.97).
The finding of this study is consistent with Thoreia Mohamed et all(2001)
conducted a study on effectiveness of among cotton mill workers to improve their
knowledge and skills. They proved that Periodic inspection, training and health
education improve the knowledge regarding respiratory problems. Main objective of
the study is teaching and guidance in order to gain the better outcomes.
The third objective of this study was to find out the difference between pretest
and post –test level of knowledge and attitude on prevention of respiratory
problems among selected cotton mill workers.
The obtained post test mean value of knowledge 15.45 was higher than the
pretest value 10.52. The mean difference between pretest and post test was 24 and the
obtained paired‘t’ test value was 7.353( p<0.001) was highly significant. The obtained
post test attitude mean value 46.95 was higher than the pretest attitude mean value 29.
The mean difference between pretest and post test attitude was 30. and obtained
paired ‘t’ test value was 11.409(p<0.001) highly significant These findings reveal that
the video teaching programme was effective and the cotton mill workers gained
adequate knowledge and attitude. Thereby research hypothesis was accepted.
The findings suggested that suggested that knowledge and attitude level was
enhanced after video teaching programme.
The findings of the study is consistent with Sateesh Satawaji(2007) conducted
a study on effectiveness of teaching programme on prevention of respiratory problems
among cotton mill workers. They found that the effectiveness of educational
programme tested by inferential statistics using the paired‘t’ test. A significance
difference was found between pre and post tests knowledge score.

45
The fourth objective of this study was to find out the association between post
test level of knowledge and attitude on prevention of respiratory problems
among selected cotton mill workers with the selected demographic variables.
The findings of the study concluded that there is no association between level
of knowledge and attitude with selected demographic variables.
The finding of the study is consistent with Jessica S Kale (2007) conducted
study on effectiveness of structured teaching programme on respiratory problems
among cotton mill workers. She identified that there was no significant association
between level of knowledge and attitude with selected demographic variables. The
investigator feels that inspite of all the variables the video teaching programme will
improve the knowledge and attitude of cotton mill workers on respiratory problems.
LIMITATIONS
1. Study is limited in assessing the knowledge on respiratory problems by
questionnaire.
2. Study is limited to the cotton mill workers who are working in selected
cotton mills, Madurai.

46
CHAPTER-VI SUMMARY AND RECOMMENDATIONS
This chapter deals with the summary and conclusion drawn. It focuses on the
implications and gives recommendations for nursing practices, nursing research,
nursing administration and nursing education.
Summary of the study
The focus of the study to evaluate the effectiveness of video teaching program
on knowledge and attitude of cotton mill workers on respiratory problems. A review
of literature helped the investigator to develop the conceptual framework,
questionnaire, likert scale and methodology. The review was done with the help of
various literatures. The conceptual frame work adopted for this study was derived
from Nola pender’s Health promotion model.
Research design adopted for the study was pre experimental design. A
questionnaire was developed and used for collecting data about knowledge and
attitude of cotton mill workers on respiratory problems. The tool was found to be
reliable and feasible. The reliability of the tool was established by test-retest method.
The tool was administered among 6 cotton mill workers at Madurai. After a gap of
one week, a retest was given. Karl parson’s coefficient of correlation was computed
and reliability of the knowledge found to be 0.99% and the reliability for attitude
found to be 0.99%. The tool was found to be reliable. Data gathered were analyzed
and interpreted terms of the study objectives.
The main study was conducted in selected cotton mills, Madurai for a period
of six weeks. Purposive sampling technique was used to collect data from the
respondents of the study. Data were organized and interpreted by using both
descriptive and inferential statistics.

47
Main findings of the study
Regarding level of knowledge and attitude in the pre test among cotton mill
workers, 40(66%) had inadequate knowledge and 10(17%) had moderate knowledge
about respiratory problems. Regarding level of attitude 56(93%) had unfavorable
attitude and remaining 4(7%) of the total cotton mill workers had favorable attitude
towards respiratory problems.
Regarding the effectiveness of video teaching program, mean score for post
test knowledge was higher than pretest knowledge. It was 10.52 in pretest and 15.45
in post test. The mean score of attitude in posttest is 24 increased from pretest mean
score 10.52. This shows that there was significant difference between pretest and
posttest knowledge and attitude regarding respiratory problems among cotton mill
workers. This shows that the video teaching program was effective. It was observed
that the video teaching program plays a vital role in improving the knowledge and
attitude of cotton mill workers.
Regarding association between level of knowledge and attitude with selected
demographic variables, there was no significant association between levels of
knowledge and level of attitude with demographic variables like age, sex,
occupational experience, overtime work, place of work and habits etc.
CONCLUSION
The main conclusion of this present study is that education plays fundamental
role in bringing changes in knowledge and attitude of the cotton mill worker. The
investigator hopes that the video teaching program could increase their knowledge
and attitude among cotton mill workers.

48
IMPLICATIONS
The findings of the study have several implications in following field. It can
be discussed on four areas namely nursing practice, nursing administration, nursing
education and nursing research.
Implications of nursing practice
• The study findings will help the occupational health nurse to create awareness
to the cotton mill workers regarding the early identification of respiratory
problems with the help of effective audio-visual aids
• The findings emphasize the need for early detection regarding respiratory
problems through the medical professionals to increase the knowledge and
attitude.
• The nurses can help the workers to get periodical medical examination
• Nursing personnel are in the best position to teach protective measure of
workers .
• Rotation of work from more dusty area to the less dusty area must be ensured.
Implications of nursing administration
• The present study will help the nursing administrative authority to recognize
the need for developing appropriate education program on respiratory
problems among cotton mill workers.
• Nursing administration should provide necessary facilities to conduct
awareness program on respiratory problems with nearby cotton mills.
• The administration should allocate budgets for developing educational
materials like pamphlets, posters, slides, cassettes, etc. which contain
information about respiratory problems in cotton mills.
Implications of nursing education
• The study emphasize the need for educating the nursing personnel through in-
service or continuing education program to update their knowledge regarding
respiratory problems in cotton mills to assess, plan and care for occupational
health problems

49
• Occupational health can be offered as a selected speciality of community
health nursing in higher studies
Implications of nursing research
• The findings of the study help to expand the scientific body of professional
knowledge upon which further research.
• Based upon this study, in-depth research studies of various factors contributes
for respiratory problems among cotton mill workers can be conducted
• Large scale studies can be conducted in consideration of other contributing
variables.
• This study helps the nurse researcher to develop insight in the development of
other research methods and set information for various workers towards
promotion of healthy life and prevention of diseases.
RECOMMENDATIONS
• A similar study can be undertaken with large number of samples which might
lead to generalization
• A similar study can be conducted in another setting
• A similar study can be undertaken by utilizing other domain like practice
• Experimental study can be conducted on effectiveness of protocols on
prevention of respiratory problems.

REFERENCES
BOOKS
• Albert Francis ,M.T.(1998),Respiratory Hazards in an occupational Institute ,
(2nd ed) Nor Publications,(150-153)
• Anderson,C.L.(1973), Community Health ,(2nd ed ), Louise C.V.Mosby and
Co,(78-80)
• Mahajan,B.K. and GuptaM.C.(1992),Textbook of social and preventive
medicine 1st ed, Jaypee brothers(47-61)
• Craig L (1990), Egan’s Fundamentals of respiratory care, Mosby company,6th
edition California.
• Chandrasekar N.K.(1988), Respiratory disease in cotton Industry workers, 94-
96.
• Dr.A.P.Kulkarni(2002),Textbook of community medicine,(2nded)Vora medical
publications.(261-273)
• Edwards RW, Bouchier IAD (1991). Davidson’s Principles and Practice of
Medicine London: ELBS with Churchill Livingstone.(501–503).
• Hutcheson,Jones et all (1981), Occupational hygiene an introduction
guide,London croom hein Ltd(11-12,70-80)
• Murray J.F and Nadel J.A.(1994),Textbook of respiratory medicine, (2nd
ed)W.B saunders publisher
• Park K., (2009), Park’s text book of Preventive and Social Medicine 20th ed.
Jabalpur: Banarsidas Bhanot Publishers.(708–711).
• Polit F Denise, Hungler.P Bernadette(1999), Nursing research principles and
methods,Lippincott,Philadelphia.
• Roberta Hunt (2005), Introduction of community based nursing, 3rd ed
Lippincott company(323-325)
JOURNALS
• Abebe Y, Seboxa T. Byssinosis and other respiratory disorders among textile
mill workers in Bahir Dar North West Ethiopia. Ethiop Med J 1995;13(1):33-
39.
• Abdel Rahman, A.H.; Mohamed, K.M.; Athia, M.N.; Mohamed, W.; Kamal,
A. and Saleh, A.M. (1990): Clinical and immunological responses to cotton

dust exposure among workers in cotton industry. The Egyptian Journal of
Community Medicine, Cairo, Egypt, 7 (2): 111.
• Ahasan, M.R.; Ahmed, S.A. and Khan, T.P (2000): Occupational exposure
and respiratory illness symptoms among textile industry workers in a
developing country. Appl. Occup. Environ. Hyg., 15 (3): 313-320.
• Ahmad, E.F (1988): Knowledge of textile workers about industrial hazards
and their prevention. Thesis submitted for partial fulfillment of master degree
of public health nursing. Alexandria Faculty of Nursing.
• Allan, H. (1981): Primary care medicine, J. B. Lipp in cott. Company. U.S.A:
151.
• Baker, F. (1986): Occupational Health Nursing Mirror, 82 (19): 25-29.
• Barjatiya MK, Mathur RN, Swaroop A (1990). Byssinosis in cotton textile
workers of Kishangarh. Indian J. Chest Dis. Allied. Sci., 32: 215-223.
• Berry G, McKerrow C, Molyneux M, Rossiter C, Tombleson J (1973). A
study of the acute and chronic changes in ventilatory capacity of
workers in Lancashire cotton mills. Br. J. Ind. Med., 30: 25-36.
• Blix, A. (1999): Integrating occupational health protection and health
promotion AAOHN J., 47 (4): 168-171.
• Beverly S, Susanne V. (1995) Air sampling instruments for evaluation of
atmospheric contaminants. 8th edition. ACGIH, Cincinnati, Ohio,.
• Bureau of Labor Statistics (BLS) (1995): Work injuries and illnesses by
selected characteristic, BLS New publication: 95- 142, April 26.
• Centers For Disease Control and Prevention (CDC) (1996): National
Occupation Research Agenda, morbidity and mortality weekly report 45: 445-
446.
• Gupta S, .( 1986)A study of byssinosis and associated respiratory disorders in
cotton mill workers. Indian J Chest Dis Allied Sci;28:183–8. [PubMed:
3610244]
• Gulani KK (2005). Conceptual Aspects of community Health. In :
Community Health Nursing Principles & Practices, Chapter 1, 1st edition,
Kumar Publishers, Delhi,10-12.

• Hayes G. B., (1994) Respiratory Disease in Cotton Textile Workers:
Epidemiologic Assessment of Small Airway Function,Environmental
ResearchVolume 66, Issue 1,31-43
• Howard JK, (1987) Tyrer FH. Text book of occupational medicine, Churchill
Livingstone Longman group U K Ltd., 235-236.
• Ina.O, Ozkan Y(1988)Geographical distribution of Turkish textile industry
and localization trents Bursa IV symposium of textile machine.
• International Labor Organization (ILO) (1981): Education and Training in
Occupational Health Safety and Ergonomics, Eighth report of the joint
ILO/WHO committee on occupational health. Technical report series No 663,
Geneva, 24- 30.
• James, S. and William, F. (1985): An overview of occupational safety and
health guides for superfund sites, American Journal of Industrial Hygiene
Association April, 46 (4): 175- 180.
• Jiang, C.A.; Lam, T.H.; Kong, C.; Cui, C.A.; Huang, H.K.; Chen, D.C.; et all
(1995): Byssinosis in Guangzhou, China. Occup. Environ. Med. J., 52: 268-
272.
• Joseph Mberikunashe1, (2010)Prevalence and risk factors for obstructive
respiratory conditions among textile industry workers in Zimbabwe,
2006,Received: 30/06/2010 - Accepted: 11/07/2010 - Published: 17/07/2010
• Koskela, R-S (1990)Mortality and disability among cotton mill workers,
British Journal of Industrial Medicine 1990;47:384-391
• Lammers, b. et all (1963)A study of byssinosis, chronic respiratory symptoms,
and ventilatory capacity in english and dutch cotton workers, with special
reference to atmospheric pollution, the Netherlands Brit. J. industr. Med.,
1964, 21, 124.
• Lane SR, Sewell RD. (2007) The bacterial profile of cotton lint from
worldwide origins, and links with occupational lung disease. Am J Ind Med.
Jan;50(1):42-7.
• Ma Q, Li D, Zhong Y. (1997) A prospective study on respiratory symptoms
and functions in new employees exposed to cotton dust Zhonghua Yu Fang Yi
Xue Za Zhi. Nov;31(6):355-7.

• Mentesinot Woldeyohannes,(1991)Respiratory problems among cotton textile
mill workers in Ethiopia, British Journal of Industrial Medicine 1991;48:110-
115
• Ministry of Manpower and Training (MMT), (1991): Occupational injury rate
by industry groups in Egypt, 1989.
• Murlidhar V, Murlidhar VJ, Kanhere V. Byssinosis in a Bombay textile mill.
Natl Med J India. 1997 Sep-Oct; 8(5):204-7.
• National Institute for Occupational Safety and Health NIOSH Pocket Guide to
chemical hazards. (1997) National Institute for Occupational Safety and
Health, Cincinnati, Ohio, USA; (NIOSH):97– 140.
• Osibogun A, Oseji MI, Isah EC, Iyawe V. Prevalence of byssinosis and other
respiratory problems among textile mill workers in Asaba, Nigeria. Niger
Postgrad Med J. 2006 Dec;13(4):333-8.
• Occupational Health Directorate (OHD), (1998): The occupational health
directorate of the Ministry of Manpower and Training.
• Occupational Safety and Health Administration (OSHA), (1995): Cotton dust.
U. S. department of labor fact sheet no. 95. V. 23: 1-3.
• Ossler, C.C.; Stanhope, M. and Lancaster, J. (1996): Community health nurse
in occupational health. In: Community health nursing Stanhope, M. and
Lancaster, J. (eds). Mosby-Year Book, inc: 907-920.
• Pneumol JB, Paulo S. Respiratory diseases morbidity and mortality among
adults in their work environment. J Bras Pneumol 2009 Aug.;35(8):1806-
1810.
• Pravin N Respiratory disease and cardiovascular morbidity, Indian J Occup
Environ Med. 2010 Sep-Dec; 14(3): 94–96. doi: 10.4103/0019-278.75697.
• Parikh JR, Et all Prevalence of byssinosis in textile mills at Ahmedabad, India.
Br J Ind Med. 1989;46:789–90.
• Raza, N.S.; Fletcher, M.A.; Pickering, A.C.; Niven, M.R. and Faragher, B.E
(1999): Respiratory symptoms in Lancashire textile weavers. Occup. Environ.
Med., 56: 514- 519.
• Richards. F. Schilling(1963) Epidemiological studies of chronic respiratory
disease Among cotton operatives, London School of Hygiene and Tropical

Medicine, Yale University, 21 November 1963. Received for publication 4
March 1964.
• Rojas P, Stark R, Tembo P. Nurses bring primary health care to industrial
workers. World Health Forum 1990;11(1):108-13.
• Rogers, B. (1994): Roles of the occupational health nurse. In: Occupational
health nursing concepts and practice. W.B. Saunders Co.: 48-64.
• Salazar, M.K. (1997): Core curriculum for occupational health nursing.
American Association of Occupational Health Nursing Inc. 1st ed. W.B.
Saunder Company Philadelphia:3-4.
• Schachter EN, Zuskin E.et.al. Airway responses to the inhalation of cotton
dust and cotton bract extracts. Respiration. 2006;73(1):41-7. Epub 2005 Sep
20.
• Sigsgaard T Respiratory disorders and atopy in cotton, wool, and other textile
mill workers in Denmark. Am J Ind Med. 1992;22(2):163-84.
• Singh AB, Singh A, Pandit T. Respiratory diseases among agricultural
industry workers in India : A cross-sectional epidemiological study. Ann
Agric Environ Med 1999;6:115-126.
• Singh MB, Fotedar R, Lakshminarayana J. Occupational morbidities and
their association with nutrition and environmental factors among textile
workers of desert areas of Rajasthan, India. J Occup Health. 2005
Sep;47(5):371-7.
• Su YM, Su JR, Sheu JY, Loh CH, Liou SH. Additive effect of smoking and
cotton dust exposure on respiratory symptoms and pulmonary function of
cotton textile workers. Ind Health. 2003 Apr;41(2):109-15.
• Tricia D, Dust, and Smoke Exposure in Relation to Adult-Onset Asthma and
Chronic Respiratory Symptoms, The Singapore Chinese Health Study
American Journal of Epidemiology 2006;163(12):1118-1128.
• Venkatakrishna-Bhatt H, Mohan-Rao N, Panchal GM. Differential diagnosis
of byssinosis by blood histamine and pulmonary function test: a review and an
appraisal. Int J Toxicol. 2001 Sep-Oct;20(5):321-7.
• Wang XR, Zhang HX.et.al. A 20-year follow-up study on chronic respiratory
effects of exposure to cotton dust. Eur Respir J. 2005 Nov;26(5):881-6.

• Wang XR, Eisen EAet.al. Respiratory symptoms and cotton dust exposure;
results of a 15 year follow up observation. Occup Environ Med. 2003
Dec;60(12):935-41.
• Wolfson, R. L. M.D.; Byssinosis in Cotton Mill Workers. International
Journal of Sociology and Anthropology Vol. 3(3), pp.109–114, March 2011
• Xy L, Hu N, Huang ZJ, Jiang Y, Wu F. Mortality and death cause proportion
of respiratory diseases in China, 2004-2005. Am Ind Hyg Assoc J
• 1996Nov.;57(11):1002-12.
NET
• American lung association occupational lung disease. An introduction, 1983
[cited 2004 Oct]; Available from: URL: http//www.lungusa.org) (accessed
Oct, 2004).
• Calvin,S. B. Joseph : Occupational Related accidents in selected Garment
Industries in Bangalore city : Indian journal of community medicine Vol. 31,
No. 3, July-September, 2006. URL: http://www.novapdf.co.
• Farooque MI, Khan B, Aziz E, Moosa M, Raheel M, Kumar S, Mansuri FA.
Community Health Sciences, Karachi Medical and Dental College, Karachi. J
Pak Med Assoc. 2008 Feb;58(2):95-8.Byssinosis: as in cotton spinning mill
workers of Karachi. Available from URL:
http://www.ncbi.nlm.nih.gov/pubmed
• Hollander, AG (December 1953). "Byssinosis". Chest 24 (6): 674–678.
American College of Chest Physicians. doi:10.1378/chest.24.6.674 (inactive
2008-06-23). PMID 13107566. Retrieved on 2008-01-
31.http://medind.nic.in/laa/t09/i4/laat09i4p152.pdf
• Lakshmi Prasanna A. Comparative study to develop health education module
on prevention and control of health problems among male and female cotton
mill workers based on their learning needs in selected cotton industries
raichur.Navodaya College of nursing . Raichur Nov 2007.[cited on 2010 jul
6] URL http://www.rguhs.ac.in/.
• Mahmoud TM. S. Hosnia. Abd El – Maged et al : A study of occupational
health hazards among assuit spinning factory workers ; Ass. Univ. Bull

Enviro. Res. Vol. No. 1, March 2004[cited on2010 Aug 8]. URL:
http://www.aun.edu.eg/env_enc/env%20mar/63-76.PDF .
• Neil E, Chter S. Respiratory effect and other disease patterns in textile
industry. Available from:URL: http://www. ilo.org/encyclopedia/?
doc&nd=857200488&nh=0.
• Occupational Safety and Health (OSH), (2000): Healthy people 2010. Centers
for Disease control and prevention. http://www. health.gov/healthy
people/Document/ HTML/ Volume 2/20 Occ. S. H.htm.
• Paramasvam Parimalam, Narayani Kamalamma and Anind kumar
Ganaguli.knowledge, attitude and practices related to occupational health
problems among Garment workers in Tamilnadu, India. Journal of
occupational health;49: 534 [ serial online] 2007, Jul [ cited on 2010 Aug 10]
URL http://www.jstage.jst.go.jp/article/joh/49/6/49_528/_article.




















