+233 21 519394 - INDEPTH Network
14
INDEPTH NETWORK 11 Mensah Wood Street, East Legon P. O. Box KD 213, Kanda Accra, Ghana [email protected] www.indepth-network.org Tel.: +233 21 519394 Fax: +233 21 519395 _____________________________________________________________ QUESTIONNAIRE _____________________________________________________________ Application for Full Membership The purpose of this questionnaire is to enable the INDEPTH Board of Trustees and the Executive Director to have sufficient information on the applicant health and demographic surveillance system (HDSS) site as they review the application for full membership into the Network. Please return the fully completed questionnaire to the INDEPTH Secretariat. The questionnaire is in two parts: PART A is the “MAIN QUESTIONNAIRE” and PART B is an additional module : PART B - HUMAN RESOURCE APPRAISAL AT INDEPTH SITES. To consider your application for full membership, it suffices to submit a fully completed PART A. However, the Secretariat would encourage all applicants to complete and submit PART B either together with PART A or at a later date.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of +233 21 519394 - INDEPTH Network
INDEPTH NETWORK
11 Mensah Wood Street, East Legon P. O. Box KD 213, Kanda
Accra, Ghana [email protected] www.indepth-network.org
Tel.: +233 21 519394 Fax: +233 21 519395
_____________________________________________________________
QUESTIONNAIRE _____________________________________________________________
Application for Full Membership The purpose of this questionnaire is to enable the INDEPTH Board of Trustees and the Executive Director to have sufficient information on the applicant health and demographic surveillance system (HDSS) site as they review the application for full membership into the Network. Please return the fully completed questionnaire to the INDEPTH Secretariat. The questionnaire is in two parts: PART A is the “MAIN QUESTIONNAIRE” and PART B is an additional module: PART B - HUMAN RESOURCE APPRAISAL AT INDEPTH SITES. To consider your application for full membership, it suffices to submit a fully completed PART A. However, the Secretariat would encourage all applicants to complete and submit PART B either together with PART A or at a later date.
PART A – MAIN QUESTIONNAIRE DEFINING INFORMATION REGARDING INDEPTH
INSTITUTIONS
Please note: Responses to these questions should be with specific reference to the health and demographic surveillance system (HDSS) operated at your site, and not to the wider portfolio of research that may be based thereon.
1. Identifying details a) Name of site/project/programme: Kisumu West Health and Demographic Surveillance System (KWHDSS)
Kombewa Clinical Research Center
Walter Reed Project/KEMRI
b) Geographic location: (be as specific as possible i.e. include country, province/region, district/sub-district as appropriate) The Kisumu West HDSS is located in Kenya, Kisumu West District of Nyanza
Province in the western parts of the country. It is situated about 40 km West of
Kisumu city, the administrative capital of Kisumu County. The site covers an
area of about 369km2 bordering the North Eastern shores of Lake Victoria. The
District lies between longitudes 34024’00”E – 34041’30”E and latitude 0011’30” N-
0011’30”S at an average altitude of 1400 m above sea level. The District is divided
into 2 sub-districts (Divisions), each with four (4) further Sub-divisions
(Locations).
The site has a monitored population of 123,477 (KWHDSS Census, 2012).
Females comprise of 54% and Males 46% of the entire HDSS population. The
population is rural and lacks access to many basic healthcare services. Malaria,
HIV, and TB are endemic in this region (western Kenya) with the prevalence of
each being higher than in other parts of the country. Other preventable diseases
(pneumonia, diarrheal disease, schistosomiasis, etc ) are also highly prevalent,
infrastructure is poor and healthcare delivery services are limited. Economic
activities in the area include small scale farming and fishing restricted to
populations bordering the Lake.

KWHDSS GEOGRAPHIC LOCATION
KISUMU WEST HDSS STUDY AREA c) Base institution(s): (e.g. university, Ministry of Health (MOH), research council, etc or multiple of these)
• Kenya Medical Research Institute (KEMRI)
• US Army Medical Research Unit-Kenya (USAMRU-K)
• Kenya Ministry of Health (KMOH)
d) Primary purpose(s) of the HDSS
The overall goal for the program is to provide a unified and exhaustive health
and demographic data set to support USAMRU-K’s work in clinical trials and
disease surveillance.
i) To conduct longitudinal health and demographic surveillance for the
catchment population
ii) To conduct local disease surveillance
iii) To assist in the design of community-based epidemiological studies
iv) To provide a platform for monitoring intervention outcomes in the
community
e) Priority Research Areas
• Malaria Vaccine Clinical Trials
• Malaria Drug Trials
• Tuberculosis Vaccine Trials
• Infectious disease epidemiology and transmission patterns (tuberculosis, diarrheal disease, HIV/AIDS, sexually transmitted infections)
• Human Influenza surveillance
• Maternal and infant health
f) Full contact details (Mailing and email addresses, Tel. and Fax)
The Kisumu West HDSS Walter Reed Project/KEMRI P.O Box 54, 40100 Kisumu, Kenya Telephone: +254-57-20 22942 Fax: +254-57-20 22903 Email: [email protected]
2. Key descriptive features: surveillance a) Size of population under continuous surveillance: 123,477 b) Year when surveillance was introduced:
2007-Initiation of the project
2008-2010-Cartographic Mapping and Census Piloting
2011- Baseline Census
2012-Round 1 of updates
c) Has there been any interruption? If yes, when was surveillance continued?
No
d) Indicate key variables under continuous surveillance: Y/N Frequency of update (monthly, Quarterly, annually)
•••• Births Y Monthly
•••• Deaths Y Monthly
•••• Migration Y Bi-annually
•••• Other variable(s) under continuous surveillance (please list, including frequency of update)
� Immunization status for children <2 years old (Bi-annually)
� Surveillance of use of bed nets, other interventions (Bi-annually)
� Socio-Economic and educational status surveys (every 2 years)
� Pregnancy and Outcomes (Bi-annually)
e) Do you collect information on cause of death? If Yes, how? Yes. During routine household surveys, deaths that have occurred to registered
HDSS members are recorded using a standard validated questionnaire.
Information captured includes date of death, place of death and cause of death
by broad causes i.e. illness, injuries, and accidents among others. All reported
deaths are then visited by a member of the Vital Events team from 3 weeks after
the death to conduct a Verbal Autopsy to identify a probable cause of death.
f) Verbal Autopsy (VA) is a method used in the absence of clinical autopsy to
elicit information on cause of death [See for details: INDEPTH Network (2002).
Population and Health in Developing Countries. Volume 1, Population, Health and
Survival at INDEPTH Sites. IDRC, Canada. This book is available online at
www.idrc.ca]
i) Are Verbal Autopsies conducted?
Yes. Verbal Autopsy questionnaires are completed electronically and returned to
the data room for downloading. Hard copies of the forms are then produced and
sent to two physicians who review the Verbal Autopsy independently and assign
a probable cause of death. If the resulting two codes are discordant, the VA is
coded by a third physician and the code selected by two physicians is entered
into the database. If there are three discordant codes, the cause is entered as
uncertain.
ii) If yes, are the VAs on all deaths, or a sample? Verbal autopsies are conducted on all reported deaths that occur to registered
HDSS members.
g) Database:
i) Are all individual records linked prospectively within the database? Comment if necessary:
Yes. Individual records are linked to their respective dwelling units. The
individual unique identifiers are contingent to the unique household number.
ii) Give brief details on the type of database used, and whether this was custom-designed or is based on a system used elsewhere (e.g. HRS 1 or 2) Data generated from the KWHDSS is stored on an SQL database which was
custom designed in-house.
iii) Comment on data entry capability (e.g. number of resident data typist(s), contracted out to private sector etc):
• in-house capability; If yes, specify: Yes.
The KWHDSS has employed the use of mobile handheld Personal Digital
Assistants (PDAs) for collecting data. The collected data is downloaded daily by
the data team onto the Database. The PDA’s have been preprogrammed with
Quality Assurance and Quality control measures that have considerably
improved the ease at which data is cleaned and assessed.
• contracted out; If Yes, specify: No.
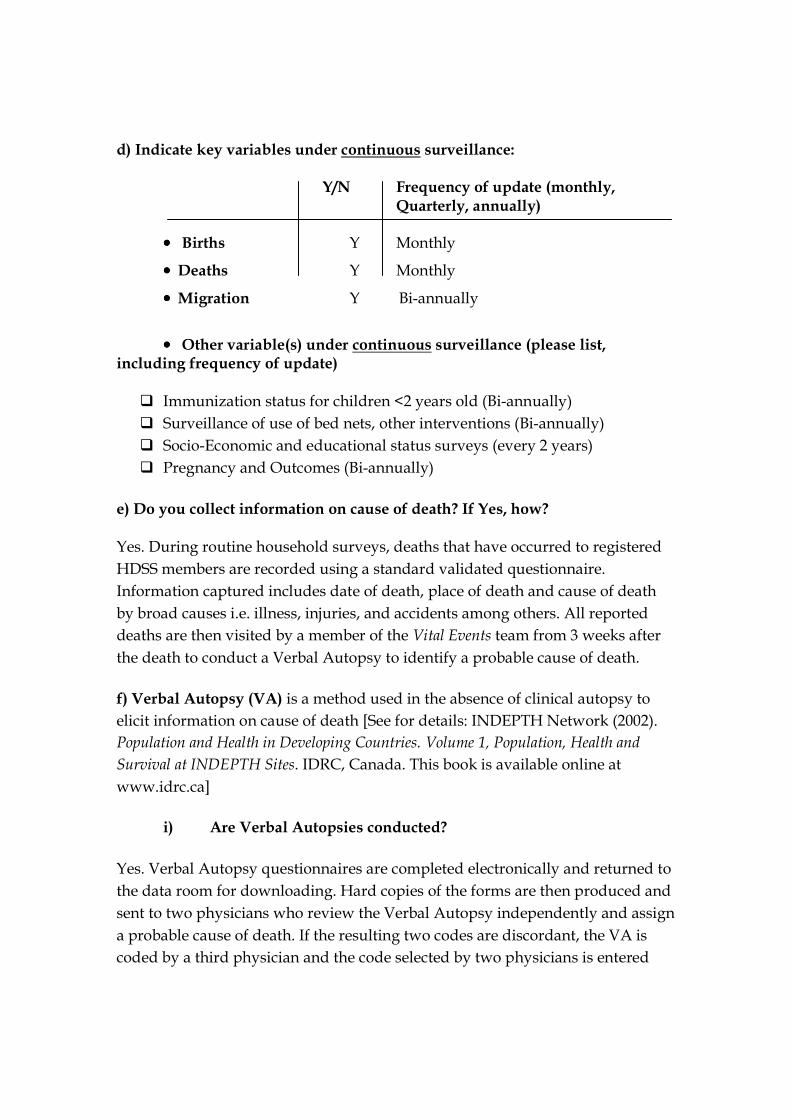
3. Key results (These results may be preliminary in case the HDSS has just been established. Please attached pages if necessary) a) Population pyramid (include as a separate page) included Attached: Appendix 1 b) Mortality rates*, by age and sex ---
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75
De
ath
s P
er
10
00
Age (Years)
KWHDSS Mortality Rates by Age, Sex
Female Male
Source:Kisumu West HDSS
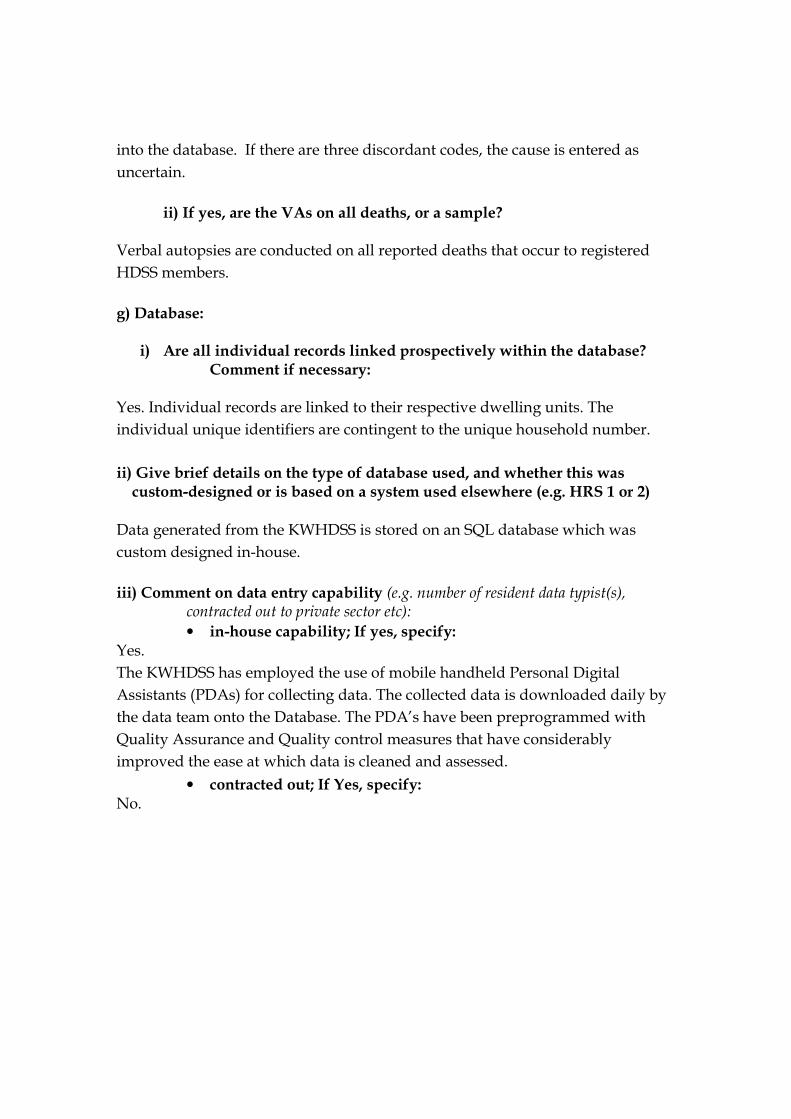
c) Fertility rates*
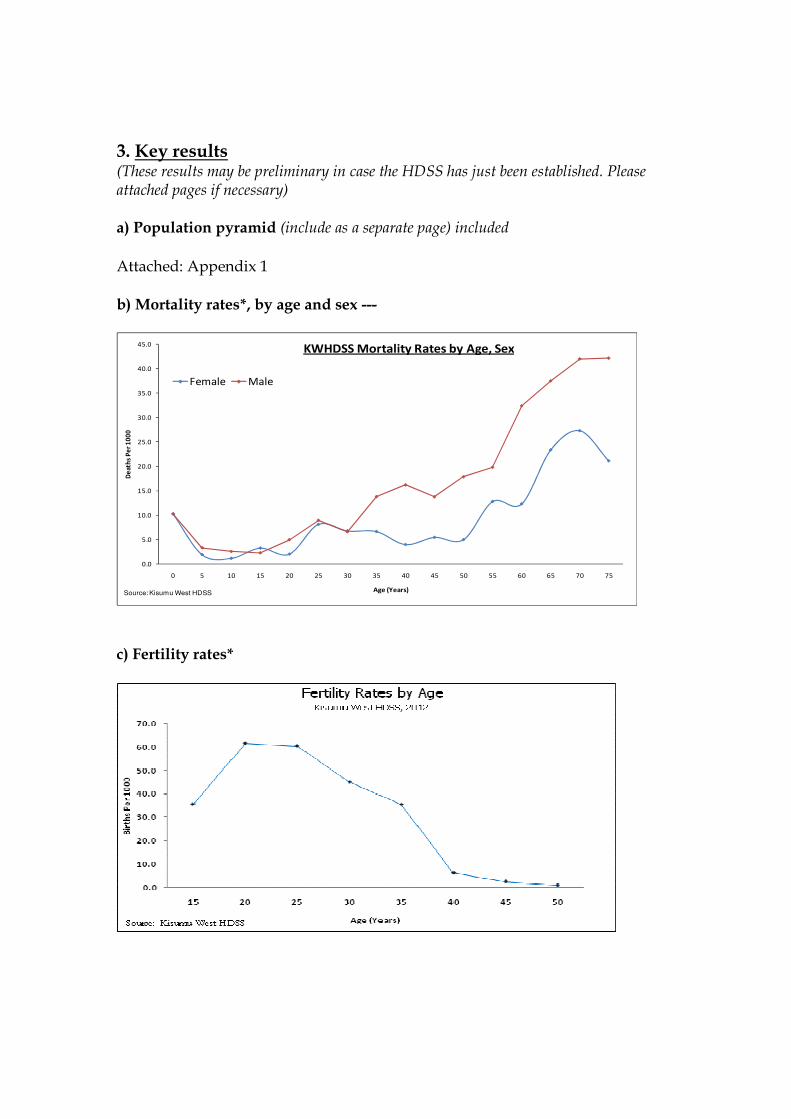
d) Include in- and out-migration rates by age and sex (preferably on the same graph) (* with mortality and fertility rates include trend lines, if available, based on retrospective and prospective analyses) Out-Migrations
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
180.0
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80+
Po
pu
lati
on
Pe
r 1
00
0
Age (Years)
Out-Migration By Age and Sex
Female Male
Kisumu West HDSS, 2012
Source: Kisumu west HDSS
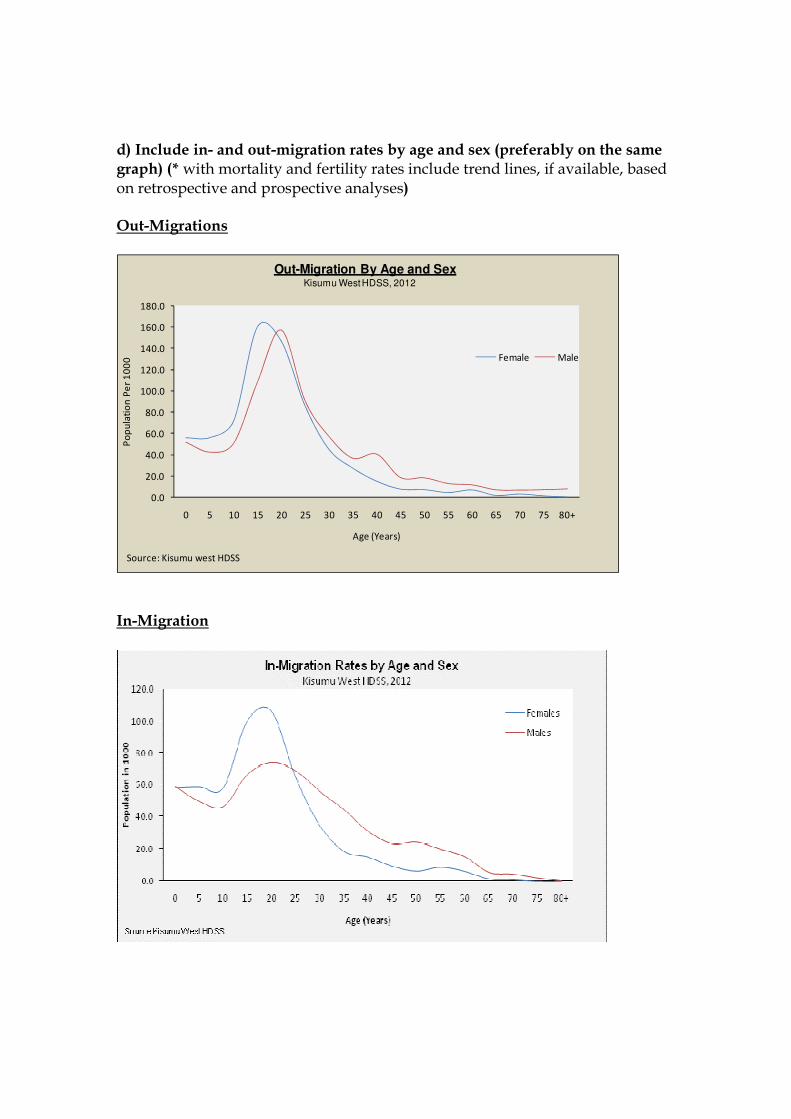
In-Migration
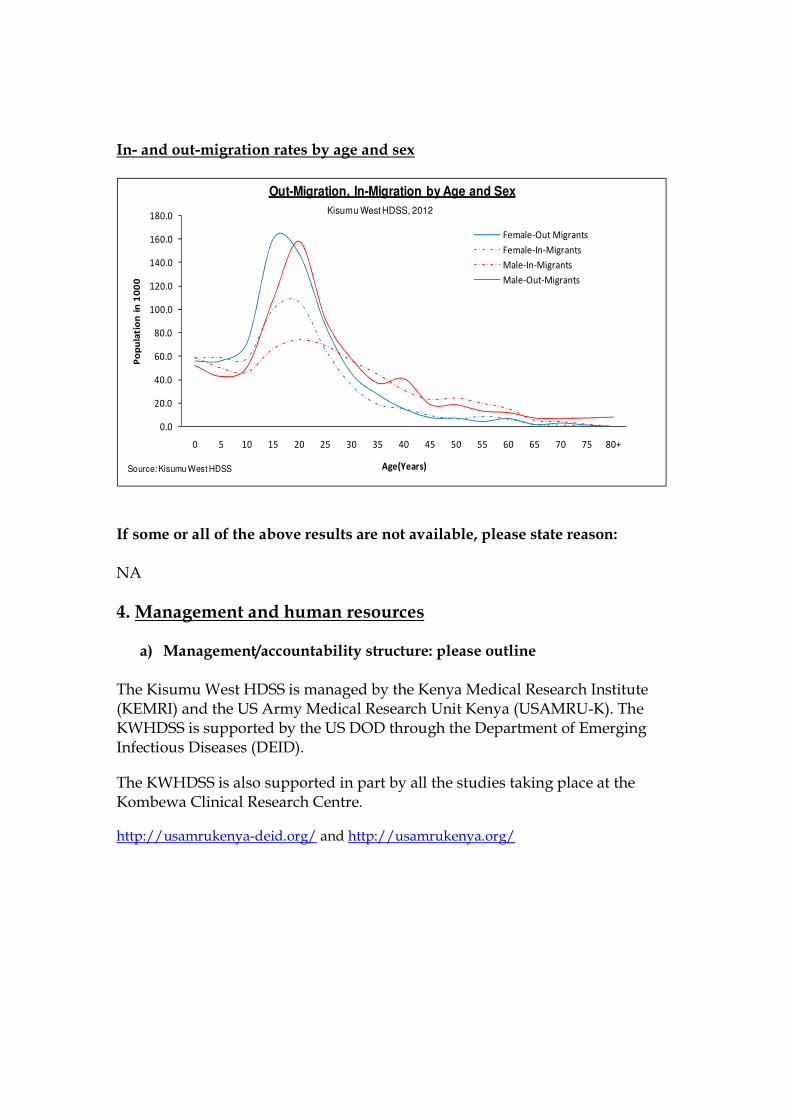
In- and out-migration rates by age and sex
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
180.0
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80+
Po
pu
lati
on
in
10
00
Age(Years)
Out-Migration, In-Migration by Age and Sex
Female-Out Migrants
Female-In-Migrants
Male-In-Migrants
Male-Out-Migrants
Source: Kisumu West HDSS
Kisumu West HDSS, 2012
If some or all of the above results are not available, please state reason:
NA
4. Management and human resources
a) Management/accountability structure: please outline
The Kisumu West HDSS is managed by the Kenya Medical Research Institute (KEMRI) and the US Army Medical Research Unit Kenya (USAMRU-K). The KWHDSS is supported by the US DOD through the Department of Emerging Infectious Diseases (DEID).
The KWHDSS is also supported in part by all the studies taking place at the Kombewa Clinical Research Centre.
http://usamrukenya-deid.org/ and http://usamrukenya.org/
b) Project /director/Manager Mr. Peter Sifuna Project Manager, Kisumu West HDSS Walter Reed Project/KEMRI P.O Box 54, 40100 Kisumu, KENYA Email: [email protected] Tel: 0724 500 607
c) Alternate contact persons
Dr. Walter Otieno, MBChB, M.Med (Paeds) PhD
Site Leader, Kombewa Clinical Research Center, Walter Reed Project/KEMRI P.O Box 54, 40100 Kisumu, KENYA Email: [email protected] Tel: +254 733 905494, +254 714 481488
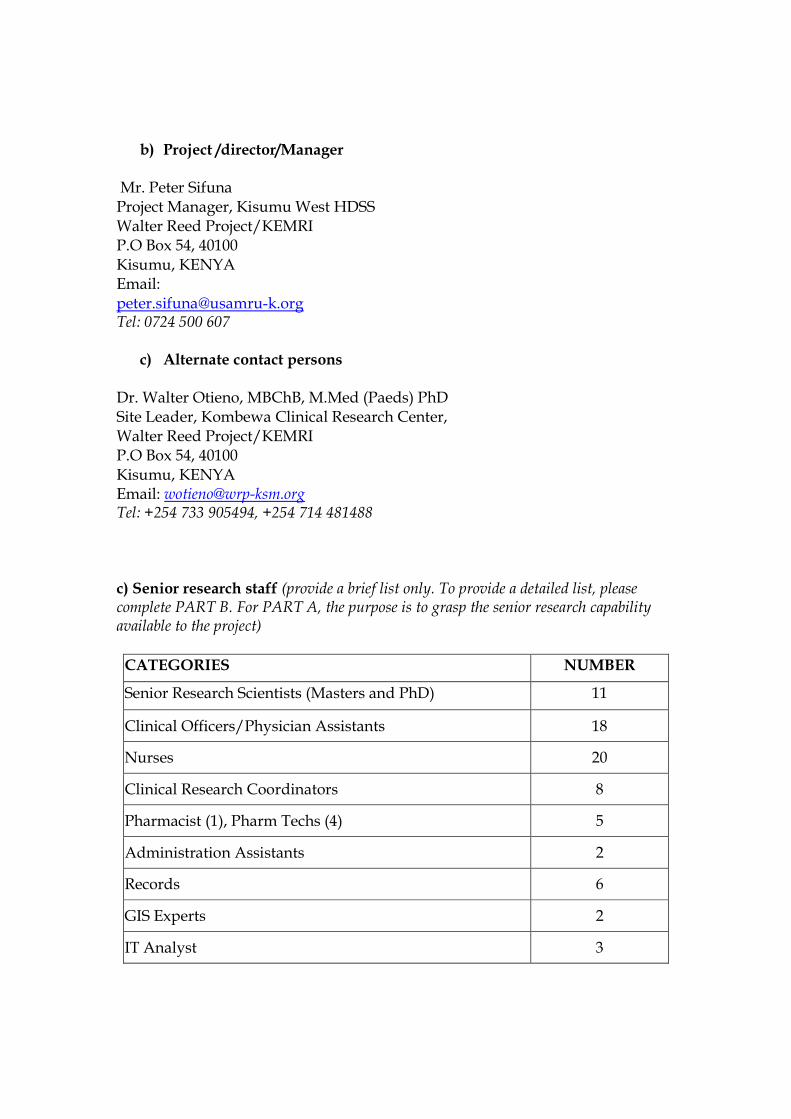
c) Senior research staff (provide a brief list only. To provide a detailed list, please complete PART B. For PART A, the purpose is to grasp the senior research capability available to the project)
CATEGORIES NUMBER
Senior Research Scientists (Masters and PhD) 11
Clinical Officers/Physician Assistants 18
Nurses 20
Clinical Research Coordinators 8
Pharmacist (1), Pharm Techs (4) 5
Administration Assistants 2
Records 6
GIS Experts 2
IT Analyst 3
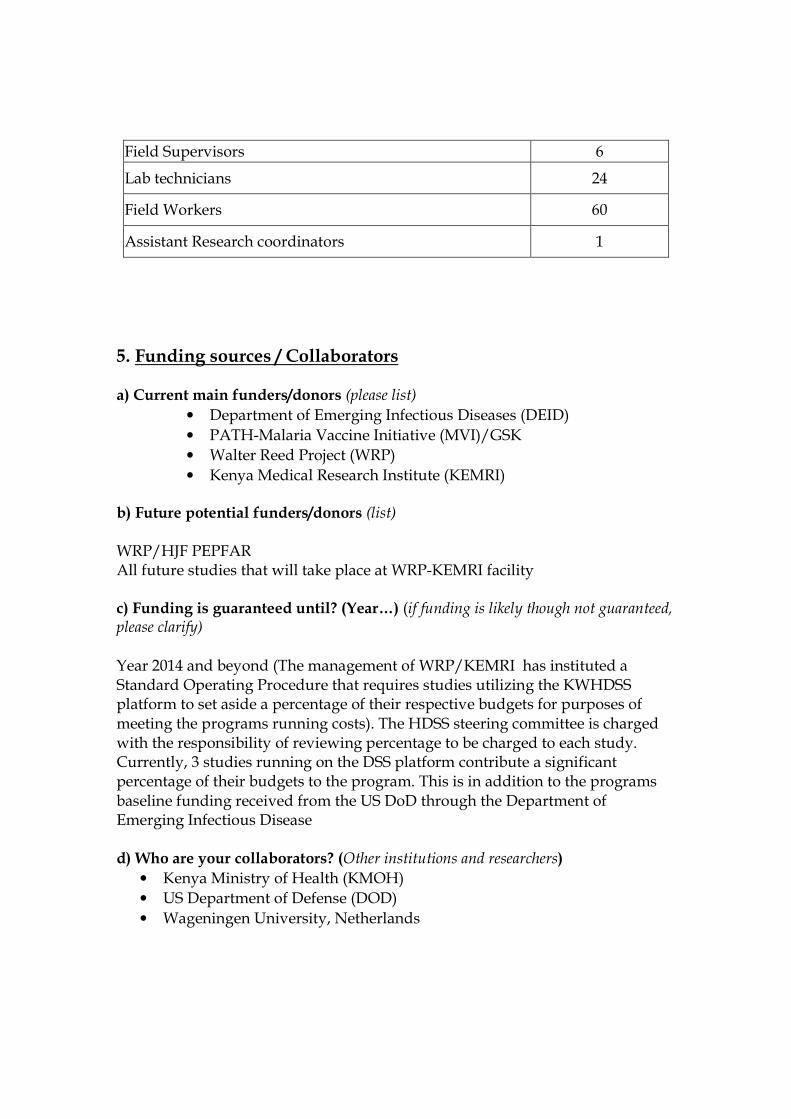
Field Supervisors 6
Lab technicians 24
Field Workers 60
Assistant Research coordinators 1
5. Funding sources / Collaborators a) Current main funders/donors (please list)
• Department of Emerging Infectious Diseases (DEID)
• PATH-Malaria Vaccine Initiative (MVI)/GSK
• Walter Reed Project (WRP)
• Kenya Medical Research Institute (KEMRI) b) Future potential funders/donors (list)
WRP/HJF PEPFAR All future studies that will take place at WRP-KEMRI facility c) Funding is guaranteed until? (Year…) (if funding is likely though not guaranteed, please clarify) Year 2014 and beyond (The management of WRP/KEMRI has instituted a Standard Operating Procedure that requires studies utilizing the KWHDSS platform to set aside a percentage of their respective budgets for purposes of meeting the programs running costs). The HDSS steering committee is charged with the responsibility of reviewing percentage to be charged to each study. Currently, 3 studies running on the DSS platform contribute a significant percentage of their budgets to the program. This is in addition to the programs baseline funding received from the US DoD through the Department of Emerging Infectious Disease d) Who are your collaborators? (Other institutions and researchers)
• Kenya Ministry of Health (KMOH)
• US Department of Defense (DOD)
• Wageningen University, Netherlands

6. Role/contribution of an international network of field sites Focus first on what would be of particular benefit to your own site and its work; thereafter, if appropriate, consider some of the broader roles and contributions such a network might make. a) Contributions of the Network to particular site/project
The INDEPTH Network provides an ideal platform for pooling data generated by the site and other HDSS sites worldwide. This pooling of knowledge leads to greater impact on policy formulation. The KWHDSS envisages that the technical support and leveraging of strengths through this network partnership will further strengthen our young site and will improve the quality of the nested studies we conduct in the future. The site also anticipates competing for multi site studies and trials within the INDEPTH membership.
b) Broader contributions
We hope that joining the network allows data from the KWHDSS to be pooled together with data from other network members for extrapolation. This will be helpful in disseminating results from our HDSS. As a member of the INDEPTH network, our data will have a larger audience and the data generated will be more broadly utilized.
c) What contributions do you envisage your site to make to the Network?
The KWHDSS will share results, research findings and publications within the network under the established framework. The KWHDSS will participate in the INDEPTH scientific conferences (By attendance, posters and oral presentations), Annual General Meetings (AGM) and interest/working groups within the network. The KWHDSS welcomes any cross site studies or data analysis by interested members and will also provide technical support to new members. The Centre will jointly with the others on the platform formulate joint proposals to answer cross site demographic and health issues
d) The INDEPTH Network is keen on taking the lead on public access to data that we generate. Tools are being developed for data access to be possible at various levels to ensure that we strike the right collaborations as well as ensure our work has the greatest impact. Please share with us your thoughts on public access to data that you are generating at your site.
We are favorable to the sharing of HDSS data with the public once the various ethical issues that guarantee the rights and privacy of the participants and their communities are addressed. The centre will be willing through our regulatory team to review and provide any input on the tools being developed for data sharing.
8. Publications a) Please list at most five (5) key publications that have resulted from your
HDSS. (Provide full details of publications and enclose copies if possible.)
i) Oyieko J, Andagalu B, Sifuna P, Otieno A, Otsyula N, Ogutu B, Otieno L,
Otieno W; Using the HDSS to link bacteremia in hospitalized children to the community(To be published)
ii) Sifuna Peter, Carol Tungwony, John Waitumbi; Spatial Analysis of Pediatric Malaria in western Kenya (To be published)
iii) Milton Omondi, Everlyne Nyagaya, Maria Bovill, Shon Remich, George Kodak, Peter Sifuna; Mapping of HIV/AIDS Occurrence in Kisumu West District, Kenya (To be published)
b) Please include your latest annual report. Attached

9. Other considerations Although this enquiry does not aim to be comprehensive, it may be that we have omitted certain key issues or concerns. If so, please list or describe these in this section.
PART B: INDEPTH HUMAN RESOURCE APPRAISAL
See attached Appendix