Death in the Bolivian High Plateau: Burials and Tiwanaku Society
Upload
independentCategory
view
4download
0
Pediatric Exercise Science, 1995, 7, 203-21 0 O 1995 Human Kinetics Publishers, Inc.
Reliability of vOpmax in Adolescent Runners: A Comparison Between Plateau Achievers
and Nonachievers
Anita M. Rivera-Brown, Miguel A. Rivera, and Walter R. Frontera
This study examined the test-retest reliability of ~ 0 , m a x in adolescent VO, plateau achievers and nonachievers. Nineteen male long-distance runners completed a modified Taylor running protocol to volitional fatigue twice within a one-week period. Results showed that 10 subjects did not achieve a plateau in either test (No P), and 9 achieved a plateau in at least one of the tests (P). The ~ 0 , m a x differed (p < .05) between tests (Test 1 and Test 2) for the entire sample (Test 1 = 70.4 + 6.0, Test 2 = 71.7 f 6.3) but not within the groups (No P, Test 1 = 72.1 f 4.4, Test 2 = 73.2 + 4.2; P, Test 1 = 68.5 + 7.3, Test 2 = 70.1 + 7.9). ~ 0 , m a x was similar for plateau achievers and nonachievers in both Test 1 and Test 2 (p > .05). Interclass correlation coefficients for ~ 0 , m a x were high for both the No P (R = 37) and P (R = .97) groups. A high test-retest reliability coefficient for ~ 0 , m a x can be obtained evenq when a plateau in ~ 0 , is not achieved.
A test that measures a physiological variable must be valid and reliable. It must measure what it is intended to measure consistently and in a reproducible manner when properly administered (10). The inherent day-to-day variability of a useful and reliable physiological measurement is smaller than the effects of interventions such as training. Maximal oxygen consumption (V02max) during progressive treadmill exercise is considered a reliable measure of cardiorespira- tory capacity. Reliability coefficients ranging from r =. .81 to r = .97 and R = .90 have been reported for repeated measurements of V02max in children and adolescents during running treadmill exercise (3, 4, 7, 12, .14). However, these studies do not report the frequency of achievement of the V02 plateau criterion in relation to the reliability of V02max.
The ~0~ plateau phenomenon is the most frequently utilized criterion to define a "true" \jo2max during exercise tests to volitional fatigue. However, studies with children and adolescents have shown that a high percentage of those who perform maximal treadmill exercise tests to volitional fatigue satisfy the respiratory exchange ratio and heart rate criteria for V02max, but do not exhibit
Anita M. Rivera-Brown, Miguel A. Rivera, and Walter R. Frontera are with the Exercise Physiology Unit, Center for Sports Health and Exercise Sciences, Albergue Olimpico, Box 2004, Salinas, PR 00751.

204 - Rivera-Brown, Rivera, and Frontera
a plateau in VO, (1, 5, 6, 11, 15, 16, 17, 19). Furthermore, Myers et al. (13) have demonstrated that the occurrence of a plateau is a random event. Therefore, by definition, the V02 plateau is not a consistent and reproducible phenomenon. It seems inappropriate to base the definition of a reliable measure such as V0,max on an inconsistent or random hen omen on.
Children and adolescents who do not reach a plateau have demonstrated VO, and other indicators of maximal effort at peak exercise similar to those who achieve a plateau (5, 6, 11, 16, 17, 20). Green and Patla (9) postulated that additional factors other than oxygen availability, such as an inability to activate the appropriate muscles at peak exercise or an impairment in the excitation- contraction process of the active muscles, may limit the exercise capacity of those who reach volitional fatigue without exhibiting a plateau in VO,.
We found only one study that reported a higher V0,max test-retest reliability when the plateau criterion was achieved during maximal exercise compared to when it was not achieved (8). However, that study was limited to ~o-~ear-old prepubescent boys, and these subjects were measured twice 4-5 months apart. Such a long period of time between tests is not recommended for accurate reliability estimation since the subjects may have changed between testing ses- sions (2). Further research is needed to adequately address this issue in active adolescents.
The purpose of the present study was to compare the test-retest reliability of ~ 0 , m a x in male adolescent long-distance runners who achieved a plateau in VO, and those who did not achieve a plateau. Also, a comparison was made between these groups on variables indicative of maximal effort.
Methodology
Subjects
A group of 19 male adolescents 14-18 years of age who participated in a specialized training program for long-distance running was recruited. These sub- jects attended a school with a special emphasis on the development of athletic skills, and they were selected because they were accustomed to strenuous running exercise and its discomforts and were highly motivated to exercise to fatigue. They had been training in long-distance running for 2 hourslday, 5 dayslweek, 9 monthslyear for an average of 3 years. Their average one-mile time was 329.1 f 21.2 s. Training sessions included a long continuous run of 4-5 miles, interval training, and a fast continuous run or fartlek running. Exercise training intensities yaried from moderate (approximately 70-75% of V0,max) to high (80-95% of V0,max) according to the distances covered each day and the time of the year.
Procedures
All tests were performed in the morning in an air-conditioned laboratory at an average temperature of 23 "C. Subjects were instructed not to exercise vigorously the previous day and not to eat for at least 2 hr before each test. Preceding the first exercise test, testing procedures were explained, parental written consent was obtained, and height was measured with a stadiometer (Detecto Co.). Weight was measured using an electronic scale (Model 2424, Ancaster Co.) the day of

pO,max in Adolescent Runners - 205
each exercise test. All subjects had been previously familiarized with testing procedures and apparatus by performing an exercise test using either the Bruce protocol or the modified Taylor protocol. Ten of the subjects had participated in a similar investigation one year previous to the present study (17).
Each runner completed the modified Taylor continuous running exercise test protocol on a motor-driven treadmill (Model 1800, Marquette Instruments) to volitional fatigue twice, at least 48 hr apart, within a 1-week period. This protocol starts with a 3-min warm-up at 7 mph and 0% grade. The inclination is then increased 2.5% every 2 min, and the speed is kept constant until volitional fatigue. This protocol constitutes a modification of the original Taylor protocol (21), which consists of 3-min stages. Strong verbal encouragement was provided by experienced technicians, and the tests were terminated when the subject indicated that he could not continue. Handrail support was not permitted.
Exercise Measurements
Subjects breathed through a low-resistance nonrebreathing valve (Hans Rudolph 2700) supported by headgear. Expired air was analyzed using an AMETEK metabolic cart (Applied Electrochemistry Model S-3A oxygen analyzer and Model CD-3A carbon dioxide analyzer) that was-calibrated before each test with certified calibration gases. Minute ventilation (VE) was measured using a flow transducer (Model K 520, KL Engineering Co.) attached to the nonrebreathing valve. Gas concentrations were sampled from a mixing chamber, and the 15-s mean V02 and carbon dioxide production (VCO,) values were averaged over 60 s and used for analysis. Respiratory exchange ratio (RER) was calculated as VC02/V02. Heart rate (HR) was recorded during the last 10 s of each minute of exercise using a Marquette electrocardiographic system (MAC 12, Marquette Instruments). If a-subject was unable to complete the final stage of a test, the last 60-s or 30-s VO, average of that final stage was compared to the last 60-s average of the previous work stage for plateau determination. The criteria for V02max were (a) RER 2 1.0, (b) HR 2 95% predicted max (220 - age), and (c) increase in VO, I 2.1 ml.kg-'.min-' with an increase in workload (plateau) (21).
The reported ~ 0 , m a x and maximal RER, HR, and V , for each subject was the highest 60-s V0, average of the test. If a test ended at 30 s into a stage, and the VO,, RER, HR, and VE, measured during those last 30 s were the highest values of the test, these last 30-s averages of the variables were considered maximal. Five subjects (out of 19) during Test 1 and 8 subjects (out of 19) during Test 2 completed the final stage of the exercise test. In 9 of the 38 tests, 30,max did not correspond with the end of a stage. In only 2 of these tests, the highest ~0~ was not figured into the plateau determination.
Statistical Analysis
Means and standard deviations were calculated for the maximal exercise values of the total sample, for those who achieved a plateau in at least one of the tests (P), and for those who did not achieve a plateau in either test (No P). A paired t test was used to compare repeated measurements of maximal exercise values for the total sample and within each group. A one-way analysis of variance was used to compare maximal exercise values between plateau achievers and

206 - Rivera-Brown, Rivera, and Frontera
nonachievers for Test 1 and Test 2 and to calculate intraclass correlation coeffi- cients (R) to determine test-retest reliability of maximal exercise values for the total sample and for each group. R was estimated as MS, - M~,/MSb, where MSb = mean square between subjects and MS, = mean square within subjects (2). An alpha level of p I .05 was considered significant.
Results
The mean (2 SD) age, weight, and height of the subjects was 15.6 + 1.4 years (range = 14-18 years), 53.3 .f 8.7 kg, and 165.9 f 6.4 cm, respectively. These athletes exhibited average VO, values of 71.0 ml.kg-'.min-' during maximal exercise typical of well-trained adult long-distance runners (18).
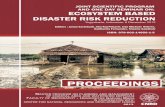
The frequency of achievement for each criterion during Test 1 and Test 2 is shown in Figure 1. All subjects attained the RER criterion, and 95% attained the HR criterion during both Test 1 and Test 2. The frequency of plateau achieve- ment was 42% and 21% during Test 1 and Test 2, respectively. Ten subjects (52%) did not achieve a plateau in either test, and 9 subjects (47%) achieved a plateau in either Test 1 or Test 2 (3 of these [16%] achieved a plateau in both tests).
RER 2 1 .O HR 2 95% vo plateau 2
TEST 1 TEST 2
Figure 1 - Percentage of adolescent long-distance runners achieving the criteria for V0,max during Test 1 and Test 2.

VO,rnax in Adolescent Runners - 207
Maximal exercise variables and intraclass correlation coefficients of the entire sample for Test 1 and Test 2 are presented in Table 1; those of the No P . group are presented in Table 2; and those of the P group are presented in Table 3. V02max differed between Test 1 and Test 2 for the entire sample 07 < .05) but not within the groups. Maximal HR and RER were similar between Tesf 1 and Test 2 for the entire sample and within the groups (p > .05). Maximal VE differed between Test 1 and Test 2 for the entire sample and within the No P group (p < -05) but was similarlwithin the P group 0, > .05). Maximal test duration differed between Test 1 and Test 2 for the entire sample and within the groups 0, < .05). No differences were found in VO,, HR, RER, v,, or test duration during maximal exercise between plateau achievers and nonachievers during Test 1 or Test 2 0, > .05). High reliability coefficients were obtained for all maximal exercise variables during Test 1 and Test 2 for the entire sample and for the P and No P groups.
Discussion Maximal oxygen consumption has been shown to be a reliable measure of the cardiorespiratory capacity of children and adolescents (3 ,4 ,7 , 12, 14). Few data
Table 1 Maximal Exercise Values and Intraclass Correlation Coefficients for the Entire Sample
Test 1 Test 2 M SD M SD P R
602 (ml.kg-l.min-I) 70.4 6.0 71.7 6.2 .032 .94 HR (beats.min-I) 206.3 6.9 207.2 8.1 .312 .92 RER 1.2 0.1 1.2 0.1 .629 .83 vE (L.min-I) 122.5 21.4 126.2 22.2 .003 .98 Test duration (s) 587.4 73.0 618.9 73.6 .OOO .90
Table 2 Maximal Exercise Values and Intraclass Correlation Coefficients for the No Plateau Group
Test 1 Test 2 M SD M SD P R
VO, (ml.kg-l.min-') 72.1 4.4 73.2 4.2 .246 .87 HR (beats.min-I) 206.3 5.9 207.7 7.1 .338 .87 RER 1.2 0.1 1.2 0.5 .881 .75 V, (L.min-') 124.2 18.4 129.0 18.5 .011 .97 Test duration (s) 585.0 72.4 621.0 69.3 .008 .88

208 - Rivera-Brown, Rivera, and Frontera
Table 3 Maximal Exercise Values and Intraclass Correlation Coefficients for the Plateau Group
Test 1 Test 2 M SD M SD P R
~0~ (ml.kg-'.min-I) 68.5 7.3 70.1 7.9 .067 .97 HR (beats.min-I) 206.2 8.1 206.5 9.5 .754 .97 RER 1.2 0.1 1.2 0.1 .356 .98 \jE (L.min-I) 120.6 25.3 123.1 26.6 .I50 .99 Test duration (s) 590.0 77.9 616.7 82.3 .035 .93
are available regarding the influence that achieving a VO* plateau may have on the reliability of V02max in adolescents. The major finding of the present study was that a high test-retest reliability coefficient for V02max was seen in both groups of subjects, the plateau achievers and the nonachievers.
Several investigators have questioned the usefulness of the plateau criterion to identify a true V0,max value in children and adolescents for several reasons: (a) A low percentage (1 1.5-56%) of trained and untrained children and adoles- cents achieve a plateau in VOz (1, 5, 6, 16, 17, 19); (b) plateau achievers and nonachievers demonstrate similar responses during maximal exercise (5, 6, 11, 16); and (c) the achievement of the criterion-may be protocol and population specific (17). It has been suggested that peak V02 values can be considered true V02max in these populations (1 1, 16, 17, 19, 20).
In the present study, the rates of plateau achievement were 42% and 21% for Test 1 and Test 2, respectively. This finding agrees with previous reports that indicate a plateau is not frequently achieved during maximal exercise in adolescents (1, 5, 15, 16, 17). Additionally, even though more than half of our subjects had completed at least four maximal exercise tests previous to the present study, a higher percentage of them failed to achieve a plateau during the second test compared to the first test. This suggests that familiarity performing the test was not a factor affecting the achievement of a plateau in VOz. The decrease in the number of subjects who achieved a plateau during Test 2 and the absence of a plateau in one of the two tests in several of the subjects of the P group support the argument that the plateau phenomenon is inconsistent and therefore unreliable.
Previous studies with adolescents failed to demonstrate differences between those who achieve a plateau and those who do not in t e q s of anthropometrical characteristics (16); maximal exercise variables such as V02, HR, and RER (5, 6, 16, 17); and isokinetic power of the knee extensor and flexor muscle groups (16). The findings of the present study agree with these observations. No differ- ences were found in any of the maximal exercise variables between those who achieved a plateau and those who did not.
We found only one study that reported a higher ~ 0 ~ m a x reliability in children who achieved a V02 plateau compared to those who did not. Cunningham et al. (8) studied 10-year-old male ice hockey players and reported a higher

V02max in Adolescent Runners - 209
correlation between two treadmill continuous running tests, performed 4-5 months apart, when a plateau was achieved in both tests (r = .74) compared to when it was achieved in only one of the tests (r = .60) or when it was not achieved in either test (r = .27). In our study, the reliability of V02max for plateau achievers and nonachievers is much higher than the values reported by Cunningham et al. (8). This may be due to one or more of the following reasons: (a) We used intraclass correlation coefficients to estimate reliability instead of Pearson correlation coefficients; (b) the period of time between our two tests is much shorter than that used by Cunningham et al. (8); and (c) adolescents may respond differently than children. -.
The use of the intraclass correlation coefficient is considered the best statistical method to estimate test-retest reliability (2). Nevertheless, the differ- ence between the R in our study and the Pearson correlation coefficient in the study of Cunningham et al. (8) for those who did not achieve a plateau is too large to be explained only by statistical theories. The subjects in the study of Cunningham et al. were measured twice, 4-5 months apart. Such a long period of time is not recommended for a test-retest reliability study. It is possible that the subjects may have changed between testing sessions due to the natural growth and maturation process and/or other environmental influences (2). .Finally, it is also conceivable that in adolescents the absence of a plateau in V02 may not affect the reliability of V02max to the same degree that it does in children. Further research is needed to confirm these findings.
In summary, a low frequency of achievement of the plateau criterion was observed in active adolescents who satisfied both the HR and the RER criteria during two identical maximal exercise tests performed on separate days. The reliability of ~ 0 , m a x was high even when a V02 plateau was not achieved. Those who achieved a plateau and those who did not demonstrated similar values during maximal running exercise. These data provide further evidence to~uggest that the plateau criterion should not be a requisite for establishing a true V02max in adolescents.
References 1. Armstrong, N., J. Balding, P. Gentle, and B. Kirby. Estimation of coronary risk factors
in British schoolchildren: A preliminary report. Br. J. Sports Med. 24:61-65, 1990. 2. Baumgartner, T.A., and A.S. Jackson. Measurement for Evaluation in Physical Educa-
tion and Exercise Science (4th ed.). Dubuque, IA: Brown, 1991. 3. Boileau, R.A., A. Bonen, V.H. Heyward, and B.H. Massey. Maximal aerobic capacity
on the treadmill and bicycle ergometer of boys 11-14 years of age. J. Sports Med. 17~153-162, 1977.
4. Bonen, A., V.H. Heyward, K.J. Cureton, R.A. Boileau, and B.H. Massey. Prediction of maximal oxygen uptake in boys, ages 7-15 years. Med. Sci. Sports 11:24-29, 1979.
5. Cooper, D.M., D. Weiler-Ravell, B.J. Whipp, and K. Wasserman. Aerobic parameters of exercise as a function of body size during growth in children. J. Appl. Physiol. 56~628-634, 1984.
6. Curnming, G.R., and W. Friesen. Bicycle ergometer measurement of maximal oxygen uptake in children. Can. J. Physiol. Pharmacol. 45:937-946, 1967.
7. Cunningham, D.A., P. Telford, and G.T. Swart. The cardiopulmonary capacities of young hockey players: Age 10. Med. Sci. Sports 8:23-25, 1976.

21 0 - Rivera-Brown, Rivera, and Frontera
8. Cunningham, D.A., B.M.V. Waterschoot, D.H. Paterson, M. Lefcoe, and S.P. Sangal. Reliability and reproducibility of maximal oxygen uptake measurement in children. Med. Sci. Sports 9: 104-108, 1977.
9. Green, H.J., and A.E. Patla. Maximal aerobic power: Neuromuscular and metabolic considerations. Med. Sci. Sports Exerc. 24:38-46, 1992.
10. Johnston, M.V., Keith, R.A., and Hinderer, S.R. Measurement standards for inter- disciplinary medical rehabilitation. Arch. Phys. Med. Rehabll. 73:S3-S23, 1992.
11. Mahon, A.D., and M.L. Marsh. Ventilatory threshold and V02 plateau at maximal exercise in 8- to 11-year-old children. Ped. Exer. Sci. 5:332-338, 1993.
12. Miyamura, M., H. Kuroda, K. Hirata, and Y. Honda. Evaluations of the step test scores based on the measurements of maximal aerobic powers. J. Sports Med. 15:316- 322, 1975.
13. Myers, J., D. Walsh, N. Buchanan, and V.F. Froelicher. Can maximal cardiopulmonary capacity be recognized by a plateau in oxygen uptake? Chest 96:1312-1316, 1989.
14. Paterson, D.H., D.A. Cunningham, and A. Donner. The effect of different treadmill speeds on the variability of V02max in children. Eur. J. Appl. Physiol. 47:113-122, 1981.
15. Ritmeester, J.W., H.C. Kemper, and R. Verschuur. Is a leveling-off criterion in oxygen uptake a prerequisite for a maximal performance in teenagers? In: International Series on Sport Sciences (Vol. XI), 1985, pp. 161-169.
16. Rivera-Brown, A.M., M.A. Rivera, and W.R. Frontera. Applicability of criteria for V02max in active adolescents. Ped. Exer. Sci. 4:331-339, 1992.
17. Rivera-Brown, A.M., M.A. Rivera, and W.R. Frontera. Achievement of vo2max criteria in adolescent runners: Effects of testing protocol. Ped. Exer. Sci. 6:236-245, 1994.
18. Rowland, T.W. Aerobic responses to physical training in children. In: Endurance in Sport, R.J. Shephard and P.O. Astrand (Eds.). Oxford: Blackwell Scientific, 1992, p. 380.
19. Rowland, T.W. Does peak VO, reflect vozmax in children? Evidence from supra- maximal testing. Med. Sci. Sports Exerc. 25:689-693, 1993.
20. Rowland, T.W., and L.N. Cunningham. Oxygen uptake plateau during maximal tread- mill exercise in children. Chest 2:485-489, 1992.
21. Taylor, H.L., E. Buskirk, and A. Henshell. Maximum oxygen intake as an objective measure of cardiorespiratory performance. J. Appl. Physiol. 8:73-80, 1955.
Acknowledgments
The authors thank Edgar Lopategui, MS, and Reynaldo Soler, BS, for their technical assistance during exercise testing, and the subjects and their coach, Freddy Ramos, for their enthusiastic participation in the study.
Copyright © 2022 FDOKUMEN